Attached files
| file | filename |
|---|---|
| 8-K - FORM 8-K - Orexigen Therapeutics, Inc. | d655004d8k.htm |
 January
2014 1
Exhibit 99.1 |
 Forward Looking
Statements 2
This presentation contains forward-looking statements about Orexigen Therapeutics, Inc. and
its lead product candidate, NB 32. Words such as "believes,"
"anticipates," "plans," "expects," "indicates," "will," "should," "intends," "potential," "suggests," "assuming," "designed" and
similar expressions are intended to identify
forward-looking statements. These statements are based on the Company's current beliefs and
expectations. These forward-looking statements include
statements regarding: the timing of potential approval of the NDA for NB 32; the benefit
risk profile for NB 32; Orexigen’s plans to seek a commercialization partner in territories outside of North America; and the timing of
the submission of the CSR for the interim analysis. The inclusion of forward-looking statements should not be regarded as a representation by
Orexigen that any of its plans will be achieved. Actual results may differ materially from
those expressed or implied in this release due to the risk and uncertainties inherent in
the Orexigen business, including, without limitation: the SPA is not binding on the FDA if public health
concerns unrecognized at the time the SPA agreement was entered into become evident, other new
scientific concerns regarding product safety or efficacy arise, or if Orexigen fails to
comply with the agreed upon trial protocol; the potential for the FDA to not approve NB 32 even
after meeting the prespecified threshold and resubmitting the NDA; the possibility that the
public announcement of the results of the interim analysis would later be deemed to
jeopardize the integrity of the Light Study potentially resulting in the requirement to conduct additional,
costly studies; additional analysis of the interim results or new data from the continuing
Light Study, including safety-related data, may produce negative or inconclusive
results, or may be inconsistent with the conclusion that the interim analysis was successful; the potential
that the interim analysis may not be predictive of future results in the Light Study; the
potential for early termination of Orexigen’s North American collaboration
agreement with Takeda Pharmaceutical Company Limited; the results from the interim analysis may not be sufficient
to satisfy or respond to the Day 120 List of Questions from the EMA or any other data
requirements of the EMA in connection with the review of the MAA; even if the NDA is
approved by the FDA, the final results of the Light Study may not support continued approval of NB 32; the
