Attached files
| file | filename |
|---|---|
| 8-K - PHARMACYCLICS INC | form8k207380_11052012.htm |
| EX-99.9 - PHARMACYCLICS INC | ex999to8k207380_11052012.htm |
| EX-99.4 - PHARMACYCLICS INC | ex994to8k207380_11052012.htm |
| EX-99.8 - PHARMACYCLICS INC | ex998to8k207380_11052012.htm |
| EX-99.1 - PHARMACYCLICS INC | ex991to8k207380_11052012.htm |
| EX-99.2 - PHARMACYCLICS INC | ex992to8k207380_11052012.htm |
| EX-99.5 - PHARMACYCLICS INC | ex995to8k207380_11052012.htm |
| EX-99.7 - PHARMACYCLICS INC | ex997to8k207380_11052012.htm |
| EX-99.3 - PHARMACYCLICS INC | ex993to8k207380_11052012.htm |
| EX-99.12 - PHARMACYCLICS INC | ex9912to8k207380_11052012.htm |
| EX-99.18 - PHARMACYCLICS INC | ex9918to8k207380_11052012.htm |
| EX-99.15 - PHARMACYCLICS INC | ex9915to8k207380_11052012.htm |
| EX-99.10 - PHARMACYCLICS INC | ex9910to8k207380_11052012.htm |
| EX-99.16 - PHARMACYCLICS INC | ex9916to8k207380_11052012.htm |
| EX-99.13 - PHARMACYCLICS INC | ex9913to8k207380_11052012.htm |
| EX-99.14 - PHARMACYCLICS INC | ex9914to8k207380_11052012.htm |
| EX-99.17 - PHARMACYCLICS INC | ex9917to8k207380_11052012.htm |
| EX-99.11 - PHARMACYCLICS INC | ex9911to8k207380_11052012.htm |
Exhibit 99.6
Multiple Myeloma Poster Presentation
Title: Early Changes in Cytokines, Chemokines and Indices of Bone Metabolism in a Phase 2 Study of the Bruton Tyrosine Kinase (Btk) Inhibitor, Ibrutinib (PCI-32765) in Patients with Relapsed or Relapsed/Refractory MM
Session: 653. Myeloma - Therapy, excluding Transplantation: Poster III
Date/Time: Monday, December 10, 2012, 6:00 PM - 8:00 PM
Location: Georgia World Congress Center, Hall B1-B2
Presenter: Ravi Vij
Ravi Vij, MD1, Betty Y. Chang, PhD2*, Jesus G. Berdeja, MD3, Carol Ann Huff, M.D.4, Nikoletta Lendvai, MD PhD5,6, Yu-Tzu Tai, PhD7, Stella Chang8*, Davina Moussa9*, Joseph J. Buggy, PhD9*, Laurence Elias, MD2 and Paul G. Richardson, MD10
1Department of Medicine, Division of Oncology, Washington University School of Medicine, Saint Louis, MO
2Research, Pharmacyclics, Sunnyvale, CA
3Sarah Cannon Research Institute, Nashville, TN
4Oncology, Johns Hopkins University, Baltimore, MD
5Myeloma/Lymphoma Service, Memorial Sloan-Kettering Cancer Center, New York, NY
6Weill Medical College of Cornell University, New York, NY
7Medical Oncology, Dana Farber Cancer Institute, Boston, MA
8Research, Pharmacycylics, Sunnyvale, CA
9Pharmacyclics, Inc., Sunnyvale, CA
10Department of Medical Oncology, Dana-Farber Cancer Institute, Boston, MA
ABSTRACT:
Introduction: Bruton tyrosine kinase (Btk) is essential in the development and function of B cells through normal B cell receptor signaling, and it is down-regulated in non-malignant plasma cells. This is not the case in malignant plasma cells of patients with MM where robust Btk gene expression is usual. In addition, Btk is expressed and functional in osteoclasts and their precursors, which play a pathogenic role in MM-related bone disease, as well as growth and survival of MM in the microenvironment. Researchers in our group (Tai, Chang et al, Blood, 2012) recently demonstrated that the Btk inhibitor ibrutinib (PCI-32765) inhibited the interaction of MM cells with stromal cells, and inhibited the growth in vitro of MM colony forming cells from patient explants. Ibrutinib suppressed in vitro osteoclast differentiation and production of multiple cytokines and chemokines including CCL3, CCL4, IL-8, and TGF-β. Ibrutinib furthermore decreased MM progression and accompanying bone destruction in an in vivo SCID-Hu myeloma model. Based on these observations, we initiated a clinical trial of ibrutinib in patients with relapsed (R) and relapsed/refractory (R/R) MM. This report of early marker changes is based upon 7 patients who have completed 3 cycles of treatment.
