Attached files
| file | filename |
|---|---|
| EX-23.1 - EXHIBIT 23.1 - REPROS THERAPEUTICS INC. | v403265_ex23-1.htm |
| EX-31.2 - EXHIBIT 31.2 - REPROS THERAPEUTICS INC. | v403265_ex31-2.htm |
| EX-32.1 - EXHIBIT 32.1 - REPROS THERAPEUTICS INC. | v403265_ex32-1.htm |
| EX-32.2 - EXHIBIT 32.2 - REPROS THERAPEUTICS INC. | v403265_ex32-2.htm |
| EXCEL - IDEA: XBRL DOCUMENT - REPROS THERAPEUTICS INC. | Financial_Report.xls |
| EX-31.1 - EXHIBIT 31.1 - REPROS THERAPEUTICS INC. | v403265_ex31-1.htm |
UNITED
STATES SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
Form 10-K
x ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
For the fiscal year ended December 31, 2014
or
¨ TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
For the transition period from to
Commission File No. 001-15281
Repros Therapeutics Inc.
(Exact name of registrant as specified in its charter)
| Delaware | 76-0233274 |
| (State or other jurisdiction of | (I.R.S. Employer |
| incorporation or organization) | Identification No.) |
| 2408 Timberloch Place, Suite B-7 | 77380 |
| The Woodlands, Texas | (Zip Code) |
| (Address of principal executive offices) |
(281) 719-3400
(Registrant's telephone number, including area code)
Securities registered pursuant to Section 12(b) of the Act:
| Title of Each Class | Name of Each Exchange on Which Registered | |
| Common Stock, $.001 par value | The Nasdaq Stock Market LLC | |
| Series A Warrants | The Nasdaq Stock Market LLC | |
| Series B Warrants | The Nasdaq Stock Market LLC | |
| Rights to purchase Series One Junior | The Nasdaq Stock Market LLC | |
| Participating Preferred Stock |
Indicate by check mark whether the registrant is a well-known seasoned issuer (as defined in Rule 405 of the Securities Act). Yes ¨ No x
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Securities Act.
Yes ¨ No x
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes x No ¨
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Website, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes x No ¨
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of registrant's knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. ¨
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See definitions of "large accelerated filer,” accelerated filer" and “smaller reporting company” in Rule 12b-2 of the Exchange Act.:
| Large accelerated filer ¨ | Accelerated filer x |
| Non-accelerated filer ¨(Do not check if smaller reporting company) | Smaller reporting company ¨ |
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes ¨ No x
The aggregate market value of the common stock held by non-affiliates of the registrant was approximately $304,915,821 as of June 30, 2014, the last business day of the registrant's most recently completed second fiscal quarter, based on the closing sales price of the registrant's common stock on the Nasdaq Capital Market on such date of $17.30 per share. For purposes of the preceding sentence only, all directors, executive officers and beneficial owners of ten percent or more of the shares of the registrant's common stock are assumed to be affiliates.
As of February 27, 2015, there were 24,276,173 shares of the registrant's common stock outstanding.
Documents incorporated by reference: Portions of the registrant's definitive proxy statement relating to the registrant's 2015 Annual Meeting of Shareholders, which proxy statement will be filed under the Exchange Act within 120 days of the end of the registrant's fiscal year ended December 31, 2014, are incorporated by reference into Part III of this Form 10-K.
REPROS THERAPEUTICS INC
2014 FORM 10-K ANNUAL REPORT
TABLE OF CONTENTS
This Annual Report on Form 10-K contains "forward-looking statements" within the meaning of Section 27A of the Securities Act of 1933, as amended, and Section 21E of the Securities Exchange Act of 1934, as amended. The words "may," "anticipate," "believe," "expect," "estimate," "project," "suggest," "intend" and similar expressions are intended to identify forward-looking statements. Such statements reflect our current views with respect to future events and financial performance and are subject to certain risks, uncertainties and assumptions, including those discussed in "Item 1A. Risk Factors." Should one or more of these risks or uncertainties materialize, or should underlying assumptions prove incorrect, actual results may vary materially from those anticipated, believed, expected, estimated, projected, suggested or intended.
Overview
Repros Therapeutics Inc. (the “Company,” “Repros,” or “we,” “us” or “our”) was organized on August 20, 1987. We are a biopharmaceutical company focused on the development of new drugs to treat hormonal and reproductive system disorders. Both of our product candidates have exhibited strong efficacy results in every study completed to date, and we believe the studies presently underway will place both programs on a clear late stage clinical development path.
We are developing Androxal®, a single isomer of clomiphene citrate which is an orally active proprietary small molecule compound. Androxal® is for the treatment of secondary hypogonadism in overweight men wishing to restore normal testicular function. Men with secondary hypogonadism exhibit low testosterone levels due to under stimulated testes but they are generally fertile. Androxal® is designed to treat the underlying mechanism, insufficient stimulation of the testes by the pituitary, which causes secondary hypogonadism. Secondary hypogonadism due to being overweight or obese is the single greatest cause of hypogonadism in general. Through 2013, sales of preparations for the treatment of low testosterone have exceeded $2 billion in the U.S. and first tier pharmaceutical companies are active participants in the low testosterone marketplace.
In December 2011, we completed a Phase 2B study of Androxal® in men with secondary hypogonadism, but naïve to testosterone treatment, at the recommendation of the Food and Drug Administration (the “FDA”). Top line results of this study demonstrated that Androxal® was generally well tolerated compared to placebo and that there were no drug related serious adverse events that led to discontinuation. We met with the FDA in May 2012 to discuss the design of pivotal Phase 3 efficacy studies for Androxal® as well as the components of the overall drug development program required for a New Drug Application (“NDA”) submission and agreed on registration requirements for Androxal® oral therapy for the treatment of secondary hypogonadism. In July 2012, we announced that we reached an agreement with the FDA for the design of the pivotal efficacy studies for Androxal® for the treatment of secondary hypogonadism. The pivotal studies were conducted under a Special Protocol Assessment (“SPA”). We have completed both Phase 3 pivotal efficacy studies. On March 27, 2013, we announced that the top-line results from our first pivotal Phase 3 study, ZA-301, met both co-primary endpoints mandated by the FDA, and we announced on September 16, 2013, that we met both co-primary endpoints in the second pivotal study, ZA-302. Additionally, on September 16, 2013, we announced the results from ZA-300, a six-month safety study. This study identified no new safety issues. On October 22, 2013, we announced that we received guidance from the FDA instructing the Company to request a meeting to discuss the adequacy of studies ZA-301 and ZA-302. In addition to this guidance, the FDA further noted that they would allow us to run head-to-head studies against approved testosterone replacement products. These head-to-head studies, ZA-304 and ZA-305, were initiated in January 2014 and subsequently completed in September and August 2014, respectively. Both of these head-to-head studies achieved superiority for both co-primary endpoints and most secondary endpoints as compared to the approved testosterone replacement product. On October 21, 2014, we announced the results from ZA-303, a 52 week, single-blind, placebo-controlled Phase 3 study to evaluate the effects on bone mineral density. In this study, no new safety signals were identified, including no evidence of negative effects on bone mineral density. On February 2, 2015, we announced that we electronically submitted our NDA to the FDA for Androxal®. The NDA includes a collection of data on safety and efficacy from over 20 studies, including four Phase 3 efficacy studies.
We are also developing Proellex®, an orally administered selective blocker of the progesterone receptor in women, for the treatment of uterine fibroids and endometriosis. Uterine fibroids and endometriosis affect millions of women of reproductive age. Proellex® has shown statistically significant results in previous Phase 2 studies for endometriosis and uterine fibroids. We completed a low dose escalating study as permitted by the FDA in late 2011, to determine both signals of efficacy and safety for low oral doses of the drug. There was no evidence of elevations of liver enzymes over baseline, suggesting these lower doses avoid the type of adverse events seen at much higher doses in earlier studies. On October 8, 2012, we announced that the FDA has agreed to a reclassification of the full clinical hold to a partial clinical hold on low dose oral Proellex® to allow us to conduct a Phase 2 study in the treatment of endometriosis. We initiated this study in November 2012. To date, we have experienced difficulty enrolling subjects into this study due to changes in the current treatment of this disorder. We believe we can have this study full enrolled in 2015.
On October 31, 2013, the Company held a meeting with the FDA to discuss the clinical development plan for low dose oral Proellex® in the treatment of uterine fibroids. During the meeting, the FDA provided guidance for endpoints it believed acceptable for the treatment of uterine fibroids in an efficacy study and instructed the Company to submit a request for lifting the full clinical hold. The Company has followed the FDA’s recommendations and submitted the study protocol and the request for the full hold lift. Additionally, on March 17, 2014, we announced that the FDA indicated that we may proceed to conduct Phase 1 and Phase 2 studies of low dose oral Proellex® for endometriosis and uterine fibroids while remaining on partial clinical hold. This guidance indicated that the highest allowed dose will be 12 mg daily. On December 29, 2014, we announced that we have initiated a Phase 2B study for low dose oral Proellex® in the treatment of uterine fibroids.
| -2- |
The Company has an active Investigational New Drug Application (“IND”) for the vaginal delivery of Proellex® for the treatment of uterine fibroids. Since the clinical hold relates only to oral delivery of Proellex®, this IND has no clinical hold issues. In the first quarter of 2012, we initiated a Phase 2 vaginal administration study for the treatment of uterine fibroids and subsequently reported the final study results in January 2013. We held an end of Phase 2 meeting with the FDA in May 2013, to discuss a Phase 3 study design for vaginally delivered Proellex as a treatment for uterine fibroids. The FDA recommended that a Phase 2B study should be conducted prior to commencing a Phase 3 program. On December 29, 2014, we announced that we have initiated a Phase 2B study for vaginally delivered Proellex® in the treatment of uterine fibroids.
As of December 31, 2014, we had accumulated losses of $273.1 million, approximately $46.6 million in cash and cash equivalents, and accounts payable and accrued expenses of approximately $2.9 million, in the aggregate. We anticipate that our current liquidity will be sufficient to continue the development of our product candidates into the second half of 2016.In the normal course of business we continue to explore potential corporate partnering opportunities, however, there can be no assurance that an acceptable corporate partnering opportunity will be successfully completed or that our current liquidity will be sufficient to fund all of our product development needs.
Our Research and Development Program
Our product development pipeline, with milestone dates as expected as of the date of this report, is summarized in the table below:
Product Candidate (Indication) Androxal® |
Status | Next Expected Milestone(s) | ||
| Secondary Hypogonadism | NDA submitted | FDA acceptance of NDA
| ||
| Proellex® | ||||
| Uterine Fibroids | Phase 2 | Complete first course of treatment in a Phase 2B study (oral delivery) (YE 2015)
Compete first course of treatment in a Phase 2B study (vaginal delivery) (YE 2015)
| ||
Endometriosis
|
Phase 2 | Fully enroll Phase 2 study (oral delivery) (YE 2015) |
Androxal®
Product Overview
We are developing Androxal®, a single isomer of clomiphene citrate which is an orally active proprietary small molecule compound. Androxal® is for the treatment of secondary hypogonadism in overweight men wishing to restore normal testicular function. Men with secondary hypogonadism exhibit low testosterone levels due to under stimulated testes but they are generally fertile. Androxal® is designed to treat the underlying mechanism, insufficient stimulation of the testes by the pituitary, which causes secondary hypogonadism. Secondary hypogonadism due to being overweight or obese is the single greatest cause of hypogonadism in general.
Testosterone is an important male hormone. Testosterone deficiency in men is linked to several negative physical and mental conditions, including loss of muscle tone, reduced sexual desire and deterioration of memory and certain other cognitive functions. Testosterone production normally decreases as men age and this decline can be accelerated by obesity, sometimes leading to testosterone deficiency. The leading therapy for low testosterone is AndroGel®, a commercially available testosterone replacement cream marketed by Abbott Laboratories (“Abbott”) for the treatment of low testosterone, which we believe has had and continues to have significant sales in North America.
Based on our own clinical trial screening data, we believe over 70% of men that have low testosterone suffer from secondary hypogonadism, a pituitary defect which is characterized by suboptimal levels of LH (luteinizing hormone) and FSH (follicle stimulating hormone). LH and FSH are the pituitary hormones that stimulate testicular testosterone and sperm production, respectively. Men with secondary hypogonadism can be readily distinguished from those that have primary testicular failure via assessment of the levels of secretions of pituitary hormones, as men with primary testicular failure experience elevated secretions of pituitary hormones. In secondary hypogonadism, the low levels of LH and FSH fail to provide adequate hormone signaling to the testes, causing testosterone levels to drop to a level where we believe pituitary secretions fall under the influence of estrogen, which is enhanced in obese men, thus further suppressing the testicular stimulation from the pituitary.
| -3- |
Androxal® acts centrally to restore testicular function and, hence, normal testosterone in the body. The administration of exogenous testosterone can restore serum testosterone levels, but does not restore testicular function and thereby generally leads to the cessation of, or significant reduction in, sperm production. Androxal®, by contrast, restores levels of both LH and FSH, which stimulate testicular testosterone and sperm production, respectively.
Androxal® is in the midst of a full regulatory approval process, including pivotal Phase 3 trials, long-term open label safety studies and a dual-energy X-ray absorptiometry (DEXA) study, as well as other requirements. Androxal® is closely related chemically to the drug, Clomid®, which is approved for use in women to treat certain infertility disorders. Clomid® contains both the trans and cis isomers of clomiphene citrate; Androxal® contains only the trans isomer. The FDA has indicated that testicular tumors, gynecomastia and adverse ophthalmologic events, which have been reported in males taking Clomid®, are potential risks that should be included in informed consent forms for our Androxal® clinical trials. We do not believe that Androxal® will present with the same adverse events given its reduced half-life and lack of cis isomer as compared to Clomid®. In our preclinical studies and our clinical trials to date, we have observed no evidence of any of these events except for certain ophthalmologic events in our preclinical dog study at doses significantly higher than those administered in the clinical trials. All clinical trial results are subject to review by the FDA and the FDA may disagree with our conclusions about safety and efficacy.
Treatment for Secondary Hypogonadism in Men Wishing to Preserve Testicular Function (Reproductive Status)
On November 8, 2010, we held a Type B meeting with the FDA to discuss whether the FDA would review our protocols for a Phase 3 trial of Androxal® in men with secondary hypogonadism under an SPA. In the meeting, the FDA recommended that a Phase 2B study in men with secondary hypogonadism but naïve to testosterone treatment be conducted if we desired the protocols to be reviewed under an SPA. The FDA further opined that such Phase 2B study would provide for a more solid data base for design of Phase 3 studies and eventual approval of such studies under an SPA.
We completed the Phase 2B trial which consisted of four arms; placebo, two doses of Androxal® and topical testosterone. In this study, at baseline the men exhibited morning testosterone less than 250 ng/dl and there was no statistical difference between the groups in testosterone at baseline. At the end of the three month dosing period, median morning testosterone levels were placebo (196 ng/dl), 12.5 mg Androxal® (432 ng/dl), 25 mg Androxal® (416 ng/dl) and Testim® (393 ng/dl). A comparison of final median morning testosterone in all three of the active arms to placebo showed them to be highly statistically different and there was no statistical difference observed between these active arms. This trial also showed that Androxal® was able to maintain sperm counts in men being treated for their low testosterone levels, whereas Testim® resulted in suppressed sperm levels.
On July 9, 2012, we announced that we reached an agreement with the FDA for the design of the pivotal efficacy studies for Androxal® for the treatment of secondary hypogonadism. The pivotal studies were conducted under an SPA. On March 27, 2013, we announced that the top-line results from our first pivotal Phase 3 study, ZA-301, met both co-primary endpoints mandated by the FDA and we announced on September 16, 2013, that we met both co-primary endpoints in the second pivotal study, ZA-302.
The 500 subject, six month, open label safety study, ZA-300, completed enrollment in February 2013 at 28 U.S. clinical sites. On September 16, 2013, we reported top-line results of this study. Additionally, we completed enrollment into a one year, 150 subject DEXA study, ZA-303, in January 2013 at 10 U.S. clinical sites. On October 21, 2014, we announced that this study identified no new safety signals, including no evidence of negative effects on bone mineral density.
On October 22, 2013, we announced that we received guidance from the FDA instructing the Company to request a meeting to discuss the adequacy of studies ZA-301 and ZA-302. In addition to this guidance, the FDA further noted they would allow us to run head-to-head studies against approved testosterone replacement products. These head-to-head studies, ZA-304 and ZA-305, were initiated in January 2014 and subsequently completed in September and August 2014, respectively. Both of these head-to-head studies achieved superiority for both co-primary endpoints and most secondary endpoints as compared to the approved testosterone replacement product.
On February 2, 2015, we announced that we electronically submitted our NDA to the FDA for Androxal®. The NDA includes a collection of data on safety and efficacy from over 20 studies, including four Phase 3 efficacy studies.
Unlike testosterone replacement therapies, Androxal® maintains the normal daily rhythm of testosterone peaks and valleys. We previously conducted three studies in which 24 hour testosterone levels were obtained and, unlike topical testosterone, morning testosterone was the maximum concentration observed, consistent with the normal circadian rhythm in men. These studies provide evidence that one assessment of testosterone between 8 a.m. and 10 a.m. correlates to the maximum value of testosterone for a given subject on a given day. Additionally, we conducted one additional 24-hour study which showed that Androxal®’s action in maintaining the normal rhythm is both predictable and dose-dependent.
| -4- |
In addition, the Company continues to consider the potential for use of Androxal® as an adjuvant therapy in hypogonadal men with Type 2 diabetes. The Company has an active IND open with the Division of Endocrine and Metabolic Products at the FDA for this indication. We believe there may be an association between the restoration of normal pituitary function and improvement of metabolic conditions such as Type 2 diabetes. Research has been published which demonstrates that increased insulin resistance, a characteristic implicated in Type 2 diabetes, is associated with the onset of secondary hypogonadism. Based on our own clinical trial screening data from our previously conducted Phase 2 study, we have found hypogonadism, obesity and Type 2 diabetes to be co-morbid conditions in a significant number of men. The results from this Phase 2 study indicated that the Androxal® treated subjects showed statistically significant improvement in HbA1c and insulin, as well as HOMA-IR compared to placebo in men less than 65 years of age.
We believe the advantages of oral delivery, maintenance of testicular function and additional metabolic benefits will be important differentiating factors for Androxal®, should it be approved. There can be no assurance, however, that we will be successful in implementing this strategy or that the FDA will approve our drug for commercial use.
Proellex®
Product Overview
Proellex®, our product candidate for female reproductive health, is a new chemical entity that acts as a selective blocker of the progesterone receptor and is being developed for the treatment of symptoms associated with uterine fibroids and endometriosis. There are currently no FDA-approved orally administered drug treatments for the long-term treatment of either uterine fibroids or endometriosis. The National Uterine Fibroids Foundation estimates that 80% of all women in the U.S. have uterine fibroids, and one in four of these women have symptoms severe enough to require treatment. According to the Endometriosis Association, endometriosis affects 6.3 million women in the U.S. and Canada and millions more worldwide.
The current standards of care for uterine fibroids and endometriosis consist of surgery or short-term treatment with gonadotropin-releasing hormone (“GnRH”) agonists drugs, such as Lupron®. GnRH agonists induce a low estrogen, menopausal-like state and promote bone loss and are not recommended for use for more than six months.
We have conducted numerous studies with Proellex® dosing approximately 700 women with the drug. All Proellex® studies completed to date exhibited strong efficacy signals, whether in uterine fibroids or endometriosis. In a 120 patient study of Proellex® as a treatment of uterine fibroids conducted in the United States (roughly 40 subjects per arm), both a 12.5 and 25 mg dose of Proellex® were compared to placebo. In this study each of the 12.5 and 25 mg doses achieved highly statistically significant results when compared to placebo when menstrual bleeding was assessed (p<0.0001). The two doses also achieved highly statistically significant improvement in quality of life measures using the Uterine Fibroid Symptom Quality of Life questionnaire developed and validated by Georgetown University and used in the development of device like treatments of uterine fibroids such as uterine artery embolization. There was no statistical difference in efficacy measures between the two doses. Importantly, in the Phase 2 U.S. trial a significant percentage of women stopped menstruating. Proellex® resulted in the induction of amenorrhea (cessation of menses), which we believe is a strong surrogate signal of efficacy. Over 80% of women on both the 12.5 and 25 mg doses exhibited no menses during the three month trial, whereas all women on placebo exhibited at least one menses.
Up until the summer of 2009, all side effects exhibited in the studies were considered manageable and the benefit of Proellex® far outweighed the risk. However, in Phase 3 efficacy and larger Phase 3 safety studies in diverse populations, a small number of subjects exhibited serious adverse effects associated with elevated liver enzymes. As a result of these findings, we elected to stop the trials and the FDA subsequently placed Proellex® on full clinical hold. All women that experienced elevated liver enzymes and returned for follow-up visits returned to baseline conditions with no overnight hospitalization necessary. An analysis of all the subjects that experienced such serious adverse effects showed that the effect only occurred in a small percentage of subjects that were exposed to the 50 mg dose of the drug for any period of time. Based on these findings, we petitioned the FDA to allow us to conduct a low dose study to demonstrate both safety and signals of efficacy in low oral doses of Proellex®, up to 12 mg administered per day. The FDA upgraded the full clinical hold to a partial hold to allow the low dose study to be conducted. In addition, we are exploring vaginal delivery as an alternative administrative route to bypass first-pass liver effects and reduce systemic exposure, which is currently in a Phase 2 study.
Low Dose Oral Study
Pursuant to the terms of the partial clinical hold currently in place as a result of the liver toxicity exhibited by Proellex®, the FDA allowed us to run a single study to test low oral doses of Proellex® for signals of safety and efficacy. The study tested five different doses of Proellex® (1, 3, 6, 9 and 12 mg), with 1 mg being the first dose tested. Each dose was then compared to placebo with weekly assessments of liver function during both the placebo and drug period. Subjects were dosed with the active drug for 10 weeks, which allowed for adequate time to determine the impact of a given dose on trends in liver function. Each dose was tested in up to 12 different subjects and assessment of pharmacokinetic parameters was obtained at the start of dosing and the end of the dosing period to determine overall and maximum drug exposure for a given dose. We also monitored changes in menstrual bleeding patterns and ovulation as well as changes in endometrial thickness. The FDA required that an independent Drug Safety Monitoring Board be established and that the informed consent clearly state the liver toxicity previously experienced with Proellex®. We have completed this study and have announced that there was no evidence of elevations of liver enzymes over baseline, suggesting these lower doses avoid the type of adverse events seen at much higher doses in earlier studies.
| -5- |
On July 16, 2012, we announced that we held a teleconference with the FDA to discuss the development of low dose oral Proellex® as a treatment for endometriosis. Subsequently, on October 8, 2012, we announced that the FDA has agreed to reclassify the full clinical hold to a partial clinical hold on low dose oral Proellex® to allow us to conduct a Phase 2 study in the treatment of endometriosis. We initiated this 60 subject, four month active dosing study in November 2012. To date, we have experienced difficulty enrolling subjects into this study due to changes in the current treatment of this disorder. We believe we can have this study fully enrolled in 2015.
On October 31, 2013, the Company held a meeting with the FDA to discuss the clinical development plan for low dose oral Proellex® in the treatment of uterine fibroids. During the meeting, the FDA provided guidance for endpoints it believed acceptable for the treatment of uterine fibroids in an efficacy study and instructed the Company to submit a request for lifting the full clinical hold. The Company has followed the FDA’s recommendations and submitted the study protocol and the request for the full hold lift. Additionally, on March 17, 2014, we announced that the FDA indicated that we may proceed to conduct Phase 1 and Phase 2 studies of low dose oral Proellex® for endometriosis and uterine fibroids while remaining on partial clinical hold. This guidance indicated that the highest allowed dose will be 12 mg daily. On December 29, 2014, we announced that we have initiated a Phase 2B study for low dose oral Proellex® in the treatment of uterine fibroids.
Vaginal Administration
We are assessing vaginal administration of Proellex® to avoid first pass liver effects and achieve higher reproductive tract concentrations of the drug while minimizing systemic exposure. We reported results from two in vivo animal studies which confirmed reduced maximum circulating concentrations of the drug when administered vaginally, as well as efficacy signals at substantially lower doses than oral administration. The Company has an active IND for the vaginal delivery of Proellex® for the treatment of uterine fibroids. Since the clinical hold relates only to the oral delivery of Proellex®, this IND has no clinical hold issues. In the first quarter of 2012, we initiated a Phase 2 vaginal administration study for the treatment of uterine fibroids. In January 2013, we reported the final study results which indicated the 12 mg dose achieved statistically significant improvement in menstrual bleeding, uterine fibroid symptoms and reduction in fibroid volume even with the low number of subjects enrolled into the study (n=12 @ 12 mg). Based on these findings, the Company believes the 12 mg dose is appropriate for further development. We held an end of Phase 2 meeting with the FDA in May 2013, to discuss a Phase 3 study design for the vaginally delivered Proellex as a treatment for uterine fibroids. The FDA recommended that a Phase 2B study should be conducted prior to commencing a Phase 3 program. On December 29, 2014, we announced that we have initiated a Phase 2B study for vaginally delivered Proellex® in the treatment of uterine fibroids.
Other Products
VASOMAX® has been on partial clinical hold in the U.S. since 1998, and no further development activities are planned.
Business Strategy
We plan to focus our clinical program on (i) conducting a Phase 2B study for low dose oral Proellex® in the treatment of uterine fibroids, (ii) conducting a Phase 2B vaginal administration study for Proellex® in the treatment of uterine fibroids and (iii) conducting a Phase 2 study for low dose oral Proellex® for the treatment of endometriosis. With respect to Androxal®, on February 2, 2015, we reported that the NDA was electronically submitted to the FDA. We anticipate that our current liquidity will be sufficient to continue the development of our product candidates into the second half of 2016. In the normal course of business we continue to explore potential corporate partnering opportunities for assistance in the clinical development funding and commercialization of our products, as appropriate; however, there can be no assurance that an acceptable corporate partnering opportunity will be successfully completed or that our current liquidity will be sufficient to fund all of our product development needs.
