Attached files
| file | filename |
|---|---|
| 8-K - 8-K - VIVUS INC | a10-13137_18k.htm |
| EX-99.1 - EX-99.1 - VIVUS INC | a10-13137_1ex99d1.htm |
| EX-99.2 - EX-99.2 - VIVUS INC | a10-13137_1ex99d2.htm |
| EX-99.5 - EX-99.5 - VIVUS INC | a10-13137_1ex99d5.htm |
| EX-99.4 - EX-99.4 - VIVUS INC | a10-13137_1ex99d4.htm |
Exhibit 99.3
Below is a graphical representation of the poster entitled “Low-Dose, Controlled-Release Phentermine/Topiramate and Markers of Type 2 Diabetes Mellitus”:
Below is a reproduction of the contents of the poster entitled “Low-Dose, Controlled-Release Phentermine/Topiramate and Markers of Type 2 Diabetes Mellitus”:
Authors: Donna H. Ryan, MD(a); Kishore M. Gadde, MD(b); Peter Tam(c); Barbara Troupin, MD(c)
(a)Pennington Biomedical Research Center, Baton Rouge, Louisiana, United States of America; (b)Duke University Medical Center, Durham, North Carolina, United States of America; (c)VIVUS, Inc., Mountain View, California, United States of America
· Introduction
· Obesity is an epidemic in the United States associated with comorbidities such as cardiovascular disease and type 2 diabetes mellitus (T2DM), as well as increased mortality.(1)-(4)
· Impaired fasting glucose (IFG) and impaired glucose tolerance (IGT) often lead to T2DM and can be exacerbated by weight gain. Research has demonstrated that IFG and IGT can both be improved with weight loss and therefore may potentially delay or prevent the progression to T2DM.(5),(6)
· Phentermine (PHEN) and topiramate (TPM) are 2 pharmacologic agents with demonstrated weight-loss properties. PHEN is currently approved in the United States for short-term weight loss (recommended dose is 37.5 mg) as an adjunct to lifestyle modifications. TPM is indicated for treatment of seizures (recommended dose: 400 mg/day) and prevention of migraines (recommended dose: 100 mg/day).(7),(8)
· A previous extended-release formulation of TPM at doses titrated up to 175 mg/day (range 50 mg/day to 175 mg/day) demonstrated weight loss in clinical trials, although side effects were significant, and prevented further development of that formulation as monotherapy.(9),(10) Therefore, a combination of low-dose, controlled-release (CR) PHEN/TPM for once-daily oral dosing was developed to maximize weight loss and comorbid benefits, while minimizing adverse events.
· Objective
· To evaluate the treatment effects of PHEN/TPM CR on glycemic parameters across multiple patient populations including normoglycemic, prediabetic, and diabetic.
· Methods
· 3 clinical studies are included in this evaluation:
· CONQUER: double-blind, placebo-controlled Phase 3 trial of 2487 overweight/obese adult subjects (BMI >27 kg/m2 and <45 kg/m2) with >2 weight-related comorbidities randomly assigned to placebo, PHEN 7.5 mg/TPM CR 46 mg (7.5/46), or PHEN 15 mg/TPM CR 92 mg (15/92) for 56 weeks. All subjects received lifestyle and exercise guidance. Subjects with T2DM at baseline (n=388 [15.8%]) were either antidiabetic drug-naïve or on metformin only for their diabetes.
· EQUIP: double-blind, placebo-controlled Phase 3 trial of 1267 obese subjects (BMI >35 kg/m2), excluding subjects with T2DM, randomly assigned to placebo, PHEN 3.75 mg/TPM CR 23 mg (3.75/23), or 15/92 for 56 weeks.
· DM-230: 28-week extension of a 28-week double-blind, placebo-controlled Phase 2 trial (56 weeks total). In total, 130 subjects with T2DM mostly for >5 years continued in this trial extension; 60% were on >2 antidiabetic medications. Subjects remained on their originally assigned dose of placebo or 15/92 during the 28-week extension.
· This analysis of data from CONQUER, EQUIP, and DM-230 was carried out in order to determine the effects of PHEN/TPM CR over a broad range of subjects stratified by glycemic status. The rationale for integrated analysis includes similar subjects, standardized endpoints, and consistent doses of PHEN/TPM CR in all trials.
· Assessments
· A primary efficacy endpoint for both Phase 3 studies was percent weight loss at Week 56 with last observation carried forward (LOCF) for the intent-to-treat (ITT) set and for study completers, with the corresponding treatment comparisons. For EQUIP, the change at 56 weeks for fasting glucose in subjects with the highest baseline fasting glucose is reported. For CONQUER, the change at 56 weeks in HbA1c and fasting insulin in the ITT and T2DM subset is reported. For DM-230, the changes in HbA1c, fasting glucose, and fasting insulin at 56 weeks in all subjects with T2DM are reported.
· Statistical methods: Analysis of the first primary efficacy variable, percent weight loss at endpoint, was performed using an analysis of covariance (ANCOVA) model with treatment, study, and gender as fixed effects and baseline weight as a covariate. Data are presented at Week 56 with LOCF. The ITT and study completer sets were the primary analysis populations for efficacy presentations.
