Attached files
| file | filename |
|---|---|
| EXCEL - IDEA: XBRL DOCUMENT - KERYX BIOPHARMACEUTICALS INC | Financial_Report.xls |
| EX-31.2 - EXHIBIT 31.2 - KERYX BIOPHARMACEUTICALS INC | v302731_ex31-2.htm |
| EX-21.1 - EXHIBIT 21.1 - KERYX BIOPHARMACEUTICALS INC | v302731_ex21-1.htm |
| EX-31.1 - EXHIBIT 31.1 - KERYX BIOPHARMACEUTICALS INC | v302731_ex31-1.htm |
| EX-32.1 - EXHIBIT 32.1 - KERYX BIOPHARMACEUTICALS INC | v302731_ex32-1.htm |
| EX-32.2 - EXHIBIT 32.2 - KERYX BIOPHARMACEUTICALS INC | v302731_ex32-2.htm |
| EX-23.1 - EXHIBIT 23.1 - KERYX BIOPHARMACEUTICALS INC | v302731_ex23-1.htm |
| EX-10.20 - EXHIBIT 10.20 - KERYX BIOPHARMACEUTICALS INC | v302731_ex10-20.htm |
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
x ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
For the fiscal year ended December 31, 2011.
OR
¨ TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
For the transition period from ________ to ________.
Commission File Number 000-30929
KERYX BIOPHARMACEUTICALS, INC.
(Exact name of registrant as specified in its charter)
|
Delaware (State or other jurisdiction of incorporation or organization) |
13-4087132 (I.R.S. Employer Identification No.) |
|
750 Lexington Avenue New York, New York (Address of principal executive offices) |
10022 (Zip Code) |
Registrant’s telephone number, including area code: (212) 531-5965
Securities registered pursuant to Section
12(b) of the Act:
|
Common Stock, Par Value $0.001 Per Share (Title of Class) |
NASDAQ Capital Market (Name of Each Exchange on Which Registered) |
Securities registered pursuant to Section 12(g) of the Act:
None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act.
Yes ¨ No x
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act.
Yes ¨ No x
Indicate by check mark whether the registrant: (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes x No ¨
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes x No ¨
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. £
Indicate by check mark whether the registrant is a large accelerated filed, an accelerated filer, a non-accelerated filer or a smaller reporting company. See definitions of “large accelerated filer,” “accelerated filer,” and “smaller reporting company” in Rule 12b-2 of the Exchange Act). (Check one):
| Large accelerated filer ¨ | Accelerated filer x | |
| Non-accelerated filer ¨ | Smaller reporting company ¨ |
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act).
Yes ¨ No x
The aggregate market value of voting common stock held by non-affiliates of the registrant (assuming, for purposes of this calculation, without conceding, that all executive officers and directors are “affiliates”) was $324,028,092 as of June 30, 2011, based on the closing sale price of such stock as reported on the NASDAQ Capital Market.
There were 71,022,951 shares of the registrant’s common stock outstanding as of February 23, 2012.
DOCUMENTS INCORPORATED BY REFERENCE
Portions of the registrant’s Proxy Statement for the 2012 Annual Meeting of Stockholders are incorporated by reference in Part III of this Annual Report on Form 10-K.
KERYX BIOPHARMACEUTICALS, INC.
ANNUAL REPORT ON FORM 10-K
FOR THE FISCAL YEAR ENDED DECEMBER 31, 2011
TABLE OF CONTENTS
| Page | ||
| SPECIAL CAUTIONARY NOTICE REGARDING FORWARD-LOOKING STATEMENTS | 1 | |
| PART I | ||
| ITEM 1 | Business | 2 |
| ITEM 1A | Risk Factors | 21 |
| ITEM 1B | Unresolved Staff Comments | 33 |
| ITEM 2 | Properties | 33 |
| ITEM 3 | Legal Proceedings | 33 |
| ITEM 4 | Mine Safety Disclosures | 34 |
| PART II | ||
| ITEM 5 | Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities | 34 |
| ITEM 6 | Selected Financial Data | 36 |
| ITEM 7 | Management’s Discussion and Analysis of Financial Condition and Results of Operations | 37 |
| ITEM 7A | Quantitative and Qualitative Disclosure About Market Risk | 45 |
| ITEM 8 | Financial Statements and Supplementary Data | 45 |
| ITEM 9 | Changes in and Disagreements With Accountants on Accounting and Financial Disclosure | 45 |
| ITEM 9A | Controls and Procedures | 45 |
| ITEM 9B | Other Information | 46 |
| PART III | ||
| ITEM 10 | Directors, Executive Officers and Corporate Governance | 46 |
| ITEM 11 | Executive Compensation | 46 |
| ITEM 12 | Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters | 47 |
| ITEM 13 | Certain Relationships and Related Transactions and Director Independence | 47 |
| ITEM 14 | Principal Accountant Fees and Services | 47 |
| PART IV | ||
| ITEM 15 | Exhibits and Financial Statement Schedules | 48 |
This Annual Report on Form 10-K contains trademarks and trade names of Keryx Biopharmaceuticals, Inc., including our name and logo. All other trademarks, service marks, or trade names referenced in this Annual Report on Form 10-K are the property of their respective owners.
SPECIAL CAUTIONARY NOTICE REGARDING FORWARD-LOOKING STATEMENTS
Certain matters discussed in this report, including matters discussed under the caption “Management’s Discussion and Analysis of Financial Condition and Results of Operations,” may constitute forward-looking statements for purposes of the Securities Act of 1933, as amended, or the Securities Act, and the Securities Exchange Act of 1934, as amended, or the Exchange Act, and involve known and unknown risks, uncertainties and other factors that may cause our actual results, performance or achievements to be materially different from the future results, performance or achievements expressed or implied by such forward-looking statements. The words "anticipate," "believe," "estimate," "may," "expect" and similar expressions are generally intended to identify forward-looking statements. Our actual results may differ materially from the results anticipated in these forward-looking statements due to a variety of factors, including, without limitation, those discussed under the captions “Risk Factors,” “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and elsewhere in this report, as well as other factors which may be identified from time to time in our other filings with the Securities and Exchange Commission, or the SEC, or in the documents where such forward-looking statements appear. All written or oral forward-looking statements attributable to us are expressly qualified in their entirety by these cautionary statements. Such forward-looking statements include, but are not limited to, statements about our:
| · | expectations for increases or decreases in expenses; |
| · | expectations for the pre-clinical and clinical development, manufacturing, regulatory approval, and commercialization of KRX-0401 (perifosine) and ZerenexTM (ferric citrate) or any other products we may acquire or in-license; |
| · | expectations for incurring capital expenditures to expand our research and development and manufacturing capabilities; |
| · | expectations for generating revenue or becoming profitable on a sustained basis; |
| · | expectations or ability to enter into marketing and other partnership agreements; |
| · | expectations or ability to enter into product acquisition and in-licensing transactions; |
| · | expectations or ability to build our own commercial infrastructure to manufacture, market and sell our drug candidates; |
| · | estimates of the sufficiency of our existing cash and cash equivalents and investments to finance our operating requirements, including expectations regarding the value and liquidity of our investments; |
| · | expected losses; and |
| · | expectations for future capital requirements. |
The forward-looking statements contained in this report reflect our views and assumptions only as of the date this report is signed. Except as required by law, we assume no responsibility for updating any forward-looking statements.
We qualify all of our forward-looking statements by these cautionary statements. In addition, with respect to all of our forward-looking statements, we claim the protection of the safe harbor for forward-looking statements contained in the Private Securities Litigation Reform Act of 1995.
| 1 |
PART I
Unless the context requires otherwise, references in this report to “Keryx,” “Company,” “we,” “us” and “our” refer to Keryx Biopharmaceuticals, Inc. and our subsidiaries.
ITEM 1. BUSINESS.
OVERVIEW
We are a biopharmaceutical company focused on the acquisition, development and commercialization of medically important pharmaceutical products for the treatment of cancer and renal disease. We are developing KRX-0401 (perifosine), a novel, potentially first-in-class, oral anti-cancer agent that inhibits Akt activation in the phosphoinositide 3-kinase, or PI3K, pathway, and also affects a number of other key signal transduction pathways, including the JNK pathway, all of which are pathways associated with programmed cell death, growth, differentiation and survival. KRX-0401 is currently in Phase 3 clinical development for both refractory advanced colorectal cancer and relapsed / refractory multiple myeloma, and in Phase 1 and Phase 2 clinical development for several other tumor types. Each of the KRX-0401 Phase 3 programs is being conducted under Special Protocol Assessment, or SPA, agreements with the Food and Drug Administration, or FDA, and with Fast-Track Designation.
We are also developing Zerenex™ (ferric citrate), an oral, ferric iron-based compound that has the capacity to bind to phosphate in the gastrointestinal tract and form non-absorbable complexes. Zerenex is currently in Phase 3 clinical development in the United States, under an SPA, as a treatment for hyperphosphatemia (elevated phosphate levels) in patients with end-stage renal disease, or ESRD, on dialysis. In April 2011, our Japanese partner for Zerenex (ferric citrate), Japan Tobacco Inc., or JT, and Torii Pharmaceutical Co., Ltd., or Torii, commenced its Phase 3 clinical program for ferric citrate in Japan.
We also engage in business development activities that include seeking strategic relationships for our product candidates, as well as evaluating compounds and companies for in-licensing or acquisition. To date, we have not received approval for the sale of any of our drug candidates in any market and, therefore, have not generated any product sales from our drug candidates. We have generated, and expect to continue to generate, revenue from the licensing of rights to Zerenex in Japan to JT and Torii.
The table below summarizes the status of our product pipeline.
| Product candidate | Target indication | Development status |
| KRX-0401 (perifosine) |
Colorectal cancer Multiple myeloma Several other forms of cancer |
Phase 3 trial ongoing, under SPA Phase 3 trial ongoing, under SPA Phase 1 & 2 trials ongoing |
| Zerenex™ (ferric citrate) | Hyperphosphatemia in patients with end-stage renal disease |
U.S. Phase 3 program ongoing, under SPA Japan Phase 3 program ongoing by sublicensee (JT and Torii) |
OUR STRATEGY
Our mission is to create long-term stockholder value by acquiring, developing and commercializing medically important, pharmaceutical products for the treatment of life-threatening diseases, focusing on cancer and renal disease. Our strategy to achieve this mission is to:
| · | utilize our clinical development capabilities to manage and drive our drug candidates through the clinical development process to approval; |
| · | identify and explore licensing and partnership opportunities for our current drug candidates; |
| · | seek to acquire medically important drug candidates in early clinical development; and |
| · | commercialize our drug candidates, either alone or in partnership, which we believe can provide maximum stockholder value. |
| 2 |
CORPORATE INFORMATION
We were incorporated in Delaware in October 1998. We commenced operations in November 1999, following our acquisition of substantially all of the assets and certain of the liabilities of Partec Ltd., our predecessor company that began its operations in January 1997. Our executive offices are located at 750 Lexington Avenue, New York, New York 10022. Our telephone number is 212-531-5965, and our e-mail address is info@keryx.com.
We maintain a website with the address www.keryx.com. We make available free of charge through our Internet website our annual reports on Form 10-K, quarterly reports on Form 10-Q and current reports on Form 8-K, and any amendments to these reports, as soon as reasonably practicable after we electronically file such material with, or furnish such material to, the SEC. We are not including the information on our website as a part of, nor incorporating it by reference into, this report. You may read and copy any materials we file at the SEC’s Public Reference Room at 100 F Street, N.E., Washington, D.C. 20549 on official business days during the hours of 10:00 a.m. to 3:00 p.m. Please call the SEC at 1-800-SEC-0330 for information on the Public Reference Room. Additionally, the SEC maintains a website that contains annual, quarterly, and current reports, proxy statements, and other information that issuers (including us) file electronically with the SEC. The SEC’s website address is http://www.sec.gov.
PRODUCTS UNDER DEVELOPMENT
KRX-0401 (perifosine)
Overview
KRX-0401 (perifosine) is a novel, potentially first-in-class, oral anti-cancer agent that inhibits Akt activation in the PI3K pathway, and also affects a number of other key signal transduction pathways, including the JNK pathway, all of which are pathways associated with programmed cell death, cell growth, cell differentiation and cell survival. The effects of KRX-0401 on Akt are of particular interest because of the importance of this pathway in the development of most cancers, with evidence that it is often activated in tumors that are resistant to other forms of anticancer therapy, and the difficulty encountered thus far in the discovery of drugs that will inhibit this pathway without causing excessive toxicity. High levels of activated Akt, or pAkt, are seen frequently in many types of cancer and have been correlated with poor prognosis.
To date, over 2,000 patients have been treated with KRX-0401 in trials conducted in the U.S., Canada, Europe and Israel. Its safety profile is distinctly different from that of most cytotoxic agents. In clinical trials, KRX-0401 does not appear to cause flu-like symptoms, thrombocytopenia (decrease in platelets that may result in bleeding) or alopecia (hair loss). The main side effects of KRX-0401, as seen in clinical trials, are nausea, vomiting, diarrhea and fatigue, but these are generally well-managed particularly at lower daily doses (50 mg or 100 mg) that have induced tumor regression. Responses have been seen with both daily and weekly regimens. At the doses studied, the daily regimens were better tolerated.
Pre-Clinical and Clinical Data Overview
In vitro, KRX-0401 inhibits the growth of a variety of human tumor cell lines and has demonstrated activity in vivo against a number of murine tumor models and human xenografts. Investigators at the U.S. National Cancer Institute, or NCI, were among the first to study the effects of KRX-0401 on Akt using a prostate cell line, PC-3, that is known to have constitutively activated Akt. Their results demonstrated that KRX-0401 blocked phosphorylation of Akt but did not decrease the total amount of Akt present in the cell. Additional in-vitro and in-vivo studies were conducted in several model systems, including colorectal, multiple myeloma, prostate, neuroblastoma and gastric cell lines. In these studies, KRX-0401 appeared to be additive or synergistic with cytotoxics, antimetabolites and targeted agents such as cisplatin, 5- fluorouracil (5FU), doxorubicin, proteasome inhibitor bortezomib (Velcade®), tyrosine kinase inhibitor sorafenib (Nexavar®), mTOR inhibitor temsirolimus (Torisel®), EGFR antibody cetuximab (Erbitux®) and cyclophosphamide.
Seven Phase 1 single agent studies of KRX-0401 have been conducted; three in Europe by AEterna Zentaris Inc., the licensor of KRX-0401, and four in the U.S. by the NCI, a department of the National Institutes of Health, or NIH, as part of a Cooperative Research and Development Agreement, or CRADA, and by us. These trials demonstrated that KRX-0401 can be safely given to humans with a manageable toxicity profile. The dose limiting toxicity in the Phase 1 studies was gastrointestinal: nausea, vomiting and diarrhea. Additionally, one Phase 1 study in the U.S. is being conducted to evaluate the safety of KRX-0401 in pediatric patients, and another is being conducted to evaluate the effect of KRX-0401 on electrocardiogram parameters, including QTc intervals, as well as the effect of food on KRX-0401 bioavailability.
| 3 |
Fourteen Phase 1 and Phase 2 studies of KRX-0401 in combination with other drugs have been conducted by Keryx. Agents that have been included in these combinations include capecitabine (Xeloda®), gemcitabine, paclitaxel, docetaxel, prednisone, doxorubicin, pemetrexed, irinotecan, Doxil® (doxorubicin HCl liposome injection), trastuzumab, various endocrine therapies, imatinib, bortezomib (Velcade®), lenalidomide, sorafenib, and sunitinib. KRX-0401 has generally been well tolerated when used as a low daily dose (50 mg or 100 mg) in combination with these approved agents.
The NCI has conducted a number of Phase 2 clinical trials studying KRX-0401 as a single agent, including studies in prostate, breast, head and neck and pancreatic cancers, as well as melanoma and sarcomas. In total, nine NCI clinical trials have been conducted across these six tumor types.
KRX-0401 has also been evaluated in eleven Phase 2 clinical studies conducted by Keryx evaluating the single agent activity in various tumor types where patients have progressed on standard treatments. Clinical trials where responses have been reported have been conducted in patients with renal cell carcinoma, advanced brain tumors, soft-tissue sarcomas, hepatocellular carcinoma, as well as in hematologic malignancies including multiple myeloma and Waldenstrom’s macroglobulinemia. As illustrated in the previous NCI trials, the lower daily doses (50 mg or 100 mg) have been better tolerated than the intermittent higher doses.
Colorectal Cancer Clinical Data
In June 2010, we announced updated results from a randomized, multi-center, double-blind, placebo-controlled, Phase 2 study of KRX-0401 (perifosine) in combination with capecitabine (Xeloda®) versus capecitabine plus placebo in patients with second-line, third-line or greater metastatic colorectal cancer. The data was presented at the 46th Annual Meeting of the American Society of Clinical Oncology, or ASCO, in Chicago. In October 2011, the results of the Phase 2 study were published in the Journal of Clinical Oncology, or JCO, (J Clin Oncol. 2011 Nov 20;29(33):4394-400. Epub 2011 Oct 3). The study was designed as part of a larger Phase 2 clinical protocol that included several prospectively defined perifosine + chemotherapy regimens.
In this randomized, double-blind, placebo-controlled study conducted at multiple centers across the U.S., heavily pre-treated patients with second-line, third-line or greater metastatic colorectal cancer were randomized to receive capecitabine (a chemotherapy used in advanced metastatic colorectal cancer which is marketed by Roche as Xeloda®) at a starting dose of 825 mg/m2, twice daily (total daily dose of 1650 mg/m2) on days 1 – 14 every 21 days plus either perifosine at 50 mg daily or placebo. The study enrolled a total of 38 patients, 34 of whom were third-line or greater. Median age of patients was 65 (32-83); 61% of the patients were male.
The results published in the JCO reported on the safety and efficacy for the Intent-to-Treat population, as per the protocol statistical criteria, defined as all patients who received at least one dose of study drug, which included all 38 patients enrolled. Overall Response Rate, or ORR, was measured in any patient who completed one cycle of therapy, and included 35 evaluable patients (20 patients on the perifosine + capecitabine arm and 15 patients on the placebo + capecitabine arm). Three patients on the placebo + capecitabine arm were not evaluable for response due to coming off treatment within the first cycle of therapy. All patients in the perifosine + capecitabine arm were evaluable for response.
The patients in the study were heavily pre-treated, with the arms well-balanced in terms of prior treatment regimens. The prior treatment regimens for all 38 patients are shown in the table below. Notably, all of the patients (with the exception of one CAP arm patient) had been treated with FOLFIRI and/or FOLFOX, almost 80% treated with Avastin®, and approximately half treated with an EGFR antibody.
| Prior RX | P-CAP (n=20) | CAP (n=18) | All Patients (n=38) | |||
| FOLFIRI | 18 (90%) | 16 (89%) | 34 (89%) | |||
| FOLFOX | 15 (75%) | 13 (72%) | 28 (74%) | |||
| FOLFIRI & FOLFOX | 13 (65%) | 12 (67%) | 25 (66%) | |||
| Avastin® | 15 (75%) | 15 (83%) | 30 (79%) | |||
| EGFR Antibody (1) | 9 (45%) | 10 (56%) | 19 (50%) | |||
| 5-FU Refractory Status | 14 (70%) | 13 (72%) | 27 (71%) | |||
| Third Line or > | 18 (90%) | 16 (89%) | 34 (89%) |
(1) Prior treatment with Erbitux® and/or Vectibix®
| 4 |
The primary endpoint of this study was to measure Time to Progression, or TTP. ORR, defined as Complete Response, or CR, + Partial Response, or PR, by Response Evaluation Criteria in Solid Tumors, or RECIST, and Overall Survival, or OS, were measured as secondary endpoints. The efficacy results illustrated by ORR, TTP and OS, broken down by all evaluable patients and 5-FU refractory patients, are as follows:
OVERALL RESPONSE RATE:
| ALL EVALUABLE PATIENTS (n=35) | 5-FU REFRACTORY PATIENTS (n=25) | |||||||||||||||||||
| Group | n | CR n (%) |
PR n (%) |
Duration of Response |
>
SD n (%) P = 0.036 |
Group | n | PR n (%) |
Duration of Response |
>
SD n (%) P = 0.066 | ||||||||||
| P-CAP | 20 | 1 (5%) | 3 (15%) | CR: 36 m | 11 (55%) | P-CAP | 14 | 1 (7%) | 19 m | 8 (57%) | ||||||||||
| PR: 21, 19, 11 m | ||||||||||||||||||||
| CAP | 15 | 0 | 1 (7%) | PR: 7 m | 5 (33%) | CAP | 11 | 0 | - | 3 (27%) | ||||||||||
TIME TO PROGRESSION AND OVERALL SURVIVAL
| ALL EVALUABLE PATIENTS (n=38) | 5-FU REFRACTORY PATIENTS (n=27) | |||||||||||||
| Group | n | Median TTP Weeks P < 0.001 HR: 0.254 |
Median OS* Months P = 0.0052 HR: 0.370 |
Group | n | Median TTP Weeks P < 0.001 HR: 0.170 |
Median OS* Months P = 0.0061 HR: 0.295 | |||||||
| P-CAP | 20 | 27.5 [95% CI (12.1-48.1)] |
17.7 [95% CI (8.5-24.6)] |
P-CAP | 14 | 17.6 [95% CI (12.0-36.0)] |
15.1 [95% CI (7.2-22.3)] | |||||||
| CAP | 18 | 10.1 [95% CI (6.6-13.0)] |
7.6 [95% CI (5.0-16.3)] |
CAP | 13 | 9.0 [95% CI (6.6-11.0)] |
6.5 [95% CI (4.8-10.9)] | |||||||
*Survival is calculated from date of randomization until the date of death from any cause, whether or not additional therapies were received after removal from treatment.
All 38 patients in the study were evaluable for safety. The P-CAP combination was well-tolerated with Grade 3 and 4 adverse events of > 10% incidence for the P-CAP arm versus CAP arm as follows: hand-foot syndrome (30% vs. 0%), anemia (15% vs. 0%), fatigue (0% vs. 11%), bowel obstruction (0% vs. 11%) and abdominal pain (5% vs. 11%). Of note, incidence of Grade 1 and 2 hand-foot syndrome was similar in both the P-CAP and CAP arms (25% vs. 22%, respectively). Hand-foot syndrome is a reported adverse event with capecitabine monotherapy. We believe that patients who remained on treatment longer in the Phase 2 study had a greater chance to develop hand-foot syndrome as illustrated by a median time to onset of Grade 3 and 4 hand-foot syndrome in the P-CAP arm of 19 weeks.
Metastatic Colorectal Cancer Phase 3 “X-PECT” Registration Clinical Trial
In April 2010, we initiated a Phase 3 registration clinical trial for KRX-0401 (perifosine) for the treatment of patients with refractory advanced colorectal cancer. In July 2011, we announced the completion of patient enrollment. This Phase 3 trial is being conducted pursuant to an SPA with the FDA and with Fast-Track Designation. The Phase 3 trial, entitled the “X-PECT” (Xeloda® + Perifosine Evaluation in Colorectal cancer Treatment) trial, is a randomized (1:1), double-blind trial comparing the efficacy and safety of perifosine + capecitabine vs. placebo + capecitabine in approximately 465 patients with refractory advanced colorectal cancer. Patients must have failed available therapy including 5-fluorouracil (5-FU), oxaliplatin (Eloxatin®), irinotecan (Camptosar®), bevacizumab (Avastin®) and, if KRAS wild-type, failed therapy with prior cetuximab (Erbitux®) and/or panitumumab (Vectibix®). For oxaliplatin-based therapy, failure of therapy will also include patients who discontinued due to toxicity. The primary endpoint is overall survival, with secondary endpoints including ORR, progression-free survival and safety. The median overall survival for the X-PECT study's targeted patient population, that has failed prior therapies as described above, is expected to be approximately 5 months. The X-PECT study is powered at 90% to detect a statistically significant difference in overall survival, with an assumed median overall survival for the control arm of 5-6 months and 7-8 months for the perifosine arm. Approximately 360 events of death will trigger the un-blinding of the study. On July 27, 2011, we announced the completion of patient enrollment and on August 31, 2011, we announced that the independent Data Safety Monitoring Board, or DSMB, for the Phase 3 “X-PECT” trial completed a pre-specified interim analysis for safety and futility. The independent DSMB recommended that the Phase 3 study continue to completion, as planned.
| 5 |
Dr. Johanna Bendell, Director of GI Oncology Research for the Sarah Cannon Research Institute, Nashville, Tennessee, is leading the Phase 3 investigational team that includes Dr. Cathy Eng, Associate Medical Director for the Colorectal Center at MD Anderson Cancer Center in Houston, Texas. Approximately 65 U.S. sites are participating in the study.
KRX-0401 has been granted Fast Track designation for the treatment of refractory advanced colorectal cancer.
Colorectal Cancer Market Opportunity
According to the American Cancer Society, colorectal cancer is the third most common form of cancer diagnosed in the U.S. It is estimated that approximately 143,000 people will be diagnosed with some form of colorectal cancer with approximately 51,000 patients dying from colorectal cancer in 2012. Surgery is often the main treatment for early stage colorectal cancer. When colorectal cancer metastasizes (spreads to other parts of the body such as the liver) chemotherapy is commonly used. Treatment of patients with recurrent or advanced colorectal cancer depends on the location of the disease. Chemotherapy regimens (i.e. FOLFOX or FOLFIRI either with or without bevacizumab) have been shown to increase survival rates in patients with metastatic/advanced colorectal cancer. Currently, there are seven approved drugs for patients with metastatic colorectal cancer: 5-fluorouracil (5-FU), capecitabine (Xeloda®), irinotecan (Camptosar®), oxaliplatin (Eloxatin®), bevacizumab (Avastin®), cetuximab (Erbitux®), and panitumumab (Vectibix®). Depending on the stage of the cancer, two or more of these types of treatment may be combined at the same time or used after one another. For example, FOLFOX combines 5-FU, leucovorin and oxaliplatin, whereas FOLFIRI combines 5-FU, leucovorin and irinotecan. Bevacizumab, a VEGF monoclonal antibody, is commonly administered with chemotherapy. Typically, patients who fail 5-FU, oxaliplatin, irinotecan, and bevacizumab-containing therapies, and who have wild-type KRAS status receive EGFR monoclonal antibody therapy with either cetuximab or panitumumab. Once patients progress on these agents, there are no further standard treatment options.
Multiple Myeloma Clinical Data
In December 2011, at the American Society of Hematology, or ASH, annual meeting, in a presentation by Dr. Paul Richardson, Clinical Director of the Multiple Myeloma Center at Dana-Farber Cancer Institute in Boston, we announced results (updated from a presentation at ASH in December 2009) on the clinical activity of KRX-0401 (perifosine) in combination with bortezomib (with or without dexamethasone) in patients with relapsed / refractory multiple myeloma. This trial was designed as a Phase 1 and Phase 2 study. In October 2011, the results of the study were published in the JCO (J Clin Oncol. 2011 Nov 10;29(32):4243-9. Epub 2011 Oct 11).
The Phase 1 portion of the study enrolled 18 patients and the Phase 2 portion enrolled 66 patients (for a total of 84 patients), all with advanced multiple myeloma.
The patients enrolled were heavily pre-treated with a median of 5 prior lines of therapy (range 1 - 13), including;
| · | 100% of patients had been treated with bortezomib (55% of the patients were previously treated with at least two bortezomib-based therapies (range 1 - 4) and 81% were previously treated with bortezomib plus dexamethasone); |
| · | 98% of patients were previously treated with dexamethasone; |
| · | 94% of patients were previously treated with lenalidomide (Revlimid®) and/or thalidomide (Thalomid®); and |
| · | 58% of patients had prior stem cell transplant. |
ORR, defined as the percentage of patients achieving a CR, PR or minor response, or MR, was the primary endpoint, with TTP, Progression-Free Survival, or PFS, OS and safety as secondary endpoints.
| 6 |
Seventy-three patients were evaluable for efficacy. Evaluable patients were defined as those patients who had received at least two cycles of therapy on the combination of perifosine with bortezomib. Of the 73 evaluable patients, 53 patients (73%) were previously refractory to bortezomib (defined as progression on or within 60 days of treatment with a bortezomib-based regimen), including 44 patients who were refractory to the combination of bortezomib + dexamethasone. Twenty evaluable patients (27%) were relapsed to a prior bortezomib-based regimen. Best response for all 73 evaluable patients was as follows:
| Evaluable Patients | CR /nCR* | PR | MR | ORR | SD** | |||||||||||||||||||||||||||||||||||
| All Evaluable Patients (n=73) | 3 | 4% | 13 | 18% | 14 | 19% | 30 | 41% | 30 | 41% | ||||||||||||||||||||||||||||||
| Bortezomib Relapsed (n=20) | 2 | 10% | 7 | 35% | 4 | 20% | 13 | 65% | 7 | 35% | ||||||||||||||||||||||||||||||
| Bortezomib Refractory (n=53) | 1 | 2% | 6 | 11% | 10 | 19% | 17 | 32% | 23 | 43% | ||||||||||||||||||||||||||||||
| * | nCR = Near Complete Response is defined as meeting the criteria for CR (non-detectable monoclonal protein by serum and urine), except with detectable monoclonal protein by immunofixation. |
| ** | SD = Stable Disease for a minimum of 3 months. |
Median PFS and OS data for all evaluable patients was as follows:
| Evaluable Patients | Median PFS* | Median OS* | ||
| All Evaluable Patients (n=73) |
6.4 months 95% CI (5.3 - 7.1) |
25 months 95% CI (16.3 - 31.1) |
| * | Median PFS and median TTP were identical, as no patient deaths occurred prior to progression. Kaplan Meier methodology was used to determine PFS and OS figures. |
Median PFS and OS for bortezomib relapsed vs. refractory were as follows:
| Bortezomib Relapsed vs. Refractory | Median PFS* | Median OS* | ||
| Bortezomib Relapsed (n=20) |
8.8 months 95% CI (6.3 - 11.2) |
30.4 months 95% CI (17.8 - NR**) | ||
| Bortezomib Refractory (n=53) |
5.7 months 95% CI (4.3 - 6.4) |
22.5 months 95% CI (14.2 - 31.1) |
| * | Median PFS and median TTP were identical, as no patient deaths occurred prior to progression. Kaplan Meier methodology was used to determine PFS and OS figures. |
| ** | NR = Not reached as of December 2011. |
No unexpected adverse events have been observed. Toxicities were manageable with supportive care.
In December 2010, at the ASH annual meeting, we announced updated results from a Phase 1 study of perifosine + lenalidomide (Revlimid®) + dexamethasone in patients with relapsed or refractory multiple myeloma. The data showed a 73% objective response rate (MR or better) with a 50% PR or better rate, a median PFS of 10.8 months, and a median duration for OS of 30.6 months. The myeloma investigators concluded that perifosine in combination with lenalidomide + dexamethasone was well tolerated, even at the highest doses used, and demonstrated encouraging clinical activity and survival.
Multiple Myeloma Phase 3 Registration Clinical Trial
In December 2009, we initiated a Phase 3 registration clinical trial for KRX-0401 (perifosine) in relapsed / refractory multiple myeloma patients. The trial, entitled, "A Phase 3 Randomized Study to Assess the Efficacy and Safety of Perifosine Added to the Combination of Bortezomib (Velcade®) and Dexamethasone in Multiple Myeloma Patients Previously Treated with Bortezomib" is a randomized (1:1), double-blind, placebo-controlled trial comparing the efficacy and safety of perifosine vs. placebo when combined with bortezomib (Velcade®) and dexamethasone. The trial will enroll approximately 400 patients with relapsed or relapsed / refractory multiple myeloma. Patients will be randomized to bortezomib at 1.3 mg/m2 days 1, 4, 8 and 11 every 21 days in combination with dexamethasone 20 mg on the day of and day after bortezomib treatment, and either perifosine 50 mg daily or placebo. Patients eligible for the Phase 3 trial must have been previously treated with both bortezomib (Velcade® ) and an immunomodulatory agent (Revlimid® and/or Thalomid®), and been previously treated with one to four prior lines of therapy. The primary endpoint is PFS and secondary endpoints include ORR, OS and safety. Patients can be relapsed from and refractory to all non-bortezomib based therapies, however, patients can only be relapsed (progressed > 60 days after discontinuing therapy) from prior bortezomib-based therapies. The study is powered at 90% to demonstrate a 50% improvement in PFS between the two arms. Approximately 265 events (defined as disease progression or death) will trigger the un-blinding of the data. This trial is being conducted pursuant to an SPA with the FDA. Additionally, the FDA has granted perifosine Orphan Drug and Fast Track designations in this indication.
| 7 |
The Phase 3 trial is being led by the Principal Investigator, Dr. Paul Richardson, Clinical Director of the Jerome Lipper Multiple Myeloma Center, at Dana-Farber Cancer Institute, or DFCI, in Boston, MA and Dr. Kenneth C, Anderson, Chief, Division of Hematologic Neoplasia at DFCI. Approximately 80 sites throughout North America, Western and Eastern Europe, Israel and South Korea are currently participating in this Phase 3 trial.
Multiple Myeloma Market Opportunity
Multiple myeloma, a cancer of the plasma cell, is an incurable but treatable disease. Multiple myeloma is the second most-common hematologic cancer, representing 1% of all cancer diagnoses and 2% of all cancer deaths. According to the American Cancer Society, in 2012 there will be an estimated 21,700 new cases of multiple myeloma and an estimated 10,710 deaths from multiple myeloma in the U.S. To date, several FDA approved therapies exist for the treatment of multiple myeloma. Despite this progress, patients continue to relapse, become refractory to prior treatments and eventually die from their disease. Thus, new therapies are needed to treat these patients and extend their survival.
