Attached files
| file | filename |
|---|---|
| EXCEL - IDEA: XBRL DOCUMENT - ACURA PHARMACEUTICALS, INC | Financial_Report.xls |
| EX-32 - EXHIBIT 32 - ACURA PHARMACEUTICALS, INC | v303016_ex32.htm |
| EX-31.2 - EXHIBIT 31.2 - ACURA PHARMACEUTICALS, INC | v303016_ex31-2.htm |
| EX-31.1 - EXHIBIT 31.1 - ACURA PHARMACEUTICALS, INC | v303016_ex31-1.htm |
| EX-23.1 - EXHIBIT 23.1 - ACURA PHARMACEUTICALS, INC | v303016_ex23-1.htm |
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
| (Mark One) | |
| x |
ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 FOR THE FISCAL YEAR ENDED DECEMBER 31, 2011 |
| Or | |
| ¨ |
TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 For the transition period from _____ to _____ |
Commission file number 1-10113
ACURA PHARMACEUTICALS, INC.
(Exact name of registrant as specified in its charter)
| New York | 11-0853640 |
| (State or other jurisdiction of Incorporation or organization) | (I.R.S. Employer Identification No.) |
| 616 N. North Court, Suite 120, Palatine, Illinois | 60067 |
| (Address of principal administrative office) | (Zip code) |
Registrant's telephone number, including area code: 847 705 7709
| Securities registered pursuant to section 12(b) of the Act: | Name of each exchange on which registered: |
| Common Stock, par value $0.01 per share | NASDAQ Capital Market |
Securities registered pursuant to section 12(g) of the Act:
(Title of Class)
None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act.
Yes ¨ No x
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act.
Yes ¨ No x
Indicate by check mark whether the registrant: (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes x No ¨
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes x No ¨
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K (§229.405 of this chapter is not contained herein, and will not be contained, to the best of registrant's knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. x
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company.
¨ Large Accelerated Filer ¨ Accelerated Filer x Non-Accelerated Filer ¨ Smaller Reporting Company.
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes o No x
Based on the last sale price on the NASDAQ Capital Market of the Common Stock on June 30, 2011 $3.87 (the last business day of the registrant's most recently completed second fiscal quarter), the aggregate market value of the voting stock held by non-affiliates of the registrant was approximately $45.9 million.
As of February 29, 2012, the registrant had 45,861,120 shares of Common Stock, par value $0.01, outstanding.
DOCUMENTS INCORPORATED BY REFERENCE: Portions of the Proxy Statement for the registrant’s Annual Meeting of Shareholders to be held on or about April 27, 2012 are incorporated by reference into Part III of this Annual Report on Form 10-K.
Acura Pharmaceuticals, Inc.
Form 10-K
For the Fiscal Year Ended December 31, 2011
Tablet of Contents
| PAGE | |||
| PART I | |||
| Item 1. | Business | 1 | |
| Item 1A. | Risk Factors | 24 | |
| Item 1B. | Unresolved Staff Comments | 40 | |
| Item 2. | Properties | 40 | |
| Item 3. | Legal Proceedings | 41 | |
| Item 4. | Mine Safety Disclosure | 42 | |
| PART II | |||
| Item 5. | Market for Registrant's Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities | 43 | |
| Item 6. | Selected Financial Data | 43 | |
| Item 7. | Management's Discussion and Analysis of Financial Condition and Results of Operations | 44 | |
| Item 7A. | Quantitative and Qualitative Disclosures About Market Risk | 52 | |
| Item 8. | Financial Statements and Supplementary Data | 52 | |
| Item 9. | Changes in and Disagreement with Accountants on Accounting and Financial Disclosure | 52 | |
| Item 9A. | Controls and Procedures | 53 | |
| Item 9B. | Other Information | 53 | |
| PART III | |||
| Item 10. | Directors, Executive Officers and Corporate Governance | 54 | |
| Item 11. | Executive Compensation | 54 | |
| Item 12. | Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters | 54 | |
| Item 13. | Certain Relationships and Related Transactions, and Director Independence | 54 | |
| Item 14. | Principal Accountant Fees and Services | 54 | |
| PART IV | |||
| Item 15. | Exhibits and Financial Statement Schedules | 54 | |
| Signatures | 55 | ||
| Index to Financial Statements | F-1 | ||
Forward-Looking Statements
Certain statements in this Report constitute “forward-looking statements” within the meaning of the Private Securities Litigation Reform Act of 1995. Such forward-looking statements involve known and unknown risks, uncertainties and other factors which may cause our actual results, performance or achievements to be materially different from any future results, performance, or achievements expressed or implied by such forward-looking statements. Forward-looking statements may include, but are not limited to, our and our licensee’s ability to successfully launch and commercialize our products and technologies including Oxecta® Tablets and Nexafed™ Tablets, the price discounting that may be offered by Pfizer for Oxecta®, the ability of us or our licensee’s to obtain necessary regulatory approvals and commercialize products utilizing our technologies and the market acceptance of any products, expectations regarding potential market share for our products and the timing of first sales, our ability to enter into additional license agreements for our other product candidates, the ability to avoid infringement of patents, trademarks and other proprietary rights of third parties, and the ability of our patents to protect our products from generic competition, and the ability to fulfill the U.S. Food and Drug Administration’s, or FDA, requirements for approving our product candidates for commercial manufacturing and distribution in the United States, including, without limitation, the adequacy of the results of the laboratory and clinical studies completed to date, the results of laboratory and clinical studies we may complete in the future to support FDA approval of our product candidates and the sufficiency of our development to meet over-the-counter, or OTC, Monograph standards as applicable, the adequacy of the development program for our product candidates, including whether additional clinical studies will be required to support FDA approval of our product candidates, changes in regulatory requirements, adverse safety findings relating to our product candidates, whether the FDA will agree with our analysis of our clinical and laboratory studies and how it may evaluate the results of these studies or whether further studies of our product candidates will be required to support FDA approval, whether or when we are able to obtain FDA approval of labeling for our product candidates for the proposed indications and will be able to promote the features of our abuse discouraging technologies, whether our product candidates will ultimately deter abuse in commercial settings and whether our Impede technology will disrupt the processing of pseudoephedrine into methamphetamine. In some cases, you can identify forward-looking statements by terms such as “may,” “will,” “should,” “could,” “would,” “expects,” “plans,” “anticipates,” “believes,” “estimates,” “projects,” “predicts,” “potential” and similar expressions intended to identify forward-looking statements. These statements reflect our current views with respect to future events and are based on assumptions and subject to risks and uncertainties. Given these uncertainties, you should not place undue reliance on these forward-looking statements. We discuss many of these risks in greater detail in Item 1A of this Report.
In light of these risks, uncertainties and assumptions, the forward-looking events and circumstances discussed in this Report may not occur and actual results could differ materially and adversely from those anticipated or implied in the forward-looking statements. Accordingly, readers are cautioned not to place undue reliance on such forward-looking statements.
PART I
ITEM 1. BUSINESS
Overview
We are a specialty pharmaceutical company engaged in the research, development and commercialization of products intended to address medication abuse and misuse, utilizing our proprietary Aversion® and Impede™ Technologies. Our products and product candidates are based on widely-used commercial products and do not alter the safety and efficacy of the active pharmaceutical ingredients.
Our lead product, Oxecta® Tablets CII, or Oxecta (formerly Acurox), was approved for marketing by the United States Food and Drug Administration, or FDA, on June 17, 2011. Oxecta represents the first immediate-release oxycodone product approved by the FDA that applies our Aversion Technology. Aversion is a mixture of inactive ingredients incorporated into pharmaceutical tablets and capsules designed to address some common methods of product tampering associated with abuse. Oxecta will be manufactured and commercialized by Pfizer under our October 2007 license agreement with a subsidiary of Pfizer and was made commercially available by Pfizer on January 23, 2012. We are eligible to receive tiered royalties ranging from 5% to 25% on net sales of Oxecta pursuant to our agreement with Pfizer. The royalties commence one year from the first anniversary of the first commercial sale of Oxecta which occurred on February 2, 2012. On June 30, 2011, we received a $20.0 million milestone payment from Pfizer as a result of the FDA approval of Oxecta. The trademark Oxecta® is owned by Pfizer or its affiliate.
| 1 |
In addition to Oxecta, we have licensed to Pfizer the rights to develop, manufacture and commercialize three other immediate-release opioid products utilizing our Aversion Technology in the United States, Canada and Mexico, including:
| · | hydrocodone bitartrate / acetaminophen tablets; |
| · | oxycodone HCl / acetaminophen tablets; and |
| · | an undisclosed opioid analgesic tablet product. |
The development of these additional products may follow a program consistent with that of Oxecta.
We believe our Aversion Technology can also be used to develop and commercialize unique formulations of non-opioid pharmaceutical products associated with abuse and intentional misuse. Our initial non-opioid product candidate is a stimulant product for the treatment of attention deficit disorder.
We are also developing Nexafed™, an over-the-counter, or OTC, immediate-release pseudoephedrine HCl tablet, utilizing our proprietary Impede™ Technology. Pseudoephedrine HCl, or PSE, is a widely-used nasal decongestant available in many non-prescription and prescription cold, sinus and allergy products, including Johnson & Johnson’s Sudafed® product. Our Impede Technology is a proprietary mixture of inactive ingredients designed to impede the extraction of pseudoephedrine from tablets for producing methamphetamine or disrupt the direct conversion of PSE in tablets into methamphetamine.
Oxecta is a Schedule II narcotic indicated for the management of acute and chronic moderate to severe pain where the use of an opioid analgesic is appropriate. The safety and efficacy of Oxecta 5mg and 7.5mg tablets was established by demonstrating bioequivalence to commercially available oxycodone immediate-release tablets in the fasted state. Oxecta differs from oxycodone tablets when taken with a high fat meal though these differences are not considered clinically relevant, and Oxecta can be taken without regard to food. The FDA-approved label for Oxecta describes elements unique to our Aversion Technology, which differs from current commercially available oxycodone immediate-release tablets. The label for Oxecta includes the results from a clinical study that evaluated the effects of nasally snorting crushed Oxecta and commercially available oxycodone tablets, and limitations on exposing Oxecta tablets to water and other solvents and administration through feeding tubes. The clinical study (Study K###-##-####) evaluated 40 non-dependent recreational opioid users, who self-administered the equivalent of 15mg of oxycodone. After accounting for a first sequence effect, the study demonstrated:
| · | 30% of subjects exposed to Oxecta responded that they would not take the drug again compared to 5% of subjects exposed to immediate-release oxycodone; |
| · | subjects taking Oxecta reported a higher incidence of nasopharyngeal and facial adverse events compared to immediate-release oxycodone; |
| · | a decreased ability to completely insufflate two crushed Oxecta tablets within a fixed time period (21 of 40 subjects), while all subjects were able to completely insufflate the entire dose of immediate-release oxycodone; and |
| · | small numeric differences in the median and mean drug liking scores, which were lower in response to Oxecta than immediate-release oxycodone. |
Although we believe these abuse deterrent characteristics differentiate Oxecta from immediate-release oxycodone products currently on the market, consistent with FDA guidance which requires epidemiology studies to support a claim of abuse deterrence, the clinical significance of the difference in drug liking and difference in response to taking the drug again in this study has not been established. There is no evidence that Oxecta has a reduced liability compared to immediate release oxycodone. Pfizer has agreed to a post-approval commitment with the FDA to perform an epidemiology study to assess the actual impact on abuse of Oxecta tablets.
| 2 |
Further, the Oxecta product label guides patients not to crush and dissolve the tablets or pre-soak, lick or otherwise wet the tablets prior to administration. Similarly, caregivers are advised not to crush and dissolve the tablets or otherwise use Oxecta for administration via nasogastric, gastric or other feeding tubes as it may cause an obstruction. Our laboratory studies demonstrated that the Oxecta tablet characteristics may change when Oxecta is exposed to certain solvents, including water.
The misuse and abuse of pharmaceutical products in general, and opioid analgesics in particular, is a significant societal problem. Opioid analgesics, which are used to treat both acute and chronic pain, are the most widely-prescribed and most often abused pharmaceutical products in the United States. It is estimated that 75 million people in the United States suffer from pain, and, according to U.S. government surveys, 35 million people, or more than 10% of the U.S. population, have used prescription opioid analgesics for non-medical purposes at some point in their lifetime. We expect our Aversion Technology opioid products to compete primarily in the market for immediate-release opioid products, or IR Opioid Products. In 2011, IMS Health reported 260 million prescriptions dispensed for opioid analgesic tablets and capsules, of which approximately 244 million were for IR Opioid Products and 16 million were for extended-release opioid tablet and capsule products, or ER Opioid Products. The IR Opioid market has significant generic competition, which are offered at substantial discounts to branded products.
In October 2007, we entered into a License, Development and Commercialization Agreement, or the Pfizer Agreement, with King Pharmaceuticals Research and Development, Inc., now a subsidiary of Pfizer, covering the United States, Canada and Mexico. Under the Pfizer Agreement, Pfizer will manufacture and commercialize Oxecta in the United States and develop and commercialize three additional opioid analgesic products utilizing our proprietary Aversion Technology, including hydrocodone / acetaminophen, oxycodone / acetaminophen and an undisclosed opioid analgesic tablet product. As of December 31, 2011, we had received an aggregate of $78.5 million in payments from Pfizer in the form of a $30.0 million upfront cash payment, milestone payments, option fees and reimbursement for research and development expenses, including a $20.0 million milestone fee relating to the receipt of FDA approval of the New Drug Application, or NDA, for Oxecta. In addition, we are eligible to receive milestone payments based on future regulatory events and product sales achievements, reimbursement for certain research and development expenses and tiered royalties of 5%-25% on combined annual net sales of all products commercialized under the Pfizer Agreement. Royalty payments under the Pfizer Agreement commence one year after the first commercial sale of Oxecta.
Our pipeline of IR Opioid Products and non-opioid products utilize our Aversion Technology, which is intended to deliver the known effectiveness of an FDA-approved active pharmaceutical ingredient and a similar side effect profile while incorporating ingredients that are designed to discourage some of the common methods of abuse and intentional misuse, including:
| · | intravenous injection by forming a viscous gelatinous mixture when tablets and capsules are dissolved in solvents suitable for injection; and |
| · | nasal snorting by inducing disliked nasal discomfort when tablets and capsules are crushed and snorted. |
The extent and manner in which these features are described in the FDA-approved label for these pipeline products will be dependent on the results of and acceptance by the FDA of our, or our licensees’, studies for each of these products.
Our Nexafed product is an immediate-release pseudoephedrine HCl tablet which utilizes our patent pending Impede Technology. In addition to being a widely-used nasal decongestant available in many non-prescription and prescription cold, sinus and allergy products, PSE is also the starting material in the illicit manufacture of methamphetamine, a highly addictive drug that has been used for non-medical purposes by an estimated 13 million people at some point in their lifetime. Our Impede Technology, a proprietary mixture of inactive ingredients, is designed to impede the extraction of PSE from tablets for producing methamphetamine or disrupting the direct conversion of PSE in tablets into methamphetamine. We are developing Nexafed 30mg tablets and have demonstrated that our product is bioequivalent to Johnson & Johnson’s Sudafed® 30mg Tablets and a 30mg generic store brand. Laboratory tests, sponsored by us at an independent laboratory and confirmed by a law enforcement agency, demonstrated our Impede Technology prevents the extraction of PSE from tablets for conversion into methamphetamine using what we believe are the two most common extraction methods. A third, newer method of methamphetamine production, or “one-pot” method, involves the direct conversion of PSE from tablets into methamphetamine without first extracting and purifying the PSE. Laboratory tests conducted on our behalf by an independent CRO using the “one-pot” method demonstrated that our Impede Technology disrupted the direct conversion of PSE from the tablets into methamphetamine. The study compared the amount of pure methamphetamine hydrochloride produced from Nexafed and Sudafed® tablets. Using one hundred 30 mg tablets of both products, multiple one-pot tests and a variety of commonly used solvents, the study demonstrated an average of 38% of the maximum 2.7 grams of pure methamphetamine hydrochloride was recovered from Nexafed. Comparatively, approximately twice as much pure methamphetamine hydrochloride was recovered from Sudafed® tablets. Both products yielded a substantial amount of additional solids such that the purity of the total powder provided contained approximately 65% methamphetamine hydrochloride. We expect to make Nexafed available to pharmacies later this year.
| 3 |
We expect our Impede Technology products containing PSE to compete in the highly competitive market for cold, sinus and allergy products generally available to consumers without a prescription. In 2009, AC Nielsen reported approximately $1.0 billion in sales of non-prescription products containing either PSE or phenylephrine as a nasal decongestant, of which approximately 47% contained PSE. Products in this category consist of many different formulations containing different active ingredients such as analgesics, cough suppressants and antihistamines and have strong consumer brand recognition. Commencing in 2006, the Federal Combat Methamphetamine Epidemic Act, or CMEA, has required all non-prescription PSE products to be held securely behind the pharmacy counter, has set monthly consumer purchase volume limits, and has necessitated consumer interaction with pharmacy personnel to purchase PSE-containing products. We intend to capitalize on this consumer-pharmacist interaction at the point of sale by soliciting distribution to pharmacies and educating and encouraging pharmacists to recommend Nexafed to their customers. In our 2012 survey of 215 chain and independent pharmacists, 164 indicated they had influence over the pharmacies’ product offerings. Of such pharmacists, 70% indicated they were likely to stock or recommend stocking Nexafed in their pharmacies.. The 215 surveyed pharmacists also indicated a willingness to recommend Nexafed to over 50% of their customers who seek a pharmacist’s advise for a single ingredient nasal decongestant. We also may create Nexafed product awareness through television, radio, and print advertising.
All of our Aversion Technology opioid products are covered by two issued U.S. patents, which, in combination with our product labeling and drug product listing strategies, are anticipated to provide our opioid products with barriers to market entry for generic competition through the expiration of our patents in 2025. In July 2011 we receive a U.S. patent covering our Aversion Technology with certain other non-opioid abused drugs. In January 2012 we received a U.S. patent covering an extended release abuse deterrent dosage form of oxycodone or a pharmaceutically acceptable salt thereof. We have numerous additional U.S. and international patent applications pending, including applications covering our Impede Technology.
We conduct research, development, laboratory, manufacturing, and warehousing activities at our operations facility in Culver, Indiana and lease an administrative office in Palatine, Illinois. In addition to internal capabilities and activities, we engage numerous clinical research organizations, or CROs, with expertise in regulatory affairs, clinical trial design and monitoring, clinical data management, biostatistics, medical writing, laboratory testing and related services. We have also contracted with a third-party pharmaceutical product manufacturer and packager to supply our commercial requirements for Nexafed.
Our Strategy
Our goal is to become a leading specialty pharmaceutical company focused on addressing the growing societal problem of pharmaceutical drug abuse by developing a broad portfolio of products with abuse deterrent features and benefits. Specifically, we intend to:
| · | Capitalize on our Experience and Expertise in the Research and Development of Pharmaceutical Products with Abuse Deterrent Features and Benefits. We intend to facilitate product development and minimize risk by utilizing active pharmaceutical ingredients with proven safety and efficacy profiles and known potential for abuse and misuse. |
| · | Emerge as a Leader in Developing and Commercializing Products with Abuse Deterrent Features and Benefits. We believe that Oxecta Tablets and our opioid products in development have demonstrated that the Aversion Technology allows products to provide the analgesic benefit they were intended to deliver, while simultaneously having features that are intended to address tampering associated with abuse and misuse. |
| 4 |
| · | License our Product Candidates to Strategically Focused Pharmaceutical Companies in the United States and Other Geographic Territories. We believe opportunities exist to enter into licensing agreements for our Aversion opioid products outside the United States, Canada and Mexico, which geographies are covered by the Pfizer Agreement, and for developing additional Aversion Technology and Impede Technology product candidates for other abused drugs. We will continue to leverage our expertise, intellectual property rights and Aversion and Impede Technologies without the need to invest in and build a costly physician-focused sales and manufacturing infrastructure. |
| · | Apply our Aversion and Impede Technologies to Other Pharmaceutical Products Susceptible to Abuse. We intend to first develop a portfolio of Aversion Technology opioid analgesic products, and thereafter we intend to expand our focus to other pharmaceutical product categories containing potentially abusable active ingredients. Further, we intend to develop a portfolio of cold, allergy and sinus products containing PSE as a nasal decongestant (similar to brand products such as Zyrtec-D®, Allegra-D®, and Claritin-D®). |
| · | Maintain our Efficient Internal Cost Structure. We maintain a streamlined and highly efficient cost structure focused on: (1) selection, formulation development, laboratory evaluation, manufacture, quality assurance, and stability testing of certain finished dosage form product candidates; (2) development and prosecution of our patent applications; (3) negotiation and execution of license and development agreements with strategically focused pharmaceutical companies and; (4) utilizing third-party contract manufacturers/packagers to supply our specialized development needs and commercial requirements for Nexafed. By outsourcing the high cost elements of our product development and commercialization process, we believe that we substantially minimize required fixed overhead and capital investment and thereby reduce our business risk. We currently do not intend to use a physician-focused sales force to commercialize products on our own but may develop a small national account sales force to sell Nexafed to regional and national retail drug chains. |
| · | In-license or Acquire Alternative Technologies and Product Candidates to Expand or Compliment our Portfolio of Technologies and Products. We intend to pursue the in-license or acquisition of product candidates and technologies that will allow us to expand our portfolio of products. Such in-licensing or acquisition transactions, if successfully completed, of which no assurance can be given, may include product candidates or technologies for pain relief, addiction, and other drugs. |
Product Portfolio Overview
Oxecta represents the first FDA approval for our Aversion Technology opioid products and we believe it demonstrates the FDA’s willingness to consider label differentiation compared to currently marketed immediate-release opioid products when the product features are supported by scientifically derived and supported studies. Following Oxecta, we have the following product candidates in development:
| · | three Aversion Technology opioids products in development by and licensed to Pfizer; |
| · | one Aversion Technology non-opioid product wholly owned by us; |
| · | Nexafed PSE tablets utilizing our Impede Technology wholly owned by us; and |
| · | combination cold, allergy and sinus products containing PSE utilizing our Impede Technology being evaluated for feasibility. |
| 5 |
Opioid Products Utilizing our Aversion Technology
Our Aversion Technology IR Opioid Products being developed and commercialized by Pfizer under the Pfizer Agreement include both an approved product and products in development and are summarized in the table below:
| Aversion Technology Opioid Products | Comparable Brand Name1 |
Status |
| Oxecta (oxycodone HCl) Tablets (formerly Acurox) |
Roxicodone®, Oxy IR® |
FDA Approved on June 17, 2011 First commercial sale on February 2, 2012 |
| Oxycodone HCl/acetaminophen Tablets | Percocet® | Under development by Pfizer Proof of Concept2 attained on Acura-developed formulation containing niacin |
| Hydrocodone bitartrate/acetaminophen) Tablets | Vicodin®, Lortab®, Norco® |
Under development by Pfizer Proof of Concept2 attained on Acura-developed formulation containing niacin |
| Undisclosed opioid analgesic tablet product | -- | Under development by Pfizer Proof of Concept2 attained on Acura-developed formulation containing niacin |
1 Comparable Brand Name refers to currently marketed prescription products in the United States containing the
same active analgesic ingredient as in the corresponding Aversion Technology product.
2 Proof of Concept is attained upon demonstration of certain product stability and bioavailability parameters defined in the Pfizer Agreement.
Pfizer has licensed all opioid products listed in the table above and has marketing rights in the United States, Canada and Mexico.
U.S. Market Opportunity for Opioid Analgesic Products Utilizing Aversion Technology
The misuse and abuse of prescription drug products in general, and opioid analgesics in particular, is a significant societal problem that has been described as epidemic in nature by Joseph A. Califano, Jr., Chairman and President, National Center for Addiction and Substance Abuse at Columbia University, July 2005. Results from the 2009 National Survey on Drug Use and Health indicate prescription drug abusers have supplanted abusers of all illicit drugs except marijuana. The survey estimated that 35 million people in the United States, or more than 10% of the population, have engaged in the non-medical use of prescription opioid analgesics at some point in their lifetime. IR Opioid Products comprise the vast majority of this abuse compared with ER Opioid Products. In addition, it is estimated that more than 75 million people in the United States suffer from pain, which is more than the number of people with diabetes, heart disease and cancer combined. For many pain sufferers, opioid analgesics provide their only pain relief. As a result, opioid analgesics are among the largest prescription drug classes in the United States with over 260 million tablet and capsule prescriptions dispensed in 2011 of which approximately 244 million were for IR Opioid Products and 16 million were for ER Opioid Products. However, physicians and other health care providers at times are reluctant to prescribe opioid analgesics for fear of misuse, abuse, and diversion of legitimate prescriptions for illicit use.
We expect our Aversion Technology opioid product(s), to compete primarily in the IR Opioid Product segment of the United States opioid analgesic market. IR Opioid Product prescriptions have grown at a 3.8% compounded annual rate over the last five years. Because IR Opioid Products are used for both acute and chronic pain, a prescription, on average, contains 62 tablets or capsules. According to IMS Health, in 2011, sales in the IR Opioid Product segment were approximately $2.1 billion, of which ~97% was attributable to generic products. Due to fewer identified competitors and the significantly larger market for dispensed prescriptions for IR Opioid Products compared to ER Opioid Products, we have initially focused on developing IR Opioid Products utilizing our Aversion Technology. Oxecta and our Aversion Technology products in development include the active opioid ingredients representing approximately 78% of the U.S. IR Opioid Product segment.
| 6 |
| 2011 US | ||||||||
| Prescriptions | % | |||||||
| IR Opioid Products(1) | (Millions)(2) | of Total | ||||||
| Hydrocodone | 137 | 56 | ||||||
| Oxycodone | 54 | 22 | ||||||
| Tramadol | 37 | 15 | ||||||
| Codeine | 13 | 5 | ||||||
| 3 others | 3 | 2 | ||||||
| Total (Average) | 244 | 100 | ||||||
| 1 Includes all salts and esters of the opioid and opioids in combination with other active ingredients such as acetaminophen. |
2 IMS Health, 2011
Despite considerable publicity regarding the abuse of OxyContin® extended-release tablets and other ER Opioid Products, U.S. government statistics suggest that far more people have used IR Opioid Products non-medically than ER Opioid Products. These statistics estimate that nearly four times as many people have misused the IR Opioid Products Vicodin®, Lortab® and Lorcet® (hydrocodone bitartrate/acetaminophen brands and generics) than OxyContin®. We estimate 60-95% of the 35 million lifetime U.S. opioid abusers have engaged in the non-medical use of the active ingredients in our IR Opioid product candidates. As indicated in the following chart, the top five abused opioid products are available only as IR Opioid Products.
Lifetime Non-Medical Use of Selected Pain Relievers, Age 12 or Older: 2009
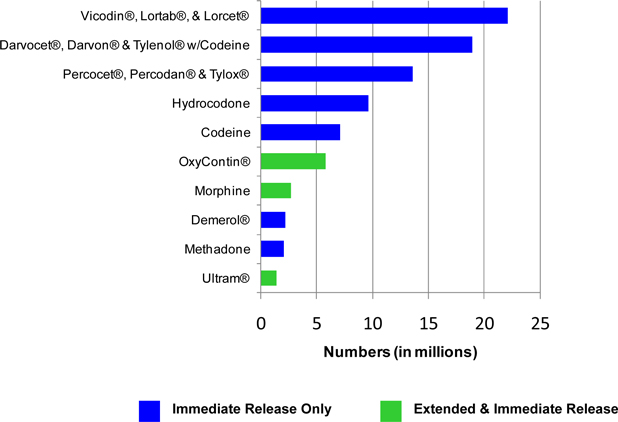
Source: SAMHSA, Office of Applied Studies, 2009 National Survey on Drug Use and Health.
| 7 |
In a 2011 survey of 400 opioid prescribing physicians conducted for us by an independent research firm, 39% of physicians indicated they were highly concerned with the diversion of their opioid prescriptions for non-medical purposes and 42% were highly concerned about opioid misuse by their patients. However, less than 17% of these same physicians indicated they were confident they could adequately identify patients who are diverting or misusing their opioid prescriptions. Further, 77% and 66% of the physicians indicated that abuse of their opioid prescription by injection and snorting, respectively, would likely lead to serious adverse health consequences for the abuser as compared to only 38% for abuse by oral administration.
A majority of pharmaceutical products in the United States are paid for by third-party payers such as insurers, pharmacy benefit managers, self-insured companies and the federal and state governments through Medicare, Medicaid and other health care programs. We believe our product candidates must demonstrate a clinical benefit to the patient and/or an economic benefit to third-party payers and/or a benefit to health care providers to receive favorable reimbursement status by the third-party payers, of which no assurance can be given.
Several independent organizations have estimated the potential cost impact of prescription opioid abuse to insurers. An analysis of health and pharmacy insurance claims between 1998 and 2002 for almost two million Americans conducted by Analysis Group, Inc. and others indicated that enrollees with a diagnosis of opioid abuse had average claims of approximately $14,000 per year higher than an age-gender matched non-opioid abuse sample. A 2007 report by the Coalition Against Insurance Fraud, after adjusting for inflation, estimated this excess cost per patient at more than $16,000 for 2007. By applying the U.S. government’s estimated 4.4 million annual opioid abusers, this organization concluded that abuse of IR and ER Opioid Products could cost health insurers up to $72.5 billion a year.
Aversion Technology Overview
Aversion Technology is our proprietary platform technology intended to address medication abuse and misuse of orally administered pharmaceutical drug products containing potentially abusable active ingredients. Our focus has been to utilize our Aversion Technology with opioid analgesics administered in tablet form. In addition, we believe Aversion Technology is a versatile technology which may be applicable to non-opioid active ingredients susceptible to abuse and misuse and administered in tablet or capsule form.
Our Aversion Technology is a unique composition of inactive pharmaceutical ingredients that when utilized with an opioid or non-opioid active pharmaceutical ingredient provide non-therapeutic functionality. When Aversion Technology is utilized, it is intended that the resulting product provides the same therapeutic benefits as the non-Aversion Technology product containing the same active pharmaceutical ingredient, while simultaneously discouraging the common methods of pharmaceutical product misuse and abuse described below.
The extent and manner in which any of the features described below will be described in the FDA approved label for our pipeline products will be dependent on the results of and the acceptance by the FDA of our and our licensees’ studies for each pipeline product.
