Attached files
| file | filename |
|---|---|
| 8-K - SUCAMPO PHARMACEUTICALS, INC. 8-K - Sucampo Pharmaceuticals, Inc. | a50246853.htm |
Exhibit 99.1
Future Leaders in the Biotech Industry James J. Egan, Chief Operating Officer Cary J. Claiborne, Chief Financial Officer Gregory Deener, Senior Vice President, Global Marketing and Product Planning April 20, 2012
2 Forward-Looking Statements This presentation contains “forward-looking statements” as that term is defined in the Private Securities Litigation Reform Act of 1995. These statements are based on management’s current expectations and involve risks and uncertainties which may cause results to differ materially from expectations and involve risks and uncertainties, which may cause results to differ materially from those set forth in the statements. The forward-looking statements may include statements regarding product development, product potential, future financial and operating results, and other statements that are not historical facts. The following factors, among others, could cause actual results to differ from those set forth in the forward-looking statements: the impact of pharmaceutical industry regulation and health care legislation; Sucampo’s ability to accurately predict future market conditions; dependence on the effectiveness of Sucampo’s patents and other protections for innovative products; the risk of new and changing regulation and health policies in the US and internationally and the exposure to litigation and/or regulatory actions. No forward-looking statement can be guaranteed and actual results may differ materially from those projected. Sucampo undertakes no obligation to publicly update any forward-looking statement, whether as a result of new information, future events, or otherwise. Forward-looking statements in this presentation should be evaluated together with the many uncertainties that affect Sucampo’s business, particularly those mentioned in the risk factors and cautionary statements in Sucampo s business, particularly those mentioned in the risk factors and cautionary statements in Sucampo’s Form 10-K for the year ended Dec. 31, 2011, which the Company incorporates by reference
3 Sucampo Snapshot Two approved drugs from proprietary ion channel activator technology AMITIZA® (lubiprostone) AMITIZA (lubiprostone) FDA approved for CIC in adult men/women and IBS-C in adult women aged 18+; sNDA for treatment of OBD to be filed mid-year 2012 Marketed in US by Takeda: 2011 royalty $41 5M on net sales of $226 4M Marketed in US by Takeda: 2011 royalty $41.5M on net sales of $226.4M Limited marketing in Switzerland; CIC filed in UK Partnered with Abbott in Japan; NDA approval expected 2012 Patent coverage through 2022 RESCULA® (unoprostone isopropyl) (un-partnered) sNDA filed with FDA to update label; MAAs to be filed in 2012 Deep pipeline includes prostones and in-licensed candidates Cash balance of $93.4M as of Dec. 31, 2011
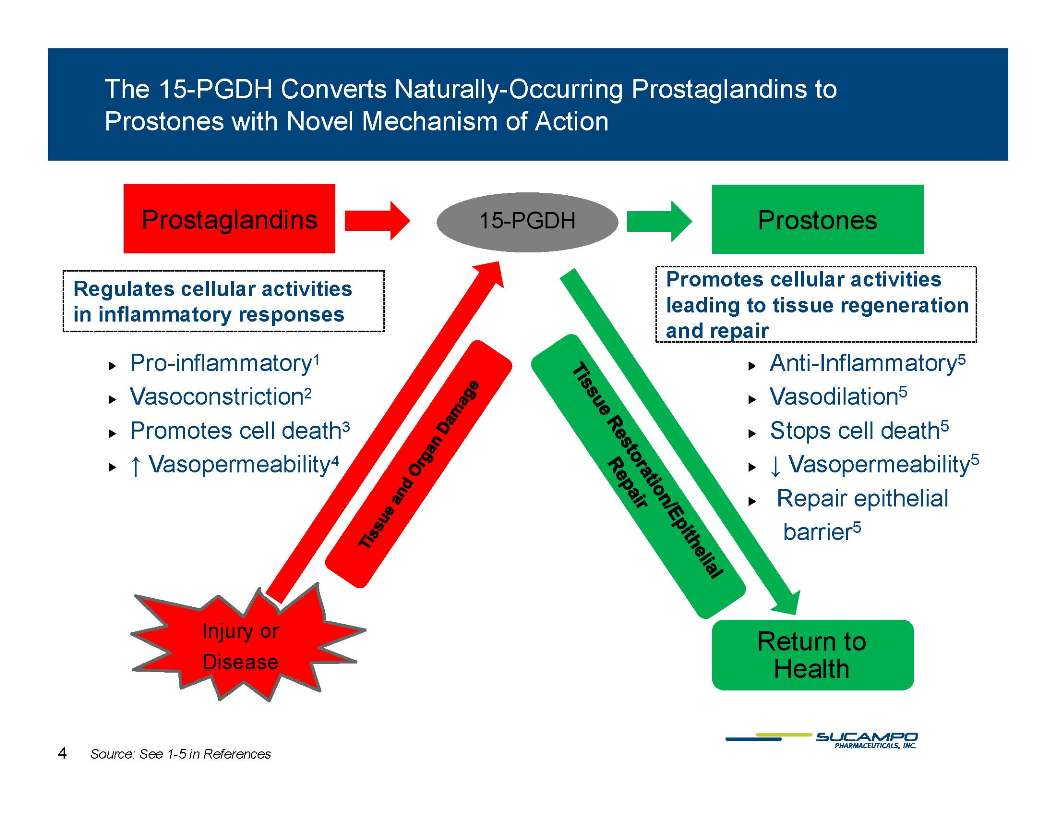
4 Prostaglandins Prostones The 15-PGDH Converts Naturally-Occurring Prostaglandins to Prostones with Novel Mechanism of Action 15-PGDH Prostones Prostaglandins Promotes cellular activities leading to tissue regeneration and repair Regulates cellular activities in inflammatory responses Pro-inflammatory1 Vasoconstriction2 Promotes cell death3 Anti-Inflammatory5 Vasodilation5 Stops cell death5 Vasopermeabilit 5 Vasopermeability4 Vasopermeability5 Repair epithelial barrier5 Injury or Disease Return to Health Source: See 1-5 in References
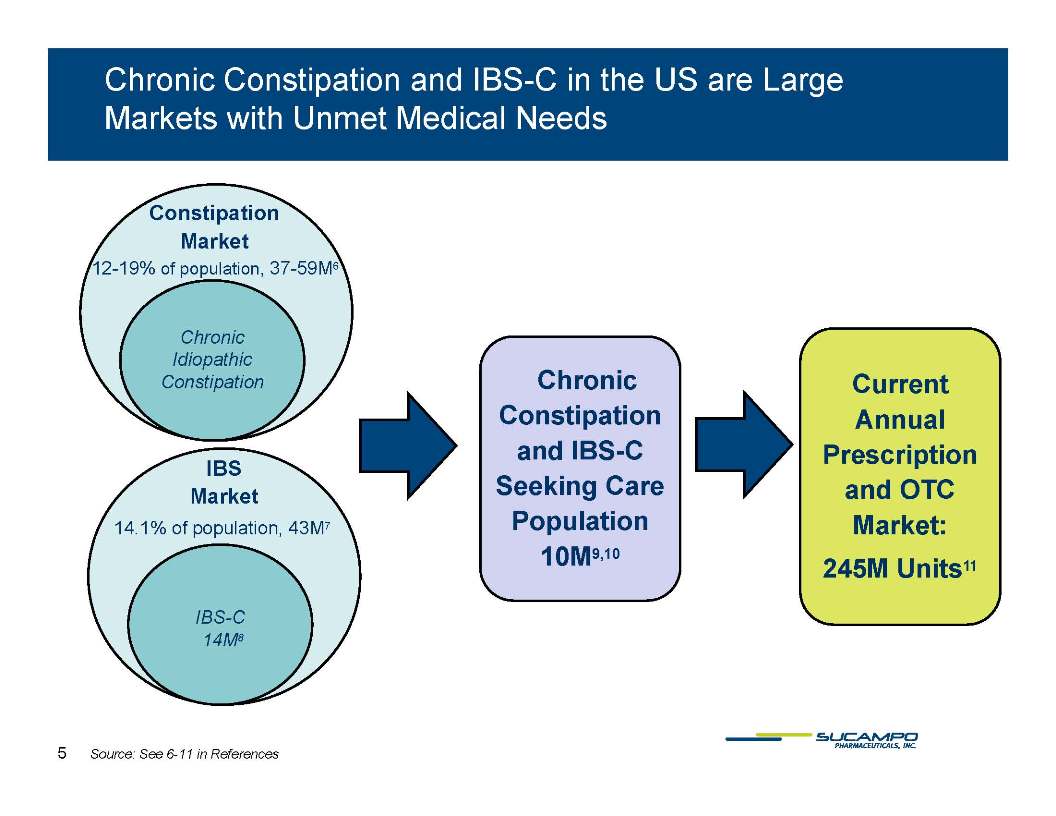
5 Chronic Constipation and IBS-C in the US are Large Markets with Unmet Medical Needs Constipation Market 12-19% of population, 37-59M6 Chronic Idiopathic Chronic Constipation and IBS-C Current Annual Prescription Constipation IBS Market a d S Seeking Care Population 10M9,10 and OTC Market: 245M U it 11 14.1% of population, 43M7 10M Units11 IBS-C 14M8 5 Source: See 6-11 in References
