Attached files
| file | filename |
|---|---|
| EX-21 - EXHIBIT 21 - Cardiff Oncology, Inc. | exhibit21q42015.htm |
| EX-31.2 - EXHIBIT 31.2 - Cardiff Oncology, Inc. | exhibit312q42015.htm |
| EX-32.1 - EXHIBIT 32.1 - Cardiff Oncology, Inc. | exhibit321q42015.htm |
| EX-23.1 - EXHIBIT 23.1 - Cardiff Oncology, Inc. | exhibit231q42015.htm |
| EX-31.1 - EXHIBIT 31.1 - Cardiff Oncology, Inc. | exhibit311q42015.htm |
| EX-10.32 - EXHIBIT 10.32 - Cardiff Oncology, Inc. | exhibit1032q42015.htm |
| EX-10.30 - EXHIBIT 10.30 - Cardiff Oncology, Inc. | exhibit1030q42015.htm |
| EX-10.28 - EXHIBIT 10.28 - Cardiff Oncology, Inc. | exhibit1028q42015.htm |
| EX-10.31 - EXHIBIT 10.31 - Cardiff Oncology, Inc. | exhibit1031q42015.htm |
| EX-10.29 - EXHIBIT 10.29 - Cardiff Oncology, Inc. | exhibit1029q42015.htm |
| EX-32.2 - EXHIBIT 32.2 - Cardiff Oncology, Inc. | exhibit322q42015.htm |
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
Form 10-K
(Mark One)
x ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
FOR THE FISCAL YEAR ENDED DECEMBER 31, 2015
o TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
FOR THE TRANSITION PERIOD FROM TO
COMMISSION FILE NUMBER 000-54556
TROVAGENE, INC.
(Exact name of registrant as specified in its charter)
Delaware | 27-2004382 | |
(State or other jurisdiction of | (I.R.S. Employer | |
incorporation or organization) | Identification No.) | |
11055 Flintkote Avenue, Suite B, San Diego, California 92121
(Address of principal executive offices) (Zip Code)
Registrant’s telephone number, including area code: (858) 952-7570
Securities registered pursuant to Section 12(b) of the Act:
Title of each class | Name of each exchange on which registered | |||
Units, each consisting of two shares of Common Stock and one Warrant to purchase one share of Common Stock | The NASDAQ Capital Market | |||
Common Stock, $0.0001 par value | The NASDAQ Capital Market | |||
Warrants to purchase Common Stock | The NASDAQ Capital Market | |||
Securities registered pursuant to Section 12(g) of the Act: None.
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act Yes o No x
Indicate by check if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes o No x
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes x No o
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§ 232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes x No o
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K (§229.405 of this chapter) is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. x
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See the definitions of “large accelerated filer”, “accelerated filer”, and “smaller reporting company” in Rule 12b-2 of the Exchange Act.
Large accelerated filer o | Accelerated filer x | |
Non-accelerated filer o | Smaller reporting company o | |
(Do not check if a smaller reporting company) | ||
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Act). Yes o No x
The aggregate market value of the voting and non-voting common equity held by non-affiliates based on a closing sale price of $10.15 per share, which was the last sale price of the common stock as of June 30, 2015, the last business day of the registrant’s most recently completed second fiscal quarter, was $195,681,564.
As of February 29, 2016, 29,757,810 shares of the registrant’s common stock, $0.0001 par value per share, were issued and outstanding.
DOCUMENTS INCORPORATED BY REFERENCE
Portions of the Proxy Statement for the registrant’s 2016 Annual Meeting of Stockholders (the “Proxy Statement”), to be filed within 120 days of the end of the fiscal year ended December 31, 2015, are incorporated by reference in Part III hereof. Except with respect to information specifically incorporated by reference in this Form 10-K, the Proxy Statement is not deemed to be filed as part hereof.
TABLE OF CONTENTS
Page | ||
2
PART I
ITEM 1. BUSINESS
We are a molecular diagnostic company that focuses on the development and commercialization of a proprietary molecular diagnostic technology for use in disease detection and monitoring across a variety of medical disciplines. Our primary internal focus is to leverage our novel cell-free molecular diagnostic platform to facilitate improvements in the field of oncology, while our external focus includes entering into license agreements or collaborations to develop our technology in areas such as infectious disease, transplant medicine and prenatal genetics.
We are leveraging our proprietary molecular diagnostic technology for the detection of cell-free DNA originating from diseased cell death that can be isolated and detected from urine, blood, and tissue samples to improve disease management. These genetic materials are also collectively referred to as “cell-free nucleic acids”, which result when cells in the body die and release their DNA contents into the bloodstream. The circulating fragments of genetic material are eventually filtered through the kidneys, and therefore, can be detected and measured in urine. Cell-free nucleic acids can be used as genetic markers of disease. As such, the contents of urine or blood samples represent systemic liquid biopsies that allow for simple, non-invasive or minimally-invasive sample collection methods.
Our fundamental cell-free molecular diagnostic platform for oncology applications, also known as our “Precision Cancer Monitoring®” (“PCM”) platform, is protected by a strong intellectual property portfolio. We have developed significant intellectual property around cell-free nucleic acids in urine, and the extraction of cell-free nucleic acids from urine, as well as novel assay designs, particularly our proprietary non-naturally occurring primers. Through this proprietary technology, we believe that we are at the forefront of a shift in the way diagnostic medicine is practiced, using simple, non-invasive or minimally invasive sampling and analysis of nucleic acids, which we believe will ultimately lead to more effective treatment monitoring, better management of serious illnesses such as cancer, and the ability to detect the success of cancer treatment, the recurrence of cancer, or the progression of cancer earlier. As of December 31, 2015, our intellectual property portfolio consisted of over 85 issued patents and over 60 pending patent applications in the U.S. and abroad. Our patent estate includes the detection of cell-free nucleic acids that pass through the kidney into the urine, as well as their application in specific disease areas, including oncology, infectious disease, transplantation, and prenatal genetics.
We believe that our proprietary PCM platform is uniquely positioned to address a high unmet clinical need in the field of oncology. Our PCM platform is designed to offer better cancer monitoring by tracking and quantifying levels of cell-free DNA from either urine or blood samples, and is intended to provide important clinical information beyond the current standard of care. Using urine as a sample, our cancer monitoring technology enables frequent, non-invasive monitoring of oncogene mutation status, disease progression and disease recurrence. Our extensive research and development efforts were strengthened, due to investments to expand our intellectual property portfolio, and were made commercially feasible following improved next-generation sequencing (“NGS”) technologies, which are now available at a significantly lower cost. This combined with our extensive patent portfolio around cell-free DNA in urine gives us a competitive advantage to leverage an emerging trend of monitoring cancer using cell-free DNA as a marker of disease status. Our proprietary sample preparation process forms the basis of our PCM platform. It includes novel technology for the extraction and isolation of cell-free DNA from either a urine or blood sample, proprietary non-naturally occurring primers to enrich the sample for mutant alleles and the ability to detect nucleic acids of interest using one of several leading gene sequencing technologies such as NGS or droplet digital polymerase chain reaction (“ddPCR”). We believe that our quantitative cell-free DNA detection and monitoring platform offers industry leading sensitivity, featuring single nucleic acid molecule detection.
Our PCM platform is poised to overcome a significant clinical dilemma in the area of cancer treatment. Recent scientific evidence supports the molecular basis of cancer and has resulted in a paradigm shift in the way cancer is diagnosed and treated. Researchers and clinicians are now focused on specific oncogene mutations and alterations that are believed to be the drivers of cancer at the molecular level, and, as a result, there is a trend in the pharmaceutical research community toward developing targeted therapies. As such, there is a need for oncologists to have an ability to track the mutational status of their patients and to assess a given patient’s response to treatments designed to target driver oncogene mutations. Current monitoring tools such as imaging procedures, tissue biopsy and circulating tumor cells are insufficient to meet the challenge of monitoring oncogene mutations. Imaging only provides a rough indication of tumor size and is an important tool for surgeons, but provides little practical information to oncologists regarding mutational status and appropriate treatment options, especially for molecular targeted therapies. Tissue biopsy usually involves a surgical procedure and, in many cases, is not repeatable as there are limitations related to access for serial biopsies. In some cases, biopsies may not be available, significantly increasing the need to determine mutational status using an alternative method. In addition, tumor heterogeneity is important, as the surgeon may not obtain the proper tissue from the tumor sample. In the case of circulating tumor cells, which are typically measured using blood tests, sensitivity is traditionally low, and such tests can be technically difficult and expensive to conduct.
3
Targeted drug therapies themselves are not without issues. Targeted therapies are typically very expensive, can have significant side effects and are not effective in every patient. In order to measure effectiveness, repeated monitoring is needed and serial biopsies can be difficult to obtain. If resistance develops, fast and accurate detection of emerging or changing oncogene mutation status is critical. Our PCM platform provides a novel solution using urine, a non-invasive, plentiful sample source, and we are continuing to build a growing body of evidence supporting the clinical utility of our technology to monitor cancer using cell-free DNA.
Our goal is to improve treatment outcomes for cancer patients using our proprietary technology to detect and quantitatively monitor cell-free DNA using a urine or blood sample.
Developing a Market for Molecular Diagnostic Tests based on Liquid Biopsies using Cell-free DNA
We intend to develop and expand our cell-free molecular diagnostic technology into a pipeline of potentially groundbreaking commercial molecular detection and monitoring products. Our Clinical Laboratory Improvement Amendments (“CLIA”)-certified, College of American Pathologists (“CAP”)-accredited laboratory in San Diego, California will enable us to initially commercialize our testing services and launch our platform technology and associated innovative molecular monitoring tests. Urine-based cell-free molecular diagnostics can provide relevant information across multiple therapeutic and clinical areas, and may lead to improvements in patient management. We are focused on the oncology treatment market and the opportunity to enable clinicians to track oncogene mutational status in cancer patients. Repeat testing is expected with most cancer patients, and there also exists a need to chronically monitor for the re-emergence of oncogenenic mutations in people that are cancer survivors.
In order to facilitate early availability and use of our products and technologies, in February 2012, we acquired the CLIA laboratory assets of MultiGEN Diagnostics, Inc. (“MultiGEN”), which included CLIA approval and licensing documentation, laboratory procedures, customer lists and marketing materials. A CLIA lab is a clinical reference laboratory that can perform high complexity diagnostic assays (e.g., those requiring polymerase chain reaction (“PCR”) amplification). Through this CLIA laboratory, we are able to offer laboratory developed tests (“LDTs”) in compliance with CLIA guidelines.
Targeting cell-free nucleic acid markers will allow for the development of genetic tests that use non-invasive and easy-to-obtain urine samples, rather than other more traditional and more invasive methods. These methods include medical imaging, blood testing, and tissue biopsies. We are exploring a broad range of clinical utilities where cell-free nucleic acid technology holds the potential to replace more complex, less robust existing technologies. We are developing more effective, non-invasive diagnostics, which align with the current industry shift toward highly personalized medicine. Urine-based cell-free nucleic acid molecular tests can make it easier to address important health problems and may lead to significant advancements in patient care.
Our patented technology uses safe, non-invasive, cost effective, and simple urine collection, which can be applied to a broad range of testing, including tumor mutation detection and monitoring, infectious disease monitoring, transplantation monitoring and prenatal genetic diagnostics. We believe that our technology is ideally suited to be used in developing molecular diagnostic assays that will allow physicians to provide simple, non-invasive, and convenient screening and monitoring tests for their patients by identifying specific biomarkers involved in a disease process. Our novel urine-based assays can facilitate improved testing compliance, resulting in a more effective use of targeted therapies, earlier detection of disease and disease progression or recurrence, and improvements in both patient outcomes and cost of care.
The material terms of certain of our clinical collaboration, research and development, and technology license agreements that we have entered into are as follows:
In September 2015, we established Trovagene Srl, also known as the Trovagene Research Institute (“TRI”), a European subsidiary focused on expanding the capabilities and adoption of the PCM platform. Alberto Bardelli, Ph.D., an internationally recognized leader in cell-free DNA cancer research, is the Scientific Chair of TRI. Concurrent with the establishment of TRI, we entered into a collaboration agreement with the Department of Oncology at the University of Torino, a leading research center in Southern Europe. The collaboration seeks to leverage the superior benefits of urine as a specimen for the detection and monitoring of oncogenic mutations, along with the capabilities and relationships of the University of Torino and Dr. Bardelli’s team. Under the terms of the agreement, we may pay our collaborator in the study approximately $529,000 for services provided. As of December 31, 2015, we incurred approximately $188,000 related to this agreement.
4
In September 2014, under the strategic partnership we established in March 2014 with Catholic Health Initiatives Center for Translational Research, we entered into a Sponsored Research Agreement with Catholic Health Initiatives Center for Translational Research to conduct clinical studies to evaluate the use of our PCM technology in the management of cancer patients. Under the terms of the agreement, we may pay our collaborator in the study approximately $151,000 for services provided. During the years ended December 31, 2015 and 2014, we incurred approximately $39,000 and $30,000, respectively, related to this agreement.
In June 2014, we entered into a Sponsored Research Agreement with Dana Farber Cancer Institute to conduct a clinical study to evaluate the use of our precision cancer monitoring technology in the management of lung cancer patients. Under the agreement, we may pay our collaborator in the study approximately $42,000 for services provided. During the years ended December 31, 2015 and 2014, we incurred approximately $1,000 and $8,000, respectively, related to this agreement.
In June 2014, we entered into a Sponsored Research Agreement with Memorial Sloan Kettering Cancer Center to conduct a clinical study for the detection of oncogenic tumor mutations in the urine of lung cancer patients. Under the agreement with Memorial Sloan Kettering Cancer Center, we may pay our collaborator approximately $146,000 for services provided. During the years ended December 31, 2015 and 2014, we incurred approximately $35,000 and $25,000, respectively, related to this agreement.
In May 2014, we entered into a Strategic Research Alliance with the Robert H. Lurie Comprehensive Cancer Center of Northwestern University to conduct one or more research agreements to evaluate the use of our precision cancer monitoring technology in the management of cancer patients. Under the agreement, each party is responsible for its own costs and obligations under the agreement. No services or costs had been incurred by us as of December 31, 2015.
In May 2014, we entered into a Patent Assignment and License Agreement, effective as of April 23, 2014, with GenSignia IP Ltd., a United Kingdom company (“GenSignia”), pursuant to which we assigned to GenSignia all of our miRNA patents, including methods of using miRNA for detection of in vivo cell death and detecting cell-free miRNA in urine and blood. Concurrent with the assignment, GenSignia granted to us an exclusive, world-wide, royalty-free, fully paid, perpetual license under the transferred patents in the urine field. Pursuant to the agreement, GenSignia will pay us a low single digit royalty on net sales and will pay an aggregate of $6.5 million in milestone payments upon the achievement of up to $150 million in net sales. GenSignia is responsible for the preparation, filing and maintenance of all patents under the agreement. During the years ended December 31, 2015 and 2014, we recorded $0 and $10,000, respectively, in license fee revenue related to the agreement. Costs have been incurred through December 31, 2015 and reimbursed by GenSignia.
In December 2013, we entered into a Clinical Trial Agreement with US Oncology Research LLC (“USOR”), pursuant to which USOR will provide the principal investigator and conduct a clinical study related to examining the utility of cell-free quantitative KRAS testing to monitor disease in patients with metastatic pancreatic cancer. Under the agreement, we committed to pay USOR approximately $270,000 for services provided. During the years ended December 31, 2015, 2014, and 2013, we incurred and recorded approximately $59,000, $16,000, and $29,000, respectively, of research and development expense related to this agreement.
In August 2013, we entered into a Clinical Trial Agreement with the University of Southern California (“USC”), pursuant to which USC will provide the principal investigator and conduct a clinical study related to the genetic characterization of metastatic colorectal cancers. Under the agreement, we are committed to pay USC approximately $232,000 for services provided. In June 2015, we entered into an amendment to the agreement that increased the total fees to be paid to USC for services provided to $277,000. During the years ended December 31, 2015, 2014, and 2013 we incurred approximately $28,000, $38,000, and $0, respectively, for expenses related to this agreement.
During 2012, we entered into research agreements with the University of Texas MD Anderson Cancer Center (“MDACC”) to provide samples and evaluate methods used by us to identify pancreatic cancer mutations, as well as to measure the degree of concordance between the results of cell-free DNA mutation analysis from urine samples and tumor tissue. An amendment in 2013 increased the scope of the research agreements. We have committed to pay approximately $451,000 for the services performed by MDACC under the research agreement. During the years ended December 31, 2015, 2014, and 2013, we incurred and recorded approximately $71,000, $124,000 and $142,000, respectively, of research and development expense related to these agreements.
In December 2012, we entered into a sublicense agreement with Genoptix, Inc. for non-exclusive worldwide rights to develop and market laboratory testing services for nucleophosmin protein (“NPM1”) for the diagnosis and monitoring of patients with acute myeloid leukemia (“AML”). Under this agreement, we granted a license to Genoptix, Inc. to certain NPM1 patents in exchange for a one time license fee of $100,000 due upon execution of the agreement and royalty payments on net
5
revenues. During the years ended December 31, 2015, 2014 and 2013, we recorded royalty and license fee revenues of approximately $40,000, $30,000 and $10,000, respectively.
In November 2012, we entered into a sublicense agreement with Duke University and Duke University Health Systems for non-exclusive rights to develop and market laboratory testing services for NPM1 for the diagnosis and monitoring of patients with AML. Under this agreement, we granted a license to Duke University and Duke University Health Systems to certain NPM1 patents in exchange for a one time license fee of $5,000 due upon execution of the agreement and royalty payments on net revenues. During the years ended December 31, 2015, 2014 and 2013, we recorded $2,000, $1,000 and $0, respectively, for royalty and license fee revenues related to this agreement.
In September 2012, we entered into a collaboration and license agreement with Strand Life Sciences Pvt. Ltd. (“Strand Life Sciences”) related to the validation and commercial launch of a urine-based DNA test for Human Papillomavirus (“HPV”). Under this agreement, we granted a license to Strand Life Sciences for the use of our tests in exchange for royalty payments on net sales earned in the territory specified in the agreement. During the years ended December 31, 2015, 2014, and 2013, no royalties or license fees were received under this agreement.
In September 2012, we entered into a sublicense agreement with Quest Diagnostics Incorporated for non-exclusive rights to develop and market laboratory testing services for NPM1 for the diagnosis and monitoring of patients with AML. Under this agreement, we granted a license to Quest Diagnostics Incorporated to certain NPM1 patents in exchange for a one time license fee of $20,000 due upon execution of the agreement and royalty payments on net sales of Quest Diagnostics Incorporated and its affiliates. During the years ended December 31, 2015, 2014 and 2013, we recorded royalty and license revenues of approximately $26,000, $26,000 and $14,000, respectively.
In December 2011, we entered into an exclusive license agreement with Columbia University to license the patent rights to hairy cell leukemia biomarkers. In consideration for the license, we paid $1,000 as an upfront license fee and agreed to make royalty payments as a single digit percentage of net sales if sales are made by us or a single digit royalty rate as a percentage on sublicense income received by us if sales are made by sublicensees. The license agreement will continue in effect until May 10, 2021, which is the date of the last to expire of the licensed patent rights covering the license product. The license agreement may also be terminated upon a material breach by Columbia University or by us if we determine that it is not commercially or scientifically appropriate to further develop the license product rights. No royalty expense was recorded related to this agreement during the years ended December 31, 2015, 2014 and 2013.
In October 2011, we entered into an exclusive license agreement with Gianluca Gaidano, Robert Foa and Davide Rossi for the patent rights to a specific gene mutation with respect to chronic lymphoblastic leukemia. In consideration for the license, we paid $1,000 as an upfront license fee and agreed to make royalty payments as a single digit percentage of net sales if sales are made by us or a single digit royalty rate as a percentage of sublicense income received by us if sales are made by sublicensees. We have an option to purchase the licensed patent rights in the event the licensor decides to sell such licensed patent rights. The license agreement will continue in effect until September 29, 2031, which is the date of the last to expire of the licensed patent rights covering the license product. The license agreement may also be terminated upon a material breach by any party or by us if it is determined that it is not commercially or scientifically appropriate to further develop the license product rights. No royalty expense was recorded related to this agreement during the years ended December 31, 2015, 2014 and 2013.
In July 2011, we entered into a sublicense agreement with Fairview Health Services (“Fairview”) for the non-exclusive rights to develop and market laboratory testing services for NPM1 for the diagnosis and monitoring of patients with AML. Fairview paid an initial license fee of $10,000 upon execution of the agreement and also agreed to pay us a royalty on any net revenues during the term of the agreement, subject to certain minimums. Fairview is obligated to pay a royalty with annual minimums of $1,000 each year. During the years ended December 31, 2015, 2014, and 2013, we recorded royalty and license fee revenues of approximately $1,000, $2,000 and $1,000, respectively.
In February 2011, we entered into a sublicense agreement with MLL Münchner Leukämielabor (“MLL”) for the non-exclusive rights to develop and market laboratory testing services for NPM1 for the diagnosis and monitoring of patients with AML. MLL paid an initial license fee of $20,000 upon execution of the agreement and agreed to pay us a royalty on any net revenues during the term of the agreement, subject to certain minimums. MLL was obligated to pay a minimum royalty of $15,000 for the first year and is currently obligated to pay a royalty with annual minimums of $20,000. The term of the license ends on October 28, 2025, which is the date of expiration of the issued patent rights. During the years ended December 31, 2015, 2014, and 2013, we recorded royalty and license fee revenues of approximately $69,000, $81,000 and $85,000, respectively.
6
In June 2010, we signed a sublicensing agreement with Skyline Diagnostics BV for the non-exclusive rights to develop, commercialize and market research and diagnostic laboratory services for the stratification and monitoring of patients with AML. Skyline Diagnostics BV paid an initial licensing fee of $10,000 upon execution of the agreement and may make future payments to us upon the attainment of certain regulatory and commercial milestones. Skyline Diagnostics BV is also obligated to pay us a royalty on any net revenues during the term of the agreement, subject to certain minimums. The term of the license ends on October 28, 2025, which is the date of expiration of the issued patent rights. During the years ended December 31, 2015, 2014 and 2013, we recorded no royalty and license revenues and no license fee expenses.
In December 2008, we signed a sublicensing agreement with InVivoScribe Technologies, Inc. for the non-exclusive rights to develop and market lab testing services for NPM1 for the diagnosis and monitoring of patients with AML. InVivoScribe Technologies paid an initial licensing fee of $10,000 upon execution of the agreement. InVivoScribe Technologies also agreed to pay us a royalty on any net revenues during the term of the agreement, subject to certain minimums. The term of the license ends on October 28, 2025, which is the expiration date of the issued patent rights. We recorded royalty revenues of approximately $25,000 during each of the years ended December 31, 2015, 2014 and 2013. During those same periods, we did not record any license fee expenses.
In August 2008, we signed a sublicensing agreement with Laboratory Corporation of America Holdings (“LabCorp”) for the non-exclusive rights to develop and market laboratory testing services for NPM1 for the diagnosis and monitoring of patients with AML. LabCorp paid an initial licensing fee of $20,000 upon execution of the agreement. LabCorp also agreed to pay us a royalty on any net revenues during the term of the agreement, subject to certain minimums. The term of the license ends August 25, 2018. During the years ended December 31, 2015, 2014 and 2013, we recorded royalty and license fee revenues of approximately $30,000, $28,000 and $20,000, respectively. During those same periods, we did not record any license fee expenses.
In October 2007, we signed a co-exclusive license agreement with ASURAGEN, Inc. for the co-exclusive rights to develop, manufacture and market research and diagnostic products for the stratification and monitoring of patients with AML. ASURAGEN paid an initial licensing fee of $120,000 upon execution of the agreement and may make future payments to us upon the attainment of certain regulatory and commercial milestones. In June 2010, we signed an amendment no. 1 to the co-exclusive license agreement. The amendment provides that we may require a license from a third-party to perform laboratory testing services. ASURAGEN also agreed to pay us a royalty on any net revenues during the term of the agreement, subject to certain minimums. The term of the license ends on October 28, 2025, which is the date of expiration of the issued patent rights. In March 2013, we signed an amendment no. 2 to the co-exclusive sublicense agreement with ASURAGEN, pursuant to which the field of use was limited to research use only (“RUO”) kits. ASURAGEN was also granted a non-exclusive sublicense for NPM1 laboratory testing services. We recorded royalty and license fee revenues of approximately $50,000 during each of the years ended December 31, 2015, 2014 and 2013. During those same periods, we had no license fee expenses related to this agreement.
In August 2007, we signed a sublicensing agreement with IPSOGEN SAS, a leading molecular diagnostics company with operations in France and the U.S. for the co-exclusive rights to develop, manufacture and market research and diagnostic products for the stratification and monitoring of patients with AML. Upon execution of this agreement, IPSOGEN SAS paid an initial licensing fee of $120,000 and may make milestone payments upon the attainment of certain regulatory and commercial milestones. IPSOGEN SAS also agreed to pay us a royalty on any net revenues during the term of the agreement, subject to certain minimums. The term of the license ends on October 28, 2025, which is the date of expiration of the issued patent rights. In September 2010, we signed an amendment no. 1 to the sublicensing agreement. Pursuant to the amendment, we may require a license from a third-party to perform laboratory testing services. During the years ended December 31, 2015, 2014 and 2013, we recorded royalty, milestone and license fee revenues of approximately $52,000, $60,000 and $60,000, respectively. During those same periods, we had no license fee expenses.
In May 2006, we entered into a license agreement with Drs. Falini and Mecucci, pursuant to which we obtained the exclusive rights for the genetic marker for AML with the intention to utilize these rights for the development of new diagnostic tools. In connection with this agreement, we paid $70,000 to Drs. Falini and Mecucci in the aggregate. In August 2010, we signed an amendment no.1 to the license agreement, pursuant to which we agreed to pay royalties of 6% on royalty revenues and/or 10% of any sublicense income to Drs. Falini and Mecucci. During the years ended December 31, 2015, 2014 and 2013, we recorded royalty expenses of approximately $22,000, $23,000 and $30,000, respectively.
7
History
On April 26, 2002, we were incorporated in the State of Florida. In January 2010, we re-incorporated from the State of Florida to the State of Delaware and changed our name to Trovagene, Inc. In June 2012, our common stock was listed on The NASDAQ Capital Market under the ticker symbol TROV.
Our corporate website address is www.trovagene.com. Our annual reports on Form 10-K, quarterly reports on Form 10-Q, proxy statements, current reports on Form 8-K and amendments to those reports filed or furnished pursuant to Section 13(a) or 15(d) of the Securities Exchange Act of 1934, as amended, are available free of charge at www.trovagene.com as soon as reasonably practicable after electronically filing such reports with the Securities and Exchange Commission. Any information contained on, or that can be accessed through, our website is not incorporated by reference into, nor is it in any way a part of, this Annual Report on Form 10-K.
Operating Segment and Geographic Information
We operate in one business segment, using one measurement of profitability to manage our business. We do not assess the performance of our geographic regions on measures of revenue or comprehensive income or expense. In addition, all of our principal operations, assets and decision-making functions are located in the U.S. We do not produce reports for, or measure the performance of, our geographic regions on any asset-based metrics. Therefore, geographic information is not presented for revenues or long-lived assets.
The Basis for Our Urine-based Molecular Diagnostic Technology
Cell-free nucleic acids have been found in a variety of human bodily fluids, with the nucleic acids isolated from urine having been extensively characterized. Cell-free nucleic acids in urine have been proven to contain mutated DNA and other markers of disease, including microRNA. In contrast to other bodily fluids (e.g., blood plasma), urine allows for truly non-invasive collection of the sample, provides a larger sample size, and allows for frequent collection. Importantly, urine enables the collection of nucleic acid material from the systemic circulation over a period of time, and those DNA and RNA fragments remain stable in urine. These factors, combined with recently developed technologies to sequence, count, and track nucleic acids with low relative abundance, make the development of our non-invasive diagnostics commercially practical and scalable.
In the human body, about 1011 - 1012 cells die each day primarily as a consequence of natural physiological processes for tissue and organ maintenance, but also as a result of disease. Together, these dead and dying cells contain more than one gram of DNA, which is mostly degraded into short fragments by specific enzymes. A small proportion of these cell-free nucleic acids escapes complete degradation and appears in the bloodstream. Our scientists were the first to discover that circulating cell-free nucleic acids cross the kidney barrier and can be found in the urine as cell-free DNA. This simple yet remarkable discovery that genetic information from various cells throughout the body is present in urine enabled the development of new, non-invasive techniques for molecular diagnostics and genetic testing.
To unlock the full potential of cell-free nucleic acids, we have developed a proprietary method for the isolation of the short fragmented nucleic acids that pass through the kidneys, and proprietary “ultra-short” amplicon assays necessary for the efficient detection of cell-free nucleic acids, which can be analyzed at our San Diego-based CLIA laboratory.
Because of the small size of cell-free nucleic acids in urine, having an isolation method that efficiently captures short nucleic acids is critical. We have multiple methods (patents and pending patents) for the isolation of nucleic acids from bodily fluids, including urine. Many nucleic isolation methods are not properly suited for the isolation of cell-free nucleic acids in urine. For example, many DNA isolation kits only capture DNA greater than 200 base-pairs (“bp”) in length, with a few claiming 100 bp or longer. No manufacturer states that their product is suitable to capture DNA sequences shorter than 80 bp in length.
When compared to leading kits for the isolation of DNA from bodily fluids, we have observed, by conducting internal studies, that our method is three to twenty times more efficient in isolating a 50 bp target. Our method is also suitable for the isolation of RNA, including miRNAs.
In addition to our cell-free nucleic acid isolation method, we have developed our technology for detecting ultra-short amplicons (patents pending). By combining our proprietary nucleic acid isolation method with our ultra-short amplicon assays, we are able to detect at least six times more mutations in a urine-based cell-free DNA sample than any other PCR-based assay, according to our internal test data. We believe that these methods are also applicable to other small or fragmented nucleic acids, including cell-free DNA from blood and formalin-fixed, paraffin-embedded samples.
8
Determining DNA and RNA signatures using urine as a “systemic biopsy” may provide a more powerful and effective tool for following and uncovering both pre-clinical and clinical changes, which may include:
• | monitoring cancer patients to determine therapeutic response or non-response and disease recurrence; |
• | determining mutational status when tissue biopsy is unavailable or infeasible; |
• | monitoring for minimal residual disease (“MRD”) after surgical resection of a malignant tumor, following organ transplant status to watch for rejection; |
• | non-invasively securing samples for the clinical diagnosis of infectious diseases; and |
• | screening and testing expectant mothers, whose fetuses may be at risk for certain genetic abnormalities. |
Currently, these clinical needs are addressed by the use of invasive blood and bone marrow tests, tissue biopsies, and amniocentesis, as well as costly CT, MRI, and PET scans.
Urine is a relatively simple aqueous solution and, unlike plasma, contains few components that can attack and break down cell-free nucleic acid fragments. Cell-free nucleic acid fragments can be accurately analyzed using conventional methods that are either in use or in development within many molecular genomics laboratories.
Our urine-based cell-free nucleic acid tests are based upon a proprietary method of nucleic acid isolation, followed by detection of specific genetic markers. These proven and well-established detection methods can also be used to detect nucleic acids in blood, stool, and other specimen types. Using enhancements of these techniques, cell-free nucleic acid markers can be isolated from easily obtained urine specimens.
Our urine-based cell-free nucleic acid technology may be applied to the detection and monitoring of a broad spectrum of medical conditions.
Characteristics of Urine-based Cell-free Nucleic Acid Testing
• | The kidney acts as a filter, passing cell-free nucleic acids from complex, multicellular, multicomponent blood into urine, a less complex aqueous environment. |
• | The collection procedure is non-invasive and does not require the involvement of trained medical staff. |
• | Urine as a sample type supports repeated testing when required and poses no discomfort for the patient. |
• | Cell-free nucleic acids in urine are stable at room temperature for extended periods of time with the addition of a simple preservative. Nucleic acids in blood and many other traditional samples are not. |
• | Sample processing and tests can often be easily automated. |
• | Isolation of cell-free markers from large sample volumes increases sensitivity of the tests. This cannot be done as easily using blood or tissue specimens, which have inherent volume limitations. |
• | Blood or sputum samples for detection of infectious diseases may not be easily obtained from certain patients, including small children and the elderly. Urine specimens typically present minimal acquisition concerns. |
• | Blood and other bodily fluids can be highly infectious by nature, urine is not. |
• | Blood and other bodily fluids are legally considered biohazardous, urine is not. |
Clinical Applications
We believe that our urine-based cell-free molecular diagnostic tests will make it easier to address important health problems worldwide and will lead to significant advances in personalized medicine for improved patient care. We intend to
9
develop clinical evidence for our cancer monitoring tests in three distinct and potentially overlapping stages. Stage 1 studies are qualitative in nature and are designed to determine the mutational status of actionable biomarkers in urine especially when biopsy is not an option. These studies demonstrate concordance (agreement) of the oncogene mutation status between a urine sample and a tumor tissue sample. These studies are considered to have diagnostic value and are designed to prove that urine-based molecular test results match the tissue biopsy closely. The clinical utility of such studies validate that mutational status of actionable biomarkers can be determined in urine when a tissue biopsy is not an option or is infeasible. Stage 2 studies are quantitative in nature and are designed to assess patient mutational status in urine longitudinally (over time) as an indicator of responsiveness to therapy and disease status of the patient. Stage 3 studies are conducted with the goal to demonstrate improved patient outcomes and eventually could lead to changing medical guidelines and establishment of a new clinical standard of care for managing certain cancers. Demonstrated clinical utility includes quantitatively assessing patient mutational status in urine longitudinally for mutational status as well as early detection of resistance to therapy as a decision tool for therapy selection. Generating clinical data with our technology that supports better patient outcomes and more efficient use of healthcare resources is a key component of Stage 3.
