Attached files
| file | filename |
|---|---|
| EX-99.2 - EXHIBIT 99.2 - CALADRIUS BIOSCIENCES, INC. | v244785_ex99-2.htm |
| EX-99.3 - EXHIBIT 99.3 - CALADRIUS BIOSCIENCES, INC. | v244785_ex99-3.htm |
| 8-K - CURRENT REPORT - CALADRIUS BIOSCIENCES, INC. | v244785_8-k.htm |

NeoStem, Inc. (“NBS”) Investor Presentation January 2012
2 Included in this presentation are “forward - looking” statements within the meaning of the Private Securities Litigation Reform Ac t of 1995, as well as historical information. Such forward - looking statements involve known and unknown risks, uncertainties and other factors which may cause the actual resu lts, performance or achievements of NeoStem, Inc. and its subsidiaries (collectively, the “Company”), or industry results, to be materially different from antici pat ed results, performance or achievements expressed or implied by such forward - looking statements. When used in this presentation, statements that are not statements of c urrent or historical fact may be deemed to be forward - looking statements. Without limiting the foregoing, the words "plan," "intend," "may," "will," "expect," "believe, " "could," "anticipate," "estimate," or "continue" or similar expressions or other variations or comparable terminology are intended to identify such forward - looking st atements, although some forward looking statements are expressed differently. Additionally, statements regarding our ability to successfully develop, integrate and g row the businesses at home and abroad, including with regard to the Company’s research and development efforts in cellular therapy, its adult stem cell and umbilica l c ord blood collection, processing and storage business, contract manufacturing and process development of cellular based medicines, and the pharmaceuticals manufacturing o per ations conducted in China, the future of regenerative medicine and the role of stem cells in that future, the future use of stem cells as a treatment option and th e r ole of VSEL™ Technology in that future and the potential revenue growth of such businesses, are forward - looking statements. Our future operating results are dependent upo n many factors and our further development is highly dependent on future medical and research developments and market acceptance, which is outside our contr ol. Forward - looking statements, including with respect to the successful execution of the Company’s strategy, may not be realized due to a variety of factors an d we cannot guarantee their accuracy or that our expectations about future events will prove to be correct. Such factors include, without limitation, ( i ) our ability to manage the business despite operating losses and cash outflows; (ii) our ability to obtain sufficient capital or strategic business arrangements to fund our operations and ex pan sion plans, including meeting our financial obligations under various licensing and other strategic arrangements and the successful commercialization of the relev ant technology; (iii) our ability to build the management and human resources and infrastructure