Attached files
| file | filename |
|---|---|
| EX-10.5 - EXHIBIT 10.5 - Cardiovascular Systems Inc | ex105-fy18execincentiveplan.htm |
| EX-32.2 - EXHIBIT 32.2 - Cardiovascular Systems Inc | ex322-63017.htm |
| EX-32.1 - EXHIBIT 32.1 - Cardiovascular Systems Inc | ex321-63017.htm |
| EX-31.2 - EXHIBIT 31.2 - Cardiovascular Systems Inc | ex312-63017.htm |
| EX-31.1 - EXHIBIT 31.1 - Cardiovascular Systems Inc | ex311-63017.htm |
| EX-23.1 - EXHIBIT 23.1 - Cardiovascular Systems Inc | ex231-63017.htm |
| EX-10.58 - EXHIBIT 10.58 - Cardiovascular Systems Inc | ex1058-koehnseparationagre.htm |
| EX-10.57 - EXHIBIT 10.57 - Cardiovascular Systems Inc | ex1057-healthtrustamendment.htm |
| EX-10.46 - EXHIBIT 10.46 - Cardiovascular Systems Inc | ex1046-2014planperformance.htm |
| EX-10.6 - EXHIBIT 10.6 - Cardiovascular Systems Inc | ex106-fy18directorcomp.htm |
| EX-10.4 - EXHIBIT 10.4 - Cardiovascular Systems Inc | ex104-fy18basesalaries.htm |
UNITED STATES SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
FORM 10-K
x | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the fiscal year ended June 30, 2017
OR
o | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
Commission file number: 000-52082
CARDIOVASCULAR SYSTEMS, INC.
(Exact name of registrant as specified in its charter)
Delaware | 41-1698056 | |
(State or other jurisdiction of incorporation or organization) | (I.R.S. Employer Identification No.) | |
1225 Old Highway 8 Northwest St. Paul, Minnesota | 55112-6416 | |
(Address of principal executive offices) | (Zip Code) | |
Registrant’s telephone number, including area code:
(651) 259-1600
Securities registered pursuant to Section 12(b) of the Act:
Title of each class | Name of each exchange on which registered | |
Common Stock, One-tenth of One Cent ($0.001) Par Value Per Share | The NASDAQ Stock Market LLC | |
Securities registered pursuant to Section 12(g) of the Act:
None.
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes o No þ
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Exchange Act. Yes o No þ
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes þ No o
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§ 232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes þ No o
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K (§ 229.405 of this chapter) is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. o
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer or a smaller reporting company. See the definitions of “large accelerated filer,” “accelerated filer” and “smaller reporting company” in Rule 12b-2 of the Exchange Act.
Large accelerated filer x | Accelerated filer o | Non-accelerated filer o | Smaller reporting company o | |||
Emerging growth company o | (Do not check if a smaller reporting company) | |||||
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act o
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes o No þ
As of December 31, 2016, the aggregate market value of the registrant’s common stock held by non-affiliates of the registrant was approximately $765.8 million based on the closing sale price as reported on the NASDAQ Global Market.
The number of shares of the registrant’s common stock outstanding as of August 18, 2017 was 32,991,788.
DOCUMENTS INCORPORATED BY REFERENCE
Portions of the proxy statement for the registrant’s 2017 Annual Meeting of Stockholders are incorporated by reference into Items 10, 11, 12, 13 and 14 of Part III of this report.
Table of Contents
Page No. | ||
Item 1. | ||
Item 1A. | ||
Item 1B. | ||
Item 2. | ||
Item 3. | ||
Item 4. | ||
Item 5. | ||
Item 6. | ||
Item 7. | ||
Item 7A. | ||
Item 8. | ||
Item 9. | ||
Item 9A. | ||
Item 9B. | ||
Item 10. | ||
Item 11. | ||
Item 12. | ||
Item 13. | ||
Item 14. | ||
Item 15. | ||
We make available, free of charge, copies of our annual report on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K and amendments to those reports filed or furnished pursuant to Section 13(a) or 15(d) of the Securities Exchange Act on our website, http://www.csi360.com, as soon as reasonably practicable after filing such material electronically or otherwise furnishing it to the Securities and Exchange Commission (“SEC”). We are not including the information on our website as a part of, or incorporating it by reference into, our Form 10-K.
The SEC maintains a website that contains reports, proxy and information statements, and other information regarding issuers, including the Company, that file electronically with the SEC. The public can obtain any documents that we file with the SEC at http://www.sec.gov. We file annual reports, quarterly reports, proxy statements, and other documents with the SEC under the Securities Exchange Act of 1934, as amended (the “Exchange Act”). The public may read and copy any materials that we file with the SEC at the SEC’s Public Reference Room at 100 F Street, N.E., Room 1580, Washington, D.C. 20549. The public may obtain information on the operation of the Public Reference Room by calling the SEC at 1-800-SEC-0330.
PART I
Item 1. Business.
Special Note Regarding Forward Looking Statements
This report contains plans, intentions, objectives, estimates and expectations that constitute forward-looking statements within the meaning of Section 27A of the Securities Act of 1933, as amended, and Section 21E of the Exchange Act, which are subject to the “safe harbor” created by those sections. Forward-looking statements are based on our management’s beliefs and assumptions and on information currently available to our management. In some cases, you can identify forward-looking statements by terms such as “may,” “will,” “intend,” “should,” “could,” “would,” “expect,” “plans,” “anticipates,” “believes,” “estimates,” “projects,” “predicts,” “potential” and similar expressions intended to identify forward-looking statements. Examples of these statements include, but are not limited to, any statements regarding our future financial performance, results of operations or sufficiency of capital resources to fund our operating requirements, and other statements that are other than statements of historical fact. Our actual results could differ materially from those discussed in these forward-looking statements due to a number of factors, including the risks and uncertainties that are described more fully by us in Part I, Item 1A and Part II, Item 7 of this report and in our other filings with the Securities and Exchange Commission. You should not place undue reliance on these forward-looking statements, which apply only as of the date of this report. You should read this report completely and with the understanding that our actual future results may be materially different from what we expect. Except as required by law, we assume no obligation to update these forward-looking statements publicly, or to update the reasons actual results could differ materially from those anticipated in these forward-looking statements, even if new information becomes available in the future.
Corporate Information
Cardiovascular Systems, Inc. (“CSI”) was incorporated in Delaware in 2000. Our principal executive office is located at 1225 Old Highway 8 Northwest, St. Paul, Minnesota 55112. Our telephone number is (651) 259-1600, and our website is www.csi360.com. The information contained in or accessible through our website is not incorporated by reference into, and should not be considered part of, this Annual Report on Form 10-K.
We have received 19 federal registrations in the U.S. Patent and Trademark Office (“USPTO”) of certain marks, including “Diamondback®,” a first “CSI®,” a second “CSI®,” “CSIQ®,” “Stealth 360°®,” a first “CSI®” logo, a second “CSI®” logo, “TAKE A STAND AGAINST AMPUTATION®,” “ViperWire®,” “ViperWire Advance®,”“Viperwire Advance® (Stylized),” “Viperslide®,” Viperslide® (Stylized),” “ViperTrack®,” “Vipertrack® (Stylized),” a first “Diamondback 360®,” a second “Diamondback 360®,” “Diamondback 360® (Stylized) Logo,” and “Stay A Step Ahead of PAD®”. We have applied for federal trademark registration with the USPTO of certain marks, including “CSIQ (Stylized),” “GLIDEASSIST”, and “TAKE A STAND AGAINST AMPUTATION (and Design).” All other trademarks, trade names and service marks appearing in this Form 10-K are the property of their respective owners.
Business Overview
We are a medical technology company leading the way in the effort to successfully treat patients suffering from peripheral and coronary artery diseases, including those with arterial calcium, the most difficult arterial disease to treat. We are committed to clinical rigor, constant innovation and a defining drive to set the industry standard to deliver safe and effective medical devices that improve lives of patients facing this difficult disease state.
We have developed a patented orbital atherectomy technology for both peripheral and coronary commercial applications. Our systems are catheter-based platforms capable of treating a broad range of vessel sizes and plaque types, including calcified plaque, and address many of the limitations associated with other treatment alternatives. We refer to the Diamondback 360® Peripheral Orbital Atherectomy Systems (“OAS”) (“Diamondback 360 Peripheral”), the Stealth 360® OAS (“Stealth 360”), and the products included in the chart below collectively in this annual report on Form 10-K as the “Peripheral OAS.”
1
The United States Food and Drug Administration (“FDA”) granted us 510(k) clearance for the following Peripheral OAS as a therapy in patients with peripheral artery disease (“PAD”):
FDA 510(k) Clearance Granted | Product | Commercial Introduction | ||
August 2007 | Diamondback 360 Peripheral(1) | September 2007 | ||
March 2009 | Predator 360(1) | April 2009 | ||
March 2011 | Stealth 360 | March 2011 | ||
February 2014 | Diamondback 360 60cm Peripheral | April 2014 | ||
April 2015 | Diamondback 360 Low Profile Peripheral | July 2015 | ||
October 2015 | Diamondback 360 1.50 Peripheral | January 2016 | ||
October 2015 | Diamondback 360 2.00 Peripheral | January 2016 | ||
June 2017 | Diamondback 360 200cm Peripheral | Expected 2018 | ||
June 2017 | Diamondback 360 180cm Peripheral | Expected 2018 | ||
(1) We are not currently marketing this product. | ||||
As of June 30, 2017, over 292,000 of our Peripheral OAS have been sold to leading institutions across the United States. Sales of Peripheral OAS during the fiscal year ended June 30, 2017 represented 69% of revenue.
Our coronary product, the Diamondback 360® Coronary OAS (“Coronary OAS”), is a catheter-based platform designed to facilitate stent delivery in patients with coronary artery disease (“CAD”) who are acceptable candidates for percutaneous transluminal coronary angioplasty or stenting due to de novo, severely calcified coronary artery lesions. The Coronary OAS design is similar to technology used in our Peripheral OAS, customized specifically for the coronary application. In October 2013, we received premarket approval (“PMA”) from the FDA to market the Coronary OAS as a treatment for severely calcified coronary arteries. We commenced a commercial launch that same month and, as of June 30, 2017, over 31,000 Coronary OAS have been sold to leading institutions across the United States. Sales of Coronary OAS during the fiscal year ended June 30, 2017 represented approximately 23% of revenue. In March 2017, the Company received approval from the FDA to market its Diamondback360® Coronary OAS Micro Crown, which is the only atherectomy device designed to both pilot tight, calcific lesions and treat 2.5 to 4mm vessels with a single device. We are planning a limited release of the Coronary OAS Micro Crown in the U.S. in fiscal 2018.
In addition to the Peripheral and Coronary OAS, we offer multiple accessory products required for use with the Peripheral and Coronary OAS. Sales of accessory products, primarily guide wires, represented 8% of revenue during the fiscal year ended June 30, 2017.
In November 2016, we signed an exclusive distribution agreement with Medikit Co., Ltd. to sell the Diamondback 360® Coronary OAS Micro Crown in Japan. In March 2017, we received approval from Japan’s Ministry of Health, Labor and Welfare (“MHLW”) of our Diamondback 360® Coronary OAS Micro Crown. Pending reimbursement approval, Japan will become the first international market for any CSI product and represents a significant milestone for us.
We will continue to evaluate options for additional international markets to expand the coronary and peripheral opportunities.
Market Overview
Peripheral Artery Disease (“PAD”)
Peripheral artery disease is widespread and can be life threatening. The disease is characterized by narrowed, hardened arteries in the legs, limiting blood flow to the legs and feet. If left untreated, PAD may continue to progress to Critical Limb Ischemia (“CLI”), a condition in which the amount of oxygenated blood being delivered to the limb is insufficient to keep the tissue alive. CLI may lead to non-healing ulcers, infections, gangrene, limb amputation or death. According to estimates by the American Heart Association (“AHA”), as many as 8 to 12 million Americans have PAD. An aging population, coupled with increasing incidence of diabetes and obesity, is likely to continue to increase the prevalence of PAD. In many older PAD patients, particularly those with diabetes, PAD is characterized by fibrotic (moderately hard) or calcified (extremely hard) plaque deposits that can be very challenging to treat. Although we believe the rate of PAD diagnoses is increasing, we also believe that under-diagnosis continues, due to patients failing to display symptoms or physicians misinterpreting symptoms as normal aging. Emphasis on PAD education from industry, medical associations, insurance companies and other groups, coupled
2
with publications in medical journals and public news channels, is increasing physician and patient awareness of PAD risk factors, symptoms, and treatment options. Physicians manage a significant portion of the PAD diagnosed population by recommending lifestyle changes, such as diet and exercise, and by prescribing prescription drugs, such as statins. While medications, diet and exercise may improve blood flow, they do not treat the underlying obstructions, and many patients have difficulty maintaining lifestyle changes. As a result of these challenges, many medically managed patients develop more severe symptoms that require procedural intervention.
Coronary Artery Disease (“CAD”)
Heart disease is the leading cause of death in both men and women in the United States. Coronary artery disease is the most common type of heart disease in the U.S. and is a life-threatening condition. CAD occurs when a fatty material called plaque builds up on the walls of arteries that supply blood to the heart. The plaque buildup causes the arteries to harden and narrow (atherosclerosis), reducing blood flow. The risk of CAD increases if a person has one or more of the following: high blood pressure, abnormal cholesterol levels, diabetes, or family history of early heart disease. According to the AHA, 15.5 million people in the U.S. (or 6.2% of the adult population) suffer from CAD, the most common form of heart disease. According to the U.S. Centers for Disease Control and Prevention, over 370,000 lives are claimed in the U.S. each year from CAD. According to estimates, significant arterial calcium is present in nearly 40% of patients (Genereux et al., 2014; Bourantas et al., 2014), and severe calcium affects up to 20% of patients (Bourantas et al., 2014), undergoing a percutaneous coronary intervention (“PCI”). Significant calcium contributes to poor outcomes and higher treatment costs in coronary interventions when traditional therapies are used, including a significantly higher occurrence of death and major adverse cardiac events (“MACE”).
Our Peripheral OAS and Coronary OAS
Our orbital atherectomy systems represent an innovative approach to the treatment of PAD and CAD that provide physicians and patients with a procedure that addresses many of the limitations of other treatment alternatives. The Peripheral OAS and Coronary OAS devices are single-use catheters that incorporate a control handle and flexible drive shaft with an eccentrically mounted diamond-coated crown. The peripheral device is often used for vessel preparation to enable low pressure percutaneous transluminal angioplasty, including the use of drug-coated balloons (“DCB”), and results in lower use of bailout stents. The coronary device is used to treat severe calcium prior to stent delivery to help facilitate optimal stent expansion and prevent malapposition of stent struts. The OAS treats atherosclerotic plaque, which is harder than a normal vessel wall. The OAS is designed to differentiate between hard, diseased plaque and healthy, compliant arterial tissue, a concept that we refer to as “differential sanding.” The diamond-coated crown preferentially engages and sands away harder material, but is designed not to damage more compliant parts of the artery, which flex away from the crown. Physicians position the crown at the site of a lesion containing arterial plaque and orbit the crown against it to sand away the superficial, or surface, plaque and create a smooth lumen, or channel, in the vessel. In addition, the crown’s rotating eccentric mass and orbital motion deliver pulsatile mechanical energy into the vessel wall. These pulsatile forces may break up deeper plaque and contribute to compliance change of the diseased segment of the artery.
Components of the OAS
Our OAS uses a single-use, low-profile catheter that travels over our proprietary ViperWire guide wires and is electrically powered by a saline infusion pump that also helps cool the system and remove debris. The Peripheral OAS reduces plaque on peripheral vessel walls by using an orbiting, diamond-coated crown within peripheral arteries. Similarly, the Coronary OAS uses the same method to reduce severely calcified plaque on coronary vessel walls within coronary arteries in order to facilitate stent delivery.
Catheter. The catheter for our OAS consists of:
• | an electrically-powered control handle, which allows movement of the crown and predictable crown location; |
• | a flexible drive shaft with an eccentrically mounted diamond-coated crown, which tracks and orbits over the guide wire; and |
• | a sheath, which covers the drive shaft and permits delivery of saline or medications to the treatment area. |
ViperWire Advance Peripheral Guide Wire, ViperWire Advance Peripheral Guide Wire with Flex Tip and ViperWire Advance Coronary Guide Wire. The ViperWire guide wires are required for using the OAS and were designed to offer the ability to maneuver through tortuous, twisting blood vessels and cross challenging lesions. The OAS travels over this wire to the lesion and operates on this wire.
ViperSlide Lubricant. ViperSlide is an exclusive lubricant designed to optimize the smooth operation of the OAS.
3
OAS Pump. The saline infusion pump bathes the OAS shaft and crown and provides an electric power supply for the operation of the catheter. The constant flow of saline during orbit reduces the risk of heat generation and improves the flush of particulates.
Mechanism of Action
The mechanism of action is a function of the centrifugal force generated by the eccentrically mounted crown as it rotates and orbits inside the vessel. As the speed of the crown’s rotation increases, centrifugal force increases the crown’s radius of orbit and presses the diamond-coated crown against the lesion or plaque, removing a small amount of plaque with each orbit. The centrifugal force exerted onto the vessel wall decreases as the orbital radius increases, reducing the likelihood of adverse events during treatment. The characteristics of the orbit and the resulting lumen size can be adjusted by modifying the following two variables:
• | Speed. An increase in speed creates a larger orbital radius, thus accommodating larger diameter vessels. Our Peripheral OAS allows the user to choose between three rotational speeds and our Coronary OAS Classic Crown allows the user to choose between two rotational speeds. |
• | Crown Characteristics. The crowns for the OAS are designed with various weights (as determined by crown geometry and material density) and are coated with diamond particles. The Peripheral OAS crowns are available in three configurations: classic, micro and solid. Physicians select crown sizes and configurations based on several case criteria, including reference vessel size, lesion length and degree of stenosis, stenosis morphology, and anatomy tortuosity. The crown for the Diamondback 360 Coronary OAS is available in two configurations: 1.25 millimeter classic crown and the recently-approved 1.25 millimeter micro crown which is designed to both pilot through tight, severely calcified coronary lesions and treat 2.5 to 4mm vessels with a single device. |
Centrifugal force propels the crown outward against the arterial wall as the crown rotates. This force is offset by the counterforce exerted by the arterial wall and the guidewire. Normal arteries are compliant and have the ability to expand and contract as needed to supply blood flow. If the tissue is compliant, it flexes away, minimizing the engagement of the diamond-grit and protecting the integrity of the healthy tissue. Diseased tissue is less flexible or non-compliant and provides resistance to the centrifugal force, which generates an opposing force that enables the diamond-coated crown to engage and sand the plaque. The sanded plaque and calcium is broken down into particles generally smaller than circulating red blood cells that are washed away downstream with the patient’s natural blood flow.
The small particle size and short treatment time minimizes the risk of vascular bed overload, or a saturation of the peripheral or coronary vessels with large particles, which may cause slow or reduced blood flow. The small size of the particles allows them to be naturally cleared from the blood via various types of white blood cells and macrophages.
We believe the OAS offers the following key benefits:
Strong Safety Profile
• | Differential Sanding Reduces Risk of Adverse Events. The OAS is designed to differentiate between hard, non-compliant plaque and soft, compliant arterial tissue. Arteries are composed of three tissue layers (from inside to out): the intima, media, and adventitia. The eccentrically mounted diamond-coated crown at the working end of the device engages and removes plaque from the artery wall with minimal likelihood of penetrating or damaging the fragile intima, or inner layer of the arterial wall because soft, compliant tissue flexes away from the crown. |
• | Eliminates Need for Distal Protection. The small size of the particles produced during sanding avoids the need for ancillary distal protection devices, commonly used with directional cutting atherectomy devices. The small particulate size also significantly reduces the risk of macroembolization, or larger pieces of removed plaque capable of blocking blood flow downstream. |
• | Allows Continuous Blood Flow During Procedure. The OAS allows for continuous blood flow while orbiting, as well as constant flushing of particulates during treatment. Other devices may restrict blood flow due to the size of the catheter required or the use of distal protection devices, which could result in complications such as excessive heat and tissue damage. |
4
• | Benefits of Smaller Sheaths. The Diamondback 360 Peripheral OAS portfolio is uniquely compatible with 4 French (“Fr”) to 6Fr sheaths. Centrifugal force enables the OAS to treat large vessels through small sheaths; for example, it can treat up to 5mm vessel through a 4Fr sheath. Smaller sheaths may be associated with less femoral bleeding, shortened post-procedure ambulation time and reduced radiation exposure. In addition, the primary complication in peripheral interventions is a vascular access site complication. Exchanging to a larger sheath has been shown to be the strongest predictor of bleeding complication during peripheral interventions. |
Proven Efficacy
• | Efficacy Demonstrated for Both Peripheral OAS and Coronary OAS. |
◦ | Peripheral OAS - Our pivotal OASIS clinical trial was a prospective 20-center study that involved 124 patients with 201 lesions treated by the Diamondback 360 Peripheral OAS. Performance targets were established cooperatively with the FDA before the trial began. Despite 55% of the lesions consisting of calcified plaque, the Diamondback 360 Peripheral OAS successfully met the study endpoints. |
◦ | Coronary OAS - Our pivotal ORBIT II coronary OAS trial was designed to evaluate the safety and efficacy of OAS in treating de novo severely calcified coronary lesions. The trial met both the primary safety and efficacy endpoints by significant margins. Preparation of severely calcified plaque with the Coronary OAS not only helped facilitate stent delivery, but also improved both peri-procedural and 30-day clinical outcomes compared with the outcomes of historic control subjects in this difficult-to-treat patient population. |
• | Treats Difficult, Fibrotic and Calcified Lesions. The OAS enables physicians to remove plaque from long, fibrotic, calcified or bifurcated lesions, as well as lesions with softer plaque, in peripheral arteries both above and below the knee. In the coronary arteries, the OAS enables physicians to treat complex, severely calcified lesions, enabling stent placement in these difficult to treat lesions. To date, the Coronary OAS is the only FDA-approved device approved specifically for treatment of severely calcified coronary lesions. |
• | Orbital Motion Improves Lesion Compliance. The orbiting action of the OAS removes the hard plaque in the artery by sanding, while the centrifugal motion of the eccentrically mounted crown creates pulsatile forces. Compliance change is achieved as the OAS differentiates between hard, diseased plaque and healthy, compliant arterial tissue, a concept that we refer to as “differential sanding.” The diamond-coated crown preferentially engages and sands away harder material, but is designed not to damage more compliant parts of the artery, which flex away from the crown. Physicians position the crown at the site of a lesion containing arterial plaque and orbit the crown against it to sand away the superficial, or surface, plaque and create a smooth lumen, or channel, in the vessel. In addition, the crown’s rotating eccentric mass and orbital motion deliver pulsatile mechanical energy into the vessel wall. These pulsatile forces may break up deeper plaque and contribute to compliance change of the diseased segment of the artery. Together, these mechanistic components sufficiently remove or modify hard plaque, allowing for low pressure balloon inflation. The orbital motion and speed of the eccentrically mounted crown increases, thus allowing for continuous reduction of plaque with differential sanding and pulsatile forces, as the opening of the lumen increases during the operation of the devices. |
• | Differential Sanding Creates Smooth Lumens. The differential sanding of the OAS creates a smooth lumen surface, or channel, inside the vessel. We believe that the smooth lumens created by the device increase the velocity of blood flow and decrease the resistance to blood flow, which may decrease the potential for restenosis, or re-narrowing of the arteries. |
Ease of Use
• | Set Up Time. Given the relative simplicity of the OAS, physicians and lab staff can usually set up and begin using the device in under two minutes. |
• | Utilizes Familiar Techniques. Physicians using the OAS employ techniques similar to those used in angioplasty, which are familiar to interventional cardiologists, vascular surgeons and interventional radiologists who are trained in endovascular techniques. The devices’ simple user interfaces require minimal additional training. |
• | Single Crown Treats Multiple Lesions in Various Sized Vessels. Centrifugal force unique to OAS allows for a single access site to treat multiple lesions, in most cases. In the coronary arteries, Coronary OAS is the only atherectomy device able to treat 2.5 to 4mm vessels with one device through a 6Fr radial approach. In the peripheral vasculature, |
5
the OAS device is capable of treating multiple lesions in multiple arteries through a single access site, thus reducing the need for multiple devices or the need for multiple access sites.
• | No Need for Collection Reservoir. Because the particles of plaque sanded away are of such small sizes, the OAS does not require a collection reservoir that needs to be repeatedly emptied or cleaned during the procedure, which would potentially add time and cost to the procedure. |
Multiple Applications
The unique OAS mechanism of action used in both the Peripheral OAS and Coronary OAS can be used to treat multiple anatomic locations.
• | Below-the-Knee and Behind-the-Knee Peripheral Artery Disease. Arteries below and behind the knee are small in diameter and may be diffusely stenosed, calcified or both. Reaching and treating these small vessels requires a low profile, which most competitive devices do not offer. Behind-the-knee, or popliteal, lesions also present challenges if a stent is used because stents frequently fracture in this area due to the forces exerted on the vessels when the knee bends or flexes. The Diamondback 360 Peripheral OAS is effective in treating those vessels. The Peripheral OAS offers a shorter shaft length (60cm), a smaller profile and a more flexible shaft than the predecessors for improved ease of use, and includes a 4 Fr catheter that enables physicians to access lesions below-the-knee using retrograde access (access through the ankle or foot). |
• | Above-the-Knee Peripheral Artery Disease. Arteries above the knee are typically longer, straighter and wider than below-the-knee vessels. Plaque in these arteries may also be diffuse, fibrotic and calcific. Physicians often use higher speeds or larger crown sizes of our products to treat lesions above the knee. |
• | Coronary Artery Disease. The individuals more at risk for being diagnosed with CAD are those that are suffering from high blood pressure, abnormal cholesterol levels, diabetes, renal insufficiency, or have a family history of heart disease. The pathogenesis of CAD is marked by the accumulation of a fatty material called plaque on the walls of arteries that supply blood to the heart. The plaque buildup causes the arteries to harden and narrow (atherosclerosis), reducing blood flow. The Diamondback 360 Coronary OAS is the only atherectomy device specifically indicated for severe coronary calcium. |
Cost and Time Efficient Procedure
• | Short Procedure Time. The OAS has a short treatment time, typically less than two minutes. |
• | Single Crown Can Treat Various Lumen Sizes Helping Limit Hospital Costs. The OAS orbital mechanism of action allows one device to treat various diameter lumens inside the artery. Adjusting the rotational speed of the crown changes the orbit to create the desired lumen diameter, thereby potentially avoiding the need to use multiple catheters of different sizes to treat multiple lesions. |
• | Trans-Radial Access Provides Multiple Benefits. Treating complex, calcified lesions in the peripheral or coronary arteries remains difficult, particularly where patients may present challenging access sites. The OAS allows for trans-radial access with benefits to both physicians and patients. For physicians, this smaller access site provides lower vascular and bleeding complication rates, faster patient recovery time, and the ability to treat bilateral disease in one setting, address obese patients and work around previous, compromised access sites. For patients, this contributes to comfort during- and post-operation, earlier ambulation, reduced risk of infection, and faster healing. |
• | Retrograde Access Treatment Option Benefits. Many of the patients treated with the Peripheral OAS have advanced PAD and suffer from CLI. These patients often have complex, calcified lesions in their lower leg, which are challenging to access and treat using the traditional femoral artery access site. If left untreated, these cases may result in lower limb amputation. CSI’s family of 1.25mm Peripheral OASs with 4Fr compatibility allows for more options to treat those lesions by providing a low-profile system that is fully compatible with alternative access sites in the foot or ankle. Smaller sheaths have been shown to reduce procedure times and decrease complications. |
6
Our OAS Strategy
Our goal is to be the leading provider of low profile solutions for the treatment of peripheral and coronary artery disease. The key elements of our strategy include:
• | Drive Adoption through Our Direct U.S. Sales Organization, Medical Education and Key Opinion Leaders. We expect to continue to drive adoption of the OAS through our direct U.S. sales force in both hospital and office-based lab settings, which targets interventional cardiologists, vascular surgeons, and interventional radiologists. As a key element of our strategy, we focus on educating physicians about the disease states and our clinical data, and training physicians regarding the proper use and application of OAS technology through physician faculty, our direct sales force and through seminars where physician industry leaders discuss case studies and treatment techniques using the devices. |
• | Collect Additional Clinical Evidence on Safety, Effectiveness and Economic Benefits of the OAS. Physicians and payers are increasingly requesting clinical and economic evidence to allow them to make decisions regarding optimal treatment of patients. We are focused on collecting clinical and economic evidence to demonstrate the advantages of the OAS in treating complex disease states such as peripheral and coronary artery disease. We believe that the clinical advantages and cost effectiveness of our OAS technology will help drive physician utilization of the OAS and sustain ongoing reimbursement coverage for our devices. |
• | Enhance OAS and Expand Product Portfolio within the Market for Treatment of Peripheral and Coronary Arteries. In addition to enhancing the OAS, we offer multiple accessory devices for use with the OAS. We are continuing product development to further expand our portfolio of PAD and CAD treatment solutions. |
• | International Expansion. In March 2017, we received regulatory approval for our coronary OAS Micro Crown device in Japan. We are evaluating options for further international expansion to maximize the coronary and peripheral market opportunities. |
• | Strategic Acquisitions and Partnerships. In addition to adding to our product portfolio through internal development efforts, we intend to explore the acquisition of other product lines, technologies or companies that may leverage our sales force or complement our strategic objectives. We also intend to explore distribution agreements, licensing transactions, manufacturing agreements and other strategic partnerships. |
Research and Development Activities
Clinical Studies Summary
We study the most challenging patient populations and are committed to providing relevant clinical evidence that enables physicians to select and utilize the best treatment options for their patients. A total of 5,735 subjects (4,764 PAD and 971 CAD) have been enrolled in our clinical studies as of June 30, 2017. Our clinical studies incorporate rigorous long-term clinical and healthcare economic data that are critical to improving patient care and ongoing healthcare changes.
We have completed numerous clinical studies to demonstrate the safety and efficacy of the Peripheral OAS. The results of these studies consistently demonstrate that the Peripheral OAS provides predictable, repeatable and durable results that differentiate it from other PAD treatments.
The following PAD clinical studies were completed or in process during fiscal 2017:
• | LIBERTY 360°. This prospective, observational, multi-center clinical study is evaluating the procedural and long-term clinical, quality of life and economic outcomes of endovascular device interventions, including orbital atherectomy, for the treatment of PAD. We expect the results from this study to increase our understanding of the clinical and economic outcomes of endovascular treatment for PAD patients, including those with the most advanced form of the disease, Rutherford Class 6. Enrollment of 1,204 subjects at 51 sites in the U.S. was completed in February 2016. |
7
LIBERTY 360° data were presented in February and August 2017. The majority of devices used in the study were balloons and/or atherectomy, and the Peripheral OAS was the most frequently used atherectomy device. The LIBERTY 360° data through one year demonstrated that peripheral interventions can be used successfully across all Rutherford classes, including the most challenging Rutherford Class 6 subjects. Overall, the results of this novel all-comers PAD study suggest that peripheral vascular intervention (“PVI”) is an alternative to “primary amputation” in Rutherford Class 6 patients. Additionally, data from the LIBERTY 360° study provide further evidence to support PVI treatment in Rutherford 2-5 patients.
• | OPTIMIZE BTK. This post-market, multi-center, randomized clinical study conducted in Europe is designed to evaluate the acute and long-term clinical outcomes of orbital atherectomy with adjunctive DCB angioplasty versus DCB angioplasty alone in PAD patients with calcified, below-the-knee lesions. Fifty evaluable subjects will be enrolled in OPTIMIZE BTK and will be followed for up to two years. |
We have conducted two clinical studies to evaluate the safety and efficacy of the Coronary OAS Classic Crown device: the ORBIT I feasibility study and the ORBIT II pivotal study. The safety and efficacy of the Coronary OAS Micro Crown device were evaluated in the COAST study. In fiscal 2017, we launched ECLIPSE, as described below.
