Attached files
| file | filename |
|---|---|
| 8-K - FORM 8-K - INFINITY PHARMACEUTICALS, INC. | d395797d8k.htm |
 Building a Fully Integrated
Biopharmaceutical Company
August 14, 2012
Exhibit 99.1 |
 Forward Looking Statements
2
•
This presentation contains forward-looking statements within the meaning of The
Private Securities Litigation Reform Act of 1995. •
These statements involve risks and uncertainties that could cause actual results to
be materially different from historical results or from any future results
expressed or implied by such forward-looking statements. •
Such forward-looking statements include those regarding the expectation that
Infinity will begin a Phase 2a study of IPI-145 in patients with
rheumatoid arthritis during the fourth quarter of 2012, the expectation that
Infinity’s Phase 1 trial of IPI-145 in patients with advanced hematologic
malignancies will expand to additional cohorts (T-cell lymphomas, diffuse large
B-cell lymphoma, acute lymphocytic leukemia and myeloproliferative
neoplasms)
once
the
maximum
tolerated
dose
is
determined,
the
expectation
that
Infinity
will
present
data
from
its
Phase
1
trial
of IPI-145 in patients with advanced hematologic malignancies in the second
half of 2012, the expectation that Infinity will present additional details
from its Phase 1 study in healthy volunteers at a medical meeting in the second half of 2012, the expectation that enrollment of the trial
evaluating retaspimycin HCl and docetaxel will complete this fall and that Infinity
will report data from this trial in the first half of 2013, the expectation
that Infinity will present top-line data from the dose escalation portion of its Phase 1b/2 trial evaluating retaspimycin HCl and
everolimus,
potential first-in-class and best-in-class opportunities, market
size projections, the expectation that Infinity will receive $27.5 million
from
the
planned
equity
investment
by
Purdue
Pharma
L.P.
and
the
expectation
that
Infinity’s
cash
runway
will
extend
into
2014.
•
For example, there can be no guarantee that Infinity will be able to complete the
transactions contemplated in the securities purchase agreement with
Purdue Pharma L.P.
and certain associated entities, that any product candidate Infinity is developing
will successfully complete necessary preclinical and clinical development
phases or that development of any of Infinity’s product candidates will continue. Further, there can be no
guarantee that any positive developments in Infinity’s product portfolio will
result in stock price appreciation. Management’s expectations could
also be affected by risks and uncertainties relating to: Infinity’s results of