Research and Development
We have limited resources and utilize consultants and outside entities to perform clinical development and limited research activities in connection with preclinical studies and clinical trials. Our primary research and development (“R&D”) expenses for 2014 were for the payment for salaries and related employee expenses, contracted regulatory affairs activities, insurance coverage for clinical trials and prior product sales, contracted research and consulting fees, facility costs, fees associated with our patent portfolio and internal research and development supplies. We believe that these expenses will continue to be our primary R&D expenses in 2014.
Proellex® License Agreement with the National Institutes of Health
In 1999, we licensed rights to Proellex® from the National Institutes of Health (“NIH”), under an exclusive, worldwide license in the field of treatment of human endocrinologic pathologies or conditions in steroid-sensitive tissues which expires upon the expiration of the last licensed patent, currently 2017. This license agreement contains numerous detailed performance obligations, with time sensitive dates for compliance, relating to clinical development and commercialization activities required by us or our designated third-party providers, as well as additional financial milestones and royalties. If we fail to achieve the benchmarks specified in the commercial development plan attached to the license agreement or meet payment obligations, the NIH can terminate the license agreement and we lose our rights to develop and commercialize Proellex®. We and the NIH periodically update the commercial development plan. There can be no assurance that we will be able to meet any or all of the performance objectives in the future on a timely basis or at all, or that, if we fail to meet any of such objectives, the NIH will agree to revised objectives. The NIH also has the ability to terminate the agreement for an uncured material breach of the agreement, if we do not keep Proellex® reasonably available to the public after commercial launch or if we cannot reasonably satisfy unmet health and safety needs, among other reasons.
| -6- |
We provide annual updates to the NIH on the progress of our development of Proellex®. Based on our interaction with the NIH to date, we believe our license and relationship with the NIH are in good standing.
The NIH retains, on behalf of the government, a nonexclusive, nontransferable, worldwide license to practice the inventions licensed under the licensed patents by or on behalf of the government. For the purpose of encouraging basic research, the NIH retains the right to grant nonexclusive research licenses to third parties. Due to the work that was done on Proellex® at the NIH prior to our license agreement, the government also has certain rights to use the product in the event of a national emergency pursuant to the Patent and Trademark Laws Amendments Act of 1980, as amended.
Manufacturing
We have identified multiple potential suppliers for the bulk active pharmaceutical ingredient (“API”) used in Androxal®, though we have not yet contracted with one. We have not faced any material problems obtaining the necessary quantities of Androxal® for our clinical trials and, therefore, do not anticipate any material problems obtaining the API necessary for commercial production if Androxal® is approved for sale. Additionally, we have contracted with Gregory Pharmaceutical Holdings, Inc., doing business as UPM Pharmaceuticals, for the finished drug product and packaging of Androxal® for commercial production, if approved by the FDA for sale.
Gedeon Richter was our third-party manufacturer of the active pharmaceutical ingredient for Proellex®. Due to the clinical hold, we cancelled our development and supply contract with Gedeon Richter; however, we have a sufficient supply of Proellex® currently available for our current and planned clinical trial efforts. In the event we require an additional supply of Proellex®, we believe that we have maintained a good relationship with Gedeon Richter and that an agreement could be reached with Gedeon Richter to provide such supply when and if needed.
For the foreseeable future, we expect to continue to rely on third-party manufacturers and other third parties to produce, package and store sufficient quantities of Androxal® and Proellex®. These product candidates are complicated and expensive to manufacture. If our third-party manufacturers fail to deliver our product candidates for clinical use on a timely basis, with sufficient quality, and at commercially reasonable prices, we may be required to delay or suspend clinical trials or otherwise discontinue development and production of our product candidates. While we may be able to identify replacement third-party manufacturers or develop our own manufacturing capabilities for these product candidates, this process would likely cause a delay in the availability of our product candidates and an increase in costs. In addition, third-party manufacturers may have a limited number of facilities in which our product candidates can be produced, and any interruption of the operation of those facilities due to events such as equipment malfunction or failure or damage to the facility could result in the cancellation of shipments, loss of product in the manufacturing process or a shortfall in available product candidates.
Sales and Marketing
We have no experience in the sales, marketing and distribution of pharmaceutical products. We anticipate that we will outsource the bulk of such activities to larger pharmaceutical companies, who may also conduct later stage pivotal trials of our product candidates. These companies are more capable of distributing the products to the market place. In the normal course of business we continue to explore possible partnerships with various pharmaceutical companies. If in the future we fail to reach or elect not to enter into an arrangement with a collaborative partner with respect to the sales and marketing of any of our product candidates, we would need to develop a sales and marketing organization with supporting distribution capability in order to market such products directly. Significant additional expenditures would be required for us to develop such a sales and marketing organization.
Patents and Proprietary Information
Our ability to compete effectively with other companies is materially dependent on the proprietary nature of our patents and technologies. We actively seek patent protection for our proprietary technology in the United States and abroad.
Under a license agreement with the NIH, we have exclusive rights to four issued U.S. patents, which expire in 2017, two pending U.S. patent applications, and several foreign patents and pending applications made by the NIH regarding Proellex®. We also have two issued U.S. patents and seven pending U.S. patent applications, 111 foreign pending patent applications and 39 granted foreign patents that cover various formulations of Proellex® and methods for using Proellex®.
| -7- |
Therapeutic uses of our Androxal® product candidate are covered in the United States by nine issued U.S. patents and seven pending patent applications. Foreign coverage of therapeutic uses of our Androxal® product candidate includes 71 issued foreign patents and 99 foreign pending patent applications. The issued patents and pending applications relate to methods for treating certain conditions including the treatment of testosterone deficiency in men, the treatment of diabetes mellitus Type 2, the treatment of metabolic syndrome and conditions associated therewith, and the treatment of infertility in hypogonadal men. Androxal® (the trans-isomer of clomiphene) is purified from clomiphene citrate. A third party individual holds two issued patents related to the use of anti-estrogen such as clomiphene citrate and others for use in the treatment of androgen deficiency and disorders related thereto. We requested re-examination of one of these patents by the U.S. Patent and Trademark Office (“PTO”) based on prior art. The patent holder amended the claims in the re-examination proceedings, which led the PTO to determine that the amended claims were patentable in view of those publications under consideration and a re-examination certificate was issued. We subsequently filed a second request for re-examination by the PTO in light of a number of additional publications. The request was granted and all of the claims were finally rejected by the PTO in the re-examination. The patent holder appealed the rejections to the PTO Board of Patent Appeals and Interferences (the “PTO Board”) which ultimately reversed the rejections of several dependent claims in view of those publications under consideration. The patent holder filed a Notice of Appeal to the Federal Circuit on September 28, 2010 contesting the rejections maintained by the PTO Board. A decision was rendered by the Court of Appeals for the Federal Circuit on December 12, 2011, affirming the rejection of the appealed claims. The PTO issued an Ex Parte Reexamination Certificate on April 29, 2013, canceling the rejected claims and confirming the patentability of the remaining claims. Nevertheless, we believe that our development of Androxal® does not infringe any of the remaining claims and that all of the remaining claims are invalid on various grounds including additional prior art publications. We also believe that the second of these two patents is invalid in view of published prior art not considered by the PTO. If necessary, we intend to vigorously defend any and all claims that may be brought by the holder of such patents in a court of competent jurisdiction in order to develop Androxal® further. Adverse determinations in litigation proceedings could require us to seek licenses which may not be available on commercially reasonable terms, or at all, or subject us to significant liabilities, in which case we may not be able to successfully commercialize or out-license Androxal® until such patents expire or are otherwise no longer in force.
All of our employees and consultants have signed assignment of invention and confidentiality agreements, and each corporate partner we enter into discussions with or engage to assist in our clinical trials or manufacturing process is also required to execute appropriate confidentiality and assignment agreements protecting our intellectual property.
Competition
We are engaged in pharmaceutical product development, an industry that is characterized by extensive research efforts and rapid technological progress. Many established pharmaceutical and biotechnology companies, universities and other research institutions with financial, scientific and other resources significantly greater than ours are marketing or may develop products that directly compete with any products we may develop. These entities may succeed in developing products that are safer, more effective or less costly than products we may develop. Even if we can develop products which should prove to be more effective than those developed by other companies, other companies may be more successful than us because of greater financial resources, greater experience in conducting preclinical studies and clinical trials and in obtaining regulatory approval, stronger sales and marketing efforts, earlier receipt of approval for competing products and other factors. If we commence significant commercial sales of any products, we or our collaborators may compete in areas in which we have no experience, such as manufacturing and marketing. There can be no assurance that our products, if commercialized, will be accepted and prescribed by healthcare professionals.
Our main competitors for the treatment of testosterone deficiency are the testosterone replacement therapies currently being marketed. The current standard of care is AndroGel®, a topical gel for the replacement of testosterone. AndroGel® is marketed by Abbott. There is another topical gel, Testim®, currently marketed by Endo International PLC, and a transdermal patch, AndroDerm®, marketed by Watson Pharmaceuticals. Eli Lilly and Company also entered into a licensing agreement with a third party for a late stage topical testosterone treatment called Axiron®, which has recently become available in pharmacies. In addition, other companies such as Apricus Biosciences, Inc. and Clarus Therapeutics, Inc. are developing other products that would compete with Androxal®. We believe we can compete with AndroGel® and the other replacement therapies because we believe that Androxal® is the only drug with an NDA submitted that normalizes testicular function and may provide additional metabolic benefits. Based on our clinical trial supply cost to date, we currently expect that Androxal®, if approved, can compete favorably on a cost basis with current testosterone replacement therapies.
Our main competitors for the treatment of uterine fibroids and endometriosis are GnRH agonists, especially Lupron®, the current therapeutic standard of care for uterine fibroids. Lupron® is marketed by Abbott, which has far greater resources and marketing capabilities than we have. Recently Abbott has licensed a Phase 3-ready molecule from Neurocrine Biosciences for the treatment of endometriosis. Gedeon Richter and Watson Pharmaceuticals have also entered into an exclusive license agreement to develop and market Esmya™ (an orally active selective progesterone receptor modulator) in the U.S. and Canada. In addition, surgical treatment of both uterine fibroids and endometriosis competes with Proellex® by removing uterine fibroids and by removing misplaced tissue in women with endometriosis. We believe we can potentially compete with Lupron® and other GnRH agonists because we believe that Proellex® will not present the same side effect of a decrease in bone mineral density given its specific focus on progesterone inhibition, which differentiates it from GnRH agonists that create a low estrogen state. There are additional companies developing similar progesterone-blocking technology.
| -8- |
Government Regulation
Our research and development activities, preclinical studies and clinical trials, and the manufacturing, marketing and labeling of any products we may develop, are subject to extensive regulation by the FDA and other regulatory authorities in the United States and other countries. The U.S. Federal Food, Drug, and Cosmetic Act and the regulations promulgated thereunder and other federal and state statutes and regulations govern, among other things, the testing, manufacture, storage, record keeping, labeling, advertising, promotion, marketing and distribution of any products we may develop. Preclinical study and clinical trial requirements and the regulatory approval process take many years and require the expenditure of substantial resources. Additional government regulation may be established that could prevent or delay regulatory approval of our product candidates. Delays in obtaining or rejections of regulatory approvals would adversely affect our ability to commercialize any product candidate we develop and our ability to receive product revenues or to receive milestone payments or royalties from any product rights we might license to others. If regulatory approval of a product candidate is granted, the approval may include significant limitations on the indicated uses for which the product may be marketed or may be conditioned on the conduct of post-marketing surveillance studies.
The standard process required by the FDA before a pharmaceutical agent may be marketed in the United States includes: (1) preclinical tests; (2) submission to the FDA of an IND application which must become effective before human clinical trials may commence; (3) adequate and well-controlled human clinical trials to establish the safety and efficacy of the drug for its intended application; (4) submission of a new drug application (an “NDA”), to the FDA; and (5) FDA approval of the NDA prior to any commercial sale or shipment of the drug.
Clinical trials typically are conducted in three sequential phases, but the phases may overlap. Phase 1 typically involves the initial introduction of the drug into human subjects. In Phase 1, the drug is tested for safety and, as appropriate, for absorption, metabolism, distribution, excretion, pharmacodynamics and pharmacokinetics. Phase 2 usually involves studies in a limited patient population to evaluate preliminarily the efficacy of the drug for specific targeted indications, determine dosage tolerance and optimal dosage and identify possible adverse effects and safety risks.
Phase 3 clinical trials are undertaken to further evaluate clinical efficacy and to test further for safety within an expanded patient population at geographically dispersed clinical study sites. Phase 1, Phase 2 or Phase 3 testing may not be completed successfully within any specific time period, if at all, with respect to any products being tested by a sponsor. Furthermore, the FDA or the Investigational Review Board may suspend clinical trials at any time on various grounds, including a finding that the healthy volunteers or patients are being exposed to an unacceptable health risk. This was evidenced when Proellex®, our product candidate for uterine fibroids and endometriosis, was placed on clinical hold by the FDA in summer 2009 due to liver toxicity data resulting from our clinical trials. Though the full clinical hold has been upgraded to a partial clinical hold, there can be no assurance that the partial hold will be lifted at any time.
Even if regulatory approvals for any products we may develop are obtained, we, our potential collaborators, our products, and the facilities manufacturing our products would be subject to continual review and periodic inspection. The FDA will require post-marketing reporting to monitor the safety of our products. Each drug-manufacturing establishment supplying the United States must be registered with the FDA. Manufacturing establishments are subject to periodic inspections by the FDA and must comply with the FDA’s requirements regarding current Good Manufacturing Practices (“GMP”). In complying with current GMP, manufacturers must expend funds, time and effort in the area of production and quality control to ensure full technical compliance. We do not have any drug manufacturing capabilities and must rely on outside firms for this capability. The FDA stringently applies regulatory standards for manufacturing. Identification of previously unknown problems with respect to a product, manufacturer or facility may result in restrictions on the product, manufacturer or facility, including warning letters, suspensions of regulatory approvals, operating restrictions, delays in obtaining new product approvals, withdrawal of the product from the market, product recalls, fines, injunctions and criminal prosecution.
Before any products we develop could be marketed outside of the United States, they would be subject to regulatory approval similar to FDA requirements in the United States, although the requirements governing the conduct of clinical trials, product licensing, pricing, and reimbursement vary widely from country to country. No action can be taken to market any drug product in a country until the regulatory authorities in that country have approved an appropriate application. FDA approval does not assure approval by other regulatory authorities. The current approval process varies from country to country, and the time spent in gaining approval varies from that required for FDA approval. In some countries, the sale price of a drug product must also be approved. The pricing review period often begins after market approval is granted. Even if a foreign regulatory authority approves any products we develop, no assurance can be given that it will approve satisfactory prices for the products.
Our research and development involves the controlled use of hazardous materials and chemicals. Although we believe that our procedures for handling and disposing of those materials comply with state and federal regulations, the risk of accidental contamination or injury from these materials cannot be eliminated. If such an accident occurs, we could be held liable for resulting damages, which could be material to our financial condition and business. We are also subject to numerous environmental, health and workplace safety laws and regulations, including those governing laboratory procedures, exposure to blood-borne pathogens, and the handling of biohazardous materials. Additional federal, state and local laws and regulations affecting us may be adopted in the future. Any violation of, and the cost of compliance with, these laws and regulations could materially and adversely affect us.
| -9- |
Third-Party Reimbursement and Pricing Controls
In the United States and elsewhere, sales of pharmaceutical products depend in significant part on the availability of reimbursement to the consumer from third-party payers, such as government and private insurance plans. Third-party payers are increasingly challenging the prices charged for medical products and services. Should any of our product candidates be approved for any commercial sales, it will be time consuming and expensive for us to go through the process of seeking reimbursement from Medicaid, Medicare and private payers.
Our products may not be considered cost effective, and coverage and reimbursement may not be available or sufficient to allow us to sell our products on a competitive and profitable basis. The passage of the Medicare Prescription Drug and Modernization Act of 2003 imposes requirements for the distribution and pricing of prescription drugs which may affect the marketing of our products.
In many foreign markets, including the countries in the European Union, pricing of pharmaceutical products is subject to governmental control. In the United States, there have been, and we expect that there will continue to be, a number of federal and state proposals to implement similar governmental pricing control. While we cannot predict whether such legislative or regulatory proposals will be adopted, the adoption of such proposals could have a material adverse effect on our profitability.
The Hatch-Waxman Act
Under the U.S. Drug Price Competition and Patent Term Restoration Act of 1984, known as the Hatch-Waxman Act, newly approved drugs and indications benefit from a statutory period of non-patent marketing exclusivity. The Hatch-Waxman Act provides five year marketing exclusivity to the first applicant to gain approval of an NDA for a new chemical entity (“NCE”), meaning that the FDA has not previously approved any other new drug containing the same active ingredient. Both of our current product candidates are considered NCEs. The Hatch-Waxman Act prohibits approval of an abbreviated new drug application (“ANDA”), for a generic version of the drug during the five-year exclusivity period. Protection under the Hatch-Waxman Act will not prevent the filing or approval of another full NDA, however, the applicant would be required to conduct its own adequate and well-controlled clinical trials to demonstrate safety and effectiveness. The Hatch-Waxman Act also provides three years of marketing exclusivity for the approval of new NDAs with new clinical trials for previously approved drugs and supplemental NDAs, for example, for new indications, dosages, or strengths of an existing drug, if new clinical investigations are essential to the approval. This three year exclusivity covers only the new changes associated with the supplemental NDA and does not prohibit the FDA from approving ANDAs for drugs containing the original active ingredient or indications.
The Hatch-Waxman Act also permits a patent extension term of up to five years as compensation for patent term lost during product development and the FDA regulatory review process. However, patent extension cannot extend the remaining term of a patent beyond a total of 14 years. The patent term restoration period is generally one-half the time between the effective date of an IND and the submission date of an NDA, plus time of active FDA review between the submission date of an NDA and the approval of that application. Only one patent applicable to an approved drug is eligible for the extension and it must be applied for prior to expiration of the patent and within 60 days of the approval of the NDA. The PTO, in consultation with the FDA, reviews and approves or rejects the application for patent term extension.
Litigation
See Item 3 of Part I of this Form 10-K.
Employees and Consultants
Employees
At December 31, 2014, we had 28 full-time employees. We also utilize consultants as well as contract research organizations and other outside specialty firms for various services such as preclinical and clinical trial support, manufacturing, regulatory approval advice and accounting and human resource management. We believe our relationship with our employees is good.
Scientific Advisors and Consultants
We benefit from consultation with prominent scientists active in fields related to our technology. For this purpose, we have part-time consulting relationships with a number of scientific advisors. At our request, these advisors review the feasibility of product development programs under consideration, provide advice about advances in areas related to our technology and aid in recruiting personnel. All of the advisors are employed by academic institutions or other entities and may have commitments to or advisory agreements with other entities that limit their availability to us. Our advisors are required to sign an agreement providing that, if appropriate, they are to disclose and assign to us any ideas, discoveries and inventions they develop in the course of providing consulting services. We also use consultants for various administrative needs. None of our advisors are otherwise affiliated with us.
| -10- |
In addition to the advisors described above, we continue to engage U.S. contract research organizations for data management for the conduct of clinical trials. Under our arrangements with these contract research organizations, we design the protocols for the clinical trials and direct the contract research organizations in their efforts. We own all of the data associated with the clinical trials.
Available Information
Our Internet site (www.reprosrx.com) makes available free of charge to all interested parties our annual reports on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K, and all amendments to those reports, as well as all other reports and schedules filed electronically with the Securities and Exchange Commission (the “SEC” or “Commission”), as soon as reasonably practicable after such material is electronically filed with or furnished to the SEC. Interested parties may also find reports, proxy and information statements and other information on issuers that file electronically with the SEC at the SEC's Internet site (http://www.sec.gov). In addition, we have made available on our Internet website under the heading “Corporate Governance” our Code of Business Conduct and Ethics and Code of Ethics for Senior Financial Officers. We intend to make available on our website any future amendments or waivers to our Code of Business Conduct and Ethics and Code of Ethics for Senior Financial Officers within four business days after any such amendments or waivers. The information on our Internet website is not part of this Form 10-K.
| -11- |
You should carefully consider the risks described below before making an investment decision. You should also refer to the other information in this report, including our financial statements and the related notes incorporated by reference. The risks and uncertainties described below are not the only risks and uncertainties we face. Additional risks and uncertainties not presently known to us or that we currently deem immaterial also may impair our business operations. If any of the following risks actually occur, our business, results of operations and financial condition could suffer. In that event the trading price of our common stock could decline, and you may lose all or part of your investment in our common stock. The risks discussed below also include forward-looking statements and our actual results may differ substantially from those discussed in these forward-looking statements.
Risks Relating to Our Business
If we fail to obtain the capital necessary to fund our operations when needed, we may have to delay, reduce or eliminate our research and development programs or commercialization efforts, dispose of assets or liquidate.
We expect to make additional capital outlays and to increase operating expenditures over the next several years to support our preclinical development and clinical trial activities, particularly with respect to ongoing clinical trials for Proellex®. On February 2, 2015, we announced that we submitted the NDA for Androxal® to the FDA. Based on our current and planned clinical programs, we anticipate that our current liquidity will be sufficient to continue the development of our product candidates into the second half of 2016. However, it is possible that our clinical trial activities will be more costly and take longer than we anticipate; accordingly, there can be no assurance that additional capital will not be necessary prior to the time anticipated. In the normal course of business we continue to explore possible partnerships with various pharmaceutical companies. If in the future we fail to reach or elect not to enter into an arrangement with a collaborative partner with respect to the sales and marketing of any of our product candidates, we would need to develop a sales and marketing organization with supporting distribution capability in order to market such products directly. Significant additional expenditures would be required for us to develop such a sales and marketing organization. We may continue to seek additional funding through public or private financings, including equity or debt financings, and/or through other means, including collaborations and license agreements, as appropriate. We do not know whether additional financing will be available when needed, or that, if available, we will obtain financing on terms favorable to our stockholders or us. We anticipate that if we are able to secure additional financing, that such financing will result in significant dilution of the ownership interests of our stockholders and may provide certain rights to the new investors senior to the rights of our current stockholders, including but not limited to, voting rights and rights to proceeds in the event of a sale or liquidation of the Company. We expect to continue to incur significant losses for the foreseeable future, and we may never achieve or sustain profitability. In the event that we are unable to obtain adequate financing to conduct operations, we may need to cease our business operations and begin liquidation proceedings. If we need to liquidate our assets, we would likely realize significantly less from them than the values at which they are carried on our financial statements. The funds resulting from the liquidation of our assets would be used first to pay off the debt owed to any secured and unsecured creditors before any funds would be available to pay our stockholders, and any shortfall in the proceeds would directly reduce the amounts available for distribution, if any, to our creditors and to our stockholders. In the event we were required to liquidate, it is highly unlikely that stockholders would receive any value for their shares.
In recent years, the general economic and capital market conditions in the United States have varied significantly and have increased the cost of capital in many circumstances, and there is no certainty that economic conditions will permit us to raise capital in an amount to sufficiently fund our long-term plans, in 2015 or beyond. If economic conditions become worse, our future cost of equity or debt capital and access to the capital markets could be adversely affected. If we cannot raise adequate funds, we may be required to:
| · | delay, reduce the scope of or eliminate one or more of our development programs; | |
| · | relinquish, license or otherwise dispose of rights to technologies, product candidate or products that we would otherwise seek to develop or commercialize ourselves at an earlier stage or on terms that are less favorable than might otherwise be available; or | |
| · | liquidate and dissolve our company. |
Our future capital requirements will depend upon a number of factors, including:
| · | the size, complexity, results and timing of our clinical programs; | |
| · | the cost to obtain sufficient supply of the compounds necessary for our product candidates at a reasonable cost; | |
| · | the time and cost involved in obtaining regulatory approvals; | |
| · | the costs involved in preparing, filing, prosecuting, maintaining, defending and enforcing patent claims; and | |
| · | competing technological and market developments. |
These factors could result in variations from our currently projected operating and liquidity requirements.
| -12- |
Because the data from our preclinical studies and clinical trials for our product candidates are not necessarily predictive of future results, we can provide no assurances that any of them will have favorable results in clinical trials or receive regulatory approval.
Before we can obtain regulatory approval for the commercial sale of any product candidate that we develop, we are required to complete preclinical development and extensive clinical trials in humans to demonstrate its safety and efficacy. To date, regulatory approval has not been obtained for any of our product candidates and, in fact, our product candidate Proellex® is currently on partial clinical hold with the FDA due to safety issues experienced in our earlier Phase 2 and Phase 3 clinical trials for endometriosis and uterine fibroids, respectively.
Unfavorable results from ongoing preclinical studies or clinical trials could result in delays, modifications or abandonment of ongoing or future clinical trials. Clinical results are frequently susceptible to varying interpretations that may delay, limit or prevent regulatory approvals. Negative or inconclusive results or adverse medical events during a clinical trial could cause a clinical trial to be delayed, repeated or terminated. In addition, we may report top-line data from time to time, which is based on a preliminary analysis of key efficacy and safety data; such data may be subject to change following a more comprehensive review of the data related to the applicable clinical trial. If Androxal®, Proellex®, or any other potential future product candidate fails to demonstrate sufficient safety and efficacy in any clinical trial, we would experience potentially significant delays in, or be required to abandon, development of that product candidate. If we delay or abandon our development efforts related to Androxal® or Proellex®, we may not be able to generate sufficient revenues or raise the additional capital necessary to continue operations or become profitable.
We have a history of operating losses, and we expect to incur increasing net losses and may not achieve or maintain profitability for some time or at all.
