Attached files
| file | filename |
|---|---|
| 8-K - FORM 8-K - Panbela Therapeutics, Inc. | snbp20210615_8k.htm |
Exhibit 99.1

Company Overview June 2021
Cautionary Statements Certain statements in this presentation are forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995 and are provided under the protection of the safe harbor for forward-looking statements provided by that Act. Forward-looking statements are based on current expectations of future events and often can be identified by words such as “anticipate,” “believe,” “continue,” “estimate,” “expect,” “future,” “intend,” “may,” “plan,” “potential,” “target,” or other words of similar meaning or the use of future dates. Examples of forward-looking statements include future determinations of the characteristics of SBP-101 and its effectiveness, removal of the partial clinical hold, publication of results, other trial activities and the timing of the same, and expected financial or operating results. Forward-looking statements are neither historical facts nor assurances of future performance. Instead, they are based only on our beliefs, expectations, and assumptions regarding the future of our business, future plans and strategies, projections, anticipated events and trends, the economy and other future conditions. Because forward-looking statements relate to the future, they are subject to inherent uncertainties, risks and changes in circumstances that are difficult to predict and many of which are outside of our control. Our actual results and financial condition may differ materially and adversely from the forward-looking statements. Therefore, you should not rely on any of these forward-looking statements. Important factors that could cause our actual results and financial condition to differ materially from those indicated in the forward-looking statements include, among others, the following: (i) our ability to obtain additional funding to complete a randomized clinical trial; (ii) progress and success of our Phase 1 clinical trial; (iii) the impact of the current COVID-19 pandemic on our ability to complete monitoring and reporting in our current clinical trial and procure the active ingredient; (iv) our ability to demonstrate the safety and effectiveness of our SBP-101 product candidate (v) our ability to obtain regulatory approvals for our SBP-101 product candidate in the United States, the European Union or other international markets; (vi) the market acceptance and level of future sales of our SBP-101 product candidate; (vii) the cost and delays in product development that may result from changes in regulatory oversight applicable to our SBP-101 product candidate; (viii) the rate of progress in establishing reimbursement arrangements with third-party payors; (ix) the effect of competing technological and market developments; (x) the costs involved in filing and prosecuting patent applications and enforcing or defending patent claims; and (xi) such other factors as discussed in Part I, Item 1A under the caption “Risk Factors” in our most recent Annual Report on Form 10-K, any additional risks presented in our Quarterly Reports on Form 10-Q and our Current Reports on Form 8-K. Any forward-looking statement made by us in this presentation is based on information currently available to us and speaks only as of the date on which it is made. We undertake no obligation to publicly update any forward-looking statement or reasons why actual results would differ from those anticipated in any such forward-looking statement, whether written or oral, whether as a result of new information, future developments or otherwise. This presentation includes information about investigational agents. The efficacy and safety of such investigational agents have not yet been established. Drug development is uncertain and investigative agents may be terminated along the development process. All trademarks, company and product names or logos are the property of their respective owners.
