Attached files
| file | filename |
|---|---|
| EX-21 - LIST OF SUBSIDIARIES - RadNet, Inc. | radnet_10ka2-ex21.htm |
| EX-23.1 - CONSENT - RadNet, Inc. | radnet_10ka2-ex2301.htm |
| EX-32.2 - CERTIFICATIONS - RadNet, Inc. | radnet_10ka2-ex3202.htm |
| EX-23.2 - CONSENT - RadNet, Inc. | radnet_10ka2-ex2302.htm |
| EX-32.1 - CERTIFICATIONS - RadNet, Inc. | radnet_10ka2-ex3201.htm |
| EX-31.1 - CERTIFICATIONS - RadNet, Inc. | radnet_10ka2-ex3101.htm |
| EX-31.2 - CERTIFICATIONS - RadNet, Inc. | radnet_10ka2-ex3102.htm |
| EXCEL - IDEA: XBRL DOCUMENT - RadNet, Inc. | Financial_Report.xls |
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington D.C. 20549
FORM 10-K/A
AMENDMENT NO. 2
ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
For the fiscal year ended December 31, 2012
Commission File Number 001-33307
RadNet, Inc.
(Exact name of registrant as specified in charter)
| Delaware | 13-3326724 |
|
(State or other jurisdiction of incorporation or organization) |
(I.R.S. Employer Identification No.) |
| 1510 Cotner Avenue | |
| Los Angeles, California | 90025 |
| (Address of principal executive offices) | (Zip Code) |
Registrant’s telephone number, including area code: (310) 478-7808
Securities registered pursuant to Section 12(b) of the Act:
| Title of Each Class | Name of each exchange on which registered |
| Common Stock, $.0001 par value | NASDAQ Global Market |
Securities registered pursuant to Section 12(g) of the Act: None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ¨ No x
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) or the act. Yes ¨ No x
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities and Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes x No ¨
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Website, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes x No ¨
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. x
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See the definitions of “large accelerated filer,” “accelerated filer” and “smaller reporting company” in Rule 12b-2 of the Exchange Act.
| Large Accelerated Filer ¨ | Accelerated Filer x | ||
| Non-Accelerated Filer ¨ (Do not check if a smaller reporting company) | Smaller Reporting Company ¨ |
Indicate by check mark whether the registrant is a shell company (as defined in Exchange Act Rule 12b-2). Yes ¨ No x
The aggregate market value of the registrant’s common stock held by non-affiliates of the registrant was approximately $81,917,304 on June 29, 2012 (the last business day of the registrant’s most recently completed second quarter) based on the closing price for the common stock on the NASDAQ Global Market on June 29, 2012.
The number of shares of the registrant’s common stock outstanding on March 8, 2013, was 38,990,482 shares.
DOCUMENTS INCORPORATED BY REFERENCE
The information required by Part III of the Form 10-K, to the extent not set forth herein, is incorporated herein by reference from the registrant’s definitive proxy statement for the Annual Meeting of Stockholders, to be filed with the Securities and Exchange Commission pursuant to Regulation 14A not later than 120 days after the close of the registrant’s fiscal year.
EXPLANATORY NOTE
This Amendment No. 2 on Form 10-K/A (“Amendment No. 2) amends our Annual Report on Form 10-K for the fiscal year ended December 31, 2012 of RadNet, Inc. (the “Company”), originally filed with the U.S. Securities and Exchange Commission on March 18, 2013 (the "Original Filing"), as amended on April 1, 2013 by that certain Amendment No. 1 to the Original Filing which includes the information required to comply with Rule 3-09 of Regulation S-X (“Amendment No. 1” and together with the Original Filing, the “Amended Original Filing”). On November 8, 2013, the Company filed a Current Report on Form 8-K to disclose that the Company had overstated certain deferred tax assets in the financial statements included in the Original Filing and that the Company would be restating those financial statements. Accordingly, this Amendment No. 2 is being filed to reflect certain adjustments to the Company’s consolidated financial statements for the year ended December 31, 2012 with respect to the impact of an overstatement of a deferred tax asset associated with the Company’s interest rate swaps. The impact of the restatement is more fully described in Note 1A to the Consolidated Financial Statements contained in this Amendment No. 2. In addition to the adjustments in the Company’s consolidated financial statements, this Amendment No. 2 also includes a correction to the report of the independent registered public accounting firm that was included in Item 8 of Amendment No. 1 concerning the financial statements of certain unconsolidated joint ventures in which the Company holds equity interests of 50% or less. No other changes have been made to Amendment No. 1.
This Amendment No 2. is intended to supersede, and replace in its entirety, the Amended Original Filing. This Amendment No. 2 amends and restates in their entirety Items 6, 7, 8 and 9A of Part II and Item 15 of Part IV of the Amended Original Filing, and no other information included in the Amended Original Filing has been amended. Accordingly, this Amendment No. 2 should be read in conjunction with the Company’s filings made with the Securities and Exchange Commission subsequent to the filing of the Original Filing.
| 2 |
RADNET, INC.
TABLE OF CONTENTS
| FORM 10-K ITEM | PAGE | |
| PART I. | ||
| Item 1. | Business | 4 |
| Item 1A. | Risk Factors | 22 |
| Item 1B. | Unresolved Staff Comments | 32 |
| Item 2. | Properties | 32 |
| Item 3. | Legal Proceedings | 32 |
| Item 4. | Mine Safety Disclosures. | 32 |
| PART II. | ||
| Item 5. | Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities | 33 |
| Item 6. | Selected Consolidated Financial Data | 35 |
| Item 7. | Management’s Discussion and Analysis of Financial Condition and Results of Operations | 36 |
| Item 7A. | Quantitative and Qualitative Disclosures About Market Risk | 51 |
| Item 8. | Financial Statements and Supplementary Data | 51 |
| Item 9. | Changes in and Disagreements with Accountants on Accounting and Financial Disclosure | 105 |
| Item 9A. | Controls and Procedures | 105 |
| Item 9B. | Other Information | 108 |
| PART III. | ||
| Item 10. | Directors, Executive Officers and Corporate Governance | 108 |
| Item 11. | Executive Compensation | 108 |
| Item 12. | Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters | 108 |
| Item 13. | Certain Relationships and Related Transactions, and Director Independence | 108 |
| Item 14. | Principal Accountant Fees and Services | 108 |
| PART IV. | ||
| Item 15. | Exhibits and Financial Statement Schedules | 109 |
Cautionary Note Regarding Forward-Looking Statements
This annual report contains forward-looking statements within the meaning of Section 27A of the Securities Act of 1933, as amended and Section 21E of the Securities Exchange Act of 1934, as amended. Forward-looking statements reflect current views about future events and are based on our currently available financial, economic and competitive data and on current business plans. Actual events or results may differ materially depending on risks and uncertainties that may affect our operations, markets, services, prices and other factors.
Statements in this annual report concerning our ability to successfully acquire and integrate new operations, to grow our contract management business, our financial guidance, our future cost saving efforts, our increased business from new equipment or operations and our ability to finance our operations are forward-looking statements. In some cases, you can identify forward-looking statements by terminology such as “may,” “will,” “should,” “expect,” “intend,” “plan,” “anticipate,” “believe,” “estimate,” “predict,” “potential,” “continue,” “assumption” or the negative of these terms or other comparable terminology.
Forward-looking statements involve known and unknown risks, uncertainties and other factors that may cause our actual results, levels of activity, performance or achievements to be materially different from any future results, levels of activity, performance or achievements expressed or implied by these forward-looking statements. These risks include those factors listed in Item 1 — “Business,” Item 1A— “Risk Factors,” Item 3— “Legal Proceedings,” Item 7 — “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and elsewhere in this annual report and in other reports that we file with the Securities and Exchange Commission.
We do not undertake any responsibility to release publicly any revisions to these forward-looking statements to take into account events or circumstances that occur after the date of this annual report. Additionally, we do not undertake any responsibility to update you on the occurrence of any unanticipated events which may cause actual results to differ from those expressed or implied by the forward-looking statements contained in this annual report.
| 3 |
PART I
| Item 1. | Business |
Business Overview
We are the leading national provider of freestanding, fixed-site outpatient diagnostic imaging services in the United States based on number of locations and annual imaging revenue. At December 31, 2012, we operated directly or indirectly through joint ventures, 246 centers located in California, Maryland, Florida, Delaware, New Jersey, Rhode Island and New York. Our centers provide physicians with imaging capabilities to facilitate the diagnosis and treatment of diseases and disorders and may reduce unnecessary invasive procedures, often reducing the cost and amount of care for patients. Our services include magnetic resonance imaging (MRI), computed tomography (CT), positron emission tomography (PET), nuclear medicine, mammography, ultrasound, diagnostic radiology (X-ray), fluoroscopy and other related procedures. The vast majority of our centers offer multi-modality imaging services, a key point of differentiation from our competitors. Our multi-modality strategy diversifies revenue streams, reduces exposure to reimbursement changes and provides patients and referring physicians one location to serve the needs of multiple procedures.
We seek to develop leading positions in regional markets in order to leverage operational efficiencies. Our scale and density within selected geographies provides close, long-term relationships with key payors, radiology groups and referring physicians. Each of our center-level and regional operations teams is responsible for managing relationships with local physicians and payors, meeting our standards of patient service and maintaining profitability. We provide training programs, standardized policies and procedures and sharing of best practices among the physicians in our regional networks.
In late 2010 and early 2011 we expanded our offering of imaging related services with our acquisition of eRAD and Imaging On Call. eRAD develops and sells computerized systems for the imaging industry, including Picture Archiving Communications Systems (“PACS”) and Radiology Information Systems (“RIS”). Imaging On Call provides teleradiology services for remote interpretation of images on behalf of radiology groups, hospitals and imaging center customers. Teleradiology is the process of taking radiological patient images, such as X-rays, CTs, and MRIs, from one location to another for the purposes of interpretation and/or consultation. Teleradiology allows radiologists to provide services without actually having to be at the location of the patient and allows trained specialists to be available 24/7. In addition to providing alternative revenue sources for us, the capabilities of both eRAD and Imaging On Call can make the RadNet imaging center operations more efficient and cost effective.
We derive substantially all of our revenue from fees charged for the diagnostic imaging services performed at our facilities. For the years ended December 31, 2012, 2011 and 2010, we performed 4,142,267 , 3,740,443 and 3,315,019 diagnostic imaging procedures and generated net revenue of $647.2 million , $585.1 million and $518.7 million, respectively . Additional information concerning RadNet, Inc., including our consolidated subsidiaries, for each of the years ended December 31, 2012, December 31, 2011 and December 31, 2010 is included in the consolidated financial statements and notes thereto in this annual report.
We typically experience some seasonality to our business. During the first quarter of each year we generally experience the lowest volumes of procedures and the lowest level of revenue for any quarter during the year. This is primarily the result of two factors. First, our volumes and revenue are typically impacted by winter weather conditions in our northeastern operations. It is common for snowstorms and other inclement weather to result in patient appointment cancellations and, in some cases, imaging center closures. Second, in recent years, we have observed greater participation in high deductible health plans by patients. As these high deductibles reset in January for most of these patients, we have observed that patients utilize medical services less during the first quarter, when securing medical care will result in significant out-of-pocket expenditures.
History of our Business
We are incorporated in Delaware and have been in business since 1985.
We develop our medical imaging business through a combination of organic growth and acquisitions. For a discussion of acquisitions, see Item 7 - “Management’s Discussion and Analysis and Results of Operations—Recent Developments and Facility Acquisitions” below.
In addition to our imaging business, our eRAD, Inc. subsidiary (see Note 4 to the consolidated financial statements to this annual report) is a provider of Picture Archiving and Communications Systems (PACS) and related workflow solutions to the radiology industry. Over 250 hospitals, teleradiology businesses, imaging centers and specialty physician groups use eRAD’s technology to distribute, visualize, store and retrieve digital images taken from all diagnostic imaging modalities. eRAD has approximately 30 employees, including a Research and Development team of 11 software engineers in Budapest, Hungary.
We have also assembled an industry leading team of software developers, based out of Prince Edward Island, Canada, to create radiology workflow solutions known as Radiology Information Systems (“RIS”) focused exclusively on RadNet’s internal use. All members of this Canadian based team have significant software development expertise in radiology, and together with eRAD and its PACS technology, are creating fully integrated solutions to manage all aspects of RadNet’s internal information needs. eRAD and the Canadian software development team form a Radiology Information Technology division of RadNet.
| 4 |
In January 2011, we entered into a new line of business with the acquisition of Imaging On Call, LLC, a provider of teleradiology services to radiology groups, hospitals and imaging centers located in Poughkeepsie, New York. The addition of the teleradiology business added a new component to our portfolio of solutions, whereby we provide interpretation services to approximately 50 hospitals and hospital-based radiology groups.
References to “RadNet,” “we,” “us,” “our” or the “Company” in this report refer to RadNet, Inc., its subsidiaries and affiliated entities. See “Management’s Discussion and Analysis and Results of Operations—Overview.”
Company Website
We maintain a website at www.radnet.com . We make available, free of charge, on our website our annual report on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K and all amendments to those reports as soon as is reasonably practicable after the material is electronically filed with the Securities and Exchange Commission. References to our website in this report are provided as a convenience and do not constitute, and should not be viewed as, an incorporation by reference of the information contained on, or available through, the website. Therefore, such information should not be considered part of this report.
Industry Overview
Diagnostic imaging involves the use of non-invasive procedures to generate representations of internal anatomy and function that can be recorded on film or digitized for display on a video monitor. Diagnostic imaging procedures facilitate the early diagnosis and treatment of diseases and disorders and may reduce unnecessary invasive procedures, often minimizing the cost and amount of care for patients. Diagnostic imaging procedures include MRI, CT, PET, nuclear medicine, ultrasound, mammography, X-ray and fluoroscopy. We estimate that the national imaging market in the United States is $100 billion annually, with projected mid-single digit growth for MRI, CT and PET/CT over the next several years, driven by the aging of the U.S. population, wider physician and payor acceptance for imaging technologies, and greater consumer and physician awareness of diagnostic screening capabilities.
While X-ray remains the most commonly performed diagnostic imaging procedure, the fastest growing and higher margin procedures are MRI, CT and PET. The rapid growth in PET scans is attributable to the increasing recognition of the efficacy of PET scans in the diagnosis and monitoring of cancer. The number of MRI and CT scans performed annual in the United States continues to grow due to their wider acceptance by physicians and payors, an increasing number of applications for their use and a general increase in demand due to the aging population.
Diagnostic Imaging Settings
Diagnostic imaging services are typically provided in one of the following settings:
Fixed-site, freestanding outpatient diagnostic facilities
These facilities range from single-modality to multi-modality facilities and are generally not owned by hospitals or clinics. These facilities depend upon physician referrals for their patients and generally do not maintain dedicated, contractual relationships with hospitals or clinics. In fact, these facilities may compete with hospitals or clinics that have their own imaging systems to provide services to these patients. These facilities bill third-party payors, such as managed care organizations, insurance companies, Medicare or Medicaid. All of our facilities are in this category.
Hospitals
Many hospitals provide both inpatient and outpatient diagnostic imaging services, typically on site. These inpatient and outpatient centers are owned and operated by the hospital or clinic, or jointly by both, and are primarily used by patients of the hospital or clinic. The hospital or clinic bills third-party payors, such as managed care organizations, insurance companies, Medicare or Medicaid.
Mobile Imaging
While many hospitals own or lease their own equipment, certain hospitals provide diagnostic imaging services by contracting with providers of mobile imaging equipment. Using specially designed trailers, mobile imaging service providers transport imaging equipment and provide services to hospitals and clinics on a part-time or full-time basis, thus allowing small to mid-size hospitals and clinics that do not have the patient demand to justify fixed on-site access to advanced diagnostic imaging technology. Diagnostic imaging providers contract directly with the hospital or clinic and are typically reimbursed directly by them.
| 5 |
Diagnostic Imaging Modalities
The principal diagnostic imaging modalities we use at our facilities are:
MRI
MRI has become widely accepted as the standard diagnostic tool for a wide and fast-growing variety of clinical applications for soft tissue anatomy, such as those found in the brain, spinal cord, abdomen, heart and interior ligaments of body joints such as the knee. MRI uses a strong magnetic field in conjunction with low energy electromagnetic waves that are processed by a computer to produce high-resolution, three-dimensional, cross-sectional images of body tissue. A typical MRI examination takes from 20 to 45 minutes. MRI systems can have either open or closed designs, routinely have magnetic field strength of 0.2 Tesla to 3.0 Tesla and are priced in the range of $0.6 million to $2.5 million. As of December 31, 2012, we had 205 MRI systems in operation.
CT
CT provides higher resolution images than conventional X-rays, but generally not as well defined as those produced by MRI. CT uses a computer to direct the movement of an X-ray tube to produce multiple cross-sectional images of a particular organ or area of the body. CT is used to detect tumors and other conditions affecting bones and internal organs. It is also used to detect the occurrence of strokes, hemorrhages and infections. A typical CT examination takes from 15 to 45 minutes. CT systems are priced in the range of $0.3 million to $1.2 million. As of December 31, 2012, we had 118 CT systems in operation.
PET
PET scanning involves the administration of a radiopharmaceutical agent with a positron-emitting isotope and the measurement of the distribution of that isotope to create images for diagnostic purposes. PET scans provide the capability to determine how metabolic activity impacts other aspects of physiology in the disease process by correlating the reading for the PET with other tools such as CT or MRI. PET technology has been found highly effective and appropriate in certain clinical circumstances for the detection and assessment of tumors throughout the body, the evaluation of some cardiac conditions and the assessment of epilepsy seizure sites. The information provided by PET technology often obviates the need to perform further highly invasive or diagnostic surgical procedures. PET systems are priced in the range of $0.8 million to $2.5 million. In addition, we employ combined PET/CT systems that blend the PET and CT imaging modalities into one scanner. These combined systems are priced in the range of $1.1 million to $2.8 million. As of December 31, 2012, we had 43 PET or combination PET/CT systems in operation.
Nuclear Medicine
Nuclear medicine uses short-lived radioactive isotopes that release small amounts of radiation that can be recorded by a gamma camera and processed by a computer to produce an image of various anatomical structures or to assess the function of various organs such as the heart, kidneys, thyroid and bones. Nuclear medicine is used primarily to study anatomic and metabolic functions. Nuclear medicine systems are priced in the range of $300,000 to $400,000. As of December 31, 2012, we had 45 nuclear medicine systems in operation.
X-ray
X-rays use roentgen rays to penetrate the body and record images of organs and structures on film. Digital X-ray systems add computer image processing capability to traditional X-ray images, which provides faster transmission of images with a higher resolution and the capability to store images more cost-effectively. X-ray systems are priced in the range of $95,000 to $440,000. As of December 31, 2012, we had 253 X-ray systems in operation.
Ultrasound
Ultrasound imaging uses sound waves and their echoes to visualize and locate internal organs. It is particularly useful in viewing soft tissues that do not X-ray well. Ultrasound is used in pregnancy to avoid X-ray exposure as well as in gynecological, urologic, vascular, cardiac and breast applications. Ultrasound systems are priced in the range of $90,000 to $250,000. As of December 31, 2012, we had 357 ultrasound systems in operation.
Mammography
Mammography is a specialized form of radiology using low dosage X-rays to visualize breast tissue and is the primary screening tool for breast cancer. Mammography procedures and related services assist in the diagnosis of and treatment planning for breast cancer. Analog mammography systems are priced in the range of $70,000 to $100,000, and digital mammography systems are priced in the range of $250,000 to $400,000. As of December 31, 2012, we had 181 mammography systems in operation.
| 6 |
Fluoroscopy
Fluoroscopy uses ionizing radiation combined with a video viewing system for real time monitoring of organs. Fluoroscopy systems are priced in the range of $100,000 to $400,000. As of December 31, 2012, we had 138 fluoroscopy systems in operation.
Industry Trends
We believe the diagnostic imaging services industry will continue to grow as a result of a number of factors, including the following:
Escalating Demand for Healthcare Services from an Aging Population
Persons over the age of 65 comprise one of the fastest growing segments of the population in the United States. According to the United States Census Bureau, this group is expected to increase as much as 33% from 2010 to 2020. Because diagnostic imaging use tends to increase as a person ages, we believe the aging population will generate more demand for diagnostic imaging procedures .
New Effective Applications for Diagnostic Imaging Technology
New technological developments are expected to extend the clinical uses of diagnostic imaging technology and increase the number of scans performed. Recent technological advancements include:
| · | MRI spectroscopy, which can differentiate malignant from benign lesions; |
| · | MRI angiography, which can produce three-dimensional images of body parts and assess the status of blood vessels; |
| · | enhancements in teleradiology systems, which permit the digital transmission of radiological images from one location to another for interpretation by radiologists at remote locations; and |
| · | the development of combined PET/CT scanners, which combine the technology from PET and CT to create a powerful diagnostic imaging system. |
Additional improvements in imaging technologies, contrast agents and scan capabilities are leading to new non-invasive methods of diagnosing blockages in the heart’s vital coronary arteries, liver metastases, pelvic diseases and vascular abnormalities without exploratory surgery. We believe that the use of the diagnostic capabilities of MRI and other imaging services will continue to increase because they are cost-effective, time-efficient and non-invasive, as compared to alternative procedures, including surgery, and that newer technologies and future technological advancements will further increase the use of imaging services. At the same time, the industry has increasingly used upgrades to existing equipment to expand applications, extend the useful life of existing equipment, improve image quality, reduce image acquisition time and increase the volume of scans that can be performed. We believe this trend toward equipment upgrades rather than equipment replacements will continue, as we do not foresee new imaging technologies on the near-term horizon that will displace MRI, CT or PET as the principal advanced diagnostic imaging modalities.
Wider Physician and Payor Acceptance of the Use of Imaging
During the last 30 years, there has been a major effort undertaken by the medical and scientific communities to develop higher quality, cost-effective diagnostic imaging technologies and to minimize the risks associated with the application of these technologies. The thrust of product development during this period has largely been to reduce the hazards associated with conventional X-ray and nuclear medicine techniques and to develop new, less harmful imaging technologies. As a result, the use of advanced diagnostic imaging modalities, such as MRI, CT and PET, which provide superior image quality compared to other diagnostic imaging technologies, has increased rapidly in recent years. These advanced modalities allow physicians to diagnose a wide variety of diseases and injuries quickly and accurately without exploratory surgery or other surgical or invasive procedures, which are usually more expensive, involve greater risk to patients and result in longer rehabilitation time. Because advanced imaging systems are increasingly seen as a tool for reducing long-term healthcare costs, they are gaining wider acceptance among payors.
| 7 |
Greater Consumer Awareness of and Demand for Preventive Diagnostic Screening
Diagnostic imaging, such as elective full-body scans, is increasingly being used as a screening tool for preventive care procedures. Consumer awareness of diagnostic imaging as a less invasive and preventive screening method has added to the growth in diagnostic imaging procedures. We believe that further technological advancements allowing for early diagnosis of diseases and disorders using less invasive procedures will create additional demand for diagnostic imaging.
Expansion of Teleradiology Services
As hiring radiologists has become more difficult, the use of teleradiology is expected to continue to expand to provide patients better, more specialized care and 24/7 services.
Our Competitive Strengths
Our Scale and Position as the Largest Provider of Freestanding, Fixed-site Outpatient Diagnostic Imaging Services in the United States, Based on Number of Centers and Revenue
As of December 31, 2012, we operated 246 centers in California, Maryland, Florida, Delaware, New Jersey, Rhode Island and New York. Our size and scale allow us to achieve operating, sourcing and administrative efficiencies, including equipment and medical supply sourcing savings and favorable maintenance contracts from equipment manufacturers and other suppliers. Our specific knowledge of our geographic markets drives strong relationships with key payors, radiology groups and referring physicians within our markets.
Our Comprehensive "Multi-Modality" Diagnostic Imaging Offering
The vast majority of our centers offer multi-modality procedures, driving strong relationships with referring physicians and payors in our markets and a diversified revenue base. At each of our multi-modality facilities, we offer patients and referring physicians one location to serve their needs for multiple procedures. Furthermore, we have complemented many of our multi-modality sites with single-modality sites to accommodate overflow and to provide a full range of services within a local area consistent with demand. This prevents multiple patient visits or unnecessary travel between facilities, thereby increasing patient throughput and decreasing costs and time delays. Our revenue is generated by a broad mix of modalities. We believe our multi-modality strategy lessens our exposure to reimbursement changes in any specific modality.
Our Competitive Pricing
We believe our fees are generally lower than hospital fees for the services we provide.
Our Facility Density in Many Highly Populated Areas of the United States
The strategic organization of our diagnostic imaging facilities into regional networks concentrated in major population centers in seven states offers unique benefits to our patients, our referring physicians, our payors and us. We are able to increase the convenience of our services to patients by implementing scheduling systems within geographic regions, where practical. For example, many of our diagnostic imaging facilities within a particular region can access the patient appointment calendars of other facilities within the same regional network to efficiently allocate time available and to meet a patient's appointment, date, time, or location preferences. The grouping of our facilities within regional networks enables us to easily move technologists and other personnel, as well as equipment, from under-utilized to over-utilized facilities on an as-needed basis, and drive referrals. Our organization of referral networks results in increased patient throughput, greater operating efficiencies, better equipment utilization rates and improved response time for our patients. We believe our networks of facilities and tailored service offerings for geographic areas drives local physician referrals, makes us an attractive candidate for selection as a preferred provider by third-party payors, creates economies of scale and provides barriers to entry by competitors in our markets.
Our Strong Relationships with Payors and Diversified Payor Mix
Our revenue is derived from a diverse mix of payors, including private payors, managed care capitated payors and government payors, which should mitigate our exposure to possible unfavorable reimbursement trends within any one payor class. In addition, our experience with capitation arrangements over the last several years has provided us with the expertise to manage utilization and pricing effectively, resulting in a predictable and recurring stream of revenue. We believe that third-party payors representing large groups of patients often prefer to enter into managed care contracts with providers that offer a broad array of diagnostic imaging services at convenient locations throughout a geographic area. As of December 31, 2012, we received approximately 56% of our payments from commercial insurance payors, 13% from managed care capitated payors, 21% from Medicare and 3% from Medicaid. With the exception of Blue Cross/Blue Shield, which are managed by different entities in each of the states in which we operate, and Medicare, no single payor accounted for more than 5% of our net revenue for the twelve months ended December 31, 2012.
| 8 |
Our Strong Relationships with Experienced and Highly Regarded Radiologists
Our contracted radiologists have outstanding credentials, strong relationships with referring physicians, and a broad mix of sub-specialties. The collective experience and expertise of these radiologists translates into more accurate and efficient service to patients. Our close relationship with Howard G. Berger, M.D., our President and Chief Executive Officer, and Beverly Radiology Medical Group (“BRMG”) in California and our long-term arrangements with radiologists outside of California enable us to better ensure that medical service provided at our facilities is consistent with the needs and expectations of our referring physicians, patients and payors.
Our Experienced and Committed Management Team
Our senior management group has more than 100 years of combined healthcare management experience. Our executive management team has created our differentiated approach based on their comprehensive understanding of the diagnostic imaging industry and the dynamics of our regional markets. We have a track record of successful acquisitions and integration of acquired businesses into RadNet, and have managed the business through a variety of economic and reimbursement cycles. Our management beneficially owns (either directly or indirectly) approximately 28% of our common stock.
Our Technologically Advanced Imaging Systems
In late 2010 and early 2011 we expanded our offering of imaging related services with our acquisition of eRad (development and sale of computerized imaging systems for the imaging industry) and Imaging On Call (teleradiology services for interpretation of images for radiology groups, hospitals and others after business hours, for overflow and specialty work). In addition, we have assembled an industry leading team of software developers to create radiology workflow solutions for our internal use.
Business Strategy
Maximize Performance at Our Existing Facilities
We intend to enhance our operations and increase scan volume and revenue at our existing facilities by expanding physician relationships and increasing the procedure offerings.
Expansion Into Related Businesses
With our acquisition of eRad we entered the business of development and sale of software systems essential to the imaging business. Similarly, with our acquisition of Imaging On Call on January 3, 2011, we entered the teleradiology business. We intend to regularly evaluate potential acquisitions of other businesses to the extent they complement our imaging business.
Focus on Profitable Contracting
We regularly evaluate our contracts with third-party payors, industry vendors and radiology groups, as well as our equipment and real property leases, to determine how we may improve the terms to increase our revenues and reduce our expenses. Because many of our contracts with third party payors are short-term in nature, we can regularly renegotiate these contracts, if necessary. We believe our position as a leading provider of diagnostic imaging services and our long-term relationships with physician groups in our markets enable us to obtain more favorable contract terms than would be available to smaller or less experienced imaging services providers.
Expand MRI, CT and PET Applications
We intend to continue to use expanding MRI, CT and PET applications as they become commercially available. Most of these applications can be performed by our existing MRI, CT and PET systems with upgrades to software and hardware, thereby minimizing capital expenditure requirements. We intend to introduce applications that will decrease scan and image-reading time and increase our productivity.
| 9 |
Optimize Operating Efficiencies
We intend to maximize our equipment utilization by adding, upgrading and re-deploying equipment where we experience excess demand. We will continue to trim excess operating and general and administrative costs where it is feasible to do so. We may also continue to use, where appropriate, highly trained radiology physician assistants to perform, under appropriate supervision of radiologists, basic services traditionally performed by radiologists. We will continue to upgrade our advanced information technology system to create cost reductions for our facilities in areas such as image storage, support personnel and financial management.
Expand Our Networks
We intend to continue to expand the number of our facilities both organically and through targeted acquisitions, using a disciplined approach for evaluating and entering new areas, including consideration of whether we have adequate financial resources to expand. Our current plans are to strengthen our market presence in geographic areas where we currently have existing operations and to expand into neighboring and other areas which we determine to be appropriate. We perform extensive due diligence before developing a new facility or acquiring an existing facility, including surveying local referral sources and radiologists, as well as examining the demographics, reimbursement environment, competitive landscape and intrinsic demand of the geographic market. We generally will only enter new markets where:
| · | there is sufficient patient demand for outpatient diagnostic imaging services; |
| · | we believe we can gain significant market share; |
| · | we can build key referral relationships or we have already established such relationships; and |
| · | payors are receptive to our entry into the market. |
Our Services
We offer a comprehensive set of imaging services including MRI, CT, PET, nuclear medicine, X-ray, ultrasound, mammography, fluoroscopy and other related procedures. We focus on providing standardized high quality imaging services, regardless of location, to ensure patients, physicians and payors consistency in service and quality. To ensure the high quality of our services, we monitor patient satisfaction, timeliness of services to patients and reports to physicians.
The key features of our services include:
| · | patient-friendly, non-clinical environments; |
| · | a 24-hour turnaround on routine examinations; |
| · | interpretations within one to two hours, if needed; |
| · | flexible patient scheduling, including same-day appointments; |
| · | extended operating hours, including weekends; |
| · | reports delivered by courier, facsimile or email; |
| · | availability of second opinions and consultations; |
| · | availability of sub-specialty interpretations at no additional charge; and |
| · | standardized fee schedules by region. |
| 10 |
Radiology Professionals
In the states in which we provide services (except Florida), a lay person or any entity other than a professional corporation or similar professional organization is not allowed to practice medicine, including by employing professional persons or by having any ownership interest or profit participation in or control over any medical professional practice. This doctrine is commonly referred to as the prohibition on the “corporate practice” of medicine. In order to comply with this prohibition, we contract with radiologists to provide professional medical services in our facilities, including the supervision and interpretation of diagnostic imaging procedures. The radiology practice maintains full control over the physicians it employs. Pursuant to each management contract, we make available the imaging facility and all of the furniture and medical equipment at the facility for use by the radiology practice, and the practice is responsible for staffing the facility with qualified professional medical personnel. In addition, we provide management services and administration of the non-medical functions relating to the professional medical practice at the facility, including among other functions, provision of clerical and administrative personnel, bookkeeping and accounting services, billing and collection, provision of medical and office supplies, secretarial, reception and transcription services, maintenance of medical records, and advertising, marketing and promotional activities. As compensation for the services furnished under contracts with radiologists, we generally receive an agreed percentage of the medical practice billings for, or collections from, services provided at the facility, typically varying between 75% to 85% of global net service fee revenue or collections after deduction of the professional component of the medical practice billings.
At all but 8 of our California facilities, we contract for the provision of professional medical services directly with BRMG, or indirectly through BRMG with other radiology groups.
Many states have also enacted laws prohibiting a licensed professional from splitting fees derived from the practice of medicine with an unlicensed person or business entity. We do not believe that the management, administrative, technical and other non-medical services we provide to each of our contracted radiology groups violate the corporate practice of medicine prohibition or that the fees we charge for such services violate the fee splitting prohibition. However, the enforcement and interpretation of these laws by regulatory authorities and state courts vary from state to state. If our arrangements with our independent contractor radiology groups are found to violate state laws prohibiting the practice of medicine by general business corporations or fee splitting, our business, financial condition and ability to operate in those states could be adversely affected.
BRMG in California
Howard G. Berger, M.D., is our President and Chief Executive Officer, a member of our Board of Directors and is deemed to be the beneficial owner, directly and indirectly, of approximately 14.0% of our outstanding common stock as of December 31, 2012. Dr. Berger also owns, indirectly, 99% of the equity interests in BRMG. BRMG provides all of the professional medical services at 101 of our facilities located in California under a management agreement with us, and contracts with various other independent physicians and physician groups to provide the professional medical services at most of our other California facilities. We obtain professional medical services from BRMG in California, rather than provide such services directly or through subsidiaries, in order to comply with California’s prohibition against the corporate practice of medicine. However, as a result of our close relationship with Dr. Berger and BRMG, we believe that we are able to better ensure that medical service is provided at our California facilities in a manner consistent with our needs and expectations and those of our referring physicians, patients and payors than if we obtained these services from unaffiliated physician groups.
We believe that physicians are drawn to BRMG and the other radiologist groups with whom we contract by the opportunity to work with the state-of-the-art equipment we make available to them, as well as the opportunity to receive specialized training through our fellowship programs, and engage in clinical research programs, which generally are available only in university settings and major hospitals.
As of December 31, 2012, BRMG employed 83 full-time and 9 part-time radiologists. Under our management agreement with BRMG, we are paid a percentage of the amounts collected for the professional services BRMG physicians render as compensation for our services and for the use of our facilities and equipment. For the year ended December 31, 2012, this percentage was 79%. The percentage may be adjusted, if necessary, to ensure that the parties receive the fair value for the services they render. The following are the other principal terms of our management agreement with BRMG:
| · | The agreement expires on January 1, 2014. However, the agreement automatically renews for consecutive 10-year periods, unless either party delivers a notice of non-renewal to the other party no later than six months prior to the scheduled expiration date. Either party may terminate the agreement if the other party defaults under its obligations, after notice and an opportunity to cure. We may terminate the agreement if Dr. Berger no longer owns at least 60% of the equity of BRMG; as of December 31, 2012, he owned 99% of the equity of BRMG. |
| · | At its expense, BRMG employs or contracts with an adequate number of physicians necessary to provide all professional medical services at all of our California facilities, except for 8 facilities for which we contract with separate medical groups. |
| 11 |
| · | At our expense, we provide all furniture, furnishings and medical equipment located at the facilities and we manage and administer all non-medical functions at, and provide all nurses and other non-physician personnel required for the operation of, the facilities. |
| · | If BRMG wants to open a new facility, we have the right of first refusal to provide the space and services for the facility under the same terms and conditions set forth in the management agreement. |
| · | If we want to open a new facility in California, BRMG must use its best efforts to provide medical personnel under the same terms and conditions set forth in the management agreement. If BRMG cannot provide such personnel, we have the right to contract with other physicians to provide services at the facility. |
| · | BRMG must maintain medical malpractice insurance for each of its physicians with coverage limits not less than $1 million per incident and $3 million in the aggregate per year. BRMG also has agreed to indemnify us for any losses we suffer that arise out of the acts or omissions of BRMG and its employees, contractors and agents. |
Non-California Locations and 8 California Locations
At the 8 centers in California where BRMG does not provide professional medical services, and at all of the centers which are located outside of California, we have entered into long-term contracts with prominent third-party radiology groups in the area to provide physician services at those facilities. These arrangements also allow us to comply with the prohibition against the “corporate practice” of medicine in other states in which we operate (except in Florida which does not have an equivalent statute prohibiting the corporate practice of medicine).
These third-party radiology practice groups provide professional services, including supervision and interpretation of diagnostic imaging procedures, in our diagnostic imaging centers. The radiology practices maintain full control over the provision of professional services. The contracted radiology practices have outstanding physician and practice credentials and reputations; strong competitive market positions; a broad sub-specialty mix of physicians; a history of growth and potential for continued growth. In these facilities we have entered into long-term agreements (typically 10-40 years in length) under which, in addition to obtaining technical fees for the use of our diagnostic imaging equipment and the provision of technical services, we provide management services and receive a fee based on the practice group’s professional revenue. We typically receive 100% of the technical reimbursements associated with imaging procedures plus certain fees paid to us for providing additional management services. The radiology practice groups retain the professional reimbursements associated with imaging procedures after deducting management service fees paid to us.
Additionally, we perform certain management services for a portion of the professional groups with whom we contract who provide professional radiology services at local hospitals. For performing these management services, which include billing, collecting, transcription and medical coding, we receive management fees.
Payors
The fees charged for diagnostic imaging services performed at our facilities are paid by a diverse mix of payors, as illustrated for the following periods presented in the table below:
| % of Net Revenue | ||||||||||||
| Year Ended December 31, 2012 | Year Ended December 31, 2011 | Year Ended December 31, 2010 | ||||||||||
| Commercial Insurance (1)(2) | 56% | 55% | 56% | |||||||||
| Managed Care Capitated Payors | 13% | 15% | 15% | |||||||||
| Medicare& Medicaid | 24% | 23% | 23% | |||||||||
(1) Includes Blue Cross/Blue Shield plans, which represented 20% of our net service fee revenue for the year ended December 31, 2012, 19% of our net service fee revenue for the year ended December 31, 2011 and 19% of our net service fee revenue for the year ended December 31, 2010.
(2) Includes co-payments, direct patient payments and payments through contracts with physician groups and other non-insurance company payors.
We have described below the types of reimbursement arrangements we have with third-party payors.
| 12 |
Commercial Insurance
Generally, insurance companies reimburse us, directly or indirectly, including through BRMG in California or through the contracted radiology groups elsewhere, on the basis of agreed upon rates. These rates are negotiated and may differ materially with rates set forth in the Medicare Physician Fee Schedule for the particular service. The patients may be responsible for certain co-payments or deductibles.
Managed Care Capitation Agreements
Under these agreements, which are generally between BRMG in California and outside of California between the contracted radiology group (typically an independent physician group or other medical group) and the payor (which in most cases are large medical groups or Independent Practice Associations), the payor pays a pre-determined amount per-member per-month in exchange for the radiology group providing all necessary covered services to the managed care members included in the agreement. These contracts pass much of the financial risk of providing outpatient diagnostic imaging services, including the risk of over-use, from the payor to the radiology group and, as a result of our management agreement with the radiology group, to us.
We believe that through our comprehensive utilization management, or UM, program we have become highly skilled at assessing and moderating the risks associated with the capitation agreements, so that these agreements are profitable for us. Our UM program is managed by our UM department, which consists of administrative and nursing staff as well as BRMG medical staff who are actively involved with the referring physicians and payor management in both prospective and retrospective review programs. Our UM program includes the following features, all of which are designed to manage our costs while ensuring that patients receive appropriate care:
| · | Physician Education |
At the inception of a new capitation agreement, we provide the new referring physicians with binders of educational material comprised of proprietary information that we have prepared and third-party information we have compiled, which are designed to address diagnostic strategies for common diseases. We distribute additional material according to the referral practices of the group as determined in the retrospective analysis described below.
| · | Prospective Review |
Referring physicians are required to submit authorization requests for non-emergency high-intensity services: MRI, CT, special procedures and nuclear medicine studies. The UM medical staff, according to accepted practice guidelines, considers the necessity and appropriateness of each request. Notification is then sent to the imaging facility, referring physician and medical group. Appeals for cases not approved are directed to us. The capitated payor has the final authority to uphold or deny our recommendation.
| · | Retrospective Review |
We collect and sort encounter activity by payor, place of service, referring physician, exam type and date of service. The data is then presented in quantitative and analytical form to facilitate understanding of utilization activity and to provide a comparison between fee-for-service and Medicare equivalents. Our Medical Director prepares a quarterly report for each payor and referring physician. When we find that a referring physician is over utilizing services, we work with the physician to modify referral patterns.
Medicare/Medicaid
Medicare is the federal health insurance program for people age 65 or older and people under age 65 with certain disabilities. Medicaid, funded by both the federal government and states, is a state-administered health insurance program for qualifying low-income and medically needy persons. For services for which we bill Medicare directly or indirectly, including through contracted radiologists, we are paid under the Medicare Physician Fee Schedule. Medicare patients usually pay a 20% co-payment unless they have secondary insurance. Medicaid rates are set by the individual states for each state program and Medicaid patients may be responsible for a modest co-payment.
Contracts with Physician Groups and Other Non-Insurance Company Payors
For some of our contracts with physician groups and other providers, we do not bill payors, but instead accept agreed upon rates for our radiology services. These rates are typically at or below the rates set forth in the current Medicare Fee Schedule for the particular service. However, we often agree to a specified rate for MRI and CT procedures that is not tied to the Medicare Fee Schedule.
| 13 |
Facilities
Through our wholly owned subsidiaries, we operate 109 fixed-site, freestanding outpatient diagnostic imaging facilities in California, 62 in the Maryland, 25 in the Rochester and Hudson Valley areas of New York, 7 in Manhattan, New York, 15 in Delaware, 5 in Rhode Island, 19 in New Jersey, as well as 4 individual facilities in Florida. We lease the premises at which these facilities are located.
Our facilities are primarily located in geographic networks that we refer to as regions. The majority of our facilities are multi-modality sites, offering various combinations of MRI, CT, PET, nuclear medicine, ultrasound, X-ray, fluoroscopy services and other related procedures. A portion of our facilities are single-modality sites, offering either X-ray or MRI services. Consistent with our regional network strategy, we locate our single-modality facilities near multi-modality facilities, to help accommodate overflow in targeted demographic areas.
The following table sets forth the number of our facilities for each year during the five-year period ended December 31, 2012:
| Year Ended | ||||||||||||||||||||
| December 31, | ||||||||||||||||||||
| 2008 | 2009 | 2010 | 2011 | 2012 | ||||||||||||||||
| Total facilities owned or managed (at beginning of the year) | 141 | 164 | 180 | 201 | 233 | |||||||||||||||
| Facilities added by: | ||||||||||||||||||||
| Acquisition | 24 | 14 | 28 | 33 | 25 | |||||||||||||||
| Internal development | 4 | 3 | 8 | 2 | – | |||||||||||||||
| Facilities closed or sold | -5 | -1 | -15 | -3 | -12 | |||||||||||||||
| Total facilities owned (at year end) | 164 | 180 | 201 | 233 | 246 | |||||||||||||||
Diagnostic Imaging Equipment
The following table indicates, as of December 31, 2012, the quantity of principal diagnostic equipment available at our facilities, by region:
| MRI | Open/MRI | CT | PET/CT | Mammo | Ultrasound | X-ray | NucMed | Fluoroscopy | Total | |||||||||||
| California | 60 | 21 | 36 | 21 | 74 | 152 | 103 | 19 | 75 | 561 | ||||||||||
| Florida | 3 | 1 | 3 | 1 | 3 | 5 | 3 | 3 | 5 | 27 | ||||||||||
| Delaware | 8 | 7 | 5 | 18 | 17 | 2 | 4 | 61 | ||||||||||||
| New Jersey | 14 | 1 | 8 | 2 | 8 | 16 | 13 | 2 | 11 | 75 | ||||||||||
| New York | 23 | 4 | 20 | 5 | 29 | 58 | 31 | 4 | 10 | 184 | ||||||||||
| Maryland | 58 | 8 | 41 | 14 | 59 | 105 | 74 | 15 | 33 | 407 | ||||||||||
| Rhode Island | 3 | 1 | 3 | - | 3 | 3 | 12 | 25 | ||||||||||||
| Total | 169 | 36 | 118 | 43 | 181 | 357 | 253 | 45 | 138 | 1,340 |
The average age of our MRI and CT units is less than six years, and the average age of our PET units is less than four years. The useful life of our MRI, CT and PET units is typically ten years.
Facility Acquisitions
Information regarding our facility acquisitions can be found within Item 7 - “Management’s Discussion and Analysis of Financial Condition and Results of Operations”, as well as Note 4 to our consolidated financial statements included in this annual report on Form 10-K.
Information Technology
Our corporate headquarters and many of our facilities are interconnected through a state-of-the-art information technology system. This system, which is compliant with the Health Insurance Portability and Accountability Act of 1996, is comprised of a number of integrated applications and provides a single operating platform for billing and collections, electronic medical records, practice management and image management.
| 14 |
This technology has created cost reductions for our facilities in areas such as image storage, support personnel and financial management and has further allowed us to optimize the productivity of all aspects of our business by enabling us to:
| · | capture patient demographic, history and billing information at point-of-service; |
| · | automatically generate bills and electronically file claims with third-party payors; |
| · | record and store diagnostic report images in digital format; |
| · | digitally transmit in real-time diagnostic images from one location to another, thus enabling networked radiologists to cover larger geographic markets by using the specialized training of other networked radiologists; |
| · | perform claims, rejection and collection analysis; and |
| · | perform sophisticated financial analysis, such as analyzing cost and profitability, volume, charges, current activity and patient case mix, with respect to each of our managed care contracts. |
Diagnostic reports and images are currently accessible via the Internet by our California referring providers. We have worked with some of the larger medical groups in California with whom we have contracts to provide access to this content through their web portals. We are in the process of making such services available outside of California.
We also utilize a third party software for our front desk patient tracking system, or Radiology Information System. We intend to develop our own RIS through our team of software development engineers. With our acquisition of eRad we believe we will be able to develop and implement programs which improve the systems we utilize in the operation of our business by providing systems which meet our specific needs as opposed to being limited to systems developed for the imaging industry in general.
Personnel
At December 31, 2012, we had a total of 4,253 full-time, 737 part-time and 956 per diem employees, including those employed by BRMG. These numbers include 102 full-time and 9 part-time physicians and 1,209 full-time, 455 part-time and 577 per-diem technologists.
We employ site managers who are responsible for overseeing day-to-day and routine operations at each of our facilities, including staffing, modality and schedule coordination, referring physician and patient relations and purchasing of materials. These site managers report to regional managers and directors, who are responsible for oversight of the operations of all facilities within their region, including sales, marketing and contracting. The regional managers and directors, along with our directors of contracting, marketing, facilities, management/purchasing and human resources report to our chief operating officers. These officers, our chief financial officer, our director of information services and our medical director report to our chief executive officer.
None of our employees is subject to a collective bargaining agreement nor have we experienced any work stoppages. We believe our relationship with our employees is good.
Sales and Marketing
At December 31, 2012, our California sales and marketing team consisted of one director of marketing and 39 customer service representatives. Our eastern marketing team consisted of one director of marketing and 77 customer sales representatives. Our sales and marketing team employs a multi-pronged approach to marketing, including physician, payor and sports marketing programs.
Physician Marketing
Each customer service representative on our physician marketing team is responsible for marketing activity on behalf of one or more facilities. The representatives act as a liaison between the facility and referring physicians, holding meetings periodically and on an as-needed basis with them and their staff to present educational programs on new applications and uses of our systems and to address particular patient service issues that have arisen. In our experience, consistent hands-on contact with a referring physician and his or her staff generates goodwill and increases referrals to our facilities. The representatives also continually seek to establish referral relationships with new physicians and physician groups. In addition to a base salary, each representative receives a bonus based upon success.
Payor Marketing
Our marketing team regularly meets with managed care organizations and insurance companies to solicit contracts and meet with existing contracting payors to solidify those relationships. The comprehensiveness of our services, the geographic location of our facilities and the reputation of the physicians with whom we contract all serve as tools for obtaining new or repeat business from payors.
| 15 |
Sports Marketing Program
We have a sports marketing program designed to increase our public profile. We provide X-ray equipment and a technician for all of the basketball games of the Lakers, Clippers and Sparks held at the Staples Center in Los Angeles, Kings hockey games held at the Honda Center in Anaheim, and University of Southern California football games held in the Los Angeles Coliseum. In exchange for this service, we receive game tickets and an advertisement in each team program throughout the season.
Suppliers
Historically, we have acquired our diagnostic imaging equipment from large suppliers such as GE Medical Systems, Inc., Hologic, Phillips, Hitachi, Carestream and others, and we purchase medical supplies from various national vendors. We believe that we have excellent working relationships with all of our major vendors. There are several comparable vendors for our supplies that would be available to us if one of our current vendors becomes unavailable.
We primarily acquire our equipment with cash or through various financing arrangements with equipment vendors and third party equipment finance companies involving the use of capital leases with purchase options at minimal prices at the end of the lease term. At December 31, 2012, capital lease obligations, excluding interest, totaled approximately $7.7 million through 2017, including current installments totaling approximately $3.9 million. If we open or acquire additional imaging facilities, we may have to incur material capital lease obligations.
Timely, effective maintenance is essential for achieving high utilization rates of our imaging equipment. We have an arrangement with GE Medical Systems, Inc. under which it has agreed to be responsible for the maintenance and repair of a majority of our equipment for a fee that is based upon a percentage of our revenue, subject to a minimum payment.
Competition
The market for diagnostic imaging services is highly competitive. We compete locally with groups of radiologists, established hospitals, clinics and other independent organizations that own and operate imaging equipment. Our competitors include Alliance Healthcare Services, Inc., Diagnostic Imaging Group and several smaller regional competitors. Some of our competitors may now or in the future have access to greater financial resources than we do and may have access to newer, more advanced equipment. In addition, some physician practices have established their own diagnostic imaging facilities within their group practices to compete with us. We experience additional competition as a result of those activities.
We compete principally on the basis of our reputation, our ability to provide multiple modalities at many of our facilities, the location of our facilities, the quality of our diagnostic imaging services and technologists and the ability to establish and maintain relationships with healthcare providers and referring physicians. See “Competitive Strengths” above.
Each of the non-BRMG contracted radiology practices has entered into agreements with its physician shareholders and full-time employed radiologists that generally prohibit those shareholders and radiologists from competing for a period of two years within defined geographic regions after they cease to be owners or employees, as applicable. In certain states, like California, a covenant not to compete is enforced in limited circumstances involving the sale of a business. In other states, a covenant not to compete will be enforced only:
| · | to the extent it is necessary to protect a legitimate business interest of the party seeking enforcement; |
| · | if it does not unreasonably restrain the party against whom enforcement is sought; and |
| · | if it is not contrary to public interest. |
Enforceability of a non-compete covenant is determined by a court based on all of the facts and circumstances of the specific case at the time enforcement is sought. For this reason, it is not possible to predict whether or to what extent a court will enforce the contracted radiology practices’ covenants. The inability of the contracted radiology practices or us to enforce radiologist’s non-compete covenants could result in increased competition from individuals who are knowledgeable about our business strategies and operations.
