Attached files
| file | filename |
|---|---|
| EX-14.1 - EXHIBIT 14.1 - Nobilis Health Corp. | exhibit14-1.htm |
| EXCEL - IDEA: XBRL DOCUMENT - Nobilis Health Corp. | Financial_Report.xls |
| EX-31.1 - EXHIBIT 31.1 - Nobilis Health Corp. | exhibit31-1.htm |
| EX-31.2 - EXHIBIT 31.2 - Nobilis Health Corp. | exhibit31-2.htm |
| EX-32.2 - EXHIBIT 32.2 - Nobilis Health Corp. | exhibit32-2.htm |
| EX-32.1 - EXHIBIT 32.1 - Nobilis Health Corp. | exhibit32-1.htm |
| EX-21.1 - EXHIBIT 21.1 - Nobilis Health Corp. | exhibit21-1.htm |
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C.
20549
FORM 10-K
(Mark One)
[X] ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
For the fiscal year ended
December 31, 2014
[ ] TRANSITION REPORT UNDER SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
For the transition period from [ ] to [ ]
Commission file number 000-55274
NOBILIS HEALTH CORP.
(Exact name of registrant as specified in its charter)
| British Columbia | 98-1188172 |
| (State or other jurisdiction of incorporation or | (I.R.S. Employer Identification No.) |
| organization) |
| 4120 Southwest Freeway, Suite 150, Houston, Texas | 77027 |
| (Address of principal executive offices) | (Zip Code) |
Registrant’s telephone number, including area code: (713) 355-8614
Securities registered pursuant to Section 12(b) of the Act:
| Title of Each Class | Name of Each Exchange On Which Registered |
| N/A | N/A |
Securities registered pursuant to Section 12(g) of the Act:
Common Stock, No par value
(Title of class)
Indicate by check mark if the registrant is a well-known
seasoned issuer, as defined in Rule 405 the Securities Act.
Yes
[ ] No [ x ]
Indicate by check mark if the registrant is not required
to file reports pursuant to Section 13 or Section 15(d) of the Act
Yes [ ] No [ x ]
Indicate by check mark whether the registrant: (1) has
filed all reports required to be filed by Section 13 or 15(d) of the Securities
Exchange Act of 1934 during the preceding 12 months (or for such shorter period
that the registrant was required to file such reports) and (2) has been subject
to such filing requirements for the last 90 days.
Yes [ x ] No
[ ]
Indicate by check mark whether the registrant has submitted
electronically and posted on its corporate Website, if any, every Interactive
Data File required to be submitted and posted pursuant to Rule 405 of Regulation
S-K (§229.405 of this chapter) during the preceding 12 months (or for such
shorter period that the registrant was required to submit and post such files).
Yes [ x ] No [ ]
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K (§229.405 of this chapter) is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. [ ]
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See definition of "large accelerated filer," "accelerated filer" and "smaller reporting company" in Rule 12b-2 of the Exchange Act.
| Large accelerated filer [ ] | Accelerated filer [ ] |
| Non-accelerated filer [ ] | Smaller reporting company [ x ] |
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes [ ] No [ x ]
The aggregate market value of Common Stock held by non-affiliates of the Registrant on June 30, 2014 was $23,254,102 based on a $0.98 average bid and asked price of such common equity, as of the last business day of the registrant’s most recently completed second fiscal quarter.
Indicate the number of shares outstanding of each of the
registrant’s classes of common stock as of the latest practicable date.
61,135,631 common shares as of March 25, 2015.
DOCUMENTS INCORPORATED BY REFERENCE
None.
TABLE OF CONTENTS
PART I
| Item 1. | Business |
This annual report contains forward-looking statements. These statements relate to future events or our future financial performance. In some cases, you can identify forward-looking statements by terminology such as "may", "should", "expects", "plans", "anticipates", "believes", "estimates", "predicts", "potential" or "continue" or the negative of these terms or other comparable terminology. These statements are only predictions and involve known and unknown risks, uncertainties and other factors, including the risks in the section entitled "Risk Factors" that may cause our or our industry’s actual results, levels of activity, performance or achievements to be materially different from any future results, levels of activity, performance or achievements expressed or implied by these forward-looking statements.
Although we believe that the expectations reflected in the forward-looking statements are reasonable, we cannot guarantee future results, levels of activity, performance or achievements. Except as required by applicable law, including the securities laws of the United States, we do not intend to update any of the forward-looking statements to conform these statements to actual results.
All dollar amounts are expressed in United States dollars as "$" and "C$" refers to Canadian dollars. The financial statements and summaries of financial information contained in this annual report are also reported in United States dollars unless otherwise stated. All such financial statements have been prepared in accordance with United States Generally Accepted Accounting Principles ("US GAAP"), unless expressly stated otherwise.
All references to "common shares" refer to the Common Shares in our capital stock.
As used in this current report and unless otherwise indicated, the terms "we", "us" and "our" and "our company" mean Nobilis Health Corp. and our subsidiaries, unless otherwise stated. References to "Nobilis" refer to Nobilis Health Corp. excluding our subsidiaries.
General Overview
Nobilis Health Corp. was incorporated on March 16, 2007 under the name "Northstar Healthcare Inc." pursuant to the provisions of the British Columbia Business Corporations Act ("BCBCA"). On December 5, 2014, Northstar Healthcare Inc. changed its name to Nobilis Health Corp. Our registered office is located at Suite 400, 570 Granville Street, Vancouver, British Columbia V6C 3P1 and our corporate office is located at 4120 Southwest Freeway, Suite 150, Houston, Texas 77027. Our common shares are and have been publicly traded on the Toronto Stock Exchange under the symbol "NHC" since May 2007.
We are an "emerging growth company" as defined in the Jumpstart Our Business Startups Act, referred to as the "JOBS Act".
Inter-corporate Relationships
The following chart illustrates our corporate structure as at January 1, 2015.
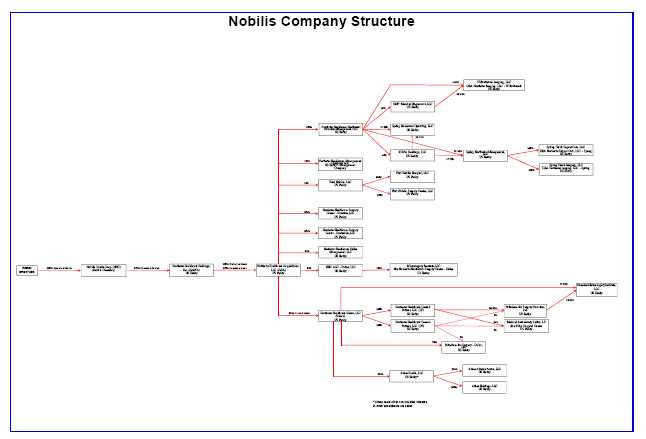
Investors own and/or manage nine healthcare facilities (the "Nobilis Facilities") in Texas and Arizona; two MRI centers, an urgent care center, one hospital and five ambulatory surgery centers, referred to as the "Nobilis ASCs" of which three are located in Houston, Texas, one in Dallas, Texas and one in Scottsdale, Arizona.
First Nobilis Hospital is a 19 bed acute-care hospital, with four operating rooms and one procedure room. We have an investment in the Oak Bend Medical Center.
The Nobilis ASCs are licensed ambulatory surgery centers that provide scheduled surgical procedures in a limited number of clinical specialties, which enables them to develop routines, procedures and protocols to maximize operating efficiency and productivity while offering an enhanced healthcare experience for both physicians and patients.
The Nobilis ASCs consist of the NHSC-H ASC, the MSID ASC, the NHSC-S ASC, the Kirby ASC, and the First Nobilis Surgery Center. We have investments in two other ASCs, the Elite Orthopedic Spine & Surgery Center and the Elite Sinus Spine and Ortho.
Together as of December 31, 2014, the First Nobilis Hospital and the Nobilis ASCs have 22 surgical suites, 6 procedure or treatment rooms typically used by pain management specialists or for colonoscopies, 39 pre-operation beds, 36 post-operation or recovery beds, 27 overnight beds, and 476 physicians with medical staff privileges (198 of whom performed surgeries in 2013).
The Nobilis ASCs do not offer the full range of services typically found in traditional hospitals, but instead focus on certain clinical specialties, including orthopedic surgery, podiatric surgery, ENT, pain management, gastro- intestinal, gynecology, and general surgery. First Nobilis Hospital focuses on these same specialties with the ability to take on more complex cases and cases that may require an overnight stay.
General Development of the Business
The following presents a summary of the general development of our business over the past five years. For a complete chart of the subsidiaries and entities referred to in this section, please refer to the diagram above which illustrates the various inter-corporate relationships in greater detail.
Pre-2010 Developments
At the time of completion of our company's initial public offering in 2007, we acquired a 70% controlling partnership interest in the The Palladium for Surgery – Houston, Ltd. (the "Palladium Partnership" or "PFSH") and a 60% partnership interest in the Medical Ambulatory Surgical Suites, L.P. (the "Kirby Partnership"). PFSH and the Kirby Partnership operated two ASCs, located in Houston, Texas.
In February 2009, Dr. Donald Kramer, our current director who was then Chief Executive Officer and also a director of our company, tendered his resignation from both positions.
2010 Developments
On September 30, 2010, we completed a private placement of common shares which resulted in a change of control. Pursuant to this private placement, we issued 14,583,417 shares of our common stock to Canada Healthcare Acquisitions, Inc. ("CHA") for C$5 million and 4,195,029 shares of our common stock to Healthcare Ventures, Ltd. ("Ventures") in exchange for all of its Class B Units in Northstar Healthcare Subco, LLC ("Northstar Subco") and Northstar Healthcare Acquisitions, LLC ("NHA"), along with the forgiveness of the related liabilities. Both CHA and Ventures were at the time indirectly controlled by Donald Kramer, M.D. In conjunction with the closing of the private placement, our company's then board of directors resigned and was replaced with a new board of directors. The newly appointed board named Dr. Kramer as Chairman. On October 27, 2010, our company's board announced that Dr. Kramer and Ms. Donna Alexander rejoined our senior management team in their previous capacities as Chief Executive Officer and Chief Operating Officer, respectively. The appointments took effect immediately.
On November 1, 2010, we formed a joint venture with certain physician partners, known as The Houston Microsurgery Institute, LLC ("MSIH"). As of November 1, 2010, the PFSH Partnership ceased performing cases and entered into a lease agreement with MSIH pursuant to which MSIH utilized the PFSH Partnership’s facility and equipment in exchange for 25% interest in the equity of MSIH.
2011 Developments
In January 2011, our company acquired Palladium for Surgery – Dallas ("PFSD") for $2.2 million. In conjunction with the acquisition the Company formed Microsurgery Institute, LLC ("MSID") to operate the ASC controlled by PFSD. PFSD became a 25% owner of MSID and subleased the ASC facility to MSID. MSID was syndicated with physician investors who owned the remaining 75%.
In January 2011, we also purchased 18% of the 27.5% non-controlling interest in the PFSH Partnership from Dr. Donald Kramer for $0.3 million, thereby increasing our interest in the PFSH Partnership to 90.5% . In August, 2011, we purchased additional non-controlling interests from two limited partners and as a result of these transactions, our interest in MSIH increased to 22.9% from 18.1% . In February 2011, we formed Gulf Coast Toxicology, LLC ("GCT") in partnership with Pioneer Laboratories, LLC. We have a 20% ownership interest in GCT, a Dallas-based drug screening laboratory. The laboratory screens and quantifies narcotics and other drugs in urine samples. GCT has partnered with a number of physicians in Houston who will supply the urine samples to be tested in the GCT’s laboratory. GCT commenced operations in early May 2011.
In November, 2011, two limited partners in the Kirby Partnership forfeited their ownership interests due to violations of the partnership agreement. The ownership percentages were distributed to the remaining partners, effectively increasing our interest in the Kirby Partnership to 65.5% from 60%.
2012 Developments
In January 2012, the Company issued 2,000,000 common shares to Dr. Kenneth Alo at a price of C$0.20 under a private placement agreement. Dr. Alo serves as a Medical Director of North American Spine (“NAS”), a subsidiary of Athas Health, LLC. The total purchase price approximated $0.4 million.
In February 2012, the Company acquired additional ownership interests from all of the physician limited partners at Houston Microsurgery Institute, LLC (“MSIH”), effectively increasing the Company’s ownership interest to 90.6% .
In March 2012, the Company sold 18.4% of its ownership interest in the Kirby Partnership to existing physician limited partners, effectively decreasing the Company’s ownership interest to 47.1% .
In April 2012, the Company returned partner capital contributions to all physician limited partners of South Texas Procedure Suites, LLC (“STPS”). The transaction effectively increased the Company’s ownership interest in STPS to 100.0% . STPS ceased operations and the Company abandoned the procedure suites model.
In August 2012, the Company purchased ownership interests from all of the physician limited partners at MSID, increasing the Company’s ownership interest to 100.0% . The Company then facilitated the closing of a private placement offering for equity at MSID to a physician group. The net result of these transactions is that Nobilis has increased its equity ownership in MSID from 25.0% to 50.0% . In conjunction with this transaction, Northstar ASC Management, LLC (“NASC”) was created to provide management services to the re-syndicated partnership. The Company’s ownership interest in NASC is 50.0% .
In November 2012, the Company sold 6.9% of its ownership interest in the Kirby Partnership to one existing physician limited partner and one new physician limited partner, effectively decreasing the Company’s ownership interest to 40.1% .
In December 2012, the Company facilitated the closing of a private placement offering for equity at MSID to three new physician limited partners, effectively decreasing the Company’s ownership interest to 36.5% .
2013 Developments
In March 2013, the Company redeemed the remaining equity interests held by physician limited partners at MSIH, effectively increasing the Company’s ownership interests to 97.7% . In August 2013, the Company formed a limited liability company, Northstar Healthcare Surgery Center – Houston, LLC (“NHSC-H”), which is owned 100% by Northstar Healthcare Acquisitions, LLC. In October 2013, MSIH ceased operating as an ASC and NHSC-H took over all existing operations of MSIH.
In July of 2013, the Company formed a limited liability company, NHC ASC – Dallas, LLC (“NHC ASC – Dallas”) which is owned 100% by NHA. In August 2013, the Company purchased ownership interest from all of the physician limited partners at MSID, increasing the Company’s ownership interest to 100%. In October 2013, the Company syndicated a partnership with certain physician partners for NHC ASC – Dallas. The Company assigned 100% of its equity interest in MSID to NHC ASC – Dallas, of which the Company owns 35% as a result of syndication.
In November 2013, the Company sold 15.1% of its ownership interest in the Kirby Partnership to existing physician limited partners, effectively decreasing the Company’s ownership interest to 25%.
In December 2013, NHA formed a wholly owned limited liability company, Northstar Healthcare Surgery Center – Scottsdale, LLC (“NHSC-S”), to operate as and ASC utilizing assets purchased from a former Brown Hand Center outpatient surgery center. These Assets (the “Scottsdale Assets”) were acquired through a business combination in December of 2013. Operations commenced subsequent to December 31, 2013.
In December 2013, the Company completed a capital raise through the private placement of common shares and warrants (the “Units”). The Company issued 5,862,500 Units, at a price of C$0.80 per Unit. Each Unit consists of one common share in the capital of the Company and one-half of one common share purchase warrant exercisable for one additional share at a price of C$1.10. Through the private placement, the Company raised $4.1 million, net of offering costs of $0.3 million. The Company utilized some of the proceeds to acquire the Scottsdale Assets.
2014 Developments
In January 2014, the Company invested in two imaging centers and one urgent care clinic in Houston. The aggregate investment was comprised of $0.3 million in cash, net of acquired cash, and 431,711 shares of NHC stock representing a combined value of $0.9 million, net of acquired cash.
On October 2, 2014 the Company’s shareholders approved a special resolution changing the name of the Company to “Nobilis Health Corp.”, and in December the Company amended its Articles of Incorporation.
On September 26, 2014, the Company closed a brokered private placement, with PI Financial Corp. as the Company’s Agent, of up to 6,153,846 Units at a price of C$1.30 per unit, for gross proceeds of $8,000,000, with the potential to raise a total of up to $10,000,000 (the “Private Placement”). . Each Unit consists of one common share in the capital of the Company and one-half of one common share purchase warrant exercisable for one additional share at a price of C$1.80 for 24 months from the closing date. The warrants are subject to an early acceleration provision in the event that, at any time following four months from the Closing date, the ten day volume weighted average price of the common shares equals or exceeds C$2.20. The proceeds of the Private Placement were used for general working capital purposes in connection with an agreement with First Surgical Partners Holdings, Inc. (“First Surgical”).
On September 29, 2014, the Company executed an agreement with First Surgical. Per the Agreement, the Company and First Surgical formed a new limited liability company, owned 51% by Nobilis and 49% by First Surgical, to jointly own and operate a hospital and surgical center. NHA manages the operations of the hospital and surgical center under a management agreement. The Company contributed $7.5 million to the new entity, which was raised by the Private Placement.
On December 1, 2014 the Company closed an agreement in which the Company would acquire all the individual member interests of Athas Health, LLC ("Athas") for a total consideration of approximately $31.2 million to expand the Company’s marketing services. The “aggregate consideration” for the Athas ownership interests consisted of $3 million in cash upon closing, the issuance of a promissory note by Company to the sellers for $12 million, the issuance at closing of 6,666,666 shares of Nobilis common stock that are subject to a lock up of up to 2 years, and the issuance of an additional 4,666,666 shares of Nobilis common stock issued over two years with half issued on the first anniversary of the closing and the remaining stock issued on the second anniversary of the closing. After the purchase, Chris Lloyd, Athas’ CEO, was named CEO of Company.
Competition
Within the Texas market, we currently compete with traditional hospitals, specialty hospitals and other ASCs to attract both physicians and patients. Hospitals generally have an advantage over ASCs with respect to the negotiation of insurance contracts and competition for physicians’ inpatient and outpatient practices. Hospitals also offer a much broader and specialized range of medical services (enabling them to service a broader patient population) and generally have longer operating histories and greater financial resources, and are better known in the general community.
The competition among ASCs and hospitals for physicians and patients has intensified in recent years. As a result, some hospitals have been acquiring physician practices and employing the physicians to work for the hospital. These hospitals incentivize these physicians to utilize the hospitals' facilities. Further, some traditional hospitals have recently formed joint ventures with physicians whereby the hospital manages, but the hospital and physicians jointly own, an ASC.
In addition, there are several large, publicly traded companies, divisions or subsidiaries of large publicly traded companies, and several private companies that develop and acquire ASCs and hospitals. These companies include United States Surgical Partners, Inc., AmSurg Corp., and Surgical Care Affiliates, Inc. These companies may compete with our company in the acquisition of additional ASCs and hospitals. Further, many physician groups develop ASCs without a corporate partner, using consultants who typically perform corporate services for a fee and who may take a small equity interest in the ongoing operations of such ASCs. See "Risk Factors – Risks Relating to Our Business – We Face Significant Competition From Other Healthcare Providers."
Cycles
Net patient service revenues are slightly seasonal in nature. Generally, revenues have been highest from October to December as physicians return from summer vacations and patients attempt to maximize the benefits afforded by third-party payors that renew health insurance deductibles at the beginning of each calendar year.
Facility Operations
-
Northstar Healthcare Surgical Center – Houston, LLC
Northstar Healthcare Surgical Center – Houston, LLC ("NHSC-H") operates an ASC located at 4120 Southwest Freeway, Suite 200, in Houston, Texas, within minutes of the Texas Medical Center. Operations at this location began in December 2003 with specialties in pain management, ENT, podiatry, orthopedics, general surgery, gastrointestinal and chiropractic medicine. As of December 31, 2013, 45 physicians had staff privileges at NHSC-H (22 of which performed surgeries in 2013). MSIH and PFSH each previously operated the ASC at this location. As of January 1, 2015, NHA directly held a 100% interest in NHSC-H. -
PFSD/MSID/NHC ASC-Dallas, LLC
The MSID ASC is located at 5920 Forest Park Road, Suite 700, in Dallas, Texas. The facility was acquired on January 1, 2011 with specialties in pain management, ENT, podiatry, orthopedics and general surgery. As of December 31, 2013, 170 physicians had staff privileges at MSID ASC (46 of which performed surgeries in 2013). The facility is operated by NHC ASC - Dallas. As of January 1, 2015, Northstar Subco, held an indirect 35.0% interest in the NHC ASC - Dallas. PFSD and MSID each previously operated the ASC at this location.
-
Medical Ambulatory Suites, LP
The Kirby Partnership owns and operates an ASC located at 9300 Kirby Drive, in Houston, Texas, less than four miles from the Texas Medical Center. Operations at this location began in June 2003 and, as of December 31, 2013, 30 physicians had staff privileges (14 of which performed surgeries in 2013). As of January 1, 2015, Northstar Subco held an indirect 25.0% interest in the Kirby Partnership while the remaining 75.0% is owned by Kirby's Physician Limited Partners. -
Northstar Healthcare Surgical Center – Scottsdale, LLC
NHSC-S is located at 9377 E Bell Rd, Suite 201, Scottsdale, Arizona 85260. The facility was acquired in December, 2013. Operations at the facility began in early 2014. As of January 1, 2015, Northstar Acquisitions directly held a 100% interest in NHSC-S. -
First Nobilis Surgical Center, LLC
First Nobilis Surgical Center, LLC (“FNSC”) operates and ASC located at 411 North 1st Street, Bellaire, Texas 77401. The facility began as part of the joint venture with First Surgical. FNSC is a wholly owned subsidiary of First Nobilis, LLC, the joint venture entity owned 51% by NHA and 49% by First Surgical. As of January 1, 2015, Northstar Acquisitions held 51% of First Nobilis Surgical Center’s parent company First Nobilis, LLC. -
First Nobilis Hospital, LLC
First Nobilis Hospital, LLC (“FNH”) operates a hospital at 4801 Bissonnet St, Bellaire, Texas 77401. The facility began as part of the joint venture with First Surgical. FNH is a wholly owned subsidiary of First Nobilis, LLC, the joint venture entity owned 51% by NHA and 49% by First Surgical. As of January 1, 2015, Northstar Acquisitions held 51% of First Nobilis Surgical Center’s parent company First Nobilis, LLC. -
Spring Northwest Management, LLC ("SNWM") Spring Creek Urgent Care, LLC ("SCUC") and Spring Creek Imaging LLC ("SCI")
The Company independently owns 31.78% of SNWM of derived through both a direct and indirect investment. The Company also indirectly owns 31.78% interest in both of SNWM’s wholly owned subsidiaries, Spring Creek Urgent Care, LLC ("SCUC") and Spring Creek Imaging LLC ("SCI"), which operate urgent care facilities. -
Willowbrook Imaging, LLC ("WIM")
WIM operates a diagnostic imaging facility located at 13652 Breton Ridge Street, Suite B, Houston, Texas 77070. The Company directly and indirectly owns a 22.22% interest in WIMt. -
Elite Orthopedic Spine & Surgery Center LLC
Elite Orthopedic Spine & Surgery Center LLC is located at 1605 Airport Freeway Bedford, Texas 76021. The Company indirectly owns thirty-five (35) membership interest units, which represents 35% of Elite Orthopedic Spine & Surgery Center LLC’s anticipated outstanding membership interest units (this private offering remains open). -
Elite Sinus Spine and Ortho LLC
Elite Sinus Spine and Ortho LLC operates and ASC located at 4120 Southwest Freeway, Suite 100, Houston, Texas 77027. The Company owns fifteen (15) membership interest units, which represent approximately 15% of Elite Sinus Spine and Ortho LLC’s outstanding membership interest units.
Employees
As of March 25, 2015, we had approximately 452 employees, of which 322 are full time.
Intellectual Property
| Mark | Type | Owner | Status | App./Reg. # |
| NOBILIS HEALTH |
Service Mark |
Nobilis Health |
Application Pending |
App. No. 86375409 |
| Mark | Type | Owner | Status | App./Reg. # |
| NORTHSTAR HEALTHCARE |
Service Mark |
Nobilis Health Corp. |
Registered |
App. No. 77892043 |
 |
Service Mark |
Northstar Healthcare Acquisitions, LLC |
Registered | Reg. No. 3444878 |
 |
Service Mark | Nobilis Health Corp. | Registered | Reg. No. 4,555,939 |
| NUESTEP | Service Mark | Nobilis Health Corp. | Registered | Reg. No. 4,555,938 |
| STEP AWAY FROM FOOT PAIN |
Service Mark |
Nobilis Health Corp. |
Registered |
Reg. No. 4,555,937 |
| AccuraScope | Trade Mark | Athas Health, LLC | Registered | Reg. No. 4,041,538 |
Enforcement of Civil Liabilities
Our subsidiaries are organized under the laws of the states of Arizona, Delaware and Texas. Substantially all of our assets and all of the assets of our subsidiaries are located in the United States. Furthermore, all of our current officers and directors reside in the United States. As a result, investors should not find it difficult to effect service of process within the United States upon us or these persons or to enforce judgments obtained against us or these persons in U.S. courts, including judgments in actions predicated upon the civil liability provisions of the U.S. federal securities laws. It may, however, be difficult for an investor to bring an original action or an action to enforce a judgment obtained in a U.S. court in a Canadian or other foreign court predicated upon the civil liability provisions of the U.S. federal securities laws against us or these persons. Conversely, it may be difficult for an investor to bring an original action or an action to enforce a judgment obtained in a Canadian or other foreign court predicated upon the civil liability provisions of the U.S. federal securities laws against us or these persons. There is uncertainty as to whether Canadian courts would: (i) enforce judgments of United States courts obtained against our company or our directors and officers predicated upon the civil liability provisions of the United States federal securities laws, or (ii) entertain original actions brought in Canadian courts against our company or such persons predicated upon the federal securities laws of the United States, as such laws may conflict with Canadian laws. In Canada, such rights are within the legislative jurisdiction of the Provinces and Territories. The Province of British Columbia, where our company is domiciled, does not have laws for the reciprocal enforcement of judgments of United States courts.
Emerging Growth Company
We are an Emerging Growth Company as defined in the JOBS Act.
We will continue to be deemed an emerging growth company until the earliest of:
| (A) |
the last day of the fiscal year of the issuer during which it had total annual gross revenues of $1,000,000,000 (as such amount is indexed for inflation every 5 years by the Commission to reflect the change in the Consumer Price Index for All Urban Consumers published by the Bureau of Labor Statistics, setting the threshold to the nearest 1,000,000) or more; |
| (B) |
the last day of the fiscal year of the issuer following the fifth anniversary of the date of the first sale of common equity securities of the issuer pursuant to an effective registration statement under this title; |
| (C) |
the date on which such issuer has, during the previous 3-year period, issued more than $1,000,000,000 in non-convertible debt; or |
| (D) |
the date on which such issuer is deemed to be a ‘large accelerated filer’, as defined in section 240.12b-2 of title 17, Code of Federal Regulations, or any successor thereto. |
As an emerging growth company we are exempt from Section 404(b) of Sarbanes Oxley. Section 404(a) requires companies to publish information in their annual reports concerning the scope and adequacy of the internal control structure and procedures for financial reporting as well as an assessment of the effectiveness of such internal controls and procedures.
Section 404(b) requires that the registered accounting firm shall, in the same report, attest to and report on the assessment on the effectiveness of the internal control structure and procedures for financial reporting.
As an emerging growth company we are exempt from Section 14A and B of the Securities Exchange Act of 1934 which require the shareholder approval of executive compensation and golden parachutes.
We have elected not to opt out of the extended transition period for complying with any new or revised accounting standards pursuant to Section 107(b) of the JOBS Act.