We believe that there are several specific applications of our PCM platform technology with regard to helping oncologists monitor a patient’s mutational status, thereby optimizing the treatment approach and improving outcomes. Our technology can be used to determine a patient’s mutational status for the first time when a tissue biopsy is not feasible, or it can be used to monitor changes in mutational load over time to provide information that can be useful to direct treatment regimens. Should a patient have their tumor removed surgically, our technology can be used to broadly search for minimal residual disease, which can confirm a successful procedure or enable early detection of recurrent disease for improved patient management. Treatment-emergent mutations can also be a major problem and may be drivers of resistance to first-line therapy. Examples of this include the emergent mutation epidermal growth factor receptor (“EGFR”) T790M in lung cancer or KRAS mutations in colorectal cancer. Because our platform uses a non-invasive, easy to obtain sample from the patient, the ability to monitor more accurately and more often with fewer barriers to doing so can provide us with key competitive advantages in the marketplace, particularly with regard to monitoring for treatment-emergent mutations.
Oncology
Urine may offer an alternative to biopsy, medical imaging, and less optimal blood-based tests such as those that use circulating tumor cells. By tracking mutations, we can inform medical practice. Our initial pilot study was focused on the BRAF mutation because of its link to discreet cancers and associated treatments, as well as the KRAS mutation because of its broad applicability in many cancers. We are now developing oncogene tracking tests using ddPCR and NGS for a variety of mutations seen in many cancer types. We believe the potential exists to expand the use of these tracking tests across many cancer types for multiple mutations in test panels.
During 2015, we had over 25 ongoing clinical studies with leading cancer centers and pharmaceutical companies to demonstrate the qualitative and quantitative clinical utility of our tests. Clinical study sites include MD Anderson Cancer Center, Memorial Sloane Kettering Cancer Center, USC Norris Cancer Center, US Oncology, pharmaceutical collaborators, and other top cancer centers. In 2014 and 2015, we entered into clinical study collaboration agreements with Memorial Sloan Kettering Cancer Center, Dana-Farber Cancer Institute, City of Hope Comprehensive Care Center, and Genomac International Ltd. (also known as the Center for Applied Genomics of Solid Tumors, Genomac Research Institute), among others.
Clinical proof of concept for KRAS and BRAF mutation assays
The MD Anderson Cancer Center clinical study is focused on detecting and monitoring BRAF and KRAS tumor mutations in cell-free DNA from urine in metastatic cancer patients. BRAF mutations are common in melanoma, thyroid, and other cancers. Within the U.S., it is estimated that nearly 730,000 patients have tumors with BRAF mutations. Several targeted therapies are either on the market or in development for BRAF-mutation positive cancers. Pancreatic cancer represents an additional diagnostic and treatment challenge. Each year, more than 43,000 new cases of pancreatic cancer are diagnosed, and 37,000 patients succumb to this disease. It is estimated that KRAS mutations occur in greater than 90% of pancreatic cancers and 11%-17% of these patients do not express the CA19-9 marker, which makes their disease more difficult to track.
Results from the MD Anderson Cancer Center clinical study were published at the AACR-NCI-EROTC International Conference in October 2013. During the study, urine samples from metastatic cancer patients known to have BRAF V600E, KRAS G12D or KRAS G12V mutations were assessed. Our researchers analyzed the urine samples using our urine-based cell-free molecular diagnostic assays. Results demonstrated high concordance between urine and tissue mutational status. In addition, preliminary results indicate that cell-free BRAF V600E mutation monitoring in urine correlates with clinical response to therapy. The clinical study demonstrated that BRAF V600E mutations were detected in urine irrespective of the cancer type, and a multitude of different cancer types, including brain cancer (“glioblastoma”), were included in the initial study results.
10
The BRAF V600E assay demonstrated 95% concordance vs. tissue biopsy (both detected and borderline), and also demonstrated that urinary DNA can be used to detect DNA fragments from circulation that harbor tumor mutations. The following cancers were detected during the study: non-small cell lung cancer (“NSCLC”), papillary thyroid carcinoma, melanoma, colorectal cancer, glioblastoma, adenocarcinoma of unknown primary, ovarian cancer, and appendiceal cancer. In addition, preliminary results indicate that cell-free BRAF V600E mutation monitoring in urine longitudinally correlates with clinical response to therapy.
The study also evaluated the feasibility of using massively parallel deep sequencing (i.e., NGS) to identify DNA mutations in the urine of metastatic cancer patients harboring known KRAS mutations. Leveraging proprietary enrichment methods, our researchers were able to detect mutant cell-free DNA in the urine of cancer patients with verified KRAS mutations.
CLIA validated BRAF mutation assay
In October 2013, our first urine test for cancer mutation monitoring was made available to clinicians through our CLIA laboratory. The robustness of our ultra-sensitive assay procedure has been demonstrated for the detection of the BRAF V600E mutation from cell-free DNA in urine. This mutation commonly occurs in melanoma. Of the more than 70,000 cases of melanoma diagnosed each year in the U.S., up to 70 percent harbor a BRAF-type mutation and of those, 80 percent may be positive specifically for BRAF V600E. There are several approved targeted therapies for the treatment of BRAF-positive melanoma, making mutational status monitoring an area of clinical interest among treating physicians.
Our cell-free BRAF test is a laboratory deleloped test (“LDT”), designed to detect and monitor this mutation in metastatic cancer patients with biopsy-proven V600E BRAF mutation in their tumor. It is the first and only commercial assay within our cancer monitoring portfolio performed using a ddPCR platform. Using urine as a non-invasive, systemic sample, the cell-free BRAF test could help physicians monitor changes in mutation status for patients requiring therapy for cancers that have this mutation. For patients with difficult-to-biopsy metastatic tumors, urine-based mutation testing may also provide a viable alternative to gauge mutation status as part of the initial treatment workup.
In April 2014, we announced the presentation of clinical study results at the American Association for Cancer Research (“AACR”) Annual Meeting. Of the 33 patients enrolled in the study, our BRAF V600E oncogene mutation assay was able to identify the mutation in 29 patients (88%) at least one time during the study, demonstrating a high level of concordance with tissue biopsy.
Longitudinal analysis was performed in 17 patients who had more than one urine-based test during the monitoring period. Of these patients, 13 (76%) showed a correlation between response to treatment and mutational status observed by the urine-based test. The results were presented by Filip Janku, M.D., Ph.D., University of Texas MD Anderson Cancer Center.
In June 2014, we announced that expanded clinical study results demonstrating the utility of our PCM platform were released at the 50th Annual Meeting of the American Society of Clinical Oncology (“ASCO”). Data from a study in multiple cancer types were published in the 2014 ASCO Annual Meeting Proceedings, a Journal of Clinical Oncology by Filip Janku, M.D., Ph.D., University of Texas MD Anderson Cancer. In this study, longitudinal analysis of sequential urine samples demonstrated a statistically significant correlation between changes in the amount of BRAF V600E mutation load and treatment response with targeted drug therapy (p=0.002), per RECIST 1.1 criteria. Results also demonstrated that patients with a decrease in BRAF V600E mutation load had a longer median time to treatment failure compared to those that did not (259 days versus 61 days; p=0.002). Patients in the study had melanoma (n=7), NSCLC (n=3), colorectal cancer (n=2) and other forms of cancer (n=5). Additionally, clinical results from a study in patients with histiocytic disease were presented by Eli Diamond, M.D., Memorial Sloan Kettering Cancer Center. In this study, our PCM technology demonstrated 93% concordance for identifying the BRAF V600E mutation and confirmed the absence of the mutation in the six patients whose biopsies tested negative. Our assay also detected the BRAF V600E mutation in two patients for whom tissue biopsy material was inadequate to determine mutational status, and these results were subsequently confirmed with follow-up biopsies. Our PCM platform showed 100% concordance in monitoring response to therapy in six study subjects who tested positive for the mutation and were treated with a BRAF inhibitor. Results from this study were published in the medical journal, Cancer Discovery, and in clinical consensus guidelines for the diagnosis and treatment of patients with the histiocytic disease, Erdheim-Chester disease.
CLIA validated KRAS mutation assay
In March 2014, our urine based test for KRAS mutations became available to clinicians through our CLIA laboratory. This assay detects and monitors the seven most commonly encountered mutations of the KRAS oncogene and is our first multiplexed oncogene mutation assay utilizing next-generation sequencing as a mutation detection platform. The robustness of
11
our ultra-sensitive assays has been demonstrated for the detection of KRAS mutations from cell-free DNA in urine. This mutation commonly occurs in patients diagnosed with either colorectal cancer, pancreatic cancer, or lung cancer. Of the more than 1.1 million estimated cases of colorectal cancer in the U.S., up to 40% are estimated to harbor KRAS mutations. In pancreatic cancer and lung cancer, approximately 90% and 15% of patients harbor KRAS mutations, respectively. Because of the prevalence of this mutation in several important cancer types, detecting and quantitatively monitoring KRAS mutational status is an area of clinical interest among treating physicians.
The clinical study being conducted at the USC Norris Cancer Center is focused on mutation monitoring and the emergence of KRAS resistant mutations in colorectal cancer. With multiple targeted therapies for colorectal cancer on the market, detection of KRAS mutations in tissue has a direct impact on the initial treatment selection for these patients. The primary purpose of the collaborative study is to determine whether KRAS mutations can be evaluated in urine to monitor treatment response in patients that test either positive or negative for the mutation.
The U.S. Oncology clinical study will test detection and monitoring of KRAS mutations in pancreatic cancer patients. In addition to the U.S. Oncology Research-affiliated community cancer care sites participating in this study, additional academic research institutions that specialize in oncology have also elected to participate. CT scans and CA19-9 blood levels are currently the only two methods available to clinicians to monitor metastatic pancreatic cancer tumor burden and response to therapy. However, approximately 11%-17% of patients will not display elevated CA 19-9, even with high tumor load. For patients that test negative for CA19-9, our method to follow disease status by detecting and monitoring KRAS mutations could be distinctly beneficial.
In November 2015, we presented clinical results at the EORTC-AACR-NCI International Symposium highlighting our ability to detect and quantitate KRAS mutations in blood and urine samples from patients with advanced colorectal cancer. Results showed a highly correlated response. Of the blinded retrospective plasma cell-free DNA samples evaluated, 95% displayed the KRAS mutation concordant with tumor tissue, and for evaluable urine samples in the study, 92% displayed the KRAS mutation concordant with tumor tissue. The majority of patients in the study underwent surgery and received neo-adjuvant or adjuvant therapy, and serial monitoring of KRAS mutations using our assay showed a clear correlation between blood and urine samples. An estimated analytical limit of detection of two copies per ~100,000 genome equivalents, or 0.002% was observed in the study, demonstrating very high analytical sensitivity.
CLIA validated EGFR mutation assays
In the first quarter of 2015, our urine-based tests for the activating mutations, EGFR L858 and EGFR Exon 19 Deletion, as well as the resistance mutation, EGFR T790M, became available to clinicians through our CLIA laboratory. These assays detect and monitor three critical mutations that are believed to drive the progression of NSCLC. The robustness of our ultra-sensitive assays has been demonstrated for the detection of these three EGFR mutations from cell-free DNA in urine.
While lung cancer is one of the most aggressive malignancies, progress has been made in the advancement of therapeutic strategies against the disease. In particular, epidermal growth factor receptor tyrosine kinase inhibitors (EGFR-TKIs), such as gefitinib and erlotinib, in NSCLC patients with activating EGFR mutations have demonstrated clinical response rates as high as 80%. However, after approximately six to twelve months, most tumors develop acquired resistance to these targeted therapies. Research into such resistance has identified the secondary EGFR T790M mutation, which occurs in approximately 60% of patients with acquired resistance to EGFR-TKIs and is reported to negate the benefits of treatment. In November 2015, the first targeted treatment for EGFR T790M mutation-positive NSCLC, Tagrisso, was approved by the U.S. Food and Drug Administration (“FDA”). Additional drug candidates such as rociletinib are in advanced clinical development for this indication. We believe that our non-invasive assays for the detection and monitoring of both activating and resistance EGFR mutations have potential to play an important role in the treatment of NSCLC.
A clinical study being conducted at UC San Diego Moores Cancer Center (“UCSD”) is focused on the determination and monitoring of EGFR T790 resistance mutations in lung cancer patients. With new targeted therapies for EGFR T790M mutation-positive lung cancer on the market or in late-stage clinical development, detection of this resistance mutation has a direct impact on treatment selection for patients who are progressing on first-line targeted therapy. The primary purpose of this collaborative study is to determine whether EGFR T790M mutations can be evaluated in urine to monitor treatment response in patients that are found to be positive for the mutation.
In April 2015, we presented clinical results at the European Lung Cancer Conference demonstrating that our urine-based PCM platform outperformed tissue biopsy for the detection and monitoring of EGFR T790M mutations in metastatic lung cancer patients. In an interim analysis of 34 patients from an ongoing clinical study, our PCM platform detected the EGFR T790M mutation in all patients who were positive for the mutation in tissue biopsy. Our urine-based assay identified additional
12
patients as EGFR T790M-positive, including those who had clinical suspicion of EGFR T790M-progressive disease, but were either negative by tissue biopsy or had not yet undergone tissue biopsy for confirmation. Based on the study results, our PCM platform detected EGFR T790M resistance mutations months earlier than radiologic detection of progression in patients. Early pharmacodynamic events occurring within hours or days of anti-EGFR drug treatment were evaluated in the study by implementing daily monitoring of urinary ctDNA. Initial results demonstrated that immediate changes in EGFR mutational load using a urine specimen may identify patients who respond to anti-EGFR therapy much earlier than follow-up CT-scans.
We have several programs to evaluate the detection and monitoring of EGFR mutational status in lung cancer patients. A focus of these studies is the emergence of the resistant mutation EGFR T790M in lung cancer patients, which can be important for therapeutic selection when this mutation type is or becomes present. In addition to our studies with UCSD, our collaborators for evaluating our technology in NSCLC include Memorial Sloan Kettering Cancer Center, City of Hope Comprehensive Cancer Center, Clovis Oncology, and Genomac Research Institute.
Additional mutation assays and clinical programs
We remain focused on expanding the mutation coverage of our platform to address the relevant clinically actionable driver and resistance mutations in cancers for which the National Comprehensive Cancer Network guidelines recommend targeted therapies, such as lung cancer, colorectal cancer, pancreatic cancer, and melanoma. In addition to our assays for the BRAF, KRAS, and EGFR oncogenes, we are also developing more comprehensive mutation coverage for these other cancers and are adding additional oncogenes with an initial focus on lung cancer, as well as targeting clinically validated gene rearrangements such as ALK, RET, and ROS. The primary objective of our clinical development program is to demonstrate utility for non-invasive, near real-time detection and monitoring of oncogene mutations for any tumor type with our highly sensitive urine- and blood-based platform. Our clinical programs with top-tier cancer centers will continue to drive multiple opportunities for data presentations and publications in peer-reviewed journals. We believe that data from our clinical studies, and those from peer-reviewed manuscripts, once published, will help support our ongoing commercial efforts to build physician demand and health insurance reimbursement for our cancer monitoring platform.
Infectious Disease
Following the completion of a pilot clinical study with a urine-based DNA test for high-risk HPV, our first HPV-HR Detection assay became commercially available in March 2013. Initial data from the pilot study showed that our assay provided superior performance to the current leading HPV assay. Our HPV-HR Detection assay showed a sensitivity of 93.0% and specificity of 96.0% for the detection of HPV in a comparative study of 320 high-risk individuals.
In August 2014, we presented results from two clinical studies at the 29th International Papillomavirus conference for our urine-based diagnostic test for the detection of high risk strains of HPV. Results from both pilot studies consistently demonstrated that our urine-based HPV assay had sensitivity greater than 90% for identifying women with high grade cervical intraepithelial neoplasia (CIN2/3). Assay performance was comparable to traditional HPV testing with commercially available tests in patient-matched cervical samples. In one of the studies, urine collection was examined to establish standardization of urine as a clinical specimen for high-risk HPV testing.
In February 2015, clinical results from the PREDICTORS 4 trial were presented at the European Research Organization on Genital Infection and Neoplasia (EUROGIN) 2015 Congress, which demonstrated high sensitivity for our non-invasive, urine-based HPV assay when determining HPV types and cervical lesions or cervical intraepithelial neoplasia (CIN) Grade 2/3. Within the PREDICTORS 4 trial, urine and cervical samples were collected from 501 women, and data from this large patient subset demonstrated that sensitivity with our HPV assay for cervical samples was comparable to established cervical screening tests. Sensitivity of our HPV assay using cervical samples was 96.3% for CIN Grade 3+ and 94.5% for CIN Grade 2+. Sensitivity for urine samples was 91.4% for CIN Grade 3+ and 89.0% for CIN Grade 2+. Furthermore, detection of high risk HPV in urine was not different from cervical samples for all age groups of women in the study (18-29 years, 30-39 years and 40-69 years). The study authors concluded that while there is a small loss of sensitivity in urine, the greater than 90% sensitivity for CIN Grade 3+ is still better than conventional Pap cytology, which makes this assay a good candidate in our efforts to increase adoption of HPV testing, especially for women who are not currently being screened for cervical cancer.
Urine-based HPV testing may offer a significant advantage over the traditional cervical swab sample, which can present a logistic, invasive or privacy concern. A urine-based assay also makes both female and male carrier screening feasible.
Through licensing agreements, we are pursuing commercialization of our HPV-HR Detection test, particularly in those geographies where compliance with cervical cell sampling is problematic.
13
Prenatal Genetics
The combination of NGS or ddPCR with our proprietary cell-free nucleic acid technology would allow for truly non-invasive prenatal screening of aneuploidies and monogenic disorders. We may pursue the development of our technology for use in prenatal genetics through licensing agreements.
Transplant
Patients who receive solid organ or bone marrow transplants are at risk of rejection, particularly during the first few months following surgery. Non-invasive monitoring of transplant status could replace repeated biopsies and blood tests, while keeping both the patient and the physician informed about potential problems.
Changing the Molecular Diagnostic Paradigm
Diagnosis and detection of severe and life-threatening diseases are among the most important outcomes of the Human Genome Project (“HGP”). There are four requirements to realize the full benefit of the HGP in relation to advances in the war on cancer: (1) large catalogues of cancer mutations, (2) affordable sequencing of patient samples, (3) detection technologies capable of identifying and quantifying rare instances of mutations at affordable prices, and (4) abundant samples that can be collected easily and frequently in order to monitor an individual’s cancer.
The first requirement has been met through the Sanger Centre’s Catalogue of Somatic Mutations in Cancer database, which has documented more than 233,000 mutations in more than 20,948 genes, and by the National Institutes of Health’s (“NIH”) The Cancer Genome Atlas, which has data on more than 20 cancer types and provides a host of tools for their analysis. The second requirement has been met through the dramatic and continuing decrease in the cost of both conventional sequencing and NGS. NGS and ddPCR, capable of detecting rare mutations among thousands of wild type molecules at a reasonable cost, fulfill the third requirement.
Our proprietary methods provide the fourth and final requirement, the provision of an abundant systemic sample that allows the purification of cell-free nucleic acids in amounts necessary to detect rare mutations. Furthermore, the “liquid biopsy” provided by urine can be collected frequently, is truly non-invasive, and requires no specialized personnel to collect it.
Taken together, these developments will increase the effectiveness of cancer diagnostics, improve healthcare spending efficiency and overall enable better patient care. These developments have made the era of personalized precision medicine in cancer possible.
The Market
The global molecular diagnostics market is forecast to reach nearly $8.0 billion by 2018, a compound annual growth rate (“CAGR”) of 9.7%, from 2013-2018. This molecular diagnostics market is segmented on the basis of application, technology, end user, product, and geography. Based on application, the market is further segmented into infectious diseases, oncology, genetics, blood screening, microbiology, and others. Infectious diseases secured the largest market share, whereas oncology was the fastest growing segment amongst the rest. The driving forces of the molecular diagnostics market include the rising incidences of infectious diseases, genetic disorders, and cancer, as well as technological advancements such as assay improvements, new diagnostic tests with novel clinical utility, and portability of equipment. The technology segment of the molecular diagnostics market is comprised of polymerase chain reaction (“PCR”), Isothermal Nucleic Acid Amplification Technology, hybridization, DNA sequencing and NGS, microarray, and others.
Based on products, the molecular diagnostics market is segmented into instruments, reagents, services and software. Reagents occupy the largest market share and will also register the maximum growth rate in the forecasted period of 2013 to 2018. These reagents include assays that detect and diagnose diseases and are also used as biomarkers that predict the biological properties of potential drug compounds.
North America accounts for the largest share of the market and is poised to grow at a high rate in the forecast period from 2013 to 2018. The growth can be attributed to the rising incidences of infectious diseases, cancer prevalence, and genetic disorders that are further adding to the overall prevalence of chronic diseases. Europe is the second leading contributor to the molecular diagnostics market. However, the growth of this region is expected to be sluggish in the forecast period and is estimated to grow at a lower CAGR than North America, due to factors such as the uneven reimbursement policies and the European economic crisis. Asia is the most promising region for molecular diagnostics in the coming five years. It is expected
14
to grow at a higher CAGR than North America and Europe over the forecast period. The large population base and improved purchasing power of patients are the major drivers of this market.
Cell-free molecular diagnostics from urine and plasma provide relevant information that can lead to improvements in personalized patient management. Most major pharmaceutical companies have active pharmacogenomic programs included in their clinical studies, anticipating the need to utilize diagnostic testing to stratify patients for clinical response. We believe that our broad intellectual property portfolio positions us to work within these markets, either alone or in partnership with other companies, to develop and market cell-free molecular diagnostic products, all of which we expect would address the large unmet market needs of abundance, simplicity, patient convenience and privacy, accuracy, and cost effectiveness. Such products could play key roles in their applications to improve testing compliance and as such, reduce morbidity and mortality. The use of urine as a sample should provide a paradigm shift in screening and monitoring practices as it provides an easier sample to acquire in a truly non-invasive fashion, with more nucleic acid targets present in the sample leading to greater sensitivity. We believe these modified testing practices will most likely meet with wide physician and patient acceptance in oncology, infectious disease, transplantation, and potentially, prenatal diagnostics.
Commercial Markets — Internal Focus
Oncology
Cancer mutation testing and monitoring is the priority area for our scientists and commercial personnel. Early data from ongoing clinical studies have shown that cell-free nucleic acid analysis may be useful for determining the presence or absence of actionable mutations, and for monitoring therapeutic response and recurrence in metastatic cancers. Such testing could serve to help physicians monitor ongoing response to therapy or minimal residual disease after surgery, identify signs of early progression, or see markers of resistance emerge prior to clinical presentation. Once therapy is completed, a simple urine test can be used to monitor for early signs of disease recurrence over time. The market for these tests, which is diagnosed cancer patients possessing mutations known to have clinical or therapeutic importance, is already established. Use of urine-based testing could be disruptive and change the pattern of use of other cancer monitoring tools, including imaging technologies, such as PET, CT and MRI scans.
According to the American Cancer Society’s (“ACS”) 2015 report, there are approximately 565,000 patients that die every year from cancer, not including cancers of the blood, bone marrow or lymphatic system. Using this number as a proxy for metastatic cancers, it can be assumed that all of these patients are being treated within 12 months of death for their disease. Testing and monitoring these patients for response to therapy or progression while on therapy, or for markers of resistance to therapy (like EGFR T790M for lung cancer), would be a natural extension of our technology. The average lung, breast, or colon cancer patient receives between 18-21 radiographic imaging procedures (PET, CT, MRI, etc.) during the two years following their diagnosis. This averages to approximately nine to ten scans per patient per year. Use of a urine-based monitoring test at the start of therapy, at several points in time during therapy, and at the completion of therapy would represent approximately six to ten separate testing events that could occur within a 12 month period. At a reimbursed price of approximately $1,000 per test, the total available market (“TAM”) for treatment response monitoring in the U.S. could be worth between $3.0 billion and $5.0 billion annually.
Once patients with cancer, primary or metastatic, have completed therapy, they will require monitoring for possible progression and for the appearance of resistance markers, since many metastatic patients may remain on lower-dose “maintenance therapy” during the remainder of their lives, or until treatment is no longer considered an option. According to the ACS, as of January 2014, there were nearly 14.5 million patients alive in the U.S. who had been treated for cancers that have metastatic potential. Use of a urine-based mutation monitoring test once a year at $1,000 per test would equate to a TAM for recurrence monitoring in the U.S. of approximately $14.5 billion annually.
Both of these markets, treatment response and recurrence monitoring, are sizeable economic opportunities. Capturing 10% of the response monitoring market would produce annual revenues of between $300 million and $500 million, and 5% of the recurrence monitoring market would yield annual revenues of over $700 million.
Beyond cancer patients being actively treated or monitored over time, cell-free nucleic acid testing may eventually emerge as a viable option for pre-cancerous screening. This was recently evaluated in a cancer clinical study at Thomas Jefferson University, funded jointly by the NIH and the National Cancer Institute (“NCI”). The study demonstrated that DNA fragments carrying a specific mutation (KRAS), and released from pre-cancerous colon polyps, can be detected in the urine of patients.
Studies have shown that cancer patients who have KRAS mutations do not respond successfully to treatment with anti-
15
EGFR drugs such as Erbitux, Iressa, Tarceva, Tykerb, and Vectibix.
These anti-EGFR agents, particularly Erbitux and Vectibix, are a mainstay of treatment for colorectal cancer. It has been estimated that 17%-25% of all human cancers have been found to harbor KRAS mutations, with mutation rates as high as 59%-90% in pancreatic cancers and 35%-40% in colorectal cancers. These tumors have a low probability of responding to anti-EGFR drugs. By first testing for KRAS mutations, physicians will be able to better manage their patients and avoid costly treatments that are unlikely to have a positive clinical response.
Screening and monitoring for KRAS and other key biomarker mutations (i.e. BRAF, EGFR, NRAS, PIK3CA, etc.) using urine-based tests would provide a simple, non-invasive, cost effective, and convenient testing alternative for physicians and patients. Urine samples may even be collected in the patient’s home as required, or as requested by the physician.
Simple urine-based assays would likely lead to improved personalized medicine for patients, resulting in the right drug being prescribed for the right disease at the right time. We believe this technology will lead to an improved quality of life for patients and will become part of a new standard of care for those patients and physicians fighting the war on cancer.
Drug Development and Monitoring of Therapeutic Outcomes
Cell-free DNA diagnostic technology has significant potential as a simple, quick, non-invasive way of monitoring clinical responses to drugs in clinical development and evaluating patient-specific responses to already approved and marketed therapies. Specific target applications include, but are not limited to, the detection of metastasis following tumor surgery, monitoring of response and tumor progression during chemotherapy, immunotherapy, and/or radiation therapy, development of optimal hormonal and chemotherapeutic treatment protocols, and monitoring of transplantation patients on immunosuppressive drugs.
With cancer treatment today, it is often difficult to determine if a particular patient is responding to their current therapeutic regimen. Generally, patients are re-examined periodically to determine if a tumor has grown in size, reduced in size (i.e., partial response), disappeared (i.e. no sign of disease - complete response) or remained the same (stable disease). If the tumor has grown in size or remained the same, treatment may be adjusted. By measuring and monitoring tumor specific genetic markers in a patient’s urine pre-, peri- and post-chemotherapy, it may be possible to more quickly determine whether a patient is responding to therapy. Use of cell-free DNA diagnostics may permit more rapid and real-time therapeutic decisions on a patient-specific basis. Approximately 1.7 million new cancer cases are diagnosed annually, and there are several hundred companies developing therapeutic agents in the U.S. alone. We believe this indicates a large potential application to use cell-free DNA diagnostic technology for both drug development and the monitoring of therapeutic outcomes.
One of the largest costs associated with development of a new therapy is the size of human clinical studies required to identify the cohort of responders, and the resulting statistical power required. By measuring specific genetic markers, it may be possible to pre-identify, and subsequently screen, for the most likely responders to the therapy, and to limit patient recruitment to this subset. This strategy could significantly reduce the cost to develop a drug and improve development timelines. We believe that there is a significant commercial potential for our urine-based cell-free molecular diagnostic technology to be incorporated into these clinical trial protocols, and ultimately into post-approval patient identification protocol.
Commercial Markets — External Focus
We will seek to license and/or partner with other companies who have vested interests or commercial strengths in the following areas in order to develop applicable diagnostic and/or monitoring tests using our cell-free molecular diagnostic technology.
Infectious Diseases — HPV
The rationale for screening for HPV is that high-risk subtypes cause virtually all cases of cervical cancer. We have developed a urine-based HPV test capable of screening for known high-risk HPV types that are associated with the development of cervical cancer. Cervical cancer is the third most commonly diagnosed cancer, and the fourth leading cause of cancer deaths in females, worldwide. Deaths due to cervical cancer are a significant global problem, especially in developing countries where screening practices are inadequate.
According to the ACS, India alone accounts for 27% (77,100) of total worldwide cervical cancer deaths. A recent clinical trial conducted in rural India found that a single round of HPV DNA testing was associated with an approximately 50% reduction in the risk of developing advanced cervical cancer and associated deaths. In the U.S., better patient compliance and
16
screening guidelines reduced cervical cancer death rates to only 4,290 cases in 2011. The major drivers of poor screening in these developing regions are cultural acceptance, limited screening resources and funding, and poor cytology proficiency. Further exacerbating the compliance hurdles is that the primary screening mechanism involves an invasive cervical scraping procedure (e.g., Pap smear). It is generally agreed that the early detection of cervical cancer leads to much higher recovery rates and lower rates of invasive disease.
There is a tremendous unmet need for a new non-invasive, simple, private, and cost effective test to simplify the HPV screening process for patients and, in turn, improve compliance. We believe our urine-based HPV test has the potential to address these market needs.
Other areas beyond HPV detection and monitoring include those infectious diseases caused by viruses, bacteria, fungi, and parasites. Cell-free nucleic acid assays that detect molecular targets in organisms can provide a quick, accurate, simple, and cost effective method for screening and monitoring disease. Specific areas of interest include testing for molecular targets from organisms that cause Lyme disease, John Cunningham Virus, valley fever, and various fungal infections. These organisms all tend to be difficult to identify with current technology, making differential diagnosis especially challenging, thus delaying the start of potentially curative anti-infective treatment.
Transplantation
According to government statistics, there are approximately 28,000 solid organ transplants performed in the U.S. annually. Post-transplant monitoring for organ rejection episodes requires a highly invasive tissue biopsy. Approximately ten such biopsies are taken over a period of one year per patient. Because organ rejection is marked by the early death of cells, we believe that an early indication of rejection can be identified by measuring a unique series of genetic markers characteristic of the organ donor that can be easily detected in random urine specimens from the transplant recipient. Providing early evidence of tissue rejection is key to the administration and monitoring of immunosuppressive therapies used to prevent rejection. Given the annual number of transplants performed in the U.S. and the annual number of corresponding biopsies performed per patient, this would equate to a market opportunity in the U.S. of roughly 300,000 urine-based tests per year. Transplantation monitoring with our technology offers opportunities for partnering with companies developing drugs for controlling tissue rejection, developing cell transplantation, or developing novel transplantation technologies. This illustrates the breadth of commercial potential of our cell-free molecular testing platform technology, and we intend to leverage such potential applications to maximize stockholder value.
Technologies for the collection, shipment and storage of urine specimens, and cell-free nucleic acid extraction
Successful implementation of our cell-free nucleic acid technology in molecular testing is tightly linked to the availability of techniques and procedures for cell-free nucleic acid preservation, purification, and analysis. Our strategic plan includes the allocation of sufficient resources for the creation of robust, feasible, and inexpensive approaches to improve the efficiency of working with urine samples.
We intend to invest in the research and development of new nucleic acid preservatives or methods, which improve the stability of urine as a cell-free nucleic acid specimen. We will also explore the feasibility of automating cell-free nucleic acid extraction from urine in collaboration with industry leaders in robotics, liquid handling, and other applicable technologies. Upon the completion of such projects, it is our expectation that a simple and streamlined method can be “kitted” as a stand-alone product to provide academic researchers with reagents that they can purchase and utilize in their own laboratories.
This program serves three primary purposes: it will (1) accelerate the rate of publications and development of the body of evidence supporting urine as a viable specimen and, therefore, market acceptance of urine-based nucleic acid testing, (2) create an RUO product for direct sale, and (3) provide a foundation for our technology transfer programs to partner reference laboratories seeking to bring cell-free nucleic acid testing technology in-house.
Expansion of Analytically Validated Instrumentation, Systems, and Platforms
A unique element of our cell-free nucleic acid testing method is its design, which is focused on “counting” the target molecules already enriched through our initial proprietary specimen collection, isolation, and amplification procedures. This molecular counting is currently achieved in our Clinical Services Laboratory by using Illumina MiSeq systems as the detection platform; however, this molecular counting is not limited to just this type of system. Alternative NGS systems, Mass Spectrometry-based systems, ddPCR, or MicroArray reading systems may also be used in conjunction with our front-end sample preparation technology. As we expand our menu of targeted biomarker tests, we will also broaden the available platforms that can be used as detectors. When coupled with the RUO kitting program referenced above, the benefit of multiple
17
analytically validated detection systems will increase the addressable market for our technology transfer program and future commercial partnerships.
Our Business Strategy
We plan to leverage our cell-free nucleic acid technology to develop and market, either independently or in conjunction with corporate partners, molecular diagnostic products in our core market, oncology, as well as other markets including infectious disease, transplantation, and prenatal diagnostics. Our marketing strategy includes approaches across multiple fronts. In the U.S. market, we have acquired a CLIA laboratory. At the late stages of development for each product, while collecting clinical data for regulatory submissions, we intend to market the products as LDTs through our CLIA laboratory. CLIA laboratories can develop and offer their own in-house tests that receive reimbursement under the provisions of LDT rules.
