Attached files
| file | filename |
|---|---|
| 8-K - FORM 8-K - HERON THERAPEUTICS, INC. /DE/ | d626911d8k.htm |
| EX-99.1 - EX-99.1 - HERON THERAPEUTICS, INC. /DE/ | d626911dex991.htm |
| EX-99.2 - EX-99.2 - HERON THERAPEUTICS, INC. /DE/ | d626911dex992.htm |
 Company Overview
OTCBB: APPA
November 2013
Exhibit 99.3 |
 Legal
Disclaimer This presentation contains "forward-looking statements"
as defined by the Private Securities Litigation Reform Act of 1995.
These forward-looking statements involve risks and uncertainties,
including uncertainties associated with timely development, approval, launch
and acceptance of new products, satisfactory completion of clinical studies,
establishment of new corporate alliances, progress in research and
development programs and other risks and uncertainties identified in the
Company's filings with the Securities and Exchange Commission. Actual
results may differ materially from the results expected in our forward looking
statements. We caution investors that forward-looking statements
reflect our analysis only on their stated date. We do not intend to
update them except as required by law.
2
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved. |
 Company:
A.P. Pharma, Inc.
Ticker:
OTCBB: APPA.OB
Stock Price:
$0.46 (11/8/2013)
Market Capitalization:
$237
million
1
Cash:
$23
million
2
Debt:
$5
million
2
Stock Summary
1
Based on 516 million fully diluted, as-converted common shares assuming the
full conversion of convertible debt outstanding and 80 million warrants
using treasury stock method; not including options
2
As of September 30, 2013
3
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved. |
 Barry
D. Quart, PharmD Chief Executive Officer
Ardea Biosciences
Agouron Pharmaceuticals
Pfizer
Robert Rosen
President &
Chief Commercial Officer
Bayer Healthcare
Sanofi-Synthèlabo
Imclone
Stephen Davis
Chief Operating Officer
Ardea Biosciences
Neurogen
Mark Gelder, M.D.
Senior Vice President &
Chief Medical Officer
GE Healthcare
Bayer Healthcare
Wyeth
Paul Marshall
Senior Vice President
Technical Operations
Amylin
Amgen
Baxter International
Brian Drazba
Vice President, Finance &
Chief Financial Officer
ISTA Pharmaceuticals
Insight Health Corp
Arthur Andersen & Co
Senior Management
4
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved. |
 Highlights
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved.
5
Lead product candidate, SUSTOL™
(formerly known as APF530), is long-
acting, injectable product for chemotherapy-induced nausea and vomiting
(CINV)
Incorporates
widely
used
5-HT3
antagonist
-
granisetron
(Kytril
®
)
5-day delivery profile
Reduces both acute-
and delayed-onset CINV with single injection
Patent coverage into 2024; however, effective exclusivity actually longer due to
polymer SUSTOL
shown
to
be
non-inferior
to
market
leader
Aloxi
®
1,341-patient, randomized, controlled, Phase 3 study
SUSTOL targets a large market opportunity, with approximately 7 million
doses of chemotherapy annually in US alone*
Recent competitive setbacks could enhance commercial uptake
Could be second, long-acting, injectable product on market
Plans to leverage our Biochronomer™
drug delivery technology,
development capacity and commercial expertise for other opportunities:
Long-acting anesthetic for post-surgical pain
Triple-combination for CINV is under evaluation
Potential for several others
*TDR August 2006 internal report |
 Strategic Product Development
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved.
6
Framework
Large, established markets with high unmet need
Rapid
development
&
approval
pathway
based
on
reformulations
and
505(b)(2)
strategy
Premium pricing through innovation and product differentiation
Clearly defined value proposition
Opportunities to optimize ROI through life cycle management (franchise
extension) Low cost of entry
Pipeline
Chemotherapy-induced nausea and vomiting
SUSTOL
Potential for triple-drug combination
Post-operative pain management
Long-acting local anesthetic
Potential for several others |
 SUSTOL Clinical Summary
7
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved. |
 APF530
Pivotal Phase 3 Study Overview Randomized, controlled, multi-center
study 1,341 patients in primary efficacy population
Two doses of APF530 (5 mg and 10 mg granisetron) compared
to the approved dose of Aloxi (results from 10 mg dose group
presented)
Patients stratified by type of chemotherapy regimen (moderately
or highly emetogenic)
Primary end point compared complete response between
groups in both the acute (day 1) and delayed (days 2-5) phase
Complete response defined as no emesis and no rescue medications
A ±15% margin was used to establish non-inferiority
8
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved. |
 5-Day Profile: APF530 Pharmacokinetics
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved.