The following CAD clinical studies were completed or in process during fiscal 2017:
• | COAST. This prospective, single-arm, multi-center, global Investigational Device Exemption (“IDE”) study was conducted to evaluate the safety and efficacy of the Coronary OAS Micro Crown in treating de novo, severely calcified lesions prior to stent implantation. Enrollment of 100 patients, including 74 patients at 12 sites in the U.S. and 26 patients at five sites in Japan, was completed in July 2015. The study results through one year were presented in February 2017. The overall one-year MACE rate, defined as the composite of myocardial infarction (“MI”), cardiac death, and target vessel revascularization, was 22.2%. The COAST MI rate did not increase from 30 days to one year, and low rates of one-year cardiac death (1.0%) and target lesion revascularization (6.3%) were reported. |
• | MACE. This prospective, multi-center, non-randomized study assessed the outcomes of current standard of care treatment in none/mild, moderate, and severely calcified coronary lesions. Treatment of the target lesion excluded use of OAS. Enrollment of 350 subjects was completed in September 2015. The one-year results of the MACE study were presented in February 2017. The MACE data through one year indicate that severe calcium is associated with higher short and long-term major adverse cardiac event rates compared to both none/mild and moderate calcification. |
• | ECLIPSE. This post-market, randomized one-to-one, multi-center trial is designed to evaluate vessel preparation with OAS compared to conventional angioplasty technique prior to drug-eluting stent implantation for the treatment of severely calcified lesions. Approximately 2,000 subjects will be enrolled at approximately 150 sites in the U.S. and subjects will be followed for up to two years. The co-primary endpoints of acute minimum stent area (assessed by optical coherence tomography in a subset of 400 subjects) and one-year target vessel failure are powered to demonstrate superiority of OAS vessel preparation vs. conventional angioplasty. |
Our clinical portfolio is expanding as we develop future studies to answer difficult questions about PAD and CAD treatment. Our clinical research continues to highlight the safety and efficacy of the OAS and current and new research illustrates our versatility in the emerging vascular market.
Development Activities
Our product research and development activities are dedicated to the development and commercialization of products that serve the peripheral and coronary vascular disease space, with emphasis towards high margin products and complex arterial disease states treated by our primary customers. The focus and value proposition of our products is to enable positive acute and long-term clinical outcomes, with efficiency and predictability, in challenging patient subsets.
Research and development resources have been strategically allocated between opportunities that maximize the clinical effectiveness and user satisfaction of our OAS product line and the development of additional products that offer portfolio diversification and incremental revenue opportunities.
Specific to the peripheral vascular disease market, we will continue our commitment to patients suffering from CLI through a breadth of above-the-knee and below-the-knee differentiated products that treat or uniquely expand the ability of our devices to treat obstructive lesions throughout the leg and foot. Most recently, we launched the Diamondback 360 Low Profile Peripheral, a line of next generation low profile orbital atherectomy devices that enable physicians to intervene through 4Fr and 5Fr access
8
sheaths. Low profile devices offer numerous benefits, including a reduction in access site complications, improved device deliverability, compatibility with alternative access sites and a reduction in post-procedure time to ambulation. Specific to the coronary vascular disease market, we are building a portfolio of differentiated products that are used to treat complex CAD. Emphasis in both franchises is placed on novel and differentiated devices that address unmet or under-met clinical or technical needs.
Research and development expenses for the years ended June 30, 2017, 2016, and 2015 were $22.9 million, $25.9 million and $31.0 million, respectively.
Sales and Marketing
We market and sell our products through a direct sales force in the United States. Revenues for the years ended June 30, 2017, 2016, and 2015 were $204.9 million, $178.2 million and $181.5 million, respectively. We have targeted sales and marketing efforts to interventional cardiologists, vascular surgeons and interventional radiologists with experience using similar catheter-based procedures, such as angioplasty, stenting, and directional or laser atherectomy. Professional education is also a key element of our sales strategy.
We target our marketing efforts to practitioners through medical conferences, seminars, peer-reviewed journals and marketing materials. Our sales and marketing program focuses on:
• | clinical results showing safety and efficacy of our products; |
• | educating physicians on the prevalence and complications of calcium in PAD and CAD; and |
• | developing relationships with key opinion leaders. |
We sell the majority of our products through direct shipment to hospitals or clinics. We are party to a Purchasing Agreement with HealthTrust Purchasing Group, L.P. (“HPG”) which became effective on August 1, 2014 and expires on January 31, 2018. HPG acts as a group purchasing organization for the healthcare providers belonging to HPG as participants. Under the Purchasing Agreement, all of HPG’s participants located in the U.S. or its territories are eligible to purchase our products at prices set forth in the Purchasing Agreement.
Manufacturing
We use internally-manufactured and externally-sourced components to manufacture the OAS. Most of the externally-sourced components are available from multiple suppliers; however, certain key components, including the diamond-grit-coated crown and our ViperSlide Lubricant, are single sourced. We have strategies and arrangements in place for procuring our key components from alternative suppliers in the event that one or more of our single source suppliers were to discontinue supplying us with a key component. We assemble the shaft, crown and handle components on-site, and test, pack, seal and label the finished assembly before sending the packaged product to a contract sterilization facility. Upon return from the sterilizer, the product is held in inventory prior to shipping to our customers.
We are located in a 125,000-square-foot corporate headquarters in Minnesota, which we now lease. This custom-designed building has space for more than 500 employees and contains dedicated research and development, training and education, and manufacturing facilities. Depending on staffing, the facility has the annual capacity to produce in excess of 75,000 devices per shift. The finished goods storage has capacity for approximately 20,000 devices and more than 500 saline infusion pumps, as well as other accessory products.
Our Pearland, Texas facility is 46,000 square feet and includes a custom-built clean room and production space for future expansion of value-add processes, including machining and electronics assembly. The facility, when fully staffed and equipped, also has the annual capacity to produce approximately 75,000 devices per shift. This facility has finished goods storage capacity for greater than 15,000 devices and other accessory products and over 500 saline infusion pumps.
We believe that our facilities in Minnesota and Texas will provide adequate production, assembly, and warehousing capacity for the foreseeable future.
We are registered with the FDA as a medical device manufacturer. We have opted to maintain quality assurance and quality management certifications to enable us to market our products in the member states of the European Union (“EU”), the European Free Trade Association and countries that have entered into Mutual Recognition Agreements with the EU. We are ISO 13485:2003 certified, and our renewal is due by December 2018. Under these registrations, our plants are audited by the
9
FDA and our Notified Body for the EU CE Mark. Our Stealth 360 has received CE Mark. We are registered as a Foreign Medical Device Manufacturer in Japan and our registration certificate renewal is due by June 2021.
Third-Party Reimbursement and Pricing
Third-party payors, including private insurers, and government insurance programs, such as Medicare and Medicaid, pay for a significant portion of patient care provided in the United States. The single largest payor in the U.S. is the Medicare program, a federal governmental health insurance program administered by the Centers for Medicare and Medicaid Services (“CMS”). Medicare covers certain medical care expenses for eligible elderly and disabled individuals, including a large percentage of the population with PAD and CAD who could be treated with the OAS. In addition, private insurers often follow the coverage and reimbursement policies of Medicare. Consequently, Medicare’s coverage and reimbursement policies are important to our operations.
CMS has established Medicare reimbursement codes describing atherectomy products and procedures using atherectomy products. We believe that physicians and hospitals that treat PAD and CAD with the respective OAS will generally be eligible to receive reimbursement from Medicare, as well as private insurers, for the cost of the single-use catheter and the physician’s services.
Competition
The medical device industry is highly competitive, subject to rapid change and significantly affected by new product introductions and other activities of industry participants. Our OAS devices compete with a variety of other products or devices for the treatment of vascular disease, including stents, balloon angioplasty catheters and atherectomy catheters, as well as products used in vascular surgery. Large competitors in the stent and balloon angioplasty market segments include Abbott Laboratories, Boston Scientific, Cook Medical, Johnson & Johnson, BARD, and Medtronic. We also compete against manufacturers of atherectomy catheters including, among others, Medtronic, Spectranetics, Boston Scientific, Philips, and Avinger, as well as manufacturers that may enter the market due to the increasing demand for treatment of vascular disease. Other competitors include pharmaceutical companies that manufacture drugs for the treatment of PAD and CAD and companies that provide products used by surgeons in peripheral and coronary bypass procedures. We are not aware of any competing high-speed rotational atherectomy systems either currently on the market or in development that also generate an orbital motion with an eccentric solid abrasive crown to create lumens with diameters that are larger than the diameter of the abrasive crown itself.
Because of the size of the peripheral opportunities, competitors and potential competitors have historically dedicated significant resources to aggressively promote their products. We believe that our Peripheral OAS and Coronary OAS compete primarily on the basis of:
• | safety and efficacy, even in calcified plaque (or severely calcified plaque in the coronaries); |
• | low profile and alternative access site capabilities; |
• | predictable clinical performance; |
• | availability of clinical data; |
• | ease of use; |
• | economic benefit; |
• | key opinion leader support and customer base; and |
• | customer service and support. |
Patents and Intellectual Property
We rely on a combination of patent, copyright and other intellectual property laws, trade secrets, nondisclosure agreements and other measures to protect our proprietary rights. As of June 2017, we held 44 issued U.S. patents and have 39 U.S. patent applications pending, as well as 262 issued or granted foreign patents and 187 foreign patent applications, each of which corresponds to aspects of our U.S. patents and applications. Our issued U.S. patents expire between 2017 and 2035, and our patents covering the core technology begin to expire in 2023 while providing core technology coverage through 2035. We have many additional patents relating to our core technology currently pending in the USPTO, which will extend our key covered subject matter and coverage dates significantly. Our issued patents and patent applications relate primarily to the design and operation of interventional atherectomy devices, including the Peripheral OAS and Coronary OAS. These patents and applications include claims covering key aspects of orbital atherectomy devices, including the design, manufacture and therapeutic use of certain atherectomy abrasive heads, drive shafts, control systems, handles and couplings. As we continue to research and develop our atherectomy technology, we intend to file additional U.S. and foreign patent applications related to
10
the design, manufacture and therapeutic uses of atherectomy devices. In addition, we hold 19 registered U.S. trademarks, 12 registered marks in the Madrid Protocol with protection granted within at least one of Australia, Europe, China, Japan and Mexico, six registered marks in Europe, five registered marks in Canada, five registered marks in Mexico, and eight registered marks in Hong Kong. We have three trademark applications pending in the U.S., eight trademark applications pending in Canada and 12 trademark applications pending in India.
We also rely on trade secrets, technical know-how and continuing innovation to develop and maintain our competitive position. We seek to protect our proprietary information and other intellectual property by requiring our employees, consultants, contractors, outside scientific collaborators and other advisors to execute non-disclosure and assignment of invention agreements on commencement of their employment or engagement. Agreements with our employees also forbid them from bringing the proprietary rights of third parties to us. We also require confidentiality or material transfer agreements from third parties that receive our confidential data or materials.
Government Regulation of Medical Devices
Governmental authorities in the U.S. at the federal, state and local levels and in other countries extensively regulate, among other things, the development, testing, manufacture, labeling, promotion, advertising, distribution, marketing and export and import of medical devices such as the Peripheral OAS and Coronary OAS.
Failure to obtain approval to market our products under development and to meet the ongoing requirements of these regulatory authorities could prevent us from marketing and continuing to market our products.
United States
The Federal Food, Drug, and Cosmetic Act (“FDCA”) and the FDA’s implementing regulations govern medical device design and development, preclinical and clinical testing, premarket clearance or approval, registration and listing, manufacturing, labeling, storage, advertising and promotion, sales and distribution, export and import, and post market surveillance. Medical devices and their manufacturers are also subject to inspection by the FDA. The FDCA, supplemented by other federal and state laws, also provides civil and criminal penalties for violations of its provisions.
Unless an exemption applies, each medical device we wish to commercially distribute in the U.S. will require marketing authorization from the FDA prior to distribution. The two primary types of FDA marketing authorization are premarket notification (also called 510(k) clearance) and PMA.
510(k) Clearance. To obtain 510(k) clearance for a medical device, an applicant must submit a premarket notification to the FDA demonstrating that the device is “substantially equivalent” to a predicate device legally marketed in the United States. A device is substantially equivalent if, with respect to the predicate device, it has the same intended use and has either (i) the same technological characteristics or (ii) different technological characteristics and the information submitted demonstrates that the device is as safe and effective as a legally marketed device and does not raise different questions of safety or effectiveness. A showing of substantial equivalence sometimes, but not always, requires clinical data. Generally, the 510(k) clearance process can exceed 90 days and may extend to a year or more.
After a device has received 510(k) clearance for a specific intended use, any modification that could significantly affect its safety or effectiveness, such as a significant change in the design, materials, method of manufacture or intended use, will require a new 510(k) clearance or PMA (if the device as modified is not substantially equivalent to a legally marketed predicate device). The determination as to whether new authorization is needed is initially left to the manufacturer; however, the FDA may review this determination to evaluate the regulatory status of the modified product at any time and may require the manufacturer to cease marketing the modified device until 510(k) clearance or PMA is obtained. The manufacturer may also be subject to significant regulatory fines or penalties.
We received 510(k) clearance for use of the Diamondback 360 Peripheral as a therapy in patients with PAD in the U.S. in August 2007. We received additional 510(k) clearances for the control unit used with the Diamondback 360
Peripheral on October 25, 2007 and for the solid crown version of the Diamondback 360 Peripheral in November 2007.
We were granted 510(k) clearance of the Predator 360 in March 2009 and Stealth 360 in March 2011. We received 510(k)
clearance of the Diamondback 360 Peripheral 1.25 Micro in November 2013 and the Diamondback 360 60cm Peripheral
in February 2014. The Diamondback 360 Low Profile Peripheral received FDA clearance in April 2015. We received
clearance of the ViperWire Advance Flex Tip Guide Wire in June 2015. The Diamondback 360 1.50 Peripheral and
Diamondback 360 2.00 Peripheral were each granted 510(k) clearance in October 2015.
11
Premarket Approval. A PMA application requires the payment of significant user fees and must be supported by valid scientific evidence, which typically requires extensive data, including technical, preclinical, clinical and manufacturing data, to demonstrate to the FDA’s satisfaction the safety and efficacy of the device. A PMA application must also include a complete description of the device and its components, a detailed description of the methods, facilities and controls used to manufacture the device, and proposed labeling. After a PMA application is submitted and found to be sufficiently complete, the FDA begins an in-depth review of the submitted information. During this review period, the FDA may request additional information or clarification of information already provided. Also during the review period, an advisory panel of experts from outside the FDA may be convened to review and evaluate the application and provide recommendations to the FDA as to the approvability of the device. In addition, the FDA will conduct a pre-approval inspection of the manufacturing facilities to ensure compliance with the FDA’s Quality System Regulation (“QSR”), which requires manufacturers to follow design, testing, control, documentation and other quality assurance procedures.
FDA review of a PMA application is required by statute to take no longer than 180 days, although the process typically takes significantly longer, and may require several years to complete. The FDA can delay, limit, or deny approval of a PMA application for many reasons, including:
• | the systems may not be safe or effective to the FDA’s satisfaction; |
• | the data from preclinical studies and clinical trials may be insufficient to support approval; |
• | the manufacturing process or facilities used may not meet applicable requirements; and |
• | changes in FDA approval policies or adoption of new regulations may require additional data. |
If the FDA evaluations of both the PMA application and the manufacturing facilities are favorable, the FDA will either issue an approval letter or an approvable letter, which usually contains a number of conditions that must be met in order to secure final approval of the PMA. When and if those conditions have been fulfilled to the satisfaction of the FDA, the agency will issue a PMA letter authorizing commercial marketing of the device for certain indications. If the FDA’s evaluation of the PMA application or manufacturing facilities is not favorable, the FDA will deny PMA or issue a not approvable letter. The FDA may also determine that additional clinical trials are necessary, in which case the PMA may be delayed for several months or years while the trials are conducted and then the data submitted in an amendment to the PMA application. Even if a PMA application is approved, the FDA may approve the device with an indication that is narrower or more limited than originally sought. The agency can also impose restrictions on the sale, distribution or use of the device as a condition of approval, or impose post approval requirements such as continuing evaluation and periodic reporting on the safety, efficacy, and reliability of the device for its intended use.
New PMA applications or PMA supplements may be required for modifications to the manufacturing process, labeling, device specifications, materials or design of a device that is approved through the PMA process. PMA supplements often require submission of the same type of information as an initial PMA application, except that the supplement is limited to information needed to support any changes from the device covered by the original PMA application and may not require as extensive clinical data or the convening of an advisory panel.
Clinical Trials. Clinical trials are almost always required to support a PMA application and are sometimes required for a 510(k) clearance. These trials generally require submission of an application for an IDE to the FDA. The IDE application must be supported by appropriate data, such as animal and laboratory testing results, showing that it is safe to test the device in humans and that the testing protocol is scientifically sound. The IDE application must be approved in advance by the FDA for a specified number of patients, unless the product is deemed a non-significant risk device and eligible for more abbreviated IDE requirements. Generally, clinical trials for a significant risk device may begin once the IDE application is approved by the FDA and the study protocol and informed consent are approved by appropriate institutional review boards at the clinical trial sites.
FDA approval of an IDE allows clinical testing to go forward but does not bind the FDA to accept the results of the trial as sufficient to prove the product’s safety and efficacy, even if the trial meets its intended success criteria. With certain exceptions, changes made to an investigational plan after an IDE is approved must be submitted in an IDE supplement and approved by FDA (and by governing institutional review boards when appropriate) prior to implementation.
All clinical trials must be conducted in accordance with regulations and requirements collectively known as Good Clinical Practice. Good clinical practices include the FDA’s IDE regulations, which describe the conduct of clinical trials with medical devices, including the recordkeeping, reporting and monitoring responsibilities of sponsors and investigators, and labeling of investigational devices. They also prohibit promotion, test marketing or commercialization of an investigational device and any representation that such a device is safe or effective for the purposes being investigated. Good clinical practices also include the FDA’s regulations for institutional review board approval and for protection of human subjects (such as informed consent), as well as disclosure of financial interests by clinical investigators.
12
Required records and reports are subject to inspection by the FDA. The results of clinical testing may be unfavorable or, even if the intended safety and efficacy success criteria are achieved, may not be considered sufficient for the FDA to grant approval or clearance of a product. The commencement or completion of any clinical trials may be delayed or halted, or be inadequate to support approval of a PMA application or clearance of a premarket notification for numerous reasons.
Continuing Regulation. After a device is cleared or approved for use and placed in commercial distribution, numerous regulatory requirements continue to apply. These include:
• | establishment registration and device listing upon the commencement of manufacturing; |
• | the QSR, which requires manufacturers, including third-party manufacturers, to follow design, testing, control, documentation and other quality assurance procedures during medical device design and manufacturing processes; |
• | labeling regulations, which prohibit the promotion of products for unapproved or “off-label” uses and impose other restrictions on labeling and promotional activities; |
• | medical device reporting regulations, which require that manufacturers report to the FDA if a device may have caused or contributed to a death or serious injury or malfunctioned in a way that would likely cause or contribute to a death or serious injury if malfunctions were to recur; |
• | corrections and removal reporting regulations, which require that manufacturers report to the FDA field corrections; and |
• | product recalls or removals if undertaken to reduce a risk to health posed by the device or to remedy a violation of the FDCA caused by the device that may present a risk to health. |
In addition, the FDA may require a company to conduct post market surveillance studies or order it to establish and maintain a system for tracking its products through the chain of distribution to the patient level.
Failure to comply with applicable regulatory requirements, including those applicable to the conduct of clinical trials, can result in enforcement action by the FDA, which may lead to any of the following sanctions:
• | warning letters or untitled letters; |
• | fines, injunctions and civil penalties; |
• | product recall or seizure; |
• | unanticipated expenditures; |
• | delays in clearing or approving or refusal to clear or approve products; |
• | withdrawal or suspension of FDA approval; |
• | orders for physician notification or device repair, replacement or refund; |
• | operating restrictions, partial suspension or total shutdown of production or clinical trials; or |
• | criminal prosecution. |
We and our contract manufacturers, specification developers and suppliers are also required to manufacture our products in compliance with Current Good Manufacturing Practice requirements set forth in the QSR.
The QSR requires a quality system for the design, manufacture, packaging, labeling, storage, installation and servicing of marketed devices, and includes extensive requirements with respect to quality management and organization, device design, buildings, equipment, purchase and handling of components, production and process controls, packaging and labeling controls, device evaluation, distribution, installation, complaint handling, servicing and record keeping. The FDA enforces the QSR through periodic announced and unannounced inspections that may include the manufacturing facilities of subcontractors. If the FDA believes that we or any of our contract manufacturers or regulated suppliers is not in compliance with these requirements, it can shut down our manufacturing operations, require recall of our products, refuse to clear or approve new marketing applications, institute legal proceedings to detain or seize products, enjoin future violations or assess civil and criminal penalties against us or our officers or other employees. Any such action by the FDA would have a material adverse effect on our business.
In April 2017, we initiated a voluntary recall of one type of our saline infusion pumps. We plan to recall and
replace approximately 900 units that were in customer inventory at the time the recall commenced. As of June 30,
2017, we had approximately 338 pumps remaining to be replaced.
13
Fraud and Abuse
Our operations are directly, or indirectly through our customers, subject to various state and federal fraud and abuse laws, including, without limitation, the FDCA, the federal Anti-Kickback Statute and the False Claims Act. These laws may impact, among other things, our sales, marketing, education and clinical programs. In addition, these laws may require us to screen individuals and other companies, suppliers and vendors in order to ensure that they are not “debarred” by the federal government and, therefore, prohibited from doing business in the healthcare industry.
The federal Anti-Kickback Statute prohibits persons from knowingly and willfully soliciting, offering, receiving or providing remuneration, directly or indirectly, in exchange for or to induce either the referral of an individual, or the furnishing or arranging for a good or service, for which payment may be made under a federal healthcare program, such as the Medicare and Medicaid programs. Several courts have interpreted the statute’s intent requirement to mean that if any one purpose of an arrangement involving remuneration is to induce referrals of federal healthcare covered business, the statute has been violated. The Anti-Kickback Statute is broad and prohibits many arrangements and practices that are lawful in businesses outside of the healthcare industry. Many states have also adopted laws similar to the federal Anti-Kickback Statute, some of which apply to the referral of patients for healthcare items or services reimbursed by any source, not only the Medicare and Medicaid programs.
The federal False Claims Act prohibits persons from knowingly filing or causing to be filed a false claim to, or the knowing use of false statements to obtain payment from, the federal government. Various states have also enacted laws modeled after the federal False Claims Act.
In addition to the laws described above, the Health Insurance Portability and Accountability Act of 1996 created two new federal crimes: healthcare fraud and false statements relating to healthcare matters. The healthcare fraud statute prohibits knowingly and willfully executing a scheme to defraud any healthcare benefit program, including private payors. The false statements statute prohibits knowingly and willfully falsifying, concealing or covering up a material fact or making any materially false, fictitious or fraudulent statement in connection with the delivery of or payment for healthcare benefits, items or services.
On June 28, 2016, we entered into a Settlement Agreement with the U.S. government, acting through the U.S. Attorney’s Office for the Western District of North Carolina (the “DOJ”) and on behalf of the Office of Inspector General of the Department of Health and Human Services (the “OIG”) and Travis Thams to resolve the DOJ investigation of whether we violated the False Claims Act. In connection with the resolution of this matter, we entered into a five-year corporate integrity agreement (the “Corporate Integrity Agreement”) with the OIG. The Corporate Integrity Agreement requires that we maintain our existing compliance programs and imposes certain expanded compliance-related requirements during the term of the Corporate Integrity Agreement, including establishment of specific procedures and requirements regarding consulting activities, co-marketing activities and other interactions with healthcare professionals and healthcare institutions and the sale and marketing of our products; ongoing monitoring, reporting, certification and training obligations; and the engagement of an independent review organization to perform certain auditing and reviews and prepare certain reports regarding our compliance with federal health care programs.
The federal Physician Payments Sunshine Act, or the Sunshine Act, and certain state laws require persons to collect and report certain data on payments and other transfers of value to physicians and teaching hospitals. It is widely anticipated that public reporting under the Sunshine Act and implementing Open Payment regulations will result in increased scrutiny of the financial relationships between industry, physicians and teaching hospitals.
Voluntary industry codes, federal guidance documents and a variety of state laws address the tracking and reporting of marketing practices relative to gifts given and other expenditures made to doctors and other healthcare professionals. In addition to impacting our marketing and educational programs, our internal business processes are and will continue to be affected by the numerous legal requirements and regulatory guidance at the state, federal and industry levels.
International Regulation
International sales of medical devices are subject to foreign government regulations, which may vary substantially from country to country. The time required to obtain approval in a foreign country may be longer or shorter than that required for FDA approval and the requirements may differ. For example, the primary regulatory environment in Europe with respect to medical devices is that of the EU, which includes most of the major countries in Europe. Other countries, such as Switzerland, have voluntarily adopted laws and regulations that mirror those of the EU with respect to medical devices. The EU has adopted numerous directives and standards regulating the design, manufacture, clinical trials, labeling and adverse event reporting for
14
medical devices. Devices that comply with the requirements of a relevant directive will be entitled to bear the CE conformity marking, indicating that the device conforms to the essential requirements of the applicable directives and, accordingly, can be commercially distributed throughout the EU, although actual implementation of these directives may vary on a country-by-country basis. The method of assessing conformity varies depending on the class of the product, but normally involves a combination of submission of a design dossier, self-assessment by the manufacturer, a third-party assessment, and review of the design dossier by a “Notified Body.” This third-party assessment generally consists of an audit of the manufacturer’s quality system and manufacturing site, as well as review of the technical documentation used to support application of the CE Mark to one’s product and possibly specific testing of the manufacturer’s product. An assessment by a Notified Body of one country within the EU is required in order for a manufacturer to commercially distribute the product throughout the EU.
In July 2016, we submitted an application to Japan’s Pharmaceuticals and Medical Devices Agency (“PMDA”) for approval of our Coronary OAS Micro Crown and received approval in March 2017. Pending reimbursement approval, Japan will become the first international market for any CSI product. As part of our anticipated Japan commercialization process we will be subject to the requirements of the Japanese Act on Securing Quality, Efficacy and Safety of Pharmaceuticals, Medical Devices, Regenerative and Cellular Therapy Products, Gene Therapy Products, and Cosmetics (the “PMD Act”). Our quality management system and products will be subject to review and examination by PMDA and subject to approval and enforcement by Japan’s MHLW. The critical suppliers named in our application will also be subject to this review and examination for the activities they perform for us. Non-compliance with the PMD Act could result in revocation or suspension of our license, revocation of approvals, and criminal sanctions such as fines and/or imprisonment.
In addition, any international expansion, operations and sales that we undertake will require us to comply with the U.S. Foreign Corrupt Practices Act and similar anti-bribery laws in other jurisdictions and with U.S. and foreign export control, trade embargo and custom laws.
Environmental Regulation
Our operations are subject to regulatory requirements relating to the environment, waste management and health and safety matters, including measures relating to the release, use, storage, treatment, transportation, discharge, disposal and remediation of hazardous substances. We are currently classified and licensed as a Very Small Quantity Hazardous Waste Generator within Ramsey County, Minnesota. There are no regulated wastes requiring licensing in our Texas facility.
Employees
As of June 30, 2017, we had 579 full-time employees. None of our employees are represented by a labor union or are parties to a collective bargaining agreement, and we believe that our employee relations are good.
Executive Officers of the Registrant
The names, ages and positions of our current executive officers are as follows:
Name | Age | Position | |
Scott R. Ward | 57 | Chairman, President and Chief Executive Officer | |
Laurence L. Betterley | 63 | Chief Financial Officer | |
Kevin J. Kenny | 52 | Chief Operating Officer | |
Laura Gillund | 56 | Chief Talent Officer | |
Alexander Rosenstein | 45 | General Counsel and Corporate Secretary | |
Sandra Sedo | 53 | Chief Compliance Officer | |
Scott R. Ward, Chairman President and Chief Executive Officer. Mr. Ward has been a member of our Board of Directors since 2013 and has served as Chairman of our Board of Directors since November 2014. Mr. Ward served as our Interim President and Chief Executive Officer commencing in November 2015, and in August 2016, Mr. Ward was appointed as our regular full-time President and Chief Executive Officer. Since 2013, Mr. Ward has been one of the Managing Directors at SightLine Partners. Following his appointment as our President and Chief Executive Officer, Mr. Ward will continue to be a Managing Director of Sightline Opportunity Management Fund II, LLC and may provide limited advisory and consulting services to Sightline Partners in this capacity. From 1981 to 2010, Mr. Ward was employed by Medtronic, Inc. and held a number of senior leadership positions. Mr. Ward was Senior Vice President and President of Medtronic’s CardioVascular business from May 2007 to November 2010. Prior to that he was Senior Vice President and President of Medtronic’s Vascular business from May
15
2004 to May 2007, Senior Vice President and President of Medtronic’s Neurological and Diabetes Business, from February 2002 to May 2004, and was President of Medtronic’s Neurological business from January 2000 to January 2002. He was Vice President and General Manager of Medtronic’s Drug Delivery Business from 1995 to 2000. Prior to that, Mr. Ward led Medtronic’s Neurological Ventures in the successful development of new therapies. Mr. Ward serves on the boards of several private companies. Until April 2016, Mr. Ward was the Chairman of the Board of Creganna Medical. Mr. Ward served as a member of the Board of Surmodics, Inc. from September 2010 to March 2015.
Laurence L. Betterley, Chief Financial Officer. Mr. Betterley joined us in April 2008 as our Chief Financial Officer. Previously, Mr. Betterley was Chief Financial Officer at Cima NanoTech, Inc. from May 2007 to April 2008, Senior Vice President and Chief Financial Officer of PLATO Learning, Inc. from 2004 to 2007, Senior Vice President and Chief Financial Officer of Diametrics Medical, Inc. from 1996 to 2003, and Chief Financial Officer of Cray Research Inc. from 1994 to 1996.
Kevin J. Kenny, Chief Operating Officer. Mr. Kenny joined us in May 2011 as Executive Vice President of Sales and Marketing and was promoted to Chief Operating Officer in February 2015. From 2002 to 2011, Mr. Kenny served in various positions with Medtronic, Inc.’s U.S. Spine and Biologics division, including Vice President of Sales. Previously, Mr. Kenny served as Vice President of U.S. Sales for Bausch and Lomb and held various sales and marketing leadership roles with B. Braun/McGaw and Smithkline Beecham.
Laura Gillund, Chief Talent Officer. Ms. Gillund joined us in September 2013 as Vice President of Human Resources and Professional Development and was promoted to Chief Talent Officer in April 2016. Previously, Ms. Gillund was Vice President of Human Resources for C.H. Robinson Worldwide, Inc. from August 2002 to May 2012. Ms. Gillund serves as a member of the Board of Allina Health System and as Chair of the College Possible Board.
Alexander Rosenstein, General Counsel and Corporate Secretary. Mr. Rosenstein joined us in September 2014 as Corporate Legal and Compliance Counsel, became Corporate Secretary in November 2014, and was promoted to General Counsel in March 2015. From October 2005 to September 2014, Mr. Rosenstein was an attorney at Fredrikson & Byron, P.A., which provides legal services to us from time to time, and from September 1998 to September 2005, he was an attorney
practicing in New York City.
Sandra Sedo, Chief Compliance Officer. Ms. Sedo joined us in June 2016 as Corporate Compliance Officer, and was promoted to Chief Compliance Officer in July 2017. Prior to joining us, Ms. Sedo consulted for medical device companies in the legal and compliance areas. From 2005 to 2015, Ms. Sedo was employed by Medtronic, Inc. in various legal and compliance roles, and prior to that was a partner at Dorsey & Whitney LLP, which provides legal services to us from time to time.
16
Item 1A. Risk Factors.
Risks Relating to Our Business and Operations
We have a history of net losses and a short commercialization experience, and we are likely to continue to incur losses.
We are not profitable and have incurred net losses in each fiscal year since our formation in 1989. In particular, we had net losses of $1.8 million, $56.0 million, and $32.8 million for the years ended June 30, 2017, 2016, and 2015, respectively. As of June 30, 2017, we had an accumulated deficit of approximately $329.3 million. We commenced commercial sales of the Peripheral OAS in September 2007 and the Coronary OAS in October 2013, and our short commercialization experience makes it difficult for us to predict future performance. We expect to continue to incur significant expenses for sales and marketing, research and development, and manufacturing as we continue to commercialize the Peripheral OAS and the Coronary OAS and develop and commercialize future versions of the Peripheral OAS, the Coronary OAS, and any future products. Additionally, we expect that our general and administrative expenses may increase to support business growth. We instituted a number of cost reduction initiatives in the year ended June 30, 2016, which, combined with revenue growth, significantly reduced our net loss in fiscal 2017 and may reduce our net losses in future periods. However, if we are unable to balance revenue growth and cost management, our operating losses are likely to continue.
We may be unable to sustain our historical revenue growth.