The U.S. Congress passed the CLIA in 1988 to regulate development, evaluation, and use of LDTs. The CLIA states that laboratories must demonstrate how well an LDT performs using certain performance standards. Laboratories that perform testing on human specimens for the diagnosis, prevention, or treatment of disease, or for the assessment of health, must comply with all applicable CLIA regulations. These regulations, which were finalized in 2003, establish standards to help ensure the quality and accuracy of laboratory testing. While most common laboratory tests are commercial tests, manufactured and marketed to multiple laboratories, some new tests are developed, evaluated, and validated within one particular laboratory. These LDTs are used solely within that laboratory and are not distributed or sold to any other laboratories or health care facilities.
Because LDTs are not marketed to other laboratories or facilities, they do not require approval for marketing from the FDA as do commercially developed and marketed tests. However, these types of tests must go through rigorous validation procedures and must meet several criteria before results can be used for decisions regarding patient care. These include demonstration of test accuracy, precision, sensitivity, and specificity.
We may pursue FDA review and approval for our products as clinical studies are completed. Assuming we receive FDA clearance or approval for our products, we plan to market such urine-based test kits through a U.S. commercial organization directly to national and regional CLIA medical testing laboratories. We also intend to complete business partnerships (out-license agreements) with diagnostic and pharmaceutical companies in the U.S., Europe, Asia Pacific and the rest of the world as appropriate given market conditions and opportunities. This strategy would provide both short term (license fees) and long term (royalty) revenue streams. Licensees of our technology will use our platform technology in the clinical development of their products, to monitor patients taking their marketed products (i.e., TNF inhibitors) and in certain situations to develop, market and sell our cell-free molecular diagnostic technology in predefined fields of use and geographic territories. We plan to become a fully vertically integrated business in which we develop, manufacture, register, market, and sell our products.
The major advantages of our cell-free nucleic acids tests, when commercially available, will be the ease of sample collection, anticipated higher levels of sensitivity and specificity, larger quantities of genetic material for analysis (allowing for the detection of oncogene mutations that are low in abundance), patient convenience, non-invasiveness, and the ability to provide more efficient and effective monitoring protocols. Our cell-free nucleic molecular diagnostic technology must be cost effective, and we believe the process to make, sell, and process our assays is relatively simple and suitable for automation.
During the last decade, medical laboratory operating margins have declined in the face of Medicare fee schedule reductions, managed care contracts, competitive bidding, and other cost containment measures. Our technology is commercially available and reimbursement is available under the current procedural terminology (“CPT”) codes for molecular-based testing. We are marketing our tests directly to physicians, and we process those tests through our CLIA laboratory. We are working with public and private payors for appropriate reimbursement of processed tests. We believe this strategy, coupled with strong clinical results supporting the use of our cell-free molecular diagnostic technology, will lead to broad market adoption of our technology.
Research and Development
As of December 31, 2015, we had 41 dedicated scientists located in our office in San Diego, California. We plan to continue to grow our research and development organization as needed to support our product development goals and expect that our research and development team will represent a good mix of senior lead researchers and scientists (Ph.Ds.), laboratory associate scientists, and experts in clinical development and regulatory affairs of molecular diagnostics. We plan to rapidly introduce new products to the market that can be used as LDTs within our CLIA lab, and simultaneously continue funding and
18
collaborating on the necessary clinical studies that can support the utility of our tests, and potentially support regulatory submissions for marketing approval or clearance of our tests depending upon the nature of the product. We currently have sufficient resources to complete these projects extending into 2017. We plan to seek additional funding as required to supplement current commercial and licensing revenue. Information and documentation systems infrastructure (e.g., design history files and firewalls) must be in place to support the confidentiality of multiple partnering programs and the rigorous scientific and regulatory oversight needed for products in the in-vitro diagnostics markets. Research and development expenses for the years ended December 31, 2015, 2014 and 2013 were approximately $10.6 million, $6.7 million and $3.9 million, respectively.
Intellectual Property
We consider the protection of our proprietary technologies and products to be a critical element in the success of our business. As of December 31, 2015, our wholly-owned and licensed intellectual property included over 85 issued patents and over 60 pending patent applications in the U.S. and abroad. The pending applications include multiple international applications filed under the Patent Cooperation Treaty (“PCT applications”) that will be used as the basis for multiple additional patent applications.
One group of patents and patent applications includes seven U.S. patents, with 30 counterpart patents in Japan, Hong Kong and Europe, including the major markets of the European countries. These patents are directed to the detection of nucleic acid sequences in urine and nucleic acid modifications and alterations in urine. This patent family includes claims directed to prenatal analysis of fetal DNA, the determination of the sex of a fetus and the detection of diseases such as Down Syndrome caused by genetic alterations. Other patented claims are directed to detecting and monitoring cancer through urine-based testing, nucleic acid screening, and monitoring in cases of transplantation and infectious diseases, including infection by viruses and pathogens, and other potential diagnostic and genetic testing applications. Members of this patent group expire between 2018 and 2026. Additional pending claims are directed to the preparation of cell-free nucleic acids, as well as detection of short cell-free nucleic acid molecules which, if granted, will expire between 2028 and 2033.
A second group is directed to the detection of specific gene mutations and indicators of disease. These include NPM1 mutations, BRAF mutations, SF3B1 mutations, HPV, AML, and hairy cell leukemia. The detection includes analysis of cell-free nucleic acid molecules. This group includes U.S. patent numbers 8,222,370 B1, 8,501,924 B1, 8,642,261 B1, and 9,222,137 B1 as well as seven pending U.S. patent applications. There are also 25 pending non-U.S. and PCT patent applications. Members of this patent group expire between 2025 and 2034.
A third group is directed to our molecular detection platform utilizing proprietary probe chemistry on optical detectors such as CMOS (complementary metal-oxide semiconductors). This platform technology utilizes a conjugated probe and optical detection of analytes in medical diagnostics. This group includes one issued patent in Japan and patents in the major markets of Europe, with pending applications in the U.S., Europe, and Hong Kong. Members of this patent group expire beginning in 2022.
Applications are also pending that are directed to detecting and enriching small concentrations of short nucleic acid sequences, detecting and monitoring mutations in histiocytosis, and detecting and monitoring mutations in diseases, such as cancer, over time.
Wherever possible, we seek to protect our inventions by filing U.S. patents as well as foreign counterpart applications in select other countries. Because patent applications in the U.S. are maintained in secrecy for at least eighteen months after the applications are filed, and since publication of discoveries in the scientific or patent literature often lags behind actual discoveries, we cannot be certain that we were the first to make the inventions covered by each of our issued or pending patent applications, or that we were the first to file for protection of inventions set forth in such patent applications. Our planned or potential products may be covered by third-party patents or other intellectual property rights, in which case continued development and marketing of our products would require a license. Required licenses may not be available to us on commercially acceptable terms, if at all. If we do not obtain these licenses, we could encounter delays in product introductions while we attempt to design around the patents, or we could find that the development, manufacture or sale of products requiring such licenses are not possible.
We may rely on trade secrets to protect our technology, which are difficult to protect. We seek to protect our proprietary technology and processes by entering into confidentiality agreements with our employees, certain consultants, and contractors. These agreements may be breached, we may not have adequate remedies for any breach and our trade secrets may otherwise become known or be independently discovered by competitors. To the extent that our employees or our consultants
19
or contractors use intellectual property owned by others in their work for us, disputes may also arise as to the rights in related or resulting know-how and inventions.
Manufacturing and Distribution
In 2016, we plan to continue introducing our LDTs into the marketplace through our CLIA licensed and CAP accredited laboratory. We source all reagents and consumables needed for our LDTs from third party vendors, and we currently do not manufacture reagents kits for use in our own laboratory, or to distribute to third party laboratories.
We have established a sales and marketing organization to directly market our LDTs for oncogene mutations to end users in the oncology market segment. As of December 31, 2015, we had 16 employees dedicated to the sales and marketing of our LDTs in the U.S. market. We intend to add additional employees as needed to support the introduction of new LDTs planned for 2016.
Reimbursement
Medicare and other third-party payors will independently evaluate our technologies by, among other things, a cost/benefit analysis, assessing other available options and reviewing the published literature with respect to the results obtained from our clinical studies. Currently, CPT codes are available for molecular testing, which we believe will allow our technologies to be billed following completion of a test that has been prescribed by a physician for a patient. We believe that the existence of current CPT codes with applicability to our tests will help facilitate Medicare’s reimbursement process, as well as that for third party insurance providers.
Reimbursement of our novel tests is a top priority, as physician and patient access to our technology is essential for widespread adoption of our products. To gain initial reimbursement, our qualitative tests will be billed and reimbursed under established Tier I codes for their respective mutation (i.e., BRAF, KRAS, and EGFR). These are CPT codes from the American Medical Association (MoPath system), which should enable us to bill and obtain reimbursement for our tests without delay. As we develop our tests and demonstrate novel clinical utility in cancer monitoring, supported by our high analytical sensitivity, quantitative performance over a large dynamic range, and clinical experience, we will pursue a Not Otherwise Classified (“NOC”) code for billing and reimbursement. Under these conditions, premium pricing is expected. Over time, we intend to pursue permanent CPT codes unique to our cancer monitoring diagnostics once sufficient value is assigned under the NOC code system. We will engage with third party payors including integrated healthcare networks and Medicare, for reimbursement of our tests, with the goals of obtaining strong adoption of our tests, positive coverage decisions and appropriate valuation of our tests on a widespread basis over time. In 2016, we plan to continue developing clinical evidence around the utility and performance of our testing platform and interacting with payors for the reimbursement of our commercially available urine-based cell-free nucleic acid diagnostics.
Government Regulation
Regulation by governmental authorities in the U.S. and other countries will be a significant factor in the development, production and marketing of any products that we may develop. The nature and extent to which such regulation may apply will vary depending on the nature of any such products and the policy of each country. Virtually all of our potential products will require regulatory allowance or approval by governmental agencies prior to commercialization, except for our LDTs. We may submit and obtain FDA approval or clearance for some or all of our diagnostic products. Pursuing and receiving FDA approval or clearance may be vital to maximizing our customer base and revenue potential for our numerous products.
FDA clearance for our products may be obtained through submission of a 510(k) statement of equivalency. Another regulatory option, albeit more complicated and expensive, is to pursue FDA approval by submitting a Pre-Market Approval (“PMA”) application. A 510(k) submission requires that we show equivalency of results in a clinical study with parallel comparison against an existing and FDA-recognized reference method (predicate device).
The FDA also regulates the sale of certain reagents, including our potential reagents, used by laboratories under the LDT rules to perform tests. The FDA refers to such reagents as Analyte-Specific Reagents (“ASRs”). ASR’s generally do not require FDA pre-market approval or clearance if they are (1) sold to clinical laboratories certified under the CLIA to perform high complexity testing and (2) are labeled in accordance with FDA requirements, including a statement that their analytical and performance characteristics have not been established. Prior to, or in lieu of, FDA approval, we can sell our reagents to laboratories that meet the established criteria. The FDA also regulates all promotional materials and specifically prohibits medical and efficacy claims.
20
Assuming that FDA approval or clearance is received for our products, a number of other FDA requirements would apply to our manufacturing and distribution efforts. Medical device manufacturers must be registered and their products listed with the FDA, and certain adverse events, such as reagent failures, significant changes in quality control and other events requiring correction and/or replacement or removal of reagents must be documented and reported to the FDA. The FDA also regulates product labeling, promotion and, in some cases, advertising, of medical devices. As discussed above, we must comply with the FDA’s Quality System Regulation that establishes extensive requirements for design control, quality control, validation, and manufacturing. Thus, even with FDA approval or clearance, we must continue to be diligent in maintaining compliance with these various regulations, as failure to do so can lead to enforcement action. The FDA periodically inspects facilities to determine compliance with these and other requirements.
Competition
The medical diagnostic industry is characterized by rapidly evolving technology and intense competition. Our competitors include medical diagnostic companies, many of which have financial, technical, and marketing resources significantly greater than our resources. In addition, there are a significant number of biotechnology companies working on evolving technologies that may supplant our technology or make it obsolete. Academic institutions, government agencies, and other public and private research organizations are also conducting research activities and seeking patent protection and may commercialize products on their own or through joint ventures. We are aware of certain development projects for products to prevent or treat certain diseases targeted by us. The existence of these potential products or other products or treatments of which we are not aware, or products or treatments that may be developed in the future, may adversely affect the marketability of our products or product candidates.
We believe that direct competition in the area of cell-free DNA detection and analysis is precluded by our growing patent estate. However, there are other companies working in the area of cell-free nucleic acids and circulating tumor cell (“CTC”) collection and analysis in blood plasma that could compete in similar clinical areas, including disease detection, therapeutic response monitoring and minimal disease detection. These companies include Johnson & Johnson (Veridex), Illumina, Inc., Genomic Health, Inc., Sequenom, Inc., Cepheid, Qiagen N.V., Quest Diagnostics Incorporated, LabCorp, Biocept, Inc., Exact Sciences Corporation, Boreal Genomics Inc., Sysmex-Inostics GmbH and numerous other smaller companies, both in the research and development and early commercial development phases. However, we believe that the advantages of urine as a specimen (large amounts of cell-free nucleic acid material, ease of collection, continuous collection over time and virtually no limit on sample size and frequency) position us favorably even among such competing companies.
Employees
As of February 29, 2016 we had a total of 72 employees, all of whom were full-time.
ITEM 1A. RISK FACTORS
An investment in our securities involves a high degree of risk. An investor should carefully consider the risks described below as well as other information contained in this Annual Report on Form 10-K. The risks and uncertainties described below are not the only ones we face. Additional risks and uncertainties not presently known to us or that we currently believe are immaterial may also impair our business operations. If any of the following risks actually occur, our business, financial condition or results of operations could be materially adversely affected, the value of our securities could decline, and investors in our company may lose all or part of their investment.
Risks Related to Our Business
We are a development stage company and may never earn a profit.
We are a development stage company and have incurred losses since our formation. As of December 31, 2015, we have an accumulated total deficit of approximately $108.9 million. For the fiscal year ended December 31, 2015, we had a net loss and comprehensive loss attributable to common stockholders of approximately $27.5 million. To date, we have experienced negative cash flow from development of our cell-free molecular diagnostic technology. We have not generated any revenue from operations except for licensing, milestone and royalty income, and we expect to incur substantial net losses for the foreseeable future as we seek to further develop and commercialize our cell-free molecular diagnostic technology. We cannot predict the extent of these future net losses, or when we may attain profitability, if at all. If we are unable to generate significant revenue from our cell-free molecular diagnostic technology or attain profitability, we will not be able to sustain operations.
21
Because of the numerous risks and uncertainties associated with developing and commercializing our cell-free molecular diagnostic technology and any future tests, we are unable to predict the extent of any future losses or when we will attain profitability, if ever. We may never become profitable and you may never receive a return on an investment in our common stock. An investor in our common stock must carefully consider the substantial challenges, risks and uncertainties inherent in the attempted development and commercialization of tests in the medical diagnostic industry. We may never successfully commercialize our cell-free molecular diagnostic technology or any future tests we may develop, and our business may not be successful.
We will need to raise substantial additional capital to commercialize our cell-free molecular diagnostic technology, and our failure to obtain funding when needed may force us to delay, reduce or eliminate our product development programs or collaboration efforts.
As of December 31, 2015, our cash balance was approximately $67.5 million and our working capital was approximately $60.2 million. Due to our recurring losses from operations and the expectation that we will continue to incur losses in the future, we will be required to raise additional capital to complete the development and commercialization of our current product candidates. We have historically relied upon private and public sales of our equity, as well as debt financings to fund our operations. At December 31, 2015 we had $16.5 million outstanding under debt agreements. In order to raise additional capital, we may seek to sell additional equity and/or debt securities or obtain a credit facility or other loan, which we may not be able to do on favorable terms, or at all. Our ability to obtain additional financing will be subject to a number of factors, including market conditions, our operating performance and investor sentiment. If we are unable to raise additional capital when required or on acceptable terms, we may have to significantly delay, scale back or discontinue the development and/or commercialization of one or more of our product candidates, restrict our operations or obtain funds by entering into agreements on unfavorable terms.
Our Loan and Security Agreement with Oxford Finance LLC, or Oxford, and Silicon Valley Bank, or SVB, and our Loan and Security Agreement with SVB for equipment, each contain certain covenants that could adversely affect our operations. Additionally, if an event of default were to occur, we could be forced to repay the outstanding indebtedness sooner than expected and possibly at a time when we do not have sufficient capital to meet these obligations, which could materially adversely affect our business, prospects and financial condition.
We have entered into a Loan and Security Agreement, dated as of June 30, 2014, with Oxford and SVB, or the Lenders, as amended, or the Loan and Security Agreement, for a term loan of $15.0 million. The term loan is secured by all of our assets, other than our intellectual property. In addition, we have entered into a Loan and Security Agreement, dated as of November 17, 2015, with SVB that provides for cash borrowings for equipment of up to $2.0 million, secured by the equipment financed, or the Equipment Line of Credit. The Loan and Security Agreement and the Equipment Line of Credit each contain affirmative and negative covenants that, among other things, restrict our ability to:
• | incur additional indebtedness or guarantees; |
• | incur liens; |
• | make investments, loans and acquisitions; |
• | consolidate or merge with or into other entities; |
• | sell or assign any part of our business or property; |
• | engage in transactions with affiliates; and |
• | pay dividends. |
Additionally, we may be deemed to be in default under the Loan and Security Agreement and the Equipment Line of Credit upon the occurrence of certain events, including, among other things, payment defaults; breaches of representations, warranties or covenants; certain insolvency events; and the occurrence of certain material adverse changes. Upon the occurrence of an event of default and following any cure period (if applicable), a default interest rate of an additional 5.0% per annum may be applied to the outstanding loan balance, and the Lenders may declare all outstanding obligations immediately due and payable and take certain other actions set forth in the Loan and Security Agreement and the Equipment Line of Credit.
22
The Loan and Security Agreement and the Equipment Line of Credit could prevent us from taking certain actions without the consent of the Lenders and, if an event of default should occur, we could be required to immediately repay the outstanding indebtedness. If we are unable to repay this debt, the Lenders may elect to foreclose on the secured collateral, including our cash accounts, and take other remedies permitted under the Loan and Security Agreement and the Equipment Line of Credit, as applicable. Even if we are able to repay the indebtedness upon the occurrence of an event of default, the repayment of these sums may significantly reduce our working capital and impair our ability to operate as planned. The occurrence of any of these events could materially adversely affect our business, prospects and financial condition.
The commercial success of our product candidates will depend upon the degree of market acceptance of these product candidates among physicians, patients, healthcare payors and the medical community and on our ability to successfully market our product candidates.
The use of our cell-free molecular diagnostic technology has never been commercialized for any indication. Even if approved for sale by the appropriate regulatory authorities, physicians may not order diagnostic tests based upon our cell-free molecular diagnostic technology, in which event we may be unable to generate significant revenue or become profitable. Acceptance of our cell-free molecular diagnostic technology by physicians, patients, healthcare payors and the medical community will depend on a number of factors, including, but not limited to:
• | successful integration into clinical practice; |
• | adequate reimbursement by third parties; |
• | cost effectiveness; |
• | potential advantages over alternative treatments; and |
• | relative convenience and ease of administration. |
We will need to make leading physicians aware of the benefits of tests using our technology through published papers, presentations at scientific conferences and favorable results from our clinical studies. In addition, we will need to gain support from thought leaders who believe that testing a urine specimen for molecular markers will provide superior performance. Ideally, we will need these individuals to publish support papers and articles which will be necessary to gain acceptance of our products. There is no guarantee that we will be able to obtain this support. Our failure to be successful in these efforts would make it difficult for us to convince medical practitioners to order cell-free molecular diagnostic tests for their patients and, consequently, would limit our revenue and profitability.
We currently have limited experience in marketing our products. If we are unable to expand our marketing and sales capabilities or enter into agreements with third parties to market and sell our product candidates, we may not be able to generate product revenue.
We have limited experience in marketing our products. We intend to expand our in-house marketing organization and sales force, which will require significant capital expenditures, management resources and time. We will have to compete with other molecular diagnostic companies to recruit, hire, train and retain marketing and sales personnel.
If we are unable or later decide not to expand our internal sales, marketing and distribution capabilities, we will pursue collaborative arrangements for the sales and marketing of our product candidates or future products; however, we may not be able to establish or maintain such collaborative arrangements or, if we are able to do so, we cannot guarantee that any sales force we use through such arrangements will be effective. Any revenue we receive will depend upon the efforts of such third parties, which may not be successful. We may have little or no control over the marketing and sales efforts of such third parties and our revenue from product sales may be lower than if we had commercialized our product candidates internally. We also face competition in our search for third parties to assist us with the sales and marketing of our product candidates, which may negatively impact our ability to enter into favorable collaborative arrangements for the sale and marketing of our product candidates.
If our potential medical diagnostic tests are unable to compete effectively with current and future medical diagnostic tests targeting similar markets as our product candidates, our commercial opportunities will be reduced or eliminated.
The medical diagnostic industry is intensely competitive and characterized by rapid technological progress. In each of our potential product areas, we face significant competition from large biotechnology, medical diagnostic and other companies.
23
The technologies associated with the molecular diagnostics industry are evolving rapidly and there is intense competition within the industry. Certain molecular diagnostics companies have established technologies that may be competitive to our product candidates and any future tests that we develop. Some of these tests may use different approaches or means to obtain diagnostic results, which could be more effective or less expensive than our tests for similar indications. Moreover, these and other future competitors have or may have considerably greater resources than we do in terms of technology, sales, marketing, commercialization and capital. These competitors also may have substantial advantages over us in terms of research and development expertise, experience in clinical studies, experience in regulatory issues, brand name exposure and expertise in sales and marketing as well as in operating central laboratory services. Many of these organizations have greater financial, marketing and human resources than we do; therefore, there can be no assurance that we can successfully compete with current or potential competitors, and any such competition could materially adversely affect our business, financial position or results of operations.
Since our cell-free molecular diagnostic technology is under development, we cannot predict the relative competitive position of any product based upon our cell-free molecular diagnostic technology. However, we expect that the following factors, among others, will determine our ability to compete effectively: safety and efficacy; product price; turnaround time; ease of administration; performance; reimbursement; and marketing and sales capabilities.
We believe that many of our competitors spend significantly more on research and development-related activities than we do. Our competitors may discover new diagnostic tools or develop existing technologies to compete with our cell-free molecular diagnostic technology. Our commercial opportunities will be reduced or eliminated if these competing products are more effective, are more convenient or are less expensive than our product candidates
Our failure to obtain human urine samples from medical institutions for our clinical studies will adversely impact the development of our cell-free molecular diagnostic technology.
We will need to establish relationships with medical institutions in order to obtain urine specimens from patients that test positive for a relevant infectious disease or from patients who have been diagnosed with solid tumors. We must obtain a sufficient number of samples in order to statistically prove the equivalency of the performance of our assays versus existing assays that are already on the market.
Cell-free nucleic acids in urine are stable at room temperature for extended periods of time with the addition of a simple preservative. Successful implementation of our cell-free nucleic acid technology in molecular testing is closely linked to the availability of techniques and procedures for cell-free nucleic acid preservation, purification and analysis. In the event urine specimens are not adequately preserved or are improperly stored or contaminated, we may be delayed in pursuing our clinical studies, and we may incur additional costs associated with procuring new human urine samples.
If the validity of an informed consent from a subject was to be challenged, we could be forced to stop using some of our resources, which would hinder our product development efforts.
We have measures in place to ensure that all clinical data and other samples that we receive from our clinical collaborators have been collected from subjects who have provided appropriate informed consent for the data and samples provided to be used for purposes that include commercial diagnostic product and test development activities. We have measures in place to ensure that data and samples that have been collected by our clinical collaborators are provided to us on a subject de-identified manner. We also have measures in place to ensure that the subjects from whom our data and samples are collected do not retain or have conferred on them any proprietary or commercial rights to the data or any discoveries derived from them. We rely on our clinical collaborators for appropriate compliance with the informed consent provided by each subject and with applicable regulations. A subject’s informed consent could be challenged in the future, and any informed consent could prove invalid, unlawful or otherwise inadequate for our purposes. Any findings against us, or our clinical collaborators, could deny us access to or force us to stop using some of our clinical samples, which would hinder our diagnostic product and test development efforts. We could become involved in legal challenges relating to the validity of one or more informed consents from subjects, which could require substantial dedication of time and financial resources.
If our clinical studies do not prove that our technologies are superior and demonstrate the clinical utility of our technology, we may never commercialize our product candidates and services.
The results of our clinical studies may not show that tests using our cell-free molecular diagnostic technology are superior to existing testing methods and may not demonstrate clinical utility. In that event, we will have to devote significant financial and other resources to further research and development, and commercialization of tests using our technologies will be delayed or may never occur. Our earlier clinical studies were small and included samples from high-risk patients. The results
24
from these earlier studies may not be representative of the results we may obtain from any future studies, including our next two clinical studies, which will include substantially more samples and a larger percentage of normal-risk patients.
We have limited experience in establishing strong business relationships with leading clinical reference laboratories to perform cell-free molecular diagnostic tests using our technologies, which could limit our revenue growth.
A key step in our strategy is to sell diagnostic products that use our proprietary technologies to leading clinical reference laboratories that will perform cell-free molecular diagnostic tests. We have limited experience in establishing these business relationships. If we are unable to establish and maintain these business relationships, we may not be able to generate revenue beyond the revenue we can generate from our limited in-house test processing capabilities.
We depend upon our officers and other key employees, and if we are not able to retain them or recruit additional qualified personnel, the commercialization of our product candidates and any future tests that we develop could be delayed or negatively impacted.
Our success is largely dependent upon the continued contributions of our officers, especially Dr. Antonius Schuh, our Chief Executive Officer, and other key employees. Our success also depends in part on our ability to attract and retain highly qualified scientific, commercial and administrative personnel. The specialized nature of our industry results in an inherent scarcity of experienced personnel in the field and, in order to pursue our test development and commercialization strategies, we will need to attract, hire and retain, or engage as consultants, additional personnel with specialized experience in a number of disciplines, including assay development, bioinformatics and statistics, laboratory and clinical operations, clinical affairs and studies, government regulation, sales and marketing, billing and reimbursement and information systems. Additionally, there is intense competition for personnel in the fields in which we operate. If we are unable to attract new employees and retain existing employees, the development and commercialization of our product candidates and any tests we may develop in the future could be delayed or negatively impacted.
We will need to increase the size of our organization, and we may experience difficulties in managing growth.
We are a small company with 67 full-time employees as of December 31, 2015. Future growth of our company will impose significant additional responsibilities on members of management, including the need to identify, attract, retain, motivate and integrate highly skilled personnel. We may increase the number of employees in the future depending on the progress of our development of cell-free molecular diagnostic technology. Our future financial performance and our ability to commercialize cell-free molecular diagnostic tests and to compete effectively will depend, in part, on our ability to manage any future growth effectively. To that end, we must be able to:
• | manage our clinical studies effectively; |
• | integrate additional management, administrative, manufacturing and regulatory personnel; |
• | maintain sufficient administrative, accounting and management information systems and controls; and |
• | hire and train additional qualified personnel. |
There is no guarantee that we will be able to accomplish these tasks, and our failure to accomplish any of them could materially adversely affect our business, prospects and financial condition.
All of our diagnostic technology and services are performed at a single laboratory, and in the event this facility is affected by a termination of the lease or a man-made or natural disaster, our operations could be severely impaired.
We are performing all of our diagnostic services in our laboratory located in San Diego, California. Despite precautions taken by us, any future natural or man-made disaster at this laboratory, such as a fire, flood, earthquake or terrorist act, could cause substantial delays in our operations, damage or destroy our equipment and urine samples or cause us to incur additional expenses.
In addition, we are leasing the facilities where our laboratory operates. We are currently in compliance with all of our lease obligations, but should the lease terminate for any reason, or if the laboratory is moved due to conditions outside of our control, it could cause substantial delay in our diagnostics operations, damage or destroy our equipment and biological samples or cause us to incur additional expenses. In the event of an extended shutdown of our laboratory, we may be unable to perform
25
our services in a timely manner or at all and therefore would be unable to operate in a commercially competitive manner. This could materially adversely affect our operating results and financial condition.
Further, if we have to use a substitute laboratory while our facility is closed, we could only use another facility with established state licensure and accreditation under CLIA. We may not be able to find another CLIA-certified facility and comply with applicable procedures, or find any such laboratory that would be willing to perform the tests for us on commercially reasonable terms. Additionally, any new laboratory opened by us would be subject to certification under CLIA and licensure by various states, which would take a significant amount of time and expense and result in delays in our ability to continue our personalized medicine services operations.
Security threats to our information technology infrastructure and/or our physical buildings could expose us to liability and damage our reputation and business.
It is essential to our business strategy that our technology and network infrastructure and our physical buildings remain secure and are perceived by our customers and corporate partners to be secure. Despite security measures, however, any network infrastructure may be vulnerable to cyber-attacks by hackers and other security threats. We may face cyber-attacks that attempt to penetrate our network security, sabotage or otherwise disable our research, products and services, misappropriate our or our customers’ and partners’ proprietary information, which may include personally identifiable information, or cause interruptions of our internal systems and services. Despite security measures, we also cannot guarantee security of our physical buildings. Physical building penetration or any cyber-attacks could negatively affect our reputation, damage our network infrastructure and our ability to deploy our products and services, harm our relationship with customers and partners that are affected, and expose us to financial liability.
Additionally, there are a number of state, federal and international laws protecting the privacy and security of health information and personal data. For example, the Health Insurance Portability and Accountability Act, or HIPAA, imposes limitations on the use and disclosure of an individual’s healthcare information by healthcare providers, healthcare clearinghouses, and health insurance plans, or, collectively, covered entities, and also grants individuals rights with respect to their health information. HIPAA also imposes compliance obligations and corresponding penalties for non-compliance on individuals and entities that provide services to healthcare providers and other covered entities. As part of the American Recovery and Reinvestment Act of 2009, or ARRA, the privacy and security provisions of HIPAA were amended. ARRA also made significant increases in the penalties for improper use or disclosure of an individual’s health information under HIPAA and extended enforcement authority to state attorneys general. As amended by ARRA and subsequently by the final omnibus rule adopted in 2013, HIPAA also imposes notification requirements on covered entities in the event that certain health information has been inappropriately accessed or disclosed: notification requirements to individuals, federal regulators, and in some cases, notification to local and national media. Notification is not required under HIPAA if the health information that is improperly used or disclosed is deemed secured in accordance with encryption or other standards developed by the U.S. Department of Health and Human Services. Most states have laws requiring notification of affected individuals and/or state regulators in the event of a breach of personal information, which is a broader class of information than the health information protected by HIPAA. Many state laws impose significant data security requirements, such as encryption or mandatory contractual terms, to ensure ongoing protection of personal information. Activities outside of the U.S. implicate local and national data protection standards, impose additional compliance requirements and generate additional risks of enforcement for non-compliance. We may be required to expend significant capital and other resources to ensure ongoing compliance with applicable privacy and data security laws, to protect against security breaches and hackers or to alleviate problems caused by such breaches.
General economic or business conditions may have a negative impact on our business.
Continuing concerns over U.S. health care reform legislation and energy costs, geopolitical issues, the availability and cost of credit and government stimulus programs in the U.S. and other countries have contributed to increased volatility and diminished expectations for the global economy. If the economic climate does not improve, or if it deteriorates, our business, including our access to patient samples and the addressable market for tests that we may successfully develop, as well as the financial condition of our suppliers and our third-party payors, could be negatively impacted, which could materially adversely affect our business, prospects and financial condition.
We incur significant costs as a result of operating as a public company and our management expects to continue to devote substantial time to public company compliance programs.
As a public company, we incur significant legal, accounting and other expenses due to our compliance with regulations and disclosure obligations applicable to us, including compliance with the Sarbanes-Oxley Act of 2002, or the
26
Sarbanes-Oxley Act, as well as rules implemented by the Securities and Exchange Commission, or the SEC, and The NASDAQ Stock Market LLC. The SEC and other regulators have continued to adopt new rules and regulations and make additional changes to existing regulations that require our compliance. For example, in July 2010, the Dodd-Frank Wall Street Reform and Consumer Protection Act, or the Dodd-Frank Act, was enacted. There is significant corporate governance and executive compensation related provisions in the Dodd-Frank Act that have required the SEC to adopt additional rules and regulations in these areas. Stockholder activism, the current political environment and the current high level of government intervention and regulatory reform may lead to substantial new regulations and disclosure obligations, which may lead to additional compliance costs and impact (in ways we cannot currently anticipate) the manner in which we operate our business. Our management and other personnel devote a substantial amount of time to these compliance programs and monitoring of public company reporting obligations and, as a result of the new corporate governance and executive compensation related rules, regulations and guidelines prompted by the Dodd-Frank Act and further regulations and disclosure obligations expected in the future, we will likely need to devote additional time and costs to comply with such compliance programs and rules. These rules and regulations will continue to cause us to incur significant legal and financial compliance costs and will make some activities more time-consuming and costly.
We may become subject to federal and state tax assessments, penalties and interest with respect to past compensation paid to certain of our executives.
During our internal review process, contingencies were identified regarding various federal and state tax exposures with respect to past compensation paid to certain of our executives. We have not recorded any accrued liabilities related to the potential federal and state tax exposure. If we become subject to any material tax assessment, penalties and interest by federal and state tax authorities in the future, our results of operations, financial performance and cash flows could be materially adversely affected.
Risks Related to Our Regulatory Environment
Our ability to successfully commercialize our technology will depend largely upon the extent to which third-party payors reimburse our current and future tests.
Physicians and patients may decide not to order our products unless third-party payors, such as managed care organizations, as well as government payors such as Medicare and Medicaid, pay a substantial portion of the test price.