necessary to support the growth of the business; (iv) our ability to integr ate the Company’s acquired businesses successfully and grow such acquired businesses as anticipated; (v) whether a large global market is established for our cellu lar - based products and services and our ability to capture a share of this market; (vi) competitive factors and developments beyond our control; (vii) scientific and medical de velopments beyond our control; (viii) our ability to obtain appropriate governmental licenses, accreditations or certifications or comply with healthcare laws and regu lat ions or any other adverse effect or limitations caused by government regulation of the business; (ix) whether any of our current or future patent applications result in issu ed patents and our ability to obtain and maintain other rights to technology required or desirable for the conduct of our business; (x) whether any potential strategi c b enefits of various licensing transactions will be realized and whether any potential benefits from the acquisition of these licensed technologies will be realized; (xi) the results of our development activities, including the timing, enrollment, outcome and/or results of any clinical trials; (xii) our ability to successfully divest our 51% ownership of our Erye subsidiary; (xiii) factors regarding our business and initiatives in China and, generally, regarding doing business in China, including through our variable interest entity structure, including (a) costs related to funding these initiatives, (b) the successful application under Chinese law of the variable interest entity structure to the Com pany’s business, which structure the Company is relying on to conduct its business in China, (c) the ability to integrate the Company and the business operations in China su ccessfully and grow such integrated businesses as anticipated, (d) the need for outside financing to meet capital requirements, and (e) the ability of the Company to realiz e o n its investment in Erye through distributions, divestiture or other strategic alternatives; and ( xiv) other risk factors disclosed in the Company’s definitive proxy statement filed September 16, 2011 and in the Company’s periodic filings with the Securities and Exchange Commission which are available for review at www.sec.gov under “Search for Company F ili ngs.” All forward - looking statements attributable to us are expressly qualified in their entirety by these and other factors. We under take no obligation to update or revise these forward - looking statements, whether to reflect events or circumstances after the date initially filed or published, to reflect t he occurrence of unanticipated events or otherwise, except to the extent required by federal securities laws. The contents of this PowerPoint presentation reflect the merger of Amorcyte , Inc., a clinical stage therapeutics company pursuing cell - based therapies for cardiovascular diseases, with and into a wholly - owned subsidiary of NeoStem, which closed on October 17, 2011. Forward - Looking Statements
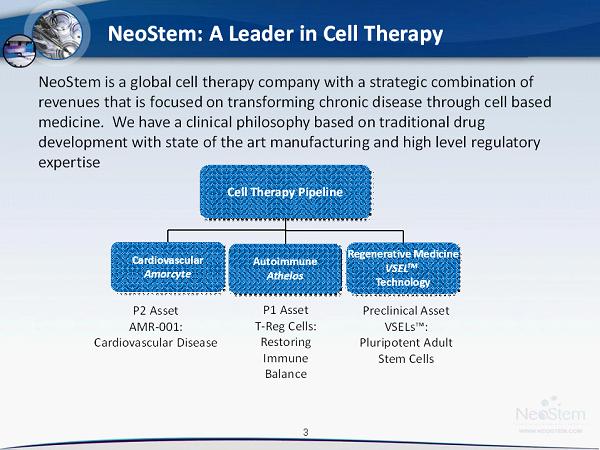
