Attached files
| file | filename |
|---|---|
| EX-32.2 - EX-32.2 - Clovis Oncology, Inc. | clvs-20171231ex3222b5bda.htm |
| EX-32.1 - EX-32.1 - Clovis Oncology, Inc. | clvs-20171231ex32156c0fa.htm |
| EX-31.2 - EX-31.2 - Clovis Oncology, Inc. | clvs-20171231ex3126aa7a0.htm |
| EX-31.1 - EX-31.1 - Clovis Oncology, Inc. | clvs-20171231ex3111fe53e.htm |
| EX-23.1 - EX-23.1 - Clovis Oncology, Inc. | clvs-20171231ex231509864.htm |
| EX-12.1 - EX-12.1 - Clovis Oncology, Inc. | clvs-20171231ex1212dd759.htm |
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
☒ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934.
For the fiscal year ended December 31, 2017.
☐TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934.
For the transition period from to .
Commission file number: 001-35347
Clovis Oncology, Inc.
(Exact name of Registrant as specified in its charter)
|
Delaware |
|
90-0475355 |
|
(State or other jurisdiction of |
|
(I.R.S. Employer |
|
|
|
|
|
5500 Flatiron Parkway, Suite 100 |
|
80301 |
|
(Address of principal executive offices) |
|
(Zip Code) |
(303) 625-5000
(Registrant’s telephone number, including area code)
Securities registered pursuant to Section 12(b) of the Act:
|
Title of each class |
|
Name of each exchange on which registered |
|
Common Stock par value $0.001 per share |
|
The NASDAQ Global Select Market |
Securities registered pursuant to Section 12(g) of the Act: None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ☒ No ☐
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes ☐ No ☒
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes ☒ No ☐
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§ 232.405) of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes ☒ No ☐
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. ☐
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, smaller reporting company, or an emerging growth company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company, and “emerging growth company” in Rule 12b-2 of the Exchange Act.
|
Large accelerated filer |
☒ |
Accelerated filer |
☐ |
|
Non-accelerated filer |
☐ (Do not check if a smaller reporting company) |
Smaller reporting company |
☐ |
|
Emerging growth company |
☐ |
|
|
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes ☐ No ☒
The aggregate market value of the registrant’s common stock, par value $0.001 per share, held by non-affiliates of the registrant on June 30, 2017, the last business day of the registrant’s most recently completed second quarter, was $4,220,084,525 based on the closing price of the registrant’s common stock on the NASDAQ Global Market on that date of $93.63 per share.
The number of outstanding shares of the registrant’s common stock, par value $0.001 per share, as of February 21, 2018 was 50,573,183.
DOCUMENTS INCORPORATED BY REFERENCE Portions of the registrant’s definitive proxy statement to be filed with the Securities and Exchange Commission pursuant to Regulation 14A in connection with the registrant’s 2017 Annual Meeting of Stockholders, which is to be filed within 120 days after the end of the registrant’s fiscal year ended December 31, 2017, are incorporated by reference into Part III of this Annual Report on Form 10-K to the extent stated therein.
2
This Annual Report filed on Form 10-K and the information incorporated herein by reference includes statements that are, or may be deemed, “forward-looking statements.” In some cases, these forward-looking statements can be identified by the use of forward-looking terminology, including the terms “believes,” “estimates,” “anticipates,” “expects,” “plans,” “intends,” “may,” “could,” “might,” “will,” “should,” “approximately” or, in each case, their negative or other variations thereon or comparable terminology, although not all forward-looking statements contain these words. They appear in a number of places throughout this Annual Report on Form 10-K and include statements regarding our intentions, beliefs, projections, outlook, analyses or current expectations concerning, among other things, the market acceptance and commercial viability of our approved product, the development of our sales and marketing capabilities, the performance of our third party manufacturers, our ongoing and planned non-clinical studies and clinical trials, the timing of and our ability to make regulatory filings and obtain and maintain regulatory approvals for our product candidates, including our ability to confirm the clinical benefit of our approved product through confirmatory trials and other post-marketing requirements, the degree of clinical utility of our products, particularly in specific patient populations, expectations regarding clinical trial data, expectations regarding sales of our products, our results of operations, financial condition, liquidity, prospects, growth and strategies, the industry in which we operate, including our competition, and the trends that may affect the industry or us.
By their nature, forward-looking statements involve risks and uncertainties because they relate to events, competitive dynamics and industry change and depend on the economic circumstances that may or may not occur in the future or may occur on longer or shorter timelines than anticipated. We caution you that forward-looking statements are not guarantees of future performance and that our actual results of operations, financial condition and liquidity and the development of the industry in which we operate may differ materially from the forward-looking statements contained herein.
Any forward-looking statements that we make in this Annual Report on Form 10-K speak only as of the date of such statement, and we undertake no obligation to update such statements to reflect events or circumstances after the date of this Annual Report on Form 10-K or to reflect the occurrence of unanticipated events. For all forward-looking statements, we claim the protection of the safe harbor for forward-looking statements contained in the Private Securities Litigation Reform Act of 1995.
You should also read carefully the factors described in the “Risk Factors” section of this Annual Report on Form 10-K to better understand the risks and uncertainties inherent in our business and underlying any forward-looking statements. You are advised, however, to consult any further disclosures we make on related subjects in our Quarterly Reports on Form 10-Q, Current Reports on Form 8-K and our website.
Clovis Oncology®, the Clovis logo and Rubraca® are trademarks of Clovis Oncology, Inc. in the United States and in other selected countries. All other brand names or trademarks appearing in this report are the property of their respective holders. Unless the context requires otherwise, references in this report to “Clovis,” the “Company,” “we,” “us” and “our” refer to Clovis Oncology, Inc., together with its consolidated subsidiaries.
Overview
We are a biopharmaceutical company focused on acquiring, developing and commercializing innovative anti-cancer agents in the United States, Europe and additional international markets. We target our development programs for the treatment of specific subsets of cancer populations, and simultaneously develop, with partners, diagnostic tools intended to direct a compound in development to the population that is most likely to benefit from its use.
Our marketed product Rubraca® (rucaparib) is approved on an accelerated basis in the United States by the Food and Drug Administration (“FDA”) as monotherapy for the treatment of patients with deleterious BRCA (human genes associated with the repair of damaged DNA) mutation (germline and/or somatic) associated advanced ovarian cancer who have been treated with two or more chemotherapies, and selected for therapy based on an FDA-approved companion diagnostic for Rubraca. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials. We launched Rubraca in the United States in December 2016 for this indication.
3
The FDA is currently reviewing on a priority review timeline our supplemental New Drug Application (“sNDA”) for Rubraca as maintenance treatment of adult patients with recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer who are in a complete or partial response to platinum-based chemotherapy.
Our Marketing Authorization Application (“MAA”) submitted to the European Union’s European Medicines Agency (“EMA”) for an ovarian cancer treatment indication for Rubraca is currently under review by the EMA’s Committee for Medicinal Products for Human Use (“CHMP”). Following a Scientific Advisory Group - Oncology meeting and an oral explanation by us before the CHMP in February 2018, the CHMP has communicated a positive trend vote for the MAA and their intention to hold a final vote on the treatment indication at their March 2018 meeting.
Beyond our labeled indication, we have a robust Rubraca clinical development program underway in a variety of solid tumor types, also including prostate and bladder cancers, and in July 2017, we entered into a broad clinical collaboration with Bristol-Myers Squibb Company to evaluate the combination of their immunotherapy Opdivo® (nivolumab) with Rubraca in several tumor types. We hold worldwide rights for Rubraca.
In addition, we have two other product candidates: lucitanib, an oral inhibitor of the tyrosine kinase activity of vascular endothelial growth factor receptors (“VEGFR”) 1-3, platelet-derived growth factor receptors (“PDGFR”) alpha and beta and fibroblast growth factor receptors (“FGFR”) 1-3, and rociletinib, an oral mutant-selective inhibitor of epidermal growth factor receptor (“EGFR”). While we have stopped enrollment in ongoing trials for each of these candidates, we continue to provide drug to patients whose clinicians recommend continuing therapy. We maintain certain development and commercialization rights for lucitanib and global development and commercialization rights for rociletinib.
Clovis was founded in 2009. We have built our organization to support innovative oncology drug development for the treatment of specific subsets of cancer populations. To implement our strategy, we have assembled an experienced team with core competencies in global clinical and non-clinical development, regulatory operations and commercialization in oncology, as well as conducting collaborative relationships with companies specializing in companion diagnostic development.
Rubraca – a PARP Inhibitor
Overview
Rubraca (rucaparib) is an oral, small molecule poly ADP-ribose polymerase (“PARP”) inhibitor of PARP1, PARP2 and PARP3. We in-licensed Rubraca from Pfizer Inc. in June 2011. In the United States, Rubraca is approved by the FDA for the treatment of patients with deleterious BRCA mutation (germline and/or somatic) associated advanced ovarian cancer who have been treated with two or more chemotherapies, and selected for therapy by an FDA-approved companion diagnostic for Rubraca. The indication is approved under the FDA’s accelerated approval program based on objective response rate and duration of response, and is based on results from two multicenter, single-arm, open-label clinical trials. Continued approval for this indication may be contingent upon verification and description of clinical benefit in ARIEL3 and/or ARIEL4, our confirmatory trials. Foundation Medicine, Inc. has developed two companion diagnostics that are FDA-approved and commercially available for selection of patients for treatment with Rubraca in this indication: FoundationFocus™ CDxBRCA and FoundationOne CDx™.
In October 2017 we submitted a sNDA for Rubraca for the maintenance treatment of adult patients with recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer who are in a complete or partial response to platinum-based chemotherapy. In December 2017, the FDA accepted our sNDA for Rubraca and granted priority review status to the application with a Prescription Drug User Free Act (“PDUFA”) goal date of April 6, 2018. If approved, we expect that diagnostic testing would not be required for patients to be prescribed Rubraca in this maintenance treatment indication. We have approximately 150 field-based personnel in the United States, and these commercial and medical affairs organizations already in place will support the commercial launch of Rubraca, if approved in this expanded maintenance treatment indication.
The second-line maintenance treatment paradigm in ovarian cancer is being rapidly adopted in the U.S. following the approval of two other PARP inhibitors in this setting during 2017. If Rubraca is approved in this setting, with no requirement for diagnostic testing as supported by the ARIEL3 data, it would be possible to address a patient population
4
approximately four times larger than our initial niche treatment indication, which is limited to women with ovarian cancer in the third-line setting with a BRCA mutation. BRCA mutations are believed to occur in approximately 25 percent of women with ovarian cancer.
Our MAA submitted to the EMA for an ovarian cancer treatment indication is currently under review. Following a Scientific Advisory Group - Oncology meeting and an oral explanation before the CHMP in February 2018, the CHMP communicated to us that they held a trend vote for the MAA and the result was positive. The CHMP also communicated to us their intention to hold a final vote on the treatment indication at their March 2018 meeting. The CHMP’s trend vote is not binding on the CHMP with respect to the final vote. The indication currently under consideration by the CHMP focuses on a subset of platinum-sensitive ovarian cancer where there is particular unmet need. If Rubraca receives a favorable opinion from the CHMP in March, a potential approval from the European Commission is expected during the second quarter of 2018. In the event of such an approval for the treatment indication, we intend to submit a variation to the marketing authorization (“MA”) for the maintenance treatment of adult patients with recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer who are in a complete or partial response to platinum-based chemotherapy, for which we anticipate a CHMP opinion may come during the fourth quarter of 2018. The EMA’s Committee for Orphan Medicinal Products (“COMP”) will meet in March 2018 to review and issue a final opinion on our application to maintain the orphan drug designation for Rubraca submitted as part of the MAA review process. While Rubraca currently has orphan drug designation in the EU, there is no assurance that COMP will maintain such designation post-approval. In the event of a negative opinion for the treatment indication, we expect to file a new MAA for the maintenance treatment indication during the second quarter of 2018. If approved in the EU, we intend to commercialize Rubraca on our own and we are building our commercial and medical affairs infrastructure in Europe. The leadership of those teams is in place, and we intend to hire field sales personnel as pricing and reimbursement decisions are made and approvals are received.
The Role of PARP Inhibition in Cancer Therapy
Cells in the human body are under constant attack from agents that can cause damage to DNA, including sunlight and other forms of radiation, as well as DNA-binding chemicals that can cause changes in the composition of DNA. Cells have evolved multiple mechanisms to enable such DNA repair, and these mechanisms are complementary to each other, each driving repair of specific types of DNA damage. If a cell’s DNA damage repair system is overwhelmed, then the cell will die undergoing a form of suicide termed apoptosis. A fundamental principle of cancer therapy is to damage cells profoundly with radiation or DNA-binding drugs, such as alkylating agents or platinums, to induce apoptosis and, subsequently, cancer cell death. Multiple DNA repair mechanisms active in the cell may reduce the activity of these anti-cancer therapies.
The PARP family comprises 17 structurally related proteins that have been identified on the basis of sequence similarity. PARP1, PARP2, and PARP3 play a central role in DNA repair. They are rapidly recruited to the sites of DNA damage and catalyze the recruitment of additional proteins that initiate the repair of damaged DNA. The breast cancer 1 (BRCA1) and breast cancer 2 (BRCA2) genes also have important roles in DNA repair pathways such as homologous recombination. According to the National Cancer Institute, BRCA1 and BRCA2 mutations are associated with an increased risk of ovarian, breast, prostate, and pancreatic cancers.
Rubraca is an inhibitor of PARP enzymes, including PARP1, PARP2, and PARP3. PARP inhibitors have shown activity in BRCA1/2 mutant and homologous recombination (“HR”) repair deficient cancer cell lines through a mechanism known as synthetic lethality in which the loss of two genes/pathways is required for cell death. The inhibition/inactivation of repair pathways by administration of a PARP inhibitor in the context of an underlying genetic defect such as a BRCA mutation results in tumor cell death through accumulation of unrepaired DNA damage.
Alterations in DNA repair genes other than BRCA1/2 have been observed in, and contribute to the hereditary risk of, ovarian, breast, prostate and pancreatic cancers. PARP inhibitors have shown evidence of nonclinical and clinical activity in tumors with alterations in non-BRCA HR genes. DNA repair deficiencies resulting from genetic and epigenetic alterations can result in a “BRCA-like” phenotype that may also render tumor cells sensitive to PARP inhibitors. One approach to identify patients with DNA repair deficiencies due to mechanisms other than a mutation in BRCA or other non-BRCA HR genes is to assess loss of heterozygosity (“LOH”), or the loss of one normal copy of a gene, which arises from error-prone DNA repair pathways when HR is compromised.
5
On the basis of these scientific observations, we initially developed Rubraca in ovarian cancer patients with tumors having BRCA mutations or other homologous recombination deficiencies (“HRD”). These molecular markers also may be used to select patients with other tumors for treatment with Rubraca. Thus, in addition to ovarian trials, studies open for enrollment or under consideration to further evaluate Rubraca, either alone or in combination with other agents, include prostate, breast, pancreatic, bladder, gastroesophageal and lung cancers.
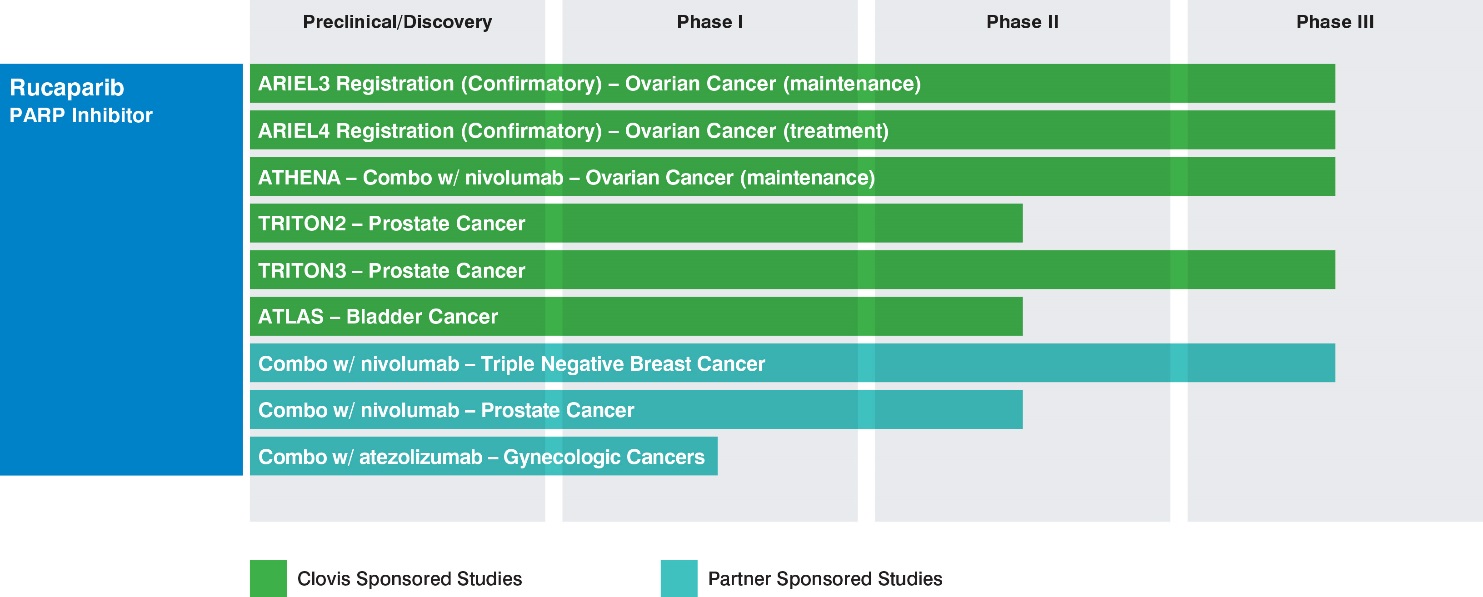
Rubraca Clinical Development
We are developing Rubraca for selected patient populations and collaborating with partners for companion diagnostic development. We have focused our development strategy for Rubraca on indications where we believe patient populations exhibit higher frequencies of mutant BRCA tumors or HRD, where PARP inhibitors have demonstrated clinical or pre-clinical activity in tumors. In certain of these trials, we or our partners will have access to interim data on a periodic or continuing basis that will not be made available publicly on the same timeframe as such data becomes available to us, or at all. The following table summarizes the ongoing Clovis- or partner-sponsored studies:
Ovarian cancer
According to the American Cancer Society, an estimated more than 22,000 women were diagnosed with ovarian cancer in the United States in 2017, and according to GLOBOCAN in 2012, an estimated more than 65,000 women in Europe are diagnosed each year with ovarian cancer, and ovarian cancer is among those cancers with the highest rate of deaths. Approximately 80% to 85% of ovarian cancer cases are not diagnosed, and therefore remain untreated, until the disease has spread to other parts of the body, or metastasized. Most women with ovarian cancer will relapse after surgery and/or chemotherapy. BRCA mutations, either germline or somatic, are believed to occur in approximately 25 percent of women with ovarian cancer according to an article published in Clinical Cancer Research in 2014.
The ARIEL (Assessment of Rucaparib In Ovarian CancEr TriaL) program is a novel, integrated translational-clinical program designed to accurately and prospectively identify ovarian cancer patients with tumor genotypes associated with benefit from Rubraca therapy.
ARIEL2 (NCT01891344) is a two-part single-arm open label study designed to identify pre-specified tumor characteristics that predict sensitivity to Rubraca using DNA sequencing to evaluate each patient’s tumor. Part 1 enrolled 204 platinum-sensitive patients and updated results were presented in June 2016. Part 2 enrolled 286 patients with advanced ovarian cancer who have received at least three prior chemotherapy regimens and includes platinum-sensitive, -resistant and -refractory patients. ARIEL2 is evaluating clinical response in patients classified into molecularly-defined subgroups, including germline BRCA-mutant, somatic BRCA-mutant and HRD by a prospectively defined genomic signature.
The efficacy of Rubraca in the ovarian cancer treatment setting was assessed in 106 patients from ARIEL2 and Study 10 (NCT01482715, a multicenter, single-arm, open-label clinical trial of Rubraca), in patients with advanced BRCA-
6
mutant ovarian cancer who had progressed after two or more prior chemotherapies. Median age was 59 years and median number of prior chemotherapy regimens was three. All 106 patients received the starting dose of Rubraca 600 mg twice daily. The major efficacy outcome measure of both trials was objective response rate (ORR) and duration of response (DOR) as assessed by the investigator according to Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1. All responses were confirmed. ORR assessed by investigator was 54% (95% Confidence Interval, or CI: 44, 64), with a median DOR of 9.2 months (95% CI: 6.6, 11.6). ORR by independent radiology review was 42% (95%: 32, 52), with a median DOR of 6.7 months (95% CI: 5.5, 11.1).
The overall safety evaluation of Rubraca in the advanced ovarian cancer treatment setting is based on data from 377 patients with ovarian cancer from ARIEL2 and Study 10. The most common adverse reactions (≥ 20% of patients; Grade 1-4) were nausea, asthenia/fatigue, vomiting, anemia, constipation, dysgeusia, decreased appetite, diarrhea, abdominal pain, thrombocytopenia and dyspnea. The most common laboratory abnormalities (≥ 35% of patients; Grade 1-4) were increase in creatinine, increase in aspartate aminotransferase (“AST”) levels, increase in alanine aminotransferase (“ALT”) levels, decrease in hemoglobin, decrease in lymphocytes, increase in cholesterol, decrease in platelets and decrease in absolute neutrophil count. Elevations in ALT/AST concentrations were generally self-limiting and not associated with other signs of liver toxicity. Rubraca requires monitoring of complete blood counts at baseline, and monthly thereafter. The most common Grade 3-4 adverse reaction was anemia, and the most common Grade 3-4 laboratory abnormality was a decrease in hemoglobin. Myelodysplastic Syndrome/Acute Myeloid Leukemia, or MDS/AML, was reported in two of the 377 (0.5%) patients with ovarian cancer treated with Rubraca. Both of these patients had received prior treatment with platinum and other DNA damaging agents. In addition, AML was reported in two (<1%) patients with ovarian cancer enrolled in ARIEL3. One case of AML was fatal. Both patients had received prior treatment with platinum and other DNA damaging agents.
The data from the two studies formed the basis of our submission of a New Drug Application (“NDA”) in the United States to the FDA in late June 2016. The application was granted priority review and approved under FDA’s accelerated approval program on December 19, 2016 as monotherapy for the treatment of patients with deleterious BRCA mutation (germline and/or somatic) associated advanced ovarian cancer, who have been treated with two or more chemotherapies, and selected for therapy based on an FDA-approved companion diagnostic for Rubraca. Continued approval for this indication may be contingent upon verification and description of clinical benefit in ARIEL3 and/or ARIEL4, our confirmatory trials.
The efficacy of Rubraca in the ovarian cancer maintenance treatment setting was investigated in ARIEL3 (NCT01968213), a double-blind, multicenter clinical trial in which 564 patients with recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer who were in response to platinum-based chemotherapy were randomized (2:1) to receive Rubraca tablets 600 mg orally twice daily (n=375) or placebo (n=189). Treatment was continued until disease progression or unacceptable toxicity. All patients had achieved a response (complete or partial) to their most recent platinum-based chemotherapy. Randomization was stratified by best response to last platinum (complete or partial), time to progression following the penultimate platinum therapy (6 to < 12 months and ≥ 12 months), and tumor biomarker status. The major efficacy outcome was investigator-assessed progression-free survival (“PFS”) evaluated according to RECISTv1.1.
The primary efficacy analysis evaluated three prospectively defined molecular sub-groups in a step-down manner: 1) tumor BRCA mutant (tBRCAmut) patients, inclusive of germline and somatic BRCA mutations (n=196); 2) HRD patients, including tBRCAmut patients and BRCA wild-type with high LOH (n=354), and, finally, 3) the intent-to-treat population, or all patients treated in ARIEL3 (n=564). ARIEL3 demonstrated a statistically significant improvement in PFS for patients randomized to Rubraca as compared with placebo in all patients, and in the HRD and tBRCAmut subgroups. Median PFS in the tBRCAmut patients was 16.6 months (95% CI: 13.4–22.9) in the Rubraca group (n=130) versus 5.4 months (95% CI: 3.4–6.7) in the placebo group (n=66) (Hazard Ratio, or HR: 0.23 [95% CI: 0.16–0.34]; p<0.0001). Median PFS in the HRD patients was 13.6 months (95% CI: 10.9–16.2) in the Rubraca group (n=236) versus 5.4 months (95% CI: 5.1–5.6) in the placebo group (n=118) (HR: 0.32 [95% CI: 0.24–0.42]; p<0·0001). Median PFS in the intent-to-treat population was 10.8 months (95% CI: 8.3–11.4) in the Rubraca group (n=375) versus 5.4 months (95% CI: 5.3–5.5) in the placebo group (n=189) (HR: 0.36 [95% CI: 0.30–0.45]; p<0·0001).
Results from a blinded independent radiology review (“BICR”) were consistent. In a pre-specified analysis of the key stand-alone secondary endpoint of progression-free survival assessed by BICR, PFS was also improved in the Rubraca group compared with placebo in all three populations. Median PFS in the tBRCAmut patients was 26.8 months (95% CI: 19.2 to not reached) in the Rubraca group versus 5.4 months (95% CI: 4.9–8.1) in the placebo group (HR: 0.20 [95%
7
CI: 0.13–0.32]; p<0.0001). Median PFS in the HRD patients was 22.9 months (95% CI: 16.2 to not reported) in the Rubraca group versus 5.5 months (95% CI: 5.1–7.4) in the placebo group (HR: 0.34 [95% CI: 0.24–0.47]; p<0.0001). Median PFS in the intent-to-treat population was 13.7 months (95% CI: 11.0–19.1) versus 5.4 months (95% CI: 5.1–5.5) in the placebo group (HR: 0.35 [0.28–0.45]; p<0.0001).
Enrollment in ARIEL3 included one-third of patients who had achieved a complete response to their prior platinum-based therapy, and two-thirds of patients who had achieved a partial response to their prior platinum-based therapy. Of those with a partial response, 37% had measurable disease at the time of enrollment and were therefore evaluable for response. The confirmed overall response rate by investigator-assessed RECISTv1.1 in the tBRCAmut group treated with Rubraca was 37.5% (15/40), of these, 17.5% (7/40) were complete responses. This compared with 9% (2/23) in the placebo group (p=0.0055). No complete responses were seen in the tBRCAmut placebo group. RECIST responses were also observed in BRCA wild-type HRD-positive and BRCA wild-type HRD-negative subgroups. RECIST responses were not assessed by independent blinded review.
Safety data from ARIEL3 demonstrated consistency with prior Rubraca studies. Treatment emergent adverse events (“TEAEs”) in the ARIEL3 Rubraca group were generally managed with dose modifications and not associated with increased mortality or morbidity compared with the placebo group. The most common (occurring in ≥5% of patients) TEAEs of grade ≥3 reported in patients treated with Rubraca in the ARIEL3 study were anemia/decreased hemoglobin (21%), increase in ALT/AST (10%), neutropenia (7%), asthenia/fatigue (7%) and thrombocytopenia (5%). The discontinuation rate for TEAEs (excluding disease progression) was 15% for Rubraca-treated patients and 2% for the placebo arm. In ARIEL3, the rate of treatment-emergent myelodysplastic syndrome (“MDS”)/acute myeloid leukemia (“AML”) in the Rubraca arm was <1% (3/372), and no patients on the placebo arm experienced treatment-emergent MDS/AML. In approximately 1,100 patients treated with Rubraca, MDS/AML occurred in 10 patients (0.9%), including those in long term follow-up. Of these, 5 occurred during treatment or during the 28 day safety follow-up (0.5%). The duration of Rubraca treatment prior to the diagnosis of MDS/AML ranged from 1 month to approximately 28 months. The cases were typical of secondary MDS/cancer therapy-related AML; in all cases, patients had received previous platinum-containing chemotherapy regimens and/or other DNA damaging agents.
At the time of the analysis of PFS, overall survival (OS) data were not mature (with 22% of events). The comprehensive dataset for ARIEL3 was presented at the 2017 European Society of Medical Oncology (“ESMO”) Congress in early September 2017 and subsequently published in The Lancet.
Based on the ARIEL3 dataset, in October 2017 we submitted a supplemental NDA for Rubraca as maintenance treatment in adult patients with recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer who are in a complete or partial response to platinum-based chemotherapy. The application was granted priority review status by the FDA and has a PDUFA date of April 6, 2018.
The ARIEL4 confirmatory study (NCT 02855944), which is open for enrollment, is a Phase 3 multicenter, randomized study of Rubraca versus chemotherapy in relapsed ovarian cancer patients with BRCA mutations (inclusive of germline and/or somatic) who have failed two prior lines of therapy. The primary endpoint of the study is PFS.
The Phase 1 RUCA-J study, sponsored by us, recently initiated with the first patient dosed with Rubraca in Japan. The Phase 1 study seeks to identify the recommended dose of rucaparib in Japanese patients.
Prostate cancer
The American Cancer Society estimates that more than 164,000 men in the United States will be diagnosed with prostate cancer in 2018, and the GLOBOCAN Cancer Fact Sheets estimated that approximately 345,000 men in Europe were diagnosed with prostate cancer in 2012. Castrate-resistant prostate cancer has a high likelihood of developing metastases. Metastatic castrate-resistant prostate cancer, or mCRPC, is an incurable disease, usually associated with poor prognosis. According to the American Cancer Society, the five-year survival rate for mCRPC is approximately 29%. Germline or somatic mutations in BRCA, ATM and other DNA repair genes are believed to be present at frequencies of 20 percent or higher in mCRPC, according to an article published in JCO Precision Oncology in 2017. These molecular markers may be used to select patients for treatment with a PARP inhibitor. Additionally, preclinical studies of rucaparib have demonstrated activity in prostate cell cancer lines deficient in BRCA or ATM.
8
The TRITON (Trial of Rucaparib in Prostate Indications) program in prostate cancer initiated in the second half of 2016, and currently includes two Clovis-sponsored potential registration studies currently open for enrollment:
|
· |
The TRITON2 study (NCT02952534), a Phase 2 single-arm study of Rubraca in men with mCRPC enrolling patients with BRCA mutations and ataxia-telangiectasia mutations, or ATM, (both inclusive of germline and/or somatic) or other deleterious mutations in other homologous recombination repair genes. All patients will have progressed after receiving one line of taxane-based chemotherapy and one or two lines of androgen receptor (“AR”) targeted therapy in the castrate-resistant setting. The primary endpoints of the study are radiologic ORR in patients with measurable disease and protein-specific antigen (“PSA”) response rate in patients who do not have measurable disease. TRITON2 initiated during the fourth quarter of 2016, and interim data are expected at a medical meeting during the second half of 2018. The estimated primary completion date for TRITON2 is the second half of 2019. Pending positive data, TRITON2 could potentially serve as the basis for an accelerated approval in the U.S. |
|
· |
The TRITON3 study (NCT02975934), a Phase 3 comparative study in men with mCRPC enrolling BRCA mutant and ATM (both inclusive of germline and/or somatic) patients who have progressed on AR-targeted therapy and who have not yet received chemotherapy in the castrate-resistant setting. TRITON3 will compare Rubraca to physician’s choice of AR-targeted therapy or chemotherapy in these patients. The planned primary endpoint of the study is radiologic PFS. TRITON3 initiated during the first quarter of 2017, and this earlier-line comparative study could potentially serve as a confirmatory study in the advanced prostate setting. |
Bladder cancer
According to GLOBOCAN Cancer Fact Sheets, bladder cancer was one of the top six most common cancers in the United States as of 2012, with an estimated 79,000 new cases of bladder cancer diagnosed in the United States in 2017, according to the National Cancer Institute. Approximately 20% to 30% of newly diagnosed bladder cancer patients have disease that has invaded the muscle, according to the National Cancer Institute. Muscle-invasive bladder cancer is a disease with poor prognosis. Overall survival of these patients after initial cisplatin-containing chemotherapy is 13-15 months, with most patients experiencing relapse of disease in 9 months, according to an article published in the European Journal of Cancer in 2006. After the first one or two lines of anti-cancer treatments, options for these patients are limited, with platinum therapy as the current standard of care. Based an analysis of The Cancer Genome Atlas (“TCGA”), bladder cancer data set, we believe approximately 60% of bladder cancer tumors have alterations in homologous recombination repair genes or other genomic features associated with HRD.
We initiated a potential registration study in bladder cancer during the first quarter of 2018, called ATLAS (A Study of Rucaparib in Patients with Locally Advanced or Metastatic Urothelial Carcinoma). ATLAS (NCT03397394) is a phase 2 single-arm study enrolling patients with relapsed metastatic urothelial carcinoma following one or two prior standard of care regimens, with measurable disease, and no prior PARP treatment. The planned primary endpoint is overall response rate, and the study will enroll all comers, with no selection based on HRD status. Pending positive data, we believe this trial design could support a sNDA in an all comers population, without regard to biomarker status.
Combination trials
In July 2017, we and Bristol-Myers Squibb Company (“BMS”) announced a broad clinical collaboration evaluating the combination of Rubraca with BMS’s immunotherapy Opdivo® (nivolumab) in multiple tumor types. Three trials are underway or expected to initiate in the first half of 2018:
|
· |
The ATHENA study, a phase 3 study in advanced ovarian cancer, sponsored by Clovis; |
|
· |
A phase 3 study in advanced triple-negative breast cancer (TNBC), sponsored by BMS; and |
|
· |
A phase 2 study in mCRPC sponsored by BMS. |
We believe that a preclinical rationale supports the conduct of clinical trials of the combination of our PARP inhibitor Rubraca with immune checkpoint inhibitors such as the PD-1 inhibitor Opdivo. BRCA1 and BRCA2 and other HRD mutations are associated with increased tumor mutational burden, which may create additional tumor-specific antigens or “neoepitopes.” Increased tumor mutation burden has been shown to correlate with increased benefit from immune checkpoint blockade. In addition, cell death that is induced by a PARP inhibitor is considered immunogenic, and stimulates a “STING-like” pathway due to fragmented DNA release into cytosol. In mice studies, rucaparib and an anti-
9
PD-1 antibody demonstrated anti-tumor activity in BRCA1 mutant ovarian tumors. The combination of rucaparib and either an anti-PD-L1 or anti-CTLA-4 antibody were equally compelling in preclinical studies.
ATHENA is a four-arm first-line maintenance treatment study to evaluate Rubraca and Opdivo, Rubraca, Opdivo and placebo in an estimated 1,000 newly diagnosed patients with stage III/IV high-grade ovarian, fallopian tube, or primary peritoneal cancer who have completed platinum-based chemotherapy. The primary objectives are to determine if the combination of Rubraca and Opdivo meaningfully extends PFS versus Rubraca monotherapy, or versus placebo, and to determine if Rubraca extends PFS versus placebo. The analysis of the study results will evaluate, in a step-down manner, the tBRCA/HRD and intent-to-treat subpopulations. We are the sponsor, and will also conduct and fund the ATHENA study, which is expected to initiate in the first half of 2018.
The combination study of Rubraca and Opdivo in patients with advanced TNBC will be sponsored and conducted by BMS, with study costs to be shared by Clovis and BMS. The study is expected to initiate in the first half of 2018.
The mCRPC study is a three-arm study evaluating Opdivo + Rubraca, Opdivo + docetaxel + prednisone, and Opdivo + enzalutamide, with the objective of determining how the combination affects objective response rate and PSA response. The study will enroll patients with biomarker negative or positive disease, and tumor tissue samples will be used to determine biomarker status. BMS is sponsoring, conducting and funding the 300 patient study in mCRPC, which initiated in the fourth quarter of 2017.
In addition, a Phase 1b study (WO39409; NCT NCT03101280) sponsored by Hoffman-La Roche (Genentech) is underway evaluating the combination of cancer immunotherapy Tecentriq® (atezolizumab; anti-PDL1) and Rubraca for the treatment of advanced gynecological cancers and TNBC in patients with a tumor BRCA or HRD mutation. This study began enrolling patients in the first half of 2017.
Companion Diagnostics
We partnered with Foundation Medicine, Inc. to co-develop a companion diagnostic test, the FDA approved FoundationFocus™ CDx BRCA, to select patients for treatment with Rubraca in the ovarian cancer treatment indication. FoundationFocus CDx BRCA is a next-generation sequencing (“NGS”) assay that assesses tumor BRCA mutations from tumor tissue samples from patients with ovarian cancer.
On November 30, 2017, Foundation announced FDA approval of its comprehensive companion diagnostic test for solid tumors, FoundationOne™ CDx, a NGS based in vitro diagnostic device for detection of substitutions, insertion and deletion alterations, and copy number alterations in 324 genes and select gene rearrangements, as well as genomic signatures including microsatellite instability and tumor mutational burden. Among the genes assessed by the test are BRCA1/2, and FoundationOne™ CDx is approved as a companion diagnostic to select patients for treatment with Rubraca in the advanced ovarian cancer treatment indication.
As part of our collaboration with Foundation, we also developed an NGS test to use as a diagnostic to assess genomic LOH in tumor samples, and this biomarker has the potential to expand the clinical utility of Rubraca in ovarian cancer and other indications. This test, FoundationFocus™ CDx BRCA HRD test, was used to assess HRD status in patient tumor samples in the ARIEL3 study.
We also have a companion diagnostic collaboration with Myriad Genetics, Inc. (“Myriad”) to support a post-marketing regulatory commitment related to Rubraca’s initial approval in the ovarian cancer treatment setting. Myriad will submit a supplementary premarket approval (“sPMA”) application under its existing PMA for BRACAnalysis CDx to include Rubraca. BRACAnalysis CDx is Myriad’s blood-based assay for the qualitative detection and classification of germline mutations in BRCA1/2 genes.
10
Lucitanib – a VEGFR, PDGFR and FGFR Inhibitor
Lucitanib is an oral inhibitor of the tyrosine kinase activity of vascular endothelial growth factor receptors (VEGFR) 1-3, platelet-derived growth factor receptors (PDGFR) alpha and beta and fibroblast growth factor receptors (FGFR) 1-3. Lucitanib was previously evaluated in breast and lung cancers. Development in those indications has ceased and we continue to provide drug to patients whose clinicians recommend continuing lucitanib therapy. We are continuing to evaluate what, if any, further development of lucitanib will be pursued. We hold development and commercialization rights in the U.S. and Japan and have sublicensed rights to Europe and rest of world markets, excluding China, to Servier.
Rociletinib - an Oral EGFR Mutant-Selective Inhibitor
Rociletinib is an oral mutant-selective inhibitor of epidermal growth factor receptor (“EGFR”). We terminated enrollment in all sponsored clinical studies, although we continue to provide drug to patients whose clinicians recommend continuing rociletinib therapy. We are continuing analyses of rociletinib data to determine whether certain populations of patients may represent an opportunity for a partner committed to investing in further clinical development. We hold global development and commercialization rights for rociletinib.
Competition
The development and commercialization of new drugs is competitive, and we face competition from major pharmaceutical and biotechnology companies worldwide. Our competitors may develop or market products or other novel technologies that are more effective, safer or less costly than any that have been or will be commercialized by us, or may obtain regulatory approval for their products more rapidly than we may obtain approval for ours.
The acquisition or licensing of pharmaceutical products is also very competitive, and a number of more established companies, which have acknowledged strategies to license or acquire products, may have competitive advantages over us, as may other emerging companies taking similar or different approaches to product acquisitions. Many of our competitors have substantially greater financial, technical and human resources than we have. Additional mergers and acquisitions in the pharmaceutical industry may result in even more resources being concentrated in our competitors. Competition may increase further as a result of advances made in the commercial applicability of technologies and greater availability of capital for investment in these fields. Our success will be based in part on our ability to build and actively manage a portfolio of drugs that addresses unmet medical needs and creates value in patient therapy.
Rubraca Competition
Lynparza®/olaparib (AstraZeneca) was the first PARP inhibitor to market and has been approved in the US in the following indications:
|
· |
as monotherapy for the treatment of adult patients who have deleterious or suspected deleterious germline BRCA-mutated (gBRCAm) advanced ovarian cancer who have been treated with three or more prior lines of chemotherapy; |
|
· |
as monotherapy for the maintenance treatment of adult patients with recurrent epithelial, fallopian tube or primary peritoneal cancer, who are in a complete or partial response to platinum-based chemotherapy; and |
|
· |
as monotherapy in patients with deleterious or suspected deleterious gBRCAm, human epidermal growth factor 2 (HER2)-negative metastatic breast cancer who have been treated with chemotherapy in the neoadjuvant, adjuvant, or metastatic setting. |
Lynparza is approved in the EU for use as monotherapy for the maintenance treatment of adult patients with platinum-sensitive relapsed BRCA-mutated (germline and/or somatic) high grade serous epithelial ovarian, fallopian tube, or primary peritoneal cancer who are in response (complete response or partial response) to platinum-based chemotherapy. In February 2018, the CHMP adopted a positive opinion recommending this label be changed and expanded to remove the limitation of use in BRCA-mutated patients. Lynparza has indications for ovarian cancer across 57 countries (as of year-end 2017).
11
In July 2017, AstraZeneca and Merck & Co., Inc. announced a global strategic oncology collaboration to co-develop and co-commercialise Lynparza for multiple cancer types. Lynparza is being investigated, alone and in combination with other agents, in multiple indications across several tumor types, including breast, prostate, and pancreatic cancers.
Zejula®/niraparib (Tesaro) was approved in March 2017 in the United States as monotherapy for the maintenance treatment of adult patients with recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer who are in a complete or partial response to platinum-based chemotherapy. Zejula was approved in November 2017 in the EU for the same indication. Additional clinical investigations of Zejula in ovarian, breast and lung cancers are ongoing or planned. Janssen Biotech has licensed rights to develop and commercialize niraparib specifically for patients with prostate cancer worldwide, except in Japan.
There are a number of PARP inhibitors in clinical development including AbbVie’s veliparib and ABT-767, Pfizer’s talazoparib, BeiGene’s BGB-290, and Checkpoint Therapeutics’ CK-102. While most PARP inhibitor development focuses on ovarian, breast and prostate cancers, additional efforts are aimed toward bladder, lung, and pancreatic cancers as well.
In addition, combination approaches that include PARP inhibitors, including Lynparza or Zejula, with other anticancer agents are in various phases of clinical development across a variety of oncology indications. These combination therapies may result in future competitive pressure on Rubraca, and multiple data readouts for such studies are anticipated throughout 2018 and beyond.
Outside of the PARP class, Avastin®/bevacizumab is approved in the US for recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer that is platinum-resistant in combination with paclitaxel, pegylated liposomal doxorubicin, or topotecan, and was approved in December 2016 in the US for recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer that is platinum-sensitive in combination with carboplatin and paclitaxel or in combination with carboplatin and gemcitabine, followed by Avastin as a single agent. Other out of class agents approved for use in advanced ovarian cancer include chemotherapeutic agents (e.g. platinum-based doublets, platinum monotherapy, non-platinum chemotherapy, etc.), Doxil® (Janssen), and Hycamtin® (Novartis). There are additional out-of-class agents in clinical development that may pose a future competitive threat to Rubraca.
License Agreements
Pfizer Inc.
In June 2011, we entered into a license agreement with Pfizer Inc. (“Pfizer”) to obtain the exclusive global rights to develop and commercialize Rubraca. The exclusive rights are exclusive even as to Pfizer and include the right to grant sublicenses. Pursuant to the terms of the license agreement, we made a $7.0 million upfront payment to Pfizer and are required to make additional payments to Pfizer for the achievement of certain development and regulatory and sales milestones and royalties on sales as required by the license agreement. Prior to the FDA approval of Rubraca, we made milestones payments of $1.4 million, which were recognized as acquired in-process research and development expense.
On August 30, 2016, we entered into a first amendment to the worldwide license agreement with Pfizer, which amends the June 2011 existing worldwide license agreement to permit us to defer payment of the milestone payments payable upon (i) FDA approval of an NDA for 1st Indication in US and (ii) European Commission approval of an MAA for 1st Indication in EU, to a date that is 18 months after the date of achievement of such milestones. In the event that we defer such milestone payments, we have agreed to pay an additional $3.0 million related to the achievement of each such milestone.
On December 19, 2016, the FDA approved Rubraca as monotherapy for the treatment of patients with deleterious BRCA mutation (germline and/or somatic) associated advanced ovarian cancer, who have been treated with two or more chemotherapies, and selected for therapy based on an FDA-approved companion diagnostic for Rubraca. The FDA approval resulted in a $0.75 million milestone payment to Pfizer as required by the license agreement, which was made in the first quarter of 2017. The FDA approval also resulted in the obligation to pay a $20.0 million milestone payment, for which we have exercised the option to defer payment by agreeing to pay $23.0 million within 18 months after the date of the FDA approval. These payments were recognized as intangible assets and amortized over the estimated remaining useful life of Rubraca.
12
We are obligated under the license agreement to use commercially reasonable efforts to develop and commercialize Rubraca and we are responsible for all ongoing development and commercialization costs for Rubraca. We are required to make regulatory milestone payments to Pfizer of up to an additional $69.75 million in aggregate if specified clinical study objectives and regulatory filings, acceptances and approvals are achieved. In addition, we are obligated to make sales milestone payments to Pfizer if specified annual sales targets for Rubraca are met, which relate to annual sales targets of $250.0 million and above, which, in the aggregate, could amount to total milestone payments of $170.0 million, and tiered royalty payments at a mid-teen percentage rate on our net sales, with standard provisions for royalty offsets to the extent we need to obtain any rights from third parties to commercialize Rubraca.
The license agreement with Pfizer will remain in effect until the expiration of all of our royalty and sublicense revenue obligations to Pfizer, determined on a product-by-product and country-by-country basis, unless we elect to terminate the license agreement earlier. If we fail to meet our obligations under the agreement and are unable to cure such failure within specified time periods, Pfizer can terminate the agreement, resulting in a loss of our rights to Rubraca and an obligation to assign or license to Pfizer any intellectual property rights or other rights we may have in Rubraca, including our regulatory filings, regulatory approvals, patents and trademarks for Rubraca.
AstraZeneca UK Limited
In April 2012, we entered into a license agreement with AstraZeneca UK Limited (“AstraZeneca”) to acquire exclusive rights associated with Rubraca under a family of patents and patent applications that claim methods of treating patients with PARP inhibitors in certain indications. The license enables the development and commercialization of Rubraca for the uses claimed by these patents. Pursuant to the terms of the license agreement, we made an upfront payment of $0.25 million upon execution of the agreement. During the second quarter of 2016, we made a milestone payment of $0.3 million to AstraZeneca upon the NDA submission for Rubraca. These payments were recognized as acquired in-process research and development expense. The FDA approval of Rubraca on December 19, 2016 resulted in a final $0.35 million milestone payment to AstraZeneca as required by the license agreement. This payment was recognized as intangible assets and amortized over the estimated remaining useful life of Rubraca. AstraZeneca also receives royalties on net sales of Rubraca.
Advenchen Laboratories LLC
In October 2008, Ethical Oncology Science, S.p.A. (“EOS”) (now known as Clovis Oncology Italy S.r.l.) entered into an exclusive license agreement with Advenchen Laboratories LLC (“Advenchen”) to develop and commercialize lucitanib on a global basis, excluding China. We are obligated to pay Advenchen tiered royalties at percentage rates in the mid-single digits on net sales of lucitanib, based on the volume of annual net sales achieved. In addition, after giving effect to the first and second amendments to the license agreement, we are required to pay to Advenchen 25% of any consideration, excluding royalties, we receive from sublicensees, in lieu of the milestone obligations set forth in the agreement. We are obligated under the agreement to use commercially reasonable efforts to develop and commercialize at least one product containing lucitanib, and we are also responsible for all remaining development and commercialization costs for lucitanib.
The license agreement with Advenchen will remain in effect until the expiration of all of our royalty obligations to Advenchen, determined on a product-by-product and country-by-country basis, unless we elect to terminate the agreement earlier. If we fail to meet our obligations under the agreement and are unable to cure such failure within specified time periods, Advenchen can terminate the agreement, resulting in a loss of our rights to lucitanib.
