Attached files
| file | filename |
|---|---|
| EX-99.1 - EX-99.1 - Recro Pharma, Inc. | d152376dex991.htm |
| 8-K - 8-K - Recro Pharma, Inc. | d152376d8k.htm |
 Relieving pain…….Improving lives
Exhibit 99.2 |
 Special
Note Regarding Forward-Looking Statements
This presentation includes forward-looking statements within the meaning of Section
27A of the Securities Act of 1933 and Section 21E of the Securities
Exchange Act of 1934. These statements, among other things, relate
to our business strategy, goals and expectations concerning our product
candidates, future operations, prospects, plans and objectives of
management. The words "anticipate", "believe", "could", "estimate", "expect", "intend", "may", "plan", "predict", "project", "will" and
similar terms and phrases are used to identify forward-looking
statements in this presentation. Our operations involve risks and
uncertainties, including the integration of our recently acquired assets,
many of which are outside our control, and any one of which, or a
combination of which, could materially affect our results of operations and whether the
forward-looking statements ultimately prove to be correct. These
forward-looking statements should be considered together with the
risks and uncertainties that may affect our business and future results
included in our filings with the Securities and Exchange Commission at
www.sec.gov. These forward-looking statements are based on
information currently available to us, and we assume no obligation to update any forward-looking statements except as required by applicable law. 2 |
 Company
Highlights •
Multiple non-opioid therapeutics in advanced clinical
development for acute post operative pain
• IV/IM meloxicam Phase III ready – long acting, demonstrated efficacy in successful Ph II trials • Dex-IN – proprietary, intranasal therapeutic with recently announced positive Ph II results • Revenue and cashflow positive manufacturing & royalty business • Experienced management team with significant development, regulatory and commercial experience 3 |
 Experienced Management and Board
• Gerri Henwood – President and CEO Founded Auxilium Pharmaceuticals (AUXL, NASDAQ) and IBAH (former NASDAQ Co. – acquired 1998); GSK • Chuck Garner – CFO, CBO and Treasurer Over 14 years of life sciences investment banking experience – Deutsche Bank, Burrill & Co., Inverness Advisors; PwC • Randy Mack – SVP, Development Over 20 years of clinical development experience – Adolor, Auxilium, Abbott Labs and Harris Labs Board of Directors Wayne B. Weisman – Chairman SCP VitaLife Partners Winston J. Churchill SCP VitaLife Partners Gerri Henwood – CEO William L. Ashton Harrison Consulting Group; frmly Amgen Abraham Ludomirski, M.D. SCP VitaLife Partners Alfred Altomari CEO, Agile Therapeutics Michael Berelowitz, M.D. Former SVP, Specialty Care Business Unit, Pfizer 4 |
 Recent
Transformative Transaction •
Acquired IV/IM meloxicam and manufacturing & royalty
business from Alkermes