Renal Cell Carcinoma Clinical Data
On September 26, 2009, Dr. Thomas E. Hutson, Director of the Genitourinary Oncology Program at Baylor-Sammons Cancer Center in Dallas, TX, presented updated Phase 2 results demonstrating KRX-0401 (perifosine) single agent efficacy in patients with metastatic renal cell carcinoma, in a presentation entitled, "Phase 2 Study of Perifosine in Patients with Metastatic Renal Cell Carcinoma Progressing After Prior Therapy with both a VEGF Receptor Inhibitor and an mTOR Inhibitor." Data from this study were first presented at the ASCO annual meeting in May 2009. The presentation included results from a subgroup of patients who failed both a VEGF receptor inhibitor (sunitinib or sorafenib) and an mTOR inhibitor (temsirolimus or everolimus). Evaluable patients (n=16) were defined as those who had greater than 7 days of treatment (2 additional patients withdrew consent within 7 days). Patients received 100 mg of perifosine daily until progression or unacceptable toxicity. The primary endpoint of this study was clinical benefit, defined as response rate (CR / PR by RECIST) or percent of patients progression-free for at least 3 months. Median PFS and OS were also analyzed for efficacy. Safety was a secondary endpoint. Perifosine was well-tolerated with the most common adverse events being gastrointestinal discomfort and fatigue. Best response to single agent perifosine was as follows:
| n | PR n (%) |
SD > 12 wks n (%) |
PD < 12 wks n (%) |
Median PFS | Overall Survival | |||||
| 16 | 1 (6%) | 7 (44%) | 8 (50%) | 16 wks [95% CI (11.7, 28)] | Not Reached (14/16 alive) at 22+ months |
PD: Progressive disease
Waldenstrom’s Macroglobulinemia Clinical Data
In an article entitled “Clinical and Translational Studies of a Phase II Trial of the Novel Oral Akt Inhibitor Perifosine in Relapsed or Relapsed/Refractory Waldenstrom’s Macroglobulinemia” which appeared in the February 1, 2010 issue of Clinical Cancer Research, we reported Phase 2 data demonstrating the single agent activity of KRX-0401 (perifosine) for the treatment of advanced Waldenstrom’s Macroglobulinemia, or Waldenstrom’s. In the Phase 2 study, 37 patients were treated with KRX-0401 (perifosine) 150 mg daily for 6 cycles. In this study, 41% of the patients had 3 or more lines of prior therapy and 78% had 2 or more prior lines of therapy. Such prior therapies include nucleoside analogues, bortezomib, alkylating agents and rituximab (Rituxan®), which are not approved for, but are often used in the treatment of Waldenstrom’s. Stable or responding patients were allowed to continue therapy until progression. Of the 37 patients, 4 achieved a PR (11%), 9 achieved a MR (24%), and 20 showed SD (54%). Overall, 89% (33/37) of patients treated with single agent perifosine were reported to have SD or better, while 11% (4 patients) demonstrated progression. The median progression-free survival in the study was 12.6 months (90% C.I. (10.2, 22.7)), with a median overall survival of 26 months (90% C.I. (26 – upper limit not reached)). Perifosine was generally well-tolerated with gastrointestinal symptoms and fatigue reported as the most common adverse events related to therapy.
Also described in the article are translational studies using gene expression profiling and immunohistochemistry on pre- versus post-treatment patient samples. Results showed that in the majority of samples tested, there was a significant reduction of phospho-GSK3/b (downstream from Akt) using immunohistochemistry. Similarly, results demonstrated that perifosine significantly inhibited the expression of multiple members of the NF-kB family of genes, confirming previous in vitro studies showing activity of perifosine targeting this pathway.
| 8 |
Recurrent Pediatric Solid Tumors, Including Neuroblastoma
In June 2010, we announced interim data from a Phase 1 clinical trial of KRX-0401 (perifosine) in recurrent pediatric solid tumors. The data was presented in the pediatric solid tumor poster discussion session held at the 46th Annual Meeting of ASCO in Chicago. The study is being conducted by the Memorial Sloan-Kettering Cancer Center pediatric group and represents the first time that KRX-0401 has been administered in a pediatric patient setting.
This Phase 1 study is a single center, open-label, dose-escalating study to assess safety, tolerability, pharmacokinetics, or PK, and to identify any dose limiting toxicity, or DLT, of single agent perifosine in pediatric patients with any solid tumor that has failed standard therapy. Eleven patients (4 males, 7 females), at a median age of 13 years (5-18) were treated in this study as of June 2010. The following tumor types were treated: high-grade glioma (5), medulloblastoma (2), neuroblastoma (3), and ependymoma (1). Most patients were heavily pretreated, with a median of three prior lines of therapy. Cohorts of three patients were treated at three dose levels: 25mg/m2/day, 50mg/m2/day and 75mg/m2/day using 50mg tablets of perifosine after a loading dose on day 1, and taking into account the drug’s long half-life (>100hrs). No DLTs were observed at any of the three dose levels. PK data thus far suggests similar drug absorption by pediatric patients relative to adult patients treated with single agent perifosine.
Of particular interest were the early signs of clinical activity observed in two of the three patients with Stage 4 refractory neuroblastoma. Both patients were refractory to prior treatments upon entering the study and achieved stable disease for 48 weeks and 55+ weeks (ongoing). The investigators concluded that perifosine is well-tolerated in children with recurrent solid tumors and that these early signals of activity warrant further investigation in patients with advanced neuroblastoma and select brain tumors. In May 2010, NCI investigators published, in the Journal of the National Cancer Institute, in vitro and in vivo data demonstrating that perifosine targets the activation of Akt in neuroblastoma cells and xenografts, significantly inhibits tumor growth in vivo and improves the survival of mice bearing neuroblastoma tumors.
In July 2010, we announced that perifosine received Orphan-Drug designation from the FDA for the treatment of neuroblastoma.
Other Indications
In December 2010, at the ASH annual meeting, we announced encouraging clinical activity, safety and tolerability of perifosine in patients with advanced chronic lymphocytic leukemia, or CLL, and Hodgkin's lymphoma, or HL. In this Phase 2 study, 26 patients were enrolled with advanced lymphoma (6 NHL, 4 CLL, 1 Waldenstroms and 15 HL). 73% of patients were previously refractory to their prior therapy, with 85% of patients having had 4 or more prior therapies. Perifosine (50 mg, twice daily) was started as a single agent for 28 days. After 28 days, patients achieving a PR or better were continued on single agent perifosine. Patients achieving less than a PR were given the combination of perifosine (50 mg, twice daily) plus sorafenib (Nexavar®) at 400 mg, twice daily.
All of the four CLL patients in the study achieved a PR on single-agent perifosine within one month of treatment and remained on perifosine single agent. As of December 2010, response durations for each of the 4 patients were 4, 8, 9+ and 12 months. The remaining 22 patients were administered the combination with sorafenib, where 5 of the 15 (33%) HL patients achieved a PR with a median response duration of 9 months. An additional 6 patients receiving the combination (40%) achieved SD. The combination was well tolerated with no unexpected safety events. The investigators concluded that perifosine in combination with sorafenib has significant anti-lymphoma activity in relapsed/refractory HL, and that perifosine as a single agent induced prolonged responses in high-risk, heavily pretreated CLL patients.
In December 2010, at the ASH annual meeting, we also announced interim results of another Phase 2 study of perifosine in patients with relapsed or refractory CLL. In this Phase 2 study, 12 patients with advanced CLL began treatment with single agent perifosine at 50mg, twice daily. Patients on study were heavily pre-treated having had a median of 4 prior lines of therapy with 75% of patients classified as Rai stage IV. One patient achieved a PR (5 months on treatment) and five additional patients achieved stable disease (median duration of 4.25 months), for an overall 50% clinical benefit rate (PR + SD). Perifosine was well tolerated with minimal dose modifications.
Zerenex™ (ferric citrate)
Overview
Zerenex (ferric citrate) is an oral, ferric iron-based compound that has the capacity to bind to phosphate in the gastrointestinal tract and form non-absorbable complexes. Zerenex is in an ongoing Phase 3 program as a treatment for elevated serum phosphorus levels, or hyperphosphatemia, in patients with ESRD on dialysis, under an SPA agreement with the FDA. Pursuant to the SPA agreement, the Zerenex Phase 3 registration program in the U.S. consists of a short-term efficacy study, and a 58-week long-term safety and efficacy study. In April 2011, we reported the final dataset from the Phase 3 short-term efficacy study. Positive top-line results from this Phase 3 short-term study were announced in November 2010. The long-term Phase 3 study is ongoing.
| 9 |
Zerenex (ferric citrate) is also in Phase 3 development in Japan by JT and Torii.
On May 2, 2011, we announced positive Scientific Advice from the European Medicines Agency, or EMA, for the development of Zerenex for the management and control of serum phosphorus in ESRD patients undergoing dialysis, and in pre-dialysis chronic kidney disease, or CKD, patients. The Scientific Advice from the EMA indicates that our current Phase 3 program in the U.S., if successful, in conjunction with safety data generated from other clinical studies with Zerenex, is considered sufficient to support a European marketing authorization application, or MAA, to the EMA for the indication in ESRD patients on dialysis. As a result, we believe that we will not need to conduct any additional clinical trials with Zerenex in order to obtain European approval in the dialysis setting. The Scientific Advice also provided us with a regulatory path forward in the pre-dialysis CKD setting in Europe.
Market Opportunity
In the U.S., according to data from the U.S. Renal Data System, there are approximately 600,000 patients with ESRD and the number of ESRD patients is projected to continue to rise in the future. The majority of ESRD patients, over 380,000, require dialysis. Phosphate retention and the resulting hyperphosphatemia in patients with ESRD on dialysis are usually associated with secondary hyperparathyroidism, renal osteodystrophy, soft tissue mineralization and the progression of renal failure. ESRD patients usually require treatment with phosphate-binding agents to lower and maintain serum phosphorus at acceptable levels.
Aluminum-type phosphate binders were widely used in the past. However, the systemic absorption of aluminum from these agents and the potential toxicity associated with their use no longer make this type of binder a viable long-term treatment option.
Calcium-type phosphate binders are commonly used to bind dietary phosphate; however, they promote positive net calcium balance and an increased risk of metastatic calcification in many patients, especially in those patients taking vitamin D analogs and those with adynamic bone disease.
Non-calcium-based, non-absorbed phosphate binders, including sevelamer hydrochloride and sevelamer carbonate are among the most prescribed phosphate binders in the U.S. Compared to the calcium-type binders, fewer coronary and aortic calcifications have been documented, however, there is a risk of metabolic acidosis with sevelamer hydrochloride, as well as the potential for gastrointestinal problems, and sevelamer can affect concomitant vitamin K and vitamin D treatment.
Lanthanum-type phosphate binders are another alternative. Lanthanum is a rare earth element and is minimally absorbed in the gastrointestinal tract. Lower level tissue deposition, particularly in bone and liver, has been observed in animals. However, the long-term effects due to the accumulation of lanthanum in these tissues have not been clearly determined.
The need for alternative phosphate-binding agents has long been recognized, especially given the increasing prevalence of ESRD as well as shortcomings with current therapies. Zerenex has the potential to be an effective and safe treatment in lowering and/or maintaining serum phosphorus levels between 3.5 and 5.5 mg/dL, the recommended range under the National Kidney Foundation KDOQI Clinical Practice Guidelines, in patients with ESRD and hyperphosphatemia.
Phase 3 Registration Clinical Program – Short-Term Study
On April 28, 2011, we reported the final dataset from the Phase 3 short-term clinical trial of Zerenex for the treatment of hyperphosphatemia in end-stage renal disease patients on dialysis. Top-line results from this Phase 3 short-term study were announced in November 2010. The final dataset was presented at the National Kidney Foundation Spring Clinical Meetings held in Las Vegas, Nevada, in an oral presentation. In this study, conducted pursuant to a SPA with the FDA, Zerenex met the study’s primary endpoint, described below, demonstrating a highly statistically significant dose response. In addition, key secondary endpoints were also met.
| 10 |
The Phase 3 short-term study was a multicenter, randomized, open-label trial with a two-week washout period, following which patients were randomized 1:1:1 to receive a fixed dose of Zerenex of either 1 gram, 6 grams or 8 grams per day for a treatment period of 28 days. Zerenex was administered using a 1 gram oral caplet formulation, and the fixed-dose arms of 1 gram, 6 grams and 8 grams per day represented 1, 6 and 8 pills per day, respectively. One hundred fifty-one dialysis patients were enrolled into the study. The Intent-to-Treat, or ITT, group included 146 patients, representing all patients who took at least one dose of Zerenex and provided a Baseline (at the end of washout) and at least one post-Baseline efficacy assessment. Efficacy assessments were taken weekly starting at Baseline and subsequently at days 7, 14, 21 and 28. The primary endpoint of the study was to determine whether there was a dose response in the change in serum phosphorus from Baseline to Day 28 in the ITT group, using a regression analysis to evaluate this objective.
The study met the primary endpoint, with the regression analysis indicating a highly statistically significant dose response (p<0.0001). Additional efficacy results are as follows:
|
Mean Serum Phosphorus (mg/dL) ITT (n=146) |
1g/Day (n=50) |
6g/Day (n=51) |
8g/Day (n=45) |
||||||
| Baseline (End of Washout) | 7.3 | 7.6 | 7.5 | ||||||
| Day 28 (End of Treatment) | 7.4 | 5.6 | 5.3 | ||||||
| Change from Baseline at Day 28 P-Value |
0.1 | -2.0 <0.0001 |
-2.2 <0.0001 |
||||||
| % Change from Baseline at Day 28 | 0.5% | -25.7% | -29.6% |
In addition, a statistically significant dose response increase in serum bicarbonate was observed in the study, indicating the potential ability of Zerenex to address metabolic acidosis. Metabolic acidosis is a condition that occurs in many dialysis patients when the kidneys do not remove sufficient acid from the body, leading to low blood pH. The consequences of metabolic acidosis can be severe. The inability to manage metabolic acidosis is believed to be a drawback for some of the currently marketed phosphate binders.
Importantly, no clinically meaningful change in serum calcium was observed in the study. Additionally, a statistically significant dose response reduction in calcium-phosphorus product was also observed in the study. Elevated levels of serum calcium (hypercalcemia) and high levels of calcium-phosphorus product, both of which are believed to be drawbacks from the use of some of the currently marketed phosphate binders, increase the risk of soft tissue calcification and may contribute to the substantial morbidity and mortality seen in patients with ESRD.
Certain iron parameters, including ferritin and TSAT, were measured in the study. Modest upward trends in ferritin and TSAT levels were observed in the 6 grams/day and 8 grams/day dose groups, which further support our belief that Zerenex may have the potential to reduce the need for intravenous, or IV, iron supplements and/or erythropoiesis-stimulating agents, or ESAs, in dialysis patients. Ferritin and TSAT levels, as well as, IV iron and ESA use, are under evaluation in the ongoing Phase 3 long-term study.
Zerenex appeared to be safe and well-tolerated in the study, with no serious adverse events deemed to be drug-related by the Data Safety Monitoring Committee, which further supports Zerenex’s favorable safety profile seen in prior clinical trials.
Phase 3 Registration Clinical Program – Long-Term Study
In September 2010, we announced the initiation of the long-term Phase 3 study of Zerenex in patients with ESRD on dialysis. The initiation of this study marked the commencement of the final component of our Phase 3 registration program for Zerenex, which is being conducted in accordance with a SPA agreement with the FDA. In September 2011, we announced the completion of patient enrollment in the study. The Phase 3 long-term study is a multicenter, randomized, open-label, safety and efficacy clinical trial in approximately 440 ESRD patients on hemodialysis or peritoneal dialysis. The study consists of a 2-week washout period followed by a 52-week safety assessment in which patients are randomized 2:1 to receive either Zerenex or an active control. The 52-week safety assessment period is followed by a 4-week efficacy assessment. During the 4-week efficacy assessment, only those patients randomized to treatment with Zerenex during the safety assessment period will be randomized in a 1:1 ratio to either continue treatment with Zerenex or to be switched to placebo for a 4-week period. Approximately, 60 sites in the U.S. and select non-U.S. sites are participating in the study.
| 11 |
Phase 2 Clinical Data – Long-Term Open-Label Extension Study
In April 2010, we reported updated long-term efficacy and safety data on Zerenex from an open-label extension study that was conducted in Taiwan in patients with ESRD who were on dialysis. This data was presented at the National Kidney Foundation 2010 Spring Clinical Meeting in a poster entitled “Long-Term Use of Ferric Citrate in End-Stage Renal Disease Patients.” After the completion of a 28-day fixed dose Phase 2 clinical trial of ferric citrate in ESRD patients, 29 patients who had participated in this trial at the site in Taiwan were offered to continue onto an Open-Label Extension, or OLE, trial for up to one year. There was approximately a two month period between the completion of the Phase 2 dose-ranging trial and enrollment into the OLE trial. During this time interval, no patient was exposed to ferric citrate as a phosphate binder. Patients were immediately switched back to ferric citrate from other phosphate binders and there was no washout period prior to starting ferric citrate treatment in the OLE trial. Of the 29 patients enrolled, 28 were exposed to ferric citrate. The patients were started on doses of ferric citrate of 2 to 6 g/day. The maximum allowed dose was 6 g/day. The average dose per patient throughout the study was approximately 4.5 g/day. The average duration of the patient’s participation in the trial was 306 +/- 85 days. The primary objective of this OLE trial of ferric citrate was to assess the long-term efficacy and safety of ferric citrate as a phosphate binder in ESRD patients for up to one year. The secondary objective of this OLE trial was to assess for the potential for iron absorption.
The therapeutic goal of the OLE study was to achieve and maintain a serum phosphorus level below 5.5 mg/dL. The mean levels of serum phosphorus, or SP, and phosphorus x calcium product, or PxC, for the evaluable patients at each time point over the treatment period were as follows:
| SP (mg/dL) | PxC (mg/dL)2 | |||
| Baseline (sd) | 5.63 (1.22) | 50.79 (12.74) | ||
| 3 months (sd) | 5.48 (1.33) | 51.84 (12.67) | ||
| 6 months (sd) | 5.16 (1.20) | 48.40 (9.60) | ||
| 9 months (sd) | 5.24 (1.20) | 48.72 (12.04) | ||
| 12 months (sd) | 5.21 (1.09) | 50.05 (11.82) |
Iron parameters were measured at baseline and then quarterly through month nine. On average, slight increases were observed over time, across all key parameters, as follows:
| Baseline (sd) | 9 Months (sd) | |||
| Ferritin (ng/mL) | 520 (328) | 781 (364) | ||
| TSAT (%) | 39.2 (19.7) | 45.5 (21.1) | ||
| Iron (mcg/dL) | 87.8 (37.9) | 88.3 (37.2) | ||
| HCT (%) | 30.8 (6.9) | 32.9 (9.7) |
If a patient had a ferritin greater than 600 ng/mL and a TSAT greater than 50%, the use of IV iron was withheld until the patient’s ferritin and TSAT were below the above levels during the treatment period. If a patient had a hematocrit, or HCT, greater than 36%, the use of an ESA was withheld until the HCT was less than 36% during the treatment period.
There were 8 patients who had IV iron supplements withheld for approximately 3 to 6 months and there were 8 patients who had an ESA withheld for approximately 1 to 10 months during the OLE trial. Out of the 16 patients in the two groups, three patients had both IV iron and ESAs withheld.
Ferric citrate was well-tolerated throughout the OLE study. There were no patient deaths during the OLE and no serious adverse events reported related to ferric citrate.
The investigators concluded that in this OLE trial of ferric citrate with doses as high as 6 g/day, ferric citrate demonstrated the potential to be used long-term as a phosphate binder in ESRD patients. Ferric citrate appeared to be efficacious in controlling serum phosphorus and well-tolerated and safe for up to one year. Additionally, it is the investigators’ opinion that this OLE trial, along with data from both animal studies and the Phase 2 high dose trial, supports the notion that some modest iron absorption may be occurring over time with the use of ferric citrate as a phosphate binder in ESRD patients and that if a reduction in the use of IV-iron supplements and/or ESAs are documented in future long-term clinical trials, the cost-benefit and cost-effectiveness of ferric citrate as a phosphate binder, as compared to currently marketed phosphate binders, would be significant.
Phase 2 Clinical Data – Short-Term Studies
In June 2009, we announced results of the U.S. Phase 2 study of Zerenex for the treatment of elevated serum phosphorus levels, or hyperphosphatemia, in patients with ESRD on thrice weekly hemodialysis. The study was a multicenter, open-label clinical trial, which enrolled 55 patients. The primary objective of this study was to assess the tolerability and safety of Zerenex with doses ranging from approximately 1 gram per day to 12 grams per day.
| 12 |
In the first part of the Phase 2 study, 34 ESRD patients who were taking approximately 6 to 15 tablets/capsules per day of calcium acetate, calcium carbonate, lanthanum carbonate or sevelamer hydrochloride or any combination of these agents were eligible for enrollment and immediately switched to a starting dose of 4.5 grams per day of Zerenex. In the second part of the study, 21 ESRD patients who were taking greater than 12 tablets/capsules per day of calcium acetate, calcium carbonate, lanthanum carbonate or sevelamer hydrochloride or any combination of these agents were eligible for enrollment and immediately switched to a starting dose of 6.0 grams per day of Zerenex. Patients were treated with Zerenex for four weeks and were titrated weekly to achieve and maintain normal serum phosphorus levels, between 3.5 to 5.5 mg/dL, the therapeutic goal.
Although designed primarily as a safety study, key efficacy parameters were evaluated, with results as follows:
At baseline:
| · | Baseline mean +/- standard deviation, or SD, serum phosphorus was approximately 5.9 +/- 1.5 mg/dL immediately prior to the switch to Zerenex; |
| · | The average daily dose of PhosLo(R) (calcium acetate) was 6.9 grams per day and for Renagel(R) (sevelamer hydrochloride) was 9.9 grams per day, for patients not on combination therapy prior to the switch to Zerenex. |
Following the treatment period (four weeks on Zerenex):
| · | At the end of the treatment period (after four weeks on Zerenex) the mean +/- SD serum phosphorus was approximately 5.4 +/- 1.3 mg/dL; |
| · | The average daily dose of Zerenex at the end of four weeks of treatment was 6.8 grams per day; |
In the subset of 29 patients who had a serum phosphorus above the normal range (> 5.5 mg/dL) at baseline, immediately prior to the switch to Zerenex, the mean (standard deviation) baseline serum phosphorus was 7.0 (1.1) mg/dL, and at the end of treatment with Zerenex the mean (SD) serum phosphorus was 5.6 (1.6) mg/dL.
In the Phase 2 study, there were four serious adverse events which were deemed unrelated to Zerenex. Darkened stool was reported in the study and was associated with the presence of iron in the gastrointestinal tract. With the exception of the reporting of darkened stool as an (asymptomatic) adverse event, the gastrointestinal adverse event profile was similar in incidence to that reported for other currently marketed phosphate binders. There was no increase in serum calcium noted in the study.
Following the results of the U.S. Phase 2 study of Zerenex announced in June 2009, the top line efficacy and safety results from this Phase 2 study were submitted to the FDA. The FDA also reviewed the final reports for the 90-day rat and 16-week canine toxicology studies. The FDA indicated that the results of the Phase 2 study and the toxicology studies were adequate to support entry into a Phase 3 program. The FDA also reviewed the protocols for the ongoing chronic toxicology studies (6-month rat and 42-week canine), which were completed and submitted to the FDA in 2010.
In June 2006, we announced final results from the Phase 2 multi-center study entitled: “A randomized, double-blind, placebo-controlled, dose ranging study of the effects of Zerenex on serum phosphate in patients with end stage renal disease (ESRD).” This Phase 2 study was conducted under an investigational new drug application, or IND, sponsored by our licensor in both the U.S. and Taiwan.
From this Phase 2 study, the investigators concluded that Zerenex appeared to have an acceptable safety and tolerability profile at the 2, 4, and 6g/day dose. The optimum dose of Zerenex in this study was 6g/day at which it appeared to be efficacious, safe and well tolerated as treatment for hyperphosphatemia in hemodialysis patients. Additionally, the investigators found that Zerenex therapy for up to 28 days had no statistically significant effect on serum iron, ferritin, transferrin saturation, or total iron binding capacity.
The Phase 2 study was designed to determine the safety and efficacy of several doses of Zerenex in patients with ESRD who were undergoing hemodialysis. In this study, each of three Zerenex doses (2g, 4g and 6g) administered daily with meals was compared to placebo. Patients who had been on other phosphate binders prior to enrolling in this study underwent a 1-2-week washout period prior to randomization. Patients who had a serum phosphorus level greater than or equal to 5.5 mg/dl and less than or equal to 10 mg/dl by the end of this washout period were eligible to be randomized to one of four treatment groups at a ratio of 2:2:2:1, (Zerenex 2g, 4g, 6g and placebo, respectively) and were treated for 28 days. The primary endpoint for this study was the change in serum phosphorus concentration at day 28 relative to baseline.
| 13 |
Of the 116 patients randomized in the study, 111 patients were evaluable for efficacy at 28 days and were included in the analysis. At day 28, there was a statistically significant dose response to Zerenex in reducing serum phosphorus concentration (p=0.0073).
Changes in Serum Phosphorus Concentration (mg/dL) on day 28 compared to day 0 (baseline) at Zerenex doses of 2, 4 and 6 g/day
|
Placebo (n=16) |
2g/day (n=31) |
4g/day (n=32) |
6g/day (n=32) | |||||
| Day 0 (Baseline)* | 7.2 (1.4) | 7.2 (1.2) | 7.1 (1.3) | 7.3 (1.3) | ||||
| Day 28 (End of Treatment Period)* | 7.2 (1.2) | 6.9 (2.2) | 6.0 (1.3) | 5.8 (1.8) | ||||
| Placebo Comparison: | ||||||||
| Mean Difference from Placebo | -0.02 | -1.1 | -1.5 | |||||
| P-value | NS | 0.06 | 0.0119 | |||||
| Baseline Comparison: | ||||||||
| Mean Difference from Baseline | -0.1 | -0.3 | -1.1 | -1.5 | ||||
| P-value | NS | NS | NS | <0.01 |
*mean (standard deviation)
There was also a statistically significant dose response to Zerenex in the calcium x phosphorus (Ca x P) product at day 28 (p=0.0158). In the 6g/day Zerenex group the mean decrease in Ca x P product when compared with placebo was statistically significant (p=0.0378).
There were no deaths over the course of the 28 day study and there were no serious adverse events that were deemed by the investigators to be related to Zerenex. Safety was assessed in 16, 33, 34 and 33 patients, in the placebo, 2, 4, and 6 grams per day groups, respectively. Possibly or probably related adverse events occurred in 4 (25.0%), 7 (21.2%), 8 (23.5%), and 7 (21.2%) patients in the placebo, 2, 4, and 6 grams per day treatment groups, respectively. The majority of adverse events were of mild severity, with 1 (6.3%), 0 (0.0%), 2 (5.9%), and 1 (3.0%) patients, of the placebo, 2, 4, and 6 grams per day groups, respectively, experiencing at least one severe adverse event.
In addition, Zerenex has been studied in two previous Phase 2 clinical trials using single fixed dose regimens. In both studies, Zerenex was able to significantly reduce serum phosphorus (p <0.005), and the degree of reduction appeared to be generally comparable to calcium-based products which were used as positive control arms in those studies. The studies were not designed to compare Zerenex to calcium-based products, therefore, no formal assessment can be made of the comparative efficacy.
COSTS AND TIME TO COMPLETE PRODUCT DEVELOPMENT
The information below provides estimates regarding the costs associated with the completion of the current development phase and our current estimated range of the time that will be necessary to complete that development phase for our key pipeline products. We also direct your attention to the risk factors which could significantly affect our ability to meet these cost and time estimates found in this report in Item 1A under the heading “Risks Associated with Our Product Development Efforts.”
| Product candidate | Target indication | Development status | Expected completion of phase |
Estimated
cost to complete phase | ||||
| KRX-0401 (perifosine) | Colorectal cancer Multiple myeloma |
Phase 3, under SPA Phase 3, under SPA |
1H 2012 1H 2013 |
$2 - $3 million $10 - $13 million* | ||||
| Zerenex™ (ferric citrate) | Hyperphosphatemia in patients with end-stage renal disease |
Phase 3, under SPA |
2H 2012 | $6 - $7 million |
* Includes estimated cost of Velcade® in those non-U.S. countries where Velcade® is not reimbursed.
Completion dates and costs in the above table are estimates and are subject to the uncertainties associated with clinical trials and the related requirements of development. In the cases where the requirements for clinical trials and development programs have not been fully defined, or are dependent on the success of other trials, we cannot estimate trial completion or cost with any certainty. The actual spending on each trial during the year is also dependent on our ability to fund such clinical trials. We therefore direct your attention to Item 7 under the heading “Liquidity and Capital Resources.”
| 14 |
INTELLECTUAL PROPERTY AND PATENTS
General
Patents and other proprietary rights are very important to the development of our business. We will be able to protect our proprietary technologies from unauthorized use by third parties only to the extent that our proprietary rights are covered by valid and enforceable patents supported by regulatory exclusivity or are effectively maintained as trade secrets. It is our intention to seek and maintain patent and trade secret protection for our drug candidates and our proprietary technologies. As part of our business strategy, our policy is to actively file patent applications in the U.S. and, when appropriate, internationally to cover methods of use, processes of manufacture, new chemical compounds, pharmaceutical compositions and dosing of the compounds and compositions and improvements in each of these. We also rely on trade secret information, technical know-how, innovation and agreements with third parties to continuously expand and protect our competitive position. We have a number of patents and patent applications related to our compounds and other technology, but we cannot guarantee the scope of protection of the issued patents, or that such patents will survive a validity or enforceability challenge, or that any of the pending patent applications will issue as patents.
Generally, patent applications in the U.S. are maintained in secrecy for a period of 18 months or more. Since publication of discoveries in the scientific or patent literature often lag behind actual discoveries, we are not certain that we were the first to make the inventions covered by each of our pending patent applications or that we were the first to file those patent applications. The patent positions of biotechnology and pharmaceutical companies are highly uncertain and involve complex legal and factual questions. Therefore, we cannot predict the breadth of claims allowed in biotechnology and pharmaceutical patents, or their enforceability. To date, there has been no consistent policy regarding the breadth of claims allowed in biotechnology patents. Third parties or competitors may challenge or circumvent our patents or patent applications, if issued. If our competitors prepare and file patent applications in the U.S. that claim technology also claimed by us, we may have to participate in interference proceedings declared by the U.S. Patent and Trademark Office to determine priority of invention, which could result in substantial cost, even if the eventual outcome is favorable to us. Because of the extensive time required for development, testing and regulatory review of a potential product, it is possible that before we commercialize any of our products, any related patent may expire or remain in existence for only a short period following commercialization, thus reducing any advantage of the patent. However, the life of a patent covering a product that has been subject to regulatory approval may have the ability be extended through the patent restoration program, although any such extension could still be minimal.
If a patent is issued to a third party containing one or more preclusive or conflicting claims, and those claims are ultimately determined to be valid and enforceable, we may be required to obtain a license under such patent or to develop or obtain alternative technology. In the event of a litigation involving a third party claim, an adverse outcome in the litigation could subject us to significant liabilities to such third party, require us to seek a license for the disputed rights from such third party, and/or require us to cease use of the technology. Further, our breach of an existing license or failure to obtain a license to technology required to commercialize our products may seriously harm our business. We also may need to commence litigation to enforce any patents issued to us or to determine the scope and validity of third-party proprietary rights. Litigation would involve substantial costs.
Pursuant to our license for KRX-0401 (perifosine) with AEterna Zentaris Inc., we have the exclusive commercial rights to a series of patents and patent applications in the U.S., Canada and Mexico. These patents and patent applications include a composition of matter patent expiring in the second half of 2013 (with possible patent term extension through the second half of 2018, which is the maximum term of extension under the patent term restoration program), as well as a method of use patent application, directed to the use of perifosine in combination with various other anticancer agents, which would expire in 2023. We have also filed a patent application relating to the combination use of perifosine and capecitabine, which would expire in 2031.
Pursuant to our license for Zerenex (ferric citrate) with Panion & BF Biotech, Inc., or Panion, we have the exclusive commercial rights to a series of patent applications worldwide, excluding certain Asian-Pacific countries. These patents and patent applications cover a composition of matter and method of treatment of hyperphosphatemia in patients with ESRD (expiring in the second half of 2017, with possible patent term extension through 2020 or later), as well as a method for the manufacture of ferric citrate (expiring 2023). We have also filed a patent application relating to the formulation of ferric citrate drug product.
| 15 |
The patent rights that we own or have licensed relating to our product candidates are limited in ways that may affect our ability to exclude third parties from competing against us if we obtain regulatory approval to market these product candidates. In particular:
| · | Our composition of matter patent covering KRX-0401 (perifosine) expires in the second half of 2013 and we cannot assure you that we can obtain an extension to the second half of 2018 (the maximum term of extension under the patent term restoration program). Our composition of matter patent covering Zerenex expires in the second half of 2017 and we cannot assure you that we can obtain an extension to 2022 (the maximum term of extension under the patent term restoration program). Composition of matter patents can provide protection for pharmaceutical products to the extent that the specifically covered compositions are important. Upon expiration of our composition of matter patents for KRX-0401 and Zerenex, competitors who obtain the requisite regulatory approval can offer products with the same composition as our products so long as the competitors do not infringe any other patents that we may hold, such as method of use patents. |
| · | Our method of use patents only protect the products when used or sold for the specified method. However, this type of patent does not limit a competitor from making and marketing a product that is identical to our product that is labeled for an indication that is outside of our patented method, or for which there is a substantial use in commerce outside our patented method. |
| · | Our pending patent applications may not issue as patents and may not issue in all countries in which we develop, manufacture or potentially sell our products or in countries where others develop, manufacture and potentially sell products using our technologies. Moreover, our pending patent applications, if issued as patents, may not provide additional protection for our products. |
| · | Because clinical trials for KRX-0401 and Zerenex are ongoing, and because any potential date for regulatory approval is currently unknown, it is possible that the life of these patents following regulatory approval will be minimal, even if the above-discussed extensions are obtained. |
Proof of direct infringement by a competitor for method of use patents can prove difficult because the competitors making and marketing a product typically do not engage in the patented use. Additionally, proof that a competitor contributes to or induces infringement of a patented method of use by another can also prove difficult because an off-label use of a product could prohibit a finding of contributory infringement and inducement of infringement requires proof of intent by the competitor.
Moreover, physicians may prescribe such a competitive identical product for indications other than the one for which the product has been approved, or off-label indications, that are covered by the applicable patents. Although such off-label prescriptions may directly infringe or contribute to or induce infringement of method of use patents, such infringement is difficult to prevent or prosecute.
In addition, the limited patent protection described above may adversely affect the value of our product candidates and may inhibit our ability to obtain a corporate partner at terms acceptable to us, if at all.