Les Laboratoires Servier
In September 2012, EOS entered into a collaboration and license agreement with Les Laboratoires Servier and Institut de Recherches Internationales Servier (collectively, “Servier”), whereby EOS sublicensed to Servier exclusive rights to develop and commercialize lucitanib in all countries outside of the U.S., Japan and China. In exchange for these rights, EOS received an upfront payment of €45.0 million. We are entitled to receive additional payments on the achievement of specified development, regulatory and commercial milestones up to €100.0 million in the aggregate, €10.0 million of which was received in the first quarter of 2014. In addition, we are entitled to receive sales milestone payments if specified annual sales targets for lucitanib are met, each of which relates to annual sales targets of €250.0 million and above, which, in the aggregate, could amount to a total of €250.0 million. We are also entitled to receive royalties at percentage rates ranging from low-to-mid teens on sales of lucitanib by Servier.
13
We and Servier are developing lucitanib pursuant to a development plan agreed to between the parties. Servier is responsible for all of the development costs for lucitanib up to €80.0 million. Cumulative global development costs in excess of €80.0 million, if any, will be shared equally between us and Servier. During the second quarter of 2016, we and Servier agreed to discontinue the development of lucitanib for breast cancer. During 2017, we completed the committed on-going development activities and received full reimbursement of our development costs from Servier. Reimbursements are recorded as reduction to research and development expense on the Consolidated Statement of Operations.
The collaboration and license agreement will remain in effect until the expiration of all of Servier’s royalty obligations to us, determined on a product-by-product and country-by-country basis, unless Servier elects to terminate the agreement earlier. If we fail to meet our obligations under the agreement and are unable to cure such failure within specified time periods, Servier can terminate the agreement, resulting in the granting of a perpetual license to Servier of rights to lucitanib.
Celgene Corporation
In May 2010, we entered into an exclusive worldwide license agreement with Avila Therapeutics, Inc. (now Celgene Avilomics Research Inc., part of Celgene Corporation (“Celgene”)) to discover, develop and commercialize a covalent inhibitor of mutant forms of the EGFR gene product. Rociletinib was identified as the lead inhibitor candidate under the license agreement. We are responsible for all non-clinical, clinical, regulatory and other activities necessary to develop and commercialize rociletinib.
We made an upfront payment of $2.0 million upon execution of the license agreement, a $4.0 million milestone payment in the first quarter of 2012 upon the acceptance by the FDA of our Investigational New Drug (“IND”) application for rociletinib and a $5.0 million milestone payment in the first quarter of 2014 upon the initiation of the Phase II study for rociletinib. In the third quarter of 2015, we made milestone payments totaling $12.0 million upon acceptance of the NDA and MAA for rociletinib by the FDA and EMA, respectively. We recognized all payments prior to commercial approval as acquired in-process research and development expense.
We are obligated to pay royalties at percentage rates ranging from mid-single digits to low teens on the volume of annual net sales achieved. We are required to pay up to an additional aggregate of $98.0 million in development and regulatory milestone payments if certain clinical study objectives and regulatory filings, acceptances and approvals are achieved. In addition, we are required to pay up to an aggregate of $120.0 million in sales milestone payments if certain annual sales targets are achieved.
We have full sublicensing rights under the license agreement, subject to our sharing equally with Celgene any upfront payments from any sub-licensing arrangements relating to Japan, or Japan and any one or more of China, South Korea and Taiwan, which we refer to herein as an Asian Partnership, and subject to our paying royalties on sales in Asia equal to the greater of the royalty rates contained in our license agreement or 50% of the royalties we receive from our Asian Partnership.
The license agreement will remain in effect until the expiration of all of our royalty and sublicense revenue obligations to Celgene, determined on a product-by-product and country-by-country basis, unless we elect to terminate the license agreement earlier. If we fail to meet our obligations under the agreement and are unable to cure such failure within specified time periods, Celgene can terminate the agreement, resulting in a loss of our rights to rociletinib and an obligation to assign or license to Celgene any intellectual property rights or other rights we may have in rociletinib, including our regulatory filings, regulatory approvals, patents and trademarks for rociletinib.
Government Regulation
Government authorities in the United States (including federal, state and local authorities) and in other countries, extensively regulate, among other things, the manufacturing, research and clinical development, marketing, labeling and packaging, storage, distribution, post-approval monitoring and reporting, advertising and promotion, pricing and export and import of pharmaceutical products. The process of obtaining regulatory approvals and the subsequent compliance with appropriate federal, state, local and foreign statutes and regulations require the expenditure of substantial time and financial resources. Moreover, failure to comply with applicable regulatory requirements may result in, among other
14
things, warning letters, clinical holds, civil or criminal penalties, recall or seizure of products, injunction, disbarment, partial or total suspension of production or withdrawal of the product from the market.
U.S. Government Regulation
In the United States, the FDA regulates drugs under the Federal Food, Drug and Cosmetic Act (“FDCA”) and its implementing regulations. Drugs are also subject to other federal, state and local statutes and regulations. The process required by the FDA before product candidates may be marketed in the United States generally involves the following:
|
· |
completion of extensive non-clinical laboratory tests and non-clinical animal studies, all performed in accordance with the FDA’s Good Laboratory Practice regulations; |
|
· |
submission to the FDA of an IND which must become effective before human clinical trials may begin and must be updated at least annually; |
|
· |
performance of adequate and well-controlled human clinical trials to establish the safety and efficacy of the product candidate for each proposed indication; |
|
· |
submission to the FDA of a marketing authorization application in the form of an NDA for the initial commercial sale of a product, or of a sNDA, for approval of a new indication if the product is already approved for another indication; |
|
· |
satisfactory completion of an FDA pre-approval inspection of the manufacturing facilities at which the active pharmaceutical ingredient (“API”) and finished drug product are produced and tested to assess compliance with Current Good Manufacturing Practices (“cGMP”) and/or sites involved in clinical studies to assess compliance with Good Clinical Practices (“GCP”); |
|
· |
if FDA convenes an advisory committee, satisfactory completion of the advisory committee review; and |
|
· |
FDA review and approval of the marketing authorization application and product prescribing information prior to any commercial marketing or sale of the drug for the intended use. |
An IND is a request for authorization from the FDA to administer a product candidate to humans. The central focus of an IND submission is on the general investigational plan and the protocol(s) for human studies. The IND also includes results of animal studies or other human studies, as appropriate, as well as manufacturing information, analytical data and any available clinical data or literature to support the use of the product candidate. An IND must become effective before human clinical trials may begin. An IND will automatically become effective 30 days after receipt by the FDA, unless before that time the FDA raises concerns or questions related to the proposed clinical trials, including concerns that human research subjects will be exposed to unreasonable health risks. In such a case, the IND may be placed on clinical hold requiring delay of a proposed clinical investigation, and the IND sponsor and the FDA must resolve any outstanding concerns or questions before clinical trials can begin. Accordingly, submission of an IND may or may not result in the FDA allowing clinical trials to commence.
Clinical trials involve the administration of the drug candidate to human subjects under the supervision of qualified investigators in accordance with GCP, which include the requirement that all research subjects provide their informed consent for their participation in any clinical trial. Clinical trials are conducted under protocols detailing, among other things, the objectives of the study, the parameters to be used in monitoring safety and the efficacy criteria to be evaluated. A protocol for each clinical trial and any subsequent protocol amendments must be submitted to the FDA as part of the IND. Additionally, approval must also be obtained from an Institutional Review Board (“IRB”) for each medical center proposing to conduct the clinical trial before the trials may be initiated, and the IRB must monitor the study until completed. Clinical trials are subject to central registration and results reporting requirements, such as on www.clinicaltrials.gov.
The clinical investigation of a drug is generally divided into three phases. Although the phases are usually conducted sequentially, they may overlap or be combined. The three phases of an investigation are as follows:
|
· |
Phase 1. Phase 1 includes the initial introduction of the product candidate into humans. Phase 1 clinical trials are typically closely monitored and may be conducted in patients with the target disease or condition or in healthy volunteers. These studies are designed to evaluate the safety, dosage tolerance, metabolism and pharmacologic actions of product candidate in humans, the side effects associated with increasing doses, and if possible, to gain early evidence on effectiveness. During Phase 1 clinical trials, sufficient information about the |
15
product candidate’s pharmacokinetics and pharmacological effects may be obtained to permit the design of well-controlled and scientifically valid Phase 2 clinical trials. The total number of participants included in Phase 1 clinical trials varies, but is generally in the range of 20 to 80. |
|
· |
Phase 2. Phase 2 includes controlled clinical trials conducted to preliminarily or further evaluate the effectiveness of the product candidate for a particular indication(s) in patients with the disease or condition under study, to determine dosage tolerance and optimal dosage, and to identify possible adverse side effects and safety risks associated with the drug. Phase 2 clinical trials are typically well-controlled, closely monitored, and conducted in a limited patient population, usually involving no more than several hundred participants. |
|
· |
Phase 3. Phase 3 clinical trials are generally controlled clinical trials conducted in an expanded patient population generally at geographically dispersed clinical trial sites. They are performed after preliminary evidence suggesting effectiveness of the drug has been obtained and are intended to further evaluate dosage, clinical effectiveness and safety, to establish the overall benefit-risk relationship of the investigational drug product and to provide an adequate basis for product approval. Phase 3 clinical trials usually involve several hundred to several thousand participants. |
A pivotal study is a clinical study which adequately meets regulatory agency requirements for the evaluation of a drug candidate’s efficacy and safety such that it can be used to justify the approval of the product. Generally, pivotal studies are also Phase 3 studies but may be Phase 2 studies if the trial design provides a well-controlled and reliable assessment of clinical benefit, particularly in situations where there is an unmet medical need.
The FDA, an IRB or the clinical trial sponsor may suspend or terminate a clinical trial at any time on various grounds, including a finding that the research subjects are being exposed to an unacceptable health risk. Additionally, some clinical trials are overseen by an independent group of qualified experts organized by the clinical trial sponsor, known as an Independent Data Monitoring Committee (“IDMC”). The IDMC receives special access to un-blinded data during the clinical trial and may halt the clinical trial if it determines that there is an unacceptable safety risk for subjects or other grounds, such as no demonstration of efficacy. We may also suspend or terminate a clinical trial based on evolving business objectives and/or competitive climate.
Assuming successful completion of all required testing in accordance with all applicable regulatory requirements, detailed product development information is submitted to the FDA in the form of an NDA or sNDA requesting approval to market the product for one or more indications.
The application includes all relevant data available from pertinent non-clinical and clinical trials, including negative or ambiguous results, as well as positive findings, together with detailed information relating to the product’s chemistry, manufacturing, controls and proposed labeling, among other things. Data can come from company-sponsored clinical trials intended to test the safety and effectiveness of a use of a product, or from a number of alternative sources, including studies initiated by investigators. To support marketing approval, the data submitted must be sufficient in quality and quantity to establish the safety and effectiveness of the product candidate to the satisfaction of the FDA.
Once the marketing application submission has been accepted for filing, the FDA’s goal is to review applications within 10 months of acceptance for filing or, if the application relates to treatment of a serious or life-threatening condition and is granted fast track priority review designation, six months from acceptance for filing. The review process is often significantly extended by FDA requests for additional information or clarification. The FDA may refer the application to an advisory committee for review, evaluation and recommendation as to whether the application should be approved. The FDA is not bound by the recommendation of an advisory committee, but it typically follows such recommendations.
After the FDA evaluates the NDA or sNDA and conducts inspections of clinical research facilities and/or manufacturing facilities where the drug product and/or its API will be produced, it may issue an approval letter or a Complete Response Letter. An approval letter authorizes commercial marketing of the drug with specific prescribing information for specific indications. A Complete Response Letter indicates that the review cycle of the application is complete, and the application is not ready for approval. A Complete Response Letter may require additional clinical data and/or an additional pivotal Phase 3 clinical trial(s), and/or other significant, expensive and time-consuming requirements related to clinical trials, non-clinical studies or manufacturing. Even if such additional information is submitted, the FDA may ultimately decide that the application does not satisfy the criteria for approval. The FDA could also approve the NDA with a Risk Evaluation and Mitigation Strategies plan to mitigate risks, which could include
16
medication guides, physician communication plans or elements to assure safe use, such as restricted distribution methods, patient registries and other risk minimization tools. The FDA also may condition approval on, among other things, changes to proposed labeling, development of adequate controls and specifications or a commitment to conduct one or more post-market studies or clinical trials. Such post-market testing may include Phase IV clinical trials and surveillance to further assess and monitor the product’s safety and effectiveness after commercialization. Regulatory approval of oncology products often requires that patients in clinical trials be followed for long periods to determine the overall survival benefit of the drug.
Products manufactured or distributed pursuant to FDA approvals are subject to continuing regulation by the FDA, including recordkeeping requirements and reporting of adverse experiences with the drug. Adverse event experience with the product must be reported to the FDA in a timely fashion and pharmacovigilance programs to proactively look for these adverse events are mandated by the FDA. Newly discovered or developed safety or effectiveness data may require changes to a product’s approved labeling, including the addition of new warnings and contraindications and also may require the implementation of other risk management measures.
Drug manufacturers and their subcontractors are required to register their establishments with the FDA and certain state agencies, and are subject to periodic unannounced inspections by the FDA and certain state agencies for compliance with GMP, which impose certain procedural and documentation requirements upon us and our third-party manufacturers. Following such inspections, the FDA may issue notices on Form FDA 483 and Warning Letters that could cause us to modify certain activities. A Form FDA 483 notice, if issued at the conclusion of an FDA inspection, can list conditions the FDA investigators believe may have violated cGMP or other FDA regulations or guidance. Failure to adequately and promptly correct the observations(s) can result in further regulatory enforcement action. In addition to Form FDA 483 notices and Warning Letters, failure to comply with the statutory and regulatory requirements can subject a manufacturer to possible legal or regulatory action, such as suspension of manufacturing, seizure of product, injunctive action or possible civil penalties. In addition, changes to the manufacturing process are strictly regulated, and, depending on the significance of the change, may require prior FDA approval before being implemented. FDA regulations also require investigation and correction of any deviations from cGMP and impose reporting and documentation requirements upon us and any third-party manufacturers that we may decide to use. Accordingly, manufacturers must continue to expend time, money and effort in the area of production and quality control to maintain compliance with cGMP and other aspects of regulatory compliance.
Government Regulation Outside of the United States
In addition to regulations in the United States, we are subject to a variety of regulations in other jurisdictions governing, among other things, clinical trials and any commercial sales and distribution of our products. The approval process and requirements governing the conduct of clinical trials, product licensing, pricing, and reimbursement vary greatly from country to country, and the time may be longer or shorter than that required for FDA approval.
Regardless of whether we hold FDA approval for a product, we must obtain the requisite approvals from regulatory authorities in foreign countries prior to the commencement of clinical trials or marketing of the product in those countries. Certain countries outside of the United States have a similar process that requires the submission of a clinical trial application much like the IND prior to the commencement of human clinical trials. In Europe, for example, a clinical trial application, (“CTA”) must be submitted to each country’s national health authority and an independent ethics committee, much like the FDA and IRB, respectively. Once the CTA is approved in accordance with a country’s requirements, clinical trial development may proceed.
Medicines can be authorized in the European Union by using either the centralized authorization procedure or national authorization procedures. Under the centralized procedure, marketing authorization applications are submitted to the EMA whose CHMP reviews the application and issues an opinion on it. The opinion is considered by the European Commission (“EC”) which is responsible for deciding applications. If the application is approved, the EC grants a single marketing authorization that is valid for all European Union member states as well as Iceland, Liechtenstein and Norway. The centralized procedure is compulsory for human medicines that contain a new active substance indicated for the treatment of certain diseases, including cancer.
The national authorization procedures, the decentralized and mutual recognition procedures, are available for products for which the centralized procedure is not compulsory. Using the decentralized procedure, an applicant may apply for simultaneous authorization in more than one European Union country of medicinal products that have not yet
17
been authorized in any European Union country and that do not fall within the mandatory scope of the centralized procedure. Under the mutual recognition procedure, a medicine is first authorized in one European Union Member State, in accordance with the national procedures of that country. Following this, further marketing authorizations can be sought from other European Union countries in a procedure whereby the countries concerned agree to recognize the validity of the original, national marketing authorization
Available Special Regulatory Procedures
Formal Meetings
We are encouraged to engage and seek guidance from health authorities relating to the development and review of investigational drugs, as well as marketing applications. In the United States, there are different types of official meetings that may occur between us and the FDA. Each meeting type is subject to different procedures. Conclusions and agreements from each of these meetings are captured in the official final meeting minutes issued by the FDA.
The EMA also provides the opportunity for dialogue with us. This is usually done in the form of Scientific Advice, which is given by the Scientific Advice Working Party of CHMP. A fee is incurred with each Scientific Advice meeting.
Advice from either the FDA or EMA is typically provided based on questions concerning, for example, quality (chemistry, manufacturing and controls testing), nonclinical testing and clinical studies and pharmacovigilance plans and risk-management programs. Such advice is not legally binding on the sponsor. To obtain binding commitments from the FDA in the United States, Special Protocol Assessment (“SPA”) procedures are available. A SPA is an evaluation by the FDA of a protocol with the goal of reaching an agreement with the sponsor that the protocol design, clinical endpoints and statistical analyses are acceptable to support regulatory approval of the product candidate with respect to effectiveness in the indication studied. The FDA’s agreement to a SPA is binding upon the FDA except in limited circumstances, such as if the FDA identifies a substantial scientific issue essential to determining the safety or effectiveness of the product after clinical studies begin, or if the study sponsor fails to follow the protocol that was agreed upon with the FDA. There is no guarantee that a study will ultimately be adequate to support an approval even if the study is subject to a SPA.
Orphan Drug Designation
The FDA may grant orphan drug designation to drugs intended to treat a rare disease or condition that affects fewer than 200,000 individuals in the United States, or if it affects more than 200,000 individuals in the United States and there is no reasonable expectation that the cost of developing and making the drug for this type of disease or condition will be recovered from sales in the United States. In the European Union, the EMA’s Committee for Orphan Medicinal Products grants orphan drug designation to promote the development of products that are intended for the diagnosis, prevention or treatment of life-threatening or chronically debilitating conditions affecting not more than five in 10,000 persons in the European Union Community. Additionally, designation is granted for products intended for the diagnosis, prevention or treatment of a life-threatening, seriously debilitating or serious and chronic condition and when, without incentives, it is unlikely that sales of the drug in the European Union would be sufficient to justify the necessary investment in developing the drug or biological product.
In the United States, orphan drug designation entitles a party to financial incentives such as opportunities for grant funding towards clinical trial costs, tax advantages and user-fee waivers. In addition, if a product receives the first FDA approval for the indication for which it has orphan designation, the product is entitled to orphan drug exclusivity, which means the FDA may not approve any other application to market the same drug for the same indication for a period of seven years, except in limited circumstances, such as a showing of clinical superiority over the product with orphan exclusivity.
In the European Union, orphan drug designation also entitles a party to financial incentives such as reduction of fees or fee waivers and 10 years of market exclusivity is granted following drug or biological product approval. This period may be reduced to six years if the orphan drug designation criteria are no longer met, including where it is shown that the product is sufficiently profitable not to justify maintenance of market exclusivity.
Orphan drug designation must be requested before submitting an application for marketing approval. Orphan drug designation does not convey any advantage in, or shorten the duration of, the regulatory review and approval process.
18
Pediatric Development
In the United States, the FDCA provides for an additional six months of marketing exclusivity for a drug if reports are filed of investigations studying the use of the drug product in a pediatric population in response to a written request from the FDA. Separate from this potential exclusivity benefit, NDAs must contain data (or a proposal for post-marketing activity) to assess the safety and effectiveness of an investigational drug product for the claimed indications in all relevant pediatric populations in order to support dosing and administration for each pediatric subpopulation for which the drug is safe and effective. The FDA may, on its own initiative or at the request of the applicant, grant deferrals for submission of some or all pediatric data until after approval of the product for use in adults or full or partial waivers if certain criteria are met. Discussions about pediatric development plans can be discussed with the FDA at any time, but usually occur any time between the end-of-Phase II meeting and submission of the NDA.
For the EMA, a Pediatric Investigation Plan, and/or a request for waiver or deferral, is required for submission prior to submitting a marketing authorization application.
Breakthrough Therapy Designation in the United States
The U.S. Congress created the Breakthrough Therapy designation program as a result of the passage of the Food and Drug Administration Safety and Innovation Act of 2012. FDA may grant Breakthrough Therapy status to a drug intended for the treatment of a serious condition when preliminary clinical evidence indicates that the drug may demonstrate substantial improvement over existing therapies on one or more clinically significant endpoints. The Breakthrough Therapy designation, which may be requested by a sponsor when filing or amending an IND, is intended to facilitate and expedite the development and FDA review of a product candidate. Specifically, the Breakthrough Therapy designation may entitle the sponsor to more frequent meetings with the FDA during drug development, intensive guidance on clinical trial design and expedited FDA review by a cross-disciplinary team comprised of senior managers. The designation does not guarantee a faster development or review time as compared to other drugs, however, nor does it assure that the drug will obtain ultimate marketing approval by the FDA. Once granted, the FDA may withdraw this designation at any time.
Expedited Review and Approval in the United States
The FDA has various programs, including Fast Track, priority review and accelerated approval, which are intended to expedite or simplify the process for reviewing drugs and biologics, and/or provide for the approval of a drug or biologic on the basis of a surrogate endpoint. Even if a drug qualifies for one or more of these programs, the FDA may later decide that the drug no longer meets the conditions for qualification or that the time period for FDA review or approval will be shortened. Generally, drugs that are eligible for these programs are those for serious or life-threatening conditions, those with the potential to address unmet medical needs and those that offer meaningful benefits over existing treatments. For example, based on results of the Phase 3 clinical trial(s) submitted in an NDA, upon the request of an applicant, the FDA may grant the NDA a priority review designation, which sets the target date for FDA action on the application at six months from the 60-day filing date, if the drug is anew molecular entity, rather than to the standard FDA review period of 10 months. Priority review is granted where preliminary estimates indicate that a product, if approved, has the potential to provide a safe and effective therapy where no satisfactory alternative therapy exists, or a significant improvement compared to marketed products is possible. Priority review designation does not change the scientific/medical standard for approval or the quality of evidence necessary to support approval.
Accelerated approval provides for an earlier approval for a new drug that is intended to treat a serious or life-threatening disease or condition upon a determination that the product has an effect on a surrogate endpoint that is reasonably likely to predict clinical benefit and is better than available therapy. A surrogate endpoint is a laboratory measurement or physical sign used as an indirect or substitute measurement representing a clinically meaningful outcome. The FDA will also take into account the severity, rarity or prevalence of the condition. As a condition of approval for drugs granted accelerated approval, one or more post-marketing confirmatory studies are required to confirm as predicted by the surrogate marker trial an effect on clinical benefit, which is defined as having a positive effect on how a patient feels, functions or survives.
19
Accelerated Review in the European Union
Under the Centralized Procedure in the European Union, the maximum timeframe for the evaluation of a marketing authorization application is 210 days (excluding clock stops, when additional written or oral information is to be provided by the applicant in response to questions asked by the CHMP). Accelerated evaluation might be granted by the CHMP in exceptional cases, when a medicinal product is expected to be of a major public health interest, defined by three cumulative criteria: the seriousness of the disease (e.g. heavy disabling or life-threatening diseases) to be treated; the absence or insufficiency of an appropriate alternative therapeutic approach; and anticipation of high therapeutic benefit. In this circumstance, EMA ensures that the opinion of the CHMP is given within 150 days of submission of the MAA, excluding clock stops.
Pharmaceutical Coverage, Pricing and Reimbursement
Significant uncertainty exists as to the coverage and reimbursement status of any drug products for which we obtain regulatory approval. In the United States and markets in other countries, sales of any products for which we receive regulatory approval for commercial sale depend in part on the availability of reimbursement from third-party payors. Third-party payors include government health administrative authorities, managed care providers, private health insurers and other organizations. The process for determining whether a payor will provide coverage for a drug product may be separate from the process for setting the price or reimbursement rate that the payor will pay for the drug product. Third-party payors may limit coverage to specific drug products on an approved list, or formulary, which might not include all of the FDA-approved drugs for a particular indication. Third-party payors are increasingly challenging the price and examining the medical necessity and cost-effectiveness of medical products and services, in addition to their safety and efficacy. We may need to conduct expensive pharmacoeconomic studies in order to demonstrate the medical necessity and cost effectiveness of our products, in addition to the costs required to obtain FDA approvals. The development of a product dossier and a Budget Impact Model may be helpful in assisting the payors in evaluating cost effectiveness. Our approved products may not be considered medically necessary or cost-effective. A payor’s decision to provide coverage for a drug product does not imply that an adequate reimbursement rate will be established. Adequate third-party reimbursement may not be available to enable us to maintain price levels sufficient to realize an appropriate return on our investment in product development.
There have been a number of federal and state proposals in recent years regarding the pricing of pharmaceutical products, government control and other changes to the healthcare system of the United States. The U.S. government enacted legislation providing a partial prescription drug benefit for Medicare beneficiaries. Government payment for some of the costs of prescription drugs may increase demand for any products for which we receive marketing approval; however, to obtain payments under this program, we are required to sell products to Medicare recipients through prescription drug plans operating pursuant to this legislation. These plans will likely negotiate discounted prices for our products. Additionally, the Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act (collectively, the “Affordable Care Act”) was enacted in 2010 with a goal of reducing the cost of healthcare and substantially changing the way healthcare is financed by both government and private insurers. Among other cost containment measures, the Affordable Care Act established:
|
· |
An annual, nondeductible fee on any entity that manufactures or imports certain branded prescription drugs and biologic agents; |
|
· |
A Medicare Part D coverage gap discount program, in which pharmaceutical manufacturers who wish to have their drugs covered under Part D must offer discounts to eligible beneficiaries during their coverage gap period (the “donut hole”); and |
|
· |
A formula that increases the rebates a manufacturer must pay under the Medicaid Drug Rebate Program. |
Since its enactment, there have been judicial and Congressional challenges to certain aspects of the Affordable Care Act. We expect that the current presidential administration and U.S. Congress will likely continue to seek to modify, repeal, or otherwise invalidate all, or certain provisions of, the Affordable Care Act. Most recently, the Tax Cuts and Jobs Act was enacted, which, among other things, removes penalties for not complying with Affordable Care Act’s individual mandate to carry health insurance. There is still uncertainty with respect to the impact President Trump’s administration and the U.S. Congress may have, if any, and any changes will likely take time to unfold, and could have an impact on coverage and reimbursement for healthcare items and services covered by plans that were authorized by the Affordable Care Act.
20
In addition, other legislative changes have been proposed and adopted since the Affordable Care Act was enacted. These changes include aggregate reductions to Medicare payments to providers of 2% per fiscal year, which went into effect on April 1, 2013 and, due to subsequent legislative amendments to the statute, will stay in effect through 2025 unless additional Congressional action is taken. Additionally, in January 2013, the American Taxpayer Relief Act of 2012 was signed into law, which, among other things, further reduced Medicare payments to several types of providers and increased the statute of limitations period for the government to recover overpayments to providers from three to five years. Recently there has been heightened governmental scrutiny over the manner in which manufacturers set prices for their marketed products, which has resulted in several Congressional inquiries and proposed bills designed to, among other things, reform government program reimbursement methodologies. Individual states in the United States have also become increasingly active in implementing regulations designed to control pharmaceutical product pricing, including price or patient reimbursement constraints, discounts, restrictions on certain product access and marketing cost disclosure and transparency measures, and, in some cases, designed to encourage importation from other countries and bulk purchasing. We expect that federal, state and local governments in the United States will continue to consider legislation to limit the growth of healthcare costs, including the cost of prescription drugs. Future legislation could limit payments for pharmaceuticals such as our products.
Moreover, payment methodologies, including payment for companion diagnostics, have been subject to changes due to healthcare legislation and regulatory initiatives. For example, CMS began bundling the Medicare payments for certain laboratory tests ordered while a patient received services in a hospital outpatient setting. Additionally, on April 1, 2014, the Protecting Access to Medicare Act of 2014, or PAMA, was signed into law, which, among other things, significantly alters the current payment methodology under the Clinical Laboratory Fee Schedule. Beginning on January 1, 2018, the Medicare payment rate for each clinical diagnostic lab test, with some exceptions, is equal to the weighted median private payer payment for the test, as calculated using data collected by applicable laboratories during the data collection period and reported to CMS during a specified data reporting period. Also under PAMA, CMS is required to adopt temporary billing codes to identify new clinical diagnostic laboratory tests and advanced diagnostic laboratory tests that do not already have unique diagnostic codes, and that have been cleared or approved by the FDA.
Different pricing and reimbursement schemes exist in other countries. In the European Community, governments influence the price of pharmaceutical products through their pricing and reimbursement rules and control of national health care systems that fund a large part of the cost of those products to consumers. Some jurisdictions operate positive and negative list systems under which products may only be marketed once a reimbursement price has been agreed. To obtain reimbursement or pricing approval, some of these countries may require the completion of clinical trials that compare the cost-effectiveness of a particular product candidate to currently available therapies. Other member states allow companies to fix their own prices for medicines, but monitor and control company profits. The downward pressure on health care costs in general, particularly prescription drugs, has become very intense. As a result, increasingly high barriers are being erected to the entry of new products. In addition, in some countries, cross-border imports from low-priced markets exert a commercial pressure on pricing within a country.
The marketability of any products for which we receive regulatory approval for commercial sale may suffer if the government and third-party payors fail to provide adequate coverage and reimbursement. In addition, emphasis on reducing the rate of healthcare spending in the United States has increased, and we expect will continue to increase the pressure on pharmaceutical pricing. There has been particular and increasing legislative interest in the United States with respect to drug pricing practices, particularly with respect to drugs that have been subject to relatively large price increases over relatively short time periods. Certain independent charitable foundations operate programs that provide grants to defray medical expenses (including cost-sharing obligations for drug treatments and health insurance premiums) for patients who meet certain financial need criteria and suffer from specific chronic illnesses or rare disorders. There has been recent enforcement interest regarding donations by pharmaceutical manufacturers to such foundations on the bases that such donations were used in part to guide patients to those donors’ products or that the donors obtained data on how the donations were used, including how often donations correlate to the frequency of referrals to donors’ products. There have been several U.S. Congressional inquiries and proposed bills designed to, among other things, bring more transparency to drug pricing, review the relationship between pricing and manufacturer patient programs, and reform government program reimbursement methodologies for drugs. Coverage policies and third-party reimbursement rates may change at any time. Even if favorable coverage and reimbursement status is attained for one or more products for which we receive regulatory approval, less favorable coverage policies and reimbursement rates may be implemented in the future. The implementation of cost containment measures or other healthcare reforms may prevent us from being able to generate revenue, attain profitability or commercialize our products.
21
Advertising and Promotion
The FDA and other U.S. federal regulatory agencies closely regulate the marketing and promotion of drugs through, among other things, the FDCA and the FDA’s implementing regulations and standards. The FDA’s review of marketing and promotional activities encompasses, but is not limited to, direct-to-consumer advertising, healthcare provider-directed advertising and promotion, sales representative communications to healthcare professionals, communications regarding unapproved or “off-label” uses, industry-sponsored scientific and educational activities and promotional activities involving the internet. A product cannot be commercially promoted before it is approved. After approval, product promotion can include only those claims relating to safety and effectiveness that are consistent with the labeling approved by the FDA. FDA regulations impose stringent restrictions on manufacturers’ communications regarding off-label uses. Failure to comply with applicable FDA requirements and restrictions regarding unapproved uses of a drug or for other violations of its advertising and labeling laws and regulations, may result in adverse publicity and enforcement action by the FDA, the Department of Justice or the Office of the Inspector General of the Department of Health and Human Services, as well as state authorities. A range of penalties are possible that could have significant commercial consequences, including product seizures, injunctions, civil and/or criminal fines and agreements that materially restrict the manner in which a company promotes or distributes its products or regulatory letters, which may require corrective advertising or other corrective communications to healthcare professionals.
Other Healthcare Laws and Compliance Requirements
We are subject to various laws targeting fraud and abuse in the healthcare industry, including anti-kickback laws and false claims laws. For example, in the United States, there are federal and state anti-kickback laws that prohibit the payment or receipt of kickbacks, bribes or other remuneration intended to induce the purchase or recommendation of healthcare products and services or reward past purchases or recommendations. Violations of these laws can lead to civil and criminal penalties, including fines, imprisonment and exclusion from participation in federal healthcare programs.
The federal Anti-Kickback Statute prohibits persons from knowingly and willfully soliciting, receiving, offering or paying remuneration, directly or indirectly, to induce either the referral of an individual, or the furnishing, recommending, or arranging for a good or service, for which payment may be made under a federal healthcare program, such as the Medicare and Medicaid programs. The reach of the Anti-Kickback Statute was broadened by the Affordable Care Act, which, among other things, amended the intent requirement of the federal Anti-Kickback Statute and the applicable criminal healthcare fraud statutes contained within 42 U.S.C. § 1320a-7b. Pursuant to the statutory amendment, a person or entity no longer needs to have actual knowledge of this statute or specific intent to violate it in order to have committed a violation. In addition, the Affordable Care Act provides that the government may assert that a claim including items or services resulting from a violation of the federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the civil False Claims Act (discussed below) or the civil monetary penalties statute. Many states have adopted laws similar to the federal Anti-Kickback Statute, some of which apply to the referral of patients for healthcare items or services reimbursed by any source, not only the Medicare and Medicaid programs.
The federal False Claims Act imposes liability on any person who, among other things, knowingly presents, or causes to be presented, a false or fraudulent claim for payment by a federal program, including federal healthcare programs. The “qui tam” provisions of the False Claims Act allow a private individual to bring civil actions on behalf of the federal government alleging that the defendant has submitted a false claim to the federal government, and to share in any monetary recovery. In addition, various states have enacted false claims laws analogous to the False Claims Act. Many of these state laws apply where a claim is submitted to any third-party payor and not merely a federal healthcare program. When an entity is determined to have violated the False Claims Act, it may be required to pay up to three times the actual damages sustained by the government, plus civil penalties.
In addition, a person who offers or transfers to a Medicare or Medicaid beneficiary any remuneration, including waivers of co-payments and deductible amounts (or any part thereof), that the person knows or should know is likely to influence the beneficiary’s selection of a particular provider, practitioner or supplier of Medicare or Medicaid payable items or services may be liable for civil monetary penalties of up to $15,270 for each wrongful act. Moreover, in certain cases, providers who routinely waive copayments and deductibles for Medicare and Medicaid beneficiaries can also be held liable under the Anti-kickback Statute and civil False Claims Act, which can impose additional penalties associated with the wrongful act. One of the statutory exceptions to the prohibition is non-routine, unadvertised waivers of copayments or deductible amounts based on individualized determinations of financial need or exhaustion of reasonable
22
collection efforts. The Office of Inspector General of the Department of Health and Human Services emphasizes, however, that this exception should only be used occasionally to address special financial needs of a particular patient. Although this prohibition applies only to federal healthcare program beneficiaries, the routine waivers of copayments and deductibles offered to patients covered by commercial payers may implicate applicable state laws related to, among other things, unlawful schemes to defraud, excessive fees for services, tortious interference with patient contracts and statutory or common law fraud. To the extent our patient assistance programs are found to be inconsistent with applicable laws, we may be required to restructure or discontinue such programs, or be subject to other significant penalties.
In addition to the laws described above, the Affordable Care Act also imposed new reporting requirements on drug manufacturers for payments made to physicians and teaching hospitals, as well as ownership and investment interests held by physicians and their immediate family members. Failure to submit required information may result in civil monetary penalties of up to an aggregate of $165,786 per year (or up to an aggregate of $1.105 million per year for “knowing failures”), for all payments, transfers of value or ownership or investment interests that are not timely, accurately and completely reported in an annual submission. Applicable drug manufacturers are required to collect data for each calendar year and submit reports to CMS by March 31st of each subsequent calendar year. In addition, there are also an increasing number of state laws that require manufacturers to make reports to states on pricing and marketing information. These laws may affect our sales, marketing, and other promotional activities by imposing administrative and compliance burdens on us.
For those marketed products which are covered in the United States by the Medicaid programs, we have various obligations, including government price reporting and rebate requirements, which generally require products be offered at substantial rebates/discounts to Medicaid and certain purchasers (including “covered entities” purchasing under the 340B Drug Discount Program). We are also required to discount such products to authorized users of the Federal Supply Schedule of the General Services Administration, under which additional laws and requirements apply. These programs require submission of pricing data and calculation of discounts and rebates pursuant to complex statutory formulas, as well as the entry into government procurement contracts governed by the Federal Acquisition Regulations, and the guidance governing such calculations is not always clear. Compliance with such requirements can require significant investment in personnel, systems and resources, but failure to properly calculate our prices, or offer required discounts or rebates could subject us to substantial penalties. One component of the rebate and discount calculations under the Medicaid and 340B programs, respectively, is the “additional rebate”, a complex calculation which is based, in part, on the rate at which a branded drug price increases over time more than the rate of inflation (based on the CPI-U). This comparison is based on the baseline pricing data for the first full quarter of sales associated with a branded drug’s NDA, and baseline data cannot generally be reset, even on transfer of the NDA to another manufacturer. This “additional rebate” calculation can, in some cases where price increase have been relatively high versus the first quarter of sales of the NDA, result in Medicaid rebates up to 100% of a drug’s “average manufacturer price” and 340B prices of one penny. Subject to the control of Directive 89/105/EEC, pricing and reimbursement in the EU/EEA (European Economic Area) is governed by national rules and policy and may vary from Member State to Member State.
Also, the Health Insurance Portability and Accountability Act of 1996 (“HIPAA”) created several new federal crimes, including health care fraud and false statements relating to health care matters. Most healthcare providers who are expected to prescribe our products and from whom we obtain patient health information are subject to privacy and security requirements under HIPAA. Although we are not directly subject to HIPAA, we could be subject to criminal penalties if we knowingly obtain individually identifiable health information from a HIPAA-covered entity in a manner that is not authorized or permitted by HIPAA. Similar to the federal Anti-Kickback Statute, a person or entity does not need to have actual knowledge of the statute or specific intent to violate it in order to have committed a violation. Other countries also have, or are developing, laws governing the collection, use and transmission of personal information. For example, the EU Data Privacy Directive (95/46/EC), which will be replaced on May 28, 2018 by the more restrictive General Data Protection Regulation (Regulation (EU) 2016/679) and the Swiss Federal Act on Data Protection, regulate the processing of personal data within the European Union and between countries in the European Union and countries outside of the European Union, including the U.S. Failure to provide adequate privacy protections and maintain compliance with the new EU-U.S. Privacy Shield framework, which will replace the previous safe harbor mechanisms, could jeopardize business transactions across borders and result in significant penalties, These laws could create liability for us or increase our cost of doing business.
23
Regulation of Diagnostic Tests
In the United States, the FDCA and its implementing regulations, and other federal and state statutes and regulations govern, among other things, medical device design and development, non-clinical and clinical testing, premarket clearance or approval, registration and listing, manufacturing, labeling, storage, advertising and promotion, sales and distribution, export and import, and post-market surveillance. Diagnostic tests are classified as medical devices under the FDCA. Unless an exemption applies, diagnostic tests require marketing clearance or approval from the FDA prior to commercial distribution. The two primary types of FDA marketing authorization applicable to a medical device are premarket notification, also called 510(k) clearance, and premarket approval, or PMA approval. Because the diagnostic tests being developed by our third-party collaborators are of substantial importance in preventing impairment of human health, they are subject to the PMA approval process.
PMA applications must be supported by valid scientific evidence, which typically requires extensive data, including technical, non-clinical, clinical and manufacturing data, to demonstrate to the FDA’s satisfaction the safety and effectiveness of the device. For diagnostic tests, a PMA application typically includes data regarding analytical and clinical validation studies. As part of its review of the PMA, the FDA will conduct a pre-approval inspection of the manufacturing facility or facilities to ensure compliance with the Quality System Regulation, or QSR, which requires manufacturers to follow design, testing, control, documentation and other quality assurance procedures. FDA review of an initial PMA application is required by statute to take between six to ten months, although the process typically takes longer, and may require several years to complete. If the FDA evaluations of both the PMA application and the manufacturing facilities are favorable, the FDA will either issue an approval letter or an approvable letter, which usually contains a number of conditions that must be met in order to secure the final approval of the PMA. If the FDA’s evaluation of the PMA or manufacturing facilities is not favorable, the FDA will deny approval of the PMA or issue a not approvable letter. A not approvable letter will outline the deficiencies in the application and, where practical, will identify what is necessary to make the PMA approvable. The FDA may also determine that additional clinical trials are necessary, in which case the PMA approval may be delayed for several months or years while the trials are conducted and then the data submitted in an amendment to the PMA. Once granted, PMA approval may be withdrawn by the FDA if compliance with post approval requirements, conditions of approval or other regulatory standards is not maintained or problems are identified following initial marketing.
We and our third-party collaborators who are developing companion diagnostics work cooperatively to generate the data required for submission with a PMA application, and remain in close contact with the Center for Devices and Radiological Health (“CDRH”) at the FDA to ensure that any changes in requirements are incorporated into the development plans. Meetings with the FDA with regard to our drug product candidates, as well as companion diagnostic product candidates, typically include representatives from the Center for Drug Evaluation and Research and CDRH when appropriate to ensure that the NDA and PMA submissions are coordinated to enable FDA to conduct a parallel review of both submissions. The FDA has issued guidance documents addressing the development and approval process for “In Vitro Companion Diagnostic Devices.” According to these guidance documents, for novel therapeutic products such as our product candidates, the PMA for a companion diagnostic device should generally be developed and approved or cleared contemporaneously with the therapeutic.
In the EEA, in vitro medical devices are required to conform to the essential requirements of the E.U. Directive on in vitro diagnostic medical devices (Directive No 98/79/EC, as amended). To demonstrate compliance with the essential requirements, the manufacturer must undergo a conformity assessment procedure. The conformity assessment varies according to the type of medical device and its classification. For low-risk devices, the conformity assessment can be carried out internally, but for higher risk devices it requires the intervention of an accredited EEA Notified Body. If successful, the conformity assessment concludes with the drawing up by the manufacturer of an EC Declaration of Conformity entitling the manufacturer to affix the CE mark to its products and to sell them throughout the EEA. The data generated for the U.S. registration will be sufficient to satisfy the regulatory requirements for the European Union and other countries.
Patents and Proprietary Rights
The proprietary nature of, and protection for, our product candidates, processes and know-how are important to our business. Our success depends in part on our ability to protect the proprietary nature of our product candidates, technology, and know-how, to operate without infringing on the proprietary rights of others, and to prevent others from infringing our proprietary rights. We seek patent protection in the United States and internationally for our product
24
candidates and other technology. Our policy is to patent or in-license the technology, inventions and improvements that we consider important to the development of our business. We also rely on trade secrets, know-how and continuing innovation to develop and maintain our competitive position. We cannot be sure that patents will be granted with respect to any of our pending patent applications or with respect to any patent applications filed by us in the future, nor can we be sure that any of our existing patents or any patents granted to us in the future will be commercially useful in protecting our technology.
In June 2011, we obtained an exclusive, worldwide license from Pfizer to develop and commercialize rucaparib. U.S. Patent 6,495,541, and its equivalent counterparts issued in dozens of countries, directed to the rucaparib composition of matter, expire in 2020 and are potentially eligible for up to five years patent term extension in various jurisdictions. We believe that patent term extension under the Drug Price Competition and Patent Term Restoration Act of 1984 (the “Hatch-Waxman Act”) could be available to extend our patent exclusivity for rucaparib to the fourth quarter of 2023 in the United States. In Europe, we believe that patent term extension under a supplementary protection certificate could be available for an additional five years to at least 2025. In April 2012, we obtained an exclusive license from AstraZeneca under a family of patents and patent applications which will permit the development and commercialization of rucaparib for certain methods of treating patients with PARP inhibitors. Additionally, other patents and patent applications are directed to methods of making, methods of using, dosing regimens, various salt and polymorphic forms and formulations and have expiration dates ranging from 2020 through potentially 2035, including the camsylate salt/polymorph patent family licensed from Pfizer, which expires in 2031 and a patent application directed to high dosage strength rucaparib tablets that, if issued, will expire in 2035. As of February 27, 2018, the rucaparib camsylate salt patent was issued in 47 countries to date (including US and Europe), with applications pending in 9 countries, and the rucaparib composition of matter patent was issued in 48 countries. We are aware of a number of challenges of salt and polymorph patents. Two oppositions were filed in the granted European counterpart of the rucaparib camsylate salt/polymorph patent on June 20, 2017. European oppositions are commonly filed against patents related to pharmaceutical products. The grounds of opposition related to Rubraca were lack of novelty and lack of inventive step. The novelty and inventive step challenges are based on prior art references (or closely related disclosures) that were previously raised by the European patent examiner during prosecution of the application. The claims of the granted patent were found to be patentable over this prior art. While the ultimate results of patent challenges can be difficult to predict, we believe a number of factors, including a constellation of unexpected properties, support the novelty and non-obviousness of our rucaparib camsylate salt/polymorph composition of matter patent. Based on these facts, we believe, a successful challenge of that patent would be difficult.
We obtained rights to lucitanib by acquiring EOS in November 2013, along with its license agreements with Advenchen and Servier. In October 2008, EOS entered into an exclusive license agreement with Advenchen to develop and commercialize lucitanib on a global basis, excluding China. In September 2012, EOS entered into a collaboration and license agreement with Servier whereby EOS sublicensed to Servier exclusive rights to develop and commercialize lucitanib in all countries outside of the U.S., Japan and China. Composition of matter and method of use patent protection for lucitanib and a group of structurally-related compounds is issued in the U.S., Europe and Japan and is issued or pending in other jurisdictions. In the U.S., the composition of matter patent will expire in 2030, and in other jurisdictions, it expires in 2028. We believe that patent term extension could be available to extend our composition of matter patent up to five years beyond the scheduled expiration under the Hatch-Waxman Act. Additionally, patents or patent applications directed to methods of manufacturing lucitanib are issued or pending in the United States, Europe, Japan, and China.
In May 2010, we acquired an exclusive, worldwide license to rociletinib from Celgene. U.S. Patent 8,975,927, directed to rociletinib composition of matter, expires in 2032 and U.S. Patent 9,108,927, directed to rociletinib HBr salts and polymorphs, expires in 2033. Other patent applications are pending that claim rociletinib generically that, if issued, would have expiration dates in 2029. In January 2013, we acquired from Gatekeeper Pharmaceuticals, Inc. an exclusive worldwide sub-license to a Dana Farber patent family having claims directed to wild-type sparing irreversible EGFR inhibitors, such as rociletinib. We or our licensors have filed additional patent applications related to rociletinib methods of use, metabolites, combinations, diagnostic methods and dosing regimens.
In addition, we intend to seek patent protection whenever available for any products or product candidates and related technology we acquire in the future.
The patent positions of pharmaceutical firms like us are generally uncertain and involve complex legal, scientific and factual questions. In addition, the coverage claimed in a patent application can be significantly reduced before the patent
25
is issued. Consequently, we do not know whether any of the product candidates we acquire or license will gain patent protection or, if any patents are issued, whether they will provide significant proprietary protection or will be challenged, circumvented or invalidated. Because patent applications in the United States and certain other jurisdictions are maintained in secrecy for 18 months, and since publication of discoveries in the scientific or patent literature often lags behind actual discoveries, until that time we cannot be certain that we were the first to file any patent application related to our product candidates. Moreover, we may have to participate in interference proceedings declared by the United States Patent and Trademark Office (“U.S. PTO”) to determine priority of invention or in opposition or other third-party proceedings in the U.S. or a foreign patent office, either of which could result in substantial cost to us, even if the eventual outcome is favorable to us. There can be no assurance that the patents, if issued, would be held valid by a court of competent jurisdiction. An adverse outcome in a third-party patent dispute could subject us to significant liabilities to third parties, require disputed rights to be licensed from third parties or require us to cease using specific compounds or technology.
The term of individual patents depends upon the legal term of the patents in the countries in which they are obtained. In most countries in which we file, the patent term is 20 years from the earliest date of filing a non-provisional patent application. In the United States, a patent’s term may be lengthened by patent term adjustment, which compensates a patentee for administrative delays by the U.S. PTO in granting a patent, or may be shortened if a patent is terminally disclaimed over another patent.