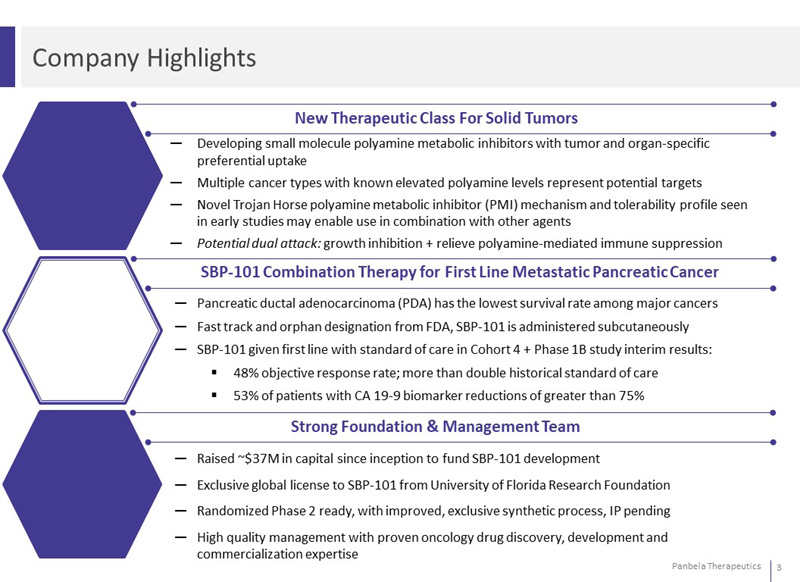
Company Highlights New Therapeutic Class For Solid Tumors Developing small molecule polyamine metabolic inhibitors with tumor and organ-specific preferential uptake Multiple cancer types with known elevated polyamine levels represent potential targets Novel Trojan Horse polyamine metabolic inhibitor (PMI) mechanism and tolerability profile seen in early studies may enable use in combination with other agents Potential dual attack: growth inhibition + relieve polyamine-mediated immune suppression SBP-101 Combination Therapy for First Line Metastatic Pancreatic Cancer Pancreatic ductal adenocarcinoma (PDA) has the lowest survival rate among major cancers Fast track and orphan designation from FDA, SBP-101 is administered subcutaneously SBP-101 given first line with standard of care in Cohort 4 + Phase 1B study interim results: 48% objective response rate; more than double historical standard of care 53% of patients with CA 19-9 biomarker reductions of greater than 75% Strong Foundation & Management Team Raised ~$37M in capital since inception to fund SBP-101 development Exclusive global license to SBP-101 from University of Florida Research Foundation Randomized Phase 2 ready, with improved, exclusive synthetic process, IP pending High quality management with proven oncology drug discovery, development and commercialization expertise
Panbela Leadership Team and Board of Directors Collectively developed 10 FDA-approved therapies generating billions in sales Leadership Team Jennifer K. Simpson, PhD, MSN, CRNP President & CEO Susan Horvath, CPA (inactive), CMA VP of Finance & CFO Thomas X. Neenan, PhD Co-Founder, Chief Scientific Officer Suzanne Gagnon, MD, FACP Chief Medical Officer Board of Directors Michael T. Cullen, MD, MBA, ABIM Jennifer K. Simpson, PhD, MSN, CRNP Art Fratamico, MBA Suzanne Gagnon, MD, FACP Jeff Mathiesen, CPA Paul W. Schaffer, PharmD D. Robert Schemel Proven oncology drug discovery, development and commercialization expertise
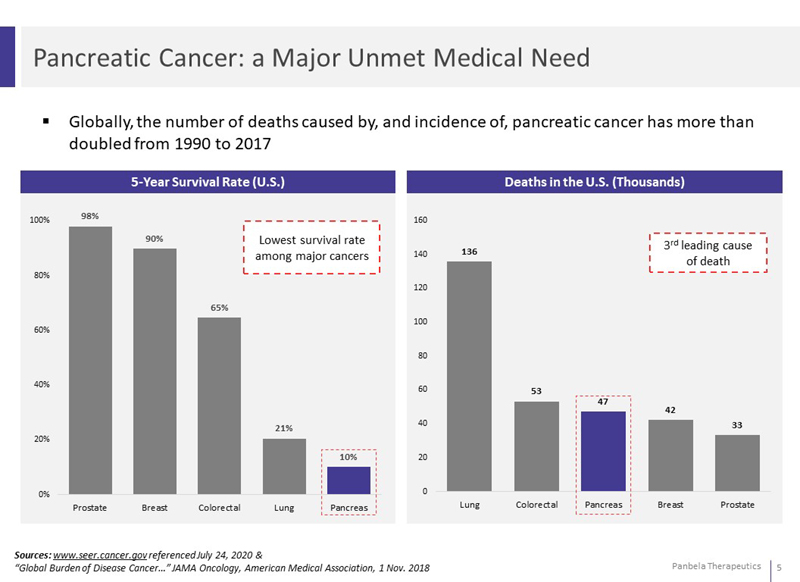
Pancreatic Cancer: a Major Unmet Medical Need Globally, the number of deaths caused by, and incidence of, pancreatic cancer has more than doubled from 1990 to 2017 5-Year Survival Rate (U.S.) Lowest survival rate among major cancers 98% 90% 65% 21% 10% Sources: www.seer.cancer.gov referenced July 24, 2020 & “Global Burden of Disease Cancer…” JAMA Oncology, American Medical Association, 1 Nov. 2018 Prostate Breast Colorectal Lung Pancreas Deaths in the U.S. (Thousands) Lung 135.72 Colorectal 53.2 Pancreas 47.05 Breast 42.17 Prostate 33.33 3rd leading cause of death
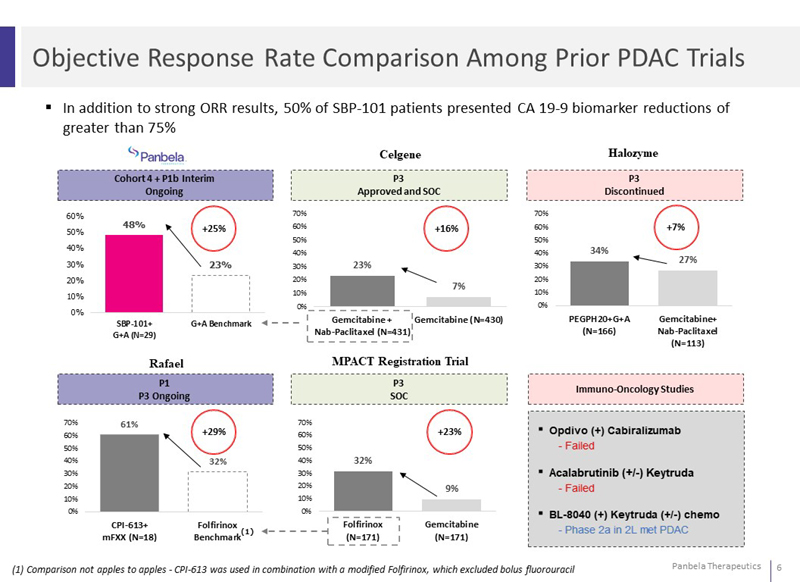
Objective Response Rate Comparison Among Prior PDAC Trials In addition to strong ORR results, 50% of SBP-101 patients presented CA 19-9 biomarker reductions of greater than 75% Cohort 4 + P1b Interim Ongoing P3 Approved and SOC P3 Discontinued Celgene Halozyme 70% 60% 50% 40% 30% 20% 10% 0% 48% +25% 23% 23% +16% 7% 34% +7% 27% "SBP-101+ G+A (N=29)" G+A Benchmark "Gemcitabine + Nab-Paclitaxel (N=431)" Gemcitabine (N=430) "PEGPH20+G+A (N=166)" "Gemcitabine+ Nab-Paclitaxel (N=113)" Rafael MPACT Registration Trial P1 P3 Ongoing P3 SOC Immuno-Oncology Studies 61% +29% 32% 32% +23% 9% (1) Comparison not apples to apples CPI-613 was used in combination with a modified Folfirinox, which excluded bolus fluorouracil "CPI-613+ mFXX (N=18)" Folfirinox Benchmark "Folfirinox (N=171)" Gemcitabine (N=171) Opdivo (+) Cabiralizumab - Failed ▪ Acalabrutinib (+/-) Keytruda Failed BL-8040 (+) Keytruda (+/-) chemo Phase 2a in 2L met PDAC
