Attached files
| file | filename |
|---|---|
| 8-K - 8-K - Cardiff Oncology, Inc. | a14-1253_28k.htm |
Exhibit 99.1
|
|
Better Cancer Monitoring with Cell-Free DNA in Urine Antonius Schuh, Ph.D. | Chief Executive Officer January 2014 |
|
|
Forward-Looking Statements Statements in this presentation about the Company's expectations, applications of its technology, markets, launch of tests and other statements that are not historical facts are "forward-looking statements" within the meaning of Section 27A of the Securities Act of 1933 and Section 21E of the Securities Exchange Act of 1934 and are based on management's current beliefs, assumptions, estimates and projections. Actual results may differ materially from those projected in the forward-looking statements for various reasons, including risks associated with product and test development, test transfer to contracting labs, government regulation, market acceptance, limited commercial experience, dependence on key personnel, obtaining financing and other factors discussed in the Company's periodic reports filed with the Securities and Exchange Commission. DISCLAIMER |
|
|
Our Goal: Improve Treatment Outcomes For Cancer Patients INTRODUCTION Trovagene’s technology is designed to detect and quantitatively monitor DNA mutations in the urine of cancer patients to improve disease management Our diagnostic platform provides important clinical information beyond the current standard of care |
|
|
Key Assets Cancer monitoring technology addresses high unmet clinical need Enables more frequent, non-invasive monitoring of oncogene mutation status, disease progression, and recurrence Feasible now that improved PCR and next generation sequencing (NGS) platforms are available at significantly lower cost Significant patent portfolio around cell-free DNA in urine Competitive advantages of urine include ease of sampling and large volume Growing body of evidence supporting clinical utility CLIA certified, CAP accredited lab to offer diagnostic services Technology collaborations with leading corporate partners INTRODUCTION NASDAQ: TROV $180 M market cap* Molecular Diagnostic Specialist founded in 1999 NASDAQ listing 2012 $55M invested in R&D and IP ~$26 M cash on hand (12/31/13) Focused on cancer management *as of 08 January 2014 Company Overview |
|
|
Experienced Leadership Team INTRODUCTION Thomas Adams, PhD (Chair) John P. Brancaccio, CPA Gary S. Jacob, PhD Paul Billings, MD, PhD Carlo M. Croce, MD Riccardo Dalla-Favera, MD Brunangelo Falini, MD Kunwar Shailubhai, PhD Antonius Schuh, PhD Stanley Tennant, MD Chris McGuigan, PhD Scientific Advisors Antonius Schuh PhD CEO Sorrento Therapeutics, AviaraDx, Arcturus Biosciences, Sequenom PhD Pharm. Chem Stephen Zaniboni CFO Mark Erlander PhD CSO Michael Terry EVP, Comm Ops Keith McCormick VP, Sales/Mktg Awarepoint, XIFIN, Sorrento Therapeutics, AviaraDx, Arcturus, Sequenom CPA, BS Accounting, MBA Boston College bioTheranostics, AviaraDx, Arcturus Biosciences, J&J, Scripps Research Institute BS, MS Biochem; Ph.D. Neuroscience bioTheranostics, AviaraDx, Biogen Idec, Schering Plough, Dianon Systems BBA – Marketing MBA – Int’l Business Ligand DX, EVP Sequenom, EVP Lumenis, GE Healthcare Medical BS Econ & Business, AD Int’l Business Mary Barry VP, Clinical Ops Promethus Labs, AviaraDx, Cypress Bio, Verinata, Scripps Research Institute, Healthcare Medical MBA, Clinical Laboratory Scientist Board of Directors |