– $50M up-front cash payment; meloxicam milestones and royalties – Warrants issued to Alkermes and OrbiMed – Non-dilutive up-front financed by loan from OrbiMed • IV/IM meloxicam – long acting preferential COX-2 inhibitor for moderate to severe acute pain ready for Ph III – Widely prescribed, approved oral chronic pain therapeutic – Multiple Phase II studies successfully completed in acute pain models – Dosing advantages over existing acute pain therapeutics, including long action • Manufacturing, royalty and formulation business – 87,000 sq. ft. facility (DEA licensed) manufactures 5 commercial products marketed by partners – $75M in revenues and cashflow positive (2014) 5 |
 Positive
Dex-IN Ph II Results (REC-14-013
– Post Op Day 1 Dosing) • Randomized, placebo controlled Phase II bunionectomy study (168 patients) – Randomized, placebo controlled study – 50 mcg of Dex-IN or placebo every 6 hours – Primary endpoint – SPID48 (p=0.0214) – Oral opioid rescue therapy allowed • 6 patients discontinued for lack of efficacy (3 in each treatment group) and 1 patient due to serious adverse event of hypotension • Most common adverse events observed in the study were: – blood pressure decrease / hypotension – nausea (similar incidences to placebo) – nasal discomfort and headache • Adverse event of bradycardia was reported in 3 subjects in the Dex-IN treatment group 6 |
 Clinical
Stage Pipeline Product
PC I II III Rights Meloxicam WW IV formulation Acute post operative pain Phase III ready IM formulation Acute pain Dexmedetomidine (“Dex”)
WW, exc. Europe, Turkey, CIS
Dex-IN (intranasal)
Acute post operative pain
Cancer breakthrough pain
Dex-SL (sublingual)
Fadolmidine (“Fado”)
WW, exc. Europe, Turkey, CIS
Intrathecal Topical 7 |
 Post Op
Pain Market Underserved •
$5.9 billion market (1) • Predominantly opioid use • Significant side effects / issues associated with opioids • Dearth of non-opioid drugs in development Inpatient procedures Total procedures (2009) 47.9M Addressable >25M Ambulatory procedures Total procedures (2006) 53.3M Addressable >25M Note: Addressable includes procedures expected to utilize pain medication. Source: National Center for Health Statistics and management estimates. (1) GBI Research, 2010 sales. 8 |
 Limited
Pain Relief Options for Patients Pain
Severity Class Compounds Advantages Disadvantages Mild Acetaminophen Antipyretic properties; Oral; no opioid AEs Only effective for mild pain; short acting NSAIDs Ketorolac, ibuprofen, aspirin Mild to moderate analgesia; oral; no opioid AEs Bleeding risk; GI and renal complications; short acting Moderate Sodium channel blockers Bupivacaine, lidocaine Use directly at pain site; mostly peri- operative Limited duration of action; some are concerned about local tissue impact Moderate to Severe Long-acting preferential COX-2 IV/IM meloxicam (Recro Pharma) Long acting; fast onset, high pain relief, and less constipation Bleeding risk; GI and renal complications Alpha 2 agonists Dexmedetomidine (Recro Pharma) Good pain relief; anxiolytic properties; no respiratory depression, impaired GI or addictive properties In development – potential for first in class to be approved for post- operative pain Opioids Morphine, hydrocodone, oxycodone, fentanyl Good pain relief Respiratory depression, impaired GI motility after even one dose; frequent nausea and vomiting; abuse/addiction potential Note: Pain severity based upon market research / physician feedback 9 |