Liability Insurance
We maintain insurance policies with coverage we believe is appropriate in light of the risks attendant to our business and consistent with industry practice. However, adequate liability insurance may not be available to us in the future at acceptable costs or at all. We maintain general liability insurance and professional liability insurance in commercially reasonable amounts. Additionally, we maintain workers’ compensation insurance on all of our employees. Coverage is placed on a statutory basis and corresponds to individual state’s requirements.
| 16 |
Pursuant to our agreements with physician groups with whom we contract, including BRMG, each group must maintain medical malpractice insurance for each physician in the group, having coverage limits of not less than $1.0 million per incident and $3.0 million in the aggregate per year.
California’s medical malpractice cap further reduces our exposure. California places a $250,000 limit on non-economic damages for medical malpractice cases. Non-economic damages are defined as compensation for pain, suffering, inconvenience, physical impairment, disfigurement and other non-pecuniary injury. The cap applies whether the case is for injury or death, and it allows only one $250,000 recovery in a wrongful death case. No cap applies to economic damages. Other states in which we now operate do not have similar limitations and in those states we believe our insurance coverage to be sufficient.
Regulation
General
The healthcare industry is highly regulated, and we can give no assurance that the regulatory environment in which we operate will not change significantly in the future. Our ability to operate profitably will depend in part upon us, and the contracted radiology practices and their affiliated physicians obtaining and maintaining all necessary licenses and other approvals, and operating in compliance with applicable healthcare regulations. We believe that healthcare regulations will continue to change. Therefore, we monitor developments in healthcare law and modify our operations from time to time as the business and regulatory environment changes.
Licensing and Certification Laws
Ownership, construction, operation, expansion and acquisition of diagnostic imaging facilities are subject to various federal and state laws, regulations and approvals concerning licensing of facilities and personnel. In addition, free-standing diagnostic imaging facilities that provide services not performed as part of a physician office must meet Medicare requirements to be certified as an independent diagnostic testing facility before it can be authorized to bill the Medicare program. We have experienced a slowdown in the credentialing of our physicians over the last several years which has lengthened our billing and collection cycle.
Corporate Practice of Medicine
In the states in which we operate, other than Florida, a lay person or any entity other than a professional corporation or other similar professional organization is not allowed to practice medicine, including by employing professional persons or by having any ownership interest or profit participation in or control over any medical professional practice. The laws of such states also prohibit a lay person or a non-professional entity from exercising control over the medical judgments or decisions of physicians and from engaging in certain financial arrangements, such as splitting professional fees with physicians. We structure our relationships with the radiology practices, including the purchase of diagnostic imaging facilities, in a manner that we believe keeps us from engaging in the practice of medicine, exercising control over the medical judgments or decisions of the radiology practices or their physicians, or violating the prohibitions against fee-splitting.
Medicare and Medicaid Fraud and Abuse – Federal Anti-kickback Statute
During the year ended December 31, 2012, approximately 21% of our revenue generated at our diagnostic imaging centers was derived from federal government sponsored healthcare programs (Medicare) and 3% from state sponsored programs (Medicaid).
Federal law known as the Anti-kickback Statute prohibits the knowing and willful offer, payment, solicitation or receipt of any form of remuneration in return for, or to induce, (i) the referral of a person, (ii) the furnishing or arranging for the furnishing of items or services reimbursable under the Medicare, Medicaid or other governmental programs or (iii) the purchase, lease or order or arranging or recommending purchasing, leasing or ordering of any item or service reimbursable under the Medicare, Medicaid or other governmental programs. Enforcement of this anti-kickback law is a high priority for the federal government, which has substantially increased enforcement resources and is scheduled to continue increasing such resources. Noncompliance with the federal Anti-kickback Statute can result in exclusion from the Medicare, Medicaid or other governmental programs and civil and criminal penalties.
The Anti-kickback Statute is broad, and it prohibits many arrangements and practices that are lawful in businesses outside of the healthcare industry. Recognizing that the Anti-kickback Statute is broad and may technically prohibit many innocuous or beneficial arrangements within the healthcare industry, the Office of the Inspector General of the U.S. Department of Health and Human Services issued regulations in July of 1991, which the Department has referred to as “safe harbors.” These safe harbor regulations set forth certain provisions which, if met in form and substance, will assure healthcare providers and other parties that they will not be prosecuted under the federal Anti-kickback Statute. Additional safe harbor provisions providing similar protections have been published intermittently since 1991. Our arrangements with physicians, physician practice groups, hospitals and other persons or entities who are in a position to refer may not fully meet the stringent criteria specified in the various safe harbors. Although full compliance with these provisions ensures against prosecution under the federal Anti-kickback Statute, the failure of a transaction or arrangement to fit within a specific safe harbor does not necessarily mean that the transaction or arrangement is illegal or that prosecution under the federal Anti-kickback Statute will be pursued.
| 17 |
Although some of our arrangements may not fall within a safe harbor, we believe that such business arrangements do not violate the Anti-kickback Statute because we are careful to structure them to reflect fair value and ensure that the reasons underlying our decision to enter into a business arrangement comport with reasonable interpretations of the Anti-kickback Statute. However, even though we continuously strive to comply with the requirements of the Anti-kickback Statute, liability under the Anti-kickback Statute may still arise because of the intentions or actions of the parties with whom we do business. While we are not aware of any such intentions or actions, we have only limited knowledge regarding the intentions or actions underlying those arrangements. Conduct and business arrangements that do not fully satisfy one of these safe harbor provisions may result in increased scrutiny by government enforcement authorities such as the Office of the Inspector General.
Medicare and Medicaid Fraud and Abuse – Stark Law
Congress has placed significant legal prohibitions against physician referrals including the Ethics in Patient Referral Act of 1989 which is commonly known as the Stark Law. The Stark Law prohibits a physician from referring Medicare patients to an entity providing designated health services, as defined under the Stark Law, including, without limitation, radiology services, in which the physician (or immediate family member) has an ownership or investment interest or with which the physician (or immediate family member) has entered into a compensation arrangement. The Stark Law also prohibits the entity from billing for any such prohibited referral. The penalties for violating the Stark Law include a prohibition on payment by these governmental programs and civil penalties of as much as $15,000 for each violation referral and $100,000 for participation in a circumvention scheme. We believe that, although we receive fees under our service agreements for management and administrative services, we are not in a position to make or influence referrals of patients.
Under the Stark Law, radiology and certain other imaging services and radiation therapy services and supplies are services included in the designated health services subject to the self-referral prohibition. Such services include the professional and technical components of any diagnostic test or procedure using X-rays, ultrasound or other imaging services, CT, MRI, radiation therapy and diagnostic mammography services (but not screening mammography services). PET and nuclear medicine procedures are also included as designated health services under the Stark Law. The Stark Law, however, excludes from designated health services: (i) X-ray, fluoroscopy or ultrasound procedures that require the insertion of a needle, catheter, tube or probe through the skin or into a body orifice; (ii) radiology procedures that are integral to the performance of, and performed during, non-radiological medical procedures; and (iii) invasive or interventional radiology, because the radiology services in these procedures are merely incidental or secondary to another procedure that the physician has ordered.
The Stark Law provides that a request by a radiologist for diagnostic radiology services or a request by a radiation oncologist for radiation therapy, if such services are furnished by or under the supervision of such radiologist or radiation oncologist pursuant to a consultation requested by another physician, does not constitute a referral by a referring physician. If such requirements are met, the Stark Law self-referral prohibition would not apply to such services. The effect of the Stark Law on the radiology practices, therefore, will depend on the precise scope of services furnished by each such practice’s radiologists and whether such services derive from consultations or are self-generated.
We believe that, other than self-referred patients, all of the services covered by the Stark Law provided by the contracted radiology practices derive from requests for consultation by non-affiliated physicians. Therefore, we believe that the Stark Law is not implicated by the financial relationships between our operations and the contracted radiology practices. In addition, we believe that we have structured our acquisitions of the assets of existing practices, and we intend to structure any future acquisitions, so as not to violate the Anti-kickback Statute and Stark Law and regulations. Specifically, we believe the consideration paid by us to physicians to acquire the tangible and intangible assets associated with their practices is consistent with fair value in arms’ length transactions and is not intended to induce the referral of patients or other business generated by such physicians. Should any such practice be deemed to constitute an arrangement designed to induce the referral of Medicare or Medicaid patients, then our acquisitions could be viewed as possibly violating anti-kickback and anti-referral laws and regulations. A determination of liability under any such laws could have a material adverse effect on our business, financial condition and results of operations.
Medicare and Medicaid Fraud and Abuse – General
The federal government embarked on an initiative to audit all Medicare carriers, which are the companies that adjudicate and pay Medicare claims. These audits are expected to intensify governmental scrutiny of individual providers. An unsatisfactory audit of any of our diagnostic imaging facilities or contracted radiology practices could result in any or all of the following: significant repayment obligations, exclusion from the Medicare, Medicaid or other governmental programs, and civil and criminal penalties.
| 18 |
Federal regulatory and law enforcement authorities have increased enforcement activities with respect to Medicare, Medicaid fraud and abuse regulations and other reimbursement laws and rules, including laws and regulations that govern our activities and the activities of the radiology practices. The federal government also has increased funding to fight healthcare fraud and is coordinating its enforcement efforts among various agencies, such as the U.S. Department of Justice, the U.S. Department of Health and Human Services Office of Inspector General, and state Medicaid fraud control units. The government may investigate our or the radiology practices’ activities, claims may be made against us or the radiology practices and these increased enforcement activities may directly or indirectly have an adverse effect on our business, financial condition and results of operations.
State Anti-kickback and Physician Self-referral Laws
Many states have adopted laws similar to the federal Anti-kickback Statute. Some of these state prohibitions apply to referral of patients for healthcare services reimbursed by any source, not only the Medicare and Medicaid programs. Although we believe that we comply with both federal and state Anti-kickback laws, any finding of a violation of these laws could subject us to criminal and civil penalties or possible exclusion from federal or state healthcare programs. Such penalties would adversely affect our financial performance and our ability to operate our business.
Federal False Claims Act
The federal False Claims Act provides, in part, that the federal government may bring a lawsuit against any person who it believes has knowingly presented, or caused to be presented, a false or fraudulent request for payment from the federal government, or who has made a false statement or used a false record to get a claim approved. The federal False Claims Act further provides that a lawsuit thereunder may be initiated in the name of the United States by an individual, a “whistleblower,” who is an original source of the allegations. The government has taken the position that claims presented in violation of the federal anti-kickback law or Stark Law may be considered a violation of the federal False Claims Act. Penalties include civil penalties of not less than $5,500 and not more than $11,000 for each false claim, plus three times the amount of damages that the federal government sustained because of the act of that person.
Recently, the number of suits brought against healthcare providers by private individuals has increased dramatically. Further, on May 20, 2009, President Obama signed into law the Fraud Enforcement and Recovery Act of 2009 (FERA), which greatly expanded the types of entities and conduct subject to the False Claims Act. Also, various states are considering or have enacted laws modeled after the federal False Claims Act. Under the Deficit Reduction Act of 2005, or DRA, states are being encouraged to adopt false claims acts similar to the federal False Claims Act, which establish liability for submission of fraudulent claims to the State Medicaid program and contain whistleblower provisions. Even in instances when a whistleblower action is dismissed with no judgment or settlement, we may incur substantial legal fees and other costs relating to an investigation. Future actions under the False Claims Act may result in significant fines and legal fees, which would adversely affect our financial performance and our ability to operate our business.
We believe that we are in compliance with the rules and regulations that apply to the federal False Claims Act as well as its state counterparts.
Healthcare Reform Legislation
Healthcare reform legislation enacted in the first quarter of 2010 by the Patient Protection and Affordable Care Act or PPACA, specifically requires the U.S. Department of Health and Human Services, in computing physician practice expense relative value units, to increase the equipment utilization factor for advanced diagnostic imaging services (such as MRI, CT and PET) from a presumed utilization rate of 50% to 65% for 2010 through 2012, 70% in 2013, and 75% thereafter. Excluded from the adjustment are low-technology imaging modalities such as ultrasound, X-ray and fluoroscopy. The Health Care and Education Reconciliation Act of 2010 (H.R. 4872) or Reconciliation Act, which was passed by the Senate and approved by the President on March 30, 2010, amends the provision for higher presumed utilization of advanced diagnostic imaging services to a presumed rate of 75%. The higher utilization rate was fully implemented in the beginning of 2011 and replaced the phase-in approach provided in the PPACA. This utilization rate was further increased to 90% by the American Taxpayer Relief Act of 2012 (“ATRA”), to be effective as of January 1, 2014.
The aim of increased utilization of diagnostic imaging services is to spread the cost of the equipment and services over a greater number of scans, resulting in a lower cost per scan. These changes will precipitate reductions in federal reimbursement for medical imaging and result in decreased revenue for the scans we perform for Medicare beneficiaries. Other changes in reimbursement for services rendered by Medicare Advantage plans may also reduce the revenues we receive for services rendered to Medicare Advantage enrollees.
| 19 |
Health Insurance Portability and Accountability Act of 1996
Congress enacted the Health Insurance Portability and Accountability Act of 1996, or HIPAA, in part, to combat healthcare fraud and to protect the privacy and security of patients’ individually identifiable healthcare information. HIPAA, among other things, amends existing crimes and criminal penalties for Medicare fraud and enacts new federal healthcare fraud crimes, including actions affecting non-government healthcare benefit programs. Under HIPAA, a healthcare benefit program includes any private plan or contract affecting interstate commerce under which any medical benefit, item or service is provided. A person or entity that knowingly and willfully obtains the money or property of any healthcare benefit program by means of false or fraudulent representations in connection with the delivery of healthcare services is subject to a fine or imprisonment, or potentially both. In addition, HIPAA authorizes the imposition of civil money penalties against entities that employ or enter into contracts with excluded Medicare or Medicaid program participants if such entities provide services to federal health program beneficiaries. A finding of liability under HIPAA could have a material adverse effect on our business, financial condition and results of operations.
Further, HIPAA requires healthcare providers and their business associates to maintain the privacy and security of individually identifiable protected health information (“PHI”). HIPAA imposes federal standards for electronic transactions, for the security of electronic health information and for protecting the privacy of PHI. The Health Information Technology for Economic and Clinical Health Act of 2009 (“HITECH”), signed into law on February 17, 2009, dramatically expanded, among other things, (1) the scope of HIPAA to now apply directly to “business associates,” or independent contractors who receive or obtain PHI in connection with providing a service to a covered entity, (2) substantive security and privacy obligations, including new federal security breach notification requirements to affected individuals, DHHS and prominent media outlets, of certain breaches of unsecured PHI, (3) restrictions on marketing communications and a prohibition on covered entities or business associates from receiving remuneration in exchange for PHI, and (4) the civil and criminal penalties that may be imposed for HIPAA violations, increasing the annual cap in penalties from $25,000 to $1.5 million per year.
In addition, many states have enacted comparable privacy and security statutes or regulations that, in some cases, are more stringent than HIPAA requirements. In those cases it may be necessary to modify our operations and procedures to comply with the more stringent state laws, which may entail significant and costly changes for us. We believe that we are in compliance with such state laws and regulations. However, if we fail to comply with applicable state laws and regulations, we could be subject to additional sanctions.
We believe that we are in compliance with the current HIPAA requirements, as amended by HITECH, and comparable state laws, but we anticipate that we may encounter certain costs associated with future compliance. Moreover, we cannot guarantee that enforcement agencies or courts will not make interpretations of the HIPAA standards that are inconsistent with ours, or the interpretations of our contracted radiology practices or their affiliated physicians. A finding of liability under the HIPAA standards may result in significant criminal and civil penalties. Noncompliance also may result in exclusion from participation in government programs, including Medicare and Medicaid. These actions could have a material adverse effect on our business, financial condition, and results of operations.
U.S. Food and Drug Administration or FDA
The FDA has issued the requisite pre-market approval for all of the MRI and CT systems we use. We do not believe that any further FDA approval is required in connection with the majority of equipment currently in operation or proposed to be operated, except under regulations issued by the FDA pursuant to the Mammography Quality Standards Act of 1992, as amended by the Mammography Quality Standards Reauthorization Acts of 1998 and 2004 (collectively, the MQSA). All mammography facilities are required to meet the applicable MQSA requirements, including quality standards, be accredited by an approved accreditation body or state agency and certified by the FDA or an FDA-approved certifying state agency. Pursuant to the accreditation process, each facility providing mammography services must comply with certain standards that include, among other things, annual inspection of the facility's equipment, personnel (interpreting physicians, technologists and medical physicists) and practices.
Compliance with these MQSA requirements and standards is required to obtain Medicare payment for services provided to beneficiaries and to avoid various sanctions, including monetary penalties, or suspension of certification. Although the Mammography Accreditation Program of the American College of Radiology is an approved accreditation body and currently accredits all of our facilities which provide mammography services, and although we anticipate continuing to meet the requirements for accreditation, if we lose such accreditation, the FDA could revoke our certification. Congress has extended Medicare benefits to include coverage of screening mammography but coverage is subject to the facility performing the mammography meeting prescribed quality standards described above. The Medicare requirements to meet the standards apply to diagnostic mammography and image quality examination as well as screening mammography.
| 20 |
Radiologist Licensing
The radiologists providing professional medical services at our facilities are subject to licensing and related regulations by the states in which they provide services. As a result, we require BRMG and the other radiology groups with which we contract to require those radiologists to have and maintain appropriate licensure. We do not believe that such laws and regulations will either prohibit or require licensure approval of our business operations, although no assurances can be made that such laws and regulations will not be interpreted to extend such prohibitions or requirements to our operations.
Insurance Laws and Regulation
States in which we operate have adopted certain laws and regulations affecting risk assumption in the healthcare industry, including those that subject any physician or physician network engaged in risk-based managed care to applicable insurance laws and regulations. These laws and regulations may require physicians and physician networks to meet minimum capital requirements and other safety and soundness requirements. Implementing additional regulations or compliance requirements could result in substantial costs to the contracted radiology practices, limiting their ability to enter into capitated or other risk-sharing managed care arrangements and indirectly affecting our revenue from the contracted practices.
Sequestration
We derive a substantial portion of our revenue from direct billings to governmental healthcare programs, such as Medicare and Medicaid, and private health insurance companies and/or health plans, including but not limited to those participating in the Medicare Advantage program. As a result, any negative changes in governmental capitation or fee-for-service rates or methods of reimbursement for the services we provide could have a significant adverse impact on our revenue and financial results.
Congress has a strong interest in reducing the federal debt, which may lead to new proposals designed to achieve savings by altering payment policies. The Budget Control Act of 2011 (“BCA”) established a Joint Select Committee on Deficit Reduction, which had the goal of achieving a reduction in the federal debt level of at least $1.2 trillion. As a result of the Joint Select Committee’s failure to draft a proposal by the BCA’s deadline, automatic cuts in various federal programs (excluding cuts to Medicaid but including cuts to Medicare provider reimbursement in an amount not to exceed 2%) were scheduled to commence on January 1, 2013. However, as a result of the enactment of ATRA on January 2, 2013, any such cuts were delayed until March 1, 2013 so as to allow the Congress sworn in on January 3, 2013 to consider whether to allow sequestration to take place or replace it with other cuts in federal spending and/or higher taxes.
On March 1, 2013, Congress failed to act and prevent the automatic cuts from taking effect, and CMS has stated that a 2% cut to Medicare payments will begin starting April 1, 2013, which will have a negative impact on our revenues. In addition, certain Congressional members have stated that the automatic federal spending cuts under the BCA are insufficient to achieve the BCA’s goals of reducing federal spending and, in turn, the federal deficit. Such members have said that the way to achieve these additional cuts is to implement changes to federal entitlement programs, such as Medicare. Therefore it is not possible at this time to estimate what further impact, if any, other federal Medicare provider reimbursement cuts will have on our integrated care business or results of operations.
Because governmental healthcare programs generally reimburse on a fee schedule basis rather than on a charge-related basis, we generally cannot increase our revenues from these programs by increasing the amount of charges for services. Moreover, if our costs increase, we may not be able to recover our increased costs from these programs. Government and private payors have taken and may continue to take steps to control the cost, eligibility for, use, and delivery of healthcare services as a result of budgetary constraints, cost containment pressures and other reasons. We believe that these trends in cost containment will continue. These cost containment measures, and other market changes in non-governmental insurance plans have generally restricted our ability to recover, or shift to non-governmental payors, any increased costs that we experience. Our integrated care business and financial operations may be materially affected by these developments.
Environmental Matters
The facilities we operate or manage generate hazardous and medical waste subject to federal and state requirements regarding handling and disposal. We believe that the facilities that we operate and manage are currently in compliance in all material respects with applicable federal, state and local statutes and ordinances regulating the handling and disposal of such materials. We do not believe that we will be required to expend any material additional amounts in order to remain in compliance with these laws and regulations or that compliance will materially affect our capital expenditures, earnings or competitive position.
| 21 |
Compliance Program
We maintain a program to monitor compliance with federal and state laws and regulations applicable to healthcare entities. We have a compliance officer who is charged with implementing and supervising our compliance program, which includes the adoption of (i) Standards of Conduct for our employees and affiliates and (ii) a process that specifies how employees, affiliates and others may report regulatory or ethical concerns to our compliance officer. We believe that our compliance program meets the relevant standards provided by the Office of Inspector General of the Department of Health and Human Services.
An important part of our compliance program consists of conducting periodic audits of various aspects of our operations and that of the contracted radiology practices. We also conduct mandatory educational programs designed to familiarize our employees with the regulatory requirements and specific elements of our compliance program.
| Item 1A. | Risk Factors |
If BRMG or any of our other contracted radiology practices terminate their agreements with us, our business could substantially diminish.
Our relationship with BRMG is an integral part of our business. Through our management agreement, BRMG provides all of the professional medical services at 101 of our 109 California facilities. Professional medical services are provided at our other facilities through management contracts with other radiology groups. BRMG and these other radiology groups contract with various other independent physicians and physician groups to provide all of the professional medical services at most of our facilities, and they must use their best efforts to provide the professional medical services at any new facilities that we open or acquire in their areas of operation. In addition, BRMG and the other radiology groups’ strong relationships with referring physicians are largely responsible for the revenue generated at the facilities they service. Although our management agreement with BRMG runs until 2014, and for terms as long, if not longer, with the other groups, BRMG and the other radiology groups have the right to terminate the agreements if we default on our obligations and fail to cure the default. Also, the various radiology groups’ ability to continue performing under the management agreements may be curtailed or eliminated due to the groups’ financial difficulties, loss of physicians or other circumstances. If the radiology groups cannot perform their obligations to us, we would need to contract with one or more other radiology groups to provide the professional medical services at the facilities serviced by the group. We may not be able to locate radiology groups willing to provide those services on terms acceptable to us, if at all. Even if we were able to do so, any replacement radiology group’s relationships with referring physicians may not be as extensive as those of the terminated group. In any such event, our business could be seriously harmed. In addition, the radiology groups are party to substantially all of the managed care contracts from which we derive revenue. If we were unable to readily replace these contracts, our revenue would be negatively affected.
Our ability to generate revenue depends in large part on referrals from physicians.
We derive substantially all of our net revenue, directly or indirectly, from fees charged for the diagnostic imaging services performed at our facilities. We depend on referrals of patients from unaffiliated physicians and other third parties who have no contractual obligations to refer patients to us for a substantial portion of the services we perform. If a sufficiently large number of these physicians and other third parties were to discontinue referring patients to us, our scan volume could decrease, which would reduce our net revenue and operating margins. Further, commercial third-party payors have implemented programs that could limit the ability of physicians to refer patients to us. For example, prepaid healthcare plans, such as health maintenance organizations, sometimes contract directly with providers and require their enrollees to obtain these services exclusively from those providers. Some insurance companies and self-insured employers also limit these services to contracted providers. These “closed panel” systems are now common in the managed care environment. Other systems create an economic disincentive for referrals to providers outside the system’s designated panel of providers. If we are unable to compete successfully for these managed care contracts, our results and prospects for growth could be adversely affected.
If our contracted radiology practices, including BRMG, lose a significant number of their radiologists, our financial results could be adversely affected.
At times, there has been a shortage of qualified radiologists in some of the regional markets we serve. In addition, competition in recruiting radiologists may make it difficult for our contracted radiology practices to maintain adequate levels of radiologists. If a significant number of radiologists terminate their relationships with our contracted radiology practices and those radiology practices cannot recruit sufficient qualified radiologists to fulfill their obligations under our agreements with them, our ability to maximize the use of our diagnostic imaging facilities and our financial results could be adversely affected. Increased expenses to BRMG will impact our financial results because the management fee we receive from BRMG, which is based on a percentage of BRMG’s collections, is adjusted annually to take into account the expenses of BRMG. Neither we, nor our contracted radiology practices, maintain insurance on the lives of any affiliated physicians.
| 22 |
We may become subject to professional malpractice liability, which could be costly and negatively impact our business.
The physicians employed by our contracted radiology practices are from time to time subject to malpractice claims. We structure our relationships with the practices under our management agreements in a manner that we believe does not constitute the practice of medicine by us or subject us to professional malpractice claims for acts or omissions of physicians employed by the contracted radiology practices. Nevertheless, claims, suits or complaints relating to services provided by the contracted radiology practices have been asserted against us in the past and may be asserted against us in the future. In addition, we may be subject to professional liability claims, including, without limitation, for improper use or malfunction of our diagnostic imaging equipment or for accidental contamination or injury from exposure to radiation. We may not be able to maintain adequate liability insurance to protect us against those claims at acceptable costs or at all.
Any claim made against us that is not fully covered by insurance could be costly to defend, result in a substantial damage award against us and divert the attention of our management from our operations, all of which could have an adverse effect on our financial performance. In addition, successful claims against us may adversely affect our business or reputation. Although California places a $250,000 limit on non-economic damages for medical malpractice cases, no limit applies to economic damages and no such limits exist in the other states in which we provide services.
We may not receive payment from some of our healthcare provider customers because of their financial circumstances.
Some of our healthcare provider customers do not have significant financial resources, liquidity or access to capital. If these customers experience financial difficulties they may be unable to pay us for the equipment and services that we provide. A significant deterioration in general or local economic conditions could have a material adverse effect on the financial health of certain of our healthcare provider customers. As a result, we may have to increase the amounts of accounts receivables that we write-off, which would adversely affect our financial condition and results of operations.
Capitation fee arrangements could reduce our operating margins.
For the year ended December 31, 2012, we derived approximately 13% of our payments from capitation arrangements, and we intend to increase the revenue we derive from capitation arrangements in the future. Under capitation arrangements, the payor pays a pre-determined amount per-patient per-month in exchange for us providing all necessary covered services to the patients covered under the arrangement. These contracts pass much of the financial risk of providing diagnostic imaging services, including the risk of over-use, from the payor to the provider. Our success depends in part on our ability to negotiate effectively, on behalf of the contracted radiology practices and our diagnostic imaging facilities, contracts with health maintenance organizations, employer groups and other third-party payors for services to be provided on a capitated basis and to efficiently manage the utilization of those services. If we are not successful in managing the utilization of services under these capitation arrangements or if patients or enrollees covered by these contracts require more frequent or extensive care than anticipated, we would incur unanticipated costs not offset by additional revenue, which would reduce operating margins.
Pressure to control healthcare costs could have a negative impact on our results.
One of the principal objectives of health maintenance organizations and preferred provider organizations is to control the cost of healthcare services. Healthcare providers participating in managed care plans may be required to refer diagnostic imaging tests to certain providers depending on the plan in which a covered patient is enrolled. In addition, managed care contracting has become very competitive, and reimbursement schedules are at or below Medicare reimbursement levels. The expansion of health maintenance organizations, preferred provider organizations and other managed care organizations within the geographic areas covered by our network could have a negative impact on the utilization and pricing of our services, because these organizations will exert greater control over patients’ access to diagnostic imaging services, the selections of the provider of such services and reimbursement rates for those services.
We experience competition from other diagnostic imaging companies and hospitals, and this competition could adversely affect our revenue and business.
The market for diagnostic imaging services is highly competitive. We compete principally on the basis of our reputation, our ability to provide multiple modalities at many of our facilities, the location of our facilities and the quality of our diagnostic imaging services. We compete locally with groups of radiologists, established hospitals, clinics and other independent organizations that own and operate imaging equipment. Our competitors include Alliance Healthcare Services, Inc., Diagnostic Imaging Group and several smaller regional competitors. Some of our competitors may now or in the future have access to greater financial resources than we do and may have access to newer, more advanced equipment. In addition, some physician practices have established their own diagnostic imaging facilities within their group practices and compete with us. We are experiencing increased competition as a result of such activities, and if we are unable to successfully compete, our business and financial condition would be adversely affected.
| 23 |
Our success depends in part on our key personnel and loss of key executives could adversely affect our operations. In addition, former employees and radiology practices we have previously contracted with could use the experience and relationships developed while employed or under contract with us to compete with us.
Our success depends in part on our ability to attract and retain qualified senior and executive management, managerial and technical personnel. Competition in recruiting these personnel may make it difficult for us to continue our growth and success. The loss of their services or our inability in the future to attract and retain management and other key personnel could hinder the implementation of our business strategy. The loss of the services of Dr. Howard G. Berger, our President and Chief Executive Officer, and Norman R. Hames or Stephen M. Forthuber, our Chief Operating Officers, west and east coast, respectively, could have a significant negative impact on our operations. We believe that they could not easily be replaced with executives of equal experience and capabilities. We do not maintain key person insurance on the life of any of our executive officers with the exception of a $5.0 million policy on the life of Dr. Berger. Also, if we lose the services of Dr. Berger, our relationship with BRMG could deteriorate, which would materially adversely affect our business.
Many of the states in which we operate do not enforce agreements that prohibit a former employee from competing with a former employer. As a result, many of our employees whose employment is terminated are free to compete with us, subject to prohibitions on the use of trade secret information and, depending on the terms of the employee’s employment agreement, on solicitation of existing employees and customers (if enforceable). A former executive, manager or other key employee who joins one of our competitors could use the relationships he or she established with third party payors, radiologists or referring physicians while our employee and the industry knowledge he or she acquired during that tenure to enhance the new employer’s ability to compete with us.
The agreements with most of our radiology practices contain non-compete provisions; however the enforceability of these provisions is determined by a court based on all the facts and circumstances of the specific case at the time enforcement is sought. Our inability to enforce radiologists’ non-compete provisions could result in increased competition from individuals who are knowledgeable about our business strategies and operations.
Our failure to integrate the businesses we acquire successfully and on a timely basis could reduce our profitability.
We may never realize expected synergies, business opportunities and growth prospects in connection with our acquisitions. We may experience increased competition that limits our ability to expand our business. We may not be able to capitalize on expected business opportunities, assumptions underlying estimates of expected cost savings may be inaccurate, or general industry and business conditions may deteriorate. In addition, integrating operations will require significant efforts and expenses on our part. Personnel may leave or be terminated because of an acquisition. Our management may have its attention diverted while trying to integrate an acquisition. If these factors limit our ability to integrate the operations of an acquisition successfully or on a timely basis, our expectations of future results of operations, including certain cost savings and synergies as a result of the acquisition, may not be met. In addition, our growth and operating strategies for a target’s business may be different from the strategies that the target company pursued prior to our acquisition. If our strategies are not the proper strategies, they could have a material adverse effect on our business, financial condition and results of operations.
We may not be able to successfully grow our business, which would adversely affect our financial condition and results of operations.
Historically, we have experienced substantial growth through acquisitions that have increased our size, scope and geographic distribution. During the past two fiscal years, we have completed 21 acquisitions. These acquisitions have added 58 centers to our fixed-site outpatient diagnostic imaging services. Our ability to successfully expand through acquiring facilities, developing new facilities, adding equipment at existing facilities, and directly or indirectly entering into contractual relationships with high-quality radiology practices depends upon many factors, including our ability to:
| · | identify attractive and willing candidates for acquisitions; |
| · | identify locations in existing or new markets for development of new facilities; |
| · | comply with legal requirements affecting our arrangements with contracted radiology practices, including state prohibitions on fee-splitting, corporate practice of medicine and self-referrals; |
| · | obtain regulatory approvals where necessary and comply with licensing and certification requirements applicable to our diagnostic imaging facilities, the contracted radiology practices and the physicians associated with the contracted radiology practices; |
| · | recruit a sufficient number of qualified radiology technologists and other non-medical personnel; |
| 24 |
| · | expand our infrastructure and management; and |
| · | compete for opportunities. We may not be able to compete effectively for the acquisition of diagnostic imaging facilities. Our competitors may have more established operating histories and greater resources than we do. Competition may also make any acquisitions more expensive. |
Managing our recent acquisitions, as well as any other future acquisitions, will entail numerous operational and financial risks, including:
| · | inability to obtain adequate financing; |
| · | possible adverse effects on our operating results; |
| · | diversion of management’s attention and resources; |
| · | failure to retain key personnel; |
| · | difficulties in integrating new operations into our existing infrastructure; and |
| · | amortization or write-offs of acquired intangible assets, including goodwill. |
If we are unable to successfully grow our business through acquisitions it could have an adverse effect on our financial condition and results of operations. Further we cannot ensure we will be able to receive the required regulatory approvals for any future acquisitions, expansions or replacements, and the failure to obtain these approvals could limit the market for our services and have an adverse effect on our financial condition and results of operations.
The acquisitions of eRAD, Inc. and Imaging On Call, LLC have resulted in new lines of business for us that could be difficult to integrate, disrupt our business or harm our results of operations.
The acquisition of eRAD, Inc. has provided us with a new line of business that has a large research and development component that is new to our business. The acquisition of Imaging On Call, LLC has provided us with a new teleradiology division, a line of business in which we have not previously provided services. The process of integrating the acquired business, technology, service and research and development component into our business and operations and entry into a new line of business in which we are inexperienced may result in unforeseen operating difficulties and expenditures. In developing the new line of business as a result of the eRAD, Inc. and Imaging On Call, LLC acquisitions, we may invest significant time and resources, such as our investment in the team of software developers in Canada, the attention of management’s time that would otherwise be available for ongoing development of our business that may affect our results of operations and we may not be able to take full advantage of the business opportunities available to us as we expand these new lines of business. Additionally, there are competitors in the same business as eRAD, Inc. and Imaging On Call, LLC. Failure to successfully manage these risks in the development and implementation of new lines of business could have a material, adverse effect on the Company’s business, financial condition, and results of operations.
We have experienced operating losses and we have a substantial accumulated deficit. If we are unable to improve our financial performance, we may be unable to pay our obligations.
Although we had net income of $ 59.8 million and $7.2 million for the years ended December 31, 2012 and 2011, respectively, we did incur a net loss of $12.9 million for the year ended December 31, 2010 and have generated net losses in three of our previous five years of operations. As of December 31, 2012, our stockholders’ equity deficit was $ 6.7 million. If we cannot continue to generate income from operations in sufficient amounts, we will not be able to pay our obligations as they become due, which could adversely impact our business, financial condition and results of operations.
| 25 |
Our substantial debt could adversely affect our financial condition and prevent us from fulfilling our obligations under our outstanding indebtedness.
Our current substantial indebtedness and any future indebtedness we incur could adversely affect our financial condition. We are highly leveraged. As of December 31, 2012, our total indebtedness was $582.4 million, $551.2 million of which constituted senior secured indebtedness. Our substantial indebtedness could also:
| · | make it difficult for us to satisfy our obligations with respect to our outstanding indebtedness; |
| · | require us to dedicate a substantial portion of our cash flow from operations to payments on our debt, reducing the availability of our cash flow to fund working capital, capital expenditures, acquisitions and other general corporate purposes; |
| · | expose us to the risk of interest rate increases on our variable rate borrowings, including borrowings under our new senior secured credit facilities; |
| · | increase our vulnerability to adverse general economic and industry conditions; |
| · | limit our flexibility in planning for, or reacting to, changes in our business and the industry in which we operate; |
| · | place us at a competitive disadvantage compared to our competitors that have less debt; and |
| · | limit our ability to borrow additional funds on terms that are satisfactory to us or at all. |
We may not be able to finance future needs or adapt our business plan to changes because of restrictions placed on us by our credit facilities, the indenture governing our senior unsecured notes and instruments governing our other indebtedness.
The indenture governing the senior unsecured notes and our credit facilities contain affirmative and negative covenants which restrict, among other things, our ability to:
| · | pay dividends or make certain other restricted payments or investments; |
| · | incur additional indebtedness and issue preferred stock; |
| · | create liens (other than permitted liens) securing indebtedness or trade payables unless the notes are secured on an equal and ratable basis with the obligations so secured, and, if such liens secure subordinated indebtedness, the notes are secured by a lien senior to such liens; |
| · | sell certain assets or merge with or into other companies or otherwise dispose of all or substantially all of our assets; |
| · | enter into certain transactions with affiliates; |
| · | create restrictions on dividends or other payments by our restricted subsidiaries; and |
| · | create guarantees of indebtedness by restricted subsidiaries. |
All of these restrictions could affect our ability to operate our business and may limit our ability to take advantage of potential business opportunities as they arise. A failure to comply with these covenants and restrictions would permit the relevant creditors to declare all amounts borrowed under the applicable agreement governing such indebtedness, together with accrued interest and fees, to be immediately due and payable. If the indebtedness our credit facilities or the senior unsecured notes is accelerated, we may not have sufficient assets to repay amounts due under the credit facilities, the senior unsecured notes or on other indebtedness then outstanding.
A failure to meet our capital expenditure requirements could adversely affect our business.
We operate in a capital intensive, high fixed-cost industry that requires significant amounts of capital to fund operations, particularly the initial start-up and development expenses of new diagnostic imaging facilities and the acquisition of additional facilities and new diagnostic imaging equipment. We incur capital expenditures to, among other things, upgrade and replace equipment for existing facilities and expand within our existing markets and enter new markets. If we open or acquire additional imaging facilities, we may have to incur material capital lease obligations. To the extent we are unable to generate sufficient cash from our operations, funds are not available from our lenders or we are unable to structure or obtain financing through operating leases, long-term installment notes or capital leases, we may be unable to meet our capital expenditure requirements.
The regulatory framework in which we operate is uncertain and evolving.
Although we believe that we are operating in compliance with applicable federal and state laws, neither our current or anticipated business operations nor the operations of the contracted radiology practices have been the subject of judicial or regulatory interpretation. We cannot assure you that a review of our business by courts or regulatory authorities will not result in a determination that could adversely affect our operations or that the healthcare regulatory environment will not change in a way that restricts our operations. In addition, healthcare laws and regulations may change significantly in the future. We continuously monitor these developments and modify our operations from time to time as the regulatory environment changes. We cannot assure you however, that we will be able to adapt our operations to address new regulations or that new regulations will not adversely affect our business.
| 26 |
Certain states have enacted statutes or adopted regulations affecting risk assumption in the healthcare industry, including statutes and regulations that subject any physician or physician network engaged in risk-based managed care contracting to applicable insurance laws and regulations. These laws and regulations, if adopted in the states in which we operate, may require physicians and physician networks to meet minimum capital requirements and other safety and soundness requirements. Implementing additional regulations or compliance requirements could result in substantial costs to us and the contracted radiology practices and limit our ability to enter into capitation or other risk-sharing managed care arrangements.
State and federal anti-kickback and anti-self-referral laws may adversely affect income.
Various federal and state laws govern financial arrangements among healthcare providers. The federal Anti-Kickback Law prohibits the knowing and willful offer, payment, solicitation or receipt of any form of remuneration in return for, or to induce, the referral of Medicare, Medicaid, or other federal healthcare program patients, or in return for, or to induce, the purchase, lease or order of items or services that are covered by Medicare, Medicaid, or other federal healthcare programs. Similarly, many state laws prohibit the solicitation, payment or receipt of remuneration in return for, or to induce the referral of patients in private as well as government programs. Violation of these Anti-Kickback Laws may result in substantial civil or criminal penalties for individuals or entities and/or exclusion from federal or state healthcare programs. We believe we are operating in compliance with applicable law and believe that our arrangements with providers would not be found to violate the Anti-Kickback Laws. However, these laws could be interpreted in a manner inconsistent with our operations.
Federal law prohibiting physician self-referrals, known as the Stark Law, prohibits a physician from referring Medicare or Medicaid patients to an entity for certain “designated health services” if the physician has a prohibited financial relationship with that entity, unless an exception applies. Certain radiology services are considered “designated health services” under the Stark Law. Although we believe our operations do not violate the Stark Law, our activities may be challenged. If a challenge to our activities is successful, it could have an adverse effect on our operations. In addition, legislation may be enacted in the future that further addresses Medicare and Medicaid fraud and abuse or that imposes additional requirements or burdens on us.
In addition, under the DRA, states enacting false claims statutes similar to the federal False Claims Act, which establish liability for submission of fraudulent claims to the State Medicaid program and contain qui tam or whistleblower provisions, receive an increased percentage of any recovery from a State Medicaid judgment or settlement. Adoption of new false claims statutes in states where we operate may impose additional requirements or burdens on us.
Changes in the method or rates of third-party reimbursement could have a negative impact on our results.
From time to time, changes designed to contain healthcare costs have been implemented, some of which have resulted in decreased reimbursement rates for diagnostic imaging services that impact our business. For services for which we bill Medicare directly, we are paid under the Medicare Physician Fee Schedule, which is updated on an annual basis. Under the Medicare statutory formula, payments under the Physician Fee Schedule would have decreased for the past several years if Congress failed to intervene.
Medicare program reimbursements for physician services as well as other services to Medicare beneficiaries who are not enrolled in Medicare Advantage plans are based upon the fee-for-service rates set forth in the Medicare Physician Fee Schedule, which relies, in part, on a target-setting formula system called the SGR. Each year, on January 1st, the Medicare program updates the Medicare Physician Fee Schedule reimbursement rates. Many private payors use the Medicare Physician Fee Schedule to determine their own reimbursement rates. Based on the SGR, the annual fee schedule update is adjusted to reflect the comparison of actual expenditures to target expenditures. Because one of the factors for calculating the SGR is linked to the growth in the U.S. gross domestic product (“GDP”), the SGR formula may result in a negative payment update if growth in Medicare beneficiaries’ use of services exceeds GDP growth, a situation which has occurred every year since 2002 and the reoccurrence of which we cannot predict.
CMS determined that, effective January 1, 2013, the SGR formula results in a decrease to the physician Medicare fee schedule reimbursement by 26.5%. Congress, however, enacted ATRA which provides, in part, that Medicare physician fee schedule rates for 2012 are extended through December 31, 2013. Therefore, the Medicare fee schedule rates for 2013 are neither subject to the 26.5% SGR formula-driven reduction nor are they subject to any increase over and above the 2012 fee schedule rates.
While Congress has repeatedly intervened to mitigate the negative reimbursement impact associated with the SGR formula, there is no guarantee that Congress will continue to do so in the future. Moreover, the existing methodology may result in significant yearly fluctuations in the Medicare Physician Fee Schedule amounts, which may be unrelated to changes in the actual costs of providing physician services. Unless Congress enacts a change to the SGR methodology, the uncertainty regarding reimbursement rates and fluctuation will continue to exist. Moreover, if Congress does change the SGR methodology or substitute a new system for physician fee-for-service payments, it may require reductions in other Medicare programs including Medicare Advantage to offset such additional costs.
| 27 |
Another provision that affects physician payments under the Medicare Physician Fee Schedule is an adjustment under the Medicare statute to reflect the geographic variation in the cost of delivering physician services, by comparing those costs to the national average. Medicare payments to physicians under the Medicare Physician Fee Schedule are geographically adjusted to reflect the varying cost of delivering physician services across areas. The adjustments are made by indices, known as the Geographic Practice Cost Indices (“GPCI”) that reflect how each geographic area compares to the national average. In 2003, Congress established that for three years there would be a floor of 1.0 on the work component of the Medicare Physician Fee Schedule formula used to determine physician payments, which meant that physician payments would not be reduced in a geographic area just because the relative cost of physician work in that area fell below the national average. Congress extended the GPCI work floor several times since its enactment in 2003. ATRA provides another extension through December 31, 2013. Although Congress has extended the GPCI work floor several times, there is no guarantee that Congress will block the adjustment in the future, which could result in a decrease in payments for physician services.
The 2013 Medicare Physician Fee Schedule also expanded a reduction in reimbursement for multiple images on contiguous body parts to new services, namely diagnostic cardiovascular services and ophthalmology services. Medicare has a longstanding policy to reduce payment by 50% for the second and subsequent procedures furnished to the same beneficiary by a single physician or physicians in the same group practice on the same day, largely based on the presence of efficiencies in the practice expense and physician work. This policy already applies to the technical and professional component of advanced imaging services. Under the new expansion CMS shall apply a 25% reduction to the technical component of second and subsequent diagnostic cardiovascular services, and a 20% reduction to the technical component of second and subsequent diagnostic ophthalmology services, furnished by the same physician (or physicians in the same group practice) to the same beneficiary, on the same day. This further reduces payments for physician services relating to diagnostic imaging, and our associated revenues. Regulatory updates to payment rates for which we bill the Medicare program directly are published annually by CMS in the Federal Register. Current payment rates for certain diagnostic services using equipment costing more than $1 million are subject to usage assumptions at a usage rate of 75%. However, as part of ATRA, Congress paid for part of the SGR freeze by increasing the equipment utilization threshold for advanced imaging modalities from the current 75% to 90% beginning January 2014.
Complying with federal and state regulations is an expensive and time-consuming process, and any failure to comply could result in substantial penalties.
We are directly or indirectly through the radiology practices with which we contract subject to extensive regulation by both the federal government and the state governments in which we provide services, including:
| · | the federal False Claims Act; |
| · | the federal Medicare and Medicaid Anti-Kickback Laws, and state anti-kickback prohibitions; |
| · | federal and state billing and claims submission laws and regulations; |
| · | the federal Health Insurance Portability and Accountability Act of 1996, as amended by the Health Information Technology for Economic and Clinical Health Act of 2009, and comparable state laws; |
| · | the federal physician self-referral prohibition commonly known as the Stark Law and the state equivalent of the Stark Law; |
| · | state laws that prohibit the practice of medicine by non-physicians and prohibit fee-splitting arrangements involving physicians; |
| · | federal and state laws governing the diagnostic imaging and therapeutic equipment we use in our business concerning patient safety, equipment operating specifications and radiation exposure levels; and |
| · | state laws governing reimbursement for diagnostic services related to services compensable under workers compensation rules. |
If our operations are found to be in violation of any of the laws and regulations to which we or the radiology practices with which we contract are subject, we may be subject to the applicable penalty associated with the violation, including civil and criminal penalties, damages, fines and the curtailment of our operations. Any penalties, damages, fines or curtailment of our operations, individually or in the aggregate, could adversely affect our ability to operate our business and our financial results. The risks of our being found in violation of these laws and regulations is increased by the fact that many of them have not been fully interpreted by the regulatory authorities or the courts, and their provisions are open to a variety of interpretations. Any action brought against us for violation of these laws or regulations, even if we successfully defend against it, could cause us to incur significant legal expenses and divert our management’s attention from the operation of our business.
| 28 |
If we fail to comply with various licensure, certification and accreditation standards, we may be subject to loss of licensure, certification or accreditation, which would adversely affect our operations.
Ownership, construction, operation, expansion and acquisition of our diagnostic imaging facilities are subject to various federal and state laws, regulations and approvals concerning licensing of personnel, other required certificates for certain types of healthcare facilities and certain medical equipment. In addition, freestanding diagnostic imaging facilities that provide services independent of a physician’s office must be enrolled by Medicare as an independent diagnostic treatment facility, or IDTF, to bill the Medicare program. Medicare carriers have discretion in applying the IDTF requirements and therefore the application of these requirements may vary from jurisdiction to jurisdiction. In addition, federal legislation requires all suppliers that provide the technical component of diagnostic MRI, PET/CT, CT, and nuclear medicine to be accredited by an accreditation organization designated by CMS (which currently include the American College of Radiology (ACR), the Intersocietal Accreditation Commission (IAC) and the Joint Commission) by January 1, 2012. Our MRI, CT, nuclear medicine, ultrasound and mammography facilities are currently accredited by the American College of Radiology. We may not be able to receive the required regulatory approvals or accreditation for any future acquisitions, expansions or replacements, and the failure to obtain these approvals could limit the opportunity to expand our services.
Our facilities are subject to periodic inspection by governmental and other authorities to assure continued compliance with the various standards necessary for licensure and certification. If any facility loses its certification under the Medicare program, then the facility will be ineligible to receive reimbursement from the Medicare and Medicaid programs. For the year ended December 31, 2012, approximately 24% of our net revenue came from the Medicare and Medicaid programs. A change in the applicable certification status of one of our facilities could adversely affect our other facilities and in turn us as a whole. We have experienced a slowdown in the credentialing of our physicians over the last several years which has lengthened our billing and collection cycle, and could negatively impact our ability to collect revenue from patients covered by Medicare. Credentialing of physicians is required by our payors prior to commencing payment.
Our agreements with the contracted radiology practices must be structured to avoid the corporate practice of medicine and fee-splitting.
State law prohibits us from exercising control over the medical judgments or decisions of physicians and from engaging in certain financial arrangements, such as splitting professional fees with physicians. These laws are enforced by state courts and regulatory authorities, each with broad discretion. A component of our business has been to enter into management agreements with radiology practices. We provide management, administrative, technical and other non-medical services to the radiology practices in exchange for a service fee typically based on a percentage of the practice’s revenue. We structure our relationships with the radiology practices, including the purchase of diagnostic imaging facilities, in a manner that we believe keeps us from engaging in the practice of medicine or exercising control over the medical judgments or decisions of the radiology practices or their physicians, or violating the prohibitions against fee-splitting. There can be no assurance that our present arrangements with BRMG or the physicians providing medical services and medical supervision at our imaging facilities will not be challenged, and, if challenged, that they will not be found to violate the corporate practice of medicine or fee splitting prohibitions, thus subjecting us to potential damages, injunction and/or civil and criminal penalties or require us to restructure our arrangements in a way that would affect the control or quality of our services and/or change the amounts we receive under our management agreements. Any of these results could jeopardize our business.
Newly enacted and future federal legislation could limit the prices we can charge for our services, which would reduce our revenue and adversely affect our operating results.
New legislation has introduced certain changes that may result in decreased revenue for the scans we perform. Among other things, the new legislation will adjust Medicare payment rates for physician imaging services in an attempt to better reflect actual usage, by revising upward the assumed usage rate for diagnostic imaging equipment costing more than $1 million to 90% starting January, 1, 2014. Other changes in reimbursement for services rendered by Medicare Advantage plans may reduce the revenues we receive for services rendered to Medicare Advantage enrollees.
Some of our imaging modalities use radioactive materials, which generate regulated waste and could subject us to liabilities for injuries or violations of environmental and health and safety laws.
Some of our imaging procedures use radioactive materials, which generate medical and other regulated wastes. For example, patients are injected with a radioactive substance before undergoing a PET scan. Storage, use and disposal of these materials and waste products present the risk of accidental environmental contamination and physical injury. We are subject to federal, state and local regulations governing storage, handling and disposal of these materials. We could incur significant costs and the diversion of our management’s attention in order to comply with current or future environmental and health and safety laws and regulations. Also, we cannot completely eliminate the risk of accidental contamination or injury from these hazardous materials. Although we believe that we maintain professional liability insurance coverage consistent with industry practice in the event of an accident, we could be held liable for any resulting damages, and any liability could exceed the limits of or fall outside the coverage of our professional liability insurance.
| 29 |
Technological change in our industry could reduce the demand for our services and require us to incur significant costs to upgrade our equipment.