3 Cell Therapy Pipeline Regenerative Medicine VSEL TM Technology Cardiovascular Amorcyte P1 Asset T - Reg Cells: Restoring Immune Balance Preclinical Asset VSELs™: Pluripotent Adult Stem Cells P2 Asset AMR - 001: Cardiovascular Disease Autoimmune Athelos NeoStem is a global cell therapy company with a strategic combination of revenues that is focused on transforming chronic disease through cell based medicine. We have a clinical philosophy based on traditional drug development with state of the art manufacturing and high level regulatory expertise NeoStem: A Leader in Cell Therapy

4 Commercial Scale Manufacturin g • Industry leader in commercial cell therapy manufacturing • 50,000 square feet of cGMP manufacturing capability located in North America and China • Manufactured 30,000+ cell therapy product procedures and delivered 6,000+ cell therapies to patients worldwide for over 100 clients • Cost - efficient cell therapy development platform • Diversified revenue stream from cell therapy manufacturing contracts
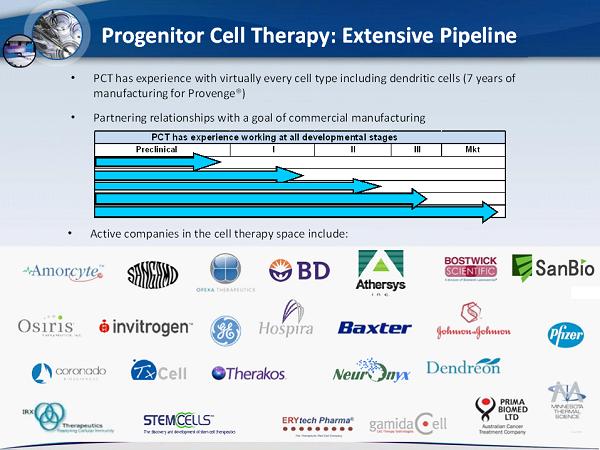
5 Progenitor Cell Therapy: Extensive Pipeline • PCT has experience with virtually every cell type including dendritic cells (7 years of manufacturing for Provenge ®) • Partnering relationships with a goal of commercial manufacturing • Active companies in the cell therapy space include: Preclinical I II III Mkt PCT has experience working at all developmental stages

6 • An autologous pharmaceutical grade product: purified and enriched natural cell population derived from patients’ bone marrow and intended to preserve heart muscle function and limit MACE following acute myocardial infarction • Clinical biologic dosing threshold established in clinical trial • Defined mechanism of action: CD34 + CXCR4 + homing & integration • Dominant IP position with both composition of matter and method patents • Pharmacoeconomic value
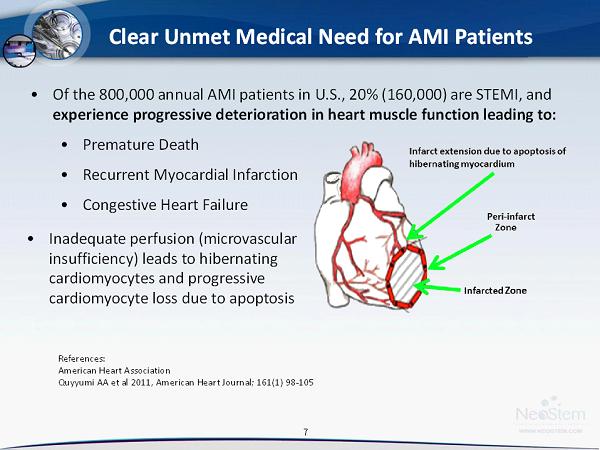
7 7 7 • Of the 800,000 annual AMI patients in U.S., 20% (160,000) are STEMI, and experience progressive deterioration in heart muscle function leading to: • Premature Death • Recurrent Myocardial Infarction • Congestive Heart Failure Clear Unmet Medical Need for AMI Patients References: American Heart Association Quyyumi AA et al 2011, American Heart Journal; 161(1) 98 - 105 • Inadequate perfusion ( microvascular insufficiency) leads to hibernating cardiomyocytes and progressive cardiomyocyte loss due to apoptosis
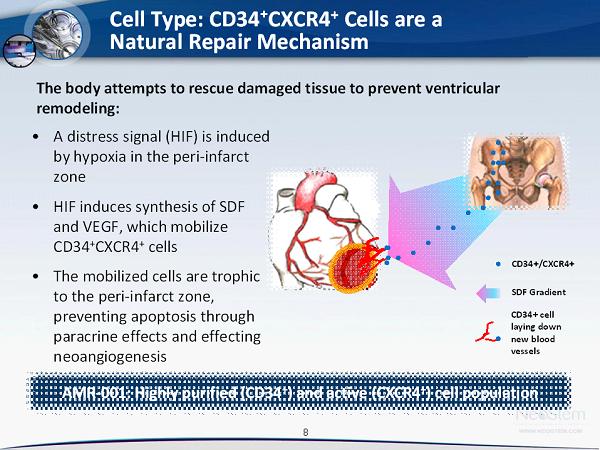
8 Cell Type: CD34⁺CXCR4 + Cells are a Natural Repair Mechanism • A distress signal (HIF) is induced by hypoxia in the peri - infarct zone • HIF induces synthesis of SDF and VEGF, which mobilize CD34 + CXCR4 + cells • The mobilized cells are trophic to the peri - infarct zone, preventing apoptosis through paracrine effects and effecting neoangiogenesis The body attempts to rescue damaged tissue to prevent ventricular remodeling: CD34+/CXCR4+ SDF Gradient CD34+ cell laying down new blood vessels AMR - 001: Highly purified (CD34 + ) and active (CXCR4 + ) cell population
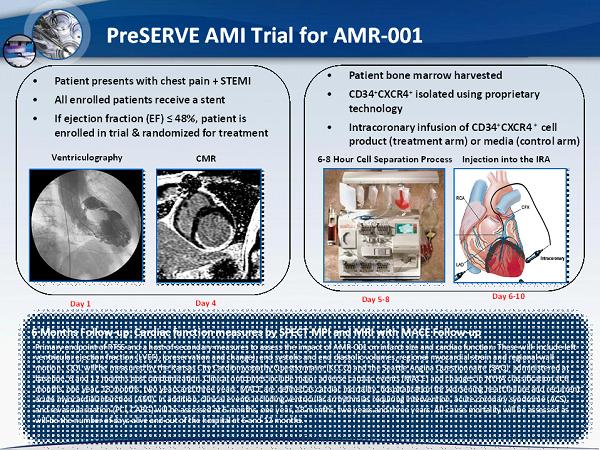