9
Granisetron is released rapidly following injection of APF530 and continues to be
released over a 5-day period, providing long-acting coverage for
CINV Minimum
therapeutic
concentration of
granisetron*
*Data from patent application 20120258164 for transdermal granisetron
0
5
10
15
20
0
24
48
72
96
120
144
168
Time after Dosing (h)
All subjects (n= 18)
mean ±
SEM |
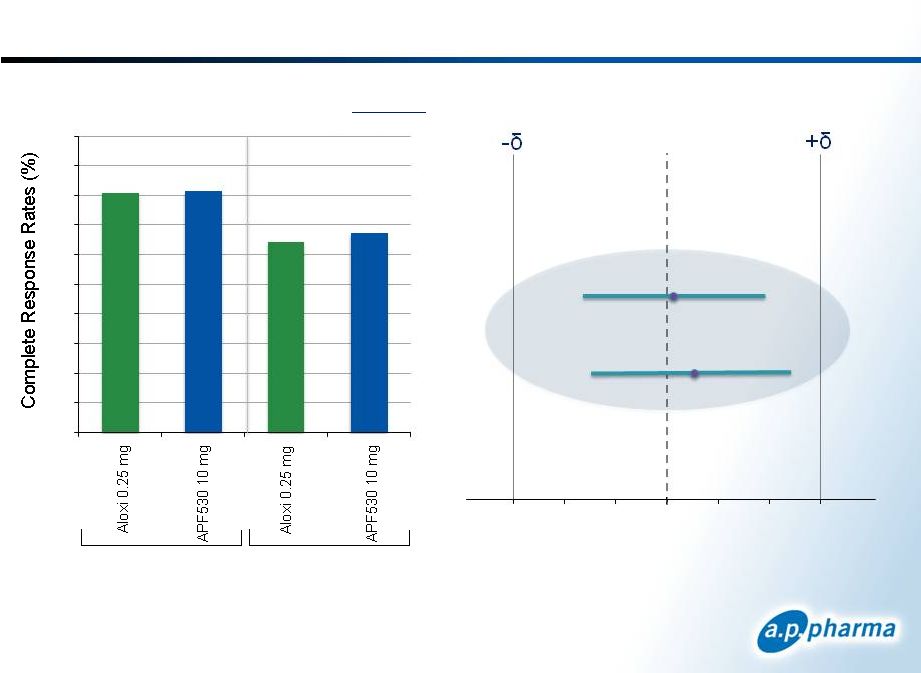
 Primary Efficacy Results: Complete Response
Patients Receiving Moderately
Emetogenic Chemotherapy
Acute
Delayed
APF530 10mg
Acute
Delayed
Difference in Complete Response
APF530-Aloxi (97.5% CI)
-15
-10
-5
0
5
10
15
10
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved.
75.0
76.9
57.2
58.5
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0 |
 Primary Efficacy Results: Complete Response
Difference in Complete Response
APF530-Aloxi (98.33% CI)
-15
-10
-5
0
5
10
15
Patients Receiving Highly
Emetogenic Chemotherapy
Acute
Delayed
11
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved.
0
10
20
30
40
50
60
70
80
90
100
Acute
Delayed
APF530 10mg
80.7
81.3
64.3
67.1 |
 Safety Summary
1
Safety results with the 5 mg dose of APF530 studied in separate arm of the phase 3
study are not included 2
>90% of injection site reactions were reported as mild; one patient
discontinued due to injection site reaction Reported in Cycle 1
12
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved.