therapeutic and commercial value of NB 32; Orexigen’s ability to maintain sufficient
capital to fund its operations through potential approval of NB 32 in 2014; and other
risks described in Orexigen’s filings with the Securities and Exchange Commission. You are cautioned not to place
undue reliance on these forward-looking statements, which
speak only as of the date hereof, and Orexigen undertakes no obligation to revise or
update this news release to reflect events or circumstances after the date hereof. Further information regarding these and other risks is
included under the heading "Risk Factors" in Orexigen's Current Report on Form 8-K
filed with the Securities and Exchange Commission on December 2, 2013 and its
other reports, which are available from the SEC's website (www.sec.gov) and on Orexigen's website
(www.orexigen.com) under the heading "Investor Relations." All forward-looking statements are qualified in their entirety by this cautionary
statement. This caution is made under the safe harbor provisions of Section 21E of the Private
Securities Litigation Reform Act of 1995. |
 2000
303m
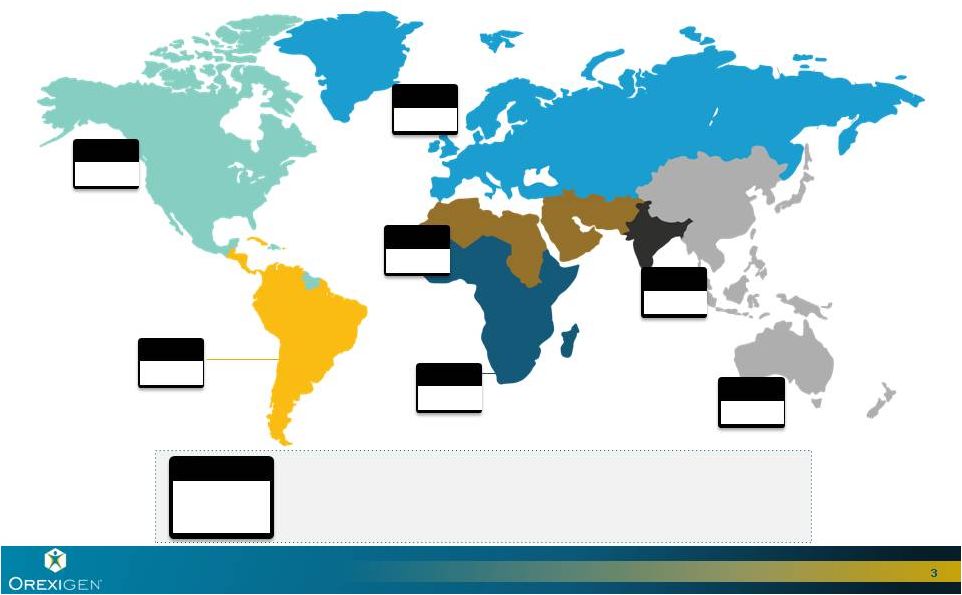
Obesity is a Growing Global Epidemic
3
2000
86m
North America and Caribbean (NAC)
South and Central America (SACA)
Africa (AFR)
Western Pacific (WP)
SE Asia
(SEA)
Europe (EUR)
Middle East and
North Africa (MENA)
millions of people
2000
2020
2000
95m
2000
2000
30m
2000
2000
5m
46m
2000
2000
9m
2000
2000
32m
Source: EuroMonitor,
2010;
WHO Statistics
2000 |
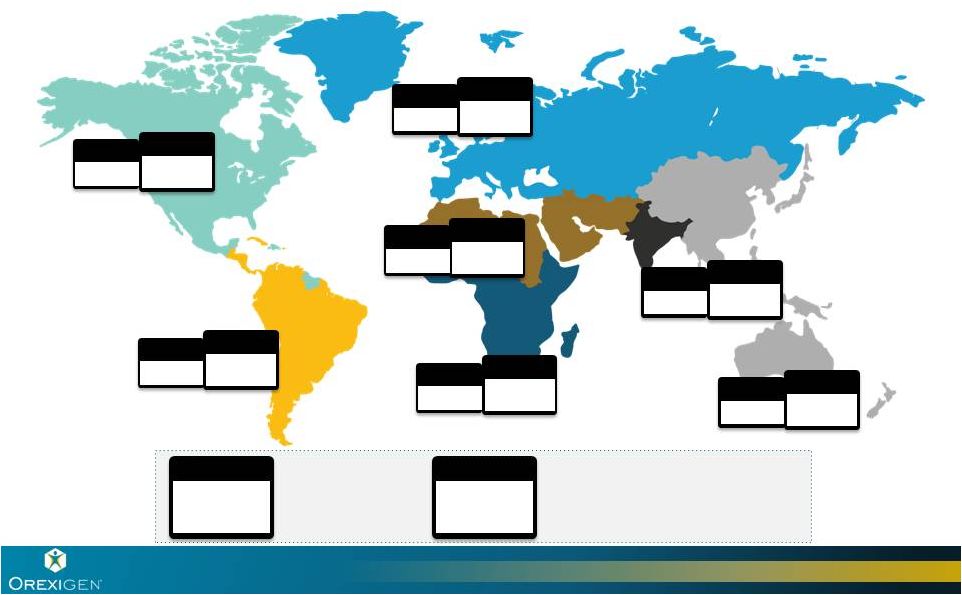 2010
2000
472m
303m
Obesity is a Growing Global Epidemic
4
2000
86m
2010
110m
North America and Caribbean (NAC)
South and Central America (SACA)
Africa (AFR)
Western Pacific (WP)
SE Asia
(SEA)
Europe (EUR)
Middle East and
North Africa (MENA)
millions of people
2000
2020
2000
2010
122m
95m
2000
2000
2010
51m
30m
2000
2000
2010
16m
5m
2000
2010
99m
46m
2000
2000
2010
15m
9m
2000
2000
2010
59m
32m
Source: EuroMonitor,
2010;
WHO Statistics |
 2010
2000
472m
303m
Obesity is a Growing Global Epidemic
5
2020
672m
2000
86m
2010
110m
2020
149m
North America and Caribbean (NAC)
South and Central America (SACA)
Africa (AFR)
Western Pacific (WP)
SE Asia
(SEA)
Europe (EUR)
Source: EuroMonitor,
2010;
WHO Statistics
Middle East and
North Africa (MENA)
millions of people
2000
2020
2000
2010
2020
122m
144m
95m
2000
2000
2010
2020
51m
71m
30m
2000
2000
2010
2020
16m
35m
5m
2000
2000
2010
99m
156m
46m
2000
2000
2010
2020
15m
24m
9m
2000
2000
2010
2020
59m
93m
32m |
 Obesity
and
Co-Morbid
Diabetes
Increase
Risk
of
Coronary
Heart
Disease
6
Source: Obesity: Volume 18, Issue 2, pages 377-383, 6 SEP 2012 DOI: 10.1038/oby.2009.223
http://onlinelibrary.wiley.com/doi/10.1038/oby.2009.223/full#f1 Annual Cost
in US:
$245B
