Attached files
| file | filename |
|---|---|
| EX-12.1 - EX-12.1 - GENOMIC HEALTH INC | ghdx-20171231ex1213d64fd.htm |
| EX-32.2 - EX-32.2 - GENOMIC HEALTH INC | ghdx-20171231ex322af110a.htm |
| EX-32.1 - EX-32.1 - GENOMIC HEALTH INC | ghdx-20171231ex3214aad71.htm |
| EX-31.2 - EX-31.2 - GENOMIC HEALTH INC | ghdx-20171231ex312713e32.htm |
| EX-31.1 - EX-31.1 - GENOMIC HEALTH INC | ghdx-20171231ex311830d98.htm |
| EX-23.1 - EX-23.1 - GENOMIC HEALTH INC | ghdx-20171231ex231ba5cd8.htm |
| EX-21.1 - EX-21.1 - GENOMIC HEALTH INC | ghdx-20171231ex21174557f.htm |
| EX-10.5.1 - EX-10.5.1 - GENOMIC HEALTH INC | ghdx-20171231ex1051b0d0b.htm |
| EX-10.5 - EX-10.5 - GENOMIC HEALTH INC | ghdx-20171231ex10585ba8b.htm |
taxane
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
Form 10‑K
|
(Mark One) |
|
|
☒ |
ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
|
For the fiscal year ended: December 31, 2017 |
|
|
or |
|
|
☐ |
TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
|
For the transition period from to . |
|
Commission File Number: 000‑51541
GENOMIC HEALTH, INC.
(Exact name of Registrant as specified in its charter)
|
Delaware |
77‑0552594 |
|
301 Penobscot Drive |
94063 |
(650) 556‑9300
(Registrant’s telephone number, including area code)
Securities registered pursuant to Section 12(b) of the Act:
|
Title of Each Class |
Name of Each Exchange on Which Registered: |
|
Common Stock, par value $0.0001 per share |
The Nasdaq Stock Market LLC |
Securities registered pursuant to Section 12(g) of the Act and Title of Class: None
Indicate by check mark if the registrant is a well‑known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ☐ No ☒
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes ☐ No ☒
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes ☒ No ☐
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Website, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S‑T during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes ☒ No ☐
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S‑K is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10‑K or any amendment to this Form 10‑K. ☐
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non‑accelerated filer, or a smaller reporting company. See the definitions of “large accelerated filer,” “accelerated filer” and “smaller reporting company” in Rule 12b‑2 of the Exchange Act. (Check one):
|
Large accelerated filer ☐
Non‑accelerated filer ☐ |
Accelerated filer ☒ Smaller reporting company ☐ Emerging growth company ☐ |
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b‑2 of the Act). Yes ☐ No ☒
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
As of June 30, 2017, the aggregate market value of voting and non‑voting common stock held by non‑affiliates of the registrant was approximately $646.5 million, based on the closing price of the common stock as reported on The Nasdaq Global Select Market for that date.
There were 35,324,394 shares of the registrant’s Common Stock outstanding on February 28, 2018.
DOCUMENTS INCORPORATED BY REFERENCE
Items 10 (as to directors and Section 16(a) Beneficial Ownership Reporting Compliance), 11, 12, 13 and 14 of Part III incorporate by reference information from the registrant’s proxy statement to be filed with the Securities and Exchange Commission in connection with the solicitation of proxies for the registrant’s 2018 Annual Meeting of Stockholders to be held on June 6, 2018.
2
This report contains forward‑looking statements within the meaning of the Private Securities Litigation Reform Act of 1995. When used in this report, the words “expects,” “anticipates,” “intends,” “estimates,” “plans,” “believes,” and similar expressions are intended to identify forward‑looking statements. These are statements that relate to future periods and include statements about our expectation that, for the foreseeable future, a significant amount of our revenues will be derived from our Oncotype DX invasive breast cancer test; the factors that may impact our financial results; our ability to achieve sustained profitability; our business strategy and our ability to achieve our strategic goals; our expectations regarding product revenues and the sources of those revenues; the amount of future revenues that we may derive from Medicare patients or categories of patients; our belief that we may become more dependent on Medicare reimbursement in the future; our plans to pursue reimbursement on a case‑by‑case basis; our ability, and expectations as to the amount of time it will take, to achieve reimbursement from third‑party payors and government insurance programs for new indications of tests, new tests or in new markets; the potential impact of changes in reimbursement levels for our tests; our expectations regarding our international expansion and opportunities; the potential effects of foreign currency exchange rate fluctuations and our efforts to hedge such effects; our beliefs with respect to the benefits and attributes of our tests or collaborations or tests we may seek to develop or collaborate on in the future; the factors we believe drive demand for our tests and our ability to sustain or increase such demand; our success in increasing patient and physician demand as a result of our direct sales approach and our salesforce’s capacity to sell our tests; plans for, and the timeframe for the development or commercial launch of future tests, test enhancements or new technologies; the factors that we believe will drive reimbursement and the establishment of coverage policies; the capacity of our clinical reference laboratory to process tests and our expectations regarding capacity; our dependence on collaborative relationships to develop tests and the success of those relationships; whether any additional tests will result from our collaborations or license agreements; the applicability of clinical results to actual outcomes; our estimates and assumptions with respect to disease incidence and potential market opportunities; the occurrence, timing, outcome or success of clinical trials or studies; our expectations regarding timing of the announcement or publication of research results; the benefits of our technology platform; the economic benefits of our tests to the healthcare system; the ability of our tests to impact treatment decisions; our beliefs regarding our competitive position; our expectations regarding new and future technologies, including non‑invasive test technology, and their potential benefits; our belief that multi‑gene analysis provides superior analytical information; our beliefs regarding the benefits of genomic analysis in various patient populations; our expectations regarding our research and development, general and administrative and sales and marketing expenses and our anticipated uses of our funds; our expectations regarding capital expenditures; our ability to comply with the requirements of being a public company; our expectations regarding billing and collections; our ability to attract and retain experienced personnel; the adequacy of our product liability insurance; our anticipated cash needs and our estimates regarding our capital requirements; our expected future sources of cash; our compliance with federal, state and foreign regulatory requirements; the potential impact resulting from the regulation of our tests by the U.S. Food and Drug Administration, or FDA, and other similar non‑U.S. regulators; our belief that our tests are properly regulated under the Clinical Laboratory Improvement Amendments of 1988, or CLIA; the impact of new or changing policies, regulation or legislation, or of judicial decisions, on our business and reimbursement for our tests; the impact of seasonal fluctuations on our business; our belief that we have taken reasonable steps to protect our intellectual property; the impact of changing interest rates; our beliefs regarding unrecognized tax benefits or our valuation allowance; the impact of accounting pronouncements and our critical accounting policies, judgments, estimates, models and assumptions on our financial results; the impact of the economy on our business, patients and payors; and anticipated trends and challenges in our business and the markets in which we operate.
Forward‑looking statements are subject to risks and uncertainties that could cause actual results to differ materially from those expected. These risks and uncertainties include, but are not limited to, those risks discussed in Item 1A of this report, as well as our ability to develop and commercialize new products and product enhancements; the risk of unanticipated delays in research and development efforts; the risk that we may not obtain or maintain reimbursement for our existing tests or any future tests we may develop; the risk that reimbursement pricing or coverage may change; the risks and uncertainties associated with the regulation of our tests by the FDA or regulatory agencies outside of the U.S.; the success of our new technology; the results of clinical studies; the applicability of clinical results to actual outcomes; the impact of new legislation or regulations, or of judicial decisions, on our business; our ability to compete against third parties; the success of our collaborations; our ability to obtain capital when needed; the economic environment; and our history of operating losses. These forward‑looking statements speak only as of the date hereof. We expressly disclaim any obligation or undertaking to update any forward‑looking statements contained herein to reflect any change in our expectations with regard thereto or any change in events, conditions or circumstances on which any such statement is based.
3
This report contains statistical data attributable to both the Kantar Health, Inc.’s CancerMPact epidemiology database (December 2015) and the American Cancer Society, Global Cancer Facts and Figures, 2016, or data that we derived from these sources. These sources generally indicate that they believe their information is reliable but do not guarantee the accuracy and completeness of their information. Although we believe that the sources are reliable, we have not independently verified their data.
In this report, all references to “Genomic Health,” “we,” “us,” or “our” mean Genomic Health, Inc.
Genomic Health, the Genomic Health logo, Oncotype, Oncotype DX, Recurrence Score, DCIS Score, Genomic Prostate Score, Oncotype SEQ, Oncotype IQ, Oncotype DX AR-V7 Nucleus Detect, Oncotype SEQ Liquid Select, and Genomic Intelligence Platform are trademarks or registered trademarks of Genomic Health, Inc. We also refer to trademarks of other corporations and organizations in this report.
Company Overview
Genomic Health is a global provider of genomic-based diagnostic tests that address both the overtreatment and optimal treatment of early stage cancer, one of the greatest issues in healthcare today. With our Oncotype DX IQ Genomic Intelligence Platform we are applying our world-class scientific and commercial expertise and infrastructure to lead the translation of clinical and genomic big data into clinically actionable results for treatment planning throughout the cancer patient's journey, from [screening and surveillance, through] diagnosis, treatment selection and monitoring. Our Oncotype IQ Genomic Intelligence Platform is currently comprised of our flagship line of Oncotype DX gene expression tests, as well as our expanded platform of additional liquid- and tissue-based tests, including our recently launched Oncotype DX AR-V7 Nucleus Detect test.
Our testing services are made available through our clinical reference laboratory located in Redwood City, California, which is accredited under the Clinical Laboratory Improvement Amendments of 1988, or CLIA, and certified by the College of American Pathologists, or CAP.
In 2017, approximately 1.7 million people in the United States and 15.3 million people worldwide were diagnosed with cancer. Common types of cancer include breast, prostate, lung and colon. Cancer treatment decisions may include whether to perform surgery and whether to administer chemotherapy, radiation therapy or utilize other targeted therapies.
To treat cancer effectively, physicians diagnose and gauge the stage of a patient’s disease to determine the best course of therapy. For many cancer patients, surgery, radiation therapy, and chemotherapy are commonly used as treatment options, with varying degrees of benefit and side effects that may not always justify the cost of the therapy or the physical and mental burden patients endure.
Historically, physicians have used tumor pathology grade and stage when predicting whether a cancer will recur, as the key determinant in treatment decisions. Because tumor pathology grade and staging are heavily dependent on visual assessment and human interpretation, physicians and patients may make treatment decisions that rely on subjective and qualitative information and may not account for the molecular nature of the patient’s cancer. As a result, many patients may be misclassified as high risk for disease recurrence when in fact they are low risk or, conversely, low risk for disease recurrence when they are high risk, resulting in over‑treatment for some and under‑treatment for others.
We offer our tissue-based invasive breast, DCIS, prostate and colon Oncotype DX tests as clinical laboratory services, where we analyze the expression levels of genes in tumor tissue samples and provide physicians with a gene expression profile expressed as a single quantitative score. We refer to this score as a Recurrence Score for our invasive breast cancer and colon cancer tests, a DCIS Score for our ductal carcinoma in situ, or DCIS test, and a Genomic Prostate Score, or GPS, for our prostate cancer test. These tests utilize a quantitative genomic analysis known as reverse transcription polymerase chain reaction, or RT‑PCR, in standard tumor pathology specimens to provide tumor‑specific information, or the “oncotype” of a tumor. Our Oncotype DX cancer tests further analyze the expression levels of multiple genes across multiple biological pathways to predict cancer aggressiveness. We have also introduced non-invasive liquid biopsy tests that we plan to continue delivering through our Oncotype IQ Genomic Intelligence Platform.
The Oncotype DX invasive breast cancer test has extensive clinical evidence validating its ability to predict the likelihood of breast cancer recurrence and the likelihood of chemotherapy benefit. We also provide an Oncotype DX test for patients with DCIS, a pre‑invasive form of breast cancer. Our Oncotype DX colon cancer test is the first multigene expression test developed to assess the risk of recurrence in patients with stage II disease, and is also available for use in patients with
4
stage III disease treated with oxaliplatin‑containing adjuvant therapy. Finally, our Oncotype DX prostate cancer test has demonstrated that the multi‑gene Oncotype DX Genomic Prostate Score assessed in prostate needle biopsy tumor tissue, is a predictor of adverse pathology, that is, the likelihood of aggressive disease upon prostatectomy, for patients with early‑ or intermediate-stage prostate cancer.
We have expanded in both the U.S. and international markets and continue to publish new studies supporting the clinical validity, clinical utility and positive health economics of our Oncotype DX tests. As of January 2018, we have published more than 120 peer-reviewed papers and completed over 100 clinical studies involving more than 65,000 breast, colon and prostate cancer patients worldwide. In the United States, our Oncotype DX breast cancer test is the only test incorporated in published American Society of Clinical Oncologists, or ASCO, and National Comprehensive Cancer Network, or NCCN, breast cancer treatment guidelines for patients with node negative, or N-, breast cancer that is estrogen receptor positive, or ER+, and/or progesterone receptor positive, or PR+. The test is also recognized in international guidelines issued by the St. Gallen International Breast Cancer Expert Panel and European Society for Medical Oncology, or ESMO. In addition, in guidance that is currently in the course of a routine triennial review, the National Institute for Health and Care Excellence (NICE) in England recommended Oncotype DX as the only multi‑gene breast cancer test for use in clinical practice to guide chemotherapy treatment decisions for certain patients with early‑stage, N-, hormone receptor‑positive, human epidermal growth factor receptor 2, or HER2, negative, invasive breast cancer. Also, each of the Gynecologic Oncology Working Group (AGO) in Germany and the Japan Breast Cancer Society updated their guidelines to recommend Oncotype DX as the only breast cancer gene expression test to predict chemotherapy benefit in early-stage, hormone receptor-positive invasive breast cancer. Finally, the Oncotype DX breast cancer test is included in the Eighth Edition of the American Joint Committee on Cancer, or AJCC, Cancer Staging Manual, a guidebook that serves to ensure consistent cancer diagnoses and data collection across the range of U.S. cancer care providers and facilities. The AJCC Cancer Staging Manual identifies Oncotype DX as the only multi-gene assay that provides Level I evidence to determine formal staging of breast cancer patients. Specifically, the Oncotype DX Breast Recurrence Score, hormonal status (ER, PR) and HER2 status have been added to nodal status, tumor size and tumor grade as standard AJCC criteria for staging breast cancer.
As of December 31, 2017, more than 19,000 physicians in over 90 countries had ordered more than 850,000 Oncotype DX tests. We have a direct commercial presence with employees and consultants in the United States and certain other countries, and our tests are also available outside of the United States through a network of distributors. See our consolidated financial statements and the related notes in Item 8 of this Annual Report for segment-related information.
Scientific Background
Use of Genomics to Understand Cancer
Genetics and genomics are playing an increasingly critical role throughout all stages of cancer care. While genomics and genetics may sound similar and are related, each focuses on different information. Genetics involve the study of individual genes and how genes pass on hereditary traits from one generation to the next and how new traits may develop from genetic mutations or changes. Examples of traits include physical traits, predisposition to certain conditions or drug metabolism. Certain genes, which normally help control healthy cell growth, can pass on predispositions to certain types of diseases, including cancer.
Cancer can result from inheriting mutated genes or from developing mutations in otherwise normal cells. Such mutations can be the cause of cancer. For most solid tumors, there is great heterogeneity between patients in the tumor mutations that are observed, regardless of the cause. The ability to detect mutations and their functional results and to understand whether the mutation contributes to disease can be crucial to better diagnosis and ultimately more rational and effective treatment.
Genomics on the other hand, is the study of complex sets of genes, such as the entire set of genes of an organism, their germline and somatic genetics, their expression and their function in a particular organism or disease, such as cancer. Genomics can be used to understand diseases at the molecular level. Diseases can occur when mutated or defective genes inappropriately activate or block molecular pathways that are important for normal biological function.
The key to utilizing genomics in cancer is identifying specific sets of genes and gene interactions that are important in diagnosing different subsets of cancers. Using our RT‑PCR platform, we have performed studies linking the likelihood of recurrence or response to therapy to the pattern of gene expression in tumors. We used these results to develop our Oncotype DX tests that quantify gene expression within an individual’s tumor, allowing physicians to better understand what treatments are most likely to work for an individual patient or how likely a cancer is to recur.
5
Our Oncotype DX tests utilize existing technologies, such as RT‑PCR, in concert with information technologies to optimize and integrate them into new processes. We are incorporating new technologies in our research and development laboratory, and expect to continue to extend the capabilities of various technologies into proprietary platforms to create new products.
Extract RNA from FPE‑Tumor Biopsies
Our Oncotype DX product development process includes quantifying the relative amounts of ribonucleic acid, or RNA, in fixed paraffin-embedded, or FPE, tissue. We have developed proprietary technology, intellectual property and know‑how for this process and continue to develop new and improved technologies for optimized and automated methods for extraction and analysis of RNA from FPE tissue.
Amplify and Detect Diminished Amounts of RNA Consistently
We currently use RT‑PCR as the basis for our tissue-based Oncotype DX breast, colon and prostate cancer tests. This technology uses reverse transcription, or RT, coupled to a polymerase chain reaction, or PCR, along with fluorescent detection methods to quantify the relative amount of RNA in a biological specimen. We believe our technology platform has the following advantages:
|
· |
Sensitivity. We have developed protocols for extracting and quantifying RNA utilizing RT‑PCR. Our method for amplifying small fragmented RNA is designed to allow us to conduct future studies with hundreds to thousands of genes from 10 micron sections of FPE tissue for our breast and colon cancer tests and significantly smaller tissue samples from needle biopsies for our prostate cancer test. |
|
· |
Specificity. Our RT‑PCR platform is highly specific because it works only when certain test reagents, called DNA primers and probes, independently match each target RNA sequence to be measured. In addition, we have designed and implemented proprietary software to select optimal probe and primer sequences in an automated, high‑throughput process. The ability to utilize these sequences allows us to design highly specific assays for closely related sequences. |
|
· |
Precision and Reproducibility. The reagents, materials, instruments and controls in our processes are used by trained personnel following validated standard operating procedures. Validation studies have shown that these standard operating procedures precisely quantify tested RNA with minimal variability in the assay system across days, instruments and operators. This enables our clinical laboratory to produce consistently precise and accurate gene expression results. Our quality control methods for our reagents and processes, along with our software for automation, sample tracking, data quality control and statistical analysis, add to the reproducibility and precision of our tests. |
|
· |
Dynamic Range. Because our RT‑PCR platform can amplify small amounts of RNA in proportion to the amount present in each sample, we are able to measure RNA levels across as much as a hundred thousand-fold range of differing RNA expression. Having a broad range of high resolution testing capability increases the quality of our correlations with clinical outcomes and therefore the predictive power of our tests. |
Analyze Thousands of Biomarkers from Small Amounts of Biological Material
The methods and know‑how we have developed allow us to expand RT‑PCR technology to a scale that enables screening of hundreds of genes at a time while using minimal amounts of tissue. With continued investment in instrumentation, automation, and informatics we believe that our technology will be capable of continued increases in throughput.
We have developed technologies for assaying low liquid volumes and amplifying trace amounts of RNA in order to develop products that can evaluate minimal amounts of tissue, including breast core biopsies and prostate needle biopsies.
Our proprietary methods also include the extraction of DNA from FPE tissue and blood and subsequent complete and targeted genome analyses by next-generation sequencing, or NGS. We have explored the combination and superimposition of certain whole transcriptome derived RNA information (standardized expression; univariate biomarker direction of association) on genomic information to reveal the genomic landscapes of cancers.
6
Technology
Next Generation Technologies
When the presence of tumor-derived DNA in blood or urine is high and persists or increases over time, the cancer is likely growing and a new course of treatment may be appropriate. We plan on monitoring this tumor-derived DNA through a variety of technologies to expand our focus beyond early‑stage treatment decision support toward patients with later‑stage disease to help guide therapeutic choices, monitor progression and response to therapeutics, and monitor disease recurrence. We may pursue additional research and development opportunities and leverage our existing and future collaborations using other analytes such as circulating tumor cells, or CTCs, RNA, and proteins. Additionally, we may also use a number of other technologies across our various development programs and to implement our products. While early‑stage cancer continues to represent a significant opportunity with near‑term revenue potential, we believe we also have an opportunity to expand our business further along the patient’s cancer journey, both through our research and development process and strategic collaborations.
Advanced Information Technology
We have developed computer programs to automate our RT‑PCR assay processes. We have also developed and optimized laboratory information management systems to track our gene‑specific reagents, instruments, assay processes and the data generated. Similarly, we have automated data analysis, storage and process quality control. We use statistical methods to optimize and monitor assay performance and to analyze data from our development studies. We are investigating methods to further automate our workflow.
We are also working with a number of different technologies, such as digital PCR and detection and capture methods for CTCs and circulating tumor DNA, or ctDNA, to expand our capabilities, and continue to develop methods to enable genomic testing using a variety of biological materials such as blood and urine.
Oncotype DX Tests
Our tissue-based Oncotype DX tests utilize our RT‑PCR approach to improve cancer treatment decisions. Our diagnostic approach correlates gene expression to clinical outcomes and provides an individualized analysis of each patient’s tumor. We have built an infrastructure that allows us to move from research into development through to processing actual patient samples in our clinical reference laboratory. We have optimized this technology for quantitative gene expression on FPE tissue by developing methods and processes for screening hundreds of genes at a time using minimal amounts of tissue.
We believe that our multi‑gene analysis, as opposed to single‑gene analysis, provides a more powerful approach to distinguish cancer as being more or less likely to recur or progress. This information ultimately allows the physician and patient to choose a course of treatment that is individualized for each patient.
We currently offer Oncotype DX tests as clinical laboratory services, utilizing existing technologies such as RT‑PCR and information technologies and optimize and integrate them into new processes. We expect to continue to extend the capabilities of the various components of our process to develop effective products, including providing these products through different technology platforms. Our technologies allow us to analyze tumor tissue samples in our clinical reference laboratory and provide physicians with genomic information specific to the patient’s tumor. We analyze tissues that are handled, processed and stored under routine clinical pathology laboratory practices.
We believe our tests provide information that has the following benefits:
|
· |
Improved Quality of Treatment Decisions. We believe our approach to genomic‑based cancer analysis improves the quality of cancer treatment decisions by providing an individualized analysis of each patient’s tumor that is correlated to clinical outcome, rather than solely using subjective, anatomic and qualitative factors to determine treatments. Oncotype DX has been consistently shown, in more than 30 breast cancer, colon cancer and prostate cancer clinical studies, to classify many patients into recurrence risk categories different than classifications based primarily on tumor pathology grade and stage, and to generally change treatment decisions in more than 30% of patients. As a result, we believe our tests enable patients and physicians to make more informed decisions about the risks and benefits of various treatments, and consequently design an individualized treatment plan. |
7
|
· |
Improved Economics of Cancer Care. We believe that improving the quality of treatment decisions can result in significant economic benefits. For example, in early stage invasive breast cancer, our data shows that many patients are misclassified as high or low risk using traditional pathological and other measures. As a result, many low risk patients misclassified as high risk receive toxic and expensive chemotherapy or radiation treatment regimens, the cost of which may exceed $20,000, as compared to the significantly lower cost of an Oncotype DX test. On the other hand, some high risk breast cancer patients misclassified as low risk are not provided chemotherapy or radiation treatment, possibly necessitating future treatment costing up to $50,000 or more if the cancer recurs. |
Oncotype DX Breast Cancer Tests
Oncotype DX for Early-Stage, Invasive Breast Cancer
Our Oncotype DX invasive breast cancer test is designed to help identify those patients with higher risk disease who are most likely to benefit from chemotherapy and to identify those patients with lower risk disease who may receive minimal clinical benefit from chemotherapy.
In 2017, approximately 249,000 people in the United States and 1.9 million people worldwide were diagnosed with breast cancer, including both invasive and the pre‑invasive form, DCIS. Breast cancer tumors are classified as stage 0, I, II, III or IV. Stage 0, which includes DCIS, generally refers to a pre‑invasive tumor with reduced risk of recurrence. DCIS is typically not treated with chemotherapy but may be treated with lumpectomy or mastectomy, followed by radiation therapy and hormonal therapy. Stage 0, I and II are generally referred to as early stage breast cancer, and stage III and IV are generally referred to as late stage breast cancer.
Following diagnosis, a physician determines the stage of the breast cancer by examining the pathology of the tumor, the size of the tumor, nodal status, referred to as N+, where the tumor has spread to the lymph nodes, and N−, where the tumor has not spread to the lymph nodes, and the extent to which the cancer has spread to other parts of the body.
Prior to the inclusion of our Oncotype DX invasive breast cancer test in clinical guidelines, standard treatment guidelines weighed the stage of the cancer and additional factors to predict cancer recurrence and determine treatment protocol such as estrogen receptor status, referred to as ER+, where estrogen receptors are present, and ER−, where estrogen receptors are not present, the abundance of HER2, genes or protein in the tumor, the age of the patient, and the histological type and grading of the tumor as reported by the pathologist.
Because these diagnostic factors have limited capability to predict future recurrence and treatment benefit, and some are subjective, a large percentage of breast cancer patients received aggressive treatment while others were undertreated. Most early stage breast cancer patients have N−, ER+ tumors. These patients have been demonstrated to respond well to hormonal therapy, such as tamoxifen or an aromatase inhibitor. Identifying which of these patients to treat with radiation therapy or chemotherapy was a difficult decision.
Development of Oncotype DX Breast Cancer Test and Scientific Studies
To develop our Oncotype DX breast cancer test, we evaluated 250 genes in three independent clinical studies which identified a 21‑gene panel whose composite gene expression profile can be represented by a Breast Recurrence Score. Our clinical validation study with the NSABP B‑14 population, published by The New England Journal of Medicine in December 2004, demonstrated that the Breast Recurrence Score correlated with an individual’s likelihood of distant recurrence within 10 years of invasive breast cancer diagnosis. The NSABP B-14 study also demonstrated that the incremental survival benefit of chemotherapy in N−, ER+ patients also treated with tamoxifen is only 4%. Moreover, our study with the NSABP B‑20 population, published in the Journal of Oncology in May 2006, demonstrated that the Breast Recurrence Score also correlates with the likelihood of chemotherapy benefit for invasive breast cancer patients.
We expanded the utility of our Oncotype DX breast cancer test to patients diagnosed with N+ breast cancer that may not benefit from chemotherapy or may have other health issues that increase the risk of chemotherapy treatment. Results from studies of our Oncotype DX breast cancer test in N+ patients utilizing tumor samples from chemotherapy treated patients (anthracycline plus Cytoxan or anthracycline plus Taxotere), completed in collaboration with the Eastern Cooperative Oncology Group, or ECOG, and Aventis, Inc., were published in the Journal of Clinical Oncology in 2008. The results of this study suggest that the Breast Recurrence Score result of our test provides accurate recurrence risk information for patients with
8
ER+ breast cancer, regardless of whether they are N+ or N−. In December 2007, we presented results from a second study conducted in conjunction with SWOG, that reinforced the conclusion that chemotherapy does not appear to benefit patients with either 1‑3 or 4 or more positive nodes for disease‑free survival over 10 years, if their tumors had a low Breast Recurrence Score result. The results were published in The Lancet Oncology in December 2009.
We conducted studies of our Oncotype DX breast cancer test with clinical samples from postmenopausal women with invasive breast cancer who were treated with aromatase inhibitors. Aromatase inhibitors and tamoxifen are both used as standard treatment for early stage ER+ breast cancer patients. In March 2010, the Journal of Clinical Oncology published results from a European study using our test to analyze tumor samples from over 1,200 patients in the ATAC (Arimedix, Tamoxifen, Alone or in Combination) trial, which established the wide use of aromatase inhibitors for adjuvant treatment of postmenopausal women with hormone receptor‑positive breast cancer. The study demonstrated that, along with other standard measures such as tumor size, our Oncotype DX breast cancer test contributes independently to provide a more complete picture of prognosis for N− and N+ patients treated with aromatase inhibitors.
In 2015, the results of two large independent prospective studies were announced. In September 2015, initial results from the TAILORx trial demonstrated that a group of trial participants with a Breast Recurrence Score of 10 or less who received hormonal therapy alone without chemotherapy had less than 1% chance of recurrence at five years. In December 2015, we announced results from the Surveillance, Epidemiology and End Results (SEER) program of the National Cancer Institute, a large population-based observational study based on the SEER registry of more than 40,000 node-negative and 4,500 node-positive patients, demonstrating breast cancer specific mortality at five years was less than 0.5% in node-negative disease and 1% in node positive disease (up to three positive nodes) where the patient’s Breast Recurrence Score result was less than 18.
Clinical Decision Studies and Health Economic Benefits of Oncotype DX Breast Cancer Test
We have conducted numerous clinical decision studies intended to support the adoption and reimbursement of our Oncotype DX invasive breast cancer test, both in the United States and in numerous countries outside of the United States. Among these studies is a meta-analysis of seven studies with a total of 912 patients that demonstrated a consistent and large impact of the Recurrence Score on invasive breast cancer adjuvant treatment decisions. In these studies, physicians who use the Oncotype DX invasive breast cancer test in clinical practice changed their treatment decisions in over a third of patients, leading to an overall reduction in chemotherapy use of approximately 28% with the use of the Breast Recurrence Score. The Breast Recurrence Score also led to the addition of chemotherapy to hormonal treatment in approximately 4% of patients who, prior to obtaining a Breast Recurrence Score, were considered low risk but were subsequently identified by their Recurrence Score as having high risk disease. The results of this meta-analysis indicate that the Breast Recurrence Score provides key information for treatment decision making that cannot be ascertained from traditional measures.
In addition to clinical decision studies, we sponsor third party studies conducted by researchers affiliated with academic institutions to examine the health economic implications of our Oncotype DX breast cancer test. One such study, which was conducted in the United States and published in The American Journal of Managed Care in May 2005, demonstrated that our test provided a more accurate classification of risk than the NCCN guidelines in place at that time as measured by 10-year distant recurrence free survival. Based on these results, a model was designed to forecast quality adjusted survival and expected costs, or the net present value of all costs of treatment until death, if our Oncotype DX breast cancer test was used in patients classified as low risk or high risk by NCCN guidelines. The model, when applied to a hypothetical population of 100 patients with the demographic and disease characteristics of the patients entered in the NSABP B-14 Study, demonstrated an increase to quality adjusted survival in this population of 8.6 years and a reduction in projected aggregate costs of approximately $200,000. Furthermore, the model showed that as the expected costs and anticipated toxicity of chemotherapy regimens increase, the use of the Breast Recurrence Score test result to identify which patients would benefit from chemotherapy should lead to larger reductions in projected overall costs. According to this model, if all early stage invasive breast cancer patients and their physicians used our test and acted on the information provided by the Breast Recurrence Score test result, there would be significant economic benefit to the healthcare system.
These studies reinforce the impact of the Oncotype DX invasive breast cancer test on changing treatment decisions for invasive breast cancer patients and demonstrate its cost effectiveness across multiple healthcare systems. We plan to conduct or support additional clinical decision studies and health economic studies of our breast cancer test with clinical researchers domestically and abroad as we expand distribution of our test.
9
Oncotype DX for Ductal Carcinoma in Situ (DCIS) Stage 0, Pre-Invasive Breast Cancer
In December 2011, we further expanded the utility of our Oncotype DX tests to include DCIS patients. The DCIS test provides an individualized prediction of the 10‑year risk of local recurrence (DCIS or invasive carcinoma), represented by a DCIS Score result, to help guide treatment decision‑making in women with DCIS treated by local excision, with or without tamoxifen. In the United States alone, one out of every five new breast cancer patients each year is diagnosed with DCIS. After breast‑conserving surgery, local recurrences of DCIS or a new invasive breast cancer occur in 20‑25% of patients at 10 years, on average, with surgery alone. The addition of radiation therapy and its attendant costs has been shown in clinical trials to reduce local recurrence risk, but has not been shown to prolong survival.
Development of Oncotype DX DCIS Test and Scientific Studies
Development of our Oncotype DX DCIS test was based on published results for the Oncotype DX invasive breast cancer test that showed similarity in the expression profiles of the invasive Breast Recurrence Score genes between DCIS and invasive breast cancer when both are present within the same patient tumor. The DCIS Score algorithm was developed based on published data obtained from the Kaiser Permanente and NSABP B‑14 studies in which the proliferation gene group was found to predict distant recurrence regardless of whether adjuvant tamoxifen therapy was given.
In 2011, we presented positive results from the Eastern Cooperative Oncology Group, or ECOG, E5194 DCIS clinical validation study at the San Antonio Breast Cancer Symposium, or SABCS. The study demonstrated that a pre‑specified Oncotype DX DCIS Score can predict the risk of local recurrence, defined as either the development of a new invasive breast cancer or the recurrence of DCIS in the same breast. The study further demonstrated that 75% of patients have a low DCIS Score and may be able to forego radiation therapy. Conversely, the study demonstrated that patients with a high DCIS Score had a 27% likelihood of local recurrence, of which approximately half were likely to develop a new invasive breast cancer. The DCIS Score also demonstrated consistent association with local recurrence across subgroups regardless of lesion size, grade, surgical margins, or menopausal status. This information can assist physicians and patients in deciding on the appropriate course of treatment based on a more complete understanding of the recurrence risk involved. In May 2013, this clinical validation study was published online in the Journal of the National Cancer Institute.
In 2014, we announced positive top line results of an additional clinical validation study conducted in collaboration with the Ontario DCIS Study Group to confirm and extend the observations of the first DCIS clinical validation study. Representing the largest genomic study in DCIS to date, the results confirmed and extended the conclusions of the previously published validation study. Additionally, for the first time, the Oncotype DX DCIS Score was shown to predict the risk of local recurrence in a group of patients treated with radiation therapy in clinical practice. In December 2014, we presented the study results at the SABCS.
Oncotype DX Colon Cancer Test
In 2017, approximately 98,000 people in the United States and one million people worldwide were diagnosed with colon cancer. Colon cancer tumors are classified as stage 0, I, II, III or IV. Stage 0 generally refers to a pre‑invasive tumor with reduced risk of recurrence that is typically not treated with chemotherapy but may be treated with surgery.
Following diagnosis, a physician determines the stage of the colon cancer by examining the following the pathology of the tumor, the size of the tumor, nodal status, and the extent to which the cancer has spread to other parts of the body.
Standard treatment guidelines weigh the stage of the cancer and additional factors to predict cancer recurrence and determine treatment protocol including the age of the patient, the histological type and grading of the tumor as reported by the pathologist, the level of mismatch repair, also known as microsatellite instability, and T‑stage, an index of tumor penetration through the bowel.
In 2017, stage II and stage III colon cancer affected approximately 28,000 and 29,000 people, respectively, in the United States, and the current treatment paradigm is unclear. The decision to treat patients with chemotherapy following surgery is based on an assessment of how likely their disease is to recur. However, accurately identifying those patients with high recurrence risk is a critical issue for physicians because the available markers to determine likelihood of disease recurrence are limited, resulting in both over‑treatment and under‑treatment of patients following surgery. Research indicates that the survival benefit of chemotherapy treatment is only 5% in stage II disease and 10% in stage III disease, however all chemotherapy‑treated colon cancer patients are at risk of significant drug‑related toxicity. While there are existing clinical markers associated
10
generally with higher risk in colon cancer patients, there was no clinically validated genomic test available that predicted the likelihood of recurrence for individual patients prior to the availability of our test.
Development of Oncotype DX Colon Cancer Test and Scientific Studies
In developing our colon cancer test, we used the same rigorous clinical development strategy and standardized quantitative technology designed for our Oncotype DX invasive breast cancer test. We developed our gene panel by identifying 761 cancer‑related genes through review of existing research literature and computer analysis of genomic databases. The NSABP conducted three development studies and the Cleveland Clinic Foundation conducted one development study, which we funded, analyzing the 761 candidate genes in over 1,800 patients with stage II colon cancer. Detailed analysis of gene expression and colon cancer recurrence was performed to identify specific genes with the potential to predict the likelihood of cancer recurrence and response to chemotherapy.
We selected a final set of 12 genes which were then independently evaluated in a validation study of over 1,400 stage II colon cancer patients. Gene expression was quantified by RT‑PCR from manually micro-dissected FPE primary colon cancer tissue, and recurrence‑free interval, disease‑free survival and overall survival were analyzed.
In 2009, we presented positive results from this clinical validation study. In 2010, we presented additional results from a study demonstrating that the Oncotype DX colon cancer test result and number of nodes examined are independent predictors of recurrence in stage II colon cancer and both should be considered when assessing individual recurrence risk in this patient population. In June 2011, a second large study confirming that the Oncotype DX colon cancer test independently predicts individualized recurrence risk for stage II colon cancer was presented.
We believe these studies and publications will help to support adoption of and further reimbursement for our Oncotype DX colon cancer test.
Clinical Decision Studies and Health Economic Benefits of Oncotype DX Colon Cancer Test
In January 2012, we presented positive results of the first clinical decision-making study of the Oncotype DX colon cancer test that show that a colon Recurrence Score result has a significant impact on treatment recommendations for stage II colon cancer patients. The data demonstrated that knowledge of a patient’s Recurrence Score changes medical oncologists’ treatment recommendations in 29% of cases, with two‑thirds of the changes being decreases in treatment intensity, further confirming the test’s clinical utility as an independent predictor of recurrence in stage II colon cancer.
As with our breast cancer test, we sponsor third‑party studies conducted by researchers affiliated with academic institutions to examine the health economic implications of our Oncotype DX colon cancer test. The results of one such study, announced in January 2013, demonstrated after receiving the colon Recurrence Score for their stage II colon cancer patients, physician recommendations for adjuvant chemotherapy in patients with low risk of recurrence decreased by 22%, resulting in direct medical care cost savings of $4,200 per patient.
In November 2013, positive results from the Partnership for Health Analytic Research clinical utility analysis of the Oncotype DX colon cancer test were published, demonstrating that use of our test changed treatment recommendations in 29% of stage II colon cancer patients.
These studies reinforce the impact of the Oncotype DX colon cancer test on changing treatment decisions for stage II and stage III colon cancer patients and demonstrate its cost effectiveness.
Oncotype DX Prostate Cancer Test
The tissue-based Oncotype DX prostate cancer test analyzes 17 genes across four biological pathways from tumor tissue removed during biopsy to provide an individual Genomic Prostate Score, that, in combination with other clinical factors, further clarifies a man's risk prior to treatment intervention. The test enables confident treatment decisions and an opportunity for low-and intermediate-risk patients to avoid prostatectomy or radiation - and their side effects - while identifying men who need immediate invasive treatment.
In 2017, approximately 228,000 men in the United States and 1.2 million men worldwide were diagnosed with prostate cancer. The vast majority of these patients receive aggressive treatment, including surgery and radiation therapy, and more than
11
half of these patients suffer incontinence and/or impotence after surgery. Less than 10% of patients choose active surveillance even though, for most prostate cancer patients, their disease will not cause clinical symptoms or death.
Development of Oncotype DX Prostate Cancer Test and Scientific Studies
In 2011, we presented positive full results from our prostate cancer gene identification study. The study, which applied the same RT‑PCR technology used in our Oncotype DX invasive breast and colon cancer tests, identified 295 genes strongly associated with clinical recurrence of prostate cancer following radical prostatectomy. In June 2012, we presented results of our first development study in prostate tissue obtained from needle biopsies. The study, an analysis of biopsy samples from men with conventionally defined low/intermediate risk prostate cancer, showed that genes and biological pathways associated with clinically‑aggressive prostate cancer in radical prostatectomy specimens can be reliably measured by quantitative RT‑ PCR from fixed prostate needle biopsies.
In 2012, we announced positive top line results from a clinical validation study of our tissue biopsy‑based prostate cancer test. As a result of this clinical validation study meeting its primary end point, we launched our Oncotype DX prostate cancer test in May 2013, and made the test available worldwide. The test provides a GPS that predicts disease aggressiveness in men with low risk disease. This test may be used to improve treatment decisions for prostate cancer patients, in conjunction with the Gleason score, or tumor grading. In May 2014, the positive results from our two development studies, as well as our clinical validation study of diagnostic biopsies from 395 men who were candidates for active surveillance were published, demonstrating that the use of the GPS can potentially increase the percentage of men who could confidently choose active surveillance from 20% to 30%.
We use our proprietary RT‑PCR process for analyzing very small amounts of prostate tissue obtained by needle biopsy to determine, whether a patient has high grade disease or disease that has extended beyond the prostate—versus low grade disease or disease confined to the prostate. Our test is intended to address the well‑known limitations of biopsy sampling, which leads to overtreatment based on the potential of a patient’s tumor being upgraded or upstaged following radical prostatectomy. Our test allows more patients to appropriately select active surveillance, avoiding radical surgery and its lifelong complications.
In August 2014, we announced positive top line results of a second Oncotype DX prostate cancer clinical validation study, demonstrating the ability of our test’s GPS to predict multiple clinical endpoints related to disease aggressiveness among low/intermediate risk patients, as a predictor of biochemical recurrence. The study also confirmed the earlier validation study presented in 2013 and published in May 2014. The results from this clinical validation study were presented at ESMO in September 2014, and at the Society of Urologic Oncology meeting in December 2014.
In November 2016, in collaboration with Kaiser Permanente, we demonstrated that the Oncotype DX prostate cancer test is a strong predictor of the development of metastasis and prostate cancer death in patients with early-stage prostate cancer, which met the primary study endpoint. With these results, the Oncotype DX prostate cancer test became the first genomic test validated in all major short- and long-term end points: adverse pathology, biochemical recurrence, metastasis and prostate cancer-specific death.
Clinical Decision Studies and Health Economic Benefits of Oncotype DX Prostate Cancer Test
In December 2014, we announced results of the first Oncotype DX prostate cancer test decision impact study, which showed that the use of the test significantly changed urologists’ treatment recommendations across patient risk categories, leading to an overall decrease in treatment intensity and a substantial increase in the number of men for whom active surveillance would be recommended. Additionally, use of the test increased physician confidence in treatment planning. We also announced results from two studies of the Oncotype DX prostate cancer test demonstrating its value in low- and intermediate-risk prostate cancer to enable physicians and patients to avoid over- and under-treatment of the disease.
In April 2015, Urology Practice published the positive results of our prostate cancer test’s decision impact study. This prospective study involving 158 newly diagnosed prostate cancer patients showed that incorporation of our test’s GPS changed modality and/or intensity of treatment recommendations in 26% of patients across multiple urology practice settings. Additionally, 85% of urologists were more confident in their treatment recommendation following review of the patient’s GPS.
In July 2015, a second utility study focused on the Oncotype DX prostate cancer test was published in Urology Practice. This study analyzed the medical charts from 211 men diagnosed with prostate cancer across 10 different sites and compared physician recommendations and the actual treatment received between patients who received the Oncotype DX
12
prostate cancer test and those who did not. The observed net increase in physicians recommending active surveillance was consistent with the previously published prospective clinical study in Urology Practice. In addition, when actual treatment received was determined, patients who received an Oncotype DX GPS had an absolute increase of 24% and a relative increase of 56% in use of active surveillance when compared to patients in the same practices with similar traditional risk factors but without an Oncotype DX GPS.
In May 2015, the MolDx program of Palmetto, GBA, or Palmetto, released a draft local coverage determination, or LCD, supporting reimbursement for the Oncotype DX prostate cancer test for men with very low and low risk disease, as defined by NCCN guidelines. In August 2015, Palmetto issued its final LCD for our Oncotype DX prostate cancer test, approving nationwide coverage of our prostate cancer test for qualified Medicare patients throughout the United States. Palmetto initiated reimbursement for our Oncotype DX prostate cancer test for patients with low- and very-low-risk disease effective October 2015 and for patients with favorable intermediate-risk disease effective October 2017.
We expect to continue to invest substantial resources related to continued clinical studies and the global adoption of and reimbursement for our prostate cancer test.
Oncotype DX AR-V7 Nucleus Detect Test
In June 2016, we entered into a collaboration agreement with Epic Sciences, Inc., or Epic Sciences, under which we have been granted exclusive distribution rights to commercialize the Oncotype DX AR-V7 Nucleus Detect test in the United States.