APF530 10 mg
1
Aloxi 0.25 mg
N
%
N
%
Drug Related Serious Adverse Events
0
0
0
0
Discontinued Due to Adverse Event
1
0.2
0
0
Frequent Adverse Events
Gastrointestinal Disorders
Constipation
Diarrhea
Abdominal pain
72
44
13
15.4
9.4
2.8
62
39
28
13.4
8.4
6.0
Nervous System
Headache
47
10.0
45
9.7
Injection Site
Placebo (NaCl)
Bruising
Erythema (redness)
Nodule (lump)
Pain
93
51
50
33
19.9
10.9
10.7
7.1
41
14
3
5
8.9
3.0
0.6
1.1
2 |
 FDA
Requested ASCO 2011 Reanalysis Improves Difference Between SUSTOL and
Aloxi Protocol Specified HEC Population
Acute
Delayed
13
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved.
Acute
Delayed
ASCO 2011 Guideline HEC Population
81
81
64
67
0
10
20
30
40
50
60
70
80
90
100
67
75
51
56
0
10
20
30
40
50
60
70
80
90
100 |
 Largest Differences Between Arms is Seen With
Most Difficult Chemo Regimens
1
CR Rates by Treatment
Chemotherapeutic Regimen
APF530 10 mg
Aloxi 0.25 mg
Moderately
Emetogenic
Acute
Cyclophosphamide/Doxorubicin
70.7%
65.7%
All other regimens
84.4%
85.0%
Delayed
Cyclophosphamide/Doxorubicin
47.4%
46.3%
All other regimens
72.9%
70.0%
Highly
Emetogenic
Acute
Cisplatin regimens
81.1%
75.5%
Carboplatin/Paclitaxel
85.4%
89.8%
All other regimens
75.4%
67.6%
Delayed
Cisplatin regimens
66.0%
60.4%
Carboplatin/Paclitaxel
70.8%
71.4%
All other regimens
65.2%
57.4%
1
Data from post-hoc analysis. Not statistically significant.
Highlighted HEC regimens were considered HEC in both protocol specified Hesketh and
2011 ASCO Guidelines
14
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved. |
 Summary of Clinical Results
Bio-erodible polymer technology releases granisetron to prevent CINV
over at least 5 days
Large, randomized, Phase 3 study conducted: APF530 10 mg showed
non-inferiority to Aloxi
For both acute-
and delayed-onset CINV
With both moderately and highly emetogenic chemotherapy
APF530 was well-tolerated
Incidence of adverse events comparable to Aloxi
Injection site reactions where predominately mild
Good response rates were observed in difficult chemotherapy
regimens
Efficacy was maintained with reanalysis using ASCO 2011 guidelines
and through multiple cycles of chemotherapy
TQT study showed APF530 has no clinically significant effect on QT;
differentiated from Zofran(ondansetron) and Anzemet(dolasetron)
15
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved. |
 SUSTOL Regulatory Status
16
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved. |
 SUSTOL NDA Status
Submitted NDA in May 2009 under 505(b)(2) filing pathway
Received Complete Response Letter in March 2010
FDA raised major issues in multiple areas
Resubmitted NDA in September 2012
Received Complete Response Letter March 2013 raising three
main issues:
17
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved.
CMC: correction of PAI issues and revision of one in-vitro release
method Requirement for Human Factors Validation Study with commercial
product Re-analysis of the existing Phase 3 study using the ASCO 2011
guidelines for categorization of MEC and HEC |
 New
Management Team Is Addressing the CRL Chemistry, Manufacturing, and
Controls Sites with PAI issues are being eliminated from the supply chain,
with work transferred to well established site with no PAI issues
Transition is almost complete
Secondary benefit of consolidating manufacturing and release efforts is that
there has been a substantial improvement in the COGS
New in-vitro release method has been developed and being validated
Plan to produce three validation batches of finished product in advance of
re-filing to supply Human Factors Study
Human Factors Validation Study
Will be conducted as soon as commercial material available
Re-analysis of Phase 3 using new ASCO 2011 Guidelines
Re-analysis complete
Complete dataset and programs supplied to FDA and found acceptable
Re-submission is now planned for late 1Q2014
18
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved. |
 SUSTOL Life-Cycle Management
Plans to Obtain Post-Approval Indication for
“Delayed HEC”
19
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved. |
 Palonosetron lacks an indication in delayed HEC because
it was unable to demonstrate superiority vs. ondansetron
©
2013. A.P. Pharma, Inc. All rights reserved.
20
Goal for New HEC Study is a
Differentiated Target Product Profile*
“Well, it appears to be certainly longer-acting, and the real
differentiator appears to be in the delayed setting”
–Oncologist, Suburban, Large Private Practice
“We’d probably try a few patients on it and as long as
we’re getting the sense that it is doing what it’s claimed to
do, then we may make the full switchover...