Other than a 4.9% decline in revenue from sales of our Peripheral OAS during fiscal 2016, our revenue from sales of our OAS devices has grown in each of the fiscal years since we began commercialization in September 2007. Our ability to increase our revenues in future periods will depend on our ability to increase sales of the OAS devices and improved products we introduce, which will, in turn, depend in part on our success in growing our customer base and reorders from those customers. We may not be able to generate, sustain or increase revenues on a quarterly or annual basis. If we cannot achieve or sustain revenue growth for an extended period, our financial results will be adversely affected and our stock price may decline.
Economic conditions may adversely affect our business.
Adverse worldwide economic conditions may negatively impact our business. A significant change in the liquidity or financial condition of our customers could cause unfavorable trends in their purchases and also in our receivable collections and additional allowances may be required, which could adversely affect our operating results. Adverse worldwide economic conditions may also adversely impact our suppliers’ ability to provide us with materials and components, which could adversely affect our business and operating results.
The Peripheral OAS, the Coronary OAS and future products may never achieve broad market acceptance.
The Peripheral OAS, the Coronary OAS, and future products we may develop or market may never gain broad market acceptance among physicians, patients and the medical community. The degree of market acceptance of any of our products will depend on a number of factors, including:
• | the actual and perceived effectiveness and reliability of our products; |
• | the prevalence and severity of any adverse patient events involving our products; |
• | the results of any clinical trials relating to use of our products; |
• | the availability, relative cost and perceived advantages and disadvantages of alternative technologies or treatment methods for conditions treated by our products; |
• | the degree to which treatments using our products are approved for reimbursement by public and private insurers; |
• | the degree to which physicians adopt the Peripheral OAS and Coronary OAS; |
• | the extent to which we are successful in educating physicians about PAD and CAD in general and the existence and benefits of the Peripheral OAS and the Coronary OAS in particular; |
• | the strength of our marketing and distribution infrastructure; |
• | the level of education and awareness among physicians and hospitals concerning our products; and |
• | our reputation among physicians and hospitals. |
Failure of the Peripheral OAS and Coronary OAS to significantly penetrate current or new markets would negatively impact our business, financial condition and results of operations.
17
Our customers may not be able to achieve adequate reimbursement for using the Peripheral OAS and the Coronary OAS, which could affect the acceptance of our products and cause our business to suffer.
The availability of insurance coverage and reimbursement for newly approved medical devices and procedures is uncertain. The commercial success of our products is substantially dependent on whether third-party insurance coverage and reimbursement for the use of such products and related services are available. We expect our products to continue to be purchased by hospitals and other providers who will then seek reimbursement from various public and private third-party payors, such as Medicare, Medicaid and private insurers, for the services provided to patients. While third-party payors are currently providing reimbursement for our products, we can give no assurance that these third-party payors will continue to provide adequate reimbursement for use of the Peripheral OAS and the Coronary OAS to permit hospitals and doctors to consider the products cost-effective for patients requiring treatment, or that current reimbursement levels for our products will continue. In addition, the overall amount of reimbursement available for PAD and CAD treatment could decrease in the future. Failure by hospitals and other users of our products to obtain sufficient reimbursement could cause our business to suffer.
Medicare, Medicaid, health maintenance organizations and other third-party payors are increasingly attempting to contain healthcare costs by limiting both coverage and the level of reimbursement, and, as a result, they may not cover or provide adequate payment for use of our products. In order to position our products for acceptance by third-party payors, we may have to agree to lower prices than we might otherwise charge.
Governmental and private sector payors have instituted initiatives to limit the growth of healthcare costs using, for example, price regulation or controls and competitive pricing programs. Some third-party payors also require demonstrated superiority, on the basis of randomized clinical trials, or pre-approval of coverage, for new or innovative devices or procedures before they will reimburse healthcare providers who use such devices or procedures. It is uncertain whether our current products or any future products we may develop will be viewed as sufficiently cost-effective to warrant adequate coverage and reimbursement levels.
In addition, in June 2016, we entered into a Settlement Agreement with the U.S. government, acting through the U.S. Attorney for the Western District of North Carolina (the “DOJ”) and on behalf of the Office of Inspector General of the Department of Health and Human Services (the “OIG”), and Travis Thams, and a five-year Corporate Integrity Agreement with the OIG. In the event of a breach of the Settlement Agreement or the Corporate Integrity Agreement, we could be excluded from participation in federal health care programs. If third-party coverage and reimbursement for our products is limited or not available, the acceptance of our products and, consequently, our business will be substantially harmed.
Healthcare reform legislation could adversely affect our operating results and financial condition.
There have been and continue to be proposals by the federal government, state governments, regulators and third-party payors to control healthcare costs and, more generally, to reform the U.S. healthcare system, some of which have been enacted into law, such as the Patient Protection and Affordable Care Act, or the Patient Act. The Patient Act and any additional healthcare proposals and laws that may be enacted in the future could also limit the prices we are able to charge for our products or the amounts of reimbursement available for our products and could limit the acceptance and availability of our products. The Patient Act and future healthcare legislation could adversely affect our revenue and financial condition. The U.S. Congress has been considering legislation to repeal, modify or replace the Patient Act. We cannot predict the outcome of these efforts and, as a result, we cannot predict the effect that any such repeal, modification or replacement will have on our business and results of operations.
Our financial performance may be adversely affected by medical device tax provisions in the health care reform legislation.
The imposition of the 2.3% medical device excise tax enacted as part of the Patient Act has adversely affected our financial results and has required, and will continue to require, us to identify ways to reduce spending in other areas or raise additional capital to offset the increased expense. Although the excise tax has been suspended by Congress until the end of 2017, its status is unclear for 2018 and subsequent years. We have not been able to pass along the cost of the tax to our customers or offset the cost of the tax through higher sales volumes resulting from the expansion of health insurance coverage and do not expect to be able to do so in the future. Ongoing implementation of this legislation could have a material adverse effect on our results of operations and cash flows.
18
We have limited data and experience regarding the safety and efficacy of the Peripheral OAS and Coronary OAS. Any long-term data that is generated may not be positive or consistent with our limited short-term data, which would affect market acceptance of these products.
Because our technology is relatively new in the treatment of PAD and CAD, we have performed clinical trials only with limited patient populations. The long-term effects of using the Peripheral OAS and the Coronary OAS in a large number of patients have not been studied and the results of short-term clinical use of the Peripheral OAS or the Coronary OAS do not necessarily predict long-term clinical benefits or reveal long-term adverse effects. We are conducting and developing several clinical trials, and there are substantial risks and uncertainties involved in these trials. We must devote substantial resources to our clinical trials, clinical trials often take several years to develop and conduct, there are difficulties involved in locating sites and patients to participate in our clinical trials, and the results of every trial are uncertain until the trial is completed. These uncertainties could adversely impact our financial results, our reputation and the reputation of our products.
Clinical trials conducted with the Peripheral OAS and the Coronary OAS have involved procedures performed by physicians who are very technically proficient. Consequently, both short and long-term results reported in these studies may be significantly more favorable than typical results achieved by physicians, which could negatively impact market acceptance of the Peripheral OAS and the Coronary OAS and materially harm our business.
We face significant competition, must innovate to stay competitive, and may be unable to sell the Peripheral OAS or the Coronary OAS at profitable levels.
The market for medical devices is highly competitive, dynamic and marked by rapid and substantial technological development and product innovation. Our ability to compete depends on our ability to innovate successfully, and, while certain barriers exist to entry into our market, we cannot assure that new entrants or existing competitors will not be able to develop products that compete directly with our products. We compete against very large and well-known stent and balloon angioplasty device manufacturers, atherectomy catheter manufacturers, pharmaceutical companies, and companies that provide products used by surgeons in peripheral and coronary bypass procedures. We may have difficulty competing effectively with these competitors because of their well-established positions in the marketplace, significant financial and human capital resources, established reputations and worldwide distribution channels.
Our competitors may:
• | develop and patent processes or products earlier than we will; |
• | obtain regulatory clearances or approvals for competing medical device products more rapidly than we will; |
• | market their products more effectively than we will; |
• | sell their products at lower prices than we do; or |
• | develop more effective or less expensive products or technologies that render our technology or products obsolete or non-competitive. |
We have encountered and expect to continue to encounter potential customers who, due to existing relationships with our competitors, are committed to or prefer the products offered by these competitors. In addition, increased consolidation in the healthcare industry has resulted in companies with greater market power, which increases competition for goods and services.
We experience significant competition on the pricing of our products and expect to continue to experience pressure from our customers to lower our prices. Our customers may require lower pricing in connection with contract renewals or otherwise for us to continue to sell our products to them. Our Purchasing Agreement with HealthTrust Purchasing Group, L.P. expires on January 31, 2018. If we are unable to renew this agreement at favorable pricing levels or at all, our financial results will be materially adversely affected.
If we are unable to compete successfully, our revenue will suffer. Increased competition might lead to price reductions and other concessions that might adversely affect our operating results. Competitive pressures may decrease the demand for our products and could adversely affect our financial results.
19
We have limited commercial manufacturing experience and could experience difficulty in producing the Peripheral OAS and the Coronary OAS or may need to depend on third parties to manufacture the products.
We have limited experience in commercially manufacturing the Peripheral OAS, even less experience in commercially manufacturing the Coronary OAS and no experience manufacturing these products in the volume that we anticipate will be required if we achieve planned levels of commercial sales. As a result, we may not be able to develop and implement efficient, low-cost manufacturing capabilities and processes that will enable us to manufacture the Peripheral OAS and the Coronary OAS or future products in significant volumes, while meeting the legal, regulatory, quality, price, durability, engineering, design and production standards required to market our products successfully.
The forecasts of demand we use to determine order quantities and lead times for components purchased from outside suppliers may be incorrect. Our failure to obtain required components or subassemblies when needed and at a reasonable cost would adversely affect our business.
In addition, we may in the future need to depend upon third parties to manufacture the Peripheral OAS and Coronary OAS and future products. Any difficulties in locating and hiring third-party manufacturers, or in the ability of third-party manufacturers to supply quantities of our products at the times and in the quantities we need, could have a material adverse effect on our business.
We depend upon third-party suppliers, including single source suppliers to us and our customers, making us vulnerable to supply problems and price fluctuations.
We rely on third-party suppliers to provide us with certain components of our products and to provide key components or supplies to our customers for use with our products. We rely on single source suppliers for certain components of the Peripheral OAS and the Coronary OAS, including the diamond-grit-coated crown and our ViperSlide Lubricant. In some cases, we do not have long-term supply agreements with, or guaranteed commitments from, our suppliers, including single source suppliers. We depend on our suppliers to provide us and our customers with materials in a timely manner that meet our and their quality, quantity and cost requirements. These suppliers may encounter problems during manufacturing for a variety of reasons, any of which could delay or impede their ability to meet our demand and our customers’ demands. These suppliers may cease producing the components we purchase from them or otherwise decide to cease doing business with us.
Any supply interruption from our suppliers or failure to obtain additional suppliers for any of the components used in our products would limit our ability to manufacture our products and could have a material adverse effect on our business, financial condition and results of operations.
We are dependent on our senior management team and highly skilled personnel, and our business could be harmed if we are unable to attract and retain personnel necessary for our success.
We are highly dependent on our senior management and other key personnel. Our success will depend on our ability to retain senior management and to attract and retain qualified personnel in the future, including sales and marketing professionals, scientists, clinical specialists, engineers and other highly skilled personnel and to integrate current and additional personnel in all departments. The loss of members of our senior management, sales and marketing professionals, scientists, clinical and regulatory specialists and engineers could prevent us from achieving our objectives of continuing to grow our company. We do not carry key person life insurance on any of our employees.
We have increased the size of our organization and may need to do so in the future, and we may experience difficulties managing growth. If we are unable to manage the anticipated growth of our business, our future revenue and operating results may be adversely affected.
We have significantly expanded the size of our organization over the past three years, particularly in the number of sales and marketing personnel, and may need to do so in the future. The growth we may experience in the future may provide challenges to our organization, requiring us to also rapidly expand other aspects of our business, including our manufacturing operations. Rapid expansion in personnel may result in less experienced people producing and selling our products, which could result in unanticipated costs and disruptions to our operations. If we cannot scale and manage our business appropriately, our anticipated growth may be impaired and our financial results will suffer.
20
We intend to sell our products internationally in the future, but we may experience difficulties in obtaining approval to do so or in successfully marketing our products internationally even if approved.
Currently, all of our revenues are in the United States; however, we intend to sell internationally in the future. There can be no guarantee that we will receive approval to sell our products internationally, nor can there be any guarantee that any sales would result even if such approval is received. In addition, we will incur substantial expenses in connection with international expansion. Our inability to successfully enter international markets and manage business on a global scale could negatively affect our financial results.
We may require additional financing, and our failure to obtain additional financing when needed could force us to delay, reduce or eliminate our product development programs or commercialization efforts.
We may be dependent on additional financing to execute our business plan. Additional funds may not be available when we need them on terms that are acceptable to us, or at all. In the event we need or desire additional financing, we may be unable to obtain it by borrowing money in the credit markets or raising money in the capital markets. If adequate funds are not available on a timely basis, we may terminate or delay the development of one or more of our products, or delay establishment of sales and marketing capabilities or other activities necessary to commercialize our products.
We face a risk of non-compliance with the financial covenants in our loan and security agreement with Silicon Valley Bank.
We are party to a loan and security agreement with Silicon Valley Bank. This agreement requires us to maintain, among other things, either (i) minimum unrestricted cash at Silicon Valley Bank and unused availability on our line of credit of at least $10.0 million or (ii) minimum trailing three-month Adjusted EBITDA of $1.0 million and contains customary events of default, including, among others, the failure to comply with certain covenants or other agreements. Upon the occurrence and during the continuation of an event of default, amounts due under the agreements may be accelerated by Silicon Valley Bank. If we are unable to meet the financial or other covenants under the current loan and security agreement or negotiate future waivers or amendments of such covenants, events of default could occur under the agreement. Upon the occurrence and during the continuance of an event of default under the agreement, Silicon Valley Bank has available a range of remedies customary in these circumstances, including declaring all outstanding debt, together with accrued and unpaid interest thereon, to be due and payable, foreclosing on the assets securing the agreement and/or ceasing to provide additional loans under our line of credit, which could have a material adverse effect on us.
The restrictive covenants under this agreement could limit our ability to obtain future financing, withstand a future downturn in our business or the economy in general or otherwise conduct necessary corporate activities. The financial and restrictive covenants contained in this agreement could also adversely affect our ability to respond to changing economic and business conditions and place us at a competitive disadvantage relative to other companies that may be subject to fewer restrictions. Transactions that we may view as important opportunities, such as acquisitions, may be subject to the consent of Silicon Valley Bank, which consent may be withheld or granted subject to conditions specified at the time that may affect the attractiveness or viability of the transaction.
We lease our corporate headquarters, which subjects us to ongoing payment obligations and compliance with certain covenants.
On March 30, 2017, we completed the sale of our corporate headquarters. In connection with such sale, we entered into a lease agreement for our corporate headquarters, which has an initial term of fifteen years, with four consecutive renewal options of five years each. Under this lease, we are obligated to pay a base annual rent in the first year of $1,637,500 with annual escalations of 3%. If we are unable to make such rent payments or comply with the other covenants contained in the lease, the landlord could take certain actions against us, up to and including termination of the lease, which could have an adverse impact on our business, results of operations or financial conditions.
Our stock price is volatile and subject to significant fluctuations.
The market price of our common stock could be subject to significant fluctuations. Market prices for securities of early-stage pharmaceutical, medical device, biotechnology and other life sciences companies have historically been particularly volatile. Our common stock traded as low as $18.00 and as high as $33.11 per share during the 12-month period ended June 30, 2017. Factors that may cause the market price of our common stock to fluctuate include, but are not limited to:
• | announcements of technological or medical innovations for the treatment of vascular disease; |
• | quarterly variations in our or our competitors’ results of operations; |
21
• | failure to meet estimates or recommendations by securities analysts who cover our stock; |
• | failure to meet our own financial estimates; |
• | accusations that we have violated a law or regulation; |
• | recalls of our products; |
• | significant litigation; |
• | sales of large blocks of our common stock, including sales by our executive officers, directors and significant stockholders; |
• | changes in accounting principles; |
• | actual or anticipated changes in healthcare policy and reimbursement levels; |
• | developments relating to our competitors and markets; and |
• | general market conditions and other factors, including factors unrelated to our operating performance or the operating performance of our competitors. |
Moreover, the stock markets in general have experienced substantial volatility that has often been unrelated to the operating performance of individual companies. These broad market fluctuations may also adversely affect the trading price of our common stock.
We currently are involved in litigation, and may face future claims, that could adversely affect our business and financial results, divert management’s attention from our business, and subject us to significant liabilities.
We are party to Shoemaker v. Cardiovascular Systems, Inc. et al., a stockholder securities lawsuit. On March 29, 2017, the court granted our motion to dismiss the complaint in this action and dismissed the plaintiffs’ amended complaint without prejudice. The court granted the plaintiffs’ request for leave to amend their complaint, and on June 27, 2017, the plaintiffs filed an amended complaint. The amended complaint makes similar allegations as the original complaint, namely, that we made materially false and misleading statements and failed to disclose material adverse facts about our business, operational and financial performance, in violation of federal securities laws, relating to alleged kickbacks to health care providers. The plaintiffs seek unspecified monetary damages on behalf of the alleged class, interest, and attorney’s fees and costs of litigation. We filed a motion to dismiss the amended complaint on August 11, 2017.
Although we believe that this lawsuit is without merit and intend to defend ourselves vigorously, we are not able to predict the ultimate outcome of this lawsuit. It is possible that it could cause us to incur substantial costs and that it could be resolved adversely to us, result in substantial damages, result in or be connected to additional claims, and divert management’s attention and resources, any of which could harm our business. While we maintain director and officer liability insurance, the amount of insurance coverage may not be sufficient to cover these claims and other claims to which we may become subject, and the continued availability of this insurance cannot be assured. Protracted litigation, including any adverse outcomes, may have an adverse impact on our business, results of operations or financial condition and could subject us to adverse publicity and require us to incur significant legal fees.
The outcome of recent employment litigation recently decided against us could adversely affect our business and financial results, divert management’s attention from our business, and subject us to significant liabilities.
We are party to Steven Babyak v. Cardiovascular Systems, Inc., a lawsuit originally filed in the Superior Court of California, County of Los Angeles, on November 16, 2015. The plaintiff, a former Regional Sales Manager, made claims under California law relating to whistleblower retaliation; defamation; discrimination on the basis of association with protected group; harassment on the basis of sex in violation of FEHA; retaliation for exercising rights under FEHA; failure to prevent discrimination, harassment and retaliation in violation of FEHA; wrongful termination in violation of public policy; and violation of business and professions code. Following an April 2017 trial, a jury awarded the plaintiff $2.7 million in compensatory damages with respect to his claims for whistleblower retaliation and wrongful termination in violation of public policy. The jury also awarded the plaintiff $22.4 million in punitive damages with respect to the same claims. We filed post-trial motions for judgment notwithstanding the verdict and a new trial, on the grounds that this case was incorrectly decided as to liability, the compensatory and punitive damages were not appropriate and were excessive, and we were prevented from a fair trial by the improper exclusion of critical evidence. On June 29, 2017, the Court partially granted our motions, reducing the punitive damages award from $22.4 million to $2.7 million but denied our other motions. We filed a Notice of Appeal on July 24, 2017.
Although we believe that this case was incorrectly decided and intend to vigorously challenge the verdict, we are not able to predict the ultimate outcome of this case. This case has generated negative publicity against us, which could cause us reputational harm. Following our challenges and appeals, it is possible that this case could ultimately be resolved adversely to us, result in substantial damages, result in or be connected to additional claims, result in additional publicity, and divert
22
management’s attention and resources, any of which could harm our business. Protracted litigation, both with respect to the challenge and appeal of this case and any new claims that may arise relating to this case, including any adverse outcomes, may have an adverse impact on our business, results of operations or financial condition and could subject us to additional adverse publicity and reputational harm and require us to incur significant legal fees. While we have insurance coverage relating to this case, there can be no assurance that the amounts available under such insurance will be sufficient to cover any payments we may ultimately be required to make.
Our ability to use our net operating loss carryforwards and certain other tax attributes may be limited.
Under Sections 382 and 383 of the Internal Revenue Code of 1986, as amended, if a corporation undergoes an “ownership change,” the corporation’s ability to use its pre-change net operating loss carryforwards and other pre-change tax attributes, such as research tax credits, to offset its post-change income or taxes may be limited. In general, an “ownership change” will occur if there is a cumulative change in our ownership by “5-percent shareholders” that exceeds 50 percentage points over a rolling three-year period. Similar rules may apply under state tax laws. We may have experienced an ownership change in the past and we may also experience ownership changes in the future as a result of future transactions in our stock, some of which may be outside our control. As a result, if we earn net taxable income, our ability to use our pre-change net operating loss carryforwards or other pre-change tax attributes to offset U.S. federal and state taxable income or taxes may be subject to limitations.
An interruption in or breach of security of our information or manufacturing systems could cause a loss of business or damage to our reputation.
We rely on information and communication systems in our manufacturing and in the conduct our business. If there is any failure or interruption of these systems, such an incident could cause failures or disruptions in our customer relationship systems or product manufacturing. In addition, we could be subject to a cyber incident, such as an intentional attack or an unintentional event that involves a third party gaining unauthorized access to our systems, which could disrupt our operations, corrupt our data, or result in release of our confidential information. The occurrence of any failures, interruptions or cyber incidents could cause a loss of business or damage to our reputation and have a material effect on our business, financial condition, results of operations and cash flows.
Risks Related to Government Regulation
Our ability to market the Peripheral OAS in the United States is limited to use as a therapy in patients with PAD and our ability to market the Coronary OAS in the United States is limited to use as a therapy in patients with severely calcified CAD, and if we want to expand our marketing claims, we will need to file for additional FDA clearances or approvals and conduct further clinical trials, which would be expensive and time consuming and may not be successful.
We received FDA 510(k) clearances in the U.S. for use of the Peripheral OAS as a therapy in patients with PAD, and we received PMA to use the Coronary OAS as a therapy in patients with severely calcified CAD. These general clearances and approvals restrict our ability to market or advertise the Peripheral OAS and the Coronary OAS beyond these uses and could affect our growth.
If we determine to market our orbital technology in the U.S. for other uses, we would need to conduct further clinical trials and obtain premarket approval from the FDA. Clinical trials are complex, expensive, time consuming, uncertain and subject to substantial and unanticipated delays. There is no assurance that we will be able to obtain FDA approval to use our orbital atherectomy technology for applications other than the treatment of PAD and CAD.
We are or will be subject to an extensive set of post-market controls that apply to us as we commercialize our products, including annual PMA reports, Medical Device Reports on serious adverse events, complaint handling and analysis under the FDA’s QSR, export controls, advertising and promotion requirements, and potential post-market studies required by the FDA.
We and our suppliers are also subject to regulation by various state authorities, which may inspect our or our suppliers’ facilities and manufacturing processes and enforce state regulations. Failure to comply with applicable state regulations may result in seizures, injunctions or other types of enforcement actions.
Our promotion of the Peripheral OAS and the Coronary OAS is closely controlled by the FDA and enforcement activities could limit our ability to inform potential customers of the features of the products.
23
The Peripheral OAS or the Coronary OAS may in the future be subject to product recalls that could harm our reputation and product liability claims that could exceed the limits of available insurance coverage.
The FDA and similar governmental authorities in other countries have the authority to require the recall of commercialized products in the event of material regulatory deficiencies or defects in design or manufacture. For example, since commercialization of the Peripheral OAS, we have had minor instances of recalls, including, in the year ended June 30, 2017 minor recalls involving guidewires and the OAS saline infusion pump recall discussed below. Any recalls of our products or products that we distribute would divert managerial and financial resources, harm our reputation with customers and have an adverse effect on our financial condition and results of operations.
Also, if the Peripheral OAS or the Coronary OAS is defectively designed, manufactured or labeled, contain defective components or are misused, we may become subject to costly litigation by our customers or their patients. The use, misuse or off-label use of the Peripheral OAS or the Coronary OAS may result in injuries that lead to product liability suits, which could be costly to our business. We cannot prevent a physician from using the Peripheral OAS or the Coronary OAS for off-label applications. While we have product liability insurance coverage for our products and intend to maintain such insurance coverage in the future, there can be no assurance that we will be adequately protected from claims that are brought against us.
The recall of our saline infusion pumps could adversely affect our business and financial results, harm our reputation and result in legal claims against us.
In April 2017, we initiated a voluntary recall of one type of our saline infusion pumps. We plan to recall and replace approximately 900 units that were in customer inventory at the time the recall commenced. While we have made design changes to this pump to address the issues that led to the recall, it is possible that we did not adequately assess the cause and effect of these issues and we may not have adequately modified the pump design in order to prevent these issues from happening in the future. We cannot predict or control any future actions by the FDA and other regulatory bodies with respect to this recall. We may experience delays in obtaining components of the pump from suppliers, which could cause delays in manufacturing replacement pumps, and we may not be able to replace all affected pumps in a timely manner. We could also discover additional versions or lots of our pumps that could be subject to recall. There can be no assurance that the FDA will approve any future designs and versions of the pump. Any of these matters could cause delays in the ability of our customers to perform procedures using our devices and prevent us from adding new customers who may not have access to other pumps that can be used in procedures, which could harm our reputation with customers, adversely affect our ability to generate revenue, and have an adverse effect on our financial condition and results of operations. The existence of the recall could harm our reputation, which could result in loss of both current and potential customers. This recall is diverting managerial and sales force attention and financial resources from other aspects of our business and may require us to incur more expense than we currently anticipate. In addition, this recall and any effects of it could subject us to legal claims or proceedings that would divert managerial and financial resources and could adversely impact our business and financial condition. While we carry liability insurance coverage and intend to maintain such insurance coverage in the future, there can be no assurance that we will be adequately protected from claims that are brought against us with respect to this recall.
We are subject to many laws and governmental regulations and any adverse regulatory action may materially adversely affect our financial condition and business operations.
The Peripheral OAS and the Coronary OAS and related manufacturing processes, clinical data, adverse events, recalls and corrections and promotional activities are subject to extensive regulation by the FDA and other regulatory bodies. In particular, we are required to comply with the QSR and other regulations, which cover the methods and documentation of the design, testing, production, control, quality assurance, labeling, packaging, storage and shipping of any product for which we obtain marketing clearance or approval. We are also responsible for the quality of components received by our suppliers. Failure to comply with the QSR requirements or other statutes and regulations administered by the FDA and other regulatory bodies, or failure to adequately respond to any observations, could result in, among other things:
• | warning or other letters from the FDA; |
• | fines, injunctions and civil penalties; |
• | product recall or seizure; |
• | unanticipated expenditures; |
• | delays in clearing or approving or refusal to clear or approve products; |
• | withdrawal or suspension of approval or clearance by the FDA or other regulatory bodies; |
• | orders for physician notification or device repair, replacement or refund; |
• | operating restrictions, partial suspension or total shutdown of production or clinical trials; and |
• | criminal prosecution. |
24
If any of these actions were to occur, it would harm our reputation and cause our product sales to suffer.
Our operations are also subject to regulatory requirements relating to the environment, waste management and health and safety matters, including measures relating to the release, use, storage, treatment, transportation, discharge, disposal and remediation of hazardous substances. Environmental laws and regulations could become more stringent over time, imposing greater compliance costs and increasing risks and penalties associated with violations.
In addition, our relationships with physicians, hospitals and the marketers of our products are subject to scrutiny under various federal anti-kickback, self-referral, false claims and similar laws, often referred to collectively as healthcare fraud and abuse laws, as further described below.
If our operations are found to be in violation of these laws, we, as well as our employees, may be subject to penalties, including monetary fines, civil and criminal penalties, exclusion from federal and state healthcare programs, including Medicare, Medicaid, Veterans Administration health programs, workers’ compensation programs and TRICARE (the healthcare system administered by or on behalf of the U.S. Department of Defense for uniformed services beneficiaries, including active duty and their dependents, retirees and their dependents), and forfeiture of amounts collected in violation of such prohibitions, which could materially adversely affect our financial condition and business operations.
In addition, we have agreements with federal, state and local government agencies, such as the Veterans Administration, and third-party healthcare providers that receive government funding to sell our products. We are subject to extensive regulatory compliance obligations in the award, performance and administration of our government contracts, including regulations relating to procurement integrity, pricing protection, export control, government security, employment practices, accuracy of records and the recording of costs. The other parties to these agreements have the right to audit us to determine whether we are in compliance with these agreements. Failure to comply with these regulations and requirements could result in reductions of the value of contracts, contract modifications or termination, repayment of amounts, the assessment of penalties and fines, and/or suspension or debarment from government contracting or subcontracting in the future, any of which could negatively affect our financial condition and results of operations.
We are subject to federal and state laws prohibiting “kickbacks” and false and fraudulent claims which, if violated, could subject us to substantial penalties. Additionally, any challenges to or investigations into our practices under these laws could cause adverse publicity and be costly to respond to, and thus could harm our business.
The federal healthcare program Anti-Kickback Statute, and similar state laws, prohibit payments that are intended to induce health care professionals or others either to refer patients or to purchase, lease, order or arrange for or recommend the purchase, lease or order of healthcare products or services. A number of states have enacted laws that require pharmaceutical and medical device companies to monitor and report payments, gifts and other remuneration made to physicians and other health care professionals and health care organizations. In addition, some state statutes, most notably laws in Massachusetts and Vermont, impose outright bans on certain gifts to physicians as well as requiring reporting of payments to physicians. Some of these laws, referred to as “aggregate spend” or “gift” laws, carry substantial fines if they are violated. The federal Physician Payments Sunshine Act, or the Sunshine Act, requires us to collect and report certain data on payments and other transfers of value to physicians and teaching hospitals.
It is widely anticipated that public reporting under the Sunshine Act and implementing Open Payments regulations will result in increased scrutiny of the financial relationships between industry, physicians and teaching hospitals. These anti-kickback, public reporting and aggregate spend laws affect our sales, marketing, promotional and clinical activities by limiting the kinds of financial arrangements, including sales programs, we may have with hospitals, physicians or other potential purchasers or users of medical devices. They also impose additional administrative and compliance burdens on us. In particular, these laws influence, among other things, how we structure our sales offerings, including discount practices, customer support, education and training programs, physician consulting and other service arrangements, and clinical trials. If we were to offer or pay inappropriate inducements to purchase our products, we could be subject to a claim under the federal healthcare program Anti-Kickback Statute or similar state laws. If we fail to comply with particular reporting requirements, we could be subject to penalties under applicable federal or state laws. Other federal and state laws generally prohibit individuals or entities from knowingly presenting, or causing to be presented, claims for payments to Medicare, Medicaid or other third-party payors that are false or fraudulent, or for items or services that were not provided as claimed. Although we do not submit claims directly to government healthcare programs or other payors, manufacturers can be held liable under these laws if they are deemed to “cause” the submission of false or fraudulent claims by providing inaccurate billing or coding information to customers, by providing improper financial inducements, or through certain other activities.
25
In providing billing and coding information to customers, we make every effort to ensure that the billing and coding information furnished is accurate and that treating physicians understand that they are responsible for all treatment decisions. Nevertheless, we cannot provide assurance that the government will regard any billing errors that may be made as inadvertent or that the government will not examine our role in providing information to our customers and physicians concerning the benefits of therapy with our devices. Likewise, our financial relationships with customers, physicians, or others in a position to influence the purchase or use of our products may be subject to government scrutiny or be alleged or found to violate applicable fraud and abuse laws. False claims laws prescribe civil, criminal and administrative penalties for noncompliance, which can be substantial. Moreover, an unsuccessful challenge or investigation into our practices could cause adverse publicity, and be costly to respond to, and thus could harm our business and results of operations.
On May 8, 2014, we received a letter from the DOJ stating that it is investigating us to determine whether we had violated the False Claims Act, and on June 28, 2016, we entered into a Settlement Agreement with the United States of America, acting through the DOJ and on behalf of the OIG, and Travis Thams, who filed the qui tam complaint underlying the DOJ’s investigation (the “Civil Action”), to resolve the investigation by the DOJ and the Civil Action. The existence of the investigation and subsequent settlement could negatively affect our reputation and harm our business and results of operations. In addition, the release we received from the government in the Settlement Agreement related to particular conduct alleged in the complaint underlying the investigation. If the government determines that other conduct alleged in the complaint for which the government did not grant us a release merits additional investigation or if the government pursues any action against us relating to this other alleged conduct, then we may need to expend additional amounts to defend ourselves, our management would undergo the distraction of additional investigation and potential litigation, our reputation could be harmed, and our business and results of operations could be materially adversely affected.
Compliance with the terms and conditions of our Corporate Integrity Agreement requires significant resources and management time and, if we fail to comply, we could be subject to penalties or, under certain circumstances, excluded from government healthcare programs, which would materially adversely affect our business.