The patent term of a patent that covers an FDA-approved drug may also be eligible for patent term extension, which permits patent term restoration as compensation for the patent term lost during the FDA regulatory review process. The Hatch-Waxman Act permits a patent term extension of up to five years beyond the expiration of the patent. The length of the patent term extension is related to the length of time the drug is under regulatory review. Patent extension cannot extend the remaining term of a patent beyond a total of 14 years from the date of product approval and only one patent applicable to an approved drug may be extended. Similar provisions are available in Europe and other non-U.S. jurisdictions to extend the term of a patent that covers an approved drug. In the future, if and when our pharmaceutical products receive FDA approval, we expect to apply for patent term extensions on patents covering those products.
To protect our rights to any of our issued patents and proprietary information, we may need to litigate against infringing third parties, or avail ourselves of the courts or participate in hearings to determine the scope and validity of those patents or other proprietary rights. These types of proceedings are often costly and could be very time-consuming to us, and we cannot assure you that the deciding authorities will rule in our favor. An unfavorable decision could allow third parties to use our technology without being required to pay us licensing fees or may compel us to license needed technologies to a third-party. Such a decision could even result in the invalidation or a limitation in the scope of our patents or forfeiture of the rights associated with our patents or pending patent applications. To the extent prudent, we intend to bring litigation against third parties that we believe are infringing one or more of our patents.
In addition, we have sought and intend to continue seeking orphan drug status whenever it is available. If a product which has an orphan drug designation subsequently receives the first regulatory approval for the indication for which it has such designation, the product is entitled to orphan exclusivity, meaning that the applicable regulatory authority may not approve any other applications to market the same drug for the same indication, except in certain very limited circumstances, for a period of seven years in the United States and ten years in the European Union. Orphan drug designation does not prevent competitors from developing or marketing different drugs for an indication.
We also rely on trade secret protection for our confidential and proprietary information. No assurance can be given that others will not independently develop substantially equivalent proprietary information and techniques or otherwise gain access to our trade secrets or disclose such technology, or that we can meaningfully protect our trade secrets. However, we believe that the substantial costs and resources required to develop technological innovations will help us to protect the competitive advantage of our products.
It is our policy to require our employees, consultants, outside scientific collaborators, sponsored researchers and other advisors to execute confidentiality agreements upon the commencement of employment or consulting relationships with us. These agreements provide that all confidential information developed or made known to the individual during the course of the individual’s relationship with us is to be kept confidential and not disclosed to third parties except in specific circumstances. In the case of employees, the agreements provide that all inventions conceived by the individual
26
shall be our exclusive property. There can be no assurance, however, that these agreements will provide meaningful protection or adequate remedies for our trade secrets in the event of unauthorized use or disclosure of such information.
Manufacturing
We currently contract with third parties for the manufacture of our product candidates for non-clinical studies and clinical trials and intend to do so in the future. We currently have long-term agreements with third-party contract manufacturing organizations (“CMOs”) for the production of the active ingredient and final product for Rubraca. We do not own or operate manufacturing facilities for the production of clinical quantities of our product candidates. We currently have no plans to build our own clinical or commercial scale manufacturing capabilities. To meet our projected needs for commercial manufacturing, we are working with our current third party suppliers to increase their scale of production and we are in the process of evaluating additional second source suppliers. Although we rely on contract manufacturers, we have personnel with extensive manufacturing experience to oversee the relationships with our contract manufacturers.
We have developed the process for manufacturing Rubraca’s active pharmaceutical ingredient (“API”) to a degree sufficient to meet clinical demands and, as production capacity is increased as described below under “Lonza Agreement,” projected commercial requirements. Manufacturing of Rubraca API is being performed at a single CMO. The Rubraca drug product formulation and manufacturing process to produce that formulation have been developed to a degree sufficient to meet clinical demands and projected commercial requirements. A single third-party CMO capable of both formulation development and drug product manufacturing is currently producing Rubraca drug product. Our operating plan for the next 12 months includes a significant investment in inventory to meet the projected commercial requirements for Rubraca.
To date, our third-party manufacturers have met our manufacturing requirements. We expect third-party manufacturers to be capable of providing sufficient quantities of our product candidates to meet anticipated full scale commercial demands.
Lonza Agreement
On October 3, 2016, we entered into an agreement with Lonza Ltd (“Lonza”) for the long-term manufacture and supply of the API for rucaparib.
Under this agreement, Lonza will be a non-exclusive manufacturer of the rucaparib API during the 10 year term of the agreement. Lonza will construct, in an existing Lonza facility, a production train that will be exclusively dedicated to the manufacture of the rucaparib API. The dedicated production train will provide manufacturing capacity to meet our currently anticipated needs for commercial supply of rucaparib API. We are obligated to make scheduled capital program fee payments towards capital equipment and other costs associated with the construction of the dedicated production train and, once the facility is operational, to pay a fixed facility fee each quarter for the duration of the term of the agreement. The dedicated production train is estimated to be completed during the fourth quarter of 2018 at which time Lonza will begin producing API under this agreement.
Lonza will manufacture and store an advanced intermediate to be used in the subsequent production of the rucaparib API. We will pay fixed fees on a per kilogram basis for quantities of the advanced intermediate and the rucaparib API ordered by us, subject to certain adjustments. Until the dedicated facility is completed and operationally qualified, Lonza will manufacture the rucaparib API in existing Lonza facilities at pricing established in the agreement.
Either party may terminate the agreement due to a material breach of the agreement by the other party, subject to prior written notice and a cure period. We may terminate the agreement, subject to 90 days’ prior written notice, in the event rucaparib is withdrawn from the market for certain reasons. In the event of such a termination by us, or termination by Lonza due to material breach by us, we are obligated to compensate Lonza for any services rendered, or for which costs have been incurred by Lonza in anticipation of services to be provided to us, and to pay to Lonza the remaining amount of any capital program fees and quarterly fixed facility fees for the remainder of the term of the agreement. In the event we terminate the agreement due to material breach by Lonza, Lonza is obligated to repay all or a portion of the capital program fees previously paid by us.
27
The active pharmaceutical ingredient for lucitanib is currently being produced by a third-party supplier. To date, the current production process has been sufficient to satisfy immediate clinical demands. We may undertake additional development work to further optimize the active pharmaceutical ingredient manufacturing process. The finished drug product for lucitanib is currently being manufactured at a CMO. The current product and process are sufficiently developed to meet immediate clinical demands. Additional scale-up work and/or additional production capacity will be necessary to support larger clinical development or commercialization requirements.
The active pharmaceutical ingredient for rociletinib is currently being manufactured by one CMO. The current drug substance production process has already been sufficiently developed to satisfy immediate clinical demands. We have engaged a single CMO capable of both formulation development and drug product manufacturing. The current drug product production process has already been sufficiently developed to satisfy immediate clinical demands. Additional scale-up work and/or additional production capacity may be necessary to support larger clinical development or commercialization requirements.
Commercial Operations
Our commercial organization in the U.S. is in place and supporting the commercial sale of Rubraca. We believe the U.S. oncology market for Rubraca in both of its approved indications is addressable with a targeted sales and marketing organization, with capabilities that include the management of key accounts such as managed care organizations, group-purchasing organizations, oncology group networks and government accounts. We sell Rubraca through a limited distribution network consisting of select number of specialty pharmacies and distributors. Healthcare providers prescribe Rubraca to patients and the specialty pharmacies and distributors dispense Rubraca directly to patients. We intend to continue promoting Rubraca ourselves in the U.S. for its current indications and any additional indications we may obtain in the future. We retain the rights to Rubraca in the rest of the world. The MAA submission with the EMA for an ovarian cancer treatment indication is currently under review. If approved in the EU, we intend to commercialize rucaparib on our own and we are building our commercial and medical affairs infrastructure in Europe. The leadership of those teams is in place, and we will hire field sales personnel as pricing and reimbursement decisions are made and approvals are received.
Customers
We are currently approved to sell Rubraca in the U.S. market. We distribute our product principally through a limited number of specialty distributor and specialty pharmacy providers, collectively, our customers. Our customers subsequently sell our products to patients and health care providers, at which time we recognize the associated revenue.
Our customers, which distribute our product, consist of three specialty distributors and four specialty pharmacy providers. Furthermore, we do not believe the loss of one of these customers would significantly impact the ability to distribute our product as we expect that sales volume would be absorbed evenly by the remaining customers.
Employees
As of February 16, 2018, we employed 360 full-time employees. None of our employees is represented by labor unions, and a very small number of international employees are covered by collective bargaining agreements. We consider our relationship with our employees to be good.
As part of the Compensation Committee’s annual review of overall employee compensation, effective March 1, 2018, in order to align their base salary compensation with the 50th percentile of similarly situated employees at the Company’s peer group companies, the Compensation Committee approved for Mr. Mahaffy a base salary increase of 7.1% to $696,300, for Mr. Muehl a base salary increase of 15.7% to $433,800, for Ms. Ivers-Read a base salary increase of 3.0% to $450,246, for Dr. Rolfe a base salary increase of 4.1% to $489,300 and for Mr. Hooks a base salary increase of 5.3% to $421,300. Also, the Compensation Committee approved new bonus targets (as a percentage of their new annual base salaries) for each of these executive officers as follows: for Mr. Mahaffy, 70%; for Ms. Ivers-Read and Dr. Rolfe, 50%; and for Messrs. Muehl and Hooks, 45%. In addition, as part of the annual grants of equity awards to employees of the Company, the Compensation Committee approved the following equity awards to such executive officers to be made on March 1, 2018: Mr. Mahaffy, options to purchase 120,000 shares of the Company’s common stock; Mr. Muehl, options to purchase 9,000 shares of the Company’s common stock and 9,000 restricted stock units (“RSUs”); Ms. Ivers-Read, options to purchase 11,000 shares of the Company’s common stock and 11,000 restricted
28
stock units; Dr. Rolfe, options to purchase 11,000 shares of the Company’s common stock and 11,000 restricted stock units; and Mr. Hooks, options to purchase 9,000 shares of the Company’s common stock and 9,000 restricted stock units.
Research and Development
We invested $142.5 million, $251.1 million and $269.3 million in research and development during the years ended December 31, 2017, 2016 and 2015, respectively.
About Clovis
We were incorporated under the laws of the State of Delaware in April 2009 and completed our initial public offering of our common stock in November 2011. Our common stock is listed on the NASDAQ Global Select Market under the symbol “CLVS.” Our principal executive offices are located at 5500 Flatiron Parkway, Suite 100, Boulder, Colorado 80301, and our telephone number is (303) 625-5000. We maintain additional offices in San Francisco, California, Cambridge, UK, and Milan, Italy. Our website address is www.clovisoncology.com. Our website and the information contained on, or that can be accessed through, the website will not be deemed to be incorporated by reference in, and are not considered part of, this report.
Available Information
As a public company, we file reports and proxy statements with the Securities and Exchange Commission (“SEC”). These filings include our annual reports on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K and proxy statements on Schedule 14A, as well as any amendments to those reports and proxy statements, and are available free of charge through our website as soon as reasonably practicable after we file them with, or furnish them to, the SEC. Once at www.clovisoncology.com, go to Investors & News/SEC Filings to locate copies of such reports. You may also read and copy materials that we file with SEC at the SEC’s Public Reference Room at 100 F Street, NE, Washington, DC 20549. You may obtain information on the operation of the Public Reference Room by calling the SEC at 1-800-SEC-0330. The SEC also maintains a website at www.sec.gov that contains reports, proxy statements and other information regarding us and other issuers that file electronically with the SEC.
Our business faces significant risks and uncertainties. Certain factors may have a material adverse effect on our business prospects, financial condition and results of operations, and you should carefully consider them. Accordingly, in evaluating our business, we encourage you to consider the following discussion of risk factors, in its entirety, in addition to other information contained in or incorporated by reference into this Annual Report on Form 10-K and our other public filings with the SEC. Other events that we do not currently anticipate or that we currently deem immaterial may also affect our business, prospects, financial condition and results of operations.
Risks Related to Our Financial Position and Capital Requirements
We have incurred significant losses since our inception and anticipate that we will continue to incur losses for the foreseeable future. We have generated only modest historical revenues, which makes it difficult to assess our future viability.
We are a biopharmaceutical company with a limited operating history. Biopharmaceutical product development is a highly speculative undertaking and involves a substantial degree of risk. We have focused primarily on in-licensing and developing our product candidates. We are not profitable and have incurred losses in each year since our inception in April 2009. We have only a limited operating history upon which you can evaluate our business and prospects. There are many risks and uncertainties frequently encountered by companies in new and rapidly evolving fields, particularly in the biopharmaceutical area. Three of our product candidates, CO-101, CO-1686 (rociletinib) and CO-3810 (lucitanib), encountered development and/or regulatory setbacks after initial promising data, leading us to discontinue enrollment in then-ongoing clinical trials. We have received regulatory approval to market Rubraca in the U.S., but we do not yet know whether it will be approved in other jurisdictions or whether it will achieve market acceptance and be commercially successful. We have generated only modest revenues from product sales to date. We continue to incur
29
significant research and development and other expenses related to our ongoing operations. For the years ended December 31, 2017, 2016 and 2015, we had net losses of $346.4 million, $349.1 million and $352.9 million, respectively. As of December 31, 2017, we had an accumulated deficit of $1,447.4 million. We expect to continue to incur losses for the foreseeable future. As such, we are subject to all of the risks incident to the development of new biopharmaceutical products and related companion diagnostics, and we may encounter unforeseen expenses, difficulties, complications, regulatory scrutiny, delays and other unknown factors that may adversely affect our business. If any of our product candidates fail in clinical trials or do not gain regulatory approval, or if Rubraca or any of our product candidates, if approved, fail to achieve market acceptance, we may never become profitable. Even if we achieve profitability in the future, we may not be able to sustain profitability in subsequent periods. Our prior losses, combined with expected future losses, have had and will continue to have an adverse effect on our stockholders’ equity and working capital.
We will require substantial additional funding which may not be available to us on acceptable terms, or at all. If we fail to obtain additional financing, we may be unable to complete the development and commercialization of our product candidates or continue our development programs.
Our operations have consumed substantial amounts of cash since inception. We expect to continue to spend substantial amounts to advance the clinical development of our product candidates and launch and commercialize any product candidates for which we receive regulatory approval, including building our own commercial organizations to address certain markets.
Based on current estimates, we believe that our existing cash, cash equivalents and available-for-sale securities will allow us to fund our operating plan through at least the next 12 months. We do not have any material committed external source of funds or other support for our development efforts.
Until we can generate a sufficient amount of product revenue to finance our cash requirements, which we may never do in sufficient amounts, we expect to finance future cash needs through a combination of public or private equity offerings, collaborations, strategic alliances and other similar licensing arrangements. We cannot be certain that additional funding will be available on acceptable terms, or at all. If we are unable to raise additional capital in sufficient amounts or on terms acceptable to us, we may have to significantly delay, scale back or discontinue the development or commercialization of one or more of our product candidates, or our plans for acquisition or in-license of new product candidates. We may also seek collaborators for one or more of our current or future product candidates on terms that are less favorable than might otherwise be available. Any of these events could significantly harm our business, financial condition and prospects.
Servicing our long-term debt requires a significant amount of cash, and we may not have sufficient cash flow from our business to pay our substantial debt.
In September 2014, we completed a private placement of $287.5 million aggregate principal amount of 2.5% convertible senior notes due 2021 (the “Notes”), resulting in net proceeds to the Company of $278.3 million after deducting offering expenses. The Notes are governed by the terms of the indenture between the Company, as issuer, and The Bank of New York Mellon Trust Company, N.A., as trustee. Interest is payable on the Notes semi-annually, and the Notes mature on September 15, 2021, unless redeemed, repurchased or converted prior to that date. In addition, if, as defined by the terms of the indenture, a fundamental change occurs, holders of the Notes may require us to repurchase for cash all or any portion of their Notes at a purchase price equal to 100% of the principal amount of the Notes to be repurchased plus accrued and unpaid interest, if any, to, but excluding, the fundamental change repurchase date. As of December 31, 2017, all $287.5 million principal amount of the Notes remained outstanding.
Our ability to make scheduled payments of interest and principal on the Notes, or to pay the repurchase price for the Notes on a fundamental change, depends on our future performance, which is subject to economic, financial, competitive and other factors beyond our control. We may not have sufficient cash in the future to service our debt. If we are unable to generate such cash flow or secure additional sources of funding, we may be required to adopt one or more alternatives, such as restructuring debt or obtaining additional equity capital on terms that may be onerous or highly dilutive. Our ability to refinance our indebtedness will depend on the capital markets and our financial condition at such time. We may not be able to engage in any of these activities or engage in these activities on desirable terms, which could result in a default on our debt obligations.
30
We and certain of our officers and directors have been named as defendants in several lawsuits that could result in substantial costs and divert management’s attention.
We and certain of our officers have been named as defendants in a number of lawsuits that generally allege that we and certain of our officers violated federal securities laws by making allegedly false and misleading statements regarding the progress toward FDA approval and the potential for market success of rociletinib. Some of these lawsuits have been settled while others remain outstanding and others may still be brought. See “Part I, Item 3-Legal Proceedings” in this report.
We intend to engage in a vigorous defense of these lawsuits; however, we are unable to predict the outcome of these matters at this time. If we are not successful in our defense of these litigation matters, we could be forced to make significant payments to, or enter into other settlements with, our security holders and their lawyers (and in certain circumstances reimburse costs and expenses incurred by the underwriters), and such payments or settlement arrangements could have a material adverse effect on our business, operating results and financial condition. For example, we could suffer a significant adverse impact on our reputation and divert management’s attention and resources from other priorities, any of which could have a material adverse effect on our business. In addition, any of these matters could require payments that are not covered by, or exceed the limits of, our available directors’ and officers’ liability insurance, which could have a material adverse effect on our operating results or financial condition. We will not receive any further contributions from our insurance carriers for any amounts (including damages, settlement costs or legal fees) relating to the Company’s regulatory update announcement in November 2015 that the FDA requested additional clinical data on the efficacy and safety of rociletinib.
Additional lawsuits with similar claims may be filed by other parties against us and our officers and directors. Even if such claims are not successful, these lawsuits or other future similar actions, or other regulatory inquiries or investigations, may result in substantial costs and have a significant adverse impact on our reputation and divert management’s attention and resources, which could have a material adverse effect on our business, operating results or financial condition.
The recently passed comprehensive tax reform bill could adversely affect our business and financial condition.
On December 22, 2017, President Trump signed into law new legislation that significantly revises the Internal Revenue Code of 1986, as amended. The newly enacted federal income tax law, among other things, contains significant changes to corporate taxation, including reduction of the corporate tax rate from a top marginal rate of 35% to a flat rate of 21%, limitation of the tax deduction for interest expense to 30% of adjusted earnings (except for certain small businesses), limitation of the deduction for net operating losses to 80% of current year taxable income and elimination of net operating loss carrybacks, one time taxation of offshore earnings at reduced rates regardless of whether they are repatriated, elimination of U.S. tax on foreign earnings (subject to certain important exceptions), immediate deductions for certain new investments instead of deductions for depreciation expense over time, and modifying or repealing many business deductions and credits (including reducing the business tax credit for certain clinical testing expenses incurred in the testing of certain drugs for rare diseases or conditions generally referred to as “orphan drugs”). Notwithstanding the reduction in the corporate income tax rate, the overall impact of the new federal tax law is uncertain, and our business and financial condition could be adversely affected. In addition, it is uncertain if and to what extent various states will conform to the newly enacted federal tax law. The impact of this tax reform on holders of our common stock is also uncertain and could be adverse. Investors should consult with their legal and tax advisors with respect to this legislation and the potential tax consequences of investing in or holding our common stock.
Risks Related to Our Business and Industry
We are highly dependent on the commercial success of Rubraca in the U.S.; Rubraca may not achieve market acceptance and may not be commercially successful and we may not attain profitability and positive cash flow from operations.
On December 19, 2016, the FDA granted approval for Rubraca as monotherapy for the treatment of patients with deleterious BRCA mutation (germline and/or somatic) associated advanced ovarian cancer, who have been treated with two or more chemotherapies, and selected for therapy based on an FDA approved companion diagnostic for Rubraca. Our MAA submitted to the EMA for an ovarian cancer treatment indication is currently under review by the CHMP, and in February 2018, the CHMP communicated to us their intention to hold a final vote on the treatment indication at their
31
March 2018 meeting. Rubraca is commercially available in the U.S. The degree of market acceptance and the commercial success of Rubraca will depend on a number of factors, including:
|
· |
the effectiveness of our sales and marketing strategy and operations; |
|
· |
maintaining compliance with all regulatory requirements applicable to Rubraca and our commercial activities, including the post-marketing requirements and post-marketing commitments required by the FDA and, if approved in Europe, the EMA, to verify Rubraca’s clinical benefit or safety by completing certain confirmatory trials, pharmacology studies and additional diagnostic development; |
|
· |
the acceptance of Rubraca by patients and the medical community and the availability, perceived advantages and relative cost, safety and efficacy of alternative and competing products and therapies; |
|
· |
the continued acceptable safety profile of Rubraca and the occurrence of any unexpected side effects, adverse reactions or misuse, or any unfavorable publicity in these areas; |
|
· |
the ability of our third-party manufacturers to manufacture commercial supplies of Rubraca, to remain in good standing with regulatory agencies, and to develop, validate and maintain commercially viable manufacturing processes that are, to the extent required, compliant with current good manufacturing practice (“cGMP”) regulations; |
|
· |
the availability of coverage and adequate reimbursement from managed care plans, private health insurers and other third party payors and the willingness and ability of patients to pay for Rubraca; |
|
· |
the development or commercialization of competing products or therapies; |
|
· |
marketing and distribution support for Rubraca, including the degree to which the approved labeling supports promotional initiatives for commercial success; |
|
· |
the actual market size for Rubraca, which may be different than expected; |
|
· |
our ability to enforce our intellectual property rights in and to Rubraca; |
|
· |
our ability to avoid third party patent interference or patent infringement claims; and |
|
· |
our ability to obtain regulatory approvals to commercialize Rubraca in markets outside of the U.S. |
As many of these factors are beyond our control, we cannot assure you that we will ever be able to generate meaningful revenue through the sale of Rubraca. In addition, we may experience significant fluctuations in sales of Rubraca from period to period. We currently do not have any other product candidates in active development though we are exploring rucaparib in other indications. Any inability on our part to successfully commercialize Rubraca in the United States and any foreign territories where it may be approved, or any significant delay in such approvals, could have a material adverse impact on our ability to execute upon our business strategy and, ultimately, to generate sufficient revenues from Rubraca to reach or maintain profitability or sustain our anticipated levels of operations.
Rubraca may cause undesirable side effects or have other properties that could limit its commercial potential.
If we or others identify previously unknown side effects or if known side effects are more frequent or severe than in the past, then:
|
· |
sales of Rubraca may decline; |
|
· |
regulatory approvals for Rubraca may be restricted or withdrawn; |
|
· |
we may decide to, or be required to, send product warning letters or field alerts to physicians, pharmacists and hospitals; |
|
· |
additional nonclinical or clinical studies, changes in labeling or changes to manufacturing processes, specifications and/or facilities may be required; |
|
· |
government investigations or lawsuits, including class action suits, may be brought against us; and |
|
· |
our reputation may suffer. |
32
Any of the above occurrences would harm or prevent sales of Rubraca, increase our expenses and impair our ability to successfully commercialize Rubraca. As Rubraca is commercially available, it may be used in a wider population and in a less rigorously controlled environment than in clinical studies. As a result, regulatory authorities, healthcare practitioners, third-party payors or patients may perceive or conclude that the use of Rubraca is associated with previously unknown serious adverse effects, undermining our commercialization efforts.
If our sales, marketing and distribution capabilities for Rubraca or our product candidates for which we obtain marketing approval are inadequate, we may be unable to generate revenue from sales of our products.
Prior to the launch of Rubraca, we had not commercialized any drug products as a company. To achieve commercial success for Rubraca and any product candidate that may be approved by the FDA or comparable foreign regulatory authorities, we must continue to expand our sales, marketing, managerial and other nontechnical capabilities or make arrangements with third parties to perform these services. We will be competing with companies that currently have extensive, well-funded, and more experienced sales and marketing operations. We may be unable to compete successfully against these more established companies.
We have recently built a field organization and other capabilities for the sales, marketing and distribution of Rubraca in the United States and have hired the commercial infrastructure in the European Union, and there are significant risks involved with building and managing a sales organization. Factors that may inhibit our efforts to effectively commercialize Rubraca on our own include:
|
· |
our inability to recruit, train, retain and incentivize adequate numbers of qualified and effective sales and marketing personnel; |
|
· |
the inability of sales personnel to generate sufficient sales leads and to obtain access to physicians or persuade adequate numbers of physicians to use or prescribe Rubraca; |
|
· |
our inability to effectively manage a geographically dispersed sales and marketing team. |
If we are unable to maintain effective sales, marketing and distribution capabilities for Rubraca or if we are unable to establish and maintain sales, marketing and distribution capabilities for Rubraca outside of the United States, if approved, or for any other product candidate for which we obtain marketing approval, whether independently or with third parties, we may not be able to generate product revenue or may not become profitable. If the cost of establishing and maintaining a sales and marketing organization exceeds the cost-effectiveness of doing so, we may not become profitable.
With respect to our product candidates, we may elect to collaborate with third parties that have direct sales forces and established distribution systems, either to augment our own sales force and distribution systems or in lieu of our own sales force and distribution systems in certain territories. To the extent that we enter into licensing or co-promotion arrangements for any of our product candidates, our product revenue may be lower than if we directly marketed or sold our approved products. In addition, any revenue we receive as a result of such arrangements would depend in whole or in part upon the efforts of such third parties, which may not be successful and are generally not within our control. If we are unable to enter into such arrangements on acceptable terms or at all, we may not be able to successfully commercialize our product candidates that receive regulatory approval. If we are not successful in commercializing our product candidates, either on our own or through collaborations with one or more third parties, our future product revenue will suffer and we may incur significant additional losses.
We cannot give any assurance that rucaparib will receive regulatory approval outside the United States or that the rucaparib development program in other lines of therapies and indications will be successful or that our other product candidates will receive regulatory approval.
To date, we have invested a significant portion of our efforts and financial resources in the acquisition and development of our product candidates. Our business depends entirely on the successful development and commercialization of our product candidates.
Each of our product candidates requires clinical development, management of clinical, non-clinical and manufacturing activities, regulatory approval in multiple jurisdictions, obtaining manufacturing supply, building of a commercial organization and significant marketing efforts in order to generate any revenues from product sales. We are not permitted to market or promote any of our product candidates before we receive regulatory approval from the FDA
33
or comparable foreign regulatory authorities. To date, we have received regulatory approval from the FDA to market Rubraca in the United States for a certain limited indication. We may not receive similar regulatory approvals outside the United States and we may never receive regulatory approval for any of our other product candidates. In addition, our product development programs contemplate the development of companion diagnostics by third-party collaborators. Companion diagnostics are subject to regulation as medical devices and must themselves be approved for marketing by the FDA or certain other foreign regulatory agencies before our product candidates may be commercialized.
We cannot be certain that rucaparib will be successfully developed in other lines of therapy, tumor types or other indications or that any of our product candidates will be successful in clinical trials or receive regulatory approval. Further, our product candidates may not receive regulatory approval even if they are successful in clinical trials. Three of our product candidates, CO-101, rociletinib and lucitanib encountered development and regulatory setbacks after initial promising data, leading us to discontinue enrollment in ongoing clinical trials. Even if we successfully obtain regulatory approvals to market one or more of our product candidates, our revenues will be dependent, in part, upon our diagnostic collaborators’ ability to obtain regulatory approval of the companion diagnostics to be used with our product candidates, as well as the size of the markets in the territories for which we gain regulatory approval and have commercial rights. If the markets for patient subsets that we are targeting are not as significant as we estimate, we may not generate significant revenues from sales of such products, if approved.
We plan to seek regulatory approval to commercialize our product candidates, and for other lines of therapies, indications or tumor types for rucaparib, in the United States, the European Union and in additional foreign countries. While the scope of regulatory approval is similar in other countries, obtaining separate regulatory approval in many other countries requires compliance with numerous and varying regulatory requirements of such countries regarding safety and efficacy and governing, among other things, clinical trials and commercial sales, pricing and distribution of our product candidates, and we cannot predict success in these jurisdictions.
Clinical drug development involves a lengthy and expensive process with an uncertain outcome, and results of earlier studies and trials may not be predictive of future trial results.
Clinical testing is expensive and can take many years to complete, and its outcome is inherently uncertain. Failure can occur at any time during the clinical trial process. The results of non-clinical studies and early clinical trials of our product candidates may not be predictive of the results of later-stage clinical trials. Product candidates in later stages of clinical trials may fail to show the desired safety and efficacy traits despite having progressed through non-clinical studies and initial clinical trials. It is not uncommon for companies in the biopharmaceutical industry to suffer significant setbacks in advanced clinical trials due to lack of efficacy or adverse safety profiles, notwithstanding promising results in earlier trials. Indeed, based on the negative results of a pivotal study, we ceased further development of our previous product candidate CO-101, and we decided to discontinue ongoing development of rociletinib as a result of the issuance of a Complete Response Letter by the FDA. Additionally, our future clinical trial results may not be successful.
Although we have clinical trials ongoing, we may experience delays in our ongoing clinical trials, and we do not know whether planned clinical trials will begin on time, need to be redesigned, enroll patients on time or be completed on schedule, if at all. Clinical trials can be delayed for a variety of reasons, including delays related to:
|
· |
obtaining regulatory approval to commence a trial; |
|
· |
reaching agreement on acceptable terms with prospective contract research organizations (“CROs”) and clinical trial sites, the terms of which can be subject to extensive negotiation and may vary significantly among different CROs and trial sites; |
|
· |
obtaining institutional review board (“IRB”) approval at each site; |
|
· |
recruiting suitable patients to participate in a trial; |
|
· |
developing and validating companion diagnostics on a timely basis; |
|
· |
having patients complete a trial or return for post-treatment follow-up; |
|
· |
clinical sites deviating from trial protocol or dropping out of a trial; |
|
· |
adding new clinical trial sites; or |
|
· |
manufacturing sufficient quantities of product candidate for use in clinical trials. |
34
Patient enrollment, a significant factor in the timing of clinical trials, is affected by many factors including the size and nature of the patient population, the proximity of patients to clinical sites, the eligibility criteria for the trial, the design of the clinical trial, competing clinical trials and clinicians’ and patients’ perceptions as to the potential advantages of the drug being studied in relation to other available therapies, including any new drugs that may be approved for the indications we are investigating. Furthermore, we rely on CROs and clinical trial sites to ensure the proper and timely conduct of our clinical trials, and while we have agreements governing their committed activities, we have limited influence over their actual performance.
We could encounter delays if a clinical trial is suspended or terminated by us, by the IRBs of the institutions in which such trials are being conducted, by the Data Safety Monitoring Board for such trial or by the FDA or other regulatory authorities. Such authorities may impose a suspension or termination due to a number of factors, including failure to conduct the clinical trial in accordance with regulatory requirements or our clinical protocols, inspection of the clinical trial operations or trial site by the FDA or other regulatory authorities resulting in the imposition of a clinical hold, unforeseen safety issues or adverse side effects, failure to demonstrate a benefit from using a drug, changes in governmental regulations or administrative actions or lack of adequate funding to continue the clinical trial. If we experience delays in the completion of, or termination of, any clinical trial of our product candidates, the commercial prospects of our product candidates will be harmed, and our ability to generate product revenues from any of these product candidates will be delayed. In addition, any delays in completing our clinical trials will increase our costs, slow down our product candidate development and approval process and jeopardize our ability to commence product sales and generate revenues. Any of these occurrences may harm our business, financial condition and prospects significantly. In addition, many of the factors that cause, or lead to, a delay in the commencement or completion of clinical trials may also ultimately lead to the denial of regulatory approval of our product candidates.
The regulatory approval processes of the FDA and comparable foreign authorities are lengthy, time consuming and inherently unpredictable, and if we are ultimately unable to obtain regulatory approval for rucaparib in other indications and lines of therapy or for our other product candidates, our business will be substantially harmed.
The time required to obtain approval by the FDA and comparable foreign authorities is unpredictable, but typically takes many years following the commencement of clinical trials and depends upon numerous factors, including the substantial discretion of the regulatory authorities. In addition, approval policies, regulations or the type and amount of clinical data necessary to gain approval may change during the course of a product candidate’s clinical development and may vary among jurisdictions. We have obtained regulatory approval for Rubraca in the United States for a specific indication, and it is possible that Rubraca may not obtain regulatory approval outside the United States or for broader indications and lines of therapy or other tumor types or that any of our other existing product candidates or any product candidates we may seek to develop in the future will ever obtain regulatory approval. Indeed, with the issuance of a Complete Response Letter by the FDA with respect to the rociletinib NDA, we decided to discontinue ongoing development of rociletinib.
Our product candidates could fail to receive regulatory approval or approval may be delayed for many reasons, including the following:
|
· |
the FDA or comparable foreign regulatory authorities may disagree with the design or implementation of our clinical trials; |
|
· |
we may be unable to demonstrate to the satisfaction of the FDA or comparable foreign regulatory authorities that a product candidate is safe and effective for its proposed indication; |
|
· |
the results of clinical trials may not meet the level of statistical significance required by the FDA or comparable foreign regulatory authorities for approval; |
|
· |
the FDA or comparable foreign regulatory authorities may disagree with our interpretation of data from non-clinical studies or clinical trials; |
|
· |
the data collected from clinical trials of our product candidates may not be sufficient to support the submission of an NDA or other submission or to obtain regulatory approval in the United States or elsewhere; |
|
· |
the FDA or comparable foreign regulatory authorities may fail to approve the manufacturing processes or facilities of third-party manufacturers with which we contract for clinical and commercial supplies; |
35
|
· |
the FDA or comparable foreign regulatory authorities may fail to approve the companion diagnostics we contemplate developing with partners; and |
|
· |
the approval policies or regulations of the FDA or comparable foreign regulatory authorities may significantly change in a manner rendering our clinical data insufficient for approval. |
This lengthy approval process, as well as the unpredictability of future clinical trial results, may result in our failing to obtain regulatory approval to market our product candidates, which would significantly harm our business, results of operations and prospects.
Even if we receive regulatory approval for our product candidates, we will be subject to ongoing obligations and continued regulatory review, which may result in significant additional expense. Additionally, our product candidates, if and when approved, could be subject to labeling and other restrictions and market withdrawal, and we may be subject to penalties if we fail to comply with regulatory requirements or experience unanticipated problems with our products.
Any regulatory approvals that we receive for our product candidates may also be subject to limitations on the approved indicated uses for which the product may be marketed or to the conditions of approval, or contain requirements for potentially costly post-marketing testing and clinical trials and surveillance to monitor the safety and efficacy of the product candidate. In addition, if the FDA or comparable foreign regulatory authority approves any of our product candidates, the manufacturing processes, pricing, labeling, packaging, distribution, adverse event reporting, storage, advertising, promotion and recordkeeping for the product will be subject to extensive and ongoing regulatory requirements. These requirements include submissions of safety and other post-marketing information and reports, registration, as well as continued compliance with current good manufacturing practices and good clinical practices for any clinical trials that we conduct post-approval. Later discovery of previously unknown problems with a product, including adverse events of unanticipated severity or frequency, or with our third-party manufacturers or manufacturing processes or failure to comply with regulatory requirements, may result in, among other things:
|
· |
restrictions on the marketing or manufacturing of the product, withdrawal of the product from the market or voluntary or mandatory product recalls; |
|
· |
refusal by the FDA and comparable foreign authorities to approve pending applications or supplements to approved applications filed by us, or suspension or revocation of product license approvals; |
|
· |
injunctions or the imposition of civil or criminal penalties. |
All of the foregoing limitations, obligations, and requirements also apply to Rubraca, for which we have received regulatory approval in the United States for certain limited indications.
We may seek approval from U.S. and foreign regulatory authorities for one or more product candidates on a conditional basis with full approval conditioned upon fulfilling the requirements of regulators. For example, we received accelerated approval from the FDA for the initial indication for Rubraca and are seeking conditional marketing authorization from the E.U. for rucaparib. Each of these approval pathways has certain conditions to approval, some of which may be post-approval, such as the conduct of a post-approval, or confirmatory, trial using due diligence. For example, continued approval of Rubraca by the FDA may be contingent upon verification and description of clinical benefit in ARIEL3 and/or ARIEL4, our confirmatory trials. If we are unable to fulfill the requirements of regulators that are conditions of a product’s accelerated or conditional approval, if the confirmatory trial shows unfavorable results or increased or additional undesirable side effects, or if regulators re-evaluate the data or risk-benefit profile of our product candidate, the availability of accelerated or conditional approval may be withdrawn or our conditional approval may not result in full approval or may be revoked or not renewed. Alternatively, we may be required to change a product candidate’s labeled indications or even withdraw the product, if approved, from the market.
The FDA’s and comparable foreign authorities’ policies may change and additional government regulations may be enacted that could prevent, limit or delay regulatory approval of our product candidates. We cannot predict the likelihood, nature or extent of government regulation that may arise from future legislation or administrative action, either in the United States or abroad. If we are slow or unable to adapt to changes in existing requirements or the
36
adoption of new requirements or policies, or if we are not able to maintain regulatory compliance, we may lose any marketing approval that we may have obtained, and we may not achieve or sustain profitability, which would adversely affect our business. Any of the foregoing scenarios could materially harm the commercial prospects for our product candidates.
Rubraca and our other product candidates may cause undesirable side effects or have other properties that could delay or prevent their regulatory approval, limit the commercial profile of an approved label or result in significant negative consequences following marketing approval, if any.
Adverse events (“AEs”) attributable to our product candidates could cause us or regulatory authorities to interrupt, delay or halt clinical trials and could result in a more restrictive label or the delay or denial of regulatory approval by the FDA or other comparable foreign authorities. Clinical studies conducted to date have generated AEs related to our product candidates, some of which have been serious. Patients treated with Rubraca have commonly experienced nausea, vomiting, constipation, dysgeusia, anemia/decreased hemoglobin, decreased appetite, diarrhea, abdominal pain, thrombocytopenia and fatigue/asthenia. In studies of lucitanib, hypertension, proteinuria and subclinical hypothyroidism requiring supplementation are the most common AEs observed. The most notable AEs experienced by patients treated with rociletinib include hyperglycemia and OTc prolongation. As is the case with all oncology drugs, it is possible that there may be other potentially harmful characteristics associated with their use in future trials, including larger and lengthier Phase III clinical trials. As we evaluate the use of our product candidates in combination with other active agents, we may encounter safety issues as a result of the combined safety profiles of each agent, which could pose a substantial challenge to that development strategy.
Results of our trials could reveal a high and unacceptable severity and prevalence of these or other side effects. In such an event, our trials could be suspended or terminated and the FDA or comparable foreign regulatory authorities could order us to cease further development of or deny approval of our product candidates for any or all targeted indications. The drug-related AEs could affect patient recruitment or the ability of enrolled patients to complete the trial or result in potential product liability claims. Any of these occurrences may harm our business, financial condition and prospects significantly.
Additionally, if we or others later identify undesirable side effects caused by such products, a number of potentially significant negative consequences could result, including:
|
· |
regulatory authorities may withdraw approvals of such product; |
|
· |
regulatory authorities may require additional warnings on the label; |
|
· |
we may be required to create a medication guide outlining the risks of such side effects for distribution to patients; |
|
· |
we could be sued and held liable for harm caused to patients; and |
|
· |
our reputation may suffer. |
Any of these events could prevent us from achieving or maintaining market acceptance of the particular product candidate, if approved, and could significantly harm our business, results of operations and prospects.
Failure to successfully validate, develop and obtain regulatory approval for companion diagnostics could harm our drug development strategy.
As one of the key elements of our clinical development strategy, we seek to identify patient subsets within a disease category who may derive selective and meaningful benefit from the product candidates we are developing. In collaboration with partners, we plan to develop companion diagnostics to help us to more accurately identify patients within a particular subset, both during our clinical trials and in connection with the commercialization of our product candidates. Companion diagnostics are subject to regulation by the FDA and comparable foreign regulatory authorities as medical devices and require separate regulatory approval prior to commercialization. We do not develop companion diagnostics internally and thus we are dependent on the sustained cooperation and effort of our third-party collaborators in developing and obtaining approval for these companion diagnostics. We and our collaborators may encounter difficulties in developing and obtaining approval for the companion diagnostics, including issues relating to selectivity/specificity, analytical validation, reproducibility, or clinical validation. Any delay or failure by our
37
collaborators to develop or obtain regulatory approval of the companion diagnostics could delay or prevent approval of our product candidates. In addition, our collaborators may encounter production difficulties that could constrain the supply of the companion diagnostics, and both they and we may have difficulties gaining acceptance of the use of the companion diagnostics in the clinical community. If such companion diagnostics fail to gain market acceptance, it would have an adverse effect on our ability to derive revenues from sales of our products. In addition, the diagnostic company with whom we contract may decide to discontinue selling or manufacturing the companion diagnostic that we anticipate using in connection with development and commercialization of our product candidates or our relationship with such diagnostic company may otherwise terminate. We may not be able to enter into arrangements with another diagnostic company to obtain supplies of an alternative diagnostic test for use in connection with the development and commercialization of our product candidates or do so on commercially reasonable terms, which could adversely affect and/or delay the development or commercialization of our product candidates.
We rely on third parties to conduct our non-clinical and clinical trials. If these third parties do not successfully carry out their contractual duties or meet expected deadlines, we may not be able to obtain regulatory approval for or commercialize our product candidates and our business could be substantially harmed.
We have relied upon and plan to continue to rely upon third-party CROs to monitor and manage data for our ongoing non-clinical and clinical programs. We rely on these parties for execution of our non-clinical and clinical trials, and control only certain aspects of their activities. Nevertheless, we are responsible for ensuring that each of our studies is conducted in accordance with the applicable protocol, legal, regulatory and scientific standards, and our reliance on the CROs does not relieve us of our regulatory responsibilities. We and our CROs are required to comply with GCP, which are regulations and guidelines enforced by the FDA, the EEA and comparable foreign regulatory authorities for all of our products in clinical development. Regulatory authorities enforce these GCPs through periodic inspections of trial sponsors, principal investigators and trial sites. If we or any of our CROs fail to comply with applicable GCPs, the clinical data generated in our clinical trials may be deemed unreliable and the FDA, the EMA or comparable foreign regulatory authorities may require us to perform additional clinical trials before approving our marketing applications. We cannot assure you that upon inspection by a given regulatory authority, such regulatory authority will determine that any of our clinical trials comply with GCP regulations. In addition, our clinical trials must be conducted with product produced under current GMP regulations. Our failure to comply with these regulations may require us to repeat clinical trials, which would delay the regulatory approval process.
Our CROs have the right to terminate their agreements with us in the event of an uncured material breach. In addition, some of our CROs have an ability to terminate their respective agreements with us if it can be reasonably demonstrated that the safety of the subjects participating in our clinical trials warrants such termination, if we make a general assignment for the benefit of our creditors or if we are liquidated.
If any of our relationships with these third-party CROs terminate, we may not be able to enter into arrangements with alternative CROs or to do so on commercially reasonable terms. In addition, our CROs are not our employees, and except for remedies available to us under our agreements with such CROs, we cannot control whether or not they devote sufficient time and resources to our on-going clinical and non-clinical programs. If CROs do not successfully carry out their contractual duties or obligations or meet expected deadlines, if they need to be replaced or if the quality or accuracy of the clinical data they obtain is compromised due to the failure to adhere to our clinical protocols, regulatory requirements or for other reasons, our clinical trials may be extended, delayed or terminated and we may not be able to obtain regulatory approval for or successfully commercialize our product candidates. As a result, our results of operations and the commercial prospects for our product candidates would be harmed, our costs could increase and our ability to generate revenues could be delayed.
Switching or adding additional CROs involves additional cost and requires management time and focus. In addition, there is a natural transition period when a new CRO commences work. As a result, delays occur, which can materially influence our ability to meet our desired clinical development timelines. Though we carefully manage our relationships with our CROs, there can be no assurance that we will not encounter similar challenges or delays in the future or that these delays or challenges will not have a material adverse effect on our business, financial condition and prospects.
38
We rely completely on third parties to manufacture our clinical drug supplies and we intend to rely on third parties to produce commercial supplies of any approved product candidate, and our commercialization of any of our product candidates could be stopped, delayed or made less profitable if those third parties fail to obtain approval of the FDA or comparable foreign regulatory authorities, fail to provide us with sufficient quantities of drug product or fail to do so at acceptable quality levels or prices.
We do not currently have nor do we plan to acquire the infrastructure or capability internally to manufacture our clinical drug supplies for use in the conduct of our clinical trials, and we lack the resources and the capability to manufacture any of our product candidates on a clinical or commercial scale. We do not control the manufacturing process of, and are completely dependent on, our contract manufacturing partners for compliance with the GMP regulatory requirements for manufacture of both active drug substances and finished drug products. If our contract manufacturers cannot successfully manufacture material that conforms to the strict regulatory requirements of the FDA or others, they will not be able to secure and/or maintain regulatory approval for their manufacturing facilities. In addition, we have no control over the ability of our contract manufacturers to maintain adequate quality control, quality assurance and qualified personnel. If the FDA or a comparable foreign regulatory authority does not approve these facilities for the manufacture of our product candidates or if it withdraws any such approval in the future, we may need to find alternative manufacturing facilities, which would significantly affect our ability to develop, obtain regulatory approval for or market our product candidates, if approved.
We rely on our manufacturers to purchase from third-party suppliers the materials necessary to produce our product candidates for our clinical trials. There are a limited number of suppliers of raw materials that we use to manufacture our drugs and there may be a need to assess alternate suppliers to prevent a possible disruption of the manufacture of the materials necessary to produce our product candidates for our clinical trials, and if approved, ultimately for commercial sale. We do not have any control over the process or timing of the acquisition of these raw materials by our manufacturers. Moreover, we currently do not have any agreements for the commercial production of these raw materials. Any significant delay in the supply of a product candidate, or the raw material components thereof, for an ongoing clinical trial due to the need to replace a third-party manufacturer could considerably delay completion of our clinical trials, product testing and potential regulatory approval of our product candidates. If our manufacturers or we are unable to purchase these raw materials after regulatory approval has been obtained for our product candidates, the commercial launch of our product candidates would be delayed or there would be a shortage in supply, which would impair our ability to generate revenues from the sale of our product candidates.
We are dependent on our third party manufacturers to conduct process development and scale-up work necessary to support greater clinical development and commercialization requirements for our product candidates. Carrying out these activities in a timely manner, and on commercially reasonable terms, is critical to the successful development and commercialization of our product candidates. We expect that our third-party manufacturers are capable of providing sufficient quantities of our product candidates to meet anticipated clinical and full-scale commercial demands, however if third parties with whom we currently work are unable to meet our supply requirements, we will need to secure alternate suppliers. While we believe that there are other contract manufacturers having the technical capabilities to manufacture our product candidates, we cannot be certain that identifying and establishing relationships with such sources would not result in significant delay or material additional costs.
We expect to continue to depend on third-party contract manufacturers for the foreseeable future. While we have long-term agreements with Lonza for the manufacture of API for Rubraca and with the manufacturer of the finished drug product, we have not entered into agreements with any alternate suppliers. We currently obtain our supplies of finished drug product through individual purchase orders.
Our commercial success depends upon attaining significant market acceptance of our product candidates, if approved, among physicians, patients, healthcare payors and major operators of cancer clinics.
Even if we obtain regulatory approval for our other product candidates, the product may not gain market acceptance among physicians, health care payors, patients and the medical community, which are critical to commercial success. Market acceptance of any product candidate for which we receive approval depends on a number of factors, including:
|
· |
the efficacy and safety as demonstrated in clinical trials; |
|
· |
the timing of market introduction of such product candidate as well as competitive products; |
39
|
· |
the clinical indications for which the drug is approved and the product label approved by regulatory authorities, including any warnings that may be required on the label; |
|
· |
the approval, availability, market acceptance and reimbursement for the companion diagnostic; |
|
· |
acceptance by physicians, major operators of cancer clinics and patients of the drug as a safe and effective treatment; |
|
· |
the potential and perceived advantages of such product candidate over alternative treatments, especially with respect to patient subsets that we are targeting with such product candidate; |
|
· |
the safety of such product candidate seen in a broader patient group, including its use outside the approved indications; |
|
· |
the cost, safety and efficacy of the product in relation to alternative treatments; |
|
· |
the availability of adequate reimbursement and pricing by third-party payors and government authorities; |
|
· |
relative convenience and ease of administration; |
|
· |
the prevalence and severity of adverse side effects; and |
|
· |
the effectiveness of our sales and marketing efforts. |
If our product candidates are approved but fail to achieve an adequate level of acceptance by physicians, healthcare payors and patients, we will not be able to generate significant revenues, and we may not become or remain profitable.