clinical trials and preclinical studies, including subsequent analysis of
existing
data
and
new
data
received
from
ongoing
and
future
studies;
the
content
and
timing
of
decisions
made
by
the
U.S.
FDA
and
other
regulatory authorities, investigational review boards at clinical trial sites and
publication review bodies; Infinity’s ability to enroll patients in its
clinical trials; unplanned cash requirements and expenditures, including in
connection with business development activities; development of agents by
Infinity’s competitors for diseases in which Infinity is currently developing its product candidates; and Infinity’s ability to obtain, maintain
and enforce patent and other intellectual property protection for any product
candidates it is developing. •
These
and
other
risks
which
may
impact
management’s
expectations
are
described
in
greater
detail
under
the
caption
“Risk
Factors”
included
in
Infinity’s
quarterly
report
on
Form
10-Q
for
the
quarter
ended
June
30,
2012,
filed
with
the
Securities
and
Exchange
Commission
on
August
7,
2012.
•
Further, any forward-looking statements contained in this presentation speak
only as of the date hereof, and Infinity expressly disclaims any obligation
to update any forward-looking statements, whether as a result of new information, future events or otherwise. |
 Building a Fully Integrated
Biopharmaceutical Company
Focused
pipeline
Near-term
value
inflection
points
Global rights
to all products
Substantial
market
opportunities
3
Sustainable Model for Value Creation |
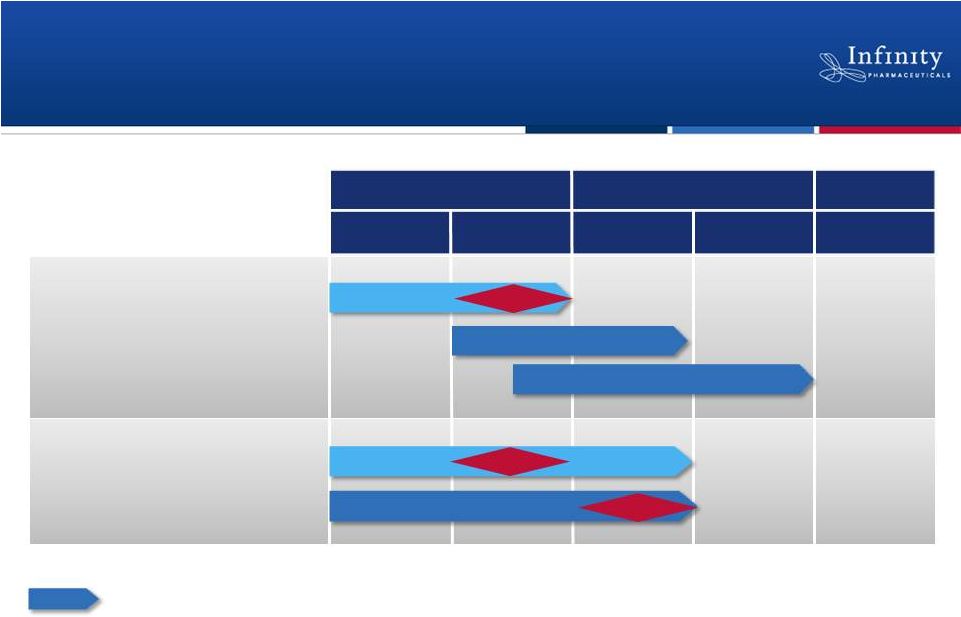 Pipeline with Multiple Near-Term Data
Readouts
4
1H’12
1H’13
2H’13
2H’12
PI3K: IPI-145
NSCLC (mKRAS)
NSCLC (Heavy smokers)
Hematologic Malignancies
2012
2013
2014+
Hsp90: Retaspimycin HCl
Asthma
Rheumatoid arthritis
Randomized, double-blind, placebo-controlled trial
Data
Phase 2
Data
Phase
1
Data
Phase 2a
Phase 2a
Phase 1b/2 |
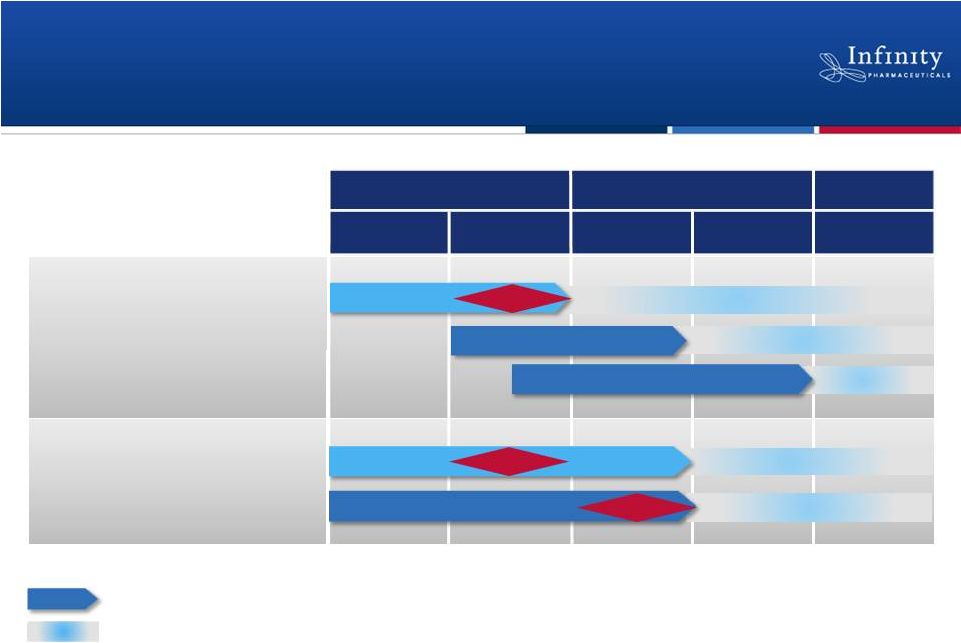 Pipeline with Multiple Near-Term Data
Readouts
5
1H’12
1H’13
2H’13
2H’12
PI3K: IPI-145
NSCLC (mKRAS)
NSCLC (Heavy smokers)
Hematologic Malignancies
2012
2013
2014+
Hsp90: Retaspimycin HCl
Asthma
Rheumatoid arthritis
Randomized, double-blind, placebo-controlled trial
Phase 3
Phase 3
Data
Data
Expansions >>> Phase 2
Data
Phase 2
Phase 2
Next step and approximate timing, if data are positive.
Phase
1
Phase 1b/2
Phase 2
Phase 2a
Phase 2a |
 IPI-145:
First
PI3K-
,
Inhibitor
in Clinical Development |
 IPI-145: First-
and Best-in-Class Potential
Profile:
Therapeutic Focus:
Intellectual Property:
Commercial Rights:
7
•
Dual development path in hematologic malignancies and inflammation
•
Composition patent issued in U.S.; pending broadly ex-U.S.