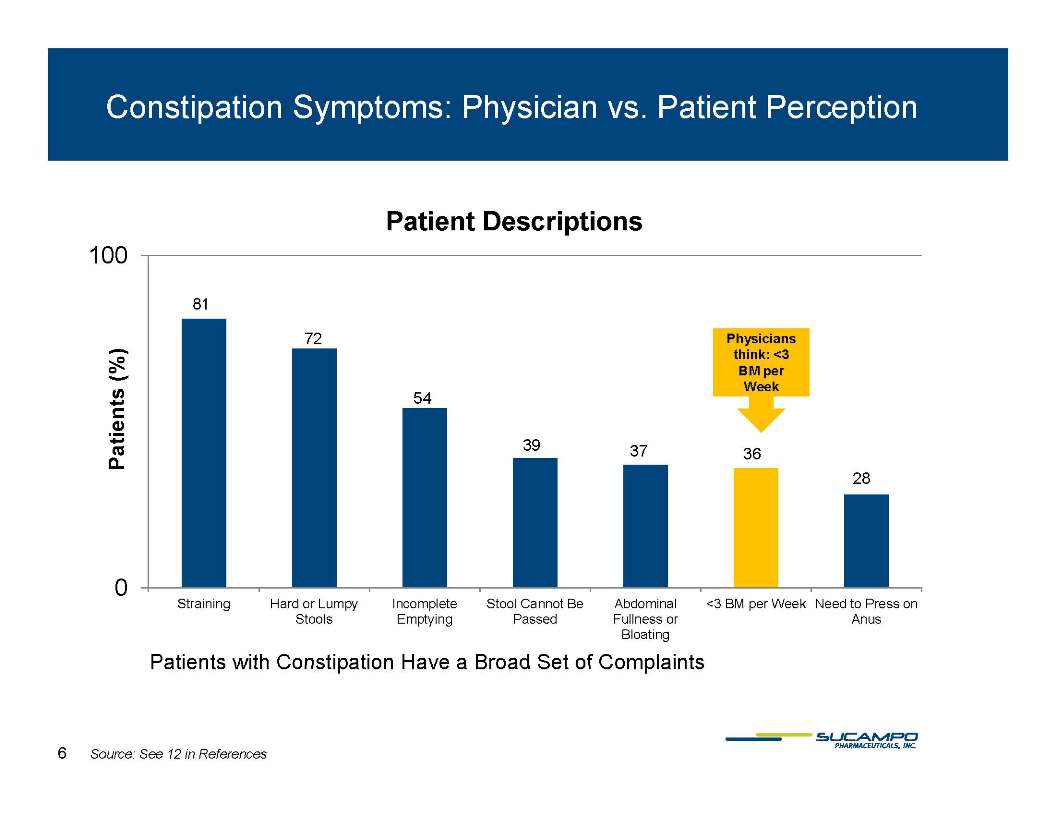
6 Constipation Symptoms: Physician vs. Patient Perception Patients (%) Patient Descriptions 100 81 72 54 39 37 36 28 0 Straining Hard or Lumpy Incomplete Stool Cannot Be Abdominal <3 BM per Week Need to Press on Stools Emptying Passed Fullness or Anus Bloating Patients with Constipation Have a Broad Set of Complaints Source: See 12 in References
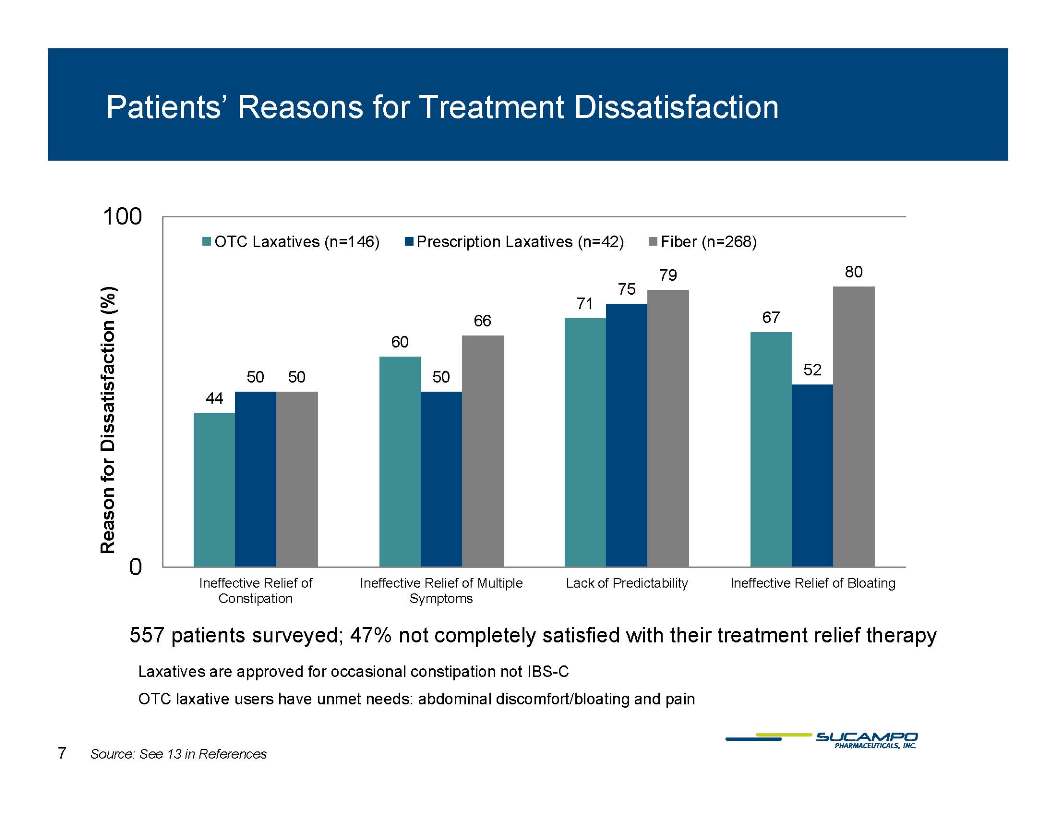
7 Patients’ Reasons for Treatment Dissatisfaction Reason for Dissatisfaction (%) 100 OTC Laxatives (n=146) Prescription Laxatives (n=42) Fiber (n=268) 79 80 75 71 67 66 60 52 50 50 50 44 0 0 Ineffective Relief of Ineffective Relief of Multiple Lack of Predictability Ineffective Relief of Bloating Constipation Symptoms 557 patients surveyed; 47% not completely satisfied with their treatment relief therapy Laxatives are approved for occasional constipation not
IBS-C OTC laxative users have unmet needs: abdominal discomfort/bloating and pain Source: See 13 in References
8 ACG* Evidence Based Review of IBS- 2009 AMITIZA 1B-Highest Grade; Laxatives 2C –Worst Grade Recommendations were graded using a formalized system that quantifies the strength of evidence Each recommendation was classified as strong (grade 1) or weak (grade 2); The strength of evidence classified as strong (level A), moderate (level B), or weak (level C) Highest ranking 1A and lowest ranking 2C Effectiveness of dietary fiber, bulking agents, and laxatives in the Gd2C management of irritable bowel syndrome: Grade 2C No placebo-controlled, randomized study of laxatives in IBS published No effect on pain intensity Effectiveness of the CIC-2 chloride channel activators in management of IBS C: highest score given to a marketed product Source: See 14 in References
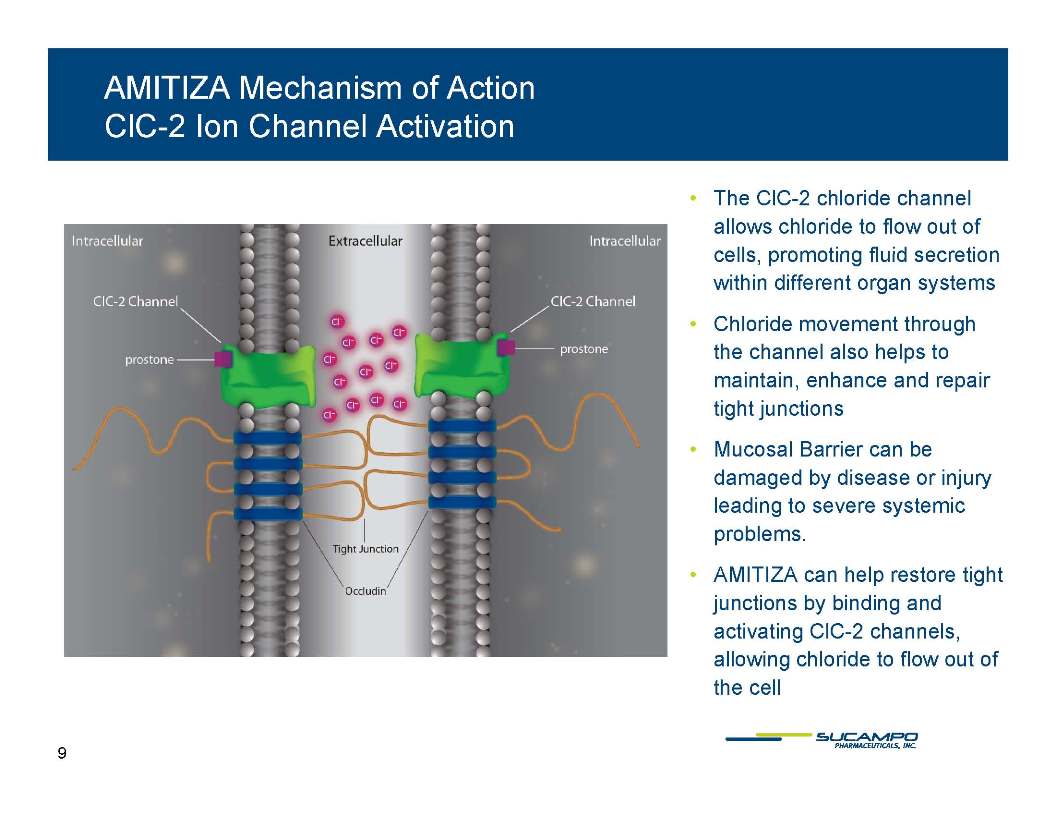
9 AMITIZA Mechanism of Action CIC-2 Ion Channel Activation The CIC-2 chloride channel allows chloride to flow out of cells promoting fluid secretion cells, promoting fluid secretion within different organ systems Chloride movement through the channel also helps to the channel also helps to maintain, enhance and repair tight junctions Mucosal Barrier can be damaged by disease or injury leading to severe systemic problems. AMITIZA can help restore tight junctions by binding and activating ClC-2 channels, allowing chloride to flow out of allowing chloride to flow out of the cell
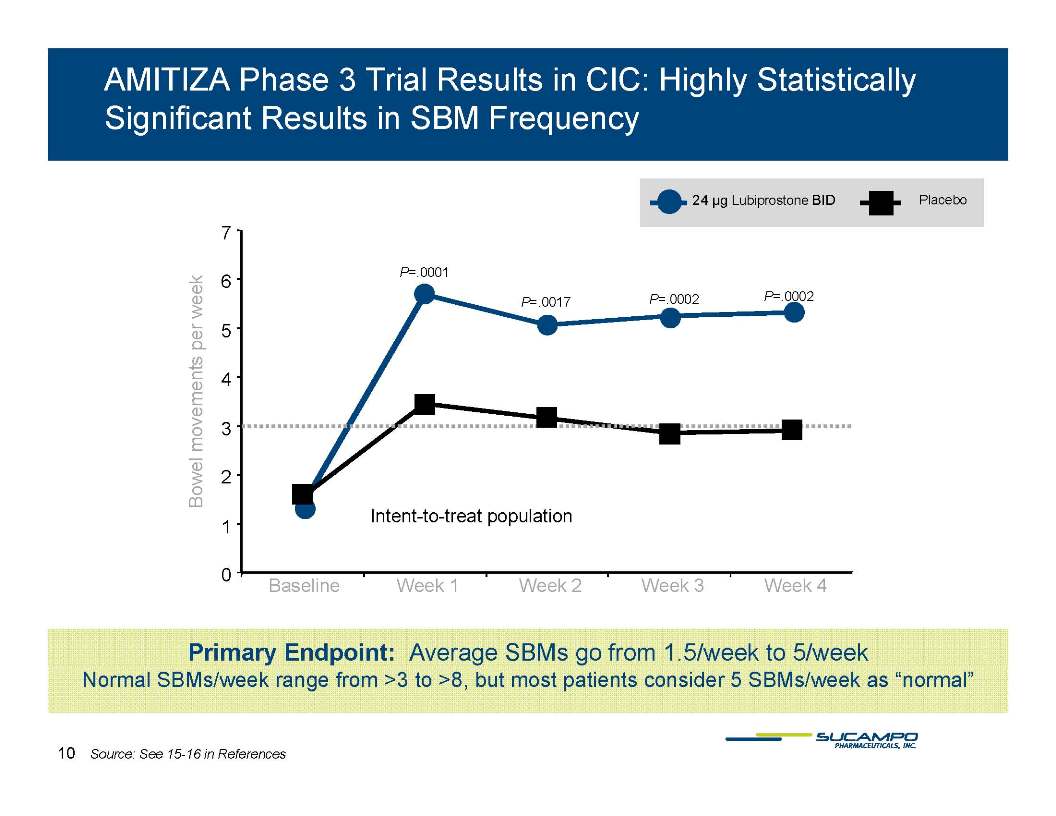
10 AMITIZA Phase 3 Trial Results in CIC: Highly Statistically Significant Results in SBM Frequency 24 µg Lubiprostone BID Placebo 7 P=.0001 P=.0017 P=.0002 P=.0002 5 6 Bowel movements per week 3 4 Intent-to-treat population 1 2 0 Baseline Week 1 Week 2 Week 3 Week 4 Primary Endpoint: Average SBMs go from 1.5/Week to 5/Week Normal SBMs/week range from >3 to >8, but most patients consider 5 SBMs/week as “normal” Source: See 15-16 in References
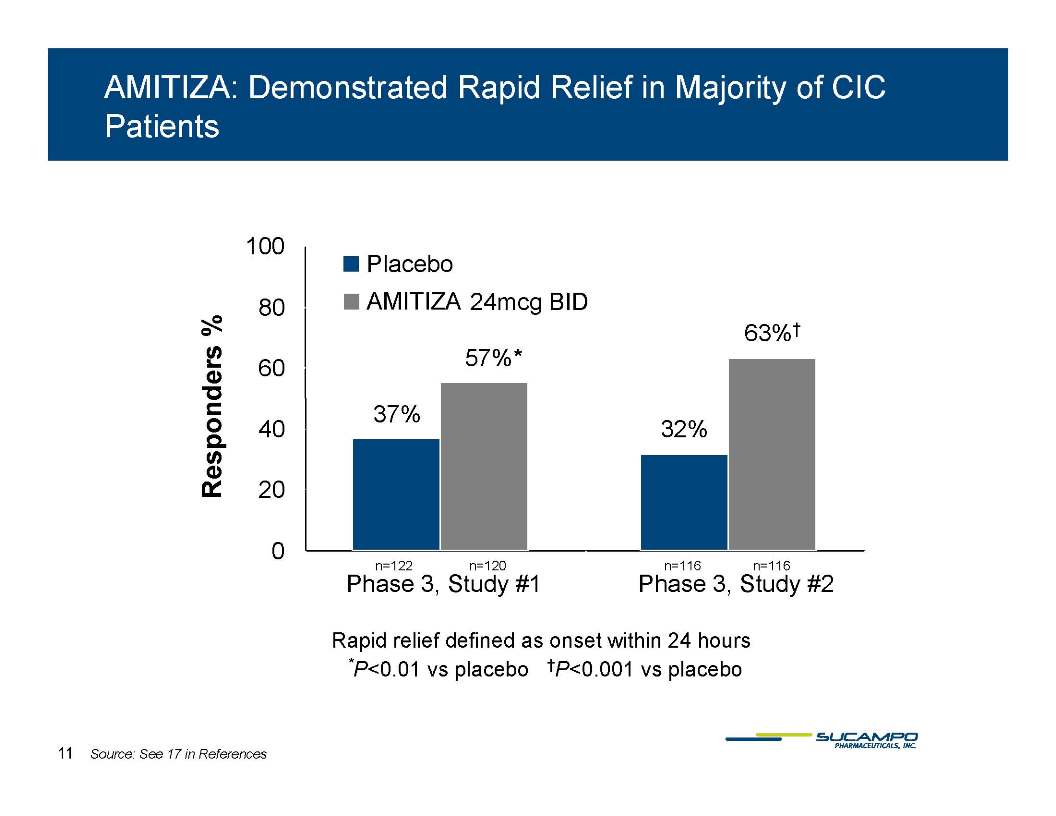
11 AMITIZA: Demonstrated Rapid Relief in Majority of CIC Patients Responders % 100 Placebo AMITIZA 24mcg BID 80 63% 57% 57% 60 37% 40 32% 20 0122 n=120 n=116 116 Phase 3, Study #1 Phase 3, Study #2 Rapid relief defined as onset within 24 hours P<0.01 vs placebo. P<0 001 vs placebo P<0 01 vs placebo P<0.001 vs placebo. 100 57% 63% 80 % 37% 57% 40 60 32% 0 20 n=122 n=120 n=116 n=116 Phase 3-1 Phase 3-2 Rapid relief defined as onset within 24 hours Source: See 17 in References
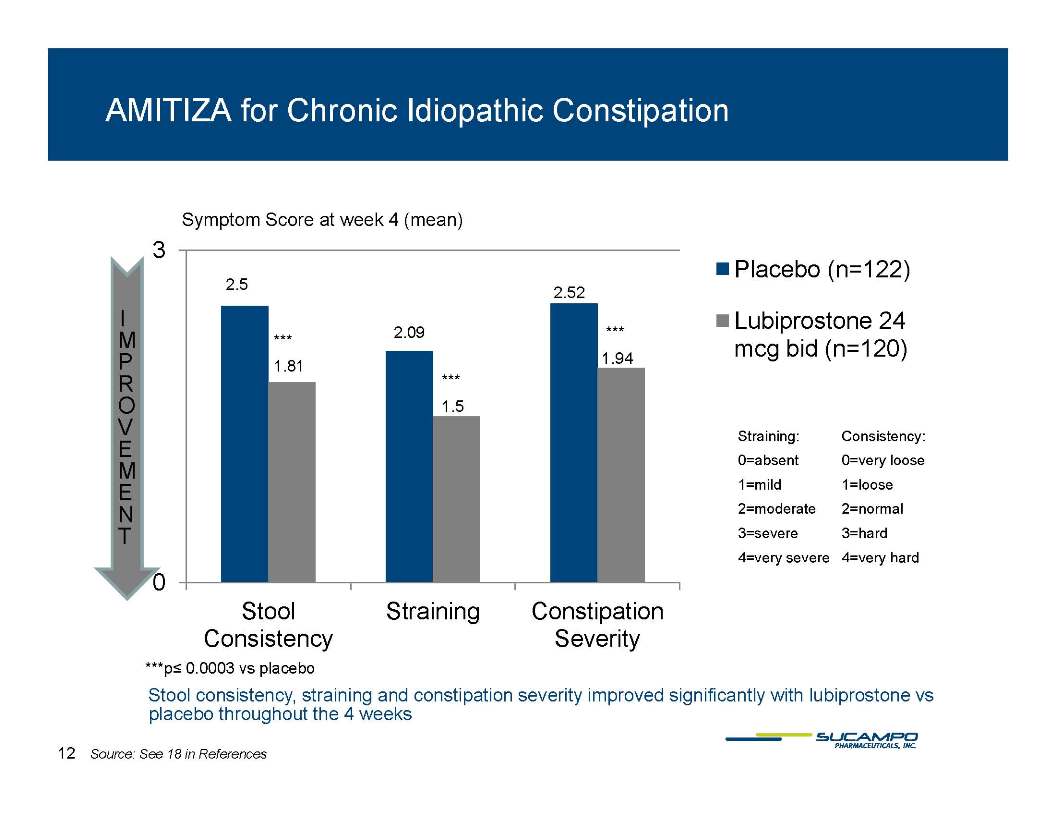
12 AMITIZA for Chronic Idiopathic Constipation Symptom Score at week 4 (mean) 3 Placebo (n=122) 2.5 2.52 Lubiprostone 24 2.09 mcg bid (n=120) g 194 1.94 1.81 1.5 Straining: Consistency: 0=absent 0=very loose 0=absent 0=very loose 1=mild 1=loose 2=moderate 2=normal 3=severe 3=hard 4=very severe 4=very hard 0 Stool Straining Constipation Consistency Severity p= 0.0003 vs placebo Stool consistency, straining and constipation severity improved significantly with lubiprostone vs placebo throughout the 4 weeks 12 Source: See 18 in References