We face significant competition from other biotechnology and pharmaceutical companies, and our operating results will suffer if we fail to compete effectively.
The biotechnology and pharmaceutical industries are intensely competitive and subject to rapid and significant technological change. In addition, the competition in the oncology market is intense. We have competitors both in the United States and internationally, including major multinational pharmaceutical companies, biotechnology companies and universities and other research institutions.
Lynparza™ (olaparib) is approved in the U.S. as monotherapy in patients with germline BRCA mutated advanced ovarian cancer who have been treated with three or more prior lines of chemotherapy, as monotherapy for the maintenance treatment of adult patients with recurrent epithelial, fallopian tube or primary peritoneal cancer, who are in a complete or partial response to platinum-based chemotherapy and as monotherapy in patients with deleterious or suspected deleterious gBRCAm, human epidermal growth factor 2 (HER2)-negative metastatic breast cancer who have been treated with chemotherapy in the neoadjuvant, adjuvant, or metastatic setting. Lynparza is also approved in the EU for the maintenance treatment of BRCA mutated platinum-sensitive relapsed serous ovarian cancer. In February 2018, the CHMP adopted a positive opinion recommending this label be changed and expanded to remove the limitation of use in BRCA-mutated patients. Lynparza has indications for ovarian cancer across 57 countries (as of year-end 2017). In July 2017, AstraZeneca and Merck & Co., Inc. announced a global strategic oncology collaboration to co-develop and co-commercialise Lynparza for multiple cancer types. Lynparza is being investigated, alone and in combination with other agents, in multiple indications across several tumor types, including breast, prostate, and pancreatic cancers.
Zejula®/niraparib (Tesaro) was approved in March 2017 in the United States as monotherapy for the maintenance treatment of adult patients with recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer who are in a complete or partial response to platinum-based chemotherapy. Zejula was approved in November 2017 in the EU for the same indication. Additional clinical investigations of Zejula in ovarian, breast and lung cancers are ongoing or planned. Janssen Biotech has licensed rights to develop and commercialize niraparib specifically for patients with prostate cancer worldwide, except in Japan.
There are a number of PARP inhibitors in clinical development including AbbVie’s veliparib and ABT-767, Pfizer’s talazoparib, BeiGene’s BGB-290, and Checkpoint Therapeutics’ CK-102. While most PARP inhibitor development focuses on ovarian, breast and prostate cancers, additional efforts are aimed toward bladder, lung, and pancreatic cancers as well.
40
In addition, combination approaches that include PARP inhibitors, including Lynparza or Zejula, with other anticancer agents are in various phases of clinical development across a variety of oncology indications. These combination therapies may result in future competitive pressure on Rubraca, and multiple data readouts for such studies are anticipated throughout 2018 and beyond.
Many of our competitors have substantially greater financial, technical and other resources, such as larger research and development staff and experienced marketing and manufacturing organizations. Additional mergers and acquisitions in the biotechnology and pharmaceutical industries may result in even more resources being concentrated in our competitors. As a result, these companies may obtain regulatory approval more rapidly than we are able and may be more effective in selling and marketing their products as well. Smaller or early-stage companies may also prove to be significant competitors, particularly through collaborative arrangements with large, established companies. Competition may increase further as a result of advances in the commercial applicability of technologies and greater availability of capital for investment in these industries. Our competitors may succeed in developing, acquiring or licensing on an exclusive basis drug products that are more effective or less costly than any drug candidate that we are currently developing or that we may develop. If approved, our product candidates will face competition from commercially available drugs, as well as drugs that are in the development pipelines of our competitors and later enter the market.
Established pharmaceutical companies may invest heavily to accelerate discovery and development of novel compounds or to in-license novel compounds that could make our product candidates less competitive. In addition, any new product that competes with an approved product must demonstrate compelling advantages in efficacy, convenience, tolerability and safety in order to overcome price competition and to be commercially successful. Accordingly, our competitors may succeed in obtaining patent protection, receiving FDA, European Commission or other regulatory approval or discovering, developing and commercializing medicines before we do, which would have a material adverse effect on our business.
Reimbursement may be limited or unavailable in certain market segments for our product candidates, which could make it difficult for us to sell our products profitably.
There is significant uncertainty related to the third-party coverage and reimbursement of newly approved drugs. We have received approval for Rubraca in the United States for a limited indication. We intend to seek additional approvals to market Rubraca and other product candidates in the United States, Europe and other selected foreign jurisdictions. Market acceptance and sales of our product candidates in both domestic and international markets will depend significantly on the availability of adequate coverage and reimbursement from third-party payors for any of our product candidates and may be affected by existing and future healthcare reform measures. Government and other third-party payors are increasingly attempting to contain healthcare costs by limiting both coverage and the level of reimbursement for new drugs and, as a result, they may not cover or provide adequate payment for our product candidates. These payors may conclude that our product candidates are less safe, less effective or less cost-effective than existing or later introduced products, and third-party payors may not approve our product candidates for coverage and reimbursement or may cease providing coverage and reimbursement for these product candidates.
Obtaining coverage and reimbursement approval for a product from a government or other third-party payor is a time consuming and costly process that could require us to provide to the payor supporting scientific, clinical and cost-effectiveness data for the use of our products. We may not be able to provide data sufficient to gain acceptance with respect to coverage and reimbursement. We cannot be sure that coverage or adequate reimbursement will be available for any of our product candidates. Even if we obtain coverage for our product candidates, third-party payors may not establish adequate reimbursement amounts, which may reduce the demand for, or the price of, our products. If reimbursement of our future products is unavailable or limited in scope or amount, or if pricing is set at unsatisfactory levels, we may be unable to achieve or sustain profitability.
In both the United States and certain foreign jurisdictions, there have been and we expect there will continue to be a number of legislative and regulatory changes to the health care system that could affect our ability to sell our products profitably. The U.S. government and other governments have shown significant interest in pursuing healthcare reform. In particular, the Medicare Modernization Act of 2003 revised the payment methodology for many products under the Medicare program in the United States. This has resulted in lower rates of reimbursement. In 2010, the Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act (collectively, the “Affordable Care Act”), was enacted. The Affordable Care Act substantially changed the way healthcare is financed by both governmental and private insurers. Such government-adopted reform measures may adversely affect the pricing of
41
healthcare products and services in the United States or internationally and the amount of reimbursement available from governmental agencies or other third-party payors.
Moreover, payment methodologies, including payment for companion diagnostics, may be subject to changes in healthcare legislation and regulatory initiatives. For example, the CMS has begun bundling the Medicare payments for certain laboratory tests ordered while a patient received services in a hospital outpatient setting and, in 2018, the CMS began paying for clinical laboratory services based on a weighted average of reported prices that private payors, Medicare Advantage plans, and Medicaid Managed Care plans pay for laboratory services.
There have been, and likely will continue to be, legislative and regulatory proposals at the federal and state levels directed at broadening the availability of healthcare and containing or lowering the cost of healthcare. Recently there has also been heightened governmental scrutiny over the manner in which manufacturers set prices for their marketed products, which has resulted in several Congressional inquiries and proposed bills designed to, among other things, reform government program reimbursement methodologies. Individual states in the United States have also become increasingly active in implementing regulations designed to control pharmaceutical product pricing, including price or patient reimbursement constraints, discounts, restrictions on certain product access and marketing cost disclosure and transparency measures, and, in some cases, designed to encourage importation from other countries and bulk purchasing. We cannot predict the initiatives that may be adopted in the future. The continuing efforts of the government, insurance companies, managed care organizations and other payors of healthcare services to contain or reduce costs of healthcare may adversely affect the demand for any drug products for which we may obtain regulatory approval, as well as our ability to set satisfactory prices for our products, to generate revenues, and to achieve and maintain profitability.
In some foreign countries, particularly in the European Union, the pricing of prescription pharmaceuticals is subject to governmental control. In these countries, pricing negotiations with governmental authorities can take considerable time after the receipt of marketing approval for a product candidate. To obtain reimbursement or pricing approval in some countries, we may be required to conduct additional clinical trials that compare the cost-effectiveness of our product candidates to other available therapies. If reimbursement of our product candidates is unavailable or limited in scope or amount in a particular country, or if pricing is set at unsatisfactory levels, we may be unable to achieve or sustain profitability of our products in such country.
If we are not successful in attracting and retaining highly qualified personnel, we may not be able to successfully implement our business strategy. Further, we will need to grow our organization, and we may experience difficulties in managing this growth, which could disrupt our operations.
Our industry has experienced a high rate of turnover of management personnel in recent years. Our ability to compete in the highly competitive biotechnology and pharmaceuticals industries depends upon our ability to attract and retain highly qualified managerial, scientific and medical personnel. We are highly dependent on our management, scientific and medical personnel, especially Patrick J. Mahaffy, our President and Chief Executive Officer, Lindsey Rolfe, our Executive Vice President of Clinical and Preclinical Development and Pharmacovigilance and Chief Medical Officer, Dale Hooks, our Senior Vice President and Chief Commercial Officer and Gillian C. Ivers-Read, our Executive Vice President, Technical Operations and Chief Regulatory Officer, whose services are critical to the successful implementation of our product candidate acquisition, development and regulatory strategies.
Despite our efforts to retain valuable employees, members of our management, scientific, development and commercial teams may terminate their employment with us on short notice. Pursuant to their employment arrangements, each of our executive officers may voluntarily terminate their employment at any time by providing as little as thirty days advance notice. Our employment arrangements with all of our employees provide for at-will employment, which means that any of our employees could leave our employment at any time, with or, other than our executive officers, without notice. For example, Andrew R. Allen, our former Executive Vice President of Clinical and Pre-Clinical Development and Chief Medical Officer, resigned in July 2015, and Steven L. Hoerter, our former Executive Vice President and Chief Commercial Officer, resigned in January 2016 and Erle T. Mast, our former Executive Vice President and Chief Financial Officer, resigned in March 2016. The loss of the services of any of our executive officers or other key employees and our inability to find suitable replacements could potentially harm our business, financial condition and prospects. Our success also depends on our ability to continue to attract, retain and motivate highly skilled junior, mid-level and senior managers as well as junior, mid-level and senior scientific and medical personnel.
42
As of February 16, 2018, we employed 360 full-time employees. As our development plans and strategies develop, we expect to expand our employee base for managerial, operational, financial and other resources. Future growth will impose significant added responsibilities on members of management, including the need to identify, recruit, maintain, motivate and integrate additional employees. Also, our management may need to divert a disproportionate amount of its attention away from our day-to-day activities and devote a substantial amount of time to managing these growth activities. We may not be able to effectively manage the expansion of our operations which may result in weaknesses in our infrastructure, give rise to operational mistakes, loss of business opportunities, loss of employees and reduced productivity among remaining employees. Our expected growth could require significant capital expenditures and may divert financial resources from other projects. If our management is unable to effectively manage our expected growth, our expenses may increase more than expected, our ability to generate revenues could be reduced and we may not be able to implement our business strategy.
We may not be able to attract or retain qualified management and scientific personnel in the future due to the intense competition for a limited number of qualified personnel among biopharmaceutical, biotechnology, pharmaceutical and other businesses. Many of the other pharmaceutical companies that we compete against for qualified personnel have greater financial and other resources, different risk profiles and a longer history in the industry than we do. They also may provide more diverse opportunities and better chances for career advancement. Some of these characteristics may be more appealing to high quality candidates than what we have to offer. In order to induce valuable employees to continue their employment with us, we have provided stock options that vest over time. The value to employees of stock options that vest over time is significantly affected by movements in our stock price that are beyond our control, and may at any time be insufficient to counteract more lucrative offers from other companies. If we are unable to continue to attract and retain high quality personnel, the rate and success at which we can develop and commercialize product candidates will be limited.
Our employees may engage in misconduct or other improper activities, including noncompliance with regulatory standards and requirements, which could have a material adverse effect on our business.
We are exposed to the risk of employee fraud or other misconduct. Misconduct by employees could include intentional failures to comply with FDA regulations, provide accurate information to the FDA, comply with manufacturing standards we have established, comply with federal and state health-care fraud and abuse laws and regulations, report financial information or data accurately or disclose unauthorized activities to us. In particular, sales, marketing and business arrangements in the healthcare industry are subject to extensive laws and regulations intended to prevent fraud, kickbacks, self-dealing and other abusive practices. These laws and regulations may restrict or prohibit a wide range of pricing, discounting, marketing and promotion, sales commission, customer incentive programs and other business arrangements. Employee misconduct could also involve the improper use of information obtained in the course of clinical trials, which could result in regulatory sanctions and serious harm to our reputation. We have adopted a Code of Business Ethics and other compliance policies, but it is not always possible to identify and deter employee misconduct, and the precautions we take to detect and prevent this activity may not be effective in controlling unknown or unmanaged risks or losses or in protecting us from governmental investigations or other actions or lawsuits stemming from a failure to be in compliance with such laws or regulations. If any such actions are instituted against us, and we are not successful in defending ourselves or asserting our rights, those actions could have a significant effect on our business and results of operations, including the imposition of significant fines or other sanctions.
Our relationships with healthcare professionals, investigators, consultants, customers (actual and potential) and third-party payors are and will continue to be subject, directly or indirectly, to federal and state healthcare fraud and abuse laws, false claims laws, transparency and disclosure (or “sunshine”) laws, government price reporting, and health information privacy and security laws. If we are unable to comply, or have not fully complied, with such laws, we could face substantial penalties.
Our operations may be directly, or indirectly through our customers, subject to various federal and state fraud and abuse laws, including, without limitation, the federal Anti-Kickback Statute and the federal False Claims Act. These laws may affect, among other things, our current activities with clinical study investigators and research subjects, as well as proposed and future sales, marketing, disease awareness, and patient assistance programs. In addition, we may be subject to patient privacy regulation by both the federal government and the states in which we conduct our business. The laws that may affect our ability to operate include, but are not limited to:
|
· |
the federal Anti-Kickback Statute, which prohibits, among other things, persons from knowingly and willfully soliciting, receiving, offering or paying remuneration, including any kickback, bribe, or certain rebate, directly |
43
or indirectly, to induce, or in return for, either the referral of an individual, or the purchase, lease, order or recommendation of any good, facility, item or service for which payment will be made, in whole or in part, under a federal healthcare program, such as the Medicare and Medicaid programs. A person or entity does not need to have actual knowledge of the federal Anti-Kickback Statute or special intent to violate the law in order to have committed a violation; in addition, the government may assert that a claim including items or services resulting from a violation of the federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the federal False Claims Act; |
|
· |
federal false claims laws, including the False Claims Act, which impose criminal and civil penalties, including through civil “qui tam” or “whistleblower” actions, against individuals or entities from knowingly presenting, or causing to be presented, claims for payment or approval from federal programs, such as Medicare and Medicaid, that are false or fraudulent, or knowingly making a false statement to improperly avoid, decrease or conceal an obligation to pay money to the federal government; |
|
· |
the Health Insurance Portability and Accountability Act of 1996, or HIPAA which imposes criminal and civil liability for, among other things, willfully executing, or attempting to execute, a scheme to defraud any healthcare benefit program and making false statements relating to healthcare matters. Similar to the federal Anti-Kickback Statute, a person or entity does not need to have actual knowledge of the statute or specific intent to violate it in order to have committed a violation; |
|
· |
HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act and its implementing regulations, which also imposes certain requirements on certain covered healthcare providers, health plans, and healthcare clearinghouses, as well as their respective business associates that perform services for them that involve the use, or disclosure of, individually identifiable health information, with respect to safeguarding the privacy, security and transmission of individually identifiable health information; |
|
· |
the federal civil monetary penalties statute, which prohibits, among other things, the offering or giving of remuneration to a Medicare or Medicaid beneficiary that the person knows or should know is likely to influence the beneficiary’s election of a particular supplier of items or services reimbursable by a Federal or state governmental program; |
|
· |
the federal Physician Payment Sunshine Act, which requires certain manufacturers of drugs, devices, biologics and medical supplies for which payment is available under Medicare, Medicaid or the Children’s Health Insurance Program (with certain exceptions) to report annually to the Centers for Medicare and Medicaid Services, or CMS, information related to payments or other transfers of value made to physicians (defined to include doctors, dentists, optometrists, podiatrists and chiropractors) and teaching hospitals, as well as ownership and investment interests held by the physicians described above and their immediate family members; |
|
· |
federal consumer protection and unfair competition laws, which broadly regulate marketplace activities and activities that potentially harm consumers; |
|
· |
federal government price reporting laws, which require drug manufacturers to calculate and report complex pricing metrics to government agencies, including CMS, where such reported prices may be used in the calculation of reimbursement and/or discounts on marketed products. Participation in these programs and compliance with the applicable requirements may result in potentially significant discounts on products subject to reimbursement under federal healthcare programs and increased infrastructure costs, and may potentially limit a drug manufacturer’s ability to offer certain marketplace discounts; and |
|
· |
analogous state laws and regulations, such as state anti-kickback, false claims, consumer protection and unfair competition laws which may apply to pharmaceutical business practices, including but not limited to, research, distribution, sales and marketing arrangements as well as submitting claims involving healthcare items or services reimbursed by any third-party payer, including commercial insurers; state laws that require pharmaceutical companies to comply with the pharmaceutical industry’s voluntary compliance guidelines and the relevant compliance guidance promulgated by the federal government that otherwise restricts payments that may be made to healthcare providers and other potential referral sources; state laws that require drug manufacturers to file reports with states regarding pricing and marketing information, such as the tracking and reporting of gifts, compensations and other remuneration and items of value provided to healthcare professionals and entities; and state laws governing the privacy and security of health information in certain circumstances, many of which differ from each other in significant ways and may not have the same effect, thus complicating compliance efforts. |
44
In addition, the research and development of our product candidates outside the United States, and any sales of our products or product candidates once commercialized outside the United States will also likely subject us to foreign equivalents of the healthcare laws mentioned above, among other foreign laws.
Efforts to ensure that our business arrangements will comply with applicable healthcare laws may involve substantial costs, including investments in infrastructure and additional resources. Because of the breadth of these laws and the narrowness of the statutory exceptions and safe harbors available, it is possible that some of our business activities, including our consulting agreements and other relationships with physicians, could be subject to challenge under one or more of such laws. Governmental and enforcement authorities may conclude that our business practices do not comply with current or future statutes, regulations or case law interpreting applicable fraud and abuse or other healthcare laws and regulations. If our operations are found to be in violation of any of the laws described above or any other governmental regulations that apply to us, we may be subject to, without limitation, civil, criminal, and administrative penalties, damages, monetary fines, disgorgement, possible exclusion from participation in Medicare, Medicaid and other federal healthcare programs, contractual damages, reputational harm, diminished profits and future earnings and curtailment or restructuring of our operations, any of which could adversely affect our ability to operate our business and our results of operations.
If product liability lawsuits are brought against us, we may incur substantial liabilities and may be required to limit commercialization of our product candidates.
We face an inherent risk of product liability. For example, we may be sued if any product we develop allegedly causes injury or is found to be otherwise unsuitable during product testing, manufacturing, marketing or sale. Any such product liability claims may include allegations of defects in manufacturing, defects in design, a failure to warn of dangers inherent in the product, negligence, strict liability and a breach of warranties. Claims could also be asserted under state consumer protection acts. If we cannot successfully defend ourselves against product liability claims, we may incur substantial liabilities or be required to limit commercialization of our product candidates, if approved. Even successful defense would require significant financial and management resources. Regardless of the merits or eventual outcome, liability claims may result in:
|
· |
decreased demand for our product candidates or products that we may develop; |
|
· |
injury to our reputation; |
|
· |
withdrawal of clinical trial participants; |
|
· |
initiation of investigations by regulators; |
|
· |
costs to defend the related litigation; |
|
· |
a diversion of management’s time and our resources; |
|
· |
substantial monetary awards to trial participants or patients; |
|
· |
increase in insurance premiums; |
|
· |
product recalls, withdrawals or labeling, marketing or promotional restrictions; |
|
· |
loss of revenues from product sales; |
|
· |
the inability to commercialize our product candidates; and |
|
· |
a decline in our stock price. |
Our inability to obtain and retain sufficient product liability insurance at an acceptable cost to protect against potential product liability claims could prevent or inhibit the commercialization of products we develop. We have a program of product liability insurance covering our ongoing clinical trials; however, the amount of insurance we maintain may not be adequate to cover all liabilities that we may incur. Although we maintain such insurance, any claim that may be brought against us could result in a court judgment or settlement in an amount that is not covered, in whole or in part, by our insurance or that is in excess of the limits of our insurance coverage. Our insurance policies also have various exclusions, and we may be subject to a product liability claim for which we have no coverage. We will have to pay any
45
amounts awarded by a court or negotiated in a settlement that exceed our coverage limitations or that are not covered by our insurance, and we may not have, or be able to obtain, sufficient capital to pay such amounts.
Our internal computer systems, or those used by our CROs or other contractors or consultants, may fail or suffer security breaches.
We and our business partners maintain sensitive company data on our computer networks, including our intellectual property and proprietary business information, as well as certain clinical trial information. Cybersecurity attacks are becoming more commonplace and include, but are not limited to, malicious software, attempts to gain unauthorized access to data and other electronic security breaches that could lead to disruptions in systems, misappropriation of information and corruption of data. Despite the implementation of security measures, our internal computer systems and those of our CROs and other contractors and consultants are vulnerable to damage from computer viruses, unauthorized access, natural disasters, terrorism, war and telecommunication and electrical failures. While we have not experienced any such material system failure, accident or security breach to date, if such an event were to occur and cause interruptions in our operations, it could result in a material disruption of our development programs and business operations. For example, the loss of clinical trial data from completed or ongoing or planned clinical trials could result in delays in our regulatory approval efforts and significantly increase our costs to recover or reproduce the data. To the extent that any disruption or security breach were to result in a loss of or damage to our data or applications, or inappropriate disclosure of confidential or proprietary information, we could incur liability and the further development of our product candidates could be delayed.
Risks Related to Our Intellectual Property
If our efforts to protect the proprietary nature of the intellectual property related to our technologies are not adequate, we may not be able to compete effectively in our market.
We rely upon a combination of patents, trade secret protection and confidentiality agreements to protect the intellectual property related to our technologies. Any disclosure to or misappropriation by third parties of our confidential proprietary information could enable competitors to quickly duplicate or surpass our technological achievements, thus eroding our competitive position in our market.
The strength of patents in the biotechnology and pharmaceutical field involves complex legal and scientific questions and can be uncertain. The patent applications that we own or license may fail to result in issued patents in the United States or in other foreign countries. Even if the patents do successfully issue, third parties may challenge the validity, enforceability or scope thereof, which may result in such patents being narrowed, invalidated or held unenforceable. Two oppositions were filed in the granted European counterpart of the rucaparib camsylate salt/polymorph patent on June 20, 2017. Furthermore, even if they are unchallenged, our patents and patent applications may not adequately protect our intellectual property or prevent others from designing around our claims. If the breadth or strength of protection provided by the patent applications we hold or pursue with respect to our product candidates is threatened, it could threaten our ability to commercialize our product candidates. Further, if we encounter delays in our clinical trials, the period of time during which we could market our product candidates under patent protection would be reduced. Since patent applications in the United States and most other countries are confidential for a period of time after filing, we cannot be certain that we were the first to file any patent application related to our product candidates. Furthermore, an interference proceeding can be provoked by a third-party or instituted by the United States Patent and Trademark Office (“U.S. PTO”) to determine who was the first to invent any of the subject matter covered by the patent claims of our applications.
In addition to the protection afforded by patents, we seek to rely on trade secret protection and confidentiality agreements to protect proprietary know-how that is not patentable, processes for which patents are difficult to enforce and any other elements of our drug development processes that involve proprietary know-how, information or technology that is not covered by patents. Although we require all of our employees to assign their inventions to us, and all of our employees, consultants, advisors and any third parties who have access to our proprietary know-how, information or technology to enter into confidentiality agreements, we cannot be certain that our trade secrets and other confidential proprietary information will not be disclosed or that competitors will not otherwise gain access to our trade secrets or independently develop substantially equivalent information and techniques. Further, the laws of some foreign countries do not protect proprietary rights to the same extent or in the same manner as the laws of the United States. As a result, we may encounter significant problems in protecting and defending our intellectual property both in the United
46
States and abroad. If we are unable to prevent material disclosure of the intellectual property related to our technologies to third parties, we will not be able to establish or maintain a competitive advantage in our market, which could materially adversely affect our business, results of operations and financial condition.
Third-party claims of intellectual property infringement may prevent or delay our drug discovery and development efforts.
Our commercial success depends in part on our avoiding infringement of the patents and proprietary rights of third parties. There is a substantial amount of litigation involving patent and other intellectual property rights in the biotechnology and pharmaceutical industries, including interference, inter parties review and reexamination proceedings before the U.S. PTO or oppositions and other comparable proceedings in foreign jurisdictions. Numerous United States and foreign issued patents and pending patent applications, which are owned by third parties, exist in the fields in which we are developing product candidates. As the biotechnology and pharmaceutical industries expand and more patents are issued, the risk increases that our product candidates may give rise to claims of infringement of the patent rights of others.
Third parties may assert that we are employing their proprietary technology without authorization. There are or may be third-party patents with claims to materials, formulations, methods of manufacture or methods for treatment related to the use or manufacture of our product candidates. Because patent applications can take many years to issue, there may be currently pending patent applications, which may later result in issued patents that our product candidates may infringe. In addition, third parties may obtain patents in the future and claim that use of our technologies infringes upon these patents. If any third-party patents were held by a court of competent jurisdiction to cover the manufacturing process of any of our product candidates, any molecules formed during the manufacturing process or any final product itself, the holders of any such patents may be able to block our ability to commercialize such product candidate unless we obtain a license under the applicable patents, or until such patents expire or they are finally determined to be held invalid or unenforceable. Similarly, if any third-party patent were held by a court of competent jurisdiction to cover aspects of our formulations, processes for manufacture or methods of use, including combination therapy or patient selection methods, the holders of any such patent may be able to block our ability to develop and commercialize the applicable product candidate unless we obtain a license, limit our uses, or until such patent expires or is finally determined to be held invalid or unenforceable. In either case, such a license may not be available on commercially reasonable terms or at all.
Parties making claims against us may obtain injunctive or other equitable relief, which could effectively block our ability to further develop and commercialize one or more of our product candidates. Defense of these claims, regardless of their merit, would involve substantial litigation expense and would be a substantial diversion of employee resources from our business. In the event of a successful claim of infringement against us, we may have to pay substantial damages, including treble damages and attorneys’ fees for willful infringement, obtain one or more licenses from third parties, limit our uses, pay royalties or redesign our infringing product candidates, which may be impossible or require substantial time and monetary expenditure. We cannot predict whether any such license would be available at all or whether it would be available on commercially reasonable terms. Furthermore, even in the absence of litigation, we may need to obtain licenses from third parties to advance our research or allow commercialization of our product candidates. We may fail to obtain any of these licenses at a reasonable cost or on reasonable terms, if at all. In that event, we would be unable to further develop and commercialize one or more of our product candidates, which could harm our business significantly.
The patent protection, patent prosecution and patent enforcement for some of our product candidates is dependent on third parties.
While we normally seek and gain the right to fully prosecute, maintain and enforce the patents relating to our product candidates, there may be times when platform technology patents that relate to our product candidates are controlled by our licensors. This is the case with the method of use patents licensed under the AstraZeneca license. This is also the case with our license to rociletinib, under which Celgene holds the right to prosecute and maintain the patents and patent applications covering its core discovery technology, including molecular backbones, building blocks and classes of compounds generated by that technology, aspects of which relate to rociletinib. We have the right to jointly prosecute and maintain, and the first right to enforce, the patent rights for the composition of matter for rociletinib. If AstraZeneca, Celgene or any of our future licensing partners fail to appropriately prosecute, maintain or enforce, as applicable, patent protection for patents covering any of our product candidates, our ability to develop and commercialize those product
47
candidates may be adversely affected and we may not be able to prevent competitors from making, using and selling competing products.
We may be involved in lawsuits to protect or enforce our patents or the patents of our licensors, which could be expensive, time consuming and unsuccessful.
Competitors may infringe our patents or the patents of our licensors. To counter infringement or unauthorized use, we may be required to file infringement claims, which can be expensive and time-consuming. In addition, in an infringement proceeding, a court may decide that a patent of ours or our licensors is not valid or is unenforceable, or may refuse to stop the other party from using the technology at issue on the grounds that our patents do not cover the technology in question. An adverse result in any litigation or defense proceedings could put one or more of our patents at risk of being invalidated, held unenforceable or interpreted narrowly and could put our patent applications at risk of not issuing.
Interference proceedings provoked by third parties or brought by the U.S. PTO may be necessary to determine the priority of inventions with respect to our patents or patent applications or those of our licensors. An unfavorable outcome could require us to cease using the related technology or to attempt to license rights to it from the prevailing party. Our business could be harmed if the prevailing party does not offer us a license on commercially reasonable terms. Litigation or interference proceedings may fail and, even if successful, may result in substantial costs and distract our management and other employees.
We may not be able to prevent, alone or with our licensors, misappropriation of our trade secrets or confidential information, particularly in countries where the laws may not protect those rights as fully as in the United States. Furthermore, because of the substantial amount of discovery required in connection with intellectual property litigation, there is a risk that some of our confidential information could be compromised by disclosure during this type of litigation. In addition, there could be public announcements of the results of hearings, motions or other interim proceedings or developments. If securities analysts or investors perceive these results to be negative, it could have a substantial adverse effect on the price of our common stock.
We may not be able to protect our intellectual property rights throughout the world.
Filing, prosecuting and defending patents on all of our product candidates throughout the world would be prohibitively expensive. Competitors may use our technologies in jurisdictions where we have not obtained patent protection to develop their own products and further, may export otherwise infringing products to territories where we have patent protection, but enforcement is not as strong as that in the United States. These products may compete with our products in jurisdictions where we do not have any issued patents and our patent claims or other intellectual property rights may not be effective or sufficient to prevent them from so competing.
Many companies have encountered significant problems in protecting and defending intellectual property rights in foreign jurisdictions. The legal systems of certain countries, particularly certain developing countries, do not favor the enforcement of patents and other intellectual property protection, particularly those relating to biopharmaceuticals, which could make it difficult for us to stop the infringement of our patents or marketing of competing products in violation of our proprietary rights generally. Proceedings to enforce our patent rights in foreign jurisdictions could result in substantial cost and divert our efforts and attention from other aspects of our business.
If we breach any of the agreements under which we license commercialization rights to our product candidates from third parties, we could lose license rights that are important to our business.
We license the use, development and commercialization rights for all of our product candidates, and may enter into similar licenses in the future. Under each of our existing license agreements we are subject to commercialization and development, diligence obligations, milestone payment obligations, royalty payments and other obligations. If we fail to comply with any of these obligations or otherwise breach our license agreements, including by failing to use commercially reasonable efforts to develop or commercialize the product candidate, our licensing partners may have the right to terminate the license in whole or in part. Generally, the loss of any one of our licenses or other licenses in the future could materially harm our business, prospects, financial condition and results of operations.
48
Intellectual property rights do not necessarily address all potential threats to our competitive advantage.
The degree of future protection afforded by our intellectual property rights is uncertain because intellectual property rights have limitations, and may not adequately protect our business, or permit us to maintain our competitive advantage. The following examples are illustrative:
|
· |
others may be able to make compounds that are similar to our product candidates but that are not covered by the claims of the patents that we own or have exclusively licensed; |
|
· |
we or our licensors or strategic partners might not have been the first to make the inventions covered by the issued patent or pending patent application that we own or have exclusively licensed; |
|
· |
we or our licensors or strategic partners might not have been the first to file patent applications covering certain of our inventions; |
|
· |
others may independently develop similar or alternative technologies or duplicate any of our technologies without infringing our intellectual property rights; |
|
· |
it is possible that our pending patent applications will not lead to issued patents; |
|
· |
issued patents that we own or have exclusively licensed may not provide us with any competitive advantages, or may be held invalid or unenforceable, as a result of legal challenges by our competitors; |
|
· |
our competitors might conduct research and development activities in countries where we do not have patent rights and then use the information learned from such activities to develop competitive products for sale in our major commercial markets; |
|
· |
we may not develop additional proprietary technologies that are patentable; and |
|
· |
the patents of others may have an adverse effect on our business. |
Should any of these events occur, they could significantly harm our business, results of operations and prospects.
Risks Related to Ownership of our Common Stock and Convertible Senior Notes
There may not be a viable public market for our common stock and as a result it may be difficult for you to sell your shares of our common stock.
Our common stock had not been publicly traded prior to our initial public offering in November 2011. An active trading market for our common stock on the NASDAQ Global Select Market may not be sustained. As a result of these and other factors, you may be unable to resell your shares at a price that is attractive to you or at all. Further, an inactive market may also impair our ability to raise capital by selling shares of our common stock and may impair our ability to enter into strategic partnerships or acquire companies or products by using our shares of common stock as consideration.
The price of our stock has been, and may continue to be, volatile, and you could lose all or part of your investment.
The trading price of our common stock has been, and may continue to be, volatile and could be subject to wide fluctuations in response to various factors, some of which are beyond our control. During the 12-month period ended December 31, 2017, the price of our common stock on the NASDAQ Global Select Market ranged from $39.83 per share to $99.45 per share. In addition to the factors discussed in this “Risk Factors” section and elsewhere in this report, these factors include:
|
· |
adverse results of regulatory actions or decisions; |
|
· |
our failure to successfully commercialize our product candidates, if approved; |
|
· |
actual or anticipated adverse results or delays in our clinical trials; |
|
· |
unanticipated serious safety concerns related to the use of any of our product candidates; |
|
· |
changes in laws or regulations applicable to our product candidates, including but not limited to clinical trial requirements for approvals; |
49
|
· |
disputes or other developments relating to proprietary rights, including patents, litigation matters and our ability to obtain patent protection for our product candidates; |
|
· |
our decision to initiate a clinical trial, not to initiate a clinical trial or to terminate an existing clinical trial; |
|
· |
inability to obtain adequate product supply for any approved drug product or inability to do so at acceptable prices; |
|
· |
our dependence on third parties, including CMOS and CROs, as well as our partners that provide us with companion diagnostic products; |
|
· |
additions or departures of key scientific or management personnel; |
|
· |
failure to meet or exceed any financial guidance or expectations regarding development milestones that we may provide to the public; |
|
· |
actual or anticipated variations in quarterly operating results; |
|
· |
failure to meet or exceed the estimates and projections of the investment community; |
|
· |
overall performance of the equity markets and other factors that may be unrelated to our operating performance or the operating performance of our competitors, including changes in market valuations of similar companies; |
|
· |
conditions or trends in the biotechnology and biopharmaceutical industries; |
|
· |
introduction of new products offered by us or our competitors; |
|
· |
announcements of significant acquisitions, strategic partnerships, joint ventures or capital commitments by us or our competitors; |
|
· |
issuances of debt or equity securities; |
|
· |
significant lawsuits, including patent or stockholder litigation; |
|
· |
sales of our common stock by us or our stockholders in the future; |
|
· |
trading volume of our common stock; |
|
· |
publication of research reports about us or our industry or positive or negative recommendations or withdrawal of research coverage by securities analysts; |
|
· |
ineffectiveness of our internal controls; |
|
· |
general political and economic conditions; |
|
· |
effects of natural or man-made catastrophic events; and |
|
· |
other events or factors, many of which are beyond our control. |
In addition, the stock market in general, and the NASDAQ Global Select Market and biotechnology companies in particular, have experienced extreme price and volume fluctuations that have often been unrelated or disproportionate to the operating performance of these companies. Broad market and industry factors may negatively affect the market price of our common stock, regardless of our actual operating performance. The realization of any of the above risks or any of a broad range of other risks, including those described in these “Risk Factors,” could have a dramatic and material adverse effect on the market price of our common stock.
Because our outstanding Notes are convertible into shares of our common stock, volatility or depressed prices of our common stock could have a similar effect on the trading price of our Notes. In addition, the existence of the Notes may encourage short selling in our common stock by market participants because the conversion of the Notes could depress the price of our common stock.
The conversion of some or all of the Notes may dilute the ownership interest of existing stockholders. Holders of the outstanding Notes are able to convert them at any time prior to the close of business on the business day immediately preceding September 15, 2021. Upon conversion, holders of the Notes will receive shares of common stock. Any sales in the public market of shares of common stock issued upon conversion of such Notes could adversely affect the trading price of our common stock. We cannot predict the size of future issuances or the effect, if any, that they may have on the
50
market price of our common stock. The issuance and sale of substantial amounts of common stock, or the perception that such issuances and sales may occur, could adversely affect the market price of our common stock and impair our ability to raise capital through the sale of additional equity or convertible debt securities.
Following periods of volatility in a company’s stock price, litigation has often been initiated against companies. Following the decline in our stock price related to the rociletinib regulatory update in November 2015, a number of lawsuits have been filed against us (see “Part I, Item 3-Legal Proceedings”). These proceedings and other similar litigation, if instituted against us, could result in substantial costs and diversion of management’s attention and resources, which could materially and adversely affect our business and financial condition.
Certain members of management and their affiliates own a significant percentage of our stock and will be able to exert influence over matters subject to stockholder approval.
Our executive officers, directors and their respective affiliates known to us beneficially owned approximately 6.7% of our voting stock as of February 21, 2018. These stockholders may have the ability to influence the outcome of matters submitted to our stockholders for approval. The interests of our executive officers, directors, and their affiliates might not coincide with the interests of the other holders of our capital stock which may prevent or discourage unsolicited acquisition proposals or offers for our common stock that you may feel are in your best interest as one of our stockholders.
Sales of a substantial number of shares of our common stock in the public market could cause our stock price to fall.
Shares of common stock that are either subject to outstanding options or reserved for future issuance under our equity incentive plans will become eligible for sale in the public market to the extent permitted by the provisions of various vesting schedules. If these additional shares of common stock are sold, or if it is perceived that they will be sold, in the public market, the trading price of our common stock could decline.
Future sales and issuances of our common stock or rights to purchase common stock, including pursuant to our equity incentive plans, could result in additional dilution of the percentage ownership of our stockholders and could cause our stock price to fall.
We expect that significant additional capital will be needed in the future to continue our planned operations. To raise capital, we may sell common stock, convertible securities or other equity securities in one or more transactions at prices and in a manner we determine from time to time. If we sell common stock, convertible securities or other equity securities in more than one transaction, investors may be materially diluted by subsequent sales. Such sales may also result in material dilution to our existing stockholders, and new investors could gain rights, preferences and privileges senior to those of holders of our common stock.
Pursuant to our equity incentive plan(s), our compensation committee (or its designee) is authorized to grant equity-based incentive awards to our employees, directors and consultants. As of December 31, 2017, the number of shares of our common stock available for future grant under our 2011 Stock Incentive Plan (“2011 Plan”) is 3,147,903. The number of shares of our common stock reserved for issuance under our 2011 Plan will be increased (i) from time to time by the number of shares of our common stock forfeited upon the expiration, cancellation, forfeiture, cash settlement or other termination of awards under our 2009 Equity Incentive Plan, and (ii) at the discretion of our board of directors, on the date of each annual meeting of our stockholders, by up to the lesser of (x) a number of additional shares of our common stock representing 4% of our then-outstanding shares of common stock on such date and (y) 2,758,621 shares of our common stock. Future option and restricted stock unit, or RSU, grants and issuances of common stock under our 2011 Plan may have an adverse effect on the market price of our common stock. In addition, a substantial number of shares of our common stock are reserved for issuance upon conversion of the Notes.
Some provisions of our charter documents and Delaware law may have anti-takeover effects that could discourage an acquisition of us by others, even if an acquisition would be beneficial to our stockholders and may prevent attempts by our stockholders to replace or remove our current management.
Provisions in our amended and restated certificate of incorporation and bylaws, as well as provisions of Delaware law, could make it more difficult for a third-party to acquire us or increase the cost of acquiring us, even if doing so would benefit our stockholders or remove our current management. These provisions include:
51
|
· |
authorizing the issuance of “blank check” preferred stock, the terms of which may be established and shares of which may be issued without stockholder approval; |
|
· |
limiting the removal of directors by the stockholders; |
|
· |
creating a staggered board of directors; |
|
· |
prohibiting stockholder action by written consent, thereby requiring all stockholder actions to be taken at a meeting of our stockholders; |
|
· |
eliminating the ability of stockholders to call a special meeting of stockholders; |
|
· |
permitting our board of directors to accelerate the vesting of outstanding option grants upon certain transactions that result in a change of control; and |
|
· |
establishing advance notice requirements for nominations for election to the board of directors or for proposing matters that can be acted upon at stockholder meetings. |
These provisions may frustrate or prevent any attempts by our stockholders to replace or remove our current management by making it more difficult for stockholders to replace members of our board of directors, which is responsible for appointing the members of our management. Because we are incorporated in Delaware, we are governed by the provisions of Section 203 of the Delaware General Corporation Law, which may discourage, delay or prevent someone from acquiring us or merging with us whether or not it is desired by or beneficial to our stockholders. Under Delaware law, a corporation may not, in general, engage in a business combination with any holder of 15% or more of its capital stock unless the holder has held the stock for three years or, among other things, the board of directors has approved the transaction. Any provision of our certificate of incorporation or bylaws or Delaware law that has the effect of delaying or deterring a change in control could limit the opportunity for our stockholders to receive a premium for their shares of our common stock, and could also affect the price that some investors are willing to pay for our common stock. Additionally, certain provisions of our outstanding Notes could make it more difficult or more expensive for a third party to acquire us. The repurchase price of the Notes must be paid in cash, and this obligation may have the effect of discouraging, delaying or preventing an acquisition of the Company that would otherwise be beneficial to our security holders.
If securities or industry analysts do not publish research or publish inaccurate or unfavorable research about our business, our stock price and trading volume could decline.
The trading market for our common stock depends in part on the research and reports that securities or industry analysts publish about us or our business. If one or more of the analysts who cover us downgrades our stock or publishes inaccurate or unfavorable research about our business, our stock price would likely decline. If one or more of these analysts ceases coverage of our company or fails to publish reports on us regularly, demand for our stock could decrease, which might cause our stock price and trading volume to decline.
We may not be able to raise the funds necessary to repurchase the Notes upon a fundamental change, and our future debt may contain limitations on our ability to repurchase the Notes.
If we undergo a fundamental change, as defined in the indenture, prior to the maturity date of the Notes, holders may require us to repurchase for cash all or any portion of the Notes at a fundamental change repurchase price equal to 100% of the principal amount of the Notes to be repurchased, plus accrued and unpaid interest to, but excluding, the fundamental change repurchase date. We may not have or be able to borrow the funds required to repurchase the Notes on the fundamental change repurchase date. In addition, our ability to repurchase the Notes may otherwise be limited by law, regulatory authority or agreements governing our future indebtedness. Our failure to repurchase the Notes at a time when the repurchase is required by the indenture would constitute a default under the indenture. A default under the indenture or the fundamental change itself could also lead to a default under agreements governing our future indebtedness. If the repayment of the related indebtedness were to be accelerated after any applicable notice or grace periods, we may not have sufficient funds to repay the indebtedness and repurchase the Notes when required.
We may incur substantially more debt or take other actions which would intensify the risks discussed above; and we may not generate cash flow from operations in the future sufficient to satisfy our obligations under the Notes and any future indebtedness we may incur.
52
We may incur substantial additional debt in the future, subject to the restrictions contained in any debt instruments that we enter into in the future, some of which may be secured debt. We are not restricted under the terms of the indenture governing the Notes from incurring additional debt, securing existing or future debt, recapitalizing our debt or taking a number of other actions that are not limited by the terms of the indenture governing the Notes that could have the effect of diminishing our ability to make payments on the Notes when due. Our ability to refinance the Notes or future indebtedness will depend on the capital markets and our financial condition at such time. In addition, agreements that govern any future indebtedness that we may incur may contain financial and other restrictive covenants that will limit our ability to engage in activities that may be in our long-term best interests. Our failure to comply with those covenants could result in an event of default that, if not cured or waived, could result in the acceleration of some or all of our debt.
ITEM 1B.UNRESOLVED STAFF COMMENTS
Not applicable.
Our principal offices are located at five leased facilities, a 29,177 square foot facility in Boulder, Colorado used primarily for corporate functions, a 24,877 square foot facility in San Francisco, California and a 32,660 square foot facility in Oakland, CA used for clinical development operations and research laboratory space, a 3,350 square foot facility in Cambridge, United Kingdom used for our European regulatory and clinical operations and a 416 square foot facility in Milan, Italy used for clinical operations. These leases expire in January 2023, December 2021, April 2028, May 2019 and March 2018, respectively. We believe that our existing facilities are sufficient for our needs for the foreseeable future.
Rociletinib-Related Litigation
Following Clovis’ regulatory announcement in November 2015 of adverse developments in its ongoing clinical trials for rociletinib, Clovis and certain of its current and former executives were named in various securities lawsuits, the largest of which was a putative class action lawsuit in the District of Colorado (the “Medina Action”) which was settled on October 26, 2017 (the “Medina Settlement”). The open actions currently pending against Clovis are discussed below. While other entities have threatened to bring claims relating to rociletinib and the November 2015 announcement, none have commenced litigation as of the date of this filing.
On January 22, 2016, the Electrical Workers Local #357 Pension and Health & Welfare Trusts, a purported shareholder of Clovis, filed a purported class action complaint (the “Electrical Workers Complaint”) against Clovis and certain of its officers, directors, investors and underwriters in the Superior Court of the State of California, County of San Mateo (the “Electrical Workers Court”). The Electrical Workers Complaint purports to be asserted on behalf of a class of persons who purchased stock in the July 2015 Offering. The complaint asserted claims under certain provisions of the Securities Act of 1933 (the “Securities Act”) relating to a July 2015 follow-on offering of Clovis securities (the “July 2015 Offering”) based on substantially similar allegations to those asserted in the Medina Action. On June 30, 2016, the Electrical Workers Plaintiffs filed an amended complaint adding new allegations (the “Amended Complaint”).
On July 28, 2016, the defendants filed a motion to stay the Electrical Workers action pending resolution of the Medina Action and a demurrer to the Amended Complaint. On September 23, 2016, after hearing oral argument, the Electrical Workers Court granted the motion to stay and reserved on issuing a ruling on defendants’ pending demurrer.
The Company believes that the claims asserted in the Electrical Workers Action are released and barred by operation of law through the Medina Settlement, and accordingly plans to seek dismissal of the Electrical Workers Action on that basis.
On November 10, 2016, Antipodean Domestic Partners (“Antipodean”) filed a complaint (the “Antipodean Complaint”) against Clovis and certain of its officers, directors and underwriters in New York Supreme Court, County of New York. The Antipodean Complaint alleges that the defendants violated certain sections of the Securities Act by making allegedly false statements to Antipodean and in the offering materials for the July 2015 Offering relating to the
53
efficacy of rociletinib, its safety profile, and its prospects for market success. In addition to the Securities Act claims, the Antipodean Complaint also asserts Colorado state law claims and common law claims. Both the state law and common law claims are based on allegedly false and misleading statements regarding rociletinib’s progress toward FDA approval. The Antipodean Complaint seeks compensatory, recessionary, and punitive damages.
On December 15, 2016, the Antipodean Plaintiffs filed an amended complaint (the “Antipodean Amended Complaint”) asserting substantially the same claims against the same defendants and purporting to correct certain details in the original Antipodean Complaint.
On January 31, 2017, Defendants filed a motion to stay the Antipodean action pending resolution of the Medina Action in the District of Colorado. Defendants also filed a motion to dismiss the Antipodean Amended Complaint on March 29, 2017.
On March 14, 2017, the Clovis Defendants and Antipodean participated in a mediation, which did not result in a settlement.
On August 8, 2017, the parties participated in a scheduled hearing on Defendants’ motion to stay and motion to dismiss before Justice Masley of the New York Supreme Court, County of New York. At the hearing, Justice Masley granted Defendants’ motion to stay. Per the Court’s August 10, 2017 order, Defendants’ motion to dismiss was held in abeyance and deemed submitted on November 1, 2017. On November 1, 2017, the Defendants provided a status update to the Court regarding the outcome of the hearing. The update informed the Court that Antipodean had excluded itself from the Medina Settlement, as memorialized in the final judgment entered by the Medina Court. No date has been scheduled for argument on Defendants’ motion to dismiss.