|
|
THE CLINICAL UTILITY OF CELL-FREE DNA FROM URINE Treatment Response and Resistance Monitoring Metastatic cancer patients per year: ~525,000 Price Per Test: $1,000 Tests Per Year: 6 TAM patients: 3.2M TAM $: ~$3.2B Average patient receives 8-10 imaging studies during initial 12 month period post-diagnosis Over 170M cancer screening and diagnostic procedures performed annually in the U.S. Cancer survivors: ~11M Price Per Test: $1,000 Tests Per Year: 1 TAM patients: ~11M TAM $: ~$11B Recurrence Monitoring Large Addressable Market; Est. 45% Rise in U.S. Cancer Incidence by 2030* *Smith, B.D. et al. Future of Cancer Incidence in the United States: Burdens Upon Ageing, Changing Nation, Journal of Clinical Oncology, Vol. 27, No. 17, June 10, 2009. ᶲCancer Facts and Figures 2013, American Cancer Society, p. 4 ⱡ American Cancer Society Website; http://www.cancer.org/cancer/cancerbasics/cancer-prevalence. ◊ Table 2 in Dinan, et. Al. Changes in the Use and Costs of Diagnostic Imaging Among Medicare Beneficiaries With Cancer, 1999-2006, JAMA, April 2010. ◊ ᶲ ⱡ |
|
|
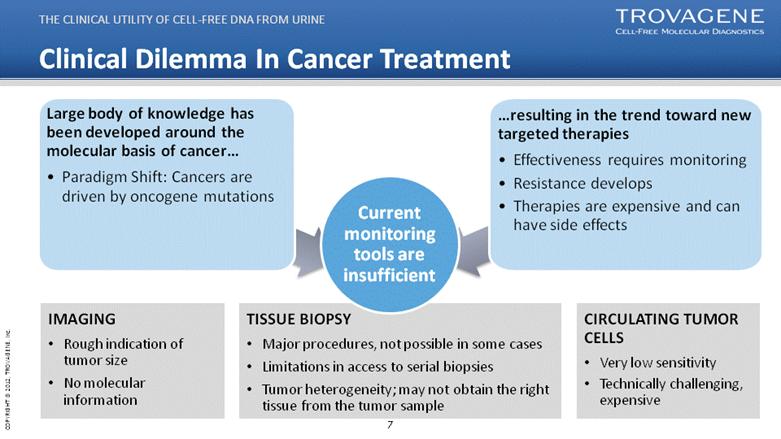
Clinical Dilemma In Cancer Treatment Large body of knowledge has been developed around the molecular basis of cancer... Paradigm Shift: Cancers are driven by oncogene mutations... resulting in the trend toward new targeted therapies Effectiveness requires monitoring Resistance develops Therapies are expensive and can have side effects THE CLINICAL UTILITY OF CELL-FREE DNA FROM URINE IMAGING Rough indication of tumor size No molecular information TISSUE BIOPSY Major procedures, not possible in some cases Limitations in access to serial biopsies Tumor heterogeneity; may not obtain the right tissue from the tumor sample CIRCULATING TUMOR CELLS Very low sensitivity Technically challenging, expensive Current monitoring tools are insufficient |
|
|
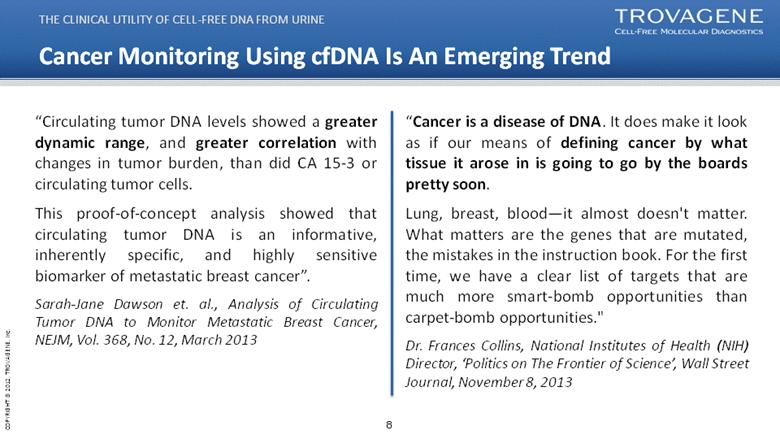
Cancer Monitoring Using cfDNA Is An Emerging Trend THE CLINICAL UTILITY OF CELL-FREE DNA FROM URINE “Circulating tumor DNA levels showed a greater dynamic range, and greater correlation with changes in tumor burden, than did CA 15-3 or circulating tumor cells. This proof-of-concept analysis showed that circulating tumor DNA is an informative, inherently specific, and highly sensitive biomarker of metastatic breast cancer”. Sarah-Jane Dawson et. al., Analysis of Circulating Tumor DNA to Monitor Metastatic Breast Cancer, NEJM, Vol. 368, No. 12, March 2013 “Cancer is a disease of DNA. It does make it look as if our means of defining cancer by what