Attached files
| file | filename |
|---|---|
| 8-K - 8-K - SYNERGY PHARMACEUTICALS, INC. | a14-21617_28k.htm |
Exhibit 99.1
|
|
Corporate Presentation |

|
|
2 Safe Harbor Statement This presentation may contain forward-looking statements within the meaning of Section 27A of the Securities Act of 1933 and Section 21E of the Securities Exchange Act of 1934. Such forward-looking statements are characterized by future or conditional verbs such as “may,” “will,” “expect,” “intend,” “anticipate,” believe,” “estimate” and “continue” or similar words. You should read statements that contain these words carefully because they discuss future expectations and plans, which contain projections of future results of operations or financial condition or state other forward-looking information. Such statements are only predictions and our actual results may differ materially from those anticipated in these forward-looking statements. We believe that it is important to communicate future expectations to investors. However, there may be events in the future that we are not able to accurately predict or control. Factors that may cause such differences include, but are not limited to, those discussed under Risk Factors and elsewhere in our Offering Memorandum and our Annual Report on Form 10-K for the year ended December 31, 2013, as filed with the Securities and Exchange Commission, including the uncertainties associated with product development, the risk that products that appeared promising in early clinical trials do not demonstrate safety and efficacy in larger-scale clinical trials, the risk that we will not obtain approval to market our products, the risks associated with dependence upon key personnel and the need for additional financing. We do not assume any obligation to update forward-looking statements as circumstances change. This presentation does not constitute an offer or invitation for the sale or purchase of securities or to engage in any other transaction with Synergy or its affiliates. The information in this presentation is not targeted at the residents of any particular country or jurisdiction and is not intended for distribution to, or use by, any person in any jurisdiction or country where such distribution or use would be contrary to local law or regulation. |
|
|