 IV/IM
Meloxicam |
 IV/IM
Meloxicam Overview •
FDA approved, oral preferential COX-2 inhibitor
used in a wide variety of indications
• Proprietary long acting injectable form for moderate to severe acute pain – Incorporates Alkermes’ NanoCrystal™ technology • Phase III ready – multiple Phase II studies completed on IV and a Phase I on IM – Positive Ph II hysterectomy and dental pain studies with demonstrated efficacy • IP issued through 2022 and additional IP could extend protection through 2030 NanoCrystal ® is a registered trademark of Alkermes plc. 11 |
 Favorable
Dosing Profile Attribute
Meloxicam Ketorolac Caldolor (ibuprofen) Ofirmev (APAP) Route IV/IM IV/IM IV IV Onset of pain relief < 10 min 30 min N/A N/A Time to peak analgesic effect 40 min 1-2 hrs N/A N/A Duration of pain relief 18-24 hrs 4-6 hrs 4-6 hrs 4-6 hrs Admin. IV bolus / pre- filled syringe (later) Ready to use IV bolus (15 sec) Dilution required, 30 min infusion Ready to use, 15 min infusion 12 |
 IV/IM
Meloxicam Clinical Overview •
Elan/ALKS conducted 5 IV and 1 IM clinical trials
– Two Phase 1 IV PK & Safety trials – One Phase 1 IM PK & Safety trial – Three Phase 2 IV efficacy trials in various acute pain models • Good safety & tolerability across large dose range IV/IM • Demonstrated efficacy using various measures in multiple pain models 13 |
 Multiple
Successful IV Phase 2 Trials •
Elan/ALKS have conducted 5 IV and 1 IM clinical trials
Trial Design Outcome Phase II Study N1539-02 Acute pain following dental surgery (N = 230) Statistically significant differences for all doses compared to placebo were seen in SPID24, pain relief and onset of pain relief Phase II Study N1539-04 Acute pain following open abdominal hysterectomy surgery (N = 486) Statistically significant differences for all doses compared to placebo were seen in multiple efficacy analyses, including SPID24. meloxicam 30 mg and 60 mg produced the greatest response with no difference between doses Phase II Study N1539-05 Acute pain following laparoscopic abdominal surgery (N =50) Study stopped early (planned N = 250) for business reasons. However, statistically significant differences in SPID48 observed for 30mg QD dose despite small sample size 14 |
 Phase II
Abdominal Hysterectomy Study •
Multicenter, single-dose, randomized, double-blind,
placebo- & active-controlled study in Eastern Europe • In double-blind period, single doses of: – Placebo – IV Morphine (10-15 mg) – Meloxicam 5 mg, 7.5 mg, 15 mg, 30 mg, 60 mg – After 24 hours, open-label Meloxicam was available • Standard analgesia study design – Pain Intensity assessments (SPID24 = Primary Endpoint) – Pain Relief – Rescue mediation – Time to onset 15 |
 Robust
Efficacy (Abdominal
Hysterectomy Trial – IV Meloxicam) *** p < 0.001 vs. Placebo *** *** *** *** *** *** 16 (10,000) - 10,000 20,000 30,000 40,000 50,000 60,000 Placebo n=64 Morphine n=62 5 mg n=60 7.5 mg n=91 15 mg n=60 30 mg n=60 60 mg n=89 |
 Confirmed
Efficacy in Multiple Studies Summary of Pain Intensity Differences
(SPID) *** p < 0.001 vs.
Placebo Dental Pain Study
p = 0.0682
p = 0.0392
