Attached files
| file | filename |
|---|---|
| EX-32.2 - EX-32.2 - REATA PHARMACEUTICALS INC | reta-ex322_10.htm |
| EX-32.1 - EX-32.1 - REATA PHARMACEUTICALS INC | reta-ex321_7.htm |
| EX-31.2 - EX-31.2 - REATA PHARMACEUTICALS INC | reta-ex312_6.htm |
| EX-31.1 - EX-31.1 - REATA PHARMACEUTICALS INC | reta-ex311_9.htm |
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, DC 20549
FORM 10-Q
(Mark One)
|
☒ |
QUARTERLY REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the quarterly period ended March 31, 2017
OR
|
☐ |
TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the transition period from to
Commission File Number: 001-37785
Reata Pharmaceuticals, Inc.
(Exact Name of Registrant as Specified in its Charter)
|
DELAWARE |
|
11-3651945 |
|
( State or other jurisdiction of incorporation or organization) |
|
(I.R.S. Employer |
|
|
|
|
|
2801 Gateway Dr, Suite 150 |
|
75063 |
|
(Address of principal executive offices) |
|
(Zip Code) |
Registrant’s telephone number, including area code: (972) 865-2219
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes ☒ No ☐
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§ 232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes ☒ No ☐
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, an emerging growth company, or a smaller reporting company. See the definitions of “large accelerated filer,” “accelerated filer” and “smaller reporting company” in Rule 12b-2 of the Exchange Act.
|
Large accelerated filer |
|
☐ |
|
Accelerated filer |
|
☐ |
|
Non-accelerated filer |
|
☒ (Do not check if a small reporting company) |
|
Smaller reporting company |
|
☐ |
|
Emerging growth company |
|
☒ |
|
|
|
|
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☒
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes ☐ No ☒
As of May 8, 2017, the registrant had 13,991,575 shares of Class A common stock, $0.001 par value per share, and 8,374,032 shares of Class B common stock, $0.001 par value per share, outstanding.
|
|
|
Page |
|
3 |
||
|
PART I. |
|
|
|
Item 1. |
4 |
|
|
|
4 |
|
|
|
5 |
|
|
|
6 |
|
|
|
7 |
|
|
Item 2. |
Management’s Discussion and Analysis of Financial Condition and Results of Operations |
14 |
|
Item 3. |
31 |
|
|
Item 4. |
32 |
|
|
PART II. |
|
|
|
Item 1. |
33 |
|
|
Item 1A. |
33 |
|
|
Item 2. |
34 |
|
|
Item 3. |
34 |
|
|
Item 4. |
34 |
|
|
Item 5. |
34 |
|
|
Item 6. |
35 |
|
|
36 |
||
|
|
|
|
2
CAUTIONARY NOTE REGARDING FORWARD-LOOKING STATEMENTS
This Quarterly Report on Form 10-Q contains forward-looking statements that involve substantial risks and uncertainties. We make such forward-looking statements pursuant to the safe harbor provisions of the Private Securities Litigation Reform Act of 1995 and other federal securities laws. All statements, other than statements of historical facts, contained in this Quarterly Report on Form 10-Q, including statements regarding our strategy, future operations, future financial position, future revenues, projected costs, prospects, plans, and objectives of management, are forward-looking statements. The words “anticipate,” “believe,” “goals,” “continue,” “could,” “estimate,” “expect,” “intend,” “may,” “might,” “plan,” “potential,” “predict,” “project,” “seek,” “should,” “target,” “will,” “would,” “could,” “should,” and similar expressions are intended to identify forward-looking statements. These forward-looking statements include, but are not limited to, statements about:
|
|
• |
our expectations regarding the timing, costs, conduct, and outcome of our clinical trials, including statements regarding the timing of the initiation and availability of data from such trials; |
|
|
• |
the timing and likelihood of regulatory filings and approvals for our product candidates; |
|
|
• |
our expectations regarding the potential market size and the size of the patient populations for our product candidates, if approved for commercial use, and the potential market opportunities for commercializing our product candidates; |
|
|
• |
our expectations related to the use of our available cash; |
|
|
• |
estimates of our expenses, future revenue, capital requirements, and our needs for additional financing; |
|
|
• |
our ability to develop, acquire, and advance product candidates into, and successfully complete, clinical trials; |
|
|
• |
the initiation, timing, progress, and results of future preclinical studies and clinical trials, and our research and development programs; |
|
|
• |
the scope of protection we are able to establish and maintain for intellectual property rights covering our product candidates; |
|
|
• |
our ability to maintain and establish collaborations or obtain additional funding; |
|
|
• |
our ability to maintain and establish relationships with third parties, such as contract research organizations, suppliers, and distributors; |
|
|
• |
our expectations regarding the time during which we will be an emerging growth company under the JOBS Act; |
|
|
• |
our ability to establish and maintain arrangements for manufacture of our product candidates; |
|
|
• |
the impact of governmental laws and regulations; |
|
|
• |
developments and projections relating to our competitors and our industry; and |
|
|
• |
other risks and uncertainties, including those described under the heading “Risk Factors” included in our Annual Report on Form 10-K for the year ended December 31, 2016. |
Any forward-looking statements in this Quarterly Report on Form 10-Q reflect our current views with respect to future events or to our future financial performance and involve known and unknown risks, uncertainties, and other factors that may cause our actual results, performance, or achievements to be materially different from any future results, performance, or achievements expressed or implied by these forward-looking statements. Factors that may cause actual results to differ materially from current expectations include, among other things, those described under the heading “Risk Factors” in our Annual Report on Form 10-K for the year ended December 31, 2016, and discussed elsewhere in this Quarterly Report on Form 10-Q. Given these uncertainties, you should not place undue reliance on these forward-looking statements.
You should read this Quarterly Report on Form 10-Q and the documents that we have filed as exhibits to this Quarterly Report on Form 10-Q completely and with the understanding that our actual future results may be materially different from what we expect. Except as required by law, we assume no obligation to update or revise these forward-looking statements for any reason, even if new information becomes available in the future.
3
PART I - FINANCIAL INFORMATION
Reata Pharmaceuticals, Inc.
(in thousands, except share data)
|
|
|
March 31, 2017 (unaudited) |
|
|
December 31, 2016 |
|
||
|
Assets |
|
|
|
|
|
|
|
|
|
Cash and cash equivalents |
|
$ |
82,676 |
|
|
$ |
84,732 |
|
|
Prepaid expenses and other current assets |
|
|
3,041 |
|
|
|
2,551 |
|
|
Total current assets |
|
|
85,717 |
|
|
|
87,283 |
|
|
Property and equipment, net |
|
|
703 |
|
|
|
819 |
|
|
Other assets |
|
|
1,760 |
|
|
|
991 |
|
|
Total assets |
|
$ |
88,180 |
|
|
$ |
89,093 |
|
|
Liabilities and stockholders’ deficit |
|
|
|
|
|
|
|
|
|
Accounts payable |
|
$ |
541 |
|
|
$ |
3,830 |
|
|
Accrued direct research liabilities |
|
|
5,443 |
|
|
|
6,151 |
|
|
Other current liabilities |
|
|
3,885 |
|
|
|
3,047 |
|
|
Current portion of deferred revenue |
|
|
41,323 |
|
|
|
46,603 |
|
|
Total current liabilities |
|
|
51,192 |
|
|
|
59,631 |
|
|
Other long-term liabilities |
|
|
51 |
|
|
|
72 |
|
|
Term loan, net of discounts and debt issuance costs |
|
|
19,753 |
|
|
|
— |
|
|
Deferred revenue, net of current portion |
|
|
237,489 |
|
|
|
244,438 |
|
|
Total noncurrent liabilities |
|
|
257,293 |
|
|
|
244,510 |
|
|
Commitments and contingencies |
|
|
|
|
|
|
|
|
|
Stockholders’ deficit: |
|
|
|
|
|
|
|
|
|
Common stock A, $0.001 par value: 500,000,000 shares authorized; issued and outstanding – 13,988,839 and 11,687,974 shares at March 31, 2017 and December 31, 2016 |
|
|
14 |
|
|
|
12 |
|
|
Common stock B, $0.001 par value: 150,000,000 shares authorized; issued and outstanding – 8,376,768 and 10,656,920 shares at March 31, 2017 and December 31, 2016 |
|
|
9 |
|
|
|
11 |
|
|
Additional paid-in capital |
|
|
76,252 |
|
|
|
74,298 |
|
|
Shareholder notes receivable |
|
|
(15 |
) |
|
|
(15 |
) |
|
Accumulated deficit |
|
|
(296,565 |
) |
|
|
(289,354 |
) |
|
Total stockholders’ deficit |
|
|
(220,305 |
) |
|
|
(215,048 |
) |
|
Total liabilities and stockholders’ deficit |
|
$ |
88,180 |
|
|
$ |
89,093 |
|
See accompanying notes.
4
Unaudited Consolidated Statements of Operations
(in thousands, except share and per share data)
|
|
|
Three Months ended |
|
|||||
|
|
|
March 31, |
|
|||||
|
|
|
2017 |
|
|
2016 |
|
||
|
Collaboration revenue |
|
|
|
|
|
|
|
|
|
License and milestone |
|
$ |
12,729 |
|
|
$ |
12,365 |
|
|
Other revenue |
|
|
3 |
|
|
|
73 |
|
|
Total collaboration revenue |
|
|
12,732 |
|
|
|
12,438 |
|
|
Expenses |
|
|
|
|
|
|
|
|
|
Research and development |
|
|
14,603 |
|
|
|
9,306 |
|
|
General and administrative |
|
|
5,173 |
|
|
|
3,207 |
|
|
Depreciation and amortization |
|
|
130 |
|
|
|
188 |
|
|
Total expenses |
|
|
19,906 |
|
|
|
12,701 |
|
|
Other income (expense) |
|
|
|
|
|
|
|
|
|
Investment income |
|
|
81 |
|
|
|
23 |
|
|
Interest expense |
|
|
(5 |
) |
|
|
— |
|
|
Total other income (expense) |
|
|
76 |
|
|
|
23 |
|
|
Loss before provision for taxes on income |
|
|
(7,098 |
) |
|
|
(240 |
) |
|
Provision for taxes on income |
|
|
— |
|
|
|
18 |
|
|
Net loss |
|
$ |
(7,098 |
) |
|
$ |
(258 |
) |
|
Net loss per share—basic and diluted |
|
$ |
(0.32 |
) |
|
$ |
(0.02 |
) |
|
Weighted-average number of common shares used in net loss per share basic and diluted |
|
|
22,350,436 |
|
|
|
15,990,766 |
|
See accompanying notes.
5
Unaudited Consolidated Statements of Cash Flows
(in thousands)
|
|
|
Three Months ended |
|
|||||
|
|
|
March 31, |
|
|||||
|
|
|
2017 |
|
|
2016 |
|
||
|
Operating activities |
|
|
|
|
|
|
|
|
|
Net loss |
|
$ |
(7,098 |
) |
|
$ |
(258 |
) |
|
Adjustments to reconcile net loss to net cash used in operating activities: |
|
|
|
|
|
|
|
|
|
Depreciation and amortization |
|
|
130 |
|
|
|
188 |
|
|
Stock-based compensation expense |
|
|
1,603 |
|
|
|
289 |
|
|
Changes in operating assets and liabilities: |
|
|
|
|
|
|
|
|
|
Prepaid expenses and other current assets |
|
|
(490 |
) |
|
|
(482 |
) |
|
Other assets |
|
|
(769 |
) |
|
|
— |
|
|
Accounts payable |
|
|
(3,289 |
) |
|
|
(2,985 |
) |
|
Accrued direct research and other current liabilities |
|
|
84 |
|
|
|
1,211 |
|
|
Federal income tax receivable/payable |
|
|
— |
|
|
|
15,218 |
|
|
Deferred revenue |
|
|
(12,229 |
) |
|
|
(12,364 |
) |
|
Net cash (used in) provided by operating activities |
|
|
(22,058 |
) |
|
|
817 |
|
|
Investing activities |
|
|
|
|
|
|
|
|
|
Purchases of property and equipment |
|
|
(34 |
) |
|
|
(16 |
) |
|
Net cash used in investing activities |
|
|
(34 |
) |
|
|
(16 |
) |
|
Financing activities |
|
|
|
|
|
|
|
|
|
Proceeds from long-term debt, net of discount |
|
|
19,840 |
|
|
|
— |
|
|
Payments on deferred offering costs |
|
|
— |
|
|
|
(911 |
) |
|
Exercise of options |
|
|
241 |
|
|
|
— |
|
|
Payment of capital lease obligation |
|
|
(45 |
) |
|
|
(45 |
) |
|
Net cash provided by (used in) financing activities |
|
|
20,036 |
|
|
|
(956 |
) |
|
Net decrease in cash and cash equivalents |
|
|
(2,056 |
) |
|
|
(155 |
) |
|
Cash and cash equivalents at beginning of year |
|
|
84,732 |
|
|
|
42,008 |
|
|
Cash and cash equivalents at end of period |
|
$ |
82,676 |
|
|
$ |
41,853 |
|
|
Supplemental disclosures |
|
|
|
|
|
|
|
|
|
Cash paid for interest |
|
$ |
5 |
|
|
$ |
— |
|
|
Unpaid debt issuance costs |
|
$ |
87 |
|
|
$ |
— |
|
|
Income taxes paid |
|
$ |
— |
|
|
$ |
18 |
|
|
Purchases of equipment in accounts payable and other current liabilities |
|
$ |
— |
|
|
$ |
24 |
|
|
Accrued deferred offering costs |
|
$ |
— |
|
|
$ |
887 |
|
See accompanying notes.
6
Notes to Unaudited Consolidated Financial Statements
1. Description of Business
Reata Pharmaceuticals, Inc. (the Company) is a clinical stage biopharmaceutical company located in Irving, Texas focused on identifying, developing, and commercializing product candidates to address rare and life-threatening diseases with few or no approved therapies by targeting molecular pathways that regulate cellular metabolism and inflammation. The Company operates as a single segment of business.
The Company’s lead product candidates, bardoxolone methyl and omaveloxolone, are Nrf2 activators that target the important transcription factor Nrf2 to restore mitochondrial function, reduce oxidative stress, and resolve inflammation. Bardoxolone methyl is in Phase 3 clinical development for the treatment of pulmonary arterial hypertension associated with connective tissue disease (CTD-PAH), and Phase 2 clinical development for the treatment of PAH and pulmonary hypertension due to interstitial lung disease (PH-ILD). The Company began enrolling patients in its Phase 3 trial in CTD-PAH in October 2016. In addition, bardoxolone methyl is being studied in a single, pivotal Phase 2/3 trial in chronic kidney disease (CKD) caused by Alport syndrome, in which the Company began enrolling patients in March 2017. Omaveloxolone is being studied in separate two-part Phase 2 trials for the treatment of Friedreich’s ataxia (FA) and mitochondrial myopathies (MM), known as MOXIe and MOTOR, respectively. The Company has completed enrollment of part one in MOXIe and is currently dosing patients in part one of MOTOR, both of which are dose ranging. Data from part two of each of the trials have the potential to be used for registration. Omaveloxolone is also being studied in a Phase 1b/2 trial for the treatment of metastatic melanoma, known as REVEAL. In addition to its lead product candidates, the Company is in Phase 1 development for RTA 901. Beyond our clinical programs, the Company has additional promising preclinical development programs. The Company believes its product candidates and preclinical programs have the potential to improve clinical outcomes in numerous underserved patient populations.