The Company intends to vigorously defend against the allegations in the Antipodean Amended Complaint. However, there can be no assurance that the defense will be successful.
In March 2017, two putative shareholders of the Company, Macalinao and McKenry (the “Derivative Plaintiffs”), filed shareholder derivative complaints against certain directors and officers of the Company in the Court of Chancery of the State of Delaware. On May 4, 2017, the Macalinao and McKenry actions were consolidated for all purposes in a single proceeding under the caption In re Clovis Oncology, Inc. Derivative Litigation, Case No, 2017-0222 (the “Consolidated Derivative Action”).
On May 18, 2017, the Derivative Plaintiffs filed a Consolidated Verified Shareholder Derivative Complaint (the “Consolidated Derivative Complaint”). The Consolidated Derivative Complaint generally alleged that the defendants breached their fiduciary duties owed to the Company by allegedly causing or allowing misrepresentations of the Company’s business operations and prospects, failing to ensure that the TIGER-X clinical trial was being conducted in accordance with applicable rules, regulations and protocols, and engaging in insider trading. The Consolidated Derivative Complaint purported to rely on documents produced by the Company in response to prior demands for inspection of the Company’s books and records served on the Company by each of Macalinao and McKenry under 8 Del. C. § 220. The Consolidated Derivative Complaint sought, among other things, an award of money damages.
On July 31, 2017, the defendants filed a motion to dismiss the Consolidated Derivative Complaint. Plaintiffs filed an opposition to the motion to dismiss on August 31, 2017, and the defendants filed a reply in further support of the motion to dismiss on September 26, 2017. No date has been scheduled for argument on Defendants’ motion to dismiss the Consolidated Derivative Complaint.
The Company intends to vigorously defend against the allegations in the Consolidated Derivative Complaint, but there can be no assurance that the defense will be successful.
On March 20, 2017, a purported shareholder of the Company, filed a shareholder derivative complaint (the “Guo Complaint”) against certain officers and directors of the Company in the United States District Court for the District of Colorado. The Guo Complaint generally alleged that the defendants breached their fiduciary duties owed to the Company by either recklessly or with gross negligence approving or permitting misrepresentations of the Company’s business operations and prospects. The Guo Complaint also alleged claims for waste of corporate assets and unjust enrichment. Finally, the Guo Complaint alleged that certain of the individual defendants violated Section 14(a) of the Securities Exchange Act, by allegedly negligently issuing, causing to be issued, and participating in the issuance of
54
materially misleading statements to stockholders in the Company’s Proxy Statement on Schedule DEF 14A in connection with the 2015 Annual Meeting of Stockholders, held on June 11, 2015. The Guo Complaint sought, among other things, an award of money damages.
On June 19, 2017, the parties filed a joint motion to stay the Guo action pending resolution of the motion to dismiss the Consolidated Derivative Complaint. On June 20, 2017, the court granted the motion to stay.
The Company intends to vigorously defend against the allegations in the Guo Complaint, but there can be no assurance that the defense will be successful.
In addition, the Company has received inquiries and requests for information from governmental agencies, including the U.S. Securities and Exchange Commission and the U.S. Department of Justice, relating to the Company’s regulatory update announcement in November 2015 that the FDA requested additional clinical data on the efficacy and safety of rociletinib. The Company is continuing to cooperate with these agencies with respect to their investigations. The Medina Settlement does not resolve these inquiries and the Company cannot predict their timing or outcome.
Director Compensation Litigation
On May 10, 2017, John Solak, a purported shareholder of the Company, filed a shareholder derivative complaint in the Court of Chancery of the State of Delaware (the “Solak Complaint”) against certain directors and an officer of the Company. The Solak Complaint generally alleged that the defendants breached their fiduciary duties owed to the Company by adopting a compensation plan that overcompensated the non-employee director defendants, in relation to companies of comparable market capitalization and size. The Solak Complaint also alleged claims of waste of corporate assets and unjust enrichment due to this allegedly wrongful compensation plan. The Solak Complaint sought, among other things, an award of money damages and the imposition of corporate governance reforms.
The Court has entered a number of orders extending the defendants’ time to respond to the Solak Complaint based on, among other factors, the fact that the parties are engaged in discussions in an effort to resolve the Solak action. On February 14, 2018, the parties filed a joint letter to the Court requesting that all deadlines in the action be held in abeyance while the parties engaged in final settlement discussions.
On February 26, 2018, the defendants entered into a stipulation of compromise and settlement with plaintiff that is intended to settle the Solak action. The proposed settlement is subject to Court approval upon the conclusion of a settlement hearing concerning the fairness of the terms of the proposed settlement, which will be scheduled following the provision of notice to shareholders of the Company.
In accordance with the terms of the proposed settlement, the Company will present a new non-employee director compensation policy for shareholder vote at the next annual shareholder meeting. Under the proposed new non-employee director compensation policy, annual base compensation for incumbent non-employee directors would be set at an amount between $350,000 and $425,000, which would remain in place for a period between two and five years. Additionally, the proposed policy sets annual base compensation for new non-employee directors at an amount between $525,000 and $637,500 and includes fixed annual fees for board and committee service. The proposed settlement also sets forth a number of corporate governance reforms that the Company will undertake, including, enhanced proxy disclosures, the codification of the Company’s stock ownership guidelines for directors, and enhanced disclosure requirements for certain forms of director compensation. While no cash payments will be made to investors as part of the proposed settlement, plaintiff’s counsel is expected to file a fee application which the Company has agreed not to oppose up to an agreed-upon amount. The proposed settlement contains no admission of wrongdoing.
ITEM 4.MINE SAFETY DISCLOSURES
Not applicable.
55
ITEM 5.MARKET FOR REGISTRANT’S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES
Market Information and Holders
Our common stock trades on the NASDAQ Global Select Market under the symbol “CLVS.” The following table sets forth, for the periods indicated, the high and low sales prices for our common stock as reported on the NASDAQ Global Select Market:
|
|
|
HIGH |
|
LOW |
|
||
|
Balance, December 31, 2017 |
|
|
|
|
|
|
|
|
First Quarter |
|
$ |
74.94 |
|
$ |
39.83 |
|
|
Second Quarter |
|
$ |
96.92 |
|
$ |
45.42 |
|
|
Third Quarter |
|
$ |
99.45 |
|
$ |
64.61 |
|
|
Fourth Quarter |
|
$ |
86.26 |
|
$ |
57.33 |
|
|
Balance, December 31, 2016 |
|
|
|
|
|
|
|
|
First Quarter |
|
$ |
34.75 |
|
$ |
16.78 |
|
|
Second Quarter |
|
$ |
20.90 |
|
$ |
11.57 |
|
|
Third Quarter |
|
$ |
40.29 |
|
$ |
13.43 |
|
|
Fourth Quarter |
|
$ |
46.97 |
|
$ |
25.50 |
|
On February 21, 2018, there were approximately 24 holders of record of our common stock. The holders of record number does not include a substantially greater number of holders whose shares are held of record in nominee or street name accounts through banks, brokers and/or other financial institutions.
Dividends
We have never declared or paid any cash dividends on our capital stock. We currently intend to retain all available funds and any future earnings to support our operations and finance the growth and development of our business. We do not intend to pay cash dividends on our common stock for the foreseeable future. Any future determination related to our dividend policy will be made at the discretion of our board of directors and will depend upon, among other factors, our results of operations, financial condition, capital requirements, contractual restrictions, business prospects and other factors our board of directors may deem relevant.
Securities Authorized for Issuance Under Equity Compensation Plans
Equity Compensation Plan Information
As of December 31, 2017
|
|
|
|
|
|
|
|
Number of |
|
|
|
|
|
|
|
|
|
securities |
|
|
|
|
|
|
|
|
|
remaining |
|
|
|
|
|
|
|
|
|
available |
|
|
|
|
|
|
|
|
|
for issuance |
|
|
|
|
|
|
|
|
|
under equity |
|
|
|
|
|
|
|
|
|
compensation |
|
|
|
|
|
|
Weighted- |
|
plans |
|
|
|
|
|
Number of securities to |
|
average |
|
(excluding |
|
|
|
|
|
be issued upon exercise |
|
exercise price |
|
securities |
|
|
|
|
|
of outstanding options |
|
of outstanding |
|
reflected |
|
|
|
|
|
and restricted stock |
|
options |
|
in column (a)) |
|
|
|
Plan Category |
|
(a) |
|
(b) |
|
(c) |
|
|
|
Equity compensation plans approved by security holders (1) (2) |
|
6,379,264 |
|
$ |
46.77 |
|
3,147,903 |
|
|
Equity compensation plans not approved by security holders |
|
— |
|
|
— |
|
— |
|
|
Total |
|
6,379,264 |
|
$ |
46.77 |
|
3,147,903 |
|
56
(1)As of December 31, 2017, 9,590,378 shares were authorized for issuance under our 2011 Stock Incentive Plan (“2011 Plan”), which became effective upon closing of our initial public offering in November 2011, including 192,185 remaining shares available for future issuance under the 2009 Equity Incentive Plan (“2009 Plan”), which were transferred to the 2011 Plan. The number of shares of our common stock reserved for issuance under the 2011 Plan will be increased (i) from time to time by the number of shares of our common stock forfeited upon the expiration, cancellation, forfeiture, cash settlement or other termination of awards under the 2009 Plan and (ii) at the discretion of our board of directors, on the date of each annual meeting of our stockholders, by up to the lesser of (x) a number of additional shares of our common stock representing 4% of our then-outstanding shares of common stock on such date and (y) 2,758,621 shares of our common stock.
(2)As of December 31, 2017, 558,870 shares were reserved for issuance under our 2011 Employee Stock Purchase Plan (“ESPP”), which became effective upon closing of our initial public offering in November 2011. The number of shares of our common stock reserved for issuance under the ESPP will be increased at the discretion of our board of directors, on the date of each annual meeting of our stockholders, by up to the lesser of (x) a number of additional shares of our common stock representing 1% of our then-outstanding shares of common stock on such date and (y) 344,828 shares of our common stock.
Performance Graph (1)
The following graph shows a comparison from December 31, 2012 through December 31, 2017 of the cumulative total return on an assumed investment of $100 in cash in our common stock, the NASDAQ Composite Index and the NASDAQ Biotechnology Index. Such returns are based on historical results and are not intended to suggest future performance. Data for the NASDAQ Composite Index and the NASDAQ Biotechnology Index assume reinvestment of dividends.

(1)This performance graph shall not be deemed “soliciting material” or to be “filed” with the SEC for purposes of Section 18 of the Securities and Exchange Act of 1934, as amended, or otherwise subject to the liabilities under that Section, and shall not be deemed incorporated by reference into any filing of Clovis Oncology, Inc. under the Securities Act of 1933, as amended.
57
ITEM 6.SELECTED FINANCIAL DATA
The following table sets forth certain of our selected historical financial data at the dates and for the periods indicated. The selected historical statement of operations data presented below for the years ended December 31, 2017, 2016 and 2015 and the historical balance sheet data as of December 31, 2017 and 2016 have been derived from our audited financial statements, which are included elsewhere in this Annual Report on Form 10-K. The historical statement of operations data presented below for the years ended December 31, 2014 and 2013 and the historical balance sheet data as of December 31, 2015, 2014 and 2013 have been derived from our audited financial statements that do not appear in this report.
Our historical results are not necessarily indicative of results expected in any future period.
The selected historical financial data presented below should be read in conjunction with “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and our financial statements and the related notes thereto, which are included elsewhere in this Annual Report on Form 10-K. The selected historical financial information in this section is not intended to replace our financial statements and the related notes thereto.
Statement of Operations Data:
|
|
|
Year Ended December 31, |
|
|||||||||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|
2014 |
|
2013 |
|
|||||
|
|
|
(in thousands, except per share amounts) |
|
|||||||||||||
|
Revenues: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Product revenue, net |
|
$ |
55,511 |
|
$ |
78 |
|
$ |
— |
|
$ |
— |
|
$ |
— |
|
|
License and milestone revenue |
|
|
— |
|
|
— |
|
|
— |
|
|
13,625 |
|
|
— |
|
|
Total revenues |
|
|
55,511 |
|
|
78 |
|
|
— |
|
|
13,625 |
|
|
— |
|
|
Operating expenses: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cost of sales - product |
|
|
10,251 |
|
|
70 |
|
|
— |
|
|
— |
|
|
— |
|
|
Cost of sales - intangible asset amortization |
|
|
1,486 |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
Research and development |
|
|
142,498 |
|
|
251,129 |
|
|
269,251 |
|
|
137,705 |
|
|
66,545 |
|
|
Selling, general and administrative |
|
|
138,907 |
|
|
40,731 |
|
|
30,524 |
|
|
21,457 |
|
|
16,567 |
|
|
Acquired in-process research and development |
|
|
— |
|
|
1,300 |
|
|
12,000 |
|
|
8,806 |
|
|
250 |
|
|
Impairment of intangible asset |
|
|
— |
|
|
104,517 |
|
|
89,557 |
|
|
3,409 |
|
|
— |
|
|
Change in fair value of contingent purchase consideration |
|
|
— |
|
|
(24,936) |
|
|
(24,611) |
|
|
707 |
|
|
405 |
|
|
Total expenses |
|
|
293,142 |
|
|
372,811 |
|
|
376,721 |
|
|
172,084 |
|
|
83,767 |
|
|
Operating loss |
|
|
(237,631) |
|
|
(372,733) |
|
|
(376,721) |
|
|
(158,459) |
|
|
(83,767) |
|
|
Other income (expense): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Interest expense |
|
|
(10,428) |
|
|
(8,491) |
|
|
(8,372) |
|
|
(2,604) |
|
|
— |
|
|
Foreign currency gain (loss) |
|
|
(82) |
|
|
(580) |
|
|
2,740 |
|
|
3,580 |
|
|
(535) |
|
|
Legal settlement loss |
|
|
(105,477) |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
Other income (expense) |
|
|
3,643 |
|
|
633 |
|
|
416 |
|
|
(240) |
|
|
(178) |
|
|
Other income (expense), net |
|
|
(112,344) |
|
|
(8,438) |
|
|
(5,216) |
|
|
736 |
|
|
(713) |
|
|
Loss before income taxes |
|
|
(349,975) |
|
|
(381,171) |
|
|
(381,937) |
|
|
(157,723) |
|
|
(84,480) |
|
|
Income tax benefit (expense) |
|
|
3,578 |
|
|
32,034 |
|
|
29,076 |
|
|
(2,308) |
|
|
(52) |
|
|
Net loss |
|
$ |
(346,397) |
|
$ |
(349,137) |
|
$ |
(352,861) |
|
$ |
(160,031) |
|
$ |
(84,532) |
|
|
Basic and diluted net loss per common share |
|
$ |
(7.36) |
|
$ |
(9.07) |
|
$ |
(9.79) |
|
$ |
(4.72) |
|
$ |
(2.95) |
|
|
Basic and diluted weighted average common shares outstanding |
|
|
47,047 |
|
|
38,478 |
|
|
36,026 |
|
|
33,889 |
|
|
28,672 |
|
58
Balance Sheet Data:
|
|
|
As of December 31, |
|
|||||||||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|
2014 |
|
2013 |
|
|||||
|
|
|
(in thousands) |
|
|||||||||||||
|
Cash, cash equivalents and available-for-sale securities |
|
$ |
563,731 |
|
$ |
266,183 |
|
$ |
528,588 |
|
$ |
482,677 |
|
$ |
323,228 |
|
|
Working capital |
|
|
545,423 |
|
|
213,813 |
|
|
464,125 |
|
|
443,400 |
|
|
307,644 |
|
|
Total assets |
|
|
735,230 |
|
|
364,557 |
|
|
713,386 |
|
|
786,206 |
|
|
649,635 |
|
|
Convertible senior notes |
|
|
282,406 |
|
|
281,126 |
|
|
279,885 |
|
|
278,680 |
|
|
— |
|
|
Common stock and additional paid-in capital |
|
|
1,887,249 |
|
|
1,174,989 |
|
|
1,130,016 |
|
|
785,123 |
|
|
762,204 |
|
|
Total stockholders’ equity (deficit) |
|
|
367,636 |
|
|
(3,634) |
|
|
300,650 |
|
|
331,630 |
|
|
497,886 |
|
59
ITEM 7.MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS
You should read the following discussion and analysis of our financial condition and results of operations together with our financial statements and related notes appearing at the end of this Annual Report on Form 10-K. Some of the information contained in this discussion and analysis or set forth elsewhere in this Annual Report on Form 10-K, including information with respect to our plans and strategy for our business and related financing, includes forward-looking statements that involve risks and uncertainties. You should read the “Risk Factors” section of this report for a discussion of important factors that could cause actual results to differ materially from the results described in or implied by the forward-looking statements contained in the following discussion and analysis.
Overview
We are a biopharmaceutical company focused on acquiring, developing and commercializing innovative anti-cancer agents in the United States, Europe and additional international markets. We target our development programs for the treatment of specific subsets of cancer populations, and simultaneously develop, with partners, diagnostic tools intended to direct a compound in development to the population that is most likely to benefit from its use.
Our marketed product Rubraca® (rucaparib) is approved on an accelerated basis in the United States by the Food and Drug Administration (“FDA”) as monotherapy for the treatment of patients with deleterious BRCA (human genes associated with the repair of damaged DNA) mutation (germline and/or somatic) associated advanced ovarian cancer who have been treated with two or more chemotherapies, and selected for therapy based on an FDA-approved companion diagnostic for Rubraca. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials. We launched Rubraca in the United States in December 2016 for this indication.
The FDA is currently reviewing on a priority review timeline our sNDA for Rubraca as maintenance treatment of adult patients with recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer who are in a complete or partial response to platinum-based chemotherapy.
Our MAA submitted to the EMA for an ovarian cancer treatment indication for Rubraca is currently under review by the EMA’s CHMP. Following a Scientific Advisory Group - Oncology meeting and an oral explanation by us before the CHMP in February 2018, the CHMP has communicated a positive trend vote for the MAA and their intention to hold a final vote on the treatment indication at their March 2018 meeting.
In addition, we have two other product candidates: lucitanib, an oral inhibitor of the tyrosine kinase activity of vascular endothelial growth factor receptors (“VEGFR”) 1-3, platelet-derived growth factor receptors (“PDGFR”) alpha and beta and fibroblast growth factor receptors (“FGFR”) 1-3, and rociletinib, an oral mutant-selective inhibitor of epidermal growth factor receptor (“EGFR”). While we have stopped enrollment in ongoing trials for each of these candidates, we continue to provide drug to patients whose clinicians recommend continuing therapy. We maintain certain development and commercialization rights for lucitanib and global development and commercialization rights for rociletinib.
We commenced operations in April 2009. To date, we have devoted substantially all of our resources to identifying and in-licensing product candidates, performing development activities with respect to those product candidates and the general and administrative support of these operations. Through December 31, 2017, we have generated $13.6 million in license and milestone revenue related to our collaboration and license agreement with Servier and for the year ended December 31, 2017 have generated $55.5 million product revenue related to sales of Rubraca, which we began to commercialize on December 19, 2016. We have principally funded our operations using the net proceeds from the sale of convertible preferred stock, the issuance of convertible promissory notes, public offerings of our common stock and our convertible senior notes offering.
We have never been profitable and, as of December 31, 2017, we had an accumulated deficit of $1,447.4 million. We incurred net losses of $346.4 million, $349.1 million and $352.9 million for the years ended December 31, 2017, 2016 and 2015, respectively, and had cash, cash equivalents and available-for-sale securities totaling $563.7 million at December 31, 2017.
60
We expect to incur significant losses for the foreseeable future, as we incur costs related to commercial activities associated with Rubraca. In January 2017, we sold 5,750,000 shares of our common stock in a public offering at $41.00 per share. The net proceeds from the offering were $221.2 million, after deducting underwriting discounts and commissions and offering expenses. In June 2017, we sold 3,920,454 shares of our common stock in a public offering at $88.00 per share. The net proceeds from the offering were $324.6 million, after deducting underwriting discounts and commissions and offering expenses. Based on our current estimates, we believe that our cash, cash equivalents and available-for-sale securities will allow us to fund activities through at least the next 12 months. Until we can generate a sufficient amount of revenue from Rubraca, we expect to finance our operations in part through additional public or private equity or debt offerings and may seek additional capital through arrangements with strategic partners or from other sources. Adequate additional financing may not be available to us on acceptable terms, or at all. Our failure to raise capital as and when needed would have a negative impact on our financial condition and our ability to pursue our business strategy. We will need to generate significant revenues to achieve profitability, and we may never do so.
Product License Agreements
For a discussion of our product license agreements, see Note 13, License Agreements, in the Notes to Consolidated Financial Statements included in Part II, Item 8, Financial Statements and Supplementary Data, of this Annual Report on Form 10-K.
Financial Operations Overview
Revenue
During 2017, we recorded $55.5 million in revenue related to sales of Rubraca, which we began to commercialize on December 19, 2016. In addition, we distributed free drug to eligible patients through our patient assistance program that represented approximately $14.1 million in commercial value. For further discussion of our revenue recognition policy, see “Critical Accounting Policies and Significant Judgments and Estimates” below. Our ability to generate revenue and become profitable depends upon our ability to successfully commercialize products. Any inability on our part to successfully commercialize Rubraca in the United States and any foreign territories where it may be approved, or any significant delay in such approvals, could have a material adverse impact on our ability to execute upon our business strategy and, ultimately, to generate sufficient revenues from Rubraca to reach or maintain profitability or sustain our anticipated levels of operations.
Currently, we only recognize revenue on product sales once the product is sold to the patient or healthcare provider by the specialty distributor or specialty pharmacy provider, therefore reducing the significance of estimates made for product returns. Effective January 1, 2018, we adopted Accounting Standards Codification (“ASC”), Topic 606, “Revenue from Contracts with Customers”. Upon adoption, we will begin recognizing revenue when our customers, the specialty distributors and specialty pharmacy providers, take control of our product. This will have the impact of us recognizing revenue approximately two to four weeks earlier than before adopting the new standard and will also increase the significance of estimating variable consideration, including product returns, rebates and chargebacks.
We used the modified retrospective method to adopt the new standard. This means that we will not restate previously issued financial statements, but will record a one-time adjustment to retained earnings of $2.3 million. This adjustment represents the sales of our product to our customers prior to January 1, 2018, that have not been sold to patients or healthcare providers, offset by related gross-to-net adjustments and other direct costs, including royalties and sales incentive compensation.
During 2017, revenue was recognized for U.S. tax purposes when our product was sold to the specialty distributors and pharmacies, a method that differs from book treatment. This difference in revenue recognition resulted in the establishment of the deferred tax asset for the sales value of our product held by our specialty distributor and pharmacy providers at December 31, 2017. The deferred tax asset was offset by a full valuation allowance and has no impact to our statement of operations. With the adoption of ASC 606 effective January 1, 2018, revenue will be recognized when our product is sold to the specialty distributors pharmacies, which will match the tax treatment resulting in no deferred tax asset.
61
For a complete discussion of this adoption and the accounting for net product revenue, see Note 2, Summary of Significant Accounting Policies in the “Recently Issued Accounting Standards” section and Note 11, Revenue Recognition.
Research and Development Expenses
Research and development expenses consist of costs incurred for the development of our product candidates and companion diagnostics, which include:
|
· |
license fees and milestone payments related to the acquisition of in-licensed products, which are reported on our Consolidated Statements of Operations and Comprehensive Loss as acquired in-process research and development; |
|
· |
employee-related expenses, including salaries, benefits, travel and share-based compensation expense; |
|
· |
expenses incurred under agreements with CROs and investigative sites that conduct our clinical trials; |
|
· |
the cost of acquiring, developing and manufacturing clinical trial materials; |
|
· |
costs associated with non-clinical activities and regulatory operations; |
|
· |
market research, disease education and other commercial product planning activities, including the hiring of a U.S. sales and marketing and medical affairs organization in preparation for commercial launch of rucaparib; and |
|
· |
activities associated with the development of companion diagnostics for our product candidates. |
Research and development costs are expensed as incurred. License fees and milestone payments related to in-licensed products and technology are expensed if it is determined that they have no alternative future use. Costs for certain development activities, such as clinical trials and manufacturing of clinical supply, are recognized based on an evaluation of the progress to completion of specific tasks using data such as patient enrollment, clinical site activations or information provided to us by our vendors. As a result of the FDA approval of Rubraca and the discontinuation of enrollment in rociletinib, our research and development expenses decreased for 2017 as commercialization related expenses are classified as selling, general and administrative expenses and not research and development costs. Our research and development expenses will increase in 2018 as our ongoing rucaparib studies progress.
The following table identifies research and development and acquired in-process research and development costs on a program-specific basis for our products under development. Personnel-related costs, depreciation and share-based compensation are not allocated to specific programs, as they are deployed across multiple projects under development and, as such, are separately classified as personnel and other expenses in the table below.
|
|
|
Year Ended December 31, |
|
|||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|
|||
|
|
|
(in thousands) |
|
|||||||
|
Rucaparib Expenses |
|
|
|
|
|
|
|
|
|
|
|
Research and development |
|
$ |
72,901 |
|
$ |
101,598 |
|
$ |
58,922 |
|
|
Acquired in-process research and development |
|
|
— |
|
|
1,300 |
|
|
— |
|
|
Rucaparib Total |
|
|
72,901 |
|
|
102,898 |
|
|
58,922 |
|
|
Lucitanib Expenses |
|
|
|
|
|
|
|
|
|
|
|
Research and development (a) |
|
|
(1,187) |
|
|
(1,337) |
|
|
1,923 |
|
|
Lucitanib Total |
|
|
(1,187) |
|
|
(1,337) |
|
|
1,923 |
|
|
Rociletinib Expenses |
|
|
|
|
|
|
|
|
|
|
|
Research and development |
|
|
7,712 |
|
|
43,768 |
|
|
122,912 |
|
|
Acquired in-process research and development |
|
|
— |
|
|
— |
|
|
12,000 |
|
|
Rociletinib Total |
|
|
7,712 |
|
|
43,768 |
|
|
134,912 |
|
|
Personnel and other expenses |
|
|
63,072 |
|
|
107,100 |
|
|
85,494 |
|
|
Total |
|
$ |
142,498 |
|
$ |
252,429 |
|
$ |
281,251 |
|
(a)This amount reflects actual costs incurred less amounts due from Servier for reimbursable development expenses pursuant to the collaboration and license agreement described in Note 13, License Agreements, to our audited consolidated financial statements included in this Annual Report on Form 10-K.
For 2017 and 2016, research and development expenses have continued to decrease primarily due to decreased development activities for the rociletinib program.
62
Selling, General and Administrative Expenses
Selling, general and administrative expenses consist principally of salaries and related costs for personnel in executive, finance, legal, investor relations, human resources and information technology functions. Other general and administrative expenses include facilities expenses, communication expenses, information technology costs, corporate insurance and professional fees for legal, consulting and accounting services. With the FDA approval of Rubraca on December 19, 2016, all sales and marketing expenses associated with Rubraca are included in selling, general and administrative expenses. We anticipate that our selling, general and administrative expenses will continue to increase in the future in support of our commercial activities related to Rubraca in the U.S. and Europe.
Acquired In-Process Research and Development Expenses
Acquired in-process research and development expenses consist of upfront payments to acquire a new drug compound, as well as subsequent milestone payments. Acquired in-process research and development payments are immediately expensed provided that the drug has not achieved regulatory approval for marketing and, absent obtaining such approval, has no alternative future use. Once regulatory approval is received, payments to acquire rights, and the related milestone payments, are capitalized and the amortization of such assets recorded to product cost of sales.
Impairment of Intangible Asset
In connection with the acquisition of EOS in November 2013, we recorded intangible assets to reflect the fair value of acquired in-process research and development (“IPR&D”) as of the acquisition date. The fair value was established based upon discounted cash flow models using assumptions related to the timing of development, probability of development and regulatory success, sales and commercialization factors and estimated product life. During the second quarter of 2016, we recorded a $104.5 million impairment charge due to our and our development partner’s decision to discontinue the development of lucitanib for breast cancer. During the fourth quarter of 2015, we recorded an $89.6 million impairment charge to the IPR&D intangible assets. At December 31, 2017, the IPR&D intangible asset recorded on the Consolidated Balance Sheets was zero.
Change in Fair Value of Contingent Purchase Consideration
In connection with the acquisition of EOS in November 2013, we also recorded a purchase consideration liability equal to the estimated fair value of future payments that are contingent upon the achievement of various regulatory and sales milestones. Subsequent to the acquisition date, we re-measure contingent consideration arrangements at fair value each reporting period and record changes in fair value to change in fair value of contingent purchase consideration and foreign currency gains (losses) for changes in the foreign currency translation rate on the Consolidated Statements of Operations and Comprehensive Loss. Changes in fair value are primarily attributed to new information about the likelihood of achieving such milestones and the passage of time. In the absence of new information, changes to fair value reflect only the passage of time as we progress towards the achievement of future milestones. During the second quarter of 2016, we recorded a $25.5 million reduction in the fair value of the contingent purchase consideration liability due to our and our development partner’s decision to discontinue the development of lucitanib for breast cancer. During the fourth quarter of 2015, we recorded a $26.9 million reduction in the fair value of the contingent purchase consideration liability due to a change in the estimated probability-weighted future milestone payments, as well as the timing of such payments, for the lucitanib program. At December 31, 2017, the contingent purchase consideration liability recorded on the Consolidated Balance Sheets remained at zero due to the uncertainty of achieving any of the lucitanib regulatory milestones, and therefore the remote likelihood of future milestone payout amounts to the former EOS shareholders.
Other Income and Expense
Other income and expense is primarily comprised of foreign currency gains and losses resulting from transactions with CROs, investigational sites and contract manufacturers where payments are made in currencies other than the U.S. dollar. Other expense also includes interest expense recognized related to our convertible senior notes.
63
Critical Accounting Policies and Significant Judgments and Estimates
Our discussion and analysis of our financial condition and results of operations are based on our financial statements, which have been prepared in accordance with U.S. generally accepted accounting principles. The preparation of these financial statements requires us to make estimates and judgments that affect the reported amounts of assets, liabilities, expenses and revenue and related disclosures. On an ongoing basis, we evaluate our estimates and judgments, including those related to revenue, intangible asset impairment, clinical trial accruals and share-based compensation expense. We base our estimates on historical experience, known trends and events and various other factors that are believed to be reasonable under the circumstances, the results of which form the basis for making judgments about the carrying values of assets and liabilities that are not readily apparent from other sources. Actual results may differ from these estimates under different assumptions or conditions.
Our significant accounting policies are described in more detail in the notes to our consolidated financial statements appearing elsewhere in this Annual Report on Form 10-K. We believe the following accounting policies to be most critical to the judgments and estimates used in the preparation of our financial statements.
Revenue Recognition
We are currently approved to sell Rubraca in the United States markets. We distribute our product principally through a limited number of specialty distributor and specialty pharmacy providers, collectively, our customers. Our customers subsequently sell our products to patients and health care providers. Separately, we have arrangements with certain payors and other third parties that provide for government-mandated and privately-negotiated rebates, chargebacks and discounts.
Revenues from product sales are recognized when persuasive evidence of an arrangement exists, delivery has occurred and title of the product and associated risk of loss has passed to the customer, the price is fixed or determinable, collection from the customer has been reasonably assured and all performance obligations have been met and returns and allowances can be reasonably estimated. Product sales are recorded net of estimated rebates, chargebacks, discounts and other deductions as well as estimated product returns. Estimating rebates, chargebacks, discounts, product returns and other deductions requires significant judgments about future events and uncertainties, and requires us to rely heavily on assumptions, as well as historical experience. We only recognize revenue on product sales once the product is sold to the patient or healthcare provider by the specialty distributor or specialty pharmacy provider, therefore reducing the significance of estimates made for product returns.
For the year ended December 31, 2017, we recognized $55.5 million of product revenue. Based on our policy to expense costs associated with the manufacture of our products prior to regulatory approval, certain of the costs of Rubraca units recognized as revenue during the year ended December 31, 2017 were expensed prior to the December 19, 2016 FDA approval, and a minimal amount is included in cost of sales during the current period. We expect cost of sales to increase in relation to product revenues as we deplete these inventories. The majority of products sales were of pre-commercialization inventory in 2017.
Revenue is recognized from milestone payments when the following criteria have been met: (1) persuasive evidence of an arrangement exists; (2) delivery has occurred or services have been rendered; (3) the price is fixed or determinable; and (4) collectability is reasonably assured. We exercise judgment in determining that collectability is reasonably assured or that services have been delivered in accordance with the arrangement. We assess whether the fee is fixed or determinable based on the payment terms associated with the transaction and whether the sales price is subject to refund or adjustment. We assess collectability based primarily on the customer’s payment history and creditworthiness of the customer. Payments that are contingent upon the achievement of a milestone will be recognized in the period in which the milestone is achieved.
Accrued Research and Development Expenses
As part of the process of preparing our financial statements, we are required to estimate our accrued expenses. This process involves reviewing open contracts and purchase orders, communicating with our personnel to identify services that have been performed on our behalf and estimating the level of service performed and the associated cost incurred for the service when we have not yet been invoiced or otherwise notified of the actual cost. The majority of our service providers invoice us monthly in arrears for services performed or when contractual milestones are met. We make
64
estimates of our accrued expenses as of each balance sheet date in our financial statements based on facts and circumstances known to us at that time. We periodically confirm the accuracy of our estimates with the service providers and make adjustments if necessary. Examples of estimated accrued research and development expenses include:
|
· |
fees paid to CROs in connection with clinical studies; |
|
· |
fees paid to investigative sites in connection with clinical studies; |
|
· |
fees paid to vendors in connection with non-clinical development activities; |
|
· |
fees paid to vendors associated with the development of companion diagnostics; and |
|
· |
fees paid to vendors related to product manufacturing, development and distribution of clinical supplies. |
We base our expenses related to clinical studies on our estimates of the services received and efforts expended pursuant to contracts with multiple CROs that conduct and manage clinical studies on our behalf. The financial terms of these agreements are subject to negotiation, vary from contract to contract and may result in uneven payment flows. There may be instances in which payments made to our vendors will exceed the level of services provided and result in a prepayment of the clinical expense. Payments under some of these contracts depend on factors such as the successful enrollment of patients and the completion of clinical trial milestones. In accruing service fees, we estimate the time period over which services will be performed, enrollment of patients, number of sites activated and the level of effort to be expended in each period. If the actual timing of the performance of services or the level of effort varies from our estimate, we adjust the accrual or prepaid accordingly. Although we do not expect our estimates to be materially different from amounts actually incurred, our understanding of the status and timing of services performed relative to the actual status and timing of services performed may vary and may result in us reporting amounts that are too high or too low in any particular period.
Share-Based Compensation
Determining the amount of share-based compensation to be recorded requires us to develop estimates of the fair value of stock options as of their grant date. Compensation expense is recognized over the vesting period of the award. Calculating the fair value of share-based awards requires that we make highly subjective assumptions. We use the Black-Scholes option pricing model to value our stock option awards. Use of this valuation methodology requires that we make assumptions as to the expected dividend yield, price volatility of our common stock, the risk-free interest rate for a period that approximates the expected term of our stock options and the expected term of our stock options. We utilize a dividend yield of zero based on the fact that we have never paid cash dividends and have no current intention to pay cash dividends.
The fair value of stock options for the years ended December 31, 2017, 2016 and 2015 was estimated at the grant date using the following weighted average assumptions for the respective periods:
|
|
|
Year Ended December 31, |
|
||||
|
|
|
2017 |
|
2016 |
|
2015 |
|
|
Dividend yield |
|
— |
|
— |
|
— |
|
|
Volatility (a) |
|
89 |
% |
93 |
% |
72 |
% |
|
Risk-free interest rate (b) |
|
2.16 |
% |
1.77 |
% |
1.77 |
% |
|
Expected term (years) (c) |
|
5.8 |
|
5.8 |
|
6.1 |
|
(a)Volatility: The expected volatility was estimated using our historical data.
(b)Risk-free interest rate: The rate is based on the yield on the grant date of a zero-coupon U.S. Treasury bond whose maturity period approximates the option’s expected term.
(c)Expected term: The expected term of the award was estimated using our historical data.
We recognized share-based compensation expense of approximately $44.7 million, $39.8 million and $40.4 million for the years ended December 31, 2017, 2016 and 2015, respectively. As of December 31, 2017, we had $89.4 million in total unrecognized share-based compensation expense, net of related forfeiture estimates, which is expected to be recognized over a weighted-average remaining vesting period of 3.3 years. We expect our share-based compensation to continue to grow in future periods due to the potential increases in the value of our common stock and headcount.
We estimate the level of forfeitures expected to occur and record compensation expense only for those awards that we ultimately expect will vest.
65
Valuation of Contingent Consideration Resulting from a Business Combination
Contingent consideration resulting from a business combination is reported at its fair value on the acquisition date. Each subsequent reporting period, the contingent consideration obligations are revalued and changes in fair value are recorded to change in fair value of contingent purchase consideration and foreign currency gains (losses) for changes in the foreign currency translation rate on the Consolidated Statements of Operations and Comprehensive Loss.
Changes to contingent consideration obligations can result from adjustments to discount rates and time periods, updates in the assumed achievement or timing of any development milestone or changes in the probability of certain clinical events and regulatory approvals. The assumptions related to determining the value of contingent consideration require significant judgment and changes to the assumptions may have a material impact on the amount of expense recorded in any given period. The acquisition of EOS resulted in the recognition of a contingent consideration liability, based on assumptions related to potential future payout amounts, estimated discount rate, probability of success for each milestone achievement and the estimated timing of the milestone payments to the former EOS shareholders.
During the second quarter 2016, we recorded $25.5 million reduction in fair value of the contingent purchase consideration due to our and our development partner’s decision to discontinue the development of lucitanib for breast cancer. At December 31, 2017, the contingent purchase consideration liability recorded on the Consolidated Balance Sheets remained at zero due to the uncertainty of achieving any of the lucitanib regulatory milestones, and therefore the remote likelihood of future milestone payout amounts to the former EOS shareholders.
Intangible Assets
Definite-lived intangible assets related to capitalized milestones under license agreements are amortized on a straight-line basis over their remaining useful lives, which are estimated to be the remaining patent life. If our estimate of the product’s useful life is shorter than the remaining patent life, then a shorter period is used. Amortization expense is recorded as a component of cost of sales in the Consolidated Statements of Operations and Comprehensive Loss.
IPR&D assets were established as part of the acquisition of EOS in November 2013 and have not been amortized, but have been assessed for impairment.
Intangible assets are evaluated for impairment at least annually in the fourth quarter or more frequently if impairment indicators exist. Events that could result in an impairment, or trigger an interim impairment assessment, include the decision to discontinue the development of a drug, the receipt of additional clinical or nonclinical data regarding our drug candidate or a potentially competitive drug candidate, changes in the clinical development program for a drug candidate, or new information regarding potential sales for the drug. In connection with any impairment assessment, the fair value of the intangible assets as of the date of assessment is compared to the carrying value of the intangible asset. Impairment losses are recognized if the carrying value of an intangible asset is both not recoverable and exceeds its fair value. During the second quarter of 2016, we recorded a $104.5 million impairment charge to the IPR&D intangible assets due to our and our development partner’s decision to discontinue the development of lucitanib for breast cancer, thereby reducing the remaining carrying value to zero.
66
Results of Operations
Comparison of the Year Ended December 31, 2017 to the Year Ended December 31, 2016
|
|
|
|
|
|
|
|
|
Change |
|
||||
|
|
|
Year ended December 31, |
|
Favorable/(Unfavorable) |
|
||||||||
|
|
|
2017 |
|
2016 |
|
$ |
|
% |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Product revenue, net |
|
$ |
55,511 |
|
$ |
78 |
|
$ |
55,433 |
|
|
71,068 |
% |
|
Operating expenses: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cost of sales - product |
|
|
10,251 |
|
|
70 |
|
|
10,181 |
|
|
14,544 |
% |
|
Cost of sales - intangible asset amortization |
|
|
1,486 |
|
|
— |
|
|
1,486 |
|
|
100 |
% |
|
Research and development |
|
|
142,498 |
|
|
251,129 |
|
|
(108,631) |
|
|
(43) |
% |
|
Selling, general and administrative |
|
|
138,907 |
|
|
40,731 |
|
|
98,176 |
|
|
241 |
% |
|
Acquired in-process research and development |
|
|
— |
|
|
1,300 |
|
|
(1,300) |
|
|
(100) |
% |
|
Impairment of intangible asset |
|
|
— |
|
|
104,517 |
|
|
(104,517) |
|
|
(100) |
% |
|
Change in fair value of contingent purchase consideration |
|
|
— |
|
|
(24,936) |
|
|
24,936 |
|
|
(100) |
% |
|
Total expenses |
|
|
293,142 |
|
|
372,811 |
|
|
(79,669) |
|
|
(21) |
% |
|
Operating loss |
|
|
(237,631) |
|
|
(372,733) |
|
|
135,102 |
|
|
(36) |
% |
|
Other income (expense): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Interest expense |
|
|
(10,428) |
|
|
(8,491) |
|
|
(1,937) |
|
|
23 |
% |
|
Foreign currency gain (loss) |
|
|
(82) |
|
|
(580) |
|
|
498 |
|
|
(86) |
% |
|
Legal settlement loss |
|
|
(105,477) |
|
|
— |
|
|
(105,477) |
|
|
100 |
% |
|
Other income (expense) |
|
|
3,643 |
|
|
633 |
|
|
3,010 |
|
|
476 |
% |
|
Other income (expense), net |
|
|
(112,344) |
|
|
(8,438) |
|
|
(103,906) |
|
|
1,231 |
% |
|
Loss before income taxes |
|
|
(349,975) |
|
|
(381,171) |
|
|
31,196 |
|
|
(8) |
% |
|
Income tax benefit |
|
|
3,578 |
|
|
32,034 |
|
|
(28,456) |
|
|
(89) |
% |
|
Net loss |
|
$ |
(346,397) |
|
$ |
(349,137) |
|
$ |
2,740 |
|
|
(1) |
% |
Product Revenue, Net. Product revenue for the year ended December 31, 2017 was due to the recognition of $55.5 million of net product revenue from the sale of Rubraca, which was approved for sale in the United States markets on December 19, 2016. Revenue is recorded net of sales deductions comprised of rebates, chargebacks and other discounts. Sales deductions represented approximately 8.1% of the gross product revenue recognized in the year ended December 31, 2017 and summarized as follows:
|
|
|
Year ended |
|
||||
|
|
|
December 31, 2017 |
|
||||
|
|
|
$ |
|
% of Gross Sales |
|
||
|
|
|
(in thousands) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Gross product revenue |
|
$ |
60,384 |
|
|
100.0% |
|
|
Sales deductions: |
|
|
|
|
|
|
|
|
Government rebates and chargebacks |
|
|
2,575 |
|
|
4.3% |
|
|
Discounts and fees |
|
|
2,298 |
|
|
3.8% |
|
|
Total sales deductions |
|
|
4,873 |
|
|
8.1% |
|
|
Product revenue, net |
|
$ |
55,511 |
|
|
91.9% |
|
Cost of Sales - Product. Product cost of sales for the year ended December 31, 2017 relate to freight and royalties costs associated with Rubraca sales for the period. Based on our policy to expense costs associated with the manufacture of our products prior to regulatory approval, certain of the costs of Rubraca units recognized as revenue during the year ended December 31, 2017 were expensed prior to the December 19, 2016 FDA approval, and therefore are not included in costs of sales during the current period. We expect cost of sales to increase in relation to product revenues as we deplete these inventories. The majority of product sales were of pre-commercialization inventory in 2017.
Cost of Sales – Intangible Asset Amortization. For the year ended December 31, 2017, we recognized cost of sales of $1.5 million associated with the amortization of capitalized milestone payments related to the FDA approval of Rubraca.
67
Prior to the FDA approval on December 19, 2016, all acquired license and milestone payments were expensed as incurred.
Research and Development Expenses. Research and development expenses decreased during the year ended December 31, 2017 compared to 2016 primarily due to lower research and development costs for rucaparib and rociletinib and classification of commercialization related expenses associated with Rubraca in selling, general and administrative expenses rather than research and development expenses. In the year ended December 31, 2017, Rubraca commercialization costs included in selling, general and administrative expenses were $95.2 million.
Clinical trial costs for rucaparib were $0.3 million lower compared to the same period a year ago due to completed enrollment in our ARIEL2 and ARIEL 3 studies, partially offset by higher costs from enrollment in ARIEL4, our confirmatory ovarian cancer trials, and enrollment in our TRITON2 and TRITON3 studies for prostate cancer. Diagnostic development costs were $4.4 million lower compared to the prior year as the prior year included the costs associated with our collaboration with Foundation Medicine, Inc. to develop a novel companion diagnostic test to identify patients most likely to respond to rucaparib. Finally, clinical supply and related manufacturing development costs were $15.9 million lower than 2016 due to the capitalization of these costs subsequent to the FDA approval of rucaparib.
Clinical trial costs for rociletinib were $23.6 million lower than 2016 primarily due to the completion of patient enrollment for all of the TIGER studies in non-small cell lung cancer. Clinical supply and related manufacturing development costs were $6.6 million lower than 2016 driven by timing of production to support our clinical studies.
Selling, General and Administrative Expenses. Selling, general and administrative expenses increased during the year ended December 31, 2017 compared to 2016 primarily due to classification of commercialization related expenses associated with Rubraca in selling, general and administrative expenses rather than research and development expenses.
Acquired In-Process Research and Development Expenses. During 2016, we made a milestone payment of $0.3 million to AstraZeneca upon the NDA submission for rucaparib and we made milestone payments totaling $1.0 million to Pfizer upon acceptance of the NDA and MAA for rucaparib by the FDA and EMA, respectively. No such payments occurred during 2017.
Impairment of Intangible Asset. During the second quarter of 2016, we recorded a $104.5 million impairment charge to the IPR&D intangible asset relating to our lucitanib product candidate which reduced the carrying value of the intangible assets related to the product to zero. This reduction in the estimated fair value of lucitanib was the result of our and our development partner’s decision to discontinue the development of lucitanib for breast cancer.
Change in Fair Value of Contingent Purchase Consideration. The fair value of contingent purchase consideration decreased $24.9 million for the year ended December 31, 2016, which is due to a $25.5 million reduction in the fair value of the contingent purchase consideration liability we recorded during the second quarter of 2016 due to our and our development partner’s decision to discontinue the development of lucitanib for breast cancer.
Legal Settlement Loss, Net of Insurance Receivable. During 2017, we recorded a $105.5 million legal settlement loss, net of insurance receivable, related to a stipulation agreement of settlement whereby we issued the plaintiff and participating class members a total consideration comprised of $25.0 million in cash and the issuance of 1.5 million shares. The cash portion of the consideration was funded by Clovis’ insurance carriers.
Other Income (Expense). Other income increased for the year ended December 31, 2017 compared to 2016 due to interest income earned on our available-for-sale securities.
Income Tax Benefit (Expense). For the year ended December 31, 2016, we recognized a $28.4 million deferred tax benefit associated with the impairment of the IPR&D intangible assets recorded in the second quarter of 2016. In addition, during the first quarter 2016, we recognized a $3.6 million deferred tax benefit due to a reduction in the enacted corporate tax rate of a foreign jurisdiction in which we operate.