Intended to Deter I.V. Injection of Opioids Extracted from Dissolved Tablets
Drug abusers may dissolve currently marketed tablets or capsules containing abused drugs in water, alcohol, or other common solvents, filter the dissolved solution, and then inject the resulting fluid intravenously to obtain euphoric effects. In product candidates utilizing Aversion Technology, extracting the active ingredient using generally available solvents, including water or alcohol, into a volume and form suitable for intravenous injection, converts the tablet into a viscous gel mixture and traps the active ingredient in the gel. Additionally, it is not possible, without difficulty, to draw this viscous gel through a needle into a syringe for a single I.V. injection. We believe that this gel forming feature will limit or impede the ability of I.V. drug abusers from extracting and injecting opioid active ingredients from product candidates developed utilizing Aversion Technology. The FDA approved Oxecta label does not contain a description of the studies we performed to characterize these abuse deterrent features and benefits and there can be so assurance that the label for an Aversion Technology product approved by the FDA, if any, in the future will contain such a description. The FDA approved Oxecta label contains limitations on exposing Oxecta tablets to water and other solvents and administration through feeding tubes.
| 8 |
Intended to Deter Nasal Snorting
Drug abusers may crush or grind currently marketed pharmaceutical tablets or capsules and snort the resulting powder. The abused active ingredient in the powder is absorbed through the lining of the nasal passages providing the abuser with a rapid onset of euphoric effects. The combination of Aversion Technology inactive ingredients is intended to induce nasal passage discomfort and disliking effects if the tablets are crushed and snorted. We believe products which utilize Aversion Technology will discourage prospective nasal drug abusers from snorting crushed tablets. The FDA approved Oxecta label contains the results of a study evaluating the effects of nasally snorting crushed Oxecta tablets.
Development of Aversion Opioid Products
We and/or our partners are required by the FDA to scientifically support the safety, efficacy and other characteristics of our products to support approval for marketing and inclusion of information in our product label. Development of future Aversion Technology opioid products may follow a development program consistent with the program for Oxecta. The clinical and laboratory development program for Oxecta took approximately 12 months from inception to NDA submission, although the Oxecta formulation development and manufacturing scale up benefited from the earlier development program for our Aversion oxycodone with niacin tablets product candidate. The Oxecta clinical and laboratory program is outlined below:
|
Studies in the Oxecta Tablets 505(b)(2) NDA Submission
|
No. of Subjects | |
|
AP-ADD-100
|
Bioequivalence to currently marketed oxycodone HCl Reference Listed Drug | 40 |
|
K###-##-####
|
Dose Proportionality and the Effects of Food on the Bioavailability | 40 |
|
K###-##-####
|
Evaluate effects of nasal snorting in subjects with a history of snorting and nasal drug abuse | 40 |
| PR-381 | Laboratory test quantifying I.V. abuse deterrent properties (syringe test) |
-- |
| PR-382 | Laboratory tests quantifying I.V. abuse deterrent properties (extraction test) |
-- |
Study K###-##-####: Study 1002 is entitled “Randomized, Double-Blind, Active-Controlled Study to Evaluate the Relative Abuse Potential and Safety of Intranasally Administered Crushed Oxecta Tablets (formerly Acurox) in Non-Dependent Recreational Opioid Users”. A total of 40 adult subjects with a history of recreational drug abuse successfully completed screening, a naloxone challenge (demonstrating no addiction to opioids), and a discrimination test (demonstrating the ability to discern drug liking between snorting oxycodone HCl 15mg and placebo) and were randomized into the treatment phase of the study.
In the treatment phase, subjects intranasally administered crushed tablets of: (a) 3 x 5mg Roxicodone® tablets, and (b) 2 x 7.5mg Oxecta tablets. Subjects received all doses in a randomized, cross-over manner with 48 hours between doses. Subjects rated each dose for 6 hours post-administration for drug liking/disliking on a 100mm bipolar visual analogue scale (100mm bi-polar VAS where 100 = “like a lot”, 50 = “neutral”, and 0 = “dislike a lot”) as well as six-point measures of several nasal discomfort measures. At eight hours, subjects rated their Overall Drug Liking and Take Drug Again measures (both 100mm bipolar VAS).
Study PR-382 – Extraction Test: Study PR-382 is entitled “Evaluation of the Potential for Extraction of Oxycodone HCl from Dissolved Oxecta tablets (formerly Acurox) for the Preparation of an Intravenous Solution Suitable for Injection in Humans”. An independent pharmaceutical laboratory utilizing a professionally trained pharmaceutical chemist attempted to extract the oxycodone HCl from: (a) 8 x 5mg generic oxycodone HCl tablets and (b) 8 x 5mg Oxecta Tablets. The chemist was allowed to use any processes, procedures and equipment to prepare a solution of 10mL suitable for injection that could be drawn through a hypodermic needle into a syringe. The chemist was limited to eight hours of laboratory time per drug. Endpoints in the study were the percent of oxycodone HCl extracted from each drug, a chemist rating of the ease / difficulty of the extraction procedure (1 = easy to execute; 10 = complex to execute) and the relative availability of the equipment or materials used (1 = readily available; 10 = difficult to obtain).
| 9 |
Study PR-381 – Syringe Test: Study PR-381 is entitled “Demonstration of the Ability of Oxecta (oxycodone HCl, USP) Tablets (formerly Acurox) to Resist Direct Conversion into an Injectable Solution”. An independent pharmaceutical laboratory attempted to prepare a solution suitable for intravenous injection from: (a) 2 x 5mg generic oxycodone HCl tablets and (b) 2 x 5mg Oxecta Tablets. The tablets were crushed and dissolved in increasing amounts of seven different common solvents safe for humans to inject until at least 3mL of the resulting mixture could be drawn through a hypodermic needle into a syringe.
Pfizer may choose to change the study designs used in the Oxecta development program or run additional studies to facilitate the FDA’s review of future NDAs, to supplement the label for Oxecta, or to provide enhanced information in the label of future Aversion Technology opioid products. These studies are simulations of drug abuse behavior and may not be predictive of actual impact on abuse and misuse. The clinical significance of the difference in drug liking and difference in response to taking the drug again reported in these studies has not yet been established. There is no evidence that Oxecta has a reduced abuse liability compared to immediate-release oxycodone.
Product Labeling for Aversion Technology Products
The FDA has indicated abuse deterrence claims must be supported by either (a) double-blind controlled clinical studies demonstrating an actual reduction in product abuse by patients or drug abusers or (b) robust, long-term epidemiological data supporting a change in levels of abuse in the community over a reasonably long period of time. We believe the cost, time and practicality of designing and implementing controlled clinical studies to support abuse deterrent labeling claims are prohibitive. Pfizer has committed to the FDA to complete an epidemiology study to address whether Oxecta results in a decrease of the consequences of misuse and abuse. The timing and results of such study will be dependent on the level of sales of Oxecta and may require Pfizer to track illegal drug abuse activity and results specific to Oxecta. No assurance can be given that the epidemiological study will be successful or that the results of such study will support an abuse deterrent label claim for Oxecta.
The FDA has allowed scientifically derived data and information describing the physical characteristics of a product candidate and/or the results of laboratory and clinical studies simulating product abuse to be included in the product label. Pfizer may seek similar descriptions of abuse liability studies in the labels of the other Aversion Technology products in development. Pfizer may also undertake additional studies to submit to the FDA seeking inclusion of new data into the Oxecta label. Pfizer also has committed to the FDA to undertake epidemiological studies to assess the actual consequences of abuse of Oxecta in the market. The extent to which a description of the abuse deterrent characteristics, laboratory or clinical studies or results of epidemiological studies will be added to or included in the FDA approved product label for our products will be the subject of our discussions with the FDA as part of the NDA review process, even after having obtained approval of Oxecta. Further, because the FDA closely regulates promotional materials, even if FDA initially approves labeling that includes a description of the abuse deterrent characteristics of the product, such as in the case of Oxecta Tablets, the FDA’s Office of Prescription Drug Promotion, or OPDP, will continue to review the acceptability of promotional labeling claims and product advertising campaigns for our marketed products, if any.
Pfizer Agreement
On October 30, 2007, we and King Pharmaceuticals Research and Development, Inc., now a wholly-owned subsidiary of Pfizer, entered into the Pfizer Agreement to develop and commercialize in the United States, Canada and Mexico certain opioid analgesic products utilizing our proprietary Aversion Technology. The Pfizer Agreement initially provided Pfizer with an exclusive license in the United States, Canada and Mexico, or the Pfizer Territory, for Oxecta (oxycodone HCl) Tablets and oxycodone HCl/acetaminophen tablets utilizing Aversion Technology. In addition, the Pfizer Agreement provides Pfizer with an option to license in the Pfizer Territory certain future opioid analgesic products developed utilizing Aversion Technology. As of December 31, 2011, Pfizer exercised its option to license two additional product candidates including an an undisclosed immediate-release opioid analgesic tablet product and hydrocodone bitartrate/acetaminophen tablets, each of which utilize our Aversion Technology. The Pfizer Agreement provides that we or Pfizer may develop additional opioid analgesic product candidates utilizing our Aversion Technology and, if Pfizer exercises its option to license such additional product candidates, they will be subject to the milestone and royalty payments and other terms of the Pfizer Agreement.
| 10 |
Pursuant to the Pfizer Agreement, we and Pfizer formed a joint steering committee to oversee development and commercialization strategies for Aversion opioid analgesic products licensed to Pfizer. For all products licensed by Pfizer, including Oxecta, or for which Pfizer exercises its option to license, Pfizer will be responsible, at its own expense, for development, regulatory, and commercialization activities in all Pfizer Territories. All products developed pursuant to the Pfizer Agreement will be manufactured by Pfizer or a third party contract manufacturer under the direction of Pfizer. Subject to the Pfizer Agreement, Pfizer will have final decision making authority with respect to all development and commercialization activities for all licensed products.
As of December 31, 2011, we had received aggregate payments of $78.5 million from Pfizer, consisting of a $30.0 million non-refundable upfront cash payment, $17.5 million in reimbursed research and development expenses relating to licensed products, $6.0 million in fees relating to Pfizer’s exercise of its option to license an undisclosed immediate-release opioid analgesic tablet product and hydrocodone bitartrate/acetaminophen tablets, a $5.0 million milestone fee relating to our successful achievement of the primary endpoints for our pivotal Phase III clinical study for Aversion oxycodone HCl with niacin tablets and a $20.0 million milestone fee relating to the FDA’s approval of the Oxecta Tablets NDA. The Pfizer Agreement also provides for Pfizer’s payment to us of a $3.0 million fee upon Pfizer’s exercise of its option for each future opioid analgesic utilizing Aversion Technology. In the event that Pfizer does not exercise its option for a Future Product, Pfizer may be required to reimburse us for certain of our expenses relating to such Future Product. Further, we may receive up to $23 million in additional non-refundable milestone payments for each active opioid analgesic ingredient licensed to Pfizer which achieves certain regulatory milestones in specific countries in the Pfizer Territory. An opioid analgesic product candidate formulated with and without niacin is considered a single product candidate for purposes of the option fees and milestone payments payable under the Pfizer Agreement. We can also receive a one-time $50 million sales milestone payment upon the first attainment of $750 million in net sales of all of our licensed products across all Pfizer Territories. In addition, for sales occurring on and following February 2, 2013 (the one year anniversary of the first commercial sale of Oxecta), Pfizer will pay us a royalty at one of six rates ranging from 5% to 25% based on the level of combined annual net sales for all products licensed by us to Pfizer across all Pfizer Territories, with the highest applicable royalty rate applied to such combined annual sales.
Pfizer’s royalty payment obligations expire on a product-by-product and country-by-country basis upon the later of (i) the expiration of the last valid patent claim covering such product in such country, or (ii) 15 years from the first commercial sale of such product in such country. No minimum annual fees are payable by either party under the Pfizer Agreement. If Pfizer, after consultation with us, enters into a license agreement with a third party to avoid or settle such third party’s allegations or claims regarding freedom to operate against a licensed Aversion Technology product, Pfizer may deduct 50% of any royalties or other license payments it pays to such third party under such license, provided that the royalties payable to us are no less than 80% of the royalties otherwise due to us under the Pfizer Agreement.
The Pfizer Agreement expires upon the expiration of Pfizer’s royalty payment and other payment obligations under the Pfizer Agreement. Pfizer may terminate the Pfizer Agreement (i) in its entirety at any time by written notice to us, and (ii) with respect to any product at any time upon the provision of not less than 12 months’ prior written notice. We may terminate the Pfizer Agreement with respect to a product in the United States in the event such product is not commercially launched by Pfizer within 120 days after receipt of regulatory approval of such product or in its entirety if Pfizer commences any interference or opposition proceeding challenging the validity or enforceability of any of our patent rights licensed to Pfizer under the Pfizer Agreement. Either party has the right to terminate the Pfizer Agreement on a product by product and country-by-country basis if the other party is in material breach of its obligations under the Pfizer Agreement relating to such product and such country, and to terminate the Agreement in its entirety in the event the other party makes an assignment for the benefit of creditors, files a petition in bankruptcy or otherwise seeks relief under applicable bankruptcy laws, in each case subject to applicable cure periods.
In the event of termination, no payments are due except those royalties and milestones that have accrued prior to termination under the Pfizer Agreement and all licenses under the Pfizer Agreement are terminated. For all Acura terminations and termination by Pfizer where we are not in breach, the Pfizer Agreement provides for the transition of development and marketing of the licensed products from Pfizer to us, including the conveyance by Pfizer to us of the trademarks and all regulatory filings and approvals solely used in connection with the commercialization of such licensed products and, in certain cases, for Pfizer’s supply of such licensed products for a transitional period at Pfizer’s cost plus a mark-up.
| 11 |
The foregoing description of the Pfizer Agreement contains forward-looking statements about Oxecta Tablets, and other product candidates being developed pursuant to the Pfizer Agreement. As with any pharmaceutical products under development or proposed to be developed, substantial risks and uncertainties exist in development, regulatory review and commercialization process. There can be no assurance that the Pfizer Agreement will not be terminated by its terms prior to receipt of regulatory approval for any product being developed pursuant to the Pfizer Agreement. Further, there can be no assurance that any product developed pursuant to the Pfizer Agreement will prove to be commercially successful. Accordingly, there is no assurance that the Company will receive the milestone payments or royalty revenues described in the Pfizer Agreement or even if such milestones are achieved, that the related products will be successfully commercialized and that any royalty revenues payable to us by Pfizer will materialize. For further discussion of other risks and uncertainties associated with the Company, see Item 1A in this Report under the heading “Risks Factors”.
Aversion Technology Non-Opioid Products in Development
We are developing the following non-opioid Aversion Technology product:
| Aversion Technology Non-opioid Products | Status | |
| Stimulant immediate-release tablet for treatment of attention deficit disorder | Formulation development |
Our stimulant product in development utilizes our Aversion Technology and is intended for the treatment of attention deficit disorder. Stimulant products are classified as Schedule II controlled substances by the DEA. According to Drugs of Abuse, published by the DEA, stimulants are abused in manners similar to opioid analgesics. The 2009 National Survey on Drug Use and Health estimates that 9.1 million people have abused prescription stimulants at some point in their lifetime and 1.9 million have abused stimulants in the past year. In 2008, IMS Health reported 21.2 million prescriptions were dispensed for stimulant products.
Our stimulant product is intended to be encompassed by our U.S. patent issued in July 2011.
Impede Technology Product Candidates in Development
We are developing the following Impede Technology products:
| Impede Technology Product | Status | |
| Nexafed (pseudoephedrine HCl) 30mg immediate-release tablets | Bioequivalence to Sudafed demonstrated, Abuse deterrent testing and commercial assessment being finalized | |
| Immediate-release pseudoephedrine HCl in combination with other cold and allergy active ingredients | Feasibility studies initiated |
We are developing Nexafed, a 30mg PSE tablet product, utilizing our patent pending Impede Technology. Impede Technology utilizes a proprietary mixture of inactive ingredients intended to impede the extraction of PSE from the tablets for producing methamphetamine or disrupting the direct conversion of PSE in tablets into methamphetamine. Specifically, the Impede Technology forms a viscous, gelatinous mixture when our tablets are dissolved in solvents typically used in the PSE extraction or methamphetamine production processes and trapping the PSE or converted methamphetamine to prevent its isolation or purification. The unique mixture of inactive ingredients in Nexafed is generally recognized as safe by the FDA.
| 12 |
We have demonstrated that our Nexafed 30mg tablets is bioequivalent to Johnson & Johnson’s Sudafed® 30mg Tablets and a 30mg generic store brand. Laboratory tests, sponsored by us at an independent laboratory and confirmed by a law enforcement agency, demonstrated our Impede Technology prevents the extraction of PSE from tablets for conversion into methamphetamine using what we believe are the two most common extraction methods. A third, newer method of methamphetamine production, or “one-pot” method, involves the direct conversion of PSE from tablets into methamphetamine without first extracting and purifying the PSE. Laboratory tests conducted on our behalf by an independent CRO using the “one-pot” method demonstrated that our Impede Technology disrupted the direct conversion of PSE from the tablets into methamphetamine. The study compared the amount of pure methamphetamine hydrochloride provided from Nexafed and Sudafed® tablets. Using one hundred 30mg tablets of both products, multiple one-pot tests and a variety of commonly used solvents, the study demonstrated an average of 38% of the maximum 2.7 grams of pure methamphetamine hydrochloride was recovered from Nexafed. Comparatively, approximately twice as much pure methamphetamine hydrochloride was recovered from Sudafed® tablets. Both products yielded a substantial amount of additional solids such that the purity of the total powder provided contained approximately 65% methamphetamine hydrochloride. We expect to make Nexafed available to pharmacies later this year.
Most PSE-containing products are classified by the FDA for OTC sale, or without a doctor’s prescription, and many product formulations do not require the approval of an NDA or an Abbreviated New Drug Application, or ANDA, by the FDA for commercial distribution and marketing. Tablet products containing 60 mg or less of PSE are considered by the FDA to be safe and effective for use by the general public without a prescription. We believe 30mg Nexafed developed utilizing Impede Technology meets or will meet the FDA’s requirements for “Over-the-Counter Human Drugs Which are Generally Recognized as Safe and Effective and Not Misbranded” as set forth in the FDA’s regulations applicable to OTC Monograph products. As such, we intend to commercialize Nexafed without submitting a NDA or ANDA to the FDA. We have contracted with a third party manufacturer for the scale up and commercial manufacture of Nexafed.
The chemical structure of PSE is very similar to methamphetamine, facilitating a straight-forward chemical conversion to methamphetamine. There are multiple known processes to convert PSE to methamphetamine, all of which are not complex and do not require specialized equipment; however, many do require readily available but uncommon ingredients. Two of the three most popular processes follow two general processing steps: (1) dissolving the PSE tablets in a solvent to isolate purified PSE and (2) a chemical reduction of the PSE into methamphetamine for drying into crystals. The third method, or the “one-pot” method, involves the direct chemical reduction of the PSE to methamphetamine in the presence of the tablet’s inactive ingredients. All the solvents used are ultimately dried off or otherwise removed so a vast range of solvents are amenable to the process.
Methamphetamine is a highly addictive illicit drug used non-medically by an estimated 13 million people at some point in their lifetime. In 2006 regulations relating to over-the counter sale of PSE products were amended with the enactment of the Federal Combat Methamphetamine Epidemic Act, or CMEA. The CMEA was enacted in response to an alarming increase in and widespread conversion of PSE containing products into methamphetamine. Among other things, the CMEA requires retail stores to maintain their inventory of PSE containing products in a secured location and restricts the amount of PSE products a store can sell to an individual customer. Implementation of the CMEA initially reduced the number of illegal methamphetamine laboratory seizures reported by the Drug Enforcement Administration, or DEA, as the then most commonly used process for conversion of PSE to methamphetamine required substantial quantities of PSE. However, a newer process for converting PSE to methamphetamine requires less PSE. Possibly as a result of this new conversion process, the DEA reported 2010 clandestine methamphetamine laboratory seizures increased 84% over the low reported in 2007. Impede Technology is designed to deter the conversion of PSE to methamphetamine, including by use of both the older and newer conversion processes. In response to the ongoing methamphetamine problem, several local jurisdictions (state, counties and/or local municipalities) have enacted or propose to enact legislation to require a physician’s prescription to obtain a PSE-containing product.
PSE is a widely-used nasal decongestant available in many non-prescription and prescription cold, sinus and allergy products. PSE is sold in products as the only active ingredient in both immediate and extended-release products. In addition, PSE is combined with other cold, sinus and allergy ingredients such as pain relievers, cough suppressants and antihistamines. PSE also competes against phenylephrine, an alternate nasal decongestant available in non-prescription products. Our 2010 market research study showed that 93% of the 204 pharmacists surveyed believe that PSE has superior efficacy as a nasal decongestant compared to phenylephrine. Due to the CMEA, many cold, sinus and allergy products replaced PSE with phenylephrine to avoid the security and consumer sales volume restrictions imposed by the CMEA on PSE products.
| 13 |
We expect our Impede Technology products containing PSE to compete in the highly competitive market for cold, sinus and allergy products generally available to consumers without a prescription. In 2009, AC Nielsen reported approximately $1.0 billion in sales of non-prescription products containing either PSE or phenylephrine as a nasal decongestant, of which approximately 47% contained PSE. Products in this category (such as Sudafed®, Claritin-D®, and Zyrtec-D®) have strong consumer brand recognition and, in some cases, prescription drug heritage. Category leading brands are often supported by national mass marketing and promotional efforts. Consumers often have a choice to purchase a less expensive store brand. Store brands contain the same active ingredients as the more popular national brands but are not supported by large marketing campaigns and are offered at a lower price. Non-prescription products are typically distributed through retail outlets including drug store chains, food store chains, independent pharmacies and mass merchandisers. The distribution outlets for PSE products are highly consolidated. According to Chain Drug Review, the top 50 drug, food and mass merchandising chains operate approximately 40,000 pharmacies in the U.S., of which 58% are operated by the four largest chains. Our survey of PSE 30mg tablet prices at these top four drug chains indicates that branded PSE products were priced, on average, to the consumer at approximately $0.25 per tablet as compared to approximately $0.12 per tablet for the corresponding store brand.
In our 2012 survey of 215 chain and independent pharmacists, 164 indicated they had influence over the pharmacies’ product offerings. Of such pharmacists, 70% indicated they were likely to stock or recommend stocking Nexafed in their pharmacies.. The 215 surveyed pharmacists also indicated a willingness to recommend Nexafed to over 50% of their customers who seek a pharmacist’s advise for a single ingredient nasal decongestant. A separate market study conducted on our behalf showed that approximately one-third of consumers seek a pharmacist’s recommendation for their nasal decongestant and, as a result of the CMEA, are required to do so to purchase PSE containing products. We intend to capitalize on this consumer-pharmacist interaction at the point of sale by soliciting distribution to the pharmacies and engaging pharmacists to recommend Nexafed to their customers. We may form a small national account sales staff to sell Nexafed to regional and national retail drug chains. We are also considering creating Nexafed product awareness through local television, radio, and print advertising. No assurance can be given, however, that pharmacy chains will stock our Nexafed product or that consumers will purchase our Nexafed product.
Product Labeling for Impede Technology Products
We intend to market our Nexafed product pursuant to the FDA’s OTC Monograph regulations, which require that our product have labeling as specified in the regulations. We believe, however, we can advertise the extraction characteristics and benefits of our Nexafed product which is supported by our research studies.
We expect that our other Impede Technology products marketed pursuant to an NDA or ANDA will be subject to a label approved by the FDA. We expect that such a label will require submission of our scientifically derived abuse liability data and we intend to seek descriptions of our abuse liability studies in the FDA approved product label, although there can be no assurance that this will be the case.
Competition
Our products and technologies will, if marketed, compete to varying degrees against both brand and generic products offering similar therapeutic benefits and being developed and marketed by small and large pharmaceutical (for prescription products) and consumer packaged goods (for OTC products) companies. Many of our competitors have substantially greater financial and other resources and are able to expend more funds and effort than us in research, development and commercialization of their competitive technologies and products. Prescription generic products and OTC store brand products will offer cost savings to third party payers and/or consumers that will create pricing pressure on our products. Also, these competitors may have a substantial sales volume advantage over our products which may result in our costs of manufacturing being higher than our competitors’ costs.
We believe potential competitors may be developing opioid abuse deterrent technologies and products. Such potential competitors include, but may not be limited to, Pain Therapeutics, in collaboration with Pfizer, Purdue Pharma, Atlantic Pharmaceuticals, Egalet a/s, KemPharm and Collegium Pharmaceuticals, Inc. These companies appear to be focusing their development efforts on ER opioid Products, except for Atlantic Pharmaceuticals, while the majority of our Aversion Technology opioid analgesic product candidates under development, are IR opioid Products. Pfizer, our partner in developing and commercializing Aversion Technology immediate-release opioid products, is also developing and/or marketing ER opioid Products, other analgesic products and non-analgesic products, all of which will compete for development and commercialization resources with our products, which may delay development or adversely impact the sales of our products.
| 14 |
Our Impede Technology products containing PSE will compete in the highly competitive market for cold, sinus and allergy products generally available to the consumer without a prescription. Some of our competitors will have multiple consumer product offerings both within and outside the cold, allergy and sinus category providing them with substantial leverage in dealing with a highly consolidated pharmacy distribution network. The competing products may have well established brand names and may be supported by national or regional advertising. Nexafed will compete directly with Johnson & Johnson’s Sudafed® brand as well as generic formulations manufactured by Perrigo Company and others.
We are aware that some large pharmaceutical companies in the past have sought to develop PSE technologies or products that resist conversion into methamphetamine, but believe those efforts have been discontinued, although there can be no assurance that this is the case. Highland Pharmaceuticals has recently publicized a PSE product that resists PSE extraction in aqueous solutions. We may consider licensing our Impede Technology or products utilizing such technology for commercialization.
Patents and Patent Applications
In April 2007, the United States Patent and Trademark Office, or USPTO, issued to us U.S. Patent No. 7,201,920 titled “Methods and Compositions for Deterring Abuse of Opioid Containing Dosage Forms,” or the 920 Patent. The 54 allowed claims in the 920 Patent encompass certain pharmaceutical compositions intended to deter the most common methods of prescription opioid analgesic product misuse and abuse. These patented pharmaceutical compositions include the mixture of functional inactive ingredients and specific opioid analgesics such as oxycodone HCl and hydrocodone bitartrate among others.
In January 2009, the USPTO issued to us U.S. Patent No. 7,476,402, or the 402 Patent, with 18 allowed claims. The 402 Patent encompasses certain combinations of kappa and mu opioid receptor agonists and other ingredients intended to deter opioid analgesic product misuse and abuse.
In March 2009, the USPTO issued to us U.S. Patent No. 7,510,726, or the 726 Patent, with 20 allowed claims. The ‘726 Patent encompasses a wider range of abuse deterrent compositions than our ’920 Patent.
Neither of the ’920 Patent, ’402 Patent or ‘726 Patent requires niacin to be a constituent of a product for the product to be within the scope of the patent claims.
In July 2011, the USPTO issued to us U.S. Patent No. 7,981,439, or the 439 Patent, with 7 allowed claims. The 439 Patent encompasses certain compositions including any water soluble drug of abuse intended to deter the most common methods of prescription opioid analgesic product misuse and abuse. We believe our stimulant product candidate currently in development is encompassed by the 439 Patent.
In January 2012, the USPTO issued to us U.S. Patent No. 8,101,630, or the 630 Patent with a single claim that encompasses an extended release abuse deterrent dosage form of oxycodone or a pharmaceutically acceptable salt thereof.
In addition to our issued U.S. patents, we have filed multiple U.S. patent applications and international patent applications relating to compositions containing abusable active pharmaceutical ingredients as well as applications covering our Impede Technology. Except for those rights conferred in the Pfizer Agreement, we have retained all intellectual property rights to our Aversion Technology, Impede Technology, and related product candidates.
Reference is made to the Risk Factors contained in Item 1A of this Report for a discussion, among other things, of patent applications and patents owned by third parties including claims that may encompass our Aversion Technology and Oxecta tablets.
| 15 |
Government Regulation
All pharmaceutical firms, including us, are subject to extensive regulation by the federal government, principally by the FDA under the Federal Food, Drug and Cosmetic Act, or the FD&C Act, and, to a lesser extent, by state and local governments. Before our prescription products, and some OTC products may be marketed in the U.S., they must be approved by the FDA for commercial distribution. Other OTC products must comply with applicable FDA regulations, known as OTC Monographs, in order to be marketed, but do not require FDA review and approval before marketing. Additionally, we are subject to extensive regulation by the DEA under the Controlled Substances Act, the Combat Methamphetamine Act of 2005, and related laws and regulations for research, development, manufacturing, marketing and distribution of controlled substances and certain other pharmaceutical active ingredients that are regulated as Listed Chemicals. Extensive FDA, DEA, and state regulation of our products and commercial operations continues after drug product approvals, and the requirements for our continued marketing of our products may change even after initial approval. We are also subject to regulation under federal, state and local laws, including requirements regarding occupational safety, laboratory practices, environmental protection and hazardous substance control, and may be subject to other present and future local, state, federal and foreign regulations, including possible future regulations of the pharmaceutical industry. We cannot predict the extent to which we may be affected by legislative and other regulatory developments concerning our products and the healthcare industry in general.
The FD&C Act, the Controlled Substances Act and other federal statutes and regulations govern the testing, manufacture, quality control, export and import, labeling, storage, record keeping, approval, pricing, advertising, promotion, sale and distribution of pharmaceutical products. Noncompliance with applicable requirements both before and after approval, can subject us, our third party manufacturers and other collaborative partners to administrative and judicial sanctions, such as, among other things, warning letters, fines and other monetary payments, recall or seizure of products, criminal proceedings, suspension or withdrawal of regulatory approvals, interruption or cessation of clinical trials, total or partial suspension of production or distribution, injunctions, limitations on or the limitation of claims we can make for our products, and refusal of the government to enter into supply contracts for distribution directly by governmental agencies, or delay in approving or refusal to approve new drug applications. The FDA also has the authority to revoke or withhold approvals of new drug applications.
FDA approval is required before any "new drug," can be marketed. A "new drug" is one not generally recognized, by experts qualified by scientific training and experience, as safe and effective for its intended use. Our products not subject to and in compliance with an OTC Monograph are new drugs and require prior FDA approval. Such approval must be based on extensive information and data submitted in a NDA, including but not limited to adequate and well controlled laboratory and clinical investigations to demonstrate the safety and effectiveness of the drug product for its intended use(s). In addition to providing required safety and effectiveness data for FDA approval, a drug manufacturer's practices and procedures must comply with cGMPs, which apply to manufacturing, receiving, holding and shipping. Accordingly, manufacturers must continue to expend time, money and effort in all applicable areas relating to quality assurance and regulatory compliance, including production and quality control to comply with cGMPs. Failure to so comply risks delays in approval of drug products and possible FDA enforcement actions, such as an injunction against shipment of products, the seizure of non-complying products, criminal prosecution and/or any of the other possible consequences described above. We are subject to periodic inspection by the FDA and DEA, which inspections may or may not be announced in advance.