9 PreSERVE AMI Trial for AMR - 001 • Patient presents with chest pain + STEMI • All enrolled patients receive a stent • If ejection fraction (EF) ≤ 48%, patient is enrolled in trial & randomized for treatment Day 1 Day 4 • Patient bone marrow harvested • CD34 + CXCR4 + isolated using proprietary technology • Intracoronary infusion of CD34 + CXCR4 + cell product (treatment arm) or media (control arm) Day 5 - 8 6 - 8 Hour Cell Separation Process Ventriculography 9 CMR Day 6 - 10 6 Months Follow - up : Cardiac function measures by SPECT MPI and MRI with MACE Follow - up Primary endpoint of RTSS and a host of secondary measures to assess the impact of AMR - 001 on infarct size and cardiac function. These will include left ventricular ejection fraction (LVEF), (preservation and change), end systolic and end diastolic volumes, regional myocardial str ain and regional wall motion. QOL will be measured by the Kansas City Cardiomyopathy Questionnaire (KCCQ) and the Seattle Angina Questionnaire (SAQ) administered at baseline, 6 and 12 months post randomization. Clinical outcomes include major adverse cardiac events (MACE) and changes in NY HA classification at 6 months, one year, 18 months, two years and three years. MACE are defined as cardiac mortality, hospitalization for worsening hea rt failure and recurrent acute myocardial infarction (AMI). In addition, clinical events including ventricular arrhythmias requiring intervention, acute coronary syndrome (ACS), and revascularization (PCI, CABG) will be assessed at 6 months, one year, 18 months, two years and three years. All - cause mortal ity will be assessed as will be the number of days alive and out of the hospital at 6 and 12 months. Injection into the IRA
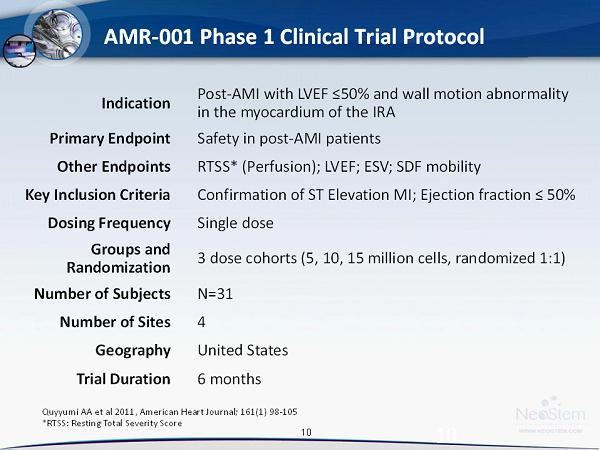
10 AMR - 001 Phase 1 Clinical Trial Protocol 10 Indication Post - AMI with LVEF ≤50% and wall motion abnormality in the myocardium of the IRA Primary Endpoint Safety in post - AMI patients Other Endpoints RTSS* (Perfusion); LVEF; ESV; SDF mobility Key Inclusion Criteria Confirmation of ST Elevation MI; Ejection fraction ≤ 50% Dosing Frequency Single dose Groups and Randomization 3 dose cohorts (5, 10, 15 million cells, randomized 1:1) Number of Subjects N=31 Number of Sites 4 Geography United States Trial Duration 6 months Quyyumi AA et al 2011, American Heart Journal; 161(1) 98 - 105 *RTSS: Resting Total Severity Score
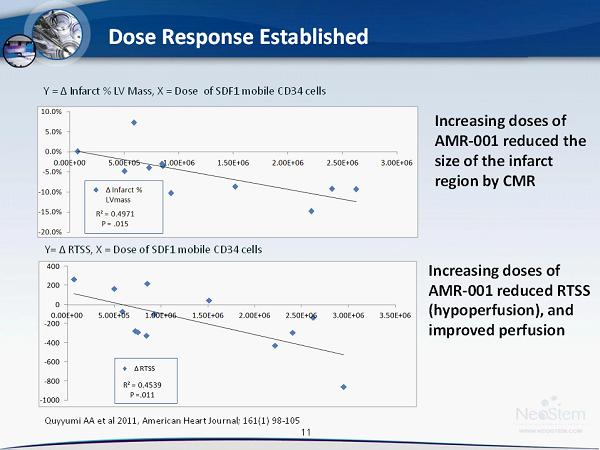
11 11 11 Dose Response Established Y = Δ Infarct % LV Mass, X = Dose of SDF1 mobile CD34 cells Increasing doses of AMR - 001 reduced the size of the infarct region by CMR Increasing doses of AMR - 001 reduced RTSS ( hypoperfusion ), and improved perfusion Y= Δ RTSS, X = Dose of SDF1 mobile CD34 cells Quyyumi AA et al 2011, American Heart Journal; 161(1) 98 - 105
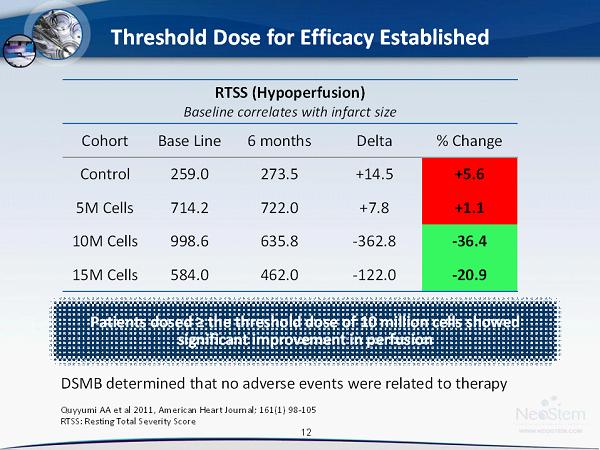