3 Our Team: GI Expertise & Proven Track Record of Execution Gary Jacob, Ph.D. Chairman & CEO Over 25 years of experience in pharma and biotech across multiple disciplines, including: R & D, operations and business development Kunwar Shailubhai, PhD Chief Scientific Officer Major discoverer of Plecanatide and SP-333 for GI indications Over 20 years experience at G.D. Searle/Monsanto Co. and NIH Patrick Griffin, MD Chief Medical Officer Board-certified, internal medicine and gastroenterology Over 25 years of experience; Sanofi-Aventis, Forest Laboratories, Private practice Laura Barrow, PharmD SVP, Clinical Operations Over 25 years experience in clinical development Hoffmann La-Roche, Bristol-Myers Squibb, Pfizer Paul Eng, PhD SVP, Drug Development Former Director of GI Clinical Development, Forest Laboratories Successfully led CIC/IBS-C phase 3 trials to NDA and drug approval Marino Garcia SVP, Corporate Development Former VP of Global BD, Aptalis Pharmaceuticals Aspreva Pharmaceuticals, Eli Lily, Schering Plough, Pfizer Bernard Denoyer, CPA SVP, Finance Former CFO of META Group Inc. SVP, Finance and Secretary, Callisto Pharmaceuticals |
|
|
4 Our Focus: Pioneering GI Research & Development NATURAL PHYSIOLOGY MEETS BREAKTHROUGH SCIENCE Advanced clinical programs with multiple value drivers Unique mechanism-of-action based on a naturally occurring human GI hormone Exclusive worldwide rights Strong patent portfolio Experienced management team |
|
|
5 Our Platform: Discovered & Developed by Synergy COMPOUND INDICATION PHASE 1 PHASE 2 PHASE 3 PLECANATIDE Chronic Idiopathic Constipation (CIC) Irritable Bowel Syndrome with Constipation (IBS-C) SP-333 Opioid-Induced Constipation (OIC) Ulcerative Colitis (UC) |
|
|
6 Our Approach: Based on a Natural Human GI Hormone - Uroguanylin UROGUANYLIN (Natural GI Hormone) PLECANATIDE CIC/IBS-C SP-333 OIC/UC |
|
|
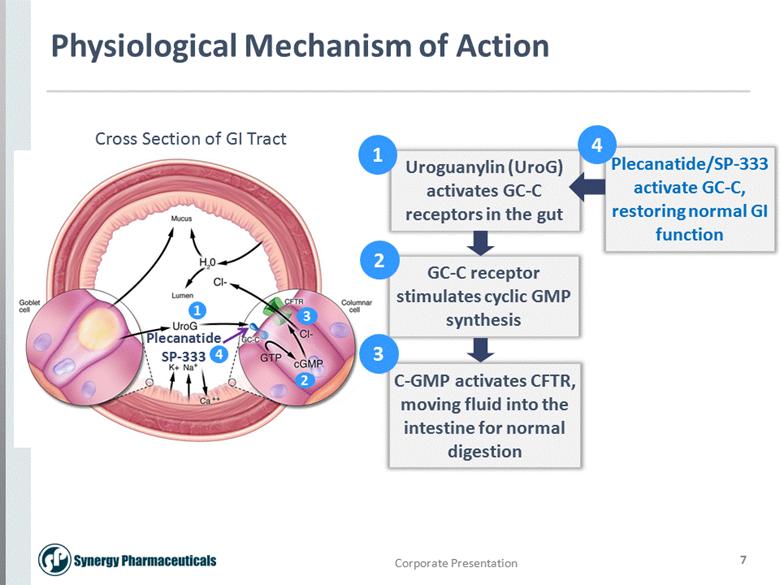
7 Physiological Mechanism of Action 1 2 3 Plecanatide SP-333 Uroguanylin (UroG) activates GC-C receptors in the gut GC-C receptor stimulates cyclic GMP synthesis C-GMP activates CFTR, moving fluid into the intestine for normal digestion Plecanatide/SP-333 activate GC-C, restoring normal GI function Cross Section of GI Tract 2 3 4 4 1 |
|
|
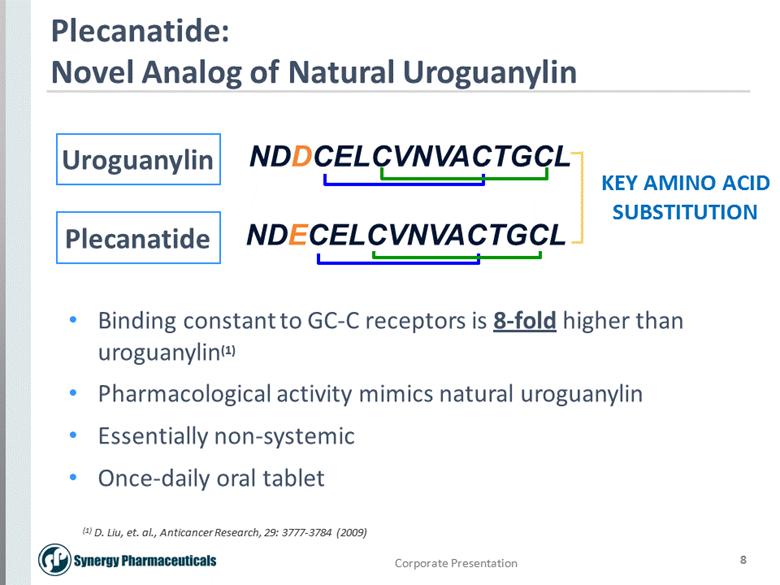
8 Plecanatide: Novel Analog of Natural Uroguanylin NDDCELCVNVACTGCL NDECELCVNVACTGCL KEY AMINO ACID SUBSTITUTION (1) D. Liu, et. al., Anticancer Research, 29: 3777-3784 (2009) Uroguanylin Plecanatide Binding constant to GC-C receptors is 8-fold higher than uroguanylin(1) Pharmacological activity mimics natural uroguanylin Essentially non-systemic Once-daily oral tablet |