Abdominal Laparoscopic Pain Study
17 0 20000 40000 60000 80000 100000 120000 140000 160000 180000 200000 - 10,000 20,000 30,000 40,000 50,000 60,000 70,000 80,000 *** *** *** *** |
 Single 30
mg Dose Performance over 24 hrs (Abdominal Hysterectomy
Trial – IV Meloxicam) Baseline Pain Level 60 18 -10 0 10 20 30 40 50 60 0 4 8 12 16 20 24 Time (Hours) Placebo n=64 Morphine n=62 15 mg n=60 30 mg n=60 60 mg n=89 |
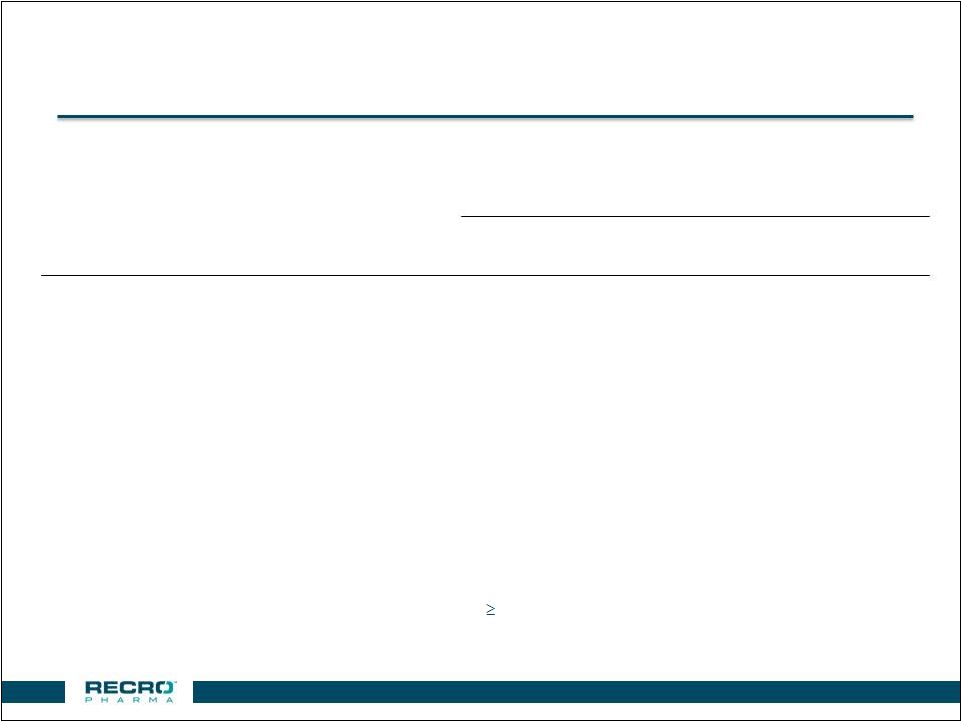 Well
Tolerated (Abdominal
Hysterectomy Trial – IV Meloxicam) **Reported in 3% of Subjects in any group and greater than Placebo
Meloxicam
Placebo
n=64
Morphine
n=62
5 mg
n=60
7.5 mg
n=91
15 mg
n=60
30 mg
n=60
60 mg
n=89
Anemia
3.1
4.8
3.3
13.2
3.3
1.7
10.1
Anemia Postoperative
-
1.6
-
-
-
3.3
-
Constipation
-
4.8
5.0
1.1
1.7
-
-
Flatulence
-
4.8
1.7
1.1
3.3
-
-
Hypokalaemia
-
3.2
1.7
1.1
-
1.7
-
Insomnia
4.7
8.1
10.0
4.4
5.0
5.0
4.5
Ketonuria
7.8
9.7
6.7
9.9
15
10
10.1
Leukocytosis
-
-
1.7
-
-
3.3
-
Pyrexia
1.6
3.2
3.3
2.2
-
-
-
Sinus Tachycardia
-
-
3.3
-
-
-
1.1
Percent of Subjects Reporting an Adverse Event
** 19 |
 Next
Steps for IV Meloxicam •
Production of a clinical supply batch
• Conduct Phase III Pivotal Study in hard and soft tissue models • Verify need for additional safety studies to meet adequate exposures / special populations 20 |
 Dexmedetomidine (“Dex”)
|
 Dex Has Demonstrated Analgesia & Safety • Alpha 2 agonist (non-opioid) – Injectable form (Precedex) marketed by Hospira in US as sedative – Multiple studies demonstrating analgesia of alpha 2 agonists • Intranasal formulation in clinical development for acute pain – In-licensed non-IV rights from Orion – Worldwide rights except Europe, Turkey, and CIS • Multiple studies demonstrate Dex pain relief and safe profile – Including our completed placebo controlled trials • Expect strong IP position – Pending IP coverage could run through 2030 • Expect to file 505(b)(2) NDA after completion of Ph III 22 |
 Dex Efficacy and Safety in Multiple Studies Beneficial effects Source Approved sedative and safe profile NDA filing / pivotal trials - Abbott/Hospira, Orion Morphine sparing NDA studies plus Literature Analgesia by IV route Chan, 2010; Grosu, 2010; Lin, 2009, Arain, 2010 Demonstration of pain relief (VAS) Placebo controlled trials; L. Webster, MD (Utah) CLBP study (Recro sponsored) Positive PK/PD plasma levels demonstrating analgesic potential Clinical trials run by Recro Relieves morphine
“Max” (‘hyperalgesia’)
University of Minnesota; M. Belgrade, MD
23 |
 Significant Advantages Over Opioids
Dex Fast-acting Opioids Non-opioid (Not controlled substance) Opioid - DEA scheduled product No habituation effects Addictive Does not cause respiratory depression Respiratory depression Not associated with constipation, nausea, or vomiting Unwanted side-effects of constipation, nausea and vomiting Enhances morphine effectiveness without morphine dose increase Additive effect requires higher dose More cognitively intact Frequently “Foggy”/
may be confused Anxiolytic
properties Not anxiolytic Effective Analgesic Effective Analgesic 24 |