68
Comparison of the Year Ended December 31, 2016 to the Year Ended December 31, 2015
|
|
|
|
|
|
|
|
|
Change |
|
||||
|
|
|
Year ended December 31, |
|
Favorable/(Unfavorable) |
|
||||||||
|
|
|
2016 |
|
2015 |
|
$ |
|
% |
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Product revenue, net |
|
$ |
78 |
|
$ |
— |
|
$ |
78 |
|
|
100 |
% |
|
Operating expenses: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cost of sales - product |
|
|
70 |
|
|
— |
|
|
70 |
|
|
100 |
% |
|
Research and development |
|
|
251,129 |
|
|
269,251 |
|
|
(18,122) |
|
|
(7) |
% |
|
Selling, general and administrative |
|
|
40,731 |
|
|
30,524 |
|
|
10,207 |
|
|
33 |
% |
|
Acquired in-process research and development |
|
|
1,300 |
|
|
12,000 |
|
|
(10,700) |
|
|
(89) |
% |
|
Impairment of intangible asset |
|
|
104,517 |
|
|
89,557 |
|
|
14,960 |
|
|
17 |
% |
|
Change in fair value of contingent purchase consideration |
|
|
(24,936) |
|
|
(24,611) |
|
|
(325) |
|
|
1 |
% |
|
Total expenses |
|
|
372,811 |
|
|
376,721 |
|
|
(3,910) |
|
|
(1) |
% |
|
Operating loss |
|
|
(372,733) |
|
|
(376,721) |
|
|
3,988 |
|
|
(1) |
% |
|
Other income (expense): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Interest expense |
|
|
(8,491) |
|
|
(8,372) |
|
|
(119) |
|
|
1 |
% |
|
Foreign currency gain (loss) |
|
|
(580) |
|
|
2,740 |
|
|
(3,320) |
|
|
(121) |
% |
|
Other income (expense) |
|
|
633 |
|
|
416 |
|
|
217 |
|
|
52 |
% |
|
Other income (expense), net |
|
|
(8,438) |
|
|
(5,216) |
|
|
(3,222) |
|
|
62 |
% |
|
Loss before income taxes |
|
|
(381,171) |
|
|
(381,937) |
|
|
766 |
|
|
(0) |
% |
|
Income tax benefit |
|
|
32,034 |
|
|
29,076 |
|
|
2,958 |
|
|
10 |
% |
|
Net loss |
|
$ |
(349,137) |
|
$ |
(352,861) |
|
$ |
3,724 |
|
|
(1) |
% |
Product Revenue, Net. Product revenue for the year ended December 31, 2016 was due to the recognition of $0.1 million of net product revenue from the sale of Rubraca, which was approved for sale in the United States markets on December 19, 2016.
Cost of Sales - Product. Product cost of sales for the year ended December 31, 2016 relate to freight and royalties costs associated with Rubraca sales for the period. Based on our policy to expense costs associated with the manufacture of our products prior to regulatory approval, certain of the costs of Rubraca units recognized as revenue during the year ended December 31, 2016 were expensed prior to the December 19, 2016 FDA approval, and therefore are not included in costs of sales during the current period.
Research and Development Expenses. The decrease in research and development expenses for the year ended December 31, 2017 compared to 2016 was primarily due to decreased development activities for the rociletinib program partially offset by higher expenses related to the rucaparib program.
Clinical trial costs for rucaparib were $14.0 million higher in 2016 than the prior year primarily due to higher enrollment in the ARIEL2 and ARIEL3 studies in ovarian cancer. Market research, disease education and other commercial product planning activities were $16.6 million higher than the prior year due to the preparation for the potential regulatory approval and commercial launch of rucaparib. Clinical supply and related manufacturing development costs were $9.2 million higher than the prior year, as we increased production to support the expanded clinical studies. In addition, diagnostic development costs for rucaparib were $0.9 million higher than the prior year due to the advancement of our collaboration with Foundation Medicine, Inc. to develop a novel companion diagnostic test to identify patients most likely to respond to rucaparib.
Salaries, share-based compensation expense and other personnel-related costs were $24.0 million higher in 2016 driven by increased headcount to support our expanded development and commercial planning activities. During the third quarter of 2015, we completed the hiring of our U.S. sales and marketing and medical affairs organization in preparation for the potential regulatory approval and commercial launch of rociletinib.
Clinical trial costs for rociletinib were $41.0 million lower in 2016 than the prior year primarily due to the completion of patient enrollment in the TIGER-1, TIGER-2 and TIGER-X studies in non-small cell lung cancer. This decrease was
69
partially offset by higher clinical trial costs for the TIGER-3 study, which began enrolling patients during the second quarter of 2015. Market research, disease education and other commercial planning activities were $19.7 million lower than the prior year. We incurred higher costs during 2015 due to the preparation for the potential regulatory approval and commercial launch of rociletinib. In addition, clinical supply and related manufacturing development costs were $17.2 million lower than the prior year driven by timing of production to support our clinical studies.
Selling, General and Administrative Expenses. The increase in selling, general and administrative expenses for the year ended December 31, 2016 over 2015 was primarily due to $3.1 million of selling expenses related to the commercialization of Rubraca, $5.3 million higher legal expense and, to a lesser extent, higher personnel costs. Pre-commercialization activities for Rubraca were included in research and development expenses.
Acquired In-Process Research and Development Expenses. Acquired in-process research and development expenses decreased for the year ended December 31, 2016 compared to 2015. During the third quarter of 2015, we made milestone payments totaling $12.0 million to Celgene upon acceptance of the NDA and MAA for rociletinib by the FDA and EMA, respectively. During the second quarter of 2016, we made a milestone payment of $0.3 million to AstraZeneca upon the NDA submission for rucaparib. During 2016, we made milestone payments totaling $1.0 million to Pfizer upon acceptance of the NDA and MAA for rucaparib by the FDA and EMA, respectively.
Impairment of Intangible Asset. During the second quarter of 2016, we recorded a $104.5 million impairment charge to the IPR&D intangible asset relating to our lucitanib product candidate which reduced the carrying value of the intangible assets related to the product to zero. This reduction in the estimated fair value of lucitanib was the result of our and our development partner’s decision to discontinue the development of lucitanib for breast cancer. During the fourth quarter of 2015, we recorded an $89.6 million impairment charge to the IPR&D intangible asset relating to our lucitanib product candidate. This reduction in the estimated fair value of lucitanib was the result of our and our development partner’s decision to terminate the development of lucitanib for lung cancer, as well as updates to the probability-weighted discounted cash flow assumptions for the breast cancer indication.
Change in Fair Value of Contingent Purchase Consideration. Change in fair value of contingent purchase consideration was a decrease of $24.9 million for the year ended December 31, 2016 compared to a decrease of $24.6 million for the year ended December 31, 2015. During the second quarter of 2016, we recorded a $25.5 million reduction in the fair value of the contingent purchase consideration liability due to our and our development partner’s decision to discontinue the development of lucitanib for breast cancer. During the fourth quarter of 2015, we recorded a $26.9 million reduction in the fair value of the contingent purchase consideration liability due to a change in the estimated probability-weighted future milestone payments, as well as the timing of such payments, for the lucitanib program.
Other Income (Expense), Net. Other expense increased for the year ended December 31, 2016 compared to 2015. During 2016, we recognized $0.6 million of foreign currency losses compared with $2.7 million of gains in 2015. The change in the foreign currency gains and losses was driven by fluctuations in the foreign currency rate utilized to translate our Euro-denominated contingent purchase consideration liability into U.S. dollars.
Income Tax Benefit (Expense). For the year ended December 31, 2016, we recognized a $28.4 million deferred tax benefit associated with the impairment of the IPR&D intangible assets recorded in the second quarter of 2016. In addition, during the first quarter 2016, we recognized a $3.6 million deferred tax benefit due to a reduction in the enacted corporate tax rate of a foreign jurisdiction in which we operate.
For the year ended December 31, 2015, we recognized a $29.1 million deferred tax benefit primarily associated with the impairment of the IPR&D intangible assets recorded in the fourth quarter of 2015.
Liquidity and Capital Resources
To date, we have funded our operations through the public offering of our common stock and the private placement of convertible debt securities and preferred stock. In January 2017, we sold 5,750,000 shares of our common stock in a public offering at $41.00 per share. The net proceeds from the offering were $221.2 million, after deducting underwriting discounts and commissions and offering expenses. In June 2017, we sold 3,920,454 shares of our common stock in a public offering at $88.00 per share. The net proceeds from the offering were $324.6 million, after deducting underwriting discounts and commissions and offering expenses. As of December 31, 2017, we had cash, cash equivalents and available-for-sale securities totaling $563.7 million.
70
The following table sets forth the primary sources and uses of cash for each of the periods set forth below:
|
|
|
Year Ended December 31, |
|
|||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|
|||
|
|
|
(in thousands) |
|
|||||||
|
Net cash used in operating activities |
|
$ |
(260,904) |
|
$ |
(266,680) |
|
$ |
(253,066) |
|
|
Net cash (used in) provided by investing activities |
|
|
(54,102) |
|
|
199,299 |
|
|
(254,578) |
|
|
Net cash provided by financing activities |
|
|
562,075 |
|
|
5,176 |
|
|
304,480 |
|
|
Effect of exchange rate changes on cash and cash equivalents |
|
|
943 |
|
|
(365) |
|
|
(757) |
|
|
Net increase (decrease) in cash and cash equivalents |
|
$ |
248,012 |
|
$ |
(62,570) |
|
$ |
(203,921) |
|
Operating Activities
Net cash used in operating activities for the year ended December 31, 2017 decreased by $5.8 million compared to 2016 due to a decrease in net loss adjusted for non-cash items of $63.3 million, primarily due the recognition of $55.5 million of revenue during 2017, partially offset by inventory purchases and deposits of $48.0 million and the recognition of $6.2 million in accounts receivable in 2017.
Net cash used in operating activities increased $13.6 million for the year ended December 31, 2016 compared to 2015 driven by an increase in payments for other accrued expenses related to the rociletinib program of non-clinical and clinical development studies, for which enrollment was completed in 2016.
Investing Activities
Net cash used in investing activities for the year ended December 31, 2017 includes $263.5 million in purchases of available-for-sale securities compared to no purchases in 2016.
Net cash provided by investing activities for the year ended December 31, 2016 includes $200.0 million in sales of available-for-sale securities compared to $251.5 million in net purchases in 2015.
Financing Activities
Net cash provided by financing activities for the year ended December 31, 2017 includes $545.8 million in net proceeds received from our common stock offerings in January and June 2017 and $16.2 million received from employee stock option exercises and stock purchases under the employee stock purchase plan.
Net cash provided by financing activities for the year ended December 31, 2016 is due to $5.2 million received from employee stock option exercises and stock purchases under the employee stock purchase plan.
Net cash provided by financing activities for the year ended December 31, 2015 includes $298.5 million in net proceeds received from our common stock offering in July 2015 and $6.0 million received from employee stock option exercises and stock purchases under the employee stock purchase plan.
Operating Capital Requirements
On December 19, 2016, the FDA approved Rubraca tablets as monotherapy for the treatment of patients with deleterious BRCA mutation (germline and/or somatic) associated with advanced ovarian cancer, who have been treated with two or more chemotherapies, and selected for therapy based on FDA-approved companion diagnostic for Rubraca. We expect to incur significant losses for the foreseeable future, as we commercialize Rubraca and expand our selling, general and administrative functions to support the growth in our commercial organization. Additionally, our operating plan for the next 12 months includes a significant investment in inventory to meet the projected commercial requirements for Rubraca. We receive the active pharmaceutical ingredient in Rubraca from one supplier and we experience long lead times associated with its production. Accordingly, we expect to experience a decrease in our liquidity at the beginning of a production cycle and an increase as the inventory produced is sold.
71
As of December 31, 2017, we had cash, cash equivalents and available-for-sale securities totaling $563.7 million and total current liabilities of $81.5 million. In January 2017, we sold 5,750,000 shares of our common stock in a public offering at $41.00 per share. The net proceeds from the offering were $221.2 million, after deducting underwriting discounts and commissions and offering expenses. In June 2017, we sold 3,920,454 shares of our common stock in a public offering at $88.00 per share. The net proceeds from the offering were $324.6 million, after deducting underwriting discounts and commissions and offering expenses. We intend to use the net proceeds of the offerings for general corporate purposes, including commercial planning and sales and marketing expenses associated with the launch of Rubraca in the United States and, if approved by the European Commission in Europe, funding of its development programs, selling, general and administrative expenses, acquisition or licensing of additional product candidates or businesses and working capital. Based on current estimates, we believe that our existing cash, cash equivalents and available-for-sale securities will allow us to fund our operating plan through at least the next 12 months.
Because of the numerous risks and uncertainties associated with research, development and commercialization of pharmaceutical products, we are unable to estimate the exact amounts of our working capital requirements. Our future funding requirements will depend on many factors, including but not limited to:
|
· |
the number and characteristics of the product candidates, companion diagnostics and indications we pursue; |
|
· |
the achievement of various development, regulatory and commercial milestones resulting in required payments to partners pursuant to the terms of our license agreements; |
|
· |
the scope, progress, results and costs of researching and developing our product candidates and related companion diagnostics and conducting clinical and non-clinical trials; |
|
· |
the timing of, and the costs involved in, obtaining regulatory approvals for our product candidates and companion diagnostics; |
|
· |
the cost of commercialization activities, including marketing and distribution costs; |
|
· |
the cost of manufacturing any of our product candidates we successfully commercialize; |
|
· |
the costs involved in preparing, filing, prosecuting, maintaining, defending and enforcing patent claims, including litigation costs and outcome of such litigation; and |
|
· |
the timing, receipt and amount of sales, if any, of our product candidates. |
Contractual Obligations and Commitments
The following table summarizes our contractual obligations at December 31, 2017 (in thousands):
|
|
|
Less than 1 |
|
|
|
|
|
|
|
More Than 5 |
|
|
|
|
||
|
|
|
Year |
|
1 to 3 Years |
|
3 to 5 Years |
|
Years |
|
Total |
|
|||||
|
Convertible senior notes |
|
$ |
— |
|
$ |
— |
|
$ |
287,500 |
|
$ |
— |
|
$ |
287,500 |
|
|
Interest on convertible senior notes |
|
|
7,187 |
|
|
14,376 |
|
|
5,091 |
|
|
— |
|
|
26,654 |
|
|
Operating lease commitments |
|
|
3,050 |
|
|
7,646 |
|
|
6,374 |
|
|
11,563 |
|
|
28,633 |
|
|
Milestone payments (a) |
|
|
23,000 |
|
|
— |
|
|
— |
|
|
— |
|
|
23,000 |
|
|
Purchase and other commitments (b) |
|
|
137,154 |
|
|
25,179 |
|
|
24,630 |
|
|
36,945 |
|
|
223,908 |
|
|
Total |
|
$ |
170,391 |
|
$ |
47,201 |
|
$ |
323,595 |
|
$ |
48,508 |
|
$ |
589,695 |
|
(a)Amount relates to a $20 million milestone payment, which we have exercised the option to defer payment by agreeing to pay $23 million within 18 months after the date of the FDA approval of Rubraca on December 19, 2016.
(b)On October 3, 2016, we entered into a Manufacturing and Services Agreement (the “Agreement”) with a non-exclusive third-party supplier for the production of the active ingredient for rucaparib. Under the terms of the Agreement, we will provide the third-party supplier a rolling forecast for the supply of the active ingredient in rucaparib that will be updated by us on a quarterly basis. We are obligated to order material sufficient to satisfy an initial quantity specified in any forecast. In addition, the third-party supplier will construct, in its existing facility, a production train that will be exclusively dedicated to the manufacture of the rucaparib active ingredient. We are obligated to make scheduled capital program fee payments toward capital equipment and other costs associated with the construction of the dedicated production train. Further, once the facility is operational, we are obligated to pay a fixed facility fee each quarter for the duration of the Agreement, which expires on December 31, 2025, unless extended by mutual consent of the parties.
72
Royalty and License Fee Commitments
We have certain obligations under licensing agreements with third parties contingent upon achieving various development, regulatory and commercial milestones. On August 30, 2016, we entered into a first amendment to the worldwide license agreement with Pfizer, which amends the June 2011 existing worldwide license agreement to permit us to defer payment of the milestone payments payable upon (i) FDA approval of an NDA for 1st Indication in US and (ii) European Commission approval of an MAA for 1st Indication in EU, to a date that is 18 months after the date of achievement of such milestones. In the event that we defer such milestone payments, we have agreed to certain higher payments related to the achievement of such milestones.
On December 19, 2016, the FDA approved Rubraca tablets as monotherapy for the treatment of patients with deleterious BRCA mutation (germline and/or somatic) associated with advanced ovarian cancer, who have been treated with two or more chemotherapies, and selected for therapy based on FDA-approved companion diagnostic for Rubraca. The FDA approval resulted in a $0.75 million milestone payment to Pfizer as required by the license agreement. The FDA approval also resulted in the obligation to pay a $20.0 million milestone payment, in which we have exercised the option to defer payment by agreeing to pay $23.0 million within 18 months after the date of the FDA approval. These payments were recognized as intangible assets and will be amortized over the estimated remaining useful life of rucaparib.
Pursuant to our license agreements for the development of rucaparib, we are required to make regulatory milestone payments up to an additional $69.75 million in aggregate if specified clinical study objectives and regulatory filings, acceptances and approvals are achieved. In addition, we are obligated to make sales milestone payments if specified annual sales targets for rucaparib are met, which relate to annual sales targets of $250.0 million and above, which, in aggregate, could amount to total milestone payments of $170.0 million, and tiered royalty payments at a mid-teen percentage rate on our net sales, with standard provisions for royalty offsets to the extent we need to obtain any rights from third parties to commercialize rucaparib.
We are obligated to pay additional consideration to the former EOS shareholders if certain future regulatory and lucitanib-related sales milestones are achieved. The estimated fair value of these payments was recorded as contingent purchase consideration on our Consolidated Balance Sheets. The potential contingent milestone payments range from a zero payment, which assumes lucitanib fails to achieve any of the regulatory milestones, to $186.0 million ($65.0 million and €115.0 million) if all regulatory and sales milestones are met, utilizing the translation rate at December 31, 2017. The estimated fair value of the liability was zero at December 31, 2017 due to the uncertainty of achieving any of the lucitanib regulatory milestones, and therefore the remote likelihood of future milestone payout amounts to the former EOS shareholders. We are also obligated to pay to Advenchen 25% of any consideration, excluding royalties, received pursuant to any sublicense agreements for lucitanib, including the agreement with Servier.
Pursuant to our license agreement for the development and commercialization of rociletinib, we may be required to pay up to an additional aggregate of $98.0 million in regulatory milestone payments if certain clinical study objectives and regulatory filings, acceptance and approvals are achieved. Further, we may be required to pay up to an aggregate of $120.0 million in sales milestone payments if certain annual sales targets are met for rociletinib.
Finally, pursuant to terms of each of our product license agreements, we will pay royalties to our licensors on sales, if any, of the respective products.
Off-Balance Sheet Arrangements
We did not have during the periods presented, and we do not currently have, any off-balance sheet arrangements, as defined under the rules promulgated by the U.S. Securities and Exchange Commission.
Tax Loss Carryforwards
As of December 31, 2017, we have net operating loss (“NOL”) carryforwards of approximately $1.0 billion to offset future federal income taxes. We also have research and development and orphan drug tax credit carryforwards of $245.1 million to offset future federal income taxes. The federal net operating loss carryforwards and research and development and orphan drug tax credit carryforwards expire at various times through 2037.
73
We believe that a change in ownership as defined under Section 382 of the U.S. Internal Revenue Code occurred as a result of our public offering of common stock completed in April 2012. Future utilization of the federal net operating losses and tax credit carryforwards accumulated from inception to the change in ownership date will be subject to annual limitations to offset future taxable income. At this time, we do not believe this limitation will prevent the utilization of the federal NOL or credit carryforward prior to expiration. It is possible that a change in ownership will occur in the future, which will limit the NOL amounts generated since the last estimated change in ownership. At December 31, 2017, we recorded a 100% valuation allowance against our net deferred tax assets in the U.S. of approximately $561.1 million and a $3.0 million valuation allowance against tax assets in foreign jurisdictions, as we believe it is more likely than not that the tax benefits will not be fully realized. In the future, if we determine that a portion or all of the tax benefits associated with our tax carryforwards will be realized, net income would increase in the period of determination.
Recently Adopted and Issued Accounting Standards
For a discussion of recently adopted and issued accounting standards, see Note 2, Summary of Significant Accounting Policies, in the Notes to Consolidated Financial Statements included in Part II, Item 8, Financial Statements and Supplementary Data, of this Annual Report on Form 10-K.
ITEM 7A.QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK
We are exposed to market risk related to changes in interest rates. As of December 31, 2017, we had cash, cash equivalents and available-for-sale securities of $563.7 million, consisting of bank demand deposits, money market funds and U.S. treasury securities. The primary objectives of our investment policy are to preserve principal and maintain proper liquidity to meet operating needs. Our investment policy specifies credit quality standards for our investments and limits the amount of credit exposure to any single issue, issuer or type of investment. Our primary exposure to market risk is interest rate sensitivity, which is affected by changes in the general level of U.S. interest rates, particularly because our investments are in short-term securities. Our available-for-sale securities are subject to interest rate risk and will decline in value if market interest rates increase. Due to the short-term duration of our investment portfolio and the low risk profile of our investments, an immediate 100 basis point change in interest rates would not have a material effect on the fair value of our portfolio.
We contract with contract research organizations, investigational sites and contract manufacturers globally where payments are made in currencies other than the U.S. dollar. In addition, on October 3, 2016, we entered into a Manufacturing and Services Agreement with a Swiss company for the production and supply of the active ingredient for rucaparib. Under the terms of this agreement, payments for the supply of the active ingredient in rucaparib as well as scheduled capital program fee payment toward capital equipment and other costs associated with the construction of a dedicated production train will be made in Swiss francs. Once the production facility is operational, we are obligated to pay a fixed facility fee each quarter for the duration of the agreement, which expires on December 31, 2025.
As of December 31, 2017, $223.9 million of purchase commitments exist under the Swiss Manufacturing and Services Agreement and we are required to remit amounts due in Swiss francs. Due to other variables that may exist, it is difficult to quantify the impact of a particular change in exchange rates. However, we estimate that if the value of the US dollar was to strengthen by 10% compared to the value of Swiss franc as of December 31, 2017, it would decrease the total US dollar purchase commitment under the Swiss Manufacturing and Services Agreement by approximately $20.4 million. Similarly, a 10% weakening of the US dollar compared to the Swiss franc would increase the total US dollar purchase commitment by approximately $24.9 million.
While we periodically hold foreign currencies, primarily Euro and Pound Sterling, we do not use other financial instruments to hedge our foreign exchange risk. Transactions denominated in currencies other than the functional currency are recorded based on exchange rates at the time such transactions arise. As of December 31, 2017 and 2016, approximately 1% of our total liabilities were denominated in currencies other than the functional currency.
74
ITEM 8.FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA
The financial statements required by this Item are included in Item 15 of this report and are presented beginning on page F-1.
ITEM 9.CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE
None.
ITEM 9A.CONTROLS AND PROCEDURES
Conclusion Regarding the Effectiveness of Disclosure Controls and Procedures
Our disclosure controls and procedures are designed to ensure that information required to be disclosed in the reports we file or submit under the Securities Exchange Act of 1934, as amended (“Exchange Act”) is recorded, processed, summarized and reported within the time periods specified in the Securities and Exchange Commission’s rules and forms, and that such information is accumulated and communicated to our management, including the Chief Executive Officer and the Principal Financial and Accounting Officer, to allow timely decisions regarding required disclosures. Any controls and procedures, no matter how well designed and operated, can provide only reasonable assurance of achieving the desired control objective.
As of December 31, 2017, our management, with the participation of our Chief Executive Officer and Principal Financial and Accounting Officer, performed an evaluation of the effectiveness of the design and operation of our disclosure controls and procedures as defined in Rules 13a-15(e) and 15d-15(e) of the Exchange Act. Based on this evaluation, our Chief Executive Officer and Principal Financial and Accounting Officer concluded that, as of December 31, 2017, the design and operation of our disclosure controls and procedures were effective at the reasonable assurance level.
Management’s Report on Internal Control Over Financial Reporting
Our management is responsible for establishing and maintaining effective internal control over financial reporting and for the assessment of the effectiveness of internal control over financial reporting. Internal control over financial reporting is a process designed by, or under the supervision of, a company’s principal executive officer and principal financial officer and affected by our board of directors, management and other personnel, to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. Our internal control over financial reporting includes those policies and procedures that:
|
· |
pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of our assets; |
|
· |
provide reasonable assurance that transactions are recorded as necessary to permit preparation of the consolidated financial statements in accordance with generally accepted accounting principles, and that our receipts and expenditures are being made only in accordance with authorizations of our management and directors; and |
|
· |
provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use or disposition of our assets that could have a material effect on the consolidated financial statements. |
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions or the degree of compliance with the policies or procedures may deteriorate.
As of December 31, 2017, our management, with the participation of our Chief Executive Officer and Principal Financial and Accounting Officer, assessed the effectiveness of our internal control over financial reporting as defined in Rules 13a-15(f) or 15d-15(f) of the Exchange Act. In making its assessment, management used the criteria established in Internal Control—Integrated Framework (2013 framework) issued by the Committee of Sponsoring Organizations of the Treadway Commission. Based on its assessment, our management determined that, as of December 31, 2017, we maintained effective internal control over financial reporting based on those criteria.
75
In addition, the effectiveness of our internal control over financial reporting as of December 31, 2017 has been audited by Ernst & Young, LLP, an independent registered public accounting firm.
Changes in Internal Control Over Financial Reporting
There were no changes in our internal controls over financial reporting during the quarter ended December 31, 2017 that have materially affected, or are reasonably likely to materially affect, our internal controls over financial reporting.
76
Report of Independent Registered Public Accounting Firm
The Stockholders and Board of Directors of Clovis Oncology, Inc.
Opinion on Internal Control over Financial Reporting
We have audited Clovis Oncology, Inc.’s internal control over financial reporting as of December 31, 2017, based on criteria established in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (2013 framework) (the COSO criteria). In our opinion, Clovis Oncology Inc. (the Company) maintained, in all material respects, effective internal control over financial reporting as of December 31, 2017, based on the COSO criteria.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States) (PCAOB), the consolidated balance sheets of the Company, as of December 31, 2017 and 2016, and the related consolidated statements of operations and comprehensive loss, stockholders' equity (deficit), and cash flows for each of the three years in the period ended December 31, 2017, and the related notes and our report dated February 27, 2018 expressed an unqualified opinion thereon.
Basis for Opinion
The Company’s management is responsible for maintaining effective internal control over financial reporting, and for its assessment of the effectiveness of internal control over financial reporting included in the accompanying Management’s Report on Internal Control over Financial Reporting. Our responsibility is to express an opinion on the Company’s internal control over financial reporting based on our audit. We are a public accounting firm registered with the PCAOB and are required to be independent with respect to the Company in accordance with the U.S federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audit in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects.
Our audit included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, testing and evaluating the design and operating effectiveness of internal control based on the assessed risk, and performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
Definition and Limitations of Internal Control Over Financial Reporting
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
/s/ Ernst & Young LLP
Denver, Colorado
February 27, 2018
77
None.
Certain information required by Part III is omitted from this Annual Report on Form 10-K and is incorporated herein by reference from our definitive proxy statement relating to our 2018 annual meeting of stockholders, pursuant to Regulation 14A of the Securities Exchange Act of 1934, as amended, also referred to in this Form 10-K as our 2018 Proxy Statement, which we expect to file with the SEC no later than April 30, 2018.
ITEM 10.DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE
Information regarding our directors, including the audit committee and audit committee financial experts, and executive officers and compliance with Section 16(a) of the Exchange Act will be included in our 2018 Proxy Statement and is incorporated herein by reference.
We have adopted a Code of Business Ethics for all of our directors, officers and employees as required by NASDAQ governance rules and as defined by applicable SEC rules. Stockholders may locate a copy of our Code of Business Ethics on our website at www.clovisoncology.com or request a copy without charge from:
Clovis Oncology, Inc.
Attention: Investor Relations
5500 Flatiron Parkway, Suite 100
Boulder, CO 80301
We will post to our website any amendments to the Code of Business Ethics and any waivers that are required to be disclosed by the rules of either the SEC or NASDAQ.
ITEM 11.EXECUTIVE COMPENSATION
The information required by this item regarding executive compensation will be included in our 2018 Proxy Statement and is incorporated herein by reference.
ITEM 12.SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS
The information required by this item regarding security ownership of certain beneficial owners and management will be included in the 2018 Proxy Statement and is incorporated herein by reference.
ITEM 13.CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE
The information required by this item regarding certain relationships and related transactions and director independence will be included in the 2018 Proxy Statement and is incorporated herein by reference.
ITEM 14.PRINCIPAL ACCOUNTING FEES AND SERVICES
The information required by this item regarding principal accounting fees and services will be included in the 2018 Proxy Statement and is incorporated herein by reference.
78
ITEM 15.EXHIBITS AND FINANCIAL STATEMENT SCHEDULES
(a)The following documents are being filed as part of this report:
(1) Financial Statements.
Reference is made to the Index to Financial Statements of Clovis Oncology, Inc. appearing on page F-1 of this report.
(2) Financial Statement Schedules.
All financial statement schedules have been omitted because they are not applicable or not required or because the information is included elsewhere in the Financial Statements or the Notes thereto.
(3) Exhibits.
Reference is made to the Index to Exhibits filed as a part of this Annual Report on Form 10-K.
79
INDEX TO EXHIBITS
|
Exhibit |
|
Exhibit Description |
|
|
|
|
|
3.1(5) |
|
Amended and Restated Certificate of Incorporation of Clovis Oncology, Inc. |
|
|
|
|
|
3.2(5) |
|
|
|
|
|
|
|
4.1(3) |
|
|
|
|
|
|
|
4.2(8) |
|
|
|
|
|
|
|
10.1*(4) |
|
|
|
|
|
|
|
10.2*(4) |
|
License Agreement, dated as of June 2, 2011, by and between Clovis Oncology, Inc. and Pfizer Inc. |
|
|
|
|
|
10.3+(1) |
|
|
|
|
|
|
|
10.4+(4) |
|
|
|
|
|
|
|
10.5+(1) |
|
Form of Clovis Oncology, Inc. 2009 Equity Incentive Plan Stock Option Agreement. |
|
|
|
|
|
10.6+(4) |
|
Form of Clovis Oncology, Inc. 2011 Stock Incentive Plan Stock Option Agreement. |
|
|
|
|
|
10.7+(3) |
|
|
|
|
|
|
|
10.8+(3) |
|
|
|
|
|
|
|
10.9+(1) |
|
|
|
|
|
|
|
10.10+(1) |
|
|
|
|
|
|
|
10.11+(1) |
|
|
|
|
|
|
|
10.12+(1) |
|
|
|
|
|
|
|
10.13+(1) |
|
|
|
|
|
|
|
10.14+(1) |
|
|
|
|
|
|
|
10.15+(1) |
|
|
|
|
|
|
|
10.16+(1) |
|
Indemnification Agreement, dated as of May 12, 2009, between Clovis Oncology, Inc. and Erle T. Mast. |
|
|
|
|
|
10.17+(1) |
|
|
|
|
|
|
80
|
Exhibit |
|
Exhibit Description |
|
10.18+(1) |
|
|
|
|
|
|
|
10.19+(4) |
|
|
|
|
|
|
|
10.20+(4) |
|
|
|
|
|
|
|
10.21+(6) |
|
|
|
|
|
|
|
10.22+(2) |
|
|
|
|
|
|
|
10.23+(2) |
|
|
|
|
|
|
|
10.24(7) |
|
|
|
|
|
|
|
10.25*(7) |
|
|
|
|
|
|
|
10.26*(7) |
|
|
|
|
|
|
|
10.27+(12) |
|
|
|
|
|
|
|
10.28+(12) |
|
|
|
|
|
|
|
10.29+(12) |
|
|
|
|
|
|
|
10.30+(12) |
|
|
|
|
|
|
|
10.31+(9) |
|
|
|
|
|
|
|
10.32+(15) |
|
|
|
|
|
|
|
10.33+(10) |
|
|
|
|
|
|
|
10.34*(11) |
|
|
|
|
|
|
|
10.35+(13) |
|
Form of Clovis Oncology, Inc. 2011 Stock Incentive Plan RSU Agreement. |
|
|
|
|
|
10.36*(13) |
|
|
|
|
|
|
81
|
Exhibit |
|
Exhibit Description |
|
10.37*(14) |
|
|
|
|
|
|
|
12.1 |
|
|
|
|
|
|
|
21.1(16) |
|
|
|
|
|
|
|
23.1 |
|
|
|
|
|
|
|
31.1 |
|
|
|
|
|
|
|
31.2 |
|
|
|
|
|
|
|
32.1 |
|
|
|
|
|
|
|
32.2 |
|
|
|
|
|
|
|
101.INS |
|
XBRL Instance Document |
|
|
|
|
|
101.SCH |
|
XBRL Taxonomy Extension Schema Document |
|
|
|
|
|
101.CAL |
|
XBRL Taxonomy Extension Calculation Linkbase Document |
|
|
|
|
|
101.LAB |
|
XBRL Taxonomy Extension Label Linkbase Document |
|
|
|
|
|
101.PRE |
|
XBRL Taxonomy Extension Presentation Linkbase Document |
|
|
|
|
|
101.DEF |
|
XBRL Taxonomy Extension Definition Linkbase Document |
|
(1) |
Filed as an exhibit with the Registrant’s Registration Statement on Form S-1 (File No. 333-175080) on June 23, 2011. |
|
(2) |
Filed as an exhibit with the Registrant’s Current Report on Form 8-K (File No. 001-35347) on June 14, 2013. |
|
(3) |
Filed as an exhibit with Amendment No. 2 to the Registrant’s Registration Statement on Form S-1 (File No. 333-175080) on August 31, 2011. |
|
(4) |
Filed as an exhibit with Amendment No. 3 to the Registrant’s Registration Statement on Form S-1 (File No. 333-175080) on October 31, 2011. |
|
(5) |
Filed as an exhibit with the Registrant’s Annual Report on Form 10-K on March 15, 2012. |
|
(6) |
Filed as an exhibit with the Registrant’s Registration Statement on Form S-1 (File No. 333-180293) on March 23, 2012. |
|
(7) |
Filed as an exhibit with the Registrant’s Current Report on Form 8-K (File No. 001-35347) on November 19, 2013. |
|
(8) |
Filed as an exhibit with the Registrant’s Current Report on Form 8-K (File No. 001-35347) on September 9, 2014. |
|
(9) |
Filed as an exhibit with the Registrant’s Current Report on Form 8-K (File No. 001-35347) on April 1, 2016. |
|
(10) |
Filed as an exhibit with the Registrant’s Quarterly Report on Form 10-Q on May 9, 2016. |
|
(11) |
Filed as an exhibit with the Registrant’s Quarterly Report on Form 10-Q on November 4, 2016. |
|
(12) |
Filed as an exhibit with the Registrant’s Annual Report on Form 10-K on February 29, 2016. |
|
(13) |
Filed as an exhibit with the Registrant’s Annual Report on Form 10-K on February 23, 2017. |
|
(14) |
Filed as an exhibit with the Registrant’s Quarterly Report on Form 10-Q on May 4, 2017. |
|
(15) |
Filed as an exhibit with the Registrant’s Current Report on Form 8-K (File No. 001-35347) on July 7, 2017. |
|
(16) |
Filed as an exhibit with the Registrant’s Quarterly Report on Form 10-Q on August 3, 2017. |
+ Indicates management contract or compensatory plan.
* Confidential treatment has been sought or granted with respect to portions of this exhibit, which portions have been omitted and filed separately with the Securities and Exchange Commission.
82
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
|
|
CLOVIS ONCOLOGY, INC. |
|
|
|
|
|
|
|
By: |
/S/ PATRICK J. MAHAFFY |
|
|
|
Patrick J. Mahaffy |
|
Date: February 27, 2018 |
|
President and Chief Executive Officer; Director |
Pursuant to the requirements of the Securities Exchange Act of 1934, as amended, this report has been signed by the following persons on behalf of the registrant and in the capacities and on the dates indicated:
|
Name |
|
Title |
|
Date |
|
|
|
|
|
|
|
/S/ PATRICK J. MAHAFFY |
|
President and Chief Executive Officer; Director |
|
February 27, 2018 |
|
Patrick J. Mahaffy |
||||
|
|
|
|
|
|
|
/S/ DANIEL W. MUEHL Daniel W. Muehl |
|
Senior Vice President of Finance (Principal Financial Officer and Principal Accounting Officer) |
|
February 27, 2018 |
|
|
|
|
|
|
|
/S/ BRIAN G. ATWOOD Brian G. Atwood |
|
Director |
|
February 27, 2018 |
|
|
|
|
|
|
|
/S/ M. JAMES BARRETT M. James Barrett |
|
Director |
|
February 27, 2018 |
|
|
|
|
|
|
|
/S/ JAMES C. BLAIR James C. Blair |
|
Director |
|
February 27, 2018 |
|
|
|
|
|
|
|
/S/ KEITH FLAHERTY Keith Flaherty |
|
Director |
|
February 27, 2018 |
|
|
|
|
|
|
|
/S/ GINGER L. GRAHAM Ginger L. Graham |
|
Director |
|
February 27, 2018 |
|
|
|
|
|
|
|
/S/ PAUL KLINGENSTEIN Paul Klingenstein |
|
Director |
|
February 27, 2018 |
|
|
|
|
|
|
|
/S/ EDWARD J. MCKINLEY Edward J. McKinley |
|
Director |
|
February 27, 2018 |
|
|
|
|
|
|
|
/S/ THORLEF SPICKSCHEN Thorlef Spickschen |
|
Director |
|
February 27, 2018 |
83
INDEX TO CONSOLIDATED FINANCIAL STATEMENTS
|
Index to Consolidated Financial Statements |
|
|
|
|
|
F-2 |
|
|
|
|
|
Consolidated Statements of Operations and Comprehensive Loss |
F-3 |
|
|
|
|
F-4 |
|
|
|
|
|
F-5 |
|
|
|
|
|
F-6 |
|
|
|
|
|
F-7 |
F-1
Report of Independent Registered Public Accounting Firm
The Stockholders and Board of Directors of Clovis Oncology, Inc.
Opinion on the Financial Statements
We have audited the accompanying consolidated balance sheets of Clovis Oncology, Inc. (the Company) as of December 31, 2017 and 2016, and the related consolidated statements of operations and comprehensive loss, stockholders' equity (deficit), and cash flows for each of the three years in the period ended December 31, 2017, and the related notes (collectively referred to as the consolidated “financial statements”). In our opinion, the consolidated financial statements present fairly, in all material respects, the consolidated financial position of the Company at December 31, 2017 and 2016, and the consolidated results of its operations and its cash flows for each of the three years in the period ended December 31, 2017, in conformity of U.S. generally accepted accounting principles.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States) (PCAOB), the Company’s internal control over financial reporting as of December 31, 2017, based on criteria established in Internal Control-Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (2013 framework) and our report dated February 27, 2018 expressed an unqualified opinion thereon.
Basis for Opinion
These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on the Company’s financial statements based on our audits. We are a public accounting firm registered with the PCAOB and are required to be independent with respect to the Company in accordance with the U.S federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement, whether due to error or fraud. Our audits included performing procedures to assess the risks of material misstatement of the financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the financial statements. We believe that our audits provide a reasonable basis for our opinion.
/s/ Ernst & Young LLP
We have served as the Company’s auditor since 2009.
Denver, Colorado
February 27, 2018
F-2
CLOVIS ONCOLOGY, INC.
Consolidated Statements of Operations and Comprehensive Loss
|
|
|
For the Year ended December 31, |
|
|||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|
|||
|
|
|
(in thousands, except per share amounts) |
|
|||||||
|
Revenues: |
|
|
|
|
|
|
|
|
|
|
|
Product revenue, net |
|
$ |
55,511 |
|
$ |
78 |
|
$ |
— |
|
|
Operating expenses: |
|
|
|
|
|
|
|
|
|
|
|
Cost of sales - product |
|
|
10,251 |
|
|
70 |
|
|
— |
|
|
Cost of sales - intangible asset amortization |
|
|
1,486 |
|
|
— |
|
|
— |
|
|
Research and development |
|
|
142,498 |
|
|
251,129 |
|
|
269,251 |
|
|
Selling, general and administrative |
|
|
138,907 |
|
|
40,731 |
|
|
30,524 |
|
|
Acquired in-process research and development |
|
|
— |
|
|
1,300 |
|
|
12,000 |
|
|
Impairment of intangible asset |
|
|
— |
|
|
104,517 |
|
|
89,557 |
|
|
Change in fair value of contingent purchase consideration |
|
|
— |
|
|
(24,936) |
|
|
(24,611) |
|
|
Total expenses |
|
|
293,142 |
|
|
372,811 |
|
|
376,721 |
|
|
Operating loss |
|
|
(237,631) |
|
|
(372,733) |
|
|
(376,721) |
|
|
Other income (expense): |
|
|
|
|
|
|
|
|
|
|
|
Interest expense |
|
|
(10,428) |
|
|
(8,491) |
|
|
(8,372) |
|
|
Foreign currency gain (loss) |
|
|
(82) |
|
|
(580) |
|
|
2,740 |
|
|
Legal settlement loss |
|
|
(105,477) |
|
|
— |
|
|
— |
|
|
Other income |
|
|
3,643 |
|
|
633 |
|
|
416 |
|
|
Other income (expense), net |
|
|
(112,344) |
|
|
(8,438) |
|
|
(5,216) |
|
|
Loss before income taxes |
|
|
(349,975) |
|
|
(381,171) |
|
|
(381,937) |
|
|
Income tax benefit |
|
|
3,578 |
|
|
32,034 |
|
|
29,076 |
|
|
Net loss |
|
$ |
(346,397) |
|
$ |
(349,137) |
|
$ |
(352,861) |
|
|
Other comprehensive income (loss): |
|
|
|
|
|
|
|
|
|
|
|
Foreign currency translation adjustments, net of tax |
|
|
5,517 |
|
|
(357) |
|
|
(22,629) |
|
|
Net unrealized gain (loss) on available-for-sale securities, net of tax |
|
|
(110) |
|
|
237 |
|
|
(383) |
|
|
Other comprehensive income (loss) |
|
|
5,407 |
|
|
(120) |
|
|
(23,012) |
|
|
Comprehensive loss |
|
$ |
(340,990) |
|
$ |
(349,257) |
|
$ |
(375,873) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Loss per basic and diluted common share: |
|
|
|
|
|
|
|
|
|
|
|
Basic and diluted net loss per common share |
|
$ |
(7.36) |
|
$ |
(9.07) |
|
$ |
(9.79) |
|
|
Basic and diluted weighted average common shares outstanding |
|
|
47,047 |
|
|
38,478 |
|
|
36,026 |
|
See accompanying Notes to Consolidated Financial Statements.
F-3
CLOVIS ONCOLOGY, INC.
|
|
|
December 31, |
|
December 31, |
|
||
|
|
|
2017 |
|
2016 |
|
||
|
|
|
|
|
|
|
|
|
|
ASSETS |
|
|
|
|
|
|
|
|
Current assets: |
|
|
|
|
|
|
|
|
Cash and cash equivalents |
|
$ |
464,198 |
|
$ |
216,186 |
|
|
Accounts receivable, net |
|
|
6,181 |
|
|
121 |
|
|
Inventories |
|
|
27,508 |
|
|
— |
|
|
Available-for-sale securities |
|
|
99,533 |
|
|
49,997 |
|
|
Prepaid research and development expenses |
|
|
1,559 |
|
|
6,427 |
|
|
Deposit on inventory |
|
|
20,461 |
|
|
— |
|
|
Other current assets |
|
|
7,500 |
|
|
6,679 |
|
|
Total current assets |
|
|
626,940 |
|
|
279,410 |
|
|
Property and equipment, net |
|
|
4,007 |
|
|
4,440 |
|
|
Intangible assets, net |
|
|
19,561 |
|
|
21,047 |
|
|
Goodwill |
|
|
65,217 |
|
|
57,192 |
|
|
Other assets |
|
|
19,505 |
|
|
2,468 |
|
|
Total assets |
|
$ |
735,230 |
|
$ |
364,557 |
|
|
LIABILITIES AND STOCKHOLDERS' EQUITY (DEFICIT) |
|
|
|
|
|
|
|
|
Current liabilities: |
|
|
|
|
|
|
|
|
Accounts payable |
|
$ |
15,147 |
|
$ |
10,912 |
|
|
Accrued research and development expenses |
|
|
18,465 |
|
|
35,198 |
|
|
Milestone liability |
|
|
22,022 |
|
|
— |
|
|
Other accrued expenses |
|
|
25,883 |
|
|
19,487 |
|
|
Total current liabilities |
|
|
81,517 |
|
|
65,597 |
|
|
Milestone liability |
|
|
— |
|
|
20,062 |
|
|
Convertible senior notes |
|
|
282,406 |
|
|
281,126 |
|
|
Deferred rent, long-term |
|
|
3,671 |
|
|
1,406 |
|
|
Total liabilities |
|
|
367,594 |
|
|
368,191 |
|
|
Commitments and contingencies (Note 14) |
|
|
|
|
|
|
|
|
Stockholders' equity (deficit): |
|
|
|
|
|
|
|
|
Preferred stock, par value $0.001 per share; 10,000,000 shares authorized, no shares issued and outstanding at December 31, 2017 and December 31, 2016 |
|
|
— |
|
|
— |
|
|
Common stock, $0.001 par value per share, 100,000,000 shares authorized at December 31, 2017 and December 31, 2016; 50,565,119 and 38,724,090 shares issued and outstanding at December 31, 2017 and December 31, 2016 respectively |
|
|
51 |
|
|
39 |
|
|
Additional paid-in capital |
|
|
1,887,198 |
|
|
1,174,950 |
|
|
Accumulated other comprehensive loss |
|
|
(42,173) |
|
|
(47,580) |
|
|
Accumulated deficit |
|
|
(1,477,440) |
|
|
(1,131,043) |
|
|
Total stockholders' equity (deficit) |
|
|
367,636 |
|
|
(3,634) |
|
|
Total liabilities and stockholders' equity (deficit) |
|
$ |
735,230 |
|
$ |
364,557 |
|
See accompanying Notes to Consolidated Financial Statements.
F-4
CLOVIS ONCOLOGY, INC.
Consolidated Statements of Stockholders’ Equity (Deficit)
|
|
|
|
|
|
|
|
|
|
|
Accumulated |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Additional |
|
Other |
|
|
|
|
|
|
|
||
|
|
|
Common Stock |
|
Paid-In |
|
Comprehensive |
|
Accumulated |
|
|
|
|
||||||
|
|
|
Shares |
|
Amount |
|
Capital |
|
Income (Loss) |
|
Deficit |
|
Total |
|
|||||
|
|
|
(in thousands, except for share amounts) |
|
|||||||||||||||
|
Balance at January 1,2015 |
|
33,977,187 |
|
$ |
34 |
|
$ |
785,089 |
|
$ |
(24,448) |
|
$ |
(429,045) |
|
$ |
331,630 |
|
|
Issuance of common stock, net of issuance costs of $17,741 |
|
4,054,487 |
|
|
4 |
|
|
298,505 |
|
|
— |
|
|
— |
|
|
298,509 |
|
|
Issuance of common stock under employee stock purchase plan |
|
32,021 |
|
|
— |
|
|
493 |
|
|
— |
|
|
— |
|
|
493 |
|
|
Exercise of stock options |
|
295,759 |
|
|
— |
|
|
5,534 |
|
|
— |
|
|
— |
|
|
5,534 |
|
|
Share-based compensation expense |
|
— |
|
|
— |
|
|
40,357 |
|
|
— |
|
|
— |
|
|
40,357 |
|
|
Net unrealized loss on available-for-sale securities |
|
— |
|
|
— |
|
|
— |
|
|
(383) |
|
|
— |
|
|
(383) |
|
|
Foreign currency translation adjustments |
|
— |
|
|
— |
|
|
— |
|
|
(22,629) |
|
|
— |
|
|
(22,629) |
|
|
Net loss |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
(352,861) |
|
|
(352,861) |
|
|
Balance at December 31, 2015 |
|
38,359,454 |
|
|
38 |
|
|
1,129,978 |
|
|
(47,460) |
|
|
(781,906) |
|
|
300,650 |
|
|
Issuance of common stock under employee stock purchase plan |
|
110,508 |
|
|
— |
|
|
1,965 |
|
|
— |
|
|
— |
|
|
1,965 |
|
|
Exercise of stock options |
|
247,431 |
|
|
1 |
|
|
3,268 |
|
|
— |
|
|
— |
|
|
3,269 |
|
|
Issuance of common stock from vesting of restricted stock units, net of shares withheld for taxes |
|
6,697 |
|
|
— |
|
|
(57) |
|
|
— |
|
|
— |
|
|
(57) |
|
|
Share-based compensation expense |
|
— |
|
|
— |
|
|
39,796 |
|
|
— |
|
|
— |
|
|
39,796 |
|
|
Net unrealized gain on available-for-sale securities |
|
— |
|
|
— |
|
|
— |
|
|
237 |
|
|
— |
|
|
237 |
|
|
Foreign currency translation adjustments |
|
— |
|
|
— |
|
|
— |
|
|
(357) |
|
|
— |
|
|
(357) |
|
|
Net loss |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
(349,137) |
|
|
(349,137) |
|
|
Balance at December 31, 2016 |
|
38,724,090 |
|
|
39 |
|
|
1,174,950 |
|
|
(47,580) |
|
|
(1,131,043) |
|
|
(3,634) |
|
|
Issuance of common stock, net of issuance costs |
|
9,670,454 |
|
|
10 |
|
|
545,828 |
|
|
— |
|
|
— |
|
|
545,838 |
|
|
Issuance of common stock under employee stock purchase plan |
|
51,681 |
|
|
— |
|
|
2,312 |
|
|
— |
|
|
— |
|
|
2,312 |
|
|
Exercise of stock options |
|
465,690 |
|
|
1 |
|
|
13,924 |
|
|
— |
|
|
— |
|
|
13,925 |
|
|
Issuance of common stock from vesting of restricted stock units, net of shares withheld for taxes |
|
180,912 |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
Share-based compensation expense |
|
— |
|
|
— |
|
|
44,707 |
|
|
— |
|
|
— |
|
|
44,707 |
|
|
Legal settlement |
|
1,472,324 |
|
|
1 |
|
|
105,477 |
|
|
— |
|
|
— |
|
|
105,478 |
|
|
Net unrealized loss on available-for-sale securities |
|
— |
|
|
— |
|
|
— |
|
|
(110) |
|
|
— |
|
|
(110) |
|
|
Foreign currency translation adjustments |
|
— |
|
|
— |
|
|
— |
|
|
5,517 |
|
|
— |
|
|
5,517 |
|
|
Net loss |
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
(346,397) |
|
|
(346,397) |
|
|
Balance at December 31, 2017 |
|
50,565,151 |
|
$ |
51 |
|
$ |
1,887,198 |
|
$ |
(42,173) |
|
$ |
(1,477,440) |
|
$ |
367,636 |
|
See accompanying Notes to Consolidated Financial Statements.