The Oncotype DX AR-V7 Nucleus Detect test is performed by Epic Sciences in its centralized laboratory in San Diego, California, which is accredited under CLIA and certified by CAP. This blood-based test detects the V7 variant of the androgen receptor, or AR, protein in the nucleus of CTCs, and provides information to help guide treatment selection in patients with metastatic castration-resistant prostate cancer, or mCRPC.
Development of Oncotype DX AR-V7 Nucleus Detect Test and Scientific Studies
In January 2017, investigators from Memorial Sloan Kettering Cancer Center and Epic Sciences published findings in European Urology, that only nuclear localization of AR-V7 protein in CTCs from mCRPC patient blood samples is predictive of therapeutic benefit. Previous work by the same team, reported in JAMA Oncology, demonstrated that nuclear localized AR-V7 protein in CTCs was predictive of a 76% reduction of risk of death for mCRPC patients who received taxane chemotherapy versus Androgen Receptor Signaling Inhibitors. We began making the Oncotype DX AR-V7 Nucleus Detect test available through a clinical utility program in July 2017, and commercially available in February 2018.
We believe that this collaboration is complementary to our product development efforts for our other Oncotype tests and allows us to leverage our commercial channel in a way that we believe may generate growth across our business in the United States. We may also pursue additional collaboration opportunities that are intended to complement our expanding product portfolio.
Commercial Collaborations
In September 2017, we entered into an exclusive license and development agreement with Biocartis N.V., or Biocartis, a molecular diagnostics company based in Belgium, to develop and commercialize an in vitro diagnostic, or IVD, version of the Oncotype DX invasive breast cancer test on Biocartis' Idylla platform that can be performed locally by laboratory partners and in hospitals around the world. The Idylla platform offers a unique solution in the localization of complex molecular diagnostics. Using Biocartis’ proprietary Idylla platform, we intend to enable local pathology labs to generate Oncotype DX Breast Recurrence Score results. Under the terms of the license and development agreement, we have an exclusive, worldwide, royalty-bearing, license to develop and commercialize an IVD version of our Oncotype DX invasive breast cancer test on Biocartis’ Idylla platform, and an option to expand the collaboration to include additional tests in oncology and urology. We have primary responsibility for developing, validating and registering our IVD tests to be performed on the Idylla platform, and are also responsible for manufacturing and commercialization activities with respect to such tests.
In November 2017, we entered into an exclusive license agreement with Cleveland Diagnostics, Inc., or Cleveland Diagnostics, a biotechnology company based in Cleveland, Ohio, whereby we were granted exclusive global rights to develop and commercialize early- and late-stage cancer diagnostic tests based on Cleveland Diagnostics’ proprietary IsoPSA reagent
13
and solvent interaction analysis technology platform. We intend to develop and commercialize our first test based on the IsoPSA technology as an IVD blood-based test that can be integrated into the workflow of any urology laboratory practice to distinguish cancer-related PSA isoforms from benign isoforms to detect prostate cancer more precisely than standard PSA testing alone.
Product Development
We internally developed our tissue-based tests generally using the following multi‑phased clinical development program that we are also using to develop future products for breast, prostate and other cancers:
|
· |
Research phase. We conduct studies that are designed to associate genes, pathways or biology with important clinical challenges or endpoints to discover biomarkers that will ultimately prove to have clinical utility in oncology. These studies establish technological feasibility to determine potential clinical and commercial opportunities. |
|
· |
Development phase. In this phase, we establish a product definition and development plan and perform gene identification either by selecting candidate genes from the approximately 25,000 genes in the human genome or by applying NGS technology to explore both coding and non‑coding regions that could influence tumor biology. Typically, we secure access to archival tumor biopsy samples correlated with clinical data to identify genes that correlate with specific clinical outcomes. If early clinical development studies successfully identify genes, we may conduct additional clinical studies to refine the gene set in the specific patient population of interest. We typically select the final gene panel through statistical modeling of the gene expression and outcome data and considerations of analytical performance. Following establishment of a gene panel, we finalize the remaining assay parameters. |
|
· |
Validation phase. Once the genomic panel, assay chemistry and processes, automation and analysis specifications are finalized, tested and analytically validated, we typically begin clinical validation. In this phase, we conduct one or more validation studies with prospectively designed endpoints to test our candidate gene panel and the corresponding quantitative expression score. We are often able to conduct large validation studies using archived samples with years of clinical outcomes, thus saving clinical development time. |
|
· |
Clinical utility and product expansion phase. Once a test is commercially available, we may perform additional studies designed to support the test’s clinical utility and to broaden its use in additional patient populations or for additional indications. Clinical utility studies may include a variety of studies, including retrospective surveys and prospective studies to verify that our test being studied is changing physician behavior and to determine the impact on patient care and health economics. In addition, further studies may be performed to test a commercial product in new patient populations. Finally, through our investigator sponsored trial program, we provide physicians with our tests for use in specific patient populations. |
Product Development Opportunities
In addition to developing products to address new cancer areas, we seek to expand the clinical utility and addressable patient populations for our existing tests, including expanding our current test offerings to include tests that are performed as IVDs. These developments efforts may lead to a variety of possible new products covering various treatment decisions, including risk assessment, screening and prevention, early disease diagnosis, adjuvant and/or neoadjuvant disease treatment, metastatic disease treatment selection and patient monitoring.
Breast Cancer
We have continued to conduct and present a variety of development studies to expand the reach of our products for breast cancer. For example, we presented results from a clinical study summarizing the gene signatures of male patients for whom the Oncotype DX breast cancer test was used to guide chemotherapy treatment, indicating that breast cancer in men displays similar gene signatures to female breast cancer. We also presented a study demonstrating that there were significant differences in gene expression between hormone receptor negative, or triple negative, breast cancer compared with hormone receptor positive disease.
14
Other studies presented include results of our clinical outcomes study for biomarker discovery using NGS. In addition to re‑confirming the original 21 Oncotype DX invasive breast cancer genes originally identified by RT‑PCR, this study also revealed more than 1,800 new biological relationships associated with breast cancer recurrence. In addition, the results of a large study of early‑stage, node‑positive breast cancer patients treated with anthracycline‑containing chemotherapy as part of the NSABP B‑28 trial were also presented, supporting the Oncotype DX Breast Recurrence Score results as a predictor of distant recurrence, disease‑free survival and overall survival in this patient population.
At the December 2013 SABCS, we presented results of a study examining our Oncotype DX invasive breast cancer test and two other commercially available genomic tests, in which we evaluated whether the information those tests provide is equivalent to the Oncotype DX Breast Recurrence Score results. Specifically, the results indicated a more than 44% discordance with the other assays studied when they were compared to Oncotype DX, highlighting the potential of these other tests to misclassify and mistreat patients if they are used to determine chemotherapy treatment. Two additional studies were presented at the December 2013 SABCS, including one demonstrating the importance of accurate assessment of ER status to ensure appropriate hormonal treatment, and one that presented the results of a pilot clinical study that demonstrated the feasibility of the large ongoing clinical trial of early endocrine sensitivity prediction by the Oncotype DX invasive breast cancer test and conventional parameters in clinical practice.
Colorectal Cancer
We have conducted a variety of development studies that could support certain additional opportunities in colon cancer. For example, in the NSABP C‑07 clinical trial, which validated the Oncotype DX colon cancer test as a predictor of recurrence in stage III disease, we also performed a gene identification study which analyzed over 700 new genes, and identified 16 genes as being predictive of oxaliplatin benefit for use in patients with stage III disease.
In 2013, we conducted a clinical validation study to identify the potential use of our Oncotype DX colon cancer test in patients diagnosed with rectal cancer, a cancer that has pathologic features similar to colon cancer and was diagnosed in approximately 40,000 patients in the United States in 2014. The study, conducted by the Department of Surgery at the Leiden University Medical Centre, evaluated the Oncotype DX colon cancer score and recurrence risk in rectal cancer patients.
Prostate Cancer
In August 2014, we announced positive top line results of a second clinical study, demonstrating the ability of our test’s GPS to predict multiple clinical endpoints related to disease aggressiveness among low/intermediate risk patients. The study also confirmed the earlier validation study published in May 2014. The results from the clinical validation study were presented at ESMO in September 2014, and at the Society of Urologic Oncology meeting in December 2014.
We plan to continue conducting development studies to support the relationship of our Oncotype DX prostate cancer test and its benefit in predicting prostate cancer clinical recurrence and biochemical recurrence, as well as its ability to add value in following patients on active surveillance. Also, as with breast and colon cancer, we will explore opportunities to expand the use of genomic testing in prostate cancer to address additional populations. These additional populations may include high-risk patients, based on clinical and pathologic features at the time of diagnosis, the large number of patients with negative biopsies, and patients who receive treatment with radical prostatectomy or radiation who may be considering additional adjuvant therapy with some of the new treatment modalities that are available for advanced disease.
Pipeline Products
In addition to extending the market opportunities for our existing tests, we are also developing products to address new cancer areas. These development efforts may lead to possible new products covering various treatment decisions, including risk assessment, screening and prevention, early disease diagnosis, adjuvant and/or neoadjuvant disease treatment, metastatic disease treatment selection and patient monitoring.
Potential new products may address a variety of specific clinical needs by leveraging one or multiple technological capabilities including NGS and digital PCR. Additionally, we believe potential new products can be implemented in the form of non‑invasive tests performed on blood or urine, similar to the Oncotype DX AR-V7 Nucleus Detect test.
We have also begun development of an IVD version of the Oncotype DX breast cancer test on Biocartis' Idylla platform that can be performed locally by laboratory partners and in hospitals around the world. Finally, we also plan to
15
continue to expand our product footprint through collaborations, including the development of additional prostate tests using technology licensed to us from our collaboration with Cleveland Diagnostics.
As new clinical evidence continues to be introduced, we intend to incorporate such evidence into additional iterations of these tests, which could include additional genes or updated interpretations of genes already included in such tests.
Commercial Operations
United States
Our commercial infrastructure, including our sales force, managed care group, and patient support network, is critical to our future success. We continue to build a strong domestic sales, marketing and reimbursement effort by interacting directly with medical, radiation, and surgical oncologists, urologists, pathologists and payors. Because oncology and urology are distinct concentrated specialties, we believe that a focused marketing organization and specialized sales force with regional and local experience in the U.S. for each of oncology and urology is necessary to effectively serve both specialties. We employ a direct sales approach that targets oncologists, cancer surgeons and urologists, and utilizes medical education and scientific liaisons who target key opinion leaders. We also plan to continue conducting clinical studies with the objective of having results published in peer‑reviewed journals. We believe the combination of these approaches is our best means to increase patient and physician demand and the number of favorable reimbursement coverage decisions by third‑party payors. Due to significant overlap between breast and colon oncologists and surgeons, we believe our current oncology salesforce has sufficient capacity to market our Oncotype DX breast and colon cancer tests. In 2017, we continued to expand our urology sales team in the United States to market our prostate cancer test to urologists, and we believe our current urology salesforce has sufficient capacity to market our Oncotype DX prostate cancer test. Going forward, we intend to leverage our existing sales capabilities and channels to introduce and commercialize new products, such as the Oncotype DX AR-V7 Nucleus Detect.
Our managed care group works with our contract and reimbursement teams to encourage adoption of our tests under payor medical policy and to ensure our tests are appropriately reimbursed. These teams, along with our customer service group and patient support network, handle benefits investigation, preauthorization, and other administrative matters for patients who use our tests. We have the infrastructure, if needed, to appeal claims for our tests that are denied by third‑party payors. In addition, we provide patient and physician education through our website, material provided to local advocacy groups, local, national and social media campaigns and materials provided to oncologists, urologists and surgeons.
All internally developed Oncotype tests are currently processed in our clinical reference laboratory facilities in Redwood City, California. The Oncotype DX AR-V7 Nucleus Detect test, which was designed and validated by Epic Sciences, is performed in its CLIA-certified, CAP-accredited clinical reference laboratory facility in San Diego, California. Our current clinical laboratory processing capacity in Redwood City is approximately 150,000 tests annually, and it has significant expansion capacity with incremental increases in laboratory personnel and equipment, including expansion capacity for laboratory facilities. We believe that we currently have sufficient capacity to process all of our tests. We have recently completed the construction of an additional laboratory facility on our Redwood City, California campus that will increase capacity for sample processing and research and development. We may require additional facilities in the future as we expand our business and believe that additional space, when needed, will be available on commercially reasonable terms.
International
We have a direct commercial presence with employees in Canada, Japan and six European countries. Additionally, we have exclusive distribution agreements for one or more of our Oncotype DX tests with distributors covering more than 90 countries outside of the United States.
We believe our future success is dependent on our ability to continue to expand our international commercial presence and achieve adequate reimbursement for our tests. However, there are significant differences between countries that need to be considered. For example, regulatory or reimbursement requirements vary from country to country, and different countries may have a public healthcare system, a combination of public and private healthcare system or a cash‑based payment system. Treatment costs outside of the United States may be lower, which may impact the cost savings of our tests, and therefore impact the reimbursement amount we can achieve in certain countries.
We expect that international sales of our tests will be heavily dependent on the availability of reimbursement and sample access. In many countries, governments are primarily responsible for financing diagnostic tests. Governments often
16
have significant discretion in determining whether a test will be reimbursed at all, and if so, how much will be paid. In addition, certain countries such as China have prohibitions against exporting tissue samples, which will limit our ability to offer our tests in those countries without local laboratories or a method of test delivery that does not require samples to be transported to our U.S. laboratory.
Coverage, Coding and Reimbursement
U.S. Coverage
Medicare coverage for our tests is currently subject to the discretion of the local Medicare Administrative Contractors, or MACs. Palmetto, the MAC that establishes the coverage and coding policies for the majority of our tests under Medicare, developed the Molecular Diagnostic Services Program, or MolDx, to identify and establish Medicare coverage for molecular diagnostic tests that fall within the scope of its Molecular Diagnostic Test LCD. To obtain coverage under the MolDx program, developers of molecular diagnostic tests must submit a detailed dossier of analytical and clinical data to substantiate that a test meets Medicare’s requirements for coverage. To date, Palmetto has determined that our invasive breast and colon cancer tests will be covered, and that our prostate cancer test will be covered for patients with specified risk levels. Coverage determinations for our tests made by Palmetto under the MolDx program have been adopted by Noridian Healthcare Solutions, the MAC that processes Medicare claims submitted by us.
In December 2015, Palmetto determined that it was appropriate to establish a unique identifier code and independent coverage for the Oncotype DX DCIS test. We obtained that unique identifier code for the Oncotype DX DCIS test, and have submitted to Palmetto additional validation and clinical utility data generated since its previous decision in May 2013, to cover our Oncotype DX DCIS test for all qualified Medicare patients with DCIS. On January 19, 2017, Palmetto announced that it would cover the Oncotype DX DCIS test under a new LCD with Coverage with Data Development, or CDD, for tests performed beginning March 6, 2017. Between January 26, 2017 and March 5, 2017, Palmetto provided coverage consistent with the criteria under the LCD.
The Protecting Access to Medicare Act of 2014, or PAMA, codified coverage rules for laboratory tests by requiring that any Medicare local coverage policy be issued in accordance with the requirements for the LCD process.
PAMA also authorizes CMS to consolidate coverage policies for clinical laboratory tests among one to four laboratory-specific MACs. These same contractors may also be designated to process claims if CMS determines that such a model is appropriate. To date, CMS has not exercised this authority, however, if the MolDx Program is eliminated, or the administrator of the program is changed, it could impact Medicare coverage for our current tests and our ability to obtain Medicare coverage for products for which we do not currently have coverage or any products that we may launch in the future.
State Medicaid programs typically make their own decisions with respect to coverage for our tests. Similarly, private payors make their own decisions whether to cover our tests.
Coding and Reimbursement
We have specific Current Procedural Terminology, or CPT, codes for our Oncotype DX invasive breast and colon cancer tests. Our other tests, however, are currently billed with an unlisted procedure code. Providers use an unlisted procedure code to bill for a service when no existing specific code accurately describes the service.
Reimbursement for clinical laboratory tests may come from several sources, including commercial third‑party payors, such as insurance companies and health maintenance organizations, government payors, such as Medicare and Medicaid in the United States, patient self‑pay and, in some cases, from hospitals or referring laboratories who, in turn, may bill third‑party payors for testing.
Reimbursement of our tests by third‑party payors is essential to our commercial success. Where there is a payor policy, contract or agreement in place, we bill the third‑party payor, the hospital or referring laboratory and/or the patient (for deductibles and coinsurance or copayments, where applicable) in accordance with established policy, contract or agreement terms. Where there is no payor policy in place, we pursue third-party reimbursement on behalf of each patient on a case‑by‑case basis. Our efforts on behalf of these patients involve a substantial amount of time and expense, and bills may not be paid for many months, if at all. Furthermore, if a third‑party payor denies coverage after final appeal, it may take a substantial amount of time to collect from the patient, if we are able to collect at all.
17
We received a specific CPT code for our Oncotype DX invasive breast cancer test effective January 1, 2015. Medicare established a national limitation amount for this code under the gapfill process that maintained the contractor amount then in effect through 2017. The new rate calculated using the methodology required under PAMA was adopted in January 2018 and represents an increase of approximately 12% as compared to the 2017 rate.
We also received a specific CPT code for our Oncotype DX colon cancer test, effective January 1, 2016. For 2016, Medicare claims were paid at the rate established by the local MACs under the gapfill process. Medicare established a national limitation amount for this code that maintained the contractor amount through 2017. The new rate calculated using the methodology required under PAMA was adopted in January 2018 and represents a less than 1% reduction as compared to the 2017 rate.
There have also been recent and substantial changes to the payment structure for physicians, including those passed as part of the Medicare Access and CHIP Reauthorization Act of 2015, or MACRA, which was signed into law on April 16, 2015. MACRA created the Merit-Based Incentive Payment System which, beginning in 2019, more closely aligns physician payments with composite performance on performance metrics similar to three existing incentive programs (i.e., the Physician Quality Reporting System, the Value-based modifier program and the Electronic Health Record Meaningful Use program) and incentivizes physicians to enroll in alternative payment methods. At this time, we do not know whether these changes to the physician payment systems will have any impact on orders or payments for our tests.
Under PAMA, many laboratories that receive the majority of their Medicare revenues from payments made under the Clinical Laboratory Fee Schedule, or CLFS, or the Physician Fee Schedule, will be required to report private payor payment rates and volumes for their tests. CMS will use the rates and volumes reported by laboratories to develop Medicare payment rates for the tests equal to the volume-weighted median of the private payor payment rates for the tests. Laboratories that fail to report the required payment information may be subject to substantial civil money penalties. Rates for “advanced diagnostic laboratory tests” must be reported annually; rates for other diagnostic tests must be reported every three years.
The payment rates calculated under PAMA apply effective January 1, 2018. In general, any reductions to payment rates compared to rates paid under the CLFS in 2017 resulting from the new methodology are limited to 10% per test per year in each of the years 2018 through 2020 and to 15% per test per year in each of the years 2021 through 2023. Rates for 2021 through 2023 will be established following collection of data on private payor rates from the first half of 2019 that will be reported in the first quarter of 2020. The initial payment rate under PAMA for a new advanced diagnostic laboratory test will be set at the “actual list charge” for the test as reported by the laboratory, for a period not to exceed nine months. If the actual list charge exceeds private payor rates by more than 30%, CMS will have the ability to recoup excess payments made during the initial nine-month payment period.
In June 2016, CMS issued a final rule that outlines how the agency will implement the PAMA payment system. We believe the reporting policy articulated in the final rule requires us to report information annually on rates paid by private payors for each of our Oncotype DX tests if we seek designation for our tests as advanced diagnostic laboratory tests. Under the criteria outlined in the final rule, we believe all of our Oncotype DX tests are eligible for designation as advanced diagnostic laboratory tests, although we may or may not seek to have our existing tests designated as advanced diagnostic laboratory tests. In the final rule, CMS finalized a six-month data collection period for all tests (including advanced diagnostic laboratory tests), spanning the first six months of each data collection year. CMS also provided that the data collection period would be immediately followed by a six-month period during which we may verify and validate our private payor rate data before the data is due to CMS between January 1 and March 31 of the following year.
With respect to pricing of existing tests, CMS further defines the rate-setting methodology by indicating that it will assess every payment rate, by payor, submitted by laboratories and to determine the median of the payment rates for each test, listing each distinct private payor rate the same number of times in the array as its volume. The PAMA rate-setting process follows the current timeline for CLFS rate-setting, which is publication of preliminary rates in September with final rates published in November to become effective the following January, and will update the payment rates every three years, or annually for advanced diagnostic laboratory tests. Any reductions to payment rates resulting from the new methodology are limited to 10% per test per year in each of the years 2018 through 2020 and to 15% per test per year in each of 2021 through 2023.
With respect to pricing of new advanced diagnostic laboratory tests, the initial payment rate, for a period not to exceed nine months, will be set at the “actual list charge” for the test as reported by the laboratory. The “actual list charge” is the lowest publicly available price on the first date at which the test is available for purchase by a private payor, as evidenced by sources such as websites, test registries or price listings for patients. If the actual list charge exceeds the rate calculated using the new
18
methodology by more than 30%, CMS will recoup excess payments made during the initial nine-month payment period.
In 2014, CMS began to bundle payment for most clinical laboratory tests together with other services performed during hospital outpatient visits under the Hospital Outpatient Prospective Payment System, or HOPPS. While CMS exempted molecular diagnostic tests from this bundling provision, it is possible that CMS could propose to bundle payment for such tests in the future. Our tests are generally not furnished in the hospital outpatient setting, and insofar as they are furnished in that setting they likely would be considered molecular tests if billed under specific procedure codes, but it is possible that payment for our tests could be bundled if furnished in a hospital outpatient setting in the future.
In the 2018 Medicare HOPPS Final Rule, CMS finalized revisions to its billing rules that will allow us to directly bill Medicare more frequently. Specifically, under the revised billing rules, a laboratory that performs molecular pathology tests on specimens collected during a hospital outpatient stay may bill Medicare directly for such tests if the test was performed following a hospital outpatient's discharge from the hospital outpatient department. To the extent these revisions to Medicare’s billing policy permit us to bill Medicare directly for tests previously billed to hospitals under the previous Medicare billing rules, we will no longer bill hospitals for such tests. We continue to be subject to previous Medicare billing rules, however, where we perform tests on specimens collected during a hospital inpatient stay.
On several occasions Congress has considered various cost reduction alternatives, including imposing a 20% co‑insurance amount on clinical laboratory services, which would require beneficiaries to pay a portion of the cost of their clinical laboratory testing. Although these changes have not been enacted at this time, Congress could decide to impose these or other fee reductions or taxes at some point in the future. If so, these additional coinsurance payments for our Oncotype DX tests could be difficult to collect and any new fee reductions or taxes would impact our revenues.
State Medicaid agencies will assign a reimbursement rate equal to or less than the prevailing Medicare rate, often determined by state law as a percentage of the Medicare reimbursement rate.
International Coverage and Reimbursement
The majority of our international Oncotype DX breast and colon cancer test revenues come from direct payor reimbursement, payments from our distributors, and patient self‑pay. We have obtained coverage for our invasive breast cancer test outside of the United States, including coverage for certain patients in Canada, France, Ireland, Israel, Saudi Arabia, Switzerland, and the United Kingdom. We expect that broadening coverage and reimbursement for our Oncotype DX breast, colon and prostate cancer tests outside of the United States will take years.
Oncotype DX Invasive Breast Cancer Test
We expect to continue to focus substantial resources on pursuing global adoption of and reimbursement for our Oncotype DX invasive breast cancer test. We believe increased demand for our Oncotype DX invasive breast cancer test is the result of our ongoing commercial efforts, expanded utility for new breast cancer patient groups, continued publication of peer-reviewed articles on studies we sponsored, conducted or collaborated on that support the use of and reimbursement for the test, clinical presentations at major symposia, and the inclusion of our breast cancer test in clinical practice guidelines for N−, ER+ invasive disease. However, this increased demand is not necessarily indicative of future growth rates, and we cannot provide assurance that this level of increased demand can be sustained or that publication of articles, future appearances or presentations at medical conferences, increased commercial efforts or expansion of utility to new breast cancer patient groups will have a similar impact on demand for our invasive breast cancer test in the future. Sequential quarterly demand for our breast cancer test may also be impacted by other factors, including the economic environment and seasonal variations that have historically impacted physician office visits, any shift in commercial focus, patient enrollment in clinical studies and the number of clinical trials in process by cooperative groups or makers of other tests conducting experience studies.
Most national and regional third‑party payors in the United States, along with the designated regional Medicare contractor for our tests, have issued positive coverage determinations for our Oncotype DX invasive breast cancer test for patients with N−, ER+ invasive disease through contracts, agreements or policy decisions. The local carrier with jurisdiction for claims submitted by us for Medicare patients also provides coverage for our invasive breast cancer test for ER+ patients with N+ disease (up to three positive lymph nodes) and invasive breast cancer patients where a lymph node status is unknown or not accessible due to a prior surgical procedure, or when the test is used to guide a neoadjuvant treatment decision. Additionally, some payors provide policy coverage for the use of our test in ER+ patients with N+ disease, including lymph node micro‑metastasis. However, we may not be able to obtain reimbursement coverage from other payors for our test for breast cancer patients with N+, ER+ disease.
19
We have established limited reimbursement coverage for the use of our Oncotype DX DCIS test for some private third‑party payors. In many instances our test is covered under existing breast cancer coverage policies with the addition of the indicated diagnosis code for DCIS. We also received an LCD with Coverage with Data Development for our DCIS test in March 2017, and we intend to continue to devote resources to gaining Medicare and expanded private reimbursement for this test in its intended patient population. We believe it may take several years to achieve reimbursement with a majority of third‑party payors for the use of our DCIS test. However, we cannot predict whether, or under what circumstances, payors will reimburse for this test.
We have established coverage for our Oncotype DX invasive breast cancer test in more than 90% of state Medicaid programs for N− disease. In addition, the Veterans Administration and the Department of Defense hospitals have processes in place that provide coverage for this test.
Oncotype DX Colon Cancer Test
We are working with public and private payors and health plans to secure coverage for our Oncotype DX colon cancer test based upon our published and presented results in clinical validation studies and the completed and ongoing studies designed to demonstrate the treatment decision impact of the test in clinical practice. In September 2011, the local carrier with jurisdiction for claims submitted by us for Medicare patients established coverage for our colon cancer test for patients with stage II colon cancer. Additionally, the Veterans Administration, Department of Defense hospitals and a few additional private payors provide coverage and reimbursement. We intend to pursue reimbursement while seeking to obtain formal coverage policies with payors and expect that this test will continue to be reviewed on a case‑by‑case basis until policy decisions have been established. We believe it may take several years to achieve additional reimbursement with third‑party payors for our colon cancer test. However, we cannot predict whether, or under what circumstances, payors will reimburse for this test.
Oncotype DX Prostate Cancer Test
We expect to continue to focus substantial resources on pursuing global adoption of and reimbursement for our Oncotype DX prostate cancer test. We believe the key factors that will drive adoption of this test include publication of the clinical validation study conducted in collaboration with the University of California, San Francisco and other studies we sponsored, conducted or collaborated on that support the use of and reimbursement for the test, clinical presentations at major symposia and our ongoing commercial efforts.
In August 2015, Palmetto issued its final LCD, approving nationwide coverage of our prostate cancer test for qualified male Medicare patients with low and very low risk disease, as defined by NCCN guidelines, throughout the United States. The LCD includes specific requirements for certification and training of physicians who order the test and requirements for collection and reporting of specific data elements related to the use of our test and patient outcomes. Palmetto initiated reimbursement of the Oncotype DX prostate cancer test for patients with low-risk disease effective October 2015.
In August 2017, Palmetto issued its final LCD, recommending Medicare coverage for use of our prostate cancer test in qualified patients with favorable intermediate-risk prostate cancer, as defined by American Urological Association, or AUA, guidelines. Effective October 2017, Palmetto expanded their reimbursement coverage of our Oncotype DX prostate cancer test to include qualified patients with favorable intermediate-risk prostate cancer.
Other than Medicare coverage, we have obtained some reimbursement coverage from third‑party payors for our Oncotype DX prostate cancer test. As a new test, our prostate cancer test may be considered investigational by payors and therefore may not be covered under their reimbursement policies. Consequently, we intend to pursue case‑by‑case reimbursement and expect that this test will continue to be reviewed on this basis until policy decisions have been made by individual payors. We plan to work with public and private payors and health plans to secure coverage for this Oncotype DX prostate cancer test based upon clinical evidence demonstrating the utility of the test. We believe it may take several years to achieve reimbursement with a majority of third‑party payors for our prostate cancer test. However, we cannot predict whether, or under what circumstances, payors will reimburse for this test. We plan to hire additional commercial, scientific, technical and other personnel to support this process.
Competition
We compete in a rapidly evolving and highly competitive industry, and there are a number of private and public companies that offer products or have conducted research to profile genes and gene expression in breast, colon and prostate
20
cancer, including companies such as Agendia Inc., BioTheranostics, Exact Sciences, Inc. GenomeDx Biosciences Inc., Hologic Inc., Myriad Genetics Inc. (and its Sividon Diagnostics subsidiary), NanoString Technologies Inc., NeoGenomics, Inc., and Qiagen N.V. As we look to expand our research, development and commercialization efforts, we may face competition from companies such as Danaher Corporation (and its Cepheid, Inc. subsidiary), Exosome Diagnostics, Inc., Foundation Medicine, Grail, Guardant Health, MDxHealth, Metamark Genetics, Inc., Natera Inc. and Personal Genome Diagnostics, Inc. Historically, our principal competition for our Oncotype DX tests has also come from existing diagnostic methods used by pathologists and oncologists, and such traditional diagnostic methods can be difficult to change or supplement. We also compete with companies offering capital equipment and kits or reagents to local pathology laboratories. These kits are used directly by the pathologist, which facilitates adoption more readily than tests like ours that are performed outside the pathology laboratory.
We also potentially face competition from commercial laboratories with strong distribution networks for diagnostic tests, such as Laboratory Corporation of America Holdings and Quest Diagnostics Incorporated. Other potential competitors include companies that develop diagnostic tests such as Roche Diagnostics, a division of Roche Holding, Ltd, Siemens AG, as well as other companies and academic and research institutions.
In our prostate cancer market, we face comparatively greater competition than in our breast cancer market, including competition from products which were on the market prior to our product launch and which are supported by clinical studies and published data. This existing direct and indirect competition for tests and procedures may make it difficult to gain additional market share, impact our ability to obtain reimbursement or result in a substantial increase in resources necessary for us to continue to successfully commercialize our Oncotype DX prostate cancer test.
As more information regarding cancer genomics becomes available to the public, we anticipate that more products aimed at identifying targeted treatment options will be developed and that these products may compete with ours. In addition, competitors may develop their own versions of our tests in countries where we did not apply for patents, where our patents have not issued or where our intellectual property rights are not recognized and compete with us in those countries, including encouraging the use of their test by physicians or patients in other countries. Many of our present and potential competitors have widespread brand recognition and substantially greater financial and technical resources and development, production and marketing capabilities than we do. Others may develop lower‑priced, less complex tests that could be viewed by physicians and payors as functionally equivalent to our tests.
We believe that we compete primarily on the basis of the value of the quantitative information our Oncotype DX tests provide; the clinical validation of the utility of our tests; the level of adoption and reimbursement coverage for our tests; the inclusion of our tests in clinical practice guidelines; our ability to commercialize products through our clinical development platform; our ability to expand our sales efforts into new areas of medical practice as we launch new products; our collaborations with clinical study groups; the quality of our clinical reference laboratory; and the level of customer service we provide.
While we believe that we compete favorably with respect to these factors, in order to continue to do so we must continue to innovate and adopt advanced technology; successfully market, sell and enhance our Oncotype DX tests for use in types of cancer other than breast, colon and prostate; obtain peer-reviewed publications of our clinical studies in a timely manner; continue to obtain positive reimbursement determinations; continue to expand in countries outside of the United States; continue to develop our technological and clinical operations; encourage physician participation in Medicare-required information collection efforts; and, successfully expand our reach into additional product markets including through collaborations with third parties.
Regulation
United States
Clinical Laboratory Improvement Amendments of 1988 (CLIA)
We and our collaboration partners are required to hold certain federal, state and local licenses, certificates and permits to conduct our business. Under CLIA, we are required to hold a certificate applicable to the types of tests we perform and to comply with standards covering personnel qualifications, facilities administration, quality systems, inspections and proficiency testing.
We have a current Certificate of Accreditation under CLIA to perform high complexity testing and are accredited by the College of American Pathologists, or CAP. To renew our CLIA certificate, we are subject to survey and inspection every
21
two years to assess compliance with program standards and may be subject to additional inspections without prior notice. The standards applicable to the tests we perform may change over time. We cannot assure that we will operate profitably should it become substantially costlier to comply with regulatory requirements in the future.
If our laboratory is out of compliance with CLIA requirements, we may be subject to sanctions such as suspension, limitation or revocation of our CLIA certificate, as well as directed plan of correction, state on‑site monitoring, civil money penalties, civil injunctive suit or criminal penalties. CMS may also cancel our laboratory’s approval to receive Medicare payments if we are found to be out of compliance with CLIA requirements. If we are to be found out of compliance with CLIA program requirements and sanctions are imposed, our business could be harmed.
U.S. Food and Drug Administration (FDA)
Diagnostic test kits that are sold and distributed through interstate commerce are regulated as medical devices by the FDA. Devices subject to FDA regulation must undergo pre‑market review prior to commercialization unless the device is exempt from such review. In addition, manufacturers of medical devices must comply with various regulatory requirements under the Federal Food, Drug and Cosmetic Act and regulations promulgated under that Act, including quality system regulations, unless they are exempt. Entities that fail to comply with FDA requirements can be liable for criminal or civil penalties, such as recalls, detentions, orders to cease manufacturing, and restrictions on labeling and promotion, among other potential sanctions.
Clinical laboratory tests like ours are regulated under CLIA, as administered by CMS, as well as by applicable state laws. Clinical laboratory tests that are developed and validated by a laboratory for its own use, which are referred to as laboratory developed tests, or LDTs, are generally not currently subject to FDA regulation, although reagents or software provided by third parties and used to perform LDTs may be subject to regulation. We do not believe that our current tests are diagnostic kits and believe that they are properly classified as LDTs. As a result, we believe our current tests should not be subject to regulation at this time under established FDA policies. The container we provide for collection and transport of tumor samples from a pathology laboratory to our clinical reference laboratory may be considered a medical device subject to regulation but is currently exempt from pre‑market review by the FDA.
At various times since 2006, the FDA has issued guidance documents or announced draft guidance regarding initiatives that may require varying levels of FDA oversight of our tests. In October 2014, the FDA issued draft guidance that sets forth a proposed risk-based regulatory framework that would apply varying levels of FDA oversight to LDTs. The FDA has indicated that it does not intend to implement its proposed framework until the draft guidance documents are finalized. On January 13, 2017, the FDA published a discussion paper in which the FDA outlined a substantially revised possible approach to the oversight of LDTs. The discussion paper explicitly states that it is not a final version of the 2014 draft guidance and that it does not represent the FDA’s formal position. It is unclear at this time if or when the FDA will finalize its plans to end enforcement discretion for LDTs, and even then, the new regulatory requirements are expected to be phased-in over time. However, the FDA may decide to regulate certain LDTs on a case-by-case basis at any time.
Legislative proposals addressing oversight of genetic testing and LDTs have been introduced in previous Congresses and we expect that new legislative proposals will be introduced from time to time in the future. We cannot provide any assurance that FDA regulation, including pre-market review, will not be required in the future for our tests, whether through finalization of guidance issued by the FDA, new enforcement policies adopted by the FDA or new legislation enacted by Congress. It is possible that legislation will be enacted into law or guidance could be issued by the FDA which may result in increased regulatory burdens for us to continue to offer our tests or to develop and introduce new tests.
We cannot predict the ultimate form of any statutes, regulations or guidance and the potential impact on our existing tests, our tests in development or materials used to perform our tests. If pre‑market review is required, our business could be negatively impacted until such review is completed and clearance or approval is obtained, and the FDA could require that we stop selling our tests pending pre‑market clearance or approval. If our tests are allowed to remain on the market but there is uncertainty about the regulatory status of our tests, if they are labeled investigational by the FDA, or if labeling claims the FDA allows us to make are more limited than the claims we currently make, orders or reimbursement may decline. The regulatory review process may involve, among other things, successfully completing additional clinical trials and submitting a pre‑market clearance notice or filing a pre-market approval application with the FDA. If pre‑market review is required by the FDA, there can be no assurance that our tests will be cleared or approved on a timely basis, if at all, nor can there be assurance that the labeling claims cleared or approved by the FDA will be consistent with our current claims or adequate to support continued adoption of and reimbursement for our tests. Ongoing compliance with FDA regulations would increase the cost of conducting
22
our business, and subject us to inspection by the FDA and to the regulatory requirements of the FDA, and potentially subject us to penalties for failure to comply with these requirements.
We may also decide voluntarily to pursue FDA pre‑market review of our tests if we determine that doing so would be appropriate from a strategic reimbursement or other standpoint. In November 2017, CMS published a draft national coverage determination, or NCD, for NGS tests for patients with advanced cancer. Under this NCD, CMS proposes to provide full coverage for FDA-approved tests performed in patients that fall within that test’s FDA-approved labeling, but places significant limits on coverage for NGS-based tests offered as LDTs, effectively limiting coverage of NGS tests to those that are FDA-approved.
While we qualify all materials used in our tests according to CLIA regulations, we cannot be certain that the FDA will not enact rules or guidance that could impact our ability to purchase certain materials necessary for the performance of our tests, such as products labeled for research use only. Should the availability of any of the reagents obtained by us from vendors and used in conducting our tests be affected by future regulatory actions, our business could be adversely affected by those actions, including increasing the cost of testing or delaying, limiting or prohibiting the purchase of reagents necessary to perform testing.
Health Insurance Portability and Accountability Act
The Health Insurance Portability and Accountability Act of 1996, or HIPAA, required the Department of Health and Human Services, or HHS, to issue regulations to protect the privacy and security of protected health information. HIPAA’s privacy and security requirements are broad in scope and apply to “covered entities,” which include healthcare providers like us who transmit health information in connection with electronic healthcare transactions. In 2009, HIPAA was amended by the Health Information Technology for Economic and Clinical Health Act, or HITECH. The implementing regulations of HIPAA, as amended by HITECH, were last modified in 2013 and resulted in significant changes to the privacy, security, breach notification, and enforcement requirements with which we must comply. Among these changes, covered entities are now vicariously liable for violations of HIPAA that result from acts or omissions of their business associates where the business associate is an agent of the covered entity and was acting within the scope of its agency, regardless of whether the covered entity and business associate entered into a business associate agreement in compliance with HIPAA. Penalties for violations of HIPAA include civil money and criminal penalties.
As a covered entity, we are required to develop and maintain extensive policies and procedures to comply with the HIPAA privacy, security and breach notification requirements. We may not use or disclose protected health information in any form, including electronic, written, or oral, in a way that is not permitted under HIPAA, and we are required to implement security measures to ensure the confidentiality, integrity, and availability of the electronic protected health information that we create, receive, maintain, or transmit. While we have some flexibility in determining which security safeguards are reasonable and appropriate to implement for our operations, it nonetheless requires significant effort and expense to ensure continuing compliance with the HIPAA security rule. Moreover, the requirements under HIPAA’s privacy, security, and breach notification regulations may change periodically and could have an effect on our business operations if compliance becomes substantially costlier than under current requirements. We are also required to comply with the administrative simplification standards under HIPAA when we conduct the electronic transactions regulated by HIPAA, including by using standard code sets and formats and standardized identifiers for health plans and providers.
In addition to HIPAA, a number of state and international laws impose requirements regarding the protection of health or other personal information that are applicable to our operations. Many state laws are not preempted by HIPAA because they are more stringent or are broader in scope than HIPAA. Further, we are required to comply with international personal data protection laws and regulations. Under the current European Union Data Protection Directive, or E.U. Directive, we are required to self-certify as to our adherence to its principles of data protection and security. Effective May 25, 2018, the E.U. Directive will be superseded by the General Data Protection Regulation, or GDPR, a more prescriptive, detailed, and punitive regulation. While companies are afforded some flexibility in determining how to comply with the GDPR’s various requirements, it has and will continue to require significant effort and expense to ensure continuing compliance with the GDPR. Moreover, the requirements under the GDPR as to documentation, breach notification, access rights, and security, and breach notification regulations may change periodically or may be modified by E.U. national law, and could have an effect on our business operations if compliance becomes substantially costlier than under current requirements. It is possible that each of these privacy laws may be interpreted and applied in a manner that is inconsistent with our practices. If so, this could result in government imposed fines or orders requiring that we change our practices, which could adversely affect our business.
23
Complying with these various laws could cause us to incur substantial costs or require us to change our business practices and compliance procedures in a manner adverse to our business.
Under the E.U. Directive, and the GDPR, personal information about E.U. citizens can only be transferred from the E.U. to countries with adequate data protection. The U.S.-E.U. Privacy Shield, or the Privacy Shield, has been open to registrants as of August 1, 2016. We have self-certified compliance with the Privacy Shield, which we believe will mitigate customer concerns about overseas data transfers. However there continue to be concerns about whether the Privacy Shield will face additional challenges (similar to those that invalidated the Safe Harbor Framework), and it is not guaranteed that companies who have self-certified under the Privacy Shield will be free of additional ongoing scrutiny by E.U. data protection authorities.
Federal and State Physician Self‑Referral Prohibitions
We are subject to the federal physician self‑referral prohibitions, commonly known as the Stark Law. We are also subject to similar restrictions under the self-referral prohibitions of certain states in which we operate. Such state laws are generally interpreted by regulators and the courts in a manner similar to the Stark Law. Together these restrictions generally prohibit us from billing a patient or any governmental or private payor for any test when the physician ordering the test, or any member of such physician’s immediate family, has a financial interest in or compensation arrangement with us, unless the arrangement meets an exception.
For example, under the personal services exception of both the Stark Law and California’s Physician Ownership and Referral Act, or PORA, billing for tests is permitted when the orders for such tests came from physicians whose compensation arrangement with us is for personal services and meets certain written contractual requirements. We have compensation arrangements with a number of physicians for personal services, such as speaking engagements and consulting services. We have structured these arrangements with terms intended to comply with the requirements of the personal services exception of the Stark Law and PORA. However, we cannot be certain that regulators would find these arrangements to be in compliance with the exceptions of the Stark Law, PORA or similar laws in other states. If the arrangements were found to not be in compliance with these exceptions and prohibited referrals were made, we would be required to refund any payments we received pursuant to a prohibited referral to the patient, the payor or the Medicare program, as applicable.
Sanctions for a violation of the Stark Law include the following:
|
· |
denial of payment for the services provided in violation of the prohibition; |
|
· |
refunds of amounts collected by an entity in violation of the Stark Law; |
|
· |
a civil penalty of up to $24,253 (as of 2017) for each claim submitted in violation of the Stark; |
|
· |
possible exclusion from federal healthcare programs, including Medicare and Medicaid; and |
|
· |
a civil penalty of up to $161,692 (as of 2017) for each scheme to circumvent the Stark Law. |
These prohibitions apply regardless of the reasons for the financial relationship and the referral. No finding of intent to violate the Stark Law is required for a violation. In addition, knowing violations of the Stark Law may also serve as the basis for liability under the Federal False Claims Act, which prohibits the knowing presentation of a false, fictitious or fraudulent claim for payment to the U.S. Government or knowingly retaining an overpayment from the U.S. Government.
Further, a violation of the self-referral prohibitions of states in which we operate could lead to additional liability. For example, a violation of PORA is a misdemeanor and could result in civil penalties and criminal fines. While we believe we comply with the Stark Law, PORA and similar laws of other states, it is possible that our claims for tests ordered by physicians with whom we have a financial relationship could be subject to regulatory scrutiny at some point in the future, and we cannot provide assurance that we will be found to be in compliance following any such regulatory review.