|
|
9 Natural GC-C Agonist vs. Bacterial Enterotoxin Linaclotide: Enterotoxin Analog NDDCELCVNVACTGCL NDECELCVNVACTGCL NSSNYCCELCCNPACTGCY CCEYCCNPACTGCY ST Peptide: Produced by E. coli Bacteria Uroguanylin: Natural GC-C Agonist Plecanatide: Uroguanylin Analog Linaclotide is a truncated version of a bacterial enterotoxin |
|
|
CIC/IBS-C Market Overview |

|
|
11 Growing US Market Opportunity Millions of US adults with CIC/IBS-C Around 35 million US adults with CIC Estimated 13 million US adults with IBS-C CIC population expected to grow CIC affects around 50% of the US elderly – 74% nursing home residents 65+ population expected to reach 80 million by 2040 – accounting for 21% of the US population New therapy launch and multi-million dollar marketing campaign is building the CIC/IBS-C market Only two FDA approved CIC/IBS-C drugs currently available – latest drug launched in Dec. 2012 Multi-million dollar direct-to-consumer awareness campaign started in April 2014 1. Wald A, Scarpignato C, Kamm MA, et al. The burden of constipation on quality of life: results of a multinational survey. Aliment Pharmacol Ther. 2007;26(2);227-236. 2. Rao SC, Go JT. Update on the management of constipation in the elderly: new treatment options. Clin Interv Aging. 2010;5:163-171. 3. A profile of Older Americans: 2012, Administration on Aging Adminisration for Community Living, US Department of Health and Human Services (1) (2) (3) |

|
|
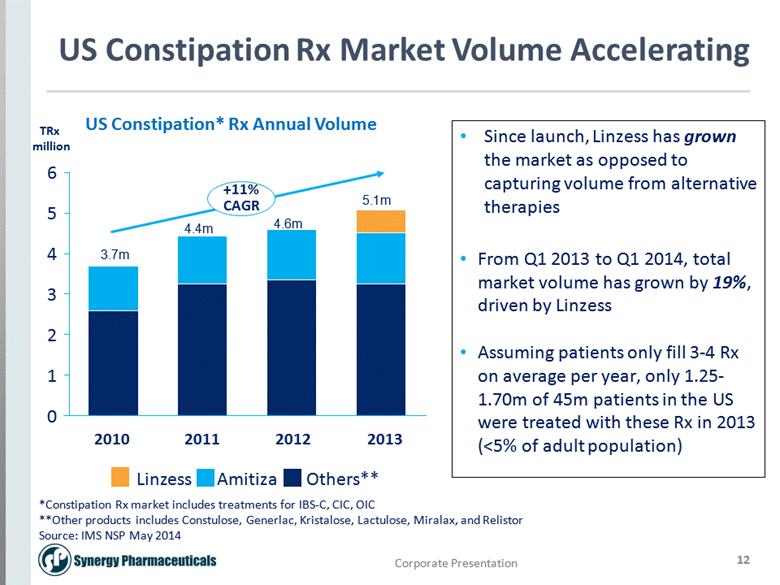
12 US Constipation Rx Market Volume Accelerating US Constipation* Rx Annual Volume 6 5 4 3 0 2 1 2013 +11% CAGR 2011 2012 2010 Linzess Amitiza Others** Since launch, Linzess has grown the market as opposed to capturing volume from alternative therapies From Q1 2013 to Q1 2014, total market volume has grown by 19%, driven by Linzess Assuming patients only fill 3-4 Rx on average per year, only 1.25-1.70m of 45m patients in the US were treated with these Rx in 2013 (<5% of adult population) 5.1m 4.6m 4.4m 3.7m *Constipation Rx market includes treatments for IBS-C, CIC, OIC **Other products includes Constulose, Generlac, Kristalose, Lactulose, Miralax, and Relistor Source: IMS NSP May 2014 TRx million |
|
|