The Company’s consolidated financial statements include the accounts of all majority-owned subsidiaries that are required to be consolidated. Accordingly, the Company’s share of net earnings and losses from these subsidiaries is included in the consolidated statements of operations. Intracompany profits, transactions, and balances have been eliminated in consolidation.
On May 25, 2016, the Company’s registration statement on Form S-1 (File No. 333-208843) relating to its initial public offering (IPO) of its common stock was declared effective by the U.S. Securities and Exchange Commission (SEC). The shares began trading on The NASDAQ Global Market on May 26, 2016. The public offering price of the shares sold in the offering was $11.00 per share. The IPO closed on June 1, 2016, for 6,325,000 shares of its Class A common stock, which included 825,000 shares of its Class A common stock issued pursuant to the over-allotment option granted to the underwriters. The Company received total proceeds from the offering of $60.9 million, net of underwriting discounts and commissions and offering expenses.
2. Summary of Significant Accounting Policies
Basis of Presentation
The accompanying unaudited consolidated financial statements have been prepared in accordance with accounting principles generally accepted in the United States (U.S. GAAP) for interim financial information and with the instructions to Form 10-Q and Article 10 of Regulation S-X. Accordingly, they do not include all of the information and notes required by U.S. GAAP for complete financial statements. In the opinion of management, all adjustments (consisting of normal recurring adjustments) considered necessary for a fair presentation have been included. Operating results for the three months ended March 31, 2017, are not necessarily indicative of the results that may be expected for the year ending December 31, 2017. The consolidated balance sheet at December 31, 2016, has been derived from the audited consolidated financial statements at that date but does not include all of the information and footnotes required by U.S. GAAP for complete financial statements. For further information, refer to the annual consolidated financial statements and footnotes thereto of the Company.
Revenue Recognition
The Company’s revenue to date has been generated primarily through collaborative licensing agreements with AbbVie Ltd. (AbbVie) and Kyowa Hakko Kirin Co., Ltd. (KHK). Revenues for periods shown consist of the recognition of deferred revenue from upfront payments and milestone payments received in 2012 and prior years. The Company has not generated any revenue based on the sale of products.
7
Reata Pharmaceuticals, Inc.
Notes to Unaudited Consolidated Financial Statements (continued)
In June 2013, the Company entered into a research collaboration with a disease advocacy organization. Under the agreement, the Company may be provided milestone payments to fund research and development activities estimated over a two-year period. The Company recorded collaboration revenue totaling $500,000 related to milestone payments during the three months ended March 31, 2017.
Research and Development Costs
AbbVie is not currently participating in the development of bardoxolone methyl for the treatment of CKD caused by Alport syndrome, PAH, or PH-ILD, and we are therefore incurring all costs for this program. With respect to its omaveloxolone programs and its collaboration agreement with AbbVie, the Company was responsible for a certain initial amount in early development costs before AbbVie began sharing development costs equally. As of April 2016, the Company had incurred all of these initial costs, after which payments from AbbVie with respect to research and development costs incurred by the Company were recorded as a reduction in research and development expenses.
In September 2016, the Company and AbbVie mutually agreed that the Company would continue unilateral development of omaveloxolone. Therefore, AbbVie no longer co-funds the exploratory development costs of this program, but retains the right to opt back in at certain points in development. Depending upon what point, if any, AbbVie opts back into development, AbbVie may retain its right to commercialize a product outside the U.S., or the Company may be responsible for commercializing the product on a worldwide basis. Upon opting back in, AbbVie would be required to pay an agreed upon amount of all development costs accumulated up to the point of exercising their opt-in right, after which development costs incurred and product revenue worldwide would be split equally. For the quarters ended March 31, 2017 and 2016, no payments related to shared research and developments costs were received.
The Company bases its expense accruals related to clinical trials on its estimates of the services received and efforts expended pursuant to contracts with multiple research institutions and contract research organizations that conduct and manage clinical trials on its behalf. The financial terms of these agreements vary from contract to contract and may result in uneven payment flows. Payments under some of these contracts depend on factors such as the successful enrollment of patients and the completion of clinical trial milestones. In accruing costs, the Company estimates the time period over which services will be performed and the level of effort to be expended in each period. If the Company does not identify costs that it has begun to incur or if the Company underestimates or overestimates the level of services performed or the costs of these services, its actual expenses could differ from its estimates.
To date, the Company has not experienced significant changes in its estimates of accrued research and development expenses after a reporting period. However, due to the nature of estimates, the Company cannot assure that it will not make changes to its estimates in the future as the Company becomes aware of additional information about the status or conduct of its clinical trials and other research activities.
Stock-Based Compensation
The Company accounts for its equity-based compensation awards in accordance with Accounting Standard Codification ASC 718 Compensation—Stock Compensation (ASC 718). ASC 718 requires companies to recognize compensation expense using a fair value based method for costs related to stock-based payments, including stock options. The expense is measured based on the grant date fair value of the awards that are expected to vest, and the expense is recorded over the applicable requisite service period.
The Company uses the Black-Scholes option-pricing model to estimate the fair value of stock option awards, which takes into consideration various factors, including the exercise price of the award, the expected term of the award, the current price of the underlying shares, the expected volatility of the underlying share price based on peer companies, and the risk-free interest rate. The Company accounts for forfeitures of share-based awards when they occur.
Prior to the Company’s IPO of its common stock, the fair values of the shares of common stock underlying the Company’s share-based awards were estimated on each grant date using a probability-weighted expected return method. Following the close of its IPO in June 2016, the fair values of its common stock underlying its share-based awards were estimated using observable market prices.
8
Reata Pharmaceuticals, Inc.
Notes to Unaudited Consolidated Financial Statements (continued)
The Company has experienced losses and negative operating cash flows for many years since inception and has no marketed drug or other products. The Company’s ability to generate future revenue depends upon the results of its development programs, the success of which cannot be guaranteed. The Company will need to raise additional equity or debt capital in the future in order to fund its operations.
Use of Estimates
The preparation of consolidated financial statements in conformity with U.S. GAAP requires management to make estimates and assumptions that affect the amounts reported in the consolidated financial statements and accompanying notes. Actual results could differ from those estimates.
Fair Value of Financial Instruments
The fair values of the Company’s stockholder notes receivable were approximately $30,000 and $28,000 at March 31, 2017 and December 31, 2016, respectively. The fair value was calculated using an income approach to estimate the present value of expected future cash flows to be received under the notes. The measurement is considered to be based primarily on Level 3 inputs used in the calculation, including the discount rate applied and the estimate of future cash flows.
Net Loss per Share
Basic and diluted net loss per common share is calculated by dividing net loss attributable to common stockholders by the weighted average number of common shares outstanding during the period, without consideration for common stock equivalents. The Company’s potentially dilutive shares, which include unvested restricted stock and options to purchase common stock, are considered to be common stock equivalents and are only included in the calculation of diluted net income (loss) per share when their effect is dilutive. For periods in which the Company reports a net loss attributable to common stockholders, diluted net loss per share attributable to common stockholders is the same as basic net loss per share attributable to common stockholders, since dilutive common shares are not assumed to have been issued if their effect is anti-dilutive.
The Company uses the two-class method to compute net loss per common share attributable to common stockholders because the Company has issued securities, other than Class A and Class B common stock, that contractually entitle the holders to participate in dividends and earnings of the Company. The two-class method requires earnings for the period to be allocated between common stock and participating securities based upon their respective rights to receive distributed and undistributed earnings. Holders of restricted common stock are entitled to the dividend amount paid to common stockholders on an as-if-converted-to-common stock basis when declared by the Company’s Board of Directors. As a result, all restricted common stock are considered to be participating securities.
Deferred Offering Costs
Deferred offering costs, which primarily consist of direct incremental accounting, legal, and printing fees relating to the IPO, were initially capitalized. The deferred offering costs totaling $3,489,000 were subsequently offset against IPO proceeds upon the completion of the IPO on June 1, 2016.
Debt Issuance Costs
The Company defers costs related to debt issuance and amortizes these cost to interest expense over the term of the debt, using the effective interest method. Debt issuance costs are presented in the balance sheet as a deduction from the carrying amount of the debt liability.
Recent Accounting Pronouncements
The Company is an “emerging growth company,” as defined in the Jumpstart Our Business Startups Act of 2012 (the JOBS Act). Under the JOBS Act, emerging growth companies can delay adopting new or revised accounting standards issued subsequent to the enactment of the JOBS Act until such time as those standards apply to private companies. The Company has irrevocably elected not to avail itself of this exemption from new or revised accounting standards, and, therefore, will be subject to the same new or revised accounting standards as public companies that are not emerging growth companies.
9
Reata Pharmaceuticals, Inc.
Notes to Unaudited Consolidated Financial Statements (continued)
In May 2014, the Financial Accounting Standards Board (FASB) issued Accounting Standards Update (ASU) No. 2014-09, Revenue from Contracts with Customers (Topic 606) (ASU 2014-09), which supersedes the revenue recognition requirements in ASC 605, Revenue Recognition. The FASB has subsequently issued a number of amendments to ASU 2014-09. The new standard, as amended, provides a single comprehensive model based on the principle that revenue is recognized to depict the transfer of goods or services to customers in an amount that reflects the consideration to which the entity expects to be entitled in exchange for those goods or services. To achieve this principle, ASU 2014-09 defines a five-step process, which may include more judgment and estimates than are required under existing GAAP, including identifying performance obligations in a contract, estimating the amount of variable consideration to include in the transaction price, and allocating the transaction price to each performance obligation.
The new standard is effective for interim and annual periods beginning after December 15, 2017, with early application for interim and annual periods beginning after December 15, 2016, permitted, and allows two methods of adoption: the full retrospective method, which requires the standard to be applied to each prior period presented, or the modified retrospective method, which requires the cumulative effect of adoption to be recognized as an adjustment to opening retained earnings in the period of adoption. The Company has begun an initial review of its existing contracts with AbbVie and KHK and has not yet determined what, if any, effect ASU 2016-09 will have on its consolidated results of operations or financial position.
In April 2015, the FASB issued ASU No. 2015-03, Interest-Imputation of Interest: Simplifying the Presentation of Debt Issuance Costs (ASU 2015-03), which requires that debt issuance costs related to a recognized debt liability be presented in the balance sheets as a direct deduction from the carrying amount of that debt liability, consistent with debt discounts. The Company adopted ASU 2015-03 as of January 1, 2017. The recognition and measurement guidance for debt issuance costs were not affected by the amendments in ASU No. 2015-03. In March 2017, upon entering into a loan and security agreement, $87,000 of debt issuance costs was netted against the principal balance of our outstanding term loan of $20,000,000.
In February 2016, the FASB issued ASU No. 2016-02, Leases (Topic 842) (ASU 2016-02), which supersedes ASC 840, Leases. ASU 2016-02 requires the recognition of lease assets and lease liabilities by lessees for those leases previously classified as operating leases. The standard is effective for public companies for fiscal years, and for interim periods within those fiscal years, beginning after December 15, 2018. Early adoption is permitted. The Company will apply the guidance and disclosure provisions of the new standard upon adoption. The Company is currently evaluating this standard and has not yet determined what, if any, effect ASU 2016-02 will have on its consolidated operations or financial position but anticipates the recognition of additional assets and corresponding liabilities related to leases on its balance sheet.
In March 2016, the FASB issued ASU No. 2016-09, Compensation – Stock Compensation: Improvements to Employee Share-Based Payment Accounting (Topic 718) (ASU 2016-09) which modifies U.S. GAAP by requiring the following, among others: (1) all excess tax benefits and tax deficiencies are to be recognized as income tax expense or benefit on the income statement (excess tax benefits are recognized regardless of whether the benefit reduces taxes payable in the current period); (2) excess tax benefits are to be classified along with other income tax cash flows as an operating activity in the statement of cash flows; (3) in the area of forfeitures, an entity can still follow the current U.S. GAAP practice of making an entity-wide accounting policy election to estimate the number of awards that are expected to vest or may instead account for forfeitures when they occur; and (4) classification as a financing activity in the statement of cash flows of cash paid by an employer to the taxing authorities when directly withholding shares for tax withholding purposes. ASU 2016-09 is effective for annual periods beginning after December 15, 2016. The Company adopted ASU 2016-09 as of January 1, 2017, which resulted in an adjustment to retained earnings of $110,000 related to the cumulative effect of the accounting policy election to account for forfeitures of share-based awards when they occur, and an adjustment of $115,000 to recognize excess tax benefits as a component of the provision for income taxes on a prospective basis. For the three months ended March 31, 2017, the effect on the provision for income taxes included in the consolidated statement of operations was not significant.
In August 2016, the FASB issued ASU No. 2016-15, Statement of Cash Flows: Classification of Certain Cash Receipts and Cash Payments (Topic 230) (ASU 2016-15). This update addresses eight specific cash flow issues with the objective of reducing the existing diversity in practice. The ASU is effective for public companies for fiscal years, and interim periods within those fiscal years, beginning after December 15, 2017. The Company is currently evaluating this standard and has not yet determined what, if any, effect ASU 2016-15 will have on its consolidated results of operations or financial position.
In January 2017, the FASB issued ASU No. 2017-03, Accounting Changes and Error Corrections (Topic 250) and Investments—Equity Method and Joint Ventures (Topic 323) (ASU 2017-03). This ASU amends the disclosure requirements for ASU No. 2014-09, Revenue from Contracts with Customers (Topic 606), ASU No. 2016-02, Leases (Topic 842) and ASU No. 2016-13, Financial Instruments—Credit Losses (Topic 326): Measurement of Credit Losses on Financial Instruments. This ASU states that if a registrant does not know or cannot reasonably estimate the impact that the adoption of the above ASUs is expected to have on the financial
10
Reata Pharmaceuticals, Inc.
Notes to Unaudited Consolidated Financial Statements (continued)
statements, then in addition to making a statement to that effect, the registrant should consider additional qualitative financial statement disclosures to assist the reader in assessing the significance of the impact that the standard will have on the financial statements of the registrant when adopted. ASU 2017-03 was effective upon issuance. The adoption did not have a material impact on the Company’s financial statements.