The development of new technologies or refinements of existing modalities may require us to upgrade and enhance our existing equipment before we may otherwise intend. Many companies currently manufacture diagnostic imaging equipment. Competition among manufacturers for a greater share of the diagnostic imaging equipment market may result in technological advances in the speed and imaging capacity of new equipment. This may accelerate the obsolescence of our equipment, and we may not have the financial ability to acquire the new or improved equipment and may not be able to maintain a competitive equipment base. In addition, advances in technology may enable physicians and others to perform diagnostic imaging procedures without us. If we are unable to deliver our services in the efficient and effective manner that payors, physicians and patients expect our revenue could substantially decrease.
Because we have high fixed costs, lower scan volumes per system could adversely affect our business.
The principal components of our expenses, excluding depreciation, consist of debt service, capital lease payments, compensation paid to technologists, salaries, real estate lease expenses and equipment maintenance costs. Because a majority of these expenses are fixed, a relatively small change in our revenue could have a disproportionate effect on our operating and financial results depending on the source of our revenue. Thus, decreased revenue as a result of lower scan volumes per system could result in lower margins, which could materially adversely affect our business.
We may be unable to effectively maintain our equipment or generate revenue when our equipment is not operational.
Timely, effective service is essential to maintaining our reputation and high use rates on our imaging equipment. Although we have an agreement with GE Medical Systems pursuant to which it maintains and repairs the majority of our imaging equipment, this agreement does not compensate us for loss of revenue when our systems are not fully operational and our business interruption insurance may not provide sufficient coverage for the loss of revenue. Also, GE Medical Systems may not be able to perform repairs or supply needed parts in a timely manner, which could result in a loss of revenue. Therefore, if we experience more equipment malfunctions than anticipated or if we are unable to promptly obtain the service necessary to keep our equipment functioning effectively, our ability to provide services would be adversely affected and our revenue could decline.
Disruption or malfunction in our information systems could adversely affect our business.
Our information technology system is vulnerable to damage or interruption from:
| · | earthquakes, fires, floods and other natural disasters; |
| · | power losses, computer systems failures, internet and telecommunications or data network failures, operator negligence, improper operation by or supervision of employees, physical and electronic losses of data and similar events; and |
| · | computer viruses, penetration by hackers seeking to disrupt operations or misappropriate information and other breaches of security. |
We rely on our information systems to perform functions critical to our ability to operate, including patient scheduling, billing, collections, image storage and image transmission. Accordingly, an extended interruption in the system’s function could significantly curtail, directly and indirectly, our ability to conduct our business and generate revenue.
Adverse changes in general domestic and worldwide economic conditions and instability and disruption of credit markets could adversely affect our operating results, financial condition, or liquidity.
We are subject to risk arising from adverse changes in general domestic and global economic conditions, including recession or economic slowdown and disruption of credit markets. Continued concerns about the systemic impact of potential long-term and wide-spread recession, inflation, energy costs, geopolitical issues, the availability and cost of credit have contributed to increased market volatility and diminished expectations for the United States economy. The United States, and other western countries have responded to this economic situation by exercising monetary policy to keep interest rates low. Any significant change in economic conditions or change in fiscal monetary policy could result in material changes in interest rates.
| 30 |
Continued turbulence in the United States and international markets and economies may adversely affect our liquidity and financial condition, and the liquidity and financial condition of our patients. If these market conditions continue, they may increase expenses associated with borrowing, limit our ability, and the ability of our patients, to timely replace maturing liabilities, and access the capital markets to meet liquidity needs, resulting in adverse effects on our financial condition and results of operations.
The California budget crisis, if not successfully resolved could have an impact on our revenue.
California is experiencing a budget crisis which has resulted in significant state government cutbacks. 109 of our 246 facilities are located in California. One to one-and-one-half percent (1% to 1.5%) of our revenues come from the California Medicaid program ($6.5 million to $9.7 million). To the extent California is unable to provide these payments on a timely basis, or at all, our revenues will be negatively impacted.
We are vulnerable to earthquakes, harsh weather and other natural disasters.
Our corporate headquarters and 109 of our facilities are located in California, an area prone to earthquakes and other natural disasters. Several of our facilities are located in areas of Florida and the east coast that have suffered from hurricanes. Most recently, our operations in Maryland, Delaware, New York and New Jersey were negatively impacted when Hurricane Sandy made landfall on the east coast in late October 2012, resulting in site closures, loss of power and other related business disruptions. In addition, some of our facilities have been affected by snow and other harsh weather conditions particularly in February 2010, when winter snow storms in the mid-Atlantic region, including Maryland, Delaware and New Jersey, caused us to close many of our facilities for up to five business days. An earthquake, harsh weather conditions or other natural disaster could decrease scan volume during affected periods and seriously impair our operations. Damage to our equipment or interruption of our business would adversely affect our financial condition and results of operations.
Possible volatility in our stock price could negatively affect us and our stockholders.
The trading price of our common stock on the NASDAQ Global Market has fluctuated significantly in the past. During the period from January 1, 2011 through December 31, 2012, the trading price of our common stock fluctuated from a high of $3.58 per share to a low of $1.94 per share. In the past, we have experienced a drop in stock price following an announcement of disappointing earnings or earnings guidance. Any such announcement in the future could lead to a similar drop in stock price. The price of our common stock could also be subject to wide fluctuations in the future as a result of a number of other factors, including the following:
| · | changes in expectations as to future financial performance or buy/sell recommendations of securities analysts; |
| · | our, or a competitor’s, announcement of new services, or significant acquisitions, strategic partnerships, joint ventures or capital commitments; and |
| · | the operating and stock price performance of other comparable companies. |
In addition, the U.S. securities markets have experienced significant price and volume fluctuations. These fluctuations often have been unrelated to the operating performance of companies in these markets. Broad market and industry factors may lead to volatility in the price of our common stock, regardless of our operating performance. Moreover, our stock has limited trading volume, and this illiquidity may increase the volatility of our stock price.
In the past, following periods of volatility in the market price of an individual company’s securities, securities class action litigation often has been instituted against that company. The institution of similar litigation against us could result in substantial costs and a diversion of management’s attention and resources, which could negatively affect our business, results of operations or financial condition.
Provisions of the Delaware General Corporation Law and our organizational documents may discourage an acquisition of us.
In the future, we could become the subject of an unsolicited attempted takeover of our company. Although an unsolicited takeover could be in the best interests of our stockholders, our organizational documents and the General Corporation Law of the State of Delaware both contain provisions that will impede the removal of directors and may discourage a third-party from making a proposal to acquire us. For example, the provisions:
| · | permit the board of directors to increase its own size, within the maximum limitations set forth in the bylaws, and fill the resulting vacancies; |
| · | authorize the issuance of shares of preferred stock in one or more series without a stockholder vote; |
| 31 |
| · | establish an advance notice procedure for stockholder proposals to be brought before an annual meeting of our stockholders, including proposed nominations of persons for election to the board of directors; and |
| · | prohibit transfers and/or acquisitions of stock (without consent of the Board of Directors ) that would result in any stockholder owning greater than 5% of the currently outstanding stock resulting in a limitation on net operating loss carryovers, capital loss carryovers, general business credit carryovers, alternative minimum tax credit carryovers and foreign tax credit carryovers, as well as any loss or deduction attributable to a “net unrealized built-in loss” within the meaning of Section 382 of the internal revenue code of 1986, as amended. |
We are subject to Section 203 of the Delaware General Corporation Law, which could have the effect of delaying or preventing a change in control.
We have identified material weaknesses in our internal controls over financial reporting.
Maintaining effective internal controls over financial reporting is necessary for us to produce reliable financial statements. The Board of Directors of the Company concluded on November 8, 2013 that material weaknesses in the internal control over financial reporting exist at the Company, and consequently the Board of Directors determined that management’s report on internal control over financial reporting as of December 31, 2012, included in the Company’s Annual Report on Form 10-K for the year then ended, should no longer be relied upon. These material weaknesses led to the need for the restatement of the Company’s financial statements for the year ended December 31, 2012. These material weaknesses are discussed further within Item 9A “Controls and Procedures” of this Annual Report on Form 10-K/A. The existence of one or more material weaknesses precludes a conclusion by management that a corporation’s internal control over financial reporting is effective.
The Company is currently in the process of remediating this material weakness in internal control over financial reporting by, among other things, designing and implementing additional controls to ensure the quality of information delivered to, and improve the review of completed work received from, our outside tax consultant and improve controls over our identification and assessment of uncertain tax positions. If we fail to remediate this material weakness or fail to otherwise maintain effective controls over financial reporting in the future, it could result in a material misstatement of our financial statements that would not be prevented or detected on a timely basis. Management continues to devote significant time and attention to remediating this material weakness and improving our internal controls, and we expect to continue to incur costs associated with implementing appropriate processes, which could include fees for additional audit and consulting services, which could negatively affect our financial condition and operating results.
| Item 1B. | Unresolved Staff Comments |
None.
| Item 2. | Properties |
Our corporate headquarters is located in adjoining premises at 1508, 1510 and 1516 Cotner Avenue, Los Angeles, California 90025, in approximately 21,500 square feet occupied under leases, which expire (with options to extend) on June 30, 2017. In addition, we lease approximately 60,000 square feet of warehouse and other space under leases nationwide, which expire at various dates through August 2020. We also have a regional office of approximately 39,000 square feet in Baltimore, Maryland under a lease, which expires September 30, 2018.
We operate 109 fixed-site, freestanding outpatient diagnostic imaging facilities in California, 62 in Maryland, 25 in the Rochester and Hudson Valley areas of New York, 7 in Manhattan, New York, 15 in Delaware, 5 in Rhode Island, 19 in New Jersey, as well as 4 individual facilities in Florida. We lease the premises at which these facilities are located. Our facility lease terms vary in length from month to month to 15 years with renewal options upon prior written notice, from 1 year to 15 years depending upon the agreed upon terms with the local landlord. Rents under our facility lease amounts generally increase from 1% to 6% on an annual basis. We do not have options to purchase the facilities we rent.
| Item 3. | Legal Proceedings |
We are engaged from time to time in the defense of lawsuits arising out of the ordinary course and conduct of our business. We believe that the outcome of our current litigation will not have a material adverse impact on our business, financial condition and results of operations. However, we could be subsequently named as a defendant in other lawsuits that could adversely affect us.
| Item 4. | Mine Safety Disclosures |
Not applicable.
| 32 |
PART II
| Item 5. | Market for the Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities |
Our common stock is quoted on the NASDAQ Global Market under the symbol “RDNT.” The following table indicates the high and low prices for our common stock for the periods indicated based upon information supplied by the NASDAQ Global Market.
| Low | High | |||||||
| Quarter Ended | ||||||||
| December 31, 2012 | $ | 2.29 | $ | 2.75 | ||||
| September 30, 2012 | 2.30 | 2.86 | ||||||
| June 30, 2012 | 2.33 | 3.32 | ||||||
| March 31, 2012 | 1.94 | 3.58 | ||||||
| December 31, 2011 | $ | 1.94 | $ | 2.79 | ||||
| September 30, 2011 | 2.30 | 4.58 | ||||||
| June 30, 2011 | 3.40 | 5.19 | ||||||
| March 31, 2011 | 2.87 | 4.00 | ||||||
The last low and high prices for our common stock on the NASDAQ Global Market on March 8, 2013 were $2.68 and $2.77, respectively.
Holders
As of March 8, 2013, the number of holders of record of our common stock was 835. However, Cede & Co., the nominee for The Depository Trust Company, the clearing agency for most broker-dealers, owned a substantial number of our outstanding shares of common stock of record on that date. Our management believes that the number of beneficial owners of our common stock is approximately 4,000.
Dividends
We have never declared or paid cash dividends on our capital stock and we do not expect to pay any dividends in the foreseeable future. We currently intend to retain future earnings, if any, to finance the growth and development of our business. Our current credit facilities place restrictions on our ability to issue dividends. See discussion under “Liquidity and Capital Resources” regarding our current credit facilities. Payment of future dividends, if any, will be at the discretion of our board of directors and will depend on our financial condition, results of operations, capital requirements and such other factors as the board of directors deems relevant.
Equity Compensation Plans Information
The information required by this item will be contained in our definitive proxy statement, to be filed with the SEC in connection with our 2013 annual meeting of stockholders, which is expected to be filed not later than 120 days after the end of our fiscal year ended December 31, 2012, and is incorporated in this report by reference.
Stock Performance Graph
The following graph compares the yearly percentage change in cumulative total stockholder return of our common stock during the period from 2007 to 2012 with (i) the cumulative total return of the S&P500 index and (ii) the cumulative total return of the S&P500 – Healthcare Sector index. The comparison assumes $100 was invested in December 31, 2007 in our common stock and in each of the foregoing indices and the reinvestment of dividends through January 1, 2013. The stock price performance on the following graph is not necessarily indicative of future stock price performance.
This graph shall not be deemed incorporated by reference by any general statement incorporating by reference this Form 10-K into any filing under the Securities Act or under the Exchange Act, except to the extent that RadNet specifically incorporates this information by reference, and shall not otherwise be deemed filed under such Acts.
| 33 |
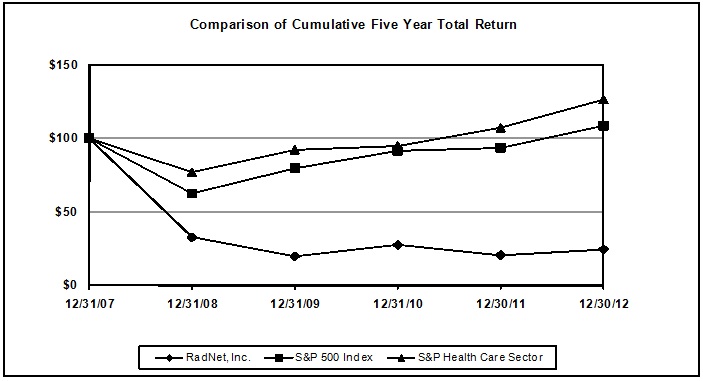
| ANNUAL RETURN PERCENTAGE | ||||||
| Years Ending | ||||||
| Company / Index | 12/31/08 | 12/31/09 | 12/31/10 | 12/30/11 | 12/30/12 | |
| RadNet, Inc. | -67.00 | -39.10 | 38.24 | -24.47 | 18.78 | |
| S&P 500 Index | -37.00 | 26.46 | 15.06 | 2.11 | 16.00 | |
| S&P Health Care Sector | -22.81 | 19.70 | 2.90 | 12.73 | 17.89 | |
| INDEXED RETURNS | ||||||
| Base | Years Ending | |||||
| Period | ||||||
| Company / Index | 12/31/07 | 12/31/08 | 12/31/09 | 12/31/10 | 12/30/11 | 12/30/12 |
| RadNet, Inc. | 100 | 33.00 | 20.10 | 27.78 | 20.99 | 24.93 |
| S&P 500 Index | 100 | 63.00 | 79.67 | 91.68 | 93.61 | 108.59 |
| S&P Health Care Sector | 100 | 77.19 | 92.40 | 95.07 | 107.18 | 126.35 |
Recent Sales of Unregistered Securities
None.
| 34 |
| Item 6. | Selected Consolidated Financial Data |
The following table sets forth our selected historical consolidated financial data. The selected consolidated statements of operations data set forth below for the years ended December 31, 2012, 2011 and 2010, and the consolidated balance sheet data as of December 31, 2012 and 2011, are derived from our audited consolidated financial statements and notes thereto included elsewhere herein. The selected historical consolidated statements of operations data set forth below for the years ended December 31, 2009 and 2008, and the consolidated balance sheet data set forth below as of December 31, 2010, 2009 and 2008, are derived from our audited consolidated financial statements not included herein. This data should be read in conjunction with and is qualified in its entirety by reference to the audited consolidated financial statements and the related notes included elsewhere in this annual report and Item 7 - “Management’s Discussion and Analysis of Financial Condition and Results of Operations.”
The financial data set forth below and discussed in this annual report are derived from the consolidated financial statements of RadNet, its subsidiaries and certain affiliates. As a result of the contractual and operational relationship among BRMG, Dr. Berger and us, we are considered to have a controlling financial interest in BRMG pursuant to applicable accounting guidance. Due to the deemed controlling financial interest, we are required to include BRMG as a consolidated entity in our consolidated financial statements. This means, for example, that revenue generated by BRMG from the provision of professional medical services to our patients, as well as BRMG’s costs of providing those services, are included as net revenue and cost of operations in our consolidated statement of operations, whereas the management fee that BRMG pays to us under our management agreement with BRMG is eliminated as a result of the consolidation of our results with those of BRMG. Also, because BRMG is a consolidated entity in our financial statements, any borrowings or advances we have received from or made to BRMG have been eliminated in our consolidated balance sheet. If BRMG were not treated as a consolidated entity in our consolidated financial statements, the presentation of certain items in our income statement, such as net service fee revenue and costs and expenses, would change but our net income would not, because in operation and historically, the annual revenue of BRMG from all sources closely approximates its expenses, including Dr. Berger’s compensation, fees payable to us and amounts payable to third parties.
| Years Ended | ||||||||||||||||||||
| December 31, | ||||||||||||||||||||
| 2012 | 2011 | 2010 | 2009 | 2008 | ||||||||||||||||
| (Restated) 1. | ||||||||||||||||||||
| (in thousands, except per share data) | ||||||||||||||||||||
| Statement of Operations Data: | ||||||||||||||||||||
| Net revenue | $ | 647,153 | $ | 585,121 | $ | 518,657 | $ | 494,911 | $ | 471,286 | ||||||||||
| Operating expenses: | ||||||||||||||||||||
| Cost of operations, excluding depreciation and amortization | 542,993 | 477,828 | 420,973 | 397,753 | 384,297 | |||||||||||||||
| Depreciation and amortization | 57,740 | 57,481 | 53,997 | 53,800 | 53,548 | |||||||||||||||
| Loss (gain) on sale and disposal of equipment, net | 456 | (2,240 | ) | 1,136 | 523 | 516 | ||||||||||||||
| Gain from sale of joint venture interests | – | – | – | – | – | |||||||||||||||
| Gain on de-consolidation of joint venture | (2,777 | ) | – | – | (1,387 | ) | – | |||||||||||||
| Loss on extinguishment of debt | – | – | 9,871 | – | – | |||||||||||||||
| Net income (loss) | 59,834 | 7,231 | (12,852 | ) | (2,267 | ) | (12,836 | ) | ||||||||||||
| Basic income (loss) per share | 1.58 | 0.19 | (0.35 | ) | (0.06 | ) | (0.36 | ) | ||||||||||||
| Diluted income (loss) per share | 1.52 | 0.19 | (0.35 | ) | (0.06 | ) | (0.36 | ) | ||||||||||||
| Balance Sheet Data: | ||||||||||||||||||||
| Cash and cash equivalents | $ | 362 | $ | 2,455 | $ | 627 | $ | 10,094 | $ | – | ||||||||||
| Total assets | 710,864 | 619,188 | 539,514 | 480,671 | 495,572 | |||||||||||||||
| Total long-term liabilities | 598,507 | 566,615 | 516,723 | 456,727 | 469,994 | |||||||||||||||
| Total liabilities | 717,548 | 688,995 | 621,987 | 555,432 | 576,602 | |||||||||||||||
| Working capital | 36,859 | 29,947 | 5,761 | 9,204 | 2,720 | |||||||||||||||
| Stockholders' equity deficit | ( 6,684 | ) | (69,807 | ) | (82,473 | ) | (74,761 | ) | (81,030 | ) | ||||||||||
1. See Note 1A of the Consolidated Financial Statements contained in Item 8 for further detail regarding the restatement of the amounts included in the above table as of and for the year ended December 31, 2012.
| 35 |
| Item 7. | Management’s Discussion and Analysis of Financial Condition and Results of Operations |
Overview
We are filing this Amendment No. 2 of our annual report on Form 10-K to reflect certain adjustments to our consolidated financial statements as of and for the year ended December 31, 2012 with respect to the impact of an overstatement of a deferred tax asset associated with our interest rate swaps. The impact of the restatement is more fully described in Note 1A to the Consolidated Financial Statements contained in Item 8 of this Amendment No. 2.
We are the leading national provider of freestanding, fixed-site outpatient diagnostic imaging services in the United States based on number of locations and annual imaging revenue. At December 31, 2012, we operated directly or indirectly through joint ventures, 246 centers located in California, Maryland, Florida, Delaware, New Jersey, Rhode Island and New York. Our centers provide physicians with imaging capabilities to facilitate the diagnosis and treatment of diseases and disorders and may reduce unnecessary invasive procedures, often reducing the cost and amount of care for patients. Our services include magnetic resonance imaging (MRI), computed tomography (CT), positron emission tomography (PET), nuclear medicine, mammography, ultrasound, diagnostic radiology (X-ray), fluoroscopy and other related procedures. As of December 31, 2012, we had in operation 205 MRI systems, 118 CT systems, 43 PET or combination PET/CT systems, 45 nuclear medicine systems, 253 X-ray systems, 181 mammography systems, 357 ultrasound systems, and 138 fluoroscopy systems.
We derive substantially all of our revenue from fees charged for the diagnostic imaging services performed at our facilities. For the years ended December 31, 2012, 2011 and 2010, we performed 4,142,267 , 3,740,443 and 3,315,019 diagnostic imaging procedures and generated net revenue of $647.2 million , $585.1 million and $518.7 million, respectively. Additional information concerning RadNet, Inc., including our consolidated subsidiaries, for each of the years ended December 31, 2012, December 31, 2011 and December 31, 2010 is included in the consolidated financial statements and notes thereto in this annual report .
Our revenue is derived from a diverse mix of payors, including private payors, managed care capitated payors and government payors. We believe our payor diversity mitigates our exposure to possible unfavorable reimbursement trends within any one-payor class. In addition, our experience with capitation arrangements over the last several years has provided us with the expertise to manage utilization and pricing effectively, resulting in a predictable stream of revenue. As of December 31, 2012, we received approximately 56% of our payments from commercial insurance payors, 13% from managed care capitated payors, 21% from Medicare and 3% from Medicaid. With the exception of Blue Cross/Blue Shield and government payors, no single payor accounted for more than 5% of our net revenue for the twelve months ended December 31, 2012.
We have developed our medical imaging business through a combination of organic growth and acquisitions. For a discussion of acquisitions and dispositions of facilities, see “Recent Developments and Facility Acquisitions and Dispositions” below.
We typically experience some seasonality to our business. During the first quarter of each year we generally experience the lowest volumes of procedures and the lowest level of revenue for any quarter during the year. This is primarily the result of two factors. First, our volumes and revenue are typically impacted by winter weather conditions in our northeastern operations. It is common for snowstorms and other inclement weather to result in patient appointment cancellations and, in some cases, imaging center closures. Second, in recent years, we have observed greater participation in high deductible health plans by patients. As these high deductibles reset in January for most of these patients, we have observed that patients utilize medical services less during the first quarter, when securing medical care will result in significant out-of-pocket expenditures.
The consolidated financial statements in this annual report include the accounts of Radnet Management and BRMG. The consolidated financial statements also include Radnet Management I, Inc., Radnet Management II, Inc., Radiologix, Inc., Radnet Management Imaging Services, Inc., Delaware Imaging Partners, Inc., New Jersey Imaging Partners, Inc. and Diagnostic Imaging Services, Inc. (DIS), all wholly owned subsidiaries of Radnet Management. Accounting Standards Codification Section 810-10-15-14 stipulates that generally any entity with a) insufficient equity to finance its activities without additional subordinated financial support provided by any parties, or b) equity holders that, as a group, lack the characteristics specified in the Codification which evidence a controlling financial interest, is considered a Variable Interest Entity (“VIE”). We consolidate all voting interest entities in which we own a majority voting interest and all VIEs for which we are the primary beneficiary. We determine whether we are the primary beneficiary of a VIE through a qualitative analysis that identifies which variable interest holder has the controlling financial interest in the VIE. The variable interest holder who has both of the following has the controlling financial interest and is the primary beneficiary: (1) the power to direct the activities of the VIE that most significantly impact the VIE’s economic performance and (2) the obligation to absorb losses of, or the right to receive benefits from, the VIE that could potentially be significant to the VIE. In performing our analysis, we consider all relevant facts and circumstances, including: the design and activities of the VIE, the terms of the contracts the VIE has entered into, the nature of the VIE’s variable interests issued and how they were negotiated with or marketed to potential investors, and which parties participated significantly in the design or redesign of the entity.
Recent Developments and Facility Acquisitions
On October 10, 2012 we completed the refinancing of our senior secured credit facilities for an aggregate of $451.25 million. The refinancing includes a new credit agreement providing for a $350 million senior secured term loan and a $101.25 million senior secured revolving credit facility. See Note 8 to our consolidated financial statements included in this annual report on Form 10-K for further details regarding this debt refinancing.
On December 31, 2012, we completed our acquisition of Lenox Hill Radiology, consisting of three multi-modality imaging centers as well as three additional X-Ray facilities all located in Manhattan, New York. We also acquired in this transaction a 31.5% interest in a joint venture multi-modality imaging center in Manhattan, New York and an option to purchase a 50% interest in a multi-modality imaging center located in Brooklyn, New York for $1.00. The purchase price consisted of approximately $29.0 million in cash. We have made a preliminary fair value determination of the acquired assets and assumed liabilities and approximately $4.5 million of working capital, $7.2 million of fixed assets, $648,000 of joint venture interests, $2.5 million in a $1.00 joint venture purchase option, $100,000 of intangible assets $15.7 million of goodwill and the assumption of approximately $400,000 of other liabilities and $1.3 million of capital lease debt was recorded with respect to this transaction. Our preliminary fair value determination will be made final with the help of an outside valuation expert which we expect to have completed by the end of our first quarter of 2013.
On January 30, 2013, we purchased an additional 20.9% interest in a joint venture multi-modality imaging center located in Manhattan, New York of which we initially held a 31.5% interest from our December 31, 2012 acquisition of Lenox Hill Radiology. This additional 20.9% interest gave us a controlling interest in the center and so accordingly, we will be consolidating its financial statements in the first quarter of 2013.
| 36 |
On February 28, 2013, we completed our acquisition of a multi-modality imaging center located in Brooklyn, New York by exercising a $1.00 purchase option to acquire an initial 50% interest (we acquired this option through our December 31, 2012 acquisition of Lenox Hill Radiology) and then by purchasing the remaining 50% interest from the existing partner for approximately $2.7 million in cash.
On December 3, 2012, we completed our acquisition of a multi-modality imaging center, Clinical Radiologists Medical Imaging located in Silver Spring, Maryland, for $2.8 million in cash. We have made a fair value determination of the acquired assets and assumed liabilities and approximately $65,000 of working capital, $1.8 million of fixed assets, $71,000 of other assets, $1.8 million of goodwill and the assumption of approximately $938,000 of capital lease debt was recorded with respect to this transaction.
On November 5, 2012, we completed our acquisition of a multi-modality imaging center, Vanowen Radiology located in Van Nuys, California, for cash consideration of $550,000. We have made a fair value determination of the acquired assets and approximately $164,000 of fixed assets and $386,000 of goodwill was recorded with respect to this transaction.
On November 9, 2012, we completed our acquisition of a multi-modality imaging center, Pueblo Radiology located in Ventura, California, for cash consideration of $750,000. This center is located in an area of Ventura where we operate an existing center and compete directly with Pueblo Radiology. We plan on closing our existing center and serving this location from this acquired center. We have made a fair value determination of the acquired assets and approximately $1.6 million of fixed assets and no goodwill was recorded with respect to this transaction. In accordance with accounting standards, any excess of fair value of acquired net assets over the acquisition consideration results in a gain on bargain purchase. Prior to recording a gain, the acquiring entity must reassess whether all acquired assets and assumed liabilities have been identified and recognized and perform re-measurements to verify that the consideration paid, assets acquired, and liabilities assumed have been properly valued. We undertook such a reassessment, and as a result, have recorded a gain on bargain purchase of approximately $810,000, which is included in Other Income within our consolidated statement of income for the year ended December 31, 2012. We believe that the gain on bargain purchase resulted from various factors that impacted the sale. The seller, a group of Radiologists some of whom own the building where the imaging center is based, were planning to close the imaging center, which was facing competition pressure from our existing RadNet center, and were facing possible expenses to renovate the building to make it available for a non-imaging center tenant. They saw the sale of these assets to RadNet and RadNet’s assumption of an operating lease for the building as a way to avoid costly renovation expense, get out of a location where they were competing directly with a RadNet center and immediately establish a rental revenue stream. We believe that the seller was willing to accept a bargain purchase price from us in return for our ability to enter into a long-term lease agreement for the facility and establish an immediate rental revenue stream with no investment on their part.
On October 1, 2012 we acquired a 100% controlling interest in one of our non-consolidated joint venture imaging centers in which we previously held a 50% non-consolidated equity investment. As a result of this transaction, we began consolidating this imaging center, recording all of its assets and liabilities at their fair value at October 1, 2012. We have made a fair value determination of the acquired assets and assumed liabilities and $2.1 million of fixed assets and $1.8 million of goodwill was recorded with respect to this transaction. We also assumed approximately $1.9 million of capital lease debt and $200,000 of other liabilities.
On August 6, 2012 we formed a limited liability company with Barnabas Health, a New Jersey owner and operator of a large New Jersey hospital system, for the purpose of creating a New Jersey imaging network under our management. Our first endeavor was to establish a multi-modality imaging center located in Cedar Knolls, New Jersey, of which we own 49%. Our initial investment of approximately $1.8 million was recorded to investment in non-consolidated joint ventures.
On July 23, 2012, we completed our acquisition of a multi-modality imaging center, Orthopedic Imaging Center, LLC. located in Redlands, California, for cash consideration of $700,000. We have made a fair value determination of the acquired assets and approximately $373,000 of fixed assets, $25,000 of other assets and $302,000 of goodwill was recorded with respect to this transaction.
On July 1, 2012, we completed the sale of a 41% portion of our ownership interest of one of our consolidated joint ventures to our existing partner in that joint venture for $1.8 million. After the sale, we retained a 49% ownership interest in this joint venture. As a result of this transaction we de-consolidated this joint venture and recorded the fair value of our remaining interest as an investment in non-consolidated joint venture accounted for under the equity method. We recorded a gain on de-consolidation of a joint venture of approximately $2.8 million with respect to this transaction. Approximately $1.4 million of this gain is related to the re-measurement to current fair value of our remaining 49% interest, using a market based valuation approach. The main input used in our valuation model was the $1.8 million sale price of a 41% interest.
On May 1, 2012, we completed our acquisition of Advanced Medical Imaging of Stuart, L.P., which consists of two multi-modality imaging centers located in Stuart, Florida, for cash consideration of $1.0 million. We have made a fair value determination of the acquired assets and approximately $39,000 of fixed assets, $88,000 of other current assets and $923,000 of goodwill was recorded with respect to this transaction.
On April 1, 2012, we completed our acquisition of West Coast Radiology, which consists of five multi-modality imaging centers in Orange County, California, for cash consideration of $8.1 million. The centers are located in Anaheim, Santa Ana/Tustin, Irvine and Mission Viejo/Laguna Niguel and operate a combination of MRI, CT, ultrasound, mammography, X-ray and other related modalities. We have made a fair value determination of the acquired assets and assumed liabilities and approximately $715,000 of working capital, $3.1 million of fixed assets, $5.4 million of goodwill, $200,000 of intangible assets and the assumption of approximately $1.3 million of capital lease debt was recorded with respect to this transaction.
| 37 |
On February 29, 2012, we completed the acquisition of a multi-modality imaging center from TODIC, L.P. located in Camarillo, California for cash consideration of $350,000. The facility provides MRI, CT, mammography, ultrasound and X-ray services. We have made a fair value determination of the acquired assets and assumed liabilities and approximately $425,000 of fixed assets and $86,000 of goodwill was recorded with respect to this transaction as well as the assumption of approximately $40,000 of accrued liabilities and approximately $121,000 of capital lease debt.
On February 29, 2012, we completed the acquisition of a multi-modality imaging center from Progressive MRI, LLC located in Frederick, Maryland for cash consideration of $230,000. The facility provides MRI, CT, mammography, ultrasound and X-ray services. We have made a fair value determination of the acquired assets and approximately $230,000 of fixed assets was recorded with respect to this transaction.
Results of Operations
The following table sets forth, for the periods indicated, the percentage that certain items in the statements of operations bears to net revenue before provision for bad debts .
RADNET, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF OPERATIONS
(IN THOUSANDS EXCEPT SHARE DATA)
| Years Ended December 31, | ||||||||||||
| 2012 | 2011 | 2010 | ||||||||||
| (Restated) | ||||||||||||
| NET REVENUE | ||||||||||||
| Service fee revenue, net of contractual allowances and discounts | 91.8 | % | 91.4 | % | 90.5 | % | ||||||
| Provision for bad debts | -3.8 | % | -3.7 | % | -4.1 | % | ||||||
| Net service fee revenue | 88.0 | % | 87.7 | % | 86.4 | % | ||||||
| Revenue under capitation arrangements | 8.2 | % | 8.6 | % | 9.5 | % | ||||||
| Total net revenue | 96.2 | % | 96.3 | % | 95.9 | % | ||||||
| OPERATING EXPENSES | ||||||||||||
| Cost of operations, excluding depreciation and amortization | 80.7 | % | 78.7 | % | 77.9 | % | ||||||
| Depreciation and amortization | 8.6 | % | 9.5 | % | 10.0 | % | ||||||
| Loss (gain) on sale and disposal of equipment | 0.1 | % | -0.4 | % | 0.2 | % | ||||||
| Severance costs | 0.1 | % | 0.2 | % | 0.2 | % | ||||||
| Total operating expenses | 89.4 | % | 88.0 | % | 88.2 | % | ||||||
| INCOME FROM OPERATIONS | 6.7 | % | 8.3 | % | 7.7 | % | ||||||
| OTHER INCOME AND EXPENSES | ||||||||||||
| Interest expense | 8.0 | % | 8.7 | % | 9.0 | % | ||||||
| Loss on extinguishment of debt | 0.0 | % | 0.0 | % | 1.8 | % | ||||||
| Gain on de-consolidation of joint venture | -0.4 | % | 0.0 | % | 0.0 | % | ||||||
| Other (income) expenses | -0.5 | % | -0.8 | % | 0.1 | % | ||||||
| Total other expenses | 7.0 | % | 7.9 | % | 10.9 | % | ||||||
| (LOSS) INCOME BEFORE INCOME TAXES AND EQUITY IN EARNINGS OF JOINT VENTURES | -0.3 | % | 0.5 | % | -3.2 | % | ||||||
| Benefit from (provision for) income taxes | 8.2 | % | -0.1 | % | -0.1 | % | ||||||
| Equity in earnings of joint ventures | 1.0 | % | 0.9 | % | 0.9 | % | ||||||
| NET INCOME (LOSS) | 8.9 | % | 1.2 | % | -2.3 | % | ||||||
| Net (loss) income attributable to noncontrolling interests | 0.0 | % | 0.0 | % | 0.0 | % | ||||||
| NET INCOME (LOSS) ATTRIBUTABLE TO RADNET, INC. COMMON STOCKHOLDERS | 8.9 | % | 1.2 | % | -2.4 | % | ||||||
Year Ended December 31, 2012 Compared to the Year Ended December 31, 2011
Service Fee Revenue , net of contractual allowances and discounts
Service fee revenue , net of allowances and discounts for the year ended December 31, 2012 was $ 618.0 million compared to $ 555.0 million for the year ended December 31, 2011, an increase of $ 63.0 million, or 11.4 %.
Service fee revenue , net of allowances and discounts , including only those centers which were in operation throughout the full fiscal years of both 2012 and 2011, decreased $6. 3 million, or 1. 2%. This 1. 2 % decrease is primarily the result of a similar percentage decrease in procedure volumes. This comparison excludes revenue contributions from centers that were acquired subsequent to January 1, 2011. For the year ended December 31, 2012, service fee revenue , net of contractual allowances and discounts, from centers that were acquired subsequent to January 1, 2011 and excluded from the above comparison was $ 96.3 million. For the year ended December 31, 2011, net revenue from centers that were acquired subsequent to January 1, 2011 and excluded from the above comparison was $27.0 million.
| 38 |
Provision for Bad Debts
Provision for bad debts increased $3.6 million, or 16.0%, to $25.9 million, or 3.8% of net revenue, for the year ended December 31, 2012 compared to $22.3 million, or 3.7% of net revenue, for the year ended December 31, 2011. This increase is in line with the increase in service fee revenues.
Revenue Under Capitation Arrangements
Revenue under capitation arrangements for the year ended December 31, 2012 was $55.1 million compared to $52.5 million for the year ended December 31, 2011, an increase of $2.6 million, or 5.0%.
Revenue under capitation arrangements, including only those centers which were in operation throughout the full fiscal years of both 2012 and 2011, increased $174,000, or 0.3%. This comparison excludes revenue contributions from centers that were acquired subsequent to January 1, 2011. For the year ended December 31, 2012, revenue under capitation arrangements from centers that were acquired subsequent to January 1, 2011 and excluded from the above comparison was $2.5 million. For the year ended December 31, 2011, net revenue from centers that were acquired subsequent to January 1, 2011 and excluded from the above comparison was $46,000.
Operating Expenses
Cost of operations for the year ended December 31, 2012 increased approximately $65.2 million, or 13.6%, from $477.8 million for the year ended December 31, 2011 to $543.0 million for the year ended December 31, 2012. The following table sets forth our operating expenses for the years ended December 31, 2012 and 2011 (in thousands):
| Years Ended December 31, | ||||||||
| 2012 | 2011 | |||||||
| Salaries and professional reading fees, excluding stock-based compensation | $ | 298,409 | $ | 264,465 | ||||
| Stock-based compensation | 2,736 | 3,110 | ||||||
| Building and equipment rental | 60,624 | 53,251 | ||||||
| Medical supplies | 38,879 | 34,014 | ||||||
| Other operating expenses * | 142,345 | 122,988 | ||||||
| Cost of operations | 542,993 | 477,828 | ||||||
| Depreciation and amortization | 57,740 | 57,481 | ||||||
| Loss (gain) on sale and disposal of equipment | 456 | (2,240 | ) | |||||
| Severance costs | 736 | 1,391 | ||||||
| Total operating expenses | $ | 601,925 | $ | 534,460 | ||||
* Includes billing fees, office supplies, repairs and maintenance, insurance, business tax and license, outside services, utilities, marketing, travel and other expenses.
| · | Salaries and professional reading fees, excluding stock-based compensation and severance |
Salaries and professional reading fees increased $33.9 million, or 12.8%, to $298.4 million for the year ended December 31, 2012, compared to $264.5 million for the year ended December 31, 2011.
Salaries and professional reading fees, including only those centers which were in operation throughout the full fiscal years of both 2012 and 2011, increased $3.8 million, or 1.5%. This 1.5% increase is primarily due to the fact that there was one additional work day during the year ended December 31, 2012 when compared to the prior year. There were also bonuses paid to certain members of management during the year ended December 31, 2012 that were not paid in the prior year. This comparison excludes contributions from centers that were acquired subsequent to January 1, 2011. For the year ended December 31, 2012, salaries and professional reading fees from centers that were acquired subsequent to January 1, 2011 and excluded from the above comparison was $40.4 million. For the year ended December 31, 2011, salaries and professional reading fees from centers that were acquired subsequent to January 1, 2011, and excluded from the above comparison was $10.2 million.
| · | Stock-based compensation |
Stock-based compensation decreased $374,000, or 12.0%, to $2.7 million for the year ended December 31, 2012 compared to $3.1 million for the year ended December 31, 2011. The decrease is due to fewer equity compensation instruments being issued in 2012 compared to the prior year.
| · | Building and equipment rental |
Building and equipment rental expenses increased $7.4 million, or 13.8%, to $60.6 million for the year ended December 31, 2012, compared to $53.2 million for the year ended December 31, 2011.
| 39 |
Building and equipment rental expenses, including only those centers which were in operation throughout the full fiscal years of both 2012 and 2011, increased $1.2 million, or 2.5%. This 2.5% increase is primarily due to equipment lease buy-outs occurring in the third quarter of 2012. This comparison excludes contributions from centers that were acquired subsequent to January 1, 2011. For the year ended December 31, 2012, building and equipment rental expenses from centers that were acquired subsequent to January 1, 2011, and excluded from the above comparison, was $8.8 million. For the year ended December 31, 2011, building and equipment rental expenses from centers that were acquired subsequent to January 1, 2011, and excluded from the above comparison, was $2.6 million.
| · | Medical supplies |
Medical supplies expense increased $4.9 million, or 14.3%, to $38.9 million for the year ended December 31, 2012, compared to $34.0 million for the year ended December 31, 2011.
Medical supplies expenses, including only those centers which were in operation throughout the full fiscal years of both 2012 and 2011, decreased $441,000, or 1.4%. This 1.4% decrease is in line with our decrease in service fee revenue. This comparison excludes contributions from centers that were acquired or divested subsequent to January 1, 2011. For the year ended December 31, 2012, medical supplies expense from centers that were acquired subsequent to January 1, 2011, and excluded from the above comparison was $7.6 million. For the year ended December 31, 2011, medical supplies expense from centers that were acquired subsequent to January 1, 2011, and excluded from the above comparison was $2.3 million.
| · | Other Operating Expenses |
Other operating expenses increased $19.3 million, or 15.7%, to $142.3 million for the year ended December 31, 2012 compared to $123.0 million for the year ended December 31, 2011.
Other operating expenses, including only those centers which were in operation throughout the full fiscal years of both 2012 and 2011, increased $2.3 million, or 1.9%. This 1.9% increase is primarily due to an increase in insurance costs as well as increases in certain outside accounting and consulting services. This comparison excludes contributions from centers that were acquired or divested subsequent to January 1, 2011. For the year ended December 31, 2012, other operating expense from centers that were acquired subsequent to January 1, 2011, and excluded from the above comparison was $22.3 million. For the year ended December 31, 2011, other operating expense from centers that were acquired subsequent to January 1, 2011, and excluded from the above comparison was $5.3 million.
| · | Depreciation and amortization expense |
Depreciation and amortization expense increased $259,000, or 0.4%, to $57.7 million for the year ended December 31, 2012 when compared to the same period last year. The increase is due to property and equipment additions for existing centers as well as newly acquired centers. Offsetting this is a catch-up reduction to depreciation of approximately $1.4 million recorded in September of 2012 related to our finalization of purchase accounting for our acquisition of Raven Holdings U.S., Inc.
| · | Loss (gain) on sale and disposal of equipment |
Loss on sale of equipment was approximately $456,000 for the year ended December 31, 2012 and resulted primarily from the sale of imaging equipment for scrap value upon acquisition of upgraded equipment. Gain on sale of equipment was approximately $2.2 million for the year ended December 31, 2011 and was primarily related to the difference between the net book value of certain equipment damaged in a fire at one of our imaging facilities and insurance proceeds we received from claims filed on this damaged equipment.
| · | Severance costs |
During the year ended December 31, 2012, we recorded severance costs of $736,000 compared to $1.4 million recorded during the year ended December 31, 2011. In each period, these costs were primarily associated with the integration of acquired operations.
Interest expense
Interest expense increased approximately $1.0 million, or 1.9%, to $53.8 million for the year ended December 31, 2012compared to $52.8 million for the year ended December 31, 2011. Interest expense for the year ended December 31, 2012 included $3.6 million of amortization of deferred financing costs and discount on issuance of debt as well as $918,000 of amortization of Accumulated Other Comprehensive Loss associated with fair value adjustments to our interest rate swaps accumulated prior to April 6, 2010, the date we established our credit facilities. Interest expense for the year ended December 31, 2011 included $3.2 million of amortization of deferred financing costs and discount on issuance of debt as well as $1.2 million of amortization of Accumulated Other Comprehensive Loss associated with fair value adjustments to our interest rate swaps accumulated prior to April 6, 2010. See “Liquidity and Capital Resources” below for more details on our credit facilities. Excluding these adjustments to interest expense for each period, interest expense increased approximately $900,000 for the year ended December 31, 2012 compared to the year ended December 31, 2011. This increase was primarily due to interest expense on the additional borrowings.
| 40 |
Gain on de-consolidation of joint venture
On July 1, 2012, we completed the sale of a 41% portion of our ownership interest of one of our consolidated joint ventures to our existing partner in that joint venture for $1.8 million. After the sale, we retained a 49% ownership interest in this joint venture. As a result of this transaction we no longer include the financials of this joint venture in our consolidated financial statements and we recorded the fair value of our remaining interest as an investment in non-consolidated joint venture accounted for under the equity method. We recorded a gain on de-consolidation of a joint venture of approximately $2.8 million with respect to this transaction. Approximately $1.4 million of this gain is related to the re-measurement to current fair value of our remaining 49% interest, using a market based valuation approach. The main input used in our valuation model was the $1.8 million sale price of a 41% interest.
Other income
For the year ended December 31, 2012 we recorded approximately $3.7 million of other income primarily consisting of approximately $5.1 million of fair value adjustments on our interest rate swaps and an $810,000 bargain purchase gain related to our November 9, 2012 acquisition of Pueblo Radiology (see “Recent Developments and Facility Acquisitions” above), offset by the write-off of approximately $2.2 million of other non-operating receivables. For the year ended December 31, 2011 we recorded approximately $5.1 million of other income primarily related to fair value adjustments on our interest rate swaps.
Income tax benefit / expense
For the year ended December 31, 2012, we recorded a benefit from income taxes of approximately $ 55.2 million primarily related to reversing the valuation allowance against our deferred tax assets (see Note 11 to our consolidated financial statements for more details). For the year ended December 31, 2011, we recorded $820,000 for state income tax expense primarily related to taxable income generated in the states of California, Maryland and Delaware.
Equity in earnings from unconsolidated joint ventures
Equity in earnings from our unconsolidated joint ventures increased $1.3 million, or 24.0% to $6.5 million for the year ended December 31, 2012 compared to $5.2 million for the year ended December 31, 2011. This increase primarily related to an increase in procedure volumes at these joint venture imaging centers.
Year Ended December 31, 2011 Compared to the Year Ended December 31, 2010
Service Fee Revenue , net of contractual allowances and discounts
Service fee revenue , net of allowances and discounts for the year ended December 31, 2011 was $ 555.0 million compared to $ 489.3 million for the year ended December 31, 2010, an increase of $ 65.7 million, or 13 .4%.
Service fee revenue , net of contractual allowances and discounts , including only those centers which were in operation throughout the full fiscal years of both 2011 and 2010, increased $ 2.6 million, or 0. 6%. This 0. 6 % increase is primarily the result of increases in our procedure volumes. This comparison excludes revenue contributions from centers that were acquired subsequent to January 1, 2010. This comparison excludes revenue contributions from centers that were acquired subsequent to January 1, 2010. For the year ended December 31, 2011, service fee revenue, net of contractual allowances and discounts, from centers that were acquired subsequent to January 1, 2010 and excluded from the above comparison was $ 95.8 million. For the year ended December 31, 2010, net revenue from centers that were acquired subsequent to January 1, 2010 and excluded from the above comparison was $32. 7 million.
Provision for Bad Debts
Provision for bad debts increased $300,000, or 1.4%, to $22.3 million, or 3.7% of net revenue, for the year ended December 31, 2011 compared to $22.0 million, or 4.1% of net revenue, for the year ended December 31, 2010.
| 41 |
Revenue Under Capitation Arrangements
Revenue under capitation arrangements for the year ended December 31, 2011 was $52.5 million compared to $51.4 million for the year ended December 31, 2010, an increase of $1.1 million, or 2.1%.
Revenue under capitation arrangements, including only those centers which were in operation throughout the full fiscal years of both 2011 and 2010, increased $687,000, or 1.3%. This comparison excludes revenue contributions from centers that were acquired subsequent to January 1, 2010. For the year ended December 31, 2011, revenue under capitation arrangements from centers that were acquired subsequent to January 1, 2010 and excluded from the above comparison was $500,000. For the year ended December 31, 2010, net revenue from centers that were acquired subsequent to January 1, 2010 and excluded from the above comparison was $36,000.
Operating Expenses
Cost of operations for the year ended December 31, 2011 increased approximately $56.8 million, or 13.5%, from $421.0 million for the year ended December 31, 2010 to $477.8 million for the year ended December 31, 2011. The following table sets forth our operating expenses for the years ended December 31, 2011 and 2010 (in thousands):
| Years Ended December 31, | ||||||||
| 2011 | 2010 | |||||||
| Salaries and professional reading fees, excluding stock-based compensation | $ | 264,465 | $ | 231,922 | ||||
| Stock-based compensation | 3,110 | 3,718 | ||||||
| Building and equipment rental | 53,251 | 47,938 | ||||||
| Medical supplies | 34,014 | 30,413 | ||||||
| Other operating expenses * | 122,988 | 106,982 | ||||||
| Cost of operations | 477,828 | 420,973 | ||||||
| Depreciation and amortization | 57,481 | 53,997 | ||||||
| Loss (gain) on sale and disposal of equipment | (2,240 | ) | 1,136 | |||||
| Severance costs | 1,391 | 838 | ||||||
| Total operating expenses | $ | 534,460 | $ | 476,944 | ||||
* Includes billing fees, office supplies, repairs and maintenance, insurance, business tax and license, outside services, utilities, marketing, travel and other expenses.
| · | Salaries and professional reading fees, excluding stock-based compensation and severance |
Salaries and professional reading fees increased $32.6 million, or 14.0%, to $264.5 million for the year ended December 31, 2011, compared to $231.9 million for the year ended December 31, 2010.
Salaries and professional reading fees, including only those centers which were in operation throughout the full fiscal years of both 2011 and 2010, increased $4.8 million, or 2.2%. This 2.2% increase is primarily due to expansion of our existing breast care centers.
This comparison excludes contributions from centers that were acquired subsequent to January 1, 2010. For the year ended December 31, 2011, salaries and professional reading fees from centers that were acquired subsequent to January 1, 2010 and excluded from the above comparison was $42.6 million. For the year ended December 31, 2010, salaries and professional reading fees from centers that were acquired subsequent to January 1, 2010, and excluded from the above comparison was $14.8 million.
| · | Stock-based compensation |
Stock-based compensation decreased $608,000, or 16.4%, to $3.1 million for the year ended December 31, 2011 compared to $3.7 million for the year ended December 31, 2010. The decrease is primarily due to a larger number of options granted during the first three quarters of 2010 that vested on the date of grant compared to the same period of 2011.
| · | Building and equipment rental |
Building and equipment rental expenses increased $5.3 million, or 11.1%, to $53.2 million for the year ended December 31, 2011, compared to $47.9 million for the year ended December 31, 2010.
Building and equipment rental expenses, including only those centers which were in operation throughout the full fiscal years of both 2011 and 2010, decreased $246,000, or 0.6%. This 0.6% decrease is primarily due to equipment lease buy-outs occurring in the third quarter of 2011. This comparison excludes contributions from centers that were acquired subsequent to January 1, 2010. For the year ended December 31, 2011, building and equipment rental expenses from centers that were acquired subsequent to January 1, 2010, and excluded from the above comparison, was $9.1 million. For the year ended December 31, 2010, building and equipment rental expenses from centers that were acquired subsequent to January 1, 2010, and excluded from the above comparison, was $3.5 million.
| · | Medical supplies |
Medical supplies expense increased $3.6 million, or 11.8%, to $34.0 million for the year ended December 31, 2011, compared to $30.4 million for the year ended December 31, 2010.
| 42 |
Medical supplies expenses, including only those centers which were in operation throughout the full fiscal years of both 2011 and 2010, increased $265,000, or 0.9%. This 0.9% increase is in line with the increase in our procedure volumes. This comparison excludes contributions from centers that were acquired or divested subsequent to January 1, 2010. For the year ended December 31, 2011, medical supplies expense from centers that were acquired subsequent to January 1, 2010, and excluded from the above comparison was $ 4.7 million. For the year ended December 31, 2010, medical supplies expense from centers that were acquired subsequent to January 1, 2010, and excluded from the above comparison was $1.4 million.
| · | Other Operating Expenses |
Other operating expenses increased $16.0 million, or 15.0%, to $123.0 million for the year ended December 31, 2011 compared to $107.0 million for the year ended December 31, 2010.