Reimbursement by a third-party payor may depend on a number of factors, including a payor’s determination that our product candidates are:
• | not experimental or investigational; |
• | effective; |
• | medically necessary; |
• | appropriate for the specific patient; |
• | cost-effective; |
• | supported by peer-reviewed publications; and |
• | included in clinical practice guidelines. |
Market acceptance, sales of products based upon our cell-free molecular diagnostic technology, and our profitability may depend on reimbursement policies and healthcare reform measures. Several entities conduct technology assessments of medical tests and devices and provide the results of their assessments for informational purposes to other parties. These assessments may be used by third-party payors and healthcare providers as grounds to deny coverage for a test or procedure. The levels at which government authorities and third-party payors, such as private health insurers and health maintenance organizations, may reimburse the price patients pay for such products could affect whether we are able to commercialize our product candidates. Our product candidates may receive negative assessments that may impact our ability to receive reimbursement for our current and future tests. Since each payor makes its own decision as to whether to establish a policy to reimburse a test, seeking these approvals may be a time-consuming and costly process. We cannot be sure that reimbursement
27
in the U.S. or elsewhere will be available for any of our product candidates in the future. If reimbursement is not available or is limited, we may not be able to commercialize our product candidates.
In addition, if we are unable to obtain reimbursement approval from private payors and Medicare and Medicaid programs for our product candidates, or if the amount reimbursed is inadequate, our ability to generate revenues could be limited. Even if we are able to obtain reimbursement for our tests, insurers may withdraw their coverage policies or cancel their contracts with us at any time, stop paying for our tests or reduce the payment rate for our tests, each of which would reduce our revenue. Moreover, we may depend upon a limited number of third-party payors for a significant portion of our test revenues and if these or other third-party payors stop providing reimbursement or decrease the amount of reimbursement for our tests, our revenues could decline.
If we do not receive regulatory approvals, we may not be able to develop and commercialize our cell-free molecular diagnostic technology.
We may need approval from the U.S. Food and Drug Administration, or the FDA, to market products based on our cell-free molecular diagnostic technology for diagnostic uses in the U.S. and approvals from foreign regulatory authorities to market products based on our cell-free molecular diagnostic technology outside the U.S. We have not yet filed an application with the FDA to obtain approval to market any of our proposed products. If we fail to obtain regulatory approval for the marketing of products based on our cell-free molecular diagnostic technology, we will be unable to sell such product candidates and will not be able to sustain operations.
We believe the estimated molecular diagnostics market for many diseases in Europe is approximately as large as that of the U.S. If we seek to market products or services such as a urine-based Human Papillomavirus, or HPV, high-risk, or HR, Detection test in Europe, we will need to receive a CE Mark. If we do not obtain a CE Mark for our urine-based HPV HR Detection test, we will be unable to sell this product candidate in Europe and countries that recognize the CE Mark.
The regulatory review and approval process, which may include evaluation of preclinical studies and clinical studies of product candidates based on our cell-free molecular diagnostic technology, as well as the evaluation of manufacturing processes and contract manufacturers’ facilities, is lengthy, expensive and uncertain. Securing regulatory approval for products based on our cell-free molecular diagnostic technology may require the submission of extensive preclinical and clinical data and supporting information to regulatory authorities to establish such product candidates’ safety and effectiveness for each indication. We have limited experience in filing and pursuing applications necessary to gain regulatory approvals.
Regulatory authorities generally have substantial discretion in the approval process and may either refuse to accept one or more of our applications or may decide after review of an application that the data submitted is insufficient to allow for approval of any product based upon our cell-free molecular diagnostic technology. If regulatory authorities do not accept or approve our applications, they may require that we conduct additional preclinical, clinical or manufacturing studies and submit that data before regulatory authorities will reconsider such application. We may need to expend substantial resources to conduct further studies to obtain data that regulatory authorities believe is sufficient. Depending on the extent of these studies, approval of applications may be delayed by several years or may require us to expend substantially more resources than we had budgeted for such applications. It is also possible that additional studies may not suffice in helping us obtain approval of our applications. If any of these outcomes occur, we may be forced to abandon our applications for approval, which may force us to cease or curtail operations.
If we do not comply with governmental regulations applicable to our Clinical Laboratory Improvement Amendments, or CLIA, certified laboratory, we may not be able to continue our operations.
The establishment and operation of our laboratory is subject to regulation by numerous federal, state and local governmental authorities in the U.S. Our laboratory holds a CLIA certificate of compliance and is licensed by every state (other than the State of New York) and the District of Columbia, as required, which enables us to provide testing services to residents of almost every state. Failure to comply with state regulations or changes in state regulatory requirements could result in a substantial curtailment or even prohibition of the operations of our laboratory and could materially adversely affect our business. CLIA is a federal law that regulates clinical laboratories that perform testing on human specimens for the purpose of providing information for the diagnosis, prevention or treatment of disease. To renew CLIA certification, laboratories are subject to survey and inspection every two years. Moreover, CLIA inspectors may make unannounced inspections of these laboratories. If we were to lose our CLIA certification or our state licenses, whether as a result of a revocation, suspension or limitation of our license, we would no longer be able to continue our testing operations, which would materially adversely affect our business, prospects and financial condition. Potential sanctions for violations of these statutes and regulations also
28
include significant fines, the suspension or loss of various licenses, certificates and authorizations, or product suspension or recalls.
If we use biological and hazardous materials in a manner that causes injury, we could be liable for damages.
Our activities currently require the controlled use of potentially harmful biological materials and chemicals. We cannot eliminate the risk of accidental contamination or injury to employees or third parties from the use, storage, handling or disposal of these materials. In the event of contamination or injury, we could be held liable for any resulting damages, and any liability could exceed our resources or any applicable insurance coverage we may have. Additionally, we are subject to, on an ongoing basis, federal, state and local laws and regulations governing the use, storage, handling and disposal of these materials and specified waste products. The cost of compliance with these laws and regulations may become significant and could materially adversely affect our business, prospects and financial condition. Moreover, in the event of an accident or if we otherwise fail to comply with applicable regulations, we could lose our permits or approvals or be held liable for damages or penalized with fines.
Changes in healthcare policy could subject us to additional regulatory requirements that may delay the commercialization of our tests and increase our costs.
The U.S. government and other governments have shown significant interest in pursuing healthcare reform. Any government-adopted reform measures could adversely impact the pricing of our diagnostic products and tests in the U.S. or internationally and the amount of reimbursement available from governmental agencies or other third party payors. The continuing efforts of the U.S. and foreign governments, insurance companies, managed care organizations and other payors of healthcare services to contain or reduce healthcare costs may adversely affect our ability to set prices for our products and services that we believe are fair, which may impact our ability to generate revenues and achieve and maintain profitability.
New laws, regulations and judicial decisions, or new interpretations of existing laws, regulations and judicial decisions, that relate to healthcare availability, methods of delivery or payment for products and services, or sales, marketing or pricing, may limit our potential revenue or force us to revise our research and development programs. The pricing and reimbursement environment may change in the future and become more challenging due to several reasons, including policies advanced by the current executive administration in the U.S., new healthcare legislation or fiscal challenges faced by government health administration authorities. Specifically, in both the U.S. and certain foreign jurisdictions, there have been a number of legislative and regulatory proposals to change the healthcare system in ways that could affect our ability to sell our products profitably.
For example, the Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act, or the PPACA, has substantially changed the way healthcare is financed by both government health plans and private insurers. The PPACA contains a number of provisions that are expected to impact our business and operations in ways that may negatively affect our revenues in the future. While it is too early to predict all the specific effects the PPACA or any future healthcare reform legislation will have on our business, such provisions could materially adversely affect our business, prospects and financial condition.
The Food and Drug Administration Amendments Act of 2007 gives the FDA enhanced post-marketing authority, including the authority to require post-marketing studies and clinical studies of products, labeling changes based on new safety information, and compliance with risk evaluations and mitigation strategies approved by the FDA. The FDA’s exercise of this authority could result in delays or increased costs during product development, clinical studies and regulatory review, increased costs to assure compliance with post-approval regulatory requirements, and potential restrictions on the sale and/or distribution of approved products, all of which could materially adversely affect our business, prospects and financial condition.
If the FDA were to begin regulating laboratory developed tests, or LDTs, or if we decide to market our product candidates as a medical device rather than a LDT, we could be forced to delay commercialization of our current product candidates, experience significant delays in commercializing any future tests, incur substantial costs and time delays associated with meeting requirements for pre-market clearance or approval and/or experience decreased demand for or reimbursement of our test.
We intend to develop products that are considered to be medical devices and are subject to federal regulations, including, but not limited to, those covering the FDA’s Quality System Regulation, or QSR, and Medical Device Reporting, or MDR.
29
The QSR includes requirements related to the methods used in and the facilities and controls used for designing, purchasing, manufacturing, packaging, labeling, storing, installing and servicing of medical devices. Manufacturing facilities undergo FDA inspections to assure compliance with the QSR. The quality systems for FDA-regulated products are known as current good manufacturing practices, or cGMPs, as described in the Code of Federal Regulations, part 820 (21 CFR part 820). Among the cGMP requirements are those requiring manufacturers to have sufficient appropriate personnel to implement required design controls and other portions of the QSR guidelines.
Design controls include procedures that describe the product design requirements (design goals) and compare actual output to these requirements, including documented Design Reviews. Required Design History Files, or DHFs, for each device will document the records necessary to demonstrate that the design was developed in accordance with the approved design plan and the requirements of the QSR.
The QSR also includes stipulation for control of all documents used in design and production, including history of any changes made. Production and process controls include stipulations to ensure products are in fact produced as specified by controlled documents resulting from the controlled design phase, using products and services purchased under controlled purchasing procedures.
Incidents in which a device may have caused or contributed to a death or serious injury must be reported to the FDA under the MDR program. In addition, certain malfunctions must also be reported. The MDR regulation is a mechanism for the FDA and manufacturers to identify and monitor significant adverse events involving medical devices. The goals of the MDR regulation are to detect and correct problems in a timely manner.
We are subject to MDR through two routes. As a manufacturer of products for sale within the U.S., we are required to report to the FDA any deaths, serious injuries, malfunctions or events requiring remedial action to prevent an unreasonable risk of substantial harm to the public health. Our CLIA laboratory, which offers services for sale, is already currently required to report suspected medical device related deaths to both the FDA and the relevant manufacturers of products we purchase and use.
Clinical laboratory tests like our current product offerings are regulated in the U.S. under CLIA as well as by applicable state laws. Diagnostic kits that are sold and distributed through interstate commerce are regulated as medical devices by the FDA. Clinical laboratory tests that are developed and validated by a laboratory for its own use are called LDTs. Most LDTs currently are not subject to FDA regulation, although reagents or software provided by third parties and used to perform LDTs may be subject to regulation. We expect that, upon the commencement of commercialization, our product candidates will be an LDT and not a diagnostic kit. As a result, we believe that our product candidates should not be subject to regulation under current FDA policies; however, there is no assurance that our product candidates will not be subject to such regulation in the future. If we decide to market our product candidates as a diagnostic kit rather than as a LDT, our products would be subject to FDA regulation as a medical device. Further, the container we expect to provide for collection and transport of tumor samples from a pathology laboratory to our clinical reference laboratory may be a medical device subject to FDA regulation, and while we expect that it will be exempt from pre-market review by the FDA, there is no certainty in that respect.
We cannot provide any assurance that FDA regulation, including pre-market review, will not be required in the future for our LDT product candidates, either through new policies adopted by the FDA or new legislation enacted by Congress. It is possible that legislation that results in increased regulatory burdens for us to offer or continue to offer our product as a clinical laboratory service will be signed into law, which could materially adversely affect our business, prospects and financial condition.
If pre-market review is required, our business could be negatively impacted until such review is completed and clearance to market or approval is obtained, and the FDA could require that we stop selling our product. If pre-market review of our LDTs is required by the FDA, there can be no assurance that our product offerings will be cleared or approved on a timely basis, if at all. Ongoing compliance with FDA regulations, such as the QSR and MDR, would increase the cost of conducting our business and subject us to inspection by the FDA and penalties for failure to comply with these requirements. We may also decide voluntarily to pursue FDA pre-market review of our product offerings if we determine that doing so would be appropriate. Some competitors may develop competing tests cleared for marketing by the FDA. There may be a marketing differentiation or perception that an FDA-cleared test is more desirable than our product offerings, and that could discourage adoption and reimbursement of our test.
We may be required to conduct clinical studies and we may find it difficult to enroll patients in such clinical studies, which could delay or prevent clinical studies of our product candidates.
30
If the FDA decides to regulate our LDTs, it may require that we conduct extensive pre-market clinical studies prior to submitting a regulatory application for commercial sales. If we are required to conduct pre-market clinical studies, whether using retrospectively collected and banked samples or prospectively collected samples, delays in the commencement or completion of clinical studies could significantly increase our test development costs and delay commercialization. Many of the factors that may cause or lead to a delay in the commencement or completion of clinical studies may also ultimately lead to delay or denial of regulatory clearance or approval. The commencement and completion of clinical trials may be delayed by factors such as unforeseen safety issues, lack of effectiveness during clinical trials, inability to monitor patients adequately during or after testing and slower than expected rates of patient recruitment.
Insufficient patient enrollment is a function of many factors, including the size of the patient population, the nature of the protocol, the proximity of patients to clinical sites and the eligibility criteria for the clinical trial. We may find it necessary to engage contract research organizations to perform data collection and analysis and other aspects of our clinical studies, which may increase the cost of the studies. We will also depend on clinical investigators, medical institutions and contract research organizations to perform the studies properly. If these parties do not successfully carry out their contractual duties or obligations or meet expected deadlines, or if the quality, completeness or accuracy of the clinical data they obtain is compromised due to failure to adhere to our clinical protocols or FDA requirements, or for other reasons, our clinical studies may have to be extended, delayed or terminated. Many of these factors could be beyond our control. We may not be able to enter into replacement arrangements without undue delays or considerable expenditures. If there are delays in testing as a result of the failure to perform by third parties, our research and development costs would increase and we may not be able to obtain regulatory clearance or approval for our test. In addition, we may not be able to establish or maintain relationships with these parties on favorable terms, if at all. Each of these outcomes would harm our ability to market our test or to become profitable.
In addition, in the event we are required to conduct clinical trials, it may be very expensive and difficult to design and implement clinical trials due to the rigorous regulatory requirements to which clinical trials are subject. Clinical trials are also time consuming and there is no certainty as to when we may be able to complete the clinical trial process.
The testing, manufacturing and marketing of medical diagnostic devices entails an inherent risk of product liability and personal injury claims.
To date, we have experienced no product liability or personal injury claims, but any such claims arising in the future could materially adversely affect our business, prospects and financial condition. Potential product liability or personal injury claims may exceed the amount of our insurance coverage or may be excluded from coverage under the terms of our policy or limited by other claims under our umbrella insurance policy. Additionally, we may not be able to renew our existing insurance at a cost and level of coverage comparable to that presently in effect, if at all. In the event that we are held liable for a claim against which we are not insured or for damages exceeding the limits of our insurance coverage, such claim could negatively impact our cash flow and materially adversely affect our business, prospects and financial condition.
Some of our activities may subject us to risks under federal and state laws prohibiting “kickbacks” and false or fraudulent claims.
In addition to FDA marketing restrictions, several other types of state and federal healthcare fraud and abuse laws have been applied in recent years to restrict certain marketing practices in the healthcare product and service industry and to regulate billing practices and financial relationships with physicians, hospitals and other healthcare providers. These laws include the Federal False Claims Act and the Anti-Kickback Statute and several similar state laws, which prohibit payments intended to induce physicians or others to refer patients or to acquire or arrange for or recommend the acquisition of healthcare products or services. While the federal law applies only to referrals, products or services for which payment may be made by a federal healthcare program, state laws often apply regardless of whether federal funds may be involved. These laws constrain the sales, marketing and other promotional activities of manufacturers of medical devices and providers of laboratory services by limiting the kinds of financial arrangements, including sales programs, that may be used with hospitals, physicians, laboratories and other potential purchasers or prescribers of medical devices and laboratory services. Other federal and state laws generally prohibit individuals or entities from knowingly presenting, or causing to be presented, claims for payment from Medicare, Medicaid or other third-party payors that are false or fraudulent, or are for items or services that were not provided as claimed. Anti-kickback and false claims laws prescribe civil and criminal penalties (including fines) for noncompliance that can be substantial. Interpretations of the applicability of these laws to marketing and billing practices is constantly evolving and even an unsuccessful challenge could cause adverse publicity and be costly to respond to, and therefore could materially adversely affect our business, prospects and financial condition. Our failure to comply with applicable laws could result in various adverse consequences which could harm our business, including the exclusion of our products and services from government programs and the imposition of civil or criminal sanctions.
31
Our business could be adversely impacted by adoption of new coding for molecular genetic tests.
If our technology were commercially available today, reimbursement would be available under the current procedural terminology, or CPT, codes, for molecular-based testing. The American Medical Association CPT® Editorial Panel is continuing its process of establishing analyte specific billing codes to replace codes that describe procedures used in performing molecular testing. The adoption of analyte specific codes will allow payors to better determine tests being performed. This could lead to limited coverage decisions or payment denials for our product candidates or products we may develop in the future, which could materially adversely affect our business, prospects and financial condition.
Risks Related to Our Intellectual Property
If we are unable to protect our intellectual property effectively, we may be unable to prevent third parties from using our technologies, which would impair our competitive advantage.
We rely on patent protection as well as a combination of trademark, copyright and trade secret protection, and other contractual restrictions, to protect our proprietary technologies, all of which provide limited protection and may not adequately protect our rights or permit us to gain or keep any competitive advantage. We may not be successful in defending challenges made in connection with our patents and patent applications. If we fail to protect our intellectual property, we will be unable to prevent third parties from using our technologies and they will be able to compete more effectively against us.
In addition to our patents, we rely on contractual restrictions to protect our proprietary technology. We require our employees and third parties to sign confidentiality agreements and our employees are also required to sign agreements assigning to us all intellectual property arising from their work for us. Nevertheless, we cannot guarantee that these measures will be effective in protecting our intellectual property rights. Any failure to protect our intellectual property rights could materially adversely affect our business, prospects and financial condition.
Our currently pending or future patent applications may not result in issued patents and any patents issued to us may be challenged, invalidated or held unenforceable. Furthermore, we cannot be certain that we were the first to make the invention claimed in our issued patents or pending patent applications in the U.S., or that we were the first to file for protection of the inventions claimed in our foreign issued patents or pending patent applications. In addition, there are numerous recent changes to the patent laws and proposed changes to the rules of the U.S. Patent and Trademark Office, or the PTO, which may have a significant impact on our ability to protect our technology and enforce our intellectual property rights. For example, in September 2011, the U.S. enacted sweeping changes to the U.S. patent system under the Leahy-Smith America Invents Act, including changes that would transition the U.S. from a “first-to-invent” system to a “first-to-file” system and alter the processes for challenging issued patents. These changes could increase the uncertainties and costs surrounding the prosecution of our patent applications and the enforcement or defense of our issued patents. In addition, we may become subject to interference proceedings conducted in the patent and trademark offices of various countries to determine our entitlement to patents, and these proceedings may conclude that other patents or patent applications have priority over our patents or patent applications. It is also possible that a competitor may successfully challenge our patents through various proceedings and those challenges may result in the elimination or narrowing of our patents, and therefore reduce our patent protection. Accordingly, rights under any of our issued patents, patent applications or future patents may not provide us with commercially meaningful protection for our products or afford us a commercial advantage against our competitors or their competitive products or processes.
The patents issued to us may not be broad enough to provide any meaningful protection, one or more of our competitors may develop more effective technologies, designs or methods without infringing our intellectual property rights and one or more of our competitors may design around our proprietary technologies.
If we are not able to protect our proprietary technology, trade secrets and know-how, our competitors may use our inventions to develop competing products. We own certain patents relating to our cell-free molecular diagnostic technology. However, these patents may not protect us against our competitors, and patent litigation is very expensive. We may not have sufficient cash available to pursue any patent litigation to its conclusion because we currently do not generate revenues other than licensing, milestone and royalty income.
We cannot rely solely on our current patents to be successful. The standards that the PTO and foreign patent offices use to grant patents, and the standards that U.S. and foreign courts use to interpret patents, are not the same, are not always applied predictably or uniformly and can change, particularly as new technologies develop. As such, the degree of patent protection obtained in the U.S. may differ substantially from that obtained in various foreign countries. In some instances, patents have been issued in the U.S. while substantially less or no protection has been obtained in Europe or other countries.
32
We cannot be certain of the level of protection, if any, that will be provided by our patents if they are challenged in court, where our competitors may raise defenses such as invalidity, unenforceability or possession of a valid license. In addition, the type and extent of any patent claims that may be issued to us in the future are uncertain. Any patents that are issued may not contain claims that will permit us to stop competitors from using similar technology.
We may incur substantial costs as a result of litigation or other proceedings relating to patent and other intellectual property rights and we may be unable to protect our rights to, or use, our cell-free molecular diagnostic technology.
Third parties may challenge the validity of our patents and other intellectual property rights, resulting in costly litigation or other time-consuming and expensive proceedings, which could deprive us of valuable rights. If we become involved in any intellectual property litigation, interference or other judicial or administrative proceedings, we will incur substantial expenses and the attention of our technical and management personnel will be diverted. An adverse determination may subject us to significant liabilities or require us to seek licenses that may not be available from third parties on commercially favorable terms, if at all. Further, if such claims are proven valid, through litigation or otherwise, we may be required to pay substantial monetary damages, which can be tripled if the infringement is deemed willful, or be required to discontinue or significantly delay development, marketing, selling and licensing of the affected products and intellectual property rights. In our European patent that covers using microRNAs to detect in vivo cell death, an anonymous third party has recently filed an opposition against the claims in the patent. Oppositions against the patentability of claims in a European patent are considered by a panel of examiners at the European Patent Office, and we are considering the full range of options available for defending against the opposition.
Our competitors may have filed, and may in the future file, patent applications covering technology similar to ours. Any such patent application may have priority over our patent applications and could further require us to obtain rights to issued patents covering such technologies. There may be third-party patents, patent applications and other intellectual property relevant to our potential products that may block or compete with our potential products or processes. If another party has filed a U.S. patent application on inventions similar to ours, we may have to participate in an interference proceeding declared by the PTO to determine priority of invention in the U.S. The costs of these proceedings could be substantial, and it is possible that such efforts would be unsuccessful, resulting in a loss of our U.S. patent position with respect to such inventions. In addition, we cannot assure you that we would prevail in any of these suits or that the damages or other remedies that we are ordered to pay, if any, would not be substantial. Claims of intellectual property infringement may require us to enter into royalty or license agreements with third parties that may not be available on acceptable terms, if at all. We may also be subject to injunctions against the further development and use of our technology, which could materially adversely affect our business, prospects and financial condition.
Some of our competitors may be able to sustain the costs of complex patent litigation more effectively than we can because they have substantially greater resources. In addition, any uncertainties resulting from the initiation and continuation of any litigation could materially adversely affect our ability to raise the funds necessary to continue our operations.
Risks Related to Ownership of Our Common Stock
If we discover material weaknesses and other deficiencies in our internal control and accounting procedures, our stock price could decline significantly and raising capital could be more difficult.
If we fail to comply with the rules under the Sarbanes-Oxley Act, related to disclosure controls and procedures, or if we discover additional material weaknesses and other deficiencies in our internal control and accounting procedures, our stock price could decline significantly and raising capital could be more difficult. Moreover, effective internal controls are necessary for us to produce reliable financial reports and are important in helping prevent financial fraud. If we cannot provide reliable financial reports or prevent fraud, our business and operating results could be harmed, investors could lose confidence in our reported financial information, and the trading price of our common stock could drop significantly. We previously identified a material weakness in our internal control over financial reporting as of December 31, 2012, which was remedied in the year ended December 31, 2013. We cannot be certain that additional material weaknesses or significant deficiencies in our internal controls will not be discovered in the future.
The rights of the holders of our common stock may be impaired by the potential issuance of preferred stock.
Our certificate of incorporation gives our board of directors the right to create one or more new series of preferred stock. As a result, the board of directors may, without stockholder approval, issue preferred stock with voting, dividend, conversion, liquidation or other rights that could adversely affect the voting power and equity interests of the holders of our
33
common stock. Preferred stock, which could be issued with the right to more than one vote per share, could be used to discourage, delay or prevent a change of control of our company, which could materially adversely affect the price of our common stock. Without the consent of the holders of the outstanding shares of our Series A Convertible Preferred Stock, we may not adversely alter or change the rights of the holders of the Series A Convertible Preferred Stock or increase the number of authorized shares of Series A Convertible Preferred Stock, create a class of stock that is senior to or on parity with the Series A Convertible Preferred Stock, amend our certificate of incorporation in breach of these provisions or agree to any of the foregoing.
Our common stock price may be volatile and could fluctuate widely in price, which could result in substantial losses for investors.
The market price of our common stock historically has been, and we expect will continue to be, subject to significant fluctuations over short periods of time. For example, during the year ended December 31, 2015, the closing price of our common stock ranged from a low of $4.21 to a high of $13.58. These fluctuations may be due to various factors, many of which are beyond our control, including:
• | technological innovations or new products and services introduced by us or our competitors; |
• | clinical trial results relating to our tests or those of our competitors; |
• | announcements or press releases relating to the industry or to our own business or prospects; |
• | coverage and reimbursement decisions by third party payors, such as Medicare and other managed care organizations; |
• | regulation and oversight of our product candidates and services, including by the FDA, Centers for Medicare & Medicaid Services and comparable foreign agencies; |
• | the establishment of partnerships with clinical reference laboratories; |
• | healthcare legislation; |
• | intellectual property disputes; |
• | additions or departures of key personnel; |
• | sales of our common stock; |
• | our ability to integrate operations, technology, products and services; |
• | our ability to execute our business plan; |
• | operating results below expectations; |
• | loss of any strategic relationship; |
• | industry developments; |
• | economic and other external factors; and |
• | period-to-period fluctuations in our financial results. |
In addition, market fluctuations, as well as general political and economic conditions, could materially adversely affect the market price of our securities. Because we are a development stage company with no revenue from operations to date, other than licensing, milestone and royalty income, you should consider any one of these factors to be material. Our stock price may fluctuate widely as a result of any of the foregoing.
Because certain of our stockholders control a significant number of shares of our common stock, they may have effective control over actions requiring stockholder approval.
34
As of December 31, 2015, our directors, executive officers and principal stockholders, and their respective affiliates, beneficially owned approximately 33.4% of our outstanding shares of common stock. As a result, these stockholders, acting together, would have the ability to control the outcome of matters submitted to our stockholders for approval, including the election of directors and any merger, consolidation or sale of all or substantially all of our assets. In addition, these stockholders, acting together, would have the ability to control the management and affairs of our company. Accordingly, this concentration of ownership may harm the market price of our common stock by:
• | delaying, deferring or preventing a change in control of our company; |
• | impeding a merger, consolidation, takeover or other business combination involving us; or |
• | discouraging a potential acquirer from making a tender offer or otherwise attempting to obtain control of us. |
We have not paid dividends on our common stock in the past and do not expect to pay dividends on our common stock for the foreseeable future. Any return on investment may be limited to the value of our common stock.
We have never paid any cash dividends on our common stock. We expect that any income received from operations will be devoted to our future operations and growth. We do not expect to pay cash dividends on our common stock in the near future. Payment of dividends would depend upon our profitability at the time, cash available for those dividends, and other factors that our board of directors may consider relevant. If we do not pay dividends, our common stock may be less valuable because a return on an investor’s investment will only occur if our stock price appreciates. In addition, under the terms of our Loan and Security Agreement and the Equipment Line of Credit, we are precluded from paying cash dividends without the prior written consent of the Lenders, and the terms of the Series A Convertible Preferred Stock prohibit us from paying dividends to the holders of our common stock so long as any dividends due on the Series A Convertible Preferred Stock remain unpaid. Investors in our common stock should not rely on an investment in our company if they require dividend income.
If securities or industry analysts do not publish research or reports about our business, or if they adversely change their recommendations regarding our stock, our stock price and trading volume could decline.
The trading market for our common stock will be influenced by the research and reports that industry or securities analysts publish about us or our business. If one or more of the analysts who cover us downgrade our stock or publish inaccurate or unfavorable research about our business, our stock price would likely decline. In addition, if our operating results fail to meet the forecast of analysts, our stock price would likely decline. If one or more of these analysts cease coverage of our company or fail to publish reports on us regularly, we could lose visibility in the financial markets, which in turn could cause our stock price or trading volume to decline.
Delaware law and our corporate charter and bylaws contain anti-takeover provisions that could delay or discourage takeover attempts that stockholders may consider favorable.
Provisions in our certificate of incorporation and bylaws may have the effect of delaying or preventing a change of control of our company or changes in our management. For example, our board of directors has the authority to issue up to 20,000,000 shares of preferred stock in one or more series and to fix the powers, preferences and rights of each series without stockholder approval. The ability to issue preferred stock could discourage unsolicited acquisition proposals or make it more difficult for a third party to gain control of our company, or otherwise could materially adversely affect the market price of our common stock.
Furthermore, because we are incorporated in Delaware, we are governed by the provisions of Section 203 of the General Corporation Law of the State of Delaware. This provision may prohibit or restrict large stockholders, in particular those owning 15% or more of our outstanding voting stock, from merging or combining with us, which could discourage potential takeover attempts, reduce the price that investors may be willing to pay for shares of our common stock in the future and result in our market price being lower than it would without these provisions.
A sale of a substantial number of shares of our common stock may cause the price of our common stock to decline and may impair our ability to raise capital in the future.
Our common stock is traded on The NASDAQ Capital Market and could be considered “thinly-traded,” meaning that the number of investors interested in purchasing our common stock at or near bid prices at any given time may be relatively small or non-existent. Finance transactions resulting in a large amount of newly issued shares that become readily tradable, or
35
other events that cause current stockholders to sell shares, could place downward pressure on the trading price of our common stock. In addition, the lack of a robust resale market may require a stockholder who desires to sell a large number of shares of common stock to sell the shares in increments over time to mitigate any adverse impact of the sales on the market price of our stock.
If our stockholders sell, or the market perceives that our stockholders may sell for various reasons, including the ending of restriction on resale, substantial amounts of our common stock in the public market, including shares issued upon the exercise of outstanding options or warrants, the market price of our common stock could fall. Sales of a substantial number of shares of our common stock may make it more difficult for us to sell equity or equity-related securities in the future at a time and price that we deem reasonable or appropriate.
We may be subject to stockholder litigation, thereby diverting our resources, which could materially adversely affect our profitability and results of operations.
The market for our common stock is characterized by significant price volatility, and we expect that our share price will continue to be at least as volatile for the indefinite future. In the past, plaintiffs have often initiated securities class action litigation against a company following periods of volatility in the market price for its securities. In addition, stockholders may bring actions against companies relating to past transactions or other matters. Any such actions could give rise to substantial damages and thereby materially adversely affect our consolidated financial position, liquidity or results of operations. Even if an action is not resolved against us, the uncertainty and expense associated with stockholder actions could materially adversely affect our business, prospects and financial condition. Litigation can be costly, time-consuming and disruptive to business operations. The defense of lawsuits could also result in diversion of our management’s time and attention away from business operations, which could harm our business.
ITEM 1B. UNRESOLVED STAFF COMMENTS
None.
ITEM 2. PROPERTIES
We currently lease approximately 22,600 square feet of laboratory and office space for our headquarters in San Diego, California under a lease agreement that expires in December 2021. In November 2015, we also entered into a lease agreement pursuant to which we will lease approximately 2,300 square feet of office space in Torino, Italy. The lease agreement commenced on January 1, 2016 and expires on December 31, 2018. We believe that our facilities are adequate for our needs for the immediate future and that, should it be needed, suitable additional space will be available to accommodate expansion of our operations on commercially reasonable terms.
ITEM 3. LEGAL PROCEEDINGS
From time to time, we may become involved in litigation relating to claims arising out of its operations in the normal course of business. We are not involved in any pending legal proceeding or litigation and, to the best of our knowledge, no governmental authority is contemplating any proceeding to which we are a party or to which any of our properties is subject, which would reasonably be likely to have a material adverse effect on us.
ITEM 4. MINE SAFETY DISCLOSURES
Not applicable.
PART II
ITEM 5. MARKET FOR REGISTRANT’S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES
Our common stock has traded on the NASDAQ Capital Market (“NASDAQ”) under the symbol “TROV” since May 30, 2012.
Our common stock was traded over the counter on the pink sheets under the symbol TROV.PK from June 15, 2007 until May29, 2012. From July 27, 2004 until June 14, 2007, our common stock was quoted on the OTC Bulletin Board under the symbol “XNOM.OB”. Prior to July 27, 2004, our common stock was quoted on the OTC Bulletin Board under the symbol
36
“UKAR.OB”, but never traded. The following table sets forth the range of high and low per share sales prices of our common stock during the periods indicated, as reported on NASDAQ.
2015 | 2014 | |||||||||||||||
High | Low | High | Low | |||||||||||||
First Quarter | $ | 8.04 | $ | 4.33 | $ | 6.74 | $ | 5.13 | ||||||||
Second Quarter | $ | 13.58 | $ | 6.50 | $ | 6.01 | $ | 3.50 | ||||||||
Third Quarter | $ | 10.46 | $ | 4.85 | $ | 6.30 | $ | 3.00 | ||||||||
Fourth Quarter | $ | 7.18 | $ | 4.21 | $ | 5.17 | $ | 4.01 | ||||||||
The closing price of our common stock on NASDAQ on February 29, 2016 was $5.15 per share.
Number of Stockholders
As of February 29, 2016, we had approximately 59 stockholders of record of our common stock.
Dividend Policy
Historically, we have not paid any dividends to the holders of shares of our common stock and we do not expect to pay any such dividends in the foreseeable future as we expect to retain our future earnings for use in the operation and expansion of our business. Pursuant to the terms of our outstanding shares of Series A Convertible Preferred Stock, dividends cannot be paid to the holders of shares of our common stock so long as any dividends due on the Series A Convertible Preferred Stock remain unpaid.