13 AMITIZA IBS-C Study Design “Rigorous 7 Point Scale” Balanced 7-point Likert scale . Demonstrates overall symptom relief . More restrictive definition than other global outcome measures “How would you rate your relief of IBS symptoms (abdominal discomfort/pain, bowel habits, and other IBS symptoms) over the past week compared to how you felt before entering the study?” Significantly relieved No Change A little bit worse Moderately relieved Moderately worse A little bit relieved Significantly worse Monthly Responder – subject reported a symptom rating off at least “moderately” relieved or greater for 4 of 4 weeks within a month or “significantly relieved” for at least 2 of 4 weeks within a month.
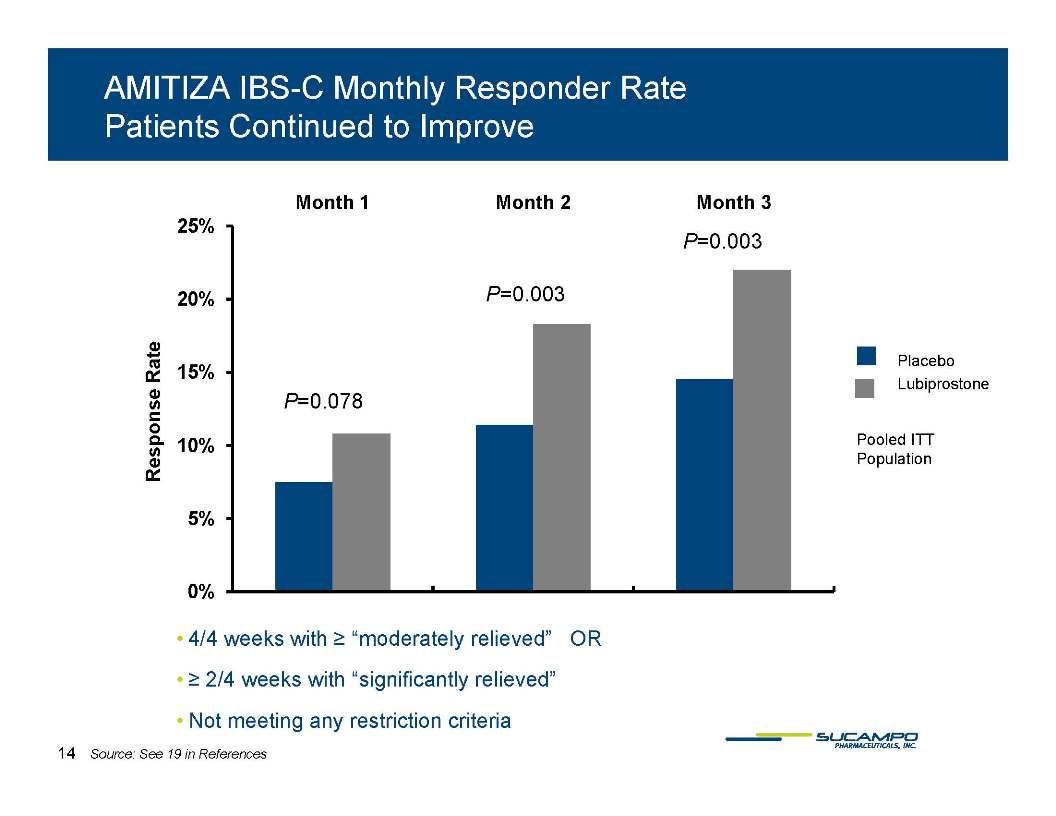
14 AMITIZA IBS-C Monthly Responder Rate Patients Continued to Improve Month 1 Month 2 Month 3 Response Rate 25% P=0.003 P=0.003 20% Placebo 15% Lubiprostone P=0.078 Pooled ITT 10% Population Population 5% 0% 4/4 weeks with = “moderately relieved” OR = 2/4 weeks with “significantly relieved” Not meeting any restriction criteria 14 Source: See 19 in References
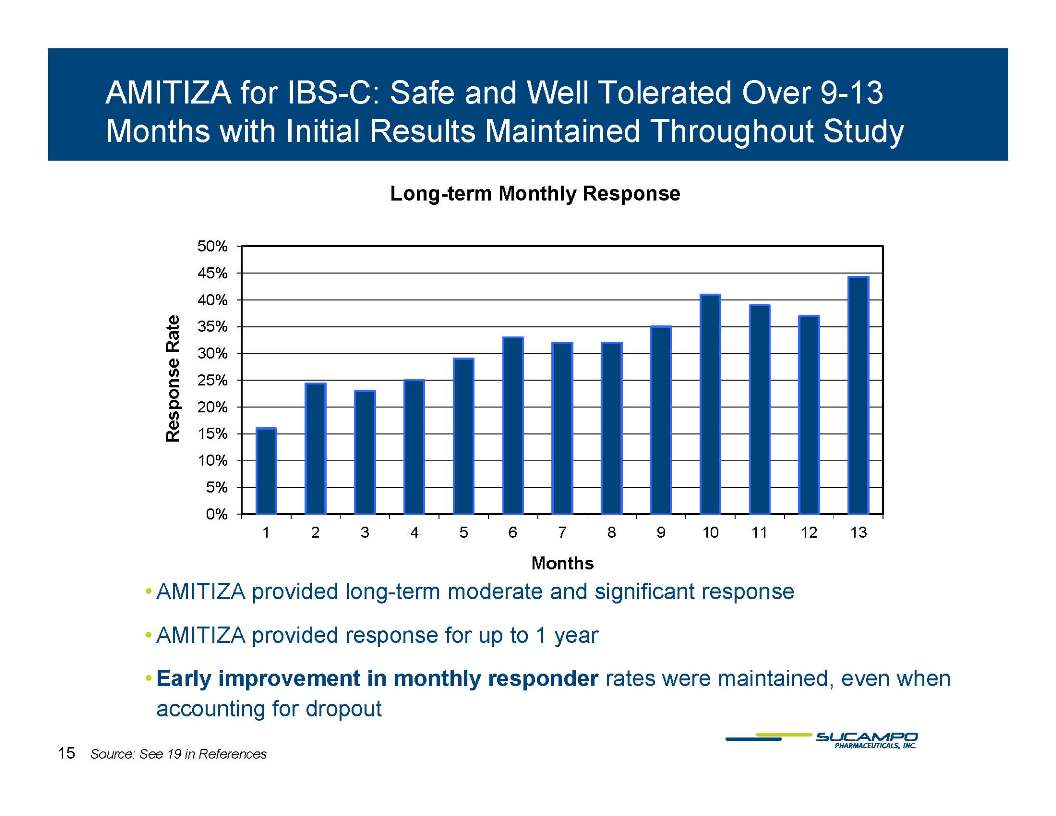
15 AMITIZA for IBS-C: Safe and Well Tolerated Over 9-13 Months with Initial Results Maintained Throughout Study Response Rate Long-term Monthly Response 50% 45% 40% 35% 30% 25% 20% 15% 10% 5% 0% 1 2 3 4 5 6 7 8 9 10 11 12 13 Months AMITIZA provided long-term moderate and significant response AMITIZA provided response for up to 1 year Early improvement in monthly responder rates were maintained, even when accounting for dropout Source: See 19 in References
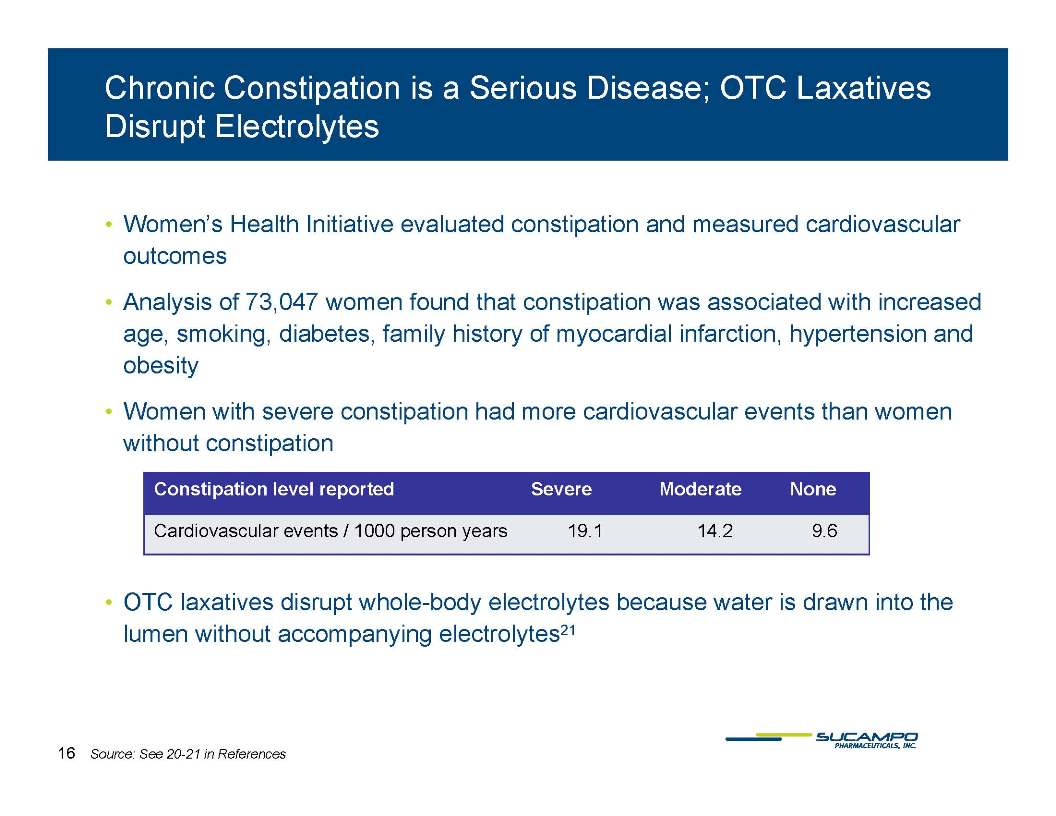
16 Chronic Constipation is a Serious Disease; OTC Laxatives Disrupt Electrolytes Women’s Health Initiative evaluated constipation and measured cardiovascular outcomes Analysis of 73,047 women found that constipation was associated with increased age, smoking, diabetes, family history of myocardial infarction, hypertension and obesity Women with severe constipation had more cardiovascular events than women without constipation OTC laxatives disrupt whole-body electrolytes because water is drawn into the lumen without accompanying electrolytes21 Source: See 20-21 in Reference
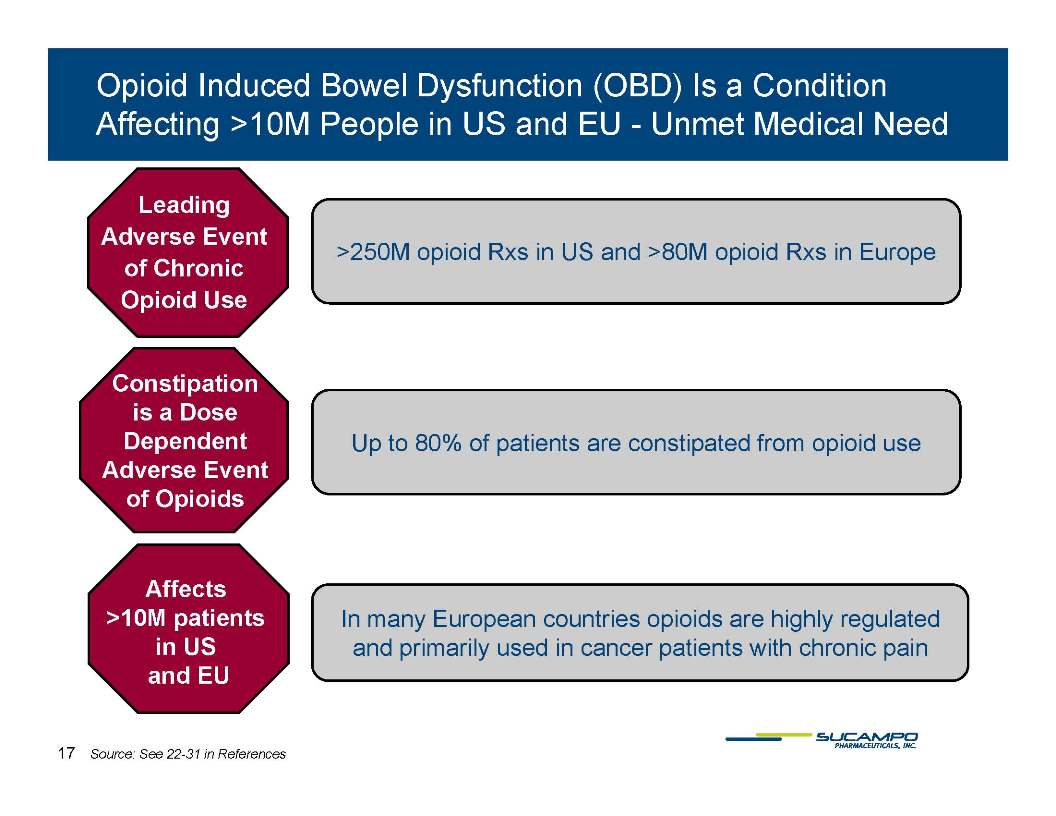
17 Opioid Induced Bowel Dysfunction (OBD) Is a Condition Affecting >10M People in US and EU - Unmet Medical Need >250M opioid Rxs opioid Rxs Europe Leading Adverse Event in US and >80M in of Chronic Opioid Use Constipation is a Dose Dependent Up to 80% of patients are constipated from opioid use Adverse Event of Opioids Affects >10M patients in US and EU In many European countries opioids are highly regulated and primarily used in cancer patients with chronic pain Affects >10M patients in US 17 Source: See 22-31 in References and EU
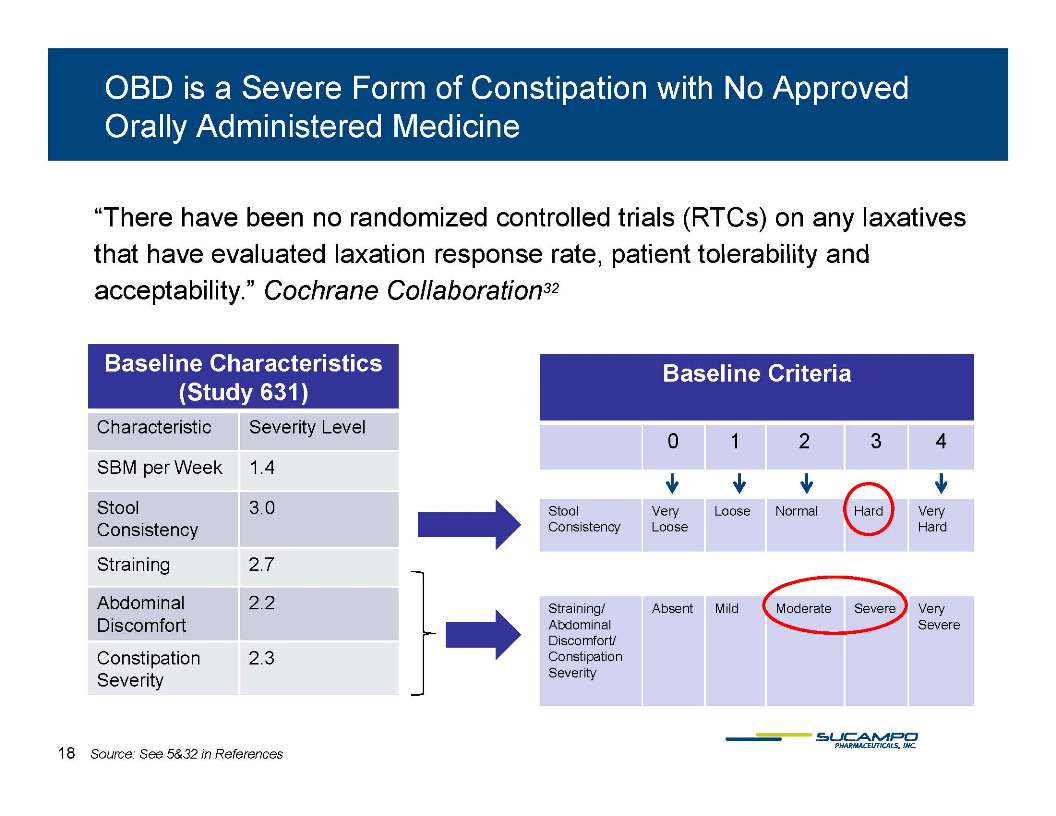
18 OBD is a Severe Form of Constipation with No Approved Orally Administered Medicine “There have been no randomized controlled trials (RTCs) on any laxatives that have evaluated laxation response rate patient tolerability and that have evaluated laxation response rate, patient tolerability and acceptability.” Cochrane Collaboration32 Baseline Characteristics (Study 631) Characteristic Severity Level Baseline Criteria 0 1 2 3 4 SBM per Week 1.4 Stool Consistency 3.0 Straining 2.7 Very Loose Loose Normal Hard Very Hard Abdominal Discomfort 2.2 Constipation 2.3 Straining/Abdominal Discomfort/ Constipation Absent Mild Moderate Severe Very Severe Severity Source: See 5&32 in References