tissue it arose in is going to go by the boards pretty soon. Lung, breast, blood—it almost doesn't matter. What matters are the genes that are mutated, the mistakes in the instruction book. For the first time, we have a clear list of targets that are much more smart-bomb opportunities than carpet-bomb opportunities.” Dr. Frances Collins, National Institutes of Health (NIH) Director, ‘Politics on The Frontier of Science’, Wall Street Journal, November 8, 2013 |
|
|
Cell-free DNA Filters Into The Urine THE CLINICAL UTILITY OF CELL-FREE DNA FROM URINE Large volume can be collected High frequency of collection possible Truly non-invasive Patient can self-sample at home or clinic No medical professional required for specimen No refrigeration required No infection risk Lower cost Cell-free DNA stable in urine Urine sample Tracking-cell free DNA Cells in the body die continuously; cancer cells die at an accelerated rate DNA is released into the bloodstream, which is then broken down into smaller segments and filtered by the kidney. Small, stable DNA fragments collect in urine where Trovagene technology can identify and quantify mutations of interest. |
|
|
A Decade of Scientific Work Validates Our Novel Approach 15 peer reviewed publications covering all nucleic acid types in urine DNA RNA miRNA Methylation Fields of Study Oncology Prenatal Infectious Disease Transplant TROVAGENE PLATFORM See appendix for details |
|
|
Genetic Sequencing Advancements Enable TROV Technology Detecting rare DNA mutation events in urine made commercially feasible by NGS & ddPCR Trovagene IP Next Gen sequencing Digital Droplet PCR TROVAGENE PLATFORM Decline in cost for gene sequencing outpacing Moore’s Law since 2008; reflects transition from Sanger-based to next generation sequencing Source: National Human Genome Research Institute |
|
|
Trovagene Proprietary Technology Leverages NGS/ddPCR NGS ddPCR TROVAGENE PLATFORM + Resulting in Unparalleled Sensitivity (Analytical Detection to 0.03%) Novel Extraction Process Enrichment of DNA from circulation Enrichment of DNA containing tumor mutations ~100-fold enrichment Because highly degraded need to preferentially pre-amplify ~30bp footprint of DNA having mutation (M) Enriched for Circulating DNA Preferentially isolate short DNA Trovagene IP Portfolio & Know How |
|
|
Short Sequences in Urine & Novel Primers Solidify IP Position Determining mutational status of short DNAs limits the DNA sequences available for amplification; therefore enabling IP of surrounding DNA that is difficult to navigate around Use of non-human DNA contiguous with primers used to amplify short regions indicates use of non-naturally occurring DNA to interrogate mutations Shorter DNA footprints leads to increased sensitivity of assays PROPRIETARY ADVANTAGE Interrogating BRAF V600E Mutation DNA sequences available to amplify region are restrictive Single-base Mutation of A→T A G C T A C A G T G A A A T C C T A C A G A G A A A T C T C C T A G C T A C A G T G A A