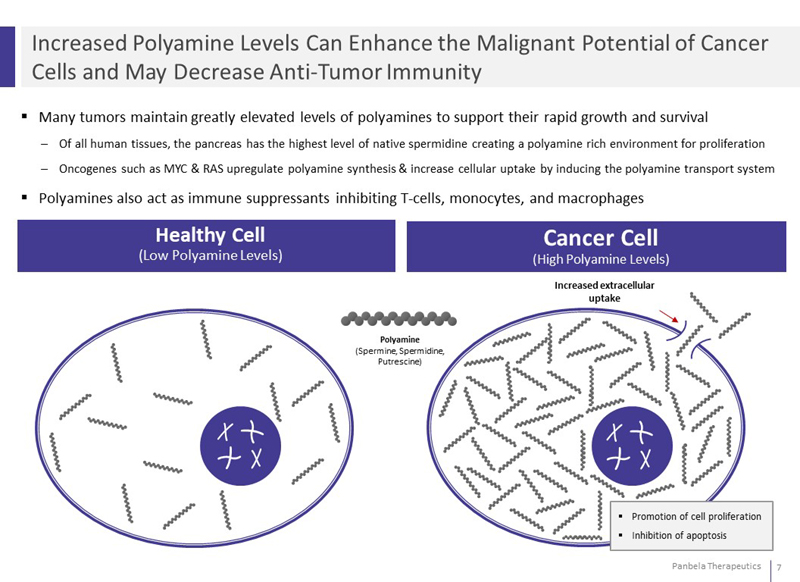
Increased Polyamine Levels Can Enhance the Malignant Potential of Cancer Cells and May Decrease Anti-Tumor Immunity Many tumors maintain greatly elevated levels of polyamines to support their rapid growth and survival Of all human tissues, the pancreas has the highest level of native spermidine creating a polyamine rich environment for proliferation Oncogenes such as MYC & RAS upregulate polyamine synthesis & increase cellular uptake by inducing the polyamine transport system Polyamines also act as immune suppressants inhibiting T-cells, monocytes, and macrophages Healthy Cell (Low Polyamine Levels) Cancer Cell (High Polyamine Levels) Polyamine (Spermine, Spermidine, Putrescine) Increased extracellular uptake Promotion of cell proliferation Inhibition of apoptosis
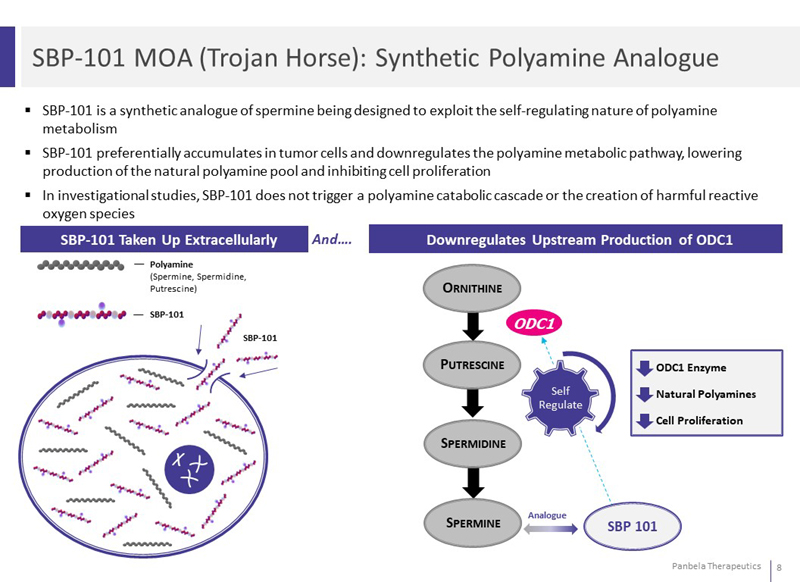
SBP-101 MOA (Trojan Horse): Synthetic Polyamine Analogue SBP-101 is a synthetic analogue of spermine being designed to exploit the self-regulating nature of polyamine metabolism SBP-101 preferentially accumulates in tumor cells and downregulates the polyamine metabolic pathway, lowering production of the natural polyamine pool and inhibiting cell proliferation In investigational studies, SBP-101 does not trigger a polyamine catabolic cascade or the creation of harmful reactive oxygen species SBP-101 Taken Up Extracellularly And Downregulates Upstream Production of ODC1 Polyamine (Spermine, Spermidine, Putrescine) SBP-101 Ornithine Putrescine Spermidine Spermine ODC1 Self Regulate ODC1 Enzyme Natural Polyamines Cell Proliferation Analogue
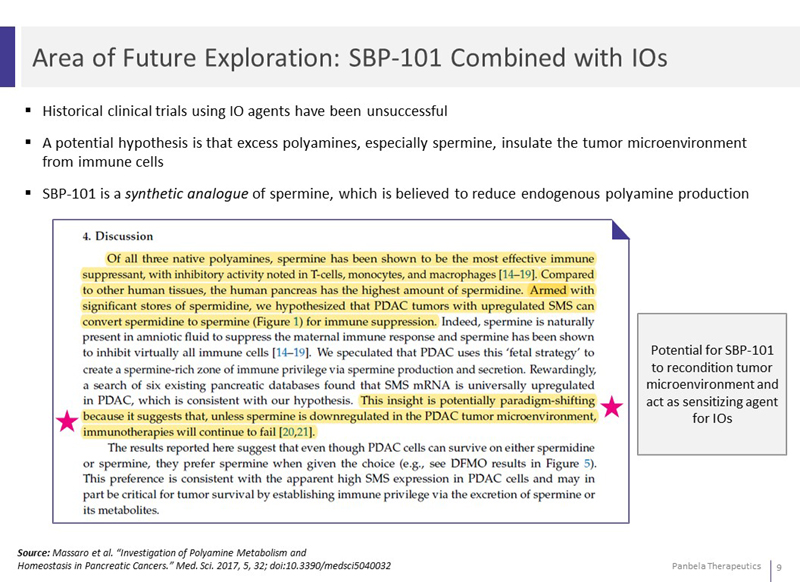
Area of Future Exploration: SBP-101 Combined with IOs Historical clinical trials using IO agents have been unsuccessful A potential hypothesis is that excess polyamines, especially spermine, insulate the tumor microenvironment from immune cells SBP-101 is a synthetic analogue of spermine, which is believed to reduce endogenous polyamine production Potential for SBP-101 to recondition tumor microenvironment and act as sensitizing agent for IOs Source: Massaro et al. “Investigation of Polyamine Metabolism and Homeostasis in Pancreatic Cancers.” Med. Sci. 2017, 5, 32; doi:10.3390/medsci5040032 4. Discussion Of all three native polyamines, spermine has been shown to be the most effective immune suppressant, with inhibitory activity noted in T-cells, monocytes, and macrophages [14-19]. Compared to other human tissues, the human pancreas has the highest amount of spermidine. Armed with significant stores of spermidine, we hypothesized that PDAC tumors with upregulated SMS can convert spermidine to spermine (Figure 1) for immune suppression. Indeed, spermine is naturally present in amniotic fluid to suppress the maternal immune response and spermine has been shown to inhibit virtually all immune cells [14-19]. We speculated that PDAC uses this fetal strategy to create a spermin-rich zone of immune privilege via spermine production and secretion. Rewardingly, a search of six existing pancreatic databases found that sms mrna is universally upregulated in PDAC, which is consistent with our hypothesis. This insight is potentially paradigm-shifting because it suggests that, unless spermine is downregulated in the PDAC tumor microenvironment, immunotherapies will continue to fail [20,21]. The results reported here suggest that even though PDAC cells can survive on either spermidine or spermine, they prefer spermine when given the choice {e.g., see dfmo results in Figure 5). This preference is consistent with the apparent high sms expression in PDAC cells and may in part be critical for tumor survival by establishing immune privilege via the excretion of spermine or its metabolites.