We have experienced significant operating losses in each fiscal year since our inception. As of December 31, 2014, we had accumulated losses of $273.1 million, approximately $46.6 million in cash and cash equivalents, and accounts payable and accrued expenses of approximately $2.9 million, in the aggregate. We expect to continue incurring net losses and we may not achieve or maintain profitability for some time, if at all. As we increase expenditures for the clinical development of our products, we expect our total operating losses to increase for at least the next few years. Our ability to achieve profitability will depend on, among other things, successfully completing the development of our products, obtaining regulatory approvals, establishing marketing, sales and manufacturing capabilities or collaborative arrangements with others that possess such capabilities, and raising sufficient funds to finance our activities. There can be no assurance that we will be able to achieve profitability or that profitability, if achieved, can be sustained.
Raising additional funds by issuing securities or through collaboration and licensing arrangements may cause dilution to our stockholders, restrict our operations or require us to relinquish proprietary rights.
We may raise additional funds through public or private equity offerings, debt financings or potential corporate collaborations and licensing arrangements. We cannot be certain that additional funding will be available on acceptable terms, or at all. To the extent that we raise additional capital by issuing equity securities, our stockholders’ ownership will be diluted. Any debt financing we enter into may involve covenants that restrict our operations. These restrictive covenants may include limitations on borrowing and specific restrictions on the use of our assets, as well as prohibitions on our ability to create liens, pay dividends, redeem capital stock or make investments. In addition, if we raise additional funds through collaboration and licensing arrangements, it may be necessary to relinquish potentially valuable rights to our potential products or proprietary technologies, or grant licenses on terms that are not favorable to us. For example, we might be forced to relinquish all or a portion of our sales and marketing rights with respect to Androxal®, Proellex®, or other potential products or license intellectual property that enables licensees to develop competing products.
Our stock price could decline significantly based on the results and timing of clinical trials of, and regulatory and other decisions affecting, our product candidates.
Results of clinical trials and preclinical studies of our current and potential product candidates may not be viewed favorably by us or third parties, including the FDA or other regulatory authorities, investors, analysts and potential collaborators. The same may be true of how we design the clinical trials of our product candidates and regulatory decisions affecting those clinical trials. Biopharmaceutical company stock prices have declined significantly when such results and decisions were unfavorable or perceived negatively or when a product candidate did not otherwise meet expectations. The final results from our clinical development programs may be negative, may not meet expectations or may be perceived negatively. The designs of our clinical trials (which may change significantly and be more expensive than currently anticipated depending on our clinical results and regulatory decisions) may also be viewed negatively by third parties. We may not be successful in completing these clinical trials on our projected timetable, if at all.
Failure to initiate additional clinical trials or delays in existing clinical trials of Proellex®, and failure of the FDA to lift the partial clinical hold on Proellex®, or unfavorable results or decisions or negative perceptions regarding any of such clinical trials, could cause our stock price to decline significantly. Additionally, we have submitted an NDA for Androxal® to the FDA. Failure to achieve FDA approval for Androxal® could cause our stock price to decline significantly.
| -13- |
We are thinly staffed and highly dependent on a limited number of management persons and key personnel, and if we lose these members of our team or are unable to attract and retain additional qualified personnel, our future growth and ability to compete would suffer.
The competition for qualified personnel in the biopharmaceutical field is intense, and our future success depends upon our ability to attract, retain and motivate highly skilled scientific, technical and managerial employees. We had only 28 full-time employees at December 31, 2014, including our President and Chief Executive Officer, Joseph S. Podolski. We are highly dependent on Mr. Podolski and our professional staff for the management of our company and the development of our technologies. Mr. Podolski has an employment agreement with us. There can be no assurance that any of these employees will remain with us through development of our current product candidates. The loss of the services of any of our employees could delay or curtail our research and product development efforts.
If our employees commit fraud or other misconduct, including noncompliance with regulatory standards and requirements and insider trading, our business may experience serious adverse consequences.
We are exposed to the risk of employee fraud or other misconduct. Misconduct by employees could include intentional failures to comply with FDA regulations, to provide accurate information to the FDA, to comply with manufacturing standards we have established, to comply with federal and state healthcare fraud and abuse laws and regulations, to report financial information or data accurately or to disclose unauthorized activities to us. In particular, sales, marketing and business arrangements in the healthcare industry are subject to extensive laws and regulations intended to prevent fraud, kickbacks, self-dealing and other abusive practices. These laws and regulations may restrict or prohibit a wide range of pricing, discounting, marketing and promotion, sales commission, customer incentive programs and other business arrangements. Employee misconduct could also involve the improper use of information obtained in the course of clinical trials, which could result in regulatory sanctions and serious harm to our reputation. We have adopted a Code of Business Conduct and Ethics, but it is not always possible to identify and deter employee misconduct, and the precautions we take to detect and prevent this activity may not be effective in controlling unknown or unmanaged risks or losses or in protecting us from governmental investigations or other actions or lawsuits stemming from a failure to be in compliance with such laws or regulations. If any such actions are instituted against us, and we are not successful in defending ourselves or asserting our rights, those actions could have a significant impact on our business, including the imposition of significant fines or other sanctions.
We are increasingly dependent on information technology systems to operate our business and a cyber attack or other breach of our systems, or those of third parties on whom we may rely, could subject us to liability or interrupt the operation of our business.
We are increasingly dependent on information technology systems to operate our business. A breakdown, invasion, corruption, destruction or interruption of critical information technology systems by employees, others with authorized access to our systems or unauthorized persons could negatively impact operations. In the ordinary course of business, we collect, store and transmit confidential information and it is critical that we do so in a secure manner to maintain the confidentiality and integrity of such information. Additionally, we outsource certain elements of our information technology systems to third parties. As a result of this outsourcing, our third party vendors may or could have access to our confidential information making such systems vulnerable. Data breaches of our information technology systems, or those of our third party vendors, may pose a risk that sensitive data may be exposed to unauthorized persons or to the public. While we believe that we have taken appropriate security measures to protect our data and information technology systems, and have been informed by our third party vendors that they have as well, there can be no assurance that our efforts will prevent breakdowns or breaches in our systems, or those of our third party vendors, that could adversely affect our business.
Our plan to use collaborations to leverage our capabilities may not be successful.
As part of our business strategy, we may enter into collaboration arrangements with strategic partners to develop and commercialize our product candidates. For our collaboration efforts to be successful, we must identify partners whose competencies complement ours. We must also successfully enter into collaboration agreements with them on terms attractive to us and integrate and coordinate their resources and capabilities with our own. We may be unsuccessful in entering into collaboration agreements with acceptable partners or negotiating favorable terms in these agreements. In addition, we may face a disadvantage in seeking to enter into or negotiating collaborations with potential partners because other potential collaborators may have greater management and financial resources than we do. Also, we may be unsuccessful in integrating the resources or capabilities of these collaborators. In addition, our collaborators may prove difficult to work with or less skilled than we originally expected. If we are unsuccessful in our collaborative efforts, our ability to develop and market product candidates could be severely limited.
Our rights agreement and certain provisions in our charter documents and Delaware law could delay or prevent a change in management or a takeover attempt that you may consider to be in your best interest.
We have adopted certain anti-takeover provisions, including a rights agreement. The rights agreement will cause substantial dilution to any person who attempts to acquire us in a manner or on terms not approved by our board of directors.
| -14- |
The rights agreement and certain provisions in our certificate of incorporation and bylaws and under Delaware law could delay or prevent the removal of directors and other management and could make more difficult a merger, tender offer or proxy contest involving us that you may consider to be in your best interest. For example, these provisions:
| · | allow our board of directors to issue preferred stock without stockholder approval; | |
| · | limit who can call a special meeting of stockholders; and | |
| · | establish advance notice requirements for nomination for election to the board of directors or for proposing matters to be acted upon at stockholder meetings. |
Risks Relating to Our Product Development Efforts
Changes in existing regulations and the adoption of new regulations may increase our costs and otherwise adversely affect our business, results of operations and financial condition.
Our research and development activities, preclinical studies and clinical trials, and the manufacturing, marketing and labeling of any products we may develop, are subject to extensive regulation by the FDA and other regulatory authorities in the United States and other countries. Additional government regulation may be established that could prevent or delay regulatory approval of our product candidates or materially increase our costs. Delays in obtaining or rejections of regulatory approvals would adversely affect our ability to commercialize any product candidate we develop and our ability to receive product revenues or to receive milestone payments or royalties from any product rights we might license to others. If regulatory approval of a product candidate is granted, the approval may include significant limitations on the indicated uses for which the product may be marketed or may be conditioned on the conduct of post-marketing surveillance studies.
Delays in the commencement of clinical trials testing of our current and potential product candidates could result in increased costs to us and delay our ability to generate revenues.
Our product candidates will require continued extensive clinical trials prior to the submission of a regulatory application for commercial sales. Because of the nature of clinical trials, we do not know whether future planned clinical trials will begin on time, if at all. Delays in the commencement of clinical trials could significantly increase our product development costs and delay any product commercialization. In addition, many of the factors that may cause, or lead to, a delay in the commencement of clinical trials may also ultimately lead to denial of regulatory approval of a product candidate.
The commencement of clinical trials can be delayed for a variety of reasons, including delays in:
| · | demonstrating sufficient safety and efficacy in past clinical trials to obtain regulatory approval to commence a further clinical trial;
| |
| · | convincing the FDA that we have selected valid endpoints for use in proposed clinical trials;
| |
| · | reaching agreements on acceptable terms with prospective contract manufacturers for manufacturing sufficient quantities of a product candidate; and
| |
| · | obtaining institutional review board approval to conduct a clinical trial at a prospective site. |
In addition, the commencement of clinical trials may be delayed due to insufficient patient enrollment, which is a function of many factors, including the size of the patient population, the nature of the protocol, the proximity of patients to clinical sites, the availability of effective treatments for the relevant disease, and the eligibility criteria for the clinical trial.
Delays in the completion of, or the termination of, clinical testing of our current and potential product candidates could result in increased costs to us, and could delay or prevent us from generating revenues.
Once a clinical trial has begun, it may be delayed, suspended or terminated by us or the FDA or other regulatory authorities due to a number of factors, including:
| · | lack of adequate funding to continue clinical trials; | |
| · | lack of effectiveness of any product candidate during clinical trials; | |
| · | side effects experienced by trial participants or other safety issues; | |
| · | slower than expected rates of patient recruitment and enrollment or lower than expected patient retention rates; |
| -15- |
| · | delays or inability to manufacture or obtain sufficient quantities of materials for use in clinical trials; | |
| · | inadequacy of or changes in our manufacturing process or compound formulation; | |
| · | delays in obtaining regulatory approvals to commence a trial, or “clinical holds” or delays requiring suspension or termination of a trial by a regulatory agency, such as the FDA, after a trial is commenced; | |
| · | changes in applicable regulatory policies and regulations; | |
| · | delays in identifying and reaching agreement on acceptable terms with prospective clinical trial sites; | |
| · | uncertainty regarding proper dosing; | |
| · | unfavorable results from on-going clinical trials and preclinical studies; | |
| · | failure of our clinical research organizations to comply with all regulatory and contractual requirements or otherwise fail to perform their services in a timely or acceptable manner; | |
| · | scheduling conflicts with participating clinicians and clinical institutions; | |
| · | failure to construct appropriate clinical trial protocols; | |
| · | insufficient data to support regulatory approval; | |
| · | inability or unwillingness of medical investigators to follow our clinical protocols; | |
| · | difficulty in maintaining contact with subjects during or after treatment, which may result in incomplete data; | |
| · | the timing of discussions and meetings with the FDA or other regulatory authorities regarding the scope or design of our clinical trials; and | |
| · | acceptability to the FDA of data obtained from clinical studies conducted in Europe or other non-United States jurisdictions. |
Many of these factors that may lead to a delay, suspension or termination of clinical testing of a current or potential product candidate may also ultimately lead to denial of regulatory approval of a current or potential product candidate. In fact, the FDA placed Proellex® on clinical hold in summer 2009 due to liver toxicity data resulting from our clinical trials. Though the full clinical hold has been upgraded to a partial clinical hold, there can be no assurance that the partial hold will be lifted at any time.
If we experience delays in the completion of, or termination of, clinical testing of any product candidates in the future, our financial results and the commercial prospects for our product candidates will be harmed, and our ability to generate product revenues will be delayed.
Even if we successfully complete clinical trials for Proellex®, there are no assurances that we will be able to submit, or obtain FDA approval of, a new drug application.
There can be no assurance that, if our clinical trials for Proellex® are successfully completed, we will be able to submit an NDA to the FDA or that any NDA we submit will be approved by the FDA in a timely manner, if at all. After completing clinical trials for a product candidate in humans, a drug dossier is prepared and submitted to the FDA as an NDA, and includes all preclinical studies and clinical trial data relevant to the safety and effectiveness of the product at the suggested dose and duration of use for the proposed indication, in order to allow the FDA to review such drug dossier and to consider a product candidate for approval for commercialization in the United States. If we are unable to submit an NDA with respect to Proellex®, or if any NDA we submit is not approved by the FDA, we will be unable to commercialize that product. The FDA can and does reject NDAs and requires additional clinical trials, even when drug candidates achieve favorable results in large-scale Phase 3 clinical trials. If we fail to commercialize Proellex®, we may be unable to generate sufficient revenues to continue operations or attain profitability and our reputation in the industry and in the investment community would likely be damaged.
Our success in obtaining regulatory approval to market Androxal® in the U.S. or elsewhere depends on our ability to address any issues the FDA or foreign regulatory agencies may raise, including with respect to our NDA filing for Androxal, and ultimately to obtain approval by the FDA or foreign regulatory agencies.
On February 2, 2015, we announced that we submitted the NDA for Androxal® to the FDA. If the NDA is accepted for filing, the NDA will then assign a team to evaluate our research on Androxal®’s safety and efficacy, including a review of labeling information and the manufacturing process. We would expect this evaluation and review, which would be under the Prescription Drug User Fee Act, to take approximately 12 months after submission. Ultimately, FDA reviewers will either approve the NDA or issue a response letter with comments. If the FDA is not satisfied with the information we provide, the FDA may require the addition of labeling statements or other warnings or contraindications, require us to perform additional clinical trials or studies or provide additional information, or redesign Androxal® in order to secure approval. Any such requirement could have a material adverse effect on our business and financial condition.
| -16- |
Even if Androxal® is approved, the FDA may limit the indications for which it may be used, include extensive warnings on the product labeling, or require costly ongoing requirements for post-marketing clinical studies and surveillance or other risk management measures to monitor the safety or efficacy of Androxal®. Further, in the event that we seek regulatory approval of Androxal® outside the United States, such markets also have requirements for approval of drug candidates with which we must comply prior to marketing. Obtaining regulatory approval for marketing of Androxal® in one country does not ensure we will be able to obtain regulatory approval in other countries but a failure or delay in obtaining regulatory approval in one country may have a negative effect on the regulatory process in other countries.
Any regulatory approval of Androxal®, once obtained, may be withdrawn. Ultimately, the failure to obtain and maintain regulatory approvals would prevent Androxal® from being marketed and would have a material and adverse effect on our business.
We rely on third parties to conduct clinical trials for our product candidates, and their failure to timely and properly perform their obligations may result in costs and delays that prevent us from obtaining regulatory approval or successfully commercializing our product candidates.
We rely on independent contractors, including researchers at clinical research organizations (“CROs”), and universities, in certain areas that are particularly relevant to our research and product development plans, such as for data management for the conduct of clinical trials. The competition for these relationships is intense, and we may not be able to maintain our relationships with them on acceptable terms. Independent contractors generally may terminate their engagements at any time, subject to notice. As a result, we can control their activities only within certain limits, and they will devote only a certain amount of their time conducting research on and trials of our product candidates and assisting in developing them. If they do not successfully carry out their duties under their agreements with us, fail to inform us if these trials fail to comply with clinical trial protocols, or fail to meet expected deadlines, our clinical trials may need to be extended, delayed or terminated. We may not be able to enter into replacement arrangements without undue delays or excessive expenditures. If there are delays in testing or regulatory approvals as a result of the failure to perform by our independent contractors or other outside parties, our drug development costs will increase and we may not be able to attain regulatory approval for or successfully commercialize our product candidates.
In addition, we have no control over the financial health of our independent contractors. Several of our independent contractors are in possession of valuable and sensitive information relating to the safety and efficacy of our product candidates, and several others provide services to a significant percentage of the patients enrolled in the respective clinical trials in which such independent contractors participate. Should one or more of these independent contractors become insolvent, or otherwise are not able to continue to provide services to us, the clinical trial in which such contractor participates could become significantly delayed and we may be adversely affected as a result of the delays and additional expenses associated with such event.
Any of our future product candidates may cause adverse effects or have other properties that could delay or prevent their regulatory approval or limit the scope of any approved label or market acceptance.
Adverse events, or AEs, caused by our future product candidates could cause us, other reviewing entities, clinical trial sites or regulatory authorities to interrupt, delay or halt clinical trials and could result in the denial of regulatory approval.
If AEs are observed in any clinical trials of our future product candidates, including those that our strategic partners may develop under our alliance agreements, our or our partners’ ability to obtain regulatory approval for product candidates may be negatively impacted.
Further, if any of our future products, if and when approved for commercial sale, cause serious or unexpected side effects, a number of potentially significant negative consequences could result, including:
| · | regulatory authorities may withdraw their approval of the product or impose restrictions on its distribution in the form of a modified risk evaluation and mitigation strategy; | |
| · | regulatory authorities may require the addition of labeling statements, such as warnings or contraindications; | |
| · | we may be required to change the way the product is administered or conduct additional clinical trials; | |
| · | we could be sued and held liable for harm caused to patients; or | |
| · | our reputation may suffer. |
Any of these events could prevent us or our partners from achieving or maintaining market acceptance of the affected product and could substantially increase the costs of commercializing our future products and impair our ability to generate revenues from the commercialization of these products either by us or by our strategic alliance partners.
| -17- |
The risk of accidental contamination or injury resulting from our handling and disposing of hazardous materials and chemicals may expose us to litigation.
Our research and development involves the controlled use of hazardous materials and chemicals. Although we believe that our procedures for handling and disposing of those materials comply with state and federal regulations, the risk of accidental contamination or injury from these materials cannot be eliminated. If such an accident occurs, we could be held liable for resulting damages, which could have a material adverse effect on us.
Risks Relating to Manufacturing Our Products
We currently rely on third-party manufacturers and other third parties for production of our product candidates, and our dependence on these manufacturers may impair the development of our product candidates.
Currently, we do not have the ability internally to manufacture the product candidates that we need to conduct our clinical trials. We terminated our supply agreement with Gedeon Richter for the manufacturing of Proellex® due to the clinical hold imposed by the FDA in August 2009; however, we believe that we have a sufficient supply of Proellex® currently available for our current and planned clinical trial efforts. In the event we require an additional supply of Proellex®, we believe that we have maintained a good relationship with Gedeon Richter and that an agreement could be reached with Gedeon Richter to provide such supply when and if needed, but we cannot assure you this will be the case.
We have identified multiple potential suppliers for the bulk active pharmaceutical ingredient (“API”) used in Androxal®, though we have not yet contracted with one. We have not faced any material problems obtaining the necessary quantities of Androxal® for our clinical trials and, therefore, do not anticipate any material problems obtaining the API necessary for commercial production if Androxal® is approved for sale. Additionally, we have contracted with Gregory Pharmaceutical Holdings, Inc., doing business as UPM Pharmaceuticals, for the finished drug product and packaging of Androxal® for commercial production, if approved by the FDA for sale.
For the foreseeable future, we expect to continue to rely on third-party manufacturers and other third parties to produce, package and store sufficient quantities of Androxal®, Proellex®, and any future product candidates for use in our clinical trials or commercialization, if appropriate. These product candidates are complicated and expensive to manufacture. If our third-party manufacturers fail to deliver our product candidates for clinical use on a timely basis, with sufficient quality, and at commercially reasonable prices, we may be required to delay or suspend clinical trials or otherwise discontinue development and production of our product candidates. While we may be able to identify replacement third-party manufacturers or develop our own manufacturing capabilities for these product candidates, this process would likely cause a delay in the availability of our product candidates and an increase in costs. In addition, third-party manufacturers may have a limited number of facilities in which our product candidates can be produced, and any interruption of the operation of those facilities due to events such as equipment malfunction or failure or damage to the facility by natural disasters could result in the cancellation of shipments, loss of product in the manufacturing process or a shortfall in available product candidates.
Identification of previously unknown problems with respect to a product, manufacturer or facility may result in restrictions on the product, manufacturer or facility.
The FDA stringently applies regulatory standards for the manufacturing of our products. Identification of previously unknown problems with respect to a product, manufacturer or facility may result in restrictions on the product, manufacturer or facility, including warning letters, suspensions of regulatory approvals, operating restrictions, delays in obtaining new product approvals, withdrawal of the product from the market, product recalls, fines, injunctions and criminal prosecution. Any of the foregoing could have a material adverse effect on us.
Our product candidates have only been manufactured in small quantities to date, and we may face delays or complications in manufacturing quantities of our product candidates in sufficient quantities to meet the demands of late stage clinical trials and marketing.
We cannot assure that we will be able to successfully increase the manufacturing capacity or scale-up manufacturing volume per batch, whether on our own or in reliance on third-party manufacturers, for any of our product candidates in a timely or economical manner, or at all. To date our product candidates have been manufactured exclusively by third parties in small quantities for preclinical studies and clinical trials. Future clinical trials of our product candidates, if any, will require increased quantities for future commercial sales in the event that such product candidates are approved by the FDA or foreign regulatory bodies. Significant scale-up of manufacturing requires certain additional developmental work, which the FDA must review and approve to assure product comparability. If we or our third-party manufacturers are unable to successfully increase the manufacturing capacity for a product candidate, the regulatory approval or commercial launch of that product candidate may be delayed or there may be a shortage in supply of that product candidate.
| -18- |
Our product candidates require precise, high-quality manufacturing which may not be available at acceptable costs.
Androxal® and Proellex® are novel compounds that have never been produced in large scale. As in the development of any new compound, there are underlying risks associated with their manufacture. These risks include, but are not limited to, cost, process scale-up, process reproducibility, construction of a suitable process plant, timely availability of raw materials, as well as regulatory issues associated with the manufacture of an active pharmaceutical agent. Any of these risks may prevent us from successfully developing Androxal® or Proellex®. Our failure, or the failure of our third-party manufacturers to achieve and maintain these high manufacturing standards, including the incidence of manufacturing errors and reliable product packaging for diverse environmental conditions, could result in patient injury or death, product recalls or withdrawals, delays or failures in product testing or delivery, cost overruns or other problems that could seriously hurt our business.
We may experience delays in the development of our product candidates if the third-party manufacturers of our product candidates cannot meet FDA requirements relating to Good Manufacturing Practices.
Our third-party manufacturers are required to produce our product candidates under FDA current Good Manufacturing Practices in order to meet acceptable standards for our clinical trials. If such standards change, the ability of third-party manufacturers to produce our product candidates on the schedule we require for our clinical trials may be affected. In addition, third-party manufacturers may not perform their obligations under their agreements with us or may discontinue their business before the time required by us to gain approval for or commercialize our product candidates. Any difficulties or delays in the manufacturing and supply of our product candidates could increase our costs or cause us to lose revenue or postpone or cancel clinical trials.
The FDA also requires that we demonstrate structural and functional comparability between the same drug product produced by different third-party manufacturers. Because we may use multiple sources to manufacture Androxal® and Proellex®, we may need to conduct comparability studies to assess whether manufacturing changes have affected the product safety, identity, purity or potency of any commercial product candidate compared to the product candidate used in clinical trials. If we are unable to demonstrate comparability, the FDA could require us to conduct additional clinical trials, which would be expensive and significantly delay commercialization of our product candidates.
Risks Relating to Product Commercialization
If commercialized, our product candidates may not be approved for sufficient governmental or third-party reimbursements, which would adversely affect our ability to market our product candidates.
In the United States and elsewhere, sales of pharmaceutical products depend in significant part on the availability of reimbursement to the consumer from third-party payers, such as government and private insurance plans. Third-party payers are increasingly challenging the prices charged for medical products and services. It will be time consuming and expensive for us to go through the process of seeking reimbursement from Medicaid, Medicare and private payers for Proellex® and Androxal®. Our products may not be considered cost effective, and coverage and reimbursement may not be available or sufficient to allow us to sell our products on a competitive and profitable basis. The passage of the Medicare Prescription Drug and Modernization Act of 2003 imposes requirements for the distribution and pricing of prescription drugs, which may negatively affect the marketing of our potential products.
If we successfully develop products but those products do not achieve and maintain market acceptance, our business will not be profitable.
Even if our product candidates are approved for commercial sale by the FDA or other regulatory authorities, the degree of market acceptance of any approved product by physicians, healthcare professionals and third-party payers and our profitability and growth will depend on a number of factors, including:
| · | relative convenience and ease of administration; | |
| · | the prevalence and severity of any adverse side effects; | |
| · | availability, effectiveness and cost of alternative treatments; | |
| · | pricing and cost effectiveness of our drugs; | |
| · | effectiveness of our or collaborators’ sales and marketing strategies; and | |
| · | our ability to obtain sufficient third-party insurance coverage or reimbursement. |
If Androxal® does not provide a treatment regime that is more beneficial than AndroGel®, the current standard of care for the treatment of testosterone deficiency, or otherwise provide patient benefit, it likely will not be accepted favorably by the market. If any products we may develop do not achieve market acceptance, then we will not generate sufficient revenue to achieve or maintain profitability.
| -19- |
In addition, even if our products achieve market acceptance, we may not be able to maintain that market acceptance over time if:
| · | new products or technologies are introduced that are more favorably received than our products, are more cost effective or render our products obsolete;
| |
| · | unforeseen complications arise with respect to use of our products; or
| |
| · | sufficient third-party insurance coverage or reimbursement does not remain available. |
In many foreign markets, including the countries in the European Union, pricing of pharmaceutical products is subject to governmental control. In the United States, there have been, and we expect that there will continue to be, a number of federal and state proposals to implement similar governmental pricing controls. While we cannot predict whether such legislative or regulatory proposals will be adopted, the adoption of such proposals could have a material adverse effect on our profitability.
