Attached files
| file | filename |
|---|---|
| EX-32.2 - EX-32.2 - SUNLINK HEALTH SYSTEMS INC | d213211dex322.htm |
| EX-32.1 - EX-32.1 - SUNLINK HEALTH SYSTEMS INC | d213211dex321.htm |
| EX-31.2 - EX-31.2 - SUNLINK HEALTH SYSTEMS INC | d213211dex312.htm |
| EX-31.1 - EX-31.1 - SUNLINK HEALTH SYSTEMS INC | d213211dex311.htm |
| EX-23.1 - EX-23.1 - SUNLINK HEALTH SYSTEMS INC | d213211dex231.htm |
| EX-21.1 - EX-21.1 - SUNLINK HEALTH SYSTEMS INC | d213211dex211.htm |
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
Form 10-K
| x | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the Fiscal Year Ended June 30, 2016
OR
| ¨ | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the transition period from to
Commission File No. 1-12607
SunLink Health Systems, Inc.
(Exact name of registrant as specified in its charter)
| Ohio | 31-0621189 | |
| (State or other jurisdiction of incorporation or organization) |
(I.R.S. Employer Identification No.) |
900 Circle 75 Parkway, Suite 1120, Atlanta, Georgia 30339
(Address of principal executive offices)
Registrant’s telephone number, including area code: (770) 933-7000
Securities Registered Pursuant to Section 12(b) of the Act:
| Title of each Class |
Name of each Exchange on which registered | |
| Common Shares without par value | NYSE Amex Equities |
Indicate by check mark whether if the registrant is a well-known seasoned issuer, as defined in Rule 405 of Securities Act. Yes ¨ No x
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes ¨ No x
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes x No ¨
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§ 232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes x No ¨
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K (§ 229.405 of this chapter) is not contained herein, and will not be contained, to the best of the registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K Yes ¨ No x
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, or a non-accelerated filer, or a smaller reporting company. See definition of “large accelerated filer”, “accelerated filer” and “smaller reporting company” in Rule 12b-2 of the Exchange Act.
| Large accelerated filer | ¨ | Accelerated filer | ¨ | |||
| Non-accelerated filer | ¨ (Do not check if a smaller reporting company) | Smaller reporting company | x | |||
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Act). Yes ¨ No x
At the close of business on September 29, 2016, there were 9,443,408 shares of the registrant’s common shares without par value outstanding. The aggregate market value of the voting and non-voting common equity held by non-affiliates computed by reference to the closing price on December 31, 2015 of the registrant’s common shares as reported by NYSE Amex Equities stock exchange amounted to $4,837,749.
DOCUMENTS INCORPORATED BY REFERENCE
Portions of the registrant’s definitive Proxy Statement to be filed under Regulation 14A in connection with the Annual Meeting of Shareholders of SunLink Health Systems, Inc., scheduled to be held on November 7, 2016, have been incorporated by reference into Part III of this Report. The Proxy Statement or an amendment to this Annual Report will be filed with the Securities and Exchange Commission within 120 days after June 30, 2016.
Certain Cautionary Statements
FORWARD-LOOKING STATEMENTS
This Annual Report and the documents that are incorporated by reference in this Annual Report contain certain forward-looking statements within the meaning of the safe harbor for forward-looking statements contained in the Private Securities Litigation Reform Act of 1995. Forward-looking statements include all statements that do not relate solely to historical or current facts and may be identified by the use of words such as “may,” “believe,” “will,” “expect,” “project,” “estimate,” “anticipate,” “plan” or “continue.” These forward-looking statements are based on current plans and expectations and are subject to a number of risks, uncertainties and other factors which could significantly affect current plans and expectations and our future financial condition and results. These factors, which could cause actual results, performance and achievements to differ materially from those anticipated, include, but are not limited to:
General Business Conditions
| • | general economic and business conditions in the U.S., both nationwide and in the states in which we operate; |
| • | increases in uninsured and/or underinsured patients due to unemployment or other conditions, higher deductibles and co-insurance, or other terms of health insurance coverage resulting in higher bad debt amounts; |
| • | the competitive nature of the U.S. community hospital, nursing home and pharmacy businesses; |
| • | demographic changes in areas where we operate; |
| • | the availability of cash or borrowings to fund working capital, renovations, replacements, expansions and capital improvements at existing healthcare and pharmacy facilities and for acquisitions and replacement of such facilities; |
| • | changes in accounting principles generally accepted in the U.S.; and, |
| • | fluctuations in the market value of equity securities including SunLink common shares. |
Operational Factors
| • | ability or inability to operate profitably in one or more segments of the healthcare business; |
| • | the availability of, and our ability to attract and retain, sufficient qualified staff physicians, management, nurses, pharmacists and staff personnel for our operations; |
| • | timeliness and amount of reimbursement payments received under government programs; |
| • | the ability or inability to obtain external financing for working capital included under lending agreements; |
| • | changes in interest rates under lending agreements and other indebtedness; |
| • | the ability or inability to refinance former or existing indebtedness and potential defaults under existing indebtedness; |
| • | restrictions imposed by existing or future lending and other indebtedness; |
| • | the cost and availability of insurance coverage including professional liability (e.g., medical malpractice) and general liability insurance; |
| • | the efforts of insurers, healthcare providers, government payors and others to contain healthcare costs; |
| • | the impact on hospital services of the treatment of patients in lower acuity healthcare settings, whether with drug therapy or in alternative healthcare settings, such as surgery centers or urgent care centers; |
2
| • | changes in medical and other technology; |
| • | risks of changes in estimates of self insurance claims and reserves; |
| • | changes in prices of materials and services utilized in our Healthcare Facilities and Pharmacy Segments; |
| • | changes in wages as a result of inflation or competition for management, physician, nursing, pharmacy and staff positions; |
| • | changes in the amount and risk of collectability of accounts receivable, including deductibles and co-pay amounts; |
| • | the functionality or costs with respect to our information systems for our Healthcare Facilities and Pharmacy Segments and our corporate office, including both software and hardware; and |
| • | the availability of and competition from alternative drugs or treatments provided by our Pharmacy Segment; and |
| • | the restrictions, processes and conditions relating to our Pharmacy Segment imposed by pharmacy benefit providers, drug manufacturers and distributors. |
Liabilities, Claims, Obligations and Other Matters
| • | claims under leases, guarantees, disposition agreements, and other obligations relating to discontinued operations, including claims from sold or leased facilities, retained liabilities, or retained subsidiaries; |
| • | potential adverse consequences of known and unknown government investigations; |
| • | claims for product and environmental liabilities from continuing and discontinued operations; |
| • | professional, general and other claims which may be asserted against us; and, |
| • | natural disasters and weather-related events such as earthquakes, hurricanes, flooding, snow, ice and wind damage and population evacuations affecting areas in which we operate. |
Regulation and Governmental Activity
| • | existing and proposed governmental budgetary constraints; |
| • | Federal and state insurance exchanges and their rules on reimbursement terms; |
| • | the decision by states in which we operate hospitals (Georgia and Mississippi) to not expand Medicaid; |
| • | the regulatory environment for our businesses, including state certificate of need laws and regulations, pharmacy licensing laws and regulations, rules and judicial cases relating thereto; |
| • | adverse changes in the levels and terms of government (including Medicare, Medicaid and other programs) and private reimbursement for SunLink’s healthcare services including the payment arrangements and terms of managed care agreements; EHR reimbursement and indigent care reimbursements (Medicare Upper Payment Limit “UPL” and Disproportionate Share Hospital “DSH” adjustments); |
| • | changes in or failure to comply with Federal, state or local laws and regulations affecting our Healthcare Facilities and Pharmacy Segments; and, |
| • | the possible enactment of additional Federal healthcare reform laws or reform laws in states where our subsidiaries operate hospital and pharmacy facilities (including Medicaid waivers, bundled payments, accountable care and similar organizations, competitive bidding, and other reforms). |
3
Dispositions, Acquisitions, and Renovation Related Matters
| • | the ability to dispose of underperforming facilities; |
| • | the availability and terms of capital to fund acquisitions, improvements, renovations or replacement facilities; and |
| • | competition in the market for acquisitions of hospitals, pharmacy facilities and healthcare businesses. |
The foregoing are significant factors we think could cause our actual results to differ materially from expected results. However, there could be additional factors besides those listed herein that also could affect SunLink in an adverse manner.
You should read this Annual Report completely and with the understanding that actual future results may be materially different from what we expect. You are cautioned not to unduly rely on forward-looking statements when evaluating the information presented in this Annual Report or our other disclosures because current plans, anticipated actions, and future financial conditions and results may differ from those expressed in any forward-looking statements made by or on behalf of SunLink.
We have not undertaken any obligation to publicly update or revise any forward-looking statements. All of our forward-looking statements speak only as of the date of the document in which they are made or, if a date is specified, as of such date. We disclaim any obligation or undertaking to provide any updates or revisions to any forward-looking statement to reflect any change in our expectations or any changes in events, conditions, circumstances or information on which the forward-looking statement is based. All subsequent written and oral forward-looking statements attributable to us or persons acting on our behalf are expressly qualified in their entirety by the foregoing factors and the other risk factors set forth elsewhere in this report.
4
PART I
| Item 1. | Business (all dollar amounts in thousands except share, per share and revenue per equivalent admission amounts) |
Overview
SunLink Health Systems, Inc., through subsidiaries, owns businesses which are a provider of healthcare services in certain markets in the United States. Unless the context indicates otherwise, all references to “SunLink,” “we,” “our,” “ours,” “us” and the “Company” refer to SunLink Health Systems, Inc. and our consolidated subsidiaries. References to our specific operations refer to operations conducted through our subsidiaries and references to “we,” “our,” “ours,” and “us” in such context refer to the operations of our subsidiaries. Our business is composed of the ownership of two business segments, the Healthcare Facilities Segment and the Specialty Pharmacy Segment. Our Healthcare Facilities Segment subsidiaries own and operate a 84 bed community hospital and a 66 bed nursing home in Mississippi and a 100 bed nursing home in Georgia. A subsidiary also leases the emergency department and certain auxiliary space of a closed hospital facility in Georgia to a non-affiliated healthcare operator. Two of our subsidiaries each own a medical office building which are leased to third parties. A subsidiary also owns a closed hospital building that is currently vacant except for one rented medical office. Our Specialty Pharmacy Segment subsidiary operates a specialty pharmacy business in Louisiana with four service lines.
SunLink’s executive offices are located at 900 Circle 75 Parkway, Suite 1120, Atlanta, Georgia 30339, and our telephone number is (770) 933-7000. Our website address is www.sunlinkhealth.com. Information contained on our website does not constitute part of this report. Any materials we file with the Securities and Exchange Commission (“SEC”) may be read at the SEC’s Public Reference Room at 100 F Street, NE, Room 1580 Washington, DC 20549. Information on the operation of the Public Reference Room may be obtained by calling the SEC at 1-800-SEC-0330. Certain materials we file with the SEC may also be read and copied at or through our website or at the Internet website maintained by the SEC at www.sec.gov.
History
We are an Ohio corporation incorporated in June 1959. In 2001, we redirected our business strategy toward healthcare services in the United States. On February 1, 2001, we purchased five community hospitals, leasehold rights for a sixth hospital and the related businesses of all six hospitals. We subsequently have acquired two hospitals and sold four hospitals and three home health businesses. We also sold the operations of one hospital to a buyer who leased the hospital building from us but which subsequently ceased its hospital operations. In 2008, a wholly-owned subsidiary acquired Carmichael’s Cashway Pharmacy, Inc. (“Carmichael”) which provides retail and institutional pharmacy services to various communities in southwest Louisiana and eastern Texas.
Business Strategy: Operations, Dispositions and Acquisitions
The business strategy of SunLink is to focus its efforts on improving internal operations of the existing pharmacy business and healthcare facilities subsidiaries and on the sale or disposition of its subsidiaries’ underperforming assets. The Company considers the disposition of facilities and operations based on a variety of factors in addition to under-performance, including asset values, return on investments and competition from existing and potential competitors, capital improvement needs, prevailing reimbursement rates for drugs and medical services under various Federal and state programs (e.g., Medicare and Medicaid) and by private payors, corporate strategy and other corporate objectives. The Company also is considering, subject to available funds, potential healthcare facility upgrades and improvements.
On August 19, 2016, a subsidiary of the Company sold substantially all assets and certain liabilities of its Chestatee Regional Hospital in Dahlonega, GA (“Dahlonega”), for approximately $15,000 subject to adjustment for the book value of certain assets and liabilities at the sale date. In addition, the Company has entered into an agreement to lease the emergency department and certain ancillary space in its former hospital,
5
North Georgia Medical Center, which is now closed, to a regional healthcare system. The lease transaction is subject to a number of conditions precedent including regulatory approval and negotiation of definitive leases. The Company continues to operate its 100-bed skilled nursing facility which is located adjacent to such hospital. The Company believes its specialty pharmacy business continues to under-perform, and the Company has engaged advisors to assist it in evaluating the possible sale of its specialty pharmacy business and one medical office building. The Company’s recent or possible uses of net proceeds from the Dahlonega sale and other possible transactions include or may include, among other things, a prepayment of long-term debt, a return of capital to shareholders via a repurchase of shares or a dividend, improvements to existing facilities, and other general corporate purposes. However, there can be no assurance any further sale or lease transaction will be authorized by the Board of Directors or completed or, if completed, that there will be sufficient proceeds to repay the Company’s long-term debt, or return capital to shareholders or for future development or general corporate purposes.
Healthcare Facilities Operations
SunLink’s Healthcare Facilities Segment includes:
| • | Trace Regional Hospital (“Trace”), owned and operated by a subsidiary, located in Houston, Chickasaw County, Mississippi, consists of a JCAHO accredited 84-licensed-bed, acute care hospital, which includes an 18-bed geriatric psychiatric unit (“GPU”), Trace is the only hospital in Chickasaw County. |
| • | Floy Dyer Manor Nursing Home, a 66-bed nursing home, owned by the same subsidiary as, and located adjacent to, Trace. |
| • | Gilmer Nursing Home (“Gilmer”), owned and operated by a subsidiary, located in Ellijay, Gilmer County, Georgia, which operates a 100-bed nursing facility. This subsidiary also owns a hospital building and has agreed to lease the portion of that building occupied by the former emergency department to an unaffiliated healthcare provider. |
| • | Two separate subsidiaries which own medical buildings, in Dahlonega and Ellijay, Georgia, respectively, which are leased to unaffiliated healthcare providers. |
| • | A subsidiary which owns the Careside Medical Park (“Careside”) located in Clanton, Chilton County, Alabama. Careside includes a closed hospital and medical office building in which it currently rents office space to one unaffiliated healthcare provider. |
Hospital Operations
Utilization of Local Hospital Management Team
We believe that the potential of the Trace Hospital is dependent on its ability to offer appropriate healthcare services and effectively recruit and retain employees and physicians. The hospital has developed and continuously seeks to implement an operating plan designed to improve efficiency and increase revenue including, but not limited to, the expansion of services offered by the hospital and the recruitment of physicians to the community.
The Trace Hospital management team is comprised of a chief executive officer, chief financial officer and chief nursing officer. The quality of the on-site hospital management team is critical to the success of the hospital. The on-site management team is responsible for implementing the operating plan under the guidance of the board of directors of the subsidiary which owns and operates Trace. The Trace Hospital management team participates in a performance-based compensation program based upon the achievement of operational, clinical and financial goals set forth in the operating plan.
The Trace Hospital management team is responsible for the day-to-day operations of the hospital and has access to support services, assistance, and advice in certain areas, including strategic planning and physician
6
recruiting, supplies and equipment purchasing, corporate compliance, reimbursement, information systems, human resources, accounting, cash management, capital financing, tax and insurance, some of which may be provided by SunLink or other SunLink subsidiaries. Financial controls are maintained through the utilization of policies and procedures and monitoring by the subsidiary board of directors.
Expansion of Services and Facilities
The subsidiary which owns and operates Trace Hospital seeks to add services on an as-needed basis in order to improve access to quality healthcare services in the communities it serves, with the ultimate goal of reducing the out-migration of patients to other hospitals or alternate service providers. Additional and expanded services and programs, which may include specialty inpatient and outpatient services, are often dependent on recruiting physicians and other healthcare professionals; therefore recruiting goals are important to the hospital’s ability to expand services. Capital investments in technology and facilities are often necessary to increase the quality and scope of services provided to the communities and to add to the Trace Hospital’s reputation in the community, reducing out-migration and increasing patient referrals and revenue. The hospital endeavors to provide a quality, urgent care clinic or rural health clinic as a critical component of its local service offering and which is intended to function as each facility’s “window to the community”.
Medical Staff
The number and quality of physicians affiliated with a hospital directly affect the quality and availability of patient care and the reputation of the hospital. Physicians generally may terminate their affiliation with a hospital at any time. Our Trace Hospital seeks to retain primary care physicians of varied specialties on its medical staff to attract other qualified physicians. Physicians generally refer patients to a hospital primarily on the basis of the perceived quality of services the hospital renders to patients and physicians; the quality of other physicians on the medical staff; the location of the hospital; and the quality of the hospital’s facilities, equipment and employees. Accordingly, Trace Hospital strives to provide suitable facilities, equipment, employees and services for physicians and their patients.
Recruiting Physicians and Healthcare Professionals
The Trace Hospital management team is responsible for assessing the need for additional physicians and other healthcare professionals including the number and specialty of additional physicians needed by the hospital’s community. The local hospital management team, with the assistance of outside recruiting firms, identifies and seeks to attract specific physicians to the hospital’s medical staff and other hospital professionals to work under the direction of staff physicians. Our Trace Hospital has employed physicians to better align physician performance with hospital goals through employment relationships. Many hospitals and hospital systems are attempting to improve clinical and financial results by employing physicians. For newly recruited non-employed physicians, the hospital may guarantee such physicians a minimum level of gross receipts during an initial period, generally one year, and assist the physician’s transition into the community. The physician is required to repay some or all of the amounts paid under such guarantee if the physician leaves the community within a specified period. The hospital periodically evaluates each physician and may terminate employment based on performance and the needs of each facility. Physician recruiting has become more challenging, and will continue to remain challenging due to various factors including healthcare reform and market forces, including competition for physicians. The costs of recruiting and retaining physicians are also expected to increase as more physicians are employed and salaries and support costs continue to increase.
Quality Assurance
The Trace Hospital implements quality assurance procedures to monitor the level and quality of care provided to its patients. Each hospital has a medical director who supervises and is responsible for the quality of medical care provided and a medical advisory committee comprised of physicians who review the professional
7
credentials of physicians applying for medical staff privileges at the hospital. The medical advisory committee also reviews the quality of the logistical, medical and technological support provided to the physicians. Trace Hospital periodically conducts surveys of its patients, either during their stay at the hospital or subsequently, to identify potential areas of improvement. Trace Hospital is accredited by the JCAHO.
Operating Statistics
The following table sets forth certain operating statistics for SunLink’s healthcare facility subsidiaries included in continuing operations as of June 30 for the periods indicated. The table includes Trace Regional Hospital and Floy Dyer Nursing Home in Houston, Mississippi and North Georgia Medical Center (which was closed in June 2016) and Gilmer Nursing Home in Ellijay, Georgia.
| Fiscal Years Ended June 30, | ||||||||||||
| 2016 | 2015 | 2014 | ||||||||||
| Hospitals owned or leased at end of period |
2 | 2 | 2 | |||||||||
| Licensed hospital beds (at end of period) |
134 | 134 | 134 | |||||||||
| Hospital beds in service (at end of period) |
54 | 94 | 94 | |||||||||
| Nursing home beds in service (at end of period) |
166 | 166 | 166 | |||||||||
| Admissions |
607 | 1,442 | 1,422 | |||||||||
| Equivalent Admissions (1) |
3,546 | 4,756 | 5,074 | |||||||||
| Average Length of Stay (2) |
7.4 | 5.2 | 4.7 | |||||||||
| Patient days |
4,476 | 7,477 | 6,728 | |||||||||
| Adjusted patient days (3) |
19,531 | 22,552 | 24,035 | |||||||||
| Occupancy rate (% of licensed beds) (4) |
9.13 | % | 15.29 | % | 13.76 | % | ||||||
| Occupancy rate (% of beds in service) (5) |
22.65 | % | 21.79 | % | 19.61 | % | ||||||
| Net patient service revenues (in thousands) |
$ | 30,462 | $ | 39,933 | $ | 39,986 | ||||||
| Net outpatient service revenues (in thousands) |
$ | 7,852 | $ | 11,370 | $ | 11,556 | ||||||
| Net revenue per equivalent admissions |
$ | 8,590 | $ | 8,396 | $ | 7,880 | ||||||
| Net outpatient service revenues (as a % of net patient service revenues) |
25.78 | % | 28.47 | % | 28.90 | % | ||||||
| (1) | Equivalent admissions are a statistic used by management (and certain investors) as a general approximation of combined inpatient and outpatient volume. Equivalent admissions are computed by multiplying admissions (inpatient volume) by the sum of gross inpatient revenues and gross outpatient revenues and dividing the result by gross inpatient revenues. The equivalent admissions computation is intended to relate outpatient revenues to the volume measure (admissions) used to measure inpatient volume resulting in a general approximation of combined inpatient and outpatient volume. |
| (2) | Average length of stay is calculated based on the number of patient days divided by the number of admissions. |
| (3) | Adjusted patient days have been calculated based on a revenue-based formula of multiplying actual patient days by the sum of gross inpatient revenues and gross outpatient revenues and dividing the result by gross inpatient revenues for each subsidiary hospital. Adjusted patient days is a statistic (which is used generally in the industry) designed to communicate an approximate volume of service provided to inpatients and outpatients by converting total patient revenues to a number representing adjusted patient days. |
| (4) | Percentages are calculated by dividing average daily census by the average number of licensed hospital beds. |
| (5) | Percentages are calculated by dividing average daily census by the average number of hospital beds in service. |
8
Healthcare Facilities Revenue Sources Allocation
Sources of Revenue
Our Trace Hospital and our nursing homes receive payments for patient care from Federal Medicare programs, State Medicaid programs, private insurance carriers, health maintenance organizations, preferred provider organizations, TriCare, and from employers and patients directly. Medicare is a federal program that provides certain hospital and medical insurance benefits to persons age 65 and over, some disabled persons and persons with end-stage renal disease. Medicaid is a federal-state program, administered by the states, that provides hospital and nursing home benefits to qualifying individuals who are unable to afford care. Trace Hospital is certified as a healthcare services provider for persons covered by Medicare and Medicaid programs. TriCare is a federal program for the healthcare of certain U.S. military personnel and their dependants. See “Item 7 Management’s Discussion and Analysis of Financial Condition and Results of Operations”.
The following table sets forth the percentage of patient days from various payors in SunLink’s healthcare facilities for the periods indicated. The table includes Trace Regional Hospital and Floy Dyer Nursing Home in Houston, Mississippi and North Georgia Medical Center (which was closed in June 2016) and Gilmer Nursing Home in Ellijay, Georgia.
| Fiscal Years Ended June 30, | ||||||||||||
| 2016 | 2015 | 2014 | ||||||||||
| Source |
||||||||||||
| Medicare |
92.8 | % | 83.7 | % | 83.2 | % | ||||||
| Medicaid |
1.8 | % | 5.0 | % | 4.9 | % | ||||||
| Private and Other Sources |
5.4 | % | 11.3 | % | 11.9 | % | ||||||
|
|
|
|
|
|
|
|||||||
| 100.0 | % | 100.0 | % | 100.0 | % | |||||||
|
|
|
|
|
|
|
|||||||
The following table sets forth the percentage of the net patient revenues from major payors in SunLink’s healthcare facilities.
| Fiscal Years Ended June 30, | ||||||||||||
| 2016 | 2015 | 2014 | ||||||||||
| Source |
||||||||||||
| Medicare |
37.1 | % | 39.0 | % | 40.4 | % | ||||||
| Medicaid |
37.7 | % | 30.3 | % | 28.8 | % | ||||||
| Private and Other Sources |
25.2 | % | 30.7 | % | 30.8 | % | ||||||
|
|
|
|
|
|
|
|||||||
| 100.0 | % | 100.0 | % | 100.0 | % | |||||||
|
|
|
|
|
|
|
|||||||
Sources of Revenue
Our Trace Hospital and our nursing centers receive payments for patient care from Federal Medicare programs, State Medicaid programs, private insurance carriers, health maintenance organizations, preferred provider organizations, TriCare, and from employers and patients directly. Medicare is a federal program that provides certain hospital and medical insurance benefits to persons age 65 and over, some disabled persons and persons with end-stage renal disease. Medicaid is a federal-state program, administered by the states, that provides hospital and nursing home benefits to qualifying individuals who are unable to afford care. Trace Hospital and our nursing centers are certified as healthcare services providers for persons covered by Medicare and Medicaid programs. TriCare is a federal program for the healthcare of certain U.S. military personnel and their dependants. See “Item 7 Management’s Discussion and Analysis of Financial Condition and Results of Operations”.
Hospital patients generally are not responsible for any difference between established hospital charges and amounts reimbursed for such services under Medicare, Medicaid and some private insurer plans, health maintenance organization (“HMO”) plans and preferred provider organizations (“PPO”) plans, but are
9
responsible to the extent of any exclusions, deductibles or co-insurance features of their coverage. The amount of such exclusions, deductibles and co-insurance has been increasing in recent years. Collection of amounts due from individuals typically is more difficult than from governmental or third-party payors. Further, amounts received under the Medicare and Medicaid programs generally are significantly less than the established charges of most hospitals, including our own, for the services provided. Likewise, HMOs and PPOs generally seek and obtain discounts from the established charges of most hospitals. See “Item 1. Business—Government Reimbursement Programs—Hospitals—Medicare/Medicaid Reimbursement”.
Nursing Center Operations
Our nursing centers consist of two skilled nursing facilities (collectively “nursing centers”) and form part of our healthcare facilities segment.
Utilization of Local Nursing Center Management Team
Each of our nursing centers is managed by a state-licensed executive director who is supported by other professional personnel, including, but not limited to, a director of nursing, nursing assistants, licensed practical nurses, staff development coordinator, activities director, social services director, clinical liaisons, admissions coordinator, and business office manager. The directors of nursing are state-licensed nurses who supervise our nursing staffs that include, but are not limited to, registered nurses, licensed practical nurses, and nursing assistants. Staff size and composition vary depending on the size and occupancy of each nursing center, the types of services provided and the acuity level of the patients and residents. The nursing centers contract with physicians who provide medical director services and serve on performance improvement committees. We provide our nursing center subsidiaries with centralized administrative services in the areas of information systems, clinical operations, regulatory guidance, reimbursement guidance, state licensing, and Medicare and Medicaid certification, and maintenance support, as well as legal, finance, accounting, purchasing, human resources management, and facilities management support. The centralization of these services improves operating efficiencies, promotes the standardization of certain processes and permits the healthcare staff to of our nursing centers to focus on the delivery of quality care.
Quality Assurance
Quality of care is monitored and enhanced by our clinical operations personnel, as well as family satisfaction surveys. The Improving Medicare Post-Acute Care Transformation Act of 2014 (the “IMPACT Act”), passed on October 6, 2014, requires standardized assessment data for quality improvement, payment, and discharge planning purposes across the spectrum of post acute-care providers (“PACs”), including skilled nursing facilities.
Sources of Revenue
Nursing center revenues are derived principally from the Medicare and Medicaid programs and private and other payors. Consistent with the nursing centers industry, changes in the mix of the patient and resident population among these categories could significantly affect the profitability of our nursing centers operations. A substantial portion of our nursing centers’ revenues are derived from patients covered by the Medicare and Medicaid programs. We could be adversely affected by the continuing efforts of governmental and private third-party payors to contain healthcare costs. We cannot assure you that reimbursement payments under governmental and private third-party payor programs, including Medicare supplemental insurance policies, will remain at levels comparable to present levels or will be sufficient to cover the costs allocable to patients eligible for reimbursement pursuant to these programs. Medicare reimbursement in nursing centers is subject to fixed payments under the Medicare prospective payment systems. In accordance with Medicare laws, CMS makes annual adjustments to Medicare payment rates in many prospective payment systems under what is commonly known as a “market basket update.” Each year, the Medicare Payment Advisory Commission (“Med PAC”), a
10
commission chartered by Congress to advise it on Medicare payment issues, makes payment policy recommendations to Congress for a variety of Medicare payment systems. Congress is not obligated to adopt Med PAC recommendations, and, based upon outcomes in previous years, there can be no assurance that Congress will adopt Med Pac’s recommendations in a given year. Medicaid reimbursement rates in many states in which we operate nursing centers also are based upon fixed payment systems. Generally, these rates are adjusted annually for inflation. However, these adjustments may not reflect the actual increase in the costs of providing healthcare services. In addition, Medicaid reimbursement can be impacted negatively by state budgetary pressures, which may lead to reduced reimbursement or delays in receiving payments. Moreover, we cannot assure you that the nursing centers operated by us, or the provision of goods and services offered by us, will meet the requirements for participation in such programs.
Healthcare Facilities Competition
Among the factors which we believe influence patient selection among our healthcare in our subsidiary hospital and nursing center markets are:
| • | The appearance and functionality of the healthcare facilities; |
| • | The quality and demeanor of professional staff and physicians; and |
| • | The participation of the facility in plans which pays all or a portion of the patient’s bill. |
Such factors are influenced heavily by the quality and scope of medical services, strength of hospital referral networks, location and the price of services.
Trace Hospital may face less competition in its immediate patient service area than would be expected in larger communities because it is the primary provider of hospital services in its community. Our Trace hospital faces competition from larger tertiary care centers and, in most cases, other rural, exurban, suburban or, in limited circumstances, urban hospitals, some of which offer more specialized services. The competing hospitals may be owned by governmental agencies or not-for-profit entities supported by endowments and charitable contributions and may be able to finance capital expenditures on a tax-exempt basis. Such governmental-owned and not-for-profit hospitals, as well as various for-profit hospitals operating in the broader service area of our subsidiary hospital, likely have greater access to financial resources than does our subsidiary hospital.
Our nursing centers compete with other nursing centers and similar long-term care facilities primarily on the basis of quality of care, reputation, location, and physical appearance and, in the case of private payment residents, the charges for our services. Our nursing centers also compete on a local and regional basis with other facilities providing similar services, including hospitals, extended care centers, assisted living facilities, home health agencies, and similar institutions. Some competitors may operate newer facilities and may provide services, including skilled nursing services that we may not offer at our nursing centers. Our competitors include government-owned, religious organization-owned, secular nonprofit and for-profit institutions. Many of these competitors have greater financial and other resources than we do. Although there is limited, if any, price competition with respect to Medicare and Medicaid residents (since revenues received for services provided to these residents are generally based on pre-established rates), there is substantial price competition for private payment residents. Historically our nursing centers have been located adjacent to acute care hospitals owned and operated by one of our subsidiaries. Currently, however, one of our two nursing centers operates in environment where we no longer own an adjacent hospital and such former hospital has ceased operations, although an unaffiliated healthcare provider intends to re-open an emergency department adjacent to our Gilmer Nursing Home.
Managed Care
Our subsidiary hospital is affected by its ability to negotiate service contracts with purchasers of group healthcare services. HMOs and PPOs attempt to direct and control the use of hospital services through managed care programs. In addition, employers and traditional health insurers increasingly are seeking to contain costs
11
through negotiations with hospitals for managed care programs and discounts from established charges. Generally, hospitals compete for service contracts with group healthcare service purchasers on the basis of market reputation, geographic location, quality and range of services, quality of medical staff, convenience and price.
The importance of obtaining contracts with managed care organizations varies from market to market, depending on the market strength of such organizations. Nevertheless, a significant portion of hospital patients in our hospital community are covered by managed care or other reimbursement programs, all of which generally pay less than established charges for hospital services.
The healthcare industry as a whole faces the challenge of continuing to provide quality patient care while managing rising costs, facing strong competition for patients, and adjusting to a continued general reduction of reimbursement rates by both private and government payors. Both private and government payors continually seek to reduce the nature and scope of services which may be reimbursed. Healthcare reform at both the federal and state level generally has created pressure to reduce reimbursement rates. Changes in medical technology, existing and future legislation, regulations and interpretations, and competitive contracting for provider services by private and government payors, have required and in the future may further require changes in our facility, equipment, personnel, rates and/or services.
Efforts to Control Healthcare Costs
Rural hospitals, including the Trace Hospital owned and operated by SunLink’s subsidiary, continue to have significant unused capacity. Inpatient utilization and average inpatient occupancy rates continue to be affected negatively by payor-required pre-admission authorization, utilization review, and payment mechanisms designed to maximize outpatient and alternative healthcare delivery services for less acutely ill patients and to limit the cost of treating inpatients. Admissions constraints, payor pressures, and increased competition are likely to continue. Historically, hospitals owned and operated by SunLink’s subsidiaries have responded to such trends by adding and expanding outpatient services, upgrading facilities and equipment, offering new programs (such as geriatric psychiatric units) and adding or expanding certain inpatient and ancillary services. In addition, our hospitals have reduced services and taken beds out of service in response to such trends. Currently we expect our Trace Hospital will continue to respond to such trends in a similar manner subject to the availability of capital resources and our evaluation of the continued utility of such historical responses.
Health Care Reform
The Patient Protection and Affordable Care Act and the Health Care Education Reconciliation Act of 2010 (collectively, the “Affordable Care Act” or “ACA”) were signed into law by President Obama on March 23, 2010, and March 30, 2010, respectively. The ACA alters the United States health care system and is intended to decrease the number of uninsured Americans and reduce overall health care costs. The ACA attempts to achieve these goals by, among other things, requiring most Americans to obtain health insurance or pay a tax penalty, expanding Medicare and Medicaid eligibility, reducing Medicare and Medicaid payments including disproportionate share payments, expanding the Medicare program’s use of value-based purchasing programs, tying hospital payments to the satisfaction of certain quality criteria, and bundling payments to hospitals and other providers. The ACA also contains a number of measures that are intended to reduce fraud and abuse in the Medicare and Medicaid programs, such as requiring the use of recovery audit contractors in the Medicaid program and generally prohibiting physician-owned hospitals from adding new physician owners or increasing the number of beds and operating rooms for which they are licensed. We believe the implementation or interpretation of rules and regulations or the provisions of the ACA may have and may continue to have an adverse effect on our financial condition and results of our operations, especially since the one state in which we operate our hospital has decided not to set up state exchanges and not to expand Medicaid.
12
SPECIALTY PHARMACY OPERATIONS
Our Specialty Pharmacy Segment is operated through SunLink ScriptsRx, LLC (“Scripts”), a wholly-owned subsidiary, and composed of four material service lines:
| 1. | Retail Pharmacy Products and Services, consisting of pharmacy sales at our three retail locations in Louisiana and including complementary products such as uniforms, vitamins, supplements and nutritionals. |
| 2. | Institutional Pharmacy Services, consisting of the provision of specialty and non-specialty pharmaceuticals and biological products to institutional clients or to patients in institutional settings, such as nursing homes, specialty hospitals, hospices and correctional facilities; |
| 3. | Specialty Pharmacy Services, which ordinarily include one or more of the following elements: |
| • | The provision of products relating to infusion therapy, enteral feeding services, oncology and chemotherapy drug administration, and cardiac, diabetes, pain management, wound care and psychiatric services; |
| • | Pharmaceutical or biological products administered via non-oral means, which are frequently through injectable or infusion therapies; |
| • | Products delivered to patients via express package or hand delivery and requiring special handling, such as constant refrigeration or having an extremely limited shelf life; |
| • | Products that generally are administered in a non-hospital setting, including physicians’ offices, specialty clinics or patients’ homes; |
| • | The provision of pharmaceuticals or biological products not managed under traditional outpatient prescription drug benefits; and, |
| • | Therapies that require complex care, patient education and continuous monitoring. |
The major conditions these drugs treat include, but are not limited to, respiratory system weakness, cancer, HIV/AIDS, hemophilia, hepatitis C, multiple sclerosis, infertility, Crohn’s disease, rheumatoid arthritis and growth hormone deficiency.
| 4. | Durable Medical Equipment Services, consisting primarily of products for patient-administered home care such as oxygen concentrator services, continuous and variable/bi-level positive airway pressure (“CPAP” and “VPAP”/“BPAP”) machines, nebulizers, diabetes management products and prosthetics. |
Pharmacy Competition
There are many companies which provide one or more of the healthcare operations which comprise or may compete with our specialty pharmacy operations of Scripts. For example, home healthcare business companies, which may compete with our specialty pharmacy services, our durable medical equipment services operations or both, range in size from small entrepreneurial companies to rapidly expanding companies with strategies for national operations, such as Amedisys, Inc., Apria Healthcare Group, Inc., Kindred Healthcare, Inc., and Walgreen Co. Specialty pharmacy companies range from local or regional pharmacies to large public companies, such as CVS Health Corporation (CVS Specialty), Express Scripts (Accredo Health Group, Inc.), Walgreen Co. and BioScript Inc. Institutional pharmacy companies likewise range from local or regional pharmacies to large public companies including CVS Health Corporation (Omnicare, Inc.) and PharMerica Corporation.
GOVERNMENT REIMBURSEMENT PROGRAMS
Government Reimbursement Programs—Hospitals
A significant portion of SunLink’s healthcare facilities net revenues are dependent upon reimbursement from Medicare and Medicaid. The Centers for Medicare and Medicaid Services or “CMS” is the federal agency
13
which administers Medicare, Medicaid and the Children’s Health Insurance Program (“CHIP”). The federal government generally reviews payment rates under its various programs annually, and changes in reimbursement rates under such programs, including Medicare and Medicaid, generally occur based on the fiscal year of the federal government which currently begins on October 1 and ends on September 30 of each year.
Medicare Inpatient Reimbursement
The Medicare program currently pays hospitals under the provisions of a prospective payment system for most inpatient services. Under the inpatient prospective payment system, a hospital receives a fixed amount for inpatient hospital services based on the established fixed payment amount per discharge for categories of hospital treatment, known as diagnosis related groups (“DRGs”). Each patient admitted for care is assigned to a DRG based upon a primary admitting diagnosis. Every DRG is assigned a payment rate by the government based upon the estimated intensity of hospital resources necessary to treat the average patient with that particular diagnosis. DRG payments do not consider a specific hospital’s costs, but are national rates adjusted for area wage differentials and case-mix indices.
DRG rates are usually adjusted by an update factor each federal fiscal year (“FFY”). The percentage increases to DRG payment rates for the last several years have been lower than the percentage increases in the related cost of goods and services provided by general hospitals. The index used to adjust the DRG payment rates is based on a price statistic, known as the CMS Market Basket Index, reduced by congressionally mandated reduction factors and other factors imposed by CMS.