12 12 12 Threshold Dose for Efficacy Established RTSS ( Hypoperfusion ) Baseline correlates with infarct size Cohort Base Line 6 months Delta % Change Control 259.0 273.5 +14.5 +5.6 5M Cells 714.2 722.0 +7.8 +1.1 10M Cells 998.6 635.8 - 362.8 - 36.4 15M Cells 584.0 462.0 - 122.0 - 20.9 Patients dosed ≥ the threshold dose of 10 million cells showed significant improvement in perfusion DSMB determined that no adverse events were related to therapy Quyyumi AA et al 2011, American Heart Journal; 161(1) 98 - 105 RTSS: Resting Total Severity Score

13 13 13 Subgroup Analyses: Additional Cardiac Function Test Results RTSS ( Hypoperfusion ) 6 month Base Line 6 Mo. Δ % Δ Below Threshold 385.4 398.1 +12.6 +3.3 Above Threshold 814.3 558.6 - 255.8 - 31.4 (p=0.01)* * change in 10M/15M cells cohorts significant compared to 5M cells/Control cohorts Ejection Fraction 6 month BL 6 Mo. Δ % % Δ Below Threshold 51.0 51.8 0.7 +1.3 Above Threshold 48.2 52.7 +4.5 +9.4 End Systolic Volume 6 month BL 6 Mo. Δ ml % Δ Below Threshold 77.7 81.3 +3.6 +4.6 Above Threshold 94.1 88.4 - 5.7 - 6.1 The overall composite data and individual scores (EF) support potential best in class product Drop in Ejection Fraction 30% 40% Above Threshold Ejection Fraction [ Improvement +9.4% ] Quyyumi AA et al 2011, American Heart Journal; 161(1) 98 - 105
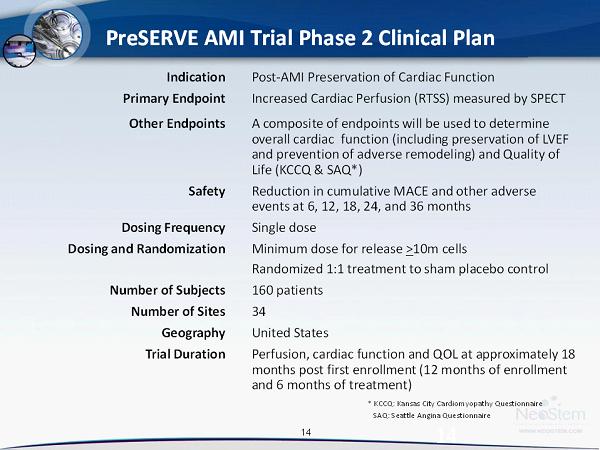
14 PreSERVE AMI Trial Phase 2 Clinical Plan 14 Indication Post - AMI Preservation of Cardiac Function Primary Endpoint Increased Cardiac Perfusion (RTSS) measured by SPECT Other Endpoints A composite of endpoints will be used to determine overall cardiac function (including preservation of LVEF and prevention of adverse remodeling) and Quality of Life (KCCQ & SAQ*) Safety Reduction in cumulative MACE and other adverse events at 6, 12, 18, 24, and 36 months Dosing Frequency Single dose Dosing and Randomization Minimum dose for release > 10m cells Randomized 1:1 treatment to sham placebo control Number of Subjects 160 patients Number of Sites 34 Geography United States Trial Duration Perfusion, cardiac function and QOL at approximately 18 months post first enrollment (12 months of enrollment and 6 months of treatment) * KCCQ: Kansas City Cardiomyopathy Questionnaire SAQ: Seattle Angina Questionnaire

15 15 15 Clinical Development Stage PII PII PI PI PII PII PII PI PII Field of Use AMI AMI AMI AMI AMI AMI HF HF CMI Defined Mechanism of Action x x x x x Autologous x x x x x x Potential Toxicities /Safety Signals x x x Centralized Manufacturing x x x x x x x x cGMP Defined Product x x x x x x x Threshold Dose x x x x x Cells Expanded x x x x Strong IP x AMI = Acute Myocardial Infarction HF = Heart Failure CMI = Chronic Myocardial Ischemia AMR - 001 Advantages in the Landscape AMR - 001 Advantages • Functionality of CD34 + CXCR4 + cells • Confirmed mechanism of action • cGMP processing and manufacturing that stabilizes the CD34 + CXCR4 + cells • Potency, viability, stability, sterility, and variability assays • Threshold dose is established at 10 million cells • Dominant IP • composition of matter • methods and processes • catheter delivery
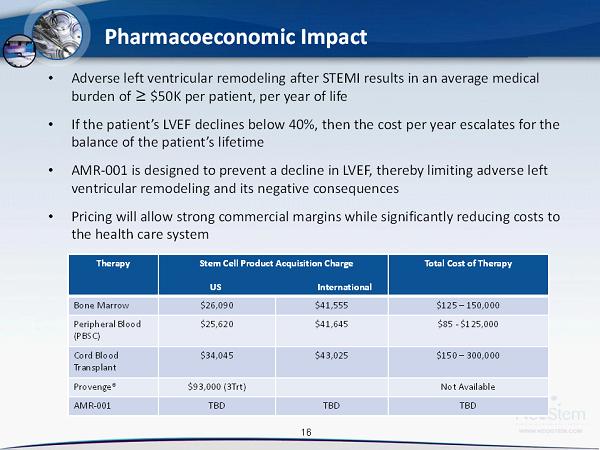