Corporate Performance Graph
The following corporate performance graph and related information shall not be deemed “soliciting material” or to be “filed” with the Securities and Exchange Commission, nor shall such information be incorporated by reference into any future filing under the Securities Act of 1933, as amended, or the Securities Exchange Act of 1934, as amended, except to the extent that we specifically incorporate it by reference into such filing.
The following corporate performance graph compares our total stockholder returns from May 30, 2012 through December 31, 2015 against the NASDAQ Stock Market (U.S.), the NASDAQ Pharmaceutical Index and the Russell 3000 Index, assuming a $100 investment made on May 30, 2012. Each of the comparative measures of cumulative total return assumes reinvestment of dividends. The corporate performance shown on the graph below is not necessarily indicative of future price performance.
37
COMPARISON OF CUMULATIVE TOTAL RETURN
Among the NASDAQ Stock Market (U.S.),
The NASDAQ Pharmaceutical Index, the Russell 3000 Index
and Trovagene, Inc.
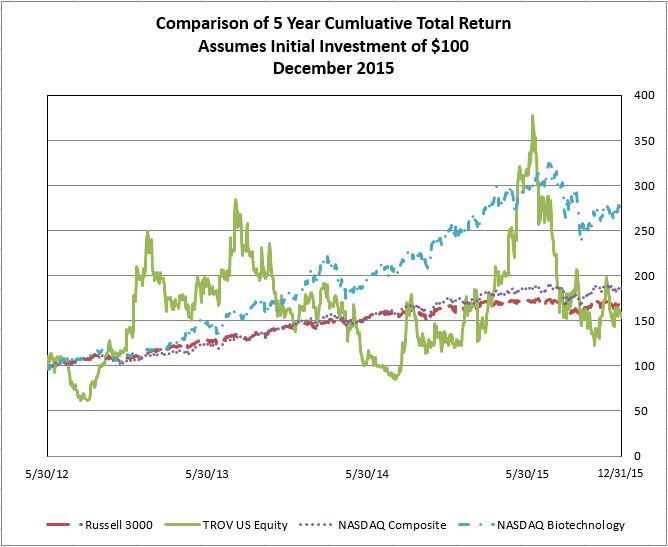
ITEM 6. SELECTED FINANCIAL DATA
The following tables set forth our selected consolidated financial data and have been derived from our audited consolidated financial statements. Consolidated balance sheets as of December 31, 2015 and 2014, as well as consolidated statements of operations for the years ended December 31, 2015, 2014, and 2013, and the reports thereon are included elsewhere in this Annual Report on Form 10-K. The information should be read in conjunction with our audited consolidated financial statements and the notes to such statements, included below in Item 8 “Financial Statements and Supplementary Data”, and “Management’s Discussion and Analysis of Financial Condition and Results of Operations” included in Item 7. Historical results are not necessarily indicative of the results to be expected in the future.
38
Year ended December 31, | ||||||||||||||||||||
2015 | 2014 | 2013 | 2012 | 2011 | ||||||||||||||||
(in thousands, except for share and per share data) | ||||||||||||||||||||
Consolidated Statement of Operations Data: | ||||||||||||||||||||
Revenues | $ | 313 | $ | 280 | $ | 259 | $ | 450 | $ | 258 | ||||||||||
Costs and Expenses: | ||||||||||||||||||||
Cost of revenues | 629 | 15 | — | — | — | |||||||||||||||
Research and development | 10,594 | 6,665 | 3,948 | 1,920 | 911 | |||||||||||||||
Selling and marketing | 6,444 | 2,735 | 1,530 | 506 | — | |||||||||||||||
General and administrative | 7,920 | 5,810 | 5,472 | 2,873 | 2,324 | |||||||||||||||
Total operating expenses | 25,587 | 15,225 | 10,950 | 5,299 | 3,235 | |||||||||||||||
Loss from operations | (25,274 | ) | (14,945 | ) | (10,691 | ) | (4,849 | ) | (2,977 | ) | ||||||||||
Other (income) loss, net | (3 | ) | 25 | (23 | ) | 4 | — | |||||||||||||
Net interest expense | (1,468 | ) | (831 | ) | (13 | ) | — | (56 | ) | |||||||||||
Gain (loss) on change in fair value of derivative instruments-warrants | (726 | ) | 1,426 | (1,084 | ) | (6,721 | ) | 171 | ||||||||||||
Gain on extinguishment of debt | — | — | — | — | 623 | |||||||||||||||
Net loss and comprehensive loss | (27,471 | ) | (14,325 | ) | (11,811 | ) | (11,566 | ) | (2,239 | ) | ||||||||||
Preferred stock dividends | (24 | ) | (23 | ) | (30 | ) | (38 | ) | (38 | ) | ||||||||||
Net loss and comprehensive loss attributable to common stockholders | $ | (27,495 | ) | $ | (14,348 | ) | $ | (11,841 | ) | $ | (11,604 | ) | $ | (2,277 | ) | |||||
Net loss per common share - basic | $ | (1.05 | ) | $ | (0.76 | ) | $ | (0.70 | ) | $ | (0.89 | ) | $ | (0.23 | ) | |||||
Net loss per common share - diluted | $ | (1.21 | ) | $ | (0.88 | ) | $ | (0.70 | ) | $ | (0.89 | ) | $ | (0.23 | ) | |||||
Weighted average shares outstanding - basic* | 26,201,713 | 18,904,280 | 16,978,212 | 13,066,600 | * | 9,711,519 | * | |||||||||||||
Weighted average shares outstanding - diluted* | 26,452,165 | 19,071,112 | 16,978,212 | 13,066,600 | * | 9,711,519 | * | |||||||||||||
(*) Weighted average shares outstanding reflects retroactive change of a one for six (1:6) reverse stock split effective on May 29, 2012
December 31, | |||||||||||||||||||
2015 | 2014 | 2013 | 2012 | 2011 | |||||||||||||||
($ in thousands) | |||||||||||||||||||
Consolidated Balance Sheet Data: | |||||||||||||||||||
Cash and cash equivalents | $ | 67,493 | $ | 27,294 | $ | 25,837 | $ | 10,820 | $ | 700 | |||||||||
Working capital | 60,180 | 23,232 | 24,060 | 10,318 | (588 | ) | |||||||||||||
Total assets | 71,446 | 28,897 | 27,156 | 11,665 | 1,039 | ||||||||||||||
Total stockholders’ equity (deficit) | 48,701 | 8,350 | 20,392 | 2,169 | (4,231 | ) | |||||||||||||
ITEM 7. MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS
Forward-Looking Statements
The information in this report contains forward-looking statements. All statements other than statements of historical fact made in this report are forward looking. In particular, the statements herein regarding industry prospects and future results of operations or financial position are forward-looking statements. These forward-looking statements can be identified by the use of words such as “believes,” “estimates,” “could,” “possibly,” “probably,” “anticipates,” “projects,” “expects,” “may,” “will,” or “should” or other variations or similar words. No assurance can be given that the future results anticipated by the
39
forward-looking statements will be achieved. Forward-looking statements reflect management’s current expectations and are inherently uncertain. Our actual results may differ significantly from management’s expectations.
The following discussion and analysis should be read in conjunction with our financial statements, included herewith. This discussion should not be construed to imply that the results discussed herein will necessarily continue into the future, or that any conclusion reached herein will necessarily be indicative of actual operating results in the future. Such discussion represents only the best present assessment of our management.
Overview
We are focused on developing and commercializing our precision cancer monitoring technology, which can inform oncologists and guide treatment decisions by determining a tumor’s mutational status and enabling physicians to track therapeutic response and resistance over time.
We are expanding the body of clinical evidence supporting our urine-based cell-free molecular diagnostic platform through collaborations with major cancer treatment centers and integrated healthcare networks. We expect that the benefits of our precision cancer monitoring technology will become more apparent in terms of its clinical utility and impact on patient outcomes. Our intellectual property estate protecting our technology includes methods of extracting, purifying, preparing, and detecting cell-free DNA and RNA mutations in urine.
Through December 31, 2015, our cumulative total deficit was $108,887,243. To date, we have generated minimal revenues and expect to incur additional losses to perform further research and development activities and commercial expansion. During 2015, we advanced our business with the following activities:
• | We formed the Trovagene Research Institute in Europe with Alberto Bardelli, Ph.D., an internationally recognized leader in cell-free DNA cancer research, and currently affiliated with the Department of Oncology, Torino Medical School and the Candiolo Cancer Institute in Italy. We appointed Dr. Bardelli as the Scientific Director and transferred core technologies from the University of Torino. Trovagene Research Institute intends to improve cancer care through advanced genomic solutions with the mission of accelerating adoption of our PCM platform in translational research and clinical applications. |
• | Clinical study results were presented by Hatim Husain, M.D., from the University of California, San Diego Moores Cancer Center at the 2015 European Lung Cancer Conference. In that study, our urinary ctDNA assay identified 100% of tissue biopsy confirmed EGFR T790M mutations (n=10) in metastatic lung cancer patients. Our assay also detected T790M mutations in three subjects that Dr. Husain speculated may have been tissue biopsy false negatives. In addition, data from the study suggest that our assay may be capable of detecting cancer progression earlier than standard imaging and may be useful in determining patient response to novel EGFR T790M inhibitors. |
• | Clinical study results from a second large-scale clinical trial for our urine-based HPV test were presented by Adriana Lorenzi, a research fellow at the Institute of Education and Research and Molecular Oncology Research Center, Barretos Cancer Hospital - Pio XII Foundation, Barretos, Brazil at the 30th International Papillomavirus Conference. In the trial, urine samples collected from women prior to treatment of cervical pre-cancer lesions (referral population) were tested with our HPV HR Test, and results were compared to Roche’s cobas® HPV Test results from cervical samples. The trial results were consistent with previously reported Predictors 4 data, which demonstrated that sensitivity with our HPV HR Test for the detection of cervical intraepithelial neoplasia Grade Two or higher (“CIN2+”) and Grade Three or higher (“CIN3+”) were comparable to other established cervical cancer screening tests. In the Brazilian cohort, 271 cases of CIN2+ and 202 cases of CIN3+ disease were tested. |
• | Clinical study results for our PCM platform were presented by Julia Johansen, M.D. at Herlev Hospital, Copenhagen, and Hatim Husain, M.D., from the University of California, San Diego Moores Cancer Center at the European Cancer Congress. Results demonstrated that quantitative detection and monitoring of ctDNA and driver mutations can be used to rapidly detect treatment response. |
• | We completed an underwritten public offering of 4,600,000 shares of common stock with net proceeds of approximately $37.4 million in July 2015. |
• | We entered into a clinical collaboration with Memorial Sloan Kettering Cancer Center to monitor response to immunotherapy in melanoma patients using our PCM platform. |
40
• | We launched our “Yellow Is The New Red” marketing campaign for our PCM service at the 2015 American Society of Clinical Oncology Annual Meeting. The campaign is centered on our Clinical Experience Program, in which qualified oncologists can gain hands on clinical experience with our proprietary urinary liquid biopsy tests. |
• | We completed an underwritten public offering of 5,111,110 shares of common stock with net proceeds of approximately $21.3 million in February 2015. |
• | We recruited Matthew Posard to our Executive Management Team as Chief Commercial Officer to lead our commercial operations. |
• | We entered into a clinical collaboration with University of California, San Diego Moores Cancer Center to determine the utility of detecting and monitoring EGFR mutations in lung cancer patients using our PCM platform. |
• | We entered into a clinical collaboration with City of Hope to conduct studies to determine the clinical utility of detecting and monitoring EGFR mutations in lung cancer patients using our PCM platform. |
• | Two sets of clinical study results were presented at the 2015 Gastrointestinal Cancer Symposium supporting the potential utility of our PCM platform in colorectal and pancreatic cancer patients. Results demonstrated the ability of our PCM platform to detect and quantitate KRAS mutations at diagnosis and longitudinally in ctDNA obtained from colorectal and pancreatic cancer patients. We also showed data demonstrating that our proprietary KRAS assay may allow physicians to determine mutational status, monitor treatment response, and use genomics to aid in predicting patient prognosis. |
• | Two sets of clinical study results and one set of analytical data were presented at the 2015 American Association for Cancer Research (“AACR”) Annual Meeting that demonstrated potential clinical utilities and advantages of our PCM platform. Our liquid biopsy technology features single molecule sensitivity and the ability to obtain significantly more ctDNA from urine samples as compared to plasma. |
• | Clinical results from the PREDICTORS 4 trial were presented by Jack Cuzick, Ph.D., Director, Wolfson Institute of Preventive Medicine and Head, Centre for Cancer Prevention at Queen Mary University of London at the European Research Organization on Genital Infection and Neoplasia 2015 Congress. Based on our analysis of more than 500 samples, the results showed high sensitivity (>90%) for our non-invasive, urine-based HPV assay for the detection of high-risk HPV types and cervical intraepithelial neoplasia (“CIN”) Grade 2 or higher lesions. |
• | Clinical data from four studies utilizing our PCM platform were presented at the 2015 American Society of Clinical Oncology Annual Meeting in Chicago, Illinois. Results demonstrated that our PCM technology offers advantages over tissue biopsy and demonstrates the ability to monitor tumor dynamics in lung, pancreatic, and colon cancers. |
Our product development and commercialization efforts are in their early stages, and we cannot make estimates of the costs or the time our development efforts will take to complete, or the timing and amount of revenues related to the sale of our tests and revenues related to our license agreements. The risk of failing to complete of any program is high because of the many uncertainties involved in bringing new diagnostic products to market, including the long duration of clinical testing, the specific performance of proposed products under stringent clinical trial protocols and/or CLIA requirements, the extended regulatory approval and review cycles, our ability to raise additional capital, the nature and timing of research and development expenses, and competing technologies being developed by organizations with significantly greater resources.
CRITICAL ACCOUNTING POLICIES
Financial Reporting Release No. 60 requires all companies to include a discussion of critical accounting policies or methods used in the preparation of financial statements. Our accounting policies are described in Item 8. Financial Statements—Note 2 Basis of Presentation and Summary of Significant Accounting Policies in this Annual Report on Form 10-K. The preparation of financial statements in conformity with accounting principles generally accepted in the United States of America requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of expenses during the reporting period. Actual results could differ from those estimates. We believe that the following discussion represents our critical accounting policies.
41
Revenue Recognition
Historically, our revenues have been generated from royalty, license and milestones related to agreements we have with other healthcare companies, medical laboratories and biotechnology partners. We also have revenues from our diagnostics services.
We recognize revenues when persuasive evidence that an arrangement exists, delivery has occurred, the price is fixed or determinable, and collection is reasonably assured.
Milestone, Royalty and License Revenues
We license and sublicense our patent rights to healthcare companies, medical laboratories and biotechnology partners. These agreements may involve multiple elements such as license fees, royalties and milestone payments. Revenue is recognized when the criteria described above have been met as well as the following:
• | Up-front nonrefundable license fees pursuant to agreements under which we have no continuing performance obligations are recognized as revenues on the effective date of the agreement and when collection is reasonably assured. |
• | Minimum royalties are recognized as earned, and royalties in excess of minimum amounts are recognized upon receipt of payment when collection is assured. |
• | Milestone payments are recognized when both the milestone is achieved and the related payment is received. |
Diagnostic Service Revenue
Diagnostic service revenue, which consists of fees for clinical laboratory tests may come from several sources, including commercial third-party payors, such as insurance companies and health maintenance organizations, government payors, such as Medicare and Medicaid in the U.S., patient self-pay and, in some cases, from hospitals or referring laboratories who, in turn, bill third-party payors for testing.
Diagnostic service revenue will be recognized when the criteria described above has been met as well as upon cash collection until we can reliably estimate the amount that will be ultimately collected for our LDTs, at which time we will recognize revenues on an accrual basis.
Derivative Financial Instruments—Warrants
Our derivative liabilities are related to warrants issued in connection with financing transactions and are therefore not designated as hedging instruments. All derivatives are recorded on our balance sheet at fair value in accordance with current accounting guidelines for such complex financial instruments.
We have issued common stock warrants in connection with the execution of certain equity and debt financings. Such warrants are classified as derivative liabilities under the provisions of the Financial Accounting Standards Board (“FASB”) Accounting Standards Codification (“ASC”) Topic 815, Derivatives and Hedging (“ASC 815”) and are recorded at their fair market value as of each reporting period. Such warrants do not meet the exemption that a contract should not be considered a derivative instrument if it is (1) indexed to its own stock and (2) classified in stockholders’ equity. Changes in fair value of derivative liabilities are recorded in the consolidated statement of operations under the caption “Change in fair value of derivative instruments.”
The fair value of warrants is determined using the Black-Scholes option-pricing model using assumptions regarding volatility of our common stock price, remaining life of the warrant, and risk-free interest rates at each period end. Therefore we use model-derived valuations where inputs are observable in active markets to determine the fair value and accordingly classify such warrants in Level 3 per ASC Topic 820, Fair Value Measurements and Disclosures (“ASC 820”). At December 31, 2015 and 2014, the fair value of such warrants was $3,297,077 and $3,006,021, respectively, which is included in the derivative financial instruments’ liability on our balance sheet.
42
Cost of Revenue
Cost of revenue represents the cost of materials, personnel costs and costs associated with processing specimens including pathological review, quality control analyses, and delivery charges necessary to render an individualized test result. Costs associated with performing tests are recorded as the tests are processed.
Research and Development
Research and development expense, which includes expenditures in connection with an in-house research and development laboratory, salaries and staff costs, application and filing for regulatory approval of proposed products, regulatory and scientific consulting fees and clinical samples, as well as clinical collaborators and insurance, are accounted for in accordance with FASB ASC Topic 730-10-55-2, Research and Development. Also, as prescribed by this guidance, patent filing and maintenance expenses are considered legal in nature and therefore classified as general and administrative expense. We are providing the following summary of our research and development expense to supplement the more detailed discussions under “Results of Operations” below. Costs are not allocated to projects as the majority of the costs relate to employees and facilities costs and we do not track employees’ hours by project or allocate facilities costs on a project basis.
For the years ended December 31, | |||||||||||
2015 | 2014 | 2013 | |||||||||
Salaries and staff costs | $ | 5,365,045 | $ | 3,465,211 | $ | 2,063,474 | |||||
Outside services, consultants and lab supplies | 4,211,251 | 2,435,917 | 1,301,190 | ||||||||
Facilities | 748,466 | 628,535 | 466,138 | ||||||||
Other | 269,107 | 135,243 | 116,787 | ||||||||
Total Research and Development | $ | 10,593,869 | $ | 6,664,906 | $ | 3,947,589 | |||||
While certain of our research and development costs may have future benefits, our policy of expensing all research and development expenditures is predicated on the fact that we have no history of successful commercialization of molecular diagnostic products to base any estimate of the number of future periods that would be benefited.
FASB ASC Topic 730, Research and Development requires that non-refundable advance payments for goods or services that will be used or rendered for future research and development activities be deferred and capitalized. As the related goods are delivered or the services are performed, or when the goods or services are no longer expected to be provided, the deferred amounts are recognized as an expense. There are no non-refundable advance payments that are deferred and capitalized as of December 31, 2015, 2014 and 2013.
Stock-based Compensation
We rely heavily on incentive compensation in the form of stock options to recruit, retain and motivate directors, executive officers, employees and consultants. Incentive compensation in the form of stock options and warrants is designed to provide long-term incentives, develop and maintain an ownership stake and conserve cash. Stock-based compensation expense for employees and directors is recognized in the statement of operations based on estimated amounts, including the grant date fair value and the expected service period. For stock options, we estimate the grant date fair value using a Black-Scholes model. Stock-based compensation recorded in our statement of operations is based on awards expected to ultimately vest and has been reduced for estimated forfeitures. We recognize the value of the awards on a straight-line basis over the awards’ requisite service periods. The requisite service period is generally the time over which our stock-based awards vest.
We account for equity instruments granted to non-employees in accordance with FASB ASC Topic 505-50 “Equity-Based Payment to Non-Employees”, where the value of the stock-based compensation is based upon the measurement date as determined at either: (1) the date at which a performance commitment is reached, or (2) the date at which the necessary performance to earn the equity instruments is complete. Accordingly, the fair value of these options is being “marked to market” quarterly until the measurement date is determined.
Fair Value of Financial Instruments
Financial instruments consist of cash and cash equivalents, accounts receivable, accounts payable, debt and derivative liabilities. We have adopted ASC 820 for financial assets and liabilities that are required to be measured at fair value and non-financial assets and liabilities that are not required to be measured at fair value on a recurring basis. These financial instruments
43
are stated at their respective historical carrying amounts, which approximate fair value due to their short term nature as they reflect current market interest rates. Debt is stated at its respective historical carrying amounts, which approximate fair value as they reflect current market interest rates.
ASC 820 provides that the measurement of fair value requires the use of techniques based on observable and unobservable inputs. Observable inputs reflect market data obtained from independent sources, while unobservable inputs reflect our market assumptions. The inputs create the following fair value hierarchy:
• | Level 1 — Quoted prices for identical instruments in active markets. |
• | Level 2 — Quoted prices for similar instruments in active markets; quoted prices for identical or similar instruments in markets that are not active; and model-derived valuations where inputs are observable or where significant value drivers are observable. |
• | Level 3 — Instruments where significant value drivers are unobservable to third parties. |
Off-Balance Sheet Arrangements
As of December 31, 2015, we did not have any off-balance sheet arrangements as described by Item 303(a)(4) of Regulation S-K.
Recent Accounting Pronouncements
See Item 8. Financial Statements—Note 2 Basis of Presentation and Summary of Significant Accounting Policies in this Annual Report on Form 10-K for a discussion of recent accounting pronouncements.
Results of Operations
YEARS ENDED DECEMBER 31, 2015 AND 2014
Revenues
Our total revenues were $312,812 and $280,178 for the years ended December 31, 2015 and 2014, respectively. Total revenues consisted of the following:
For the years ended December 31, | |||||||||||
2015 | 2014 | (Decrease)/Increase | |||||||||
Royalty income | $ | 274,648 | $ | 270,178 | $ | 4,470 | |||||
License fees | — | 10,000 | (10,000 | ) | |||||||
Diagnostic service revenue | 13,789 | — | 13,789 | ||||||||
Other income | $ | 24,375 | $ | — | $ | 24,375 | |||||
Total revenues | $ | 312,812 | $ | 280,178 | $ | 32,634 | |||||
The $4,470 increase in royalty income in the year ended December 31, 2015 is primarily a result of certain licensees’ payments exceeding their minimum royalties as compared to the prior year. According to our revenue recognition policy, we do not record royalty revenues in excess of minimum royalty amounts until we have received payment of such royalties.
In the year ended December 31, 2014, we received a $10,000 license fee related to a licensing agreement signed in the second quarter of 2014. There were no license fees earned during the year ended December 31, 2015.
Diagnostic service revenue is recognized when payment is received for the test results. We received $13,789 in diagnostic service revenue in the year ended December 31, 2015, primarily as a result of our clinical laboratory tests. There was no diagnostic service revenue for the year ended December 31, 2014 as no payments were received.
Other revenue consists primarily of revenue from the sale of collection kits. In the year ended December 31, 2015, we entered into supply agreements with our customers to sell specimen collection kits. Revenue was recognized when kits were delivered. There was no such revenue for the year ended December 31, 2014.
44
We expect our royalty income to fluctuate as the royalties are based on the minimum royalty payments as well as the timing of when payments are received for royalties in excess of minimum royalties. Milestone and license fee revenues are difficult to predict and can vary significantly from period to period. In addition, we expect our diagnostic service revenue to increase in future periods, but as revenue recognition is based on cash receipts, the timing of these revenues is also uncertain. We expect other revenue to fluctuate based on timing of supply agreements.
Cost of Revenues
Our total cost of revenues was $629,191 in the year ended December 31, 2015, compared to $15,441 in the year ended December 31, 2014. The increase in cost of revenues in the year ended December 31, 2015 compared to the prior year is primarily due to an increase in the volume of tests processed. Cost of revenues primarily relates to the costs of our diagnostic service revenue. The costs are recognized at the completion of testing. Due to revenue being recognized when cash is received, costs incurred in one period may relate to revenue recognized in a later period. Gross margins are negative as we begin to build test volume to cover costs associated with running our diagnostic tests as well as inefficiencies in realizing capacity related issues.
Research and Development Expenses
Research and development expenses consisted of the following:
For the years ended December 31, | |||||||||||
2015 | 2014 | Increase/(Decrease) | |||||||||
Salaries and staff costs | $ | 3,866,036 | $ | 2,669,203 | $ | 1,196,833 | |||||
Stock-based compensation | 1,499,009 | 796,008 | 703,001 | ||||||||
Outside services, consultants and lab supplies | 4,211,251 | 2,435,917 | 1,775,334 | ||||||||
Facilities | 748,466 | 628,535 | 119,931 | ||||||||
Travel and scientific conferences | 228,490 | 119,562 | 108,928 | ||||||||
Other | 40,617 | 15,681 | 24,936 | ||||||||
Total research and development expenses | $ | 10,593,869 | $ | 6,664,906 | $ | 3,928,963 | |||||
Research and development expenses increased by $3,928,963 to $10,593,869 for the year ended December 31, 2015 from $6,664,906 for the year ended December 31, 2014. Substantially all of the increase resulted from an increased number of samples processed and validated in connection with our clinical collaborations. We utilize our clinical collaborations to provide data that summarizes the accuracy of our tests to detect certain types of cancer in urine samples. We also enter into clinical studies to provide data that supports our technology for the monitoring of responsiveness to therapy and the status of diseases. We were party to twenty-six active collaborations or studies during the year ended December 31, 2015, while during the year ended December 31, 2014, we were party to twenty-three collaborations or studies. To support the expansion of our collaboration efforts, we increased the average number of our internal research and development personnel from seventeen to twenty-two, and purchased additional laboratory equipment, lab supplies and clinical samples. To date our research and development expenses have related to validating our tests and supporting clinical collaborations. These costs are expected to increase as we expand current collaborations or enter into new collaborations to support our research and development activities.
45
Selling and Marketing Expenses
Selling and marketing expenses consisted of the following:
For the years ended December 31, | |||||||||||
2015 | 2014 | Increase/(Decrease) | |||||||||
Salaries and staff costs | $ | 2,628,822 | $ | 1,139,855 | $ | 1,488,967 | |||||
Stock-based compensation | 768,146 | 145,240 | 622,906 | ||||||||
Outside services and consultants | 932,237 | 902,181 | 30,056 | ||||||||
Facilities and insurance | 283,809 | 115,713 | 168,096 | ||||||||
Trade shows, conferences and marketing | 1,282,059 | 258,658 | 1,023,401 | ||||||||
Travel | 449,294 | 139,710 | 309,584 | ||||||||
Other | 99,211 | 33,546 | 65,665 | ||||||||
Total selling and marketing expenses | $ | 6,443,578 | $ | 2,734,903 | $ | 3,708,675 | |||||
Selling and marketing expenses increased by $3,708,675 to $6,443,578 for the year ended December 31, 2015, from $2,734,903 for the year ended December 31, 2014. The significant components of the increase were primarily increased salaries and staff costs, stock-based compensation, and trade shows, conferences and marketing costs. For the year ended December 31, 2015, we increased our average internal headcount in this functional area from five to thirteen to support our sales and marketing activities, resulting in the increase in salaries and staff costs. In addition to the increased trade shows and conferences costs, costs related to our clinical experience program, where we offer new clinicians a series of tests for no charge, are included in marketing expenses. We expect our selling and marketing expenses to increase as we add new personnel to our commercial team that are focused on increasing market acceptance of our commercially available tests.
General and Administrative Expenses
General and administrative expenses consisted of the following:
For the years ended December 31, | |||||||||||
2015 | 2014 | Increase/(Decrease) | |||||||||
Personnel and outside services costs | $ | 3,509,844 | $ | 2,245,801 | $ | 1,264,043 | |||||
Stock-based compensation | 1,639,196 | 1,128,948 | 510,248 | ||||||||
Board of Directors’ fees | 457,865 | 328,184 | 129,681 | ||||||||
Legal and accounting fees | 1,182,427 | 1,314,960 | (132,533 | ) | |||||||
Facilities and insurance | 524,763 | 336,154 | 188,609 | ||||||||
Travel | 266,410 | 208,651 | 57,759 | ||||||||
Fees, licenses, taxes and other | 339,321 | 247,389 | 91,932 | ||||||||
Total general and administrative expenses | $ | 7,919,826 | $ | 5,810,087 | $ | 2,109,739 | |||||
General and administrative expenses increased by $2,109,739 to $7,919,826 for the year ended December 31, 2015 from $5,810,087 for the year ended December 31, 2014. This increase was primarily due to an increase in personnel and outside services costs and stock-based compensation, partially offset by a decrease in legal and accounting fees. We have increased our average internal headcount from four to seven, as well as utilized outside services and consultants, to support our growth in both research and development and sales and marketing, resulting in the increase in personnel and outside services costs during the year ended December 31, 2015 as compared to the prior year. Stock-based compensation, a non-cash expense, will fluctuate based on the timing and amount of options granted, as well as the fair value of the options at the time of grant or remeasurement. In January 2016, our CEO was granted 350,000 non-qualified stock options which have an exercise price of $5.18 per share and vested immediately upon grant. The fair value of the options which is approximately $1.4 million will be expensed in full in the first quarter of 2016. We expect our general and administrative costs to increase to support the growth of our sales and marketing and research and development teams and from the additional costs we will incur in the billing and collection of revenues from the sales of our diagnostic tests.
46
Interest Expense
Interest expense was $1,525,482 and $843,259 for the years ended December 31, 2015 and 2014, respectively. The increase in the year ended December 31, 2015 resulted primarily from the $15.0 million term loan we entered into in June 2014. We paid twelve months of interest only payments in the year ended December 31, 2015 as compared to six months of interest only payments in the year ended December 31, 2014. If we complete the anticipated refinancing of our debt to include an additional period of interest only payments, our interest expense will increase.
Change in Fair Value of Derivative Instruments - Warrants
We have issued securities that are accounted for as derivative liabilities. As of December 31, 2015, the derivative liabilities related to securities issued were revalued to $3,297,077, resulting in a net increase in value of $291,056 from December 31, 2014, based primarily upon the change in our stock price from $4.30 at December 31, 2014 to $5.40 at December 31, 2015, and the changes in the expected term, volatility and risk-free interest rates for the expected term, offset by fair value of warrants reclassified from a liability to additional paid-in capital upon exercise of warrants. The increase in value was recorded as non-operating loss for the year ended December 31, 2015.
Net Loss
Net loss and per share amounts were as follows:
For the years ended December 31, | |||||||||||
2015 | 2014 | Increase/(Decrease) | |||||||||
Net loss and comprehensive loss attributable to common stockholders | $ | (27,495,334 | ) | $ | (14,348,499 | ) | $ | 13,146,835 | |||
Net loss per common share - basic | $ | (1.05 | ) | $ | (0.76 | ) | $ | 0.29 | |||
Net loss per common share - diluted | $ | (1.21 | ) | $ | (0.88 | ) | $ | 0.33 | |||
Weighted-average shares outstanding - basic | 26,201,713 | 18,904,280 | 7,297,433 | ||||||||
Weighted-average shares outstanding - diluted | 26,452,165 | 19,071,112 | 7,381,053 | ||||||||
The increase in net loss and comprehensive loss attributable to common stockholders of $13,146,835 to $27,495,334 for the year ended December 31, 2015 from $14,348,499 for the year ended December 31, 2014 resulted primarily from a slight increase in revenues, offset by an increase in operating expenses, interest expense, and loss from the change in fair value of derivative liabilities. Basic and diluted net loss per share for the year ended December 31, 2015 were impacted by the increase in both basic and diluted weighted-average shares outstanding resulting from the sale and issuance of approximately 10.0 million shares of common stock through underwritten public offerings and a controlled equity offering through our agreement with Cantor Fitzgerald & Co., as well as the issuance of approximately 838,000 shares of common stock in connection with the exercise of stock options and warrants.
YEARS ENDED DECEMBER 31, 2014 AND 2013
Revenues
Our total revenues were $280,178 and $259,246 for the years ended December 31, 2014 and 2013, respectively. Total revenues consisted of the following:
Years ended December 31, | |||||||||||
2014 | 2013 | Increase | |||||||||
Royalty income | $ | 270,178 | $ | 259,246 | $ | 10,932 | |||||
License fees | 10,000 | — | 10,000 | ||||||||
Total revenues | $ | 280,178 | $ | 259,246 | $ | 20,932 | |||||
47
Royalty income increased by $10,932 in the year ended December 31, 2014, primarily as a result of certain licensees exceeding their minimum royalties as compared to the prior year. In accordance with our revenue recognition policy, we do not record royalty revenues in excess of minimum royalty amounts until we have received payment of such royalties.
In the year ended December 31, 2014, we received a $10,000 license fee related to a licensing agreement signed in the second quarter of 2014. There were no license fees earned during the year ended December 31, 2013.
Cost of Revenues
Cost of revenues relates to the costs of our diagnostic services revenues and is recognized at the completion of testing. Gross margins on diagnostic tests are affected by test volumes, the timing of collections and overall reimbursement for the amount paid per test.
Research and Development Expenses
Research and development expenses consisted of the following:
For the years ended December 31, | |||||||||||
2014 | 2013 | Increase/(Decrease) | |||||||||
Salaries and staff costs | $ | 2,669,203 | $ | 1,514,009 | $ | 1,155,194 | |||||
Stock-based compensation | 796,008 | 549,465 | 246,543 | ||||||||
Outside services, consultants and lab supplies | 2,435,917 | 1,301,190 | 1,134,727 | ||||||||
Facilities | 628,535 | 466,138 | 162,397 | ||||||||
Travel and scientific conferences | 119,562 | 95,399 | 24,163 | ||||||||
Other | 15,681 | 21,388 | (5,707 | ) | |||||||
Total research and development expenses | $ | 6,664,906 | $ | 3,947,589 | $ | 2,717,317 | |||||
Research and development expenses increased by $2,717,317 to $6,664,906 for the year ended December 31, 2014 from $3,947,589 for the year ended December 31, 2013. Substantially all of the increase resulted from the expansion of our research and development efforts as we increased the average number of our internal research and development personnel from nine to seventeen, and purchased additional laboratory equipment to support the increase in clinical collaborations for the commercialization of our tests. The clinical collaborations with external parties involve validation of our tests to detect certain types of cancer in urine samples.