Federal and State Anti‑Kickback Laws
The federal Anti‑kickback Law makes it a felony for a provider or supplier, including a laboratory, to knowingly and willfully offer, pay, solicit or receive remuneration, directly or indirectly, in order to induce business that is reimbursable under any federal health care program. A violation of the Anti‑kickback Law may result in criminal penalties including fines of up to
24
$100,000, imprisonment for up to ten years, or both. Convictions under the Anti‑kickback Law result in mandatory exclusion from federal health care programs. In addition, HHS has the authority to impose civil assessments and fines and to exclude health care providers and others engaged in prohibited activities from Medicare, Medicaid and other federal health care programs. Actions that violate the Anti‑kickback Law or similar laws may also involve liability under the Federal False Claims Act.
Although the Anti‑kickback Law applies only to federal health care programs, a number of states in which we operate have passed statutes generally similar to the Anti‑kickback Law. For example, both California’s general anti-kickback statute, Business and Professions Code Section 650, and its Medi‑Cal anti‑kickback statute, Welfare and Institutions Code Section 14107.2, have been interpreted by the California Attorney General and California courts in generally the same way that HHS and courts have interpreted the federal Anti‑kickback Law. A violation of Section 650 is punishable by imprisonment and fines of up to $50,000. A violation of Section 14107.2 is punishable by imprisonment and fines of up to $10,000.
Federal and state law enforcement authorities may scrutinize arrangements between health care providers and potential referral sources to ensure that the arrangements are not designed as a mechanism to induce patient care referrals and opportunities. Law enforcement authorities, the courts and Congress have also demonstrated a willingness to look behind the formalities of a transaction to determine the underlying purpose of payments between health care providers and actual or potential referral sources. Generally, courts have taken a broad interpretation of the scope of the Anti‑kickback Law, holding that the statute may be violated if merely one purpose of a payment arrangement is to induce future referrals.
In addition to statutory exceptions to the Anti‑kickback Law, regulations provide for a number of safe harbors to the law. If an arrangement meets all the provisions of a safe harbor, it is deemed not to violate the Anti‑kickback Law. An arrangement must fully comply with each element of an applicable safe harbor in order to qualify for protection. However, failure to meet the terms of the safe harbor does not render an arrangement illegal. Rather, the arrangement must be evaluated under the language of the statute, taking into account all facts and circumstances.
Among the Anti‑kickback Law safe harbors that may be relevant to us is the discount safe harbor. The discount safe harbor potentially applies to discounts provided by providers and suppliers, including laboratories, to physicians or institutions where the physician or institution bills the payor for the test, not when the laboratory bills the payor directly. If the terms of the discount safe harbor are met, the discounts will not be considered prohibited remuneration under the Anti‑kickback Law. This safe harbor may therefore be potentially applicable to our agreements to sell tests to hospitals where the hospital submits a claim to the payor.
Another safe harbor to the Anti-kickback Law that may be relevant to us is the personal services safe harbor. This safe harbor provides that remuneration paid to a referral source for personal services will be deemed not to violate the Anti‑kickback Law provided all the elements of that safe harbor are met. One element is that, if the agreement is intended to provide for the services of the physician on a periodic, sporadic or part‑time basis, the agreement must specify the schedule of such intervals, their precise length, and the exact charge for such intervals. Our personal services arrangements with some physicians do not meet the specific requirement of this safe harbor in that the agreements do not specify exactly the schedule of the intervals of time to be spent on the services. The reason for this is that the nature of the services, such as speaking engagements, does not lend itself to exact scheduling and therefore meeting this element of the personal services safe harbor is impractical. However, as noted above, failure to meet the terms of the safe harbor does not render an arrangement illegal, as such arrangements are evaluated under the language of the statute, taking into account all facts and circumstances.
Many state anti-kickback statutes have analogous exceptions or safe harbors to those of the Anti-kickback Law. As noted above, these state anti-kickback statutes have generally been interpreted consistently with the Anti‑kickback Law.
While we believe that we are in compliance with the Anti‑kickback Law and similar anti-kickback statutes in the states in which we operate, there can be no assurance that our relationships with physicians, hospitals and other customers will not be subject to investigation or a successful challenge under such laws. If imposed for any reason, sanctions under these laws could have a negative effect on our business.
Many other countries in which we offer our tests also have anti‑kickback regulations, which are discussed below.
25
Other Federal and State Fraud and Abuse Laws
In addition to the requirements discussed above, there are several other health care fraud and abuse laws that could have an impact on our business. For example, provisions of the Social Security Act permit Medicare and Medicaid to exclude an entity that charges the federal health care programs substantially in excess of its usual charges for its services. The terms “usual charge” and “substantially in excess” are ambiguous and subject to varying interpretations.
Further, as stated above, the Federal False Claims Act prohibits a person from knowingly submitting a false claim or making a false record or statement in order to secure payment or retain an overpayment by the federal government. In addition to actions initiated by the government itself, the statute authorizes actions to be brought on behalf of the federal government by a private party having knowledge of the alleged fraud. These lawsuits are known as qui tam or whistleblower lawsuits. Because complaints related to such actions are initially filed under seal, the action may be pending for some time before the defendant is even aware of the action. If the government is ultimately successful in obtaining redress in the matter or if the plaintiff succeeds in obtaining redress without the government’s involvement, then the whistleblower plaintiff will receive a percentage of the recovery.
Finally, the Social Security Act includes its own provisions that prohibit the filing of false claims or submitting false statements in order to obtain payment. Violation of these provisions may result in fines, imprisonment or both, and possible exclusion from Medicare or Medicaid programs. Many states also have analogous false claims prohibitions, including California, which has a false claims provision applicable to all payors.
Laboratory Licensing
In addition to federal certification requirements for laboratories under CLIA, certain state laws, including those of California, New York, Maryland, Pennsylvania, Rhode Island and Florida, require us and certain laboratories with whom we collaborate to maintain certain licenses to either operate in the state or accept specimens from the state. These laws establish standards for the day‑to‑day operation of our clinical reference laboratory and those of certain of our collaborators, including the training and skills required of personnel and quality control. In addition, California laws require us to participate in a state-approved proficiency testing program, which involves testing of known specimens to verify the accuracy and reliability of our laboratory’s tests. We maintain a license in good standing with the California Department of Public Health, the New York State Department of Health, and relevant authorities in Florida, Maryland, Pennsylvania and Rhode Island.
If our clinical laboratory is out of compliance with California standards, the California Department of Public Health may suspend, restrict or revoke our license to operate our clinical laboratory, assess substantial civil money penalties, or impose specific corrective action plans, among other potential penalties. If our laboratory is out of compliance with New York statutory or regulatory standards, the New York State Department of Health may suspend, limit, revoke or annul the laboratory’s New York license, censure the holder of the license or assess civil money penalties, among other potential penalties. If imposed, any such penalties could materially affect our business.
From time to time, we may become aware of other states that require out‑of‑state laboratories to obtain a license in order to accept specimens from the state, and it is possible that other states already have such requirements or will have such requirements in the future. If we identify any other state with such requirements or if we are contacted by any other state advising us of such requirements, we intend to follow instructions from the state regulators as to how we should comply with such requirements.
Environmental Laws
We are subject to regulation under federal, state and local laws and regulations governing environmental protection and the use, storage, handling and disposal of hazardous substances. The cost of complying with these laws and regulations may be significant. Our activities currently require the controlled use of potentially harmful biological materials, hazardous materials and chemicals. We cannot eliminate the risk of accidental contamination or injury to employees or third parties from the use, storage, handling or disposal of these materials. In the event of contamination or injury, we could be held liable for any resulting damages, and any liability could exceed our resources or any applicable insurance coverage we may have.
26
International
Many countries in which we offer our tests in have anti‑kickback regulations prohibiting providers from offering, paying, soliciting or receiving remuneration, directly or indirectly, in order to induce business that is reimbursable under any national health care program. In situations involving physicians employed by state‑funded institutions or national health care agencies, violation of the local anti‑kickback law may also constitute a violation of the U.S. Foreign Corrupt Practices Act, or FCPA.
The FCPA prohibits any U.S. individual, business entity or employee of a U.S. business entity from offering or providing, directly or through a third party, including the distributors we rely on in certain markets, anything of value to a foreign government official with corrupt intent to influence an award or continuation of business or to gain an unfair advantage, whether or not such conduct violates local laws. In addition, it is illegal for a company that reports to the SEC to have false or inaccurate books or records or to fail to maintain a system of internal accounting controls. We are also required to maintain accurate information and control over sales and distributors’ activities that may fall within the purview of the FCPA, its books and records provisions and its anti‑bribery provisions.
The standard of intent and knowledge in the Anti‑Bribery cases is minimal, and intent and knowledge are usually inferred from that fact that bribery took place. The accounting provisions do not require intent. Violations of the FCPA’s anti‑bribery provisions for corporations and other business entities may result in a fine of up to $2 million and officers, directors, stockholders, employees, and agents are subject to a fine of up to $100,000 and imprisonment for up to five years. Other countries, including the United Kingdom and other OECD Anti‑Bribery Convention members, have similar anti‑corruption regulations, such as the United Kingdom Bribery Act.
When marketing our tests outside of the United States, we are subject to foreign regulatory requirements governing human clinical testing, export of tissue, marketing approval for our products and performance and reporting of tests on a local basis. These requirements vary by jurisdiction, differ from those in the United States and may require us to perform additional pre‑clinical or clinical testing. In many countries outside of the United States, coverage, pricing and reimbursement approvals are also required in order for our tests to be made available to patients.
Patents and Proprietary Technology
We rely on a combination of patents, patent applications, copyrights and trademarks, as well as contracts, such as confidentiality, material data transfer, license and invention assignment agreements, to protect our intellectual property rights. We also rely upon trade secret laws to protect unpatented know‑how and continuing technological innovation.
As of December 31, 2017, we had 40 issued patents in the United States and 349 issued patents outside of the United States, which includes validated patents issued by the European Patent Office in key European Union countries, covering genes and methods that are components of the Oncotype DX breast, colon and prostate cancer tests or research methods and platform technologies. In addition, we have a number of pending patent applications in the United States and in other countries, including provisional and non‑provisional filings. Our issued U.S. patents expire at various times between 2023 and 2033. Some of these U.S. patent applications also have corresponding pending or granted applications under the Patent Cooperation Treaty in Canada, Europe, Japan, Australia and other jurisdictions. In these patent applications, we have either sole or joint ownership positions. In certain cases where joint ownership positions were created, we have negotiated contractual provisions providing us with the opportunity to acquire exclusive rights under the patent applications. Under some patent applications, we have elected to allow exclusive options to lapse without exercising the option. The joint ownership agreements generally are in the form of material data transfer agreements that were executed at the onset of our collaborations with third parties.
Our patent applications relate to two main areas: gene expression and sequencing technology methods, and gene biomarkers and methods for predicting cancer recurrence and drug response in certain forms of cancer.
We have in the past, and may in the future, receive notices of claims of infringement and misappropriation or misuse of other parties’ proprietary rights and may from time to time receive additional notices. Assertions of misappropriation, infringement or misuse, or actions seeking to establish the validity of our patents could materially or adversely affect our business, financial condition and results of operations.
An adverse determination in litigation or interference proceedings to which we may become a party relating to any patents issued to us in the future, or any patents owned by third parties, could subject us to significant liabilities to third parties
27
or require us to seek licenses from third parties. Furthermore, if we are found to willfully infringe these patents, we could, in addition to other penalties, be required to pay treble damages. If certain aspects of our Oncotype DX tests or other tests are found to infringe the intellectual property rights of others, we may not be able to redesign our Oncotype DX tests or other tests to avoid infringement, or such redesign may take considerable time, and force us to reassess our business plans or obtain a license in order to continue to utilize the Oncotype DX tests as is, which license may not be available on satisfactory or commercially feasible terms, if at all.
All employees and consultants working for us are required to execute confidentiality agreements in connection with their employment and consulting relationships with us. Confidentiality agreements provide that all confidential information developed or made known to others during the course of the employment, consulting or business relationship shall be kept confidential except in specified circumstances. In addition, agreements with employees provide that all inventions conceived by the individual while employed by us are our exclusive property. Despite measures taken to protect our intellectual property, unauthorized parties might copy aspects of our technology or obtain and use information that we regard as proprietary.
Roche License Agreement
On October 28, 2016, we provided notice of termination of a license agreement with Roche Molecular Systems, Inc., or Roche, whereby we non-exclusively licensed from Roche a number of U.S. patents claiming nucleic acid amplification processes known as PCR, homogeneous polymerase chain reaction, and RT‑PCR. We determined to terminate this license agreement because we believe we satisfied all obligations under the agreement.
Research and Development Expenses
Research and development expenses were $62.8 million, $60.2 million and $58.4 million for the years ended December 31, 2017, 2016, and 2015, respectively. In 2015, we made a one-time $5.5 million payment to wind down a previous license agreement and development program. We also continued to conduct research and development studies in breast, prostate and other cancers, including proprietary platforms that incorporate emerging molecular technologies to develop non‑invasive tests that can be performed on blood or urine.
Employees
As of December 31, 2017, we had 863 employees, including 174 in clinical reference laboratory operations, 144 in research and development, including bioinformatics, 345 in sales and marketing, 100 in information technology and systems and 100 in general and administrative functions. None of our U.S.-based employees are covered by collective bargaining arrangements, and we consider our relationship with our employees to be good.
Available Information
We were incorporated in Delaware in August 2000, and our website is located at www.genomichealth.com. We make available free of charge on our website our annual reports on Form 10‑K, quarterly reports on Form 10‑Q, current reports on Form 8‑K and amendments to those reports, as soon as reasonably practicable after we electronically file or furnish such materials to the Securities and Exchange Commission. Our website and the information contained therein or connected thereto are not intended to be incorporated into this Annual Report on Form 10‑K.
Risks Relating to our Business and Business Strategy
We have a history of net losses, we may incur net losses in the future, and we expect to continue to incur significant expenses to develop and market our tests and enter into collaborations, which may make it difficult for us to achieve sustained profitability.
We have historically incurred substantial net losses. From our inception in August 2000 through December 31, 2017, we had an accumulated deficit of $245.9 million. We expect to continue to invest in our product pipeline, including our current Oncotype DX tests and future commercialized products, and to invest in our global commercial infrastructure, our laboratory operations, commercial collaborations and next generation sequencing, or NGS, and other technologies. For the year ended December 31, 2017, our research and development expenses were $62.8 million and our selling and marketing expenses were
28
$157.0 million. We expect our expense levels to continue to increase for the foreseeable future as we seek to globally expand the clinical utility of our Oncotype DX breast and prostate cancer tests, drive adoption of and reimbursement for our Oncotype DX colon cancer and prostate cancer tests and develop and commercialize new tests, including Oncotype DX AR-V7 Nucleus Detect, the in-vitro diagnostic, or IVD, version of our Oncotype DX breast cancer test, and the potential IsoPSA IVD test for high-risk prostate cancer. As a result, we will need to generate significant growth in revenues in order to achieve sustained profitability. Our failure to achieve increased revenue or sustained profitability in the future could cause the market price of our common stock to decline.
If third‑party payors, including managed care organizations and Medicare, do not provide reimbursement, breach, rescind or modify their contracts or reimbursement policies or delay payments for our tests, or we are unable to successfully renegotiate reimbursement contracts, our commercial success could be compromised.
Physicians and patients might not order our tests unless third‑party payors, such as managed care organizations as well as government payors such as Medicare and Medicaid and government payors outside of the United States, pay a substantial portion of the test price. Reimbursement by a payor may depend on a number of factors, including a payor’s determination that tests using our technologies are not experimental or investigational, and that they are medically necessary, cost-effective, supported by peer-reviewed publications and included in clinical practice guidelines. There is uncertainty concerning third-party payor reimbursement of any test incorporating new technology, including tests developed using our Oncotype platform.
Our Oncotype DX invasive breast cancer test has received certain negative assessments in the past relating to technology criteria for clinical effectiveness and appropriateness for use in patients with N+ disease, and our tests may receive similar negative assessments in the future. Since each payor makes its own decision as to whether to establish a policy to reimburse our tests, seeking these approvals is a time-consuming and costly process. To date, we have positive coverage determinations for our Oncotype DX breast cancer test for N‑, ER+ patients from most third‑party payors in the United States through contracts, agreements or policy decisions. We cannot be certain that coverage for this test will be provided in the future by additional third‑party payors or that existing contracts, agreements or policy decisions or reimbursement levels, including tests processed as out of network, will remain in place or be fulfilled within existing terms and provisions. From time to time payors change processes that may affect timely payment. These changes may result in uneven cash flow or impact the timing of revenue recognized with these payors.
We have obtained limited reimbursement from private third-party payors in the United States for our Oncotype DX colon cancer test and for our Oncotype DX breast cancer test for N+ and DCIS patients. Until further clinical data is presented, our N+ and DCIS indication for our breast cancer test and our colon cancer test may be considered investigational by payors and therefore may not be covered under their reimbursement policies.
We have obtained Medicare reimbursement coverage for our prostate cancer test for low and very-low risk patients and for favorable intermediate-risk patients. However, we may not be able to obtain Medicare reimbursement coverage for our prostate cancer test for patients with different risk profiles or obtain other third-party payor reimbursement for patients with colon or prostate cancer or with N+ breast cancer patients that is similar to the coverage we have obtained for our invasive breast cancer test for N-, ER- patients. We believe that it may take several years to achieve reimbursement with a majority of third-party payors for our tests. If we fail to establish broad adoption of and reimbursement for all of our tests and any future tests we may develop, our reputation could be harmed and our future prospects and our business could suffer.
Under the terms of the coverage determinations for our Oncotype DX prostate cancer test, coverage for the test for patients with certain risk profiles is limited to tests ordered by physicians who agree to participate in a Certification and Training Registry, or CTR, and to provide certain information about Medicare beneficiaries who receive our test. If physicians do not timely submit necessary information as part of participating in the CTR, the timeframe in which we are reimbursed and recognize revenue for those tests may be accordingly delayed and negatively affect our results of operations.
Changes in payment rates may result in delays receiving payments and a related increase in accounts receivable balances as payors update their billing systems to reflect the changes. Additionally, on a five-year rotational basis, Medicare requests bids for its regional Medicare Administrative Contractor, or MAC, services. In September 2013, the claims processing function for our jurisdiction transitioned from Palmetto to Noridian Healthcare Solutions, although coverage determinations for our tests remain with Palmetto at this time through the MolDx Program. Future changes in the MAC with jurisdiction over our tests may affect our ability to obtain Medicare coverage and reimbursement for products for which we have coverage, for products for which we do not yet have coverage or for any products we may launch in the future or delay payments.
If we are unable to obtain or maintain reimbursement from both private and public payors for our existing tests or new
29
tests or test enhancements we may develop in the future, our ability to generate revenues could be limited. We have in the past, and will likely in the future, experience delays and temporary interruptions in the receipt of payments from third-party payors due to modifications in existing contracts or arrangements, contract implementation matters, documentation requirements and other issues, which could cause our revenues to fluctuate from period to period.
Our financial results depend largely on the sales of one test, our Oncotype DX invasive breast cancer test, and we will need to generate sufficient revenues from this and other tests to run our business and achieve profitability.
For the near future, we expect to continue to derive a substantial majority of our revenues from sales of one test, our Oncotype DX invasive breast cancer test. While we launched our test for colon cancer in January 2010, we do not expect to recognize significant revenues from this test. We are in various stages of research and development for other tests that we may offer as well as for enhancements to our existing tests. We may not be able to successfully commercialize tests for other cancers or diseases. If we are unable to increase sales of our Oncotype DX invasive breast cancer test, establish expanded adoption of and reimbursement for our prostate cancer or DCIS tests, or successfully develop and commercialize new products or product enhancements to our currently commercialized tests, our revenues and our ability to achieve sustained profitability would be impaired.
The prices at which our tests are reimbursed may be reduced by Medicare and private and other payors, and any such changes could have a negative impact on our revenues.
Even if we are being reimbursed for our tests, Medicare, Medicaid and other payors may withdraw their coverage policies, cancel their contracts with us at any time, review and adjust the rate of reimbursement, require co-payments from patients or stop paying for our tests, which would reduce our revenues. In addition, insurers, including managed care organizations as well as government payors such as Medicare and Medicaid, have increased their efforts to control the cost, utilization and delivery of healthcare services. These measures have resulted in reduced payment rates for and decreased utilization of clinical laboratory services, as well as an increase in the administrative requirements for reimbursement of claims. Noridian Healthcare Solutions and Palmetto GBA, the MACs, that process Medicare claims and set Medicare coverage policies, respectively, for most tests billed by our laboratory and other MACs review coverage decisions regularly.
The Protecting Access to Medicare Act of 2014, or PAMA, implements a substantial new payment system for clinical laboratory tests under the Clinical Laboratory Fee Schedule, or CLFS. Under PAMA, Medicare payment rates for tests are equal to the volume-weighted median of the private payor payment rates for such tests. The payment rates calculated under PAMA apply to our tests effective as of January 1, 2018, and will be reviewed annually for “advanced diagnostic laboratory tests” (and every three years for other tests), based on private payor payment rates and volumes. Laboratories that fail to report or erroneously report the required payment information may be subject to substantial civil money penalties. We believe our Oncotype DX tests each meet the criteria to be considered advanced diagnostic laboratory tests. We may or may not, however, seek designation as an advanced diagnostic laboratory test for any of our established tests. There can be no assurance under PAMA that adequate Medicare payment rates will continue to be assigned to our tests.
If we are unable to obtain or maintain adequate reimbursement for our tests outside of the United States, our ability to expand internationally will be compromised.
The majority of our international Oncotype DX breast and colon cancer test revenues come from direct payor reimbursement, payments from our distributors, and patient self‑pay. In many countries outside of the United States, various coverage, pricing and reimbursement approvals are required for our tests to be available to patients. We expect that it will take several years to establish broad coverage and reimbursement for our tests with payors in countries outside of the United States, and our efforts may not be successful. Even if public or private reimbursement is obtained, it may cover competing tests, or the reimbursement may be conditioned upon local performance of the tests or other requirements we may have difficulty satisfying. Reimbursement levels outside of the United States may vary considerably from the domestic reimbursement amounts we receive. In addition, because we rely on distributors to obtain reimbursement for our tests outside of the United States, to the extent we do not have direct reimbursement arrangements with payors, we may not be able to retain reimbursement coverage in certain countries with a particular payor if our agreement with a distributor is terminated or expires, if a distributor fails to pay us or for other reasons. We may also be negatively affected by the financial instability of, and austerity measures implemented by, several countries in the European Union and elsewhere.
30
We depend on Medicare for a significant portion of our product revenues and if Medicare or other significant payors stop providing reimbursement or decrease the amount of reimbursement for our tests, our revenues could decline.
Reimbursement on behalf of patients covered by Medicare accounted for 22%, 21% and 20% of our product revenues for the years ended December 31, 2017, 2016 and 2015, respectively. Accounts receivable on behalf of patients directly covered by Medicare represented 23%, 24% and 14% of our total accounts receivable at December 31, 2017, 2016 and 2015, respectively. While there were no other third-party payors representing 10% or more of our product revenues for these periods, there have been in the past, and may be in the future, payors accounting for 10% or more of our product revenues. Because the majority of stage II and stage III colon cancer patients and prostate cancer patients in the United States are age 65 and over, and thus eligible for Medicare, we may become more dependent on Medicare reimbursement in the future. It is possible that Medicare or other third-party payors that provide reimbursement for our tests may suspend, revoke or discontinue coverage at any time, may require co-payments from patients, or may reduce the reimbursement rates payable to us. Any such action could have a negative impact on our revenues.
Because of Medicare billing rules or changes in Medicare billing rules and processes, we may not receive reimbursement for all tests provided to Medicare patients or may experience delays of receiving payments.
Effective January 1, 2018, for Medicare beneficiaries who were hospital outpatients at the time the tumor tissue samples were obtained, we may bill for tests that are performed following an outpatient encounter. Payment for our Oncotype DX tests performed on Medicare beneficiaries who were hospital inpatients at the time the tumor tissue or blood samples were obtained and whose tests were ordered less than 14 days from discharge must be bundled into the payment that the hospital receives for the services provided. In these circumstances, hospitals are required to furnish services such as our tests as “services furnished under arrangements between a provider and an outside vendor” and only the hospital may bill Medicare for such tests. Under these circumstances, for us to obtain payment for these services, we are required to bill individual hospitals for tests ordered for Medicare beneficiaries. Such hospitals have generally been unwilling to enter into written agreements with us to assume the financial responsibility for these tests ordered for Medicare beneficiaries and consequently we generally cancel such orders when received within the 14-day timeframe when written agreements from such hospitals are not in place.
These billing rules may lead to confusion regarding whether Medicare provides adequate reimbursement for our tests, and could discourage providers from ordering our tests for Medicare patients. In addition, compared to our breast cancer tests, a greater proportion of eligible patients for our colon and prostate tests are covered by Medicare. We cannot assure you that Medicare will continue these billing rules in their current form, that Medicare not will seek to expand the scope of its payment bundling rules in the future, or that other payors will not adopt similar billing rules. In addition, changes in Medicare billing rules and processes could result in delays in receiving payments and any such delays could affect our results of operations.
If our Oncotype laboratory facilities become inoperable, we will be unable to perform our tests and our business will be harmed.
We do not have redundant clinical reference laboratory facilities outside of Redwood City, California for our Oncotype DX tests. Redwood City is situated near active earthquake fault lines. Our facilities and the equipment we use to perform our tests would be costly to replace and could require substantial lead time to repair or replace. Our facilities may be harmed or rendered inoperable by natural or man‑made disasters, including earthquakes, flooding and power outages, which may render it difficult or impossible for us to perform our tests for some period of time. The inability to perform our tests or the backlog of tests that could develop if our facility is inoperable for even a short period of time may result in the loss of customers or harm our reputation, and we may be unable to regain those customers in the future. Although we possess insurance for damage to our property and the disruption of our business, this insurance may not be sufficient to cover all of our potential losses and may not continue to be available to us on acceptable terms, if at all.
In order to rely on a third party to perform our tests, we could only use another facility with established state licensure and CLIA accreditation under the scope of which Oncotype tests could be performed following validation and other required procedures. We cannot assure you that we would be able to find another CLIA‑certified facility willing to comply with the required procedures, that this laboratory would be willing to perform the tests for us on commercially reasonable terms, or that it would be able to meet our quality standards. In order to establish a redundant clinical reference laboratory outside of our Redwood City, California facilities, we would have to spend considerable time and money securing adequate space, constructing the facility, recruiting and training employees, and establishing the additional operational and administrative infrastructure necessary to support a second facility. We may not be able, or it may take considerable time, to replicate our testing processes or results in a new facility. Additionally, any new clinical reference laboratory facility opened by us would
31
be subject to certification under CLIA and licensing by several states, including California and New York, which could take a significant amount of time and result in delays in our ability to resume operations.
We may acquire other businesses, form joint ventures or make investments in other companies or technologies that could harm our operating results, dilute our stockholders’ ownership, increase our debt or cause us to incur significant expense.
As part of our business strategy, we may pursue acquisitions of complementary businesses and assets, as well as technology licensing arrangements or other collaborations. We also may pursue strategic alliances that leverage our core technology and industry experience to expand our product offerings or distribution, or make investments in other companies. We have in the past and may in the future experience losses related to the recognition of our portion of the net losses of equity method investees, and we may in the future experience impairment losses related to our investments in companies if we determine that the value of an investment is impaired. Losses related to our investments in other companies could have a material negative effect on our results of operations. We have no experience with respect to acquiring other companies and only recent experience with respect to the formation of strategic alliances and joint ventures. If we make any acquisitions, we may not be able to integrate these acquisitions successfully into our existing business, and we could assume unknown or contingent liabilities. Any future acquisitions by us also could result in significant write‑offs or the incurrence of debt and contingent liabilities, any of which could harm our operating results. Integration of an acquired company also may require management resources that otherwise would be available for ongoing development of our existing business. We may not identify or complete these transactions in a timely manner, on a cost‑effective basis, or at all, and we may not realize the anticipated benefits of any acquisition, technology license, strategic alliance, joint venture or investment. Additionally, although we are not currently a majority investor in any other company, we cannot guarantee that a company in whom we invest in the future will not be considered a variable interest entity, or VIE, under relevant accounting standards and guidance. If an entity in which we invest is determined to be a VIE, and we are determined to be the primary beneficiary of that VIE, we may have to consolidate that entity’s financial results with ours, and such consolidation could have a negative effect on our financial results.
To finance any acquisitions or investments, we may choose to issue shares of our common stock as consideration, which would dilute the ownership of our stockholders. Periods of upheaval in the capital markets and world economy have in the past, and may in the future, cause volatility in the market price of our common stock. If the price of our common stock is low or volatile, we may not be able to acquire other companies for stock. Alternatively, it may be necessary for us to raise additional funds for acquisitions through public or private financings. Additional funds may not be available on terms that are favorable to us, or at all.
International expansion of our business exposes us to business, regulatory, political, operational, financial, compliance and economic risks associated with doing business outside of the United States.
Our business strategy incorporates international expansion, including increasing the size of and maintaining direct sales and physician outreach and education capabilities outside of the United States and expanding our relationships with international payors and distributors. Doing business internationally involves a number of risks, including:
|
· |
difficulties in complying with multiple, conflicting and changing laws and regulations such as tax laws, export and import restrictions, employment laws, data protection laws, regulatory requirements and other governmental approvals, permits and licenses; |
|
· |
significant competition from local and regional product offerings; |
|
· |
difficulties in complying with unclear product regulations in various jurisdictions; |
|
· |
difficulties in staffing and managing foreign operations; |
|
· |
complexities associated with managing multiple payor reimbursement regimes, government payors or patient self‑pay systems; |
|
· |
logistics and regulations associated with shipping tissue samples or complying with local regulations concerning the analysis of tissue, including infrastructure conditions and transportation delays; |
|
· |
limits in our ability to penetrate international markets if we are not able to process tests locally; |
32
|
· |
lack of intellectual property protection in certain markets; |
|
· |
financial risks, such as longer payment cycles, difficulty collecting accounts receivable, the impact of local and regional financial crises on demand and payment for our tests and exposure to foreign currency exchange rate fluctuations; |
|
· |
natural disasters, political and economic instability, including wars, terrorism, and political unrest, outbreak of disease, boycotts, curtailment of trade and other business restrictions; and |
|
· |
regulatory and compliance risks that relate to maintaining accurate information and control over the activities of our salesforce and distributors that may fall within the purview of the U.S. Foreign Corrupt Practices Act, or FCPA, its books and records provisions or its anti‑bribery provisions. |
Any of these factors could significantly harm our future international expansion and operations and, consequently, our revenues and results of operations.
We face risks associated with currency exchange rate fluctuations, which could adversely affect our operating results.
We receive a portion of our revenues and pay a portion of our expenses in currencies other than the U.S. dollar, such as the Euro, the Swiss franc, the British pound and the Canadian dollar. As a result, we are at risk from exchange rate fluctuations between such foreign currencies and the U.S. dollar, which could affect our results of operations. For the year ended December 31, 2017, approximately 9% of our product revenues came from foreign denominated currencies. If the U.S. dollar strengthens against foreign currencies, the translation of these foreign currency denominated transactions will result in decreased revenues and operating expenses and increased net losses. We may not be able to offset adverse foreign currency impact with increased revenues. In September 2017, we entered into forward contracts to mitigate the impact of adverse movements in foreign exchange rates related to the re-measurement of monetary assets and liabilities and hedge our foreign currency exchange rate exposure. Even with this strategy in place to mitigate balance sheet foreign currency risk, we will not eliminate our exposure to foreign exchange rate fluctuations on our financial results.
If it became necessary and we were unable to raise additional capital on acceptable terms in the future, it may limit our ability to develop and commercialize new tests and technologies and expand our operations.
We expect capital outlays and operating expenditures to increase over the next several years as we expand our infrastructure, commercial operations and research and development activities. Specifically, we may need to raise capital to, among other things, expand and fund the commercialization of our products, increase our selling and marketing efforts, further expand our clinical laboratory operations, technologies and research and development activities, invest in complementary businesses or assets or finance capital expenditures and general and administrative expenses.
Our present and future funding requirements will depend on many factors, including establishing and maintaining reimbursement arrangements with third-party payors, costs associated with expanding our commercial and laboratory operations, spending on research and development activities, costs associated with acquiring, licensing or investing in new technologies or complementary businesses, costs associated with protecting our intellectual property rights, costs associated with international expansion, and the costs and potential delays involved with regulatory clearances and approvals.
We cannot assure you that we would be able to obtain additional funds on acceptable terms, or at all. If we raise funds by issuing equity securities, dilution to our stockholders could result. Any equity or debt securities issued also may provide for rights, preferences or privileges senior to those of holders of our common stock and could impose significant restrictions on our operations. If we raise funds through collaborations and licensing arrangements, we might be required to relinquish significant rights to our technologies or products, or grant licenses on terms that are not favorable to us. If we are not able to secure additional funding when needed, we may have to delay, reduce the scope of or eliminate one or more research and development programs or selling and marketing initiatives. Any or all of these factors could harm our business, operating results and financial condition.
33
We may be unable to manage our future growth and operational expansion effectively, which could make it difficult to execute our business strategy.
Future growth will impose significant added responsibilities on management, including the need to identify, recruit, train and integrate additional employees. In addition, rapid and significant growth may place strain on our administrative and operational infrastructure, including customer service and our clinical laboratory. Our ability to manage our operations and growth will require us to continue to improve our operational, financial and management controls, reporting systems and procedures. If we are unable to manage our growth effectively, it may be difficult for us to execute our business strategy.
The implementation and transition to a new enterprise resource planning system to streamline a broad range of business processes and functional areas including order fulfillment, sample processing, customer service, supply chain management, and others has, in some cases, resulted in delays in access to, or could result in errors in, critical business and financial information. Unexpected errors or delays could also harm our ability to operate certain aspects of our business or to file our periodic reports in a timely manner.
We are dependent on our information technology and telecommunications systems, and any failure of these systems could harm our business.
We depend on information technology, or IT, and telecommunications systems for significant aspects of our operations. In addition, our third‑party billing and collections provider is dependent upon telecommunications and data systems provided by outside vendors and information it receives from us on a regular basis. These IT and telecommunications systems support a variety of functions, including test processing, sample tracking, quality control, customer service and support, billing and reimbursement, research and development activities, and our general and administrative activities. Failures or significant downtime of our IT or telecommunications systems or those used by our third‑party service providers could prevent us from processing tests, providing test results to physicians, billing payors, processing reimbursement appeals, handling patient or physician inquiries, conducting research and development activities, and managing the administrative aspects of our business. Any disruption or loss of IT or telecommunications systems on which critical aspects of our operations depend could have an adverse effect on our business and our product revenues.
Security breaches, loss of data and other disruptions could compromise sensitive information related to our business or prevent us from accessing critical information and expose us to liability, which could adversely affect our business and our reputation.
In the ordinary course of our business, we and our third-party billing and collections provider collect and store sensitive data, including legally protected health information, sensitive personal data, credit card information, personally identifiable information about our employees, customers and patients, intellectual property, and our proprietary business information and that of our customers, payors and collaboration partners. We manage and maintain our applications and data utilizing a combination of on‑site systems, managed data center systems and cloud‑based data center systems. These applications and data encompass a wide variety of business-critical information including research and development information, commercial information and business and financial information. We face four primary risks relative to protecting this critical information, including loss of access risk, inappropriate disclosure risk and inappropriate modification risk combined with the risk of our ability to identify and audit our controls over the first three risks.
The secure processing, storage, maintenance and transmission of this critical information is vital to our operations and business strategy, and we devote significant resources to protecting such information. Although we take measures to protect sensitive information from unauthorized access or disclosure, our information technology and infrastructure, and that of our third-party billing and collections provider, may be vulnerable to attacks by hackers or viruses or breached due to employee error, malfeasance or other disruptions. Any such breach or interruption could compromise our networks and the information stored there could be accessed by unauthorized parties, publicly disclosed, lost or stolen. Any such access, disclosure or other loss of information could result in legal claims or proceedings, liability under laws that protect the privacy of personal information, such as the Health Insurance Portability and Accountability Act of 1996, similar state data protection regulations, the E.U. General Data Protection Regulation, or GDPR, and other regulations, the breach of which could result in significant penalties. Unauthorized access, loss or dissemination could also disrupt our operations, including our ability to process tests, provide test results, bill payors or patients, process claims and appeals, provide customer assistance services, conduct research and development activities, collect, process and prepare company financial information, provide information about our tests and other patient and physician education and outreach efforts through our website, manage the administrative aspects of our business and damage our reputation, any of which could adversely affect our business.
34
In addition, the interpretation and application of consumer, health‑related and data protection laws in the U.S., Europe and elsewhere are often uncertain, contradictory and in flux. For example, in October 2015, the European Court of Justice invalidated the U.S./E.U. Safe Harbor Framework regarding the overseas transfer of E.U. residents’ personal data, under which we held certification. Companies, such as us, who relied upon the invalid Safe Harbor Framework were exposed to additional scrutiny from the E.U. data protection authorities without the protection of the Safe Harbor Framework. The U.S.-E.U. Privacy Shield, or the Privacy Shield, has been open to registrants as of August 1, 2016. We have self-certified with the Department of Commerce for compliance with the Privacy Shield, which we believe will mitigate customer concerns about overseas data transfers. However there continue to be concerns about whether the Privacy Shield will face additional challenges (similar to those that invalidated the Safe Harbor Framework), and it is not guaranteed that companies who have self-certified under the Privacy Shield will be free of additional ongoing scrutiny by E.U. data protection authorities. Compliance with Privacy Shield requirements does not, in addition, equate to compliance with the stringent requirements of the GDPR. European data protection authorities could interpret or apply European data protection law in a manner that is inconsistent with our practices. If so, this could result in prohibitions on processing of data required to perform our tests in Europe or government-imposed fines, or both, which could adversely affect our business. Complying with these various laws could in addition cause us to incur substantial costs or require us to change our business practices and compliance procedures in a manner adverse to our business.
If we were sued for product liability or professional liability, we could face substantial liabilities that exceed our resources.
The marketing, sale and use of our tests could lead to the filing of product liability claims if someone were to allege that our tests failed to perform as designed. We may also be subject to liability for errors in the test results we provide to physicians or for a misunderstanding of, or inappropriate reliance upon, the information we provide. For example, physicians sometimes order our Oncotype DX breast cancer test for patients who do not have the specific clinical attributes indicated on the report form as those for whom the test provides clinical information validated by studies. It is our practice to offer medical consultation to physicians ordering our test for such patients, including patients with ER‑ breast cancers. A product liability or professional liability claim could result in substantial damages and be costly and time consuming for us to defend. Although we maintain product and professional liability insurance, we cannot assure you that our insurance would protect us from the financial impact of defending against product liability or professional liability claims or any judgments, fines or settlement costs arising out of any such claims. Any product liability or professional liability claim brought against us, with or without merit, could increase our insurance rates or prevent us from securing insurance coverage in the future. Additionally, any product liability lawsuit could cause injury to our reputation, result in the recall of our products, or cause current clinical partners to terminate existing agreements and potential clinical partners to seek other partners, any of which could impact our results of operations.
If we use hazardous materials in a manner that causes injury, we could be liable for damages.
Our activities currently require the use of hazardous materials and medical specimens. We cannot eliminate the risk of accidental contamination or injury to employees or third parties from the use, storage, handling or disposal of these materials or specimens. In the event of contamination or injury, we could be held liable for any resulting damages, and any liability could exceed our resources or any applicable insurance coverage we may have. Additionally, we are subject on an ongoing basis to federal, state and local laws and regulations governing the use, storage, handling and disposal of these materials and specified waste products, as well as regulations relating to the safety and health of laboratory employees. The cost of compliance with these laws and regulations may become significant and could negatively affect our operating results.
We incur increased costs as a result of operating as a public company, and must continually implement additional and expensive business systems, procedures and controls to satisfy public company reporting requirements.
As a public reporting company, we are required to comply with the Sarbanes-Oxley Act of 2002 and the related rules and regulations of the Securities and Exchange Commission. Compliance with Section 404 of the Sarbanes-Oxley Act and other requirements has increased our costs and required additional management resources. We will need to continue to implement additional finance, accounting, and business operating systems, procedures, and controls as we grow our business and organization and to satisfy existing reporting requirements. If we fail to maintain or implement adequate controls, if we are unable to complete the required Section 404 assessment as to the adequacy of our internal control over financial reporting in future Form 10-K filings, or if our independent registered public accounting firm is unable to provide us with an unqualified report as to the effectiveness of our internal control over financial reporting in future Form 10-K filings, the market price of our stock could decline and we could be subject to sanctions or investigations by the SEC, Nasdaq or other regulatory authorities which could require additional financial and management resources.
35
Risks Related to Governmental Regulation
Healthcare policy changes, including legislation reforming the U.S. healthcare system, may have a material adverse effect on our financial condition and results of operations.
The Patient Protection and Affordable Care Act, as amended by the Health Care and Education Affordability Reconciliation Act, collectively, the Affordable Care Act, or ACA, enacted in March 2010, makes changes that significantly impact the pharmaceutical and medical device industries and clinical laboratories. For example, beginning in 2013 through December 31, 2015, each medical device manufacturer was required to pay sales tax in an amount equal to 2.3% of the price for which such manufacturer sells its medical devices that are listed with the FDA. The medical device tax has been suspended since 2016, but is scheduled to be re-imposed in 2020. Various proposals have been put forth, including by the FDA, to regulate LDTs, as medical devices. Although none of our LDTs, such as our Oncotype DX breast, colon and prostate cancer tests, are currently listed with the FDA, we cannot assure you that the tax will not apply to services such as ours in the future.
Other significant measures contained in the ACA include, for example, coordination and promotion of research on comparative clinical effectiveness of different technologies and procedures, initiatives to revise Medicare payment methodologies, such as bundling of payments across the continuum of care by providers and physicians, and initiatives to promote quality indicators in payment methodologies. The ACA also includes significant new fraud and abuse measures, including required disclosures of financial arrangements with physician customers, lower thresholds for violations and increasing potential penalties for such violations. In addition to the ACA, various healthcare reform proposals have also emerged from federal and state governments. The current U.S. President and other U.S. lawmakers have made statements about potentially repealing and/or replacing the ACA and efforts are currently underway in the U.S. Congress to consider legislative actions to that end. Notably, Congress enacted legislation in 2017 that eliminates the ACA’s individual insurance mandate beginning in 2019, which may significantly impact the number of covered lives participating in exchange plans. We are monitoring the impact of the ACA and proposals to repeal, replace or refine the ACA to enable us to determine the trends and changes that may potentially impact our business over time.
Under the Budget Control Act of 2011, which went into effect for dates of service on or after April 1, 2013, Medicare payments, including payments to clinical laboratories, are subject to a 2% reduction due to implementation of the automatic expense reductions (sequester). Reductions made by the Congressional sequester are applied to total claims payment made. The sequester reductions do not result in a rebasing of the negotiated or established Medicare or Medicaid reimbursement rates.
Although individual states’ reimbursement methodology has not materially affected the payment rate for our tests recently, we cannot be certain that future changes will not affect payment rates. We also cannot predict whether future healthcare initiatives will be implemented at the federal or state level or in countries outside of the United States in which we may do business, or the effect any future legislation or regulation will have on us. The taxes imposed by new legislation, cost reduction measures and the expansion in government’s role in the U.S. healthcare industry may result in decreased profits to us, lower reimbursements by payors for our products or reduced medical procedure volumes, all of which may adversely affect our business, financial condition and results of operations. In addition, sales of our tests outside the United States make us subject to foreign regulatory requirements and cost‑reduction measures, which may also change over time.
If the FDA were to begin regulating our laboratory developed tests, we could incur substantial costs and time delays associated with meeting requirements for pre‑market clearance or approval or we could experience decreased demand for or reimbursement of our tests.