DRG rate increases were 1.4% , 0.9% and 0.95% for FFY 2015 , 2016, and 2017 respectively. The Balanced Budget Act of 1997 originally set the increase in DRG payment rates for future FFYs at rates that would be based on the market basket index, which in certain years have been, and in the future may be, subject to reduction factors. If the update factor does not adequately reflect increases in the cost of providing inpatient services by our subsidiary’s hospital, our financial condition or results of operations could be negatively affected.
The ACA combined with the America Taxpayer Relief Act of 2012 (“ATRA”) and the Medicare Access and CHIP Reauthorization Act of 2015 (“MARA”) made a number of changes to Medicare which include but are not limited to:
| • | Reduction of market basket updates in Medicare payment rates for providers, to incorporate an adjustment for expected productivity gains. The market basket was reduced by 0.25% for both FFY 2010 and 2011, 0.10% for FFY 2012, 0.10% in FFY 2013 and 0.30% in FFY 2014; and will be reduced by 0.20% in 2015 and 2016, and by 0.75% in FFYs 2017-2019. |
| • | Reduction of Medicare payments that would otherwise be made to hospitals by specified percentages to account for preventable hospital readmissions, as defined by CMS, effective October 1, 2012. |
| • | Extension of the Medicare Dependent Hospital Program until September 30, 2017. |
| • | Expansion, on a temporary basis, of the low volume hospital inpatient payment adjustment to include hospitals that are more than 15 miles from other healthcare facilities and have less than 1,600 discharges per year. The new temporary criteria were effective for FFYs 2011 through 2013 and further expanded through September 30, 2017. Effective FFY 2018, the low-volume hospital definition and payment adjustment methodology is scheduled to return to the pre-FFY 2011 definition and methodology. |
| • | Hospitals that do not successfully participate in the Hospital IQR Program and do not submit the required quality data will be subject to a one-fourth reduction of the market basket update. |
| • | A requirement that any hospital which is not a meaningful electronic health records user will be reduced by one-half of the market basket update in FY 2016. Our subsidiary hospital does not expect to attest as a meaningful electronic records user for FY 2016. |
14
SunLink’s subsidiary hospital is an eligible hospital under one or more provisions of ACA, ATRA and MARA.
Medicare Outpatient Reimbursement
Most outpatient services provided by general hospitals are reimbursed by Medicare under the outpatient prospective payment system. This outpatient prospective payment system is based on a system of Ambulatory Payment Classifications (“APC”). Each APC is designed to represent a “bundle” of outpatient services, and each APC is assigned a fully prospective reimbursement rate. Medicare pays a set price or rate for each APC group, regardless of the actual cost incurred in providing care. Each APC rate generally is subject to adjustment each year by an “update factor” based on a market basket of services index. For calendar year 2015, the update factor was 2.4% and for calendar year 2016 it was (0.3%). For calendar year 2017 is expected to be 1.55%. If the update factor for current and future periods does not adequately reflect increases in SunLink’s subsidiary hospital cost of providing outpatient services, our financial condition or results of operations could be negatively affected.
Medicare Bad Debt Reimbursement
Under Medicare, the costs attributable to the deductible and coinsurance amounts that remain unpaid by Medicare beneficiaries can be partially added to, and reimbursed as a portion of, the Medicare share of allowable costs as cost reports are filed. Bad debts must meet specific criteria to be allowable. Hospitals generally receive interim pass-through payments during the cost report year which are determined by the respective Medicare Audit Contractor (“MAC”) from the prior cost report filing, and which are finally adjusted when cost reports are filed and audited.
Amounts uncollectible from specific beneficiaries are charged off as bad debts in the accounting period in which the accounts are deemed to be worthless. In some cases, an amount previously written off as a bad debt and allocated to the program may be recovered in a subsequent accounting period. In these cases, the recoveries must be used to reduce the cost of beneficiary services for the period in which the collection is made. In determining reasonable costs for hospitals, the amount of bad debts otherwise treated as allowable costs was reduced by 35% beginning FFY 2014.
Medicare Disproportionate Share Payments
In addition to the standard DRG payment, the Social Security Act requires that additional Medicare payments be made to hospitals with a disproportionate share of low income patients. Beneficiary Improvement and Protection Act (“BIPA”) provisions stipulate that rural facilities with fewer than 100 beds with a disproportionate share percentage greater than 15% will be classified as a disproportionate share hospital and is entitled to receive a supplemental disproportionate share payment based on gross DRG payments. Since April 1, 2004, the effective rate has been 12.0% of DRG payments. Trace Hospital is classified as a disproportionate share hospital as of July 1, 2016. The Affordable Care Act provides for material reductions in Medicare DSH funding. We estimate that Medicare disproportionate share payments represented approximately 1% of our net patient service revenues for the years ended June 30, 2016, 2015 and 2014.
Medicaid Inpatient and Outpatient Reimbursement
Each state operates a Medicaid program funded jointly by the state and the federal government. Federal law governs the general management of the Medicaid program, but there is wide latitude for states to customize Medicaid programs to fit local needs and resources. As a result, each state Medicaid plan has its own payment formula and recipient eligibility criteria.
In the recent past, the state in which our subsidiary operates its hospital has initiated increased efforts to reduce Medicaid assistance payments. These efforts and reductions often are triggered by one or more of the
15
following factors: an increased effort by CMS to decrease the federal share of payments for Medicaid beneficiaries or significant increases in program utilization resulting from increased enrollment or budgetary pressures on the applicable states. The federal government’s percentage share of each state’s medical assistance expenditures under Medicaid is determined by a formula specified in Medicaid law referred to as the Federal Medical Assistance Percentage (“FMAP”).
The states in which SunLink subsidiaries have operated hospitals have implemented initiatives to decrease the Medicaid funds paid to providers. Medicaid pays providers for inpatient services in a manner similar to the Medicare prospective payment system in that hospitals receive a fixed fee for inpatient hospital services based on the established fixed payment amount per discharge for categories of hospital treatment, also known as DRGs. These Medicaid DRG payments do not consider a specific hospital’s costs, but are statewide rates adjusted for each subsidiaries’ hospitals’ capital cost allotment.
Medicaid outpatient services are reimbursed with interim rates based on a facility specific cost to charge ratio. These interim payments are then adjusted subsequent to the end of the cost reporting period to an amount equal to 85.6% of the costs associated with providing care to the Medicaid outpatient population.
If SunLink or our subsidiaries or any of their facilities were found to be in violation of federal or state laws relating to Medicare, Medicaid or similar programs, SunLink or the applicable subsidiary or facility could be subject to substantial monetary fines, civil penalties and exclusion from future participation in the Medicare and Medicaid programs. Any such sanctions could have a material adverse effect on our financial condition or results of operations.
Adoption of Electronic Health Records
Electronic Health Records (“EHR”) incentive reimbursements are payments received under the Health Information Technology for Economic and Clinical Health Act (the “HITECH Act”) which was enacted into law in 2009 as part of ARRA. The HITECH Act includes provisions designed to increase the use of EHR by both physicians and hospitals. Beginning with federal fiscal year 2011 and extending through federal fiscal year 2016, eligible hospitals participating in the Medicare and Medicaid programs are eligible for reimbursement incentives based on successfully demonstrating meaningful use of their certified EHR technology. Conversely, those hospitals that do not successfully demonstrate meaningful use of EHR technology are subject to payment penalties or downward adjustments to their Medicare payments beginning in federal fiscal year 2015.
The Company accounts for EHR incentive payments in accordance with Financial Accounting Standards Board (“FASB”) Accounting Standards Codification (“ASC”) 450-30, “Gain Contingencies” (“ASC 450-30”). In accordance with ASC 450-30, the Company recognizes a gain for EHR incentive payments when the applicable eligible subsidiary hospital has demonstrated meaningful use of certified EHR technology for the applicable period and when the cost report information needed for the full cost report year used for the final calculation of the EHR incentive reimbursement payment is available. The demonstration of meaningful use is based on meeting a series of objectives and varies among hospitals, between the Medicare and Medicaid programs, and within the Medicaid program from state to state. Additionally, meeting the series of objectives in order to demonstrate meaningful use becomes progressively more stringent as its implementation is phased in through stages as outlined by the CMS.
16
Attestation of Medicare meaningful use requirements was successful for each of SunLink’s hospital subsidiaries’ including certain discontinued operations for fiscal years ended June 30, 2014. SunLink’s hospital subsidiaries have also successfully attested to the meaningful use requirements for the Medicaid program for continuing and certain discontinued operations for the fiscal years ended June 30, 2016, 2015 and 2014. EHR incentive payments received (repaid) were as follows:
| 2016 | 2015 | 2014 | ||||||||||
| Continuing Operations |
||||||||||||
| Medicare |
$ | (7 | ) | $ | 0 | $ | 1,468 | |||||
| Medicaid |
0 | 21 | 312 | |||||||||
|
|
|
|
|
|
|
|||||||
| $ | (7 | ) | $ | 21 | $ | 1,780 | ||||||
|
|
|
|
|
|
|
|||||||
| Discontinued Operations |
||||||||||||
| Medicare |
$ | 0 | $ | 703 | $ | 1,026 | ||||||
| Medicaid |
(93 | ) | 29 | 281 | ||||||||
|
|
|
|
|
|
|
|||||||
| $ | (93 | ) | $ | 732 | $ | 1,307 | ||||||
|
|
|
|
|
|
|
|||||||
| Combined Operations |
||||||||||||
| Medicare |
$ | (7 | ) | $ | 703 | $ | 2,494 | |||||
| Medicaid |
(93 | ) | 50 | 593 | ||||||||
|
|
|
|
|
|
|
|||||||
| $ | (100 | ) | $ | 753 | $ | 3,087 | ||||||
|
|
|
|
|
|
|
|||||||
The amounts in the table above represent actual funds received from meeting the meaningful use requirements for Medicare and Medicaid programs. The discontinued operations Medicare funds received in fiscal 2015 were for attestation of the meaningful use requirements in fiscal 2014. Amounts recognized may differ due to year-end adjustments and final settlement of cost reports.
The Company received no Medicare meaningful use payments in continuing operations in fiscal 2016 and 2015 because, based on its cost-benefit evaluation, it chose not to attest for such payments. We currently believe we will receive no Medicare incentive payments and minimal Medicaid incentive payments in future years.
Government Reimbursement Program Administration and Adjustments
The Medicare, Medicaid and TriCare programs are subject to statutory and regulatory changes, administrative rulings, interpretations and determinations, requirements for utilization review and changing governmental funding restrictions, all of which may materially increase or decrease program payments as well as affect the cost of providing services and the timing of payments under such programs.
All hospitals participating in the Medicare and Medicaid programs are required to meet certain financial reporting requirements. Federal and, where applicable, state regulations require the submission of annual cost reports covering the revenues, costs and expenses associated with the services provided by each subsidiary hospital to Medicare beneficiaries and Medicaid recipients.
Annual cost reports required under the Medicare and Medicaid programs are subject to routine audits which may result in adjustments to the amounts ultimately determined to be due under these reimbursement programs. These audits often require several years to reach the final determination of amounts due. Providers have rights of appeal and it is common to contest issues raised in audits. Although the final outcome of these audits and the nature and amounts of any adjustments are difficult to predict, we believe that we have made adequate provisions in our financial statements for adjustments that may result from these audits and that final resolution of any contested issues should not have a material adverse effect upon our financial condition or results of operations. Until final adjustment, however, significant issues may remain unresolved and previously determined allowances could become either inadequate or greater than ultimately required.
17
In 2005, CMS began using recovery audit contractors (“RACs”) to detect Medicare overpayments not identified through existing claims review mechanisms. The RAC program relies on private companies to examine Medicare claims filed by healthcare providers. The RAC program was made permanent by the Tax Relief and Health Care Act of 2006. The ACA expanded the RAC program’s scope to include managed Medicare and Medicaid claims, and required all states to establish programs to contract with RACs by 2011. Currently all states where our subsidiaries operate have RAC programs, and all their facilities have had requests from the various RACs to review claims.
RACs perform post-discharge audits of medical records to identify Medicare overpayments resulting from incorrect payment amounts, non-covered services, incorrectly coded services, and duplicate services. CMS has given RACs the authority to look back at claims up to three years old, provided that the claim was paid on or after October 1, 2007. Claims review strategies used by RACs generally include a review of high dollar claims, including inpatient hospital claims. As a result, a large majority of the total amounts recovered by RACs has come from hospitals. Claims identified as overpayments are subject to an appeals process and the Company’s hospitals routinely appeal RAC overpayment determinations. Under the RAC program, SunLink has experienced losses in the aggregate from audit adjustments of approximately $0, $86 and $153 for the fiscal years ended June 30, 2016, 2015 and 2014, respectively.
RACs are paid a contingency fee based on the overpayments they identify and collect. We expect that the RACs will continue to look closely at claims submitted by our subsidiary facility in an attempt to identify possible overpayments. Although we believe the claims for reimbursement submitted to the Medicare program are accurate, we cannot predict the results of any future RAC audits.
In addition, CMS employs Medicaid Integrity Contractors (“MICs”) to perform post-payment audits of Medicaid claims and identify overpayments. The ACA increases federal funding for the MIC program for federal fiscal year 2011 and later years. In addition to RACs and MICs, the state Medicaid agencies and other contractors have also increased their review activities.
Government Reimbursement Programs—Nursing Centers
Medicare—The Medicare Part A program provides reimbursement for extended-care services furnished to Medicare beneficiaries who are admitted to nursing centers after at least a three-day stay in an acute care hospital. Covered services include supervised nursing care, room and board, social services, physical, speech, and occupational therapies, certain pharmaceuticals and supplies, and other necessary services provided by nursing centers. Medicare payments to our nursing centers are based upon certain resource utilization grouping (“RUG”) payment rates developed by CMS that provide various levels of reimbursement based upon patient acuity.
The Balanced Budget Act established a Medicare prospective payment system (“PPS”) for nursing centers in 1998. The payments received under PPS cover substantially all services for Medicare residents including all ancillary services, such as respiratory therapy, physical therapy, occupational therapy, speech therapy, and certain covered pharmaceuticals.
Medicare Part B provides reimbursement for certain physician services, limited drug coverage, and other outpatient services, such as therapy and other services, outside of a Medicare Part A covered patient stay. Payment for these services is determined according to the Medicare Physician Fee Schedule (“MPFS”). Annually since 1997, the MPFS has been subject to the sustainable growth rate adjustment (“SGR”) reduction, which is intended to keep spending growth in line with allowable spending. Each year since the SGR was enacted, this adjustment produced a scheduled negative update to payment for physicians, therapists, and other healthcare providers paid under the MPFS. Annually, since 2002, Congress has stepped in with so-called “doc fix” legislation to suspend payment cuts to physicians. Subsequent legislation annually suspended the payment cut with the Protecting Access to Medicare Act of 2014, enacted on April 1, 2014 (“PAMA”) most recently
18
suspending the payment cut until March 31, 2015.The Medicare Access and CHIP Reauthorization Act of 2015 (“MACRA”) permanently replaces the SGR formula previously used to determine updates to Medicare physician reimbursement, replacing these updates with quality and value measurements and participation in alternative payment models.
Since 2006, federal legislation has provided for an annual Medicare Part B outpatient therapy cap. In years since 2006, CMS has increased the amount of the therapy cap. In addition, legislation was passed that required CMS to implement a broad process for reviewing medically necessary therapy claims, creating an exception to the cap. Legislation has annually extended the Medicare Part B outpatient therapy cap exception process. MACRA further extended the therapy cap exception process until December 31, 2017. This review process has had an adverse effect on the provision and billing of services for patients and can negatively impact therapist productivity. Patients whose stay is not reimbursed by Medicare Part A must seek reimbursement for their therapy under Medicare Part B and are subject to the therapy cap.
In 2006, the Medicare Prescription Drug, Improvement, and Modernization Act of 2003 (“Medicare Part D”) implemented a major expansion of the Medicare program through the introduction of a prescription drug benefit. Under Medicare Part D, dual-eligible patients have their outpatient prescription drug costs covered by this Medicare benefit, subject to certain limitations. Most of our nursing center patients are dual-eligible patients who qualify for the Medicare drug benefit. Accordingly, Medicaid is no longer a primary payor for the pharmacy services provided to these patients.
On July 31, 2013, CMS issued final regulations updating Medicare payment rates for nursing centers effective October 1, 2013. These final regulations implement a net market basket increase of 1.3% consisting of: (1) a 2.3% market basket inflation increase, less (2) a 0.5% adjustment to account for the effect of a productivity adjustment, and less (3) a 0.5% market basket forecast error adjustment.
On April 1, 2014, PAMA was enacted, which directed CMS to create a value-based purchasing initiative applicable to nursing centers beginning October 1, 2018. The initiative will focus on a preventable hospital readmission measure to be provided on or before October 1, 2015 and corresponding preventable hospital readmission rates to be provided on or before October 1, 2016. Nursing centers will be ranked according to performance on this preventable hospital readmission rate, with corresponding incentive payments based upon such ranking. CMS also will reduce the Medicare per diem rate by 2% beginning October 1, 2018 in connection with the launch of this initiative.
On July 31, 2014, CMS issued final regulations updating Medicare payment rates for nursing centers effective October 1, 2014. These final regulations implement a net market basket increase of 2.0% consisting of: (1) a 2.5% market basket inflation increase, less (2) a 0.5% adjustment to account for the effect of a productivity adjustment.
On July 30, 2015, CMS issued final regulations updating Medicare payment rates for nursing centers effective October 1, 2015. These final regulations implement a net market basket increase of 1.2% consisting of: (1) a 2.3% market basket increase, less (2) a 0.6% market basket forecast error adjustment and (3) a 0.5% productivity adjustment.
In February 2012, the Middle Class Tax Relief Act of 2012 was enacted, which provides that certain Medicare Part B therapy services exceeding a threshold of $3,700 would be subject to a pre-payment manual medical review process effective October 1, 2012. The review process for these services continues to be used by CMS. This review process has had an adverse effect on the provision and billing of services for patients and can negatively impact therapist productivity.
In February 2012, Congress passed The Job Creation Act of 2012 (the “Job Creation Act”), which provides for reductions in reimbursement of Medicare bad debts for nursing centers. The Job Creation Act provides for a
19
phase-in of the reduction in the rate of reimbursement for bad debts of patients that are dually eligible for Medicare and Medicaid. The rate of reimbursement for bad debts for these dually eligible patients were reduced from 100% to 88% for cost reporting periods beginning on or after October 1, 2012 and was reduced to 76% for cost reporting periods beginning on or after October 1, 2013, and was reduced to 65% for cost reporting periods beginning on or after October 2, 2014. The rate of reimbursement for bad debts for patients not dually eligible for both Medicare and Medicaid was reduced from 70% to 65%, effective for cost reporting periods beginning on or after October 1, 2012.
The Budget Control Act of 2011 (as amended by the Taxpayer Relief Act) instituted an automatic 2% reduction on each claim submitted to Medicare beginning April 1, 2013.
Medicaid—Medicaid is a state-administered program financed by state funds and matching federal funds. The program provides for medical assistance to the indigent and certain other eligible persons. Although administered under broad federal regulations, states are given flexibility to construct programs and payment methods consistent with their individual goals. Accordingly, these programs differ in many respects from state to state.
Our subsidiary nursing centers provide Medicaid-covered services consisting of nursing care, room and board, and social services to eligible individuals. In addition, states may at their option cover other services such as physical, occupational, and speech therapies, and pharmaceuticals. Medicaid programs also are subject to statutory and regulatory changes, administrative rulings, interpretations of policy by the state agencies, and certain government funding limitations, all of which may materially increase or decrease the level of program payments to our subsidiary nursing centers. We believe that the payments under many of these programs may not be sufficient on an overall basis to cover the costs of serving certain patients participating in these programs. In addition, many states are experiencing budgetary pressures which have resulted in further reductions to Medicaid payments to our nursing centers.
There continue to be legislative and regulatory proposals that would impose further limitations on government and private payments to providers of healthcare services. Many states are considering or have enacted measures that are designed to reduce their Medicaid expenditures and to make certain changes to private healthcare insurance. As states face budgetary issues, we anticipate further pressure on Medicaid rates that could negatively impact payments to our nursing centers.
In addition, some states seek to increase the levels of funding contributed by the federal government to their Medicaid programs through a mechanism known as a provider tax. Under these programs, states levy a tax on healthcare providers, which increases the amount of state revenue available to expend on the Medicaid program. This increase in program revenues increases the payment made by the federal government to the state in the form of matching funds. Consequently, the state then has more funds available to support Medicaid rates for providers of Medicaid covered services. However, states may not necessarily use these funds to increase payments to nursing center providers. Provider tax plans are subject to approval by the federal government. Although some of these plans have been approved in the past, we cannot assure you that such plans will be approved by the federal government in the future.
Nongovernment payments—Although our nursing centers seek to maximize the number of nongovernment payment residents admitted to our nursing centers, including those covered under private insurance and managed care health plans, nongovernment payment residents in our nursing centers are limited. Nongovernment payment residents typically have financial resources (including insurance coverage) to pay for their services and do not rely on government programs for support. It is important to our business to establish relationships with commercial insurers, managed care health plans, and other private payors and to maintain our reputation with such payors as a provider of quality patient and resident care. We negotiate contracts with purchasers of group healthcare services, including private employers, commercial insurers, and managed care companies. Most payor organizations attempt to obtain discounts from established charges. We focus on
20
demonstrating to these payors how our services can provide them and their customers with the most viable pricing arrangements in circumstances where they may otherwise be faced with funding treatment at higher rates at other healthcare providers. The importance of obtaining contracts with commercial insurers, managed care health plans and other private payors varies among markets, depending on such factors as the number of commercial payors and their relative market strength. Failure to obtain contracts with certain commercial insurers and managed care health plans or reductions in lengths of stay or payments for our services provided to individuals covered by commercial insurance could have a material adverse effect on our business, financial position, results of operations, and liquidity.
Government Reimbursement Programs—Pharmacy
The operations of our Specialty Pharmacy Segment are subject to certain rules implemented by the Medicare Modernization Act (“MMA”) and, in the future, may be subject to other rules previously implemented by MMA with respect to urban providers. Regulations implementing cost containment mandates under MMA reduced the reimbursement for healthcare providers in urban areas for a number of products and services which are also provided by our pharmacy operations and established a competitive bidding program for certain durable medical equipment provided under Medicare Part B in urban areas. Competitive bidding is intended to further reduce reimbursement for certain products and will likely decrease the number of companies permitted to serve Medicare beneficiaries in the competitive bidding areas (“CBAs”). CMS had planned to implement the competitive bidding program for Medicare durable medical equipment, prosthetics, orthotics, and supplies (“DMEPOS”) products and services with the goal of offering beneficiaries access to quality with lower out-of-pocket costs. Prior to January 1, 2016, our Scripts operations were exempted under the Deficit Reduction Act of 2005 from the proposed competitive acquisition program for DMEPOS. However, on October 31, 2014, the CMS released Final Rule 1614-F, “Medicare Program: End-Stage Renal Disease Prospective Payment System, Quality Incentive Program, and Durable Medical Equipment, Prosthetics, Orthotics, and Supplies,” which, in conjunction with Sections 1834(a)(1)(F) and 1842(s)(3)(B) of the Social Security Act, established the methodology to expand competitive bidding to non-bid areas and to implement national price adjustments to payments for DMEPOS and enteral nutrition products previously paid under fee schedules. Under these rules and the resulting expansion plan, CMS applied competitive bidding prices to claims for DMEPOS and enteral nutrition products in previously non-bid areas currently covered in Rounds One and Two of the Competitive Bidding Program (CBP). An un-weighted average of all of the single payment amounts from the CBAs in each of the eight distinct CBAs was used to determine a regional single payment amount (RSPA) for each covered item in each CBA. From January 1, 2016 to June 30, 2016, reimbursement rates for affected product categories were reduced significantly, based on the sum of 50 percent of the current unadjusted fee schedule amount plus 50 percent of the RSPAs. Then, on July 1, 2016, the reimbursement rates were reduced further to fully implement the bidding-derived rates (i.e., 100% of the adjusted fee schedule amount, based on regional competitive bidding rates). We cannot assure you that Scripts will be able to operate its DMEPOS and enteral nutrition products operations profitably in the future at either existing or at the July 1, 2016 lower reimbursement rates. The MMA also created a Medicare prescription drug benefit (which began in 2006) and a prescription drug card program. Final rules implementing the portions of the MMA relating to the prescription drug benefit were adopted in 2005.
Under MMA Medicare Part B, covered drugs and biological products generally are paid based on the average sales price (“ASP”) methodology. The ASP methodology uses quarterly drug pricing data submitted to CMS by drug manufacturers. CMS will supply contractors with the ASP drug pricing files for Medicare Part B drugs on a quarterly basis. Principal products paid under the ASP methodology include certain oncology and renal dialysis drugs. Although, there are exceptions to this general rule which are listed in the latest ASP quarterly change request document and which exceptions generally are paid on a cost basis, such exceptions have not been and are not expected to be material to our operations.
Beginning in January 2008, CMS’s outpatient prospective payment system began paying for most separately payable Medicare Part B drugs administered in a hospital outpatient setting at a reimbursement level of ASP plus 5% and ASP plus 6% in other settings. Such outpatient price represented a decrease from ASP plus 6%.
21
Section 303(d) of the MMA also requires the implementation of a competitive acquisition program (the “Part B CAP”) for Medicare Part B drugs and biological not paid on a cost or prospective payment system basis. The Part B CAP is an alternative to the ASP methodology for acquiring certain Part B drugs which are administered incident to a physician’s services. Currently, the Part B CAP is a voluntary program that offers physicians the option to acquire many injectable and infused drugs they use in their practice from an approved Part B CAP vendor, thus reducing the time and cost of buying and billing for drugs. Currently, the CAP for Part B Drugs and Biologicals is only for injectable and infused drugs currently billed under Part B that are administered in a physician’s office, “incident to” a physician’s service.
In late 2005, CMS conducted the first round of bidding for approved Part B CAP vendors. The Part B CAP was implemented on July 1, 2006. The 2009-2011 CAP vendor bidding period concluded on February 15, 2008. CMS received several qualified bids; however, contractual issues with the successful bidders resulted in the 2009 program being postponed by CMS in September 2008. As a result, CAP drugs were not available from an approved CAP vendor for dates of service after December 31, 2008.
At least one Medicaid program has adopted, and other Medicaid programs, some states and some private payors may be expected to adopt, those aspects of the MMA that either result in or appear to result in price reductions for drugs covered by such programs. Adoption of ASP as the measure for determining reimbursement by Medicare and Medicaid programs for additional drugs sold by our specialty pharmacy operations could reduce revenue and gross margins and could materially affect our current average wholesale price (“AWP”) based reimbursement structure with private payors.
We cannot assure you that the ASP reimbursement methodology will not be extended to the provision of all specialty pharmaceuticals or to the specialty pharmaceuticals most often sold by our Scripts specialty pharmacy operations or that Scripts will be able to operate its specialty pharmacy operations profitably at either existing or at lower reimbursement rates. Likewise, we cannot assure you that the Part B CAP program will not be extended to rural or exurban areas in general or to the areas in which it operates, or may seek to operate, in particular or that Scripts would be able to meet the qualifications to become a Part B CAP vendor either now or at any time in the future.
HEALTHCARE REGULATION
Overview
The healthcare industry is governed by an extremely complex framework of federal, state and local laws, rules and regulations, and there continue to be federal and state proposals that would, and actions that do, impose limitations on government and private payments to providers, including community hospitals, nursing homes and pharmacy operations. In addition, there regularly are proposals to increase co-payments and deductibles from program and private patients. Hospital facilities also are affected by controls imposed by government and private payors designed to reduce admissions and lengths of stay. Such controls include what is commonly referred to as “utilization review”. Utilization review entails the review of a patient’s admission and course of treatment by a third party. Historically, utilization review has resulted in a decrease in certain treatments and procedures being performed. Utilization review is required in connection with the provision of care which is to be funded by Medicare and Medicaid and is also required under many managed care arrangements.
Many states have enacted, or are considering enacting, additional measures that are designed to reduce their Medicaid expenditures and to make changes to private healthcare insurance. Various states have applied, or are considering applying, for a waiver from current Medicaid regulations in order to allow them to serve some of their Medicaid participants through managed care providers. These proposals also may attempt to include coverage for some people who presently are uninsured, and generally could have the effect of reducing payments to hospitals, physicians and other providers for the same level of service provided under Medicaid.
22
Healthcare Facility Regulation
Certificate of Need Requirements
A number of states require approval for the purchase, construction or expansion of various healthcare facilities, including findings of need for additional or expanded healthcare facilities or services. Certificates of Need (“CONs”), which are issued by governmental agencies with jurisdiction over applicable healthcare facilities, are at times required for capital expenditures exceeding a prescribed amount, changes in bed capacity or the addition of services and certain other matters. The state in which a SunLink subsidiary currently operates a hospital (Mississippi) has a CON law that applies to such facility. The two states (Georgia and Mississippi) in which SunLink subsidiaries currently operate nursing homes/skilled nursing facilities also have CON laws that apply to nursing homes and other skilled nursing facilities. States periodically review, modify and revise their CON laws and related regulations.
SunLink is unable to predict whether its subsidiaries’ healthcare facilities will be able to obtain any CONs that may be necessary to accomplish their business objectives in any jurisdiction where such certificates of need are required. Violation of these state laws may result in the imposition of civil sanctions or the revocation of licenses for such facilities. In addition, future healthcare facility acquisitions also may occur in states that require CONs.
Future healthcare facility acquisitions also may occur in states that do not require CONs or which have less stringent CON requirements than the states in which SunLink subsidiaries currently operate healthcare facilities. Any healthcare facility operated by SunLink in such states may face increased competition from new or expanding facilities operated by competitors, including physicians.
Utilization Review Compliance and Hospital Governance
Healthcare facilities are subject to, and comply with, various forms of utilization review. In addition, under the Medicare prospective payment system, each state must have a peer review organization to carry out a federally mandated system of review of Medicare patient admissions, treatments and discharges in hospitals. Medical and surgical services and physician practices are supervised by committees of staff doctors at each healthcare facility, are overseen by each healthcare facility’s local governing board, the primary voting members of which are physicians and community members, and are reviewed by quality assurance personnel. The local governing boards also help maintain standards for quality care, develop long-range plans, establish, review and enforce practices and procedures and approve the credentials and disciplining of medical staff members.
Emergency Medical Treatment and Active Labor Act
The Emergency Medical Treatment and Active Labor Act (“EMTALA”) is a federal law that requires any hospital that participates in the Medicare program to conduct an appropriate medical screening examination of every person who presents to the hospital’s emergency department for treatment and, if the patient is suffering from an emergency medical condition or is in active labor, to either stabilize that condition or make an appropriate transfer of the patient to a facility that can handle the condition. The obligation to screen and stabilize emergency medical conditions exists regardless of a patient’s ability to pay for treatment. There are severe penalties under EMTALA if a hospital fails to screen or appropriately stabilize or transfer a patient or if the hospital delays appropriate treatment in order to first inquire about the patient’s ability to pay. Penalties for violations of EMTALA include civil monetary penalties and exclusion from participation in the Medicare program, the Medicaid program or both. In addition, an injured patient, the patient’s family or a medical facility that suffers a financial loss as a direct result of another hospital’s violation of the law can bring a civil suit against that other hospital. Although we believe that our subsidiaries’ hospitals comply with EMTALA, we cannot predict whether CMS will implement new requirements in the future and whether our subsidiaries’ hospitals will be able to comply with any new requirements.
23
Specialty Pharmacy Segment Regulation
Overview
Much like our subsidiaries’ healthcare facility operations, the operations of our Specialty Pharmacy Segment subsidiary are subject to various federal and state statutes and regulations governing their operations, including laws and regulations with respect to operation of pharmacies, repackaging of drug products, wholesale distribution, dispensing of controlled substances, cross-jurisdictional sale and distribution of pharmacy products, medical waste disposal, clinical trials and non-discriminatory access. Federal statutes and regulations govern the labeling, packaging, advertising and adulteration of prescription drugs, as well as the dispensing of controlled substances. Federal controlled substance laws require us to register our pharmacies and repackaging facilities with the United States Drug Enforcement Administration (“DEA”) and to comply with security, recordkeeping, inventory control and labeling standards in order to dispense controlled substances. Although we believe that the operations of our Specialty Pharmacy Segment have obtained the permits and/or licenses required to conduct its specialty pharmacy business as currently conducted, a failure to have the necessary permits and licenses could have a material adverse effect on its specialty pharmacy business, and our financial condition or results of operations.
Pharmaceutical Distribution
Scripts conducts the operations of our Specialty Pharmacy Segment. In addition to walk-in customers at its retail centers, it distributes pharmaceuticals through a variety of delivery methods, including by mail and express delivery services. Many states in which Scripts delivers or may seek to deliver pharmaceuticals have laws and regulations that require out-of-state mail service pharmacies to register with, or be licensed by, the boards of pharmacy or similar regulatory bodies in those states. These states generally permit the dispensing pharmacy to follow the laws of the state within which the dispensing pharmacy is located.
However, various state Medicaid programs have enacted laws and/or adopted rules or regulations directed at restricting or prohibiting the operation of out-of-state pharmacies by, among other things, requiring compliance with all laws of the states into which the out-of-state pharmacy dispenses medications, whether or not those laws conflict with the laws of the state in which the pharmacy is located, or requiring the pharmacist-in-charge to be licensed in that state. To the extent that such laws or regulations are found to be applicable to the specialty pharmacy operations of Scripts, we believe its specialty pharmacy operations comply with them in all material respects. To the extent that any of the foregoing laws or regulations prohibit or restrict the operation of mail service pharmacies and are found to be applicable to the specialty pharmacy operations of Scripts, they could have an adverse effect on its ability to expand our pharmacy operations, which currently are concentrated in Louisiana. A number of state Medicaid programs prohibit the participation in such state’s Medicare program by either out-of-state retail pharmacies or mail order pharmacies, whether located in-state or out-of-state.
Advertising and Marketing Regulations
There are also other statutes and regulations which may affect advertising, marketing and distribution of pharmacy products. The Federal Trade Commission requires mail order sellers of goods generally to engage in truthful advertising, to stock a reasonable supply of the products to be sold, to fill mail orders within 30 days, and to provide clients with refunds, when appropriate.
General Healthcare Regulations
Drugs and Controlled Substances
Various licenses and permits are required by our subsidiaries’ healthcare facilities and by the specialty pharmacy operations of Scripts in order to dispense narcotics and operate pharmacies. All of our subsidiaries are required to register our pharmacy operations for permits and/or licenses with, and comply with certain operating
24
and security standards of, the United States DEA, the Food and Drug Administration (“FDA”), state Boards of Pharmacy, state health departments and other state agencies in states where we operate or may seek to operate.
State controlled substance laws require registration and compliance with state pharmacy licensure, registration or permit standards promulgated by the state’s pharmacy licensing authority. Such standards often address the qualification of an applicant’s personnel, the adequacy of its prescription fulfillment and inventory control practices and the adequacy of its facilities. In general, pharmacy licenses are renewed annually. Pharmacists and pharmacy technicians employed at each of our dispensing locations also must satisfy applicable state licensing requirements.
Fraud and Abuse, Anti-Kickback and Self-Referral Regulations
Participation in the Medicare and/or Medicaid programs is heavily regulated by federal statutes and regulations. If a hospital fails to comply substantially with the numerous federal laws governing a facility’s activities, the hospital’s participation in the Medicare and/or Medicaid programs may be terminated and/or civil or criminal penalties may be imposed. For example, a hospital may lose its ability to participate in the Medicare and/or Medicaid programs if it:
| • | makes claims to Medicare and/or Medicaid for services not provided or misrepresents actual services provided in order to obtain higher payments; |
| • | pays money to induce the referral of patients or the purchase of items or services where such items or services are reimbursable under a federal or state health program; |
| • | fails to report or repay improper or excess payments; or |
| • | fails to provide appropriate emergency medical screening services to any individual who comes to a hospital’s campus or otherwise fails to properly treat and transfer emergency patients. |
Hospitals continue to be one of the primary focus areas of the Office of the Inspector General (“OIG”) of the United States and other governmental fraud and abuse programs. In January 2005, the OIG issued Supplemental Compliance Program Guidance for Hospitals that focuses on hospital compliance risk areas. Some of the risk areas highlighted by the OIG include correct outpatient procedure coding, revising admission and discharge policies to reflect current CMS rules, submitting appropriate claims for supplemental payments such as pass-through costs and outlier payments and a general discussion of the fraud and abuse risks related to financial relationships with referral sources. Each federal fiscal year, the OIG also publishes a General Work Plan that provides a brief description of the activities that the OIG plans to initiate or continue with respect to the programs and operations of Department of Health and Human Services (“HHS”) and details the areas that the OIG believes are prone to fraud and abuse.
Sections of the Anti-Fraud and Abuse Amendments to the Social Security Act, commonly known as the “anti-kickback” statute, prohibit certain business practices and relationships that might influence the provision and cost of healthcare services reimbursable under Medicare, Medicaid, TriCare or other healthcare programs, including the payment or receipt of remuneration for the referral of patients whose care will be funded by Medicare or other government programs. Sanctions for violating the anti-kickback statute include criminal penalties and civil sanctions, including fines and possible exclusion from future participation in government programs, such as Medicare and Medicaid. Pursuant to the Medicare and Medicaid Patient and Program Protection Act of 1987, HHS issued regulations that create safe harbors under the anti-kickback statute. A given business arrangement that does not fall within an enumerated safe harbor is not per se illegal; however, business arrangements that fail to satisfy the applicable safe harbor criteria are subject to increased scrutiny by enforcement authorities.
The Health Insurance Portability and Accountability Act of 1996 (“HIPAA”) broadened the scope of the fraud and abuse laws by adding several criminal statutes that are not related to receipt of payments from a federal healthcare program. HIPAA created civil penalties for proscribed conduct, including upcoding and billing for
25
medically unnecessary goods or services. These laws cover all health insurance programs, private as well as governmental. In addition, HIPAA broadened the scope of certain fraud and abuse laws, such as the anti-kickback statute, to include not just Medicare and Medicaid services, but all healthcare services reimbursed under a federal or state healthcare program. Finally, HIPAA established enforcement mechanisms to combat fraud and abuse. These mechanisms include a bounty system where a portion of the payment recovered is returned to the government agencies, as well as a whistleblower program, where a portion of the payment received is paid to the whistleblower. HIPAA also expanded the categories of persons that may be excluded from participation in federal and state healthcare programs.