•
U.S. patent expiry: 2030, excluding patent term extension
•
Global rights to IPI-145
•
Potent oral PI3K-
inhibitor |
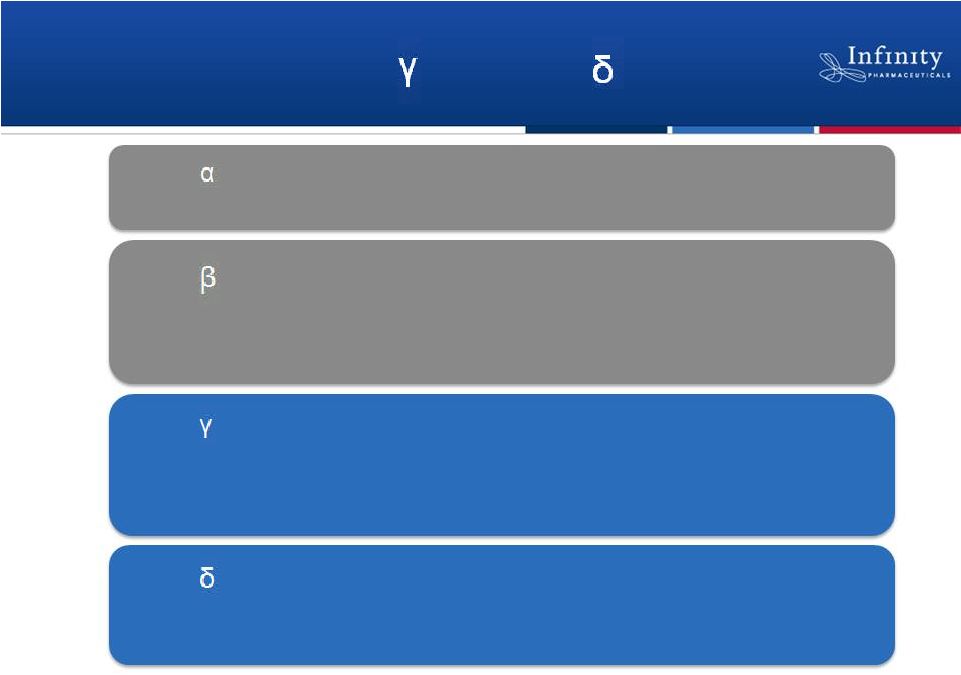 IPI-145 Targets PI3K-
and PI3K-
•
Insulin signaling
•
Mutated in solid tumors
PI3K-
•
Platelet activation
•
Insulin signaling
•
Neutrophil function
•
Solid tumors
PI3K-
•
Mast cell activation
•
Innate immune function
•
Immune cell trafficking (chemokines)
•
Solid tumors
PI3K-
•
B-cell activation and function
•
T-cell activation and function
•
Fc receptor signaling in mast cells
PI3K-
8
Ali
et
al.,
J
Immunol
2008;
Ferrandi
et
al.,
JPET,
2007;
Fruman,
D.,
Current
Opinion
in
Immunology,
2004;
Hirsch
et
al.,
Journal
of
Endocrinology,
2007;
Kulkarni
et
al.,
Sci
Signaling
2011;
Ni
et
al.,
Cancer
Disc,
2012;
Schmid
et
al.,
Cancer
Cell,
2011 |
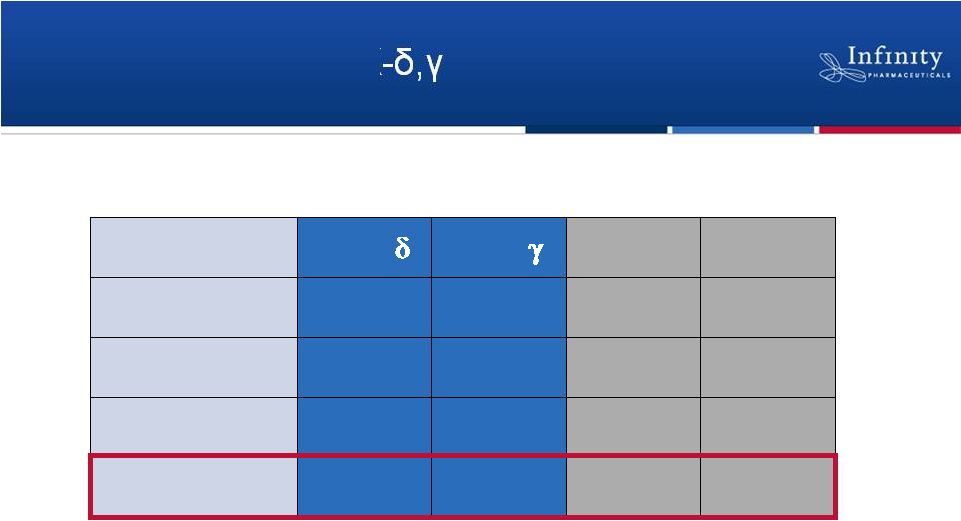 IPI-145: A Potent PI3K Inhibitor
PI3K-
PI3K-
PI3K-ß
PI3K-a
k
off
(h
-1
)
0.9
3.0
15.5
> 1800
k
on
(10
6
M
-1
s
-1
)
15.2
3.4
2.7
4.2
t
1/2
(min)
46
14
2.7
0.1
K
i
=(k
off
/k
on
)
23 pM
243 pM
1,564 pM
25,900 pM
9
Palombella. New York Academy of Sciences 2012. |
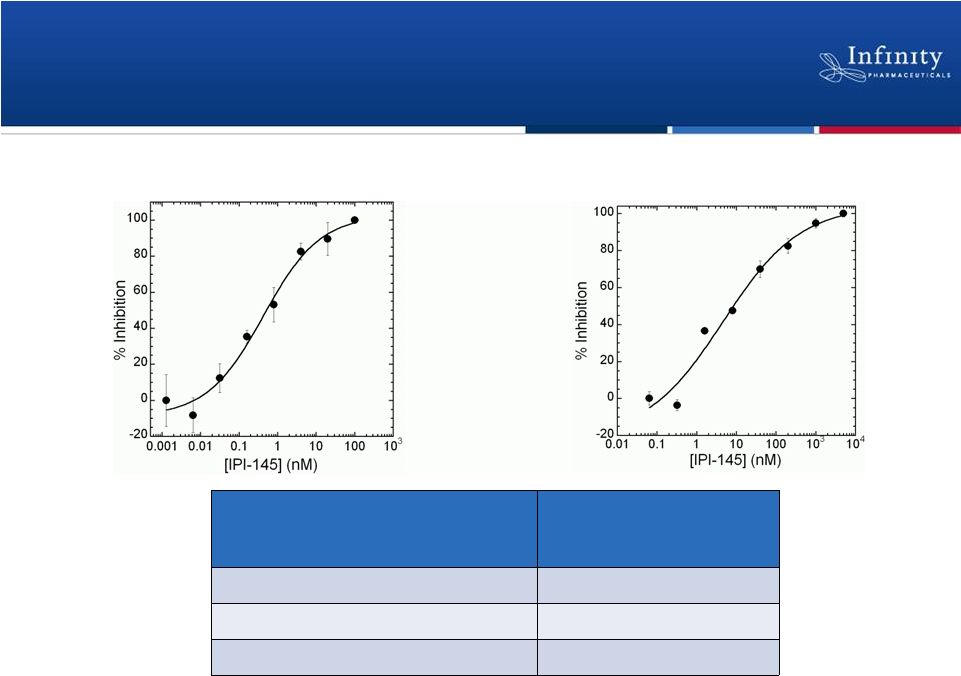 IPI-145 Inhibits B-cell and T-cell Proliferation
Functional Cellular Activity
IPI-145 (EC
50
)
Murine B-cell proliferation
0.5 nM