On June 28, 2016, we entered into a five-year Corporate Integrity Agreement with the OIG. The Corporate Integrity Agreement requires that we maintain our existing compliance programs and imposes certain expanded compliance-related requirements during the term of the Corporate Integrity Agreement, including establishment of specific procedures and requirements regarding consulting activities, co-marketing activities and other interactions with healthcare professionals and healthcare institutions and the sale and marketing of our products; ongoing monitoring, reporting, certification and training obligations; and the engagement of an independent review organization to perform certain auditing and reviews and prepare certain reports regarding our compliance with federal health care programs. Maintaining the broad array of processes, policies and procedures necessary to comply with the Corporate Integrity Agreement will require a significant portion of management’s attention and the application of significant resources. The costs associated with implementation of and compliance with the Corporate Integrity Agreement could be substantial and may be greater than we currently anticipate. In addition, while we have developed and instituted a corporate compliance program, we cannot guarantee that we, our employees, our consultants or our contractors are or will be in compliance with all potentially applicable U.S. federal and state regulations and/or laws, all potentially applicable foreign regulations and/or laws and/or all requirements of the Corporate Integrity Agreement. In the event of a breach of the Corporate Integrity Agreement, we could become liable for payment of certain stipulated penalties or could be excluded from participation in federal health care programs. The costs associated with compliance with the Corporate Integrity Agreement, or any liability or consequences associated with its breach, could have an adverse effect on our business, revenues, earnings and cash flows.
Regulations related to “conflict minerals” may force us to incur additional expenses, may result in damage to our business reputation and may adversely impact our ability to conduct our business.
Pursuant to the Dodd-Frank Wall Street Reform and Consumer Protection Act, the SEC promulgated final rules regarding disclosure of the use of certain minerals, known as conflict minerals, that are mined from the Democratic Republic of the Congo and adjoining countries, as well as procedures regarding a manufacturer’s efforts to prevent the sourcing of such minerals and metals produced from those minerals. These disclosure requirements require ongoing due diligence efforts and disclosure obligations. There are costs associated with complying with these disclosure requirements, including for diligence in regards to the sources of any conflict minerals used in our products, in addition to the cost of remediation and other changes to products, processes, or sources of supply as a consequence of such verification activities. In addition, our ongoing implementation of these rules could adversely affect the sourcing, supply, and pricing of materials used in our products.
26
Our anticipated international expansion will subject us to increased legal and regulatory requirements, which could have a material effect on our business.
We intend to sell internationally in the future. In November 2016, we signed an exclusive distribution agreement with Medikit to sell our Diamondback 360® Coronary and Peripheral OAS in Japan, and in March 2017, we received approval from Japan’s Ministry of Health, Labor and Welfare for our Diamondback 360® Coronary OAS Micro Crown. Movement into international markets will subject us and our products to different and increased laws and regulations, including foreign medical device regulations; tax laws; increased financial accounting and reporting burdens and complexities; export laws; and the Foreign Corrupt Practices Act and similar anti-corruption laws. Although we have and will continue to implement policies and procedures designed to ensure compliance with these laws, there can be no assurance that all of our employees, contractors, and agents, as well as those companies to which we will outsource certain aspects of our business operations, including those based in foreign countries where practices that violate such U.S. laws may be customary, will comply with our internal policies. We will incur additional compliance costs associated with global operations, and any alleged or actual violations of these laws and regulations could subject us to government scrutiny, severe criminal or civil fines, sanctions and other liabilities, and prohibitions on business conduct, and could negatively affect our business, reputation, operating results, and financial condition.
Risks Relating to Our Intellectual Property
Our inability to adequately protect our intellectual property could allow our competitors and others to produce products based on our technology, which could substantially impair our ability to compete.
Our success and ability to compete depends, in part, upon our ability to maintain the proprietary nature of our technologies. We rely on a combination of patents, copyrights and trademarks, as well as trade secrets and nondisclosure agreements, to protect our intellectual property. Our issued patents and related intellectual property may not be adequate to protect us or permit us to gain or maintain a competitive advantage. Also, we cannot assure you that any of our pending patent applications will result in the issuance of patents to us. Further, if any patents we obtain or license are deemed invalid and unenforceable, or have their scope narrowed, it could impact our ability to commercialize or license our technology and achieve competitive advantages.
Changes in either the patent laws or in interpretations of patent laws in the United States and other countries may diminish the value of our intellectual property. In addition, the laws of some foreign countries may not protect our intellectual property rights to the same extent as the laws of the United States, if at all.
We may, in the future, need to assert claims of infringement against third parties to protect our intellectual property. The outcome of litigation to enforce our intellectual property rights in patents, copyrights, trade secrets or trademarks is highly unpredictable, could result in substantial costs and diversion of resources, and could have a material adverse effect on our financial condition, reputation and results of operations regardless of the final outcome of such litigation.
Despite our efforts to safeguard our unpatented and unregistered intellectual property rights, we may not be successful in doing so or the steps taken by us in this regard may not be adequate to detect or deter misappropriation of our technology or to prevent an unauthorized third party from copying or otherwise obtaining and using our products, technology or other information that we regard as proprietary. In addition, we may not have sufficient resources to litigate, enforce or defend our intellectual property rights. Additionally, third parties may be able to design around our patents.
We also rely on trade secrets, technical know-how and continuing innovation to develop and maintain our competitive position. In this regard, we seek to protect our proprietary information and other intellectual property by having a policy that our employees, consultants, contractors, outside scientific collaborators and other advisors execute non-disclosure and assignment of invention agreements on commencement of their employment or engagement. We cannot provide any assurance that employees and third parties will abide by the confidentiality or assignment terms of these agreements, or that we will be effective in securing necessary assignments from these third parties.
Claims of infringement or misappropriation of the intellectual property rights of others could prohibit us from commercializing products, require us to obtain licenses from third parties or require us to develop non-infringing alternatives, and subject us to substantial monetary damages and injunctive relief.
The medical technology industry is characterized by extensive litigation and administrative proceedings over patent and other intellectual property rights. The likelihood that patent infringement or misappropriation claims may be brought against us increases as we achieve more visibility in the marketplace and introduce products to market. We are aware of numerous patents issued to third parties that relate to the manufacture and use of medical devices for the treatment of vascular disease. The
27
owners of each of these patents could assert that the manufacture, use or sale of our products infringes one or more claims of their patents. There could also be existing patents of which we are unaware that one or more aspects of our technology may inadvertently infringe. In some cases, litigation may be threatened or brought by a patent-holding company or other adverse patent owner who has no relevant product revenues and against whom our patents may provide little or no deterrence.
Any infringement or misappropriation claim could cause us to incur significant costs, place significant strain on our financial resources, divert management’s attention from our business and harm our reputation. If the relevant patents were upheld in litigation as valid and enforceable and we were found to infringe, we could be prohibited from commercializing any infringing products unless we could obtain licenses to use the technology covered by the patent or are able to design around the patent. We may be unable to obtain a license on terms acceptable to us, if at all, and we may not be able to redesign any infringing products to avoid infringement.
Item 1B. Unresolved Staff Comments.
None.
Item 2. Properties.
Our principal executive offices are located in our headquarters, a 125,000 square foot facility in St. Paul, Minnesota, which contains dedicated research and development, training and education, and manufacturing facilities, and our central administrative offices. In March 2017, we sold the Minnesota facility and entered into an agreement to lease the facility through March 2032.
In September 2009, we entered into an agreement to lease a 46,000 square foot production facility in Pearland, Texas beginning in April 2010 and continuing through March 2020. This facility primarily accommodates additional manufacturing activities.
We believe that our current facilities are substantially adequate for our current and anticipated future needs for the foreseeable future.
Item 3. Legal Proceedings.
Employment Litigation
We are party to Steven Babyak v. Cardiovascular Systems, Inc., a lawsuit originally filed in the Superior Court of California, County of Los Angeles, on November 16, 2015. The plaintiff was a former Regional Sales Manager in Southern California whose employment terminated on June 1, 2015. In late 2014 and early 2015, the plaintiff raised concerns and complained about a variety of alleged improper activities and claims his termination was in retaliation for these actions. We investigated and addressed each of plaintiff’s concerns and complaints and deny his assertion. Following the termination of his employment, the plaintiff made claims under California law relating to whistleblower retaliation; defamation; discrimination on the basis of association with protected group; harassment on the basis of sex in violation of FEHA; retaliation for exercising rights under FEHA; failure to prevent discrimination, harassment & retaliation in violation of FEHA; wrongful termination in violation of public policy; and violation of business and professions code. The plaintiff’s complaint did not demand any specific dollar amount, but generally sought compensatory damages, together with prejudgment interest; general damages; reasonable attorney’s fees; exemplary and punitive damages; costs of suit; permanent injunction; disgorgement of profits; civil penalties; pre-judgment and post-judgment relief; and such other and further relief as the court deems just and proper. Prior to trial, the plaintiff voluntarily dismissed his claim for defamation and dropped his claims for emotional distress damages. In addition, the plaintiff’s claims for discrimination, discrimination on the basis of association with a protected group, failure to prevent discrimination, and violation of business and professions code were dismissed on motion for summary judgment. Following an April 2017 trial, a jury awarded the plaintiff $2.7 million in compensatory damages with respect to his claims for whistleblower retaliation and wrongful termination in violation of public policy. The jury also awarded the plaintiff $22.4 million in punitive damages with respect to the same claims. The jury did not find any liability with respect to the plaintiff’s other remaining claims or grant the plaintiff any other relief sought. We filed post-trial motions for judgment notwithstanding the verdict and a new trial, on the grounds that this case was incorrectly decided as to liability, the compensatory and punitive damages were not appropriate and were excessive, and we were prevented from a fair trial by the improper exclusion of critical evidence. On June 29, 2017, the Court partially granted our motions, reducing the punitive damages award from $22.4 million to $2.7 million but denied our other motions. We believe that this case was incorrectly decided as to liability and the appropriateness and amount of any damages, and we filed a Notice of Appeal on July 24, 2017.
28
Stockholder Securities Litigation
On February 12, 2016, a stockholder purporting to represent a class of persons who purchased our securities between September 12, 2011 and January 21, 2016 filed a lawsuit against us and certain of our officers in the United States District Court for the Central District of California, Paradis v. Cardiovascular Systems, Inc., et al., 2:16-cv-01011 (C.D. Cal.). The lawsuit alleges that we made materially false and misleading statements and failed to disclose material adverse facts about our business, operational and financial performance, in violation of federal securities laws, relating to (1) alleged kickbacks to health care providers, (2) alleged off-label promotion of medical devices, and (3) alleged violations of the FDCA and related regulations in connection with our medical devices. On March 4, 2016, a second stockholder filed a similar lawsuit against us and certain of our officers in the United States District Court for the District of Minnesota, Shoemaker v. Cardiovascular Systems, Inc. et al., 0:16-cv-00568 (D. Minn.). The plaintiffs seek unspecified monetary damages on behalf of the alleged class, interest, and attorney’s fees and costs of litigation. On April 12, 2016, four motions for appointment as lead plaintiff were filed in the Paradis action and three of the four proposed plaintiffs also filed a motion for appointment as lead plaintiff in the Shoemaker action. On April 26, 2016, the Paradis action was voluntarily dismissed by plaintiffs in favor of the Shoemaker action. That same day, the Shoemaker court entered an order appointing the City of Miami Fire Fighters’ & Police Officers’ Retirement Trust and the County Retirement Systems as Co-Lead Plaintiffs for representing the putative class. On June 28, 2016, the Co-Lead Plaintiffs filed a new complaint. We filed a motion to dismiss the complaint in this action on August 29, 2016. A hearing was held on the motion to dismiss on December 2, 2016. On March 29, 2017, the court granted our motion to dismiss the complaint and dismissed the plaintiffs’ amended complaint without prejudice. The court granted the plaintiffs’ request for leave to amend their complaint, and on June 27, 2017, the plaintiffs filed an amended complaint. The amended complaint makes similar allegations as the original complaint, namely, that we made materially false and misleading statements and failed to disclose material adverse facts about our business, operational and financial performance, in violation of federal securities laws, relating to alleged kickbacks to health care providers. The plaintiffs seek unspecified monetary damages on behalf of the alleged class, interest, and attorney’s fees and costs of litigation. We filed a motion to dismiss the amended complaint on August 11, 2017. We believe that this lawsuit is without merit and we intend to defend ourselves vigorously.
Item 4. Mine Safety Disclosures.
None.
29
PART II
Item 5. | Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities. |
Price Range of Common Stock and Dividend Policy
We trade on the Nasdaq Global Market under the symbol “CSII.” The following table sets forth the high and low sales prices for our common stock (based upon intra-day trading) as reported by the Nasdaq Global Market:
Common Stock | |||||||
High | Low | ||||||
Fiscal Year Ended June 30, 2017 | |||||||
First quarter | $ | 25.22 | $ | 18.00 | |||
Second quarter | 27.38 | 21.29 | |||||
Third quarter | 29.70 | 23.28 | |||||
Fourth quarter | 33.11 | 27.73 | |||||
Fiscal Year Ended June 30, 2016 | |||||||
First quarter | $ | 32.91 | $ | 14.91 | |||
Second quarter | 17.53 | 11.80 | |||||
Third quarter | 15.14 | 7.50 | |||||
Fourth quarter | 18.90 | 11.45 | |||||
The number of record holders of our common stock on August 18, 2017 was approximately 144. No cash dividends have been previously paid on our common stock and none are anticipated during fiscal year 2018.
Recent Sales of Unregistered Securities
None.
Issuer Purchases of Equity Securities
None.
Securities Authorized For Issuance Under Equity Compensation Plans
For information on our equity compensation plans, refer to Item 12, “Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters.”
30
Performance Graph
The following graph compares the cumulative total stockholder return of our common stock (“CSII”) with the return of the Standard & Poor’s 500 Stock Index (“S&P”) and the S&P Health Care Index (“S&P HC”) from June 30, 2012 through June 30, 2017. The comparisons assume $100 was invested on June 30, 2012 in our common stock, the S&P 500 Stock Index and the S&P Health Care Index and also assumes that any dividends are reinvested. The returns set forth on the following graph are based on historical results and are not intended to suggest future performance.
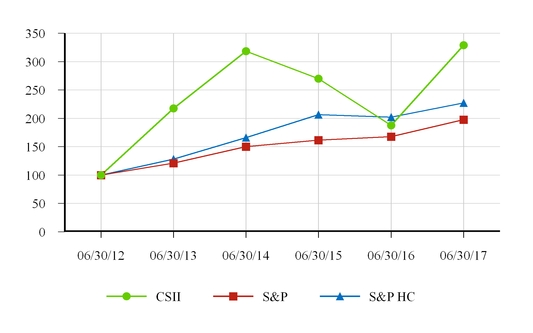
31
Item 6. Selected Financial Data.
Five-Year Selected Financial Data
(in thousands, except per share amounts)
2017 | 2016 | 2015 | 2014 | 2013 | |||||||||||||||
SUMMARY OF OPERATIONS FOR THE FISCAL YEAR: | |||||||||||||||||||
Net revenues | $ | 204,906 | $ | 178,184 | $ | 181,544 | $ | 136,612 | $ | 103,897 | |||||||||
Loss from operations | $ | (1,542 | ) | $ | (56,077 | ) | $ | (32,637 | ) | $ | (33,489 | ) | $ | (22,419 | ) | ||||
Net loss | $ | (1,792 | ) | $ | (56,024 | ) | $ | (32,822 | ) | $ | (35,290 | ) | $ | (24,037 | ) | ||||
Basic and diluted earnings per share | $ | (0.06 | ) | $ | (1.72 | ) | $ | (1.04 | ) | $ | (1.25 | ) | $ | (1.11 | ) | ||||
Cash dividends declared per share | $ | — | $ | — | $ | — | $ | — | $ | — | |||||||||
FINANCIAL POSITION AT YEAR END: | |||||||||||||||||||
Total assets | $ | 193,940 | $ | 142,406 | $ | 171,328 | $ | 181,901 | $ | 96,897 | |||||||||
Total long-term liabilities | $ | 34,579 | $ | 6,010 | $ | 2,005 | $ | 117 | $ | 7,652 | |||||||||
Stockholders’ equity | $ | 118,389 | $ | 100,897 | $ | 139,435 | $ | 152,055 | $ | 66,832 | |||||||||
Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations.
You should read the following discussion and analysis of financial condition and results of operations together with our consolidated financial statements and the related notes included elsewhere in this Form 10-K. This discussion and analysis contains forward-looking statements about our business and operations, based on current expectations and related to future events and our future financial performance, that involve risks and uncertainties. Our actual results may differ materially from those we currently anticipate as a result of many important factors, including the factors we describe under “Risk Factors” and elsewhere in this Form 10-K.
OVERVIEW
We are a medical technology company leading the way in the effort to successfully treat patients suffering from peripheral and coronary artery diseases, including those with arterial calcium, the most difficult arterial disease to treat. We are committed to clinical rigor, constant innovation and a defining drive to set the industry standard to deliver safe and effective medical devices that improve lives of patients facing this difficult disease state.
Our peripheral arterial disease (“PAD”) products, the Diamondback 360® Peripheral Orbital Atherectomy System (“OAS”) (“Diamondback 360 Peripheral”), the Diamondback 360 60cm Peripheral OAS, the Diamondback 360 4 French 1.25 Peripheral OAS, the Diamondback 360 1.50 Peripheral OAS, the Diamondback 360 2.00 Peripheral OAS, and the Stealth 360® Peripheral OAS (“Stealth 360”), are catheter-based platforms capable of treating a broad range of plaque types in leg arteries both above and below the knee, including calcified plaque, and address many of the limitations associated with existing surgical, catheter and pharmacological treatment alternatives. The micro-invasive devices use small access sheaths that can provide procedural benefits and allow physicians to treat PAD patients in even the small and tortuous vessels located below the knee through alternative access sites in the ankle and foot as well as in the groin. We refer to each of the products above in this report as the “Peripheral OAS.”
The FDA has granted us multiple 510(k) clearances for our Peripheral OAS devices as a therapy in patients with peripheral artery disease. See Item 1 in Part I of this Annual Report on Form 10-K for additional detail.
Our coronary arterial disease (“CAD”) product, Diamondback 360® Coronary OAS (“Coronary OAS”), is marketed as a treatment for severely calcified coronary arteries. The Coronary OAS is a catheter-based platform designed to facilitate stent delivery in patients with CAD who are acceptable candidates for percutaneous transluminal coronary angioplasty or stenting due to de novo, severely calcified coronary artery lesions. The Coronary OAS design is similar to technology used in our Peripheral OAS, customized specifically for the coronary application.
32
A coronary application required us to conduct a clinical trial and file a premarket approval (“PMA”) application and obtain approval from the FDA. In March 2013, we completed submission of our PMA application to the FDA for our orbital atherectomy system to treat calcified coronary arteries. In October 2013, we received PMA from the FDA to market the Coronary OAS as a treatment for severely calcified coronary arteries. We commenced a commercial launch of our Coronary OAS following receipt of PMA. In March 2017, the Company received approval from the FDA to market its Diamondback360® Coronary OAS Micro Crown, which is the only atherectomy device designed to both pilot tight, calcific lesions and treat 2.5 to 4mm vessels with a single device.
We market the Peripheral and Coronary OAS in the U.S. through a direct sales force and expend significant capital on our sales and marketing efforts to expand our customer base and utilization per customer. At our facilities, we assemble the saline infusion pump and the single-use catheter used in the Peripheral OAS and Coronary OAS with components purchased from third-party suppliers, as well as with components manufactured in-house. Ancillary products are purchased from third-party suppliers.
International
In November 2016, we signed an exclusive distribution agreement with Medikit Co., Ltd. (“Medikit”) to sell our Diamondback 360® Coronary and Peripheral OAS in Japan. In March 2017, we received approval from Japan’s Ministry of Health, Labor and Welfare for our Diamondback 360® Coronary OAS Micro Crown. Pending reimbursement approval, Japan will be the first international market for any of our products. We are currently evaluating options for additional international markets to expand the coronary and peripheral opportunities.
FINANCIAL OVERVIEW
Net Revenues. We derive substantially all of our revenues from the sale of Peripheral OAS, the Coronary OAS and ancillary products. The Peripheral OAS and Coronary OAS each use a disposable, single-use, low-profile catheter that travels over our proprietary ViperWire guide wire. The systems use a saline infusion pump as a power supply for the operation of the catheter. Additional ancillary products include the ViperSlide Lubricant and ViperTrack Radiopaque Tape.
Cost of Goods Sold. We assemble the single-use catheter with components purchased from third-party suppliers, as well as with components manufactured in-house. The infusion pump and guide wires are purchased from third-party suppliers. Our cost of goods sold consists primarily of raw materials, direct labor, and manufacturing overhead.
Selling, General and Administrative Expenses. Selling, general and administrative expenses include compensation for executive, sales, marketing, finance, information technology, human resources and administrative personnel, including stock-based compensation. Other significant expenses include the medical device excise tax, bad debt expense, travel, marketing costs, professional fees and professional education.
Research and Development Expenses. Research and development expenses include costs associated with the design, development, testing, enhancement and regulatory approval of our products. Research and development expenses include employee compensation including stock-based compensation, supplies and materials, patent expenses, consulting expenses, travel and facilities overhead. We also incur significant expenses to operate clinical trials, including trial design, third-party fees, clinical site reimbursement, data management and travel expenses. All research and development expenses are expensed as incurred. Approved patent applications are capitalized and amortized using the straight-line method over their remaining estimated lives. Patent amortization begins at the time of patent application approval, and does not exceed 20 years.
Other (Income) and Expense, Net. Other (income) and expense, net primarily includes interest expense from amounts owed under the Facility lease and DOJ settlement, and interest income from money market funds.
Net Operating Loss Carryforwards. We have established valuation allowances to fully offset our deferred tax assets due to the uncertainty about our ability to generate the future taxable income necessary to realize these deferred assets, particularly in light of our historical losses. The future use of net operating loss carryforwards is dependent on us attaining profitable operations and will be limited in any one year under Internal Revenue Code Section 382 due to significant ownership changes (as defined in Section 382) resulting from our equity financings. At June 30, 2017, we had net operating loss carryforwards for federal and state income tax reporting purposes of approximately $239.3 million, which will expire at various dates through fiscal 2036.
33
CRITICAL ACCOUNTING POLICIES AND SIGNIFICANT JUDGMENTS AND ESTIMATES
Our management’s discussion and analysis of our financial condition and results of operations are based on our consolidated financial statements, which have been prepared in accordance with accounting principles generally accepted in the United States. The preparation of our consolidated financial statements requires us to make estimates, assumptions and judgments that affect amounts reported in those statements. Our estimates, assumptions and judgments, including those related to revenue recognition, allowance for doubtful accounts, excess and obsolete inventory, and stock-based compensation are updated as appropriate at least quarterly. We use authoritative pronouncements, our technical accounting knowledge, cumulative business experience, valuation specialists, judgment and other factors in the selection and application of our accounting policies. While we believe that the estimates, assumptions and judgments that we use in preparing our consolidated financial statements are appropriate, these estimates, assumptions and judgments are subject to factors and uncertainties regarding their outcome. Therefore, actual results may materially differ from these estimates.
Some of our significant accounting policies require us to make subjective or complex judgments or estimates. An accounting estimate is considered to be critical if it meets both of the following criteria: (1) the estimate requires assumptions about matters that are highly uncertain at the time the accounting estimate is made, and (2) different estimates that reasonably could have been used, or changes in the estimate that are reasonably likely to occur from period to period, would have a material impact on the presentation of our financial condition, results of operations, or cash flows.
Revenue Recognition. We sell the majority of our products via direct shipment to hospitals or clinics. We recognize revenue when all of the following criteria are met: persuasive evidence of an arrangement exists; delivery has occurred; the sales price is fixed or determinable; and collectability is reasonably assured. Revenue recognition may occur upon shipment or upon delivery to the customer site, based on the contract terms. We record estimated sales returns, discounts and rebates as a reduction of net sales.
Costs related to products delivered are recognized in the period the revenue is recognized. Cost of goods sold consists primarily of raw materials, direct labor, and manufacturing overhead.
Allowance for Doubtful Accounts. We maintain an allowance for doubtful accounts. This allowance is an estimate and is regularly evaluated for adequacy by taking into consideration factors such as past experience, credit quality of the customer base, age of the receivable balances, both individually and in the aggregate, and current economic conditions that may affect a customer’s ability to pay. Provisions for the allowance for doubtful accounts attributed to bad debt are recorded in general and administrative expenses. During the years ended June 30, 2017, 2016 and 2015, we recorded bad debt expense of $465,000, $725,000, and $1.1 million, respectively.
Excess and Obsolete Inventory. We have inventories that are principally comprised of capitalized direct labor and manufacturing overhead, raw materials and components, and finished goods. Due to the technological nature of our products, there is a risk of obsolescence for changes in our technology and the market, which is impacted by technological developments and events. Accordingly, we write down our inventories as we become aware of any situation where the carrying amount exceeds the estimated realizable value based on assumptions about future demands and market conditions. The evaluation includes analysis of inventory levels, expected product lives, product at risk of expiration, sales levels by product and projections of future sales demand. During the years ended June 30, 2017, 2016 and 2015, we wrote off $128,000, $140,000, and $797,000 respectively, of inventory.
Stock-Based Compensation. We have stock-based compensation plans, which include stock options, nonvested share awards, and an employee stock purchase plan. We determine the fair value of our option awards using option-pricing models. We determine the fair value of nonvested share awards with market conditions using the Monte Carlo simulation. Fair value of nonvested share awards that vest based upon performance or time conditions is determined by the closing market price of our stock on the date of grant. Stock-based compensation expense is recognized ratably over the requisite service period for the awards expected to vest. Management’s key assumptions are developed with input from independent third-party valuation advisors. During the years ended June 30, 2017, 2016 and 2015, we recorded stock-based compensation expense of $10.4 million, $13.0 million, and $14.7 million, respectively.
Legal Proceedings. In accordance with FASB guidance, we record a liability in our consolidated financial statements related to legal proceedings when a loss is known or considered probable and the amount can be reasonably estimated. If the reasonable estimate of a known or probable loss is a range, and no amount within the range is a better estimate than any other, the minimum amount of the range is accrued. If a loss is reasonably possible, but not known or probable, and can be reasonably estimated, the estimated loss or range of loss is disclosed in the notes to the consolidated financial statements. In most cases, significant judgment is required to estimate the amount and timing of a loss to be recorded.
34
During fiscal 2017 we accrued $2.6 million related to current legal proceedings based on the estimate of the range of the loss that we believe is probable of occurring and recorded a receivable of $1.3 million associated with our present assessment of the probable amount of insurance proceeds we would receive related to the claim, based on the accrued amount of loss referenced above. We estimate insurance receivables based on an analysis of our policies, including their exclusions, an assessment of the nature of each claim and remaining coverage, information from its insurance carrier, and the probable loss range referenced above. We will continue to assess the probable amount of insurance proceeds expected to be received in this matter each reporting period and make adjustments, if necessary, based on additional facts as they arise.
In fiscal 2016 we recorded $8.0 million in connection with the Settlement Agreement we entered into with the United States of America, acting through the U.S. Attorney’s Office for the Western District of North Carolina and on behalf of the Office of Inspector General of the Department of Health and Human Services, and Travis Thams.
Financing Obligation. In connection with the sale of our headquarters (the “Facility”) in March 2017, we entered into an agreement to lease the Facility. The Lease Agreement has an initial term of fifteen years, with four consecutive renewal options of five years each at our option. As the lease terms resulted in a capital lease classification, we accounted for the sale and leaseback of the Facility as a financing transaction where the assets remain on our balance sheet and a financing obligation was recorded for $20.9 million. As lease payments are made, they will be allocated between interest expense and a reduction of the financing obligation, resulting in a value of the financing obligation that is equivalent to the net book value of the assets at the end of the lease term. At the end of the lease (including any renewal option terms), we will remove the assets and financing obligation from its balance sheet. The key assumptions used in the lease analysis were related to the Facility’s fair value and the interest rate.
• | Fair value - We used the most recent appraisal of the Facility, performed during the buyers’ due diligence, as its fair value at the inception of the lease agreement. As the present value of minimum lease payments was more than 90% of this fair value, the lease was determined to be a capital lease. We reviewed all possible values and believe that the appraised value is the most appropriate for use in the lease analysis. |
• | Interest rate - We used our incremental borrowing rate based on a prior proposal for a term loan. Management reviewed various factors and determined that the interest rate used in the calculation is reasonable. |
RESULTS OF OPERATIONS
The following table sets forth, for the periods indicated, our results of operations expressed as dollar amounts (in thousands), and, for certain line items, the changes between the specified periods:
Comparison of Fiscal Year Ended June 30, 2017 with Fiscal Year Ended June 30, 2016
Year Ended June 30, | |||||||||||||
2017 | 2016 | Change | Percent Change | ||||||||||
Net revenues | $ | 204,906 | $ | 178,184 | $ | 26,722 | 15.0 | % | |||||
Cost of goods sold | 39,441 | 35,421 | 4,020 | 11.3 | |||||||||
Gross profit | 165,465 | 142,763 | 22,702 | 15.9 | |||||||||
Gross margin | 80.8 | % | 80.1 | % | 0.7 | % | 0.9 | ||||||
Expenses: | |||||||||||||
Selling, general and administrative | 144,096 | 162,542 | (18,446 | ) | (11.3 | ) | |||||||
Research and development | 22,911 | 25,934 | (3,023 | ) | (11.7 | ) | |||||||
Restructuring | — | 2,364 | (2,364 | ) | 100.0 | ||||||||
Legal settlement | — | 8,000 | (8,000 | ) | 100.0 | ||||||||
Total expenses | 167,007 | 198,840 | (31,833 | ) | (16.0 | ) | |||||||
Loss from operations | (1,542 | ) | (56,077 | ) | 54,535 | (97.3 | ) | ||||||
Other (income) and expense, net | 164 | (145 | ) | 309 | (213.1 | ) | |||||||
Loss before income taxes | $ | (1,706 | ) | $ | (55,932 | ) | $ | 54,226 | (96.9 | ) | |||
Provision for income taxes | $ | 86 | $ | 92 | $ | (6 | ) | (6.5 | ) | ||||
Net loss | $ | (1,792 | ) | $ | (56,024 | ) | $ | 54,232 | (96.8 | ) | |||
35
Net Revenues. Net revenues increased by $26.7 million, or 15.0%, from $178.2 million for the year ended June 30, 2016, to $204.9 million for the year ended June 30, 2017. Revenues from our Peripheral OAS increased $13.5 million, or 10.5%, primarily reflecting an 11.5% increase in the number of devices sold. Sales of our Coronary OAS increased by approximately $11.2 million, or 31.2%, reflecting 32.2% more devices sold. The increase in Peripheral and Coronary OAS sales are primarily due to the expansion of our customer base. Other product revenue increased $2.0 million, or 14.1%, during the year ended June 30, 2017, driven by increased sales of our Peripheral and Coronary OAS, which the other products support. Currently, all of our revenues are in the U.S.; however, we intend to sell internationally in the future. In November 2016, we signed an exclusive distribution agreement with Medikit to sell our Diamondback 360® Coronary and Peripheral OAS in Japan, and in March 2017, we received approval from Japan’s Ministry of Health, Labor and Welfare for our Diamondback 360® Coronary OAS Micro Crown. We expect our revenue to increase as we continue to increase the number of physicians using the devices, increase the usage per physician, introduce new and improved products, generate additional clinical data, and expand into new geographies.
Cost of Goods Sold. Cost of goods sold increased by $4.0 million, or 11.3%, from $35.4 million for the year ended June 30, 2016 to $39.4 million for the year ended June 30, 2017. These amounts represent the cost of materials, labor and overhead for single-use catheters, guide wires, pumps, and other ancillary products. The increase was primarily due to increased sales levels and a one-time charge of $1.5 million related to the initiation of a voluntary recall of one type of our saline infusion pumps, partially offset by lower costs per unit driven by manufacturing efficiencies and cost reductions. Gross margin increased to 80.8% for the year ended June 30, 2017 from 80.1% for the year ended June 30, 2016 due to lower costs per unit, as discussed above. Cost of goods sold for the years ended June 30, 2017 and 2016 includes $689,000 and $794,000, respectively, for stock-based compensation. We expect that gross margin in fiscal 2018 will be comparable to the year ended June 30, 2017. Quarterly margin fluctuations could occur based on production volumes, timing of new product introductions, sales mix, pricing changes, or other unanticipated circumstances.