The FDA Drug Approval Process
The process of drug development is complex and lengthy. The activities undertaken before a new pharmaceutical product may be marketed in the U.S. generally include, but are not limited to, preclinical studies; submission to the FDA of an Investigational New Drug application, or IND, which must become active before human clinical trials may commence; adequate and well-controlled human clinical trials to establish the safety and efficacy of the product; submission to the FDA of an NDA; acceptance for filing of the NDA by FDA; satisfactory completion of an FDA pre-approval inspection of the clinical trial sites and manufacturing facility or facilities at which the both the active ingredients and finished drug product are produced to assess compliance with, among other things, patient informed consent requirements, the clinical trial protocols, current Good Clinical Practices, or GCP, and cGMPs; and FDA review and approval of the NDA prior to any commercial sale and distribution of the product in the U.S.
| 16 |
Preclinical studies include laboratory evaluation of product chemistry and formulation, and in some cases, animal studies and other studies to preliminarily assess the potential safety and efficacy of the product candidate. The results of preclinical studies together with manufacturing information, analytical data, and detailed information including protocols for proposed human clinical trials are then submitted to the FDA as a part of an IND. An IND must become effective, and approval must be obtained from an Institutional Review Board, or IRB, must be obtained, prior to the commencement of human clinical trials. The IND becomes effective 30 days following its receipt by the FDA unless the FDA objects to, or otherwise raises concerns or questions and imposes a clinical hold. We, the FDA or the IRB may suspend or terminate a clinical trial at any time after it has commenced due to safety or efficacy concerns or for commercial reasons. In the event that FDA objects to the IND and imposes a clinical hold, the IND sponsor must address any outstanding FDA concerns or questions to the satisfaction of the FDA before clinical trials can proceed or resume. There can be no assurance that submission of an IND will result in FDA authorization to commence clinical trials.
Human clinical trials are typically conducted in three phases that may sometimes overlap or be combined:
Phase 1: This phase is typically the first involving human participants, and involves the smallest number of human participants (typically, 20-50). The investigational drug is initially introduced into healthy human subjects or patients and tested for safety, dosage tolerance, absorption, metabolism, distribution and excretion. In addition, it is sometimes possible to gain a preliminary indication of efficacy.
Phase 2: Once the preliminary safety and tolerability of the drug in humans is confirmed during phase 1, phase 2 involves studies in a somewhat larger group of study subjects. Unlike phase 1 studies, which typically involve healthy subjects, participants in phase 2 studies may be affected by the disease or condition for which the product candidate is being developed. Phase 2 studies are intended to identify possible adverse effects and safety risks, to evaluate the efficacy of the product for specific targeted diseases, and to determine appropriate dosage and tolerance.
Phase 3: Phase 3 trials typically involve a large numbers of patients affected by the disease or condition for which the product candidate is being developed. Phase 3 clinical trials are undertaken to evaluate clinical efficacy and safety under conditions resembling those for which the product will be used in actual clinical practice after FDA approval of the NDA. Phase 3 trials are typically the most costly and time-consuming of the clinical phases.
Phase 4: Phase 4 trials may be required by FDA after the approval of the NDA for the product, as a condition of the approval, or may be undertaken voluntarily by the sponsor of the trial. The purpose of phase 4 trials is to continue to evaluate the safety and efficacy of the drug on a long-term basis and in a much larger and more diverse patient population than was included in the prior phases of clinical investigation.
After clinical trials have been completed, and if they were considered successful, the sponsor may submit a NDA or ANDA to the FDA including the results of the preclinical and clinical testing, together with, among other things, detailed information on the chemistry, manufacturing, quality controls, and proposed product labeling. There are two types of NDAs; a 505(b)(1) NDA and a 505(b)(2) NDA. A 505(b)(1) NDA is also known as a "full NDA" and is described by section 505(b)(1) of the FD&C Act as an application containing full reports of investigations of safety and effectiveness, in addition to other information. The data in a full NDA is either owned by the applicant or are data for which the applicant has obtained a right of reference. A 505(b)(2) application is one described under section 505(b)(2) of the FD&C Act as an application for which information, or one or more of the investigations relied upon by the applicant for approval "were not conducted by or for the applicant and for which the applicant has not obtained a right of reference or use from the person by or for whom the investigations were conducted". This provision permits the FDA to rely for approval of an NDA on data not developed by the applicant, such as published literature or the FDA's finding of safety and effectiveness of a previously approved drug. 505(b)(2) applications are submitted under section 505(b)(1) of the FD&C Act and are therefore subject to the same statutory provisions that govern 505(b)(1) applications that require among other things, "full reports" of safety and effectiveness. Pfizer’s submission for Oxecta Tablets was accepted for filing by FDA as a 505(b)(2) NDA.
505(b)(2) NDAs must include one of several different types of patent certifications to each patent that is listed in the FDA publication known as the Orange Book in connection with any previously approved drug, the approval of which is relied upon for approval of the 505(b)(2) NDA. Depending on the type of certification made, the approval of the 505(b)(2) NDA may be delayed until the relevant patent(s) expire, or in the case of a Paragraph IV Certification may lead to patent litigation against the applicant and a potential automatic approval delay of 30 months or more.
| 17 |
Each NDA requires payment of a user fee, pursuant to the requirements of the Prescription Drug User Fee Act, or PDUFA, as periodically amended. According to FDA’s fee schedule, effective on October 1, 2011, for the 2012 fiscal year, the user fee for an application fee requiring clinical data, such as an NDA is $1,841,000. The FDA adjusts PDUFA user fees on an annual basis. PDUFA also imposes annual product and facility fees. The annual product fee for prescription drugs and biologics for the 2012 fiscal year is $98,970 and the annual facility fee for facilities used to manufacture prescription drugs and biologics for the 2012 fiscal year is $520,100. A written request can be submitted for a waiver of the application fee for the first human drug application that is filed by a small business, but no waivers for product or establishment fees are available. Where we are subject to these fees, they are significant expenditures that may be incurred in the future and must be paid at the time of submission of each application to FDA. The Pfizer Agreement provides that Pfizer will pay the NDA application and user fees for the products licensed by the Company to Pfizer pursuant to the Pfizer Agreement.
After an NDA is submitted by an applicant, and if it is accepted for filing by the FDA, the FDA will then review the NDA and, if and when it determines that the data submitted are adequate to show that the product is safe and effective for its intended use, the FDA will approve the product for commercial distribution in the U.S. There can be no assurance that any of our products in development will receive FDA approval or that even if approved, they will be approved with labeling that includes descriptions of its abuse deterrent features. Moreover, even if our products in development are approved with labeling that includes descriptions of the abuse deterrent features of our products, advertising and promotion for the products will be limited to the specific claims and descriptions in the FDA approved product labeling.
The FDA requires drug manufacturers to establish and maintain quality control procedures for manufacturing, processing and holding drugs and investigational products, and products must be manufactured in accordance with defined specifications. Before approving an NDA, the FDA usually will inspect the facility(ies) at which the active pharmaceutical ingredients and finished drug product is manufactured, and will not approve the product unless it finds that cGMP compliance at those facility(ies) are satisfactory. If the FDA determines the NDA is not acceptable, the FDA may outline the deficiencies in the NDA and often will request additional information, thus delaying the approval of a product. Notwithstanding the submission of any requested additional testing or information, the FDA ultimately may decide that the application does not satisfy the criteria for approval. After a product is approved, changes to the approved product, such as adding new indications, manufacturing changes, or changes in or additions to the approved labeling for the product, may require submission of a new NDA or, in some instances, an NDA amendment, for further FDA review. Post-approval marketing of products in larger or different patient populations than those that were studied during development can lead to new findings about the safety or efficacy of the products. This information can lead to a product sponsor’s requesting approval for and/or the FDA requiring changes in the labeling of the product or even the withdrawal of the product from the market.
The Best Pharmaceuticals for Children Act, or BPCA, became law in 2002 and was subsequently reauthorized and amended by FDAAA. The reauthorization of BPCA provides an additional six months of market exclusivity beyond the expiration date of existing market exclusivities or eligible patents to NDA applicants that conduct acceptable pediatric studies of new and currently-marketed drug products for which pediatric information would be beneficial, as identified by FDA in a Pediatric Written Request. The FD&C Act, as amended by the Pediatric Research Equity Act, or PREA, requires that most applications for drugs and biologics include a pediatric assessment (unless waived or deferred) to ensure the drugs' and biologics' safety and effectiveness in children. Such pediatric assessment must contain data, gathered using appropriate formulations for each age group for which the assessment is required, that are adequate to assess the safety and effectiveness of the drug or the biological product for the claimed indications in all relevant pediatric subpopulations, and to support dosing and administration for each pediatric subpopulation for which the drug or the biological product is safe and effective. The pediatric assessments can only be deferred provided there is a timeline for the completion of such studies. FDA may waive (partially or fully) the pediatric assessment requirement for several reasons, including if the applicant can demonstrate that reasonable attempts to produce a pediatric formulation necessary for that age group have failed. The FDA has indicated Pfizer is exempt from the pediatric studies requirement of the PREA for Oxecta.
The terms of approval of any NDA for our product candidates, including the indication and product labeling (and, consequently permissible advertising and promotional claims we can make) may be more restrictive than what is sought in the NDA or what is desired by us. Additionally, the FDA conditioned approval of Oxecta Tablets on Pfizer’s commitment to conduct Phase 4 epidemiological studies to assess the actual abuse levels of Oxecta in the market. The testing and FDA approval process for our product candidates requires substantial time, effort, and financial resources, and we cannot be sure that any approval will be granted on a timely basis, if at all.
| 18 |
Further, drug products by FDA may be subject to continuing obligations intended to assure safe use of the products. Specifically, under the FD&C Act, as amended by the Food and Drug Administration Amendments Act of 2007, or FDAAA, FDA may require Risk Evaluation and Mitigation Strategies, or REMS, to manage known or potential serious risks associated with drugs or biological products. If FDA finds, at the time of approval or afterward, that a REMS is necessary to ensure that the benefits of our products outweigh the risks associated with the products, FDA will require a REMS and, consequently, that we take additional measures to ensure safe use of the product. Components of a REMS may include, but are not limited to, a Medication Guide and/or Patient Package Insert, a marketing and sales communication plan for patients or healthcare providers concerning the drug, Elements To Assure Safe Use, or ETASUs such as, but not limited to, patient, prescriber, and pharmacy registries, and restrictions on the extent or methods of distribution, a REMS implementation system, and a timetable for assessment of the effectiveness of the REMS. The FDA has indicated Pfizer is not required to maintain a REMS for Oxecta.
In addition, we, our suppliers and our licensees are required to comply with extensive FDA requirements both before and after approval. For example, we or our licensees are required to report certain adverse reactions and production problems, if any, to the FDA, and to comply with certain requirements concerning the advertising and promotion of our products, which, as discussed above, may significantly affect the extent to which we can include statements or claims referencing our abuse deterrent technology in product labeling and advertising. Also, quality control and manufacturing procedures must continue to conform to cGMP after approval to avoid the product being rendered misbranded and/or adulterated under the FD&C Act as a result of manufacturing problems. In addition, discovery of any material safety issues may result in changes to product labeling or restrictions on a product manufacturer, potentially including removal of the product from the market.
Whether or not FDA NDA approval in the U.S. has been obtained, approvals from comparable governmental regulatory authorities in foreign countries must be obtained prior to the commencement of commercialization of our drug products in those countries. The approval procedure varies in complexity from country to country, and the time required may be longer or shorter than that required for FDA approval.
FDA’s OTC Monograph Process
The FDA regulates certain non-prescription drugs using an OTC Monograph which, when final, is published in the Code of Federal Regulations at 21 C.F.R. Parts 330-358. For example, 21 C.F.R. Part 341 sets forth the products, such as pseudoephedrine hydrochloride, that may be marketed as an OTC cold, cough, allergy, bronchodilator, or antiasthmatic drug product in a form suitable for oral, inhalant, or topical administration and is generally recognized as safe and effective and is not misbranded. Such products that meet each of the conditions established in the OTC Monograph regulations and the other applicable regulations may be marketed without prior approval by the FDA.
The general conditions set forth for OTC Monograph products include, among other things:
| · | the product is manufactured at FDA registered establishments and in accordance with cGMPs; |
| · | the product label meets applicable format and content requirements including permissible “Indications” and all required dosing instructions and limitations, warnings, precautions and contraindications that have been established in an applicable OTC Monograph; |
| · | the product contains only permissible active ingredients in permissible strengths and dosage forms; |
| · | the product contains only suitable inactive ingredients which are safe in the amounts administered and do not interfere with the effectiveness of the preparation; and |
| · | the product container and container components meet FDA’s requirements. |
The advertising for OTC drug products is regulated by the Federal Trade Commission, or FTC, which generally requires that advertising claims be truthful, not misleading, and substantiated by adequate and reliable scientific evidence. False, misleading, or unsubstantiated OTC drug advertising may be subject to FTC enforcement action and may also be challenged in court by competitors or others under the federal Lanham Act or similar state laws. Penalties for false or misleading advertising may include monetary fines or judgments as well as injunctions against further dissemination of such advertising claims.
| 19 |
A product marketed pursuant to an OTC Monograph must be registered with the FDA and have a National Drug Code listing which is required for all marketed drug products. After marketing, the FDA may test the product or otherwise investigate the manufacturing and development of the product to ensure compliance with the OTC Monograph. Should the FDA determine that a product is not marketed in compliance with the OTC Monograph or is advertised outside of its regulations, the FDA may require corrective action up to and including market withdrawal and recall.
DEA Regulation
Several of our products, if approved and marketed, will be regulated as “controlled substances” as defined in the CSA, which establishes registration, security, recordkeeping, reporting, storage, distribution and other requirements administered by the DEA. The DEA is concerned with the loss and diversion of potentially abused drugs into illicit channels of commerce and closely monitors and regulates handlers of controlled substances, and the equipment and raw materials used in their manufacture and packaging.
The DEA designates controlled substances as Schedule I, II, III, IV or V or as List I Chemicals. Schedule I substances by definition have no established medicinal use, and may not be marketed or sold in the United States. A pharmaceutical product may be listed as Schedule II, III, IV or V, with Schedule II substances considered to present the highest risk of abuse and Schedule V substances the lowest relative risk of abuse among such substances. List I Chemicals are used to regulate potentially abused raw materials, such as pseudoephedrine HCl. We believe all of our products will receive DEA Scheduling consistent with current DEA Scheduling standards. For example, Oxecta Tablets are listed as a Schedule II controlled substances under the CSA, the same as all other oxycodone HCl products. Consequently, their manufacture, shipment, storage, sale and use will be subject to a high degree of regulation. For example, generally, all Schedule II drug prescriptions must be signed by a physician, physically presented to a pharmacist and may not be refilled without a new prescription.
Annual DEA registration is required for any facility that manufactures, tests, distributes, dispenses, imports or exports any controlled substance or List I Chemical. Except for certain DEA defined co-incidental activities, each registration is specific to a particular location and activity. For example, separate registrations are needed for import and manufacturing, and each registration must specify which schedules of controlled substances are authorized.
The DEA typically inspects a facility to review its security measures prior to issuing a registration and, thereafter, on a periodic basis. Security requirements vary by controlled substance schedule, with the most stringent requirements applying to Schedule I and Schedule II substances. Required security measures include, among other things, background checks on employees and physical control of inventory through measures such as vaults, cages, surveillance cameras and inventory reconciliations. Records must be maintained for the handling of all controlled substances and List I Chemicals, and periodic reports made to the DEA, for example distribution reports for Schedule I and II controlled substances, Schedule III substances that are narcotics, and other designated substances. Reports must also be made for thefts or significant losses of any controlled substance and List I Chemicals, and to obtain authorization to destroy any controlled substance and List I Chemicals. In addition, special authorization, notification and permit requirements apply to imports and exports.
In addition, a DEA quota system controls and limits the availability and production of controlled substances in Schedule I or II and List I Chemicals. Distributions of any Schedule I or II controlled substance must also be accomplished using special order forms, with copies provided to the DEA. Because Oxecta Tablets are Schedule II they are subject to the DEA’s production and procurement quota scheme. The DEA establishes annually an aggregate quota for how much oxycodone active ingredient may be produced in total in the United States based on the DEA’s estimate of the quantity needed to meet legitimate scientific and medicinal needs. This limited aggregate amount of oxycodone that the DEA allows to be produced in the United States each year is allocated among individual companies, who must submit applications annually to the DEA for individual production and procurement quotas. We or our licensees must receive an annual quota from the DEA in order to produce or procure any Schedule I or Schedule II substance and List I Chemicals. The DEA may adjust aggregate production quotas and individual production and procurement quotas from time to time during the year, although the DEA has substantial discretion in whether or not to make such adjustments. Our or our licensees’ quota of an active ingredient may not be sufficient to meet commercial demand or complete the manufacture or purchase of material required for clinical trials. Any delay or refusal by the DEA in establishing our or our licensees’ quota for controlled substances or List I Chemicals could delay or stop our clinical trials or product launches, or interrupt commercial sales of our products which could have a material adverse effect on our business, financial position and results of operations.
| 20 |
The DEA also regulates Listed Chemicals, which are chemicals that may be susceptible to abuse, diversion, and use in the illicit manufacture of controlled substances. Some Listed Chemicals, including pseudoephedrine, are used in various prescription and OTC drug products. DEA and state laws and regulations impose extensive recordkeeping, security, distribution, and reporting requirements for companies that handle, manufacture, or distribute Listed Chemicals, including lawful drug products containing Listed Chemicals. In particular, OTC drug products containing certain Listed Chemicals, including pseudoephedrine, are required to be secured behind the pharmacy counter and dispensed to customers directly by a pharmacist only in limited quantities. Pharmacists must obtain proof of identity from customers, and must keep detailed records and make reports to the DEA regarding sales of such products. Individual states may, and in some cases have, imposed stricter requirements on the sale of drug products containing Listed Chemicals, including requiring a doctor’s prescription prior to dispensing such products to a customer.
The DEA conducts periodic inspections of registered establishments that handle controlled substances and Listed Chemicals. Failure to maintain compliance with applicable requirements, particularly as manifested in loss or diversion, can result in enforcement action that could have a material adverse effect on our business, results of operations and financial condition. The DEA may seek civil penalties, refuse to renew necessary registrations, or initiate proceedings to revoke those registrations. In certain circumstances, violations could lead to criminal prosecution.
Individual states also regulate controlled substances and List I Chemicals, and we or our licensees are subject to such regulation by several states with respect to the manufacture and future distribution of these products.
Pharmaceutical Coverage, Pricing and Reimbursement
In the United States, the commercial success of our product candidates will depend, in part, upon the availability of coverage and reimbursement from third-party payers at the federal, state and private levels. Government payer programs, including Medicare and Medicaid, private health care insurance companies and managed care plans may deny coverage or reimbursement for a product or therapy in whole or in part if they determine that the product or therapy is not medically appropriate or necessary. Also, third-party payers have attempted to control costs by limiting coverage and the amount of reimbursement for particular procedures or drug treatments. The United States Congress and state legislatures from time to time propose and adopt initiatives aimed at cost containment, which could impact our ability to sell our products profitably.
For example, in March 2010, President Obama signed into law the Patient Protection and Affordable Care Act, as amended by the Health Care and Education Reconciliation Act, which we refer to collectively as the Health Care Reform Law, a sweeping law intended to broaden access to health insurance, reduce or constrain the growth of healthcare spending, enhance remedies against fraud and abuse, add new transparency requirements for healthcare and health insurance industries, impose new taxes and fees on the health industry and impose additional health policy reforms. Among other cost containment measures, the Healthcare Reform Law establishes:
| · | An annual, nondeductible fee on any entity that manufactures or imports certain branded prescription drugs and biologic agents; |
| · | A new Medicare Part D coverage gap discount program, in which pharmaceutical manufacturers who wish to have their drugs covered under Part D must offer discounts to eligible beneficiaries during their coverage gap period (the “donut hole”); and |
| · | A new formula that increases the rebates a manufacturer must pay under the Medicaid Drug Rebate Program. |
| 21 |
We will not know the full effects of the Health Care Reform Law until applicable federal and state agencies issue regulations or guidance under the new law. Although it is too early to determine the effect of the Health Care Reform Law, the new law appears likely to continue the pressure on pharmaceutical pricing, especially under government programs, and may also increase our or our licensees’ regulatory burdens and operating costs. Moreover, in the coming years, additional changes could be made to governmental healthcare programs that could significantly impact the success of our products.
The cost of pharmaceuticals continues to generate substantial governmental and third-party payer interest. We expect that the pharmaceutical industry will experience pricing pressures due to the trend toward managed healthcare, the increasing influence of managed care organizations and additional legislative proposals. Our or our licensees’ results of operations could be adversely affected by current and future healthcare reforms.
In international markets, reimbursement and healthcare payment systems vary significantly by country, and many countries have instituted price ceilings on specific products and therapies. There can be no assurance that our products will be considered medically reasonable and necessary for a specific indication, that our products will be considered cost-effective by third-party payers, that an adequate level of coverage or payment will be available so that the third-party payers’ reimbursement policies will not adversely affect our ability to sell our products profitably.
Other Healthcare Laws and Compliance Requirements
Our licensees that commercialize our products are subject to various federal and state laws targeting fraud and abuse in the healthcare industry. For example, the federal Anti-Kickback Statute prohibits persons from knowingly and willfully soliciting, receiving, offering or paying remuneration, directly or indirectly, to induce either the referral of an individual, or the furnishing, recommending, or arranging for a good or service, for which payment may be made under a federal healthcare program, such as the Medicare and Medicaid programs. The reach of the Anti-Kickback Statute was broadened by the Health Care Reform Law, which, among other things, amends the intent requirement of the statute so that a person or entity no longer needs to have actual knowledge of this statute or specific intent to violate it in order to have committed a violation. The Healthcare Reform Law also provides that the government may assert that a claim including items or services resulting from a violation of the federal Anti-Kickback Statute constitutes a false or fraudulent claim for purposes of the civil False Claims Act or the civil monetary penalties statute. The civil False Claims Act imposes liability on any person who, among other things, knowingly presents, or causes to be presented, a false or fraudulent claim for payment by a federal healthcare program. The “qui tam” provisions of the False Claims Act allow a private individual to bring civil actions on behalf of the federal government alleging that the defendant has submitted a false claim to the federal government, and to share in any monetary recovery. Violations of these laws or any other federal or state fraud and abuse laws may subject our licensees to civil and criminal penalties, including fines, imprisonment and exclusion from participation in federal healthcare programs, which could harm the commercial success of our products and materially affect our business, financial condition and results of operations.
Facilities for Research, Development, and Manufacturing
We conduct research, development, laboratory, clinical supplies manufacturing and related activities for product candidates utilizing our technologies at our Culver, Indiana facility. The 25,000 square foot facility is registered with the DEA to perform research, development and manufacture of certain DEA-scheduled active pharmaceutical ingredients and finished dosage form products. We obtain quotas for supply of DEA-scheduled active pharmaceutical ingredients from the DEA and develop finished dosage forms in our Culver facility. We manufacture clinical trial supplies of drug products in our Culver facility in volumes sufficient to meet FDA standards for NDAs. Pfizer is responsible for commercial manufacture of the product candidates licensed under the Pfizer Agreement. We expect that future product candidates developed and licensed by us will be commercially manufactured by our licensees or other qualified third party contract manufacturers.
We expect to rely on contract manufacturers to manufacture, package and supply our commercial quantities of our Nexafed PSE Tablet product once commercialized. Initially, we will source our commercial requirements of Nexafed PSE Tablets from a single manufacturer and will not have a second source for this product. Although we believe that there are alternate sources of supply that can satisfy our commercial requirements, replacing or adding a contract manufacturer will result in additional costs and may delay or interrupt the supply of our Nexafed PSE Tablet.
| 22 |
Segment Reporting
We operate in one business segment; the research, development and manufacture of innovative abuse deterrent, orally administered pharmaceutical products.
Environmental Compliance
We are subject to regulation under federal, state and local environmental laws and believe we are in material compliance with such laws. We incur the usual waste disposal cost associated with a pharmaceutical research, development and manufacturing operation.
Raw Materials
To purchase certain active ingredients required for our development and manufacture of product candidates utilizing our Aversion and Impede Technologies, we are required to file for and obtain supply quotas from the DEA. No assurance can be given that we will be successful in obtaining adequate DEA quotas in a timely manner. Even assuming adequate and timely DEA quotas, there can be no assurances that the approved manufacturers of raw materials for our product candidates will supply us with our requirements for the active or inactive ingredients required for the development and manufacture of our product candidates.
Subsidiaries
Our Culver, Indiana research, development, and manufacturing operations are conducted by Acura Pharmaceutical Technologies, Inc., an Indiana corporation and our wholly-owned subsidiary.
Employees
The Company has 15 full-time employees, nine of whom are engaged in the research, development and manufacture of product candidates utilizing our proprietary Aversion® and Impede™ Technologies. The remaining employees are engaged in administrative, legal, accounting, finance, market research, and business development activities. All of our senior management and most of our other employees have had prior experience in pharmaceutical or biotechnology companies. None of our employees is covered by collective bargaining agreements. We believe that our relations with our employees are good.
| 23 |
ITEM 1A. RISK FACTORS
Our future operating results may vary substantially from anticipated results due to a number of factors, many of which are beyond our control. The following discussion highlights some of these factors and the possible impact of these factors on future results of operations. If any of the following factors actually occur, our business, financial condition or results of operations could be materially harmed. In that case, the value of our common stock could decline substantially.
Risks Relating to Our Business and Industry
We are largely dependent on the commercial success of Oxecta and we have not generated any revenue from sales of Oxecta.
We anticipate that, for at least the next several years, our ability to generate revenues and become profitable will depend in large part on the commercial success of our only FDA approved product, Oxecta, which in turn, will depend on several factors, including:
| · | the successful launch of Oxecta in the United States by Pfizer, to whom we have licensed Oxecta; |
| · | Pfizer’s obtaining and increasing market demand for, and sales of, Oxecta; |
| · | obtaining acceptance of Oxecta by physicians and patients; |
| · | obtaining and maintaining adequate levels of coverage and reimbursement for Oxecta from commercial health plans and government health programs, which we refer to collectively as third-party payors, particularly in light of the availability of other branded and generic competitive products; |
| · | maintaining compliance with regulatory requirements; |
| · | Pfizer’s establishing and maintaining agreements with wholesalers and distributors on commercially reasonable terms; |
| · | Pfizer’s manufacture and supply of adequate supplies of Oxecta to meet commercial demand; and |
| · | maintaining intellectual property protection for Oxecta and obtaining favorable drug listing treatment by the FDA to minimize generic competition. |
There can be no assurance that Pfizer will devote sufficient resources to the marketing and commercialization of Oxecta. Pfizer’s marketing of Oxecta may result in low market acceptance and insufficient demand for, and sales of, the product. If Pfizer fails to successfully commercialize Oxecta and increase sales, we may be unable to generate sufficient revenues to sustain or grow our business and we may never become profitable, and our business, financial condition and results of operations will be materially affected.
If Pfizer is not successful in commercializing Oxecta and other licensed product candidates incorporating the Aversion Technology our revenues and our business will suffer.
Pursuant to our license, development and commercialization agreement with a subsidiary of Pfizer, or the Pfizer Agreement, Pfizer is responsible for manufacturing, marketing, pricing, promoting, selling, and distributing Oxecta and certain of our product candidates in development in the United States, Canada and Mexico, or the Pfizer Territory. If such agreement is terminated in accordance with its terms, including due to a party’s failure to perform its obligations or responsibilities under the agreement, then we would need to commercialize the products ourselves for which we currently have no infrastructure, or alternatively enter into a new agreement with another pharmaceutical company, of which no assurance can be given. If we are unable to build the necessary infrastructure to commercialize the products ourselves, which would substantially increase our expenses and capital requirements that we might not be able to fund, or are unable to find a suitable replacement development and commercialization partner, we would be unable to generate any revenues from these products. Even if we are successful at replacing the commercialization capabilities of Pfizer, our revenues and/or royalties for these products could be adversely impacted.
| 24 |
Pfizer’s manufacturing facility is currently the sole commercial source of supply for Oxecta and our other product candidates licensed to Pfizer. If Pfizer’s manufacturing facility fails to obtain sufficient DEA quotas for the opioid active ingredients contained in such product candidates, fails to source adequate quantities of active and inactive ingredients, fails to comply with regulatory requirements, or otherwise experiences disruptions in commercial supply of our product candidates, product revenue and our royalties could be adversely impacted.
Pfizer has a diversified product line for which Oxecta Tablets and our other product candidates licensed to Pfizer will vie for Pfizer’s promotional, marketing, and selling resources. If Pfizer fails to commit sufficient promotional, marketing and selling resources to our products, product revenue and our royalties could be adversely impacted. Additionally, in view of Pfizer’s recent acquisition of King Pharmaceuticals in February 2011, there can be no assurance that Pfizer will commit the resources required for the successful commercialization of Oxecta Tablets or the development and commercialization of our licensed product candidates.
The market for our opioid product candidates is highly competitive with many marketed non-abuse deterrent brand and generic products and other abuse deterrent product candidates in development. If Pfizer prices our product candidates inappropriately, fails to position our products properly, targets inappropriate physician specialties, or otherwise does not provide sufficient promotional support, product revenue and our royalties could be adversely impacted.
Pfizer’s promotional, marketing and sales activities in connection with Oxecta and our other product candidates licensed to Pfizer are subject to various federal and state fraud and abuse laws, including, without limitation, the federal Anti-Kickback Statute and the federal False Claims Act. The federal Anti-Kickback Statute prohibits persons from knowingly and willfully soliciting, receiving, offering or paying remuneration, directly or indirectly, to induce, or in return for, the purchase or recommendation of an item or service reimbursable under a federal healthcare program. The federal False Claims Act imposes liability on any person who, among other things, knowingly presents, or causes to be presented, a false or fraudulent claim for payment by a federal healthcare program. If Pfizer’s activities are found to be in violation of these laws or any other federal and state fraud and abuse laws, Pfizer may be subject to penalties, including civil and criminal penalties, damages, fines and the curtailment or restructuring of its activities with regard to the commercialization of our products, which could harm the commercial success of our products and materially affect our business, financial condition and results of operations.
We have a history of operating losses and may not achieve profitability sufficient to generate a positive return on shareholders’ investment.