Other Intellectual Property Rights
We depend upon trademarks, trade secrets, know-how and continuing technological advances to develop and maintain our competitive position. To maintain the confidentiality of trade secrets and proprietary information, we require our employees, scientific advisors, consultants and collaborators, upon commencement of a relationship with us, to execute confidentiality agreements and, in the case of parties other than our research and development collaborators, to agree to assign their inventions to us. These agreements are designed to protect our proprietary information and to grant us ownership of technologies that are developed in connection with their relationship with us. These agreements may not, however, provide protection for our trade secrets in the event of unauthorized disclosure of such information.
| 16 |
In addition to patent protection, we may utilize orphan drug regulations or other provisions of the Food, Drug and Cosmetic Act of 1938, as amended, or FDCA, to provide market exclusivity for certain of our drug candidates. Orphan drug regulations provide incentives to pharmaceutical and biotechnology companies to develop and manufacture drugs for the treatment of rare diseases, currently defined as diseases that exist in fewer than 200,000 individuals in the U.S., or, diseases that affect more than 200,000 individuals in the U.S. but that the sponsor does not realistically anticipate will generate a net profit. Under these provisions, a manufacturer of a designated orphan-drug can seek tax benefits, and the holder of the first FDA approval of a designated orphan product will be granted a seven-year period of marketing exclusivity for such FDA-approved orphan product. In September 2009, we announced that KRX-0401 (perifosine) has received Orphan-Drug designation from the FDA for the treatment of multiple myeloma, and in July 2010, we announced that KRX-0401 has received Orphan-Drug designation from the FDA for the treatment of neuroblastoma. We believe that KRX-0401 may be eligible for additional orphan drug designations; however, we cannot assure that KRX-0401, or any other drug candidates we may acquire or in-license, will obtain such orphan drug designations. Additionally, upon FDA approval, we believe that perifosine would qualify as a New Chemical Entity, or NCE, which provides for five years of exclusivity following approval.
We cannot assure that any other drug candidates we may acquire or in-license, will obtain such orphan drug designation or that we will be the first to receive FDA approval for such drugs so as to be eligible for market exclusivity protection.
LICENSING AGREEMENTS AND COLLABORATIONS
We have formed strategic alliances with a number of companies for the manufacture and commercialization of our products. Our current key strategic alliances are discussed below.
AEterna Zentaris Inc.
In September 2002, we signed a commercial license agreement with Zentaris AG, a wholly-owned subsidiary of AEterna Zentaris Inc., or Zentaris, relating to the development of perifosine covering composition of matter and methods of treatment. This agreement grants us the exclusive rights to KRX-0401 (perifosine) in the U.S., Canada and Mexico. To date, we have paid an aggregate of $1.8 million to Zentaris and Zentaris is eligible to receive additional payments of up to an aggregate of $17.0 million upon our successful achievement of certain clinical development, regulatory and sales milestones, in addition to royalty payments on net sales of perifosine. The license terminates upon the later of the expiration of all underlying patent rights or ten years from the first commercial sale of KRX-0401 in any of the covered territories.
Panion & BF Biotech, Inc.
In November 2005, we entered into a license agreement with Panion & BF Biotech, Inc., or Panion. Under the license agreement, we have acquired the exclusive worldwide rights, excluding certain Asian-Pacific countries, for the development and marketing of Zerenex (ferric citrate). To date, we have paid an aggregate of $3.6 million to Panion and Panion is eligible to receive additional payments of up to an aggregate of $8.0 million upon our successful achievement of certain clinical development and regulatory milestones, in addition to royalty payments on net sales of Zerenex. The license terminates upon the expiration of all underlying patent rights.
Japan Tobacco Inc. and Torii Pharmaceutical Co., Ltd.
In September 2007 (amended and restated in June 2009), we entered into a sublicense agreement with JT and Torii, JT's pharmaceutical business subsidiary, under which JT and Torii obtained the exclusive rights for the development and commercialization of Zerenex (ferric citrate) in Japan. The licensing arrangement calls for JT and Torii to pay us up to $100 million in up-front license fees and payments upon the achievement of pre-specified milestones, of which we have received $28 million, including the milestone payment of $5.0 million in April 2011 for the achievement of the Phase 3 commencement milestone. In addition, upon commercialization, JT and Torii will make royalty payments to Keryx on net sales of ferric citrate in Japan. JT and Torii are responsible for the development and commercialization costs in Japan.
COMPETITION
Competition in the pharmaceutical and biotechnology industries is intense. Our competitors include pharmaceutical companies and biotechnology companies, as well as universities and public and private research institutions. In addition, companies that are active in different but related fields represent substantial competition for us. Many of our competitors have significantly greater capital resources, larger research and development staffs and facilities and greater experience in drug development, regulation, manufacturing and marketing than we do. These organizations also compete with us to recruit qualified personnel, attract partners for joint ventures or other collaborations, and license technologies that are competitive with ours. To compete successfully in this industry we must identify novel and unique drugs or methods of treatment and then complete the development of those drugs as treatments in advance of our competitors.
| 17 |
The drugs that we are attempting to develop will have to compete with existing therapies. In addition, a large number of companies are pursuing the development of pharmaceuticals that target the same diseases and conditions that we are targeting. Other companies have products or drug candidates in various stages of pre-clinical or clinical development to treat diseases for which we are also seeking to discover and develop drug candidates. Some of these potential competing drugs are further advanced in development than our drug candidates and may be commercialized earlier. Additional information can be found under Item 1A - Risk Factors – Other Risks Related to Our Business within this report.
SUPPLY AND MANUFACTURING
We have limited experience in manufacturing products for clinical or commercial purposes.
We have established contract manufacturing relationships for the supply of KRX-0401 (perifosine). We have also established contract manufacturing relationships for the supply of Zerenex (ferric citrate) to ensure that we will have sufficient material for clinical trials. In addition, we are establishing the basis for commercial production capabilities. As with any supply program, obtaining raw materials of the correct quality cannot be guaranteed and we cannot ensure that we will be successful in this endeavor.
At the time of commercial sale, to the extent possible and commercially practicable, we would seek to engage a back-up supplier for each of our product candidates. Until such time, we expect that we will rely on a single contract manufacturer to produce each of our product candidates under current Good Manufacturing Practice, or cGMP, regulations. Our third-party manufacturers have a limited number of facilities in which our product candidates can be produced and will have limited experience in manufacturing our product candidates in quantities sufficient for commercialization. Our third-party manufacturers will have other clients and may have other priorities that could affect their ability to perform the work satisfactorily and/or on a timely basis. Both of these occurrences would be beyond our control.
We expect to similarly rely on contract manufacturing relationships for any products that we may in-license or acquire in the future. However, there can be no assurance that we will be able to successfully contract with such manufacturers on terms acceptable to us, or at all.
Contract manufacturers are subject to ongoing periodic and unannounced inspections by the FDA, the Drug Enforcement Administration and corresponding state agencies to ensure strict compliance with cGMP and other state and federal regulations. Our contractors in Europe face similar challenges from the numerous European Union and member state regulatory agencies and authorized bodies. We do not have control over third-party manufacturers’ compliance with these regulations and standards, other than through contractual obligations and periodic auditing. If they are deemed out of compliance with cGMPs, approvals could be delayed, product recalls could result, inventory could be destroyed, production could be stopped and supplies could be delayed or otherwise disrupted.
If we need to change manufacturers after commercialization, the FDA and corresponding foreign regulatory agencies must approve these new manufacturers in advance, which will involve testing and additional inspections to ensure compliance with FDA regulations and standards and may require significant lead times and delay, and disruption of supply. Furthermore, switching manufacturers may be difficult because the number of potential manufacturers is limited. It may be difficult or impossible for us to find a replacement manufacturer quickly or on terms acceptable to us, or at all.
GOVERNMENT AND INDUSTRY REGULATION
Numerous governmental authorities, principally the FDA and corresponding state and foreign regulatory agencies, impose substantial regulations upon the clinical development, manufacture and marketing of our drug candidates, as well as our ongoing research and development activities. None of our drug candidates have been approved for sale in any market in which we have marketing rights. Before marketing in the U.S., any drug that we develop must undergo rigorous pre-clinical testing and clinical trials and an extensive regulatory approval process implemented by the FDA under the FDCA. The FDA regulates, among other things, the pre-clinical and clinical testing, safety, efficacy, approval, manufacturing, record keeping, adverse event reporting, packaging, labeling, storage, advertising, promotion, export, sale and distribution of biopharmaceutical products.
The regulatory review and approval process is lengthy, expensive and uncertain. We are required to submit extensive pre-clinical and clinical data and supporting information to the FDA for each indication or use to establish a drug candidate’s safety and efficacy before we can secure FDA approval to market or sell a product in the U.S. The approval process takes many years, requires the expenditure of substantial resources and may involve ongoing requirements for post-marketing studies or surveillance. Before commencing clinical trials in humans, we must submit an IND to the FDA containing, among other things, pre-clinical data, chemistry, manufacturing and control information, and an investigative plan. Our submission of an IND may not result in FDA authorization to commence a clinical trial.
| 18 |
The FDA may permit expedited development, evaluation, and marketing of new therapies intended to treat persons with serious or life-threatening conditions for which there is an unmet medical need under its fast track drug development programs. A sponsor can apply for fast track designation at the time of submission of an IND, or at any time prior to receiving marketing approval of the new drug application, or NDA. To receive Fast Track designation, an applicant must demonstrate:
| · | that the drug is intended to treat a serious or life-threatening condition; |
| · | that the drug is intended to treat a serious aspect of the condition; and |
| · | that the drug has the potential to address unmet medical needs, and this potential is being evaluated in the planned drug development program. |
The FDA must respond to a request for fast track designation within 60 calendar days of receipt of the request. Over the course of drug development, a product in a fast track development program must continue to meet the criteria for fast track designation. Sponsors of products in fast track drug development programs must be in regular contact with the reviewing division of the FDA to ensure that the evidence necessary to support marketing approval will be developed and presented in a format conducive to an efficient review. Sponsors of products in fast track drug development programs ordinarily are eligible for priority review of a completed application in six months or less and also may be permitted to submit portions of a NDA to the FDA for review before the complete application is submitted.
Sponsors of drugs designated as fast track also may seek approval under the FDA’s accelerated approval regulations. Under this authority, the FDA may grant marketing approval for a new drug product on the basis of adequate and well-controlled clinical trials establishing that the drug product has an effect on a surrogate endpoint that is reasonably likely, based on epidemiologic, therapeutic, pathophysiologic, or other evidence, to predict clinical benefit or on the basis of an effect on a clinical endpoint other than survival or irreversible morbidity. Approval will be subject to the requirement that the applicant study the drug further to verify and describe its clinical benefit where there is uncertainty as to the relation of the surrogate endpoint to clinical benefit or uncertainty as to the relation of the observed clinical benefit to ultimate outcome. Post-marketing studies are usually underway at the time an applicant files the NDA. When required to be conducted, such post-marketing studies must also be adequate and well-controlled. The applicant must carry out any such post-marketing studies with due diligence. Many companies who have been granted the right to utilize an accelerated approval approach have failed to obtain approval. Moreover, negative or inconclusive results from the clinical trials we hope to conduct or adverse medical events could cause us to have to repeat or terminate the clinical trials. Accordingly, we may not be able to complete the clinical trials within an acceptable time frame, if at all, and, therefore, could not submit the NDA to the FDA or foreign regulatory authorities for marketing approval.
Clinical testing must meet requirements for institutional review board oversight, informed consent and good clinical practices, and must be conducted pursuant to an IND, unless exempted.
For purposes of NDA approval, clinical trials are typically conducted in the following sequential phases:
| · | Phase 1: The drug is administered to a small group of humans, either healthy volunteers or patients, to test for safety, dosage tolerance, absorption, metabolism, excretion, and clinical pharmacology. |
| · | Phase 2: Studies are conducted on a larger number of patients to assess the efficacy of the product, to ascertain dose tolerance and the optimal dose range, and to gather additional data relating to safety and potential adverse events. |
| · | Phase 3: Studies establish safety and efficacy in an expanded patient population. |
| · | Phase 4: The FDA may require Phase 4 post-marketing studies to find out more about the drug’s long-term risks, benefits, and optimal use, or to test the drug in different populations. |
| 19 |
The length of time necessary to complete clinical trials varies significantly and may be difficult to predict. Clinical results are frequently susceptible to varying interpretations that may delay, limit or prevent regulatory approvals. Additional factors that can cause delay or termination of our clinical trials, or that may increase the costs of these trials, include:
| · | slow patient enrollment due to the nature of the clinical trial plan, the proximity of patients to clinical sites, the eligibility criteria for participation in the study or other factors; |
| · | inadequately trained or insufficient personnel at the study site to assist in overseeing and monitoring clinical trials or delays in approvals from a study site’s review board; |
| · | longer treatment time required to demonstrate efficacy or determine the appropriate product dose; |
| · | insufficient supply of the drug candidates; |
| · | adverse medical events or side effects in treated patients; and |
| · | ineffectiveness of the drug candidates. |
In addition, the FDA, equivalent foreign regulatory authority, or a data safety monitoring committee for a trial may place a clinical trial on hold or terminate it if it concludes that subjects are being exposed to an unacceptable health risk, or for futility. Any drug is likely to produce some toxicity or undesirable side effects in animals and in humans when administered at sufficiently high doses and/or for a sufficiently long period of time. Unacceptable toxicity or side effects may occur at any dose level at any time in the course of studies in animals designed to identify unacceptable effects of a drug candidate, known as toxicological studies, or clinical trials of drug candidates. The appearance of any unacceptable toxicity or side effect could cause us or regulatory authorities to interrupt, limit, delay or abort the development of any of our drug candidates and could ultimately prevent approval by the FDA or foreign regulatory authorities for any or all targeted indications.
Sponsors of drugs may apply for an SPA from the FDA. The SPA process is a procedure by which the FDA provides official evaluation and written guidance on the design and size of proposed protocols that are intended to form the basis for a new drug application. However, final marketing approval depends on the results of efficacy, the adverse event profile and an evaluation of the benefit/risk of treatment demonstrated in the Phase 3 trial. The SPA agreement may only be changed through a written agreement between the sponsor and the FDA, or if the FDA becomes aware of a substantial scientific issue essential to product safety or efficacy.
Before receiving FDA approval to market a product, we must demonstrate that the product is safe and effective for its intended use by submitting to the FDA an NDA containing the pre-clinical and clinical data that have been accumulated, together with chemistry and manufacturing and controls specifications and information, and proposed labeling, among other things. The FDA may refuse to accept an NDA for filing if certain content criteria are not met and, even after accepting an NDA, the FDA may often require additional information, including clinical data, before approval of marketing a product. Whether or not the FDA requests additional information, there is no assurance that the NDA will be approved.
It is also becoming more common for the FDA to request a Risk Evaluation and Mitigation Strategy, or REMS, as part of a NDA. The REMS plan contains post-market obligations of the sponsor to train prescribing physicians, monitor off-label drug use, and conduct sufficient Phase 4 follow-up studies and registries to ensure the continued safe use of the drug.
As part of the approval process, the FDA must inspect and approve each manufacturing facility. Among the conditions of approval is the requirement that a manufacturer’s quality control and manufacturing procedures conform to cGMP. Manufacturers must expend significant time, money and effort to ensure continued compliance, and, in addition to preapproval inspections, the FDA conducts periodic inspections to evaluate continued compliance with cGMP and other requirements. It may be difficult for our manufacturers or us to comply with the applicable cGMP, as interpreted by the FDA, and other FDA regulatory requirements. If we, or our contract manufacturers, fail to comply, then the FDA may not allow us to market products that have been affected by the failure.
If the FDA grants approval, the approval will be limited to those disease states, conditions and patient populations for which the product is deemed to be safe and effective, as demonstrated through clinical studies and other data submitted in the NDA. Further, a product may be marketed only in those dosage forms and for those indications approved in the NDA. Certain changes to an approved NDA, including, with certain exceptions, any significant changes to manufacturing, drug product, or labeling, require approval of a supplemental application before the drug may be marketed as changed. Any products that we manufacture or distribute pursuant to FDA approvals are subject to continuing monitoring and regulation by the FDA, including compliance with cGMP and the reporting of adverse experiences with the drugs. The nature of marketing claims that the FDA will permit us to make in the labeling and advertising of our products will generally be limited to those specified in FDA approved labeling, and the advertising of our products will be subject to comprehensive monitoring, review and regulation by the FDA. Drugs whose review was accelerated may carry additional restrictions on marketing activities, including the requirement that all promotional materials are pre-submitted to the FDA. Claims exceeding or deemed inconsistent with those contained in approved labeling, or deemed to be false or misleading, may constitute a violation of the FDCA. Violations of the FDCA or regulatory requirements at any time during the product development process, approval process, or marketing and sale following approval may result in agency enforcement actions, including withdrawal of approval, recall, seizure of products, warning letters, injunctions, fines and/or civil or criminal penalties. Any agency enforcement action could have a material adverse effect on our business.
| 20 |
Should we wish to market our products outside the U.S., we must receive marketing authorization from the appropriate foreign regulatory authorities. The requirements governing the conduct of clinical trials, marketing authorization, pricing and reimbursement vary widely from country to country. At present, companies are typically required to apply for foreign marketing authorizations at a national level. However, within the European Union, registration procedures are available to companies wishing to market a product in more than one European Union member state. Typically, if the regulatory authority is satisfied that a company has presented adequate evidence of safety, quality and efficacy, then the regulatory authority will grant a marketing authorization. This foreign regulatory approval process, however, involves risks similar or identical to the risks associated with FDA approval discussed above, and therefore we cannot guarantee that we will be able to obtain the appropriate marketing authorization for any product in any particular country.
Failure to comply with applicable federal, state and foreign laws and regulations would likely have a material adverse effect on our business. In addition, federal, state and foreign laws and regulations regarding the manufacture and sale of new drugs are subject to future changes. We cannot predict the likelihood, nature, effect or extent of adverse governmental regulation that might arise from future legislative or administrative action, either in the U.S. or abroad.
RESEARCH AND DEVELOPMENT
Company-sponsored research and development expenses (excluding non-cash compensation and discontinued operations) totaled $7,372,000 in 2009, $13,728,000 in 2010 and $26,209,000 in 2011. “Other research and development expenses” consist primarily of salaries and related personnel costs, fees paid to consultants and outside service providers for clinical and laboratory development, facilities-related and other expenses relating to the design, development, manufacture, testing, and enhancement of our drug candidates and technologies, as well as expenses related to in-licensing of new product candidates. See “Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations—Overview.”
EMPLOYEES
As of February 23, 2012, we had 29 full- and part-time employees. None of our employees are represented by a collective bargaining agreement, and we have never experienced a work stoppage. We consider our relations with our employees to be good.
ITEM 1A. RISK FACTORS.
You should carefully consider the following risks and uncertainties. If any of the following occurs, our business, financial condition and/or operating results could be materially harmed. These factors could cause the trading price of our common stock to decline, and you could lose all or part of your investment.
Risks Related to Our Business
We have a limited operating history and have incurred substantial operating losses since our inception. We expect to continue to incur losses in the future and may never become profitable.
We have a limited operating history. You should consider our prospects in light of the risks and difficulties frequently encountered by early stage companies. In addition, we have incurred substantial operating losses since our inception and expect to continue to incur operating losses for the foreseeable future and may never become profitable. As of December 31, 2011, we had an accumulated deficit of $369.9 million. As we continue our research and development efforts, we will incur increasing losses. We may continue to incur substantial operating losses even if we begin to generate revenues from our drug candidates.
We have not yet commercialized any of our drug candidates and cannot be sure that we will ever be able to do so. Even if we commercialize one or more of our drug candidates, we may not become profitable. Our ability to achieve profitability depends on a number of factors, including our ability to complete our development efforts, obtain regulatory approval for our drug candidates, successfully complete any post-approval regulatory obligations and successfully commercialize our drug candidates.
| 21 |
Risks Associated with Our Product Development Efforts
If we are unable to successfully complete our clinical trial programs, or if such clinical trials take longer to complete than we project, our ability to execute our current business strategy will be adversely affected.
Whether or not and how quickly we complete clinical trials is dependent in part upon the rate at which we are able to engage clinical trial sites and, thereafter, the rate of enrollment of patients, and the rate we collect, clean, lock and analyze the clinical trial database. Patient enrollment is a function of many factors, including the size of the patient population, the proximity of patients to clinical sites, the eligibility criteria for the study, the existence of competitive clinical trials, and whether existing or new drugs are approved for the indication we are studying. We are aware that other companies are currently conducting or planning clinical trials that seek to enroll patients with the same diseases that we are studying. Certain clinical trials are designed to continue until a pre-determined number of events have occurred in the patients enrolled. Trials such as this are subject to delays stemming from patient withdrawal and from lower than expected event rates. They may also incur additional costs if enrollment is increased in order to achieve the desired number of events. If we experience delays in identifying and contracting with sites and/or in patient enrollment in our clinical trial programs, we may incur additional costs and delays in our development programs, and may not be able to complete our clinical trials in a cost-effective or timely manner or at all. In addition, conducting multi-national studies adds another level of complexity and risk. We are subject to events affecting countries outside the U.S.
Negative or inconclusive results from the clinical trials we conduct or unanticipated adverse medical events could cause us to have to repeat or terminate the clinical trials. We may also opt to change the delivery method, formulation or dosage which could affect efficacy results for the drug candidate. Accordingly, we may not be able to complete the clinical trials within an acceptable time frame, if at all.
In December 2009, we initiated a Phase 3 clinical trial for KRX-0401 (perifosine) in relapsed / refractory multiple myeloma patients pursuant to a SPA with the FDA. In April 2010, we initiated a Phase 3 clinical trial for KRX-0401 (perifosine) in patients with refractory advanced colorectal cancer also pursuant to a SPA with the FDA. In May 2010 and in September 2010, we initiated two Phase 3 clinical trials for Zerenex (ferric citrate) as a treatment of hyperphosphatemia in patients with end-stage renal disease pursuant to a SPA with the FDA. Many companies which have been granted SPAs and/or the right to utilize Fast Track or accelerated approvals have ultimately failed to obtain final approval to market their drugs. Since we are seeking approvals under SPAs, based on protocol designs negotiated with the FDA, we may be subject to enhanced scrutiny. Additionally, even if the primary endpoint in a Phase 3 clinical trial is achieved, a SPA does not guarantee approval. The FDA may raise issues of safety, study conduct, bias, deviation from the protocol, statistical power, patient completion rates, changes in scientific or medical parameters or internal inconsistencies in the data prior to making its final decision. The FDA may also seek the guidance of an outside advisory committee prior to making its final decision. Additionally, the regulatory approval of new therapies could invalidate our SPA, or require us to conduct additional, expensive clinical trials to obtain regulatory approval.
Even though our product candidate, KRX-0401, is designated for “Fast Track” in the indications of metastatic colorectal cancer and relapsed / refractory multiple myeloma, we cannot assure you that we will receive “priority review” status. Even with “Fast Track” or “priority review” status, such designations do not necessarily mean a faster development process or regulatory review process or necessarily confer any advantage with respect to approval compared to conventional FDA procedures.
In May 2011, we announced positive Scientific Advice from the European Medicines Agency, or EMA, for the development of Zerenex for the management and control of serum phosphorus in ESRD patients undergoing dialysis, and in pre-dialysis chronic kidney disease, or CKD, patients. The Scientific Advice from the EMA indicates that our current Phase 3 program in the U.S., if successful, in conjunction with safety data generated from other clinical studies with Zerenex, is considered sufficient to support a European marketing authorization application, or MAA, to the EMA for the indication in ESRD patients on dialysis. As a result, we believe that we will not need to conduct any additional clinical trials to assess the safety or efficacy of Zerenex in order to obtain European approval in the dialysis setting. The Scientific Advice also provided us with a regulatory path forward in the pre-dialysis CKD setting in Europe. Scientific Advice is legally non-binding and is based on the current scientific knowledge, which may be subject to future changes. Many companies which have been provided with Scientific Advice by the EMA have ultimately failed to obtain approval of an MAA for their drugs. Additionally, even if the primary endpoint in a Phase 3 clinical trial is achieved, the Scientific Advice does not guarantee approval. The EMA may raise issues of safety, study conduct, bias, deviation from the protocol, statistical power, patient completion rates, changes in scientific or medical parameters or internal inconsistencies in the data prior to making its final decision.
| 22 |
Additionally, we have never filed a NDA or similar application for approval in the U.S., or in any country, which may result in a delay in, or the rejection of, our filing of an NDA or similar application. We are currently compiling data from all historical KRX-0401 clinical studies, which for some studies date back over 10 years, as well as data relating to non-clinical studies and Chemistry, Manufacturing and Controls, or CMC. We cannot guarantee that we can successfully compile such data to the satisfaction of the FDA, which may result in a delay in, or the rejection of, our filing of an NDA or similar application for KRX-0401. In addition, there are several obligations outside of our ongoing Phase 3 studies for KRX-0401 which we believe are required by the FDA for our NDA filing, including, but not limited to, our ongoing food effect study with a QTc component, and, potentially, additional studies, which we may never be able to complete to the satisfaction of the FDA. Moreover, when the data that we are currently compiling are submitted to the FDA, the FDA could request more information and possibly additional studies, in response to the submitted data, and this could potentially result in a substantial delay in approval.
During the drug development process, regulatory agencies will typically ask questions of drug sponsors. While we endeavor to answer all such questions in a timely fashion, or in the NDA filing, some questions may remain unanswered by the time we file our NDA, or may be difficult or impossible to answer to the satisfaction of the regulatory authorities. Unless the FDA, or similar regulatory authority in other countries, opts not to pursue these questions, submission of a NDA may be delayed or rejected.
Pre-clinical testing and clinical development are long, expensive and uncertain processes. If our drug candidates do not receive the necessary regulatory approvals, we will be unable to commercialize our drug candidates.
We have not received, and may never receive, regulatory approval for the commercial sale of any of our drug candidates. We will need to conduct significant additional research and human testing before we can apply for product approval with the FDA or with regulatory authorities of other countries. Pre-clinical testing and clinical development are long, expensive and uncertain processes. Satisfaction of regulatory requirements typically depends on the nature, complexity and novelty of the product. It requires the expenditure of substantial resources. Data obtained from pre-clinical and clinical tests can be interpreted in different ways, which could delay, limit or prevent regulatory approval. The FDA, or regulatory authority of another country as applicable, may pose additional questions or request further clinical substantiation. It may take us many years to complete the testing of our drug candidates and failure can occur at any stage of this process. Negative or inconclusive results or medical events during a pre-clinical or clinical trial could cause us to delay or terminate our development efforts. Furthermore, interim results of preclinical or clinical studies do not necessarily predict their final results, and acceptable results in early studies might not be obtained in later studies.
Safety signals detected during clinical studies and pre-clinical animal studies, such as the gastrointestinal bleeding and liver toxicities that have been seen in some high-dose, ferric citrate canine studies, may require us to perform additional safety studies or analyses, which could delay the development of the drug or lead to a decision to discontinue development of the drug. We have submitted to the FDA data from our short-term and long-term rat and canine pre-clinical studies for Zerenex. While the FDA has reviewed the data from these studies and has permitted us to continue with our Phase 3 clinical program, we can provide no assurance that the FDA will not raise any safety concerns in the future from these studies. Drug candidates in the later stages of clinical development may fail to show the desired traits of safety and efficacy despite positive results in earlier clinical testing. The risk remains that a pivotal program may generate efficacy data that will be insufficiently persuasive for the approval of the drug, or may raise safety concerns that may prevent approval of the drug. The risk also remains that a clinical program conducted by one of our partners may raise efficacy or safety concerns that may prevent approval of the drug. Interpretation of the prior pre-clinical and clinical safety and efficacy data of our drug candidates may be flawed. There can be no assurance that safety and/or efficacy concerns from the prior data were not overlooked or misinterpreted, which in subsequent, larger studies might appear and prevent approval of such drug candidates. Top-line results are based on a preliminary analysis of then available data (both safety and efficacy) and there is the risk that that such findings and conclusions could change following a more comprehensive review of the data.
We may not be able to replicate in our Phase 3 clinical program for Zerenex, the efficacy and safety results for Zerenex observed in the previous Phase 3 and Phase 2 clinical trials and the Open-Label Extension, or OLE, clinical trial. The positive effects of Zerenex on intravenous iron and erythropoiesis-stimulating agent, or ESA, use observed in the OLE clinical trial may not be reproducible. Further, any negative effects of the potential absorption and/or accumulation of ferric iron or citrate would significantly limit the likelihood of obtaining regulatory approval for Zerenex. In addition, we may not be able to replicate in the Phase 3 trials for KRX-0401, the efficacy and safety results for KRX-0401 observed in previous clinical trials. In addition, we will need to re-input our safety information on KRX-0401 into a database compliant with Good Clinical Practice. We can provide no assurance that safety concerns will not subsequently arise.
| 23 |
Independent Data Safety Monitoring Boards, or DSMBs, are monitoring the safety of our Phase 3 clinical trials for KRX-0401 (perifosine) and Zerenex (ferric citrate) and, in accordance with the protocols for the clinical trials, will periodically assess whether the Phase 3 trials should continue as planned. The DSMBs have the authority to recommend placing a trial on clinical hold, temporarily or permanently, or recommend termination of the clinical trial, based on an evaluation of safety and efficacy. The DSMBs are independent from us and we have no control or influence on their decisions. In accordance with the protocol, in August 2011, the independent DSMB overseeing our Phase 3 trial in refractory advanced colorectal cancer completed a pre-specified interim analysis for safety and futility. The independent DSMB recommended that the Phase 3 study continue to completion, as planned. We can provide no assurance that the Phase 3 study in refractory advanced colorectal cancer will be successful despite the DSMB recommendation to continue to completion. Additionally, we can provide no assurance that future meetings of our DSMBs will result in a positive outcome.
Clinical trials have a high risk of failure. A number of companies in the pharmaceutical industry, including biotechnology companies, have suffered significant setbacks in advanced clinical trials, even after achieving what appeared to be promising results in earlier trials. If we experience delays in the testing or approval process or if we need to perform more or larger clinical trials than originally planned, our financial results and the commercial prospects for our drug candidates may be materially impaired. In addition, we have limited experience in conducting and managing the clinical trials necessary to obtain regulatory approval in the U.S. and abroad. Accordingly, we may encounter unforeseen problems and delays in the approval process. Although we engage, from time to time, clinical research organizations with experience in conducting regulatory trials, errors in the conduct, monitoring and/or auditing could potentially invalidate the results.
Because all of our proprietary technologies are licensed to us by third parties, termination of these license agreements would prevent us from developing our drug candidates.
We do not own any of our drug candidates. We have licensed the rights, patent or otherwise, to our drugs candidates from third parties. These license agreements require us to meet development milestones and impose development and commercialization due diligence requirements on us. In addition, under these agreements, we must pay royalties on sales of products resulting from licensed technologies and pay the patent filing, prosecution and maintenance costs related to the licenses. If we do not meet our obligations in a timely manner or if we otherwise breach the terms of our license agreements, our licensors could terminate the agreements, and we would lose the rights to our drug candidates. From time to time, we may have disagreements with our licensors or collaborators, or they and/or we may have disagreements with the original inventors, regarding the terms of our agreements or ownership of proprietary rights, which could lead to delays in the research, development and commercialization of our drug candidates, could require or result in litigation or arbitration, which would be time-consuming and expensive, or could lead to the termination of a license, or force us to negotiate a revised or new license agreement on terms less favorable than the original.
We rely on third parties to manufacture and analytically test our products. If these third parties do not successfully manufacture and test our products, our business will be harmed.
We have limited experience in manufacturing products for clinical or commercial purposes. We intend to continue, in whole or in part, to use third parties to manufacture and analytically test our products for use in clinical trials and for future sales. We may not be able to enter into future contract agreements with these third-parties on terms acceptable to us, if at all.
Our ability to conduct clinical trials and commercialize our product candidates will depend on the ability of such third parties to manufacture our products on a large scale at a competitive cost and in accordance with current Good Manufacturing Practices, or cGMP, and other regulatory requirements, including requirements from federal and state environmental and safety regulatory agencies. Prior to approval, we will need to complete validation studies that the FDA must review and approve. Significant scale-up of manufacturing may result in unanticipated technical challenges and may require additional validation studies that the FDA must review and approve. Contract manufacturers often encounter difficulties in scaling up production, including problems involving raw material supplies, production yields, scaled-up product characteristics, quality control and assurance, shortage of qualified personnel, compliance with FDA and foreign regulations, production costs and development of advanced manufacturing techniques and process controls. Any of these difficulties, if they occur, and are not overcome to the satisfaction of the FDA or other regulatory agency, could lead to significant delays and possibly the termination of the development program for any of our drug candidates. These risks become more acute as we scale up for commercial quantities, where a reliable source of raw material supplies becomes critical to commercial success. For example, given the large quantity of materials required for ferric citrate production, as we approach commercialization for Zerenex we will need to ensure an adequate supply of starting materials that meet quality, quantity and cost standards. Failure to achieve this level of supply can jeopardize the successful commercialization of the product. Moreover, issues that may arise in our current transition to a commercial batch manufacturer for Zerenex can lead to delays in our planned clinical trials and development timelines, and could affect our ability to complete our clinical trials on a cost-effective or timely basis, if at all.
| 24 |
Our third-party manufacturers may not perform as agreed or may not remain in the contract manufacturing business for the time required by us to successfully produce and market our drug candidates. In addition, our contract manufacturers will be subject to ongoing periodic and unannounced inspections by the FDA and corresponding foreign governmental agencies to ensure strict compliance with cGMP, as well as other governmental regulations and corresponding foreign standards. While we periodically audit our contractors for adherence to regulatory requirements, we cannot assure you that unforeseen changes at these contractors may occur that change their regulatory standing. The same issues apply to contract analytical services which we use for testing of our products. We will not have control over, other than by contract and periodic oversight, third-party manufacturers' compliance with these regulations and standards. We are currently developing analytical tools for KRX-0401 (perifosine) and ferric citrate active pharmaceutical ingredient and drug product testing. Failure to develop effective analytical tools could result in regulatory or technical delay or could jeopardize our ability to complete Phase 3 clinical trials and/or obtain FDA approval. Switching or engaging multiple third-party contractors to produce our products may be difficult because the number of potential manufacturers may be limited and the process by which multiple manufacturers make the drug substance must meet established specifications at each manufacturing facility. It may be difficult for us to find and engage replacement or multiple manufacturers quickly and on terms acceptable to us, if at all. For Zerenex, we currently rely on one supplier to source the ferric citrate active pharmaceutical ingredient. The loss of this source of supply would result in significant additional costs and delays in our development program. Moreover, if we need to change manufacturers after commercialization, the FDA and corresponding foreign regulatory agencies must approve these manufacturers in advance, which will involve testing and additional inspections to ensure compliance with FDA and foreign regulations and standards.