Methods: Patients with progressive disease (PD) after at least 2 prior lines of therapy received a fixed dose of oral ibrutinib 420 mg orally once daily, with a cycle defined as 28 days. Dexamethasone 40 mg weekly could be added if no response or PD was observed by cycle 2. Blood levels of cytokines, chemokines and bone markers (bone-specific alkaline phosphatase (bAP), sclerostin and RANKL) were assessed centrally at Days 1, 2, 8, and 15 of Cycle 1, Cycle 2 Day 1 and every 2 cycles thereafter, by single or multiplexed immunoassays. Serum cross-linked C-terminal peptide of collagen I (sCTx) was determined by a central lab at the start of Cycles 1 and 2 and every other cycle thereafter. Responses were assessed following the International Myeloma Working Group criteria (modified to include minimal response).
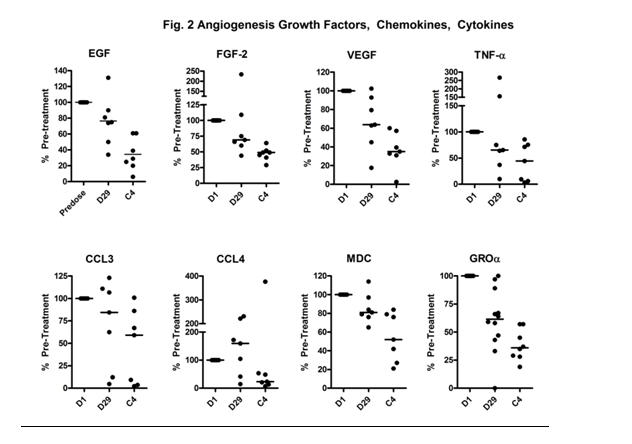
Results: Thirteen patients [M/F: 8/5; median age 62, range 49-74 years] were enrolled between March 21 and June 6, 2012. All patients had received prior treatment with lenalidomide, bortezomib, alkylators and dexamethasone. 7 were refractory to their last treatment. At the time of data cut off, 7 of the 13 patients enrolled had completed 3 cycles of therapy and were the ones used for analysis. Over the course of three cycles, several markers relevant to bone metabolism exhibited gradual decreases. At Cy4D1 plasma RANKL, sclerostin, and bAP exhibited (median) decreases of 47%, 39%, and 36%, respectively. Relative changes in sCTx were more variable at Cy2D1, but there appeared to be a trend towards subject-by-subject decreases at C4D1 (Fig. 1). Factors promoting growth and angiogenesis (e.g. VEGF, EGF, and FGF) and cytokines and chemokines (CCL3, CCL4, TNFα, Groα and MDC) with roles in MM micro-environmental interactions exhibited similar reductions (Fig. 2). Among these the most dramatic and consistent changes were in CCL3 and CCL4, chemokines enhancing adhesive interactions contributing to osteolysis in MM, which showed median decreases of 43% and 77% at Cy4D1, respectively. Ibrutinib has been uniformly well tolerated and the safety experience to date has been similar to that noted in other studies of ibrutinib in lymphoma and CLL.
Conclusions: Early reductions in blood levels of cytokines, chemokines, markers of bone metabolism, and pro-angiogenic and growth factors, were observed among MM patients treated with ibrutinib, which were consistent with pre-clinical studies. Among markers related to bone metabolism, it appeared that changes in regulatory molecules (sclerostin, RANKL) were more marked and perhaps preceded changes in markers of osteoclast (sCTx) or osteoblast (bAP) activity. Elucidation of these patterns and their significance will require longer follow-up of a larger number of patients. These results indicate that ibrutinib can exert significant biologic effects on the microenvironment in MM. Clinical correlations will be forthcoming based upon maturing results over the next several months.
FIGURES

Disclosures: Vij: Millennium: Speakers Bureau; Celgene: Research Funding, Speakers Bureau; Onyx: Honoraria, Research Funding. Chang: Pharmacyclics, Inc.: Employment, Equity Ownership. Huff: Celgene: Membership on an entity’s Board of Directors or advisory committees; Novartis: Consultancy. Chang: Pharmacyclics, Inc.: Employment, Equity Ownership. Moussa: Pharmacyclics, Inc.: Employment, Equity Ownership. Buggy: Pharmacyclics: Employment, Equity Ownership. Elias: Pharmacyclics, Inc.: Employment, Equity Ownership. Richardson: Millenium Pharmaceuticals: Membership on an entity’s Board of Directors or advisory committees; Celgene Corporation: Membership on an entity’s Board of Directors or advisory committees; Novartis Pharmaceuticals: Membership on an entity’s Board of Directors or advisory committees; Johnson & Johnson: Membership on an entity’s Board of Directors or advisory committees; Bristol Myers Squibb: Membership on an entity’s Board of Directors or advisory committees.