–
Oncologist, Urban, Group Practice
Physician Feedback
Source: August 2013 qualitative market research with n=30 oncologists
Nov 2013
*Text in blue is based on the successful outcome to the
planned HEC trial
“[The
delayed
HEC
study]
solidifies
my
impression
of
[APF530]
&
gives
even
more
confidence
in
its
clinical
profile.
–Oncologist,
Urban,
Mid-sized,
Multi-specialty
Practice
SUSTOL
Indication
MEC –
acute
and
delayed
CINV
HEC –
acute
and
delayed
CINV
Dosing
SC
injection
once
per
cycle
Duration
of action
Bioerodible
polymer technology maintains
super
therapeutic levels of granisetron
over 5 to 7 days
-
Study
SUSTOL vs. palonosetron
SUSTOL + fosaprepitant
ondansetron
fosaprepitant
•
•
vs.
+
Efficacy
Results
•
Non
inferior to palonosetron
•
Effective
in prevention of acute & delayed CINV in
MEC and acute CINV in HEC
•
SUSTOL superior to ondansetron
•
Effective
in prevention of delayed CINV in HEC
-
Safety
esults
•
Headache, constipation, injection site bruising and
pain. Majority of AEs were mild
•
Clean QT profile
R |
 Planned Phase 3 “Delayed”
HEC Study Schematic
1000 patients
scheduled to receive
HEC* randomized
1:1
Ondansetron 0.15 mg/kg
IV (up to 16 mg IV) d1 +
Fosaprepitant 150 mg IV
d1 + Placebo SC d1
SUSTOL SC d1 +
Fosaprepitant 150 mg IV
d1 + Placebo IV d1
Cycle 1
1)
All subjects will receive dexamethasone 12 mg IV on day 1 and 8 mg PO on days 2-
4
2)
All subjects will be allowed to receive “rescue”
medications as needed at the discretion of their
treating physician
©
2013. A.P. Pharma, Inc. All rights reserved.
21
* HEC agents as defined in the 2011 ASCO CINV Guidelines
•
Study design has been accepted by FDA for obtaining expanded
indication
•
Study is powered to show superiority (10% difference) to three drug
“standard of care”
for HEC
•
Study planned to complete late 2014
Nov 2013 |
 45
65
67
0
10
20
30
40
50
60
70
80
90
100
New SUSTOL Study in Delayed HEC Has a High
Likelihood of Success Based on Previous Results
^^Average
Complete
Response
rate
improvement
when
adding
an
NK-1
RA
to
a
5-HT3
RA
and
Dex
is
~15
-
20%
in
the
delayed
phase
* Poll-Bigelli; Cancer, 97:12, 3090, 2003
Projected
Response
with addition
of NK1
^^
Study
powered
to show 10%
difference:
65% vs 75%
APF530 + Dex
+ Fosaprepitant**
APF530+Dex
Ondansetron + Dex
+ Fosaprepitant*
Ondansetron + Dex*
87%
Standard of Care
Phase 3 Study
HEC Study
67%
65%
45%
Study powered for a 10% difference between arms
20% difference is expected with the addition of fosaprepitant,
©
2013. A.P. Pharma, Inc. All rights reserved.
22 |
 SUSTOL Commercial Opportunity
23
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved. |
 Continuing Unmet Need in CINV
Need for long-acting antiemetic
therapies
Delayed CINV (days 2-5) remains
particularly challenging to manage
Significant portion of patients fail to respond
to palonosetron
Need for antiemetic therapies with
sustained efficacy
CINV risk increases over multiple
chemotherapy cycles
1
Available at:
http://www.cancer.gov/cancertopics/pdq/supportivecare/nausea/HealthProfessional/page6#Section_183
“Despite the use of both first-generation
and
second-generation
5-HT
3
receptor
antagonists, the control of acute CINV, and
especially delayed nausea and vomiting, is
suboptimal,
and
there
is
considerable
opportunity for improvement
with either
the addition or substitution of new agents in
current regimens.”