There is increasing scrutiny by law enforcement authorities, the OIG, the courts and the U.S. Congress of arrangements between healthcare providers and potential referral sources to ensure that the arrangements are not designed as mechanisms to exchange remuneration for patient-care referrals and opportunities. Investigators also have demonstrated a willingness to look behind the formalities of a business transaction and to reinterpret the underlying purpose of payments between healthcare providers and potential referral sources. Enforcement actions have increased, as is evidenced by highly publicized enforcement investigations of certain hospital activities.
In addition, provisions of the Social Security Act, known as the Stark Act, also prohibit physicians from referring Medicare and Medicaid patients to providers of a broad range of designated health services with which the physicians or their immediate family members have ownership or certain other financial arrangements. Certain exceptions are available for employment agreements, leases, physician recruitment and certain other physician arrangements. A person making a referral, or seeking payment for services referred, in violation of the Stark Act is subject to civil monetary penalties of up to $15 for each service; restitution of any amounts received for illegally billed claims; and/or exclusion from future participation in the Medicare program, which can subject the person or entity to exclusion from future participation in state healthcare programs.
Further, if any physician or entity enters into an arrangement or scheme that the physician or entity knows or should have known has the principal purpose of assuring referrals by the physician to a particular entity, and the physician directly makes referrals to such entity, then such physician or entity could be subject to a civil monetary penalty of up to $100. In addition, the monitoring of compliance with and the enforcing of penalties for violations of these laws and regulations is changing and increasing. For example, in 2010, CMS issued a “self-referral disclosure protocol” for hospitals and other providers that wish to self-disclose potential violations of the Stark Act and attempt to resolve those potential violations and any related overpayment liabilities at levels below the maximum penalties and amounts set forth in the statute. In light of the provisions of the Affordable Care Act that created potential liabilities under the federal False Claims Act (discussed below) for failing to report and repay known overpayments and return an overpayment within sixty (60) days of the identification of the overpayment or the date by which a corresponding cost report is due, whichever is later, hospitals and other healthcare providers are encouraged to disclose potential violations of the Stark Act to CMS. It is likely that self-disclosure of Stark Act violations will increase in the future. Finally, many states have adopted or are considering similar legislative proposals, some of which extend beyond the Medicaid program, to prohibit the payment or receipt of remuneration for the referral of patients and physician self-referrals regardless of the source of the payment for the care.
The Federal False Claims Act and Similar State Laws
The Federal False Claims Act prohibits providers from, among other things, knowingly submitting false or fraudulent claims for payment to the federal government. The False Claims Act defines the term “knowingly” broadly, and while simple negligence generally will not give rise to liability, submitting a claim with reckless disregard to its truth or falsity can constitute the “knowing” submission of a false or fraudulent claim for the purposes of the False Claims Act. The “qui tam” or “whistleblower” provisions of the False Claims Act allow private individuals to bring actions under the False Claims Act on behalf of the government. These private parties are entitled to share in any amounts recovered by the government, and, as a result, the number of “whistleblower”
26
lawsuits that have been filed against providers has increased significantly in recent years. When a private party brings a qui tam action under the False Claims Act, the defendant will generally not be aware of the lawsuit until the government makes a determination whether it will intervene and take a lead in the litigation. If a provider is found to be liable under the False Claims Act, the provider may be required to pay up to three times the actual damages sustained by the government plus mandatory civil monetary penalties of between $5 to $11 for each separate false claim. The government has used the False Claims Act to prosecute Medicare and other government healthcare program fraud such as coding errors, billing for services not provided, submitting false cost reports, and providing care that is not medically necessary or that is substandard in quality.
HIPAA Transaction, Privacy and Security Requirements
HIPAA and federal regulations issued pursuant to HIPAA contain, among other measures, provisions that have required SunLink and our subsidiaries to implement modified or new computer systems, employee training programs and business procedures. The federal regulations are intended to encourage electronic commerce in the healthcare industry, provide for the confidentiality and privacy of patient healthcare information and ensure the security of healthcare information.
A violation of the HIPAA regulations could result in civil money penalties of $1 per incident, up to a maximum of $25 per person, per year, per standard violated. HIPAA also provides for criminal penalties of up to $50 and one year in prison for knowingly and improperly obtaining or disclosing protected health information, up to $100 and five years in prison for obtaining protected health information under false pretenses and up to $250 and ten years in prison for obtaining or disclosing protected health information with the intent to sell, transfer or use such information for commercial advantage, personal gain or malicious harm. Since there is limited history of enforcement efforts by the federal government at this time, it is difficult to ascertain the likelihood of enforcement efforts in connection with the HIPAA regulations or the potential for fines and penalties, which may result from any violation of the regulations.
HIPAA Privacy Regulations
HIPAA privacy regulations protect the privacy of individually identifiable health information. The regulations provide increased patient control over medical records, mandate substantial financial penalties for violation of a patient’s right to privacy and, with a few exceptions, require that an individual’s individually identifiable health information only be used for healthcare-related purposes. These privacy standards apply to all health plans, all healthcare clearinghouses and healthcare providers, such as our subsidiaries’ facilities, that transmit health information in an electronic form in connection with standard transactions, and apply to individually identifiable information held or disclosed by a covered entity in any form. These standards impose extensive administrative requirements on our subsidiaries’ facilities and require compliance with rules governing the use and disclosure of such health information, and they require our subsidiaries’ facilities to impose these rules, by contract, on any business associate to whom we disclose such information in order to perform functions on behalf of our subsidiaries’ facilities. In addition, our subsidiaries’ facilities are subject to any state laws that are more restrictive than the privacy regulations issued under HIPAA. These laws vary by state and could impose stricter standards and additional penalties.
The HIPAA privacy regulations also require healthcare providers to implement and enforce privacy policies to ensure compliance with the regulations and standards. In conjunction with a private HIPAA consultant and HIPAA coordinators at each facility, individually tailored policies and procedures were developed and implemented and HIPAA privacy educational programs are presented to all employees and physicians at each facility. We believe all of our subsidiaries’ facilities are in compliance with current HIPAA privacy regulations.
HIPAA Electronic Data Standards
The Administrative Simplification Provisions of HIPAA require the use of uniform electronic data transmission standards for all healthcare related electronic data interchange. These provisions are intended to
27
streamline and encourage electronic commerce in the healthcare industry. Among other things, these provisions require healthcare facilities to use standard data formats and code sets established by HHS when electronically transmitting information in connection with certain transactions, including health claims and equivalent encounter information, healthcare payment and remittance advice and health claim status.
The HHS regulations establish electronic data transmission standards that all healthcare providers and payors must use when submitting and receiving certain electronic healthcare transactions. The uniform data transmission standards are designed to enable healthcare providers to exchange billing and payment information directly with the many payors thereby eliminating data clearinghouses and simplifying the interface programs necessary to perform this function. We believe that the management information systems at our subsidiaries comply with HIPAA’s electronic data regulations and standards.
HIPAA Security Standards
The Administrative Simplification Provisions of HIPAA require the use of a series of security standards for the protection of electronic health information. The HIPAA security standards rule specifies a series of administrative, technical and physical security procedures for covered entities to use to assure the confidentiality of electronic protected health information. The standards are delineated into either required or addressable implementation specifications.
In conjunction with a consortium of rural hospitals, private HIPAA security consultants and HIPAA security officers at each facility, our subsidiaries have performed security assessments, and implemented individually tailored plans to apply required or addressable solutions and implemented a set of security policies and procedures. In addition, our subsidiaries developed and adopted an individually tailored comprehensive disaster contingency plan for each facility and presented a HIPAA security training program to all applicable personnel. We believe SunLink and our subsidiaries are in compliance with all aspects of the HIPAA security regulations.
HIPAA National Provider Identifier
HIPAA also required HHS to issue regulations establishing standard unique health identifiers for individuals, employers, health plans and healthcare providers to be used in connection with standard electronic transactions. All healthcare providers, including our facilities, were required to obtain a new National Provider Identifier (“NPI”) to be used in standard transactions instead of other numerical identifiers by May 23, 2007. Our facilities implemented use of a standard unique healthcare identifier by utilizing their employer identification number. HHS has not yet issued proposed rules that establish the standard for unique health identifiers for health plans or individuals. Once these regulations are issued in final form, we expect to have approximately one to two years to become fully compliant, but cannot predict the impact of such changes at this time. We cannot predict whether our facilities may experience payment delays during the transition to the new identifiers. HHS is currently working on the standards for identifiers for health plans; however, there are currently no proposed timelines for issuance of proposed or final rules. The issuance of proposed rules for individuals is on hold indefinitely.
Medical Waste Regulations
Our operations, especially our healthcare facility operations, generate medical waste that must be disposed of in compliance with federal, state and local environmental laws, rules and regulations. Our operations are also generally subject to various other environmental laws, rules and regulations. Based on our current level of operations, we do not anticipate that such compliance costs will have a material adverse effect on our cash flows, financial position or results of operations.
28
Regulatory Compliance Program
Our subsidiaries maintain compliance programs under the direction of a risk manager. The compliance programs are directed at all areas of regulatory compliance, including physician recruitment, reimbursement and cost reporting practices, as well as pharmacy and home healthcare operations. Each hospital and the specialty pharmacy operations designates a compliance officer and develops plans to correct problems should they arise. In addition, all employees are provided with a copy of and given an introduction to the subsidiary’s Code of Conduct, which includes ethical and compliance guidelines and instructions about the proper resources to utilize in order to address any concerns that may arise. Each hospital and the specialty pharmacy operations conduct annual training to re-emphasize its Code of Conduct and monitor its compliance program to respond to developments in healthcare regulations and the industry. A toll-free hotline is also maintained to permit employees to report compliance concerns on an anonymous basis.
Professional Liability
As part of our business, our subsidiaries are subject to claims of liability for events occurring in the ordinary course of operations. To cover a portion of these claims, professional malpractice liability insurance and general liability insurance are maintained in amounts which are commercially available and believed to be sufficient for operations as currently conducted, although some claims may exceed the scope or amount of the coverage in effect.
The recorded liability for professional liability risks of our subsidiaries’ operations includes an estimate of liability for claims assumed at the acquisition and for claims incurred after the acquisition of healthcare businesses. These estimates are based on actuarially determined amounts.
Environmental Regulation
We believe our subsidiaries are in substantial compliance with applicable federal, state and local environmental regulations. To date, compliance with federal, state and local laws regulating the discharge of material into the environment or otherwise relating to the protection of the environment have not had a material effect upon our consolidated results of operations, consolidated financial condition or competitive position. Similarly, we have not had to make material capital expenditures to comply with such regulations.
29
EXECUTIVE OFFICERS OF THE REGISTRANT
Our executive officers, as of September 27, 2016, their positions with the Company or its subsidiaries and their ages are as follows:
| Name |
Offices |
Age | ||||
| Robert M. Thornton, Jr. |
Director, Chairman of the Board of Directors, President and Chief Executive Officer | 67 | ||||
| Mark J. Stockslager |
Chief Financial Officer and Principal Accounting Officer | 57 | ||||
| Byron D. Finn |
President—SunLink ScriptsRx, LLC | 66 | ||||
All of our executive officers hold office for an indefinite term, subject to the discretion of the Board of Directors.
Robert M. Thornton, Jr. has been Chairman and Chief Executive Officer of SunLink Health Systems, Inc. since September 10, 1998, President since July 16, 1996 and was Chief Financial Officer from July 18, 1997 to August 31, 2002. From March 1995 to the present, Mr. Thornton has been a private investor in and Chairman and Chief Executive Officer of CareVest Capital, LLC, a private investment and management services firm. Mr. Thornton was President, Chief Operating Officer, Chief Financial Officer and a director of Hallmark Healthcare Corporation (“Hallmark”) from November 1993 until Hallmark’s merger with Community Health Systems, Inc. in October 1994. From October 1987 until November 1993, Mr. Thornton was Executive Vice President, Chief Financial Officer, Secretary, Treasurer and a director of Hallmark.
Mark J. Stockslager has been Chief Financial Officer of SunLink Health Systems, Inc. since July 1, 2007. He was interim Chief Financial Officer from November 6, 2006 until June 30, 2007. He has been the Principal Accounting Officer since March 11, 1998 and was Corporate Controller from November 6, 1996 to June 4, 2007. He has been associated continuously with our accounting and finance operations since June 1988 and has held various positions, including Manager of U.S. Accounting, from June 1993 until November 1996. From June 1982 through May 1988, Mr. Stockslager was employed by Price Waterhouse & Co.
Byron D. Finn was named President of SunLink ScriptsRx, LLC on October 1, 2010. Mr. Finn was most recently president of Byron D. Finn, CPA, PC, which provided accounting, financial consulting and litigation support services to its clients, including numerous healthcare clients. His experience also includes various positions with The Coca-Cola Company, where he served in a number of financial-related positions and in connection with special projects, and he was previously employed by Ernst & Young. Mr. Finn is a licensed CPA and received his BA in Business Administration and Master in Accountancy degrees from the University of Georgia.
| Item 1A. | Risk Factors |
In addition to other information contained in this Annual Report, including certain cautionary and forward-looking statements, you should carefully consider the following factors in evaluating an investment in SunLink:
Consolidated Operations Risks
If our operating results continue to decline, we may not be able to generate sufficient cash flows to meet our liquidity needs.
We rely upon cash on hand, cash from operations and asset sales to fund our cash requirements for working capital, capital expenditures, commitments and payments of principal and interest on borrowings. Our ability to generate cash from operations has been negatively impacted by reduced Federal and state reimbursements, uncollectible self-pay net revenues of our Healthcare Facilities Segment, increased salary expenses for employed
30
physicians and decreased patient volume at our facilities as a result of economic conditions in the locations we serve as well as decreased sales volume and earning experienced by our Specialty Pharmacy Segment. We expect that these factors will continue to have a negative impact on our business for the foreseeable future. Further deterioration would negatively impact our results of operations and cash flows.
SunLink would require additional debt or equity capital in order to make significant capital investments or expand our operations and the inability to make significant capital investments or expand our operations may negatively affect SunLink’s competitive position, reduce earnings, and negatively affect our results of operations.
SunLink’s operations strategy may require significant capital investments from time to time. Significant capital investments may be required for on-going and planned capital improvements at existing facilities and/or in connection with future capital projects either in connection with existing properties or future acquired properties. SunLink’s ability to make capital investments depends on numerous factors such as the availability of funds from operations and access to additional debt and equity financing. No assurance can be given that the necessary funds will be available. Moreover, incurrence of additional debt financing, if available, may involve additional restrictive covenants that could negatively affect SunLink’s ability to operate its business in the desired manner, and raising additional equity likely would be dilutive to shareholders. The failure to obtain funds necessary for the realization of SunLink’s operating strategy could impair SunLink’s existing operations and could force SunLink to forego opportunities that may arise in the future. This could, in turn, have a negative impact on the competitive position of our operating subsidiaries.
Indebtedness of one or more of our subsidiaries which we have guaranteed could be subject to prepayment which could require a substantial amount of our cash and any such repayment could restrict our current and future operations, which could adversely affect our ability to respond to manage our operations and liquidity.
The RDA loans at two of our subsidiaries contain various terms and conditions, including financial restrictions and limitations, and affirmative and negative covenants. Currently, Trace is not in compliance with the debt service coverage, fixed charge ratio and funded debt to EBITDA ratios under its RDA loan. The loan is guaranteed by SunLink and SunLink and Trace continue to discuss a modification or waiver of this non-compliance with the lender. In the event the lender were to declare an event of default and accelerate the maturity of the indebtedness, either Trace or SunLink under its guarantee could be required to repay such loan in advance of its maturity which could require a substantial amount of our cash and any such repayment could restrict our current and future operations, which could adversely affect our ability to respond to manage our operations and liquidity.
Healthcare reform has initiated significant changes to the United States healthcare system some of which may adversely affect our business.
Various healthcare reform provisions became law upon enactment of the ACA. The reforms contained in the ACA have impacted each of our businesses in some manner. Several of the reforms are very significant and could ultimately change the nature of our services, the methods of payment for our services, and the underlying regulatory environment. The reforms include the possible modifications to the conditions of qualification for payment, bundling payments to cover both acute and post-acute care, and the imposition of enrollment limitations on new providers. The ACA also provides for: (1) reductions to the annual market basket payment updates for additional annual “productivity adjustment” reductions to the annual market basket payment update as determined by CMS for nursing centers (beginning in federal fiscal year 2012); (2) new transparency, reporting, and certification requirements for nursing centers, including disclosures regarding organizational structure, officers, directors, trustees, managing employees, and financial, clinical, and other related data; (3) a quality reporting system for hospitals beginning in federal fiscal year 2014; and (4) reductions in Medicare payments to hospitals beginning in federal fiscal year 2014 for failure to meet certain quality reporting standards or to comply with standards in new value-based purchasing demonstration project programs.
31
In addition, a primary goal of healthcare reform is to reduce costs, which includes reductions in the reimbursement paid to us and other healthcare providers. Moreover, healthcare reform could negatively impact insurance companies, other third-party payors, our customers, as well as other healthcare providers, which may in turn negatively impact our business. As such, healthcare reforms and changes resulting from the ACA, as well as other similar healthcare reforms, could have a material adverse effect on our business, financial position, results of operations, and liquidity.
SunLink conducts business in a heavily regulated industry; changes in regulations or violations of regulations may result in increased costs or sanctions that could reduce revenue and profitability.
The healthcare industry is subject to extensive federal, state and local laws and regulations relating to:
| • | licensure; |
| • | conduct of operations including patient referrals, physician recruiting practices, cost reporting and billing practices; |
| • | ownership, condition and operation of facilities; |
| • | addition of facilities and services; |
| • | confidentiality, maintenance, and security issues associated with medical records; |
| • | billing for services; and |
| • | prices for services. |
These laws and regulations are extremely complex and, in many instances, the industry does not have the benefit of significant regulatory or judicial interpretation of these laws and regulations, including in particular, Medicare and Medicaid anti-fraud and abuse amendments, codified in Section 1128B(b) of the Social Security Act and known as the “anti-kickback statute.” This law prohibits providers and others from soliciting, receiving, offering or paying, directly or indirectly, any remuneration with the intent to generate referrals of orders for services or items reimbursable under Medicare, Medicaid, and other federal healthcare programs.
HHS regulations describe some of the conduct and business relationships immune from prosecution under the anti-kickback statute. The fact that a given business arrangement does not fall within one of these “safe harbor” provisions does not render the arrangement illegal. However, business arrangements of healthcare service providers that fail to satisfy the applicable safe harbor criteria risk increased scrutiny by enforcement authorities.
We have a variety of financial relationships with physicians who refer patients to our subsidiaries’ hospitals. We have contracts with physicians providing services under a variety of financial arrangements such as employment contracts and professional service agreements. We also provide financial incentives, including loans and minimum revenue guarantees, to recruit physicians into the communities served by our subsidiaries’ hospitals.
HIPAA broadened the scope of the fraud and abuse laws to include all healthcare services, whether or not they are reimbursed under a federal program. In addition, provisions of the Social Security Act, known as the Stark Act, also prohibit physicians from referring Medicare and Medicaid patients to providers of a broad range of designated health services in which the physicians or their immediate family members have an ownership interest or certain other financial arrangements.
In addition, SunLink’s facilities will continue to remain subject to any state laws that are more restrictive than the regulations issued under HIPAA, which vary by state and could impose additional penalties. In recent years, both federal and state government agencies have announced plans for or implemented heightened and coordinated civil and criminal enforcement efforts.
32
Government officials charged with responsibility for enforcing healthcare laws could assert that SunLink or any of the transactions in which the Company or its subsidiaries or their predecessors is or was involved, are in violation of these laws. It is also possible that these laws ultimately could be interpreted by the courts in a manner that is different from the interpretations made by the Company or others. A determination that either SunLink or its subsidiaries or their predecessors is or was involved in a transaction that violated these laws, or the public announcement that SunLink or its subsidiaries or their predecessors is being investigated for possible violations of these laws, could have a material adverse effect on SunLink’s business, financial condition, results of operations or prospects and SunLink’s business reputation could suffer significantly.
The laws, rules, and regulations described above are complex and subject to interpretation. In the event of a determination that we are in violation of any of these laws, rules or regulations, or if further changes in the regulatory framework occur, our results of operations could be significantly harmed.
The industry trend towards value-based purchasing may negatively impact our revenues.
There is a trend in the healthcare industry toward “value-based” purchasing of healthcare services. These value-based purchasing programs include both public reporting of quality data and preventable adverse events tied to the quality and efficiency of care provided by facilities. Governmental programs including Medicare and Medicaid currently require healthcare facilities to report certain quality data to receive full reimbursement updates. In addition, Medicare does not reimburse for care related to certain preventable adverse events. Many large commercial payors currently require hospitals to report quality data, and several commercial payors do not reimburse hospitals for certain preventable adverse events.
The ACA contains a number of provisions intended to promote value-based purchasing. Effective July 1, 2011, the ACA prohibits the use of federal funds under the Medicaid program to reimburse providers for medical assistance provided to treat hospital acquired conditions (“HACs”). An HAC is a condition that is acquired by a patient while admitted as an inpatient at a hospital, such as a surgical site infection. Beginning in federal fiscal year 2015, hospitals that fall into the top 25% of national risk-adjusted HAC rates for all hospitals in the previous year will receive a 1% reduction in their total Medicare payments. Hospitals with excessive readmissions for conditions designated by HHS will receive reduced payments for all inpatient discharges, not just discharges relating to the conditions subject to the excessive readmission standard.
The ACA also requires HHS to implement a value-based purchasing program for inpatient hospital services. The Affordable Care Act requires HHS to reduce inpatient hospital payments for all discharges by a percentage beginning at 1% in federal fiscal year 2013 and increasing by 0.25% each fiscal year up to 2% in federal fiscal year 2017 and subsequent years. HHS will pool the amount collected from these reductions to fund payments to reward hospitals that meet or exceed certain quality performance standards established by HHS. HHS will determine the amount each of our subsidiaries’ hospital that meets or exceeds the quality performance standards will receive from the pool of dollars created by these payment reductions.
We expect value-based purchasing programs, including programs that condition reimbursement on patient outcome measures, to become more common and to involve a higher percentage of reimbursement amounts. We are unable at this time to predict how this trend will affect our results of operations, but it could negatively impact our financial condition or results of operations.
The lingering effects of the economic recession could adversely affect our cash flows, financial position, or results of operations.
The United States economy experienced a major economic recession beginning in 2008, the economy remains relatively weak and there is a risk that the economy could lapse back into recession. Much healthcare spending is discretionary and can be significantly impacted by economic downturns. When patients are experiencing personal financial difficulties or have concerns about general economic conditions, they may
33
choose to defer or forego elective surgeries and other non-emergent procedures, which are generally more profitable lines of business for hospitals. In addition, employers may impose or patients may select a high-deductible insurance plan or no insurance at all, which increases a hospital’s dependence on self-pay revenue. Moreover, a greater number of uninsured patients may seek care in our emergency rooms.
We are unable to quantify the specific impact of recent or continued adverse economic conditions on our business; however we believe that the lingering effects of the economic recession have had an adverse impact on our operations. Such impact can be expected to continue to affect not only the healthcare decisions of our patients and potential patients but could also have an adverse impact on the solvency of certain managed care providers and other counterparties to transactions with us.
Our subsidiaries are subject to potential claims for professional liability, including claims based on the acts or omissions of third parties, which claims may not be covered by insurance.
Our subsidiaries are subject to potential claims for professional liability (medical malpractice) in connection with current operations, as well as potentially acquired or discontinued operations. To cover such claims, professional malpractice liability insurance and general liability insurance is maintained in amounts believed to be sufficient for operations, although some claims may exceed the scope or amount of the coverage in effect. The assertion of a significant number of claims, either within a self-insured retention (deductible) or individually or in the aggregate in excess of available insurance, could have a material adverse effect on our results of operations or financial condition. Premiums for professional liability insurance have historically been volatile and we cannot assure you that professional liability insurance will continue to be available on terms acceptable to us, if at all. The operations of hospitals also depend on the professional services of physicians and other trained healthcare providers and technicians in the conduct of their respective operations, including independent laboratories and physicians rendering diagnostic and medical services. There can be no assurance that any legal action stemming from the act or omission of a third party provider of healthcare services, would not be brought against one of our subsidiaries’ hospitals or SunLink, resulting in significant legal expenses in order to defend against such legal action or to obtain a financial contribution from the third-party whose acts or omissions occasioned the legal action.
SunLink depends heavily on its management personnel and the loss of the services of one or more of SunLink’s key senior management personnel could weaken SunLink’s management team.
SunLink has been, and will continue to be, dependent upon the services and management experience of its executive officers. If any of SunLink’s executive officers were to resign their positions or otherwise be unable to serve, SunLink’s management could be weakened.
SunLink is and in the future could be subject to claims related to discontinued operations, including discontinued healthcare operations.
SunLink has discontinued operations carried on by its former life sciences and engineering segment and certain of our healthcare operations which have been sold or closed. SunLink currently does not purchase insurance policies to reduce discontinued operations exposures and does not anticipate it will purchase such insurance in the future. Based upon an evaluation of information currently available and consultation with legal counsel, management has not reserved any amounts for contingencies related to the discontinued operations.
34
Risks Related to Our Healthcare Facility Operations
SunLink depends heavily on its subsidiaries’ healthcare facility management personnel and the loss of the services of one or more of SunLink’s key local management personnel could weaken SunLink’s management team and its ability to deliver healthcare services.
The success of our healthcare subsidiaries depends on their ability to attract and retain managers and related health care employees and on the ability of hospital-based officers and key employees to manage growth successfully. SunLink’s subsidiaries have not had any material difficulties in attracting healthcare facility management; however, if a hospital is unable to attract and retain affective local management, the operating performance of that facility could decline.
SunLink’s success depends on the ability of our operating subsidiaries to attract and retain qualified healthcare professionals. A shortage of qualified healthcare professionals in certain markets could weaken the ability of our subsidiaries to deliver healthcare services.
In addition to the management personnel which each subsidiary employs, our healthcare operations are dependent on the efforts, ability, and experience of other healthcare professionals, such as physicians, nurses, therapists, pharmacists and lab technicians. Nurses, pharmacists, lab technicians and other healthcare professionals are generally employees of an individual subsidiaries’ hospital. Each subsidiary’s success has been, and will continue to be, influenced by its ability to attract and retain these skilled employees. A shortage of healthcare professionals in certain markets, the loss of some or all of its key employees or the inability to attract or retain sufficient numbers of qualified healthcare professionals could cause the operating performance of one or more of our subsidiaries to decline.
A significant portion of SunLink’s revenue is dependent on Medicare and Medicaid payments to its subsidiaries and possible reductions in Medicare or Medicaid payments or the implementation of other measures to reduce reimbursements may reduce our revenues.
A significant portion of SunLink’s consolidated revenues are derived from the Medicare and Medicaid programs, which are highly regulated and subject to frequent and substantial changes. Approximately 95% of consolidated patient days and 75% of consolidated net patient revenues were derived from the Medicare and Medicaid programs for the year ended June 30, 2016. Previous legislative changes have resulted in, and future legislative changes may result in, limitations on and reduced levels of payment and reimbursement for a substantial portion of hospital procedures and costs. Georgia and Mississippi have not expanded Medicaid or set-up exchanges.
Future healthcare legislation or other changes in the administration or interpretation of governmental healthcare programs may have a material adverse effect on our consolidated business, financial condition, results of operations or prospects.
Revenue and profitability of our subsidiaries’ healthcare facility operations may be constrained by future cost containment initiatives undertaken by purchasers of healthcare services.
Our subsidiaries’ have been affected by the increasing number of initiatives undertaken during the past several years by all major purchasers of healthcare, including (in addition to federal and state governments) insurance companies and employers, to revise payment methodologies and monitor healthcare expenditures in order to contain healthcare costs. Our community hospital operations derived approximately 25% of their consolidated net patient revenues for the fiscal year ended June 30, 2016 from private payors and other non-governmental sources who contributed approximately 5% of consolidated patient days. Initiatives such as managed care organizations offering prepaid and discounted medical services packages have adversely affected hospital revenue growth throughout the country and such packages represent an increasing portion of our
35
subsidiary’s hospital’s admissions and outpatient revenues and have resulted in reduced revenue growth at our current and former subsidiaries’ hospitals. In addition, private payers increasingly are attempting to control healthcare costs through direct contracting with hospitals to provide services on a discounted basis, increased utilization review and greater enrollment in managed care programs such as health maintenance organizations and preferred provider organizations, referred to as PPOs. If our subsidiaries, specifically our hospital subsidiary operations, are unable to contain costs through increased operational efficiencies and the trend toward declining reimbursements and payments continues, the results of healthcare facility segment operations and cash flow will be adversely affected and the results of our consolidated operations and our consolidated cash flow similarly likely would be adversely affected.
Our healthcare subsidiaries face intense competition from other hospitals and nursing centers which directly affect such segment and consolidated revenues and profitability.
Although Trace Hospital operates in a community where it is currently the only general, acute care hospital, it faces substantial competition from other hospitals, including larger tertiary care centers. Although these competing hospitals may be as far as 30 to 50 miles away, patients in these markets may migrate to these competing facilities as a result of local physician referrals, managed care plan incentives or personal choice.
Our nursing centers also compete on a local and regional basis with other facilities providing similar services, including hospitals, extended care centers, assisted living facilities, home health agencies, and similar institutions. Some competitors may operate newer facilities and may provide services, including skilled nursing services that we do not offer at all of our nursing centers. Our competitors include government-owned, religious organization-owned, secular nonprofit and for-profit institutions. Many of these competitors have greater financial and other resources than we do. Although there is limited, if any, price competition with respect to Medicare and Medicaid residents (since revenues received for services provided to these residents are generally based on pre-established rates), there is substantial price competition for private payment residents. Historically our nursing centers have been located adjacent to acute care hospitals owned and operated by one of our subsidiaries. Currently, however, one of our two nursing homes operate in environment where we no longer own an adjacent hospital and the former hospital has ceased operations which could subject such centers to greater competition from nursing centers located closer to hospital facilities.
The healthcare business is highly competitive and competition among hospitals, nursing homes and other healthcare providers for patients has intensified in recent years. Some of these competing facilities offer services which are not offered by SunLink’s subsidiaries’ facilities. Some of the competing facilities are owned or operated by tax-supported governmental bodies or by private not-for-profit entities supported by endowments and charitable contributions which can finance capital expenditures on a tax-exempt basis and are exempt from sales, property, and income taxes. SunLink’s subsidiaries also face competition from other for-profit healthcare companies, some of which have substantially greater resources, as well as other providers such as outpatient surgery and diagnostic centers and home health agencies.
The intense competition from other healthcare providers directly affects the market share of our subsidiaries’ facilities, as well as their and our revenues and profitability.
Changes in market demographics may increase competition for certain of our healthcare subsidiaries.
Some of our subsidiaries’ facilities are located in exurban areas which are becoming more suburban or metropolitan. Such markets are likely to attract additional competitors. We cannot assure you that we will have the financial resources to fund capital improvements to our subsidiaries’ existing facilities, which may face additional competition or that even if financial resources are available to us, projected operating results will justify such expenditures. An inability to fund or the infeasibility of funding capital improvements could directly or indirectly have an adverse impact on our revenues through lower patient utilization, increased difficulty in physician recruitment and otherwise as a result of increased competition.
36
SunLink’s subsidiaries’ healthcare facilities may be subject to, and depend on, certificate of need laws which could affect their ability to operate profitably.
All states in which SunLink subsidiaries currently operate have laws requiring approval for the purchase, construction or expansion of various healthcare facilities including hospitals, nursing homes and ambulatory surgery centers and the provision of various services. Under such certificate of need (“CON”) laws, prior state approval is required for the acquisition of major medical equipment or the purchase, lease, construction, expansion, sale or closure of covered healthcare facilities, based on a determination of need for additional or expanded facilities or services. The failure to obtain any required CON may impair SunLink’s subsidiaries’ ability to operate profitably.
In addition, the elimination or modification of CON laws in states in which SunLink subsidiaries operate or in the future may operate covered healthcare facilities could subject such facilities to greater competition making it more difficult to operate profitably.
If our healthcare subsidiaries fail to effectively and timely implement electronic health record systems, our consolidated operations could be adversely affected.
As required by ARRA, HHS has adopted an incentive payment program for eligible hospitals and healthcare professionals that implement certified EHR technology and use it consistently with “meaningful use” requirements. If our subsidiary hospital and employed or contracted professionals do not meet the Medicare or Medicaid EHR incentive program requirements, the hospital and clinics will not receive Medicare or Medicaid incentive payments to offset some of the costs of implementing the EHR systems. Further, beginning in federal fiscal year 2015, eligible hospitals and physicians that fail to demonstrate meaningful use of certified EHR technology are subject to reduced payments from Medicare. Failure to implement EHR systems effectively and in a timely manner could have a material, adverse effect on our consolidated financial position and results of operations.
The success of SunLink’s hospital subsidiary depends upon that subsidiary’s hospital’s ability to maintain good relationships with the physicians and, if the hospital is unable to successfully maintain good relationships with physicians, admissions and outpatient revenues may decrease and operating performance could decline.
Because physicians generally direct the majority of hospital admissions and outpatient services, a hospital’s success is, in part, dependent upon the number and quality of physicians on the medical staffs, the admissions and referrals practices of the physicians at our subsidiaries’ hospitals, and the ability to maintain good relations with physicians. Many physicians are not employees of the hospitals at which they practice and, in many of the markets, most physicians have admitting privileges at other hospitals. If one or more of the hospitals operated by our subsidiaries is unable to successfully maintain good relationships with physicians, admissions may decrease and operating performance could decline.
Changes in the laws and regulations regarding payments for hospice services and “room and board” provided to hospice patients residing in skilled nursing facilities could reduce our net patient service revenue and profitability.
For hospice patients receiving nursing center care under certain state Medicaid programs who elect hospice care under Medicare or Medicaid, the state must pay, in addition to the applicable Medicare or Medicaid hospice per diem rate, an amount equal to at least 95% of the Medicaid per diem skilled nursing facility rate for “room and board” furnished to the patient by the skilled nursing facility. The reduction or elimination of Medicare payments for hospice patients residing in skilled nursing facilities could adversely affected the revenues of our skilled nursing facility.
37
Risks Relating to our Specialty Pharmacy Business
The operations of our Specialty Pharmacy Segment may be adversely affected by changes in government reimbursement regulations and payment levels.
For the year ended June 30, 2016, the operation by Scripts of our Specialty Pharmacy Segment derived approximately 26% of its net revenues from government payors, principally Medicare and Medicaid. The Deficit Reduction Act of 2005 exempted rural providers of home care related services from the competitive acquisition program to which urban providers are subject.
We cannot assure you that the ASP reimbursement methodology will not be extended to the provision of all specialty pharmaceuticals or to the specialty pharmaceuticals most often sold by the Scripts or that Scripts will continue to be able to operate our Specialty Pharmacy Segment profitably at either existing or at lower reimbursement rates. Likewise, we cannot assure you that the Part B CAP program will not be extended to rural or exurban areas in general or to the areas in which Scripts operates, or may seek to operate, in particular or that Scripts would be able to meet the qualifications to become a Part B CAP vendor either now or at any time in the future.
The operations of our Specialty Pharmacy Segment could be harmed by further changes in government purchasing methodologies and reimbursement rates for Medicare or Medicaid.
In addition to the impact of MMA, in order to deal with budget shortfalls, some states are attempting to create state administered prescription drug discount plans, to limit the number of prescriptions per person that are covered, and to raise Medicaid co-pays and deductibles, and are proposing more restrictive formularies and reductions in pharmacy reimbursement rates. Any reductions in amounts reimbursable by other government programs for pharmacy services or changes in regulations governing such reimbursements could materially and adversely affect our pharmacy business, financial condition and results of operations.
The durable medical equipment service line of Scripts may be adversely affected by further changes in government reimbursement regulations and payment levels, especially if the durable medical equipment service line becomes subject to additional competitive bidding procedures.
Scripts is currently subject to the expanded provisions of the Medicare competitive acquisition program. The current provisions could be expanded or changed in the future. Any additional changes in government reimbursement or payment amounts could have an adverse effect on our consolidated results of operations.
The operations of our Specialty Pharmacy Segment depend on a continuous supply of key products. Any shortages of key products could adversely affect the business of Scripts.
Many of the products distributed by the operations of our Specialty Pharmacy Segment are manufactured with ingredients that are susceptible to supply shortages. In addition, the manufacturers of these products may not have adequate manufacturing capability to meet rising demand. If any products distributed by Scripts are in short supply for long periods of time, this could result in a material adverse effect on our business and results of operations.
The operations of our Specialty Pharmacy Segment are highly dependent on relationships with key suppliers and the loss of any of such key suppliers could adversely affect the business of Scripts.
Any termination of, or adverse change in, our relationships with our key suppliers, or the loss of supply of one of our key products for any other reason, could have a material adverse effect on the business of Scripts and our consolidated results of operations. The largest supplier for Scripts accounted for approximately 76% of the segment’s cost of goods sold in the fiscal year ended June 30, 2016. In addition, Scripts has few long-term contracts with its suppliers. Arrangements with most of its suppliers may be canceled by either party, without cause and on minimal notice; and many of these arrangements are not governed by written agreements.
38
The loss of one or more of larger institutional pharmacy customers could hurt our business by reducing the revenues and profitability of the operations of our Specialty Pharmacy Segment.
As is customary in the institutional pharmacy industry, our Specialty Pharmacy Segment generally does not have long-term contracts with its institutional pharmacy customers. Significant declines in the level of purchases by one or more of the larger institutional pharmacy customers could have a material adverse effect on the business of Scripts and our consolidated results of operations.
The failure of Scripts to maintain eligibility as a Medicare and Medicaid supplier could materially adversely affect its competitive position. Likewise, its failure to maintain and expand relationships with private payors, who can effectively determine the pharmacy source for their members, could materially adversely affect its competitive position.
Changes in average wholesale prices could reduce our pricing and margins.
Many government payors, including Medicare and Medicaid, have paid, or continue to pay, the operations of our Specialty Pharmacy Segment directly or indirectly at a rate based upon a drug’s AWP less a percentage factor. Scripts also has contracted with some private payors to sell drugs at AWP or at AWP less a percentage factor. For most drugs, AWP is compiled and published by several private companies, including First DataBank, Inc. Several states have filed lawsuits against pharmaceutical manufacturers for allegedly inflating reported AWP for prescription drugs. In addition, class action lawsuits have been brought by consumers against pharmaceutical manufacturers alleging overstatement of AWP. We are not responsible for such calculations, reports or payments; however, there can be no assurance that the ability of our Specialty Pharmacy Segment to negotiate discounts from drug manufacturers will not be materially adversely affected by such investigations or lawsuits.