Diabetes
Cardiovascular
Disease (CVD):
$444B
18.5-22.9
23.0-24.9
25.0-26.9
27.0-29.9
30.0+
Body Mass Index (BMI)
Excess Weight and the Risk of
Coronary Heart Disease Among Men
0
1
2
3
4
5
6
7
8 |
 7
* Insulin excluded
Weight
Loss
Improves
Cardiometabolic
Risk
Factors
Therapeutic Class
Cardiometabolic Risk
Factors Adversely Impacted
by Excess Weight
US 2011 Total
Rx Expenditures
(billions)
Global 2011
Total Rx
Expenditures
(billions)
Anti-hypertension
Blood Pressure
$14.2
$51.3
Anti-diabetes
agents*
Blood Glucose
$10.3
$20.3
Lipid Modifiers
Triglycerides
$22.0
$39.0
HDL-cholesterol
LDL-cholesterol |
 How Will Obesity
Therapeutics Become a Blockbuster Category?
8
Global approvals
A clear safety profile established by positive outcomes
trial data
Large, skilled primary care marketing efforts
Increased access and coverage for therapeutics and
programs
Continued investment in outcomes data establishing long
term health and economic benefits
Investment in key life cycle opportunities |
 NB32 -
Our Lead Investigational Medicine
naltrexone sustained release (SR)/bupropion SR
9
A Unique Combination with Unexpected Results
Placebo
(N=60)
Naltrexone
(N=33)
Bupropion
(N=44)
NB32
(N=45)
Phase 2b Completers
Weight loss at 24 weeks
-7.1%
-3.1%
-1.7%
-1.1%
Orexigen is seeking approval for NB32 for weight loss and maintenance of weight loss.
NB32:
A fixed dose combination of two drugs
that demonstrates an unexpected and
significant impact on weight loss
–
Bupropion:
Indications for depression, smoking
cessation
–
Naltrexone:
Indications in anti-addiction |
 NB32: Issued
Patents and Pending Applications 10
2033
2031
2031
2029
2027
2027
2027
2026
2026
2024/25
Light Study (methods)
Binge Eating (methods)
Major Depression (methods)
Visceral Fat (methods)
Titration / Dose Pack (methods & devices)
Trilayer (methods & compositions)
Nal SR (methods & compositions)
Food Cravings / Titration (methods)
Insulin Sensitivity (methods & compositions)
Weber / Cowley (methods & compositions)
Pending
Issued in some territories,
pending in others |
 NB32 Studies
Have Included More Than 13,000 Patients
Phase 3 trials met co-primary and key
secondary endpoints
Reduction in body weight
Improvements in CV and metabolic
risk factors
Improvements in food craving
measures
Generally well tolerated with overall
safety profile consistent with
components
Reduction in HbA1C in COR-Diabetes
trial
Greater weight loss observed when
combined with intensive behavioral
modification (BMOD)
11
Interim results achieved goal set by
FDA
No new safety signals observed
Results clearly address single approval
deficiency of CRL
Phase 2 & 3 clinical trials in
4,500+ patients established efficacy
and safety profile
Light Study CVOT evaluating NB32 vs.