Other operating expenses, including only those centers which were in operation throughout the full fiscal years of both 2011 and 2010, increased $1.8 million, or 1.8%. This 1.8% increase is primarily due to an increase in insurance costs as well as increases in certain outside accounting and consulting services. This comparison excludes contributions from centers that were acquired or divested subsequent to January 1, 2010. For the year ended December 31, 2011, other operating expense from centers that were acquired subsequent to January 1, 2010, and excluded from the above comparison was $21.8 million. For the year ended December 31, 2010, other operating expense from centers that were acquired subsequent to January 1, 2010, and excluded from the above comparison was $7.6 million.
| · | Depreciation and amortization expense |
Depreciation and amortization expense increased $3.5 million, or 6.5%, to $57.5 million for the year ended December 31, 2011 when compared to the same period last year. The increase is primarily due to property and equipment additions for existing centers as well as newly acquired centers.
| · | Loss (gain) on sale and disposal of equipment |
Gain on sale of equipment was approximately $2.2 million for the year ended December 31, 2011 and was primarily from insurance proceeds received on equipment lost in a fire at one of our west coast imaging centers. Loss on sale of equipment was approximately $1.1 million for the year ended December 31, 2010 and resulted primarily from the sale of imaging equipment for scrap value upon acquisition of upgraded equipment.
| · | Severance costs |
During the year ended December 31, 2011, we recorded severance costs of $1.4 million compared to $838,000 recorded during the year ended December 31, 2010. In each period, these costs were primarily associated with the integration of acquired operations.
Interest expense
Interest expense increased approximately $4.4 million, or 9.1%, to $52.8 million for the year ended December 31, 2011 compared to $48.4 million for the year ended December 31, 2010. Interest expense for the year ended December 31, 2011 included $3.2 million of amortization of deferred financing costs as well as $1.2 million of amortization of Accumulated Other Comprehensive Loss associated with fair value adjustments to our interest rate swaps accumulated prior to April 6, 2010, the date of our debt refinancing. Interest expense for the year ended December 31, 2010 included $3.0 million of amortization of deferred financing costs as well as $917,000 of amortization of Accumulated Other Comprehensive Loss associated with fair value adjustments to our interest rate swaps accumulated prior to April 6, 2010, the date of our debt refinancing. See “Liquidity and Capital Resources” below for more details on our debt refinancing. Excluding these adjustments to interest expense for each period, interest expense increased $3.9 million. This increase was primarily due to interest expense on the additional borrowings under the debt refinancing completed April 6, 2010.
Loss on extinguishment of debt
For the year ended December 31, 2010, we recorded a $9.9 million loss on extinguishment of debt related to our debt refinancing completed on April 6, 2010. This loss included a $7.6 million write-off of deferred loan costs associated with our GE debt settled on April 6, 2010, as well as approximately $2.3 million to settle a call premium associated with our prior credit facilities and for interest rate swap related expenses. There was no similar expense for the year ended December 31, 2011.
Other expenses
For the year ended December 31, 2011 we recorded approximately $5.1 million of other income primarily related to fair value adjustments on our interest rate swaps. For the year ended December 31, 2010, we recorded approximately $505,000 of other expenses which consisted of approximately $132,000 related to fair value adjustments on our interest rate swaps as well as $373,000 related to litigation.
Income tax expense
For the years ended December 31, 2011 and 2010, we recorded $820,000 and $576,000, respectively, for state income tax expense primarily related to taxable income generated in the states of California, Maryland and Delaware.
Equity in earnings from unconsolidated joint ventures
Equity in earnings from our unconsolidated joint ventures increased $272,000, or 5.5% to $5.2 million for the year ended December 31, 2011 compared to $4.9 million for the year ended December 31, 2010. The 5.5% increase is primarily due to an improvement in collection rates during the end 2010.
| 43 |
Adjusted EBITDA
We use both GAAP and non-GAAP metrics to measure our financial results. We believe that, in addition to GAAP metrics, these non-GAAP metrics assist us in measuring our cash generated from operations and ability to service our debt obligations. We believe this information is useful to investors and other interested parties because we are highly leveraged and our non-GAAP metrics removes non-cash and nonrecurring charges that occur in the affected period and provides a basis for measuring the Company's financial condition against other quarters.
One non-GAAP measure we believe assists us is Adjusted EBITDA. We define Adjusted EBITDA as earnings before interest, taxes, depreciation and amortization, each from continuing operations as adjusted to exclude losses or gains on the disposal of equipment, other income or loss, loss on debt extinguishments, bargain purchase gains, loss on de-consolidation of joint ventures and non-cash equity compensation. Adjusted EBITDA includes equity earnings in unconsolidated operations and subtracts allocations of earnings to non-controlling interests in subsidiaries, and is adjusted for non-cash or extraordinary and one-time events taken place during the period.
Adjusted EBITDA is a non-GAAP financial measure used as an analytical indicator by us and the healthcare industry to assess business performance, and is a measure of leverage capacity and ability to service debt. Adjusted EBITDA should not be considered a measure of financial performance under GAAP, and the items excluded from Adjusted EBITDA should not be considered in isolation or as alternatives to net income, cash flows generated by operating, investing or financing activities or other financial statement data presented in the consolidated financial statements as an indicator of financial performance or liquidity. As Adjusted EBITDA is not a measurement determined in accordance with GAAP and is therefore susceptible to varying methods of calculation, this metric, as presented, may not be comparable to other similarly titled measures of other companies.
The following is a reconciliation of the nearest comparable GAAP financial measure, net income (loss), to Adjusted EBITDA for the years ended December 31, 2012, 2011, and 2010, respectively (in thousands):
Years Ended December 31, | ||||||||||||
| 2012 | 2011 | 2010 | ||||||||||
| (Restated) | ||||||||||||
| Net income (loss) attributable to RadNet, Inc. common stockholders | $ | 59,834 | $ | 7,231 | $ | (12,852 | ) | |||||
| Plus Benefit from (provision for) income taxes | (55,227 | ) | 820 | 576 | ||||||||
| Plus Other (income) expenses | (3,679 | ) | (5,075 | ) | 505 | |||||||
| Plus Interest expense | 53,783 | 52,798 | 48,398 | |||||||||
| Plus Severence costs | 736 | 1,391 | 838 | |||||||||
| Plus Loss (gain) on sale and disposal of equipment | 456 | (2,240 | ) | 1,136 | ||||||||
| Gain on de-consolidation of joint venture | (2,777 | ) | – | – | ||||||||
| Plus Loss on extinguishment of debt | – | – | 9,871 | |||||||||
| Plus Depreciation and amortization | 57,740 | 57,481 | 53,997 | |||||||||
| Plus Non-cash employee stock based compensation | 2,736 | 3,110 | 3,718 | |||||||||
| Adjusted EBITDA | $ | 113,602 | $ | 115,516 | $ | 106,187 | ||||||
Liquidity and Capital Resources
We had cash and cash equivalents of $362,000 and accounts receivable of $129.2 million at December 31, 2012, compared to cash of $2.5 million and accounts receivable of $128.4 million at December 31, 2011. We had a working capital balance of $ 36.9 million and $29.9 million at December 31, 2012 and 2011, respectively. We had net income attributable to RadNet, Inc.’s common stockholders of $ 59.8 million and $7.2 million, and a net loss of $12.9 million for the years ended December 31, 2012, 2011 and 2010, respectively. We also had a stockholders’ equity deficit of $ 6.7 million and $69.8 million at December 31, 2012 and 2011, respectively.
We operate in a capital intensive, high fixed-cost industry that requires significant amounts of capital to fund operations. In addition to operations, we require a significant amount of capital for the initial start-up and development of new diagnostic imaging facilities, the acquisition of additional facilities and new diagnostic imaging equipment. Because our cash flows from operations have been insufficient to fund all of these capital requirements, we have depended on the availability of financing under credit arrangements with third parties.
Based on our current level of operations, we believe that cash flow from operations and available cash, together with available borrowings from our senior secured credit facilities, will be adequate to meet our short-term and long-term liquidity needs. Our future liquidity requirements will be for working capital, capital expenditures, debt service and general corporate purposes. Our ability to meet our working capital and debt service requirements, however, is subject to future economic conditions and to financial, business and other factors, many of which are beyond our control. If we are not able to meet such requirements, we may be required to seek additional financing. There can be no assurance that we will be able to obtain financing from other sources on the terms acceptable to us, if at all.
| 44 |
On a continuing basis, we also consider various transactions to increase shareholder value and enhance our business results, including acquisitions, divestitures and joint ventures. These types of transactions may result in future cash proceeds or payments but the general timing, size or success of any acquisition, divestiture or joint venture effort and the related potential capital commitments cannot be predicted. We expect to fund any future acquisitions primarily with cash flow from operations and borrowings, including borrowing from amounts available under our senior secured credit facilities or through new equity or debt issuances.
We and our subsidiaries or affiliates may from time to time, in our or their sole discretion, continue to purchase, repay, redeem or retire any of our outstanding debt or equity securities in privately negotiated or open market transactions, by tender offer or otherwise. However, we have no formal plan of doing so at this time.
Sources and Uses of Cash
Cash provided by operating activities was $75.3 million, $57.6 million and $66.9 million for the years ended December 31, 2012, 2011 and 2010, respectively.
Cash used in investing activities was $87.2 million, $87.7 million and $101.4 million for the years ended December 31, 2012, 2011 and 2010, respectively. For the year ended December 31, 2012, we purchased property and equipment for approximately $44.5 million, acquired the assets and businesses of additional imaging facilities for approximately $45.6 million (see Note 4 to the consolidated financial statements of this annual report), and purchased additional equity interests in non-consolidated joint ventures of $2.8 million. Offsetting our cash used in investing activities was $2.3 million in proceeds from the sale of an acquired imaging center that was classified on our consolidated balance sheet at December 31, 2011 as an asset held for sale, $1.8 million of proceeds from the sale of joint venture interests, and $1.5 million of proceeds from the sale of imaging equipment.
Cash provided by financing activities was $9.7 million, $31.9 million and $25.0 million for the years ended December 31, 2012, 2011 and 2010, respectively. The cash provided by financing for the year ended December 31, 2012, was primarily due to our refinancing of our Credit Facilities originally entered into on April 6, 2010.
2010 Credit Agreements
On April 6, 2010, we completed a series of transactions which we refer to as our "debt refinancing plan" for an aggregate of $585.0 million. As part of the debt refinancing plan, our wholly owned subsidiary, Radnet Management, Inc., issued and sold $200.0 million in 10 3/8% senior unsecured notes due 2018 (the “senior notes”). All payments of the senior notes, including principal and interest, are guaranteed jointly and severally on a senior unsecured basis by RadNet, Inc. and all of Radnet Management’s current and future domestic wholly owned restricted subsidiaries. The senior notes were issued under an indenture agreement dated April 6, 2010 (the “Indenture”), by and among Radnet Management, as issuer, RadNet, Inc., as parent guarantor, the subsidiary guarantors thereof and U.S. Bank National Association, as trustee, in a private placement that was not subject to the registration requirements of the Securities Act. The senior notes initially issued on April 6, 2010 in a private placement were subsequently publicly offered for exchange enabling holders of the outstanding senior notes to exchange the outstanding notes for publicly registered exchange notes with nearly identical terms. The exchange offer was completed on February 14, 2011.
In addition to the issuance of senior notes, Radnet Management entered into a Credit and Guaranty Agreement with a syndicate of lenders (the “Credit Agreement”), whereby Radnet Management obtained $385.0 million in senior secured first-lien bank financing, consisting of (i) a $285.0 million, six-year term loan facility and (ii) a $100.0 million, five-year revolving credit facility, including a swing line subfacility and a letter of credit subfacility (collectively, the “Credit Facilities”).
Radnet Management’s obligations under the Credit Agreement were unconditionally guaranteed by RadNet, Inc., all of Radnet Management’s current and future domestic subsidiaries as well as certain affiliates, including Beverly Radiology Medical Group III and its equity holders (Beverly Radiology Medical Group, Inc., BreastLink Medical Group, Inc. and ProNet Imaging Medical Group, Inc.). The Credit Facilities created by the Credit Agreement were secured by a perfected first-priority security interest in all of Radnet Management’s and the guarantors’ tangible and intangible assets, including, but not limited to, pledges of equity interests of Radnet Management and all of our current and future domestic subsidiaries.
| 45 |
2012 Refinancing
On October 10, 2012 we completed the refinancing of the Credit Facilities by entering into a new Credit and Guaranty Agreement with a syndicate of banks and other financial institutions (the “Refinance Agreement”). The total amount of refinancing was $451.25 million, consisting of (i) a $350 million senior secured term loan and (ii) a $101.25 million senior secured revolving credit facility. The obligations of Radnet Management, Inc. under the Refinance Agreement are guaranteed by RadNet, Inc. and all of Radnet Management’s current and future domestic subsidiaries and certain of our affiliates. The obligations under the Refinance Agreement, including the guarantees, are secured by a perfected first-priority security interest in all of Radnet Management’s and the guarantors’ tangible and intangible assets, including, but not limited to, pledges of equity interests of Radnet Management and all of our current and future domestic subsidiaries.
The termination date for the $350 million term loan is the earliest to occur of (i) the sixth anniversary of the closing date (October 10, 2012), (ii) the date on which all of the term loans shall become due and payable in full under the Refinance Agreement whether by acceleration or otherwise and (iii) October 1, 2017 if our senior notes due 2018 have not been refinanced by such date. The termination date for the $101.25 million revolving credit facility is the earliest to occur of (i) the fifth anniversary of the closing date, (ii) the date the revolving credit facility is permanently reduced to zero pursuant to section 2.13(b) of the Refinance Agreement, (iii) the date of the termination of the revolving credit facility pursuant to section 8.01 of the Refinance Agreement and (iv) October 1, 2017 if our senior notes due 2018 have not been refinanced by such date.
In connection with the refinancing of the Credit Facilities, Radnet Management used the net proceeds to repay in full its existing six year term loan facility for $277.9 million in principal amount outstanding, which would have matured on April 6, 2016, and its revolving credit facility for $59.8 million in principal amount outstanding, which would have matured on April 6, 2015.
At December 31, 2012, we had $200.0 million aggregate principal amount of senior notes outstanding, $349.13 million aggregate principal amount of senior secured term loan debt outstanding and $33.0 million aggregate principal amount outstanding under the revolving credit facility.
Refinance Agreement
On October 10, 2012, we used the proceeds under the Refinance Agreement to refinance the indebtedness under the Credit Agreement. Under the Refinance Agreement, we obtained $451.25 million in senior secured financing, consisting of a $350 million, six-year term loan facility and a $101.25 million, five-year revolving credit facility.
Interest. The Refinance Agreement bears interest through maturity at a rate determined by adding the applicable margin to either (a) the Base Rate, which is defined in the Refinance Agreement as the highest of (i) the prime rate quoted in the Wall Street Journal, (ii) the rate which is 0.5% in excess of the federal funds rate, (iii) (with respect to term loans only) 2.25% and (iv) 1.00% in excess of the one-month Adjusted Eurodollar Rate at such time, or (b) the Adjusted Eurodollar Rate, which is defined in the Refinance Agreement as the higher of (i) the London interbank offered rate, adjusted for statutory reserve requirements, for the respective interest period, as determined by the administrative agent and (ii) (with respect to term loans only) 1.25%. As used in the Refinance Agreement, applicable margin means (i) (a) with respect to term loans that are Eurodollar Rate Loans, 4.25% per annum and (b) with respect to term loans that are Base Rate Loans, 3.25% per annum; and (ii) (a) with respect to revolving loans that are Eurodollar Rate Loans, 4.25% per annum and (b) with respect to revolving loans and swing line loans that are Base Rate Loans, 3.25% per annum.
Payments. Commencing on December 31, 2012 we began making quarterly amortization payments on the term loan facility under the Refinance Agreement, each in the amount of $875,000, with the remaining principal balance paid at maturity. Under the Refinance Agreement, we are also required to make mandatory prepayments, subject to specified exceptions, from consolidated excess cash flow, and upon certain events, including, but not limited to, (i) the receipt of net cash proceeds from the sale or other disposition of any property or assets by us or any of our subsidiaries, (ii) the receipt of net cash proceeds from insurance or condemnation proceeds paid on account of any loss of any property or assets of us or any of our subsidiaries, and (iii) the receipt of net cash proceeds from the incurrence of indebtedness by us or any of our subsidiaries (other than certain indebtedness otherwise permitted under the Refinance Agreement).
Guarantees and Collateral. The obligations under the Refinance Agreement are guaranteed by us, all of our current and future domestic subsidiaries and certain of our affiliates. The obligations under the Refinance Agreement and the guarantees are secured by a perfected first priority security interest in all of Radnet Management’s and the guarantors’ tangible and intangible assets, including, but not limited to, pledges of equity interests of Radnet Management and all of our current and future domestic subsidiaries.
Restrictive Covenants. In addition to certain customary covenants, the Refinance Agreement places limits on our ability to declare dividends or redeem or repurchase capital stock, prepay, redeem or purchase debt, incur liens and engage in sale-leaseback transactions, make loans and investments, incur additional indebtedness, amend or otherwise alter debt and other material agreements, engage in mergers, acquisitions and asset sales, enter into transactions with affiliates and alter the business we and our subsidiaries currently conduct.
| 46 |
Financial Covenants. The Refinance Agreement contains financial covenants including a maximum total leverage ratio and a limit on annual capital expenditures.
Events of Default. In addition to certain customary events of default, events of default under the Refinance Agreement include failure to pay principal or interest when due, a material breach of any representation or warranty contained in the loan documents, covenant defaults, events of bankruptcy and a change of control. The occurrence of an event of default could permit the lenders under the Refinance Agreement to declare all amounts borrowed, together with accrued interest and fees, to be immediately due and payable and to exercise other default remedies.
Senior Notes
On April 6, 2010, we issued $200 million in aggregate amount of unsecured senior notes which have a coupon of 10.375% and were issued at a price of 98.680%. The senior notes were issued by Radnet Management, Inc. and guaranteed jointly and severally on a senior unsecured basis by us and all of our current and future wholly-owned domestic restricted subsidiaries. The senior notes were offered and sold in a private placement exempt from registration under the Securities Act to qualified institutional buyers pursuant to Rule 144A and Regulation S under the Securities Act. We pay interest on the senior notes on April 1 and October 1, commencing October 1, 2010, and they will expire on April 1, 2018. The senior notes are governed under the Indenture. Under the terms of the indenture, we agreed to file a registration statement with the SEC relating to an offer to exchange the senior notes for registered publicly tradable notes that have substantially identical terms as the senior notes. On August 30, 2010, we filed a registration statement on Form S-4 with the SEC relating to the offer to exchange the senior notes. On January 13, 2011, our registration statement was declared effective by the SEC. On February 14, 2011, we completed an exchange offer whereby all senior notes were exchanged for registered publicly tradable notes.
Ranking. The senior notes and the guarantees:
| · | rank equally in right of payment with any existing and future unsecured senior indebtedness of the guarantors; |
| · | rank senior in right of payment to all existing and future subordinated indebtedness of the guarantors; |
| · | are effectively subordinated in right of payment to any secured indebtedness of the guarantors (including indebtedness under the Refinance Agreement) to the extent of the value of the assets securing such indebtedness; and |
| · | are structurally subordinated in right of payment to all existing and future indebtedness and other liabilities of any of the Company’s subsidiaries that is not a guarantor of the senior notes. |
Optional Redemption. Radnet Management may redeem the senior notes, in whole or in part, at any time on or after April 1, 2014, at the redemption prices specified under the Indenture. Prior to April 1, 2013, we may redeem up to 35% of aggregate principal amount of the senior notes issued under the Indenture from the net proceeds of one or more equity offerings at a redemption price equal to 110.375% of the senior notes redeemed, plus accrued and unpaid interest, if any. Radnet Management is also permitted to redeem the senior notes prior to April 1, 2014, in whole or in part, at a redemption price equal to 100% of the principal amount redeemed, plus a make-whole premium and accrued and unpaid interest, if any.
Change of Control and Asset Sales. If a change in control of Radnet Management occurs, Radnet Management must give holders of the senior notes the opportunity to sell their senior notes at 101% of their face amount, plus accrued interest. If we or one of our restricted subsidiaries sells assets under certain circumstances, Radnet Management will be required to make an offer to purchase the senior notes at their face amount, plus accrued and unpaid interest to the purchase date.
Restrictive Covenants. The Indenture contains covenants that limit, among other things, the ability of us and our restricted subsidiaries, to:
| · | pay dividends or make certain other restricted payments or investments; |
| · | incur additional indebtedness and issue preferred stock; |
| · | create liens (other than permitted liens) securing indebtedness or trade payables unless the notes are secured on an equal and ratable basis with the obligations so secured, and, if such liens secure subordinated indebtedness, the notes are secured by a lien senior to such liens; |
| · | sell certain assets or merge with or into other companies or otherwise dispose of all or substantially all of our assets; |
| 47 |
| · | enter into certain transactions with affiliates; |
| · | create restrictions on dividends or other payments by our restricted subsidiaries; and |
| · | create guarantees of indebtedness by restricted subsidiaries. |
However, these limitations are subject to a number of important qualifications and exceptions, as described in the Indenture. As of December 31, 2012, we were in compliance with all covenants.
Contractual Commitments
Our future obligations for notes payable, equipment under capital leases, lines of credit, equipment and building operating leases and purchase and other contractual obligations for the next five years and thereafter include (dollars in thousands):
| 2013 | 2014 | 2015 | 2016 | 2017 | Thereafter | Total | ||||||||||||||||||||||
| Notes payable (1) | $ | 47,225 | $ | 44,873 | $ | 45,596 | $ | 45,405 | $ | 77,580 | $ | 555,783 | $ | 816,462 | ||||||||||||||
| Capital leases (2) | 4,232 | 2,553 | 734 | 532 | 185 | – | 8,236 | |||||||||||||||||||||
| Operating leases (3) | 54,571 | 45,975 | 38,949 | 30,668 | 21,131 | 50,465 | 241,759 | |||||||||||||||||||||
| Total | $ | 106,028 | $ | 93,401 | $ | 85,279 | $ | 76,605 | $ | 98,896 | $ | 606,248 | $ | 1,066,457 | ||||||||||||||
(1) Includes variable rate debt for which the contractual obligation was estimated using the applicable rate at December 31, 2012.
(2) Includes interest component of capital lease obligations.
(3) Includes all operating leases through the end of their lease term.
We have an arrangement with GE Medical Systems under which it has agreed to be responsible for the maintenance and repair of a majority of our equipment for a fee that is based on the type and age of the equipment. Under this agreement, we are committed to minimum payments of approximately $23.0 million per year through 2016.
Critical Accounting Policies
Use of Estimates
Our discussion and analysis of financial condition and results of operations are based on our consolidated financial statements that were prepared in accordance with U.S. generally accepted accounting principles, or GAAP. Management makes estimates and assumptions when preparing financial statements. These estimates and assumptions affect various matters, including:
| · | our reported amounts of assets and liabilities in our consolidated balance sheets at the dates of the financial statements; |
| · | our disclosure of contingent assets and liabilities at the dates of the financial statements; and |
| · | our reported amounts of net revenue and expenses in our consolidated statements of operations during the reporting periods. |
These estimates involve judgments with respect to numerous factors that are difficult to predict and are beyond management’s control. As a result, actual amounts could differ materially from these estimates.
The SEC defines critical accounting estimates as those that are both most important to the portrayal of a company’s financial condition and results of operations and require management’s most difficult, subjective or complex judgment, often as a result of the need to make estimates about the effect of matters that are inherently uncertain and may change in subsequent periods. In note 2 to our consolidated financial statements, we discuss our significant accounting policies, including those that do not require management to make difficult, subjective or complex judgments or estimates. The most significant areas involving management’s judgments and estimates are described below.
| 48 |
Revenues
Service fee revenue, net of contractual allowances and discounts, consists of net patient fees received from various payers and patients themselves based mainly upon established contractual billing rates, less allowances for contractual adjustments and discounts. As it relates to BRMG centers, this service fee revenue includes payments for both the professional medical interpretation revenue recognized by BRMG as well as the payment for all other aspects related to our providing the imaging services, for which we earn management fees from BRMG. As it relates to non-BRMG centers, this service fee revenue is earned through providing the use of our diagnostic imaging equipment and the provision of technical services as well as providing administration services such as clerical and administrative personnel, bookkeeping and accounting services, billing and collection, provision of medical and office supplies, secretarial, reception and transcription services, maintenance of medical records, and advertising, marketing and promotional activities.
Service fee revenues are recorded during the period the services are provided based upon the estimated amounts due from the patients and third-party payers. Third-party payers include federal and state agencies (under the Medicare and Medicaid programs), managed care health plans, commercial insurance companies and employers. Estimates of contractual allowances under managed care health plans are based upon the payment terms specified in the related contractual agreements. Contractual payment terms in managed care agreements are generally based upon predetermined rates per discounted fee-for-service rates. We also record a provision for doubtful accounts (based primarily on historical collection experience) related to patients and copayment and deductible amounts for patients who have health care coverage under one of our third-party payers.
Under capitation arrangements with various health plans, we earn a per-enrollee amount each month for making available diagnostic imaging services to all plan enrollees under the capitation arrangement. Revenue under capitation arrangements is recognized in the period which we are obligated to provide services to plan enrollees under contracts with various health plans.
Our revenue, net of contractual allowances , discounts and provision for bad debts for the years ended December 31, are summarized in the following table (in thousands):
| Years Ended December 31, | ||||||||||||
| 2012 | 2011 | 2010 | ||||||||||
| Commercial Insurance | $ | 409,114 | $ | 376,107 | $ | 337,980 | ||||||
| Medicare | 122,971 | 107,613 | 103,055 | |||||||||
| Medicaid | 20,101 | 17,756 | 16,118 | |||||||||
| Workers' Compensation/Personal Injury | 26,604 | 23,137 | 21,002 | |||||||||
| Other | 39,192 | 30,367 | 11,140 | |||||||||
| Service fee revenue, net of contractual allowances and discounts | 617,982 | 554,979 | 489,294 | |||||||||
| Provision for bad debts | (25,904 | ) | (22,339 | ) | (21,995 | ) | ||||||
| Net service fee revenue | 592,078 | 532,640 | 467,299 | |||||||||
| Revenue under capitation arrangements | 55,075 | 52,481 | 51,358 | |||||||||
| Total net revenue | $ | 647,153 | $ | 585,121 | $ | 518,657 | ||||||
The break-out of our service fee revenue, net of contractual allowances and discounts, is calculated based upon global payments received from consolidated imaging centers from dates of service from each respective period illustrated.
Provision for Bad Debts
We provide for an allowance against accounts receivable that could become uncollectible to reduce the carrying value of such receivables to their estimated net realizable value. We estimate this allowance based on the aging of our accounts receivable by each type of payer over an 18-month look-back period and other relevant factors. A significant portion of our provision for bad debt relates to co-payments and deductibles owed to us from patients with insurance. Although we attempt to collect deductibles and co-payments due from patients with insurance at the time of service, this attempt to collect at the time of service is not an assessment of the patient’s ability to pay nor are revenues recognized based on an assessment of the patient’s ability to pay. There are various factors that can impact collection trends, such as changes in the economy, which in turn have an impact on the increased burden of co-payments and deductibles to be made by patients with insurance. These factors continuously change and can have an impact on collection trends and our estimation process.
Accounts Receivable
Substantially all of our accounts receivable are due under fee-for-service contracts from third party payors, such as insurance companies and government-sponsored healthcare programs, or directly from patients. Services are generally provided pursuant to one-year contracts with healthcare providers. Receivables generally are collected within industry norms for third-party payors. We continuously monitor collections from our payors and maintain an allowance for bad debts based upon specific payor collection issues that we have identified and our historical experience.
| 49 |
Depreciation and Amortization of Long-Lived Assets
We depreciate our long-lived assets over their estimated economic useful lives with the exception of leasehold improvements where we use the shorter of the assets useful lives or the lease term of the facility for which these assets are associated.
Deferred Tax Assets
We evaluate the realizability of the net deferred tax assets and assess the valuation allowance periodically. If future taxable income or other factors are not consistent with our expectations, an adjustment to our allowance for net deferred tax assets may be required. For net deferred tax assets we consider estimates of future taxable income, including tax planning strategies, in determining whether our net deferred tax assets are more likely than not to be realized.
Valuation of Goodwill and Long-Lived Assets
Goodwill at December 31, 2012 totaled $193.9 million. Goodwill is recorded as a result of business combinations. Management evaluates goodwill, at a minimum, on an annual basis and whenever events and changes in circumstances suggest that the carrying amount may not be recoverable in accordance with ASC 350, Intangibles – Goodwill and Other. Impairment of goodwill is tested at the reporting unit level by comparing the reporting unit’s carrying amount, including goodwill, to the fair value of the reporting unit. The fair value of a reporting unit is estimated using a combination of the income or discounted cash flows approach and the market approach, which uses comparable market data. If the carrying amount of the reporting unit exceeds its fair value, goodwill is considered impaired and a second step is performed to measure the amount of impairment loss, if any. We tested goodwill for impairment on October 1, 2012. Based on our test, we noted no impairment related to goodwill as of October 1, 2012 as the estimated fair value of each reporting unit exceeded its carrying value by no less than 38%. Our largest reporting unit, which is our California Operations, has goodwill of $67.5 million and an estimated fair value in excess of carrying value of 43% as of October 1, 2012. However, if estimates or the related assumptions change in the future, we may be required to record impairment charges to reduce the carrying amount of goodwill.
We evaluate our long-lived assets (property and equipment) and intangibles, other than goodwill, for impairment whenever indicators of impairment exist. The accounting standards require that if the sum of the undiscounted expected future cash flows from a long-lived asset or definite-lived intangible is less than the carrying value of that asset, an asset impairment charge must be recognized. The amount of the impairment charge is calculated as the excess of the asset’s carrying value over its fair value, which generally represents the discounted future cash flows from that asset or in the case of assets we expect to sell, at fair value less costs to sell. No indicators of impairment were identified with respect to our long-lived assets as of December 31, 2012.
Recent Accounting Standards
On January 1, 2012, we adopted ASU 2011-05, “Comprehensive Income (Topic 220): Presentation of Comprehensive Income,” which updates existing guidance on comprehensive income. This guidance eliminates the option to present the components of other comprehensive income as part of our Condensed Consolidated Statements of Equity and Comprehensive Income, which was our previous presentation. It requires companies to present the total of comprehensive income, the components of net income and the components of other comprehensive income either in a single continuous statement of comprehensive income or in two separate but consecutive statements. In the two statement approach which we have adopted, the first statement presents total net income and its components followed consecutively by a second statement that presents total other comprehensive income, the components of other comprehensive income and the total of comprehensive income. The adoption of this pronouncement did not have any effect on our financial condition or results of operations, though it did change our financial statement presentation.
On January 1, 2012, we adopted ASU 2011-07, “Health Care Entities (Topic 954): Presentation and Disclosure of Patient Service Revenue, Provision for Bad Debts, and the Allowance for Doubtful Accounts for Certain Health Care Entities,” which requires health care entities to present the provision for doubtful accounts relating to patient service revenue as a deduction from patient service revenue in the statement of operations rather than as an operating expense. Additional disclosures relating to sources of patient revenue and the allowance for doubtful accounts related to patient accounts receivable are also required. Such additional disclosures are included in Note 2 of our consolidated financial statements. The adoption of this ASU had no impact on our financial condition, results of operations or cash flows, although it did change our financial statement presentation.
On January 1, 2012, we adopted ASU 2011-08, “Intangibles—Goodwill and Other (Topic 350): Testing Goodwill for Impairment”, simplifying how a company is required to test goodwill for impairment. Companies will now have the option to first assess qualitative factors to determine whether it is more likely than not that the fair value of a reporting unit is less than its carrying amount. If the company determines that it is not more likely than not that the fair value of a reporting unit is less than its carrying amount, then performing the two-step impairment test is unnecessary. This qualitative assessment was not performed as of December 31, 2012.
| 50 |
In July 2012, the FASB modified existing rules to allow entities to use a qualitative approach to test indefinite-lived intangible asset for impairment. The revised standard allows an entity the option to first assess qualitatively whether it is more likely than not (that is, a likelihood of more than 50 percent) that an indefinite-lived intangible asset is impaired. An entity is not required to calculate the fair value of an indefinite-lived intangible asset and perform the quantitative impairment test unless the entity determines that it is more likely than not that the asset is impaired. This guidance will be effective for the Company in 2013, but early adoption is permitted. Adoption of this standard will not have a material impact on our results of operations, cash flows, or financial position.
In February 2013, the FASB issued new guidance which requires disclosure of information about significant reclassification adjustments from accumulated other comprehensive income in a single note or on the face of the financial statements. This guidance will be effective for the Company in 2013. Adoption of this standard, which is related to disclosure only, will not have an impact on the Company’s consolidated financial position, results of operations, or cash flows.
| Item 7A. | Quantitative and Qualitative Disclosures About Market Risk |
Foreign Currency Exchange Risk. We sell our services exclusively in the United States and receive payment for our services exclusively in United States dollars. As a result, our financial results are unlikely to be affected by factors such as changes in foreign currency, exchange rates or weak economic conditions in foreign markets.
After the completion of the acquisition of Image Medical Corporation, the parent of eRAD, Inc. on October 1, 2010, we maintain research and development facilities in Prince Edward Island, Canada and Budapest, Hungary for which expenses are paid in the local currency. Accordingly, we do have currency risk resulting from fluctuations between such local currency and the United States Dollar. At the present time, we do not have any foreign exchange currency contracts to mitigate this risk. Fluctuations in foreign exchange rates could impact future operating results. A hypothetical 1% increase in the rate of exchange of foreign currencies against the dollar for 2012 would have resulted in an increase of approximately $10,000 in our operating expenses for the year.
Interest Rate Sensitivity. Radnet Inc. pays interest on various types of debt instruments to its suppliers, investors and lending institutions. The agreements entail either fixed or variable interest rates. Instruments which have fixed rates include leases on equipment and interest due on our $200 million outstanding senior notes. Variable rate interest obligations relate primarily to amounts borrowed under our outstanding credit facilities, which allows elections of either LIBOR or prime rates of interest. Under the Refinance Agreement’s LIBOR election facility, borrowed funds bear a 1.25% floor or 6 month LIBOR plus an applicable margin of 4.25%. At December 31, 2012, we had $348.3 million outstanding subject to a LIBOR election. As the LIBOR floor exceeds the current spot rate of 6 month LIBOR, the spot rate would have to increase more than 74 basis points before an additional interest expense would be accrued. An increase of 174 basis points would be necessary to realize a hypothetical 1% increase in the borrowing rate and a resultant $3.5 million of additional interest expense. At December 31, 2012, an additional $33.9 million was tied to the prime rate. A hypothetical 1% increase in the prime rate for 2012 would have resulted in an increase of approximately $339,000 in interest expense for the year ended December 31, 2012.
| Item 8. | Financial Statements and Supplementary Data |
The Financial Statements are attached hereto and begin on page 53 .
| 51 |
Report of Independent Registered Public Accounting Firm
The Board of Directors and Stockholders of RadNet, Inc.
We have audited the accompanying consolidated balance sheets of RadNet, Inc. and subsidiaries (the “Company” or “RadNet”) as of December 31, 2012 and 2011, and the related consolidated statements of operations, comprehensive income (loss), equity deficit, and cash flows for each of the three years in the period ended December 31, 2012. Our audits also included the financial statement schedule listed in the Index at Item 15(a)(2). These financial statements and schedule are the responsibility of the Company’s management. Our responsibility is to express an opinion on these financial statements and schedule based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements. An audit also includes assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the financial statements referred to above present fairly, in all material respects, the consolidated financial position of RadNet, Inc. and subsidiaries at December 31, 2012 and 2011, and the consolidated results of their operations and their cash flows for each of the three years in the period ended December 31, 2012, in conformity with U.S. generally accepted accounting principles. Also, in our opinion, the related financial statement schedule when considered in relation to the basic financial statements taken as a whole, presents fairly in all material respects the information set forth therein.
As discussed in Note 1A to the consolidated financial statements, the 2012 financial statements have been restated to correct an error in accounting for income taxes.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), RadNet’s internal control over financial reporting as of December 31, 2012, based on criteria established in Internal Control-Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission and our report dated March 18, 2013, except for the effects of the material weakness described in the sixth paragraph as to which the date is November 13, 2013, expressed an adverse opinion thereon.
/s/ Ernst & Young LLP
Los Angeles, California
March 18, 2013 , except for Note 1A, as to which the date is November 13, 2013.
| 52 |
RADNET, INC. AND SUBSIDIARIES
CONSOLIDATED BALANCE SHEETS
(IN THOUSANDS EXCEPT SHARE DATA)
| December 31, | December 31, | |||||||||||||
| 2012 | 2011 | |||||||||||||
| (Restated) | ||||||||||||||
| ASSETS | ||||||||||||||
| CURRENT ASSETS | ||||||||||||||
| Cash and cash equivalents | $ | 362 | $ | 2,455 | ||||||||||
| Accounts receivable, net | 129,194 | 128,432 | ||||||||||||
| Asset held for sale | – | 2,300 | ||||||||||||
| Current portion of deferred tax assets | 7,607 | – | ||||||||||||
| Prepaid expenses and other current assets | 18,737 | 19,140 | ||||||||||||
| Total current assets | 155,900 | 152,327 | ||||||||||||
| PROPERTY AND EQUIPMENT, NET | 216,560 | 215,527 | ||||||||||||
| OTHER ASSETS | ||||||||||||||
| Goodwill | 193,871 | 159,507 | ||||||||||||
| Other intangible assets | 51,674 | 53,105 | ||||||||||||
| Deferred financing costs | 11,977 | 13,490 | ||||||||||||
| Investment in joint ventures | 28,598 | 22,326 | ||||||||||||
| Deferred tax assets, net of current portion | 48,535 | – | ||||||||||||
| Deposits and other | 3,749 | 2,906 | ||||||||||||
| Total assets | $ | 710,864 | $ | 619,188 | ||||||||||
| LIABILITIES AND STOCKHOLDERS' EQUITY DEFICIT | ||||||||||||||
| CURRENT LIABILITIES | ||||||||||||||
| Accounts payable, accrued expenses and other | $ | 106,357 | $ | 103,101 | ||||||||||
| Due to affiliates | 1,602 | 3,762 | ||||||||||||
| Deferred revenue | 1,273 | 1,076 | ||||||||||||
| Current portion of notes payable | 4,703 | 6,608 | ||||||||||||
| Current portion of deferred rent | 1,164 | 999 | ||||||||||||
| Current portion of obligations under capital leases | 3,942 | 6,834 | ||||||||||||
| Total current liabilities | 119,041 | 122,380 | ||||||||||||
| LONG-TERM LIABILITIES | ||||||||||||||
| Deferred rent, net of current portion | 15,850 | 12,407 | ||||||||||||
| Deferred tax liabilities, net | – | 277 | ||||||||||||
| Line of credit | 33,000 | 58,000 | ||||||||||||
| Notes payable, net of current portion | 537,009 | 484,046 | ||||||||||||
| Obligations under capital lease, net of current portion | 3,753 | 3,338 | ||||||||||||
| Other non-current liabilities | 8,895 | 8,547 | ||||||||||||
| Total liabilities | 717,548 | 688,995 | ||||||||||||
| STOCKHOLDERS' EQUITY DEFICIT | ||||||||||||||
| Common stock - $.0001 par value, 200,000,000 shares authorized; 38,540,482, and 37,426,460 shares issued and outstanding at December 31, 2012 and December 31, 2011, respectively | 4 | 4 | ||||||||||||
| Paid-in-capital | 168,415 | 165,796 | ||||||||||||
| Accumulated other comprehensive income (loss) | 39 | (946 | ) | |||||||||||
| Accumulated deficit | (175,776 | ) | (235,610 | ) | ||||||||||
| Total RadNet, Inc.'s stockholders' equity deficit | (7,318 | ) | (70,756 | ) | ||||||||||
| Noncontrolling interests | 634 | 949 | ||||||||||||
| Total stockholders' equity deficit | (6,684 | ) | (69,807 | ) | ||||||||||
| Total liabilities and stockholders' equity deficit | $ | 710,864 | $ | 619,188 | ||||||||||
The accompanying notes are an integral part of these financial statements.
| 53 |
RADNET, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF OPERATIONS
(IN THOUSANDS EXCEPT SHARE DATA)
| Years Ended December 31, | ||||||||||||
| 2012 | 2011 | 2010 | ||||||||||
| (Restated) | ||||||||||||
| NET REVENUE | ||||||||||||
| Service fee revenue, net of contractual allowances and discounts | $ | 617,982 | $ | 554,979 | $ | 489,294 | ||||||
| Provision for bad debts | (25,904 | ) | (22,339 | ) | (21,995 | ) | ||||||
| Net service fee revenue | 592,078 | 532,640 | 467,299 | |||||||||
| Revenue under capitation arrangements | 55,075 | 52,481 | 51,358 | |||||||||
| Total net revenue | 647,153 | 585,121 | 518,657 | |||||||||
| OPERATING EXPENSES | ||||||||||||
| Cost of operations, excluding depreciation and amortization | 542,993 | 477,828 | 420,973 | |||||||||
| Depreciation and amortization | 57,740 | 57,481 | 53,997 | |||||||||
| Loss (gain) on sale and disposal of equipment | 456 | (2,240 | ) | 1,136 | ||||||||
| Severance costs | 736 | 1,391 | 838 | |||||||||
| Total operating expenses | 601,925 | 534,460 | 476,944 | |||||||||
| INCOME FROM OPERATIONS | 45,228 | 50,661 | 41,713 | |||||||||
| OTHER INCOME AND EXPENSES | ||||||||||||
| Interest expense | 53,783 | 52,798 | 48,398 | |||||||||
| Loss on extinguishment of debt | – | – | 9,871 | |||||||||
| Gain on de-consolidation of joint venture | (2,777 | ) | – | – | ||||||||
| Other (income) expenses | (3,679 | ) | (5,075 | ) | 505 | |||||||
| Total other expenses | 47,327 | 47,723 | 58,774 | |||||||||
| (LOSS) INCOME BEFORE INCOME TAXES AND EQUITY | ||||||||||||
| IN EARNINGS OF JOINT VENTURES | (2,099 | ) | 2,938 | (17,061 | ) | |||||||
| Benefit from (provision for) income taxes | 55,227 | (820 | ) | (576 | ) | |||||||
| Equity in earnings of joint ventures | 6,476 | 5,224 | 4,952 | |||||||||
| NET INCOME (LOSS) | 59,604 | 7,342 | (12,685 | ) | ||||||||
| Net (loss) income attributable to noncontrolling interests | (230 | ) | 111 | 167 | ||||||||
| NET INCOME (LOSS) ATTRIBUTABLE TO RADNET, INC. | ||||||||||||
| COMMON STOCKHOLDERS | $ | 59,834 | $ | 7,231 | $ | (12,852 | ) | |||||
| BASIC NET INCOME (LOSS) PER SHARE | ||||||||||||
| ATTRIBUTABLE TO RADNET, INC. COMMON STOCKHOLDERS | $ | 1.58 | $ | 0.19 | $ | (0.35 | ) | |||||
| DILUTED NET INCOME (LOSS) PER SHARE | ||||||||||||
| ATTRIBUTABLE TO RADNET, INC. COMMON STOCKHOLDERS | $ | 1.52 | $ | 0.19 | $ | (0.35 | ) | |||||
| WEIGHTED AVERAGE SHARES OUTSTANDING | ||||||||||||
| Basic | 37,751,170 | 37,367,736 | 36,853,477 | |||||||||
| Diluted | 39,244,686 | 38,785,675 | 36,853,477 | |||||||||
The accompanying notes are an integral part of these financial statements.
| 54 |
RADNET, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF COMPREHENSIVE INCOME (LOSS)
(IN THOUSANDS)
| Years Ended December 31, | ||||||||||||
| 2012 | 2011 | 2010 | ||||||||||
| (Restated) | ||||||||||||
| NET INCOME (LOSS) | $ | 59,604 | $ | 7,342 | $ | (12,685 | ) | |||||
| Foreign currency translation adjustments | 67 | (34 | ) | 6 | ||||||||
| Change in fair value of cash flow hedge | – | – | (1,472 | ) | ||||||||
| Reclassification of net cash flow hedge losses included in net income during the period | 918 | 1,225 | 917 | |||||||||
| COMPREHENSIVE INCOME (LOSS) | 60,589 | 8,533 | (13,234 | ) | ||||||||
| Less comprehensive (loss) income attributible to non-controlling interests | (230 | ) | 111 | 167 | ||||||||
| COMPREHENSIVE INCOME (LOSS) ATTRIBUTIBLE TO RADNET, INC. COMMON STOCKHOLDERS | $ | 60,359 | $ | 8,644 | $ | (13,067 | ) | |||||
The accompanying notes are an integral part of these financial statements.
| 55 |
RADNET, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENT OF STOCKHOLDERS' EQUITY DEFICIT
(IN THOUSANDS EXCEPT SHARE DATA)
| Accumulated Other | Total | |||||||||||||||||||||||
| Common Stock | Paid-in | Accumulated | Comprehensive | Radnet, Inc.'s | Noncontrolling | Total | ||||||||||||||||||
| Shares | Amount | Capital | Deficit | Income (Loss) | Equity Deficit | Interests | Equity Deficit | |||||||||||||||||
| BALANCE - JANUARY 1, 2010 | 36,259,279 | $ | 4 | $ | 156,758 | $ | (229,989 | ) | $ | (1,588 | ) | $ | (74,815 | ) | $ | 54 | $ | (74,761 | ) | |||||
| Issuance of common stock to sellers of Truxtun Imaging | 375,000 | – | 1,238 | – | – | 1,238 | – | 1,238 | ||||||||||||||||
| Issuance of common stock to sellers of Union Imaging | 75,000 | – | 153 | – | – | 153 | – | 153 | ||||||||||||||||
| Issuance of warrant to sellers of Rutherford Imaging | – | – | 306 | – | – | 306 | – | 306 | ||||||||||||||||
| Issuance of common stock upon exercise of options/warrants | 514,196 | – | 271 | – | – | 271 | – | 271 | ||||||||||||||||
| Stock-based compensation | – | 3,718 | – | – | 3,718 | – | 3,718 | |||||||||||||||||
| Non-controlling interests assumed from the acquisition of Progressive imaging | (33 | ) | (33 | ) | ||||||||||||||||||||
| Dividends paid to noncontrolling interests | – | – | – | – | – | – | (131 | ) | (131 | ) | ||||||||||||||
| Change in cumulative foreign currency translation adjustment | – | – | – | – | 6 | 6 | – | 6 | ||||||||||||||||
| Change in fair value of cash flow hedge | – | – | – | – | (1,472 | ) | (1,472 | ) | – | (1,472 | ) | |||||||||||||
| Change in fair value of cash flow hedge from prior periods reclassified to earnings | – | – | – | – | 917 | 917 | – | 917 | ||||||||||||||||
| Net loss | – | – | – | (12,852 | ) | – | (12,852 | ) | 167 | (12,685 | ) | |||||||||||||
| BALANCE - DECEMBER 31, 2010 | 37,223,475 | $ | 4 | $ | 162,444 | $ | (242,841 | ) | $ | (2,137 | ) | $ | (82,530 | ) | $ | 57 | $ | (82,473 | ) | |||||
| Issuance of common stock upon exercise of options/warrants | 202,985 | – | 242 | – | – | 242 | – | 242 | ||||||||||||||||
| Stock-based compensation | – | – | 3,110 | – | – | 3,110 | – | 3,110 | ||||||||||||||||
| Noncontrolling interests assumed from Radar joint venture | – | – | – | – | – | – | 961 | 961 | ||||||||||||||||
| Distributions paid to noncontrolling interests | – | – | – | – | – | – | (154 | ) | (154 | ) | ||||||||||||||
| Purchase of non-controlling interests | – | – | – | – | – | – | (26 | ) | (26 | ) | ||||||||||||||
| Change in cumulative foreign currency translation adjustment | – | – | – | – | (34 | ) | (34 | ) | – | (34 | ) | |||||||||||||
| Change in fair value of cash flow hedge from prior periods reclassified to earnings | – | – | – | – | 1,225 | 1,225 | – | 1,225 | ||||||||||||||||
| Net income | – | – | – | 7,231 | – | 7,231 | 111 | 7,342 | ||||||||||||||||
| BALANCE - DECEMBER 31, 2011 | 37,426,460 | $ | 4 | $ | 165,796 | $ | (235,610 | ) | $ | (946 | ) | $ | (70,756 | ) | $ | 949 | $ | (69,807 | ) | |||||
| Issuance of common stock upon exercise of options/warrants | 74,022 | – | – | – | – | – | – | – | ||||||||||||||||
| Stock-based compensation | – | – | 2,736 | – | – | 2,736 | – | 2,736 | ||||||||||||||||
| Purchase of non-controlling interests | – | – | (117 | ) | – | – | (117 | ) | – | (117 | ) | |||||||||||||
| De-consolidation of joint venture | – | – | – | – | – | – | (14 | ) | (14 | ) | ||||||||||||||
| Issuance of restricted stock | 1,040,000 | – | – | – | – | – | – | – | ||||||||||||||||
| Dividends paid to noncontrolling interests | – | – | – | – | – | – | (71 | ) | (71 | ) | ||||||||||||||
| Change in cumulative foreign currency translation adjustment | – | – | – | – | 67 | 67 | – | 67 | ||||||||||||||||
| Change in fair value of cash flow hedge from prior periods reclassified to earnings | – | – | – | – | 918 | 918 | – | 918 | ||||||||||||||||
| Net income (Restated) | – | – | – | 59,834 | – | 59,834 | (230 | ) | 59,604 | |||||||||||||||
| BALANCE - DECEMBER 31, 2012 (Restated) | 38,540,482 | $ | 4 | $ | 168,415 | $ | (175,776 | ) | $ | 39 | $ | (7,318 | ) | $ | 634 | $ | (6,684 | ) | ||||||
The accompanying notes are an integral part of these financial statements.
| 56 |
RADNET, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF CASH FLOWS (IN THOUSANDS)
| Years Ended December 31, | ||||||||||||
| 2012 | 2011 | 2010 | ||||||||||
| CASH FLOWS FROM OPERATING ACTIVITIES | (Restated) | |||||||||||
| Net income (loss) | $ | 59,604 | $ | 7,342 | $ | (12,685 | ) | |||||
| Adjustments to reconcile net income (loss) to net cash provided by operating activities: | ||||||||||||
| Depreciation and amortization | 57,740 | 57,481 | 53,997 | |||||||||
| Provision for bad debts | 25,904 | 22,339 | 21,995 | |||||||||
| Equity in earnings of joint ventures | (6,476 | ) | (5,224 | ) | (4,952 | ) | ||||||
| Distributions from joint ventures | 6,477 | 4,993 | 7,639 | |||||||||
| Deferred rent amortization | 3,608 | 2,282 | 1,848 | |||||||||
| Amortization of deferred financing cost | 2,474 | 2,940 | 2,797 | |||||||||
| Amortization of bond and term loan discounts | 1,163 | 244 | 164 | |||||||||
| Loss (gain) on sale and disposal of equipment | 456 | (2,240 | ) | 1,136 | ||||||||
| Gain on bargain purchase | (810 | ) | – | – | ||||||||
| Loss on extinguishment of debt | – | – | 9,871 | |||||||||
| Gain on de-consolidation of joint venture | (2,777 | ) | – | – | ||||||||
| Amortization of cash flow hedge | 918 | 1,225 | 917 | |||||||||
| Stock-based compensation | 2,736 | 3,110 | 3,718 | |||||||||
| Changes in operating assets and liabilities, net of assets acquired and liabilities assumed in purchase transactions: | ||||||||||||
| Accounts receivable | (17,350 | ) | (45,014 | ) | (24,822 | ) | ||||||
| Other current assets | 3,565 | (3,935 | ) | (3,226 | ) | |||||||
| Other assets | (578 | ) | 43 | 24 | ||||||||
| Deferred taxes | (56,142 | ) | – | – | ||||||||
| Deferred revenue | 197 | (492 | ) | 207 | ||||||||
| Accounts payable and accrued expenses | (5,440 | ) | 12,542 | 8,256 | ||||||||
| Net cash provided by operating activities | 75,269 | 57,636 | 66,884 | |||||||||
| CASH FLOWS FROM INVESTING ACTIVITIES | ||||||||||||
| Purchase of imaging facilities | (45,493 | ) | (42,990 | ) | (61,774 | ) | ||||||
| Purchase of property and equipment | (44,448 | ) | (42,720 | ) | (40,293 | ) | ||||||
| Proceeds from sale of equipment | 1,549 | 325 | 685 | |||||||||
| Proceeds from insurance claims on damaged equipment | – | 2,740 | – | |||||||||
| Proceeds from sale of imaging facilities | 2,300 | – | – | |||||||||
| Proceeds from sale of joint venture interests | 1,800 | – | – | |||||||||
| Purchase of equity interest in joint ventures | (2,756 | ) | (5,094 | ) | – | |||||||
| Net cash used in investing activities | (87,048 | ) | (87,739 | ) | (101,382 | ) | ||||||
| CASH FLOWS FROM FINANCING ACTIVITIES | ||||||||||||
| Principal payments on notes and leases payable | (22,223 | ) | (18,756 | ) | (21,463 | ) | ||||||
| Proceeds from borrowings upon refinancing | 344,485 | – | 478,313 | |||||||||
| Repayment of debt | (277,875 | ) | – | (412,000 | ) | |||||||
| Deferred financing costs | (3,753 | ) | (944 | ) | (13,566 | ) | ||||||
| Proceeds from, net of payments on, line of credit | (25,000 | ) | 58,000 | – | ||||||||
| Payments to counterparties of interest rate swaps, net of amounts received | (5,823 | ) | (6,455 | ) | (6,382 | ) | ||||||
| Distributions to noncontrolling interests | (71 | ) | (154 | ) | (131 | ) | ||||||
| Equity attributable to non-controlling interests | (117 | ) | – | – | ||||||||
| Proceeds from issuance of common stock upon exercise of options/warrants | – | 242 | 271 | |||||||||
| Net cash provided by financing activities | 9,623 | 31,933 | 25,042 | |||||||||
| EFFECT OF EXCHANGE RATE CHANGES ON CASH | 63 | (2 | ) | (11 | ) | |||||||
| NET (DECREASE) INCREASE IN CASH AND CASH EQUIVALENTS | (2,093 | ) | 1,828 | (9,467 | ) | |||||||
| CASH AND CASH EQUIVALENTS, beginning of period | 2,455 | 627 | 10,094 | |||||||||
| CASH AND CASH EQUIVALENTS, end of period | $ | 362 | $ | 2,455 | $ | 627 | ||||||
| SUPPLEMENTAL DISCLOSURE OF CASH FLOW INFORMATION | ||||||||||||
| Cash paid during the period for interest | $ | 47,806 | $ | 47,310 | $ | 40,352 | ||||||
| Cash paid during the period for income taxes | $ | 918 | $ | 514 | $ | 659 | ||||||
The accompanying notes are an integral part of these financial statements.
| 57 |
RADNET, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF CASH FLOWS (CONTINUED)
Supplemental Schedule of Non-Cash Investing and Financing Activities
We acquired equipment and certain leasehold improvements for approximately $14.4 million, $9.3 million and $12.2 million during the years ended December 31, 2012, 2011 and 2010, respectively, that we had not paid for as of December 31, 2012, 2011 and 2010, respectively. The offsetting amount due was recorded in our consolidated balance sheet under “accounts payable, accrued expenses and other.”