19 AMITIZA: Expansion Strategy Well Underway; Results of Third Phase 3 Trial in OBD Third Phase 3 Trial (OBD1033) design:. Primary endpoint: Overall SBM response rate in non-cancer, non-methadone pain patients Randomized and treated ~440 patients in a placebo-controlled, multi-center trial Almost the same protocol as used in the previous phase 3 trial (OBD0631) reported at DDW 2010, except for FDA-requested new primary endpoint and exclusion of patients on DDW 2010 , except for FDA-requested new primary endpoint and exclusion of patients on methadone. One 24-mcg gel capsule of lubiprostone or placebo twice each day, over 12 weeks Met Primary Endpoint of at least 9 weeks with > 3 SBMs/week and on all non-missing treatment weeks having > 1 SBM over baseline, p=0.035 Aim to File mid sNDA in mid-year 2012 Data to be presented at DDW 2012 and submitted to a peer-reviewed publication Source: See 33 in References
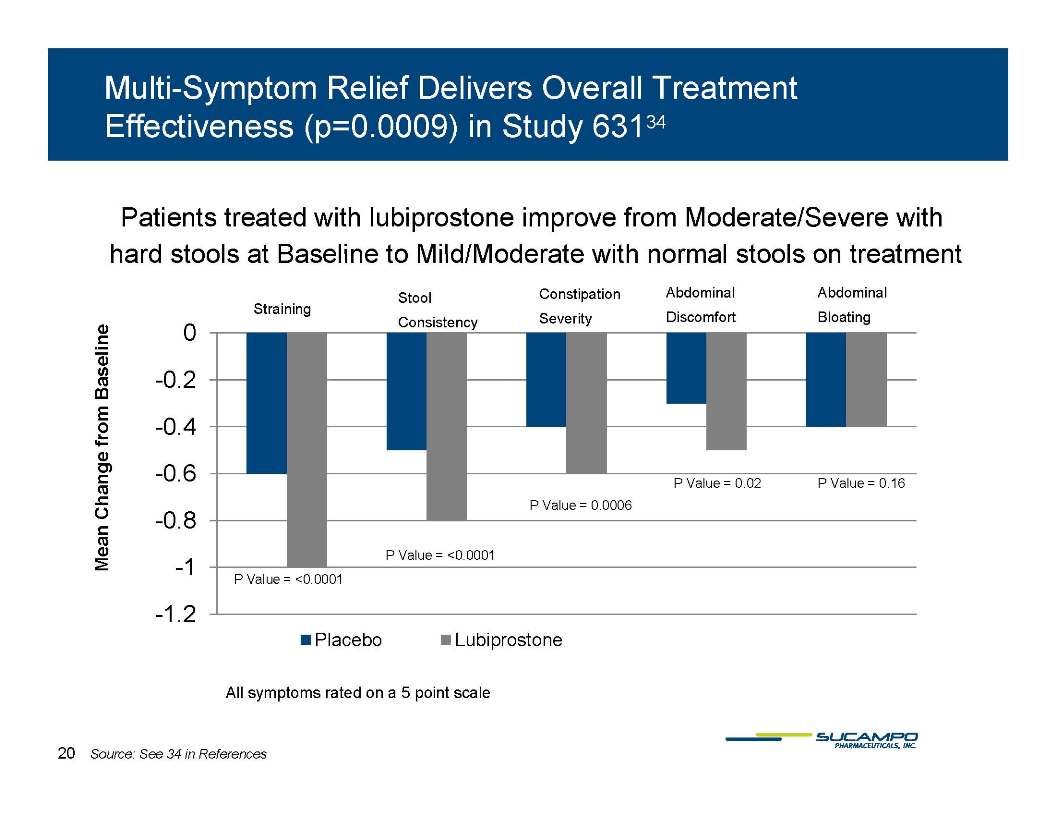
20 Multi-Symptom Relief Delivers Overall Treatment Effectiveness (p=0.0009) in Study 63134 Patients treated with lubiprostone improve from Moderate/Severe with hard stools at Baseline to Mild/Moderate with normal stools on treatment 0 Mean Change from Baseline Straining Stool Consistency Constipation Severity Abdominal Bloating Abdominal Discomfort -0.4 -0.2 -1 -0.8 -0.6 P Value = <0.0001 P Value = 0.0006 P Value = 0.02 P Value = 0.16 P Value = <0.0001 -1.2 Placebo Lubiprostone All symptoms rated on a 5 point scale Source: See 34 in References
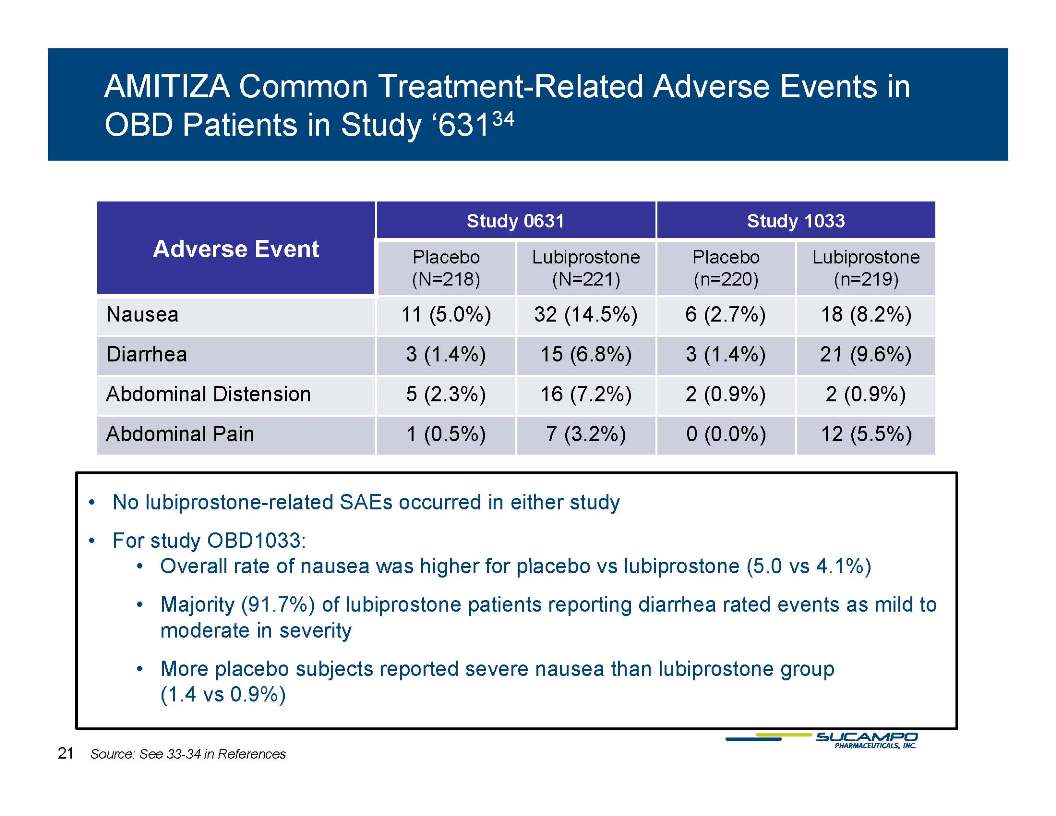
21 AMITIZA Common Treatment-Related Adverse Events in OBD Patients in Study ‘63134 Study 0631 Study 1033 Placebo Lubiprostone Placebo Lubiprostone Adverse Event (N=218) (N=221) (n=220) (n=219) Nausea 11 (5.0%) 32 (14.5%) 6 (2.7%) 18 (8.2%) Diarrhea 3 (1.4%) 15 (6.8%) 3 (1.4%) 21 (9.6%) (1.4%) (6.8%) (1.4%) (9.6%) Abdominal Distension 5 (2.3%) 16 (7.2%) 2 (0.9%) 2 (0.9%) Abdominal Pain 1 (0.5%) 7 (3.2%) 0 (0.0%) 12 (5.5%) No lubiprostone-related SAEs occurred in either study For study OBD1033: Overall rate of nausea was higher for placebo vs lubiprostone (5.0 vs 4.1%) Majority (91.7%) of lubiprostone patients reporting diarrhea rated events as mild to moderate in severity placebo More subjects reported severe nausea than lubiprostone group (1.4 vs 0.9%) Source: See 33-34 in References
22 Terms of Sucampo’s AMITIZA Agreement with Takeda Takeda shall exert best efforts to promote, market, and sell and to maximize net sales revenue AMITIZA in the US and Canada Sucampo’s Sucampo s tiered royalty rate: 18% to 26% of annual net sales Sucampo earned $20M in upfront and $130M in development milestone payments, as of Dec. 31, 2011 We are disappointed by our partner’s performance Arbitration hearing was held in December 2011; expect decision by April 30, 2012 but it is not known how long thereafter the arbitration proceedings will conclude
23 RESCULA® (unoprostone isopropyl) Indication: FDA approved for the lowering of intraocular pressure (IOP) in open-angle open glaucoma and ocular hypertension in patients who are intolerant of or insufficiently responsive to other IOP-lowering medication Global status: label Updating US via sNDA; Conducting trials to drive label expansion - dry AMD; Seeking re-approvals in EU and Switzerland Conducting reformulation trials Patent Life (registered formulated drug product patent): US coverage extends to 2018
24 US Glaucoma Market Overview On the surface, large, mature “satisfied” Rx market 2.5M patients35, 19.2M TRxs, 67% of the market is generic36 IOP is associated with slowing the progression of visual field degeneration Limited new products vs. reformulations In reality, unsatisfied patients IOP improvement does not guarantee visual field maintenance Compliance and adherence are unmet needs 50% of new patients drop off therapy within one year of initiation Prostaglandins are inflammatory agents which depolarize cell membranes #1 reason for discontinuation of prostaglandins is hyperemia37 Source: See 35-39 in References