placebo in ~8,900 overweight and
obese patients |
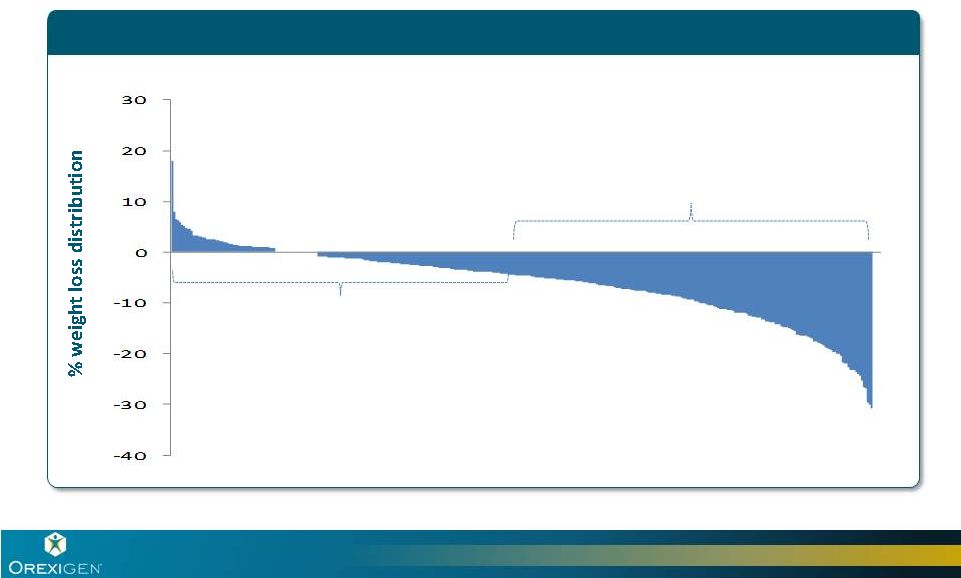 Our Focus is on
Responders to Therapy Illustrative : Typical distribution of weight loss response to
obesity therapy Our Focus:
Responders
Non-responders discontinue
drug therapy |
 NB32 Responders
Achieved Significant Weight Loss
5 -
<10
%
-16 lbs
10 -
<15
%
-27 lbs
15
%
-43 lbs
0 –
<5
%
-6 lbs
COR-I and COR-II Responders
Represents one year data for responders (patients with
5% weight loss at week 16)
|
 Combining NB32
with Behavioral Modification Drives Better Results
COR-I and COR-II Responders
COR-BMOD Responders
In COR-BMOD, 47% of responders
completing one year of treatment lost at
least 15% of body weight.
Represents
one
year
data
for
responders
(patients
with
5%
weight
loss
at
week
16)
-43 lbs
-6 lbs
-16 lbs
5 -
<10
%
10 -
<15
%
-27 lbs
15
%
-7 lbs
-18 lbs
5 -
<10
%
10 -
<15
%
-27 lbs
-45 lbs
15
%
0 –
<5
%
0 –
<5
% |
 NB32 Well
Established Safety Profile Safety profile consistent with bupropion and naltrexone
labels
Well tolerated in Phase 3 trials
Most common AEs:
–
Mild to moderate and transient nausea during dose escalation
–
Low frequency reports of dry mouth, headache, dizziness,
insomnia
Phase 3 SAEs infrequent and similar to placebo
15 |
 The Light Study
Will Supplement the NB32 Profile with Cardiovascular Outcomes Data
16
Light Study Randomized Approximately 8,900 Patients
With History of CV Disease or Diabetes + CV Risk Factors
Primary endpoint is ITT analysis of MACE (MI, stroke, CV death)
Real-world
test
-
long
term
exposure
to
study
drug
only
in
patients
demonstrating
early
potential
to
benefit from therapy
WEEK -2
DAY 1
Lead-in
Placebo + WeightMate™
NB32 + WeightMate™
WEEK 16
Treatment Period
~8,900
patients
randomized
Evaluation of
appropriateness of treatment
Interim analysis after 87 events
Trial continues blinded to final analysis |
 Light Study
Interim Analysis Met Goal Set by FDA and Clearly Satisfied CRL
17
Category
Criteria
Result
CV Outcomes
Interim Analysis to Rule out excess
cardiovascular risk (H/R < 2.0, 95% CI)
Overall Safety
No new safety signals observed |
 Orexigen is
Confident Light Study Interim Results Support a Favorable Benefit : Risk Assessment
18
Time to first occurrence of MACE, the primary endpoint
Time to first occurrence of the three components of MACE: non fatal
heart attack, non fatal stroke, and cardiovascular death
Death from any cause
Unstable angina requiring hospitalization
Coronary revascularization procedures
Blood pressure, heart rate, waist circumference, and body weight
Use of concomitant medications
Extensive comparisons to placebo regarding treatment emergent
serious adverse events
New information provided by Light Study includes: |
 19
Source: Table 4,5, and 6, DMC Summary Report of Light Study interim analysis * Numbers are
rounded Characteristics
Mean
All*
(N=8905)
Average age (years)
61
Gender (M/F)
45.5 / 54.5%
Race
White
7436
Other races/not reported
1466
BMI (kg/m
)
37
Current Tobacco Smoker
800
History of Depression
2000
Use of SSRI
1400
Use of other antidepressants
700
All Diabetes (T2DM)
7600
All Cardiovascular Disease
2900
Diabetes and CV Disease
1500
Diabetes without CV Disease
6000
CVD without Diabetes
1300
History of Hypertension and using BP lowering meds
8300
Dyslipidemia and using lipid lower meds
8200
Light Study Data are Generalizable to the Broader