16 16 16 Pharmacoeconomic Impact • Adverse left ventricular remodeling after STEMI results in an average medical burden of ≥ $50K per patient, per year of life • If the patient’s LVEF declines below 40%, then the cost per year escalates for the balance of the patient’s lifetime • AMR - 001 is designed to prevent a decline in LVEF, thereby limiting adverse left ventricular remodeling and its negative consequences • Pricing will allow strong commercial margins while significantly reducing costs to the health care system Therapy Stem Cell Product Acquisition Charge US International Total Cost of Therapy Bone Marrow $26,090 $41,555 $125 – 150,000 Peripheral Blood (PBSC) $25,620 $41,645 $85 - $125,000 Cord Blood Transplant $34,045 $43,025 $150 – 300,000 Provenge ® $93,000 (3Trt) Not Available AMR - 001 TBD TBD TBD
17 Additional Potential Indications for AMR - 001 • AMR - 001 platform can be applied to other conditions resulting from underlying ischemia • Chronic Myocardial Ischemia post - AMI • Cardiomyopathy : – Ischemic – Chemotherapy Induced • Congestive Heart Failure • Critical Limb Ischemia • Cryopreserved preparations of AMR - 001 AMR - 001 platform can be applied to other conditions resulting from underlying ischemia • AMR - 001: Composition of matter patent (2028) • NeoStem’s patent estate includes patents for Amorcyte , Athelos & VSELs™ Over 30 issued patents and over 90 pending patent applications, including composition of matter and methods claims. Geographic breadth of filings includes North America, Europe, Asia, Australia, Israel and South Africa
18 18 18 Athelos: T - reg Cells - Restoring Immune Balance • Partnership with Becton Dickinson which owns 20% of the Athelos subsidiary • Immune mediated diseases, such as GVHD, autoimmune diseases and allergic diseases, are a result of an imbalance between T - effector cells and T - regulatory cells (T - reg ) • T - reg therapy represents a novel approach for restoring immune balance by enhancing T - regulatory cell number and function • T - reg cells are collected by apheresis , isolated using surface markers (for example: CD4+, CD25+, FoxP3+), activated and expanded ex vivo approximately 500 fold in 20 days 1 • Phase 1 work is ongoing globally under several independent physician INDs, results of which will inform NeoStem’s future clinical direction 1) Chai, Jian - Guo et al, Journal of Immunology 2008; 180;858 - 869

19 19 19 VSEL™ Pluripotent Adult Stem Cells heart neuron pancreas VSEL™ • VSEL™ (Very Small Embryonic - Like) technology is NeoStem’s proprietary adult stem cell technology platform • Believed to be naturally pluripotent – no manipulation required • iPSCs (induced pluripotent stem cells) are recognized as manipulated and destroyed by the immune system (even as an autologous product) • VSELs™ have been shown in animal research to home to sites of injury, up - regulate angiogenesis, down - regulate inflammation (the “paracrine effect”), BUT, importantly, go one step further and differentiate into target cell types VSELs™ potentially represent the most powerful regenerative cell as they are pluripotent, autologous, “ natural,” powerful “paracrine” cells. Rodgerson DO, Harris AG, “A Comparison of Stem Cells for Therapeutic Use”, Stem Cell Rev. 2011 Mar 2.