If we do not establish or maintain manufacturing, drug development and marketing arrangements with third parties, we may be unable to commercialize our products.
We do not possess all of the capabilities to fully commercialize our products on our own. From time to time, we may need to contract with third parties to:
| · | manufacture our product candidates; |
| · | assist us in developing, testing and obtaining regulatory approval for and commercializing some of our compounds and technologies; and |
| · | market and distribute our drug products. |
We can provide no assurance that we will be able to successfully enter into agreements with such third parties on terms that are acceptable to us, if at all. If we are unable to successfully contract with third parties for these services when needed, or if existing arrangements for these services are terminated, whether or not through our actions, or if such third parties do not fully perform under these arrangements, we may have to delay, scale back or end one or more of our drug development programs or seek to develop or commercialize our products independently, which could result in delays. Furthermore, such failure could result in the termination of license rights to one or more of our products. If these manufacturing, development or marketing agreements take the form of a partnership or strategic alliance, such arrangements may provide our collaborators with significant discretion in determining the efforts and resources that they will apply to the development and commercialization of our products. Accordingly, to the extent that we rely on third parties to research, develop or commercialize our products, we are unable to control whether such products will be scientifically or commercially successful. Additionally, if these third parties fail to perform their obligations under our agreements with them or fail to perform their work in a satisfactory manner, in spite of our efforts to monitor and ensure the quality of such work, we may face delays in achieving the regulatory milestones required for commercialization of one or more drug candidates.
If, in the future, the market conditions for raising capital deteriorate, we may be forced to rely predominantly or entirely on our ability to contract with third parties for our manufacturing, drug development and marketing. If we are unable to contract with such third parties, we may be forced to limit or suspend or terminate the development of some or all of our product candidates.
Our reliance on third parties, such as clinical research organizations, or CROs, may result in delays in completing, or a failure to complete, clinical trials if such CROs fail to perform under our agreements with them.
In the course of product development, we engage CROs to conduct and manage clinical studies and to assist us in guiding our products through the FDA review and approval process. If the CROs fail to perform their obligations under our agreements with them or fail to perform clinical trials in a satisfactory manner, we may face significant delays in completing our clinical trials, as well as commercialization of one or more drug candidates. Furthermore, any loss or delay in obtaining contracts with such entities may also delay the completion of our clinical trials and the market approval of drug candidates.
| 25 |
Other Risks Related to Our Business
If we are unable to develop adequate sales, marketing or distribution capabilities or enter into agreements with third parties to perform some of these functions, we will not be able to commercialize our products effectively.
In the event that one or more of our drug candidates are approved by the FDA, we may conduct our own sales and marketing effort to support the drugs. We currently have limited experience in sales, marketing or distribution. To directly market and distribute any products, we must build a sales and marketing organization with appropriate technical expertise and distribution capabilities. We may attempt to build such a sales and marketing organization on our own or with the assistance of a contract sales organization. For some market opportunities, we may want or need to enter into co-promotion or other licensing arrangements with larger pharmaceutical or biotechnology firms in order to increase the commercial success of our products. We may not be able to establish sales, marketing and distribution capabilities of our own or enter into such arrangements with third parties in a timely manner or on acceptable terms. To the extent that we enter into co-promotion or other licensing arrangements, our product revenues are likely to be lower than if we directly marketed and sold our products, and some or all of the revenues we receive will depend upon the efforts of third parties, and these efforts may not be successful. Additionally, building marketing and distribution capabilities may be more expensive than we anticipate, requiring us to divert capital from other intended purposes or preventing us from building our marketing and distribution capabilities to the desired levels.
From time to time we may consider offers or hold discussions with companies for partnerships or the acquisition of our company or any of our products. Any accepted offer may preclude us from commercializing our products effectively.
Even if we obtain FDA approval to market our drug products, if they fail to achieve market acceptance, we may never record meaningful revenues.
Even if our products are approved for sale, they may not be commercially successful in the marketplace. Market acceptance of our drug products will depend on a number of factors, including:
| · | perceptions by members of the health care community, including physicians, of the safety and efficacy of our product candidates, including, but not limited to, the perception of the long-term effects of the potential absorption and/or accumulation of ferric iron or citrate resulting from the use of Zerenex; |
| · | the rates of adoption of our products by medical practitioners and the target populations for our products; |
| · | the potential advantages that our products offer over existing treatment methods; |
| · | the cost-effectiveness of our products relative to competing products; |
| · | the availability of government or third-party payor reimbursement for our products; |
| · | the side effects or unfavorable publicity concerning our products or similar products; and |
| · | the effectiveness of our sales, marketing and distribution efforts. |
Because we expect sales of our products, if approved, to generate substantially all of our revenues in the long-term, the failure of our drugs to find market acceptance would harm our business and could require us to seek additional financing or other sources of revenue.
If our competitors develop and market products that are less expensive, more effective or safer than our drug products, our commercial opportunities may be reduced or eliminated.
The pharmaceutical industry is highly competitive. Our competitors include pharmaceutical companies and biotechnology companies, as well as universities and public and private research institutions. In addition, companies that are active in different but related fields represent substantial competition for us. Many of our competitors have significantly greater capital resources, larger research and development staffs and facilities and greater experience in drug development, regulation, manufacturing and marketing than we do. These organizations also compete with us to recruit qualified personnel, attract partners for joint ventures or other collaborations, and license technologies that are competitive with ours. As a result, our competitors may be able to more easily develop technologies and products that could render our drug products obsolete or noncompetitive. To compete successfully in this industry we must identify novel and unique drugs or methods of treatment and then complete the development of those drugs as treatments in advance of our competitors.
| 26 |
The drugs that we are attempting to develop will have to compete with existing therapies. For example, KRX-0401 (perifosine), if approved in the U.S. would compete with other anti-cancer agents, such as mTOR inhibitors. Pfizer Inc., Novartis AG and Ariad Pharmaceuticals are developing mTOR inhibitors for use in cancer and Pfizer’s mTOR inhibitor, temsirolimus, and Novartis’ mTOR inhibitor, everolimus, have been FDA approved to treat patients with advanced kidney disease (everolimus is also FDA approved for pancreatic neuroendocrine tumors and a specific type of brain tumor). Biotechnology and pharmaceutical companies such as Amgen Inc., Bayer AG, Biogen-Idec, Inc., ImClone Systems, Inc. (a wholly-owned subsidiary of Eli Lilly and Company), Merck & Co., Inc., Millennium Pharmaceuticals, Inc. (a wholly-owned subsidiary of Takeda Pharmaceutical Company), Novartis AG, Onyx Pharmaceuticals, Inc. and OSI Pharmaceuticals, Inc. are developing and, in some cases, marketing drugs to treat various diseases, including cancer, by inhibiting cell-signaling pathways. In addition, we are aware of a number of small and large companies developing competitive products that target Akt and the PI3K pathway. Bayer HealthCare, a subgroup of Bayer AG, recently announced positive results from its Phase 3 trial evaluating its investigational compound, regorafenib (BAY 73-4506), for the treatment of patients with metastatic colorectal cancer whose disease has progressed after approved standard therapies. If approved by the FDA, regorafenib could have a material effect on the market opportunity of KRX-0401 (perifosine). Zerenex, if approved in the U.S., would compete with other FDA approved phosphate binders such as Renagel® (sevelamer hydrochloride) and Renvela® (sevelamer carbonate), both marketed by Genzyme Corporation (a wholly-owned subsidiary of Sanofi-Aventis), PhosLo® (calcium acetate), marketed by Fresenius Medical Care, and Fosrenol® (lanthanum carbonate), marketed by Shire Pharmaceuticals Group plc, as well as over-the-counter calcium carbonate products such as TUMS® and metal-based options such as aluminum and magnesium. A generic formulation of PhosLo® manufactured by Roxane Laboratories, Inc. was launched in the U.S. in October 2008. In addition, upon the expiration of their core patents (expected in the U.S. in 2014), generic formulations of Renagel® and Renvela® may be launched, which could have a material effect on the pricing of phosphate binders.
Our commercial opportunities may be reduced or eliminated if our competitors develop and market products that are less expensive, more effective or safer than our drug products. Other companies have drug candidates in various stages of pre-clinical or clinical development to treat diseases for which we are also seeking to discover and develop drug products. Some of these potential competing drugs are further advanced in development than our drug candidates and may be commercialized earlier. Even if we are successful in developing effective drugs, our products may not compete successfully with products produced by our competitors.
If we lose our key personnel or are unable to attract and retain additional personnel, our operations could be disrupted and our business could be harmed.
As of February 23, 2012, we had 29 full and part-time employees. To successfully develop our drug candidates, we must be able to attract and retain highly skilled personnel. Our limited resources may hinder our efforts to attract and retain highly skilled personnel. In addition, if we lose the services of our current personnel, in particular, Ron Bentsur, our Chief Executive Officer, our ability to continue to execute on our business plan could be materially impaired. Although we have an employment agreement with Mr. Bentsur, such agreement does not prevent him from terminating his employment with us.
Any acquisitions we make may require a significant amount of our available cash and may not be scientifically or commercially successful.
As part of our business strategy, we may effect acquisitions to obtain additional businesses, products, technologies, capabilities and personnel. If we make one or more significant acquisitions in which the consideration includes cash, we may be required to use a substantial portion of our available cash.
Acquisitions involve a number of operational risks, including:
| · | difficulty and expense of assimilating the operations, technology and personnel of the acquired business; |
| · | our inability to retain the management, key personnel and other employees of the acquired business; |
| · | our inability to maintain the acquired company's relationship with key third parties, such as alliance partners; |
| · | exposure to legal claims for activities of the acquired business prior to the acquisition; |
| · | the diversion of our management's attention from our core business; and |
| · | the potential impairment of goodwill and write-off of in-process research and development costs, adversely affecting our reported results of operations. |
| 27 |
The status of reimbursement from third-party payors for newly approved health care drugs is uncertain and failure to obtain adequate reimbursement could limit our ability to generate revenue.
Our ability to commercialize pharmaceutical products may depend, in part, on the extent to which reimbursement for the products will be available from:
| · | government and health administration authorities; |
| · | private health insurers; |
| · | managed care programs; and |
| · | other third-party payors. |
Significant uncertainty exists as to the reimbursement status of newly approved health care products. Third-party payors, including Medicare, are challenging the prices charged for medical products and services. Government and other third-party payors increasingly are attempting to contain health care costs by limiting both coverage and the level of reimbursement for new drugs and by refusing, in some cases, to provide coverage for uses of approved products for disease indications for which the FDA has not granted labeling approval. In 2003, Congress passed the Medicare Prescription Drug, Improvement and Modernization Act of 2003, which for the first time established prescription drug coverage for Medicare beneficiaries, under Medicare Part D. Under this program, beneficiaries purchase insurance coverage from private insurance companies to cover the cost of their prescription drugs. However, third-party insurance coverage may not be available to patients for our products. If government and other third-party payors do not provide adequate coverage and reimbursement levels for our products, their market acceptance may be reduced.
Health care reform measures could adversely affect our business.
The business prospects and financial condition of pharmaceutical and biotechnology companies are affected by the efforts of governmental and third-party payors to contain or reduce the costs of health care. In the U.S. and in foreign jurisdictions there have been, and we expect that there will continue to be, a number of legislative and regulatory proposals aimed at changing the health care system, such as proposals relating to the pricing of healthcare products and services in the U.S. or internationally, the reimportation of drugs into the U.S. from other countries (where they are then sold at a lower price), and the amount of reimbursement available from governmental agencies or other third party payors. For example, drug manufacturers are required to have a national rebate agreement with the Department of Health and Human Services, or HHS, in order to obtain state Medicaid coverage, which requires manufacturers to pay a rebate on drugs dispensed to Medicaid patients. On January 27, 2012, the Centers for Medicare and Medicaid Services, or CMS, issued a proposed regulation covering the calculation of Average Manufacturer Price, or AMP, which is the key variable in the calculation of these rebates.
Furthermore, in the U.S., health care reform legislation titled the Patient Protection and Affordable Care Act was signed into law on March 23, 2010. This comprehensive legislation will affect the terms of public and private health insurance and have a substantial impact on the pharmaceutical industry. For example, the new law will impose an annual fee on manufacturers of branded prescription pharmaceuticals that will impact our products. Regulations to implement this and other provisions related to the research, marketing and sale of prescription pharmaceutical products could result in a decrease in our stock price or limit our ability to raise capital or to obtain strategic partnerships or licenses. Government-financed comparative efficacy research could also result in new practice guidelines, labeling or reimbursement policies that discourages use of our products.
For example, in July 2010, CMS released its final rule to implement a bundled prospective payment system for end-stage renal disease facilities as required by the Medicare Improvements for Patients and Providers Act, or MIPPA. The final rule delayed the inclusion of oral medications without IV equivalents, such as phosphate binders, in the bundle until January 1, 2014. If phosphate binders are included in the bundle beginning in 2014, separate Medicare reimbursement will no longer be available for phosphate binders, as it is today under Medicare Part D. While it is too early to project the impact bundling may have on the phosphate binder industry, the impact could potentially cause dramatic price reductions for phosphate binders.
| 28 |
On September 27, 2007, the Food and Drug Administration Amendments Act of 2007 was enacted, giving the FDA enhanced post-market authority, including the authority to require post-marketing studies and clinical trials, labeling changes based on new safety information, and compliance with risk evaluations and mitigation strategies approved by the FDA. The FDA's exercise of this authority may result in delays or increased costs during the period of product development, clinical trials and regulatory review and approval, which may also increase costs related to complying with new post-approval regulatory requirements, and increase potential FDA restrictions on the sale or distribution of approved products.
We face product liability risks and may not be able to obtain adequate insurance.
The use of our drug candidates in clinical trials, and the future sale of any approved drug candidates and new technologies, exposes us to liability claims. Although we are not aware of any historical or anticipated product liability claims against us, if we cannot successfully defend ourselves against product liability claims, we may incur substantial liabilities or be required to cease clinical trials of our drug candidates or limit commercialization of any approved products.
We intend to expand our insurance coverage to include the commercial sale of any approved products if marketing approval is obtained; however, insurance coverage is becoming increasingly expensive. We may not be able to maintain insurance coverage at a reasonable cost. We also may not be able to obtain additional insurance coverage that will be adequate to cover product liability risks that may arise. Regardless of merit or eventual outcome, product liability claims may result in:
| · | decreased demand for a product; |
| · | injury to our reputation; |
| · | our inability to continue to develop a drug candidate; |
| · | withdrawal of clinical trial volunteers; and |
| · | loss of revenues. |
Consequently, a product liability claim or product recall may result in losses that could be material.
In connection with the clinical trial management and site recruitment services we previously provided, we may be exposed to liability that could have a material adverse effect on our financial condition and results of operations.
Online Collaborative Oncology Group, Inc., or OCOG, a subsidiary we acquired through our acquisition of ACCESS Oncology, Inc. in 2004, previously provided clinical trial management and site recruitment services to us as well as other biotechnology and pharmaceutical companies. OCOG entered into its last third-party service contract in 2005 and its business was discontinued as of December 2011. In conducting the activities of OCOG, any failure on our part to comply with applicable governmental regulations or contractual obligations could expose us to liability to our clients and could have a material adverse effect on us. We also could be held liable for errors or omissions in connection with the services we performed. In addition, the wrongful or erroneous delivery of health care information or services may expose us to liability. If we were required to pay damages or bear the costs of defending any such claims, the losses could be material.
Our corporate compliance efforts cannot guarantee that we are in compliance with all potentially applicable regulations.
The development, manufacturing, pricing, sales, and reimbursement of our products, together with our general operations, are subject to extensive regulation by federal, state and other authorities within the U.S. and numerous entities outside of the U.S. We are a relatively small company with 29 full and part-time employees as of February 23, 2012. We also have significantly fewer employees than many other companies that have a product candidate in clinical development, and we rely heavily on third parties to conduct many important functions. While we believe that our corporate compliance program is sufficient to ensure compliance with applicable regulations, we cannot assure you that we are or will be in compliance with all potentially applicable regulations. If we fail to comply with any of these regulations we could be subject to a range of regulatory actions, including suspension or termination of clinical trials, the failure to approve a product candidate, restrictions on our products or manufacturing processes, withdrawal of products from the market, significant fines, or other sanctions or litigation.
| 29 |
Risks Related to Our Financial Condition
Our cash, cash equivalents and investment securities may not be adequate to finance our operating cash requirements for the length of time that we have estimated.
Depending on the outcome of our Phase 3 study for KRX-0401 in refractory advanced colorectal cancer, our operating cash requirements may vary dramatically. In the event of a negative outcome, we currently anticipate that our cash, cash equivalents and investment securities as of December 31, 2011, exclusive of our anticipated milestone payments to be received, are sufficient to fund our anticipated operating cash requirements for approximately 18 to 20 months from December 31, 2011. Our forecast of the period of time through which our cash, cash equivalents and investment securities will be adequate to support our current operations is a forward-looking statement that involves risks and uncertainties. The actual amount of funds we will need to operate is subject to many factors, some of which are beyond our control. These factors include, but are not limited to, the following:
| · | the timing, design and conduct of, and results from, clinical trials for our drug candidates; |
| · | the timing of expenses associated with manufacturing and product development of the proprietary drug candidates within our portfolio and those that may be in-licensed, partnered or acquired; |
| · | the timing of the in-licensing, partnering and acquisition of new product opportunities; |
| · | the progress of the development efforts of parties with whom we have entered, or may enter, into research and development agreements; |
| · | our ability to achieve our milestones under our licensing arrangements; and |
| · | the costs involved in prosecuting and enforcing patent claims and other intellectual property rights. |
If our cash is insufficient to meet future operating requirements, we will have to raise additional funds. If we are unable to obtain additional funds on terms favorable to us or at all, we may be required to cease or reduce our operating activities or sell or license to third parties some or all of our intellectual property. If we raise additional funds by selling additional shares of our capital stock, the ownership interests of our stockholders will be diluted. If we need to raise additional funds through the sale or license of our intellectual property, we may be unable to do so on terms favorable to us, if at all.
Risks Related to Our Intellectual Property and Third-Party Contracts
If we are unable to adequately protect our intellectual property, third parties may be able to use our intellectual property, which could adversely affect our ability to compete in the market.
Our commercial success will depend in part on our ability and the ability of our licensors to obtain and maintain patent protection on our drug products and technologies and successfully defend these patents against third-party challenges. The patent positions of pharmaceutical and biotechnology companies can be highly uncertain and involve complex legal and factual questions. No consistent policy regarding the breadth of claims allowed in biotechnology patents has emerged to date. Accordingly, the patents we use may not be sufficiently broad to prevent others from practicing our technologies or from developing competing products. Furthermore, others may independently develop similar or alternative drug products or technologies or design around our patented drug products and technologies. The patents we use may be challenged or invalidated or may fail to provide us with any competitive advantage.
We rely on trade secrets to protect our intellectual property where we believe patent protection is not appropriate or obtainable. Trade secrets are difficult to protect. While we require our employees, collaborators and consultants to enter into confidentiality agreements, this may not be sufficient to adequately protect our trade secrets or other proprietary information. In addition, we share ownership and publication rights to data relating to some of our drug products and technologies with our research collaborators and scientific advisors. If we cannot maintain the confidentiality of this information, our ability to receive patent protection or protect our trade secrets or other proprietary information will be at risk.
| 30 |
The intellectual property that we own or have licensed relating to our product candidates is limited, which could adversely affect our ability to compete in the market and adversely affect the value of our product candidates.
The patent rights that we own or have licensed relating to our product candidates are limited in ways that may affect our ability to exclude third parties from competing against us if we obtain regulatory approval to market these product candidates. In particular:
| · | Our composition of matter patent covering KRX-0401 (perifosine) expires in the second half of 2013 and we cannot assure you that we can obtain an extension to the second half of 2018 (the maximum term of extension under the patent term restoration program). Our composition of matter patent covering Zerenex expires in the second half of 2017 and we cannot assure you that we can obtain an extension to 2022 (the maximum term of extension under the patent term restoration program). Composition of matter patents can provide protection for pharmaceutical products to the extent that the specifically covered compositions are important. Upon expiration of our composition of matter patents for KRX-0401 and Zerenex, competitors who obtain the requisite regulatory approval can offer products with the same composition as our products so long as the competitors do not infringe any other patents that we may hold, such as method of use patents. |
| · | Our method of use patents only protect the products when used or sold for the specified method. However, this type of patent does not limit a competitor from making and marketing a product that is identical to our product that is labeled for an indication that is outside of our patented method, or for which there is a substantial use in commerce outside our patented method. |
| · | Our pending patent applications may not issue as patents and may not issue in all countries in which we develop, manufacture or potentially sell our products or in countries where others develop, manufacture and potentially sell products using our technologies. Moreover, our pending patent applications, if issued as patents, may not provide additional protection for our products. |
| · | Because clinical trials for KRX-0401 and Zerenex are ongoing, and because any potential date for regulatory approval is currently unknown, it is possible that the life of these patents following regulatory approval will be minimal, even if the above-discussed extensions are obtained. |
Proof of direct infringement by a competitor for method of use patents can prove difficult because the competitors making and marketing a product typically do not engage in the patented use. Additionally, proof that a competitor contributes to or induces infringement of a patented method of use by another can also prove difficult because an off-label use of a product could prohibit a finding of contributory infringement and inducement of infringement requires proof of intent by the competitor.
Moreover, physicians may prescribe such a competitive identical product for indications other than the one for which the product has been approved, or off-label indications, that are covered by the applicable patents. Although such off-label prescriptions may directly infringe or contribute to or induce infringement of method of use patents, such infringement is difficult to prevent or prosecute.
In addition, the limited patent protection described above may adversely affect the value of our product candidates and may inhibit our ability to obtain a corporate partner at terms acceptable to us, if at all.
In addition to patent protection, we may utilize orphan drug regulations or other provisions of the FDCA to provide market exclusivity for certain of our drug candidates. Orphan drug regulations provide incentives to pharmaceutical and biotechnology companies to develop and manufacture drugs for the treatment of rare diseases, currently defined as diseases that exist in fewer than 200,000 individuals in the U.S., or, diseases that affect more than 200,000 individuals in the U.S. but that the sponsor does not realistically anticipate will generate a net profit. Under these provisions, a manufacturer of a designated orphan drug can seek tax benefits, and the holder of the first FDA approval of a designated orphan product will be granted a seven-year period of marketing exclusivity for such FDA-approved orphan product. In September 2009, we announced that KRX-0401 (perifosine) has received Orphan-Drug designation from the FDA for the treatment of multiple myeloma, and in July 2010, we announced that KRX-0401 has received Orphan-Drug designation from the FDA for the treatment of neuroblastoma. We believe that KRX-0401 may be eligible for additional orphan-drug designations; however, we cannot assure you that KRX-0401, or any other drug candidates we may acquire or in-license, will obtain such orphan-drug designations. Additionally, upon FDA approval, we believe that perifosine would qualify as a New Chemical Entity, which provides for five years of exclusivity following approval, however; we cannot assure you that perifosine will qualify and gain the additional five-year exclusivity period.
| 31 |
Litigation or third-party claims could require us to spend substantial time and money defending such claims and adversely affect our ability to develop and commercialize our products.
We may be forced to initiate litigation to enforce our contractual and intellectual property rights, or we may be sued by third parties asserting claims based on contract, tort or intellectual property infringement. In addition, third parties may have or may obtain patents in the future and claim that our drug products or technologies infringe their patents. If we are required to defend against suits brought by third parties, or if we sue third parties to protect our rights, we may be required to pay substantial litigation costs, and our management's attention may be diverted from operating our business. In addition, any legal action against our licensors or us that seeks damages or an injunction of our commercial activities relating to our drug products or technologies could subject us to monetary liability and require our licensors or us to obtain a license to continue to use our drug products or technologies. We cannot predict whether our licensors or we would prevail in any of these types of actions or that any required license would be made available on commercially acceptable terms, if at all.
Risks Related to Our Common Stock
Future sales or other issuances of our common stock could depress the market for our common stock.
Sales of a substantial number of shares of our common stock, or the perception by the market that those sales could occur, could cause the market price of our common stock to decline or could make it more difficult for us to raise funds through the sale of equity in the future.
We currently have two shelf registration statements on Form S-3, filed and declared effective by the SEC, providing for the offering of up to approximately $79 million of common stock and warrants in the aggregate.
| · | On August 28, 2009, we filed with the SEC a shelf registration statement on Form S-3 (File No. 333-161607) and declared effective by the SEC on September 23, 2009. The registration statement provided for the offering of up to $40 million of our common stock and warrants. Subsequent to the registered direct offering completed on September 30, 2009, there remains approximately $12 million of our common stock and warrants available for sale under the shelf registration statement. |
| · | On January 3, 2011, we filed with the SEC a shelf registration statement on Form S-3 (File No. 333-171517) that was declared effective by the SEC on January 28, 2011, providing for the offering of up to $100 million of our common stock and warrants to purchase our common stock. Subsequent to the registered offering in May 2011, there remains approximately $67 million of our common stock and warrants available for sale under the shelf registration statement. |
Future sales pursuant to these registration statements could depress the market for our common stock.
If we make one or more significant acquisitions in which the consideration includes stock or other securities, our stockholders’ holdings may be significantly diluted. In addition, stockholders’ holdings may also be diluted if we enter into arrangements with third parties permitting us to issue shares of common stock in lieu of certain cash payments upon the achievement of milestones.
Our stockholders would also experience dilution if we are required to issue up to 2,872,422 shares of our common stock to former stockholders of ACCESS Oncology, Inc. upon the achievement of certain development and sales milestones related to KRX-0401.
Our stock price can be volatile, which increases the risk of litigation, and may result in a significant decline in the value of your investment.
The trading price of our common stock is likely to be highly volatile and subject to wide fluctuations in price in response to various factors, many of which are beyond our control. These factors include:
| · | developments concerning our drug candidates, including the safety and efficacy results from clinical trials, such as the results from the Phase 3 study for KRX-0401 (perifosine) in advanced refractory colorectal cancer expected to be available in the first half of 2012; |
| · | announcements of technological innovations by us or our competitors; |
| · | introductions or announcements of new products by us or our competitors; |
| · | announcements by us of significant acquisitions, strategic partnerships, joint ventures or capital commitments; |
| · | changes in financial estimates by securities analysts; |
| · | actual or anticipated variations in quarterly operating results; |
| · | expiration or termination of licenses, research contracts or other collaboration agreements; |
| · | conditions or trends in the regulatory climate and the biotechnology and pharmaceutical industries; |
| · | changes in the market valuations of similar companies; |
| · | negative comments and sentiment in the media; and |
| · | additions or departures of key personnel. |
| 32 |
In addition, equity markets in general, and the market for biotechnology and life sciences companies in particular, have experienced extreme price and volume fluctuations that have often been unrelated or disproportionate to the operating performance of companies traded in those markets. These broad market and industry factors may materially affect the market price of our common stock, regardless of our development and operating performance. In the past, following periods of volatility in the market price of a company's securities, securities class-action litigation has often been instituted against that company. Such litigation, if instituted against us, could cause us to incur substantial costs to defend such claims and divert management's attention and resources, which could seriously harm our business.
Certain anti-takeover provisions in our charter documents and Delaware law could make a third-party acquisition of us difficult. This could limit the price investors might be willing to pay in the future for our common stock.
Provisions in our amended and restated certificate of incorporation and bylaws could have the effect of making it more difficult for a third party to acquire, or of discouraging a third party from attempting to acquire, or control us. These factors could limit the price that certain investors might be willing to pay in the future for shares of our common stock. Our amended and restated certificate of incorporation allows us to issue preferred stock without the approval of our stockholders. The issuance of preferred stock could decrease the amount of earnings and assets available for distribution to the holders of our common stock or could adversely affect the rights and powers, including voting rights, of such holders. In certain circumstances, such issuance could have the effect of decreasing the market price of our common stock. Our amended and restated bylaws eliminate the right of stockholders to call a special meeting of stockholders, which could make it more difficult for stockholders to effect certain corporate actions. Any of these provisions could also have the effect of delaying or preventing a change in control.
ITEM 1B. UNRESOLVED STAFF COMMENTS.
None.
ITEM 2. PROPERTIES.
Our corporate and executive office is located in New York, New York. Our New York facility consists of approximately 11,700 square feet of leased space at 750 Lexington Avenue, New York, New York 10022, with a lease term through September 30, 2013. We are a party to an office sharing agreement with a third-party for a portion of our leased space through the term of our lease.
ITEM 3. LEGAL PROCEEDINGS.
We, and our subsidiaries, are not a party to, and our property is not the subject of, any material pending legal proceedings, other than as noted below.
In October 2009, we filed a statement of claim with the Financial Institution Regulatory Authority, or FINRA, to commence an arbitration proceeding against an SEC registered broker-dealer. In this arbitration proceeding, we seek damages arising from that broker-dealer’s recommendations and purchases of auction rate securities for our cash management account. The claim will be determined by a panel of three FINRA arbitrators. In January 2010, the broker-dealer filed an answer to the statement of claim and denied liability. The hearing concerning our claims against the broker-dealer commenced in October 2011, and is scheduled to be completed in March 2012.
| 33 |
ITEM 4. MINE SAFETY DISCLOSURES.
Not applicable
PART II
ITEM 5. MARKET FOR REGISTRANT’S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES.
Market Information
Our common stock is listed on the NASDAQ Capital Market and trades under the symbol “KERX.”
The following table sets forth the high and low closing sale prices of our common stock for the periods indicated.
| Fiscal Year Ended December 31, 2011 | High | Low | ||||||
| Fourth Quarter | $ | 3.37 | $ | 2.38 | ||||
| Third Quarter | $ | 4.94 | $ | 2.99 | ||||
| Second Quarter | $ | 5.42 | $ | 4.28 | ||||
| First Quarter | $ | 5.19 | $ | 3.81 | ||||
| Fiscal Year Ended December 31, 2010 | High | Low | ||||||
| Fourth Quarter | $ | 5.47 | $ | 4.58 | ||||
| Third Quarter | $ | 4.87 | $ | 3.39 | ||||
| Second Quarter | $ | 6.51 | $ | 2.74 | ||||
| First Quarter | $ | 3.00 | $ | 2.27 | ||||
Holders
The number of record holders of our common stock as of February 23, 2012 was 55.
Dividends
We have never declared or paid any cash dividends on our common stock and do not anticipate paying any cash dividends in the foreseeable future. Any future determination to pay dividends will be at the discretion of our board of directors.
Securities Authorized for Issuance Under Equity Compensation Plans
The following table provides information as of December 31, 2011, regarding the securities authorized for issuance under our equity compensation plans, consisting of the 1999 Stock Option Plan, as amended, the 2000 Stock Option Plan, as amended, the 2004 Long-Term Incentive Plan, the 2007 Incentive Plan and the 2009 CEO Incentive Plan.
| Equity Compensation Plan Information | ||||||||||||
| Plan Category | Number of securities to be issued upon exercise of outstanding options | Weighted-average exercise price of outstanding options | Number of securities remaining available for future issuance under equity compensation plans (excluding securities reflected in column (a)) | |||||||||
| (a) | (b) | (c) | ||||||||||
| Equity compensation plans approved by security holders | 2,917,000 | $ | 7.64 | 3,351,445 | ||||||||
| Equity compensation plans not approved by security holders | 600,000 | 0.35 | – | |||||||||
| Total | 3,517,000 | $ | 6.40 | 3,351,445 | ||||||||
For information about all of our equity compensation plans, see Note 11 to our Consolidated Financial Statements included in this report.
| 34 |
COMMON STOCK PERFORMANCE GRAPH
The following graph compares the cumulative total stockholder return on our common stock for the period from December 31, 2006 through December 31, 2011, with the cumulative total return over such period on (i) the U.S. Index of The NASDAQ Stock Market and (ii) the Biotechnology Index of The NASDAQ Stock Market. The graph assumes an investment of $100 on December 31, 2006, in our common stock (at the closing market price) and in each of the indices listed above, and assumes the reinvestment of all dividends. Measurement points are December 31 of each year.
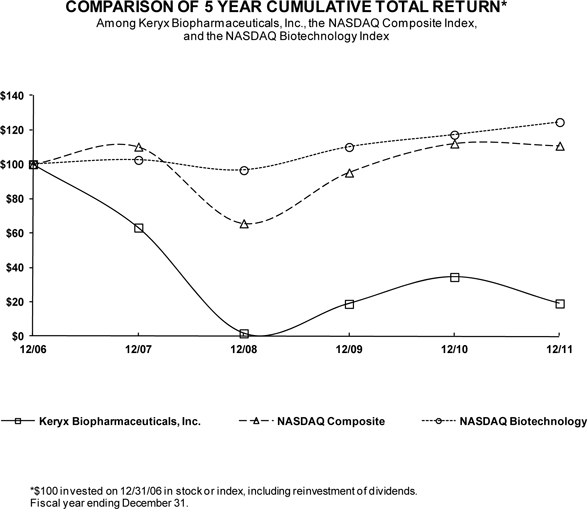
| 35 |
ITEM 6. SELECTED FINANCIAL DATA.