A T C T A G C T A C A G A G A A A T C C T A G C T A C A G T G A A A T 69 ° C C T A G C T A C A G T G A A A T C 71 ° C 20 A T G T C A C T T T A G A G C T A C 68 ° C G A T G T C A C T T T A G A G C T A C 70 ° C (R2) T A G G T G A T T T T G G T C T A G C T A C A G T G A A A T C T C G A T G G A G T G G G T C C A T C C A C T A A A A C C A G A T C G A T G T C A C T T T A G A G C T A C C T C A C C C A G G G A ~ (R2) A A G A T A G SHORTEST SHT FTPT FTPT 35 36.4 13 G T G A T T T T G G T C T C T A C C T C A C C C A G 13 43.1 35 34 32.1 12 T G A T T T T G G T C T C T A C C T C A C C C A 12 40.1 34 35 37.4 14 G T G A T T T T G G T C T A C T A C C T C A C C C 11 35.7 33 34 33.5 13 T G A T T T T G G T C T A G C T A C C T C A C C C A G 14 48.2 35 33 29.0 12 G A T T T T G G T C T A G C T A C C T C A C C C A 13 45.9 34 33 36.9 14 T G A T T T T G G T C T A G G C T A C C T C A C C C 12 42.2 33 32 33.0 13 G A T T T T G G T C T A G A G C T A C C T C A C C C A 14 48.8 34 33 39.2 14 G A T T T T G G T C T A G C A G C T A C C T C A C C C 13 45.5 33 32 36.1 13 A T T T T G G T C T A G C A G C T A C C T C A C C 12 40.4 32 31 33.8 12 T T T T G G T C T A G C G A G C T A C C T C A C C C 14 47.8 33 33 42.1 15 G A T T T T G G T C T A G C T G A G C T A C C T C A C C 13 43.3 32 32 39.4 14 A T T T T G G T C T A G C T G A G C T A C C T C A C 12 38.2 31 31 37.5 13 T T T T G G T C T A G C T A G A G C T A C C T C A C C 14 46.2 32 30 34.9 12 T T T G G T C T A G C T A G A G C T A C C T C A C 13 41.6 31 32 40.1 15 A T T T T G G T C T A G C T A A G A G C T A C C T C A 12 37.9 30 31 38.4 14 T T T T G G T C T A G C T A T A G A G C T A C C T C A C 13 43.2 31 30 36.1 13 T T T G G T C T A G C T A T A G A G C T A C C T C A 14 39.9 30 29 33.3 12 T T G G T C T A G C T A T A G A G C T A C C T C 12 35.8 29 30 39.7 14 T T T G G T C T A G C T A C T T A G A G C T A C C T C A 14 42.0 30 29 37.6 13 LNA1-4 T T G G T C T A G C T A C x x x T T A G A G C T A C C T C 13 38.3 29 28 35.0 12 T G G T C T A G C T A C T T A G A G C T A C C T 12 34.8 28 29 41.3 14 T T G G T C T A G C T A C A T T T A G A G C T A C C T C 14 40.4 29 28 39.2 13 T G G T C T A G C T A C A T T T A G A G C T A C C T vv 13 37.4 28 27 35.0 12 G G T C T A G C T A C A T T T A G A G C T A C C 12 33.6 27 A G C T A C A G T G A A A T C C T A C A G A G A A A T C T C C T A G C T A C A G T G A A A T C T A G C T A C A G A G A A A T C C T A G C T A C A G T G A A A T 69 ° C C T A G C T A C A G T G A A A T C 71 ° C 20 A T G T C A C T T T A G A G C T A C 68 ° C G A T G T C A C T T T A G A G C T A C 70 ° C (R2) T A G G T G A T T T T G G T C T A G C T A C A G T G A A A T C T C G A T G G A G T G G G T C C A T C C A C T A A A A C C A G A T C G A T G T C A C T T T A G A G C T A C C T C A C C C A G G G A ~ (R2) A A G A T A G SHORTEST SHT FTPT FTPT 35 36.4 13 G T G A T T T T G G T C T C T A C C T C A C C C A G 13 43.1 35 34 32.1 12 T G A T T T T G G T C T C T A C C T C A C C C A 12 40.1 34 35 37.4 14 G T G A T T T T G G T C T A C T A C C T C A C C C 11 35.7 33 34 33.5 