Clinical laboratory tests like ours are regulated under the Clinical Laboratory Improvement Amendments of 1988, or CLIA, as well as by applicable state laws. Diagnostic kits that are sold and distributed through interstate commerce are regulated as medical devices by the FDA. Most LDTs are not currently subject to FDA regulation, although reagents or software provided by third parties and used to perform LDTs may be subject to regulation. We believe that our Oncotype tests are not diagnostic kits and also believe that they are LDTs. As a result, we believe our tests should not be subject to regulation at this time under established FDA policies. The container we provide for collection and transport of tumor samples from a pathology laboratory to our clinical reference laboratory may be a medical device subject to FDA regulation but is currently exempt from pre‑market review by the FDA.
At various times since 2006, the FDA has issued documents outlining its intent to require varying levels of FDA oversight of many LDTs, including our tests. In October 2014, the FDA issued draft guidance that sets forth a proposed risk-based regulatory framework that would apply varying levels of FDA oversight to LDTs. The FDA has indicated that it does not intend to implement its proposed framework until the draft guidance documents are finalized. On January 13, 2017, the
36
FDA published a discussion paper in which the FDA outlined a substantially revised possible approach to the oversight of LDTs. The discussion paper explicitly states that it is not a final version of the 2014 draft guidance and that it does not represent the FDA’s formal position. It is unclear at this time if or when the FDA will finalize its plans to end enforcement discretion for LDTs, and even then, the new regulatory requirements are expected to be phased-in over time. However, the FDA may decide to regulate certain LDTs on a case-by-case basis at any time.
Legislative proposals addressing oversight of genetic testing and LDTs have been introduced in previous Congresses, and we expect that new legislative proposals will be introduced from time to time in the future. We cannot provide any assurance that FDA regulation, including pre-market review, will not be required in the future for our tests, whether through finalization of guidance issued by the FDA, new enforcement policies adopted by the FDA or new legislation enacted by Congress. It is possible that legislation will be enacted into law or guidance could be issued by the FDA which may result in increased regulatory burdens for us to continue to offer our tests or to develop and introduce new tests.
If pre-market review is required for our current LDTs, our business could be negatively impacted until such review is completed and clearance or approval is obtained, and the FDA could require that we stop selling our tests pending pre‑market clearance or approval. If our tests are allowed to remain on the market but there is uncertainty about the regulatory status of our tests, if they are labeled investigational by the FDA, or if labeling claims the FDA allows us to make are more limited than the claims we currently make, orders or reimbursement may decline. The regulatory approval process may involve, among other things, successfully completing additional clinical trials and submitting a pre‑market clearance notice or filing a pre‑market approval application with the FDA. If pre‑market review is required by the FDA, there can be no assurance that our tests will be cleared or approved on a timely basis, if at all, nor can there be assurance that the labeling claims cleared or approved by the FDA will be consistent with our current claims or adequate to support continued adoption of and reimbursement for our tests. Ongoing compliance with FDA regulations would increase the cost of conducting our business, and subject us to inspection by and the regulatory requirements of the FDA, for example registration and listing and medical device reporting, and penalties in the event we fail to comply with these requirements. We may also decide voluntarily to pursue FDA pre‑market review of our tests if we determine that doing so would be appropriate.
We cannot predict the ultimate timing or form of final FDA guidance, legislation or regulation of LDTs and the potential impact on our existing tests, our tests in development or the materials used to perform our tests. While we qualify all materials used in our tests according to CLIA regulations, we cannot be certain that the FDA will not enact rules or guidance documents which could impact our ability to purchase certain materials necessary for the performance of our tests, such as products labeled for research use only. Should any of the reagents obtained by us from suppliers and used in conducting our tests be affected by future regulatory actions, our business could be adversely affected by those actions, including increasing the cost of testing or delaying and limiting or prohibiting the purchase of reagents necessary to perform testing.
If we were required to conduct additional clinical trials prior to continuing to sell our current tests or launching any other tests we may develop, those trials could result in delays or failure to obtain necessary regulatory approvals or clearances, which could harm our business.
If the FDA decides to regulate any of our LDTs, it may require additional pre-market clinical testing before clearing or approving such tests for commercial sales. Such pre-market clinical testing could delay the commencement or completion of other clinical testing, significantly increase our test development costs, delay commercialization of any future tests, and interrupt sales of our current tests. Many of the factors that may cause or lead to a delay in the commencement or completion of clinical trials may also ultimately lead to delay or denial of regulatory clearance or approval. The commencement of clinical trials may be delayed due to insufficient patient enrollment, which is a function of many factors, including the size of the patient population, the nature of the protocol, the proximity of patients to clinical sites and the eligibility criteria for the clinical trial.
We may find it necessary to engage contract research organizations to perform data collection and analysis and other aspects of our clinical trials, which might increase the cost and complexity of those trials. We may also depend on clinical investigators, medical institutions and contract research organizations to perform certain aspects of the trials. If these parties do not successfully carry out their contractual duties or obligations or meet expected deadlines, or if the quality, completeness or accuracy of the clinical data they obtain is compromised due to the failure to adhere to our clinical protocols or for other reasons, our clinical trials may have to be extended, delayed or terminated. Many of these factors would be beyond our control. We may not be able to enter into replacement arrangements without undue delays or considerable expenditures. If there are delays in testing or approvals as a result of the failure to perform by third parties, our research and development costs would increase, and we may not be able to obtain regulatory clearance or approval for our tests. In addition, we may not be able to establish or maintain relationships with these parties on favorable terms, if at all. Each of these outcomes would harm our ability to market our LDTs, or to achieve sustained profitability.
37
Our business could be harmed by the loss, suspension, or other restriction on a license, certification, or accreditation, or by the imposition of a fine or penalties, under CLIA, its implementing regulations, or other state, federal and foreign laws and regulations affecting licensure or certification, or by future changes in these laws or regulations.
We and certain laboratories with whom we collaborate are subject to CLIA, a federal law that regulates clinical laboratories that perform testing on specimens derived from humans for the purpose of providing information for the diagnosis, prevention or treatment of disease. CLIA regulations mandate specific standards in the areas of personnel qualifications, facilities administration, quality systems, inspections, and proficiency testing. We have a current certificate of accreditation under CLIA to perform testing through our accreditation by the College of American Pathologists, or CAP. To renew this certificate, we are subject to survey and inspection every two years. Inspectors may also make random inspections of our clinical reference laboratory.
Although we are required to hold a certificate of accreditation or compliance under CLIA to perform high complexity testing, we are not required to hold a certificate of accreditation through CAP. We could alternatively maintain a certificate of accreditation from another accrediting organization or a certificate of compliance through inspection by surveyors acting on behalf of the CLIA program. If our accreditation under CAP were to terminate, either voluntarily or involuntarily, we would need to convert our certification under CLIA to a certificate of compliance (or to a certificate of accreditation with another accreditation organization) in order to maintain our ability to perform our clinical tests and to continue commercial operations. Whether we would be able to successfully maintain operations through either of these alternatives would depend upon the facts and circumstances surrounding the termination of our CAP accreditation, such as whether any deficiencies were identified by CAP as the basis for termination and, if so, whether these deficiencies were addressed to the satisfaction of the surveyors for the CLIA program (or another accrediting organization).
We and certain laboratories with whom we collaborate are also required to maintain a California clinical laboratory license to conduct testing in California. California laws establish standards for day‑to‑day operation of our clinical reference laboratory, including the training and skills required of personnel and quality control. In addition, our clinical reference laboratory is required to be licensed on a test‑specific basis by New York State. New York law also mandates proficiency testing for laboratories licensed under New York state law, regardless of whether or not such laboratories are located in New York. Moreover, Pennsylvania, Maryland and Rhode Island require that we hold licenses to test specimens from patients in those states and Florida requires that we hold a license when we receive specimens from clinical laboratories in that state. Other states may have similar requirements or may adopt similar requirements in the future. Finally, we may be subject to regulation in foreign jurisdictions as we seek to expand international distribution of our tests, which may require regulatory review of our tests in order for them to be offered, or may have other limitations such as prohibitions on the export of tissue necessary for us to perform our tests that may limit our ability to distribute outside of the United States.
If we were to lose our CLIA accreditation or California license, whether as a result of a revocation, suspension or limitation, we would no longer be able to sell our tests, which would limit our revenues and harm our business. If we were to lose our license in New York or in other states where we are required to hold licenses, we would not be able to test specimens from those states.
We are subject to numerous U.S. and foreign laws and governmental regulations, and any governmental enforcement action may materially affect our financial condition and business operations.
We are subject to regulation in the United States by both the federal government and the states in which we conduct our business, as well as in other jurisdictions outside of the United States, including:
|
· |
Medicare billing and payment regulations applicable to clinical laboratories; |
|
· |
the Federal Anti‑kickback Law and state anti‑kickback prohibitions; |
|
· |
the Federal physician self‑referral prohibition, commonly known as the Stark Law, and the state equivalents; |
|
· |
the Federal Health Insurance Portability and Accountability Act of 1996 (as amended); |
|
· |
the Medicare civil money penalty and exclusion requirements; |
38
|
· |
the Federal False Claims Act civil and criminal penalties and state equivalents; and |
|
· |
the Foreign Corrupt Practices Act, the United Kingdom Anti‑bribery Act, the European Data Protection Directive, the GDPR, and the E.U. In Vitro Diagnostic Device Regulation, all of which apply or will apply to our international activities. |
The U.S. Attorney’s Offices have increased their scrutiny over the healthcare industry in recent years. The U.S. Congress, Department of Justice, Office of Inspector General of the Department of Health and Human Services, and Department of Defense have all issued subpoenas and other requests for information to conduct investigations of, and commenced civil and criminal litigation against, healthcare companies, related to financial arrangements with health care providers, regulatory compliance, product promotional practices, and documentation, coding and billing practices. In addition, the Federal False Claims Act has led to whistleblowers filing numerous qui tam civil lawsuits against healthcare companies, in part, because a whistleblower can receive a portion of any amount obtained by the government through such a lawsuit.
Governmental enforcement action or qui tam civil litigation against us may result in material costs and occupy significant management resources, even if we ultimately prevail. In addition, governmental enforcement action may result in substantial fines, penalties or administrative remedies, including exclusion from government reimbursement programs and entry into corporate integrity agreements with governmental agencies, which would entail significant obligations and costs.
We have adopted policies and procedures designed to comply with these laws. In the ordinary course of our business, we conduct internal reviews of our compliance with these laws. Our compliance is also subject to governmental review. The growth of our business and sales organization and our expansion outside of the United States may increase the potential of violating these laws or our internal policies and procedures. The risk of our being found in violation of these or other laws and regulations is further increased by the fact that many of them have not been fully interpreted by the regulatory authorities or the courts, and their provisions are open to a variety of interpretations. Any action brought against us for violation of these or other laws or regulations, even if we successfully defend against it, could cause us to incur significant legal expenses and divert our management’s attention from the operation of our business. If our operations are found to be in violation of any of these laws and regulations, we may be subject to any applicable penalty associated with the violation, including civil and criminal penalties, damages and fines, we could be required to refund payments received by us, and we could be required to curtail or cease our operations. Any of the foregoing consequences could seriously harm our business and our financial results.
We are subject to increasingly complex taxation rules and practices, which may affect how we conduct our business and our results of operations.
As our business grows, we are required to comply with increasingly complex taxation rules and practices. We are subject to tax in multiple U.S. tax jurisdictions and in foreign tax jurisdictions as we expand internationally. The development of our tax strategies requires additional expertise and may impact how we conduct our business. Our future effective tax rates could be unfavorably affected by changes in, or interpretations of, tax rules and regulations in the jurisdictions in which we do business or by changes in the valuation of our deferred tax assets and liabilities. Furthermore, we provide for certain tax liabilities that involve significant judgment. We are subject to the examination of our tax returns by federal, state and foreign tax authorities, which could focus on our intercompany transfer pricing methodology as well as other matters. If our tax strategies are ineffective or we are not in compliance with domestic and international tax laws, our financial position, operating results and cash flows could be adversely affected.
Risks Relating to Product Development, Commercialization and Sales of our Products
New test development involves a lengthy and complex process, and we may be unable to commercialize on a timely basis, or at all, any new tests we may develop.
We have tests in development, including an IVD version of our invasive breast cancer test, and devote considerable resources to research and development. There can be no assurance that our new Oncotype tests or IVD versions of our current tests will be capable of reliably predicting the recurrence of cancers with the sensitivity and specificity necessary to be clinically useful and commercially viable. We also cannot be certain that the products we launch will attain widespread use among the intended target of community oncologists. In addition, before we can develop diagnostic tests for new cancers or other diseases and commercialize any new products, we will need to:
|
· |
conduct substantial research and development; |
39
|
· |
conduct validation studies; |
|
· |
expend significant funds; |
|
· |
develop and scale our laboratory processes to accommodate different tests; and |
|
· |
develop and scale our infrastructure to be able to analyze increasingly large amounts of data and to add new capabilities, such as inventory management. |
Our product development process involves a high degree of risk and may take several years. Our product development efforts may fail for many reasons, including:
|
· |
failure of the product at the research or development stage; |
|
· |
difficulty in accessing tissue and blood samples; |
|
· |
challenges in timely patient enrollment in future clinical trials; or |
|
· |
lack of clinical validation data to support the effectiveness of the product. |
Few research and development projects result in commercial products, and success in early clinical trials often is not replicated in later studies. At any point, we may abandon development of a product candidate or we may be required to expend considerable resources repeating clinical trials, which would adversely impact the timing for generating potential revenues from those product candidates. If a clinical validation study fails to demonstrate the prospectively defined endpoints of the study, we might choose to abandon the development of the product or product feature that was the subject of the clinical trial, which could harm our business. In addition, competitors may develop and commercialize competing products faster than we are able to do so.
If we are unable to support demand for our tests, including successfully managing the evolution of our technology and business systems, our business could suffer.
As our test volume grows and we examine additional means through which we can provide our tests, we will need to continue to ramp up our testing capacity, implement increases in scale and related processing, customer service, billing and systems process improvements, and expand our internal quality assurance program, technology and manufacturing platforms to support testing on a larger scale. We will also need additional certified laboratory scientists and other scientific and technical personnel to process higher volumes of our tests. We cannot assure you that any increases in scale, related improvements and quality assurance will be successfully implemented or that appropriate personnel will be available. As additional products are commercialized, we will need to bring new equipment on‑line, implement new systems, technology, controls and procedures and hire personnel with different qualifications. We cannot assure you that any such efforts will not result in delays. Failure to implement necessary procedures, transition to new equipment or processes or to hire the necessary personnel could result in higher cost of processing or an inability to meet market demand. There can be no assurance that we will be able to perform tests on a timely basis at a level consistent with demand, that our efforts to scale our commercial operations will not negatively affect the quality of test results, or that we will be successful in responding to the growing complexity of our testing operations. If we encounter difficulty meeting market demand or quality standards for our tests, our reputation could be harmed and our future prospects and our business could suffer.
We may experience limits on our revenues if physicians or patients decide not to order our tests.
If medical practitioners do not order our Oncotype tests or any future tests developed or offered by us, we will likely not be able to create or maintain demand for our products in sufficient volume for us to achieve sustained profitability. To generate demand, we will need to continue to make oncologists, urologists, surgeons and pathologists aware of the benefits of each type of test through published papers, presentations at scientific conferences and one‑on‑one education by our salesforce. In addition, we will need to demonstrate our ability to obtain and maintain adequate reimbursement coverage from third‑party payors.
Prior to the inclusion of our Oncotype DX invasive breast cancer test in clinical guidelines for treatment of N−, ER+ breast cancer, guidelines and practices regarding the treatment of breast cancer recommended that chemotherapy be considered in most cases, including many cases in which our test might indicate that, based on our clinical trial results, chemotherapy would be of little or no benefit. For these historical reasons, physicians may be reluctant to order a test that may suggest
40
recommending against chemotherapy in treating breast cancer. Moreover, our test provides quantitative information not currently provided by pathologists and it is performed at our facility rather than by the pathologist in a local laboratory, so pathologists may be reluctant to support our test. These facts may make it difficult for us to convince medical practitioners to order our test for their patients, which could limit our ability to generate revenues and achieve sustained profitability.
We will need to continue to educate physicians, patients and payors about the benefits and cost‑effectiveness of our tests and to establish reimbursement arrangements for these tests with payors. We have and expect to continue to hire additional commercial, sales, scientific, technical and other personnel to support this process. If our marketing and educational efforts do not result in sufficient physician or patient demand, we may not be able to obtain adequate reimbursement for our tests. If we fail to successfully establish adoption of and additional reimbursement beyond Medicare for our colon and prostate cancer tests, our reputation could be harmed and our business could suffer.
Some patients may decide not to use our Oncotype tests due to their price, all or part of which may be payable directly by the patient if the applicable payor denies reimbursement in full or in part. Even if medical practitioners recommend that their patients use our tests, patients may still decide not to use our tests, either because they do not want to be made aware of the likelihood of recurrence or they wish to pursue a particular course of therapy regardless of test results. Additionally, the current economic environment in the United States and abroad could continue to negatively impact patients, resulting in higher co‑payments and insurance premiums or the loss of healthcare coverage, which may result in delayed medical checkups or an inability to pay for our tests. If only a small portion of the patient population decides to use our tests, we will experience limits on our revenues and our ability to achieve sustained profitability.
Our dependence on distributors for sales of our Oncotype tests outside of the U.S. could limit or prevent us from selling our test in foreign markets and impact our revenue.
As of December 31, 2017, we have entered into exclusive distribution agreements for the sale of our tests with distributors covering more than 90 countries. We may enter into other similar arrangements to distribute our tests in other countries in the future. We intend to continue to grow our business internationally, and to do so we may need to attract additional distributors to expand the territories in which we sell our tests. Despite contractual obligations, distributors may not commit the necessary resources to market and sell our tests to the level of our expectations. If current or future distributors do not perform adequately, or we are unable to enter into arrangements with distributors to market our tests in particular geographic areas, we may not realize long‑term international revenue growth. In addition, our revenue from distributors could be negatively impacted as a result of changes in business cycles, business or economic conditions, reimbursement rates, changes in foreign currency exchange rates that make our tests more expensive in our distributors’ local currencies or other factors that could affect their ability to pay us for tests on a timely basis or at all.
Our rights to use technologies licensed from third parties are not within our control, and we may not be able to sell our products if we lose our existing rights or cannot obtain new rights on reasonable terms.
We license from third parties technology necessary to develop our products. In return for the use of a third party’s technology, we may agree to pay the licensor royalties based on sales of our products. Royalties are a component of cost of product revenues and impact the margins on our tests. We may need to license other technologies to commercialize future products. We may also need to negotiate licenses to patents and patent applications after launching any of our commercial products. Our business may suffer if these licenses terminate, if the licensors fail to abide by the terms of the license, determine to unilaterally stop supplying technologies or products subject to a license, or fail to prevent infringement by third parties, if the licensed patents or other rights are found to be invalid, if the patents or patent applications are unavailable for license or if we are unable to enter into necessary licenses on acceptable terms.
If we are unable to develop products to keep pace with rapid technological, medical and scientific change, our operating results and competitive position could be harmed.
In recent years, there have been numerous advances in technologies relating to the diagnosis and treatment of cancer. For example, technologies in addition to ours now permit measurement of gene expression in fixed paraffin‑embedded tissue specimens or blood or urine. There have also been advances in methods used to analyze very large amounts of genomic information, specifically NGS. These advances require us to continuously develop our technology, develop new products and enhance existing products to keep pace with evolving standards of care. Our tests could become obsolete unless we continually innovate and expand our products to demonstrate recurrence and treatment benefit in patients treated with new therapies. New treatment therapies typically have only a few years of clinical data associated with them, which limits our ability to perform clinical studies and correlate sets of genes to a new treatment’s effectiveness. Additionally, as new products are developed, evolving industry standards and metrics may slow the widespread adoption of any new products we may introduce. If we are
41
unable to demonstrate the applicability of our tests to new treatments or to keep pace with new industry standards, sales of our test could decline, which would harm our revenues.
If we are unable to compete successfully, we may be unable to increase or sustain our revenues or achieve sustained profitability.
We compete in a rapidly evolving and highly competitive industry, and there are a number of private and public companies that offer products or have conducted research to profile genes and gene expression in breast, colon and prostate cancer, including companies such as Agendia Inc., BioTheranostics, Exact Sciences, Inc. GenomeDx Biosciences Inc., Hologic Inc., Myriad Genetics Inc. (and its Sividon Diagnostics subsidiary), NanoString Technologies Inc., NeoGenomics, Inc. and Qiagen N.V. As we look to expand our research, development and commercialization efforts, we may face competition from companies such as Danaher Corporation (and its Cepheid, Inc. subsidiary), Exosome Diagnostics, Inc., Foundation Medicine, Grail, Guardant Health, MDxHealth, Metamark Genetics, Inc., Natera Inc. and Personal Genome Diagnostics, Inc. Historically, our principal competition for our Oncotype tests has also come from existing diagnostic methods used by pathologists and oncologists, and such traditional diagnostic methods can be difficult to change or supplement. We also face competition from commercial laboratories with strong distribution networks for diagnostic tests, such as Laboratory Corporation of America Holdings and Quest Diagnostics Incorporated. Other potential competitors include companies that develop diagnostic tests such as Roche Diagnostics, a division of Roche Holding, Ltd, and Siemens AG, as well as other companies and academic and research institutions.
In our more recently established prostate cancer market, we face comparatively greater competition than in our breast cancer market, including competition from products which were on the market prior to our product launch and which are supported by clinical studies and published data. This existing direct and indirect competition for tests and procedures may make it difficult to gain market share, impact our ability to obtain reimbursement or result in a substantial increase in resources necessary for us to successfully continue to commercialize our Oncotype DX prostate test and the recently launched Oncotype DX AR-V7 Nucleus Detect test.
As more information regarding cancer genomics becomes available to the public, we anticipate that more products aimed at identifying targeted treatment options will be developed and that these products may compete with ours. In addition, competitors may develop their own versions of our tests in countries where we did not apply for patents, where our patents have not issued or where our intellectual property rights are not recognized and compete with us in those countries, including encouraging the use of their test by physicians or patients in other countries. We have changed the list price of our tests in the past and we expect to change prices for our tests in the future. Any increase or decrease in pricing could impact reimbursement of and demand for our tests. Many of our present and potential competitors have widespread brand recognition and substantially greater financial and technical resources and development, production and marketing capabilities than we do. Others may develop lower‑priced tests that could be viewed by physicians and payors as functionally equivalent to our tests, or offer tests at prices designed to promote market penetration, which could force us to lower the list prices of our tests and impact our operating margins and our ability to achieve sustained profitability. Some competitors have developed tests cleared or approved for marketing by the FDA. There may be a marketing differentiation or perception that an FDA‑cleared or approved test is more desirable than Oncotype tests, which are LDTs, and that may discourage adoption of and reimbursement for our tests. If we are unable to compete successfully against current or future competitors, we may be unable to increase market acceptance for and sales of our tests, which could prevent us from increasing or sustaining our revenues or achieving sustained profitability and could cause the market price of our common stock to decline.
Our research and development efforts will be hindered if we are not able to contract with third parties for access to tissue or complete timely enrollment in future clinical trials.
Under standard clinical practice, tumor biopsies removed from patients are typically chemically preserved and embedded in paraffin wax and stored. Our clinical development relies on our ability to secure access to these archived tumor biopsy samples, as well as information pertaining to their associated clinical outcomes. Generally, the agreements under which we gain access to archival samples are nonexclusive. Other companies study archival samples and often compete with us for access. Additionally, the process of negotiating access to archived samples is lengthy since it typically involves numerous parties and approval levels to resolve complex issues such as usage rights, institutional review board approval, privacy rights, publication rights, intellectual property ownership and research parameters. If we are not able to negotiate access to clinical samples with hospitals, clinical partners, pharmaceutical companies, or companies developing therapeutics on a timely basis, or at all, or if other laboratories or our competitors secure access to these samples before us, our ability to research, develop and commercialize future products will be limited or delayed. Finally, we may not be able to conduct or complete clinical trials on a timely basis if we are not able to enroll sufficient numbers of patients in such trials, and our failure to do so could have an adverse effect on our research and development and product commercialization efforts.
42
If we cannot successfully maintain or manage our current collaborations or enter into new collaborations, our product development could be delayed and our introduction of new products into the market could be adversely affected which could have an adverse effect on our financial results.
We rely on and expect to continue to rely on clinical collaborators to perform a substantial portion of our clinical trial functions. If any of our collaborators were to breach or terminate its agreement with us or otherwise fail to conduct the contracted activities successfully and in a timely manner, the research, development or commercialization of the products contemplated by the collaboration could be delayed or terminated. If any of our clinical collaboration agreements are terminated, or if we are unable to renew those agreements on acceptable terms, we would be required to seek alternatives. We may not be able to negotiate agreements with alternate collaborators on acceptable terms, if at all, and these collaborations may not be successful.
In the past, we have entered into clinical trial collaborations with highly regarded organizations in the cancer field. Our success in the future depends in part on our ability to enter into agreements with other leading cancer organizations. This can be difficult due to internal and external constraints placed on these organizations. Some organizations may limit the number of collaborations they have with any one company so as to not be perceived as biased or conflicted. Organizations may also have insufficient administrative and related infrastructure to enable collaborations with many companies at once, which can prolong the time it takes to develop, negotiate and implement collaboration. Additionally, organizations often insist on retaining the rights to publish the clinical data resulting from the collaboration. We have found the publication of clinical data in peer‑reviewed journals to be a crucial step in commercializing and obtaining reimbursement for tests such as ours, and our inability to control when, if ever, results are published may delay or limit our ability to derive sufficient revenues from any product that may result from a collaboration.
We have only recent experience in commercializing products through collaborations with third parties, which includes our commercial collaboration with Epic Sciences, our in-licensing rights granted by Cleveland Diagnostics, and our license and development agreement with Biocartis. The collaboration with Epic Sciences poses a number of risks, including, among others, whether we will be able to obtain adequate reimbursement for Oncotype DX AR-V7 Nucleus Detect with both public and private payors, whether our commercial channel will be successful in creating market demand for Oncotype DX AR-V7 Nucleus Detect, whether Epic Sciences is able to obtain and maintain appropriate state laboratory licensure, and whether our information technology and reporting systems are adequately and securely integrated with those of Epic Sciences. We are also subject to legal, regulatory, and governmental risks with regards to the performance and delivery of Oncotype DX AR-V7 Nucleus Detect tests, given that Epic Sciences is a centralized CLIA laboratory performing such tests.
The loss of key members of our senior management team or our inability to attract and retain highly skilled scientists, software engineers, clinicians and salespeople could adversely affect our business.
Our success depends largely on the skills, experience and performance of key members of our executive management team and others in key management positions. The efforts of each of these persons together will be critical to us as we continue to develop our technologies and testing processes, continue our international expansion and transition to a company with multiple commercialized products. If we were to lose one or more of these key employees, we may experience difficulties in competing effectively, developing our technologies and implementing our business strategies.
Our research and development programs, commercial laboratory operations and information technology infrastructure depend on our ability to attract and retain highly skilled scientists, technicians and engineers, including licensed laboratory technicians, chemists, biostatisticians and software engineers. We may not be able to attract or retain qualified scientists, technicians and software engineers in the future due to the competition for qualified personnel among life science and technology businesses, particularly in the San Francisco Bay Area. We also face competition from universities and public and private research institutions in recruiting and retaining highly qualified scientific personnel. In addition, our success depends on our ability to attract and retain salespeople with extensive experience in oncology and urology and close relationships with medical oncologists, urologists, surgeons, pathologists and other hospital personnel. All of our employees in the United States are at-will, which means that either we or the employee may terminate their employment at any time. If we are not able to attract and retain the necessary personnel to accomplish our business objectives, our business and operating results could be harmed.
43
We rely on a limited number of suppliers or, in many cases, a sole supplier, for some of our laboratory instruments and materials and may not be able to find replacement suppliers or immediately transition to alternative suppliers.
We rely on many sole suppliers to supply and service some of the laboratory equipment on which we perform our tests. We believe that there are relatively few equipment manufacturers that are currently capable of supplying and servicing the equipment necessary for our tests. Although we have identified alternative suppliers, transition to a new supplier would be time consuming and expensive, and there can be no assurance that we would be able to secure alternative equipment and bring that equipment on line without experiencing interruptions in testing. If we should encounter delays or difficulties in securing the quality and quantity of equipment we require for our tests, we may need to reconfigure our test processes, which could result in an interruption in sales. If any of these events occur, our business and operating results could be harmed.
We also rely on several sole suppliers for certain laboratory reagents and materials which we use to perform our tests. While we have developed alternate sourcing strategies for these materials, we cannot be certain that these strategies will be effective. If we should encounter delays or difficulties in securing these laboratory materials, if the materials do not meet our quality specifications, or if we cannot obtain acceptable substitute materials, an interruption in test processing could occur. Any such interruption may significantly affect future product revenues.
Risks Related to Our Intellectual Property
If we are unable to maintain intellectual property protection, our competitive position could be harmed.
Our ability to compete and to achieve sustained profitability is impacted by our ability to protect our proprietary discoveries and technologies. We currently rely on a combination of issued patents, patent applications, copyrights, trademarks, and confidentiality, material data transfer, license and invention assignment agreements to protect our intellectual property rights. We also rely upon trade secret laws to protect unpatented know‑how and continuing technological innovation. Our intellectual property strategy is intended to develop and maintain our competitive position.
Our pending patent applications may not result in issued patents, and we cannot assure you that our issued patents or any patents that might ultimately be issued by the U.S. Patent and Trademark Office, or USPTO, will protect our technology. In addition, we do not file patent applications in every country nor is patent protection available in every country. We may face competition internationally in jurisdictions where we do not have intellectual property protection. Any patents that may be issued to us might be challenged by third parties as being invalid or unenforceable, or third parties may independently develop similar or competing technology that avoids our patents.
We cannot be certain that the steps we have taken will prevent the misappropriation and use of our intellectual property, particularly in foreign countries where the laws may not protect our proprietary rights as fully as in the United States.
If patent regulations or standards are modified, such changes could have a negative impact on our business.
From time to time, the U.S. Supreme Court, other federal courts, the U.S. Congress or the USPTO may change the standards of patentability and validity of patents within the genomic diagnostic space, and any such changes could have a negative impact on our business. In addition, competitors may develop their own versions of our test in countries where we did not apply for patents or where our patents have not issued and compete with us in those countries, including encouraging the use of their test by physicians or patients in other countries.
There have been several cases involving “gene patents” and diagnostic claims that have been considered by the U.S. Supreme Court. In March 2012, the Supreme Court in Mayo Collaborative v. Prometheus Laboratories, or Prometheus, found a patented diagnostic method claim unpatentable because the relationship between a metabolite concentration and optimized dosage was a patent‑ineligible “law of nature.” In June 2013, the Supreme Court ruled in ACLU v. Myriad Genetics, or Myriad, that an isolated genomic DNA sequence is not patent eligible while cDNA is eligible. Both the Prometheus and Myriad decisions affect the legal concept of subject matter eligibility by seemingly narrowing the scope of the statute defining patentable inventions.
In December 2014, the USPTO published revised guidelines for patent examiners to apply when examining process claims for patent eligibility in view of several recent Supreme Court decisions, including Mayo Collaborative Services v. Prometheus Laboratories, Inc., Association for Molecular Pathology v. Myriad Genetics, Inc., and Alice Corporation Pty. Ltd. V. CLS Bank International, et al. The guidance indicates that claims directed to a law of nature, a natural phenomenon, or an
44
abstract idea that do not meet the eligibility requirements should be rejected as non‑statutory, patent ineligible subject matter. We cannot assure you that our patent portfolio will not be negatively impacted by the decisions described above, rulings in other cases or changes in guidance or procedures issued by the USPTO.
Additional substantive changes to patent law, whether new or associated with the America Invents Act, may affect our ability to obtain, enforce or defend our patents. Accordingly, it is not clear what, if any, impact the new law will ultimately have on the cost of prosecuting our patent applications, our ability to obtain patents based on our discoveries and our ability to enforce or defend our issued patents, all of which could have a material adverse effect on our business.
We may face intellectual property infringement claims that could be time‑consuming and costly to defend, and could result in our loss of significant rights and the assessment of treble damages.
We have in the past, and may in the future, receive notices of claims of infringement and misappropriation or misuse of other parties’ proprietary rights and may from time to time receive additional notices. Some of these claims may lead to litigation. We cannot assure you that we will prevail in such actions, or that other actions alleging misappropriation or misuse by us of third‑party trade secrets, alleging infringement by us of third‑party patents and trademarks or challenging the validity of our patents, will not be asserted or prosecuted against us. If there is a successful claim of infringement against us, we may be required to pay substantial damages (including treble damages if that infringement were found to be willful) to the party claiming infringement, develop non‑infringing technology, stop selling our tests or using technology that contains the allegedly infringing intellectual property or enter into royalty or license agreements that may not be available on acceptable or commercially practical terms, if at all. Our failure to develop non‑infringing technologies or license the proprietary rights on a timely basis could harm our business.
We may also initiate claims to defend our intellectual property or to seek relief on allegations that we use, sell, or offer to sell technology that incorporates third-party intellectual property. Intellectual property litigation, regardless of outcome, is expensive and time‑consuming, could divert management’s attention from our business and have a material negative effect on our business, operating results or financial condition. In addition, revising our tests to include the non‑infringing technologies would require us to re‑validate our tests, which would be costly and time consuming. Also, we may be unaware of pending third-party patent applications that relate to our tests. Parties making infringement claims on future issued patents may be able to obtain an injunction that could prevent us from selling our tests or using technology that contains the allegedly infringing intellectual property, which could harm our business.
It is possible that a third party or patent office might take the position that one or more patents or patent applications constitute prior art in the field of genomic-based diagnostics. In such a case, we might be required to pay royalties, damages and costs to firms who own the rights to these patents, or we might be restricted from using any of the inventions claimed in those patents.
ITEM 1B. Unresolved Staff Comments.
None.
We currently lease approximately 180,700 square feet of laboratory and office space in Redwood City, California under operating leases that expire between March 2021 and March 2023, with options for us to extend the term of each lease for an additional five years. We also lease approximately 7,500 square feet of office space in Geneva, Switzerland under an operating lease that expires in May 2021. Additionally, we have offices in France, Germany, Ireland, Italy, Japan and the United Kingdom with short‑term rental agreements. We may need additional facilities in the future as we expand our business and believe that additional space, when needed, will be available on commercially reasonable terms.
We were not a party to any material legal proceedings at December 31, 2017, or at the date of this report. We may from time to time become involved in various legal proceedings arising in the ordinary course of business.
ITEM 4. Mine Safety Disclosures.
Not applicable.
45
Executive Officers of the Registrant
The names of our executive officers and their ages as of March 1, 2018, are as follows:
|
|
|
|
|
|
|
|
Name |
|
Age |
|
Position |
|
|
Kimberly J. Popovits |
|
59 |
|
President and Chief Executive Officer |
|
|
G. Bradley Cole |
|
62 |
|
Chief Financial Officer |
|
|
Phillip Febbo, M.D. |
|
51 |
|
Chief Medical Officer |
|
|
Laura Leber Kammeyer |
|
55 |
|
Chief Communications Officer |
|
|
Kim McEachron |
|
62 |
|
Chief People Officer |
|
|
Frederic Pla, Ph.D. |
|
58 |
|
Chief Operating Officer |
|
|
Jason W. Radford |
|
36 |
|
Chief Legal Officer and Secretary |
|
|
Steven Shak, M.D. |
|
67 |
|
Chief Scientific Officer |
|
|
James Vaughn |
|
55 |
|
Chief Commercial Officer |
|
Kimberly J. Popovits has served as our President and Chief Executive Officer since January 2009, and as Chairman of the Board since March 2012. Prior to that, Ms. Popovits served as our President and Chief Operating Officer since February 2002 and as a director since March 2002. From November 1987 to February 2002, Ms. Popovits served in various roles at Genentech, Inc., a biotechnology company, most recently serving as Senior Vice President, Marketing and Sales from February 2001 to February 2002, and as Vice President, Sales from October 1994 to February 2001. Prior to joining Genentech, she served as Division Manager, Southeast Region, for American Critical Care, a division of American Hospital Supply, a supplier of health care products to hospitals. Ms. Popovits serves as a director of MyoKardia, Inc., a precision medicine company. Ms. Popovits holds a B.A. in Business from Michigan State University.
G. Bradley Cole has served as our Chief Financial Officer since June 2014, and from July 2004 until January 2011. Mr. Cole also served as our Chief Operating Officer from January 2009 until March 2018. Prior to these roles, Mr. Cole served as Executive Vice President, Operations from January 2008 until January 2009. Mr. Cole also served as our Secretary from February 2005 until July 2012. From December 1997 to May 2004, he served in various roles at Guidant Corporation, a medical device company, most recently serving as Vice President, Finance and Business Development for the Endovascular Solutions Group from January 2001 until May 2004. From July 1994 to December 1997, Mr. Cole was Vice President, Finance and Chief Financial Officer of Endovascular Technologies, Inc., a medical device company that was acquired by Guidant Corporation. From December 1988 to February 1994, he served as Vice President, Finance and Chief Financial Officer of Applied Biosystems Incorporated, a life sciences systems company. Mr. Cole holds a B.S. in Business from Biola University and an M.B.A. from San Jose State University.
Phillip Febbo, M.D., has served as our Chief Medical Officer since August 2013. From July 2010 to August 2013, Dr. Febbo served as Director of Applied Genomics at the University of California, San Francisco. While at UCSF, Dr. Febbo was the Co-Leader of the Prostate Cancer Program at the UCSF Helen Diller Family Comprehensive Cancer Center and the Program Principal Investigator of the Translational Research Program for the Alliance for Clinical Trials in Oncology. From September 2004 to June 2010, Dr. Febbo served as Associate Professor of Medicine and Molecular Genetics and Microbiology at Duke University Medical Center’s Institute of Genome Sciences and Policy. Dr. Febbo holds a B.A. in Biology from Dartmouth College and an M.D. from the University of California, San Francisco, and completed his internal medicine residency at the Brigham and Women’s Hospital.
Laura Leber Kammeyer has served as our Chief Communications Officer since December 2014. Prior to that, Ms. Kammeyer served as our Senior Vice President, Communications beginning in November 2002. From 1992 to 2001, Ms. Kammeyer served in various roles at Genentech, Inc., a biotechnology company, most recently as Vice President, Corporate Communications. Ms. Kammeyer holds a Bachelor of Journalism from the University of Missouri, Columbia.
Kim McEachron has served as our Chief People Officer since December 2014. Prior to that, Ms. McEachron served as our Senior Vice President, Human Resources from March 2012 to November 2014. From November 2010 to January 2012, Ms. McEachron served as the Vice President of Human Resources, Engagement and Inclusion for Medtronic, a medical technology company, for their Cardiac and Vascular division. Ms. McEachron holds a B.A. in Sociology and Anthropology from Carleton College and a Master’s degree in Industrial Relations from the University of Minnesota.
Frederic Pla, Ph.D., has served as our Chief Operating Officer since March 2018. Prior to that, Dr. Pla served as our Chief Business and Product Development Officer from January 2015 to March 2018. From July 2005 to February 2014, Dr. Pla served in various roles at Life Technologies Corporation (now part of Thermo Fisher Scientific), a global life sciences company, most recently serving as Vice President, Corporate Business Development from July 2008 to February 2014, and as
46
Vice President and General Manager of the Diagnostics Business from July 2005 to July 2008. Prior to joining Life Technologies, Dr. Pla served in various roles at GE Healthcare, most recently serving as General Manager for the Enterprise IT and Cardiology IT businesses. Dr. Pla holds an Engineering degree from the University of Technology of Compiegne, France, a Master’s degree from The University of Southampton, United Kingdom and a Ph.D. in Acoustics from the Pennsylvania State University.
Jason W. Radford has served as our Chief Legal Officer since May 2015. From May 2014 to May 2015, Mr. Radford served as Executive Vice President and General Counsel at Accumen Inc. Prior to joining Accumen, he served in various roles in the legal department at Life Technologies Corporation (now part of Thermo Fisher Scientific), a global life sciences company, from March 2010 to March 2014 including Division Lead Counsel for the Genetic and Medical Sciences business. Before joining Life Technologies, Mr. Radford was an attorney in the Corporate and Securities Group of DLA Piper LLP, where he served as outside counsel to public and private companies in a variety of commercial transactions. Mr. Radford holds a B.A. in Political Science from the University of California, Los Angeles, a J.D. from Boston College Law School and an M.B.A. from the Wallace E. Carroll Graduate School of Management at Boston College.
Steven Shak, M.D., has served as our Chief Scientific Officer since January 2015 and has also served as our Executive Vice President of Research and Development from July 2012 to December 2014 and as our Chief Medical Officer from December 2000 to August 2013. From July 1996 to October 2000, Dr. Shak served in various roles in Medical Affairs at Genentech, most recently as Senior Director and Staff Clinical Scientist. From November 1989 to July 1996, Dr. Shak served as a Director of Discovery Research at Genentech, where he was responsible for Pulmonary Research, Immunology, and Pathology. Prior to joining Genentech, Dr. Shak was an Assistant Professor of Medicine and Pharmacology at the New York University School of Medicine. Dr. Shak holds a B.A. in Chemistry from Amherst College and an M.D. from the New York University School of Medicine, and completed his post‑doctoral training at the University of California, San Francisco.
James Vaughn has served as our Chief Commercial Officer since December 2014. Prior to that, Mr. Vaughn served as our Senior Vice President, Worldwide Commercial from August 2011 to December 2014, and as our Vice President, International, from November 2008 to August 2011. From July 2004 to November 2008, Mr. Vaughn served as our Managed Care and Western U.S. Sales Director. Prior to 2004, Mr. Vaughn served as Vice President of Cerus Corporation, a biomedical products company, and held a number of positions in sales, sales management, and marketing. Mr. Vaughn holds a B.S. in Pharmacy from Creighton University and an M.B.A. from Northwestern University, Kellogg School of Business.
ITEM 5. Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities.
Our common stock, par value $0.0001 per share, is traded on The Nasdaq Global Select Market under the symbol “GHDX.” The following table sets forth the range of high and low sales prices for our common stock for the periods indicated:
|
|
|
2017 |
|
||||||||||
|
|
|
First |
|
Second |
|
Third |
|
Fourth |
|
||||
|
|
|
Quarter |
|
Quarter |
|
Quarter |
|
Quarter |
|
||||
|
Stock price—high |
|
$ |
32.52 |
|
$ |
33.97 |
|
$ |
33.95 |
|
$ |
37.50 |
|
|
Stock price—low |
|
$ |
26.37 |
|
$ |
28.64 |
|
$ |
27.60 |
|
$ |
26.54 |
|
|
|
|
2016 |
|
||||||||||
|
|
|
First |
|
Second |
|
Third |
|
Fourth |
|
||||
|
|
|
Quarter |
|
Quarter |
|
Quarter |
|
Quarter |
|
||||
|
Stock price—high |
|
$ |
35.79 |
|
$ |
28.99 |
|
$ |
30.57 |
|
$ |
33.96 |
|
|
Stock price—low |
|
$ |
22.00 |
|
$ |
23.57 |
|
$ |
25.56 |
|
$ |
28.16 |
|
According to the records of our transfer agent, we had 44 stockholders of record as of February 28, 2018.
Dividends
We have never declared or paid any cash dividends on our capital stock, and we do not currently intend to pay any cash dividends on our common stock in the foreseeable future. We expect to retain any future earnings to fund the development and growth of our business. Our board of directors will determine future cash dividends, if any. There are currently no contractual restrictions on our ability to pay dividends.
47
Stock Performance Graph
The following information is not deemed to be “soliciting material” or to be “filed” with the Securities and Exchange Commission or subject to Regulation 14A or 14C under the Securities Exchange Act of 1934 or to the liabilities of Section 18 of the Securities Exchange Act of 1934, and will not be deemed to be incorporated by reference into any filing under the Securities Act of 1933 or the Securities Exchange Act of 1934, except to the extent we specifically incorporate it by reference into such a filing.
Set forth below is a line graph showing the cumulative total stockholder return (change in stock price plus reinvested dividends) assuming the investment of $100 on December 31, 2012 in each of our common stock, the Nasdaq Market Index and the Nasdaq Biotechnology Index for the period commencing on December 31, 2012 and ending on December 31, 2017. The comparisons in the table are required by the Securities and Exchange Commission and are not intended to forecast or be indicative of future performance of our common stock.