3. Term Loan
On March 31, 2017, the Company entered into a loan and security agreement (Loan Agreement) with Oxford Finance LLC and Silicon Valley Bank (collectively, Lenders), under which the Lenders agreed to lend the Company up to $35,000,000, issuable in two separate term loans of $20,000,000 (Term A Loan) and $15,000,000 (Term B Loan). On March 31, 2017, the Company borrowed $20,000,000 from the Term A Loan. Beginning July 1, 2017, under the Term of the Loan Agreement, the Company may, as its sole discretion, borrow $15,000,000 under Term B Loan following the achievement of first patient enrollment in either (a) the Phase 3 portion of the ongoing Phase 2/3 clinical trial of bardoxolone methyl in CKD caused by Alport syndrome or (b) Part 2 of the ongoing two-part clinical trial, or a separate Phase 3 clinical trial, of omavaloxolone in FA until the earlier of 90 days thereafter or March 31, 2018.
All outstanding Term Loans will mature on March 1, 2022. Under the Term A Loan, the Company will make interest-only payments for 18 months through November 1, 2018; however, if the Company draws the Term B Loan, the Company will make interest-only payments for 24 months through May 1, 2019. The interest-only payment period will be followed by 41 equal monthly payments, or 35 equal monthly payments if the Company draws the Term B Loan, of principal and interest payments. The Term Loans will bear interest at a floating per annum rate calculated as 7.40% plus the greater of the 30-day U.S. Dollar LIBOR rate reported in The Wall Street Journal on the last business day of the month that immediately precedes the month in which the interest will accrue or 0.75%, with a minimum rate of 8.15% and maximum rate of 10.15%.
The Company has the option to prepay all, but not less than all, of the borrowed amounts, provided that the Company will be obligated to pay a prepayment fee equal to (a) 3.0% of the outstanding principal balance of the applicable Term Loan if prepayment is made prior to the first anniversary of the applicable funding date of the Term Loan, (b) 2.0% of the outstanding principal balance of the applicable Term Loan if prepayment is made prior to the second anniversary of the applicable funding date of the Term Loan, or (c) 1.0% of the outstanding principal balance of the applicable Term Loan if prepayment is made prior to the third anniversary of the applicable funding date of the Term Loan. The Company will also be required to make a final exit fee payment of 2.95% of the principal balance of all Term Loans outstanding, payable on the earliest of the prepayment of the Term Loans, acceleration of any Term Loan, or at maturity of the Term Loans.
The Company may use the proceeds from the Term Loans for working capital and to fund its general business requirements. The Company’s obligations under the Loan Agreement are secured by a first priority security interest in substantially all of its current and future assets, other than its owned intellectual property. The Company has also agreed not to encumber its intellectual property assets, except as permitted by the Loan Agreement.
As of March 31, 2017, the Company had $20,000,000 outstanding under the Term A Loan, which was recorded at its initial carrying value of $20,000,000, less discount and debt issuance costs totaling approximately $247,000. In connection with the Term A Loan, the discount and debt issuance costs were recorded as a reduction to debt on its balance sheet and are being accreted to interest expense over the life of the Term A Loan. Additionally, the final exit fee of approximately $590,000 is being accrued over the life of the Term A Loan through interest expense. The Term A Loan has a current effective interest rate of 9.94%. The Company is in compliance with all covenants under the Loan Agreement as of March 31, 2017.
The future principal payments for the Company’s Term A Loan as of March 31, 2017 are as follows (in thousands):
|
2017 |
|
$ |
— |
|
|
2018 |
|
|
975 |
|
|
2019 |
|
|
5,854 |
|
|
2020 |
|
|
5,854 |
|
|
2021 |
|
|
5,854 |
|
|
2022 |
|
|
1,463 |
|
|
|
|
$ |
20,000 |
|
11
Reata Pharmaceuticals, Inc.
Notes to Unaudited Consolidated Financial Statements (continued)
4. Income Taxes
The Company’s effective tax rate varies with the statutory rate due primarily to the impact of nondeductible stock-based compensation and the changes in valuation allowance related to certain deferred tax assets generated or utilized in the applicable period. The Company’s deferred tax assets have been fully offset by a valuation allowance at March 31, 2017, and the Company expects to maintain this valuation allowance until there is sufficient evidence that future earnings can be achieved, which is uncertain at this time.
5. Stock-Based Compensation
Stock Options
The following table summarizes stock-based compensation expense reflected in the consolidated statements of operations (in thousands):
|
|
|
Three Months ended |
|
|||||
|
|
|
March 31, |
|
|||||
|
|
|
2017 |
|
|
2016 |
|
||
|
Research and development |
|
$ |
570 |
|
|
$ |
138 |
|
|
General and administrative |
|
|
1,033 |
|
|
|
151 |
|
|
|
|
$ |
1,603 |
|
|
$ |
289 |
|
The following table summarizes stock option activity as of March 31, 2017, and changes during the three months ended March 31, 2017, under the 2007 Long Term Incentive Plan (the 2007 LTIP) and standalone option agreements:
|
|
|
Number of Options |
|
|
Weighted- Average Exercise Price |
|
||
|
Outstanding at January 1, 2017 |
|
|
2,311,146 |
|
|
|
17.18 |
|
|
Granted |
|
|
60,169 |
|
|
|
26.31 |
|
|
Exercised |
|
|
(20,713 |
) |
|
|
11.62 |
|
|
Forfeited |
|
|
(2,225 |
) |
|
|
11.98 |
|
|
Expired |
|
|
— |
|
|
|
— |
|
|
Outstanding at March 31, 2017 |
|
|
2,348,377 |
|
|
|
17.46 |
|
|
Exercisable at March 31, 2017 |
|
|
552,887 |
|
|
|
16.72 |
|
The total intrinsic value of all outstanding options and exercisable options at March 31, 2017 was $13,901,000 and $4,686,000, respectively.
6. Related-Party Transactions
During the three months ended March 31, 2017, the Company did not have any related party transactions. During the three months ended March 31, 2016, the Company paid approximately $115,000 to AbbVie, a greater than 10% shareholder of the Company at that time, for manufacturing services. The payments are recorded in research and development expense in the accompanying consolidated statements of operations.
12
Reata Pharmaceuticals, Inc.
Notes to Unaudited Consolidated Financial Statements (continued)
The following table sets forth the computation of basic and diluted net loss per share attributable to common stockholders:
|
|
|
Three Months ended |
|
|||||
|
|
|
March 31, |
|
|||||
|
|
|
2017 |
|
|
2016 |
|
||
|
Numerator |
|
|
|
|
|
|
|
|
|
Net loss (in thousands) |
|
$ |
(7,098 |
) |
|
$ |
(258 |
) |
|
Denominator |
|
|
|
|
|
|
|
|
|
Weighted-average number of common shares used in net loss per share – basic |
|
|
22,350,436 |
|
|
|
15,990,766 |
|
|
Dilutive potential common shares |
|
|
— |
|
|
|
— |
|
|
Weighted-average number of common shares used in net loss per share – diluted |
|
|
22,350,436 |
|
|
|
15,990,766 |
|
|
Net loss per share – basic |
|
|
(0.32 |
) |
|
|
(0.02 |
) |
|
Net loss per share – diluted |
|
|
(0.32 |
) |
|
|
(0.02 |
) |
The number of weighted average options that were not included in the diluted earnings per share calculation because the effect would have been anti-dilutive represented 2,348,377 and 2,311,146 shares for the three months ended March 31, 2017 and 2016, respectively.
13
Item 2. MANAGEMENT’S DISCUSSION AND ANALYSIS
OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS
You should read the following discussion and analysis of our financial condition and results of operations together with our consolidated financial statements and related notes and other financial information appearing in this Quarterly Report on Form 10-Q. Some of the information contained in this discussion and analysis or set forth elsewhere in this Quarterly Report on Form 10-Q, including information with respect to our plans and strategy for our business, operations, and product candidates, includes forward-looking statements that involve risks and uncertainties. Factors that may cause actual results to differ materially from current expectations include, among other things, those described under the heading “Risk Factors” and discussed elsewhere in this Quarterly Report on Form 10-Q.
Overview
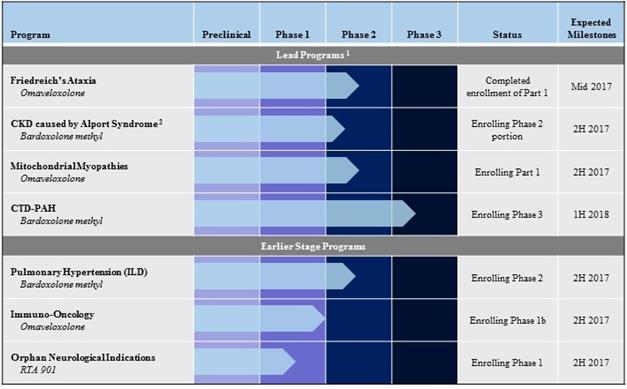
We are a clinical stage biopharmaceutical company focused on identifying, developing, and commercializing product candidates to address rare and life-threatening diseases with few or no approved therapies by targeting molecular pathways that regulate cellular metabolism and inflammation. Our lead product candidates, bardoxolone methyl and omaveloxolone, are Nrf2 activators that target the important transcription factor Nrf2 to restore mitochondrial function, reduce oxidative stress, and resolve inflammation. Bardoxolone methyl is currently being studied in a Phase 3 trial, known as CATALYST, for the treatment of CTD-PAH as well as a Phase 2 trial, known as LARIAT, for the treatment of PH-ILD and PAH. In addition, bardoxolone methyl is currently being studied in a single, pivotal Phase 2/3 trial, known as CARDINAL, for the treatment of CKD caused by Alport syndrome. We began enrolling patients in CARDINAL in March 2017. Omaveloxolone is being studied in separate two-part Phase 2 trials for the treatment of FA and MM, known as MOXIe and MOTOR, respectively. We have completed enrollment of part one in MOXIe and are currently dosing patients in part one of MOTOR, both of which are dose ranging. Data from part two of each of the trials have the potential to be used for registration. Omaveloxolone is also being studied in a Phase 1b/2 trial for the treatment of metastatic melanoma, known as REVEAL. In addition to our lead product candidates, we are also conducting a Phase 1 trial of RTA 901. Beyond our clinical programs, we have additional promising preclinical development programs. We believe that our product candidates and preclinical programs have the potential to improve clinical outcomes in numerous underserved patient populations.
To date, we have focused most of our efforts and resources on developing our product candidates and conducting preclinical studies and clinical trials. We have historically financed our operations primarily through revenue generated from our collaborations with AbbVie and KHK, from sales of our securities, and from our secured term loan. We have not received any payments or revenue from collaborations other than nonrefundable upfront, milestone, and cost sharing payments from our collaborations with AbbVie and KHK and reimbursements of expenses under the terms of our agreement with KHK. We have incurred losses in each year since our inception, other than in 2014. As of March 31, 2017, we had approximately $82.7 million of cash and cash equivalents and an accumulated deficit of $296.6 million. We continue to incur significant research and development and other expenses related to our ongoing operations. Despite contractual product development commitments and the potential to receive future payments from our collaborators, we anticipate that, without taking into account deferred revenue, we will continue to incur losses for the foreseeable future, and we anticipate that our losses will increase as we continue our development of, and seek regulatory approval for, our product candidates. If we do not successfully develop and obtain regulatory approval of our existing product candidates or any future product candidates and effectively manufacture, market, and sell any products that are approved, we may never generate revenue from product sales. Furthermore, even if we do generate revenue from product sales, we may never again achieve or sustain profitability on a quarterly or annual basis. Our prior losses, combined with expected future losses, have had and will continue to have an adverse effect on our stockholders’ equity and working capital. Our failure to become and remain profitable could depress the market price of our Class A common stock and could impair our ability to raise capital, expand our business, diversify our product offerings, or continue our operations.
The probability of success for each of our product candidates and clinical programs and our ability to generate product revenue and become profitable depend upon a variety of factors, including the quality of the product candidate, clinical results, investment in the program, competition, manufacturing capability, commercial viability, and our collaborators’ ability to successfully execute our development and commercialization plans. We will also require additional capital through equity or debt financings in order to fund our operations and execute on our business plans, and there is no assurance that such financing will be available to us on commercially reasonable terms or at all. For a description of the numerous risks and uncertainties associated with product development and raising additional capital, see “Risk Factors” included in this Form 10-Q and our Annual Report on Form 10-K for the year ended December 31, 2016.
14
The chart below is a summary of our current clinical programs:
|
1. |
Our lead programs include programs for which we have received guidance from the FDA on registrational endpoints and trial design, and for which the ongoing trial may support registration. |
|
2. |
We have initiated the Phase 2 portion of an integrated Phase 2/3 clinical trial in the first half of 2017, with Phase 2 data expected in the second half of 2017. Additionally, the one year withdrawal data, which could support accelerated approval, are expected in the first half of 2019. |
Bardoxolone Methyl
Bardoxolone methyl activates molecular pathways that promote the resolution of inflammation by restoring mitochondrial function, reducing oxidative stress, and inhibiting pro-inflammatory signaling. Bardoxolone methyl binds to Keap1, which activates Nrf2, a transcription factor that promotes normal mitochondrial function by making reducing equivalents available for ATP production, and increases cellular antioxidant content. This reduces mitochondrial reactive oxygen species (ROS) production and ROS-mediated activation of inflammatory signaling complexes. Binding to Keap1 and activation of Nrf2 also inhibit NF-κB, the primary transcription factor producing proteins that promote inflammation and the production of ROS. Bardoxolone methyl is currently being tested in a Phase 3 trial in CTD-PAH, a Phase 2 trial in several forms of PH-ILD and PAH, and a single, pivotal Phase 2/3 trial in CKD caused by Alport syndrome.
CTD-PAH and CKD caused by Alport syndrome are our most advanced indications with bardoxolone methyl. Although CTD-PAH and Alport syndrome have different causes and inflammatory stimuli, at a molecular level, mitochondrial dysfunction, inflammation, and proliferative signaling are common to the pathophysiology of both diseases. The anti-inflammatory and anti-fibrotic properties of bardoxolone methyl may therefore have the potential to prevent remodeling of the pulmonary vasculature in CTD-PAH as well as inhibit structural alterations and fibrosis of the glomerulus in the kidney in Alport syndrome.
PAH and PH-ILD
We are currently focused on the treatment of CTD-PAH, a subset of PAH, and PH-ILD. PAH results in a progressive increase in pulmonary vascular resistance, which ultimately leads to right ventricular heart failure and death. Female PAH patients outnumber males by a factor of 2:1, and the onset of PAH generally occurs between the ages of 40 and 60, with the average age of onset being 53. CTD-PAH represents approximately 30% of the overall PAH population.