Human B-cell proliferation
0.5 nM
Human T-cell proliferation
9.5 nM
Human B-cell
proliferation Human T-cell
proliferation Anti-IgM and anti-CD40 stimulation
Concanavalin A stimulation
10
Palombella. New York Academy of Sciences 2012. |
 IPI-145: First-in-Class Opportunity in
Inflammatory Diseases |
 Completed Phase 1 Trial in Healthy Subjects
•
Phase 1 single ascending and multiple ascending dose study
completed
–
Proportional increase in plasma exposure with increased dose
–
Rapid, dose dependent, and durable inhibition of ex vivo basophil
activation at all dose levels
–
Well tolerated
•
Abstracts submitted for data presentation at American College of
Rheumatology Annual Scientific Meeting in Washington, D.C. in
November
12
1
June 27, 2012 Infinity press release; ClinicalTrials.gov NCT01549106.
1 |
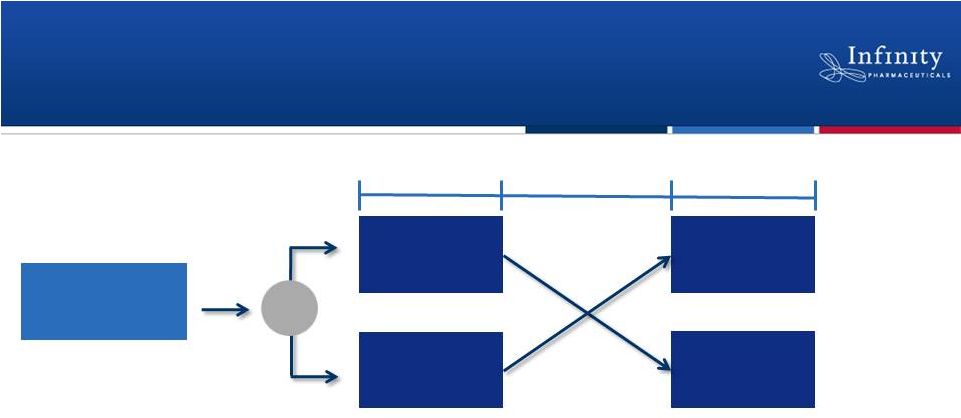 Initiated Phase 2a Trial in Asthma
•
Double-blind, randomized, placebo-controlled, crossover study
•
Approximately 30 subjects with mild, allergic asthma
•
Multiple-dose study designed to evaluate safety, PK, and activity
–
Efficacy endpoints include FEV
1
, markers of inflammation
and airway hyperresponsiveness
13
~30 subjects
IPI-145
Placebo
IPI-145
Placebo
14 Days
14 Days
7-12 Day Washout
ClinicalTrials.gov NCT01653756.