COMPARISON OF 5 YEAR CUMULATIVE TOTAL RETURN*
AMONG GENOMIC HEALTH, THE NASDAQ COMPOSITE INDEX
AND THE NASDAQ BIOTECHNOLOGY INDEX
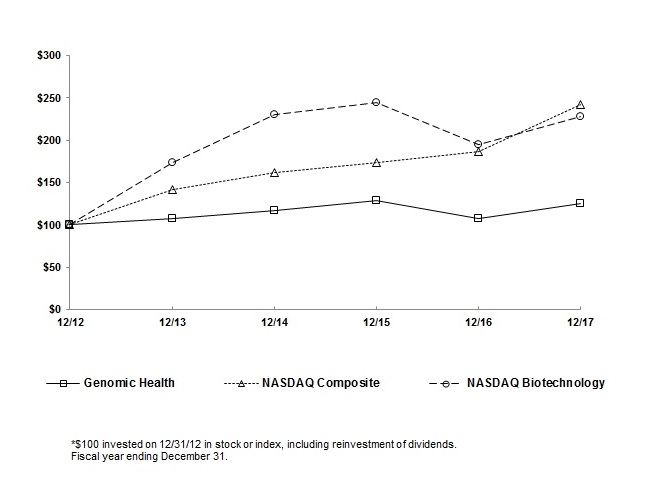
|
|
|
December 31, |
|
December 31, |
|
December 31, |
|
December 31, |
|
December 31, |
|
December 31, |
|
||||||
|
|
|
2012 |
|
2013 |
|
2014 |
|
2015 |
|
2016 |
|
2017 |
|
||||||
|
Genomic Health |
|
$ |
100.00 |
|
$ |
107.45 |
|
$ |
117.36 |
|
$ |
129.22 |
|
$ |
107.89 |
|
$ |
125.55 |
|
|
Nasdaq Composite |
|
$ |
100.00 |
|
$ |
141.63 |
|
$ |
162.09 |
|
$ |
173.33 |
|
$ |
187.19 |
|
$ |
242.29 |
|
|
Nasdaq Biotechnology |
|
$ |
100.00 |
|
$ |
174..05 |
|
$ |
230.33 |
|
$ |
244.29 |
|
$ |
194.95 |
|
$ |
228.29 |
|
48
ITEM 6. Selected Financial Data.
The following selected consolidated financial data should be read together with “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and our consolidated financial statements and related notes included elsewhere in this report. The selected consolidated balance sheet data at December 31, 2017 and 2016 and the selected consolidated statements of operations data for each year ended December 31, 2017, 2016 and 2015 have been derived from our audited consolidated financial statements that are included elsewhere in this report. The selected consolidated balance sheet data at December 31, 2015, 2014, and 2013 and the selected consolidated statements of operations data for the years ended December 31, 2014 and 2013 have been derived from our audited consolidated financial statements not included in this report. Historical results are not necessarily indicative of the results to be expected in the future.
|
|
|
Year Ended December 31, |
|
|||||||||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|
2014 |
|
2013 |
|
|||||
|
|
|
(In thousands, except per share data) |
|
|||||||||||||
|
Consolidated Statements of Operations Data: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Revenues: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Product revenues |
|
$ |
340,451 |
|
$ |
326,918 |
|
$ |
287,458 |
|
$ |
275,706 |
|
$ |
259,192 |
|
|
Contract revenues |
|
|
299 |
|
|
950 |
|
|
— |
|
|
— |
|
|
2,403 |
|
|
Total revenues |
|
|
340,750 |
|
|
327,868 |
|
|
287,458 |
|
|
275,706 |
|
|
261,595 |
|
|
Operating expenses(1): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cost of product revenues |
|
|
54,718 |
|
|
58,828 |
|
|
55,135 |
|
|
50,129 |
|
|
42,100 |
|
|
Research and development |
|
|
62,811 |
|
|
60,158 |
|
|
58,445 |
|
|
51,689 |
|
|
64,177 |
|
|
Selling and marketing |
|
|
157,001 |
|
|
151,042 |
|
|
143,557 |
|
|
137,846 |
|
|
112,758 |
|
|
General and administrative |
|
|
72,670 |
|
|
73,272 |
|
|
64,348 |
|
|
59,669 |
|
|
54,392 |
|
|
Total operating expenses |
|
|
347,200 |
|
|
343,300 |
|
|
321,485 |
|
|
299,333 |
|
|
273,427 |
|
|
Loss from operations |
|
|
(6,450) |
|
|
(15,432) |
|
|
(34,027) |
|
|
(23,627) |
|
|
(11,832) |
|
|
Impairment on investments |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
(643) |
|
|
Interest income, net |
|
|
934 |
|
|
418 |
|
|
221 |
|
|
192 |
|
|
222 |
|
|
Gain on sale of equity securities |
|
|
2,807 |
|
|
3,208 |
|
|
— |
|
|
— |
|
|
— |
|
|
Other income (expense), net |
|
|
356 |
|
|
(732) |
|
|
(498) |
|
|
(764) |
|
|
(158) |
|
|
Loss before income taxes |
|
|
(2,353) |
|
|
(12,538) |
|
|
(34,304) |
|
|
(24,199) |
|
|
(12,411) |
|
|
Income tax expense (benefit) |
|
|
1,504 |
|
|
1,381 |
|
|
(996) |
|
|
393 |
|
|
346 |
|
|
Net loss |
|
$ |
(3,857) |
|
$ |
(13,919) |
|
$ |
(33,308) |
|
$ |
(24,592) |
|
$ |
(12,757) |
|
|
Basic and diluted net loss per share |
|
$ |
(0.11) |
|
$ |
(0.42) |
|
$ |
(1.03) |
|
$ |
(0.78) |
|
$ |
(0.42) |
|
|
Weighted-average shares used in computing basic and diluted net loss per share |
|
|
34,495 |
|
|
33,264 |
|
|
32,382 |
|
|
31,453 |
|
|
30,512 |
|
|
(1) |
Includes non‑cash charges for employee stock‑based compensation expense as follows: |
|
|
|
Year Ended December 31, |
|
|||||||||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|
2014 |
|
2013 |
|
|||||
|
|
|
(In thousands) |
|
|||||||||||||
|
Cost of product revenues |
|
$ |
741 |
|
$ |
664 |
|
$ |
584 |
|
$ |
564 |
|
$ |
483 |
|
|
Research and development |
|
|
5,469 |
|
|
4,860 |
|
|
4,169 |
|
|
4,076 |
|
|
4,486 |
|
|
Selling and marketing |
|
|
5,730 |
|
|
5,551 |
|
|
4,526 |
|
|
4,822 |
|
|
4,756 |
|
|
General and administrative |
|
|
8,316 |
|
|
7,228 |
|
|
6,726 |
|
|
7,076 |
|
|
7,732 |
|
|
Total |
|
$ |
20,256 |
|
$ |
18,303 |
|
$ |
16,005 |
|
$ |
16,538 |
|
$ |
17,457 |
|
|
|
|
At December 31, |
|
|||||||||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|
2014 |
|
2013 |
|
|||||
|
|
|
(In thousands) |
|
|||||||||||||
|
Consolidated Balance Sheet Data: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cash, cash equivalents and marketable securities |
|
$ |
129,575 |
|
$ |
96,989 |
|
$ |
94,943 |
|
$ |
103,660 |
|
$ |
105,350 |
|
|
Working capital |
|
|
134,744 |
|
|
104,789 |
|
|
100,278 |
|
|
110,182 |
|
|
115,160 |
|
|
Total assets |
|
|
231,617 |
|
|
201,114 |
|
|
184,617 |
|
|
185,921 |
|
|
177,034 |
|
|
Accumulated deficit |
|
|
(245,945) |
|
|
(242,088) |
|
|
(228,169) |
|
|
(194,861) |
|
|
(170,269) |
|
|
Total stockholders’ equity |
|
|
188,291 |
|
|
156,105 |
|
|
139,535 |
|
|
145,513 |
|
|
144,981 |
|
49
ITEM 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations.
The following discussion of our financial condition and results of operations should be read in conjunction with our consolidated financial statements and the related notes included in Item 8 of this report. Historical results are not necessarily indicative of future results.
Business Overview
We are a global healthcare company that provides clinically-actionable genomic information to personalize cancer treatment. We develop and globally commercialize genomic-based clinical laboratory services that analyze the underlying biology of cancer, allowing physicians and patients to make individualized treatment decisions. We are translating significant amounts of genomic data that will be useful for treatment planning throughout the cancer patient’s journey, from diagnosis to treatment selection and monitoring. We offer our Oncotype tests as clinical laboratory services, where we analyze the expression levels of genes in tumor tissue samples and provide physicians with a quantitative gene expression profile expressed as a single quantitative score, which we call a Recurrence Score for invasive breast cancer and colon cancer, a DCIS Score for ductal carcinoma in situ, or DCIS, and a Genomic Prostate Score, or GPS, for prostate cancer.
In January 2004, we launched our first Oncotype DX test, which is used to predict the likelihood of cancer recurrence and the likelihood of chemotherapy benefit in early stage invasive breast cancer patients. In January 2010, we launched our second Oncotype DX test, the first multigene expression test developed to assess risk of recurrence in stage II colon cancer patients. In late December 2011, we made Oncotype DX available for patients with DCIS, a pre-invasive form of breast cancer. In June 2012, we extended our offering of the Oncotype DX colon cancer test to patients with stage III disease treated with oxaliplatin-containing adjuvant therapy. In May 2013, we launched our Oncotype DX prostate cancer test, which is used to predict disease aggressiveness in men with low and intermediate risk disease. In July 2017, the Oncotype DX AR-V7 Nucleus Detect test for men with metastatic castration-resistant prostate cancer, or mCRPC, became available as part of a clinical utility program, and we commercially launched the test in February 2018. As of February 28, 2018, the list price of our Oncotype DX invasive breast cancer and DCIS tests in the United States was $4,620, the list price of our Oncotype DX colon cancer test was $4,420, the list price of our Oncotype DX prostate cancer test was $4,520 and the list price of the Oncotype DX AR-V7 Nucleus Detect test was $3,950. There was no increase in 2017 to the list prices of our Oncotype DX invasive breast, colon and prostate cancer tests and our DCIS test. The substantial majority of our historical revenues have been derived from the sale of Oncotype DX invasive breast cancer tests ordered by physicians in the United States.
For the year ended December 31, 2017, more than 126,740 Oncotype test reports were delivered for use in treatment planning, compared to more than 118,750 and 107,030 test reports delivered for the years ended December 31, 2016 and 2015, respectively. All of our internally-developed tests are conducted at our clinical reference laboratory in Redwood City, California. Our clinical reference laboratory processing capacity is currently approximately 150,000 tests annually, and has significant expansion capacity with incremental increases in laboratory personnel and equipment. The Oncotype DX breast, colon, and prostate cancer tests analyze different genes. However, all of the tests performed in our laboratory are based on a similar Oncotype DX reverse transcription polymerase chain reaction, or RT-PCR, platform and require both histology and pathology assessments. We believe that we currently have sufficient capacity to process current demand for our tests.
We expect our continued commercialization efforts of our tests will result in increased costs for laboratory testing, including staffing-related costs, incremental sales and marketing personnel to introduce our products to physicians and patients, costs for clinical utility studies and costs associated with obtaining reimbursement coverage.
We depend upon third-party payors, both public and private, to provide reimbursement for our tests. Accordingly, we have and expect to continue to focus substantial resources on obtaining and maintaining reimbursement coverage from third-party payors. Sales of our tests in the United States and other countries are dependent upon the coverage decisions and reimbursement policies established by government healthcare programs and private health insurers. Market acceptance of our tests has and will continue to depend upon the ability to obtain an appropriate level of coverage for, and reimbursement from, third-party payors for our tests. We have had Medicare coverage for our Oncotype DX invasive breast cancer test since 2006 and for our Oncotype DX colon cancer test since 2011. In October 2015, we obtained Medicare coverage for our Oncotype DX prostate cancer test for patients with low and very-low risk as defined by National Comprehensive Cancer Network, or NCCN, guidelines. Under the terms of the coverage determination for our prostate cancer test, reimbursement for such patients is limited to tests ordered by physicians who agree to participate in a Certification Training Registry and to provide certain information about Medicare beneficiaries who receive our test, also referred to as Coverage with Data Development, or CDD. In August 2017, Palmetto GBA, a Medicare Administrative Contractor that processes Medicare claims and sets Medicare
50
coverage policies for certain tests performed by our laboratory, issued its final local coverage determination, or LCD, recommending Medicare coverage for use of our prostate cancer test in qualified patients with favorable intermediate-risk prostate cancer. Effective October 2017, Palmetto expanded their reimbursement coverage of our Oncotype DX prostate cancer test to include qualified patients with favorable intermediate-risk prostate cancer.
On December 16, 2015, Palmetto informed us that they believe it was appropriate to establish a unique identifier code and independent coverage for the Oncotype DX DCIS test. We have obtained a unique identifier code for this test, and we submitted to Palmetto additional validation and clinical utility data generated since its previous decision in May 2013, to cover the Oncotype DX DCIS test for all qualified Medicare patients with DCIS. The Oncotype DX DCIS test became covered under a new LCD with Coverage with Data Development for services furnished beginning in March 2017.
We have continued to expand our business, both in the United States and internationally. There are significant differences between countries that need to be considered. For example, operational requirements generally vary from country to country, and different countries may have a public healthcare system, a combination of public and private healthcare system or a cash-based payment system. We have a direct commercial presence with employees in Canada, Japan and six European counties, including our European headquarters in Geneva, Switzerland. Additionally, we have exclusive distribution agreements for the sale of our breast and colon cancer tests with distributors covering more than 90 countries outside of the United States.
As our international business expands, our financial results become more sensitive to the effect of fluctuations in foreign currency exchange rates. For example, in countries where we have a direct commercial presence, our tests are sold in local currency, which results in foreign currency exchange rate fluctuations affecting our U.S.-dollar reported revenues. In other markets where we sell our tests in U.S. dollars to distribution partners, the demand for our tests may be impacted by the change in U.S. dollar exchange rates affecting partners’ costs or local market price adjustments.
We expect that international sales of our Oncotype tests will be heavily dependent on the availability of reimbursement and sample access. In many countries, governments are primarily responsible for reimbursing diagnostic tests. Governments often have significant discretion in determining whether a test will be reimbursed at all, and if so, on what conditions, for which other competing products, and how much will be paid. In addition, certain countries, such as China, have prohibitions against exporting tissue samples which will limit our ability to offer our tests in those countries without local laboratories or a method of test delivery which does not require samples to be transported to our U.S. laboratory.
The majority of our international Oncotype DX breast and colon cancer test revenues come from direct payor reimbursement, payments from our distributors and patient self-pay. We have obtained some coverage, which varies substantially from country to country, for our breast cancer test outside of the United States, including in Canada, the Czech Republic, Germany, Greece, Hungary, Ireland, Israel, Saudi Arabia, Spain, Switzerland and the United Kingdom.
We established reimbursement with NHS England following NICE’s recommendation for our breast cancer test, and in 2015 we began to receive payments from NHS England trusts with whom we have completed contractual arrangements. In 2014, the Gynecologic Oncology Working Group in Germany updated their guidelines to recommend Oncotype DX as the only breast cancer gene expression test to predict chemotherapy benefit in early-stage, hormone receptor-positive invasive breast cancer. We expect that it will take several years to establish broad coverage and reimbursement for our Oncotype DX breast, colon and prostate cancer tests with payors in countries outside of the United States and there can be no assurance that our efforts will be successful.
Economic Environment
Continuing concerns over entitlement and health care reform efforts, regulatory changes and taxation issues, and geopolitical issues have contributed to uncertain expectations both for the U.S. and global economies. These factors, combined with uncertainties in business and consumer confidence and continued concerns regarding the stability of some European Union member countries, have contributed to the expectations of slower domestic and global economic growth in the near term. We periodically evaluate the impact of the economic environment on our cash management, cash collection activities and volume of tests delivered.
As of the date of this report, we have not experienced a loss of principal on any of our short-term marketable securities, and we expect that we will continue to be able to access or liquidate these investments as needed to support our business activities. We periodically monitor the financial position of our significant third-party payors, which include Medicare and managed care companies. As of the date of this report, we do not expect the current economic environment to have a material
51
negative impact on our ability to collect payments from third-party payors in the foreseeable future. We believe the economic environment and changes in the healthcare system continued to impact product payment cycles, growth in tests delivered and product revenue generated during the year ended December 31, 2017. We intend to continue to assess the impact of the economic environment on our business activities. If the economic environment does not improve or deteriorates, our business including our patient population, government and third-party payors and our distributors and suppliers could be negatively affected, resulting in a negative impact on our product revenues.
U.S. Healthcare Reimbursement and Regulatory Environment
The healthcare industry has undergone significant change driven by various efforts to reduce costs, both in the U.S. and in many foreign countries. The effect of the implementation of the Affordable Care Act, or ACA, or any future changes to the ACA on our business is uncertain and, could among other things limit the use of our tests and reduce reimbursement. We also expect that pricing of medical products and services will remain under pressure as alternative payment models such as bundling, value-based purchasing and accountable care organizations develop in the United States. Additionally, the ACA requires medical device manufacturers to pay a 2.3% excise tax on U.S. sales of certain medical devices that are listed with the FDA starting in January 2013; this tax has been suspended through 2019, but is scheduled for re-imposition in 2020. Various proposals have been put forth, including by the FDA, to regulate laboratory developed tests, or LDTs, as medical devices. Although none of our LDTs, such as our Oncotype DX breast, colon and prostate cancer tests, are currently listed with the FDA, we cannot assure you that the tax will not apply to services such as ours in the future.
In addition, the Protecting Access to Medicare Act of 2014, or PAMA requires CMS to implement a substantial new payment system for certain clinical laboratory tests, which became effective in 2018. Under PAMA, laboratories that receive the majority of their Medicare revenues from payments made under the Clinical Laboratory Fee Schedule, or CLFS, or the Physician Fee Schedule will be required to report every three years (or annually for “advanced diagnostic laboratory tests”), private payor payment rates and volumes for their tests. CMS will use the rates and volumes reported by laboratories to develop Medicare payment rates for the tests equal to the volume-weighted median of the private payor payment rates for the tests.
There have also been recent and substantial changes to the payment structure for physicians, including those passed as part of the Medicare Access and CHIP Reauthorization Act of 2015, or MACRA, which was signed into law on April 16, 2015. MACRA created the Merit-Based Incentive Payment System which, beginning in 2019, more closely aligns physician payments with composite performance for the Physician Quality Reporting System, the Value-based modifier program and the Electronic Health Record Meaningful Use program, and incentivizes physicians to enroll in alternative payment methods. At this time, we do not know whether these changes to the physician payment systems will have any impact on orders or payments for our tests.
Changes in Medicare Administrative Contractor (MAC) services
On a five-year rotational basis, Medicare requests bids for its regional MAC services. In September 2013, the claims processing function for our jurisdiction transitioned from Palmetto GBA, to Noridian, our current MAC. Palmetto GBA under their MolDx Program is continuing to establish coverage and coding policies for molecular diagnostic tests performed in our jurisdiction, including our tests, which is not subject to the same five-year rotation as for regional MAC services. The elimination of the MolDx Program or a change in the administrator of that program could impact the current coverage for our existing tests and our ability to obtain Medicare coverage for products for which we do not yet have coverage or any products we may launch in the future, or delay payments for our tests.
Critical Accounting Policies and Significant Judgments and Estimates
This discussion and analysis of our financial condition and results of operations is based on our consolidated financial statements, which have been prepared in accordance with accounting principles generally accepted in the United States. The preparation of these financial statements requires management to make estimates and judgments that affect the reported amounts of assets and liabilities and the disclosure of contingent assets and liabilities at the date of the financial statements, as well as revenues and expenses during the reporting periods. We evaluate our estimates and judgments on an ongoing basis. We base our estimates on historical experience and on various other factors we believe are reasonable under the circumstances, the results of which form the basis for making judgments about the carrying value of assets and liabilities that are not readily apparent from other sources. Actual results could therefore differ materially from those estimates under different assumptions or conditions.
52
We believe the following critical accounting policies reflect our more significant estimates and assumptions used in the preparation of our financial statements. There have been no material changes to our critical accounting policies during the year ended December 31, 2017, other than the adoption of Accounting Standards Update (“ASU”) 2016-09 described below.
Revenue Recognition
We determine whether revenue is recognized on an accrual basis when test results are delivered or on a cash basis when cash is received from the payor. Our revenues for tests performed are recognized on an accrual basis when the following criteria are met: (1) persuasive evidence that an arrangement exists; (2) delivery has occurred or services have been rendered; (3) the fee is fixed or determinable; and (4) collectability is reasonably assured. When evaluating whether the fee is fixed or determinable and collectible, we consider whether we have sufficient history to reliably estimate the total fee that will be received from a payor and a payor’s individual payment patterns. Based upon at least several months of payment history, we review the number of tests paid against the number of tests billed and the payor’s outstanding balance for unpaid tests to determine whether payments are being made at a consistently high percentage of tests billed and at appropriate amounts given the arrangement or contracted payment amount. The estimated accrual amounts per test, recorded upon delivery of a patient report, are calculated for each accrual payor and are based on the arrangement or contracted price adjusted for individual payment patterns resulting from co-payment amounts and excluded services in healthcare plans.
To the extent all criteria set forth above are not met, including where there is no evidence of payment history at the time test results are delivered, product revenues are recognized on a cash basis when cash is received from the payor.
We enter into exclusive distribution agreements for the sale of one or more of our Oncotype DX tests with distributors outside of the United States. In these countries, the distributor generally provides us with certain marketing and administrative services within its territory. As a condition of these agreements, the distributor generally pays us an agreed upon fee per test and we process the tests. The same revenue recognition criteria described above generally apply to tests delivered through distributors. To the extent all criteria set forth above are not met when test results are delivered, product revenues are generally recognized when cash is received from the distributor.
Test revenue recognized on an accrual basis is recorded upon delivery of each test performed, net of any contractual discount, at the amount that we expect to collect. We determine the amount we expect to collect on a per payor, per contract or arrangement basis, based on our analysis of historical average payments. This average amount is typically lower than the agreed upon amount due to several factors, such as the amount of patient co-payments, the existence of secondary payors and claim denials. We typically review our analysis annually, or at the time a contractual price change is implemented or when information comes to our attention that leads us to believe an adjustment may be warranted.
As of December 31, 2017, amounts outstanding for tests delivered, net of write-downs and adjustments, which were not recognized as revenue upon delivery because our accrual revenue recognition criteria were not met and which had not been collected totaled approximately $70.4 million. We cannot provide any assurance as to when, if ever, and to what extent these amounts will be collected.
From time to time, we receive requests for refunds of payments, generally due to overpayments made by third‑party payors. Upon becoming aware of a refund request, we establish an accrued liability for tests covered by the refund request until such time as we determine whether or not a refund is due. If we determine that a refund is due, we credit cash and reduce the accrued liability. Accrued refunds were $87,000 and $487,000 at December 31, 2017 and 2016, respectively.
Contract revenues are generally derived from studies conducted with biopharmaceutical and pharmaceutical companies and are recognized on a contract-specific basis. Under certain contracts, revenues are recognized as costs are incurred or assays are processed. We may exercise judgment when estimating full-time equivalent level of effort, costs incurred and time to project completion. For certain contracts, we utilize the performance-based method of revenue recognition, which requires that we estimate the total amount of costs to be expended for a project and recognize revenue equal to the portion of costs expended to date. The estimated total costs to be expended are necessarily subject to revision from time-to-time as the underlying facts and circumstances change.
Allowance for Doubtful Accounts
We accrue an allowance for doubtful accounts against our accounts receivable based on estimates consistent with historical payment experience. Our allowance for doubtful accounts is evaluated quarterly and adjusted when trends or
53
significant events indicate that a change in estimate is appropriate. Historically, the amounts of uncollectible accounts receivable that have been written off have been consistent with management’s expectations. We cannot assure you that we will not experience higher than expected write-offs in the future. As of December 31, 2017, and 2016, our allowance for doubtful accounts was $3.9 million and $4.5 million, respectively. See “Liquidity and Capital Resources” for additional information, including a summary of accounts receivable aging by payor mix.
Results of Operations
Comparison of Years Ended December 31, 2017, 2016 and 2015
We recorded a net loss of $3.9 million for the year ended December 31, 2017, compared to net losses of $13.9 million and $33.3 million for the years ended December 31, 2016 and 2015, respectively. On a basic and diluted basis, net loss per share was $0.11, $0.42 and $1.03 for the years ended December 31, 2017, 2016 and 2015, respectively. We may incur net losses in future periods due to future spending and fluctuations in our business, and we may not achieve or maintain sustained profitability in the future.
Revenues
We derive our revenues primarily from product sales and, to a lesser extent, from contract research arrangements. We operate in one industry segment. As of December 31, 2017, the substantial majority of our product revenues have been derived from the sale of our Oncotype invasive breast cancer test. Payors are billed upon generation and delivery of test results to the physician. Product revenues are recorded on a cash basis unless a contract or arrangement to pay is in place with the payor at the time of billing and collectability is reasonably assured. Contract revenues are derived from studies conducted with biopharmaceutical and pharmaceutical companies and are recorded as contractual obligations are completed.
|
|
|
Year Ended December 31, |
|
|||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|
|||
|
|
|
(In thousands) |
||||||||
|
Product revenues |
|
$ |
340,451 |
|
$ |
326,918 |
|
$ |
287,458 |
|
|
Contract revenues |
|
|
299 |
|
|
950 |
|
|
— |
|
|
Total revenues |
|
$ |
340,750 |
|
$ |
327,868 |
|
$ |
287,458 |
|
|
Period over period dollar increase in product revenues |
|
$ |
13,533 |
|
$ |
39,460 |
|
|
|
|
|
Period over period percentage increase in product revenues |
|
|
4 |
% |
|
14 |
% |
|
|
|
The year over year increases in product revenues resulted, in part, from increased adoption. Test volume increased by 7% for the year ended December 31, 2017 compared to the year ended December 31, 2016. Of the growth in test volume, approximately 4% was from breast cancer tests and 3% from prostate cancer tests delivered worldwide. Test volume increased by 11% for the year ended December 31, 2016 compared to the year ended December 31, 2015. Of the growth in test volume, approximately 10% was from breast cancer tests delivered worldwide. In addition, the stronger U.S. dollar in 2016 and 2015 resulted in a negative impact on product revenues as described below.
International product revenue increased to $53.1 million or by 13% for the year ended December 31, 2017 compared to the year ended December 31, 2016 due to revenue growth in Germany, Switzerland and the United Kingdom, offset by the impact of a stronger U.S. dollar compared to the United Kingdom pound. International product revenues increased to $46.8 million or by 13% for the year ended December 31, 2016 compared to the year ended December 31, 2015 due to revenue growth in the United Kingdom and Japan offset by the impact of a stronger U.S. dollar on the translation of revenue from foreign denominated currencies.
Approximately $242.4 million, or 71%, of product revenues for the year ended December 31, 2017, was recorded on an accrual basis and recognized at the time the test results were delivered, compared to $231.3 million, or 71%, and $211.7 million, or 74%, of product revenues for the years ended December 31, 2016 and 2015, respectively. For all periods, the balance of product revenues was recognized upon cash collection as payments were received. The timing of recognition of revenues related to third-party payors may cause fluctuations in product revenues from period to period.
Product revenues related to Medicare patients for the year ended December 31, 2017 were $75.2 million, or 22%, of product revenues, compared to $70.2 million, or 21%, and $58.9 million or 20%, of product revenues for the years ended
54
December 31, 2015 and 2014, respectively. No other third‑party payors comprised product revenues of 10% or more for those years.
Contract revenues were $299,000 for the year ended December 31, 2017 compared to $950,000 and $0 for the years ended December 31, 2016 and 2015. We expect that our contract revenues will continue to fluctuate based on the number and timing of studies being conducted.
Cost of Product Revenues
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year Ended December 31, |
|
|||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|
|||
|
|
|
(In thousands) |
||||||||
|
Tissue sample processing costs |
|
$ |
53,663 |
|
$ |
52,905 |
|
$ |
45,316 |
|
|
Stock-based compensation |
|
|
741 |
|
|
664 |
|
|
584 |
|
|
Total tissue sample processing costs |
|
|
54,404 |
|
|
53,569 |
|
|
45,900 |
|
|
License fees |
|
|
314 |
|
|
5,259 |
|
|
9,235 |
|
|
Total cost of product revenues |
|
$ |
54,718 |
|
$ |
58,828 |
|
$ |
55,135 |
|
|
Period over period dollar increase in tissue sample processing costs |
|
$ |
758 |
|
$ |
7,589 |
|
|
|
|
|
Period over period percentage increase in tissue sample processing costs |
|
|
1 |
% |
|
17 |
% |
|
— |
|
Cost of product revenues includes the cost of materials, direct labor, equipment and infrastructure expenses associated with processing tissue samples (including sample accessioning, histopathology, anatomical pathology, paraffin extraction, RT- PCR, quality control analysis and shipping charges to transport tissue samples) and license fees. Infrastructure expenses include allocated facility occupancy and information technology costs. Costs associated with performing our tests are recorded as tests are processed. Costs recorded for tissue sample processing represent the cost of all the tests processed during the period regardless of whether revenue was recognized with respect to that test. Historically, royalties for licensed technology calculated as a percentage of product revenues and fixed annual payments relating to the launch and commercialization of Oncotype DX tests are recorded as license fees in cost of product revenues at the time product revenues are recognized or in accordance with other contractual obligations. For the years ended December 31, 2017 and 2016, the decrease in license fees is primarily due to the satisfaction of certain royalty payment obligations for the license of PCR patents under a license agreement with Roche Molecular Systems, Inc., or Roche, during 2016. In previous periods, license fees were generally calculated as a percentage of product revenues; however, the percentage change in license fees does not correlate exactly to the percentage change in product revenues because certain agreements contain provisions for fixed annual payments and other agreements have tiered rates and payments that may be capped at annual minimum or maximum amounts. As a result of the termination of the Roche license agreement during the year ended December 31, 2016, we expect license fees expense to be consistent with the levels recognized during the year ended December 31, 2017 in future periods.
Tissue sample processing costs increased $758,000 or 1%, in 2017 compared to 2016. The increase was primarily due to a $2.4 million increase in materials and reagents primarily due to a 7% increase in test volumes, a $2.3 million increase in personnel-related expenses due to increased headcount, an increase of $440,000 in infrastructure costs and a $437,000 increase in the cost of contract labor, offset by a $4.3 million decrease of net cost allocations and a $554,000 decrease in bonus expense. Tissue sample processing costs increased $7.6 million, or 17%, in 2016 compared to 2015, driven primarily by increases in test volume of 11% in 2016, as well as an increase in information technology cost allocation associated with the implementation of new systems.
We expect the cost of product revenues to increase in future periods as we process more tests.
55
Research and Development Expenses
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year Ended December 31, |
|
|||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|
|||
|
|
|
(In thousands) |
||||||||
|
Personnel-related expenses |
|
$ |
35,121 |
|
$ |
32,177 |
|
$ |
29,137 |
|
|
Stock-based compensation |
|
|
5,469 |
|
|
4,860 |
|
|
4,169 |
|
|
Collaboration expenses |
|
|
6,785 |
|
|
3,337 |
|
|
8,088 |
|
|
Reagents and laboratory supplies |
|
|
3,204 |
|
|
2,302 |
|
|
2,861 |
|
|
Allocated information technology, facilities and other costs |
|
|
6,284 |
|
|
10,905 |
|
|
7,771 |
|
|
Other costs |
|
|
5,948 |
|
|
6,577 |
|
|
6,419 |
|
|
Total research and development expenses |
|
$ |
62,811 |
|
$ |
60,158 |
|
$ |
58,445 |
|
|
Period over period dollar increase |
|
$ |
2,653 |
|
$ |
1,713 |
|
|
|
|
|
Period over period percentage increase |
|
|
4 |
% |
|
3 |
% |
|
|
|
Research and development expenses represent costs incurred to develop our technology, our proprietary liquid platform and continuous process improvement, and carry out clinical studies. Research and development expenses include personnel related expenses, reagents and supplies used in research and development laboratory work, collaboration expenses, infrastructure expenses, including allocated overhead and facility occupancy costs, contract services and other outside costs.
The $2.7 million, or 4%, increase in research and development expenses for 2017 compared to 2016 was primarily due to a $3.4 million increase in collaboration expenses, a $2.9 million increase in personnel-related expense, a $902,000 increase in reagents and laboratory supplies and a $609,000 increase in stock-based compensation offset by a $4.6 million decrease in allocated information technology, facilities and other costs, and a $629,000 decrease in other costs. The $6.8 million of collaboration expenses for the year ended December 31, 2017 includes a $3.2 million one-time upfront license and option fee under the exclusive license and development agreement with Biocartis. Exclusive of this one-time expense, collaboration expenses for the year ended December 31, 2017 compared to the year ended December 31, 2016 increased by $200,000, or 6%.
The $2.9 million increase in personnel-related expenses was primarily attributable to a $3.7 million increase in salaries, benefits and related expenses due to increased headcount during the year and higher benefits costs offset by a decrease of $943,000 in bonuses. The $4.6 million decrease in allocated information technology, facilities and other costs is primarily due to $2.5 million increase in research and development support allocated to other functional areas and a $2.1 million decrease in post-implementation projects for our enterprise resource planning system completed in 2016.
The $1.7 million, or 3%, increase in research and development expenses for 2016 compared to 2015 was primarily due to a $3.0 million increase in personnel-related expense, a $3.1 million increase in allocated information technology facilities and other costs and a $692,000 increase in stock-based compensation partially offset by a $4.8 million decrease in collaboration expenses and a $560,000 decrease in reagents and laboratory supplies. The $8.1 million of collaboration expenses for the year ended December 31, 2015 includes a one-time $5.5 million cost for the wind-down of a license agreement and development program. Exclusive of this one-time expense, research and development expenses for the year ended December 31, 2016 compared to the year ended December 31, 2015 increased by $7.2 million, or 14%.
We expect our research and development expenses, exclusive of the one-time expenses described above, to increase in future periods due to increased investment in our new product pipeline for breast, prostate and other cancers.
56
Selling and Marketing Expenses
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year Ended December 31, |
|
|
|||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|
|
|||
|
|
|
(In thousands) |
|
||||||||
|
Personnel-related expenses |
|
$ |
80,411 |
|
$ |
79,719 |
|
$ |
77,570 |
|
|
|
Stock-based compensation |
|
|
5,730 |
|
|
5,551 |
|
|
4,526 |
|
|
|
Promotional and marketing materials |
|
|
14,119 |
|
|
14,758 |
|
|
17,492 |
|
|
|
Travel, meetings and seminars |
|
|
15,527 |
|
|
16,003 |
|
|
15,715 |
|
|
|
Collaboration expenses |
|
|
528 |
|
|
1,290 |
|
|
3,030 |
|
|
|
Allocated information technology, facilities and other costs |
|
|
36,458 |
|
|
26,783 |
|
|
20,612 |
|
|
|
Other costs |
|
|
4,228 |
|
|
6,938 |
|
|
4,612 |
|
|
|
Total selling and marketing expenses |
|
$ |
157,001 |
|
$ |
151,042 |
|
$ |
143,557 |
|
|
|
Period over period dollar increase |
|
$ |
5,959 |
|
$ |
7,485 |
|
|
|
|
|
|
Period over period percentage increase |
|
|
4 |
% |
|
5 |
% |
|
|
|
|
Our selling and marketing expenses consist primarily of personnel related expenses, education and promotional expenses, market analysis and development expenses and infrastructure expenses, including allocated facility occupancy and information technology costs. These expenses include the costs of educating physicians, laboratory personnel and other healthcare professionals regarding our genomic technologies, how our tests are developed and validated and the value of the quantitative information that our tests provide. Selling and marketing expenses also include the costs of sponsoring continuing medical education, medical meeting participation and dissemination of scientific and economic publications related to our tests. Our salesforce compensation includes annual salaries and eligibility for quarterly commissions based on the achievement of predetermined sales goals and other management objectives.
The $6.0 million, or 4% increase in selling and marketing expenses for 2017 compared to 2016 was primarily due to a $9.7 million increase in allocated information technology, facilities and other costs primarily associated with the realignment of core business functions and a $692,000 increase in personnel-related expenses offset by a $2.7 million decrease in other costs primarily due to the write off of previously capitalized software development costs in 2016, a $762,000 decrease in collaboration costs, a $639,000 decrease in promotional and marketing materials and a $476,000 decrease in travel, meetings and seminars.
The $9.7 million increase in allocated information technology, facilities and other costs is primarily due to a $10.5 million expense associated with the realignment of core business support functions, a $1.3 million decrease in allocations to research and development associated with a reduction in support to research and development, an $823,000 increase in allocations from information technology and a $383,000 increase in facilities allocations offset by a $3.4 million decrease in allocations associated with the implementation of new systems.
The $7.5 million, or 5% increase in selling and marketing expenses for 2016 compared to 2015 was primarily due to U.S. and international sales and operations support and included a $6.2 million increase in allocated information technology, facilities and other costs primarily associated with the implementation of new systems, a $2.3 million increase in other costs from the write off of previously capitalized software development costs, a $2.1 million increase in personnel-related expenses and a $1.0 million increase in stock-based compensation partially offset by a $2.7 million decrease in promotional and marketing materials and a $1.7 million decrease in collaboration expenses.
We expect selling and marketing expenses will continue to increase in future periods due to our efforts to establish adoption of and reimbursement for our new products, continued investment in our global commercial infrastructure and increases in our salesforce.
57
General and Administrative Expenses
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year Ended December 31, |
|
|||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|
|||
|
|
|
(In thousands) |
||||||||
|
Personnel-related expenses |
|
$ |
52,324 |
|
$ |
56,412 |
|
$ |
45,645 |
|
|
Stock-based compensation |
|
|
8,316 |
|
|
7,228 |
|
|
6,726 |
|
|
Occupancy and equipment expenses |
|
|
32,695 |
|
|
29,491 |
|
|
23,156 |
|
|
Billing and collection fees |
|
|
12,285 |
|
|
11,234 |
|
|
9,949 |
|
|
Bad debt expense |
|
|
6,794 |
|
|
7,886 |
|
|
5,971 |
|
|
Professional fees and other expenses |
|
|
10,504 |
|
|
10,513 |
|
|
9,922 |
|
|
Information technology, facilities and other cost allocations |
|
|
(50,248) |
|
|
(49,492) |
|
|
(37,021) |
|
|
Total general and administrative expenses |
|
$ |
72,670 |
|
$ |
73,272 |
|
$ |
64,348 |
|
|
Period over period dollar (decrease) increase |
|
$ |
(602) |
|
$ |
8,924 |
|
|
|
|
|
Period over period percentage (decrease) increase |
|
|
(1) |
% |
|
14 |
% |
|
|
|
Our general and administrative expenses consist primarily of personnel-related expenses, occupancy and equipment expenses, including rent and depreciation expenses, billing and collection fees, bad debt expense, professional fees and other expenses, including intellectual property defense and prosecution costs, and other administrative costs, partially offset by cost allocations to our commercial laboratory operations, research and development, and sales and marketing functions, including allocated information technology and facility occupancy costs.
The $602,000 or 1%, decrease in general and administrative expenses for 2017 compared to 2016 included a $4.1 million decrease in personnel‑related expenses, a $1.1 million decrease in bad debt expense driven by improved cash collection and an increase of $756,000 in information technology, facilities and other costs allocated to other functional areas offset by a $3.2 million increase in occupancy and equipment expenses driven by increased software license expenses and facility expansion, an $1.1 million increase in stock-based compensation and a $1.1 million increase in billing and collection fees. Of the $4.1 million decrease in personnel-related expenses, $3.8 million was attributable to decreases in contract labor primarily due to completing post-implementation projects for our enterprise resource planning system in 2016 and $1.2 million was attributable to decreases in bonus expenses offset by increases of $889,000 attributable to higher salaries, benefits and related expenses.
The $8.9 million, or 14%, increase in general and administrative expenses for 2016 compared to 2015 included a $10.8 million increase in personnel‑related expenses, a $6.3 million increase in occupancy and equipment expenses driven by increased software license expenses and increased depreciation expense related to our new enterprise resource planning system, a $1.9 million increase in bad debt expense and a $1.3 million increase in billing and collection fees partially offset by a $12.5 million increase in information technology, facilities and other costs allocated to other functional areas. Of the $10.8 million increase in personnel-related expenses, $8.4 million was attributable to an increase in salaries and benefits expenses due to increased headcount and higher benefits costs, $2.1 million was attributable to an increase in bonuses and $324,000 was attributable to higher contract labor and consulting expenses to support growth of our business.
We expect general and administrative expenses to increase in future periods as we hire additional staff and incur other expenses to support the growth of our business, and to the extent we spend more on billing and collections fees.
Interest Income
Interest income was $934,000 for the year ended December 31, 2017, compared to $418,000 and $221,000 for years ended December 31, 2016 and 2015, respectively. We expect our interest income will remain nominal if the current low interest rate environment continues.
Gain on sale of equity securities
We realized gain on sale of equity securities of $2.8 million for the year ended December 31, 2017 in connection with the sale of a portion of our holdings of common stock of Invitae Corporation, or Invitae. We realized gain on the sale of equity
58
securities of $3.2 million during the years ended December 31, 2016 and none in 2015. As of December 31, 2017, we had sold all of our remaining shares of common stock of Invitae.
Other Income (Expense), Net
Other income (expense), net was $356,000 for the year ended December 31, 2017, compared to other income (expense), net of $(732,000) and $(498,000) for the years ended December 31, 2016 and 2015, respectively. Other income (expense), net for the years ended December 31, 2017, 2016 and 2015 was primarily related to $317,000, $(782,000) and $(551,000) of net foreign currency transaction gains (losses), respectively, resulting from valuation adjustments to our international accounts receivable balance. We expect other income (expense), net to continue to fluctuate based on fluctuations in exchange rates that impact our foreign exchange transaction gains and losses.
Income Tax Expense (Benefit)
For the years ended December 31, 2017, 2016, and 2015, we recorded an income tax expense of $1.5 million, an income tax expense of $1.4 million and income tax benefit of $996,000, respectively. The 2017, 2016 and 2015 income tax expense or benefit is principally comprised of the deferred tax impact for available-for-sale marketable securities, miscellaneous state income tax expense and foreign tax expense on earnings of our foreign subsidiaries.
As a result of historical losses and based on all current available evidence, we believe that it is more likely than not that our recorded net deferred tax assets will not be realized. Accordingly, we recorded a full valuation allowance on our net deferred tax assets for the years ended December 31, 2017, 2016 and 2015, respectively. We will continue to maintain a full valuation allowance on our net deferred tax assets until there is sufficient evidence to support the reversal of all or some portion of this allowance.
On December 22, 2017, the 2017 Tax Cut and Jobs Act (the Act) was enacted into law. The new legislation contains several key tax provisions, including a one-time mandatory transition tax on accumulated foreign earnings and a reduction of the corporate income tax rate to 21% effective January 1, 2018, among others. We are required to recognize the effect of the tax law changes in the period of enactment, such as determining the estimated transition tax, re-measuring our U.S. deferred tax assets and liabilities at a 21% rate as well as reassessing the net realizability of our deferred tax assets and liabilities. The one-time transition tax does not generate a tax liability as the deemed distribution is offset by tax attributes. The provisional amount related to the re-measurement of our deferred tax balance is a reduction of approximately $31.4 million. Due to the corresponding valuation allowance fully offsetting deferred taxes, there is no income statement impact.
In December 2017, the SEC staff issued Staff Accounting Bulletin No. 118 Income Tax Accounting Implications of the Tax Cuts and Jobs Act (SAB 118) which allows companies to record provisional amounts during a measurement period not to extend beyond one year of the enactment date. Since the Act was passed late in the fourth quarter of 2017, and ongoing guidance and accounting interpretation are expected over the next 12 months, we consider the accounting of the transition tax and deferred tax re-measurements to be incomplete. Additional work will be necessary for a more detailed analysis of our deferred tax assets and liabilities and our historical foreign earnings as well as potential correlative adjustments. We expect to complete our analysis within the measurement period in accordance with SAB 118. We do not expect any material subsequent adjustment to these amounts. Adjustment if any will have no impact to the income statement due to our loss position and valuation allowance.