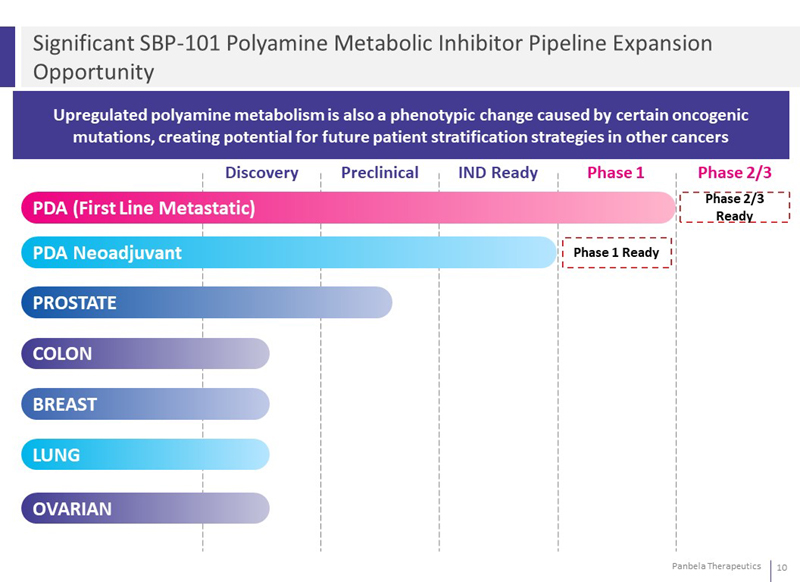
Significant SBP-101 Polyamine Metabolic Inhibitor Pipeline Expansion Opportunity Upregulated polyamine metabolism is also a phenotypic change caused by certain oncogenic mutations, creating potential for future patient stratification strategies in other cancers Discovery Preclinical IND Ready Phase 1 Phase 2/3 PDA (First Line Metastatic) Phase 2/3 Ready PDA Neoadjuvant Phase 1 Ready PROSTATE COLON BREAST LUNG OVARIAN
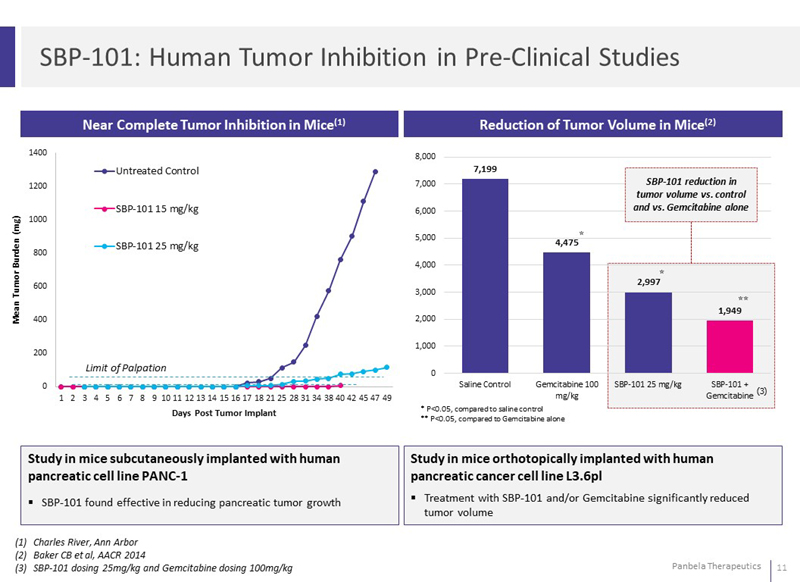
SBP-101: Human Tumor Inhibition in Pre-Clinical Studies Near Complete Tumor Inhibition in Mice(1) Reduction of Tumor Volume in Mice(2) Study in mice subcutaneously implanted with human pancreatic cell line PANC-1 SBP-101 found effective in reducing pancreatic tumor growth Study in mice orthotopically implanted with human pancreatic cancer cell line L3.6pl Treatment with SBP-101 and/or Gemcitabine significantly reduced tumor volume Charles River, Ann Arbor Baker CB et al, AACR 2014 SBP-101 dosing 25mg/kg and Gemcitabine dosing 100mg/kg Days Post Tumor Implant Mean Tumor Burden (mg) 0 200 400 600 800 1000 1200 1400 Untreated Control SBP-101 15 mg/kg SBP-101 25mg/kg SBP-101 reduction in tumor volume vs. control and vs. Gemcitabine alone 7199 4475 2997 1949 Saline Control Gemcitabine 100 mg/kg SBP-101 25mg/kg SBP-101 Gemcitabine * P<0.05, compared to saline control ** P<0.05, compared to Gemcitabine alone
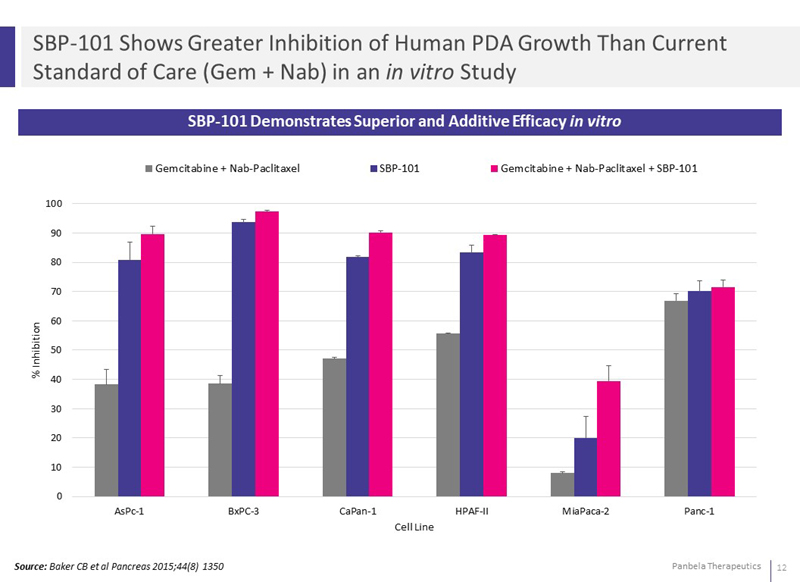
SBP-101 Shows Greater Inhibition of Human PDA Growth Than Current Standard of Care (Gem + Nab) in an in vitro Study SBP-101 Demonstrates Superior and Additive Efficacy in vitro Gemcitabine Nab-Paclitaxel SBP-101 emcitabine + Nab-Paclitaxel + SBP-101 AsPc-1 BxPC-3 CaPan-1 HPAF-II MiaPaca-2 Panc-1 % Inhibition0 10 20 30 40 50 60 70 80 90 100 Cell Line Source: Baker CB et al Pancreas 2015;44(8) 1350
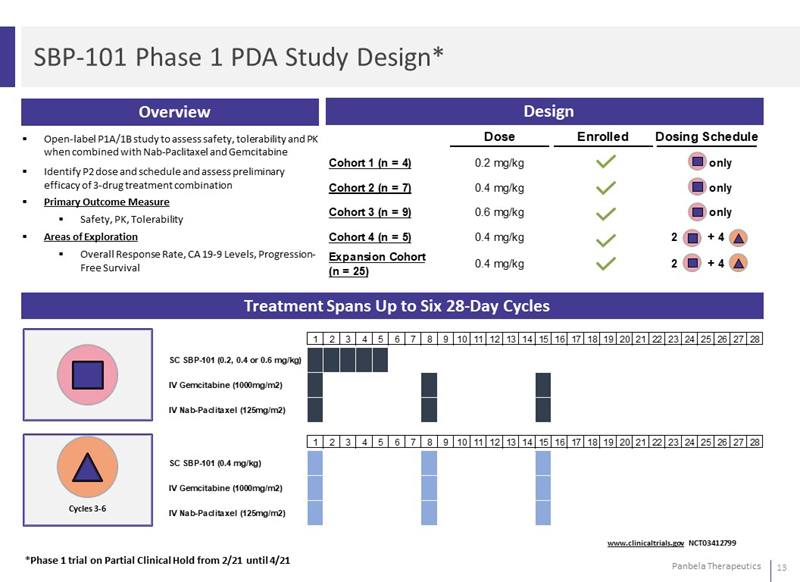
SBP-101 Phase 1 PDA Study Design* Overview Design Open-label P1A/1B study to assess safety, tolerability and PK when combined with Nab-Paclitaxel and Gemcitabine Identify P2 dose and schedule and assess preliminary efficacy of 3-drug treatment combination Primary Outcome Measure Safety, PK, Tolerability Areas of Exploration Overall Response Rate, CA 19-9 Levels, Progression-Free Survival Dose Enrolled Dosing Schedule Cohort 1 (n=4) 0.2 mg/kg Cohort 2 (n=7) 0.4 mg/kg Cohort 3 (n=9) 0.6 mg/kg Cohort 4 (n=5) 0.4 mg/kg Expansion Cohort (n=25) only 2 + 4 Treatment Spans Up to Six 28-Day Cycles *Phase 1 trial on Partial Clinical Hold from 2/21 until 4/21 www.clinicaltrials.gov NCT03412799 SC SBP-101 (0.2, 0.4 or 0.6 mg/kg) IV Gemcitabine (1000mg/m2) IV Nab-Paclitaxel (125mg/m2) SC SBP-101 (0.4 mg/kg) IV Gemcitabine (1000mg/m2) IV Nab-Paclitaxel (125mg/m2)