Our liability insurance may neither provide adequate coverage nor may it always be available on favorable terms or at all.
Neither Androxal® nor Proellex® has been approved for commercial sale. However, the current and future use of our product candidates by us and potential corporate collaborators in clinical trials, and the sale of any approved products in the future, may expose us to liability claims. These claims might be made directly by consumers or healthcare providers or indirectly by pharmaceutical companies, potential corporate collaborators or others selling such products. We may experience financial losses in the future due to product liability claims. We have obtained limited general commercial liability insurance coverage for our clinical trials. We intend to expand our insurance coverage to include the sale of commercial products if we obtain marketing approval for any of our product candidates. However, we may not be able to maintain insurance coverage at a reasonable cost or in sufficient amounts to protect us against losses. If a successful product liability claim or series of claims is brought against us for uninsured liabilities or for liabilities in excess of our insurance limits, our assets may not be sufficient to cover such claims and our business operations could be impaired.
We face significant competition from many companies with substantially greater resources than we have and other possible advantages.
We are engaged in biopharmaceutical product development, an industry that is characterized by extensive research efforts and rapid technological progress. The biopharmaceutical industry is also highly competitive. Our success will depend on our ability to acquire, develop and commercialize products and our ability to establish and maintain markets for any products for which we receive marketing approval. Potential competitors in North America, Europe and elsewhere include major pharmaceutical companies, specialty pharmaceutical companies and biotechnology firms, universities and other research institutions and government agencies. Many of our competitors have substantially greater research and development and regulatory capabilities and experience, and substantially greater management, manufacturing, distribution, marketing and financial resources, than we do. Accordingly, our competitors may:
| · | develop or license products or other novel technologies that are more effective, safer or less costly than the product candidates that we are developing; | |
| · | obtain regulatory approval for products before we do; or | |
| · | commit more resources than we can to developing, marketing and selling competing products. |
Our main competitors for the treatment of testosterone deficiency are the testosterone replacement therapies currently being marketed. The current standard of care is AndroGel®, a topical gel for the replacement of testosterone developed by Solvay Pharmaceuticals (which was acquired by Abbott Laboratories). Abbott is a much larger company than we are, with greater resources and marketing ability. Androxal® would also compete with other forms of testosterone replacement therapies such as oral treatments, patches, injectables and a tablet applied to the upper gum. There is another topical gel currently marketed by Endo International PLC called Testim®, and a transdermal patch marketed by Watson Pharmaceuticals called AndroDerm®. Eli Lilly and Company also entered into a licensing agreement with a third party for a late stage topical testosterone treatment called Axiron®, which has recently become available in pharmacies. There can be no assurance that our product candidates will be more successful than competitive products. In addition, other potential competitors may be developing testosterone therapies similar to ours.
The main therapeutic products competitive with Proellex® for the treatment of uterine fibroids and endometriosis are GnRH agonists, including Lupron® and the use of approved progestin-based contraceptives for the treatment of endometriosis. In addition, surgical treatment of both uterine fibroids and endometriosis would compete with Proellex®, if approved, by removing uterine fibroids and by removing misplaced tissue in women with endometriosis. Furthermore, Abbott has recently licensed a Phase 3–ready molecule from Neurocrine Biosciences Inc. for the treatment of endometriosis. Gedeon Richter and Watson Pharmaceuticals have also entered into an exclusive license agreement to develop and market Esmya™ (an orally selective progesterone receptor modulator) in the U.S. and Canada.
| -20- |
Risks Relating to Our Intellectual Property
A third party individual holds two issued patents related to the use of an anti-estrogen such as clomiphene citrate in the treatment of disorders related to androgen deficiency.
We requested re-examination of one of these patents by the U.S. Patent and Trademark Office (“PTO”) based on prior art. The patent holder amended the claims in the re-examination proceedings, which led the PTO to determine that the amended claims were patentable in view of those publications under consideration and a re-examination certificate was issued. We subsequently filed a second request for re-examination by the PTO in light of a number of additional publications. The request was granted and all of the claims were finally rejected by the PTO in the re-examination. The patent holder appealed the rejections to the PTO Board of Patent Appeals and Interferences (the “PTO Board”) which ultimately reversed the rejections of several dependent claims in view of those publications under consideration. The patent holder filed a Notice of Appeal to the Federal Circuit on September 28, 2010 contesting the rejections maintained by the PTO Board. A decision was rendered by the Court of Appeals for the Federal Circuit on December 12, 2011, affirming the rejection of the appealed claims. The PTO issued an Ex Parte Reexamination Certificate on April 29, 2013, canceling the rejected claims and confirming the patentability of the remaining claims. Nevertheless, we believe that our development of Androxal® does not infringe any of the remaining claims and that all of the remaining claims are invalid on various grounds including additional prior art publications. We also believe that the second of these two patents is invalid in view of published prior art not considered by the PTO. If necessary, we intend to vigorously defend any and all claims that may be brought by the holder of such patents in a court of competent jurisdiction in order to develop Androxal® further. Adverse determinations in litigation proceedings could require us to seek licenses which may not be available on commercially reasonable terms, or at all, or subject us to significant liabilities, in which case we may not be able to successfully commercialize or out-license Androxal® until such patents expire or are otherwise no longer in force.
We licensed our rights to Proellex® from the NIH and our inability to fulfill our commitments and obligations under such license may result in forfeiture of our rights.
Our rights to Proellex® are licensed exclusively to us from the NIH under a license agreement. This license agreement contains numerous detailed performance obligations, with time sensitive dates for compliance, relating to clinical development and commercialization activities required by us or our designated third-party providers, as well as additional financial milestones and royalties. Failure to achieve the benchmarks specified in the commercial development plan attached to the license agreement or meet payment obligations could result in termination of the license agreement and the loss of our rights to develop and commercialize Proellex®. We periodically update the commercial development plan as such plans evolve. There can be no assurance that we will be able to meet any or all of the performance objectives in the future on a timely basis or at all, or that, if we fail to meet any of such objectives, the NIH will agree to revised objectives. The NIH also has the ability to terminate the agreement for an uncured material breach of the agreement, if we do not keep Proellex® reasonably available to the public after commercial launch or if we cannot reasonably satisfy unmet health and safety needs, among other reasons.
There can be no assurance that our manufacture, use or sale of our product candidates will not infringe on the patent rights of others.
There can be no assurance that the manufacture, use or sale of any of our product candidates will not infringe the patent rights of others. We may be unable to avoid infringement of the patent rights of others and may be required to seek a license, defend an infringement action or challenge the validity of the patents in court. There can be no assurance that a license to the allegedly infringed patents will be available to us on terms and conditions acceptable to us, if at all, or that we will prevail in any patent litigation. Patent litigation is extremely costly and time-consuming, and there can be no assurance that we will have sufficient resources to defend any possible litigation related to such infringement. If we do not obtain a license on acceptable terms under such patents, or are found liable for infringement, or are not able to have such patents declared invalid, we may be liable for significant money damages, may encounter significant delays in bringing our product candidates to market, or may be precluded from participating in the manufacture, use or sale of any such product candidates, any of which would materially and adversely affect our business.
A dispute regarding the infringement or misappropriation of our proprietary rights or the proprietary rights of others could be costly and result in delays in our research and development activities.
Our commercial success depends upon our ability to develop and manufacture our product candidates and market and sell drugs, if any, and conduct our research and development activities without infringing or misappropriating the proprietary rights of others. We may be exposed to future litigation by others based on claims that our product candidates, technologies or activities infringe the intellectual property rights of others. Numerous United States and foreign issued patents and pending patent applications owned by others also exist in the therapeutic areas in, and for the therapeutic targets for, which we are developing drugs. These could materially affect our ability to develop our product candidates or sell drugs, and our activities, or those of our licensor or future collaborators, could be determined to infringe these patents. Because patent applications can take many years to issue, there may be currently pending applications, unknown to us, which may later result in issued patents that our drug candidates or technologies may infringe. There also may be existing patents, of which we are not aware, that our product candidates or technologies may infringe. Further, there may be issued patents and pending patent applications in fields relevant to our business, of which we are or may become aware, that we believe we do not infringe or that we believe are invalid or relate to immaterial portions of our overall drug discovery and development efforts. We cannot assure you that others holding any of these patents or patent applications will not assert infringement claims against us for damages or seeking to enjoin our activities. We also cannot assure you that, in the event of litigation, we will be able to successfully assert any belief we may have as to non-infringement, invalidity or immateriality, or that any infringement claims will be resolved in our favor.
| -21- |
In addition, others may infringe or misappropriate our proprietary rights, and we may have to institute costly legal action to protect our intellectual property rights. We may not be able to afford the costs of enforcing or defending our intellectual property rights against others. There could also be significant litigation and other administrative proceedings in our industry that affect us regarding patent and other intellectual property rights. Any legal action or administrative action against us, or our collaborators, claiming damages or seeking to enjoin commercial activities relating to our drug discovery and development programs could:
| · | require us, or potential collaborators, to obtain a license to continue to use, manufacture or market the affected drugs, methods or processes, which may not be available on commercially reasonable terms, if at all; | |
| · | prevent us from importing, making, using, selling or offering to sell the subject matter claimed in patents held by others and subject us to potential liability for damages; or | |
| · | consume a substantial portion of our managerial, scientific and financial resources; or be costly, regardless of the outcome. |
Furthermore, because of the substantial amount of pre-trial documents and witness discovery required in connection with intellectual property litigation, there is risk that some of our confidential information could be compromised by disclosure during this type of litigation. In addition, during the course of this kind of litigation, there could be public announcements of the results of hearings, motions or other interim proceedings or developments. If securities analysts or investors perceive these results to be negative, it could have a substantial adverse effect on the trading price of our common stock or warrants.
We face substantial uncertainty in our ability to protect our patents and proprietary technology.
Our ability to commercialize our products will depend, in part, on our or our licensor’s ability to obtain patents, to enforce those patents and preserve trade secrets, and to operate without infringing on the proprietary rights of others. The patent positions of biopharmaceutical companies are highly uncertain and involve complex legal and factual questions. There can be no assurance that:
| · | Patent applications for and relating to our products candidates, Androxal® and Proellex®, will result in issued patents; | |
| · | Patent protection will be secured for any particular technology; | |
| · | Any patents that have been or may be issued to us, such as our issued patents and/or pending patent applications relating to Proellex® or Androxal®, or any patents that have been or may be issued to our licensor, such as the patent(s) and application(s) underlying our Proellex® compound, when issued, will be valid and enforceable; | |
| · | any patents will provide meaningful protection to us; | |
| · | others will not be able to design around the patents; or | |
| · | our patents will provide a competitive advantage or have commercial application. |
The failure to obtain and maintain adequate patent protection would have a material adverse effect on us and may adversely affect our ability to enter into, or affect the terms of, any arrangement for the marketing of any product.
We cannot assure that our patents will not be challenged by others.
There can be no assurance that patents owned by or licensed to us will not be challenged by others. We could incur substantial costs in proceedings, including interference proceedings before the PTO and comparable proceedings before similar agencies in other countries in connection with any claims that may arise in the future. These proceedings could result in adverse decisions about the patentability of our or our licensor’s inventions and products, as well as about the enforceability, validity or scope of protection afforded by the patents. Any adverse decisions about the patentability of our product candidates could cause us to either lose rights to develop and commercialize our product candidates or to license such rights at substantial cost to us. In addition, even if we were successful in such proceedings, the cost and delay of such proceedings would most likely have a material adverse effect on our business.
| -22- |
Confidentiality agreements with employees and others may not adequately prevent disclosure of trade secrets and other proprietary information, may not adequately protect our intellectual property, and will not prevent third parties from independently discovering technology similar to or in competition with our intellectual property.
We rely on trade secrets and other unpatented proprietary information in our product development activities. To the extent we rely on trade secrets and unpatented know-how to maintain our competitive technological position, there can be no assurance that others may not independently develop the same or similar technologies. We seek to protect trade secrets and proprietary knowledge, in part, through confidentiality agreements with our employees, consultants, advisors, collaborators and contractors. Nevertheless, these agreements may not effectively prevent disclosure of our confidential information and may not provide us with an adequate remedy in the event of unauthorized disclosure of such information. If our employees, scientific consultants, advisors, collaborators or contractors develop inventions or processes independently that may be applicable to our technologies, product candidates or products, disputes may arise about ownership of proprietary rights to those inventions and processes. Such inventions and processes will not necessarily become our property, but may remain the property of those persons or their employers. Protracted and costly litigation could be necessary to enforce and determine the scope of our proprietary rights. If we fail to obtain or maintain trade secret protection for any reason, the competition we face could increase, reducing our potential revenues and adversely affecting our ability to attain or maintain profitability.
We may be subject to claims that our employees have wrongfully used or disclosed alleged trade secrets of their former employers.
As is common in the biotechnology and pharmaceutical industries, we employ individuals who were previously employed at other biotechnology or pharmaceutical companies, including our competitors or potential competitors. We may be subject to claims that we, or our employees, independent contractors or consultants, have inadvertently or otherwise used or disclosed trade secrets or other proprietary information of their former employers. Litigation may be necessary to defend against these claims. Even if we are successful in defending against these claims, litigation could result in substantial costs and be a distraction to management.
We cannot protect our intellectual property rights throughout the world.
Filing, prosecuting, and defending patents on all of our drug discovery technologies and all of our potential drug candidates throughout the world would be prohibitively expensive. Competitors may use our technologies to develop their own drugs in jurisdictions where we have not obtained patent protection. These drugs may compete with our drugs, if any, and may not be covered by any of our patent claims or other intellectual property rights. The laws of some foreign countries do not protect intellectual property rights to the same extent as the laws of the United States, and many companies have encountered significant problems in protecting and defending such rights in foreign jurisdictions. Many countries, including certain countries in Europe, have compulsory licensing laws under which a patent owner may be compelled to grant licenses to third parties (for example, the patent owner has failed to “work” the invention in that country or the third party has patented improvements). In addition, many countries limit the enforceability of patents against government agencies or government contractors. In these countries, the patent owner may have limited remedies, which could materially diminish the value of the patent. Compulsory licensing of life-saving drugs is also becoming increasingly popular in developing countries either through direct legislation or international initiatives. Such compulsory licenses could be extended to include some of our drug candidates, which could limit our potential revenue opportunities. Moreover, the legal systems of certain countries, particularly certain developing countries, do not favor the aggressive enforcement of patents and other intellectual property protection, particularly those relating to biotechnology and/or pharmaceuticals, which makes it difficult for us to stop the infringement of our patents. Proceedings to enforce our patent rights in foreign jurisdictions could result in substantial cost and divert our efforts and attention from other aspects of our business.
Risks Related to our Common Stock and Warrants
The trading price of our common stock has been volatile and is likely to be volatile in the future.
The trading price of our common stock has been highly volatile. Since January 1, 2013 through February 27, 2015, the sale price of our stock price has fluctuated from a low of $5.92 to a high of $29.79. The market price for our common stock and warrants will be affected by a number of factors, including:
| · | the denial or delay of regulatory clearances or approvals of our drug candidates or receipt of regulatory approval of competing products; | |
| · | our ability to accomplish clinical, regulatory and other product development milestones; | |
| · | the ability of our product candidates, if they receive regulatory approval, to achieve market success; | |
| · | the performance of third-party manufacturers and suppliers; | |
| · | actual or anticipated variations in our results of operations or those of our competitors; | |
| · | developments with respect to patents and other intellectual property rights; |
| -23- |
| · | sales of common stock or other securities by us or our stockholders in the future; | |
| · | additions or departures of key scientific or management personnel; | |
| · | disputes or other developments relating to proprietary rights, including patents, litigation matters and our ability to obtain patent protection for our products; | |
| · | trading volume of our common stock and warrants; | |
| · | investor perceptions about us and our industry; | |
| · | public reaction to our press releases, other public announcements and SEC and other filings; | |
| · | the failure of analysts to cover our common stock, or changes in analysts’ estimates or recommendations; | |
| · | the failure by us to meet analysts’ projections or guidance; | |
| · | general market conditions and other factors unrelated to our operating performance or the operating performance of our competitors; and | |
| · | the other factors described elsewhere in these “Risk Factors” or the section titled “Risk Factors” contained in our other public filings. |
The stock prices of many companies in the biotechnology industry have experienced wide fluctuations that have often been unrelated to the operating performance of these companies. Following periods of volatility in the market price of a company’s securities, securities class action litigation often has been initiated against a company. If any class action litigation is initiated against us, we may incur substantial costs and our management’s attention may be diverted from our operations, which could significantly harm our business.
Our common stock is thinly traded and in the future, may continue to be thinly traded, and our stockholders may be unable to sell at or near asking prices or at all if they need to sell their shares to raise money or otherwise desire to liquidate such shares.
To date, we have a low volume of daily trades in our common stock on NASDAQ. For example, the average daily trading volume in our common stock on NASDAQ during the fourth quarter of 2014 was approximately 938,900 shares per day. Our stockholders may be unable to sell their common stock at or near their asking prices or at all, which may result in substantial losses to our stockholders.
The market for our common stock may be characterized by significant price volatility when compared to seasoned issuers, and we expect that our share price will be more volatile than a seasoned issuer for the indefinite future. As noted above, our common stock may be sporadically and/or thinly traded. As a consequence of this lack of liquidity, the trading of relatively small quantities of shares by our stockholders may disproportionately influence the price of those shares in either direction. The price for our shares could, for example, decline significantly in the event that a large number of our common stock are sold on the market without commensurate demand, as compared to a seasoned issuer that could better absorb those sales without adverse impact on its share price.
Our inability to comply with the listing requirements of the Nasdaq Capital Market could result in our common stock and/or warrants being delisted, which could affect their market price and liquidity and reduce our ability to raise capital.
We are required to meet certain qualitative and financial tests (including a minimum closing bid price of $1.00 per share for our common stock) to maintain the listing of our common stock and/or warrants on the Nasdaq Capital Market. If we do not maintain compliance with the continued listing requirements for the Nasdaq Capital Market within specified periods and subject to permitted extensions, our common stock and/or warrants may be recommended for delisting (subject to any appeal we would file). If our common stock or warrants are delisted, it could be more difficult to buy or sell our common stock and/or our warrants and to obtain accurate quotations, and the price of our common stock and/or warrants could suffer a material decline. Delisting would also impair our ability to raise capital.
The market price of our common stock may fall below the exercise price of our Series B Warrants.
The Series B Warrants are exercisable at any time at or prior to 5:00 p.m. Eastern time on February 8, 2016. The market price of our common stock may fall below the exercise price for such warrants prior to their expiration. Any Series B Warrants not exercised by such date of expiration will expire and be worthless and we will be under no further obligation to the holders of such warrants.
| -24- |
Our ability to use our net operating loss carryforwards and certain other tax attributes may be limited.
The Tax Reform Act of 1986 provided for a limitation on the use of NOL and tax credit carryforwards following certain ownership changes that could limit the Company’s ability to utilize these NOLs and tax credits. The limitation is generally referred to as the “section 382 limit” after the IRC section. The issuance of stock, together with changes in stock ownership, resulted in multiple ownership changes for federal income tax purposes. During 2013, the Company completed an analysis of its section 382 limit. Based on this analysis, the Company concluded that the amount of NOL carryforwards and the credits available to offset taxable income is limited under section 382. Accordingly, if the Company generates taxable income in any year in excess of its then annual limitation, the Company may be required to pay federal income taxes even though it has unexpired NOL carryforwards. Additionally, because U.S. tax laws limit the time during which NOLs and tax credit carryforwards may be applied against future taxable income and tax liabilities, the Company may not be able to take full advantage of its NOLs and tax credit carryforwards for federal income tax purposes. Future public and private stock placements may create additional limitations on the Company’s NOLs, credits and other tax attributes.
We do not intend to pay dividends on our common stock so any returns will be limited to the value of our stock.
We have never declared or paid any cash dividends on our common stock. We currently anticipate that we will retain future earnings for the development, operation and expansion of our business and do not anticipate declaring or paying any cash dividends for the foreseeable future. Any return to stockholders will therefore be limited to the appreciation of their stock.
Item 1B. Unresolved Staff Comments
None.
We lease our current property under a lease agreement that expires in June 2015. This lease is for approximately 7,100 square feet of our laboratory and office space located in The Woodlands, Texas. We do not own or lease any other property and believe that our current facilities are sufficient for our needs for the foreseeable future.
Therapeutic uses of our Androxal product candidate are covered in the United States by nine issued U.S. patents and seven pending patent applications. Foreign coverage of therapeutic uses of our Androxal product candidate includes 71 issued foreign patents and 99 foreign pending patent applications. The issued patents and pending applications relate to methods for treating certain conditions including the treatment of testosterone deficiency in men, the treatment of diabetes mellitus Type 2, the treatment of metabolic syndrome and conditions associated therewith, and the treatment of infertility in hypogonadal men. Androxal (the trans-isomer of clomiphene) is purified from clomiphene citrate. A third party individual holds two issued patents related to the use of anti-estrogen such as clomiphene citrate and others for use in the treatment of androgen deficiency and disorders related thereto. We requested re-examination of one of these patents by the U.S. Patent and Trademark Office (“PTO”) based on prior art. The patent holder amended the claims in the re-examination proceedings, which led the PTO to determine that the amended claims were patentable in view of those publications under consideration and a re-examination certificate was issued. We subsequently filed a second request for re-examination by the PTO in light of a number of additional publications. The request was granted and all of the claims were finally rejected by the PTO in the re-examination. The patent holder appealed the rejections to the PTO Board of Patent Appeals and Interferences (the “PTO Board”) which ultimately reversed the rejections of several dependent claims in view of those publications under consideration. The patent holder filed a Notice of Appeal to the Federal Circuit on September 28, 2010 contesting the rejections maintained by the PTO Board. A decision was rendered by the Court of Appeals for the Federal Circuit on December 12, 2011, affirming the rejection of the appealed claims. The PTO issued an Ex Parte Reexamination Certificate on April 29, 2013, cancelling the rejected claims and confirming patentability of the remaining claims. Nevertheless, we believe that our development of Androxal does not infringe any of the remaining claims and that all of the remaining claims are invalid on various grounds including additional prior art publications. We also believe that the second of these two patents is invalid in view of published prior art not considered by the PTO. If necessary, we intend to vigorously defend any and all claims that may be brought by the holder of such patents in a court of competent jurisdiction in order to develop Androxal further. Adverse determinations in litigation proceedings could require us to seek licenses from patent holders which may not be available on commercially reasonable terms, or at all, or may subject us to significant liabilities, in which case we may not be able to successfully commercialize or out-license Androxal until such patents expire or are otherwise no longer in force.
On July 19, 2013, we received a letter from Dr. Harry Fisch threatening to file a lawsuit against us and two of our executive officers (Joseph S. Podolski, President and Chief Executive Officer and Ron Wiehle, Executive Vice President), seeking addition of Dr. Harry Fisch as an inventor on three of our patents, U.S. Patent Nos. 7,173,064, 7,737,185 and 7,759,360, covering therapeutic uses of Androxal®. We believe that these allegations are without merit and on August 2, 2013, we commenced a lawsuit against Dr. Fisch in the U.S. District Court for the Southern District of Texas seeking a declaratory judgment that he should not be added as inventor to any of these patents. On October 2, 2013, Dr. Fisch filed counterclaims to our complaint seeking correction of inventorship of the three patents at issue to name Dr. Fisch as a co-inventor of the applications leading these patents. Dr. Fisch subsequently stipulated that he does not claim to be a co-inventor of U.S. Patent No. 7,173,064. The court granted summary judgment in favor of the Company on separate equitable and legal grounds, and entered judgment on December 23, 2014. Our request for attorney’s fees was denied. On February 9, 2015, Dr. Fisch filed a notice of appeal of the summary judgment rulings to the United States Court of Appeals for the Federal Circuit.
| -25- |
ITEM 4. MiNE SAFETY DISCLOSURES
Not applicable.
| -26- |
ITEM 5. Market for the Registrant's Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities
Our common stock is quoted on the Nasdaq Capital Market under the symbol “RPRX”. The following table shows the high and low sale prices per share of our common stock as reported by the Nasdaq Stock Market during the periods presented
| Price Range | ||||||||
| High | Low | |||||||
| 2013 | ||||||||
| First Quarter | $ | 19.12 | $ | 8.42 | ||||
| Second Quarter | 21.02 | 14.10 | ||||||
| Third Quarter | 29.79 | 18.15 | ||||||
| Fourth Quarter | 27.52 | 14.09 | ||||||
| 2014 | ||||||||
| First Quarter | $ | 22.57 | $ | 15.27 | ||||
| Second Quarter | 18.40 | 13.93 | ||||||
| Third Quarter | 22.55 | 8.86 | ||||||
| Fourth Quarter | 11.21 | 5.92 | ||||||
All of the foregoing prices reflect interdealer quotations, without retail mark-up, markdowns or commissions and may not necessarily represent actual transactions in the common stock.
On February 27, 2015, the last sale price of our common stock, as reported by the Nasdaq Capital Market, was $9.21 per share. On February 27, 2015, there were approximately 104 holders of record and approximately 8,300 beneficial holders of our common stock.
Dividend Policy
General
We have never declared or paid cash dividends on our capital stock. We currently intend to retain our future earnings, if any, for use in our business and therefore do not anticipate paying cash dividends in the foreseeable future. Payment of future dividends, if any, will be at the discretion of our board of directors after taking into account various factors, including our financial condition, operating results, current and anticipated cash needs.