The following Statement of Operations Data for the years ended December 31, 2011, 2010, 2009, 2008 and 2007, and Balance Sheet Data as of December 31, 2011, 2010, 2009, 2008 and 2007, as set forth below are derived from our audited consolidated financial statements. This financial data should be read in conjunction with “Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations” and “Item 8. Financial Statements and Supplementary Data.”
| Years ended December 31, | ||||||||||||||||||||
| 2011 | 2010 | 2009 | 2008 | 2007 | ||||||||||||||||
| (in thousands, except per share data) | ||||||||||||||||||||
| Statement of Operations Data: | ||||||||||||||||||||
| Revenue: | ||||||||||||||||||||
| License revenue | $ | 5,000 | $ | – | $ | 21,616 | $ | 1,180 | $ | 204 | ||||||||||
| Other revenue | – | – | 3,575 | – | 727 | |||||||||||||||
| Total revenue | 5,000 | – | 25,191 | 1,180 | 931 | |||||||||||||||
| Operating expenses: | ||||||||||||||||||||
| Research and development: | ||||||||||||||||||||
| Non-cash compensation | 803 | 1,236 | 1,233 | (67 | ) | 3,574 | ||||||||||||||
| Other research and development | 26,209 | 13,728 | 7,372 | 38,075 | 74,883 | |||||||||||||||
| Total research and development | 27,012 | 14,964 | 8,605 | 38,008 | 78,457 | |||||||||||||||
| General and administrative: | ||||||||||||||||||||
| Non-cash compensation | 1,289 | 1,237 | 1,867 | 6,815 | 7,086 | |||||||||||||||
| Other general and administrative | 5,448 | 5,014 | 4,904 | 7,474 | 9,141 | |||||||||||||||
| Total general and administrative | 6,737 | 6,251 | 6,771 | 14,289 | 16,227 | |||||||||||||||
| Total operating expenses | 33,749 | 21,215 | 15,376 | 52,297 | 94,684 | |||||||||||||||
| Operating (loss) income | (28,749 | ) | (21,215 | ) | 9,815 | (51,117 | ) | (93,753 | ) | |||||||||||
| Other income (expense): | ||||||||||||||||||||
| Interest and other income (expense), net | 380 | 764 | 667 | (1,665 | ) | 4,555 | ||||||||||||||
| Income taxes | – | – | – | – | (36 | ) | ||||||||||||||
| (Loss) income from continuing operations | (28,369 | ) | (20,451 | ) | 10,482 | (52,782 | ) | (89,234 | ) | |||||||||||
| Gain (loss) from discontinued operations | 246 | 120 | 3 | (99 | ) | (828 | ) | |||||||||||||
| Net (loss) income | $ | (28,123 | ) | $ | (20,331 | ) | $ | 10,485 | $ | (52,881 | ) | $ | (90,062 | ) | ||||||
| Basic and diluted (loss) income per common share: | ||||||||||||||||||||
| Continuing operations | $ | (0.42 | ) | $ | (0.34 | ) | $ | 0.21 | $ | (1.18 | ) | $ | (2.05 | ) | ||||||
| Discontinued operations | – | * | – | * | – | * | (–) | * | (0.02 | ) | ||||||||||
| Basic and diluted (loss) income per common share | $ | (0.42 | ) | $ | (0.34 | ) | $ | 0.21 | $ | (1.18 | ) | $ | (2.07 | ) | ||||||
* Amount less than one cent per share.
| As of December 31, | ||||||||||||||||||||
| 2011 | 2010 | 2009 | 2008 | 2007 | ||||||||||||||||
| (in thousands) | ||||||||||||||||||||
| Balance Sheet Data: | ||||||||||||||||||||
| Cash, cash equivalents, interest receivable and short-term investment securities | $ | 39,470 | $ | 28,512 | $ | 34,000 | $ | 15,467 | $ | 62,386 | ||||||||||
| Long-term investment securities | – | – | 1,914 | 7,185 | 2,296 | |||||||||||||||
| $ | 39,470 | $ | 28,512 | $ | 35,914 | $ | 22,652 | $ | 64,682 | |||||||||||
| Working capital | 30,237 | 22,520 | 29,489 | 9,282 | 42,319 | |||||||||||||||
| Total assets | 43,488 | 32,114 | 40,818 | 26,634 | 81,061 | |||||||||||||||
| Deferred revenue, net of current portion | – | – | – | 17,308 | 11,022 | |||||||||||||||
| Other liabilities | 35 | 35 | 50 | 118 | 202 | |||||||||||||||
| Contingent equity rights | 2,639 | 2,639 | 2,639 | 4,004 | 4,004 | |||||||||||||||
| Total stockholders’ equity (deficiency) | 31,047 | 23,248 | 32,097 | (1,489 | ) | 44,422 | ||||||||||||||
| 36 |
ITEM 7. MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS.
The following discussion and analysis contains forward-looking statements about our plans and expectations of what may happen in the future. Forward-looking statements are based on a number of assumptions and estimates that are inherently subject to significant risks and uncertainties, and our results could differ materially from the results anticipated by our forward-looking statements as a result of many known or unknown factors, including, but not limited to, those factors discussed in “Item 1A. Risk Factors.” See also the “Special Cautionary Notice Regarding Forward-Looking Statements” set forth at the beginning of this report.
You should read the following discussion and analysis in conjunction with “Item 6. Selected Financial Data,” “Item 8. Financial Statements and Supplementary Data,” and our consolidated financial statements beginning on page F-1 of this report.
Overview
We are a biopharmaceutical company focused on the acquisition, development and commercialization of medically important pharmaceutical products for the treatment of cancer and renal disease. We are developing KRX-0401 (perifosine), a novel, potentially first-in-class, oral anti-cancer agent that inhibits Akt activation in the PI3K pathway, and also affects a number of other key signal transduction pathways, including the JNK pathway, all of which are pathways associated with programmed cell death, growth, differentiation and survival. KRX-0401 is currently in Phase 3 clinical development for both refractory advanced colorectal cancer and relapsed / refractory multiple myeloma, and in Phase 1 and Phase 2 clinical development for several other tumor types. Each of the KRX-0401 Phase 3 programs is being conducted under SPA agreements with the FDA and with Fast-Track Designation.
We are also developing Zerenex™ (ferric citrate), an oral, ferric iron-based compound that has the capacity to bind to phosphate in the gastrointestinal tract and form non-absorbable complexes. Zerenex is currently in Phase 3 clinical development in the United States, under an SPA agreement, as a treatment for hyperphosphatemia (elevated phosphate levels) in patients with ESRD on dialysis. In April 2011, our Japanese partner for Zerenex (ferric citrate), JT and Torii, commenced its Phase 3 clinical program for ferric citrate in Japan. Under the terms of the license agreement with JT and Torii, we received a non-refundable milestone payment of $5.0 million in April 2011 from JT and Torii for the achievement of the Phase 3 commencement milestone.
We also engage in business development activities that include seeking strategic relationships for our product candidates, as well as evaluating compounds and companies for in-licensing or acquisition. To date, we have not received approval for the sale of any of our drug candidates in any market and, therefore, have not generated any product sales from our drug candidates. We have generated, and expect to continue to generate, revenue from the licensing of rights to Zerenex in Japan to JT and Torii.
We have devoted substantially all of our efforts to the identification, in-licensing, development and partnering of drug candidates. We have incurred negative cash flow from operations each year since our inception. We anticipate incurring negative cash flows from operating activities for the foreseeable future. We have spent, and expect to continue to spend, substantial amounts in connection with implementing our business strategy, including our product development efforts, our clinical trials, partnership and licensing activities.
Our license revenues currently consist of license fees and milestone payments arising from our agreement with JT and Torii. We recognize license revenue in accordance with the revenue recognition guidance of the Financial Accounting Standards Board, or FASB, Accounting Standards Codification, or the Codification. We analyze each element of our licensing agreement to determine the appropriate revenue recognition. The terms of the license agreement may include payment to us of non-refundable up-front license fees, milestone payments if specified objectives are achieved, and/or royalties on product sales. We recognize revenue from upfront payments over the period of significant involvement under the related agreements unless the fee is in exchange for products delivered or services rendered that represent the culmination of a separate earnings process and no further performance obligation exists under the contract. We recognize milestone payments as revenue upon the achievement of specified milestones only if (1) the milestone payment is non-refundable, (2) substantive effort is involved in achieving the milestone, (3) the amount of the milestone is reasonable in relation to the effort expended or the risk associated with achievement of the milestone, and (4) the milestone is at risk for both parties. If any of these conditions are not met, we defer the milestone payment and recognize it as revenue over the estimated period of performance under the contract.
| 37 |
Our other revenues consist of fees and payments arising from technology transfer, termination and settlement agreements related to our prior license agreements.
We have not earned any revenues from the commercial sale of any of our drug candidates.
Our research and development expenses consist primarily of salaries and related personnel costs, fees paid to consultants and outside service providers for clinical and laboratory development, facilities-related and other expenses relating to the design, development, manufacture, testing, and enhancement of our drug candidates and technologies, as well as expenses related to in-licensing of new product candidates. We expense our research and development costs as they are incurred. Other research and development expenses, which exclude non-cash compensation and discontinued operations, for the years ended December 31, 2011, 2010 and 2009 were $26,209,000, $13,728,000 and $7,372,000, respectively.
The following table sets forth the other research and development expenses per project, for the periods presented.
| Years ended December 31, | ||||||||||||
| 2011 | 2010 | 2009 | ||||||||||
| KRX-0401 (perifosine) | $ | 12,119,000 | $ | 5,952,000 | $ | 1,930,000 | ||||||
| Zerenex (ferric citrate) | 13,007,000 | 6,771,000 | 3,647,000 | |||||||||
| Other | 1,102,000 | 1,112,000 | 679,000 | |||||||||
| Terminated programs | (19,000 | ) | (107,000 | ) | 1,116,000 | |||||||
| Total | $ | 26,209,000 | $ | 13,728,000 | $ | 7,372,000 | ||||||
Amounts in the above table exclude discontinued operations.
Our general and administrative expenses consist primarily of salaries and related expenses for executive, finance and other administrative personnel, recruitment expenses, professional fees and other corporate expenses, including investor relations, legal activities and facilities-related expenses.
Our results of operations include non-cash compensation expense as a result of the grants of stock options and restricted stock. Compensation expense for awards of options and restricted stock granted to employees and directors represents the fair value of the award recorded over the respective vesting periods of the individual awards. The expense is included in the respective categories of expense in the consolidated statements of operations. We expect to continue to incur significant non-cash compensation expenses.
For awards of options and restricted stock to consultants and other third-parties, compensation expense is determined at the “measurement date.” The expense is recognized over the vesting period of the award. Until the measurement date is reached, the total amount of compensation expense remains uncertain. We record compensation expense based on the fair value of the award at the reporting date. The awards to consultants and other third-parties are then revalued, or the total compensation is recalculated based on the then current fair value, at each subsequent reporting date. This results in a change to the amount previously recorded in respect of the equity award grant, and additional expense or a reversal of expense may be recorded in subsequent periods based on changes in the assumptions used to calculate fair value, such as changes in market price, until the measurement date is reached and the compensation expense is finalized.
In addition, certain options and restricted stock issued to employees, consultants and other third-parties vest upon the achievement of certain milestones, therefore the total expense is uncertain until the milestone is met.
Our ongoing clinical trials are lengthy and expensive. Even if these trials show that our drug candidates are effective in treating certain diseases or conditions, there is no guarantee that we will be able to record commercial sales of any of our drug candidates in the near future. In addition, we expect losses to continue as we continue to fund in-licensing and development of new drug candidates. As we continue our development efforts, we may enter into additional third-party collaborative agreements and may incur additional expenses, such as licensing fees and milestone payments. In addition, we may need to establish the commercial infrastructure required to manufacture, market and sell our drug candidates following approval, if any, by the FDA or regulatory authorities of other countries, which would result in us incurring additional expenses. As a result, our quarterly results may fluctuate and a quarter-by-quarter comparison of our operating results may not be a meaningful indication of our future performance.
| 38 |
RESULTS OF OPERATIONS
Years Ended December 31, 2011 and 2010
License Revenue. License revenue for the year ended December 31, 2011 was $5,000,000 due to the recognition of a non-refundable milestone payment received in April 2011 from JT and Torii for their commencement of a Phase 3 clinical program in Japan. There was no license revenue for the year ended December 31, 2010. We expect to recognize additional license revenue in future periods from our sublicense agreement with JT and Torii, provided their Phase 3 program is successful.
Non-Cash Compensation Expense (Research and Development). Non-cash compensation expense (research and development) related to equity incentive grants decreased by $433,000 to $803,000 for the year ended December 31, 2011, as compared to $1,236,000 for the year ended December 31, 2010. The decrease in non-cash compensation expense in the year ended December 31, 2011, as compared to the year ended December 31, 2010, was primarily related to the recording of the fair value of equity awards granted to research and development personnel, which are expensed over the vesting periods of the individual awards.
Other Research and Development Expenses. Other research and development expenses increased by $12,481,000 to $26,209,000 for the year ended December 31, 2011, as compared to $13,728,000 for the year ended December 31, 2010. The increase in other research and development expenses was due primarily to a $6,167,000 increase in research and development expenses related to our two KRX-0401 Phase 3 clinical trials, as well as to a $6,236,000 increase in research and development expenses related to our Zerenex Phase 3 clinical program. We expect our other research and development costs to decrease modestly in 2012 due to the completion of our Phase 3 clinical programs for KRX-0401 and Zerenex, partially offset by expenses associated with our potential filings of new drug applications.
Non-Cash Compensation Expense (General and Administrative). Non-cash compensation expense (general and administrative) related to equity incentive grants increased by $52,000 to $1,289,000 for the year ended December 31, 2011, as compared to $1,237,000 for the year ended December 31, 2010. The decrease in non-cash compensation expense in the year ended December 31, 2011, as compared to the year ended December 31, 2010, was primarily related to the recording of the fair value of equity awards granted to general and administrative personnel and directors, which are expensed over the vesting periods of the individual awards.
Other General and Administrative Expenses. Other general and administrative expenses increased by $434,000 to $5,448,000 for the year ended December 31, 2011, as compared to $5,014,000 for the year ended December 31, 2010. The increase was due primarily to an increase in miscellaneous general and administrative expenses, including market research initiatives, partially offset by a decrease in legal expenses. Depending on the outcome of our Phase 3 study for KRX-0401 in refractory advanced colorectal cancer, our other general and administrative costs could vary dramatically over the next year. In the event of a negative outcome, we would expect our other general and administrative costs to remain at a comparable level to 2011. With a positive outcome, our other general and administrative costs may increase in order to scale-up our operations and infrastructure to prepare to commercialize KRX-0401, subject to our business development activities.
Interest and Other Income, Net. Interest and other income, net, decreased by $384,000 to $380,000 for the year ended December 31, 2011, as compared to $764,000 for the year ended December 31, 2010. The decrease was primarily due to a one-time $489,000 grant, received in November 2010, under The Patient Protection and Affordable Care Act of 2010 for our drug candidates, KRX-0401 (perifosine) and Zerenex (ferric citrate).
Gain from Discontinued Operations. For the year ended December 31, 2011, we recorded a $246,000 reversal of previously recorded estimated liabilities associated with the discontinued operations of our services business. See Note 8 – Discontinued Operations.
Years Ended December 31, 2010 and 2009
License Revenue. There was no license revenue for the year ended December 31, 2010, as compared to license revenue of $21,616,000 for the year ended December 31, 2009. The decrease in license revenue was due primarily to the recognition in 2009 of all remaining deferred revenue related to the JT and Torii sublicense agreement originally signed in September 2007, and amended and restated in June 2009, and due to the recognition in the year ended December 31, 2009, of a $3.0 million milestone payment received from JT and Torii due to their initiation in 2009 of a Phase 2 clinical study of Zerenex in Japan.
| 39 |
Other Revenue. There was no other revenue for the year ended December 31, 2010, as compared to other revenue of $3,575,000 for the year ended December 31, 2009. The other revenue in the year ended December 31, 2009, was due to the $3,500,000 settlement of our dispute with Alfa Wassermann S.p.A., in July 2009, over issues arising from the terminated license agreement for Sulonex (sulodexide) and was also related to a $75,000 payment earned in June 2009 from a December 2008 license termination agreement for KRX-0501. Payments associated with these license terminations are recognized as earned since we have no on-going responsibilities under the terminated license agreement or the termination agreement.
Non-Cash Compensation Expense (Research and Development). Non-cash compensation expense (research and development) related to equity incentive grants increased by $3,000 to $1,236,000 for the year ended December 31, 2010, as compared to $1,233,000 for the year ended December 31, 2009. Non-cash compensation expense is related to grants of equity awards to research and development personnel and the recording of the related fair value of the awards over the respective vesting periods of the individual awards.
Other Research and Development Expenses. Other research and development expenses increased by $6,356,000 to $13,728,000 for the year ended December 31, 2010, as compared to $7,372,000 for the year ended December 31, 2009. The increase in other research and development expenses was due primarily to a $4,022,000 increase in research and development expenses related to KRX-0401 due to the two ongoing Phase 3 clinical trials, as well as to a $3,123,000 increase in research and development expenses related to the Zerenex Phase 3 clinical program. The year ended December 31, 2009, included a one-time $1,460,000 accrual for a terminated early-stage pipeline product candidate.
Non-Cash Compensation Expense (General and Administrative). Non-cash compensation expense (general and administrative) related to equity incentive grants decreased by $630,000 to $1,237,000 for the year ended December 31, 2010, as compared to $1,867,000 for the year ended December 31, 2009. The decrease in non-cash compensation expense was primarily related to an expense in the year ended December 31, 2009, of approximately $660,000 associated with the equity modifications of outstanding stock options and shares of restricted stock of our former chief executive officer, whose employment was terminated in April 2009.
Other General and Administrative Expenses. Other general and administrative expenses increased by $110,000 to $5,014,000 for the year ended December 31, 2010, as compared to $4,904,000 for the year ended December 31, 2009. The increase was due to a $943,000 increase in miscellaneous general and administrative expenses, including investor outreach initiatives, partially offset by an expense in the year ended December 31, 2009, of approximately $833,000 for severance, pro rata bonus and notice pay related to the termination of our former chief executive officer in April 2009.
Interest and Other Income, Net. Interest and other income, net, increased by $97,000 to $764,000 for the year ended December 31, 2010, as compared to $667,000 for the year ended December 31, 2009. The increase was primarily due to a one-time $489,000 grant, received in November 2010, under The Patient Protection and Affordable Care Act of 2010 for our drug candidates, KRX-0401 (perifosine) and Zerenex (ferric citrate), partially offset by lower effective interest earned on our investment portfolio in 2010, as well as a realized loss of $82,000 related to the sale, in May 2010, of our last auction rate security investment.
Gain from Discontinued Operations. For the year ended December 31, 2010, we recorded a $120,000 reversal of previously recorded estimated liabilities associated with the discontinued operations of our diagnostic business that was terminated in September 2008. See Note 8 – Discontinued Operations.
LIQUIDITY AND CAPITAL RESOURCES
Our major sources of cash have been proceeds from various private placements of equity securities, option and warrant exercises, public offerings of our common stock, interest income, and from the upfront and milestone payments from our sublicense agreement with JT and Torii and miscellaneous payments from our other prior licensing activities. We have not yet commercialized any of our drug candidates and cannot be sure if we will ever be able to do so. Even if we commercialize one or more of our drug candidates, we may not become profitable. Our ability to achieve profitability depends on a number of factors, including our ability to obtain regulatory approval for our drug candidates, successfully complete any post-approval regulatory obligations and successfully commercialize our drug candidates alone or in partnership. We may continue to incur substantial operating losses even if we begin to generate revenues from our drug candidates.
| 40 |
In April 2011, we received a non-refundable milestone payment of $5.0 million from JT and Torii.
On May 4, 2011, we announced the pricing of an underwritten registered offering of 7,021,277 shares of our common stock at a price of $4.70 per share for gross proceeds of approximately $33 million. Net proceeds from this offering were approximately $30.7 million, net of underwriting discounts and offering expenses of approximately $2.3 million.
As December 31, 2011, we had $39.5 million in cash, cash equivalents, interest receivable, and investment securities, an increase of $11.0 million from December 31, 2010. Depending on the outcome of our Phase 3 study for KRX-0401 in refractory advanced colorectal cancer, our operating cash requirements may vary dramatically. In the event of a negative outcome, we currently anticipate that our cash, cash equivalents and investment securities as of December 31, 2011, exclusive of our anticipated milestone payments to be received, are sufficient to fund our anticipated operating cash requirements for approximately 18 to 20 months from December 31, 2011. The actual amount of cash that we will need to operate is subject to many factors, including, but not limited to, the timing, design and conduct of clinical trials for our drug candidates. We are dependent upon significant financing to provide the cash necessary to execute our current operations, including the commercialization of any of our drug candidates.
We currently have two shelf registration statements on Form S-3, filed and declared effective by the SEC, providing for the offering of up to approximately $79 million of common stock and warrants in the aggregate.
| · | On August 28, 2009, we filed with the SEC a shelf registration statement on Form S-3 (File No. 333-161607) and declared effective by the SEC on September 23, 2009. The registration statement provided for the offering of up to $40 million of our common stock and warrants. Subsequent to the registered direct offering completed in September 2009, there remains approximately $12 million of our common stock and warrants available for sale under the shelf registration statement. |
| · | On January 3, 2011, we filed with the SEC a shelf registration statement on Form S-3 (File No. 333-171517) that was declared effective by the SEC on January 28, 2011, providing for the offering of up to $100 million of our common stock and warrants to purchase our common stock. Subsequent to the registered offering in May 2011, there remains approximately $67 million of our common stock and warrants available for sale under the shelf registration statement. |
We may offer the securities under our shelf registration statements from time to time in response to market conditions or other circumstances if we believe such a plan of financing is in our best interests and the best interests of our stockholders. We believe that these shelf registration statements provide us with the flexibility to efficiently raise additional capital to finance our operations as needed.
Net cash used in operating activities of continuing operations for the year ended December 31, 2011 was $22.8 million, as compared to $16.2 million for the year ended December 31, 2010. This increase in cash used in operating activities was due primarily to increased expenditures associated with our Phase 3 clinical programs for KRX-0401 and Zerenex, partially offset by the $5.0 million non-refundable milestone payment received from JT and Torii in April 2011.
For the year ended December 31, 2011, net cash used in investing activities of $4.2 million was primarily the result of investments in held-to-maturity short-term securities, partially offset by maturities of held-to-maturity short-term securities. For the year ended December 31, 2011, net cash provided by financing activities of $33.8 million was related to net proceeds of $30.7 million received from the underwritten registered offering in May 2011 and $3.1 million in net proceeds from the exercise of stock options.
OFF-BALANCE SHEET ARRANGEMENTS
We have not entered into any transactions with unconsolidated entities whereby we have financial guarantees, subordinated retained interests, derivative instruments or other contingent arrangements that expose us to material continuing risks, contingent liabilities, or any other obligations under a variable interest in an unconsolidated entity that provides us with financing, liquidity, market risk or credit risk support.
OBLIGATIONS AND COMMITMENTS
As of December 31, 2011, we have known contractual obligations, commitments and contingencies of $14,395,000. Of this amount, $13,439,000 relates to research and development agreements (relating to our KRX-0401 and Zerenex clinical programs), of which $9,251,000 is due within the next year. Most of these commitments are contingent upon our continuing development of our drug candidates. The additional $956,000 relates to our operating lease obligations, of which $526,000 is due within the next year.
| 41 |
| Payment due by period | ||||||||||||||||||||
| Contractual obligations | Total | Less than 1 year | 1-3 years | 3-5 years | More than 5 years | |||||||||||||||
| Research and development agreements | $ | 13,439,000 | $ | 9,251,000 | $ | 4,188,000 | $ | – | $ | – | ||||||||||
| Operating leases | 956,000 | 526,000 | 430,000 | – | – | |||||||||||||||
| Total | $ | 14,395,000 | $ | 9,777,000 | $ | 4,618,000 | $ | – | $ | – | ||||||||||
In August 2010, we signed an amendment to the lease on our corporate and executive office located in New York City extending its term through September 30, 2013. We also executed an amendment to our office sharing agreement with a third party for a portion of our leased space through September 29, 2013, whereby the third party pays us $13,400 per month. This sublet income is not included as an offset to our operating lease obligations in the table above.
We have undertaken to make contingent milestone payments to certain of our licensors of up to approximately $25.0 million over the life of the licenses, of which approximately $22.0 million will be due upon or following regulatory approval of the licensed drugs. We have also committed to pay to the former stockholders of ACCESS Oncology, Inc. certain contingent equity rights (up to 2,872,422 shares of our common stock) if KRX-0401 meets certain development milestones. The contingent equity rights have been recognized as a non-current liability on the consolidated balance sheet. The uncertainty relating to the timing of the commitments described in this paragraph prevents us from including them in the table above.
CRITICAL ACCOUNTING POLICIES
The discussion and analysis of our financial condition and results of operations is based upon our consolidated financial statements, which have been prepared in accordance with GAAP. The preparation of these financial statements requires us to make estimates and judgments that affect the reported amount of assets and liabilities and related disclosure of contingent assets and liabilities at the date of our financial statements and the reported amounts of revenues and expenses during the applicable period. Actual results may differ from these estimates under different assumptions or conditions.
We define critical accounting policies as those that are reflective of significant judgments and uncertainties and which may potentially result in materially different results under different assumptions and conditions. In applying these critical accounting policies, our management uses its judgment to determine the appropriate assumptions to be used in making certain estimates. These estimates are subject to an inherent degree of uncertainty. Our critical accounting policies include the following:
Stock Compensation. We have granted stock options and restricted stock to employees, directors and consultants, as well as warrants to other third parties. For employee and director grants, the value of each option award is estimated on the date of grant using the Black-Scholes option-pricing model. The Black-Scholes model takes into account volatility in the price of our stock, the risk-free interest rate, the estimated life of the option, the closing market price of our stock and the exercise price. We base our estimates of our stock price volatility on the historical volatility of our common stock and our assessment of future volatility; however, these estimates are neither predictive nor indicative of the future performance of our stock. For purposes of the calculation, we assumed that no dividends would be paid during the life of the options and warrants. The estimates utilized in the Black-Scholes calculation involve inherent uncertainties and the application of management judgment. In addition, we are required to estimate the expected forfeiture rate and only recognize expense for those equity awards expected to vest. As a result, if other assumptions had been used, our recorded stock-based compensation expense could have been materially different from that reported. In addition, because some of the options and warrants issued to employees, consultants and other third-parties vest upon the achievement of certain milestones, the total expense is uncertain.
Total compensation expense for options and restricted stock issued to consultants is determined at the “measurement date.” The expense is recognized over the vesting period for the options and restricted stock. Until the measurement date is reached, the total amount of compensation expense remains uncertain. We record stock-based compensation expense based on the fair value of the equity awards at the reporting date. These equity awards are then revalued, or the total compensation is recalculated based on the then current fair value, at each subsequent reporting date. This results in a change to the amount previously recorded in respect of the equity award grant, and additional expense or a reversal of expense may be recorded in subsequent periods based on changes in the assumptions used to calculate fair value, such as changes in market price, until the measurement date is reached and the compensation expense is finalized.
| 42 |
Accruals for Clinical Research Organization and Clinical Site Costs. We make estimates of costs incurred in relation to external clinical research organizations, or CROs, and clinical site costs. We analyze the progress of clinical trials, including levels of patient enrollment, invoices received and contracted costs when evaluating the adequacy of the amount expensed and the related prepaid asset and accrued liability. Significant judgments and estimates must be made and used in determining the accrued balance and expense in any accounting period. We review and accrue CRO expenses and clinical trial study expenses based on work performed and rely upon estimates of those costs applicable to the stage of completion of a study. Accrued CRO costs are subject to revisions as such trials progress to completion. Revisions are charged to expense in the period in which the facts that give rise to the revision become known. With respect to clinical site costs, the financial terms of these agreements are subject to negotiation and vary from contract to contract. Payments under these contracts may be uneven, and depend on factors such as the achievement of certain events, the successful recruitment of patients, the completion of portions of the clinical trial or similar conditions. The objective of our policy is to match the recording of expenses in our financial statements to the actual services received and efforts expended. As such, expense accruals related to clinical site costs are recognized based on our estimate of the degree of completion of the event or events specified in the specific clinical study or trial contract.
Revenue Recognition. We recognize license revenue in accordance with the revenue recognition guidance of the Codification. We analyze each element of our licensing agreement to determine the appropriate revenue recognition. The terms of the license agreement may include payment to us of non-refundable up-front license fees, milestone payments if specified objectives are achieved, and/or royalties on product sales. We recognize revenue from upfront payments over the period of significant involvement under the related agreements unless the fee is in exchange for products delivered or services rendered that represent the culmination of a separate earnings process and no further performance obligation exists under the contract. We recognize milestone payments as revenue upon the achievement of specified milestones only if (1) the milestone payment is non-refundable, (2) substantive effort is involved in achieving the milestone, (3) the amount of the milestone is reasonable in relation to the effort expended or the risk associated with achievement of the milestone, and (4) the milestone is at risk for both parties. If any of these conditions are not met, we defer the milestone payment and recognize it as revenue over the estimated period of performance under the contract.
We recognize other revenues at the time such fees and payments are earned.
Accounting Related to Goodwill. As of December 31, 2011, there was approximately $3.2 million of goodwill on our consolidated balance sheet. Goodwill is reviewed for impairment annually, or when events arise that could indicate that an impairment exists. We test for goodwill impairment using a two-step process. The first step compares the fair value of the reporting unit with the unit's carrying value, including goodwill. When the carrying value of the reporting unit is greater than fair value, the unit’s goodwill may be impaired, and the second step must be completed to measure the amount of the goodwill impairment charge, if any. In the second step, the implied fair value of the reporting unit’s goodwill is compared with the carrying amount of the unit’s goodwill. If the carrying amount is greater than the implied fair value, the carrying value of the goodwill must be written down to its implied fair value.
We are required to perform impairment tests annually, at December 31, and whenever events or changes in circumstances suggest that the carrying value of an asset may not be recoverable. For all of our acquisitions, various analyses, assumptions and estimates were made at the time of each acquisition that were used to determine the valuation of goodwill and intangibles. In future years, the possibility exists that changes in forecasts and estimates from those used at the acquisition date could result in impairment indicators.
Impairment of Investment Securities. In May 2010, we sold our one remaining auction rate security investment for $1.6 million, representing a loss of $82,000. Auction rate securities were recorded at their fair value and were classified as long-term investments. In prior quarters, we assessed the fair value of our auction rate securities portfolio. As a result of this valuation process, as described below, we reported an other comprehensive loss of $180,000 in the year ended December 31, 2010, for a reduction of a temporary unrealized gain related to the estimated fair value of our last auction rate security, and recorded impairment charges of $32,000 and $68,000 in the years ended December 31, 2010 and 2009, respectively, for other-than-temporary declines in the value of our auction rate securities, all of which were included in interest and other income, net.
The valuation methods used to estimate the auction rate securities’ fair value were (1) a discounted cash flow model, where the expected cash flows of the auction rate securities are discounted to the present using a yield that incorporates compensation for illiquidity, and (2) a market comparables method, where the auction rate securities are valued based on indications, from the secondary market, of what discounts buyers demand when purchasing similar auction rate securities. The valuation also included assessments of the underlying structure of each security, expected cash flows, discount rates, credit ratings, workout periods, and overall capital market liquidity. These assumptions, assessments and the interpretations of relevant market data are subject to uncertainties, are difficult to predict and require significant judgment. The use of different assumptions, applying different judgment to inherently subjective matters and changes in future market conditions could result in significantly different estimates of fair value of our prior investments in auction rate securities. In addition, the estimated fair value of the auction rates securities may differ from the values that would have been used had a ready market existed, and the differences could be material to the consolidated financial statements.
| 43 |
We review investment securities for impairment and to determine the classification of the impairment as temporary or other-than-temporary. Losses are recognized in our consolidated statement of operations when a decline in fair value is determined to be other-than-temporary. We review our investments on an ongoing basis for indications of possible impairment. Once identified, the determination of whether the impairment is temporary or other-than-temporary requires significant judgment. The primary factors we consider in classifying an impairment include the extent and time the fair value of each investment has been below cost and our ability to hold such investment to maturity.
Impairment of Long-Lived Assets. We recognize an impairment loss when circumstances indicate that the carrying value of long-lived tangible and intangible assets with finite lives may not be recoverable. Management’s policy in determining whether an impairment indicator exists, a triggering event, comprises measurable operating performance criteria as well as qualitative measures. If an analysis is necessitated by the occurrence of a triggering event, we make certain assumptions in determining the impairment amount. Recoverability of assets to be held and used is measured by a comparison of the carrying amount of an asset to future cash flows expected to be generated by the asset or used in its disposal. If the carrying amount of an asset exceeds its estimated future cash flows, an impairment charge is recognized for the excess of the carrying value of the asset above its fair value.
Accounting For Income Taxes. In preparing our consolidated financial statements, we are required to estimate our income taxes in each of the jurisdictions in which we operate. This process involves management estimation of our actual current tax exposure and assessment of temporary differences resulting from differing treatment of items for tax and accounting purposes. These differences result in deferred tax assets and liabilities. We must then assess the likelihood that our deferred tax assets will be recovered from future taxable income and, to the extent we believe that recovery is not likely, we must establish a valuation allowance. To the extent we establish a valuation allowance or increase this allowance in a period, we must include an expense within the tax provision in the consolidated statement of operations. Significant management judgment is required in determining our provision for income taxes, our deferred tax assets and liabilities and any valuation allowance recorded against our net deferred tax assets. We have fully offset our deferred tax assets with a valuation allowance. Our lack of earnings history and the uncertainty surrounding our ability to generate taxable income prior to the reversal or expiration of such deferred tax assets were the primary factors considered by management in maintaining the valuation allowance.
RECENTLY ISSUED ACCOUNTING STANDARDS
In September 2011, the FASB issued Accounting Standards Update, or ASU, 2011-08, “Intangibles — Goodwill and Other,” which amends current guidance to allow a company to first assess qualitative factors to determine whether it is necessary to perform the two-step quantitative goodwill impairment test. The amendment also improves previous guidance by expanding upon the examples of events and circumstances that an entity should consider between annual impairment tests in determining whether it is more likely than not that the fair value of a reporting unit is less than its carrying amount. ASU 2011-08 is effective for annual and interim goodwill impairment tests performed for fiscal years beginning after December 15, 2011, which for us means January 1, 2012. We do not expect that the adoption of ASU 2011-08 will have an impact upon our financial position and results of operations.