The federal government also has entered into settlement agreements with several drug manufacturers relating to the calculation and reporting of AWP pursuant to which the drug manufacturers, among other things, have agreed to report new pricing information, the “average sales price”, to government healthcare programs. The average sales price is calculated differently than AWP.
Scripts faces numerous competitors and potential competitors in the market in which our Specialty Pharmacy Segment operates, many of whom are significantly larger and who have significantly greater financial resources.
Large national companies operate in the existing market in which our Specialty Pharmacy Segment operates. We cannot assure you that one or more of such companies or other healthcare companies will not seek to compete or intensify their level of competition in the areas in which we conduct or may seek to conduct one or more of the components of the operations of our Specialty Pharmacy Segment.
The operations of our Specialty Pharmacy Segment may be adversely affected by industry trends in managed care contracting and consolidation.
A growing number of health plans are contracting with a single provider of specialty pharmacy services. Likewise, manufacturers may not be eager to contract with regional providers of specialty pharmacy services. If Scripts is unable to obtain managed care contracts in the areas in which we provide specialty pharmacy services or are unable to obtain specialty pharmacy products at reasonable costs or at all, the business operations of our Specialty Pharmacy Segment could be adversely affected.
The specialty pharmacy market may grow slower than expected, which could adversely affect our revenues.
We cannot predict the rate of actual future growth in product availability and spending, the extent to which patient demand or spending for specialty drug services in rural or exurban areas will match national averages or whether government payors will provide reimbursement for new products under Medicare or Medicaid on a timely basis, at what rates or at all. Adverse developments in any of these areas could have an adverse impact on the business operations of our Specialty Pharmacy Segment.
39
The profitability of our Specialty Pharmacy Segment can be adversely affected by a decrease in the introduction of new brand name and generic prescription drugs.
Sales and profit margins of Scripts are materially affected by the introduction of new brand name and generic drugs. New brand name drugs can result in increased drug utilization and associated sales revenues, while the introduction of lower priced generic alternatives typically result in relatively lower sales revenues, but higher gross profit margins. Accordingly, a decrease in the number of significant new brand name drugs or generics successfully introduced could adversely affect our business and results of operations.
Other Risks
Future developments could affect our ability to maintain adequate liquidity. Additionally, our ability to access alternative sources of capital is limited.
Historically our available capital has been sufficient to meet our operating expenses, lease obligations, debt service requirements, and capital expenditures and we have managed our liquidity such that our aggregate unrestricted cash at June 30, 2016, was $3,261. Future circumstances could require us to materially increase our revenues, materially reduce our expenses, or otherwise materially improve operating results, dispose of existing assets or obtain material new sources of capital in order to maintain adequate liquidity.
The Company is currently limited in its ability to raise capital, debt or equity, in the public or private markets on what it considers acceptable terms. Two of the Company’s subsidiaries have been able to borrow money through facility based mortgages, each of which is guaranteed by the Company, utilizing USDA Rural Development Authority guaranties, (individually, an “RDA Loan” and collectively, the “RDA Loans”). The Company and its subsidiaries currently must fund working capital needs from cash from operations or from the sale of additional assets, and we cannot assure you that we would be successful in improving our results of operations, reducing our costs, obtaining additional credit facilities or selling additional assets.
If we were to go private, holders of our securities would be subject to the risks of an investment in a private rather than a public company.
From time to time the Company has considered the advisability of deregistering it common shares under the Exchange Act. In the event the Company were able to deregister its common shares under the Exchange Act, holders of our securities would be subject to the risks of an investment in a private rather than a public company. Upon any such deregistration of our shares, our duty to file periodic reports with the SEC would be suspended for as long as we had fewer than 300 record shareholders, and we would no longer be a public reporting company. In addition, we would be relieved of the obligation to comply with the requirements of the proxy rules under Section 14 of the Exchange Act. When and if the Company were to deregister, SunLink shares would no longer be listed on the NYSE Amex Equities stock exchange, and there might not be a sufficient number of shares outstanding and publicly traded following any deregistration to ensure a continued trading market in the shares in any over-the-counter market. The continued quotation of our common shares as well as the availability of any over-the-counter trading in our common shares would depend, in part, on the nature and extent of continued publicly available information about SunLink. Shareholders also could be adversely affected by a reduction in our “public float,” that is, the number of shares owned by outside shareholders and available for trading in the securities markets, especially if the Company makes future tender offers or private or open market purchases of its common shares. The suspension of our reporting obligations under the Exchange Act might further reduce the existing limited trading market for the Company’s shares and may result in a decline in the price of the Company’s shares and reduced liquidity in any trading market for our shares in the future. We might also have less access to capital markets and not be able to use the Company’s shares to effect acquisitions as a non-reporting company. Although the Company is not currently pursuing an effort to deregister our common shares under the Exchange Act, there is no assurance that our Board may not again determine to pursue going private in the future.
40
Forward-looking statements in this annual report may prove inaccurate.
This document contains forward-looking statements about SunLink that are not historical facts but, rather, are statements about future expectations. Forward-looking statements in this document are based on management’s current views and assumptions and may be influenced by factors that could cause actual results, performance or events to be materially different from those projected. These forward-looking statements are subject to numerous risks and uncertainties. Important factors, some of which are beyond the control of SunLink, could cause actual results, performance or events to differ materially from those in the forward-looking statements. These factors include those described above under “Risk Factors” and elsewhere in this report under “Forward-Looking Statements.”
| Item 1B. | Unresolved Staff Comments |
None.
41
| Item 2. | Properties |
Our principal properties as of the date of filing of this report are listed below:
| Name or function (licensed beds) |
Location City and State |
Square Footage |
Date of Acquisition/ Lease Inception |
Ownership Type |
||||||||||||
| Healthcare Facilities |
||||||||||||||||
| Trace Regional Hospital (84) |
Houston, MS | 111,050 | February 1, 2001 | Owned | ||||||||||||
| Floy Dyer Nursing Home (66) |
Houston, MS | 70,429 | February 1, 2001 | Owned | ||||||||||||
| Gilmer Nursing Home (100) |
Ellijay, GA | 32,000 | February 1, 2001 | Owned | ||||||||||||
| Ellijay, GA Hospital (closed) |
Ellijay, GA | 38,500 | February 1, 2001 | Owned | ||||||||||||
| Medical Office of North Georgia & Community Center of North Georgia |
Ellijay, GA | 47,500 | (1) | October 31, 2013 | Owned | |||||||||||
| Dahlonega Medical Office Building |
Dahlonega, GA | 10,000 | (1) | February 1, 2001 | Owned | |||||||||||
| Specialty Pharmacy Operations |
||||||||||||||||
| Carmichael Cashway Pharmacy, Inc. |
Crowley, LA | 22,500 | (2) | April 22, 2008 | Leased | |||||||||||
| Carmichael Cashway Pharmacy, Inc. |
Lafayette, LA | 5,900 | (3) | April 22, 2008 | Leased | |||||||||||
| Specialty Pharmacy Operations |
||||||||||||||||
| Carmichael Cashway Pharmacy, Inc. |
Crowley, LA | 22,500 | (2) | April 22, 2008 | Leased | |||||||||||
| Carmichael Cashway Pharmacy, Inc. |
Lafayette, LA | 5,900 | (3) | April 22, 2008 | Leased | |||||||||||
| Carmichael Cashway Pharmacy, Inc. |
Lake Charles, LA | 7,800 | (4) | April 22, 2008 | Leased | |||||||||||
| Other |
||||||||||||||||
| Careside Medical Park |
Clanton, AL | 62,013 | (5) | February 1, 2001 | Owned | |||||||||||
| Fulton, MO land |
Fulton, MO | 11.4 acres | November 2003 | Owned | ||||||||||||
| Corporate Offices |
Atlanta, GA | 4,800 | (6) | June 1, 1998 | Leased | |||||||||||
| (1) | This property is leased to outside healthcare operator. |
| (2) | Lease of approximately 18,800 square feet of store location, warehouse and office space. The lease expires in April 2018 and provides for a renewal of the lease for a five-year term. Additional lease, commencing in April 2013, of approximately 1,300 square feet of office space. This lease expired in April 2015 and continuing on a month-to-month lease continuation. Additional lease of approximately 2,400 square feet of warehouse space. This lease expires in March 2021 |
| (3) | This lease is for store location and warehouse space and expires in August 2021. |
| (4) | This lease is for store location and warehouse space and expires in December 2018. |
| (5) | The building is currently vacant except for an office which is rented by a nonaffiliated healthcare provider. |
| (6) | This lease is for office space for corporate staff. The lease expires in June 2020. |
| Item 3. | Legal Proceedings |
None.
| Item 4. | Not Applicable |
42
PART II
| Item 5. | Market for Registrant’s Common Equity and Related Stockholder Matters |
SunLink common shares are listed on the NYSE Amex Equities exchange. SunLink’s ticker symbol is “SSY”. The following table shows, for the calendar quarters indicated, based on published financial sources, the high and low sale prices of SunLink common shares as reported on the NYSE Amex Equities exchange.
| Sales Price of SunLink Common Shares |
||||||||
| High | Low | |||||||
| Fiscal 2016 (July 1, 2015—June 30, 2016) |
||||||||
| Fourth Quarter |
$ | 0.77 | $ | 0.45 | ||||
| Third Quarter |
0.98 | 0.36 | ||||||
| Second Quarter |
1.82 | 0.86 | ||||||
| First Quarter |
1.83 | 1.51 | ||||||
| Fiscal 2015 (July 1, 2014—June 30, 2015) |
||||||||
| Fourth Quarter |
$ | 1.70 | $ | 1.36 | ||||
| Third Quarter |
1.74 | 1.30 | ||||||
| Second Quarter |
1.84 | 1.25 | ||||||
| First Quarter |
1.62 | 1.13 | ||||||
American Stock Transfer & Trust Company is the Transfer Agent and Registrar for our common shares. For all shareholder inquiries, call American Stock Transfer & Trust’s Shareholder Services Department at 1-888-937-5449.
Tax Benefits Protection Rights Plan
On September 29, 2016, SunLink entered into a Tax Benefits Preservation Rights Plan (the “Tax Benefits Protection Rights Plan”). Effective September 29, 2016, the Board declared a dividend in the form of one preferred stock purchase right for each of the Company’s issued and outstanding common shares. The purpose of the Tax Benefits Protection Rights Plan is to diminish the risk that the Company’s ability to use its net operating losses and certain other tax assets to reduce potential future federal income tax obligations would become subject to limitations by reason of the Company experiencing an “ownership change,” as defined in Section 382 of the Code.
Dividends
SunLink does not currently pay cash dividends. SunLink has historically retained its earnings for use in the operation and improvement of its business and for other corporate purposes. While the Company currently does not anticipate declaring or paying regular cash dividends in the foreseeable future, the board of directors has discussed returning capital to shareholders as funds are available from asset sales or otherwise, any future determination to declare or pay cash dividends will be determined by SunLink’s board of directors and will depend on SunLink’s financial condition, results of operations, business, prospects, capital requirements, credit agreements and such other matters as the board of directors may consider relevant at this time.
Holders
As of June 30, 2016 there were approximately 408 registered holders of SunLink common shares.
43
Securities Authorized for Issuance under Equity Compensation Plans
The following provides tabular disclosure of the number of securities at June 30, 2016 to be issued upon the exercise of outstanding options, the weighted average exercise price of outstanding options and the number of securities remaining available for future issuance under equity compensation plans, reported by two categories- plans that have been approved by shareholders and plans that have not been so approved:
| (a) | (b) | (c) | ||||||||||
| Plan Category |
Number of securities to be issued upon exercise of outstanding options |
Weighted average exercise price of outstanding options |
Number of securities remaining available for future issuance under equity compensation plans (excluding securities reflected in column (a)) |
|||||||||
| Equity compensation plans approved by security holders: |
||||||||||||
| 2005 Equity Incentive Plan |
407,642 | $ | 2.46 | 0 | ||||||||
| 2011 Director Stock Option Plan |
228,000 | 1.37 | 72,000 | |||||||||
|
|
|
|
|
|
|
|||||||
| 635,642 | $ | 2.07 | 72,000 | |||||||||
|
|
|
|
|
|
|
|||||||
| Equity compensation plans not approved by security holders: |
||||||||||||
| None |
0 | 0.00 | 0 | |||||||||
|
|
|
|
|
|
|
|||||||
| Total |
635,642 | $ | 2.07 | 72,000 | ||||||||
|
|
|
|
|
|
|
|||||||
44
Performance Graph
The following graph presents a comparison of five years cumulative total return for SunLink, the NYSE Amex Equities exchange Composite Index and a self constructed peer group. The peer group consists of Amsurg Corp., Community Health Systems Inc., Dynacq Healthcare Inc., Lifepoint Hospitals Inc., Magellan Health Services Inc., Tenet Healthcare Corp., and Universal Health Services Inc. There is no assurance the Hospital Index peer group or NYSE Amex Equities Composite is comparable to SunLink, because, among other reasons, both consist of larger companies than SunLink.
COMPARISON OF 5 YEAR CUMULATIVE TOTAL RETURN*
Among SunLink Health Systems, Inc., the NYSE MKT Composite Index,
and Hospitals Index
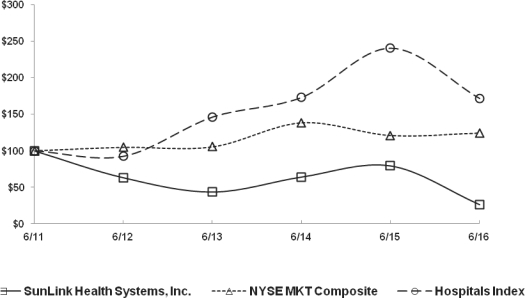
| * | $100 invested on 6/30/11 in stock or index, including reinvestment of dividends. Fiscal year ending June 30. |
| 6/11 | 6/12 | 6/13 | 6/14 | 6/15 | 6/16 | |||||||||||||||||||
| SunLink Health Systems, Inc. |
100.00 | 63.16 | 43.68 | 64.21 | 79.47 | 26.31 | ||||||||||||||||||
| NYSE MKT Composite |
100.00 | 104.79 | 105.46 | 138.56 | 121.07 | 124.53 | ||||||||||||||||||
| Hospitals Index |
100.00 | 92.58 | 146.13 | 172.94 | 240.26 | 171.53 | ||||||||||||||||||
45
| Item 6. | Selected Financial Data |
Selected historical financial data presented below as of and for the fiscal years ended June 30, 2016, 2015, 2014, 2013 and 2012. The following financial information reflects the disposition of Chestatee, Fulton, Dexter, Chilton operations (exclusive of the physical facility), Memorial and three home health agencies. This data should be read in conjunction with “Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations,” and the Consolidated Financial Statements of SunLink and the notes thereto included in Item 8 of this Annual Report.
SunLink Selected Historical Financial Data
(All amounts in thousands, except per share amounts)
| 2016 | 2015 | 2014 | 2013 | 2012 | ||||||||||||||||
| Net Revenues |
$ | 63,433 | $ | 73,746 | $ | 73,769 | $ | 75,174 | $ | 82,709 | ||||||||||
| Earnings (loss) from continuing operations |
(11,914 | ) | 487 | (484 | ) | (2,517 | ) | (2,378 | ) | |||||||||||
| Earnings (loss) from discontinued operations |
(2,169 | ) | (242 | ) | (61 | ) | 7,005 | 3,459 | ||||||||||||
| Net income (loss) |
(14,083 | ) | 245 | (545 | ) | 4,488 | 1,081 | |||||||||||||
| Earnings (loss) per share from continuing operations |
||||||||||||||||||||
| Basic |
(1.26 | ) | 0.05 | (0.05 | ) | (0.27 | ) | (0.25 | ) | |||||||||||
| Diluted |
(1.26 | ) | 0.05 | (0.05 | ) | (0.27 | ) | (0.25 | ) | |||||||||||
| Earnings (loss) per share from discontinued operations |
||||||||||||||||||||
| Basic |
(0.23 | ) | (0.02 | ) | (0.01 | ) | 0.75 | 0.37 | ||||||||||||
| Diluted |
(0.23 | ) | (0.02 | ) | (0.01 | ) | 0.75 | 0.37 | ||||||||||||
| Net earnings (loss) per share: |
||||||||||||||||||||
| Basic |
(1.49 | ) | 0.03 | (0.06 | ) | 0.48 | 0.12 | |||||||||||||
| Diluted |
(1.49 | ) | 0.03 | (0.06 | ) | 0.48 | 0.12 | |||||||||||||
| Total Assets |
44,841 | 57,128 | 63,847 | 68,003 | 79,172 | |||||||||||||||
| Long-term debt, including current maturities |
11,188 | 12,045 | 12,509 | 13,305 | 18,643 | |||||||||||||||
| Shareholders’ equity |
$ | 19,489 | $ | 33,560 | $ | 33,318 | $ | 33,743 | $ | 29,291 | ||||||||||
46
| Item 7. | Management’s Discussion and Analysis of Financial Condition and Results of Operations (all dollar amounts in thousands, except per share and revenue per equivalent admissions amounts) |
This Annual Report and the documents that are incorporated by reference in this Annual Report contain certain forward-looking statements within the meaning of the safe harbor for forward-looking statements contained in the Private Securities Litigation Reform Act of 1995. Forward-looking statements include all statements that do not relate solely to historical or current facts and may be identified by the use of words such as “may,” “believe,” “will,” “seeks to”, “expect,” “project,” “estimate,” “anticipate,” “plan” or “continue.” These forward-looking statements are based on the current plans and expectations and are subject to a number of risks, uncertainties and other factors which could significantly affect current plans and expectations and our future financial condition and results. For a listing and a discussion of such factors, which could cause actual results, performance and achievements to differ materially from those anticipated, see Certain Cautionary Statements—Forward Looking Information and Item 1A.
Critical Accounting Estimates
The preparation of financial statements in accordance with U.S. generally accepted accounting principles requires us to make estimates and assumptions that affect reported amounts and related disclosures. We consider an accounting estimate to be critical if:
| • | it requires assumptions to be made that were uncertain at the time the estimate was made; and |
| • | changes in the estimate or different estimates that could have been made could have a material impact on our consolidated statement of earnings or financial condition. |
The table of critical accounting estimates that follows is not intended to be a comprehensive list of all of our accounting policies that require estimates. We believe that of our significant accounting policies, as discussed in Note 2 of our Notes to Consolidated Financial Statements included in this Annual Report on Form 10-K for the fiscal year ended June 30, 2016, the estimates discussed below involve a higher degree of judgment and complexity. We believe the current assumptions and other considerations used to estimate amounts reflected in our consolidated financial statements are appropriate. However, if actual experience differs from the assumptions and other considerations used in estimating amounts reflected in our consolidated financial statements, the resulting changes could have a material adverse effect on our consolidated results of operations and financial condition.
47
The table that follows presents information about our critical accounting estimates, as well as the effects of hypothetical changes in the material assumptions used to develop each estimate:
| Balance Sheet or Income Statement Caption/Nature of Critical Estimate Item (dollar amounts in thousands, except per share) |
Assumption / Approach Used (dollar amounts in thousands, except per share) |
Sensitivity Analysis (dollar amounts in thousands, except per share) | ||
|
Receivables-net and Provision for Bad Debts |
||||
| Receivables-net for our Healthcare Facilities Segment primarily consists of amounts due from third-party payors and patients from providing healthcare services to healthcare facility patients. Receivables-net for our Specialty Pharmacy Segment primarily consists of amounts due from third-party payors; institutions such as nursing homes, home health, hospice, hospitals; pharmacy stores; Medicaid Part D program; and customers from the sale of pharmacy services and merchandise. Our ability to collect outstanding receivables is critical to our results of operations and cash flows. To provide for accounts receivable that could become uncollectible in the future, we establish an allowance for doubtful accounts to reduce the carrying value of such receivables to their estimated net realizable value. The primary uncertainty lies with accounts for which patients are responsible, which we refer to as patient responsibility accounts. These accounts include both amounts payable by uninsured patients and co-payments and deductibles payable by insured patients. Our allowance for doubtful accounts, included in our balance sheets as of June 30 was as follows:
2016—$991; and 2015—$2,770.
Our provision for bad debts, included in our results of continuing operations for the years ended June 30, was as follows:
2016—$2,068 2015—$4,041; and 2014—$4,050 |
The largest component of bad debts in our patient accounts receivable for our healthcare facilities and Specialty Pharmacy Segments relates to accounts for which patients are responsible, which we refer to as patient responsibility accounts. These accounts include both amounts payable by uninsured patients and co-payments and deductibles payable by insured patients. In general, we attempt to collect deductibles, co-payments and self-pay accounts prior to the time of service for non-emergency care. If we do not collect these patient responsibility accounts prior to the delivery of care, the accounts are handled through our billing and collections processes.
We attempt to verify each patient’s insurance coverage as early as possible before a scheduled non-emergency admission or procedure, including with respect to eligibility, benefits and authorization/pre-certification requirements, in order to notify patients of the estimated amounts for which they will be responsible. We attempt to verify insurance coverage within a reasonable amount of time for all emergency room visits and non-emergency urgent admissions in compliance with the Emergency Medical Treatment and Active Labor Act. |
A significant increase in our provision for doubtful accounts (as a percentage of revenues) would lower our earnings. This would adversely affect our results of operations, financial condition, liquidity and potentially our future access to capital.
If net revenues during fiscal year 2016 were changed by 1%, our 2016 after-tax income from continuing operations would change by approximately $634 or diluted earnings per share of $0.07.
This is only one example of reasonably possible sensitivity scenarios. The process of determining the allowance requires us to estimate uncollectible patient accounts that are highly uncertain and requires a high degree of judgment. It is impacted by, among other things, changes in regional economic conditions, business office operations, payor mix and trends in private and federal or state governmental healthcare coverage. | ||
48
| Balance Sheet or Income Statement Caption/Nature of Critical Estimate Item (dollar amounts in thousands, except per share) |
Assumption / Approach Used (dollar amounts in thousands, except per share) |
Sensitivity Analysis (dollar amounts in thousands, except per share) | ||
| In general, we utilize the following steps in collecting accounts receivable: if possible, cash collection of all or a portion of deductibles, co-payments and self-pay accounts prior to or at the time service is provided; billing and follow-up with third party payors; collection calls; utilization of collection agencies; sue to collect if the patient has the means to pay and chooses not to pay; and if collection efforts are unsuccessful, write off the accounts. | ||||
| Our policy is to write off accounts after all collection efforts have failed, which is typically no longer than 120 days after the date of discharge of the patient or service to the patient or customer. Patient responsibility accounts represent the majority of our write-offs. All of our subsidiaries’ hospitals retain third-party collection agencies for billing and collection of delinquent accounts. At most of our subsidiaries’ hospitals, more than one collection agency is used to promote competition and improved performance. The selection of collection agencies and the timing of the referral of an account to a collection agency vary among hospitals. Generally, we do not write off accounts prior to utilizing the services of a collection agency. Once collection efforts have proven unsuccessful, an account is written off from our patient accounting system against the allowance for doubtful accounts. | ||||
49
| Balance Sheet or Income Statement Caption/Nature of Critical Estimate Item (dollar amounts in thousands, except per share) |
Assumption / Approach Used (dollar amounts in thousands, except per share) |
Sensitivity Analysis (dollar amounts in thousands, except per share) | ||
| We determine the adequacy of the allowance for doubtful accounts utilizing a number of analytical tools and benchmarks. No single statistic or measurement alone determines the adequacy of the allowance.
We monitor our revenue trends by payor classification on a quarter-by-quarter basis along with the composition of our accounts receivable agings. This review is focused primarily on trends in self-pay revenues, accounts receivable, co-payment receivables and historic payment patterns.
In addition, we analyze other factors such as day’s revenue in accounts receivable and we review admissions and charges by physicians, primarily focusing on recently recruited physicians. |
50
HEALTHCARE FACILITIES SEGMENT NET ACCOUNTS RECEIVABLE
JUNE 30, 2016
| Days Outstanding1 | ||||||||||||||||||||||||||||||||
| Payor Class |
0 - 30 | 31 - 60 | 61 - 90 | 91 - 120 | 121 - 150 | 151 - 180 | >180 | Total | ||||||||||||||||||||||||
| Medicare |
$ | 783 | $ | 67 | $ | 43 | $ | 14 | $ | 17 | $ | 10 | $ | 98 | $ | 1,032 | ||||||||||||||||
| Medicaid |
389 | 16 | 12 | 8 | 1 | 4 | 13 | 443 | ||||||||||||||||||||||||
| Commercial |
264 | 61 | 28 | 10 | 14 | 11 | 68 | 456 | ||||||||||||||||||||||||
| Self Pay |
14 | 10 | 8 | 6 | 21 | 7 | 41 | 107 | ||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
| $ | 1,450 | $ | 154 | $ | 91 | $ | 38 | $ | 53 | $ | 32 | $ | 220 | $ | 2,038 | |||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
| 1 | The above table shows, as of June 30, 2016, net Healthcare Facilities Segment accounts receivable aged from patient date of service and are grouped by classification of verified insurance coverage. The receivables are net of contractual allowances and allowance for doubtful accounts. Contractual allowances and the allowance for doubtful accounts are calculated by payor class and are not calculated by the aging of the patient billing date; therefore, these allowances have been allocated within the aging of the various payor classes based upon gross patient receivable amounts. |
SPECIALTY PHARMACY SEGMENT NET ACCOUNTS RECEIVABLE
JUNE 30, 2016
| Days Outstanding2 | ||||||||||||||||||||||||
| Payor Class |
0 - 30 | 31 - 60 | 61 - 90 | 91 - 120 | 121 - 150 | Total | ||||||||||||||||||
| Medicare |
$ | 133 | $ | 72 | $ | 66 | $ | 45 | $ | 225 | $ | 541 | ||||||||||||
| Medicaid |
136 | 88 | 35 | 32 | 107 | 398 | ||||||||||||||||||
| Private insurance and institutions |
739 | 236 | 99 | 110 | 360 | 1,544 | ||||||||||||||||||
| Other |
867 | 106 | 74 | 190 | 408 | 1,645 | ||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
| $ | 1,875 | $ | 502 | $ | 274 | $ | 377 | $ | 1,100 | $ | 4,128 | |||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
| 2 | The above table shows, as of June 30, 2016, net Specialty Pharmacy Segment accounts receivable aged from the date of sale or services performed and are grouped by classification of verified payer class. The receivables are net of contractual allowances and allowance for doubtful accounts. |
51
| Balance Sheet or Income Statement Caption/Nature of Critical Estimate Item |
Assumption / Approach Used (dollar amounts in thousands, except per share) |
Sensitivity
Analysis per share) | ||||||||
| Revenue recognition / Net Patient Service Revenues |
||||||||||
| For our Healthcare Facilities Segment, we recognize revenues in the period in which services are provided. For our Specialty Pharmacy Segment, we recognize revenues in the period in which services are provided and at the time the customer takes possession of merchandise. Patient receivables primarily consist of amounts due from third-party payors and patients. Amounts we receive for treatment of patients covered by governmental programs, such as Medicare and Medicaid, and other third-party payors, such as HMOs, PPOs and other private insurers, are determined pursuant to contracts or established government rates and are generally less than our established billing rates. Accordingly, our gross revenues and patient receivables are reduced to net amounts receivable pursuant to such contracts or government payment rates through an allowance for contractual discounts. Approximately 96.6%, 92.8% and 91.5% of our revenues during the years ended June 30, 2016, 2015 and 2014, respectively, relate to discounted charges. The sources of these revenues were as follows for the year ended June 30, 2016 (as a percentage of total revenues):
Medicare—37.1%; Medicaid—37.7%; and Commercial insurance and other sources—25.2%. |
|
Revenues are recorded at estimated amounts due from patients, third- party payors, institutions, pharmacies, and others for healthcare and pharmacy services and goods provided net of contractual discounts pursuant to contract or government payment rates. Estimates for contractual allowances are calculated using computerized and manual processes depending on the type of payor involved. In certain hospitals, the contractual allowances are calculated by a computerized system based on payment terms for each payor. In other hospitals, the contractual allowances are estimated manually using historical collections for each type of payor. For all hospitals, certain manual estimates are used in calculating contractual allowances based on historical collections from payors that are not significant or have not entered into a contract with us. All contractual adjustments regardless of type of payor or method of calculation are reviewed and compared to actual experience on a periodic basis.
Accounts receivable primarily |
|
|||||||
52
| Balance Sheet or Income Statement Caption/Nature of Critical Estimate Item |
Assumption / Approach Used (dollar amounts in thousands, except per share) |
Sensitivity
Analysis per share) | ||||||
| Governmental payors | Governmental payors | |||||||
| The majority of services performed on Medicare and Medicaid patients are reimbursed at predetermined reimbursement rates. The differences between the established billing rates (i.e., gross charges) and the predetermined reimbursement rates are recorded as contractual discounts and deducted from gross charges. Under this prospective reimbursement system, there is no adjustment or settlement of the difference between the actual cost to provide the service and the predetermined reimbursement rates.
Discounts for retrospectively
Final settlements under all |
Because the laws and regulations governing the Medicare and Medicaid programs are complex and subject to change, the estimates of contractual discounts we record could change by material amounts. Adjustments related to final settlements for revenues retrospectively increased (decreased) our revenues from continuing operations by the following amounts for the years ended June 30:
2016—$(786); 2015—$(540) and 2014—$624. | |||||||
| Commercial Insurance | Commercial Insurance | |||||||
| For most managed care plans, contractual allowances estimated at the time of service are adjusted to actual contractual allowances as cash is received and claims are reconciled. We evaluate the following criteria in developing the estimated contractual allowance percentages: historical contractual allowance trends based on actual claims paid by managed care payors; review of contractual allowance information reflecting current contract terms; consideration and analysis of changes in payor mix |
If our overall estimated contractual discount percentage on all of our commercial revenues during 2016 were changed by 1%, our 2016 after-tax income from continuing operations would change by approximately $69. This is only one example of reasonably possible sensitivity scenarios. The process of determining the allowance requires us to estimate the amount expected to be received and requires a high degree of judgment. It is impacted by changes in managed care contracts and other related factors.
| |||||||
53
| Balance Sheet or Income Statement Caption/Nature of Critical Estimate Item |
Assumption / Approach Used (dollar amounts in thousands, except per share) |
Sensitivity
Analysis per share) | ||||||||||
| reimbursement levels; and other issues that may impact contractual allowances. |
A significant increase in our estimate of contractual discounts would lower our earnings. This would adversely affect our results of operations, financial condition, liquidity and future access to capital. | |||||||||||
| Goodwill, other intangible assets and accounting for business combinations | ||||||||||||
| Goodwill represents the excess of the purchase price over the fair value of the net assets (including separately identified intangible assets) of acquired companies. The Company has one reportable business segment with goodwill. Goodwill included in our consolidated balance sheets as of June 30 for the following years was as follows:
|
|
In accordance with FASB Accounting Standards Codification 350-10, “Intangibles—Goodwill and Other,” (“ASC 350-10”) goodwill and intangible assets with indefinite lives are reviewed by us at least annually for impairment. For purposes of these analyses, the estimate of fair value is based on the income approach, which estimates the fair value based on future discounted cash flows. The estimate of future discounted cash flows is based on assumptions and projections that are believed to be currently reasonable and supportable. If it is determined the carrying value of goodwill or other intangible assets to be impaired, then the carrying value is reduced. |
||||||||||
| 2016 | 2015 | |||||||||||
| Pharmacy |
$ | 461 | $ | 461 | ||||||||
|
|
|
|
|
|||||||||
| The goodwill resulted from the 2008 acquisition of our specialty pharmacy business.
The Company’s other intangible assets relate to Certificates of Need (“CON”), non-competition agreements, trade name, customer relationships and Medicare licenses. CON, Non-competition agreements, customer relationships, and Medicare licenses are amortized over the terms of the agreements. The trade name has been determined to have an indefinite life and, accordingly, is not amortized. |
|
The purchase price of acquisitions is allocated to the assets acquired and liabilities assumed based upon their respective fair values and are subject to change during the twelve month period subsequent to the acquisition date. We engage independent third-party valuation firms to assist us in determining the fair values of assets acquired and liabilities assumed at the time of acquisition. Such valuations require us to make significant estimates and assumptions, |
||||||||||
54
| Balance Sheet or Income Statement Caption/Nature of Critical Estimate Item |
Assumption / Approach Used (dollar amounts in thousands, except per share) |
Sensitivity
Analysis per share) | ||||||||||||
| Our other intangible assets by business segment included in our consolidated balance sheets as of June 30 for the following years was as follows:
|
|
|
including projections of future events and operating performance.
Fair value estimates are derived |
|
||||||||||
| 2016 | 2015 | |||||||||||||
| Pharmacy |
||||||||||||||
| Trade name |
$ | 2,000 | $ | 2,000 | ||||||||||
| Customer relationships |
1,089 | 1,089 | ||||||||||||
| Medicare License |
769 | 769 | ||||||||||||
|
|
|
|
|
|||||||||||
| 3,858 | 3,858 | |||||||||||||
| Accumulated amortization |
(1,163 | ) | (1,021 | ) | ||||||||||
|
|
|
|
|
|||||||||||
| Total |
$ | 2,695 | $ | 2,837 | ||||||||||
|
|
|
|
|
|||||||||||
| Professional and general liability claims | ||||||||||||||
| We are subject to potential medical malpractice lawsuits and other claims as part of providing healthcare services. To mitigate a portion of this risk, we have maintained insurance for individual malpractice claims exceeding a self-insured retention amount. Our self-insurance retention amount was $1,000 on individual malpractice claims for each contract year commencing March 1, 2011.
Each year, we obtain quotes from various malpractice insurers with respect to the cost of obtaining medical malpractice insurance coverage. We compare these quotes to our most recent actuarially determined estimates of losses at various self-insured retention levels. Accordingly, changes in insurance costs affect the self-insurance retention level we choose each year. As insurance costs increase, we may accept a higher level of risk in self-insured retention levels.
|
|
|
The reserve for professional and general liability claims is based upon independent actuarial calculations, which consider historical claims data, demographic considerations, severity factors and other actuarial assumptions in the determination of reserve estimates.
The reserve for professional
and
We revise our reserve estimation |
|
Actuarial calculations include a large number of variables that may significantly impact the estimate of ultimate losses recorded during a reporting period. In determining loss estimates, professional judgment is used by each actuary by selecting factors that are considered appropriate by the actuary for our specific circumstances. Changes in assumptions used by our independent actuary with respect to demographics and geography, Industry trends, development patterns and judgmental selection of other factors may impact our recorded reserve levels and our results of operations.
Changes in our initial estimates of professional and general liability claims are non-cash charges and accordingly, there would be no material impact currently on our liquidity or capital resources.
| |||||||||
55
| Balance Sheet or Income Statement Caption/Nature of Critical Estimate Item |
Assumption / Approach Used (dollar amounts in thousands, except per share) |
Sensitivity
Analysis per share) | ||||||
| The reserve for professional and general liability claims included in our consolidated balance sheets as of June 30 was as follows:
2016—$1,391; and 2015—$979
The total increases (decreases) for professional and general liability coverage, included in our consolidated results of operations for the years ended June 30, was as follows:
2016—$678; 2015—$78; and 2014—$(272). |
Our estimated reserve for professional and general liability claims will be significantly affected if current and future claims differ from historical trends. While we monitor reported claims closely and consider potential outcomes as estimated by our independent actuaries when determining our professional and general liability reserves, the complexity of the claims, the extended period of time to settle the claims and the wide range of potential outcomes complicates the estimation process. In addition, certain states, including Georgia, have passed varying forms of tort reform which attempt to limit the number and types of claims and the amount of some medical malpractice awards. If enacted limitations remain in place or if similar laws are passed in the states where our other hospitals are located, our loss estimates could decrease. Conversely, liberalization of the number and type of claims and damage awards permitted under any such law applicable to our operations could cause our loss estimates to increase. |
|||||||
| Accounting for income taxes | ||||||||
| Deferred tax assets generally represent items that will result in a tax deduction in future years for which we have already recorded the tax benefit in our income statement. We assess the likelihood that deferred tax assets will be recovered from future taxable income. To the extent we believe that recovery is not probable, a valuation allowance is established. To the extent we establish a valuation allowance or increase this allowance, we must include an expense as part of the income tax provision in our results of | The first step in determining the deferred tax asset valuation allowance is identifying reporting jurisdictions where we have a history of tax and operating losses or are projected to have losses in future periods as a result of changes in operational performance. We then determine if a valuation allowance should be established against the deferred tax assets for that reporting jurisdiction.
|
Our deferred tax assets were $12,974 and our deferred tax liabilities were $0 at June 30, 2016, excluding the impact of valuation allowances. At June 30, 2016, the Company evaluated the need for a valuation against our deferred tax assets and determined that it was more likely than not that $2,322 of our deferred tax assets would be realized. As a result, in accordance with ASC | ||||||
56
| Balance Sheet or Income Statement Caption/Nature of Critical Estimate Item |
Assumption / Approach Used (dollar amounts in thousands, except per share) |
Sensitivity
Analysis per share) | ||||||
| operations. Our net deferred tax asset balance (net of valuation allowance) in our consolidated balance sheets as of June 30 for the following years was as follows:
2016—$2,322; and 2015—$6,852.
Our valuation allowances for deferred tax assets in our consolidated balance sheets as of June 30 for the following years were as follows:
2016—$10,652; and 2015—$2,564.
In addition, significant judgment is required in determining and assessing the impact of certain tax-related contingencies. We establish accruals when, despite our belief that our tax return positions are fully supportable, it is probable that we have incurred a loss related to tax contingencies and the loss or range of loss can be reasonably estimated.
We adjust the accruals related to tax contingencies as part of our provision for income taxes in our results of operations based upon changing facts and circumstances, such as the progress of a tax audit, development of industry related examination issues, as well as legislative, regulatory or judicial developments. A number of years may elapse before a particular matter, for which we have established an accrual, is audited and resolved. |
The second step is to determine the amount of the valuation allowance. We will generally establish a valuation allowance equal to the net deferred tax asset (deferred tax assets less deferred tax liabilities) related to the jurisdiction identified in the first step of the analysis. In certain cases, we may not reduce the valuation allowance by the amount of the deferred tax liabilities depending on the nature and timing of future taxable income attributable to deferred tax liabilities.
In assessing tax contingencies, we
During each reporting period,
we |
740, we recognized a total valuation allowance of $10,652 against the deferred tax asset so that the net tax asset was $2,322 at June 30, 2016. We conducted our evaluation by considering available positive and negative evidence to determine our ability to realize our deferred tax assets. In our evaluation, we gave more significant weight to evidence that was objective in nature as compared to subjective evidence. Also, more significant weight was given to evidence that directly related to our current financial performance as compared to less current evidence and future plans.