Liquidity and Capital Resources
As of December 31, 2017, we had an accumulated deficit of $245.9 million. We may incur net losses in the future, and we cannot provide assurance as to when, if ever, we will achieve sustained profitability. We expect that our research and development expenses, selling and marketing and general and administrative expenses will increase in future periods and, as a result, we will need to continue to generate significant product revenues to achieve sustained profitability.
|
|
|
December 31, |
|
December 31, |
||
|
|
|
2017 |
|
2016 |
||
|
|
|
(in thousands) |
||||
|
Cash, cash equivalents and short-term marketable securities |
|
$ |
129,575 |
|
$ |
96,989 |
|
Working capital |
|
|
134,744 |
|
|
104,789 |
59
Sources (Uses) of Liquidity
Historically we have financed our operations primarily through sales of our equity securities and cash received in payment for our tests. At December 31, 2017, we had cash, cash equivalents and short‑term investments of $129.6 million compared to $97.0 million at December 31, 2016. The $32.6 million increase was primarily attributable to increased cash collections from increased sales of our tests, sales of marketable securities and net sales proceeds from the issuance of common stock under our stock plans, offset by investments in the growth of our business, including research and development, global expansion, and activities related to reimbursement coverage of our tests. In accordance with our investment policy, available cash is invested in short-term and long-term, low-risk, investment-grade debt instruments. Other than our equity investments in Biocartis, our cash and marketable securities are held in a variety of interest-bearing instruments including money market accounts and high-grade commercial paper and corporate bonds.
Accounts Receivable
At December 31, 2017 and 2016, $31.2 million, or 13%, and $35.2 million, or 17%, respectively, of our total assets consisted of accounts receivable. The $4.0 million year over year decrease in accounts receivable was primarily attributable to increased cash collections. Days sales outstanding, or DSOs, is a measure of the average number of days it takes for us to collect our accounts receivable, calculated from the date that tests are billed. At December 31, 2017 and 2016, our weighted average DSOs were 62 days and 71 days, respectively. The timing of our billing and cash collections may also cause fluctuations in our monthly DSOs and accounts receivable.
The following tables summarize accounts receivable by payor mix at December 31, 2017 and 2016:
|
|
|
December 31, 2017 |
|
|||||||||||||||||||||
|
|
|
|
|
|
% of |
|
|
|
|
31 - 60 |
|
61 - 90 |
|
91 - 120 |
|
121 to 180 |
|
Over 180 |
|
|||||
|
|
|
Total |
|
Total |
|
Current |
|
Days |
|
Days |
|
Days |
|
Days |
|
Days |
|
|||||||
|
|
|
(In thousands) |
|
|||||||||||||||||||||
|
Managed care and other |
|
$ |
27,017 |
|
77 |
% |
$ |
12,501 |
|
$ |
5,028 |
|
$ |
2,225 |
|
$ |
1,771 |
|
$ |
1,775 |
|
$ |
3,717 |
|
|
Medicare |
|
|
8,028 |
|
23 |
|
|
6,170 |
|
|
564 |
|
|
94 |
|
|
258 |
|
|
467 |
|
|
475 |
|
|
Total |
|
|
35,045 |
|
100 |
% |
$ |
18,671 |
|
$ |
5,592 |
|
$ |
2,319 |
|
$ |
2,029 |
|
$ |
2,242 |
|
$ |
4,192 |
|
|
Allowance for doubtful accounts |
|
|
(3,884) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Net accounts receivable |
|
$ |
31,161 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
December 31, 2016 |
|
|||||||||||||||||||||
|
|
|
|
|
|
% of |
|
|
|
|
31 - 60 |
|
61 - 90 |
|
91 - 120 |
|
121 to 180 |
|
Over 180 |
|
|||||
|
|
|
Total |
|
Total |
|
Current |
|
Days |
|
Days |
|
Days |
|
Days |
|
Days |
|
|||||||
|
|
|
(In thousands) |
|
|||||||||||||||||||||
|
Managed care and other |
|
$ |
30,209 |
|
76 |
% |
$ |
12,061 |
|
$ |
5,108 |
|
$ |
2,298 |
|
$ |
1,792 |
|
$ |
2,608 |
|
$ |
6,342 |
|
|
Medicare |
|
|
9,478 |
|
24 |
|
|
6,043 |
|
|
997 |
|
|
119 |
|
|
281 |
|
|
511 |
|
|
1,527 |
|
|
Total |
|
|
39,687 |
|
100 |
% |
$ |
18,104 |
|
$ |
6,105 |
|
$ |
2,417 |
|
$ |
2,073 |
|
$ |
3,119 |
|
$ |
7,869 |
|
|
Allowance for doubtful accounts |
|
|
(4,508) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Net accounts receivable |
|
$ |
35,179 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cash Flows
|
|
|
|
2017 |
|
2016 |
|
2015 |
|
|||
|
|
|
|
(In thousands) |
|
|||||||
|
For the year ended December 31, |
|
|
|
|
|
|
|
|
|
|
|
|
Cash provided by (used in): |
|
|
|
|
|
|
|
|
|
|
|
|
Operating activities |
|
|
$ |
30,593 |
|
$ |
13,456 |
|
$ |
(11,831) |
|
|
Investing activities |
|
|
|
(42,558) |
|
|
(19,126) |
|
|
6,283 |
|
|
Financing activities |
|
|
|
17,079 |
|
|
13,541 |
|
|
8,355 |
|
|
Capital expenditures (included in investing activities above) |
|
|
|
(13,276) |
|
|
(19,786) |
|
|
(23,483) |
|
Cash Provided by (Used in) Operating Activities
Cash provided by operating activities was $30.6 million in 2017 and consisted primarily of net loss of $3.9 million, adjusted for non-cash items of $34.2 million, gain on sale of equity securities of $2.8 million and $3.1 million related to changes in operating assets and liabilities.
60
Cash provided by operating activities was $13.5 million in 2016 and consisted primarily of net loss of $13.9 million, adjusted for non-cash items of $30.9 million, offset by a gain on sale of equity securities of $3.2 million and $269,000 related to changes in operating assets and liabilities.
Cash used in operating activities was $11.8 million in 2015 and consisted primarily of net loss of $33.3 million, adjusted for non-cash items of $22.4 million and $927,000 related to changes in operating assets and liabilities.
Cash (Used in) Provided by Investing Activities
Cash used in investing activities was $42.6 million in 2017 and consisted of $37.4 million in net purchases of marketable securities, $13.3 million in capital expenditures related to the expansion of our business and $2.0 million in other investments related to our collaboration agreement with Cleveland Diagnostics, offset by $10.2 million in sales of marketable securities.
Cash used in investing activities was $19.1 million in 2016 and consisted primarily of $19.8 million capital expenditures related to the expansion of our business, $6.1 million in other investments related to our collaboration agreement with Epic Sciences and $3.0 million in net purchase of marketable securities offset by $9.7 million in sales of marketable securities.
Cash provided by investing activities was $6.3 million in 2015 and consisted primarily of $29.7 million in net maturities and $23.5 million in capital expenditures.
Cash Provided by Financing Activities
Cash provided by financing activities was $17.1 million in 2017 and consisted $21.8 million in proceeds from the issuance of our common stock upon the exercise of employee stock options and stock purchased pursuant to our ESPP, partially offset by cash paid for tax withholdings in the amount of $4.7 million related to net share settlements of restricted stock units and awards.
Cash provided by financing activities was $13.5 million in 2016 and consisted $17.0 million in proceeds from the issuance of our common stock upon the exercise of employee stock options and stock purchased pursuant to our ESPP, partially offset by cash paid for tax withholdings in the amount of $3.5 million related to net share settlements of restricted stock units and awards.
Cash provided by financing activities was $8.4 million in 2015 and consisted $12.2 million in proceeds from the issuance of our common stock upon the exercise of employee stock options and stock purchased pursuant to our ESPP, partially offset by cash paid for tax withholdings in the amount of $3.8 million related to net share settlements of restricted stock units and awards.
Contractual Obligations
The following table summarizes our significant contractual obligations as of December 31, 2017 and the effect those obligations are expected to have on our liquidity and cash flows in future periods:
|
|
|
Payments Due by Period |
|
|||||||||||||
|
|
|
|
|
|
Less Than |
|
|
|
|
|
|
|
More Than |
|
||
|
|
|
Total |
|
1 Year |
|
1 - 3 Years |
|
3 - 5 Years |
|
5 Years |
|
|||||
|
|
|
(In thousands) |
|
|||||||||||||
|
Non-cancelable operating lease obligations |
|
$ |
29,718 |
|
$ |
5,958 |
|
$ |
13,821 |
|
$ |
8,904 |
|
$ |
1,035 |
|
Our non‑cancelable operating lease obligations are for laboratory and office space. We lease various facilities in Redwood City, California, totaling approximately 180,700 square feet. The lease terms expire between March 2021 and March 2023, each with an option for us to extend the terms of the lease for an additional five years. We also lease 7,500 square feet of space in Geneva, Switzerland. This lease expires in May 2021.
61
We have also committed to make potential future payments to third parties as part of our collaboration and licensing agreements. Payments under these agreements generally become due and payable only upon achievement of specific project milestones. Because the achievement of these milestones is generally neither probable nor reasonably estimable, such contingencies have not been recorded on our Consolidated Balance Sheets and have not been included in the table above.
Off‑Balance Sheet Activities
As of December 31, 2017, we had no material off‑balance sheet arrangements.
Operating Capital and Capital Expenditure Requirements
We currently anticipate that our cash, cash equivalents and short-term marketable securities, together with payments for our tests, will be sufficient to fund our operations and facilities expansion plans for at least the next 12 months, including our research and development programs, our commercialization efforts related to Oncotype DX AR-V7 Nucleus Detect, our efforts to expand adoption of and reimbursement for our tests, our international expansion efforts and our development of our IVD product and capabilities. We expect to spend approximately $9 million over the next 12 months for planned laboratory equipment, information technology and facilities expansion. We may also use cash to acquire or invest in complementary businesses, technologies, services or products. We expect that our cash, cash equivalents and short term marketable securities will also be used to fund working capital and for other general corporate purposes, such as licensing technology rights, distribution arrangements for our tests both within and outside of the United States or expanding our direct sales capabilities worldwide.
The amount and timing of actual expenditures may vary significantly depending upon a number of factors, such as the amount of cash provided by our operations, the progress of our commercialization efforts, product development, regulatory requirements, progress in reimbursement for our tests and available strategic opportunities for acquisition of or investment in complementary businesses, technologies, services or products.
We cannot be certain that our international expansion plans, efforts to expand adoption of and reimbursement for our tests or the development of future products will be successful or that we will be able to raise sufficient additional funds to see these activities through to a successful result. It may take years to move any one of a number of product candidates in research through development and validation to commercialization.
Our future funding requirements will depend on many factors, including the following:
|
· |
the rate of progress in establishing and maintaining reimbursement arrangements with domestic and international third-party payors; |
|
· |
costs associated with expanding our commercial and laboratory operations, including our selling and marketing efforts; |
|
· |
the rate of progress and cost of research and development activities associated with expansion of our current tests and the development of new tests; |
|
· |
the rate of progress and cost of selling and marketing activities associated with expanding adoption of our Oncotype tests; |
|
· |
costs associated with acquiring, licensing or investing in technologies; |
|
· |
costs associated with acquiring or investing in complementary businesses or assets; |
|
· |
expenditures in connection with strategic relationships and license agreements, including our agreements with Epic Sciences, Biocartis and Cleveland Diagnostics; |
|
· |
costs related to future product launches; |
|
· |
costs related to acquiring or achieving access to tissue samples and technologies; |
|
· |
costs related to filing, prosecuting, defending and enforcing any patent claims and other intellectual property rights; |
|
· |
the effect of competing technological and market developments; |
62
|
· |
costs related to international expansion; |
|
· |
costs and delays in product development as a result of any changes in regulatory oversight applicable to our products or operations; |
|
· |
the impact of changes in Federal, state and international taxation; and |
|
· |
the economic and other terms and timing of any collaborations, licensing or other arrangements into which we may enter or investments or acquisitions we might seek to effect. |
If we are not able to generate and maintain sustained product revenues to finance our cash requirements, we will need to finance future cash needs primarily through public or private equity offerings, debt financings, borrowings or strategic collaborations or licensing arrangements. If we raise funds by issuing equity securities, dilution to stockholders may result. Any equity securities issued may also provide for rights, preferences or privileges senior to those of holders of our common stock. If we raise funds by issuing debt securities, these debt securities would have rights, preferences and privileges senior to those of holders of our common stock. The terms of debt securities or borrowings could impose significant restrictions on our operations. If we raise funds through collaborations and licensing arrangements, we might be required to relinquish significant rights to our technologies or products, or grant licenses on terms that are not favorable to us. The credit market and financial services industry have in the past, and may in the future, experience periods of upheaval that could impact the availability and cost of equity and debt financing. If we are not able to secure additional funding when needed, on acceptable terms, we may have to delay, reduce the scope of or eliminate one or more research and development programs or selling and marketing initiatives. In addition, we may have to work with a partner on one or more of our product or market development programs, which could lower the economic value of those programs to us.
Recently Issued Accounting Pronouncements
In May 2014, the Financial Accounting Standards Board (“FASB”) issued Accounting Standards Update (“ASU”) No. 2014-09, Revenue from Contracts with Customers (Topic 606). Topic 606 supersedes the revenue recognition requirements in Accounting Standards Codification Topic 605, Revenue Recognition, and requires entities to recognize revenue when they transfer control of promised goods or services to customers in an amount that reflects the consideration to which the entity expects to be entitled to in exchange for those goods or services. In addition, Topic 606 requires more detailed disclosures to enable users of financial statements to understand the nature, amount, timing, and uncertainty of revenue and cash flows arising from contracts with customers. Topic 606 will be effective for us in the first quarter of 2018. We adopted Topic 606 effective January 1, 2018, using the modified retrospective transition method. We will also elect the practical expedient of applying the new guidance only to contracts that are not completed as of the date of initial application. Upon adoption, we will recognize the cumulative effect of adopting this guidance as an adjustment to our opening accumulated deficit balance. We expect this adjustment to be approximately $14 million. Prior periods will not be retrospectively adjusted.
We have completed our assessment of the impact Topic 606 will have on our consolidated financial statements and related disclosures. The assessment included the analysis of our current portfolio of customer contracts, including a review of historical accounting policies and practices to identify potential differences in applying Topic 606. Based on the assessment, we expect the timing of revenue recognition from certain payors who are not currently accrual payors to be accelerated. In addition, certain amounts that were historically classified as bad debt expense will be considered an implicit price concession in determining the transaction price and therefore as a reduction in net revenues when historically these amounts were classified as bad debt expenses within general and administrative expenses.
In January 2016, the FASB issued ASU No. 2016-01, Financial Instruments-Overall (Subtopic 825-10): Recognition and Measurement of Financial Assets and Financial Liabilities. This ASU changes accounting for equity investments, financial liabilities under the fair value option and the presentation and disclosure requirements for financial instruments. In addition, it clarified guidance related to the valuation allowance assessment when recognizing deferred tax assets resulting from unrealized losses on available-for-sale debt securities. The new guidance could result in volatility of other income (expense), net, in future periods as a result of the remeasurement of the equity securities through earnings upon the occurrence of future observable price changes. The guidance will become effective for us beginning in the first quarter of 2018 and must be adopted using a modified retrospective approach, with certain exceptions. We will adopt this new guidance on January 1, 2018. We expect an impact related to the recognition and measurement of our equity investment in Biocartis. We will reclassify the unrealized loss from accumulated other comprehensive income (loss) to accumulated deficit as of the date of the adoption, which comprises
63
of $180,000 of unrealized loss based on the fair value of the equity investment in Biocartis as of December 31, 2017.
In February 2016, the FASB issued ASU No. 2016-2, Leases (Topic 842). Topic 842 generally requires entities to recognize operating and financing lease liabilities and corresponding right-of-use assets on the balance sheet. Topic 842 is effective for our interim and annual reporting periods during the year ending December 31, 2019, and all annual and interim reporting periods thereafter. Early adoption is permitted. Entities are required to use a modified retrospective approach for leases that exist or are entered into after the beginning of the earliest comparative period in the financial statements, and there are certain optional practical expedients that an entity may elect to apply. Full retrospective application is prohibited and early adoption by public entities is permitted. We are currently evaluating the impact that the adoption of Topic 842 will have on our consolidated financial statements and related disclosures.
In March 2016, the FASB issued ASU No. 2016-09, Improvements to Employee Share-Based Payment Accounting, which simplifies several aspects of the accounting for share-based payments, including immediate recognition of all excess tax benefits and deficiencies in the income statement, changing the threshold to qualify for equity classification up to the employees' maximum statutory tax rates, allowing an entity-wide accounting policy election to either estimate the number of awards that are expected to vest or account for forfeitures as they occur, and clarifying the classification on the statement of cash flows for the excess tax benefit and employee taxes paid when an employer withholds shares for tax-withholding purposes. The standard is effective for interim and annual reporting periods beginning after December 15, 2016, although early adoption is permitted. We adopted this ASU in the first quarter of 2017 and elected to continue to estimate forfeitures expected to occur to estimate the amount of compensation cost to be recognized in each period. As the result, in the first quarter of 2017, we recorded an $11.6 million cumulative-effect adjustment decrease in accumulated deficit and an offsetting increase in deferred tax assets for previously unrecognized excess tax benefits that existed as of December 31, 2016. However, as all of our deferred tax assets, net of deferred tax liabilities, are subject to a valuation allowance and the realization of these assets is not more likely than not to be achieved, we recorded an $11.6 million valuation allowance against these deferred tax assets with an offsetting increase in accumulated deficit. The presentation requirement for cash flows related to employee taxes paid for withheld shares will not impact the statements of cash flows since such amounts have historically been presented as a financing activity. The adoption was on a prospective basis and therefore had no impact on prior periods.
ITEM 7A. Quantitative and Qualitative Disclosures About Market Risk.
Interest Rate Risk
Our exposure to market risk for changes in interest rates relates primarily to interest earned on our cash equivalents and marketable securities. The primary objective of our investment activities is to preserve our capital to fund operations. We also seek to maximize income from our investments without assuming significant risk. Our investment policy provides for investments in short-term, low-risk, investment-grade debt instruments. Our investments in marketable securities, which are comprised primarily of money market funds, commercial paper and corporate bonds, are subject to default, changes in credit rating and changes in market value. These investments are subject to interest rate risk and will decrease in value if market interest rates increase.
At December 31, 2017, we had cash, cash equivalents and short-term marketable securities of $129.6 million. We currently do not hedge interest rate exposure, and we do not have any foreign currency or other derivative financial instruments. The securities in our investment portfolio are classified as available for sale and are, due to their short-term nature, subject to minimal interest rate risk. To date, we have not experienced a loss of principal on any of our investments. Although we currently expect that our ability to access or liquidate these investments as needed to support our business activities will continue, we cannot ensure that this will not change. We believe that, if market interest rates were to change immediately and uniformly by 10% from levels at December 31, 2017, the impact on the fair value of these securities or our cash flows or income would not be material.
Foreign Currency Exchange Risk
Substantially all of our revenues are recognized in U.S. dollars, although a growing percentage is denominated in foreign currency as we continue to expand into markets outside of the United States. Certain expenses related to our international activities are payable in foreign currencies. As a result, factors such as changes in foreign currency exchange rates or weak economic conditions in foreign markets will affect our financial results.
We recognized net foreign exchange transaction gains (losses) of $317,000, $(782,000) and $(551,000) for the years ended December 31, 2017, 2016 and 2015, respectively. The functional currency of our wholly-owned subsidiaries is the U.S.
64
dollar, so we are not currently subject to gains and losses from foreign currency translation of the subsidiary financial statements. In September 2017, we entered into forward contracts to mitigate the impact of adverse movements in foreign exchange rates related to the re-measurement of monetary assets and liabilities and hedge our foreign currency exchange rate exposure. As of December 31, 2017, we had open foreign currency forward contracts with notional amounts of $16.1 million. Although the impact of currency fluctuations on our financial results has been immaterial in the past, there can be no guarantee that the impact of currency fluctuations related to our international activities will not be material in the future.
65
ITEM 8. Financial Statements and Supplementary Data.
Genomic Health, Inc.
Index to Consolidated Financial Statements
66
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Stockholders and the Board of Directors of Genomic Health, Inc.
Opinion on the Financial Statements
We have audited the accompanying consolidated balance sheets of Genomic Health, Inc. (the Company) as of December 31, 2017 and 2016, the related consolidated statements of operations, comprehensive income (loss), stockholders’ equity, and cash flows for each of the three years in the period ended December 31, 2017, and the related notes and financial statement schedule listed in the Index at Item 15(a)(2) (collectively referred to as the “consolidated financial statements”). In our opinion, the consolidated financial statements present fairly, in all material respects, the financial position of the Company at December 31, 2017 and 2016, and the results of its operations and its cash flows for each of the three years in the period ended December 31, 2017, in conformity with U.S. generally accepted accounting principles.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States) (PCAOB), the Company's internal control over financial reporting as of December 31, 2017, based on criteria established in Internal Control-Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (2013 framework) and our report dated March 14, 2018 expressed an unqualified opinion thereon.
Basis for Opinion
These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on the Company’s financial statements based on our audits. We are a public accounting firm registered with the PCAOB and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement, whether due to error or fraud. Our audits included performing procedures to assess the risks of material misstatement of the financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures include examining, on a test basis, evidence regarding the amounts and disclosures in the financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the financial statements. We believe that our audits provide a reasonable basis for our opinion.
/s/ Ernst & Young LLP
We have served as the Company’s auditor since 2002.
Redwood City, California
March 14, 2018
67
GENOMIC HEALTH, INC.
(In thousands, except share and per share amounts)
|
|
|
December 31, |
||||
|
|
|
2017 |
|
2016 |
||
|
ASSETS |
|
|
|
|
|
|
|
Current assets: |
|
|
|
|
|
|
|
Cash and cash equivalents |
|
$ |
45,518 |
|
$ |
40,404 |
|
Short-term marketable securities |
|
|
84,057 |
|
|
56,585 |
|
Accounts receivable (net of allowance for doubtful accounts; 2017—$3,884, 2016—$4,508) |
|
|
31,161 |
|
|
35,179 |
|
Prepaid expenses and other current assets |
|
|
13,524 |
|
|
13,796 |
|
Total current assets |
|
|
174,260 |
|
|
145,964 |
|
Property and equipment, net |
|
|
46,440 |
|
|
45,688 |
|
Other assets |
|
|
10,917 |
|
|
9,462 |
|
Total assets |
|
$ |
231,617 |
|
$ |
201,114 |
|
LIABILITIES AND STOCKHOLDERS’ EQUITY |
|
|
|
|
|
|
|
Current liabilities: |
|
|
|
|
|
|
|
Accounts payable |
|
$ |
156 |
|
$ |
2,864 |
|
Accrued compensation and employee benefits |
|
|
24,953 |
|
|
27,900 |
|
Accrued expenses and other current liabilities |
|
|
14,084 |
|
|
10,180 |
|
Other current liabilities |
|
|
323 |
|
|
231 |
|
Total current liabilities |
|
|
39,516 |
|
|
41,175 |
|
|
|
|
|
|
|
|
|
Other liabilities |
|
|
3,810 |
|
|
3,834 |
|
Commitments and contingencies |
|
|
|
|
|
|
|
Stockholders’ equity: |
|
|
|
|
|
|
|
Preferred stock, $0.0001 par value, 5,000,000 shares authorized, no shares issued and outstanding |
|
|
— |
|
|
— |
|
Common stock, $0.0001 par value; 100,000,000 shares authorized, 36,110,767 and 34,893,329 shares issued and 35,049,436 and 33,831,998 shares outstanding at December 31, 2017 and 2016, respectively |
|
|
|
|
|
|
|
Common stock |
|
|
3 |
|
|
3 |
|
Additional paid-in capital |
|
|
464,637 |
|
|
427,102 |
|
Accumulated other comprehensive (loss) income |
|
|
(294) |
|
|
1,198 |
|
Accumulated deficit |
|
|
(245,945) |
|
|
(242,088) |
|
Treasury stock, at cost, 1,061,331 shares at December 31, 2017 and 2016 |
|
|
(30,110) |
|
|
(30,110) |
|
Total stockholders’ equity |
|
|
188,291 |
|
|
156,105 |
|
Total liabilities and stockholders’ equity |
|
$ |
231,617 |
|
$ |
201,114 |
See accompanying notes.
68
GENOMIC HEALTH, INC.
Consolidated Statements of Operations
(In thousands, except per share data)
|
|
|
|
|
|||||||
|
|
|
|
December 31, |
|||||||
|
|
|
|
2017 |
|
2016 |
|
2015 |
|||
|
Revenues: |
|
|
|
|
|
|
|
|
|
|
|
Product revenues |
|
|
$ |
340,451 |
|
$ |
326,918 |
|
$ |
287,458 |
|
Contract revenues |
|
|
|
299 |
|
|
950 |
|
|
— |
|
Total revenues |
|
|
|
340,750 |
|
|
327,868 |
|
|
287,458 |
|
Operating expenses: |
|
|
|
|
|
|
|
|
|
|
|
Cost of product revenues |
|
|
|
54,718 |
|
|
58,828 |
|
|
55,135 |
|
Research and development |
|
|
|
62,811 |
|
|
60,158 |
|
|
58,445 |
|
Selling and marketing |
|
|
|
157,001 |
|
|
151,042 |
|
|
143,557 |
|
General and administrative |
|
|
|
72,670 |
|
|
73,272 |
|
|
64,348 |
|
Total operating expenses |
|
|
|
347,200 |
|
|
343,300 |
|
|
321,485 |
|
Loss from operations |
|
|
|
(6,450) |
|
|
(15,432) |
|
|
(34,027) |
|
Interest income |
|
|
|
934 |
|
|
418 |
|
|
221 |
|
Gain on sale of equity securities |
|
|
|
2,807 |
|
|
3,208 |
|
|
— |
|
Other income (expense), net |
|
|
|
356 |
|
|
(732) |
|
|
(498) |
|
Loss before income taxes |
|
|
|
(2,353) |
|
|
(12,538) |
|
|
(34,304) |
|
Income tax expense (benefit) |
|
|
|
1,504 |
|
|
1,381 |
|
|
(996) |
|
Net loss |
|
|
$ |
(3,857) |
|
$ |
(13,919) |
|
$ |
(33,308) |
|
Basic and diluted net loss per share |
|
|
$ |
(0.11) |
|
$ |
(0.42) |
|
$ |
(1.03) |
|
Shares used in computing basic and diluted net loss per share |
|
|
|
34,495 |
|
|
33,264 |
|
|
32,382 |
See accompanying notes.
69
GENOMIC HEALTH, INC.
Consolidated Statements of Comprehensive Income (Loss)
(In thousands)
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year Ended December 31, |
|||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|||
|
Net loss |
|
$ |
(3,857) |
|
$ |
(13,919) |
|
$ |
(33,308) |
|
Other comprehensive Loss: |
|
|
|
|
|
|
|
|
|
|
Unrealized gain (loss), net, on available-for-sale marketable securities, net of tax of $0, $0, and $1,548 for the years ended December 31, 2017, 2016 and 2015 respectively. |
|
|
(366) |
|
|
300 |
|
|
2,767 |
|
Reclassification adjustment for net gain on sale of equity securities included in net loss |
|
|
(1,126) |
|
|
(1,854) |
|
|
— |
|
Comprehensive loss |
|
$ |
(5,349) |
|
$ |
(15,473) |
|
$ |
(30,541) |
See accompanying notes.
70
Consolidated Statements of Stockholders’ Equity
(In thousands)
|
|
|
|
|
|
|
|
|
|
Accumulated |
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
Additional |
|
Other |
|
|
|
Treasury |
|
Total |
|||||
|
|
|
Common Stock |
|
Paid-In |
|
Comprehensive |
|
Accumulated |
|
Stock |
|
Stockholders’ |
||||||||
|
|
|
Shares |
|
Amount |
|
Capital |
|
Income (Loss) |
|
Deficit |
|
at Cost |
|
Equity |
||||||
|
Balance at December 31, 2014 |
|
31,911 |
|
$ |
3 |
|
$ |
370,496 |
|
$ |
(15) |
|
$ |
(194,861) |
|
$ |
(30,110) |
|
$ |
145,513 |
|
Issuance of common stock upon exercise of stock options for cash and vesting of restricted stock units |
|
678 |
|
|
— |
|
|
3,664 |
|
|
— |
|
|
— |
|
|
— |
|
|
3,664 |
|
Issuance of common stock upon settlement of employee stock purchase plan |
|
204 |
|
|
— |
|
|
4,694 |
|
|
— |
|
|
— |
|
|
— |
|
|
4,694 |
|
Issuance of restricted stock to directors in lieu of fees |
|
7 |
|
|
— |
|
|
200 |
|
|
— |
|
|
— |
|
|
— |
|
|
200 |
|
Stock-based compensation expense related to employee stock options, restricted stock units and employee stock purchase plan |
|
— |
|
|
— |
|
|
16,005 |
|
|
— |
|
|
— |
|
|
— |
|
|
16,005 |
|
Net loss |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
(33,308) |
|
|
— |
|
|
(33,308) |
|
Unrealized gain on investments, net of tax |
|
— |
|
|
— |
|
|
— |
|
|
2,767 |
|
|
— |
|
|
— |
|
|
2,767 |
|
Balance at December 31, 2015 |
|
32,800 |
|
|
3 |
|
|
395,059 |
|
|
2,752 |
|
|
(228,169) |
|
|
(30,110) |
|
|
139,535 |
|
Issuance of common stock upon exercise of stock options for cash and vesting of restricted stock units |
|
799 |
|
|
— |
|
|
8,385 |
|
|
— |
|
|
— |
|
|
— |
|
|
8,385 |
|
Issuance of common stock upon settlement of employee stock purchase plan |
|
226 |
|
|
— |
|
|
5,155 |
|
|
— |
|
|
— |
|
|
— |
|
|
5,155 |
|
Issuance of restricted stock to directors in lieu of fees |
|
7 |
|
|
— |
|
|
200 |
|
|
— |
|
|
— |
|
|
— |
|
|
200 |
|
Stock-based compensation expense related to employee stock options, restricted stock units and employee stock purchase plan |
|
— |
|
|
— |
|
|
18,303 |
|
|
— |
|
|
— |
|
|
— |
|
|
18,303 |
|
Unrealized gain on investments, net of tax |
|
— |
|
|
— |
|
|
— |
|
|
300 |
|
|
— |
|
|
— |
|
|
300 |
|
Net loss |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
(13,919) |
|
|
— |
|
|
(13,919) |
|
Reclassification adjustment for net gain on sale of investments, net of tax |
|
— |
|
|
— |
|
|
— |
|
|
(1,854) |
|
|
— |
|
|
— |
|
|
(1,854) |
|
Balance at December 31, 2016 |
|
33,832 |
|
|
3 |
|
|
427,102 |
|
|
1,198 |
|
|
(242,088) |
|
|
(30,110) |
|
|
156,105 |
|
Issuance of common stock upon exercise of stock options for cash and vesting of restricted stock units |
|
1,000 |
|
|
— |
|
|
11,636 |
|
|
— |
|
|
— |
|
|
— |
|
|
11,636 |
|
Issuance of common stock upon settlement of employee stock purchase plan |
|
211 |
|
|
— |
|
|
5,443 |
|
|
— |
|
|
— |
|
|
— |
|
|
5,443 |
|
Issuance of restricted stock to directors in lieu of fees |
|
6 |
|
|
— |
|
|
200 |
|
|
— |
|
|
— |
|
|
— |
|
|
200 |
|
Stock-based compensation expense related to employee stock options, restricted stock units and employee stock purchase plan |
|
— |
|
|
— |
|
|
20,256 |
|
|
— |
|
|
— |
|
|
— |
|
|
20,256 |
|
Net loss |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
(3,857) |
|
|
— |
|
|
(3,857) |
|
Unrealized loss on investments, net of tax |
|
— |
|
|
— |
|
|
— |
|
|
(366) |
|
|
— |
|
|
— |
|
|
(366) |
|
Reclassification adjustment for net gain on sale of investments, net of tax |
|
— |
|
|
— |
|
|
— |
|
|
(1,126) |
|
|
— |
|
|
— |
|
|
(1,126) |
|
Balance at December 31, 2017 |
|
35,049 |
|
$ |
3 |
|
$ |
464,637 |
|
$ |
(294) |
|
$ |
(245,945) |
|
$ |
(30,110) |
|
$ |
188,291 |
See accompanying notes.
71
GENOMIC HEALTH, INC.
Consolidated Statements of Cash Flows
(In thousands)
|
|
|
|
|||||||
|
|
|
December 31, |
|||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|||
|
Operating activities |
|
|
|
|
|
|
|
|
|
|
Net loss |
|
$ |
(3,857) |
|
$ |
(13,919) |
|
$ |
(33,308) |
|
Adjustments to reconcile net loss to net cash provided by operating activities: |
|
|
|
|
|
|
|
|
|
|
Depreciation and amortization |
|
|
11,759 |
|
|
8,933 |
|
|
7,069 |
|
Employee stock-based compensation |
|
|
20,256 |
|
|
18,303 |
|
|
16,005 |
|
Write-off of previously capitalized software costs |
|
|
76 |
|
|
2,600 |
|
|
635 |
|
Impairment of assets held for sale and long-lived assets |
|
|
22 |
|
|
56 |
|
|
123 |
|
Gain (loss) on disposal of property and equipment |
|
|
35 |
|
|
33 |
|
|
(80) |
|
Outside director restricted stock awarded in lieu of fees |
|
|
200 |
|
|
200 |
|
|
200 |
|
Gain on sale of equity securities |
|
|
(2,807) |
|
|
(3,208) |
|
|
— |
|
Discount on convertible promissory note |
|
|
671 |
|
|
— |
|
|
— |
|
Discount on equity investment |
|
|
322 |
|
|
— |
|
|
— |
|
Unrealized gain on revaluation of equity investment |
|
|
(7) |
|
|
— |
|
|
— |
|
Deferred tax benefit from unrealized gain on available-for-sale marketable securities, net |
|
|
820 |
|
|
727 |
|
|
(1,548) |
|
Changes in assets and liabilities: |
|
|
|
|
|
|
|
|
|
|
Accounts receivable |
|
|
4,018 |
|
|
1,985 |
|
|
(2,248) |
|
Prepaid expenses and other assets |
|
|
55 |
|
|
(4,550) |
|
|
(1,292) |
|
Accounts payable |
|
|
(2,308) |
|
|
(4,579) |
|
|
949 |
|
Accrued compensation and employee benefits |
|
|
(2,947) |
|
|
5,661 |
|
|
4,531 |
|
Accrued expenses and other liabilities |
|
|
4,164 |
|
|
1,645 |
|
|
(2,963) |
|
Deferred revenues |
|
|
121 |
|
|
(431) |
|
|
96 |
|
Net cash provided by (used in) operating activities |
|
|
30,593 |
|
|
13,456 |
|
|
(11,831) |
|
Investing activities |
|
|
|
|
|
|
|
|
|
|
Purchases of property and equipment |
|
|
(13,276) |
|
|
(19,786) |
|
|
(23,483) |
|
Proceeds from sale of property and equipment |
|
|
10 |
|
|
8 |
|
|
70 |
|
Purchases of marketable securities |
|
|
(109,249) |
|
|
(69,722) |
|
|
(76,743) |
|
Maturities of marketable securities |
|
|
71,802 |
|
|
66,757 |
|
|
106,439 |
|
Proceeds from sales of marketable securities |
|
|
10,155 |
|
|
9,717 |
|
|
— |
|
Other investments |
|
|
(2,000) |
|
|
(6,100) |
|
|
— |
|
Net cash (used) in provided by investing activities |
|
|
(42,558) |
|
|
(19,126) |
|
|
6,283 |
|
Financing activities |
|
|
|
|
|
|
|
|
|
|
Proceeds from issuance of common stock under stock plans |
|
|
21,776 |
|
|
17,010 |
|
|
12,197 |
|
Withholding taxes related to restricted stock units net share settlement |
|
|
(4,697) |
|
|
(3,469) |
|
|
(3,842) |
|
Net cash provided by financing activities |
|
|
17,079 |
|
|
13,541 |
|
|
8,355 |
|
Net increase in cash and cash equivalents |
|
|
5,114 |
|
|
7,871 |
|
|
2,807 |
|
Cash and cash equivalents at the beginning of period |
|
|
40,404 |
|
|
32,533 |
|
|
29,726 |
|
Cash and cash equivalents at the end of period |
|
$ |
45,518 |
|
$ |
40,404 |
|
$ |
32,533 |
|
Supplemental disclosure of cash flow information |
|
|
|
|
|
|
|
|
|
|
Cash paid for income taxes |
|
$ |
1,093 |
|
$ |
428 |
|
$ |
459 |
|
Non-cash investing and financing activities |
|
|
|
|
|
|
|
|
|
|
Accrued purchases of property and equipment |
|
$ |
717 |
|
$ |
1,452 |
|
$ |
3,847 |
|
Change in fair value of equity investment |
|
$ |
(495) |
|
$ |
(316) |
|
$ |
4,269 |
See accompanying notes.
72
Note 1. Organization and Summary of Significant Accounting Policies
The Company
Genomic Health, Inc. (the “Company”) is a global healthcare company that provides actionable genomic information to personalize cancer treatment decisions. The Company develops and globally commercializes genomic‑based clinical laboratory services that analyze the underlying biology of cancer, allowing physicians and patients to make individualized treatment decisions. The Company was incorporated in Delaware in August 2000. The Company’s first product, the Oncotype DX invasive breast cancer test, was launched in 2004 and is used for early stage invasive breast cancer patients to predict the likelihood of breast cancer recurrence and the likelihood of chemotherapy benefit. In January 2010, the Company launched its second product, the Oncotype DX colon cancer test, which is used to predict the likelihood of colon cancer recurrence in patients with stage II disease. The tests for invasive breast and colon cancers result in a quantitative score referred to as a Recurrence Score. In December 2011, the Company made Oncotype DX available for patients with ductal carcinoma in situ (“DCIS”), a pre‑invasive form of breast cancer. This test provides a DCIS Score that is used to predict the likelihood of local recurrence. In June 2012, the Company began offering the Oncotype DX colon cancer test for use in patients with stage III disease treated with oxaliplatin‑containing adjuvant therapy. In May 2013, the Company launched the Oncotype DX prostate cancer test, which provides a Genomic Prostate Score, or GPS, to predict disease aggressiveness in men with low risk prostate cancer and to improve treatment decisions for prostate cancer patients in conjunction with the Gleason score, or tumor grading. In July 2017, the Oncotype DX AR-V7 Nucleus Detect test, for men with metastatic castration-resistant prostate cancer, or mCRPC, became commercially available as part of a clinical utility program.
Principles of Consolidation
These consolidated financial statements include all the accounts of the Company and its wholly‑owned subsidiaries. The Company had two wholly-owned subsidiaries at December 31, 2017: Genomic Health International Holdings, LLC, which was established in Delaware in 2010 and supports the Company’s international sales and marketing efforts; and Oncotype Laboratories, Inc., which was established in 2012, and is inactive. Genomic Health International Holdings, LLC has nine wholly-owned subsidiaries. The functional currency for the Company’s wholly-owned subsidiaries incorporated outside the United States is the U.S. dollar. All significant intercompany balances and transactions have been eliminated.
Basis of Presentation and Use of Estimates
The accompanying consolidated financial statements have been prepared in accordance with accounting principles generally accepted in the United States (“GAAP”). The preparation of financial statements in conformity with GAAP requires management to make judgments, assumptions and estimates that affect the reported amounts of assets, liabilities, revenues and expenses, and related disclosures in the Company’s consolidated financial statements and accompanying notes. Actual results could differ materially from those estimates.
There have been no material changes in the Company’s significant accounting policies, other than the adoption of Accounting Standards Update ("ASU") 2016-09 described below, as compared to the significant accounting policies described in the Company’s Annual Report on Form 10-K for the year ended December 31, 2016.
Certain reclassifications have been made to prior period amounts to conform to the current year presentation. For the years ended December 31, 2016 and 2015, a reclassification of certain expenses from research and development to cost of product revenue was made in the consolidated statements of operations to conform to the current-year presentation.
Cash Equivalents
The Company considers all highly liquid investments with maturities of three months or less when purchased to be cash equivalents.
73
GENOMIC HEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
December 31, 2017
Marketable Securities
The Company invests in marketable securities, primarily money market funds, obligations of U.S. Government agencies and government‑sponsored entities, corporate bonds, commercial paper and equity securities. The Company considers all investments with a maturity date of less than one year as of the balance sheet date to be short‑term investments. Those investments with a maturity date greater than one year as of the balance sheet date are considered to be long‑term investments.
In December 2017, the Company invested €3.4 million or $4.0 million in 270,000 shares of the common stock of Biocartis N.V. (“Biocartis”), a public company listed on the Euronext exchange. This investment was accounted for as an available-for-sale marketable security and valued at €3.0 million or $3.5 million at December 31, 2017. Unrealized gains or losses resulting from changes in the fair value of this investment will be recognized in other comprehensive income until the securities are sold. During the year ended December 31, 2017, $180,000 of unrealized losses relating to changes in the fair value of this investment were recorded in other comprehensive income. These securities are subject to a lock-up agreement which expires in December 2018. During the year ended December 31, 2017, a discount of $322,000 relating to the lock-up agreement was recognized in research and development expense, and a foreign currency revaluation gain of $7,000 was recorded in other income.
Beginning in 2011, the Company made investments in various tranches of the preferred stock of Invitae Corporation (“Invitae”), which at the time was a privately-held company, such that the carrying value of this investment was $13.9 million at December 31, 2014. On February 18, 2015, Invitae completed an initial public offering of its common stock and the Company’s preferred stock investment automatically converted into 2,207,793 shares of Invitae common stock. This investment was accounted for on the cost method as an available-for-sale marketable security and valued at $18.1 million at December 31, 2015.
During the year ended December 31, 2017, the Company sold its remaining shares of the common stock of Invitae for net proceeds of $10.2 million based on a cost of $6.28 per share, resulting in a realized gain of $2.8 million. During the year ended December 31, 2016, the Company sold a portion of its shares of the common stock of Invitae for proceeds of $9.7 million based on a cost of $6.28 per share, resulting in a realized gain of $3.2 million. There were no shares sold during the year ended December 31, 2015. The fair value of the remaining investment was $9.3 million at December 31, 2016. This investment, which is accounted for under the cost method, was valued at $7.3 million at December 31, 2016. Unrealized gains or losses resulting from changes in the fair value of this investment were recognized in other comprehensive income until the securities were sold. During the years ended December 31, 2017 and 2016, $1.1 million of unrealized gains, net of tax of $820,000, and $1.9 million of unrealized gains, net of tax of $727,000, respectively, related to the shares sold were reclassified out of accumulated other comprehensive income into earnings. There was no unrealized gain reclassified out of accumulated other comprehensive income into earnings during the year ended December 31, 2015.
As of December 31, 2017, and 2016, respectively, all investments in marketable securities were classified as available for sale. These securities are carried at estimated fair value with unrealized gains and losses included in stockholders’ equity.
Realized gains and losses and declines in value, if any, judged to be other than temporary on available‑for‑sale securities are reported in other income or expense. When securities are sold, any associated unrealized gain or loss initially recorded as a separate component of stockholders’ equity is reclassified out of stockholders’ equity on a specific‑identification basis and recorded in earnings for the period. The cost of securities sold is determined using specific identification.
Fair Value of Financial Instruments
The Company’s financial instruments consist principally of cash and cash equivalents, marketable securities, trade receivables and accounts payable. The carrying amounts of certain of these financial instruments, including cash and cash equivalents, trade receivables, note receivables and accounts payable, approximate fair value due to their short maturities.