25 Current AAO/AOA Treatment Guidelines AAO Guidelines40 for treatment of POAG: To identify and treat POAG and to To preserve visual function while minimizing adverse effects of therapy, thereby enhancing the patient’s health and quality of life. “The ophthalmologist should consider the balance between side effects and effectiveness in choosing a regimen of maximal effectiveness and tolerance to achieve the desired IOP reduction for each patient.” The goals of managing patients with POAG are to achieve the following: Stable visual fields Stable optic nerve/retinal nerve fiber layer status Controlled IOP in the target pressure range Maintenance of quality of life Objective of AOA Guidelines41: To provide the patient with their individualized target pressure, with the understanding that multiple treatments may be necessary as glaucoma is a progressive degenerative disease Source: See 40-41 in References
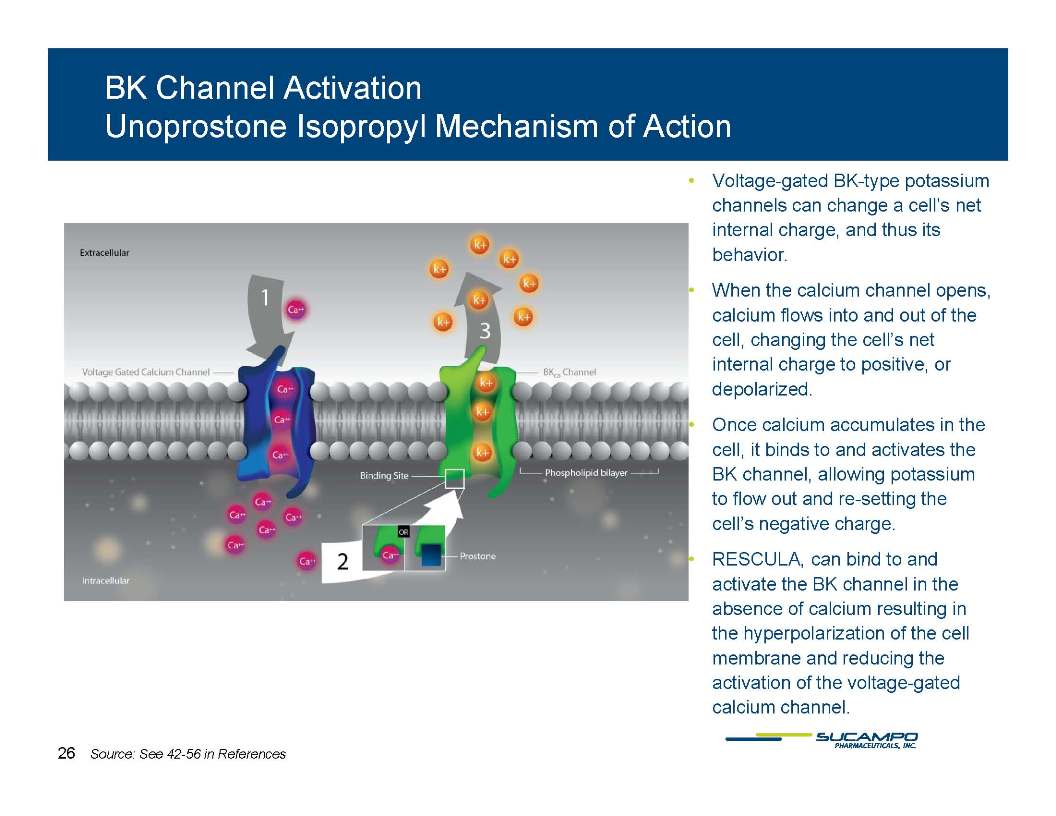
26 BK Channel Activation Unoprostone Isopropyl Mechanism of Action Voltage-gated BK-type potassium channels can change a cell’s net internal charge, and thus it’s behavior behavior. When the calcium channel opens, calcium flows into and out of the cell, changing the cell’s net internal charge to positive, or depolarized. Once calcium accumulates in the cell, it binds to and activates the BK channel, allowing potassium to flow out and re-setting the cell’s negative charge. Prostones RESCULA Prostones, like RESCULA, can bind to and activate the BK channel in the absence of calcium resulting in the hyperpolarization of the cell membrane and reducing the activation of the voltage-gated calcium channel. Source: See 42-56 in References
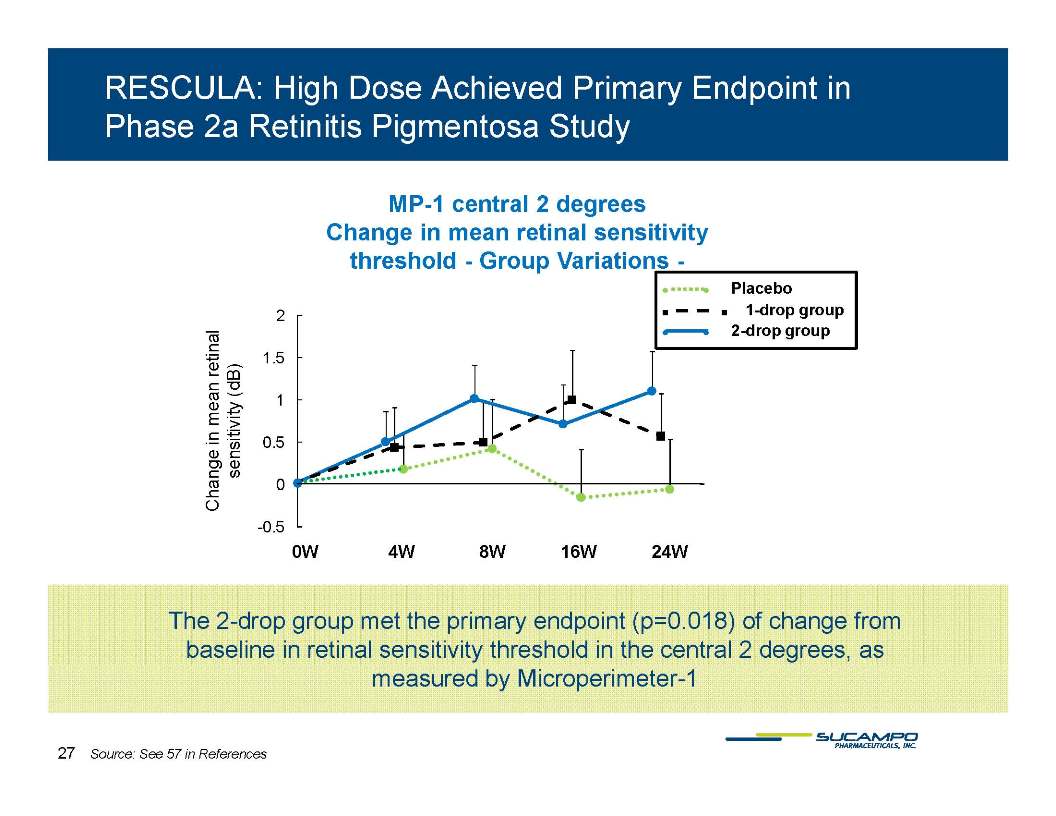
27 RESCULA: High Dose Achieved Primary Endpoint in Phase 2a Retinitis Pigmentosa Study MP-1 central 2 degrees Change in mean retinal sensitivity threshold - Group Variations - 2 1.5 Placebo 1-drop group 2-drop group -0.5 0.5 1 1.5 2 (dB) 0 0W 4W 8W 16W 24W The 2-drop group met the primary endpoint (p=0.018) of change from baseline in retinal sensitivity threshold in the central 2 degrees, as measured by Microperimeter-1. Source: See 57 in References
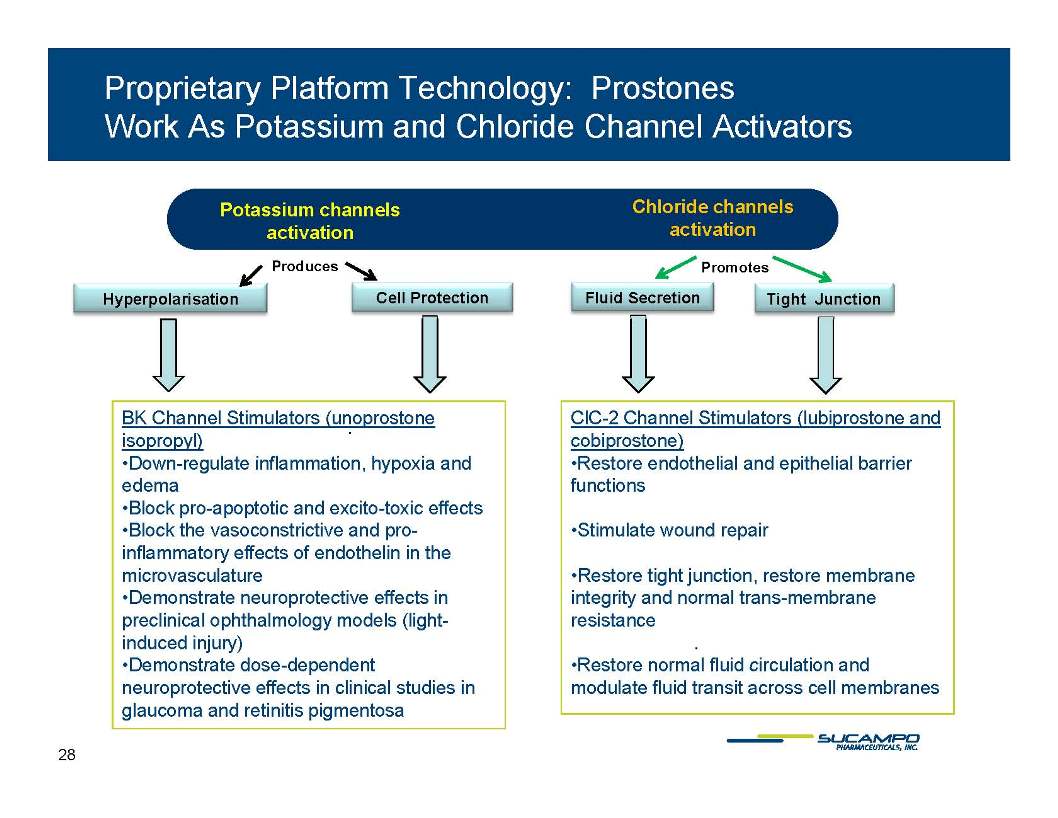
28 Proprietary Platform Technology: Prostones Work As Potassium and Chloride Channel Activators Chloride channels activation Potassium channels activation Hyperpolarisation Cell Protection Fluid Secretion Tight Junction Produces Promotes BK Channel Stimulators (unoprostone isopropyl) Down regulate inflammation hypoxia ClC-2 Channel Stimulators (lubiprostone and cobiprostone) Restore endothelial and epithelial Down-inflammation, and edema Block pro-apoptotic and excito-toxic effects Block the vasoconstrictive and proinflammatory effects of endothelin in the barrier functions Stimulate wound repair microvasculature Demonstrate neuroprotective effects in preclinical ophthalmology models (lightinduced injury) Demonstrate dose-dependent Restore tight junction, restore membrane integrity and normal trans-membrane resistance Restore normal fluid neuroprotective effects in clinical studies in glaucoma and retinitis pigmentosa circulation and modulate fluid transit across cell membranes
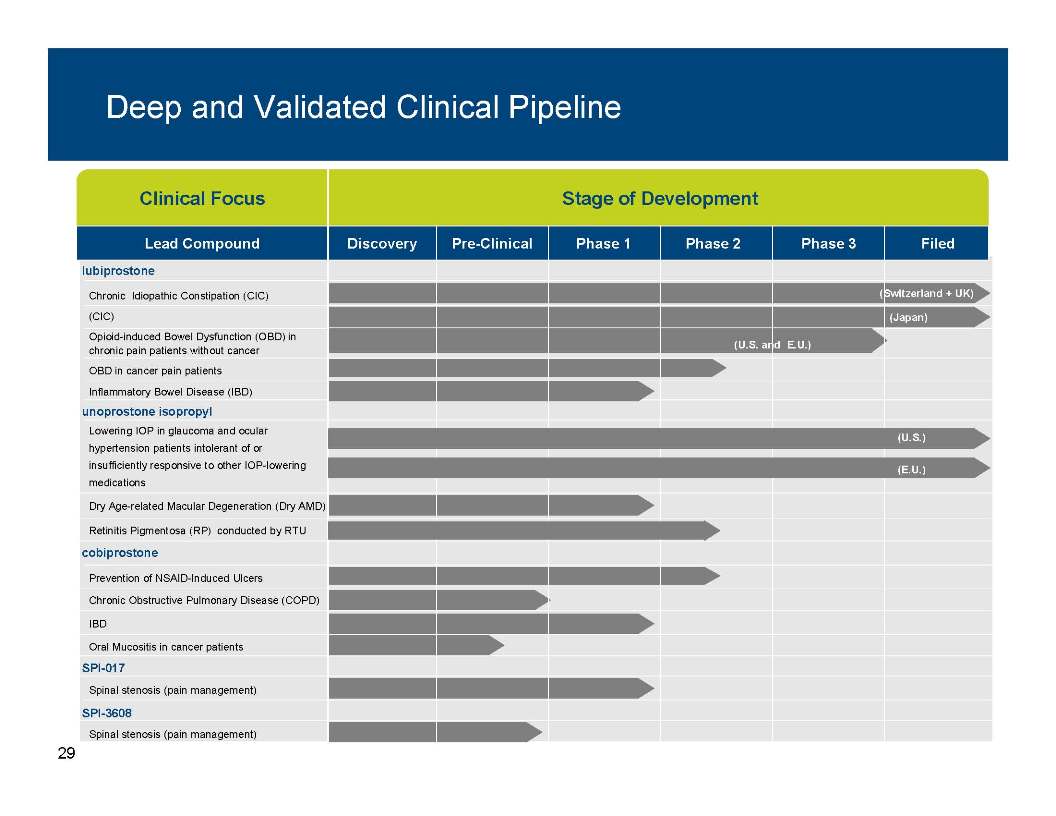
29 Deep and Validated Clinical Pipeline Clinical Focus Stage of Development Lead Compound Discovery Pre-Clinical Phase 1 Phase 2 Phase 3 Filed lubiprostone Chronic Idiopathic Constipation (CIC) (CIC) Opioid-induced Bowel Dysfunction (OBD) in chronic pain patients without cancer (U.S. and E.U.) (Japan) (Switzerland + UK) unoprostone isopropyl OBD in cancer pain patients Inflammatory Bowel Disease (IBD) Lowering IOP in glaucoma and ocular hypertension patients intolerant of or (U.S.) cobiprostone insufficiently responsive to other IOP-lowering medications Dry Age-related Macular Degeneration (Dry AMD) Retinitis Pigmentosa (RP) conducted by RTU (E.U.) SPI 017 Prevention of NSAID-Induced Ulcers Chronic Obstructive Pulmonary Disease (COPD) IBD Oral Mucositis in cancer patients SPI-Spinal stenosis (pain management) SPI-3608 Spinal stenosis (pain management)
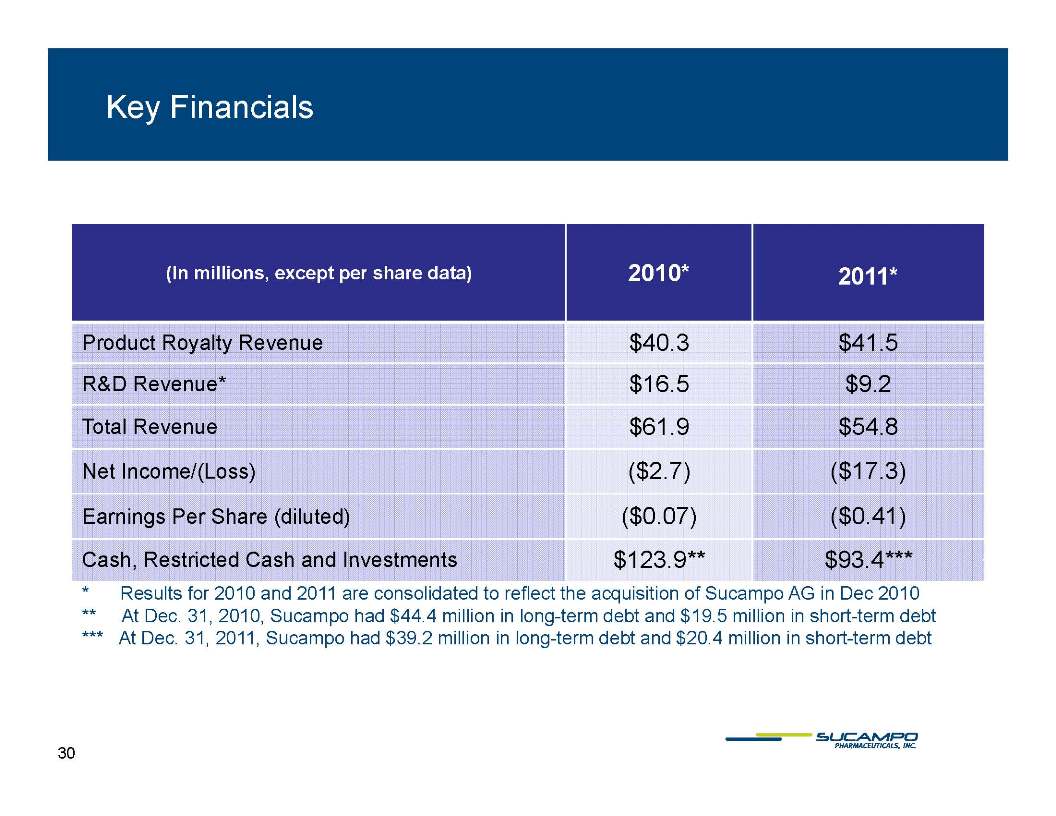