The IRS may propose adjustments for items we have failed to identify as tax contingencies. If the IRS were to propose and sustain assessments equal to 10% of our taxable income for 2016, we would incur approximately $0 of additional tax expense for 2016 plus applicable penalties and interest. | ||||||
57
Financial Summary
The results of continuing operations shown in the historical summary below are for our two business segments, Healthcare Facilities and Specialty Pharmacy. The results of the Company’s Chestatee Regional Hospital (“Chestatee”) which sold on August 19, 2016, have been reclassified as discontinued operations in our consolidated financial statements for the fiscal years ended June 30, 2016, 2015 and 2014. As a result, their results are not included in Healthcare Facilities Segment results discussed.
| Years Ended June 30, | ||||||||||||
| 2016 | 2015 | 2014 | ||||||||||
| Net Revenues—Healthcare Facilities |
$ | 30,462 | $ | 39,933 | $ | 39,986 | ||||||
| Net Revenues—Specialty Pharmacy |
32,216 | 33,175 | 33,322 | |||||||||
| Net Revenues—Corporate and Other |
755 | 638 | 461 | |||||||||
|
|
|
|
|
|
|
|||||||
| Total Net Revenues |
63,433 | 73,746 | 73,769 | |||||||||
| Costs and expenses |
(69,091 | ) | (71,555 | ) | (75,001 | ) | ||||||
| Electronic health records incentives |
(7 | ) | 29 | 2,274 | ||||||||
| Impairment of plant, property and equipment |
(858 | ) | 0 | 0 | ||||||||
|
|
|
|
|
|
|
|||||||
| Operating Profit (Loss) |
(6,523 | ) | 2,220 | 1,042 | ||||||||
| Interest Expense |
(843 | ) | (861 | ) | (944 | ) | ||||||
| Gain (Loss) on sale of assets |
10 | 21 | (41 | ) | ||||||||
|
|
|
|
|
|
|
|||||||
| Earnings (Loss) from continuing operations before income taxes |
$ | (7,356 | ) | $ | 1,380 | $ | 57 | |||||
|
|
|
|
|
|
|
|||||||
| Healthcare Facilities Segment: |
||||||||||||
| Admissions |
607 | 1,442 | 1,422 | |||||||||
|
|
|
|
|
|
|
|||||||
| Equivalent Admissions |
3,546 | 4,756 | 5,074 | |||||||||
|
|
|
|
|
|
|
|||||||
| Surgeries |
486 | 950 | 1,040 | |||||||||
|
|
|
|
|
|
|
|||||||
| Revenue per Equivalent Admission |
$ | 8,590 | $ | 8,396 | $ | 7,880 | ||||||
|
|
|
|
|
|
|
|||||||
Equivalent admissions—Equivalent admissions is used by management (and certain investors) as a general approximation of combined inpatient and outpatient volume. Equivalent admissions are computed by multiplying admissions (inpatient volume) by the sum of gross inpatient revenues and gross outpatient revenues and dividing the result by gross inpatient revenues. The equivalent admissions computation is intended to relate outpatient revenues to the volume measure (admissions) used to measure inpatient volume to result in a general approximation of combined inpatient and outpatient volume (equivalent admissions).
Results of Operations
Our net revenues are from our two business segments, Healthcare Facilities and Specialty Pharmacy.
Healthcare Facilities Segment
The following table sets forth the percentage of net patient revenues from major payors for the Healthcare Facilities Segment for the periods indicated:
| Fiscal Years Ended June 30, | ||||||||||||
| 2016 | 2015 | 2014 | ||||||||||
| Source |
||||||||||||
| Medicare |
37.1 | % | 39.0 | % | 40.4 | % | ||||||
| Medicaid |
37.7 | % | 30.3 | % | 28.7 | % | ||||||
| Self pay |
3.4 | % | 7.2 | % | 8.5 | % | ||||||
| Managed Care Insurance & Other |
21.8 | % | 23.5 | % | 22.4 | % | ||||||
|
|
|
|
|
|
|
|||||||
| 100.0 | % | 100.0 | % | 100.0 | % | |||||||
|
|
|
|
|
|
|
|||||||
58
Healthcare Facilities net revenues decreased $9,471 or 23.7% in the year ended June 30, 2016 compared to the year ended June 30, 2015. Net revenue from all payer sources decreased compared to last year. Medicare and Managed Care net revenues decreased 30.5% and 32.5%, respectively, from the prior year. Medicaid net revenues decreased 9.0% from the prior year while Self-pay net revenues decreased 64.9%. The lower revenues were generally due to lower in-patient volumes and the emergency department at one hospital closing. The lower patient volumes for the periods above result from several factors. One facility does not accept the insurance provided by Health Insurance Marketplace plan offered through the Federal government due to the low reimbursement rates offered by the plan in calendar 2015. This facility also made renovations at the facility (now completed) which disrupted the patient areas resulting in lower volume. This facility also closed its emergency department in September 2014 in order to reduce its bad debt experience from self-pay admissions. The change resulted in a loss of physicians, which have not yet been replaced, and in decreased admissions. Another hospital facility had reduced admissions due to changes in physician staffing as well as the negative perception and publicity resulting from a proposal to lease the emergency room and medical office building to a regional healthcare system and discontinue inpatient services. An agreement was reached in early June 2016 and the facility will lease a portion of the hospital building and a medical office building to an unaffiliated healthcare provider. Inpatient services at the hospital were discontinued in June 2016. The medical office building lease began in July 2016 and the emergency room lease is expected to begin by November 2016.
Healthcare Facilities net revenues decreased $54 in the year ended June 30, 2015 compared to the year ended June 30, 2014. Medicare and Self-pay net revenues decreased 3.8% and 15.9%, respectively, from the prior year. Medicaid new revenues increased 4.9% from the prior year while Managed Care net revenues increased 4.7%.
Specialty Pharmacy Segment
Net revenues for the year ended June 30, 2016 decreased 2.9% from the prior year, with decreased institutional pharmacy revenues and infusion therapy revenues somewhat offset by increased durable medical equipment (DME) revenues and retail pharmacy revenues. Institutional pharmacy revenues decreased 11.0% and infusion therapy pharmacy revenues decreased by 25.1% while retail pharmacy revenues increased 3.3% and DME increased 10.4% in 2016 as compared to 2015.
Net revenues for the year ended June 30, 2015 decreased 0.4% from the prior year, with decreased infusion therapy revenues somewhat offset by increased institutional and retail pharmacy and DME revenues. Revenue from the sale of one infusion drug which is primarily sold to Medicaid covered customers decreased by approximately $3,695 due to Louisiana Medicaid restricting both the number of eligible customers and number of approved doses of the drug. Institutional pharmacy revenues increased 29.3%, retail pharmacy revenues increased 3.4% and DME increased 8.2% in 2015 as compared to 2014.
Net revenues for the year ended June 30, 2014 remained consistent with the prior year net revenues; however, fiscal 2014 included a net increase in pharmacy net revenues of $957 due primarily to additional institutional pharmacy contracts and a net decline in durable medical equipment sales of $949 due primarily to the elimination of certain unprofitable items. Although fiscal 2014 retail and institutional pharmacy script volumes increased 8.7% as compared to fiscal 2013, the corresponding pharmacy net revenues decreased 4.1%, primarily as a result of decreases in reimbursement rates, including Medicare, Medicaid and managed care; the negative effects of significant brand-to-generic conversion activity; and, a significant increase in exclusive preferred provider network arrangements between major pharmacy benefit managers and certain retail chain pharmacies. Fiscal 2014 infusion therapy net revenues increased 2.0% as compared to fiscal 2013, primarily related to certain higher reimbursed specialty pharmacy services.
59
Healthcare Facilities Segment Cost and Expenses
Costs and expenses for our Healthcare Facilities, including depreciation and amortization, were $33,534, $35,369, and $35,980, for the fiscal years ended June 30, 2016, 2015 and 2014, respectively.
| Cost and Expenses as a % of Net Revenue Years Ended June 30, |
||||||||||||
| 2016 | 2015 | 2014 | ||||||||||
| Salaries, wages and benefits |
70.2 | % | 59.7 | % | 59.7 | % | ||||||
| Supplies |
10.5 | % | 10.6 | % | 10.1 | % | ||||||
| Purchased services |
8.8 | % | 7.1 | % | 8.1 | % | ||||||
| EHR incentive payments |
0.0 | % | -0.1 | % | -5.7 | % | ||||||
| Other operating expenses |
17.3 | % | 12.5 | % | 14.7 | % | ||||||
| Rent and lease expense |
1.3 | % | 1.0 | % | 1.2 | % | ||||||
| Depreciation and amortization expense |
2.0 | % | 1.7 | % | 1.8 | % | ||||||
Salaries, wages and benefits expense, purchased services expense and other operating expenses increased as a percentage of net revenue in the year ended June 30, 2016 primarily due to the 23.7% decrease in net revenues from the prior year. Salaries, wages and benefits expense as a percentage of total net revenues were relatively unchanged in the year ended June 30, 2015 compared to the prior year. Other operating expenses increased $274 in fiscal 2016 due to professional liability expense.
Purchased services decreased as a percentage of net revenues for the fiscal year ended June 30, 2015 compared to the prior fiscal year due reduced legal fees, medical professional fees and outside collection expense.
EHR incentive payments as a percentage of net revenue are 0.0%, (0.1%) and (5.7%) for the fiscal years ended June 30, 2016, 2015 and 2014, respectively. No Medicare incentive payments were received in the fiscal years 2016 and 2015. We believe we will receive minimal EHR incentive payments in future periods.
Depreciation and amortization expense was $618, $664, and $737 for the years ended June 30, 2016, 2015, and 2014, respectively. The decreases in depreciation and amortization expense resulted from assets being fully over depreciated the past several years.
Specialty Pharmacy Segment Cost and Expenses
Cost and expenses for our Specialty Pharmacy Segment, including depreciation and amortization, was $32,258, $32,681 and $32,769 for the fiscal years ended June 30, 2016, 2015 and 2014, respectively.
| Cost and Expenses as a % of Net Revenue Years Ended June 30, |
||||||||||||
| 2016 | 2015 | 2014 | ||||||||||
| Cost of goods sold |
63.3 | % | 63.4 | % | 66.4 | % | ||||||
| Salaries, wages and benefits |
23.1 | % | 22.7 | % | 20.6 | % | ||||||
| Provision for bad debts |
2.0 | % | 1.1 | % | 0.8 | % | ||||||
| Supplies |
0.4 | % | 0.4 | % | 0.5 | % | ||||||
| Purchased services |
3.5 | % | 3.9 | % | 3.8 | % | ||||||
| Other operating expenses |
3.8 | % | 3.6 | % | 3.3 | % | ||||||
| Rent and lease expense |
1.0 | % | 1.0 | % | 0.9 | % | ||||||
| Depreciation and amortization expense |
3.0 | % | 2.4 | % | 2.2 | % | ||||||
Cost of goods sold as a percent of net revenues decreased slightly in the fiscal years ended June 30, 2016 and 2015 as compared to the respective prior fiscal years due to changes in sales product mix and favorable
60
pricing negotiations and discounts earned with certain suppliers. The 53% decrease in infusion therapy products revenues in 2015 was the primary cause of decrease for 2015 compared to 2014.
Salaries, wages and benefits as a percent of net revenues increased in the fiscal years ended June 30, 2016, 2015 and 2014 as compared to the respective prior fiscal years primarily due to expansion of services and increased compliance and documentation requirements.
Other operating expenses as a percent of net revenues increased during the fiscal years ended June 30, 2016 and 2015 as compared to the prior fiscal year primarily due to office and related expenses incurred in connection with new institutional customers and an additional retail location in fiscal 2015. Purchased services decreased $368 in fiscal year ended June 30, 2016 compared to the prior year due to lower freight and advertising expenses.
Depreciation and amortization expense as a percent of net revenues increased during the fiscal years ended June 30, 2016 and 2015 as compared to the prior fiscal year due to increased depreciation expense related to additions and improvements to owned and leased properties. Depreciation and amortization expense was $954, $796 and $730 for the fiscal years ended June 30, 2016, 2015 and 2014.
Corporate Overhead Costs and Expenses
Cost and expenses for Corporate Overhead including depreciation and amortization, was $3,306, $3,477 and $3,978 for the fiscal years ended June 30, 2016, 2015 and 2014, respectively. The decrease in the fiscal year ended June 30, 2016 from the prior year was due primarily to decreased salaries and legal expense. The decrease in the fiscal year ended June 30, 2015 from the prior year was due to decreased depreciation and amortization expense resulting from assets becoming fully depreciated or transferred to the Healthcare Facilities Segment.
Impairment of Long-Lived Assets
A facility composed of a closed hospital building and a medical office building formerly leased to an unaffiliated third party hospital operator, is currently vacant with the exception of one rented office. The net realizable value of the facility was evaluated at June 30, 2016 and an impairment charge of $858 was recognized in the fiscal year ended June 30, 2016.
Insurance settlement
In January 2015, the Company received a $1,000 settlement on a claim made under its insurance policy covering, among other things, employee theft relating to misappropriation of funds by two now former employees over an eight year period beginning in 2006. Income of $1,000 was recognized in the year ended June 30, 2015.
Operating Profit (Loss)
Operating loss was $6,523 for the year ended June 30, 2016 and operating profit was $2,220 and $1,042 for the years ended June 30, 2015 and 2014. The operating loss resulted from the decreased Healthcare Facilities Segment net revenues, increased professional liability expense, asset impairment charge and the non-recurrence of the $1,000 insurance settlement. The increased operating profit for the year ended June 30, 2015 results lower operating expenses and the $1,000 insurance settlement.
Interest Expense-net
Interest expense was $843, $861, and $944 for the years ended June 30, 2016, 2015 and, 2014, respectively. The decreases in interest expense for the years ended June 30, 2016 and 2015 was due to lower outstanding debt.
61
Income Taxes
We recorded income tax expense of $4,558 ($4,134 federal tax expense and $424 state tax expense) for the year ended June 30, 2016 compared to income tax expense of $893 ($414 federal tax expense and $479 state tax expense) for the year ended June 30, 2015 and income tax expense of $541 ($50 federal tax expense and $491 state tax expense) for the year ended June 30, 2014.
In accordance with the Financial Accounting Standards Board Accounting Standards Codification (‘ASC”) 740, we evaluate our deferred taxes quarterly to determine if adjustments to our valuation allowance are required based on the consideration of available positive and negative evidence using a “more likely than not” standard with respect to whether deferred tax assets will be realized. Our evaluation considers, among other factors, our historical operating results, our expectation of future results of operations, the duration of applicable statuary carryforward periods and conditions of the healthcare industry. The ultimate realization of our deferred tax assets depends primarily on our ability to generate future taxable income during the periods in which the related temporary differences in the financial basis and the tax basis of the assets become deductible. The value of our deferred tax assets will depend on applicable income tax rates.
At December 31, 2015 and again at March 31, 2016 and June 30, 2016, in accordance with the process, we evaluated the need for a valuation against our deferred tax assets and determined that it was more likely than not that none of our deferred tax assets would be realized. Subsequent to year end, we sold Dahlonega at a gain. We determined that it was more likely than not that a portion of our deferred tax assets would be realized during the fiscal year ended June 30, 2017 and accordingly recorded a valuation allowance of $10,652 during 2016 representing the amount of our net deferred tax assets not expected to be realized. We conducted our evaluation by considering available positive and negative evidence to determine our ability to realize our deferred tax assets. In our evaluation, we gave more significant weight to evidence that was objective in nature as compared to subjective evidence. Also, more significant weight was given to evidence that directly related to our current financial performance as compared to less current evidence and future plans. The principal negative evidence that led us to determine at June 30, 2016 that substantially all the deferred tax assets should have a full valuation allowances was the three-year cumulative pre-tax loss from continuing operations as well as the underlying negative business conditions for rural hospital businesses in which our Healthcare Facilities Segment businesses operate.
We had an estimated net operating loss carry-forward for federal income tax purposes of approximately $13,700 at June 30, 2016. Use of this net operating loss carry-forward is subject to the limitation provisions of Internal Revenue Code Section 382.
Earnings (Loss) After Taxes
Loss from continuing operations was $11,914 (a loss of $1.26 per fully diluted share) for the year ended June 30, 2016 compared to earnings from continuing operations of $487 ($0.05 per fully diluted share) for the year ended June 30, 2015 and a loss from continuing operations of $484 (a loss of $0.05 loss per fully diluted share) for the year ended June 30, 2014. The loss from continuing operations in fiscal year 2016 resulted from the recording of a full valuation allowance for the gross deferred tax asset and lower Healthcare Facilities Segment net revenues. The net earnings in fiscal year 2015 resulted from decrease operating expenses for the Healthcare Facilities and decreased cost of goods sold of the Specialty Pharmacy Segment as compared to fiscal 2014.
62
Losses from discontinued operations were $2,169 for the year ended June 30, 2016; $242 for the year ended June 30, 2015 and $61 for the year ended June 30, 2014. The results of all the businesses in discontinued operations are presented below:
Discontinued Operations—Summary Statement of Earnings Information
| Years Ended June 30, | ||||||||||||
| 2016 | 2015 | 2014 | ||||||||||
| Earnings (Loss) Before Income Taxes: |
||||||||||||
| Chestatee Hospital |
$ | (1,961 | ) | $ | 315 | $ | 261 | |||||
| Fulton Hospital |
84 | (1,170 | ) | (1,621 | ) | |||||||
| Dexter Hospital |
(115 | ) | 727 | 1,548 | ||||||||
| Memorial of Adel |
4 | 15 | (94 | ) | ||||||||
| Life sciences and engineering |
(181 | ) | (105 | ) | (158 | ) | ||||||
|
|
|
|
|
|
|
|||||||
| Loss before income taxes |
(2,169 | ) | (218 | ) | (64 | ) | ||||||
|
|
|
|
|
|
|
|||||||
| Loss on Sale: |
||||||||||||
| Fulton Hospital |
0 | (197 | ) | 0 | ||||||||
|
|
|
|
|
|
|
|||||||
| Loss on Sale |
0 | (197 | ) | 0 | ||||||||
|
|
|
|
|
|
|
|||||||
| Income tax benefit |
0 | (173 | ) | (3 | ) | |||||||
|
|
|
|
|
|
|
|||||||
| Loss from discontinued operations |
$ | (2,169 | ) | $ | (242 | ) | $ | (61 | ) | |||
|
|
|
|
|
|
|
|||||||
A net loss for the year ended June 30, 2016 was $14,083 (a loss of $1.49 per fully diluted share) compared to net earnings for the year ended June 30, 2015 of $245 ($0.03 earnings per fully diluted share) and a net loss of $545 (a loss of $0.06 earnings per fully diluted share) for the year ended June 30, 2014.
Adjusted Earnings Before Income Taxes, Interest, Depreciation and Amortization
Earnings before income taxes, interest, depreciation and amortization (“EBITDA”) represent the sum of income before income taxes, interest, depreciation and amortization. We understand that certain industry analysts and investors generally consider EBITDA to be one measure of the liquidity of a company, and it is presented to assist analysts and investors in analyzing the ability of a company to generate cash, service debt and meet capital requirements. We believe increased EBITDA is an indicator of improved ability to service existing debt and to satisfy capital requirements. EBITDA, however, is not a measure of financial performance under accounting principles generally accepted in the United States of America and should not be considered an alternative to net income as a measure of operating performance or to cash liquidity. Because EBITDA is not a measure determined in accordance with accounting principles generally accepted in the United States of America and is thus susceptible to varying calculations, EBITDA, as presented, may not be comparable to other similarly titled measures of other corporations. Where we adjust EBITDA for non-cash charges we refer to such measurement as “Adjusted EBITDA”, which we report on a company wide basis. Non-cash adjustments in Adjusted EBITDA are not intended to be identified or characterized in any respect as “non-recurring, infrequent or unusual,” if we believe such charge is reasonably likely to recur within two years, or if there was a similar charge (or gain) within the prior two years. Where we report Adjusted EBITDA, we typically also report Hospital Facilities Segment Adjusted EBITDA and Specialty Pharmacy Segment Adjusted EBITDA which is the EBITDA for the applicable segments without any allocation of corporate overhead, which we report as a separate line item, and without any allocation of the non-cash adjustments, which we also report as a separate line item in Adjusted EBITDA. Net cash provided by operations for the years ended June 30, 2016, 2015 and 2014, respectively, is shown below.
63
| Years ended June 30, | ||||||||||||
| 2016 | 2015 | 2014 | ||||||||||
| Healthcare Facilities Adjusted EBITDA |
$ | (2,454 | ) | $ | 5,227 | $ | 4,742 | |||||
| Specialty Pharmacy Adjusted EBITDA |
912 | 1,290 | 1,283 | |||||||||
| Corporate overhead costs |
(2,245 | ) | (2,460 | ) | (2,661 | ) | ||||||
| Taxes and net interest expense |
(5,401 | ) | (1,754 | ) | (1,485 | ) | ||||||
| Other non-cash expenses and net changes in operating assets and liabilities |
8,762 | 635 | 2,013 | |||||||||
|
|
|
|
|
|
|
|||||||
| Net cash provided by (used in) operations |
$ | (426 | ) | $ | 2,938 | $ | 3,892 | |||||
|
|
|
|
|
|
|
|||||||
Liquidity and Capital Resources
Overview
Our primary source of liquidity is currently cash on hand. The Company’s ability to raise capital (debt or equity) in the public or private markets on what it considers acceptable terms is uncertain. On August 19, 2016, a subsidiary of the Company sold substantially all assets and certain liabilities of its Chestatee Regional Hospital in Dahlonega, GA, for approximately $15,000 subject to adjustment for the book value of certain assets and liabilities at the sale date. In addition, the Company has entered into an agreement to lease the emergency department and certain ancillary space in its former hospital, North Georgia Medical Center, which is now closed, to a regional healthcare system. The lease transaction is subject to a number of conditions precedent including regulatory approval and negotiation of definitive leases. The Company continues to operate its 100-bed skilled nursing facility which is located adjacent to the closed hospital. The Company believes its specialty pharmacy business continues to under-perform, and the Company has engaged advisors to assist it in evaluating the possible sale of its specialty pharmacy business and one medical office building. The Company’s possible use of net proceeds from the Dahlonega sale and possible future transactions may include, among other things, a prepayment of long-term debt, a return of capital to shareholders via a repurchase of shares or a dividend, and other general corporate purposes. However, there can be no assurance any further sale or lease transaction will be authorized by the Board of Directors or completed and , if so, that there will be sufficient proceeds to return capital to shareholders or for future development or other general corporate purposes.
Subject to the risks and uncertainties discussed herein, we believe we have adequate financing and liquidity to support our current level of operations through the next twelve months.
Subsidiary Loans
Trace RDA Loan and Trace Working Capital Loan—SunLink and two wholly owned subsidiaries of the Company, closed a $9,975 Mortgage Loan Agreement (“Trace RDA Loan”) and a Working Capital Loan Agreement, both dated as of July 5, 2012 (“Trace Working Capital Loan”).
The Trace RDA Loan has a term of 15 years with monthly payments of principal and interest. The Trace RDA Loan bears a floating rate of interest equal to the greater of (i) the prime rate (as published in The Wall Street Journal) plus 1.5%, or (ii) 6% (6.0% at June 30, 2016). The Trace RDA Loan is collateralized by real estate and equipment of Trace Regional Hospital in Houston, MS and is partially guaranteed under the U.S. Department of Agriculture, Rural Development Business and Industry Program.
The Trace Working Capital Loan as amended provided for a revolving line of credit to Trace equal to the lesser of (i) a Borrowing Base equal to eighty percent (80%) of Eligible Accounts Receivable (as defined in the Working Capital Loan Agreement dated July 5, 2012) or (ii) $500. The Trace Working Capital Loan expired July 2, 2016 and was not renewed. At June 30, 2016 and 2015, there were no outstanding borrowings under the Trace Working Capital Loan.
The Trace RDA Loan contains various terms and conditions, including financial restrictions and limitations, and affirmative and negative covenants. The covenants include financial covenants measured on a quarterly basis
64
which require Trace to comply with a ratio of current assets to current liabilities, debt service coverage, fixed charge coverage, and funded debt to EBITDA, all as defined in the Trace RDA Loan. At March 31, 2016 and June 30, 2016, Trace was not in compliance with the debt service coverage, fixed charge ratio and funded debt to EBITDA ratios. The Company received a waiver from the lender dated August 10, 2016 of this non-compliance for March 31, 2016. No modification or waiver for the June 30, 2016 non-compliance has been obtained as of September 28, 2016 and the $7,698 of indebtedness under the Trace RDA Loan is presented in current liabilities in the condensed consolidated balance sheet as of June 30, 2016. The Company continues to discuss a modification or waiver of this non-compliance with the lender. The ability of Trace to continue to make the required debt service payments under the Trace RDA Loan depends on, among other things, its ability to generate sufficient cash flows, including from operating activities. If Trace is unable to generate sufficient cash flow from operations to meet debt service payments on the Trace RDA Loan, including in the event the lender were to declare an event of default and accelerate the maturity of the indebtedness, such failure could have material adverse effects on the Company. The Trace RDA Loan is guaranteed by the Company and one subsidiary.
SHPP RDA Loan—SunLink Healthcare Professional Property, LLC, a subsidiary of the Company which owns a medical office building, entered into and closed on $2,100 term loan dated as of October 31, 2012 (the “SHPP RDA Loan”). SHPP formerly leased a medical office building to Southern Health Corporation of Ellijay, Inc. (“SHC Ellijay”), but effective July 1, 2016, SHPP entered into a 10 year lease with a third-party lessee.
The SHPP RDA Loan has a term of 25 years with monthly payments of principal and interest until repaid. The SHPP RDA Loan bears interest at a floating rate of interest equal to the greater of (i) the prime rate (as published in The Wall Street Journal) plus 2.0%, or (ii) 5% (5.50% at June 30, 2016). The SHPP RDA Loan is collateralized by SHPP’s real estate, equipment and leases and is partially guaranteed under the U.S. Department of Agriculture, Rural Development Business and Industry Program The SHPP RDA Loan contains certain financial covenants with respect to the ratio of current assets to current liabilities and debt service coverage, all as defined in the SHPP RDA Loan Agreement, which SHPP must maintain and that are measured at the end of each fiscal year. The SHPP RDA Loan is guaranteed by the Company and one subsidiary. As of June 30, 2016, the Company was in compliance with all financial covenants under the SHPP RDA Loan.
Carmichael Notes—The Carmichael Note was paid off on September 9, 2016 and the Company expects to recognize a gain on the early repayment of approximately $47 in its fiscal quarter ending September 30, 2106. On April 22, 2008, SunLink Scripts Rx, LLC issued a $3,000 promissory note with an interest rate of 8% to the former owners of Carmichael as part of the acquisition purchase price (the “Carmichael Note”). Under amendments and modifications to the Carmichael Note during fiscal 2013 and 2014, the Company made payments of principal and interest with additional notes and extended the maturity date to October 22, 2017. The Carmichael Note was payable in semi-annual installments of $185 of principal and accrued interest, with the remaining balance of $1,255 due October 22, 2017. The Carmichael Note was guaranteed by the Company.
Contractual Obligations, Commitments and Contingencies
Contractual obligations related to long-term debt, non-cancelable operating leases and interest on outstanding debt from continuing operations at June 30, 2016 is shown in the following table. The interest on variable interest debt is calculated at the interest rate in effect at June 30, 2016.
65
| Payments due in: |
Long-Term Debt |
Operating Leases |
Interest on Long-Term Debt |
|||||||||
| 1 year |
$ | 8,012 | $ | 472 | $ | 685 | ||||||
| 2 years |
1,310 | 314 | 136 | |||||||||
| 3 years |
46 | 196 | 101 | |||||||||
| 4 years |
49 | 155 | 99 | |||||||||
| 5 years |
51 | 31 | 96 | |||||||||
| More than 5 years |
1,720 | 0 | 1,015 | |||||||||
|
|
|
|
|
|
|
|||||||
| $ | 11,188 | $ | 1,168 | $ | 2,132 | |||||||
|
|
|
|
|
|
|
|||||||
Long-term Debt—At June 30, 2016, we had outstanding long-term debt of $11,188 of which $7,698 was incurred under the Trace RDA Loan, $1,950 was incurred under the SHPP RDA Loan, $1,508 was incurred under the Carmichael Notes, and $32 was related to capital leases and other obligations.
Tax Benefits Protection Rights Plan—On September 29, 2016, SunLink entered into a Tax Benefits Preservation Rights Plan (the “Tax Benefits Protection Rights Plan”). Effective September 29, 2016, the Board declared a dividend in the form of one preferred stock purchase right for each of the Company’s issued and outstanding common shares. The purpose of the Tax Benefits Protection Rights Plan is to diminish the risk that the Company’s ability to use its net operating losses and certain other tax assets to reduce potential future federal income tax obligations would become subject to limitations by reason of the Company experiencing an “ownership change,” as defined in Section 382 of the Code.
Recent Accounting Pronouncements
In April 2015, the Financial Accounting Standards Board (“FASB”) issued Accounting Standards Update (“ASU”) 2015-3, “Simplifying the Presentation of Debt Issuance Costs” (“ASU 2015-3”). ASU 2015-3 requires that debt issuance costs related to a recognized debt liability be presented in the balance sheet as a direct deduction from the carrying amount of that debt liability, consistent with debt discounts, rather than separately as an asset. ASU 2015-3 is effective for annual reporting periods beginning after December 15, 2015, including interim periods within those years, and is to be applied retrospectively. Early adoption is permitted. The Company does not expect the adoption of ASU 2015-3 will have an impact on its results of operations or cash flows.
In February 2015, the FASB issued ASU 2015-2 “Consolidation” (“ASU 2015-2”). ASU 2015-2 includes amendments that are intended to improve targeted areas of consolidation for legal entities including reducing the number of consolidation models from four to two and simplifying the FASB Accounting Standards Codification (“ASC”). The provisions of ASU 2015-2 are effective for annual reporting periods beginning after December 15, 2015. The amendments may be applied retrospectively in previously issued financial statements for one or more years with a cumulative effect adjustment to retained earnings as of the beginning of the first year restated. Early adoption is permitted. The Company does not expect the adoption of ASU 2015-2 will have an impact on its results of operations or cash flows.
In August 2014, the FASB issued ASU 2014-15 “Disclosure of Uncertainties about an Entity’s Ability to Continue as a Going Concern” (“ASU 2014-15”). ASU 2014-15 will explicitly require management to assess an entity’s ability to continue as a going concern, and to provide related footnote disclosure in certain circumstances. The new standard will be effective for all entities in the first annual period ending after December 15, 2016. Earlier adoption is permitted. The Company is currently evaluating the impact of the adoption of ASU 2014-15.
In September 2015, the Financial Accounting Standards Board (“FASB”) issued Accounting Standards Update (“ASU”) 2015-16, “Business Combinations: Simplifying the Accounting for Measurement-Period Adjustments” (“ASU 2015-16”). ASU 2015-16 eliminates the requirement for an acquirer to retrospectively adjust its financial statements for changes to provisional amounts that are identified during the measurement-period following the consummation of a business combination. Instead, ASU 2015-16 requires these types of
66
adjustments to be made during the reporting period in which they are identified and would require additional disclosure or separate presentation of the portion of the adjustment that would have been recorded in the previously reported periods as if the adjustment to the provisional amounts had been recognized as of the acquisition date. ASU 2015-16 is effective for annual reporting periods beginning after December 15, 2015, including interim periods within those years, and is to be applied retrospectively. The Company does not expect the adoption of ASU 2015-16 will have an impact on its results of operations or cash flows.
In April 2015, the FASB issued ASU 2015-5, “Intangibles—Goodwill and Other—Internal-Use Software” (“ASU 2015-5”). ASU 2015-5 provides guidance to customers about whether a cloud computing arrangement includes a software license. If a cloud computing arrangement includes a software license, ASU 2015-5 specifies that the customer should account for the software license element of the arrangement consistent with the acquisition of other software licenses. ASU 2015-5 further specifies that the customer should account for a cloud computing arrangement as a service contract if the arrangement does not include a software license. ASU 2015-5 is effective for annual reporting periods beginning after December 15, 2015, including interim periods within those years, and is to be applied retrospectively. The Company does not expect the adoption of ASU 2015-5 will have an impact on its results of operations or cash flows.
In March 2016, the FASB issued ASU 2016-9 “Compensation—Stock Compensation: Improvements to Employee Share-Based Payment Accounting” (“ASU 2016-9”). ASU 2016-9 changes certain aspects of accounting for share-based payment awards to employees, including the accounting for income taxes, application of estimated rates of forfeiture and statutory tax withholding requirements. ASU 2016-9 is effective for annual reporting periods beginning after December 15, 2016, including interim periods within those years. Early adoption is permitted. The Company is currently evaluating the impact that the adoption of this standard will have on its financial position, results of operations and cash flows.
In February 2016, the FASB issued ASU 2016-2 “Leases” (“ASU 2016-2”). ASU 2016-2 requires the rights and obligations arising from lease contracts, including existing and new arrangements, to be recognized as assets and liabilities on the balance sheet. ASU 2016-2 is effective for annual reporting periods beginning after December 15, 2018, including interim periods within those years. Early adoption is permitted. The Company anticipates that the adoption of ASU 2016-2 will result in an increase in both total assets and total liabilities. The Company is still evaluating the impact that the adoption of this standard will have on its policies, procedures and control framework.
In May 2014, the FASB issued ASU 2014-9, “Revenue from Contracts with Customers” (“ASU 2014-9”). ASU 2014-9 provides for a single comprehensive principles-based standard for the recognition of revenue across all industries through the application of the following five-step process:
Step 1: Identify the contract(s) with a customer.
Step 2: Identify the performance obligations in the contract.
Step 3: Determine the transaction price.
Step 4: Allocate the transaction price to the performance obligations in the contract.
Step 5: Recognize revenue when (or as) the entity satisfies a performance obligation.
Among other provisions and in addition to expanded disclosure about the nature, amount, timing and uncertainty of revenue as well as certain additional quantitative and qualitative disclosures, ASU 2014-9 changes the healthcare industry specific presentation guidance under ASU 2011-7, “Presentation and Disclosure of Patient Service Revenue, Provision for Bad Debts, and the Allowance for Doubtful Accounts for Certain Health Care Entities.” The provisions of ASU 2014-9 are effective for annual periods beginning after December 15, 2017, including interim periods within those years. Early adoption is permitted starting with annual periods beginning after December 31, 2016. The Company is still evaluating the impact that the adoption of this standard will have on its revenue recognition policies, procedures, financial position, results of operations, cash flows, financial disclosures and control framework.
67
Related Party Transactions
A director of the Company and the Company’s former company secretary are members of two different law firms, each of which provides services to SunLink. The Company has expensed an aggregate of $275, $334 and $689 to these law firms in the fiscal years ended June 30, 2016, 2015 and 2014, respectively. Included in the Company’s consolidated balance sheets at June 30, 2016 and 2015 is $75 and $89, respectively, of amounts payable to these law firms.
Inflation
During periods of inflation and labor shortages, employee wages increase and suppliers pass along rising costs to us in the form of higher prices for their supplies and services. We have not always been able to offset increases in operating costs by increasing prices for our services and products or by implementing cost control measures. We are unable to predict our ability to control future cost increases or offset future cost increases by passing along the increased cost to customers.
| Item 8. | Financial Statements and Supplementary Data. |
Index to Financial Statements and Supplementary Data
| Page | ||||
| F-1 | ||||
| F-2 | ||||
| F-3 | ||||
| F-4 | ||||
| Consolidated Statements of Cash Flows—for each of the three years ended June 30, 2016, 2015 and 2014 |
F-5 | |||
| F-6 | ||||
| Item 9A. | Controls and Procedures. |
Evaluation of Disclosure Controls and Procedures
As required by Rule 13a-15 under the Securities Exchange Act of 1934 (the “Exchange Act”), as of the end of the period covered by this report, we carried out an evaluation of the effectiveness of the design and operation of our Company’s disclosure controls and procedures (as such term is defined in Rules 13a-15(e) and 15d-15(e) under the Exchange Act. Under the direction of our principal executive officer and principal financial officer, we evaluated our disclosure controls and procedures and internal control over financial reporting and concluded that our disclosure controls and procedures were effective as of June 30, 2016.
Disclosure controls and procedures and other procedures are designed to ensure that information required to be disclosed in our reports or submitted under the Exchange Act, such as this Annual Report on Form 10-K, is recorded, processed, summarized and reported within the time period specified in the SEC’s rules and forms. Disclosure controls and procedures include, without limitation, controls and procedures designed to ensure that information required to be disclosed in our reports filed under the Exchange Act is accumulated and communicated to management, including our principal executive and principal financial officers, as appropriate to allow timely decisions regarding required disclosure.
Based on an evaluation of the effectiveness of disclosure controls and procedures performed in connection with this Annual Report on Form 10-K, our chief executive officer and chief financial officer concluded that our disclosure controls and procedures were effective as of June 30, 2016.
68
Management’s Responsibility for Financial Statements
Our management is responsible for the integrity and objectivity of all information presented in this Annual Report on Form 10-K. The consolidated financial statements contained herein were prepared in conformity with accounting principles generally accepted in the United States of America and include amounts based on management’s best estimates and judgments. Management believes the consolidated financial statements fairly reflect the form and substance of transactions and that the financial statements fairly represent the Company’s financial position and results of operations.
The Audit Committee of the Board of Directors, which is composed solely of independent directors, meets regularly with the Company’s independent registered public accounting firm and representatives of management to review accounting, financial reporting, internal control and audit matters, as well as the nature and extent of the audit effort. The Audit Committee is responsible for the engagement of the independent registered public accounting firm. The independent registered public accounting firm has free access to the Audit Committee.
Management’s Report on Internal Control Over Financial Reporting
The management of the Company is responsible for establishing and maintaining adequate internal control over financial reporting as such term is defined in Rule 13a-15(f) under the Exchange Act. Our internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of our financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. Our internal control over financial reporting includes those policies and procedures that (i) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the Company; (ii) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the Company are being made only in accordance with authorizations of management and directors of the Company; and (iii) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the Company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Management assessed the effectiveness of the Company’s internal control over financial reporting as of June 30, 2016. In making this assessment, we used the criteria set forth by the Committee of Sponsoring Organizations of the Treadway Commission (COSO) in Internal Control—Integrated Framework (2013). Based on our assessment we concluded that, as of June 30, 2016, the Company’s internal control over financial reporting was effective based on those criteria.