F-5
CLOVIS ONCOLOGY, INC.
Consolidated Statements of Cash Flows
|
|
|
Year ended December 31, |
|
|||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|
|||
|
|
|
(in thousands) |
|
|||||||
|
Operating activities |
|
|
|
|
|
|
|
|
|
|
|
Net loss |
|
$ |
(346,397) |
|
$ |
(349,137) |
|
$ |
(352,861) |
|
|
Adjustments to reconcile net loss to net cash used in operating activities: |
|
|
|
|
|
|
|
|
|
|
|
Share-based compensation expense |
|
|
44,707 |
|
|
39,796 |
|
|
40,357 |
|
|
Depreciation and amortization |
|
|
2,504 |
|
|
1,141 |
|
|
761 |
|
|
Amortization of premiums and discounts on available-for-sale securities |
|
|
354 |
|
|
211 |
|
|
1,400 |
|
|
Amortization of debt issuance costs |
|
|
1,279 |
|
|
1,242 |
|
|
1,205 |
|
|
Legal settlement loss |
|
|
105,477 |
|
|
— |
|
|
— |
|
|
Impairment of intangible asset |
|
|
— |
|
|
104,517 |
|
|
89,557 |
|
|
Change in fair value of contingent purchase consideration |
|
|
— |
|
|
(24,661) |
|
|
(27,792) |
|
|
Loss on disposal of property and equipment |
|
|
— |
|
|
105 |
|
|
39 |
|
|
Deferred income taxes |
|
|
(3,218) |
|
|
(31,771) |
|
|
(28,874) |
|
|
Changes in operating assets and liabilities: |
|
|
|
|
|
|
|
|
|
|
|
Accounts receivable |
|
|
(6,061) |
|
|
(121) |
|
|
— |
|
|
Inventory |
|
|
(27,508) |
|
|
— |
|
|
— |
|
|
Prepaid and accrued research and development expenses |
|
|
(17,297) |
|
|
(15,364) |
|
|
14,122 |
|
|
Deposit on inventory |
|
|
(20,461) |
|
|
— |
|
|
— |
|
|
Other operating assets |
|
|
(6,476) |
|
|
1,039 |
|
|
(4,380) |
|
|
Accounts payable |
|
|
5,637 |
|
|
(1,544) |
|
|
8,105 |
|
|
Other accrued expenses |
|
|
6,556 |
|
|
7,867 |
|
|
5,295 |
|
|
Net cash used in operating activities |
|
|
(260,904) |
|
|
(266,680) |
|
|
(253,066) |
|
|
Investing activities |
|
|
|
|
|
|
|
|
|
|
|
Purchases of property and equipment |
|
|
(487) |
|
|
(766) |
|
|
(3,035) |
|
|
Proceeds from sale of property and equipment |
|
|
— |
|
|
65 |
|
|
— |
|
|
Deposits for purchases of property and equipment |
|
|
(2,515) |
|
|
— |
|
|
— |
|
|
Purchases of available-for-sale securities |
|
|
(263,500) |
|
|
— |
|
|
(392,540) |
|
|
Sales of available-for-sale securities |
|
|
213,500 |
|
|
200,000 |
|
|
140,997 |
|
|
Acquired in-process research and development - milestone payment |
|
|
(1,100) |
|
|
— |
|
|
— |
|
|
Net cash (used in) provided by investing activities |
|
|
(54,102) |
|
|
199,299 |
|
|
(254,578) |
|
|
Financing activities |
|
|
|
|
|
|
|
|
|
|
|
Proceeds from the sale of common stock, net of issuance costs |
|
|
545,838 |
|
|
— |
|
|
298,509 |
|
|
Proceeds from the exercise of stock options and employee stock purchases |
|
|
16,237 |
|
|
5,176 |
|
|
5,971 |
|
|
Net cash provided by financing activities |
|
|
562,075 |
|
|
5,176 |
|
|
304,480 |
|
|
Effect of exchange rate changes on cash and cash equivalents |
|
|
943 |
|
|
(365) |
|
|
(757) |
|
|
Increase (decrease) in cash and cash equivalents |
|
|
248,012 |
|
|
(62,570) |
|
|
(203,921) |
|
|
Cash and cash equivalents at beginning of period |
|
|
216,186 |
|
|
278,756 |
|
|
482,677 |
|
|
Cash and cash equivalents at end of period |
|
$ |
464,198 |
|
$ |
216,186 |
|
$ |
278,756 |
|
|
Supplemental disclosure of cash flow information: |
|
|
|
|
|
|
|
|
|
|
|
Cash paid for interest |
|
$ |
7,188 |
|
$ |
7,188 |
|
$ |
7,307 |
|
|
Non-cash investing and financing activities: |
|
|
|
|
|
|
|
|
|
|
|
Acquired in-process research and development - milestone not paid as of period end |
|
$ |
— |
|
$ |
21,100 |
|
$ |
— |
|
|
Vesting of restricted stock units |
|
$ |
12,170 |
|
$ |
175 |
|
$ |
— |
|
|
|
|
|
|
|
|
|
|
|
|
|
See accompanying Notes to Consolidated Financial Statements.
F-6
CLOVIS ONCOLOGY, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
1. Nature of Business
We are a biopharmaceutical company focused on acquiring, developing and commercializing innovative anti-cancer agents in the United States, Europe and additional international markets. We target our development programs for the treatment of specific subsets of cancer populations, and simultaneously develop, with partners, diagnostic tools intended to direct a compound in development to the population that is most likely to benefit from its use. We have and intend to continue to license or acquire rights to oncology compounds in all stages of clinical development. In exchange for the right to develop and commercialize these compounds, we generally expect to provide the licensor with a combination of upfront payments, milestone payments and royalties on future sales. In addition, we generally expect to assume the responsibility for future drug development and commercialization costs. We currently operate in one segment. Since inception, our operations have consisted primarily of developing in-licensed compounds, evaluating new product acquisition candidates and general corporate activities.
Our marketed product Rubraca® (rucaparib) is approved on an accelerated basis in the United States by the FDA as monotherapy for the treatment of patients with deleterious BRCA (human genes associated with the repair of damaged DNA) mutation (germline and/or somatic) associated advanced ovarian cancer who have been treated with two or more chemotherapies, and selected for therapy based on an FDA-approved companion diagnostic for Rubraca. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trials. We launched Rubraca in the United States in December 2016 for this indication.
The FDA is currently reviewing on a priority review timeline our sNDA for Rubraca as maintenance treatment of adult patients with recurrent epithelial ovarian, fallopian tube, or primary peritoneal cancer who are in a complete or partial response to platinum-based chemotherapy.
Our MAA submitted to the European Union’s EMA for an ovarian cancer treatment indication for Rubraca is currently under review by the EMA’s CHMP. Following a Scientific Advisory Group - Oncology meeting and an oral explanation by us before the CHMP in February 2018, the CHMP has communicated a positive trend vote for the MAA and their intention to hold a final vote on the treatment indication at their March 2018 meeting.
Liquidity
We have incurred significant net losses since inception and have relied on our ability to fund our operations through debt and equity financings. We expect operating losses and negative cash flows to continue for the foreseeable future. As we continue to incur losses, transition to profitability is dependent upon achieving a level of revenue from Rubraca adequate to support our cost structure. We may never achieve profitability, and unless and until it does, we will continue to need to raise additional cash.
In January 2017, we sold 5,750,000 shares of our common stock in a public offering at $41.00 per share. The net proceeds from the offering were $221.2 million, after deducting underwriting discounts and commissions and offering expenses. In June 2017, we sold 3,920,454 shares of our common stock in a public offering at $88.00 per share. The net proceeds from the offering were $324.6 million, after deducting underwriting discounts and commissions and offering expenses. We intend to use the net proceeds of the offerings for general corporate purposes, including commercial planning and sales and marketing expenses associated with the launch of Rubraca in the United States and, if approved by the European Commission in Europe, funding of its development programs, selling, general and administrative expenses, acquisition or licensing of additional product candidates or businesses and working capital. Based on our current estimates, we believe that our cash, cash equivalents and available-for-sale securities will allow us to fund activities through the next 12 months.
F-7
2. Summary of Significant Accounting Policies
Basis of Presentation
The accompanying financial statements have been prepared in accordance with U.S. generally accepted accounting principles (“U.S. GAAP”). The consolidated financial statements include our accounts and our wholly-owned subsidiaries. All significant intercompany balances and transactions have been eliminated in consolidation.
Use of Estimates
The preparation of financial statements in conformity with U.S. GAAP requires management to make estimates and assumptions that affect the reported amounts of assets, liabilities, expenses and revenue and related disclosures. On an ongoing basis, we evaluate our estimates, including estimates related to revenue, intangible asset impairment, clinical trial accruals and share-based compensation expense. We base our estimates on historical experience and other market-specific or other relevant assumptions that we believe to be reasonable under the circumstances. Actual results may differ from those estimates or assumptions.
Revenue Recognition
We are currently approved to sell Rubraca in the United States market. We distribute our product principally through a limited number of specialty distributor and specialty pharmacy providers, collectively, our customers. Our customers subsequently sell our products to patients and health care providers. Separately, we have arrangements with certain payors and other third-parties that provide for government-mandated and privately-negotiated rebates, chargebacks and discounts.
Revenues from product sales are recognized when persuasive evidence of an arrangement exists, delivery has occurred and title of the product and associated risk of loss has passed to the customer, the price is fixed or determinable, collection from the customer has been reasonably assured and all performance obligations have been met and returns and allowances can be reasonably estimated. Product sales are recorded net of estimated rebates, chargebacks, discounts and other deductions as well as estimated product returns. Estimating rebates, chargebacks, discounts, product returns and other deductions requires significant judgments about future events and uncertainties, and requires us to rely heavily on assumptions, as well as historical experience. We only recognize revenue on product sales once the product is sold to the patient or healthcare provider by the specialty distributor or specialty pharmacy provider, therefore reducing the significance of estimates made for product returns.
For the year ended December 31, 2017, we recognized $55.5 million of product revenue. Based on our policy to expense costs associated with the manufacture of our products prior to regulatory approval, certain of the costs of Rubraca units recognized as revenue during the year ended December 31, 2017 were expensed prior to the December 19, 2016 FDA approval, and a minimal amount is included in cost of sales during the current period. We expect cost of sales to increase in relation to product revenues as we deplete these inventories. The majority of products sales were of pre-commercialization inventory in 2017.
Product revenue from each of our customers who individually accounted for 10% or more of total revenues consisted of the following:
|
|
|
December 31, |
|
|
|
2017 |
|
Customer A |
|
35% |
|
Customer B |
|
27% |
|
Customer C |
|
12% |
|
Customer D |
|
10% |
Effective January 1, 2018, we adopted ASC 606, the new revenue recognition standard, using the modified retrospective method. For a complete discussion of this adoption and the accounting for net product revenue, see the Recently Issued Accounting Standards section below and Note 11, Revenue Recognition.
F-8
Fair Value of Financial Instruments
Cash, cash equivalents, available-for-sale securities and contingent purchase consideration are carried at fair value. Financial instruments, including other current assets and accounts payable, are carried at cost, which approximates fair value given their short-term nature (see Note 4, Fair Value Measurements).
Cash, Cash Equivalents and Available-for-Sale Securities
We consider all highly liquid investments with original maturities at the date of purchase of three months or less to be cash equivalents. Cash and cash equivalents include bank demand deposits and money market funds that invest primarily in certificate of deposits, commercial paper and U.S. government and U.S. government agency obligations.
Marketable securities are considered to be available-for-sale securities and consist of U.S. treasury securities. Available-for-sale securities are reported at fair value on the Consolidated Balance Sheets and unrealized gains and losses are included in accumulated other comprehensive loss on the Consolidated Balance Sheets. Realized gains and losses, amortization of premiums and discounts and interest and dividends earned are included in other income (expense) on the Consolidated Statements of Operations and Comprehensive Loss. The cost of investments for purposes of computing realized and unrealized gains and losses is based on the specific identification method. Investments with maturities beyond one year are classified as short-term based on our intent to fund current operations with these securities or to make them available for current operations.
A decline in the market value of a security below its cost that is deemed to be other than temporary is charged to earnings and results in the establishment of a new cost basis for the security. Factors evaluated to determine if an investment is other-than-temporarily impaired include significant deterioration in earnings performance, credit rating, asset quality or business prospects of the issuer; adverse changes in the general market conditions in which the issuer operates; and our intent and ability to hold the security until an anticipated recovery in value occurs.
Accounts Receivable
As of December 31, 2017 and 2016, we had no allowance for doubtful accounts. We provide an allowance for doubtful accounts based on experience and specifically identified risks. Accounts receivable are carried at fair value and charged off against the allowance for doubtful accounts when we determine that recovery is unlikely and we cease collection efforts.
Property and Equipment
Property and equipment are stated at cost, less accumulated depreciation. Property and equipment are depreciated using the straight-line method over the estimated useful lives of the assets. Equipment purchased for use in manufacturing and clinical trials is evaluated to determine whether the equipment is solely beneficial for a drug candidate in the development stage or whether it has an alternative use. Equipment with an alternative use is capitalized. Leasehold improvements are amortized over the economic life of the asset or the lease term, whichever is shorter. Maintenance and repairs are expensed as incurred. The estimated useful lives of our capitalized assets are as follows:
|
|
|
Estimated |
|
|
|
|
Useful Life |
|
|
Computer hardware and software |
|
3 to 5 years |
|
|
Leasehold improvements |
|
6 years |
|
|
Laboratory, manufacturing and office equipment |
|
5 to 7 years |
|
|
Furniture and fixtures |
|
10 years |
|
Long-Lived Assets
We review long-lived assets for impairment when events or changes in circumstances indicate that the carrying value of the assets may not be recoverable. Recoverability is measured by comparison of the assets’ book value to future net undiscounted cash flows that the assets are expected to generate. If the carrying value of the assets exceed their future net undiscounted cash flows, an impairment charge is recognized for the amount by which the carrying value of the assets exceeds the fair value of the assets.
F-9
Intangible Assets, Net
Definite-lived intangible assets related to capitalized milestones under license agreements are amortized on a straight-line basis over their remaining useful lives, which are estimated to be the remaining patent life. If our estimate of the product’s useful life is shorter than the remaining patent life, then a shorter period is used. Amortization expense is recorded as a component of cost of sales on the Consolidated Statements of Operations and Comprehensive Loss.
Intangible acquired in-process research and development (“IPR&D”) assets were established as part of the acquisition of Ethical Oncology Science, S.p.A. (“EOS”) in November 2013 and were not amortized.
Intangible assets are evaluated for impairment at least annually in the fourth quarter or more frequently if impairment indicators exist. Events that could result in an impairment, or trigger an interim impairment assessment, include the decision to discontinue the development of a drug, the receipt of additional clinical or nonclinical data regarding our drug candidate or a potentially competitive drug candidate, changes in the clinical development program for a drug candidate, or new information regarding potential sales for the drug. In connection with any impairment assessment, the fair value of the intangible assets as of the date of assessment is compared to the carrying value of the intangible asset. Impairment losses are recognized if the carrying value of an intangible asset is both not recoverable and exceeds its fair value. During the second quarter of 2016, we recorded a $104.5 million impairment charge to the IPR&D intangible assets, reducing the remaining carrying value to zero (see Note 6, Intangible Assets and Goodwill). Previously, the Company recorded an $89.6 million impairment charge to the IPR&D intangible assets during the fourth quarter of 2015.
Goodwill
Goodwill represents the excess of the purchase price over the fair value of net assets acquired in a business combination accounted for under the acquisition method of accounting and is not amortized, but is subject to impairment testing at least annually in the fourth quarter or when a triggering event is identified that could indicate a potential impairment. We are organized as a single reporting unit and perform impairment testing by comparing the carrying value of the reporting unit to the fair value of the Company. Goodwill was recorded as a result of the EOS acquisition.
Other Current Assets
Other current assets are comprised of the following (in thousands):
|
|
|
December 31, |
|
December 31, |
|
||
|
|
|
2017 |
|
2016 |
|
||
|
Receivable from partners |
|
$ |
9 |
|
$ |
2,882 |
|
|
Prepaid insurance |
|
|
1,926 |
|
|
1,234 |
|
|
Prepaid expenses - other |
|
|
3,355 |
|
|
2,109 |
|
|
Receivable - other |
|
|
2,023 |
|
|
364 |
|
|
Other |
|
|
187 |
|
|
90 |
|
|
Total |
|
$ |
7,500 |
|
$ |
6,679 |
|
F-10
Other Accrued Expenses
Other accrued expenses are comprised of the following (in thousands):
|
|
|
December 31, |
|
December 31, |
|
||
|
|
|
2017 |
|
2016 |
|
||
|
Accrued personnel costs |
|
$ |
13,889 |
|
$ |
15,850 |
|
|
Accrued interest payable |
|
|
2,096 |
|
|
2,096 |
|
|
Income tax payable |
|
|
— |
|
|
556 |
|
|
Accrued corporate legal fees and professional services |
|
|
415 |
|
|
589 |
|
|
Accrued royalties |
|
|
2,984 |
|
|
— |
|
|
Accrued sales deductions |
|
|
1,008 |
|
|
— |
|
|
Payable to third party logistics provider |
|
|
2,661 |
|
|
— |
|
|
Accrued expenses - other |
|
|
2,830 |
|
|
396 |
|
|
Total |
|
$ |
25,883 |
|
$ |
19,487 |
|
Valuation of Contingent Consideration Resulting from a Business Combination
Subsequent to the acquisition date, we re-measure contingent consideration arrangements at fair value each reporting period and record changes in fair value to change in fair value of contingent purchase consideration and foreign currency gains (losses) for changes in the foreign currency translation rate on the Consolidated Statements of Operations and Comprehensive Loss. Changes in fair value are primarily attributed to new information about the IPR&D assets, including changes in timeline and likelihood of success, and the passage of time. In the absence of new information, changes in fair value reflect only the passage of time. During the fourth quarter of 2015, we recorded a $26.9 million reduction in the fair value of the contingent purchase consideration liability due to a change in the estimated probability-weighted future discounted milestone payments, as well as the timing of such payments, for the lucitanib program. Then, during the second quarter of 2016, we recorded a $25.5 million reduction in the fair value of the contingent purchase consideration liability due to our and our development partner’s decision to discontinue the development of lucitanib for breast cancer. At December 31, 2017, the contingent purchase consideration liability recorded on the Consolidated Balance Sheets remained at zero due to the uncertainty of achieving any of the lucitanib regulatory milestones, and therefore the remote likelihood of future milestone payouts.
Research and Development Expense
Research and development costs are charged to expense as incurred and include, but are not limited to, salary and benefits, share-based compensation, clinical trial activities, drug development and manufacturing, companion diagnostic development and third-party service fees, including contract research organizations and investigative sites. During 2015, we completed the hiring of our U.S. sales and marketing and medical affairs organizations in preparation for the potential commercial launch of Rubraca. These costs were also included in research and development expense before the FDA approval of Rubraca.
Costs for certain development activities, such as clinical trials, are recognized based on an evaluation of the progress to completion of specific tasks using data such as patient enrollment, clinical site activations or information provided to us by our vendors on their actual costs incurred. Payments for these activities are based on the terms of the individual arrangements, which may differ from the pattern of costs incurred and are reflected on the Consolidated Balance Sheets as prepaid or accrued research and development expenses.
Acquired In-Process Research and Development Expense
We have acquired and expect to continue to acquire the rights to develop and commercialize new drug candidates. The upfront payments to acquire a new drug compound, as well as subsequent milestone payments, are immediately expensed as acquired in-process research and development provided that the drug has not achieved regulatory approval for marketing and, absent obtaining such approval, has no alternative future use. Once regulatory approval is received, payments to acquire rights, and the related milestone payments, are capitalized and the amortization of such assets recorded to product cost of sales.
F-11
Share-Based Compensation Expense
Share-based compensation is recognized as expense for all share-based awards made to employees and directors and is based on estimated fair values. We determine equity-based compensation at the grant date using the Black-Scholes option pricing model. The value of the award that is ultimately expected to vest is recognized as expense on a straight-line basis over the requisite service period. Any changes to the estimated forfeiture rates are accounted for prospectively.
Inventory
Inventories are stated at the lower of cost or estimated net realizable value, on a first-in, first-out, or FIFO, basis. Prior to the regulatory approval of Rubraca, we incurred expenses for the manufacture of drug that could potentially be available to support the commercial launch of Rubraca. Until the first reporting period when regulatory approval has been received, we record all such costs as research and development expense. We periodically analyze our inventory levels, and write down inventory that has become obsolete, inventory that has a cost basis in excess of its estimated realizable value and/or inventory in excess of expected sales requirements as cost of product revenues. Expired inventory would be disposed of and the related costs would be written off as cost of product revenues.
The active pharmaceutical ingredient in Rubraca is currently produced by a single supplier.
At December 31, 2017, deposit on inventory on the Consolidated Balance Sheets is a cash deposit of $20.5 million made to a manufacturer for the purchase of inventory which we expect to be converted to finished goods within the next twelve months.
Concentration of Credit Risk
Financial instruments that potentially subject us to concentrations of credit risk are primarily cash, cash equivalents and available-for-sale securities. We maintain our cash and cash equivalent balances in the form of money market accounts with financial institutions that we believe are creditworthy. Available-for-sale securities are invested in accordance with our investment policy. The investment policy includes guidelines on the quality of the institutions and financial instruments and defines allowable investments that we believe minimizes the exposure to concentration of credit risk. We have no financial instruments with off-balance sheet risk of accounting loss.
Foreign Currency
The assets and liabilities of our foreign operations are translated into U.S. dollars at current exchange rates and the results of operations are translated at the average exchange rates for the reported periods. The resulting translation adjustments are included in accumulated other comprehensive loss on the Consolidated Balance Sheets. Transactions denominated in currencies other than the functional currency are recorded based on exchange rates at the time such transactions arise. Transaction gains and losses are recorded to foreign currency gains (losses) on the Consolidated Statements of Operations and Comprehensive Loss. As of December 31, 2017 and 2016, approximately 1% of our total liabilities were denominated in currencies other than the functional currency.
Income Taxes
We account for income taxes under the asset and liability method. Deferred tax assets and liabilities are recognized for the future tax consequences attributable to differences between the financial statement carrying amounts of existing assets and liabilities and their respective tax bases using enacted tax rates in effect for the year in which the differences are expected to affect taxable income. Tax benefits are recognized when it is more likely than not that a tax position will be sustained during an audit. Deferred tax assets are reduced by a valuation allowance if current evidence indicates that it is considered more likely than not that these benefits will not be realized.
Recently Adopted Accounting Standards
In March 2016, the FASB issued Accounting Standards Update No. 2016-09, Compensation – Stock Compensation (Topic 718): Improvements to Employee Share-Based Payment Accounting" (ASU 2016-09). ASU 2016-09 simplifies how several aspects of share-based payments are accounted for and presented in the financial statements. ASU 2016-09 is effective for public companies for annual reporting periods beginning after December 15, 2016. We adopted this ASU
F-12
in the first quarter of 2017. We had excess tax benefits for which a benefit could not be previously recognized of approximately $18.2 million. Upon adoption the balance of the unrecognized excess tax benefits were reversed with the impact recorded to retained earnings including any change to the valuation allowance as a result of the adoption. Due to the full valuation allowance on the U.S. deferred tax assets, there is no impact to the financial statements as a result of this adoption.
Recently Issued Accounting Standards
In May 2014, the Financial Accounting Standards Board (“FASB”) issued ASU No. 2014-09, “Revenue from Contracts with Customers” and has subsequently issued several supplemental and/or clarifying ASUs (collectively, “ASC 606”). ASC 606 prescribes a single common revenue standard that replaces most existing U.S. GAAP revenue recognition guidance. ASC 606 is intended to provide a more consistent interpretation and application of the principles outlined in the standard across filers in multiple industries and within the same industries compared to current practices, which should improve comparability. Adoption of ASC 606 is required for annual and interim periods beginning after December 15, 2017. Upon adoption, we must elect to adopt either retrospectively to each prior reporting period presented or use the modified retrospective transition method with the cumulative effect of initial adoption recognized at the date of initial application. We have elected to apply the new standard using the modified retrospective method upon its adoption date on January 1, 2018.
Under ASC 606, an entity recognizes revenue when its customer obtains control of promised goods or services, in an amount that reflects the consideration which the entity expects to receive in exchange for those goods or services. To determine revenue recognition for arrangements that an entity determines are within the scope of ASC 606, the entity performs the following five steps: (i) identify the contract(s) with a customer; (ii) identify the performance obligations in the contract; (iii) determine the transaction price; (iv) allocate the transaction price to the performance obligations in the contract; and (v) recognize revenue when (or as) the entity satisfies a performance obligation. ASC 606 also impacts certain other areas, such as the accounting for costs to obtain or fulfill a contract. The standard also requires disclosure of the nature, amount, timing and uncertainty of revenue and cash flows arising from contracts with customers.
We have examined our revenue recognition policy specific to revenue streams from representative contracts governing product sales from Rubraca and have come to conclusions on the impact of the new standard using the 5-step process prescribed by ASC 606. We have reviewed a representative sample of contracts, including our collaboration agreements with Servier and Bristol-Myers Squibb discussed in Note 13, License Agreements, and determined the potential impact to our accounting policies, financial controls and operations. Our conclusions include recognizing revenue on product sales once the product is sold to the specialty distributor and specialty pharmacy providers. Currently, we anticipate the effects of adoption to be as described in Note 11, Revenue Recognition.
In February 2016, the FASB issued ASU No. 2016-02, “Leases (Topic 842),” which requires lessees to recognize assets and liabilities for the rights and obligations created by most leases on their balance sheet. The guidance is effective for fiscal years beginning after December 15, 2018, including interim periods within those fiscal years. Early application is permitted. We plan to adopt on January 1, 2019. ASU 2016-02 requires modified retrospective adoption for all leases existing at, or entered into after, the date of initial application, with an option to use certain transition relief. We are currently evaluating the impact the standard may have on our consolidated financial statements and related disclosures.
In January 2017, the FASB issued ASU No. 2017-01, “Clarifying the Definition of a Business,” which clarifies the definition of a business in ASC 805. The guidance is effective for fiscal years beginning after December 15, 2017, including interim periods within those fiscal years. Early application is permitted. We adopted this standard on January 1, 2018 and the adoption resulted in no change to our consolidated financial statements and related disclosures.
In May 2017, the FASB issued ASU 2017-09, “Compensation – Stock Compensation (Topic 718): Scope of Modification Accounting”, which amends the scope of modification accounting for share-based payment arrangements. The ASU provides guidance on the types of changes to the terms or conditions of share-based payment awards to which we would be required to apply modification accounting under ASC 718. Specifically, we would not apply modification accounting if the fair value, vesting conditions, and classification of the awards are the same immediately before and after the modification. The guidance is effective for annual reporting periods, including interim periods within those annual periods, beginning after December 15, 2017. Early adoption is permitted, including adoption in any interim
F-13
period. We adopted this standard on January 1, 2018 and the adoption resulted in no change to our consolidated financial statements and related disclosures.
3. Property and Equipment
Property and equipment consisted of the following (in thousands):
|
|
|
December 31, |
|
||||
|
|
|
2017 |
|
2016 |
|
||
|
Laboratory, manufacturing and office equipment |
|
$ |
2,853 |
|
$ |
2,555 |
|
|
Leasehold improvements |
|
|
2,285 |
|
|
2,276 |
|
|
Furniture and fixtures |
|
|
1,416 |
|
|
1,411 |
|
|
Computer hardware and software |
|
|
1,141 |
|
|
855 |
|
|
Total property and equipment |
|
|
7,695 |
|
|
7,097 |
|
|
Less: accumulated depreciation |
|
|
(3,688) |
|
|
(2,657) |
|
|
Total property and equipment, net |
|
$ |
4,007 |
|
$ |
4,440 |
|
Depreciation expense related to property and equipment was approximately $1.0 million, $1.1 million and $0.8 million for the years ended December 31, 2017, 2016 and 2015, respectively.
4. Fair Value Measurements
Fair value is defined as the exchange price that would be received to sell an asset or paid to transfer a liability (at exit price) in the principal or most advantageous market for the asset or liability in an orderly transaction between market participants on the measurement date. The three levels of inputs that may be used to measure fair value include:
|
Level 1: |
Quoted prices in active markets for identical assets or liabilities. Our Level 1 assets consist of money market investments. We do not have Level 1 liabilities. |
|
|
|
|
Level 2: |
Observable inputs other than Level 1 prices, such as quoted prices for similar assets or liabilities in active markets or other inputs that are observable or can be corroborated by observable market data for substantially the full term of the assets or liabilities. Our Level 2 assets consist of U.S. treasury securities. We do not have Level 2 liabilities. |
|
|
|
|
Level 3: |
Unobservable inputs that are supported by little or no market activity. We do not have Level 3 assets. The contingent purchase consideration related to the undeveloped lucitanib product rights acquired with the purchase of EOS in November 2013 is a Level 3 liability. The fair value of this liability is based on unobservable inputs and includes valuations for which there is little, if any, market activity. During the second quarter of 2016, we recorded a $25.5 million reduction in the fair value of the contingent purchase consideration liability due to our and our development partner’s decision to discontinue the development of lucitanib for breast cancer, reducing the remaining fair value to zero. The fair value and carrying value remained at zero as of December 31, 2017.
The change in the fair value of Level 3 instruments is included in change in fair value of contingent purchase consideration and foreign currency gains (losses) for changes in the foreign currency translation rate on the Consolidated Statements of Operations and Comprehensive Loss.
|
F-14
The following table identifies our assets that were measured at fair value on a recurring basis (in thousands):
|
|
|
Balance |
|
Level 1 |
|
Level 2 |
|
Level 3 |
|
||||
|
December 31, 2017 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Assets: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Money market |
|
$ |
433,136 |
|
$ |
433,136 |
|
$ |
— |
|
$ |
— |
|
|
U.S. treasury securities |
|
|
99,533 |
|
|
— |
|
|
99,533 |
|
|
— |
|
|
Total assets at fair value |
|
$ |
532,669 |
|
$ |
433,136 |
|
$ |
99,533 |
|
$ |
— |
|
|
December 31, 2016 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Assets: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Money market |
|
$ |
202,361 |
|
$ |
202,361 |
|
$ |
— |
|
$ |
— |
|
|
U.S. treasury securities |
|
|
49,997 |
|
|
— |
|
|
49,997 |
|
|
— |
|
|
Total assets at fair value |
|
$ |
252,358 |
|
$ |
202,361 |
|
$ |
49,997 |
|
$ |
— |
|
There were no liabilities that were measured at fair value on a recurring basis as of December 31, 2017. There were no transfers between the Level 1 and Level 2 categories or into or out of the Level 3 category during the year ended December 31, 2017.
Financial instruments not recorded at fair value include our convertible senior notes. At December 31, 2017, the carrying amount of the convertible senior notes was $282.4 million, which represents the aggregate principal amount net of remaining debt issuance costs, and the fair value was $388.3 million. The fair value was determined using Level 2 inputs based on the indicative pricing published by certain investment banks or trading levels of the convertible senior notes, which are not listed on any securities exchange or quoted on an inter-dealer automated quotation system. See Note 7, Convertible Senior Notes for discussion of the convertible senior notes. The carrying amounts of accounts payable and accrued expenses approximate their fair value due to their short-term maturities.
5. Available-for-Sale Securities
As of December 31, 2017, available-for-sale securities consisted of the following (in thousands):
|
|
|
|
|
|
Gross |
|
Gross |
|
Aggregate |
|
|||
|
|
|
Amortized |
|
Unrealized |
|
Unrealized |
|
Fair |
|
||||
|
|
|
Cost |
|
Gains |
|
Losses |
|
Value |
|
||||
|
U.S. treasury securities |
|
$ |
99,650 |
|
$ |
— |
|
$ |
(117) |
|
$ |
99,533 |
|
As of December 31, 2017, the fair value and gross unrealized losses of available-for-sale securities that have been in a continuous unrealized loss position for less than 12 months were as follows (in thousands):
|
|
|
Aggregate |
|
Gross |
|
||
|
|
|
Fair |
|
Unrealized |
|
||
|
|
|
Value |
|
Losses |
|
||
|
U.S. treasury securities |
|
$ |
99,533 |
|
$ |
(117) |
|
Our investments have been in an unrealized loss position for two months. Based upon our evaluation of all relevant factors, we believe that the decline in fair value of securities held at December 31, 2017 below cost is temporary, and we intend to retain our investment in these securities for a sufficient period of time to allow for recovery of the fair value.
As of December 31, 2017, the amortized cost and fair value of available-for-sale securities by contractual maturity were (in thousands):
|
|
|
Amortized |
|
Fair |
|
||
|
|
|
Cost |
|
Value |
|
||
|
Due in one year or less |
|
$ |
99,650 |
|
$ |
99,533 |
|
|
Due in one year to two years |
|
|
— |
|
|
— |
|
|
Total |
|
$ |
99,650 |
|
$ |
99,533 |
|
F-15
6. Inventories
The following table presents inventories as of December 31, 2017 and December 31, 2016 (in thousands):
|
|
|
December 31, |
|
||||
|
|
|
2017 |
|
2016 |
|
||
|
Work in process |
|
$ |
24,721 |
|
$ |
— |
|
|
Finished goods |
|
|
2,787 |
|
|
— |
|
|
Total |
|
$ |
27,508 |
|
$ |
— |
|
At December 31, 2017, deposit on inventory on the Consolidated Balance Sheets is a cash deposit of $20.5 million made to a manufacturer for the purchase of inventory which we expect to be converted to finished goods within the next twelve months.
7. Intangible Assets and Goodwill
At December 31, 2017 and 2016, intangible assets related to capitalized milestones under license agreements consisted of the following (in thousands):
|
|
|
December 31, |
|
||||
|
|
|
2017 |
|
2016 |
|
||
|
Intangible asset - milestones |
|
$ |
21,100 |
|
$ |
21,100 |
|
|
Accumulated amortization |
|
|
(1,539) |
|
|
(53) |
|
|
Total intangible asset, net |
|
$ |
19,561 |
|
$ |
21,047 |
|
The estimated useful lives of these intangibles assets extended through 2031.
We recorded an amortization expense of $1.5 million and $0.053 million related to capitalized milestone payments during the year ended December 31, 2017 and December 31, 2016, respectively. Estimated future amortization expense for intangible assets as of December 31, 2017 is as follows (in thousands):
|
2018 |
|
|
|
|
$ |
1,486 |
|
|
2019 |
|
|
|
|
|
1,486 |
|
|
2020 |
|
|
|
|
|
1,486 |
|
|
2021 |
|
|
|
|
|
1,486 |
|
|
2022 |
|
|
|
|
|
1,486 |
|
|
Thereafter |
|
|
|
|
|
12,131 |
|
|
|
|
|
|
|
$ |
19,561 |
|
IPR&D assets and goodwill were established as part of the purchase accounting of EOS in November 2013, and consisted of the following (in thousands):
|
|
|
December 31, |
|
||||
|
|
|
2017 |
|
2016 |
|
||
|
IPR&D assets: |
|
|
|
|
|
|
|
|
Balance at beginning of period |
|
$ |
— |
|
$ |
101,500 |
|
|
Impairment of intangible asset (a) |
|
|
— |
|
|
(104,517) |
|
|
Change in foreign currency gains and losses |
|
|
— |
|
|
3,017 |
|
|
Balance at end of period |
|
$ |
— |
|
$ |
— |
|
|
|
|
|
|
|
|
|
|
|
Goodwill: |
|
|
|
|
|
|
|
|
Balance at beginning of period |
|
$ |
57,192 |
|
$ |
59,327 |
|
|
Change in foreign currency gains and losses |
|
|
8,025 |
|
|
(2,135) |
|
|
Balance at end of period |
|
$ |
65,217 |
|
$ |
57,192 |
|
F-16
|
(a) |
During the second quarter of 2016, we recorded a $104.5 million impairment charge due to our and our development partner’s decision to discontinue the development of lucitanib for breast cancer. At December 31, 2017, the IPR&D intangible asset recorded on the Consolidated Balance Sheets was zero. |
During the fourth quarter of 2015, we recorded an $89.6 million impairment charge due to our and our development partner’s decision to terminate the development of lucitanib for lung cancer, as well as updates to the probability-weighted discounted cash flow assumptions for the breast cancer indication.
These reductions were included in impairment of intangible asset on the Consolidated Statements of Operations and Comprehensive Loss.
As of December 31, 2017, no impairment to the carrying value of the goodwill was identified.
8. Convertible Senior Notes
On September 9, 2014, we completed a private placement of $287.5 million aggregate principal amount of 2.5% convertible senior notes due 2021 (the “Notes”) resulting in net proceeds of $278.3 million after deducting offering expenses. In accordance with the accounting guidance, the conversion feature did not meet the criteria for bifurcation, and the entire principal amount was recorded as a long-term liability on the Consolidated Balance Sheets.
The Notes are governed by the terms of the indenture between the Company, as issuer, and The Bank of New York Mellon Trust Company, N.A., as trustee. The Notes are senior unsecured obligations and bear interest at a rate of 2.5% per year, payable semi-annually in arrears on March 15 and September 15 of each year. The Notes will mature on September 15, 2021, unless earlier converted, redeemed or repurchased.
Holders may convert all or any portion of the Notes at any time prior to the close of business on the business day immediately preceding the maturity date. Upon conversion, the holders will receive shares of our common stock at an initial conversion rate of 16.1616 shares per $1,000 in principal amount of Notes, equivalent to a conversion price of approximately $61.88 per share. The conversion rate is subject to adjustment upon the occurrence of certain events described in the indenture, but will not be adjusted for any accrued and unpaid interest. In addition, following certain corporate events that occur prior to the maturity date or upon our issuance of a notice of redemption, we will increase the conversion rate for holders who elect to convert the Notes in connection with such a corporate event or during the related redemption period in certain circumstances.
On or after September 15, 2018, we may redeem the Notes, at our option, in whole or in part, if the last reported sale price of our common stock has been at least 150% of the conversion price then in effect for at least 20 trading days (whether or not consecutive) during any 30 consecutive trading day period ending not more than two trading days preceding the date on which we provide written notice of redemption at a redemption price equal to 100% of the principal amount of the Notes to be redeemed plus accrued and unpaid interest to, but excluding, the redemption date. No sinking fund is provided for the Notes.
If we undergo a fundamental change, as defined in the indenture, prior to the maturity date of the Notes, holders may require us to repurchase for cash all or any portion of the Notes at a fundamental change repurchase price equal to 100% of the principal amount of the Notes to be repurchased, plus accrued and unpaid interest to, but excluding, the fundamental change repurchase date.
The Notes rank senior in right of payment to any of our indebtedness that is expressly subordinated in right of payment to the Notes; equal in right of payment to all of our liabilities that are not so subordinated; effectively junior in right of payment to any secured indebtedness to the extent of the value of the assets securing such indebtedness; and structurally junior to all indebtedness and other liabilities (including trade payables) of our subsidiaries.
In connection with the issuance of the Notes, we incurred $9.2 million of debt issuance costs. The debt issuance costs are amortized as interest expense over the expected life of the Notes using the effective interest method. We determined the expected life of the debt was equal to the seven-year term of the Notes. As of December 31, 2017 and 2016, the
F-17
balance of unamortized debt issuance costs was $5.1 million and $6.4 million, respectively, and is recorded as a reduction to the convertible senior notes at the Consolidated Balance Sheets.
The following table sets forth total interest expense to the Notes and the milestone liability during the years ended December 31, 2017 and 2016 (in thousands):
|
|
|
Year ended December 31, |
|||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|||
|
Contractual interest expense |
|
$ |
7,188 |
|
$ |
7,187 |
|
$ |
7,167 |
|
Accretion of interest on milestone liability |
|
|
1,961 |
|
|
62 |
|
|
— |
|
Amortization of debt issuance costs |
|
|
1,279 |
|
|
1,242 |
|
|
1,205 |
|
Total interest expense |
|
$ |
10,428 |
|
$ |
8,491 |
|
$ |
8,372 |
9. Stockholders’ Equity
Common Stock
In July 2015, we sold 4,054,487 shares of our common stock in a public offering at $78.00 per share. The net proceeds from the offering were $298.5 million, after deducting underwriting discounts and commissions and offering expenses.
In January 2017, we sold 5,750,000 shares of our common stock in a public offering at $41.00 per share. The net proceeds from the offering were $221.2 million, after deducting underwriting discounts and commissions and offering expenses.
In June 2017, we sold 3,920,454 shares of our common stock in a public offering at $88.00 per share. The net proceeds from the offering were $324.6 million, after deducting underwriting discounts and commissions and offering expenses.
The holders of common stock are entitled to one vote per share on all matters to be voted upon by our stockholders. Subject to the preferences that may be applicable to any outstanding shares of preferred stock, the holders of common stock are entitled to receive ratably such dividends, if any, as may be declared by our Board of Directors.
Accumulated Other Comprehensive Loss
Accumulated other comprehensive loss consists of changes in foreign currency translation adjustments, which includes changes in a subsidiary’s functional currency, and unrealized gains and losses on available-for-sale securities.
The accumulated balances related to each component of other comprehensive income (loss) are summarized as follows (in thousands):
|
|
|
Foreign Currency |
|
Unrealized |
|
Total Accumulated |
|||
|
|
|
Translation Adjustments |
|
(Losses) Gains |
|
Other Comprehensive Loss |
|||
|
Balance at December 31, 2015 |
|
$ |
(47,077) |
|
$ |
(383) |
|
$ |
(47,460) |
|
Other comprehensive income (loss) |
|
|
(1,693) |
|
|
224 |
|
|
(1,469) |
|
Total before tax |
|
|
(48,770) |
|
|
(159) |
|
|
(48,929) |
|
Tax effect |
|
|
1,336 |
|
|
13 |
|
|
1,349 |
|
Balance at December 31, 2016 |
|
|
(47,434) |
|
|
(146) |
|
|
(47,580) |
|
Other comprehensive income (loss) |
|
|
8,735 |
|
|
(110) |
|
|
8,625 |
|
Total before tax |
|
|
(38,699) |
|
|
(256) |
|
|
(38,955) |
|
Tax effect |
|
|
(3,218) |
|
|
— |
|
|
(3,218) |
|
Balance at December 31, 2017 |
|
$ |
(41,917) |
|
$ |
(256) |
|
$ |
(42,173) |
The other comprehensive income (loss) related to foreign currency translation adjustments was primarily due to the currency translation of the IPR&D intangible assets, goodwill and deferred income taxes (see Note 7, Intangible Assets
F-18
and Goodwill). There were no reclassifications out of accumulated other comprehensive loss in the years ended December 31, 2017, 2016 and 2015.
10. Share-Based Compensation
Stock Options
In August 2011, our Board of Directors approved the 2011 Stock Incentive Plan (the “2011 Plan”), which became effective upon the closing of our initial public offering in November 2011. The 2011 Plan provides for the granting of incentive and nonqualified stock options, stock appreciation rights, restricted stock, restricted stock units, performance awards and other share-based awards to our employees, directors and consultants. Common shares authorized for issuance under the 2011 Plan were 9,590,378 at December 31, 2017, which represents the initial reserve of 1,250,000 shares of common stock plus 192,185 shares of common stock remaining for future grant from the 2009 Equity Incentive Plan (the “2009 Plan”), which was terminated upon the closing of our initial public offering in November 2011, and 8,148,193 new shares authorized by the Board of Directors at the annual meetings of stockholders. Future forfeitures and cancellations of options previously granted under the 2009 Plan were transferred to and also available for grant under the 2011 Plan. Stock options granted vest ratably over either a one-year period or three-year period for Board of Director grants. Employee stock options generally vest over a four-year period with 25% of the options cliff-vesting after year one and the remaining options vesting ratably over each subsequent month. All stock options expire 10 years from the date of grant.
Share-based compensation expense for the years ended December 31, 2017, 2016 and 2015, respectively, was recognized in the accompanying Consolidated Statements of Operations and Comprehensive Loss as follows (in thousands):
|
|
|
Year ended December 31, |
|
|||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|
|||
|
Research and development |
|
$ |
20,335 |
|
$ |
27,558 |
|
$ |
27,321 |
|
|
Selling, general and administrative |
|
|
24,372 |
|
|
12,238 |
|
|
13,036 |
|
|
Total share-based compensation expense |
|
$ |
44,707 |
|
$ |
39,796 |
|
$ |
40,357 |
|
We did not recognize a tax benefit related to share-based compensation expense during the years ended December 31, 2017, 2016 and 2015 as we maintain net operating loss carryforwards and have established a valuation allowance against the entire net deferred tax asset as of December 31, 2017.
The following table summarizes the activity relating to our options to purchase common stock:
|
|
|
|
|
|
|
|
Weighted |
|
|
|
|
|
|
|
|
|
Weighted |
|
Average |
|
Aggregate |
|
||
|
|
|
|
|
Average |
|
Remaining |
|
Intrinsic |
|
||
|
|
|
Number of |
|
Exercise |
|
Contractual |
|
Value |
|
||
|
|
|
Options |
|
Price |
|
Term (Years) |
|
(Thousands) |
|
||
|
Outstanding at December 31, 2016 |
5,520,482 |
$ |
42.00 |
||||||||
|
Granted |
1,048,700 |
66.09 |
|||||||||
|
Exercised |
(465,690) |
29.90 |
|||||||||
|
Forfeited |
(313,757) |
49.20 |
|||||||||
|
Outstanding at December 31, 2017 (a) |
5,789,735 |
$ |
46.77 |
7.1 |
$ |
145,067 |
|||||
|
Vested and expected to vest at December 31, 2017 |
5,505,557 |
$ |
46.52 |
7.0 |
$ |
139,526 |
|||||
|
Vested and exercisable at December 31, 2017 |
3,481,931 |
$ |
44.60 |
6.1 |
$ |
95,463 |
|||||
|
(a) |
Includes 33,750 performance-based stock options granted to our executives in the first quarter of 2015, which vested on approval by the FDA in December 19, 2016 to commercially distribute, sell or market Rubraca. Related stock compensation expense was recognized on that date. |
The aggregate intrinsic value in the table above represents the pretax intrinsic value, based on our closing stock price of $68.00 as of December 31, 2017, which would have been received by the option holders had all option holders with in-the-money options exercised their options as of that date.