As discussed in Note 10, we entered into interest rate swap modifications in the first quarter of 2009. These modifications include a significant financing element and, as such, all cash inflows and outflows subsequent to the date of modification are presented as financing activities. Also, as a result of our debt refinancing completed on April 6, 2010, our interest rate swaps are no longer effective. Accordingly, all changes in their fair value after April 6, 2010, and through November 15, 2012, their maturity date, were recognized in earnings as other expense.
Detail of investing activity related to acquisitions can be found in Note 4.
| 58 |
RADNET, INC. AND AFFILIATES
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
NOTE 1 – NATURE OF BUSINESS
At December 31, 2012, we operated directly or indirectly through joint ventures, 246 centers located in California, Maryland, Florida, Delaware, New Jersey, Rhode Island and New York. We provide diagnostic imaging services including magnetic resonance imaging (MRI), computed tomography (CT), positron emission tomography (PET), nuclear medicine, mammography, ultrasound, diagnostic radiology, or X-ray, fluoroscopy and other related procedures. Our operations comprise a single segment for financial reporting purposes.
The consolidated financial statements include the accounts of Radnet Management, Inc. (or “Radnet Management”) and Beverly Radiology Medical Group III, a professional partnership (“BRMG”). The consolidated financial statements also include Radnet Management I, Inc., Radnet Management II, Inc., Radiologix, Inc., Radnet Managed Imaging Services, Inc., Delaware Imaging Partners, Inc., New Jersey Imaging Partners, Inc. and Diagnostic Imaging Services, Inc. (“DIS”), all wholly owned subsidiaries of Radnet Management. All of these affiliated entities are referred to collectively as “RadNet”, “we”, “us”, “our” or the “Company” in this report.
Accounting Standards Codification (“ASC”) Section 810-10-15-14 stipulates that generally any entity with a) insufficient equity to finance its activities without additional subordinated financial support provided by any parties, or b) equity holders that, as a group, lack the characteristics specified in the Codification which evidence a controlling financial interest, is considered a Variable Interest Entity (“VIE”). We consolidate all voting interest entities in which we own a majority voting interest and all VIEs for which we are the primary beneficiary. We determine whether we are the primary beneficiary of a VIE through a qualitative analysis that identifies which variable interest holder has the controlling financial interest in the VIE. The variable interest holder who has both of the following has the controlling financial interest and is the primary beneficiary: (1) the power to direct the activities of the VIE that most significantly impact the VIE’s economic performance and (2) the obligation to absorb losses of, or the right to receive benefits from, the VIE that could potentially be significant to the VIE. In performing our analysis, we consider all relevant facts and circumstances, including: the design and activities of the VIE, the terms of the contracts the VIE has entered into, the nature of the VIE’s variable interests issued and how they were negotiated with or marketed to potential investors, and which parties participated significantly in the design or redesign of the entity.
Howard G. Berger, M.D. is our President and Chief Executive Officer, a member of our Board of Directors and is deemed to be the beneficial owner, directly and indirectly, of approximately 14.0% of our outstanding common stock. Dr. Berger also owns, indirectly, 99% of the equity interests in BRMG. BRMG provides all of the professional medical services at the majority of our facilities located in California under a management agreement with us, and employs physicians or contracts with various other independent physicians and physician groups to provide the professional medical services at most of our other California facilities. We generally obtain professional medical services from BRMG in California, rather than provide such services directly or through subsidiaries, in order to comply with California’s prohibition against the corporate practice of medicine. However, as a result of our close relationship with Dr. Berger and BRMG, we believe that we are able to better ensure that medical service is provided at our California facilities in a manner consistent with our needs and expectations and those of our referring physicians, patients and payors than if we obtained these services from unaffiliated physician groups. BRMG is a partnership of ProNet Imaging Medical Group, Inc., Breastlink Medical Group, Inc. and Beverly Radiology Medical Group, Inc., each of which are 99% or 100% owned by Dr. Berger. RadNet provides non-medical, technical and administrative services to BRMG for which it receives a management fee, per the management agreement. Through the management agreement and our relationship with Dr. Berger, we have exclusive authority over all non-medical decision making related to the ongoing business operations of BRMG. Through our management agreement with BRMG we determine the annual budget of BRMG and make all physician employment decisions. BRMG has insignificant operating assets and liabilities, and de minimis equity. Through the management agreement with us, all of BRMG’s cash flows are transferred to us.
We have determined that BRMG is a variable interest entity, and that we are the primary beneficiary, and consequently, we consolidate the revenue and expenses of BRMG. BRMG recognized $53.4 million, $53.9 million and $51.5 million of revenue, net of management service fees to RadNet, for the years ended December 31, 2012, 2011 and 2010, respectively, and $53.4 million, $53.9 million and $51.5 million of operating expenses for the years ended December 31, 2012, 2011 and 2010, respectively. RadNet recognized $208.7 million, $196.7 million and $186.3 million of net revenues for the years ended December 31, 2012, 2011 and 2010, respectively, for management services provided to BRMG relating primarily to the technical portion of total billed revenue. The cash flows of BRMG are included in the accompanying consolidated statements of cash flows. All intercompany balances and transactions have been eliminated in consolidation. In our consolidated balance sheets at December 31, 2012 and 2011, we have included approximately $51.8 million and $49.1 million, respectively, of accounts receivable and approximately $6.3 million and $5.5 million, respectively, of accounts payable and accrued liabilities, related to BRMG.
| 59 |
The creditors of BRMG do not have recourse to our general credit and there are no other arrangements that could expose us to losses. However, BRMG is managed to recognize no net income or net loss and, therefore, RadNet may be required to provide financial support to cover any operating expenses in excess of operating revenues.
Aside from centers in California where we contract with BRMG for the provision of professional medical services, at the remaining centers in California and at all of the centers which are located outside of California, we have entered into long-term contracts with independent radiology groups in the area to provide physician services at those facilities. These third party radiology practices provide professional services, including supervision and interpretation of diagnostic imaging procedures, in our diagnostic imaging centers. The radiology practices maintain full control over the provision of professional services. The contracted radiology practices generally have outstanding physician and practice credentials and reputations; strong competitive market positions; a broad sub-specialty mix of physicians; a history of growth and potential for continued growth. In these facilities we enter into long-term agreements with radiology practice groups (typically 40 years). Under these arrangements, in addition to obtaining technical fees for the use of our diagnostic imaging equipment and the provision of technical services, we provide management services and receive a fee based on the practice group’s professional revenue, including revenue derived outside of our diagnostic imaging centers. We own the diagnostic imaging equipment and, therefore, receive 100% of the technical reimbursements associated with imaging procedures. The radiology practice groups retain the professional reimbursements associated with imaging procedures after deducting management service fees paid to us. We have no financial controlling interest in the independent (non-BRMG) radiology practices; accordingly, we do not consolidate the financial statements of those practices in our consolidated financial statements.
NOTE 1A – RESTATEMENT
The Company is restating its previously issued consolidated financial statements as of and for the year ended December 31, 2012 to correct the following:
In the fourth quarter of 2012, the Company recorded a benefit from income taxes of approximately $60.4 million primarily resulting from the release of a valuation allowance against its deferred tax assets. In November 2013, during a review of the Company’s work papers supporting its deferred tax assets, management discovered an error in the historical tax treatment of certain mark-to-market adjustments recorded in relation to its interest rate swaps, dating back as far as 2009. This error caused the Company’s deferred tax assets to be overstated by approximately $4.3 million and unrecognized tax benefit liability (included in accounts payable, accrued expenses and other) to be understated by approximately $0.4 million at December 31, 2012. Periods prior to the fourth quarter of 2012 were not significantly impacted by the overstatement, as the Company had a valuation allowance established against the overstated deferred tax assets.
To correct the income tax benefit overstatement described above, the Company is restating the following line items in its consolidated financial statements:
| As Previously Reported | Restatement Adjustments | As Restated | ||||||||
| As of and for the year ended December 31, 2012 | ||||||||||
| Current portion of deferred tax assets | $ | 7,607 | $ | – | $7,607 | |||||
| Deferred tax assets, net of current portion | 52,790 | (4,255 | ) | 48,535 | ||||||
| Total deferred tax assets | 60,397 | (4,255 | ) | 56,142 | ||||||
| Total Assets | 715,119 | (4,255 | ) | 710,864 | ||||||
| Accounts payable, accrued expenses and other | 105,929 | 428 | 106,357 | |||||||
| Total current liabilities | 118,613 | 428 | 119,041 | |||||||
| Total liabilities | 717,120 | 428 | 717,548 | |||||||
| Accumulated deficit | (171,093 | ) | (4,683 | ) | (175,776) | |||||
| Total stockholders' deficit | (2,001 | ) | (4,683 | ) | (6,684) | |||||
| Benefit from income taxes | 59,910 | (4,683 | ) | 55,227 | ||||||
| Net income | 64,287 | (4,683 | ) | 59,604 | ||||||
| Net income attributable to RadNet, Inc. common stockholders | 64,517 | (4,683 | ) | 59,834 | ||||||
| Basic net income per share attributable to RadNet, Inc. common stockholders | 1.71 | (0.13 | ) | 1.58 | ||||||
| Diluted net income per share attributable to RadNet, Inc. common stockholders | 1.64 | (0.12 | ) | 1.52 | ||||||
| Comprehensive income | 65,502 | (4,683 | ) | 60,819 | ||||||
| Comprehensive income attributable to RadNet, Inc. common stockholders | 65,272 | (4,683 | ) | 60,589 |
In addition to the restated line items above, certain information in Note 2 (earnings per share), Note 11, Note 15 and Note 16 has been restated to reflect the restated amounts above.
The restate adjustments had no impact on cash flows from operating, investing or financing activities.
| 60 |
NOTE 2 - SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES
PRINCIPLES OF CONSOLIDATION - The operating activities of subsidiaries are included in the accompanying consolidated financial statements from the date of acquisition. Investments in companies in which the Company has the ability to exercise significant influence, but not control, are accounted for by the equity method. All intercompany transactions and balances, including the unsettled amount of intercompany transactions with our equity method investees, have been eliminated in consolidation.
USE OF ESTIMATES - The preparation of the financial statements in conformity with U.S. generally accepted accounting principles requires management to make estimates and assumptions that affect the amounts reported in the financial statements and accompanying notes. These estimates and assumptions affect various matters, including our reported amounts of assets and liabilities in our consolidated balance sheets at the dates of the financial statements; our disclosure of contingent assets and liabilities at the dates of the financial statements; and our reported amounts of revenues and expenses in our consolidated statements of operations during the reporting periods. These estimates involve judgments with respect to numerous factors that are difficult to predict and are beyond management’s control. As a result, actual amounts could materially differ from these estimates.
RECLASSIFICATION – Certain reclassifications have been made to the December 31, 2011 and 2010 consolidated financial statements and accompanying notes to conform to the December 31, 2012 presentation. We have adjusted the prior year’s presentation as a result of the adoption of ASU 2011-07, Health Care Entities (Topic 954). In connection with this adjustment, we identified certain mechanical errors in our historical calculation of the provision for bad debts, resulting in the gross up of the provision for bad debts and revenues by $12.3 million and $11.2 million for the years ended December 31, 2011 and 2010, respectively. The error has been corrected in these financial statements and upon adoption of the new guidance, resulted in no impact to net service fee revenue.
REVENUES - Service fee revenue, net of contractual allowances and discounts, consists of net patient fees received from various payers and patients themselves based mainly upon established contractual billing rates, less allowances for contractual adjustments and discounts. As it relates to BRMG centers, this service fee revenue includes payments for both the professional medical interpretation revenue recognized by BRMG as well as the payment for all other aspects related to our providing the imaging services, for which we earn management fees from BRMG. As it relates to non-BRMG centers, this service fee revenue is earned through providing the use of our diagnostic imaging equipment and the provision of technical services as well as providing administration services such as clerical and administrative personnel, bookkeeping and accounting services, billing and collection, provision of medical and office supplies, secretarial, reception and transcription services, maintenance of medical records, and advertising, marketing and promotional activities.
Service fee revenues are recorded during the period the services are provided based upon the estimated amounts due from the patients and third-party payers. Third-party payers include federal and state agencies (under the Medicare and Medicaid programs), managed care health plans, commercial insurance companies and employers. Estimates of contractual allowances under managed care health plans are based upon the payment terms specified in the related contractual agreements. Contractual payment terms in managed care agreements are generally based upon predetermined rates per discounted fee-for-service rates. We also record a provision for doubtful accounts (based primarily on historical collection experience) related to patients and copayment and deductible amounts for patients who have health care coverage under one of our third-party payers.
Under capitation arrangements with various health plans, we earn a per-enrollee amount each month for making available diagnostic imaging services to all plan enrollees under the capitation arrangement. Revenue under capitation arrangements is recognized in the period which we are obligated to provide services to plan enrollees under contracts with various health plans.
Our service fee revenue, net of contractual allowances and discounts, the provision for bad debts, and revenue under capitation arrangements for the years ended December 31, are summarized in the following table (in thousands):
| 61 |
| Years Ended December 31, | ||||||||||||
| 2012 | 2011 | 2010 | ||||||||||
| Commercial Insurance | $ | 409,114 | $ | 376,107 | $ | 337,980 | ||||||
| Medicare | 122,971 | 107,613 | 103,055 | |||||||||
| Medicaid | 20,101 | 17,756 | 16,118 | |||||||||
| Workers' Compensation/Personal Injury | 26,604 | 23,137 | 21,002 | |||||||||
| Other | 39,192 | 30,367 | 11,140 | |||||||||
| Service fee revenue, net of contractual allowances and discounts | 617,982 | 554,979 | 489,294 | |||||||||
| Provision for bad debts | (25,904 | ) | (22,339 | ) | (21,995 | ) | ||||||
| Net service fee revenue | 592,078 | 532,640 | 467,299 | |||||||||
| Revenue under capitation arrangements | 55,075 | 52,481 | 51,358 | |||||||||
| Total net revenue | $ | 647,153 | $ | 585,121 | $ | 518,657 | ||||||
The break-out of our service fee revenue, net of contractual allowances and discounts, is calculated based upon global payments received from consolidated imaging centers from dates of service from each respective period illustrated.
PROVISION FOR BAD DEBTS - We provide for an allowance against accounts receivable that could become uncollectible to reduce the carrying value of such receivables to their estimated net realizable value. We estimate this allowance based on the aging of our accounts receivable by each type of payer over an 18-month look-back period and other relevant factors. A significant portion of our provision for bad debt relates to co-payments and deductibles owed to us from patients with insurance. Although we attempt to collect deductibles and co-payments due from patients with insurance at the time of service, this attempt to collect at the time of service is not an assessment of the patient’s ability to pay nor are revenues recognized based on an assessment of the patient’s ability to pay. There are various factors that can impact collection trends, such as changes in the economy, which in turn have an impact on the increased burden of co-payments and deductibles to be made by patients with insurance. These factors continuously change and can have an impact on collection trends and our estimation process.
ACCOUNTS RECEIVABLE - Substantially all of our accounts receivable are due under fee-for-service contracts from third party payors, such as insurance companies and government-sponsored healthcare programs, or directly from patients. Services are generally provided pursuant to one-year contracts with healthcare providers. Receivables generally are collected within industry norms for third-party payors. We continuously monitor collections from our payors and maintain an allowance for bad debts based upon specific payor collection issues that we have identified and our historical experience.
SOFTWARE REVENUE RECOGNITION - On October 1, 2010, we completed our acquisition of Image Medical Corporation, the parent of eRAD, Inc. eRAD sells Picture Archiving Communications Systems (“PACS”) and related services, primarily in the United States. The PACS systems sold by eRAD are primarily composed of certain elements: hardware, software, installation and training, and support. Sales are made primarily through eRAD’s sales force. These sales are multiple-element arrangements that generally include hardware, software, software installation, configuration, system installation, training and first-year warranty support. Hardware, which is not unique or special purpose, is purchased from a third-party and resold to eRAD’s customers with a small mark-up.
We have determined that our core software products, such as PACS, are essential to most of our arrangements as hardware, software and related services are sold as an integrated package. Therefore, these transactions are accounted for under ASC 605-25, Multiple-Element Arrangements (as modified by ASU 2009-13). Non-essential software and related services, and essential software sold on a stand-alone basis without hardware, would continue to be accounted for under ASC 985-605, Software.
We recognize revenue for four units of accounting, hardware, software, installation (including manufacturing and configuration, training, implementation and project management) and post-contract support (“PCS”), as follows:
| • | Hardware – Revenue is recognized when the hardware is shipped. The hardware qualifies as a separate unit of accounting under ASC 605-25-25-5, as it meets the following criteria: |
| o | The hardware has standalone value as it is sold separately by other vendors and the customer could resell the hardware on a standalone basis; and |
| o | Delivery or performance of the undelivered items is probable and substantially within our control. |
| • | Software– We sell essential software. This software revenue is recognized along with the related hardware revenue. |
| • | Installation – Installation revenue related to essential software that is sold with hardware, is recognized when the installation is completed, as it qualifies as a separate unit of accounting once delivered as it can be provided by a third party. |
| • | Post-Contract Support – Revenue is recognized over the term of the agreement, usually one year. |
| 62 |
Our transactions do not generally contain refund provisions. We allocate the transaction price to each unit of accounting using relative selling price. We consider historical pricing, list price and market considerations in determining estimated selling price in the allocation.
For the years ended December 31, 2012, 2011 and 2010, we recorded approximately $4.9 million, $4.8 million and $998,000, respectively, in revenue related to our eRAD business which is included in net service fee revenue in our consolidated statement of operations. At December 31, 2012 we had a deferred revenue liability of approximately $1.3 million associated with eRAD sales which we expect to recognize into revenue over the next 12 months.
SOFTWARE DEVELOPMENT COSTS - Costs related to the research and development of new software products and enhancements to existing software products are expensed as incurred until technological feasibility of the product has been established, at which time such costs are capitalized, subject to expected recoverability.
We utilize a variety of computerized information systems in the day to day operation of our 246 diagnostic imaging facilities. One such system is our front desk patient tracking system or Radiology Information System (“RIS”). We currently utilize third party RIS software solutions and pay monthly fees to outside third party software vendors for the use of this software. We intend to develop our own RIS solution from the ground up through our wholly owned subsidiary, Radnet Management Information Systems (“RMIS”). Beginning August 1, 2010, RMIS directly employs a team of software development engineers to develop from the ground up a RIS system specifically tailored for RadNet, Inc. and the operation of our 246 imaging centers.
By following the accounting guidance under ASC 350-40, Accounting for the Costs of Computer Software Developed for Internal Use, the development costs incurred by RMIS, which began on August 1, 2010, will be capitalized and amortized over the useful life of the developed RIS system which we determined to be 5 years. The development stage will run for approximately 36 months ending on or around August 1, 2013. We have estimated total costs to be capitalized will be approximately $4.6 million and will start to be amortized in August of 2013 at approximately $77,000 per month.
As of December 31, 2012 and 2011 we capitalized approximately $3.4 million and $2.6 million, respectively, in costs associated with the development of our RIS system to a construction in progress account which is a component of our total Property and Equipment at December 31, 2012 and 2011.
CONCENTRATION OF CREDIT RISKS - Financial instruments that potentially subject us to credit risk are primarily cash equivalents and accounts receivable. We have placed our cash and cash equivalents with one major financial institution. At times, the cash in the financial institution is temporarily in excess of the amount insured by the Federal Deposit Insurance Corporation, or FDIC. Substantially all of our accounts receivable are due under fee-for-service contracts from third party payors, such as insurance companies and government-sponsored healthcare programs, or directly from patients. Services are generally provided pursuant to one-year contracts with healthcare providers. Receivables generally are collected within industry norms for third-party payors. We continuously monitor collections from our clients and maintain an allowance for bad debts based upon our historical collection experience.
CASH AND CASH EQUIVALENTS - We consider all highly liquid investments that mature in three months or less when purchased to be cash equivalents. The carrying amount of cash and cash equivalents approximates their fair market value.
DEFERRED FINANCING COSTS - Costs of financing are deferred and amortized on a straight-line basis over the life of the associated loan, which approximates the effective interest rate method.
INVENTORIES - Inventories, consisting of mainly medical supplies, are stated at the lower of cost or market with cost determined by the first-in, first-out method. Reserves for slow-moving and obsolete inventories are provided based on historical experience and product demand. We evaluate the adequacy of these reserves periodically.
PROPERTY AND EQUIPMENT - Property and equipment are stated at cost, less accumulated depreciation and amortization. Depreciation and amortization of property and equipment are provided using the straight-line method over the estimated useful lives, which range from 3 to 15 years. Leasehold improvements are amortized at the lesser of lease term or their estimated useful lives, whichever is lower, which range from 3 to 30 years. Only a few leasehold improvements are deemed to have a life greater than 15 to 20 years. Maintenance and repairs are charged to expense as incurred.
GOODWILL - Goodwill at December 31, 2012 totaled $193.9 million. Goodwill is recorded as a result of business combinations. Management evaluates goodwill, at a minimum, on an annual basis and whenever events and changes in circumstances suggest that the carrying amount may not be recoverable. Impairment of goodwill is tested at the reporting unit level by comparing the reporting unit’s carrying amount, including goodwill, to the fair value of the reporting unit. The fair value of a reporting unit is estimated using a combination of the income or discounted cash flows approach and the market approach, which uses comparable market data. If the carrying amount of the reporting unit exceeds its fair value, goodwill is considered impaired and a second step is performed to measure the amount of impairment loss, if any. We tested goodwill for impairment on October 1, 2012. Based on our test, we noted no impairment related to goodwill as of October 1, 2012 as the estimated fair value of each reporting unit exceeded its carrying value by no less than 38%. Our largest reporting unit, which is our California Operations, has goodwill of $67.5 million and an estimated fair value in excess of carrying value of 43% as of October 1, 2012. However, if estimates or the related assumptions change in the future, we may be required to record impairment charges to reduce the carrying amount of goodwill.
| 63 |
LONG-LIVED ASSETS - We evaluate our long-lived assets (property and equipment) and intangibles, other than goodwill, for impairment whenever indicators of impairment exist. The accounting standards require that if the sum of the undiscounted expected future cash flows from a long-lived asset or definite-lived intangible is less than the carrying value of that asset, an asset impairment charge must be recognized. The amount of the impairment charge is calculated as the excess of the asset’s carrying value over its fair value, which generally represents the discounted future cash flows from that asset or in the case of assets we expect to sell, at fair value less costs to sell. No indicators of impairment were identified with respect to our long-lived assets as of December 31, 2012.
INCOME TAXES - Income tax expense is computed using an asset and liability method and using expected annual effective tax rates. Under this method, deferred income tax assets and liabilities result from temporary differences in the financial reporting bases and the income tax reporting bases of assets and liabilities. The measurement of deferred tax assets is reduced, if necessary, by the amount of any tax benefit that, based on available evidence, is not expected to be realized. When it appears more likely than not that deferred taxes will not be realized, a valuation allowance is recorded to reduce the deferred tax asset to its estimated realizable value. For net deferred tax assets we consider estimates of future taxable income, including tax planning strategies, in determining whether our net deferred tax assets are more likely than not to be realized. Income taxes are further explained in Note 11.
UNINSURED RISKS – Prior to November 1, 2006 we maintained a self-insured workers’ compensation insurance program for which our third party administrator over this program continues to make payments on behalf of the Company for claims incurred from November 1, 2004 through October 31, 2006. We are required to maintain a cash collateral account with this administrator as guarantee of our submission of full reimbursement of claims paid on our behalf. We record this collateral deposit as restricted cash and include it as other assets in our consolidated balance sheet which amounted to approximately $529,000 as of both December 31, 2012 and 2011.
With respect to the above-mentioned claims incurred from November 1, 2004 through October 31, 2006, the estimated future cash obligation associated with the unpaid portion of those claims that remain open but have not yet been resolved is recorded to accrued expenses in our consolidated balance sheet. This current liability is determined by the administrator’s estimate of loss development of open claims and was approximately $188,000 and $225,000 at December 31, 2012 and 2011, respectively.
For the two years from November 1, 2006 through October 31, 2008, we pre-funded our anticipated workers’ compensation claims’ losses through a third party administrator. As of December 31, 2012, we anticipate that the loss development on the claims for the latter of these two years will exceed what has already been paid and expensed. Accordingly, we have recorded a reserve of $200,000 for estimated costs exceeding the actuary’s original estimate on open claims from this period which we recorded to accrued expenses in our consolidated balance sheet at December 31, 2012.
On November 1, 2008 we obtained a fully funded and insured workers’ compensation policy, thereby eliminating any uninsured risks for employee injuries occurring on or after that date.
We and our affiliated physicians carry an annual medical malpractice insurance policy that protects us for claims that are filed during the policy year and that fall within policy limits. The policy has a deductible for which we have recorded liabilities and included it in our consolidated balance sheets at December 31, 2012 and December 31, 2011 of approximately $457,000 and $304,000, respectively.
In December 2008, in order to eliminate the exposure for claims not reported during the regular malpractice policy period, we purchased a medical malpractice tail policy, which provides coverage for any claims reported in the event that our medical malpractice policy expires. As of December 31, 2012, this policy remains in effect.
On January 1, 2008 we entered into an arrangement with Blue Shield to administer and process claims under a new self-insured plan that provides health insurance coverage for our employees and dependents. We have recorded liabilities as of December 31, 2012 and December 31, 2011 of $2.8 million and $2.6 million, respectively, for the estimated future cash obligations associated with the unpaid portion of the medical and dental claims incurred by our participants. Additionally, we entered into an agreement with Blue Shield for a stop loss policy that provides coverage for any claims that exceed $200,000 up to a maximum of $1.0 million in order for us to limit our exposure for unusual or catastrophic claims.
LOSS CONTRACTS – We assess the profitability of our contracts to provide management services to our contracted physician groups and identify those contracts where current operating results or forecasts indicate probable future losses. Anticipated future revenue is compared to anticipated costs. If the anticipated future cost exceeds the revenue, a loss contract accrual is recorded. In connection with the acquisition of Radiologix in November 2006, we acquired certain management service agreements for which forecasted costs exceeds forecasted revenue. As such, an $8.9 million loss contract accrual was established in purchase accounting, and is included in other non-current liabilities. The recorded loss contract accrual is being accreted into operations over the remaining term of the acquired management service agreements. As of December 31, 2012 and 2011, the remaining accrual balance is $6.8 million, and $7.2 million, respectively. In addition, we have certain operating lease commitments for facilities that are not in use. Accordingly, we have recorded a loss contract accrual related to the remaining payments under these lease commitments. As of December 31, 2012 and 2011, the remaining loss contract accrual for these leases is $3.3 million and $2.1 million, respectively.
| 64 |
EQUITY BASED COMPENSATION – We have two long-term incentive plans which we refer to as the 2000 Plan and the 2006 Plan. The 2000 Plan was terminated as to future grants when the 2006 Plan was approved by the stockholders in 2006. As of December 31, 2012, we have reserved for issuance under the 2006 Plan 11,000,000 shares of common stock. Certain options granted under the 2006 Plan to employees are intended to qualify as incentive stock options under existing tax regulations. In addition, we may issue non-qualified stock options and warrants under the 2006 Plan from time to time to non-employees, in connection with acquisitions and for other purposes and we may also issue restricted stock under the 2006 Plan. Stock options and warrants generally vest over two to five years and expire five to ten years from date of grant.
The compensation expense recognized for all equity-based awards is net of estimated forfeitures and is recognized over the awards’ service periods. Equity-based compensation is classified in operating expenses within the same line item as the majority of the cash compensation paid to employees.
FOREIGN CURRENCY TRANSLATION - The functional currency of our foreign subsidiaries is the local currency. In accordance with ASC 830, Foreign Currency Matters, assets and liabilities denominated in foreign currencies are translated using the exchange rate at the balance sheet dates. Revenues and expenses are translated using average exchange rates prevailing during the reporting period. Any translation adjustments resulting from this process are shown separately as a component of accumulated other comprehensive income (loss). Foreign currency transaction gains and losses are included in the determination of net income.
COMPREHENSIVE INCOME (LOSS) - ASC 220, Comprehensive Income, establishes rules for reporting and displaying comprehensive income and its components. Unrealized gains or losses on the change in fair value of the Company’s cash flow hedging activities are included in comprehensive income (loss). Also included are foreign currency translation adjustments. The components of comprehensive income (loss) for the three years in the period ended December 31, 2012 are included in the consolidated statements of comprehensive income (loss).
FAIR VALUE MEASUREMENTS – Assets and liabilities subject to fair value measurements are required to be disclosed within a fair value hierarchy. The fair value hierarchy ranks the quality and reliability of inputs used to determine fair value. Accordingly, assets and liabilities carried at, or permitted to be carried at, fair value are classified within the fair value hierarchy in one of the following categories based on the lowest level input that is significant to a fair value measurement:
Level 1—Fair value is determined by using unadjusted quoted prices that are available in active markets for identical assets and liabilities.
Level 2—Fair value is determined by using inputs other than Level 1 quoted prices that are directly or indirectly observable. Inputs can include quoted prices for similar assets and liabilities in active markets or quoted prices for identical assets and liabilities in inactive markets. Related inputs can also include those used in valuation or other pricing models such as interest rates and yield curves that can be corroborated by observable market data.
Level 3—Fair value is determined by using inputs that are unobservable and not corroborated by market data. Use of these inputs involves significant and subjective judgment.
The table below summarizes the estimated fair values of certain of our financial liabilities that are subject to fair value measurements, and the classification of these liabilities on our consolidated balance sheets, as follows (in thousands):
| As of December 31, 2011 | ||||||||||||||||
| Level 1 | Level 2 | Level 3 | Total | |||||||||||||
| Accounts payable, accrued expenses and other: | ||||||||||||||||
| Interest Rate Swaps | $ | – | $ | 5,064 | $ | – | $ | 5,064 | ||||||||
The estimated fair value of these swaps, which are discussed in Note 10, was determined using Level 2 inputs. More specifically, the fair value was determined by calculating the value of the difference between the fixed interest rate of the interest rate swaps and the counterparty’s forward LIBOR curve. The forward LIBOR curve is readily available in the public markets or can be derived from information available in the public markets.
| 65 |
The table below summarizes the estimated fair value and carrying amount of our long-term debt as follows (in thousands):
| As of December 31, 2012 | ||||||||||||||||||||
| Level 1 | Level 2 | Level 3 | Total Fair Value | Total Carrying Value | ||||||||||||||||
| Senior Secured Term Loan | $ | – | $ | 352,180 | $ | – | $ | 352,180 | $ | 349,125 | ||||||||||
| Senior Notes | – | 204,500 | – | 204,500 | 200,000 | |||||||||||||||
| As of December 31, 2011 | ||||||||||||||||||||
| Level 1 | Level 2 | Level 3 | Total | Total Carrying Value | ||||||||||||||||
| Senior Secured Term Loan | $ | – | $ | 264,600 | $ | – | $ | 264,600 | $ | 280,000 | ||||||||||
| Senior Notes | – | 180,000 | – | 180,000 | 200,000 | |||||||||||||||
The carrying value of our line of credit at December 31, 2012 and 2011 of $33.0 million and $58.0 million, respectively, approximated its fair value.
The estimated fair value of our long-term debt, which is discussed in Note 8, was determined using Level 2 inputs primarily related to comparable market prices.
We consider the carrying amounts of cash and cash equivalents, receivables, other current assets and current liabilities to approximate their fair value because of the relatively short period of time between the origination of these instruments and their expected realization or payment. Additionally, we consider the carrying amount of our capital lease obligations to approximate their fair value because the weighted average interest rate used to formulate the carrying amounts approximates current market rates.
EARNINGS PER SHARE - Earnings per share is based upon the weighted average number of shares of common stock and common stock equivalents outstanding, net of common stock held in treasury, as follows (in thousands except share and per share data):
| Years Ended December 31, | ||||||||||||
| 2012 | 2011 | 2010 | ||||||||||
| (Restated) | ||||||||||||
| Net income (loss) attributable to RadNet, Inc.'s common stockholders | $ | 59,834 | $ | 7,231 | $ | (12,852 | ) | |||||
| BASIC NET INCOME (LOSS) PER SHARE ATTRIBUTABLE TO RADNET, INC.'S COMMON STOCKHOLDERS | ||||||||||||
| Weighted average number of common shares outstanding during the period | 37,751,170 | 37,367,736 | 36,853,477 | |||||||||
| Basic net income (loss) per share attributable to RadNet, Inc.'s common stockholders | $ | 1.58 | $ | 0.19 | $ | (0.35 | ) | |||||
| DILUTED NET INCOME (LOSS) PER SHARE ATTRIBUTABLE TO RADNET, INC.'S COMMON STOCKHOLDERS | ||||||||||||
| Weighted average number of common shares outstanding during the period | 37,751,170 | 37,367,736 | 36,853,477 | |||||||||
| Add nonvested restricted stock subject only to service vesting | 533,014 | – | – | |||||||||
| Add additional shares issuable upon exercise of stock options and warrants | 960,502 | 1,417,939 | – | |||||||||
| Weighted average number of common shares used in calculating diluted net income (loss) per share | 39,244,686 | 38,785,675 | 36,853,477 | |||||||||
| Diluted net income (loss) per share attributable to RadNet, Inc.'s common stockholders | $ | 1.52 | $ | 0.19 | $ | (0.35 | ) | |||||
For the year ended December 31, 2010 we excluded all options and warrants in the calculation of diluted earnings per share because their effect would be antidilutive.
INVESTMENT IN JOINT VENTURES – We have nine unconsolidated joint ventures with ownership interests ranging from 31% to 50%. These joint ventures represent partnerships with hospitals, health systems or radiology practices and were formed for the purpose of owning and operating diagnostic imaging centers. Professional services at the joint venture diagnostic imaging centers are performed by contracted radiology practices or a radiology practice that participates in the joint venture. Our investment in these joint ventures is accounted for under the equity method. We evaluate our investment in joint ventures for impairment whenever indicators of impairment exist. No indicators of impairment exist as of December 31, 2012. Investment in joint ventures increased approximately $6.3 million to $28.6 million at December 31, 2012 compared to $22.3 million at December 31, 2011. This increase is summarized as follows (in thousands):
| 66 |
| Investment in joint ventures at December 31, 2011 | $ | 22,326 | ||
| Fair value of remaining interest in de-consolidated joint venture (see Note 2) | 1,936 | |||
| Initial investment in joint venture imaging center located in Cedar Knolls, New Jersey (see Note 2) | 1,836 | |||
| Additional investment in an existing joint venture imaging center | 920 | |||
| Final purchase accounting adjustment to the fair value of joint venture interests acquired | ||||
| with our acquisition of Raven Holdings (see Note 2) | 933 | |||
| Fair value of joint venture interests acquired through our acquisition of | ||||
| Lenox Hill Radiology (see Note 2) | 648 | |||
| Equity in earnings of joint ventures for the year ended December 31, 2012 | 6,476 | |||
| Distributions from joint ventures received during the year ended December 31, 2012 | (6,477 | ) | ||
| Investment in joint ventures at December 31, 2012 | $ | 28,598 |
We received management service fees from the centers underlying these joint ventures of approximately $8.5 million, $6.8 million and $6.8 million for the years ended December 31, 2012, 2011 and 2010, respectively. We offset the portion of the fees earned from our service revenue associated with our ownership with an increase to our equity earnings.
The following table is a summary of key financial data for these joint ventures as of December 31, 2012 and 2011, respectively, and for the years ended December 31, 2012, 2011 and 2010, respectively, (in thousands):
| December 31, | ||||||||
| Balance Sheet Data: | 2012 | 2011 | ||||||
| Current assets | $ | 17,026 | $ | 16,869 | ||||
| Noncurrent assets | 49,163 | 41,928 | ||||||
| Current liabilities | (7,419 | ) | (9,575 | ) | ||||
| Noncurrent liabilities | (8,997 | ) | (9,370 | ) | ||||
| Total net assets | $ | 49,773 | $ | 39,852 | ||||
| Book value of RadNet joint venture interests | $ | 24,712 | $ | 18,566 | ||||
| Cost in excess of book value of acquired joint venture interests | 3,511 | 3,511 | ||||||
| Elimination of intercompany profit remaining on Radnet's consolidated balance sheet | 375 | 249 | ||||||
| Total value of Radnet joint venture interests | $ | 28,598 | $ | 22,326 | ||||
| Total book value of other joint venture partner interests | $ | 25,061 | $ | 21,286 | ||||
| Income statement data for the years ended December 31, | 2012 | 2011 | 2010 | |||||||||
| Net revenue | $ | 85,036 | $ | 76,076 | $ | 76,937 | ||||||
| Net income | $ | 14,031 | $ | 11,655 | $ | 12,639 | ||||||
NOTE 3 – RECENT ACCOUNTING STANDARDS
On January 1, 2012, we adopted ASU 2011-05, “Comprehensive Income (Topic 220): Presentation of Comprehensive Income,” which updates existing guidance on comprehensive income. This guidance eliminates the option to present the components of other comprehensive income as part of our Consolidated Statements of Equity Deficit and Comprehensive Income (Loss), which was our previous presentation. It requires companies to present the total of comprehensive income, the components of net income and the components of other comprehensive income either in a single continuous statement of comprehensive income or in two separate but consecutive statements. In the two statement approach which we have adopted, the first statement presents total net income and its components followed consecutively by a second statement that presents total other comprehensive income, the components of other comprehensive income and the total of comprehensive income. The adoption of this pronouncement did not have any effect on our financial condition or results of operations, though it did change our financial statement presentation.
| 67 |
On January 1, 2012, we adopted ASU 2011-07, “Health Care Entities (Topic 954): Presentation and Disclosure of Patient Service Revenue, Provision for Bad Debts, and the Allowance for Doubtful Accounts for Certain Health Care Entities,” which requires health care entities to present the provision for doubtful accounts relating to patient service revenue as a deduction from patient service revenue in the statement of operations rather than as an operating expense. Additional disclosures relating to sources of patient revenue and the allowance for doubtful accounts related to patient accounts receivable are also required. Such additional disclosures are included in Note 2. The adoption of this ASU had no impact on our financial condition, results of operations or cash flows, although it did change our financial statement presentation.
On January 1, 2012, we adopted ASU 2011-08, “Intangibles—Goodwill and Other (Topic 350): Testing Goodwill for Impairment”, simplifying how a company is required to test goodwill for impairment. Companies will now have the option to first assess qualitative factors to determine whether it is more likely than not that the fair value of a reporting unit is less than its carrying amount. If the company determines that it is not more likely than not that the fair value of a reporting unit is less than its carrying amount, then performing the two-step impairment test is unnecessary. This qualitative assessment was not performed as of December 31, 2012.
In July 2012, the FASB modified existing rules to allow entities to use a qualitative approach to test indefinite-lived intangible asset for impairment. The revised standard allows an entity the option to first assess qualitatively whether it is more likely than not (that is, a likelihood of more than 50 percent) that an indefinite-lived intangible asset is impaired. An entity is not required to calculate the fair value of an indefinite-lived intangible asset and perform the quantitative impairment test unless the entity determines that it is more likely than not that the asset is impaired. This guidance will be effective for the Company in 2013, but early adoption is permitted. Adoption of this standard will not have a material impact on our results of operations, cash flows, or financial position.
In February 2013, the FASB issued new guidance which requires disclosure of information about significant reclassification adjustments from accumulated other comprehensive income in a single note or on the face of the financial statements. This guidance will be effective for the Company in 2013. Adoption of this standard, which is related to disclosure only, will not have an impact on the Company’s consolidated financial position, results of operations, or cash flows.
NOTE 4 – FACILITY ACQUISITIONS
On December 31, 2012, we completed our acquisition of Lenox Hill Radiology, consisting of three multi-modality imaging centers as well as three additional x-Ray facilities all located in Manhattan, New York. We also acquired in this transaction a 31.5% interest in a joint venture multi-modality imaging center in Manhattan, New York and an option to purchase a 50% interest in a multi-modality imaging center located in Brooklyn, New York for $1.00. The purchase price consisted of approximately $29.0 million in cash. We have made a preliminary fair value determination of the acquired assets and assumed liabilities and approximately $4.5 million of working capital, $7.2 million of fixed assets, $648,000 of joint venture interests, $2.5 million in a $1.00 joint venture purchase option, $100,000 of intangible assets $15.7 million of goodwill and the assumption of approximately $400,000 of other liabilities and $1.3 million of capital lease debt was recorded with respect to this transaction. Our preliminary fair value determination will be made final with the help of an outside valuation expert which we expect to have completed by the end of our first quarter of 2013.
On December 3, 2012, we completed our acquisition of a multi-modality imaging center, Clinical Radiologists Medical Imaging located in Silver Spring, Maryland, for $2.8 million in cash. We have made a fair value determination of the acquired assets and assumed liabilities and approximately $65,000 of working capital, $1.8 million of fixed assets, $71,000 of other assets, $1.8 million of goodwill and the assumption of approximately $938,000 of capital lease debt was recorded with respect to this transaction.
On November 5, 2012, we completed our acquisition of a multi-modality imaging center, Vanowen Radiology located in Van Nuys, California, for cash consideration of $550,000. We have made a fair value determination of the acquired assets and approximately $164,000 of fixed assets and $386,000 of goodwill was recorded with respect to this transaction.
On November 9, 2012, we completed our acquisition of a multi-modality imaging center, Pueblo Radiology located in Ventura, California, for cash consideration of $750,000. This center is located in an area of Ventura where we operate an existing center and compete directly with Pueblo Radiology. We plan on closing our existing center and serving this location from this acquired center. We have made a fair value determination of the acquired assets and approximately $1.6 million of fixed assets and no goodwill was recorded with respect to this transaction. In accordance with accounting standards, any excess of fair value of acquired net assets over the acquisition consideration results in a gain on bargain purchase. Prior to recording a gain, the acquiring entity must reassess whether all acquired assets and assumed liabilities have been identified and recognized and perform re-measurements to verify that the consideration paid, assets acquired, and liabilities assumed have been properly valued. We undertook such a reassessment, and as a result, have recorded a gain on bargain purchase of approximately $810,000, which is included in Other Income within our consolidated statement of income for the year ended December 31, 2012. We believe that the gain on bargain purchase resulted from various factors that impacted the sale. The seller, a group of Radiologists some of whom own the building where the imaging center is based, were planning to close the imaging center, which was facing competition pressure from our existing RadNet center, and were facing possible expenses to renovate the building to make it available for a non-imaging center tenant. They saw the sale of these assets to RadNet and RadNet’s assumption of an operating lease for the building as a way to avoid costly renovation expense, get out of a location where they were competing directly with a RadNet center and immediately establish a rental revenue stream. We believe that the seller was willing to accept a bargain purchase price from us in return for our ability to enter into a long-term lease agreement for the facility and establish an immediate rental revenue stream with no investment on their part.
| 68 |
On October 1, 2012 we acquired a 100% controlling interest in one of our non-consolidated joint venture imaging centers in which we previously held a 50% non-consolidated equity investment. As a result of this transaction, we began consolidating this imaging center, recording all of its assets and liabilities at their fair value at October 1, 2012. We have made a fair value determination of the acquired assets and assumed liabilities and $2.1 million of fixed assets and $1.8 million of goodwill was recorded with respect to this transaction. We also assumed approximately $1.9 million of capital lease debt and $200,000 of other liabilities.
On August 6, 2012 we formed a limited liability company with Barnabas Health, a New Jersey owner and operator of a large New Jersey hospital system, for the purpose of creating a New Jersey imaging network under our management. Our first endeavor was to establish a multi-modality imaging center located in Cedar Knolls, New Jersey, of which we own 49%. Our initial investment of approximately $1.8 million was recorded to investment in non-consolidated joint ventures.
On July 23, 2012, we completed our acquisition of a multi-modality imaging center, Orthopedic Imaging Center, LLC. located in Redlands, California, for cash consideration of $700,000. We have made a fair value determination of the acquired assets and approximately $373,000 of fixed assets, $25,000 of other assets and $302,000 of goodwill was recorded with respect to this transaction.
On July 1, 2012, we completed the sale of a 41% portion of our ownership interest of one of our consolidated joint ventures to our existing partner in that joint venture for $1.8 million. After the sale, we retained a 49% ownership interest in this joint venture. As a result of this transaction we de-consolidated this joint venture and recorded the fair value of our remaining interest as an investment in non-consolidated joint venture accounted for under the equity method. We recorded a gain on de-consolidation of a joint venture of approximately $2.8 million with respect to this transaction. Approximately $1.4 million of this gain is related to the re-measurement to current fair value of our remaining 49% interest, using a market based valuation approach. The main input used in our valuation model was the $1.8 million sale price of a 41% interest.
On May 1, 2012, we completed our acquisition of Advanced Medical Imaging of Stuart, L.P., which consists of two multi-modality imaging centers located in Stuart, Florida, for cash consideration of $1.0 million. We have made a fair value determination of the acquired assets and approximately $39,000 of fixed assets, $88,000 of other current assets and $923,000 of goodwill was recorded with respect to this transaction.
On April 1, 2012, we completed our acquisition of West Coast Radiology, which consists of five multi-modality imaging centers in Orange County, California, for cash consideration of $8.1 million. The centers are located in Anaheim, Santa Ana/Tustin, Irvine and Mission Viejo/Laguna Niguel and operate a combination of MRI, CT, ultrasound, mammography, X-ray and other related modalities. We have made a fair value determination of the acquired assets and assumed liabilities and approximately $715,000 of working capital, $3.1 million of fixed assets, $5.4 million of goodwill, $200,000 of intangible assets and the assumption of approximately $1.3 million of capital lease debt was recorded with respect to this transaction.
On February 29, 2012, we completed the acquisition of a multi-modality imaging center from TODIC, L.P. located in Camarillo, California for cash consideration of $350,000. The facility provides MRI, CT, mammography, ultrasound and X-ray services. We have made a fair value determination of the acquired assets and assumed liabilities and approximately $425,000 of fixed assets and $86,000 of goodwill was recorded with respect to this transaction as well as the assumption of approximately $40,000 of accrued liabilities and approximately $121,000 of capital lease debt.