In June 2011, the FASB issued ASU No. 2011-05, “Comprehensive Income (Topic 220).” This newly issued accounting standard (1) eliminates the option to present the components of other comprehensive income as part of the statement of changes in stockholders’ equity; (2) requires the consecutive presentation of the statement of net income and other comprehensive income; and (3) requires an entity to present reclassification adjustments on the face of the financial statements from other comprehensive income to net income. The amendments in this ASU do not change the items that must be reported in other comprehensive income or when an item of other comprehensive income must be reclassified to net income nor do the amendments affect how earnings per share is calculated or presented. This ASU is required to be applied retrospectively and is effective for fiscal years and interim periods within those years beginning after December 15, 2011, which for us means January 1, 2012. As this accounting standard only requires enhanced disclosure, the adoption of this standard will not impact our financial position or results of operations.
| 44 |
ITEM 7A. QUANTITATIVE AND QUALITATIVE DISCLOSURE ABOUT MARKET RISK.
The primary objective of our investment activities is to preserve principal while maximizing our income from investments and minimizing our market risk. We invest in government and investment-grade corporate debt in accordance with our investment policy. Some of the securities in which we invest have market risk. This means that a change in prevailing interest rates, and/or credit risk, may cause the fair value of the investment to fluctuate. For example, if we hold a security that was issued with a fixed interest rate at the then-prevailing rate and the prevailing interest rate later rises, the fair value of our investment will probably decline. As of December 31, 2011, our portfolio of financial instruments consists of cash equivalents and short-term interest bearing securities, including government debt, money market funds and bank deposits. Due to the short-term nature of our investments, we believe there is no material exposure to interest rate risk, and/or credit risk, arising from our investments.
ITEM 8. FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA.
Our consolidated financial statements and the notes thereto, included in Part IV, Item 15(a), part 1, are incorporated by reference into this Item 8.
ITEM 9. CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND
FINANCIAL DISCLOSURE.
None.
ITEM 9A. CONTROLS AND PROCEDURES.
Evaluation of Disclosure Controls and Procedures. As of December 31, 2011, management carried out, under the supervision and with the participation of our Chief Executive Officer and Chief Financial Officer, an evaluation of the effectiveness of the design and operation of our disclosure controls and procedures (as defined in Rules 13a-15(e) and 15d-15(e) under the Exchange Act). Our disclosure controls and procedures are designed to provide reasonable assurance that information we are required to disclose in the reports that we file or submit under the Exchange Act is recorded, processed, summarized and reported within the time periods specified in applicable rules and forms. Based upon that evaluation, our Chief Executive Officer and Chief Financial Officer concluded that, as of December 31, 2011, our disclosure controls and procedures were effective.
Management's Report on Internal Control over Financial Reporting. Our management is responsible for establishing and maintaining adequate internal control over financial reporting (as defined in Rule 13a-15(f) or Rule 15d-15(f) under the Exchange Act). Our management assessed the effectiveness of our internal control over financial reporting as of December 31, 2011. In making this assessment, our management used the criteria set forth by the Committee of Sponsoring Organizations of the Treadway Commission, known as COSO, in Internal Control-Integrated Framework. Our management has concluded that, as of December 31, 2011, our internal control over financial reporting was effective based on these criteria. UHY LLP, our independent registered public accounting firm, has audited the accompanying consolidated balance sheets as of December 31, 2011 and 2010, and the related consolidated statements of operations, stockholders’ equity and comprehensive loss (income), and cash flows for the years ended December 31, 2011, 2010 and 2009, included in this annual report on page F-1. UHY LLP has issued an attestation report on our internal control over financial reporting as of December 31, 2011, which is found below.
Changes in Internal Control Over Financial Reporting. There were no changes in our internal control over financial reporting during the quarter ended December 31, 2011, that have materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
Limitations on the Effectiveness of Controls. Our management, including our Chief Executive Officer and Chief Financial Officer, does not expect that our disclosure controls and procedures or our internal control over financial reporting will prevent all errors and all fraud. A control system, no matter how well conceived and operated, can provide only reasonable, not absolute, assurance that the objectives of the control system are met. Further, the design of a control system must reflect the fact that there are resource constraints, and the benefits of controls must be considered relative to their costs. Because of the inherent limitations in all control systems, no evaluation of controls can provide absolute assurance that all control issues and instances of fraud, if any, within our company have been detected.
| 45 |
Report of Independent Registered Public Accounting Firm
To the Board of Directors and
Stockholders of Keryx Biopharmaceuticals, Inc.
We have audited Keryx Biopharmaceuticals, Inc.’s (the “Company”) internal control over financial reporting as of December 31, 2011, based on criteria established in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO). The Company’s management is responsible for maintaining effective internal control over financial reporting and for its assessment of the effectiveness of internal control over financial reporting included in Part II, Item 9A of this Form 10-K. Our responsibility is to express an opinion on the Company’s internal control over financial reporting based on our audit.
We conducted our audit in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects. Our audit of internal control over financial reporting included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, and testing and evaluating the design and operating effectiveness of internal control based on the assessed risk. Our audit also included performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
In our opinion, Keryx Biopharmaceuticals, Inc. maintained, in all material respects, effective internal control over financial reporting as of December 31, 2011, based on criteria established in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO).
We have also audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), the consolidated balance sheets and the related consolidated statements of operations, stockholders’ equity and comprehensive loss (income), and cash flows of Keryx Biopharmaceuticals, Inc., and our report dated March 2, 2012, expressed an unqualified opinion.
/s/ UHY LLP
New York, New York
March 2, 2012
ITEM 9B. OTHER INFORMATION.
None.
PART III
ITEM 10. DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE.
The information required by this Item is incorporated herein by reference from our Proxy Statement for our 2012 Annual Meeting of Stockholders.
ITEM 11. EXECUTIVE COMPENSATION.
The information required by this Item is incorporated herein by reference from our Proxy Statement for our 2012 Annual Meeting of Stockholders.
| 46 |
ITEM 12. SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS.
The information required by this Item is incorporated herein by reference from our Proxy Statement for our 2012 Annual Meeting of Stockholders.
ITEM 13. CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS AND DIRECTOR INDEPENDENCE.
The information required by this Item is incorporated herein by reference from our Proxy Statement for our 2012 Annual Meeting of Stockholders.
ITEM 14. PRINCIPAL ACCOUNTANT FEES AND SERVICES.
The information required by this Item is incorporated herein by reference from our Proxy Statement for our 2012 Annual Meeting of Stockholders.
| 47 |
PART IV
ITEM 15. EXHIBITS and FINANCIAL STATEMENT SCHEDULES.
| (a) 1. | Consolidated Financial Statements |
The following consolidated financial statements of Keryx Biopharmaceuticals, Inc. are filed as part of this report.
| Contents | Page |
| Report of Independent Registered Public Accounting Firm | F-1 |
| Consolidated Balance Sheets as of December 31, 2011 and 2010 | F-2 |
| Consolidated Statements of Operations for the years ended December 31, 2011, 2010 and 2009 | F-3 |
| Consolidated Statements of Stockholders’ Equity and Comprehensive Loss (Income) for the years ended December 31, 2011, 2010 and 2009 | F-4 |
| Consolidated Statements of Cash Flows for the years ended December 31, 2011, 2010 and 2009 | F-5 |
| Notes to the Consolidated Financial Statements | F-6 |
| 2. | Consolidated Financial Statement Schedules |
All schedules are omitted as the information required is inapplicable or the information is presented in the consolidated financial statements or the related notes.
| 3. | Exhibits |
| Exhibit | |
| Number | Exhibit Description |
| 2.1 | Agreement and Plan of Merger by and among Keryx Biopharmaceuticals, Inc., AXO Acquisition Corp., and ACCESS Oncology, Inc. dated as of January 7, 2004, filed as Exhibit 2.1 to the Registrant’s Current Report on Form 8-K dated January 8, 2004, filed on January 15, 2004 (File No. 000-30929), and incorporated herein by reference. |
| 2.2 | First Amendment to the Agreement and Plan of Merger by and among Keryx Biopharmaceuticals, Inc., AXO Acquisition Corp., and ACCESS Oncology, Inc. dated as of February 5, 2004, filed as Exhibit 2.2 to the Registrant’s Current Report on Form 8-K dated February 5, 2004, filed on February 20, 2004 (File No. 000-30929), and incorporated herein by reference. |
| 3.1 | Amended and Restated Certificate of Incorporation of Keryx Biopharmaceuticals, Inc., filed as Exhibit 3.1 to the Registrant's Quarterly Report on Form 10-Q for the quarter ended June 30, 2004, filed on August 12, 2004 (File No. 000-30929), and incorporated herein by reference. |
| 3.2 | Amended and Restated Bylaws of Keryx Biopharmaceuticals, Inc., filed as Exhibit 3.2 to the Registrant’s Annual Report on Form 10-K for the year ended December 31, 2001, filed on March 26, 2002 (File No. 000-30929), and incorporated herein by reference. |
| 3.3 | Amendment to Amended and Restated Certificate of Incorporation of Keryx Biopharmaceuticals, Inc., dated July 24, 2007, filed as Exhibit 3.3 to the Registrant's Quarterly Report on Form 10-Q for the quarter ended June 30, 2007, filed on August 9, 2007 and incorporated herein by reference. |
| 4.1 | Specimen Common Stock Certificate, filed as Exhibit 4.1 to the Registrant’s First Amendment to the Registration Statement on Form S-1 filed on June 30, 2000 (File No. 333-37402), and incorporated herein by reference. |
| 10.1† | 1999 Stock Option Plan, as amended, filed as Exhibit 10.2 to the Registrant’s Quarterly Report of Form 10-Q for the quarter ended March 31, 2003 filed on May 15, 2003 (File No. 000-30929) and incorporated herein by reference. |
| 48 |
| 10.2† | 2000 Stock Option Plan, as amended, filed as Exhibit 10.3 to the Registrant’s Quarterly Report of Form 10-Q for the quarter ended March 31, 2003 filed on May 15, 2003 (File No. 000-30929) and incorporated herein by reference. |
| 10.3† | 2002 CEO Incentive Stock Option Plan, filed as Exhibit 10.4 to the Registrant’s Quarterly Report of Form 10-Q for the quarter ended March 31, 2003 filed on May 15, 2003 (File No. 000-30929) and incorporated herein by reference. |
| 10.4! | License Agreement dated September 18, 2002 between Zentaris AG and AOI Pharma, Inc, filed as Exhibit 10.38 to the Registrant’s Annual Report on Form 10-K for the year ended December 31, 2003, filed on March 30, 2004, and incorporated herein by reference. |
| 10.5! | Addendum Agreement to License and Cooperation Agreement for Perifosine dated December 3, 2003 between Zentaris AG and AOI Pharma, Inc., filed as Exhibit 10.39 to the Registrant’s Annual Report on Form 10-K for the year ended December 31, 2003, filed on March 30, 2004, and incorporated herein by reference. |
| 10.6 | Cooperative Research and Development Agreement between the National Cancer Institute and ASTA Medica Inc., as amended, filed as Exhibit 10.40 to the Registrant’s Annual Report on Form 10-K for the year ended December 31, 2003, filed on March 30, 2004, and incorporated herein by reference. |
| 10.7† | Keryx Biopharmaceuticals, Inc. 2004 Long-Term Incentive Plan, filed with the Registrant’s Definitive Proxy Statement for the Annual Meeting of Stockholders on June 10, 2004, filed on April 29, 2004, and incorporated herein by reference. |
| 10.8! | License Agreement between Keryx Biopharmaceuticals, Inc. and Panion & BF Biotech, Inc. dated as of November 7, 2005, filed as Exhibit 10.21 to the Registrant’s Annual Report on Form 10-K for the year ended December 31, 2005, filed on March 8, 2006, and incorporated herein by reference. |
| 10.9† | Amendment to the Keryx Biopharmaceuticals, Inc. 2004 Long-Term Incentive Plan dated April 11, 2006, filed as Exhibit 10.1 to the Registrant’s Quarterly Report on Form 10-Q for the quarter ended June 30, 2006, filed on August 9, 2006, and incorporated herein by reference. |
| 10.10† | 2007 Incentive Plan, filed as Annex D to the Registrant’s Definitive Proxy Statement on Schedule 14A (File No. 000-30929) filed on April 30, 2007, and incorporated herein by reference. |
| 10.11! | Sub-license Agreement by and among Keryx Biopharmaceuticals, Inc., Japan Tobacco Inc., and Torii Pharmaceutical Co., Ltd. dated September 26, 2007, filed as Exhibit 10.1 to the Registrant’s Quarterly Report on Form 10-Q for the quarter ended September 30, 2007, filed on November 9, 2007, and incorporated herein by reference. |
| 10.12! | Amended and Restated License Agreement by and between Panion & BF Biotech, Inc. and Keryx Biopharmaceuticals, Inc. dated March 17, 2008, filed as Exhibit 10.1 to the Registrant’s Quarterly Report on Form 10-Q for the quarter ended March 31, 2008, filed on May 12, 2008, and incorporated herein by reference. |
| 10.13! | First Amendment to Amended and Restated License Agreement by and between Panion & BF Biotech, Inc. and Keryx Biopharmaceuticals, Inc. dated March 17, 2008. |
| 10.14! | Amended and Restated License Agreement dated June 8, 2009, by and between Keryx Biopharmaceuticals, Inc., Japan Tobacco, Inc. and Japan Torii Pharmaceutical Co. Ltd., filed as Exhibit 10.1 to the Registrant’s quarterly report on Form 10-Q for the quarter ended June 30, 2009, filed on August 8, 2009, and incorporated herein by reference. |
| 10.15 | Settlement Agreement and General Release between Keryx Biopharmaceuticals, Inc. and Alfa Wassermann S.p.A. filed as Exhibit 10.2 to the Registrant’s quarterly report on Form 10-Q for the quarter ended June 30, 2009, filed on August 8, 2009, and incorporated herein by reference. |
| 49 |
| 10.16 | Amendment to License and Cooperation Agreement for Perifosine by and among AOI Pharma, Inc. (a subsidiary of the Company) and AEterna Zentaris GmbH dated April 12, 2011, filed as Exhibit 10.1 to the Registrant's Quarterly Report on Form 10-Q for the quarter ended March 31, 2011, filed on May 10, 2011 and incorporated herein by reference. |
| 10.17† | Employment Agreement with Ron Bentsur dated September 14, 2009, filed as Exhibit 10.1 to the Registrant’s Form 8-K filed on September 16, 2009, and incorporated herein by reference. |
| 10.18† | First Amendment to Employment Agreement with Ron Bentsur dated January 13, 2012, filed as Exhibit 10.1 to the Registrant’s Form 8-K filed on January 19, 2012, and incorporated herein by reference. |
| 10.19† | Second Amended and Restated Directors Equity Compensation Plan, filed as Exhibit 10.1 to the Registrant's Quarterly Report on Form 10-Q for the quarter ended June 30, 2010, filed on August 9, 2010 and incorporated herein by reference. |
| 10.20† | Change in Control Agreement with James F. Oliviero dated October 31, 2011, as amended on November 3, 2011. |
| 21.1 | List of subsidiaries of Keryx Biopharmaceuticals, Inc. |
| 23.1 | Consent of UHY LLP. |
| 24.1 | Power of Attorney of Director and Officers of Keryx Biopharmaceuticals, Inc. (included herein). |
| 31.1 | Certification of Chief Executive Officer pursuant to Rule 13a-14(a)/15d-14(a), as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002, dated March 2, 2012. |
| 31.2 | Certification of Chief Financial Officer pursuant to Rule 13a-14(a)/15d-14(a), as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002, dated March 2, 2012. |
| 32.1 | Certification of Chief Executive Officer pursuant to 18 U.S.C. §1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002, dated March 2, 2012. |
| 32.2 | Certification of Chief Financial Officer pursuant to 18 U.S.C. §1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002, dated March 2, 2012. |
| 101 | The following financial information from Keryx Biopharmaceuticals, Inc.’s Annual Report on Form 10-K for the year ended December 31, 2011, formatted in XBRL (eXtensible Business Reporting Language): (i) Consolidated Balance Sheets, (ii) Consolidated Statements of Operations, (iii) Consolidated Statements of Stockholders’ Equity and Comprehensive Loss (Income), (iv) Consolidated Statements of Cash Flows and (v) the Notes to Consolidated Financial Statements. |
| ! | Confidential treatment has been granted with respect to the omitted portions of this exhibit. |
| † | Indicates management contract or compensatory plan or arrangement. |
| 50 |
Keryx Biopharmaceuticals, Inc.
Consolidated Financial Statements as of December 31, 2011
| Contents | Page |
| Report of Independent Registered Public Accounting Firm | F-1 |
| Consolidated Balance Sheets as of December 31, 2011 and 2010 | F-2 |
| Consolidated Statements of Operations for the years ended December 31, 2011, 2010 and 2009 | F-3 |
| Consolidated Statements of Stockholders’ Equity and Comprehensive Loss (Income) for the years ended December 31, 2011, 2010 and 2009 | F-4 |
| Consolidated Statements of Cash Flows for the years ended December 31, 2011, 2010 and 2009 | F-5 |
| Notes to the Consolidated Financial Statements | F-6 |
Report of Independent Registered Public Accounting Firm
To the Board of Directors and
Stockholders of Keryx Biopharmaceuticals, Inc.
We have audited the accompanying consolidated balance sheets of Keryx Biopharmaceuticals, Inc. (the “Company”) as of December 31, 2011 and 2010, and the related consolidated statements of operations, stockholders’ equity and comprehensive loss (income), and cash flows for each of the years in the three-year period ended December 31, 2011. The Company’s management is responsible for these financial statements. Our responsibility is to express an opinion on these financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements. An audit also includes assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the financial statements referred to above present fairly, in all material respects, the consolidated financial position of Keryx Biopharmaceuticals, Inc. as of December 31, 2011 and 2010, and the results of its consolidated operations and its cash flows for each of the years in the three-year period ended December 31, 2011 in conformity with accounting principles generally accepted in the United States of America.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), the Company’s internal control over financial reporting as of December 31, 2011, based on criteria established in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO), and our report dated March 2, 2012, expressed an unqualified opinion.
| /s/ UHY LLP | |
| New York, New York | |
| March 2, 2012 |
| F-1 |
Keryx Biopharmaceuticals, Inc.
Consolidated Balance Sheets as of December 31,
(in thousands, except share and per share amounts)
| 2011 | 2010 | |||||||
| Assets | ||||||||
| Current assets: | ||||||||
| Cash and cash equivalents | $ | 35,252 | $ | 28,412 | ||||
| Short-term investment securities | 4,211 | 100 | ||||||
| Interest receivable | 7 | — | ||||||
| Other current assets | 534 | 200 | ||||||
| Total current assets | 40,004 | 28,712 | ||||||
| Property, plant and equipment, net | 67 | 57 | ||||||
| Goodwill | 3,208 | 3,208 | ||||||
| Other assets, net | 209 | 137 | ||||||
| Total assets | $ | 43,488 | $ | 32,114 | ||||
| Liabilities and stockholders’ equity | ||||||||
| Current liabilities: | ||||||||
| Accounts payable and accrued expenses | $ | 8,870 | $ | 5,278 | ||||
| Accrued compensation and related liabilities | 897 | 669 | ||||||
| Liabilities of discontinued operations | — | 245 | ||||||
| Total current liabilities | 9,767 | 6,192 | ||||||
| Contingent equity rights | 2,639 | 2,639 | ||||||
| Other liabilities | 35 | 35 | ||||||
| Total liabilities | 12,441 | 8,866 | ||||||
| Commitments and contingencies (Note 14) | ||||||||
| Stockholders’ equity: | ||||||||
| Preferred stock, $0.001 par value per share (5,000,000 shares authorized, no shares issued and outstanding) | — | — | ||||||
| Common stock, $0.001 par value per share (95,000,000 shares authorized, 71,102,899 and 61,521,483 shares issued, 71,022,951 and 61,441,535 shares outstanding at December 31, 2011 and 2010, respectively) | 71 | 62 | ||||||
| Additional paid-in capital | 401,220 | 365,307 | ||||||
| Treasury stock, at cost, 79,948 shares at December 31, 2011 and 2010, respectively | (357 | ) | (357 | ) | ||||
| Accumulated deficit | (369,887 | ) | (341,764 | ) | ||||
| Total stockholders’ equity | 31,047 | 23,248 | ||||||
| Total liabilities and stockholders’ equity | $ | 43,488 | $ | 32,114 | ||||
The accompanying notes are an integral part of the consolidated financial statements.
| F-2 |
Keryx Biopharmaceuticals, Inc.
Consolidated Statements of Operations for the Year Ended December 31,
(in thousands, except share and per share amounts)
| 2011 | 2010 | 2009 | ||||||||||
| Revenue: | ||||||||||||
| License revenue | $ | 5,000 | $ | — | $ | 21,616 | ||||||
| Other revenue | — | — | 3,575 | |||||||||
| Total revenue | 5,000 | — | 25,191 | |||||||||
| Operating expenses: | ||||||||||||
| Research and development: | ||||||||||||
| Non-cash compensation | 803 | 1,236 | 1,233 | |||||||||
| Other research and development | 26,209 | 13,728 | 7,372 | |||||||||
| Total research and development | 27,012 | 14,964 | 8,605 | |||||||||
| General and administrative: | ||||||||||||
| Non-cash compensation | 1,289 | 1,237 | 1,867 | |||||||||
| Other general and administrative | 5,448 | 5,014 | 4,904 | |||||||||
| Total general and administrative | 6,737 | 6,251 | 6,771 | |||||||||
| Total operating expenses | 33,749 | 21,215 | 15,376 | |||||||||
| Operating (loss) income | (28,749 | ) | (21,215 | ) | 9,815 | |||||||
| Interest and other income, net | 380 | 764 | 667 | |||||||||
| (Loss) income from continuing operations before income taxes | (28,369 | ) | (20,451 | ) | 10,482 | |||||||
| Income taxes | — | — | — | |||||||||
| (Loss) income from continuing operations | (28,369 | ) | (20,451 | ) | 10,482 | |||||||
| Gain from discontinued operations | 246 | 120 | 3 | |||||||||
| Net (loss) income | $ | (28,123 | ) | $ | (20,331 | ) | $ | 10,485 | ||||
| Basic net (loss) income per common share: | ||||||||||||
| Continuing operations | $ | (0.42 | ) | $ | (0.34 | ) | $ | 0.21 | ||||
| Discontinued operations | — | * | — | * | — | * | ||||||
| Basic net (loss) income per common share | $ | (0.42 | ) | $ | (0.34 | ) | $ | 0.21 | ||||
| Diluted net (loss) income per common share: | ||||||||||||
| Continuing operations | $ | (0.42 | ) | $ | (0.34 | ) | $ | 0.21 | ||||
| Discontinued operations | — | * | — | * | — | * | ||||||
| Diluted net (loss) income per common share | $ | (0.42 | ) | $ | (0.34 | ) | $ | 0.21 | ||||
| Weighted average shares used in computing basic net (loss) income per common share | 67,370,354 | 58,987,854 | 49,940,730 | |||||||||
| Weighted average shares used in computing diluted net (loss) income per common share | 67,370,354 | 58,987,854 | 50,498,982 | |||||||||
* Amount less than one cent.
The accompanying notes are an integral part of the consolidated financial statements.
| F-3 |
Keryx Biopharmaceuticals, Inc.
Consolidated Statements of Stockholders’
Equity and Comprehensive Loss (Income)
for the Years Ended December 31, 2011, 2010 and 2009
(in thousands, except share amounts)
| Additional | Accumulated | |||||||||||||||||||||||||||||||
| Common stock | paid-in | Treasury stock | other comp | Accumulated | ||||||||||||||||||||||||||||
| Shares | Amount | capital | Shares | Amount | income (loss) | deficit | Total | |||||||||||||||||||||||||
| Balance at December 31, 2008 | 47,729,507 | $ | 48 | $ | 330,738 | 79,948 | $ | (357 | ) | $ | - | $ | (331,918 | ) | $ | (1,489 | ) | |||||||||||||||
| Issuance of common stock in public offering (net of offering costs of $1,557) | 8,000,000 | 8 | 15,553 | 15,561 | ||||||||||||||||||||||||||||
| Issuance of common stock warrants in public offering | 2,877 | 2,877 | ||||||||||||||||||||||||||||||
| Issuance of common stock in connection with acquisition | 500,000 | 1 | 1,364 | 1,365 | ||||||||||||||||||||||||||||
| Issuance of restricted stock | 578,539 | - | * | - | * | |||||||||||||||||||||||||||
| Forfeiture of restricted stock | (361,742 | ) | (- | )* | (- | )* | ||||||||||||||||||||||||||
| Issuance of common stock in connection with exercise of warrants | 64,174 | - | * | - | * | - | * | |||||||||||||||||||||||||
| Issuance of common stock in connection with exercise of options | 50,000 | - | * | 18 | 18 | |||||||||||||||||||||||||||
| Compensation in respect of options and restricted stock granted to employees, directors and third-parties | 3,100 | 3,100 | ||||||||||||||||||||||||||||||
| Comprehensive income: | ||||||||||||||||||||||||||||||||
| Net income | 10,485 | 10,485 | ||||||||||||||||||||||||||||||
| Unrealized gain on long-term investment securities | 180 | 180 | ||||||||||||||||||||||||||||||
| Total comprehensive income | 10,665 | |||||||||||||||||||||||||||||||
| Balance at December 31, 2009 | 56,560,478 | $ | 57 | $ | 353,650 | 79,948 | $ | (357 | ) | $ | 180 | $ | (321,433 | ) | $ | 32,097 | ||||||||||||||||
| Issuance of restricted stock | 695,500 | 1 | 1 | |||||||||||||||||||||||||||||
| Forfeiture of restricted stock | (7,635 | ) | (- | )* | (- | )* | ||||||||||||||||||||||||||
| Issuance of common stock in connection with the exercise of warrants from public offering (net of offering costs of $452) | 2,908,000 | 3 | 7,302 | 7,305 | ||||||||||||||||||||||||||||
| Issuance of common stock in connection with the exercise of options | 1,365,140 | 1 | 1,883 | 1,884 | ||||||||||||||||||||||||||||
| Compensation in respect of options and restricted stock granted to employees, directors and third-parties | 2,472 | 2,472 | ||||||||||||||||||||||||||||||
| Comprehensive loss: | ||||||||||||||||||||||||||||||||
| Net loss | (20,331 | ) | (20,331 | ) | ||||||||||||||||||||||||||||
| Reduction of unrealized gain on long-term investment securities | (180 | ) | (180 | ) | ||||||||||||||||||||||||||||
| Total comprehensive loss | (20,511 | ) | ||||||||||||||||||||||||||||||
| Balance at December 31, 2010 | 61,521,483 | $ | 62 | $ | 365,307 | 79,948 | $ | (357 | ) | $ | — | $ | (341,764 | ) | $ | 23,248 | ||||||||||||||||
| Issuance of common stock in public offering (net of offering costs of $2,266) | 7,021,277 | 7 | 30,727 | 30,734 | ||||||||||||||||||||||||||||
| Issuance of restricted stock | 206,450 | - | * | - | * | |||||||||||||||||||||||||||
| Forfeiture of restricted stock | (28,338 | ) | (- | )* | (- | )* | ||||||||||||||||||||||||||
| Issuance of common stock in connection with the exercise of options | 2,382,027 | 2 | 3,094 | 3,096 | ||||||||||||||||||||||||||||
| Compensation in respect of options and restricted stock granted to employees, directors and third-parties | 2,092 | 2,092 | ||||||||||||||||||||||||||||||
| Comprehensive loss: | ||||||||||||||||||||||||||||||||
| Net loss | (28,123 | ) | (28,123 | ) | ||||||||||||||||||||||||||||
| Total comprehensive loss | (28,123 | ) | ||||||||||||||||||||||||||||||
| Balance at December 31, 2011 | 71,102,899 | $ | 71 | $ | 401,220 | 79,948 | $ | (357 | ) | $ | — | $ | (369,887 | ) | $ | 31,047 | ||||||||||||||||
* Amount less than one thousand dollars.
The accompanying notes are an integral part of the consolidated financial statements.
| F-4 |
Keryx Biopharmaceuticals, Inc.
Consolidated Statements of Cash Flows for the Year Ended December 31,
(in thousands)
| 2011 | 2010 | 2009 | ||||||||||
| CASH FLOWS FROM OPERATING ACTIVITIES | ||||||||||||
| Net (loss) income | $ | (28,123 | ) | $ | (20,331 | ) | $ | 10,485 | ||||
| Gain from discontinued operations | 246 | 120 | 3 | |||||||||
| (Loss) income from continuing operations | (28,369 | ) | (20,451 | ) | 10,482 | |||||||
| Adjustments to reconcile (loss) income from continuing operations to cash flows used in operating activities of continuing operations: | ||||||||||||
| Stock compensation expense | 2,092 | 2,473 | 3,100 | |||||||||
| Depreciation and amortization | 47 | 60 | 92 | |||||||||
| Loss (gain) on sale of investment securities | — | 82 | (173 | ) | ||||||||
| Impairment of investment securities | — | 32 | 68 | |||||||||
| Changes in assets and liabilities, net of effects of acquisitions: | ||||||||||||
| (Increase) decrease in other current assets | (334 | ) | 1,321 | (1,013 | ) | |||||||
| (Increase) decrease in accrued interest receivable | (7 | ) | 66 | (41 | ) | |||||||
| Increase in security deposits | (51 | ) | (50 | ) | — | |||||||
| (Increase) decrease in other assets | (21 | ) | (6 | ) | 3 | |||||||
| Increase in accounts payable and accrued expenses | 3,592 | 376 | 388 | |||||||||
| Increase (decrease) in accrued compensation and related liabilities | 228 | (86 | ) | 259 | ||||||||
| Decrease in other liabilities | — | (15 | ) | (68 | ) | |||||||
| Decrease in deferred revenue | — | — | (18,616 | ) | ||||||||
| Net cash used in operating activities of continuing operations | (22,823 | ) | (16,198 | ) | (5,519 | ) | ||||||
| Net cash provided by (used in) operating activities of discontinued operations | 1 | (10 | ) | 3 | ||||||||
| Net cash used in operating activities | (22,822 | ) | (16,208 | ) | (5,516 | ) | ||||||
| CASH FLOWS FROM INVESTING ACTIVITIES | ||||||||||||
| Purchases of property, plant and equipment | (57 | ) | (23 | ) | (4 | ) | ||||||
| Investment in held-to-maturity short-term securities | (9,941 | ) | (18,366 | ) | (17,593 | ) | ||||||
| Proceeds from maturity of held-to-maturity short-term securities | 5,830 | 35,814 | 2,343 | |||||||||
| Proceeds from sale of available-for-sale long-term securities | — | 1,620 | 5,557 | |||||||||
| Net cash (used in) provided by investing activities | (4,168 | ) | 19,045 | (9,697 | ) | |||||||
| CASH FLOWS FROM FINANCING ACTIVITIES | ||||||||||||
| Proceeds from public offerings, net | 30,734 | — | 18,438 | |||||||||
| Proceeds from exercise of warrants from public offering, net | — | 7,305 | — | |||||||||
| Proceeds from exercise of options | 3,096 | 1,884 | 18 | |||||||||
| Net cash provided by financing activities | 33,830 | 9,189 | 18,456 | |||||||||
| NET INCREASE IN CASH AND CASH EQUIVALENTS | 6,840 | 12,026 | 3,243 | |||||||||
| Cash and cash equivalents at beginning of year | 28,412 | 16,386 | 13,143 | |||||||||
| CASH AND CASH EQUIVALENTS AT END OF YEAR | $ | 35,252 | $ | 28,412 | $ | 16,386 | ||||||
| NON-CASH TRANSACTIONS | ||||||||||||
| Issuance of common stock in connection with contingent equity rights | $ | — | $ | — | $ | 1,365 | ||||||
| Issuance of warrants to placement agent in public offering | — | — | 100 | |||||||||
The accompanying notes are an integral part of the consolidated financial statements.
| F-5 |
Keryx Biopharmaceuticals, Inc.
Notes to the Consolidated Financial Statements
Unless the context requires otherwise, references in this report to “Keryx,” “Company,” “we,” “us” and “our” refer to Keryx Biopharmaceuticals, Inc. and our subsidiaries.
NOTE 1 - ORGANIZATION AND SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES
DESCRIPTION OF BUSINESS
We are a biopharmaceutical company focused on the acquisition, development and commercialization of medically important pharmaceutical products for the treatment of cancer and renal disease. We own a 100% interest in each of ACCESS Oncology, Inc. (“ACCESS Oncology”), Neryx Biopharmaceuticals, Inc., and Accumin Diagnostics, Inc. (“ADI”), all U.S. corporations incorporated in the State of Delaware. Most of our biopharmaceutical development and substantially all of our administrative operations during 2011, 2010 and 2009 were conducted in the U.S.
LIQUIDITY AND CAPITAL RESOURCES
Except for 2009, we have incurred substantial operating losses since our inception, and expect to continue to incur operating losses for the foreseeable future and may never become profitable. As of December 31, 2011, we have an accumulated deficit of $369.9 million.
Our major sources of cash have been proceeds from various private placements of equity securities, public offerings of our common stock, option and warrant exercises, interest income, and from the upfront and milestone payments from our Sublicense Agreement with Japan Tobacco Inc. (“JT”) and Torii Pharmaceutical Co., Ltd. (“Torii”) and miscellaneous payments from our other prior licensing activities. We have not yet commercialized any of our drug candidates and cannot be sure if we will ever be able to do so. Even if we commercialize one or more of our drug candidates, we may not become profitable. Our ability to achieve profitability depends on a number of factors, including our ability to obtain regulatory approval for our drug candidates, successfully complete any post-approval regulatory obligations and successfully commercialize our drug candidates alone or in partnership. We may continue to incur substantial operating losses even if we begin to generate revenues from our drug candidates, if approved.
Depending on the outcome of our Phase 3 study for KRX-0401 in refractory advanced colorectal cancer, our operating cash requirements may vary dramatically. In the event of a negative outcome, we currently anticipate that our cash, cash equivalents and investment securities as of December 31, 2011, exclusive of our anticipated milestone payments to be received, are sufficient to fund our anticipated operating cash requirements for approximately 18 to 20 months from December 31, 2011. The actual amount of cash that we will need to operate is subject to many factors, including, but not limited to, the timing, design and conduct of clinical trials for our drug candidates. We are dependent upon significant financing to provide the cash necessary to execute our current operations, including the commercialization of any of our drug candidates.