· Results
· Baseline characteristics of pooled 1-year cohort (EQUIP and CONQUER) are presented in Table 1. Subjects were mostly female (74.3%), age <65 years (93.3%), and over-weight or obese (60.5% BMI >30 kg/m2 and <40 kg/m2; 34.7% BMI >40 kg/m2). DM-230 subjects were mostly female (69.2%) and had a mean age of 49.6 years. At baseline, mean weight was 96.3 kg, BMI was 35.3 kg/m2, and waist circumference was 109.8 cm.
Table 1. Baseline Characteristics of Pooled Analysis of EQUIP and CONQUER: ITT Set- 1 Year Cohort
|
|
|
Placebo |
|
PHEN/TPM |
|
PHEN/TPM |
|
PHEN/TPM |
|
Total |
|
|
Age (years) |
|
|
|
|
|
|
|
|
|
|
|
|
Mean (SD) |
|
48.5 (11.43) |
|
43.0 (11.05) |
|
51.1 (10.38) |
|
48.0 (11.97) |
|
48.3 (11.62) |
|
|
Age, n (%) |
|
|
|
|
|
|
|
|
|
|
|
|
<65 years |
|
1382 (93.6) |
|
230 (98.3) |
|
442 (90.6) |
|
1376 (93.0) |
|
3430 (93.3) |
|
|
Gender, n (%) |
|
|
|
|
|
|
|
|
|
|
|
|
Female |
|
1102 (74.6) |
|
194 (82.9) |
|
341 (69.9) |
|
1094 (74.0) |
|
2731 (74.3) |
|
|
Weight (kg) |
|
|
|
|
|
|
|
|
|
|
|
|
Mean (SD) |
|
107.5 (20.18) |
|
118.6 (21.94) |
|
102.8 (18.19) |
|
107.1 (19.62) |
|
107.4 (20.09) |
|
|
Waist circumference (cm) |
|
|
|
|
|
|
|
|
|
|
|
|
Mean (SD) |
|
115.8 (13.26) |
|
121.5 (15.15) |
|
112.7 (12.42) |
|
115.5 (13.51) |
|
115.7 (13.50) |
|
|
BMI (kg/m2) |
|
|
|
|
|
|
|
|
|
|
|
|
Mean (SD) |
|
38.5 (5.73) |
|
42.5 (6.54) |
|
36.3 (4.41) |
|
38.4 (5.67) |
|
38.4 (5.75) |
|
|
BMI category n (%) |
|
|
|
|
|
|
|
|
|
|
|
|
>30 and <40 kg/m2 |
|
904 (61.2) |
|
91 (38.9) |
|
344 (70.5) |
|
887 (60.0) |
|
2226 (60.5) |
|
|
>40 kg/m2 |
|
502 (34.0) |
|
143 (61.1) |
|
111 (22.7) |
|
521 (35.2) |
|
1277 (34.7) |
|
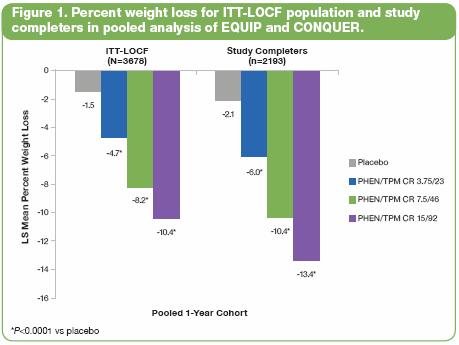
· In pooled data from Phase 3 trials EQUIP and CONQUER, least-squares (LS) mean percent weight loss in the ITT-LOCF population (N=3678) was significantly greater for all doses of PHEN/TPM CR vs placebo: 1.5%, 4.7%, 8.2%, and 10.4% for placebo, 3.75/23, 7.5/46, and 15/92, respectively; P<0.0001 (Figure 1).
· For subjects in this cohort completing 56 weeks of treatment on study drug (n=2193), LS mean percent weight loss was also significant vs placebo: 2.1%, 6.0%, 10.4%, and 13.4% for placebo, 3.75/23, 7.5/46, and 15/92, respectively; P<0.0001 (Figure 1).
· In EQUIP, the 261 subjects in the upper quartile of fasting glucose (FG) had baseline mean FG of 105.0-105.6 mg/dL across treatment groups, which is within the prediabetes range of 100-125 mg/dL. At 56 weeks, the LS mean change in FG in subjects treated with PHEN/TPM CR was -3.5 mg/dL, -9.3 mg/dL, and -6.2 mg/dL for placebo, 3.75/23, and 15/92, respectively (P<0.05 vs placebo), placing post-treatment mean values below the prediabetes threshold (Table 2).