We had net income of $10.4 million for the year ended December 31, 2011 and a net loss of $12.7 million and $15.8 million for the years ended December 31, 2010 and 2009, respectively. Our future profitability will depend on several factors, including:
| · | our receipt of milestone payments and royalties relating to our FDA approved Oxecta Tablets, for which we only receive royalties on sales occurring on and following February 2, 2013, the one year anniversary of the first commercial sale of Oxecta Tablets, and other products developed and commercialized under the Pfizer Agreement; |
| · | the receipt of FDA approval and the successful commercialization by Pfizer and other future licensees (if any) of products utilizing our Aversion Technology and our ability to commercialize our Impede Technology without infringing the patents and other intellectual property rights of third parties; and |
| · | our successful development, launch and marketing of Nexafed and other products utilizing our Impede Technology, and market acceptance, increased demand for and sales of Nexafed. |
We cannot assure you that our Oxecta or Nexafed products will be successfully commercialized or our Aversion Technology products in development will be approved for commercialization by the FDA.
| 25 |
We recognized revenues of $20.5 million, $3.3 million and $3.8 million in the years ended December 31, 2011, 2010 and 2009, respectively, from payments received under the Pfizer Agreement. However, we have not yet generated any revenues from Aversion Technology or Impede Technology product sales. Even if we or Pfizer succeed in commercializing one or more of our Aversion Technology products or if we are successful in commercializing our Impede Technology products, we expect to continue using cash reserves for the foreseeable future. Our expenses may increase in the foreseeable future as a result of continued research and development of additional product candidates, maintaining and expanding the scope of our intellectual property, commercializing our Nexafed product, and hiring of additional research and development staff.
We will need to generate revenues from direct product sales or indirectly from royalties on sales to achieve and maintain profitability. If we cannot successfully commercialize Nexafed or successfully develop, obtain regulatory approval and commercialize our products licensed to Pfizer under the Pfizer Agreement or other products under similar license agreements that we may enter into with other pharmaceutical companies in the future, of which no assurance can be given, we will not be able to generate such royalty revenues or achieve future profitability. Our failure to achieve or maintain profitability would have a material adverse impact on the market price of our common stock.
We must rely on current cash reserves, technology licensing fees and third party financing to fund operations.
Pending the receipt of milestone payments and royalties, if any, under the Pfizer Agreement or under similar license agreements that we may enter into with other pharmaceutical companies in the future, of which no assurance can be given, we must rely on our current cash reserves, revenues from sales of Nexafed, if any, and third-party financing to fund operations and product development activities. No assurance can be given that current cash reserves or revenues from Nexafed product sales will be sufficient to fund the continued operations and development of our product candidates until such time as we generate additional revenue from the Pfizer Agreement or any similar future license agreements. Moreover, no assurance can be given that we will be successful in raising additional financing or, if funding is obtained, that such funding will be sufficient to fund operations until product candidates utilizing our Aversion and Impede Technologies may be commercialized.
Our and our licensees’ ability to market and promote Oxecta and other Aversion Technology products by describing the abuse deterrent features of such products will be determined by the FDA approved label for such products.
The commercial success of our Aversion Technology products will depend upon our and our licensees’ ability to obtain FDA approved labeling describing such products’ abuse deterrent features or benefits. Our or our licensees’ failure to achieve FDA approval of product labeling containing such information will prevent or substantiality limit our and our licensees’ advertising and promotion of such abuse deterrent features in order to differentiate Aversion Technology products from other immediate release opioid products containing the same active ingredients, and would have a material adverse impact on our business and results of operations. The FDA has publicly stated that explicit indications or claims of abuse deterrence will not be permitted unless such indications or claims are supported by double blind controlled clinical studies demonstrating an actual reduction in product abuse by patients or drug abusers. Because the cost, time and practicality of designing and implementing clinical studies adequate to support explicit claims of abuse deterrence are prohibitive, we and Pfizer are not pursuing and have not conducted the clinical trials necessary to include an explicit product label claim of abuse deterrence. Instead, we will rely on certain clinical and laboratory studies to support product labeling describing the relative difficulty of abusing or misusing our products and such products’ abuse deterrent features. However, the extent to which such information is included in the FDA approved product label is the subject of our and our licensees’ discussions with, and agreement by, the FDA as part of the NDA review process for each of our product candidates. The outcome of those discussions with the FDA will determine whether we or our licensees will be able to market our products with labeling that sufficiently differentiates them from other products that have comparable therapeutic profiles. While the FDA approved label for Oxecta includes the results from a clinical study which evaluated the effects of nasally snorting crushed Oxecta and commercially available oxycodone tablets and limitations on wetting or dissolving Oxecta, it does not, however, include the results of our laboratory studies intended to evaluate Oxecta’s potential to limit extraction of oxycodone HCl from dissolved Oxecta Tablets and resist conversion into an injectable, or IV solution. The absence of the results of these extraction and syringe studies in the FDA approved label for Oxecta may substantially limit Pfizer’s ability to differentiate Oxecta from other immediate release oxycodone products, which would have a material adverse effect on market acceptance of Oxecta and on our business and results of operations.
| 26 |
Notwithstanding the FDA approved labeling for Oxecta, there can be no assurance that our Aversion Technology products in development will receive FDA approved labeling that describes the abuse deterrent features of such products. If the FDA does not approve labeling containing such information, we or our licensees will not be able to promote such products based on their abuse deterrent features, may not be able to differentiate such products from other immediate release opioid products containing the same active ingredients, and may not be able to charge a premium above the price of such other products which could materially adversely affect our business and results of operations.
Because the FDA closely regulates promotional materials and other promotional activities, even if the FDA initially approves product labeling that includes a description of the abuse deterrent characteristics of our product, as in the case of Oxecta, the FDA may object to our or our licensee’s marketing claims and product advertising campaigns. This could lead to the issuance of warning letters or untitled letters, suspension or withdrawal of Oxecta from the market, recalls, fines, disgorgement of money, operating restrictions, injunctions or criminal prosecution, which could harm the commercial success of our product and materially affect our business, financial condition and results of operations.
Our product candidates are unproven and may not be approved by the FDA.
We are committing a majority of our resources to the development of product candidates utilizing our Aversion and Impede Technologies. Notwithstanding the receipt of FDA approval of Oxecta Tablets, there can be no assurance that the FDA will approve any other product candidate utilizing Aversion Technology for commercial distribution. Further there can be no assurance that other product candidates that may be developed using Aversion Technology or Impede Technology will achieve the targeted end points in the required clinical studies or perform as intended in other pre-clinical and clinical studies or lead to an NDA submission or filing acceptance. Our failure to successfully develop and achieve final FDA approval of our product candidates in development utilizing Aversion Technology will have a material adverse effect on our financial condition.
If the FDA disagrees with our determination that certain of our products meet the over-the-counter, or OTC, requirements, once those products are commercialized, they may be removed from the market; the FDA or the U.S. Federal Trade Commission, or FTC, may object to our advertisement and promotion of the extraction characteristics and benefits of Nexafed.
Drugs that have been deemed safe and effective by the FDA for use by the general public without a prescription are classified as OTC drug products. Certain OTC drug products may be commercialized without premarket review by the FDA if the standards set forth in the applicable regulatory monograph are met. An OTC monograph provides the marketing conditions for the applicable OTC drug product, including active ingredients, labeling, and other general requirements such as compliance with cGMP and establishment registration. Any product which fails to conform to each of the general conditions and a monograph is subject to regulatory action. Further, although the FDA regulates OTC drug product labeling, the FTC regulates the advertising and marketing of OTC drug products. We believe that Nexafed is classified for OTC sale under an FDA OTC monograph which will allow us to commercialize them without submitting an NDA or ANDA to the FDA. We have also determined that, provided we adhere to the FDA’s requirements for OTC monograph products, including product labeling, we can advertise and promote the extraction characteristics and benefits of Nexafed which are supported by our research studies. No assurance can be given, however, that the FDA will agree that Nexafed may be sold under the FDA’s OTC monograph product regulations or that the FDA or FTC will not object to our advertisement and promotion of Nexafed’s extraction characteristics and benefits. If the FDA determines that Nexafed does not conform to the OTC monograph or if we fail to meet the general conditions, once commercialized, the product may be removed from the market and we may face various actions including, but not limited to, restrictions on the marketing or distribution of such products, warning letters, fines, product seizure, or injunctions or the imposition of civil or criminal penalties. Any of these actions may materially and adversely affect our financial condition and operations. If the FDA requires that we submit a NDA or ANDA to obtain marketing approval for Nexafed, this would result in substantial additional costs, delay or suspend the commercialization of Nexafed and require FDA approval prior to sale, of which no assurance can be provided. In such case, the label for Nexafed would be subject to FDA review and approval and there can be no assurance that we will be able to market Nexafed with labeling sufficient to differentiate it from products that have comparable therapeutic profiles. If we are unable to advertise and promote the extraction characteristics of Nexafed, we may be unable to compete with national brands and pharmacy chain store brands.
| 27 |
Our Aversion and Impede Technology products may not be successful in limiting or impeding abuse or misuse upon commercialization.
We are committing a majority of our resources to the development of products utilizing our Aversion and Impede Technologies. Notwithstanding the receipt of FDA approval of Oxecta Tablets and the results of our numerous clinical and laboratory studies for Oxecta and our Aversion and Impede Technology products in development, there can be no assurance that Oxecta or any other product utilizing our Aversion or Impede Technologies will perform as tested and limit or impede the actual abuse or misuse of such products in commercial settings. Moreover, there can be no assurance that the post-approval epidemiological study required by the FDA as a condition of approval of Oxecta will show a reduction in the consequences of abuse and misuse by patients for whom Oxecta is prescribed. The failure of Oxecta or other products utilizing our Aversion and Impede Technologies to limit or impede actual abuse or misuse in practice will have a material adverse impact on market acceptance for such products and on our financial condition and results of operations.
Relying on third party CROs may result in delays in our pre-clinical, clinical or laboratory testing. If pre-clinical, clinical or laboratory testing for our product candidates are unsuccessful or delayed, we will be unable to meet our anticipated development and commercialization timelines.
To obtain FDA approval to commercially sell and distribute in the United States any of our prescription product candidates, we or our licensees must submit to the FDA an NDA demonstrating, among other things, that the product candidate is safe and effective for its intended use. As we do not possess the resources or employ all the personnel necessary to conduct such testing, we rely on CROs for the majority of this testing with our product candidates. As a result, we have less control over our development program than if we performed the testing entirely on our own. Third parties may not perform their responsibilities on our anticipated schedule. Delays in our development programs could significantly increase our product development costs and delay product commercialization.
The commencement of clinical trials with our product candidates may be delayed for several reasons, including but not limited to delays in demonstrating sufficient pre-clinical safety required to obtain regulatory approval to commence a clinical trial, reaching agreements on acceptable terms with prospective CROs, clinical trial sites and licensees, manufacturing and quality assurance release of a sufficient supply of a product candidate for use in our clinical trials and/or obtaining institutional review board approval to conduct a clinical trial at a prospective clinical site. Once a clinical trial has begun, it may be delayed, suspended or terminated by us or regulatory authorities due to several factors, including ongoing discussions with regulatory authorities regarding the scope or design of our clinical trials, a determination by us or regulatory authorities that continuing a trial presents an unreasonable health risk to participants, failure to conduct clinical trials in accordance with regulatory requirements, lower than anticipated recruitment or retention rate of patients in clinical trials, inspection of the clinical trial operations or trial sites by regulatory authorities, the imposition of a clinical hold by FDA, lack of adequate funding to continue clinical trials, and/or negative or unanticipated results of clinical trials.
Clinical trials required by the FDA for commercial approval may not demonstrate safety or efficacy of our product candidates. Success in pre-clinical testing and early clinical trials does not assure that later clinical trials will be successful. Results of later clinical trials may not replicate the results of prior clinical trials and pre-clinical testing. Even if the results of our pivotal phase III clinical trials are positive, we and our licensees may have to commit substantial time and additional resources to conduct further pre-clinical and clinical studies before we or our licensees can submit NDAs or obtain regulatory approval for our product candidates.
Clinical trials are expensive and at times difficult to design and implement, in part because they are subject to rigorous regulatory requirements. Further, if participating subjects or patients in clinical studies suffer drug-related adverse reactions during the course of such trials, or if we, our licensees or the FDA believes that participating patients are being exposed to unacceptable health risks, we or our licensees may suspend the clinical trials. Failure can occur at any stage of the trials, and we or our licensees could encounter problems causing the abandonment of clinical trials or the need to conduct additional clinical studies, relating to a product candidate.
| 28 |
Even if our clinical trials and laboratory testing are completed as planned, their results may not support commercially viable product label claims. The clinical trial process may fail to demonstrate that our product candidates are safe and effective for their intended use. Such failure may cause us or our licensees to abandon a product candidate and may delay the development of other product candidates.
We have no commercial manufacturing capacity and rely on third-party contract manufacturers to produce commercial quantities of our products.
We do not have the facilities, equipment or personnel to manufacture commercial quantities of our products and therefore must rely on our licensees or other qualified third-party contract manufactures with appropriate facilities and equipment to contract manufacture commercial quantities of products utilizing our Aversion and Impede Technologies. These licensees and third- party contract manufacturers are also subject to current good manufacturing practice, or cGMP regulations, which impose extensive procedural and documentation requirements. Any performance failure on the part of our licensees or contract manufacturers could delay commercialization of any approved products, depriving us of potential product revenue.
Our drug products, including Nexafed, require precise, high quality manufacturing. Failure by our contract manufacturers to achieve and maintain high manufacturing standards could result in patient injury or death, product recalls or withdrawals, delays or failures in testing or delivery, cost overruns, or other problems that could materially adversely affect our business. Contract manufacturers may encounter difficulties involving production yields, quality control, and quality assurance. These manufacturers are subject to ongoing periodic unannounced inspection by the FDA and corresponding state and foreign agencies to ensure strict compliance with cGMP and other applicable government regulations; however, beyond contractual remedies that may be available to us, we do not have control over third-party manufacturers’ compliance with these regulations and standards.
If for some reason our contract manufacturers cannot perform as agreed, we may be required to replace them. Although we believe there are a number of potential replacements, we may incur added costs and delays in identifying and qualifying any such replacements. In addition, a new manufacturer would have to be educated in, or develop substantially equivalent processes for, production of our drug candidates.
We or our licensees may not obtain required FDA approval; the FDA approval process is time-consuming and expensive.
The development, testing, manufacturing, marketing and sale of pharmaceutical products are subject to extensive federal, state and local regulation in the United States and other countries. Satisfaction of all regulatory requirements typically takes years, is dependent upon the type, complexity and novelty of the product candidate, and requires the expenditure of substantial resources for research, development and testing. Substantially all of our operations are subject to compliance with FDA regulations. Failure to adhere to applicable FDA regulations by us or our licensees would have a material adverse effect on our operations and financial condition. In addition, in the event we are successful in developing product candidates for distribution and sale in other countries, we would become subject to regulation in such countries. Such foreign regulations and product approval requirements are expected to be time consuming and expensive.
We or our licensees may encounter delays or rejections during any stage of the regulatory review and approval process based upon the failure of clinical or laboratory data to demonstrate compliance with, or upon the failure of the product candidates to meet, the FDA’s requirements for safety, efficacy and quality; and those requirements may become more stringent due to changes in regulatory agency policy or the adoption of new regulations. After submission of an NDA the FDA may refuse to file the application, deny approval of the application, require additional testing or data and/or require post-marketing testing and surveillance to monitor the safety or efficacy of a product. For instance, the FDA’s approval of Oxecta is conditioned on Pfizer conducting a post-approval epidemiological study to assess the actual abuse levels and consequences of Oxecta in the market. The Prescription Drug User Fee Act, or PDUFA, sets time standards for the FDA’s review of NDA’s. The FDA's timelines described in the PDUFA guidance are flexible and subject to change based on workload and other potential review issues and may delay the FDA’s review of an NDA. Further, the terms of approval of any NDA, including the product labeling, may be more restrictive than we or our licensees desire and could affect the marketability of our products.
| 29 |
Even if we comply with all the FDA regulatory requirements, we or our licensees may never obtain regulatory approval for any of our product candidates in development. For example, we previously submitted an NDA to the FDA for an Aversion Technology product containing niacin, intended to provide impediments to over-ingesting the product. Such niacin containing product was not approved by the FDA. If we or our licensees fail to obtain regulatory approval for any of our product candidates in development, we will have fewer commercialized products and correspondingly lower revenues. Even if regulatory approval of our products in development is received, such approval may involve limitations on the indicated uses or promotional claims we or our licensees may make for our products, or otherwise not permit labeling that sufficiently differentiates our product candidates from competitive products with comparable therapeutic profiles but without abuse deterrent features (see risk factor above entitled “Our and our licensees ability to market and promote Oxecta and other Aversion Technology products by describing the abuse deterrent features of such products will be determined by the FDA approved label for such products”). Such events would have a material adverse effect on our operations and financial condition. We may market certain of our products without the prior application to and approval by the FDA. The FDA may subsequently require us to withdraw such products and submit NDA’s for approval prior to re-marketing.
The FDA also has the authority to revoke or suspend approvals of previously approved products for cause, to debar companies and individuals from participating in the drug-approval process, to request recalls of allegedly violative products, to seize allegedly violative products, to obtain injunctions to close manufacturing plants allegedly not operating in conformity with current cGMP and to stop shipments of allegedly violative products. In the event the FDA takes any such action relating to our products (if any are approved by the FDA), such actions would have a material adverse effect on our operations and financial condition.
We must maintain FDA approval to manufacture clinical supplies of our product candidates at our facility; failure to maintain compliance with FDA requirements may prevent or delay the manufacture of our product candidates and costs of manufacture may be higher than expected.
We have installed the equipment necessary to manufacture clinical trial supplies of our Aversion and Impede Technology product candidates in tablet formulations at our Culver, Indiana facility. To be used in clinical trials, all of our product candidates must be manufactured in conformity with cGMP regulations. All such product candidates must be manufactured, packaged, and labeled and stored in accordance with cGMPs. Modifications, enhancements or changes in manufacturing sites of marketed products are, in many circumstances, subject to FDA approval, which may be subject to a lengthy application process or which we may be unable to obtain. Our Culver, Indiana facility, and those of any third-party manufacturers that we or our licensees may use, are periodically subject to inspection by the FDA and other governmental agencies, and operations at these facilities could be interrupted or halted if the FDA deems such inspections are unsatisfactory. Failure to comply with FDA or other governmental regulations can result in fines, unanticipated compliance expenditures, recall or seizure of products, total or partial suspension of production or distribution, suspension of FDA review of our product candidates, termination of ongoing research, disqualification of data for submission to regulatory authorities, enforcement actions, injunctions and criminal prosecution.
We develop our products, and manufacture clinical supplies, at a single location. Any disruption at this facility could adversely affect our business and results of operations.
We rely on our Culver, Indiana facility for developing our product candidates and the manufacture of clinical supplies of our product candidates. If the Culver, Indiana facility were damaged or destroyed, or otherwise subject to disruption, it would require substantial lead-time to repair or replace. If our Culver facility were affected by a disaster, we would be forced to rely entirely on CROs and third-party contract manufacturers for an indefinite period of time. Although we believe we possess adequate insurance for damage to our property and for the disruption of our business from casualties, such insurance may not be sufficient to cover all of our potential losses and may not continue to be available to us on acceptable terms, or at all. Moreover, any disruptions or delays at our Culver, Indiana facility could impair our ability to develop our product candidates utilizing the Aversion or Impede Technologies, which could adversely affect our business and results of operations.
| 30 |
Our operations are subject to environmental, health and safety, and other laws and regulations, with which compliance is costly and which exposes us to penalties for non-compliance.
Our business, properties and product candidates are subject to federal, state and local laws and regulations relating to the protection of the environment, natural resources and worker health and safety and the use, management, storage and disposal of hazardous substances, waste and other regulated materials. Because we own and operate real property, various environmental laws also may impose liability on us for the costs of cleaning up and responding to hazardous substances that may have been released on our property, including releases unknown to us. These environmental laws and regulations also could require us to pay for environmental remediation and response costs at third-party locations where we dispose of or recycle hazardous substances. The costs of complying with these various environmental requirements, as they now exist or may be altered in the future, could adversely affect our financial condition and results of operations.
Our failure to successfully establish new license agreements with pharmaceutical companies for the development and commercialization of our other products in development may adversely impair our ability to develop, market and sell such products.
The Pfizer Agreement grants Pfizer an exclusive license to develop and commercialize Oxecta and certain other opioid analgesic products in the Pfizer Territory. We believe that opportunities exist to enter into agreements similar to the Pfizer Agreement with other partners for the commercialization of these same opioid products outside the Pfizer Territory and for the development and commercialization of additional Aversion Technology and Impede Technology product candidates for other abused and misused drugs, such as tranquilizers, stimulants, sedatives and nasal decongestants in the United States and worldwide. However, there can be no assurance that we will be successful in entering into such license agreements in the future. If we are unable to enter into such agreements, our ability to develop and commercialize our product candidates, and our financial condition and results of operations, would be adversely affected.
If our licensees do not satisfy their obligations, we will be unable to develop our licensed product candidates.
As part of our Pfizer Agreement or other future similar license agreements (if any), we do not and will not have day-to-day control over the activities of our licensees with respect to any product candidate. If a licensee fails to fulfill its obligations under an agreement with us, we may be unable to assume the development of the product candidate covered by that agreement or to enter into alternative arrangements with another third party. In addition, we may encounter delays in the commercialization of the product candidate that is the subject of a license agreement. Accordingly, our ability to receive any revenue from the product candidates covered by such agreements will be dependent on the efforts of our licensee. We could be involved in disputes with a licensee, which could lead to delays in or termination of, our development and commercialization programs and result in time consuming and expensive litigation or arbitration. In addition, any such dispute could diminish our licensee’s commitment to us and reduce the resources they devote to developing and commercializing our products. If any licensee terminates or breaches its agreement, or otherwise fails to complete its obligations in a timely manner, our chances of successfully developing or commercializing our product candidates would be materially adversely effected. Additionally, due to the nature of the market for our product candidates, it may be necessary for us to license all or a significant portion of our product candidates to a single company thereby eliminating our opportunity to commercialize other product candidates with other licensees.
If we fail to maintain our license agreement with Pfizer, we may have to reduce or delay our product candidate development.
Our plan for developing, manufacturing and commercializing Oxecta Tablets and certain other opioid analgesic product candidates utilizing our Aversion Technology currently requires us to maintain our license agreement with Pfizer. In addition to other customary termination provisions, the Pfizer Agreement provides that Pfizer may terminate the Pfizer Agreement at any time upon written notice to us. If Pfizer elects to terminate the Pfizer Agreement, or if we are otherwise unable to maintain our existing relationship with Pfizer, we may have to limit the size or scope of, or delay or abandon the development of, our Aversion Technology opioid analgesic product candidates or undertake and fund development of these product candidates ourselves. If we were required to fund the commercialization efforts with respect to Oxecta Tablets and the development and commercialization efforts to our other Aversion Technology opioid analgesic product candidates on our own, we may need to obtain additional financing, which may not be available on acceptable terms, or at all.
| 31 |
The market may not be receptive to products incorporating our Aversion or Impede Technologies.
The commercial success of our products will depend on acceptance by health care providers and others that such products are clinically useful, cost-effective and safe. There can be no assurance given that our products utilizing the Aversion or Impede Technologies would be accepted by health care providers and others. Factors that may materially affect market acceptance of our product candidates include but are not limited to:
| · | the relative advantages and disadvantages of our products compared to competitive products; |
| · | the relative timing to commercial launch of our products compared to competitive products; |
| · | the relative safety and efficacy of our products compared to competitive products; |
| · | the product labeling approved by the FDA for our products; |
| · | the perception of health care providers of their role in helping to prevent abuse and their willingness to prescribe abuse-deterrent products to do so; |
· the willingness of third party payers to reimburse for our prescription products;
· the willingness of pharmacy chains to stock our Impede Technology products; and
· the willingness of consumers to pay for our products.
Oxecta and our product candidates, if successfully developed and commercially launched, will compete with both currently marketed and new products launched in the future by other companies. Health care providers may not accept or utilize any of our products. Physicians and other prescribers may not be inclined to prescribe our prescription products unless our products demonstrate commercially viable advantages over other products currently marketed for the same indications. Pharmacy chains may not be willing to stock our Impede Technology products and pharmacists may not recommend such products to consumers. Further, consumers may not be willing to purchase our products. If our products do not achieve market acceptance, we may not be able to generate significant revenues or become profitable.
If we are not successful in commercializing Nexafed and other Impede Technology products our revenues and business will suffer.
We intend to market and sell Nexafed to pharmacies. Nexafed will compete in the highly competitive market for cold, sinus and allergy products generally available to the consumer without a prescription. Many of our competitors have substantially greater financial and other resources and are able to expend more funds and effort than us in marketing their competing products. Category leading brands are often supported by regional and national advertising and promotional efforts. Nexafed will compete with national brands as well as pharmacy store brands that are offered at a lower price. There can be no assurance that we will launch or succeed in commercializing Nexafed, or that even if commercialized, that the pricing of Nexafed will allow us to generate significant revenues or profit. Regulations have been enacted in several state or local jurisdictions requiring a doctor’s prescription to obtain pseudoephedrine products. An expansion of such restrictions to other jurisdictions or even nationally will adversely impact our ability to market Nexafed as an OTC product and generate revenue from Nexafed product sales.
If we, our licensees or others identify serious adverse events or deaths relating to any of our products once on the market, we may be required to withdraw our products from the market, which would hinder or preclude our ability to generate revenues.
We or our licensees are required to report to relevant regulatory authorities all serious adverse events or deaths involving our product candidates or approved products. If we, our licensees, or others identify such events, regulatory authorities may withdraw their approvals of such products; we or our licensees may be required to reformulate our products; we or our licensees may have to recall the affected products from the market and may not be able to reintroduce them onto the market; our reputation in the marketplace may suffer; and we may become the target of lawsuits, including class actions suits. Any of these events could harm or prevent sales of the affected products and could materially adversely affect our business and financial condition.
| 32 |
In the event that we or our licensees are successful in bringing any products to market, our revenues may be adversely affected if we fail to obtain insurance coverage or adequate reimbursement for our products from third-party payers.
The ability of our licensees to successfully commercialize our products may depend in part on the availability of reimbursement for our prescription products from government health administration authorities, private health insurers, and other third-party payers and administrators, including Medicaid and Medicare. We cannot predict the availability of reimbursement for newly-approved products utilizing our Aversion Technology. Third-party payers and administrators, including state Medicaid programs and Medicare, are challenging the prices charged for pharmaceutical products. Government and other third-party payers increasingly are limiting both coverage and the level of reimbursement for new drugs. Third-party insurance coverage may not be available to patients for any of our products candidates. The continuing efforts of government and third-party payers to contain or reduce the costs of health care may limit our commercial opportunity. If government and other third-party payers do not provide adequate coverage and reimbursement for any product utilizing our Aversion Technology, health care providers may not prescribe them or patients may ask their health care providers to prescribe competing products with more favorable reimbursement. In some foreign markets, pricing and profitability of pharmaceutical products are subject to government control. In the United States, we expect there may be federal and state proposals for similar controls. In addition, we expect that increasing emphasis on managed care in the United States will continue to put pressure on the pricing of pharmaceutical products. Cost control initiatives could decrease the price that we or our licensees charge for any of our products in the future. Further, cost control initiatives could impair our ability or the ability of our licensees to commercialize our products and our ability to earn revenues from commercialization.
In both the United States and certain foreign jurisdictions, there have been and we expect there will continue to be a number of legislative and regulatory changes to the health care system that could impact our or our licensees’ ability to sell our products profitably. In particular, in 2010, the Patient Protection Affordable Care Act, as amended by the Health Care and Education Reconciliation Act, collectively, the Healthcare Reform Law, was enacted. The Healthcare Reform Law substantially changes the way healthcare is financed by both governmental and private insurers and significantly affects the pharmaceutical industry. Among the provisions of the Healthcare Reform Law of greatest importance to the pharmaceutical industry are the following:
| · | An annual, nondeductible fee on any entity that manufactures or imports certain branded prescription drugs and biologic agents, beginning in 2011; |
| · | An increase in the minimum rebates a manufacturer must pay under the Medicaid Drug Rebate Program; |
| · | A new Medicare Part D coverage gap discount program, under which manufacturers must agree to offer 50 percent point-of-sale discounts off negotiated prices of applicable brand drugs to eligible beneficiaries during their coverage gap period, as a condition for the manufacturer’s outpatient drugs to be covered under Medicare Part D, beginning in 2011; |
| · | Extension of manufacturer’s Medicaid rebate liability to covered drugs dispensed to individuals who are enrolled in Medicaid managed care organizations, effective March 23, 2010; and |
| · | A new Patient-Centered Outcomes Research Institute to oversee, identify priorities in, and conduct comparative clinical effectiveness research. |
At this time, it remains uncertain what the full impact of these provisions will be on the pharmaceutical industry generally or our business in particular.
| 33 |
Consolidation in the healthcare industry could lead to demands for price concessions or for the exclusion of some suppliers from certain of our markets, which could have an adverse effect on our business, financial condition or results of operations.
Because healthcare costs have risen significantly, numerous initiatives and reforms by legislatures, regulators and third-party payers to curb these cost increases have resulted in a trend in the healthcare industry to consolidate product suppliers and purchasers. As the healthcare industry consolidates, competition among suppliers to provide products to purchasers has become more intense. This in turn has resulted and will likely continue to result in greater pricing pressures and the exclusion of certain suppliers from important market segments as group purchasing organizations, and large single accounts continue to use their market power to influence product pricing and purchasing decisions. We expect that market demand, government regulation, third-party reimbursement policies and societal pressures will continue to influence the worldwide healthcare industry, resulting in further business consolidations, which may exert further downward pressure on the prices of our anticipated products. This downward pricing pressure may adversely impact our business, financial condition or results of operations. Under our agreement with Pfizer, Pfizer controls the price of Oxecta and other licensed products and may provide price discounts and price reductions in its discretion. Such price discounts and reductions will reduce the net sales of our licensed products and, correspondingly, our royalty payments, if any, under the Pfizer Agreement.
Our success depends on our ability to protect our intellectual property.
Our success depends on our ability to obtain and maintain patent protection for products developed utilizing our technologies, in the United States and in other countries, and to enforce these patents. The patent positions of pharmaceutical firms, including us, are generally uncertain and involve complex legal and factual questions. Notwithstanding our receipt of U.S. Patent No. 7,201,920 and U.S. Patent No. 7,510,726 from the USPTO encompassing our opioid products utilizing our Aversion Technology, and U.S. Patent No. 7,981,439 encompassing certain non-opioid products utilizing our Aversion Technology, there is no assurance that any of our patent claims in our other pending non-provisional and provisional patent applications relating to our technologies will issue or if issued, that any of our existing and future patent claims will be held valid and enforceable against third-party infringement or that our products will not infringe any third-party patent or intellectual property. Moreover, any patent claims relating to our technologies may not be sufficiently broad to protect our products. In addition, issued patent claims may be challenged, potentially invalidated or potentially circumvented. Our patent claims may not afford us protection against competitors with similar technology or permit the commercialization of our products without infringing third-party patents or other intellectual property rights.