Research and Development
We have incurred $Nil in research and development expenditures over the last two fiscal years.
| Item 1A. | Risk Factors |
Our business operations are subject to a number of risks and uncertainties, including, but not limited to those set forth below:
We are impacted by general economic conditions
Our business is subject to general economic risks incident to the U.S. healthcare market and the U.S. and Canadian capital markets. The majority of our patients obtain health insurance through their employers, thus factors impacting the employment rate can increase or decrease our potential patient population. Further, because many health insurance plans require patients to pay co-insurance and/or a deductible, the ability of a patient to pay these portions impacts the patient's decision to undergo the elective surgical procedures we provide in many of our facilities. The continuing recovery from the global recessionary economic conditions that existed in 2012 had a positive financial impact on our business in 2013 which continued throughout 2014.
Because we have relied on, and will continue to rely on, outside investors and lenders for capital used for our operational capital, capital expenditures and strategic acquisitions, the general market conditions in the U.S. and Canada, such as interest rates, availability of credit, inflation rates, economic uncertainty, changes in laws and regulations, and national and international political circumstances impact our business.
We are subject to general business risks in the ASC industry
We are subject to general business risks inherent in the ASC industry, including changing physician and patient preferences, adverse changes in reimbursement by third-party payors, the inability to collect a profitable level of fees, increases in labor costs and other operating costs, possible future changes in labor relations, competition from or the oversupply of other similar surgical facilities, changes in neighborhood or location conditions and general economic conditions, health related risks (including liability for the provision of health care services), disease outbreaks and control risks, the imposition of increased taxes or new taxes, capital expenditure requirements, changes in interest rates, and changes in the availability and cost of long-term financing. Moreover, there is no assurance that the performance achieved to date at the Nobilis Facilities and expected in the future will continue or be achieved. Any one of, or a combination of, these factors may adversely affect our business, results of operations and financial condition.
We are subject to fluctuations in revenues and payor mix
We depend on payments from third-party payors, including private insurers, managed care organizations and government healthcare programs. We are dependent on private and, to a lesser extent, governmental third-party sources of payment for the procedures performed in our facilities. Our competitive position has been, and will continue to be, affected by reimbursement and co-payment initiatives undertaken by third-party payors, including insurance companies, and, to a lesser extent, employers, and Medicare and Medicaid.
As an increasing percentage of patients become subject to healthcare coverage arrangements with managed care payors, our success may depend in part on our ability to negotiate favorable contracts on behalf of our facilities with managed care organizations, employer groups and other private third-party payors. There can be no assurances that we will be able to enter into these arrangements on satisfactory terms in the future. Also, to the extent that our facilities have managed care contracts currently in place, there can be no assurance that such contracts will be renewed or the rates of reimbursement held at current levels.
Managed care plans often set their reimbursement rates based on Medicare and Medicaid rates and consequently, although only a small portion of our revenues are from Medicare and Medicaid, the rates established by these payors may influence our revenues from private payors.
As with most government reimbursement programs, the Medicare and Medicaid programs are subject to statutory and regulatory changes, possible retroactive and prospective rate adjustments, administrative rulings, freezes and funding reductions, all of which may adversely affect our revenues and results of operations. The Centers for Medicare and Medicare Services ("CMS") introduced substantial changes to reimbursement and coverage in early 2007. While the ASC final rule expanded the types of procedures eligible for payment in the ASC setting and excluded from eligibility only those procedures that pose a significant safety risk to patients or are expected to require active medical monitoring at midnight when furnished in an ASC, rule also provided a 4-year transition to the fully implemented revised ASC payment rates. Beginning with the November 2007 OPPS/ASC final rule with comment period (CMS-1392-FC), the annual update OPPS/ASC final rule with comment period provides the ASC payment rates and lists the surgical procedures and services that qualify for separate payment under the revised ASC payment system. As a result, reimbursement levels decreased but coverage expanded. These rates remain subject to change, thus our operating margins may continue to be under pressure as a result of changes in payor mix and growth in operating expenses in excess of increases in payments by third-party payors. In addition, as a result of competitive pressures, our ability to maintain operating margins through price increases to privately insured patients is limited. This could have a material adverse effect on our business, operating results and financial condition.
Net patient service revenue is reported at the estimated net realizable amounts from patients, third-party payors, and others for services rendered and is recognized upon performance of the patient service. In determining net patient service revenue, management periodically reviews and evaluates historical payment data, payor mix and current economic conditions and adjusts, as required, the estimated collections as a percentage of gross billings in subsequent periods based on final settlements and collections.
Management continues to monitor historical collections and market conditions to manage and report the effects of a change in estimates. While we believe that the current reporting and trending software provides us with an accurate estimate of net patient service revenues, any future methods of improving these estimates could have a material adverse effect on our operating results and financial condition.
Out-of-network reimbursement and contract negotiations
One of the complexities of our business navigating the increasingly hostile environment for entities that are not participants in the health insurance companies' ("Third Party Payers") provider networks (also referred to as an "out-of-network provider or facility"). Third Party Payers negotiate discounted fees with providers and facilities in return for access to the patient populations which those Third Party Payers cover. The providers and facilities that contractually agree to these rates become part of the Third Party Payer's "network". The Nobilis Facilities are currently out-of-network as to most Third Party Payers.
There are several risks associated with not participating in Third Party Payer networks. First, not all Third Party Payers offer coverage to their patients for services rendered by non-participants in that Third Party Payer's network. Further, it is typically the case that a patients with so-called "out-of-network benefits" will be obliged to pay a higher co-pays, a higher deductibles, and a larger percentage of co-insurance payments. In addition, because the out-of-network coverage often mandates payment at a "usual and customary rate", the determination of the amounts payable by the Third Party Payer can fluctuate. Healthcare providers and facilities that choose not to participate in a Third Party Payer's often face longer times for their claims to be processed and paid. Further, many Third Party Payers aggressively audit claims from out-of-network providers and facilities and continuously change their benefit policies in various ways that restrict the ability of beneficiaries to access out-of-network benefits, and to restrict out-of-network providers from treating their beneficiaries.
Consequently, it may become necessary for the Nobilis Facilities to change their out-of-network strategy and join Third Party Payer networks. This may require us to negotiate and maintain numerous contracts with various Third Party Payers. In either case, our performance is greatly dependent upon decisions that Third Party Payers make regarding their out-of-network benefits and alternatively, our ability to negotiate profitable contracts with Third Party Payers. If it becomes necessary for the Nobilis Facilities to become in-network facilities, there is no guarantee that we will be able to successfully negotiate these contracts. Further, we may experience difficulty in establishing and maintaining relationships with health maintenance organizations, preferred provider organizations, and other Third Party Payers. Out-of-network reimbursement rates are typically higher than in-network reimbursement rates, so our revenue would likely decline if we move to an in-network provider strategy and fail to increase our volume of business sufficiently to offset reduced in-network reimbursement rates. These factors could adversely affect our revenues and our business.
We depend on our physicians and other key personnel
Our success depends, in part, on our ability to attract and retain quality physicians. There can be no assurance that we can continue to attract high quality physicians, facility staff and technical staff to our facilities. In addition, notwithstanding contractual commitments given by certain of our physicians who were selling Physicians Limited Partners under the Partnership Interests Purchase Agreements to maintain certain specified volume levels, there can be no assurances that our current physicians will continue to practice at our facilities at their current levels, if at all. An inability to attract and retain physicians may adversely affect our business, results of operations and financial condition.
The Physician Limited Partners in the Kirby Partnership have agreed not to compete with Nobilis pursuant to the terms of the Kirby Partnership Interests Purchase Agreements and the partnership agreements. These covenants, however, only restrict ownership in a competing ASC, and do not prevent a Physician Limited Partner from performing procedures (and receiving remuneration for the performance of such procedures in the form of professional fees) at competing ASCs.
Our success also depends on the efforts and abilities of our management, as well as our ability to attract additional qualified personnel to manage operations and future growth. Although we have entered into employment agreements with certain of our key employees, we cannot be certain that any of these employees will not voluntarily terminate their employment. We have employment contracts with Donald Kramer (Chairman of the Board), Harry Fleming (President), and Chris Lloyd (CEO). Also, at this time, we do not maintain any key employee life insurance policies on any management personnel or Physician Limited Partners, but may do so in the future. The loss of a member of management, other key employee, Physician Limited Partners or other physicians who use our facilities could have an adverse effect on our business, operating results and financial condition.
Our business is not highly diversified
As of December 31, 2013, our only business was the ownership and operation of the three Nobilis ASCs located in Texas. Therefore, we were entirely dependent on the success of these facilities for all of our revenues. In January of 2014, we acquired ownership interests in two imaging centers and an urgent care clinic in the Houston, Texas area. Additionally, since the first of the year, we have started operations at NHSC-S in Arizona. These developments have provided some degree of diversification to our business. However, investors will not have the benefit of further diversification of operations or risk until such time, if ever, that we acquire or develop additional facilities, manage additional facilities, or undertake other related business opportunities. As a result of our geographic concentration, we are particularly susceptible to downturns in the local and regional economy, regional inclement weather, changes in local or state regulation, or to reductions in Texas’ Medicaid and/or Medicare payments to healthcare providers.
In addition, approximately 65.6% of the cases performed at the Nobilis ASCs in 2013 were concentrated among three major private insurance companies and workers' compensation payors. At December 31, 2013, more than 55.4% of the cases performed at the Nobilis ASCs were on an "out of network" basis, without any reimbursement rate protection or consistent in-network patient enrollments typically seen from an in-network agreement. Accordingly, we are susceptible to changes in reimbursement policies and procedures by third-party insurers and patients’ preference of utilizing their out of network benefits. In an effort to stabilize its payor mix, Kirby Partnership signed a multi-year in-network contract with one of the major private insurance companies commencing the first quarter of 2009 and another in-network contract with one of the major private insurance companies commencing the second quarter of 2012. These agreements have reduced the percentage of procedures performed at the Nobilis ASCs on an "out-of network" basis.
We face significant competition from other healthcare providers
We compete with other facilities and hospitals for patients, physicians, nurses and technical staff. Some of our competitors have long-standing and well-established relationships with physicians and third-party payors in the community. Some of our competitors are also significantly larger than us, may have access to greater marketing, financial and other resources and may be better known in the general community. The competition among facilities and hospitals for physicians and patients has intensified in recent years. Some hospitals have imposed restrictions on the credentials of their medical staff (called conflict of interest credentialing) where these physicians hold an ownership in a competing facility. The Nobilis Facilities face competition from other facilities and from hospitals that perform similar outpatient services, both inside and outside of the Nobilis Facilities’ primary service areas. Further, some traditional hospitals have recently begun forming joint ventures with physicians whereby the hospital manages and the hospital and physicians jointly own the facility. Patients may travel to other facilities for a variety of reasons. These reasons include physician referrals or the need for services the Nobilis Facilities do not offer. Patients and their physicians who seek services from these other facilities may subsequently shift their preferences to those facilities and away from the Nobilis Facilities.
Some of these competing facilities offer a broader array of outpatient surgery services than those available at the Nobilis Facilities. In addition, some of the Nobilis Facilities’ direct competitors are owned by non-profit or governmental entities, which may be supported by endowments and charitable contributions or by public or governmental support. These hospitals can make capital expenditures without paying sales tax, may hold the property without paying property taxes and may pay for the equipment out of earnings not burdened by income taxes. This competitive advantage may affect the Nobilis Facilities’ inability to compete effectively with these non-profit or governmental entities. There are several large, publicly traded companies, divisions or subsidiaries of large publicly held companies, and several private companies that develop and acquire multi-specialty facilities, and these companies compete with us in the acquisition of additional facilities. Further, many physician groups develop facilities without a corporate partner, using consultants who typically perform these services for a fee and who may take a small equity interest in the ongoing operations of a facility. We can give no assurances that we can compete effectively in these areas. If we are unable to compete effectively to recruit new physicians, attract patients, enter into arrangements with managed care payors or acquire new facilities, our ability to implement our growth strategies successfully could be impaired. This may have an adverse effect on our business, results of operations and financial condition.
The industry trend toward value-based purchasing may negatively impact our revenues.
We believe that value-based purchasing initiatives of both governmental and private payers tying financial incentives to quality and efficiency of care will increasingly affect the results of operations of our hospitals and other health care facilities and may negatively impact our revenues if we are unable to meet expected quality standards. The Affordable Care Act contains a number of provisions intended to promote value-based purchasing in federal health care programs. Medicare now requires providers to report certain quality measures in order to receive full reimbursement increases for inpatient and outpatient procedures that were previously awarded automatically. In addition, hospitals that meet or exceed certain quality performance standards will receive increased reimbursement payments, and hospitals that have "excess readmissions" for specified conditions will receive reduced reimbursement.
There is a trend among private payers toward value-based purchasing of health care services, as well. Many large commercial payers require hospitals to report quality data, and several of these payers will not reimburse hospitals for certain preventable adverse events. We expect value-based purchasing programs, including programs that condition reimbursement on patient outcome measures, to become more common, to involve a higher percentage of reimbursement amounts and to spread to reimbursement for ASCs and other ancillary services. We are unable at this time to predict how this trend will affect our results of operations, but it could negatively impact our revenues if we are unable to meet quality standards established by both governmental and private payers.
There are many federal, state and local laws that regulate our business.
The Nobilis Facilities are subject to numerous federal, state and local laws, rules and regulations. Regulations that may have the most significant effect on our business are:
Licensure and Accreditation
Healthcare facilities, such as the Nobilis ASCs, are subject to professional and private licensing, certification and accreditation requirements. These include, but are not limited to, requirements imposed by Medicare, Medicaid, state licensing authorities, voluntary accrediting organizations and third-party private payors. Receipt and renewal of such licenses, certifications and accreditations are often based on inspections, surveys, audits, investigations or other reviews, some of which may require affirmative compliance actions by the Nobilis ASCs that could be burdensome and expensive. We believe that the Nobilis ASCs are currently in material compliance with all applicable licensing, certification and accreditation requirements.
However, the applicable standards may change in the future. There can be no assurance that each of the Nobilis ASCs will be able to maintain all necessary licenses or certifications in good standing or that they will not be required to incur substantial costs in doing so. The failure to maintain all necessary licenses, certifications and accreditations in good standing, or the expenditure of substantial funds to maintain them, could have an adverse effect on our business, results of operations and financial condition.
In addition, in order to perform medical and surgical procedures in Texas, physicians must be licensed by the Texas Medical Board. Professional nurses and technical staff must also be licensed under state law. There can be no assurance that any particular physician, nurse or technical staff member who has medical staff privileges at the Nobilis ASCs will not have his or her license suspended or revoked by the Texas Medical Board or be sanctioned by the Department of Health and Human Services ("DHHS"), Office of Inspector General ("OIG"), for violations of federal Medicare laws. If a license is suspended or revoked, or if such physician, nurse or technical staff member is sanctioned by the OIG and excluded from the Medicare program, such physician, nurse or technical staff member may not be able to perform surgical procedures at the Nobilis ASCs, which may have an adverse affect on our operations and business.
Anti-Kickback Statute
The United States Medicare/Medicaid Fraud and Abuse Anti-kickback Statute (the "Anti-Kickback Statute") prohibits "knowingly or willfully" paying money or providing remuneration of any sort in exchange for federally-funded referrals. Because the Physician Limited Partners are in a position to generate referrals to the Nobilis Facilities, distributions of profits to these Limited Partners could come under scrutiny under the Anti-Kickback Statute. While the DHHS has issued regulations containing "safe harbors" to the Anti-Kickback Statute, including those specifically applicable to ASCs, our operations and arrangements do not comply with all of the requirements. As we do not have the benefit of the safe harbors, we are not immune from government review or prosecution. However, we believe that the business operations of the Nobilis Facilities are structured to substantially comply with applicable anti-kickback laws. To the extent safe harbour protection is not available, the agreements governing the structure and operations of the Nobilis Facilities include provisions to mitigate against alleged kickbacks or other inducements.
The State of Texas and the State of Arizona each maintain its own version of the Anti-Kickback Statute (the "Non-solicitation Laws"). In Texas the relevant law is called the Texas Patient Solicitation Act (“TPSA”). The TPSA prohibits payment of remuneration for referrals and violations can result in state criminal and civil penalties. Because the TPSA is based on the federal Anti-Kickback Statute, the risks described above also arise under this state law except that the TPSA arguably is not limited to claims for treatment of federal program beneficiaries. In Arizona, A.R.S §13-3713 makes it unlawful for a person to knowingly offer, deliver, receive, or accept any rebate, refund, commission, preference or other consideration in exchange for a patient, client or customer referral to any individual, pharmacy, laboratory, clinic or health care institution providing medical or health-related services or items under A.R.S. § 11-291 et seq., providing for indigent care, or A.R.S. § 36-2901 et seq., or providing for the Arizona Health Care Cost Containment System, other than specifically provided under those sections. A violator of the relevant Arizona laws is guilty of: a class 3 felony for payment of $1,000 or more; a class 4 felony for payment of more than $100 but less than $1,000; or a class 6 felony for payment of $100 or less.
The Non-solicitation Laws parallel in many respects the federal Anti-Kickback Statute, but they apply more broadly because they are not limited only to providers participating in federal and state health care programs. The Texas statute specifically provides that it permits any payment, business arrangement, or payment practice that is permitted under the federal Anti-Kickback Statute and regulations promulgated under that law, although failure to fall within a safe harbor does not mean that the arrangement necessarily violates Texas law. Arizona takes the same approach.
Some of the various arrangements that our company enters into with providers may not fit into a safe harbor to the federal Anti-Kickback Statute and thus may not be exempt from scrutiny under the Non-solicitation Laws. Although an arrangement that fits a federal safe harbor may also be excepted from the prohibitions of the Non-solicitation Laws, the burden is on the medical provider to prove that the questioned arrangement fits one of the federal safe harbors. Additionally, even if that burden is met, the provider must still comply with the law’s requirements to disclose to the patient the financial relationship involved.
A failure by our company to comply with the Anti-Kickback Statute, TPSA or Arizona laws could have an adverse effect on our business, results of operations and financial condition.
False Claims Legislation
Under the United States Criminal False Claims Act, individuals or entities that knowingly file false or fraudulent claims that are payable by the Medicare or Medicaid programs are subject to both criminal and civil liability. While the Nobilis Facilities have a compliance program and policies to create a corporate culture of compliance with these laws, failure to comply could result in monetary penalties (up to three times the amount of damages), fines and/or imprisonment, which could have an adverse effect on our business, results of operations and financial condition.
HIPAA
The Nobilis Facilities are subject to the Health Insurance Portability and Accountability Act ("HIPAA"), which mandates industry standards for the exchange of protected health information, including electronic health information. While we believe that we have implemented privacy and security systems to bring us into material compliance with HIPAA, we cannot ensure that the business associates to whom we provide information will comply with HIPAA standards. In addition, because Congress continues to amend HIPAA to keep pace with evolving recordkeeping technologies, we cannot guarantee compliance with future amendments. If we, for whatever reasons, fail to comply with the standards, or any state statute that governs an individual’s right to privacy that are not pre-empted by HIPAA, we could be subject to criminal penalties and civil sanctions, which could have an adverse effect on our business, financial condition and results of operations.
Patient Protection and Affordable Care Act
The Nobilis Facilities may be affected by the Patient Protection and Affordable Care Act ("PPACA"), which began taking effect June, 21, 2010. The impact on Nobilis Facilities remains uncertain. By mandating that residents obtain minimum levels of health insurance coverage, the PPACA has expanded the overall number of insured patients. However, it remains to be seen whether the cost born by employers of providing insurance coverage will result in a shift away from the types of policies that have historically provided the coverage that Nobilis has relied upon in the past. Further, as discussed above, the impact that value-based purchasing initiatives could have on Nobilis' revenues remains unclear. Nobilis continues to review the potential impact of PPACA’s provisions on its business as the out-of-network reimbursement under the policies issued by the state exchange might be substantially lower than those by the employer-sponsored polices.
Antitrust
Federal and state antitrust laws restrict the ability of competitors, including physicians and other providers, to act in concert in restraint of trade, to fix prices for services, to allocate territories, to tie the purchase of one product to the purchase of another product, or to attempt to monopolize a market for services.
Notwithstanding the Nobilis entities’ efforts to fully comply with all antitrust laws, a significant amount of ambiguity exists with respect to the application of these laws to healthcare activities. Thus, no assurance can be provided that an enforcement action or judicial proceeding will not be brought against the Nobilis Facilities or that the facilities will not be liable for substantial penalties, fines and legal expenses.
Environmental Laws and regulations
Typical health care provider operations include, but are not limited to, in various combinations, the handling, use, treatment, storage, transportation, disposal and/or discharge of hazardous, infectious, toxic, radioactive and flammable materials, wastes, pollutants or contaminants. As such, health care provider operations are particularly susceptible to the practical, financial, and legal risks associated with the obligations imposed by applicable environment laws and regulations. Such risks may (i) result in damage to individuals, property, or the environment; (ii) interrupt operations and/or increase their cost; (iii) result in legal liability, damages, injunctions, or fines; (iv) result in investigations, administrative proceedings, civil litigation, criminal prosecution, penalties, or other governmental agency actions; and (v) may not be covered by insurance. There can be no assurance that we will not encounter such risks in the future, and such risks may result in material adverse consequences to our operations or financial results.
Other regulations
In addition to the regulatory initiatives described above, healthcare facilities, including the Nobilis Facilities, are subject to a wide variety of federal, state, and local environmental and occupational health and safety laws and regulations that may affect their operations, facilities, and properties. Violations of these laws could subject us to civil penalties and fines for not investigating and remedying any contamination by hazardous substances, as well as other liability from third parties.
Although we believe the Nobilis Facilities are currently in material compliance with all applicable environmental laws and regulations, and expect such compliance will continue in the future, there can be no assurance that the Nobilis Facilities will not violate the requirements of one or more of these laws or that we will not have to expend significant amounts to remediate or ensure compliance.
We may be unable to implement our organic growth strategy
Future growth will place increased demands on our management, operational and financial information systems and other resources. Further expansion of our operations will require substantial financial resources and management resources and attention. To accommodate our anticipated future growth, and to compete effectively, we will need to continue to implement and improve our management, operational, financial and information systems and to expand, train, manage and motivate our workforce. Our personnel, systems, procedures or controls may not be adequate to support our operations in the future. Further, focusing our financial resources and management attention on the expansion of our operations may negatively impact our financial results. Any failure to implement and improve our management, operational, financial and information systems, or to expand, train, manage or motivate our workforce, could reduce or prevent our growth. We can give you no assurances that our personnel, systems, procedures or controls will be adequate to support our operations in the future or that our financial resources and management attention on the expansion of our operations will not adversely affect our business, result of operations and financial condition. In addition, direct-to-consumer marketing may not be a suitable means to attract case volume as patients may not directly seek our services, but instead may choose to consult with a non-Nobilis-affiliate physician. We can offer no guarantees that the financial resources expended on direct-to-consumer marketing campaigns will result in the expansion of our business.
We may be unable to implement our acquisition strategy
Our efforts to execute our acquisition strategy may be affected by our ability to identify suitable candidates and negotiate and close acquisition transactions. We may encounter numerous business risks in acquiring additional facilities, and may have difficulty operating and integrating these facilities. Further, the companies or assets we acquire in the future may not ultimately produce returns that justify our investment. If we are not able to execute our acquisition strategy, our ability to increase revenues and earnings through external growth will be impaired.
In addition, we will need capital to acquire other centers, integrate, operate and expand the Nobilis Facilities. We may finance future acquisition and development projects through debt or equity financings and may use Common Shares for all or a portion of the consideration to be paid in future acquisitions. To the extent that we undertake these financings or use Common Shares as consideration, our shareholders may experience future ownership dilution. To the extent debt is incurred, we may incur significant interest expense and may be subject to covenants in the related debt agreements that affect the conduct of business. In the event that our Common Shares do not maintain a sufficient valuation, or potential acquisition candidates are unwilling to accept our Common Shares as all or part of the consideration, we may be required to use more of our cash resources, if available, or to rely solely on additional financing arrangements to pursue our acquisition and development strategy. However, we may not have sufficient capital resources or be able to obtain financing on terms acceptable to us for our acquisition and development strategy, which would limit our growth. Without sufficient capital resources to implement this strategy, our future growth could be limited and operations impaired. There can be no assurance that additional financing will be available to fund this growth strategy or that, if available, the financing will be on terms that are acceptable to us.
We may incur unexpected, material liabilities as a result of acquiring ASCs or other healthcare facilities
Although we intend to conduct due diligence on any future acquisition, we may inadvertently invest in facilities or other healthcare facilities that have material liabilities, arising from, for example, the failure to comply with government regulations or other past activities. Although the Nobilis Facilities have the benefit of professional and general liability insurance, we do not currently maintain and are unlikely to acquire insurance specifically covering every unknown or contingent liability that may have occurred prior to our investment in the Nobilis Facilities, particularly those involving prior civil or criminal misconduct (for which there is no insurance). Incurring such liabilities as a result of future acquisitions could have an adverse effect on our business, operations and financial condition.
We may be subject to professional liability claims
As a healthcare provider, we are subject to professional liability claims both directly and vicariously through the malpractice of members of our medical staff. As a healthcare facility, each Nobilis Facility has direct responsibility and legal liability for the standard of care provided in its facility by its staff. The Nobilis Facilities have legal responsibility for the physical environment and appropriate operation of equipment used during surgical procedures. In addition, each Nobilis Facility has vicarious liability for the negligence of its credentialed medical staff under circumstances where it either knew or should have known of a problem leading to a patient injury. The physicians credentialed by the Nobilis Facilities are involved in the delivery of healthcare services to the public and are exposed to the risk of professional liability claims. Although the Nobilis Facilities neither control the practice of medicine by physicians nor have responsibility for compliance with certain regulatory and other requirements directly applicable to physicians and their services, as a result of the relationship between each Nobilis Facility and the physicians providing services to patients in the Nobilis Facilities, the Registrant’s other subsidiaries or even the Registrant may become subject to medical malpractice claims under various legal theories. Claims of this nature, if successful, could result in damage awards to the claimants in excess of the limits of available insurance coverage. Insurance against losses related to claims of this type can be expensive and varies widely from state to state. The Nobilis Facilities maintain and require the physicians on the medical staff of the Nobilis Facilities to maintain liability insurance in amounts and coverages believed to be adequate, presently $1 million per claim to an aggregate of $3 million per year.
In 2003, Texas passed legislation that reformed its laws related to professional liability claims by setting caps on non-economic damages in the amount of $250,000 per claimant to a per claim aggregate of $750,000 for physicians and other providers, including ASCs. Punitive damages are excluded from this cap. This tort reform legislation has resulted in a reduction in the cost of malpractice insurance because of the reduction in malpractice claims. However, there can be no assurances that this trend will continue into the future.
Most malpractice liability insurance policies do not extend coverage for punitive damages. While extremely rare in the medical area, punitive damages are those damages assessed by a jury with the intent to "punish" a tortfeasor rather than pay for a material loss resulting from the alleged injury. We cannot assure you that we will not incur liability for punitive damage awards even where adequate insurance limits are maintained. We also believe that there has been, and will continue to be, an increase in governmental investigations of physician-owned facilities, particularly in the area of Medicare/Medicaid false claims, as well as an increase in enforcement actions resulting from these investigations. Investigation activity by private third-party payors has also increased with, in some cases, intervention by the states’ attorneys general. Also possible are potential non-covered claims, or "qui tam" or "whistle blower" suits.