This annual report does not include an attestation report of the Company’s registered public accounting firm regarding internal control over financial reporting. Management’s report was not subject to attestation by the Company’s registered public accounting firm pursuant to rules of the SEC that permit the Company to provide only management’s report in this annual report.
Changes in Internal Control over Financial Reporting
During the last fiscal quarter ended June 30, 2016, there has been no significant change in the Company’s internal control over financial reporting that has materially affected, or is reasonably likely to materially affect, the Company’s internal control over financial reporting.
69
PART IV
| Item 15. | Exhibits, Financial Statement Schedules. |
(a) (1) Financial Statements
The following consolidated financial statements of the Company and its subsidiaries are set forth in Item 8 of this Annual Report on Form 10-K.
Report of Independent Registered Public Accounting Firm.
Consolidated Balance Sheets—June 30, 2016 and 2015.
Consolidated Statements of Operations and Comprehensive Earnings and Loss—For the Years Ended June 30, 2016, 2015 and 2014.
Consolidated Statements of Shareholders’ Equity—For the Years Ended June 30, 2016, 2015 and 2014.
Consolidated Statements of Cash Flows—For the Years Ended June 30, 2016, 2015 and 2014.
Notes to Consolidated Financial Statements—For the Years Ended June 30, 2016, 2015 and 2014.
(a) (2) Financial Statement Schedules
| Report of Independent Registered Public Accounting Firm | At page 75 of this Report | |
| Schedule II Valuation and Qualifying Accounts | At page 76 of this Report |
The information required to be submitted in Schedules I, III, IV and V for SunLink Health Systems, Inc. and its consolidated subsidiaries has either been shown in the financial statements or notes, or is not applicable or not required under Regulation S-X and, therefore, has been omitted.
(a) (3) See Item 15(b) below. Each management contract or compensatory plan or arrangement required to be filed as an Exhibit is identified below by an asterisk.
(b) Exhibits
The following exhibits are filed with this Form 10-K or incorporated herein by reference from the document set forth next to the exhibit in the list below. Exhibit numbers refer to Item 601 of Regulation S-K:
| 3.1 | Amended Articles of Incorporation of SunLink Health Systems, Inc. (incorporated by reference from Exhibit 3.1 of the Company’s Report on Form 10-Q for the quarter ended September 30, 2001). (Commission File No. 1789180) | |
| 3.1a | Amended Articles of Incorporation of KRUG International Corp. (incorporated by reference to Exhibit 3.1 of the Corporation’s Report on Form 10-K405 for the year ended March 31, 1998). (Commission File No. 98649171) | |
| 3.1b | Amended Articles of Incorporation of SunLink Health Systems, Inc. (incorporated by reference from Exhibit 3.2 of the Company’s Report on Form 10-Q for the quarter ended September 30, 2001). (Commission File No. 1789180) | |
| 3.1c | Certificate of Amendment to Amend Article Fourth of the Amended Articles of Incorporation of SunLink Health Systems, Inc. dated February 13, 2004 (incorporated by reference from Exhibit 3.1 of the Company’s Report on Form 10-Q for the quarter ended December 31, 2003). (Commission File No. 04610446) | |
| 3.1d | Certificate of Amendment to Amend and Restate Article Fourth of the Company’s Amended Articles of Incorporation (incorporated by reference from Exhibit 3.1d of the Company’s Report of Form 8-K filed September 29, 2016). (Commission File No. 161910046) | |
| 3.2 | Code of Regulations of SunLink Health Systems, Inc., as amended (incorporated by reference from Exhibit 3.1 of the Company’s Report on Form 10-Q for the quarter ended September 30, 2001). (Commission File No. 1789180) | |
70
| 3.3 | Certificate of Amendment to Amend Article Fourth of the Amended Articles of Incorporation of SunLink Health Systems, Inc. dated February 13, 2004 (incorporated by reference from Exhibit 3.1 of the Company’s Report on Form 10-Q for the quarter ended December 31, 2003). (Commission File No. 04610446) | |
| 4.1 | Shareholder Rights Agreement dated as of February 10, 2014, between SunLink Health Systems, Inc. and American Stock Transfer & Trust Company, LLC, as Rights Agent (incorporated by reference from Exhibit 4.1 of the Company’s Report on Form 8-K filed February 27, 2014). (Commission File No. 14647348) | |
| 4.2 | Tax Benefits Preservation Rights Plan between SunLink Health Systems, Inc. and American Stock Transfer & Trust, LLC, as Rights Agent dated as of September 29, 2016. (incorporated by reference from Exhibit 4.2 of the Company’s Report on Form 8-K filed September 29, 2016). (Commission File No. 161910046) | |
| 10.1* | Employment Letter, dated April 30, 2001, by and between SunLink Health Systems, Inc. and Mark Stockslager (incorporated by reference from Exhibit 10.29 of SunLink’s Form 10-Q for the quarter ended September 30, 2005). (Commission File No. 051197210) | |
| 10.2* | Amended and Restated Employment Agreement, dated July 1, 2005, between Robert M. Thornton, Jr. and SunLink Health Systems, Inc. (incorporated by reference from Exhibit 99.1 of the Company’s Report on Form 8-K filed December 23, 2005). (Commission File No. 051285094) | |
| 10.3* | 2005 Equity Incentive Plan (incorporated by reference from Exhibit 99.1 of the Company’s Registration Statement on Form S-8 filed September 20, 2006). (Commission File No. 061100389) | |
| 10.5 | Agreement of Understanding, dated June 28, 2007, between Christopher H. B. Mills and SunLink Health Systems, Inc. (incorporated by reference from Exhibit 99.2 of the Company’s Report on Form 8-K filed July 16, 2007). (Commission File No. 07982325) | |
| 10.6* | Employment letter dated September 23, 2010 with an effective date of September 30, 2010, by and between SunLink ScriptsRx, LLC and Byron D. Finn (incorporated by reference from the Company’s Annual Report on Form 10-K for the year ended June 30, 2011). (Commission File No. 111108066) | |
| 10.7 | Mortgage Loan Agreement dated as of July 5, 2012, by and between Stillwater National Bank and Southern Health Corporation of Houston, Inc. (incorporated by reference from the Company’s Annual Report on Form 10-K for the year ended June 30, 2012). (Commission File No. 121102676) | |
| 10.8 | Working Capital Loan Agreement dated as of July 5, 2012, by and between Stillwater National Bank and Southern Health Corporation of Houston, Inc. (incorporated by reference from the Company’s Annual Report on Form 10-K for the year ended June 30, 2012). (Commission File No. 121102676) | |
| 10.9 | Loan Agreement dated as of October 31, 2012 by and among Pioneer Bank, SSB; SunLink Healthcare Professional Property, LLC; MedCare South, LLC; and SunLink Health Systems, Inc. (incorporated by reference from the Company’s Quarterly Report on Form 10-Q for the quarter ended September 30, 2012). (Commission File No. 121203717) | |
| 10.10 | Amendment and Waiver to Mortgage Loan Agreement as of May 14, 2013, among Southern Health Corporation of Houston, Inc., MedCare South, LLC, SunLink Health Systems, Inc., and Stillwater National Bank and Trust Company. (incorporated by reference from the Company’s Quarterly Report on Form 10-Q for the quarter ended March 31, 2013). (Commission File No. 13848205) | |
| 10.11 | Amendment and Waiver to Working Capital Loan Agreement as of May 14, 2013, among Southern Health Corporation of Houston, Inc., MedCare South, LLC, SunLink Health Systems, Inc., and Stillwater National Bank and Trust Company. (incorporated by reference from the Company’s Quarterly Report on Form 10-Q for the quarter ended March 31, 2013). (Commission File No. 13848205) | |
| 10.12 | Second Amendment and Waiver to Mortgage Loan Agreement as of June 28, 2013, among Southern Health Corporation of Houston, Inc., MedCare South, LLC, SunLink Health Systems, Inc., and Stillwater National Bank and Trust Company. (incorporated by reference from the Company’s Annual Report on Form 10-K for the year ended June 30, 2013). (Commission File No. 131119753) | |
71
| 10.13 | Second Amendment and Waiver to Working Capital Loan Agreement as of June 28, 2013, among Southern Health Corporation of Houston, Inc., MedCare South, LLC, SunLink Health Systems, Inc., and Stillwater National Bank and Trust Company. (incorporated by reference from the Company’s Annual Report on Form 10-K for the year ended June 30, 2013). (Commission File No. 131119753) | |
| 10.14 | Third Amendment and Waiver to Mortgage Loan Agreement as of June 30, 2014, among Southern Health Corporation of Houston, Inc., Crown Healthcare Investments, LLC, SunLink Health Systems, Inc., and Stillwater National Bank and Trust Company. (incorporated by reference from the Company’s Annual Report on Form 10-K for the year ended June 30, 2014). (Commission File No. 1141123931) | |
| 10.15 | Third Amendment and Waiver to Working Capital Loan Agreement as of June 30, 2014, among Southern Health Corporation of Houston, Inc., Crown Healthcare Investments, LLC, SunLink Health Systems, Inc., and Stillwater National Bank and Trust Company. (incorporated by reference from the Company’s Annual Report on Form 10-K for the year ended June 30, 2014). (Commission File No. 1141123931) | |
| 10.16* | 2011 Director Stock Option Plan (incorporated by reference from Appendix A to the Company’s Schedule 14A Definitive Proxy Statement filed September 29, 2011) (Commission File No. 111115265). | |
| 10.17 | Asset Purchase Agreement dated December 3, 2014, By and Among HealthMont of Missouri, LLC, Crown Healthcare Investments, LLC and Fulton Medical, LLC, Nueterra Holdings, LLC. (incorporated by reference from the Company’s Current Report on Form 8-K filed December 8, 2014) (Commission File No. 141272980) | |
| 10.18 | Fourth Amendment effective July 5, 2015, among Southern Health Corporation of Houston, Inc., Crown Healthcare Investments, LLC, SunLink Health Systems, Inc., and Stillwater National Bank and Trust Company. (incorporated by reference from the Company’s Annual Report on Form 10-K for the year ended June 30, 2015). (Commission File No. 151125045) | |
| 10.19 | Limited Waiver to Mortgage Loan Agreement as of March 31, 2016 among Southern Health Corporation of Houston, Inc. Crown Healthcare Investments, LLC SunLink Health Systems, Inc. and Bank SNB. (incorporated by reference from the Company’s Annual Report on Form 10-Q for the quarter ended March 31, 2016). (Commission File No. 161646127) | |
| 10.20 | Limited Waiver to Working Capital Loan Agreement as of March 31, 2016 among Southern Health Corporation of Houston, Inc. Crown Healthcare Investments, LLC SunLink Health Systems, Inc. and Bank SNB. (incorporated by reference from the Company’s Annual Report on Form 10-Q for the quarter ended March 31, 2016). (Commission File No. 161646127) | |
| 10.21 | Letter Agreement dated June 3, 2016 between Piedmont Mountainside Hospital, Inc., SunLink Healthcare Professional Property, LLC and Southern Health Corporation of Ellijay, Inc. (incorporated by reference from the Company’s Current Report on Form 8-K filed June 10, 2016) (Commission File No. 161708777) | |
| 10.22 | Asset Purchase Agreement dated August 19, 2016 between Southern Health Corporation of Dahlonega, Inc. and Durall Capital Holdings, LLC. (incorporated by reference from the Company’s Current Report on Form 8-K filed August 25, 2016) (Commission File No. 161851572) | |
| 10.23 | Limited Waiver dated August 10, 2016 among Southern Health Corporation of Houston, Inc., Crown Healthcare Investments, LLC, SunLink Health Systems, Inc. and Bank SNB. (incorporated by reference from the Company’s Current Report on Form 8-K filed August 25, 2016) (Commission File No. 161851572) | |
| 10.24 | Lease Agreement dated July 1, 2016 between SunLink Healthcare Professional Property, LLC and Piedmont Mountainside Hospital, Inc. (incorporated by reference from the Company’s Current Report on Form 8-K filed August 25, 2016) (Commission File No. 161851572) | |
72
| 21.1 | List of Subsidiaries ^ | |
| 23.1 | Consent of Cherry Bekaert LLP ^ | |
| 31.1 | Chief Executive Officer’s Certification Pursuant to Rule 13a-14(a) of the Securities Exchange Act of 1934. ^ | |
| 31.2 | Chief Financial Officer’s Certification Pursuant to Rule 13a-14(a) of the Securities Exchange Act of 1934. ^ | |
| 32.1 | Chief Executive Officer’s Certification Pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002. ^ | |
| 32.2 | Chief Financial Officer’s Certification Pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002. ^ | |
| 101 | The following materials from the Company’s Year End Report on Form 10-K for the fiscal year ended June 30, 2016, formatted in eXtensible Business Reporting Language (“XBRL”): (i) Consolidated Balance Sheets as of June 30, 2016 and June 30, 2015, (ii) Consolidated Statements of Operations and Comprehensive Earnings and Loss for the fiscal years ended June 30, 2016, 2015 and 2014, (iii) Consolidated Statements of Shareholders’ Equity for the fiscal years ended June 30, 2016, 2015 and 2014 (iv) Consolidated Statements of Cash Flows for the fiscal years ended June 30, 2016, 2015 and 2014, and (v) Notes to Consolidated Financial Statements. | |
| * | Management contract or compensatory plan or arrangement. |
| ^ | Filed herewith. |
73
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, SunLink Health Systems, Inc. has duly caused this Report to be signed on its behalf by the undersigned, thereunto duly authorized, on this 30th day of September, 2016.
| SUNLINK HEALTH SYSTEMS, INC. | ||
| By: | /s/ ROBERT M. THORNTON, JR. | |
| Robert M. Thornton, Jr. Chairman and Chief Executive Officer | ||
Pursuant to the requirements of the Securities Exchange Act of 1934, this Report has been signed below by the following persons on behalf of SunLink Health Systems, Inc. and in the capacities and on the dates indicated:
| Name |
Title |
Date | ||
| /S/ ROBERT M. THORNTON, JR. Robert M. Thornton, Jr. |
Director, Chairman, President and |
September 30, 2016 | ||
| /S/ MARK J. STOCKSLAGER Mark J. Stockslager |
Chief Financial Officer and |
September 30, 2016 | ||
| /S/ STEVEN J. BAILEYS, D.D.S. Steven J. Baileys, D.D.S. |
Director |
September 30, 2016 | ||
| /S/ KAREN B. BRENNER Karen B. Brenner |
Director |
September 30, 2016 | ||
| /S/ GENE E. BURLESON Gene E. Burleson |
Director |
September 30, 2016 | ||
| /S/ C. MICHAEL FORD C. Michael Ford |
Director |
September 30, 2016 | ||
| /S/ CHRISTOPHER H. B. MILLS Christopher H. B. Mills |
Director |
September 30, 2016 | ||
| /S/ HOWARD E. TURNER Howard E. Turner |
Director |
September 30, 2016 | ||
74
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
Board of Directors and Shareholders of
SunLink Health Systems, Inc.
We have audited the consolidated financial statements of SunLink Health Systems, Inc. and subsidiaries (the “Company”) as of June 30, 2016 and 2015 and for each of the years in the three-year period ended June 30, 2016 and have issued our report thereon dated September 30, 2016; such consolidated financial statements and report are included elsewhere in this Form 10-K. Our audits also included the consolidated financial statement schedules of the Company, listed in Item 15 for each of the years in the three-year period ended June 30, 2016. These consolidated financial statement schedules are the responsibility of the Company’s management. Our responsibility is to express an opinion based on our audits. In our opinion, such consolidated financial statement schedules, when considered in relation to the basic consolidated financial statements taken as a whole, present fairly in all material respects the information set forth therein.
/s/ Cherry Bekaert LLP
Atlanta, Georgia
September 30, 2016
75
SUNLINK HEALTH SYSTEMS, INC. AND SUBSIDIARIES
SCHEDULE II—VALUATION AND QUALIFYING ACCOUNTS
(amounts in thousands)
| Column A |
Column B | Column C | Column D | Column E | ||||||||||||||||
| Allowance for Doubtful Accounts |
Balance at Beginning Of Year |
Charged to Cost and Expenses |
Currency Translation/ Acquisition/ (Disposition) |
Deductions from Reserves |
Balance at End of Year |
|||||||||||||||
| Year Ended June 30, 2016 |
$ | 5,437 | $ | 4,655 | $ | — | $ | (7,230 | ) | $ | 2,862 | |||||||||
| Year Ended June 30, 2015 |
$ | 6,903 | $ | 10,433 | $ | — | $ | (11,989 | ) | $ | 5,347 | |||||||||
| Year Ended June 30, 2014 |
$ | 7,761 | $ | 11,319 | $ | — | $ | (12,177 | ) | $ | 6,903 | |||||||||
| Deferred Income Tax Asset Valuation Allowance |
Balance at Beginning Of Year |
Charged to Cost and Expenses/ (Benefit) |
Currency Translation/ Acquisition/ (Disposition) |
Deductions from Reserves |
Balance at End of Year |
|||||||||||||||
| Year Ended June 30, 2016 |
$ | 2,564 | $ | 8,088 | $ | — | $ | — | $ | 10,652 | ||||||||||
| Year Ended June 30, 2015 |
$ | 2,577 | $ | (13 | ) | $ | — | $ | — | $ | 2,564 | |||||||||
| Year Ended June 30, 2014 |
$ | 2,151 | $ | 426 | $ | — | $ | — | $ | 2,577 | ||||||||||
76
INDEX TO EXHIBITS
| 3.1 | Amended Articles of Incorporation of SunLink Health Systems, Inc. (incorporated by reference from Exhibit 3.1 of the Company’s Report on Form 10-Q for the quarter ended September 30, 2001). (Commission File No. 1789180) | |
| 3.1a | Amended Articles of Incorporation of KRUG International Corp. (incorporated by reference to Exhibit 3.1 of the Corporation’s Report on Form 10-K405 for the year ended March 31, 1998). (Commission File No. 98649171) | |
| 3.1b | Amended Articles of Incorporation of SunLink Health Systems, Inc. (incorporated by reference from Exhibit 3.2 of the Company’s Report on Form 10-Q for the quarter ended September 30, 2001). (Commission File No. 1789180) | |
| 3.1c | Certificate of Amendment to Amend Article Fourth of the Amended Articles of Incorporation of SunLink Health Systems, Inc. dated February 13, 2004 (incorporated by reference from Exhibit 3.1 of the Company’s Report on Form 10-Q for the quarter ended December 31, 2003). (Commission File No. 04610446) | |
| 3.1d | Certificate of Amendment to Amend and Restate Article Fourth of the Company’s Amended Articles of Incorporation (incorporated by reference from Exhibit 3.1d of the Company’s Report of Form 8-K filed September 29, 2016). (Commission File No. 161910046) | |
| 3.2 | Code of Regulations of SunLink Health Systems, Inc., as amended (incorporated by reference from Exhibit 3.1 of the Company’s Report on Form 10-Q for the quarter ended September 30, 2001). (Commission File No. 1789180) | |
| 3.3 | Certificate of Amendment to Amend Article Fourth of the Amended Articles of Incorporation of SunLink Health Systems, Inc. dated February 13, 2004 (incorporated by reference from Exhibit 3.1 of the Company’s Report on Form 10-Q for the quarter ended December 31, 2003). (Commission File No. 04610446) | |
| 4.1 | Shareholder Rights Agreement dated as of February 10, 2014, between SunLink Health Systems, Inc. and American Stock Transfer & Trust Company, LLC, as Rights Agent (incorporated by reference from Exhibit 4.1 of the Company’s Report on Form 8-K filed February 27, 2014). (Commission File No. 14647348) | |
| 4.2 | Tax Benefits Preservation Rights Plan between SunLink Health Systems, Inc. and American Stock Transfer & Trust, LLC, as Rights Agent dated as of September 29, 2016. (incorporated by reference from Exhibit 4.2 of the Company’s Report on Form 8-K filed September 29, 2016). (Commission File No. 161910046) | |
| 10.1* | Employment Letter, dated April 30, 2001, by and between SunLink Health Systems, Inc. and Mark Stockslager (incorporated by reference from Exhibit 10.29 of SunLink’s Form 10-Q for the quarter ended September 30, 2005). (Commission File No. 051197210) | |
| 10.2* | Amended and Restated Employment Agreement, dated July 1, 2005, between Robert M. Thornton, Jr. and SunLink Health Systems, Inc. (incorporated by reference from Exhibit 99.1 of the Company’s Report on Form 8-K filed December 23, 2005). (Commission File No. 051285094) | |
| 10.3* | 2005 Equity Incentive Plan (incorporated by reference from Exhibit 99.1 of the Company’s Registration Statement on Form S-8 filed September 20, 2006). (Commission File No. 061100389) | |
| 10.5 | Agreement of Understanding, dated June 28, 2007, between Christopher H. B. Mills and SunLink Health Systems, Inc. (incorporated by reference from Exhibit 99.2 of the Company’s Report on Form 8-K filed July 16, 2007). (Commission File No. 07982325) | |
| 10.6* | Employment letter dated September 23, 2010 with an effective date of September 30, 2010, by and between SunLink ScriptsRx, LLC and Byron D. Finn (incorporated by reference from the Company’s Annual Report on Form 10-K for the year ended June 30, 2011). (Commission File No. 111108066) | |
77
| 10.7 | Mortgage Loan Agreement dated as of July 5, 2012, by and between Stillwater National Bank and Southern Health Corporation of Houston, Inc. (incorporated by reference from the Company’s Annual Report on Form 10-K for the year ended June 30, 2012). (Commission File No. 121102676) | |
| 10.8 | Working Capital Loan Agreement dated as of July 5, 2012, by and between Stillwater National Bank and Southern Health Corporation of Houston, Inc. (incorporated by reference from the Company’s Annual Report on Form 10-K for the year ended June 30, 2012). (Commission File No. 121102676) | |
| 10.9 | Loan Agreement dated as of October 31, 2012 by and among Pioneer Bank, SSB; SunLink Healthcare Professional Property, LLC; MedCare South, LLC; and SunLink Health Systems, Inc. (incorporated by reference from the Company’s Quarterly Report on Form 10-Q for the quarter ended September 30, 2012). (Commission File No. 121203717) | |
| 10.10 | Amendment and Waiver to Mortgage Loan Agreement as of May 14, 2013, among Southern Health Corporation of Houston, Inc., MedCare South, LLC, SunLink Health Systems, Inc., and Stillwater National Bank and Trust Company. (incorporated by reference from the Company’s Quarterly Report on Form 10-Q for the quarter ended March 31, 2013). (Commission File No. 13848205) | |
| 10.11 | Amendment and Waiver to Working Capital Loan Agreement as of May 14, 2013, among Southern Health Corporation of Houston, Inc., MedCare South, LLC, SunLink Health Systems, Inc., and Stillwater National Bank and Trust Company. (incorporated by reference from the Company’s Quarterly Report on Form 10-Q for the quarter ended March 31, 2013). (Commission File No. 13848205) | |
| 10.12 | Second Amendment and Waiver to Mortgage Loan Agreement as of June 28, 2013, among Southern Health Corporation of Houston, Inc., MedCare South, LLC, SunLink Health Systems, Inc., and Stillwater National Bank and Trust Company. (incorporated by reference from the Company’s Annual Report on Form 10-K for the year ended June 30, 2013). (Commission File No. 131119753) | |
| 10.13 | Second Amendment and Waiver to Working Capital Loan Agreement as of June 28, 2013, among Southern Health Corporation of Houston, Inc., MedCare South, LLC, SunLink Health Systems, Inc., and Stillwater National Bank and Trust Company. (incorporated by reference from the Company’s Annual Report on Form 10-K for the year ended June 30, 2013). (Commission File No. 131119753) | |
| 10.14 | Third Amendment and Waiver to Mortgage Loan Agreement as of June 30, 2014, among Southern Health Corporation of Houston, Inc., Crown Healthcare Investments, LLC, SunLink Health Systems, Inc., and Stillwater National Bank and Trust Company. (incorporated by reference from the Company’s Annual Report on Form 10-K for the year ended June 30, 2014). (Commission File No. 1141123931) | |
| 10.15 | Third Amendment and Waiver to Working Capital Loan Agreement as of June 30, 2014, among Southern Health Corporation of Houston, Inc., Crown Healthcare Investments, LLC, SunLink Health Systems, Inc., and Stillwater National Bank and Trust Company. (incorporated by reference from the Company’s Annual Report on Form 10-K for the year ended June 30, 2014). (Commission File No. 1141123931) | |
| 10.16* | 2011 Director Stock Option Plan (incorporated by reference from Appendix A to the Company’s Schedule 14A Definitive Proxy Statement filed September 29, 2011) (Commission File No. 111115265). | |
| 10.17 | Asset Purchase Agreement dated December 3, 2014, By and Among HealthMont of Missouri, LLC, Crown Healthcare Investments, LLC and Fulton Medical, LLC, Nueterra Holdings, LLC. (incorporated by reference from the Company’s Current Report on Form 8-K filed December 8, 2014) (Commission File No. 141272980) | |
| 10.18 | Fourth Amendment effective July 5, 2015, among Southern Health Corporation of Houston, Inc., Crown Healthcare Investments, LLC, SunLink Health Systems, Inc., and Stillwater National Bank and Trust Company. (incorporated by reference from the Company’s Annual Report on Form 10-K for the year ended June 30, 2015). (Commission File No. 151125045) | |
78
| 10.19 | Limited Waiver to Mortgage Loan Agreement as of March 31, 2016 among Southern Health Corporation of Houston, Inc. Crown Healthcare Investments, LLC SunLink Health Systems, Inc. and Bank SNB. (incorporated by reference from the Company’s Annual Report on Form 10-Q for the quarter ended March 31, 2016). (Commission File No. 161646127) | |
| 10.20 | Limited Waiver to Working Capital Loan Agreement as of March 31, 2016 among Southern Health Corporation of Houston, Inc. Crown Healthcare Investments, LLC SunLink Health Systems, Inc. and Bank SNB. (incorporated by reference from the Company’s Annual Report on Form 10-Q for the quarter ended March 31, 2016). (Commission File No. 161646127) | |
| 10.21 | Letter Agreement dated June 3, 2016 between Piedmont Mountainside Hospital, Inc., SunLink Healthcare Professional Property, LLC and Southern Health Corporation of Ellijay, Inc. (incorporated by reference from the Company’s Current Report on Form 8-K filed June 10, 2016) (Commission File No. 161708777) | |
| 10.22 | Asset Purchase Agreement dated August 19, 2016 between Southern Health Corporation of Dahlonega, Inc. and Durall Capital Holdings, LLC. (incorporated by reference from the Company’s Current Report on Form 8-K filed August 25, 2016) (Commission File No. 161851572) | |
| 10.23 | Limited Waiver dated August 10, 2016 among Southern Health Corporation of Houston, Inc., Crown Healthcare Investments, LLC, SunLink Health Systems, Inc. and Bank SNB. (incorporated by reference from the Company’s Current Report on Form 8-K filed August 25, 2016) (Commission File No. 161851572) | |
| 10.24 | Lease Agreement dated July 1, 2016 between SunLink Healthcare Professional Property, LLC and Piedmont Mountainside Hospital, Inc. (incorporated by reference from the Company’s Current Report on Form 8-K filed August 25, 2016) (Commission File No. 161851572) | |
| 21.1 | List of Subsidiaries ^ | |
| 23.1 | Consent of Cherry Bekaert LLP ^ | |
| 31.1 | Chief Executive Officer’s Certification Pursuant to Rule 13a-14(a) of the Securities Exchange Act of 1934. ^ | |
| 31.2 | Chief Financial Officer’s Certification Pursuant to Rule 13a-14(a) of the Securities Exchange Act of 1934. ^ | |
| 32.1 | Chief Executive Officer’s Certification Pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002. ^ | |
| 32.2 | Chief Financial Officer’s Certification Pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002. ^ | |
| 101 | The following materials from the Company’s Year End Report on Form 10-K for the fiscal year ended June 30, 2016, formatted in eXtensible Business Reporting Language (“XBRL”): (i) Consolidated Balance Sheets as of June 30, 2016 and June 30, 2015, (ii) Consolidated Statements of Operations and Comprehensive Earnings and Loss for the fiscal years ended June 30, 2016, 2015 and 2014, (iii) Consolidated Statements of Shareholders’ Equity for the fiscal years ended June 30, 2016, 2015 and 2014 (iv) Consolidated Statements of Cash Flows for the fiscal years ended June 30, 2016, 2015 and 2014, and (v) Notes to Consolidated Financial Statements. | |
| * | Management contract or compensatory plan or arrangement. |
| ^ | Filed herewith. |
79
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Board of Directors and Shareholders of
SunLink Health Systems, Inc.
We have audited the accompanying balance sheets of SunLink Health Systems, Inc. and subsidiaries (the “Company”) as of June 30, 2016 and 2015, and the related consolidated statements of operations and comprehensive earnings and loss, shareholders’ equity, and cash flows for each of the years in the three-year period ended June 30, 2016. The company’s management is responsible for these consolidated financial statements. Our responsibility is to express an opinion on these financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. The company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. Our audit included consideration of internal control over financial reporting as a basis for designing audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the company’s internal control over financial reporting. Accordingly, we express no such opinion. An audit also includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements, assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the financial position of the Company as of June 30, 2016 and 2015, and the results of its operations and its cash flows for each of the years in the three-year period ended June 30, 2016 in conformity with accounting principles generally accepted in the United States of America.
/s/ Cherry Bekaert LLP
Atlanta, Georgia
September 30, 2016
F-1
CONSOLIDATED BALANCE SHEETS
JUNE 30, 2016 AND 2015
(All Amounts in thousands)
| 2016 | 2015 | |||||||
| ASSETS | ||||||||
| CURRENT ASSETS: |
||||||||
| Cash and cash equivalents |
$ | 3,261 | $ | 5,974 | ||||
| Receivables—net |
6,166 | 7,679 | ||||||
| Inventory |
2,612 | 3,148 | ||||||
| Deferred income tax asset |
624 | 1,967 | ||||||
| Current assets held for sale |
2,461 | 2,789 | ||||||
| Prepaid expenses and other assets |
2,777 | 2,409 | ||||||
| Due from third party payors |
0 | 1,126 | ||||||
|
|
|
|
|
|||||
| Total current assets |
17,901 | 25,092 | ||||||
| PROPERTY, PLANT AND EQUIPMENT |
||||||||
| Land |
1,155 | 1,155 | ||||||
| Buildings and improvements |
14,286 | 16,062 | ||||||
| Equipment and fixtures |
18,473 | 17,769 | ||||||
|
|
|
|
|
|||||
| 33,914 | 34,986 | |||||||
| Less accumulated depreciation |
20,920 | 20,743 | ||||||
|
|
|
|
|
|||||
| Property, plant and equipment—net |
12,994 | 14,243 | ||||||
| NONCURRENT ASSETS: |
||||||||
| Intangible assets—net |
2,695 | 2,837 | ||||||
| Goodwill |
461 | 461 | ||||||
| Deferred income tax asset |
1,698 | 4,885 | ||||||
| Noncurrent assets held for sale |
7,633 | 8,090 | ||||||
| Other noncurrent assets |
1,459 | 1,520 | ||||||
|
|
|
|
|
|||||
| Total noncurrent assets |
13,946 | 17,793 | ||||||
|
|
|
|
|
|||||
| TOTAL ASSETS |
$ | 44,841 | $ | 57,128 | ||||
|
|
|
|
|
|||||
| LIABILITIES AND SHAREHOLDERS’ EQUITY | ||||||||
| CURRENT LIABILITIES: |
||||||||
| Accounts payable |
$ | 3,391 | $ | 2,688 | ||||
| Current maturities of long-term debt |
8,012 | 816 | ||||||
| Accrued payroll and related taxes |
2,872 | 3,475 | ||||||
| Due to third party payors |
1,883 | 0 | ||||||
| Income tax payable |
2 | 64 | ||||||
| Current liabilities held for sale |
2,745 | 2,343 | ||||||
| Other accrued expenses |
1,685 | 1,378 | ||||||
|
|
|
|
|
|||||
| Total current liabilities |
20,590 | 10,764 | ||||||
| LONG-TERM LIABILITIES: |
||||||||
| Long-term debt |
3,176 | 11,229 | ||||||
| Noncurrent liability for professional liability risks |
1,161 | 894 | ||||||
| Other noncurrent liabilities |
425 | 681 | ||||||
|
|
|
|
|
|||||
| Total long-term liabilities |
4,762 | 12,804 | ||||||
|
|
|
|
|
|||||
| COMMITMENTS AND CONTINGENCIES |
||||||||
| SHAREHOLDERS’ EQUITY: |
||||||||
| Preferred Shares, authorized and unissued, 2,000 shares |
0 | 0 | ||||||
| Common Shares, no par value; authorized, 12,000 shares; issued and outstanding, 9,444 shares at June 30, 2016 and 9,444 shares at June 30, 2015 |
4,722 | 4,722 | ||||||
| Additional paid-in capital |
13,539 | 13,481 | ||||||
| Retained earnings |
1,648 | 15,731 | ||||||
| Accumulated other comprehensive loss |
(420 | ) | (374 | ) | ||||
|
|
|
|
|
|||||
| Total Shareholders’ Equity |
19,489 | 33,560 | ||||||
|
|
|
|
|
|||||
| TOTAL LIABILITIES AND SHAREHOLDERS’ EQUITY |
$ | 44,841 | $ | 57,128 | ||||
|
|
|
|
|
|||||
See notes to consolidated financial statements.
F-2
CONSOLIDATED STATEMENTS OF OPERATIONS
AND COMPREHENSIVE EARNINGS AND LOSS
FOR THE YEARS ENDED JUNE 30, 2016, 2015 AND 2014
(All amounts in thousands, except per share amounts)
| Years Ended June 30, | ||||||||||||
| 2016 | 2015 | 2014 | ||||||||||
| Operating revenues (net of contractual allowances) |
$ | 64,871 | $ | 77,424 | $ | 77,564 | ||||||
| Less provision for bad debts of Healthcare Facilities Segment |
1,438 | 3,678 | 3,795 | |||||||||
|
|
|
|
|
|
|
|||||||
| Net Revenues |
63,433 | 73,746 | 73,769 | |||||||||
| Costs and expenses: |
||||||||||||
| Cost of goods sold |
20,404 | 21,042 | 22,110 | |||||||||
| Salaries, wages and benefits |
30,783 | 33,620 | 32,771 | |||||||||
| Provision for bad debts of Specialty Pharmacy Segment |
630 | 363 | 255 | |||||||||
| Supplies |
3,326 | 4,366 | 4,236 | |||||||||
| Purchased services |
3,248 | 3,616 | 3,288 | |||||||||
| Other operating expenses |
8,031 | 6,893 | 9,142 | |||||||||
| Rents and leases expense |
791 | 818 | 877 | |||||||||
| Impairment of property, plant and equipment |
858 | 0 | 0 | |||||||||
| Insurance settlement |
0 | (1,000 | ) | 0 | ||||||||
| Depreciation and amortization |
1,878 | 1,837 | 2,322 | |||||||||
| Electronic Health Records incentive payments |
7 | (29 | ) | (2,274 | ) | |||||||
|
|
|
|
|
|
|
|||||||
| Operating profit (loss) |
(6,523 | ) | 2,220 | 1,042 | ||||||||
| Other income (expense): |
||||||||||||
| Interest expense |
(843 | ) | (861 | ) | (944 | ) | ||||||
| Gain (loss) on sale of assets |
10 | 21 | (41 | ) | ||||||||
|
|
|
|
|
|
|
|||||||
| Earnings (Loss) from continuing operations before income taxes |
(7,356 | ) | 1,380 | 57 | ||||||||
| Income tax (benefit) expense |
4,558 | 893 | 541 | |||||||||
|
|
|
|
|
|
|
|||||||
| Earnings (loss) from continuing operations |
(11,914 | ) | 487 | (484 | ) | |||||||
| Loss from discontinued operations, net of income taxes |
(2,169 | ) | (242 | ) | (61 | ) | ||||||
|
|
|
|
|
|
|
|||||||
| Net earnings (loss) |
(14,083 | ) | 245 | (545 | ) | |||||||
| Other comprehensive income (loss) |
(46 | ) | (40 | ) | 72 | |||||||
|
|
|
|
|
|
|
|||||||
| Comprehensive income (loss) |
$ | (14,129 | ) | $ | 205 | $ | (473 | ) | ||||
|
|
|
|
|
|
|
|||||||
| Earnings (loss) per share: |
||||||||||||
| Continuing operations: |
||||||||||||
| Basic |
$ | (1.26 | ) | $ | 0.05 | $ | (0.05 | ) | ||||
|
|
|
|
|
|
|
|||||||
| Diluted |
$ | (1.26 | ) | $ | 0.05 | $ | (0.05 | ) | ||||
|
|
|
|
|
|
|
|||||||
| Discontinued operations: |
||||||||||||
| Basic |
$ | (0.23 | ) | $ | (0.02 | ) | $ | (0.01 | ) | |||
|
|
|
|
|
|
|
|||||||
| Diluted |
$ | (0.23 | ) | $ | (0.02 | ) | $ | (0.01 | ) | |||
|
|
|
|
|
|
|
|||||||
| Net earnings (loss): |
||||||||||||
| Basic |
$ | (1.49 | ) | $ | 0.03 | $ | (0.06 | ) | ||||
|
|
|
|
|
|
|
|||||||
| Diluted |
$ | (1.49 | ) | $ | 0.03 | $ | (0.06 | ) | ||||
|
|
|
|
|
|
|
|||||||
| Weighted-average common shares outstanding: |
||||||||||||
| Basic |
9,443 | 9,443 | 9,443 | |||||||||
|
|
|
|
|
|
|
|||||||
| Diluted |
9,443 | 9,496 | 9,456 | |||||||||
|
|
|
|
|
|
|
|||||||
See notes to consolidated financial statements.