R |
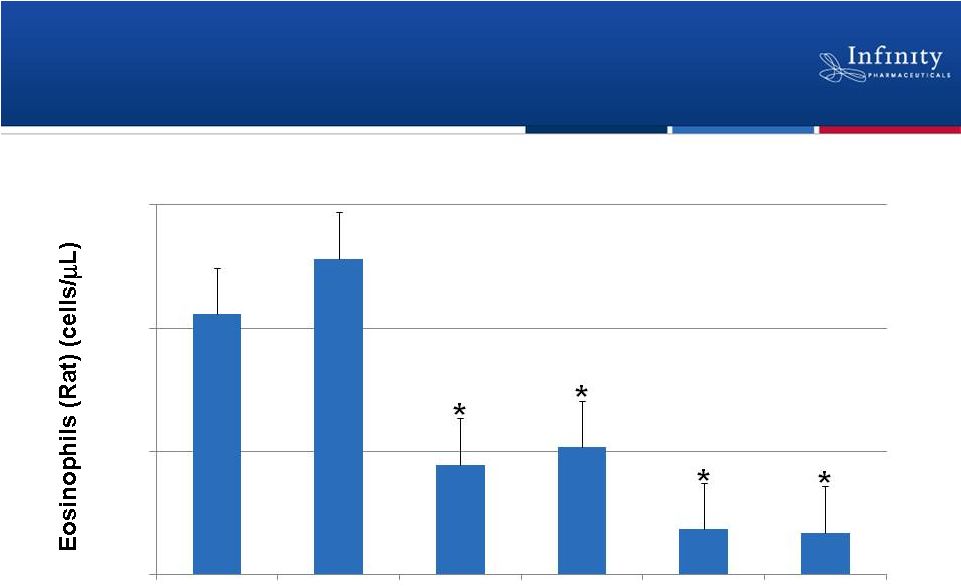 IPI-145 Inhibits Leukocyte Migration in
Preclinical Allergic Asthma Model
*p <0.05 compared to vehicle
14
0.1 mg/kg
IPI-145
0.3 mg/kg
IPI-145
1.0 mg/kg
IPI-145
10 mg/kg
IPI-145
Palombella. New York Academy of Sciences 2012.
0
250
500
750
Vehicle
10 mg/kg
Dexamethasone |
 Planning Phase 2a Trial in RA
•
Phase 2a expected to begin in 4Q’12
–
Double-blind, randomized, placebo-controlled
–
Designed to evaluate safety and activity of multiple doses
of IPI-145
15
~150 patients
Multiple doses of IPI-145
Placebo
R |
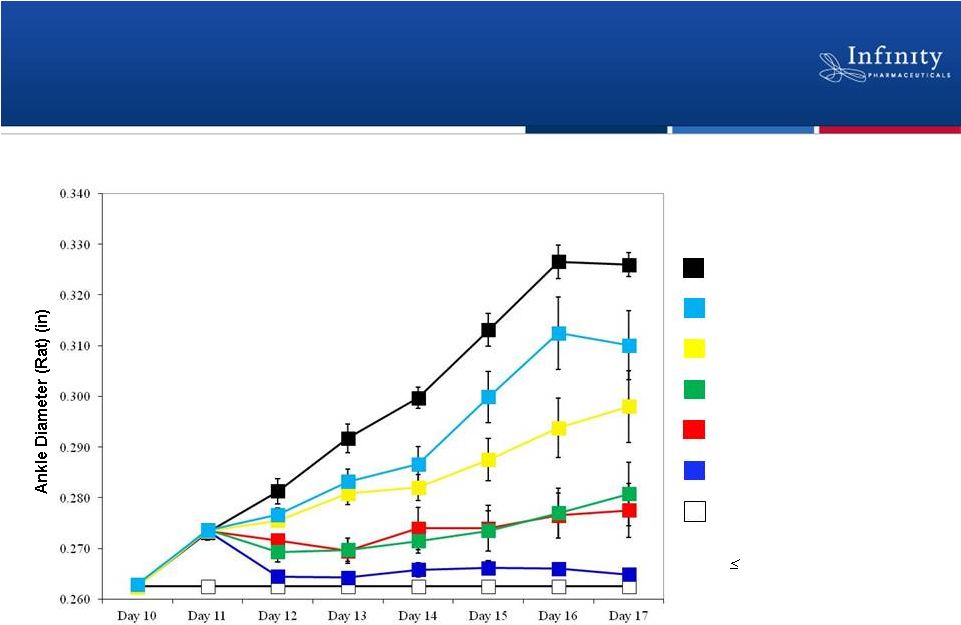 IPI-145
Demonstrates Dose-Dependent Effect in Preclinical Model of Collagen Induced Arthritis
n=4/
n=8/Treatment Group
Vehicle
0.1 mg/kg IPI-145 (*day 14)
0.5 mg/kg IPI-145 (*day 13-17)
5.0 mg/kg IPI-145 (*day 12-17)
10.0 mg/kg etanercept (*day 12-17)
10.0 mg/kg IPI-145 (*day 12-17)
Normal control (*day 11-17)
*p
0.05
16
Palombella. New York Academy of Sciences 2012.
Normal Controls |
 IPI-145: First-
and Best-in-Class
Opportunities in Hematologic
Malignancies |
 Phase 1 Dose Escalation Trial in Advanced
Hematologic Malignancies
18
Dose-escalation observations
•
Confirmed
investigator
assessments
of
clinical
response
at
the
•
Generally
well
tolerated
to
date
•
Expect
to
present
data
at
a
medical
meeting
in
2H’12
1
July 18, 2012 Infinity press release; ClinicalTrials.gov NCT01476657.