SBP-101 Phase 1 PDA Study – Hold Lifted Enrollment completed December 2020 Some patients experienced serious vision adverse events Visual changes not seen in monotherapy study Consulted with DSMB Decided not to administer SBP-101 to ongoing patients while safety information analyzed All other trial activities continue Conferred with FDA Partial clinical hold effective – February 2021 Partial clinical hold lifted – April 2021 Future clinical trials will Exclude patients with a history of retinopathy or a risk of retinal detachment Include regular ophthalmologic monitoring
Clinical Importance of CA 19-9 Biomarker Carbohydrate antigen (CA) 19-9 is a type of antigen found in the blood that is often elevated in pancreatic disease Studies have suggested that decreases in CA 19-9 levels are correlated with improved prognosis; ≥75% declines in CA 19-9 levels correlated with the greatest survival benefit in pancreatic cancer Sources: *Diaz Am J Clin Oncol 2019; 42:898-902, Chiorean, E G et al 2016: 654-60 and www.pancan.org CA 19-9 Response A Surrogate to Predict Survival in Patients With Metastatic Pancreatic Adenocarcinoma Celso L Diaz MD* Pelin Cinar MD MS Jimmy Hwang PhD Andrew H Ko MD and Mergaret A Tempero MD Objective: The objective of this study was to determine the features of carbohydrate antigen (CA) 19-9 decline that correlates best with sur-vival benefit in patients with metastatic pancreatic cancer. Methods: This is a retrospective study of 225 patients with metastatic pancreatic cancer receiving first-line therapy. Analysis was performed by the Kaplan-Meier method and Cox-proportional hazards ratios. CA 19-9 decline was grouped into Quartiles within different CA 19-9 baseline groups. Time to nadir and CA 19-9 decline at month -2 (M2) of therapy were evaluated for patients with a baseline level 1000 u/ml Results: No significant trend in survival was observed across baseline CA 19-9 levels. The greatest survival benefit was seen with a 75% decline to nadir. Among those with a 75% decline and baseline 1000u/ml 43 of 57 patients had a 50% decline at M2 of therapy and additional survival benefit was observed with a slower decline to nadir. Small sample sizes limited analysis of other baseline groups. CA 