74
GENOMIC HEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
December 31, 2017
See Note 3, “Fair Value Measurements” for further information on the fair value of the Company’s financial instruments.
Concentration of Risk
Cash equivalents, marketable securities and trade accounts receivable are financial instruments which potentially subject the Company to concentrations of credit risk. Through December 31, 2017, no material losses had been incurred related to such credit risk.
The Company is subject to credit risk from its portfolio of cash equivalents and marketable securities. The Company invests in money market funds through a major U.S. bank and is exposed to credit risk in the event of default by the financial institution to the extent of amounts recorded on the consolidated balance sheets. The Company invests in short‑term, investment‑grade debt instruments and by policy limits the amount in any one type of investment, except for securities issued or guaranteed by the U.S. government. Under its investment policy, the Company limits amounts invested in such securities by credit rating, maturity, industry group, investment type and issuer, except for securities issued by the U.S. government. The Company is not exposed to any significant concentrations of credit risk from these financial instruments. The goals of the Company’s investment policy, in order of priority, are as follows: safety and preservation of principal and diversification of risk; liquidity of investments sufficient to meet cash flow requirements; and a competitive after‑tax rate of return.
The Company is also subject to credit risk from its accounts receivable related to its product sales. The Company performs evaluations of customers’ financial condition and generally does not require collateral. The majority of the Company’s accounts receivable arise from product sales in the United States. As of December 31, 2017, the substantial majority of the Company’s product revenues have been derived from sales of one product, the Oncotype DX breast cancer test. The majority of the Company’s tests to date have been delivered to physicians in the United States. All tissue-based Oncotype DX tests are processed in the Company’s clinical reference laboratory facility in Redwood City, California. Medicare accounted for 22%, 21% and 20% of the Company’s product revenues for the years ended December 31, 2017, 2016 and 2015, respectively, and represented 23% and 24% of the Company’s total accounts receivable balance as of December 31, 2017 and 2016, respectively. No other third‑party payor represented more than 10% of the Company’s product revenues or accounts receivable balances for these periods.
Allowance for Doubtful Accounts
The Company accrues an allowance for doubtful accounts against its accounts receivable based on estimates consistent with historical payment experience. Bad debt expense is included in general and administrative expense on the Company’s consolidated statements of operations. Accounts receivable are written off against the allowance when the appeals process is exhausted, when an unfavorable coverage decision is received or when there is other substantive evidence that the account will not be paid. The Company’s allowance for doubtful accounts as of December 31, 2017 and 2016 was $3.9 million and $4.5 million, respectively. Write‑offs for doubtful accounts of $7.2 million and $7.1 million were recorded against the allowance during the years ended December 31, 2017 and 2016, respectively. Bad debt expense was $6.8 million, $7.9 million, and $6.0 million for the years ended December 31, 2017, 2016 and 2015, respectively.
Property and Equipment
Property and equipment, including purchased software, are stated at cost. Depreciation is calculated using the straight‑line method over the estimated useful lives of the assets, which generally range from three to seven years. Leasehold improvements are amortized using the straight‑line method over the estimated useful lives of the assets or the remaining term of the lease, whichever is shorter.
Internal-use Software
Costs incurred to develop software for internal use are capitalized and amortized over the estimated useful life of the software. Costs related to maintenance of internal-use software are expensed as incurred. For the years ended December 31,
75
GENOMIC HEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
December 31, 2017
2017, 2016 and 2015, the Company capitalized $5.1 million (including $2.7 million of personnel-related expenses), $3.4 million (including $1.2 million of personnel-related expenses), and $15.1 million (including $5.9 million of personnel-related expenses), respectively, of costs associated with internal-use software development. Amortization of previously capitalized amounts was $3.2 million, $2.5 million, and $380,000 for the years ended December 31, 2017, 2016, and 2015, respectively.
Intangible Assets
Intangible assets with finite useful lives are recorded at cost, less accumulated amortization. Amortization is recognized over the estimated useful lives of the assets. The Company’s intangible assets with finite lives, which are related to patent licenses, are not material and are included in non‑current other assets on the Company’s consolidated balance sheets.
Investments in Privately Held Companies
The Company determines whether its investments in privately held companies are debt or equity based on their characteristics, in accordance with the applicable accounting guidance for such investments. The Company also evaluates the investee to determine if the entity is a variable interest entity (“VIE”) and, if so, whether the Company is the primary beneficiary of the VIE, in order to determine whether consolidation of the VIE is required in accordance with accounting guidance for consolidations. If consolidation is not required and the Company owns less than 50.1% of the voting interest of the entity, the investment is evaluated to determine if the equity method of accounting should be applied. The equity method applies to investments in common stock or in‑substance common stock where the Company exercises significant influence over the investee, typically represented by ownership of 20% or more of the voting interests of an entity. If the equity method does not apply, investments in privately held companies determined to be equity securities are accounted for using the cost method. Investments in privately held companies determined to be debt securities are accounted for as available‑for‑sale or held‑to‑maturity securities, in accordance with the applicable accounting guidance for such investments.
During the years ended December 31, 2017 and 2016, the Company invested $1.4 million and $6.1 million, respectively, in the subordinated convertible promissory notes of a private company. See Note 6, “Collaboration and Commercial Technology Licensing Agreements” for additional information regarding the terms of this investment. On March 8, 2017, the subordinated convertible promissory notes were converted into preferred stock of the private company representing approximately 9% of the private entity’s voting interests, at which time the Company estimated the fair value of the subordinated convertible promissory notes to be approximately $7.1 million. The preferred stock represents a variable interest in the investee. The Company has concluded it is not the primary beneficiary and thus has not consolidated the investee pursuant to the requirements of Financial Accounting Standards Board (“FASB”) Accounting Standards Codification (“ASC”) 810. The Company determined that the Company does not have the power to direct activities of the private company that most significantly impact the private company’s economic performance. The Company will continue to assess its investment and future commitments to the investee and to the extent its relationship with the investee changes, may be required to consolidate the investee in future periods. The equity investments are accounted for using the cost method of accounting and recorded in other assets on the Company’s consolidated balance sheets.
During the year ended December 31, 2017, the Company invested $2.0 million in the convertible promissory note of a private company. See Note 6, “Collaboration and Commercial Technology Licensing Agreements” for additional information regarding the terms of this investment. The Company estimated the fair value of the convertible promissory note to be approximately $1.3 million. The investment in the convertible promissory note represents a variable interest in the investee. The Company has concluded it is not the primary beneficiary and thus has not consolidated the investee pursuant to the requirements of FASB ASC 810. The Company determined that it does not have the ability to exercise significant influence over the investee company. The Company will continue to assess its investment and future commitments to the investee and to the extent its relationship with the investee changes, may be required to consolidate the investee in future periods. The convertible promissory note is accounted for as available-for-sale debt security and recorded in other assets on the Company’s consolidated balance sheets.
76
GENOMIC HEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
December 31, 2017
Derivative Financial Instruments
The Company hedges a portion of its foreign currency exposures related to outstanding monetary assets and liabilities using foreign currency forward contracts. The foreign currency forward contracts the Company uses to hedge the exposure are not designated as hedges, and as a result, changes in their fair value are recorded in other income (expense). As of December 31, 2017, the Company had open foreign currency forward contracts with notional amounts of $16.1 million. There were no open foreign currency forward contracts at December 31, 2016.
Impairment of Long‑lived Assets
The Company reviews long‑lived assets, which include property and equipment, intangible assets and investments in privately held companies, for impairment whenever events or changes in business circumstances indicate that the carrying amounts of the assets may not be fully recoverable. For property and equipment and intangible assets, an impairment loss would be recognized when estimated undiscounted future cash flows expected to result from the use of the asset and its eventual disposition are less than its carrying amount. Impairment, if any, is assessed using undiscounted cash flows. For investments in non‑marketable equity securities, evidence of impairment might include the absence of an ability to recover the carrying amount of the investment or the inability of the investee to sustain an earnings capacity which would justify the carrying amount of the investment. The Company’s assessment as to whether any impairment is other than temporary is based on its ability and intent to hold the investment and whether evidence indicating the carrying value of the investment is recoverable within a reasonable period of time outweighs evidence to the contrary. If the fair value of the investment is determined to be less than the carrying value and the decline in value is considered to be other than temporary, the asset is written down to its fair value.
Income Taxes
The Company uses the liability method for income taxes, whereby deferred income taxes are provided on items recognized for financial reporting purposes over different periods than for income tax purposes. Valuation allowances are provided when the expected realization of tax assets does not meet a more‑likely‑than‑not criterion.
The Company accounts for uncertain income tax positions using a benefit recognition model with a two‑step approach, a more‑likely‑than‑not recognition criterion and a measurement attribute that measures the position as the largest amount of tax benefit that is greater than 50% likely of being realized upon ultimate settlement, in accordance with the accounting guidance for uncertain tax positions. If it is not more likely than not that the benefit will be sustained on its technical merits, no benefit is recorded. Uncertain tax positions that relate only to timing of when an item is included on a tax return are considered to have met the recognition threshold. The Company recognizes accrued interest and penalties related to unrecognized tax benefits in income tax expense when and if incurred. See Note 11, “Income Taxes” for additional information regarding unrecognized tax benefits.
Revenue Recognition
The Company derives its revenues from product sales and, to a lesser extent from contracts with biopharmaceutical and pharmaceutical companies. The majority of the Company’s historical product revenues have been derived from the sale of the Oncotype DX invasive breast cancer test. The Company generally bills third‑party payors upon generation and delivery of a patient report to the physician. As such, the Company takes assignment of benefits and the risk of collection with the third‑party payor. The Company generally bills the patient directly for amounts owed after multiple requests for payment have been denied or only partially paid by the insurance carrier. The Company pursues case‑by‑case reimbursement where medical policies are not in place or payment history has not been established.
The Company’s product revenues for tests performed are recognized when the following revenue recognition criteria are met: (1) persuasive evidence that an arrangement exists; (2) delivery has occurred or services have been rendered; (3) the fee is fixed or determinable; and (4) collectability is reasonably assured. Criterion (1) is satisfied when the Company has an arrangement to pay or a contract with the payor in place addressing reimbursement for the Oncotype DX test. In the absence of such arrangements, the Company considers that criterion (1) is satisfied when a third‑party payor pays the Company for the
77
GENOMIC HEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
December 31, 2017
test performed. Criterion (2) is satisfied when the Company performs the test and generates and delivers to the physician, or makes available on its web portal, a patient report. When evaluating whether the fee is fixed or determinable and collectible, the Company considers whether it has sufficient history to reliably estimate the total fee that will be received from a payor and a payor’s individual payment patterns. Determination of criteria (3) and (4) are based on management’s judgments regarding whether the fee charged for products or services delivered is fixed or determinable, and the collectability of those fees under any contract or arrangement. Based upon at least several months of payment history, the Company reviews the number of tests paid against the number of tests billed and the payor’s outstanding balance for unpaid tests to determine whether payments are being made at a consistently high percentage of tests billed and at appropriate amounts given the arrangement or contracted payment amount. The estimated accrual amounts per test, recorded upon delivery of a patient report, are calculated for each accrual payor and are based on the arrangement or contracted price adjusted for individual payment patterns resulting from co-payment amounts and excluded services in healthcare plans. The Company also reduces revenue for an estimate of amounts that qualify as patient assistance and related deductions that do not qualify for revenue recognition. When a payment received for an individual test is higher or lower than the estimated accrual amount, the Company recognizes the difference as either cash revenue, in the case of higher payments, or in the case of lower payments, a charge against either the patient assistance program and related deductions reserve or the allowance for doubtful accounts, as applicable.
To the extent all criteria set forth above are not met when test results are delivered, product revenues are recognized when cash is received from the payor.
The Company has exclusive distribution agreements for one or more of its Oncotype DX tests with distributors covering more than 90 countries outside of the United States. The distributor generally provides certain marketing and administrative services to the Company within its territory. As a condition of these agreements, the distributor generally pays the Company an agreed upon fee per test and the Company processes the tests. The same revenue recognition criteria described above generally apply to tests received through distributors. To the extent all criteria set forth above are not met when test results are delivered, product revenues are generally recognized when cash is received from the distributor.
From time to time, the Company receives requests for refunds of payments, generally due to overpayments made by third party‑payors. Upon becoming aware of a refund request, the Company establishes an accrued liability for tests covered by the refund request until such time as the Company determines whether or not a refund is due. Accrued refunds were $87,000 and $487,000 at December 31, 2017 and 2016, respectively.
Contract revenues are generally derived from studies conducted with biopharmaceutical and pharmaceutical companies. The specific methodology for revenue recognition is determined on a case‑by‑case basis according to the facts and circumstances applicable to a given contract. Under certain contracts, the Company’s input, measured in terms of full‑time equivalent level of effort or running a set of assays through its clinical reference laboratory under a contractual protocol, triggers payment obligations, and revenues are recognized as costs are incurred or assays are processed. Certain contracts have payments that are triggered as milestones are completed, such as completion of a successful set of experiments. Milestones are assessed on an individual basis and revenue is recognized when these milestones are achieved, as evidenced by acknowledgment from collaborators, provided that (1) the milestone event is substantive and its achievability was not reasonably assured at the inception of the agreement and (2) the milestone payment is non‑refundable. Where separate milestones do not meet these criteria, the Company typically defaults to a performance‑based model, such as revenue recognition following delivery of effort as compared to an estimate of total expected effort.
Advance payments received in excess of revenues recognized are classified as deferred revenue until such time as the revenue recognition criteria have been met.
Cost of Product Revenues
Cost of product revenues includes the cost of materials, direct labor, equipment and infrastructure expenses associated with processing tissue samples (including sample accessioning, histopathology, anatomical pathology, paraffin extraction, reverse transcription polymerase chain reaction (“RT‑PCR”), quality control analyses and shipping charges to transport tissue samples) and license fees. Infrastructure expenses include allocated facility occupancy and information technology costs. Costs
78
GENOMIC HEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
December 31, 2017
associated with performing the Company’s tests are recorded as tests are processed. Costs recorded for tissue sample processing and shipping charges represent the cost of all the tests processed during the period regardless of whether revenue was recognized with respect to that test. Royalties for licensed technology calculated as a percentage of product revenues and fixed annual payments relating to the launch and commercialization of the Company’s tests are recorded as license fees in cost of product revenues at the time product revenues are recognized or in accordance with other contractual obligations.
Research and Development Expenses
Research and development expenses are comprised of costs incurred to develop technology and carry out clinical studies and include salaries and benefits, reagents and supplies used in research and development laboratory work, infrastructure expenses, including allocated facility occupancy and information technology costs, contract services, and other outside costs. Research and development expenses also include costs related to activities performed under contracts with biopharmaceutical and pharmaceutical companies. Research and development costs are expensed as incurred.
The Company enters into collaboration and clinical trial agreements with clinical collaborators and records these costs as research and development expenses. The Company records accruals for estimated study costs comprised of work performed by its collaborators under contract terms. Advance payments for goods or services that will be used or rendered for future research and development activities are deferred and capitalized and recognized as expense as the goods are delivered or the related services are performed.
Stock‑based Compensation
The Company uses the Black‑Scholes option valuation model, single‑option approach, which requires the use of estimates such as stock price volatility and expected option lives, as well as expected option forfeiture rates, to value employee stock‑based compensation at the date of grant, and recognizes stock‑ based compensation expense ratably over the requisite service period.
Equity instruments granted to non‑employees are also valued using the Black‑Scholes option valuation model and are subject to periodic revaluation over their vesting terms. The Company did not grant any stock options to non‑employee consultants during any of the years presented.
401(k) Plan
Substantially all of the Company’s employees are eligible to participate in its defined contribution plan qualified under Section 401(k) of the Internal Revenue Code. The Company contributed dollar for dollar matching of employee contributions up to a maximum of $4,000, $4,000, and $3,000 for the years ended December 31, 2017, 2016 and 2015, respectively, for each employee per year based on a full calendar year of service. The match is funded concurrently with a participant’s semi‑monthly contributions to the 401(k) Plan. The Company recorded expense for its contributions under the 401(k) Plan of $2.9 million, $3.5 million and $2.8 million for the years ended December 31, 2017, 2016 and 2015, respectively.
Foreign Currency Transactions
Net foreign currency transaction gains or losses are included in other income (expense), net on the Company’s consolidated statements of operations. Net foreign currency transaction gains (losses) totaled $317,000, $(782,000) and $(551,000) for the years ended December 31, 2017, 2016 and 2015, respectively.
Comprehensive Gain or Loss
Other comprehensive gain or loss consists of unrealized gains and losses on available‑for‑sale securities.
79
GENOMIC HEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
December 31, 2017
Leases
The Company enters into lease agreements for its laboratory and office facilities. These leases are classified as operating leases. Rent expense is recognized on a straight‑line basis over the term of the lease. Incentives granted under the Company’s facilities leases, including allowances to fund leasehold improvements and rent holidays, are capitalized and are recognized as reductions to rental expense on a straight‑line basis over the term of the lease.
Guarantees and Indemnifications
The Company, as permitted under Delaware law and in accordance with its bylaws, indemnifies its officers and directors for certain events or occurrences, subject to certain limits, while the officer or director is or was serving at the Company’s request in such capacity. The term of the indemnification period is for the officer’s or director’s lifetime. The maximum amount of potential future indemnification is unlimited; however, the Company has a directors and officers insurance policy that limits its exposure and may enable it to recover a portion of any future amounts paid. The Company believes the fair value of these indemnification agreements is minimal. Accordingly, the Company has not recorded any liabilities for these agreements as of December 31, 2017 and 2016.
Recently Issued Accounting Pronouncements
In May 2014, the FASB issued Accounting Standards Update (“ASU”) No. 2014-09, Revenue from Contracts with Customers (Topic 606). Topic 606 supersedes the revenue recognition requirements in Accounting Standards Codification Topic 605, Revenue Recognition, and requires entities to recognize revenue when they transfer control of promised goods or services to customers in an amount that reflects the consideration to which the entity expects to be entitled to in exchange for those goods or services. In addition, Topic 606 requires more detailed disclosures to enable users of financial statements to understand the nature, amount, timing, and uncertainty of revenue and cash flows arising from contracts with customers. Topic 606 will be effective for the Company in the first quarter of 2018. The Company will adopt Topic 606 effective January 1, 2018, using the modified retrospective transition method. The Company will also elect the practical expedient of applying the new guidance only to contracts that are not completed as of the date of initial application. Upon adoption, the Company will recognize the cumulative effect of adopting this guidance as an adjustment to its opening accumulated deficit balance. The Company expects this adjustment to be approximately $14 million. Prior periods will not be retrospectively adjusted.
The Company has completed its assessment of the impact Topic 606 will have on its consolidated financial statements and related disclosures. The assessment included the analysis of the Company’s current portfolio of customer contracts, including a review of historical accounting policies and practices to identify potential differences in applying Topic 606. Based on the assessment, the Company expects changes to the timing of its revenue recognition from certain payors who are not currently accrual payors to be accelerated. In addition, certain amounts that were historically classified as bad debt expense will be considered an implicit price concession in determining the transaction price and therefore as a reduction in net revenues when historically these amounts were classified as bad debt expenses within general and administrative expenses.
In January 2016, the FASB issued ASU No. 2016-01, Financial Instruments-Overall (Subtopic 825-10): Recognition and Measurement of Financial Assets and Financial Liabilities. This ASU changes accounting for equity investments, financial liabilities under the fair value option and the presentation and disclosure requirements for financial instruments. In addition, it clarified guidance related to the valuation allowance assessment when recognizing deferred tax assets resulting from unrealized losses on available-for-sale debt securities. The new guidance could result to volatility of other income (expense), net, in future periods as a result of the remeasurement of the equity securities through earnings upon the occurrence of future observable price changes. The guidance will become effective for the Company beginning in the first quarter of 2018 and must be adopted using a modified retrospective approach, with certain exceptions. The Company adopted this new guidance effective January 1, 2018. The Company expects an impact related to the recognition and measurement of its equity investment in Biocartis. The Company will reclassify the unrealized loss from accumulated other comprehensive income (loss) to accumulated deficit as of the date of the adoption, which was $180,000 of unrealized loss based on the fair value of the equity investment in Biocartis as
80
GENOMIC HEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
December 31, 2017
of December 31, 2017.
In February 2016, the FASB issued ASU No. 2016-2, Leases (Topic 842). Topic 842 generally requires entities to recognize operating and financing lease liabilities and corresponding right-of-use assets on the balance sheet. Topic 842 is effective for the Company’s interim and annual reporting periods during the year ending December 31, 2019, and all annual and interim reporting periods thereafter. Early adoption is permitted. Entities are required to use a modified retrospective approach for leases that exist or are entered into after the beginning of the earliest comparative period in the financial statements, and there are certain optional practical expedients that an entity may elect to apply. Full retrospective application is prohibited and early adoption by public entities is permitted. The Company is currently evaluating the impact that the adoption of Topic 842 will have on its consolidated financial statements and related disclosures.
In March 2016, the FASB issued ASU No. 2016-09, Improvements to Employee Share-Based Payment Accounting, which simplifies several aspects of the accounting for share-based payments, including immediate recognition of all excess tax benefits and deficiencies in the income statement, changing the threshold to qualify for equity classification up to the employees' maximum statutory tax rates, allowing an entity-wide accounting policy election to either estimate the number of awards that are expected to vest or account for forfeitures as they occur, and clarifying the classification on the statement of cash flows for the excess tax benefit and employee taxes paid when an employer withholds shares for tax-withholding purposes. The standard is effective for interim and annual reporting periods beginning after December 15, 2016, although early adoption is permitted. The Company adopted this ASU in the first quarter of 2017 and elected to continue to estimate forfeitures expected to occur to estimate the amount of compensation cost to be recognized in each period. As a result, in the first quarter of 2017, the Company recorded a $11.6 million cumulative-effect adjustment decrease in accumulated deficit and an offsetting increase in deferred tax assets for previously unrecognized excess tax benefits that existed as of December 31, 2016. However, as all of the Company’s deferred tax assets, net of deferred tax liabilities, are subject to a valuation allowance and the realization of these assets is not more likely than not to be achieved, the Company recorded an $11.6 million valuation allowance against these deferred tax assets with an offsetting increase in accumulated deficit. The presentation requirement for cash flows related to employee taxes paid for withheld shares will not impact the statements of cash flows since such amounts have historically been presented as a financing activity. The adoption was on a prospective basis and therefore had no impact on prior periods.
Basic net loss per share is calculated by dividing net loss for the period by the weighted-average number of common shares outstanding for the period without consideration of potential common shares. Diluted net loss per share is calculated by dividing net loss by the weighted-average number of common shares outstanding for the period and dilutive potential common shares for the period determined using the treasury-stock method. For purposes of this calculation, options to purchase common stock and restricted stock unit (“RSU”) awards are considered to be potential common shares and are not included in the calculation of diluted net loss per share because their effect is anti-dilutive.
The following potentially dilutive common shares were excluded from the computation of diluted net loss per share for the periods presented because they would have been anti-dilutive:
|
|
|
|
Year Ended December 31, |
|
||||
|
|
|
|
2017 |
|
2016 |
|
2015 |
|
|
|
|
|
(In thousands) |
|
||||
|
Stock awards excluded from the computation |
|
|
800 |
|
828 |
|
945 |
|
|
|
|
|
|
|
|
|
|
|
81
GENOMIC HEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
December 31, 2017
Note 3. Fair Value Measurements
The Company measures certain financial assets, including cash equivalents and marketable securities, at their fair value on a recurring basis. The fair value of these financial assets was determined based on a hierarchy of three levels of inputs, of which the first two are considered observable and the last unobservable, as follows:
Level 1: Quoted prices in active markets for identical assets or liabilities.
Level 2: Observable inputs other than Level 1 inputs, such as quoted prices for similar assets or liabilities, quoted prices in markets that are not active, or other inputs that are observable or can be corroborated by observable market data for substantially the full term of the assets or liabilities.
Level 3: Unobservable inputs that are supported by little or no market activity and that are significant to the fair value of the assets or liabilities.
Assets and Liabilities Measured and Recorded at Fair Value on a Recurring Basis
Assets and liabilities measured at fair value are classified in their entirety based on the lowest level of input that is significant to the fair value measurement. The Company’s assessment of the significance of a particular input to the fair value measurement in its entirety requires management to make judgments and consider factors specific to the asset or liability. The Company did not have any non‑financial assets or liabilities that were measured or disclosed at fair value on a recurring basis at December 31, 2017 and 2016, respectively. The following tables set forth the Company’s financial instruments that were measured at fair value on a recurring basis at December 31, 2017 and 2016 by level within the fair value hierarchy:
|
|
|
Actively Quoted |
|
Significant |
|
|
|
|
|
|
||
|
|
|
Markets for |
|
Other |
|
Significant |
|
|
|
|||
|
|
|
Identical |
|
Observable |
|
Unobservable |
|
Balance at |
||||
|
|
|
Assets |
|
Inputs |
|
Inputs |
|
December 31, |
||||
|
|
|
Level 1 |
|
Level 2 |
|
Level 3 |
|
2017 |
||||
|
|
|
(In thousands) |
||||||||||
|
As of December 31, 2017: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Assets |
|
|
|
|
|
|
|
|
|
|
|
|
|
Money market deposits |
|
$ |
10,215 |
|
$ |
— |
|
$ |
— |
|
$ |
10,215 |
|
Commercial paper |
|
|
— |
|
|
30,272 |
|
|
— |
|
|
30,272 |
|
Corporate debt securities |
|
|
— |
|
|
50,260 |
|
|
— |
|
|
50,260 |
|
Corporate equity securities |
|
|
— |
|
|
3,525 |
|
|
— |
|
|
3,525 |
|
Total |
|
$ |
10,215 |
|
$ |
84,057 |
|
$ |
— |
|
$ |
94,272 |
82
GENOMIC HEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
December 31, 2017
|
|
|
Actively Quoted |
|
Significant |
|
|
|
|
|
|
||
|
|
|
Markets for |
|
Other |
|
Significant |
|
|
|
|||
|
|
|
Identical |
|
Observable |
|
Unobservable |
|
Balance at |
||||
|
|
|
Assets |
|
Inputs |
|
Inputs |
|
December 31, |
||||
|
|
|
Level 1 |
|
Level 2 |
|
Level 3 |
|
2016 |
||||
|
|
|
(In thousands) |
||||||||||
|
As of December 31, 2016: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Assets |
|
|
|
|
|
|
|
|
|
|
|
|
|
Money market deposits |
|
$ |
13,198 |
|
$ |
— |
|
$ |
— |
|
$ |
13,198 |
|
Commercial paper |
|
|
— |
|
|
32,421 |
|
|
— |
|
|
32,421 |
|
Corporate debt securities |
|
|
— |
|
|
14,869 |
|
|
— |
|
|
14,869 |
|
Corporate equity securities |
|
|
— |
|
|
9,295 |
|
|
— |
|
|
9,295 |
|
Total |
|
$ |
13,198 |
|
$ |
56,585 |
|
$ |
— |
|
$ |
69,783 |
The Company’s commercial paper and corporate bonds are classified as Level 2 as they are valued using multi-dimensional relational pricing models that use observable market inputs, including benchmark yields, reported trades, broker-dealer quotes, issuer spreads, benchmark securities, bids, offers and reference data. Not all inputs listed are available for use in the evaluation process on any given day for each security evaluation. In addition, market indicators and industry and economic events are monitored and may serve as a trigger to acquire further corroborating market data. The Company’s corporate equity securities are classified as Level 2 while subject to certain restrictions on sale. There were no transfers between Level 1 and Level 2 categories during the years ended December 31, 2017 and 2016, respectively.
All of the Company’s marketable securities are classified as available-for-sale. The following tables summarize the Company’s available‑for‑sale marketable securities as of the dates indicated:
|
|
|
December 31, 2017 |
||||||||||
|
|
|
Cost or |
|
Gross |
|
Gross |
|
Total |
||||
|
|
|
Amortized |
|
Unrealized |
|
Unrealized |
|
Estimated |
||||
|
|
|
Cost |
|
Gains |
|
Losses |
|
Fair Value |
||||
|
|
|
(In thousands) |
||||||||||
|
Commercial paper |
|
$ |
30,315 |
|
$ |
— |
|
$ |
(43) |
|
$ |
30,272 |
|
Corporate debt securities |
|
|
50,331 |
|
|
2 |
|
|
(73) |
|
|
50,260 |
|
Corporate equity securities |
|
|
4,020 |
|
|
— |
|
|
(495) |
|
|
3,525 |
|
Total |
|
$ |
84,666 |
|
$ |
2 |
|
$ |
(611) |
|
$ |
84,057 |
|
|
|
December 31, 2016 |
||||||||||
|
|
|
Cost or |
|
Gross |
|
Gross |
|
Total |
||||
|
|
|
Amortized |
|
Unrealized |
|
Unrealized |
|
Estimated |
||||
|
|
|
Cost |
|
Gains |
|
Losses |
|
Fair Value |
||||
|
|
|
(In thousands) |
||||||||||
|
Commercial paper |
|
$ |
32,350 |
|
$ |
71 |
|
$ |
— |
|
$ |
32,421 |
|
Corporate debt securities |
|
|
14,868 |
|
|
3 |
|
|
(2) |
|
|
14,869 |
|
Corporate equity securities |
|
|
7,348 |
|
|
1,947 |
|
|
— |
|
|
9,295 |
|
Total |
|
$ |
54,566 |
|
$ |
2,021 |
|
$ |
(2) |
|
$ |
56,585 |
The Company had realized gains of $2.8 million, $3.2 million and $0 for the years ended December 31, 2017, 2016 and 2015, respectively, on its available‑for‑sale marketable securities.
83
GENOMIC HEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
December 31, 2017
The following table provides the breakdown of the available‑for‑sale marketable securities with unrealized losses as of the date indicated:
|
|
|
In a Loss Position for |
||||
|
|
|
Less Than 12 Months |
||||
|
|
|
Gross |
|
|
|
|
|
|
|
Unrealized |
|
Estimated |
||
|
As of December 31, 2017: |
|
Losses |
|
Fair Value |
||
|
|
|
(In thousands) |
||||
|
Commercial paper |
|
$ |
(43) |
|
$ |
30,272 |
|
Corporate debt securities |
|
|
(73) |
|
|
45,110 |
|
Corporate equity securities |
|
|
(495) |
|
$ |
3,525 |
|
Total |
|
$ |
(611) |
|
$ |
78,907 |
All of the Company’s available‑for‑sale marketable securities had contractual maturities of one year or less as of December 31, 2017 and 2016.
Assets Measured and Recorded at Fair Value on a Nonrecurring Basis
The Company reviews the fair value of long-lived assets, which include property and equipment, intangible assets and investments in privately held companies, for impairment whenever events or changes in circumstances indicate that the carrying amounts of the assets may not be fully recoverable. During the year ended December 31, 2017 the Company wrote off $98,000 of previously capitalized equipment and software development costs. During the year ended December 31, 2016, the Company wrote off $2.6 million of previously capitalized software development costs related to a project for enhanced report delivery due to scope change. The impairment charge related to the write off is included in the selling and marketing expenses in the accompanying consolidated statements of operations. In addition, during the year ended December 31, 2016, the Company recorded impairment losses of $56,000 for equipment classified as held for sale. During the year ended December 31, 2015, the Company wrote off $635,000 of previously capitalized software costs and recorded impairment losses of $123,000 for equipment classified as held for sale.
During the year ended December 31, 2017, the Company invested $2.0 million in a convertible promissory note of Cleveland Diagnostics, Inc. (“Cleveland Diagnostics”). See Note 6, “Collaboration and Commercial Technology Licensing Agreements” for additional information regarding the terms of this investment. The Company estimated the fair value of the convertible promissory note to be approximately $1.3 million. The convertible promissory note is classified as Level 3 as it is valued using unobservable inputs that are primarily based on the Company’s estimate of the fair value of the underlying preferred stock into which the notes are convertible.
During the years ended December 31, 2017 and 2016, the Company invested $1.4 million and $6.1 million, respectively, in subordinated convertible promissory notes of Epic Sciences, Inc. (“Epic Sciences”). See Note 6, “Collaboration and Commercial Technology Licensing Agreements” for additional information regarding the terms of this investment. In March 2017, the subordinated convertible promissory notes were converted into preferred stock of Epic Sciences, Inc., with an estimated fair value of $7.1 million. The Company accounted for such preferred stock using the cost method of accounting and accordingly recorded such preferred stock in other assets. There were no identified events or changes in circumstances that may have a significant adverse effect on the fair value of the preferred stock during the remainder of the year ended December 31, 2017. As of December 31, 2016, the Company estimated the fair value of the subordinated convertible promissory notes to be approximately $5.8 million which was recorded in other assets. As of December 31, 2016, the subordinated convertible promissory notes are classified as Level 3 as they are valued using unobservable inputs that are primarily based on the Company’s estimate of the fair value of the underlying preferred stock into which the notes are convertible.
84
GENOMIC HEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
December 31, 2017
Note 4. Property and Equipment
The following table summarizes the Company’s property and equipment as of the dates indicated:
|
|
|
December 31, |
||||
|
|
|
2017 |
|
2016 |
||
|
|
|
(In thousands) |
||||
|
Laboratory equipment |
|
$ |
37,560 |
|
$ |
29,992 |
|
Computer equipment |
|
|
10,498 |
|
|
9,605 |
|
Computer software—internal use |
|
|
26,483 |
|
|
23,790 |
|
Furniture and fixtures |
|
|
4,749 |
|
|
4,055 |
|
Leasehold improvements |
|
|
29,126 |
|
|
20,756 |
|
Work in progress |
|
|
3,698 |
|
|
14,206 |
|
|
|
|
112,114 |
|
|
102,404 |
|
Less accumulated depreciation and amortization |
|
|
(65,674) |
|
|
(56,716) |
|
Total |
|
$ |
46,440 |
|
$ |
45,688 |
For the years ended December 31, 2017, 2016 and 2015, the Company recognized property and equipment depreciation and amortization expense of $11.6 million, $8.8 million and $6.9 million, respectively.
Note 5. Accrued Expenses and Other Current Liabilities
The following table summarizes the Company’s accrued expenses and other current liabilities as of the dates indicated:
|
|
|
December 31, |
||||
|
|
|
2017 |
|
2016 |
||
|
|
|
(In thousands) |
||||
|
Accrued expenses |
|
$ |
7,197 |
|
$ |
3,984 |
|
Accrued professional and other service fees |
|
|
3,114 |
|
|
1,902 |
|
Accrued refunds |
|
|
87 |
|
|
487 |
|
Accrued rebate |
|
|
407 |
|
|
588 |
|
Accrued collaboration expense |
|
|
2,532 |
|
|
2,418 |
|
Accrued taxes payable |
|
|
746 |
|
|
800 |
|
Other current liabilities |
|
|
1 |
|
|
1 |
|
Total |
|
$ |
14,084 |
|
$ |
10,180 |
Accrued professional and other service fees include third‑party billing and collections costs, legal expenses, accounting and audit fees and investor relations expenses. Accrued refunds include overpayments due to third‑party payors.
Note 6. Collaboration and Commercial Technology Licensing Agreements
The Company has entered into a variety of collaboration and specimen transfer agreements relating to its development efforts. The Company recorded collaboration expenses of $7.3 million, $4.6 million and $11.1 million for the years ended December 31, 2017, 2016 and 2015, respectively, relating to services provided by the collaborators in connection with these agreements. In addition to these expenses, some of these agreements contain provisions for royalties from inventions resulting from these collaborations. The Company has specified options and rights relating to joint inventions arising out of these collaborations.
In January 2014, the Company entered into a collaboration agreement to conduct a prostate study with a goal to determine the association between the GPS provided by the Company’s assay and the likelihood of experiencing disease progression while on active surveillance. In July 2014, the Company entered into a collaboration agreement to conduct a
85
GENOMIC HEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
December 31, 2017
prostate observational study in men who choose active surveillance at one and two years after receiving the Oncotype DX prostate cancer GPS. In August 2014, the Company entered into an agreement to provide support to conduct the main phase of a prospective study dealing with individualization of adjuvant decision-making in early-stage breast cancer. In November 2017, the Company entered into a collaboration agreement to provide support to conduct a data sweep and analysis for a mid-range recurrence score group for a prospective study which was designed to explore breast cancer recurrences in patients with early stage breast cancer. As of December 31, 2017, the estimated total remaining obligations for these agreements, including certain milestone payments, is approximately $1.3 million. All future milestone payments are contingent on certain accomplishments, and therefore the timing for any related payments cannot be estimated.
In June 2016, the Company entered into a collaboration agreement with Epic Sciences, Inc., under which the Company was granted exclusive distribution rights to commercialize Epic Sciences’ AR-V7 Nucleus Detect test in the United States, which is marketed as Oncotype DX AR-V7 Nucleus Detect. The Company has primary responsibility, in accordance with applicable laws and regulations, for marketing and promoting the test, order fulfillment, billing and collections of receivables, claims appeals, customer support, and providing and maintaining order management systems for the test. Epic Sciences is responsible for performing all tests, performing studies including analytic and clinical validation studies, and seeking Medicare coverage and a Medicare payment rate from the Centers for Medicare and Medicaid Services (“CMS”) for the test. Future revenues generated from the test will be shared by the Company and Epic Sciences in accordance with the terms of the agreement. During 2016 and 2017 the Company invested $7.5 million in subordinated promissory notes of Epic Sciences that converted into shares of Epic Sciences preferred stock in March 2017. The subordinated promissory notes had been recognized at fair value which the Company believed was approximately $7.1 million while the difference of $375,000 has been deferred as of December 31, 2017 and will be recognized as additional cost of future purchases of Oncotype DX AR-V7 Nucleus test, which the Company believes will be at a discount to fair value. Additional terms of the agreement include the Company’s obligation to pay Epic Science’s $4.0 million upon achievement of certain milestones. Also, the Company has agreed, upon achievement of one of the milestones, to invest an additional $2.5 million in Epic Sciences preferred stock. The agreement has a term of 10 years, unless terminated earlier under certain circumstances.
In November 2013, the Company entered into an exclusive license agreement to develop and commercialize a test to predict benefit from DNA damage-based chemotherapy drugs, such as anthracycline-based regimens, in high risk breast cancer. The Company made an up‑front payment of $9.0 million, which was recognized in research and development expense in the fourth quarter of 2013, and milestone payments would have been required if certain clinical and commercial endpoints were achieved in the future. With successful commercialization of a test, the Company would have been obligated to pay royalties. During the quarter ended March 31, 2015, the Company accrued $5.5 million in anticipation of the wind-down of this license agreement and development program, which was recognized as research and development expense in the accompanying consolidated statements of operations. The license agreement was terminated in May 2015 and, as a result, the Company has no future obligations under this agreement.
The Company is a party to various agreements under which it licenses technology on a non‑exclusive basis in the field of human diagnostics. Access to these licenses enables the Company to process its Oncotype DX tests. While certain agreements contain provisions for fixed annual payments, license fees are generally calculated as a percentage of product revenues, with rates that vary by agreement and may be tiered, and payments that may be capped at annual minimum or maximum amounts. The Company recognized costs under these agreements totaling $314,000, $5.3 million and $9.2 million for the years ended December 31, 2017, 2016 and 2015, respectively, which were included in cost of product revenues. The decrease in costs for these agreements for the year ended December 31, 2017 compared to the years ended December 31, 2016 and 2015, was primarily due to the satisfaction of certain royalty payment obligations. On October 28, 2016, the Company provided notice of termination of a license agreement with Roche Molecular Systems, Inc. (“Roche”), whereby the Company non-exclusively licensed from Roche a number of U.S. patents claiming nucleic acid amplification processes known as PCR, homogeneous polymerase chain reaction, and RT PCR. The effective date of the termination was November 27, 2016. The Company believes it has satisfied all obligations to make royalty payments to Roche.
In September 2017, the Company entered into an exclusive license and development agreement with Biocartis, a molecular diagnostics company based in Belgium, to develop and commercialize an in vitro diagnostic (“IVD”) version of the Oncotype DX breast cancer test on Biocartis’ Idylla platform that can be performed locally by laboratory partners and in
86
GENOMIC HEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
December 31, 2017
hospitals around the world. Under the terms of the license and development agreement, the Company has an exclusive, worldwide, royalty-bearing license to develop and commercialize an IVD version of the Oncotype DX breast cancer tests on Biocartis Idylla platform, and an option to expand the collaboration to include additional tests in oncology and urology. The Company has primary responsibility for developing, validating and obtaining regulatory authorizations and registrations for IVD Oncotype DX tests to be performed on the Idylla platform. The Company is also responsible for manufacturing and commercialization activities with respect to such tests. Pursuant to the license and development agreement, the Company recorded a one-time upfront license fee of €2.8 million or $3.2 million, which is included in research and development expenses for the year ended December 31, 2017. In December 2017, the Company purchased 270,000 ordinary shares of Biocartis at the market price of €12.50 for a total cost of €3.4 million or $4.0 million. This investment is accounted for as an available-for-sale marketable security and is subject to a lock-up agreement that expires in December 2018. The investment has been recognized at fair value, which the Company believes to be $3.5 million with the difference attributable to a $322,000 discount resulting from the lock up period and a $180,000 decrease in the market value of the Biocartis shares. Additional terms of the license and development agreement include the Company’s obligation to pay Biocartis an aggregate of €6.5 million in cash upon achievement of certain milestones, and royalties based primarily on the future sales volumes of the Company’s test performed on the Idylla platform.
In November 2017, the Company entered into an exclusive licensing agreement with Cleveland Diagnostics to develop and commercialize new prostate cancer tests based on Cleveland Diagnostics' IsoPSA reagents and technology. Initial efforts under this agreement will focus on the Company’s development of a high-PSA (prostate specific antigen) reflex test to accurately predict the presence of high-grade cancer (Gleason score > 7) prior to prostate biopsy. During the year ended December 31, 2017, the Company invested $2.0 million in a convertible promissory note of Cleveland Diagnostics. The convertible promissory note has been recognized at fair value, which the Company believes is approximately $1.3 million with the difference of $671,000 recognized as an additional cost of the license. Additional terms of the license agreement include the Company’s obligation to pay Cleveland Diagnostics up to an aggregate of $18.5 million in cash upon achievement of certain future milestones, a potential future investment in a convertible promissory note of Cleveland Diagnostics in the amount of $3.0 million upon achievement of certain future milestones, and royalties based primarily on the future sales volume of tests performed by the Company utilizing technology licensed from Cleveland Diagnostics.
Contract Research Arrangements
In November 2017, the Company entered into a multi-year research collaboration agreement with Janssen Pharmaceuticals (“Janssen”) to evaluate the Oncotype DX GPS test for its prostate cancer drug pipeline. As part of the agreement, the Company will test samples from Janssen studies to examine the association of GPS results with clinical outcomes. The Company expects the total payment to be $1.8 million. During the year ended December 31, 2017, the Company recognized $299,000 as contract revenue using a performance-based model following delivery of effort as compared to an estimate of total expected effort.
Note 7. Commitments and Contingencies
Lease Obligations
The Company leases approximately 180,700 square feet of office and laboratory space under five non-cancelable operating leases, with terms that expire between 2021 and 2023 in Redwood City, California, and 7,500 square feet of office space for the Company’s European subsidiary under a non-cancelable operating lease that expires in 2021 in Geneva, Switzerland. The Company’s Redwood City, California leases each contain options to extend the terms of such leases for an additional five years as well as tenant improvement allowances that could total as much as $2.3 million to the extent utilized by November 2018.
87
GENOMIC HEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
December 31, 2017
Rent expense under operating leases amounted to $6.3 million, $5.7 million and $4.1 million for the years ended December 31, 2017, 2016 and 2015, respectively.
Future non‑cancelable commitments under these operating leases at December 31, 2017 were as follows:
|
|
|
Annual |
|
|
|
|
Payments |
|
|
|
|
(In thousands) |
|
|
Years Ending December 31, |
|
|
|
|
2018 |
|
$ |
5,958 |
|
2019 |
|
|
6,746 |
|
2020 |
|
|
7,075 |
|
2021 |
|
|
4,822 |
|
2022 |
|
|
4,082 |
|
2023 and thereafter |
|
|
1,035 |
|
Total minimum payments |
|
$ |
29,718 |
Contingencies
From time to time, the Company may be subject to various legal proceedings and claims arising in the ordinary course of business. The Company assesses contingencies to determine the degree of probability and range of possible loss for potential accrual in its consolidated financial statements. An estimated loss contingency is accrued in the consolidated financial statements if it is probable that a liability has been incurred and the amount of the loss can be reasonably estimated. Any such accruals were not material at either December 31, 2017 or 2016.