F-19
The following table summarizes information about our stock options as of and for the years ended December 31, 2017, 2016 and 2015:
|
|
|
Year ended December 31, |
|
|||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|
|||
|
Weighted-average grant date fair value per share |
|
$ |
48.79 |
|
$ |
16.62 |
|
$ |
52.70 |
|
|
Intrinsic value of options exercised |
|
$ |
18,986,726 |
|
$ |
3,118,097 |
|
$ |
19,976,769 |
|
|
Cash received from stock option exercises |
|
$ |
13,924,174 |
|
$ |
3,267,721 |
|
$ |
5,478,211 |
|
The fair value of each share-based award is estimated on the grant date using the Black-Scholes option pricing model based upon the weighted-average assumptions provided in the following table:
|
|
|
Year ended December 31, |
|
||||
|
|
|
2017 |
|
2016 |
|
2015 |
|
|
Dividend yield |
|
— |
|
— |
|
— |
|
|
Volatility (a) |
|
89 |
% |
93 |
% |
72 |
% |
|
Risk-free interest rate (b) |
|
2.16 |
% |
1.77 |
% |
1.77 |
% |
|
Expected term (years) (c) |
|
5.8 |
|
5.8 |
|
6.1 |
|
|
(a) |
Volatility: The expected volatility was estimated using our historical data. |
|
(b) |
Risk-free interest rate: The rate is based on the yield on the grant date of a zero-coupon U.S. Treasury bond whose maturity period approximates the option’s expected term. |
|
(c) |
Expected term: The expected term of the award was estimated using our historical data. |
The total fair value of stock options vested during the years ended December 31, 2017, 2016 and 2015 was $36.0 million, $40.8 million and $36.5 million, respectively.
Restricted Stock
During 2016, we issued restricted stock units (“RSUs”) to certain employees under the 2011 Stock Incentive Plan. The RSUs vest either (i) over two years, with 50% vesting one year from the date of grant and the remaining 50% vesting two years from the date of grant or (ii) over four years, with 25% vesting one year from the date of grant and the remaining 75% vesting ratably each subsequent quarter over the following three years, as defined in the grant agreement. Vested RSUs are payable in shares of our common stock at the end of the vesting period. RSUs are measured based on the fair value of the underlying stock on the grant date. The minimum statutory tax on the value of common stock shares issued to employees upon vesting are paid by us through the sale of registered shares of our common stock.
F-20
The following table summarizes the activity related to our unvested RSUs:
|
|
|
|
|
|
|
|
|
|
|
|
|
Weighted |
|
|
|
|
|
|
|
Average |
|
|
|
|
|
Number of |
|
Grant Date |
|
|
|
|
|
Units |
|
Fair Value |
|
|
|
Unvested at December 31, 2016 |
|
562,458 |
|
$ |
24.70 |
|
|
Granted |
|
249,984 |
|
|
64.66 |
|
|
Vested |
|
(180,912) |
|
|
23.83 |
|
|
Forfeited |
|
(42,001) |
|
|
28.09 |
|
|
Unvested as of December 31, 2017 |
|
589,529 |
|
$ |
41.67 |
|
|
Expected to vest after December 31, 2017 |
|
513,069 |
|
$ |
41.40 |
|
Unrecognized share-based compensation expense related to non-vested options and RSUs, adjusted for expected forfeitures, was $89.4 million as of December 31, 2017. The unrecognized share-based compensation expense is expected to be recognized over the weighted-average remaining vesting period of 3.3 years.
Common Stock Reserved for Issuance
As of December 31, 2017, we reserved shares of common stock for future issuance as follows:
|
|
|
|
|
Available for |
|
|
|
|
|
|
|
|
Grant |
|
Total Shares of |
|
|
|
|
Common Stock |
|
or Future |
|
Common Stock |
|
|
|
|
Outstanding |
|
Issuance |
|
Reserved |
|
|
2009 Equity Incentive Plan |
|
331,213 |
|
— |
|
331,213 |
|
|
2011 Stock Incentive Plan |
|
6,048,051 |
|
2,589,033 |
|
8,637,084 |
|
|
2011 Employee Stock Purchase Plan |
|
— |
|
558,870 |
|
558,870 |
|
|
Total |
|
6,379,264 |
|
3,147,903 |
|
9,527,167 |
|
Employee Stock Purchase Plan
In August 2011, our Board of Directors approved the Clovis Oncology, Inc. 2011 Employee Stock Purchase Plan (the “Purchase Plan”). Each year, on the date of our annual meeting of stockholders and at the discretion of our board of directors, the amount of shares reserved for issuance under the Purchase Plan may be increased by up to the lesser of (1) a number of additional shares of our common stock representing 1% of our then-outstanding shares of common stock, (2) 344,828 shares of our common stock and (3) a lesser number of shares as approved by the Board. The Purchase Plan provides for consecutive six-month offering periods, during which participating employees may elect to have up to 10% of their compensation withheld and applied to the purchase of common stock at the end of each offering period. The purchase price of the common stock is 85% of the lower of the fair value of a share of common stock on the first trading date of each offering period or the fair value of a share of common stock on the last trading day of the offering period. The Purchase Plan will terminate on August 24, 2021, the tenth anniversary of the date of initial adoption of the Purchase Plan. We sold 51,681 and 110,508 shares to employees in 2017 and 2016, respectively. There were 558,870 shares available for sale under the Purchase Plan as of December 31, 2017. The weighted-average estimated grant date fair value of purchase awards under the Purchase Plan during the years ended December 31, 2017 and 2016 was $23.08 and $11.70 per share, respectively. The total share-based compensation expense recorded as a result of the Purchase Plan was approximately $1.0 million, $0.8 million and $0.9 million during the years ended December 31, 2017, 2016 and 2015, respectively.
F-21
The fair value of purchase awards granted to our employees during the years ended December 31, 2017, 2016 and 2015, respectively, was estimated using the Black-Scholes option pricing model based upon the weighted-average assumptions provided in the following table:
|
|
|
Year ended December 31, |
|
||||
|
|
|
2017 |
|
2016 |
|
2015 |
|
|
Dividend yield |
|
— |
|
— |
|
— |
|
|
Volatility (a) |
|
79 |
% |
92 |
% |
71 |
% |
|
Risk-free interest rate (b) |
|
0.90 |
% |
0.40 |
% |
0.11 |
% |
|
Expected term (years) (c) |
|
0.5 |
|
0.5 |
|
0.5 |
|
|
(a) |
Volatility: The expected volatility was estimated using our historical data. |
|
(b) |
Risk-free interest rate: The rate is based on the U.S. Treasury yield in effect at the time of grant with terms similar to the contractual term of the purchase right. |
|
(c) |
Expected term: The expected life of the award represents the six-month offering period for the Purchase Plan. |
11. Revenue Recognition
Effective January 1, 2018, we adopted ASC 606, the new revenue recognition standard, using the modified retrospective method. Upon adoption, the accounting for net product revenue is as follows:
Product Revenue, Net
We are currently approved to sell Rubraca in the United States market. We distribute our product principally through a limited number of specialty distributor and specialty pharmacy providers, collectively, our customers. Our customers subsequently sell our products to patients and health care providers. Separately, we have arrangements with certain payors and other third-parties that provide for government-mandated and privately-negotiated rebates, chargebacks and discounts.
Revenue from product sales are recognized when customers obtain control of our product, which occurs at a point in time, typically upon delivery to the customers. We expense incremental costs of obtaining a contract as and when incurred if the expected amortization period of the asset that we would have recognized is one year or less.
Reserves for Variable Consideration
Revenues from product sales are recorded at the net sales price (transaction price), which includes estimates of variable consideration for which reserves are established and which result from rebates, chargebacks, discounts, co-pay assistance, estimated product returns and other allowances that are offered within contracts between us and our customers, health care providers, payors and other indirect customers relating to the sales of our product. These reserves are based on the amounts earned or to be claimed on the related sales and are classified as reductions of accounts receivable (if the amount is payable to the customers) or a current liability (if the amount is payable to a party other than a customer). Where appropriate, these estimates take into consideration a range of possible outcomes which are probability-weighted for relevant factors such as our historical experience, current contractual and statutory requirements, specific known market events and trends, industry data and forecasted customer buying and payment patterns. Overall, these reserves reflect our best estimates of the amount of consideration to which we are entitled based on the terms of the contract. The amount of variable consideration which is included in the transaction price may be constrained, and is included in the net sales price only to the extent that it is probable that a significant reversal in the amount of the cumulative revenue recognized will not occur in a future period. Actual amounts of consideration ultimately received may differ from our estimates. If actual results in the future vary from our estimates, we adjust these estimates, which would affect net product revenue and earnings in the period such variances become known.
F-22
Rebates. Rebates include mandated discounts under the Medicaid Drug Rebate Program and the Medicare coverage gap program. Rebates are amounts owed after the final dispensing of products to a benefit plan participant and are based upon contractual agreements or legal requirements with the public-sector benefit providers. These reserves are recorded in the same period the related revenue is recognized, resulting in a reduction of product revenue and the establishment of a current liability which is included in accrued expenses on the consolidated balance sheet. We estimate our Medicaid and Medicare rebates based upon a range of possible outcomes that are probability-weighted for the estimated payor mix. The accrual for rebates is based on statutory discount rates and known sales to specialty pharmacy patients, or expected utilization for specialty distributor sales to healthcare providers. As we gain more historical experience, the accrual will be based solely on the expected utilization from historical data we have accumulated since the Rubraca product launch. Rebates are generally invoiced and paid quarterly in arrears so that the accrual balance consists of an estimate of the amount expected to be incurred for the current quarter’s activity, plus an accrual balance for known or estimated prior quarters’ unpaid rebates.
Chargebacks. Chargebacks are discounts that occur when contracted customers, which currently consist primarily of group purchasing organizations, Public Health Service organizations and federal government entities purchasing via the Federal Supply Schedule, purchase directly from our specialty distributors at a discounted price. The specialty distributor, in turn, charges back the difference between the price initially paid by the specialty distributor and the discounted price paid to the specialty distributor by the healthcare provider. These reserves are established in the same period that the related revenue is recognized, resulting in a reduction of product revenue and accounts receivable. The accrual for specialty distributor chargebacks is estimated based on known chargeback rates and known sales to specialty distributors adjusted for the estimated utilization by healthcare providers.
Discounts. Specialty distributors and specialty pharmacies are offered various forms of consideration, including service fees and prompt pay discounts for payment within a specified period. We expect these customers will earn prompt pay discounts and therefore, we deduct the full amount of these discounts from product sales when revenue is recognized. Service fees are recorded as a selling expense when product sales occur.
Co-pay assistance. Patients who have commercial insurance and meet certain eligibility requirements may receive co-pay assistance. The intent of this program is to reduce the patient’s out of pocket costs. Liabilities for co-pay assistance are based on actual program participation and estimates of program redemption using data provided by third-party administrators.
Returns. Consistent with industry practice, we generally offer customers a limited right of return for product that has been purchased based on the product’s expiration date, which lapses upon shipment to a patient. To date, we have had minimal product returns and we currently do not have an accrual for product returns. We will continue to assess our estimate for product returns as we gain additional historical experience.
Currently, we only recognize revenue on product sales once the product is sold to the patient or healthcare provider by the specialty distributor or specialty pharmacy provider, i.e. when product is sold through the channel. Effective January 1, 2018, we will begin recognizing revenue when our customers, the specialty distributors and specialty pharmacy providers, take control of our product or when product is sold into the channel. This will have the impact of us recognizing revenue approximately two to four weeks earlier than before adopting the new standard and will also increase the significance of estimating variable consideration.
We used the modified retrospective method to adopt the new standard. This means that we will not restate previously issued financial statements, but will record a one-time adjustment to retained earnings of $2.3 million. This adjustment represents the sales of our product to our customers prior to January 1, 2018, that have not been sold to patients or healthcare providers, offset by related gross-to-net adjustments and other direct costs, including royalties and sales incentive compensation.
12. Commitments and Contingencies
We lease office space in Boulder, Colorado, San Francisco, California, Oakland, California, Cambridge, UK and Milan, Italy under non-cancelable operating lease agreements that expire through 2028. The lease agreements contain periodic rent increases that result in the recording deferred rent over the terms of certain leases.
F-23
In November 2017, we entered into a ten-year lease agreement for new office space in Oakland, California. Pursuant to the terms of the lease, the landlord will reimburse us for up to $2.5 million of leasehold improvement expenditures (“Tenant Improvement Allowance”). Upon completion of construction, we will record the Tenant Improvement Allowance as deferred rent, which will be amortized as a reduction to rental expense over the lease term.
Rental expense under these leases was $2.2 million, $2.2 million and $2.4 million for the years ended December 31, 2017, 2016 and 2015, respectively.
Future minimum rental commitments, by fiscal year and in the aggregate, for our operating leases are provided below (in thousands):
|
|
|
December 31, |
|
|
|
|
|
2017 |
|
|
|
2018 |
|
$ |
3,050 |
|
|
2019 |
|
|
3,902 |
|
|
2020 |
|
|
3,744 |
|
|
2021 |
|
|
3,855 |
|
|
2022 |
|
|
2,519 |
|
|
Thereafter |
|
|
11,563 |
|
|
Total future minimum lease payments |
|
$ |
28,633 |
|
Manufacture and Services Agreement Commitments
On October 3, 2016, we entered into a Manufacturing and Services Agreement (the “Agreement”) with a non-exclusive third-party supplier for the production of the active ingredient for rucaparib. Under the terms of the Agreement, we will provide the third-party supplier a rolling forecast for the supply of the active ingredient in rucaparib that will be updated by us on a quarterly basis. We are obligated to order material sufficient to satisfy an initial quantity specified any forecast. In addition, the third-party supplier will construct, in its existing facility, a production train that will be exclusively dedicated to the manufacture of the rucaparib active ingredient. We are obligated to make scheduled capital program fee payments toward capital equipment and other costs associated with the construction of the dedicated production train. Further, once the facility is operational, we are obligated to pay a fixed facility fee each quarter for the duration of the Agreement, which expires on December 31, 2025, unless extended by mutual consent of the parties. As of December 31, 2017, $223.9 million of purchase commitments exist under the Agreement.
Legal Proceedings
We and certain of our officers were named as defendants in several lawsuits, as described below. We cannot reasonably predict the outcome of these legal proceedings, nor can we estimate the amount of loss or range of loss, if any, that may result. An adverse outcome in these proceedings could have a material adverse effect on our results of operations, cash flows or financial condition.
Rociletinib-Related Litigation
Following Clovis’ regulatory announcement in November 2015 of adverse developments in its ongoing clinical trials for rociletinib, Clovis and certain of its current and former executives were named in various securities lawsuits, the largest of which was a putative class action lawsuit in the District of Colorado (the “Medina Action”) which was settled on October 26, 2017 (the “Medina Settlement”). The open actions currently pending against Clovis are discussed below. While other entities have threatened to bring claims relating to rociletinib and the November 2015 announcement, none have commenced litigation as of the date of this filing.
On January 22, 2016, the Electrical Workers Local #357 Pension and Health & Welfare Trusts, a purported shareholder of Clovis, filed a purported class action complaint (the “Electrical Workers Complaint”) against Clovis and certain of its officers, directors, investors and underwriters in the Superior Court of the State of California, County of San Mateo (the “Electrical Workers Court”). The Electrical Workers Complaint purports to be asserted on behalf of a class of persons who purchased stock in the July 2015 Offering. The complaint asserted claims under certain provisions of the Securities Act of 1933 (the “Securities Act”) relating to a July 2015 follow-on offering of Clovis securities (the
F-24
“July 2015 Offering”) based on substantially similar allegations to those asserted in the Medina Action. On June 30, 2016, the Electrical Workers Plaintiffs filed an amended complaint adding new allegations (the “Amended Complaint”).
On July 28, 2016, the defendants filed a motion to stay the Electrical Workers action pending resolution of the Medina Action and a demurrer to the Amended Complaint. On September 23, 2016, after hearing oral argument, the Electrical Workers Court granted the motion to stay and reserved on issuing a ruling on defendants’ pending demurrer.
The Company believes that the claims asserted in the Electrical Workers Action are released and barred by operation of law through the Medina Settlement, and accordingly plans to seek dismissal of the Electrical Workers Action on that basis.
On November 10, 2016, Antipodean Domestic Partners (“Antipodean”) filed a complaint (the “Antipodean Complaint”) against Clovis and certain of its officers, directors and underwriters in New York Supreme Court, County of New York. The Antipodean Complaint alleges that the defendants violated certain sections of the Securities Act by making allegedly false statements to Antipodean and in the offering materials for the July 2015 Offering relating to the efficacy of rociletinib, its safety profile, and its prospects for market success. In addition to the Securities Act claims, the Antipodean Complaint also asserts Colorado state law claims and common law claims. Both the state law and common law claims are based on allegedly false and misleading statements regarding rociletinib’s progress toward FDA approval. The Antipodean Complaint seeks compensatory, recessionary, and punitive damages.
On December 15, 2016, the Antipodean Plaintiffs filed an amended complaint (the “Antipodean Amended Complaint”) asserting substantially the same claims against the same defendants and purporting to correct certain details in the original Antipodean Complaint.
On January 31, 2017, Defendants filed a motion to stay the Antipodean action pending resolution of the Medina Action in the District of Colorado. Defendants also filed a motion to dismiss the Antipodean Amended Complaint on March 29, 2017.
On March 14, 2017, the Clovis Defendants and Antipodean participated in a mediation, which did not result in a settlement.
On August 8, 2017, the parties participated in a scheduled hearing on Defendants’ motion to stay and motion to dismiss before Justice Masley of the New York Supreme Court, County of New York. At the hearing, Justice Masley granted Defendants’ motion to stay. Per the Court’s August 10, 2017 order, Defendants’ motion to dismiss was held in abeyance and deemed submitted on November 1, 2017. On November 1, 2017, the Defendants provided a status update to the Court regarding the outcome of the hearing. The update informed the Court that Antipodean had excluded itself from the Medina Settlement, as memorialized in the final judgment entered by the Medina Court. No date has been scheduled for argument on Defendants’ motion to dismiss.
The Company intends to vigorously defend against the allegations in the Antipodean Amended Complaint. However, there can be no assurance that the defense will be successful.
In March 2017, two putative shareholders of the Company, Macalinao and McKenry (the “Derivative Plaintiffs”), filed shareholder derivative complaints against certain directors and officers of the Company in the Court of Chancery of the State of Delaware. On May 4, 2017, the Macalinao and McKenry actions were consolidated for all purposes in a single proceeding under the caption In re Clovis Oncology, Inc. Derivative Litigation, Case No, 2017-0222 (the “Consolidated Derivative Action”).
On May 18, 2017, the Derivative Plaintiffs filed a Consolidated Verified Shareholder Derivative Complaint (the “Consolidated Derivative Complaint”). The Consolidated Derivative Complaint generally alleged that the defendants breached their fiduciary duties owed to the Company by allegedly causing or allowing misrepresentations of the Company’s business operations and prospects, failing to ensure that the TIGER-X clinical trial was being conducted in accordance with applicable rules, regulations and protocols, and engaging in insider trading. The Consolidated Derivative Complaint purported to rely on documents produced by the Company in response to prior demands for inspection of the Company’s books and records served on the Company by each of Macalinao and McKenry under 8 Del. C. § 220. The Consolidated Derivative Complaint sought, among other things, an award of money damages.
F-25
On July 31, 2017, the defendants filed a motion to dismiss the Consolidated Derivative Complaint. Plaintiffs filed an opposition to the motion to dismiss on August 31, 2017, and the defendants filed a reply in further support of the motion to dismiss on September 26, 2017. No date has been scheduled for argument on Defendants’ motion to dismiss the Consolidated Derivative Complaint.
The Company intends to vigorously defend against the allegations in the Consolidated Derivative Complaint, but there can be no assurance that the defense will be successful.
On March 20, 2017, a purported shareholder of the Company, filed a shareholder derivative complaint (the “Guo Complaint”) against certain officers and directors of the Company in the United States District Court for the District of Colorado. The Guo Complaint generally alleged that the defendants breached their fiduciary duties owed to the Company by either recklessly or with gross negligence approving or permitting misrepresentations of the Company’s business operations and prospects. The Guo Complaint also alleged claims for waste of corporate assets and unjust enrichment. Finally, the Guo Complaint alleged that certain of the individual defendants violated Section 14(a) of the Securities Exchange Act, by allegedly negligently issuing, causing to be issued, and participating in the issuance of materially misleading statements to stockholders in the Company’s Proxy Statement on Schedule DEF 14A in connection with the 2015 Annual Meeting of Stockholders, held on June 11, 2015. The Guo Complaint sought, among other things, an award of money damages.
On June 19, 2017, the parties filed a joint motion to stay the Guo action pending resolution of the motion to dismiss the Consolidated Derivative Complaint. On June 20, 2017, the court granted the motion to stay.
The Company intends to vigorously defend against the allegations in the Guo Complaint, but there can be no assurance that the defense will be successful.
In addition, the Company has received inquiries and requests for information from governmental agencies, including the U.S. Securities and Exchange Commission and the U.S. Department of Justice, relating to the Company’s regulatory update announcement in November 2015 that the FDA requested additional clinical data on the efficacy and safety of rociletinib. The Company is continuing to cooperate with these agencies with respect to their investigations. The Medina Settlement does not resolve these inquiries and the Company cannot predict their timing or outcome.
Director Compensation Litigation
On May 10, 2017, John Solak, a purported shareholder of the Company, filed a shareholder derivative complaint in the Court of Chancery of the State of Delaware (the “Solak Complaint”) against certain directors and an officer of the Company. The Solak Complaint generally alleged that the defendants breached their fiduciary duties owed to the Company by adopting a compensation plan that overcompensated the non-employee director defendants, in relation to companies of comparable market capitalization and size. The Solak Complaint also alleged claims of waste of corporate assets and unjust enrichment due to this allegedly wrongful compensation plan. The Solak Complaint sought, among other things, an award of money damages and the imposition of corporate governance reforms.
The Court has entered a number of orders extending the defendants’ time to respond to the Solak Complaint based on, among other factors, the fact that the parties are engaged in discussions in an effort to resolve the Solak action. On February 14, 2018, the parties filed a joint letter to the Court requesting that all deadlines in the action be held in abeyance while the parties engaged in final settlement discussions.
On February 26, 2018, the defendants entered into a stipulation of compromise and settlement with plaintiff that is intended to settle the Solak action. The proposed settlement is subject to Court approval upon the conclusion of a settlement hearing concerning the fairness of the terms of the proposed settlement, which will be scheduled following the provision of notice to shareholders of the Company.
In accordance with the terms of the proposed settlement, the Company will present a new non-employee director compensation policy for shareholder vote at the next annual shareholder meeting. Under the proposed new non-employee director compensation policy, annual base compensation for incumbent non-employee directors would be set at an amount between $350,000 and $425,000, which would remain in place for a period between two and five years. Additionally, the proposed policy sets annual base compensation for new non-employee directors at an amount between $525,000 and $637,500 and includes fixed annual fees for board and committee service. The proposed settlement also
F-26
sets forth a number of corporate governance reforms that the Company will undertake, including, enhanced proxy disclosures, the codification of the Company’s stock ownership guidelines for directors, and enhanced disclosure requirements for certain forms of director compensation. While no cash payments will be made to investors as part of the proposed settlement, plaintiff’s counsel is expected to file a fee application which the Company has agreed not to oppose up to an agreed-upon amount. The proposed settlement contains no admission of wrongdoing.
13. License Agreements
Rucaparib
In June 2011, we entered into a license agreement with Pfizer Inc. to obtain the exclusive global rights to develop and commercialize Rubraca. The exclusive rights are exclusive even as to Pfizer and include the right to grant sublicenses. Pursuant to the terms of the license agreement, we made a $7.0 million upfront payment to Pfizer and are required to make additional payments to Pfizer for the achievement of certain development and regulatory and sales milestones and royalties on sales as required by the license agreement. Prior to the FDA approval of Rubraca, we made milestones payments of $1.4 million, which were recognized as acquired in-process research and development expense.
On August 30, 2016, we entered into a first amendment to the worldwide license agreement with Pfizer, which amends the June 2011 existing worldwide license agreement to permit us to defer payment of the milestone payments payable upon (i) FDA approval of an NDA for 1st Indication in US and (ii) European Commission approval of an MAA for 1st Indication in EU, to a date that is 18 months after the date of achievement of such milestones. In the event that we defer such milestone payments, we have agreed to certain higher payments related to the achievement of such milestones.
On December 19, 2016, the FDA approved Rubraca as monotherapy for the treatment of patients with deleterious BRCA mutation (germline and/or somatic) associated with advanced ovarian cancer, who have been treated with two or more chemotherapies, and selected for therapy based on FDA-approved companion diagnostic for Rubraca. The FDA approval resulted in a $0.75 million milestone payment to Pfizer as required by the license agreement, which was paid in the first quarter of 2017. The FDA approval also resulted in the obligation to pay a $20.0 million milestone payment, for which we have exercised the option to defer payment by agreeing to pay $23.0 million within 18 months after the date of the FDA approval. These payments were recognized as intangible assets and amortized over the estimated remaining useful life of rucaparib.
We are obligated under the license agreement to use commercially reasonable efforts to develop and commercialize Rubraca and we are responsible for all ongoing development and commercialization costs for Rubraca. We are required to make regulatory milestone payments to Pfizer of up to an additional $69.75 million in aggregate if specified clinical study objectives and regulatory filings, acceptances and approvals are achieved. In addition, we are obligated to make sales milestone payments to Pfizer if specified annual sales targets for Rubraca are met, which relate to annual sales targets of $250.0 million and above, which, in the aggregate, could amount to total milestone payments of $170.0 million, and tiered royalty payments at a mid-teen percentage rate on our net sales, with standard provisions for royalty offsets to the extent we need to obtain any rights from third parties to commercialize Rubraca.
The license agreement with Pfizer will remain in effect until the expiration of all of our royalty and sublicense revenue obligations to Pfizer, determined on a product-by-product and country-by-country basis, unless we elect to terminate the license agreement earlier. If we fail to meet our obligations under the agreement and are unable to cure such failure within specified time periods, Pfizer can terminate the agreement, resulting in a loss of our rights to Rubraca and an obligation to assign or license to Pfizer any intellectual property rights or other rights we may have in Rubraca, including our regulatory filings, regulatory approvals, patents and trademarks for Rubraca.
In April 2012, we entered into a license agreement with AstraZeneca UK Limited to acquire exclusive rights associated with Rubraca under a family of patents and patent applications that claim methods of treating patients with PARP inhibitors in certain indications. The license enables the development and commercialization of Rubraca for the uses claimed by these patents. Pursuant to the terms of the license agreement, we made an upfront payment of $0.25 million upon execution of the agreement. During the second quarter of 2016, we made a milestone payment of $0.3 million to AstraZeneca upon the NDA submission for Rubraca. These payments were recognized as acquired in-process research and development expense. The FDA approval of Rubraca on December 19, 2016 resulted in a final $0.35 million milestone payment to AstraZeneca as required by the license agreement. This payment was recognized in
F-27
intangible assets and amortized over the estimated remaining useful life of Rubraca. AstraZeneca also receives royalties on net sales of Rubraca.
Lucitanib
In connection with our acquisition of EOS in November 2013, we gained rights to develop and commercialize lucitanib, an oral, selective tyrosine kinase inhibitor. As further described below, EOS licensed the worldwide rights, excluding China, to develop and commercialize lucitanib from Advenchen Laboratories LLC (“Advenchen”). Subsequently, rights to develop and commercialize lucitanib in markets outside the U.S. and Japan were sublicensed by EOS to Servier in exchange for upfront milestone fees, royalties on sales of lucitanib in the sublicensed territories and research and development funding commitments.
In October 2008, EOS entered into an exclusive license agreement with Advenchen to develop and commercialize lucitanib on a global basis, excluding China. We are obligated to pay Advenchen tiered royalties at percentage rates in the mid-single digits on net sales of lucitanib, based on the volume of annual net sales achieved. In addition, after giving effect to the first and second amendments to the license agreement, we are required to pay to Advenchen 25% of any consideration, excluding royalties, received pursuant to any sublicense agreements for lucitanib, including the agreement with Servier. We are obligated under the agreement to use commercially reasonable efforts to develop and commercialize at least one product candidate containing lucitanib, and we are also responsible for all remaining development and commercialization costs for lucitanib.
In the first quarter of 2014, we recognized acquired in-process research and development expense of $3.4 million, which represents 25% of the sublicense agreement consideration of $13.6 million received from Servier upon the end of opposition and appeal of the lucitanib patent by the European Patent Office.
The license agreement with Advenchen will remain in effect until the expiration of all of our royalty obligations to Advenchen, determined on a product-by-product and country-by-country basis, unless we elect to terminate the agreement earlier. If we fail to meet our obligations under the agreement and are unable to cure such failure within specified time periods, Advenchen can terminate the agreement, resulting in a loss of our rights to lucitanib.
In September 2012, EOS entered into a collaboration and license agreement with Servier whereby EOS sublicensed to Servier exclusive rights to develop and commercialize lucitanib in all countries outside of the U.S., Japan and China. In exchange for these rights, EOS received an upfront payment of €45.0 million. We are entitled to receive additional payments upon achievement of specified development, regulatory and commercial milestones up to €100.0 million in the aggregate, €10.0 million of which was received in the first quarter of 2014. In addition, we are entitled to receive sales milestone payments if specified annual sales targets for lucitanib are met, which, in the aggregate, could total €250.0 million. We are also entitled to receive royalties at percentage rates ranging from low to mid-teens on sales of lucitanib by Servier.
The development, regulatory and commercial milestones represent non-refundable amounts that would be paid by Servier to us if certain milestones are achieved in the future. These milestones, if achieved, are substantive as they relate solely to past performance, are commensurate with estimated enhancement of value associated with the achievement of each milestone as a result of our performance, which are reasonable relative to the other deliverables and terms of the arrangement, and are unrelated to the delivery of any further elements under the arrangement.
We and Servier are developing lucitanib pursuant to a development plan agreed to between the parties. Servier is responsible for all of the global development costs for lucitanib up to €80.0 million. Cumulative global development costs in excess of €80.0 million, if any, will be shared equally between us and Servier. During the second quarter of 2016, we and Servier agreed to discontinue the development of lucitanib for breast cancer. We are continuing to evaluate what, if any, further development of lucitanib will be pursued. During 2017, we completed the committed on-going development activities in 2017 and received full reimbursement of our development costs from Servier. Reimbursements are recorded as a reduction to research and development expense on the Consolidated Statements of Operations and Comprehensive Loss.
We recorded a $0.0 and $1.3 million receivable at December 31, 2017 and 2016, respectively, for the reimbursable development costs incurred under the global development plan, which is included in other current assets on the Consolidated Balance Sheets. During the years ending December 31, 2017, 2016 and 2015, we incurred ($0.2) million,
F-28
$7.7 million and $13.7 million, respectively, in research and development costs and recorded reductions in research and development expense of $1.0 million, $9.0 million and $11.8 million, respectively, for reimbursable development costs due from Servier.
Rociletinib
In May 2010, we entered into an exclusive worldwide license agreement with Celgene to discover, develop and commercialize a covalent inhibitor of mutant forms of the epidermal growth factor receptor (“EGFR”) gene product. Rociletinib was identified as the lead inhibitor candidate under the license agreement. We are responsible for all non-clinical, clinical, regulatory and other activities necessary to develop and commercialize rociletinib.
We made an upfront payment of $2.0 million upon execution of the license agreement, a $4.0 million milestone payment in the first quarter of 2012 upon the acceptance by the FDA of our Investigational New Drug application for rociletinib and a $5.0 million milestone payment in the first quarter of 2014 upon initiation of the Phase II study for rociletinib. In the third quarter of 2015, we made milestone payments totaling $12.0 million upon acceptance of the NDA and MAA for rociletinib by the FDA and EMA, respectively. We recognized all payments prior to commercial approval as acquired in-process research and development expense.
During the second quarter of 2016, we received a CRL from the FDA for the rociletinib NDA. We terminated enrollment in all sponsored clinical studies, although we continue to provide drug to patients whose clinicians recommend continuing rociletinib therapy. We are continuing analyses of rociletinib data to determine whether certain populations of patients may represent an opportunity for a partner committed to investing in further clinical development.
We are obligated to pay royalties at percentage rates ranging from mid-single digits to low teens based on the volume of annual net sales achieved. We are required to pay up to an additional aggregate of $98.0 million in development and regulatory milestone payments if certain clinical study objectives and regulatory filings, acceptances and approvals are achieved. In addition, we are required to pay up to an aggregate of $120.0 million in sales milestone payments if certain annual sales targets are achieved, which relate to annual sales targets of $500.0 million and above.
14. Net Loss Per Common Share
Basic net loss per share is calculated by dividing net loss by the weighted-average number of common shares outstanding during the period. Diluted net loss per share is computed by dividing net loss by the weighted-average number of common share equivalents outstanding using the treasury-stock method for the stock options and the if-converted method for the Notes. As a result of our net losses for the periods presented, all potentially dilutive common share equivalents were considered anti-dilutive and were excluded from the computation of diluted net loss per share.
The shares outstanding at the end of the respective periods presented in the table below were excluded from the calculation of diluted net loss per share due to their anti-dilutive effect (in thousands):
|
|
|
Year ended December 31, |
|
||||
|
|
|
2017 |
|
2016 |
|
2015 |
|
|
Common shares under option |
|
4,260 |
|
3,398 |
|
2,031 |
|
|
Convertible senior notes |
|
4,646 |
|
4,646 |
|
4,646 |
|
|
Total potential dilutive shares |
|
8,906 |
|
8,044 |
|
6,677 |
|
F-29
15. Income Taxes
We are subject to U.S. federal, state and foreign income tax. The geographical components of income (loss) before income taxes consisted of the following (in thousands):
|
|
|
Year ended December 31, |
|
|||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|
|||
|
Domestic |
|
$ |
(351,338) |
|
$ |
(277,776) |
|
$ |
(290,342) |
|
|
Foreign |
|
|
1,363 |
|
|
(103,395) |
|
|
(91,595) |
|
|
Total loss before income taxes |
|
$ |
(349,975) |
|
$ |
(381,171) |
|
$ |
(381,937) |
|
The income tax provision consists of the following current and deferred tax (benefit) expense amounts (in thousands):
|
|
|
Year ended December 31, |
|
|||||||
|
|
|
2017 |
|
2016 |
|
2015 |
|
|||
|
Current tax: |
|
|
|
|
|
|
|
|
|
|
|
U.S. Federal & State |
|
$ |
— |
|
$ |
— |
|
$ |
— |
|
|
Foreign |
|
|
(360) |
|
|
64 |
|
|
— |
|
|
Total current (benefit) expense |
|
|
(360) |
|
|
64 |
|
|
— |
|
|
Deferred tax: |
|
|
|
|
|
|
|
|
|
|
|
U.S. Federal & State |
|
|
(3,218) |
|
|
— |
|
|
— |
|
|
Foreign |
|
|
— |
|
|
(32,098) |
|
|
(29,076) |
|
|
Total deferred (benefit) |
|
|
(3,218) |
|
|
(32,098) |
|
|
(29,076) |
|
|
Total income tax (benefit) |
|
$ |
(3,578) |
|
$ |
(32,034) |
|
$ |
(29,076) |
|
A reconciliation of the U.S. federal statutory income tax rate to our effective tax rate is provided below:
|
|
|
Year ended December 31, |
|
||||
|
|
|
2017 |
|
2016 |
|
2015 |
|
|
Federal income tax benefit at statutory rate |
|
(34.0) |
% |
(34.0) |
% |
(34.0) |
% |
|
State income tax benefit, net of federal benefit |
|
(3.2) |
|
(3.6) |
|
(3.0) |
|
|
Tax credits |
|
(1.2) |
|
(10.8) |
|
(13.6) |
|
|
Limitation on future foreign tax credits |
|
— |
|
(5.9) |
|
(5.0) |
|
|
Change in uncertain tax positions |
|
0.2 |
|
4.2 |
|
— |
|
|
Other |
|
(1.1) |
|
2.3 |
|
0.4 |
|
|
Tax impact of Tax Cuts and Jobs Act of 2017 |
|
46.4 |
|
— |
|
— |
|
|
Change in valuation allowance |
|
(8.1) |
|
39.4 |
|
47.6 |
|
|
Effective income tax rate |
|
(1.0) |
% |
(8.4) |
% |
(7.6) |
% |
F-30
The significant components of our deferred tax assets and liabilities are as follows (in thousands):
|
|
|
December 31, |
|
||||
|
|
|
2017 |
|
2016 |
|
||
|
Deferred tax assets: |
|
|
|
|
|
|
|
|
Net operating loss carryforward |
|
$ |
272,710 |
|
$ |
275,898 |
|
|
Tax credit carryforwards |
|
|
222,150 |
|
|
217,948 |
|
|
Intangible assets |
|
|
29,900 |
|
|
42,745 |
|
|
Share-based compensation expense |
|
|
27,844 |
|
|
31,390 |
|
|
Foreign currency translation |
|
|
3,012 |
|
|
10,510 |
|
|
Product acquisition costs |
|
|
5,881 |
|
|
9,764 |
|
|
Accrued liabilities and other |
|
|
3,879 |
|
|
5,384 |
|
|
Total deferred tax assets |
|
|
565,376 |
|
|
593,639 |
|
|
Valuation allowance |
|
|
(564,122) |
|
|
(592,423) |
|
|
Deferred tax assets, net of valuation allowance |
|
|
1,254 |
|
|
1,216 |
|
|
Deferred tax liabilities: |
|
|
|
|
|
|
|
|
Prepaid expenses and other |
|
|
(1,254) |
|
|
(1,216) |
|
|
Total deferred tax liabilities |
|
|
(1,254) |
|
|
(1,216) |
|
|
Net deferred tax liability |
|
$ |
— |
|
$ |
— |
|
On December 22, 2017, President Trump signed into law the Tax Cuts and Jobs Act (the “Act”), a tax reform bill which, among other items, reduces the current corporate federal income tax rate to 21% from 35%. The rate reduction is effective January 1, 2018. We believe the Act will cause us to revalue our deferred tax assets and liabilities to the lower federal tax rate. Deferred income taxes result from temporary differences between the tax basis of assets and liabilities and their reported amounts in the financial statements that will result in taxable or deductible amounts in future years. Deferred tax assets and liabilities are measured using enacted tax rates expected to apply to taxable income in years in which those temporary differences are expected to be recovered or settled. As changes in tax laws or rates are enacted, deferred tax assets and liabilities are adjusted through income tax expense.
Pursuant to the SEC Staff Accounting Bulletin ("SAB") No. 118, "Income Tax Accounting Implications of the Tax Cuts and Jobs Act" ("SAB 118"), we may select one of three scenarios to determine a reasonable estimate arising from the Tax Act. Those scenarios are (i) a final estimate which effectively closes the measurement window; (ii) a reasonable estimate leaving the measurement window open for future revisions; and (iii) no estimate as the law is still being analyzed. We were able to provide a reasonable estimate for the revaluation of deferred taxes by recording a net tax provision of $162.2 million in the period ending December 31, 2017, which is offset by a change in valuation allowance with no net impact to tax expense. Other impacts of the Act including, but not limited to, provisional transition tax, expensing of qualified property and interest limitations are not expected to have a material impact to our financial statement presentation or disclosures. The final impact of the Act may be different from the provisional amounts reported due to changes in interpretations and assumptions of the current guidance available as well as the issuance of new regulatory guidance in the future. We anticipate the full financial impact will be determined at the time our 2017 U.S. corporate income tax return is filed in 2018.
The realization of deferred tax assets is dependent upon a number of factors including future earnings, the timing and amount of which is uncertain. A valuation allowance was established for the net deferred tax asset balance due to management’s belief that the realization of these assets is not likely to occur in the foreseeable future. We recorded a net decrease to the valuation allowance of $28.3 million for the year ended December 31, 2017, due to the revaluation of our net deferred tax assets resulting from the reduction to the corporate federal tax rate to 21% offset by the growth in net operating losses and credit carryforwards during the year. The increase of $143.3 million recorded to our valuation allowance during the year ended December 31, 2016 was due primarily to the increase in net operating loss and tax credit carryforwards.
In addition, the Company recognizes tax benefits if it is more likely than not to be sustained under audit by the relevant taxing authority based on technical merits. An uncertain tax position will not be recognized if it has less than a 50% likelihood of being sustained during audit. If the threshold is met, the tax benefit is measured and recognized at the largest amount above the greater than 50% likelihood threshold at time of settlement. The balance of unrecognized tax benefits at December 31, 2017 of $24.5 million, if recognized, would not impact the Company’s effective tax rate as
F-31
long as they remain subject to a full valuation allowance. The following table summarizes the gross amounts of unrecognized tax benefits (in thousands):
|
|
|
|
Year ended December 31, |
|
|||
|
|
|
|
2017 |
2016 |
|
||
|
Balance at beginning of year |
|
$ |
24,075 |
|
$ |
— |
|
|
Additions related to prior periods tax positions |
|
|
— |
|
|
17,844 |
|
|
Additions related to current period tax positions |
|
|
437 |
|
|
6,231 |
|
|
Settlements with tax authorities |
|
|
— |
|
|
— |
|
|
Expiration of statute of limitations |
|
|
— |
|
|
— |
|
|
Balance at end of year |
|
$ |
24,512 |
|
$ |
24,075 |
|
As of December 31, 2017, we had approximately $1.0 billion, $1.2 billion and $0.4 million of U.S. federal, state and foreign net operating loss carryforwards, respectively. The U.S. federal net operating losses will expire from 2029 to 2037 if not utilized and the U.S state net operating losses will expire from 2024 to 2037 if not utilized. We have research and development and orphan drug tax credit carryforwards of $245.1 million that will expire from 2029 through 2037 if not utilized.
We believe that a change in ownership as defined under Section 382 of the U.S. Internal Revenue Code occurred as a result of our public offering of common stock completed in April 2012. Future utilization of the federal net operating losses (“NOL”) and tax credit carryforwards accumulated from inception to the change in ownership date will be subject to annual limitations to offset future taxable income. At this time, we do not believe this limitation will prevent the utilization of the federal NOL or credit carryforward prior to expiration. It is possible that a change in ownership will occur in the future, which will limit the NOL amounts generated since the last estimated change. Our federal and state income taxes for the period from inception to December 31, 2017 remain open to an audit. Our foreign subsidiaries are also subject to tax audits by tax authorities in the jurisdictions where they operate for the periods from December 31, 2011 to December 31, 2017.
We may be assessed interest and penalties related to the settlement of tax positions and such amounts will be recognized within income tax expense when assessed. To date, no interest and penalties have been recognized.
16. Employee Benefit Plans
We maintain a retirement plan, which is qualified under section 401(k) of the Internal Revenue Code for our U.S. employees. The plan allows eligible employees to defer, at the employee’s discretion, pretax compensation up to the IRS annual limits. We matched contributions up to 4% of the eligible employee’s compensation or the maximum amount permitted by law. Total expense for contributions made to U.S. employees was approximately $1.9 million, $1.6 million and $0.8 million for the years ended December 31, 2017, 2016 and 2015, respectively. Our international employees participate in retirement plans or postretirement life insurance plans governed by the local laws in effect for the country in which they reside. We made contributions to the retirement plans or postretirement life insurance plans of international employees of approximately $0.3 million, $0.2 million and $0.2 million for the years ended December 31, 2017, 2016 and 2015, respectively.
F-32
17. Quarterly Information (Unaudited)
The results of operations on a quarterly basis for the years ended December 31, 2017 and 2016 were as follows (in thousands):
|
|
|
March 31, |
|
June 30, |
|
September 30, |
|
December 31, |
|
March 31, |
|
June 30, |
|
September 30, |
|
December 31, |
|
||||||||
|
|
|
2017 |
|
2017 |
|
2017 |
|
2017 |
|
2016 |
|
2016 (1) |
|
2016 |
|
2016 |
|
||||||||
|
Revenues: |
|
|
` |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Product revenue, net |
|
$ |
7,045 |
|
$ |
14,620 |
|
$ |
16,806 |
|
$ |
17,040 |
|
$ |
— |
|
$ |
— |
|
$ |
— |
|
$ |
78 |
|
|
Operating expenses: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Cost of sales - product |
|
|
1,163 |
|
|
2,730 |
|
|
3,026 |
|
|
3,332 |
|
|
— |
|
|
— |
|
|
— |
|
|
70 |
|
|
Cost of sales - intangible asset amortization |
|
|
372 |
|
|
372 |
|
|
372 |
|
|
370 |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
Research and development |
|
|
32,447 |
|
|
33,108 |
|
|
38,924 |
|
|
38,019 |
|
|
74,608 |
|
|
67,729 |
|
|
54,338 |
|
|
54,454 |
|
|
Selling, general and administrative |
|
|
29,224 |
|
|
36,149 |
|
|
35,011 |
|
|
38,523 |
|
|
9,827 |
|
|
9,552 |
|
|
9,162 |
|
|
12,190 |
|
|
Acquired in-process research and development |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
300 |
|
|
500 |
|
|
500 |
|
|
Impairment of intangible asset |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
104,517 |
|
|
— |
|
|
— |
|
|
Change in fair value of contingent purchase consideration |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
516 |
|
|
(25,452) |
|
|
— |
|
|
— |
|
|
Total expenses |
|
|
63,206 |
|
|
72,359 |
|
|
77,333 |
|
|
80,244 |
|
|
84,951 |
|
|
156,646 |
|
|
64,000 |
|
|
67,214 |
|
|
Operating loss |
|
|
(56,161) |
|
|
(57,739) |
|
|
(60,527) |
|
|
(63,204) |
|
|
(84,951) |
|
|
(156,646) |
|
|
(64,000) |
|
|
(67,136) |
|
|
Other income (expense): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Interest expense |
|
|
(2,581) |
|
|
(2,598) |
|
|
(2,618) |
|
|
(2,631) |
|
|
(2,104) |
|
|
(2,106) |
|
|
(2,108) |
|
|
(2,173) |
|
|
Foreign currency gain (loss) |
|
|
(159) |
|
|
76 |
|
|
(44) |
|
|
45 |
|
|
(551) |
|
|
183 |
|
|
(66) |
|
|
(146) |
|
|
Legal settlement loss |
|
|
— |
|
|
(117,000) |
|
|
— |
|
|
11,523 |
|
|
— |
|
|
— |
|
|
— |
|
|
— |
|
|
Other income (expense) |
|
|
354 |
|
|
594 |
|
|
1,291 |
|
|
1,404 |
|
|
25 |
|
|
196 |
|
|
252 |
|
|
160 |
|
|
Other income (expense), net |
|
|
(2,386) |
|
|
(118,928) |
|
|
(1,371) |
|
|
10,341 |
|
|
(2,630) |
|
|
(1,727) |
|
|
(1,922) |
|
|
(2,159) |
|
|
Loss before income taxes |
|
|
(58,547) |
|
|
(176,667) |
|
|
(61,898) |
|
|
(52,863) |
|
|
(87,581) |
|
|
(158,373) |
|
|
(65,922) |
|
|
(69,295) |
|
|
Income tax (expense) benefit |
|
|
83 |
|
|
1,281 |
|
|
1,234 |
|
|
980 |
|
|
4,181 |
|
|
29,059 |
|
|
227 |
|
|
(1,433) |
|
|
Net loss |
|
$ |
(58,464) |
|
$ |
(175,386) |
|
$ |
(60,664) |
|
$ |
(51,883) |
|
$ |
(83,400) |
|
$ |
(129,314) |
|
$ |
(65,695) |
|
$ |
(70,728) |
|
|
Basic and diluted net loss per common share |
|
$ |
(1.33) |
|
$ |
(3.88) |
|
$ |
(1.24) |
|
$ |
(1.04) |
|
$ |
(2.17) |
|
$ |
(3.37) |
|
$ |
(1.70) |
|
$ |
(1.83) |
|
|
Basic and diluted weighted average common shares outstanding |
|
|
44,039 |
|
|
45,176 |
|
|
48,917 |
|
|
49,973 |
|
|
38,360 |
|
|
38,389 |
|
|
38,538 |
|
|
38,624 |
|
|
(1) |
In the second quarter of 2016, we recorded a $104.5 million impairment charge to the IPR&D intangible asset related to our lucitanib product candidate. |
F-33