19-9 decline at M2 was not predictive. Conclusions: In patients with a CA 19-9 1000 u/ml, serial CA 19-9 levels may be considered as a surrogate for serial imaging to evaluate treatment response, with a 75% decline indicating the greatest survival benefit. Survival was improved further in the setting of a slower decline to nadir with the highest benefit seen in patients with a nadir occuring at 4 months or longer. From the *School of Medicine, University of California Department of Medicine Division of Hematology/Oncology, University of California and UCSF Helen Diller Family Comprehensive Cancer Center San Francisco CA CA19-9 decrease at 8 weeks as a predictor of overall survival in a randomized phase III trial (MPACT) of weekly nab-paclitaxel plus gemcitabine versus gemcitabine alone in patients with metastatic pancreatic cancer E. G. Chiorean D. D. Von Hoff M. Reni F. P. Arena J. R. Infante V. G. Bathini T. E. Wood P. N. Mainwaring R. T. Muldoon P. R. Clingan V. Kunzmann R. K. Ramanathan J. Tabernero D. Goldstein D. McGovern B. Le & A. Ko Background: A phase I/II study and subsequent phase III study (MPACT) reported significant correlations between CA19-9 decreases and prolonged overall survival (OS) with nab-paclitaxel plus gemcitabine (nab-P+Gem) treatment for metastatic pancreatic cancer (MPC). CA19-9 changes at week 8 and potential associations with efficacy were investigated as part of an exploratory analysis in the MPACT trial. Patients and methods: Untreated patients with MPC (N=861) received nab-p+Gem or Gem alone. CA19-9 was evaluated at baseline and every 8 weeks. Results: Patients with baseline and week-8 CA19-9 measurements were analyzed (nab-P+Gem:252:Gem:202). In an analysis pooling the treatments, patients with any CA19-9 decline (80%) versus those without (20%) had improved OS (median 11.1 versus 8.0 months; P=0.005). In the nab-P+Gem arm, Patients with (n=206) versus without (n=46) any CA19-9 decrease at week 8 had a confirmed overall response rate (ORR) of 40% versus 13% and a median OS of 13.2 versus 8.3 months (P=0.001) respectively. In the Gem-alone arm, patients with (n=159) versus without (n=43) CA19-9 decrease at week 8 had a confirmed ORR 15% versus 5% and a median OS of 9.4 versus 7.1 months (P=0.404) respectively. In the nab-P + Gem and Gem-alone arms by week 8, 16% (40/252) and 6% (13/202) of patients respectively had an unconfirmed radiologic response (median OS 13.7 and 14.7 months respectively) and 79% and 84% of patients