15
CTD-PAH is a late and often fatal manifestation of many types of autoimmune disease, including systemic sclerosis (scleroderma), systemic lupus erythematosus, mixed connective tissue disease, and others. Patients with CTD-PAH are generally less responsive to existing therapies and have a worse prognosis than patients with other forms of PAH. In comparison to patients with idiopathic PAH (I-PAH), patients with CTD-PAH have a higher occurrence of small vessel fibrosis and greater incidence of pulmonary veno-obstructive diseases. In the United States, the five-year survival rate for CTD-PAH patients is approximately 44% while I-PAH patients have a 68% five-year survival rate.
Currently approved therapies to treat PAH include endothelin receptor antagonists, nitric oxide pathway modulators, and prostacyclin pathway agonists, all of which are systemic vasodilators that directly modulate vasoconstrictive and vasodilatory pathways. The effects of these existing therapies are not specific to the pulmonary vasculature, so they also have systemic hemodynamic effects. These systemic hemodynamic effects can result in hypotension and syncope (fainting), which generally limits their clinical effectiveness. These hemodynamic effects can be exacerbated when a patient is prescribed multiple vasodilators. In addition, clinically significant drug-drug interactions have been observed that can further limit the ability to deliver effective drug combinations.
A meta-analysis of the response of CTD-PAH patients to vasodilator therapy in 11 registrational trials comprised of more than 2,700 PAH patients published in 2015 demonstrated that CTD-PAH patients respond less well than I-PAH patients to approved vasodilator therapies in both clinical worsening and improvements in 6-minute walk distance (6MWD) from baseline, with a response in CTD-PAH patients (9.6 meters) of approximately one-third of the response in I-PAH patients (30 meters). The meta-analysis also demonstrated that I-PAH patients were more hemodynamically impaired than CTD-PAH patients, which likely explains why vasodilator therapy is more effective in I-PAH patients. This difference also explains why CTD-PAH patients respond less well to vasodilator therapy, as their disease process is less hemodynamic and involves systemic fibrotic processes caused by the patients’ underlying autoimmune diseases, such as scleroderma, lupus, or mixed connective tissue disease.
Bardoxolone methyl directly targets the bioenergetic and inflammatory components of PAH. PAH patients experience mitochondrial dysfunction, increased activation of NF-κB and related inflammatory pathways involved in ROS-mediated signaling, cellular proliferation, and fibrosis. Bardoxolone methyl, through the combined effect of Nrf2 activation and NF-κB suppression, has the potential to inhibit inflammatory and proliferative signaling, suppress ROS production and signaling, reduce the production of enzymes related to fibrosis and tissue remodeling, and increase ATP production and cellular respiration. Bardoxolone methyl targets multiple cell types relevant to PAH, including endothelial cells, smooth muscle cells, and macrophages. Additionally, unlike current therapies, bardoxolone methyl does not have systemic hemodynamic effects or drug-drug interactions in PAH patients. Therefore, by addressing a novel pathway in PAH, we believe that bardoxolone methyl may provide additional benefits beyond current PAH therapies, including increased functional capacity, potential effects beyond functional improvements, broader applicability to underserved patients, such as those with PH-ILD, and potential as a combination therapy with other current therapies. In 2015, the FDA granted our request for orphan drug designation for the treatment of PAH.
ILD patients experience extensive pulmonary vascular remodeling, which ultimately leads to PH-ILD in approximately 30% to 40% of ILD patients. We are initially targeting the use of bardoxolone methyl in the subsets of ILD patients with sarcoidosis, idiopathic pulmonary fibrosis, CTD that has affected the lung tissue, and idiopathic interstitial pneumonia. PH-ILD patients have a one-year survival rate of approximately 63%, as compared to approximately 92% for ILD patients without PH. Recent studies have demonstrated that mitochondrial abnormalities are contributors to PH-ILD.
Currently, there are no approved therapies for PH-ILD patients. While vasodilators approved for PAH are sometimes used off-label, given the degree of remodeling and fibrosis present in the lung tissue and vasculature of PH-ILD patients, they are minimally effective. Several current PAH therapies have been tested in PH-ILD patients and have resulted in little to no reproducible clinical improvement.
Phase 3 CATALYST Trial
In October 2016, the first patient was enrolled in CATALYST, an international, randomized, double-blind, placebo-controlled Phase 3 trial examining the safety, tolerability, and efficacy of bardoxolone methyl in patients with CTD-PAH when added to standard-of-care vasodilator therapy. Patients will be on up to two background therapies and will be randomized 1:1 to bardoxolone methyl or placebo. Patients will be enrolled at approximately 100 sites in the U.S., Canada, Australia, Japan, Mexico, Europe, Israel, the Philippines, and South America, and the study drug will be administered once daily for 24 weeks. Patients randomized to bardoxolone methyl will start at 5 mg and will dose-escalate to 10 mg at Week 4 unless contraindicated clinically. The primary endpoint is the change from baseline in 6MWD relative to placebo at Week 24. Secondary endpoints include time to first clinical improvement as measured by improvement in World Health Organization/New York Heart Association (WHO/NYHA), functional class, increase from baseline in 6MWD by at least 10%, or decrease from baseline in creatine kinase, which is a surrogate biomarker for muscle injury and inflammation, by at least 10%. The trial will enroll between 130 and 200 patients. To determine the final sample
16
size, a pre-specified, blinded sample size re-calculation based on 6MWD variability and baseline characteristics will be conducted after 100 patients have been enrolled in the trial. All patients who complete the treatment period are eligible to continue into an extension trial to evaluate the intermediate and long-term safety of bardoxolone methyl. Those patients who had been receiving placebo are converted to bardoxolone methyl in the extension trial. Data from CATALYST are expected to be available during the first half of 2018.
During our interaction with the FDA in October 2015, the FDA concurred with our design of the Phase 3 trial and noted that CATALYST, together with the Phase 2 data from our LARIAT trial in PAH patients and prior clinical trials with bardoxolone methyl, would provide adequate data for a New Drug Application review of the safety profile of bardoxolone methyl. Prior to this meeting, we had completed a series of clinical pharmacology studies, including a Thorough QT study, hepatic impairment study, food effect study, mass balance study, and three drug-drug interaction studies. The FDA recommended conducting a single additional clinical drug-drug interaction study and otherwise had no clinical trial, clinical pharmacology, or preclinical study requests.
We presented initial results from cohorts 1 and 2 of LARIAT, our Phase 2 PAH trial in patients with PAH and PH-ILD, at the CHEST World Congress during October 2015. Cohorts 1 and 2 included patients with both I-PAH and CTD-PAH and enrolled only U.S. patients on approved vasodilator therapies. The data demonstrated that administration of bardoxolone methyl significantly improved the function of patients when compared to placebo as assessed by 6MWD. The placebo-corrected change in time averaged 6MWD was 21.4 meters with a p-value of 0.037. Additionally, no clinically meaningful differences were noted in safety variables including vital signs and laboratory data, and bardoxolone methyl was combined with approved vasodilator therapies without increasing the risk of hypotensive events or exacerbating their adverse event profile.
A result is considered to be statistically significant when the probability of the result occurring by random chance, rather than from the efficacy of the treatment, is sufficiently low. The conventional method for measuring the statistical significance of a result is known as the “p-value,” which represents the probability that random chance caused the result. For example, a p-value of 0.001 means that there is a 0.1% or less probability that the difference between the control group and the treatment group is purely due to random chance. A p-value of 0.05 is a commonly used criterion for statistical significance, and may be supportive of a finding of efficacy by regulatory authorities. However, regulatory authorities, including the FDA, do not rely on strict statistical significance thresholds as criteria for marketing approval and maintain the flexibility to evaluate the overall risks and benefits of a treatment. Accordingly, treatments may receive marketing approval from the FDA even if the p-value of the primary endpoint is greater than 0.05, or may fail to receive marketing approval from the FDA even if the p-value of the primary endpoint is less than 0.05.
An important finding from cohort 1 of LARIAT was that bardoxolone methyl provided the greatest improvement in 6MWD to CTD-PAH patients. Because of these data, we expanded LARIAT to include cohort 3a, a cohort of additional CTD-PAH patients. In advance of the initiation of CATALYST, we analyzed data for all CTD-PAH patients treated with doses of up to 10 mg who had completed the 16-week treatment period (or terminated early) in the ongoing LARIAT trial. A total of 22 CTD-PAH patients, including patients from cohorts 1, 2, and 3a, met these criteria, with 15 randomized to bardoxolone methyl and seven randomized to placebo.
The LARIAT statistical analysis plan defined the treatment effect as the time-averaged change from baseline in 6MWD values using a longitudinal model to assess the average of all available 6MWD timepoints, using a mixed-model repeated measures (MMRM). Change from baseline in 6MWD at Weeks 4, 8, 12, and 16 were analyzed to compare the difference between the active drug and placebo groups. The analysis showed that patients treated with bardoxolone methyl demonstrated a statistically significant mean time-averaged increase in 6MWD compared to baseline of 26.7 meters (p=0.001). Placebo-treated patients had a non-significant time-averaged mean change from baseline in 6MWD of 0.6 meters (p=0.96). The placebo-corrected time-averaged change in 6MWD was 26.1 meters (p=0.06).
Based on findings in the LARIAT trial, patients with moderate to severe anemia, which represents a small percentage of the patient population, are being excluded from CATALYST because treatment with iron supplementation or erythropoietin can affect 6MWD values independent of study drug effect. Three CTD-PAH patients enrolled in LARIAT and included in the above analysis were anemic at screening as defined by low hemoglobin values, and two of these patients, both randomized to placebo, received post-randomization anemia treatments. An analysis was conducted excluding patients with anemia at screening to estimate the treatment effect in patients who meet the final CATALYST eligibility criteria. MMRM analysis for CATALYST-eligible patients, and all patients, is shown in the table below. The pooled standard deviation of change of 6MWD was 34.1 meters.
17
Summary of Time-Averaged 6MWD Changes for CTD-PAH Patients in LARIAT
|
|
|
All Patients |
|
CATALYST-Eligible Patients |
||
|
Treatment |
N |
Change from Baseline (m) |
Placebo-corrected (m) |
N |
Change from Baseline (m) |
Placebo-corrected (m) |
|
Placebo |
7 |
0.6 p=0.96 |
— |
5 |
-10.1 p=0.39 |
— |
|
Bardoxolone Methyl |
15 |
26.7 p=0.001 |
26.1 p=0.06 |
14 |
30.2 p < 0.001 |
40.3 p=0.009 |
CATALYST will be analyzed using a different method of statistical analysis. In CATALYST, the primary endpoint is the placebo-corrected change in 6MWD from baseline to the end-of-treatment at 24 weeks. This method allows for greater separation in 6MWD values between active and placebo groups, assuming improved efficacy over time. We performed an analysis applying the MMRM statistical analysis method for CATALYST to the available end-of-treatment change in 6MWD data from CTD-PAH patients in LARIAT. The summary of our MMRM statistical analysis using change at the end of treatment period on CATALYST-eligible patients, and all patients, is shown in the table below.
Summary of End-of-Treatment 6MWD Changes for CTD-PAH Patients in LARIAT
|
|
|
All Patients |
|
CATALYST Eligible Patients |
||
|
Treatment |
N |
Change from Baseline (m) |
Placebo-corrected (m) |
N |
Change from Baseline |
Placebo-corrected |
|
Placebo |
7 |
9.8 p=0.44 |
— |
5 |
-5.8 p=0.68 |
— |
|
Bardoxolone Methyl |
15 |
38.2 p <0.001 |
28.4 p=0.07 |
14 |
42.7 p < 0.001 |
48.5 p=0.005 |
With respect to safety, bardoxolone methyl was well-tolerated in CTD-PAH patients. None of the 15 bardoxolone methyl treated patients discontinued early, whereas one of the seven placebo treated patients discontinued prematurely. The expanded data set shows no clinically meaningful differences in safety variables including vital signs and laboratory data. Bardoxolone methyl was combined with approved vasodilator therapies without increasing the risk of hypotensive events or exacerbating their adverse event profile.
CATALYST is designed to detect a minimum treatment effect of 12.5 meters versus placebo assuming a standard deviation of 50 meters. The observed treatment effect in the LARIAT CTD-PAH subgroup analyses, both with and without the anemic patients included, is meaningfully larger than the minimally detectable treatment effect in CATALYST. The standard deviation observed in LARIAT of 37 meters is lower than the estimated standard deviation of 50 meters in CATALYST.
CTD-PAH is a serious progressive disease that ultimately leads to right ventricular heart failure and death. Patients with CTD-PAH can develop serious comorbidities, such as syncope, chest pain, palpitations, fluid retention, and hypoxemia. CATALYST is overseen by a data safety monitoring board (DSMB) that reviews all data, including serious adverse event (SAE) and adverse event (AE) data, on an unblinded basis to assess safety. The DSMB has not reported any safety concerns to date.
Phase 2 LARIAT Trial
The LARIAT trial is a randomized, placebo-controlled, double-blind, dose-escalation Phase 2 trial evaluating the safety and efficacy of once daily, orally administered bardoxolone methyl in up to 486 patients with PAH or PH-ILD. LARIAT is comprised of four separate cohort groups, all of which include patients classified as WHO/NYHA, Functional Class II and III. Functional Class II patients are comfortable at rest, but ordinary physical activity results in breathlessness, fatigue, or palpitations. Functional Class III patients are comfortable at rest, but less than ordinary physical activity results in breathlessness, fatigue, or palpitations.
The primary endpoint of the LARIAT trial is change in 6MWD during a 16 week treatment period. All patients who complete the treatment period are eligible to continue into an extension trial to evaluate the intermediate and long-term safety of bardoxolone methyl. Those patients who had been receiving placebo are converted to bardoxolone methyl in the extension trial. The initial treatment period for cohorts 1 and 2 has been completed and, as discussed above, initial data from cohorts 1, 2, and 3a have been publicly presented.
18
Because bardoxolone methyl was active in patients with CTD-PAH, a fibrotic disease, we believe that bardoxolone methyl may be effective in PH-ILD patients. We are enrolling patients with PH-ILD caused by sarcoidosis, idiopathic pulmonary fibrosis, CTD, and idiopathic interstitial pneumonia in LARIAT in four separate groups in cohort 4. Data have not been presented from cohort 4. We anticipate that data from PH-ILD patients in LARIAT will be available in the second half of 2017.
We have observed no significant tolerability issues in LARIAT to date. A higher incidence of AEs related to mild, transient nausea has been observed in patients at the 20 mg dose of bardoxolone methyl. Due to the observed nausea at the 20 mg dose and the fact that signs of activity have been observed at lower dose levels, the titration design in cohorts 3 and 4 utilizes 2.5 mg, 5 mg, and 10 mg doses. In the PAH patients in this trial, all of whom receive background vasodilator therapies, there have been no observed increases in the incidence of AEs typically associated with vasodilation, such as headache or jaw pain.
PAH and PH-ILD are serious progressive diseases that ultimately lead to right ventricular heart failure and death. Patients with these diseases can develop serious comorbidities such as syncope, chest pain, palpitations, fluid retention, and hypoxemia. The trial utilizes a protocol safety review committee (PSRC) that reviews all data, including SAE and AE data, on an unblinded basis to assess safety. The PSRC has not reported any safety concerns to date.