Note 8. Capital Stock
Common Stock
As of December 31, 2017, the Company had 35,049,436 shares of common stock outstanding. Shares of common stock reserved for future issuance as of December 31, 2017 were as follows:
|
|
|
Number of |
|
|
|
Shares |
|
|
|
(In thousands) |
|
Shares to be issued upon exercise of outstanding stock options and vesting of RSUs |
|
4,424 |
|
Shares available for future stock option and RSU grants, settlement of employee stock purchase plan (ESPP) and restricted stock to be issued to outside directors in lieu of director fees |
|
4,403 |
|
Shares of common stock reserved for future issuance |
|
8,827 |
Treasury Stock
In December 2012, the Company entered into an accelerated share repurchase agreement with a financial institution to repurchase $30.0 million of its common stock on an accelerated basis. The shares of common stock repurchased under the agreement were 984,074 and 77,257 during the year ended December 31, 2012 and 2013, respectively. The average purchase price of the Company’s common stock from the accelerated share repurchase program was $28.27 per share.
Note 9. Stock‑based Compensation
2005 Stock Incentive Plan
On September 8, 2005, the Board of Directors approved the 2005 Stock Incentive Plan (the “2005 Plan”), which was later approved by the Company’s stockholders. Pursuant to the 2005 Plan, stock options, restricted shares, stock units, including
88
GENOMIC HEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
December 31, 2017
RSUs, and stock appreciation rights may be granted to employees, consultants, and outside directors of the Company. Options granted may be either incentive stock options or nonstatutory stock options. The Company initially reserved 5,000,000 shares of the Company’s common stock for issuance under the 2005 Plan, effective upon the closing of the Company’s initial public offering on October 4, 2005. On June 8, 2009, the Company’s stockholders approved an amendment to the 2005 Plan to increase the shares reserved for issuance under the 2005 Plan by 3,980,000 shares. The amended and restated plan also extends the term under which awards may be granted under the 2005 Plan until January 27, 2019. On June 11, 2015, the Company’s stockholders approved an amendment to the amended and restated 2005 Plan to increase the shares reserved for issuance under the 2005 Plan by 1,500,000 shares. On June 9, 2016, the Company’s stockholders approved an amendment to the amended and restated 2005 Plan to increase the shares reserved for issuance under the 2005 Plan by 1,500,000 shares. On June 15, 2017 the Company’s stockholders approved an amended and restated 2005 Plan to increase the shares reserved for issuance under the 2005 Plan by 1,500,000 sharers. As of December 31, 2017, a total of 3,034,000 shares remain available for future grant under the 2005 Plan.
Stock Option Activity
Stock options are governed by stock option agreements between the Company and recipients of stock options. Incentive stock options may be granted under the 2005 Plan at an exercise price of not less than 100% of the fair market value of the common stock on the date of grant, determined by the Compensation Committee of the Board of Directors. Nonstatutory stock options may be granted under the 2005 Plan at an exercise price of not less than 80% of the fair market value of the common stock on the date of grant, determined by the Compensation Committee of the Board of Directors. Options become exercisable and expire as determined by the Compensation Committee, provided that the term of incentive stock options may not exceed 10 years from the date of grant. Stock option agreements may provide for accelerated exercisability in the event of an optionee’s death, disability, or retirement or other events.
Under the 2005 Plan, each outside director who joins the board after the effective date of the 2005 Plan will receive an automatic nonstatutory stock option grant that vests at a rate of 25% at the end of the first year, with the remaining balance vesting monthly over the next three years. On the first business day following the annual meeting of the Company’s stockholders, each outside director who is continuing board service and who was not initially elected to the board at the annual meeting will receive an additional nonstatutory stock option grant, which will vest in full on the first anniversary of the date of grant or, if earlier, immediately prior to the next annual meeting of the Company’s stockholders. Nonstatutory stock options granted to outside directors must have an exercise price equal to 100% of the fair market value of the common stock on the date of grant. Nonstatutory stock options terminate on the earlier of the day before the tenth anniversary of the date of grant or the date twelve months after termination of the outside director’s service as a member of the Board of Directors.
89
GENOMIC HEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
December 31, 2017
The following table summarizes option activity for the year ended December 31, 2017:
|
|
|
|
|
|
|
|
Weighted-Average |
|
|
|
|
|
|
Outstanding Options |
|
Remaining |
|
Aggregate |
||||
|
|
|
Number of |
|
Weighted-Average |
|
Contractual |
|
Intrinsic |
||
|
|
|
Shares |
|
Exercise Price |
|
Life |
|
Value |
||
|
|
|
(In thousands) |
|
|
|
(In years) |
|
(In thousands) |
||
|
Balance at December 31, 2016 |
|
3,606 |
|
$ |
25.07 |
|
|
|
|
|
|
Options granted |
|
741 |
|
$ |
28.12 |
|
|
|
|
|
|
Options exercised |
|
(765) |
|
$ |
21.34 |
|
|
|
|
|
|
Options forfeited |
|
(87) |
|
$ |
28.22 |
|
|
|
|
|
|
Options expired |
|
(35) |
|
$ |
29.80 |
|
|
|
|
|
|
Balance at December 31, 2017 |
|
3,460 |
|
$ |
26.42 |
|
6.0 |
|
$ |
27,023 |
|
Exercisable at December 31, 2017 |
|
2,324 |
|
$ |
25.61 |
|
4.7 |
|
$ |
20,062 |
|
Vested and expected to vest at December 31, 2017 |
|
3,388 |
|
$ |
26.39 |
|
6.0 |
|
$ |
26,572 |
The total intrinsic value of stock options exercised during the years ended December 31, 2017, 2016 and 2015 was $8.0 million, $5.6 million and $6.6 million, respectively. The total fair value of stock options vested during the years ended December 31, 2017, 2016 and 2015 was $6.2 million, $5.3 million and $4.2 million, respectively.
Performance-Based Vesting Stock Options
Under the 2005 Plan, the Company grants performance-based vesting stock options (“PV stock options”) which vest upon achievement of specified performance goals. The Company recognizes the fair value of these awards to the extent the achievement of the related performance criteria is estimated to be probable. If a performance criterion is subsequently determined to not be probable of achievement, any related expense is reversed in the period such determination is made. Conversely, if a performance criterion is not currently expected to be achieved but is later determined to be probable of achievement, a “catch-up” entry is recorded in the period such determination is made for the expense that would have been recognized had the performance criterion been probable of achievement since the grant of the award.
In April 2016, the Company granted PV stock options to purchase 75,531 shares of common stock with an exercise price of $31.12 per share. The number of shares potentially issuable under PV stock options were subject to the attainment of a pre-established, corporate-level objective performance goal for the year ended December 31, 2016. In addition, the awards had a service-vesting criteria following the achievement of performance criteria through February 2019. As of December 31, 2016, the achievement of the performance criteria was estimated to be remote and the award was cancelled.
Restricted Stock Unit Activity
The Company began granting RSUs in 2011. The RSUs generally vest in three equal annual installments. As of April 2011, outside directors were given the option to elect to receive some or all of their retainers (other than retainers for serving as committee chair) in the form of fully‑vested restricted stock. Restricted shares, stock units and stock appreciation rights granted under the 2005 Plan are governed by agreements between the Company and recipients of the awards. Terms of the agreements are determined by the Compensation Committee.
90
GENOMIC HEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
December 31, 2017
A following table summarizes RSU activity for the year ended December 31, 2017:
|
|
|
|
|
Weighted-Average |
|
|
|
|
Number of |
|
Grant Date Fair |
|
|
|
|
Shares |
|
Value |
|
|
|
|
(In thousands) |
|
|
|
|
Balance at December 31, 2016 |
|
871 |
|
$ |
28.42 |
|
RSUs granted |
|
593 |
|
$ |
28.35 |
|
RSUs vested |
|
(388) |
|
$ |
28.75 |
|
RSUs cancelled |
|
(112) |
|
$ |
28.35 |
|
Balance at December 31, 2017 |
|
964 |
|
$ |
28.25 |
The weighted-average per share grant date fair values of RSUs were $28.35, $27.50 and $30.65 during the years ended December 31, 2017, 2016 and 2015, respectively. The fair value of RSUs vested were $12.0 million, $8.6 million $9.4 million for the year ended December 31, 2017, 2016 and 2015, respectively.
Performance-Based Restricted Stock Unit Activity
Under the 2005 Plan, the Company grants performance-based restricted stock units (“PVRSUs”) which vest upon achievement of specified performance goals. The fair value of each PVRSU is estimated at the date of grant or when performance objectives are defined for the grants. The Company recognizes the fair value of these awards to the extent the achievement of the related performance criteria is estimated to be probable. If a performance criteria is subsequently determined to not be probable of achievement, any related expense is reversed in the period such determination is made. Conversely, if a performance criteria is not currently expected to be achieved but is later determined to be probable of achievement, a “catch-up” entry is recorded in the period such determination is made for the expense that would have been recognized had the performance criteria been probable of achievement since the grant of the award.
There were no PVRSU activities during the year ended December 31, 2017. The weighted-average per share grant date fair values of PVRSUs were $0, $28.09 and $31.12 during the years ended December 31, 2017, 2016 and 2015, respectively. The fair value of PVRSUs vested was $0, $163,000 and $211,000 during the years ended December 31, 2017, 2016 and 2015 respectively.
Restricted Stock in Lieu of Directors’ Fees
Outside members of the Company’s Board of Directors may elect to receive fully‑vested restricted stock in lieu of cash compensation for services as a director. During the years ended December 31, 2017, 2016 and 2015, the Company issued 6,375, 6,970, and 7,365 shares of restricted stock, respectively, to outside directors, with vesting date fair values of $200,000 for each of the years, and a weighted‑average grant date fair value of $31.33, $28.65, and $27.10 per share, respectively.
Employee Stock Purchase Plan
In June 2011, the Company’s stockholders approved the Company’s Employee Stock Purchase Plan (“ESPP”). The ESPP provides eligible employees with an opportunity to purchase common stock from the Company and to pay for their purchases through payroll deductions. The ESPP is implemented through a series of offerings of purchase rights to eligible employees beginning December 1, 2011. Under the ESPP, the Compensation Committee of the Company’s Board of Directors may specify offerings with a duration of not more than 27 months, and may specify shorter purchase periods within each offering. During each purchase period, payroll deductions accumulate without interest. On the last day of the purchase period, accumulated payroll deductions are used to purchase common stock for employees participating in the offering. The purchase price is specified pursuant to the offering, but cannot, under the terms of the ESPP, be less than 85% of the fair market value per share of the Company’s common stock on either the last trading day preceding the offering date or on the purchase date, whichever is less.
91
GENOMIC HEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
December 31, 2017
The Company’s Board of Directors has determined that the purchase periods initially shall have a duration of six months and that the purchase price will be 85% of the fair market value per share of the Company’s common stock on either the last trading day preceding the offering date or the purchase date, whichever is less. The length of the purchase period applicable to U.S. employees and the purchase price may not be changed without the approval of the independent members of the Company’s Board of Directors.
A total of 1,250,000 shares of common stock were initially reserved for issuance under the ESPP. On June 15, 2017 the Company’s stockholders approved an amendment to the ESPP to increase the shares reserved for issuance under the ESPP by 1,250,000 shares. As of December 31, 2017, a total of 1,368,713 shares were available for issuance under the ESPP. During 2017, 2016 and 2015, 210,880, 226,303 and 203,842 shares were issued under the ESPP, respectively.
As of December 31, 2017, there was $587,000 of unrecognized compensation expense related to the ESPP, which is expected to be recognized over a period of five months.
Employee Stock‑Based Compensation Expense
Stock-based compensation is recognized as expense over the requisite service periods in the consolidated statements of operations using the straight-line expense attribution approach for stock options and RSUs, and using a graded vesting expense attribution approach for PV stock options and PVRSUs. The Company recognized employee stock‑based compensation expense of $20.3 million, $18.3 million and $16.0 million for the years ended December 31, 2017, 2016 and 2015, respectively. Employee stock‑based compensation expense was calculated based on awards ultimately expected to vest and has been reduced for estimated forfeitures. Forfeitures are estimated at the time of grant and revised, if necessary, in subsequent periods if actual forfeitures differ from those estimates. Employee stock‑based compensation expense includes expense related to stock options granted to outside directors of the Company as well as stock purchased under the ESPP. The following table presents the impact of employee stock‑based compensation expense on selected statement of operations line items for the periods indicated:
|
|
|
|
Year Ended December 31, |
|||||||
|
|
|
|
2017 |
|
2016 |
|
2015 |
|||
|
|
|
|
(In thousands) |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Cost of product revenues |
|
|
$ |
741 |
|
$ |
664 |
|
$ |
584 |
|
Research and development |
|
|
|
5,469 |
|
|
4,860 |
|
|
4,169 |
|
Selling and marketing |
|
|
|
5,730 |
|
|
5,551 |
|
|
4,526 |
|
General and administrative |
|
|
|
8,316 |
|
|
7,228 |
|
|
6,726 |
|
Total |
|
|
$ |
20,256 |
|
$ |
18,303 |
|
$ |
16,005 |
As of December 31, 2017, unrecognized compensation expense related to unvested stock options and RSUs net of estimated forfeitures was $10.0 million and $16.3 million, respectively. The Company expects to recognize these expenses over a weighted‑average period of 2.6 years and 1.8 years, respectively. There was no unrecognized compensation expense related to unvested PV stock options and PVRSUs.
Valuation Assumptions
Fair values of awards granted under the 2005 Plan and ESPP were estimated at grant or purchase dates using a Black‑Scholes option valuation model. Option valuation models require the input of highly subjective assumptions that can vary over time. The Company’s assumptions regarding expected volatility are based on the historical volatility of the Company’s common stock. The expected life of options granted is estimated based on historical option exercise data and assumptions related to unsettled options. The risk‑free interest rate is estimated using published rates for U.S. Treasury securities with a remaining term approximating the expected life of the options granted. The Company uses a dividend yield of
92
GENOMIC HEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
December 31, 2017
zero as it has never paid cash dividends and does not anticipate paying cash dividends in the foreseeable future. The weighted‑average fair values and assumptions used in calculating such values during each fiscal year are as follows:
|
|
|
Year Ended December 31, |
|
|||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|
|||
|
Expected volatility: |
|
|
|
|
|
|
|
|
|
|
|
Stock options |
|
|
40 |
% |
|
44 |
% |
|
44 |
% |
|
ESPP |
|
|
33 |
% |
|
44 |
% |
|
35 |
% |
|
Risk-free interest rate: |
|
|
|
|
|
|
|
|
|
|
|
Stock options |
|
|
2.01 |
% |
|
1.36 |
% |
|
1.66 |
% |
|
ESPP |
|
|
0.91 |
% |
|
0.47 |
% |
|
0.10 |
% |
|
Expected life in years: |
|
|
|
|
|
|
|
|
|
|
|
Stock options |
|
|
6.22 |
|
|
6.10 |
|
|
5.94 |
|
|
ESPP |
|
|
0.50 |
|
|
0.50 |
|
|
0.50 |
|
|
Weighted-average fair value: |
|
|
|
|
|
|
|
|
|
|
|
Stock options |
|
$ |
11.83 |
|
$ |
11.73 |
|
$ |
13.37 |
|
|
ESPP |
|
$ |
7.16 |
|
$ |
7.35 |
|
$ |
6.99 |
|
Note 10. Segment Information
The Company operates in one business segment, which primarily focuses on the development and global commercialization of genomic‑based clinical laboratory services that analyze the underlying biology of cancer, allowing physicians and patients to make individualized treatment decisions. The Company’s Oncotype DX breast, colon and prostate cancer tests have similar economic and other characteristics, including the nature of the products and production processes, type of customers, distribution methods and regulatory environment. As of December 31, 2017, the majority of the Company’s product revenues have been derived from sales of one product, the Oncotype DX breast cancer test.
As of December 31, 2017, the majority of the Company’s tests have been delivered to physicians in the United States. All tissue-based Oncotype DX tests are processed in the Company’s clinical reference laboratory facility in Redwood City, California. The following table summarizes total revenues from customers, payors and collaboration partners by geographic region (in thousands). Product revenues are attributed to countries based on ship‑to location. Contract revenues are attributed to countries based on the location of the collaboration partner.
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Year Ended December 31, |
|||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|||
|
|
|
(In thousands) |
|||||||
|
United States |
|
$ |
287,662 |
|
$ |
281,077 |
|
$ |
246,008 |
|
Outside of the United States |
|
|
53,088 |
|
|
46,791 |
|
|
41,450 |
|
Total revenues |
|
$ |
340,750 |
|
$ |
327,868 |
|
$ |
287,458 |
93
GENOMIC HEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
December 31, 2017
Note 11. Income Taxes
The components of the Company’s loss before income taxes were as follows:
|
|
|
Year Ended December 31, |
|||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|||
|
|
|
(In thousands) |
|||||||
|
Domestic |
|
$ |
(5,404) |
|
$ |
(14,676) |
|
$ |
(34,276) |
|
Foreign |
|
|
3,051 |
|
|
2,138 |
|
|
(28) |
|
Total loss before income taxes |
|
$ |
(2,353) |
|
$ |
(12,538) |
|
$ |
(34,304) |
The components of the Company’s income tax expense (benefit) were as follows:
|
|
|
Year Ended December 31, |
|||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|||
|
|
|
(In thousands) |
|||||||
|
Current expense (benefit): |
|
|
|
|
|
|
|
|
|
|
Federal |
|
$ |
(140) |
|
$ |
18 |
|
$ |
— |
|
State |
|
|
31 |
|
|
67 |
|
|
(15) |
|
Foreign |
|
|
792 |
|
|
569 |
|
|
566 |
|
|
|
|
|
|
|
|
|
|
|
|
Deferred tax expense (benefit): |
|
|
|
|
|
|
|
|
|
|
Federal |
|
|
792 |
|
|
702 |
|
|
(1,494) |
|
State |
|
|
29 |
|
|
25 |
|
|
(53) |
|
Foreign |
|
|
— |
|
|
— |
|
|
— |
|
Total income tax expense (benefit) |
|
$ |
1,504 |
|
$ |
1,381 |
|
$ |
(996) |
The income tax expense (benefit) differs from the amount computed by applying the statutory federal income tax rate as follows:
|
|
|
Year Ended December 31, |
|||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|||
|
|
|
(In thousands) |
|||||||
|
Federal tax at statutory rate |
|
$ |
(824) |
|
$ |
(4,388) |
|
$ |
(12,006) |
|
Stock-based compensation |
|
|
(687) |
|
|
867 |
|
|
782 |
|
Non-deductible meals and entertainment |
|
|
534 |
|
|
530 |
|
|
558 |
|
Net operating losses not used |
|
|
1,846 |
|
|
3,705 |
|
|
10,499 |
|
Tax effect on available-for-sale securities |
|
|
792 |
|
|
702 |
|
|
(1,494) |
|
Subpart F |
|
|
185 |
|
|
— |
|
|
— |
|
Foreign tax |
|
|
(279) |
|
|
(179) |
|
|
576 |
|
Federal AMT refundable credit |
|
|
(122) |
|
|
— |
|
|
— |
|
State tax, net of federal benefit |
|
|
39 |
|
|
68 |
|
|
(63) |
|
Other |
|
|
20 |
|
|
76 |
|
|
152 |
|
Total income tax expense (benefit) |
|
$ |
1,504 |
|
$ |
1,381 |
|
$ |
(996) |
94
GENOMIC HEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
December 31, 2017
Deferred income taxes reflect the net tax effects of temporary differences between the carrying amounts of assets and liabilities for financial reporting purposes and the amounts used for income tax purposes. Significant components of deferred tax assets and liabilities are as follows:
|
|
|
December 31, |
||||
|
|
|
2017 |
|
2016 |
||
|
|
|
(In thousands) |
||||
|
Deferred tax assets: |
|
|
|
|
|
|
|
Net operating loss carryforwards |
|
$ |
34,450 |
|
$ |
42,550 |
|
Stock-based compensation |
|
|
8,120 |
|
|
12,290 |
|
Research tax credits |
|
|
21,710 |
|
|
17,620 |
|
Fixed assets |
|
|
690 |
|
|
1,960 |
|
Accrued compensation |
|
|
3,070 |
|
|
6,080 |
|
Other |
|
|
7,150 |
|
|
7,490 |
|
Total deferred tax assets |
|
|
75,190 |
|
|
87,990 |
|
Valuation allowance |
|
|
(75,190) |
|
|
(87,990) |
|
Net deferred tax assets |
|
$ |
— |
|
$ |
— |
Based on all available objective evidence, the Company believes that it is more likely than not that the net deferred tax assets will not be fully realizable. Accordingly, the Company recorded a valuation allowance against all of its net deferred tax assets as of both December 31, 2017 and 2016. The Company will continue to maintain a full valuation allowance on its net deferred tax assets until there is sufficient evidence to support the reversal of all or some portion of this allowance. The net valuation allowance increased (decreased) by $(12.8) million, $6.1 million and $10.1 million during the years ended December 31, 2017, 2016 and 2015, respectively.
As of December 31, 2017, the Company had federal and state net operating loss carryforwards of approximately $156.0 million and $93.3 million, respectively, and federal and state research and development tax credit carryforwards of approximately $13.4 million and $13.3 million, respectively. The federal net operating loss and federal tax credit carryforwards will expire at various dates beginning in 2021. The state net operating loss carryforwards begin to expire in 2018 if not utilized. The state tax credit carryforwards have no expiration date. None of the net operating loss and tax credit carryforwards are subject to the limitations imposed by Sections 382 and 383 of the Internal Revenue Code.
The Company had $2.4 million, $2.1 million and $2.8 million of unrecognized tax benefits as of December 31, 2017, 2016 and 2015, respectively. The unrecognized tax benefits are primarily research tax credits for all years. The following table summarizes the activity related to unrecognized tax benefits:
|
|
|
Year Ended December 31, |
|||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|||
|
|
|
(In thousands) |
|||||||
|
Balance at January 1 |
|
$ |
2,078 |
|
$ |
2,847 |
|
$ |
1,600 |
|
Increase (decrease) related to prior year tax positions |
|
|
— |
|
|
(1,076) |
|
|
927 |
|
Increase related to current year tax positions |
|
|
331 |
|
|
307 |
|
|
320 |
|
Balance at December 31 |
|
$ |
2,409 |
|
$ |
2,078 |
|
$ |
2,847 |
Unrecognized tax benefits may change during the next twelve months for items that arise in the ordinary course of business. The Company does not anticipate a material change to its unrecognized tax benefits over the next twelve months that would affect the Company’s effective tax rate.
Accrued interest and penalties related to unrecognized tax benefits are recognized as part of the Company’s income tax provision in its consolidated statements of operations. For the year ended December 31, 2017, 2016 and 2015, the Company recognized $8,800, $8,000 and $7,200 in interest and penalties, respectively, related to unrecognized tax benefits.
95
GENOMIC HEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
December 31, 2017
The Company files federal, state and foreign income tax returns in many jurisdictions in the United States and abroad. The statute of limitations remains open for the years 2001 through 2017 in U.S. federal and state jurisdictions, and for the years 2012 through 2017 in foreign jurisdictions. Fiscal years outside the normal statute of limitations remain open to audit by tax authorities due to tax attributes generated in early years which have been carried forward and may be audited in subsequent years when utilized.
On December 22, 2017 the 2017 Tax Cut and Jobs Act (the Act) was enacted into law and the new legislation contains several key tax provisions, including a one-time mandatory transition tax on accumulated foreign earnings and a reduction of the corporate income tax rate to 21% effective January 1, 2018, among others. The Company is required to recognize the effect of the tax law changes in the period of enactment, such as determining the estimated transition tax, re-measuring our U.S. deferred tax assets and liabilities at a 21% rate as well as reassessing the net realizability of its deferred tax assets and liabilities. The one-time transition tax does not generate a tax liability as the deemed distribution is offset by tax attributes. The provisional amount related to the re-measurement of the Company’s deferred tax balance is a reduction of approximately $31.4 million. Due to the corresponding valuation allowance fully offsetting deferred taxes, there is no income statement impact.
In December 2017, the SEC staff issued Staff Accounting Bulletin No. 118, Income Tax Accounting Implications of the Tax Cuts and Jobs Act (SAB 118) which allows companies to record provisional amounts during a measurement period not to extend beyond one year of the enactment date. Since the Act was passed late in the fourth quarter of 2017, and ongoing guidance and accounting interpretation are expected over the next 12 months, the Company considers the accounting of the transition tax and deferred tax re-measurements to be incomplete. Additional work will be necessary for a more detailed analysis of the Company’s deferred tax assets and liabilities and its historical foreign earnings as well as potential correlative adjustments. The Company expects to complete its analysis within the measurement period in accordance with SAB 118. The Company does not expect any material subsequent adjustment to these amounts. Adjustment if any will have no impact to the income statement due to the Company’s loss position and valuation allowance.
Note 12. Selected Quarterly Financial Data (Unaudited)
The following table contains selected unaudited consolidated statement of operations information for each of the quarters in 2017 and 2016. The Company believes that the following information reflects all adjustments, consisting of only normal recurring adjustments, necessary for a fair presentation of the information for the periods presented. The operating results for any quarter are not necessarily indicative of results for any future period.
|
Quarter Ended |
|
March 31, |
|
June 30, |
|
September 30, |
|
December 31, |
|
||||
|
|
|
(In thousands, except per share data) |
|
||||||||||
|
2017: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Total revenues |
|
$ |
83,979 |
|
$ |
85,487 |
|
$ |
83,821 |
|
$ |
87,463 |
|
|
Product revenues |
|
|
83,979 |
|
|
85,487 |
|
|
83,821 |
|
|
87,164 |
|
|
Cost of product revenues |
|
|
13,672 |
|
|
13,798 |
|
|
13,433 |
|
|
13,814 |
|
|
Net income (loss) |
|
|
(806) |
|
|
(2,739) |
|
|
(2,191) |
|
|
1,879 |
|
|
Basic net income (loss) per common share |
|
$ |
(0.02) |
|
$ |
(0.08) |
|
$ |
(0.06) |
|
$ |
0.05 |
|
|
Diluted net income (loss) per common share |
|
$ |
(0.02) |
|
$ |
(0.08) |
|
$ |
(0.06) |
|
$ |
0.05 |
|
|
2016: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Total revenues |
|
$ |
80,894 |
|
$ |
81,974 |
|
$ |
82,258 |
|
$ |
82,742 |
|
|
Product revenues |
|
|
80,894 |
|
|
81,886 |
|
|
82,136 |
|
|
82,002 |
|
|
Cost of product revenues |
|
|
16,153 |
|
|
15,598 |
|
|
13,425 |
|
|
13,652 |
|
|
Net income (loss) |
|
|
(6,351) |
|
|
(6,100) |
|
|
(2,820) |
|
|
1,352 |
|
|
Basic net income (loss) per common share |
|
$ |
(0.19) |
|
$ |
(0.18) |
|
$ |
(0.08) |
|
$ |
0.04 |
|
|
Diluted net income (loss) per common share |
|
$ |
(0.19) |
|
$ |
(0.18) |
|
$ |
(0.08) |
|
$ |
0.04 |
|
The quarterly increases in product revenues during 2017 and 2016 were primarily attributable to increased adoption of the Oncotype DX breast and Oncotype DX prostate cancer tests by physicians, international expansion, increased revenues recorded on an accrual basis, and increased reimbursement for these tests by third‑party payors. Per share amounts for the
96
GENOMIC HEALTH, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
December 31, 2017
quarters and full year have been calculated separately. Accordingly, quarterly amounts may not add up to the annual amount because of differences in the weighted‑average common shares outstanding during each period, due primarily to the effect of the Company’s issuing shares of its common stock during the year.
For all of the quarters presented, except for the quarters ended December 31, 2016, and December 31, 2017, basic and diluted net loss per common share were identical as potential common shares were excluded from the calculation because their effects were anti‑dilutive.
On March 8, 2018 the Company announced its decision to no longer provide its commercial offering of Oncotype SEQ Liquid Select or any further investment in next generation sequencing (NGS) panels due to a decision to focus the Company’s efforts to develop in vitro diagnostic test solutions and other tests with more predictable reimbursement, higher proprietary value and better prospects for global adoption. With this shift in strategic direction, the Company announced a reduction of its workforce resources of approximately 10%. The Company will take a charge of approximately $10 million in the first quarter of 2018 for costs associated with personnel reductions and a write-off of certain assets associated with NGS-based panels.
97
ITEM 9. Changes in and Disagreements with Accountants on Accounting and Financial Disclosures.
Not applicable.
ITEM 9A. Controls and Procedures.
|
(a) Evaluation of disclosure controls and procedures. We maintain “disclosure controls and procedures,” as such term is defined in Rule 13a‑15(e) under the Securities Exchange Act of 1934, or the Exchange Act, that are designed to ensure that information required to be disclosed by us in reports that we file or submit under the Exchange Act is recorded, processed, summarized, and reported within the time periods specified in Securities and Exchange Commission rules and forms, and that such information is accumulated and communicated to our management, including our Chief Executive Officer and Chief Financial Officer, as appropriate, to allow timely decisions regarding required disclosure. In designing and evaluating our disclosure controls and procedures, management recognized that disclosure controls and procedures, no matter how well conceived and operated, can provide only reasonable, not absolute, assurance that the objectives of the disclosure controls and procedures are met. Our disclosure controls and procedures have been designed to meet reasonable assurance standards. Additionally, in designing disclosure controls and procedures, our management necessarily was required to apply its judgment in evaluating the cost‑benefit relationship of possible disclosure controls and procedures. The design of any disclosure controls and procedures also is based in part upon certain assumptions about the likelihood of future events, and there can be no assurance that any design will succeed in achieving its stated goals under all potential future conditions. |
Based on their evaluation as of the end of the period covered by this Annual Report on Form 10‑K, our Chief Executive Officer and Chief Financial Officer have concluded that, as of such date, our disclosure controls and procedures were effective at the reasonable assurance level.
|
(b) Management’s Annual Report on Internal Control over Financial Reporting. Our management is responsible for establishing and maintaining internal control over our financial reporting. Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Projections of any evaluation of the effectiveness of internal control to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with policies or procedures may deteriorate. Our management, with the participation of our Chief Executive Officer and Chief Financial Officer, assessed the effectiveness of our internal control over financial reporting as of December 31, 2017. In making this assessment, our management used the criteria set forth by the Committee of Sponsoring Organizations of the Treadway Commission, or COSO, in Internal Control—Integrated Framework (2013 Framework). Based on the assessment using those criteria, our management concluded that, as of December 31, 2017 our internal control over financial reporting was effective. Our independent registered public accounting firm, Ernst & Young LLP, audited the effectiveness of our internal control over financial reporting. Their report appears below. |
|
(c) Changes in internal controls. There was no change in our internal control over financial reporting (as defined in Rule 13a‑15(f) under the Exchange Act) identified in connection with the evaluation described in Item 9A(a) above that occurred during our last fiscal quarter that has materially affected, or is reasonably likely to materially affect, our internal control over financial reporting. |
98
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Stockholders and Board of Directors of Genomic Health, Inc.
Opinion on Internal Control over Financial Reporting
We have audited Genomic Health, Inc.’s internal control over financial reporting as of December 31, 2017, based on criteria established in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (2013 framework) (the COSO criteria). In our opinion, Genomic Health, Inc. (the Company) maintained, in all material respects, effective internal control over financial reporting as of December 31, 2017, based on the COSO criteria.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States) (PCAOB), the 2017 consolidated financial statements of the Company and our report dated March 14, 2018 expressed an unqualified opinion thereon.
Basis for Opinion
The Company’s management is responsible for maintaining effective internal control over financial reporting and for its assessment of the effectiveness of internal control over financial reporting included in the accompanying Management’s Annual Report on Internal Control over Financial Reporting. Our responsibility is to express an opinion on the Company’s internal control over financial reporting based on our audit. We are a public accounting firm registered with the PCAOB and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audit in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects.
Our audit included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, testing and evaluating the design and operating effectiveness of internal control based on the assessed risk, and performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
Definition and Limitations of Internal Control Over Financial Reporting
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
/s/ Ernst & Young LLP
Redwood City, California
March 14, 2018
99
On March 8, 2018, we announced our decision to no longer provide its commercial offering of Oncotype SEQ Liquid Select or any further investment in next generation sequencing (NGS) panels due to a decision to focus our efforts to develop in vitro diagnostic test solutions and other tests with more predictable reimbursement, higher proprietary value and better prospects for global adoption. With this shift in strategic direction, we announced a reduction of our workforce resources of approximately 10%. We will take a charge of approximately $10 million in the first quarter of 2018 including costs of approximately $4 million associated with personnel reductions and approximately $6 million to write-off certain assets associated with NGS-based panels.
On March 13, 2018, Frederic Pla, Ph.D. was appointed as our Chief Operating Officer. Dr. Pla previously served as Chief Business and Product Development Officer. G. Bradley Cole, formerly Chief Operating Officer and Chief Financial Officer remains as our Chief Financial Officer.
Frederic Pla, Ph.D., 58, served as our Chief Business and Product Development Officer from January 2015 to March 2018. From July 2005 to February 2014, Dr. Pla served in various roles at Life Technologies Corporation (now part of Thermo Fisher Scientific), a global life sciences company, most recently serving as Vice President, Corporate Business Development from July 2008 to February 2014, and as Vice President and General Manager of the Diagnostics Business from July 2005 to July 2008. Prior to joining Life Technologies, Dr. Pla served in various roles at GE Healthcare, most recently serving as General Manager for the Enterprise IT and Cardiology IT businesses.
ITEM 10. Directors, Executive Officers and Corporate Governance.
The information required by this item with respect to directors is incorporated by reference from the information under the caption “Election of Directors” contained in our Proxy Statement to be filed with the Securities and Exchange Commission in connection with the solicitation of proxies for our 2018 Annual Meeting of Stockholders to be held on June 6, 2018, or Proxy Statement. Certain information required by this item concerning executive officers is set forth in Part I of this Report under the caption “Executive Officers of the Registrant” and is incorporated herein by reference.
Item 405 of Regulation S‑K calls for disclosure of any known late filing or failure by an insider to file a report required by Section 16(a) of the Exchange Act. This disclosure is contained in the section entitled “Section 16(a) Beneficial Ownership Reporting Compliance” in the Proxy Statement and is incorporated herein by reference.
We have adopted a Code of Business Conduct and Ethics that applies to all of our officers and employees, including our President and Chief Executive Officer, our Chief Financial Officer and other employees who perform financial or accounting functions. The Code of Business Conduct and Ethics sets forth the basic principles that guide the business conduct of our employees. We have also adopted a Senior Financial Officers’ Code of Ethics that specifically applies to our President and Chief Executive Officer, our Chief Financial Officer, and key management employees. Stockholders may request a free copy of our Code of Business Conduct and Ethics and our Senior Financial Officers’ Code of Ethics by contacting Genomic Health, Inc., Attention: Chief Financial Officer, 301 Penobscot Drive, Redwood City, California 94063.
To date, there have been no waivers under our Code of Business Conduct and Ethics or Senior Financial Officers’ Code of Ethics. We intend to disclose future amendments to certain provisions of our Code of Business Conduct and Ethics or Senior Financial Officers’ Code of Ethics or waivers of such Codes granted to executive officers and directors on our website at http://www.genomichealth.com within four business days following the date of such amendment or waiver.
Our Board of Directors has appointed an Audit Committee, comprised of Mr. Geoffrey M. Parker, as Chairman, Dr. Fred E. Cohen and Ms. Ginger L. Graham. The Board of Directors has determined that Mr. Parker qualifies as an Audit Committee Financial Expert under the definition outlined by the Securities and Exchange Commission. In addition, each of the members of the Audit Committee qualifies as an “independent director” under the current rules of The Nasdaq Stock Market and Securities and Exchange Commission rules and regulations.
ITEM 11. Executive Compensation.
The information required by this item is incorporated by reference from the information under the captions “Election of Directors—Director Compensation” and “Executive Compensation” contained in the Proxy Statement.
100
ITEM 12. Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters.
The information required by this item is incorporated by reference from the information under the captions “Security Ownership of Certain Beneficial Owners and Management” and “Executive Compensation—Equity Compensation Plan Information” contained in the Proxy Statement.
ITEM 13. Certain Relationships and Related Transactions, and Director Independence.
The information required by this item is incorporated by reference from the information under the caption “Election of Directors—Certain Relationships and Related Transactions” and “—Director Independence” contained in the Proxy Statement.
ITEM 14. Principal Accounting Fees and Services.
The information required by this item is incorporated by reference from the information under the caption “Ratification of the Appointment of Independent Registered Public Accounting Firm” contained in the Proxy Statement.
ITEM 15. Exhibits and Financial Statement Schedules.
|
(a) |
Documents filed as part of this report: |
|
(1) |
Financial Statements |
Reference is made to the Index to Consolidated Financial Statements of Genomic Health under Item 8 of Part II hereof.
|
(2) |
Financial Statement Schedules |
The following schedule is filed as part of this Form 10‑K:
Schedule II—Valuation and Qualifying Accounts for the years ended December 31, 2017, 2016, and 2015.
SCHEDULE II
GENOMIC HEALTH, INC.
VALUATION AND QUALIFYING ACCOUNTS
Years Ended December 31, 2017, 2016 and 2015
|
|
|
Balance at |
|
|
|
|
|
|
|
Balance at |
||
|
|
|
Beginning of |
|
|
|
|
|
|
|
End of |
||
|
|
|
Period |
|
Expenses |
|
Deductions |
|
Period |
||||
|
|
|
(In thousands) |
||||||||||
|
Allowance for Doubtful Accounts: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Year ended December 31, 2017 |
|
$ |
4,508 |
|
$ |
6,554 |
|
$ |
7,178 |
|
$ |
3,884 |
|
Year ended December 31, 2016 |
|
$ |
3,988 |
|
$ |
7,654 |
|
$ |
7,134 |
|
$ |
4,508 |
|
Year ended December 31, 2015 |
|
$ |
3,628 |
|
$ |
5,542 |
|
$ |
5,182 |
|
$ |
3,988 |
All other financial statement schedules have been omitted because they are not applicable or not required or because the information is included elsewhere in the Consolidated Financial Statements or the Notes thereto.
|
(3) |
Exhibits |
See Item 15(b) below. Each management contract or compensatory plan or arrangement required to be filed has been identified.
101
|
(b) |
Exhibits |
|
Exhibit No. |
|
|
Description of Document |
|
|
|
|
|
|
|
| 3 |
(i) |
|
||
| 3 |
(ii) |
|
||
| 4.1 |
|
|
||
| 10.1 |
# |
|
||
|
|
|
|
|
|
|
10.2.1 |
# |
|
||
|
10.2.2 |
# |
|
||
|
10.2.3 |
# |
|
||
|
10.2.4 |
# |
|
||
| 10.3 |
# |
|
||
| 10.4 |
# |
|
||
| 10.5 |
#* |
|
Genomic Health, Inc. Severance Plan for Executive Management, as amended. |
|
|
10.5.1 |
#* |
|
Genomic Health, Inc. Severance Plan for Executive Management, International Version. |
|
| 10.6 |
|
|
||
|
10.6.1 |
|
|
||
|
10.6.2 |
|
|
||
| 10.7 |
|
|
||
|
10.7.1 |
|
|
||
102
|
Exhibit No. |
|
|
Description of Document |
|
|
|
|
|
|
|
|
10.7.2 |
|
|
||
| 10.8 |
|
|
||
|
10.8.1 |
|
|
||
| 10.9 |
|
|
||
|
10.9.1 |
|
|
||
|
10.9.2 |
|
|
||
| 10.10 |
|
|
||
| 10.11 |
|
|
||
| 10.12 |
# |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
| 12.1 |
* |
|
||
| 21.1 |
* |
|
||
| 23.1 |
* |
|
||
| 24.1 |
* |
|
||
| 31.1 |
* |
|
||
| 31.2 |
* |
|
Rule 13a‑14(a) Certification of the Chief Financial Officer. |
|
| 32.1 |
** |
|
||
| 32.2 |
** |
|
||
| 101 |
|
|
The following materials from Registrant’s Annual Report on Form 10‑K for the year ended December 31, 2017, formatted in Extensible Business Reporting Language (XBRL), includes: (i) Consolidated Balance Sheets at December 31, 2017 and 2016, (ii) Consolidated Statements of Income for the three years ended December 31, 2017, 2016 and 2015, (iii) Consolidated Statements of Comprehensive Income for the three years ended December 31, 2017, 2016 and 2015, (iv) Consolidated Statements of Stockholders’ Equity for the three years ended December 31, 2017, 2016 and 2015, (v) Consolidated Statements of Cash Flows for the three years ended December 31, 2017, 2016, and 2015, and (vi) Notes to Consolidated Financial Statements. |
|
103
*Filed herewith.
**In accordance with Item 601(b)(32)(ii) of Regulation S‑K and SEC Release No. 34‑47986, the certifications furnished in Exhibits 32.1 and 32.2 hereto are deemed to accompany this Form 10‑K and will not be deemed “filed” for purposes of Section 18 of the Securities Exchange Act of 1934. Such exhibits will not be deemed to be incorporated by reference into any filing under the Securities Act of 1933 or the Securities Exchange Act of 1934.
#Indicates management contract or compensatory plan or arrangement.
|
(c) |
Financial Statements and Schedules |
Reference is made to Item 15(a)(2) above.
Copies of above exhibits not contained herein are available to any stockholder, upon payment of a reasonable per page fee, upon written request to: Chief Financial Officer, Genomic Health, Inc., 301 Penobscot Drive, Redwood City, California 94063.
Not applicable.
104
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
|
|
GENOMIC HEALTH, INC. |
|
|
|
|
|
|
|
|
|
|
|
By: |
/s/ Kimberly J. Popovits
Kimberly J. Popovits |
Date: March 14, 2018
KNOW ALL PERSONS BY THESE PRESENTS, that each person whose signature appears below constitutes and appoints Kimberly J. Popovits and G. Bradley Cole, and each of them, his true and lawful attorneys‑in‑fact, each with full power of substitution, for him or her in any and all capacities, to sign any amendments to this report on Form 10-K and to file the same, with exhibits thereto and other documents in connection therewith, with the Securities and Exchange Commission, hereby ratifying and confirming all that each of said attorneys‑in‑fact or their substitute or substitutes may do or cause to be done by virtue hereof.
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
|
Signature |
Title |
Date |
||||
|
|
|
|
||||
|
/s/ KIMBERLY J. POPOVITS Kimberly J. Popovits |
President, Chief Executive Officer and Chairman of the Board (Principal Executive Officer) |
March 14, 2018 |
||||
|
|
|
|
||||
|
/s/ G. BRADLEY COLE G. Bradley Cole |
Chief Financial Officer (Principal Financial and Accounting Officer) |
March 14, 2018 |
||||
|
|
|
|
||||
|
/s/ FELIX J. BAKER Felix J. Baker |
Director |
March 14, 2018 |
||||
|
|
|
|
||||
|
/s/ JULIAN C. BAKER Julian C. Baker |
Director |
March 14, 2018 |
||||
|
|
|
|
||||
|
/s/ FRED E. COHEN, M.D., D. PHIL Fred E. Cohen, M.D., D. Phil. |
Director |
March 14, 2018 |
||||
|
|
|
|
||||
|
/s/ HENRY J. FUCHS, M.D. Henry J. Fuchs, M.D. |
Director |
March 14, 2018 |
||||
|
|
|
|
||||
|
/s/ GINGER L. GRAHAM Ginger L. Graham |
Director |
March 14, 2018 |
||||
|
|
|
|
||||
|
/s/ GEOFFREY M. PARKER Geoffrey M. Parker |
Director |
March 14, 2018 |
||||
|
|
|
|
||||
105