respectively had stable disease (SD) (median OS 11.1 and 9 months respectively). Patients with SD and any CA19-9 decrease (158/199 and 133/170) had a median OS of 13.2 and 9.4 months respectively. Conclusion: This analysis demostrated that, in patients with MPC, any CA19-9 decrease at week 8 can be an early marker for chemotherapy efficacy, including in those patients with SD. CA19-9 decrease identified more patients with survival benefit than radiologic response by week 8.
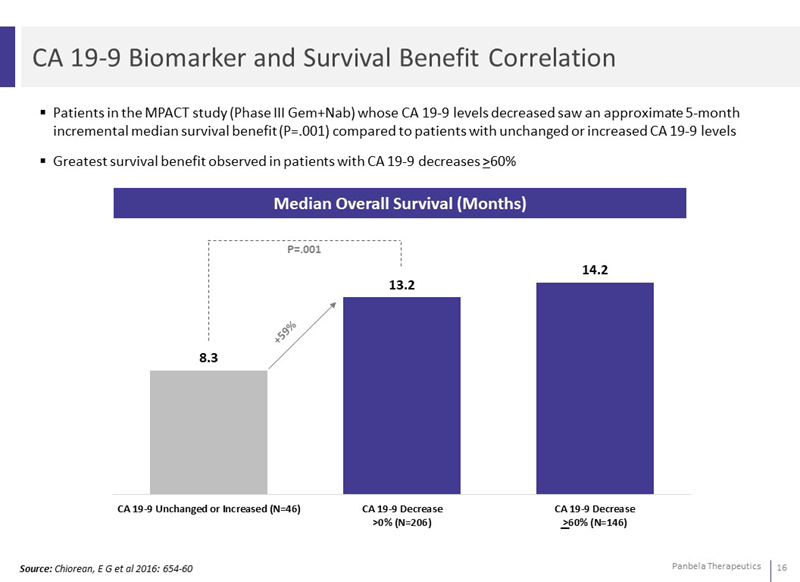
CA 19-9 Biomarker and Survival Benefit Correlation Patients in the MPACT study (Phase III Gem+Nab) whose CA 19-9 levels decreased saw an approximate 5-month incremental median survival benefit (P=.001) compared to patients with unchanged or increased CA 19-9 levels Greatest survival benefit observed in patients with CA 19-9 decreases >60% Median Overall Survival (Months) CA 19-9 Unchanged or Increased (N=46) 8.3 "CA 19-9 Decrease >0% (N=206)" 13.2 "CA 19-9 Decrease >60% (N=146)" 14.2 +59% Source: Chiorean, E G et al 2016: 654-60
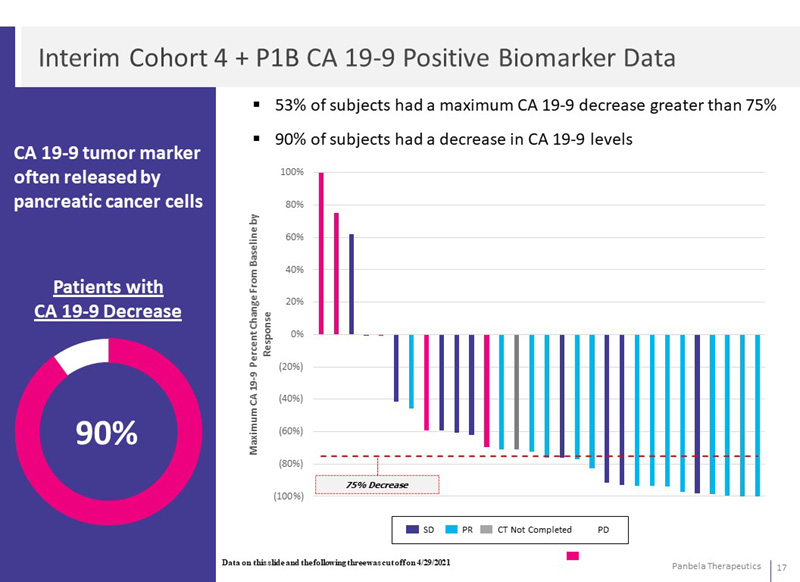
Interim Cohort 4 + P1B CA 19-9 Positive Biomarker Data CA 19-9 tumor marker often released by pancreatic cancer cells Patients with CA 19-9 Decrease 90% 53% of subjects had a maximum CA 19-9 decrease greater than 75% 90% of subjects had a decrease in CA 19-9 levels Maximum CA19-9 Percent Change From Baseline by Response 100% 80% 60% 40% 20% 0% (20%) (40%) (60%) (80%) (100%) 75% Decrease SD PR CT Not Completed PD Data on this slide and the following three was cut off on 4/29/2021
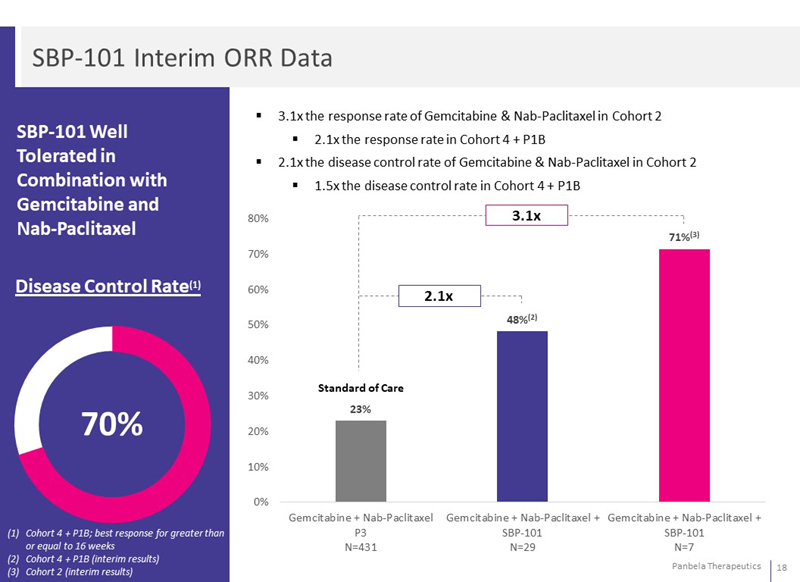
SBP-101 Interim ORR Data SBP-101 Well Tolerated in Combination with Gemcitabine and Nab-Paclitaxel Disease Control Rate(1) 70% Cohort 4 + P1B; best response for greater than or equal to 16 weeks Cohort 4 + P1B (interim results) Cohort 2 (interim results) 3.1x the response rate of Gemcitabine & Nab-Paclitaxel in Cohort 2 2.1x the response rate in Cohort 4 + P1B 2.1x the disease control rate of Gemcitabine & Nab-Paclitaxel in Cohort 2 1.5x the disease control rate in Cohort 4 + P1B 80% 70% 60% 50% 40% 30% 20% 10% 0% 3.1x 2.1x 71%(3) 48%(2) Standard of Care 23% "Gemcitabine + Nab-Paclitaxel P3 N=431" "Gemcitabine + Nab-Paclitaxel + SBP-101 N=29" "Gemcitabine + Nab-Paclitaxel + SBP-101 N=7"
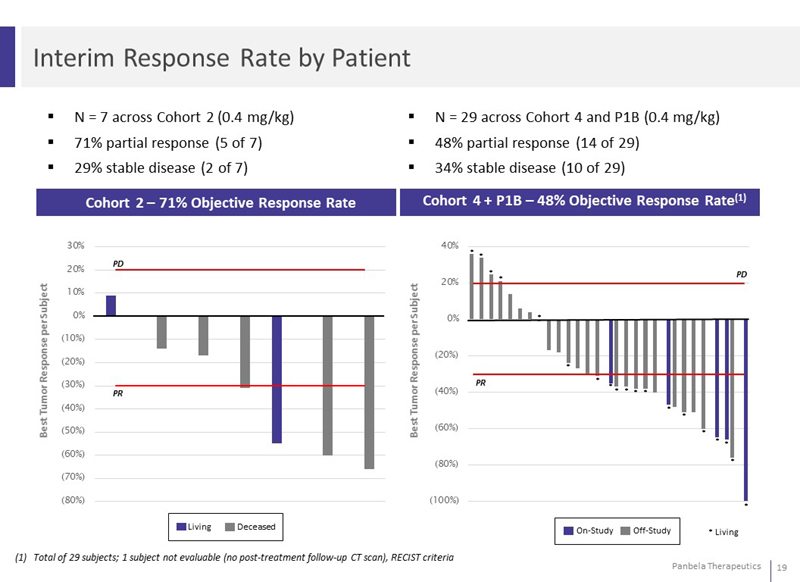