30 Key Financials (In millions, except per share data) 2010* 2011* Product Royalty Revenue $40.3 $41.5 R&D Revenue* $16.5 $9.2 Total Revenue $61.9 $54.8 Net Income/(Loss) ($2.7) ($17.3) Earnings Per Share (diluted) ($0.07) ($0.41) Cash Investments $123 9** $93 4*** Cash, Restricted Cash and 123.9 93.4 Results for 2010 and 2011 are consolidated to reflect the acquisition of Sucampo AG in Dec 2010 At Dec. 31, 2010, Sucampo had $44.4 million in long-term debt and $19.5 million in short-term debt At Dec. 31, 2011, Sucampo had $39.2 million in long-term debt and $20.4 million in short-term debt
31 Key Value Drivers in 2012 AMITIZA US File OBD sNDA mid-year 2012; request priority review Anticipate decision in Takeda arbitration by April 30, 2012 Switzerland Limited marketing commenced, pricing negotiations continue Japan Expect Japanese regulatory approval decision in June 2012, and pricing decision in 3Q12, launch in 4Q12 (CIC patient population in Japan: >25M) EU Expect approval of MAA in UK for CIC in 3Q12, to be followed by mutual recognition procedure for EU; approval will trigger filing of in UK and Switzerland RESCULA Expect data from exploratory trial in dry AMD patients US: Anticipate approval of sNDA for glaucoma indication in US (updated MOA) EUROPE: Re-approval filings in EU and Switzerland
Appendix
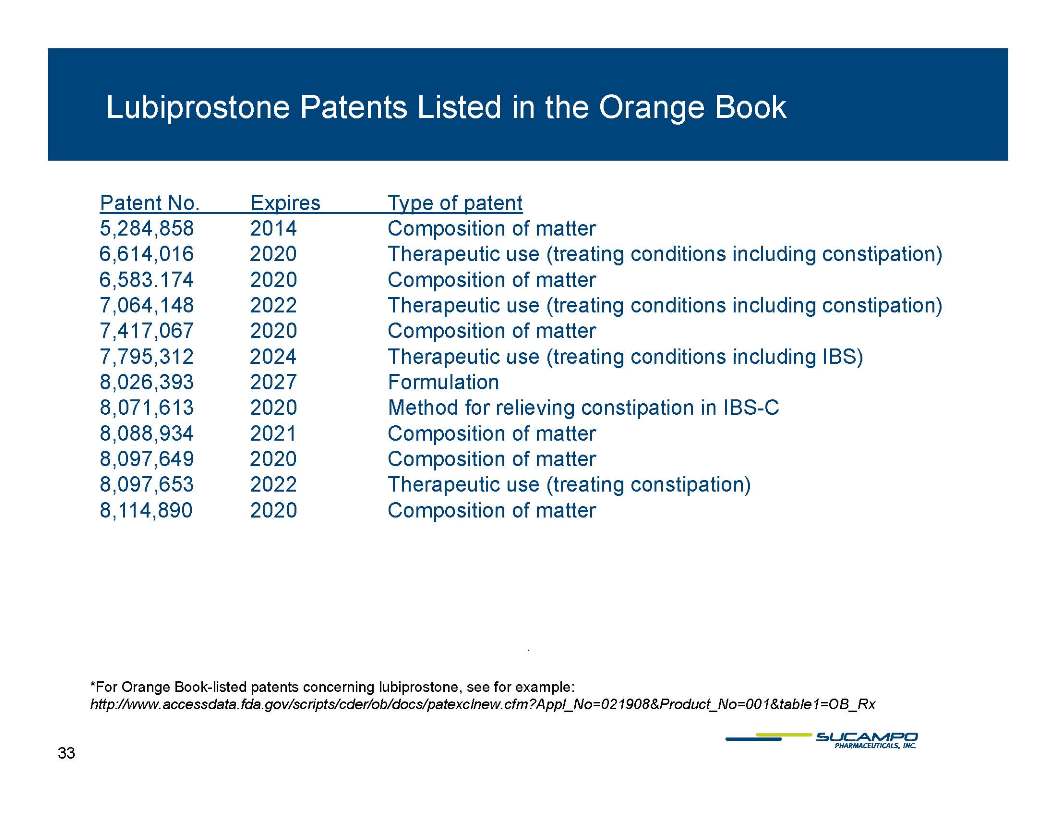
33 Lubiprostone Patents Listed in the Orange Book Patent No. Expires Type of patent 5,284,858 2014 Composition of matter 6,614,016 2020 Therapeutic use (treating conditions including constipation) 6,583,174 7,064,148 7,417,067 7,795,312 8,026,393 8,071,613 8,088,934 8,097,649 8,097,653 8,114,890 2022 2024 2027 2021 Formulation Method for relieving constipation in IBS-C For orange book-listed patents concerning lubiprostone, see example: http://www.accessdata.fda.gov/scripts/cder/ob/docs/patexclnew.cfm?Appl_no=021908&Product_No=001&table1=OB_Rx
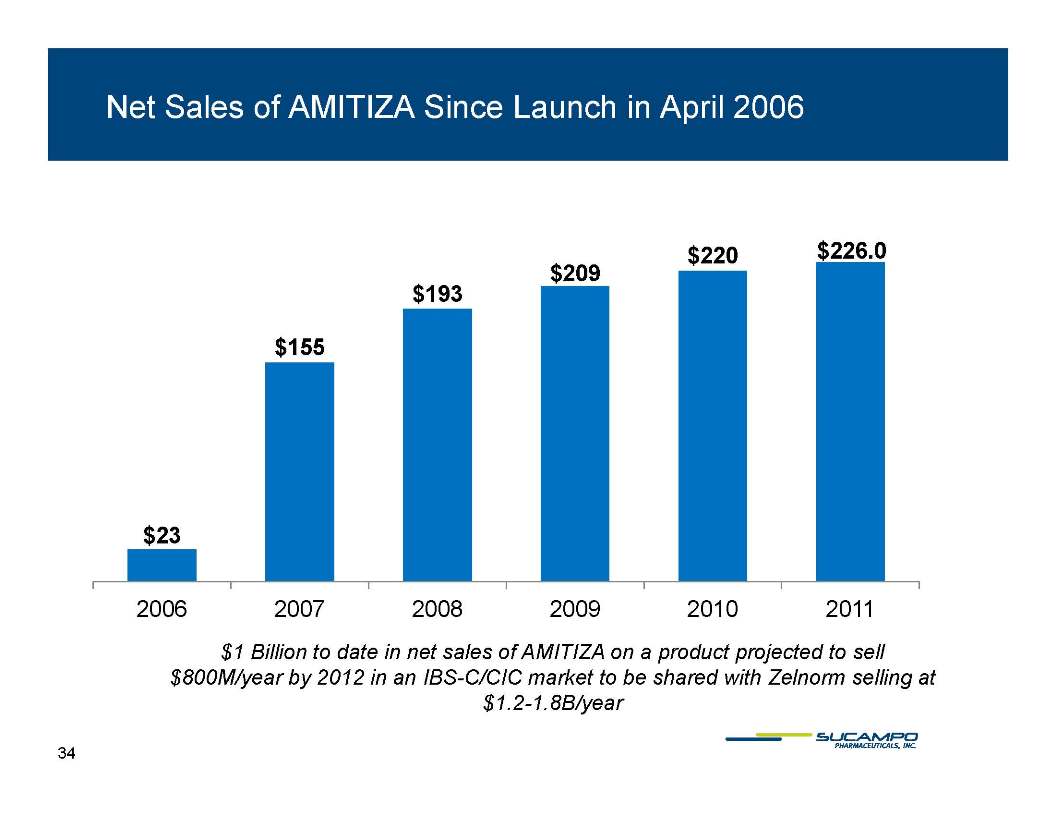
34 Net Sales of AMITIZA Since Launch in April 2006 $220 $226 0 $155 $193 $209 226.0 $23 2006 2007 2008 2009 2010 2011 $1.0B to date in net sales of AMITIZA on a product projected to sell $800M/year by 2012 in an IBS-C/CIC market to be shared with Zelnorm selling at $1.2-1.8B/year
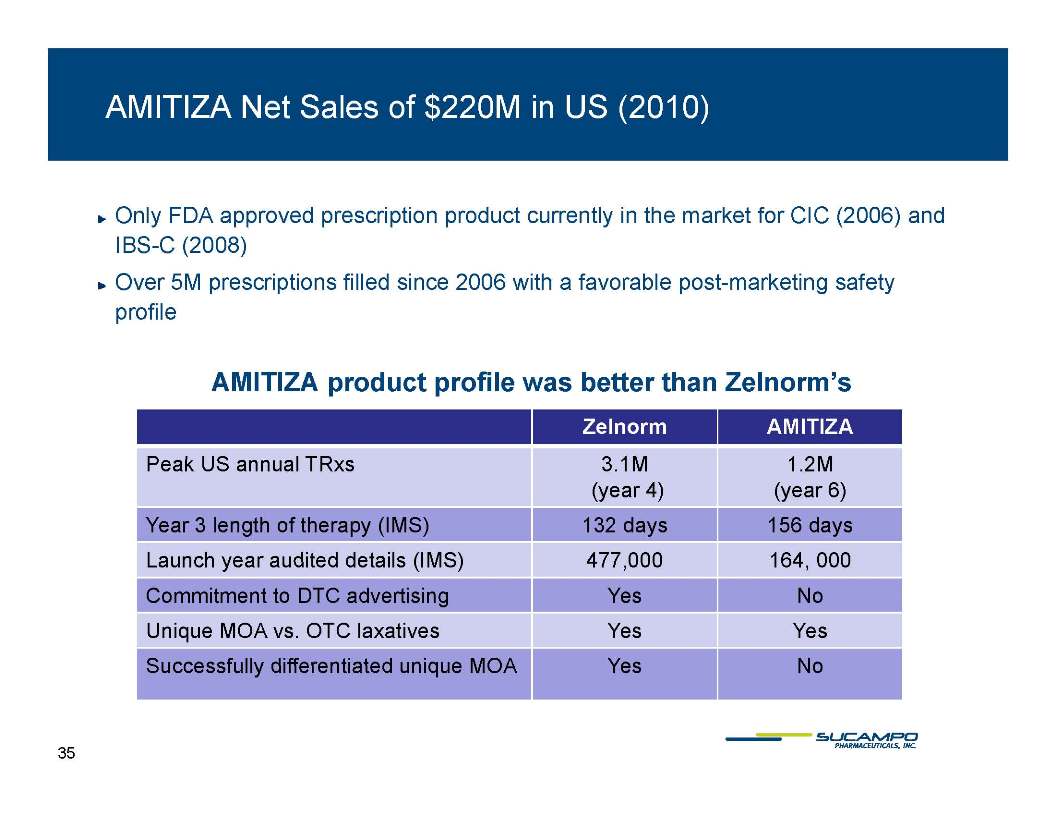
35 AMITIZA Net Sales of $220M in US (2010) Only FDA approved prescription product currently in the market for CIC (2006) and IBS-C ( 2008) ) Over 5M prescriptions filled since 2006 with a favorable post-marketing safety profile AMITIZA product profile was better than Zelnorm’s Zelnorm AMITIZA P kUS lTR 3 1M 1 2M Peak US annual TRxs 3.1M (year 4) 1.2M (year 6) Year 3 length of therapy (IMS) 132 days 156 days year audited details 477 000 164 Launch (IMS) 477,000 164, 000 Commitment to DTC advertising Yes No Unique MOA vs. OTC laxatives Yes Yes Yes No Successfully differentiated unique MOA
36 RESCULA: Exploring Potential with Phase 2a Study in Dry AMD Purpose: ̶ To study choroidal blood flow following administration of unoprostone isopropyl vs. placebo Design: ̶ A single-center, double-masked, randomized, placebo-controlled, crossover design study in 28 dry AMD patients ̶ Administer two doses (Day 1 and 8); 14 day follow-up period ̶ Choroidal blood flow measured by laser doppler flowmetery Study initiated in May 2011, expecting results in 2Q12
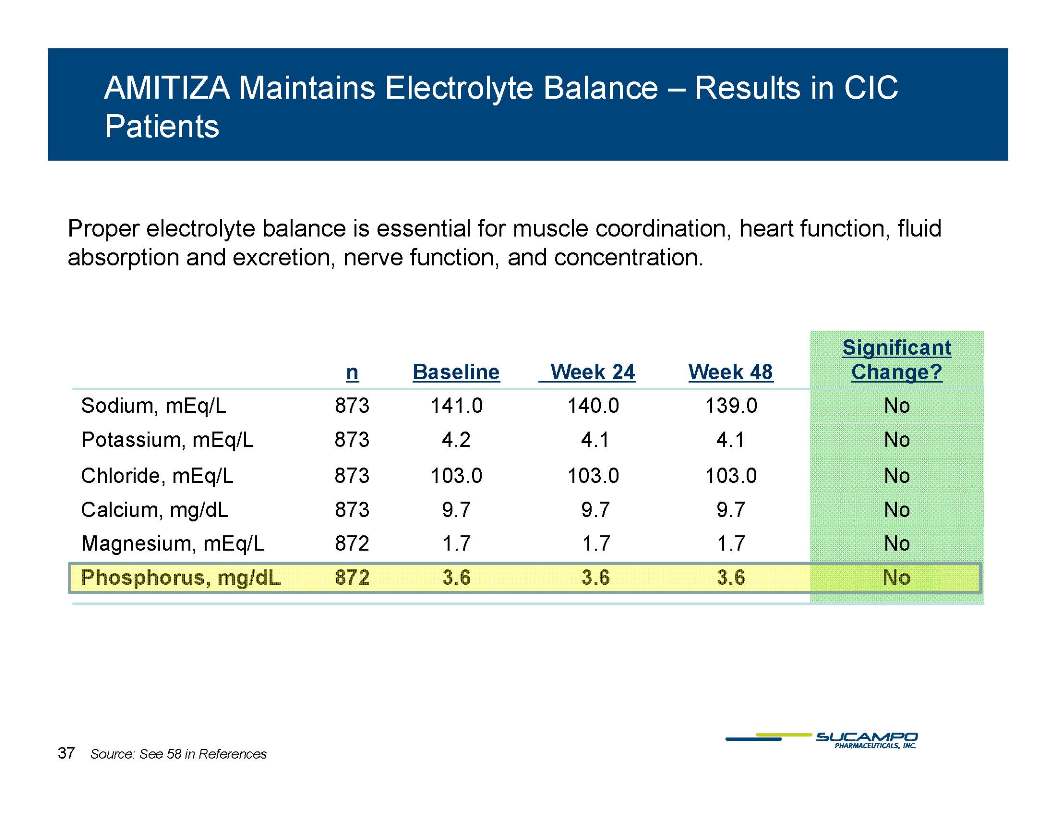
37 AMITIZA Maintains Electrolyte Balance – Results in CIC Patients Proper electrolyte balance is essential for muscle coordination, heart function, fluid absorption excretion function concentration Significant and excretion, nerve function, and concentration. n Baseline Week 24 Week 48 g Change? Sodium, mEq/L 873 141.0 140.0 139.0 No Potassium, mEq/L 873 4.2 4.1 4.1 No Chloride, mEq/L 873 103.0 103.0 103.0 No Calcium, mg/dL 873 9.7 9.7 9.7 No Magnesium, mEq/L 872 1.7 1.7 1.7 No Phosphorus, mg/dL 872 3.6 3.6 3.6 No Source: See 58 in References
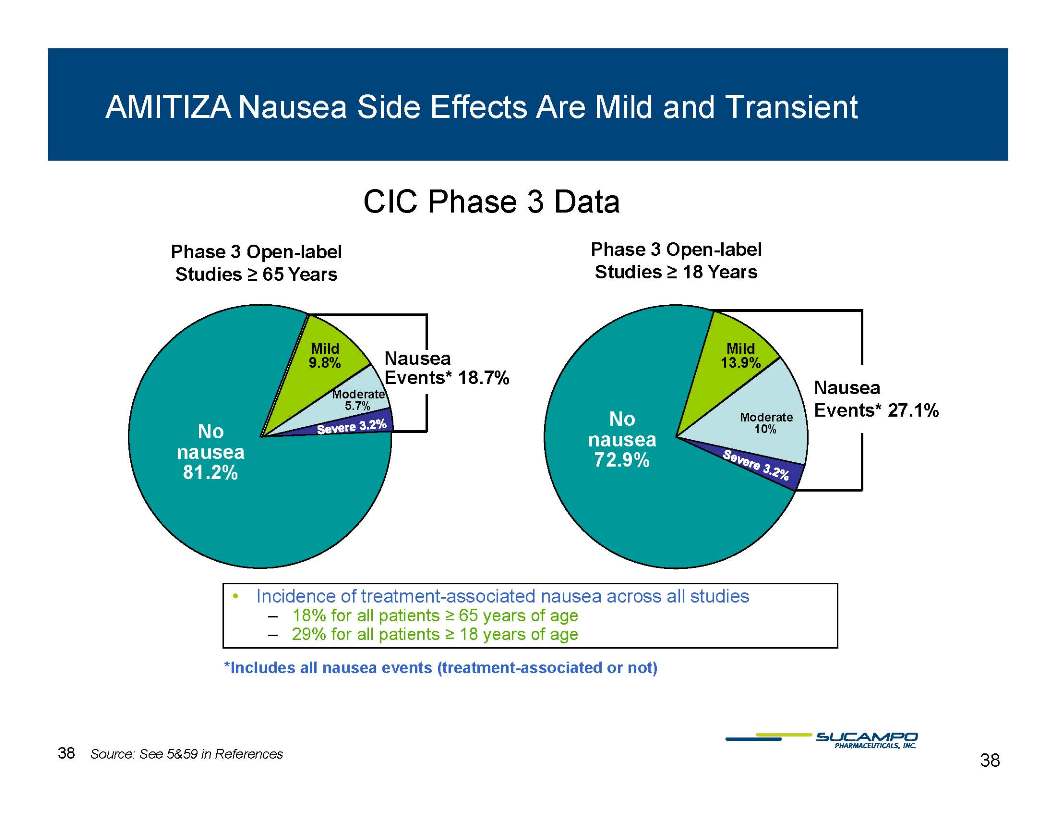