Chronic Kidney Disease Caused by Alport Syndrome
Alport syndrome is a rare and serious hereditary disease that is caused by mutations in the genes encoding type IV collagen, a major structural component of the glomerular basement membrane (GBM) in the kidney. The abnormal expression of type IV collagen causes loss of GBM integrity, abnormal leakage of proteins through the GBM, and excessive reabsorption of protein in the proximal tubules of the kidney. As in other forms of CKD, excessive reabsorption of protein in the tubules induces oxidative stress, renal interstitial inflammation, and fibrosis.
Patients with Alport syndrome are normally diagnosed with the disease in childhood to early adulthood and have average glomerular filtration rate (GFR) declines of 4.0 mL/min/1.73 m2 per year. The progressive decline of GFR in Alport syndrome leads to renal failure and end-stage renal disease (ESRD), with a median survival of approximately 55 years. Fifty percent of males with the most prevalent subtype of Alport syndrome require dialysis or kidney transplant by age 25. The incidence of renal failure in these patients increases to 90% by age 40 and nearly 100% by age 60. Similar to patients with other forms of CKD, Alport syndrome patients receiving dialysis are at increased risk for cardiovascular disease and infections, which are the most common causes of death in these patients.
The pathogenic role of inflammatory processes in Alport syndrome disease progression and declining renal function is similar to that of other chronic kidney diseases. The GBM defects and leaked proteins in Alport syndrome, the hyperglycemia in diabetes, and hypertension in cardiovascular disease all activate pro-inflammatory signaling pathways. Chronic activation of pro-inflammatory pathways in kidney cells promotes GFR loss by at least three mechanisms. First, inflammation-associated ROS reduce the amount of nitric oxide available to the endothelial cells in the blood vessels of the glomerulus. This results in a decrease of the overall surface area of the glomerulus that is available for filtration, and thus decreases GFR. Second, inflammation-associated ROS cause contraction of mesangial cells in the kidney. The primary function of these cells is to remove debris and protein from the GBM allowing proper filtration to occur. Mesangial cell contraction reduces their function, and thus reduces GFR. Third, inflammation-associated ROS lead to fibrosis, which changes the structure of the mesangial cell layer and causes thickening of the GBM, contributing to decline of GFR.
Bardoxolone methyl has the potential to address the causes of GFR loss in Alport syndrome patients because it activates molecular pathways that promote the resolution of inflammation by restoring mitochondrial function, reducing oxidative stress, and inhibiting ROS-mediated pro-inflammatory signaling. Bardoxolone methyl binds to Keap1 and activates Nrf2, a transcription factor that increases cellular antioxidant content and promotes normal mitochondrial function by making reducing equivalents available for ATP production. This reduces mitochondrial ROS production and ROS-mediated activation of inflammatory signaling complexes. Through these effects, bardoxolone methyl restores mitochondrial production of ATP, increases production of antioxidants, reduces oxidative stress, and reduces pro-inflammatory signaling.
Phase 2/3 CARDINAL Trial
During a meeting in October 2016, the FDA provided us with guidance on key elements of a single, pivotal clinical trial that would study the safety and efficacy of bardoxolone methyl in patients with CKD caused by Alport syndrome. In March 2017, we dosed the first patient in the Phase 2 portion of CARDINAL, a single, pivotal Phase 2/3 clinical trial. With the aid of international key opinion leaders and the Alport Syndrome Foundation and based on the guidance from the FDA, we designed the trial as an international, multi-center, double-blind, randomized, placebo-controlled trial that studies the safety, tolerability, and efficacy of bardoxolone methyl in qualified patients with Alport syndrome from age 12 to 60. The Phase 2 portion of the trial is open-label, will
19
test bardoxolone methyl in approximately 30 patients, and the primary endpoint will assess eGFR change at 12 weeks. These patients will be followed for two years, with eGFR measurements, including at weeks 48 and 100 on drug and 52 and 104 after withdrawal of drug for four weeks, and will not be included in the Phase 3 portion of the trial.
In designing the trial, we leveraged data from our previous clinical experience in CKD patients, including the retained eGFR analysis for BEACON and BEAM discussed below. The Phase 3 portion is designed to support registration and will enroll up to 180 patients. The patients in the Phase 3 portion of the trial are randomized 1:1 to either bardoxolone methyl or placebo. The eGFR change at one year will be measured after 48 weeks while the patient is on treatment, and after withdrawal of drug for four weeks (retained eGFR). After withdrawal, patients will be restarted on study drug with their original treatment assignments and will continue on study drug for a second year. The eGFR change at two years will also be measured after 100 weeks while the patient is on treatment and after withdrawal of drug for four weeks (retained eGFR). If the trial is successful, the year one retained eGFR data could support accelerated approval under subpart H of the Federal Food, Drug, and Cosmetic Act (the FD&C Act), and the year two retained eGFR data could support full approval under the FD&C Act. We expect to have Phase 2 data by the end of 2017. We expect to have the one year withdrawal data in the first half of 2019 that could then support accelerated approval. CARDINAL is overseen by a data monitoring committee (DMC) that reviews all data, including SAE and AE data, on an unblinded basis to assess safety. The DMC is scheduled to hold their first quarterly meeting in May 2017. In December 2016, we submitted a request to the FDA for orphan drug designation for bardoxolone methyl for the treatment of CKD caused by Alport syndrome.
There are no currently approved therapies for the treatment of CKD caused by Alport syndrome. The goal of current disease management is to slow the progression of CKD, beginning with anti-hypertensives, such as angiotensin converting enzyme inhibitors or angiotensin receptor blockers, aldosterone, and diuretics, all of which are intended to reduce the levels of protein found in patient urine. Once patients reach ESRD, they require dialysis and, in severe cases, renal transplantation.
|
|
|
|
|
|
Previous Renal Findings in Clinical Trials of Bardoxolone Methyl
Prior to initiating the current clinical development programs in PAH, PH-ILD, and CKD caused by Alport syndrome, bardoxolone methyl was evaluated in multiple trials, enrolling approximately 3,100 people, of which approximately 1,900 received bardoxolone methyl, including patients with CKD caused by diabetes, patients with solid tumors or lymphoma, and healthy volunteers.
We conducted six Phase 1 and 2 studies that demonstrated significant improvements in renal function evidenced by increases in eGFR and creatinine clearance as well as reductions in uremic solutes, such as blood urea nitrogen (BUN), uric acid, and phosphate, in inverse correlation with eGFR. These trials included the BEAM trial, a randomized, placebo-controlled 52-week Phase 2 trial in patients with CKD caused by diabetes. BEAM primarily enrolled patients with moderate or Stage 3 CKD caused by diabetes and demonstrated that eGFR improvements were sustained for 52 weeks on treatment and that eGFR at week 56, four weeks after withdrawal of drug, was greater than both baseline and placebo eGFR values. The BEAM data demonstrated that a portion of the on treatment eGFR improvement was retained after withdrawal of drug and suggested that bardoxolone methyl had disease-modifying activity in CKD caused by diabetes.
On the basis of the Phase 2 results, we conducted BEACON, a large, multinational Phase 3 trial in patients with Stage 4 CKD caused by diabetes. During October 2012, BEACON was terminated early in response to the independent data monitoring committee’s recommendation to stop the trial for safety concerns when data trends indicated a statistically significant increase in heart failure events and a non-statistically significant increase in mortality in the treatment arm. At the time, nothing was known about the cause or timing of the safety events or whether these events might worsen. After the trial was terminated, analysis revealed that there was a small but significant imbalance in heart failure events of 5.0% on placebo and 8.8% on active drug but no statistical difference in mortality. The primary reason for the increase in heart failure events was fluid overload that occurred in the first four weeks after randomization. Patients with fluid overload events who were treated with intravenous diuretics generally resolved their symptoms, and there was no increase in risk for fluid overload, as compared to placebo, after the first four weeks of treatment.
Post-hoc analysis from BEACON identified two major risk factors as predictors of fluid overload events in patients with Stage 4 CKD caused by diabetes: (a) prior hospitalization for heart failure and (b) baseline elevation in B-type natriuretic peptide (BNP), a clinical chemistry measure of fluid status. Patients without these risk factors showed no imbalance in heart failure events or mortality, which is consistent with the Phase 2 trials conducted by us that primarily enrolled patients with Stage 3 CKD caused by diabetes and did not show a risk of fluid overload. There were no other significant adverse safety findings from the BEACON trial, and patients in the treatment arm had fewer kidney and liver-related SAEs than patients in the placebo arm.
After BEACON, we instituted risk mitigation procedures for new trials which include the exclusion of patients with severe renal impairment, prior history of left-sided heart disease or heart failure, or with elevated baseline BNP levels. These risk mitigation
20
procedures have been used in all of our trials since BEACON, including LARIAT, the Phase 3 CATALYST trial in CTD-PAH, and the Phase 2/3 CARDINAL trial in CKD caused by Alport syndrome.
In April 2014, a paper in the American Journal of Nephrology was published that described the mechanisms contributing to the AEs described above in the BEACON trial. In June 2014, we gave a presentation at the European Renal Association-European Dialysis and Transplant Association on the investigation of SAEs in bardoxolone methyl patients in BEACON and in December 2014, a paper in the Journal of Cardiac Failure was published describing the risk factors discussed above.
In addition, our Asian development partner, KHK, initiated a Phase 2 trial named TSUBAKI in 2014, with bardoxolone methyl in patients in Stage 3 CKD caused by diabetes. In May 2016, KHK announced interim results from TSUBAKI showing that bardoxolone methyl treatment resulted in a significant improvement in measured GFR, as assessed by inulin clearance, after 16 weeks of treatment compared to placebo. Inulin clearance is the most rigorous technique to determine measured GFR. Moreover, the increase in inulin clearance is similar in magnitude to the changes in eGFR reported in other studies with bardoxolone methyl. KHK has recently expanded the trial to include patients in Stage 4 CKD caused by diabetes. No results from these patients have been released.
In previous trials performed by us in patients with CKD caused by diabetes, bardoxolone methyl significantly increased creatinine clearance, significantly reduced uremic solutes, such as BUN, uric acid, and phosphate, in inverse correlation to eGFR increases, and numerically reduced renal SAEs and ESRD events. These data, taken together with the KHK data, support that the increases in eGFR observed in the seven trials in patients with CKD caused by diabetes treated by bardoxolone methyl reflect actual increases in GFR and support the use of eGFR as a reliable marker of renal function. Below is an overview of renal improvements that have been shown in clinical trials with bardoxolone.
Overview of Bardoxolone Methyl Studies Demonstrating Improvements in Renal Function
|
Study |
|
Phase/Country |
|
Patient Population |
|
Mean Placebo-corrected ∆ eGFR |
|
402-C-0903 (BEACON) |
|
3/Global |
|
CKD/Diabetes |
|
6.4 (p<0.001 vs PBO) |
|
402-C-0804 (BEAM) |
|
2/US |
|
CKD/Diabetes |
|
8.6 (p<0.001 vs PBO) |
|
RTA402-005 (TSUBAKI) |
|
2/Japan |
|
CKD/Diabetes |
|
Data not yet publicly disclosed |
|
402-C-0902 |
|
2/US |
|
CKD/Diabetes |
|
6.5 (p<0.001) 2 |
|
402-C-0801 (Stratum 1) |
|
2a/US |
|
CKD/Diabetes |
|
6.7 (p<0.001) 2 |
|
402-C-0801 (Stratum 2) |
|
2b/US |
|
CKD/Diabetes |
|
7.2 (p<0.001) 2 |
|
402-C-1102 |
|
1/US |
|
CKD/Diabetes |
|
9.0 (p<0.05) 2 |
|
402-C-0501 |
|
1/US |
|
Cancer |
|
18.2 (p<0.0001) 2 |
|
402-C-0702 |
|
1/2/US |
|
Cancer |
|
32.2 (p=0.001) 2 |
|
402-C-1302 (LARIAT) |
|
2/US |
|
Pulmonary hypertension |
|
14.7 (p<0.001 vs PBO) |
|
1 |
Unless noted, data are differences between mean eGFR changes from baseline for bardoxolone methyl versus placebo groups and p- values calculated comparing the difference in means between bardoxolone methyl and placebo groups. |
|
2 |
Data are mean eGFR changes from baseline for bardoxolone methyl patients and p-values are calculated from two-sided paired t-tests comparing eGFR change to 0. |
In addition to the eGFR increase data, two separate trials, BEAM and BEACON, which included approximately 600 patients treated for one year or longer, showed that increases in eGFR in patients with CKD caused by diabetes treated with bardoxolone methyl were sustained for at least one year. In BEACON, bardoxolone methyl patients had mean increases in eGFR through Week 48 of 5.5 mL/min/1.73 m2. In contrast, placebo-treated patients experienced a mean decline in eGFR of -0.9 mL/min/1.73 m2, corresponding to a relative difference between groups of 6.4 mL/min/1.73 m2 (p<0.001).
Furthermore, in BEACON, at 48 weeks, bardoxolone methyl significantly reduced the proportion of patients with an eGFR loss of 3, 5, or 7.5 mL/min/1.73 m2, which represents losses of approximately 13%, 22%, and 33%, respectively, of baseline eGFR. The proportion of patients with a loss of eGFR of 30% from baseline at any visit was reduced by 67% (p<0.001).
After one year of treatment, a retained eGFR increase from baseline was observed in bardoxolone methyl patients after cessation of drug for four weeks, while an eGFR decline from baseline was observed in placebo patients. The table below shows the placebo-corrected eGFR change post-withdrawal. These data suggest that the abnormal structural deficits that contribute to declining kidney function may be improved over the course of longer-term treatment with bardoxolone methyl.
21
Retained eGFR Benefit After Withdrawal of Bardoxolone Methyl
|
|
|
Baseline eGFR |
|
Placebo-Corrected eGFR |
|
p-value |
|
BEAM (n=172) |
|
|
|
|
|
|
|
Low Dose |
|
33 |
|
0.6 |
|
p>0.05 |
|
Mid Dose |
|
32 |
|
4.7 |
|
p<0.05 |
|
High Dose |
|
32 |
|
5.0 |
|
p<0.05 |
|
BEACON (n=498) |
|
|
|
|
|
|
|
20mg |
|
23 |
|
l.8 |
|
p<0.00l |
Our goal in designing CARDINAL was to power the trial to replicate the BEAM mid-dose response of 4.7 mL/min/1.73m2. We have designed the trial with substantially more patients than the BEAM mid-dose, which enrolled 90 patients, to ensure that the trial could potentially be successful with an effect that is approximately 50% less than that seen with the mid-dose of BEAM.