Rights Plan
We are party to a rights agreement, as amended, pursuant to which a dividend consisting of one preferred stock purchase right was distributed for each share of our common stock held as of the close of business on September 13, 1999, and to each share of common stock issued thereafter until the earlier of (i) the distribution date which is defined in the rights plan, (ii) the redemption date which is defined in the rights plan or (iii) September 13, 2015. The rights plan is designed to deter coercive takeover tactics and to prevent an acquirer from gaining control of us without offering fair value to our stockholders. The rights will expire on September 13, 2015, subject to earlier redemption or exchange as provided in the rights plan. Each right entitles its holder to purchase from us one one-hundredth of a share of a new series of Series One Junior Participating Preferred Stock at a price of $20.00 per one one-hundredth of a share, subject to adjustment. The rights are generally exercisable only if a person acquires beneficial ownership of 20% or more of our outstanding common stock.
A complete description of the rights, the rights plan with Computershare Trust Company, Inc., as rights agent, and the Series One Junior Participating Preferred Stock is hereby incorporated by reference from the information appearing under the caption “Item 1. Description of the Registrant’s Securities to be Registered” contained in the Registration Statement on Form 8-A filed with the SEC on September 3, 1999, and as amended by amendments to such Registration Statement on Form 8-A/A filed with the SEC on September 11, 2002, October 31, 2002, June 30, 2005, January 10, 2008, October 10, 2008 and September 9, 2010.
| -27- |
Performance Graph
This information is required by Item 201(e) of Regulation S-K. Such information shall not be deemed to be “filed” or incorporated by reference in future filings with the SEC, or subject to the liabilities of Section 18 of the Securities Exchange Act of 1934, except to the extent that we specifically incorporate it by reference into a document filed under the Securities Act of 1933 or the Securities Exchange Act of 1934.
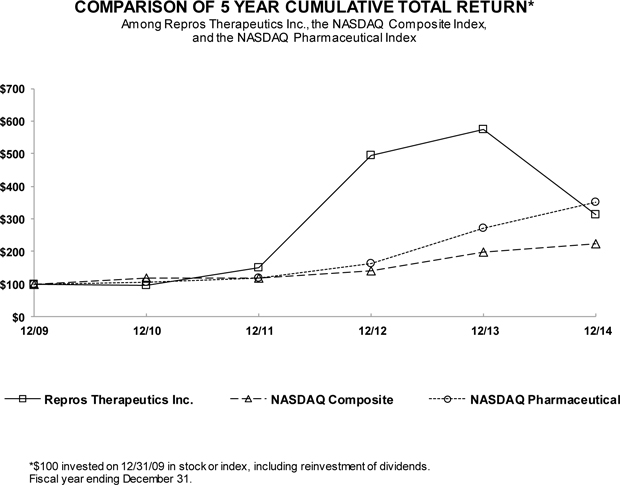
| 12/09 | 12/10 | 12/11 | 12/12 | 12 /13 | 12 /14 | |||||||||||||||||||
| Repros Therapeutics Inc. | 100.00 | 95.41 | 151.27 | 494.29 | 574.32 | 312.89 | ||||||||||||||||||
| NASDAQ Composite | 100.00 | 117.61 | 118.70 | 139.00 | 196.83 | 223.74 | ||||||||||||||||||
| NASDAQ Pharmaceutical | 100.00 | 104.24 | 117.69 | 161.80 | 271.53 | 349.75 |
| -28- |
ITEM 6. sELECTED CONSOLIDATED FINANCIAL DATA
The statement of operations data for the years ended December 31, 2014, 2013 and 2012, and the balance sheet data as of December 31, 2014 and 2013, have been derived from our financial statements, included elsewhere in this Form 10-K. The statement of operations data for the years ended December 31, 2011 and 2010, and the balance sheet data as of December 31, 2012, 2011 and 2010 have been derived from our financial statements not included in this Form 10-K. Our historical results are not necessarily indicative of results to be expected for any future period. The data presented below have been derived from financial statements that have been prepared in accordance with accounting principles generally accepted in the United States of America and should be read with our financial statements, including notes, and with "Management's Discussion and Analysis of Financial Condition and Results of Operations" included elsewhere in this Form 10-K.
STATEMENTS OF OPERATIONS DATA(1):
(In thousands, except per share data)
| 2014 | 2013 | 2012 | 2011 | 2010(3) | ||||||||||||||||
| Revenues and Other Income | ||||||||||||||||||||
| Interest income | $ | 9 | $ | 9 | $ | 3 | $ | 2 | $ | — | ||||||||||
| Other income | — | — | — | — | 421 | |||||||||||||||
| Total revenues | 9 | 9 | 3 | 2 | 421 | |||||||||||||||
| Expenses: | ||||||||||||||||||||
| Research and development | 27,107 | 23,657 | 14,120 | 8,893 | 3,192 | |||||||||||||||
| General and administrative | 5,437 | 4,818 | 4,827 | 3,811 | 2,285 | |||||||||||||||
| Total expenses | 32,544 | 28,475 | 18,947 | 12,704 | 5,477 | |||||||||||||||
| Net loss | $ | (32,535 | ) | $ | (28,466 | ) | $ | (18,944 | ) | $ | (12,702 | ) | $ | (5,056 | ) | |||||
| Net loss per share – basic and diluted (2) | $ | (1.39 | ) | $ | (1.37 | ) | $ | (1.23 | ) | $ | (1.06 | ) | $ | (0.63 | ) | |||||
| Shares used in loss per share calculation | 23,432 | 20,808 | 15,346 | 11,961 | 8,057 |
| (1) | 2010 – 2013 Statements of Operations Data has been revised. For a further description of this revision, see "Note 2. Revision of Prior Years’ Financial Statements" of the Notes to Consolidated Financial Statements. | |
| (2) | See "Note 3. Summary of Significant Accounting Policies" of the Notes to Consolidated Financial Statements for a description of the computation of loss per share. | |
| (3) | The basic and diluted net loss per share and shares used in loss per share calculation have been adjusted to reflect the one-for-four reverse stock split that was effected on October 14, 2010. |
BALANCE SHEET DATA(1):
(In thousands)
| 2014 | 2013 | 2012 | 2011 | 2010 | ||||||||||||||||
| Cash, cash equivalents and marketable securities | $ | 46,620 | $ | 75,807 | $ | 24,212 | $ | 4,565 | $ | 2,957 | ||||||||||
| Total assets | 46,941 | 76,071 | 24,670 | 4,679 | 3,292 | |||||||||||||||
| Accumulated deficit | (273,064 | ) | (240,529 | ) | (212,063 | ) | (193,119 | ) | (180,417 | ) | ||||||||||
| Total stockholders' equity | $ | 44,017 | $ | 72,519 | $ | 20,873 | $ | 3,281 | $ | 1,994 | ||||||||||
| (1) | 2010 – 2013 Balance Sheet Data has been revised. For a further description of this revision, please See "Note 2. Revision of Prior Year Financial Statements" of the Notes to Consolidated Financial Statements. |
| -29- |
ITEM 7. Management's Discussion and Analysis of Financial Condition and Results of Operations
The following management's discussion and analysis should be read in conjunction with our historical consolidated financial statements and their notes included elsewhere in this Form 10-K. This discussion contains forward-looking statements that reflect our current views with respect to future events and financial performance. Our actual results may differ materially from those anticipated in these forward-looking statements as a result of certain factors, such as those set forth under "Risk Factors" and elsewhere in this Form 10-K.
Overview
The Company was organized on August 20, 1987. We are a biopharmaceutical company focused on the development of new drugs to treat hormonal and reproductive system disorders.
We are developing Androxal®, a single isomer of clomiphene citrate which is an orally active proprietary small molecule compound. Androxal® is for the treatment of secondary hypogonadism in overweight men wishing to restore normal testicular function. Men with secondary hypogonadism exhibit low testosterone levels due to under stimulated testes but they are generally fertile. Androxal® is designed to treat the underlying mechanism, insufficient stimulation of the testes by the pituitary, which causes secondary hypogonadism. Secondary hypogonadism due to being overweight or obese is the single greatest cause of hypogonadism in general. As of 2013, sales of preparations for the treatment of low testosterone have exceeded $2 billion in the U.S. and first tier pharmaceutical companies have entered the low testosterone marketplace.
In December 2011, we completed a Phase 2B study of Androxal® in men with secondary hypogonadism, but naïve to testosterone treatment, at the recommendation of the Food and Drug Administration (the “FDA”). Top line results of this study demonstrated that Androxal® was generally well tolerated compared to placebo and that there were no drug related serious adverse events that led to discontinuation. We met with the FDA in May 2012 to discuss the design of pivotal Phase 3 efficacy studies for Androxal® as well as the components of the overall drug development program required for a New Drug Application (“NDA”) submission and agreed on registration requirements for Androxal® oral therapy for the treatment of secondary hypogonadism. In July 2012, we announced that we reached an agreement with the FDA for the design of the pivotal efficacy studies for Androxal® for the treatment of secondary hypogonadism. The pivotal studies were conducted under a Special Protocol Assessment (“SPA”). We have completed both Phase 3 pivotal efficacy studies. On March 27, 2013, we announced that the top-line results from our first pivotal Phase 3 study, ZA-301, met both co-primary endpoints mandated by the FDA, and we announced on September 16, 2013, that we met both co-primary endpoints in the second pivotal study, ZA-302. Additionally, on September 16, 2013, we announced the results from ZA-300, a six-month safety study. This study identified no new safety issues. On October 22, 2013, we announced that we received guidance from the FDA instructing the Company to request a meeting to discuss the adequacy of studies ZA-301 and ZA-302. In addition to this guidance, the FDA further noted that they would allow us to run head-to-head studies against approved testosterone replacement products. These head-to-head studies, ZA-304 and ZA-305, were initiated in January 2014 and subsequently completed in September and August 2014, respectively. Both of these head-to-head studies achieved superiority for both co-primary endpoints and most secondary endpoints as compared to the approved testosterone replacement product. On October 21, 2014, we announced the results from ZA-303, a 52 week, single-blind, placebo-controlled Phase 3 study to evaluate the effects on bone mineral density. In this study, no new safety signals were identified, including no evidence of negative effects on bone mineral density. On February 2, 2015, we announced that we electronically submitted our NDA to the FDA for Androxal®. The NDA includes a collection of data on safety and efficacy from over 20 studies, including four Phase 3 efficacy studies.
We are also developing Proellex®, an orally administered selective blocker of the progesterone receptor in women, for the treatment of uterine fibroids and endometriosis. Uterine fibroids and endometriosis affect millions of women of reproductive age. Proellex® has shown statistically significant results in previous Phase 2 studies for endometriosis and uterine fibroids. We completed a low dose escalating study as permitted by the FDA in late 2011, to determine both signals of efficacy and safety for low oral doses of the drug. There was no evidence of elevations of liver enzymes over baseline, suggesting these lower doses avoid the type of adverse events seen at much higher doses in earlier studies. On October 8, 2012, we announced that the FDA has agreed to a reclassification of the full clinical hold to a partial clinical hold on low dose oral Proellex® to allow us to conduct a Phase 2 study in the treatment of endometriosis. We initiated this study in November 2012. To date, we have experienced difficulty enrolling subjects into this study due to changes in the current treatment of this disorder. We believe we can have this study full enrolled in 2015.
On October 31, 2013, the Company held a meeting with the FDA to discuss the clinical development plan for low dose oral Proellex® in the treatment of uterine fibroids. During the meeting, the FDA provided guidance for endpoints it believed acceptable for the treatment of uterine fibroids in an efficacy study and instructed the Company to submit a request for lifting the full clinical hold. The Company has followed the FDA’s recommendations and submitted the study protocol and the request for the full hold lift. Additionally, on March 17, 2014, we announced that the FDA indicated that we may proceed to conduct Phase 1 and Phase 2 studies of low dose oral Proellex® for endometriosis and uterine fibroids while remaining on partial clinical hold. This guidance indicated that the highest allowed dose will be 12 mg daily. On December 29, 2014, we announced that we have initiated a Phase 2B study for low dose oral Proellex® in the treatment of uterine fibroids.
| -30- |
The Company has an active IND for the vaginal delivery of Proellex® for the treatment of uterine fibroids. Since the clinical hold relates only to oral delivery of Proellex®, this IND has no clinical hold issues. In the first quarter of 2012, we initiated a Phase 2 vaginal administration study for the treatment of uterine fibroids, and reported final study results in January 2013. We held an end of Phase 2 meeting with the FDA in May 2013, to discuss a Phase 3 study design for the vaginally delivered Proellex as a treatment for uterine fibroids. The FDA recommended that a Phase 2B study should be conducted prior to commencing a Phase 3 program. On December 29, 2014, we announced that we have initiated a Phase 2B study for vaginally delivered Proellex® in the treatment of uterine fibroids.
VASOMAX® has been on partial clinical hold in the U.S. since 1998, and no further development activities are planned.
The clinical development of pharmaceutical products is a complex undertaking and many products that begin the clinical development process do not obtain regulatory approval. The costs associated with our clinical trials may be impacted by a number of internal and external factors, including the number and complexity of clinical trials necessary to obtain regulatory approval, the number of eligible patients necessary to complete our clinical trials and any difficulty in enrolling these patients and the length of time to complete our clinical trials. Given the uncertainty of these potential costs, we recognize that the total costs we will incur for the clinical development of our product candidates may exceed our current estimates.
As with most biotechnology companies with drug candidates in development, the path to marketing approval by the FDA and comparable foreign agencies for each such candidate is long and uncertain. The regulatory process, both domestically and abroad, is a multi-year process with no certainty when and if a drug candidate will be approved for commercial use. The development path for a particular drug candidate typically includes a variety of clinical trials. While we have a general estimate of the timeframe for our clinical trials, the actual anticipated completion dates for each of our drug candidates are uncertain due to a wide variety of risks, including those described in the risk factors in this Form 10-K. The length of time for a clinical trial may vary substantially according to factors relating to the particular clinical trial, such as the type and intended use of the drug candidate, the clinical trial design and the ability to enroll suitable patients. A clinical hold can also result in unpredictable delays and added costs. We will not receive any revenue from commercial sales unless we, or a potential partner, complete the clinical trial process, obtain regulatory approval, and successfully commercialize one or more of our product candidates. Similarly, we do not have a reasonable basis to predict when or if material net cash inflows from the commercialization and sale of our drug candidates will occur. To date, we have not commercialized any of our drug candidates to any material extent and in fact may never do so. For a discussion of the risks and uncertainties associated with the timing and costs of completing the development of the Company’s drug candidates, see the section titled “Risk Factors.”
Our results of operations may vary significantly from year to year and quarter to quarter and depend on, among other factors, our ability to be successful in our clinical trials, the regulatory approval process in the United States and other foreign jurisdictions and the ability to complete new licenses and product development agreements. The timing of our revenues may not match the timing of our associated product development expenses. To date, research and development expenses have generally exceeded revenue in any particular period and/or fiscal year.
As of December 31, 2014, we had accumulated losses of $273.1 million, approximately $46.6 million in cash and cash equivalents, and accounts payable and accrued expenses of approximately $2.9 million, in the aggregate. We continue to explore potential corporate partnering opportunities for assistance in the clinical development funding and commercialization of our products, as appropriate; however, there can be no assurance that an acceptable corporate partnering opportunity will be successfully completed or that our current liquidity will be sufficient to fund all of our product development needs.
At December 31, 2014, we had 28 full-time employees who utilize the services of contract research organizations, contract manufacturers and various consultants to assist us in performing clinical and regulatory services for the clinical development of our products. We are substantially dependent on our various contract groups to adequately perform the activities required to obtain regulatory approval of our products.
The value of the tax asset associated with the December 31, 2014 accumulated deficit can be substantially diminished in value to us due to various tax regulations, including change in control provisions in the tax code. For additional information relating to our net operating loss carryforward, see "Note 6. Federal Income Taxes" of the Notes to Consolidated Financial Statements. Losses have resulted principally from costs incurred in conducting clinical trials for our product candidates, in research and development activities related to efforts to develop our products and from the associated administrative costs required to support those efforts. There can be no assurance that we will be able to successfully commercialize any of our drug candidates. Our ability to achieve profitability will depend on, among other things, successfully completing the clinical development of our products in a reasonable time frame and at a reasonable cost, obtaining regulatory approvals, establishing marketing, sales and manufacturing capabilities or collaborative arrangements with others that possess such capabilities, our and our partners' ability to realize value from our research and development programs through the commercialization of those products and raising sufficient funds to finance our activities. There can be no assurance that we will be able to achieve profitability or that profitability, if achieved, can be sustained. See "Item 1. Business — Risk Factors" and "Note 1. Organization and Operations" of Notes to Consolidated Financial Statements.
| -31- |
Critical Accounting Policies and the Use of Estimates
The preparation of our financial statements in conformity with accounting principles generally accepted in the United States requires management to make estimates and assumptions that affect the amounts reported in our financial statements and accompanying notes. Please see Note 3, "Summary of Significant Accounting Policies," for a detailed discussion of our critical accounting policies. A brief summary of our accounting policies is provided below.
Accrued Expenses
We estimate accrued expenses as part of our process of preparing financial statements. Examples of areas in which subjective judgments may be required include costs associated with services provided by contract organizations for clinical trials, preclinical development and manufacturing of clinical materials. We accrue for costs incurred as the services are being provided by monitoring the status of the trials or services provided and the invoices received from our external service providers. In the case of clinical trials, a portion of the estimated cost normally relates to the projected cost to treat a patient in our trials, and we recognize this cost over the estimated term of the study based on the number of patients enrolled in the trial on an ongoing basis, beginning with patient enrollment. As actual costs become known to us, we adjust our accruals. To date, our estimates have not differed significantly from the actual costs incurred. However, subsequent changes in estimates may result in a material change in our accruals, which could also materially affect our balance sheet and results of operations.
Research & Development Expenses
Research and development (“R&D”) expenses include salaries and related employee expenses, contracted regulatory affairs activities, insurance coverage for clinical trials and prior product sales, contracted research and consulting fees, fees associated with our patent portfolio, facility costs and internal research and development supplies. We expense R&D costs in the period they are incurred. These costs consist of direct and indirect costs associated with specific projects as well as fees paid to various entities that perform research on our behalf.
Share-Based Compensation
We had one stock-based compensation plan at December 31, 2014, the 2011 Equity Incentive Plan. Accounting standards generally require the recognition of the cost of employee services for share-based compensation based on the grant date fair value of the equity or liability instruments issued. We use the Black-Scholes option pricing model to estimate the fair value of our stock options. Expected volatility is determined using historical volatilities based on historical stock prices for a period equal to the expected term. The expected volatility assumption is adjusted if future volatility is expected to vary from historical experience. The expected term of options represents the period of time that options granted are expected to be outstanding and falls between the options’ vesting and contractual expiration dates. The risk-free interest rate is based on the yield at the date of grant of a zero-coupon U.S. Treasury bond whose maturity period equals the option’s expected term.
Income Taxes
We have had net operating losses since inception and, therefore, have not been subject to federal income taxes. We have accumulated approximately $1.4 million of research and development tax credits. As of December 31, 2014, we had approximately $210.2 million of net operating loss (“NOL”) carryforwards for federal income tax purposes. Additionally, approximately $12.2 million of NOLs, and approximately $838,000 of research and development tax credits, expire in 2018. Accounting standards require the recognition of a deferred tax asset. However, a valuation allowance must be recorded for deferred tax assets whose recovery is deemed unlikely. As we have incurred net operating losses since inception, and there is no certainty of future revenues, our deferred tax assets have been reserved in full in the accompanying consolidated financial statements. Additionally, during 2013, the Company completed an analysis of its section 382 limit. Based on this analysis, the Company concluded that the amount of NOL carryforwards and the credits available to offset taxable income is limited under section 382. Accordingly, if the Company generates taxable income in any year in excess of its then annual limitation, the Company may be required to pay federal income taxes even though it has unexpired NOL carryforwards. Additionally, because U.S. tax laws limit the time during which NOLs and tax credit carryforwards may be applied against future taxable income and tax liabilities, the Company may not be able to take full advantage of its NOLs and tax credit carryforwards for federal income tax purposes. Future public and private stock placements may create additional limitations on the Company’s NOLs, credits and other tax attributes.
Recent Accounting Pronouncements
In August 2014, the FASB issued Accounting Standards Update No. 2014-15, “Presentation of Financial Statements - Going Concern.” The new standard requires management to evaluate whether there are conditions or events that raise substantial doubt about an entity's ability to continue as a going concern for both annual and interim reporting periods. This guidance is effective for us for the fiscal year beginning January 1, 2016 and interim periods thereafter. The guidance is not expected to have a material impact on our consolidated financial statements.
| -32- |
In June 2014, the FASB issued Accounting Standards Update 2014-10 (“ASU 2014-10”), “Development Stage Entities (Topic 915): Elimination of Certain Financial Reporting Requirements, Including an Amendment to Variable Interest Entities Guidance in Topic 810, Consolidation.” The guidance eliminates the definition of a development stage entity thereby removing the incremental financial reporting requirements from U.S. Generally Accepted Accounting Principles for development stage entities, primarily presentation of inception to date financial information. The provisions of the amendment is effective for annual reporting periods beginning after December 15, 2015. We have elected to adopt ASU 2014-10 early and as an early adopter, we are no longer providing inception-to-date financial information in our consolidated financial statements.
In May 2014, the FASB issued Accounting Standards Update 2014-09, “Revenue from Contracts with Customers” (“ASU 2014-09”). ASU 2014-09 is a comprehensive new revenue recognition model requiring a company to recognize revenue to depict the transfer of goods or services to a customer at an amount reflecting the consideration it expects to receive in exchange for those goods or services. In adopting ASU 2014-09, companies may use either a full retrospective or a modified retrospective approach. Additionally, this guidance requires improved disclosures regarding the nature, amount, timing and uncertainty of revenue and cash flows arising from contracts with customers. ASU 2014-09 is effective for the first interim period within annual reporting periods beginning after December 15, 2016, and early adoption is not permitted. The Company is currently assessing the impact of the new standard on our consolidated financial statements.
Results of Operations
Comparison of Years Ended December 31, 2014 and 2013
Revenues and Other Income
Total revenues and other income, which consisted solely of interest income, was $9,000 for both years ended December 31, 2014 and 2013.
Research and Development Expenses
R&D expenses include contracted services relating to our clinical product development activities which include preclinical studies, clinical trials, fees associated with our patent portfolio, regulatory affairs and bulk manufacturing scale-up activities and bulk active ingredient purchases for preclinical and clinical trials primarily relating to our two product candidates, Androxal® and Proellex®. Research and development expenses also include internal operating expenses relating to our general research and development activities. R&D expenses increased 15%, or approximately $3.5 million, to $27.1 million for 2014 as compared to $23.7 million for 2013. Our primary R&D expenses for 2014 and 2013 are shown in the following table (in thousands):
| Year Ended December 31, | ||||||||||||||||
| Research and Development | 2014 | 2013 | Variance | Change (%) | ||||||||||||
| Androxal® clinical development | $ | 17,160 | $ | 14,791 | $ | 2,369 | 16 | % | ||||||||
| Proellex® clinical development | 1,883 | 1,815 | 68 | 4 | % | |||||||||||
| Payroll and benefits | 4,319 | 3,914 | 405 | 10 | % | |||||||||||
| Operating and occupancy | 3,745 | 3,137 | 608 | 19 | % | |||||||||||
| Total | $ | 27,107 | $ | 23,657 | $ | 3,450 | 15 | % | ||||||||
Operating and occupancy expense for 2013 has been revised. For a further description of the revisions, see Note 2. “Revision of Prior Years’ Financial Statements” of the Notes to Consolidated Financial Statements.
The increase in Androxal® clinical development expenses for the year ended 2014 as compared to 2013 was primarily due to the completion of the Phase 3 studies, ZA-303, ZA-304 and ZA-305, as well as costs associated with the filing of the NDA in early 2015. The clinical development expenses related to Proellex® increased for 2014 as compared to 2013 primarily due to increased expenses associated with our Phase 2 endometriosis study.
From inception through December 31, 2014 we incurred $60.3 million for the development of Androxal® and $62.8 million for the development of Proellex®. These accumulated costs exclude any internal operating expenses and related fees associated with our patent portfolio.
R&D payroll and benefits expense for both years ended December 31, 2014 and 2013 includes salaries, non-cash stock based compensation expense and fringe benefits and increased 10%, or approximately $405,000, to $4.3 million for 2014 as compared to $3.9 million for 2013. This increase was primarily due to an increase in headcount and increased salaries. Included in R&D payroll and benefit expense is a charge for non-cash stock based compensation expense of $1.9 million for 2014 as compared to $1.8 million for 2013.
R&D operating and occupancy increased 19%, or approximately $608,000, to $3.7 million for 2014 as compared to $3.1 million for 2013. This increase was primarily due to increases in legal expenses and costs associated with our patent portfolio.
| -33- |
General and Administrative Expenses
General and administrative expenses (“G&A”) increased 13%, or approximately $619,000, to $5.4 million for 2014 as compared to $4.8 million for 2013. Our primary G&A expenses for 2014 and 2013 are shown in the following table (in thousands):
| Year Ended December 31, | ||||||||||||||||
| General and Administrative | 2014 | 2013 | Variance | Change (%) | ||||||||||||
| Payroll and benefits | $ | 3,392 | $ | 2,519 | $ | 873 | 35 | % | ||||||||
| Operating and occupancy | 2,045 | 2,299 | (254 | ) | (11 | )% | ||||||||||
| Total | $ | 5,437 | $ | 4,818 | $ | 619 | 13 | % | ||||||||
G&A payroll and benefits expense for both 2014 and 2013 includes salaries, non-cash stock based compensation expense and fringe benefits and increased 35%, or approximately $873,000, to $3.4 million for 2014 as compared to $2.5 million for 2013. Included in payroll and benefit expense is a charge for non-cash stock based compensation expense of $1.9 million for 2014 as compared to $1.3 million for 2013. Additionally, salaries for 2014 were $1.4 million as compared to $1.1 million for 2013.