Obese Population
2 |
 Orexigen
Confident in Prospects for US and EU Approvals in 2014
Filings contain an unprecedented amount of pre-approval
cardiovascular outcomes information for an obesity therapeutic
June 10, 2014 PDUFA date
Anticipated European approval year end 2014*
20
Q4 2013
Q1 2014
Q2 2014
Q3 2014
DMC Report
Submit CVOT CSR to NDA
NDA Resubmission: FDA Review
PDUFA Action Date
MAA Submission: CHMP Review
Submit MAA (4 Oct)
Day 0
Day 120
List of Questions
Day 180
Opinion
or List of
Outstanding
Issues
Day 210
CHMP
Opinion
* Assumes 3 month clock stop at day 120 |
 NB32 Poised for
Commercial Success 21
Skilled partner with heavy resourcing
Differentiated product profile
Unmet need / limited competition
Large, growing market
>
>
>
> |
 Robust Market
Research Shows NB32 Preferred for Important Patient Groups
NB32 had high preference share and/or willingness to
prescribe among
–
Women
–
Obese patients with depression
–
Obese patients with diabetes
–
Obese patients reporting issues with food cravings and eating
control
Market research demonstrates importance of overall
product profile
–
Efficacy, safety, tolerability, abuse liability, teratogenicity
22
Source: Orexigen market research |
 Majority of
Obesity Prescriptions go to Women 23
Age (years)
Source: Orexigen market research; IMS Health, National Disease and Therapeutic
Index 0
500
1,000
1,500
2,000
2,500
3,000
0-19
20-39
40-59
60-64
65+
Female
Male |
 Preference Share
Separated in Favor of NB32 for Women
24
Product preference for male vs. female patients
NB32
Qsymia
Belviq
Source: Orexigen quantitative research, 2012
MALE
FEMALE
20
%
30
%
40
%
Sex
39.9%
28.1%
32.0%
32.5%
34.8%
32.7% |
 Obese Population
Often has Co-morbid Depression or is on Antidepressants
Physicians report that
approximately 1/3 of obese
patients are diagnosed and/or
treated for depression
Another 1/3 of obese patients
display signs and symptoms of
untreated depression
The probability of moderate/severe
depressive symptoms and major
depression increased progressively,
beginning at BMI of 30
Bupropion is a commonly used
antidepressant in the obese
population
25
Source: Orexigen quantitative market research 2009 Obesity (2010) 18:347-353
Antidepressants in Obese Population
74%
71%
69%
64%
59%
55%
28%
7%
5%
6%
0%
25%
50%
75%
Depressed
(diagnosed/
treated)
Depressed
(signs and
symptoms)
Not depressed |
 High Willingness
To Prescribe NB32 for Obese Patients With Co-morbid Depression
26
Utilization intent measures
indicate 92%
of physicians
would be willing to prescribe
NB32 to obese patients who:
–
Display
depressive
symptoms
but
–
Are not on an antidepressant
Utilization intent measures indicate
72%
of physicians would be
willing to prescribe NB32 to obese
patients who:
–
Display
depressive
symptoms
and
–
Are on an antidepressant
Willingness to prescribe NB32
Willingness to prescribe NB32
YES
92%
YES
72%
Source: Orexigen quantitative market research |
 Obesity Viewed
as a Driver of Diabetes 27
Obesity is increasing globally -
a key factor driving
diabetes rates
Rates of obesity have risen dramatically worldwide
and in the United States over the past several decades
Diabetes costs in the US are $245 billion annually up
41% from 2007 to 2012
41
%
79m
Americans
have
prediabetes
26m
Americans
have
diabetes
~$500B within
a decade
diabetes
rates
Modest weight loss shown to significantly reduce the risk of