We believe that the improvements in renal function noted in many studies with bardoxolone methyl coupled with the BEACON data demonstrating reduced risk of loss of kidney function suggest that bardoxolone methyl may have the potential to prevent renal function decline, which may translate to a multi-year delay in disease progression to ESRD for patients with Alport syndrome.
Omaveloxolone
Omaveloxolone is a close structural analog of bardoxolone methyl that was developed to improve tissue distribution, including blood-brain barrier penetration. To date, omaveloxolone has been administered orally to patients with FA, MM, and solid tumors, and has been administered topically to patients receiving cataract surgery and to breast cancer patients receiving radiation therapy and suffering from radiation dermatitis. We believe that an omaveloxolone-induced increase in mitochondrial energy production could have beneficial effects on multiple organ systems, with the most profound effects being in skeletal muscle, the brain, and other tissues with a high energy demand.
Friedreich’s Ataxia
Friedreich’s ataxia is an inherited, debilitating, and degenerative neuromuscular disorder that is typically diagnosed during adolescence and can ultimately lead to early death. Patients with FA experience progressive loss of coordination, muscle weakness, and fatigue, which commonly progresses to motor incapacitation and wheelchair reliance. FA patients may also experience visual impairment, hearing loss, diabetes, and cardiomyopathy. Childhood-onset FA can occur as early as age five, is more common than later-onset FA, and typically involves more rapid disease progression. The majority of FA patients have disease onset by approximately 13 to 15 years of age, and thereafter have a mean duration until wheelchair use of 10 to 15 years. The median age of death is in the mid-30s.
A mutation in the frataxin gene leads to impaired transcription and reduced expression of the mitochondrial protein frataxin. Deficiency of frataxin in cells leads to a mitochondrial iron overload and poor cellular iron regulation, increased sensitivity to oxidative stress, and impaired mitochondrial ATP production. Impaired ATP production in FA patients likely accounts for the decreased coordination, progressive muscle weakness, exercise intolerance, and fatigue observed in these patients, as well as other disease manifestations.
There are no currently approved therapies for the treatment of FA. Patients are usually given guidelines around certain lifestyle habits. They are recommended to follow a diet that is low in iron and encouraged to take vitamins and supplements. Idebenone was previously approved as a treatment for FA in Canada, but it was withdrawn five years after it was launched because no evidence could be provided for its efficacy. Despite the lack of current marketing authorization and minimal evidence of effectiveness in FA, idebenone continues to be prescribed off-label by physicians we believe in part due to the lack of other therapeutic options for FA patients.
Since patients suffering from FA experience increased sensitivity to oxidative stress and impaired mitochondrial ATP production, we believe that omaveloxolone may be effective in treating this indication. In FA patients, mitochondrial function is correlated with measures of neurologic function. Further, data demonstrate that Nrf2 signaling is significantly impaired in FA patients, resulting in impairment of antioxidant defense mechanisms, while silencing of frataxin gene expression has been linked to decreases in expression of Nrf2. Additionally, omaveloxolone has been shown in vitro to restore mitochondrial activity in fibroblasts
22
isolated from FA patients. Accordingly, we believe that Nrf2 activation through omaveloxolone may result in a clinical benefit to FA patients.
We are evaluating omaveloxolone in the MOXIe trial to evaluate the safety and efficacy of omaveloxolone in patients with Friedreich’s ataxia under an IND that we sponsored and filed in July 2014. MOXIe is being conducted at sites in the United States, Europe, and Australia. In 2014, we met with the FDA to discuss our FA program. Based on these discussions with the FDA, we designed a two-part, randomized, placebo-controlled, double-blind, dose-escalation Phase 2 trial with evaluation of a broad dose range in part one and a confirmatory evaluation of efficacy and safety in part two. Part one focuses on the evaluation of safety and efficacy of omaveloxolone doses ranging from 2.5 mg to 300 mg, and enrolled 69 patients, with enrollment completed in February 2017. Data for multiple endpoints are being collected, with the part one primary efficacy endpoint being the change in peak work, as measured by exercise testing on a recumbent bicycle. The key secondary endpoint in part one is a functional assessment based on the modified Friedreich’s Ataxia Rating Scale (mFARS). Data from MOXIe part one are expected in mid-year 2017. Part two will be designed to provide additional efficacy and safety data and it has the potential to be used to support registration. If part one is successful, we expect to evaluate the data and make any changes needed to the protocol for the second part of MOXIe, and then initiate part two of MOXIe as soon as possible.
We have observed no significant tolerability issues in MOXIe to date. The trial is being overseen by a DSMB that reviews all data, including SAE and AE data, on an unblinded basis to assess safety. The DSMB has not reported any safety concerns to date. In November 2014, we submitted a request to the FDA for orphan drug designation for omaveloxolone for the treatment of FA. The FDA has requested that we submit in vivo or human clinical data to support this application. In January 2017, we filed an amendment to the orphan application, which includes additional information.
Mitochondrial Myopathies
We are evaluating omaveloxolone in the MOTOR trial, a two-part randomized, placebo-controlled, double-blind, dose-escalation Phase 2 trial to evaluate the safety and efficacy of omaveloxolone in patients with MM. The protocol for the trial allows up to 100 patients with MM under an IND that we sponsored and filed in July 2014. MOTOR is being conducted at sites in the United States and Europe. In 2014, we met with the FDA to discuss our MM program. Based on discussions with the FDA, we designed a two-part trial with evaluation of a broad dose range in part one and confirmatory evaluation of safety and efficacy in part two. Part one focuses on the evaluation of safety and efficacy of omaveloxolone doses ranging from 2.5 mg to 160 mg. Data for multiple endpoints are being collected, with the primary efficacy endpoint being the change in peak work, as measured by exercise testing on a recumbent bicycle. The key secondary endpoint is the change from baseline in patients’ 6MWD. Part two is designed to provide additional efficacy and safety data and it has the potential to be used for registration. Data from the first part of MOTOR are expected in the second half of 2017, and if successful, we expect to evaluate the data and make any changes needed to the protocol for the second part of MOTOR and then initiate part two of MOTOR as soon as possible.
We have observed no significant tolerability issues in MOTOR to date. The trial is being overseen by a DSMB that reviews all data, including SAE and AE data, on an unblinded basis to assess safety. The DSMB has not reported any safety concerns to date. We intend to submit a request to the FDA for orphan drug designation for omaveloxolone for the treatment of MM once we have in vivo or human clinical data to support this application.
Immuno-oncology
We are evaluating omaveloxolone in the REVEAL trial, an open-label, multi-center, dose-escalation Phase 1b/2 trial under an IND that we sponsored and filed in August 2013, to evaluate the safety, pharmacodynamics, and efficacy of omaveloxolone, in combination with existing immunotherapies, in up to 102 patients with metastatic melanoma. REVEAL is being conducted at sites in the United States. In REVEAL, patients receive omaveloxolone monotherapy for one week, followed by omaveloxolone in combination with the labeled treatment course of either Yervoy® or Opdivo®. We previously evaluated omaveloxolone in the DISCOVER trial, an open-label, multi-center, dose-escalation Phase 1 trial conducted at sites in the United States under an IND that we sponsored and filed in August 2013 to evaluate the safety, pharmacokinetics, and pharmacodynamics of omaveloxolone in patients with advanced solid tumors. We have observed no significant tolerability issues in DISCOVER or REVEAL to date. The REVEAL trial is being overseen by a PSRC that reviews all data, including SAE and AE data, to assess safety. The PSRC has not reported any safety concerns to date. Data from the 1b dose escalation portion of REVEAL are expected during the second half of 2017. An orphan drug designation request was submitted in advanced malignant melanoma in November 2014. The FDA requested we submit in vivo or human clinical data to support the application, which we anticipate submitting in 2017.
23
RTA 901 for the Treatment of Orphan Neurological Indications
Our Hsp90 inhibitors, including RTA 901, are highly potent and selective C-terminal inhibitors of Hsp90. Inhibition of Hsp90 may result in activation of Hsp70, a molecular chaperone that plays a critical role in the process through which a protein assumes its functional shape and that serves as a central gatekeeper for mitochondrial protein import. Mitochondria rely on Hsp70-dependent protein import mechanisms for almost all of their activity, including the production of ATP. There are also indications that Hsp70 activation may play a profound role in neuroprotection since nerve cells are high consumers of ATP and rely on Hsp70-dependent protein import for proper mitochondrial function.
We initiated a Phase 1 clinical trial in January 2017 to evaluate the safety, tolerability, and pharmacokinetic profile of RTA 901 in healthy adult volunteers. The trial is designed in two parts, part 1 with single ascending doses, and part 2 with multiple ascending doses. In part 1, approximately 56 healthy subjects in up to 7 groups of 8 subjects each are randomized in a 3:1 ratio to receive a single dose of RTA 901 or placebo, respectively. In part 2, approximately 30 healthy subjects in up to 3 groups of 10 subjects each will be randomized in a 4:1 ratio to receive 14 daily doses of RTA 901 or placebo, respectively. We plan to complete the trial and report data in the second half of 2017. If the Phase 1 clinical trial of RTA 901 supports further development, we plan to follow it with a Phase 2 clinical trial of RTA 901 for the treatment of an orphan neurological indication or diabetic neuropathy.
Preclinical Programs
Additional Nrf2 Activator Indications
If beneficial effects are demonstrated in our ongoing PAH, PH-ILD, FA and MM trials, this could indicate that our Nrf2 activator pharmacology may also provide therapeutic benefit for patients suffering from other diseases where mitochondrial dysfunction or chronic inflammation is implicated. In addition, if therapeutic benefits are demonstrated in CKD caused by Alport syndrome, the Nrf2 activator pharmacology may also provide therapeutic benefit in other renal diseases. Some of these diseases may be treated by our current lead product candidates, bardoxolone methyl and omaveloxolone.
Additional Hsp90 Inhibitor Indications
If beneficial neuroprotective and bioenergetic effects are demonstrated in our future Phase 2 trials, this could indicate that our Hsp90 inhibitor pharmacology may also provide therapeutic benefit for patients suffering from other diseases where neurodegenerative and mitochondrial dysfunction are implicated.
RORγT Inhibitors
We are pursuing preclinical development of novel, small-molecule, orally bioavailable RORγT inhibitors. RORγT is the master regulator of human T Helper 17 (Th17) cellular differentiation, function, and cytokine production, and represents a compelling target for a variety of autoimmune and inflammatory conditions. TH17 cells produce cytokines, including IL-17, that play a critical role in driving immune-mediated inflammation and are implicated in the pathogenesis of certain autoimmune diseases. The efficacy of suppressing IL-17 as a means of treating these conditions has been demonstrated both in animal models and in humans. We have selected and are advancing a single RORγT development candidate into Good Laboratory Practices toxicology studies.
Financial Operations Overview
Revenue
Our revenue to date has been generated primarily from licensing fees received under our collaborative license agreements and reimbursements for expenses. We currently have no approved products and have not generated any revenue from the sale of products to date. In the future, we may generate revenue from product sales, royalties on product sales, reimbursements for collaboration services under our current collaboration agreements, or license fees, milestones, or other upfront payments if we enter into any new collaborations or license agreements. We expect that our future revenue will fluctuate from quarter to quarter for many reasons, including the uncertain timing and amount of any such payments and sales.
Our license and milestone revenue has been generated primarily from our collaborative licensing agreements with AbbVie and KHK and consists of upfront payments and milestone payments. Under our revenue recognition policy, license revenue associated with upfront, non-refundable license payments received under the collaboration agreements with AbbVie and KHK are recognized ratably over the expected term of the performance obligations under the agreements, which extend through various periods beginning in 2017 and ending in 2026. License revenue recorded with respect to the collaboration agreements with AbbVie consists solely of the
24
recognition of deferred revenue. License revenue recorded with respect to the collaboration agreements with KHK consists of the recognition of deferred revenue and reimbursement of supply costs.
We also have other license revenue, which consists of milestone payments from a disease advocacy organization in 2017, and other revenue, which consists of reimbursements from KHK for expenses incurred to obtain drug supplies.
Research and Development Expenses
The largest component of our total operating expenses has historically been our investment in research and development activities, including the clinical development of our product candidates. From our inception through March 31, 2017, we have incurred a total of $492.8 million in research and development expense, a majority of which relates to the development of bardoxolone methyl and omaveloxolone. We expect our research and development expense to continue to increase in the future as we advance our product candidates through clinical trials and expand our product candidate portfolio. The process of conducting the necessary clinical research to obtain regulatory approval is costly and time-consuming and we consider the active management and development of our clinical pipeline to be crucial to our long-term success. The actual probability of success for each product candidate and preclinical program may be affected by a variety of factors, including the safety and efficacy data for product candidates, investment in the program, competition, manufacturing capability, and commercial viability.
Research and development expenses include:
|
|
• |
expenses incurred under agreements with clinical trial sites that conduct research and development activities on our behalf; |
|
|
• |
expenses incurred under contract research agreements and other agreements with third parties; |
|
|
• |
employee and consultant-related expenses, which include salaries, benefits, travel, and stock-based compensation; |
|
|
• |
laboratory and vendor expenses related to the execution of preclinical and non-clinical studies and clinical trials; |
|
|
• |
the cost of acquiring, developing, manufacturing, and distributing clinical trial materials; and |
|
|
• |
facilities, depreciation, and other expenses, which include direct and allocated expenses for rent and maintenance of facilities, insurance, and other supply costs. |
Research and development costs are expensed as incurred. Costs for certain development activities such as clinical trials are recognized based on an evaluation of the progress to completion of specific tasks using information and data provided to us by our vendors and our clinical sites.
We base our expense accruals related to clinical trials on our estimates of the services received and efforts expended under contracts with multiple research institutions and contract research organizations (CROs) that conduct and manage clinical trials on our behalf. The financial terms of these agreements vary from contract to contract and may result in uneven payment flows. Payments under some of these contracts depend on factors such as the successful enrollment of patients and the completion of clinical trial milestones. In accruing costs, we estimate the time period over which services will be performed and the level of effort to be expended in each period. If we do not identify costs that we have begun to incur or if we underestimate or overestimate the level of services performed or the costs of these services, our actual expenses could differ from our estimates.
To date, we have not experienced significant changes in our estimates of accrued research and development expenses after a reporting period. However, due to the nature of estimates, we cannot assure you that we will not make changes to our estimates in the future as we become aware of additional information about the status or conduct of our clinical trials and other research activities.
Currently, AbbVie is not participating in the development of bardoxolone methyl for the treatment of CKD caused by Alport syndrome, PAH, or PH-ILD and we are therefore incurring all costs for this program. With respect to our omaveloxolone programs and our collaboration agreement with AbbVie, we were responsible for a certain initial amount in early development costs before AbbVie began sharing development costs equally. In April 2016, we had incurred all of these initial costs, after which payments from AbbVie with respect to research and development costs incurred by us were recorded as a reduction in research and development expenses.