Our success also depends on our not infringing patents issued to others. We may become aware of patents belonging to competitors and others that could require us to obtain licenses to such patents or alter our technologies. Obtaining such licenses or altering our technology could be time consuming and costly. We may not be able to obtain a license to any technology owned by or licensed to a third party that we or our licensees require to manufacture or market one or more of our products. Even if we can obtain a license, the financial and other terms may be disadvantageous.
Our success also depends on maintaining the confidentiality of our trade secrets and know-how. We seek to protect such information by entering into confidentiality agreements with employees, potential licensees, raw material suppliers, contract research organizations, contract manufacturers, consultants and other parties. These agreements may be breached by such parties. We may not be able to obtain an adequate, or perhaps, any remedy to such a breach. In addition, our trade secrets may otherwise become known or be independently developed by our competitors. Our inability to protect our intellectual property or to commercialize our products without infringing third-party patents or other intellectual property rights would have a material adverse affect on our operations and financial condition.
We also rely on or intend to rely on our trademarks, trade names and brand names to distinguish our products from the products of our competitors, and have registered or applied to register many of these trademarks. However, our trademark applications may not be approved. Third parties may also oppose our trademark applications or otherwise challenge our use of the trademarks. In the event that our trademarks are successfully challenged, we could be forced to rebrand our product, which could result in loss of brand recognition and could require us to devote resources to advertising and marketing these new brands. Further, our competitors may infringe our trademarks, or we may not have adequate resources to enforce our trademarks.
| 34 |
We may become involved in patent litigation or other intellectual property proceedings relating to our Aversion or Impede Technologies or product candidates which could result in liability for damages or delay or stop our development and commercialization efforts.
The pharmaceutical industry has been characterized by significant litigation and other proceedings regarding patents, patent applications and other intellectual property rights. The situations in which we may become parties to such litigation or proceedings may include:
| · | litigation or other proceedings we or our licensee(s) may initiate against third parties to enforce our patent rights or other intellectual property rights; |
| · | litigation or other proceedings we or our licensee(s) may initiate against third parties seeking to invalidate the patents held by such third parties or to obtain a judgment that our products do not infringe such third parties’ patents; |
| · | litigation or other proceedings third parties may initiate against us or our licensee(s) to seek to invalidate our patents or to obtain a judgment that third party products do not infringe our patents; |
| · | if our competitors file patent applications that claim technology also claimed by us, we may be forced to participate in interference or opposition proceedings to determine the priority of invention and whether we are entitled to patent rights on such invention; and |
| · | if third parties initiate litigation claiming that our products infringe their patent or other intellectual property rights, we will need to defend against such proceedings. |
The costs of resolving any patent litigation or other intellectual property proceeding, even if resolved in our favor, could be substantial. Many of our potential competitors will be able to sustain the cost of such litigation and proceedings more effectively than we can because of their substantially greater resources. Uncertainties resulting from the initiation and continuation of patent litigation or other intellectual property proceedings could have a material adverse effect on our ability to compete in the marketplace. Patent litigation and other intellectual property proceedings may also consume significant management time.
In the event that a competitor infringes upon our patent or other intellectual property rights, enforcing those rights may be costly, difficult and time consuming. Even if successful, litigation to enforce our intellectual property rights or to defend our patents against challenge could be expensive and time-consuming and could divert our management’s attention. We may not have sufficient resources to enforce our intellectual property rights or to defend our patent or other intellectual property rights against a challenge. If we are unsuccessful in enforcing and protecting our intellectual property rights and protecting our products, it could harm our business. In certain circumstances, our licensee Pfizer has the first right to control the enforcement of certain of our patents against third party infringers. Pfizer may not put adequate resources or effort into such enforcement actions or otherwise fail to restrain infringing products. In addition, in an infringement proceeding, a court may decide that a patent of ours is invalid or is unenforceable, or may refuse to stop the other party from using the technology at issue on the grounds that our patents do not cover the technology in question. An adverse result in any litigation or defense proceedings could put one or more of our patents at risk of being invalidated or interpreted narrowly and could put our patent applications at risk of not issuing.
Our technologies or products may be found to infringe claims of patents owned by others. If we determine that we are, or if we are found to be infringing a patent held by another party, we, our suppliers or our licensees might have to seek a license to make, use, and sell the patented technologies and products. In that case, we, our suppliers or our licensees might not be able to obtain such license on acceptable terms, or at all. The failure to obtain a license to any third party technology that may be required would materially harm our business, financial condition and results of operations. If a legal action is brought against us or our licensee(s), we could incur substantial defense costs, and any such action might not be resolved in our favor. If such a dispute is resolved against us, we may have to pay the other party large sums of money and use of our technology and the testing, manufacturing, marketing or sale of one or more of our products could be restricted or prohibited. Even prior to resolution of such a dispute, use of our technology and the testing, manufacturing, marketing or sale of one or more of our products could be restricted or prohibited.
| 35 |
We are aware of certain United States and international pending patent applications owned by third parties with claims potentially encompassing Oxecta and our Aversion products in development. While we do not expect the claims contained in such pending patent applications will issue in their present form, there can be no assurance that such patent applications will not issue as patents with claims encompassing one or more of our product candidates. If such patent applications result in valid and enforceable issued patents, containing claims in their current form or otherwise encompassing our products we or our licensees may be required to obtain a license to such patents, should one be available, or alternatively, alter our products so as to avoid infringing such third-party patents. If we or our licensees are unable to obtain a license on commercially reasonable terms, or at all, we or our licensees could be restricted or prevented from commercializing our products. Additionally, any alterations to our products or our technologies could be time consuming and costly and may not result in technologies or products that are non-infringing or commercially viable.
We are aware of an issued United States patent owned by a third party having claims encompassing the use of one of our Aversion inactive ingredients in a controlled release pharmaceutical preparation. We are also aware of an issued United States patent owned by a third party having claims encompassing a pharmaceutical preparation containing viscosity producing ingredients that can be drawn into a syringe when dissolved in 10mL’s or less of aqueous solution. While we believe that our Aversion products do not infringe these patents, or that such patents are otherwise invalid, there can be no assurance that we or Pfizer will not be sued for infringing these patents, and if sued, there can be no assurance that we or Pfizer will prevail in any such litigation. If we or Pfizer are found to infringe either or both of these patents, we or Pfizer may seek a license to use the patented technology. If we are unable to obtain such a license, of which no assurance can be given, we or Pfizer may be restricted or prevented from commercializing our Aversion products.
We are aware of certain issued United States patents owned by a third party having claims encompassing a process used to manufacture oxycodone HCl of high purity and pharmaceutical products resulting therefrom. As required by the FDA, Oxecta contains a similar high purity oxycodone HCl manufactured by a supplier that is not the owner or licensee of such patents. The owner of these patents has filed patent infringement actions relating to these patents against companies that have filed abbreviated new drug applications with the FDA for extended-release versions of oxycodone HCl. To our knowledge, the patent owner has not initiated any patent infringement actions against the sellers of immediate-release oxycodone HCl products or their suppliers of oxycodone HCl, however, we cannot be certain that these immediate-release products actually utilize a high purity oxycodone. We cannot provide assurance that Pfizer or its oxycodone HCl supplier will not be sued for infringing these patents. In the event of an infringement action, Pfizer and their oxycodone HCl supplier would have to either: (a) demonstrate that the manufacture of the oxycodone HCl used in Oxecta does not infringe the patent claims, (b) demonstrate the patents are invalid or unenforceable, or (c) enter into a license with the patent owner. If Pfizer or their oxycodone HCl supplier is unable to demonstrate the foregoing, or obtain a license to these patients, Pfizer may be required or choose to withdraw Oxecta from the market.
We cannot assure you that our technologies, products and/or actions in developing our products will not infringe third-party patents. Our failure to avoid infringing third-party patents and intellectual property rights in the development and commercialization of our products would have a material adverse affect on our operations and financial condition.
We may be exposed to product liability claims and may not be able to obtain or maintain adequate product liability insurance.
Our business exposes us to potential product liability risks, which are inherent in the testing, manufacturing, marketing and sale of pharmaceutical products. Product liability claims might be made by patients, or health care providers or others that sell or consume our products. These claims may be made even with respect to those products that possess regulatory approval for commercial sale. We are currently covered by clinical trial product liability insurance on a claims-made basis and expect to expand such coverage to cover Nexafed, if commercialized. This coverage may not be adequate to cover any product liability claims. Product liability coverage is expensive. In the future, we may not be able to obtain coverage for Nexafed or, if obtained, maintain such product liability insurance at a reasonable cost or in sufficient amounts to protect us against losses due to product liability claims. Any claims that are not covered by product liability insurance could have a material adverse effect on our business, financial condition and results of operations. Reference is made to the discussion under the caption “Item 3, Legal Proceedings – Reglan®/Metoclopramide Litigation” for a discussion of pending product liability litigation filed against the Company in each of Pennsylvania, New Jersey, California.
| 36 |
The pharmaceutical industry is characterized by frequent litigation. Those companies with significant financial resources will be better able to bring and defend any such litigation. No assurance can be given that we would not become involved in future litigation, in addition to the ongoing Reglan/Metoclopramide mass tort litigation. Such litigation may have material adverse consequences to our financial condition and results of operations.
We face significant competition which may result in others developing or commercializing products before or more successfully than we do.
Our products and technologies will, if marketed, compete to varying degrees against both brand and generic products offering similar therapeutic benefits and being developed and marketed by small and large pharmaceutical (for prescription products) and consumer packaged goods (for OTC products) companies. Many of our competitors have substantially greater financial and other resources and are able to expend more funds and effort than us in research, development and commercialization of their competitive technologies and products. Prescription generic products and OTC store brand products will offer cost savings to third party payers and/or consumers that will create pricing pressure on our products. Also, these competitors may have a substantial sales volume advantage over our products which may result in our costs of manufacturing being higher than our competitors’ costs. If our products are unable to capture and maintain market share, we or our licensees may not achieve significant product revenues and our financial condition and results of operations will be materially adversely affected.
We believe potential competitors may be developing opioid abuse deterrent technologies and products. Such potential competitors include, but may not be limited to, Pain Therapeutics, in collaboration with Pfizer, Purdue Pharma, Atlantic Pharmaceuticals, Egalet a/s, KemPharm and Collegium Pharmaceuticals, Inc. These companies appear to be focusing their development efforts on ER Opioid Products, except for Atlantic Pharmaceuticals, while the majority of our Aversion Technology opioid analgesic product candidates under development are IR Opioid Products. Pfizer, our partner in developing and commercializing Aversion Technology immediate-release opioid products, is also developing and/or marketing ER Opioid Products, other analgesic products and non-analgesic products, all of which will compete for development and commercialization resources with our products, which may delay development or adversely impact the sales of our products.
Our Impede Technology products containing PSE will compete in the highly competitive market for cold, sinus and allergy products generally available to the consumer without a prescription. Some of our competitors will have multiple consumer product offerings both within and outside the cold, allergy and sinus category providing them with substantial leverage in dealing with a highly consolidated pharmacy distribution network. The competing products may have well established brand names and may be supported by national or regional advertising. Nexafed will compete directly with Johnson & Johnson’s Sudafed® brand as well as generic formulations manufactured by Perrigo Company and others.
We are concentrating a substantial majority of our efforts and resources on developing product candidates utilizing our Aversion and Impede Technologies. The commercial success of products utilizing such technologies will depend, in large part, on the intensity of competition, FDA approved product labeling for our products compared to competitive products, and the relative timing and sequence for commercial launch of new products by other companies developing, marketing, selling and distributing products that compete with the products utilizing our Aversion and Impede Technologies. Alternative technologies and non-opioid products are being developed to improve or replace the use of opioid analgesics. In the event that such alternatives to opioid analgesics are widely adopted, then the market for products utilizing our Aversion and Impede Technologies may be substantially decreased thus reducing our ability to generate future profits.
| 37 |
Key personnel are critical to our business and our success depends on our ability to retain them.
We are dependent on our management and scientific team, including Robert Jones, our President and Chief Executive Officer, and Albert W. Brzeczko, Ph.D., our Vice President of Technical Affairs. We may not be able to attract and retain personnel on acceptable terms given the competition for such personnel among biotechnology, pharmaceutical and healthcare companies, universities and non-profit research institutions. While we have employment agreements with certain employees, all of our employees are at-will employees who may terminate their employment at any time. We do not have key personnel insurance on any of our officers or employees. The loss of any of our key personnel, or the inability to attract and retain such personnel, may significantly delay or prevent the achievement of our product and technology development and business objectives and could materially adversely affect our business, financial condition and results of operations.
Our products are subject in regulation by the U.S. Drug Enforcement Administration, or DEA, and such regulation may affect the development and sale of our products.
The DEA regulates certain finished drug products and active pharmaceutical ingredients, including certain opioid active pharmaceutical ingredients and pseudoephedrine HCl that are contained in our products. Consequently, their manufacture, research, shipment, storage, sale and use are subject to a high degree of regulation. Furthermore, the amount of active ingredients we can obtain for our clinical trials is limited by the DEA and our quota may not be sufficient to complete clinical trials. There is a risk that DEA regulations may interfere with the supply of the products used in our clinical trials.
In addition, we and our contract manufacturers are subject to ongoing DEA regulatory obligations, including, among other things, annual registration renewal, security, recordkeeping, theft and loss reporting, periodic inspection and annual quota allotments for the raw material for commercial production of our products. The DEA, and some states, conduct periodic inspections of registered establishments that handle controlled substances. Facilities that conduct research, manufacture, store, distribute, import or export controlled substances must be registered to perform these activities and have the security, control and inventory mechanisms required by the DEA to prevent drug loss and diversion. Failure to maintain compliance, particularly non-compliance resulting in loss or diversion, can result in regulatory action that could have a material adverse effect on our business, results of operations, financial condition and prospects. The DEA may seek civil penalties, refuse to renew necessary registrations, or initiate proceedings to revoke those registrations. In certain circumstances, violations could lead to criminal proceedings.
Individual states also have controlled substances laws. Though state controlled substances laws often mirror federal law, because the states are separate jurisdictions, they may separately schedule drugs, as well. While some states automatically schedule a drug when the DEA does so, in other states there has to be a rulemaking or a legislative action. State scheduling may delay commercial sale of any controlled substance drug product for which we obtain FDA approval and adverse scheduling could have a material adverse effect on the attractiveness of such product. We or our licensees must also obtain separate state registrations in order to be able to obtain, handle, and distribute controlled substances for clinical trials or commercial sale, and failure to meet applicable regulatory requirements could lead to enforcement and sanctions from the states in addition to those from the DEA or otherwise arising under federal law.
Prior ownership changes limit our ability to use our tax net operating loss carryforwards.
Significant equity restructuring often results in an Internal Revenue Section 382 ownership change that limits the future use of Net Operating Loss, or NOL, carryforwards and other tax attributes. We have determined that an ownership change (as defined by Section 382 of the Internal Revenue Code) did occur as a result of restructuring that occurred in 2004. Neither the amount of our NOL carryforwards nor the amount of limitation of such carryforwards claimed by us have been audited or otherwise validated by the Internal Revenue Service, which could challenge the amount we have calculated. The recognition and measurement of our tax benefit includes estimates and judgment by our management, which includes subjectivity. Changes in estimates may create volatility in our tax rate in future periods based on new information about particular tax positions that may cause management to change its estimates.
| 38 |
Risks Relating to Our Common Stock
Our quarterly results of operations will fluctuate, and these fluctuations could cause our stock price to decline.
Our quarterly and annual operating results are likely to fluctuate in the future. These fluctuations could cause our stock price to decline. The nature of our business involves variable factors, such as the timing of launch and market acceptance of our products, including those licensed to Pfizer, and the timing of the research, development and regulatory submissions of our products in development that could cause our operating results to fluctuate. The forecasting of the timing and amount of sales of our products is difficult due to market uncertainty and the uncertainty inherent in seeking FDA and other necessary approvals for our product candidates. As a result, in some future quarters or years our clinical, financial or operating results may not meet the expectations of securities analysts and investors which could result in a decline in the price of our stock.
Volatility in stock prices of other companies may contribute to volatility in our stock price.
The market price of our common stock, like the market price for securities of pharmaceutical and biotechnology companies, has historically been highly volatile. The stock market from time to time experiences significant price and volume fluctuations unrelated to the operating performance of particular companies. Factors, such as fluctuations in our operating results, future sales of our common stock, announcements of the timing and amount of product sales, of our products, announcements of technological innovations or new therapeutic products by us or our competitors, announcements regarding collaborative agreements, laboratory or clinical trial results, government regulation, FDA determinations on the approval of a product candidate NDA submission, developments in patent or other proprietary rights, public concern as to the safety of drugs developed by us or others, changes in reimbursement policies, comments made by securities analysts and general market conditions may have a substantial effect on the market price of our common stock. In the past, following periods of volatility in the market price of a company’s securities, securities class action litigation and shareholder derivative litigation has often been instituted. A securities class action suit or shareholder derivative suit against us could result in substantial costs, potential liabilities and the diversion of management’s attention and resources and result in a material adverse affect on our financial condition and results of operations. Reference is made to the discussion under “Item 3, Legal Proceedings – Securities Class Action and Derivative Litigation” for a discussion of a pending securities class action litigation filed against us in the United States District Court for the Northern District of Illinois, Eastern Division, and three shareholder derivative suits filed in the Circuit Court of Cook County, Illinois, Chancery Division.
Our stock price has been volatile and there may not be an active, liquid trading market for our common stock.
Our stock price has experienced significant price and volume fluctuations and may continue to experience volatility in the future. Factors that may have a material impact on the price of our common stock, in addition to the other issues described herein, include the launch and commercial success of Oxecta and Nexafed, results of or delays in our pre-clinical and clinical studies, any delays in, or failure to receive FDA approval of our product candidates, the success of our license agreement with Pfizer, announcements of technological innovations or new commercial products by us or others, developments in patents and other proprietary rights by us or others, future sales of our common stock by existing stockholders, regulatory developments or changes in regulatory guidance, the departure of our officers, directors or key employees, and period-to-period fluctuations in our financial results. Also, you may not be able to sell your shares at the best market price if trading in our stock is not active or if the volume is low. There is no assurance that an active trading market for our common stock will be maintained on the NASDAQ Capital Market.
The National Association of Securities Dealers, Inc., or NASD, and the Securities and Exchange Commission, or SEC, have adopted rules relating to the listing of publicly traded stock. If we were unable to continue to comply with such rules, we could be delisted from trading on the NASDAQ Capital Market and thereafter trading in our common stock, if any, would be conducted through the Over-the-Counter Bulletin Board of the NASD. As a consequence of such delisting, an investor would likely find it more difficult to dispose of, or to obtain quotations as to the price of, our common stock. Delisting of our common stock from the NASDAQ Capital Market could also result in lower prices per share of our common stock than would otherwise prevail.
| 39 |
We do not have a history of paying dividends on our common stock.
Historically we have not declared and paid any cash dividends on our common stock. We intend to retain all of our earnings for the foreseeable future to finance the operation and expansion of our business. As a result, you may only receive a return on your investment in our common stock if the market price of our common stock increases.
GCE Holdings LLC can control all matters requiring approval by shareholders.
GCE Holdings LLC beneficially owns approximately 72.5% of our outstanding common stock as of December 31, 2011 (calculated in accordance with Rule 13d-3 promulgated under the Securities Exchange Act of 1934, as amended). As a result, GCE Holdings LLC, in view of its ownership percentage of our common stock, will be able to control all matters requiring approval by our shareholders, including the approval or rejection of mergers, sales or licenses of all or substantially all of our assets, or other business combination transactions. The interests of GCE Holdings LLC may not always coincide with the interests of our other shareholders and as such we may take action in advance of its interests to the detriment of our other shareholders. Accordingly, you may not be able to influence any action we take or consider taking, even if it requires a shareholder vote.
We are currently a “Controlled Company” within the meaning of the NASDAQ Capital Market Listing Requirements and, as a result, are exempt from certain corporate governance requirements.
Because GCE Holdings LLC controls more than 50% of the voting power of our common stock, we are currently considered to be a “controlled company” for purposes of a NASDAQ Capital Market listing requirements. As such, we are permitted, and have elected, to opt out of the NASDAQ Capital Market listing requirements that would otherwise require our board of directors to have a majority of independent directors, our board nominations to be selected, or recommended for the board’s selection either by a nominating committee comprised entirely of independent directors or by a majority of independent directors, and our compensation committee to be comprised entirely of independent directors. Accordingly, you may not have the same protections afforded to stockholders of companies that are subject to all of the NASDAQ Capital Market corporate governance requirements.
Any future sale of a substantial number of shares included in our current registration statement could depress the trading price of our stock, lower our value and make it more difficult for us to raise capital.
In accordance with the terms of the Securities Purchase Agreement dated August 20, 2007 between us and the investors named therein, we filed a registration statement with and declared effective by the SEC, to register the shares included in our Units issued pursuant to the Securities Purchase Agreement, including shares underlying warrants included in the Units. In addition, pursuant to the exercise of previously granted piggyback registration rights, each of GCE Holdings, LLC, Galen Partners III, L.P., Galen Partners International III, L.P., Galen Employee Fund III, L.P., Care Capital Investments II, LP, Care Capital Offshore Investments II, LP and Essex Woodlands Health Ventures V, L.P. have exercised their piggyback registration rights to include an aggregate of 26,584,016 shares in such registration statement. As a result, 34,243,273 shares (representing approximately 65% of our shares outstanding on a fully-diluted basis – including all derivative securities, whether or not currently exercisable) are available for resale by selling stockholders under the registration statement. If some or all of the shares included in such registration statement are sold by our affiliates and others it may have the effect of depressing the trading price of our common stock. In addition, such sales could lower our value and make it more difficult for us to raise capital if needed in the future.
ITEM 1B. UNRESOLVED STAFF COMMENTS
The Company has received no written comments regarding periodic or current reports from the staff of the SEC that were issued 180 days or more preceding the end of its 2011 fiscal year that remain unresolved.
ITEM 2. PROPERTIES
We lease from an unaffiliated Lessor, approximately 1,600 square feet of administrative office space at 616 N. North Court, Suite 120, Palatine, Illinois 60067. The lease agreement has a term expiring March 31, 2013. The lease agreement provides for rent, property taxes, common area maintenance, and janitorial services on an annualized basis of approximately $29,000 per year. We utilize this lease space for our administrative, marketing and business development functions.
| 40 |
We conduct research, development, laboratory, development scale and NDA submission batch scale manufacturing and other activities relating to developing product candidates using Aversion and Impede Technologies at our facility located at 16235 State Road 17, Culver, Indiana. At this location, our wholly-owned subsidiary Acura Pharmaceutical Technologies, Inc., owns a 25,000 square foot facility with 7,000 square feet of warehouse, 8,000 square feet of manufacturing space, 4,000 square feet of research and development labs and 6,000 square feet of administrative and storage space. The facility is located on 28 acres of land.
ITEM 3. LEGAL PROCEEDINGS
Securities Class Action and Derivative Litigation
A lawsuit captioned Bang v. Acura Pharmaceuticals, et al, was filed on September 10, 2010 in the United States District Court for the Northern District of Illinois, Eastern Division (Case 1:10-cv-05757) against us and certain of our current and former officers seeking unspecified damages on behalf of a putative class of persons who purchased our common stock (the “Affected Securities”) between February 21, 2006 and April 22, 2010 (the “Plaintiff Class”). The complaint alleged that certain Company officers made false or misleading statements, or failed to disclose material facts in order to make statements not misleading, relating to our Acurox® with Niacin Tablet product candidate, resulting in violations of Section 10(b) of the Securities Exchange Act of 1934 (the “Exchange Act”), Rule 10b-5 under the Exchange Act and Section 20(a) of the Exchange Act. The complaint further alleges that such false or misleading statements or omissions had the effect of artificially inflating the price of our common stock. On March 14, 2011, an amended complaint was filed in this lawsuit. The amended complaint asserts the same claims as the initial complaint based upon the same alleged false or misleading statements, and has added three of our current directors as defendants. The Court has changed the caption of this case to In re Acura Pharmaceuticals, Inc. Securities Litigation. We filed a motion to dismiss this case on May 13, 2011.
On October 31, 2011, we entered into a Stipulation of Settlement (“Stipulation”) providing for the release of all claims against the Company and its named directors and officers (the “Defendants”) in this case, for a payment of $1.5 million. The Company and the individual defendants continue to deny all charges of wrongdoing or liability against them relating to this action and the Stipulation does not contain or constitute any admission or finding of wrongful conduct, acts or omissions on the part of any Defendant. On December 16, 2011, our insurance carrier paid the $1.5 million settlement amount into an escrow account to fund the settlement.
In consideration of the payment of the settlement amount, the Plaintiff Class has agreed, upon final approval by the court, to dismiss the class action with prejudice and release all known and unknown claims arising out of or relating to, or in connection with the purchase or acquisition of the Affected Securities during the class period which have been or could have been asserted by the members of the Plaintiff Class. On February 16, 2012, the court entered final approval of the settlement reflected in the Stipulation.
On October 25, 2010, Kiley Hill, a purported stockholder of the Company filed a shareholder derivative action in the Circuit Court of Cook County, Illinois, Chancery Division captioned Hill v. Acura Pharmaceuticals et al. (Case No. 2010-CH-46380), against our directors and certain of our executive officers, generally relating to the same events that are the subject of the class action litigation described above. The complaint purports to be brought on our behalf and names us as a nominal defendant. The complaint seeks unspecified damages from the individual defendants for breaches of fiduciary duty, abuse of control, gross mismanagement, contribution and indemnification, waste of corporate assets and unjust enrichment for actions occurring from at least February 21, 2006 through April 22, 2010. Substantively similar complaints captioned Hagan v. Acura Pharmaceuticals et al. (Case No. 2010-CH-46621) and Newell v. Reddick et al (Case No. 2010-CH-46873) were filed in the Circuit Court of Cook County, Illinois, Chancery Division, by other purported stockholders of the Company on October 27, 2010 and October 28, 2010, respectively. We filed a motion to dismiss these shareholder derivative actions on November 23, 2011.
| 41 |
Reglan®/Metoclopramide Litigation
Halsey Drug Company, as predecessor to us, has been named along with numerous other companies as a defendant in cases filed in three separate state coordinated litigations pending in Pennsylvania, New Jersey and California, respectively captioned In re: Reglan®/Metoclopramide Mass Tort Litigation, Philadelphia County Court of Common Pleas, January Term, 2010, No. 01997; In re: Reglan® Litigation, Superior Court of New Jersey, Law Division, Atlantic County, Case No. 289, Master Docket No. ATL-L-3865-10; and Reglan®/Metoclopramide Cases, Superior Court of California, San Francisco County, Judicial Council Coordination Proceeding No. 4631, Superior Court No.: CJC-10-004631. In this product liability litigation against numerous pharmaceutical product manufacturers and distributors, including us, plaintiffs claim injuries from their use of the Reglan brand of metoclopramide and generic metoclopramide. In the Pennsylvania state court mass tort proceeding, over 200 lawsuits have been filed against us and Halsey Drug Company alleging that plaintiffs developed neurological disorders as a result of their use of the Reglan brand and/or generic metoclopramide. Plaintiffs have filed approximately 150 lawsuits against us, but have served less than 50 individual lawsuits upon us in the New Jersey action. In the California action, we were not served with any complaints until the Spring of 2011 when a single complaint including over 400 plaintiffs was served. To date, Acura has not been served with any metoclopramide lawsuits in jurisdictions other than Philadelphia, New Jersey and California state courts.
In the lawsuits filed to date, plaintiffs have not confirmed they ingested any of the generic metoclopramide manufactured by us. We discontinued manufacture and distribution of generic metoclopramide more than 15 years ago. In addition, we believe the June 23, 2011 decision by the U.S. Supreme Court in PLIVA v. Mensing (“Mensing decision”) holding that state tort law failure to warn claims against generic drug companies are pre-empted by the 1984 Hatch-Waxman Act Amendments and federal drug regulations will assist us in favorably resolving these cases. We have consistently maintained the position that these claims are without merit and intend to vigorously defend these actions.
In Philadelphia, New Jersey and California, Generic Defendants, including Acura, have filed dispositive motions based on the Mensing decision. The New Jersey and California courts are expected to issue their rulings in the 1st quarter of 2012. On November 18, 2011, the Philadelphia trial court denied Generic Defendants’ dispositive motion. In December 2011, the Generic Defendants appealed this ruling, which the trial court refused to modify on reconsideration. Nonetheless, the trial court has approved certification of the federal preemption issues based on the Mensing decision for immediate appeal to the Pennsylvania Superior Court. A decision on this appeal should be issued later this year which could result in dismissal of all of the Philadelphia cases against Generic Defendants, although there can be no assurance in this regard.
ITEM 4. MINE SAFETY DISLCOSURE
Not Applicable.
| 42 |
PART II
ITEM 5. MARKET FOR REGISTRANT'S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES
Market and Market Prices of Common Stock
Set forth below for the periods indicated are the high and low sales prices for trading in our common stock on the NASDAQ Capital Market as reported by the NASDAQ Capital Market.
| Period | Sale Prices | |||||||||
| High | Low | |||||||||
| 2010 Fiscal Year | ||||||||||
| First Quarter | 6.06 | 4.33 | ||||||||
| Second Quarter | 9.13 | 2.50 | ||||||||
| Third Quarter | 2.95 | 2.25 | ||||||||
| Fourth Quarter | 3.98 | 2.20 | ||||||||
| 2011 Fiscal Year | ||||||||||
| First Quarter | 3.62 | 2.91 | ||||||||
| Second Quarter | 6.80 | 3.16 | ||||||||
| Third Quarter | 4.10 | 2.28 | ||||||||
| Fourth Quarter | 5.49 | 2.97 | ||||||||
| 2012 Fiscal Year | ||||||||||
| First Quarter (through January 31, 2012) | 4.22 | 3.17 | ||||||||
Holders
There were approximately 600 holders of record of our common stock on February 29, 2012. This number, however, does not reflect the ultimate number of beneficial holders of our common stock.
Dividend Policy
The payment of cash dividends is subject to the discretion of our Board of Directors and is dependent upon many factors, including our earnings, our capital needs and our general financial condition. Historically we have not paid any cash dividends.