25 mg BID expansion
•
Chronic
lymphocytic
leukemia
•
Indolent
non-Hodgkin’s
lymphoma
•
Mantle
cell
lymphoma
Ongoing
Dose escalation
Cohort expansions at MTD
•
Diffuse
large
B-cell
lymphoma
•
T-cell
lymphomas
•
Acute
lymphocytic
leukemia
•
Myeloproliferative
neoplasms
1
lowest dose levels, including 15 mg BID and less
1 |
 Phase 1 Dose Escalation Trial in Advanced
Hematologic Malignancies
Ongoing
Dose escalation
19
Byrd
et
al,
ASCO
2012;
Fowler
et
al,
ASH
2010;
Furman
et
al,
ASCO
2012;
Furman
et
al,
ASCO
2010;
Jaglowski,
et
al,
ASCO
2012;
Kahl
et
al
ASH
2010;
O’Brien et al, ASCO 2012; O’Brien et al, ASH 2011; Sharman et al, ASH
2011; Staudt et al, ASH 2011; de Vos et al, ASH 2011; Wang et al, ASH 2011.
Malignancy
Chronic lymphocytic leukemia
Indolent non-Hodgkin’s lymphoma
Mantle cell lymphoma
Observed Clinical Activity
PI3K-
inhibitor
BTK inhibitor
+ +
+ +
+ +
+/-
+/-
+
25 mg BID expansion
•
Chronic lymphocytic leukemia
•
Indolent non-Hodgkin’s lymphoma
•
Mantle cell lymphoma
Cohort expansions at MTD
•
Diffuse large B-cell lymphoma
•
T-cell lymphomas
•
Acute lymphocytic leukemia
•
Myeloproliferative neoplasms
|
 Phase 1 Dose Escalation Trial in Advanced
Hematologic Malignancies
20
1
BTK not expressed in T-cells
Furman et al ASCO 2010; Staudt et al ASH 2011.
Ongoing
Dose escalation
•
Diffuse large B-cell lymphoma
•
T-cell lymphomas
•
Acute lymphocytic leukemia
•
Myeloproliferative neoplasms
25 mg BID expansion
•
Chronic lymphocytic leukemia
•
Indolent non-Hodgkin’s lymphoma
•
Mantle cell lymphoma
Malignancy
Observed Clinical Activity
PI3K-
inhibitor
BTK inhibitor
Diffuse large B-
cell lymphoma
Not explored
Not explored
Acute lymphocytic leukemia
Not explored
Myeloproliferative neoplasms
Not explored
Not explored
T-cell lymphomas
+
(10 pts)
-
Not explored
1
Cohort expansions at MTD |
 21
PI3K Franchise: Potentially First-in-Class
and Best-in-Class Opportunities
RA
2
5.2M
Other
Multiple Large Opportunities
Heme
Malignancies
>600,000
Severe Asthma
3
7.1M
1
1
Decision Resources, Non-
Hodgkin’s Lymphoma, Apr 2011.
2
Decision Resources Immune and
Inflammatory Disorders Study –
Rheumatoid Arthritis, May 2012.
3
Decision Resources Immune and
Inflammatory Disorders Study –
Asthma Dec 2011.
Prevalence in G7 regions: US, UK,
IT, DE, ES, FR, JP. |
 Retaspimycin HCl (IPI-504):
Potent, Selective Inhibitor of Heat
Shock Protein 90 (Hsp90) |
 Retaspimycin HCl: Addressing Unmet Need
in NSCLC
Profile:
Therapeutic Focus:
Intellectual Property:
Commercial Rights:
23
•
Selective and potent Hsp90 inhibitor
•
Non-small cell lung cancer (NSCLC), with robust biomarker strategy
•
Composition and methods patents issued broadly worldwide
•
U.S. patent expiry: 2025, excluding patent term extension
•
Global rights to retaspimycin HCl |
 Hsp90 Plays an Important Role in Cancer
Cell Survival
Function of Hsp90
•
Chaperone necessary for stability
and function, to maintain protein
homeostasis
Function of Hsp90 in Cancer Cells
•
Many oncoproteins are hyper-
dependent on Hsp90 for function
•
Hsp90 is elevated in cancer cells
and buffers cancer specific stress
ATP
Retaspimycin HCl
Oncoprotein
Hsp90
24 |
 Phase 2 Trial in NSCLC Patients with a
Smoking History
•
Randomized, double-blind, placebo-controlled trial
•
Anticipate enrollment completion Fall 2012 and data 1H’13
25
ClinicalTrials.gov NCT01362400.