Although exposure to qui tam lawsuits is minimal since Medicare and Medicaid comprises less than 5.0% of our revenue and an even smaller percentage of our profit, many plaintiffs’ lawyers have refocused their practices on "whistle blower" lawsuits given the reduction in awards from medical malpractice claims. These whistle blower lawsuits are based on alleged violations of government law related to billing practice and kickbacks. Under federal Medicare law, these whistle blowers are entitled to receive a percentage of recoveries made if the federal government takes on the case. However, a whistle blower may pursue direct action against the healthcare entity under the applicable statutes and seek recoveries without federal government intervention. Many malpractice carriers will not insure for violations of the law although they may cover the cost of defense. Any adverse determination in a legal proceeding or governmental investigation, whether currently asserted or arising in the future, could have a material adverse effect on our financial condition. In this regard, the Registrant notes that the billing practices of one of its facilities were investigated in 2006 based upon a complaint with the CMS finding no basis to take any action, and with the complaint being dismissed.
The Nobilis Facilities may, in the ordinary course of their business, be subject to litigation claims. In particular, the Nobilis Facilities can be subject to claims, among others, relating to actions of medical personnel performing services at the Nobilis Facilities. Historically, the Nobilis Facilities have been able to obtain what we believe is adequate insurance to cover these risks. However, the cost of this insurance may increase and there can be no assurance that we will be able to obtain adequate insurance against medical liability claims in the future on economically reasonable terms, or at all. In addition, claims of this nature, if successful, could result in damage awards to the claimants in excess of the limits of any applicable insurance coverage. If the insurance that we have in place from time to time is not sufficient to cover claims that are made, the resulting shortfall could have a material adverse affect on our business and operations.
The Nobilis Facilities’ insurance coverages might not cover all claims against them or be available at a reasonable cost, if at all. If the Nobilis Facilities are unable to maintain insurance coverage, if judgments are obtained in excess of the coverage the Nobilis Facilities maintain, or if the Nobilis Facilities are required to pay uninsured punitive damages or pay fines under "qui tam" lawsuits, the Nobilis Facilities would be exposed to substantial additional liabilities. The Registrant cannot assure that each Nobilis Facility will be able to maintain insurance coverage at a reasonable premium, or at all, that coverage will be adequate to satisfy adverse determinations against the Nobilis Facilities, or that the number of claims will not increase.
Malpractice insurance premiums or claims may adversely affect our business
Should the Nobilis Facilities experience adverse risk management claims or should the market for medical malpractice dictate a large increase in rates, our business and financial results could be adversely affected.
We rely on technology
The medical technology used in our facilities is ever changing and represents a significant cost of doing business. There can be no assurance that the equipment purchased or leased by our facilities will not be enhanced or rendered obsolete by advances in medical technology, or that our facilities will be able to finance or lease additional equipment necessary to remain competitive should its medical staff physicians request such modern equipment or its existing equipment become obsolete. This could have an adverse effect on our business, operations and financial condition.
We are subject to rising costs
The costs of providing our services have been rising and are expected to continue to rise at a rate higher than that anticipated for consumer goods as a whole. Our business, operating results or financial condition could be adversely affected if we are unable to implement annual private pay increases due to market conditions, otherwise increase our revenues or, to a lesser extent, if reimbursement rates from Medicaid and Medicare sources are not adjusted to cover increases in labor and other costs.
We depend on referrals
Our success, in large part, is dependent upon referrals to our physicians from other physicians, systems, health plans and others in the communities in which we operate, and upon our medical staff’s ability to maintain good relations with these referral sources. Physicians who use our facilities and those who refer patients are not our employees and, in many cases, most physicians have admitting privileges at other hospitals and (subject to any non-competition arrangements that may have been entered into in connection with the Partnership Agreements) may refer patients to other providers. If we are unable to successfully cultivate and maintain strong relationships with our physicians and their referral sources, the number of procedures performed at our facilities may decrease and cause revenues to decline. This could adversely affect our business, results of operations and financial condition.
We may be subject to changes in current law or the enactment of future legislation
In recent years, a variety of legislative and regulatory initiatives have occurred on both the federal and state levels concerning physician ownership of healthcare entities to which physicians refer patients, third-party payment programs and other regulatory matters concerning ASCs. We anticipate that federal and state legislatures will continue to review and assess alternative healthcare delivery and payment systems. Potential approaches that have been considered include mandated basic health care benefits, controls on health care spending through limitations on the growth of private health insurance premiums and Medicare and Medicaid spending, the creation of large insurance purchasing groups, pay for performance systems, and other fundamental changes to the health care delivery system. Private sector providers and payors have embraced certain elements of reform, resulting in increased consolidation of health care providers and payors as those providers and payors seek to form alliances in order to provide cost effective, quality care. Legislative debate is expected to continue in the future, and the Company cannot predict what impact the adoption of any federal or state health care reform measures or future private sector reform may have on its business.
It is not possible to predict what federal or state initiatives, if any, may be adopted in the future or how such changes might affect us. If a federal or state agency asserts a different position or enacts new legislation regarding ASCs, we may experience a significant reduction in our revenues, be excluded from participation in third-party payor programs, or be subject to future civil and criminal penalties.
We may face a shortage of nurses
The United States is currently experiencing a shortage of nursing staff. The failure of the Nobilis Facilities to hire and retain qualified nurses could have a material adverse effect on our business operations and financial condition.
We are subject to general litigation risks
Litigation could potentially be brought against us by various individuals or entities including, but not limited to federal, state, or local governments, potential competitors, investors and current and former employees. Any such lawsuits could have an adverse effect on our operations and financial results.
We do not have control of the day-to-day medical affairs and certain other affairs of the Nobilis Facilities
At December 31, 2013, Northstar Subco held a 91.9% indirect ownership interest in the PFSH Partnership, a 25.0% indirect ownership interest in the Kirby Partnership, a 97.7% indirect ownership interest in MSIH, a 35% indirect ownership in MSID, a 35% indirect ownership in NHC ASC – Dallas, and a 40% indirect ownership interest in HPS. Although we indirectly manage the day to-day-business affairs of each Nobilis Facility under a management agreement, we only have the right to attend and observe at meetings of each Nobilis Facilities’ Medical Board. As such, we do not have the ability to direct day-to-day medical affairs of the Nobilis Facilities, but rather only its business and commercial affairs, all as set forth in the Partnership Agreements. In addition, certain actions by the Entities are subject to a veto by a written vote of a majority in interest of the Physician Limited Partners, including the approval of the annual budget and annual plan (subject to the right of Northstar Healthcare General Partner, LLC to continue to operate the Nobilis Facilities in a manner that preserves its business and goodwill, business relationships and physical plant).
We are subject to Canadian tax laws
Our company's income and our related entities must be computed in accordance with Canadian and foreign tax laws, as applicable, and we are subject to Canadian tax laws, all of which may be changed in a manner that could adversely affect the amount of distributions to shareholders. There can be no assurance that Canadian federal income tax laws, the judicial interpretation thereof or the administrative and assessing practices and policies of the Canada Revenue Agency and the Department of Finance (Canada) will not be changed in a manner that adversely affects shareholders. In particular, any such change could increase the amount of tax payable by the Registrant, reducing the amount available to pay dividends to the holders of the Common Shares.
We are subject to U.S. tax laws
There can be no assurance that United States federal income tax laws and Internal Revenue Service and Department of the Treasury administrative and legislative policies respecting the United States federal income tax consequences described herein will not be changed in a manner that adversely affects the holders of the Common Shares.
The non-solicitation, non-competition, transfer and other covenants of the Physician Limited Partners and others may not be enforceable
Under the Kirby Partnership Agreement (subject to certain limited exceptions) during the time that a Physician Limited Partner is a Partner and for two years thereafter, the Physician Limited Partner may not directly or indirectly own, control, finance or participate in the profits or revenues of any business that engages in competition with such Nobilis Facility anywhere within a 20-mile radius of such Nobilis Facility; provided, however, that a Physician Limited Partner shall not be prevented from performing surgery at another facility or otherwise practicing medicine in a private practice that may utilize such competing facility. In addition, six of the nine current Kirby Partners are bound by a similar non-competition provision contained in a Unit Transfer Agreement executed in 2012. The Limited Partners bound by this provision may not directly or indirectly own, control, finance or participate in the profits or revenues of any business that engages in competition with such Nobilis Facility anywhere within a 20- mile radius of such Nobilis Facility for a period of three years from March 30, 2012. The Unit Transfer Agreement contains certain "burn off" provisions which state that the non-competition period will be reduced by a year in the event that Kirby fails to meet certain gross revenue goals.
In addition, the Athas subsidiary is a party, either directly or indirectly, to several contracts containing non-competition provisions purporting to bind physicians to whom Athas provides marketing services.
Because non-competition provisions are enforced not as a matter of contractual law but as a matter of "equity", a court asked to enforce a non-competition provision with a Physician Limited Partner or other physicians will have broad discretion over enforcement, non-enforcement or the fashioning of relief different from that contractually agreed to by the parties. While no single physician's non-competition provision is material to Nobilis, a court decision to not enforce a physician's non-competition covenant could set a precedent with respect to physicians bound by the same or similar provisions, such that, in the aggregate, there results may be a detrimental impact on Nobilis revenues.
Future issuances of Common Shares could result in dilution
Our articles authorize the issuance of an unlimited number of shares of our common stock, on terms that the Board of Directors, without approval of any shareholders, establishes. We may issue additional common shares in the future in connection with a future financing or acquisition. The issuance of additional shares may dilute the investment of a shareholder.
We qualify as an "emerging growth company" under the JOBS Act. As a result, we are permitted to, and intend to, rely on exemptions from certain disclosure requirements. For so long as we are an emerging growth company, we will not be required to:
-
have an auditor report on our internal controls over financial reporting pursuant to Section 404(b) of the Sarbanes-Oxley Act;
-
comply with any requirement that may be adopted by the Public Company Accounting Oversight Board regarding mandatory audit firm rotation or a supplement to the auditor’s report providing additional information about the audit and the financial statements (i.e., an auditor discussion and analysis);
-
submit certain executive compensation matters to shareholder advisory votes, such as "say-on-pay" and "say-on-frequency"; and
-
disclose certain executive compensation related items such as the correlation between executive compensation and performance and comparisons of the Chief Executive's compensation to median employee compensation.
We will remain an "emerging growth company" for up to five years, or until the earliest of (i) the last day of the first fiscal year in which our total annual gross revenues exceed $1 billion, (ii) the date that we become a "large accelerated filer" as defined in Rule 12b-2 under the Securities Exchange Act of 1934, which would occur if the market value of our ordinary shares that is held by non-affiliates exceeds $700 million as of the last business day of our most recently completed second fiscal quarter or (iii) the date on which we have issued more than $1 billion in non-convertible debt during the preceding three year period.
Until such time, however, we cannot predict if investors will find our common stock less attractive because we may rely on these exemptions. If some investors find our common stock less attractive as a result, there may be a less active trading market for our common stock and our stock price may be more volatile.
Since we have elected under Section 107 of the JOBS Act to use the extended transition period with respect to complying with new or revised accounting standards, our financial statements may not be comparable to companies that comply with public company effective dates making it more difficult for an investor to compare our results with other public companies.
Section 107 of the JOBS Act provides that an emerging growth company can take advantage of the extended transition period provided in Section 102(b)(2)(B) of the JOBS Act for complying with new or revised accounting standards. In other words, as an emerging growth company we can delay the adoption of certain accounting standards until those standards would otherwise apply to private companies. We have elected to take advantage of the benefits of this extended transition period. Our financial statements may therefore not be comparable to those of companies that comply with such new or revised accounting standards.
| Item 1B. | Unresolved Staff Comments |
As a "smaller reporting company", we are not required to provide the information required by this Item.
| Item 2. | Properties |
Our corporate head office is located at 4120 Southwest Freeway, Suite 200, Houston, Texas. The 4,905 sq. ft. facility is currently leased from a third-party in Houston, Texas. The lease has a term that ends in 2023 and is currently in good standing.
Northstar Healthcare Surgical Center-Dallas
The 20,929 sq. ft. facility is currently leased from a third-party in Dallas, Texas under two leases. The first lease covering 17,205 sq. ft. has an expiration date of May 2017, and is currently in good standing. The second lease covering 3,724 sq.ft. has an expiration date of January 31, 2015, and is currently in good standing. The facility is operated by NHC ASC - Dallas.
Kirby Surgery Center
The approximately 11,000 sq. ft. facility is leased from a third-party in Houston, Texas. The lease was renewed in 2014 for an additional ten years and is currently in good standing.
Northstar Healthcare Surgical Center - Scottsdale
The 18,643 sq. ft. facility is currently leased from a third-party in Scottsdale, Arizona. The lease has a term that ends in 2022 and is currently in good standing.
Corporate /Northstar Healthcare Surgical Center - Houston
The 24,586 sq. ft. facility is currently leased from a third-party in Houston, Texas. The lease has a term that ends in 2018 and is currently in good standing.
First Nobilis Surgical Center
The 11,025 sq. ft. facility is currently leased from a third-party in Houston, Texas. The lease has a term that ends in 2033 and is currently in good standing
First Nobilis Hospital
The 23,000 sq. ft. facility is currently leased from a third-party in Houston, Texas. The lease has a term that ends in 2033 and is currently in good standing.
First Nobilis Hospital
The expanded 41,000 sq. ft. facility is currently leased from a third-party in Houston, Texas. The lease has a term that ends in 2033 and is currently in good standing.
Athas Health – Corporate
The 16,139 sq. ft. facility is currently leased from a third-party in Houston, Texas. The lease has a term that ends in 2016 and is currently in good standing.
| Item 3. | Legal Proceedings |
From time to time, we may become involved in litigation relating to claims arising out of its operations in the normal course of business. We are not involved in any pending legal proceeding or litigation and, to the best of our knowledge, no governmental authority is contemplating any proceeding to which we area party or to which any of our properties is subject, which would reasonably be likely to have a material adverse effect on us, except for the following:
Adam Lefton, our former Chief Marketing Officer, on December 27, 2013 filed suit in the 11th District Court of Harris County, Texas against us and our subsidiary, Northstar Acquisitions, alleging breach of his employment agreement and claiming to have suffered damages. We have answered the suit denying the claims. As of September 30, 2014, based on the early nature of these proceedings no provision has been made for this claim. Mr. Lefton alleges damages of $676,500 plus 1,000,000 common shares of our company.
| Item 4. | Mine Safety Disclosures |
Not applicable.
| Item 5. | Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities |
Our common stock is listed and posted for trading on the Toronto Stock Exchange under the symbol "NHC". The following table sets forth the reported high and low prices and the trading volume for our common shares on the Toronto Stock Exchange for the periods indicated in 2013 and 2014:
| Month | High (C$) | Low (C$) | Trading Volume (#) |
| 2014 Q4 | 3.60 | 1.11 | 10,345,600 |
| 2014 Q3 | 1.58 | 1.06 | 3,484,918 |
| 2014 Q2 | 1.22 | 1.02 | 2,095,400 |
| 2014 Q1 | 1.28 | 0.98 | 3,828,300 |
| 2013 Q4 | 1.64 | 0.71 | 3,441,700 |
| 2013 Q3 | 0.87 | 0.39 | 1,382,400 |
| 2013 Q2 | 0.47 | 0.28 | 729,500 |
| 2013 Q1 | 0.52 | 0.13 | 2,631,300 |
| 2012 Q4 | 0.15 | 0.09 | 542,600 |
| 2012 Q3 | 0.22 | 0.09 | 278,200 |
| 2012 Q2 | 0.25 | 0.11 | 294,800 |
| 2012 Q1 | 0.21 | 0.15 | 282,600 |
Our shares are issued in registered form. CST Trust Company, 320 Bay Street, 3rd Floor, Toronto, ON, M5H 4A6, Telephone: (416) 682-3850; Facsimile: (877) 715-0494 is the registrar and transfer agent for our common shares.
On December 31, 2014, the shareholders’ list showed 50 registered shareholders with 59,393,227 Common Shares outstanding.
Dividend Policy
We have not declared or paid any cash dividends on our common stock for over five years and we do not anticipate paying any dividends in the foreseeable future. We expect to retain any future earnings to finance our operations and expansion. The payment of cash dividends in the future will depend upon our future revenues, earnings and capital requirements and other factors the Board considers relevant.
Equity Compensation Plan Information
Restricted Share Unit Plan
During 2008, the board of directors approved the adoption of a Restricted Share Unit Plan for employees. RSUs may be granted to employees of Northstar Acquisitions at the sole discretion of the board of directors.
Subject to the board of directors’ ability to accelerate the vesting of the RSUs if it determines circumstances so warrant, each RSU will generally vest in full on the third anniversary of the date of grant; provided that if there is a change of control of our company prior to the vesting date of the RSUs and a participant is terminated (or resigns for good reason) within six months following such change of control, a pro rata portion of their unvested RSUs will vest up to the date of the change of control.
Upon vesting of his or her RSUs, a participant will be entitled to receive on the vesting date, at the discretion of the board of directors either: (a) a lump sum cash payment equal to the number of RSUs multiplied by an average closing price of the common shares on the Toronto Stock Exchange on the redemption date, net of any applicable deductions and withholdings; or (b) that number of common shares equal to the number of RSUs credited to the participant’s RSU account, such common shares to be issued from treasury of our company. The participant is to receive the benefit on, or as soon as practicable after, the vesting date, but in no event later than 90 days after the vesting date. Unlike share options, RSUs do not require the payment of any monetary consideration to our company.
Whenever cash dividends are paid on our company’s common shares, dividend equivalents in the form of additional RSUs will be credited to each Participant and will become part of his or her award under the RSU Plan. The RSUs representing dividend equivalents will vest and be paid at the same time and in the same manner as the RSUs to which the dividend equivalents pertain.
In the event of a Participant’s termination of employment, voluntary or by cause, with our company prior to any vesting date, the Participant’s rights to any unvested RSUs will be immediately and irrevocably forfeited.
If the Participant’s employment with our company terminates on account of death or disability or is terminated by our company without cause prior to any vesting date, the Participant will become vested in a prorated portion of his or her unvested RSUs, based on the number of months that have elapsed in the then current vesting period as of the date of termination.
Deferred Share Unit Plan
In May 2012, the board of directors terminated the DSU Plan. In conjunction with its termination, all outstanding DSUs previously issued to the directors were cancelled, and our company granted each director a number of RSUs equal to the number of DSUs which had been previously granted. The RSUs vested immediately. A total of 536,219 DSUs were cancelled in this manner. As the cancelled DSUs and newly granted RSUs all vested at the time of grant, no change to compensation expense occurred.
Share Option Plan
In April 2012, the board of directors approved the adoption of a Share Option Plan for insiders, employees, and service providers. In May 2012, our company’s shareholders approved the Share Option Plan, and in July 2012, the Toronto Stock Exchange approved the Share Option Plan. Options reserved under the plan consist of the right of a participant (a “Participant”) to purchase one common share per option (“Option”) may be granted at the sole discretion of the board of directors. The exercise price of an Option is determined by the board of directors at the time of grant and shall not be less than the current market price. The term of each Option is determined by the board of directors and shall not exceed 10 years.
If an Optionee shall cease to be a Participant for cause, no Option held by such Optionee shall be exercisable following the date on which such Optionee ceases to be a Participant. If an Optionee ceases to be a Participant for any reason other than for cause, any Option held by such Optionee at such time shall remain exercisable in full at any time, and in part from time to time, for a period of 90 days after the date on which the Optionee ceases to be a Participant.
If the Participant’s employment with our company terminates on account of death, any option held by such Participant at the date of death shall be exercisable in whole or in part only by the person or persons to whom the rights of the Participant’s Options by will or laws of descent.
The maximum number of RSUs and share options that may be issued under the combined plans is equal to 20.0% of our company’s issued and outstanding common shares.
Nobilis granted a total of 3,118,218 incentive stock options during the twelve months ended December 31, 2014, with exercise prices ranging from C$$0.30 - C$1.87.
Nobilis granted a total of 4,075,000 RSUs during the twelve months ended December 31, 2014.
The following table summarizes certain information regarding our equity compensation plans as at December 31, 2014:
| Equity Compensation Plan Information | |||
Plan Category |
Number of securities to be
issued upon exercise of outstanding options, warrants and rights(1) |
Weighted-average
exercise price of outstanding options, warrants and rights (C$) |
Number of securities
remaining available for future issuance under equity compensation plans(1) (2) |
| Equity compensation plans approved by
security holders (aggregated) |
6,795,000 |
1.31 |
5,083,645 |
| Equity compensation plans not approved by
security holders (aggregated) |
1,048,218 |
1.87 |
– |
| Total | 7,843,218 | 1.38 | 5,083,645 |
_____________
Notes:
| (1) |
Includes securities issued under our Restricted Share Unit Plan and Stock Option Plan up to December 31, 2014. | |
| (2) |
Excludes securities reflected in column entitled “Number of securities to be issued upon exercise of outstanding options, warrants and rights”. |
Convertible Securities
As of December 31, 2014, we had 3,118,218 incentive stock options outstanding at exercise prices ranging from C$$0.95 - C$1.87. Each incentive stock option entitles the holder to purchase, subject to adjustment, one common share of our company at the exercise price established at the time of grant of the options.
As of December 31, 2014, we had 2,784,200 warrants outstanding to purchase common shares at an exercise price of C$1.80. Each share purchase warrant entitles the holder to purchase, subject to adjustment, one common share of our company for a period of two years until September 26, 2016.
As of December 31, 2014, we had 135,620 transferable Agent’s Warrants outstanding to purchase common shares at an exercise price of C$0.95 and 332,908 transferable Agent’s Warrants outstanding to purchase common shares at an exercise price of C$1.37. Each Agent’s Warrant entitles the holder to purchase, subject to adjustment, one common share of our company for period of two years ending December 16, 2015 and September 26, 2016. The Agent’s Warrants were issued in connection with the company’s private placements in December 2013 and September 2014.
Recent Sales of Unregistered Securities; Use of Proceeds from Registered Securities
In January 2012, Nobilis issued 2,000,000 common shares to Dr. Kenneth Alo at a price of C$0.20 under a private placement agreement. Dr. Alo serves as a Medical Director of NAS, a subsidiary of Athas Health, LLC. The total purchase price approximated $0.4 million.
In December 2013, the Nobilis completed a capital raise through the private placement of Units. The Nobilis issued 5,862,500 Units, at a price of C$0.80 per Unit. Each Unit consists of one common share in the capital of the Company and one-half of one common share purchase warrant exercisable for one additional share at a price of C$1.10. Through the private placement, the Company raised $4.1 million, net of offering costs of $0.3 million. The Company utilized some of the proceeds to acquire the Scottsdale Assets. The shares were issued in reliance on an exemption from the registration requirements of the Securities Act of 1933, as amended.
On September 26, 2014, the Company closed a brokered private placement, with PI Financial Corp. as the Company’s Agent, of up to 6,153,846 Units at a price of C$1.30 per unit, for gross proceeds of $8,000,000, with the potential to raise a total of up to $10,000,000 (the “Private Placement”). . Each Unit consists of one common share in the capital of the Company and one-half of one common share purchase warrant exercisable for one additional share at a price of C$1.80 for 24 months from the closing date. The warrants are subject to an early acceleration provision in the event that, at any time following four months from the Closing date, the ten day volume weighted average price of the common shares equals or exceeds C$2.20. The proceeds of the Private Placement were used for general working capital purposes in connection with an agreement with First Surgical Partners Holdings, Inc. (“First Surgical”).
Each of the foregoing issuances was exempt from the registration requirements of the Securities Act of 1933, as amended pursuant to Section 4(2).
Purchase of Equity Securities by the Issuer and Affiliated Purchasers
We did not purchase any of our shares of common stock or other securities during our fourth quarter of our fiscal year ended December 31, 2014.
| Item 6. | Selected Financial Data |
As a "smaller reporting company", we are not required to provide the information required by this Item.
| Item 7. | Management’s Discussion and Analysis of Financial Condition and Results of Operations |
Forward-Looking Statements
The following discussion of the Company’s historical performance and financial condition should be read together with the consolidated financial statements and related notes in Item 8 of this report. This discussion contains forward-looking statements based on the views and beliefs of our management, as well as assumptions and estimates made by our management. These statements by their nature are subject to risks and uncertainties, and are influenced by various factors. As a consequence, actual results may differ materially from those in the forward-looking statements. See Item 1A. Risk Factors of this report for the discussion of risk factors.
Overview
Nobilis Health Corp. (“NHC”) together with its subsidiaries (collectively, “Nobilis,” “Company,” “us,” “we,” or “our”) was incorporated on March 16, 2007 under the name "Northstar Healthcare Inc." pursuant to the provisions of the British Columbia Business Corporations Act. On December 5, 2014, Northstar Healthcare Inc. changed its name to Nobilis Health Corp. Our registered office is located at Suite 400, 570 Granville Street, Vancouver, British Columbia V6C 3P1 and our corporate office is located at 4120 Southwest Freeway, Suite 150, Houston, Texas 77027.
The Company is a corporation formed to indirectly acquire and/or manage ambulatory surgery centers (ASCs) and healthcare facilities in the United States. We own and manage nine healthcare facilities (the “Nobilis Facilities”) in Texas and Arizona; two MRI centers, an urgent care center, one hospital and five ambulatory surgery centers, referred to as the "Nobilis ASCs" of which three are located in Houston, Texas, one in Dallas, Texas and one in Scottsdale, Arizona. In December 2014, the Company expanded its services to health care marketing when it acquired 100% interests of Athas Health, LLC (“Athas”).
Details of business developments that occurred prior to January 1, 2013, have been disclosed in the Company’s previous public filings.
Revenue Model and Case Mix
Revenues earned by the Nobilis Facilities vary depending on the procedures performed. For every medical procedure performed there are usually three separately invoiced patient billings:
- the facility fee for the use of infrastructure, surgical equipment, nursing staff, non-surgical professional services, supplies and other support services, which is earned by the Nobilis Facilities or by physician entities using the Nobilis Facilities under a use agreement and billed by the Nobilis Facilities on the physician entities’ behalf;
- the professional fee, which is separately earned, billed and collected by the physician performing the procedure, separate and apart from the fees charged by the Nobilis Facilities; and
- the anesthesiology fee, which is separately earned, billed and collected by the anesthesia provider, separate and apart from the fees charged by the Nobilis Facilities and the physicians.
Overall facility revenue depends on procedure volume, case mix and payment rates of the respective payors.