Table 2. Change in FG at Week 56 for EQUIP Subjects in Upper Quartile at Baseline (ITT-LOCF)
|
|
|
Baseline Mean |
|
LS Mean Change |
|
P value vs |
|
|
Placebo |
|
105.0 |
|
-3.5 |
|
— |
|
|
PHEN/TPM CR 3.75/23 |
|
105.6 |
|
-9.3 |
|
0.0003 |
|
|
PHEN/TPM CR 15/92 |
|
105.2 |
|
-6.2 |
|
0.0350 |
|
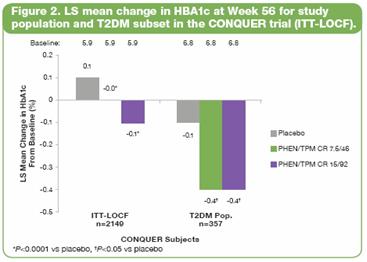
· In CONQUER, at Week 56, HbA1c was significantly reduced in both PHEN/TPM CR groups vs placebo both in subjects with T2 DM (P<0.05) and the study population as a whole (P<0.0001) (Figure 2).
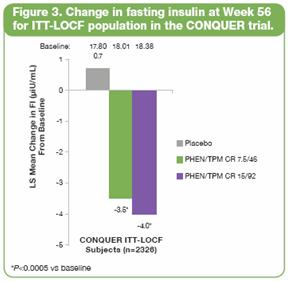
· In CONQUER, mean changes in fasting insulin showed increased values in placebo compared with significant dose-proportional improvements in both treated groups (P<0.0005 vs placebo; ITT-LOCF population) (Figure 3).
· In DM-230, PHEN/TPM CR led to significantly greater LS mean improvement from baseline to Week 56 in HbA1c (-1.6% vs -1.2% for placebo; P=0.0381), fasting glucose (-42.1 vs -27.4 mg/dL for placebo; P=0.0205), and fasting insulin (2.1 vs 5.9 µIU/mL for placebo; P=0.0296) (Table 3).
Table 3. Change in Glycemic Parameters at Week 56 in Subjects With T2DM After PHEN/TPM CR Treatment in
DM-230 (ITT-LOCF)
|
|
|
HbA1c |
|
Fasting Glucose |
|
Fasting Insulin |
|
||||||
|
|
|
Baseline |
|
LS Mean Change |
|
Baseline |
|
LS Mean Change |
|
Baseline (µIU/mL) |
|
LS Mean Change |
|
|
Placebo |
|
8.55 |
|
-1.2% |
|
170.7 |
|
-27.4 |
|
13.24 |
|
5.9 |
|
|
PHEN/TPM CR 15/92 |
|
8.76 |
|
-1.6%* |
|
176.2 |
|
-42.1* |
|
10.62 |
|
2.1* |
|
*P<0.05 vs placebo
· Conclusions
· Treatment with PHEN/TPM CR leads to weight loss and improvement in glycemic markers across multiple populations — normoglycemic, prediabetic, and diabetic (both early and more advanced disease) — compared to worsening glycemic status in untreated/placebo subjects.
· Benefits in glycemic status from PHEN/TPM CR treatment likely represent effects of significant weight loss, which may alter the natural history of diabetes as a weight-related disease. Improvements in glycemic markers demonstrate benefit above and beyond lifestyle intervention and standard of care, which was the standardized background for all subjects.
These trials are registered at ClinicalTrials.gov, number NCT00600067 (DM-230), number NCT00554216 (EQUIP), and
number NCT00553787 (CONQUER).
References: 1. Reaven GM. Importance of identifying the overweight patient who will benefit the most by losing weight. Ann Intern Med. 2003;138:420-423. 2. Flegal KM, Carroll MD, Ogden CL, Johnson CL. Prevalence and trends in obesity among US adults, 1999-2000. JAMA. 2002;288:1723-1727. 3. Haslam DW, James WP. Obesity. Lancet. 2005;366:1197-1209. 4. Adams KF, Schatzkin A, Harris TB, et al. Overweight, obesity, and mortality in a large prospective cohort of persons 50 to 71 years old. N Engl J Med. 2006;355:763-778. 5. American Diabetes Association. Standards of medical care in diabetes—2006. Diabetes Care. 2006;29(suppl 1):S4-S42. 6. Diabetes Prevention Program Research Group. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346:393-403. 7. Adipex-P [package insert]. Sellersville, PA: Teva Pharmaceuticals USA; 2005. 8. Topamax [package insert]. Titusville, NJ: Ortho-McNeil-Janssen Pharmaceuticals, Inc.;2009. 9. Rosenstock J. Hollander P, Gadde KM, Sun X, Strauss R, Leung A, for the OBD-205 Study Group. A randomized, double-blind, placebo-controlled, multicenter study to assess the efficacy and safety of topiramate controlled release in the treatment of obese type 2 diabetic patients. Diabetes Care. 2007;30:1480-1486. 10. Stenlöf K, Rössner S, Vercruysse F, Kumar A, Fitchet M, Sjöström L, for the OBDM-003 Study Group. Topiramate in the treatment of obese subjects with drug-naive type 2 diabetes. Diabetes Obes Metab. 2007;9:360-368.
Acknowledgements: We would like to acknowledge and thank the CONQUER, EQUIP, and DM-230 investigators and study coordinators, the Medpace and Synteract teams (study CROs), The Lockwood Group (for poster development assistance), and VIVUS internal contributors.