We currently have two shelf registration statements on Form S-3 filed and declared effective by the SEC, providing for the offering of up to $79 million of common stock and warrants in the aggregate. We may offer the securities under our shelf registration statements from time to time in response to market conditions or other circumstances if we believe such a plan of financing is in our best interests and the best interests of our stockholders. We believe that these shelf registration statements provide us with the flexibility to efficiently raise additional capital to finance our operations as needed.
Our common stock is listed on the NASDAQ Capital Market and trades under the symbol “KERX.”
2009 MANAGEMENT CHANGES
On April 23, 2009, our Board of Directors voted to terminate the employment of Michael S. Weiss as our Chairman and Chief Executive Officer. Under the terms of Mr. Weiss’ employment agreement with us dated December 23, 2002, as amended on December 26, 2008 (the “Employment Agreement”), he remained an employee for a period of 90 days; however, during such notice period, he did not serve as our Chairman and Chief Executive Officer.
| F-6 |
The Employment Agreement provided that Mr. Weiss was entitled to receive as severance (i) one year's base salary, (ii) payment of his salary during the 90 days following formal notice of termination of employment, and (iii) a pro rata bonus for the year of termination. In addition, under the terms of the Employment Agreement, all of Mr. Weiss’ outstanding stock options and shares of restricted stock vested, and all stock options remained exercisable for two years following termination. In the year ended December 31, 2009, we recorded approximately $833,000 of expense, in other general and administrative expenses, associated with the cash severance, pro rata bonus and salary during the notice period (of which approximately $245,000 was included in accrued compensation at December 31, 2009 and was paid in January 2010). Additionally, in the year ended December 31, 2009, we recorded approximately $660,000 in non-cash compensation expense (general and administrative) associated with the equity modifications of Mr. Weiss’ outstanding stock options and shares of restricted stock.
On May 20, 2009, we announced that we appointed Ron Bentsur as Chief Executive Officer. The terms of Mr. Bentsur’s employment are set forth in an employment agreement with us dated September 14, 2009, as amended on January 13, 2012. As an inducement to his employment, on May 20, 2009, we granted Mr. Bentsur options to purchase 600,000 shares of our common stock at an exercise price of $0.35, the fair market value of the stock as of the date of grant. The options will vest in equal annual installments over a four-year period or upon an earlier change in control of the Company. The options were granted as an inducement award and were not issued under our 2007 Incentive Plan.
On June 16, 2009, Ron Bentsur was appointed to our Board of Directors by unanimous vote of the Board of Directors, and Michael P. Tarnok was appointed Chairman of the Board by unanimous vote of the Board of Directors.
RECENTLY ISSUED ACCOUNTING STANDARDS
In September 2011, the FASB issued ASU 2011-08, “Intangibles — Goodwill and Other,” which amends current guidance to allow a company to first assess qualitative factors to determine whether it is necessary to perform the two-step quantitative goodwill impairment test. The amendment also improves previous guidance by expanding upon the examples of events and circumstances that an entity should consider between annual impairment tests in determining whether it is more likely than not that the fair value of a reporting unit is less than its carrying amount. ASU 2011-08 is effective for annual and interim goodwill impairment tests performed for fiscal years beginning after December 15, 2011, which for us means January 1, 2012. We do not expect that the adoption of ASU 2011-08 will have an impact upon our financial position and results of operations.
In June 2011, the FASB issued ASU No. 2011-05, “Comprehensive Income (Topic 220).” This newly issued accounting standard (1) eliminates the option to present the components of other comprehensive income as part of the statement of changes in stockholders’ equity; (2) requires the consecutive presentation of the statement of net income and other comprehensive income; and (3) requires an entity to present reclassification adjustments on the face of the financial statements from other comprehensive income to net income. The amendments in this ASU do not change the items that must be reported in other comprehensive income or when an item of other comprehensive income must be reclassified to net income nor do the amendments affect how earnings per share is calculated or presented. This ASU is required to be applied retrospectively and is effective for fiscal years and interim periods within those years beginning after December 15, 2011, which for us means January 1, 2012. As this accounting standard only requires enhanced disclosure, the adoption of this standard will not impact our financial position or results of operations.
PRINCIPLES OF CONSOLIDATION
The consolidated financial statements include our financial statements and those of our wholly-owned subsidiaries. Intercompany transactions and balances have been eliminated in consolidation.
| F-7 |
USE OF ESTIMATES
The preparation of financial statements in conformity with U.S. generally accepted accounting principles (“GAAP”) requires management to make estimates and judgments that affect the reported amounts of assets and liabilities and the disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenues and expenses during the applicable reporting period. Actual results could differ from those estimates. Such differences could be material to the financial statements.
CASH AND CASH EQUIVALENTS
We treat liquid investments with original maturities of less than three months when purchased as cash and cash equivalents.
INVESTMENT SECURITIES
Investment securities at December 31, 2011 consist of short-term government securities. Investment securities at December 31, 2010 consisted of a bank deposit. We classify our short-term and long-term debt securities as held-to-maturity. Held-to-maturity securities are those securities in which we have the ability and intent to hold the security until maturity. Held-to-maturity securities are recorded at amortized cost, adjusted for the amortization or accretion of premiums or discounts. Premiums and discounts are amortized or accreted over the life of the related held-to-maturity security as an adjustment to yield using the effective interest method. Available-for-sale investment securities (which were comprised of auction rate securities) are recorded at fair value. See Note 4 – Fair Value Measurements.
A decline in the market value of any investment security below cost, that is deemed to be other than temporary, results in a reduction in the carrying amount to fair value. The impairment is charged to operations and a new cost basis for the security is established. Other-than-temporary impairment charges are included in interest and other income, net, and unrealized gains, if determined to be temporary, are included in accumulated other comprehensive income in stockholders’ equity. Dividend and interest income are recognized when earned.
PROPERTY, PLANT AND EQUIPMENT
Property, plant and equipment are stated at historical cost. Depreciation is computed using the straight-line method over the estimated useful lives of the assets:
| Estimated useful life (years) | ||||
| Office furniture and equipment | 3-7 | |||
| Computers, software and related equipment | 3 | |||
Leasehold improvements are amortized over the shorter of their useful life or the remaining term of the lease exclusive of renewal options.
PATENT COSTS
We expense patent maintenance costs as incurred. We have classified our patent expenses in other general and administrative.
REVENUE RECOGNITION
We recognize license revenue in accordance with the revenue recognition guidance of the FASB Accounting Standards Codification, or the Codification. We analyze each element of our licensing agreement to determine the appropriate revenue recognition. The terms of the license agreement may include payments to us of non-refundable up-front license fees, milestone payments if specified objectives are achieved, and/or royalties on product sales. We recognize revenue from upfront payments over the period of significant involvement under the related agreements unless the fee is in exchange for products delivered or services rendered that represent the culmination of a separate earnings process and no further performance obligation exists under the contract. We recognize milestone payments as revenue upon the achievement of specified milestones only if (1) the milestone payment is non-refundable, (2) substantive effort is involved in achieving the milestone, (3) the amount of the milestone is reasonable in relation to the effort expended or the risk associated with achievement of the milestone, and (4) the milestone is at risk for both parties. If any of these conditions are not met, we defer the milestone payment and recognize it as revenue over the estimated period of performance under the contract (see Note 9 – License Agreements).
| F-8 |
Other revenue consists of fees and payments arising from technology transfer, termination and settlement agreements related to our prior license agreements. Other revenues are recognized at the time such fees and payments are earned. See Note 9 – License Agreements.
RESEARCH AND DEVELOPMENT COSTS
Research and development costs are expensed as incurred. Nonrefundable advance payments for goods or services that will be used or rendered for future research and development activities are deferred and amortized over the period that the goods are delivered or the related services are performed, subject to an assessment of recoverability. We make estimates of costs incurred in relation to external clinical research organizations, or CROs, and clinical site costs. We analyze the progress of clinical trials, including levels of patient enrollment, invoices received and contracted costs when evaluating the adequacy of the amount expensed and the related prepaid asset and accrued liability. Significant judgments and estimates must be made and used in determining the accrued balance and expense in any accounting period. We review and accrue CRO expenses and clinical trial study expenses based on work performed and rely upon estimates of those costs applicable to the stage of completion of a study. Accrued CRO costs are subject to revisions as such trials progress to completion. Revisions are charged to expense in the period in which the facts that give rise to the revision become known. With respect to clinical site costs, the financial terms of these agreements are subject to negotiation and vary from contract to contract. Payments under these contracts may be uneven, and depend on factors such as the achievement of certain events, the successful recruitment of patients, the completion of portions of the clinical trial or similar conditions. The objective of our policy is to match the recording of expenses in our financial statements to the actual services received and efforts expended. As such, expense accruals related to clinical site costs are recognized based on our estimate of the degree of completion of the event or events specified in the specific clinical study or trial contract.
INCOME TAXES
Income taxes are accounted for under the asset and liability method. Deferred tax assets and liabilities are recognized for the future tax consequences attributable to temporary differences between the financial statement carrying amounts of existing assets and liabilities and their respective tax bases, operating losses and tax credit carryforwards. Deferred tax assets and liabilities are measured using enacted tax rates expected to apply to taxable income in the years in which those temporary differences are expected to be recovered or settled. The effect on deferred tax assets and liabilities of a change in tax rates is recognized in operations in the period that includes the enactment date. If the likelihood of realizing the deferred tax assets or liability is less than “more likely than not,” a valuation allowance is then created.
We, and our subsidiaries, file income tax returns in the U.S. federal jurisdiction and in various states. We have tax net operating loss carryforwards that are subject to examination for a number of years beyond the year in which they were generated for tax purposes. Since a portion of these net operating loss carryforwards may be utilized in the future, many of these net operating loss carryforwards will remain subject to examination.
We are continuing our practice of recognizing interest and penalties related to uncertain income tax positions in income tax expense.
STOCK - BASED COMPENSATION
We recognize all share-based payments to employees and to non-employee directors as compensation for service on our board of directors as compensation expense in the consolidated financial statements based on the fair values of such payments. Stock-based compensation expense recognized each period is based on the value of the portion of share-based payment awards that is ultimately expected to vest during the period. Forfeitures are estimated at the time of grant and revised, if necessary, in subsequent periods if actual forfeitures differ from those estimates.
| F-9 |
For share-based payments to consultants and other third-parties, compensation expense is determined at the “measurement date.” The expense is recognized over the vesting period of the award. Until the measurement date is reached, the total amount of compensation expense remains uncertain. We record compensation expense based on the fair value of the award at the reporting date. The awards to consultants and other third-parties are then revalued, or the total compensation is recalculated based on the then current fair value, at each subsequent reporting date.
BASIC AND DILUTED NET (LOSS) INCOME PER COMMON SHARE
Basic net loss or income per share is based upon the weighted average number of common shares outstanding during the period. Diluted net loss or income per share is based upon the weighted average number of common shares outstanding during the period, plus the effect of additional weighted average common equivalent shares outstanding during the period when the effect of adding such shares is dilutive. Common equivalent shares result from the assumed exercise of outstanding stock options and warrants (the proceeds of which are then assumed to have been used to repurchase outstanding stock using the treasury stock method). In addition, the assumed proceeds under the treasury stock method include the average unrecognized compensation expense of stock options that are in-the-money. This results in the “assumed” buyback of additional shares, thereby reducing the dilutive impact of stock options and warrants. Common equivalent shares have not been included in the net loss per share calculations for the years ended December 31, 2011 and 2010, because the effect of including them would have been anti-dilutive.
Basic and diluted net (loss) income per share were determined as follows:
| For the year ended December 31 | ||||||||||||
| (in thousands, except share and per share amounts) | 2011 | 2010 | 2009 | |||||||||
| Basic: | ||||||||||||
| (Loss) income from continuing operations | $ | (28,369 | ) | $ | (20,451 | ) | $ | 10,482 | ||||
| Gain from discontinued operations | 246 | 120 | 3 | |||||||||
| Net (loss) income | $ | (28,123 | ) | $ | (20,331 | ) | $ | 10,485 | ||||
| Weighted average shares outstanding | 67,370,354 | 58,987,854 | 49,940,730 | |||||||||
| Basic net (loss) income per common share: | ||||||||||||
| Continuing operations | $ | (0.42 | ) | $ | (0.34 | ) | $ | 0.21 | ||||
| Discontinued operations | — | * | — | * | — | * | ||||||
| Basic net (loss) income per common share | $ | (0.42 | ) | $ | (0.34 | ) | $ | 0.21 | ||||
| Diluted: | ||||||||||||
| (Loss) income from continuing operations | $ | (28,369 | ) | $ | (20,451 | ) | $ | 10,482 | ||||
| Gain from discontinued operations | 246 | 120 | 3 | |||||||||
| Net (loss) income | $ | (28,123 | ) | $ | (20,331 | ) | $ | 10,485 | ||||
| Weighted average shares outstanding | 67,370,354 | 58,987,854 | 49,940,730 | |||||||||
| Effect of dilutive options and warrants | — | — | 558,252 | |||||||||
| Weighted average shares outstanding assuming dilution | 67,370,354 | 58,987,854 | 50,498,982 | |||||||||
| Diluted net (loss) income per common share: | ||||||||||||
| Continuing operations | $ | (0.42 | ) | $ | (0.34 | ) | $ | 0.21 | ||||
| Discontinued operations | — | * | — | * | — | * | ||||||
| Diluted net (loss) income per common share | $ | (0.42 | ) | $ | (0.34 | ) | $ | 0.21 | ||||
* Amount less than one cent.
We did not include the following securities in the computation of diluted net (loss) income per common share in the table above because the securities were anti-dilutive during the periods presented:
| For the year ended December 31 | ||||||||||||
| 2011 | 2010 | 2009 | ||||||||||
| Stock options | 3,517,000 | 7,638,403 | 8,417,920 | |||||||||
| Warrants | — | — | 2,908,000 | |||||||||
| Total | 3,517,000 | 7,638,403 | 11,325,920 | |||||||||
| F-10 |
COMPREHENSIVE (LOSS) INCOME
Comprehensive (loss) income is composed of net (loss) income and other comprehensive (loss) income. Other comprehensive (loss) income, for the years ended December 31, 2010 and 2009, is comprised of unrealized losses or gains on our available-for-sale long-term investment securities that are excluded from net (loss) income and reported separately in stockholders’ equity.
SEGMENT REPORTING
Following the discontinuation of the Diagnostic segment in September 2008 and the Services segment in December 2011, we have determined that we operate in only one reportable segment: the Products segment.
ACQUISITIONS
We adopted ASC Topic 805, Business Combinations, as of January 1, 2009. The adoption of ASC Topic 805 was effective on a prospective basis. Prior to the adoption of ASC Topic 805, we accounted for acquired businesses using the purchase method of accounting which required that the assets acquired and liabilities assumed be recorded at the date of acquisition at their respective fair values. Our consolidated financial statements and results of operations through 2008 reflected an acquired business after the completion of the acquisition and were not retroactively restated. The cost to acquire a business, including transaction costs, was allocated to the underlying net assets of the acquired business in proportion to their respective fair values. Any excess of the purchase price over the estimated fair values of the net assets acquired was recorded as goodwill. Any excess of the net assets acquired over the purchase price represented negative goodwill.
IMPAIRMENT
Long lived assets are reviewed for an impairment loss when circumstances indicate that the carrying value of long-lived tangible and intangible assets with finite lives may not be recoverable. Management’s policy in determining whether an impairment indicator exists, a triggering event, comprises measurable operating performance criteria as well as qualitative measures. If an analysis is necessitated by the occurrence of a triggering event, we make certain assumptions in determining the impairment amount. Recoverability of assets to be held and used is measured by a comparison of the carrying amount of an asset to future cash flows expected to be generated by the asset or used in its disposal. If the carrying amount of an asset exceeds its estimated future cash flows, an impairment charge is recognized.
Goodwill is reviewed for impairment annually, or when events arise that could indicate that an impairment exists. We test for goodwill impairment using a two-step process. The first step compares the fair value of the reporting unit with the unit's carrying value, including goodwill. When the carrying value of the reporting unit is greater than fair value, the unit’s goodwill may be impaired, and the second step must be completed to measure the amount of the goodwill impairment charge, if any. In the second step, the implied fair value of the reporting unit’s goodwill is compared with the carrying amount of the unit’s goodwill. If the carrying amount is greater than the implied fair value, the carrying value of the goodwill must be written down to its implied fair value. As of December 31, 2009, 2010 and 2011, management conducted its annual assessments of goodwill and concluded that there were no impairments. We will continue to perform impairment tests annually, at December 31, and whenever events or changes in circumstances suggest that the carrying value of an asset may not be recoverable.
CONCENTRATIONS OF CREDIT RISK
We do not have significant off-balance-sheet risk or credit risk concentrations. We maintain our cash and cash equivalents and held-to-maturity investments with multiple financial institutions that invest in investment-grade securities with average maturities of less than twelve months. See Note 3 – Investment Securities and Note 4 – Fair Value Measurements.
| F-11 |
NOTE 2 – CASH AND CASH EQUIVALENTS
| (in thousands) | December 31, 2011 | December 31, 2010 | ||||||
| Money market funds | $ | 16,347 | $ | 22,743 | ||||
| Checking and bank deposits | 18,905 | 5,669 | ||||||
| Total | $ | 35,252 | $ | 28,412 | ||||
Cash is maintained in Federal Deposit Insurance Corporation (“FDIC”) insured accounts at credit qualified financial institutions. At times, such amounts may exceed the FDIC insurance limits. In October 2008, the FDIC increased its insurance from $100,000 per depositor to $250,000, and to an unlimited amount for non-interest bearing accounts. The coverage increase, which is temporary, extends through December 31, 2013 for interest bearing accounts and December 31, 2012 for non-interest bearing accounts. At December 31, 2011, uninsured cash balances totaled approximately $32.8 million.
NOTE 3 - INVESTMENT SECURITIES
We record our investments as either held-to-maturity or available-for-sale. Held-to-maturity investments are recorded at amortized cost. Available-for-sale investment securities are recorded at fair value (see Note 4 – Fair Value Measurements). Other-than-temporary impairment charges are included in interest and other income, net, and unrealized gains (losses), if determined to be temporary, are included in accumulated other comprehensive income (loss) in stockholders’ equity.
The following tables summarize our investment securities at December 31, 2011 and December 31, 2010:
| December 31, 2011 | ||||||||||||||||
| (in thousands) | Amortized cost, as adjusted | Gross unrealized holding gains | Gross unrealized holding losses | Estimated fair value | ||||||||||||
| Short-term investments (held-to-maturity): | ||||||||||||||||
| Obligations of domestic governmental agencies (mature April 2012) | $ | 4,011 | $ | 2 | $ | — | $ | 4,013 | ||||||||
| Bank deposit (matures February 2012) | 200 | — | — | 200 | ||||||||||||
| Total short-term investment securities | $ | 4,211 | $ | 2 | $ | — | $ | 4,213 | ||||||||
| December 31, 2010 | ||||||||||||||||
| (in thousands) | Amortized cost, as adjusted | Gross unrealized holding gains | Gross unrealized holding losses | Estimated fair value | ||||||||||||
| Short-term investments (held-to-maturity): | ||||||||||||||||
| Bank deposit (matured January 2011) | $ | 100 | — | — | $ | 100 | ||||||||||
| Total short-term investment securities | $ | 100 | $ | — | $ | — | $ | 100 | ||||||||
NOTE 4 – FAIR VALUE MEASUREMENTS
We measure certain financial assets and liabilities at fair value on a recurring basis in the financial statements. The hierarchy ranks the quality and reliability of inputs, or assumptions, used in the determination of fair value and requires financial assets and liabilities carried at fair value to be classified and disclosed in one of the following three categories:
| · | Level 1 – quoted prices in active markets for identical assets and liabilities; |
| · | Level 2 – inputs other than Level 1 quoted prices that are directly or indirectly observable; and |
| · | Level 3 – unobservable inputs that are not corroborated by market data. |
| F-12 |
In the year ended December 31, 2010, we sold our last remaining auction rate security investment for $1.6 million, representing a loss of $82,000. In the year ended December 31, 2009, we sold four auction rate security investments for $5.6 million, representing a gain of $173,000. Auction rate securities were recorded at their fair value and classified as long-term investments.
Quarterly, we assessed the fair value of our auction rate securities portfolio. As a result of this valuation process, as described below, we reported an other comprehensive loss of $180,000 and an other comprehensive gain of $180,000, in the years ended December 31, 2010 and 2009, respectively, for the temporary unrealized loss and gain, respectively, related to the estimated fair value of our last auction rate security, and reported other-than-temporary impairment charges and net realized gains and losses in interest and other income, net, as per the following table.
| For the year ended December 31 | ||||||||||||
| (in thousands) | 2011 | 2010 | 2009 | |||||||||
| Impairment of investment securities | $ | — | $ | (32 | ) | $ | (68 | ) | ||||
| Net realized loss | — | (82 | ) | — | ||||||||
| Net realized gain | — | — | 173 | |||||||||
| $ | — | $ | (114 | ) | $ | 105 | ||||||
The valuation methods used to estimate the auction rate securities’ fair value were (1) a discounted cash flow model, where the expected cash flows of the auction rate securities are discounted to the present using a yield that incorporates compensation for illiquidity, and (2) a market comparables method, where the auction rate securities are valued based on indications, from the secondary market, of what discounts buyers demand when purchasing similar auction rate securities. The valuation also included assessments of the underlying structure of each security, expected cash flows, discount rates, credit ratings, workout periods, and overall capital market liquidity. These assumptions, assessments and the interpretations of relevant market data are subject to uncertainties, are difficult to predict and require significant judgment. The use of different assumptions, applying different judgment to inherently subjective matters and changes in future market conditions could result in significantly different estimates of fair value of our past investments in auction rate securities. In addition, the estimated fair value of the auction rate securities may differ from the values that would have been used had a ready market existed, and the differences could be material to our consolidated financial statements.
We review investment securities for impairment and to determine the classification of the impairment as temporary or other-than-temporary. Losses are recognized in our consolidated statement of operations when a decline in fair value is determined to be other-than-temporary. We review our investments on an ongoing basis for indications of possible impairment. Once identified, the determination of whether the impairment is temporary or other-than-temporary requires significant judgment. We believe that the impairment charges related to our auction rate securities investments were other-than-temporary. The primary factors we considered in classifying impairments related to these securities included the extent and time the fair value of each investment had been below cost and our ability to hold such investment to maturity.
The following table provides the fair value measurements of applicable financial assets as of December 31, 2011 and 2010:
| Financial assets at fair value as of December 31, 2011 | ||||||||||||
| (in thousands) | Level 1 | Level 2 | Level 3 | |||||||||
| Money market funds (1) | $ | 16,347 | $ | — | $ | — | ||||||
| Obligations of domestic governmental agencies (held-to-maturity) (2) | 4,011 | — | — | |||||||||
| Bank deposits (held-to-maturity) | 200 | — | — | |||||||||
| Total | $ | 20,558 | $ | — | $ | — | ||||||
| Financial assets at fair value as of December 31, 2010 | ||||||||||||
| (in thousands) | Level 1 | Level 2 | Level 3 | |||||||||
| Money market funds (1) | $ | 22,743 | $ | — | $ | — | ||||||
| Bank deposits (held-to-maturity) | 100 | — | — | |||||||||
| Total | $ | 22,843 | $ | — | $ | — | ||||||
| (1) | Included in cash and cash equivalents on our consolidated balance sheet. The carrying amount of money market funds is a reasonable estimate of fair value. |
| (2) | Amortized cost approximates fair value. |
| F-13 |
The following table summarizes the change in carrying value associated with Level 3 financial assets for the years ended December 31, 2010 and 2011:
| (in thousands) | Available-for-sale long-term investments | |||
| Balance at December 31, 2009 | $ | 1,914 | ||
| Total impairment charges included in net (loss) income | (32 | ) | ||
| Sale of security | (1,620 | ) | ||
| Realized loss on sale of security | (82 | ) | ||
| Other comprehensive loss (reduction of temporary unrealized gain) | (180 | ) | ||
| Balance at December 31, 2010 | $ | — | ||
| Balance at December 31, 2011 | $ | — | ||
NOTE 5 - PROPERTY, PLANT AND EQUIPMENT
| (in thousands) | December 31, 2011 | December 31, 2010 | ||||||
| Leasehold improvements | $ | 20 | $ | 20 | ||||
| Office furniture and equipment | 329 | 315 | ||||||
| Computers, software and related equipment | 506 | 463 | ||||||
| 855 | 798 | |||||||
| Accumulated depreciation and amortization | (788 | ) | (741 | ) | ||||
| Net book value | $ | 67 | $ | 57 | ||||
Depreciation expense for the years ended December 31, 2011, 2010 and 2009 was approximately $47,000, $60,000 and $92,000, respectively. The following table summarizes depreciation expense for the years ended December 31, 2011, 2010 and 2009.
| For the year ended December 31 | ||||||||||||
| (in thousands) | 2011 | 2010 | 2009 | |||||||||
| Depreciation expense: | ||||||||||||
| Research and development | 28 | 36 | 55 | |||||||||
| General and administrative | 19 | 24 | 37 | |||||||||
| Total | $ | 47 | $ | 60 | $ | 92 | ||||||
NOTE 6 – GOODWILL
On April 6, 2006, ADI, our wholly-owned subsidiary, completed the acquisition of AccuminTM, a novel, patent protected, diagnostic for the direct measurement of total, intact urinary albumin, from AusAm Biotechnologies, Inc. The purchase price of Accumin was $3,996,000. We accounted for the ADI transaction as a purchase. The excess of the purchase price over the net assets acquired in the ADI transaction represented goodwill of approximately $3,208,000, which was allocated to our Products segment based on the proposed synergies with our then existing drug pipeline activities. In September 2008, we terminated our license agreement related to the ADI product and ceased all operations related to the Diagnostic segment. See Note 8 – Discontinued Operations.
NOTE 7 - OTHER ASSETS
| (in thousands) | December 31, 2011 | December 31, 2010 | ||||||
| Patents and other intangible assets | $ | 352 | $ | 352 | ||||
| Deposits | 163 | 112 | ||||||
| Deferred registration fees | 46 | 25 | ||||||
| 561 | 489 | |||||||
| Accumulated amortization | (352 | ) | (352 | ) | ||||
| $ | 209 | $ | 137 | |||||
There were no amortization expenses for the years ended December 31, 2011, 2010 and 2009. We do not expect to record amortization expenses going forward, as all intangible assets are fully amortized.
| F-14 |
NOTE 8 – DISCONTINUED OPERATIONS
In December 2011, we ceased the operations of Online Collaborative Oncology Group, which was providing clinical trial management and site recruitment services and ceased all operations related to the Services segment. In September 2008, we terminated the license agreement related to the ADI product and ceased all operations related to our Diagnostic segment. The results of our Services and Diagnostic segments and the related financial positions have been reflected as discontinued operations in the consolidated financial statements. The consolidated financial statements have been reclassified to conform to discontinued operations presentation for all historical periods presented.
For the years ended December 31, 2011 and 2010, we recorded reversals of previously recorded estimated liabilities associated with our discontinued operations of $246,000 and $120,000, respectively. Summarized selected financial information for discontinued operations are as follows:
| For the year ended December 31 | ||||||||||||
| (in thousands) | 2011 | 2010 | 2009 | |||||||||
| Service revenue | $ | 156 | $ | — | $ | 3 | ||||||
| Operating expenses: | ||||||||||||
| Cost of services | (90 | ) | — | — | ||||||||
| Selling, general and administrative | — | (120 | ) | — | ||||||||
| Total operating income | 246 | 120 | 3 | |||||||||
| Gain from discontinued operations | $ | 246 | $ | 120 | $ | 3 | ||||||
The assets and liabilities of discontinued operations are stated separately on our accompanying consolidated balance sheets. The major assets and liabilities categories are as follows:
| (in thousands) | December 31, 2011 | December 31, 2010 | ||||||
| Assets | ||||||||
| Assets of discontinued operations | $ | — | $ | — | ||||
| Liabilities | ||||||||
| Accounts payable and accrued expenses | $ | — | $ | 89 | ||||
| Deferred revenue | — | 156 | ||||||
| Liabilities of discontinued operations | $ | — | $ | 245 | ||||
NOTE 9 - LICENSE AGREEMENTS
In September 2007, we entered into a Sublicense Agreement with JT and Torii, under which JT and Torii obtained the exclusive sublicense rights for the development and commercialization of ferric citrate in Japan, which is being developed in the U.S. under the trade name Zerenex. JT and Torii are responsible for the future development and commercialization costs in Japan. Effective as of June 8, 2009, we entered into an Amended and Restated Sublicense Agreement (the “Revised Agreement”) with JT and Torii, which, among other things, provided for the elimination of all significant on-going obligations under the sublicense agreement. Accordingly, in accordance with our revenue recognition policies, all remaining deferred revenue pertaining to this sublicense was recognized in the year ended December 31, 2009.
| F-15 |
Prior to the Revised Agreement, an upfront payment of $12.0 million, which was received in October 2007, was being recognized as license revenue on a straight-line basis over the life of the agreement, which is through the expiration of the last-to-expire patent covered by the agreement in 2023, and represented the estimated period over which we had certain significant ongoing responsibilities under the original sublicense agreement. An additional milestone payment of $8.0 million, for the achievement of certain milestones reached in March 2008, was received in April 2008, and was being recognized as license revenue on a straight-line basis over the life of the original agreement, as discussed above. As a result of the signing of the Revised Agreement, as discussed above, the unamortized portion of the upfront payment of $12.0 million and the additional milestone payment of $8.0 million, approximately $18.0 million, was recognized in the year ended December 31, 2009.
In March 2009, JT and Torii informed us that they had initiated a Phase 2 clinical study of ferric citrate in Japan, which triggered a $3.0 million non-refundable milestone payment, which we received in March 2009. As a result, we recorded license revenue of $3.0 million in accordance with our revenue recognition policy, which was included in the year ended December 31, 2009.
In April 2011, JT and Torii commenced a Phase 3 clinical program of ferric citrate in Japan. Under the terms of the license agreement with JT and Torii, we received a non-refundable milestone payment of $5.0 million in April 2011 for the achievement of the Phase 3 milestone. As a result, we recorded license revenue of $5.0 million in accordance with our revenue recognition policy, which is included in the year ended December 31, 2011.
We may receive up to an additional $72.0 million in payments upon the achievement of pre-specified milestones. In addition, upon commercialization, JT and Torii will make royalty payments to us on net sales of ferric citrate in Japan.
In July 2009, we settled a dispute with Alfa Wassermann S.p.A. over issues arising from the terminated license agreement for Sulonex (sulodexide). Under the terms of the settlement agreement, Alfa Wassermann paid us $3,500,000 (of which $2,750,000 was received in July 2009, and $750,000 was received in July 2010), and we were required to deliver to Alfa Wassermann all of our data, information and other intellectual property related to Sulonex.
NOTE 10 – CONTINGENT EQUITY RIGHTS
On February 5, 2004, we acquired ACCESS Oncology, a related party, for a purchase price of approximately $19,502,000. The purchase price included our assumption of certain liabilities of ACCESS Oncology equal to approximately $8,723,000, the issuance of shares of our common stock valued at approximately $6,325,000, contingent equity rights valued at approximately $4,004,000 and transaction costs of approximately $450,000.
At the effective date of the merger, each share of ACCESS Oncology common stock, including shares issuable upon the exercise of options exercised before March 1, 2004, and upon the exercise of outstanding warrants, was converted into the right to share in the contingent equity rights pro rata with the other holders of ACCESS Oncology common stock. Pursuant to the merger agreement, 623,145 shares of our common stock valued at approximately $6,325,000 have been issued to the former preferred stockholders of ACCESS Oncology. An additional 4,433 shares of our common stock are issuable to those preferred stockholders of ACCESS Oncology who have yet to provide the necessary documentation to receive shares of our common stock.
On December 16, 2009, we announced the initiation of a Phase 3 registration trial of KRX-0401 (perifosine) for the treatment of patients with relapsed / refractory multiple myeloma. The achievement of this event triggered contingent milestone stock consideration payable to the former stockholders of ACCESS Oncology in the amount of an aggregate of 500,000 shares of our common stock valued at $1,365,000.
The remaining contingent equity rights will be paid upon the achievement of the following milestones:
| · | 750,000 shares of our common stock upon the first new drug application acceptance by the Food and Drug Administration, or FDA, for KRX-0401; |
| · | 1,750,000 shares of our common stock upon the first FDA approval of KRX-0401; and |
| · | 372,422 shares of our common stock following the first 12-month period that sales of KRX-0401 exceed $100 million. |
| F-16 |
In no event will we issue more than 4,000,000 shares of our common stock pursuant to the merger agreement. These 4,000,000 shares include 1,127,578 shares issued or issuable to date and any contingent shares as described above. Accordingly, the remaining amount of our common stock deliverable to the former ACCESS Oncology stockholders as milestone consideration will be no more than 2,872,422 shares. The former preferred stockholders of ACCESS Oncology are not entitled to a share of the milestone consideration. Our stockholders approved the issuance of shares of our common stock payable as contingent milestone consideration at the 2004 annual meeting of stockholders, which took place on June 10, 2004.
We have accounted for the ACCESS Oncology acquisition as a purchase. On the date of the acquisition, the excess of the net assets acquired over the purchase price represented negative goodwill of approximately $4,004,000. Since the negative goodwill was a result of not recognizing contingent consideration (i.e., the contingent equity rights), the lesser of the negative goodwill ($4,004,000) and the maximum value of the contingent equity rights at the date of the acquisition ($34,275,000) was recorded as a liability, thereby eliminating the negative goodwill. The maximum value of the contingent equity rights at the date of acquisition of $34,275,000 was based on the volume-adjusted weighted average closing price per share of our common stock measured over the last seven trading days immediately preceding the closing of the acquisition ($10.15 per share) multiplied by 3,376,855 shares, which consisted of the sum of the unissued amount of our common stock deliverable to the ACCESS Oncology stockholders as milestone consideration (3,372,422 shares) and to those preferred stockholders of ACCESS Oncology who have yet to provide the necessary documentation to receive shares of our common stock (4,433 shares). On December 16, 2009, upon the issuance of 500,000 shares of contingent milestone consideration discussed above, the value of the contingent equity rights was reduced by $1,365,000 to $2,639,000.
NOTE 11 - STOCKHOLDERS’ EQUITY
Preferred Stock
Our amended and restated certificate of incorporation authorizes the issuance of up to 5,000,000 shares of preferred stock, $0.001 par value, with rights senior to those of our common stock.