The following table sets out the net patient service revenues, the number of procedures performed and the net patient service revenue per procedure at each of the Nobilis Facilities for last two fiscal years ended December 31, 2014, and 2013:
| Net Patient Service Revenue | Net Patient Service Revenue | ||||||||||||||||||
| ($)(in thousands) | Number of Cases (1) | ($) per Case (2) | |||||||||||||||||
| Nobilis Facility | 2014 | 2013 | 2014 | 2013 | 2014 | 2013 | |||||||||||||
| NHSC-H | $ | 22,052 | $ | 6,676 | 1,402 | 825 | $ | 15,729 | $ | 8,092 | |||||||||
| KIRBY | 12,933 | 11,503 | 3,760 | 3,491 | 3,440 | 3,295 | |||||||||||||
| MSID | 31,320 | 12,635 | 1,831 | 1,170 | 17,105 | 10,799 | |||||||||||||
| NHSC-S | 1,773 | - | 214 | - | 8,287 | - | |||||||||||||
| FNH | 10,763 | - | 659 | - | 16,333 | - | |||||||||||||
| FNSC | 1,444 | - | 450 | - | 3,209 | - | |||||||||||||
| Total | 80,285 | 30,814 | 8,316 | 5,486 | 9,654 | 5,617 | |||||||||||||
| Year over Year Growth | 161% | 52% | 72% | ||||||||||||||||
____________________
Notes
| (1) |
This table refers to all cases performed, regardless of their contribution to net patient service revenue. |
| (2) |
Calculated by dividing net patient service revenues by the number of cases. |
The Nobilis Facilities focus on a limited number of high-volume, non-emergency procedures, most of which are billed on an “out of network” basis. The case mix at each Nobilis Facility is a function of the clinical specialties of the physicians on the medical staff and the equipment and infrastructure at each facility. The Nobilis Facilities intend to continue to refine their case mix as opportunities arise. The following table sets forth the combined number of cased and procedures by medical specialty performed in 2014 and 2013 at the Nobilis Facilities:
MEDICAL SERVICES SEGMENT
CASE AND PROCEDUREMIX OF
THENOBILIS FACILITIES
FOR THEYEARS ENDED DECEMBER 31, 2014 AND 2013
| 2014 % | 2014 | 2014 % | 2013 % | 2013 | 2013 % | |||||||||||||||||||
| Specialty | 2014 Cases | Cases | Procedures | Procedures | 2013 Cases | Cases | Procedures | Procedures | ||||||||||||||||
| Pain Management | 3,415 | 41.1% | 13,246 | 51.1% | 2,877 | 52.4% | 11,928 | 60.5% | ||||||||||||||||
| Musculoskeletal Interventions | 18 | 0.2% | 18 | 0.1% | - | 0.0% | - | 0.0% | ||||||||||||||||
| Interventional Headache Procedure | - | 0.0% | - | 0.0% | - | 0.0% | - | 0.0% | ||||||||||||||||
| Orthopedics | 985 | 11.8% | 2,808 | 10.8% | 724 | 13.2% | 2,417 | 12.3% | ||||||||||||||||
| Podiatry | 361 | 4.3% | 1,800 | 6.9% | 286 | 5.2% | 1,566 | 7.9% | ||||||||||||||||
| Gastro-intestinal | 213 | 2.6% | 295 | 1.1% | 269 | 4.9% | 400 | 2.0% | ||||||||||||||||
| General Surgery | 550 | 6.6% | 1,205 | 4.6% | 415 | 7.6% | 1,095 | 5.6% | ||||||||||||||||
| Plastic & Reconstructive | 421 | 5.1% | 752 | 2.9% | - | 0.0% | - | 0.0% | ||||||||||||||||
| Bariatrics | 1,591 | 19.1% | 3,632 | 14.0% | 372 | 6.8% | 594 | 3.0% | ||||||||||||||||
| GYN | 134 | 1.6% | 163 | 0.6% | 77 | 1.4% | 98 | 0.5% | ||||||||||||||||
| Ear, Nose, Throat (E.N.T.) | 628 | 7.6% | 2,019 | 7.9% | 466 | 8.5% | 1,620 | 8.2% | ||||||||||||||||
| TOTAL | 8,316 | 100.0% | 25,938 | 100.0% | 5,486 | 100.0% | 19,718 | 100.0% |
Contracted marketing revenue is comprised of payments from hospitals, ASC’s and other ancillary service providers, other than the Nobilis Facilities, through marketing services agreements. The services include licensing, marketing, patient intake, patient outcome assessments and educational services. Revenue is recognized on a gross basis upon the performance of the marketing service and when ultimate collection is measurable and reasonably assured. Facility revenue from the cases generated by Athas under its marketing program and performed at Nobilis facilities are included under the Medical Service Segment.
Factoring revenue is comprised of revenue generated from certain accounts receivables which are purchased from third parties through the regular course of business. Purchase price is determined either by a flat fee per case, as dictated per the agreement, or as a percentage of final collections. At the time of purchase, the Company assumes all financial risk and incurs all costs related to collections without any recourse to the third party seller. Revenue is recognized based upon the date of the original service associated with the receivable.
MARKETING & FACTORING SEGMENT
CASE AND
PROCEDUREMIX OF THENOBILIS FACILITIES
FOR THEYEARS ENDED DECEMBER 31, 2014
AND 2013
| 2014 % | 2014 | 2014 % | 2013 % | 2013 | 2013 % | |||||||||||||||||||
| Specialty | 2014 Cases | Cases | Procedures | Procedures | 2013 Cases | Cases | Procedures | Procedures | ||||||||||||||||
| Pain Management | 178 | 42.0% | 178 | 42.0% | - | 0.0% | - | 0.0% | ||||||||||||||||
| Musculoskeletal Interventions | 206 | 48.6% | 206 | 48.6% | - | 0.0% | - | 0.0% | ||||||||||||||||
| Interventional Headache Procedure | 40 | 9.4% | 40 | 9.4% | - | 0.0% | - | 0.0% | ||||||||||||||||
| Orthopedics | - | 0.0% | - | 0.0% | - | 0.0% | - | 0.0% | ||||||||||||||||
| Podiatry | - | 0.0% | - | 0.0% | - | 0.0% | - | 0.0% | ||||||||||||||||
| Gastro-intestinal | - | 0.0% | - | 0.0% | - | 0.0% | - | 0.0% | ||||||||||||||||
| General Surgery | - | 0.0% | - | 0.0% | - | 0.0% | - | 0.0% | ||||||||||||||||
| Plastic & Reconstructive | - | 0.0% | - | 0.0% | - | 0.0% | - | 0.0% | ||||||||||||||||
| Bariatrics | - | 0.0% | - | 0.0% | - | 0.0% | - | 0.0% | ||||||||||||||||
| Gynecology | - | 0.0% | - | 0.0% | - | 0.0% | - | 0.0% | ||||||||||||||||
| Ear, Nose, Throat (E.N.T.) | - | 0.0% | - | 0.0% | - | 0.0% | - | 0.0% | ||||||||||||||||
| TOTAL | 424 | 100.0% | 424 | 100.0% | - | 0.0% | - | 0.0% |
CONSOLIDATED SEGMENTS
CASEAND PROCEDUREMIX OF
THENOBILIS FACILITIES
FOR THEYEARS ENDED DECEMBER 31, 2014 AND 2013
| 2014 % | 2014 | 2014 % | 2013 % | 2013 | 2013 % | |||||||||||||||||||
| Specialty | 2014 Cases | Cases | Procedures | Procedures | 2013 Cases | Cases | Procedures | Procedures | ||||||||||||||||
| Pain Management | 3,593 | 41.1% | 13,424 | 50.9% | 2,877 | 52.4% | 11,928 | 60.5% | ||||||||||||||||
| Musculoskeletal Interventions | 224 | 2.6% | 224 | 0.8% | - | 0.0% | - | 0.0% | ||||||||||||||||
| Interventional Headache Procedure | 40 | 0.5% | 40 | 0.2% | - | 0.0% | - | 0.0% | ||||||||||||||||
| Orthopedics | 985 | 11.3% | 2,808 | 10.7% | 724 | 13.2% | 2,417 | 12.3% | ||||||||||||||||
| Podiatry | 361 | 4.1% | 1,800 | 6.8% | 286 | 5.2% | 1,566 | 7.9% | ||||||||||||||||
| Gastro-intestinal | 213 | 2.4% | 295 | 1.1% | 269 | 4.9% | 400 | 2.0% | ||||||||||||||||
| General Surgery | 550 | 6.3% | 1,205 | 4.6% | 415 | 7.6% | 1,095 | 5.6% | ||||||||||||||||
| Plastic & Reconstructive | 421 | 4.8% | 752 | 2.9% | - | 0.0% | - | 0.0% | ||||||||||||||||
| Bariatrics | 1,591 | 18.2% | 3,632 | 13.8% | 372 | 6.8% | 594 | 3.0% | ||||||||||||||||
| Gynecology | 134 | 1.5% | 163 | 0.6% | 77 | 1.4% | 98 | 0.5% | ||||||||||||||||
| Ear, Nose, Throat (E.N.T.) | 628 | 7.2% | 2,019 | 7.6% | 466 | 8.5% | 1,620 | 8.2% | ||||||||||||||||
| TOTAL | 8,740 | 100.0% | 26,362 | 100.0% | 5,486 | 100.0% | 19,718 | 100.0% |
Note:
A procedure is defined as the actual surgery or surgeries that are performed on the date of service for each patient (case). Each case typically includes numerous procedures. In prior management discussion and analysis reports, the Issuer provided the number of “unique” procedures per case as the total number of procedures during the period (i.e. a patient may have three different procedures performed, however, one of the three procedures might have been performed numerous times during the case). In this annual information form, the Issuer has calculated the total quantity of procedures performed on a case, regardless of the fact that the same procedure may have been performed numerous times. These tables refer to all cases and procedures performed, regardless of their contribution to net patient service revenue.
Total cases for the twelve months ended December 31, 2014, were 8,740, representing an increase of 3,254 cases or 59.3% from the 5,486 cases in the prior corresponding period. The newly acquired marketing segment is attributable to 424 of the increase while the medical services segment increased by 2,830 cases, or 51.6%, from 5,486 the prior corresponding period. Case volume primarily increased under bariatric and pain management surgeries.
Procedure volume for the twelve months ended December 31, 2014, increased by 33.7% from 19,718 to 26,362. Since case reimbursement is based on case type, a decrease in the number of procedures per case has no effect on reimbursement and net patient service revenue per case.
The Nobilis Facilities receive payments for surgical procedures and related services from private health insurance plans, workers’ compensation, directly from patients and from government payor plans. A substantial portion of net patient service revenues generated by the Nobilis Facilities is based on payments received from private (non-government) insurance plans. The Nobilis Facilities receive a relatively small amount of revenue from Medicare or Medicaid procedures. The Nobilis Facilities also receive a relatively small portion of their revenue directly from uninsured patients, who pay out of pocket for the services they receive. Insured patients are responsible for services not covered by their health insurance plans. The amount of these deductibles, co-payments and coinsurance obligations has increased in recent years but does not represent a material component of the revenue generated by the Nobilis Facilities. The surgical center fees of the Nobilis Facilities are generated by the Physician Limited Partners and the other physicians who utilize the Nobilis Facilities to provide services. The surgical center fees are billed and collected directly by the Nobilis Facilities.
Patient and net professional fees and contracted marketing revenues are reported as the estimated net realizable amounts from patients, third-party payors, and others for services rendered. Revenue is recognized upon the performance of the patient service. The amounts actually collected by the Company from third-party payors, including private insurers vary even for identical procedures performed. An additional factor in the determination of net patient service revenue is the Company’s payor mix, as between private health insurance plans, workers’ compensation, directly from patients and from government payor plans. Management reviews and evaluates historical payment data, payor mix and current economic conditions on a periodic basis and adjusts the estimated collections as a percentage of gross billings, which are used to determine net patient service revenue, as required based on final settlements and collections.
| MEDICAL SERVICES SEGMENT |
| PATIENT AND NET PROFESSIONAL FEEREVENUEBY PAYORS OF THENOBILIS FACILITIES |
| FOR THEYEARS ENDED DECEMBER 31, 2014 AND 2013 |
| 2014 Patient and Net | 2013 Patient and Net | ||||||
| Payors | Professional Fee | Professional Fee | |||||
| Revenue by Payor Mix | Revenue by Payor Mix | ||||||
| Private insurance and other private pay | 97.0% | 92.4% | |||||
| Workers compensation | 2.3% | 4.5% | |||||
| Medicare | 0.7% | 3.1% | |||||
| Total | 100.0% | 100.0% |
| MARKETING & FACTORING SEGMENT |
| PATIENT AND NET PROFESSIONAL FEEREVENUEBY PAYORS OF THENOBILIS FACILITIES |
| FOR THEYEARS ENDED DECEMBER 31, 2014 AND 2013 |
| 2014 Patient and Net | 2013 Patient and Net | ||||||
| Payors | Professional Fee | Professional Fee | |||||
| Revenue by Payor Mix | Revenue by Payor Mix | ||||||
| Private insurance and other private pay | 100.0% | 0.0% | |||||
| Workers compensation | 0.0% | 0.0% | |||||
| Medicare | 0.0% | 0.0% | |||||
| Total | 100.0% | 0.0% |
| CONSOLIDATED SEGMENTS |
| PATIENT AND NET PROFESSIONAL FEEREVENUEBY PAYORS OF THENOBILIS FACILITIES |
| FOR THEYEARS ENDED DECEMBER 31, 2014 AND 2013 |
| 2014 Patient and Net | 2013 Patient and Net | ||||||
| Payors | Professional Fee | Professional Fee | |||||
| Revenue by Payor Mix | Revenue by Payor Mix | ||||||
| Private insurance and other private pay | 97.1% | 92.4% | |||||
| Workers compensation | 2.2% | 4.5% | |||||
| Medicare | 0.7% | 3.1% | |||||
| Total | 100.0% | 100.0% |
Results of Operations
| Year Ended December 31, 2014 Compared to Year Ended December 31, 2013 |
| RESULTS OF OPERATIONS AS A PERCENTAGEOF PATIENT AND NET PROFESSIONAL FEES |
| FOR THETWELVE MONTHS ENDED DECEMBER 31, 2014 |
| AND FOR THE TWELVEMONTHS ENDED DECEMBER 31, 2013 |
| Year ended December 31, | ||||||
| 2014 | 2013 | |||||
| Revenues: | 100% | 100% | ||||
| Cost of revenues | 0.2% | 0.0% | ||||
| Gross Profit | 99.8% | 100% | ||||
| Operating expenses: | ||||||
| Salaries and benefits | 14.2% | 17.1% | ||||
| Drugs and supplies | 13.2% | 14.2% | ||||
| General and administrative | 37.8% | 34.2% | ||||
| Amortization | 1.8% | 2.1% | ||||
| Total operating expenses | 67.0% | 67.6% | ||||
| Corporate costs: | ||||||
| Salaries and benefits | 2.8% | 7.3% | ||||
| General and administrative | 4.9% | 7.2% | ||||
| Legal expenses | 0.1% | 2.6% | ||||
| Amortization | 0.1% | 0.3% | ||||
| Total corporate costs | 7.9% | 17.4% | ||||
| Income from operations | 24.9% | 15.0% | ||||
| Other expense (income): | ||||||
| Gain on bargain purchase | 0.0% | -7.7% | ||||
| Interest expense | 0.3% | 0.3% | ||||
| Other expense (income), net | -0.2% | 0.4% | ||||
| Total other expense (income) | 0.1% | -7.0% | ||||
| Net income before income taxes and noncontrolling interests | 24.8% | 22.0% | ||||
| Income tax | 0.6% | 0.6% | ||||
| Net income | 24.2% | 21.4% | ||||
| Net income attributable to noncontrolling interests | 15.5% | 17.6% | ||||
| Net income attributable to Nobilis Health Corp. | 8.7% | 3.8% | ||||
Consolidated Revenues
Total revenues for the twelve months ended December 31, 2014, totaled $84.0 million, an increase of $52.9 million or 170.1%, compared to $31.1 million from the prior corresponding period. The newly acquired marketing segment is attributable to $3.4 million of the increase while the medical services segment increased by $49.5 million, or 159.2% compared to $31.1 million from the prior corresponding period. The increase in total revenues was due to an increase in total case volume, the addition of the newly acquired facilities, and a favorable shift in case mix to higher per revenue per case specialties.
Operating Salaries
Operating salaries and benefits for the twelve months ended December 31, 2014, totaled $11.9 million, an increase of $6.6 million or 124.5% from the prior corresponding period. This increase is primarily due to increased case volumes and the opening of the NHSC-S, FNH and FNSC locations.
Medical supplies
Drugs and medical supplies expense for the twelve months ended December 31, 2014, totaled $11.1 million, an increase of $6.7 million or 152.3% from the prior corresponding period. This increase is primarily due to an increase in case volume at all Nobilis Facilities. Additionally, the shift in case mix to include a greater percentage of orthopedic and spine cases contributes to an overall higher spend on drugs and medical supplies per case.
Operating General and Administrative
Operating general and administrative expense for the twelve months ended December 31, 2014, totaled $31.8 million, an increase of $21.2 million or an increase of 200.0% from the prior corresponding period. The newly acquired marketing segment is attributable to $1.8 million of the increase. The remaining $19.4 million increase is due to an increase in operations associated with the newly acquired medical services facilities, an increase in marketing expense, physician contracting, general infrastructure development, such as rent, telecommunication, travel, consulting, etc., and revenue cycle management expenses.
The newly acquired medical services facilities accounted for $6.4 million of the increase in operating general and administrative expense. Marketing expense, excluding the newly acquired marketing segment, increased to $6.0 million for the twelve months ended December 31, 2014, from $2.3 million for the corresponding period in 2013. For the development of the marketing programs, the Company enters into independent contractor agreements with physicians to provide services to the Company including administrative, management and marketing services. This expense increased to $4.0 million for the twelve months ended December 31, 2014 to $1.0 million in 2013. Expenses related to general infrastructure development increased by $1.7 million to $3.0 million in 2014 from $1.3 million in 2013. As a percentage of total revenues, operating general and administrative expenses increase by 3.6% from 34.2% of total revenues in 2013 to 37.8% in 2014 due to the Company’s ongoing effort to develop new marketing programs.
In addition, operating general and administrative expenses increased as a result of an increase in revenue cycle management expenses. Pursuant to the terms of this arrangement, the Company, from time to time, shall transfer to the third party certain of its accounts receivable payments on a non-recourse basis in return for advancement on payment for a faster cash collection. The advancement payment varies by specialties and on average is between 20 and 50% of the amounts transferred. The Company does not have any other relationship with this third party other than the vendor relationship described herein. For the twelve months ended December 31, 2014 and 2013 advancement payment of $1.3 million and $0.4 million was received by the Company. During the same period, $7.3 million and $2.5 million of receivables, net of advancement payment, were transferred resulting in an increase in revenue cycle management expenses of $4.8 million.
Depreciation
Depreciation for the twelve months ended December 31, 2014, totaled $1.5 million, an increase of $0.8 million or 114.3% from the prior corresponding period. This increase is primarily due to an increase in property and equipment from the NHSC-S location.
Corporate General and Administrative
In total, Corporate costs for the twelve months ended December 31, 2014, totaled $6.6 million, an increase of $1.2 million or 22.2% from the prior corresponding period. The increase was primarily attributable to additional corporate staff and legal expenses related to marketing and acquisitions. The Company presents corporate costs as a separate section from the operating expenses of the revenue generating operational facilities to illustrate the Company’s operation efficiency.
Net income attributable to non-controlling interests are based on ownership percentages in the Nobilis Facilities that are owned by outside parties.
Liquidity, Capital Resources and Financial Condition
Liquidity refers to an entity’s ability to meet its financial obligations and commitments as they become due. The Company is dependent upon cash generated from operating activities of the Nobilis entities, which are the major source of financing for its operations and for meeting its contractual obligations.
Cash and cash equivalents at December 31, 2014 and December 31, 2013 were $7.6 million and $5.6 million, respectively. For the year ended December 31, 2014, we experienced an increase in operating cash flows, net of non-controlling interests, of approximately $0.5 million, primarily attributable to increased case volumes at same store operations and the newly acquired hospital and ASC.
As of December 31, 2014, the Company had consolidated net working capital of $23.8 million compared to $8.4 million in the corresponding period of 2013. The increase is primarily due to an increase in accounts receivable of $33.9 million and assets related to the acquisition of Athas. Net cash provided by operating activities for 2014 was $4.0 million compared to $3.5 million in 2013. The cash impact from the aforementioned operating results will largely be seen during the first quarter of 2015.
In December 2013, the Company issued, through a private placement agreement, 5,862,500 Units, at a price of Cdn$0.80 per Unit. Each Unit consists of one common share in the capital of the Company and one-half of one common share purchase warrant exercisable for one additional share at a price of Cdn$1.10. Through the private placement, the Company raised USD $4.1 million, as of December 31, 2013, net of offering costs of USD $0.3 million.
In August 2014, the Company elected to accelerate the expiry date of the common share purchase warrants originally issued by Nobilis as part of its unit private placement completed on December 16, 2013 (the "2013 Private Placement"). Each Warrant entitled the holder thereof to purchase one additional common share of Nobilis at a price of Cdn$1.10. Nobilis received total gross proceeds of Cdn$3,224,375 from the exercise.
In September 2014, the Company issued, through a private placement agreement, 5,568,400 Units, at a price of Cdn$1.30 per Unit. Each Unit consists of one common share in the capital of the Company and one-half of one common share purchase warrant exercisable for one additional share at a price of Cdn$1.80. Through the private placement, the Company raised USD$6.1 million, as of December 31, 2014, net of offering costs of USD$0.5 million.
Critical Accounting Policies
The discussion and analysis of our financial condition and results of operations are based upon our consolidated financial statements, which have been prepared in accordance with accounting principles generally accepted in the United States. The preparation of our consolidated financial statements requires us to make estimates and assumptions that affect our reported results of operations and the amount of reported assets and liabilities. Some accounting policies involve judgments and uncertainties to such an extent that there is reasonable likelihood that materially different amounts could have been reported under different conditions, or if different assumptions had been used. Actual results may differ from the estimates and assumptions used in the preparation of our consolidated financial statements. Described below are the most significant policies we apply in preparing our consolidated financial statements, some of which are subject to alternative treatments under accounting principles generally accepted in the United States.
Recently Issued Accounting Standards
In May 2014, the Financial Accounting Standards Board (“FASB”) issued new guidance that introduces a new five-step revenue recognition model in which an entity should recognize revenue to depict the transfer of promised goods or services to customers in an amount that reflects the consideration to which the entity expects to be entitled in exchange for those goods or services. This guidance also requires disclosures sufficient to enable users to understand the nature, amount, timing, and uncertainty of revenue and cash flows arising from contracts with customers, including qualitative and quantitative disclosures about contracts with customers, significant judgments and changes in judgments, and assets recognized from the costs to obtain or fulfill a contract. This standard is effective for fiscal years beginning after December 15, 2016, including interim periods within that reporting period. The Company is currently evaluating the new guidance to determine the impact it will have on its consolidated financial statements.
In June 2014, the FASB issued amended guidance on the accounting for certain share-based employee compensation awards. The amended guidance applies to share-based employee compensation awards that include a performance target that affects vesting when the performance target can be achieved after the requisite service period. These targets are to be treated as a performance condition. As such, the performance target should not be reflected in estimating the grant-date fair value of the award and compensation cost should be recognized in the period in which it becomes probable that the performance target will be achieved. The amendments are effective for annual periods and interim periods within those annual periods beginning after December 15, 2015. The Company does not expect adoption will have a material impact on its consolidated financial statements.
In February 2015, the FASB issued amended guidance on the consolidation of legal entities including limited partnerships and limited liability corporations. The guidance modifies the consolidation models to be analyzed in determining whether a reporting entity should consolidate certain types of legal entities. The guidance must be applied using on of two retrospective application methods and will be effective for fiscal years beginning after December 15, 2015, and for interim periods within those fiscal years. Early adoption is permitted, including adoption in any interim period. The Company does not expect adoption will have a material impact on its consolidated financial statements.
| ITEM 7A. | QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK |
As a smaller reporting company, as defined by Rule 12b-2 of the Exchange Act and in Item 10(f)(1) of Regulation S-K, we are electing scaled disclosure reporting obligations and therefore are not required to provide the information requested by this Item.
| Item 8. | Financial Statements and Supplementary Data |
![]()
Report of Independent Registered Public Accounting Firm
To the Shareholders of
Nobilis Health Corp.
We have audited the accompanying consolidated balance sheets of Nobilis Health Corp. and subsidiaries (collectively, the “Company”) as of December 31, 2014 and 2013, and the related consolidated statements of earnings, comprehensive income, changes in shareholders’ equity, and cash flows for the years ended December 31, 2014 and 2013. These consolidated financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on these financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the consolidated financial statements are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements. An audit also includes assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the financial position of the Company as of December 31, 2014 and 2013, and the results of its operations and its cash flows for each of the years in the three-year period ended December 31, 2014, in conformity with accounting principles generally accepted in the United States of America.