Selling and Marketing Expenses
Selling and marketing expenses consisted of the following:
For the years ended December 31, | |||||||||||
2014 | 2013 | Increase/(Decrease) | |||||||||
Salaries and staff costs | $ | 1,139,855 | $ | 734,060 | $ | 405,795 | |||||
Stock-based compensation | 145,240 | 100,189 | 45,051 | ||||||||
Outside services and consultants | 902,181 | 274,625 | 627,556 | ||||||||
Facilities and insurance | 115,713 | 98,081 | 17,632 | ||||||||
Marketing | 258,658 | 193,701 | 64,957 | ||||||||
Travel | 139,710 | 92,030 | 47,680 | ||||||||
Fees, licenses, taxes and other | 33,546 | 37,474 | (3,928 | ) | |||||||
Total sales and marketing expenses | $ | 2,734,903 | $ | 1,530,160 | $ | 1,204,743 | |||||
Selling and marketing expenses increased by $1,204,743 to $2,734,903 for the year ended December 31, 2014 from $1,530,160 for the year ended December 31, 2013. The most significant increase was in outside services and related to reestablishing our corporate and product identity, a commercial update to our website, and market research related to pricing and reimbursement of our tests. We had three commercially available tests as of December 31, 2014. During the year ended
48
December 31, 2014, we increased our average internal headcount in this functional area from three to five, resulting in an increase in salaries and staff costs and stock-based compensation expense.
General and Administrative Expenses
General and administrative expenses consisted of the following:
For the years ended December 31, | |||||||||||
2014 | 2013 | Increase/(Decrease) | |||||||||
Personnel and outside services costs | $ | 2,245,801 | $ | 2,057,986 | $ | 187,815 | |||||
Stock-based compensation | 1,128,948 | 1,528,501 | (399,553 | ) | |||||||
Board of Directors’ fees | 328,184 | 241,229 | 86,955 | ||||||||
Legal and accounting fees | 1,314,960 | 995,185 | 319,775 | ||||||||
Facilities and insurance | 336,154 | 248,491 | 87,663 | ||||||||
Travel | 208,651 | 220,691 | (12,040 | ) | |||||||
Fees, licenses, taxes and other | 247,389 | 179,955 | 67,434 | ||||||||
Total general and administrative expenses | $ | 5,810,087 | $ | 5,472,038 | $ | 338,049 | |||||
General and administrative expenses increased by $338,049 to $5,810,087 for the year ended December 31, 2014 from $5,472,038 for the year ended December 31, 2013. This increase was primarily due to an increase in legal fees related to filings and maintenance of patents. We increased our average internal headcount in these functional areas from two to four, to support the growth in both research and development and sales and marketing, resulting in the increase in salaries and staff costs during the year ended December 31, 2014 as compared to the prior year. In addition, the costs associated with being a public company, such as additional costs for insurance, The NASDAQ Stock Market LLC fees, and compliance with the Sarbanes-Oxley Act of 2002, as amended, added to our general and administrative expenses, as compared to the year ended December 31, 2013. The overall increase was partially offset by decreases in stock-based compensation due to timing and quantity of stock-based awards.
Interest Expense
Interest expense was $843,259 and $17,005 for the years ended December 31, 2014 and 2013, respectively. The increase in the year ended December 31, 2014 resulted from a $15.0 million long term loan that we entered into in June 2014.
Change in Fair Value of Derivative Instruments - Warrants
The change in fair value of derivative instruments resulted in a $1,425,850 gain in the year ended December 31, 2014 compared to a loss of $1,084,114 in the prior year. The gain was a result of the revaluation of warrants based upon the change in our stock price from $5.74 at December 31, 2013 to $4.30 at December 31, 2014, and the changes in the expected term, volatility and risk-free interest rates for the expected term. The decrease in value was recorded as non-operating gain for the year ended December 31, 2014.
Net Loss
Net loss and per share amounts were as follows:
For the years ended December 31, | |||||||||||
2014 | 2013 | Increase (Decrease) | |||||||||
Net loss and comprehensive loss attributable to common stockholders | $ | (14,348,499 | ) | $ | (11,840,778 | ) | $ | 2,507,721 | |||
Net loss per common share - basic | $ | (0.76 | ) | $ | (0.70 | ) | $ | 0.06 | |||
Net loss per common share - diluted | $ | (0.88 | ) | $ | (0.70 | ) | $ | 0.18 | |||
Weighted-average shares outstanding - basic | 18,904,280 | 16,978,212 | 1,926,068 | ||||||||
Weighted-average shares outstanding - diluted | 19,071,112 | 16,978,212 | 2,092,900 | ||||||||
49
The increase in net loss and comprehensive loss attributable to common stockholders of $2,507,721 to $14,348,499 for the year ended December 31, 2014 from $11,840,778 for the year ended December 31, 2013 resulted primarily from a slight increase in revenues, offset by increases in all operating expenses. The net loss per share - basic for the year ended December 31, 2014 increased by $0.06 to a net loss of $0.76 as a result of an overall increase in net loss, slightly offset by an increase in weighted average shares outstanding during the year ended December 31, 2014 compared to the prior year. Weighted-average basic and diluted shares outstanding increased for the year ended December 31, 2014 due to 3.4 million shares issued as a result of shares sold through controlled equity offerings, the exercise of warrants and stock options during the year ended December 31, 2014, and the issuance of approximately 13,000 shares as a result of the net exercise of warrants during the year ended December 31, 2014.
Liquidity and Capital Resources
As of December 31, 2015, we had $67,493,047 in cash and cash equivalents. Net cash used in operating activities for the year ended December 31, 2015 was $22,119,025, compared to $12,727,385 for the year ended December 31, 2014. Our use of cash was primarily a result of the net loss of $27,471,094 for the year ended December 31, 2015, adjusted for non-cash items related to stock-based compensation of $3,946,027, depreciation and amortization of $378,711 and gain from the change in fair value of derivatives of $726,421. The changes in our operating assets and liabilities consisted of higher accounts payable and accrued expenses and an increase in accounts receivable. At our current and anticipated level of operating loss, we expect to continue to incur an operating cash outflow for the next several years. As of December 31, 2015 and 2014, we had working capital of $60,179,971 and $23,231,596, respectively. The increase in working capital is primarily due to the increase in cash and cash equivalents as a result of the sale and issuance of approximately 10.0 million shares of common stock through underwritten public offerings and a controlled equity offering through an agreement with Cantor Fitzgerald & Co.
Investing activities consisted of purchases for capital equipment that used $2,233,466 in cash during the year ended December 31, 2015, compared to $299,790 for the year ended December 31, 2014. We expect to invest approximately $4.6 million in capital equipment during 2016. Any such investment will be predominantly for laboratory equipment.
Net cash provided by financing activities was $64,551,740 during the year ended December 31, 2015, compared to $14,484,036 during the year ended December 31, 2014. Financing activities during the year ended December 31, 2015 included $61,215,399 from the sales of common stock, $2,250,279 from proceeds related to the exercise of warrants and options, and $1,086,062 from new borrowings on equipment lines. As of December 31, 2015, we had approximately $900,000 remaining available for borrowing under our equipment line of credit and we intend to utilize the remaining amount during 2016. Financing activities during the year ended December 31, 2014 consisted of net borrowings of $15.0 million under our debt agreement, offset by $515,964 of repayment on equipment lines.
As of February 29, 2016, our cash balance was approximately $62.9 million and our working capital was approximately $55.8 million.
Our working capital requirements will depend upon numerous factors including but not limited to, the nature, cost and timing of our research and development programs and ramp up of our sales and marketing function. To date, our sources of cash have been primarily limited to the sale of equity securities and debentures and a venture capital loan. We cannot be certain that additional funding will be available on acceptable terms, or at all. To the extent that we raise additional funds by issuing equity securities, our stockholders may experience significant dilution. Any debt financing, if available, may involve restrictive covenants that impact our ability to conduct business. If we are unable to raise additional capital when required or on acceptable terms, we may have to (1) significantly delay, scale back or discontinue the development and/or commercialization of one or more of our product candidates; (2) seek collaborators for product candidates at an earlier stage than otherwise would be desirable and on terms that are less favorable than might otherwise be available; or (3) relinquish or otherwise dispose of rights to technologies, product candidates or products that we would otherwise seek to develop or commercialize ourselves on unfavorable terms.
Controlled Equity Offering and Public Offerings
On January 25, 2013, we filed a Registration Statement on Form S-3 (the “Registration Statement”) to offer and sell in one or more offerings any combination of common stock, preferred stock, warrants, or units having an aggregate initial offering price of up to $150,000,000. If issued, the preferred stock, warrants, and units would be convertible, exercisable or exchangeable for common stock, preferred stock or other securities. The Registration Statement was declared effective on February 4, 2013. In addition, in connection with the Registration Statement, we entered into an agreement with Cantor Fitzgerald & Co. (“Agent”) on January 25, 2013 to issue and sell up to $30,000,000 of shares of common stock. As payment for its services, the Agent is entitled to a 3% commission on gross proceeds on sales of our securities. We received gross proceeds
50
of approximately $4.2 million from the sale of 488,476 shares of our common stock during the year ended December 31, 2013 under the agreement with the Agent. In addition, we received gross proceeds of approximately $15.0 million from the sale of 2,142,857 shares of our common stock through a registered direct offering that occurred in July 2013. During the year ended December 31, 2015, we also received gross proceeds of approximately $2.8 million from the sale of 285,421 shares of our common stock at a weighted-average price of $9.66 under the agreement with the Agent. During the year ended December 31, 2015, we received gross proceeds of approximately $63.2 million from the sale of 9,711,110 shares of our common stock through underwritten public offerings in February 2015 and July 2015.
Contractual Obligations and Commitments
The following table is a summary of contractual obligations that existed as of December 31, 2015, and is based on information appearing in the notes to Consolidated Financial Statements included elsewhere in this Annual Report on Form 10-K.
Payments Due by period | |||||||||||||||||||
Total | Less than 1 Year | 1-3 Years | 3-5 Years | More than 5 Years | |||||||||||||||
Operating leases | $ | 4,745,113 | $ | 683,871 | $ | 1,604,008 | $ | 1,614,705 | $ | 842,529 | |||||||||
Research agreements (1) | 1,666,544 | 1,666,544 | — | — | — | ||||||||||||||
Long-term debt (2) | 18,837,720 | 6,187,388 | 12,234,475 | 415,857 | — | ||||||||||||||
Purchase obligations - major vendors (3) | 133,623 | 133,623 | — | — | — | ||||||||||||||
Total obligations | $ | 25,383,000 | $ | 8,671,426 | $ | 13,838,483 | $ | 2,030,562 | $ | 842,529 | |||||||||
(1) | Payments under research agreements are based on the completion of activities as specified in the research agreement. The amounts in the table above assume the successful completion of the collaborative research activities contemplated by the agreements. |
(2) | Represents long-term debt and interest. |
(3) | Represents amounts that will become due upon future delivery of supplies and services from various suppliers under open purchase orders as of December 31, 2015. |
ITEM 7A. QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK
Interest Rate Risk
Our cash and cash equivalents primary consist of securities issued by the U.S. government, deposits, and money market deposits managed by commercial banks. The goals of our investment policy are preservation of capital, fulfillment of liquidity needs and fiduciary control of cash and investments. We also seek to maximize income from our investments without assuming significant risk.
Our primary exposure to market risk is interest income sensitivity, which is affected by changes in the general level of interest rates, particularly because our investments are in short-term money market funds. Due to the short-term duration of our investment portfolio and the relatively low risk profile of our investments, we believe that the fair value of our investment portfolio would not be significantly impacted by either a hypothetical 100 basis point increase or decrease in market interest rates.
We do not believe our cash and cash equivalents investments have significant risk of default or illiquidity; however, we maintain significant amounts of cash and cash equivalents at one or more financial institutions that are in excess of federally insured limits. Given the current instability of financial institutions, we cannot provide assurance that we will not experience losses on these deposits.
51
Effects of Inflation
We do not believe that inflation and changing prices during the years ended December 31, 2015, 2014, and 2013 had a significant impact on our results of operations.
ITEM 8. FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA
All financial information required by this Item is attached hereto at the end of this report beginning on page F-1 and is hereby incorporated by reference.
ITEM 9. CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE
None.
ITEM 9A. CONTROLS AND PROCEDURES
Disclosure Controls and Procedures
Our chief executive officer and chief financial officer evaluated the effectiveness of our disclosure controls and procedures as of December 31, 2015. The term “disclosure controls and procedures,” as defined in Rules 13a-15(e) and 15d-15(e) under the Securities Exchange Act of 1934, as amended, or the Exchange Act, means controls and other procedures of a company that are designed to ensure that information required to be disclosed by a company in the reports that it files or submits under the Exchange Act is recorded, processed, summarized and reported, within the time periods specified in the Securities and Exchange Commission’s rules and forms. Management recognizes that any controls and procedures, no matter how well designed and operated, can provide only reasonable assurance of achieving their objectives and management necessarily applies its judgment in evaluating the cost-benefit relationship of possible controls and procedures. Disclosure controls and procedures include, without limitation, controls and procedures designed to ensure that information required to be disclosed by a company in the reports that it files or submits under the Exchange Act is accumulated and communicated to the company’s management, including its principal executive and principal financial officers, as appropriate to allow timely decisions regarding required disclosure. Based on that evaluation, our principal executive officer and principal financial officer concluded that our disclosure controls and procedures were effective as of the end of the period covered by this Annual Report on Form 10-K.
Management’s Report on Internal Control Over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over financial reporting as such term is defined in Exchange Act Rule 13a-15(f). Internal control over financial reporting is a process designed under the supervision and with the participation of our management, including our principal executive officer and principal financial officer, to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with accounting principles generally accepted in the United States of America. All internal control systems, no matter how well designed, have inherent limitations. Therefore, even those systems determined to be effective can provide only reasonable assurance with respect to financial statement preparation and presentation.
As of December 31, 2015, under the supervision and with the participation of our management, including our principal executive officer and principal financial officer, we conducted an evaluation of the effectiveness of our internal control over financial reporting based on the Committee of Sponsoring Organizations of the Treadway Commission in Internal Control-Integrated Framework - 2013. Based on this assessment, our management concluded that, as of December 31, 2015, our internal control over financial reporting was effective based on those criteria.
The effectiveness of our internal control over financial reporting as of December 31, 2015 has been audited by BDO USA, LLP, an independent registered public accounting firm, as stated in their report which is included herein.
Changes in Internal Control Over Financial Reporting
There has been no change in our internal control over financial reporting during the quarter ended December 31, 2015 that has materially affected, or is reasonably likely to materially affect, our internal control over financial reporting.
52
Report of Independent Registered Public Accounting Firm
Board of Directors and Stockholders
Trovagene, Inc.
San Diego, California
We have audited Trovagene, Inc.’s internal control over financial reporting as of December 31, 2015, based on criteria established in Internal Control - Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission (the COSO criteria). Trovagene, Inc.’s management is responsible for maintaining effective internal control over financial reporting and for its assessment of the effectiveness of internal control over financial reporting, included in the accompanying Item 9A, Management’s Report on Internal Control Over Financial Reporting. Our responsibility is to express an opinion on the company’s internal control over financial reporting based on our audit.
We conducted our audit in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects. Our audit included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, and testing and evaluating the design and operating effectiveness of internal control based on the assessed risk. Our audit also included performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
In our opinion, Trovagene, Inc. maintained, in all material respects, effective internal control over financial reporting as of December 31, 2015, based on the COSO criteria.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), the consolidated balance sheets of Trovagene, Inc. as of December 31, 2015 and 2014, and the related consolidated statements of operations and comprehensive loss, stockholders’ equity (deficit), and cash flows for each of the three years in the period ended December 31, 2015 and our report dated March 10, 2016 expressed an unqualified opinion thereon.
/s/ BDO USA, LLP
San Diego, California
March 10, 2016
53
ITEM 9B. OTHER INFORMATION
None.
PART III
ITEM 10. DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE
The information required by this item is incorporated by reference from the information contained in our Definitive Proxy Statement to be filed with the Securities and Exchange Commission in connection with the Annual Meeting of Stockholders to be held in 2016 (the “2016 Proxy Statement”), under the headings “Election of Directors-Information with Respect to Director Nominees,” “Section 16(a) Beneficial Ownership Reporting Compliance,” “Election of Directors-Information Regarding the Board of Directors and Corporate Governance” and “Executive Officers”.
ITEM 11. EXECUTIVE COMPENSATION
The information required by this item is incorporated by reference from the information contained in the 2016 Proxy Statement under the headings “Executive Compensation,” “Summary Compensation Table,” “Grants of Plan-Based Awards During Fiscal Year 2015,” “Outstanding Equity Awards at Fiscal Year-End,” “Option Exercises and Stock Vested,” “Pension Benefits-Non-Qualified Defined Contribution and Other Nonqualified Deferred Compensation,” “Potential Payments Upon Termination or Change in Control,” “Director Compensation” and “Election of Directors-Information Regarding the Board of Directors and Corporate Governance”.
ITEM 12. SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS
The information required by this item is incorporated by reference from the information contained in the 2016 Proxy Statement under the headings “Security Ownership of Certain Beneficial Owners and Management” and “Securities Authorized for Issuance Under Equity Compensation Plans”.
ITEM 13. CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE
The information required by this item is incorporated by reference from the information contained in the 2016 Proxy Statement under the headings “Certain Relationships and Related Transactions” and “Election of Directors-Information Regarding the Board of Directors and Corporate Governance”.
ITEM 14. PRINCIPAL ACCOUNTING FEES AND SERVICES
The information required by this item is incorporated by reference from the information contained in the 2016 Proxy Statement under the heading “Proposal 2: Ratification of the Appointment of Our Independent Registered Public Accounting Firm for Fiscal Year Ending December 31, 2016”.
54
PART IV
ITEM 15. EXHIBITS, FINANCIAL STATEMENT SCHEDULES
Exhibit Number | Description of Exhibit | |
(a)(1)Financial Statements | ||
The financial statements required by this item are submitted in a separate section beginning on page F-1 of this Annual Report on Form 10-K. | ||
(b) Exhibits | ||
Exhibit Number | Description | |
1.2 | Controlled Equity OfferingSM Sales Agreement dated January 25, 2013 by and between Trovagene, Inc. and Cantor Fitzgerald & Co. (incorporated by reference to Exhibit 1.2 to the Company’s Form S-3 filed on January 25, 2013). | |
3.1 | Amended and Restated Certificate of Incorporation of Trovagene, Inc. (incorporated by reference to Exhibit 3.1 to the Company’s Form 10-12G filed on November 25, 2011). | |
3.2 | Certificate of Amendment of Amended and Restated Certificate of Incorporation of Trovagene, Inc. (incorporated by reference to Appendix B to the Company’s Proxy Statement on Schedule 14A filed on March 20, 2012). | |
3.3 | By-Laws of Trovagene, Inc. (incorporated by reference to Exhibit 3.2 to the Company’s Form 10-12G filed on November 25, 2011). | |
4.1 | Form of Common Stock Certificate of Trovagene, Inc. (incorporated by reference to Exhibit 4.1 to the Company’s Form 10-12G filed on November 25, 2011). | |
4.2+ | 2004 Stock Option Plan (incorporated by reference to Exhibit 4.3 to the Company’s Current Report on Form 8-K filed on July 19, 2004) | |
4.3 | Form of Registration Rights Agreement (incorporated by reference to Exhibit 4.2 to the Company’s Current Report on Form 8-K, filed on April 16, 2012). | |
4.4 | Form of Warrant Agency Agreement by and between Trovagene, Inc. and Broadridge Corporate Issuer Solutions, Inc. and Form of Warrant Certificate (incorporated by reference to Exhibit 4.5 to the Company’s Amendment No. 3 to Form S-1 filed on May 22, 2012). | |
4.5 | Form of Unit Agency Agreement by and between Trovagene, Inc. and Broadridge Corporate Issuer Solutions, Inc. (incorporated by reference to Exhibit 4.6 to Amendment No. 3 to the Company’s Form S-1 filed on May 22, 2012). | |
4.6 | Form of Warrant (incorporated by reference to Exhibit 4.2 to the Company’s Current Report on Form 8-K filed on November 28, 2012). | |
4.7 | Form of Warrant to Purchase Common Stock (incorporated by reference to Exhibit 4.2 to the Company’s Current Report on Form 8-K filed on July 1, 2014). | |
4.8+ | Trovagene, Inc. 2014 Equity Incentive Plan (incorporated by reference to Appendix A to the Company’s Definitive Proxy Statement on Schedule 14A filed on July 23, 2014). | |
55
10.1 | Summary of Terms of Lease Agreement dated as of October 28, 2009 between Trovagene, Inc. and BMR-Sorrento West LLC (incorporated by reference to Exhibit 10.3 to the Company’s Form 10-12G/A filed on February 15, 2012). | |
10.2 | Form of First Amendment to Standard Industrial Net Lease dated September 28, 2011 between Trovagene, Inc. and BMR-Sorrento West LLC (incorporated by reference to Exhibit 10.4 to the Company’s Form 10-12G/A filed on February 15, 2012). | |
10.3 | Form of Second Amendment to Standard Industrial Net Lease dated October 2011 between Trovagene, Inc. and BMR-Sorrento West LLC (incorporated by reference to Exhibit 10.5 to the Company’s Form 10-12G/A filed on February 15, 2012). | |
10.4 | Form of Third Amendment to Standard Industrial Net Lease dated October 22, 2012 between Trovagene, Inc. and BMR-Sorrento West, LP. (incorporated by reference to Exhibit 10.6 to the Company’s Annual Report on Form 10-K filed on March 12, 2015). | |
10.5 | Form of Fourth Amendment to Standard Industrial Net Lease dated December 2, 2013 between Trovagene, Inc. and BMR-Coast 9 LP. (incorporated by reference to Exhibit 10.7 to the Company’s Annual Report on Form 10-K filed on March 12, 2015). | |
10.6 | Form of Fifth Amendment to Standard Industrial Net Lease dated May 14, 2014 between Trovagene, Inc. and BMR-Coast 9 LP. (incorporated by reference to Exhibit 10.8 to the Company’s Annual Report on Form 10-K filed on March 12, 2015). | |
10.7 | Sixth Amendment to Standard Industrial Net Lease dated June 11, 2015 between Trovagene, Inc. and BMR-Coast 9 LP (incorporated by reference to Exhibit 10.1 to the Company’s Quarterly Report on Form 10-Q filed on August 10, 2015). | |
10.8 | Co-Exclusive Sublicense Agreement dated October 22, 2007 between Trovagene, Inc. and Asuragen, Inc. (incorporated by reference to Exhibit 10.6 to the Company’s Form 10-12G/A filed on February 15, 2012). | |
10.9 | Amendment to Co-Exclusive Sublicense Agreement dated June 1, 2010 between Trovagene, Inc. and Asuragen, Inc. (incorporated by reference to Exhibit 10.7 to the Company’s Form 10-12G/A filed on February 15, 2012). | |
10.10 | Sublicense Agreement dated as of August 27, 2007 between Trovagene, Inc. and Ipsogen SAS (incorporated by reference to Exhibit 10.8 to the Company’s Form 10-12G/A filed on February 15, 2012). | |
10.11 | Amendment to Co-Exclusive Sublicense Agreement dated as of September 1, 2010 between Trovagene, Inc. and Ipsogen SAS (incorporated by reference to Exhibit 10.9 to the Company’s Form 10-12G/A filed on February 15, 2012). | |
10.12 | Sublicense Agreement dated as of July 20, 2011 between Trovagene, Inc. and Fairview Health Services (incorporated by reference to Exhibit 10.11 to the Company’s Form 10-12G/A filed on February 15, 2012). | |
10.13 | Sublicense Agreement dated as of December 1, 2008 by and between Trovagene, Inc. and InVivoScribe Technologies, Inc. (incorporated by reference to Exhibit 10.13 to the Company’s Form 10-12G/A filed on February 15, 2012). | |
10.14 | Sublicense Agreement dated as of August 25, 2008 by and between Trovagene, Inc. and Laboratory Corporation of America Holdings (incorporated by reference to Exhibit 10.14 to the Company’s Form 10-12G/A filed on February 15, 2012). | |
56
10.15 | Form of Sublicense Agreement effective as of February 8, 2011 by and between Trovagene, Inc. and MLL Munchner Leukamielabor GmbH (incorporated by reference to Exhibit 10.15 to the Company’s Form 10-12G/A filed on February 15, 2012). | |
10.16 | Sublicense Agreement effective as of June 15, 2010 by and between Trovagene, Inc. and Skyline Diagnostics BV (incorporated by reference to Exhibit 10.16 to the Company’s Form 10-12G/A filed on February 15, 2012). | |
10.17 | Exclusive License Agreement effective as of December 12, 2011 by and between Columbia University and Trovagene, Inc. (incorporated by reference to Exhibit 10.20 to the Company’s Form 10-12G/A filed on February 15, 2012). | |
10.18 | Form of Exclusive License Agreement effective as of October 2011 by and between Gianluca Gaidano, Robert Foa and Davide Rossi and Trovagene, Inc. (incorporated by reference to Exhibit 10.21 to the Company’s Form 10-12G/A filed on February 15, 2012). | |
10.19 | Exclusive License Agreement effective as of May 2006 by and between Brunangelo Falini, Cristina Mecucci and Trovagene, Inc. (incorporated by reference to Exhibit 10.23 to the Company’s Form 10-12G/A filed on February 15, 2012). | |
10.20 | Form of First Amendment to Exclusive License Agreement effective as of August 2010 by and among Brunangelo Falini, Cristina Mecucci and Trovagene, Inc. (incorporated by reference to Exhibit 10.24 to the Company’s Form 10-12G/A filed on February 15, 2012). | |
10.21 | Form of Securities Purchase Agreement dated as of July 30, 2013 (incorporated by reference to Exhibit 10.1 to the Company’s Current Report on Form 8-K filed on July 31, 2013). | |
10.22 | Loan and Security Agreement dated as of June 30, 2014 by and among Oxford Finance LLC, Silicon Valley Bank, Trovagene, Inc. and Etherogen, Inc. (incorporated by reference to Exhibit 10.1 to the Company’s Current Report on Form 8-K filed on July 1, 2014). | |
10.23 | First Amendment to Loan and Security Agreement dated as of December 18, 2014 by and among Oxford Finance LLC, Silicon Valley Bank, Trovagene, Inc. and Etherogen, Inc. (incorporated by reference to Exhibit 10.2 to the Company’s Quarterly Report on Form 10-Q filed on August 10, 2015). | |
10.24 | Second Amendment to Loan and Security Agreement dated as of May 6, 2015 by and among Oxford Finance LLC, Silicon Valley Bank, Trovagene, Inc. and Etherogen, Inc. (incorporated by reference to Exhibit 10.3 to the Company’s Quarterly Report on Form 10-Q filed on August 10, 2015). | |
10.25 | Form of Secured Promissory Note issued by the Company and Etherogen, Inc. (incorporated by reference to Exhibit 4.1 to the Company’s Current Report on Form 8-K filed on July 1, 2014). | |
10.26+ | Form of Indemnification Agreement to be entered into between the Company and its directors and executive officers (incorporated by reference to Exhibit 10.1 to the Company’s Current Report on Form 8-K filed on December 15, 2015). | |
10.27* | Patent Assignment and License Agreement dated April 23, 2014 between Trovagene, Inc. and GenSignia IP Ltd. (incorporated by reference to Exhibit 10.1 to the Company’s Quarterly Report on Form 10-Q filed on May 12, 2014). | |
10.28+ | Employment Agreement, effective January 1, 2016, by and between the Company and Antonius Schuh, Ph.D. | |
10.29+ | Employment Agreement, effective January 1, 2016, by and between the Company and Stephen Zaniboni. | |
57
10.30+ | Offer Letter and General Employment Terms & Conditions, dated January 14, 2013, by and between the Company and Mark Erlander. | |
10.31+ | Offer Letter and General Employment Terms & Conditions, dated February 9, 2015, by and between the Company and Matthew L. Posard. | |
10.32 | Loan and Security Agreement dated as of November 17, 2015 by and between the Company and Silicon Valley Bank. | |
21 | List of Subsidiaries. | |
23.1 | Consent of BDO USA, LLP | |
24 | Power of Attorney (included on signature page hereto). | |
31.1 | Certification of Chief Executive Officer required under Rule 13a-14(a)/15d-14(a) under the Exchange Act. | |
31.2 | Certification of Principal Financial Officer required under Rule 13a-14(a)/15d-14(a) under the Exchange Act. | |
32.1 | Certification of Chief Executive Officer pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002. | |
32.2 | Certification of Principal Financial Officer pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 | |
101 | Financial statements from the Annual Report on Form 10-K of Trovagene for the year ended December 31, 2015, formatted in Extensible Business Reporting Language (XBRL): (i) the Consolidated Balance Sheets, (ii) the Consolidated Statements of Operations and Comprehensive Loss, (iii) the Consolidated Statement of Stockholders’ Equity (Deficiency), (iv) the Consolidated Statements of Cash Flows, and (v) the Notes to Consolidated Financial Statements. | |
+ Indicates a management contract or compensatory plan or arrangement.
* The U.S. Securities and Exchange Commission (SEC) has granted confidential treatment with respect to certain portions of this exhibit. Omitted portions have been filed separately with the SEC.
58
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
TROVAGENE, INC. | |
/s/ Dr. Antonius Schuh | |
March 10, 2016 | Chief Executive Officer |
POWER OF ATTORNEY
KNOW ALL PERSONS BY THESE PRESENTS, that each person whose signature appears below hereby constitutes and appoints, jointly and severally, Antonius Schuh, Ph.D., and Stephen Zaniboni, and each of them acting individually, as his attorney-in-fact, each with full power of substitution and resubstitution, for him in any and all capacities, to sign any and all amendments to this Annual Report on Form 10-K, and to file the same, with exhibits thereto and other documents in connection therewith, with the Securities and Exchange Commission, granting unto said attorneys-in-fact full power and authority to do and perform each and every act and thing requisite and necessary to be done in connection therewith as fully to all intents and purposes as he might or could do in person, hereby ratifying and confirming all that said attorneys-in-fact, or their substitute or substitutes, may lawfully do or cause to be done by virtue hereof.
Pursuant to the requirements of the Securities Exchange Act of 1934, this Report has been signed below by the following persons on behalf of the Registrant and in the capacities and on the dates indicated.
SIGNATURE | TITLE | DATE | |||
/s/ Dr. Antonius Schuh | Chief Executive Officer and Director | March 10, 2016 | |||
Dr. Antonius Schuh | (Principal Executive Officer) | ||||
/s/ Stephen Zaniboni | Chief Financial Officer | March 10, 2016 | |||
Stephen Zaniboni | (Principal Financial and Accounting Officer) | ||||
Chairman of the Board | |||||
Thomas H. Adams | |||||
/s/ John P. Brancaccio | Director | March 10, 2016 | |||
John P. Brancaccio | |||||
/s/ Gary S. Jacob | Director | March 10, 2016 | |||
Gary S. Jacob | |||||
/s/ Paul Billings | Director | March 10, 2016 | |||
Paul Billings | |||||
/s/ Stanley Tennant | Director | March 10, 2016 | |||
Stanley Tennant | |||||
/s/ Rodney S. Markin | Director | March 10, 2016 | |||
Rodney S. Markin | |||||
59
TROVAGENE, INC.
Index to Consolidated Financial Statements
F-1
Report of Independent Registered Public Accounting Firm
Board of Directors and Stockholders
Trovagene, Inc.
San Diego, California
We have audited the accompanying consolidated balance sheets of Trovagene, Inc. and Subsidiaries’ (“Trovagene”) as of December 31, 2015 and 2014 and the related consolidated statements of operations and comprehensive loss, stockholders’ equity (deficit), and cash flows for each of the three years in the period ended December 31, 2015. These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on these financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements, assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the financial statements. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the financial position of Trovagene, Inc. and Subsidiaries at December 31, 2015 and 2014, and the results of its operations and its cash flows for each of the three years in the period ended December 31, 2015, in conformity with accounting principles generally accepted in the United States of America.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), Trovagene’s internal control over financial reporting as of December 31, 2015, based on criteria established in Internal Control — Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO) and our report dated March 10, 2016 expressed an unqualified opinion thereon.
/s/ BDO USA, LLP | |
San Diego, California | |
March 10, 2016 | |
F-2
Trovagene, Inc. and Subsidiaries
Consolidated Balance Sheets
December 31, 2015 | December 31, 2014 | ||||||
Assets | |||||||
Current assets: | |||||||
Cash and cash equivalents | $ | 67,493,047 | $ | 27,293,798 | |||
Accounts receivable | 98,736 | 56,694 | |||||
Prepaid expenses and other assets | 789,285 | 369,259 | |||||
Total current assets | 68,381,068 | 27,719,751 | |||||
Property and equipment, net | 2,690,579 | 840,387 | |||||
Other assets | 374,004 | 336,708 | |||||
Total Assets | $ | 71,445,651 | $ | 28,896,846 | |||
Liabilities and Stockholders’ Equity | |||||||
Current liabilities: | |||||||
Accounts payable | $ | 1,040,868 | $ | 747,799 | |||
Accrued expenses | 1,934,411 | 1,841,808 | |||||
Current portion of long-term debt | 5,225,818 | 1,898,548 | |||||
Total current liabilities | 8,201,097 | 4,488,155 | |||||
Long-term debt, less current portion | 11,246,188 | 13,053,117 | |||||
Derivative financial instruments | 3,297,077 | 3,006,021 | |||||
Total liabilities | 22,744,362 | 20,547,293 | |||||
Commitments and contingencies (Note 10) | |||||||
Stockholders’ equity | |||||||
Preferred stock, $0.001 par value, 20,000,000 shares authorized, 60,600 shares outstanding at each of December 31, 2015 and 2014, designated as Series A Convertible Preferred Stock with liquidation preference of $606,000 at each of December 31, 2015 and 2014 | 60 | 60 | |||||
Common stock, $0.0001 par value, 150,000,000 shares authorized at December 31, 2015 and 2014; 29,737,601 and 18,915,793 issued and outstanding at December 31, 2015 and 2014, respectively | 2,974 | 1,891 | |||||
Additional paid-in capital | 157,585,498 | 89,739,511 | |||||
Accumulated deficit | (108,887,243 | ) | (81,391,909 | ) | |||
Total stockholders’ equity | 48,701,289 | 8,349,553 | |||||
Total Liabilities and Stockholders’ Equity | $ | 71,445,651 | $ | 28,896,846 | |||
The accompanying notes are an integral part of these consolidated financial statements.