Selling, General and Administrative Expenses. Selling, general, and administrative expenses decreased by $18.4 million, or 11.3%, from $162.5 million for the year ended June 30, 2016 to $144.1 million for the year ended June 30, 2017 primarily due to lower payroll-related and travel expenses from a decrease in headcount from the year ended June 30, 2016, commission plan changes, $1.5 million of prior year costs associated with the departure of our former CEO, and a reduction in medical device excise tax expense due to the suspension of the tax effective January 1, 2016. Partially offsetting the decreases was a charge of $1.3 million for employment litigation costs and an increase in incentive compensation expense due to performance. Selling, general, and administrative expenses for the years ended June 30, 2017 and 2016 include $8.7 million and $10.4 million, respectively, for stock-based compensation, which decreased due to the reduction in headcount and a change in vesting terms for our performance-based restricted stock awards granted in fiscal 2017 from those granted in fiscal 2016. We expect our selling, general and administrative expenses to increase as revenue grows in fiscal 2018, but at a rate less than the rate of revenue growth.
Research and Development Expenses. Research and development expenses decreased by $3.0 million, or 11.7%, from $25.9 million for the year ended June 30, 2016 to $22.9 million for the year ended June 30, 2017. Research and development expenses relate to the specific projects to develop new products or expand into new markets, such as the development of new versions of our Peripheral OAS and Coronary OAS, and ancillary products, and PAD and CAD clinical studies. The decrease primarily related to the completion of enrollment in several of our clinical studies and lower payroll-related expenses from a decrease in headcount from the year ended June 30, 2016. Partially offsetting these were higher patent expense and incentive compensation expense due to performance. Research and development expenses for the years ended June 30, 2017 and 2016 include $1.0 million and $1.8 million, respectively, for stock-based compensation, which decreased due to the reduction in headcount. We generally expect to incur research and development expenses higher in fiscal 2018 than amounts incurred for the year ended June 30, 2017 due to timing of projects and studies. Fluctuations could occur based on the number of projects and studies and the timing of expenditures.
Restructuring Charges. In March 2016, we announced a broad-based restructuring to reduce costs as a key part of our plan to balance revenue growth with a pathway to profitability and positive cash flow. As a result, we recorded a restructuring expense of $2.4 million during the year ended June 30, 2016, which was comprised of severance and other employee related costs. We do not anticipate additional charges related to restructuring activities.
Legal Settlement. On June 28, 2016, we entered into a Settlement Agreement with the United States of America, acting through the U.S. Attorney for the Western District of North Carolina (the “DOJ”) and on behalf of the Office of Inspector General of the Department of Health and Human Services, and Travis Thams (the “Relator”), to resolve the previously disclosed investigation by the DOJ and the qui tam complaint filed by the Relator pursuant to the False Claims Act in the United States District Court for the Western District of North Carolina, Charlotte Division. We recorded an $8.0 million legal settlement expense during the year ended June 30, 2016.
36
Comparison of Fiscal Year Ended June 30, 2016 with Fiscal Year Ended June 30, 2015
Year Ended June 30, | |||||||||||||
2016 | 2015 | Change | Percent Change | ||||||||||
Net revenues | $ | 178,184 | $ | 181,544 | $ | (3,360 | ) | (1.9 | )% | ||||
Cost of goods sold | 35,421 | 39,520 | (4,099 | ) | (10.4 | ) | |||||||
Gross profit | 142,763 | 142,024 | 739 | 0.5 | |||||||||
Gross margin | 80.1 | % | 78.2 | % | 1.9 | % | 2.4 | ||||||
Expenses: | |||||||||||||
Selling, general and administrative | 162,542 | 143,684 | 18,858 | 13.1 | |||||||||
Research and development | 25,934 | 30,977 | (5,043 | ) | (16.3 | ) | |||||||
Restructuring | 2,364 | — | 2,364 | 100.0 | |||||||||
Legal Settlement | 8,000 | — | 8,000 | 100.0 | |||||||||
Total expenses | 198,840 | 174,661 | 24,179 | 13.8 | |||||||||
Loss from operations | (56,077 | ) | (32,637 | ) | (23,440 | ) | 71.8 | ||||||
Other (income) and expense, net | (145 | ) | 71 | (216 | ) | (304.2 | ) | ||||||
Loss before income taxes | (55,932 | ) | (32,708 | ) | (23,224 | ) | 71.0 | ||||||
Provision for income taxes | 92 | 114 | (22 | ) | (19.3 | ) | |||||||
Net loss | $ | (56,024 | ) | $ | (32,822 | ) | $ | (23,202 | ) | 70.7 | |||
Net Revenues. Net revenues decreased by $3.4 million, or 1.9%, from $181.5 million for the year ended June 30, 2015, to $178.2 million for the year ended June 30, 2016. This decrease was primarily attributable to the expiration in June 2015 of our exclusive distribution agreement with Asahi to market its peripheral guidewire line in the U.S., which contributed approximately $7.5 million in sales during the year ended June 30, 2015. Revenues from our Peripheral OAS decreased $6.6 million, or 4.9%, primarily reflecting a 3.4% decrease in the average selling prices, as well as a 1.5% decrease in the number of devices sold, primarily resulting from challenges associated with the expansion of our sales force and the transition to a dual-franchise (peripheral and coronary) sales organization. Sales of our Coronary OAS increased approximately $9.2 million, or 34.2%, reflecting 35.2% more devices sold from the expansion of our customer base. Other product revenue decreased $6.0 million, or 29.5%, during the year ended June 30, 2016, driven by the absence of sales of the Asahi guidewires, partially offset by an increase of $1.6 million in other products that support our Peripheral OAS and Coronary OAS.
Cost of Goods Sold. Cost of goods sold decreased by $4.1 million, or 10.4%, from $39.5 million for the year ended June 30, 2015 to $35.4 million for the year ended June 30, 2016. These amounts represent the cost of materials, labor and overhead for single-use catheters, guide wires, pumps, and other ancillary products. The decrease was primarily due to lower indirect costs per unit sold from higher production volumes and manufacturing efficiencies. Gross margin increased to 80.1% for the year ended June 30, 2016 from 78.2% for the year ended June 30, 2015 due to lower costs per unit, as discussed above. Cost of goods sold for the years ended June 30, 2016 and 2015 includes $794,000 and $1.0 million, respectively, for stock-based compensation.
Selling, General and Administrative Expenses. Selling, general, and administrative expenses increased by $18.9 million, or 13.1%, from $143.7 million for the year ended June 30, 2015 to $162.5 million for the year ended June 30, 2016 primarily due to the expansion of our sales and administrative organizations. In addition, we incurred a $1.5 million expense associated with the departure of our former CEO and increased legal fees primarily associated with the DOJ matter discussed below. Partially offsetting the increase was a reduction in medical device excise tax expense of $1.5 million due to the suspension of the tax, effective January 1, 2016. Selling, general, and administrative expenses for the years ended June 30, 2016 and 2015 include $10.4 million and $12.2 million, respectively, for stock-based compensation, which decreased due to lower than expected attainment of performance based restricted stock award goals.
Research and Development Expenses. Research and development expenses decreased by $5.0 million, or 16.3%, from $31.0 million for the year ended June 30, 2015 to $25.9 million for the year ended June 30, 2016. Research and development expenses relate to the specific projects to develop new products or expand into new markets, such as the development of new versions of our Peripheral OAS and Coronary OAS, and ancillary products, and PAD and CAD clinical studies. The decrease primarily related to the completion of enrollment in several of our clinical studies. Research and development expenses for the years ended June 30, 2016 and 2015 include $1.8 million and $1.5 million, respectively, for stock-based compensation.
37
Restructuring Charges. In March 2016, we announced a broad-based restructuring to reduce costs as a key part of our plan to balance revenue growth with a pathway to profitability and positive cash flow. As a result, we recorded a restructuring expense of $2.4 million during the year ended June 30, 2016, which was comprised of severance and other employee related costs.
Legal Settlement. On June 28, 2016, we entered into a Settlement Agreement with the United States of America, acting through the DOJ and on behalf of the Office of Inspector General of the Department of Health and Human Services, and the Relator, to resolve the previously disclosed investigation by the DOJ and the qui tam complaint filed by the Relator pursuant to the False Claims Act in the U.S. District Court for the Western District of North Carolina, Charlotte Division. We recorded an $8.0 million legal settlement expense during the year ended June 30, 2016.
NON-GAAP FINANCIAL INFORMATION
To supplement our consolidated financial statements prepared in accordance with GAAP, our management uses a non-GAAP financial measure referred to as “Adjusted EBITDA.” The following table sets forth, for the periods indicated, a reconciliation of Adjusted EBITDA to the most comparable United States GAAP measure expressed as dollar amounts (in thousands):
Year Ended June 30, | |||||||
2017 | 2016 | ||||||
Net loss | $ | (1,792 | ) | $ | (56,024 | ) | |
Less: Other (income) and expense, net | 164 | (145 | ) | ||||
Less: Provision for income taxes | 86 | 92 | |||||
Loss from operations | (1,542 | ) | (56,077 | ) | |||
Add: Stock-based compensation | 10,354 | 12,977 | |||||
Add: Depreciation and amortization | 4,135 | 3,917 | |||||
Adjusted EBITDA | $ | 12,947 | $ | (39,183 | ) | ||
Adjusted EBITDA improved as compared to the prior year due to the lower loss from operations as a result of higher revenues and lower costs, slightly offset by lower stock based compensation as a result of reduced headcount.
Use and Economic Substance of Non-GAAP Financial Measures Used and Usefulness of Such Non-GAAP Financial Measures to Investors
We use Adjusted EBITDA as a supplemental measure of performance and believe this measure facilitates operating performance comparisons from period to period and company to company by factoring out potential differences caused by depreciation and amortization expense and non-cash charges such as stock-based compensation. Our management uses Adjusted EBITDA to analyze the underlying trends in our business, assess the performance of our core operations, establish operational goals and forecasts that are used to allocate resources and evaluate our performance period over period and in relation to our competitors’ operating results. Additionally, our management is partially evaluated on the basis of Adjusted EBITDA when determining achievement of their incentive compensation performance targets. Management does not use this Adjusted EBITDA measure as a liquidity measure or in the calculation of our financial covenants under the revolving credit facility with Silicon Valley Bank.
We believe that presenting Adjusted EBITDA provides investors greater transparency to the information used by our management for its financial and operational decision-making and allows investors to see our results “through the eyes” of management. We also believe that providing this information better enables our investors to understand our operating performance and evaluate the methodology used by our management to evaluate and measure such performance.
The following is an explanation of each of the items that management excluded from Adjusted EBITDA and the reasons for excluding each of these individual items:
• | Stock-based compensation. Our management believes that excluding this item from our non-GAAP results is useful to investors to understand the application of stock-based compensation guidance and its impact on our operational performance and ability to make additional investments in the Company, and it allows for greater transparency to certain line items in our financial statements. |
• | Depreciation and amortization expense. Our management believes that excluding these items from our non-GAAP results is useful to investors to understand our operational performance and ability to make additional investments in the company. |
38
Material Limitations Associated with the Use of Non-GAAP Financial Measures and Manner in which We Compensate for these Limitations
Non-GAAP financial measures have limitations as analytical tools and should not be considered in isolation or as a substitute for our financial results prepared in accordance with GAAP. Some of the limitations associated with our use of these non-GAAP financial measures are:
• | Items such as stock-based compensation do not directly affect our cash flow position; however, such items reflect economic costs to us and are not reflected in our Adjusted EBITDA, and therefore these non-GAAP measures do not reflect the full economic effect of these items. |
• | Non-GAAP financial measures are not based on any comprehensive set of accounting rules or principles and therefore other companies may calculate similarly titled non-GAAP financial measures differently than we do, limiting the usefulness of those measures for comparative purposes. |
• | Our management exercises judgment in determining which types of charges or other items should be excluded from the non-GAAP financial measures we use. |
We compensate for these limitations by relying primarily upon our GAAP results and using non-GAAP financial measures only supplementally.
LIQUIDITY AND CAPITAL RESOURCES
We had cash and cash equivalents of $107.9 million and $60.6 million at June 30, 2017 and 2016, respectively. During the year ended June 30, 2017, net cash provided by operations was $19.6 million. As of June 30, 2017, we had an accumulated deficit of $329.3 million. We have historically funded our operating losses primarily from the issuance of common and preferred stock, convertible promissory notes, and debt.
Facility Sale
On December 29, 2016, we entered into a Purchase and Sale Agreement, as subsequently amended (collectively, the “Sale Agreement”), with Krishna Holdings, LLC (the “Buyer”), providing for the sale to Buyer of our headquarters facility in St. Paul, Minnesota (the “Facility”), for a cash purchase price of $21.5 million. On March 30, 2017, the sale of the Facility under the Sale Agreement closed. We received proceeds of approximately $20.9 million ($21.5 million less $556,000 of transaction expenses).
We intend to use the net proceeds from the sale for working capital and general corporate purposes, which may include, but are not limited to:
• | the funding of clinical trials and studies; |
• | sales and marketing programs; |
• | expansion into international markets; and |
• | development of new products. |
We may also use a portion of the net proceeds for the potential acquisition of, or investments in, businesses, technologies and products, although we have no current understandings, commitments or arrangements to do so. We cannot specify with certainty all of the particular uses for the net proceeds. Accordingly, we will retain broad discretion over the use of these net proceeds.
Revolving Credit Facility
On March 31, 2017, we entered into a Loan and Security Agreement (the “Loan Agreement”) with Silicon Valley Bank (“SVB”). The Loan Agreement provides for a senior, secured revolving credit facility (the “Revolver”) of $40.0 million (the “Maximum Dollar Amount”).
Advances under the Revolver may be made from time to time up to the Maximum Dollar Amount, subject to certain borrowing limitations. The Revolver has a maturity date of March 31, 2020 and bears interest at a floating per annum rate equal to the Wall Street Journal prime rate, less 0.25%. Interest on borrowings is due monthly and the principal balance is due at maturity. Borrowings up to $10.0 million are available on a non-formula basis. Borrowings above $10.0 million are based on (i) 85% of eligible domestic accounts receivable, and (ii) the lesser of 50% of eligible inventory or $5.0 million, subject to adjustment as
39
defined in Loan Agreement. Upon the Revolver’s maturity, any outstanding principal balance, unpaid accrued interest, and all other obligations under the Revolver will be due and payable. We will incur a fee equal to 1% of the Maximum Dollar Amount upon termination of the Loan Agreement or the Revolver for any reason prior to the maturity date, unless refinanced with SVB.
Our obligations under the Loan Agreement are secured by certain of our assets, including, among other things, accounts receivable, deposit accounts, inventory, equipment, general intangibles and records pertaining to the foregoing. The collateral does not include our intellectual property, but we agreed not to encumber our intellectual property without the consent of SVB. The Loan Agreement contains customary covenants limiting our ability to, among other things, incur debt or liens, make certain investments and loans, enter into transactions with affiliates, undergo certain fundamental changes, dispose of assets, or change the nature of its business. In addition, the Loan Agreement contains financial covenants requiring us to maintain, at all times when any amounts are outstanding under the Revolver, either (i) minimum unrestricted cash at SVB and unused availability on the Revolver of at least $10.0 million or (ii) minimum trailing three-month Adjusted EBITDA of $1.0 million. If we do not comply with the various covenants under the Loan Agreement, the interest rate on outstanding amounts will increase by 5% and SVB may, subject to various customary cure rights, decline to provide additional advances under the Revolver, require the immediate payment of all amounts outstanding under the Revolver, and foreclose on all collateral.
Under the Loan Agreement, we paid SVB a non-refundable commitment fee of $80,000, which will be amortized to interest expense over the term of the Loan Agreement. We are required to pay a fee equal to 0.35% per annum on the unused portion of the Revolver, payable quarterly in arrears. SVB’s obligations to advance funds under the Revolver are subject to an initial collateral examination to be completed within 90 days of the effective date of the Loan Agreement. We are not obligated to draw any funds under the Revolver and no amounts are outstanding as of June 30, 2017. We currently do not have plans of borrowing under the Loan Agreement.
Changes in Liquidity
Cash and Cash Equivalents. Cash and cash equivalents was $107.9 million and $60.6 million at June 30, 2017 and 2016, respectively. The increase was primarily attributable to net cash provided by our financing and operating activities during the year ended June 30, 2017.
Operating Activities. Net cash provided by (used in) operating activities was $19.6 million, $(23.6) million, and $(22.4) million for the years ended June 30, 2017, 2016, and 2015, respectively. For the years ended June 30, 2017, 2016, and 2015, we had a net loss of $1.8 million, $56.0 million, and $32.8 million, respectively, and stock based compensation expense of $10.4 million, $13.0 million, and $14.7 million, respectively. Significant changes in working capital during these periods included:
• | Cash (used in) provided by accounts receivable of $(5.8) million, $7.3 million, and $(10.6) million during the years ended June 30, 2017, 2016, and 2015, respectively, was primarily due to the amount and timing of revenue during the periods. |
• | Cash provided by (used in) inventories was $543,000, $(3.5) million, and $(1.1) million during the years ended June 30, 2017, 2016, and 2015, respectively. Cash provided by inventory during fiscal 2017 was primarily due to lower inventory levels from better inventory management. Cash used by inventory during fiscal 2016 and 2015 was due to higher levels of inventory for future sales growth and new product launches, such as the Diamondback 360 Low Profile Peripheral OAS commercial launch in fiscal 2016 and Coronary OAS commercial launch throughout fiscal 2016 and fiscal 2015, as well as timing of inventory purchases and sales. |
• | Cash (used in) provided by prepaid expenses and other current assets was $(1.8) million, $728,000, and $(1.2) million during the years ended June 30, 2017, 2016, and 2015, respectively, primarily due to payment timing of vendor deposits and other expenditures. |
• | Cash provided by (used in) accounts payable of $1.8 million, $(970,000), and $581,000 during the years ended June 30, 2017, 2016, and 2015, respectively, was primarily due to the amount and timing of purchases and vendor payments. |
40
• | Cash provided by accrued expenses and other liabilities was $725,000, $10.9 million, and $4.4 million during the years ended June 30, 2017, 2016, and 2015, respectively. Cash provided in fiscal 2017 was primarily due to the amount and timing of compensation payments. Cash provided in fiscal 2016 was primarily due to the restructuring accrual, benefits related to our former CEO’s departure, and the Department of Justice legal settlement expense. Cash provided in fiscal 2015 was primarily due to higher accruals for the executive deferred compensation plan, higher payroll and vacation liabilities related to increased headcount, clinical study accruals for increased activity, and the general timing and payment of accruals. |
Investing Activities. Net cash used in investing activities was $1.8 million, $3.8 million, and $23.0 million for the years ended June 30, 2017, 2016, and 2015, respectively. Cash used in fiscal 2017 was primarily due to the purchase of property and equipment and patents. During fiscal 2016, cash was used primarily for the purchase of property and equipment and patents, and for the issuance of a convertible note receivable, partially offset by the sale of available-for-sale marketable securities under the deferred compensation plan. During fiscal 2015, cash was used primarily for the construction of our new headquarters and the related equipment purchases. In addition, we purchased available-for-sale marketable securities for the deferred compensation plans.
Financing Activities. Net cash provided by financing activities was $29.5 million, $4.1 million, and $2.6 million during the years ended June 30, 2017, 2016, and 2015, respectively. Cash provided by financing activities during these periods included:
• | Proceeds of $20.9 million from the sale of the Facility in March 2017. |
• | Employee stock purchase plan purchases of $3.3 million, $3.1 million, and $2.9 million during the years ended June 30, 2017, 2016, and 2015, respectively. |
• | Proceeds from the exercise of stock options of $5.3 million, $1.0 million, and $2.2 million during the years ended June 30, 2017, 2016, and 2015, respectively. |
Cash used in financing activities in these periods included payments on long-term debt of $2.4 million during the year ended June 30, 2015.
Our future liquidity and capital requirements will be influenced by numerous factors, including the extent and duration of future operating losses, the level and timing of future sales and expenditures, the results and scope of ongoing research and product development programs, working capital required to support our business operations, the receipt of and time required to obtain regulatory clearances and approvals, our sales and marketing programs, the continuing acceptance of our products in the marketplace, competing technologies, market and regulatory developments, ongoing facility requirements, potential strategic transactions (including the potential acquisition of, or investments in, businesses, technologies and products), international expansion, and the existence, defense and resolution of legal proceedings. As of June 30, 2017, we believe our current cash and cash equivalents will be sufficient to fund working capital requirements, capital expenditures and operations for the foreseeable future, including at least the next twelve months, as well as to fund payments related to the DOJ settlement, expenses relating to implementation and compliance with our Corporate Integrity Agreement, payments under our lease agreements, payments related to our restructuring and departure of our former CEO and anticipated costs relating to litigation. We intend to retain any future earnings to support operations and to finance the growth and development of our business. We do not anticipate paying any dividends in the foreseeable future.
Legal Settlement
On June 28, 2016, we entered into a Settlement Agreement with the United States of America, acting through the U.S. Attorney’s Office for the Western District of North Carolina and on behalf of the Office of Inspector General of the Department of Health and Human Services (the “OIG”), and Travis Thams, pursuant to which we will pay $8.0 million as follows: an initial payment of $3.0 million, which we paid on July 1, 2016, with the remaining $5.0 million, which bears interest at 1.8% per annum, payable in 11 equal quarterly installments, beginning January 1, 2017. Under the Settlement Agreement, if we make a single payment in excess of $2.0 million, which payment is not covered by an insurance policy, in settlement of any claims before paying the full Settlement Amount, the remaining unpaid balance of the Settlement Amount will become immediately due and payable, with interest accruing on the unpaid principal portion at an interest rate of 1.8% per annum. Accordingly, with respect to the employment litigation matter described below, in the event that a final, non-appealable judgement requires us to pay an amount more than $2.0 million that is not covered by an insurance policy, the remaining Settlement Amount, plus accrued interest, will be due and payable at the time of such payment.
In connection with the resolution of this matter, we entered into a five-year corporate integrity agreement (the “Corporate Integrity Agreement”) with the OIG. The Corporate Integrity Agreement requires that we maintain our existing compliance programs and imposes certain expanded compliance-related requirements during the term of the Corporate Integrity
41
Agreement, including establishment of specific procedures and requirements regarding consulting activities, co-marketing activities and other interactions with healthcare professionals and healthcare institutions and the sale and marketing of our products; ongoing monitoring, reporting, certification and training obligations; and the engagement of an independent review organization to perform certain auditing and reviews and prepare certain reports regarding our compliance with federal health care programs. In the event of a breach of the Corporate Integrity Agreement, we could become liable for payment of certain stipulated penalties or could be excluded from participation in federal health care programs. The Corporate Integrity Agreement requires us to invest additional amounts in our compliance program and pay fees and expenses of the independent review organization.
Restructuring
In March 2016, we announced a broad-based restructuring to reduce costs as a part of our plan to progress towards profitability and positive cash flow. As a result, we recorded a restructuring expense of $2.4 million during the year ended June 30, 2016, which was comprised of severance and other employee related costs. As of June 30, 2017, approximately $169,000 is payable over the next twelve months and $22,000 payable in subsequent periods. See Note 2 to our Consolidated Financial Statements included in Item 8 of this Annual Report on Form 10-K for additional discussion.
CEO Departure
In February, 2016, our former CEO resigned from his positions as President and CEO of the Company and as a director of the Company. The Company and the former CEO entered into a Separation Agreement with benefits consistent with our Amended and Restated Executive Officer Severance Plan. As of June 30, 2017, there was approximately $413,000 that will be paid in the next twelve months and $14,000 subsequently payable. See Note 2 to our Consolidated Financial Statements included in Item 8 of this Annual Report on Form 10-K for additional discussion.
Facility Lease
We entered into a Lease Agreement (the “Lease Agreement”) with Krishna Holdings, LLC, Apex Holdings, LLC, Kashi Associates, LLC, Keva Holdings, LLC, S&V Ventures, LLC, Polo Group LLC, SPAV Holdings LLC, Star Associates LLC, and The Global Villa, LLC. The Lease Agreement has an initial term of fifteen years, with four consecutive renewal options of five years each, with a base annual rent in the first year of $1.6 million and annual escalations of 3%. See Note 2 to our Consolidated Financial Statements included in Item 8 of this Annual Report on Form 10-K for additional discussion.
Pump Recall
In April 2017, we initiated a voluntary recall of one type of our saline infusion pumps. We plan to recall and replace approximately 900 units that were in customer inventory at the time the recall commenced and recorded a reserve for approximately $1.5 million of expenses during the year ended June 30, 2017 related to the recall and replacement of all affected saline infusion pumps. As of June 30, 2017, we had 338 pumps remaining to be replaced.
Employee Litigation
We are party to Steven Babyak v. Cardiovascular Systems, Inc., a lawsuit originally filed in the Superior Court of California, County of Los Angeles, on November 16, 2015. The plaintiff, a former Regional Sales Manager, made claims under California law relating to whistleblower retaliation; defamation; discrimination on the basis of association with protected group; harassment on the basis of sex in violation of FEHA; retaliation for exercising rights under FEHA; failure to prevent discrimination, harassment & retaliation in violation of FEHA; wrongful termination in violation of public policy; and violation of business and professions code. Following an April 2017 trial, a jury awarded the plaintiff $2.7 million in compensatory damages with respect to his claims for whistleblower retaliation and wrongful termination in violation of public policy. The jury also awarded the plaintiff $22.4 million in punitive damages with respect to the same claims. We filed post-trial motions for judgment notwithstanding the verdict and a new trial, on the grounds that this case was incorrectly decided as to liability, the compensatory and punitive damages were not appropriate and were excessive, and we were prevented from a fair trial by the improper exclusion of critical evidence. On June 29, 2017, the Court partially granted our motions, reducing the punitive damages award from $22.4 million to $2.7 million but denied our other motions. We believe that this case was incorrectly decided as to liability and the appropriateness and amount of any damages and we filed a Notice of Appeal on July 24, 2017.
We have accrued $2.6 million in the year ended June 30, 2017 based on our estimate of the range of possible losses and have recorded a receivable for $1.3 million of insurance proceeds related to the claim, under the guidance of ASC 450 and 210, respectively.
42
Contractual Cash Obligations. Our contractual obligations and commercial commitments as of June 30, 2017 are summarized below:
Payments Due by Period (in thousands) | |||||||||||||||||||
Contractual Obligations | Total | Less Than 1 Year | 1-3 Years | 3-5 Years | More Than 5 Years | ||||||||||||||
Operating leases(1) | $ | 1,377 | $ | 551 | $ | 826 | $ | — | $ | — | |||||||||
Financing obligation(2) | 30,046 | 1,650 | 3,449 | 3,660 | 21,287 | ||||||||||||||
Purchase commitments(3) | 19,054 | 19,054 | — | — | — | ||||||||||||||
Legal settlement(4) | 4,128 | 1,814 | 2,314 | — | — | ||||||||||||||
Severance payments(5) | 1,236 | 1,138 | 98 | — | — | ||||||||||||||
Other(6) | 199 | 133 | 66 | — | — | ||||||||||||||
Total | $ | 56,040 | $ | 24,340 | $ | 6,753 | $ | 3,660 | $ | 21,287 | |||||||||
(1) | The amounts represent future minimum payments under a non-cancellable operating leases for our offices and production facility along with equipment. |
(2) | The amounts represent future minimum payments due under the capital lease related to the sale leaseback of our Facility. |
(3) | The amount represents open purchase orders as of June 30, 2017. |
(4) | Consists of payments and related interest associated with the DOJ Settlement discussed above. |
(5) | Includes severance related to our former CEO, restructuring activities, and other severance agreements. |
(6) | Other includes service agreements. |
Due to the uncertainty with respect to the timing of future cash flows associated with our unrecognized tax benefits at June 30, 2017, we are unable to make reasonably reliable estimates of the period of cash settlement with the respective taxing authority. Therefore, $570,000 of unrecognized tax benefits have been excluded from the contractual obligations table above.
INFLATION
We do not believe that inflation has had a material impact on our business and operating results during the periods presented.
OFF-BALANCE SHEET ARRANGEMENTS
Since inception, we have not engaged in any off-balance sheet arrangements as defined in Item 303(a)(4) of Regulation S-K.
RECENT ACCOUNTING PRONOUNCEMENTS
In May 2014, the Financial Accounting Standards Board (“FASB”) issued amended revenue recognition guidance to clarify the principles for recognizing revenue from contracts with customers. The guidance requires an entity to recognize revenue in an amount that reflects the consideration to which an entity expects to be entitled in exchange for the transfer of goods or services. The guidance also requires expanded disclosures relating to the nature, amount, timing, and uncertainty of revenue and cash flows arising from contracts with customers. Additionally, qualitative and quantitative disclosures are required about customer contracts, significant judgments and changes in judgments, and assets recognized from the costs to obtain or fulfill a contract. We are working through an adoption plan which will include a review of customer contracts, applying the five-step model of the new standard to the customer contracts and comparing the results to our current accounting. As part of this, we are evaluating the method of adoption and assessing changes that might be necessary to information technology systems, processes, and internal controls to capture new data and address changes in financial reporting. Effective July 1, 2018, we will be revising our revenue recognition accounting policy and expanding revenue disclosures to reflect the requirements of the amended revenue recognition guidance. Because of the nature of the work that remains, at this time we are unable to reasonably estimate the impact of adoption on our consolidated financial statements.
In July 2015, the FASB issued ASU No. 2015-11, “Simplifying the Measurement of Inventory.” The guidance requires an entity to measure inventory within the scope of the ASU at the lower of cost and net realizable value. ASU 2015-11 is effective for annual periods, including interim periods within those annual periods, beginning after December 15, 2016 and should be applied prospectively. Early adoption is permitted. The guidance is effective on July 1, 2017. We do not anticipate a material impact on our financial statements upon adoption.
43
In November 2015, the FASB issued ASU 2015-17, “Balance Sheet Classification of Deferred Taxes.” The guidance requires that all deferred tax assets and liabilities, along with any related valuation allowance, be classified as noncurrent on the balance sheet. ASU 2015-17 is effective for annual periods, including interim periods within those annual periods, beginning after
December 15, 2016 and can be applied either prospectively or retrospectively. Early adoption is permitted. The guidance is effective on July 1, 2017. We do not anticipate a material impact on our financial statements upon adoption.
In February 2016, the FASB issued ASU 2016-02, “Leases.” The guidance requires lessees to recognize the assets and liabilities that arise from leases on the balance sheet. ASU 2016-02 is effective for annual periods beginning after December 15, 2018, including interim periods within those annual periods, and should be applied using a modified retrospective approach. Early adoption is permitted. The guidance is effective on July 1, 2019. We are currently evaluating the timing, method of adoption and impact of the new lease guidance on our financial statements.
In March 2016, the FASB issued ASU 2016-09, “Stock Compensation.” The guidance simplifies several aspects related to the accounting for share-based payment transactions, including the accounting for income taxes, classification on the statement of cash flows, forfeitures, and statutory withholding requirements. ASU 2016-09 is effective for annual periods beginning after December 15, 2016, and interim periods within those annual periods. Early adoption is permitted and transition requirements vary based on the amendments adopted. The guidance is effective on July 1, 2017. We are currently evaluating the impact of the stock compensation guidance on our financial statements.
In June 2016, the FASB issued ASU No. 2016-13, “Measurement of Credit Losses on Financial Instruments,” which revises guidance for the accounting for credit losses on financial instruments within its scope. The new standard introduces an approach, based on expected losses, to estimate credit losses on certain types of financial instruments and modifies the impairment model for available-for-sale debt securities. The new approach to estimating credit losses (referred to as the current expected credit losses model) applies to most financial assets measured at amortized cost and certain other instruments, including trade and other receivables, loans, held-to-maturity debt securities, net investments in leases and off-balance-sheet credit exposures. ASU 2016-13 is effective for annual periods beginning after December 15, 2019, including interim periods within those fiscal years. Early adoption is permitted and should be applied as a cumulative-effect adjustment to retained earnings as of the beginning of the first reporting period in which the guidance is adopted. The guidance is effective on July 1, 2020. We do not anticipate a material impact on our financial statements upon adoption.
In May 2017, the FASB issued ASU 2017-09, “Scope of Modification Accounting” which clarifies when changes to the terms or conditions of a share-based payment award must be accounted for as modifications. The new guidance will reduce diversity in practice and result in fewer changes to the terms of an award being accounted for as modifications. ASU 2017-09 will be applied prospectively to awards modified on or after the adoption date. The guidance is effective for annual periods, and interim periods within those annual periods beginning after December 15, 2017, with early adoption permitted. We do not anticipate a material impact on our financial statements upon adoption.