NCI Statement On The Existing
Unmet
Need
in
CINV
1
24
©
2013. A.P. Pharma, Inc. All rights reserved.
Nov 2013 |
 Addressing Debilitating Effects of CINV
©
2013. A.P. Pharma, Inc. All rights reserved.
25
More than 7 million cycles of
chemotherapy administered each
year*
~27% are highly emetogenic
~46% are moderately emetogenic
Most chemotherapy patients will
undergo 4-15 cycles of
chemotherapy
5-HT3 antagonists are standard-
of-
care for CINV
Recommended in ASCO, NCCN
and MASCC guidelines
NK-1 antagonists are only indicated
in combination with 5-HT3
antagonists
An Injectable 5-HT3 antagonist is
co-administered with more than
>80% of MEC and HEC regimens
If initial regimen is non-effective,
drugs are added or changed to
address CINV in subsequent cycles
*TDR August 2006
Nov 2013 |
 U.S.
CINV Market Dynamics 26
©
2013. A.P. Pharma, Inc. All rights reserved.
Source: WK 07/2013
Nov 2013
0
100,000
200,000
300,000
400,000
500,000
600,000
700,000
800,000
Q2'06
Q4'06
Q2'07
Q4'07
Q2'08
Q4'08
Q2'09
Q4'09
Q2'10
Q4'10
Q2'11
Q4'11
Q2'12
Q4'12
Injectable Drugs for the Prevention of CINV
Number of Package Units Sold by Quarter
ALOXI
ANZEMET
KYTRIL
KYTRIL Generic (GRANISETRON)
ZOFRAN
ZOFRAN Generic (ONDANSETRON)
EMEND
* US Oncology
data added starting 1/2009. |
 Physicians View SUSTOL As Highly Competitive
vs. Palonosetron
©
2013. A.P. Pharma, Inc. All rights reserved.
27
Physicians responded favorably to HTH
study
design
vs.
palonosetron
–
good
sample size, clinically meaningful
endpoints, & strong comparator
PK profile and efficacy results were
viewed
as
clinically
meaningful
–
SUSTOL viewed as a long-acting agent
with sustained efficacy over multiple
days
SUSTOL is perceived as a clinically
equivalent alternative to palonosetron for
most physicians
SUSTOL safety profile is similar to
palonosetron and very manageable
“Well designed, well done clinical trial, the kind of trial you
want to see. I think that’s very favorable.”
–
Oncologist, Mid-sized Community Practice
“I think it’s an incrementally better product than palonosetron.
The whole idea is probably the longer [PK profile].”
–
Oncologist, Large Community Practice
“I think [APF530] is great…we need something which has a
much longer [duration of action]…I would certainly use it.”
–
Oncologist, Urban, Community Practice
“It has [few] side effects…very comparable to medications
we are currently using.”
–
Oncologist, Suburban, Large Practice
Source: August 2013 qualitative market research with n=30 oncologists
Nov 2013 |
 Despite lack of commercial presence, a significant
portion of physicians view SUSTOL as differentiated
©
2013. A.P. Pharma, Inc. All rights reserved.
28
Question: “Based on the design and results of these studies, how do you
perceive SUSTOL vs. palonosetron?”
““The [first] study is compared with
palonosetron and it seems like they
are equivalent. I’m OK with that.”
–Oncologist, Large Community
Practice
“Well, this product in comparison to
palonosetron seems to be better. So,
I would have no problems using a
better agent …The bottom line is that
your data show that this therapy was
better than palonosetron.”