13 US Constipation Rx Market Value ($) Growing US Constipation* Rx Annual Sales 600 500 550 0 100 150 200 50 450 300 400 350 250 +21% CAGR 2013 2010 2012 2011 Others** Amitiza Linzess Both Linzess and Amitiza have driven sales growth in the market From Q1 2013 to Q1 2014, the market has grown by 55%, largely driven by Linzess sales $ million *Constipation Rx market includes treatments for IBS-C, CIC, OIC **Other products includes Constulose, Generlac, Kristalose, Lactulose, Miralax, and Relistor Source: IMS NSP May 2014 |
|
|
Plecanatide CIC Clinical Program |
|
|
15 Plecanatide Phase 2b/3 CIC Trial: Study Overview Aim: Assess the safety and efficacy of 0.3, 1.0 and 3.0 mg plecanatide doses vs. placebo in CIC patients Patient Population: 951 patients with CIC (Modified Rome III Criteria) Primary Endpoint: Proportion of Durable Overall Responders (fulfills ≥ 3 CSBMs + ≥ 1 CSBM from baseline per week, for 9/12 weeks, including ≥ 3 of the last 4 weeks) – FDA Approval Endpoint Design: Screening up to 4 weeks Baseline 2 weeks Treatment 12 weeks Post-Tx 2 weeks Patients called in daily to IVRS |
|
|
16 Placebo n=236 3.0 mg n=237 p value % CSBM Responders 10.7 19 p= <0.01 CSBM Frequency 1.03 2.13 p= <0.001 SBM Frequency 1.30 2.88 p= <0.001 Stool Consistency 0.81 2.01 p= <0.001 Mean Straining Change -1.24 -2.07 p= <0.001 Plecanatide Phase 2b/3 CIC Trial: Results Summary Plecanatide 3.0 mg dose showed statistically significant improvement in all primary and key secondary endpoints |
|
|
17 Plecanatide Phase 2b/3 CIC Trial: Results Summary % Responders * = p<0.05; ** = p < 0.01; *** = p < 0.001 Treatment Week Treatment week Bristol Stool Form Scale Score Stool Consistency (BSFS) Weekly Responder Rates Plecanatide 3.0 mg demonstrated immediate and sustained effect |
|
|
18 Plecanatide Phase 2b/3 CIC Trial: Clear Dose-Response for Efficacy * = p<0.05; ** = p < 0.01; *** = p < 0.001 *** *** *** |
|
|
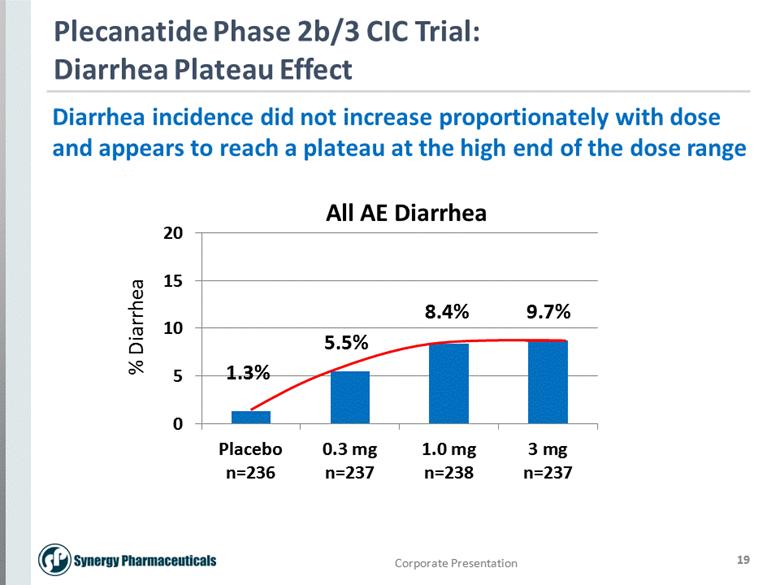
19 Plecanatide Phase 2b/3 CIC Trial: Diarrhea Plateau Effect All AE Diarrhea 9.7% 8.4% 5.5% 1.3% Diarrhea incidence did not increase proportionately with dose and appears to reach a plateau at the high end of the dose range |
|
|
20 Placebo n=236 3.0 mg n=237 Serious Adverse Events (AE) 5 (2.1%) 2 (0.8%) Treatment-emergent (TE) AEs 96 (40.7%) 106 (44.7%) AEs leading to withdrawal 8 (3.4%) 13 (5.5%) All Diarrhea TEAEs 3 (1.3%) 23 (9.7%) Severe Diarrhea TEAEs 0 1 (0.4%) Withdrawal due to Diarrhea 1 (0.4%) 7 (3.0%) Plecanatide Phase 2b/3 CIC Trial: Safety Summary Plecanatide was safe and well tolerated with <10% diarrhea at 3.0 mg dose |