PRIVATE SECURITIES LITIGATION REFORM ACT
The Private Securities Litigation Reform Act of 1995 provides a “safe harbor” for forward-looking statements. Such “forward-looking” information is included in this Form 10-K and in other materials filed or to be filed by us with the Securities and Exchange Commission (as well as information included in oral statements or other written statements made or to be made by the Company). Forward-looking statements include all statements based on future expectations. This Form 10-K contains forward-looking statements that involve risks and uncertainties, including, but not limited to, (i) the expectation of selling our products, including recently approved products, domestically and internationally in the future and the timing and structure of our plans to do so; (ii) our strategy; (iii) the competitive benefits of our products; (iv) our expectations regarding reimbursement approval for our Coronary OAS device in Japan; (v) potential strategic acquisitions and partnerships; (vi) reimbursement of our products; (vii) our intention to expand our product portfolio through internal development and external relationships; (viii) our expectation that our losses will decline as our revenues grow; (ix) our plan to balance revenue growth with a pathway to profitability and positive cash flow; (x) our current and anticipated clinical studies, including the results and timing of such studies; (xi) the stockholder and employment litigation; (xii) our expectation that our revenue will increase; (xiii) our expectation of increased selling, general and administrative expenses and the rate of such growth; (xiv) our expectation that gross margin in fiscal 2018 will be comparable to fiscal 2017; (xv) our expectation that our current facilities will be adequate for the foreseeable future; (xvi) our plans to continue to expand our sales and marketing efforts as well as our product portfolio and clinical studies; (xvii) our intention to file additional patents and our efforts to protect our intellectual property; (xviii) our expectation that we will incur research and development expenses in fiscal 2018 higher than the amounts incurred for fiscal 2017; (xix) our anticipation that we will not incur additional charges related to restructuring activities; (xx) our belief that our current cash and cash equivalents will be sufficient to fund working capital requirements, capital expenditures and operations for the foreseeable future, as well as to fund certain other anticipated expenses; (xxi) our intention
44
to retain any future earnings to support operations and to finance the growth and development of our business; (xxii) our dividend expectations; (xxiii) our plans to use the net proceeds from the sale of our headquarters facility; (xxiv) our ability to obtain regulatory approvals to market our products; (xxv) the saline infusion pump recall; (xxvi) our plan not to borrow under the Loan Agreement; and (xxvii) the anticipated impact of adoption of recent accounting pronouncements on the our financial statements.
In some cases, you can identify forward-looking statements by the following words: “anticipate,” “believe,” “continue,” “could,” “estimate,” “expect,” “intend,” “may,” “ongoing,” “plan,” “potential,” “predict,” “project,” “should,” “will,” “would,” or the negative of these terms or other comparable terminology, although not all forward-looking statements contain these words. Forward-looking statements are only predictions and are not guarantees of performance. These statements are based on our management’s beliefs and assumptions, which in turn are based on their interpretation of currently available information.
These statements involve known and unknown risks, uncertainties and other factors that may cause our results or our industry’s actual results, levels of activity, performance or achievements to be materially different from the information expressed or implied by these forward-looking statements. These factors include regulatory developments in the United States, Japan and other foreign countries; FDA and similar Japanese and other foreign clearances and approvals; approval of our products for distribution in foreign countries; approval of products for reimbursement and the level of reimbursement in the U.S., Japan and other foreign countries; dependence on market growth; agreements with third parties to sell their products; our ability to maintain third-party supplier relationships and renew existing purchase agreements; our ability to maintain our relationship with our distribution partner in Japan; experience of physicians regarding the effectiveness and reliability of our products; the reluctance of physicians, hospitals and other organizations to accept new products; the potential for unanticipated delays in enrolling medical centers and patients for clinical trials; actual clinical trial and study results; the impact of competitive products and pricing; our ability to comply with the financial covenants in our loan and security agreement and to make payments under and comply with the lease agreement for our corporate headquarters; unanticipated developments affecting our estimates regarding expenses, future revenues and capital requirements; the difficulty of successfully managing operating costs; our ability to manage our sales force strategy; actual research and development efforts and needs; our ability to obtain and maintain intellectual property protection for product candidates; fluctuations in results and expenses based on new product introductions, sales mix, unanticipated warranty claims, and the timing of project expenditures; our ability to manage costs; our actual financial resources and our ability to obtain additional financing; investigations or litigation threatened or initiated against us; future actions by the FDA and other regulatory bodies; issues relating to our saline pump recall; and general economic conditions. These and additional risks and uncertainties are described more fully in Item 1A of this Form 10-K under “Risk Factors.”
You should read these risk factors and the other cautionary statements made in this Form 10-K as being applicable to all related forward-looking statements wherever they appear in this Form 10-K. We cannot assure you that the forward looking statements in this Form 10-K will prove to be accurate. Furthermore, if our forward-looking statements prove to be inaccurate, the inaccuracy may be material. You should read this Form 10-K completely. Other than as required by law, we undertake no obligation to update these forward-looking statements, even though our situation may change in the future.
Item 7A. Quantitative and Qualitative Disclosures About Market Risk.
The primary objective of our investment activities is to preserve our capital for the purpose of funding operations while at the same time maximizing the income we receive from our investments without significantly increasing risk or availability. To achieve these objectives, our investment policy allows us to maintain a portfolio of cash equivalents and investments in a variety of marketable securities, including money market funds, United States government securities, and certain bank obligations. Our cash and cash equivalents as of June 30, 2017 include liquid money market accounts. Due to the short-term nature of these investments, we believe that there is no material exposure to interest rate risk.
Additionally, we have certain available-for-sale marketable securities under our deferred compensation plan. See Note 1 to our Consolidated Financial Statements included in Item 8 of Part II of this Annual Report on Form 10-K for additional information on these available-for-sale marketable securities.
45
Item 8. Financial Statements and Supplementary Data.
Index to Financial Statements
Page | |
F-1 | |
F-2 | |
F-3 | |
F-4 | |
F-5 | |
F-6 | |
F-7 | |
46
Report of Independent Registered Public Accounting Firm
To the Board of Directors and Shareholders of Cardiovascular Systems, Inc.
In our opinion, the accompanying consolidated balance sheets and the related consolidated statements of operations, of comprehensive loss, of changes in stockholders’ equity and of cash flows present fairly, in all material respects, the financial position of Cardiovascular Systems, Inc. and its subsidiaries as of June 30, 2017 and 2016, and the results of their operations and their cash flows for each of the three years in the period ended June 30, 2017 in conformity with accounting principles generally accepted in the United States of America. Also in our opinion, the Company maintained, in all material respects, effective internal control over financial reporting as of June 30, 2017, based on criteria established in Internal Control - Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO). The Company's management is responsible for these financial statements, for maintaining effective internal control over financial reporting and for its assessment of the effectiveness of internal control over financial reporting, included in Management’s Annual Report on Internal Control Over Financial Reporting under Item 9A. Our responsibility is to express opinions on these financial statements and on the Company's internal control over financial reporting based on our integrated audits. We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audits to obtain reasonable assurance about whether the financial statements are free of material misstatement and whether effective internal control over financial reporting was maintained in all material respects. Our audits of the financial statements included examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements, assessing the accounting principles used and significant estimates made by management, and evaluating the overall financial statement presentation. Our audit of internal control over financial reporting included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, and testing and evaluating the design and operating effectiveness of internal control based on the assessed risk. Our audits also included performing such other procedures as we considered necessary in the circumstances. We believe that our audits provide a reasonable basis for our opinions.
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (i) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (ii) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (iii) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
PricewaterhouseCoopers LLP
Minneapolis, Minnesota
August 24, 2017
F-1
Cardiovascular Systems, Inc.
Consolidated Balance Sheets
(Dollars in thousands, except per share and share amounts)
June 30, 2017 | June 30, 2016 | ||||||
ASSETS | |||||||
Current assets | |||||||
Cash and cash equivalents | $ | 107,912 | $ | 60,638 | |||
Accounts receivable, net | 28,472 | 23,128 | |||||
Inventories | 16,897 | 17,440 | |||||
Marketable securities | 704 | 684 | |||||
Prepaid expenses and other current assets | 5,074 | 2,992 | |||||
Total current assets | 159,059 | 104,882 | |||||
Property and equipment, net | 29,696 | 32,471 | |||||
Patents, net | 5,056 | 5,013 | |||||
Other assets | 129 | 40 | |||||
Total assets | $ | 193,940 | $ | 142,406 | |||
LIABILITIES AND STOCKHOLDERS’ EQUITY | |||||||
Current liabilities | |||||||
Accounts payable | 10,736 | 8,506 | |||||
Accrued expenses | 30,236 | 26,993 | |||||
Total current liabilities | 40,972 | 35,499 | |||||
Long-term liabilities | |||||||
Financing obligation | 21,100 | — | |||||
Deferred revenue | 10,000 | — | |||||
Other liabilities | 3,479 | 6,010 | |||||
Total liabilities | 75,551 | 41,509 | |||||
Commitments and contingencies | |||||||
Common stock, $0.001 par value at June 30, 2017 and 2016; authorized 100,000,000 common shares at June 30, 2017 and 2016; issued and outstanding 32,849,563 at June 30, 2017 and 32,792,497 at June 30, 2016 | 33 | 33 | |||||
Additional paid in capital | 447,559 | 428,235 | |||||
Accumulated other comprehensive income | 100 | 40 | |||||
Accumulated deficit | (329,303 | ) | (327,411 | ) | |||
Total stockholders’ equity | 118,389 | 100,897 | |||||
Total liabilities and stockholders’ equity | $ | 193,940 | $ | 142,406 | |||
The accompanying notes are an integral part of these consolidated financial statements.
F-2
Cardiovascular Systems, Inc.
Consolidated Statements of Operations
(Dollars in thousands, except per share and share amounts)
Year Ended June 30, | |||||||||||
2017 | 2016 | 2015 | |||||||||
Net revenues | $ | 204,906 | $ | 178,184 | $ | 181,544 | |||||
Cost of goods sold | 39,441 | 35,421 | 39,520 | ||||||||
Gross profit | 165,465 | 142,763 | 142,024 | ||||||||
Expenses: | |||||||||||
Selling, general and administrative | 144,096 | 162,542 | 143,684 | ||||||||
Research and development | 22,911 | 25,934 | 30,977 | ||||||||
Restructuring | — | 2,364 | — | ||||||||
Legal settlement | — | 8,000 | — | ||||||||
Total expenses | 167,007 | 198,840 | 174,661 | ||||||||
Loss from operations | (1,542 | ) | (56,077 | ) | (32,637 | ) | |||||
Other (income) and expense, net | 164 | (145 | ) | 71 | |||||||
Loss before income taxes | $ | (1,706 | ) | $ | (55,932 | ) | $ | (32,708 | ) | ||
Provision for income taxes | 86 | 92 | 114 | ||||||||
Net loss | $ | (1,792 | ) | $ | (56,024 | ) | $ | (32,822 | ) | ||
Basic and diluted earnings per share | $ | (0.06 | ) | $ | (1.72 | ) | $ | (1.04 | ) | ||
Basic and diluted weighted average shares outstanding | 32,373,709 | 32,537,621 | 31,547,711 | ||||||||
The accompanying notes are an integral part of these consolidated financial statements.
F-3
Cardiovascular Systems, Inc.
Consolidated Statements of Comprehensive Loss
(Dollars in thousands, except per share and share amounts)
Year Ended June 30, | |||||||||||
2017 | 2016 | 2015 | |||||||||
Net loss | $ | (1,792 | ) | $ | (56,024 | ) | $ | (32,822 | ) | ||
Other comprehensive income (loss): | |||||||||||
Unrealized gain on available for sale securities | 66 | 20 | 90 | ||||||||
Adjustment for net gain realized and included in interest and other, net | (6 | ) | (70 | ) | — | ||||||
Total change in unrealized gain (loss) on available for sale securities | 60 | (50 | ) | 90 | |||||||
Comprehensive loss | $ | (1,732 | ) | $ | (56,074 | ) | $ | (32,732 | ) | ||
The accompanying notes are an integral part of these consolidated financial statements.
F-4
Cardiovascular Systems, Inc.
Consolidated Statements of Changes in Stockholders’ Equity
(Dollars in thousands, except per share and share amounts)
Common Stock | Additional Paid In Capital | Accumulated Other Comprehensive Income | Accumulated Deficit | Total | ||||||||||||||||||
Shares | Amount | |||||||||||||||||||||
Balances at June 30, 2014 | 31,084,742 | $ | 31 | $ | 390,589 | $ | — | $ | (238,565 | ) | $ | 152,055 | ||||||||||
Stock-based compensation related to restricted stock awards, net | 469,575 | 1 | 14,088 | — | — | 14,089 | ||||||||||||||||
Exercise of stock options at $5.01-$12.37 per share | 222,937 | — | 2,152 | — | — | 2,152 | ||||||||||||||||
Employee stock purchase plan activity | 120,870 | — | 3,871 | — | — | 3,871 | ||||||||||||||||
Unrealized gain on marketable securities | — | — | — | 90 | — | 90 | ||||||||||||||||
Net loss | — | — | — | — | (32,822 | ) | (32,822 | ) | ||||||||||||||
Balances at June 30, 2015 | 31,898,124 | $ | 32 | $ | 410,700 | $ | 90 | $ | (271,387 | ) | $ | 139,435 | ||||||||||
Stock-based compensation related to restricted stock awards, net | 557,756 | $ | 1 | $ | 11,985 | $ | — | $ | — | $ | 11,986 | |||||||||||
Exercise of stock options at $7.90-$12.37 per share | 87,817 | — | 1,006 | — | — | 1,006 | ||||||||||||||||
Employee stock purchase plan activity | 248,800 | — | 4,544 | — | — | 4,544 | ||||||||||||||||
Unrealized gain on marketable securities | — | — | — | 20 | — | 20 | ||||||||||||||||
Net gain reclassified from accumulated other comprehensive income | — | — | — | (70 | ) | — | (70 | ) | ||||||||||||||
Net loss | — | — | — | — | (56,024 | ) | (56,024 | ) | ||||||||||||||
Balances at June 30, 2016 | 32,792,497 | $ | 33 | $ | 428,235 | $ | 40 | $ | (327,411 | ) | $ | 100,897 | ||||||||||
Stock-based compensation related to restricted stock awards, net | (635,018 | ) | $ | — | $ | 9,412 | $ | — | $ | — | $ | 9,412 | ||||||||||
Exercise of stock options at $7.90-$12.15 per share | 515,164 | — | 5,362 | — | (100 | ) | 5,262 | |||||||||||||||
Employee stock purchase plan activity | 176,920 | — | 4,550 | — | — | 4,550 | ||||||||||||||||
Unrealized gain on marketable securities | — | — | — | 66 | — | 66 | ||||||||||||||||
Net gain reclassified from accumulated other comprehensive income | — | — | — | (6 | ) | — | (6 | ) | ||||||||||||||
Net loss | — | — | — | — | (1,792 | ) | (1,792 | ) | ||||||||||||||
Balances at June 30, 2017 | 32,849,563 | $ | 33 | $ | 447,559 | $ | 100 | $ | (329,303 | ) | $ | 118,389 | ||||||||||
The accompanying notes are an integral part of these consolidated financial statements.
F-5
Cardiovascular Systems, Inc.
Consolidated Statements of Cash Flows
(Dollars in thousands)
Year Ended June 30, | |||||||||||
2017 | 2016 | 2015 | |||||||||
Cash flows from operating activities | |||||||||||
Net loss | $ | (1,792 | ) | $ | (56,024 | ) | $ | (32,822 | ) | ||
Adjustments to reconcile net loss to net cash used in operations | |||||||||||
Depreciation of property and equipment | 3,917 | 3,686 | 2,150 | ||||||||
Provision for doubtful accounts (including note receivable) | 465 | 725 | 1,121 | ||||||||
Amortization of patents | 218 | 231 | 171 | ||||||||
Write-off of patent costs | 733 | 168 | 43 | ||||||||
Loss on disposal of property and equipment | 158 | 170 | 121 | ||||||||
Stock-based compensation | 10,354 | 12,977 | 14,718 | ||||||||
Other | 138 | — | — | ||||||||
Changes in assets and liabilities | |||||||||||
Accounts receivable | (5,809 | ) | 7,327 | (10,568 | ) | ||||||
Inventories | 543 | (3,474 | ) | (1,076 | ) | ||||||
Prepaid expenses and other assets | (1,823 | ) | 728 | (1,183 | ) | ||||||
Accounts payable | 1,761 | (970 | ) | 581 | |||||||
Accrued expenses and other liabilities | 725 | 10,873 | 4,387 | ||||||||
Deferred revenue | 10,000 | — | — | ||||||||
Net cash provided by (used in) operations | 19,588 | (23,583 | ) | (22,357 | ) | ||||||
Cash flows from investing activities | |||||||||||
Expenditures for property and equipment | (981 | ) | (3,818 | ) | (20,325 | ) | |||||
Issuance of convertible note receivable | — | (350 | ) | — | |||||||
Purchases of marketable securities | — | (37 | ) | (2,112 | ) | ||||||
Sales of marketable securities | 46 | 1,249 | 365 | ||||||||
Costs incurred in connection with patents | (844 | ) | (813 | ) | (955 | ) | |||||
Net cash used in investing activities | (1,779 | ) | (3,769 | ) | (23,027 | ) | |||||
Cash flows from financing activities | |||||||||||
Proceeds from the employee stock purchase plan | 3,254 | 3,142 | 2,882 | ||||||||
Exercise of stock options | 5,263 | 1,006 | 2,152 | ||||||||
Payments on borrowings | — | — | (2,400 | ) | |||||||
Proceeds from financing | 20,944 | — | — | ||||||||
Other | 4 | — | — | ||||||||
Net cash provided by financing activities | 29,465 | 4,148 | 2,634 | ||||||||
Net change in cash and cash equivalents | 47,274 | (23,204 | ) | (42,750 | ) | ||||||
Cash and cash equivalents | |||||||||||
Beginning of period | 60,638 | 83,842 | 126,592 | ||||||||
End of period | $ | 107,912 | $ | 60,638 | $ | 83,842 | |||||
Noncash investing and financing activities | |||||||||||
Change in equipment included in accounts payable | $ | (319 | ) | $ | (374 | ) | $ | (469 | ) | ||
Change in patent costs included in accounts payable | $ | (150 | ) | $ | 87 | $ | (52 | ) | |||
Supplemental cash flow information | |||||||||||
Interest paid | $ | 500 | $ | — | $ | 23 | |||||
The accompanying notes are an integral part of these consolidated financial statements.
F-6
CARDIOVASCULAR SYSTEMS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
(dollars in thousands, except per share and share amounts)
1. Summary of Significant Accounting Policies
Company Description
Cardiovascular Systems, Inc. (the “Company”) was incorporated as Replidyne, Inc. (“Replidyne”) in Delaware in 2000. On February 25, 2009, Replidyne completed its business combination with Cardiovascular Systems, Inc., a Minnesota corporation, in accordance with the terms of the Agreement and Plan of Merger and Reorganization, dated as of November 3, 2008. At the effective time of the merger, Replidyne changed its name to Cardiovascular Systems, Inc.
The Company develops, manufactures and markets devices for the treatment of vascular diseases. The Company’s peripheral arterial disease (“PAD”) products, the Diamondback 360® Peripheral Orbital Atherectomy System (“OAS”) and the Stealth 360°® Peripheral OAS, are catheter-based platforms capable of treating a broad range of plaque types, including calcified plaque, in leg arteries both above and below the knee, and address many of the limitations associated with other surgical, catheter and pharmacological treatment alternatives. These devices use smaller access sheaths that can provide procedural benefits and allow physicians to treat PAD patients in a variety of vessel sizes, including the small and tortuous vessels located below the knee through alternative access sites in the ankle and foot as well as in the groin.
In October 2013, the Company received premarket approval from the U.S. Food and Drug Administration (“FDA”) to market the Diamondback 360® Coronary OAS as a treatment for severely calcified coronary arteries. In March 2017, the Company received approval from the FDA to market the Diamondback 360® Coronary OAS Micro Crown. The Coronary OAS Micro Crown is the only atherectomy device designed to treat both pilot tight, calcific lesions and treat 2.5 to 4mm vessels with a single device.
The Company is currently selling only in the United States. In November 2016, the Company signed an exclusive distribution agreement with Medikit Co., Ltd. (“Medikit”) to sell its Diamondback 360® Coronary and Peripheral OAS in Japan. In March 2017, the Company received approval from Japan’s Ministry of Health, Labor and Welfare for its Diamondback 360® Coronary OAS Micro Crown. Pending reimbursement approval, Japan would become the first international market for any of the Company’s products. The Company is currently evaluating options for additional international markets to expand the coronary and peripheral opportunities.
Principles of Consolidation
The consolidated balance sheets and statements of operations, comprehensive loss, changes in stockholders’ equity, and cash flows include the accounts of the Company and its wholly-owned subsidiary, after elimination of all intercompany transactions and accounts.
Cash and Cash Equivalents
The Company considers all money market funds and other investments purchased with an original maturity of three months or less to be cash and cash equivalents.
Accounts Receivable and Allowance for Doubtful Accounts
Trade accounts receivable are recorded at the invoiced amount and do not bear interest. Customer credit terms are established prior to shipment with the general standard being net 30 days. Collateral or any other security to support payment of these receivables generally is not required. The Company maintains an allowance for doubtful accounts, which is an estimate regularly evaluated by the Company for adequacy by taking into consideration factors such as past experience, credit quality of the customer base, age of the receivable balances, both individually and in the aggregate, and current economic conditions that may affect a customer’s ability to pay. Provisions for the allowance for doubtful accounts attributed to bad debt are recorded in general and administrative expenses.
F-7
CARDIOVASCULAR SYSTEMS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
The following table shows the allowance for doubtful accounts activity:
Amount | |||
Balances at June 30, 2014 | $ | 451 | |
Provision for doubtful accounts | 1,121 | ||
Write-offs | (135 | ) | |
Balance at June 30, 2015 | 1,437 | ||
Provision for doubtful accounts | 375 | ||
Write-offs | (1,100 | ) | |
Balance at June 30, 2016 | 712 | ||
Provision for doubtful accounts | 465 | ||
Write-offs | (313 | ) | |
Balance at June 30, 2017 | $ | 864 | |
Inventories
Inventories are stated at the lower of cost or market with cost determined on a first-in, first-out method of valuation. The establishment of inventory allowances for excess and obsolete inventories is based on estimated exposure on specific inventory items. We write down our inventories as we become aware of any situation where the carrying amount exceeds the estimated realizable value based on assumptions about future demands and market conditions.
Property and Equipment
Property and equipment is carried at cost, less accumulated depreciation and amortization. Depreciation is computed using the straight-line method over estimated useful lives of 40 years for the building; five to seven years for production equipment and furniture and fixtures; three years for computer equipment and software; and the shorter of their estimated useful lives or the lease term for leasehold improvements. Expenditures for maintenance and repairs and minor renewals and betterments that do not extend or improve the life of the respective assets are expensed as incurred. All other expenditures for renewals and betterments are capitalized. The assets and related depreciation accounts are adjusted for property retirements and disposals with the resulting gains or losses included in the consolidated statement of operations.
Patents
The capitalized costs incurred to obtain patents are amortized using the straight-line method over their remaining estimated lives. Patent amortization begins at the time of patent application approval, and does not exceed 20 years. The recoverability of capitalized patent costs is dependent upon the Company’s ability to derive revenue-producing products from such patents or the ultimate sale or licensing of such patent rights. Patent recoverability is regularly reviewed and any patents that are abandoned are written off at the time of abandonment.
Long-Lived Assets
The Company regularly evaluates the carrying value of long-lived assets for events or changes in circumstances that indicate that the carrying amount may not be recoverable or that the remaining estimated useful life should be changed. An impairment loss is recognized when the carrying amount of an asset exceeds the anticipated future undiscounted cash flows expected to result from the use of the asset and its eventual disposition. The amount of the impairment loss to be recorded, if any, is calculated by the excess of the asset’s carrying value over its fair value.
Operating Leases
The Company leases its Texas manufacturing facilities under an operating lease agreement. The lease contains rent escalation clauses for which the lease expense is recognized on a straight-line basis over the lease term. Rent expense that is recognized but not yet paid is included in other liabilities on the consolidated balance sheets.
F-8
CARDIOVASCULAR SYSTEMS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Financing Obligation
In March 2017, the Company entered into an agreement to lease the Minnesota facility. The Lease Agreement has an initial term of fifteen years, with four consecutive renewal options of five years each at the Company's option. As the lease terms resulted in a capital lease classification, the Company accounted for the sale and leaseback of the Minnesota facility as a financing transaction where the assets remain on the Company's balance sheet and a financing obligation was recorded for $20,944. As lease payments are made, they will be allocated between interest expense and a reduction of the financing obligation, resulting in a value of the financing obligation that is equivalent to the net book value of the assets at the end of the lease term. At the end of the lease (including any renewal option terms), the Company will remove the assets and financing obligation from its balance sheet.
Revenue Recognition
The Company sells the majority of its products via direct shipment to hospitals or clinics. The Company recognizes revenue when all of the following criteria are met: persuasive evidence of an arrangement exists; delivery has occurred; the sales price is fixed or determinable; and collectability is reasonably assured. Revenue recognition may occur upon shipment or upon delivery to the customer site, based on the contract terms. The Company records estimated sales returns, discounts and rebates as a reduction of net sales.
Costs related to products delivered are recognized in the period the revenue is recognized. Cost of goods sold consists primarily of raw materials, direct labor, and manufacturing overhead.
Warranty Costs
The Company provides its customers with the right to receive a replacement if a product is determined to be defective at the time of shipment. Warranty reserve provisions are estimated based on Company experience, volume, and expected warranty claims. Warranty reserve, provisions and claims were as follows:
Amount | |||
Balances at June 30, 2014 | $ | 116 | |
Provision | 377 | ||
Claims | (367 | ) | |
Balance at June 30, 2015 | 126 | ||
Provision | 490 | ||
Claims | (471 | ) | |
Balance at June 30, 2016 | 145 | ||
Provision | 1,733 | ||
Claims | (1,361 | ) | |
Balance at June 30, 2017 | $ | 517 | |
Pump Recall
In April 2017, the Company initiated a voluntary recall of one type of its saline infusion pumps. The Company is in the process of recalling and replacing approximately 900 units in customer inventory and recorded a reserve for approximately $1,535 of expenses during the year ended June 30, 2017, that included $1,378 of estimated costs related to the recall and replacement of all affected saline infusion pumps, accrued consulting fees, as well as an inventory reserve for pumps held in its inventory.
Litigation and Contingent Liabilities
The Company and its operations from time to time are, and in the future may be, parties to or targets of lawsuits, claims, investigations, and proceedings, which are handled and defended in the ordinary course of business. The Company accrues a liability for such matters when it is probable that a liability has been incurred and the amount can be reasonably estimated. When a single amount cannot be reasonably estimated but the cost can be estimated within a range, the Company accrues an amount based on management’s best estimate considering all facts and circumstances. The Company expenses legal costs, including those expected to be incurred in connection with a loss contingency, as incurred.
F-9
CARDIOVASCULAR SYSTEMS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Medical Device Excise Tax
The Patient Protection and Affordable Care Act of 2010 imposed a medical device excise tax on medical device manufacturers on their sales in the U.S. of certain devices, which was effective January 1, 2013. The excise tax is 2.3% of the taxable base and applies to a substantial majority of the Company’s sales. Effective January 1, 2016, the excise tax was suspended until the end of 2017. For the years ended June 30, 2017, 2016 and 2015, the Company incurred $0, $1,273, and $2,731 of expense, respectively.
Income Taxes
Deferred income taxes are recorded to reflect the tax consequences in future years of differences between the tax bases of assets and liabilities and their financial reporting amounts based on enacted tax rates applicable to the periods in which the differences are expected to affect taxable income. Valuation allowances are established when necessary to reduce deferred tax assets to the amount expected to be realized.
Developing a provision for income taxes, including the effective tax rate and the analysis of potential tax exposure items, if any, requires significant judgment and expertise in federal and state income tax laws, regulations and strategies, including the determination of deferred tax assets. The Company’s judgment and tax strategies are subject to audit by various taxing authorities.
Accounting guidance requires that accounting for uncertainty in income taxes is recognized in the financial statements. The guidance provides that a tax benefit from an uncertain tax position may be recognized when it is more likely than not that the position will be sustained upon examination, including resolutions of any related appeals or litigation processes, based on the technical merits of the position. Income tax positions must meet a more-likely-than-not recognition threshold to be recognized. The guidance also provides rules on measurement, derecognition, classification, interest and penalties, accounting in interim periods, disclosure and transition.
Research and Development Expenses
Research and development expenses include costs associated with the design, development, testing, enhancement and regulatory approval of the Company’s products. Research and development expenses include employee compensation (including stock-based compensation), supplies and materials, consulting expenses, patent amortization, travel and facilities overhead. The Company also incurs significant expenses to operate clinical trials, including trial design, third-party fees, clinical site reimbursement, data management and travel expenses. Research and development expenses are expensed as incurred. Expenses associated with patent applications are capitalized and amortized using the straight-line method over their remaining estimated lives. Patent amortization begins at the time of patent application approval, and does not exceed 20 years.
Concentration of Credit Risk
Financial instruments that potentially expose the Company to concentration of credit risk consist primarily of cash and cash equivalents, marketable securities and accounts receivable.
The Company maintains its cash balances primarily with one financial institution. These balances exceed federally insured limits. The Company has not experienced any losses in such accounts and believes it is not exposed to any significant credit risk in cash and cash equivalents.
The Company believes that the credit risk related to marketable securities is limited due to the adherence to an investment policy and that credit risk related to accounts receivable is limited due to a large customer base.
Marketable Securities
The Company’s marketable securities consist solely of available-for-sale securities and were valued in accordance with the fair value measurement guidance discussed below. Available-for-sale securities are carried at fair value with unrealized gains and losses reported as a component of stockholders’ equity as accumulated other comprehensive income (loss), net of tax. Realized gains and losses, if any, are calculated on the specific identification method and are included in interest and other, net in the consolidated statements of operations.
F-10
CARDIOVASCULAR SYSTEMS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Available-for-sale securities are reviewed for possible impairment at least quarterly, or more frequently if circumstances arise that may indicate impairment. When the fair value of the securities declines below the amortized cost basis, impairment is indicated and it must be determined whether it is other than temporary. Impairment is considered to be other than temporary if the Company: (i) intends to sell the security, (ii) will more likely than not be forced to sell the security before recovering its cost, or (iii) does not expect to recover the security’s amortized cost basis. If the decline in fair value is considered other than temporary, the cost basis of the security is adjusted to its fair market value and the realized loss is reported in earnings. Subsequent increases or decreases in fair value are reported in equity as accumulated other comprehensive income (loss).
Fair Value Measurements
Under the authoritative guidance for fair value measurements, fair value is defined as the exit price, or the amount that would be received to sell an asset or paid to transfer a liability in an orderly transaction between market participants as of the measurement date. The authoritative guidance also establishes a hierarchy for inputs used in measuring fair value that maximizes the use of observable inputs and minimizes the use of unobservable inputs by requiring that the most observable inputs be used when available. Observable inputs are inputs market participants would use in valuing the asset or liability developed based on market data obtained from sources independent of the Company. Unobservable inputs are inputs that reflect the Company’s assumptions about the factors market participants would use in valuing the asset or liability developed based upon the best information available in the circumstances. The categorization of financial assets and financial liabilities within the valuation hierarchy is based upon the lowest level of input that is significant to the fair value measurement.
The hierarchy is broken down into three levels defined as follows:
Level 1 Inputs — quoted prices in active markets for identical assets and liabilities
Level 2 Inputs — observable inputs other than quoted prices in active markets for identical assets and liabilities
Level 3 Inputs — unobservable inputs
As of June 30, 2017, the Company believes that the carrying amounts of its other financial instruments, including accounts receivable, accounts payable and accrued liabilities, approximate their fair value due to the short-term maturities of these instruments. See Note 4 for additional information.
Use of Estimates
The preparation of the Company’s consolidated financial statements in conformity with accounting principles generally accepted in the United States of America requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenues and expenses during the reporting period. Actual results could differ from those estimates and these differences could be material.
Stock-Based Compensation
The Company has stock-based compensation plans, which include stock options, nonvested share awards, and an employee stock purchase plan. Fair value of option awards is determined using option-pricing models, fair value of nonvested share awards with market conditions is determined using the Monte Carlo simulation, and fair value of nonvested share awards that vest based upon performance or service conditions is determined by the closing market price of the Company’s stock on the date of grant. Stock-based compensation expense is recognized ratably over the requisite service period for the awards expected to vest.