–
Oncologist, Community Practice
Source: August 2013 qualitative market research with n=30 oncologists
“Also…
even
if
there
were
no
delayed
data
in
HEC,
I
would
still
use
it
because
then it would be very comparable to the current medication that I'm
using." –Oncologist, Mid-sized Community Practice
Nov 2013
Clinically
Equivalent
67%
Clinically
Differentiated
33% |
 HEC
regimens represent a significant market opportunity for SUSTOL
©
2013. A.P. Pharma, Inc. All rights reserved.
29
1
IntrinsiQ data from July 2012 –
June 2013
HEC regimens account for ~20% (500K)
of palonosetron administrations
Of all HEC administrations, ~20% are given
without concomitant IV 5-HT3 –
inconsistent with clinical guidelines
Nov 2013
497,256
1,463,558
451,490
111,696
HEC
MEC
LEC
Minimal
-
200,000
400,000
600,000
800,000
1,000,000
1,200,000
1,400,000
1,600,000
497,256
317,915
188,988
-
200,000
400,000
600,000
800,000
1,000,000
1,200,000
Annual HEC
administrations
Untreated with
IV 5HT3
Treated with
generic IV
5HT3
Treated with
Aloxi |
 SUSTOL
has the potential to be the next generation 5-HT3 receptor antagonist
(RA) 30
©
2013. A.P. Pharma, Inc. All rights reserved.
5-HT3
RAs
1
st
generation
2
nd
generation
3
rd
generation
Products
ondansetron
granisetron
palonosetron
SUSTOL
Duration of
action
Short acting
~ 8 hr half-life
Longer acting
~40 hr half-life
Long acting
PK profile 5-7 days
Indications
Prevention of CINV in
emetogenic chemo including
high-dose cisplatin
MEC –
acute & delayed CINV
HEC –
acute CINV
MEC
–
acute
&
delayed
CINV
HEC
–
acute
&
delayed
CINV*
*Obtaining delayed HEC will be based on completion of new clinical trial
Nov 2013 |
 WKH Data Oct. 2012 –
Clinic Analysis
Palonosetron Clinical Use Is Highly
Concentrated
Cumulative Number of Accounts
32
1% accts
87
4% accts
161
7% accts
252
11% accts
500
22% accts
674
29% accts
904
39% accts
1246
54% accts
2305
100% accts
362
15% accts
80% of all units (2.2M) comes from community clinics
80% of clinic units (1.7M) comes from 39% of accounts (904)
50% of clinic units (1.1M) comes from 15% of accounts (362)
31
©
2013. A.P. Pharma, Inc. All rights reserved.
Nov 2013
0
200
400
600
800
1,000
1,200
1,400
1,600
1,800
2,000
2,200 |
 Summary
©
2013. A.P. Pharma, Inc. All rights reserved.
32
CINV market is a large, concentrated commercial opportunity
Over
2.7MM
annual
units
of
palonosetron
1
>80%
of
use
is
in
the
community
practice
setting
–
highly
concentrated
among
large
practices
1
Physicians view a non-inferior SUSTOL profile as highly competitive
5-7 day PK profile
Non-inferior to market leader palonosetron based on large,
head-to-head trial Good response in difficult chemotherapy regimens
including AC and cisplatin Sustained efficacy over multiple cycles of
chemotherapy Efficacy in palonosetron failures
Favorable safety profile with clean QT results
Differentiated profile would position SUSTOL as the next generation IV
5-HT3 Delayed
CINV,
especially
in
HEC
regimens,
is
the
biggest
area
of
unmet
need
No 5-HT3 drugs approved specifically for delayed CINV in HEC
Palonosetron failed to show superiority to ondansetron in delayed HEC
High likelihood of clinical success versus ondansetron
Supports differentiated value proposition vs. palonosetron
HEC regimens represent a significant market opportunity
20%
of
palonosetron
administrations
are
given
with
HEC
regimens
2
20%
of
patients
receiving
HEC
regimens
do
not
receive
concomitant
treatment
with
an
IV
5-HT3
2
1. Wolters Kluwer 2012, 2. Intrinsiq 2013
Nov 2013 |
 New
Product Initiative 33
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved. |
 SUSTOL
Product Lifecycle Considerations 34
SUSTOL covered by multiple patents
2 patents covering combination of polymer, excipients and drug expire in
2021 3 patents covering APF530 expire in 2024
Polymer-based injectable products are difficult to copy independent of
IP
ANDA FDA requirements for injectable products
Must
have
same
inactive
ingredients
in
the
same
concentration
as
the
reference listed drug
Polymers are complex mixtures of varying-length molecules, making
characterization for “sameness”
very challenging
Obtaining the delayed HEC indication will further differentiate SUSTOL
from all other 5-HT3 products
Creating additional product opportunities with SUSTOL will further
leverage our investment in the HEC program
One opportunity under evaluation is a three-drug combination
containing SUSTOL, an NK1 antagonist and dexamethasone
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved. |
 Biochronomer Triple-Drug Combination for CINV
in Dogs
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved.