In September 2016, we and AbbVie mutually agreed that we would continue unilateral development of omaveloxolone. Therefore, AbbVie no longer co-funds the exploratory development costs of this program, but retains the right to opt back in at certain points in development. Depending upon what point, if any, AbbVie opts back into development, AbbVie may retain its right to commercialize a product outside the U.S. or we may be responsible for commercializing the product on a worldwide basis. Upon
25
opting back in, AbbVie would be required to pay an agreed upon amount of all development costs accumulated up to the point of exercising their opt-in right, after which development costs incurred and product revenue worldwide would be split equally. For the quarter ended March 31, 2016, no payments related to shared research and developments costs were received.
The following table summarizes our research and development expenses incurred:
|
|
|
Three Months Ended March 31, |
|
|||||
|
|
|
2017 |
|
|
2016 |
|
||
|
|
|
(unaudited) |
|
|||||
|
|
|
(in thousands) |
|
|||||
|
Bardoxolone methyl |
|
$ |
7,467 |
|
|
$ |
3,632 |
|
|
Omaveloxolone |
|
|
1,569 |
|
|
|
1,934 |
|
|
RTA 901 |
|
|
570 |
|
|
|
817 |
|
|
Other research and development expenses |
|
|
4,997 |
|
|
|
2,923 |
|
|
Total research and development expenses |
|
$ |
14,603 |
|
|
$ |
9,306 |
|
The program-specific expenses summarized in the table above include costs that we directly allocate to our product candidates. Our other research and development expenses include research and development salaries, benefits, stock-based compensation, and preclinical, research, and discovery costs, which we do not allocate on a program-specific basis.
General and Administrative Expenses
General and administrative expenses consist primarily of employee-related expenses for executive, operational, finance, legal, compliance, and human resource functions. Other general and administrative expenses include personnel expense, facility-related costs, professional fees, accounting and legal services, depreciation expense, other external services, and expenses associated with obtaining and maintaining our intellectual property rights.
We anticipate that our general and administrative expenses will increase in the future as we increase our headcount to support our continued research and development and potential commercialization of our product candidates. We have also incurred increased expenses associated with being a public company, including exchange listing and SEC requirements, director and officer insurance premiums, legal, audit, and tax fees, regulatory compliance programs, and investor relations costs. Additionally, if and when we believe the first regulatory approval of one of our product candidates appears likely, we anticipate an increase in payroll and related expenses as a result of our preparation for commercial operations, especially for the sales and marketing of our product candidates.
Other Income
Other income represents interest and gains earned on our cash and cash equivalents, which include money market funds.
Interest expense
Commencing in March 2017, interest expense is primarily attributable to interest charges associated with borrowings under our Loan Agreement.
Provision for Taxes on Income
Provision for taxes on income consists of net loss, taxed at federal tax rates and adjusted for certain permanent differences. We maintain a valuation allowance against the majority of our net deferred tax assets. Changes in this valuation allowance also affect the tax provision.
26
Comparison of the three months ended March 31, 2017 and 2016 (unaudited)
The following table sets forth our results of operations for the three months ended March 31:
|
|
|
2017 |
|
|
2016 |
|
|
Change $ |
|
|
Change % |
|
||||
|
|
|
(unaudited) |
|
|||||||||||||
|
|
|
(in thousands, except percentage data) |
|
|||||||||||||
|
Consolidated Statements of Operations Data |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Collaboration revenue |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
License and milestone |
|
$ |
12,729 |
|
|
$ |
12,365 |
|
|
|
364 |
|
|
|
3 |
|
|
Other revenue |
|
|
3 |
|
|
|
73 |
|
|
|
(70 |
) |
|
|
(96 |
) |
|
Total collaboration revenue |
|
|
12,732 |
|
|
|
12,438 |
|
|
|
294 |
|
|
|
2 |
|
|
Expenses |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Research and development |
|
|
14,603 |
|
|
|
9,306 |
|
|
|
5,297 |
|
|
|
57 |
|
|
General and administrative |
|
|
5,173 |
|
|
|
3,207 |
|
|
|
1,966 |
|
|
|
61 |
|
|
Depreciation and amortization |
|
|
130 |
|
|
|
188 |
|
|
|
(58 |
) |
|
|
(31 |
) |
|
Total expenses |
|
|
19,906 |
|
|
|
12,701 |
|
|
|
7,205 |
|
|
|
57 |
|
|
Other income (expense) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Investment income |
|
|
81 |
|
|
|
23 |
|
|
|
58 |
|
|
|
252 |
|
|
Interest expense |
|
|
(5 |
) |
|
|
— |
|
|
|
(5 |
) |
|
|
(100 |
) |
|
Total other income (expense) |
|
|
76 |
|
|
|
23 |
|
|
|
53 |
|
|
|
230 |
|
|
Loss before provision for taxes on income |
|
|
(7,098 |
) |
|
|
(240 |
) |
|
|
(6,858 |
) |
|
|
(2,858 |
) |
|
Provision for taxes on income |
|
|
— |
|
|
|
18 |
|
|
|
(18 |
) |
|
|
(100 |
) |
|
Net loss |
|
$ |
(7,098 |
) |
|
$ |
(258 |
) |
|
|
(6,840 |
) |
|
|
(2,651 |
) |
Revenue
License and milestone revenue increased by $0.4 million, or 3%, for the three months ended March 31, 2017, compared to the three months ended March 31, 2016. The increase was primarily due to the achievement of a $0.5 million milestone from a research collaboration with a disease advocacy organization in March 2017. License revenue represented 100% and 99% of total revenue from the three months ended March 31, 2017 and 2016, respectively.
The following table summarizes the sources of our revenue for the three months ended March 31:
|
|
|
2017 |
|
|
2016 |
|
||
|
|
|
(unaudited) |
|
|||||
|
|
|
(in thousands) |
|
|||||
|
License and milestone |
|
|
|
|
|
|
|
|
|
AbbVie license agreement |
|
$ |
5,280 |
|
|
$ |
5,338 |
|
|
AbbVie collaboration agreement |
|
|
6,570 |
|
|
|
6,644 |
|
|
KHK agreement |
|
|
379 |
|
|
|
383 |
|
|
Other revenue |
|
|
500 |
|
|
|
— |
|
|
Total license and milestone |
|
|
12,729 |
|
|
|
12,365 |
|
|
Other revenue |
|
|
3 |
|
|
|
73 |
|
|
Total collaboration revenue |
|
$ |
12,732 |
|
|
$ |
12,438 |
|
Research and Development Expenses
Research and development expenses increased by $5.3 million, or 57%, for the three months ended March 31, 2017, compared to the three months ended March 31, 2016. The increase was primarily due to increases of $3.8 million in clinical activities for the start-up activities for CARDINAL, CATALYST, and the extension trial for CATALYST and LARIAT patients, increase of $0.3 million in preclinical and research activities in our RORγT program, $0.8 million in personnel expense to support growth in our development activities, and $0.4 million in stock compensation expense related to award issuances in June and December 2016.
27
General and Administrative Expenses
General and administrative expenses increased by $2.0 million, or 61%, for the three months ended March 31, 2017, compared to the three months ended March 31, 2016. The increase was primarily due to $0.5 million in personnel expense to support growth in the organization and expanded development activities, $0.9 million in stock compensation expense related to award issuances in June and December 2016, $0.3 million increased insurance coverage costs and consulting fees in connection with being a public company, and $0.1 million in increased intellectual property costs.
Investment Income
Investment income was immaterial for the three months ended March 31, 2017 and 2016.
Interest Expense
Interest expense is primarily attributable to interest charges associated with borrowings under our Loan Agreement for the three months ended March 31, 2017. We recorded no interest expense for the three months ended March 31, 2016.
Provision for Taxes on Income
Provision for taxes on income was immaterial for the three months ended March 31, 2017 and 2016.
Liquidity and Capital Resources
Since our inception, we have funded our operations primarily through collaboration and license agreements and the sale of preferred and common stock. To date, we have raised gross cash proceeds of $476.6 million through the sale of convertible preferred stock and received $750 million from payments under license and collaboration agreements, $60.9 million in net proceeds from our initial public offering of our Class A common stock, and $19.8 million in net proceeds from our Loan Agreement in March 2017. As of March 31, 2017, we had available cash and cash equivalents of approximately $82.7 million. Our cash and cash equivalents are invested in accordance with our investment policy, primarily with a view to liquidity and capital preservation.
On March 31, 2017, we entered into a Loan Agreement, under which our Lenders agreed to lend us up to $35.0 million, issuable in two separate tranches of $20.0 million (Term A Loan) and $15.0 million (Term B Loan). On March 31, 2017, we borrowed $20.0 million from the Term A Loan.
All outstanding Term Loans will mature on March 1, 2022. We will make interest-only payments for 18 months through November 1, 2018; however, if we draw the Term B Loan, we will make interest-only payment for 24 months through May 1, 2019. The interest-only payment period will be followed by principal and interest payments thereafter and through maturity. The Term A Loan bears interest at a floating per annum rate between a minimum of 8.15% and a maximum of 10.15%. The interest rate is calculated as 7.40% plus the greater of the 30-day U.S. Dollar LIBOR rate reported in The Wall Street Journal or 0.75%.
Cash Flows
The following table sets forth the primary sources and uses of cash for each of the three months ended March 31 set forth below:
|
|
|
2017 |
|
|
2016 |
|
||
|
|
|
(unaudited) |
|
|||||
|
|
|
(in thousands) |
|
|||||
|
Net cash (used in) provided by: |
|
|
|
|
|
|
|
|
|
Operating activities |
|
$ |
(22,058 |
) |
|
$ |
817 |
|
|
Investing activities |
|
|
(34 |
) |
|
|
(16 |
) |
|
Financing activities |
|
|
20,036 |
|
|
|
(956 |
) |
|
Net change in cash and cash equivalents |
|
$ |
(2,056 |
) |
|
$ |
(155 |
) |
Operating Activities
Net cash used in operating activities was $22.1 million for the three months ended March 31, 2017, consisting primarily of net loss of $7.1 million adjusted for non-cash items including stock-based compensation expense of $1.6 million, depreciation expense of $0.1 million, and a net decrease in operating assets and liabilities of $16.7 million. The significant items in the change in operating
28
assets and liabilities include an increase of prepaid expenses and other current assets of $1.3 million due to clinical trial prepayments and reimbursements due from KHK, a decrease in account payable of $3.3 million due to timing of vendor payments, and a decrease in deferred revenue of $12.2 million. The decrease in deferred revenue relates to the timing of upfront payments and ratable recognition of revenue over the expected term of the performance obligations under our collaboration agreements with AbbVie and KHK, resulting in recognition of $12.2 million of license and milestone revenue.
Net cash provided by operating activities was $0.8 million for the three months ended March 31, 2016, consisting primarily of net loss of $0.3 million adjusted for non-cash items including stock-based compensation expense of $0.3 million, depreciation expense of $0.2 million, and a net increase in operating assets and liabilities of $0.6 million. The significant items in the change in operating assets and liabilities include an increase of prepaid expenses and other current assets of $0.5 million due to prepayments on trial and other operating expenses and reimbursements due from KHK, an increase in accrued direct research and other current liabilities of $1.2 million due to clinical trial activities, a decrease in account payable of $3.0 million due to timing of vendor payments, a decrease in income tax receivable of $15.2 million due to tax refunds received, and a decrease in deferred revenue of $12.4 million. The decrease in deferred revenue relates to the timing of upfront payments and ratable recognition of revenue over the expected term of the performance obligations under our collaboration agreements with AbbVie and KHK, resulting in recognition of $12.4 million of license and milestone revenue.
Investing Activities
Net cash used in investing activities consisted of purchases and sales of property and equipment. Net cash used in investing activities for the three months ended March 31, 2017 and 2016 was not significant.
Financing Activities
Net cash provided by financing activities was $20.0 million, primarily due to net proceeds of $19.8 million from our Loan Agreement for the three months ended March 31, 2017.
Net cash used in financing activities for the three months ended March 31, 2016, primarily consisted of payments on deferred offering costs.
Operating Capital Requirements
To date, we have not generated any revenue from product sales. We do not know when or whether we will generate any revenue from product sales. We do not expect to generate significant revenue from product sales unless and until we obtain regulatory approval of and commercialize one or more of our current or future product candidates. We anticipate that we will continue to generate losses for the foreseeable future, and we expect the losses to increase as we continue the development of, and seek regulatory approvals for, our product candidates, and begin to commercialize any approved products. We are subject to all the risks related to the development and commercialization of novel therapeutics, and we may encounter unforeseen expenses, difficulties, complications, delays, and other unknown factors that may adversely affect our business. We expect to incur additional costs associated with operating as a public company. We anticipate that we will need substantial additional funding in connection with our continuing operations.
We believe our existing cash and cash equivalents, not including expected receipts from our collaborations, will be sufficient to enable us to fund our operating expenses and capital expenditure requirements for at least the next 12 months.
Our longer term liquidity requirements will require us to raise additional capital, such as through additional equity or debt financings. Our future capital requirements will depend on many factors, including the receipt of milestones under our current collaboration agreements and the timing of our expenditures related to clinical trials. In addition, we may choose to raise additional capital at any time for the further development of our existing product candidates and may also need to raise additional funds sooner to pursue other development activities related to additional product candidates. Decisions about the timing or nature of any financing will rely on, among other things, our perception of our liquidity and of the market opportunity to raise equity or debt. Additional securities may include common stock, preferred stock, or debt securities.
Until we can generate a sufficient amount of revenue from our product candidates, if ever, we expect to finance future cash needs through public or private equity or debt offerings. Additional capital may not be available on reasonable terms, if at all. If we are unable to raise additional capital in sufficient amounts or on terms acceptable to us, we may have to significantly delay, scale back, or discontinue the development or commercialization of one or more of our product candidates. If we raise additional funds through the issuance of additional equity or debt securities, it could result in dilution to our existing stockholders or increased fixed payment
29
obligations, and any such securities may have rights senior to those of our common stock. If we incur additional indebtedness, we could become subject to additional covenants that could further restrict our operations and potentially impair our competitiveness, such as limitations on our ability to incur additional debt, limitations on our ability to acquire, sell, or license intellectual property rights, and other operating restrictions that could adversely affect our ability to conduct our business, and any such debt could be secured by our owned intellectual property, in addition to assets which currently secure our debt. Any of these events could significantly harm our business, financial condition, and prospects.