 Dex Has Been Well Studied by Recro • Evaluated proprietary formulations of Dex in 10 trials Trial Form Design Outcome REC-14-013 Dex-IN Acute pain following bunionectomy surgery (n=168) Statistically significant difference of SPID48 between 50 mcg of Dex-IN vs. placebo (p=0.0214) REC-13-012 Dex-IN Acute pain following bunionectomy surgery (n=85 evaluable) Within subset of patients (n=42), with baseline pain intensity of 6 or below, there was a trend towards analgesia in 50 mcg and reduced opioid use vs placebo REC-11-010 Dex-IN Chronic lower back pain POC study (n=24) Statistically significant pain relief within 30 minutes demonstrated in placebo controlled trial – single use device REC-09-003 Dex-SL Chronic lower back pain POC study (n=21) Statistically significant reduction in pain intensity demonstrated in placebo controlled trial 25 |
 Dex-IN Study REC-14-013
(US placebo controlled trial)
• Phase II bunionectomy study – Randomized, placebo controlled study – Primary endpoint – SPID48 – Oral opioid rescue therapy allowed – Post Op Day 1 dosing • 50 mcg of Dex-IN or placebo every 6 hours – 84 patients in each treatment group (168 in total) • Additional secondary endpoints included: – Use of opioid rescue medication – SPIDs over various time intervals – Other standard efficacy analyses • Patients followed for 7 days after initial dosing 26 |
 Study
REC-14-013 (SPID48
– Primary Endpoint) 27 Note: Last Observation Carried Forward Analysis Method p = 0.0214 0 500 1000 2000 2500 3000 Placebo N = 84 DEX-IN 50 µg N = 84 1500 |
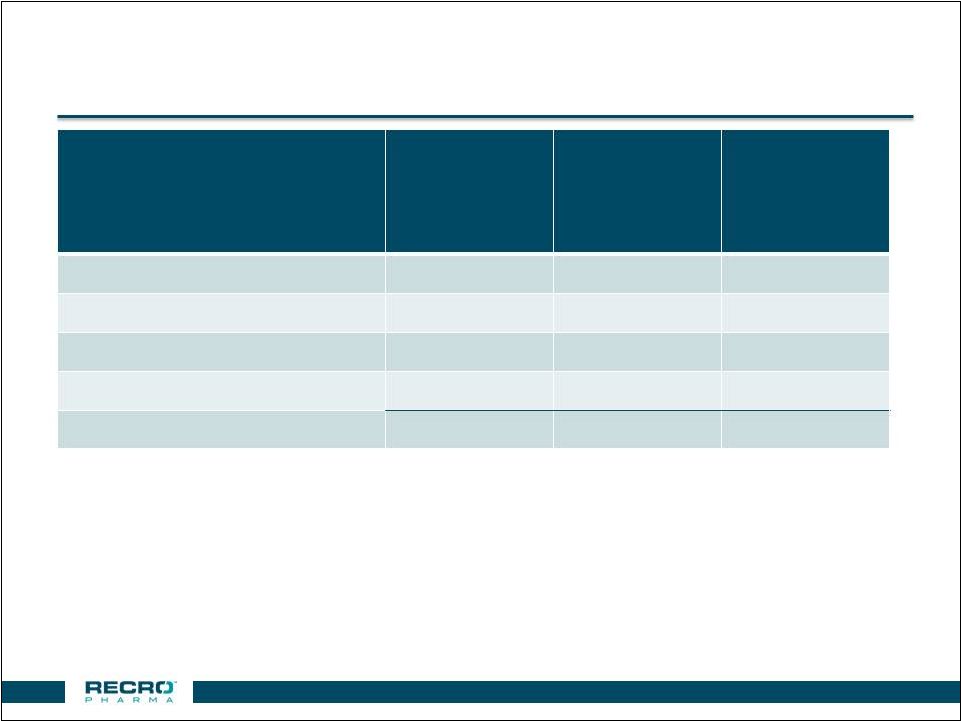
 Study
REC-14-013 (Subject Characteristics)
Placebo (N=84) DEX-IN 50 µg (N=84) Female, n (%) 75 (89.3) 79 (94.0) Age, Mean 44 43.9 (range) (46 - 70) (46 - 69) Discontinued Subjects, n (%) 3 (3.6) 4 (4.8) Lack of Efficacy 3 (3.6) 3 (3.6) Adverse Event 0 1 (1.2)** Race, n (%) White 56 (66.7) 59 (70.2) Black/African American 21 (25.0) 20 (23.8) Other 7 (8.4) 5 (6.0) Baseline PI Score, Mean 6.7 6.4 (range) (4 - 10) (4 - 10) 28 **Serious Adverse Event of Hypotension |
 Study
REC-14-013 (Adverse Events –
3 in Dex-IN Group) 29 • If IV fluid given and no symptoms present, “BP Decrease” recorded as AE • No medication given to any patient with BP or HR change • All nasal related AEs were rated as mild, except one case of nasal congestion rated as moderate Adverse Event Placebo (N=84) DEX-IN 50 µg (N=84) BP Decreased 3 (3.6%) 22 (26.2%) Nausea 14 (16.7%) 13 (15.5%) Nasal Discomfort 2 (2.4%) 7 (8.3%) Headache 4 (4.8%) 6 (7.1%) Vomiting 6 (7.1%) 4 (4.8%) Nasal Dryness 3 (3.6%) 4 (4.8%) Nasal Congestion 1 (1.2%) 4 (4.8%) Nasal Obstruction 2 (2.4%) 3 (3.6%) Bradycardia 0 3 (3.6%) Dizziness 1 (1.2%) 3 (3.6%) Hypotension 0 3 (3.6%) |
 Clinical
Pipeline Intellectual Property •
IV/IM meloxicam – formulation IP through 2022 – Additional IP filed could run to 2030 • Dex applications for methods for treating/preventing pain through intranasal and sublingual formulations without significant sedation • Fado IP in-licensed from Orion – Composition of matter – Method of administration for analgesia – Treatment and prevention of hypotension and shock – Pro-Drug • Regulatory exclusivity – 505(b)(2) – 3 years (Meloxicam, Dex-IN, Dex-SL) – 505(b)(1) – NCE, 5 years (Fado) 30 |
 Fadolmidine (“Fado”)