13 T G A T T T T G G T C T A G C T A C C T C A C C C A G 14 48.2 35 33 29.0 12 G A T T T T G G T C T A G C T A C C T C A C C C A 13 45.9 34 33 36.9 14 T G A T T T T G G T C T A G G C T A C C T C A C C C 12 42.2 33 32 33.0 13 G A T T T T G G T C T A G A G C T A C C T C A C C C A 14 48.8 34 33 39.2 14 G A T T T T G G T C T A G C A G C T A C C T C A C C C 13 45.5 33 32 36.1 13 A T T T T G G T C T A G C A G C T A C C T C A C C 12 40.4 32 31 33.8 12 T T T T G G T C T A G C G A G C T A C C T C A C C C 14 47.8 33 33 42.1 15 G A T T T T G G T C T A G C T G A G C T A C C T C A C C 13 43.3 32 32 39.4 14 A T T T T G G T C T A G C T G A G C T A C C T C A C 12 38.2 31 31 37.5 13 T T T T G G T C T A G C T A G A G C T A C C T C A C C 14 46.2 32 30 34.9 12 T T T G G T C T A G C T A G A G C T A C C T C A C 13 41.6 31 32 40.1 15 A T T T T G G T C T A G C T A A G A G C T A C C T C A 12 37.9 30 31 38.4 14 T T T T G G T C T A G C T A T A G A G C T A C C T C A C 13 43.2 31 30 36.1 13 T T T G G T C T A G C T A T A G A G C T A C C T C A 14 39.9 30 29 33.3 12 T T G G T C T A G C T A T A G A G C T A C C T C 12 35.8 29 30 39.7 14 T T T G G T C T A G C T A C T T A G A G C T A C C T C A 14 42.0 30 29 37.6 13 LNA1-4 T T G G T C T A G C T A C x x x T T A G A G C T A C C T C 13 38.3 29 28 35.0 12 T G G T C T A G C T A C T T A G A G C T A C C T 12 34.8 28 29 41.3 14 T T G G T C T A G C T A C A T T T A G A G C T A C C T C 14 40.4 29 28 39.2 13 T G G T C T A G C T A C A T T T A G A G C T A C C T vv 13 37.4 28 27 35.0 12 G G T C T A G C T A C A T T T A G A G C T A C C 12 33.6 27 |
|
|
Core IP Extends Into Assay Detection & Development Original TrNA Patent Family Term to approx. 2018 US & EP Viral and Pathogen TrNA Families Term to approx. 2026 US, EP, JP, China, Australia, Canada, India 20-50 bp TrNA Family Term to approx. 2029 US & EP 51-110 bp TrNA Family Term to approx. 2034 US provisional app filed Transrenal miRNA Detection Family Term to approx. 2028 US, EP, JP, China, Australia, Canada, India Original Anion Exchange Purification Family Term to approx. 2027 US, EP, Canada Purification with Chaotropic Salt Family Term to approx. 2034 US provisional app filed New: Sub-20 basepair Detection App PROPRIETARY ADVANTAGE |

|
|
Summary of Trovagene Techology Technology Leverages The Advantages of Cell-Free DNA In Urine Greater chance of “seeing” mutations for detection and monitoring Enabling Advantages of Urine: Specimen Volume & Frequency Oncogene mutations have low abundance in cancer patients (bigger sample, bigger dynamic range) Half-life of cell-free DNA in blood plasma is short; stable in urine Proprietary Short Sequences in Urine, Trovagene Primers, Assay Designs, Clinical Data Know-how working with transrenal DNA for years Substantial IP Analytical sensitivity among the highest in the industry Clinical Data from collaborations from leading cancer centers Practical Benefits Logistics Advantages of Urine: Truly non-invasive Integrates with the move toward home care PROPRIETARY ADVANTAGE |