Smokers
w/ 2
nd
-
or 3
rd
-line
NSCLC
(docetaxel naïve)
N = ~210
R
Docetaxel +
Retaspimycin HCl
(N = ~105)
Follow-up for OS
Docetaxel +
placebo
(N = ~105)
Follow-up for OS
–
Co-primary endpoints: Overall survival in total population and squamous
cell –
Secondary endpoints: Predictive biomarkers, progression free survival,
overall response rate |
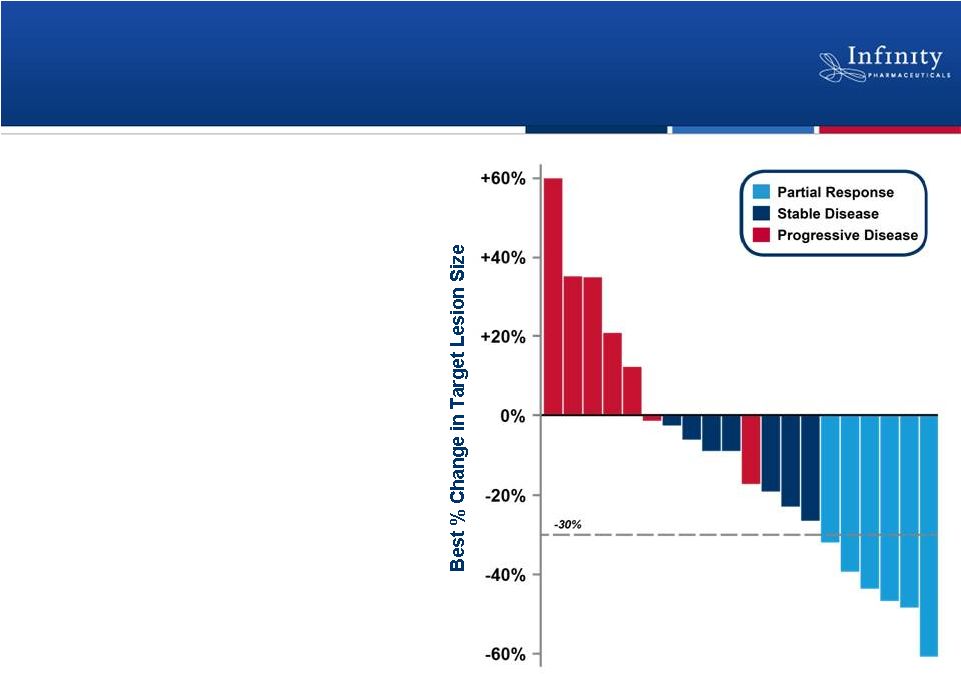 Phase 1b Trial: Clinically Active in
Combination with Docetaxel
26
•
Partial response in 6 patients
(ORR = 26%)
•
Stable disease in 7 patients
•
Well tolerated
–
No unexpected or overlapping
toxicities
–
No dose reductions or
discontinuations due to liver
function tests
–
No significant visual
disturbances
Riely et al., ASCO 2011.
PR
PR
PR
PR
PR
PR
Patients (N = 20) |
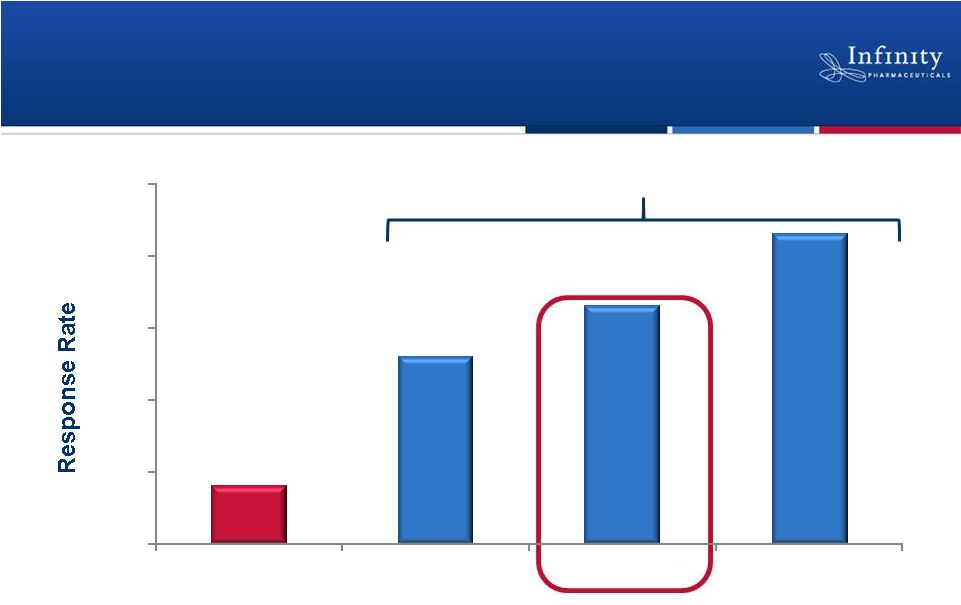 Phase 1b Trial: Responses Observed in
Patients with Historically Poor Prognoses
27
*Hanna et al, J Clin Oncol, 22:1589-97.
Riely et al., ASCO 2011.