|
 Fado Effective in Phase II for Pain Relief • Alpha 2 agonist – more potent at the alpha 2c receptor than Dex – >20 fold less potent at the alpha 1b receptor than clonidine • Fado has demonstrated analgesia in multiple animal models • Positive Phase II analgesia study in bunionectomy patients – Intrathecal route of administration • Formulation work underway for topical prototype – Potential in regional neuropathies • WW rights to all human uses except Europe, Turkey and CIS • NCE patent w/ expected extension to 2021 / pursuing add’l IP 32 |
 Corporate Overview |
 US Based
Manufacturing Facility 34 |
 Manufacturing & Royalty Overview
Manufacturing facility • 87,000 sq. ft. solid oral dosage manufacturing cGMP • DEA licensed • ~165 employees Service capabilities • Formulation, process development and optimization • Process scale-up • Clinical supply and validation • Commercial supply Ritalin LA • Once daily ADHD treatment marketed by Novartis Focalin XR • ADHD treatment marketed by Novartis Verelan / verapamil • CV/High blood pressure treatment marketed by Actavis and UCB Zohydro ER • Extended release hydrocodone marketed by Pernix • Launched in 2014 • Abuse deterrent form launched 35 |
 Strong
Historical Manufacturing Performance •
Carve-out financials
• Zohydro ER – abuse deterrent form launched • Additional capacity for new product opportunities • Positive cashflow expected to cover all debt service obligations and excess cashflows to repay loan principal 36 *EBITDA is a non-GAAP financial metric. Please see slide 38 for additional information including a
reconciliation of Net Income to EBITDA.
(in millions) 12 months ended Dec. 31, 2014 (audited) 3 months ended March 31, 2015 3 months ended March 31, 2014 Revenues $75.2 $19.4 $16.6 EBITDA* $29.2 $5.2 $6.8 |
 Company
Highlights •
Multiple non-opioid therapeutics in mid to late stage
clinical development for acute post operative pain
• IV/IM meloxicam Phase III ready – long acting, demonstrated efficacy in successful Ph II trials • Dex-IN – proprietary, intranasal therapeutic with recently announced positive Ph II results • Revenue and cashflow positive manufacturing & royalty business • Experienced management team with significant development, regulatory and commercial experience 37 |
 Supplemental Financial Information
Non-GAAP Reconciliation
(in millions) 12 months ended Dec. 31, 2014 (audited) 3 months ended March 31, 2015 3 months ended March 31, 2014 Net income $14.3 $1.8 $3.5 Income tax expense $3.3 $0.6 $0.8 Impairment of long-lived assets $1.4 $0.0 $0.0 Depreciation and amortization $10.3 $2.9 $2.5 EBITDA $29.2 $5.2 $6.8 38 The Company defines EBITDA as earnings before interest, taxes, depreciation and amortization. The
Company also presents EBITDA because it believes it is frequently used by securities
analysts, investors and other interested parties as a measure of
financial performance. EBITDA has limitations as an analytical tool, and
when assessing the Company's operating performance, investors should not
consider EBITDA in isolation, or as a substitute for net income (loss) or other
consolidated income statement data prepared in accordance with U.S. GAAP.
|