![]()
Houston, Texas
April 2, 2015
![]()
| Nobilis Health Corp. |
| Consolidated Balance Sheets |
| December 31, 2014 and 2013 |
| (In thousands) |
| December 31, | December 31, | |||||
| 2014 | 2013 | |||||
| Assets | ||||||
| Current Assets: | ||||||
| Cash | $ | 7,568 | $ | 5,602 | ||
| Trade accounts receivable, net | 42,175 | 8,281 | ||||
| Medical supplies | 1,412 | 787 | ||||
| Prepaid expenses and other current assets | 3,554 | 540 | ||||
| Total current assets | 54,709 | 15,210 | ||||
| Property and equipment, net | 9,087 | 4,833 | ||||
| Intangible assets | 19,543 | 1,097 | ||||
| Goodwill | 22,470 | 1,228 | ||||
| Notes receivable | 659 | 150 | ||||
| Investments in associates | 880 | - | ||||
| Other long-term assets | 234 | 121 | ||||
| Total Assets | $ | 107,582 | $ | 22,639 | ||
| Liabilities and Equity | ||||||
| Current Liabilities: | ||||||
| Trade accounts payable | $ | 10,528 | $ | 3,018 | ||
| Accrued liabilities | 9,112 | 1,970 | ||||
| Lines of credit | 5,420 | - | ||||
| Subordinated notes payable | 635 | - | ||||
| Current portion of debt | 3,437 | 1,693 | ||||
| Current portion of capital leases | 257 | 49 | ||||
| Other current liabilities | 1,485 | 43 | ||||
| Total current liabilities | 30,874 | 6,773 | ||||
| Long-term capital leases, net of current portion | 573 | 163 | ||||
| Long-term debt, net of current portion | 10,582 | - | ||||
| Other long-term liabilities | 252 | - | ||||
| Total liabilities | 42,281 | 6,936 | ||||
| Shareholders' Equity: | ||||||
| Common stock, no par value | - | - | ||||
| Additional paid in capital | 179,293 | 150,897 | ||||
| Accumulated deficit | (132,866 | ) | (140,052 | ) | ||
| Accumulated other comprehensive income | (111 | ) | 104 | |||
| Total shareholders’ equity attributable to Nobilis Health Corp. | 46,316 | 10,949 | ||||
| Noncontrolling interests | 18,985 | 4,754 | ||||
| Total shareholders' equity | 65,301 | 15,703 | ||||
| Total Liabilities and Shareholders' Equity | $ | 107,582 | $ | 22,639 |
The accompanying notes are an integral part of the consolidated financial statements.
| Nobilis Health Corp. |
| Consolidated Statements of Earnings |
| Years Ended December 31, 2014 and 2013 |
| (In thousands, except earnings per share) |
| Year ended December 31, | ||||||
| 2014 | 2013 | |||||
| Revenues: | ||||||
| Patient and net professional fees | $ | 80,917 | $ | 31,128 | ||
| Contracted marketing revenues | 2,171 | - | ||||
| Factoring revenues | 941 | - | ||||
| Total revenue | 84,029 | 31,128 | ||||
| Cost of revenues | 201 | - | ||||
| Gross Profit | 83,828 | 31,128 | ||||
| Operating expenses: | ||||||
| Salaries and benefits | 11,933 | 5,329 | ||||
| Drugs and supplies | 11,094 | 4,423 | ||||
| General and administrative | 31,791 | 10,648 | ||||
| Depreciation and amortization | 1,529 | 650 | ||||
| Total operating expenses | 56,347 | 21,050 | ||||
| Corporate costs: | ||||||
| Salaries and benefits | 2,386 | 2,285 | ||||
| General and administrative | 4,082 | 2,228 | ||||
| Legal expenses | 66 | 808 | ||||
| Depreciation | 114 | 81 | ||||
| Total corporate costs | 6,648 | 5,402 | ||||
| Income from operations | 20,833 | 4,676 | ||||
| Other expense (income): | ||||||
| Gain on bargain purchase | - | (2,392 | ) | |||
| Interest expense | 288 | 97 | ||||
| Other expense (income), net | (183 | ) | 120 | |||
| Total other expense (income) | 105 | (2,175 | ) | |||
| Net income before income taxes and noncontrolling interests | 20,728 | 6,851 | ||||
| Income tax | 480 | 177 | ||||
| Net income | 20,248 | 6,674 | ||||
| Net income attributable to noncontrolling interests | 13,062 | 5,476 | ||||
| Net income attributable to Nobilis Health Corp. | $ | 7,186 | $ | 1,198 | ||
| Net income per basic common share | $ | 0.15 | $ | 0.03 | ||
| Net income per fully diluted common share | $ | 0.15 | $ | 0.03 | ||
| Weighted average shares outstanding (basic) | 46,517,815 | 36,793,950 | ||||
| Weighted average shares outstanding (fully diluted) | 48,781,348 | 37,637,662 | ||||
The accompanying notes are an integral part of the consolidated financial statements.
| Nobilis Health Corp. |
| Consolidated Statements of Comprehensive Income |
| Years Ended December 31, 2014 and 2013 |
| (In thousands) |
| Year ended December 31, | ||||||
| 2014 | 2013 | |||||
| Net income | $ | 7,186 | $ | 1,198 | ||
| Other comprehensive income: | ||||||
| Foreign currency translation adjustments | (215 | ) | (32 | ) | ||
| Total other comprehensive income | (215 | ) | (32 | ) | ||
| Comprehensive income attributable to Nobilis Health Corp. | $ | 6,971 | $ | 1,166 | ||
The accompanying notes are an integral part of the consolidated financial statements.
| Nobilis Health Corp. |
| Consolidated Statements of Changes in Equity |
| Years Ended December 31, 2014 and 2013 |
| (In thousands) |
| Accumulated Other | Equity | Equity Attributable | |||||||||||||||||||
| Additional Paid In | Accumulated | Comprehensive | Attributable to | to Noncontrolling | |||||||||||||||||
| Common Stock | Capital | Deficit | Income | Nobilis Health | Interests | Total Equity | |||||||||||||||
| BALANCE — January 1, 2013 | $ | - | $ | 145,802 | $ | (141,250 | ) | $ | 136 | $ | 4,688 | $ | 4,462 | $ | 9,150 | ||||||
| Net income | - | - | 1,198 | - | 1,198 | 5,476 | 6,674 | ||||||||||||||
| Proceeds from private equity offering | - | 4,089 | - | - | 4,089 | - | 4,089 | ||||||||||||||
| Proceeds from sale of ownership interest in subsidiary | - | 303 | - | - | 303 | - | 303 | ||||||||||||||
| Purchase of additional ownership interest in subsidiary | - | 157 | - | - | 157 | (927 | ) | (770 | ) | ||||||||||||
| Distributions to noncontrolling interests | - | - | - | - | - | (4,257 | ) | (4,257 | ) | ||||||||||||
| Other comprehensive income | - | - | - | (32 | ) | (32 | ) | - | (32 | ) | |||||||||||
| Subtotal | - | 150,351 | (140,052 | ) | 104 | 10,403 | 4,754 | 15,157 | |||||||||||||
| Exercise of stock options | - | 168 | - | - | 168 | - | 168 | ||||||||||||||
| Share-based compensation, net | - | 378 | - | - | 378 | - | 378 | ||||||||||||||
| BALANCE — December 31, 2013 | $ | - | $ | 150,897 | $ | (140,052 | ) | $ | 104 | $ | 10,949 | $ | 4,754 | $ | 15,703 | ||||||
| BALANCE — January 1, 2014 | $ | - | $ | 150,897 | $ | (140,052 | ) | $ | 104 | $ | 10,949 | $ | 4,754 | $ | 15,703 | ||||||
| Net income | - | - | 7,186 | - | 7,186 | 13,062 | 20,248 | ||||||||||||||
| Proceeds from private equity offering | - | 6,100 | - | - | 6,100 | - | 6,100 | ||||||||||||||
| Proceeds from sale of ownership interest in subsidiary | - | 705 | - | - | 705 | - | 705 | ||||||||||||||
| Purchase of investment | - | 490 | - | - | 490 | - | 490 | ||||||||||||||
| Consolidation of investment | - | - | - | - | - | 522 | 522 | ||||||||||||||
| Consolidation of First Nobilis | - | - | - | - | - | 7,206 | 7,206 | ||||||||||||||
| Acquisition of Athas Health | 16,239 | - | - | 16,239 | - | 16,239 | |||||||||||||||
| Distributions to noncontrolling interests | - | - | - | - | - | (6,559 | ) | (6,559 | ) | ||||||||||||
| Other comprehensive income | - | - | - | (215 | ) | (215 | ) | - | (215 | ) | |||||||||||
| Subtotal | - | 174,431 | (132,866 | ) | (111 | ) | 41,454 | 18,985 | 60,439 | ||||||||||||
| Exercise of stock warrants | 3,188 | - | - | 3,188 | - | 3,188 | |||||||||||||||
| Exercise of stock options | - | 166 | - | - | 166 | - | 166 | ||||||||||||||
| Share-based compensation, net | - | 1,508 | - | - | 1,508 | - | 1,508 | ||||||||||||||
| BALANCE — December 31, 2014 | $ | - | $ | 179,293 | $ | (132,866 | ) | $ | (111 | ) | $ | 46,316 | $ | 18,985 | $ | 65,301 |
The accompanying notes are an integral part of the consolidated financial statements.
| Nobilis Health Corp. |
| Consolidated Statements of Cash Flows |
| Years Ended December 31, 2014 and 2013 |
| (In thousands) |
| Year ended December 31, | ||||||
| 2014 | 2013 | |||||
| CASH FLOWS FROM OPERATING ACTIVITIES: | ||||||
| Net income | $ | 7,186 | $ | 1,198 | ||
| Adjustments to reconcile net
income attributable to Nobilis to net cash provided by operating activities: |
||||||
| Depreciation | 1,642 | 731 | ||||
| Gain on sale of fixed assets | (39 | ) | (2 | ) | ||
| Noncontrolling interests | 13,062 | 5,476 | ||||
| Gain on bargain purchase of a business | - | (2,392 | ) | |||
| Foreign currency gain (loss) | (215 | ) | (32 | ) | ||
| Share-based compensation | 1,508 | 378 | ||||
| Changes in operating assets and liabilities | (19,146 | ) | (1,869 | ) | ||
| Net cash provided by operating activities | 3,998 | 3,488 | ||||
| CASH FLOWS FROM INVESTING ACTIVITIES: | ||||||
| Purchase of property and equipment | (2,023 | ) | (1,180 | ) | ||
| Purchase of investment in associate | (150 | ) | - | |||
| Purchase of interest acquired in a subsidiary | (346 | ) | - | |||
| Distributions from investments in associates | - | 159 | ||||
| Proceeds from sale of property and equipment | 39 | 2 | ||||
| Proceeds from sale of ownership interests of subsidiary | 705 | 303 | ||||
| Purchase of additional ownership interest in subsidiary | - | (770 | ) | |||
| Acquisition of a business | (3,000 | ) | (460 | ) | ||
| Net cash (used for) investing activities | (4,775 | ) | (1,946 | ) | ||
| CASH FLOWS FROM FINANCING ACTIVITIES: | ||||||
| Distributions to non controlling interests | (6,559 | ) | (4,257 | ) | ||
| Proceeds from exercise of stock options | 166 | 168 | ||||
| Proceeds from exercise of stock warrants | 3,188 | - | ||||
| Payments on capital lease obligations | (77 | ) | (12 | ) | ||
| Proceeds from debt and lines of credit | 1,300 | - | ||||
| Payments of debt and lines of credit | (1,375 | ) | - | |||
| Note receivable | - | (150 | ) | |||
| Proceeds from private placement | 6,100 | 4,089 | ||||
| Net cash provided by (used for) financing activities | 2,743 | (162 | ) | |||
| NET INCREASE IN CASH AND CASH EQUIVALENTS | 1,966 | 1,380 | ||||
| CASH AND CASH EQUIVALENTS — Beginning of period | 5,602 | 4,222 | ||||
| CASH AND CASH EQUIVALENTS — End of period | $ | 7,568 | $ | 5,602 | ||
| SUPPLEMENTAL DISCLOSURE OF CASH FLOW INFORMATION: | ||||||
| Cash paid for taxes | $ | 165 | $ | 100 | ||
| Cash paid for interest | $ | 216 | $ | 97 | ||
| SUPPLEMENTAL SCHEDULE OF NON-CASH INVESTING AND FINANCING ACTIVITIES: | ||||||
| Capital expenditures funded by capital lease borrowings | $ | 696 | $ | 224 | ||
| Non-cash acquisition of property and equipment | $ | 2,271 | $ | - | ||
| Non-cash acquisition of intangibles and goodwill | $ | 7,206 | $ | - | ||
The accompanying notes are an integral part of the consolidated financial statements.
| Nobilis Health Corp. |
| Notes to the Consolidated Financial Statements |
| (in thousands, except per share amounts and as otherwise noted) |
1. Company Description
Nobilis Health Corp. was incorporated on March 16, 2007 under the name "Northstar Healthcare Inc." pursuant to the provisions of the British Columbia Business Corporations Act ("BCBCA" ) . On December 5, 2014, Northstar Healthcare Inc. changed its name to Nobilis Health Corp. Our registered office is located at Suite 400, 570 Granville Street, Vancouver, British Columbia V6C 3P1 and our corporate office is located at 4120 Southwest Freeway, Suite 150, Houston, Texas 77027. Our common shares are and have been publicly traded on the Toronto Stock Exchange under the symbol "NHC" since May 2007.
We own and manage nine healthcare facilities (the "Nobilis Facilities") in Texas and Arizona; two MRI centers, an urgent care center, one hospital and five ambulatory surgery centers (“ASC”), referred to as the "Nobilis ASCs" of which three are located in Houston, Texas, one in Dallas, Texas and one in Scottsdale, Arizona. The Nobilis ASCs are licensed ambulatory surgery centers that provide scheduled surgical procedures in a limited number of clinical specialties, which enables them to develop routines, procedures and protocols to maximize operating efficiency and productivity while offering an enhanced healthcare experience for both physicians and patients.
The Nobilis ASCs do not offer the full range of services typically found in traditional hospitals, but instead focus on certain clinical specialties, including orthopedic surgery, podiatric surgery, ENT, pain management, gastro- intestinal, gynecology, and general surgery. Nobilis’ hospital focuses on these same specialties with the ability to take on more complex instances.
In December 2014, the Company expanded its services to health care marketing and factoring of receivables when it acquired 100% interests of Athas Health, LLC (“Athas”).
2. Summary of Significant Accounting Policies
Basis of Presentation
The Company’s consolidated financial statements have been prepared in accordance with accounting principles generally accepted in the United States of America (“U.S. GAAP”).
Principles of Consolidation
Our consolidated financial statements include the accounts of Nobilis and its subsidiaries. Subsidiaries are all entities over which the Company has the power to govern the financial and operating policies through ownership of more than one half of the voting rights or by determining that the subsidiary is a variable interest entity (“VIE”) that requires consolidation. A reporting entity with a controlling financial interest in a VIE will have both of the following characteristics: (i) the power to direct the activities of a VIE that most significantly impact the VIE’s economic performance and (ii) the obligation to absorb the losses of the VIE that could potentially be significant to the VIE or the right to receive benefit from the VIE that could potentially be significant to the VIE. See note 17 for details. All significant intercompany accounts are eliminated in consolidation.
Use of Accounting Estimates
The preparation of financial statements in conformity with U.S. GAAP requires us to make estimates and assumptions that affect the reported amounts of assets and liabilities and the disclosure of contingent assets and liabilities at the date of the consolidated financial statements and the amounts of revenues and expenses during the reporting period. Actual results may differ from those estimates. Retroactively calculated third-party contractual adjustments are accrued on an estimated basis in the period in which the related services are rendered. Net patient service revenue is adjusted as required in subsequent periods based on final settlements and collections.
Cash
We maintain our cash in bank deposit accounts that at times, may exceed federally insured limits. We have not experienced any losses in such accounts, and we believe we are not exposed to any significant credit risks on cash. At December 31, 2014 and 2013, our cash exceeded what is federally insured.
Patient and Net Professional Fees
Patient and net professional fees is reported at the estimated net realizable amounts from patients, third-party payors, and others for services rendered.
The amounts actually collected by the Company from third-party payors, including private insurers, are variable, even for identical procedures performed. An additional factor in the determination of patient and net professional fees is the Company’s payor mix, as between private health insurance plans, workers’ compensation, directly from patients, and from government payor plans. Management reviews and evaluates historical payment data, payor mix and current economic conditions on a periodic basis and adjusts the estimated collections as a percentage of gross billings (which are used to determine patient and net professional fees) as required in subsequent periods based on final settlements and collections.
Revenue is recognized upon the performance of the patient service and when ultimate collection is measurable and reasonably assured.
Contracted Marketing Revenues
Contracted marketing revenue is comprised of payments from hospitals, ASC’s and other ancillary service providers through marketing services agreements. The services include licensing, marketing, patient intake, patient outcome assessments and educational services. Revenue is recognized on a gross basis upon the performance of the marketing service and when ultimate collection is measurable and reasonably assured. Costs associated with the performance of these services is recorded in cost of revenue in the consolidated statement of earnings.
Factoring Revenues
Factoring revenue is comprised of revenue generated from certain accounts receivables which are purchased from third parties through the regular course of business. Purchase price is determined either by a flat fee per case, as dictated per the agreement, or as a percentage of final collections. At the time of purchase, the Company assumes all financial risk and incurs all costs related to collections without any recourse to the third party seller. Revenue is recognized based upon the date of the original service associated with the receivable.
Accounts Receivable
Accounts receivable consists of net patient service revenues and factoring revenues recorded at net realizable value and contracted marketing revenues recorded at the fees due from the facilities for marketing services performed.
On a periodic basis, we evaluate receivables based on the age of the receivable, history of past collections and current credit and economic conditions and adjust the carrying value accordingly. An account is written off when it is determined that all collection efforts have been exhausted. The Company does not accrue finance or interest charges on accounts receivable. An allowance for uncollectible patient receivables balances, including receivables from non-partner surgeons, is maintained at a level which the Company believes is adequate to absorb possible losses.
Medical Supplies
Medical supplies consist of various surgical supplies and medications and are valued at the lower of cost or market on the first-in, first-out method. The market value of inventories is determined based on the estimated selling price in the ordinary course of business less the estimated costs of sale, and a reasonable profit margin based on the effort required sell the inventories. The Company had no write-downs for medical supplies for the years ended December 31, 2014 or 2013.
Property and Equipment
Property and equipment is stated at cost less accumulated depreciation. Depreciation is computed using the straight-line method over the estimated useful lives of the related assets. Property under capital leases and the related obligation for future lease payments are initially recorded at an amount equal to the lesser of fair value of the property and equipment or the present value of the future lease payments. Leasehold improvements are amortized over the lesser of the estimated useful life of the asset or the term of the lease. Maintenance and repairs are charged to operations when incurred.
We evaluate our long-lived assets for possible impairment annually or whenever events or changes in circumstances indicate that the carrying amount of the asset, or related group of assets, may not be recoverable from estimated future undiscounted cash flows. If the estimated future undiscounted cash flows are less than the carrying value of the assets, we calculate the amount of impairment if the carrying value of the long-lived assets exceeds the fair value of the assets. The fair value of the assets is estimated based on appraisals, established market values of comparable assets or internal estimates of future net cash flows expected to result from the use and ultimate disposition of the asset. The estimates of these future cash flows are based on assumptions and projections we believe to be reasonable and supportable. They require our subjective judgments and take into account assumptions about revenue and expense growth rates. These assumptions may vary by type of facility and presume stable, improving or, in some cases, declining results at our hospitals, depending on their circumstances.
We report long-lived assets to be disposed of at the lower of their carrying amounts or fair values less costs to sell. In such circumstances, our estimates of fair value are based on appraisals, established market prices for comparable assets or internal estimates of future net cash flows. Gains and losses on disposals of property and equipment are determined by comparing the proceeds from disposal with the net carrying amount of property and equipment, and are recognized within other expense (income) in the consolidated statement of earnings.
The estimated useful lives for depreciation purposes are as follows:
| Property and Equipment | Estimated Useful Lives |
| Telephone equipment | 7 Years |
| Computer hardware | 5 Years |
| Computer software | 3-5 Years |
| Furniture and office equipment | 7 Years |
| Medical equipment | 5 Years |
| Leasehold improvements | Estimated usefule life or lease term |
Investments in Associates
Investments in associates which are not consolidated, but over which the Company exercises significant influence, are accounted for under the equity method of accounting. Whether or not the Company exercises significant influence with respect to an associate depends on an evaluation of several factors including, among others, representation on the associate’s board of directors, involvement in operations, and ownership level. Under the equity method of accounting, the associate’s accounts are not reflected within the Company’s consolidated balances sheets and statements of earnings; however, the Company’s share of the earnings or losses of the associate is reflected in other expense (income) in the consolidated statements of earnings. The Company’s carrying value in an equity method investment is reflected in investments in associates in the consolidated balance sheets.
When the Company’s carrying value in an equity method investment is reduced to zero, no further losses are recorded in the Company’s consolidated financial statements unless the Company guaranteed obligations of the associate or has committed additional funding. When the associate subsequently reports income, the Company will not record its share of such income until it equals the amount of its share of losses not previously recognized.
Investments in associates which are not accounted for under the equity method of accounting are accounted for under the cost method of accounting and are initially recognized at cost. Distributions received from an associate are recorded as other expense (income) in the consolidated statements of earnings. Under this method, the Company’s share of the earnings or losses of the associates is not included in the consolidated balance sheets or consolidated statements of earnings. However, the investments are reviewed for impairment at least annually and any impairment loss that is other than temporary is recognized in the consolidated statements of earnings. If circumstances suggest that the value of the associate has subsequently recovered, such recovery is not recorded. At December 31, 2014, the investments are not considered impaired.
Goodwill and Intangibles
Goodwill represents the excess of the cost of an acquisition over the fair value of the Company’s share of the net identifiable assets of an acquired subsidiary on the date of acquisition. Goodwill is reviewed for impairment on an annual basis or more frequently if events or circumstances indicate potential impairment. The Company’s goodwill evaluation is based on both qualitative and quantitative assessments regarding the fair value of goodwill relative to its carrying value. The Company assesses qualitative factors to determine if its sole reporting unit’s fair value is more likely than not to exceed its carrying value, including goodwill. In the event the Company determines that it is more likely than not that its reporting unit’s fair value is less than its carrying amount, quantitative testing is performed comparing recorded values to estimated fair values. Estimates of fair value are based on appraisals, established market prices for comparable assets or internal estimates of future net cash flows. If the fair value exceeds the carrying value, goodwill is not impaired. If the carrying value exceeds the fair value, an impairment charge is recognized through a charge to operations based upon the excess of the carrying value of goodwill over the implied fair value.
Indefinite life intangible assets consisting of trade names, trademarks, Medicare licenses, and an unfavorable lease, are not amortizable; however, are evaluated for impairment on an annual basis. Definite live intangible assets consisting of non-compete agreements, internally developed software, trade secret methodology and physician relationships, are carried at cost less accumulated amortization, which is calculated on a straight-line basis over a period of five to 20 years depending on the asset’s useful life.
Advertising and Marketing Costs
Advertising costs are expensed as they are incurred. Advertising expense for the years ended December 31, 2014 and 2013 was $9.9 million and $3.2 million, respectively. The Company utilizes many media outlets for marketing to patients which include internet, TV, radio, print, seminar and billboard advertising.
Income Taxes
The tax expense for the period comprises current and deferred tax. Tax expense is recognized in the consolidated statement of earnings, except to the extent that it relates to items recognized directly in equity. For items recognized directly in equity, the tax expense is also recognized in equity.
The current income tax charge is calculated on the basis of the tax laws enacted or substantively enacted at the balance sheet date in the countries where the Company’s subsidiaries and associates operate and generate taxable income. Management periodically evaluates positions taken in tax returns with respect to situations in which applicable tax regulations is subject to interpretation. It establishes provisions where appropriate on the basis of amounts expected to be paid to the tax authorities.
Deferred income tax is recognized, using the liability method, on temporary differences arising between the tax basis of assets and liabilities and their carrying amounts in the consolidated financial statements. Deferred income tax is determined using tax rates (and laws) that have been enacted or substantially enacted by the balance sheet date and are expected to apply when the related deferred income tax asset is realized or the deferred income tax liability is settled.
Deferred income tax assets are recognized only to the extent that it is probable that future taxable profit will be available against which the temporary difference can be utilized.
Deferred income tax is provided on temporary differences arising on investments in subsidiaries and associates, except where the timing of the reversal of the temporary difference is controlled by the Company and it is probable that the temporary difference will not reverse in the foreseeable future.
Under U.S. GAAP, the Company may recognize the tax benefit from an uncertain tax position only if it is more likely than not that the tax position will be sustained on examination by the taxing authorities, based on the technical merits of the position. The tax benefits recognized in the financial statements from such a position should be measured based on the largest benefit that has a greater than fifty (50) percent likelihood of being realized upon ultimate settlement. The Company annually evaluates tax positions to determine the need for any additional disclosures in accordance with U.S. GAAP, including de-recognition, classification, interest and penalties on income taxes and accounting in interim periods.
Leases
Certain leases are classified as capital leases whenever the terms of the lease transfer substantially all of the risks and rewards of ownership to the lessee. Leases in which a significant portion of the risks and rewards of ownership are retained by the lessor are classified as operating leases. Payments made under operating leases (net of any incentives received from the lessor) are charged to the consolidated statement of earnings on a straight-line basis over the period of the lease as rent expense.
Foreign Currency
Items included in the consolidated financial statements for each of the Company’s entities are measured using the currency of the primary economic environment in which the entity operates (the “functional currency”). Currently, all of the Company’s activities are measured using the U.S. Dollar (“USD”). The consolidated statements are presented in USD, the Company’s reporting currency.
From time to time monetary assets and liabilities may be denominated in foreign currency, and, if so, will be translated at the exchange rate in effect as the statement of financial position date, with resulting gains or losses included within the consolidated statement of comprehensive income. Revenues and expenses denominated in foreign currencies are translated into USD at the average foreign currency exchange rate for the period.
Share Based Compensation
The Company recognizes all stock-based payments to employees, including grants of employee stock options, in the consolidated financial statements based on their grant-date fair values in accordance with U.S GAAP. The Company values its stock options awarded using the Black-Scholes option pricing model. Restricted stock awards are valued at the grant date closing market price. Stock based compensation costs are recognized over the vesting period, which is the period during which the employee is required to provide service in exchange for the award. Stock-based compensation paid to non-employees are valued at the fair value at the applicable measurement date and charged to expense as services are rendered.
Net Income Per Common Share
We calculate net income per common share by dividing net income available for common shareholders by the weighted average number of common shares outstanding during the period. Fully diluted income per share is computed using the weighted average number of common and potential common shares outstanding during the period. Potential common shares include those that may be issued upon redemption of units granted under the Company’s RSU and Share Option Plans.
Comprehensive Income
Comprehensive income consists of net income and other gains and losses affecting stockholder's equity that are excluded from net income, such as unrealized gains and losses on available-for-sale investments, foreign currency translation gains and losses and minimum pension liability. The Company’s other comprehensive income represents foreign currency translation adjustments.
Noncontrolling Interests
Noncontrolling interests are classified in the consolidated statements of earnings as part of consolidated net income and the accumulated amount of noncontrolling interest in the consolidated balance sheets as part of shareholders’ equity. Changes in the ownership interest in a consolidated subsidiary that does not result in a loss of control are accounted for as an equity transaction. If a change in ownership of a consolidated subsidiary results in a loss of control and deconsolidation, any retained ownership interests are remeasured with the gain or loss reported in net earnings.
Segment Reporting
The Company reports segment information based on how the chief operating decision maker, along with other members of management, organize and utilize financial and operational data in determining how to allocate resources and assess performance.
Effective December 1, 2014, the Company’s business lines are classified into two reportable business segments which include a medical services segment and a marketing and factoring segment. The medical services segment provides the operation of hospitals, outpatient facilities and other various related health care services. The marketing and factoring segment provides direct to consumer marketing efforts which educate patients on their healthcare options. Factoring activities are included in the marketing segment, as such activities only pertain to patients which are acquired through the marketing efforts of Athas.
We evaluate performance based on income from operations of the respective business units prior to the allocation of corporate office expenses. Transactions between segments are eliminated in consolidation. Our corporate office provides general and administrative as well as support services to our two revenue-generating segments. Management allocates costs between segments for selling, general and administrative expenses and depreciation expense.
Recent Accounting Pronouncements
In May 2014, the Financial Accounting Standards Board (“FASB”) issued new guidance that introduces a new five-step revenue recognition model in which an entity should recognize revenue to depict the transfer of promised goods or services to customers in an amount that reflects the consideration to which the entity expects to be entitled in exchange for those goods or services. This guidance also requires disclosures sufficient to enable users to understand the nature, amount, timing, and uncertainty of revenue and cash flows arising from contracts with customers, including qualitative and quantitative disclosures about contracts with customers, significant judgments and changes in judgments, and assets recognized from the costs to obtain or fulfill a contract. This standard is effective for fiscal years beginning after December 15, 2016, including interim periods within that reporting period. The Company is currently evaluating the new guidance to determine the impact it will have on its consolidated financial statements.
In June 2014, the FASB issued amended guidance on the accounting for certain share-based employee compensation awards. The amended guidance applies to share-based employee compensation awards that include a performance target that affects vesting when the performance target can be achieved after the requisite service period. These targets are to be treated as a performance condition. As such, the performance target should not be reflected in estimating the grant-date fair value of the award and compensation cost should be recognized in the period in which it becomes probable that the performance target will be achieved. The amendments are effective for annual periods and interim periods within those annual periods beginning after December 15, 2015. The Company does not expect adoption will have a material impact on its consolidated financial statements.
In February 2015, the FASB issued amended guidance on the consolidation of legal entities including limited partnerships and limited liability corporations. The guidance modifies the consolidation models to be analyzed in determining whether a reporting entity should consolidate certain types of legal entities. The guidance must be applied using on of two retrospective application methods and will be effective for fiscal years beginning after December 15, 2015, and for interim periods within those fiscal years. Early adoption is permitted, including adoption in any interim period. The Company does not expect adoption will have a material impact on its consolidated financial statements.
3. Acquisitions and Business Combinations
In December 2013, the Company completed its acquisition of a former outpatient surgery center near Phoenix, Arizona. The acquisition was completed through bankruptcy court. The Company created a new subsidiary named Northstar Healthcare Surgery Center – Scottsdale, LLC and will continue to operate the surgery center in a similar capacity.
The Company concluded that the fair value of the consideration transferred in the acquisition was less than the fair value of the net identifiable assets acquired, resulting in $2.4 million gain recognized in connection with the acquisition. The gain from a bargain purchase has been presented in a separate line item in the accompanying consolidated statements of earnings.
The costs related to the transaction were $0.1 million and were expensed during the year ended December 31, 2013.