35
Profile of each component of triple-drug combo is similar to individual
agents Single shot with all three of the drugs recommended for HEC
Registration could be based primarily on bioequivalence
0
10
20
30
40
50
60
70
80
90
0
100
200
300
400
500
600
700
800
900
0
24
48
72
96
120
144
168
Hours
NK1 Antagonist
Granisetron
Dexamethasone |
 Biochronomer™
Bupivacaine/Ropivacaine:
Post-Surgical Pain Control
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved.
36
Opportunity to use our polymer for post-surgical pain control utilizing
the 505(b)(2) process
Once we have an FDA approved polymer, manufacturing site and syringe filler, the
next products using the polymer will be much easier and cheaper to develop
We believe the leading product in this market, EXPAREL, can be
substantially improved by:
Prolonging the period of anesthetic release, so peak concentration are seen at
48- 72 hours rather than 12-24 hours as seen with EXPAREL
Potentially using a better anesthetic agent, ropivacaine
|
 Greatest Benefit for
EXPAREL Is First 12 Hours Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved.
37
Adapted from EXPAREL Product Monograph
*US Package Insert
Package insert states that there was minimal
to no difference between Exparel and placebo
treatments 24-72 hours post-dose* |
 Mean
Plasma Bupivacaine Concentrations After EXPAREL From FDA Clinical Pharmacology
Review Data from FDA Clinical Pharmacology Review; NDA 22-496 EXPAREL; *
US Package Insert Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved.
38
Low concentrations of bupivacaine after 24 hr
may explain why there was minimal to no
difference between Exparel and placebo
treatments 24-72 hours post-dose* |
 Biochronomer™
Bupivacaine Has Superior PK Profile
in Dogs
*Projected from 7.5 mg/kg dose; EXPAREL data from Richard, et. al. 2012
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved.
39 |
 Biochronomer™
Ropivacaine Has Superior PK Profile
in Dogs
*Dose adjusted to match bupivacaine; EXPAREL data from Richard, et. al. 2012
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved.
40 |
 Post-Operative Pain Management
Commercial Considerations
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved.
41 |
 Post-operative pain
market represents an attractive opportunity for product development
©
2013. A.P. Pharma, Inc. All rights reserved.
42
•
Patients are typically treated with a combination of NSAIDs, opioids, local
anesthetics and/or simple analgesics
•
Strong opioids currently hold approximately half of the market sales
Treatment
Paradigm
•
As of 2012, approximately 24.8 million procedures associated with post-operative
pain were conducted in the US. Expected to grow to 32.3 million by 2022
•
US
post-operative
pain
market
sales*
are
expected
to
grow
1.6%
annually
from
~$3.1 billion in 2012 to ~$3.6 billion by 2022
•
Market growth is primarily driven by the increasing number of procedures and by
new reformulations
Market Size
•
Longer-acting local anesthetics (>3 days) with improved safety profiles
•
Potent opioid-sparing analgesics with improved tolerability and less severe side
effects compared to opioids
Unmet Needs
•
Pain is a major driver of inpatient admissions and increased length of stay
•
Reimbursement will increasingly be tied to measures of quality and ratings of
patient experience –
both of which are significantly impacted by pain
•
Costs of opioid addiction & opioid-related adverse events are significant concerns
High Cost of
Post-Operative
Pain
Source:
Decision
Resources,
Acute
Pain
Pharmacor,
December
2012;
Decision
Resources,
Post-operative
Pain
Pharmacor,
May
2006
Nov 2013 |
 Innovation in a large, growing disease area with high
unmet need will drive significant dollar market growth
43
Source: Decision Resources, Post-Operative Pain Pharmacor, May 2006; Decision
Resources, Acute Pain, December 2012 2012 Post-Op Pain Market (US
only) 2012 Total: $3.1B
By 2020, 10% penetration into the 30M procedures requiring post-op pain
management equates to $850M+ opportunity at a price of $285/unit
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved.