|
|
21 Plecanatide Pivotal Phase 3 CIC Trials: Program Overview Aim: Two, randomized, 12-week, double-blind, placebo-controlled trials to confirm the safety and efficacy of plecanatide in CIC patients Treatment Groups: 3.0 and 6.0 mg oral tablet plecanatide or placebo once-daily Estimated Enrollment: 1350 CIC patients per trial (2700 patients total) Primary Endpoint: Proportion of Durable Overall Responders Design: Screening up to 4 weeks Baseline 2 weeks Treatment 12 weeks Post-Tx 2 weeks Patients call in daily to IVRS |
|
|
Plecanatide IBS-C Clinical Program |

|
|
23 Plecanatide Phase 2b IBS-C Trial: Study Overview Screening up to 6 weeks Baseline 2 weeks Treatment 12 weeks Post-Tx 2 weeks Patients called in daily to IVRS Study Aim: Assess the efficacy and safety of 0.3, 1.0, 3.0 and 9.0 mg plecanatide doses vs. placebo in IBS-C patients Population: 424 patients with IBS-C (Rome III Criteria) Primary Endpoint: Mean change from baseline in CSBMs Study Design: |
|
|
24 Plecanatide Phase 2b IBS-C Trial: Preliminary Top-line Data 1.0, 3.0 and 9.0 mg dose groups demonstrated statistical significance for the study’s primary endpoint (CSBM frequency) Safe and well tolerated at all doses with no treatment-related serious adverse events 3.0 mg dose consistently demonstrated statistically significant improvement in key secondary endpoints, including the overall responder endpoint (FDA endpoint required for approval) 3.0 mg dose group showed < 10% diarrhea rate Full data results to be presented at ACG on October 20, 2014 |
|
|
25 41.9% * 24.7% *p< 0.05 n = 85 n = 86 Plecanatide Phase 2b IBS-C Trial: Overall Responder Endpoint (FDA Approval Endpoint) Overall Responder = fulfills both ≥ 30% reduction in worst abdominal pain and Increase of ≥ 1 CSBMs from baseline in the same week for at least 50% of the weeks (6/12 wks) |
|
|
26 Placebo n=85 3.0 mg n=86 p value CSBM frequency/ 12 weeks 1.29 2.74 p= <0.001 Worst Abdominal Pain Intensity -1.4 (-24.5%) -2.0 (-33.9%) p= <0.05 Stool Consistency 1.01 2.49 p= <0.001 Diarrhea Rate 0 9.3% Plecanatide Phase 2b IBS-C Trial: Preliminary Top-line Data Plecanatide 3.0 mg demonstrated ideal efficacy for treating IBS-C patients and excellent tolerability at <10% diarrhea |
|
|