20 20 20 Financial Highlights Key Metrics as of September 30, 2011 Revenue $56.0m (nine months ended 9/30/11) Cash Position $15.6m* Net Loss Excluding Non - Cash Charges $10.0m (nine months ended 9/30/11)* Total Stock and Equivalent Shares Common Shares 100.4m Options 17.7m Warrants 35.2m Series E Preferred Stock 4.7m *See Appendix for GAAP to Non - GAAP reconciliation
21 21 21 Key Executives Robin Smith, MD, MBA CEO & Chairman of the Board MD – Yale; MBA – Wharton Formerly President & CEO IP2M (HC multimedia), EVP & CMO HealthHelp (radiology management) Trustee of NYU Medical Center; Chairman of the Board of NYU Hospital for Joint Diseases (through November 2009) and Stem for Life Foundation Larry May Chief Financial Officer BS Business Administration – University of Missouri Formerly Treasurer & Controller at Amgen; SVP Finance & CFO at BioSource Intl Extensive experience building accounting, finance and IT operations Jason Kolbert, MBA VP of Strategic Business Development BS Chemistry – SUNY New Paltz, MBA - University of New Haven 17 years experience on Wall Street as Research Analyst in biotechnology in US and Asia 6 years in the pharmaceutical industry with Schering-Plough in Japan Andrew Pecora, MD, FACP Chief Medical Officer MD – University of Medicine and Dentistry of New Jersey Chief Innovations Officer, Professor and Vice President of Cancer Services at John Theurer Cancer Center at Hackensack University Medical Center Robert Preti, PhD President and Chief Scientific Officer of PCT PhD and MS in Cellular Biology / Hematology - New York University One of the country’s leading authorities on cell engineering and the principal investigator for a number of clinical trials relating to stem cell transplantation 10 years experience as Director of Hematopoietic Stem Cell Processing & Research Laboratory Jian Zhang General Manager, Suzhou Erye Pharmaceuticals Co., Ltd Joined Erye in 2003; extensive experience in the Chinese pharmaceutical industry Degree in Finance and Accounting from Central Television University Certified Public Accountant in China
22 22 22 • First patient enrollment in PreSERVE AMI Phase 2 trial (Q1 2012 ) • Expansion of intellectual property beyond cardiovascular disease (Q1 2012) • Start of AMR - 001 trial in congestive heart failure (2012) • Athelos – data read - out from investigator sponsored P1 trials in GVHD, diabetes, solid organ transplant, and asthma (2012) • Presentation of VSEL TM Technology data at American Society of Hematology Annual Meeting by SAB member, Dec. 10 - 13, 2011 • Monetization of 51% ownership in Suzhou Erye (2012) • Data readouts for PreServe AMI Phase 2 Trial (Q3 2013) • Additional government research grants Recent and Expected Milestones

23 23 23 Questions
24 24 24 Board of Directors Robin Smith, MD, MBA CEO & Chairman of the Board MD – Yale; MBA – Wharton Formerly President & CEO IP2M (HC multimedia), EVP & CMO HealthHelp (radiology management) Experience - Trustee of NYU Medical Center; Chairman of the Board of NYU Hospital for Joint Diseases (through November 2009) and Stem for Life Foundation Richard Berman (Independent) Over 35 years of venture capital, management, M&A experience Experience – Current Board of Directors of Apricus Biosciences, Easylink Services International, Inc., Advaxis, Inc., Broadcaster, Inc., National Investment Managers Drew Bernstein, CPA (Independent) BS – University of Maryland Business School Licensed in State of New York; member AICPA, NYSSCPA and NSA Experience – Bernstein & Pinchuk LLP (member of BDO Seidman Alliance); PRC auditing; 200+ real estate transactions with $3B+ aggregate value; accountant and business advisor Edward Geehr, MD (Independent) BS – Yale University; MD – Duke University Experience – Abraxis Bio-Science; Allez Spine; IPC-The Hospitalist Company Martyn Greenacre, MBA (Independent) BA – Harvard College; MBA – Harvard Business School Experience – Board and executive positions for multiple biopharmaceutical companies; Former CEO of Delsys Pharmaceutical Corporation and Zynaxis Inc; Chairman of the Board of BMP Sunstone Corporation Steven Myers (Independent) BS Mathematics – Stanford University Experience – Founder/Chairman/CEO SM&A (competition management services); career in aerospace and defense sectors supporting DoD & NASA programs Andrew Pecora, MD, FACP MD — University of Medicine and Dentistry of New Jersey Experience – Chief Innovations Officer, Professor and Vice President of Cancer Services at John Theurer Cancer Center at Hackensack University Medical Center, and Managing Partner of the Northern New Jersey Cancer Center Mingsheng Shi Chairman of the Board of Suzhou Erye Pharmaceutical BSc Economics & Management – Party School of the Communist Party of China Professional title of Senior Economist Extensive experience in pharmaceutical industry in China Eric Wei Managing Partner, RimAsia Capital Partners BS Mathematics & Economics – Amherst College; MBA – Wharton Experience – Founder/Managing Partner of RimAsia Capital Partners (private equity); Peregrine Capital, Prudential Securities, Lazard Freres, Citibank; Gilbert Global Equity PartnersCrimson Asia Capital Partners NeoStem Board Members
25 25 25 Eugene Braunwald, MD, FRCP Brigham & Women’s Hospital Bernard J. Gersh, MD, ChB, DPhil, FRCP The Mayo Clinic Dean J. Kereiakes, MD, FACC The Christ Hospital Heart of Greater Cincinnati Douglas L. Mann, MD, FACC Washington University School of Medicine Andrew L. Pecora, MD, FACP, CPE Chief Medical Officer, NeoStem Hackensack University Medical Center Carl J. Pepine, MD University of Florida College of Medicine Emerson C. Perin, MD, PhD, FACC Texas Heart Institute Bertram Pitt, MD University of Michigan School of Medicine Arshed Quyyumi, MD, FRCP, FACC Principal Investigator, Phase II Emory University School of Medicine Edmund K. Waller, MD, PhD, FACP Emory University School of Medicine James T. Willerson, MD University Texas Health Science Center Joseph Wu, MD, PhD Stanford University School of Medicine Amorcyte Scientific Advisory Board
26 26 26 Athelos Scientific Advisory Board Robert A. Preti, PhD, Chairman Progenitor Cell Therapy Bruce Blazar, MD University of Michigan Masonic Cancer Center Jeffrey Bluestone, PhD University of California, San Francisco, Diabetes Center David A. Horwitz, MD University of Southern California Carl June, MD Perelman School of Medicine, University of California Robert Korngold, PhD Hackensack University Medical Center Wayne A. Marasco, MD, PhD Dana-Farber Cancer Institute Robert S. Negrin, MD Stanford University David Peritt, PhD Hospira Camillo Recordi, MD University of Miami Diabetes Research Institute Noel L. Warner, PhD BD Biosciences
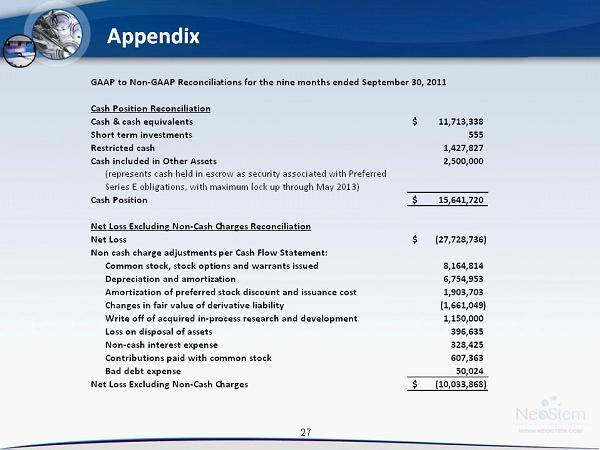
27 27 27 Appendix GAAP to Non-GAAP Reconciliations for the nine months ended September 30, 2011 Cash Position Reconciliation Cash & cash equivalents 11,713,338$ Short term investments 555 Restricted cash 1,427,827 Cash included in Other Assets 2,500,000 (represents cash held in escrow as security associated with Preferred Series E obligations, with maximum lock up through May 2013) Cash Position 15,641,720$ Net Loss Excluding Non-Cash Charges Reconciliation Net Loss (27,728,736)$ Non cash charge adjustments per Cash Flow Statement: Common stock, stock options and warrants issued 8,164,814 Depreciation and amortization 6,754,953 Amortization of preferred stock discount and issuance cost 1,903,703 Changes in fair value of derivative liability (1,661,049) Write off of acquired in-process research and development 1,150,000 Loss on disposal of assets 396,635 Non-cash interest expense 328,425 Contributions paid with common stock 607,363 Bad debt expense 50,024 Net Loss Excluding Non-Cash Charges (10,033,868)$