Our forecast of the period through which our financial resources will be adequate to support our operations is a forward-looking statement and involves risks and uncertainties, and actual results could vary as a result of a number of factors. We have based this estimate on assumptions that may prove to be wrong, and we could utilize our available capital resources sooner than we currently expect. Our future funding requirements, both near- and long-term, will depend on many factors, including, but not limited to:
|
|
• |
the scope, rate of progress, results and cost of our clinical trials, preclinical testing, and other activities related to the development of our product candidates; |
|
|
• |
the number and characteristics of product candidates that we pursue; |
|
|
• |
the costs of development efforts for our product candidates that are not subject to reimbursement from our collaborators; |
|
|
• |
the costs necessary to obtain regulatory approvals, if any, for our product candidates in the United States and other jurisdictions, and the costs of post-marketing studies that could be required by regulatory authorities in jurisdictions where approval is obtained; |
|
|
• |
the continuation of our existing collaborations and entry into new collaborations and the receipt of any collaboration payments; |
|
|
• |
the time and unreimbursed costs necessary to commercialize products in territories in which our product candidates are approved for sale; |
|
|
• |
the revenue from any future sales of our products for which we are entitled to a profit share, royalties, and milestones; |
|
|
• |
the level of reimbursement or third-party payor pricing available to our products; |
|
|
• |
the costs of obtaining third-party commercial supplies of our products, if any, manufactured in accordance with regulatory requirements; |
|
|
• |
the costs associated with being a public company; and |
|
|
• |
the costs we incur in the filing, prosecution, maintenance, and defense of our extensive patent portfolio and other intellectual property rights. |
If we cannot expand our operations or otherwise capitalize on our business opportunities because we lack sufficient capital, our business, financial condition, and results of operations could be materially adversely affected.
Contractual Obligations and Commitments
As of March 31, 2017, there have been no material changes, outside of the ordinary course of business, in our outstanding contractual obligations from those disclosed within "Management's Discussion and Analysis of Financial Condition and Results of Operations", as contained in our Annual Report on Form 10-K for year ended December 31, 2016, other than the following:
As of March 31, 2017, our contractual obligations were as follows:
|
|
|
Payments due by period |
|
|||||||||||||
|
|
|
Less than 1 year |
|
|
1 to 3 years |
|
|
4 to 5 years |
|
|
Total |
|
||||
|
|
|
(in thousands) |
|
|||||||||||||
|
Operating lease obligations |
|
$ |
600 |
|
|
$ |
356 |
|
|
$ |
— |
|
|
$ |
956 |
|
|
Outstanding Term A Loan |
|
|
— |
|
|
|
8,293 |
|
|
$ |
12,297 |
|
|
$ |
20,590 |
|
|
Total contractual obligations |
|
$ |
600 |
|
|
$ |
8,649 |
|
|
$ |
12,297 |
|
|
$ |
21,546 |
|
30
As of March 31, 2017, we have several on-going clinical trials in various stages. Under agreements with various CROs and clinical trial sites, we incur expenses related to clinical trials of our product candidates and potential other clinical candidates. The timing and amounts of these disbursements are contingent upon the achievement of certain milestones, patient enrollment, and services rendered or as expenses are incurred by the CROs or clinical trial sites. Therefore, we cannot estimate the potential timing and amount of these payments and they have been excluded from the table above.
Critical Accounting Policies and Significant Judgments and Estimates
Our management’s discussion and analysis of our financial condition and results of operations are based on our consolidated financial statements, which have been prepared in accordance with U.S. generally accepted accounting principles. The preparation of these financial statements requires us to make estimates and judgments that affect the reported amounts of assets, liabilities, and expenses and the disclosure of contingent assets and liabilities in our financial statements. On an ongoing basis, we evaluate our estimates and judgments, including those related to revenue recognition, accrued research and development expenses, income taxes, and stock-based compensation. We base our estimates on historical experience, known trends and events, and various other factors that we believe to be reasonable under the circumstances, the results of which form the basis for making judgments about the carrying values of assets and liabilities that are not readily apparent from other sources. Actual results may differ from these estimates under different assumptions or conditions. There have been no significant and material changes in our critical accounting policies during the three months ended March 31, 2017, as compared to those disclosed in “Management’s Discussion and Analysis of Financial Condition and Results of Operations-Critical Accounting Policies and Significant Judgments and Estimates” in our Annual Report on Form 10-K for the year ended December 31, 2016.
Off-Balance Sheet Arrangements
Since our inception, we have not had any relationships with unconsolidated organizations or financial partnerships, such as structured finance or special purpose entities that would have been established for the purpose of facilitating off-balance sheet arrangements, and we have not engaged in any other off-balance sheet arrangements, as defined in the rules and regulations of the SEC.
Recent Accounting Pronouncements
For a discussion of recent accounting pronouncements, please see Note 2 of Notes to Consolidated Financial Statements contained in this Quarterly Report on Form 10-Q.
Item 3. Quantitative and Qualitative Disclosures About Market Risk.
We are exposed to market risks in the ordinary course of our business. These market risks are principally limited to interest rate fluctuations. We had cash and cash equivalents of $82.7 million at March 31, 2017, consisting primarily of funds in operating cash accounts. The primary objective of our investment activities is to preserve principal and liquidity while maximizing income without significantly increasing risk. We do not enter into investments for trading or speculative purposes. Due to the short-term nature of our investment portfolio, we do not believe an immediate 1.0% increase in interest rates would have a material effect on the fair market value of our portfolio, and accordingly we do not expect a sudden change in market interest rates to affect materially our operating results or cash flows.
We also have interest rate exposure as a result of our Term A Loan. As of March 31, 2017, the outstanding principal amount of our Term A Loan was $20.0 million. Term A Loan bears interest at a floating per annum rate calculated as 7.40% plus the greater of the 30-day U.S. Dollar LIBOR rate reported in The Wall Street Journal or 0.75%, with a minimum rate of 8.15% and a maximum rate of 10.15%. Changes in the U.S. Dollar LIBOR rate may therefore affect our interest expense associated with the Term A Loan. An increase of 1.0% in interest rates would increase expense by approximately $0.2 million annually based on the amounts currently outstanding and would not materially affect our results of operations.
We contract with research, development, and manufacturing organizations and investigational sites globally. Generally, these contracts are denominated in U.S. dollars. However, we may be subject to fluctuations in foreign currency rates in connection with agreements not denominated in U.S. dollars. We do not hedge our foreign currency exchange rate risk.
31
Item 4. Controls and Procedures.
Evaluation of Disclosure Controls and Procedures
Our management, with the participation of our Chief Executive Officer and Chief Financial Officer, evaluated the effectiveness of our disclosure controls and procedures as of March 31, 2017. The term “disclosure controls and procedures,” as defined in Rules 13a-15(e) and 15d-15(e) under the Exchange Act of 1934 (Exchange Act), means controls and other procedures of a company that are designed to ensure that information required to be disclosed by a company in the reports that it files or submits under the Exchange Act is recorded, processed, summarized, and reported within the time periods specified in the Securities and Exchange Commission’s rules and forms. Disclosure controls and procedures include, without limitation, controls and procedures designed to ensure that information required to be disclosed by a company in the reports that it files or submits under the Exchange Act is accumulated and communicated to the company’s management, including its principal executive and principal financials officers, as appropriate to allow timely decisions regarding required disclosure. Management recognizes that any controls and procedures, no matter how well designed and operated, can provide only reasonable assurance of achieving their objectives and management necessarily applies its judgment in evaluating the cost-benefit relationship of possible controls and procedures. Based on the evaluation of our disclosure controls and procedures as of March 31, 2017, our Chief Executive Officer and Chief Financial Officer concluded that, as of such date, our disclosure controls and procedures were effective at the reasonable assurance level.
Changes in Internal Control over Financial Reporting
There has been no change in our internal control over financial reporting (as defined in Rules 13a-15(f) and 15d-15(f) under the Exchange Act) during the three months ended March 31, 2017, that has materially affected, or is reasonably likely to materially affect, our internal control over financial reporting.
32
We are not currently subject to any material legal proceedings.
In addition to the risks discussed below and other information set forth in this Quarterly Report on Form 10-Q, you should carefully consider the risk factors and other cautionary statements described under the heading “Risk Factors” included in our Annual Report on Form 10-K for the year ended December 31, 2016, which could materially affect our businesses, financial condition, or future results. Additional risks and uncertainties not currently known to us or that we currently deem to be immaterial also may materially adversely affect our business, financial condition, or future results. There has been no material changes in our risk factors from those described in the Annual Report on Form 10-K for the year ended December 31, 2016, other than as discussed below.
Risks Related to Our Financial Condition
Payments under the instruments governing our indebtedness may reduce our working capital. In addition, a default under our Loan Agreement could cause a material adverse effect on our financial position.
In March 2017, we entered into the Loan Agreement, under which the Lenders agreed to lend us up to $35 million, issuable in two separate tranches of $20 million (Term A Loan) and $15 million (Term B Loan). On March 31, 2017, we borrowed the $20 million from the Term A Loan. Beginning July 1, 2017, under the terms of the Loan Agreement, the Company may, at its sole discretion, borrow $15.0 million under the Term B Loan following the achievement of the first of two defined milestone events until the earlier of 90 days thereafter or March 31, 2018.
Our obligations under the Loan Agreement are secured by a first priority security interest in substantially all of our current and future assets, other than our intellectual property. We have also agreed not to encumber our intellectual property assets, except as permitted by the Loan Agreement. All outstanding Term Loans will mature on March 1, 2022. We will make interest-only payments for 18 months through November 1, 2018; however, if we draw the Term B Loan, we will make interest-only payments for 24 months through May 1, 2019. The interest-only payment period will be followed by 41 equal monthly payments, or 35 equal monthly payments if we draw the Term B Loan, of principal and interest payments. Payments under the Loan Agreement could result in a significant reduction of our working capital.
The Loan Agreement requires us, and any debt arrangements we may enter into in the future may require us, to comply with various covenants that limit our ability to, among other things:
|
|
• |
incur indebtedness; |
|
|
• |
encumber assets; |
|
|
• |
dispose of assets; |
|
|
• |
complete mergers or acquisitions; |
|
|
• |
pay dividends or make other distributions to holders of our capital stock; |
|
|
• |
make specified investments; and |
|
|
• |
engage in transactions with our affiliates. |
These restrictions could inhibit our ability to pursue our business strategies. If we default under our obligations under the Loan Agreement, the Lenders could proceed against the collateral granted to it to secure our indebtedness or declare all obligation under the Loan Agreement to be due and payable. In certain circumstances, procedures by the Lenders could result in a loss by us of all of our equipment and inventory, which are included in the collateral granted to the lenders. If any indebtedness under the Loan Agreement were to be accelerated, there can be no assurance that our assets would be sufficient to repay in full that indebtedness. In addition, upon any distribution of assets pursuant to any liquidation, insolvency, dissolution, reorganization, or similar proceeding, the holders of secured indebtedness will be entitled to receive payment in full from the proceeds of the collateral securing our secured indebtedness before the holders of other indebtedness or our common stock will be entitled to receive any distribution with respect thereto.
33
Subject to the provisions of the Loan Agreement, we may incur additional indebtedness in the future. The debt instruments governing such indebtedness may contain provisions that are as, or more, restrictive than the provisions governing our existing indebtedness under the Loan Agreement.
We may not be able to refinance, extend, or repay our indebtedness to our Lenders, which would have a material adverse effect on our financial condition and ability to continue as a going concern. Additionally, our Lenders could proceed against the collateral or force us into bankruptcy or liquidation.
Item 2. Unregistered Sales of Equity Securities and Use of Proceeds.
Unregistered Sales of Equity Securities
None.
Use of Proceeds from Initial Public Offering of Class A Common Stock
On May 25, 2016, our registration statement on Form S-1 (File No. 333-208843) relating to our IPO of our Class A common stock was declared effective by the SEC. The shares began trading on The NASDAQ Global Market on May 26, 2016. The public offering price of the shares sold in the offering was $11.00 per share. The IPO closed on June 1, 2016 and included 6,325,000 shares of Class A common stock, which included 825,000 shares of Class A common stock issued pursuant to the overallotment option granted to the underwriters, for gross proceeds of approximately $69.6 million before deducting underwriters’ discounts and commissions and offering-related expenses. Net proceeds, after deducting underwriting discounts and commissions of $4.9 million and offering expenses of approximately $3.8 million, were $60.9 million. Citigroup Global Markets Inc., Cowen and Company, LLC, and Piper Jaffray & Co. acted as joint book-running managers of this offering.
There has been no material change in the planned use of proceeds from our IPO as described in our prospectus dated May 25, 2016, filed with the SEC pursuant to Rule 424(b)(4) of the Securities Act. We invested the funds received in highly liquid money market funds. The net proceeds from the IPO have been used and will be used, together with our cash and cash equivalents, to fund continued advancement of our bardoxolone methyl, omaveloxolone, and clinical trials and preclinical studies, and to provide funds for working capital and other general purposes. None of the offering proceeds were paid directly or indirectly to any of our directors or officers, or their associates, or persons owning 10.0% or more of any class of our equity securities or to any other affiliates.
Item 3. Defaults Upon Senior Securities.
None.
Item 4. Mine Safety Disclosures.
None.
None.
34
|
Exhibit Number |
|
Description |
|
|
|
|
|
3.1 |
|
Thirteenth Amended and Restated Certificate of Incorporation (incorporated by reference to Exhibit 3.7 to the Registrant’s Registration Statement on Form S-1, File No. 333-208843, filed with the Commission on May 16, 2016). |
|
|
|
|
|
3.2 |
|
Second Amended and Restated Bylaws (incorporated by reference to Exhibit 3.1 to the Registrant’s Registration Statement on Form 8-K, File No. 001-37785, filed with the Commission on December 7, 2016). |
|
|
|
|
|
3.3 |
|
Loan and Security Agreement (incorporated by reference to Exhibit 10.1 to the Registrant’s Registration Statement on Form 8-K, File No. 001-37785, filed with the Commission on April 3, 2017). |
|
|
|
|
|
31.1* |
|
|
|
|
|
|
|
31.2* |
|
|
|
|
|
|
|
32.1* |
|
|
|
|
|
|
|
32.2* |
|
|
|
|
|
|
|
101.INS** |
|
XBRL Instance Document |
|
|
|
|
|
101.SCH** |
|
XBRL Taxonomy Extension Schema Document |
|
|
|
|
|
101.CAL** |
|
XBRL Taxonomy Extension Calculation Linkbase Document |
|
|
|
|
|
101.DEF** |
|
XBRL Taxonomy Extension Definition Linkbase Document |
|
|
|
|
|
101.LAB** |
|
XBRL Taxonomy Extension Label Linkbase Document |
|
|
|
|
|
101.PRE** |
|
XBRL Taxonomy Extension Presentation Linkbase Document |
|
|
|
|
|
* |
Filed herewith. |
|
** |
Filed electronically herewith. |
35
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
|
Date: May 10, 2017 |
REATA PHARMACEUTICALS, INC. |
||
|
|
|
|
|
|
|
By: |
|
/s/ J. Warren Huff |
|
|
Name: |
|
J. Warren Huff |
|
|
Title: |
|
Chief Executive Officer and President |
|
|
By: |
|
/s/ Jason D. Wilson |
|
|
Name: |
|
Jason D. Wilson |
|
|
Title: |
|
Chief Financial Officer |
36