Recent Accounting Pronouncements
In May 2014, the Financial Accounting Standards Board (“FASB”) issued amended revenue recognition guidance to clarify the principles for recognizing revenue from contracts with customers. The guidance requires an entity to recognize revenue in an amount that reflects the consideration to which an entity expects to be entitled in exchange for the transfer of goods or services. The guidance also requires expanded disclosures relating to the nature, amount, timing, and uncertainty of revenue and cash flows arising from contracts with customers. Additionally, qualitative and quantitative disclosures are required about customer contracts, significant judgments and changes in judgments, and assets recognized from the costs to obtain or fulfill a contract. The Company is working through an adoption plan which will include a review of customer contracts, applying the five-step model of the new standard to the customer contracts and comparing the results to the Company’s current accounting. As part of this, the Company is evaluating the method of adoption and assessing changes that might be necessary to information
F-11
CARDIOVASCULAR SYSTEMS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
technology systems, processes, and internal controls to capture new data and address changes in financial reporting. Effective July 1, 2018, the Company will be revising its revenue recognition accounting policy and expanding revenue disclosures to reflect the requirements of the amended revenue recognition guidance. Because of the nature of the work that remains, at this time the Company is unable to reasonably estimate the impact of adoption on its consolidated financial statements.
In July 2015, the FASB issued ASU 2015-11, “Simplifying the Measurement of Inventory.” The guidance requires an entity to measure inventory within the scope of the ASU at the lower of cost and net realizable value. ASU 2015-11 is effective for annual periods, including interim periods within those annual periods, beginning after December 15, 2016 and should be applied prospectively. Early adoption is permitted. The guidance is effective for the Company on July 1, 2017. The Company does not anticipate a material impact on its financial statements upon adoption.
In November 2015, the FASB issued ASU 2015-17, “Balance Sheet Classification of Deferred Taxes.” The guidance requires that all deferred tax assets and liabilities, along with any related valuation allowance, be classified as noncurrent on the balance sheet. ASU 2015-17 is effective for annual periods, including interim periods within those annual periods, beginning after December 15, 2016 and can be applied either prospectively or retrospectively. Early adoption is permitted. The guidance is effective for the Company on July 1, 2017. The Company does not anticipate a material impact on its financial statements upon adoption.
In February 2016, the FASB issued ASU 2016-02, “Leases.” The guidance requires lessees to recognize the assets and liabilities that arise from leases on the balance sheet. ASU 2016-02 is effective for annual periods beginning after December 15, 2018, including interim periods within those annual periods, and should be applied using a modified retrospective approach. Early adoption is permitted. The guidance is effective for the Company on July 1, 2019. The Company is currently evaluating the timing, method of adoption and impact of the new lease guidance on its financial statements.
In March 2016, the FASB issued ASU 2016-09, “Stock Compensation.” The guidance simplifies several aspects related to the accounting for share-based payment transactions, including the accounting for income taxes, classification on the statement of cash flows, forfeitures, and statutory withholding requirements. ASU 2016-09 is effective for annual periods beginning after
December 15, 2016, and interim periods within those annual periods. Early adoption is permitted and transition requirements vary based on the amendments adopted. The guidance is effective for the Company on July 1, 2017. The Company is currently evaluating the impact of the stock compensation guidance on its financial statements.
In June 2016, the FASB issued ASU 2016-13, “Measurement of Credit Losses on Financial Instruments,” which revises guidance for the accounting for credit losses on financial instruments within its scope. The new standard introduces an approach, based on expected losses, to estimate credit losses on certain types of financial instruments and modifies the impairment model for available-for-sale debt securities. The new approach to estimating credit losses (referred to as the current expected credit losses model) applies to most financial assets measured at amortized cost and certain other instruments, including trade and other receivables, loans, held-to-maturity debt securities, net investments in leases and off-balance-sheet credit exposures. ASU 2016-13 is effective for annual periods beginning after December 15, 2019, including interim periods within those fiscal years. Early adoption is permitted and should be applied as a cumulative-effect adjustment to retained earnings as of the beginning of the first reporting period in which the guidance is adopted. The guidance is effective for the Company on July 1, 2020. The Company does not anticipate a material impact on its financial statements upon adoption.
In May 2017, the FASB issued ASU 2017-09, “Scope of Modification Accounting” which clarifies when changes to the terms or conditions of a share-based payment award must be accounted for as modifications. The new guidance will reduce diversity in practice and result in fewer changes to the terms of an award being accounted for as modifications. ASU 2017-09 will be applied prospectively to awards modified on or after the adoption date. The guidance is effective for annual periods, and interim periods within those annual periods beginning after December 15, 2017, with early adoption permitted. The Company does not anticipate a material impact on its financial statements upon adoption.
F-12
CARDIOVASCULAR SYSTEMS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
2. Selected Consolidated Financial Statement Information
Accounts Receivable, Net
Accounts receivable consists of the following:
June 30, | |||||||
2017 | 2016 | ||||||
Accounts receivable | $ | 29,336 | $ | 23,840 | |||
Less: Allowance for doubtful accounts | (864 | ) | (712 | ) | |||
Accounts receivable, net | $ | 28,472 | $ | 23,128 | |||
Inventories
Inventories consist of the following:
June 30, | |||||||
2017 | 2016 | ||||||
Raw materials | $ | 7,898 | $ | 7,439 | |||
Work in process | 1,221 | 1,142 | |||||
Finished goods | 7,778 | 8,859 | |||||
Inventories, net | $ | 16,897 | $ | 17,440 | |||
Property and Equipment
Property and equipment consists of the following:
June 30, | |||||||
2017 | 2016 | ||||||
Land | $ | 500 | $ | 500 | |||
Building | 22,420 | 22,575 | |||||
Equipment | 16,502 | 14,141 | |||||
Furniture | 2,709 | 2,709 | |||||
Leasehold improvements | 86 | 86 | |||||
Construction in progress | 421 | 1,533 | |||||
42,638 | 41,544 | ||||||
Less: Accumulated depreciation | (12,942 | ) | (9,073 | ) | |||
Total Property and equipment, net | $ | 29,696 | $ | 32,471 | |||
On December 29, 2016, the Company entered into a Purchase and Sale Agreement, as subsequently amended (collectively, the “Sale Agreement”), with Krishna Holdings, LLC (the “Buyer”), providing for the sale to Buyer of the Company’s headquarters facility in St. Paul, Minnesota (the “Facility”), for a cash purchase price of $21,500. On March 30, 2017, the sale of the Facility under the Sale Agreement closed. The Company received proceeds of approximately $20,944 ($21,500, less $556 of transaction expenses). The net proceeds are to be used for working capital and general corporate purposes. In connection with the sale, the Company recorded an impairment charge of $158.
Under the Sale Agreement, the Company entered into a Lease Agreement (the “Lease Agreement”) with Krishna Holdings, LLC, Apex Holdings, LLC, Kashi Associates, LLC, Keva Holdings, LLC, S&V Ventures, LLC, Polo Group LLC, SPAV Holdings LLC, Star Associates LLC, and The Global Villa, LLC. As the lease terms resulted in a capital lease classification, the Company accounted for the sale and leaseback of the Facility as a financing transaction where the assets remain on the Company’s balance sheet. See Note 3 for further discussion on future payment obligations under the Lease Agreement.
F-13
CARDIOVASCULAR SYSTEMS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Patents, net
Patents, net consist of the following:
June 30, | |||||||
2017 | 2016 | ||||||
Patents | $ | 6,056 | $ | 6,049 | |||
Less: Accumulated amortization | (1,000 | ) | (1,036 | ) | |||
Total Patents, net | $ | 5,056 | $ | 5,013 | |||
As of June 30, 2017, future estimated amortization of patents is as follows:
2018 | $ | 198 | |
2019 | 190 | ||
2020 | 180 | ||
2021 | 180 | ||
2022 | 180 | ||
Thereafter | 4,128 | ||
$ | 5,056 | ||
This future amortization expense is an estimate. Actual amounts may vary from these estimated amounts due to additional intangible asset acquisitions, approval of patents-in-process, potential impairment, change in useful life or other events.
Accrued Expenses
Accrued expenses consist of the following:
June 30, | |||||||
2017 | 2016 | ||||||
Salaries and bonus | $ | 8,247 | $ | 4,305 | |||
Commissions | 8,217 | 7,788 | |||||
Accrued vacation | 3,436 | 3,498 | |||||
Accrued excise, sales and other taxes | 3,497 | 3,372 | |||||
Accrued litigation | 2,600 | — | |||||
Legal settlement | 1,814 | 3,872 | |||||
Clinical studies | 657 | 1,757 | |||||
Restructuring | 169 | 1,337 | |||||
Other accrued expenses | 1,599 | 1,064 | |||||
Total Accrued expenses | $ | 30,236 | $ | 26,993 | |||
Legal Settlement
On June 28, 2016, the Company entered into a Settlement Agreement (the “Settlement Agreement”) with the United States of America, acting through the Department of Justice (the “DOJ”) and on behalf of the Office of Inspector General of the Department of Health and Human Services, and Travis Thams, to resolve the investigation by the DOJ and the Civil Action underlying such investigation. Under the Settlement Agreement, the Company agreed to pay $8,000 (the “Settlement Amount”), as follows: an initial payment of $3,000, paid on July 1, 2016, with the remaining $5,000, which bears interest at 1.8% per annum, payable in 11 equal quarterly installments, beginning January 1, 2017. The amount payable within the next twelve months is included in accrued expenses (as noted in the table above) with the long-term portion included in other liabilities (as noted in the table below). Under the Settlement Agreement, if the Company makes a single payment in excess of $2,000, which payment is not covered by an insurance policy, in settlement of any claims before paying the full Settlement Amount, the remaining unpaid balance of the Settlement Amount will become immediately due and payable, with interest accruing on the unpaid principal portion at an interest rate of 1.8% per annum.
F-14
CARDIOVASCULAR SYSTEMS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Restructuring
On March 31, 2016, the Company announced a restructuring to reduce costs as part of its plan to progress towards profitability and positive cash flow. As a result, the Company recorded a restructuring expense of $2,364 during the year ended June 30, 2016, which was comprised of severance and other employee related costs.
The following table provides information regarding the restructuring accrual:
Severance | |||
Restructuring accrual at June 30, 2015 | $ | — | |
Restructuring charge(1) | 2,311 | ||
Cash payments | (790 | ) | |
Restructuring accrual at June 30, 2016 | 1,521 | ||
Cash payments | (1,330 | ) | |
Restructuring accrual at June 30, 2017 | $ | 191 | |
(1) Excludes $55 of restructuring expense related to other employee related costs, and $(2) related to stock-based compensation modification expense.
The Company anticipates that $169 of the restructuring accrual at June 30, 2017, will be paid within the next twelve months and is therefore recorded in accrued expenses on the consolidated balance sheet. Estimated payments of $22, representing the long-term portion of benefits, are recorded in other liabilities on the consolidated balance sheet at June 30, 2017. The Company does not anticipate additional restructuring costs.
CEO Departure
On February 26, 2016, the Company’s former Chief Executive Officer (“CEO”) resigned from his positions as President and CEO of the Company and as a director of the Company. The Company and the former CEO entered into a Separation Agreement with benefits consistent with the Company’s Amended and Restated Executive Officer Severance Plan. The total expense related to the former CEO’s departure was $1,507 and was recorded in selling, general and administrative expenses for the year ended June 30, 2016. At June 30, 2017 approximately $413 of the package benefits is recorded in accrued expenses and $14 is recorded in other liabilities on the consolidated balance sheet, representing the long-term portion of the former CEO’s benefits.
Other Liabilities
The Company’s non-current other liabilities consist of the following:
June 30, | |||||||
2017 | 2016 | ||||||
Legal settlement | $ | 2,314 | $ | 4,128 | |||
Deferred compensation | 519 | 684 | |||||
Deferred grant incentive | 473 | 486 | |||||
Accrued severance | 99 | 610 | |||||
Other liabilities | 74 | 102 | |||||
Total Other liabilities | $ | 3,479 | $ | 6,010 | |||
Deferred Revenue
In November 2016, the Company signed an exclusive distribution agreement with Medikit to sell its Diamondback 360® Coronary and Peripheral OAS in Japan. To secure exclusive distribution rights, Medikit made an upfront payment of $10,000 to the Company, which is refundable based on the occurrence of certain events during the term of the agreement. The Company has classified the upfront payment as long-term based on its expectation of when revenue will be recognized. The classification will be re-evaluated on a quarterly basis.
F-15
CARDIOVASCULAR SYSTEMS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
3. Debt
Revolving Credit Facility
On March 31, 2017, the Company entered into a Loan and Security Agreement (the “Loan Agreement”) with Silicon Valley Bank (“SVB”). The Loan Agreement provides for a senior, secured revolving credit facility (the “Revolver”) of $40,000 (the “Maximum Dollar Amount”).
Advances under the Revolver may be made from time to time up to the Maximum Dollar Amount, subject to certain borrowing limitations. The Revolver has a maturity date of March 31, 2020 and bears interest at a floating per annum rate equal to the Wall Street Journal prime rate, less 0.25%. Interest on borrowings is due monthly and the principal balance is due at maturity. Borrowings up to $10,000 are available on a non-formula basis. Borrowings above $10,000 are based on (i) 85% of eligible domestic accounts receivable, and (ii) the lesser of 50% of eligible inventory or $5,000, subject to adjustment as defined in Loan Agreement. Upon the Revolver’s maturity, any outstanding principal balance, unpaid accrued interest, and all other obligations under the Revolver will be due and payable. The Company will incur a fee equal to 1% of the Maximum Dollar Amount upon termination of the Loan Agreement or the Revolver for any reason prior to the maturity date, unless refinanced with SVB.
The Company’s obligations under the Loan Agreement are secured by certain of the Company’s assets, including, among other things, accounts receivable, deposit accounts, inventory, equipment, general intangibles and records pertaining to the foregoing. The collateral does not include the Company’s intellectual property, but the Company has agreed not to encumber its intellectual property without the consent of SVB. The Loan Agreement contains customary covenants limiting the Company’s ability to, among other things, incur debt or liens, make certain investments and loans, enter into transactions with affiliates, undergo certain fundamental changes, dispose of assets, or change the nature of its business. In addition, the Loan Agreement contains financial covenants requiring the Company to maintain, at all times when any amounts are outstanding under the Revolver, either (i) minimum unrestricted cash at SVB and unused availability on the Revolver of at least $10,000 or (ii) minimum trailing three-month Adjusted EBITDA of $1,000. If the Company does not comply with the various covenants under the Loan Agreement, the interest rate on outstanding amounts will increase by 5% and SVB may, subject to various customary cure rights, decline to provide additional advances under the Revolver, require the immediate payment of all amounts outstanding under the Revolver, and foreclose on all collateral.
Under the Loan Agreement, the Company paid SVB a non-refundable commitment fee of $80, which is being amortized to interest expense over the term of the Loan Agreement. The Company is required to pay a fee equal to 0.35% per annum on the unused portion of the Revolver, payable quarterly in arrears. SVB’s obligations to advance funds under the Revolver are subject to an initial collateral examination to be completed within 90 days of the effective date of the Loan Agreement. The Company is not obligated to draw any funds under the Revolver and no amounts were outstanding as of June 30, 2017.
Financing Obligation
In connection with the sale of the Facility, the Company entered into an agreement to lease the Facility. The Lease Agreement has an initial term of 15 years, with four consecutive renewal options of 5 years each at the Company’s option, with a base annual rent in the first year of $1,638 and annual escalations of 3% thereafter. Rent during subsequent renewal terms will be at the then fair market rental rate. The effective interest rate is 7.89%.
Future payments under the initial term of the Lease Agreement as of June 30, 2017 are as follows:
2018 | $ | 1,650 | |
2019 | 1,699 | ||
2020 | 1,750 | ||
2021 | 1,803 | ||
2022 | 1,857 | ||
Thereafter | 21,287 | ||
$ | 30,046 | ||
F-16
CARDIOVASCULAR SYSTEMS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
4. Deferred Compensation
The Company offers certain members of management and highly compensated employees the opportunity to defer up to 100% of their base salary (after 401(k), payroll tax and other deductions), performance bonus and discretionary bonus and elect to receive the deferred compensation at a fixed future date of participant’s choosing. Each participant may, at the time of his or her deferral election, choose to allocate the deferred compensation into investment alternatives set by the Human Resources and Compensation Committee. The amount payable to each participant under the plan will change in value based upon the investment selected by that participant and is classified as current or long-term on the Company’s balance sheet based on the disbursement elections made by the participants. As of June 30, 2017, $185 of the amount is included in accrued liabilities and $519 is included in other liabilities on the consolidated balance sheet.
The available-for-sale marketable securities are primarily comprised of investments with a fixed income and equity investments and consist of the following:
As of June 30, 2017 | |||||||||||||
Amortized Cost | Unrealized Gains | Unrealized Losses | Fair Value | ||||||||||
Mutual funds | $ | 604 | 100 | — | $ | 704 | |||||||
Total marketable securities | $ | 604 | 100 | — | $ | 704 | |||||||
As of June 30, 2016 | |||||||||||||
Amortized Cost | Unrealized Gains | Unrealized Losses | Fair Value | ||||||||||
Mutual funds | $ | 644 | 40 | — | $ | 684 | |||||||
Total marketable securities | $ | 644 | 40 | — | $ | 684 | |||||||
During the years ended June 30, 2017 and 2016, there were $0 and $37, respectively, in purchases of available-for-sale securities and $40 and $1,249, respectively, of available-for-sale securities that were sold. There were no other-than-temporary impairments during the years ended June 30, 2017 and 2016. During the years ended June 30, 2017 and 2016, there was a realized gain of $6 and $70 that was recorded within interest and other, net on the consolidated statement of operations.
The following tables provide information by level for the Company’s available-for-sale marketable securities that were measured at fair value on a recurring basis:
Fair Value Measurements as of June 30, 2017 Using Inputs Considered as | |||||||||||||
Fair Value | Level 1 | Level 2 | Level 3 | ||||||||||
Mutual funds | $ | 704 | 281 | 423 | $ | — | |||||||
Total marketable securities | $ | 704 | 281 | 423 | $ | — | |||||||
Fair Value Measurements as of June 30, 2016 Using Inputs Considered as | |||||||||||||
Fair Value | Level 1 | Level 2 | Level 3 | ||||||||||
Mutual funds | $ | 684 | 425 | 259 | $ | — | |||||||
Total marketable securities | $ | 684 | 425 | 259 | $ | — | |||||||
The Company’s marketable securities classified within Level 1 are valued primarily using real-time quotes for transactions in active exchange markets. Marketable securities within Level 2 are valued using readily available pricing sources. There were no transfers of assets between Level 1 and Level 2 of the fair value measurement hierarchy during the year ended June 30, 2017. Any transfers between levels are recognized on the date of the event or when a change in circumstances causes a transfer.
F-17
CARDIOVASCULAR SYSTEMS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
5. Stock Options and Restricted Stock Awards
The Company maintains the 2014 Equity Incentive Plan (the “2014 Plan”) for the purpose of granting equity awards to employees and directors. The 2014 Plan was approved by the Company’s stockholders and became effective in November 2014 and was subsequently amended in May 2015. The 2014 Plan replaced the 2007 Equity Incentive Plan (the “2007 Plan”), and no further equity awards may be granted under the 2007 Plan. The Company also maintains one other terminated plan, the 2003 Stock Option Plan (the “2003 Plan”) (the 2014 Plan, the 2007 Plan, and the 2003 Plan are collectively referred to as the “Plans”).
The 2014 Plan allows for the granting of up to 2,030,000 shares of common stock as approved by the board of directors or committees thereof in the form of nonqualified or incentive stock options, restricted stock awards, restricted stock unit awards, performance share awards, performance unit awards or stock appreciation rights to officers, directors, consultants and employees of the Company.
Stock Options
All options granted under the Plans become exercisable over periods established at the date of grant. The option exercise price is generally not less than the estimated fair market value of the Company’s common stock at the date of grant, as determined by the Company’s management and board of directors. In addition, the Company has granted nonqualified stock options to a director outside of the Plans.
Stock option activity is as follows:
Number of Options | Weighted Average Exercise Price | |||||
Options outstanding at June 30, 2014 | 922,809 | $ | 10.16 | |||
Exercised | (222,937 | ) | $ | 9.65 | ||
Options outstanding at June 30, 2015 | 699,872 | $ | 10.32 | |||
Exercised | (87,817 | ) | $ | 11.46 | ||
Forfeited or expired | (5,176 | ) | $ | 12.37 | ||
Options outstanding at June 30, 2016 | 606,879 | $ | 10.14 | |||
Exercised | (519,297 | ) | $ | 10.33 | ||
Expired | (9,381 | ) | $ | 8.83 | ||
Options outstanding at June 30, 2017 | 78,201 | $ | 9.07 | |||
As of June 30, 2017, all options were fully vested. An employee’s vested options must be exercised at or within 90 days of termination to avoid forfeiture. The Company determined the fair value of options using the Black-Scholes option pricing model. The estimated fair value of options, including the effect of estimated forfeitures, was recognized as expense on a straight-line basis over the options’ vesting periods. There were no options granted during the years ended June 30, 2017, 2016 or 2015.
The aggregate intrinsic value of a stock option award is the amount by which the market value of the underlying stock exceeds the exercise price of the award. The aggregate intrinsic value for vested and outstanding options at June 30, 2017, 2016 and 2015, was $1,811, $4,025 and $11,286, respectively. The total aggregate intrinsic value of options exercised during the years ended June 30, 2017, 2016 and 2015, was $7,955, $417, and $4,907, respectively. Cash received from option exercises was $5,363, $1,006 and $2,152 for the years ended June 30, 2017, 2016 and 2015, respectively. The weighted average remaining contractual life of options outstanding at June 30, 2017 was 0.71 years. Shares supporting option exercises are sourced from new share issuances.
Restricted Stock
The fair value of each restricted stock award was equal to the fair market value of the Company’s common stock at the date of grant. Vesting of time based restricted stock awards range from one to three years. The estimated fair value of restricted stock awards, including the effect of estimated forfeitures, is recognized on a straight-line basis over the restricted stock’s vesting period.
F-18
CARDIOVASCULAR SYSTEMS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Restricted stock award activity is as follows:
Number of Shares | Weighted Average Grant Date Fair Value | |||||
Outstanding at June 30, 2014 | 1,169,266 | $ | 18.96 | |||
Granted | 362,072 | $ | 30.30 | |||
Forfeited | (119,081 | ) | $ | 21.43 | ||
Vested | (569,163 | ) | $ | 16.46 | ||
Outstanding at June 30, 2015 | 843,094 | $ | 25.16 | |||
Granted | 522,415 | $ | 19.30 | |||
Forfeited | (230,710 | ) | $ | 24.83 | ||
Vested | (487,226 | ) | $ | 22.27 | ||
Outstanding at June 30, 2016 | 647,573 | $ | 23.24 | |||
Granted | 258,346 | $ | 21.80 | |||
Forfeited | (103,140 | ) | $ | 22.11 | ||
Vested | (316,195 | ) | $ | 24.21 | ||
Outstanding at June 30, 2017 | 486,584 | $ | 21.26 | |||
Total fair value of time-based restricted stock that vested during fiscal 2017, 2016 and 2015 was $7,655, $10,851, and $9,370, respectively. Estimated pre-vesting forfeitures are considered in determining stock-based compensation expense. As of June 30, 2017, 2016 and 2015, the Company estimated its weighted average forfeiture rate at 17.1%, 17.0% and 19.2%, respectively. As of June 30, 2017, there was approximately $7,780 of total unrecognized compensation expense, net of the effect of estimated forfeitures, related to nonvested restricted stock awards which is expected to be recognized over a weighted-average period of 2.2 years.
Performance-Based Restricted Stock
The Company also grants performance based restricted stock awards to certain executives and other management. Fiscal 2017 awards vest based on the Company’s total shareholder return relative to total shareholder return of the peer group (a market condition), as measured by the closing prices of the stock of the Company and its peer group for the 90 trading days preceding July 1, 2016 compared to the closing prices for the 90 trading days preceding July 1, 2019. Fiscal 2016 and fiscal 2015 awards included grants that vested based upon the achievement of certain thresholds measuring total shareholder return during periods within the fiscal year as compared to a pre-determined peer group of companies, and grants that vest based upon achievement of certain thresholds measuring annual revenue growth during the fiscal year as compared to a pre-determined peer group of companies. The aggregate maximum shares granted were as follows:
Performance Measurement | 2017 | 2016 | 2015 | ||||||
Total shareholder return | 336,826 | 156,509 | 76,112 | ||||||
Annual revenue growth | N/A | 156,509 | 76,112 | ||||||
The results of the Company’s performance based restricted stock awards for fiscal 2016 and 2015 were as follows:
Total Shareholder Return | Annual Revenue Growth | ||||||||||
% Achievement | Shares Vested | % Achievement | Shares Vested | ||||||||
Fiscal 2015 | 69 | % | 26,339 | 200 | % | 76,112 | |||||
Fiscal 2016 | — | % | 0 | — | % | 0 | |||||
F-19
CARDIOVASCULAR SYSTEMS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Performance-based restricted stock award activity is as follows:
Number of Shares | Weighted Average Grant Date Fair Value | |||||
Outstanding at June 30, 2014 | 107,132 | $ | 14.68 | |||
Granted | 152,224 | $ | 22.03 | |||
Vested | (107,132 | ) | $ | 14.68 | ||
Outstanding at June 30, 2015 | 152,224 | $ | 22.03 | |||
Granted | 313,018 | $ | 16.67 | |||
Forfeited | (52,680 | ) | $ | 28.64 | ||
Vested | (102,451 | ) | $ | 25.58 | ||
Outstanding at June 30, 2016 | 310,111 | $ | 16.67 | |||
Granted | 336,826 | $ | 11.97 | |||
Forfeited | (328,353 | ) | $ | 16.41 | ||
Outstanding at June 30, 2017 | 318,584 | $ | 11.97 | |||
Total fair value of performance-based restricted stock that vested during fiscal 2017, 2016 and 2015 was $0, $2,621, and $1,573, respectively. Estimated pre-vesting forfeitures are considered in determining stock-based compensation expense. As of June 30, 2017, there was approximately 2,743 of total unrecognized compensation expense, related to nonvested performance-based restricted stock awards, which is expected to be recognized over a weighted-average period of 2 years.
Restricted Stock Units
The Company grants restricted stock units to members of the Board of Directors. Restricted stock units represent the right to receive payment in the form of shares of the Company’s common stock or in cash at the Company’s option. Restricted stock unit payments would occur within 30 days following the six month anniversary of the date that the director ceases to serve on the Board or, if the restricted stock units are granted in lieu of an annual cash retainer, on the payment date selected by the director that is at least two years after the grant date. The estimated fair value of restricted stock awards is recognized on a straight-line basis over the vesting period.
Restricted stock unit activity is as follows:
Number of Shares | Weighted Average Grant Date Fair Value | |||||
Restricted stock units outstanding at June 30, 2014 | 296,131 | $ | 10.09 | |||
Granted | 41,172 | $ | 29.57 | |||
Converted to common stock | (74,360 | ) | $ | 11.90 | ||
Restricted stock units outstanding at June 30, 2015 | 262,943 | $ | 12.62 | |||
Granted | 47,586 | $ | 22.27 | |||
Converted to common stock | (5,713 | ) | $ | 22.18 | ||
Restricted stock units outstanding at June 30, 2016 | 304,816 | $ | 13.95 | |||
Granted | 54,064 | $ | 21.21 | |||
Forfeited | (2,974 | ) | $ | 21.01 | ||
Converted to common stock | (6,476 | ) | $ | 29.34 | ||
Restricted stock units outstanding at June 30, 2017 | 349,430 | $ | 14.73 | |||
F-20
CARDIOVASCULAR SYSTEMS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Stock-Based Compensation Expense
The following amounts were recognized as stock-based compensation expense in the consolidated statements of operations:
Year Ended June 30, 2017 | Restricted Stock Awards | Employee Stock Purchase Plan | Restricted Stock Units | Total | ||||||||||||
Cost of goods sold | $ | 588 | $ | 101 | $ | — | $ | 689 | ||||||||
Selling, general and administrative | 6,568 | 1,065 | 1,024 | 8,657 | ||||||||||||
Research and development | 879 | 129 | — | 1,008 | ||||||||||||
Total stock-based compensation expense | $ | 8,035 | $ | 1,295 | $ | 1,024 | $ | 10,354 | ||||||||
Year Ended June 30, 2016 | Restricted Stock Awards | Employee Stock Purchase Plan | Restricted Stock Units | Total | ||||||||||||
Cost of goods sold | $ | 679 | $ | 115 | $ | — | $ | 794 | ||||||||
Selling, general and administrative | 8,215 | 1,167 | 1,000 | 10,382 | ||||||||||||
Research and development | 1,681 | 120 | — | 1,801 | ||||||||||||
Total stock-based compensation expense | $ | 10,575 | $ | 1,402 | $ | 1,000 | $ | 12,977 | ||||||||
Year Ended June 30, 2015 | Restricted Stock Awards | Employee Stock Purchase Plan | Restricted Stock Units | Total | ||||||||||||
Cost of goods sold | $ | 937 | $ | 64 | $ | — | $ | 1,001 | ||||||||
Selling, general and administrative | 10,486 | 825 | 917 | 12,228 | ||||||||||||
Research and development | 1,388 | 101 | — | 1,489 | ||||||||||||
Total stock-based compensation expense | $ | 12,811 | $ | 990 | $ | 917 | $ | 14,718 | ||||||||
Shares Available for Grant
The following summarizes shares available for grant under the Company’s 2014 Plan:
Shares available for grant at June 30, 2014 | — | |
Reserved | 2,030,000 | |
Granted | (171,411 | ) |
Forfeited or cancelled | 5,866 | |
Shares available for grant at June 30, 2015 | 1,864,455 | |
Granted | (883,019 | ) |
Forfeited or cancelled | 133,499 | |
Shares available for grant at June 30, 2016 | 1,114,935 | |
Granted | (649,236 | ) |
Forfeited or cancelled | 415,700 | |
Shares available for grant at June 30, 2017(a) | 881,399 | |
(a) | Excludes the effect of shares granted, exercised, forfeited or expired related to activity from shares granted outside of the 2014 Plan. |
6. Employee Stock Purchase Plan
The Company maintains an employee stock purchase plan (“ESPP”) that was approved by the Company’s stockholders in November 2015 (“2015 ESPP”) and replaced the previous ESPP that expired on May 31, 2016. The plan provides eligible employees the opportunity to acquire common stock in accordance with Section 423 of the Internal Revenue Code of 1986. Stock can be purchased each 6-month period per year (twice per year). The purchase price is equal to 85% of the lower of the price at the beginning or the end of the respective period. Employees purchased 176,920 shares at an average price of $18.39 per share during the year ended June 30, 2017. Shares reserved under the plan at June 30, 2017 totaled 1,844,370.
F-21
CARDIOVASCULAR SYSTEMS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
7. Income Taxes
The components of the Company’s overall deferred tax assets and liabilities are as follows:
June 30, | |||||||
2017 | 2016 | ||||||
Deferred tax assets | |||||||
Stock-based compensation | $ | 5,107 | $ | 3,375 | |||
Accrued expenses | 1,650 | 2,795 | |||||
Inventories | 433 | 382 | |||||
Compensation accruals | 261 | 254 | |||||
Depreciation and amortization | 409 | 360 | |||||
Other | 1,019 | 487 | |||||
Research and development credit carryforwards | 4,650 | 4,483 | |||||
Net operating loss carryforwards | 87,502 | 89,081 | |||||
Total deferred tax assets | 101,031 | 101,217 | |||||
Valuation allowance | (101,031 | ) | (101,217 | ) | |||
Net deferred tax assets | $ | — | $ | — | |||
The Company has established valuation allowances to fully offset its deferred tax assets due to the uncertainty about the Company’s ability to generate the future taxable income necessary to realize these deferred assets, particularly in light of the Company’s historical losses. The future use of net operating loss carryforwards is dependent on the Company attaining profitable operations, and may be limited in any one year under Internal Revenue Code Section 382 due to significant ownership changes, as defined under such Section, as a result of the Company’s equity financings. A summary of the valuation allowances are as follows:
Balances at June 30, 2014 | $ | 68,699 | |
Additions | 15,620 | ||
Balance at June 30, 2015 | 84,319 | ||
Additions | 16,898 | ||
Balance at June 30, 2016 | 101,217 | ||
Reductions | (186 | ) | |
Balance at June 30, 2017 | $ | 101,031 | |
As of June 30, 2017 and 2016, the Company had federal tax NOL carryforwards of approximately $239,308 and $244,214, respectively. These NOL carryforwards are available to offset taxable income through 2036 and begin to expire in 2018. The Company also had various state NOL carryforwards available to offset future state taxable income. These state NOL carryforwards typically have the same expirations as the Company’s federal tax NOL carryforwards.