38 AMITIZA Nausea Side Effects Are Mild and Transient Phase 3 Open-label Phase 3 Open-label CIC Phase 3 Data Nausea Mild Studies ≥ 65 Years Mild Open Studies ≥ 18 Years Events* 18.7% No nausea 9.8% Moderate 5.7% Nausea Events* 27.1% No nausea 72 9% 13.9% Moderate 10% 81.2% 72.9% • Incidence of treatment-associated nausea across all studies – 18% for all patients ≥ 65 years of age – 29% for all patients ≥ 18 years of age *nausea events (treatment associated Includes all treatment-or not) Source: See 5&59 in References
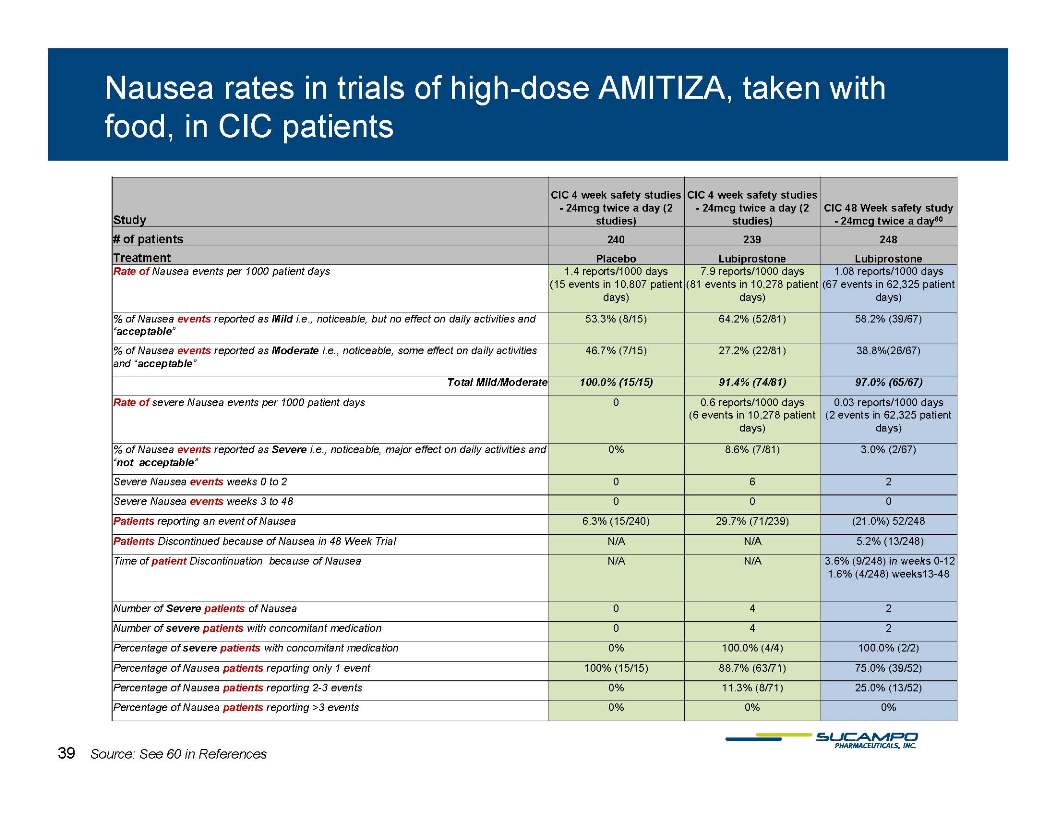
39 Nausea rates in trials of high-dose AMITIZA, taken with food, in CIC patients Study CIC 4 week safety studies - 24mcg twice a day (2 studies) CIC 4 week safety studies - 24mcg twice a day (2 studies) CIC 48 Week safety study - 24mcg twice a day60 # of patients 240 239 248 T Treatment Placebo Lubiprostone Lubiprostone Rate of Nausea events per 1000 patient days 1.4 reports/1000 days (15 events in 10,807 patient days) 7.9 reports/1000 days (81 events in 10,278 patient days) 1.08 reports/1000 days (67 events in 62,325 patient days) % of Nausea events reported as Mild i.e., noticeable, but no effect on daily activities and “acceptable” 53.3% (8/15) 64.2% (52/81) 58.2% (39/67) % of Nausea events reported as Moderate i.e., noticeable, some effect on daily activities 46.7% (7/15) 27.2% (22/81) 38.8%(26/67) and “acceptable” Total Mild/Moderate 100.0% (15/15) 91.4% (74/81) 97.0% (65/67) Rate of severe Nausea events per 1000 patient days 0 0.6 reports/1000 days (6 events in 10,278 patient days) 0.03 reports/1000 days (2 events in 62,325 patient days) % of Nausea events reported as Severe i.e., noticeable, major effect on daily activities and “ t tbl” 0% 8.6% (7/81) 3.0% (2/67) not acceptable” Severe Nausea events weeks 0 to 2 0 6 2 Severe Nausea events weeks 3 to 48 0 0 0 Patients reporting an event of nausea 6.3% (15/240) 29.7% (71/239) (21.0%) 52/248 Patients Discontinued because of Nausea in 48 Week Trial N/A N/A 5.2% (13/248) Time patient N/A N/A 3 6% 248) in 0-12 of Discontinuation because of Nausea 3.6% (9/weeks 0 1.6% (4/248) weeks13-48 Number of Severe patients of Nausea 0 4 2 Number of severe patients with concomitant medication 0 4 2 Percentage of severe patients with concomitant medication 0% 100.0% (4/4) 100.0% (2/2) 88.7% 75 0% Percentage of nausea patients reporting only 1 event 100% (15/15) 88.7% (63/71) 75.0% (39/52) Percentage of nausea patients reporting 2-3 events 0% 11.3% (8/71) 25.0% (13/52) Percentage of nausea patients reporting >3 events 0% 0% 0% 39 Source: See 60 in References
40 References 1. Yang C et al.Prostaglandin E receptors as inflammatory therapeutic targets for atherosclerosis. Life Sci. 2011 Jan 31; 88(5-6): 201-5. Epub 2010 Nov 26. 2. Wong SL et al. Prostaglandins in action indispensable roles of cyclooxygenase-1 and -2 in endothelium-dependent contractions. Adv Pharmacol. 2010;60:61-83. 3. Föller M. et al. Erythrocyte programmed cell death. IUBMB Life. 2008 Oct;60(10):661-8. 4. Kolaczkowska E et al. Enhanced early vascular permeability in gelatinase B (MMP-9)-deficient mice: putative contribution of COX- 1-derived PGE2 of macrophage origin. J Leukoc Biol. 2006 Jul;80(1):125-32. Epub 2006 May 9. 5. Sucampo Data on File 6. Higgins, P. D. R. et al. (2004) Epidemiology of Constipation in North America: A Systematic Review. American Journal of Gastroenterology, 99(4):750-9. 7. Hungin, A.P.S. et al. (2005) IBS in the United States:Prevalence, Symptom Patterns and Impact: Discussion. Alimentary Pharmacology & Therapeutic , 21(11):1365-1375. 8. Muller-Lissner, S. et al. (2001) Epidemiological Aspects of Irritable Bowel Syndrome in Europe and North America. Digestion, 64, 200-204 9. Chey, W. et al “Frequency and Bothersomeness of Symptoms, Health Care Seeking Behavior and Satisfaction with Therapy in IBS-C Patients Meeting ROME II Criteria: Results of a Population Based Survey.” 10 S h fi ld P S t F H lth C S ki B h i d S ti f ti ith Th Ch i C ti ti 10. Schoenfield, P. “System Frequency, Health Care Seeking Behavior, and Satisfaction with Therapy among Chronic Constipation Patients: Results of a Population-Based Survey” 11. IMS NPA Data, Dec 2011, current Q. annualized 12. Pare et al, Am J Gastroenterol 2001; 96: 3130–7 13 & 13. Johanson Kralstein, Aliment Pharmacol Ther 2007; 25: 599–608 14. American College of Gastroenterology, Supplement 1, January 2009 15. Barish CF, et al Dig Dis Sci 2010; 55: 1090-1097