|
|
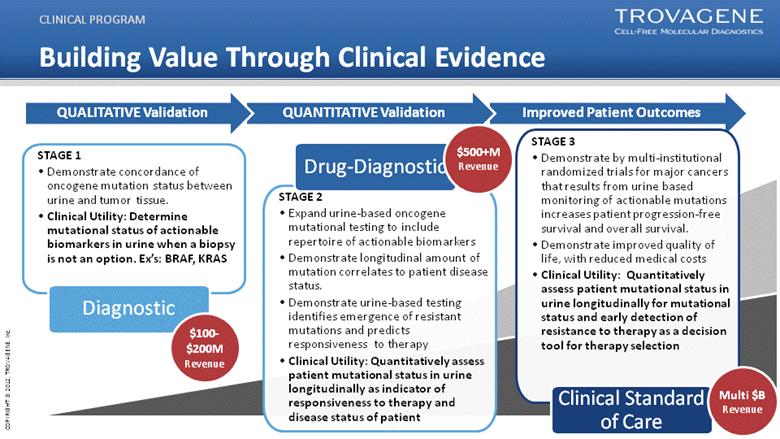
Improved Patient Outcomes Building Value Through Clinical Evidence CLINICAL PROGRAM STAGE 1 Demonstrate concordance of oncogene mutation status between urine and tumor tissue. Clinical Utility: Determine mutational status of actionable biomarkers in urine when a biopsy is not an option. Ex’s: BRAF, KRAS Diagnostic $100-$200M Revenue STAGE 2 Expand urine-based oncogene mutational testing to include repertoire of actionable biomarkers Demonstrate longitudinal amount of mutation correlates to patient disease status. Demonstrate urine-based testing identifies emergence of resistant mutations and predicts responsiveness to therapy Clinical Utility: Quantitatively assess patient mutational status in urine longitudinally as indicator of responsiveness to therapy and disease status of patient QUANTITATIVE Validation QUALITATIVE Validation Drug-Diagnostic STAGE 3 Demonstrate by multi-institutional randomized trials for major cancers that results from urine based monitoring of actionable mutations increases patient progression-free survival and overall survival. Demonstrate improved quality of life, with reduced medical costs Clinical Utility: Quantitatively assess patient mutational status in urine longitudinally for mutational status and early detection of resistance to therapy as a decision tool for therapy selection $500+M Revenue Clinical Standard of Care Multi $B Revenue |
|
|
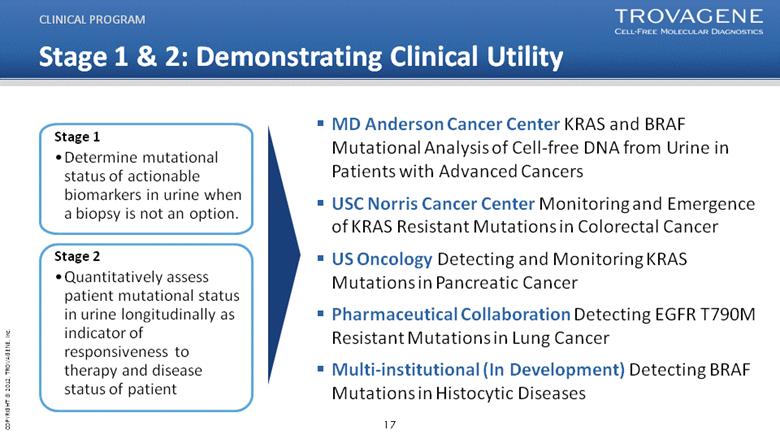
Stage 1 & 2: Demonstrating Clinical Utility MD Anderson Cancer Center KRAS and BRAF Mutational Analysis of Cell-free DNA from Urine in Patients with Advanced Cancers USC Norris Cancer Center Monitoring and Emergence of KRAS Resistant Mutations in Colorectal Cancer US Oncology Detecting and Monitoring KRAS Mutations in Pancreatic Cancer Pharmaceutical Collaboration Detecting EGFR T790M Resistant Mutations in Lung Cancer Multi-institutional (In Development) Detecting BRAF Mutations in Histocytic Diseases CLINICAL PROGRAM Stage 1 Determine mutational status of actionable biomarkers in urine when a biopsy is not an option. Stage 2 Quantitatively assess patient mutational status in urine longitudinally as indicator of responsiveness to therapy and disease status of patient |
|
|
Concordance of Urine-Based Oncogene Mutation Testing vs. Tumor Biopsy Title: KRAS and BRAF Mutational Analysis of Cell-free DNA from Urine in Patients with Advanced Cancers Principal Investigator: Filip Janku MD PhD; Investigational Cancer Therapeutics (Phase I Clinical Trials Program) MD Anderson Cancer Center Objective 1: Measure the degree of concordance between results of DNA mutation analysis from urine samples versus confirmed mutational status of tumor biopsy tissue. Objective 2: Longitudinal assessment over time of mutational status of urinary DNA in the treatment of metastatic cancer patients with correlation to therapeutic response and disease status of the patient. CLINICAL PROGRAM Clinical Study: Detecting & Monitoring Tumor Mutations in cfDNA from Urine in Metastatic Cancer Patients |