8%
26%
33%
43%
0%
10%
20%
30%
40%
50%
Historical 2nd-line
Docetaxel*
NSCLC patients in
trial (N=23)
Smokers (N=18)
Squamous Cell
Carcinoma (N=7)
Patient Populations
Retaspimycin HCl Plus Docetaxel: Response Rate |
 Phase 1b/2 Trial in NSCLC Patients
with mKRAS
Determine
recommended
Phase 2 dose in
mKRAS NSCLC
•
Small, open-label exploratory trial with option for expansion
–
Neither drug active as single agent in these patients
–
Primary efficacy endpoint: Response rate
•
Topline data from dose-escalation portion of trial anticipated 2H’12
•
Strong preclinical rationale: Evidence of substantial tumor regression in a
NSCLC model*
Expansion
Phase 1b
Phase 2
ClinicalTrials.gov NCT01427946; *De Raedt et al., 2011; Cancer Cell
13;20(3):400-13. Retaspimycin HCl
+ everolimus
(N = 12)
Retaspimycin HCl
+ everolimus
(N = additional 23)
28 |
 Retaspimycin HCl: Significant Commercial
Potential
Current NSCLC market is ~ $4.0B and is projected to grow to $6.3B in 2019*
*Decision Resources NSCLC Pharmacor Report, March 2011. G7 regions: US, UK, IT, DE,
ES, FR, JP Roberts et al., 2010; J Clin Oncol
28(31):4769-4777. Janjigian et al., 2010; Cancer
116(3):670-675.
29
Patient
Population
% of Overall
NSCLC
Population
Number of
Patients
Number of
Stage IIIb/IV
Patients
Heavy smokers
70%
~291,000
~180,000
Squamous cell
35%
~145,000
~90,000
KRAS mutant
30%
~125,000
~80,000 |
 2012 Financial Highlights
•
$104.6M in cash as of June 30, 2012 (unaudited)
–
Net proceeds of approximately $83M from public equity offering
–
Anticipate
additional
$27.5M
in
cash
from
planned
sale
of
equity
to
Purdue
1
•
Cash runway into 2014*
30
1
Subject to Hart-Scott-Rodino clearance and satisfaction of other closing
conditions. *
Includes
proceeds
from
equity
offering
and
planned
$27.5M
equity
investment
by
Purdue,
exclusive of
additional funding or business development activities and based on Infinity’s
current operating plans. |
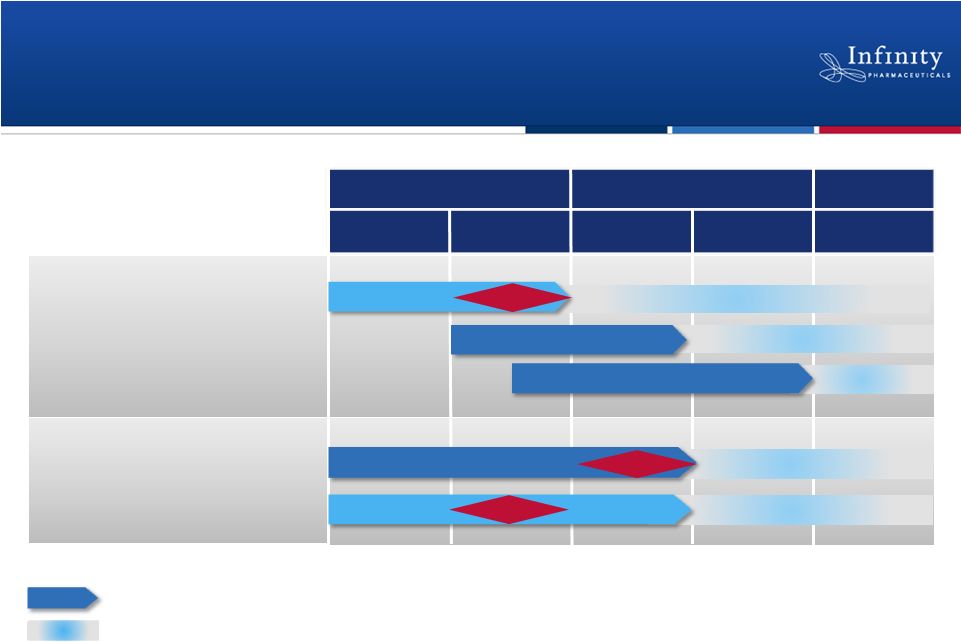 Pipeline with Multiple Near-Term Data
Readouts
31
PI3K: IPI-145
NSCLC (mKRAS)
Hematologic Malignancies
2012
2013
2014+
Hsp90: Retaspimycin HCl
Rheumatoid arthritis
Randomized, double-blind, placebo-controlled trial
Next step and approximate timing, if data are positive.
Phase 3
Phase 3
Expansions >>> Phase 2
Phase 2
Phase 2
1H’12
1H’13
2H’13
2H’12
Asthma
Phase 1b/2
Data
Phase
1
Phase 2a
Phase 2a
Data
Data
Phase
2
NSCLC (Heavy smokers) |
 Building a Fully Integrated
Biopharmaceutical Company
August 14, 2012 |
 Third Party Obligations
33
Millennium
•
Up to $21M remaining in pre-NDA filing milestones for two distinct product
candidates
•
•
Royalties on net sales of IPI-145 ranging from single- to low-double digits •
•
For next-generation PI3K inhibitors •
–
Milestones and royalties, possible co-development and co-commercial rights on
certain products in U.S. only
Mundipharma/Purdue
•
Infinity pays 4% aggregate royalty on worldwide net sales, until $260M in
royalties is paid
•
•
Thereafter, INFI pays 1% royalty on U.S. net sales •
•
Applies to PI3K, FAAH and early discovery programs
Astra Zeneca
INFI pays single-digit royalty on worldwide net sales of retaspimycin HCl
|