F-3
CONSOLIDATED STATEMENTS OF SHAREHOLDERS’ EQUITY
FOR THE YEARS ENDED JUNE 30, 2016, 2015 AND 2014
(All amounts in thousands)
| Common Shares | Additional Paid-in Capital |
Retained Earnings |
Accumulated Other Comprehensive Earnings (Loss) |
Total Shareholders’ Equity |
||||||||||||||||||||
| Shares | Amount | |||||||||||||||||||||||
| JUNE 30, 2013 |
9,444 | $ | 4,722 | $ | 13,396 | $ | 16,031 | $ | (406 | ) | $ | 33,743 | ||||||||||||
| Net loss |
0 | 0 | 0 | (545 | ) | 0 | (545 | ) | ||||||||||||||||
| Minimum pension liability adjustment, net of tax of $44 |
0 | 0 | 0 | 0 | 72 | 72 | ||||||||||||||||||
| Share-based compensation |
0 | 0 | 48 | 0 | 0 | 48 | ||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
| JUNE 30, 2014 |
9,444 | 4,722 | 13,444 | 15,486 | (334 | ) | 33,318 | |||||||||||||||||
| Net earnings |
0 | 0 | 0 | 245 | 0 | 245 | ||||||||||||||||||
| Minimum pension liability adjustment, net of tax of $25 |
0 | 0 | 0 | 0 | (40 | ) | (40 | ) | ||||||||||||||||
| Share-based compensation |
0 | 0 | 37 | 0 | 0 | 37 | ||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
| JUNE 30, 2015 |
9,444 | 4,722 | 13,481 | 15,731 | (374 | ) | 33,560 | |||||||||||||||||
| Net loss |
0 | 0 | 0 | (14,083 | ) | 0 | (14,083 | ) | ||||||||||||||||
| Minimum pension liability adjustment, net of tax of $28 |
0 | 0 | 0 | 0 | (46 | ) | (46 | ) | ||||||||||||||||
| Share-based compensation |
0 | 0 | 58 | 0 | 0 | 58 | ||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
| JUNE 30, 2016 |
$ | 9,444 | $ | 4,722 | $ | 13,539 | $ | 1,648 | $ | (420 | ) | $ | 19,489 | |||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
See notes to consolidated financial statements.
F-4
CONSOLIDATED STATEMENTS OF CASH FLOWS
FOR THE YEARS ENDED JUNE 30, 2016, 2015 AND 2014
(All amounts in thousands)
| Years Ended June 30, | ||||||||||||
| 2016 | 2015 | 2014 | ||||||||||
| CASH FLOWS FROM OPERATING ACTIVITIES |
||||||||||||
| Net earnings (loss) |
$ | (14,083 | ) | $ | 245 | $ | (545 | ) | ||||
| Adjustments to reconcile net earnings (loss) to net cash provided by (used in) operating activities: |
||||||||||||
| Depreciation and amortization |
2,436 | 2,681 | 3,662 | |||||||||
| Share-based compensation |
58 | 37 | 48 | |||||||||
| Impairment of property, plant and equipment |
858 | 0 | 0 | |||||||||
| Loss (gain) on disposal of property, plant and equipment |
(15 | ) | (21 | ) | 41 | |||||||
| Loss on sale of Fulton Hospital |
0 | 197 | 0 | |||||||||
| Change in assets and liabilities: |
||||||||||||
| Receivables |
1,513 | 444 | 1,358 | |||||||||
| Inventory |
536 | (20 | ) | (249 | ) | |||||||
| Prepaid expenses and other assets |
(309 | ) | (279 | ) | 1,393 | |||||||
| Accounts payable and accrued expenses |
374 | (1,890 | ) | (912 | ) | |||||||
| Income taxes |
(62 | ) | (9 | ) | 1,842 | |||||||
| Deferred income taxes |
4,530 | 557 | 803 | |||||||||
| Third-party payor settlements |
3,009 | 1,660 | (3,342 | ) | ||||||||
| Electronic Health Records deferred gain |
0 | 0 | (1,135 | ) | ||||||||
| Net activities of discontinued operations |
729 | (664 | ) | 928 | ||||||||
|
|
|
|
|
|
|
|||||||
| Net cash provided by (used in) operating activities |
(426 | ) | 2,938 | 3,892 | ||||||||
| CASH FLOWS FROM INVESTING ACTIVITIES |
||||||||||||
| Proceeds from sale of Fulton Hospital |
0 | 6,090 | 0 | |||||||||
| Proceeds from sale of property, plant & equipment |
21 | 34 | 0 | |||||||||
| Change in cash in escrow |
0 | 0 | (160 | ) | ||||||||
| Expenditures for property, plant and equipment – continuing operations |
(1,347 | ) | (1,235 | ) | (1,484 | ) | ||||||
| Expenditures for property, plant and equipment – discontinued operations |
(104 | ) | (78 | ) | (239 | ) | ||||||
|
|
|
|
|
|
|
|||||||
| Net cash provided by (used in) investing activities |
(1,430 | ) | 4,811 | (1,883 | ) | |||||||
| CASH FLOWS FROM FINANCING ACTIVITIES: |
||||||||||||
| Payment of long-term debt – continuing operations |
(857 | ) | (695 | ) | (795 | ) | ||||||
| Payment of long-term debt – discontinued operations |
0 | (4,842 | ) | (124 | ) | |||||||
| Proceeds from long-term debt – continuing operations |
0 | 175 | 0 | |||||||||
|
|
|
|
|
|
|
|||||||
| Net cash used in by financing activities |
(857 | ) | (5,362 | ) | (919 | ) | ||||||
| NET INCREASE (DECREASE) IN CASH AND CASH EQUIVALENTS |
(2,713 | ) | 2,387 | 1,090 | ||||||||
| CASH AND CASH EQUIVALENTS: |
||||||||||||
| Beginning of year |
5,974 | 3,587 | 2,497 | |||||||||
|
|
|
|
|
|
|
|||||||
| End of year |
$ | 3,261 | $ | 5,974 | $ | 3,587 | ||||||
|
|
|
|
|
|
|
|||||||
| SUPPLEMENTAL DISCLOSURE OF CASH FLOW INFORMATION |
||||||||||||
| Cash paid for (refunded by): |
||||||||||||
| Income taxes |
$ | 78 | $ | 57 | $ | (1,881 | ) | |||||
|
|
|
|
|
|
|
|||||||
| Interest |
$ | 768 | $ | 914 | $ | 1,128 | ||||||
|
|
|
|
|
|
|
|||||||
| Non-cash investing and financing activities: |
||||||||||||
| Assets acquired under capital lease obligation – continuing operations |
$ | 0 | $ | 56 | $ | 0 | ||||||
|
|
|
|
|
|
|
|||||||
See notes to consolidated financial statements.
F-5
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
AS OF AND FOR THE YEARS ENDED JUNE 30, 2016, 2015 AND 2014
(All amounts in thousands, except share and per share amounts)
| 1. | BUSINESS OPERATIONS |
SunLink Health Systems, Inc., through subsidiaries (“SunLink”, “we”, “our”, “ours”, “us” or the “Company”), owns businesses which are providers of healthcare services in certain markets in the United States. SunLink’s business is composed of the ownership of two business segments:
| • | The Healthcare Facilities Segments, which is composed of: |
| • | A subsidiary which owns and operates an 84-licensed-bed, acute care hospital, which includes an 18-bed GPU, and a 66-bed nursing home. |
| • | A subsidiary which owns and operates a 100-bed nursing home. This subsidiary also owns a hospital facility and leases the emergency department to outside third party. |
| • | Two separate subsidiaries which own medical buildings, which are leased to unaffiliated healthcare providers. |
| • | A subsidiary which owns a closed hospital building and a medical office building which it currently rents an office to an unaffiliated healthcare provider. |
| • | The Specialty Pharmacy Segment, which is composed of four operational areas: |
| • | Retail pharmacy products and services, all of which are conducted in rural markets; |
| • | Institutional pharmacy services; |
| • | Specialty pharmacy services; and |
| • | Durable medical equipment. |
SunLink subsidiaries have conducted the healthcare facilities business since 2001 and the specialty pharmacy operations since 2008. Our Specialty Pharmacy Segment currently is operated through Carmichael’s Cashway Pharmacy, Inc. (“Carmichael”), a subsidiary of our SunLink ScriptsRx, LLC subsidiary, and is composed of a specialty pharmacy business acquired in April 2008 with four service lines.
On August 19, 2016, a subsidiary of the Company sold substantially all assets and certain liabilities of its Chestatee Regional Hospital in Dahlonega, GA, for approximately $15,000 subject to adjustment for the book value of certain assets and liabilities at the sale date. In addition, the Company has entered into an agreement to lease the emergency department and certain ancillary space located in its former hospital, North Georgia Medical Center, which is now closed, to a regional healthcare system. The lease transaction is subject to a number of conditions precedent including regulatory approval and negotiation of definitive leases. The Company continues to operate its 100-bed skilled nursing facility which is located adjacent to the closed hospital. The Company believes its specialty pharmacy business continues to under-perform, and the Company has engaged advisors to assist it in evaluating the sale of its specialty pharmacy business and one medical office building. The Company’s possible use of net proceeds from the Dahlonega sale and possible future transactions may include, among other things, a prepayment of long-term debt, a return of capital to shareholders via a repurchase of shares or a dividend, and other general corporate purposes. However, there can be no assurance any further sale or lease transaction will be authorized by the Board of Directors or completed or, if completed, that there will be sufficient proceeds to return capital to shareholders or for future development or other general corporate purposes.
Throughout these notes to the consolidated financial statements, SunLink Health Systems, Inc., and its consolidated subsidiaries are referred to on a collective basis as “SunLink”, “we”, “our”, “ours”, “us” or the
F-6
“Company.” This drafting style is not meant to indicate that the publicly traded Company or any particular subsidiary of the Company owns or operates any asset, business or property. The Trace Hospital, pharmacy operations and businesses described in this filing are owned and operated by distinct and indirect subsidiaries of SunLink Health System, Inc.
| 2. | SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES |
Principles of Consolidation—The consolidated financial statements include the accounts of SunLink and its subsidiaries. All significant intercompany transactions and balances have been eliminated.
Management Estimates—The preparation of financial statements in conformity with accounting principles generally accepted in the United States of America requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosures of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenues and expenses during the reporting period. Some of the more significant estimates made by management involve reserves for adjustments to net patient service revenues, evaluation of the recoverability of assets, including accounts receivable and intangible assets, and the assessment of litigation and contingencies, including income taxes and related tax asset valuation allowances, all as discussed in more detail in the remainder of these notes to the consolidated financial statements. Actual results could differ materially from these estimates.
Net Patient Service Revenue—SunLink’s subsidiaries have agreements with third-party payors that provide for payments at amounts different from established charges. Payment arrangements vary and include prospectively determined rates per discharge, reimbursed costs, discounted charges and per diem payments. Patient service revenues are reported as services are rendered at the estimated net realizable amounts from patients, third-party payors, and others. Estimated net realizable amounts are estimated based upon contracts with third-party payors, published reimbursement rates, and historical reimbursement percentages pertaining to each payor type. Estimated reductions in revenues to reflect agreements with third-party payors and estimated retroactive adjustments under such reimbursement agreements are accrued during the period the related services are rendered and are adjusted in future periods as interim and final settlements are determined. Significant changes in reimbursement levels for services under government and private programs could significantly impact the estimates used to accrue such revenue deductions. At June 30, 2016, there were no material claims or disputes with third-party payors.
Charity Care—SunLink’s subsidiaries’ hospitals provide care to patients who meet certain criteria under its charity care policy without charge or at amounts less than its established rates. Because SunLink subsidiaries do not pursue collection of amounts determined to qualify as charity, they are not reported as revenue. SunLink’s subsidiaries’ hospitals provided $1,801, $2,266, and $5,632, of charity care in the fiscal years ended June 30, 2016, 2015 and 2014, respectively.
Concentrations of Credit Risk—SunLink’s Healthcare Facilities segment subsidiaries grant unsecured credit to their patients, most of who reside in the service area of the subsidiaries’ facilities and are insured under third-party agreements. Medicare and Medicaid patient accounts represent SunLink’s only significant concentrations of credit risk. For SunLink’s Healthcare Facilities Segment, Medicare net revenues were approximately 37%, 39%, and 40% of net revenues for the years ended June 30, 2016, 2015 and 2014, respectively. For SunLink’s Healthcare Facilities Segment, Medicaid was approximately 37%, 30%, and 29% of net revenues for the years ended June 30, 2016, 2015 and 2014, respectively. For SunLink’s Healthcare Facilities Segment, Medicare receivables were approximately 51% and 45% of receivables—net at June 30, 2016 and 2015, respectively, while Medicaid receivables were approximately 22% and 15% of receivables—net at June 30, 2016 and 2015, respectively.
SunLink’s Specialty Pharmacy segment subsidiary grants unsecured credit to individual customers and institutional customers. Individual customers primarily are insured under third-party agreements, including
F-7
Medicare and Medicaid, while the institutional customers are grant credit according to their determined credit risk. Medicare receivables were approximately 13% and 18% of the Specialty Pharmacy’s receivables at June 30, 2016 and 2015, respectively, while Medicaid receivables were approximately 10% and 12% of the segments receivable at June 30, 2016 and 2015, respectively. Approximately 77% and 70% of the Specialty Pharmacy’s net receivables at June 30, 2016 and 2015, respectively, were private insurance and institutional customers’ receivables. Net revenues for the Specialty Pharmacy segment for the fiscal year ended June 30, 2016 and 2015 were approximately 16% and 8% Medicare, respectively, and approximately 10% and 14% Medicaid, respectively.
Cash and Cash Equivalents—Cash and cash equivalents consist of highly liquid financial instruments, which have original maturities of three months or less when purchased. Cash is deposited with commercial banks and may have deposits totaling amounts in excess of the federally insured limits from time to time.
Inventory—Inventory consists of medical and pharmacy supplies. Medical supplies are valued at the lower of cost or market, using the first-in, first-out method. Pharmacy supplies are stated at the lower of cost (standard cost method), or market. Use of this method does not result in a material difference from the methods required by generally accepted accounting principles in the United States of America.
Allowance for Doubtful Accounts—Substantially all of SunLink’s subsidiaries’ receivables result from providing healthcare services to hospital facility patients and from providing pharmacy services and products to customers. Accounts receivable are reduced by an allowance for doubtful accounts estimated to become uncollectible in the future. For the Healthcare Facilities Segment, an allowance percentage is calculated based generally upon its historical collection experience for each type of payor. The allowance amount is computed by applying allowance percentages to receivable amounts included in specific payor categories. Significant changes in reimbursement levels for services under government and private programs could significantly impact the estimates used to determine the allowance for doubtful accounts. Accounts receivable are written off after all collection efforts have failed, normally within 120 days after the date of discharge of the patient or service to the patient or customer. For the Specialty Pharmacy Segment operations, an allowance percentage is calculated based on past credit history with customers and their current financial condition. Accounts receivable are written off against the allowance for doubtful accounts when they are deemed uncollectible.
Medicare and Medicaid Electronic Health Records (“EHR”) Incentives—The Company accounts for EHR incentive payments in accordance with Accounting Standards Codification 450-30, “Gain Contingencies”, (“ASC 450-30”). In accordance with ASC 450-30, the Company recognizes EHR incentive payments when all contingencies relating to the incentive payment have been satisfied and compliance with the EHR meaningful use criteria have been attested to. For recognition of Medicaid EHR incentive payments, recognition of the payments will be at the time of attestation to EHR meaningful use criteria since Medicaid payments for the states in which the Company operates are based upon historical cost report information with no subsequent payment adjustment. However, for Medicare EHR incentive payments, recognition is being deferred until both the Medicare federal fiscal year during which EHR meaningful use was demonstrated ends and the cost report information utilized to determine the final amount of reimbursement is known. The demonstration of meaningful use is based on meeting a series of objectives and varies among hospitals, between the Medicare and Medicaid programs, and within the Medicaid program from state to state. Additionally, meeting the series of objectives in order to demonstrate meaningful use becomes progressively more stringent as its implementation is phased in through stages as outlined by the Centers for Medicare and Medicaid Services.
Property, Plant, and Equipment—Property, plant, and equipment, including equipment subject to capital leases, is recorded at cost. Depreciation is recognized over the estimated useful lives of the assets, which range from 3 to 45 years, on a straight-line basis. Generally, furniture and fixtures are depreciated over 5 to 10 years, machinery and equipment over 10 years, and buildings over 25 to 45 years. Leasehold improvements and leased machinery and equipment are depreciated over the lease term or estimated useful life of the asset, whichever is shorter, and range from 5 to 15 years. For the Specialty Pharmacy Segment, durable medical equipment is
F-8
depreciated over 3 years. Expenditures for major renewals and replacements are capitalized. Expenditures for maintenance and repairs are charged to operating expense as incurred. When property items are retired or otherwise disposed of, amounts applicable to such items are removed from the related asset and accumulated depreciation accounts and any resulting gain or loss is credited or charged to income. Depreciation expense totaled $1,736, $1,695, and $2,180, for the years ended June 30, 2016, 2015 and 2014, respectively.
Risk Management—SunLink and its subsidiaries are exposed to various risks of loss from professional liability and other claims and casualties; theft of, damage to, and destruction of assets; business interruption; errors and omissions; employee injuries and illnesses; natural disasters (including earthquakes and hurricanes); and employee health, dental and accident benefits. Commercial insurance coverage is purchased for a portion of claims arising from such matters.
When, in management’s judgment, claims are sufficiently identified, a liability is accrued for estimated costs and losses under such claims, net of estimated insurance recoveries except where applicable laws, rules or regulations require us to report the gross estimate of potential or estimated losses.
The recorded liability for professional liability risks includes an estimate of liability for claims assumed at the acquisition and for claims incurred after the acquisition of a business. These amounts are based on actuarially determined estimates.
The Company self-insures for workers’ compensation risk. The estimated liability for workers’ compensation risk includes estimates of the ultimate costs for both reported claims and claims incurred but not reported. The Company is also self-insured for employee health risks. The estimated liability for employee health risk includes estimates of the ultimate costs for both reported claims and claims incurred but not reported.
The Company accrues an estimate of losses resulting from workers’ compensation and professional liability claims to the extent they are not covered by insurance. These accruals are estimated quarterly based upon management’s review of claims reported and historical loss data.
The Company records a liability pertaining to pending litigation if it is probable a loss has been incurred and accrues the most likely amount of loss based on the information available. If no amount within the range of losses estimated from the information available is more likely than any other amount in the range of loss, the minimum amount in the range of loss is accrued. Because of uncertainties surrounding the nature of litigation and the ultimate liability to SunLink and its subsidiaries, if any, estimates are revised as additional facts become known.
Long-lived Assets—SunLink and its subsidiaries periodically assesses the recoverability of assets based on its expectations of future profitability and the undiscounted cash flows of the related operations and, when circumstances dictate, adjust the carrying value of the asset to estimated fair value. These factors, along with management’s plans with respect to the operations, are considered in assessing the recoverability of long-lived assets.
Goodwill and Intangibles—Goodwill represents the cost of acquired businesses in excess of fair value of identifiable tangible and intangible net assets purchased. Goodwill has an indefinite life and is not subject to periodic amortization. However, goodwill is tested at least annually for impairment, using a fair value methodology, in lieu of amortization. Definite-life intangible assets are amortized on a straight-line basis over their estimated useful lives, generally for periods ranging from 2 to 30 years. SunLink and its subsidiaries evaluate the reasonableness of the useful lives of intangible assets and they are tested for impairment as conditions warrant.
Income Taxes—SunLink accounts for income taxes using an asset and liability approach and the recognition of deferred tax assets and liabilities for expected future tax consequences. SunLink considers all
F-9
expected future events other than proposed enactments of changes in the income tax law or rates. When management determines that it is more likely than not that a portion of or none of the net deferred tax asset will be realized through future taxable earnings or implementation of tax planning strategies, management provides a valuation allowance for the portion not expected to be realized.
Share-Based Compensation—The Company issues common share options to key employees and directors under various shareholder-approved plans. Share-based compensation expense of $58, $37 and $48 for the fiscal years ended June 30, 2016, 2015 and 2014, respectively, was recorded in salaries, wages and benefits expense for share options issued to employees and directors of the Company. The fair value of the share options was estimated using the Black-Scholes option pricing model. The historical volatility is used to calculate the estimated volatility in this model.
Fair Value of Financial Instruments—The recorded values of cash, receivables, and payables approximate their fair values because of the relatively short maturity of these instruments. Similarly, the fair value of long-term debt is estimated to approximate the recorded value due to its current variable interest rate.
Fair Value Measurements—Fair value is a market-based measurement, not an entity-specific measurement. Therefore, a fair value measurement should be determined based on the assumptions that market participants would use in pricing the asset or liability. As a basis for considering market participant assumptions in fair value measurements, the Company utilizes the U.S. Generally Accepted Accounting Principles (“GAAP”) fair value hierarchy that distinguishes between market participant assumptions based on market data obtained from sources independent of the reporting entity (observable inputs that are classified within Levels 1 and 2 of the hierarchy) and the reporting entity’s own assumption about market participant assumptions (unobservable inputs classified within Level 3 of the hierarchy).
The inputs used to measure fair value are classified into the following fair value hierarchy:
Level 1: Quoted market prices in active markets for identical assets or liabilities.
Level 2: Observable market-based inputs or unobservable inputs that are corroborated by market data.
Level 3: Unobservable inputs that are supported by little or no market activity and are significant to the fair value of the assets or liabilities. Level 3 includes values determined using pricing models, discounted cash flow methodologies, or similar techniques reflecting the Company’s own assumptions.
In instances where the determination of the fair value hierarchy measurement is based on inputs from different levels of the fair value hierarchy, the level in the fair value hierarchy within which the entire fair value measurement falls is based on the lowest level input that is significant to the fair value measurement in its entirety. The Company’s assessment of the significance of a particular input to the fair value measurement in its entirety requires judgment of factors specific to the asset or liability.
Earnings (Loss) per Share—Earnings (loss) per common share is based on the weighted-average number of common shares and dilutive common share equivalents outstanding for each period presented, including vested and unvested shares issued under SunLink’s 2005 Equity Incentive Plan, and the 2011 Director Stock Option Plan. Common share equivalents represent the dilutive effect of the assumed exercise of the outstanding stock options.
Recent Accounting Pronouncements—In April 2015, the Financial Accounting Standards Board (“FASB”) issued Accounting Standards Update (“ASU”) 2015-3, “Simplifying the Presentation of Debt Issuance Costs” (“ASU 2015-3”). ASU 2015-3 requires that debt issuance costs related to a recognized debt liability be presented in the balance sheet as a direct deduction from the carrying amount of that debt liability, consistent with debt discounts, rather than separately as an asset. ASU 2015-3 is effective for annual reporting periods beginning after December 15, 2015, including interim periods within those years, and is to be applied retrospectively. Early adoption is permitted. The Company does not expect the adoption of ASU 2015-3 will have an impact on its results of operations or cash flows.
F-10
In February 2015, the FASB issued ASU 2015-2 “Consolidation” (“ASU 2015-2”). ASU 2015-2 includes amendments that are intended to improve targeted areas of consolidation for legal entities including reducing the number of consolidation models from four to two and simplifying the FASB Accounting Standards Codification (“ASC”). The provisions of ASU 2015-2 are effective for annual reporting periods beginning after December 15, 2015. The amendments may be applied retrospectively in previously issued financial statements for one or more years with a cumulative effect adjustment to retained earnings as of the beginning of the first year restated. Early adoption is permitted. The Company does not expect the adoption of ASU 2015-2 will have an impact on its results of operations or cash flows.
In August 2014, the FASB issued ASU 2014-15 “Disclosure of Uncertainties about an Entity’s Ability to Continue as a Going Concern” (“ASU 2014-15”). ASU 2014-15 will explicitly require management to assess an entity’s ability to continue as a going concern, and to provide related footnote disclosure in certain circumstances. The new standard will be effective for all entities in the first annual period ending after December 15, 2016. Earlier adoption is permitted. The Company is currently evaluating the impact of the adoption of ASU 2014-15.
In September 2015, the Financial Accounting Standards Board (“FASB”) issued Accounting Standards Update (“ASU”) 2015-16, “Business Combinations: Simplifying the Accounting for Measurement-Period Adjustments” (“ASU 2015-16”). ASU 2015-16 eliminates the requirement for an acquirer to retrospectively adjust its financial statements for changes to provisional amounts that are identified during the measurement-period following the consummation of a business combination. Instead, ASU 2015-16 requires these types of adjustments to be made during the reporting period in which they are identified and would require additional disclosure or separate presentation of the portion of the adjustment that would have been recorded in the previously reported periods as if the adjustment to the provisional amounts had been recognized as of the acquisition date. ASU 2015-16 is effective for annual reporting periods beginning after December 15, 2015, including interim periods within those years, and is to be applied retrospectively. The Company does not expect the adoption of ASU 2015-16 will have an impact on its results of operations or cash flows.
In April 2015, the FASB issued ASU 2015-5, “Intangibles—Goodwill and Other—Internal-Use Software” (“ASU 2015-5”). ASU 2015-5 provides guidance to customers about whether a cloud computing arrangement includes a software license. If a cloud computing arrangement includes a software license, ASU 2015-5 specifies that the customer should account for the software license element of the arrangement consistent with the acquisition of other software licenses. ASU 2015-5 further specifies that the customer should account for a cloud computing arrangement as a service contract if the arrangement does not include a software license. ASU 2015-5is effective for annual reporting periods beginning after December 15, 2015, including interim periods within those years, and is to be applied retrospectively. The Company does not expect the adoption of ASU 2015-5 will have an impact on its results of operations or cash flows.
In March 2016, the FASB issued ASU 2016-9 “Compensation—Stock Compensation: Improvements to Employee Share-Based Payment Accounting” (“ASU 2016-9”). ASU 2016-9 changes certain aspects of accounting for share-based payment awards to employees, including the accounting for income taxes, application of estimated rates of forfeiture and statutory tax withholding requirements. ASU 2016-9 is effective for annual reporting periods beginning after December 15, 2016, including interim periods within those years. Early adoption is permitted. The Company is currently evaluating the impact that the adoption of this standard will have on its financial position, results of operations and cash flows.
In February 2016, the FASB issued ASU 2016-2 “Leases” (“ASU 2016-2”). ASU 2016-2 requires the rights and obligations arising from lease contracts, including existing and new arrangements, to be recognized as assets and liabilities on the balance sheet. ASU 2016-2 is effective for annual reporting periods beginning after December 15, 2018, including interim periods within those years. Early adoption is permitted. The Company anticipates that the adoption of ASU 2016-2 will result in an increase in both total assets and total liabilities. The Company is still evaluating the impact that the adoption of this standard will have on its policies, procedures and control framework.
F-11
In May 2014, the FASB issued ASU 2014-9, “Revenue from Contracts with Customers” (“ASU 2014-9”). ASU 2014-9 provides for a single comprehensive principles-based standard for the recognition of revenue across all industries through the application of the following five-step process:
Step 1: Identify the contract(s) with a customer.
Step 2: Identify the performance obligations in the contract.
Step 3: Determine the transaction price.
Step 4: Allocate the transaction price to the performance obligations in the contract.
Step 5: Recognize revenue when (or as) the entity satisfies a performance obligation.
Among other provisions and in addition to expanded disclosure about the nature, amount, timing and uncertainty of revenue as well as certain additional quantitative and qualitative disclosures, ASU 2014-9 changes the healthcare industry specific presentation guidance under ASU 2011-7, “Presentation and Disclosure of Patient Service Revenue, Provision for Bad Debts, and the Allowance for Doubtful Accounts for Certain Health Care Entities.” The provisions of ASU 2014-9 are effective for annual periods beginning after December 15, 2017, including interim periods within those years. Early adoption is permitted starting with annual periods beginning after December 31, 2016. The Company is still evaluating the impact that the adoption of this standard will have on its revenue recognition policies, procedures, financial position, results of operations, cash flows, financial disclosures and control framework.
| 3. | SUBSEQUENT EVENTS |
On August 19, 2016, the Company’s subsidiary Southern Health Corporation of Dahlonega, Inc. (“Chestatee”) sold substantially all of the assets and certain liabilities of Chestatee Regional Hospital in Dahlonega, Georgia through an asset purchase agreement for $15,000 subject to adjustment for the book value of certain assets and certain liabilities assumed at the sale date. A portion of the net proceeds will be allotted for the payment of debt and the balance will be retained for other possible applications including working capital and other general corporate purposes.
On September 9, 2016, the Carmichael Note, which had a principal balance of $1,508, was paid in full. The accrued interest payable of $47 was forgiven as a condition of the early repayment.
| 4. | DISCONTINUED OPERATIONS |
All of the businesses discussed below are reported as discontinued operations and the consolidated financial statements for all prior periods have been adjusted to reflect this presentation.
Chestatee Hospital—On August 19, 2016, the Company’s subsidiary Southern Health Corporation of Dahlonega, Inc. (“Chestatee”) sold substantially all of the assets and certain liabilities of Chestatee Regional Hospital in Dahlonega, Georgia through an asset purchase agreement for $15,000 subject to adjustment for the book value of certain assets and certain liabilities assumed at the sale date. A portion of the net proceeds will be allotted for the payment of debt and the balance will be retained for working capital and general corporate purposes. The total assets sold by Chestatee were approximately 19% of the Company’s total assets of the June 30, 2015 balance sheet and accordingly, the Chestatee sale constitutes a disposition of discontinued operations under ASC 205, Presentation of Financial Statements, and ASC 360, Property, Plant and Equipment. Chestatee’s results have been reclassified as discontinued operations in our consolidated financial statements for the fiscal years ended June 30, 2016, 2015 and 2014. The assets sold and liabilities assumed are shown as assets held for sale in our consolidated balances as of June 30, 2016 and 2015.
Fulton Hospital—On December 31. 2014, the Company’s subsidiary, HealthMont of Missouri, LLC (“Fulton”) sold substantially all the assets of its Callaway Community Hospital for approximately $6,090. Fulton
F-12
retained accounts receivable and certain other assets and substantially all liabilities of the hospital as of the sale closing date. A loss of $197 resulted from the sale of the Fulton assets, which includes $237 early repayment penalty resulting from the repayment of Fulton’s long-term debt. Fulton’s results have been reclassified as discontinued operations in our consolidated financial statements for the fiscal years ended June 30, 2016, 2015 and 2014.
Dexter Hospital—On December 31, 2012, the Company completed the sale of substantially all the assets and the leasehold interest of its subsidiary, Dexter Hospital, LLC (“Dexter”), to Southeast Health Center of Stoddard County, LLC, an indirect subsidiary of Southeast Missouri Hospital Association (“SoutheastHEALTH”) for approximately $9,930. Dexter’s operations have been classified as discontinued operations in our consolidated financial statements for the fiscal years ended June 30, 2015, 2015 and 2014.
Memorial Hospital of Adel—On July 2, 2012, the Company and its HealthMont of Georgia, Inc. (“Memorial”) subsidiary completed the sale of substantially all the assets of the Company’s Memorial Hospital of Adel and Memorial Convalescent Center to the Hospital Authority of Tift County, Georgia (“Tift”) for approximately $8,350. Memorial’s operations have been classified as discontinued operations in our consolidated financial statements for the fiscal years ended June 30, 2016, 2015 and 2014.
Life Sciences and Engineering Segment—SunLink retained a defined benefit retirement plan which covered substantially all of the employees of this segment when the segment was sold in fiscal 1998. Effective February 28, 1997, the plan was amended to freeze participant benefits and close the plan to new participants. Pension expense and related tax benefit or expense is reflected in the results of operations for this segment for the fiscal years ended June 30, 2016, 2015 and 2014.
Results for all the businesses included in discontinued operations are presented in the following table:
Discontinued Operations—Summary Statement of Earnings Information
| Years Ended June 30, | ||||||||||||
| 2016 | 2015 | 2014 | ||||||||||
| Net Revenues: |
||||||||||||
| Chestatee Hospital |
$ | 14,714 | $ | 18,086 | $ | 18,206 | ||||||
| Fulton Hospital |
181 | 6,869 | 13,456 | |||||||||
| Dexter Hospital |
141 | 55 | 602 | |||||||||
| Memorial of Adel |
34 | 64 | (59 | ) | ||||||||
|
|
|
|
|
|
|
|||||||
| $ | 15,070 | $ | 25,074 | $ | 32,205 | |||||||
|
|
|
|
|
|
|
|||||||
| Earnings (Loss) Before Income Taxes: |
||||||||||||
| Chestatee Hospital |
$ | (1,961 | ) | $ | 315 | $ | 261 | |||||
| Fulton Hospital |
84 | (1,170 | ) | (1,621 | ) | |||||||
| Dexter Hospital |
(115 | ) | 727 | 1,548 | ||||||||
| Memorial of Adel |
4 | 15 | (94 | ) | ||||||||
| Life sciences and engineering |
(181 | ) | (105 | ) | (158 | ) | ||||||
|
|
|
|
|
|
|
|||||||
| Loss before income taxes |
(2,169 | ) | (218 | ) | (64 | ) | ||||||
|
|
|
|
|
|
|
|||||||
| Loss on Sale: |
||||||||||||
| Fulton Hospital |
0 | (197 | ) | 0 | ||||||||
|
|
|
|
|
|
|
|||||||
| Loss on Sale |
0 | (197 | ) | 0 | ||||||||
|
|
|
|
|
|
|
|||||||
| Income tax benefit |
0 | (173 | ) | (3 | ) | |||||||
|
|
|
|
|
|
|
|||||||
| Loss from discontinued operations |
$ | (2,169 | ) | $ | (242 | ) | $ | (61 | ) | |||
|
|
|
|
|
|
|
|||||||
F-13
| 5. | REVENUE RECOGNITION AND ACCOUNTS RECEIVABLES |
SunLink’s subsidiaries have agreements with third-party payors that provide for payments at amounts different from the subsidiaries’ established rates. A summary of the payment arrangements with major third-party payors follows:
Medicare—Inpatient acute care services rendered to Medicare program beneficiaries are paid at prospectively determined rates per Diagnosis Related Group. These rates vary according to a patient classification system that is based on clinical, diagnostic, and other factors. Inpatient nonacute services, certain outpatient services, and defined capital and medical education costs related to Medicare beneficiaries are paid based on a cost reimbursement methodology. Cost reimbursable items are paid at a tentative rate, with final settlement determined after submission of annual cost reports and audits thereof by the Medicare fiscal intermediary.
Medicaid—Inpatient and outpatient services rendered to Medicaid program beneficiaries are reimbursed either under contracted rates or reimbursed for cost reimbursable items at a tentative rate, with final settlement determined after submission of annual cost reports and audits thereof by the Medicaid fiscal intermediary.
Other—SunLink’s subsidiaries have also entered into payment agreements with certain commercial insurance carriers, health maintenance organizations, and preferred provider organizations. The basis for payment under these agreements includes prospectively determined rates per discharge, discounts from established charges, and prospectively determined daily rates.
The Company’s revenues before provision for doubtful accounts by payor were as follows for the years ended June 30, 2016, 2015 and 2014:
| Years Ended June 30, | ||||||||||||
| 2016 | 2015 | 2014 | ||||||||||
| Healthcare Facilities Segment: |
||||||||||||
| Medicare |
$ | 11,781 | $ | 16,960 | $ | 17,629 | ||||||
| Medicaid |
11,977 | 13,166 | 12,554 | |||||||||
| Self-pay |
1,092 | 3,107 | 3,694 | |||||||||
| Managed Care & Other Insurance |
6,913 | 10,240 | 9,779 | |||||||||
| Other |
136 | 137 | 125 | |||||||||
|
|
|
|
|
|
|
|||||||
| Revenues before provision for doubtful accounts |
31,899 | 43,610 | 43,781 | |||||||||
| Provision for doubtful accounts |
(1,438 | ) | (3,678 | ) | (3,795 | ) | ||||||
|
|
|
|
|
|
|
|||||||
| Healthcare Facilities Segment Net Revenues |
30,461 | 39,932 | 39,986 | |||||||||
| Specialty Pharmacy Segment Net Revenues |
32,216 | 33,175 | 33,322 | |||||||||
| Other Revenues |
756 | 639 | 461 | |||||||||
|
|
|
|
|
|
|
|||||||
| Total Net Revenues |
$ | 63,433 | $ | 73,746 | $ | 73,769 | ||||||
|
|
|
|
|
|
|
|||||||
The net revenues of the Specialty Pharmacy Segment are presented net of contractual adjustments. The provision for bad debts of the Specialty Pharmacy Segment is presented as a component of operating expenses in the Consolidated Statements of Operations and Comprehensive Earning and Loss.
F-14
Summary information for receivables is as follows:
| June 30, | ||||||||
| 2016 | 2015 | |||||||
| Patient accounts receivable (net of contractual allowances) |
$ | 7,157 | $ | 10,449 | ||||
| Less allowance for doubtful accounts |
(991 | ) | (2,770 | ) | ||||
|
|
|
|
|
|||||
| Patient accounts receivable—net |
$ | 6,166 | $ | 7,679 | ||||
|
|
|
|
|
|||||
The following is a summary of the activity in the allowance for doubtful accounts for the Healthcare Facilities Segment and the Specialty Pharmacy Segment for the fiscal years ended June 30, 2016 and 2015:
| Fiscal year ended June 30, 2016 | Healthcare Facilities |
Specialty Pharmacy |
Total | |||||||||
| Balance at July 1, 2015 |
$ | 2,385 | $ | 385 | 2,770 | |||||||
| Additions recognized as a reduction to revenues: |
||||||||||||
| Continuing operations |
1,438 | 0 | 1,438 | |||||||||
| Discontinued operations |
(135 | ) | 0 | (135 | ) | |||||||
| Bad debt expense |
0 | 630 | 630 | |||||||||
| Accounts written off, net of recoveries |
(3,064 | ) | (648 | ) | (3,712 | ) | ||||||
|
|
|
|
|
|
|
|||||||
| Balance at June 30, 2016 |
$ | 624 | $ | 367 | $ | 991 | ||||||
|
|
|
|
|
|
|
|||||||
| Fiscal year ended June 30, 2015 | Healthcare Facilities |
Specialty Pharmacy |
Total | |||||||||
| Balance at July 1, 2014 |
$ | 4,178 | $ | 254 | 4,432 | |||||||
| Additions recognized as a reduction to revenues: |
||||||||||||
| Continuing operations |
3,678 | 0 | 3,678 | |||||||||
| Discontinued operations |
1,749 | 0 | 1,749 | |||||||||
| Bad debt expense |
0 | 363 | 363 | |||||||||
| Accounts written off, net of recoveries |
(7,220 | ) | (232 | ) | (7,452 | ) | ||||||
|
|
|
|
|
|
|
|||||||
| Balance at June 30, 2015 |
$ | 2,385 | $ | 385 | $ | 2,770 | ||||||
|
|
|
|
|
|
|
|||||||
Net revenues included a decrease of $786 for the year ended June 30, 2016 for the settlement of filings of prior year Medicare and Medicaid cost reports. Net revenues included increases (decreases) of ($540) and $624 for the years ended June 30, 2015 and 2014, respectively, for the settlements and filings of prior year Medicare and Medicaid cost reports.
| 6. | MEDICARE AND MEDICAID ELECTRONIC HEALTH RECORDS INCENTIVES |
EHR incentive reimbursements are payments received under the Health Information Technology for Economic and Clinical Health Act (the “HITECH Act”) which was enacted into law on February 17, 2009 as part of the American Recovery and Reinvestment Act of 2009 (“ARRA”). The HITECH Act includes provisions designed to increase the use of EHR by both physicians and hospitals. Beginning with federal fiscal year 2011 (federal fiscal year is October 1 through September 30) and extending through federal fiscal year 2016, eligible hospitals and critical access hospitals (“CAH”) participating in the Medicare and Medicaid programs are eligible for reimbursement incentives based on successfully demonstrating meaningful use of their certified EHR technology. Conversely, those hospitals that do not successfully demonstrate meaningful use of EHR technology are subject to payment penalties or downward adjustments to their Medicare payments beginning in federal fiscal year 2015.