|
|
Concordance of BRAF V600E mutations1 CLINICAL PROGRAM 1 Janku et al, AACR-NCI-EROTC International Conference, 2013 BRAF V600E mutations were detected in urine irrespective of cancer type with a multitude of different cancer types including Glioblastoma (brain cancer) BRAF V600E assay demonstrated 95% concordance vs. tissue biopsy (both detected and borderline) Study demonstrates that urine DNA can be used to detect DNA fragments from circulation that harbor tumor mutations (1) Janku et al, AACR-NCI-EROTC International Conference, 2013 |
|
|
Longitudinal Urinary cf-DNA BRAF V600E Mutation Correlates with Therapy Response CLINICAL PROGRAM Patient 5: Melanoma Progressive Disease Vemurafenib only Urinary cfDNA BRAF V600E mutuation (%) 40 35 30 25 20 15 10 5 0 BRAF V600E cfDNA 10/1/2012 11/1/2012 12/1/2012 1/1/2013 2/1/2013 3/1/2013 4/1/2013 5/1/2013 6/1/2013 7/1/2013 |
|
|
Progressing on Chemotherapy Patient 16 Colorectal Cancer Patient 44 Appendiceal Cancer Progressing on chemotherapy Longitudinal Urinary cf-DNA BRAF V600E Mutation Correlates with Therapy Response CLINICAL PROGRAM 10/1/2013 11/1/2013 12/1/2013 1/1/2013 2/1/2013 3/1/2013 4/1/2013 5/1/2013 6/1/2013 7/1/2013 8/1/2013 9/1/2013 7/23/2013 7/30/2013 8/6/2013 8/13/2013 8/20/2013 8/27/2013 9/3/2013 9/10/2013 BRAF V600E cfDNA BRAF V600E cfDNA |
|
|
Completed assays will be transferred to Trovagene’s CLIA laboratory in 2014 2014 Development Program For Cancer Monitoring Applications ASSAY DEVELOPMENT PROGRAM EGFR L858R KRAS KRAS QUANT BRAF Quant EFGR T790M EFGR Ex19Del EFGR L858R c-met amp HER-2 NRAS PIK3CA 1047 KRAS Q61H Melanoma CRC Lung, Breast, CRC Lung |
|
|
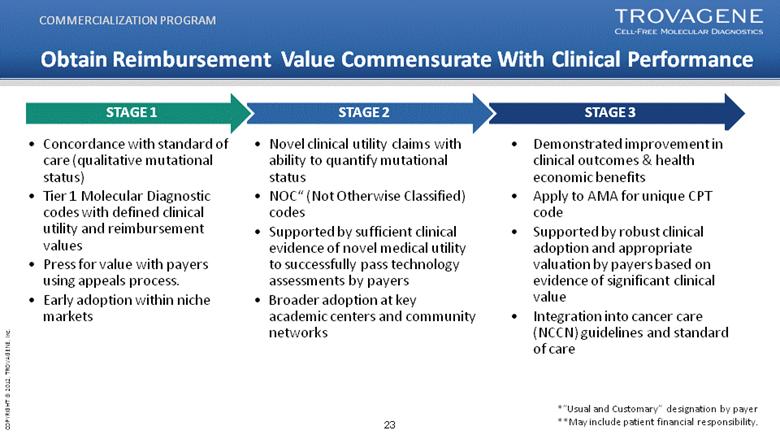
STAGE 3 Obtain Reimbursement Value Commensurate With Clinical Performance Concordance with standard of care (qualitative mutational status) Tier 1 Molecular Diagnostic codes with defined clinical utility and reimbursement values Press for value with payers using appeals process. Early adoption within niche markets Novel clinical utility claims with ability to quantify mutational status NOC“ (Not Otherwise Classified) codes Supported by sufficient clinical evidence of novel medical utility to successfully pass technology assessments by payers Broader adoption at key academic centers and community networks STAGE 2 STAGE 1 Demonstrated improvement in clinical outcomes & health economic benefits Apply to AMA for unique CPT code Supported by robust clinical adoption and appropriate valuation by payers based on evidence of significant clinical value Integration into cancer care (NCCN) guidelines and standard of care COMMERCIALIZATION PROGRAM Appeal *”Usual and Customary” designation by payer **May include patient financial responsibility. |
|
|