Common Stock
Our amended and restated certificate of incorporation authorizes the issuance of up to 95,000,000 shares of $0.001 par value common stock.
On May 4, 2011, we announced the pricing of an underwritten registered offering of 7,021,277 shares of our common stock at a price of $4.70 per share for gross proceeds of approximately $33 million. Net proceeds from this offering were approximately $30.7 million, net of underwriting discounts and offering expenses of approximately $2.3 million. The shares were sold under a shelf registration statement on Form S-3 (File No. 333-171517) that was previously filed and declared effective by the SEC on January 28, 2011.
On September 30, 2009, we completed a registered direct offering to certain investors of 8,000,000 shares of our common stock and warrants to purchase up to a total of 2,800,000 shares of our common stock for gross proceeds of approximately $20 million. The common stock and warrants were sold in units, with each unit consisting of one share of common stock and a warrant to purchase 0.35 of a share of common stock. The purchase price per unit was $2.50. Subject to certain ownership limitations, the warrants were exercisable at any time on or prior to October 1, 2010, at an exercise price of $2.65 per warrant share. In addition, the placement agent received a warrant to purchase up to 108,000 shares of common stock at an exercise price of $3.125 per warrant share, exercisable at any time on or prior to October 1, 2010. Total proceeds from this public offering were approximately $18.4 million, net of offering costs of approximately $1.6 million. As of December 31, 2010, all the warrants were exercised, which provided us with additional proceeds of approximately $7.3 million, net of offering costs of approximately $0.5 million. The shares and warrants were sold under a shelf registration statement on Form S-3 (File No. 333-161607) filed with the SEC on August 28, 2009, and declared effective by the SEC on September 23, 2009.
| F-17 |
We currently have two shelf registration statements on Form S-3, filed and declared effective by the SEC, providing for the offering of up to approximately $79 million of common stock and warrants in the aggregate.
| · | On August 28, 2009, we filed with the SEC a shelf registration statement on Form S-3 (File No. 333-161607) and declared effective by the SEC on September 23, 2009. The registration statement provided for the offering of up to $40 million of our common stock and warrants. Subsequent to the registered direct offering completed in September 2009, there remains approximately $12 million of our common stock and warrants available for sale under the shelf registration statement. |
| · | On January 3, 2011, we filed with the SEC a shelf registration statement on Form S-3 (File No. 333-171517) that was declared effective by the SEC on January 28, 2011, providing for the offering of up to $100 million of our common stock and warrants to purchase our common stock. Subsequent to the registered offering in May 2011, there remains approximately $67 million of our common stock and warrants available for sale under the shelf registration statement. |
We may offer the securities under our shelf registration statements from time to time in response to market conditions or other circumstances if we believe such a plan of financing is in our best interests and the best interests of our stockholders. We believe that these shelf registration statements provide us with the flexibility to efficiently raise additional capital to finance our operations as needed.
Treasury Stock
As of December 31, 2011 and 2010, we held a total of 79,948 shares of our common stock in treasury, at a total cost of $357,000.
Equity Incentive Plans
We have in effect the following stock option and incentive plans.
a. The 1999 Stock Option Plan was adopted in November 1999. Under the 1999 Stock Option Plan, our board of directors could grant stock-based awards to directors, consultants and employees. The plan authorizes grants to purchase up to 4,230,000 shares of authorized but unissued common stock. The plan limits the term of each option, to no more than 25 years from the date of the grant, unless otherwise authorized by the board. The plan permits the board of directors or a committee appointed by the board to administer the plan. The administrator has the authority, in its discretion, to determine the terms and conditions of any option granted to a service provider, including the vesting schedule. As of December 31, 2011, no additional shares of our common stock may be issued under the 1999 Stock Option Plan.
b. The 2000 Stock Option Plan was adopted in June 2000. Under the 2000 Stock Option Plan, the compensation committee of our board of directors is authorized to grant stock-based awards to directors, consultants and employees. The 2000 plan authorizes grants to purchase up to 4,455,000 shares of authorized but unissued common stock. The plan limits the term of each option to no more than 10 years from the date of the grant, unless authorized by the board. As of December 31, 2011, up to an additional 1,206,427 shares may be issued under the 2000 Stock Option Plan.
c. The 2004 Long-Term Incentive Plan was adopted in June 2004 by our stockholders. Under the 2004 Long-Term Incentive Plan, the compensation committee of our board of directors is authorized to grant stock-based awards to directors, consultants and employees. The 2004 plan authorizes grants to purchase up to 4,000,000 shares of authorized but unissued common stock. The plan limits the term of each option to no more than 10 years from the date of grant. As of December 31, 2011, up to an additional 1,874,872 shares may be issued under the 2004 Long-Term Incentive Plan.
d. The 2007 Incentive Plan was adopted in June 2007 by our stockholders. Under the 2007 Incentive Plan, the compensation committee of our board of directors is authorized to grant stock-based awards to directors, consultants, employees and officers. The 2007 Incentive Plan authorizes grants to purchase up to 6,000,000 shares of authorized but unissued common stock. The plan limits the term of each option to no more than 10 years from the date of grant. As of December 31, 2011, up to an additional 270,146 shares may be issued under the 2007 Incentive Plan.
e. The 2009 CEO Incentive Plan was adopted in May 2009. Under the 2009 CEO Incentive Plan, our board of directors granted an option to Ron Bentsur, our Chief Executive Officer, to purchase up to 600,000 shares of authorized but unissued common stock. The option has a term of 10 years from the date of grant. The option will vest in equal annual installments over a four-year period or upon an earlier change in control of the Company.
| F-18 |
Shares available for the issuance of stock options or other stock-based awards under our stock option and incentive plans were 3,351,445 shares at December 31, 2011.
Stock Options
The following table summarizes stock option activity for all plans for the years ended December 31, 2011, 2010 and 2009:
| Number of shares | Weighted- average exercise price | Weighted- average Contractual Term | Aggregate Intrinsic Value | |||||||||||||
| Outstanding at January 1, 2009 | 9,114,459 | $ | 7.19 | |||||||||||||
| Granted | 700,000 | 0.55 | ||||||||||||||
| Exercised | (50,000 | ) | 0.36 | $ | 85,300 | |||||||||||
| Forfeited | (159,467 | ) | 6.75 | |||||||||||||
| Expired | (251,420 | ) | 11.16 | |||||||||||||
| Outstanding at December 31, 2009 | 9,353,572 | 6.63 | ||||||||||||||
| Granted | 417,840 | 3.71 | ||||||||||||||
| Exercised | (1,365,140 | ) | 1.38 | $ | 4,943,663 | |||||||||||
| Forfeited | (2,120 | ) | 9.80 | |||||||||||||
| Expired | (765,749 | ) | 10.20 | |||||||||||||
| Outstanding at December 31, 2010 | 7,638,403 | 7.05 | ||||||||||||||
| Granted | 692,350 | 4.53 | ||||||||||||||
| Exercised | (2,382,027 | ) | 1.30 | $ | 6,604,300 | |||||||||||
| Forfeited | (98,600 | ) | 4.32 | |||||||||||||
| Expired | (2,333,126 | ) | 13.26 | |||||||||||||
| Outstanding at December 31, 2011 | 3,517,000 | $ | 6.40 | 6.9 | $ | 2,139,130 | ||||||||||
| Vested and expected to vest at December 31, 2011 | 3,473,275 | $ | 6.42 | 6.9 | $ | 2,116,924 | ||||||||||
| Exercisable at December 31, 2011 | 2,161,774 | $ | 7.42 | 6.2 | $ | 1,476,282 | ||||||||||
The following table summarizes information about stock options outstanding at December 31, 2011:
| Options outstanding | Options exercisable | |||||||||||||||||||
| Range of exercise prices | Number outstanding | Weighted- average remaining contractual life (years) | Weighed- average exercise price | Number exercisable | Weighed-average exercise price | |||||||||||||||
| $ 0.10 - $ 3.00 | 1,161,492 | 8.7 | $ | 0.69 | 779,892 | $ | 0.64 | |||||||||||||
| 3.70 - 8.90 | 1,140,458 | 7.9 | 5.00 | 341,832 | 6.18 | |||||||||||||||
| 9.96 - 14.64 | 1,215,050 | 4.2 | 13.17 | 1,040,050 | 12.92 | |||||||||||||||
| $ 0.10 - $ 14.64 | 3,517,000 | 6.9 | $ | 6.40 | 2,161,774 | $ | 7.42 | |||||||||||||
Upon the exercise of stock options, we issue new shares of our common stock. As of December 31, 2011, 235,000 options issued to employees and 50,000 options issued to consultants are unvested, milestone-based options.
| F-19 |
Restricted Stock
Certain employees, directors and consultants have been awarded restricted stock under the 2004 Long-Term Incentive Plan and 2007 Incentive Plan. The time-vesting restricted stock grants vest primarily over a period of three to four years. The following table summarizes restricted share activity for the years ended December 31, 2011, 2010 and 2009:
| Number of Shares | Weighted Average Grant Date Fair Value | Aggregate Intrinsic Value | ||||||||||
| Outstanding at January 1, 2009 | 3,982,572 | $ | 0.36 | |||||||||
| Granted | 578,539 | 0.76 | ||||||||||
| Vested | (2,707,233 | ) | 0.32 | $ | 1,325,377 | |||||||
| Forfeited | (361,742 | ) | 0.34 | |||||||||
| Outstanding at December 31, 2009 | 1,492,136 | 0.59 | $ | 3,730,340 | ||||||||
| Granted | 695,500 | 2.78 | ||||||||||
| Vested | (779,308 | ) | 0.67 | $ | 3,375,859 | |||||||
| Forfeited | (7,634 | ) | 1.41 | |||||||||
| Outstanding at December 31, 2010 | 1,400,694 | 1.63 | $ | 6,415,179 | ||||||||
| Granted | 206,450 | 4.49 | ||||||||||
| Vested | (957,225 | ) | 1.20 | $ | 4,650,171 | |||||||
| Forfeited | (28,338 | ) | 3.35 | |||||||||
| Outstanding at December 31, 2011 | 621,581 | $ | 3.16 | $ | 1,572,600 | |||||||
On September 14, 2009, we entered in an employment agreement with Ron Bentsur, our Chief Executive Officer, which was amended on January 13, 2012. The agreement, as amended, terminates on May 20, 2014, subject to certain early termination events. As of December 31, 2011, Mr. Bentsur has been granted a total of 350,000 shares of restricted stock based on the achievement of certain milestone awards described in his employment agreement. In addition, as of December 31, 2011, Mr. Bentsur has the opportunity to earn certain milestone awards as follows:
(1) 400,000 shares of restricted stock will be granted to Mr. Bentsur upon the first to occur of (a) our filing of an accepted new drug application, or NDA, with the U.S. Food and Drug Administration for Zerenex or Perifosine, or (b) our outlicensing of Zerenex or Perifosine in the U.S. to a third party. Such restricted stock will vest in equal installments over each of the first three anniversaries of the date of grant provided that Mr. Bentsur remains an employee during such vesting period. This milestone #1 may be achieved with respect to NDAs or qualifying outlicenses for multiple indications of the same product, but not for subsequent outlicenses of the product relating to an indication for which the milestone is met. Upon achievement of milestone #2 below with respect to a product, the restricted stock granted for one indication of the product under milestone #1 above will vest in full.
(2) 500,000 shares of restricted stock will be granted to Mr. Bentsur, upon the first to occur of (a) our first commercial sale of Zerenex or Perifosine in the U.S. off an approved NDA, (b) our receipt of the first royalty upon the commercial sale of Zerenex or Perifosine in the U.S. by a partner to whom we have sold exclusive or non-exclusive commercial rights, or (c) our complete outlicensing of the entire product rights of Zerenex or Perifosine in the U.S. Such restricted stock will vest on the first anniversary of the date of grant provided that Mr. Bentsur remains an employee during such vesting period.
(3) 100,000 shares of restricted stock will be granted to Mr. Bentsur upon each event of our outlicensing Zerenex in a foreign market, other than Japan, resulting in a greater than $10 million non-refundable cash payment to us with a gross deal value to us of at least $50 million. Such restricted stock will vest in equal installments over each of the first three anniversaries of the date of grant provided that Mr. Bentsur remains an employee during such vesting period.
| F-20 |
Warrants
There were no warrants outstanding during the year ended December 31, 2011. The following table summarizes warrant activity for the years ended December 31, 2010 and 2009:
| Warrants | Weighted- average exercise price | Aggregate Intrinsic Value | ||||||||||
| Outstanding at January 1, 2009 | 72,564 | 0.01 | ||||||||||
| Issued | 2,908,000 | 2.67 | ||||||||||
| Exercised | (64,174 | ) | 0.01 | $ | 134,335 | |||||||
| Expired | (8,390 | ) | 0.01 | |||||||||
| Outstanding at December 31, 2009 | 2,908,000 | 2.67 | $ | — | ||||||||
| Issued | — | — | ||||||||||
| Exercised | (2,908,000 | ) | 2.67 | $ | 5,550,820 | |||||||
| Canceled | — | — | ||||||||||
| Outstanding at December 31, 2010 | — | $ | — | $ | — | |||||||
As discussed above, as part of the registered direct offering completed in September 2009, we issued warrants to purchase up to 2,800,000 shares of our common stock, all of which were exercised as of December 31, 2010. The warrants had an exercise price of $2.65 per warrant share. The grant date fair value was $1.03 per warrant, for a total fair value of $2,877,000, which is included in additional paid-in capital on the consolidated balance sheet. In addition, we issued to the placement agent in the transaction warrants to purchase up to 108,000 shares of our common stock at an exercise price of $3.125 per warrant share, all of which were exercised as of December 31, 2010, with a grant date fair value of $0.93 per warrant. The fair values of the warrants described above were estimated at the date of grant using the Black-Scholes pricing model.
Stock-Based Compensation
The fair value of stock options granted is estimated at the date of grant using the Black-Scholes pricing model. The expected term of options granted is derived from historical data and the expected vesting period. Expected volatility is based on the historical volatility of our common stock. The risk-free interest rate is based on the U.S. Treasury yield for a period consistent with the expected term of the option in effect at the time of the grant. We have assumed no expected dividend yield, as dividends have never been paid to stock or option holders and will not be paid for the foreseeable future.
| Black-Scholes Option Valuation Assumptions | 2011 | 2010 | 2009 | |||||||||
| Risk-free interest rates | 1.4 | % | 1.7 | % | 2.0 | % | ||||||
| Dividend yield | — | — | — | |||||||||
| Volatility | 115.0 | % | 126.8 | % | 123.7 | % | ||||||
| Weighted-average expected term | 4.0 years | 4.0 years | 4.7 years | |||||||||
The weighted average grant date fair value of options granted was $3.43, $2.96 and $0.44 per option for the years ended December 31, 2011, 2010 and 2009, respectively. We used historical information to estimate forfeitures within the valuation model. As of December 31, 2011, there was $2.0 million and $1.4 million of total unrecognized compensation cost related to non-vested stock options and restricted stock, respectively, which is expected to be recognized over weighted-average periods of 2.0 years and 1.7 years, respectively. These amounts do not include, as of December 31, 2011, 285,000 options outstanding which are milestone-based and vest upon certain corporate milestones, such as FDA approval of our drug candidates, market capitalization targets, and change in control. Stock-based compensation will be measured and recorded if and when a milestone occurs.
On April 23, 2009, our Board of Directors voted to terminate the employment of Michael S. Weiss as our Chairman and Chief Executive Officer (see Note 1). Under the terms of Mr. Weiss’ employment agreement, 1,800,000 shares of restricted stock vested and all of Mr. Weiss’ outstanding stock options vested and remained exercisable for two years following termination. In the year ended December 31, 2009, we recorded approximately $660,000 in non-cash compensation expense (general and administrative) associated with the equity modifications of Mr. Weiss’ outstanding stock options and shares of restricted stock.
| F-21 |
The following table summarizes stock-based compensation expense information about stock options and restricted stock for the years ended December 31, 2011, 2010 and 2009:
| Year ended December 31, | ||||||||||||
| (in thousands) | 2011 | 2010 | 2009 | |||||||||
| Stock-based compensation expense associated with restricted stock (1) | $ | 1,044 | $ | 1,584 | $ | 1,220 | ||||||
| Stock-based compensation expense associated with option grants (2) | 1,048 | 889 | 1,880 | |||||||||
| $ | 2,092 | $ | 2,473 | $ | 3,100 | |||||||
| (1) | Includes $396,000 of non-cash compensation expense in the year ended December 31, 2009, related to equity modifications of restricted stock issued to our previous Chief Executive Officer, who was terminated in April 2009. |
| (2) | Includes $264,000 of non-cash compensation expense in the year ended December 31, 2009, related to equity modifications of stock options issued to our previous Chief Executive Officer, who was terminated in April 2009. |
NOTE 12 – INCOME TAXES
We account for income taxes under the asset and liability method. Deferred tax assets and liabilities are determined based on differences between the financial reporting and tax basis of assets and liabilities and are measured using the enacted tax rates and laws that will be in effect when the differences are expected to reverse. A valuation allowance is established when necessary to reduce deferred tax assets to the amount expected to be realized. In determining the need for a valuation allowance, management reviews both positive and negative evidence, including current and historical results of operations, future income projections and the overall prospects of our business. Based upon management's assessment of all available evidence, we believe that it is more-likely-than-not that the deferred tax assets will not be realizable; and therefore, a valuation allowance is established. The valuation allowance for deferred tax assets was $128.0 million and $141.4 million as of December 31, 2011 and 2010, respectively.
As of December 31, 2011, we have U.S. net operating loss carryforwards (“NOL’s”) of approximately $323.6 million, of which approximately $45.9 million were derived from certain stock option exercises and any such benefit realized will be credited to additional paid in capital. For income tax purposes, these NOL’s will expire in the years 2019 through 2030. Due to our various equity transactions, the utilization of certain NOL’s could be subject to annual limitations imposed by Internal Revenue Code Section 382 relating to the change of control provision and/or the separate return limitation year losses limitation.
Income tax expense differed from amounts computed by applying the US federal income tax rate of 34% to pretax loss as follows:
| For the year ended December 31, | ||||||||||||
| (in thousands) | 2011 | 2010 | 2009 | |||||||||
| (Loss) income from continuing operations before income taxes, as reported in the consolidated statements of operations | $ | (28,369 | ) | $ | (20,451 | ) | $ | 10,482 | ||||
| Computed “expected” tax (benefit) expense | (9,645 | ) | (7,158 | ) | 3,670 | |||||||
| (Decrease) increase in income taxes resulting from: | ||||||||||||
| Expected (benefit) expense from state & local taxes | (925 | ) | (1,650 | ) | 846 | |||||||
| Stock option expiration | 5,872 | (— | ) | (— | ) | |||||||
| Deferred impact rate change | 19,072 | (— | ) | 4,876 | ||||||||
| Permanent differences | (147 | ) | (153 | ) | (125 | ) | ||||||
| Other | (2 | ) | (4 | ) | 83 | |||||||
| Prior year true-up | (829 | ) | 652 | (658 | ) | |||||||
| Change in the balance of the valuation allowance for deferred tax assets allocated to income tax expense | (13,396 | ) | 8,313 | (8,692 | ) | |||||||
| $ | — | $ | — | $ | — | |||||||
The significant components of deferred income tax expense (benefit) attributable to loss from operations are as follows:
| For the year ended December 31, | ||||||||||||
| (in thousands) | 2011 | 2010 | 2009 | |||||||||
| Deferred tax expense (benefit) | $ | 13,396 | $ | (8,313 | ) | $ | 8,520 | |||||
| Federal deferred tax benefit relating to the exercise of stock options | (— | ) | (— | ) | 172 | |||||||
| (Decrease) increase in the valuation allowance for deferred tax asset | (13,396 | ) | 8,313 | (8,692 | ) | |||||||
| $ | — | $ | — | $ | — | |||||||
| F-22 |
The tax effects of temporary differences that give rise to significant portions of the deferred tax assets and deferred tax liabilities at December 31, 2011 and 2010 are presented below.
| (in thousands) | December 31, 2011 | December 31, 2010 | ||||||
| Deferred tax assets (liabilities): | ||||||||
| Net operating loss carryforwards | $ | 120,580 | $ | 128,130 | ||||
| Non-cash compensation | 4,445 | 11,483 | ||||||
| Unrealized / realized loss on securities | 1,164 | 1,359 | ||||||
| Research and development | 1,332 | — | ||||||
| Intangible assets due to different amortization methods | 262 | 371 | ||||||
| Accrued expenses | 186 | — | ||||||
| Other temporary differences | 16 | 38 | ||||||
| Deferred tax asset, excluding valuation allowance | 127,985 | 141,381 | ||||||
| Less valuation allowance | (127,985 | ) | (141,381 | ) | ||||
| Net deferred tax assets | $ | — | $ | — | ||||
We file income tax returns in the U.S federal and various state and local jurisdictions. For federal and state income tax purposes, the 2008, 2009 and 2010 tax years remain open for examination under the normal three year statute of limitations. The statute of limitations for income tax audits in the U.S. will commence upon utilization of net operating losses and will expire three years from the filing of the tax return.
There was no accrual for interest and penalties related to uncertain tax positions for 2011, 2010 and 2009. We do not believe that there will be a material change in our unrecognized tax positions over the next twelve months. All of the unrecognized tax benefits, if recognized, would be offset by the valuation allowance.
NOTE 13 – INTEREST AND OTHER INCOME, NET
The components of interest and other income, net are as follows:
| For the year ended December 31, | ||||||||||||
| (in thousands) | 2011 | 2010 | 2009 | |||||||||
| Interest income | $ | 159 | $ | 148 | $ | 315 | ||||||
| Other income | 221 | 730 | 247 | |||||||||
| (Loss) gain on sale of auction rate securities | — | (82 | ) | 173 | ||||||||
| Impairment expense of auction rate securities | — | (32 | ) | (68 | ) | |||||||
| $ | 380 | $ | 764 | $ | 667 | |||||||
In 2010 and 2009, we recorded impairment charges totaling $32,000 and $68,000 respectively, for other-than-temporary declines in the fair value of our prior investments in auction rate securities (see Note 3 – Investment Securities, and Note 4 – Fair Value Measurements). Other income consists of rental income from the sublease of a portion of our leased space and a one-time grant in the amount of $489,000 received in November 2010 under The Patient Protection and Affordable Care Act of 2010 for our drug candidates, KRX-0401 (perifosine) and Zerenex (ferric citrate).
| F-23 |
NOTE 14 - COMMITMENTS AND CONTINGENCIES
Research & Development Agreements
We have entered into various research and development agreements (relating to our development of KRX-0401 and Zerenex) under which we are obligated to make payments of approximately $13,439,000 through 2013. The following table shows future research and development payment obligations by period as of December 31, 2011.
| (in thousands) | 2012 | 2013 | 2014 | 2015 | 2016 | |||||||||||||||
| Research and development agreements | $ | 9,251 | $ | 4,188 | — | — | — | |||||||||||||
Most of the commitments in the table above are contingent upon our continuing development of our drug candidates.
Leases
In August 2010, we signed an amendment to the lease on our corporate and executive office located in New York City extending its term through September 30, 2013. We also executed an amendment to our office sharing agreement with a third party for a portion of our leased space through September 29, 2013.
Total rental expense was approximately $538,000, $537,000 and $540,000 for the years ended December 31, 2011, 2010, and 2009, respectively. We recognized sublet income of $221,000, $241,000 and $247,000 for the years ended December 31, 2011, 2010 and 2009 related to office sharing agreements.
Future minimum lease commitments as of December 31, 2011, in the aggregate total approximately $956,000 through September 2013. The following table shows future minimum lease commitments by period as of December 31, 2011.
| (in thousands) | 2012 | 2013 | 2014 | 2015 | 2016 | |||||||||||||||
| Operating leases | $ | 526 | $ | 430 | — | — | — | |||||||||||||
The sublet income is not included as an offset to our operating lease obligations in the table above.
Royalty and Contingent Milestone Payments
We have licensed the patent rights to our drug candidates from others. These license agreements require us to make contingent milestone payments to certain of our licensors. In addition, under these agreements, we must pay royalties on sales of products resulting from licensed technologies.
We have undertaken to make contingent milestone payments to certain of our licensors of up to approximately $25.0 million over the life of the licenses, of which approximately $22.0 million will be due upon or following regulatory approval of the licensed drugs. We have also committed to pay to the former stockholders of ACCESS Oncology certain contingent equity rights (up to 2,872,422 shares of our common stock) if KRX-0401 meets certain development and sales milestones. The contingent equity rights have been recognized as a non-current liability on the consolidated balance sheet. See Note 10 – Contingent Equity Rights. The uncertainty relating to the timing of the commitments described in this paragraph prevents us from including them in the tables above.
NOTE 15 - LITIGATION
In March 2010, we settled a dispute with ICON Central Laboratories (“ICON”), the central laboratory we used for the clinical development of Sulonex (sulodexide), concerning certain fees related mainly to the provision of storage services pursuant to a series of service agreements. ICON was claiming that we owed it $816,647 in unpaid invoices, much of which was made up of charges for annual storage fees incurred after the effective date of termination of the agreements. Under the terms of the settlement agreement, we paid ICON $400,000 in settlement of all claims, which, at December 31, 2009, was included in accounts payable and accrued expenses on our consolidated balance sheet.
In October 2009, we filed a statement of claim with the Financial Institution Regulatory Authority, or FINRA, to commence an arbitration proceeding against an SEC registered broker-dealer. In this arbitration proceeding, we seek damages arising from that broker-dealer’s recommendations and purchases of auction rate securities for our cash management account. The claim will be determined by a panel of three FINRA arbitrators. In January 2010, the broker-dealer filed an answer to the statement of claim and denied liability. The hearing concerning our claims against the broker-dealer commenced in October 2011, and is scheduled to be completed in March 2012.
| F-24 |
NOTE 16 – QUARTERLY CONSOLIDATED FINANCIAL DATA (UNAUDITED)
| 2011 | ||||||||||||||||
| Mar. 31 | June 30 | Sept. 30 | Dec. 31 | |||||||||||||
| (in thousands, except per share data) | ||||||||||||||||
| Revenue: | ||||||||||||||||
| License revenue | $ | — | $ | 5,000 | $ | — | $ | — | ||||||||
| Total revenue | — | 5,000 | — | — | ||||||||||||
| Operating expenses: | ||||||||||||||||
| Research and development: | ||||||||||||||||
| Non-cash compensation | 259 | 205 | 152 | 187 | ||||||||||||
| Other research and development | 4,618 | 6,295 | 8,620 | 6,676 | ||||||||||||
| Total research and development | 4,877 | 6,500 | 8,772 | 6,863 | ||||||||||||
| General and administrative: | ||||||||||||||||
| Non-cash compensation | 314 | 314 | 320 | 341 | ||||||||||||
| Other general and administrative | 1,284 | 1,404 | 1,263 | 1,497 | ||||||||||||
| Total general and administrative | 1,598 | 1,718 | 1,583 | 1,838 | ||||||||||||
| Total operating expenses | 6,475 | 8,218 | 10,355 | 8,701 | ||||||||||||
| Operating loss | (6,475 | ) | (3,218 | ) | (10,355 | ) | (8,701 | ) | ||||||||
| Other income | ||||||||||||||||
| Interest and other income, net | 70 | 122 | 108 | 80 | ||||||||||||
| Income taxes | — | — | — | — | ||||||||||||
| Loss from continuing operations | (6,405 | ) | (3,096 | ) | (10,247 | ) | (8,621 | ) | ||||||||
| Gain from discontinued operations | — | — | — | 246 | ||||||||||||
| Net loss | $ | (6,405 | ) | $ | (3,096 | ) | $ | (10,247 | ) | $ | (8,375 | ) | ||||
| Basic net loss per common share | ||||||||||||||||
| Continuing operations | (0.10 | ) | (0.05 | ) | (0.15 | ) | (0.12 | ) | ||||||||
| Discontinued operations | — | — | — | — | * | |||||||||||
| Basic net loss per common share | $ | (0.10 | ) | $ | (0.05 | ) | $ | (0.15 | ) | $ | (0.12 | ) | ||||
| Diluted net loss per common share | ||||||||||||||||
| Continuing operations | (0.10 | ) | (0.05 | ) | (0.15 | ) | (0.12 | ) | ||||||||
| Discontinued operations | — | — | — | — | * | |||||||||||
| Diluted net loss per common share | $ | (0.10 | ) | $ | (0.05 | ) | $ | (0.15 | ) | $ | (0.12 | ) | ||||
*Amount less than one cent.
| F-25 |
| 2010 | ||||||||||||||||
| Mar. 31 | June 30 | Sept. 30 | Dec. 31 | |||||||||||||
| (in thousands, except per share data) | ||||||||||||||||
| Operating expenses: | ||||||||||||||||
| Research and development: | ||||||||||||||||
| Non-cash compensation | 242 | 434 | 322 | 238 | ||||||||||||
| Other research and development | 2,554 | 3,129 | 3,901 | 4,144 | ||||||||||||
| Total research and development | 2,796 | 3,563 | 4,223 | 4,382 | ||||||||||||
| General and administrative: | ||||||||||||||||
| Non-cash compensation | 407 | 261 | 291 | 278 | ||||||||||||
| Other general and administrative | 898 | 1,356 | 1,419 | 1,341 | ||||||||||||
| Total general and administrative | 1,305 | 1,617 | 1,710 | 1,619 | ||||||||||||
| Total operating expenses | 4,101 | 5,180 | 5,933 | 6,001 | ||||||||||||
| Operating loss | (4,101 | ) | (5,180 | ) | (5,933 | ) | (6,001 | ) | ||||||||
| Other income | ||||||||||||||||
| Interest and other income, net | 86 | 26 | 85 | 567 | ||||||||||||
| Income taxes | — | — | — | — | ||||||||||||
| Loss from continuing operations | (4,015 | ) | (5,154 | ) | (5,848 | ) | (5,434 | ) | ||||||||
| Gain from discontinued operations | — | — | — | 120 | ||||||||||||
| Net loss | $ | (4,015 | ) | $ | (5,154 | ) | $ | (5,848 | ) | $ | (5,314 | ) | ||||
| Basic net loss per common share | ||||||||||||||||
| Continuing operations | (0.07 | ) | (0.09 | ) | (0.10 | ) | (0.09 | ) | ||||||||
| Discontinued operations | — | — | — | — | * | |||||||||||
| Basic net loss per common share | $ | (0.07 | ) | $ | (0.09 | ) | $ | (0.10 | ) | $ | (0.09 | ) | ||||
| Diluted net loss per common share | ||||||||||||||||
| Continuing operations | (0.07 | ) | (0.09 | ) | (0.10 | ) | (0.09 | ) | ||||||||
| Discontinued operations | — | — | — | — | * | |||||||||||
| Diluted net loss per common share | $ | (0.07 | ) | $ | (0.09 | ) | $ | (0.10 | ) | $ | (0.09 | ) | ||||
*Amount less than one cent.
| F-26 |
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
Date: March 2, 2012
| KERYX BIOPHARMACEUTICALS, INC. | ||
| By: | /s/ Ron Bentsur | |
| Ron Bentsur | ||
| Chief Executive Officer and Director | ||
POWER OF ATTORNEY
KNOW ALL MEN BY THESE PRESENTS, that each person whose signature appears below constitutes and appoints each of Ron Bentsur and James F. Oliviero, his true and lawful attorney-in-fact and agent, with full power of substitution and resubstitution, for him and his name, place and stead, in any and all capacities, to sign any or all amendments to this annual report on Form 10-K, and to file the same, with all exhibits thereto and other documents in connection therewith, with the SEC, granting unto said attorney-in-fact and agent, full power and authority to do and perform each and every act and thing requisite and necessary to be done in and about the premises, as fully to all intents and purposes as he might or could do in person, hereby ratifying and confirming all that said attorney-in-fact and agent or any of his substitutes, may lawfully do or cause to be done by virtue hereof.
Pursuant to the requirements of the Securities Exchange Act of 1934, as amended, this Form 10-K has been signed by the following persons on behalf of the Registrant on March 2, 2012, and in the capacities indicated:
| Signatures | Title | |
| /s/ Ron Bentsur | Chief Executive Officer and Director | |
| Ron Bentsur | (principal executive officer) | |
| /s/ James F. Oliviero | Chief Financial Officer | |
| James F. Oliviero, CFA | (principal financial and accounting officer) | |
| /s/ Michael P. Tarnok | Chairman of the Board of Directors | |
| Michael P. Tarnok | ||
| /s/ Kevin Cameron | Director | |
| Kevin Cameron | ||
| /s/ Joseph Feczko, M.D | Director | |
| Joseph Feczko, M.D | ||
| /s/ Senator Wyche Fowler, Jr. | Director | |
| Senator Wyche Fowler, Jr. | ||
| /s/ Jack Kaye | Director | |
| Jack Kaye |
EXHIBIT INDEX
| Exhibit | |
| Number | Exhibit Description |
| 10.20 | Change in Control Agreement with James F. Oliviero dated October 31, 2011, as amended on November 3, 2011. |
| 21.1 | List of subsidiaries of Keryx Biopharmaceuticals, Inc. |
| 23.1 | Consent of UHY LLP. |
| 24.1 | Power of Attorney of Director and Officers of Keryx Biopharmaceuticals, Inc. (included herein). |
| 31.1 | Certification of Chief Executive Officer pursuant to Rule 13a-14(a)/15d-14(a), as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002, dated March 2, 2012. |
| 31.2 | Certification of Chief Financial Officer pursuant to Rule 13a-14(a)/15d-14(a), as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002, dated March 2, 2012. |
| 32.1 | Certification of Chief Executive Officer pursuant to 18 U.S.C. §1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002, dated March 2, 2012. |
| 32.2 | Certification of Chief Financial Officer pursuant to 18 U.S.C. §1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002, dated March 2, 2012. |
| 101 | The following financial information from Keryx Biopharmaceuticals, Inc.’s Annual Report on Form 10-K for the year ended December 31, 2011, formatted in XBRL (eXtensible Business Reporting Language): (i) Consolidated Balance Sheets, (ii) Consolidated Statements of Operations, (iii) Consolidated Statements of Stockholders’ Equity and Comprehensive Loss (Income), (iv) Consolidated Statements of Cash Flows and (v) the Notes to Consolidated Financial Statements. |