Securities Authorized for Issuance under Equity Compensation Plans
Reference is made to the Company’s Proxy Statement for its 2012 Annual Meeting of Shareholders under the caption “Compensation of Executive Officers and Directors - Restricted Stock Unit Award Plan; and Securities Authorized for Issuance under Equity Compensation Plans”.
ITEM 6. SELECTED FINANCIAL DATA
The selected consolidated financial data presented below for the years ended December 31, 2011, 2010, 2009, 2008 and 2007 are derived from our audited Consolidated Financial Statements. The Consolidated Financial Statements as of December 31, 2011 and 2010 and for each of the years in the three-year period ended December 31, 2011, and the reports thereon, are included elsewhere in this Report. The selected financial information presented for our 2008 and 2007 operations and for our 2009, 2008 and 2007 balance sheets are derived from our audited Consolidated Financial Statements not presented in this Report.
| 43 |
The information set forth below is qualified by reference to, and should be read in conjunction with, the Consolidated Financial Statements and related notes thereto included elsewhere in this Report and "Item 7. Management's Discussion and Analysis of Financial Condition and Results of Operations". All share data gives effect to the 1 for 10 reverse stock split implemented December 5, 2007.
| OPERATING DATA (in thousands) except per share data | 2011 | 2010 | 2009 | 2008 | 2007 | |||||||||||||||
| Revenues | $ | 20,466 | $ | 3,311 | $ | 3,835 | $ | 44,437 | $ | 6,404 | ||||||||||
| Operating expenses: | ||||||||||||||||||||
| Research and development(1) | 4,037 | 7,177 | 5,673 | 14,322 | 7,169 | |||||||||||||||
| Marketing, general and administrative(2) | 5,895 | 8,858 | 11,662 | 9,133 | 4,141 | |||||||||||||||
| Interest expense | — | — | — | — | (1,207 | ) | ||||||||||||||
| Interest income | 32 | 42 | 147 | 780 | 268 | |||||||||||||||
| Amortization of debt discount & deferred private debt offering costs | — | — | — | — | (2,700 | ) | ||||||||||||||
| (Loss) gain on fair value change of conversion features | — | — | — | — | (3,483 | ) | ||||||||||||||
| (Loss) gain on fair value change of common stock warrants | — | — | — | — | (1,905 | ) | ||||||||||||||
| Other (expense) income | (34 | ) | (14 | ) | (3 | ) | (3 | ) | 19 | |||||||||||
| (Loss) income before income tax | 10,532 | (12,696 | ) | (13,356 | ) | 21,759 | (13,914 | ) | ||||||||||||
| Income tax expense (benefit) | 147 | 11 | 2,479 | 7,285 | (9,600 | ) | ||||||||||||||
| Net (loss) income applicable to common stockholders | $ | 10,385 | $ | (12,707 | ) | $ | (15,835 | ) | $ | 14,474 | $ | (4,314 | ) | |||||||
| (Loss) earnings per share: Basic | $ | 0.22 | $ | (0.27 | ) | $ | (0.35 | ) | $ | 0.32 | $ | (0.11 | ) | |||||||
| (Loss) earnings per share: Diluted | $ | 0.22 | $ | (0.27 | ) | $ | (0.35 | ) | $ | 0.29 | $ | (0.11 | ) | |||||||
| Weighted average shares used in computing net earnings (loss) per share: Basic | 47,496 | 47,029 | 45,932 | 45,675 | 39,157 | |||||||||||||||
| Weighted average shares used in computing net earnings (loss) per share: Diluted | 48,007 | 47,029 | 45,932 | 49,416 | 39,157 | |||||||||||||||
(1) Includes stock-based compensation expense of approximately $500, $1,700, $1,900, $600 and $400 for years 2011, 2010, 2009, 2008 and 2007, respectively.
(2) Includes stock-based compensation expense of approximately $1,900, $5,100, $7,300, $3,300 and $500 for years 2011, 2010, 2009, 2008 and 2007, respectively.
| BALANCE SHEET DATA(3) (in thousands) | 2011 | 2010 | 2009 | 2008 | 2007 | |||||||||||||||
| Working capital | $ | 35,599 | $ | 23,289 | $ | 28,750 | $ | 35,991 | $ | 22,306 | ||||||||||
| Total assets | 37,173 | 25,493 | 31,917 | 42,961 | 45,628 | |||||||||||||||
| Total liabilities | 530 | 1,152 | 2,007 | 5,897 | 26,908 | |||||||||||||||
| Accumulated deficit | (325,543 | ) | (335,928 | ) | (323,221 | ) | (307,386 | ) | (321,860 | ) | ||||||||||
| Stockholders' equity | $ | 36,643 | $ | 24,341 | $ | 29,910 | $ | 37,064 | $ | 18,720 | ||||||||||
(3) Reflects $30 million received from Pfizer in December, 2007.
ITEM 7. MANAGEMENT'S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS
This discussion and analysis should be read in conjunction with our financial statements and accompanying notes included elsewhere in this Report. Operating results are not necessarily indicative of results that may occur in the future periods. Certain statements in this Report under this Item 7, Item 1, "Business", Item 1A, “Risk Factors” and elsewhere in this Report constitute "forward-looking statements" within the meaning of the Private Securities Litigation Reform Act of 1995. Such forward-looking statements involve known and unknown risks, uncertainties and other factors which may cause our actual results, performance or achievements or industry results, to be materially different from any future results, performance, or achievements expressed or implied by such forward-looking statements. See page 1 of this Report for a description of the most significant of such factors.
| 44 |
Company Overview
We are a specialty pharmaceutical company engaged in the research, development and commercialization of products intended to address medication abuse and misuse, utilizing our proprietary Aversion and Impede technologies. Our products and product candidates are based on widely-used commercial products and do not alter the safety and efficacy of the active pharmaceutical ingredients.
Our lead product, Oxecta (oxycodone HCI, USP) Tablets CII, or Oxecta (formerly Acurox), was approved for marketing by the United States Food and Drug Administration, or FDA, on June 17, 2011. Oxecta is an immediate-release oxycodone hydrochloride, or HCl, tablet utilizing our proprietary Aversion Technology. Oxecta represents the first immediate-release oxycodone product approved by the FDA that applies our Aversion technology. Aversion is a mixture of inactive ingredients incorporated into pharmaceutical tablets and capsules designed to address some common methods of product tampering. Oxecta will be manufactured and commercialized by Pfizer under our October 2007 license agreement with a subsidiary of Pfizer and was made commercially available by Pfizer on January 23, 2012. We are eligible to receive tiered royalties ranging from 5% to 25% on net sales of Oxecta. The royalties commence February 2, 2013, the first anniversary of the first commercial sale of Oxecta,. The trademark Oxecta® is owned by Pfizer or its affiliate.
In addition to Oxecta, we have licensed to Pfizer the rights to develop, manufacture and commercialize three other immediate-release opioid products utilizing our Aversion Technology in the United States, Canada and Mexico, including:
| · | hydrocodone bitartrate / acetaminophen tablets; |
| · | oxycodone HCl / acetaminophen tablets; and |
| · | an undisclosed opioid analgesic tablet product. |
We believe our Aversion Technology can also be used to develop and commercialize unique formulations of non-opioid pharmaceutical products associated with abuse and intentional misuse. Our initial non-opioid product candidate is a stimulant product for the treatment of attention deficit disorder.
We are also developing Nexafed, an over-the-counter, or OTC, immediate-release pseudoephedrine HCl tablet, utilizing our proprietary Impede Technology. Pseudoephedrine HCl, or PSE, is a widely-used nasal decongestant available in many non-prescription and prescription cold, sinus and allergy products, including Johnson & Johnson’s Sudafed®. Our Impede Technology is a proprietary mixture of inactive ingredients designed to impede the extraction of PSE from tablets for producing methamphetamine or disrupting the direct conversion of PSE in tablets into methamphetamine.
Company’s Present Financial Condition
At December 31, 2011, we had cash and cash equivalents of $35.7 million compared to $24.0 million of cash and cash equivalents at December 31, 2010. We had working capital of $35.6 million at December 31, 2011 compared to working capital of $23.3 million at December 31, 2010. We had an accumulated deficit of approximately $325.5 million and $335.9 million at December 31, 2011 and December 31, 2010, respectively. We had income from operations of approximately $10.5 million and net income of $10.4 million for the year ended December 31, 2011, compared to a loss from operations of $12.7 million and a net loss of $12.7 million for the year ended December 21, 2010. As of February 15, 2012 we had cash and cash equivalents of approximately $34.2 million.
During the year ended December 31, 2011, we recognized revenues of $0.5 million derived from the amortized portion of the $30.0 million upfront cash payment received from Pfizer’s King Pharmaceuticals subsidiary in December 2007, and a $20.0 million milestone fee paid by Pfizer under the Pfizer Agreement relating to FDA approval of the NDA for Oxecta. During the year ended December 31, 2010, we recognized revenues of $3.3 million derived from the $1.1 million amortized portion of the $30.0 million upfront cash payment received from King in December 2007 and $2.2 million for reimbursement of research and development expenses for Oxecta Tablets. We have yet to generate any product sales or royalty revenues from product sales. To fund our continued operations, we expect to rely on our current cash resources, additional payments that may be made under Pfizer Agreement and under future license agreements with other pharmaceutical company partners, of which there can be no assurance of obtaining, and revenues, if any, from our commercialization of our Nexafed Tablets. Our cash requirements for operating activities may increase in the future as we continue to conduct pre-clinical studies and clinical trials for our product candidates, maintain, defend, if necessary and expand the scope of our intellectual property, hire additional personnel, contract with third party contract manufacturers for the commercial supply of our Nexafed Tablets, commercialize our Nexafed Tablets, or invest in other areas.
| 45 |
Our losses have resulted principally from costs incurred in connection with research and development activities, salaries and other personnel-related costs and general corporate expenses. Research and development activities include costs of pre-clinical studies, clinical trials, and clinical trial product supplies associated with our product candidates. Salaries and other personnel-related costs include non-cash, stock-based compensation associated with stock options and restricted stock units granted to employees and non-employee directors.
Results of Operations for the Years Ended December 31, 2011 and 2010
| December 31 | ||||||||||||||||
| 2011 | 2010 | Change | ||||||||||||||
| $000’s | $000’s | Percent | ||||||||||||||
| Revenues | ||||||||||||||||
| Program fee revenue | 466 | 1,088 | (622 | ) | (57 | ) | ||||||||||
| Collaboration fee revenue | — | 2,233 | (2,233 | ) | (100 | ) | ||||||||||
| Milestone revenue | 20,000 | — | 20,000 | — | ||||||||||||
| Total revenue | 20,466 | 3,311 | 17,155 | 518 | ||||||||||||
| Operating expenses | ||||||||||||||||
| Research and development | 4,037 | 7,177 | (3,140 | ) | (44 | ) | ||||||||||
| Marketing, general and administrative | 5,895 | 8,858 | (2,963 | ) | (33 | ) | ||||||||||
| Total operating expenses | 9,932 | 16,035 | (6,103 | ) | (38 | ) | ||||||||||
| Income (loss) from operations | 10,534 | (12,724 | ) | 23,258 | 183 | |||||||||||
| Other income (expense) | ||||||||||||||||
| Interest income | 32 | 12 | 20 | 167 | ||||||||||||
| Other expense | (34 | ) | (14 | ) | (20 | ) | (142 | ) | ||||||||
| Total other income (expense) | (2 | ) | 28 | (30 | ) | (107 | ) | |||||||||
| Income (loss) before income tax | 10,532 | (12,696 | ) | 23,228 | 183 | |||||||||||
| Income tax expense | 147 | 11 | 136 | 1,236 | ||||||||||||
| Net income (loss) | 10,385 | (12,707 | ) | 23,092 | 182 | |||||||||||
Revenue
In December 2007, Pfizer paid us a $30.0 million upfront fee in connection with the closing of the Pfizer Agreement. Program fee revenue recognized during 2011 from amortizing this upfront fee was $0.5 million compared to $1.1 million in 2010. We have assigned an equal portion of the program fee revenue to each of three product candidates identified under the Pfizer Agreement. We have completed our development activities on all 3 product candidates, fully amortized the portion of the upfront fee for two product candidates in 2008, and fully amortized the portion of the upfront fee for the third product candidate in 2011. We had milestone revenue of $20.0 million and $0 in 2011 and 2010, respectively.
In 2011 we incurred no development or regulatory expenses relating to the licensed products pursuant to the Pfizer Agreement, and therefore recognized no collaboration revenue for such year. We do not expect collaboration revenue from Pfizer in 2012. The Company had collaboration revenue of $2.2 million for 2010.
| 46 |
Operating Expenses
Research and development expense during 2011 and 2010 were primarily for product candidates utilizing our Aversion and Impede Technologies, including costs of preclinical studies, clinical trials, clinical supplies and related formulation and design costs, salaries and other personnel related expenses, and facility costs. Included in the 2011 and 2010 results are non-cash stock-based compensation charges of $0.5 million and $1.7 million, respectively, associated with the grant of stock options and restricted stock units. Excluding the stock-based compensation expense, in 2011 there was a $2.0 million decrease in development expenses compared to 2010 primarily attributable to a reduction in development activities for our Aversion Technology product candidates.
Marketing expenses during 2011 and 2010 consisted of market research studies on our Aversion and Impede Technologies. Our general and administrative expenses primarily consisted of legal, audit and other professional fees, corporate insurance, and payroll. Included in the 2011 and 2010 results are non-cash stock-based compensation charges of $1.9 million and $5.1 million, respectively, associated with the grant of stock options and restricted stock units. Excluding the stock-based compensation expense, in 2011 there was an increase of $0.2 million in marketing, general and administrative expenses compared to 2010.
Other Income (Expense)
During 2011 and 2010, we had no debt and cash proceeds received pursuant to the Pfizer Agreement were invested in U.S. Treasury Bills and money market funds in accordance with the investment policy approved by our Board of Directors, resulting in minimal interest income in 2011 and 2010 due to the prevailing low variable, market rates of interest.
Net Income (Loss)
In 2011, the Company was able to utilize existing net operating loss carryforwards to offset the majority of its 2011 federal and state income taxes. The income tax expense is comprised of federal alternative minimum taxes as well as state income taxes totaling $0.1 million. The Company has maintained a full valuation allowance on its deferred tax asset due to the uncertainty of future utilization of the Company’s net operating losses. The net loss of $12.7 million for 2010 includes no federal or state income tax benefit provisions due to uncertainty of their future utilization. A state tax expense was recorded for the Company’s subsidiary operations apportioned to one state jurisdiction.
| 47 |
Results of Operations for the Years Ended December 31, 2010 and 2009
| December 31 | ||||||||||||||||
| 2010 | 2009 | Change | ||||||||||||||
| $000’s | $000’s | Percent | ||||||||||||||
| Revenues | ||||||||||||||||
| Program fee revenue | 1,088 | 3,077 | (1,989 | ) | (65 | ) | ||||||||||
| Collaboration fee revenue | 2,223 | 758 | 1,465 | 193 | ||||||||||||
| Total revenue | 3,311 | 3,835 | (524 | ) | (14 | ) | ||||||||||
| Operating expenses | ||||||||||||||||
| Research and development | 7,177 | 5,673 | 1,504 | 27 | ||||||||||||
| Marketing, general and administrative | 8,858 | 11,662 | (2,804 | ) | (24 | ) | ||||||||||
| Total operating expenses | 16,035 | 17,335 | (1,300 | ) | (8 | ) | ||||||||||
| Loss from operations | (12,724 | ) | (13,500 | ) | (776 | ) | (6 | ) | ||||||||
| Other income (expense) | ||||||||||||||||
| Interest income | 42 | 147 | (105 | ) | (71 | ) | ||||||||||
| Other expense | (14 | ) | (3 | ) | 11 | 367 | ||||||||||
| Total other income | 28 | 144 | (116 | ) | (81 | ) | ||||||||||
| Loss before income tax | (12,696 | ) | (13,356 | ) | (660 | ) | (5 | ) | ||||||||
| Income tax expense | 11 | 2,479 | (2,468 | ) | (100 | ) | ||||||||||
| Net loss | (12,707 | ) | (15,835 | ) | (3,128 | ) | (20 | ) | ||||||||
Revenue
In December 2007, Pfizer paid us a $30.0 million upfront fee in connection with the closing of the Pfizer Agreement. Program fee revenue recognized during 2010 from amortizing this upfront fee was $1.1 million compared to $3.0 million in 2009. We have assigned an equal portion of the program fee revenue to each of three product candidates identified under the Pfizer Agreement. We have completed our development activities on 2 of the 3 product candidates, fully amortized the portion of the upfront fee for two product candidates in 2008. We had no milestone revenue in 2010 or 2009.
Collaboration revenue recognized in 2010 was $2.2 million for reimbursement, pursuant to the Pfizer Agreement, of our development and regulatory expenses incurred during 2010 relating to the licensed products. We invoice Pfizer in arrears on a calendar quarter basis for our reimbursable development and regulatory expenses under the Pfizer Agreement. We expect the amount and timing of collaboration revenue to fluctuate in relation to the amount and timing of the underlying research and development expenses. The Company had collaboration revenue of $0.8 million for 2009.
Operating Expenses
Research and development expense during 2010 and 2009 were primarily for product candidates utilizing our Aversion and Impede Technologies, including costs of preclinical studies, clinical trials, clinical supplies and related formulation and design costs, salaries and other personnel related expenses, and facility costs. Included in the 2010 and 2009 results are non-cash stock-based compensation charges of $1.7 million and $1.9 million, respectively, associated with the grant of stock options and restricted stock units. Excluding the stock-based compensation expense, in 2010 there was a $1.7 million increase in development expenses compared to 2009 primarily attributable to development activities for our Aversion Technology product candidate, an extended release opioid product candidate, and our Nexafed tablet product.
| 48 |
Marketing expenses during 2010 and 2009 consisted of market research studies on our Aversion and Impede Technologies. Our general and administrative expenses primarily consisted of legal, audit and other professional fees, corporate insurance, and payroll. Included in the 2010 and 2009 results are non-cash stock-based compensation charges of $5.1 million and $7.3 million, respectively, associated with the grant of stock options and restricted stock units. Excluding the stock-based compensation expense, in 2010 there was a decrease of $0.6 million in marketing, general and administrative expenses compared to 2009.
Other Income (Expense)
During 2010 and 2009, we had no debt and cash proceeds received pursuant to the Pfizer Agreement were invested in U.S. Treasury Bills and money market funds in accordance with the investment policy approved by our Board of Directors, resulting in minimal interest income in 2010 and $0.1 million in 2009 due to the prevailing low variable, market rates of interest.
Net Loss
The net loss of $12.7 million for 2010 includes no federal or state income tax benefit provisions due to uncertainty of their future utilization. A state tax provision was recorded for the Company’s subsidiary operations apportioned to one state jurisdiction. The Company’s net loss of $15.8 million for 2009 included income tax expense of $2.5 million recorded when we adjusted our deferred income tax asset valuation reserve. We determined it was more likely than not that the Company’s net operating loss carryforwards may not be utilized.
Liquidity and Capital Resources
At December 31, 2011, we had cash and cash equivalents of $35.7 million compared to $24.0 million in cash and cash equivalents at December 31, 2010. We had working capital of $35.6 million at December 31, 2011 compared to $23.3 million at December 31, 2010. The increases in our 2011 cash position and working capital of $11.6 million and $12.3 million, respectively, and the cash flows provided by operating activities of $12.3 million for the year ended December 31, 2011, are primarily due to a $20.0 million milestone fee paid by Pfizer to us pursuant to the Pfizer Agreement relating to the receipt of FDA approval of the NDA for Oxecta. Our investing activities in 2011 were less than $0.2 million in capital expenditures, and in 2010 our investing activities were less than $0.1 million in capital expenditures.
At February 15, 2012, we had cash and cash equivalents of approximately $34.2 million. We estimate that such cash reserves will be sufficient to fund the development of Aversion Technology and Impede Technology product candidates, and related operating expenses at least through the next 12 months.
Pending our receipt of milestone payments and royalties from Pfizer related to product candidates developed under the Pfizer Agreement, other milestone and royalty payments under similar license agreements anticipated to be negotiated and executed with other pharmaceutical company partners, and revenues from the commercialization of our Nexafed tablets, of which no assurance can be given, we must rely on our current cash reserves, including interest income from the investment of our cash reserves, to fund the development of our Aversion Technology, Impede Technology and related administrative and operating expenses. Our future sources of revenue, if any, will be derived from milestone payments and royalties under the Pfizer Agreement and under similar license agreements with other pharmaceutical company partners, and from the commercialization of our Nexafed tablets, for which there can be no assurance.
The amount and timing of our future cash requirements will depend on regulatory and market acceptance of our product candidates and the resources we devote to the development and commercialization of our product candidates.
| 49 |
The following table presents our expected cash payments on contractual obligations outstanding as of December 31, 2011:
| Payments due by period (in thousands) | ||||||||||||||||||||
| Total | Less than 1 year | 1-3 years | 3-5 years | More than 5 years | ||||||||||||||||
| Operating leases | $ | 31 | $ | 25 | $ | 6 | $ | — | $ | — | ||||||||||
| Marketing studies | 41 | 41 | — | — | — | |||||||||||||||
| Clinical studies | 133 | 133 | — | — | — | |||||||||||||||
| Employment agreements | 602 | 602 | — | — | — | |||||||||||||||
| Total | $ | 807 | $ | 801 | $ | 6 | $ | — | $ | — | ||||||||||
Off-Balance Sheet Arrangements
We do not engage in transactions or arrangements with unconsolidated or other special purpose entities.
Critical Accounting Policies
The preparation of our financial statements in accordance with United States generally accepted accounting principles requires us to make estimates and assumptions that affect the reported amounts of assets, liabilities, revenues and expenses in our financial statements and accompanying notes. We evaluate our estimates on an ongoing basis, including those estimates related to contract agreements, research collaborations and investments. We base our estimates on historical experience and various other assumptions that we believe to be reasonable under the circumstances, the results of which form the basis for making judgments about the carrying values of assets and liabilities that are not readily apparent from other sources. Actual results may differ from these estimates under different assumptions or conditions. The following items in our financial statements require significant estimates and judgments:
Revenue Recognition, Deferred Program Fee Revenue and Collaboration Revenue
We recognize revenue when there is persuasive evidence that an arrangement exists, delivery has occurred, the price is fixed and determinable, and collection is reasonably assured. In connection with Pfizer Agreement, we recognize program fee revenue, collaboration revenue and milestone revenue.
Program fee revenue is derived from amortized upfront payments, such as the $30.0 million upfront payment from Pfizer received in December 2007, and license fees, such as the $3.0 million option exercise fee paid by King to us in each of May 2008 and December 2008 upon the exercise of its option to license a third and fourth opioid analgesic product candidate under the Pfizer Agreement. We have assigned an equal portion of Pfizer’s $30.0 million upfront payment to each of three product candidates identified in the Pfizer Agreement and recognize the upfront payment as program fee revenue ratably over our estimate of the development period for each identified product candidate. We recognized $0.5, $1.1 million, $3.1 million and $21.9 million of this program fee revenue in 2011, 2010, 2009 and 2008, respectively.
Collaboration revenue is derived from reimbursement of development expenses, which are invoiced quarterly in arrears, and are recognized when costs are incurred pursuant to the Pfizer Agreement. The ongoing research and development services being provided to Pfizer under the collaboration are priced at fair value based upon the reimbursement of expenses incurred pursuant to the collaboration with Pfizer. We recognized $0, $2.2 million, $0.8 million and $11.5 million of collaboration revenue in 2011, 2010, 2009 and 2008, respectively.
Milestone revenue is contingent upon the achievement of certain pre-defined events in the development of Oxecta Tablets and other product candidates licensed to Pfizer under the Pfizer Agreement. Milestone payments from Pfizer are recognized as revenue upon achievement of the “at risk” milestone events, which represent the culmination of the earnings process related to that milestone. Milestone payments are triggered either by the results of our research and development efforts or by events external to us, such as regulatory approval to market a product. As such, the milestones are substantially at risk at the inception of the Pfizer Agreement, and the amounts of the payments assigned thereto are commensurate with the milestone achieved. In addition, upon the achievement of a milestone event, we have no future performance obligations related to that milestone payment. Each milestone payment is non-refundable and non-creditable when made. In June 2008, Pfizer paid us a $5.0 million milestone payment for successfully achieving the primary endpoints in our pivotal Phase III study, AP-ADF-105 for Aversion oxycodone HCl with Niacin Tablets. In June 2011, Pfizer paid us a $20.0 million milestone fee relating to the receipt of FDA approval of the NDA for Oxecta.
| 50 |
Research and Development
Research and Development, or R&D, expenses include internal R&D activities, external CRO services and their clinical research sites, and other activities. Internal R&D activity expenses include facility overhead, equipment and facility maintenance and repairs, laboratory supplies, pre-clinical laboratory experiments, depreciation, salaries, benefits, and share-based compensation expenses. CRO activity expenses include preclinical laboratory experiments and clinical trial studies. Other activity expenses include regulatory consulting, and regulatory legal counsel. Internal R&D activities and other activity expenses are charged to operations as incurred. We make payments to the CRO's based on agreed upon terms and may include payments in advance of the study starting date. We review and accrue CRO expenses and clinical trial study expenses based on services performed and rely upon estimates of those costs applicable to the stage of completion of a study as provided by the CRO. Accrued CRO costs are subject to revisions as such studies progress to completion. Revisions are charged to expense in the period in which the facts that give rise to the revision become known. We have entered into several cancelable CRO arrangements and our obligations under these arrangements were approximately $133,000 and $68,000 at December 31, 2011 and 2010, respectively, for services to be incurred as subjects are enrolled and progress through the studies.
Income Taxes
We account for income taxes under the liability method. Under this method, deferred income tax assets and liabilities are determined based on differences between financial reporting and income tax basis of assets and liabilities and are measured using the enacted income tax rates and laws that will be in effect when the differences are expected to reverse. Additionally, net operating loss and tax credit carryforwards are reported as deferred income tax assets. The realization of deferred income tax assets is dependent upon future earnings. A valuation allowance against deferred income tax assets is required if, based on the weight of available evidence, it is more likely than not that some or all of the deferred income tax assets may not be realized. Because we realized taxable income in 2011 we were able to utilize a portion of our net operating loss carryforwards. At December 31, 2011, 100% of the remaining deferred income tax assets are offset by a valuation allowance due to uncertainties with respect to future utilization of net operating loss carryforwards. We recorded adjustments by way of increase of $2.5 million to the deferred income tax asset valuation allowance during 2009. This adjustment recognized a $2.5 million tax expense from income taxes in our income for 2009. If in the future it is determined that amounts of our deferred income tax assets would likely be realized, the valuation allowance would be reduced in the period in which such determination is made and a benefit from income taxes in such period would be recognized.
Stock Compensation
Compensation cost related to stock-based payment transactions is measured based on fair value of the equity or liability instrument issued. For purposes of estimating the fair value of each stock option unit on the date of grant, we utilized the Black-Scholes option-pricing model. The Black-Scholes option valuation model was developed for use in estimating the fair value of traded options, which have no vesting restrictions and are fully transferable. In addition, option valuation models require the input of highly subjective assumptions including the expected volatility factor of the market price of our common stock (as determined by reviewing its historical public market closing prices). Our accounting for stock-based compensation for restricted stock units, or RSUs, is based on the fair-value method. The fair value of the RSUs is the market price of our common stock on the date of grant, less its exercise cost.
| 51 |
Capital Expenditures
Our capital expenditures during 2011, 2010 and 2009 were $132,000, $41,000 and $220,000, respectively. Capital expenditures in each such year were primarily attributable to the purchase of scientific equipment and improvements to the Culver, Indiana facility.
Impact of Inflation
We believe that inflation did not have a material impact on our operations for the periods reported.
ITEM 7A. QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK
Some of the securities that we invest in may be subject to market risk. Our primary objective in our cash management activities is to preserve principal while at the same time maximizing income we receive from our investments. A change in the prevailing interest rates may cause the principal amount of our investments to fluctuate. We have no holdings of derivative financial and commodity instruments. As of December 31, 2011, our investments consisted primarily of investments in U.S. Treasury Bills and money market accounts with variable, market rates of interest.
ITEM 8. FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA
The consolidated financial statements of Acura Pharmaceuticals, Inc. and Subsidiary and the Report of the Independent Registered Public Accounting Firm thereon, to be filed pursuant to Item 8 are included in Item 15.
ITEM 9. CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE
Not applicable.
| 52 |
ITEM 9A. CONTROLS AND PROCEDURES
Evaluation of Disclosure Controls and Procedures. We have conducted an evaluation, under the supervision and with the participation of our management, including our Chief Executive Officer and Chief Financial Officer of the effectiveness of the design and operation of our disclosure controls and procedures pursuant to Exchange Act Rule 13a-15(e). Based upon that evaluation, our Chief Executive Officer and Chief Financial Officer concluded that our disclosure controls and procedures are effective in timely alerting them to material information relating to the Company (including our subsidiary) required to be included in our periodic Securities and Exchange Commission filings. No significant changes were made in our internal controls or in other factors that could significantly affect these controls subsequent to the date of their evaluation. The Company’s independent registered public accounting firm was not required to and did not express an opinion on the effectiveness of the Company’s internal control over financial reporting.
Management’s Report on Internal Control Over Financial Reporting. Our management is responsible for establishing and maintaining adequate internal control over financial reporting. Internal control over financial reporting is defined in Rule 13a-15(f) and 15d-15(f) promulgated under the Exchange Act as a process designated by, or under the supervision of, our principal executive and principal financial officers and effected by our board of directors, management and other personnel, to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles and includes those policies and procedures that:
| · | Pertain to the maintenance of records that in reasonable detail accurately and fairly reflect the transactions and disposition of our assets; |
| · | Provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that our receipts and expenditures are being made only in accordance with authorizations of our management and directors; and |
| · | Provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use or disposition of our assets that could have a material effect on the financial statements. |
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Therefore, even those systems determined to be effective can provide only reasonable assurance with respect to financial statement preparation and presentation. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Our management assessed the effectiveness of our internal control over financial reporting as of December 31, 2011. In making this assessment, management used the criteria set forth by the Committee of Sponsoring Organizations of the Treadway Commission (COSO) in Internal Control – Integrated Framework. Based on our assessment, management believes that, as of December 31, 2011, our internal control over financial reporting is effective based on those criteria.
Changes in Internal Control Over Financial Reporting. There was no change in our internal control over financial reporting that occurred during the Fourth Quarter 2011 that materially affected, or is reasonably likely to materially affect, our internal control over financial reporting.