Our federal net operating losses at June 30, 2017 do not include $42,097 of income tax deductions in excess of previously recorded tax benefits related to stock compensation. These additional tax deductions are not included in the net operating losses referenced above since the related tax benefit will not be recognized until the deductions reduce our income tax payable. The tax benefit of these excess deductions will be reflected as a credit to additional paid in capital when recognized. Accordingly, our deferred tax assets are reported net of the excess tax deductions for stock compensation.
As of June 30, 2017 and 2016, the Company had approximately $4,137 and $4,078 of federal research and development credit carryforwards, respectively. As of June 30, 2017 and 2016, the Company had approximately $1,560 and $1,370 of state research and development credit carryforwards. The federal and state research and development credit carryforwards will expire through fiscal 2037 and 2032, respectively.
As required by FASB ASC Topic 740, “Income Taxes,” the Company recognizes the financial statement benefit of a tax position only after determining that the relevant tax authority would more likely than not sustain the position following an audit. For tax positions meeting the more likely than not threshold, the amount recognized in the financial statements is the largest benefit that has a greater than 50 percent likelihood of being realized upon ultimate settlement with the relevant tax
F-22
CARDIOVASCULAR SYSTEMS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
authority. The Company recorded a liability relating to unrecognized tax benefits of $570 and $545 at June 30, 2017 and 2016, respectively. Due to the Company having a full valuation allowance, this liability has been netted against the deferred tax asset. The Company recognizes interest and penalties related to uncertain tax provisions as part of the provision for income taxes. The Company has not currently reserved for any interest or penalties for such reserves due to the Company being in an NOL position. The Company does not expect to recognize any benefits from the unrecognized tax benefits within the next twelve months. A reconciliation of the beginning and ending amount of unrecognized tax benefits is as follows (in thousands):
Balances at June 30, 2014 | $ | 458 | |
Increases related to prior year tax positions | 4 | ||
Increases related to current year tax positions | 32 | ||
Balances at June 30, 2015 | 494 | ||
Increases related to prior year tax positions | 10 | ||
Increases related to current year tax positions | 41 | ||
Balance at June 30, 2016 | 545 | ||
Decreases related to prior year tax positions | (8 | ) | |
Increases related to current year tax positions | 33 | ||
Balance at June 30, 2017 | $ | 570 | |
The Company is subject to income taxes in the U.S. federal jurisdiction and various state jurisdictions. Tax regulations within each jurisdiction are subject to the interpretation of the related tax laws and regulations and require significant judgment to apply. The Company is potentially subject to income tax examinations by tax authorities for the tax years ended June 30, 2017, 2016, 2015, and 2014. The Company is not currently under examination by any taxing jurisdiction.
8. Commitments and Contingencies
Operating Leases
The Company leases manufacturing space, equipment and apartments under lease agreements that expire at various dates through March 2020. Rental expenses were $656, $1,049, and $1,760, for the years ended June 30, 2017, 2016, and 2015, respectively. The decrease in rent expense in fiscal 2017 and 2016 relates to the completion of construction of the Company’s headquarters, which replaced space previously leased by the Company. In March 2017, the Company sold the headquarters facility and began leasing that facility.
Future minimum lease payments under the agreements as of June 30, 2017 are as follows:
2018 | $ | 551 | |
2019 | 472 | ||
2020 | 354 | ||
2021 | — | ||
2022 | — | ||
Thereafter | — | ||
$ | 1,377 | ||
Employment Litigation
The Company is party to Steven Babyak v. Cardiovascular Systems, Inc., a lawsuit originally filed in the Superior Court of California, County of Los Angeles, on November 16, 2015. The plaintiff, a former Regional Sales Manager of the Company, made claims under California law relating to whistleblower retaliation; defamation; discrimination on the basis of association with protected group; harassment on the basis of sex in violation of FEHA; retaliation for exercising rights under FEHA; failure to prevent discrimination, harassment & retaliation in violation of FEHA; wrongful termination in violation of public policy; and violation of business and professions code. Following an April 2017 trial, a jury awarded the plaintiff $2,700 in compensatory damages with respect to his claims for whistleblower retaliation and wrongful termination in violation of public policy. The jury also awarded the plaintiff $22,400 in punitive damages with respect to the same claims. The Company filed post-trial motions for judgment notwithstanding the verdict and a new trial, on the grounds that this case was incorrectly decided as to liability, the compensatory and punitive damages were not appropriate and were excessive, and the Company was
F-23
CARDIOVASCULAR SYSTEMS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
prevented from a fair trial by the improper exclusion of critical evidence. On June 29, 2017, the Court partially granted the Company’s motions, reducing the punitive damages award from $22,400 to $2,700 but denied the Company’s other motions. The Company believes that this case was incorrectly decided as to liability and the appropriateness and amount of any damages and the Company filed a Notice of Appeal on July 24, 2017.
The Company has accrued $2,600 as of June 30, 2017 based on the estimate of the range of the loss that the Company believes is probable of occurring. However, it is reasonably possible that the ultimate loss, if the Company is not able to successfully challenge the verdict, could be materially different than the amount that the Company has recorded. The Company will continue to monitor the accrual associated with this matter each reporting period and make adjustments, if necessary, based on additional facts as they arise. The amounts are reflected in selling, general and administrative expenses on the Company’s consolidated statement of operations. Additionally, as of June 30, 2017, the Company has recorded a receivable of $1,300 associated with its present assessment of the probable amount of insurance proceeds the Company would receive related to the claim, based on the accrued amount of loss referenced above. The Company estimates insurance receivables based on an analysis of its policies, including their exclusions, an assessment of the nature of each claim and remaining coverage, information from its insurance carrier, and the probable loss range referenced above. The Company then records an amount it has concluded is probable. Similar to the accrual pertaining to this matter, the Company will continue to assess the probable amount of insurance proceeds expected to be received in this case each reporting period and make adjustments, if necessary, based on additional facts as they arise.
Stockholder Securities Litigation
On February 12, 2016, a stockholder purporting to represent a class of persons who purchased the Company’s securities between September 12, 2011 and January 21, 2016 filed a lawsuit against the Company and certain of its officers in the U.S. District Court for the Central District of California, Paradis v. Cardiovascular Systems, Inc., et al., 2:16-cv-01011 (C.D. Cal.). The lawsuit alleges that the Company made materially false and misleading statements and failed to disclose material adverse facts about the Company’s business, operational and financial performance, in violation of federal securities laws, relating to (1) alleged kickbacks to health care providers, (2) alleged off-label promotion of medical devices, and (3) alleged violations of the Food and Drug Administration’s laws and regulations in connection with the Company’s medical devices. On March 4, 2016, a second stockholder filed a similar lawsuit against the Company and certain of its officers in the U.S. District Court for the District of Minnesota, Shoemaker v. Cardiovascular Systems, Inc. et al., 0:16-cv-00568 (D. Minn.). The plaintiffs seek unspecified monetary damages on behalf of the alleged class, interest, and attorney’s fees and costs of litigation.
On April 12, 2016, four motions for appointment as lead plaintiff were filed in the Paradis action and three of the four proposed plaintiffs also filed a motion for appointment as lead plaintiff in the Shoemaker action.
On April 26, 2016, the Paradis action was voluntarily dismissed by plaintiffs in favor of the Shoemaker action. That same day, the Shoemaker court entered an order appointing the City of Miami Fire Fighters’ & Police Officers’ Retirement Trust and the County Retirement Systems as Co-Lead Plaintiffs for representing the putative class. On June 28, 2016, the Co-Lead Plaintiffs filed a new complaint. The Company filed a motion to dismiss the complaint in this action on August 29, 2016. A hearing was held on the motion to dismiss on December 2, 2016. On March 29, 2017, the court granted the Company’s motion to dismiss the complaint and dismissed the plaintiffs’ amended complaint without prejudice. The court granted the plaintiffs’ request for leave to amend their complaint, and on June 27, 2017, the plaintiffs filed an amended complaint. The complaint makes similar allegations as the original complaint, namely, that the Company made materially false and misleading statements and failed to disclose material adverse facts about its business, operational and financial performance, in violation of federal securities laws, relating to alleged kickbacks to health care providers. The plaintiffs seek unspecified monetary damages on behalf of the alleged class, interest, and attorney’s fees and costs of litigation. The Company filed a motion to dismiss the amended complaint on August 11, 2017. The Company believes that this lawsuit is without merit and intends to defend itself vigorously.
Other Matters
In the ordinary conduct of business, the Company is subject to various lawsuits and claims covering a wide range of matters including, but not limited to, employment claims and commercial disputes. While the outcome of these matters is uncertain, the Company does not believe there are any other significant matters as of June 30, 2017 that are probable or estimable, for which the outcome is reasonably possible of having a material adverse impact on its consolidated balance sheets or statements of operations.
F-24
CARDIOVASCULAR SYSTEMS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
9. Other (Income) and Expense, Net
Other (income) and expense, net, includes the following:
Year Ended June 30, | |||||||||||
2017 | 2016 | 2015 | |||||||||
Interest expense | $ | 500 | $ | — | $ | 23 | |||||
Interest income | (383 | ) | (163 | ) | (63 | ) | |||||
Other | 47 | 18 | 111 | ||||||||
Total Other (income) and expense, net | $ | 164 | $ | (145 | ) | $ | 71 | ||||
10. Employee Benefits
The Company offers a 401(k) plan to its employees. Eligible employees may authorize up to $18 of their annual compensation as a contribution to the plan, subject to Internal Revenue Service limitations. The plan also allows eligible employees over 50 years old to contribute an additional $6 subject to Internal Revenue Service limitations. All employees must be at least 21 years of age to participate in the plan. The Company did not provide any employer matching contributions for the years ended June 30, 2017, 2016, and 2015.
11. Earnings Per Share
The following table presents a reconciliation of the numerators and denominators used in the basic and diluted earnings per common share computations (in thousands except share and per share amounts):
Year Ended June 30, | |||||||||||
2017 | 2016 | 2015 | |||||||||
Numerator | |||||||||||
Net loss | $ | (1,792 | ) | $ | (56,024 | ) | $ | (32,822 | ) | ||
Denominator | |||||||||||
Weighted average common shares outstanding — basic | 32,373,709 | 32,537,621 | 31,547,711 | ||||||||
Effect of dilutive stock options(1) | — | — | — | ||||||||
Effect of dilutive restricted stock units(2) | — | — | — | ||||||||
Effect of performance-based restricted stock awards (3) | — | — | — | ||||||||
Weighted average common shares outstanding — diluted | 32,373,709 | 32,537,621 | 31,547,711 | ||||||||
Earnings per common share — basic and diluted | $ | (0.06 | ) | $ | (1.72 | ) | $ | (1.04 | ) | ||
(1) | At June 30, 2017, 2016, and 2015; 78,201, 606,879, and 699,872 stock options, respectively, were outstanding. The effect of the shares that would be issued upon exercise of these options has been excluded from the calculation of diluted loss per share because those shares are anti-dilutive. |
(2) | At June 30, 2017, 2016, and 2015; 349,430, 304,816 and 262,943 additional shares of common stock, respectively, were issuable upon the settlement of outstanding restricted stock units. The effect of the shares that would be issued upon settlement of these restricted stock units has been excluded from the calculation of diluted loss per share because those shares are anti-dilutive. |
(3) | At June 30, 2017, 318,584 performance-based restricted stock awards were outstanding. The effect of the shares that would be issued upon vesting of these awards has been excluded from the calculation of diluted loss per share because those shares are anti-dilutive. |
F-25
CARDIOVASCULAR SYSTEMS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
12. Quarterly Data (Unaudited)
The following table sets forth the Company’s unaudited quarterly summary consolidated statements of operations in each of the quarters for the years ended June 30, 2017 and 2016. The information for each of these quarters is unaudited and has been prepared on the same basis as the consolidated financial statements. This data should be read in conjunction with the consolidated financial statements and related notes. These operating results may not be indicative of results to be expected for any future period (amounts in thousands, except per share data).
2017 | |||||||||||||||||||
Q1 | Q2 | Q3 | Q4 | Total | |||||||||||||||
Net revenue | $ | 49,800 | $ | 50,043 | $ | 52,144 | $ | 52,919 | $ | 204,906 | |||||||||
Gross profit | $ | 40,334 | $ | 40,880 | $ | 41,005 | $ | 43,246 | $ | 165,465 | |||||||||
Net income (loss) | $ | (1,858 | ) | $ | 1,043 | $ | (1,749 | ) | $ | 772 | $ | (1,792 | ) | ||||||
Earnings per common share - basic(1) | $ | (0.06 | ) | $ | 0.03 | $ | (0.05 | ) | $ | 0.02 | $ | (0.06 | ) | ||||||
Earnings per common share - diluted(1) | $ | (0.06 | ) | $ | 0.03 | $ | (0.05 | ) | $ | 0.02 | $ | (0.06 | ) | ||||||
2016 | |||||||||||||||||||
Q1 | Q2 | Q3 | Q4 | Total | |||||||||||||||
Net revenue | $ | 43,871 | $ | 41,392 | $ | 44,461 | $ | 48,460 | $ | 178,184 | |||||||||
Gross profit | $ | 35,100 | $ | 33,321 | $ | 35,736 | $ | 38,606 | $ | 142,763 | |||||||||
Net loss | $ | (13,261 | ) | $ | (15,163 | ) | $ | (22,716 | ) | $ | (4,884 | ) | $ | (56,024 | ) | ||||
Earnings per common share (basic and diluted)(1) | $ | (0.41 | ) | $ | (0.47 | ) | $ | (0.69 | ) | $ | (0.15 | ) | $ | (1.72 | ) | ||||
(1) The summation of quarterly per share data may not equate to the calculation for the full fiscal year as quarterly calculations are performed on a discrete basis.
F-26
Item 9. Changes in and Disagreements With Accountants on Accounting and Financial Disclosure.
None.
Item 9A. Controls and Procedures.
Evaluation of Disclosure Controls and Procedures
Our Chief Executive Officer and our Chief Financial Officer, referred to collectively herein as the Certifying Officers, are responsible for establishing and maintaining our disclosure controls and procedures. The Certifying Officers have reviewed and evaluated the effectiveness of the Company’s disclosure controls and procedures (as defined in Rules 240.13a-15(e) and 15d-15(e) promulgated under the Securities Exchange Act of 1934, as amended (the “Exchange Act”)) as of June 30, 2017. Based on that review and evaluation, which included inquiries made to certain other employees of the Company, the Certifying Officers have concluded that, as of the end of the period covered by this Annual Report on Form 10-K, the Company’s disclosure controls and procedures, as designed and implemented, are effective.
Management’s Annual Report on Internal Control Over Financial Reporting
Management is responsible for establishing and maintaining adequate internal control over financial reporting (as defined in Rule 13a-15(f) under the Exchange Act) for the Company. Management conducted an evaluation of the effectiveness of internal control over financial reporting based on the framework in Internal Control — Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO). Based on this evaluation, management concluded that the Company’s internal control over financial reporting was effective as of June 30, 2017.
PricewaterhouseCoopers LLP, the independent registered public accounting firm that audited the consolidated financial statements included in this Annual Report on Form 10-K, has also audited the effectiveness of the Company’s internal control over financial reporting as of June 30, 2017, as stated in their attestation report included in Part IV, Item 15 of this Annual Report on Form 10-K.
Changes in Internal Control Over Financial Reporting
There were no changes in our internal control over financial reporting (as defined in Rules 13a-15(f) and 15d-15(f) under the Exchange Act) during the three months ended June 30, 2017 that have materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
Item 9B. Other Information.
None
47
PART III
Item 10. Directors, Executive Officers and Corporate Governance.
Other than the information included in this Form 10-K under the heading “Employees—Executive Officers of the Registrant,” which is set forth at the end of Item 1 and incorporated herein by reference, the information required by Item 10 is incorporated by reference to the sections labeled “Election of Directors,” “Information Regarding the Board of Directors and Corporate Governance” and “Section 16(a) Beneficial Ownership Reporting Compliance,” all of which will appear in our definitive proxy statement for our 2017 Annual Meeting.
Item 11. Executive Compensation.
The information required by Item 11 is incorporated herein by reference to the sections entitled “Executive Compensation,” “Director Compensation,” “Human Resources and Compensation Committee” and “Compensation Committee Interlocks and Insider Participation,” all of which will appear in our definitive proxy statement for our 2017 Annual Meeting.
Item 12. Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters.
The information required by Item 12 is incorporated herein by reference to the sections entitled “Security Ownership of Certain Beneficial Owners and Management” and “Equity Compensation Plan Information,” which will appear in our definitive proxy statement for our 2017 Annual Meeting.
Item 13. Certain Relationships and Related Transactions, and Director Independence.
The information required by Item 13 is incorporated herein by reference to the sections entitled “Independence of the Board of Directors” and “Transactions With Related Persons,” which will appear in our definitive proxy statement for our 2017 Annual Meeting.
Item 14. Principal Accounting Fees and Services.
The information required by Item 14 is incorporated herein by reference to the section entitled “Principal Accountant Fees and Services,” which will appear in our definitive proxy statement for our 2017 Annual Meeting.
48
PART IV
Item 15. Exhibits, Financial Statement Schedules.
(a) Documents filed as part of this report.
(1) | Financial Statements. The following financial statements are included in Part II, Item 8 of this Annual Report on Form 10-K: |
• | Report of Independent Registered Public Accounting Firm |
• | Consolidated Balance Sheets as of June 30, 2017 and 2016 |
• | Consolidated Statements of Operations for the years ended June 30, 2017, 2016 and 2015 |
• | Consolidated Statements of Comprehensive Loss for the years ended June 30, 2017, 2016 and 2015 |
• | Consolidated Statements of Stockholders’ Equity for the years ended June 30, 2017, 2016 and 2015 |
• | Consolidated Statements of Cash Flows for the years ended June 30, 2017, 2016 and 2015 |
• | Notes to Consolidated Financial Statements |
(2) Financial Statement Schedules.
• | All financial statement schedules have been omitted, because they are not applicable, are not required, or the information is included in the Financial Statements or Notes thereto |
(3) Exhibits. See “Exhibit Index” immediately following the signature page of this Form 10-K
49
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
CARDIOVASCULAR SYSTEMS, INC. | |||
Date: August 24, 2017 | By: | /s/ Scott R. Ward | |
Scott R. Ward | |||
Chairman, President and Chief Executive Officer | |||
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
Each person whose signature appears below constitutes and appoints Scott R. Ward and Laurence L. Betterley as the undersigned’s true and lawful attorneys-in fact and agents, each acting alone, with full power of substitution and resubstitution, for the undersigned and in the undersigned’s name, place and stead, in any and all amendments to this Annual Report on Form 10-K and to file the same, with all exhibits thereto, and other documents in connection therewith, with the Securities and Exchange Commission, granted unto said attorneys-in-fact and agents, each acting alone, full power and authority to do and perform each and every act and thing requisite and necessary to be done in and about the premises, as fully to all intents and purposes as the undersigned might or could do in person, hereby ratifying and confirming all said attorneys-in-fact and agents, each acting alone, or his substitute or substitutes, may lawfully do or cause to be done by virtue thereof.
Signature | Title | Date | ||
/s/ Scott R. Ward | Chairman, President and Chief Executive Officer(principal executive officer) | August 24, 2017 | ||
Scott R. Ward | ||||
/s/ Laurence L. Betterley | Chief Financial Officer (principal financial and accounting officer) | August 24, 2017 | ||
Laurence L. Betterley | ||||
/s/ Martha Goldberg Aronson | Director | August 24, 2017 | ||
Martha Goldberg Aronson | ||||
/s/ Scott Bartos | Director | August 24, 2017 | ||
Scott Bartos | ||||
/s/ Brent G. Blackey | Director | August 24, 2017 | ||
Brent G. Blackey | ||||
/s/ Edward Brown | Director | August 24, 2017 | ||
Edward Brown | ||||
/s/ William E. Cohn | Director | August 24, 2017 | ||
William E. Cohn | ||||
/s/ Augustine Lawlor | Director | August 24, 2017 | ||
Augustine Lawlor | ||||
50
EXHIBIT INDEX
CARDIOVASCULAR SYSTEMS, INC.
FORM 10-K
Exhibit No. | Description | |
3.1 | Restated Certificate of Incorporation, as amended (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed May 14, 2009). | |
3.2 | Amended and Restated Bylaws (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Current Report on Form 8-K filed on May 21, 2015). | |
4.1 | Specimen Common Stock Certificate (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Current Report on Form 8-K filed on March 3, 2009). | |
4.2 | Registration Rights Agreement by and among Cardiovascular Systems, Inc. and certain of its stockholders, dated as of March 16, 2009 (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Current Report on Form 8-K filed on March 18, 2009). | |
10.1† | Employment Agreement, dated April 7, 2008, by and between Cardiovascular Systems, Inc., a Minnesota corporation, and Laurence L. Betterley (previously filed with the SEC as an Exhibit to and incorporated herein by reference from CSI Minnesota, Inc.’s Registration Statement on Form S-1/A, File No. 333-148798, filed April 18, 2008). | |
10.2† | Employment Agreement, dated May 9, 2011, by and between Cardiovascular Systems, Inc. and Kevin J. Kenny (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Annual Report on Form 10-K filed September 12, 2011). | |
10.3† | Form of Standard Employment Agreement (previously filed with the SEC as an Exhibit to and incorporated herein by reference from CSI Minnesota, Inc.’s Registration Statement on Form S-1, File No. 333-148798, filed January 22, 2008). | |
10.4†* | Fiscal Year 2018 Executive Officer Base Salaries. | |
10.5†* | Fiscal 2018 Executive Officer Bonus Plan and Equity Compensation. | |
10.6†* | Fiscal Year 2018 Director Compensation Arrangements. | |
10.7† | Form of Director and Officer Indemnification Agreement (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed May 14, 2009). | |
10.8† | Cardiovascular Systems, Inc. Amended and Restated 2007 Equity Incentive Plan (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Registration Statement on Form S-8, File No. 333-158755, filed April 24, 3009). | |
10.9† | Form of Incentive Stock Option Agreement under the Amended and Restated 2007 Equity Incentive Plan (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed May 14, 2009). | |
10.10† | Form of Non-Qualified Stock Option Agreement under the Amended and Restated 2007 Equity Incentive Plan (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed May 14, 2009). | |
10.11† | Form of Restricted Stock Agreement under the Amended and Restated 2007 Equity Incentive Plan (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Annual Report on Form 10-K filed on September 12, 2011). | |
10.12† | Form of Restricted Stock Unit Agreement under the Amended and Restated 2007 Equity Incentive Plan (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Annual Report on Form 10-K filed on September 12, 2011). | |
10.13† | Form of Performance Share Award under the Amended and Restated 2007 Equity Incentive Plan (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed May 14, 2009). | |
10.14† | Form of Performance Unit Award under the Amended and Restated 2007 Equity Incentive Plan (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed May 14, 2009). | |
51
Exhibit No. | Description | |
10.15† | Form of Stock Appreciation Rights Agreement under the Amended and Restated 2007 Equity Incentive Plan (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed May 14, 2009). | |
10.16† | 2003 Stock Option Plan of Cardiovascular Systems, Inc., a Minnesota corporation, as amended (previously filed with the SEC as an Exhibit to and incorporated herein by reference from CSI Minnesota, Inc.’s Registration Statement on Form S-1, File No. 333-148798, filed January 22, 2008). | |
10.17† | Form of Incentive Stock Option Agreement under the 2003 Stock Option Plan of Cardiovascular Systems, Inc., a Minnesota corporation (previously filed with the SEC as an Exhibit to and incorporated herein by reference from CSI Minnesota, Inc.’s Registration Statement on Form S-1, File No. 333-148798, filed January 22, 2008). | |
10.18† | Form of Nonqualified Stock Option Agreement under the 2003 Stock Option Plan of Cardiovascular Systems, Inc., a Minnesota corporation (previously filed with the SEC as an Exhibit to and incorporated herein by reference from CSI Minnesota, Inc.’s Registration Statement on Form S-1, File No. 333-148798, filed January 22, 2008). | |
10.19 | Corporate Job Creation Agreement between Pearland Economic Development Corporation and Cardiovascular Systems, Inc., dated June 17, 2009 (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Annual Report on Form 10-K filed on September 28, 2009). | |
10.20 | Build-To-Suit Lease Agreement between Pearland Economic Development Corporation and Cardiovascular Systems, Inc., dated September 9, 2009 (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Annual Report on Form 10-K filed on September 28, 2009). | |
10.21+ | Supply Agreement, between Cardiovascular Systems, Inc. and Fresenius Kabi AB, effective April 4, 2011 (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed on May 13, 2011). | |
10.22 | Amendment to Corporate Job Creation Agreement, dated effective July 2, 2012, by and between the Company and Pearland Economic Development Corporation (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Annual Report on Form 10-K filed September 10, 2012). | |
10.23† | Amendment to Employment Agreement, dated December 31, 2012, by and between the Company and Laurence L. Betterley (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed February 8, 2013). | |
10.24† | Amendment to Employment Agreement, dated December 31, 2012, by and between the Company and Kevin J. Kenny (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed February 8, 2013). | |
10.25† | Cardiovascular Systems, Inc. Deferred Compensation Plan (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Current Report on Form 8-K filed December 17, 2013). | |
10.26+ | Purchasing Agreement, effective August 1, 2014, between Cardiovascular Systems, Inc. and Healthtrust Purchasing Group, L.P (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Annual Report on Form 10-K filed August 28, 2014). | |
10.27 | Development Services Agreement, dated June 11, 2014, by and between Cardiovascular Systems, Inc. and Ryan Companies US, Inc. (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Annual Report on Form 10-K filed August 28, 2014). | |
10.28 | Contract for Private Redevelopment, dated June 11, 2014, by and among Cardiovascular Systems, Inc., Ryan Companies US, Inc. and The City of New Brighton (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Annual Report on Form 10-K filed August 28, 2014). | |
10.29 | Design Build Cost Plus Construction Contract, dated June 11, 2014, by and between Cardiovascular Systems, Inc. and Ryan Companies US, Inc. (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Annual Report on Form 10-K filed August 28, 2014). | |
10.30† | Cardiovascular Systems, Inc. 2014 Equity Incentive Plan, as amended (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Annual Report on Form 10-K filed August 27, 2015). | |
10.31† | Form of Restricted Stock Agreement for Time-Based Awards under the 2014 Equity Incentive Plan (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed February 6, 2015). | |
10.32† | Form of Restricted Stock Agreement for Performance-Based Awards under the 2014 Equity Incentive Plan (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed February 6, 2015). | |
52
Exhibit No. | Description | |
10.33† | Amendment No. 2 to Employment Agreement, dated February 4, 2015, by and between Cardiovascular Systems Inc. and Kevin J. Kenny (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed May 8, 2015). | |
10.34† | Cardiovascular Systems, Inc. Amended Executive Officer Severance Plan (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Annual Report on Form 10-K filed August 25, 2016). | |
10.35† | Form of Restricted Stock Unit Agreement under the 2014 Equity Incentive Plan (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed May 8, 2015). | |
10.36† | Form of Restricted Stock Agreement under the 2014 Equity Incentive Plan (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed May 8, 2015). | |
10.37† | Cardiovascular Systems, Inc. 2015 Employee Stock Purchase Plan (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Current Report on Form 8-K filed November 19, 2015). | |
10.38† | Employment Letter, dated November 30, 2015 by and between Cardiovascular Systems, Inc. and Scott R. Ward (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed February 2, 2016). | |
10.39 | Confidentiality and Assignment of Inventions Agreement, dated November 30, 2015, by and between Cardiovascular Systems, Inc. and Scott R. Ward (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed February 2, 2016). | |
10.40 | Separation Agreement, between Cardiovascular Systems, Inc. and David Martin, dated February 26, 2016 (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Current Report on Form 8-K filed February 29, 2016). | |
10.41 | Amendment No. 1 to Supply Agreement, between Cardiovascular Systems, Inc. and Fresenius Kabi AB, effective March 17, 2016 (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed May 6, 2016). | |
10.42+ | Amendment No. 1 to Product Schedule, between Cardiovascular Systems, Inc. and Fresenius Kabi AB, effective March 27, 2016 (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed May 6, 2016). | |
10.43† | Separation Agreement, between Cardiovascular Systems, Inc. and Robert Thatcher, dated May 26, 2016 (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Annual Report on Form 10-K filed August 25, 2016). | |
10.44 | Settlement Agreement, among Cardiovascular Systems, Inc., the United States of America acting through the United States Attorney for the Western District of North Carolina and on behalf of the Office of Inspector General of the Department of Health and Human Services, and Travis Thams, dated June 28, 2016 (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Current Report on Form 8-K filed June 28, 2016). | |
10.45 | Corporate Integrity Agreement, between Cardiovascular Systems, Inc. and the Office of Inspector General of the Department of Health and Human Services, dated June 28, 2016 (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Current Report on Form 8-K filed June 28, 2016). | |
10.46†* | Form of Performance Unit Award (Cash Settled) under the 2014 Equity Incentive Plan. | |
10.47† | Form of Restricted Stock Agreement for Performance-Based Awards (3-year cliff vesting) under the 2014 Equity Incentive Plan (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Annual Report on Form 10-K filed August 25, 2016). | |
10.48† | Employment Agreement, dated August 15, 2016, by and between Cardiovascular Systems Inc. and Scott R. Ward (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Annual Report on Form 10-K filed August 25, 2016). | |
10.49 | Purchase and Sale Agreement by and between Cardiovascular Systems, Inc. and Krishna Holdings, LLC dated December 29, 2016 (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed February 3, 2017). | |
10.50 | First Amendment to Purchase and Sale Agreement, by and between Cardiovascular Systems, Inc. and Krishna Holdings, LLC, dated February 2, 2017 (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed February 3, 2017). | |
10.51 | Second Amendment to Purchase and Sale Agreement, by and between Cardiovascular Systems, Inc. and Krishna Holdings, LLC, dated February 15, 2017 (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed May 5, 2017). | |
53
Exhibit No. | Description | |
10.52 | Third Amendment to Purchase and Sale Agreement, by and between Cardiovascular Systems, Inc. and Krishna Holdings, LLC, dated February 23, 2017 (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed May 5, 2017). | |
10.53 | Fourth Amendment to Purchase and Sale Agreement, by and between Cardiovascular Systems, Inc. and Krishna Holdings, LLC, dated March 1, 2017 (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed May 5, 2017). | |
10.54 | Lease Agreement, by and between Cardiovascular Systems, Inc. and Krishna Holdings, LLC, Apex Holdings, LLC, Kashi Associates, LLC, Keva Holdings, LLC, S&V Ventures, LLC, Polo Group LLC, SPAV Holdings LLC, Star Associates LLC, and The Global Villa, LLC, dated March 30, 2017 (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed May 5, 2017). | |
10.55 | Loan and Security Agreement, by and between Cardiovascular Systems, Inc. and Silicon Valley Bank, dated March 31, 2017 (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed May 5, 2017). | |
10.56 | Amendment to Purchasing Agreement between Cardiovascular Systems, Inc. and Healthtrust Purchasing Group, L.P. (previously filed with the SEC as an Exhibit to and incorporated herein by reference from the Company’s Quarterly Report on Form 10-Q filed February 3, 2017). | |
10.57* | Amendment to Purchasing Agreement between Cardiovascular Systems, Inc. and Healthtrust Purchasing Group, L.P. | |
10.58†* | Separation Agreement, between Cardiovascular Systems, Inc. and Paul Koehn, dated June 30, 2017. | |
23.1* | Consent of PricewaterhouseCoopers LLP. | |
24.1* | Power of Attorney (included on the signature page). | |
31.1* | Certification of principal executive officer required by Rule 13a-14(a). | |
31.2* | Certification of principal financial officer required by Rule 13a-14(a). | |
32.1** | Section 1350 Certification of principal executive officer. | |
32.2** | Section 1350 Certification of principal financial officer. | |
101** | Financial statements from the Annual Report on Form 10-K of the Company for the year ended June 30, 2017, formatted, in Extensible Business Reporting Language (XBRL): (i) the Consolidated Balance Sheets, (ii) the Consolidated Statements of Operations, (iii) the Consolidated Statements of Comprehensive Loss, (iv) the Consolidated Statements of Changes in Stockholders’ Equity, (v) the Consolidated Statements of Cash Flows, and (vi) the Notes to Consolidated Financial Statements. | |
* | Filed herewith. |
** | Furnished herewith. |
† | Compensatory plan or agreement. |
+ | Confidential treatment has been granted for certain portions omitted from this exhibit pursuant to Rule 24b-2 under the Securities Exchange Act of 1934, as amended. |
54