G&A operating and occupancy expense, which includes expenses to operate as a public company, decreased 11%, or approximately $254,000, to $2.0 million for 2014 as compared to $2.3 million for 2013. The decrease was primarily due to a decrease in professional services costs.
Comparison of Years Ended December 31, 2013 and 2012
Revenues and Other Income
Interest income increased 200% to $9,000 in 2013 as compared to $3,000 for 2012. This increase was due to an increase in interest income due to higher cash balances. On June 25, 2013, we completed a public offering of 4,312,500 shares of our common stock at a price per share of $19.00. Net proceeds to us, after deducting underwriters’ fees and offering expenses, were approximately $76.8 million.
Research and Development Expenses
R&D expenses include contracted services relating to our clinical product development activities which include preclinical studies, clinical trials, fees associated with our patent portfolio, regulatory affairs and bulk manufacturing scale-up activities and bulk active ingredient purchases for preclinical and clinical trials primarily relating to our two products in clinical development, Androxal® and Proellex®. Research and development expenses also include internal operating expenses relating to our general research and development activities. R&D expenses increased 68%, or approximately $9.5 million, to $23.7 million for 2013 as compared to $14.1 million for 2012. Our primary R&D expenses for 2013 and 2012 are shown in the following table (in thousands):
| Year Ended December 31, | ||||||||||||||||
| Research and Development | 2013 | 2012 | Variance | Change (%) | ||||||||||||
| Androxal® clinical development | $ | 14,791 | $ | 8,516 | $ | 6,275 | 74 | % | ||||||||
| Proellex® clinical development | 1,815 | 1,776 | 39 | 2 | % | |||||||||||
| Payroll and benefits | 3,914 | 2,137 | 1,777 | 83 | % | |||||||||||
| Operating and occupancy | 3,137 | 1,691 | 1,446 | 86 | % | |||||||||||
| Total | $ | 23,657 | $ | 14,120 | $ | 9,537 | 68 | % | ||||||||
Operating and occupancy expense for 2013 and 2012 have been revised. For a further description of the revisions, see Note 2. “Revision of Prior Years’ Financial Statements” of the Notes to Consolidated Financial Statements.
The increase in Androxal® clinical development expenses for 2013 as compared to 2012 was primarily due to the completion of the Phase 3 studies in men with secondary hypogonadism, including two pivotal studies conducted under an SPA, a six month open label safety study and the ongoing DEXA study. Although the clinical development expenses related to Proellex® remained relatively constant, we initiated a 60 subject, Phase 2 study for the treatment of endometriosis in the fourth quarter of 2012 and completed a Phase 2 vaginal administration study for uterine fibroids in 2012.
From inception through December 31, 2013 we incurred $43.2 million for the development of Androxal® and $60.9 million for the development of Proellex®. These accumulated costs exclude any internal operating expenses and related fees associated with our patent portfolio.
| -34- |
R&D payroll and benefits expense for both years ended December 31, 2013 and 2012 includes salaries, non-cash stock based compensation expense and fringe benefits and increased 83%, or approximately $1.8 million, to $3.9 million for 2013 as compared to $2.1 million for 2012. This increase was primarily due to an increase in headcount, which included the addition of the Senior Vice President of Clinical and Regulatory and the Chief Medical Officer. Included in R&D payroll and benefit expense is a charge for non-cash stock based compensation expense of $1.8 million for 2013 as compared to $880,000 for 2012.
R&D operating and occupancy increased 86%, or approximately $1.4 million, to $3.1 million for the year ended 2013 as compared to $1.7 million for 2012. This increase was primarily due to increases in legal expenses, costs associated with our patent portfolio, other outside services and travel expenses.
General and Administrative Expenses
G&A expenses remained constant at $4.8 million for both 2013 and 2012. Our primary G&A expenses for 2013 and 2012 are shown in the following table (in thousands):
| Year Ended December 31, | ||||||||||||||||
| General and Administrative | 2013 | 2012 | Variance | Change (%) | ||||||||||||
| Payroll and benefits | $ | 2,519 | $ | 3,081 | $ | (562 | ) | (18 | )% | |||||||
| Operating and occupancy | 2,299 | 1,746 | 553 | 32 | % | |||||||||||
| Total | $ | 4,818 | $ | 4,827 | $ | (9 | ) | 0 | % | |||||||
G&A payroll and benefits expense for both 2013 and 2012 includes salaries, non-cash stock based compensation expense and fringe benefits and decreased 18%, or approximately $562,000, to $2.5 million for 2013 as compared to $3.1 million for 2012. Included in payroll and benefit expense is a charge for non-cash stock based compensation expense of $1.3 million for 2013 as compared to $1.9 million for 2012. Additionally, salaries for both 2013 and 2012 were $1.1 million.
G&A operating and occupancy expense, which includes expenses to operate as a public company, increased 32%, or approximately $553,000, to $2.3 million for 2013 as compared to $1.7 million for 2012. The increase was primarily due to an increase in professional services costs.
Off-Balance Sheet Arrangements
As of December 31, 2014, we did not have any off-balance sheet arrangements.
Liquidity and Capital Resources
Since our inception, we have financed our operations primarily with proceeds from private placements and public offerings of equity securities and with funds received under collaborative agreements.
On June 25, 2013, we completed a public offering of 4,312,500 shares of our common stock at a price per share of $19.00 (the “2013 Public Offering”). Net proceeds to us, after deducting underwriter’s fees and offering expenses, were approximately $76.8 million.
On September 7, 2012, we completed a private placement of 2,145,636 shares of our common stock at a price per share of $11.00. Net proceeds to us, after deducting offering expenses, were approximately $23 million. The private placement shares may be resold pursuant to our shelf registration statement on Form S-3, as amended (File No. 333-184159).
On February 1, 2012, we completed a registered direct offering to certain institutional investors, including certain existing shareholders, of 2,463,537 shares of our common stock at a price per share of $4.50. Net proceeds to us, after deducting the placement agent's fees and offering expenses, were approximately $10.3 million.
Our primary use of cash to date has been in operating activities to fund research and development, including preclinical studies and clinical trials, and general and administrative expenses. We had cash and cash equivalents of approximately $46.6 million as of December 31, 2014 as compared to $75.8 million as of December 31, 2013. All cash and cash equivalents as of December 31, 2014 and 2013 were held in an account backed by U.S. government securities.
Net cash of approximately $29.3 million, $25.3 million and $14.1 million was used in operating activities during 2014, 2013 and 2012, respectively. The major use of cash for operating activities during 2014 was to fund our clinical development programs and associated administrative costs. Cash used in investing activities was zero, $63,000 and $30,000 during 2014, 2013 and 2012, respectively. Cash provided by financing activities was $147,000, $77.0 million and $33.8 million during 2014, 2013 and 2012, respectively. Cash provided by financing activities during 2014 was primarily due to the exercise of 23,334 stock options for cash.
| -35- |
We have experienced negative cash flows from operations since inception. We will require substantial funds for R&D, including preclinical studies and clinical trials of our product candidates, and to commence sales and marketing efforts if appropriate, if the FDA or other regulatory approvals are obtained. Based on our current and planned clinical activities, we believe that our current liquidity will be sufficient to continue the development of our product candidates into the second half of 2016. It is possible that our clinical trial activities will be more costly and take longer than we anticipate; accordingly, there can be no assurance that additional capital will not be necessary prior to the time anticipated. Our capital requirements will depend on many factors, which are discussed in detail in “Item 1A., Risk Factors” of this Form 10-K . Additionally, as discussed in Note 11, there is a third party individual patent holder that claims priority over our patent application for Androxal®.
Our results of operations may vary significantly from quarter to quarter and year to year, and depend on, among other factors, our ability to raise additional capital on acceptable terms or at all, our ability to be successful in our clinical trials, the regulatory approval process in the United States and other foreign jurisdictions and the ability to complete strategic licenses and product development agreements. The timing of our revenues may not match the timing of our associated product development expenses. To date, R&D expenses have usually exceeded revenue in any particular period and/or fiscal year.
Contractual Obligations and Commercial Commitments
The Company leases laboratory and office space pursuant to leases accounted for as operating leases. The lease for the Company’s laboratory and office space expires in June 2015. Rental expense for the years ended December 31, 2014, 2013 and 2012, was approximately $74,000, $79,000 and $76,000, respectively. Future minimum lease payments under non-cancelable leases with original terms in excess of one year as of December 31, 2014, is approximately $27,000 for 2015.
Item 7A. Quantitative and Qualitative Disclosures About Market Risk
Interest Rate Risk. We had cash and cash equivalents of approximately $46.6 million as of December 31, 2014 which is primarily held in a money market mutual fund backed by U.S. government securities. Although this cash account is subject to fluctuations in interest rates and market conditions, no significant gain or loss on this account is expected to be recognized in earnings. We do not invest in derivative securities.
ITEM 8. Financial Statements and Supplementary Data
The financial statements required by this item are set forth in Item 15 of this Form 10-K.
ITEM 9. Changes in and Disagreements with Accountants on Accounting and Financial Disclosure
Not applicable.
Item 9A. Controls and Procedures
Evaluation of Disclosure Controls and Procedures
We maintain disclosure controls and procedures that are designed to ensure that information required to be disclosed in our reports filed with the SEC, pursuant to the Securities Exchange Act of 1934 (the “Exchange Act”) is recorded, processed, summarized and reported within the time periods specified in the rules and forms of the SEC and that such information is accumulated and communicated to our management, including our Principal Executive Officer (PEO) and Principal Financial Officer (PFO), as appropriate, to allow timely decisions regarding disclosures.
Management, with the participation of our PEO and PFO, has evaluated the effectiveness of our disclosure controls and procedures (as defined in Rules 13a-15(e) and 15d-15(e) of the Exchange Act) as of the end of the period covered by this report. Based on such evaluation, our PEO and PFO have each concluded that as of the end of such period, our disclosure controls and procedures were effective to ensure that information required to be disclosed by us in reports that we file or submit under the Exchange Act is recorded, processed, summarized and reported within the time periods specified in the SEC’s rules and forms and that such information is accumulated and communicated to our management, including the PEO and PFO, as appropriate, to allow timely decisions regarding required disclosures.
Management’s Report on Internal Control Over Financial Reporting
Management is responsible for establishing and maintaining adequate internal control over financial reporting as defined in Rule 13a-15(f) under the Exchange Act. Our internal control over financial reporting was designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles.
| -36- |
Management evaluated the effectiveness of internal control over financial reporting based on the criteria in the 2013 Internal Control - Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission. Due to its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Based on management’s evaluation, management has concluded that internal control over financial reporting was effective as of December 31, 2014.
PricewaterhouseCoopers LLP, an independent registered public accounting firm, has audited and issued their report on the effectiveness of our internal control over financial reporting as of December 31, 2014, which appears herein.
Changes in Internal Control
There have been no changes in our internal control over financial reporting during our quarter ended December 31, 2014 that have materially affected, or is reasonable likely to materially affect, our internal control over financial reporting.
Not applicable.
| -37- |
ITEM 10. Directors, Executive Officers and Corporate Governance
The information required by this item is hereby incorporated by reference from the information in our proxy statement for our 2015 annual meeting of stockholders. Such proxy statement will be filed with the SEC pursuant to the Exchange Act within 120 days of the end of our fiscal year ended December 31, 2014.
ITEM 11. Executive Compensation
The information required by this item is hereby incorporated by reference from the information in our proxy statement for our 2015 annual meeting of stockholders. Such proxy statement will be filed with the SEC pursuant to the Exchange Act within 120 days of the end of our fiscal year ended December 31, 2014.
ITEM 12. Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters
The information required by this item is hereby incorporated by reference from the information in our proxy statement for our 2015 annual meeting of stockholders. Such proxy statement will be filed with the SEC pursuant to the Exchange Act within 120 days of the end of our fiscal year ended December 31, 2014.
ITEM 13. Certain Relationships and Related Transactions, and Director Independence
The information required by this item is hereby incorporated by reference from the information in our proxy statement for our 2015 annual meeting of stockholders. Such proxy statement will be filed with the SEC pursuant to the Exchange Act within 120 days of the end of our fiscal year ended December 31, 2014.
ITEM 14. Principal Accountant Fees and Services
The information required by this item is hereby incorporated by reference from the information in our proxy statement for our 2015 annual meeting of stockholders. Such proxy statement will be filed with the SEC pursuant to the Exchange Act within 120 days of the end of our fiscal year ended December 31, 2014.
| -38- |
ITEM 15. Exhibits and Financial Statement Schedules
| (a) | Documents Filed as a Part of this Form 10-K. |
| Financial Statements | Page | |
| Report of Independent Registered Public Accounting Firm | F-1 | |
| Consolidated Balance Sheets as of December 31, 2014 and 2013 | F-2 | |
| Consolidated Statements of Operations for the Years Ended December 31, 2014, 2013 and 2012 | F-3 | |
| Consolidated Statement of Stockholders' Equity | F-4 | |
| Consolidated Statements of Cash Flows for the Years Ended December 31, 2014, 2013 and 2012 | F-5 | |
| Notes to Consolidated Financial Statements | F-6 |
All financial statement schedules are omitted because they are not applicable, not required, or because the required information is included in the financial statements or the notes thereto.
(b) Exhibits.
Exhibits to the Form 10-K have been included only with the copies of the Form 10-K filed with the SEC. Upon request to the Company and payment of a reasonable fee, copies of the individual exhibits will be furnished.
| Exhibit Number | Identification Of Exhibit | |
| 3.1(a) | Restated Certificate of Incorporation. Exhibit 3.3 to the Company's Registration Statement on Form SB-2 (No. 33-57728-FW), as amended (the "Registration Statement"), is incorporated herein by reference. | |
| 3.1(b) | Certificate of Amendment to the Company's Restated Certificate of Incorporation, dated as of May 2, 2006. Exhibit 3.1 to the Company's Current Report on Form 8-K as filed with the Commission on May 2, 2006 is incorporated herein by reference. | |
| 3.1(c) | Certificate of Designation of Series One Junior Participating Preferred Stock dated September 2, 1999. Exhibit A to Exhibit 4.1 to the Company's Registration Statement on Form 8-A as filed with the Commission on September 3, 1999 (the "Rights Plan Registration Statement"), is incorporated herein by reference. | |
| 3.1(d) | Certificate of Amendment to Restated Certificate of Incorporation, dated as of December 16, 2008. Exhibit 3.1(d) to the Company’s Current Report on Form 8-K as filed with the Commission on December 23, 2008 is incorporated herein by reference. | |
| 3.1(e) | Certificate of Amendment to Restated Certificate of Incorporation, dated as of November 18, 2009. Exhibit 3.1(e) to the Company’s Current Report on Form 8-K dated November 19, 2009 is incorporated herein by reference. | |
| 3.1(f) | Certificate of Amendment to Restated Certificate of Incorporation, dated October 14, 2010. Exhibit 3.1(f) to the Company’s Current Report on Form 8-K dated October 14, 2010 is incorporated herein by reference. | |
| 3.2 | Restated Bylaws of the Company. Exhibit 3.4 to the Registration Statement is incorporated herein by reference. | |
| 4.1 | Specimen Certificate of Common Stock, $.001 par value, of the Company. Exhibit 4.1 to the Registration Statement is incorporated herein by reference. | |
| 4.2 | Rights Agreement dated September 1, 1999 between the Company and Computershare Investor Services LLC (as successor in interest to Harris Trust & Savings Bank), as Rights Agent. Exhibit 4.1 to the Rights Plan Registration Statement is incorporated herein by reference. | |
| 4.3 | First Amendment to Rights Agreement, dated as of September 6, 2002, between the Company, Harris Trust & Savings Bank and Computershare Investor Services LLC. Exhibit 4.3 to Amendment No. 1 to the Rights Plan Registration Statement on Form 8-A/A as filed with the Commission on September 11, 2002 is incorporated herein by reference. | |
| 4.4 | Second Amendment to Rights Agreement, dated as of October 30, 2002, between the Company and Computershare Investor Services LLC. Exhibit 4.4 to Amendment No. 2 to the Rights Plan Registration Statement on Form 8-A/A as filed with the Commission on October 31, 2002 is incorporated herein by reference. |
| -39- |
| 4.5 | Third Amendment to Rights Agreement, dated as of June 30, 2005, between the Company and Computershare Trust Company, Inc. (as successor in interest to Computershare Investor Services, LLC). Exhibit 4.4 to the Company's Current Report on Form 8-K as filed with the Commission on June 30, 2005 is incorporated herein by reference. | |
| 4.6 | Fourth Amendment to Rights Agreement, dated as of January 9, 2008, between the Company and Computershare Trust Company, Inc. (as successor in interest to Computershare Investor Services, LLC). Exhibit 4.5 to the Company's Current Report on Form 8-K as filed with the Commission on January 10, 2008 is incorporated herein by reference. | |
| 4.7 | Fifth Amendment to Rights Agreement, dated as of October 10, 2008, between the Company and Computershare Trust Company, Inc. (as successor in interest to Computershare Investor Services, LLC). Exhibit 4.6 to the Company’s Current Report on Form 8-K as filed with the Commission on January 10, 2008 is incorporated herein by reference. | |
| 4.8 | Sixth Amendment to Rights Agreement, dated as of September 9, 2010, between the Company and Computershare Trust Company, Inc. (as successor in interest to Computershare Investor Services, LLC). Exhibit 4.7 to the Company’s Current Report on Form 8-K as filed with the Commission on September 10, 2010 is incorporated herein by reference. | |
| 4.9 | Form of Rights Certificate. Exhibit B to Exhibit 4.1 to the Rights Plan Registration Statement is incorporated herein by reference. | |
| 4.10 | Form of Series A Warrant Certificate. Exhibit 4.10 to the Company’s Registration Statement on Form S-1/A (No. 333-171196) as filed with the Commission on February 2, 2011 is incorporated herein by reference. | |
| 4.11 | Form of Series B Warrant Certificate. Exhibit 4.11 to the Company’s Registration Statement on Form S-1/A (No. 333-171196) as filed with the Commission on February 2, 2011 is incorporated herein by reference | |
| 4.12 | Series A Warrant Agreement dated February 8, 2011 by and among the Company and Computershare Inc. and its wholly-owned subsidiary, Computershare Trust Company, N.A. Exhibit 4.1 to the Company’s Current Report on Form 8-K as filed with the Commission on February 9, 2011 is incorporated herein by reference. | |
| 4.13 | Series B Warrant Agreement dated February 8, 2011 by and among the Company and Computershare Inc. and its wholly-owned subsidiary, Computershare Trust Company, N.A. Exhibit 4.2 to the Company’s Current Report on Form 8-K as filed with the Commission on February 9, 2011 is incorporated herein by reference. | |
| 10.1+ | Amended and Restated 1993 Employee and Consultant Stock Option Plan. Exhibit 10.3 to the Registration Statement is incorporated herein by reference. | |
| 10.2+ | First Amendment to the Repros Therapeutics Inc. Amended and Restated 1993 Stock Option Plan. Exhibit 10.22 to the Company's Annual Report on Form 10-K for the year ended December 31, 1999 is incorporated herein by reference. | |
| 10.3+ | 1994 Employee and Consultant Stock Option Plan. Exhibit 4.2 to the Company's Registration Statement on Form S-8 (File No. 033-83406) as filed with the Commission on August 29, 1994 is incorporated herein by reference. | |
| 10.4+ | 2000 Non-Employee Directors' Stock Option Plan. Appendix B to the Company's Definitive Proxy Statement filed on April 26, 2000 is incorporated herein by reference. | |
| 10.5+ | First Amendment to the Repros Therapeutics Inc. 2000 Non-Employee Directors' Stock Option Plan. Exhibit 10.21 to the 2000 Form 10-K is incorporated herein by reference. | |
| 10.6+ | Second Amendment to 2000 Non-Employee Directors' Stock Option Plan. Exhibit 10.6 to the Company's Annual Report on Form 10-K for the year ended December 31, 2002 (the "2002 Form 10-K") is incorporated herein by reference. | |
| 10.7+ | Repros Therapeutics Inc. 2004 Stock Option Plan. Exhibit 10.17 to the Company's Registration Statement on Form S-1 (No. 333-119861), as amended, is incorporated herein by reference. | |
| 10.8+ | Employment Agreement, dated June 16, 2014, between the Company and Joseph S. Podolski. Exhibit 99.1 to the Company’s Current Report on Form 8-K as filed with the Commission on June 20, 2014. |
| -40- |
| 10.9 | Lease Agreement dated May 11, 2004 between the Company and Sealy Woodlands, L.P. Exhibit 10.14 to the Company's Annual Report on Form 10-K for the year ended December 31, 2004 is incorporated herein by reference. | |
| 10.10 | Amendment to Lease Agreement between the Company and Sealy Woodlands, L.P., dated May 17, 2006. Exhibit 10.1 to the Company's Quarterly Report on Form 10-Q for the fiscal quarter ended March 31, 2006 is incorporated herein by reference. | |
| 10.11 | Second Amendment to Lease, effective as of July 1, 2010, between the Company and Columbia Texas 2408 Timberloch Industrial, L.P. Exhibit 10.1 to the Company’s Quarterly Report on Form 10-Q for the fiscal quarter ended September 30, 2010 is incorporated herein by reference. | |
| 10.12++ | Letter Agreement dated July 15, 2002 between the Company, Schering Plough Ltd. and Schering-Plough Corporation. Exhibit 10.1 to the Company's Quarterly Report on Form 10-Q for the fiscal quarter ended June 30, 2002 is incorporated herein by reference. | |
| 10.13++ | PHS Patent License Agreement dated April 16, 1999 between the Company and certain agencies of the United States Public Health Service within the Department of Health and Human Services, with amendments. Exhibit 10.1 to the Company's Quarterly Report on Form 10-Q for the fiscal quarter ended September 30, 2003 is incorporated herein by reference. | |
| 10.14 | Waiver to PHS Patent License Agreement, as amended, dated March 8, 2007 between the Company and certain agencies of the United States Public Health Service within the Department of Health and Human Services. Exhibit 10.2 to the Company’s Current Report on Form 8-K as filed with the Commission on March 19, 2007 is incorporated herein by reference. | |
| 10.15++ | Sixth Amendment to PHS Patent License Agreement, as amended, dated July 7, 2009 between the Company and certain agencies of the United States Public Health Service within the Department of Health and Human Services. Exhibit 10.1 to the Company’s Current Report on Form 8-K/A as filed with the Commission on December 22, 2009 is incorporated herein by reference. | |
| 10.16++ | Seventh Amendment to PHS Patent License Agreement, as amended, dated October 28, 2009 between the Company and certain agencies of the United States Public Health Service within the Department of Health and Human Services. Exhibit 10.21 to the Company’s Annual Report on Form 10-K as filed with the Commission on March 15, 2010 is incorporated herein by reference. | |
| 10.17 | Form of Indemnification Agreement entered into between the Company and each of its directors. Exhibit 10.1 to the Company’s Current Report on Form 8-K as filed with the Commission on May 20, 2009 is incorporated herein by reference. | |
| 10.18+ | Employment Agreement dated August 1, 2011 by and between the Company and Katherine A. Anderson. Exhibit 10.1 to the Company’s Current Report on Form 8-K as filed with the Commission on August 4, 2011 is incorporated herein by reference. | |
| 10.19+ | 2011 Equity Incentive Plan (Exhibit 4.1 to the Company's Registration Statement on Form S-8 (No. 333-200370) as filed with the Commission on November 19, 2014 is incorporated herein by reference.
| |
| 10.20+ | Offer Letter dated February 5, 2013, by and between the Company and Joachim F. Wernicke, Ph.D., M.D. Exhibit 10.1 to the Company’s Current Report on Form 8-K as filed with the Commission on February 8, 2013 is incorporated herein by reference. | |
| 10.21+ | Employment Agreement dated March 25, 2013 (but effective March 26, 2013), by and between the Company and Jaye Thompson, Ph.D. Exhibit 10.1 to the Company’s Current Report on Form 8-K as filed with the Commission on April 1, 2013 is incorporated herein by reference. | |
| 10.22 | Eighth Amendment to PHS License Agreement, as amended, dated April 20, 2010 between the Company and certain agencies of the United States Public Health Service within the Department of Health and Human Services. Exhibit 10.1 to the Company’s Current Report on Form 8-K as filed with the Commission on June 17, 2013 is incorporated herein by reference. |
| -41- |
| 10.23 | Ninth Amendment to PHS License Agreement, as amended, dated June 14, 2013 between the Company and certain agencies of the United States Public Health Service within the Department of Health and Human Services. Exhibit 10.2 to the Company’s Current Report on Form 8-K as filed with the Commission on June 17, 2013 is incorporated herein by reference. | |
| 23.1* | Consent of PricewaterhouseCoopers LLP | |
| 31.1* | Certification Pursuant to Rule 13(a)-14(a) or 15(d)-14(a) of the Exchange Act, As Adopted Pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 (Principal Executive Officer) | |
| 31.2* | Certification Pursuant to Rule 13(a)-14(a) or 15(d)-14(a) of the Exchange Act, As Adopted Pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 (Principal Financial Officer) | |
| 32.1** | Certification Furnished Pursuant to 18 U.S.C. Section 1350, As Adopted Pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 (Principal Executive Officer) (This exhibit shall not be deemed “filed” for purposes of Section 18 of the Securities Exchange Act of 1934, as amended, or otherwise subject to the liability of that section. Further, this exhibit shall not be deemed to be incorporated by reference into any filing under the Securities Act of 1933, as amended, or the Securities Exchange Act of 1934, as amended.) | |
| 32.2** | Certification Furnished Pursuant to 18 U.S.C. Section 1350, As Adopted Pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 (Principal Financial Officer) (This exhibit shall not be deemed “filed” for purposes of Section 18 of the Securities Exchange Act of 1934, as amended, or otherwise subject to the liability of that section. Further, this exhibit shall not be deemed to be incorporated by reference into any filing under the Securities Act of 1933, as amended, or the Securities Exchange Act of 1934, as amended.) | |
| 101.INS* | XBRL Instance Document | |
| 101.SCH* | XBRL Taxonomy Extension Schema Document | |
| 101.CAL* | XBRL Taxonomy Extension Calculation Linkbase Document | |
| 101.DEF* | XBRL Taxonomy Extension Definition Linkbase Document | |
| 101.LAB* | XBRL Taxonomy Extension Label Linkbase Document | |
| 101.PRE* | XBRL Taxonomy Extension Presentation Linkbase Document |
| * | Filed herewith. |
| ** | Furnished herewith. |
| + | Management contract or compensatory plan. |
| ++ | Portions of this exhibit have been omitted based on a request for confidential treatment pursuant to Rule 24b-2 of the Exchange Act. Such omitted portions have been filed separately with the Commission. |
| -42- |
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
| REPROS THERAPEUTICS INC. | ||
| Dated: March 16, 2015 | By: | /s/ Joseph S. Podolski |
| Joseph S. Podolski | ||
| President and Chief Executive Officer | ||
Pursuant to the requirements of Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
| Signature | Title | Date | ||
/s/ Joseph S. Podolski |
President, Chief Executive Officer and Director |
March 16, 2015 | ||
| Joseph S. Podolski | (Principal Executive Officer) | |||
|
||||
| /s/ Katherine A. Anderson | Chief Financial Officer and Secretary | March 16, 2015 | ||
| Katherine A. Anderson | (Principal Financial Officer and | |||
| Principal Accounting Officer) | ||||
| /s/ Nola Masterson | Chair of the Board | March 16, 2015 | ||
| Nola Masterson | ||||
| /s/ Daniel F. Cain | Director | March 16, 2015 | ||
| Daniel F. Cain | ||||
| /s/ Saira Ramasastry | Director | March 16, 2015 | ||
| Saira Ramasastry | ||||
| /s/ Michael Suesserman | Director | March 16, 2015 | ||
| Michael Suesserman | ||||
| /s/ Michael Wyllie | Director | March 16, 2015 | ||
| Michael Wyllie, Ph.D. |
| -43- |
Report of Independent Registered Public Accounting Firm
To the Board of Directors and Stockholders of Repros Therapeutics Inc.:
In our opinion, the accompanying consolidated balance sheets, and the related consolidated statements of operations, cash flows and stockholders’ equity present fairly, in all material respects, the financial position of Repros Therapeutics Inc. and its subsidiary, at December 31, 2014 and 2013, and the results of their operations and their cash flows for each of the three years in the period ended December 31, 2014 in conformity with accounting principles generally accepted in the United States of America. Also in our opinion, the Company maintained, in all material respects, effective internal control over financial reporting as of December 31, 2014, based on criteria established in Internal Control - Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO). The Company's management is responsible for these financial statements, for maintaining effective internal control over financial reporting and for its assessment of the effectiveness of internal control over financial reporting, included in Management's Report on Internal Control over Financial Reporting appearing under Item 9A. Our responsibility is to express opinions on these financial statements and on the Company's internal control over financial reporting based on our integrated audits. We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audits to obtain reasonable assurance about whether the financial statements are free of material misstatement and whether effective internal control over financial reporting was maintained in all material respects. Our audits of the financial statements included examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements, assessing the accounting principles used and significant estimates made by management, and evaluating the overall financial statement presentation. Our audit of internal control over financial reporting included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, and testing and evaluating the design and operating effectiveness of internal control based on the assessed risk. Our audits also included performing such other procedures as we considered necessary in the circumstances. We believe that our audits provide a reasonable basis for our opinions.