progression to diabetes and cardiometabolic risk factors
$245 |
 New Market
Research Suggests Strong Physician Interest in NB32 For Obese Patients with Co-morbid
Diabetes or Prediabetes
500 physicians
-
200 Primary Care physicians
-
200 OB/GYN physicians
-
100 Endocrinologists
Both users and non-users of anti-obesity agents were surveyed
Profile derived from the submitted NB32 label
30 minute computer administered quantitative internet survey
28
Source: Orexigen market research; November – December 2013 |
 Nearly 60% of
all Obese Patients have Diabetes or Prediabetes
29
Source: National Diabetes Fact Sheet, 2011; 2010 National Health and Nutrition
Survey US
Obesity
Distribution
-
2010
33.1m
35.7m
9.4m
Total Obese Patients = 78.2 Million
Obese Patients with Diabetes or
Prediabetes = 45.1m or 58%
Obese With
Diabetes
Obese with
Prediabetes
Obese Without
Diabetes or
Prediabetes |
 Use of Obesity
Therapeutics in These Groups Expected to Increase Significantly in Next Five
Years
30
Treatment of
Obese Patients with Diabetes
Treatment of
Obese Patients with Prediabetes
Future Patients
Current Patients
Future Patients
Current Patients
0
10
20
30
40
50
60
70
4X
Increase
0
5
10
15
20
25
30
35
4.6X
Increase
Source: Orexigen NB32 Market Research – 2013; Note: Future estimates of treatment reflect
physician’s reaction to full exposure to diabetes and prediabetes treatment concepts
|
 Strong Interest
in Prescribing NB32 for Obesity in Patients with Diabetes or Prediabetes
31
9.4m US Obese Patients With Diabetes
% Physicians
Interested
in Prescribing
% of Patients Likely
to be Prescribed
NB32
% Physicians
Interested in
Prescribing
% of Patients Likely
to be Prescribed
NB32
Source:
Orexigen
NB32
Market
Research
–
2013
71%
39%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
77%
41%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
35.7m US Obese Patients With Prediabetes |
 Key Factors
Influencing Physicians to Prescribe NB32 for Obesity in Patients with Diabetes or
Prediabetes 32
Overall Product Profile Impacts Likelihood to Prescribe
Efficacy:
High
proportion
of
patients
losing
5%
or
10%
body weight
Combining treatment with behavioral modification
dramatically increased weight loss response
MOA: Reduces appetite, increases metabolism, & may help
control cravings
Significantly reduced HbA1c (0.6%) and improved glycemic
control and improved cardiovascular risk factors
No abuse liability, not DEA scheduled
Source: Orexigen NB32 Market Research – 2013 |
 Faster Adoption
Expected in Obese Patients with Diabetes or Prediabetes
33
NB32 Estimated Adoption by Patient Type
Experimental
Basis
Use as soon as
approved
After most of my
colleagues have tried
Use after a few
colleagues have tried
All patients
Obese patients with diabetes or prediabetes*
0%
100%
Source: Orexigen NB32 Diabetes Opportunity Market Research – 2013, Orexigen NB32 Market
Research 2012 |
 NB32 Potential
Lifecycle Opportunities Diabetes-Obesity Fixed Dose Combination: Completed
formulation work for human bioequivalence studies
(NB32 + DPP4)
Potential for diabetes indication
–
In COR-Diabetes, NB32 demonstrated placebo corrected A1C
reductions of as much a 0.7%*
–
Single additional 26 week study in patients on stable diabetes
therapy could garner new indication
–
Light Study design expected to be adequate for diabetes guidance
Smoking cessation without weight gain