On February 29, 2012, we completed the acquisition of a multi-modality imaging center from Progressive MRI, LLC located in Frederick, Maryland for cash consideration of $230,000. The facility provides MRI, CT, mammography, ultrasound and X-ray services. We have made a fair value determination of the acquired assets and approximately $230,000 of fixed assets was recorded with respect to this transaction.
| 69 |
On November 7, 2011, we completed our acquisition of all outstanding equity interests in Raven Holdings U.S., Inc. (“RH”) from CML Healthcare, Inc. The acquisition of RH includes two operating subsidiaries, American Radiology Services (“ARS”) and The Imaging Institute (“TII”). ARS operates 15 free-standing outpatient imaging facilities in Maryland (including two facilities held in joint ventures with hospital partners) and one facility in Delaware. In addition to the imaging centers, ARS provides on-site staffing and professional interpretation services to five Maryland hospitals and teleradiology services to nine additional hospitals and radiology group customers. TII operates five imaging facilities in the Cranston, Warwick and Providence local markets in Rhode Island. Aggregate consideration for the purchase was approximately $40.4 million, consisting of approximately $28.2 million in cash and $9.0 million in a seller note. With the services of an external valuation expert, we have made a final fair value determination of the acquired assets and assumed liabilities and approximately $2.4 million of working capital, $2.3 million of assets held for sale, $22.8 million of fixed assets, which is approximately $8.1 million lower than our initial estimate, $1.9 million of investments in non-consolidated joint ventures, which is approximately $933,000 higher than our initial estimates, $2.2 million of intangible assets, $279,000 of other assets and $11.8 million of goodwill was recorded with respect to this transaction. We also assumed approximately $3.4 million of assumed equipment-related debt and $3.1 million of other liabilities relating to unfavorable lease contract reserves, which is approximately $2.2 million higher than our initial estimate. Along with our $8.1 million adjustment to the value of acquired fixed assets, we recorded catch-up reductions to depreciation of approximately $1.1 million for the period from November 7, 2011 through June 30, 2012 of which approximately $275,000 relates to the period from November 7 through December 31, 2011. Along with our adjustment to the value of other liabilities, we recorded catch-up reductions to rent expense of approximately $435,000 for the period of November 7, 2011 through June 30, 2012 of which approximately $142,000 relates to the period of November 7 through December 31, 2011.
On November 1, 2011, Image Medical Corporation, a consolidated subsidiary of the Company, acquired a 51% controlling interest in Radar Medical Systems, LLC, a Michigan limited liability company (“Radar”) for $1.1 million cash consideration. The technology acquired from Radar will enhance our existing PACS technology acquired through our acquisition of Image Medical. We have made a fair value determination of the assets acquired and liabilities assumed of this limited liability company. Approximately $1.1 million of working capital, $144,000 of intangible assets and $845,000 of goodwill was recorded with respect to this transaction. We also recorded $961,000 of non-controlling interests with respect to this transaction.
On September 1, 2011, BRMG completed its acquisition of Hematology-Oncology Medical Group located in Encino, California for cash consideration of approximately $1.4 million. BRMG has made a fair value determination of the assets acquired and liabilities assumed. Approximately $342,000 of accounts receivable and $1.0 million of goodwill was recorded with respect to this transaction.
On August 1, 2011, we completed our acquisition of a multi-modality imaging center located in San Jacinto, California from San Jacinto Imaging, LLC for the assumption of approximately $750,000 of capital leases. The center operates a combination of MRI, CT, ultrasound and X-ray modalities. We have made a fair value determination of the assets acquired and liabilities assumed. Approximately $787,000 of fixed assets and $37,000 of accrued expenses was recorded with respect to this transaction.
On July 1, 2011, we completed our acquisition of a multi-modality imaging center located in Redondo Beach, California from Pacific Imaging, LLC for cash consideration of $650,000. The center operates a combination of MRI, CT, ultrasound and X-ray modalities. We have made a fair value determination of the assets acquired and liabilities assumed. Approximately $10,000 of other current assets and $640,000 of fixed assets was recorded with respect to this transaction.
On April 4, 2011, we completed our acquisition of five multi-modality imaging centers in Maryland from Diagnostic Health Corporation for an aggregate of $5.2 million in cash. The facilities located in the cities of Bowie, Chevy Chase, Frederick, Rockville and Waldorf operate a combination of MRI, CT, ultrasound, mammography, X-ray and other related modalities. We have made a fair value determination of the assets acquired and liabilities assumed. Approximately $25,000 of other current assets, $5.0 million of fixed assets and $2.0 million of goodwill was recorded with respect to this transaction. We also assumed approximately $1.8 million of capital lease debt and $102,000 of accrued liabilities.
On February 18, 2011, we completed our acquisition of Team Radiology, Inc. from Team Health, Inc. for approximately $243,000. A provider of teleradiology services, Team Radiology will complement our teleradiology operations acquired from Imaging on Call, LLC. We have made a fair value determination of the assets acquired and liabilities assumed and approximately $93,000 of other current assets, $126,000 of fixed assets and $24,000 of intangible assets related to the value of customer relationships and trade name was recorded with respect to this transaction.
On February 16, 2011, we acquired the diagnostic imaging practice of Stuart London, MD in Oakland, CA for $600,000. Upon acquisition, we relocated the practice to a nearby existing Oakland center. We have made a fair value determination of the assets acquired and liabilities assumed and have allocated the full purchase price of $600,000 to goodwill.
On January 3, 2011, we completed our acquisition of Imaging On Call, LLC, a provider of teleradiology services to radiology groups, hospitals and imaging centers located in Poughkeepsie, New York, for $5.5 million cash plus an earn-out of up to an additional $2.5 million. We have made a fair value determination of the assets acquired and liabilities assumed. Approximately $1.6 million of accounts receivable and other current assets, $785,000 of fixed assets, $850,000 of intangible assets related to the value of customer relationships and trade name, and $3.8 million of goodwill was recorded with respect to this transaction. We also assumed approximately $1.5 million of accrued liabilities of which approximately $790,000 related to our estimated fair value of the earn-out mentioned above. Upon termination of the earn-out period, we finalized our calculation of the required earn-out payment and received final approval and agreement from the seller in the amount of $452,000. The final calculation was based on actual revenue recorded during the first year of our operation of the business. Actual revenue was lower than our estimate due to certain contract cancelations which occurred subsequent to the acquisition date and could not have been forecasted for our acquisition date fair value determination. Accordingly, we recorded an adjustment of approximately $338,000 to our accrued liabilities and recognized this subsequent adjustment in earnings during the year ended December 31, 2011.
| 70 |
On December 31, 2010, we completed our acquisition of two imaging centers from Presgar Imaging and affiliated entities located in Brooklyn and Orchard Park, New York for cash consideration of $1.6 million. Highway Imaging in Brooklyn and Parkland Diagnostic in Orchard Park are both multimodality facilities, offering a combination of MRI, CT, PET/CT, ultrasound, mammography, bone density and X-ray. We have made a fair value determination of the acquired assets and assumed liabilities and approximately $2.8 million of fixed assets, and $102,000 of goodwill was recorded with respect to this transaction. Also, we assumed approximately $700,000 of equipment notes and $610,000 of accrued expenses.
On October 1, 2010, we completed the acquisition of five medical imaging facilities located in Northern New Jersey and a 50% equity interest in a sixth center from Progressive Health, LLC and certain affiliates and related entities for an aggregate of $17.2 million in cash and a warrant to purchase our common stock, which had a fair value of approximately $306,000 on the day it was granted. We have made a fair value determination of the acquired assets and assumed liabilities and approximately $800,000 of working capital, $3.3 million of fixed assets, $500,000 of other intangible assets, and $14.2 million of goodwill was recorded with respect to this transaction. We also assumed approximately $1.3 million of equipment lease debt.
On October 1, 2010, we completed our acquisition of Image Medical Corporation, the parent of eRAD, Inc., for approximately $8.5 million in cash and a $2.2 million promissory note to the former shareholders of eRAD. eRAD, Inc., headquartered in Greenville, South Carolina, has been a premier provider of Picture Archiving and Communications Systems (PACS) and related workflow solutions to the radiology industry since 1999. We have made a fair value determination of the acquired assets and assumed liabilities and $291,000 of fixed assets, $2.1 million of other intangible assets, and $9.8 million of goodwill was recorded with respect to this transaction. We also assumed approximately $1.5 million of other liabilities primarily relating to an unearned revenue liability.
On September 10, 2010, we completed the acquisition of substantially all of the assets of Korangy Medical Equipment, LLC in Catonsville, Maryland for approximately $605,000. We have made a fair value determination of the acquired assets and assumed liabilities and $605,000 of fixed assets and no goodwill was recorded with respect to this transaction.
On August 11, 2010, we completed the acquisition of Health Diagnostics of New Jersey in Edison, New Jersey for approximately $3.5 million. We have made a fair value determination of the acquired assets and assumed liabilities and $3.0 million of fixed assets, $300,000 of other intangible assets related to covenant not to compete contracts, and $977,000 of goodwill was recorded with respect to this transaction. Also, we recorded a reserve of approximately $635,000 for obligations under an existing operating facility lease through February of 2014 that we do not intend to utilize.
On July 1, 2010, we completed the acquisition of an imaging center located in Fremont, California from Insight Health Corp. for approximately $141,000. We have made a fair value determination of the acquired assets and assumed liabilities and $170,000 of fixed assets, $150,000 of other intangible assets related to covenant not to compete contracts, and no goodwill was recorded with respect to this transaction. Also, we recorded a reserve of approximately $184,000 for obligations under an existing operating facility lease through August of 2012 that we do not intend to utilize.
On July 1, 2010, we completed the acquisition of Delaware Orthopedic Specialists in Newark, Delaware for approximately $525,000. We have made a fair value determination of the acquired assets and assumed liabilities and $430,000 of fixed assets, $95,000 of other intangible assets related to covenant not to compete contracts, and no goodwill was recorded with respect to this transaction.
On May 1, 2010, we completed the acquisition of Touchstone Imaging of Bowie, LLC in Bowie, Maryland for approximately $595,000. We have made a fair value determination of the acquired assets and assumed liabilities and $595,000 of fixed assets and no goodwill was recorded with respect to this transaction.
On April 30, 2010, we completed the acquisition of Delaware Diagnostic Services, Inc. (Limestone) in Wilmington, Delaware for approximately $87,000. We have made a fair value determination of the acquired assets and assumed liabilities and $87,000 of fixed assets and no goodwill was recorded with respect to this transaction.
On April 30, 2010, we acquired three multi-modality facilities from Sonix Medical Resources, Inc. through a bankruptcy proceeding in New York for approximately $2.3 million in cash. The facilities located in Brooklyn, New York, Chatham, New Jersey and Haddon Heights, New Jersey operate a combination of MRI, CT, mammography, ultrasound, fluoroscopy, X-ray and related modalities. We have made a fair value determination of the acquired assets and assumed liabilities and approximately $1.4 million of fixed assets and $884,000 of goodwill was recorded with respect to this transaction.
| 71 |
On April 1, 2010, we completed the acquisition of Truxtun Medical Group in Bakersfield, California for approximately $20.3 million in cash and the issuance of 375,000 shares of RadNet, Inc. common stock valued at approximately $1.2 million on the date of acquisition. Truxtun operates four multi-modality facilities in Bakersfield, a Metropolitan Statistical Area in Kern County, California. Truxtun provides a broad range of services including MRI, CT, PET/CT, mammography, nuclear medicine, fluoroscopy, ultrasound, X-ray and related procedures. We have made a fair value determination of the acquired assets and assumed liabilities and approximately $2.4 million of working capital, $6.9 million of fixed assets, $1.6 million of other intangible assets related to Trade-name and covenant not to compete contracts, and $10.7 million of goodwill was recorded with respect to this transaction.
On March 15, 2010, we acquired the imaging practice of Theodore Feit, M.D., Inc. in Burbank, California for cash consideration of $350,000. We have made a fair value determination of the acquired assets and assumed liabilities and approximately $350,000 of fixed assets and no goodwill was recorded with respect to this transaction.
On March 1, 2010, we completed the acquisition of Anaheim Open MRI in Anaheim, California for cash consideration of $910,000. The facility operates MRI, CT, ultrasound and X-ray, and has been rebranded as Anaheim Advanced Imaging. We have made a fair value determination of the acquired assets and assumed liabilities and approximately $605,000 of fixed assets and $305,000 of goodwill was recorded with respect to this transaction.
On January 1, 2010, we completed the acquisition of Union Imaging Center in Union, New Jersey from Modern Medical Modalities Corporation for approximately $5.4 million in cash and the issuance of 75,000 shares of RadNet, Inc. common stock valued at approximately $153,000 on the date of acquisition. The center operates imaging modalities including MRI, CT, PET/CT, mammography, ultrasound, nuclear medicine and X-ray. We have made a fair value determination of the acquired assets and assumed liabilities and approximately $1.9 million of fixed assets and $3.7 million of goodwill was recorded with respect to this transaction.
NOTE 5 – GOODWILL AND OTHER INTANGIBLE ASSETS
Goodwill at December 31, 2012 totaled $193.9 million. Goodwill is recorded as a result of business combinations. Activity in goodwill for the years ended December 31, 2010, 2011 and 2012, is provided below (in thousands):
| Balance as of January 1, 2010 | 106,502 | |||
| Goodwill acquired through the acquisition of Union Imaging | 3,748 | |||
| Goodwill acquired through the acquisition of Anaheim Open MRI | 305 | |||
| Goodwill acquired through the acquisition of Truxtun Medical Group | 10,652 | |||
| Goodwill acquired through the acquisition of Sonix Medical Resources | 884 | |||
| Goodwill acquired through the acquisition of Health Diagnostics | 977 | |||
| Goodwill acquired through the acquisition of Image Medical Corporation | 7,327 | |||
| Goodwill acquired through the acquisition of Progressive Health | 12,856 | |||
| Goodwill acquired through the acquisition of two imaging centers from Presgar Imaging | 102 | |||
| Balance as of December 31, 2010 | 143,353 | |||
| Goodwill acquired through the acquisition of Imaging On Call, LLC | 3,799 | |||
| Goodwill acquired through the acquisition of the imaging practice of Stuart London, MD | 600 | |||
| Goodwill acquired through the acquisition of certain imaging centers from Diagnostic Health Corp. | 2,009 | |||
| Goodwill acquired through the acquisition of Hematology-Oncology | 1,016 | |||
| Adjustments to our preliminary allocation of the purchase price of Image Medical Corp. | 2,443 | |||
| Adjustments to our preliminary allocation of the purchase price of Progressive Health | 1,369 | |||
| Adjustments to our preliminary allocation of the purchase price of Presgar Imaging | 155 | |||
| Goodwill acquired through the acquisition of our controlling interest in Radar, LLC | 845 | |||
| Goodwill acquired through the acquisition of Raven Holdings U.S., Inc. | 3,918 | |||
| Balance as of December 31, 2011 | 159,507 | |||
| Goodwill acquired through the acquisition of Camarillo Imaging | 86 | |||
| Goodwill acquired through the acquisition of West Coast Radiology | 5,395 | |||
| Goodwill acquired through the acquisition of Advanced Medical Imaging of Stuart | 923 | |||
| Goodwill acquired through the acquisition of Orthopedic Imaging | 302 | |||
| Adjustments to our preliminary allocation of the purchase price of Raven Holdings U.S., Inc. | 7,895 | |||
| Goodwill acquired through the acquisition of our controlling interest in Upper Chesapeake Imaging | 1,849 | |||
| Goodwill acquired through the acquisition of Vanowen Radiology | 386 | |||
| Goodwill acquired through the acquisition of Clinical Radiologists Medical Imaging | 1,838 | |||
| Goodwill acquired through the acquisition of Lenox Hill Radiology | 15,690 | |||
| Balance as of December 31, 2012 | $ | 193,871 |
The amount of goodwill from these acquisitions that is deductible for tax purposes is $115.5 million.
| 72 |
Other intangible assets are primarily related to the value of management service agreements obtained through our acquisition of Radiologix, Inc. in 2006 and are recorded at a cost of $57.5 million less accumulated amortization of $14.2 million at December 31, 2012. Also included in other intangible assets is the value of covenant not to compete contracts associated with our recent facility acquisitions totaling $4.6 million less accumulated amortization of $3.7 million, as well as the value of trade names associated with acquired imaging facilities totaling $7.7 million less accumulated amortization of $1.4 million. Also in connection with our purchase of eRAD and included in other intangible assets is the value of eRAD’s developed technology and its customer relationships. Amortization expense for the year ended December 31, 2012, 2011 and 2010 was $3.5 million, $3.5 million and $3.5 million, respectively. Intangible assets are amortized using the straight-line method. Management service agreements are amortized over 25 years using the straight line method. Developed technology and customer relationships are amortized over 5 years using the straight line method.
The following table shows annual amortization expense, by asset classes that will be recorded over the next five years (in thousands):
| 2013 | 2014 | 2015 | 2016 | 2017 | Thereafter | Total | Weighted average amortization period remaining in years | |||||||||||||||||||||||||
| Management service contracts | $ | 2,300 | $ | 2,300 | $ | 2,300 | $ | 2,300 | $ | 2,300 | $ | 31,814 | $ | 43,314 | 18.8 | |||||||||||||||||
| Covenant not to compete contracts | 344 | 274 | 160 | 93 | 30 | 10 | 911 | 2.5 | ||||||||||||||||||||||||
| Customer relationships | 196 | 197 | 184 | 1 | – | – | 578 | 2.9 | ||||||||||||||||||||||||
| Developed technology and in-process R&D | 188 | 189 | 149 | 24 | – | – | 550 | 3.0 | ||||||||||||||||||||||||
| Trade Names | 113 | – | – | – | – | – | 6,321 | * | 0.8 | |||||||||||||||||||||||
| Total Annual Amortization | $ | 3,141 | $ | 2,960 | $ | 2,793 | $ | 2,418 | $ | 2,330 | $ | 31,824 | $ | 51,674 | ||||||||||||||||||
* Includes approximately $6.2 million of trade name intangibles that have an indefinite life.
| 73 |
NOTE 6 - PROPERTY AND EQUIPMENT
Property and equipment and accumulated depreciation and amortization are as follows (in thousands):
| December 31, | ||||||||
| 2012 | 2011 | |||||||
| Land | $ | 250 | $ | 250 | ||||
| Medical equipment | 293,169 | 278,345 | ||||||
| Computor and Office equipment, furniture and fixtures | 80,270 | 65,280 | ||||||
| Software development costs | 3,376 | 2,626 | ||||||
| Leasehold improvements | 172,914 | 155,003 | ||||||
| Equipment under capital lease | 32,091 | 28,926 | ||||||
| 582,070 | 530,430 | |||||||
| Accumulated depreciation and amortization | (365,510 | ) | (314,903 | ) | ||||
| $ | 216,560 | $ | 215,527 | |||||
Depreciation and amortization expense on property and equipment, including amortization of equipment under capital leases, for the years ended December 31, 2012, 2011 and 2010 was $54.2 million, $54.0 million and $50.5 million, respectively.
NOTE 7 – ACCOUNTS PAYABLE AND ACCRUED EXPENSES (IN THOUSANDS)
| December 31, | ||||||||
| 2012 | 2011 | |||||||
| (Restated) | ||||||||
| Accounts payable | $ | 39,177 | $ | 29,984 | ||||
| Accrued expenses | 36,146 | 41,226 | ||||||
| Accrued payroll and vacation | 23,277 | 21,212 | ||||||
| Accrued professional fees | 7,757 | 10,679 | ||||||
| Total | $ | 106,357 | $ | 103,101 | ||||
NOTE 8 - NOTES PAYABLE, LINE OF CREDIT AND CAPITAL LEASES
2010 Credit Agreements
On April 6, 2010, we completed a series of transactions which we refer to as our "debt refinancing plan" for an aggregate of $585.0 million. As part of the debt refinancing plan, our wholly owned subsidiary, Radnet Management, Inc., issued and sold $200.0 million in 10 3/8% senior unsecured notes due 2018 (the “senior notes”). All payments of the senior notes, including principal and interest, are guaranteed jointly and severally on a senior unsecured basis by RadNet, Inc. and all of Radnet Management’s current and future domestic wholly owned restricted subsidiaries. The senior notes were issued under an indenture agreement dated April 6, 2010 (the “Indenture”), by and among Radnet Management, as issuer, RadNet, Inc., as parent guarantor, the subsidiary guarantors thereof and U.S. Bank National Association, as trustee, in a private placement that was not subject to the registration requirements of the Securities Act. The senior notes initially issued on April 6, 2010 in a private placement were subsequently publicly offered for exchange enabling holders of the outstanding senior notes to exchange the outstanding notes for publicly registered exchange notes with nearly identical terms. The exchange offer was completed on February 14, 2011.
In addition to the issuance of senior notes, Radnet Management entered into a Credit and Guaranty Agreement with a syndicate of lenders (the “Credit Agreement”), whereby Radnet Management obtained $385.0 million in senior secured first-lien bank financing, consisting of (i) a $285.0 million, six-year term loan facility and (ii) a $100.0 million, five-year revolving credit facility, including a swing line subfacility and a letter of credit subfacility (collectively, the “Credit Facilities”).
Radnet Management’s obligations under the Credit Agreement were unconditionally guaranteed by RadNet, Inc., all of Radnet Management’s current and future domestic subsidiaries as well as certain affiliates, including Beverly Radiology Medical Group III and its equity holders (Beverly Radiology Medical Group, Inc., BreastLink Medical Group, Inc. and ProNet Imaging Medical Group, Inc.). The Credit Facilities created by the Credit Agreement were secured by a perfected first-priority security interest in all of Radnet Management’s and the guarantors’ tangible and intangible assets, including, but not limited to, pledges of equity interests of Radnet Management and all of our current and future domestic subsidiaries.
| 74 |
2012 Refinancing
On October 10, 2012 we completed the refinancing of the Credit Facilities by entering into a new Credit and Guaranty Agreement with a syndicate of banks and other financial institutions (the “Refinance Agreement”). The total amount of refinancing was $451.25 million, consisting of (i) a $350 million senior secured term loan and (ii) a $101.25 million senior secured revolving credit facility. The obligations of Radnet Management, Inc. under the Refinance Agreement are guaranteed by RadNet, Inc. and all of Radnet Management’s current and future domestic subsidiaries and certain of our affiliates. The obligations under the Refinance Agreement, including the guarantees, are secured by a perfected first-priority security interest in all of Radnet Management’s and the guarantors’ tangible and intangible assets, including, but not limited to, pledges of equity interests of Radnet Management and all of our current and future domestic subsidiaries.
The termination date for the $350 million term loan is the earliest to occur of (i) the sixth anniversary of the closing date (October 10, 2012), (ii) the date on which all of the term loans shall become due and payable in full under the Refinance Agreement whether by acceleration or otherwise and (iii) October 1, 2017 if our senior notes due 2018 have not been refinanced by such date. The termination date for the $101.25 million revolving credit facility is the earliest to occur of (i) the fifth anniversary of the closing date, (ii) the date the revolving credit facility is permanently reduced to zero pursuant to section 2.13(b) of the Refinance Agreement, (iii) the date of the termination of the revolving credit facility pursuant to section 8.01 of the Refinance Agreement and (iv) October 1, 2017 if our senior notes due 2018 have not been refinanced by such date.
In connection with the refinancing of the Credit Facilities, Radnet Management used the net proceeds to repay in full its existing six year term loan facility for $277.9 million in principal amount outstanding, which would have matured on April 6, 2016, and its revolving credit facility for $59.8 million in principal amount outstanding, which would have matured on April 6, 2015.
At December 31, 2012, we had $200.0 million aggregate principal amount of senior notes outstanding, $349.13 million aggregate principal amount of senior secured term loan debt outstanding and $33.0 million aggregate principal amount outstanding under the revolving credit facility.
Refinance Agreement
On October 10, 2012, we used the proceeds under the Refinance Agreement to refinance the indebtedness under the Credit Agreement. Under the Refinance Agreement, we obtained $451.25 million in senior secured financing, consisting of a $350 million, six-year term loan facility and a $101.25 million, five-year revolving credit facility.
Interest. The Refinance Agreement bears interest through maturity at a rate determined by adding the applicable margin to either (a) the Base Rate, which is defined in the Refinance Agreement as the highest of (i) the prime rate quoted in the Wall Street Journal, (ii) the rate which is 0.5% in excess of the federal funds rate, (iii) (with respect to term loans only) 2.25% and (iv) 1.00% in excess of the one-month Adjusted Eurodollar Rate at such time, or (b) the Adjusted Eurodollar Rate, which is defined in the Refinance Agreement as the higher of (i) the London interbank offered rate, adjusted for statutory reserve requirements, for the respective interest period, as determined by the administrative agent and (ii) (with respect to term loans only) 1.25%. As used in the Refinance Agreement, applicable margin means (i) (a) with respect to term loans that are Eurodollar Rate Loans, 4.25% per annum and (b) with respect to term loans that are Base Rate Loans, 3.25% per annum; and (ii) (a) with respect to revolving loans that are Eurodollar Rate Loans, 4.25% per annum and (b) with respect to revolving loans and swing line loans that are Base Rate Loans, 3.25% per annum.
Payments. Commencing on December 31, 2012 we began making quarterly amortization payments on the term loan facility under the Refinance Agreement, each in the amount of $875,000, with the remaining principal balance paid at maturity. Under the Refinance Agreement, we are also required to make mandatory prepayments, subject to specified exceptions, from consolidated excess cash flow, and upon certain events, including, but not limited to, (i) the receipt of net cash proceeds from the sale or other disposition of any property or assets by us or any of our subsidiaries, (ii) the receipt of net cash proceeds from insurance or condemnation proceeds paid on account of any loss of any property or assets of us or any of our subsidiaries, and (iii) the receipt of net cash proceeds from the incurrence of indebtedness by us or any of our subsidiaries (other than certain indebtedness otherwise permitted under the Refinance Agreement).
Guarantees and Collateral. The obligations under the Refinance Agreement are guaranteed by us, all of our current and future domestic subsidiaries and certain of our affiliates. The obligations under the Refinance Agreement and the guarantees are secured by a perfected first priority security interest in all of Radnet Management’s and the guarantors’ tangible and intangible assets, including, but not limited to, pledges of equity interests of Radnet Management and all of our current and future domestic subsidiaries.
Restrictive Covenants. In addition to certain customary covenants, the Refinance Agreement places limits on our ability to declare dividends or redeem or repurchase capital stock, prepay, redeem or purchase debt, incur liens and engage in sale-leaseback transactions, make loans and investments, incur additional indebtedness, amend or otherwise alter debt and other material agreements, engage in mergers, acquisitions and asset sales, enter into transactions with affiliates and alter the business we and our subsidiaries currently conduct.
| 75 |
Financial Covenants. The Refinance Agreement contains financial covenants including a maximum total leverage ratio and a limit on annual capital expenditures.
Events of Default. In addition to certain customary events of default, events of default under the Refinance Agreement include failure to pay principal or interest when due, a material breach of any representation or warranty contained in the loan documents, covenant defaults, events of bankruptcy and a change of control. The occurrence of an event of default could permit the lenders under the Refinance Agreement to declare all amounts borrowed, together with accrued interest and fees, to be immediately due and payable and to exercise other default remedies.
Senior Notes
On April 6, 2010, we issued $200 million in aggregate amount of unsecured senior notes which have a coupon of 10.375% and were issued at a price of 98.680%. The senior notes were issued by Radnet Management, Inc. and guaranteed jointly and severally on a senior unsecured basis by us and all of our current and future wholly-owned domestic restricted subsidiaries. The senior notes were offered and sold in a private placement exempt from registration under the Securities Act to qualified institutional buyers pursuant to Rule 144A and Regulation S under the Securities Act. We pay interest on the senior notes on April 1 and October 1, commencing October 1, 2010, and they will expire on April 1, 2018. The senior notes are governed under the Indenture. Under the terms of the indenture, we agreed to file a registration statement with the SEC relating to an offer to exchange the senior notes for registered publicly tradable notes that have substantially identical terms as the senior notes. On August 30, 2010, we filed a registration statement on Form S-4 with the SEC relating to the offer to exchange the senior notes. On January 13, 2011, our registration statement was declared effective by the SEC. On February 14, 2011, we completed an exchange offer whereby all senior notes were exchanged for registered publicly tradable notes.
Ranking. The senior notes and the guarantees:
| · | rank equally in right of payment with any existing and future unsecured senior indebtedness of the guarantors; |
| · | rank senior in right of payment to all existing and future subordinated indebtedness of the guarantors; |
| · | are effectively subordinated in right of payment to any secured indebtedness of the guarantors (including indebtedness under the Refinance Agreement) to the extent of the value of the assets securing such indebtedness; and |
| · | are structurally subordinated in right of payment to all existing and future indebtedness and other liabilities of any of the Company’s subsidiaries that is not a guarantor of the senior notes. |
Optional Redemption. Radnet Management may redeem the senior notes, in whole or in part, at any time on or after April 1, 2014, at the redemption prices specified under the Indenture. Prior to April 1, 2013, we may redeem up to 35% of aggregate principal amount of the senior notes issued under the Indenture from the net proceeds of one or more equity offerings at a redemption price equal to 110.375% of the senior notes redeemed, plus accrued and unpaid interest, if any. Radnet Management is also permitted to redeem the senior notes prior to April 1, 2014, in whole or in part, at a redemption price equal to 100% of the principal amount redeemed, plus a make-whole premium and accrued and unpaid interest, if any.
Change of Control and Asset Sales. If a change in control of Radnet Management occurs, Radnet Management must give holders of the senior notes the opportunity to sell their senior notes at 101% of their face amount, plus accrued interest. If we or one of our restricted subsidiaries sells assets under certain circumstances, Radnet Management will be required to make an offer to purchase the senior notes at their face amount, plus accrued and unpaid interest to the purchase date.
Restrictive Covenants. The Indenture contains covenants that limit, among other things, the ability of us and our restricted subsidiaries, to:
| · | pay dividends or make certain other restricted payments or investments; |
| · | incur additional indebtedness and issue preferred stock; |
| · | create liens (other than permitted liens) securing indebtedness or trade payables unless the notes are secured on an equal and ratable basis with the obligations so secured, and, if such liens secure subordinated indebtedness, the notes are secured by a lien senior to such liens; |
| · | sell certain assets or merge with or into other companies or otherwise dispose of all or substantially all of our assets; |
| · | enter into certain transactions with affiliates; |
| · | create restrictions on dividends or other payments by our restricted subsidiaries; and |
| · | create guarantees of indebtedness by restricted subsidiaries. |
| 76 |
However, these limitations are subject to a number of important qualifications and exceptions, as described in the Indenture. As of December 31, 2012, we were in compliance with all covenants.
Notes payable, line of credit and capital lease obligations consist of the following (in thousands):
| December 31, | ||||||||
| 2012 | 2011 | |||||||
| Revolving lines of credit | $ | 33,000 | $ | 58,000 | ||||
| Senior secured term loan | 349,125 | 280,013 | ||||||
| Senior unsecured notes | 200,000 | 200,000 | ||||||
| Discounts on term loan and notes | (9,510 | ) | (5,098 | ) | ||||
| Promissory notes payable to the former shareholders of businesses acquired at interest rates ranging from 4.0% to 6.0%, due through 2016 | 1,057 | 10,470 | ||||||
| Equipment notes payable at interest rates ranging from 7.1% to 11.7%, due through 2015, collateralized by medical equipment | 1,040 | 2,403 | ||||||
| Obligations under capital leases at interest rates ranging from 10.0% to 11.7%, due through 2017, collateralized by medical and office equipment | 7,695 | 10,172 | ||||||
| 582,407 | 555,960 | |||||||
| Less: current portion | (8,645 | ) | (12,768 | ) | ||||
| $ | 573,762 | $ | 543,192 | |||||
The following is a listing of annual principal maturities of notes payable exclusive of capital leases and repayments on our revolving credit facilities for years ending December 31 (in thousands):
| 2013 | $ | 4,703 | ||
| 2014 | 4,213 | |||
| 2015 | 3,547 | |||
| 2016 | 3,500 | |||
| 2017 | 3,500 | |||
| Thereafter | 531,759 | |||
| $ | 551,222 |
We lease equipment under capital lease arrangements. Future minimum lease payments under capital leases for years ending December 31 (in thousands) is as follows:
| 2013 | $ | 4,232 | ||
| 2014 | 2,553 | |||
| 2015 | 734 | |||
| 2016 | 532 | |||
| 2017 | 186 | |||
| Total minimum payments | 8,237 | |||
| Amount representing interest | (542 | ) | ||
| Present value of net minimum lease payments | 7,695 | |||
| Less current portion | (3,942 | ) | ||
| Long-term portion | $ | 3,753 |
| 77 |
NOTE 9 – COMMITMENTS AND CONTINGENCIES
Leases – We lease various operating facilities and certain medical equipment under operating leases with renewal options expiring through 2041. Certain leases contain renewal options from two to ten years and escalation based either on the consumer price index or fixed rent escalators. Leases with fixed rent escalators are recorded on a straight-line basis. We record deferred rent for tenant leasehold improvement allowances received from certain lessors and amortize the deferred rent expense over the term of the lease agreement. Minimum annual payments under operating leases for future years ending December 31 are as follows (in thousands):
| Facilities | Equipment | Total | ||||||||||
| 2013 | $ | 44,119 | $ | 10,452 | $ | 54,571 | ||||||
| 2014 | 36,189 | 9,786 | 45,975 | |||||||||
| 2015 | 30,247 | 8,702 | 38,949 | |||||||||
| 2016 | 24,526 | 6,142 | 30,668 | |||||||||
| 2017 | 19,071 | 2,060 | 21,131 | |||||||||
| Thereafter | 50,465 | – | 50,465 | |||||||||
| $ | 204,617 | $ | 37,142 | $ | 241,759 | |||||||
Total rent expense, including equipment rentals, for the years ended December 31, 2012, 2011 and 2010 was $60.6 million, $53.3 million and $47.9 million, respectively.
Maintenance Contract – We have an arrangement with GE Medical Systems under which it has agreed to be responsible for the maintenance and repair of a majority of our equipment for a fee that is based on the type and age of the equipment. Under this agreement, we are committed to minimum payments of approximately $23.0 million per year through 2016.
Litigation – We are engaged from time to time in the defense of lawsuits arising out of the ordinary course and conduct of our business. We believe that the outcome of our current litigation will not have a material adverse impact on our business, financial condition and results of operations. However, we could be subsequently named as a defendant in other lawsuits that could adversely affect us.
NOTE 10 – DERIVATIVE INSTRUMENTS
We are exposed to certain risks relating to our ongoing business operations. The primary risk managed by us using derivative instruments is interest rate risk. We have in the past entered into interest rate swap agreements to manage interest rate risk exposure. The interest rate swap agreements utilized by us effectively modified our exposure to interest rate risk by converting our floating-rate debt to a fixed rate basis during the period of the interest rate swap, thus reducing the impact of interest-rate changes on future interest expense.
At inception, we designated our interest rate swaps as cash flow hedges of floating-rate borrowings. In accordance with ASC Topic 815, derivatives that have been designated and qualify as cash flow hedging instruments are reported at fair value. The gain or loss on the effective portion of the hedge (i.e., change in fair value) is initially reported as a component of accumulated other comprehensive income in the consolidated statement of equity deficit. The remaining gain or loss, if any, is recognized currently in earnings. Unrealized gains or losses on the change in fair value of our interest rate swaps that do not qualify as hedges are recognized in earnings.
As a result of our senior secured credit facilities that were refinanced on October 10, 2012 and the issuance of the senior notes completed on April 6, 2010, our interest rate swaps do not match the terms of our current bank debt and so accordingly, they were no longer designated as cash flow hedges after the date of refinancing. Accordingly, all changes in their fair value after April 6, 2010, and through November 15, 2012, their maturity date, were recognized in earnings as other expense.
The related Accumulated Other Comprehensive Loss (“AOCL”) of $3.1 million associated with the negative fair values of these interest rate swaps on April 6, 2010 was amortized on a straight-line basis to interest expense through November 15, 2012, the maturity date of these cash flow hedges.
A tabular presentation of the fair value of derivative instruments as of December 31, 2012 is as follows (amounts in thousands):
| Balance Sheet Location | Fair Value – Asset (Liability) Derivatives | |||||
| Derivatives | ||||||
| Interest rate contracts | Accounts payable, accrued expenses and other | $ | – |
| 78 |
A tabular presentation of the fair value of derivative instruments as of December 31, 2011 is as follows (amounts in thousands):
| Balance Sheet Location | Fair Value – Asset (Liability) Derivatives | |||||
| Derivatives | ||||||
| Interest rate contracts | Accounts payable, accrued expenses and other | $ | (5,064 | ) | ||
A tabular presentation of the effect of derivative instruments on our statement of operations is as follows (amounts in thousands):
For the Year Ended December 31, 2012
| Ineffective Interest Rate Swap | Amount of Gain (Loss) Recognized in OCI on Derivative (Effective Portion) | Amount of Gain (Loss) Recognized in Income on Derivative (Ineffective Portion) | Location of Gain (Loss) Recognized in Income on Derivative (Ineffective Portion) | Amount of Gain (Loss) Reclassified from Accumulated OCI into Income (Effective Portion) | Location of Gain (Loss) Reclassified from Accumulated OCI into Income (Effective Portion) |
| Interest rate contracts | None | $5,064 | Other income/ (expense) | * ($918) | Interest income/(expense) |
For the Year Ended December 31, 2011
| Ineffective Interest Rate Swap | Amount of Gain (Loss) Recognized in OCI on Derivative (Effective Portion) | Amount of Gain (Loss) Recognized in Income on Derivative (Ineffective Portion) | Location of Gain (Loss) Recognized in Income on Derivative (Ineffective Portion) | Amount of Gain (Loss) Reclassified from Accumulated OCI into Income (Effective Portion) | Location of Gain (Loss) Reclassified from Accumulated OCI into Income (Effective Portion) |
| Interest rate contracts | None | $5,441 | Other income/ (expense) | * ($1,225) | Interest income/(expense) |
For the Year Ended December 31, 2010
| Ineffective Interest Rate Swap | Amount of Gain (Loss) Recognized in OCI on Derivative (Effective Portion) | Amount of Gain (Loss) Recognized in Income on Derivative (Ineffective Portion) | Location of Gain (Loss) Recognized in Income on Derivative (Ineffective Portion) | Amount of Gain (Loss) Reclassified from Accumulated OCI into Income (Effective Portion) | Location of Gain (Loss) Reclassified from Accumulated OCI into Income (Effective Portion) |
| Interest rate contracts | ($1,472) | ($132) | Other income/ (expense) | * ($917) | Interest income/(expense) |
* Amortization of OCI associated with the cash flow hedges through April 6, 2010 (see discussion above).
NOTE 11 – INCOME TAXES
For the years ended December 31, 2012, 2011 and 2010, we recognized income tax (benefit) expense comprised of the following:
| Years Ended | ||||||||||||
| December 31, | ||||||||||||
| 2012 Restated | 2011 | 2010 | ||||||||||
| State current tax | $ | 1,160 | $ | 820 | $ | 576 | ||||||
| Other current tax | 32 | – | – | |||||||||
| Federal deferred tax | (46,901 | ) | – | – | ||||||||
| State deferred tax | (9,518 | ) | – | – | ||||||||
| (Benefit from) provision for income taxes | $ | (55,227 | ) | $ | 820 | $ | 576 | |||||
| 79 |
A reconciliation of the statutory U.S. federal rate and effective rates is as follows (in thousands):
| Years Ended | ||||||||||||
| December 31, | ||||||||||||
| 2012 Restated | 2011 | 2010 | ||||||||||
| Federal tax | 34.00% | 34.00% | 34.00% | |||||||||
| State franchise tax, net of federal benefit | 17.49% | 6.74% | -3.14% | |||||||||
| Non deductible expenses | 1.59% | 4.97% | 0.40% | |||||||||
| Equity compensation | 10.69% | 9.43% | -8.16% | |||||||||
| Changes in valuation allowance | -1325.53% | -45.09% | -27.86% | |||||||||
| (Benefit from) provision for income taxes | -1261.76% | 10.05% | -4.76% | |||||||||
Deferred income taxes reflect the net tax effects of temporary differences between carrying amounts of assets and liabilities for financial and income tax reporting purposes and operating loss carryforwards.
Our deferred tax assets and liabilities comprise the following (in thousands):
| December 31, | ||||||||
| Deferred tax assets: | 2012 Restated | 2011 Restated | ||||||
| Net operating losses | $ | 81,348 | $ | 76,323 | ||||
| Accrued expenses | 9,679 | 8,359 | ||||||
| Unfavorable contract liability | 3,901 | 3,559 | ||||||
| Equity compensation | 2,406 | 3,530 | ||||||
| Allowance for doubtful accounts | 1,831 | 1,820 | ||||||
| Unrealized loss on hedging agreement | – | 1,522 | ||||||
| Other | 1,194 | 1,072 | ||||||
| Valuation Allowance | (7,645 | ) | (63,854 | ) | ||||
| Total Deferred Tax Assets | $ | 92,714 | $ | 32,331 | ||||
| Deferred tax liabilities: | ||||||||
| Property Plant & Equipment | (9,680 | ) | (11,652 | ) | ||||
| Goodwill | (14,221 | ) | (12,212 | ) | ||||
| Intangibles | (10,411 | ) | (5,202 | ) | ||||
| Other | (2,260 | ) | (1,064 | ) | ||||
| Total Deferred Tax Liabilities | $ | (36,572 | ) | $ | (32,608 | ) | ||
| Net Deferred Tax Asset (Liability) | $ | 56,142 | $ | (277 | ) | |||
As of December 31, 2012, we had federal and state net operating loss carryforwards of approximately $212.6 million and $69.7 million, respectively, which expire at various intervals from the years 2017 to 2032. As of December 31, 2012, $23.5 million of our federal net operating loss carryforwards acquired in connection with the 2011 acquisition of Raven Holdings U.S., Inc. were subject to limitations related to their utilization under Section 382 of the Internal Revenue Code. Future ownership changes as determined under Section 382 of the Internal Revenue Code could further limit the utilization of net operating loss carryforwards. Cumulative excess tax benefits of $4.4 million, related to the exercise of nonqualified stock options, will be recorded in equity when realized.
We consider all evidence available when determining whether deferred tax assets are more likely-than-not to be realized, including projected future taxable income, scheduled reversals of deferred tax liabilities, prudent tax planning strategies, and recent financial operations. The evaluation of this evidence requires significant judgment about the forecasts of future taxable income and are consistent with the plans and estimates we are using to manage the underlying businesses. In evaluating the objective evidence that historical results provide, we consider three years of cumulative operating income. As of December 31, 2012, we have determined that deferred tax assets of $92.7 million are more-likely than not to be realized. We have also determined that deferred tax liabilities of $14.2 million are required related to book basis in goodwill that has an indefinite life.
Prior to 2012, we had recorded a valuation allowance on the majority of our deferred tax assets to reduce the deferred tax assets to the amount that was believed more likely than not to be realized. In assessing the need for a valuation allowance, we considered all available positive and negative evidence, including past results, the existence of cumulative losses in prior years, and forecasted future taxable income, and prudent tax planning strategies. During 2012, the majority of our valuation allowance, primarily related to net operating losses (NOLs), was reversed based on historical earnings and forecasts of future taxable income, resulting in the recognition of a $56.2 million tax benefit. The remaining valuation allowance primarily relates to state NOL’s
| 80 |
For the next five years, and thereafter, federal net operating loss carryforwards expire as follows (restated) (in thousands):
Year Ended | Total Net Operating Loss Carryforwards | Amount Subject to 382 limitation | ||||||
| 2013 | $ | – | $ | – | ||||
| 2014 | – | – | ||||||
| 2015 | – | – | ||||||
| 2016 | – | – | ||||||
| 2017 | 15,184 | – | ||||||
| Thereafter | 197,399 | 23,475 | ||||||
| $ | 212,583 | $ | 23,475 | |||||
We file consolidated income tax returns in the U.S. federal jurisdiction, and various states and foreign jurisdictions. We continue to reinvest earnings of the non-US entities for the foreseeable future and therefore have not recognized any U.S. tax expense on these earnings. With limited exceptions, we are no longer subject to U.S. federal, state and local, or non-U.S. income tax examinations by tax authorities for years before 1998. We do not anticipate the results of any open examinations would result in a material change to its financial position.
A reconciliation of the total gross amounts of unrecognized tax benefits (excluding interest, penalties and the federal tax benefit of state taxes related to unrecognized tax benefits) for the years ended December 31, 2010, 2011, and 2012 is as follows (restated) (in thousands):
| Unrecognized tax benefit at 12/31/2008 | $ | – | ||
| Additional based on current year tax positions | 2,518 | |||
| Unrecognized tax benefit at 12/31/2009 | $ | 2,518 | ||
| Additional based on current year tax positions | 405 | |||
| Unrecognized tax benefit at 12/31/2010 | 2,923 | |||
| Additional based on current year tax positions | 833 | |||
| Unrecognized tax benefit at 12/31/2011 | 3,756 | |||
| Additional based on current year tax positions | 428 | |||
| Unrecognized tax benefit at 12/31/2012 | $ | 4,184 |
We recognize accrued interest and penalties related to unrecognized tax benefits in income tax expense. We recognized no penalties and interest during the years ended December 31, 2012, 2011 and 2010, and we had assumed approximately $90,000 during the year ended December, 31, 2010 for the payment of interest and penalties. Unrecognized tax benefits of $428,000 are included in accounts payable, accrued liabilities and other and of $3,756,000 as a reduction to non-current deferred tax assets at December 31, 2012 and 2011.
NOTE 12 – STOCK-BASED COMPENSATION
Stock Incentive Plans
Options and Warrants
We have two long-term incentive plans which we refer to as the 2000 Plan and the 2006 Plan. The 2000 Plan was terminated as to future grants when the 2006 Plan was approved by the stockholders in 2006. As of December 31, 2012, we have reserved for issuance under the 2006 Plan 11,000,000 shares of common stock. Certain options granted under the 2006 Plan to employees are intended to qualify as incentive stock options under existing tax regulations. In addition, we may issue non-qualified stock options and warrants under the 2006 Plan from time to time to non-employees, in connection with acquisitions and for other purposes and we may also issue restricted stock under the 2006 Plan. Stock options and warrants generally vest over two to five years and expire five to ten years from date of grant.
As of December 31, 2012, 5,322,083, or approximately 84.3%, of the 6,231,250 outstanding stock options and warrants granted under our option plans are fully vested. During the year ended December 31, 2012, we did not grant options or warrants under the 2006 Plan.
| 81 |
We have issued warrants outside the 2006 Plan under various types of arrangements to employees, and in exchange for outside services. All warrants issued to employees or consultants after our February 2007 listing on the NASDAQ Global Market have been characterized as awards under the 2006 Plan. All warrants outside the 2006 Plan have been issued with an exercise price equal to the fair value of the underlying common stock on the date of grant. The warrants expire from five to seven years from the date of grant. Vesting terms are determined by the board of directors or the compensation committee of the board of directors at the date of grant.
As of December 31, 2012, 1,502,898, or 100%, of all the outstanding warrants outside the 2006 Plan are fully vested. During the year ended December 31, 2012, we did not grant warrants outside of our 2006 Plan.
The following summarizes all of our option and warrant transactions in 2012:
| Outstanding Options and Warrants | Weighted Average Exercise price Per | Weighted Average Remaining Contractual Life | Aggregate Intrinsic | |||||||||||||
| Under the 2006 Plan and 2000 Plan | Shares | Common Share | (in years) | Value | ||||||||||||
| Balance, December 31, 2011 | 6,656,250 | $ | 3.62 | |||||||||||||
| Granted | – | – | ||||||||||||||
| Exercised | – | – | ||||||||||||||
| Canceled or expired | (425,000 | ) | 4.19 | |||||||||||||
| Balance, December 31, 2012 | 6,231,250 | 3.58 | 1.88 | $ | 671,263 | |||||||||||
| Exercisable at December 31, 2012 | 5,322,083 | 3.64 | 1.71 | 599,754 | ||||||||||||
| Non-Plan | Weighted Average Exercise price Per | Weighted Average Remaining Contractual Life | Aggregate Intrinsic | |||||||||||||
| Outstanding Warrants | Shares | Common Share | (in years) | Value | ||||||||||||
| Balance, December 31, 2011 | 2,502,898 | $ | 2.58 | |||||||||||||
| Granted | – | – | ||||||||||||||
| Exercised | (250,000 | ) | 2.52 | |||||||||||||
| Canceled or expired | (750,000 | ) | 4.77 | |||||||||||||
| Balance, December 31, 2012 | 1,502,898 | 1.50 | 0.64 | $ | 1,653,786 | |||||||||||
| Exercisable at December 31, 2012 | 1,502,898 | 1.50 | 0.64 | 1,653,786 |
The aggregate intrinsic value in the table above represents the total pretax intrinsic value (the difference between our closing stock price on December 31, 2012 and the exercise price, multiplied by the number of in-the-money options or warrants, as applicable) that would have been received by the holder had all holders exercised their options or warrants, as applicable, on December 31, 2012. Total intrinsic value of options and warrants exercised during the years ended December 31, 2012, 2011 and 2010 was approximately $265,000, $606,000 and $1.3 million, respectively. As of December 31, 2012, total unrecognized stock-based compensation expense related to non-vested employee awards was approximately $903,000, which is expected to be recognized over a weighted average period of approximately 1.2 years.
The fair value of each option granted is estimated on the grant date using the Black-Scholes option pricing model which takes into account as of the grant date the exercise price and expected life of the option, the current price of the underlying stock and its expected volatility, expected dividends on the stock and the risk-free interest rate for the term of the option. The following is the average of the data used to calculate the fair value:
| Risk-free | Expected | Expected | Expected | |||||||||||||
| Interest Rate | Life | Volatility | Dividends | |||||||||||||
| December 31, 2011 | 1.62% | 3.4 years | 91.94% | – | ||||||||||||
| December 31, 2010 | 1.92% | 3.2 years | 90.65% | – | ||||||||||||
Because we lack detailed information about exercise behavior at this time, we have determined the expected term assumption under the “Simplified Method” as defined in ASC Topic 718, Stock Compensation. The expected stock price volatility is based on the historical volatility of our stock. The risk-free interest rate is based on the U.S. Treasury yield in effect at the time of grant with an equivalent remaining term. We have not paid dividends in the past and do not currently plan to pay any dividends in the near future.
| 82 |
The weighted-average grant date fair value of stock options and warrants granted during the years ended December 31, 2011 and 2010 was $1.92 and $1.46, respectively. No options or warrants were granted during the year ended December 31, 2012.
Restricted Stock Awards
The 2006 Plan permits the award of restricted stock. On January 3, 2012, we granted restricted stock awards (“awards”) for 525,000 shares of our common stock to certain employees and 200,000 shares of our common stock to non-employee directors of the Company. Of the awards granted, 241,667 were vested on the award date, 241,667 cliff vest after one year provided that the employees or non-employees remain continuously employed or engaged through the vesting date and 241,666 cliff vest after two years provided that the employees or non-employees remain continuously employed or engaged through the vesting date. We valued the awards based on the closing market price of our stock on January 3, 2012 which was $2.17 per share.
On May 15, 2012, we granted awards for 115,000 shares of our common stock to certain employees. Of the awards granted, 38,333 were vested on the award date, 38,333 cliff vest after one year provided that the employees remain continuously employed through the vesting date and 38,334 cliff vest after two years provided that the employees remain continuously employed through the vesting date. We valued the awards based on the closing market price of our stock on May 15, 2012 which was $3.12 per share.
On December 20, 2012, we granted awards for 200,000 shares of our common stock to certain non-employee directors of the Company. Of the awards granted, 66,667 were vested on the award date, 66,667 cliff vest after one year provided that the non-employee directors remain continuously engaged through the vesting date and 66,666 cliff vest after two years provided that the non-employee directors remain continuously engaged through the vesting date. We valued the awards based on the closing market price of our stock on December 20, 2012 which was $2.52 per share.