41 References Cont. 16. Johanson JF, et al Am J Gastroenterol. 2008:103:170-177 17. AMITIZA [package insert]. Bethesda, MD: Sucampo Pharma Americas, Inc.; 2011. 18. Johanson et al, Am J Gastroenterol 2008; 103: 170—7 19. Chey et al., 2012 Safety and patient outcomes with lubiprostone for up to 52 weeks in patients with irritable bowel syndrome with constipation. Aliment Pharmacol Therapeutics 20. Salmoirago-Blotcher E et al. Am J Med.2011 Aug:124(8):714-23. 21. Caprilli R, Frieri G, Marchetti G, Giambartolomei S. Ion transport in the colon. Minerva Gastroenterol Dietol. 1995 Dec;41(4):289- 301 22. Pappagallo, M. Prevalence and Mgmt of OBD. American Journal of Surgery, 2001 23. Panchal et a. OBD: prevalence, pathophysiology and burden. Int J Clin Pract 24. Hess, B. Attitude of Swiss Physicians towards OIC: A National Survey. European Journal of Internal Medicine, 2001 25. Reimer K et al. Meeting the Challenge of OIC in Cronic Pain MGMT—A Novel Approach. Pharmacology, 2009 26. Choung RS. OBD and Narcotic Bowel Syndrome: A Population-Based Study. AM J Gastroengerol 27. National Digestive Diseases Information Clearinghouse. Constipation. NIH Publication No. 07-2754, 2007. 28. Colluzzi, F. Opiod Therapy for Chronic non-Cancer Pain: Practice Guidelines for Initiation and Maintenance of Therapy. Minerva p py py Anestesoil, 2007 29. Thomas J. OBD. J Pain and Symptom Mgmt. 2008 30. Sloots EJ, et al. Efficacy and Safety of Prucalopride in Patients with Chronic Non-cancer Pain Suffering from OIC. Dig Dis Sci, 2010. 31. Becker G. Novel opioid antagonists for oIBD and Postoperative Ileus. Lancet, 2009. 32. The Cochrane Collaboration, 2011 Wiley Laxatives or Methylanaltrexone for the Mgmt of Constipation in Palliative Care Patients 33. Sucampo press release Feb. 2, 2012
42 References Cont. 34. Dr. Byron Cryer DDW 2010 , abstract 780 958 35. Arch Ophthalmology, 2004, 122:532-538 36. IMS Health 37. Catalina 2011 38. American Academy of Ophthalmology 39. Input from KOLs 40. 2010 AAO Preferred Practice Patterns for POAG 41. 2010 AOA Practice Guidelines 42. Yu DY et al. Invest Ophthalmol Vis Sci. 1994;35:4087-4099. 43. Kern TS. Exp Diabetes Res. 2007;2007:95013. 44 Hardy P et al Prostaglandins Acids 301 325 44. al. Leukot Essent Fatty Acids. 2005;72(5):301-325. 45. Alm A et al. Exp Eye Res. 2009;88:760-768. 46. Toris CB et al. Arch Ophthalmol. 2004;122:1782-1787. 47. Llobet A et al. News Physiol Sci. 2003;18:205-209 48. Kojima S et al. Nippon Ganka Bakkai Zasshi. 1997:101;605-610. 49. Makimoto Y et al. Jpn J Ophthalmol. 2002;46:31-35. 50. Kimura I et al. Jpn J Ophthalmol. 2005;49:287-293 51. Sugiyama T et al. Arch Ophthalmol. 2009;127:454-459 52. Inoue K et al. Clinical Ophthalmology 2011:5 1003-1005 53. Hayami K et al. Ophthalmic Res. 2001 Jul-Aug;33(4):203-9 54. Melamed S. Drugs Exp Clin Res 2002;28(2-3):63-73.
43 References Cont. 55. Ishida T al. Topical Monotherapy for Normal Tension Glaucoma-Comparison of Long-term Monotherapies in Maintaining Visual Field. Ophthalmology 47:1107-1112,2005. 56. ARVO 2011, Poster#4992,A416 57 Yamamoto S et al ARVO 2011 Microperimetry Shows Protection of Central Vision in with 57. S, al. 2011, Retinitis Pigmentosa Patients Treated UF-021: A Phase 2 Study. Poster # 4992, A416 58. NDA Filing 59. AMITIZA® (lubiprostone) [prescribing information]. Bethesda, Md: Sucampo Pharmaceuticals, Inc. 2008.\ 60 Lembo AJ al Long Term Safety and Lubiprostone ClC 2) Activator 60. Lembo, AJ, et al. Long-Effectiveness of Lubiprostone, a Chloride Channel (ClC-Activator, in Patients with Chronic Idiopathic Constipation. Dig Dis Sci (2011) 56:2639-2645