The following table summarizes the fair values of the identifiable assets acquired at the date of acquisition:
| December 16 , 2013 | |||
| Furniture and office equipment | $ | 131 | |
| Medical equipment | 495 | ||
| Leasehold improvements | 2,226 | ||
| Net assets acquired | 2,852 | ||
| Less : gain from bargain purchase | (2,392 | ) | |
| Total pu rchase price | $ | 460 |
In January 2014, the Company acquired an ownership interest in two imaging centers and one urgent care clinic in Houston. The aggregate cost of the acquisition is comprised of $0.3 million in cash, net of acquired cash, and 431,711 shares of Nobilis stock representing a combined value of $0.9 million.
The following table summarizes the fair values of the identifiable assets acquired and liabilities assumed at the date of acquisition:
| January 16, 2014 | |||
| Assets: | |||
| Property and equipment | $ | 2,271 | |
| Prepaid expenses and other assets | 129 | ||
| Goodwill | 701 | ||
| Assets acquired | $ | 3,101 | |
| Liabilities: | |||
| Accounts payable | $ | 697 | |
| Debt | 1,544 | ||
| Liabilities assumed | $ | 2,241 | |
| Consideration: | |||
| Cash, net of cash acquired | $ | 346 | |
| Stock issued for acquisition | 514 | ||
| Total Consideration | $ | 860 |
First Nobilis, LLC
In September 2014, the Company formed First Nobilis, LLC, a Texas limited liability Company (“First Nobilis”). First Nobilis is owned 51% by the Company and 49% by a third party. First Nobilis formed two subsidiary Texas limited liability companies to be the new operating entities.
Upon formation of First Nobilis, effective September 1, 2014, Nobilis contributed $7.5 million in cash to the new entity. For a 49% ownership interest, a third party contributed medical supplies, intangible assets, and certain accounts payables and accounts receivables. This transaction was treated as a business combination. The fair value of the intangible assets and liabilities acquired were determined by independent third party valuation experts. The carrying amounts of all other net assets acquired approximate their fair values due to their short term nature.
The following table summarizes the fair values of the identifiable assets acquired and liabilities assumed at the date of acquisition:
| September 1, 2014 | |||
| Assets: | |||
| Accounts receivable | $ | 6,509 | |
| Medical supplies | 598 | ||
| Trade name | 1,200 | ||
| Physician relationships | 4,000 | ||
| Goodwill | 1,249 | ||
| Assets acquired | $ | 13,556 | |
| Liabilities: | |||
| Accounts payable | $ | 6,060 | |
| Unfavorable lease | 290 | ||
| Liabilities assumed | $ | 6,350 |
Athas
On December 1, 2014, the Company completed its acquisition of Athas for total consideration of approximately $31.2 million (all $ denominations in US dollars). Athas is based in Dallas, Texas, and focuses on the delivery of specialized healthcare services in seven states through the use of contracted marketing services and factoring of receivables. The purchase price for Nobilis to acquire all of the ownership interests in Athas was broken down as follows: $3.0 million in cash upon closing, the issuance of a promissory note by Nobilis to the sellers for $12.0 million, the issuance at closing of 6,666,666 shares of Nobilis common stock that are subject to a lock up of up to two years, and the issuance of an additional 4,666,666 shares of Nobilis common stock issued over two years with half issued on the first anniversary of the closing and the second half issued on the second anniversary of the closing. Under the two year lock up period, the stock issued as part of the purchase price is subject to restrictions on transfer and may not be sold or pledged until the lock out period is released.
The fair value of the intangible assets acquired were determined by independent third party valuation experts. The carrying amounts of all other net assets acquired approximate their fair values due to their short term nature. The value of the stock issued for consideration was determined by third party valuation experts using the published stock price on the date of closing, less a discount for lack of marketability as a result of the two year lock up period on the shares issued.
Subsequent to the acquisition date of December 1, 2014, Athas had $3.4 million in revenues and $1.3 million of net income which is included in the Company’s December 31, 2014 consolidated statements of earnings.
The costs related to the transaction were $0.1 million and were expensed during the year ended December 31, 2014. These costs are included in corporate general and administrative expenses in the December 31, 2014 consolidated statements of earnings.
The following table summarizes the fair values of the identifiable assets acquired and liabilities assumed at the date of acquisition:
| December 1, 2014 | |||
| Assets: | |||
| Cash | $ | (53 | ) |
| Trade accounts receivable | 6,427 | ||
| Other receivable | 450 | ||
| Prepaid expenses | 226 | ||
| Investments in associates | 730 | ||
| PP&E | 752 | ||
| Trademark | 4,770 | ||
| Internally developed software | 1,980 | ||
| Non-compete agreements | 1,820 | ||
| Trade secret methodology | 5,120 | ||
| Goodwill | 19,292 | ||
| Assets acquired | $ | 41,514 | |
| Liabilities | |||
| Trade accounts payable | $ | 1,531 | |
| Accrued liabilities | 3,470 | ||
| Line of credit | 4,120 | ||
| Subordinated notes payable | 635 | ||
| Debt | 157 | ||
| Other current liabilities | 102 | ||
| Other long-term liabilities | 260 | ||
| Liabilities assumed | $ | 10,275 | |
| Consideration: | |||
| Cash, net of cash acquired | $ | 3,000 | |
| Debt issued for consideration | 12,000 | ||
| Stock issued for consideration | 16,239 | ||
| Total consideration | $ | 31,239 |
The following summarized pro forma information for the years ended December 31, 2014 and 2013 presents the combined results of the Company as if the business combinations occurred as of January 1, 2013.
| Nobilis Health | First Surgical | Athas | Consolidated | |||||||||
| December 31, 2014 | ||||||||||||
| Revenue | $ | 84,029 | $ | 17,577 | $ | 26,059 | $ | 127,665 | ||||
| Net income before noncontrolling interests | 20,247 | (3,364 | ) | (1,481 | ) | 15,402 | ||||||
| Net income attributable to noncontrolling interests | 13,062 | (1,275 | ) | - | 11,787 | |||||||
| Net income (loss) attributable to Nobilis Health Corp. | $ | 7,185 | $ | (2,089 | ) | $ | (1,481 | ) | $ | 3,615 | ||
| December 31, 2013 | ||||||||||||
| Revenue | $ | 31,128 | $ | 32,327 | $ | 22,731 | $ | 86,186 | ||||
| Net income before noncontrolling interests | 6,674 | (677 | ) | (139 | ) | 5,858 | ||||||
| Net income attributable to noncontrolling interests | 5,476 | 2,265 | - | 7,741 | ||||||||
| Net income (loss) attributable to Nobilis Health Corp. | $ | 1,198 | $ | (2,942 | ) | $ | (139 | ) | $ | (1,883 | ) |
The pro forma financial information has been prepared for comparative purposes only and does not purport to be indicative of the actual operating results that would have been recorded had the business combinations actually taken place at the beginning of the fiscal year 2013, and should not be taken as indicative of future consolidated operating results. Additionally, the pro forma financial results do not include any anticipated synergies or other expected benefits from the business combinations.
4. Business Segment Information
A summary of the business segment information for 2014 and 2013 is as follows:
| Year Ended December 31, 2014 | ||||||||||||
| Medical | Marketing & | |||||||||||
| Services | Factoring | Corporate | Total | |||||||||
| Revenues | $ | 80,614 | $ | 3,415 | $ | - | $ | 84,029 | ||||
| Cost of goods sold | - | 201 | - | 201 | ||||||||
| Gross Profit | 80,614 | 3,214 | - | 83,828 | ||||||||
| Operating expenses | 54,438 | 1,909 | 6,648 | 62,995 | ||||||||
| Income (loss) from operations | $ | 26,176 | $ | 1,305 | $ | (6,648 | ) | $ | 20,833 | |||
| Other data: | ||||||||||||
| Depreciation and amortization expense | $ | 1,414 | $ | 114 | $ | 115 | $ | 1,643 | ||||
| Interest expense | $ | - | $ | 23 | $ | 265 | $ | 288 | ||||
| Income tax expense | $ | 480 | $ | - | $ | - | $ | 480 | ||||
| Intabgibles assets | $ | 5,945 | $ | 13,598 | $ | - | $ | 19,543 | ||||
| Goodwill | $ | 3,178 | $ | 19,292 | $ | - | $ | 22,470 | ||||
| Capital expenditures | $ | 2,023 | $ | - | $ | - | $ | 2,023 | ||||
| Non-cash acquisition of property | $ | 2,271 | $ | - | $ | - | $ | 2,271 | ||||
| Non-cash acquisition of intangibles and goodwill | $ | 7,206 | $ | - | $ | - | $ | 7,206 | ||||
| Investment in associates | $ | 150 | $ | - | $ | - | $ | 150 | ||||
| Total assets | $ | 59,751 | $ | 43,715 | $ | 4,116 | $ | 107,582 | ||||
| Total liabilities | $ | 16,995 | $ | 11,192 | $ | 14,094 | $ | 42,281 | ||||
The Company’s Marketing & Factoring segment started in 2014 following the acquisition of Athas. Prior to the acquisition, the Company operated under one operating segment and therefore, has not presented a prior period comparison of segment information.
5. Investments in Associates
In March 2014, the Company acquired an ownership interest in Group of Pioneers Diagnostics (“GOP”), LLC, representing 40% of the outstanding share interests in GOP. The investment in GOP is accounted for using the equity method of accounting. GOP owns two Management Service Organizations (“MSOs”) which provides a suite of management services to their clients which may include, but is not be limited to, general business management, fiscal management and physician practice management. GOP originated in June of 2014 and is currently undergoing efforts to achieve operational status. The carrying value of this investment at December 31, 2014 was $0.2 million, and is reflected in investments in associates on the consolidated balance sheets.
In December 2014, as part of the Athas acquisition, the Company acquired Athas’ investment ownership in two ASC’s and one hospital: 87.5% in Elite Orthopedic and Spine Surgery Center LLC; 15.7% in Elite Sinus Spine and Ortho LLC; and 10.7% in Elite Hospital Management LLC. For these investments, the Company concluded that it did not exert significant influence over the operating and financial activities. These investments are accounted for as cost method investments and recorded at cost. The carrying value of these investments at December 31, 2014 was $.7 million, and is recorded in investments in associates in the consolidated balance sheets.
6. Financial Instruments and Concentration
In common with all other businesses, the Company is exposed to risks that arise from its use of financial instruments. This note describes the Company’s objectives, policies, and processes for managing those risks and the methods used to measure them. Further quantitative information in respect of these risks is presented throughout these consolidated financial statements.
Principal financial instruments
The principal financial instruments used by the Company, from which financial instrument risk arises, are as follows:
- Accounts receivable and other receivables
- Investments in associates
- Accounts payable, accrued liabilities and other current liabilities
- Other liabilities and notes payable
- Capital leases
- Lines of credit
- Debt
The carrying amounts of the Company’s accounts receivable and other receivables, accounts payable, accrued liabilities, other current liabilities, other liabilities, capital leases, lines of credit, and debt approximate their fair values at December 31, 2014 and 2013, respectively, due to the short-term nature, maturities or nature of interest rates. Investments in associates are carried at amortized cost or their proportionate equity basis and written down to fair value if impairment is warranted.
Financial instruments - risk management
The Company is exposed through its operations to the following financial risks:
- Credit risk
- Fair value or cash flow interest rate risk
- Foreign exchange risk
- Other market price risk
- Liquidity risk
Credit risk
Credit risk is the risk of financial loss to the Company if a patient, non-partner surgeon or insurance company fails to meet its contractual obligations. The Company, in the normal course of business, is exposed mainly to credit risk on its accounts receivable from insurance companies, other third-party payors, and doctors. Accounts receivables are net of applicable bad debt reserves, which are established based on specific credit risk associated with insurance companies and payors and other relevant information.
Liquidity risk
Liquidity risk is the risk that the Company will not be able to meet its financial obligations as they fall due and arises from the Company’s management of working capital. The Company’s objective to managing liquidity risk is to ensure that it will have sufficient cash to allow it to meet its liabilities when they become due. To achieve this objective, it seeks to maintain cash balances (or agreed facilities) to meet expected requirements. The liquidity risk of the Company and its subsidiaries is managed centrally by the Company’s finance function. The Company believes that there are currently no concerns of its ability to meet its liabilities as they become due for the foreseeable future.
A summary of certain information about our payor concentration is as follows:
MEDICAL SERVICES SEGMENT
PATIENT AND NET PROFESSIONAL FEEREVENUEBY PAYORS OF
THENOBILIS FACILITIES
FOR THEYEARS ENDED DECEMBER 31, 2014 AND 2013
| 2014 Patient and Net | 2013 Patient and Net | ||||||
| Payors | Professional Fee | Professional Fee | |||||
| Revenue by Payor Mix | Revenue by Payor Mix | ||||||
| Private insurance and other private pay | 97.0% | 92.4% | |||||
| Workers compensation | 2.3% | 4.5% | |||||
| Medicare | 0.7% | 3.1% | |||||
| Total | 100.0% | 100.0% |
| MARKETING & FACTORING SEGMENT |
| PATIENT AND NET PROFESSIONAL FEEREVENUEBY PAYORS OF THENOBILIS FACILITIES |
| FOR THEYEARS ENDED DECEMBER 31, 2014 AND 2013 |
| 2014 Patient and Net | 2013 Patient and Net | ||||||
| Payors | Professional Fee | Professional Fee | |||||
| Revenue by Payor Mix | Revenue by Payor Mix | ||||||
| Private insurance and other private pay | 100.0% | 0.0% | |||||
| Workers compensation | 0.0% | 0.0% | |||||
| Medicare | 0.0% | 0.0% | |||||
| Total | 100.0% | 0.0% |
The patient and net professional fee revenues by payors of the Nobilis facilities for the marketing and factoring segment were 0.0% for all payors in 2013, as this segment was acquired in December 2014.
Three facilities represent approximately 70.3% of the Company’s contracted marketing revenue and five facilities represent approximately 69.1% of the Company’s contracted marketing accounts receivable.
| CONSOLIDATED SEGMENTS |
| PATIENT AND NET PROFESSIONAL FEEREVENUEBY PAYORS OF THENOBILIS FACILITIES |
| FOR THEYEARS ENDED DECEMBER 31, 2014 AND 2013 |
| 2014 Patient and Net | 2013 Patient and Net | ||||||
| Payors | Professional Fee | Professional Fee | |||||
| Revenue by Payor Mix | Revenue by Payor Mix | ||||||
| Private insurance and other private pay | 97.1% | 92.4% | |||||
| Workers compensation | 2.2% | 4.5% | |||||
| Medicare | 0.7% | 3.1% | |||||
| Total | 100.0% | 100.0% |
Market risk
Market risk is the risk that the fair value of future cash flows of financial instruments will fluctuate due to changes in interest rates and/or foreign currency exchange rates.
Interest rate risk
The Company entered into a revolving line of credit that, from time to time, may increase interest rates based on market index.
Foreign exchange risk
Foreign exchange risk arises because the Company has certain expenses that are incurred in Canadian dollars.
The Company is also exposed to currency risk on purchases made from vendors based in Canada. The Company had Canadian denominated cash (“Cdn”) of $0.1 million and a nominal amount of trade payables at December 31, 2014. The Company had Cdn of $3.1 million and a nominal amount of trade payables at December 31, 2013.
7. Trade Accounts Receivable
A detail of accounts receivable as of December 31, 2014 and 2013are as follows:
| 2014 | 2013 | |||||
| Trade accounts receivable | $ | 40,985 | $ | 10,431 | ||
| Allowance for doubtful accounts | (1,391 | ) | (1,384 | ) | ||
| Receivables transferred | (873 | ) | (766 | ) | ||
| Receivables purchased | 3,454 | - | ||||
| Trade accounts receivable, net | $ | 42,175 | $ | 8,281 |
Trade receivables are non-interest bearing and are generally received within 30-90 days. Bad debt expense was nil for the years ended December 31, 2014 and 2013. The Company analyzed receivables and determined that there were no collectability issues on accounts receivable balances in the current period.
As of December 31, 2014 and 2013, there remained a balance of $0.9 million and $0.8 million, respectively, in accounts receivable of transferred receivables pursuant to the terms of the original agreement. The Company, from time to time, shall transfer to the third party certain of its accounts receivable payments on a non-recourse basis. For the years ended December 31, 2014 and 2013, advance payment of $1.3 million and $0.4 million was received by the Company. During the same period, $7.3 million and $2.5 million of receivables was transferred. Concurrently, upon collection of these transferred receivables, payment will be made to the transferee.
Athas purchases receivables from physicians, at a discount, on a nonrecourse basis. The discount and purchase price vary by speciality. These purchased receivables are billed and collected by Athas who retains 100% of what is collected after paying the discounted purchase price. Following the transfer of the receivable, the transferor has no continued involvement and there are no restrictions on the receivables, and as such, these transfers of receivables are accounted for as sales transactions. Gross revenue from purchased receivables was $1.6 million for the year ended December 31, 2014. Revenue, net of the discounted purchase price, was $0.9 million for the year ended December 31, 2014. Accounts receivable for purchased receivables was $3.5 million as of December 31, 2014.
8. Property and Equipment
Property and equipment consisted of the following as of December 31, 2014 and 2013:
| 2014 | 2013 | |||||
| Telephone equipment | $ | 51 | $ | 29 | ||
| Computer hardware | 510 | 431 | ||||
| Computer software | 569 | 444 | ||||
| Furniture and office equipment | 921 | 457 | ||||
| Medical equipment | 9,943 | 6,218 | ||||
| Leasehold improvements | 6,293 | 5,178 | ||||
| 18,287 | 12,757 | |||||
| Less: accumulated depreciation | (9,200 | ) | (7,924 | ) | ||
| Property and equipment, net | $ | 9,087 | $ | 4,833 |
Depreciation expense for the years ended December 31, 2014 and 2013 was $1.5 million and $0.7 million, respectively.
9. Intangible Assets
Intangible assets at December 31, 2014 and December 31, 2013 consist of the following:
| 2014 | 2013 | ||||||||||||||||||||||||||
| Term | Historical | Accumulated | Accumulated | Net Book | Historical | Accumulated | Accumulated | Net Book | |||||||||||||||||||
| (in years) | Cost | Amortization | Impairment | Value | Cost | Amortization | Impairment | Value | |||||||||||||||||||
| Definite Life | |||||||||||||||||||||||||||
| Non-compete agreements | 10-15 | $ | 2,661 | $ | 856 | $ | - | $ | 1,805 | $ | 841 | $ | 841 | $ | - | $ | - | ||||||||||
| Internally developed software | 5 | 1,980 | 33 | - | 1,947 | - | - | - | - | ||||||||||||||||||
| Trade secret methodology | 10 | 5,120 | 44 | - | 5,076 | - | - | - | - | ||||||||||||||||||
| Physician relationships | 15-20 | 4,000 | 62 | - | 3,938 | - | - | - | - | ||||||||||||||||||
| Indefinite Life | |||||||||||||||||||||||||||
| Tradenames | 1,200 | - | - | 1,200 | - | - | - | - | |||||||||||||||||||
| Unfavorable lease | (290 | ) | - | - | (290 | ) | - | - | - | - | |||||||||||||||||
| Trademark | 4,770 | - | - | 4,770 | - | - | - | - | |||||||||||||||||||
| Medicare license | 8,498 | - | 7,401 | 1,097 | 8,498 | - | 7,401 | 1,097 | |||||||||||||||||||
| Total | $ | 27,939 | $ | 995 | $ | 7,401 | $ | 19,543 | $ | 9,339 | $ | 841 | $ | 7,401 | $ | 1,097 | |||||||||||
Amortization expense was $0.2 million and nil for the year ended December 31, 2014 and 2013, respectively. Estimated amortization expense of intangible assets is $1.2 million for the next five years and $6.7 million thereafter.
10. Goodwill
The following table provides information on changes in the carrying amount of goodwill, which is included in the accompany consolidated balance sheets as of December 31 2014 and 2013:
| 2014 | 2013 | |||||
| Cost | $ | 36,770 | $ | 15,528 | ||
| Accumulated impairment losses | (14,300 | ) | (14,300 | ) | ||
| Total | $ | 22,470 | $ | 1,228 | ||
| Cost | 2014 | 2013 | ||||
| BALANCE - beginning of period | $ | 15,528 | $ | 15,528 | ||
| January 2014 business combination | 701 | - | ||||
| September 2014 business combination | 1,249 | - | ||||
| December 2014 business combination | 19,292 | - | ||||
| Total cost | $ | 36,770 | $ | 15,528 | ||
| Accumulated impairment | ||||||
| BALANCE - beginning of period | $ | (14,300 | ) | $ | (14,300 | ) |
| Impairment charges during the period | - | - | ||||
| Total accumulated impairment | $ | (14,300 | ) | $ | (14,300 | ) |
The Company did not record any impairment charges for the year ended December 31, 2014 or 2013.
11. Lines of Credit
Revolving Credit Facility for Northstar Houston Surgery Center, LLC. (“NHSC-H”)
On November 13, 2014, NHSC-H entered into a credit agreement with Compass Bank for a $1.0 million revolving credit facility. The one-year facility requires monthly interest payments and carries an interest rate equal to the higher of (a) the Federal Funds Rate plus 0.5%, (b) LIBOR plus 1.0%, or (c) the Prime rate. Principal is due in full upon maturity at December 31, 2014, the $1.0 million facility was fully utilized. As of December 31, 2014, the Company was in full compliance with all debt covenants.
Revolving Credit Facility for Athas
Athas maintains a $5.0 million revolving line of credit with a financial institution. The line of credit renews annually and bears variable interest at the Prime rate plus 0.75% per annum, or a floor of 4.0% . The line of credit is collateralized by the assets of the Company and is renewable annually, subject to the approval of the financial institution. As of December 31, 2014, the balance due on the revolving line of credit was $4.4 million. As of December 31, 2014, the Company was in technical default under a continuity of operations clause which was triggered when Athas was acquired by Nobilis. Despite technical default, the debt has not been called by the bank. This line of credit is classified as current on the December 31, 2014 consolidated balance sheets.
12. Debt
Purchase of Palladium for Surgery Dallas, LLC (“PFSD”)
In conjunction with the Company’s purchase of PFSD, the Company entered into a promissory note with the Company’s Chairman for a principal amount of $2.1 million on January 1, 2011.
The note was initially amended in March 2012, in conjunction with a private placement of common shares that occurred in January 2012.
The note was subsequently amended in March 2013. The amended note had a principal balance of $1.7 million at December 31, 2013 bearing an interest rate at 5.25% per annum until January 2014, when the interest rate increased to 6.25% per annum. The principal amount and any accrued and unpaid interest was due on or before December 31, 2014. Interest payments were payable on a monthly basis.
The note was then amended again in December 2014. The amended note has a principal balance of $0.4 million bearing an interest rate at 6.25% per annum. The principal amount and any accrued and unpaid interest is due on or before January 31, 2016. Outstanding interest payments have been paid as of the date of these financials.
The note is included in the consolidated balance sheets as a long-term liability. The note has a principal balance of $0.4 million as of December 31, 2014.
Term Loan for Athas
Athas secured a term loan in 2011 for $0.5 million which was assumed in the acquisition (Note 2). The Company and one of the shareholders are guarantors of the loan. The loan bears interest at 4.0% per annum. The term loan requires monthly payments of principal and interest until the loan matures in May 2016. As of December 31, 2014, the balance due on the term loan was $0.1 million. The term loan is collateralized by the assets of the Company and the guarantors.
Subordinated Notes Payable
Athas carries subordinated notes payable which were given as consideration for working capital provided by certain individuals. The subordinated notes interest is payable semi-annually with a principal due at maturity on December 31, 2015. The notes carry a 12.0% annual interest rate and payment is subordinated to all senior secured debt instruments. The outstanding balance of the subordinated notes was $0.6 million at December 31, 2014. Some of the note holders are also employees and shareholders of the Company.
Promissory Note for Spring Northwest Management, LLC (“SNWM”)
In November 2013, SNWM, a consolidated entity, entered into a promissory note with Allegiance Bank Texas. The agreement provides for a $0.9 million loan which matures in November 2018. The note bears interest at a rate of 5.5% per annum and requires monthly payments of principal and interest through November 2018. The promissory note was utilized to finance the purchase of certain medical equipment, all of which serves as collateral against the note. Nobilis is not liable under the above mentioned promissory note. The note has a principal balance of $0.7 million as of December 31, 2014.
Promissory Note for Willowbrook Imaging, LLC (“WIM”)
In January 2014, WIM, a consolidated entity, entered into a promissory note with Branch Bank and Trust Company. The agreement provides for a $0.8 million loan which matures in February 2021. The note bears interest at a fixed rate of 3.65% per annum and requires monthly payments of principal and interest through February 2021. The promissory note was utilized to finance the purchase of certain medical equipment. Nobilis is not liable under the above mentioned promissory note. The note has a principal balance of $0.7 million as of December 31, 2014.
Purchase of Athas
In conjunction with the Company’s purchase of Athas, the Company entered into a promissory note with sellers for a principal amount of $12.0 million on December 1, 2014. The sellers represent the 20 previous shareholders of Athas. Payments are to be made to the sellers as follows: (a) $1.0 million payment of principal on December 31, 2014, (b) $1.0 million payment of principal on April 1, 2015, (c) consecutive monthly payments of principal and interest of $0.3 million commencing May 1, 2015 and continuing until April 1, 2018. The note accrues interest at 11% per annum. The seller agreed to defer the principal payment of $1.0 million which was due on December 31, 2014 until the Company secures financing with a commercial lender that can provide a lower cost of interest.
Future maturities of debt as of December 31, 2014 are as follows:
| Year ending December 31, | |||
| 2015 | $ | 4,072 | |
| 2016 | 4,409 | ||
| 2017 | 4,400 | ||
| 2018 | 1,499 | ||
| 2019 | 274 | ||
| Total | $ | 14,654 |
13. Operating Leases
The Company occupies five ASCs, one hospital, one urgent care clinic, one imaging center and two corporate business spaces under operating lease agreements. The Company also leases certain medical equipment. The minimum rental commitments under non-cancellable operating leases, with terms in excess of one year subsequent to December 31, 2014, are as follows:
| Year ending December 31, | |||
| 2015 | $ | 6,737 | |
| 2016 | 7,114 | ||
| 2017 | 5,917 | ||
| 2018 | 5,748 | ||
| 2019 | 5,202 | ||
| Thereafter | 19,103 | ||
| Total future commitment | 49,821 | ||
| Less: minimum sublease income to be received | (631 | ) | |
| Total future commitment, net of sublease income | $ | 49,190 |
Rent expense was $3.5 million and $1.4 million for the years ended December 31, 2014 and 2013, respectively.
14. Capital Leases
The Company holds various capital leases for medical equipment which contain bargain purchase options at the end of the lease terms. The remaining minimum capital lease obligations, with terms in excess of one year subsequent to December 31, 2014, are as follows:
| Year ending December 31, | |||
| 2015 | $ | 290 | |
| 2016 | 290 | ||
| 2017 | 254 | ||
| 2018 | 51 | ||
| 2019 | 28 | ||
| Total minimum rentals | 913 | ||
| Less: total amounts representing interest | (83 | ) | |
| Capital lease obligations | $ | 830 |
15. Shareholders’ Equity
In total, the Company has issued 59,418,227 of its common shares. There is no par value assigned to our common shares.
In December 2013, the Company issued, through a private placement agreement, 5,862,500 Units, at a price of Cdn$0.80 per Unit. Each Unit consists of one common share in the capital of the Company and one-half of one common share purchase warrant exercisable for one additional share at a price of Cdn$1.10. Through the private placement, the Company raised $4.1 million, as of December 31, 2013, net of offering costs of $0.3 million.
Of the $4.1 million raised capital, $2.7 million was provided in exchange for stock warrants and other financial instruments, resulting in a remaining $1.4 million which was recorded as an increase to share capital for the year ended December 31, 2013.