25.3
25.9
26.5
27.1
27.8
28.5
29.2
29.9
30.6
32.5
0
5
10
15
20
25
30
35
2012
2013
2014
2015
2016
2017
2018
2019
2020
2021
Procedures Requiring Post-Operative Pain
Management |
 As a
potential development candidate, ropivacaine has advantages over
bupivacaine 44
Bupivacaine
Ropivacaine
Notes
1
KOL Feedback
Efficacy
•
Both molecules have similar
efficacy, onset of action, and
analgesic potency
“Both of these products work well for
blocking pain…
the issue is that they
are short acting.”
–
Orthopedic
Surgeon
Safety
•
Lower CV and CNS toxicity
•
Overall better side-effect profile
“Safety is where ropivacaine has a
clear advantage. It is widely known in
our institution that bupivacaine has
more cardiovascular toxicity.”
–
Anesthesiologist
MOA
•
Ropivacaine has been shown to
have shorter depth and duration
of motor block compared to
bupivacaine
“The goal is to achieve sensory
blockade without significant motor
blockade. In this way, ropivacaine
seems to perform better.”
–
Orthopedic Surgeon
Clinical
Flexibility
•
Considered more clinically
versatile by physicians
•
Approved for use in children
“For all these reasons, a long-acting
bupivacaine is a ‘hit’…
but a long-
acting ropivacaine would be a ‘home
run’.”
–
Orthopedic Surgeon
1
Sources:
1
Scott,
et
al.
Anesth
Analg
1989;
24:
514-518;
2
Knudsen
K,
et
al.
Br
J
Anesth
1997
78;
507-514;
3
Bertini,
et
al.
Reg
Anesth
Pain
Med
1999;
4
Chelly
JE,
et
al.
J
Orthop
Trauma
2003;
5
Turner
G,
et al.
Br
J
Anesth
1996;
76:606-610;
5
Writer
WDR,
et
al.
Br
J
Anaesth
1998;
81:
713-717.
6
McGlade,
et
al.
Anaesth
Intensive
Care
1998;26:515-520;
7
Arikan
OK,
et
al.
J
Otaryngol
Head
Neck
Surg
2008;
37(6):
836-43;
8
Ivani
G,
et
al.
Can
J
Anaesth
1999;
46(5):
467-469;
9
Pitimana-aree
S,
et
al.
Reg
Anesth
Pain
Med
2005;
30(5):
446-51;
http://www.naropin-us.com/about_benefits.php
2
Source:
KOL
interviews
October
2013
©
2013. A.P. Pharma, Inc. All rights reserved.
Nov 2013
2 |
 Summary –
Pipeline offers significant opportunity for
commercial value creation
Large, concentrated commercial opportunity
Physicians view a non-inferior SUSTOL
profile as highly competitive with
palonosetron
5-7 day PK profile
Non-inferior to market leader palonosetron based on
large, head-to-head trial
Sustained efficacy over multiple cycles of chemotherapy &
efficacy in palonosetron failures
Favorable safety profile with clean QT results
With successful outcome in planned HEC
trial, a differentiated profile with delayed-
HEC indication would position SUSTOL as
the next generation IV 5-HT3
HEC regimens represent a significant
market opportunity
45
Large, growing market
High unmet need
3-5 day local anesthetic depot would offer
clinical differentiation
Clear value proposition given the costs of
post-operative pain
Rapid development and approval
pathway
Potential opportunity for pain franchise
through line extensions
©
2013. A.P. Pharma, Inc. All rights reserved.
1. Wolters Kluwer 2012, 2. Intrinsiq 2013
Chemotherapy-induced nausea
and vomiting
Post-Operative Pain
Nov 2013 |
 Financial Summary
Nov 2013
©
2013. A.P. Pharma, Inc. All rights reserved.
46
Summary Statement of Operations
(In thousands, except per share data)
Nine Months Ended
September 30, 2013
Revenue
$
– Operating expenses
40,626
Other income (expenses)
(614)
Net loss
$ (41,240)
Net loss per share
$ (0.13)
Condensed Balance Sheet Data
(In thousands)
September 30, 2013
Cash and cash equivalents
$ 22,597
Total assets
$ 26,370
Total stockholders’
equity
$ 20,872
1
Based on 306.1 million weighted average common shares outstanding for the period ended
September 30, 2013.
1 |