At December 31, 2012, the total unrecognized fair value of all restricted stock awards was approximately $1.0 million, which will be recognized over the remaining vesting period of 2.0 years.
In sum, of the 11,000,000 shares of common stock reserved for issuance under the 2006 Plan, at December 31, 2012, we had 7,213,750 option, warrants and shares of restricted stock outstanding and 3,786,250 available for grant.
NOTE 13 – EMPLOYEE BENEFIT PLAN
We adopted a profit-sharing/savings plan pursuant to Section 401(k) of the Internal Revenue Code that covers substantially all non-professional employees. Eligible employees may contribute on a tax-deferred basis a percentage of compensation, up to the maximum allowable under tax law. Employee contributions vest immediately. The plan does not require a matching contribution by us. There was no expense for any periods presented in the report.
NOTE 14 – INSURANCE PROCEEDS
During the year ended December 31, 2011, we received approximately $2.4 million in insurance proceeds related to equipment lost in a fire at one of our California centers and an additional 319,000 of proceeds related to equipment lost in a flood at one of our east coast centers. Each of these amounts was recorded to gain on sale and disposal of equipment. We also received approximately $309,000 of additional proceeds related to the fire at our California center for business interruption which we recorded as an adjustment to our cost of operations.
Note 15 — SUPPLEMENTAL GUARANTOR INFORMATION
In accordance with SEC Regulation S-X, Rule 3-10, Paragraph (d), the following tables present unaudited interim condensed consolidating financial information for: (a) RadNet, Inc. (the “Parent”) on a stand-alone basis as a guarantor of the registered senior notes due 2018 ; (b) Radnet Management, Inc., the subsidiary borrower and issuer (the “Subsidiary Issuer”) of the registered senior notes due 2018; (c) on a combined basis, the guarantor subsidiaries (the “Guarantor Subsidiaries”) of the registered senior notes due 2018, which include all other 100% owned subsidiaries of the Subsidiary Issuer; (d) on a combined basis, the non-guarantor subsidiaries, which include joint venture partnerships of which the Subsidiary Issuer holds investments of 50% or greater, as well as BRMG, which we consolidate as a VIE. Separate financial statements of the Subsidiary Issuer or the Guarantor Subsidiaries are not presented because the guarantee by the Parent and each Guarantor Subsidiary is full and unconditional, joint and several.
| 83 |
RADNET, INC. AND SUBSIDIARIES
CONSOLIDATED BALANCE SHEET
December 31, 2012
(in thousands)
(Restated)
| Subsidiary | Guarantor | Non-Guarantor | ||||||||||||||||||||||
| Parent | Issuer | Subsidiaries | Subsidiaries | Eliminations | Consolidated | |||||||||||||||||||
| ASSETS | ||||||||||||||||||||||||
| CURRENT ASSETS | ||||||||||||||||||||||||
| Cash and cash equivalents | $ | – | $ | 362 | $ | – | $ | – | $ | – | $ | 362 | ||||||||||||
| Accounts receivable, net | – | – | 76,838 | 52,356 | – | 129,194 | ||||||||||||||||||
| Current portion of deferred tax assets | – | – | 7,607 | – | – | 7,607 | ||||||||||||||||||
| Prepaid expenses and other current assets | – | 9,735 | 8,308 | 694 | – | 18,737 | ||||||||||||||||||
| Total current assets | – | 10,097 | 92,753 | 53,050 | – | 155,900 | ||||||||||||||||||
| PROPERTY AND EQUIPMENT, NET | – | 48,025 | 168,401 | 134 | – | 216,560 | ||||||||||||||||||
| OTHER ASSETS | ||||||||||||||||||||||||
| Goodwill | – | 48,954 | 144,072 | 845 | – | 193,871 | ||||||||||||||||||
| Other intangible assets | – | 170 | 51,394 | 110 | – | 51,674 | ||||||||||||||||||
| Deferred financing costs | – | 11,977 | – | – | – | 11,977 | ||||||||||||||||||
| Investment in subsidiaries | (7,318 | ) | 338,113 | 9,217 | – | (340,012 | ) | – | ||||||||||||||||
| Investment in joint ventures | – | – | 28,598 | – | – | 28,598 | ||||||||||||||||||
| Deferred tax assets, net of current portion | – | – | 48,535 | – | – | 48,535 | ||||||||||||||||||
| Deposits and other | – | 1,821 | 1,928 | – | – | 3,749 | ||||||||||||||||||
| Total assets | $ | (7,318 | ) | $ | 459,157 | $ | 544,898 | $ | 54,139 | $ | (340,012 | ) | $ | 710,864 | ||||||||||
| LIABILITIES AND EQUITY (DEFICIT) | ||||||||||||||||||||||||
| CURRENT LIABILITIES | ||||||||||||||||||||||||
| Intercompany | $ | – | $ | (176,217 | ) | $ | 138,223 | $ | 37,994 | $ | – | $ | – | |||||||||||
| Accounts payable, accrued expenses and other | – | 57,939 | 42,124 | 6,294 | – | 106,357 | ||||||||||||||||||
| Due to affiliates | – | – | 1,602 | – | – | 1,602 | ||||||||||||||||||
| Deferred revenue | – | – | 1,273 | – | – | 1,273 | ||||||||||||||||||
| Current portion of notes payable | – | 3,500 | 1,203 | – | – | 4,703 | ||||||||||||||||||
| Current portion of deferred rent | – | 574 | 590 | – | – | 1,164 | ||||||||||||||||||
| Current portion of obligations under capital leases | – | 1,186 | 2,756 | – | – | 3,942 | ||||||||||||||||||
| Total current liabilities | – | (113,018 | ) | 187,771 | 44,288 | – | 119,041 | |||||||||||||||||
| LONG-TERM LIABILITIES | ||||||||||||||||||||||||
| Deferred rent, net of current portion | – | 9,579 | 6,271 | – | – | 15,850 | ||||||||||||||||||
| Line of Credit | – | 33,000 | – | – | – | 33,000 | ||||||||||||||||||
| Notes payable, net of current portion | – | 536,248 | 761 | – | – | 537,009 | ||||||||||||||||||
| Obligations under capital leases,net of current portion | – | 666 | 3,087 | – | – | 3,753 | ||||||||||||||||||
| Other non-current liabilities | – | – | 8,895 | – | – | 8,895 | ||||||||||||||||||
| Total liabilities | – | 466,475 | 206,785 | 44,288 | – | 717,548 | ||||||||||||||||||
| EQUITY (DEFICIT) | ||||||||||||||||||||||||
| Total Radnet, Inc.'s equity (deficit) | (7,318 | ) | (7,318 | ) | 338,113 | 9,217 | (340,012 | ) | (7,318 | ) | ||||||||||||||
| Noncontrolling interests | – | – | – | 634 | – | 634 | ||||||||||||||||||
| Total equity (deficit) | (7,318 | ) | (7,318 | ) | 338,113 | 9,851 | (340,012 | ) | (6,684 | ) | ||||||||||||||
| Total liabilities and equity (deficit) | $ | (7,318 | ) | $ | 459,157 | $ | 544,898 | $ | 54,139 | $ | (340,012 | ) | $ | 710,864 | ||||||||||
| 84 |
RADNET, INC. AND SUBSIDIARIES
CONSOLIDATED BALANCE SHEET
December 31, 2011
(in thousands)
| Subsidiary | Guarantor | Non-Guarantor | ||||||||||||||||||||||
| Parent | Issuer | Subsidiaries | Subsidiaries | Eliminations | Consolidated | |||||||||||||||||||
| ASSETS | ||||||||||||||||||||||||
| CURRENT ASSETS | ||||||||||||||||||||||||
| Cash and cash equivalents | $ | – | $ | 1,366 | $ | – | $ | 1,089 | $ | – | $ | 2,455 | ||||||||||||
| Accounts receivable, net | – | – | 78,229 | 50,203 | – | 128,432 | ||||||||||||||||||
| Asset held for sale | – | – | 2,300 | – | – | 2,300 | ||||||||||||||||||
| Prepaid expenses and other current assets | – | 11,858 | 6,651 | 631 | – | 19,140 | ||||||||||||||||||
| Total current assets | – | 13,224 | 87,180 | 51,923 | – | 152,327 | ||||||||||||||||||
| PROPERTY AND EQUIPMENT, NET | – | 46,445 | 168,213 | 869 | – | 215,527 | ||||||||||||||||||
| OTHER ASSETS | ||||||||||||||||||||||||
| Goodwill | – | 42,784 | 115,878 | 845 | – | 159,507 | ||||||||||||||||||
| Other intangible assets | – | 50 | 52,916 | 139 | – | 53,105 | ||||||||||||||||||
| Deferred financing costs, net | – | 13,490 | – | – | – | 13,490 | ||||||||||||||||||
| Investment in subsidiaries | (70,756 | ) | 249,763 | 9,974 | – | (188,981 | ) | – | ||||||||||||||||
| Investment in joint ventures | – | – | 22,326 | – | – | 22,326 | ||||||||||||||||||
| Deposits and other | – | 1,279 | 1,627 | – | – | 2,906 | ||||||||||||||||||
| Total assets | $ | (70,756 | ) | $ | 367,035 | $ | 458,114 | $ | 53,776 | $ | (188,981 | ) | $ | 619,188 | ||||||||||
| LIABILITIES AND EQUITY | ||||||||||||||||||||||||
| CURRENT LIABILITIES | ||||||||||||||||||||||||
| Intercompany | $ | – | $ | (160,017 | ) | $ | 124,679 | $ | 35,338 | $ | – | $ | – | |||||||||||
| Accounts payable, accrued expenses and other | – | 50,262 | 45,324 | 7,515 | – | 103,101 | ||||||||||||||||||
| Due to affiliates | – | – | 3,762 | – | – | 3,762 | ||||||||||||||||||
| Deferred revenue | – | – | 1,076 | – | – | 1,076 | ||||||||||||||||||
| Current portion of notes payable | – | 2,981 | 3,627 | – | – | 6,608 | ||||||||||||||||||
| Current portion of deferred rent | – | 502 | 497 | – | – | 999 | ||||||||||||||||||
| Current portion of obligations under capital leases | – | 2,996 | 3,838 | – | – | 6,834 | ||||||||||||||||||
| Total current liabilities | – | (103,276 | ) | 182,803 | 42,853 | – | 122,380 | |||||||||||||||||
| LONG-TERM LIABILITIES | ||||||||||||||||||||||||
| Deferred rent, net of current portion | – | 7,734 | 4,673 | – | – | 12,407 | ||||||||||||||||||
| Deferred tax liabilities, net | – | – | 277 | – | – | 277 | ||||||||||||||||||
| Line of Credit | – | 58,000 | – | – | – | 58,000 | ||||||||||||||||||
| Notes payable, net of current portion | – | 474,165 | 9,881 | – | – | 484,046 | ||||||||||||||||||
| Obligations under capital leases, net of current portion | – | 1,168 | 2,170 | – | – | 3,338 | ||||||||||||||||||
| Other non-current liabilities | – | – | 8,547 | – | – | 8,547 | ||||||||||||||||||
| Total liabilities | – | 437,791 | 208,351 | 42,853 | – | 688,995 | ||||||||||||||||||
| EQUITY DEFICIT | ||||||||||||||||||||||||
| Total Radnet, Inc.'s equity (deficit) | (70,756 | ) | (70,756 | ) | 249,763 | 9,974 | (188,981 | ) | (70,756 | ) | ||||||||||||||
| Noncontrolling interests | – | – | – | 949 | – | 949 | ||||||||||||||||||
| Total equity (deficit) | (70,756 | ) | (70,756 | ) | 249,763 | 10,923 | (188,981 | ) | (69,807 | ) | ||||||||||||||
| Total liabilities and equity deficit | $ | (70,756 | ) | $ | 367,035 | $ | 458,114 | $ | 53,776 | $ | (188,981 | ) | $ | 619,188 | ||||||||||
| 85 |
RADNET, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF OPERATIONS
For The Year Ended December 31, 2012
(in thousands)
(Restated)
| Subsidiary | Guarantor | Non-Guarantor | ||||||||||||||||||||||
| Parent | Issuer | Subsidiaries | Subsidiaries | Eliminations | Consolidated | |||||||||||||||||||
| NET REVENUE | ||||||||||||||||||||||||
| Service fee revenue, net of contractual allowances and discounts | $ | – | $ | 115,583 | $ | 453,534 | $ | 48,865 | $ | – | $ | 617,982 | ||||||||||||
| Provision for bad debts | – | (5,452 | ) | (17,888 | ) | (2,564 | ) | – | (25,904 | ) | ||||||||||||||
| Net service fee revenue | – | 110,131 | 435,646 | 46,301 | – | 592,078 | ||||||||||||||||||
| Revenue under capitation arrangements | 31,393 | 14,319 | 9,363 | 55,075 | ||||||||||||||||||||
| Total net revenue | – | 141,524 | 449,965 | 55,664 | – | 647,153 | ||||||||||||||||||
| OPERATING EXPENSES | ||||||||||||||||||||||||
| Cost of operations, excluding depreciation and amortization | – | 129,188 | 358,273 | 55,532 | – | 542,993 | ||||||||||||||||||
| Depreciation and amortization | – | 12,690 | 44,870 | 180 | – | 57,740 | ||||||||||||||||||
| Loss (gain) on sale and disposal of equipment | – | 600 | (144 | ) | – | – | 456 | |||||||||||||||||
| Severance costs | – | 69 | 641 | 26 | – | 736 | ||||||||||||||||||
| Total operating expenses | – | 142,547 | 403,640 | 55,738 | – | 601,925 | ||||||||||||||||||
| (LOSS) INCOME FROM OPERATIONS | – | (1,023 | ) | 46,325 | (74 | ) | – | 45,228 | ||||||||||||||||
| OTHER EXPENSES | ||||||||||||||||||||||||
| Interest expense | – | 31,392 | 22,391 | – | – | 53,783 | ||||||||||||||||||
| Gain on de-consolidation of joint venture | – | – | (2,777 | ) | – | – | (2,777 | ) | ||||||||||||||||
| Other (income) expenses | – | (3,873 | ) | 194 | – | – | (3,679 | ) | ||||||||||||||||
| Total other expenses | – | 27,519 | 19,808 | – | – | 47,327 | ||||||||||||||||||
| (LOSS) INCOME BEFORE INCOME TAXES AND EQUITY IN EARNINGS OF JOINT VENTURES | – | (28,542 | ) | 26,517 | (74 | ) | – | (2,099 | ) | |||||||||||||||
| Provision for income taxes | – | (21 | ) | 55,253 | (5 | ) | – | 55,227 | ||||||||||||||||
| Equity in earnings of consolidated subsidiaries | 59,834 | 88,397 | 151 | (148,382 | ) | – | ||||||||||||||||||
| Equity in earnings of joint ventures | – | – | 6,476 | – | – | 6,476 | ||||||||||||||||||
| NET INCOME (LOSS) | 59,834 | 59,834 | 88,397 | (79 | ) | (148,382 | ) | 59,604 | ||||||||||||||||
| Net loss attributable to noncontrolling interests | – | – | – | (230 | ) | – | (230 | ) | ||||||||||||||||
| NET INCOME ATTRIBUTABLE TO RADNET, INC. COMMON STOCKHOLDERS | $ | 59,834 | $ | 59,834 | $ | 88,397 | $ | 151 | $ | (148,382 | ) | $ | 59,834 | |||||||||||
| 86 |
RADNET, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF OPERATIONS
For The Year Ended December 31, 2011
(in thousands)
| Subsidiary | Guarantor | Non-Guarantor | ||||||||||||||||||||||
| Parent | Issuer | Subsidiaries | Subsidiaries | Eliminations | Consolidated | |||||||||||||||||||
| NET REVENUE | ||||||||||||||||||||||||
| Service fee revenue, net of contractual allowances and discounts | $ | – | $ | 96,002 | $ | 409,528 | $ | 49,449 | $ | – | $ | 554,979 | ||||||||||||
| Provision for bad debts | – | (4,485 | ) | (15,443 | ) | (2,411 | ) | – | (22,339 | ) | ||||||||||||||
| Net service fee revenue | – | 91,517 | 394,085 | 47,038 | – | 532,640 | ||||||||||||||||||
| Revenue under capitation arrangements | 29,914 | 13,645 | 8,922 | 52,481 | ||||||||||||||||||||
| Total net revenue | – | 121,431 | 407,730 | 55,960 | – | 585,121 | ||||||||||||||||||
| OPERATING EXPENSES | ||||||||||||||||||||||||
| Cost of operations, excluding depreciation and amortization | – | 108,530 | 314,958 | 54,340 | – | 477,828 | ||||||||||||||||||
| Depreciation and amortization | – | 13,986 | 43,268 | 227 | – | 57,481 | ||||||||||||||||||
| (Gain) loss on sale and disposal of equipment | – | (2,512 | ) | 272 | – | – | (2,240 | ) | ||||||||||||||||
| Severance costs | – | 267 | 1,124 | – | – | 1,391 | ||||||||||||||||||
| Total operating expenses | – | 120,271 | 359,622 | 54,567 | – | 534,460 | ||||||||||||||||||
| INCOME FROM OPERATIONS | – | 1,160 | 48,108 | 1,393 | – | 50,661 | ||||||||||||||||||
| OTHER EXPENSES | ||||||||||||||||||||||||
| Interest expense | – | 30,458 | 22,337 | 3 | – | 52,798 | ||||||||||||||||||
| Loss on extinguishment of debt | – | – | – | – | – | – | ||||||||||||||||||
| Other (income) expenses | – | (5,165 | ) | 90 | – | – | (5,075 | ) | ||||||||||||||||
| Total other expenses | – | 25,293 | 22,427 | 3 | – | 47,723 | ||||||||||||||||||
| (LOSS) INCOME BEFORE INCOME TAXES AND EQUITY IN EARNINGS OF JOINT VENTURES | – | (24,133 | ) | 25,681 | 1,390 | – | 2,938 | |||||||||||||||||
| Provision for income taxes | – | (46 | ) | (770 | ) | (4 | ) | – | (820 | ) | ||||||||||||||
| Equity in earnings of consolidated subsidiaries | 7,231 | 31,410 | 1,275 | – | (39,916 | ) | – | |||||||||||||||||
| Equity in earnings of joint ventures | – | – | 5,224 | – | – | 5,224 | ||||||||||||||||||
| NET INCOME | 7,231 | 7,231 | 31,410 | 1,386 | (39,916 | ) | 7,342 | |||||||||||||||||
| Net income attributable to noncontrolling interests | – | – | – | 111 | – | 111 | ||||||||||||||||||
| NET INCOME ATTRIBUTABLE TO RADNET, INC. COMMON STOCKHOLDERS | $ | 7,231 | $ | 7,231 | $ | 31,410 | $ | 1,275 | $ | (39,916 | ) | $ | 7,231 | |||||||||||
| 87 |
RADNET, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF OPERATIONS
For The Year Ended December 31, 2010
(in thousands)
| Subsidiary | Guarantor | Non-Guarantor | ||||||||||||||||||||||
| Parent | Issuer | Subsidiaries | Subsidiaries | Eliminations | Consolidated | |||||||||||||||||||
| NET REVENUE | ||||||||||||||||||||||||
| Service fee revenue, net of contractual allowances and discounts | $ | – | $ | 90,385 | $ | 350,565 | $ | 48,344 | $ | – | $ | 489,294 | ||||||||||||
| Provision for bad debts | – | (5,243 | ) | (14,293 | ) | (2,459 | ) | – | (21,995 | ) | ||||||||||||||
| Net revenue before provision for bad debts | – | 85,142 | 336,272 | 45,885 | – | 467,299 | ||||||||||||||||||
| Revenue under capitation arrangements | – | 29,274 | 13,353 | 8,731 | 51,358 | |||||||||||||||||||
| Total net revenue | – | 114,416 | 349,625 | 54,616 | – | 518,657 | ||||||||||||||||||
| OPERATING EXPENSES | ||||||||||||||||||||||||
| Cost of operations, excluding depreciation and amortization | – | 103,563 | 264,258 | 53,152 | – | 420,973 | ||||||||||||||||||
| Depreciation and amortization | – | 13,656 | 40,150 | 191 | – | 53,997 | ||||||||||||||||||
| Loss on sale and disposal of equipment | – | 141 | 995 | – | – | 1,136 | ||||||||||||||||||
| Severance costs | – | 490 | 321 | 27 | – | 838 | ||||||||||||||||||
| Total operating expenses | – | 117,850 | 305,724 | 53,370 | – | 476,944 | ||||||||||||||||||
| (LOSS) INCOME FROM OPERATIONS | – | (3,434 | ) | 43,901 | 1,246 | – | 41,713 | |||||||||||||||||
| OTHER EXPENSES | ||||||||||||||||||||||||
| Interest expense | – | 25,405 | 22,965 | 28 | – | 48,398 | ||||||||||||||||||
| Loss on extinguishment of debt | – | 9,871 | – | – | – | 9,871 | ||||||||||||||||||
| Other income | – | 362 | 143 | – | – | 505 | ||||||||||||||||||
| Total other expenses | – | 35,638 | 23,108 | 28 | – | 58,774 | ||||||||||||||||||
| (LOSS) INCOME BEFORE INCOME TAXES AND EQUITY IN EARNINGS OF JOINT VENTURES | – | (39,072 | ) | 20,793 | 1,218 | – | (17,061 | ) | ||||||||||||||||
| Provision for income taxes | – | (38 | ) | (532 | ) | (6 | ) | – | (576 | ) | ||||||||||||||
| Equity in (losses) earnings of consolidated subsidiaries | (12,852 | ) | 26,258 | 1,045 | – | (14,451 | ) | – | ||||||||||||||||
| Equity in earnings of joint ventures | – | – | 4,952 | – | – | 4,952 | ||||||||||||||||||
| NET (LOSS) INCOME | (12,852 | ) | (12,852 | ) | 26,258 | 1,212 | (14,451 | ) | (12,685 | ) | ||||||||||||||
| Net income attributable to noncontrolling interests | – | – | – | 167 | – | 167 | ||||||||||||||||||
| NET (LOSS) INCOME ATTRIBUTABLE TO RADNET, INC. COMMON STOCKHOLDERS | $ | (12,852 | ) | $ | (12,852 | ) | $ | 26,258 | $ | 1,045 | $ | (14,451 | ) | $ | (12,852 | ) | ||||||||
| 88 |
RADNET, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF CASH FLOWS
For The Year Ended December 31, 2012
(in thousands)
(Restated)
| Subsidiary | Guarantor | Non-Guarantor | ||||||||||||||||||||||
| Parent | Issuer | Subsidiaries | Subsidiaries | Eliminations | Consolidated | |||||||||||||||||||
| CASH FLOWS FROM OPERATING ACTIVITIES | ||||||||||||||||||||||||
| Net income (loss) | $ | 59,834 | $ | 59,834 | $ | 88,397 | $ | (79 | ) | $ | (148,382 | ) | $ | 59,604 | ||||||||||
| Adjustments to reconcile net income (loss) to net cash (used in) provided by operating activities: | ||||||||||||||||||||||||
| Depreciation and amortization | – | 12,690 | 44,870 | 180 | – | 57,740 | ||||||||||||||||||
| Provision for bad debt | – | 5,452 | 17,888 | 2,564 | – | 25,904 | ||||||||||||||||||
| Equity in earnings of consolidated subsidiaries | (59,834 | ) | (88,397 | ) | (151 | ) | – | 148,382 | – | |||||||||||||||
| Distributions from consolidated subsidiaries | – | – | 906 | – | (906 | ) | – | |||||||||||||||||
| Equity in earnings of joint ventures | – | – | (6,476 | ) | – | – | (6,476 | ) | ||||||||||||||||
| Distributions from joint ventures | – | – | 6,477 | – | – | 6,477 | ||||||||||||||||||
| Deferred rent amortization | – | 1,917 | 1,691 | – | – | 3,608 | ||||||||||||||||||
| Amortization of deferred financing cost | – | 2,474 | – | – | – | 2,474 | ||||||||||||||||||
| Amortization of discount on notes | – | 1,163 | – | – | – | 1,163 | ||||||||||||||||||
| Loss (gain) on sale and disposal of equipment | – | 600 | (144 | ) | – | – | 456 | |||||||||||||||||
| Gain on bargain purchase | – | – | (810 | ) | – | – | (810 | ) | ||||||||||||||||
| Gain on de-consolidation of joint venture | – | – | (2,777 | ) | – | – | (2,777 | ) | ||||||||||||||||
| Amortization of cash flow hedge | – | 918 | – | – | – | 918 | ||||||||||||||||||
| Stock-based compensation | – | 684 | 2,052 | – | – | 2,736 | ||||||||||||||||||
| Changes in operating assets and liabilities, net of assets acquired and liabilities assumed in purchase transactions: | ||||||||||||||||||||||||
| Accounts receivable | – | – | (4,051 | ) | (13,299 | ) | – | (17,350 | ) | |||||||||||||||
| Other current assets | – | 2,203 | 1,085 | 277 | – | 3,565 | ||||||||||||||||||
| Other assets | – | (542 | ) | (36 | ) | – | – | (578 | ) | |||||||||||||||
| Deferred taxes | – | – | (56,142 | ) | – | – | (56,142 | ) | ||||||||||||||||
| Deferred revenue | – | – | 197 | – | – | 197 | ||||||||||||||||||
| Accounts payable, accrued expenses and other | – | (6,524 | ) | (9,161 | ) | 10,245 | – | (5,440 | ) | |||||||||||||||
| Net cash (used in) provided by operating activities | – | (7,528 | ) | 83,815 | (112 | ) | (906 | ) | 75,269 | |||||||||||||||
| CASH FLOWS FROM INVESTING ACTIVITIES | ||||||||||||||||||||||||
| Purchase of imaging facilities | – | (10,494 | ) | (34,999 | ) | – | – | (45,493 | ) | |||||||||||||||
| Purchase of property and equipment | – | (9,173 | ) | (35,275 | ) | – | – | (44,448 | ) | |||||||||||||||
| Proceeds from sale of equipment | – | 218 | 1,331 | – | – | 1,549 | ||||||||||||||||||
| Proceeds from sale of imaging facilities | – | – | 2,300 | – | – | 2,300 | ||||||||||||||||||
| Proceeds from sale of joint venture interests | – | – | 1,800 | – | – | 1,800 | ||||||||||||||||||
| Purchase of equity interest in joint ventures | – | – | (2,756 | ) | – | – | (2,756 | ) | ||||||||||||||||
| Net cash used in investing activities | – | (19,449 | ) | (67,599 | ) | – | – | (87,048 | ) | |||||||||||||||
| CASH FLOWS FROM FINANCING ACTIVITIES | ||||||||||||||||||||||||
| Principal payments on notes and leases payable | – | (6,061 | ) | (16,162 | ) | – | – | (22,223 | ) | |||||||||||||||
| Repayment of debt upon extinguishment | – | (277,875 | ) | – | – | – | (277,875 | ) | ||||||||||||||||
| Proceeds from borrowings upon refinancing | – | 344,485 | – | – | – | 344,485 | ||||||||||||||||||
| Deferred financing costs | – | (3,753 | ) | – | – | – | (3,753 | ) | ||||||||||||||||
| Proceeds from, net of payments, on line of credit | – | (25,000 | ) | – | – | – | (25,000 | ) | ||||||||||||||||
| Payments to counterparties of interest rate swaps, net of amounts received | – | (5,823 | ) | – | – | – | (5,823 | ) | ||||||||||||||||
| Purchase of non-controlling interests | – | – | (117 | ) | – | – | (117 | ) | ||||||||||||||||
| Distributions paid to noncontrolling interests | – | – | – | (977 | ) | 906 | (71 | ) | ||||||||||||||||
| Net provided by (cash used) in financing activities | – | 25,973 | (16,279 | ) | (977 | ) | 906 | 9,623 | ||||||||||||||||
| EFFECT OF EXCHANGE RATE CHANGES ON CASH | – | – | 63 | – | – | 63 | ||||||||||||||||||
| NET DECREASE IN CASH AND CASH EQUIVALENTS | – | (1,004 | ) | – | (1,089 | ) | – | (2,093 | ) | |||||||||||||||
| CASH AND CASH EQUIVALENTS, beginning of period | – | 1,366 | – | 1,089 | – | 2,455 | ||||||||||||||||||
| CASH AND CASH EQUIVALENTS, end of period | $ | – | $ | 362 | $ | – | $ | – | $ | – | $ | 362 | ||||||||||||
| 89 |
RADNET, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF CASH FLOWS
For The Year Ended December 31, 2011
(in thousands)
| Parent | Subsidiary Issuer | Guarantor Subsidiaries | Non-Guarantor Subsidiaries | Eliminations | Consolidated | |||||||||||||||||||
| CASH FLOWS FROM OPERATING ACTIVITIES | ||||||||||||||||||||||||
| Net income | $ | 7,231 | $ | 7,231 | $ | 31,410 | $ | 1,386 | $ | (39,916 | ) | $ | 7,342 | |||||||||||
| Adjustments to reconcile net income to net cash (used in) provided by operating activities: | ||||||||||||||||||||||||
| Depreciation and amortization | – | 13,986 | 43,268 | 227 | – | 57,481 | ||||||||||||||||||
| Provision for bad debt | – | 4,485 | 15,443 | 2,411 | – | 22,339 | ||||||||||||||||||
| Equity in earnings of consolidated subsidiaries | (7,231 | ) | (31,410 | ) | (1,275 | ) | – | 39,916 | – | |||||||||||||||
| Distributions from consolidated subsidiaries | – | – | 1,597 | – | (1,597 | ) | – | |||||||||||||||||
| Equity in earnings of joint ventures | – | – | (5,224 | ) | – | – | (5,224 | ) | ||||||||||||||||
| Distributions from joint ventures | – | – | 4,993 | – | – | 4,993 | ||||||||||||||||||
| Deferred rent amortization | – | 1,811 | 471 | – | – | 2,282 | ||||||||||||||||||
| Amortization of deferred financing cost | – | 2,940 | – | – | – | 2,940 | ||||||||||||||||||
| Amortization of discount on notes | – | 244 | – | – | – | 244 | ||||||||||||||||||
| (Gain) loss on sale and disposal of equipment | – | (2,512 | ) | 272 | – | – | (2,240 | ) | ||||||||||||||||
| Amortization of cash flow hedge | – | 1,225 | – | – | – | 1,225 | ||||||||||||||||||
| Stock-based compensation | – | 778 | 2,332 | – | – | 3,110 | ||||||||||||||||||
| Changes in operating assets and liabilities, net of assets acquired and liabilities assumed in purchase transactions: | ||||||||||||||||||||||||
| Accounts receivable | – | – | (27,886 | ) | (17,128 | ) | – | (45,014 | ) | |||||||||||||||
| Other current assets | – | (3,366 | ) | (183 | ) | (386 | ) | – | (3,935 | ) | ||||||||||||||
| Other assets | – | 41 | 2 | – | – | 43 | ||||||||||||||||||
| Deferred revenue | – | – | (492 | ) | – | – | (492 | ) | ||||||||||||||||
| Accounts payable, accrued expenses and other | – | (27,252 | ) | 23,275 | 16,519 | – | 12,542 | |||||||||||||||||
| Net cash (used in) provided by operating activities | – | (31,799 | ) | 88,003 | 3,029 | (1,597 | ) | 57,636 | ||||||||||||||||
| CASH FLOWS FROM INVESTING ACTIVITIES | ||||||||||||||||||||||||
| Purchase of imaging facilities | – | (1,999 | ) | (40,991 | ) | – | – | (42,990 | ) | |||||||||||||||
| Proceeds from insurance claims on damaged equipment | – | 2,422 | 318 | – | 2,740 | |||||||||||||||||||
| Purchase of property and equipment | – | (11,125 | ) | (30,984 | ) | (611 | ) | – | (42,720 | ) | ||||||||||||||
| Proceeds from sale of equipment | – | – | 325 | – | – | 325 | ||||||||||||||||||
| Purchase of equity interest in joint ventures | – | – | (5,094 | ) | – | – | (5,094 | ) | ||||||||||||||||
| Net cash used in investing activities | – | (10,702 | ) | (76,426 | ) | (611 | ) | – | (87,739 | ) | ||||||||||||||
| CASH FLOWS FROM FINANCING ACTIVITIES | ||||||||||||||||||||||||
| Principal payments on notes and leases payable | – | (7,181 | ) | (11,575 | ) | – | – | (18,756 | ) | |||||||||||||||
| Deferred financing costs | – | (944 | ) | – | – | – | (944 | ) | ||||||||||||||||
| Proceeds from, net of payments, on line of credit | – | 58,000 | – | – | – | 58,000 | ||||||||||||||||||
| Payments to counterparties of interest rate swaps, net of payments received | – | (6,455 | ) | – | – | – | (6,455 | ) | ||||||||||||||||
| Distributions paid to noncontrolling interests | – | – | – | (1,751 | ) | 1,597 | (154 | ) | ||||||||||||||||
| Proceeds from issuance of common stock | – | 242 | – | – | – | 242 | ||||||||||||||||||
| Net cash provided by (used in) financing activities | – | 43,662 | (11,575 | ) | (1,751 | ) | 1,597 | 31,933 | ||||||||||||||||
| EFFECT OF EXCHANGE RATE CHANGES ON CASH | – | (2 | ) | (2 | ) | |||||||||||||||||||
| NET INCREASE IN CASH AND CASH EQUIVALENTS | – | 1,161 | – | 667 | – | 1,828 | ||||||||||||||||||
| CASH AND CASH EQUIVALENTS, | ||||||||||||||||||||||||
| beginning of period | – | 205 | – | 422 | – | 627 | ||||||||||||||||||
| CASH AND CASH EQUIVALENTS, | ||||||||||||||||||||||||
| end of period | $ | – | $ | 1,366 | $ | – | $ | 1,089 | $ | – | $ | 2,455 | ||||||||||||
| 90 |
RADNET, INC. AND SUBSIDIARIES
CONSOLIDATED STATEMENTS OF CASH FLOWS
For The Year Ended December 31, 2010
(in thousands)
| Parent | Subsidiary Issuer | Guarantor Subsidiaries | Non-Guarantor Subsidiaries | Eliminations | Consolidated | |||||||||||||||||||
| CASH FLOWS FROM OPERATING ACTIVITIES | ||||||||||||||||||||||||
| Net (loss) income | $ | (12,852 | ) | $ | (12,852 | ) | $ | 26,258 | $ | 1,212 | $ | (14,451 | ) | $ | (12,685 | ) | ||||||||
| Adjustments to reconcile net (loss) income to net cash (used in) provided by operating activities: | ||||||||||||||||||||||||
| Depreciation and amortization | – | 13,656 | 40,150 | 191 | – | 53,997 | ||||||||||||||||||
| Provision for bad debt | – | 5,243 | 14,293 | 2,459 | – | 21,995 | ||||||||||||||||||
| Equity in earnings of consolidated subsidiaries | 12,852 | (26,258 | ) | (1,045 | ) | – | 14,451 | – | ||||||||||||||||
| Distributions from consolidated subsidiaries | – | – | 1,247 | – | (1,247 | ) | – | |||||||||||||||||
| Equity in earnings of joint ventures | – | – | (4,952 | ) | – | – | (4,952 | ) | ||||||||||||||||
| Distributions from joint ventures | – | – | 7,639 | – | – | 7,639 | ||||||||||||||||||
| Deferred rent amortization | – | 254 | 1,594 | – | – | 1,848 | ||||||||||||||||||
| Amortization of deferred financing cost | – | 2,797 | – | – | – | 2,797 | ||||||||||||||||||
| Amortization of discount on notes | – | 164 | – | – | – | 164 | ||||||||||||||||||
| Loss on sale and disposal of equipment | – | 141 | 995 | – | – | 1,136 | ||||||||||||||||||
| Loss on extinguishment of debt | – | 9,871 | – | – | – | 9,871 | ||||||||||||||||||
| Amortization of cash flow hedge | – | 917 | – | – | – | 917 | ||||||||||||||||||
| Stock-based compensation | – | 929 | 2,789 | – | – | 3,718 | ||||||||||||||||||
| Changes in operating assets and liabilities, net of assets acquired and liabilities assumed in purchase transactions: | ||||||||||||||||||||||||
| Accounts receivable | – | – | (11,818 | ) | (13,004 | ) | – | (24,822 | ) | |||||||||||||||
| Other current assets | – | (2,552 | ) | (635 | ) | (39 | ) | – | (3,226 | ) | ||||||||||||||
| Other assets | – | 876 | (852 | ) | – | – | 24 | |||||||||||||||||
| Deferred revenue | – | – | 207 | – | – | 207 | ||||||||||||||||||
| Accounts payable, accrued expenses and other | – | (27,504 | ) | 24,615 | 11,145 | – | 8,256 | |||||||||||||||||
| Net cash (used in) provided by operating activities | – | (34,318 | ) | 100,485 | 1,964 | (1,247 | ) | 66,884 | ||||||||||||||||
| CASH FLOWS FROM INVESTING ACTIVITIES | ||||||||||||||||||||||||
| Purchase of imaging facilities | – | (1,401 | ) | (60,387 | ) | 14 | – | (61,774 | ) | |||||||||||||||
| Purchase of property and equipment | – | (12,024 | ) | (28,175 | ) | (94 | ) | – | (40,293 | ) | ||||||||||||||
| Proceeds from sale of equipment | – | 121 | 564 | – | – | 685 | ||||||||||||||||||
| Net cash used in investing activities | – | (13,304 | ) | (87,998 | ) | (80 | ) | – | (101,382 | ) | ||||||||||||||
| CASH FLOWS FROM FINANCING ACTIVITIES | ||||||||||||||||||||||||
| Principal payments on notes and leases payable | – | (8,903 | ) | (12,476 | ) | (84 | ) | – | (21,463 | ) | ||||||||||||||
| Repayment of debt upon extinguishment | – | (412,000 | ) | – | – | – | (412,000 | ) | ||||||||||||||||
| Proceeds from borrowings upon refinancing | – | 478,313 | – | – | – | 478,313 | ||||||||||||||||||
| Deferred financing costs | – | (13,566 | ) | – | – | – | (13,566 | ) | ||||||||||||||||
| Payments to counterparties of interest rate swaps, net of amounts received | – | (6,382 | ) | – | – | – | (6,382 | ) | ||||||||||||||||
| Distributions paid to noncontrolling interests | – | – | – | (1,378 | ) | 1,247 | (131 | ) | ||||||||||||||||
| Proceeds from issuance of common stock | – | 271 | – | – | – | 271 | ||||||||||||||||||
| Net cash provided by (used in) financing activities | – | 37,733 | (12,476 | ) | (1,462 | ) | 1,247 | 25,042 | ||||||||||||||||
| EFFECT OF EXCHANGE RATE CHANGES ON CASH | – | – | (11 | ) | – | – | (11) | |||||||||||||||||
| NET (DECREASE) INCREASE IN CASH AND CASH EQUIVALENTS | – | (9,889 | ) | – | 422 | – | (9,467 | ) | ||||||||||||||||
| CASH AND CASH EQUIVALENTS, | ||||||||||||||||||||||||
| beginning of period | – | 10,094 | – | – | – | 10,094 | ||||||||||||||||||
| CASH AND CASH EQUIVALENTS, | ||||||||||||||||||||||||
| end of period | $ | – | $ | 205 | $ | – | $ | 422 | $ | – | $ | 627 |
| 91 |
NOTE 16 – QUARTERLY RESULTS OF OPERATIONS (unaudited)
The following table sets forth a summary of our unaudited quarterly operating results for each of the last eight quarters in the years ended December 31, 2012 and 2011. This quarterly data has been derived from our unaudited consolidated interim financial statements which, in our opinion, have been prepared on substantially the same basis as the audited financial statements contained elsewhere in this report and include all normal recurring adjustments necessary for a fair presentation of the financial information for the periods presented. These unaudited quarterly results should be read in conjunction with our financial statements and notes thereto, included elsewhere in this report. The operating results in any quarter are not necessarily indicative of the results that may be expected for any future period (in thousands except for earnings per share).
| 2012 Quarter Ended | 2011 Quarter Ended | |||||||||||||||||||||||||||||||
| Mar 31 | June 30 | Sept 30 | Dec 31 | Mar 31 | June 30 | Sept 30 | Dec 31 | |||||||||||||||||||||||||
| Statement of Operations Data: | (Restated) | |||||||||||||||||||||||||||||||
| Net service fee revenue | $ | 162,016 | $ | 165,351 | $ | 160,453 | $ | 159,333 | $ | 139,052 | $ | 147,699 | $ | 143,021 | $ | 155,349 | ||||||||||||||||
| Total operating expenses | 150,765 | 151,886 | 146,613 | 152,661 | 129,653 | 132,562 | 132,041 | 140,204 | ||||||||||||||||||||||||
| Total other expenses | 12,420 | 12,131 | 9,738 | 13,038 | 11,544 | 12,461 | 11,736 | 11,982 | ||||||||||||||||||||||||
| Equity in earnings of joint ventures | 1,262 | 1,986 | 909 | 2,319 | 1,484 | 1,267 | 1,038 | 1,435 | ||||||||||||||||||||||||
| Provision for income taxes | (245 | ) | (421 | ) | (30 | ) | 55,923 | (147 | ) | (337 | ) | (234 | ) | (102 | ) | |||||||||||||||||
| Net income (loss) | (152 | ) | 2,899 | 4,981 | 51,876 | (808 | ) | 3,606 | 48 | 4,496 | ||||||||||||||||||||||
| Net income (loss) attributable to noncontrolling interests | (41 | ) | (47 | ) | (72 | ) | (70 | ) | 68 | 85 | 9 | (51 | ) | |||||||||||||||||||
| Net income (loss) attributable to Radnet, Inc. common stockholders | $ | (111 | ) | $ | 2,946 | $ | 5,053 | $ | 51,946 | $ | (876 | ) | $ | 3,521 | $ | 39 | $ | 4,547 | ||||||||||||||
| Basic net income (loss) attributable to Radnet, Inc. common stockholders earnings (loss) per share: | $ | (0.00 | ) | $ | 0.07 | $ | 0.13 | $ | 1.35 | $ | (0.02 | ) | $ | 0.09 | $ | 0.00 | $ | 0.12 | ||||||||||||||
| Diluted net income (loss) attributable to Radnet, Inc. common stockholders earnings (loss) per share: | $ | (0.00 | ) | $ | 0.07 | $ | 0.12 | $ | 1.30 | $ | (0.02 | ) | $ | 0.09 | $ | 0.00 | $ | 0.12 | ||||||||||||||
| Weighted average shares outstanding | ||||||||||||||||||||||||||||||||
| Basic | 37,670 | 37,761 | 38,340 | 38,349 | 37,258 | 37,358 | 37,426 | 37,426 | ||||||||||||||||||||||||
| Diluted | 37,670 | 39,431 | 39,861 | 39,796 | 37,258 | 39,820 | 38,470 | 38,059 | ||||||||||||||||||||||||
Detail regarding the restatement adjustments made to arrive at the restated amounts included in the table above for the three months ended December 31, 2012 are shown in the table below. See Note 1A for further detail regarding such restatement.
| As Previously | Restatement | |||||||||||
| Reported | Adjustments | As Restated | ||||||||||
| (unaudited) | (unaudited) | (unaudited) | ||||||||||
| For the three months ended December 31, 2012 | ||||||||||||
| Benefit from income taxes | $ | 60,606 | $ | (4,683 | ) | $ | 55,923 | |||||
| Net income | 56,559 | (4,683 | ) | 51,876 | ||||||||
| Net income attributable to RadNet, Inc. common stockholders | 56,629 | (4,683 | ) | 51,946 | ||||||||
| Basic net income per share attributable to RadNet, Inc. common stockholders | 1.47 | (0.12 | ) | 1.35 | ||||||||
| Diluted net income per share attributable to RadNet, Inc. common stockholders | 1.42 | (0.12 | ) | 1.30 | ||||||||
NOTE 17 – RELATED PARTY TRANSACTIONS
We use World Wide Express, a package delivery company owned 40% by Norman Hames, our western operations chief operating officer, to provide delivery services for us. For the years ended December 31, 2012, 2011 and 2010, we expenses approximately $948,000, $997,000 and $809,000, respectively, to World Wide Express for those services. At December 31, 2012 and 2011, we had outstanding amounts due to World Wide Express of $135,000 and $75,000, respectively.
NOTE 18 – SUBSEQUENT EVENTS
On January 30, 2013, we purchased an additional 20.9% interest in a joint venture multi-modality imaging center located in Manhattan, New York of which we initially held a 31.5% interest from our December 31, 2012 acquisition of Lenox Hill Radiology. This additional 20.9% interest gave us a controlling interest in the center and so accordingly, we will be consolidating its financial statements in the first quarter of 2013.
On February 28, 2013, we completed our acquisition of a multi-modality imaging center located in Brooklyn, New York by exercising a $1.00 purchase option to acquire an initial 50% interest (we acquired this option through our December 31, 2012 acquisition of Lenox Hill Radiology) and then by purchasing the remaining 50% interest from the existing partner for approximately $2.7 million in cash.
| 92 |
The Financial Statements for certain unconsolidated joint ventures in which we hold equity interests of 50% or less are attached hereto and begin on page 94.
Report of Independent Registered Public Accounting Firm
To the partners of:
Franklin Imaging Joint Venture;
Carroll County Radiology, LLC;
MRI at St. Joseph Medical Center, LLC; and
Greater Baltimore Diagnostic Imaging Partnership
We have audited the accompanying combined balance sheet of certain RadNet, Inc. affiliates including Franklin Imaging Joint Venture, Carroll County Radiology, LLC, MRI at St. Joseph Medical Center, LLC and Greater Baltimore Diagnostic Imaging Partnership (collectively, the “Group”), as of December 31, 2012, and the related combined statements of income, partners’ capital, and cash flows for the year ended December 31, 2012. These financial statements are the responsibility of the Group’s management. Our responsibility is to express an opinion on these financial statements based on our audit.
We conducted our audit in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. We were not engaged to perform an audit of the Group’s internal control over financial reporting. Our audit included consideration of internal control over financial reporting as a basis for designing audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the Group’s internal control over financial reporting. Accordingly, we express no such opinion. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements, assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audit provides a reasonable basis for our opinion.
In our opinion, the financial statements referred to above present fairly, in all material respects, the combined financial position of the Group at December 31, 2012, and the combined results of their operations and their cash flows for the year ended December 31, 2012, in conformity with U.S. generally accepted accounting principles.
/s/ Ernst & Young, LLP
April 1, 2013
Los Angeles, California
| 93 |
CERTAIN RADNET, INC. AFFILIATES
COMBINED BALANCE SHEETS
(IN THOUSANDS)
| December 31, | December 31, | |||||||||
| 2012 | 2011 | |||||||||
| (unaudited) | ||||||||||
| ASSETS | ||||||||||
| CURRENT ASSETS | ||||||||||
| Cash and cash equivalents | $ | 1,778 | $ | 2,089 | ||||||
| Accounts receivable, net | 8,597 | 8,326 | ||||||||
| Due from affiliates | 1,121 | 2,414 | ||||||||
| Prepaid expenses and other current assets | 602 | 337 | ||||||||
| Total current assets | 12,098 | 13,166 | ||||||||
| PROPERTY AND EQUIPMENT, NET | 19,358 | 22,074 | ||||||||
| OTHER ASSETS | ||||||||||
| Goodwill | 9,923 | 7,816 | ||||||||
| Other intangible assets | 724 | 844 | ||||||||
| Total assets | $ | 42,103 | $ | 43,900 | ||||||
| LIABILITIES AND PARTNERS' CAPITAL | ||||||||||
| CURRENT LIABILITIES | ||||||||||
| Accounts payable and accrued expenses | $ | 2,043 | $ | 3,612 | ||||||
| Current portion of deferred rent | 167 | 134 | ||||||||
| Current portion of equipment notes payable | 909 | 2,698 | ||||||||
| Current portion of obligations under capital leases | 270 | 278 | ||||||||
| Total current liabilities | 3,389 | 6,722 | ||||||||
| LONG-TERM LIABILITIES | ||||||||||
| Deferred rent, net of current portion | 1,594 | 1,749 | ||||||||
| Equipment notes payable, net of current portion | 1,006 | 1,916 | ||||||||
| Obligations under capital leases, net of current portion | 144 | 414 | ||||||||
| Total liabilities | 6,133 | 10,801 | ||||||||
| COMMITMENTS AND CONTINGENCIES | ||||||||||
| PARTNERS' CAPITAL | ||||||||||
| RadNet, Inc. | 17,717 | 16,458 | ||||||||
| Other partners | 18,253 | 16,641 | ||||||||
| Total partners' capital | 35,970 | 33,099 | ||||||||
| Total liabilities and partners' capital | $ | 42,103 | $ | 43,900 | ||||||
The accompanying notes are an integral part of these financial statements.
| 94 |
CERTAIN RADNET, INC. AFFILIATES
COMBINED STATEMENTS OF INCOME
(IN THOUSANDS)
| Years Ended December 31, | ||||||||||||
| 2012 | 2011 | 2010 | ||||||||||
| NET SERVICE FEE REVENUE | (unaudited) | (unaudited) | ||||||||||
| Service fee revenue, net of contractual allowances and discounts | $ | 58,122 | $ | 46,212 | $ | 46,321 | ||||||
| Provision for bad debts | (2,752 | ) | (2,211 | ) | (2,112 | ) | ||||||
| Net service fee revenue | 55,370 | 44,001 | 44,209 | |||||||||
| OPERATING EXPENSES | ||||||||||||
| Cost of operations | 38,161 | 31,557 | 31,291 | |||||||||
| Depreciation and amortization | 4,607 | 3,856 | 3,703 | |||||||||
| (Gain) loss on sale of equipment | (35 | ) | 195 | 125 | ||||||||
| Total operating expenses | 42,733 | 35,608 | 35,119 | |||||||||
| INCOME FROM OPERATIONS | 12,637 | 8,393 | 9,090 | |||||||||
| Net interest expense | 245 | 381 | 702 | |||||||||
| NET INCOME | $ | 12,392 | $ | 8,012 | $ | 8,388 | ||||||
The accompanying notes are an integral part of these financial statements.
| 95 |
CERTAIN RADNET, INC. AFFILIATES
COMBINED STATEMENTS OF PARTNERS' CAPITAL
(IN THOUSANDS)
| RadNet, Inc. | Other Partners | Total | ||||||||||
| BALANCE - January 1, 2010 (unaudited) | $ | 11,168 | $ | 13,393 | $ | 24,561 | ||||||
| Net Income | 3,771 | 4,617 | 8,388 | |||||||||
| Distributions | (5,957 | ) | (7,128 | ) | (13,085 | ) | ||||||
| BALANCE - December 31, 2010 (unaudited) | 8,982 | 10,882 | 19,864 | |||||||||
| Net Income | 3,714 | 4,298 | 8,012 | |||||||||
| Contributions | 6,551 | 4,652 | 11,203 | |||||||||
| Distributions | (2,789 | ) | (3,191 | ) | (5,980 | ) | ||||||
| BALANCE - December 31, 2011 (unaudited) | 16,458 | 16,641 | 33,099 | |||||||||
| Net Income | 5,757 | 6,635 | 12,392 | |||||||||
| Contributions | 920 | 1,380 | 2,300 | |||||||||
| Distributions | (5,418 | ) | (6,403 | ) | (11,821 | ) | ||||||
| BALANCE - December 31, 2012 | $ | 17,717 | $ | 18,253 | $ | 35,970 | ||||||
The accompanying notes are an integral part of these financial statements.
| 96 |
CERTAIN RADNET, INC. AFFILIATES
COMBINED STATEMENTS OF CASH FLOWS
(IN THOUSANDS)
| Years Ended December 31, | ||||||||||||
| 2012 | 2011 | 2010 | ||||||||||
| (unaudited) | (unaudited) | |||||||||||
| CASH FLOWS FROM OPERATING ACTIVITIES | ||||||||||||
| Net income | $ | 12,392 | $ | 8,012 | $ | 8,388 | ||||||
| Adjustments to reconcile net income to net cash provided by operating activities: | ||||||||||||
| Depreciation and amortization | 4,607 | 3,856 | 3,703 | |||||||||
| Provision for bad debts | 2,752 | 2,211 | 2,112 | |||||||||
| Deferred rent amortization | (122 | ) | (112 | ) | 1,048 | |||||||
| (Gain) loss on sale of equipment | (35 | ) | 195 | 125 | ||||||||
| Changes in operating assets and liabilities | ||||||||||||
| Accounts receivable | (3,022 | ) | (3,036 | ) | (2,415 | ) | ||||||
| Prepaid expenses and other current assets | (264 | ) | (31 | ) | 748 | |||||||
| Due from affiliates | 1,293 | (372 | ) | 4,110 | ||||||||
| Accounts payable and accrued expenses | (1,424 | ) | 878 | 517 | ||||||||
| Net cash provided by operating activities | 16,177 | 11,601 | 18,336 | |||||||||
| CASH FLOWS FROM INVESTING ACTIVITIES | ||||||||||||
| Purchase of property and equipment | (1,091 | ) | (2,576 | ) | (2,495 | ) | ||||||
| Purchase of imaging facilities | (2,935 | ) | – | (133 | ) | |||||||
| Proceeds from sale of equipment | 35 | – | 305 | |||||||||
| Net cash used in investing activities | (3,991 | ) | (2,576 | ) | (2,323 | ) | ||||||
| CASH FLOWS FROM FINANCING ACTIVITIES | ||||||||||||
| Principal payments on notes and leases payable | (2,976 | ) | (2,764 | ) | (2,576 | ) | ||||||
| Contributions from partners | 2,300 | – | – | |||||||||
| Distributions to partners | (11,821 | ) | (5,980 | ) | (13,085 | ) | ||||||
| Net cash used in financing activities | (12,497 | ) | (8,744 | ) | (15,661 | ) | ||||||
| NET (DECREASE) INCREASE IN CASH AND CASH EQUIVALENTS | (311 | ) | 281 | 352 | ||||||||
| CASH AND CASH EQUIVALENTS, beginning of period | 2,089 | 1,808 | 1,456 | |||||||||
| CASH AND CASH EQUIVALENTS, end of period | $ | 1,778 | $ | 2,089 | $ | 1,808 | ||||||
| SUPPLEMENTAL DISCLOSURE OF CASH FLOW INFORMATION | ||||||||||||
| Cash paid during the period for interest | $ | 245 | $ | 381 | $ | 702 | ||||||
The accompanying notes are an integral part of these financial statements.
| 97 |
CERTAIN RADNET, INC. AFFILIATES
COMBINED STATEMENTS OF CASH FLOWS (CONTINUED)
Supplemental Schedule of Non-Cash Investing and Financing Activities
The Group entered into capital leases and equipment notes for approximately $733,000 (unaudited), during the year ended December 31, 2010.