In August 2014, the Company elected to accelerate the expiry date of the common share purchase warrants originally issued by Nobilis as part of its unit private placement completed on December 16, 2013. Each Warrant entitled the holder thereof to purchase one additional common share of Nobilis at a price of Cdn$1.10. Nobilis received total gross proceeds of Cdn$3,224,375 from the exercise.
In September 2014, the Company issued, through a private placement agreement, 5,568,400 Units, at a price of Cdn$1.30 per Unit. Each Unit consists of one common share in the capital of the Company and one-half of one common share purchase warrant exercisable for one additional share at a price of Cdn$1.80. Through private placement, the Company raised $6.1 million, as of September 30, 2014, net of offering costs of $0.4 million.
Of the $6.1 million raised capital, $2.2 million was provided in exchange for stock warrants and other financial instruments, resulting in a remaining $3.9 million which was recorded as an increase to additional paid in capital in the consolidated statement of changes in shareholders’ equity.
In December 2014, as part of the consideration given for the acquisition of Athas, the Company issued 6,666,666 shares of Nobilis common stock that are subject to a lock up of up to two years, and the issuance of an additional 4,666,666 shares of Nobilis common stock issued over two years with half issued on the first anniversary of the closing and the second half issued on the second anniversary of the closing.
16. Share Based Compensation
Restricted Share Unit Plan
During 2008, the BOD approved the adoption of a Restricted Share Unit Plan (“RSU”) Plan for employees. Restricted Share Units (“RSUs”) may be granted to employees of Nobilis at the sole discretion of the Board of Directors (“BOD”).
Subject to the BOD’s ability to accelerate the vesting of the RSUs if it determines circumstances so warrant, each RSU will generally vest in full on the third anniversary of the date of grant; provided that if there is a change of control of the Company prior to the vesting date of the RSUs and a participant is terminated (or resigns for good reason) within six months following such change of control, a pro rata portion of their unvested RSUs will vest up to the date of the change of control.
Upon vesting of his or her RSUs, a participant will be entitled to receive on the vesting date, at the discretion of the BOD either: (a) a lump sum cash payment equal to the number of RSUs multiplied by an average closing price of the common shares on the Toronto Stock Exchange on the redemption date, net of any applicable deductions and withholdings; or (b) that number of common shares equal to the number of RSUs credited to the participant’s RSU account, such common shares to be issued from treasury of the Company. The participant is to receive the benefit on, or as soon as practicable after, the vesting date, but in no event later than 90 days after the vesting date. Unlike share options, RSUs do not require the payment of any monetary consideration to the Company.
Whenever cash dividends are paid on the Company’s common shares, dividend equivalents in the form of additional RSUs will be credited to each Participant and will become part of his or her award under the RSU Plan. The RSUs representing dividend equivalents will vest and be paid at the same time and in the same manner as the RSUs to which the dividend equivalents pertain.
In the event of a Participant’s termination of employment, voluntary or by cause, with the Company prior to any vesting date, the Participant’s rights to any unvested RSUs will be immediately and irrevocably forfeited.
If the Participant’s employment with the Company terminates on account of death or disability or is terminated by the Company without cause prior to any vesting date, the Participant will become vested in a prorated portion of his or her unvested RSUs, based on the number of months that have elapsed in the then current vesting period as of the date of termination.
Share Option Plan
In April 2012, the BOD approved the adoption of a Share Option Plan for insiders, employees, and service providers. In May 2012, the Company’s shareholders approved the Share Option Plan, and in July 2012, the Toronto Stock Exchange approved the Share Option Plan. Share Options may be granted at the sole discretion of the BOD. The exercise price of an Option is determined by the BOD at the time of grant and shall not be less than the current market price. The term of each Option is determined by the BOD and shall not exceed 10 years.
If an Optionee shall cease to be a Participant for cause, no Option held by such Optionee shall be exercisable following the date on which such Optionee ceases to be a Participant. If an Optionee ceases to be a Participant for any reason other than for cause, any Option held by such Optionee at such time shall remain exercisable in full at any time, and in part from time to time, for a period of 90 days after the date on which the Optionee ceases to be a Participant.
If the Participant’s employment with the Company terminates on account of death, any option held by such Participant at the date of death shall be exercisable in whole or in part only by the person or persons to whom the rights of the Participant’s Options by will or laws of descent.
The maximum number of RSUs and share options that may be issued under the combined plans is equal to 20.0% of the Company’s issued and outstanding common shares.
The maximum number of RSUs and share options that may be issued under the combined plans is equal to 20.0% of the Company’s issued and outstanding common shares. The Company granted a total of 3,068,218 stock options during the year ended December 31, 2014. Of the granted options, 1.9 million of those vest ratably over a one to three year period while the remaining 1.2 million options vest within one month of issuance.
The following table summarizes stock option activity for the nine months ended December 31, 2014.
| Shares | Weighted- | Weighted-Average | |||||||
| Underlying | Average Exercise | Remaining Life | |||||||
| Options | Price | (years) | |||||||
| Outstanding at January 1, 2013 | 150,000 | $ | 0.21 | 0.1 | |||||
| Granted | 1,275,000 | $ | 0.35 | 9.6 | |||||
| Exercised | (575,000 | ) | $ | 0.31 | - | ||||
| Forfeited | (150,000 | ) | $ | 0.21 | - | ||||
| Outstanding at December 31, 2013 | 700,000 | $ | 0.39 | 9.6 | |||||
| Exercisable at December 31, 2013 | 700,000 | $ | 0.39 | 9.6 | |||||
| Outstanding at January 1, 2014 | 700,000 | $ | 0.39 | 9.8 | |||||
| Granted | 3,068,218 | $ | 1.47 | 9.9 | |||||
| Exercised | (600,000 | ) | $ | 0.30 | - | ||||
| Forfeited | (50,000 | ) | $ | 1.31 | - | ||||
| Outstanding at December 31, 2014 | 3,118,218 | $ | 1.45 | 9.8 | |||||
| Exercisable at December 31, 2014 | 220,000 | $ | 1.16 | 9.6 |
The total intrinsic value of stock options exercised was $0.6 million and nominal for the year ended December 31, 2014 and 2013, respectively. The total intrinsic value for all in-the-money vested outstanding stock options was $0.4 million and $0.5 million during the year ended December 31, 2014 and 2013, respectively.
The Company recorded compensation expense relative to stock options of $1.1 million and $0.3 million for the year ended December 31, 2014 and 2013, respectively.
The fair values of stock options used in recording compensation expense are computed using the Black-Scholes option pricing model. The table below shows the assumptions used in the model for options awarded during the year ended December 31, 2014.
| Year ended | Year ended | |||||
| December 31, 2014 | December 31, 2013 | |||||
| Expected price volatility | 119% - 123% | 124% - 125% | ||||
| Risk free interest rate | .01% - .05% | .02% - .04% | ||||
| Expected annual dividend yield | 0% | 0% | ||||
| Expected option term (years) | 10 | 0.1 and 10 | ||||
| Expected forfeiture rate | 0% | 0% | ||||
| Grant date fair value per share | $ | 0.97 - $1.64 | $ | 0.29 - $0.89 |
For stock options, the Company recognizes share-based compensation net of estimated forfeitures and revises the estimates in the subsequent periods if actual forfeitures differ from the estimates. Forfeiture rates are estimated based on historical experience as well as expected future behavior. As of December 31, 2014, the Company utilized a forfeiture rate of 0.0% based on a minimal number of stock option issuances, only two historical forfeitures and little to no anticipated turnover rate in those positions awarded with stock based compensation.
17. Noncontrolling Interests
The following changes to noncontrolling interests in subsidiaries of the Company occurred during the year ended December 31, 2014 and 2013:
Medical Ambulatory Surgical Suites, LLC (“Kirby Partnership”)
In November 2013, the Company sold 15.1% of its ownership interest in the Kirby Partnership to existing physician limited partners, effectively decreasing the Company’s ownership interest to 25%.
Houston Microsurgery Institute, LLC (“MSIH”)
In March 2013, the Company redeemed the remaining equity interests held by physician limited partners at MSIH, effectively increasing the Company’s ownership interests to 97.7% . In October 2013, MSIH ceased operating as an ASC.
Microsurgery Institute, LLC (“MSID”)
In August 2013, the Company purchased ownership interest from all of the physician limited partners at MSID, increasing the Company’s ownership interest to 100%.
NHC ASC – Dallas, LLC (“NHC – ASC Dallas”)
In July 2013, the Company formed a limited liability company, NHC ASC – Dallas, which was owned 100% by Northstar Healthcare Acquisitions, LLC (“NHA”). In October 2013, the Company syndicated a private placement for certain physicians to become members in NHC ASC – Dallas. The Company assigned 100% of its equity interest in MSID to NHC ASC – Dallas, of which the Company owns 35% as a result of syndication.
SNWM
In January 2014, the Company acquired 31.78% ownership interest in SNWM, derived through both a direct and indirect investment. The Company also holds a 31.78% interest in both of SNWM’s fully owned subsidiaries, Spring Creek Urgent Care, LLC (“SCUC”) and Spring Creek Imaging, LLC (“SCI”).
Spring Northwest Operating, LLC (“SNWO”)
In January 2014, the Company acquired a 32.14% ownership in SNWO, derived through both a direct and indirect investment.
WIM
In January 2014, the Company acquired a 22.22% ownership interest in WIM, derived through both a direct and indirect investment.
KIRPA Holdings, LLC (“KIRPA”)
In January 2014, the Company acquired a 40% ownership interest in KIRPA. KIRPA holds a controlling interest in SNWM, SCUC, SCI, and SNWO.
GRIP Medical Diagnostics, LLC (“GRIP”)
In January 2014, the Company acquired a 40% ownership interest in GRIP. GRIP holds a controlling interest in WIM.
Northstar Healthcare Dallas Management, LLC (“NHDM”)
In April 2014, the Company formed a limited liability company, NHDM, which is owned 50% by NHA and 50% by physician limited partners. NHDM was formed to provide management services to NHC-ASC Dallas.
First Nobilis
As discussed in Note 2, in September 2014, the Company and a third party formed First Nobilis. First Nobilis is owned 51% by NHA and 49% by a third party. First Nobilis formed two subsidiary companies, First Nobilis Hospital, LLC and First Nobilis Surgical Center, LLC, as new operating entities.
Noncontrolling interests at December 31, 2014 represent an 8.1% interest in The Palladium for Surgery – Houston, Ltd, 75% interest in the Kirby Partnership, 5% interest in MSID, 2.3% interest in MSIH, 60% interest in Houston Procedure Suite, LLC, 50% in NHDM, 50% in KIRPA, 60% in GRIP, 60% in NHC ASC – Dallas, 67.9% in SNWO, 68.2% in SNWM, 68.2% in SCUC, 68.2% in SCI; 77.8% in WIM, 49%, and First Nobilis Pursuant to U.S. GAAP, notwithstanding having an ownership interest less than 50%, the Company is deemed to have the power to control each of the above mentioned entities in which it holds less than the majority voting interests based on a combination of factors which include but are not limited to (1) the Company’s hold of majority voting rights as defined through executed partnership agreements, (2) the Company’s ability and right to govern day-to-day operations as defined through executed management and cost sharing agreements, (3) the Company’s rights as lessee on all leased facility space. Based on the power to control the activities of these entities and the responsibility to absorb significant losses, the Company was deemed the primary beneficiary under U.S. GAAP and as such consolidates these entities.
18. Employee Retirement Plan
Substantially all of our employees, upon qualification, are eligible to participate in our defined contribution 401(k) plan (the “Plan”). Under the Plan, employees may contribute a portion of their eligible compensation, and the Company matches such contributions annually up to a maximum percentage for participants actively employed, as defined by the Plan documents. Plan expenses were approximately $0.1 million for both the year ended December 31, 2014 and 2013. Such amounts are reflected in operating salaries and benefits in the accompanying consolidated statements of earnings.
19. Earnings Per Share
A detail of the Company’s EPS is as follows (in thousands except for share and per share amounts):
| 2014 | 2013 | |||||
| Net income for the period | $ | 7,186 | $ | 1,198 | ||
| Issued common shares at beginning of period | 42,729,547 | 36,082,114 | ||||
| Effect of investment in subsidiary | 412,787 | - | ||||
| Effect of stock based compensation | 403,552 | 470,911 | ||||
| Effect of stock warrants | 959,419 | - | ||||
| Effect of private placement | 1,464,565 | 240,925 | ||||
| Effect of Athas acquisition | 547,945 | - | ||||
| W eighted average common shares at end of period | 46,517,815 | 36,793,950 | ||||
| Basic EPS | $ | 0.15 | $ | 0.03 |
A detail of the Company’s dilutive EPS is as follows (in thousands except for share and per share amounts):
| 2014 | 2013 | |||||
| Net income for the period | $ | 7,186 | $ | 1,198 | ||
| W eighted average common shares (basic) | 46,517,815 | 36,793,950 | ||||
| Effect of stock based compensation | 1,829,540 | 731,792 | ||||
| Effect of stock warrants | 50,431 | 111,920 | ||||
| Effect of Athas acquisition | 383,562 | - | ||||
| W eighted average common shares (diuluted) at end of period | 48,781,348 | 37,637,662 | ||||
| Dilutive EPS | $ | 0.15 | $ | 0.03 |
20. Income Taxes
The following table shows the reconciliation between income tax expense reported in our consolidated statement of earnings and comprehensive income and the income tax expense that would have resulted from applying the United States federal income tax rate of 35% to pre-tax income. Though the Company was incorporated in British Columbia, all of the Company’s subsidiaries are incorporated in the United States. Therefore, the Company reconciles the income before income taxes for U.S. tax purposes.
| 2014 | 2013 | |||||
| Net income before income tax | $ | 20,728 | $ | 6,851 | ||
| US federal income tax rate | 35% | 35% | ||||
| Expected U.S. Federal income tax (recovery) | 7,254 | 2,398 | ||||
| Permanent differences / discrete items | 312 | 92 | ||||
| State income tax (net of federal benefit) | 314 | 115 | ||||
| Valuation Allowance | (2,438 | ) | (620 | ) | ||
| Non-controlling interests | (4,572 | ) | (1,917 | ) | ||
| Others | (390 | ) | 109 | |||
| Total tax expense | $ | 480 | $ | 177 |
The table below sets forth the tax effects of temporary differences that give rise to significant portions of the deferred tax assets and deferred tax liabilities that are reported in our consolidated balance sheets:
| 2014 | 2013 | |||||
| Deferred tax assets: | ||||||
| Goodwill | $ | 17,993 | $ | 20,844 | ||
| Intangibles | 1,214 | 1,459 | ||||
| U.S. non-capital losses | 14,063 | 12,398 | ||||
| Interest carry-forward | 1,391 | 1,391 | ||||
| Non-capital losses | 9,539 | 10,735 | ||||
| Allowance for bad debts | 408 | 406 | ||||
| Reduction of carrying amount of deferred tax assets | (44,608 | ) | (47,233 | ) | ||
| Net deferred tax assets | $ | - | $ | - |
Deferred tax assets are recognized to the extent that the realization of the related tax benefit through future taxable profits is probable. The Company did not recognize deferred tax assets of $44.6 million.
The Company has Canadian non-capital losses of approximately $38.2 million which will begin to expire in 2028 and U.S. net operating losses of approximately $40.2 million which will begin to expire in 2030. On September 30, 2010 the Company issued 18,778,446 common shares to entities controlled by the Company’s Chairman resulting in a change of ownership greater than 50%. As a result, the U.S. net operating losses are limited by the Internal Revenue Code. In addition, the Company has approximately $4.0 million in interest carry-forwards that have no expiration date.
21. Related Parties
In conjunction with the Company’s purchase of PFSD, the Company entered into a promissory note with the Company’s Chairman, on January 1, 2011. The note had a principal balance of $0.4 million at December 31, 2014. The principal amount and any accrued and unpaid interest is due on or before January 31, 2016.
On June 25, 2013, the Company entered into a promissory note receivable with an executive employee of the Company for a principal amount of $0.2 million. The note bears interest at a rate of 5.5% per annum. The term provides that interest will be calculated at a daily rate and all accrued and unpaid interest shall be paid annually on the first day of July of each successive year. The unpaid principal balance together with all accrued but unpaid interest is due in full on or before June 30, 2017.
In 2013, the Company entered into a Management Services Agreement (“MSA”) with Northstar Pain Management P.A. (“NSPM”). NSPM is owned by the Company’s Chairman. Operation of NSPM is designed to support the Company’s marketing campaigns. As part of the MSA, the Company provides comprehensive management services to NSPM. At December 31, 2014, the Company is owed $0.6 million from NSPM.
Facility lease costs associated with operating leases of approximately $0.4 million were incurred with affiliated entities during the year ended December 31, 2014.
The minority interest holder of First Nobilis, a fully consolidated entity, is also a partial owner of First Street Hospital, L.P. (“First Street Hospital”) and First Street Surgical Center, L.P. (“First Street Surgical”), both of which have an ongoing business relationship with the Company. At December 31, 2014, the Company has a due from these related parties of $2.0 million which is partially offset by a due to related parties of $1.4 million for a net amount owed to the Company of $0.6 million. In addition, the Company leases certain medical equipment from First Street Hospital and First Street Surgical. Equipment lease costs of approximately $0.6 million were incurred during the year ended December 31, 2014.
At December 31, 2014, three of the investors and partial owners of SNWO, WIM and SNWM owe the Company $0.2 million for their investment into the respective entities.
Certain of the sellers of Athas are current employees of Athas, including its CEO, Chris Lloyd. The sellers of Athas entered into a promissory note with the Company for $12.0 million, as mentioned in a previous footnote.
Certain members of the Company are also members of North American Laserscopic Spine Institute (“NALSI”). In June 2014, NALSI entered into a line of credit agreement with Athas, whereby NALSI may draw up to $0.9 million. The line of credit is subject to a 10.00% interest rate and matures on June 9, 2018. The outstanding balance as of December 31, 2014 is $0.5 million.
Nobilis maintains certain consulting and marketing agreements with various physicians who are also equity owners in Nobilis entities. These agreements are paid directly out of those entities in which the physicians hold an ownership percentage.
The related party transactions mentioned above are measured at exchange amounts agreed upon by both parties.
22. Supplemental Cash Flow Information
The changes in operating assets and liabilities for the years ended December 31, 2014 and 2013 are comprised of the following:
| 2014 | 2013 | |||||
| Trade accounts receivable | $ | (20,958 | ) | $ | (4,191 | ) |
| Medical supplies | (27 | ) | (252 | ) | ||
| Prepaids and other current assets | (2,799 | ) | (253 | ) | ||
| Other long-term assets | 466 | (176 | ) | |||
| Trade accounts payable and accrued liabilities | 2,840 | 2,712 | ||||
| Other current liabilities | 1,340 | 43 | ||||
| Other long-term liabilities | (8 | ) | (2 | ) | ||
| Total | $ | (19,146 | ) | $ | (2,119 | ) |
23. Litigation
The Company is involved in disputes or legal actions arising in the ordinary course of business. Management does not believe the outcome of such disputes or legal actions will have a material adverse effect on the Company’s financial position, results of operations or cash flows.
For the year ended December 31, 2014 and 2013, the Company recorded costs of $1.1 million and $1.0 million, respectively, in connection with various legal proceedings.
24. Subsequent Events
On March 31, 2015, the Company secured a $25.0 million credit facility from General Electric Capital Corporation consisting of a $20.0 million term loan and a $5 million revolving loan. The term loan bears interest at a rate of 4% plus LIBOR per annum and amortizes over 20 years with required quarterly payments of principal and interest until the loan matures in March 2020. The revolving loan also bears interest at a rate of 4% plus LIBOR per annum and amounts borrowed under the revolver may be repaid and reborrowed periodically with a maturity of March 2020. The credit facility is collateralized by the accounts receivable and physical equipment of all 100% owned subsidiaries as well as the Company’s ownership interest in all less than wholly owned subsidiaries. The new credit facility serves to refinance all previously held debt and lines of credit and provide $5.0 million for working capital. Closing costs associated with the credit facility approximated $0.6 million.
We have evaluated subsequent events through March 31, 2015, the date the consolidated financial statements were issued.
25. Approval of Financial Statements
The consolidated financial statements were approved by the board of directors for issuance on March 31, 2015.
| Item 9. | Changes in and Disagreements With Accountants on Accounting and Financial Disclosure |
There were no disagreements with our accountants related to accounting principles or practices, financial statement disclosure, internal controls or auditing scope or procedure during the two fiscal years and subsequent interim periods.
| Item 9A. | Controls and Procedures |
Disclosure Controls and Procedures
Disclosure controls and procedures are the controls and other procedures that are designed to provide reasonable assurance that information required to be disclosed by the issuer in the reports that it files or submits under the Securities Exchange Act of 1934, as amended (the "Exchange Act") is recorded, processed, summarized and reported within the time periods specified in the Securities and Exchange Commission’s rules and forms. Disclosure controls and procedures include, without limitation, controls and procedures designed to ensure that information required to be disclosed by an issuer in the reports that it files or submits under the Exchange Act is accumulated and communicated to the issuer’s management, including the principal executive and principal financial officer, or persons performing similar functions, as appropriate, to allow timely decisions regarding required disclosure. Any controls and procedures, no matter how well designed and operated, can provide only reasonable assurance of achieving the desired control objectives.
We have carried out an evaluation, under the supervision and with the participation of our president (our principal executive officer) and our chief financial officer (our principal financial officer and principal accounting officer), of the effectiveness of our disclosure controls and procedures, as defined in Rules 13a-15(e) and 15d-15(e) of the Exchange Act as of the end of the fiscal year covered by this annual report.
Based on that evaluation, our president (our principal executive officer) and our chief financial officer (our principal financial officer and principal accounting officer) have concluded that our company’s disclosure controls and procedures were effective as of the end of the fiscal year covered by this annual report on Form 10-K.
Management’s Annual Report on Internal Control over Financial Reporting
Management is responsible for establishing and maintaining adequate internal control over financial reporting, as defined in Securities Exchange Act Rule 13a-15(f). Internal control over financial reporting is designed to provide reasonable assurance regarding the reliability of financial reporting and preparation of financial statements for external purposes in accordance with U.S. GAAP. This annual report does not include a report of management's assessment regarding internal control over financial reporting due to a transition period established by rules of the Securities and Exchange Commission for newly public companies.
Change in Internal Control over Financial Reporting
During the period covered by this report there were no changes in our internal control over financial reporting that materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
| Item 9B. | Other Information |
None.
PART III
| Item 10. | Directors, Executive Officers and Corporate Governance |
All directors of our company hold office until the next annual meeting of the security holders or until their successors have been elected and qualified. The officers of our company are appointed by our board of directors and hold office until their death, resignation or removal from office. Our directors and executive officers, their ages, positions held, and duration as such, are as follows:
56
| Name |
Position Held
with the Company |
Age |
Date First Elected or
Appointed |
| Donald Kramer, M.D. | Chairman and Director | 58 | September 30, 2010(1) |
| Harry Fleming | President and Director | 55 | September 30, 2010 |
| Thomas O. Foster III | Director | 75 | July 14, 2014(2) |
| Jennifer Pfahler | Director | 46 | June 11, 2013 |
| Richard Ganley | Director | 54 | June 11, 2013 |
| Chris Lloyd | Chief Executive Officer | 42 | December 1, 2014 |
| Andy Chen | Chief Financial Officer | 38 | July 29, 2014 |
| (1) |
Dr. Kramer was originally appointed a director on March 29, 2007 and resigned on February 6, 2009. He was again appointed on September 30, 2010. | |
| (2) |
Mr. Foster was originally appointed a director on September 30, 2010 and resigned on June 11, 2013. He was again appointed on July 14, 2014. |
Business Experience
The following is a brief account of the education and business experience during at least the past five years of each director, executive officer and key employee of our company, indicating the person’s principal occupation during that period, and the name and principal business of the organization in which such occupation and employment were carried out.
Employment Agreements
As of December 31, 2014 our company had employment agreements with three executives: Christopher Lloyd, Harry Fleming and Andy Chen. In addition, our company has an Executive Transition Agreement with Donald Kramer, which governed certain compensation terms related to Dr. Kramer’s transition from Chief Executive Officer to Executive Director.
Christopher Lloyd, Chief Executive Officer. Base compensation and Term. Mr. Lloyd’s employment agreement, effective as of November 26, 2014, has a term of 3 years and will automatically renew for additional 1 year terms unless the employment agreement is terminated by either party at least 30 days prior to the end of the initial 3-year term or any subsequent 1-year term. Mr. Lloyd’s salary is $600,000 in the first year of the initial term and increases to $625,000 and $650,000 in years 2 and 3, respectively.
Termination Provisions. Mr. Lloyd may terminate his employment agreement with "good reason" upon the occurrence of any of the following: i) a diminution in title or duties, ii) a failure by our company to substantially perform any material term in his employment agreement, iii) relocation of our company’s principal place of business more than 50 miles from its current location, iv) a reduction in salary or benefits other than as the result of adverse financial conditions of our company, or v) a change in control of our company.
The Company may terminate Mr. Lloyd’s employment agreement for "cause" upon the occurrence of any of the following: i) a failure to perform substantially all of his duties, ii) his dishonesty or gross negligence, iii) his conviction or nolo contendere plea to a felony, iv) any willful act or omission by him that is materially injurious to the financial condition or business reputation of our company, v) his failure to comply with a written directive of the Board or Chief Executive Officer, or vi) a breach of the non-competition or intellectual property confidentiality provisions contained in the employment agreement.
57
In the event that Mr. Lloyd terminates his employment agreement for "good reason" or our company terminates his employment agreement without "cause", Mr. Lloyd is entitled to receive one year’s base salary as a separation benefit.
Incentive Compensation. In addition to his base salary, Mr. Lloyd may receive certain cash and equity incentive compensation. Mr. Lloyd participates in our company’s Short Term Incentive Program, which entitles him to receive as a bonus, up to 40% of his yearly base salary if our company achieves certain financial metrics established each year by our company’s Compensation, Nomination and Corporate Governance Committee. Mr. Lloyd is also entitled to receive up to 1,500,000 Company Stock Options that vest as follows - 500,000 vested on January 1, 2015, 500,000 will vest on December 1, 2015 and 500,000 will vest on December 1, 2016.
Mr. Lloyd is entitled to participate in the Companies 401k plan. Mr. Lloyd is not entitled to any other material compensation, including without limitations, equity, bonus, or retirement benefits.
Harry Fleming, President. Base compensation and Term. Mr. Fleming’s employment agreement, effective as of October 1, 2014, has a term of 3 years and will automatically renew for additional 1 year terms unless the employment agreement is terminated by either party at least 30 days prior to the end of the initial 3-year term or any subsequent 1-year term. Mr. Fleming’s salary is $425,000 in the first year of the initial term and increase to $450,000 and $475,000 in years 2 and 3, respectively.
Termination Provisions. Mr. Fleming may terminate his employment agreement with "good reason" upon the occurrence of any of the following: i) a diminution in title or duties, ii) a failure by our company to substantially perform any material term in his employment agreement, iii) relocation of our company’s principal place of business more than 50 miles from its current location, iv) a reduction in salary or benefits other than as the result of adverse financial conditions of our company, or v) a change in control of our company.
The Company may terminate Mr. Fleming’s employment agreement for "cause" upon the occurrence of any of the following: i) a failure to perform substantially all of his duties, ii) his dishonesty or gross negligence, iii) his conviction or nolo contendere plea to a felony, iv) any willful act or omission by him that is materially injurious to the financial condition or business reputation of our company, v) his failure to comply with a written directive of the Board or Chief Executive Officer, or vi) a breach of the non-competition or intellectual property confidentiality provisions contained in the employment agreement.