27 Plecanatide Phase 2b IBS-C Trial: End-of-Phase 2 FDA Meeting Highlights Agreement reached with FDA on pivotal phase 3 IBS-C studies regarding trial duration, study population, number of trials and primary endpoint Plecanatide 3.0 mg and 6.0 mg doses selected (consistent with CIC registration trials) Pivotal phase 3 IBS-C program to be initiated 4Q 2014 and will include 2 registration trials IBS-C patients successfully completing either of the 12-week placebo-controlled registration trials will be offered enrollment into a long-term safety trial in order to support the ongoing long-term safety database for the CIC indication |
|
|
28 Plecanatide Phase 3 IBS-C Trials: Program Overview Aim: Two, randomized, 12-week, double-blind, placebo-controlled studies to confirm the safety and efficacy of plecanatide in IBS-C patients Treatment Groups: 3.0 and 6.0 mg oral tablet plecanatide or placebo once-daily Estimated Enrollment: 1,050 IBS-C patients per trial (Rome III Criteria) Primary Endpoint: Overall Responder endpoint Design: Screening up to 6 weeks Baseline 2 weeks Treatment 12 weeks Post-Tx 2 weeks Patients will call in daily to IVRS |
|
|
SP-333 Clinical Program |

|
|
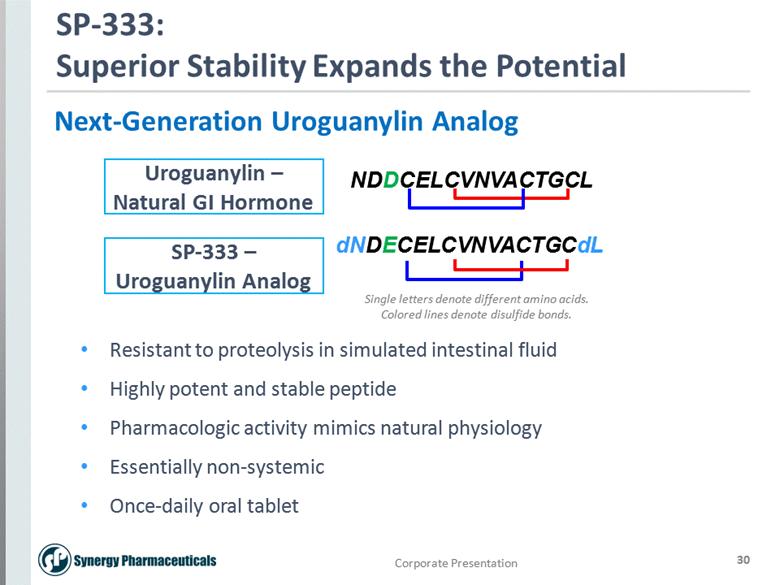
30 SP-333: Superior Stability Expands the Potential dNDECELCVNVACTGCdL NDDCELCVNVACTGCL Next-Generation Uroguanylin Analog Resistant to proteolysis in simulated intestinal fluid Highly potent and stable peptide Pharmacologic activity mimics natural physiology Essentially non-systemic Once-daily oral tablet Uroguanylin – Natural GI Hormone SP-333 – Uroguanylin Analog Single letters denote different amino acids. Colored lines denote disulfide bonds. |
|
|
31 SP-333 Phase 2 OIC Trial: Study Overview Aim: Assess the safety and efficacy of SP-333 in OIC patients receiving chronic opioid therapy for ≥ 3 months Treatment Groups: 1.0, 3.0 and 6.0 mg SP-333 vs. placebo once-daily Estimated Enrollment: 260 OIC patients Treatment Duration: 4 weeks Primary Endpoint: Mean change from baseline in the number of SBMs during week 4 of the Treatment Period Top-line data expected in the fourth quarter of this year |
|
|
Corporate Summary |

|
|
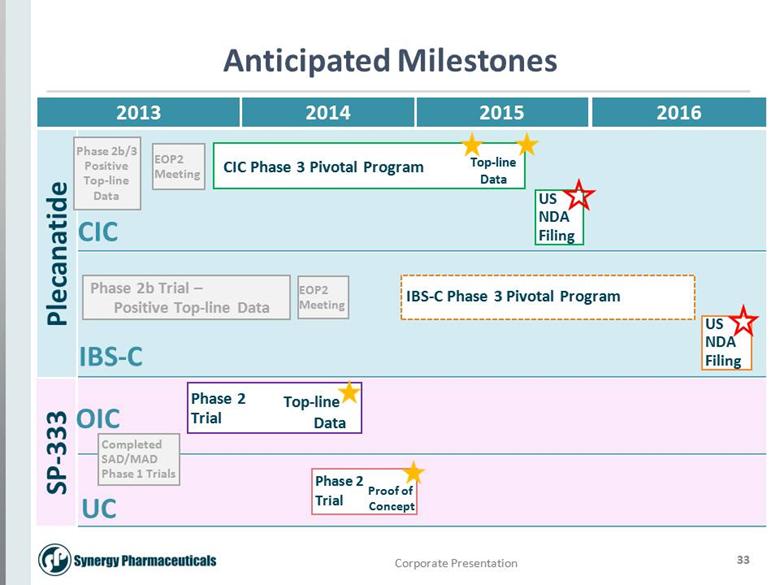
33 Anticipated Milestones 2013 Plecanatide SP-333 CIC IBS-C OIC UC EOP2 Meeting Phase 2b/3 Positive Top-line Data 2014 2015 2016 CIC Phase 3 Pivotal Program US NDA Filing Phase 2b Trial – Positive Top-line Data US NDA Filing Phase 2 Trial Top-line Data Phase 2 Trial Completed SAD/MAD Phase 1 Trials Proof of Concept EOP2 Meeting IBS-C Phase 3 Pivotal Program Top-line Data |