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (i) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (ii) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (iii) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
/s/ PricewaterhouseCoopers LLP
Houston, Texas
March 16, 2015
| F-1 |
REPROS THERAPEUTICS INC. AND SUBSIDIARY
CONSOLIDATED BALANCE SHEETS
(in thousands except share and per share amounts)
| December 31, | December 31, | |||||||
| 2014 | 2013 | |||||||
| ASSETS | ||||||||
| Current Assets | ||||||||
| Cash and cash equivalents | $ | 46,620 | $ | 75,807 | ||||
| Prepaid expenses and other current assets | 289 | 189 | ||||||
| Total current assets | 46,909 | 75,996 | ||||||
| Fixed Assets, net | 32 | 75 | ||||||
| Total assets | $ | 46,941 | $ | 76,071 | ||||
| LIABILITIES AND STOCKHOLDERS' EQUITY | ||||||||
| Current Liabilities | ||||||||
| Accounts payable | $ | 2,090 | $ | 2,966 | ||||
| Accrued expenses | 834 | 586 | ||||||
| Total current liabilities | 2,924 | 3,552 | ||||||
| Commitments and Contingencies (note 11) | ||||||||
| Stockholders' Equity | ||||||||
| Preferred Stock, $.001 par value, 5,000,000 shares authorized, none issued and outstanding | - | - | ||||||
| Common Stock, $.001 par value, 75,000,000 shares authorized, 24,388,523 and 23,125,565 shares issued, respectively; 24,276,173 and 23,013,215 shares outstanding, respectively | 24 | 23 | ||||||
| Additional paid-in capital | 318,437 | 314,405 | ||||||
| Cost of treasury stock, 112,350 shares | (1,380 | ) | (1,380 | ) | ||||
| Accumulated deficit | (273,064 | ) | (240,529 | ) | ||||
| Total stockholders' equity | 44,017 | 72,519 | ||||||
| Total liabilities and stockholders' equity | $ | 46,941 | $ | 76,071 | ||||
The accompanying notes are an integral part of these consolidated financial statements.
| F-2 |
REPROS THERAPEUTICS INC. AND SUBSIDIARY
CONSOLIDATED STATEMENTS OF OPERATIONS
(in thousands except per share amounts)
| For the Year Ended December 31, | ||||||||||||
| 2014 | 2013 | 2012 | ||||||||||
| Revenues and other income | ||||||||||||
| Interest Income | $ | 9 | $ | 9 | $ | 3 | ||||||
| Total revenues and other income | 9 | 9 | 3 | |||||||||
| Expenses | ||||||||||||
| Research and development | 27,107 | 23,657 | 14,120 | |||||||||
| General and administrative | 5,437 | 4,818 | 4,827 | |||||||||
| Total expenses | 32,544 | 28,475 | 18,947 | |||||||||
| Net loss | $ | (32,535 | ) | $ | (28,466 | ) | $ | (18,944 | ) | |||
| Loss per share - basic and diluted | $ | (1.39 | ) | $ | (1.37 | ) | $ | (1.23 | ) | |||
| Shares used in loss per share calculation: | ||||||||||||
| Basic | 23,432 | 20,808 | 15,346 | |||||||||
| Diluted | 23,432 | 20,808 | 15,346 | |||||||||
The accompanying notes are an integral part of these consolidated financial statements.
| F-3 |
REPROS THERAPEUTICS INC. AND SUBSIDIARY
CONSOLIDATED STATEMENTS OF STOCKHOLDERS' EQUITY
(in thousands except share and per share amounts)
| Additional | Total | ||||||||||||||||||||||||||
| Common Stock | Paid-in | Treasury Stock | Accumulated | Stockholders' | |||||||||||||||||||||||
| Shares | Amount | Capital | Shares | Amount | Deficit | Equity | |||||||||||||||||||||
| Balance at December 31, 2011 | 12,470,694 | $ | 12 | $ | 197,769 | 112,350 | $ | (1,380 | ) | $ | (193,119 | ) | $ | 3,282 | |||||||||||||
| Stock based option compensation | - | - | 2,785 | - | - | - | 2,785 | ||||||||||||||||||||
| Issuance of 100 shares of common stock at a share price of $5.07 | 100 | - | - | - | - | - | - | ||||||||||||||||||||
| Issuance of 2,463,537 shares of common stock at a share price of $4.50, net of offering costs of $777 | 2,463,537 | 3 | 10,307 | - | - | - | 10,310 | ||||||||||||||||||||
| Exercise of stock options to purchase common stock for cash ($1.33 to $10.88 per share) | 16,488 | - | 121 | - | - | - | 121 | ||||||||||||||||||||
| Issuance of 54,971 shares of common stock for the cashless exercise of 95,416 stock options | 54,971 | - | - | - | - | - | - | ||||||||||||||||||||
| Exercise of 121,079 Series B Warrants to purchase common stock for cash @ $2.49 per share | 121,079 | - | 301 | - | - | - | 301 | ||||||||||||||||||||
| Issuance of 2,145,636 shares of common stock at a share price of $11.00, net of offering costs of $586 | 2,145,636 | 2 | 23,016 | - | - | - | 23,018 | ||||||||||||||||||||
| Net loss | - | - | - | - | - | (18,944 | ) | (18,944 | ) | ||||||||||||||||||
| Balance at December 31, 2012 | 17,272,505 | $ | 17 | $ | 234,299 | 112,350 | $ | (1,380 | ) | $ | (212,063 | ) | $ | 20,873 | |||||||||||||
| Stock based compensation | - | - | 3,158 | - | - | - | 3,158 | ||||||||||||||||||||
| Issuance of 871,634 shares of common stock for the cashless exercise of 872,133 Series A Warrants | 871,634 | 1 | (1 | ) | - | - | - | - | |||||||||||||||||||
| Issuance of 614,837 shares of common stock for the cashless exercise of 716,767 Series B Warrants | 614,837 | 1 | (1 | ) | - | - | - | - | |||||||||||||||||||
| Exercise of 42,849 Series B Warrants to purchase common stock for cash @ $2.49 per share | 42,849 | - | 107 | - | - | - | 107 | ||||||||||||||||||||
| Issuance of 5,407 shares of common stock for the cashless exercise of 8,332 stock options | 5,407 | - | - | - | - | - | - | ||||||||||||||||||||
| Exercise of stock options to purchase common stock for cash ($10.98 to $18.74 per share) | 5,833 | - | 83 | - | - | - | 83 | ||||||||||||||||||||
| Issuance of 4,312,500 shares of common stock at $19.00 per share, net of offering costs of $5.2 million | 4,312,500 | 4 | 76,760 | - | - | - | 76,764 | ||||||||||||||||||||
| Net loss | - | - | - | - | - | (28,466 | ) | (28,466 | ) | ||||||||||||||||||
| Balance at December 31, 2013 | 23,125,565 | $ | 23 | $ | 314,405 | 112,350 | $ | (1,380 | ) | $ | (240,529 | ) | $ | 72,519 | |||||||||||||
| Stock based compensation | - | - | 3,784 | - | - | - | 3,784 | ||||||||||||||||||||
| Issuance of 72,910 shares of common stock for the cashless exercise of 98,329 stock options | 72,910 | - | - | - | - | - | - | ||||||||||||||||||||
| Exercise of stock options to purchase common stock stock for cash ($1.56 to $9.60 per share) | 23,334 | - | 147 | - | - | - | 147 | ||||||||||||||||||||
| Issuance of 836,961 shares of common stock for the cashless exercise of 837,542 Series A Warrants | 836,961 | 1 | (1 | ) | - | - | - | - | |||||||||||||||||||
| Issuance of 329,753 shares of common stock for the cashless exercise of 380,101 Series B Warrants | 329,753 | - | - | - | - | - | - | ||||||||||||||||||||
| Proceeds from a shareholder transaction | - | - | 102 | - | - | 102 | |||||||||||||||||||||
| Net loss | - | - | - | - | - | (32,535 | ) | (32,535 | ) | ||||||||||||||||||
| Balance at December 31, 2014 | 24,388,523 | $ | 24 | $ | 318,437 | 112,350 | $ | (1,380 | ) | $ | (273,064 | ) | $ | 44,017 | |||||||||||||
The accompanying notes are an integral part of these consolidated financial statements.
| F-4 |
REPROS THERAPEUTICS INC. AND SUBSIDIARY
CONSOLIDATED STATEMENTS OF CASH FLOWS
(in thousands)
| For the Year Ended December 31, | ||||||||||||
| 2014 | 2013 | 2012 | ||||||||||
| Cash Flows from Operating Activities | ||||||||||||
| Net loss | $ | (32,535 | ) | $ | (28,466 | ) | $ | (18,944 | ) | |||
| Adjustments to reconcile net loss to net cash used in operating activities: | ||||||||||||
| Depreciation and amortization | 43 | 40 | 16 | |||||||||
| Noncash stock-based compensation | 3,784 | 3,158 | 2,785 | |||||||||
| Changes in operating assets and liabilities: | ||||||||||||
| (Increase) decrease in prepaid expenses and other current assets | 3 | 216 | (307 | ) | ||||||||
| Increase (decrease) in accounts payable and accrued expenses | (629 | ) | (244 | ) | 2,377 | |||||||
| Net cash used in operating activities | (29,334 | ) | (25,296 | ) | (14,073 | ) | ||||||
| Cash Flows from Investing Activities | ||||||||||||
| Capital expenditures | - | (63 | ) | (30 | ) | |||||||
| Net cash used in investing activities | - | (63 | ) | (30 | ) | |||||||
| Cash Flows from Financing Activities | ||||||||||||
| Proceeds from issuance of common stock and warrants, net of offering costs | - | 76,764 | 33,328 | |||||||||
| Exercise of stock options & warrants | 147 | 190 | 422 | |||||||||
| Net cash provided by financing activities | 147 | 76,954 | 33,750 | |||||||||
| Net increase (decrease) in cash and cash equivalents | (29,187 | ) | 51,595 | 19,647 | ||||||||
| Cash and cash equivalents at beginning of period | 75,807 | 24,212 | 4,565 | |||||||||
| Cash and cash equivalents at end of period | $ | 46,620 | $ | 75,807 | $ | 24,212 | ||||||
The accompanying notes are an integral part of these consolidated financial statements.
| F-5 |
1. ORGANIZATION AND OPERATIONS:
Repros Therapeutics Inc. (the “Company”, “Repros,” or “we,” “us” or “our”) was organized on August 20, 1987. We are a biopharmaceutical company focused on the development of new drugs to treat hormonal and reproductive system disorders.
Our primary product candidate, Androxal®, is a single isomer of clomiphene citrate and is an orally active proprietary small molecule compound. We are developing Androxal® for the treatment of secondary hypogonadism in overweight men wishing to restore normal testicular function. Men with secondary hypogonadism exhibit low testosterone levels due to under stimulated testes but they are generally fertile. Androxal® is designed to treat the underlying mechanism, insufficient stimulation of the testes by the pituitary, which causes secondary hypogonadism. Secondary hypogonadism due to being overweight or obese is the single greatest cause of hypogonadism in general. On February 2, 2015, we announced that we electronically submitted our New Drug Application (“NDA”) to the Food and Drug Administration (“FDA”) for Androxal®.
Proellex®, our product candidate for female reproductive health, is a new chemical entity that acts as a selective blocker of the progesterone receptor and is being developed for the treatment of symptoms associated with uterine fibroids and endometriosis. On December 29, 2014, we announced that we have initiated two Phase 2B studies for low dose Proellex® in the treatment of uterine fibroids and are currently conducting a Phase 2 study in the treatment of endometriosis.
VASOMAX® has been on partial clinical hold in the U.S. since 1998, and no further development activities are planned.
As of December 31, 2014, we had accumulated losses of $273.1 million, approximately $46.6 million in cash and cash equivalents, and accounts payable and accrued expenses of approximately $2.9 million, in the aggregate. We anticipate that our current liquidity will be sufficient to continue the development of our product candidates into the second half of 2016. We continue to explore potential corporate partnering opportunities for assistance in the clinical development funding and commercialization of our products, as appropriate; however, there can be no assurance that an acceptable corporate partnering opportunity will be successfully completed or that our current liquidity will be sufficient to fund all of our product development needs.
2. REVISION OF PRIOR YEARS’ FINANCIAL STATEMENTS:
While preparing its financial statements for the year ended December 31, 2014, the Company identified a prior period error related to the accounting for patent costs. As disclosed in its prior filings, historically the Company had capitalized patent related costs associated with its drug candidates, Androxal® and Proellex®. However, the Company has now concluded that these costs should have been expensed as research and development costs since the related products were, at the time the costs were incurred, in the development phase and had not been approved by the FDA. The Company concluded this error was not material individually or in the aggregate to any of the prior reporting periods, and therefore, no restatements of previously issued financial statements were necessary. However, if the entire correction was recorded in the current period, the cumulative impact would have been material to the current period, and would have impacted the comparability to prior periods. As such, revisions for the prior periods are reflected in the financial statements herein, and will be reflected in future filings containing such information.
The effect of the error corrections on the consolidated balance sheet as of December 31, 2013 are as follows (in thousands):
| As previously reported | Correction | As revised | ||||||||||
| Other assets, net | $ | 2,906 | $ | (2,906 | ) | $ | 0 | |||||
| Total assets | 78,977 | (2,906 | ) | 76,071 | ||||||||
| Accumulated deficit | (237,623 | ) | (2,906 | ) | (240,529 | ) | ||||||
| Total stockholders’ equity | 75,425 | (2,906 | ) | 72,519 | ||||||||
At December 31, 2012, accumulated deficit and shareholders’ equity were reported as ($209,902) and $23,034, respectively, and were revised to ($212,063) and $20,873, respectively.
At December 31, 2011, accumulated deficit and shareholders’ equity were reported as ($191,735) and $4,666, respectively, and were revised to ($193,119) and $3,282, respectively.
The effects of the error correction on the consolidated statements of operations for the years ended December 31, 2013 and 2012 are as follows (in thousands):
| Year Ended December 31, 2013 | Year Ended December 31, 2012 | |||||||||||||||||||||||
| As previously reported | Correction | As revised | As previously reported | Correction | As revised | |||||||||||||||||||
| Research and development | $ | 22,912 | $ | 745 | $ | 23,657 | $ | 13,343 | $ | 777 | $ | 14,120 | ||||||||||||
| Total expenses | 27,730 | 745 | 28,475 | 18,170 | 777 | 18,947 | ||||||||||||||||||
| Net loss | (27,721 | ) | (745 | ) | (28,466 | ) | (18,167 | ) | (777 | ) | (18,944 | ) | ||||||||||||
| Loss per share – basic and diluted | (1.33 | ) | (0.04 | ) | (1.37 | ) | (1.18 | ) | (0.05 | ) | (1.23 | ) | ||||||||||||
| F-6 |
The effects of the error correction on the consolidated statements of cash flows for the years ended December 31, 2013 and 2012 are as follows (in thousands):
| Year Ended December 31, 2013 | Year Ended December 31, 2012 | |||||||||||||||||||||||
| As previously reported | Correction | As revised | As previously reported | Correction | As revised | |||||||||||||||||||
| Net cash used in operating activities | $ | (24,448 | ) | $ | (848 | ) | $ | (25,296 | ) | $ | (13,495 | ) | $ | (578 | ) | $ | (14,073 | ) | ||||||
| Net cash used in investing activities | (911 | ) | 848 | (63 | ) | (608 | ) | 578 | (30 | ) | ||||||||||||||
3. SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES:
USE OF ESTIMATES
The preparation of financial statements in conformity with accounting principles generally accepted in the United States of America requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenues and expenses during the reporting period. Actual results could differ from those estimates.
CERTAIN RISKS AND UNCERTAINTIES
Our product candidates under development require approval from the FDA or other international regulatory agencies prior to commercial sales. There can be no assurance our product candidates will receive the necessary clearance. If we are denied clearance or clearance is delayed, it may have a material adverse impact on us.
Our product candidates are concentrated in rapidly changing, highly competitive markets, which are characterized by rapid technological advances, evolving regulatory requirements and industry standards. Any failure by us to anticipate or to respond adequately to technological developments in our industry, changes in regulatory requirements or industry standards, or any significant delays in the development or introduction of products or services, could have a material adverse effect on our business, operating results and future cash flows. We have no assurance of the successful development and FDA approval or the successful commercialization of our product candidates.
CASH AND CASH EQUIVALENTS
The Company considers all cash accounts and highly liquid investments having original maturities of three months or less to be cash and cash equivalents.
PREPAID EXPENSES AND OTHER CURRENT ASSETS
Prepaid expenses and other current assets primarily consist of prepaid insurance, prepaid operating expenses and other miscellaneous assets, interest and other receivables.
FIXED ASSETS
Fixed assets include lab equipment, furniture and leasehold improvements and are recorded at cost, less accumulated depreciation and amortization. Depreciation is computed on the straight-line method over an estimated useful life of three to five years or, in the case of leasehold improvements, amortized over the shorter of the useful life or the remaining term of the lease. Maintenance and repairs that do not improve or extend the life of assets are expensed as incurred. When assets are sold or retired, the cost and accumulated depreciation are removed from the accounts and the resulting gain or loss is included in income during the period in which the transaction occurred.
RESEARCH AND DEVELOPMENT EXPENSE
Research and development (“R&D”) expenses include salaries and related employee expenses, contracted regulatory affairs activities, insurance coverage for clinical trials and prior product sales, contracted research and consulting fees, fees associated with our patent portfolio, facility costs, and internal research and development supplies. We expense R&D costs in the period they are incurred. These costs consist of direct and indirect costs associated with specific projects as well as fees paid to various entities that perform research on our behalf.
| F-7 |
We estimate accrued expenses as part of our process of preparing financial statements. Examples of areas in which subjective judgments may be required include costs associated with services provided by contract organizations for clinical trials, preclinical development and manufacturing of clinical materials. We accrue for costs incurred as the services are being provided by monitoring the status of the trials or services provided and the invoices received from our external service providers. In the case of clinical trials, a portion of the estimated cost normally relates to the projected cost to treat a patient in our trials, and we recognize this cost over the estimated term of the study based on the number of patients enrolled in the trial on an ongoing basis, beginning with patient enrollment. As actual costs become known to us, we adjust our accruals. To date, our estimates have not differed significantly from the actual costs incurred. However, subsequent changes in estimates may result in a material change in our accruals, which could also materially affect our balance sheet and results of operations.
LOSS PER SHARE
Basic loss per share is computed by dividing net loss by the weighted average number of shares of common stock outstanding during the year. Diluted loss per share is computed using the average share price for the period and applying the treasury stock method to potentially dilutive outstanding options. In applicable years all potential common stock equivalents were antidilutive and accordingly were not included in the computation.
SHARE-BASED COMPENSATION
We had one stock-based compensation plan at December 31, 2014, the 2011 Equity Incentive Plan. Accounting for stock based compensation generally requires the recognition of the cost of employee services for share-based compensation based on the grant date fair value of the equity or liability instruments issued. We use the Black-Scholes option pricing model to estimate the fair value of our stock options. Expected volatility is determined using historical volatilities based on historical stock prices for a period equal to the expected term. The expected volatility assumption is adjusted if future volatility is expected to vary from historical experience. The expected term of options represents the period of time that options granted are expected to be outstanding and falls between the options' vesting and contractual expiration dates. The risk-free interest rate is based on the yield at the date of grant of a zero-coupon U.S. Treasury bond whose maturity period equals the option's expected term.
INCOME TAXES
Our net operating losses from inception to date have resulted principally from costs incurred in conducting clinical trials and in research and development activities related to efforts to develop our products and from the associated administrative costs required to support those efforts. We have recorded a deferred tax asset for our net operating losses (“NOL”); however, as the Company has incurred net operating losses since inception, and since there is no certainty of future profits, a valuation allowance has been provided in full on our deferred tax assets in the accompanying consolidated financial statements. Additionally, during 2013, the Company completed an analysis of its section 382 limit. Based on this analysis, the Company concluded that the amount of NOL carryforwards and the credits available to offset taxable income is limited under section 382. Accordingly, if the Company generates taxable income in any year in excess of its then annual limitation, the Company may be required to pay federal income taxes even though it has unexpired NOL carryforwards. Additionally, because U.S. tax laws limit the time during which NOLs and tax credit carryforwards may be applied against future taxable income and tax liabilities, the Company may not be able to take full advantage of its NOLs and tax credit carryforwards for federal income tax purposes. Future public and private stock placements may create additional limitations on the Company’s NOLs, credits and other tax attributes.
Recent Accounting Pronouncements
In August 2014, the FASB issued Accounting Standards Update No. 2014-15, “Presentation of Financial Statements - Going Concern.” The new standard requires management to evaluate whether there are conditions or events that raise substantial doubt about an entity's ability to continue as a going concern for both annual and interim reporting periods. This guidance is effective for us for the fiscal year beginning January 1, 2016 and interim periods thereafter. The guidance is not expected to have a material impact on our consolidated financial statements.
In June 2014, the FASB issued Accounting Standards Update 2014-10, “Development Stage Entities (Topic 915): Elimination of Certain Financial Reporting Requirements, Including an Amendment to Variable Interest Entities Guidance in Topic 810, Consolidation.” The guidance eliminates the definition of a development stage entity thereby removing the incremental financial reporting requirements from U.S. Generally Accepted Accounting Principles for development stage entities, primarily presentation of inception to date financial information. The provisions of the amendment is effective for annual reporting periods beginning after December 15, 2015. We have elected to adopt ASU 2014-10 early and as an early adopter, we are no longer providing inception-to-date financial information in our consolidated financial statements.