ITEM 9B. OTHER INFORMATION
Not Applicable.
| 53 |
PART III
| ITEM 10. | DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE |
Reference is made to 2012 Proxy Statement to be filed with the SEC on or about March 9, 2012 with respect to Directors, Executive Officers and Corporate Governance, which is incorporated herein by reference and made a part hereof in response to the information required by Item 10.
| ITEM 11. | EXECUTIVE COMPENSATION. |
Reference is made to our 2012 Proxy Statement to be filed with the SEC on or about March 9, 2012 with respect to Executive Compensation, which is incorporated herein by reference and made a part hereof in response to the information required by Item 11.
| ITEM 12. | SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS. |
Reference is made to our 2012 Proxy Statement to be filed with the SEC on or about March 9, 2012 with respect to the to the security ownership of certain beneficial owners and management and related stockholder matters, which is incorporated herein by reference and made a part hereof in response to the information required by Item 12.
| ITEM 13. | CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE |
Reference is made to our 2012 Proxy Statement to be filed with the SEC on or about March 9, 2012 with respect to certain relationships and related transactions and direct independence, which is incorporated herein by reference and made a part hereof in response to the information required by Item 13.
| ITEM 14. | PRINCIPAL ACCOUNTANT FEES AND SERVICES |
Reference is made to our 2012 Proxy Statement to be filed with the SEC on or about March 9, 2012 with respect to auditor fees, which is incorporated herein by reference and made a part in response to the information required by Item 14.
PART IV
| ITEM 15. | EXHIBITS AND FINANCIAL STATEMENT SCHEDULES |
(a) The following documents are filed as part of this report:
| 1. | All Financial Statements: See Index to Financial Statements |
| 2. | Financial Statement Schedules: None |
| 3. | Exhibits: See Index to Exhibits |
| 54 |
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
| Date: March 1, 2012 | ACURA PHARMACEUTICALS, INC. | |
| By: | /s/ ROBERT B. JONES | |
| Robert B. Jones | ||
| President and Chief Executive Officer | ||
| (Principal Executive Officer) | ||
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
| Signature | Title(s) | Date | ||
| /s/Robert B. Jones | President, Chief Executive Officer and Director | March 1, 2012 | ||
| Robert B. Jones | (Principal Executive Officer) | |||
| /s/Peter A. Clemens | Senior Vice President and Chief Financial Officer | March 1, 2012 | ||
| Peter A. Clemens | (Principal Financial and Accounting Officer) | |||
| /s/William G. Skelly | Director | March 1, 2012 | ||
| William G. Skelly | ||||
| /s/Bruce F. Wesson | Director | March 1, 2012 | ||
| Bruce F. Wesson | ||||
| /s/David F. Azad | Director | March 1, 2012 | ||
| David F. Azad | ||||
| /s/Richard J. Markham | Director | March 1, 2012 | ||
| Richard J. Markham | ||||
| /s/Immanuel Thangaraj | Director | March 1, 2012 | ||
| Immanuel Thangaraj | ||||
| /s/George K. Ross | Director | March 1, 2012 | ||
| George K. Ross |
| 55 |
INDEX TO FINANCIAL STATEMENTS
| Page | |
| Report of Independent Registered Public Accounting Firm | F-2 |
| Consolidated Balance Sheets | F-3 |
| Consolidated Statements of Operations | F-4 |
| Consolidated Statements of Stockholders' Equity | F-5 |
| Consolidated Statements of Cash Flows | F-6 to F-7 |
| Notes to Consolidated Financial Statements | F-8 to F-18 |
| F-1 |
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
Board of Directors and Shareholders
Acura Pharmaceuticals, Inc.
Palatine, Illinois
We have audited the accompanying consolidated balance sheets of Acura Pharmaceuticals, Inc. and Subsidiary as of December 31, 2011 and 2010 and the related consolidated statements of operations, stockholders’ equity, and cash flows for each of the three years in the period ended December 31, 2011. These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on these financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. The Company is not required to have, nor were we engaged to perform an audit of its internal control over financial reporting. Our audits included consideration of internal control over financial reporting as a basis for designating audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no such opinion. An audit also includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements, assessing the accounting principles used and the significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the financial position of Acura Pharmaceuticals, Inc. and Subsidiary at December 31, 2011 and 2010, and the results of their operations and their cash flows for each of the three years in the period ended December 31, 2011, in conformity with accounting principles generally accepted in the United States of America.
/s/ BDO USA, LLP
Chicago, Illinois
March 1, 2012
| F-2 |
ACURA PHARMACEUTICALS, INC. AND SUBSIDIARY
CONSOLIDATED BALANCE SHEETS
DECEMBER 31, 2011 and 2010
(in thousands except par values)
| 2011 | 2010 | |||||
| Assets | ||||||
| Current assets | ||||||
| Cash and cash equivalents | $ | 35,685 | $ | 24,045 | ||
| Collaboration revenue receivable | 0 | 126 | ||||
| Income taxes refundable | 153 | 12 | ||||
| Prepaid insurance | 218 | 213 | ||||
| Prepaid expenses and other current assets | 73 | 45 | ||||
| Total current assets | 36,129 | 24,441 | ||||
| Property, plant and equipment, net | 1,044 | 1,052 | ||||
| Total assets | $ | 37,173 | $ | 25,493 | ||
| Liabilities and Stockholders’ Equity | ||||||
| Current liabilities | ||||||
| Accounts payable | $ | 53 | $ | 0 | ||
| Accrued expenses | 477 | 686 | ||||
| Deferred program fee revenue | 0 | 466 | ||||
| Total current liabilities | 530 | 1,152 | ||||
| Commitments and contingencies (Note H) | ||||||
| Stockholders’ equity | ||||||
| Common stock - $.01 par value; 100,000 shares authorized; 45,320 and 43,894 shares issued and outstanding in 2011 and 2010, respectively | 453 | 439 | ||||
| Additional paid-in capital | 361,733 | 359,830 | ||||
| Accumulated deficit | (325,543 | ) | (335,928 | ) | ||
| Total stockholders’ equity | 36,643 | 24,341 | ||||
| Total liabilities and stockholders’ equity | $ | 37,173 | $ | 25,493 | ||
See accompanying notes to the consolidated financial statements.
| F-3 |
ACURA PHARMACEUTICALS, INC. AND SUBSIDIARY
CONSOLIDATED STATEMENTS OF OPERATIONS
YEARS ENDED DECEMBER 31, 2011, 2010 and 2009
(in thousands except per share data)
| 2011 | 2010 | 2009 | |||||||
| Revenues | |||||||||
| Program fee revenue | $ | 466 | $ | 1,088 | $ | 3,077 | |||
| Collaboration revenue | 0 | 2,223 | 758 | ||||||
| Milestone revenue | 20,000 | 0 | 0 | ||||||
| Total revenue | 20,466 | 3,311 | 3,835 | ||||||
| Operating expenses | |||||||||
| Research and development | 4,037 | 7,177 | 5,673 | ||||||
| Marketing, general and administrative | 5,895 | 8,858 | 11,662 | ||||||
| Total operating expenses | 9,932 | 16,035 | 17,335 | ||||||
| Income (loss) from operations | 10,534 | (12,724 | ) | (13,500 | ) | ||||
| Other income (expense) | |||||||||
| Interest income | 32 | 42 | 147 | ||||||
| Other expense | (34 | ) | (14 | ) | (3 | ) | |||
| Total other income (expense) | (2 | ) | 28 | 144 | |||||
| Income (loss) before income tax | 10,532 | (12,696 | ) | (13,356 | ) | ||||
| Income tax expense | 147 | 11 | 2,479 | ||||||
| Net income (loss) applicable to common stockholders | $ | 10,385 | $ | (12,707 | ) | $ | (15,835 | ) | |
| Earnings (loss) per share | |||||||||
| Basic | $ | 0.22 | $ | (0.27 | ) | $ | (0.35 | ) | |
| Diluted | $ | 0.22 | $ | (0.27 | ) | $ | (0.35 | ) | |
| Weighted average shares | |||||||||
| Basic | 47,496 | 47,029 | 45,932 | ||||||
| Diluted | 48,007 | 47,029 | 45,932 | ||||||
See accompanying notes to the consolidated financial statements.
| F-4 |
ACURA PHARMACEUTICALS, INC. AND SUBSIDIARY
CONSOLIDATED STATEMENTS OF STOCKHOLDERS' EQUITY
YEARS ENDED DECEMBER 31, 2011, 2010 and 2009
(in thousands except par values)
| Common Stock $0.01 Par Value | Additional Paid-in | Accumulated | |||||||||||||
| Shares | $ Amount | Capital | Deficit | Total | |||||||||||
| Balance at Dec. 31, 2008 | 42,723 | $ | 427 | $ | 344,023 | $ | (307,386 | ) | $ | 37,064 | |||||
| Net loss for the year ended Dec. 31, 2009 | 0 | 0 | 0 | (15,835 | ) | (15,835 | ) | ||||||||
| Share-based compensation | 0 | 0 | 9,204 | 0 | 9,204 | ||||||||||
| Issuance of common stock for cashless exercise of warrants | 730 | 7 | (7 | ) | 0 | 0 | |||||||||
| Issuance of common stock for exercise of warrant | 50 | 1 | 159 | 0 | 160 | ||||||||||
| Issuance of common stock for cashless exercise of options and payroll taxes | 225 | 2 | (685 | ) | 0 | (683 | ) | ||||||||
| Balance at Dec. 31, 2009 | 43,728 | $ | 437 | $ | 352,694 | $ | (323,221 | ) | $ | 29,910 | |||||
| Net loss for the year ended Dec. 31, 2010 | 0 | 0 | 0 | (12,707 | ) | (12,707 | ) | ||||||||
| Share-based compensation | 0 | 0 | 6,746 | 0 | 6,746 | ||||||||||
| Issuance of common stock for cashless exercise of warrants | 43 | 1 | (1 | ) | 0 | 0 | |||||||||
| Issuance of common stock for exercise of warrant | 123 | 1 | 391 | 0 | 392 | ||||||||||
| Balance at Dec. 31, 2010 | 43,894 | $ | 439 | $ | 359,830 | $ | (335,928 | ) | $ | 24,341 | |||||
| Net income for the year ended Dec. 31, 2011 | 0 | 0 | 0 | 10,385 | 10,385 | ||||||||||
| Share-based compensation | 0 | 0 | 2,458 | 0 | 2,458 | ||||||||||
| Net distribution of common stock pursuant to restricted stock unit award plan | 828 | 8 | (8 | ) | 0 | 0 | |||||||||
| Common shares withheld for withholding taxes on distribution of restricted stock units | (288 | ) | (3 | ) | (945 | ) | 0 | (948 | ) | ||||||
| Net issuance of common stock pursuant to cashless exercise of stock options | 611 | 6 | (6 | ) | 0 | 0 | |||||||||
Common shares withheld for withholding taxes on cashless exercise of stock options |
(228 | ) | (2 | ) | (884 | ) | 0 | (886 | ) | ||||||
| Issuance of common stock for exercise of stock options | 167 | 2 | 215 | 0 | 217 | ||||||||||
| Issuance of common stock for exercise of warrants | 336 | 3 | 1,073 | 0 | 1,076 | ||||||||||
| Balance at Dec. 31, 2011 | 45,320 | $ | 453 | $ | 361,733 | $ | (325,543 | ) | $ | 36,643 | |||||
See accompanying notes to the consolidated financial statements.
| F-5 |
ACURA PHARMACEUTICALS, INC. AND SUBSIDIARY
CONSOLIDATED STATEMENTS OF CASH FLOWS
YEARS ENDED DECEMBER 31, 2011, 2010, and 2009
(in thousands, except supplemental data)
| 2011 | 2010 | 2009 | |||||||
| Cash flows from operating activities: | |||||||||
| Net income (loss) | $ | 10,385 | $ | (12,707 | ) | $ | (15,835 | ) | |
| Adjustments to reconcile net income (loss) to net cash provided by (used in) operating activities: | |||||||||
| Depreciation and amortization | 131 | 135 | 130 | ||||||
| Non-cash share-based compensation expense | 2,458 | 6,746 | 9,204 | ||||||
| Loss (gain) on asset disposals | 8 | 14 | (3 | ) | |||||
| Deferred income taxes | 0 | 0 | 2,479 | ||||||
| Changes in assets and liabilities | |||||||||
| Collaboration revenue receivable | 126 | 231 | 3,172 | ||||||
| Income taxes refundable | (141 | ) | 0 | 0 | |||||
| Prepaid expenses and other current assets | (33 | ) | (37 | ) | 222 | ||||
| Accounts payable | 53 | 0 | (382 | ) | |||||
| Accrued expenses | (209 | ) | 226 | (1,113 | ) | ||||
| Deferred program fee revenue | (466 | ) | (1,088 | ) | (3,077 | ) | |||
| Net cash provided by (used in) operating activities | 12,312 | (6,480 | ) | (5,203 | ) | ||||
| Cash flows from investing activities: | |||||||||
| Maturities of short-term investments | 0 | 0 | 5,039 | ||||||
| Capital expenditures | (131 | ) | (41 | ) | (220 | ) | |||
| Net cash (used in) provided by investing activities | (131 | ) | (41 | ) | 4,819 | ||||
| Cash flows from financing activities: | |||||||||
| Exercise of stock options | 217 | 0 | 0 | ||||||
| Distribution of restricted stock units | 5 | 0 | 0 | ||||||
| Net proceeds from warrant exercise | 1,076 | 392 | 160 | ||||||
| Statutory minimum withholding taxes paid on the distribution of common stock pursuant to restricted stock unit plan and exercise of stock options | (1,839 | ) | 0 | 0 | |||||
| Net cash (used in) provided by financing activities | (541 | ) | 392 | 160 | |||||
| Net increase (decrease) in cash and cash equivalents | 11,640 | (6,129 | ) | (224 | ) | ||||
| Cash and cash equivalents at beginning of period | 24,045 | 30,174 | 30,398 | ||||||
| Cash and cash equivalents at end of period | $ | 35,685 | $ | 24,045 | $ | 30,174 | |||
| Cash paid during the period: | |||||||||
| Interest | $ | 26 | $ | 0 | $ | 0 | |||
| Income taxes | $ | 284 | $ | 20 | $ | 108 | |||
See accompanying notes to the consolidated financial statements.
| F-6 |
ACURA PHARMACEUTICALS, INC. AND SUBSIDIARY
CONSOLIDATED STATEMENTS OF CASH FLOWS (CONTINUED)
YEAR ENDED DECEMBER 31, 2011, 2010, and 2009
Supplemental disclosures of noncash investing and financing activities presented on a reverse stock split basis (amounts presented are rounded to the nearest thousand):
Year ended December 31, 2011
| 1. | 829 shares of common stock were distributed pursuant to our RSU Plan utilizing various cashless exercise features of the plan and after withholding shares for $3 in exercise costs and withholding 288 shares for $948 in statutory minimum payroll taxes, 540 shares of common stock were issued. |
| 2. | Options to purchase 935 shares of common stock were exercised utilizing various cashless exercise features of our plan and after withholding 324 shares for $1,252 in exercise costs and withholding 230 shares for $886 in statutory minimum payroll taxes, 383 shares of common stock were issued. |
Year ended December 31, 2010
| 1. | Warrants to purchase 65 shares of common stock were exercised in cashless exercise transactions resulting in the net issuance of 43 shares of common stock. |
Year ended December 31, 2009
| 1. | Warrants to purchase 1,479 shares of common stock were exercised in cashless exercise transactions resulting in the issuance of 730 shares of common stock. |
| 2. | Options to purchase 525 shares of common stock were exercised in cashless exercise transactions and after withholding shares for statutory minimum payroll taxes calculated at $685, resulted in the net issuance of 225 shares of common stock. |
See accompanying notes to the consolidated financial statements.
| F-7 |
ACURA PHARMACEUTICALS, INC. AND SUBSIDIARY
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2011, 2010 and 2009
NOTE A - DESCRIPTION OF BUSINESS AND SUMMARY OF ACCOUNTING POLICIES
Acura Pharmaceuticals, Inc., a New York corporation, and its subsidiary (the “Company”, “We”, or “Our”) is a specialty pharmaceutical company engaged in research, development and commercialization of products intended to address medication abuse and misuse, utilizing its proprietary Aversion® and Impede™ Technologies.
Summary of Significant Accounting Policies
A summary of the significant accounting policies consistently applied in the preparation of the accompanying consolidated financial statements follows.
1. Principles of Consolidation
The consolidated financial statements include the accounts of the Company and its wholly-owned subsidiary, Acura Pharmaceutical Technologies, Inc. All significant intercompany accounts and transactions are eliminated in consolidation.
2. Cash and Cash Equivalents
The Company considers cash and cash equivalents to include cash in banks, U.S. Treasury Bills, and institutional money market mutual funds. The Company considers all highly liquid investments with an original maturity of three months or less to be cash equivalents. Our cash and cash equivalents are governed by our investment policy as approved by our Board of Directors. The carrying amount of cash and cash equivalents approximates its fair value due to its short-term nature.
3. Concentration of Credit Risk
We invest our excess cash in accordance with the investment policy approved by our Board of Directors that seeks both liquidity and safety of principal. The policy provides for investments in instruments issued by the United States government and by commercial institutions with strong investment grade credit ratings and places restrictions on maturity terms and concentrations by type and issuer.
4. Use of Estimates in Consolidated Financial Statements
The preparation of consolidated financial statements in conformity with accounting principles generally accepted in the United States of America requires management to make estimates and use assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent liabilities at the date of the consolidated financial statements, as well as the reported amounts of revenues and expenses during the reporting period. Actual results could differ from those estimates. Management periodically evaluates estimates used in the preparation of the consolidated financial statements for continued reasonableness. Appropriate adjustments, if any, to the estimates used are made prospectively based on such periodic evaluations.
5. Inventories
We had no inventories at each of December 31, 2011 and 2010. Purchases of active pharmaceutical ingredients and raw materials required for our development and clinical trial manufacture of product candidates utilizing our Aversion® or Impede™ Technologies are expensed as incurred.
6. Property, Plant and Equipment
Property, plant and equipment are recorded at cost. Depreciation is recorded on a straight-line basis over the estimated useful lives of the related assets. Leasehold improvements are amortized on a straight-line basis over the shorter of their useful lives or the terms of their respective leases. Betterments are capitalized and maintenance and repairs are charged to operations as incurred. The estimated lives of the major classification of depreciable assets are:
| Building and improvements | 10 - 40 years |
| Land improvements | 20 - 40 years |
| Machinery and equipment | 7 - 10 years |
| Scientific equipment | 5 - 10 years |
| Computer hardware and software | 3 - 10 years |
| Office equipment | 5 - 10 years |
| F-8 |
| 7. | Revenue Recognition, Deferred Program Fee Revenue and Collaboration Revenue |
We recognize revenue when there is persuasive evidence that an arrangement exists, delivery has occurred, the price is fixed and determinable, and collection is reasonably assured. In connection with our License, Development, and Commercialization Agreement dated October 30, 2007 with King Pharmaceuticals Research and Development, Inc., now a subsidiary of Pfizer Inc. (the “Pfizer Agreement”), we recognize program fee revenue, collaboration revenue and milestone revenue.
Program fee revenue is derived from amortized upfront payments, such as the $30.0 million upfront payment from Pfizer received in December 2007, and license fees, such as the $3.0 million option exercise fee paid by Pfizer to us in each of May 2008 and December 2008 upon the exercise of its option to license a third and fourth opioid analgesic product candidate under the Pfizer Agreement. We assigned an equal portion of Pfizer’s $30.0 million upfront payment to each of three product candidates identified in the Pfizer Agreement and recognize the upfront payment as program fee revenue ratably over our estimate of the development period for each identified product candidate. We recognized $0.5 million, $1.1 million, and $3.1 million of this program fee revenue in 2011, 2010, and 2009, respectively.
Collaboration revenue is derived from reimbursement of development expenses, which are invoiced quarterly in arrears, and are recognized when costs are incurred pursuant to the Pfizer Agreement. The ongoing research and development services being provided to Pfizer under the collaboration are priced at fair value based upon the reimbursement of expenses incurred pursuant to the collaboration with Pfizer. We recognized $2.2 million and $0.8 million of collaboration revenue in 2010 and 2009, respectively. We had no collaboration revenue in 2011.
Milestone revenue is contingent upon the achievement of certain pre-defined events in the development of Oxecta Tablets and other product candidates licensed to Pfizer under the Pfizer Agreement. Milestone payments from Pfizer are recognized as revenue upon achievement of the “at risk” milestone events, which represent the culmination of the earnings process related to that milestone. Milestone payments are triggered either by the results of our research and development efforts or by events external to us, such as regulatory approval to market a product. As such, the milestones are substantially at risk at the inception of the Pfizer Agreement, and the amounts of the payments assigned thereto are commensurate with the milestone achieved. In addition, upon the achievement of a milestone event, we have no future performance obligations related to that milestone payment. Each milestone payment is non-refundable and non-creditable when made. In June 2011, Pfizer paid us a $20 million milestone relating to the receipt of FDA approval of the NDA for Oxecta.
8. Research and Development
Research and Development (“R&D”) expenses include internal R&D activities, external Contract Research Organization (“CRO”) services and their clinical research sites, and other activities. Internal R&D activity expenses include facility overhead, equipment and facility maintenance and repairs, laboratory supplies, pre-clinical laboratory experiments, depreciation, salaries, benefits, and share-based compensation expenses. CRO activity expenses include preclinical laboratory experiments and clinical trial studies. Other activity expenses include regulatory consulting, and regulatory legal counsel. Internal R&D activities and other activity expenses are charged to operations as incurred. We make payments to the CRO's based on agreed upon terms and may include payments in advance of a study starting date. We review and accrue CRO expenses and clinical trial study expenses based on services performed and rely on estimates of those costs applicable to the stage of completion of a study as provided by the CRO. Accrued CRO costs are subject to revisions as such studies progress to completion. Revisions are charged to expense in the period in which the facts that give rise to the revision become known. At December 31, 2011 and 2010 we had accrued $28 thousand and $0.3 million, respectively of CRO and clinical trial study expenses.
| F-9 |
9. Income Taxes
We account for income taxes under the liability method. Under this method, deferred income tax assets and liabilities are determined based on differences between the financial reporting and the income tax basis of assets and liabilities and are measured using the enacted income tax rates and laws that will be in effect when the differences are expected to reverse. Additionally, net operating loss and tax credit carryforwards are reported as deferred income tax assets. The realization of deferred income tax assets is dependent upon future earnings. A valuation allowance is required against deferred income tax assets if, based on the weight of available evidence, it is more likely than not that some or all of the deferred income tax assets may not be realized. During 2009 we determined it was more likely than not that we would not be able to realize our recorded deferred income tax assets and we recorded an adjustment of $2.5 million to the deferred income tax asset valuation allowance and recognized an expense from income taxes in such period. At both December 31, 2011 and 2010, 100% of all remaining net deferred income tax assets were offset by a valuation allowance due to uncertainties with respect to future utilization of net operating loss carryforwards. If in the future it is determined that additional amounts of our deferred income tax assets would likely be realized, the valuation allowance would be reduced in the period in which such determination is made and an additional benefit from income taxes in such period would be recognized.
10. Earnings (Loss) Per Share
The computation of basic earnings (loss) per share of common stock is based upon the weighted average number of common shares outstanding during the period, including shares weighted related to vested RSUs (See Note G). The computation of diluted earnings (loss) per share is based on the same number of shares used in the basic share calculation adjusted for the effect of other potentially dilutive securities. No such adjustments were made for 2010 or 2009 as their effects would have been antidilutive.
| Year ended December 31, | |||||||||
| 2011 | 2010 | 2009 | |||||||
| (in thousands except per share data) | |||||||||
| Basic earnings per share | |||||||||
| Numerator: | |||||||||
| Net income (loss) applicable to common stockholders | $ | 10,385 | $ | (12,707 | ) | $ | (15,835 | ) | |
| Denominator: | |||||||||
| Common shares | 45,016 | 43,842 | 42,912 | ||||||
| Vested RSUs | 2,480 | 3,187 | 3,020 | ||||||
| Weighted average number of shares outstanding | 47,496 | 47,029 | 45,932 | ||||||
| Basic earnings (loss) per common share | $ | 0.22 | $ | (0.27 | ) | $ | (0.35 | ) | |
| Diluted earnings (loss) per share | |||||||||
| Denominator: | |||||||||
| Common shares | 45,016 | 43,842 | 42,912 | ||||||
| Vested RSUs | 2,489 | 3,187 | 3,020 | ||||||
| Stock options | 366 | 0 | 0 | ||||||
| Common stock warrants | 136 | 0 | 0 | ||||||
| Weighted average number of shares outstanding | 48,007 | 47,029 | 45,932 | ||||||
| Diluted earnings (loss) per common share | $ | 0.22 | $ | (0.27 | ) | $ | (0.35 | ) | |
| Excluded potentially dilutive securities: | |||||||||
| Common stock issuable (1): | |||||||||
| Stock options | 2,805 | 4,243 | 3,671 | ||||||
| Common stock warrants | 0 | 2,193 | 2,380 | ||||||
| RSUs | 0 | 49 | 204 | ||||||
| Total excluded dilutive shares | 2,805 | 6,485 | 6,255 | ||||||
| (1) The number of shares is based on maximum number of shares issuable on exercise or conversion of the related securities as of our year end. Such amounts have not been adjusted for the treasury stock method or weighted average outstanding calculations as required if the securities were dilutive. |
11. Share-Based Compensation
We have four share-based compensation plans covering stock options and RSUs for our employees and directors, which are described more fully in Note G.
| F-10 |
We measure our compensation cost related to share-based payment transactions based on fair value of the equity or liability instrument issued. For purposes of estimating the fair value of each stock option unit on the date of grant, we utilize the Black-Scholes option-pricing model. The Black-Scholes option valuation model was developed for use in estimating the fair value of traded options, which have no vesting restrictions and are fully transferable. In addition, option valuation models require the input of highly subjective assumptions including the expected volatility factor of the market price of our common stock (as determined by reviewing our historical public market closing prices).
Our accounting for share-based compensation for RSUs is based on the fair-value method. The fair value of the RSUs is the market price of our common stock on the date of grant, less its exercise cost.
Our non-cash share-based compensation expenses comprised the following:
| Year Ended December 31, | |||||||||
| 2011 | 2010 | 2009 | |||||||
| (in thousands) | |||||||||
| Research and development | |||||||||
| Stock options | $ | 457 | $ | 1,419 | $ | 1,702 | |||
| RSUs | 75 | 279 | 203 | ||||||
| 532 | 1,697 | 1,905 | |||||||
| General and administrative | |||||||||
| Stock options | 1,698 | 4,365 | 6,539 | ||||||
| RSUs | 228 | 684 | 760 | ||||||
| 1,926 | 5,049 | 7,299 | |||||||
| Total | $ | 2,458 | $ | 6,746 | $ | 9,204 | |||
| F-11 |
NOTE B – LICENSE, DEVELOPMENT, AND COMMERCIALIZATION AGREEMENT
On October 30, 2007, we and King Pharmaceuticals Research and Development, Inc., now a wholly-owned subsidiary of Pfizer, entered into the Pfizer Agreement to develop and commercialize in the United States, Canada and Mexico certain opioid analgesic products utilizing our proprietary Aversion Technology. The Pfizer Agreement initially provided Pfizer with an exclusive license in the United States, Canada and Mexico, or the Pfizer Territory, for Oxecta (oxycodone HCl) Tablets and oxycodone HCl/acetaminophen tablets utilizing Aversion Technology. In addition, the Pfizer Agreement provides Pfizer with an option to license in the Pfizer Territory certain future opioid analgesic products developed utilizing Aversion Technology. As of December 31, 2011, Pfizer exercised its option to license two additional product candidates including an undisclosed immediate-release opioid analgesic tablet product and hydrocodone bitartrate/acetaminophen tablets, each of which utilize our Aversion Technology. The Pfizer Agreement provides that we or Pfizer may develop additional opioid analgesic product candidates utilizing our Aversion Technology and, if Pfizer exercises its option to license such additional product candidates, they will be subject to the milestone and royalty payments and other terms of the Pfizer Agreement.
As of December 31, 2011, we had received aggregate payments of $78.5 million from Pfizer, consisting of a $30.0 million non-refundable upfront cash payment, $17.5 million in reimbursed research and development expenses relating to licensed products, $6.0 million in fees relating to Pfizer’s exercise of its option to license an undisclosed immediate-release opioid analgesic tablet product and hydrocodone bitartrate/acetaminophen tablets, a $5.0 million milestone fee relating to our successful achievement of the primary endpoints for our pivotal Phase III clinical study for Aversion oxycodone HCl with niacin tablets and a $20.0 million milestone fee relating to the FDA’s approval of the Oxecta Tablets NDA. The Pfizer Agreement also provides for Pfizer’s payment to us of a $3.0 million fee upon Pfizer’s exercise of its option for each future opioid analgesic utilizing Aversion Technology. In the event that Pfizer does not exercise its option for a Future Product, Pfizer may be required to reimburse us for certain of our expenses relating to such Future Product. Further, we may receive up to $23 million in additional non-refundable milestone payments for each active opioid analgesic ingredient licensed to Pfizer which achieves certain regulatory milestones in specific countries in the Pfizer Territory. An opioid analgesic product candidate formulated with and without niacin is considered a single product candidate for purposes of the option fees and milestone payments payable under the Pfizer Agreement. We can also receive a one-time $50 million sales milestone payment upon the first attainment of $750 million in net sales of all of our licensed products across all Pfizer Territories. In addition, for sales occurring on and following February 2, 2013 (the one year anniversary of the first commercial sale of Oxecta), Pfizer will pay us a royalty at one of six rates ranging from 5% to 25% based on the level of combined annual net sales for all products licensed by us to Pfizer across all Pfizer Territories, with the highest applicable royalty rate applied to such combined annual sales.
| F-12 |
Pfizer’s royalty payment obligations expire on a product-by-product and country-by-country basis upon the later of (i) the expiration of the last valid patent claim covering such product in such country, or (ii) 15 years from the first commercial sale of such product in such country. No minimum annual fees are payable by either party under the Pfizer Agreement. If Pfizer, after consultation with us, enters into a license agreement with a third party to avoid or settle such third party’s allegations or claims regarding freedom to operate against a licensed Aversion Technology product, Pfizer may deduct 50% of any royalties or other license payments it pays to such third party under such license, provided that the royalties payable to us are no less than 80% of the royalties otherwise due to us under the Pfizer Agreement.