F-3
Trovagene, Inc. and Subsidiaries
Consolidated Statements of Operations and Comprehensive Loss
Year Ended December 31, | |||||||||||
2015 | 2014 | 2013 | |||||||||
Royalty income | $ | 274,648 | $ | 270,178 | $ | 259,246 | |||||
License fees | — | 10,000 | — | ||||||||
Diagnostic service revenue | 13,789 | — | — | ||||||||
Other revenue | 24,375 | — | — | ||||||||
Total revenues | 312,812 | 280,178 | 259,246 | ||||||||
Costs and expenses: | |||||||||||
Cost of revenue | 629,191 | 15,441 | — | ||||||||
Research and development | 10,593,869 | 6,664,906 | 3,947,589 | ||||||||
Selling and marketing | 6,443,578 | 2,734,903 | 1,530,160 | ||||||||
General and administrative | 7,919,826 | 5,810,087 | 5,472,038 | ||||||||
Total operating expenses | 25,586,464 | 15,225,337 | 10,949,787 | ||||||||
Loss from operations | (25,273,652 | ) | (14,945,159 | ) | (10,690,541 | ) | |||||
Interest income | 57,261 | 12,239 | 3,663 | ||||||||
Interest expense | (1,525,482 | ) | (843,259 | ) | (17,005 | ) | |||||
Other (income) expense, net | (2,800 | ) | 24,845 | (22,941 | ) | ||||||
Gain (loss) from change in fair value of derivative instruments—warrants | (726,421 | ) | 1,425,850 | (1,084,114 | ) | ||||||
Net loss and comprehensive loss | (27,471,094 | ) | (14,325,484 | ) | (11,810,938 | ) | |||||
Preferred stock dividend | (24,240 | ) | (23,015 | ) | (29,840 | ) | |||||
Net loss and comprehensive loss attributable to common stockholders | $ | (27,495,334 | ) | $ | (14,348,499 | ) | $ | (11,840,778 | ) | ||
Net loss per common share — basic | $ | (1.05 | ) | $ | (0.76 | ) | $ | (0.70 | ) | ||
Net loss per common share — diluted | $ | (1.21 | ) | $ | (0.88 | ) | $ | (0.70 | ) | ||
Weighted-average shares outstanding — basic | 26,201,713 | 18,904,280 | 16,978,212 | ||||||||
Weighted-average shares outstanding — diluted | 26,452,165 | 19,071,112 | 16,978,212 | ||||||||
The accompanying notes are an integral part of these consolidated financial statements.
F-4
Trovagene, Inc. and Subsidiaries
Consolidated Statements of Stockholders’ Equity (Deficit)
Preferred Stock Shares | Preferred Stock Amount | Common Stock Shares | Common Stock Amount | Additional Paid-In Capital | Deficit Accumulated | Total Stockholders’ Equity (Deficit) | |||||||||||||||||||
Balance, January 1, 2013 | 95,600 | $ | 96 | 15,478,177 | $ | 1,547 | $ | 57,370,017 | $ | (55,202,632 | ) | $ | 2,169,028 | ||||||||||||
Sale of common stock, net of expenses | — | — | 2,631,332 | 263 | 18,829,381 | — | 18,829,644 | ||||||||||||||||||
Issuance of warrants in connection with services | — | — | — | — | 198,791 | — | 198,791 | ||||||||||||||||||
Stock-based compensation | — | — | — | — | 1,979,364 | — | 1,979,364 | ||||||||||||||||||
Derivative liability — Warrants reclassified to additional paid-in capital | — | — | — | — | 5,417,871 | — | 5,417,871 | ||||||||||||||||||
Issuance of common stock upon conversion of preferred stock | (35,000 | ) | (36 | ) | 36,458 | 4 | 32 | — | — | ||||||||||||||||
Issuance of common stock upon net exercise of warrant | — | — | 7,284 | 1 | (1 | ) | — | — | |||||||||||||||||
Issuance of common stock upon exercise of warrants | — | — | 715,743 | 72 | 3,599,759 | — | 3,599,831 | ||||||||||||||||||
Issuance of common stock upon net exercise of stock options | — | — | 22,955 | 2 | (2 | ) | — | — | |||||||||||||||||
Issuance of common stock upon exercise of stock options | — | — | 10,833 | 1 | 38,248 | — | 38,249 | ||||||||||||||||||
Preferred stock dividend | — | — | — | (29,840 | ) | (29,840 | ) | ||||||||||||||||||
Net loss | — | — | — | — | — | (11,810,938 | ) | (11,810,938 | ) | ||||||||||||||||
Balance, December 31, 2013 | 60,600 | 60 | 18,902,782 | 1,890 | 87,433,460 | (67,043,410 | ) | 20,392,000 | |||||||||||||||||
Trovagene, Inc. and Subsidiaries
Consolidated Statements of Stockholders’ Equity (Deficit)
Preferred Stock Shares | Preferred Stock Amount | Common Stock Shares | Common Stock Amount | Additional Paid-In Capital | Deficit Accumulated | Total Stockholders’ Equity (Deficit) | |||||||||||||||||||
Stock-based compensation | — | — | — | — | 2,070,195 | — | 2,070,195 | ||||||||||||||||||
Issuance of warrant in connection with debt agreement | — | — | — | — | 235,857 | — | 235,857 | ||||||||||||||||||
Issuance of common stock upon net exercise of warrant | — | — | 13,011 | 1 | (1 | ) | — | — | |||||||||||||||||
Preferred stock dividend | — | — | — | — | — | (23,015 | ) | (23,015 | ) | ||||||||||||||||
Net loss | — | — | — | — | — | (14,325,484 | ) | (14,325,484 | ) | ||||||||||||||||
Balance, December 31, 2014 | 60,600 | 60 | 18,915,793 | 1,891 | 89,739,511 | (81,391,909 | ) | 8,349,553 | |||||||||||||||||
Sale of common stock, net of expenses | — | — | 9,996,531 | 1,000 | 61,214,399 | — | 61,215,399 | ||||||||||||||||||
Stock-based compensation | — | — | — | — | 3,946,027 | — | 3,946,027 | ||||||||||||||||||
Derivative liability - Warrants reclassified to additional paid-in capital | — | — | — | — | 435,365 | — | 435,365 | ||||||||||||||||||
Issuance of common stock upon exercise of stock options | — | — | 265,166 | 27 | 860,825 | — | 860,852 | ||||||||||||||||||
Issuance of common stock upon net exercise of warrant | — | — | 277,136 | 28 | (28 | ) | — | — | |||||||||||||||||
Issuance of common stock upon exercise of warrants | — | — | 282,975 | 28 | 1,389,399 | — | 1,389,427 | ||||||||||||||||||
Preferred stock dividend | — | — | — | — | — | (24,240 | ) | (24,240 | ) | ||||||||||||||||
Net loss | — | — | — | — | — | (27,471,094 | ) | (27,471,094 | ) | ||||||||||||||||
Balance, December 31, 2015 | 60,600 | $ | 60 | 29,737,601 | $ | 2,974 | $ | 157,585,498 | $ | (108,887,243 | ) | $ | 48,701,289 | ||||||||||||
Trovagene, Inc. and Subsidiaries
Consolidated Statements of Cash Flows
Year ended December 31, | |||||||||||
2015 | 2014 | 2013 | |||||||||
Operating activities | |||||||||||
Net loss | $ | (27,471,094 | ) | $ | (14,325,484 | ) | $ | (11,810,938 | ) | ||
Adjustments to reconcile net loss to net cash used in operating activities: | |||||||||||
Loss (gain) on disposal of fixed assets | 4,562 | (24,845 | ) | 22,941 | |||||||
Depreciation and amortization | 378,711 | 234,813 | 130,520 | ||||||||
Stock-based compensation expense | 3,946,027 | 2,070,194 | 1,979,364 | ||||||||
Amortization of debt costs | 346,157 | 248,799 | — | ||||||||
Accretion of discount on debt | 88,123 | 57,117 | — | ||||||||
Change in fair value of financial instruments | 726,421 | (1,425,850 | ) | 1,084,114 | |||||||
Stock and warrant issued in connection with consulting services | — | — | 198,791 | ||||||||
Changes in operating assets and liabilities: | |||||||||||
Decrease (increase) in other assets | (37,296 | ) | (258 | ) | 25,631 | ||||||
Decrease (increase) in accounts receivable | (42,042 | ) | 22,300 | 89,387 | |||||||
Increase in prepaid expenses | (420,026 | ) | (216,470 | ) | (92,748 | ) | |||||
Increase in accounts payable and accrued expenses | 361,432 | 632,299 | 1,055,690 | ||||||||
Net cash used in operating activities | (22,119,025 | ) | (12,727,385 | ) | (7,317,248 | ) | |||||
Investing activities: | |||||||||||
Capital expenditures | (2,241,066 | ) | (363,290 | ) | (649,784 | ) | |||||
Proceeds from disposals of capital equipment | 7,600 | 63,500 | 500 | ||||||||
Net cash used in investing activities | (2,233,466 | ) | (299,790 | ) | (649,284 | ) | |||||
Financing activities | |||||||||||
Proceeds from sale of common stock, net of expenses | 61,215,399 | — | 18,829,644 | ||||||||
Proceeds from exercise of warrants | 1,389,427 | — | 3,599,831 | ||||||||
Proceeds from exercise of options | 860,852 | — | 38,249 | ||||||||
Borrowings under equipment line of credit | 1,086,062 | — | 515,964 | ||||||||
Repayments under equipment line of credit | — | (515,964 | ) | — | |||||||
Borrowings under debt agreement | — | 15,000,000 | — | ||||||||
Net cash provided by financing activities | 64,551,740 | 14,484,036 | 22,983,688 | ||||||||
Net change in cash and cash equivalents | 40,199,249 | 1,456,861 | 15,017,156 | ||||||||
Cash and cash equivalents—Beginning of period | 27,293,798 | 25,836,937 | 10,819,781 | ||||||||
Cash and cash equivalents—End of period | $ | 67,493,047 | $ | 27,293,798 | $ | 25,836,937 | |||||
Supplementary disclosure of cash flow activity: | |||||||||||
Cash paid for taxes | $ | 16,934 | $ | 2,400 | $ | 7,650 | |||||
Cash paid for interest | $ | 1,061,993 | $ | 425,256 | $ | 9,459 | |||||
Supplemental disclosure of non-cash investing and financing activities: | |||||||||||
Warrants issued in connection with Loan and Security Agreement | $ | — | $ | 235,857 | $ | — | |||||
Reclassification of derivative financial instruments to additional paid-in capital | $ | 435,365 | $ | — | $ | (5,417,871 | ) | ||||
Preferred stock dividends accrued | $ | 24,240 | $ | 23,015 | $ | 29,840 | |||||
The accompanying notes are an integral part of these consolidated financial statements.
F-7
Trovagene, Inc. and Subsidiaries
Notes to Consolidated Financial Statements
1. Business Overview and Liquidity
Trovagene, Inc. (“Trovagene” or the “Company”) is a molecular diagnostic company that focuses on the development and commercialization of a proprietary urine-based cell-free molecular diagnostic technology for use in disease detection and monitoring across a variety of medical disciplines. Trovagene’s primary internal focus is to leverage its novel urine-based molecular diagnostic platform to facilitate improvements in the field of oncology, while the Company’s external focus includes entering into collaborations to develop the Company’s technology in areas such as infectious disease, transplant medicine and prenatal genetics. The Company’s goal is to improve treatment outcomes for cancer patients using its proprietary technology to detect and quantitatively monitor cell-free DNA in urine.
To date, Trovagene’s efforts have been principally devoted to research and development, securing and protecting patents and raising capital. Through December 31, 2015, the Company sustained cumulative net losses attributed to common stockholders of $108,887,243. The Company’s losses have resulted primarily from expenditures incurred in connection with research and development activities, stock-based compensation expense, patent filing and maintenance expenses, outside accounting and legal services and regulatory, scientific and financial consulting fees, amortization and liquidated damages. To date, the Company has generated only limited revenue from operations and expects to incur additional losses to perform further research and development activities as well as expenses related to the commercialization of the diagnostic tests the Company had commercially available as of December 31, 2015.
Liquidity
The Company will need to continue to raise funds until it is able to generate revenues from operations sufficient to fund its development and commercial operations.
Cash used in operating activities was $22,119,025, $12,727,385, and $7,317,248 for the years ended December 31, 2015, 2014, and 2013, respectively. During the years ended December 31, 2015, 2014, and 2013, the Company incurred net loss and comprehensive loss attributable to common stockholders of $27,495,334, $14,348,499, and $11,840,778, respectively. The Company believes that it currently has adequate capital to continue operations for the next twelve months. However, to carry the Company forward beyond the next twelve months, and until it can generate adequate cash flow from operations, additional cash resources will be necessary.
To date, Trovagene’s sources of cash have been primarily limited to the sale of debt and equity securities and debt financing. Net cash provided by financing activities for the years ended December 31, 2015, 2014, and 2013 was $64,551,740, $14,484,036 and $22,983,688, respectively. The Company cannot be certain that additional funding will be available on acceptable terms, or at all. To the extent that the Company can raise additional funds by issuing equity securities, the Company’s stockholders may experience significant dilution. Any debt financing, if available, may involve restrictive covenants that impact the Company’s ability to conduct its business.
If the Company is unable to raise additional capital when required or on acceptable terms, it may have to significantly delay, scale back or discontinue the development and/or commercialization of one or more of its product candidates. The Company may also be required to:
• | Seek collaborators for product candidates at an earlier stage than otherwise would be desirable and on terms that are less favorable than might otherwise be available; and |
• | Relinquish licenses or otherwise dispose of rights to technologies, product candidates or products that the Company would otherwise seek to develop or commercialize itself. |
2. Basis of Presentation and Summary of Significant Accounting Policies
The accompanying consolidated financial statements of Trovagene, which include its wholly owned subsidiary Trovagene Srl, a subsidiary formed in Italy, have been prepared in accordance with accounting principles generally accepted in the United States of America (“GAAP”). All intercompany balances and transactions have been eliminated.
F-8
Use of Estimates
The preparation of financial statements in conformity with U.S. GAAP requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenues and expenses during the reporting period. Actual results could differ from those estimates.
Cash and Cash Equivalents
Cash and cash equivalents consist of operating and money market accounts as of December 31, 2015 and 2014 on deposit with U.S. commercial banks. Cash equivalents are considered by the Company to be highly liquid investments purchased with original maturities of three months or less from the date of purchase.
Concentration of Credit Risk
Financial instruments that potentially subject the Company to significant concentrations of credit risk consist primarily of cash and cash equivalents. The Company maintains deposit accounts that are not insured by the Federal Deposit Insurance Corporation in federally insured financial institutions. The Company has not experienced any losses in such accounts and believes it is not exposed to significant risk on its cash due to the financial position of the depository institution in which those deposits are held.
Revenues
Revenue is recognized when persuasive evidence that an arrangement exists, delivery has occurred, the price is fixed or determinable, and collection is reasonably assured.
Milestone, Royalty and License Revenues
The Company licenses and sublicenses its patent rights to healthcare companies, medical laboratories and biotechnology partners. These agreements may involve multiple elements such as license fees, royalties and milestone payments. Revenue is recognized when the criteria described above have been met as well as the following:
•Up-front nonrefundable license fees pursuant to agreements under which the Company has no continuing performance obligations are recognized as revenues on the effective date of the agreement and when collection is reasonably assured.
•Minimum royalties are recognized as earned, and royalties in excess of minimum amounts are recognized upon receipt of payment when collection is assured.
•Milestone payments are recognized when both the milestone is achieved and the related payment is received.
Diagnostic Service Revenues
Revenue for clinical laboratory tests may come from several sources, including commercial third-party payors, such as insurance companies and health maintenance organizations, government payors, such as Medicare and Medicaid in the United States, patient self-pay and, in some cases, from hospitals or referring laboratories who, in turn, might bill third-party payors for testing. The Company is recognizing diagnostic service revenue on the cash collection basis until such time as it is able to properly estimate collections on third party reimbursements.
Allowance for Doubtful Accounts
The Company reviews the collectability of accounts receivable based on an assessment of historic experience, current economic conditions, and other collection indicators. At each of December 31, 2015, 2014 and 2013, the Company had not recorded an allowance for doubtful accounts. When accounts are determined to be uncollectible, they are written off against the reserve balance and the reserve is reassessed. When payments are received on reserved accounts, they are applied to the individual’s account and the reserve is reassessed.
F-9
Derivative Financial Instruments—Warrants
The Company has issued common stock warrants in connection with the execution of certain equity financings. Such warrants are classified as derivative liabilities under the provisions of Financial Accounting Standards Board (“FASB”) Accounting Standards Codification (“ASC”) Topic 815, Derivatives and Hedging (“ASC 815”) and are recorded at their fair market value as of each reporting period. Such warrants do not meet the exemption that a contract should not be considered a derivative instrument if it is (1) indexed to its own stock and (2) classified in stockholders’ equity. Changes in fair value of derivative liabilities are recorded in the consolidated statement of operations under the caption “Change in fair value of derivative instruments.”
The fair value of warrants is determined using the Black-Scholes option-pricing model using assumptions regarding the volatility of Trovagene’s common stock price, the remaining life of the warrant, and the risk-free interest rates at each period end. The Company thus uses model-derived valuations where inputs are observable in active markets to determine the fair value and accordingly classifies such warrants in Level 3 per FASB ASC Topic 820, Fair Value Measurements (“ASC 820”). At December 31, 2015 and 2014, the fair value of these warrants was $3,297,077 and $3,006,021, respectively, and was included in the derivative financial instruments liability on the balance sheet.
Stock-Based Compensation
FASB ASC Topic 718 “Compensation—Stock Compensation” (“ASC 718”) requires companies to measure the cost of employee services received in exchange for the award of equity instruments based on the estimated fair value of the award at the date of grant. The expense is recognized over the period during which an employee is required to provide services in exchange for the award. ASC 718 did not change the way Trovagene accounts for non-employee stock-based compensation. Trovagene continues to account for shares of common stock, stock options and warrants issued to non-employees based on the fair value of the stock, stock option or warrant, if that value is more reliably measurable than the fair value of the consideration or services received. The Company accounts for stock options issued and vesting to non-employees in accordance with FASB ASC Topic 505-50 “Equity -Based Payment to Non-Employees”, and, accordingly, the value of the stock compensation to non-employees is based upon the measurement date as determined at either (1) the date at which a performance commitment is reached, or (2) the date at which the necessary performance to earn the equity instruments is complete. Therefore, the fair value of these options is being “marked to market” quarterly until the measurement date is determined.
Fair Value of Financial Instruments
Financial instruments consist of cash and cash equivalents, accounts receivable, accounts payable, debt and derivative liabilities. The Company has adopted ASC 820 for financial assets and liabilities that are required to be measured at fair value and non-financial assets and liabilities that are not required to be measured at fair value on a recurring basis. These financial instruments are stated at their respective historical carrying amounts, which approximate fair value due to their short term nature as they reflect current market interest rates. Debt is stated at its respective historical carrying amounts, which approximate fair value as they reflect current market interest rates.
In accordance with FASB ASC Subtopic 820-10, the Company measures certain assets and liabilities at fair value on a recurring basis using the three-tier fair value hierarchy, which prioritizes the inputs used in measuring fair value. The three tiers include:
• | Level 1 — Quoted prices for identical instruments in active markets. |
• | Level 2 — Quoted prices for similar instruments in active markets; quoted prices for identical or similar instruments in markets that are not active; and model-derived valuations where inputs are observable or where significant value drivers are observable. |
• | Level 3 — Instruments where significant value drivers are unobservable to third parties. |
Property, Equipment and Depreciation and Amortization
Expenditures for additions, renewals and improvements are capitalized at cost. Depreciation and amortization is generally computed on a straight-line method based on the estimated useful lives of the related assets. Amortization of leasehold improvements is computed based on the shorter of the life of the asset or the term of the lease. The estimated useful lives of the major classes of depreciable assets are three to five years for laboratory equipment and furniture and fixtures. Expenditures for repairs and maintenance are charged to operations as incurred.
F-10
Impairment of Indefinite and Long-Lived Assets
The Company reviews its long-lived and indefinite assets to determine if any event has occurred that may indicate its intangible assets with indefinite lives and other long-lived assets are potentially impaired. If indicators of impairment exist, the Company performs an impairment test to assess the recoverability of the affected assets by determining whether the carrying amount of such assets exceeds the undiscounted expected future cash flows. If the affected assets are not recoverable, the Company estimates the fair value of the assets and records an impairment loss if the carrying value of the assets exceeds the fair value. Factors that would indicate potential impairment include a significant decline in the Company’s stock price and market capitalization compared to its net book value, significant changes in the ability of a particular asset to generate positive cash flows, and significant changes in the Company’s strategic business objectives and utilization of a particular asset. The Company noted no indications of impairment for the years ended December 31, 2015, 2014, and 2013.
Income Taxes
Income taxes are determined using the asset and liability approach of accounting for income taxes. Under this approach, deferred taxes represent the future tax consequences expected to occur when the reported amounts of assets and liabilities are recovered or paid. Deferred taxes result from differences between the financial statement and tax bases of Trovagene’s assets and liabilities and are adjusted for changes in tax rates and tax laws when changes are enacted. Valuation allowances are recorded to reduce deferred tax assets when it is more likely than not that a tax benefit will not be realized. The assessment of whether or not a valuation allowance is required often requires significant judgment.
Contingencies
In the normal course of business, Trovagene is subject to loss contingencies, such as legal proceedings and claims arising out of its business, that cover a wide range of matters, including, among others, government investigations, stockholder lawsuits, product and environmental liability, and tax matters. In accordance with FASB ASC Topic 450, Accounting for Contingencies, Trovagene records such loss contingencies when it is probable that a liability has been incurred and the amount of loss can be reasonably estimated. Trovagene, in accordance with this guidance, does not recognize gain contingencies until realized.
Cost of Revenue
Cost of revenue represents the cost of materials, personnel costs, costs associated with processing specimens including pathological review, quality control analyses, and delivery charges necessary to render an individualized test result. Costs associated with performing tests are recorded as the tests are processed.
Research and Development
Research and development expenses, which include expenditures in connection with an in-house research and development laboratory, salaries and staff costs, purchased in-process research and development and regulatory and scientific consulting fees, as well as contract research and insurance, are accounted for in accordance with FASB ASC Topic 730-10-55-2, Research and Development. Also, as prescribed by this guidance, patent filing and maintenance expenses are considered legal in nature and therefore classified as general and administrative expense, if any.
While certain of the Company’s research and development costs may have future benefits, the Company’s policy of expensing all research and development expenditures is predicated on the fact that Trovagene has no history of successful commercialization of molecular diagnostic products to base any estimate of the number of future periods that would be benefited.
FASB ASC Topic 730, Research and Development requires that non-refundable advance payments for goods or services that will be used or rendered for future research and development activities be deferred and capitalized. As the related goods are delivered or the services are performed, or when the goods or services are no longer expected to be provided, the deferred amounts are recognized as an expense. There were no non-refundable advance payments as of December 31, 2015, 2014 and 2013.
F-11
Net Loss Per Share
Basic and diluted net loss per share is presented in conformity with FASB ASC Topic 260, Earnings per Share, for all periods presented. In accordance with this guidance, basic and diluted net loss per common share is determined by dividing net loss applicable to common stockholders by the weighted-average common shares outstanding during the period. Preferred dividends are included in income available to common stockholders in the computation of basic and diluted earnings per share. Shares used in calculating diluted net loss per common share exclude as anti-dilutive the following share equivalents:
December 31, | ||||||||
2015 | 2014 | 2013 | ||||||
Options to purchase Common Stock | 6,948,630 | 4,913,472 | 4,287,545 | |||||
Warrants to purchase Common stock | 4,565,947 | 5,251,660 | 6,233,483 | |||||
Series A Convertible Preferred Stock | 63,125 | 63,125 | 63,125 | |||||
11,577,702 | 10,228,257 | 10,584,153 | ||||||
The following table summarizes the Company’s diluted net loss per share:
December 31, | |||||||||||
2015 | 2014 | 2013 | |||||||||
Numerator: | |||||||||||
Net loss attributable to common stockholders | $ | (27,495,334 | ) | $ | (14,348,499 | ) | $ | (11,840,778 | ) | ||
Adjustment for change in fair value of derivative instruments - warrants | (4,396,061 | ) | (2,422,337 | ) | — | ||||||
Net loss used for diluted loss per share | $ | (31,891,395 | ) | $ | (16,770,836 | ) | $ | (11,840,778 | ) | ||
Denominator: | |||||||||||
Weighted-average shares used to compute basic net loss per share | 26,201,713 | 18,904,280 | 16,978,212 | ||||||||
Adjustments to reflect assumed exercise of warrants | 250,452 | 166,832 | — | ||||||||
Weighted-average shares used to compute diluted net loss per share | 26,452,165 | 19,071,112 | 16,978,212 | ||||||||
Net loss per share diluted | $ | (1.21 | ) | $ | (0.88 | ) | $ | (0.70 | ) | ||
Recent Accounting Pronouncements
In February 2016, the FASB issued Accounting Standards Update (“ASU”) 2016-02, Leases. The new standard establishes a right-of-use (“ROU”) model that requires a lessee to record a ROU asset and a lease liability on the balance sheet for all leases with terms longer than 12 months. Leases will be classified as either finance or operating, with classification affecting the pattern of expense recognition in the income statement. The new standard is effective for fiscal years beginning after December 15, 2018, including interim periods within those fiscal years. A modified retrospective transition approach is required for capital and operating leases existing at, or entered into after, the beginning of the earliest comparative period presented in the financial statements, with certain practical expedients available. The Company is currently evaluating the impact the adoption of the new standard will have on its consolidated financial statements.
In August 2014, the FASB issued ASU 2014-15, Presentation of Financial Statements—Going Concern, which impacts the accounting guidance related to the evaluation of an entity’s ability to continue as a going concern. The amendment establishes management’s responsibility to evaluate whether there is substantial doubt about an entity’s ability to continue as a going concern in connection with preparing financial statements for each annual and interim reporting period. The amendment also gives guidance to determine whether to disclose information about relevant conditions and events when there is substantial doubt about an entity’s ability to continue as a going concern. The amended guidance is effective prospectively for fiscal years beginning after December 15, 2016. The new guidance is not expected to have a material impact on the Company’s financial position, results of operations or cash flows.
In May 2014, the FASB issued ASU 2014-9, Revenue from Contracts with Customers (“ASU 2014-9”). ASU 2014-9 provides companies with a single model for accounting for revenue arising from contracts with customers and supersedes current revenue recognition guidance, including industry-specific revenue guidance. The core principle of the model is to
F-12
recognize revenue when control of the goods or services transfers to the customer, as opposed to recognizing revenue when the risks and rewards transfer to the customer under the existing revenue guidance. The guidance permits companies to either apply the requirements retrospectively to all prior periods presented, or apply the requirements in the year of adoption, through a cumulative adjustment. In August 2015, the FASB issued ASU 2015-14, Deferral of the Effective Date, which defers the required adoption date of ASU 2014-09 by one year. As a result of the deferred effective date, ASU 2014-09 will be effective for the Company in its first quarter of fiscal year 2018. Early adoption is permitted but not before the original effective date of the first quarter of fiscal year 2017. The Company is in the process of evaluating the transition method that will be elected and the impact of adoption of ASU 2014-09 on its consolidated financial statements.
3. Property and Equipment
Fixed assets consist of laboratory, testing and computer equipment and fixtures stated at cost. Depreciation and amortization expense for the years ended December 31, 2015, 2014, and 2013 was $378,711, $234,813, and $130,520, respectively. Property and equipment consisted of the following:
As of December 31, | |||||||
2015 | 2014 | ||||||
Furniture and office equipment | $ | 1,483,227 | $ | 365,955 | |||
Leasehold Improvements | 39,401 | 39,401 | |||||
Laboratory equipment | 2,022,733 | 968,901 | |||||
3,545,361 | 1,374,257 | ||||||
Less—accumulated depreciation and amortization | (854,782 | ) | (533,870 | ) | |||
Property and equipment, net | $ | 2,690,579 | $ | 840,387 | |||
4. Stockholders’ Equity (Deficit)
Common Stock
On January 25, 2013, the Company filed a Registration Statement on Form S-3 (the “Registration Statement”) to offer and sell in one or more offerings, any combination of common stock, preferred stock, warrants, or units having an aggregate initial offering price of up to $150,000,000. If issued, the preferred stock, warrants and units would be convertible, exercisable or exchangeable for common stock, preferred stock or other Trovagene securities. The Registration Statement was declared effective on February 4, 2013. In addition, in connection with the Registration Statement, the Company entered into an agreement with Cantor Fitzgerald & Co. (“Agent”) on January 25, 2013 to issue and sell up to $30,000,000 of shares of common stock. As payment for its services, the Agent is entitled to a 3% commission on gross proceeds on sales of the Company’s securities. The Company received gross proceeds of approximately $4.2 million from the sale of 488,476 shares of its common stock during the year ended December 31, 2013 under the agreement with the Agent. In addition, the Company received gross proceeds of approximately $15.0 million from the sale of 2,142,857 shares of its common stock through a registered direct offering that occurred in July 2013.
During the year ended December 31, 2013, the Company issued a total of 3,424,605 shares of common stock. The Company sold 2,631,332 shares of common stock for net proceeds of $18,829,644. In addition, 36,458 shares were issued upon conversion of Series A Preferred Stock, 715,743 shares were issued upon exercise of 715,743 warrants for a weighted-average price of $5.02 and 7,284 shares were issued upon net exercise of 12,745 warrants at an exercise price of $3.00. The remaining 33,788 shares include 22,955 shares that were issued upon net exercise of an option to purchase 41,667 shares of common stock at an exercise price of $4.50 and the exercise of an option to purchase 10,833 shares of common stock at a weighted-average exercise price of $3.53.
During the year ended December 31, 2014, the Company issued a total of 13,011 shares of common stock upon the net exercise of warrants at a weighted-average exercise price of $3.00.
During the year ended December 31, 2015, the Company issued a total of 10,821,808 shares of common stock. The Company received gross proceeds of approximately $63.2 million from the sale of 9,711,110 shares of its common stock through underwritten public offerings in February 2015 and July 2015. The Company also received gross proceeds of approximately $2.8 million from the sale of 285,421 shares of its common stock at a weighted-average price of $9.66 under the agreement with the Agent. In addition, 265,166 shares were issued upon exercise of options for a weighted-average price of
F-13
$3.25, 282,975 shares were issued upon exercise of warrants for a weighted-average price of $4.91, and 277,136 shares were issued upon net exercise of 449,403 warrants at a weighted-average exercise price of $3.05.
Warrants
A summary of warrant activity and changes in warrants outstanding, including both liability and equity classifications, is presented below:
Number of Warrants | Weighted-Average Exercise Price Per Share | Weighted-Average Remaining Contractual Term | ||||||
Balance outstanding, December 31, 2012 | 6,985,070 | $ | 3.96 | 5.4 | ||||
Granted | 50,000 | $ | 8.00 | |||||
Exercised | (728,488 | ) | $ | 4.99 | ||||
Expired | (73,099 | ) | $ | 4.50 | ||||
Balance outstanding, December 31, 2013 | 6,233,483 | $ | 3.87 | 4.5 | ||||
Granted | 85,470 | $ | 3.51 | |||||
Exercised | (36,666 | ) | $ | 3.00 | ||||
Expired | (16,667 | ) | $ | 10.80 | ||||
Balance outstanding, December 31, 2014 | 6,265,620 | $ | 3.85 | 3.6 | ||||
Exercised | (732,378 | ) | $ | 3.77 | ||||
Balance outstanding, December 31, 2015 | 5,533,242 | $ | 3.86 | 2.5 | ||||
The Company issued a warrant to purchase 50,000 shares of common stock at an exercise price of $8.00 per share during the year ended December 31, 2013. The warrant was issued in connection with an agreement to provide services related to investor and public relations materials and expires three years from date of grant. The estimated fair value of the warrant was determined on the date of grant using the Black-Scholes option valuation model using the following assumptions: a risk-free interest rate of 0.42%, dividend yield of 0%, expected volatility of 97% and expected term of three years. The resulting fair value of $198,791 was recorded as stock-based compensation expense.
The Company issued warrants to purchase 85,470 shares of common stock at an exercise price of $3.51 per share during the year ended December 31, 2014. The warrants were issued in connection with a $15.0 million debt agreement. The estimated fair value of the warrants was determined on the date of grant using the Black-Scholes option valuation model using the following assumptions: a risk-free interest rate of 2.53%, dividend yield of 0%, expected volatility of 73.8% and expected term of ten years. The resulting fair value of $235,857 was recorded as a debt discount and was amortized to interest expense over the term of the loan using the effective interest method.