Detail of non-cash contributions made during the year ended December 31, 2011 can be found in Note 4.
Detail of investing activity related to acquisitions can be found in Note 4.
| 98 |
CERTAIN RADNET, INC. AFFILIATES
NOTES TO COMBINED FINANCIAL STATEMENTS
NOTE 1 – DESCRIPTION OF BUSINESS
Franklin Imaging Joint Venture, Carroll County Radiology, LLC, MRI at St. Joseph Medical Center, LLC and Greater Baltimore Diagnostic Imaging Partnership, (collectively, the “Group”), are joint ventures between RadNet, Inc. and, as applicable, hospitals, health systems or radiology practices operating within the state of Maryland and were formed for the purpose of owning and operating diagnostic imaging centers. Professional services at the joint venture diagnostic imaging centers are performed by contracted radiology practices or a radiology practice that participates in the joint venture. Each joint venture within the Group is an affiliate of RadNet, Inc. as follows:
| % owned by RadNet, Inc. | ||
| Franklin Imaging Joint Venture | 49% | |
| Carroll County Radiology, LLC | 40% | |
| MRI at St. Joseph Medical Center, LLC | 49% | |
| Greater Baltimore Diagnostic Imaging Partnership | 50% |
The financial information for 2011 and 2010 included herein has been prepared by management of RadNet, Inc. without audit. Management of RadNet, Inc. believes that such financial information has been prepared in conformity with U.S. generally accepted accounting principles, and includes all adjustments necessary for a fair presentation of the financial position, results of operations and cash flows as of and for the years ended December 31, 2011 and 2010.
NOTE 2 - SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES
PRINCIPLES OF COMBINATION – Under Rule 3-09 of Regulation S-X, RadNet, Inc. is permitted to file combined financial statements for individually significant unconsolidated joint ventures which are in the same line of business. The combined financial statements include the assets, liabilities, and operations of each member of the Group. The operating activities of each of these joint ventures are completely separate from one another and are in no way affiliated with one another. Accordingly there are no intercompany transactions and balances to be eliminated when combining each together.
USE OF ESTIMATES - The preparation of these financial statements in conformity with U.S. generally accepted accounting principles requires management to make estimates and assumptions that affect the amounts reported in the financial statements and accompanying notes. These estimates and assumptions affect various matters including the Group’s reported amounts of assets and liabilities in the combined balance sheets at the dates of the financial statements; disclosure of contingent assets and liabilities at the dates of the financial statements; and reported amounts of revenues and expenses in the combined statements of income during the reporting periods. These estimates involve judgments with respect to numerous factors that are difficult to predict and are beyond management’s control. As a result, actual amounts could materially differ from these estimates.
REVENUES – Combined service fee revenue, net of contractual allowances and discounts, consists of net patient fees received from various payers and patients themselves based mainly upon established contractual billing rates, less allowances for contractual adjustments and discounts. This service fee revenue is earned through providing the use of diagnostic imaging equipment and the provision of technical services as well as providing administration services such as clerical and administrative personnel, billing and collection, provision of medical and office supplies, secretarial, reception and transcription services, maintenance of medical records, and advertising, marketing and promotional activities.
The Group's combined service fee revenues are recorded during the period the services are provided based upon the estimated amounts due from the patients and third-party payers. Third-party payers include federal and state agencies (under the Medicare and Medicaid programs), managed care health plans, commercial insurance companies and employers. Estimates of contractual allowances under managed care health plans are based upon the payment terms specified in the related contractual agreements. Contractual payment terms in managed care agreements are generally based upon predetermined rates per discounted fee-for-service rates. We also record a provision for doubtful accounts (based primarily on historical collection experience) related to patients and copayment and deductible amounts for patients who have health care coverage with third-party payers.
| 99 |
The Group’s service fee revenue, net of contractual allowances and discounts less the provision for bad debts for the years ended December 31, are summarized in the following table (in thousands):
| Years Ended December 31, | ||||||||||||
| 2012 | 2011 | 2010 | ||||||||||
| (unaudited) | (unaudited) | |||||||||||
| Commercial Insurance/Managed Care Capitation | $ | 40,220 | $ | 32,302 | $ | 32,054 | ||||||
| Medicare | 12,089 | 9,242 | 9,774 | |||||||||
| Medicaid | 1,976 | 1,525 | 1,529 | |||||||||
| Workers' Compensation/Personal Injury | 2,615 | 1,987 | 1,992 | |||||||||
| Other | 1,221 | 1,155 | 973 | |||||||||
| Service fee revenue, net of contractual allowances and discounts | 58,122 | 46,212 | 46,321 | |||||||||
| Provision for bad debts | (2,752 | ) | (2,211 | ) | (2,112 | ) | ||||||
| Net service fee revenue | $ | 55,370 | $ | 44,001 | $ | 44,209 | ||||||
The break-out of the Group’s combined service fee revenue, net of contractual allowances and discounts, is calculated based upon global payments received from consolidated imaging centers from dates of service from each respective period illustrated.
ACCOUNTS RECEIVABLE - Substantially all of the Group’s accounts receivable are due under fee-for-service contracts from third party payors, such as insurance companies and government-sponsored healthcare programs, or directly from patients. Services are generally provided pursuant to one-year contracts with healthcare providers. Receivables generally are collected within industry norms for third-party payors. The Group continuously monitors collections from payors and maintains an allowance for bad debts based upon specific payor collection issues that have been identified as well as historical collection experience.
PROVISION FOR BAD DEBTS - Although outcomes vary, the Group’s policy is to attempt to collect amounts due from patients, including co-payments and deductibles due from patients with insurance, at the time of service. The Group provides for an allowance against accounts receivable that could become uncollectible by establishing an allowance to reduce the carrying value of such receivables to their estimated net realizable value. The Group estimates this allowance based on the aging of accounts receivable by each type of payer over an 18-month look-back period, and other relevant factors. A significant portion of the provision for bad debt relates to co-payments and deductibles owed to the Group by patients with insurance. There are various factors that can impact collection trends, such as changes in the economy, which in turn have an impact on the increased burden of co-payments and deductibles to be made by patients with insurance. These factors continuously change and can have an impact on collection trends and the Group’s estimation process. The combined allowance for bad debts at December 31, 2012 and 2011 were $393,000 and $395,000 (unaudited), respectively.
CONCENTRATION OF CREDIT RISKS - Financial instruments that potentially subject the Group to credit risk are primarily cash equivalents and accounts receivable. Each joint venture places its cash and cash equivalents with one major financial institution. At times, the cash in the financial institution is temporarily in excess of the amount insured by the Federal Deposit Insurance Corporation, or FDIC. Substantially all accounts receivable are due under fee-for-service contracts from third party payors, such as insurance companies and government-sponsored healthcare programs, or directly from patients. Services are generally provided pursuant to one-year contracts with healthcare providers. Receivables generally are collected within industry norms for third-party payors. The Group continuously monitors collections from its clients and maintains an allowance for bad debts based upon any specific payor collection issues that are identified and historical experience.
CASH AND CASH EQUIVALENTS – The Group considers all highly liquid investments that mature in three months or less when purchased to be cash equivalents. The carrying amount of cash and cash equivalents approximates their fair market value.
PROPERTY AND EQUIPMENT – Property, furniture and equipment are stated at cost, less accumulated depreciation and amortization. Depreciation and amortization of property and equipment are provided using the straight-line method over the estimated useful lives, which range from 3 to 15 years. Leasehold improvements are amortized at the shorter of the related lease term or their estimated useful lives which range from 3 to 30 years.
GOODWILL – Combined goodwill of the Group at December 31, 2012 totaled $9.9 million. Goodwill is recorded by each member of the Group as a result of business combinations. Management of each member of the Group evaluates goodwill, at a minimum, on an annual basis and whenever events and changes in circumstances suggest that the carrying amount may not be recoverable. Each member of the Group adopted the provisions of ASU 2011-08 effective January 1, 2011. Each member of the Group evaluated its respective share of the combined goodwill at October 1, 2012 for signs of impairment under the provisions of ASU 2011-08. By utilizing certain qualitative measures outlined in the guidance, each member determined that its respective share of the combined goodwill was not impaired.
| 100 |
INCOME TAXES - Each member of the Group is treated
as a partnership for federal and state income tax purposes where all taxable income is allocated to the partners in accordance
with the respective partnership agreement and so accordingly federal and state taxes on income are the responsibility of the Joint
partners individually. Accordingly, no income tax provision is recorded by any joint ventures in the Group. Effective January 1,
2009, the Group adopted Accounting Standards Codification ASC 740, Income Taxes, formerly known as Financial Accounting
Standards Board (FASB) Interpretation No. 48, Accounting for Uncertainty in Income Taxes, an interpretation of FASB Statement
No. 109 (FIN 48). ASC 740 requires the impact of a tax position to be recognized in the financial statements if that position
is more-likely-than-not to be sustained by the taxing authority. Tax positions not deemed to meet the “more likely than not”
threshold would be recorded as a tax benefit or expense in the current year. Management of the Group is required to analyze all
open tax years, as defined by the statute of limitations, for all major jurisdictions, which includes federal and certain states.
Open tax years are those that are open for exam by taxing authorities, and include all returns subsequent to tax years ending after
December 31, 2009, for federal returns and December 31, 2009, for Maryland returns. The Partnership has no examinations in process
and has not been notified of any future examinations at this time. Management of the Group has reviewed all open tax years and
major jurisdictions, and has concluded that the adoption of ASC 740 did not have a material effect on the Group’s financial
position or its results of operations. There is no tax liability resulting from unrecognized tax benefits relating to uncertain-income
tax positions taken or expected to be taken in future tax returns. The Group has recognized no interest or penalties related to
uncertain tax positions taken or
expected to be taken.
FAIR VALUE MEASUREMENTS –The combined balance sheets include the following financial instruments: cash and cash equivalents, receivables, trade accounts payable, capital leases, equipment notes payable and other liabilities. The Group considers the carrying amounts of cash and cash equivalents, receivables, other current assets and current liabilities to approximate their fair value because of the relatively short period of time between the origination of these instruments and their expected realization or payment. Additionally, the Group considers the carrying amount of its equipment notes payable and capital lease obligations to approximate their fair value because the weighted average interest rate used to formulate the carrying amounts approximates current market rates.
NOTE 3 – RECENT ACCOUNTING STANDARDS
On January 1, 2012, the Group adopted ASU 2011-07, “Health Care Entities (Topic 954): Presentation and Disclosure of Patient Service Revenue, Provision for Bad Debts, and the Allowance for Doubtful Accounts for Certain Health Care Entities,” which requires health care entities to present the provision for doubtful accounts relating to patient service revenue as a deduction from patient service revenue in the statement of operations rather than as an operating expense. Additional disclosures relating to sources of patient revenue and the allowance for doubtful accounts related to patient accounts receivable are also required. Such additional disclosures are included in Note 2. The adoption of this ASU had no impact on the Group’s combined financial position, results of operations or cash flows, although it did change the financial statement presentation.
On January 1, 2012, each member of the Group adopted ASU 2011-08, “Intangibles—Goodwill and Other (Topic 350): Testing Goodwill for Impairment”, simplifying how a company is required to test goodwill for impairment. Companies will now have the option to first assess qualitative factors to determine whether it is more likely than not that the fair value of a reporting unit is less than its carrying amount. If the company determines that it is not more likely than not that the fair value of a reporting unit is less than its carrying amount, then performing the two-step impairment test is unnecessary.
In July 2012, the FASB modified existing rules to allow entities to use a qualitative approach to test indefinite-lived intangible asset for impairment. The revised standard allows an entity the option to first assess qualitatively whether it is more likely than not (that is, a likelihood of more than 50 percent) that an indefinite-lived intangible asset is impaired. An entity is not required to calculate the fair value of an indefinite-lived intangible asset and perform the quantitative impairment test unless the entity determines that it is more likely than not that the asset is impaired. This guidance will be effective for the Group in 2013.
In February 2013, the FASB issued new guidance which requires disclosure of information about significant reclassification adjustments from accumulated other comprehensive income in a single note or on the face of the financial statements. This guidance will be effective for the Group in 2013. Adoption of this standard, which is related to disclosure only, will not have an impact on the Group’s combined financial position, results of operations, or cash flows.
NOTE 4 – FACILITY ACQUISITIONS
On February 22, 2012, the members of Carroll County Radiology, LLC completed its acquisition of a multi modality imaging center from RadNet, Inc. located in Westminster, Maryland for $2.3 million. The members made a fair value determination of the assets acquired and the liabilities assumed and approximately $200,000 of fixed assets, $2.1 million of goodwill was recorded with respect to this transaction.
| 101 |
On November 1, 2012, the partners of Franklin Imaging Joint Venture completed its acquisition of a multi modality imaging center located in Baltimore, Maryland for $635,000. The members made a fair value determination of the assets acquired and the liabilities assumed and approximately $635,000 of fixed assets was recorded with respect to this transaction.
On December 31, 2011, the partners of Greater Baltimore Diagnostic Imaging Partnership (GBDIP) contributed their aggregate 100% interest in MIB Partnership, LLP, valued at $10.2 million, to GBDIP. Immediately prior to this contribution, the partners of GBDIP, who in aggregate held a 50% interest in MIB Partnership, LLP, acquired the remaining 50% interest in MIB Partnership, LLP for $5.6 million. As a result, GBDIP began consolidating this contributed partnership on December 31, 2011, recording all of its assets and liabilities at fair value on the date of contribution. As a result, $1.4 million of current assets, $2.8 million of fixed assets, $522,000 of intangible assets, and $7.6 million of goodwill was recorded with respect to this transaction. Also recorded were approximately $210,000 of accounts payable and accrued expenses, and $2.0 million of equipment notes and leases payable.
On December 31, 2011, the partners of Franklin Imaging Joint Venture (Franklin) contributed their aggregate 100% interest in Health Imaging Systems, LLC, valued at $1.0 million, to Franklin. As a result, Franklin began consolidating this contributed partnership on December 31, 2011, recording all of its assets and liabilities. As a result, $861,000 of current assets, $279,000 of fixed assets, and $137,000 of accounts payable and accrued expenses was recorded with respect to this transaction.
NOTE 5 – GOODWILL AND OTHER INTANGIBLE ASSETS
Combined goodwill of the Group at December 31, 2012 totaled $9.9 million. Goodwill is recorded as a result of business combinations. Activity in goodwill for the years ended December 31, 2011 and 2012 is provided below (in thousands):
| Balance as of January 1, 2011 (unaudited) | $ | 223 | ||
| Goodwill acquired through GBDIP's acquisition of MIB Partnership, LLP | 7,593 | |||
| Balance as of December 31, 2011 (unaudited) | 7,816 | |||
| Goodwill acquired through Carroll County Radiology's acquisition of Westminster from RadNet, Inc. | 2,107 | |||
| Balance as of December 31, 2012 | $ | 9,923 |
Other intangible assets are primarily related to the value of management service contracts on the books of MRI at St. Joseph Medical Center, LLC and covenant not to compete contracts acquired through GBDIP’s acquisition of a controlling interest of a previously held non-consolidated joint venture investment and totaled $522,000 on the date of acquisition. Accumulated amortization of the management service contract and covenant not to compete contract intangible assets through December 31, 2012 was $79,000 and $104,000, respectively. Amortization expense for the year ended December 31, 2012 was $120,000. The value of these covenant not to compete contracts are amortized using the straight-line method over five years. Management service contracts are amortized over 25 years.
The following table shows annual amortization expense, by asset classes that will be recorded over the next five years (in thousands):
| 2013 | 2014 | 2015 | 2016 | 2017 | Thereafter | Total | Weighted average amortization period remaining in years | |||||||||||||||||||||||||
| Management service contracts | 16 | 16 | 16 | 16 | 16 | 226 | 306 | 19.0 | ||||||||||||||||||||||||
| Covenant not to compete contracts | 104 | 104 | 105 | 105 | – | – | 418 | 4.0 | ||||||||||||||||||||||||
| Total annual amortization | $ | 120 | $ | 120 | $ | 121 | $ | 121 | $ | 16 | $ | 226 | $ | 724 | ||||||||||||||||||
| 102 |
NOTE 6 - PROPERTY AND EQUIPMENT
Property and equipment and accumulated depreciation and amortization are as follows (in thousands):
| December 31, | ||||||||
| 2012 | 2011 | |||||||
| (unaudited) | ||||||||
| Medical equipment | $ | 31,804 | $ | 31,514 | ||||
| Office equipment, furniture and fixtures | 2,949 | 3,051 | ||||||
| Leasehold improvements | 14,253 | 13,567 | ||||||
| Equipment under capital leases | 1,982 | 1,982 | ||||||
| 50,988 | 50,114 | |||||||
| Accumulated depreciation and amortization | (31,630 | ) | (28,040 | ) | ||||
| $ | 19,358 | $ | 22,074 | |||||
Depreciation and amortization expense on property and equipment, including amortization of equipment under capital leases, for the years ended December 31, 2012, 2011 and 2010 totaled $4.5 million, $3.8 million (unaudited) and $3.7 million (unaudited), respectively.
NOTE 7 – ACCOUNTS PAYABLE AND ACCRUED EXPENSES (IN THOUSANDS)
| December 31, | ||||||||
| 2012 | 2011 | |||||||
| (unaudited) | ||||||||
| Accounts payable | $ | 839 | $ | 873 | ||||
| Accrued expenses | 229 | 1,937 | ||||||
| Accrued payroll and vacation | 975 | 802 | ||||||
| Total | $ | 2,043 | $ | 3,612 | ||||
NOTE 8 – EQUIPMENT NOTES PAYABLE AND CAPITAL LEASES
Three members of the Group, MRI at St. Joseph Medical Center, LLC, Franklin Imaging Joint Venture, and Greater Baltimore Diagnostic Partnership hold eleven promissory notes issued by three financing companies for the purpose of acquiring imaging equipment. These notes have interest rates between 3.5% and 9.0%, mature on or before June 2016 and are collateralized by the acquired equipment.
The following is a listing of annual principal maturities of the equipment notes discussed above for years ending December 31 (in thousands):
| 2013 | $ | 909 | ||
| 2014 | 487 | |||
| 2015 | 504 | |||
| 2016 | 15 | |||
| $ | 1,915 |
The Group leases equipment under capital lease arrangements. Future minimum lease payments under capital leases for years ending December 31 (in thousands) is as follows:
| 2013 | $ | 295 | ||
| 2014 | 148 | |||
| Total minimum payments | 443 | |||
| Amount representing interest | (29 | ) | ||
| Present value of net minimum lease payments | 414 | |||
| Less current portion | (270 | ) | ||
| Long-term portion | $ | 144 |
| 103 |
NOTE 9 – COMMITMENTS AND CONTINGENCIES
Leases – The Group leases various operating facilities and certain medical equipment under operating leases with renewal options expiring through 2022. Certain leases contain renewal options from two to ten years and escalation clauses based either on the consumer price index or fixed rent escalators. Leases with fixed rent escalators are recorded on a straight-line basis. The Group records deferred rent for tenant leasehold improvement allowances received from a lessor and amortizes the deferred rent expense over the term of the lease agreement. Minimum annual payments under operating leases for future years ending December 31 follow (in thousands):
| Facilities | Equipment | Total | ||||||||||
| 2013 | $ | 2,563 | $ | 1,082 | $ | 3,645 | ||||||
| 2014 | 2,298 | 770 | 3,068 | |||||||||
| 2015 | 2,343 | 639 | 2,982 | |||||||||
| 2016 | 1,835 | 245 | 2,080 | |||||||||
| 2017 | 1,489 | – | 1,489 | |||||||||
| Thereafter | 1,028 | – | 1,028 | |||||||||
| $ | 11,556 | $ | 2,736 | $ | 14,292 | |||||||
Total rent expense, including equipment rentals, for the years ended December 31, 2012, 2011 and 2010 was $4.3 million, $3.7 million (unaudited) and $3.9 million (unaudited), respectively.
NOTE 10 – RELATED PARTY TRANSACTIONS
See Note 4 with respect to related party facility combinations.
RadNet, Inc. contracts with each joint venture within the Group to provide certain administrative services including assistance with accounting, payroll and employee benefits processing, and billing and collection functions on behalf of these joint ventures. RadNet Inc. remits to the joint ventures all amounts collected through its administration of the billing and collection functions.
RadNet, Inc., as administrator over payroll and employee benefits, pays salary and benefit obligations on behalf of these joint ventures and then bills each joint venture for its respective portion.
RadNet, Inc. contracts certain members of its contracted radiologist groups to perform professional services for the joint ventures. RadNet, Inc. assures that these radiologists are adequately covered under medical malpractice insurance policies. RadNet, Inc., on behalf of its contracted radiologist groups, bills each joint venture for its respective share of the professional fees incurred through its utilization of these contracted radiologists. RadNet, Inc. remits to its contracted radiologist groups all amounts collected from the joint ventures for the billed professional fees.
Amounts receivable from and payable to RadNet Inc. for the activities listed above are summarized in due from affiliates on the Group’s combined balance sheets and was $1.1 million and $2.4 million (unaudited) at December 31, 2012 and 2011, respectively. Due from affiliates of $1.1 million at December 31, 2012 consists of a receivable from RadNet, Inc. of $4.3 million for amounts collected through its administration of the billing and collection functions not yet remitted to the joint ventures at December 31, 2012. This receivable is offset by amounts payable to RadNet, Inc. of $525,000 for the unpaid portion of billed administrative services performed, $1.2 million for the unpaid portion of professional fees which RadNet, Inc. must in turn remit to its contracted radiologists, and $1.4 million for unpaid payroll and employee benefit costs.
NOTE 11 – SUBSEQUENT EVENTS
The member of the Group evaluated subsequent events through April, 1, 2013 and concluded that no additional disclosures were required.
| 104 |
| Item 9. | Changes In and Disagreements with Accountants on Accounting and Financial Disclosure |
None.
| Item 9A. | Controls and Procedures |
Evaluation of Disclosure Controls and Procedures
RadNet, Inc. maintains disclosure controls and procedures that are designed to ensure that information required to be disclosed in its reports under the Securities Exchange Act of 1934, as amended, is recorded, processed, summarized and reported within the time periods specified in the Commission’s rules and forms and that such information is accumulated and communicated to the Company’s management, including its Chief Executive Officer and Chief Financial Officer, as appropriate, to allow for timely decisions regarding required disclosure. In designing and evaluating the disclosure controls and procedures, management recognizes that any controls and procedures, no matter how well designed and operated, can provide only reasonable assurance of achieving the desired control objectives.
Prior to the filing of our original Annual Report on Form 10-K for the year ended December 31, 2012, RadNet, Inc. carried out a variety of procedures, under the supervision and with the participation of the Company’s management, including its Chief Executive Officer and Chief Financial Officer, to evaluate the effectiveness of the design and operation of the Company’s disclosure controls and procedures.
Based on the foregoing, the Chief Executive Officer and Chief Financial Officer of RadNet, Inc. had concluded that the Company’s disclosure controls and procedures were effective as of December 31, 2012. Subsequently, in November 2013, during the preparation of the Company’s third quarter financial statements for the three and nine months ending September 30, 2013, the Company identified a deficiency in controls relating to the accounting for income taxes resulting in the overstatement of a deferred tax asset and an understatement in an unrecognized tax benefit liability related to the historical tax treatment of certain mark-to-market adjustments recorded in relation to its interest rate swaps.
We have concluded that such deficiency represented a material weakness in internal control over financial reporting. As a result of this discovery, our Chief Executive Officer and Chief Financial Officer have now concluded that our disclosure controls and procedures were not effective as of December 31, 2012, the last day of the period covered by this Report.
Report of Management on Internal Control over Financial Reporting
The management of RadNet, Inc. is responsible for establishing and maintaining adequate internal control over financial reporting for the Company. The internal control system for RadNet, Inc. was designed to provide reasonable assurance regarding the preparation and fair presentation of published financial statements. Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Prior to the filing of the Company’s original Annual Report on Form 10-K for the year ended December 31, 2012, the management of RadNet, Inc. had assessed the effectiveness of the Company’s internal control over financial reporting. In making this assessment, it used the criteria set forth by the Committee of Sponsoring Organizations of the Treadway Commission (COSO). Based on this assessment, Company’s management had concluded that as of December 31, 2012, internal control over financial reporting was effective based on those criteria. Subsequently, in November 2013, during the preparation of the Company’s third quarter financial statements for the three and nine months ending September 30, 2013, the Company identified a deficiency in controls relating to the accounting for income taxes resulting in the overstatement of a deferred tax asset and an understatement in an unrecognized tax benefit liability related to the historical tax treatment of certain mark-to-market adjustments recorded in relation to its interest rate swaps.
A material weakness is a deficiency, or combination of deficiencies, in internal control over financial reporting such that there is a reasonable possibility that a material misstatement of the company’s annual or interim financial statements will not be prevented or detected on a timely basis.
This material weakness resulted in an error in our accounting for income taxes and contributed to our restatement of previously issued financial statements more fully described in Note 1A to the Consolidated Financial Statements. Based on our assessment, management has now concluded that, as of December 31, 2012, our internal control over the accounting for income taxes was not effective due to the identification of a material weakness.
Ernst & Young LLP, an independent registered public accounting firm, has audited the Consolidated Financial Statements included in this Annual Report on Form 10-K/A and, as part of its audit, has issued an attestation report, included herein, on the effectiveness of our internal control over financial reporting.
| 105 |
Planned Remediation Efforts to Address Material Weakness
In order to remediate the material weakness discussed above and further strengthen the overall controls surrounding the Company’s accounting for income taxes, we have taken or will take the following steps to improve the overall processes and controls in its tax function:
| • | place a senior accounting professional in a leadership position within the accounting department to ensure the quality of information delivered to, and improve the review of completed work received from, Company’s outside tax consultant; | ||
| • | improve controls over our identification and assessment of uncertain tax positions. |
Changes in Internal Control Over Financial Reporting
As previously reported, except for the material weakness described above, management did not identify any change in internal control over financial reporting occurring during the fourth quarter that materially affected, or was reasonably likely to materially affect, the Company’s internal control over financial reporting.
| 106 |
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
Board of Directors and Stockholders of RadNet, Inc.
We have audited RadNet Inc. and subsidiaries' (“ Company’s” or “ RadNet’s”) internal control over financial reporting as of December 31, 2012, based on criteria established in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (the COSO criteria). RadNet’s management is responsible for maintaining effective internal control over financial reporting, and for its assessment of the effectiveness of internal control over financial reporting included in the accompanying “Management’s Annual Report on Internal Control over Financial Reporting.” Our responsibility is to express an opinion on RadNet’s internal control over financial reporting based on our audit.
We conducted our audit in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects. Our audit included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, testing and evaluating the design and operating effectiveness of internal control based on the assessed risk, and performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
In our report dated March 18, 2013, we expressed an unqualified opinion that RadNet, Inc. and subsidiaries maintained, in all material respects, effective internal control over financial reporting as of December 31, 2012 based on the COSO criteria. Management has subsequently determined that a deficiency in controls relating to the accounting for income taxes existed as of the previous assessment date, and has further concluded that such deficiency represented a material weakness as of December 31, 2012. As a result, management has revised its assessment, as presented in Item 9A, “Report of Management on Internal Control over Financial Reporting”; to conclude that RadNet, Inc. and subsidiaries’ internal control over financial reporting was not effective as of December 31, 2012. Accordingly, our present opinion on the effectiveness of RadNet, Inc. and subsidiaries’ internal control over financial reporting as of December 31, 2012, as expressed herein, is different from that expressed in our previous report.
A material weakness is a deficiency, or combination of deficiencies, in internal control over financial reporting, such that there is a reasonable possibility that a material misstatement of the company’s annual or interim financial statements will not be prevented or detected on a timely basis. The following material weakness has been identified and included in management’s assessment. Management has identified a material weakness in controls related to the Company’s accounting for income taxes. We have also audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), the consolidated balances sheets of RadNet Inc. and subsidiaries as of December 31, 2012 and 2011, and the related consolidated statements of operations, comprehensive income (loss), equity deficit, and cash flows for each of the three years in the period ended December 31, 2012. This material weakness was considered in determining the nature, timing, and extent of audit tests applied in our audit of the 2012 consolidated financial statements and this report does not affect our report dated March 18, 2013, except for Note 1A, as to which the date is November 13, 2013, which expressed an unqualified opinion on those financial statements.
In our opinion, because of the effect of the material weakness described above on the achievement of the objectives of the control criteria, RadNet Inc. and subsidiaries has not maintained effective internal control over financial reporting as of December 31, 2012, based on the COSO criteria.
| /s/ Ernst & Young LLP |
Los Angeles, California
March 18, 2013, except for the effects of the material weakness described in the sixth paragraph as to which the date is November 13, 2013
| 107 |
| Item 9B. | Other Information |
None
PART III
| Item 10. | Directors, Executive Officers and Corporate Governance |
The information required by this Item 10 will be included under the captions “Election of Directors,” “Executive Officers,” “Board of Directors and Corporate Governance,” “Section 16(a) Beneficial Ownership Reporting Compliance” in our definitive Proxy Statement for the 2013 Annual Meeting of Stockholders to be filed with the SEC within 120 days after the end of our fiscal year (the “Proxy Statement”) and is incorporated herein by reference.
We have adopted a code of financial ethics applicable to our directors, officers and employees which is designed to deter wrongdoing and to promote:
| · | honest and ethical conduct; |
| · | full, fair, accurate, timely and understandable disclosure in reports and documents that we file with the SEC and in our other public communications; |
| · | compliance with applicable laws, rules and regulations, including insider trading compliance; and |
| · | accountability for adherence to the code and prompt internal reporting of violations of the code, including illegal or unethical behavior regarding accounting or auditing practices. |
You may obtain a copy of our Code of Financial Ethics on our website at www.radnet.com under Investors — Corporate Governance. The Audit Committee is responsible for reviewing the Code of Financial Ethics and amending as necessary. Any amendments will be disclosed on our website.
| Item 11. | Executive Compensation |
The information required by this Item 11 will be included under the captions “Compensation of Directors,” “Compensation of Executive Officers,” “Compensation Discussion and Analysis,” “Compensation Committee Interlocks and Insider Participation,” and “Compensation Committee Report “in the Proxy Statement and is incorporated herein by reference.
| Item 12. | Security Ownership of Certain Beneficial Owners and Management and Related Shareholder Matters |
The information required by this Item 12 will be included under the captions “Security Ownership of Certain Beneficial Owners and Management” and “Equity Compensation Plan Information” in the Proxy Statement and is incorporated herein by reference.
| Item 13. | Certain Relationships and Related Transactions, and Director Independence |
The information required by this Item 13 will be included under the captions “Certain Relationships and Related Party Transactions” and “Board of Directors and Corporate Governance” in the Proxy Statement and is incorporated herein by reference.
| Item 14. | Principal Accountant Fees and Services |
The information required by this Item 14 will be included under the caption “ Independent Registered Public Accounting Firm Fees” in the Proxy Statement and is incorporated herein by reference.
| 108 |
PART IV
| Item 15. Exhibits and Financial Statements Schedule | Page No. | |
| (a)(1) Financial Statements – The following financial statements are filed herewith: | ||
| Report of Independent Registered Public Accounting Firm | 52 | |
| Consolidated Balance Sheets | 53 | |
| Consolidated Statements of Operations | 54 | |
| Consolidated Statements of Comprehensive Income (Loss) | 55 | |
| Consolidated Statements of Equity Deficit | 56 | |
| Consolidated Statements of Cash Flows | 57 | |
| Notes to Consolidated Financial Statements | 58 to 93 | |
| Report of Independent Registered Public Accounting Firm | 94 | |
| Combined Balance Sheets of Certain RadNet, Inc. Affiliates | 95 | |
| Combined Statements of Income of Certain RadNet, Inc. Affiliates | 96 | |
| Combined Statements of Cash Flows of Certain RadNet, Inc. Affiliates | 97-98 | |
Notes to Combined Financial Statements |
99 | |
| (a)(2) Financial Statements Schedules |
| Schedules – The following financial statement schedules are filed herewith: | |
| Schedule II – Valuation and Qualifying Accounts |
All other schedules are omitted because they are not applicable or the required information is shown in the consolidated financial statements or notes thereto.
RADNET, INC. AND SUBSIDIARIES
SCHEDULE II – VALUATION AND QUALIFYING ACCOUNTS
| Balance at Beginning of Year | Additional Charges Against Income | Deductions from Reserve | Balance at End of Year | |||||||||||||
| Year Ended December 31, 2012 | ||||||||||||||||
| Accounts Receivable-Allowance for Bad Debts | $ | 15,688 | $ | 25,904 | $ | (24,905 | ) | $ | 16,687 | |||||||
| Year Ended December 31, 2011 | ||||||||||||||||
| Accounts Receivable-Allowance for Bad Debts | $ | 18,993 | $ | 22,339 | $ | (25,644 | ) | $ | 15,688 | |||||||
| Year Ended December 31, 2010 | ||||||||||||||||
| Accounts Receivable-Allowance for Bad Debts | $ | 12,951 | $ | 21,995 | $ | (15,953 | ) | $ | 18,993 | |||||||
| 109 |
(a)(3) Exhibits – The following exhibits are filed herewith or incorporated by reference herein:
| Exhibit No. | Description of Exhibit | ||
| 2.1 | Membership Interests Purchase Agreement dated September 7, 2010 by and among New Jersey Imaging Partners, Inc., RadNet, Inc., Progressive Health, LLC and the other parties named therein (incorporated by reference to exhibit filed with Form 8-K on January 7, 2011).† | ||
| 2.2 | Purchase Agreement dated September 7, 2010 by and between New Jersey Imaging Partners, Inc. and Progressive Medical Imaging of Rutherford, LLC (incorporated by reference to exhibit filed with Amendment No. 1 to Registration Statement on Form S-4 (File No. 333-169107)). † | ||
| 2.3 | Merger Agreement dated September 13, 2010 by and among RadNet Managed Imaging Services, Inc. INC Merger Sub, Inc. and Image Medical Corporation (incorporated by reference to exhibit filed with Amendment No. 1 to Registration Statement on Form S-4 (File No. 333-169107)).† | ||
| 2.4 | Stock Purchase Agreement dated November 7, 2011 by and between Radnet Management, Inc. and CML Healthcare Inc., and joined by RadNet, Inc. (incorporated by reference to exhibit filed with Form 8-K/A on January 18, 2012).† | ||
| 3.1 | Certificate of Incorporation of RadNet, Inc., a Delaware corporation (incorporated by reference to exhibit filed with Form 8-K on September 4, 2008). | ||
| 3.2 | Certificate of Amendment to Certificate of Incorporation of RadNet, Inc., a Delaware corporation, dated September 2, 2008 (incorporated by reference to exhibit filed with Form 8-K on September 4, 2008). | ||
| 3.3 | Bylaws of RadNet, Inc., a Delaware corporation (incorporated by reference to exhibit filed with Form 8-K on September 4, 2008). | ||
| 4.1 | Indenture, dated as of April 6, 2010, by and among Radnet Management, Inc., RadNet, Inc., the subsidiary guarantors thereunder, and U.S. Bank, National Association, as Trustee (incorporated by reference to exhibit filed with Form 8-K on April 6, 2010). | ||
| 4.2 | Form of Exchange 10 3/8% Senior Note (included in Exhibit 4.1). | ||
| 4.3 | Form of Original 10 3/8% Senior Note (included in Exhibit 4.1). | ||
| 4.4 | Registration Rights Agreement, dated April 6, 2010, by and among Radnet Management, Inc., RadNet, Inc., the subsidiary guarantors thereunder, and Deutsche Bank Securities Inc. and Barclays Capital Inc., as representatives of the initial purchasers (incorporated by reference to exhibit filed with Form 8-K on April 6, 2010). | ||
| 4.5 | Supplemental Indenture, dated as of July 6, 2010, by and between Advanced Radiology, LLC and U.S. Bank, National Association, as Trustee (incorporated by reference to exhibit filed with Registration Statement on Form S-4 (File No. 333-169107)). | ||
| 4.6 | Supplemental Indenture, dated as of August 19, 2010 by and between Health Diagnostics of New Jersey, LLC and U.S. Bank, National Association, as Trustee (incorporated by reference to exhibit filed with Registration Statement on Form S-4 (File No. 333-169107)). | ||
| 4.7 | Supplemental Indenture, dated as of January 10, 2011, by and between Image Medical Corporation and U.S. Bank, National Association, as Trustee (incorporated by reference to exhibit filed with Amendment No. 1 to Registration Statement on Form S-4 (File No. 333-169107)). | ||
| 4.8 | Supplemental Indenture, dated as of January 10, 2011, by and between eRAD, Inc. and U.S. Bank, National Association, as Trustee (incorporated by reference to exhibit filed with Amendment No. 1 to Registration Statement on Form S-4 (File No. 333-169107)). | ||
| 4.9 | Supplemental Indenture, dated as of January 10, 2011, by and between East Bergen Imaging, LLC and U.S. Bank, National Association, as Trustee (incorporated by reference to exhibit filed with Amendment No. 1 to Registration Statement on Form S-4 (File No. 333-169107)). |
| 110 |
| 4.10 | Supplemental Indenture, dated as of January 10, 2011, by and between Progressive Medical Imaging of Bloomfield, LLC and U.S. Bank, National Association, as Trustee (incorporated by reference to exhibit filed with Amendment No. 1 to Registration Statement on Form S-4 (File No. 333-169107)). | ||
| 4.11 | Supplemental Indenture, dated as of January 10, 2011, by and between Progressive Medical Imaging of Hackensack, LLC and U.S. Bank, National Association, as Trustee (incorporated by reference to exhibit filed with Amendment No. 1 to Registration Statement on Form S-4 (File No. 333-169107)). | ||
| 4.12 | Supplemental Indenture, dated as of January 10, 2011, by and between Progressive Medical Imaging of Union City, LLC and U.S. Bank, National Association, as Trustee (incorporated by reference to exhibit filed with Amendment No. 1 to Registration Statement on Form S-4 (File No. 333-169107)). | ||
| 4.13 | Supplemental Indenture, dated as of January 10, 2011, by and between Progressive X-Ray of Englewood, LLC and U.S. Bank, National Association, as Trustee (incorporated by reference to exhibit filed with Amendment No. 1 to Registration Statement on Form S-4 (File No. 333-169107)). | ||
| 4.14 | Supplemental Indenture, dated as of January 10, 2011, by and between Progressive X-Ray of Kearney, LLC and U.S. Bank, National Association, as Trustee (incorporated by reference to exhibit filed with Amendment No. 1 to Registration Statement on Form S-4 (File No. 333-169107)). | ||
| 4.15 | Supplemental Indenture, dated as of January 10, 2011, by and between Imaging On Call, LLC and U.S. Bank, National Association, as Trustee (incorporated by reference to exhibit filed with Amendment No. 1 to Registration Statement on Form S-4 (File No. 333-169107)). | ||
| 4.16 | Supplemental Indenture, dated as of January 10, 2011, by and between Advanced NA, LLC and U.S. Bank, National Association, as Trustee (incorporated by reference to exhibit filed with Amendment No. 1 to Registration Statement on Form S-4 (File No. 333-169107)). | ||
| 4.17 | Standstill Agreement, dated as of August 30, 2011, by and between RadNet, Inc. and RMCP LLC (incorporated by reference to exhibit filed with Amendment No. 1 to Schedule 13D for Red Mountain Capital Partners LLC). | ||
| 4.18 | Supplemental Indenture, dated as of November 21, 2011, among Raven Holdings U.S., Inc., Radnet Management, Inc., RadNet, Inc., U.S. Bank and the other parties named therein (incorporated by reference to exhibit filed with Form 8-K on November 22, 2011). | ||
| 4.19 | Supplemental Indenture, dated as of November 21, 2011, among American Radiology Services of Delaware, Inc., Radnet Management, Inc., RadNet, Inc., U.S. Bank and the other parties named therein (incorporated by reference to exhibit filed with Form 8-K on November 22, 2011). | ||
| 4.20 | Supplemental Indenture, dated as of November 21, 2011, among CML HealthCare Rhode Island LLC, Radnet Management, Inc., RadNet, Inc., U.S. Bank and the other parties named therein (incorporated by reference to exhibit filed with Form 8-K on November 22, 2011). | ||
| 4.21 | Supplemental Indenture, dated as of November 21, 2011, among American Radiology Services LLC, Radnet Management, Inc., RadNet, Inc., U.S. Bank and the other parties named therein (incorporated by reference to exhibit filed with Form 8-K on November 22, 2011). | ||
| 4.22 | Supplemental Indenture, dated as of November 21, 2011, among Radiology Alliance Delivery System, LLC, Radnet Management, Inc., RadNet, Inc., U.S. Bank and the other parties named therein (incorporated by reference to exhibit filed with Form 8-K on November 22, 2011). | ||
| 10.1 | Credit and Guaranty Agreement, dated October 10, 2012, by and among Radnet Management, Inc., RadNet, Inc., the guarantors thereunder, General Electric Capital Corporation, Deutsche Bank Securities, Inc., RBC Capital Markets and Barclays Bank PLC (incorporated by reference to exhibit filed with Form 8-K on October 12, 2012). | ||
| 10.2 | Pledge and Security Agreement, dated October 10, 2012, by and among Radnet Management, Inc., RadNet, Inc., the guarantors thereunder, and Barclays Bank PLC (incorporated by reference to exhibit filed with Form 8-K on October 12, 2012). | ||
| 10.3 | Form of Trademark Security Agreement by and among the guarantors thereunder and Barclays Bank PLC (filed as an exhibit to the Pledge and Security Agreement, dated October 10, 2012, by among the guarantors thereunder and Barclays Bank PLC, included as Exhibit 10.2). |
| 111 |
| 10.4 | 2000 Incentive Stock Option Plan (as amended) (incorporated by reference to exhibit filed with the Form 10-K for the year ended October 31, 2003).* | ||
| 10.5 | 2006 Equity Incentive Plan, amended and restated as of April 19, 2011 (incorporated by reference to exhibit filed with Form S-8 registration statement on August 15, 2011).* | ||
|
10.6
10.7 |
Form of Stock Option Agreement for the 2006 Equity Incentive Plan (incorporated by reference to exhibit filed with Form S-8 registration statement on August 15, 2011).* Form of Restricted Stock Award for the 2006 Equity Incentive Plan (incorporated by reference to exhibit filed with Form 10-Q for the quarter ended March 31, 2012).* | ||
| 10.8 | Form of Warrant recharacterized as under the 2006 Equity Incentive Plan – Form A (incorporated by reference to exhibit filed with Form 10-Q for the quarter ended June 30, 2008).* | ||
| 10.9 | Form of Warrant recharacterized as under the 2006 Equity Incentive Plan – Form B (incorporated by reference to exhibit filed with Form 10-Q for the quarter ended June 30, 2008).* | ||
| 10.10 | Form of Indemnification Agreement between the registrant and each of its officers and directors (incorporated by reference to exhibit filed with Form 10-Q for the quarter ended March 31, 2008).* | ||
| 10.11 | Employment Agreement dated as of June 12, 1992 with Howard G. Berger, M.D. (incorporated by reference to exhibit filed with an amendment to Form 8-K report for June 12, 1992).* | ||
| 10.12 | Amendment to Employment Agreement dated January 30, 2004 with Howard G. Berger, M.D. (incorporated by reference to exhibit filed with Form 10-Q for the quarter ended January 31, 2004).* | ||
| 10.13 | Employment Agreement dated as of April 16, 2001 with Jeffrey L. Linden (incorporated by reference to exhibit filed with Form 10-K for the year ended October 31, 2001).* | ||
| 10.14 | Amendment to Employment Agreement dated January 30, 2004 with Jeffrey L. Linden (incorporated by reference to exhibit filed with Form 10-Q for the quarter ended January 31, 2004).* | ||
| 10.15 | Employment Agreement dated as of May 1, 2001 with Norman R. Hames (incorporated by reference to exhibit filed with Form 10-K for the year ended October 31, 2001).* | ||
| 10.16 | Amendment to Employment Agreement dated January 30, 2004 with Norman R. Hames (incorporated by reference to exhibit filed with Form 10-Q for the quarter ended January 31, 2004).* | ||
| 10.17 | Employment Agreement with Mark Stolper effective January 1, 2009 (incorporated by reference to exhibit filed with Form 10-K for the year ended December 31, 2009).* | ||
| 10.18 | Retention Agreement with Stephen Forthuber dated November 15, 2006 (incorporated by reference to exhibit filed with Form 10-K/T for the year ended December 31, 2006).* | ||
| 10.19 | Amended and Restated Management and Service Agreement between Radnet Management, Inc. and Beverly Radiology Medical Group III dated January 1, 2004 (incorporated by reference to exhibit filed with Form 10-K for the year ended October 31, 2003). | ||
| 14.1 | Code of Financial Ethics (incorporated by reference to exhibit filed with Form 10-K for the year ended October 31, 2003). | ||
| 21.1 | List of Subsidiaries. | ||
| 23.1 | Consent of Registered Independent Public Accounting Firm. | ||
| 23.2 | Consent of Registered Independent Public Accounting Firm. | ||
| 24.1 | Power of Attorney (included on signature page attached hereto). |
| 112 |
| 31.1 | CEO Certification pursuant to Section 302. | ||
| 31.2 | CFO Certification pursuant to Section 302. | ||
| 32.1 | CEO Certification pursuant to Section 906. | ||
| 32.2 | CFO Certification pursuant to Section 906. | ||
| 101.INS | XBRL Instance Document | ||
| 101.SCH | XBRL Schema Document | ||
| 101.CAL | XBRL Calculation Linkbase Document | ||
| 101.LAB | XBRL Label Linkbase Document | ||
| 101.PRE | XBRL Presentation Linkbase Document | ||
| 101.DEF | XBRL Definition Linkbase Document |
* Indicates management contract or compensatory plan.
†Certain schedules to this exhibit have been omitted in accordance with Regulation S-K Item 601(b)(2). The company agrees to furnish supplementally a copy of all omitted schedules to the SEC upon its request.
| 113 |
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the Registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
| RADNET, INC. | |||
| Date: November 13 , 2013 | /s/ HOWARD G. BERGER, M.D . | ||
| Howard G. Berger, M.D., President, | |||
| Chief Executive Officer and Director | |||
POWER OF ATTORNEY
KNOW ALL PERSONS BY THESE PRESENTS, that each person whose signature appears below hereby severally constitutes and appoints Howard G. Berger, M.D. and Mark D. Stolper, and each of them, his true and lawful attorney-in-fact and agent, with full power of substitution and re-substitution for him and in his name, place and stead, in any and all capacities to sign any and all amendments to this report, and to file the same, with all exhibits thereto, and other documents in connection therewith, with the SEC, granting unto said attorney-in-fact and agents, and each of them, full power and authority to do and perform each and every act and thing requisite or necessary fully to all intents and purposes as he might or could do in person, hereby ratifying and confirming all that each said attorneys-in-fact and agents or any of them or their or his substitute or substitutes, may lawfully do or cause to be done by virtue hereof.
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of registrant in the capacities and on the dates indicated.
| By | /s/ HOWARD G. BERGER, M.D. |
| Howard G. Berger, M.D., Director, Chief Executive Officer and President | |
| Date: November 13, 2013 | |
| By | /s/ MARVIN S. CADWELL |
| Marvin S. Cadwell, Director | |
| Date: November 13, 2013 | |
| By | /s/ JOHN V. CRUES, III, M.D. |
| John V. Crues, III, M.D., Director | |
| Date: November 13, 2013 | |
| By | /s/ NORMAN R. HAMES |
| Norman R. Hames, Director | |
| Date: November 13, 2013 | |
| By | /s/ DAVID L. SWARTZ |
| David L. Swartz, Director | |
| Date: November 13, 2013 | |
| By | /s/ LAWRENCE L. LEVITT |
| Lawrence L. Levitt, Director | |
| Date: November 13, 2013 | |
| By | /s/ MICHAEL L. SHERMAN, M.D. |
| Michael L. Sherman, M.D., Director | |
| Date: November 13, 2013 | |
| By | /s/ MARK D. STOLPER |
| Mark D. Stolper, Chief Financial Officer (Principal Accounting Officer) | |
| Date: November 13, 2013 | |
| 114 |