The Pfizer Agreement expires upon the expiration of Pfizer’s royalty payment and other payment obligations under the Pfizer Agreement. Pfizer may terminate the Pfizer Agreement (i) in its entirety at any time by written notice to us, and (ii) with respect to any product at any time upon the provision of not less than 12 months’ prior written notice. We may terminate the Pfizer Agreement with respect to a product in the United States in the event such product is not commercially launched by Pfizer within 120 days after receipt of regulatory approval of such product or in its entirety if Pfizer commences any interference or opposition proceeding challenging the validity or enforceability of any of our patent rights licensed to Pfizer under the Pfizer Agreement. Either party has the right to terminate the Pfizer Agreement on a product by product and country-by-country basis if the other party is in material breach of its obligations under the Pfizer Agreement relating to such product and such country, and to terminate the Agreement in its entirety in the event the other party makes an assignment for the benefit of creditors, files a petition in bankruptcy or otherwise seeks relief under applicable bankruptcy laws, in each case subject to applicable cure periods.
NOTE C – PROPERTY, PLANT AND EQUIPMENT
Property, plant and equipment are summarized as follows:
| December 31, | ||||||
| 2011 | 2010 | |||||
| (in thousands) | ||||||
| Building and improvements | $ | 1,252 | $ | 1,243 | ||
| Land and improvements | 162 | 161 | ||||
| Machinery and equipment | 117 | 43 | ||||
| Scientific equipment | 583 | 583 | ||||
| Computer hardware and software | 270 | 251 | ||||
| Office equipment | 27 | 27 | ||||
| Other personal property | 70 | 68 | ||||
| 2,481 | 2,375 | |||||
| Less accumulated depreciation and amortization | (1,437 | ) | (1,323 | ) | ||
| Total property, plant and equipment, net | $ | 1,044 | $ | 1,052 | ||
Depreciation and amortization expense was approximately $0.1 million for each of the years ended December 31, 2011, 2010, and 2009. We lease administrative offer space in Palatine Illinois under a lease expiring March 31, 2013 for approximately $29 annually.
NOTE D – ACCRUED EXPENSES
Accrued expenses are summarized as follows:
| December 31, | ||||||
| 2011 | 2010 | |||||
| (in thousands) | ||||||
| Payroll, payroll taxes and benefits | $ | 104 | $ | 95 | ||
| Professional services | 191 | 193 | ||||
| Franchise taxes | 60 | 12 | ||||
| Property taxes | 21 | 19 | ||||
| Clinical and regulatory services | 59 | 307 | ||||
| Other fees and services | 42 | 60 | ||||
| $ | 477 | $ | 686 | |||
| F-13 |
NOTE E – COMMON STOCK WARRANTS
The Company has outstanding common stock purchase warrants at December 31, 2011 exercisable for 1.9 million shares of common stock, all of which contain a cashless exercise feature. These warrants have an exercise price of $3.40 per share and expiration date of August 2014.
NOTE F – INCOME TAXES
Provision for Income Taxes
The reconciliation between our provision for income taxes and the amounts computed by multiplying our income (loss) before taxes by the U.S. statutory tax rate is as follows:
| December 31, | |||||||||
| 2011 | 2010 | 2009 | |||||||
| (in thousands) | |||||||||
| Tax (benefit) at U.S. statutory 34% tax rate | $ | 3,510 | $ | (4,320 | ) | $ | (4,541 | ) | |
| State taxes (benefit), net of federal effect | 6 | (56 | ) | (416 | ) | ||||
| Research and development tax credits | (77 | ) | (45 | ) | (100 | ) | |||
| Wage reported share-based compensation | (307 | ) | 0 | (587 | ) | ||||
| Stock compensation | 626 | - | - | ||||||
| Other | (362 | ) | (315 | ) | (330 | ) | |||
| Change in valuation allowance | (3,863 | ) | 4,748 | 8,453 | |||||
| Provision for income taxes | $ | 147 | $ | 11 | $ | 2,479 | |||
Tax expense for 2011 is federal alternative minimum taxes (“AMT”) and current state taxes. The tax expense for 2010 is current state taxes and for 2009 it is deferred taxes.
Deferred Tax Assets and Valuation Allowance
Deferred tax assets reflect the tax effects of net operating losses (“NOLs”), tax credit carryovers, and temporary differences between the carrying amounts of assets and liabilities for financial reporting purposes and the amounts used for income tax purposes. The most significant item of our deferred tax assets is derived from our Federal NOLs. We have approximately $23.0 million federal income tax benefits at December 31, 2011 derived from $67.6 million Federal NOLs at the U.S. statutory tax rate of 34%, available to offset future taxable income, some of which have limitations for use as prescribed under IRC Section 382. Our NOLs will expire in varying amounts between 2012 and 2030 if not used, and those expirations will cause fluctuations in our valuation allowances. The components of our deferred tax assets are as follows:
| December 31, | ||||||
| 2011 | 2010 | |||||
| (in thousands) | ||||||
| Deferred tax assets: | ||||||
| Estimated future value of NOLs | ||||||
| - Federal | $ | 22,963 | $ | 25,101 | ||
| - State | 4,179 | 3,260 | ||||
| Research and development tax credits | 887 | 234 | ||||
| Deferred program fee revenue | 0 | 183 | ||||
| Share-based compensation | 4,628 | 7,704 | ||||
| Other, net | (8 | ) | 30 | |||
| Total deferred taxes | 32,649 | 36,512 | ||||
| Valuation allowance | (32,649 | ) | (36,512 | ) | ||
| Net deferred tax assets | $ | 0 | $ | 0 | ||
Realization of deferred tax assets is dependent upon future earnings, if any, and the timing and amount of which may be uncertain. Valuation allowances are placed on deferred tax assets when uncertainty exists on their near term utilization. We make periodic reviews of our valuation allowances and fluctuations can occur. Those fluctuations may be reflected as income tax expenses or benefits in the period they occur. In 2009, we increased the valuation allowance by $2.5 million for the then available deferred tax assets and also placed a valuation allowance against the 2009 and 2010 operating results. In 2011 we decreased our valuation allowance to utilize the NOLs to offset our taxable income from our 2011 operating results; however we still incurred an AMT liability. We continue to maintain full valuation allowance against all of our deferred tax assets at December 31, 2011 due to uncertainties with respect to future utilization of net operating loss carryforwards. If in the future it is determined that amounts of our deferred tax assets would likely be realized, the valuation allowance would be reduced in the period in which such determination is made and a benefit from income taxes in such period would be recognized.
| F-14 |
Uncertainty in Income Taxes
We adopted FASB’s statement regarding accounting for uncertainty in income taxes which defined the threshold for recognizing the benefits of tax-return positions in the financial statements as "more-likely-than-not" to be sustained by the taxing authorities. Our adoption of the standard did not result in establishing a contingent tax liability reserve or a corresponding charge to retained earnings. At each of December 31, 2011, 2010 and 2009, we had no liability for income tax associated with uncertain tax positions. If in the future we establish a contingent tax liability reserve related to uncertain tax positions, our practice will be to recognize the interest in interest expense and the penalties in other non-operating expense.
NOTE G – EMPLOYEE BENEFIT PLANS
401(k) and Profit-Sharing Plan
We have a 401(k) and Profit-Sharing Plan (the “Plan”) for our employees. Employees may elect to make a basic contribution of up to 15% of their annual earnings. The Plan provides that the Company can make discretionary matching contributions equal to 25% of the first 6% of employee contributions for an aggregate employee contribution of 1.5%, along with a discretionary profit-sharing contribution. We did not contribute matching or profit sharing contributions for the Plan in years 2011, 2010, and 2009.
Stock Option Plans
We maintain various stock option plans. A summary of our stock option plans as of December 31, 2011, 2010, and 2009, and for the years then ended consisted of the following:
| Years Ended December 31, | ||||||||||||||||||
| 2011 | 2010 | 2009 | ||||||||||||||||
| (in thousands except per share data) | ||||||||||||||||||
| Number of Options (000’s) | Weighted Average Exercise Price | Number of Options (000’s) | Weighted Average Exercise Price | Number of Options (000’s) | Weighted Average Exercise Price | |||||||||||||
| Outstanding, beginning | 4,243 | $ | 5.40 | 3,671 | $ | 5.90 | 2,968 | $ | 4.93 | |||||||||
| Granted | 491 | 3.63 | 649 | 3.36 | 1,312 | 6.38 | ||||||||||||
| Exercised | (1,102 | ) | 1.33 | 0 | 0 | (525 | ) | 1.30 | ||||||||||
| Forfeited or expired | (76 | ) | 3.15 | (77 | ) | 10.10 | (84 | ) | 7.95 | |||||||||
| Outstanding, ending | 3,556 | $ | 6.41 | 4,243 | $ | 5.40 | 3,671 | $ | 5.90 | |||||||||
| Options exercisable | 2,962 | $ | 7.01 | 3,528 | $ | 5.71 | 2,712 | $ | 5.49 | |||||||||
The following table summarizes information about nonvested stock options outstanding at December 31, 2011:
| Number of Options Not Exercisable (000)’s | Weighted Average Fair Value | |||||
| (in thousands except per share data) | ||||||
| Outstanding at December 31, 2010 | 715 | $ | 3.64 | |||
| Granted | 491 | 3.39 | ||||
| Vested | (546 | ) | 4.18 | |||
| Forfeited | (66 | ) | 3.02 | |||
| Outstanding at December 31, 2011 | 594 | $ | 3.22 | |||
| F-15 |
We estimate the option’s fair value on the date of grant using the Black-Scholes option-pricing model. Black-Scholes utilizes assumptions related to volatility, the risk-free interest rate, the dividend yield (which is assumed to be zero, as we have not paid any cash dividends) and employee exercise behavior. Expected volatilities utilized in the Black-Scholes model are based on the historical volatility of our common stock price. The risk-free interest rate is derived from the U.S. Treasury yield curve in effect at the time of grant. The expected life of the grants is derived from historical exercise activity. Historically, our stock options have been held until their expiration date. The assumptions used in the Black-Scholes model to determine fair value for the 2011, 2010 and 2009 stock option grants were:
| 2011 | 2010 | 2009 | |||||||
| Expected dividend yield | 0.0% | 0.0% | 0.0% | ||||||
| Risk-free interest rates | 1.9% to 3.4% | 3.5% to 3.9% | 2.4% to 3.1% | ||||||
| Average expected volatility | 114% | 119% | 124% | ||||||
| Expected term (years) | 10 | 10 | 10 | ||||||
| Weighted average grant date fair value | $ | 3.39 | $ | 3.18 | $ | 6.06 | |||
As of December 31, 2011, 2010, and 2009 the aggregate intrinsic value of the option awards vested was $0.3 million, $2.4 million and $4.8 million, respectively. In addition, the aggregate intrinsic value of option awards exercised during the year ended December 31, 2011 and 2009 was $2.7 million and $1.7 million, respectively. There were no options exercised in 2010. The total remaining unrecognized compensation cost related to the unvested option awards at December 31, 2011 was $2.0 million and is expected to be recognized in varying amounts over the 23 months remaining in the requisite service period. During 2011 options to purchase 935 shares of common stock were exercised utilizing various cashless exercise features of our stock option plan and after withholding shares for $887 in statutory minimum payroll taxes and $1,252 in exercise costs, we issued 381 shares of common stock. During 2009 options to purchase 525 shares of common stock were exercised in cashless exercise transactions and after withholding shares for statutory minimum payroll taxes calculated at $685, we issued 225 shares of common stock.
Restricted Stock Unit Award Plan
We have a Restricted Stock Unit Award Plan (“2005 RSU Plan”) for our employees and non-employee directors. Vesting of an RSU entitles the holder to receive a share of common stock of the Company on a distribution date. A summary of the RSU Plan as of December 31, 2011, 2010, and 2009, and for the years then ended consisted of the following:
| Years Ended December 31, | ||||||||||||||||||
| 2011 | 2010 | 2009 | ||||||||||||||||
| (in thousands) | ||||||||||||||||||
| Number of RSUs | Number of Vested RSUs | Number of RSUs | Number of Vested RSUs | Number of RSUs | Number of Vested RSUs | |||||||||||||
| Outstanding, beginning | 3,316 | 3,267 | 3,316 | 3,112 | 3,000 | 2,970 | ||||||||||||
| Granted | 0 | 0 | 0 | 0 | 330 | 0 | ||||||||||||
| Distributed | (829 | ) | (829 | ) | 0 | 0 | 0 | 0 | ||||||||||
| Vested | 0 | 49 | 0 | 155 | 0 | 142 | ||||||||||||
| Forfeited or expired | 0 | 0 | 0 | 0 | (17 | ) | 0 | |||||||||||
| Outstanding, ending | 2,487 | 2,487 | 3,316 | 3,267 | 3,316 | 3,112 | ||||||||||||
The share-based compensation cost to be incurred on the RSUs is the RSU’s fair value, which is the market price of the Company’s common stock on the date of grant, less its exercise cost. The fair value of the RSU grants made in 2009 and 2008 was $2.1 million and $0.4 million, respectively. The weighted average fair value of a RSU outstanding at December 31, 2011 is $3.83.
The 2005 RSU Plan provides that upon a change in control of the Company or upon termination of an employee’s employment with the Company without cause, vesting will accelerate and the RSUs will fully vest. Absent a change of control, one-fourth of vested shares of common stock underlying an RSU award will be distributed (after payment of $0.01 par value per share) on January 1 of each of 2011, 2012, 2013 and 2014. If a change in control occurs, the vested shares underlying the RSU award will be distributed at or about the time of the change in control. On January 1, 2011, 0.54 million vested shares were distributed to the holders while 0.29 million shares were withheld by the Company upon elections made to exchange RSUs in satisfaction of $1.0 million withholding tax obligations. On January 1, 2012, 0.54 million vested shares were distributed to the holders while 0.29 million shares were withheld by the Company upon elections made to exchange RSUs in satisfaction of $0.9 million withholding tax obligations.
| F-16 |
NOTE H – COMMITMENTS AND CONTINGENCIES
Securities Class Action and Derivative Litigation
A lawsuit captioned Bang v. Acura Pharmaceuticals, et al, was filed on September 10, 2010 in the United States District Court for the Northern District of Illinois, Eastern Division (Case 1:10-cv-05757) against us and certain of our current and former officers seeking unspecified damages on behalf of a putative class of persons who purchased our common stock (the “Affected Securities”) between February 21, 2006 and April 22, 2010 (the “Plaintiff Class”). The complaint alleged that certain Company officers made false or misleading statements, or failed to disclose material facts in order to make statements not misleading, relating to our Acurox® with Niacin Tablet product candidate, resulting in violations of Section 10(b) of the Securities Exchange Act of 1934 (the “Exchange Act”), Rule 10b-5 under the Exchange Act and Section 20(a) of the Exchange Act. The complaint further alleges that such false or misleading statements or omissions had the effect of artificially inflating the price of our common stock. On March 14, 2011, an amended complaint was filed in this lawsuit. The amended complaint asserts the same claims as the initial complaint based upon the same alleged false or misleading statements, and has added three of our current directors as defendants. The Court has changed the caption of this case to In re Acura Pharmaceuticals, Inc. Securities Litigation. We filed a motion to dismiss this case on May 13, 2011.
On October 31, 2011, we entered into a Stipulation of Settlement (“Stipulation”) providing for the release of all claims against the Company and its named directors and officers (the “Defendants”) in this case, for a payment of $1.5 million. The Company and the individual defendants continue to deny all charges of wrongdoing or liability against them relating to this action and the Stipulation does not contain or constitute any admission or finding of wrongful conduct, acts or omissions on the part of any Defendant. On December 16, 2011 our insurance carrier paid the $1.5 million settlement amount into an escrow account to fund the settlement.
In consideration of the payment of the settlement amount, the Plaintiff Class has agreed, upon final approval by the court, to dismiss the class action with prejudice and release all known and unknown claims arising out of or relating to, or in connection with the purchase or acquisition of the Affected Securities during the class period which have been or could have been asserted by the members of the Plaintiff Class. On February 16, 2012, the court entered final approval of the settlement reflected in the Stipulation.
On October 25, 2010, Kiley Hill, a purported stockholder of the Company filed a shareholder derivative action in the Circuit Court of Cook County, Illinois, Chancery Division captioned Hill v. Acura Pharmaceuticals et al. (Case No. 2010-CH-46380), against our directors and certain of our executive officers, generally relating to the same events that are the subject of the class action litigation described above. The complaint purports to be brought on our behalf and names us as a nominal defendant. The complaint seeks unspecified damages from the individual defendants for breaches of fiduciary duty, abuse of control, gross mismanagement, contribution and indemnification, waste of corporate assets and unjust enrichment for actions occurring from at least February 21, 2006 through April 22, 2010. Substantively similar complaints captioned Hagan v. Acura Pharmaceuticals et al. (Case No. 2010-CH-46621) and Newell v. Reddick et al (Case No. 2010-CH-46873) were filed in the Circuit Court of Cook County, Illinois, Chancery Division, by other purported stockholders of the Company on October 27, 2010 and October 28, 2010, respectively. We filed a notion to dismiss these shareholder derivative actions on November 23, 2011.
Reglan®/Metoclopramide Litigation
Halsey Drug Company, as predecessor to us, has been named along with numerous other companies as a defendant in cases filed in three separate state coordinated litigations pending in Pennsylvania, New Jersey and California, respectively captioned In re: Reglan®/Metoclopramide Mass Tort Litigation, Philadelphia County Court of Common Pleas, January Term, 2010, No. 01997; In re: Reglan® Litigation, Superior Court of New Jersey, Law Division, Atlantic County, Case No. 289, Master Docket No. ATL-L-3865-10; and Reglan®/Metoclopramide Cases, Superior Court of California, San Francisco County, Judicial Council Coordination Proceeding No. 4631, Superior Court No.: CJC-10-004631. In this product liability litigation against numerous pharmaceutical product manufacturers and distributors, including us, plaintiffs claim injuries from their use of the Reglan brand of metoclopramide and generic metoclopramide. In the Pennsylvania state court mass tort proceeding, over 200 lawsuits have been filed against us and Halsey Drug Company alleging that plaintiffs developed neurological disorders as a result of their use of the Reglan brand and/or generic metoclopramide. Plaintiffs have filed approximately 150 lawsuits against us, but have served less than 50 individual lawsuits upon us in the New Jersey action. In the California action, we were not served with any complaints until the Spring of 2011 when a single complaint including over 400 plaintiffs was served. To date, Acura has not been served with any metoclopramide lawsuits in jurisdictions other than Philadelphia, New Jersey and California state courts.
| F-17 |
In the lawsuits filed to date, plaintiffs have not confirmed they ingested any of the generic metoclopramide manufactured by us. We discontinued manufacture and distribution of generic metoclopramide more than 15 years ago. In addition, we believe the June 23, 2011 decision by the U.S. Supreme Court in PLIVA v. Mensing (“Mensing decision”) holding that state tort law failure to warn claims against generic drug companies are pre-empted by the 1984 Hatch-Waxman Act Amendments and federal drug regulations will assist us in favorably resolving these cases. We have consistently maintained the position that these claims are without merit and intend to vigorously defend these actions.
In Philadelphia, New Jersey and California, Generic Defendants, including Acura, have filed dispositive motions based on the Mensing decision. The New Jersey and California courts are expected to issue their rulings later this year. On November 18, 2011, the Philadelphia trial court denied Generic Defendants’ dispositive motion. In December 2011, the Generic Defendants appealed this ruling, which the trial court refused to modify on reconsideration. Nonetheless, the trial court has approved certification of the federal preemption issues based on the Mensing decision for immediate appeal to the Pennsylvania Superior Court. A decision on this appeal should be issued later this year which could result in dismissal of all of the Philadelphia cases against Generic Defendants, although there can be no assurance in this regard. As any potential loss is neither probable or estimable, we have not accrued for any potential loss related to this matter as of December 31, 2011. Legal fee related to this matter are currently covered by our insurance carrier.
Statutory Minimum Withholding Tax Obligations
Under our stock option plans and our 2005 RSU plan, our employees may elect to have shares withheld upon exercise of options and upon the exchange of RSUs in satisfaction of the statutory minimum withholding tax obligations of such employees relating to such option exercises or RSU exchanges. During 2011, elections were made to have 0.29 million of common shares withheld by the Company upon the exchange of RSUs in satisfaction of $1.0 million in withholding tax obligations and other elections were made to have 0.23 million common shares withheld by the Company upon the exercise of options in satisfaction of $0.9 million in withholding tax obligations. On January 1, 2012, elections were made to have 0.29 million of common shares withheld by the Company upon the exchange of RSUs in satisfaction of $1.1 million in withholding tax obligations.
Financial Advisor Agreement
In connection with our August 2007 Unit Offering, we are obligated to pay a fee to our then financial advisor upon each exercise of the warrants issued in the Unit Offering, in proportion to the number of warrants exercised. The amount of the fee assuming 100% exercise of the remaining 1.9 million warrants is $0.38 million. We have not reflected this obligation as a liability in our consolidated financial statements as the payment is contingent upon the timing and exercise of the warrants by each of the warrant holders. Such fee, if any, will be paid to the financial advisor and be offset against the equity proceeds as the warrants are exercised.
NOTE I – SELECTED QUARTERLY FINANCIAL DATA (UNAUDITED)
| Three Month Period Ended | ||||||||||||
| (in thousands except per share data) | ||||||||||||
| Calendar Year 2011 | Mar. 31 | Jun. 30 | Sept. 30 | Dec. 31 | ||||||||
| Total revenue (i) | $ | 233 | $ | 20,233 | $ | 0 | $ | 0 | ||||
| Income (loss) from operations | (2,834 | ) | 17,362 | (2,147 | ) | (1,847 | ) | |||||
| Net income (loss) | (2,857 | ) | 17,029 | (2,141 | ) | (1,646 | ) | |||||
| Income (loss) per common share Basic | $ | (0.06 | ) | $ | 0.36 | $ | (0.05 | ) | $ | (0.03 | ) | |
| Diluted | $ | (0.06 | ) | $ | 0.35 | $ | (0.05 | ) | $ | (0.03 | ) | |
| Calendar Year 2010 | Mar. 31 | Jun. 30 | Sept. 30 | Dec. 31 | ||||||||
| Total revenue (i) | $ | 2,040 | $ | 620 | $ | 292 | $ | 359 | ||||
| Loss from operations | (4,035 | ) | (3,186 | ) | (2,566 | ) | (2,937 | ) | ||||
| Net loss | (4,035 | ) | (3,192 | ) | (2,553 | ) | (2,927 | ) | ||||
| Loss per common share - basic and diluted | $ | (0.09 | ) | $ | (0.07 | ) | $ | (0.05 | ) | $ | (0.06 | ) |
(i) See Note A(7) for revenue recognition.
| F-18 |
ACURA PHARMACEUTICALS, INC.
EXHIBIT INDEX
The following exhibits are included as a part of this Annual Report on Form 10-K or incorporated herein by reference.
| Exhibit Number |
Exhibit Description | |
| 3.1 | Restated Certificate of Incorporation of the Registrant (incorporated by reference to Exhibit 3.1 to the Registrant’s Form 8-K filed on June 25, 2009). | |
| 3.2 | Certificate of Amendment Reverse Splitting Common Stock and restating but not changing text of part of Article III of Restated Certificate of Incorporation (incorporated by Reference to Exhibit 3.1 to the Form 8-K filed December 4, 2007). | |
| 3.3 | Restated Bylaws of the Registrant (incorporated by reference to Exhibit 3.1 to the Form 8-K filed on March 3, 2009). | |
| 10.1 | License, Development and Commercialization Agreement by and between the Registrant and King Pharmaceuticals Research and Development, Inc. (incorporated by reference to Exhibit 10.1 of the Form 8-K filed on November 2, 2007) (confidential treatment has been granted for portions of this Exhibit). | |
| 10.2 | Manufacturing Services Agreement dated as of July 19, 2011 between the Registrant and Patheon Pharmaceuticals Inc. (incorporated by reference to Exhibit 10.1 to our Form 8-K filed July 27, 2011) (confidential treatment has been granted for portions of this Exhibit) | |
| 10.3 | Securities Purchase Agreement dated as of August 20, 2007 (“PIPE SPA”) among the Registrant, Vivo Ventures Fund VI, L.P., Vivo Ventures VI Affiliates Fund, L.P., GCE Holdings LLC, and certain other signatories thereto (incorporated by reference to Exhibit 10.1 to the Form 8-K filed on August 21, 2007). | |
| 10.4 | Form of Warrant dated as of August 20, 2007 issued pursuant to the PIPE SPA (incorporated by reference to Exhibit 4.1 to the Form 8-K filed on August 21, 2007). | |
| 10.5 | Amended and Restated Voting Agreement dated as of February 6, 2004 among the Registrant, Care Capital Investments II, LP, Essex Woodlands Health Ventures V, L.P., Galen Partners III, L.P., and others (incorporated by reference to Exhibit 10.5 of the Form 8-K filed on February 10, 2004 (the “February 2004 Form 8-K”)). | |
| 10.6 | Joinder and Amendment to Amended and Restated Voting Agreement dated November 9, 2005 between the Registrant, GCE Holdings, Essex Woodlands Health Ventures V, L.P., Care Capital Investments II, LP, Galen Partners III, L.P. and others (incorporated by reference to Exhibit 10.1 to the Form 8-K filed November 10, 2005). | |
| 10.7 | Second Amendment to Amended and Restated Voting Agreement dated as of January 24, 2008 between the Registrant and GCE Holdings, LLC (incorporated by reference to Exhibit 10.1 to the Form 8-K filed January 28, 2008). | |
| 10.8 | Registrant’s 1995 Stock Option and Restricted Stock Purchase Plan (incorporated by reference to Exhibit 4.1 to the Registrant's Registration Statement on Form S-8, File No. 33-98396). | |
| 10.9 | Registrant’s 1998 Stock Option Plan, as amended (incorporated by reference to Appendix C to the Registrant’s Proxy Statement filed on May 12, 2009). |
| E-1 |
| Exhibit Number |
Exhibit Description | |
| 10.10 | Registrant’s 2005 Restricted Stock Unit Award Plan, as amended (incorporated by reference to Appendix B to the Registrant’s Proxy Statement filed on April 2, 2008). | |
| 10.11 | Registrant’s 2008 Stock Option Plan, as amended on June 25, 2009 (incorporated by reference to Appendix B to our Proxy Statement filed on May 12, 2009). | |
| 10.12 | Executive Employment Agreement dated as of August 26, 2003 between the Registrant and Andrew D. Reddick (“Reddick”) (incorporated by reference to Exhibit 10.2 to the Form 10-Q for the quarter ended June 30, 2004 filed on August 9, 2004 (the “June 2004 10-Q”)). | |
| 10.13 | Amendment to Executive Employment Agreement between the Registrant and Reddick, dated May 27, 2004 (incorporated by reference to Exhibit 10.4 to the June 2004 10-Q). | |
| 10.14 | Second Amendment to Executive Employment Agreement between the Registrant and Reddick, dated May 24, 2005 incorporated by reference to Exhibit 10.116 to the Form 10-K for the year ending December 31, 2005 filed on February 21, 2006 (the “2005 Form 10-K”)). | |
| 10.15 | Third Amendment to Executive Employment Agreement between the Registrant and Reddick, dated December 22, 2005 (incorporated by reference to Exhibit 10.1 to the Form 8-K filed December 23, 2005 (the “December 2005 Form 8-K”)). | |
| 10.16 | Fourth Amendment to Executive Employment Agreement between the Registrant and Reddick dated December 16, 2007 (incorporated by reference to Exhibit 10.20 to the Form 10-K for the year ending December 31, 2007, filed on March 5, 2008). | |
| 10.17 | Fifth Amendment to Executive Employment Agreement between the Registrant and Reddick executed July 9, 2008 (incorporated by reference to Exhibit 10.1 to our Form 8-K filed on July 10, 2008) | |
| 10.18 | Employment Agreement dated as of March 10, 1998 between the Registrant and Peter Clemens (“Clemens”) (incorporated by reference to Exhibit 10.44 to the Form 10-K for the period ending December 31, 2007, filed on April 15, 1998). | |
| 10.19 | First Amendment to Employment Agreement made as of June 28, 2000 between the Registrant and Clemens (incorporated by reference to Exhibit 10.44A to the Registrant’s 2005 Form 10-K). | |
| 10.20 | Second Amendment to Executive Employment Agreement between Registrant and Clemens, dated as of January 5, 2005 (incorporated by reference to Exhibit 99.1 to the Registrant's Form 8-K filed January 31, 2005). | |
| 10.21 | Third Amendment to Executive Employment Agreement dated December 22, 2005 between Registrant and Clemens (incorporated by reference to Exhibit 10.3 to the December 2005 Form 8-K). | |
| 10.22 | Fourth Amendment to Executive Employment Agreement dated December 16, 2007 between Registrant and Clemens (incorporated by reference to Exhibit 10.28 to the Form 10-K for the year ending December 31, 2007, filed on March 5, 2008). | |
| 10.23 | Fifth Amendment to Executive Employment Agreement executed July 9, 2008 between Registrant and Clemens (incorporated by reference to Exhibit 10.4 to our Form 8-K filed on July 10, 2008). |
| E-2 |
| Exhibit Number |
Exhibit Description | |
| 10.24 | Employment Agreement dated as of March 18, 2008 between the Registrant and Robert B. Jones (incorporated by reference to Exhibit 10.1 to our Form 8-K filed on March 24, 2008). | |
| 10.25 | Amendment to Executive Employment Agreement dated as of April 28, 2011 between the Registrant and Robert B. Jones (incorporated by reference to Exhibit 10.1 to our Form 10-Q filed July 28, 2011) | |
| 10.26 | Stipulation of Settlement dated October 31, 2011 re: Class Action Litigation (incorporated by reference to Exhibit 10.1 to our Form 8-K filed November 4, 2011) | |
| 14.1 | Code of Ethics (incorporated by reference to Exhibit 14.1 of the Form 8-K filed on December 10, 2007). | |
| 21 | Subsidiaries of the Registrant (incorporated by reference to Exhibit 21 to the Form 10-K for the fiscal year ended December 31, 2006 filed on March 15, 2007). | |
| *23.1 | Consent of BDO USA LLP, Independent Registered Public Accounting Firm. | |
| *31.1 | Certification of Periodic Report by Chief Executive Officer pursuant to Rule 13a-14 and 15d-14 of the Securities Exchange Act of 1934. | |
| *31.2 | Certification of Periodic Report by Chief Financial Officer pursuant to Rule 13a-14 and 15d-14 of the Securities Exchange Act of 1934. | |
| *32 | Certification of Chief Executive Officer and Chief Financial Officer pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002. | |
| *101.INS | XBRL Instance Document | |
| *101.SCH | XBRL Taxonomy Extension Schema Document | |
| *101.CAL | XBRL Extension Calculation Linkbase | |
| *101.LAB | XBRL Extension Label Linkbase | |
| *101.PRE | XBRL Extension Presentation Linkbase | |
| *101.DEF | XBRL Taxonomy Extension Definition Linkbase |
*Filed or furnished herewith.
| E-3 |