Series A Convertible Preferred Stock
The material terms of the Series A Convertible Preferred Stock consist of:
1) Dividends. Holders of the Company’s Series A Convertible Preferred Stock are entitled to receive cumulative dividends at the rate per share of 4% per annum, payable quarterly on March 31, June 30, September 30 and December 31, beginning with September 30, 2005. Dividends are payable, at the Company’s sole election, in cash or shares of common stock. As of December 31, 2015, 2014, and 2013, the Company had $268,295, $244,055, and $221,040, respectively in accrued cumulative unpaid preferred stock dividends, included in Accrued Expenses in the Company’s consolidated balance sheets, and $24,240, $23,015, and $29,840 of accrued dividends was recorded during the years ended December 31, 2015, 2014, and 2013, respectively.
2) Voting Rights. Shares of the Series A Convertible Preferred Stock have no voting rights. However, so long as any shares of Series A Convertible Preferred Stock are outstanding, the Company may not, without the affirmative vote of the holders of the shares of Series A Convertible Preferred Stock then outstanding, (a) adversely change the powers, preferences or rights given to the Series A Convertible Preferred Stock, (b) authorize or create any class of stock senior or equal to the Series A Convertible Preferred Stock, (c) amend its certificate of incorporation or other charter documents, so as to affect adversely any rights of the holders of Series A Convertible Preferred Stock or (d) increase the authorized number of shares of Series A Convertible Preferred Stock.
F-14
3) Liquidation. Upon any liquidation, dissolution or winding-up of the Company, the holders of the Series A Convertible Preferred Stock are entitled to receive an amount equal to the Stated Value per share, which is currently $10 per share plus any accrued and unpaid dividends.
4) Conversion Rights. Each share of Series A Convertible Preferred Stock is convertible at the option of the holder into that number of shares of common stock determined by dividing the Stated Value, currently $10 per share, by the conversion price, originally $2.15 per share.
5) Subsequent Equity Sales. The conversion price is subject to adjustment for dilutive issuances for a period of 12 months beginning upon registration of the common stock underlying the Series A Convertible Preferred Stock. The relevant registration statement became effective on March 17, 2006 and during the following twelve month period the conversion price was adjusted to $9.60 per share.
6) Automatic Conversion. If the price of the Company’s common stock equals $25.80 per share for 20 consecutive trading days, and an average of 8,333 shares of common stock per day are traded during the 20 trading days, the Company will have the right to deliver a notice to the holders of the Series A Convertible Preferred Stock, requesting the holders to convert any portion of the shares of Series A Convertible Preferred Stock into shares of common stock at the applicable conversion price. As of the date of these financial statements, such conditions have not been met.
During the year ended December 31, 2013, 35,000 shares of Series A Convertible Preferred Stock were converted into 36,458 shares of common stock, on a net converted basis. As of each of December 31, 2015, 2014, and 2013, there were 60,600 shares of Series A Convertible Preferred Stock outstanding.
5. Stock Option Plan
In June 2004, the Company adopted the Trovagene Stock Option Plan, as amended (the “2004 Plan”), under which up to 6,000,000 shares common stock were reserved for issuance to directors and eligible employees, including executive officers and consultants. Generally, vesting for options granted under the Plan was from three to four years, and options expired after a 10-year period. Options were granted at an exercise price not less than the fair market value at the date of grant. As of December 31, 2014, the 2004 Plan was expired. As of December 31, 2013, there were 1,788,921 shares available for issuance under the 2004 Plan.
During 2013, the Company issued 260,000 options over the authorized number of options in the 2004 Plan. As per FASB ASC Topic 815-40, the options were accounted for as liabilities and recorded at fair value with the changes in fair value being recorded in the Company’s statement of operations. Stockholder approval was obtained on July 18, 2013 to increase the number of authorized shares in the 2004 Plan from 3,666,667 to 6,000,000. Accordingly, the options were remeasured as of the date of stockholder approval with the change recorded in stock based compensation expense and the $23,024 liability was reclassified to additional paid-in capital.
In July 2013, an option to purchase 90,000 shares of common stock was granted to a member of the Board for services provided outside of routine Board activities. This option was vested in full upon grant. The fair value of this option was approximately $500,000 and is included in general and administrative expenses.
The Trovagene, Inc. 2014 Equity Incentive Plan (the “2014 EIP’), authorizing up to 2,500,000 shares of common stock for issuance under the 2014 EIP, was approved by the Board in June 2014 and approved by the stockholders of the Company at the September 17, 2014 Annual Meeting of Stockholders. An additional 2,500,000 shares of common stock was authorized for issuance by the Board in March 2015 and was approved by the stockholders at the June 10, 2015 Annual Meeting of Stockholders.
As of December 31, 2015, there were 1,361,832 shares available for issuance under the 2014 EIP.
F-15
Stock-based compensation has been recognized in operating results as follows:
Years ended December 31, | |||||||||||
2015 | 2014 | 2013 | |||||||||
In cost of revenue | $ | 39,676 | $ | — | $ | — | |||||
In research and development expenses | 1,499,009 | 796,008 | 549,465 | ||||||||
In selling and marketing expense | 768,146 | 145,239 | 70,626 | ||||||||
In general and administrative expenses | 1,639,196 | 1,128,947 | 1,359,273 | ||||||||
Total stock-based compensation | $ | 3,946,027 | $ | 2,070,194 | $ | 1,979,364 | |||||
The estimated fair value of stock option awards was determined on the date of grant using the Black-Scholes option valuation model with the following assumptions during the years indicated below:
Years ended December 31, | |||||
2015 | 2014 | 2013 | |||
Risk-free interest rate | 1.35% - 2.15% | 1.42% - 2.1% | 0.74% - 1.5% | ||
Dividend yield | 0% | 0% | 0% | ||
Expected volatility (range) | 73% - 77% | 81% - 86% | 82% - 100% | ||
Expected volatility (weighted-average) | 75% | 85% | 91% | ||
Expected term (in years) | 6.0 years | 5.8 years | 5.0 years | ||
Risk-free interest rate — Based on the daily yield curve rates for U.S. Treasury obligations with maturities that correspond to the expected term of the Company’s stock options.
Dividend yield — Trovagene has not paid any dividends on common stock since its inception and does not anticipate paying dividends on its common stock in the foreseeable future.
Expected volatility — Based on the historical volatility of a group of peer companies with attributes similar to Trovagene.
Expected term — The expected option term represents the period that stock-based awards are expected to be outstanding based on the simplified method provided in Staff Accounting Bulletin (“SAB”) No. 107, Share-Based Payment (“SAB No. 107”), which averages an award’s weighted-average vesting period and expected term for “plain vanilla” share options. Under SAB No. 107, options are considered to be “plain vanilla” if they have the following basic characteristics: (1) are granted “at-the-money”; (2) exercisability is conditioned upon service through the vesting date; (3) termination of service prior to vesting results in forfeiture; (4) limited exercise period following termination of service; and (5) are non-transferable and non-hedgeable.
Forfeitures — FASB ASC Topic 718 (“ASC 718”) requires forfeitures to be estimated at the time of grant and revised, if necessary, in subsequent periods if actual forfeitures differ from those estimates. The Company estimates forfeitures based on its historical experience.
The weighted-average fair value per share of all options granted during the years ended December 31, 2015, 2014, and 2013, estimated as of the grant date using the Black-Scholes option valuation model, was $4.60, $3.16 and $4.54 per share, respectively.
The unrecognized compensation cost related to non-vested stock options outstanding at December 31, 2015 and 2014 was $10,430,604 and $4,862,030, respectively. The weighted-average remaining contractual term at December 31, 2015 and 2014 for options outstanding and vested options was 3.1 years and 3.0 years, respectively.
The total intrinsic value of stock options exercised was $1,382,255, $0 and $275,492 during the years ended December 31, 2015, 2014 and 2013, respectively. The total fair value of shares vested during the years ended December 31, 2015, 2014 and 2013 was $2,634,688, $1,960,256 and $1,633,071, respectively.
F-16
A summary of stock option activity and of changes in stock options outstanding is presented below:
Number of Options | Weighted-Average Exercise Price Per Share | Intrinsic Value | Weighted-Average Remaining Contractual Life | |||||||||
Balance outstanding, December 31, 2012 | 3,711,303 | $ | 4.69 | $ | 8,301,484 | 6.3 years | ||||||
Granted | 1,144,760 | $ | 6.33 | |||||||||
Exercised | (52,500 | ) | $ | 4.30 | ||||||||
Forfeited | (516,018 | ) | $ | 4.35 | ||||||||
Balance outstanding, December 31, 2013 | 4,287,545 | $ | 5.18 | $ | 5,896,329 | 6.7 years | ||||||
Granted | 1,410,038 | $ | 4.42 | |||||||||
Forfeited | (784,111 | ) | $ | 7.08 | ||||||||
Balance outstanding, December 31, 2014 | 4,913,472 | $ | 4.66 | $ | 2,808,083 | 7.6 years | ||||||
Granted | 2,688,500 | $ | 7.02 | |||||||||
Exercised | (265,166 | ) | $ | 3.25 | ||||||||
Forfeited | (388,176 | ) | $ | 7.75 | ||||||||
Balance outstanding, December 31, 2015 | 6,948,630 | $ | 5.45 | $ | 5,903,466 | 7.8 years | ||||||
Vested and exercisable, December 31, 2015 | 2,825,398 | $ | 4.38 | $ | 4,194,205 | 6.0 years | ||||||
ASC 718 requires that cash flows resulting from tax deductions in excess of the cumulative compensation cost recognized for options exercised (excess tax benefits) be classified as cash inflows from financing activities and cash outflows from operating activities. Due to Trovagene’s accumulated deficit position, no tax benefits have been recognized in the cash flow statement.
6. Derivative Financial Instruments — Warrants
Based upon the Company’s analysis of the criteria contained in ASC Topic 815-40, Contracts in Entity’s Own Equity (“ASC 815-40”), Trovagene has determined that certain warrants issued in connection with its private placements must be recorded as derivative liabilities with a charge to additional paid-in capital as they were issued with other equity instruments. In accordance with ASC 815-40, the warrants are also being re-measured at each balance sheet date based on estimated fair value, and any resultant change in fair value is being recorded in the Company’s statement of operations. The Company estimates the fair value of these warrants using the Black-Scholes option pricing model.
The range of assumptions used to determine the fair value of the warrants valued using the Black-Scholes option pricing model during the periods indicated was:
Year ended December 31 | |||||
2015 | 2014 | 2013 | |||
Estimated fair value of Trovagene common stock | $5.40 - $10.15 | $3.00 - $6.74 | $5.74 - $7.18 | ||
Expected warrant term | 3.0-3.8 years | 4.0 years | 1 month to 5.8 years | ||
Risk-free interest rate | 0.89%-1.31% | 1.38% | .03%-1.75% | ||
Expected volatility | 73%-77% | 86.4% | 82%-100% | ||
Dividend yield | —% | —% | —% | ||
Expected volatility is based on the volatility of a peer group of companies with attributes similar to Trovagene. The warrants have a transferability provision and based on guidance provided in SAB No. 107 for instruments issued with such a provision, Trovagene used the full contractual term as the expected term of the warrants. The risk-free interest rate is based on the U.S. Treasury security rates consistent with the expected remaining term of the warrants at each balance sheet date.
The following table sets forth the components of changes in the Company’s derivative financial instruments liability balance, valued using the Black-Scholes option pricing method, for the periods indicated.
F-17
Date | Description | Number of Warrants | Derivative Instrument Liability | ||||||
December 31, 2013 | Balance of derivative financial instruments liability | 1,013,961 | $ | 4,431,871 | |||||
Change in fair value of warrants during the year recognized as a gain in the statement of operations | — | (1,425,850 | ) | ||||||
December 31, 2014 | Balance of derivative financial instruments liability | 1,013,961 | 3,006,021 | ||||||
Exercised warrants | (46,666 | ) | (435,365 | ) | |||||
Change in fair value of warrants during the year recognized as a loss in the statement of operations | — | 726,421 | |||||||
December 31, 2015 | Balance of derivative financial instruments liability | 967,295 | $ | 3,297,077 | |||||
The weighted-average remaining contractual term of all of the Company’s warrants outstanding at December 31, 2015 and 2014 was approximately 2.5 and 3.6 years, respectively.
At December 31, 2015 and 2014, the total fair value of the above warrants accounted for as derivative financial instruments, valued using the Black-Scholes option pricing model, was $3,297,077 and $3,006,021, respectively, and is classified as derivative financial instruments liability on the balance sheet.
7. Fair Value Measurements
The following table presents the Company’s assets and liabilities that are measured and recognized at fair value on a recurring basis classified under the appropriate level of the fair value hierarchy as of December 31, 2015 and 2014:
Fair Value Measurements at December 31, 2015 | |||||||||||||||
Quoted Prices in Active Markets for Identical Assets and Liabilities (Level 1) | Significant Other Observable Inputs (Level 2) | Significant Unobservable Inputs (Level 3) | Total | ||||||||||||
Assets: | |||||||||||||||
Money market fund (1) | $ | 65,016,222 | $ | — | $ | — | $ | 65,016,222 | |||||||
Total Assets | $ | 65,016,222 | $ | — | $ | — | $ | 65,016,222 | |||||||
Liabilities: | |||||||||||||||
Derivative liabilities related to warrants | $ | — | $ | — | $ | 3,297,077 | $ | 3,297,077 | |||||||
Total Liabilities | $ | — | $ | — | $ | 3,297,077 | $ | 3,297,077 | |||||||
Fair Value Measurements at December 31, 2014 | |||||||||||||||
Quoted Prices in Active Markets for Identical Assets and Liabilities (Level 1) | Significant Other Observable Inputs (Level 2) | Significant Unobservable Inputs (Level 3) | Total | ||||||||||||
Assets: | |||||||||||||||
Money market fund (1) | $ | 27,123,587 | $ | — | $ | — | $ | 27,123,587 | |||||||
Total Assets | $ | 27,123,587 | $ | — | $ | — | $ | 27,123,587 | |||||||
Liabilities: | |||||||||||||||
Derivative liabilities related to warrants | $ | — | $ | — | $ | 3,006,021 | $ | 3,006,021 | |||||||
Total Liabilities | $ | — | $ | — | $ | 3,006,021 | $ | 3,006,021 | |||||||
(1)Included as a component of cash and cash equivalents on the accompanying consolidated balance sheet.
F-18
The following table sets forth a summary of changes in the fair value of the Company’s Level 3 liabilities for the years ended December 31, 2015 and 2014:
Description | Balance at December 31, 2014 | Fair Value of Warrants Reclassified to Additional Paid-in Capital | Unrealized (gains) or losses | Balance at December 31, 2015 | ||||||||||||
Derivative liabilities related to Warrants | $ | 3,006,021 | $ | (435,365 | ) | $ | 726,421 | $ | 3,297,077 | |||||||
Description | Balance at December 31, 2013 | Unrealized (gains) or losses | Balance at December 31, 2014 | |||||||||
Derivative liabilities related to Warrants | $ | 4,431,871 | $ | (1,425,850 | ) | $ | 3,006,021 | |||||
The unrealized gains or losses on the derivative liabilities are recorded as a change in fair value of derivative liabilities in the Company’s statement of operations. A financial instrument’s level within the fair value hierarchy is based on the lowest level of any input that is significant to the fair value measurement. At each reporting period, the Company reviews the assets and liabilities that are subject to ASC Topic 815-40. At each reporting period, all assets and liabilities for which the fair value measurement is based on significant unobservable inputs or instruments that trade infrequently and therefore have little or no price transparency are classified as Level 3.
8. Debt
Equipment Line of Credit
In November 2015, the Company entered into a Loan and Security Agreement (“Equipment Line of Credit”) with Silicon Valley Bank that provided for cash borrowings for equipment (“Equipment Advances”) of up to $2.0 million, secured by the equipment financed. Under the terms of the agreement, interest is equal to 1.25% above the Prime Rate. Interest only payments are due on borrowings through November 30, 2016, with both interest and principal payments commencing in December 2016. Any equipment advances after November 30, 2016 are subject to principal and interest payments immediately over a 36-month period following the advance. All unpaid principal and interest on each Equipment Advance will be due on November 1, 2019. The Company has an obligation to make a final payment equal to 7% of total amounts borrowed at the loan maturity date and the final payment is being accrued over the term of the loans using the effective-interest method.
The Company is also subject to certain affirmative and negative covenants under the Equipment Line of Credit. As of December 31, 2015, the Company was in compliance with all covenants.
As of December 31, 2015, $1,086,062 has been borrowed under the Equipment Line of Credit. As of December 31, 2015, amounts due under the Equipment Line of Credit included $30,168 in current liabilities and $1,058,709 in long-term liabilities, which includes $2,815 of accrued financial payment. The Company recorded $5,702 in interest expense related to the Equipment Line of Credit during the year ended December 31, 2015.
Future maturities of long-term debt at December 31, 2015 are as follows:
2016 | $ | 30,168 | |
2017 | 362,021 | ||
2018 | 362,021 | ||
2019 | 331,852 | ||
Total principal | 1,086,062 | ||
Plus final fee premium accretion | 2,815 | ||
Total long-term obligations | $ | 1,088,877 | |
Loan and Security Agreement
In June 2014, the Company entered into a $15,000,000 loan and security agreement (“Agreement”) with two banks pursuant to which the lenders provided the Company with a term loan, which was funded at closing. A portion of the proceeds
F-19
were used to repay the existing outstanding amount under the Equipment Line of Credit entered into in June 2013. The repayment with the same lender was accounted for as a debt extinguishment under FASB ASC Topic 470-50, Debt. The interest rate on the new loan is 7.07% per annum. The Company made interest only payments on the outstanding amount of the loan on a monthly basis through July 2015, after which equal monthly payments of principal and interest were scheduled to become due until the loan maturity date of July 1, 2018. However, included in the Agreement is a provision to extend the interest only payments through January 1, 2016 upon the Company’s receipt of unrestricted net cash proceeds from the sale of equity securities of not less than $30 million by June 30, 2015. In June 2015, the Company entered into an amendment to the Agreement (“Amendment”), which reduced the amount of unrestricted net cash proceeds to not less than $21 million from the sale of equity securities to qualify for an interest-only extension. The Company met the conditions in the Amendment related to the interest-only extension and, as a result, the interest only payments that were to expire on August 1, 2015 were extended for six months to February 1, 2016, when both interest and principal payments will commence. The loan is secured by a security interest in all of the Company’s assets except intellectual property, which is subject to a negative pledge. In connection with the loan, each of the lenders received a warrant to purchase up to an aggregate of 85,470 shares of the Company’s common stock at an exercise price of $3.51 per share, which such warrants are exercisable for ten years from the date of issuance. The original value of the warrants, totaling $235,857, was recorded as debt discount and additional paid-in capital as the warrants were equity classified. As of December 31, 2015, a warrant to purchase 42,735 shares of common stock remains outstanding.
At the Company’s option, it may prepay all of the outstanding principal balance, subject to certain pre-payment fees ranging from 1% to 3% of the prepayment amount. In the event of a final payment of the loans under the loan agreement, either in the event of repayment of the loan at maturity or upon any prepayment, the Company is obligated to pay the amortized portion of the final fee of $1,050,000.
The Company is also subject to certain affirmative and negative covenants under the Agreement, including limitations on its ability to: undergo certain change of control events; convey, sell, lease, license, transfer or otherwise dispose of any equipment financed by loans under the loan agreement; create, incur, assume, guarantee or be liable with respect to indebtedness, subject to certain exceptions; grant liens on any equipment financed under the loan agreement; make or permit any payment on specified subordinated debt; and pay dividends. In addition, under the Agreement, subject to certain exceptions, the Company is required to maintain with the lender its primary operating, other deposit and securities accounts. Furthermore, under the Amendment, the Company is required to be in compliance with healthcare laws and regulations and terms and conditions of healthcare permits. The Company was in compliance with all covenants under the Agreement, as amended, as of December 31, 2015.
As of December 31, 2015, amounts due under the Agreement include $5,195,650 in current liabilities and $10,187,479 in long-term liabilities, which include $535,024 of accrued financial payment. The Company recorded $1,590,750 in interest expense related to the Agreement during the year ended December 31, 2015. Closing costs are being accreted over the life of the loan to interest expense.
Future maturities of long-term debt at December 31, 2015 are as follows:
2016 | $ | 5,195,650 | |
2017 | 6,064,315 | ||
2018 | 3,740,035 | ||
Total principal | 15,000,000 | ||
Less discount | (151,895 | ) | |
Plus final fee premium accretion | 535,024 | ||
Total long-term obligations | $ | 15,383,129 | |
9. Income Taxes
At December 31, 2015, Trovagene had federal net operating loss carryforwards (NOLs) of approximately $72.6 million, which, if not used, expire beginning in 2020. Trovagene also has California NOLs of approximately $52.6 million that will begin to expire in 2021 and New Jersey NOLs of approximately $6.9 million that begin to expire on January 31, 2016. Trovagene also has research and development tax credits available for federal and California purposes of approximately $1.2 million and $0.5 million, respectively. The federal research and development tax credits will begin to expire on January 31, 2025. The California research and development tax credits are not set to expire. The utilization of these NOLs and research and development tax credits is subject to limitations based on past and future changes in ownership of Trovagene pursuant to Section 382 (“Section 382”) of the Internal Revenue Code of 1986, as amended (the “Code”). The Company has determined
F-20
that ownership changes have occurred for purposes of Section 382 and, therefore, the ability of the Company to utilize its NOLs is limited.
The provision for income taxes based on losses from continuing operations consists of the following at December 31 (in thousands):
Years ended December 31, | |||||||||||
2015 | 2014 | 2013 | |||||||||
Deferred benefit | |||||||||||
Federal | $ | (9,602 | ) | $ | (5,651 | ) | $ | (3,806 | ) | ||
State | (1,742 | ) | (449 | ) | (593 | ) | |||||
Total deferred benefit | (11,344 | ) | (6,100 | ) | (4,399 | ) | |||||
Valuation allowance | 11,344 | 6,100 | 4,399 | ||||||||
Total income tax provision | $ | — | $ | — | $ | — | |||||
Significant components of the Company’s taxes and the rates as of December 31 are shown below (in thousands, except percentages):
Years ended December 31, | |||||||||||||
2015 | 2014 | ||||||||||||
Tax computed at the federal statutory rate | $ | (9,340 | ) | 34 | % | $ | (4,871 | ) | 35 | % | |||
State tax, net of federal tax benefit | (1,559 | ) | 6 | % | (891 | ) | 6 | % | |||||
Permanent Items | 258 | (1 | )% | (320 | ) | 2 | % | ||||||
Tax credits | (997 | ) | 3 | % | — | — | % | ||||||
Valuation allowance increase | 11,638 | (42 | )% | 6,081 | (43 | )% | |||||||
Other | — | — | % | 1 | — | % | |||||||
Provision for income taxes | $ | — | — | % | $ | — | — | % | |||||
Significant components of the Company’s deferred tax assets and liabilities from federal and state income taxes as of December 31 are shown below:
Years ended December 31, | |||||||
2015 | 2014 | ||||||
Deferred tax assets | |||||||
Tax loss carryforwards | $ | 27,962,000 | $ | 19,010,900 | |||
Research and development credits and other tax credits | 1,698,300 | 698,000 | |||||
Stock-based compensation | 3,225,200 | 2,193,900 | |||||
Other | 782,000 | 420,800 | |||||
Total deferred tax assets | 33,667,500 | 22,323,600 | |||||
Valuation allowance | (33,667,500 | ) | (22,323,600 | ) | |||
Net deferred tax asset | $ | — | $ | — | |||
Trovagene records a valuation allowance against deferred tax assets to the extent that it is more likely than not that some portion, or all of, the deferred tax assets will not be realized. Due to the substantial doubt related to Trovagene’s ability to utilize its deferred tax assets, the Company recorded a valuation allowance against the deferred tax.
FASB ASC Topic 740-10-30-7, Accounting for Income Taxes had no effect on Trovagene’s financial position, cash flows or results of operations upon adoption, as Trovagene does not have any unrecognized tax benefits. Trovagene’s practice is to recognize interest and/or penalties related to income tax matters in income tax expense, and none have been incurred to date.
F-21
10. Commitments and Contingencies
Research and Development and License Agreements
The Company has entered into a variety of collaboration and specimen transfer agreements relating to its development efforts. Included in research and development expense, the Company has incurred and recorded approximately $1,362,000, $712,000, and $217,000 as of December 31, 2015, 2014 and 2013, respectively, relating to services provided by the collaborators in connection with these agreements.
The Company is a party to various agreements under which it licenses technology on an exclusive basis in the field of human diagnostics. License fees are generally calculated as a percentage of product revenues, with rates that vary by agreement. To date, payments have not been material.
Litigation
Trovagene does not believe that the Company has legal liabilities that are probable or reasonably possible that require either accrual or disclosure. From time to time, the Company may become involved in various lawsuits and legal proceedings that arise in the ordinary course of business. However, litigation is subject to inherent uncertainties, and an adverse result in these or other matters may arise from time to time that may harm the Company’s business.
The Company is not currently a party to any material legal proceedings.
Employment and Consulting Agreements
The Company has longer-term contractual commitments with various consultants and employees, including the Company’s CEO and CFO. The executive agreements with the CEO, CFO and CCO provide for severance payments. The executive agreement with the CEO also provides for a bonus payment in cash or stock upon the earlier of meeting certain trading volumes and market price of Trovagene’s common stock for a minimum period of ninety days or in the event of a change in control where the Company’s per share enterprise value equal or exceeds $7.50. If the market price and volume target is realized, the bonus is approximately $3.5 million. If a change of control occurs at the targeted enterprise values, the bonus is equal to 4% of the enterprise value. The executive agreements with the CEO and CFO were replaced by the employment agreements that became effective in January 2016. See Note 14. Subsequent Events.
Lease Agreements
The Company leases laboratory and office spaces under various non-cancelable lease agreements. The Company is headquartered in San Diego, California and leases facilities in San Diego and Italy. The Company currently leases its facilities in San Diego under an operating lease that expires in 2017. On June 11, 2015, the Company entered into an amendment to the lease agreement which expands the square footage leased by the Company to approximately 22,600 square feet at a monthly rental rate of approximately $60,000. The amended lease expires on December 31, 2021. The amended monthly rental rate will be effective when the Company commences business operations in the expanded premises, expected to occur in the second quarter of 2016.
In November 2015, the Company entered into a lease agreement, under the terms of which the Company will lease certain office building in Torino, Italy, consisting of approximately 2,300 square feet at a monthly rental rate of approximately $3,100. The lease is for a period of three years with an effective date of January 1, 2016.
Rent expense for the years ended December 31, 2015, 2014, and 2013 was approximately $471,000, $315,000 and $294,000, respectively. The Company is also a party to various operating lease agreements for office equipment.
Total annual commitments under non-cancelable lease agreements for each of the years ended December 31 are as follows:
F-22
2016 | $ | 683,871 | |
2017 | 792,221 | ||
2018 | 811,797 | ||
2019 | 796,716 | ||
2020 | 817,989 | ||
Thereafter | 842,529 | ||
Total | $ | 4,745,123 | |
11. Employee Benefit Plan
The Company has a retirement savings plan under Section 401(k) of the Code covering its employees. The plan allows employees to defer, up to the maximum allowed, a percentage of their income on a pre-tax basis through contributions to the plans, plus any employee age 50 and over can participate in the caught-up dollars as allowed by Internal Revenue Service codes. The Company also has a Roth investment plan that is taken after taxes. The Company does not currently make matching contributions.
12. Related Party Transactions
In January 2015, the Company entered into a one year consulting agreement with Thomas H. Adams, Ph.D., the Chairman of the Board, pursuant to which Dr. Adams provides consulting services to the Company in connection with applying the Company’s technology in the field of infectious disease with the first application to be detection of John Cunningham virus mutants in the presence of wild type in human urine as a prognostic indicator of the development of progressive multifocal leukoencephalopathy disease. Under the agreement, the Company committed to pay $9,500 per month for the services performed by Dr. Adams. During the year ended December 31, 2015, the Company incurred and recorded $114,000 of consulting fees related to the agreement.
In September 2015, the Company entered into a research agreement with the University of Torino (“University”) to collaborate on a program of research to develop, optimize and test molecular profiling tools for plasma and urine ctDNA in cancer. Dr. Alberto Bardelli, the Principal Investigator of the University who oversees this research program, is also a member of the Scientific Advisory Board of the Company. Under the agreement, the Company committed to pay up to $529,000 for the services performed by the University. In addition, the Company may pay royalties to the University on revenue generated by the Company from the commercialization of any tools developed during the collaboration. During the year ended December 31, 2015, the Company incurred and recorded approximately $188,000 of research and development expenses related to the agreement. No royalty expense has been incurred as of December 31, 2015.
13. Selected Quarterly Financial Data (Unaudited)
The following is a summary of the quarterly results of operations of the Company for years ended December 31, 2015 and 2014:
F-23
Quarter Ended(1) | |||||||||||||||
March 31 | June 30 | September 30 | December 31 | ||||||||||||
(dollars in thousands, except per share data) | |||||||||||||||
2015 | |||||||||||||||
Revenues | $ | 127 | $ | 49 | $ | 58 | $ | 79 | |||||||
Operating expenses | $ | 4,975 | $ | 6,682 | $ | 6,467 | $ | 7,463 | |||||||
Net loss and comprehensive loss attributable to common stockholders | $ | (7,180 | ) | $ | (10,186 | ) | $ | (2,742 | ) | $ | (7,387 | ) | |||
Net loss per common share - basic | $ | (0.33 | ) | $ | (0.41 | ) | $ | (0.10 | ) | $ | (0.25 | ) | |||
Net loss per common share - diluted | $ | (0.33 | ) | $ | (0.41 | ) | $ | (0.23 | ) | $ | (0.26 | ) | |||
Shares used in the calculation of net loss attributable to common stockholders - basic | 21,817,710 | 24,592,883 | 28,560,211 | 29,723,254 | |||||||||||
Shares used in the calculation of net loss attributable to common stockholders - diluted | 21,817,710 | 24,592,883 | 29,128,235 | 30,157,038 | |||||||||||
2014 | |||||||||||||||
Revenues | $ | 111 | $ | 56 | $ | 57 | $ | 56 | |||||||
Operating expenses | $ | 3,371 | $ | 3,297 | $ | 3,997 | $ | 4,560 | |||||||
Net loss and comprehensive loss attributable to common stockholders | $ | (3,198 | ) | $ | (1,079 | ) | $ | (5,382 | ) | $ | (4,689 | ) | |||
Net loss per common share - basic | $ | (0.17 | ) | $ | (0.06 | ) | $ | (0.28 | ) | $ | (0.25 | ) | |||
Net loss per common share - diluted | $ | (0.17 | ) | $ | (0.17 | ) | $ | (0.28 | ) | $ | (0.25 | ) | |||
Shares used in the calculation of net loss attributable to common stockholders - basic | 18,902,783 | 18,902,783 | 18,902,783 | 18,904,280 | |||||||||||
Shares used in the calculation of net loss attributable to common stockholders - diluted | 18,902,783 | 19,232,760 | 18,902,783 | 19,071,112 | |||||||||||
(1) Basic and diluted net loss per common share are computed independently for each of the periods presented. Accordingly, the sum of the quarterly net loss per common share amount may not agree to the total for the year.
14. Subsequent Events
Employment Agreements
In January 2016, the Company entered into an employment agreement with Antonius Schuh, Ph.D. in which he agreed to serve as our Chief Executive Officer. The term of the agreement is effective as of January 1, 2016 and continues until January 1, 2020 and is automatically renewed for successive one year periods at the end of each term. Dr. Schuh’s base compensation is $488,800 per year. Dr. Schuh is eligible to receive an annual bonus of up to 50% of his base compensation based on meeting certain performance objectives and bonus criteria. Upon entering the agreement, Dr. Schuh was granted 450,000 non-qualified stock options which have an exercise price of $5.18 per share and vest monthly in equal amounts over a period of four years. Dr. Schuh was also granted 350,000 non-qualified stock options which have an exercise price of $5.18 per share and vested immediately upon grant.
If the employment agreement is terminated by the Company without cause, Dr. Schuh is entitled to receive a severance payment equal to base compensation for twenty-four months and the potential bonus and any benefits Dr. Schuh would be eligible during such twenty-four month period. If the employment agreement is terminated as a result of a change of control, in addition to the severance payment described above, all unvested equity awards would immediately vest and become fully exercisable for a period of six months following the date of termination.
In January 2016, the Company entered into an employment agreement with Stephen Zaniboni in which he agreed to serve as our Chief Financial Officer. The term of the agreement is effective as of January 1, 2016 and continues until January 1, 2020 and is automatically renewed for successive one year periods at the end to each term. Mr. Zaniboni’s base compensation
F-24
is $357,500 per year. Mr. Zaniboni is eligible to receive an annual bonus of up to 50% of his base compensation based on meeting certain performance objectives and bonus criteria. Upon entering the agreement, Mr. Zaniboni was granted 150,000 non-qualified stock options which have an exercise price of $5.18 per share and vest monthly in equal amounts over a period of four years.
If the employment agreement is terminated by the Company without cause, Mr. Zaniboni is entitled to receive a severance payment equal to base compensation for twelve months and the potential bonus and any benefits Mr. Zaniboni would be eligible during such twelve month period. If the employment agreement is terminated as a result of a change of control, in addition to the severance payment, all unvested equity awards would immediately vest and become fully exercisable for a period of six months following the date of termination.
Debt Agreement
In February 2016, the Company signed a term sheet to refinance its existing term loan entered into on June 2014. Under the term sheet, interest would be equal to 3.75% plus the Wall Street Journal Prime Rate, subject to a floor of 7.25%. Interest only payments would be for 12 months, followed by equal monthly payments of principal and interest over the following 30 months. The Company would also have an obligation to make a final payment equal to 7.50% of total funded amounts at the loan maturity date. In addition, the lenders would receive a warrant to purchase such number of shares of the Company’s common stock as is equal to 1% of the funded amount divided by an average closing price of the Company’s common stock.
Registration Statement
Effective February 4, 2016, the Registration Statement expired and the Company therefore will no longer be able to issue securities pursuant to the Registration Statement, including pursuant to its agreement with the Agent.
F-25