Corporate Development Strategies Collaborations with large strategic companies Accelerate our core strategic mission in cancer monitoring Create out-licensing opportunities with potential for incremental revenue streams 2014/14 R&D collaborations include PerkinElmer (NYSE PKI) and Illumina (Nasdaq – ILMN) Pharmaceutical collaborations Integrate TROV’s oncogene monitoring technology in trials for targeted cancer therapies Paid collaboration means immediate revenue generation Very strong value proposition based on logistical benefits and better endpoint measurement 1st major collaboration announced in Q4 13 Out-licensing strategy for non-core IP assets Hem biomarker portfolio New licensees include Novartis and Duke University HPV test out-licensing strategy BUISENESS DEVELOPMENT |
|
|
Collaborations With Leading MDx/Life Science Companies PerkinElmer R&D collaboration TROV to develop a urine-based assay for the liver cancer market - PKI option for commercialization Companies will collaborate on automation of TROV’s urine-based DNA isolation method Financial terms not disclosed; potential for milestone payments to TROV Illumina R&D collaboration Develop sequencing library using urine-based cell free nucleic acids (cfNAs) with focus on cancer Establish NGS as an analytical platform for the analysis of urine-based cfNA Illumina to provide sample sets and sequencing services BUSINESS DEVELOPMENT Both strategic collaborations with industry leaders provide 3rd party validation, will accelerate our core mission in cancer monitoring and will create multiple product opportunities with potential for incremental revenue streams |
|
|
2013 Achievements Validated single oncogene mutation detection assay in CLIA lab Launched BRAF-cf assay Released first prospective data Identified the presence of BRAF, KRAS in multiple cancer types Demonstrated that oncology mutation signal in urine correlates with response to therapy Completed $15 million registered direct offering CORPORATE SUMMARY Extended oncogene mutation detection development program Began second study at MD Anderson cancer center focusing on BRAF and KRAS mutations in 2013 Initiated prospective colorectal cancer study with USC Norris Cancer Center US Oncology Initiated R&D partnerships Illumina Collaborate to apply NGS for the analysis of transrenal sequence signals PerkinElmer Collaborate to develop test for liver cancer risk |
|
|
2014 Goals & Expected Milestones Conduct additional clinical studies with our diagnostic technology at major oncology centers Enter into additional clinical collaborations with pharmaceutical companies Expand and enter into new partnerships with Life Science/MDx technology companies Publish clinical results for studies using our oncogene detection and monitoring technology Expand mutation detection portfolio availability in the CLIA lab Adoption of Trovagene technology in key cancer centers nationwide Develop a health economic model supporting appropriate value and reimbursement levels for Trovagene testing CORPORATE SUMMARY |
|
|
For further information Please contact: Antonius Schuh, CEO aschuh@trovagene.com Stephen Zaniboni, CFO szaniboni@trovagene.com |