In May 2014, the FASB issued Accounting Standards Update 2014-09, “Revenue from Contracts with Customers” (“ASU 2014-09”). ASU 2014-09 is a comprehensive new revenue recognition model requiring a company to recognize revenue to depict the transfer of goods or services to a customer at an amount reflecting the consideration it expects to receive in exchange for those goods or services. In adopting ASU 2014-09, companies may use either a full retrospective or a modified retrospective approach. Additionally, this guidance requires improved disclosures regarding the nature, amount, timing and uncertainty of revenue and cash flows arising from contracts with customers. ASU 2014-09 is effective for the first interim period within annual reporting periods beginning after December 15, 2016, and early adoption is not permitted. The Company is currently assessing the impact of the new standard on our consolidated financial statements.
| F-8 |
4. FIXED ASSETS:
Fixed assets are as follows (in thousands):
| December 31, | ||||||||
| 2014 | 2013 | |||||||
| Laboratory equipment | $ | 20 | $ | 20 | ||||
| Office equipment | 101 | 101 | ||||||
| Furniture and fixtures | 18 | 18 | ||||||
| Leasehold improvements | 77 | 77 | ||||||
| Total fixed assets | 216 | 216 | ||||||
| Less — Accumulated depreciation and amortization | 184 | 141 | ||||||
| Net Fixed Assets | $ | 32 | $ | 75 | ||||
Depreciation was $43,000, $40,000 and $17,000 for the years ended December 31, 2014, 2013 and 2012, respectively.
5. OPERATING LEASES:
The Company leases laboratory and office space, pursuant to leases accounted for as operating leases. The lease for the Company’s laboratory and office space expires in June 2015. Rental expense for the years ended December 31, 2014, 2013 and 2012, was approximately $74,000, $79,000 and $76,000, respectively. Future minimum lease payments under non-cancelable leases with original terms in excess of one year as of December 31, 2014, is approximately $27,000 for 2015.
6. ACCRUED EXPENSES:
Accrued expenses consist of the following (in thousands):
| December 31, | ||||||||
| 2014 | 2013 | |||||||
| Personnel related costs | $ | 458 | $ | 196 | ||||
| Research and development costs | 284 | 277 | ||||||
| Other | 92 | 113 | ||||||
| Total | $ | 834 | $ | 586 | ||||
7. FEDERAL INCOME TAXES:
The Company has had net operating losses since inception and, therefore, has not been subject to federal income taxes. As of December 31, 2014, the Company has accumulated approximately $1.4 million of research and development tax credits. As of December 31, 2014, the Company had approximately $210.2 million of NOL carryforwards for federal income tax purposes. Additionally, approximately $12.2 million of NOLs and approximately $838,000 of research and development tax credits will expire in 2018. The NOL’s will expire from 2018 through 2034. The research and development credits will expire from 2018 through 2022.
The Tax Reform Act of 1986 provided for a limitation on the use of NOL and tax credit carryforwards following certain ownership changes that could limit the Company’s ability to utilize these NOLs and tax credits. The limitation is generally referred to as the “section 382 limit” after the IRC section. The issuance of stock, together with changes in stock ownership, resulted in multiple ownership changes for federal income tax purposes. During 2013, the Company completed an analysis of its section 382 limit. Based on this analysis, the Company concluded that the amount of NOL carryforwards and the credits available to offset taxable income is limited under section 382. Accordingly, if the Company generates taxable income in any year in excess of its then annual limitation, the Company may be required to pay federal income taxes even though it has unexpired NOL carryforwards. Additionally, because U.S. tax laws limit the time during which NOLs and tax credit carryforwards may be applied against future taxable income and tax liabilities, the Company may not be able to take full advantage of its NOLs and tax credit carryforwards for federal income tax purposes. Future public and private stock placements may create additional limitations on the Company’s NOLs, credits and other tax attributes.
| F-9 |
The Company’s net operating losses from inception to date have resulted principally from costs incurred in conducting clinical trials and in research and development activities related to efforts to develop products and from the associated administrative costs required to support those efforts. The Company has recorded a deferred tax asset for its net operating losses; however, as the Company has incurred operating losses since inception, and since there is no certainty of future profits, a valuation allowance has been provided in full on the deferred tax assets in the accompanying consolidated financial statements.
The tax effects of temporary differences that give rise to significant portions of the deferred tax assets are as follows (in thousands):
| December 31, | ||||||||
| 2014 | 2013 | |||||||
| Net operating loss carryforwards | $ | 71,472 | $ | 61,714 | ||||
| Research and development tax credits | 1,384 | 1,384 | ||||||
| Inventory reserve | 1,510 | 1,510 | ||||||
| Total deferred tax assets | 74,366 | 64,608 | ||||||
| Less — Valuation allowance | (74,366 | ) | (64,608 | ) | ||||
| Net deferred tax assets | $ | — | $ | — | ||||
The Company adopted FIN 48 in 2007. The Company has no unrecognized tax benefits that should be accrued under FIN 48. The Company’s policy is to record interest and penalties on income taxes as a component of the income tax provision.
The Company’s only taxing jurisdictions are the United States and Texas. The Company’s tax years from 1998 to the present remain open for federal examination due to the net operating loss carryforwards. Texas has a four year statute of limitations so that returns filed since 2011 remain open for state examination.
8. STOCKHOLDERS’ EQUITY:
OFFERINGS
On June 25, 2013, we completed a public offering of 4,312,500 shares of our common stock at a price per share of $19.00. Net proceeds to us, after deducting underwriters’ fees and offering expenses, were approximately $76.8 million.
On September 7, 2012, we completed a private placement of 2,145,636 shares of our common stock at a purchase price of $11.00 per share for aggregate proceeds after expenses of approximately $23 million. The private placement shares may be resold pursuant to our shelf registration statement on Form S-3, as amended (File No. 333-184159).
On February 1, 2012, we completed a direct registered offering of 2,463,537 shares of our common stock at a purchase price of $4.50 per share for aggregate proceeds after expenses of approximately $10.3 million.
On February 8, 2011, we completed an underwritten public offering of 690,000 units (including the exercise of the underwriter’s over-allotment option), consisting of an aggregate of 2,760,000 shares of our common stock, Series A Warrants to purchase 2,070,000 shares of our common stock and Series B Warrants to purchase 1,690,500 shares of our common stock, at a price per unit of $17.15. Each unit consisted of four shares of our common stock, Series A Warrants exercisable for three shares of our common stock at an exercise price of $0.01 per share and Series B Warrants exercisable for 2.45 shares of our common stock at an exercise price of $2.49 per share. Net proceeds to us, after the underwriting discount and offering expenses, were approximately $10.7 million. The fair value of the Series A and Series B Warrants was determined using a Black-Scholes model with the following assumptions: risk-free interest rate of 0.18%; no dividend yield; volatility of 131.66% and an expected term of six months. This resulted in a fair value of the Series A and Series B Warrants of approximately $5.4 million and a fair value of the common stock of approximately $5.3 million, which has been recorded in Additional Paid-In Capital on our Condensed Consolidated Balance Sheet. As of December 31, 2014, 2,029,325 shares of our common stock have been issued from the exercise of the Series A Warrants at $0.01 per share and 1,108,518 shares of our common stock have been issued from the exercise of the Series B Warrants at $2.49 per share. The Series A and B Warrants have a five year term from the date of issuance. The Series B Warrants are callable by the Company in the event that the Company’s stock trades at $8.00 or more for a period of 20 trading days over any consecutive 30 trading day period. As of the date of this filing, our common stock reached this price threshold, however, we have not yet required the exercise of the Series B Warrants pursuant to this provision. The Series A and B Warrants are also exercisable on a cashless basis. In addition, in no event may the Warrants be exercised if the holder would own 20% or more of the outstanding shares of the Company’s common stock following the exercise.
| F-10 |
LOSS PER SHARE
The following table presents information necessary to calculate loss per share for the three years ended December 31, 2014, 2013 and 2012 (in thousands, except per share amounts):
| 2014 | 2013 | 2012 | ||||||||||
| Net loss | $ | (32,535 | ) | $ | (28,466 | ) | $ | (18,944 | ) | |||
| Weighted average common shares outstanding | 23,432 | 20,808 | 15,346 | |||||||||
| Basic loss per share | $ | (1.39 | ) | $ | (1.37 | ) | $ | (1.23 | ) | |||
| Weighted average common and dilutive potential common shares outstanding: | ||||||||||||
| Weighted average common shares outstanding | 23,432 | 20,808 | 15,346 | |||||||||
| Assumed exercise of stock options | — | — | — | |||||||||
| 23,432 | 20,808 | 15,346 | ||||||||||
| Diluted loss per share | $ | (1.39 | ) | $ | (1.37 | ) | $ | (1.23 | ) |
Net loss and basic and diluted loss per share have been revised for 2013 and 2012. For a further description of the revisions, see Note 2. “Revision of Prior Years’ Financial Statements” in the Notes to Consolidated Financial Statements.
Other potential common stock of 2,910,157, 4,031,793 and 5,204,374, common shares underlying stock options and warrants for the periods ended December 31, 2014, 2013 and 2012, respectively, were excluded from the above calculation of diluted loss per share because such issuance would have been anti-dilutive. Potential common stock includes Series A Warrants issued in our February 8, 2011 public offering to purchase 39,595, 877,137 and 1,749,270 shares of our common stock at an exercise price of $0.01, for the periods ended December 31, 2014, 2013 and 2012, respectively. Additionally, potential common stock for periods ended December 31, 2014, 2013 and 2012 includes Series B Warrants issued in our February 8, 2011 public offering to purchase 429,704, 809,805 and 1,569,421 shares, respectively, of our common stock at an exercise price of $2.49.
9. STOCK OPTION PLANS:
As of December 31, 2014, there were 905,479 options available to grant under the 2011 Equity Incentive Plan. Typically, options are granted with an exercise price per share which is equal to the fair market value per share of common stock on the date of grant. Vesting provisions for each grant are determined by the board of directors and typically vest over a three year period. All options expire no later than the tenth anniversary of the grant date.
A summary of the status of the Company’s outstanding options at December 31, 2014, 2013, and 2012 and changes during the years then ended is presented in the tables below:
| Stock Options | Weighted Average Exercise Price | Remaining Weighted Average Contractual Term (Years) | Aggregate Intrinsic Value (In Thousands) | |||||||||||||
| Outstanding at December 31, 2011 | 1,960,003 | 6.79 | ||||||||||||||
| Granted | 246,000 | 10.08 | ||||||||||||||
| Exercised | (111,904 | ) | 4.08 | $ | 870.8 | |||||||||||
| Forfeited/cancelled | (208,416 | ) | 9.69 | |||||||||||||
| Outstanding at December 31, 2012 | 1,885,683 | 6.92 | ||||||||||||||
| Granted | 505,000 | 13.37 | ||||||||||||||
| Exercised | (14,165 | ) | 10.31 | $ | 144.4 | |||||||||||
| Forfeited/cancelled | (31,667 | ) | 11.87 | |||||||||||||
| Outstanding at December 31, 2013 | 2,344,851 | 8.22 | ||||||||||||||
| Granted | 351,000 | 17.24 | ||||||||||||||
| Exercised | (121,663 | ) | 5.27 | $ | 1,721.1 | |||||||||||
| Forfeited/cancelled | (133,330 | ) | 11.65 | |||||||||||||
| Outstanding at December 31, 2014 | 2,440,858 | 9.48 | 7.01 | $ | 1,202.5 | |||||||||||
| Exercisable at December 31, 2014 | 1,936,186 | 7.61 | 6.36 | $ | 4,204.2 | |||||||||||
| F-11 |
The following table summarizes information about stock options outstanding at December 31, 2014:
| Range Of Exercise Prices | Number Outstanding | Weighted Average Remaining Life | Weighted Average Exercise Price | Number Exercisable | Weighted Average Exercise Price | |||||||||||||||||||||
| $ | 1.33 to | $ | 4.00 | 253,138 | 5.5 | $ | 2.32 | 253,138 | $ | 2.32 | ||||||||||||||||
| 4.01 to | 5.00 | 762,312 | 6.2 | 4.50 | 758,980 | 4.50 | ||||||||||||||||||||
| 5.01 to | 10.00 | 569,908 | 7.0 | 6.74 | 500,727 | 6.42 | ||||||||||||||||||||
| 10.01 to | 20.00 | 749,000 | 8.6 | 15.62 | 346,923 | 15.04 | ||||||||||||||||||||
| 21.00 to | 50.80 | 106,500 | 5.2 | 33.54 | 76,418 | 38.58 | ||||||||||||||||||||
| 2,440,858 | 1,936,186 | |||||||||||||||||||||||||
Stock-based compensation is outlined in the following table (in thousands):
| 2014 | 2013 | 2012 | ||||||||||
| R&D expense | $ | 1,924 | $ | 1,839 | $ | 880 | ||||||
| G&A expense | 1,860 | 1,319 | 1,905 | |||||||||
| Total expense | $ | 3,784 | $ | 3,158 | $ | 2,785 | ||||||
At December 31, 2014, there was approximately $5.5 million of total unrecognized compensation cost related to non-vested stock options. This compensation cost is expected to be recognized over a weighted-average period of approximately 1.9 years.
Estimated fair values of stock options granted have been determined using the Black-Scholes option pricing model with the following weighted average assumptions:
| 2014 | 2013 | 2012 | ||||||||||
| Risk-free interest rate | 2.2 | % | 1.5 | % | 0.97 | % | ||||||
| Expected term | 7 years | 7 years | 6 years | |||||||||
| Volatility | 89 | % | 94 | % | 95 | % | ||||||
| Dividend yield | — | — | — | |||||||||
| Fair value | $ | 13.41 | $ | 10.53 | $ | 7.75 | ||||||
Expected term represents the period that the Company’s stock-based awards are expected to be outstanding. The Company’s historical stock option exercise experience does not provide a reasonable basis upon which to estimate expected term. As such, the simplified method was used to calculate the expected term.
Due to our net operating loss position there are no anticipated windfall tax benefits upon exercise of options.
The Black-Scholes option pricing model and other existing models were developed for use in estimating the fair value of traded options that have no vesting restrictions and are fully transferable. In addition, option valuation models require the input of and are highly sensitive to subjective assumptions including the expected stock price volatility. The Company’s employee stock options have characteristics significantly different from those of traded options and changes in the subjective input assumptions can materially affect the fair value estimate.
10. LICENSE, RESEARCH AND DEVELOPMENT AGREEMENTS:
NATIONAL INSTITUTES OF HEALTH (NIH)
In 1999, we licensed rights to Proellex® from the National Institutes of Health (“NIH”) under an exclusive, worldwide license in the field of treatment of human endocrinologic pathologies or conditions in steroid-sensitive tissues which expires upon the expiration of the last licensed patent. Under the terms of the agreement, we are obligated to meet certain developmental milestones as outlined in a commercial development plan, which has been amended and revised from time to time as circumstances warrant. We have recently amended the agreement to provide us with rights to certain second generation compounds under certain circumstances.
We provide annual updates to the NIH on the progress of our development of Proellex®. The NIH has the ability to terminate the agreement for lack of payment or if we are not meeting milestones as outlined in the commercial development plan and for other reasons as outlined in the agreement. Although we believe that we have a good working relationship with the NIH, there can be no assurance that all of the objectives and conditions in the commercial development plan will be met on a timely basis or at all, or that, if we fail to meet any of such objectives, the NIH will agree to amend this agreement to our satisfaction. Failure to comply with the material terms contained in the license agreement could result in termination of such agreement, which would prohibit us from further development of Proellex® and severely harm our business prospects. The NIH retains, on behalf of the government, a nonexclusive, nontransferable, worldwide license to practice the inventions licensed under the licensed patents by or on behalf of the government. For the purpose of encouraging basic research, the NIH retains the right to grant nonexclusive research licenses to third parties. Due to the work that was done on Proellex® at the NIH prior to our license agreement, the government also has certain rights to use the product in the event of a national emergency pursuant to the Patent and Trademark Laws Amendments Act of 1980, as amended.
| F-12 |
11. COMMITMENTS AND CONTINGENCIES:
See footnote 5 for a discussion of our operating lease commitments.
Therapeutic uses of our Androxal® product candidate are covered in the United States by nine issued U.S. patents and seven pending patent applications. Foreign coverage of therapeutic uses of our Androxal® product candidate includes 71 issued foreign patents and 99 foreign pending patent applications. The issued patents and pending applications relate to methods for treating certain conditions including the treatment of testosterone deficiency in men, the treatment of diabetes mellitus Type 2, the treatment of metabolic syndrome and conditions associated therewith, and the treatment of infertility in hypogonadal men. Androxal® (the trans-isomer of clomiphene) is purified from clomiphene citrate. A third party individual holds two issued patents related to the use of anti-estrogen such as clomiphene citrate and others for use in the treatment of androgen deficiency and disorders related thereto. We requested re-examination of one of these patents by the U.S. Patent and Trademark Office (“PTO”) based on prior art. The patent holder amended the claims in the re-examination proceedings, which led the PTO to determine that the amended claims were patentable in view of those publications under consideration and a re-examination certificate was issued. We subsequently filed a second request for re-examination by the PTO in light of a number of additional publications. The request was granted and all of the claims were finally rejected by the PTO in the re-examination. The patent holder appealed the rejections to the PTO Board of Patent Appeals and Interferences (the “PTO Board”) which ultimately reversed the rejections of several dependent claims in view of those publications under consideration. The patent holder filed a Notice of Appeal to the Federal Circuit on September 28, 2010 contesting the rejections maintained by the PTO Board. A decision was rendered by the Court of Appeals for the Federal Circuit on December 12, 2011, affirming the rejection of the appealed claims. The PTO issued an Ex Parte Reexamination Certificate on April 29, 2013, canceling the rejected claims and confirming the patentability of the remaining claims. Nevertheless, we believe that our development of Androxal® does not infringe any of the remaining claims and that all of the remaining claims are invalid on various grounds including additional prior art publications. We also believe that the second of these two patents is invalid in view of published prior art not considered by the PTO. If necessary, we intend to vigorously defend any and all claims that may be brought by the holder of such patents in a court of competent jurisdiction in order to develop Androxal® further. Adverse determinations in litigation proceedings could require us to seek licenses which may not be available on commercially reasonable terms, or at all, or subject us to significant liabilities, in which case we may not be able to successfully commercialize or out-license Androxal® until such patents expire or are otherwise no longer in force.
On July 19, 2013, we received a letter from Dr. Harry Fisch threatening to file a lawsuit against us and two of our executive officers (Joseph S. Podolski, President and Chief Executive Officer and Ron Wiehle, Executive Vice President), seeking addition of Dr. Harry Fisch as an inventor on three of our patents, U.S. Patent Nos. 7,173,064, 7,737,185 and 7,759,360, covering therapeutic uses of Androxal®. We believe that these allegations are without merit and on August 2, 2013, we commenced a lawsuit against Dr. Fisch in the U.S. District Court for the Southern District of Texas seeking a declaratory judgment that he should not be added as inventor to any of these patents. On October 2, 2013, Dr. Fisch filed counterclaims to our complaint seeking correction of inventorship of the three patents at issue to name Dr. Fisch as a co-inventor of the applications leading these patents. Dr. Fisch subsequently stipulated that he does not claim to be a co-inventor of U.S. Patent No. 7,173,064. The court granted summary judgment in favor of the Company on separate equitable and legal grounds, and entered judgment on December 23, 2014. Our request for attorney’s fees was denied. On February 9, 2015, Dr. Fisch filed a notice of appeal of the summary judgment rulings to the United States Court of Appeals for the Federal Circuit.
Rights Plan
We are party to a rights agreement, as amended, pursuant to which a dividend consisting of one preferred stock purchase right was distributed for each share of our common stock held as of the close of business on September 13, 1999, and to each share of common stock issued thereafter until the earlier of (i) the distribution date which is defined in the rights plan, (ii) the redemption date which is defined in the rights plan or (iii) September 13, 2015. The rights plan is designed to deter coercive takeover tactics and to prevent an acquirer from gaining control of us without offering fair value to our stockholders. The rights will expire on September 13, 2015, subject to earlier redemption or exchange as provided in the rights plan. Each right entitles its holder to purchase from us one one-hundredth of a share of a new series of Series One Junior Participating Preferred Stock at a price of $20.00 per one one-hundredth of a share, subject to adjustment. The rights are generally exercisable only if a person acquires beneficial ownership of 20% or more of our outstanding common stock.
12. QUARTERLY FINANCIAL INFORMATION (UNAUDITED):
Quarterly financial information for the quarters ended March 31, June 30 and September 30, 2014 and for 2013 have been revised. For a further description of this revision, see “Note 2. Revision of Prior Years’ Financial Statements” of the Notes to Consolidated Financial Statements.
| AS REPORTED | First Quarter Ended March 31, 2014 | Second Quarter Ended June 30, 2014 | Third Quarter Ended September 30, 2014 | Fourth Quarter Ended December 31, 2014 | ||||||||||||
| (In thousands except per share amounts) | ||||||||||||||||
| Revenues and other income: | ||||||||||||||||
| Interest income | $ | 2 | $ | 2 | $ | 2 | $ | 3 | ||||||||
| Total revenues and other income | 2 | 2 | 2 | 3 | ||||||||||||
| Expenses: | ||||||||||||||||
| Research and development | 7,325 | 7,450 | 6,107 | 5,771 | ||||||||||||
| General and administrative | 1,226 | 1,256 | 1,277 | 1,678 | ||||||||||||
| Total expenses | 8,551 | 8,706 | 7,384 | 7,449 | ||||||||||||
| Net loss | $ | (8,549 | ) | $ | (8,704 | ) | $ | (7,382 | ) | $ | (7,446 | ) | ||||
| Net loss per share – basic and diluted | $ | (0.37 | ) | $ | (0.38 | ) | $ | (0.32 | ) | $ | (0.31 | ) | ||||
| Shares used in loss per share calculation | 23,033 | 23,102 | 23,347 | 24,234 | ||||||||||||
| F-13 |
| AS REVISED | First Quarter Ended March 31, 2014 | Second Quarter Ended June 30, 2014 | Third Quarter Ended September 30, 2014 | Fourth Quarter Ended December 31, 2014 | ||||||||||||
| (In thousands except per share amounts) | ||||||||||||||||
| Revenues and other income: | ||||||||||||||||
| Interest income | $ | 2 | $ | 2 | $ | 2 | $ | 3 | ||||||||
| Total revenues and other income | 2 | 2 | 2 | 3 | ||||||||||||
| Expenses: | ||||||||||||||||
| Research and development | 7,569 | 7,491 | 6,276 | 5,771 | ||||||||||||
| General and administrative | 1,226 | 1,256 | 1,277 | 1,678 | ||||||||||||
| Total expenses | 8,795 | 8,747 | 7,553 | 7,449 | ||||||||||||
| Net loss | $ | (8,793 | ) | $ | (8,745 | ) | $ | (7,551 | ) | $ | (7,446 | ) | ||||
| Net loss per share – basic and diluted | $ | (0.38 | ) | $ | (0.38 | ) | $ | (0.32 | ) | $ | (0.31 | ) | ||||
| Shares used in loss per share calculation | 23,033 | 23,102 | 23,347 | 24,234 | ||||||||||||
| AS REPORTED | First Quarter Ended March 31, 2013 | Second Quarter Ended June 30, 2013 | Third Quarter Ended September 30, 2013 | Fourth Quarter Ended December 31, 2013 | ||||||||||||
| (In thousands except per share amounts) | ||||||||||||||||
| Revenues and other income: | ||||||||||||||||
| Interest income | $ | 1 | $ | 1 | $ | 3 | $ | 4 | ||||||||
| Total revenues and other income | 1 | 1 | 3 | 4 | ||||||||||||
| Expenses: | ||||||||||||||||
| Research and development | 6,308 | 6,037 | 4,786 | 5,781 | ||||||||||||
| General and administrative | 1,067 | 1,171 | 1,215 | 1,365 | ||||||||||||
| Total expenses | 7,375 | 7,208 | 6,001 | 7,146 | ||||||||||||
| Net loss | $ | (7,374 | ) | $ | (7,207 | ) | $ | (5,998 | ) | $ | (7,142 | ) | ||||
| Net loss per share – basic and diluted | $ | (0.41 | ) | $ | (0.38 | ) | $ | (0.26 | ) | $ | (0.31 | ) | ||||
| Shares used in loss per share calculation | 18,182 | 18,958 | 23,006 | 23,012 | ||||||||||||
| AS REVISED | First Quarter Ended March 31, 2013 | Second Quarter Ended June 30, 2013 | Third Quarter Ended September 30, 2013 | Fourth Quarter Ended December 31, 2013 | ||||||||||||
| (In thousands except per share amounts) | ||||||||||||||||
| Revenues and other income: | ||||||||||||||||
| Interest income | $ | 1 | $ | 1 | $ | 3 | $ | 4 | ||||||||
| Total revenues and other income | 1 | 1 | 3 | 4 | ||||||||||||
| Expenses: | ||||||||||||||||
| Research and development | 6,467 | 6,262 | 4,975 | 5,953 | ||||||||||||
| General and administrative | 1,067 | 1,171 | 1,215 | 1,365 | ||||||||||||
| Total expenses | 7,534 | 7,433 | 6,190 | 7,318 | ||||||||||||
| Net loss | $ | (7,533 | ) | $ | (7,432 | ) | $ | (6,187 | ) | $ | (7,314 | ) | ||||
| Net loss per share – basic and diluted | $ | (0.41 | ) | $ | (0.39 | ) | $ | (0.27 | ) | $ | (0.32 | ) | ||||
| Shares used in loss per share calculation | 18,182 | 18,958 | 23,006 | 23,012 | ||||||||||||
| F-14 |
13. SUBSEQUENT EVENTS
On January 6, 2015, we paid a filing fee to the FDA associated with the submission of our NDA for Androxal® in the amount of $2.3 million.
On January 28, 2015, the Board of Directors approved grants of a total of 189,000 stock options to certain employees. These options have an exercise price of $8.33, which was the closing price of our common stock on the date of grant, and will vest in equal annual installments on the first three year anniversaries of the date of grant.
On February 5, 2015, the Compensation Committee of the Board of Directors approved grants of a total of 180,000 stock options to non-employee Board Members and the Chief Financial Officer. These options have an exercise price of $8.44, which was the closing price of our common stock on the date of grant, and will vest in equal annual installments on the first three year anniversaries of the date of grant.
| F-15 |