In the event that Mr. Fleming terminates his employment agreement for "good reason" or our company terminates his employment agreement without "cause", Mr. Fleming is entitled to receive any earned by unpaid base salary, accrued but unused vacation pay, and any incurred but unreimbursed business expenses.
Incentive Compensation. In addition to his base salary, Mr. Fleming may receive certain cash and equity incentive compensation. Mr. Fleming participates in our company’s Short Term Incentive Program, which entitles him to receive as a bonus, up to 40% of his yearly base salary if our company achieves certain financial metrics established each year by our company’s Compensation, Nomination and Corporate Governance Committee. Per the agreement, our company awarded Mr. Fleming 1,000,000 RSUs that vest in 10 years regardless of Mr. Fleming’s employment status with our company (the "First Fleming Grant of RSUs"). The these RSUs will immediately vest, however, upon the occurrence of any of the following: i) the termination of Mr. Fleming’s employment (for any reason), ii) a change in control of our company, or iii) at Mr. Fleming’s election if there is a formal offer from a third party to buy or to merge our company. In addition, the agreement (later amended as described below) contained an additional award of 1,000,000 RSUs (the "Second Fleming Grant of RSUs") which would have been awarded in the event of a consummated change in control or in the event that our company terminated Mr. Fleming’s employment agreement without cause (defined in the agreement) or Mr. Fleming terminated his employment with good reason (defined in the agreement). Due to the acquisition of Athas Health, LLC and the change in Mr. Fleming’s role with our company as the result of the anticipated scope of Mr. Lloyd’s duties, the Board approved amendments to Mr. Fleming’s employment agreement such that the Second Fleming Grant of RSUs was deleted in its entirety and the First Fleming Grant of RSUs was increased from 1,000,000 RSUs to 2,000,000 RSUs.
58
Mr. Fleming is entitled to participate in the Companies 401k plan. Mr. Fleming is not entitled to any other material compensation, including without limitations, equity, bonus, or retirement benefits.
Andy Chen, Chief Financial Officer. Base compensation and Term. Mr. Chen’s employment agreement, effective as of November 26, 2014, has a term of 3 years and will automatically renew for additional 1 year terms unless the agreement is terminated by either party at least 30 days prior to the end of the initial 3-year term or any subsequent 1-year term. Mr. Chen’s salary was $170,000 in 2014 and increased, per his employment agreement, to $200,000 on January 1, 2015.
Termination Provisions. Mr. Chen may terminate his employment agreement with good reason upon the occurrence of any of the following: i) a diminution in title or duties, ii) a failure by our company to substantially perform any material term in his employment agreement, iii) relocation of our company’s principal place of business more than 50 miles from its current location, iv) a reduction in salary or benefits other than as the result of adverse financial conditions of our company, or v) a change in control of our company.
The Company may terminate Mr. Chen’s employment agreement for cause upon the occurrence of any of the following: i) a failure to perform substantially all of his duties, ii) his dishonesty or gross negligence, iii) his conviction or nolo contendere plea to a felony, iv) any willful act or omission by him that is materially injurious to the financial condition or business reputation of our company, v) his failure to comply with a written directive of the Board or Chief Executive Officer, or vi) a breach of the non-competition or intellectual property confidentiality provisions contained in the employment agreement.
In the event that Mr. Chen terminates his employment agreement for "good reason" or our company terminates his employment agreement without "cause", Mr. Chen is entitled to receive one year’s base salary as a separation benefit.
Incentive Compensation. In addition to his base salary, Mr. Chen may receive certain cash and equity incentive compensation. Mr. Chen participates in our company’s Short Term Incentive Program, which entitles him to receive as a bonus, up to 40% of his yearly base salary if our company achieves certain financial metrics established each year by our company’s Compensation, Nomination and Corporate Governance Committee. Mr. Chen has received 200,000 Company Stock Options. The Board has accelerated the vesting of the 200,000 Stock Options issued to Mr. Chen from vesting in one-third increments on May 9, 2015, May 9, 2016 and May 9, 2017, respectively, to all such Stock Options vesting on February 3, 2015.
Mr. Chen is entitled to participate in the Companies 401k plan. Mr. Chen is note entitled to any other material compensation, including without limitations, equity, bonus, or retirement benefits.
Donald Kramer, Executive Director. As the result of the Athas Health, LLC acquisition, Dr. Kramer resigned as Chief Executive Officer of our company and assumed the role of Executive Director. Dr. Kramer’s compensation as Executive Director remains at $450,000 per year, which was the salary he received as Chief Executive Officer. The Company and Dr. Kramer executed a Confidential Executive Transition Agreement, in which the parties agreement that Dr. Kramer would receive, in lieu of any incentive or separation compensation due under his employment agreement, 2,000,000 RSUs will vest the sooner of i) ten years or ii) the termination of his role as Executive Director.
Dr. Kramer is not entitled to any other material compensation, including without limitations, equity, bonus, or retirement benefits.
Family Relationships
There are no family relationships between any of our directors, executive officers and proposed directors or executive officers.
Involvement in Certain Legal Proceedings
To the best of our knowledge, none of our directors or executive officers has, during the past ten years:
| 1. |
been convicted in a criminal proceeding or been subject to a pending criminal proceeding (excluding traffic violations and other minor offences); |
59
| 2. |
had any bankruptcy petition filed by or against the business or property of the person, or of any partnership, corporation or business association of which he was a general partner or executive officer, either at the time of the bankruptcy filing or within two years prior to that time; | |
| 3. |
been subject to any order, judgment, or decree, not subsequently reversed, suspended or vacated, of any court of competent jurisdiction or federal or state authority, permanently or temporarily enjoining, barring, suspending or otherwise limiting, his involvement in any type of business, securities, futures, commodities, investment, banking, savings and loan, or insurance activities, or to be associated with persons engaged in any such activity; | |
| 4. |
been found by a court of competent jurisdiction in a civil action or by the SEC or the Commodity Futures Trading Commission to have violated a federal or state securities or commodities law, and the judgment has not been reversed, suspended, or vacated; | |
| 5. |
been the subject of, or a party to, any federal or state judicial or administrative order, judgment, decree, or finding, not subsequently reversed, suspended or vacated (not including any settlement of a civil proceeding among private litigants), relating to an alleged violation of any federal or state securities or commodities law or regulation, any law or regulation respecting financial institutions or insurance companies including, but not limited to, a temporary or permanent injunction, order of disgorgement or restitution, civil money penalty or temporary or permanent cease- and-desist order, or removal or prohibition order, or any law or regulation prohibiting mail or wire fraud or fraud in connection with any business entity; or | |
| 6. |
been the subject of, or a party to, any sanction or order, not subsequently reversed, suspended or vacated, of any self-regulatory organization (as defined in Section 3(a)(26) of the Exchange Act (15 U.S.C. 78c(a)(26)), any registered entity (as defined in Section 1(a)(29) of the Commodity Exchange Act (7 U.S.C. 1(a)(29)), or any equivalent exchange, association, entity or organization that has disciplinary authority over its members or persons associated with a member. |
Compliance with Section 16(A) of the Securities Exchange Act of 1934
Section 16(a) of the Securities Exchange Act of 1934, as amended (the "Exchange Act"), requires our executive officers and directors and persons who own more than 10% of a registered class of our equity securities to file with the SEC initial statements of beneficial ownership, reports of changes in ownership and annual reports concerning their ownership of our shares of common stock and other equity securities, on Forms 3, 4 and 5, respectively. Executive officers, directors and greater than 10% shareholders are required by the SEC regulations to furnish us with copies of all Section 16(a) reports they file.
As at our fiscal year ended December 31, 2014, our common stock was not registered pursuant to Section 12 of the Exchange Act. Accordingly, as at December 31, 2014, our officers, directors, and principal stockholders were not subject to the beneficial ownership reporting requirements of Section 16(a) of the Exchange Act. Our officers, directors, and principal stockholders will be required to make filings under Section 16(a) of the Exchange Act beginning fiscal 2015.
Code of Ethics
Effective May 14, 2014, our Company’s board of directors adopted a Code of Business Conduct and Ethics that applies to, among other persons, our company’s principal executive officer and our principal financial and accounting officer, as well as persons performing similar functions. As adopted, our Code of Business Conduct and Ethics sets forth written standards that are designed to deter wrongdoing and to promote:
| 1. |
compliance with applicable governmental laws, rules and regulations; | |
| 2. |
honest and ethical conduct, including the ethical handling of actual or apparent conflicts of interest between personal and professional relationships; | |
| 3. |
health and safety; |
60
| 4. |
full, fair, accurate, timely, and understandable disclosure in reports and documents that we file with, or submit to, the regulatory authorities and in other public communications made by us; | |
| 5. |
the prompt internal reporting of violations of the Code of Business Conduct and Ethics to an appropriate person or persons identified in the Code of Business Conduct and Ethics; and | |
| 6. |
accountability for adherence to the Code of Business Conduct and Ethics. |
Code of Business Conduct and Ethics emphasizes that all personnel are required to talk to supervisors, managers or other appropriate personnel about observed illegal or unethical behavior and when in doubt about the best course of action in a particular situation. The failure to report such information may itself be deemed a violation of the Code of Business Conduct and Ethics. It is our policy not to allow retaliation for reports of misconduct by others made in good faith.
Our Code of Business Conduct and Ethics is attached as an exhibit to this annual report. We will provide a copy of the Code of Business Conduct and Ethics to any person without charge, upon request. Requests can be sent to: Corporate Counsel, Nobilis Health Corp., 4120 Southwest Freeway, Suite 150, Houston, TX 77027.
Board and Committee Meetings
Our board of directors held 5 formal meetings during the year ended December 31, 2014. The board of directors also conducted proceedings resolutions consented to in writing by all the directors and filed with the minutes of the proceedings of the directors. Such resolutions consented to in writing by the directors entitled to vote on that resolution at a meeting of the directors are, according to the Business Corporations Act (British Columbia) and our Articles, as valid and effective as if they had been passed at a meeting of the directors duly called and held.
Compensation, Nominating and Corporate Governance Committee
Our Compensation, Nominating and Corporate Governance Committee consists of Jennifer Pfahler (Chair), Thomas O. Foster, III and Richard Ganley. The committee is governed by a Compensation, Nominating and Corporate Governance Committee Charter adopted by our board and which is available in the corporate governance section of our website at http://www.nobilishealth.com/.
Members of the committee are appointed by our board to assist in:
| 1. |
the evaluation of the performance of our executives; | |
| 2. |
the oversight and evaluation of compensation, including benefits, off our executives; | |
| 3. |
developing and recommending criteria for selecting new board members and identifying and considering candidates; | |
| 4. |
recommending the applicable board nominees for each annual meeting of shareholders, and making recommendations concerning membership of each committee of the board; | |
| 5. |
developing appropriate corporate governance guidelines for our company; and | |
| 6. |
the annual review of our board's performance. |
Our Compensation, Nominating and Corporate Governance Committee held 1 meeting during the year ended December 31, 2014.
As of December 31, 2014, we did not effect any material changes to the procedures by which our shareholders may recommend nominees to our Compensation, Nominating and Corporate Governance Committee.
61
If shareholders wish to recommend candidates directly to our Compensation, Nominating and Corporate Governance Committee, they may do so by sending communications to the Chair of the committee at the address on the cover of this annual report.
Audit Committee
Our Audit Committee discusses with management and our outside auditors the financial information developed by us, our systems of internal controls and our audit process. Our Audit Committee is solely and directly responsible for appointing, evaluating, retaining and, when necessary, terminating the engagement of the independent auditor. The independent auditors meet with our Audit Committee (both with and without the presence of management) to review and discuss various matters pertaining to our Audit, including our financial statements, the report of the independent auditors on the results, scope and terms of their work, and their recommendations concerning the financial practices, controls, procedures and policies employed by us. Our Audit Committee preapproves all audit services to be provided to us, whether provided by the principal auditor or other firms, and all other services (review, attest and non-audit) to be provided to us by the independent auditor. Our Audit Committee coordinates our board of directors’ oversight of our internal control over financial reporting, disclosure controls and procedures and code of conduct. Our Audit Committee is charged with establishing procedures for (i) the receipt, retention and treatment of complaints received by us regarding accounting, internal accounting controls or auditing matters; and (ii) the confidential, anonymous submission by employees of our company of concerns regarding questionable accounting or auditing matters. Our Audit Committee reviews all related party transactions on an ongoing basis, and all such transactions must be approved by our Audit Committee. Our Audit Committee is authorized, without further action by our board, to engage such independent legal, accounting and other advisors as it deems necessary or appropriate to carry out its responsibilities. Our board has adopted a written charter for our Audit Committee, which is available in the corporate governance section of our website at http://www.nobilishealth.com/.
Our Audit Committee currently consists of Jennifer Pfahler (Chair), Thomas O. Foster, III and Richard Ganley, each of whom is independent within the meaning of The NASDAQ Marketplace Rules and Rule 10A-3 under the Exchange Act. Our board has determined that Jennifer Pfahler (Chair), Thomas O. Foster, III and Richard Ganley are each an "audit committee financial expert" as defined in Item 407(d)(5) of Regulation S-K. Our Audit Committee held 4 meetings during the fiscal year ended December 31, 2014.
| Item 11. | Executive Compensation |
The information regarding executive compensation set forth in the 2015 Proxy Statement is incorporated herein by reference.
| Item 12. | Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters |
The following table sets forth, as of December 31, 2014, certain information with respect to the beneficial ownership of our common shares by each shareholder known by us to be the beneficial owner of more than 5% of our common shares, as well as by each of our current directors and executive officers as a group. Each person has sole voting and investment power with respect to the shares of common stock, except as otherwise indicated. Beneficial ownership consists of a direct interest in the shares of common stock, except as otherwise indicated.
| Name and Address of Beneficial Owner
|
Amount and Nature of
Beneficial Ownership |
Percentage of Class(1) |
| Donald Kramer 4120 Southwest Freeway, Suite 150 Houston TX 77027 |
19,372,282 Common |
32.2% |
| Harry Fleming 4120 Southwest Freeway, Suite 150 Houston TX 77027 |
4,996,755 Common |
8.3%
|
62
| Name and Address of Beneficial Owner
|
Amount and Nature of
Beneficial Ownership |
Percentage of Class(1) |
| Chris Lloyd 4120 Southwest Freeway, Suite 150 Houston TX 77027 |
3,566,434 Common |
6.0% |
| Richard Ganley 4120 Southwest Freeway, Suite 150 Houston TX 77027 |
55,200 Common |
0.1% |
| Thomas O. Foster, III 4120 Southwest Freeway, Suite 150 Houston TX 77027 |
126,788 Common |
0.2% |
| Andy Chen 4120 Southwest Freeway, Suite 150 Houston TX 77027 |
303,000 Common |
0.5% |
| Directors and Executive Officers as a Group | 28,470,456 Common Shares | 47.1% |
| (1) |
Under Rule 13d-3, a beneficial owner of a security includes any person who, directly or indirectly, through any contract, arrangement, understanding, relationship, or otherwise has or shares: (i) voting power, which includes the power to vote, or to direct the voting of shares; and (ii) investment power, which includes the power to dispose or direct the disposition of shares. Certain shares may be deemed to be beneficially owned by more than one person (if, for example, persons share the power to vote or the power to dispose of the shares). In addition, shares are deemed to be beneficially owned by a person if the person has the right to acquire the shares (for example, upon exercise of an option) within 60 days of the date as of which the information is provided. In computing the percentage ownership of any person, the amount of shares outstanding is deemed to include the amount of shares beneficially owned by such person (and only such person) by reason of these acquisition rights. As a result, the percentage of outstanding shares of any person as shown in this table does not necessarily reflect the person’s actual ownership or voting power with respect to the number of shares of common stock actually outstanding on March 25, 2015. As of March 25, 2015 there were 61,135,631 shares of our company’s common stock issued and outstanding. |
Changes in Control
We are unaware of any contract or other arrangement or provisions of our Articles of Incorporation or Bylaws the operation of which may at a subsequent date result in a change of control of our company. There are not any provisions in our Articles of Incorporation or Bylaws, the operation of which would delay, defer, or prevent a change in control of our company.
| Item 13. | Certain Relationships and Related Transactions, and Director Independence |
Except as disclosed herein, no director, executive officer, shareholder holding at least 5% of shares of our common stock, or any family member thereof, had any material interest, direct or indirect, in any transaction, or proposed transaction since the year ended December 31, 2014, in which the amount involved in the transaction exceeded or exceeds the lesser of $120,000 or one percent of the average of our total assets at the year-end for the last three completed fiscal years.
On January 1, 2011 and as amended and restated on March 6, 2012, Northstar Subco entered into a promissory note with Donald Kramer, our Chief Executive Officer in the amount of $1,692,565.00 with interest accruing at 5.25% . This note is in good standing.
On June 20, 2013, Northstar Acquisitions entered into a promissory note with Harry Fleming, our then Chief Financial Officer in the amount of $150,000 with interest accruing at 5.5% . Per the terms of the note, no payment on the principal is owed until June 30, 2017. The note currently is in good standing.
Director Independence
We currently act with five directors, consisting of Donald Kramer, M.D., Harry Fleming, Thomas O. Foster III, Jennifer Pfahler and Richard Ganley.
63
We have determined that Thomas O. Foster III, Jennifer Pfahler and Richard Ganley are independent directors, as that term is used in Rule 4200(a)(15) of the Rules of National Association of Securities Dealers.
Currently our audit committee consists of Thomas O. Foster III, Richard Ganley and Jennifer Pfahler. We currently do not have nominating, compensation committees or committees performing similar functions. There has not been any defined policy or procedure requirements for shareholders to submit recommendations or nomination for directors.
From inception to present date, we believe that the members of our audit committee and the board of directors have been and are collectively capable of analyzing and evaluating our financial statements and understanding internal controls and procedures for financial reporting.
| Item 14. | Principal Accounting Fees and Services |
The aggregate fees billed for the most recently completed fiscal year ended December 31, 2014 and for fiscal year ended December 31, 2013 for professional services rendered by the principal accountant for the audit of our annual financial statements and review of the financial statements included in our quarterly reports on Form 10-Q and services that are normally provided by the accountant in connection with statutory and regulatory filings or engagements for these fiscal periods were as follows:
| Year Ended | ||
| December 31, 2014 | December 31, 2013 | |
| Audit Fees | 226,000 | 110,000 |
| Audit Related Fees | 184,000 | 63,000 |
| Tax Fees | 102,000 | 57,000 |
| All Other Fees | 24,000 | - |
| Total | 536,000 | 230,000 |
Our board of directors pre-approves all services provided by our independent auditors. All of the above services and fees were reviewed and approved by the board of directors either before or after the respective services were rendered.
Our board of directors has considered the nature and amount of fees billed by our independent auditors and believes that the provision of services for activities unrelated to the audit is compatible with maintaining our independent auditors’ independence.
PART IV
| Item 15. | Exhibits, Financial Statement Schedules |
| (a) |
Financial Statements | ||
| (1) |
Financial statements for our company are listed in the index under Item 8 of this document. | ||
| (2) |
All financial statement schedules are omitted because they are not applicable, not material or the required information is shown in the financial statements or notes thereto. | ||
| (b) |
Exhibits | ||
| Exhibit | Description |
| Number | |
| (3) | Articles of Incorporation |
64
| Exhibit | Description |
| Number | |
| 3.1(1) | Certificate of Incorporation. |
| 3.2(1) | Notice of Articles. |
| 3.3(1) | Articles. |
| (10) | Material Contracts |
| 10.1(1) | Sale and Repurchase Agreement between Northstar Healthcare Inc. and Northstar Healthcare Holding, Inc, dated May 17, 2007. |
| 10.2(1) | Employment Agreement between Northstar Healthcare Acquisitions and Donald Kramer, dated October 1, 2014 |
| 10.3(1) | Second Amended and Restated Promissory Note between Northstar Healthcare Subco and Donald Kramer, dated March 6, 2013. |
| 10.4(1) | Promissory Note between Northstar Healthcare Acquisitions and Harry Fleming, dated June 30, 2013. |
| 10.5 (1) | Employment Agreement between Northstar Healthcare Acquisitions and Harry Fleming, dated October 1, 2014. |
| 10.6(1) | Employment Agreement between Northstar Healthcare Acquisitions and Chris Lloyd, dated November 26, 2014. |
| 10.7(1) | Agency Agreement between Northstar Healthcare Inc. and PI Financial Corp. dated December 16, 2013. |
| 10.8(1) | Agency Agreement between Northstar Healthcare Inc. and PI Financial Corp. dated September 26, 2014. |
| 10.9(1) | Master Agreement by and between First Surgical Partners Holdings, Inc. and Northstar Healthcare Inc. dated September 2, 2014. |
| 10.10(1) | Amendment to Master Agreement by and between First Surgical Partners Holdings, Inc. and Northstar Healthcare Inc. dated September 2, 2014. |
| 10.11(1) | Lease Agreement between Cole River Oaks, Ltd. and Northstar Healthcare, Inc. |
| 10.12(1) | Assignment and Assumption of Base Year Medical Office Building between NHSC-Scottsdale, LLC and Brown Medical Center, Inc, dated January 8, 2014. |
| 10.13(1) | Medical Office Building Lease Agreement between Southwest Professional Building, Ltd. and Microsurgery Institute LLC dated June 1, 2012. |
| 10.14(1) | Assignment and Assumptions of Lease between Microsurgery Institute LLC and Northstar Healthcare Inc. dated December 1, 2013. |
| 10.15(1) | Sublease between Northstar Healthcare Inc. and NHS ASC- Dallas, LLC dated December 1, 2013. |
| 10.16(1) | Retail Lease Bissonnett Shopping Center, Suite 4811 4803-B Bissonnet, Houston, Texas 77401 between Lenox Hill Holdings, Ltd. and First Street Surgical Center dated January 2005. |
| 10.17(1) | First Amendment to Lease between Lenox Hill Holdings, Ltd. and First Street Surgical Center dated August 25, 2010. |
| 10.18(1) | Second Amendment to Lease between Lenox Hill Holdings, Ltd. and First Street Surgical Center dated February 1, 2012. |
65
| Exhibit | Description |
| Number | |
| 10.19(1) | Second Amendment to Lease between Lenox Hill Holdings, Ltd. and First Street Surgical Center dated November 29, 2013. |
| 10.20(1) | Assignment of Lease between First Street Surgical Center and First Nobilis, LLC date September 29, 2014. |
| 10.21(1) | Building Lease between First Street Holdings, Ltd. and First Street Hospital LP dated September 17, 2006. |
| 10.22(1) | Second Amendment to Lease Agreement First Street Holdings, Ltd. and First Street Hospital LP dated December 1, 2013. |
| 10.23(1) | Assignment of Lease between First Street Hospital LP and First Nobilis, LLC date September 29, 2014. |
| 10.24(1) | Lease Agreement between Lenox Hill Holdings, Ltd. and First Street Hospital, LP dated December 1, 2103. |
| 10.25(1) | Assignment of Lease between First Street Hospital LP and First Nobilis, LLC date September 29, 2014. |
| 10.26(1) | Building Lease between Islington, Ltd. and First Street Surgical Center, LP dated April 1, 2013. |
| 10.27(1) | First Amendment to Lease between First Street Holdings, Ltd. and First Street Surgical Center, LP dated April 1, 2013. |
| 10.28(1) | Second Amendment to Lease between First Street Holdings, Ltd. and First Street Surgical Center, LP dated December 1, 2013. |
| 10.29(1) | Assignment of Lease between First Street Surgical Center, LP and First Nobilis, LLC date September 29, 2014. |
| 10.30(1) | Office Space lease between Texas Institute for Eyes, LLC and North American Spine, LLC dated August 5, 2009. |
| 10.31(1) | First Amendment to Office Space lease between Texas Institute for Eyes, LLC and North American Spine, LLC dated June 22, 2010. |
| 10.32(1) | Second Amendment to Office Space lease between Texas Institute for Eyes, LLC and North American Spine, LLC dated October 7, 2010. |
| 10.33(1) | Third Amendment to Office Space lease between Texas Institute for Eyes, LLC and North American Spine, LLC dated June 30, 2011. |
| 10.34(1) | Membership Interest Purchase Agreement between Northstar Healthcare Subco, LLC, Northstar Healthcare Inc., Athas Health, LLC and the Individual Seller Parties dated November 26, 2014. |
| 10.35(1) | Security Agreement dated November 26, 2014. |
| 10.36(1) | Secured Promissory Note dated November 26, 2014. |
| 10.37(1) | Registration of Rights Agreement dated November 26, 2014. |
| 10.38(1) | NHC ASC – Dallas, LLC Company Agreement. |
| 10.39(1) | Third Amended and Restated Agreement of Limited Partnership of Medical Ambulatory Surgical Suite, LP. |
| 10.40(1) | Credit Agreement between Northstar Healthcare Surgery Center- Houston, LLC and Compass Bank. |
| 10.41(2) | First Amended Employment Agreement between Northstar Healthcare Acquisitions and Harry |
66
| Exhibit | Description |
| Number | |
| Fleming, dated October 1, 2014. | |
| 10.42(2) | Confidential Executive Transition Agreement between Northstar Healthcare Acquisitions and Donald Kramer, dated December 1, 2014. |
| 10.43(2) | Employment Agreement between Northstar Healthcare Acquisitions and Andy Chen, dated August 1, 2014. |
| (14) | Code of Ethics |
| 14.1* | Code of Business Conduct and Ethics. |
| (21) | Subsidiaries of the Registrant |
| 21.1* | Subsidiaries of the Registrant |
| (31) | Rule 13a-14 (d)/15d-14d) Certifications |
| 31.1* | Section 302 Certification by the Principal Executive Officer. |
| 31.2* | Section 302 Certification by the Principal Financial Officer and Principal Accounting Officer. |
| (32) | Section 1350 Certifications |
| 32.1* | Section 906 Certification by the Principal Executive Officer. |
| 32.2* | Section 906 Certification by Principal Financial Officer and Principal Accounting Officer. |
| (101)* | Interactive Data File |
| 101.INS | XBRL Instance Document. |
| 101.SCH | XBRL Taxonomy Extension Schema Document. |
| 101.CAL | XBRL Taxonomy Extension Calculation Linkbase Document. |
| 101.DEF | XBRL Taxonomy Extension Definition Linkbase Document. |
| 101.LAB | XBRL Taxonomy Extension Label Linkbase Document. |
| 101.PRE | XBRL Taxonomy Extension Presentation Linkbase Document. |
| * filed herewith | |
| (1) | Incorporated by reference to our Form 10, Registration of Securities filed on December 23, 2014 |
| (2) | Incorporated by reference to our Form 10/A, Registration of Securities filed on January 29, 2015 |
67
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereto duly authorized.
| NOBILIS HEALTH CORP. | |
| (Registrant) | |
| Dated: April 1, 2015 | /s/ Chris Lloyd |
| Chris Lloyd | |
| Chief Executive Officer | |
| (Principal Executive Officer) | |
| Dated: April 1, 2015 | /s/ Andy Chen |
| Andy Chen | |
| Chief Financial Officer | |
| (Principal Financial Officer) |
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
| Dated: April 1, 2015 | /s/ Harry Fleming |
| Harry Fleming | |
| President and Director | |
| Dated: April 1, 2015 | /s/ Thomas O. Foster |
| Thomas O. Foster | |
| Director | |
| Dated: April 1, 2015 | /s/ Donald Kramer |
| Donald Kramer, M.D. | |
| Director, Chairman of the Board |
68