34
* Before rescue medications |
 Strong
Partnership with Takeda
35
$50M upfront payment
20 –
35% tiered royalty on net sales
$1 billion potential milestones, including $100M between
approval and launch
Takeda covers all commercialization costs
Takeda shares in post approval clinical development costs
Orexigen retains a right to co-promote which survives change of control
Multi-year contractual commercial commitments provide right
resources, alignment and incentives for successful NB32 launch
Primary detail equivalents (sales calls)
Marketing spend
Sales force compensation structure |
 Takeda
Commercial Expertise and Resources Across All
Commercial Functions
36
Integrated
Launch
Execution
Channel Fill
Strategy
Professional
Strategy
Sales
Strategy
Managed
Market
Strategy
Patient
Strategy |
 Targeting
Optimal Physician Audiences with Skill and Scale
for Successful Launch
Takeda has 2,000+ field personnel in the US
Assuming approval, an appropriate number of them will detail NB32 to
provide the reach and frequency required to effectively launch a
product in primary care
Takeda’s
size and commitments to NB32 will deliver MARKET
LEADING reach and frequency levels
Sales force effort will be fully supported by Takeda’s integrated
infrastructure including a comprehensive Managed Care effort
Takeda has deep experience in diabetes with Actos and the recently
launched Nesina family of products
37 |
 From Q3 2012
– Q2 2013, ~40% of branded obesity therapeutics claims
were covered for patients with commercial insurance
Medicare now covers obesity counseling; legislation introduced to cover
obesity therapeutics
Public policy pressure and legislative efforts are increasing to
address the
obesity epidemic
Working with payors and employers to increase access and coverage are
strengths of Takeda
Many managed Care Companies now have >50% Coverage for Branded
Obesity Therapeutics
Access and Coverage are Increasing
Sources: Amundsen 2013; Medicare.gov
(http://www.medicare.gov/coverage/obesity-screening-and-counseling.html);HR 2415, Treat and Reduce Obesity Act 2013 |
 EU and ROW
Opportunity for Obesity Therapeutics is Large
39
Historic Worldwide Anti-Obesity Sales in 2007
Historic Anti-Obesity Sales in 2007 ~ $1.7 billion
Source: IMS
US
19%
Europe
35%
ROW
46% |
 Rates of Obesity
Have Risen Dramatically in Several Key Regions Over the Past Several
Decades
40
Source: EuroMonitor, 2010; WHO Statistics
All sales are from2007 in $ USD (Millions)
millions of people
BRAZIL
$130.4
28.2m
26.9m
6.4m
4.8m
2010
2020
42.0m
25.4m
$48.8
RUSSIA
2010
2020
S. KOREA
$74.2
2010
2020
7.5m
5.0m
AUS
$53.5
33
%
65
%
50
%
5
%
2010
2020 |
 Orexigen
Financial Position is Strong 41
Revenue drivers
$100M in milestones to Orexigen between approval and first
commercial sale
Tiered royalties of 20-35% on net sales in North America
Potential sales milestones up to $880M
Proceeds from potential ROW partnership
Expenses
Corporate: Orexigen runs lean with ~50 employees
Takeda pays for all commercialization costs
Post
approval
development
–
Takeda
responsible
for
majority
of
costs
Cash
~$177M in cash, cash equivalents and marketable securities
(unaudited 12.31.13 balance) |
 Near Term
Catalysts and Financial Strength Position Orexigen for Transformational Year
42
Potential Key Catalysts for 2014
ROW partnership progress
EU approval
US launch
US approval |
 |