Interim Response Rate by Patient N = 7 across Cohort 2 (0.4 mg/kg) 71% partial response (5 of 7) 29% stable disease (2 of 7) N = 29 across Cohort 4 and P1B (0.4 mg/kg) 48% partial response (14 of 29) 34% stable disease (10 of 29) Cohort 2 – 71% Objective Response Rate Cohort 4 + P1B – 48% Objective Response Rate(1) Best Tumor Response per Subject 30% 20% 10% 0% (10%) (20%) (30%) (40%) (50%) (60%) (70%) (80%) 40% 20% 0% (20%) (40%) (60%) (80%) (100%) Living Deceased On-Study Off-Study *Living Total of 29 subjects; 1 subject not evaluable (no post-treatment follow-up CT scan), RECIST criteria
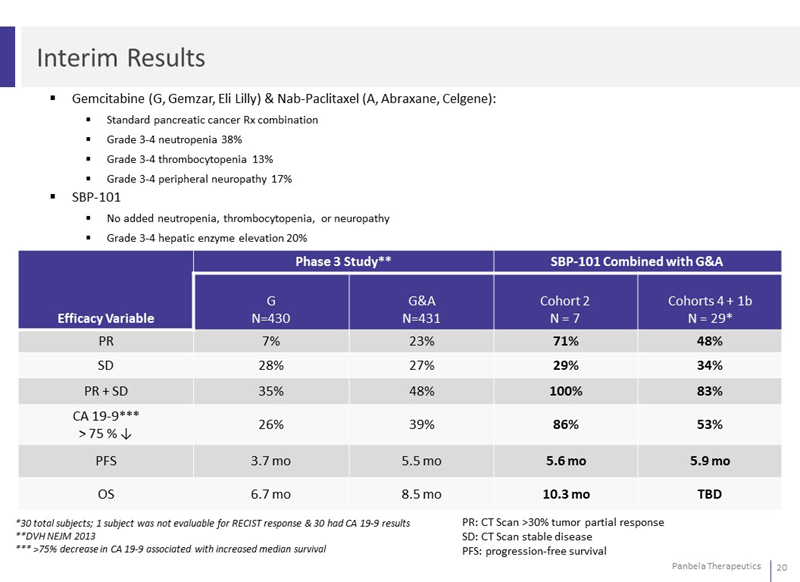
Interim Results Gemcitabine (G, Gemzar, Eli Lilly) & Nab-Paclitaxel (A, Abraxane, Celgene): Standard pancreatic cancer Rx combination Grade 3-4 neutropenia 38% Grade 3-4 thrombocytopenia 13% Grade 3-4 peripheral neuropathy 17% SBP-101 No added neutropenia, thrombocytopenia, or neuropathy Grade 3-4 hepatic enzyme elevation 20% Phase 3 Study** SBP-101 Combined with G&A Efficacy Variable G N=430 G&A N=431 Cohort 2 N = 7 Cohorts 4 + 1b N = 29* PR 7% 23% 71% 48% SD 28% 27% 29% 34% PR + SD 35% 48% 100% 83% CA 19-9*** > 75 % 26% 39% 86% 53% PFS 3.7 mo 5.5 mo 5.6 mo 5.9 mo OS 6.7 mo 8.5 mo 10.3 mo TBD *30 total subjects; 1 subject was not evaluable for RECIST response & 30 had CA 19-9 results **DVH NEJM 2013 *** >75% decrease in CA 19-9 associated with increased median survival PR: CT Scan >30% tumor partial response SD: CT Scan stable disease PFS: progression-free survival
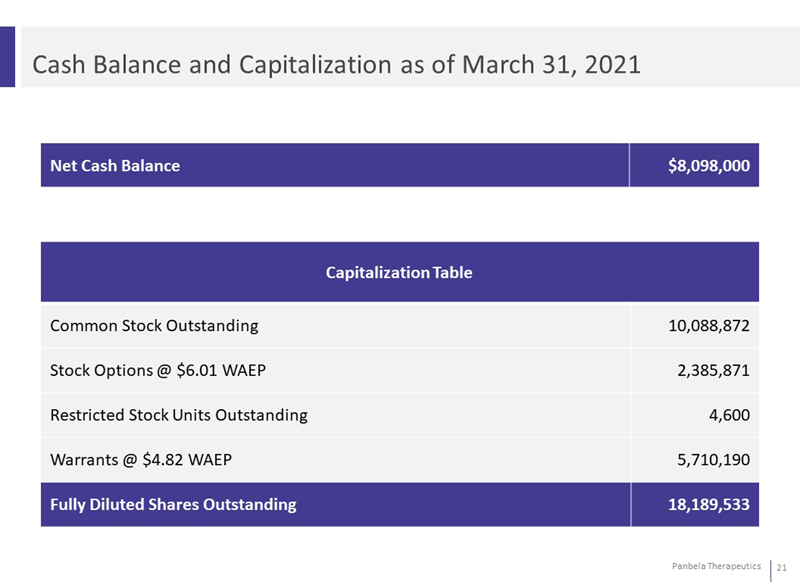
Cash Balance and Capitalization as of March 31, 2021 Net Cash Balance $8,098,000 Capitalization Table Common Stock Outstanding 10,088,872 Stock Options @ $6.01 WAEP 2,385,871 Restricted Stock Units Outstanding 4,600 Warrants @ $4.82 WAEP 5,710,190 Fully Diluted Shares Outstanding 18,189,533
Milestones 2021 Data from phase 1 trial (1H'21) Initiation of randomized phase 2 study (2H ‘21) Pre-Clinical Data (2H’21) Conference presentation (1H'21 or 2H'21)
SBP-101 Summary Unique dual-attack MOA is synergistic with other agents, potentially enhancing anti-tumor response Favorable safety & tolerability profile and subcutaneous administration in clinical studies to date supports potential ease of use Encouraging interim efficacy and tumor marker signals consistent with preferential uptake of SBP-101 in tumor cells Potential to expand SBP-101 into other cancers with known elevated levels of polyamine metabolism (Pre-Clinical Data 2H’21) Interim data from Phase 1a/1b trial presented at ASCO annual meeting Q2 21 Advancing SBP-101 clinical development to create significant shareholder value