Attestation of Medicare meaningful use requirements was successful for each of SunLink’s hospital subsidiaries’ and certain discontinued operations for the fiscal year ended June 30, 2014. SunLink’s hospital
F-15
subsidiaries have also successfully attested to the meaningful use requirements for the Medicaid program for continuing and certain discontinued operations for the fiscal years ended June 30, 2016, 2015 and 2014. EHR incentive payments received were as follows:
| 2016 | 2015 | 2014 | ||||||||||
| Continuing Operations |
||||||||||||
| Medicare |
$ | (7 | ) | $ | — | $ | 1,468 | |||||
| Medicaid |
— | 21 | 312 | |||||||||
|
|
|
|
|
|
|
|||||||
| $ | (7 | ) | $ | 21 | $ | 1,780 | ||||||
|
|
|
|
|
|
|
|||||||
| Discontinued Operations |
||||||||||||
| Medicare |
$ | — | $ | 703 | $ | 1,026 | ||||||
| Medicaid |
(93 | ) | 29 | 281 | ||||||||
|
|
|
|
|
|
|
|||||||
| $ | (93 | ) | $ | 732 | $ | 1,307 | ||||||
|
|
|
|
|
|
|
|||||||
| Combined Operations |
||||||||||||
| Medicare |
$ | (7 | ) | $ | 703 | $ | 2,494 | |||||
| Medicaid |
(93 | ) | 50 | 593 | ||||||||
|
|
|
|
|
|
|
|||||||
| $ | (100 | ) | $ | 753 | $ | 3,087 | ||||||
|
|
|
|
|
|
|
|||||||
| 7. | INVENTORY |
Inventory consisted of the following:
| June 30, | ||||||||
| 2016 | 2015 | |||||||
| Healthcare Facilities Segment, supplies inventory |
$ | 373 | $ | 795 | ||||
| Specialty Pharmacy Segment, goods held for sale |
2,239 | 2,353 | ||||||
|
|
|
|
|
|||||
| $ | 2,612 | $ | 3,148 | |||||
|
|
|
|
|
|||||
| 8. | IMPAIRMENT OF LONG-LIVED ASSETS |
Impairment of Long-Lived Assets—A hospital facility formerly leased to a third party hospital operator is currently vacant with the exception of one rented office. The net realizable value of the facility was evaluated at June 30, 2016 and an impairment charge of $858 was recognized in the fiscal year ended June 30, 2016.
Impairment analysis—For the purposes of these analyses, our estimates of fair value are based on a combination of the income approach, which estimates the fair value based on future discounted cash flows, and the market approach, which estimates the fair value of based on comparable market prices. Estimates of fair value for reporting units fall under Level 3 of the fair value hierarchy. Estimates of future discounted cash flows are based on assumptions and projections we believe to be currently reasonable and supportable. These assumptions take into account revenue and expense growth rates, patient volumes, changes in payor mix, and changes in legislation and other payor payment patterns.
F-16
| 9. | GOODWILL AND INTANGIBLE ASSETS |
SunLink’s Specialty Pharmacy Segment has goodwill and intangible assets related to its Carmichael acquisition, which consists of:.
| Goodwill: |
||||||||
| June 30, | ||||||||
| 2016 | 2015 | |||||||
| Specialty Pharmacy Segment |
$ | 461 | $ | 461 | ||||
|
|
|
|
|
|||||
| Intangible assets : | June 30, | |||||||
| 2016 | 2015 | |||||||
| Specialty Pharmacy Segment |
||||||||
| Trade Name |
$ | 2,000 | $ | 2,000 | ||||
| Customer Relationships |
1,089 | 1,089 | ||||||
| Medicare License |
769 | 769 | ||||||
|
|
|
|
|
|||||
| 3,858 | 3,858 | |||||||
| Accumulated Amortization |
(1,163 | ) | (1,021 | ) | ||||
|
|
|
|
|
|||||
| Total |
$ | 2,695 | $ | 2,837 | ||||
|
|
|
|
|
|||||
The Trade Name intangible asset under the Specialty Pharmacy Segment is a non-amortizing intangible asset. Customer Relationships intangible asset is being amortized over 12 years and Medicare License intangible asset is being amortized over 15 years.
Amortization expense was $142 for each of the fiscal years ended June 30, 2016, 2015 and 2014, respectively.
Annual amortization of amortizing intangibles for the next five years and thereafter is as follows:
| 2017 |
$ | 142 | ||
| 2018 |
142 | |||
| 2019 |
142 | |||
| 2020 |
125 | |||
| 2021 |
51 | |||
| 2022 and thereafter |
93 | |||
|
|
|
|||
| Total |
$ | 695 | ||
|
|
|
| 10. | LONG-TERM DEBT |
Long-term debt consisted of the following:
| June 30, | ||||||||
| 2016 | 2015 | |||||||
| Trace RDA Loan |
$ | 7,698 | $ | 8,175 | ||||
| SHPP RDA Loan |
1,950 | 1,992 | ||||||
| Carmichael Note |
1,508 | 1,741 | ||||||
| Capital lease obligations and other |
32 | 137 | ||||||
|
|
|
|
|
|||||
| Total |
11,188 | 12,045 | ||||||
| Less current maturities |
(8,012 | ) | (816 | ) | ||||
|
|
|
|
|
|||||
| $ | 3,176 | $ | 11,229 | |||||
|
|
|
|
|
|||||
F-17
Trace RDA Loan and Trace Working Capital Loan—SunLink and two wholly owned subsidiaries of the Company, closed on a $9,975 Mortgage Loan Agreement (“Trace RDA Loan”) and a Working Capital Loan Agreement, both dated as of July 5, 2012 (“Trace Working Capital Loan”).
The Trace RDA Loan has a term of 15 years with monthly payments of principal and interest. The Trace RDA Loan bears a floating rate of interest equal to the greater of (i) the prime rate (as published in The Wall Street Journal) plus 1.5%, or (ii) 6% (6.0% at June 30, 2016). The Trace RDA Loan is collateralized by real estate and equipment of Trace Regional Hospital in Houston, MS and is partially guaranteed under the U.S. Department of Agriculture, Rural Development Business and Industry Program.
The Trace Working Capital Loan as amended provided for a revolving line of credit to Trace equal to the lesser of (i) a Borrowing Base equal to eighty percent (80%) of Eligible Accounts Receivable (as defined in the Working Capital Loan Agreement dated July 5, 2012) or (ii) $500. The Trace Working Capital Loan expired July 2, 2016 and was not renewed. At June 30, 2016 and 2015, there were no outstanding borrowings under the Trace Working Capital Loan.
The Trace RDA Loan contains various terms and conditions, including financial restrictions and limitations, and affirmative and negative covenants. The covenants include financial covenants measured on a quarterly basis which require Trace to comply with a ratio of current assets to current liabilities, debt service coverage, fixed charge coverage, and funded debt to EBITDA, all as defined in the Trace RDA Loan. At March 31, 2016 and June 30, 2016, Trace was not in compliance with the debt service coverage, fixed charge ratio and funded debt to EBITDA ratios. The Company received a waiver from the lender dated August 10, 2016 of this non-compliance from the lender for March 31, 2016. No modification or waiver for the June 30, 2016 non-compliance has been obtained as of September 28, 2016 and the $7,698 of indebtedness under the Trace RDA Loan is presented in current liabilities in the condensed consolidated balance sheet as of June 30, 2016. The Company continues to discuss a modification or waiver of this non-compliance with the lender. The ability of Trace to continue to make the required debt service payments under the Trace RDA Loan depends on, among other things, its ability to generate sufficient cash flows, including from operating activities. If Trace is unable to generate sufficient cash flow from operations to meet debt service payments on the Trace RDA Loan, including in the event the lender were to declare an event of default and accelerate the maturity of the indebtedness, such failure could have material adverse effects on the Company. The Trace RDA Loan is guaranteed by the Company and one subsidiary.
SHPP RDA Loan—SunLink Healthcare Professional Property, LLC, a subsidiary of the Company which owns a medical office building, closed a $2,100 term loan dated as of October 31, 2012 (the “SHPP RDA Loan”) with a bank. SHPP owns and formerly leased a medical office building to Southern Health Corporation of Ellijay, Inc. (“SHC Ellijay”), but effective July 1, 2016, SHPP entered into a 10 year lease with a third-party lessee.
The SHPP RDA Loan has a term of 25 years with monthly payments of principal and interest until repaid. The SHPP RDA Loan bears interest at a floating rate of interest equal to the greater of (i) the prime rate (as published in The Wall Street Journal) plus 2.0%, or (ii) 5% (5.50% at June 30, 2016). The SHPP RDA Loan is collateralized by SHPP’s real estate, equipment and leases and is partially guaranteed under the U.S. Department of Agriculture, Rural Development Business and Industry Program. The SHPP RDA Loan contains certain financial covenants with respect to the ratio of current assets to current liabilities and debt service coverage, all as defined in the SHPP RDA Loan Agreement, which SHPP must maintain and that are measured at the end of each fiscal year. The SHPP RDA Loan is guaranteed by the Company and one subsidiary. As of June 30, 2016, the Company was in compliance with all financial covenants under the SHPP RDA Loan.
Carmichael Note—On April 22, 2008, SunLink Scripts Rx, LLC issued a $3,000 promissory note with an interest rate of 8% to the former owners of Carmichael as part of the acquisition purchase price (the “Carmichael Note”). Under amendments and modifications to the Carmichael Note during fiscal 2013 and 2014, the Company made payments of principal and interest with additional notes (which have been paid) and extended the maturity date to October 22, 2017. The Carmichael Note currently was payable in semi-annual installments of $185 of
F-18
principal and accrued interest, with the remaining balance of $1,255 due October 22, 2017. The Carmichael Note was guaranteed by the Company. The Carmichael note was paid off on September 9, 2016.
Debt Commitments—Annual required payments of debt and contractual commitments for interest on long-term debt are shown in the following table. The interest rate on variable interest debt is calculated at the interest rate at June 30, 2016.
| Debt | Interest | |||||||
| 2017 |
$ | 8,012 | $ | 685 | ||||
| 2018 |
1,310 | 136 | ||||||
| 2019 |
46 | 101 | ||||||
| 2020 |
49 | 99 | ||||||
| 2021 |
51 | 96 | ||||||
| 2022 and thereafter |
1,720 | 1,015 | ||||||
|
|
|
|
|
|||||
| Total |
$ | 11,188 | $ | 2,132 | ||||
|
|
|
|
|
|||||
| 11. | SHAREHOLDERS’ EQUITY |
Employee and Directors Stock Option Plans—The 2011 Director Stock Option Plan was approved by SunLink’s shareholders at the Annual Meeting of Shareholders on November 7, 2011. This plan permits the grant of options to non-employee directors of SunLink for the purchase of up to 300,000 common shares through November 2021. Options for 30,000 and 198,000 shares were granted during the fiscal years ended June 30, 2016 and 2015, respectively. No options have been exercised under this plan. Options outstanding under the plan were 228,000 at June 30, 2016. Options available for future issuance under the plan were 72,000 at June 30, 2016.
The 2005 Equity Incentive Plan was approved by SunLink’s shareholders at the Annual Meeting of Shareholders on November 7, 2005. This plan permitted the grant of options to employees, non-employee directors and service providers of SunLink for the purchase of up to 800,000 common shares plus the number of unused shares under the 2001 Plans, which is 30,675, by November 2015. This Plan restricted the number of Incentive Stock Options to 700,000 shares and Restricted Stock Awards to 200,000 shares. The combination of Incentive Stock Options and Restricted Stock Awards cannot exceed 800,000 shares plus the number of unused shares under the 2001 Plans. Each award of Restricted Shares reduces the number of share options to be granted by four option shares for each Restricted Share awarded. No options have been exercised under this Plan. Options to purchase 45,000 and 90,000 shares were granted during the fiscal years ended June 30, 2016 and 2015, respectively. Options outstanding under this Plan were 407,642 at June 30, 2016. No additional awards may be granted under this Plan.
F-19
The activity of Company’s share options is shown in the following table:
| Number of Shares |
Weighted- Average Exercise Price |
Range of Exercise Prices |
||||||||||
| Options outstanding June 30, 2012 |
400,499 | $ | 2.62 | $ | 1.67 - $9.63 | |||||||
| Granted |
260,000 | 1.22 | 1.22 | |||||||||
| Forfeited |
(43,000 | ) | 2.13 | 2.09 - 2.65 | ||||||||
|
|
|
|||||||||||
| Options outstanding June 30, 2013 |
617,499 | 1.92 | 1.22 - 9.63 | |||||||||
| Granted |
21,000 | 0.71 | 0.71 | |||||||||
| Forfeited |
(89,500 | ) | 2.15 | 1.22 - 2.90 | ||||||||
|
|
|
|||||||||||
| Options outstanding June 30, 2014 |
548,999 | 2.71 | 0.71 - 9.63 | |||||||||
| Granted |
90,000 | 1.49 | 1.49 | |||||||||
| Forfeited |
(48,857 | ) | 3.50 | 0.71 - 9.63 | ||||||||
|
|
|
|||||||||||
| Options outstanding June 30, 2015 |
590,142 | 2.46 | 0.71 - 9.63 | |||||||||
| Granted |
75,000 | 1.79 | 1.79 | |||||||||
| Forfeited |
(29,500 | ) | 9.15 | 2.51 - 9.63 | ||||||||
|
|
|
|||||||||||
| Options outstanding June 30, 2016 |
635,642 | $ | 2.07 | $ | 0.71 - $8.00 | |||||||
|
|
|
|
|
|
|
|||||||
| Options exercisable June 30, 2014 |
448,998 | $ | 2.97 | $ | 0.71 - $9.63 | |||||||
|
|
|
|
|
|
|
|||||||
| Options exercisable June 30, 2015 |
470,142 | $ | 2.73 | $ | 0.71 - $9.63 | |||||||
|
|
|
|
|
|
|
|||||||
| Options exercisable June 30, 2016 |
530,642 | $ | 2.16 | $ | 0.71 - $8.00 | |||||||
|
|
|
|
|
|
|
|||||||
The weighted-average fair value of each option granted during the years ended June 30, 2016, 2015 and 2014 was $1.79, $1.49 and $0.71, respectively. The fair value of each stock option grant was estimated using the Black-Scholes option pricing model with the following weighted-average assumptions used for grants during the year ended June 30, 2016: estimated volatility of 80%; risk-free interest rate of 1.63%; dividend yield of 0%; and an expected life of 6 years. The fair value of each stock option grant was estimated using the Black-Scholes option pricing model with the following weighted-average assumptions used for grants during the year ended June 30, 2015: estimated volatility of 84%; risk-free interest rate of 2.03%; dividend yield of 0%; and an expected life of 6 years. The fair value of each stock option grant was estimated using the Black-Scholes option pricing model with the following weighted-average assumptions used for grants during the year ended June 30, 2014: estimated volatility of 93%; risk-free interest rate of 0.89%; dividend yield of 0%; and an expected life of 5 years. The expected life of each stock option grant was determined to be the midpoint between the vesting period and the contractual term of the grants. The estimate of the forfeited options in the compensation expense calculation was determined as the weighted-average forfeitures for the last three years. For the years ended June 30, 2016, 2015, and 2014, the Company recognized $58, $37 and $48, respectively, of compensation expense for share options issued. As of June 30, 2016, there was $25 of unrecognized compensation cost related to nonvested share-based compensation arrangements granted under the Plans. That cost is expected to be recognized during the fiscal years ended June 30, 2017, 2018 and 2019.
F-20
Information with respect to stock options outstanding and exercisable at June 30, 2016 is as follows:
| Exercise Prices |
Number Outstanding |
Weighted-Average Remaining Contractual Life (in years) |
Number Exercisable |
|||||||||
| $0.71 |
18,000 | 7.22 | 18,000 | |||||||||
| $1.22 |
210,000 | 6.18 | 210,000 | |||||||||
| $1.49 |
90,000 | 8.19 | 30,000 | |||||||||
| $1.67 |
60,000 | 5.37 | 60,000 | |||||||||
| $1.79 |
75,000 | 9.20 | 30,000 | |||||||||
| $2.09 |
120,000 | 5.20 | 120,000 | |||||||||
| $2.51 |
6,000 | 2.23 | 6,000 | |||||||||
| $6.55 |
27,500 | 0.87 | 27,500 | |||||||||
| $8.00 |
29,142 | 1.23 | 29,142 | |||||||||
|
|
|
|
|
|
|
|||||||
| 635,642 | 6.10 | 530,642 | ||||||||||
|
|
|
|
|
|
|
|||||||
No options were exercised during the years ended June 30, 2016, 2015 and 2014. As of June 30, 2016 and 2015, the aggregate intrinsic value of options outstanding and options exercisable were $0 and $67, respectively.
Shareholder Rights Plan—On February 10, 2014, the Board of Directors of the Company adopted a new Shareholder Rights Plan (the “Plan”). The Plan is intended to encourage fair treatment of shareholders should a take-over bid be made for the Company and provide the Board of Directors of the Company (the “Board”) and the shareholders more time to consider any unsolicited take-over bid. Unless otherwise terminated in accordance with its terms, the Plan will terminate on February 9, 2021.
The Rights issued under the Plan will become exercisable only when a person (including any party related to it) acquires or announces its intention to acquire 20% or more of the outstanding shares of the Company. Should such acquisition occur, each right will, upon exercise, entitle a right holder other than the acquiring person or related persons to purchase shares of SunLink Health Systems at a substantial discount to the market price at that time.
Tax Benefits Protection Rights Plan—On September 29, 2016, SunLink entered into a Tax Benefits Preservation Rights Plan (the “Tax Benefits Protection Rights Plan”). Effective September 29, 2016, the Board declared a dividend in the form of one preferred stock purchase right for each of the Company’s issued and outstanding common shares. The purpose of the Tax Benefits Protection Rights Plan is to diminish the risk that the Company’s ability to use its net operating losses and certain other tax assets to reduce potential future federal income tax obligations would become subject to limitations by reason of the Company experiencing an “ownership change,” as defined in Section 382 of the Code.
Accumulated Other Comprehensive Loss—Information with respect to the balances of each classification within accumulated other comprehensive loss is as follows:
| Minimum Pension Liability Adjustment |
Accumulated Other Comprehensive Loss |
|||||||
| June 30, 2013 |
$ | (406 | ) | $ | (406 | ) | ||
| Current period change |
72 | 72 | ||||||
|
|
|
|
|
|||||
| June 30, 2014 |
(334 | ) | (334 | ) | ||||
| Current period change |
(40 | ) | (40 | ) | ||||
|
|
|
|
|
|||||
| June 30, 2015 |
(374 | ) | (374 | ) | ||||
| Current period change |
(46 | ) | (46 | ) | ||||
|
|
|
|
|
|||||
| June 30, 2016 |
$ | (420 | ) | $ | (420 | ) | ||
|
|
|
|
|
|||||
F-21
| 12. | INCOME TAXES |
The provision (benefit) for income taxes on continuing operations are as follows:
| Year ended June 30, | ||||||||||||
| 2016 | 2015 | 2014 | ||||||||||
| Current |
$ | 2 | $ | 38 | $ | 95 | ||||||
| Deferred |
4,556 | 855 | 446 | |||||||||
|
|
|
|
|
|
|
|||||||
| Total income tax expense |
$ | 4,558 | $ | 893 | $ | 541 | ||||||
|
|
|
|
|
|
|
|||||||
Net deferred income tax assets recorded in the consolidated balance sheets are as follows:
| June 30, | ||||||||
| 2016 | 2015 | |||||||
| Net operating loss carryforward |
$ | 8,529 | $ | 4,096 | ||||
| Depreciation expense |
11 | (556 | ) | |||||
| Allowances for receivables |
714 | 1,365 | ||||||
| Accrued expenses |
1,155 | 1,365 | ||||||
| Intangible assets |
2,147 | 2,627 | ||||||
| Pension liabilities |
282 | 238 | ||||||
| Other |
136 | 281 | ||||||
|
|
|
|
|
|||||
| 12,974 | 9,416 | |||||||
| Less valuation allowance |
(10,652 | ) | (2,564 | ) | ||||
|
|
|
|
|
|||||
| Net deferred income tax assets |
$ | 2,322 | $ | 6,852 | ||||
|
|
|
|
|
|||||
The differences between income taxes on continuing operations at the Federal statutory rate and the effective tax rate were as follows:
| Year ended June 30, | ||||||||||||
| 2016 | 2015 | 2014 | ||||||||||
| Income tax at Federal statutory rate |
$ | (2,501 | ) | $ | 469 | $ | 20 | |||||
| Changes in valuation allowance—continuing operations |
7,350 | 215 | 460 | |||||||||
| U.S. state income taxes, net of federal benefit |
(405 | ) | 116 | 32 | ||||||||
| Share option expense |
20 | 12 | 16 | |||||||||
| Other |
94 | 81 | 13 | |||||||||
|
|
|
|
|
|
|
|||||||
| Total income tax expense—continuing operations |
$ | 4,558 | $ | 893 | $ | 541 | ||||||
|
|
|
|
|
|
|
|||||||
In accordance with the Financial Accounting Standards Board Accounting Standards Codification (‘ASC”) 740, we evaluate our deferred taxes quarterly to determine if adjustments to our valuation allowance are required based on the consideration of available positive and negative evidence using a “more likely than not” standard with respect to whether deferred tax assets will be realized. Our evaluation considers, among other factors, our historical operating results, our expectation of future results of operations, the duration of applicable statuary carryforward periods and conditions of the healthcare industry. The ultimate realization of our deferred tax assets depends primarily on our ability to generate future taxable income during the periods in which the related temporary differences in the financial basis and the tax basis of the assets become deductible. The value of our deferred tax assets will depend on applicable income tax rates.
At December 31, 2015 and again at March 31, 2016 and June 30, 2016, consistent with the above process, we evaluated the need for a valuation against our deferred tax assets and determined that it was more likely than not that none of our deferred tax assets would be realized. Subsequent to year end, we sold one of our facilities at
F-22
a gain. (See Note 3.) We determined that it was more likely than not that a portion of our deferred tax assets would be realized during the fiscal year ended June 30, 2017 and accordingly recorded a valuation allowance of $10,652 during 2016 representing the amount of our net deferred tax assets not expected to be realized. We conducted our evaluation by considering available positive and negative evidence to determine our ability to realize our deferred tax assets. In our evaluation, we gave more significant weight to evidence that was objective in nature as compared to subjective evidence. Also, more significant weight was given to evidence that directly related to our current financial performance as compared to less current evidence and future plans. The Company provided a $2,564 deferred tax valuation allowance as of June 30, 2015 so that the net deferred income tax assets were $6,852 as of June 30, 2015.
The principal negative evidence that led us to determine at June 30, 2016 that substantially all the deferred tax assets should have a full valuation allowances was the three-year cumulative pre-tax loss from continuing operations as well as the underlying negative business conditions for rural hospital businesses in which our Healthcare Facilities Segment businesses operate.
For Federal income tax purposes, at June 30, 2016, the Company had approximately $13,700 of estimated net operating loss carry-forwards available for use in future years subject to the limitations of the provisions of Internal Revenue Code Section 382. The net operating loss carryforwards expire in 2024. The Company’s tax returns for the periods prior to the fiscal year ended June 30, 2013 are no longer subject to potential federal and state income tax examination.
| 13. | EMPLOYEE BENEFITS |
Defined Benefit Plans—No defined benefit plan is maintained for employees of either the Healthcare Facilities Segment or the Specialty Pharmacy Segment. Prior to 1997, SunLink maintained defined benefit retirement plans covering substantially all of its domestic employees. Effective February 28, 1997, SunLink amended its domestic retirement plan to freeze participant benefits and close the plan to new participants. Benefits under the frozen plan are based on years of service and level of earnings. SunLink funds the frozen plan, which is noncontributory, at a rate that meets or exceeds the minimum amounts required by the Employee Retirement Income Security Act of 1974.
Since the sale of SunLink’s life sciences and engineering segment businesses in the fiscal year ended March 31, 1999, net pension expense has been classified as an expense of discontinued operations.
At June 30, 2016, the plan’s assets were invested 57% in cash and short term investments, 27% in equity investments and 16% in fixed income investments. The plan’s current investment policy of primarily investing in cash and short term investments is in response to the poor returns on investment of the past 5 years in the equity markets, the returns available in the fixed income markets and the possible need for immediate liquidity as participants retire or withdraw from the plan. The expected return on investment of 4% is based upon the plan’s historical return on assets. The plan expects to pay $94, $68, $65, $62, and $62 in pension benefits in the years ending June 30, 2017 through 2021, respectively. The plan expects to pay $431 in pension benefits for the years June 30, 2022 through 2026, in the aggregate. This assumes the plan participants elect to take monthly pension benefits as opposed to a lump sum payout when they reach age 65. The Company made a contribution of $128 to the plan for the year ended June 30, 2016 and plans to make a contribution of $140 to the plan for the year ended June 30, 2017
F-23
The components of net pension expense for all plans (comprised solely of one domestic plan) were as follows:
| Years Ended June 30, | ||||||||||||
| 2016 | 2015 | 2014 | ||||||||||
| Service cost |
$ | 0 | $ | 0 | $ | 0 | ||||||
| Interest cost |
65 | 60 | 59 | |||||||||
| Expected return on assets |
(35 | ) | (34 | ) | (30 | ) | ||||||
| Amortization of prior service cost |
113 | 100 | 129 | |||||||||
| Settlement cost |
38 | 0 | 0 | |||||||||
|
|
|
|
|
|
|
|||||||
| Net pension expense |
$ | 181 | $ | 126 | $ | 158 | ||||||
|
|
|
|
|
|
|
|||||||
| Weighted-average assumptions: |
||||||||||||
| Discount rate |
4.50 | % | 4.50 | % | 4.50 | % | ||||||
| Expected return on plan assets |
4.00 | % | 4.00 | % | 4.00 | % | ||||||
| Rate of compensation increase |
0.00 | % | 0.00 | % | 0.00 | % | ||||||
Summary information for the plans (comprised solely of one domestic plan) is as follows:
| 2016 | 2015 | |||||||
| Change in Benefit Obligation: |
||||||||
| Benefit obligation at beginning of year |
$ | 1,476 | $ | 1,366 | ||||
| Interest cost |
65 | 60 | ||||||
| Actuarial loss |
169 | 117 | ||||||
| Benefits paid |
(127 | ) | (67 | ) | ||||
|
|
|
|
|
|||||
| Benefit obligation end of year |
$ | 1,583 | $ | 1,476 | ||||
|
|
|
|
|
|||||
| Change in Fair Value of Plan Assets: |
||||||||
| Beginning fair value |
$ | 848 | $ | 816 | ||||
| Actual return on plan assets |
(23 | ) | (13 | ) | ||||
| Employer contribution |
128 | 112 | ||||||
| Benefits paid |
(127 | ) | (67 | ) | ||||
|
|
|
|
|
|||||
| Plan assets at end of year |
$ | 826 | $ | 848 | ||||
|
|
|
|
|
|||||
| Funded status of the plans |
(757 | ) | (628 | ) | ||||
| Unrecognized actuarial loss |
676 | 600 | ||||||
|
|
|
|
|
|||||
| Prepaid (accrued) benefit cost |
$ | (81 | ) | $ | (28 | ) | ||
|
|
|
|
|
|||||
| Amounts Recognized in Consolidated Balance Sheets |
||||||||
| Prepaid (accrued) benefit cost |
(81 | ) | (28 | ) | ||||
| Accumulated other comprehensive loss* |
676 | 600 | ||||||
|
|
|
|
|
|||||
| Net amount recognized |
$ | (757 | ) | $ | (628 | ) | ||
|
|
|
|
|
|||||
* Accumulated other comprehensive loss represents pretax minimum pension liability adjustments.
Defined Contribution Plan—SunLink has a defined contribution plan pursuant to IRS Section 401(k) covering substantially all domestic employees. SunLink matches a specified percentage of the employee’s contribution as determined periodically by its management. A match of $120 was provided for the fiscal year ended June 30, 2014. No match was provided for the fiscal years ended June 30, 2016 and 2015. Plan expense for the defined contribution plan was $0 for the years ended June 30, 2016, 2015 and 2014.
F-24
| 14. | INSURANCE SETTLEMENT |
In January 2015, the Company received a $1,000 settlement on a claim made under its insurance policy covering, among other things, employee theft relating to misappropriation of funds by two now former employees over an eight year period beginning in 2006. Income of $1,000 was recognized in the year ended June 30, 2015.
| 15. | COMMITMENTS AND CONTINGENCIES |
Leases—The Company leases various land, buildings, and equipment under operating lease obligations having noncancelable terms ranging from one to 7 years. Rent expense was $791, $818, and $877, for the years ended June 30, 2016, 2015 and 2014, respectively. Minimum lease commitments as of June 30, 2016 are as follows:
| Fiscal year ending June 30: |
||||
| 2017 |
$ | 472 | ||
| 2018 |
314 | |||
| 2019 |
196 | |||
| 2020 |
155 | |||
| 2021 |
31 | |||
|
|
|
|||
| $ | 1,168 | |||
|
|
|
| 16. | RELATED PARTIES |
A director of the Company and the Company’s former company secretary are members of two different law firms, each of which provides services to SunLink. The Company has expensed an aggregate of $275, $334 and $689 to these law firms in the fiscal years ended June 30, 2016, 2015 and 2014, respectively. Included in the Company’s consolidated balance sheets at June 30, 2016 and 2015 is $75 and $89, respectively, of amounts payable to these law firms.
| 17. | FINANCIAL INFORMATION BY SEGMENTS |
Under ASC Topic No. 280, Segment Reporting, operating segments are defined as components of an enterprise about which separate financial information is available that is evaluated regularly by the chief operating decision maker, or decision-making group, in deciding how to allocate resources and in assessing performance. Our chief operating decision-making group is composed of the chief executive officer and members of senior management. Our two reportable operating segments are Healthcare Facilities and Specialty Pharmacy.
F-25
We evaluate performance of our operating segments based on revenue and operating profit (loss). During the current year, the Company modified the approach to certain expense allocations to calculate segment operating profit. All prior year amounts have been changed to consistently apply the changed allocation method used in the current year. Segment information for the fiscal years ended June 30, 2016, 2015 and 2014 is as follows:
| Healthcare Facilities |
Specialty Pharmacy |
Corporate and Other |
Total | |||||||||||||
| 2016 |
||||||||||||||||
| Net Revenues from external customers |
$ | 30,462 | $ | 32,216 | $ | 755 | $ | 63,433 | ||||||||
| Operating profit (loss) |
(3,072 | ) | (42 | ) | (3,409 | ) | (6,523 | ) | ||||||||
| Depreciation and amortization |
618 | 954 | 306 | 1,878 | ||||||||||||
| Assets |
23,060 | 11,656 | 10,125 | 44,841 | ||||||||||||
| Expenditures for property, plant and equipment |
93 | 1,224 | 30 | 1,347 | ||||||||||||
| 2015 |
||||||||||||||||
| Net Revenues from external customers |
$ | 39,933 | $ | 33,175 | $ | 638 | $ | 73,746 | ||||||||
| Operating profit (loss) |
4,564 | 494 | (2,838 | ) | 2,220 | |||||||||||
| Depreciation and amortization |
663 | 796 | 378 | 1,837 | ||||||||||||
| Assets |
28,856 | 12,344 | 15,928 | 57,128 | ||||||||||||
| Expenditures for property, plant and equipment |
158 | 1,008 | 69 | 1,235 | ||||||||||||
| 2014 |
||||||||||||||||
| Net Revenues from external customers |
$ | 39,986 | $ | 33,322 | $ | 461 | $ | 73,769 | ||||||||
| Operating profit (loss) |
4,006 | 553 | (3,517 | ) | 1,042 | |||||||||||
| Depreciation and amortization |
736 | 730 | 856 | 2,322 | ||||||||||||
| Assets |
37,481 | 11,321 | 15,045 | 63,847 | ||||||||||||
| Expenditures for property, plant and equipment |
420 | 711 | 352 | 1,483 | ||||||||||||
F-26
| 18. | EARNINGS PER SHARE |
(Share Amounts in Thousands)
| Years Ended June 30, | ||||||||||||||||||||||||
| 2016 | 2015 | 2014 | ||||||||||||||||||||||
| Amount | Per Share Amount |
Amount | Per Share Amount |
Amount | Per Share Amount |
|||||||||||||||||||
| Earnings (loss) from continuing operations |
$ | (11,914 | ) | $ | 487 | $ | (484 | ) | ||||||||||||||||
|
|
|
|
|
|
|
|||||||||||||||||||
| Basic: |
||||||||||||||||||||||||
| Weighted-average shares outstanding |
9,443 | $ | (1.26 | ) | 9,443 | $ | 0.05 | 9,443 | $ | (0.05 | ) | |||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
| Diluted: |
||||||||||||||||||||||||
| Weighted-average shares outstanding |
9,443 | $ | (1.26 | ) | 9,496 | $ | 0.05 | 9,456 | $ | (0.05 | ) | |||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
| Earnings (loss) from discontinued operations |
$ | (2,169 | ) | $ | (242 | ) | $ | (61 | ) | |||||||||||||||
|
|
|
|
|
|
|
|||||||||||||||||||
| Basic: |
||||||||||||||||||||||||
| Weighted-average shares outstanding |
9,443 | $ | (0.23 | ) | 9,443 | $ | (0.02 | ) | 9,443 | $ | (0.01 | ) | ||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
| Diluted: |
||||||||||||||||||||||||
| Weighted-average shares outstanding |
9,443 | $ | (0.23 | ) | 9,496 | $ | (0.02 | ) | 9,456 | $ | (0.01 | ) | ||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
| Net Earnings (loss) |
$ | (14,083 | ) | $ | 245 | $ | (545 | ) | ||||||||||||||||
|
|
|
|
|
|
|
|||||||||||||||||||
| Basic: |
||||||||||||||||||||||||
| Weighted-average shares outstanding |
9,443 | $ | (1.49 | ) | 9,443 | $ | 0.03 | 9,443 | $ | (0.06 | ) | |||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
| Diluted: |
||||||||||||||||||||||||
| Weighted-average shares outstanding |
9,443 | $ | (1.49 | ) | 9,496 | $ | 0.03 | 9,456 | $ | (0.06 | ) | |||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
| Weighted-average number of shares outstanding—basic |
9,443 | 9,443 | 9,443 | |||||||||||||||||||||
|
|
|
|
|
|
|
|||||||||||||||||||
| Effect of dilutive director, employee and guarantor options and outstanding common share warrants |
0 | 53 | 13 | |||||||||||||||||||||
|
|
|
|
|
|
|
|||||||||||||||||||
| Weighted-average number of shares outstanding—diluted |
9,443 | 9,496 | 9,456 | |||||||||||||||||||||
|
|
|
|
|
|
|
|||||||||||||||||||
Share options of 636 for the year ended June 30, 2016 are not included in the computation of diluted earnings per share because their effect would be antidilutive.
F-27
| 19. | SELECTED QUARTERLY FINANCIAL DATA (UNAUDITED) |
(All amounts in thousands, except per share amount)
The following selected quarterly data for the years ended June 30, 2016 and 2015, respectively, are unaudited.
| Fourth Quarter |
Third Quarter |
Second Quarter |
First Quarter |
|||||||||||||||
| NET REVENUE |
Year Ended June 30, 2016 | $ | 14,060 | $ | 16,205 | $ | 16,585 | $ | 16,583 | |||||||||
| Year Ended June 30, 2015 | $ | 18,474 | $ | 19,288 | $ | 18,504 | $ | 17,480 | ||||||||||
| EARNINGS (LOSS) FROM |
||||||||||||||||||
| CONTINUING OPERATIONS |
Year Ended June 30, 2016 | (823 | ) | (1,392 | ) | (8,566 | ) | (1,133 | ) | |||||||||
| Year Ended June 30, 2015 | (7 | ) | (940 | ) | 1,633 | (199 | ) | |||||||||||
| NET EARNINGS (LOSS) |
Year Ended June 30, 2016 | (1,234 | ) | (1,835 | ) | (9,346 | ) | (1,668 | ) | |||||||||
| Year Ended June 30, 2015 | 92 | (411 | ) | 977 | (413 | ) | ||||||||||||
| EARNINGS (LOSS) PER SHARE: |
||||||||||||||||||
| Continuing operations |
||||||||||||||||||
| Basic |
Year Ended June 30, 2016 | (0.09 | ) | (0.15 | ) | (0.91 | ) | (0.12 | ) | |||||||||
| Year Ended June 30, 2015 | (0.00 | ) | (0.10 | ) | 0.17 | (0.02 | ) | |||||||||||
| Diluted |
Year Ended June 30, 2016 | (0.09 | ) | (0.15 | ) | (0.91 | ) | (0.12 | ) | |||||||||
| Year Ended June 30, 2015 | (0.00 | ) | (0.10 | ) | 0.17 | (0.02 | ) | |||||||||||
| NET EARNINGS (LOSS): |
||||||||||||||||||
| Basic |
Year Ended June 30, 2016 | (0.13 | ) | (0.19 | ) | (0.99 | ) | (0.18 | ) | |||||||||
| Year Ended June 30, 2015 | 0.01 | (0.04 | ) | 0.10 | (0.04 | ) | ||||||||||||
| Diluted |
Year Ended June 30, 2016 | $ | (0.13 | ) | $ | (0.19 | ) | $ | (0.99 | ) | $ | (0.18 | ) | |||||
| Year Ended June 30, 2015 | $ | 0.01 | $ | (0.04 | ) | $ | 0.10 | $ | (0.04 | ) | ||||||||
| WEIGHTED-AVERAGE COMMON SHARES OUTSTANDING: |
||||||||||||||||||
| Basic |
Year Ended June 30, 2016 | 9,443 | 9,443 | 9,443 | 9,443 | |||||||||||||
| Year Ended June 30, 2015 | 9,443 | 9,443 | 9,443 | 9,443 | ||||||||||||||
| Diluted |
Year Ended June 30, 2016 | 9,443 | 9,443 | 9,443 | 9,443 | |||||||||||||
| Year Ended June 30, 2015 | 9,490 | 9,443 | 9,497 | 9,443 | ||||||||||||||
F-28