Attached files
| file | filename |
|---|---|
| EXCEL - IDEA: XBRL DOCUMENT - Synthetic Biologics, Inc. | Financial_Report.xls |
| EX-32.1 - EXHIBIT 32.1 - Synthetic Biologics, Inc. | v239387_ex32-1.htm |
| EX-31.2 - EXHIBIT 31.2 - Synthetic Biologics, Inc. | v239387_ex31-2.htm |
| EX-31.1 - EXHIBIT 31.1 - Synthetic Biologics, Inc. | v239387_ex31-1.htm |
UNITED STATES SECURITIES AND EXCHANGE COMMISSION
Washington, DC 20549
FORM 10-Q
(Mark One)
|
x
|
QUARTERLY REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934
|
|
|
For the quarterly period ended September 30, 2011
|
OR
|
o
|
TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES ACT OF 1934
|
|
|
For the transition period from ____________ to ____________
|
Commission File Number: 1-12584
ADEONA PHARMACEUTICALS, INC.
(Name of small business issuer in its charter)
|
Nevada
|
13-3808303
|
|
|
(State or other jurisdiction of incorporation or organization)
|
(IRS Employer Identification Number)
|
|
|
3985 Research Park Drive, Suite 200
|
||
|
Ann Arbor, MI
|
48108
|
|
|
(Address of principal executive offices)
|
(Zip Code)
|
Registrant’s telephone number, including area code:
(734) 332-7800
Securities registered pursuant to Section 12(b) of the Act:
Common Stock, $0.001 par value per share
Securities registered pursuant to Section 12(g) of the Act:
None.
(Title of Class)
Indicate by check mark whether the issuer: (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes x No o
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes x No o
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated file, a non-accelerated file, or a smaller reporting company. See the definitions of “large accelerated filer, “accelerated filer” and “smaller reporting company” in Rule 12b-2 of the Exchange Act. (Check one):
|
Large accelerated filer o
|
Accelerated filer o
|
|
|
Non-Accelerated filer o
|
Smaller reporting company x
|
|
|
(Do not check if a smaller reporting company)
|
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes o No x
As of November 10, 2011, the registrant had 28,209,126 shares of common stock outstanding.
ADEONA PHARMACEUTICALS, INC.
FORM 10-Q
TABLE OF CONTENTS
|
Page
|
|||
|
PART I. — FINANCIAL INFORMATION
|
|||
|
Item 1.
|
Financial Statements
|
||
|
Consolidated Balance Sheets as of September 30, 2011 (Unaudited) and December 31, 2010
|
3
|
||
|
Consolidated Statements of Operations (Unaudited)
|
4
|
||
|
Consolidated Statements of Cash Flows (Unaudited)
|
5
|
||
|
Notes to Consolidated Financial Statements (Unaudited)
|
6
|
||
|
Item 2.
|
Management’s Discussion and Analysis of Financial Information and Results of Operations
|
15
|
|
|
Item 3.
|
Quantitative and Qualitative Disclosures About Market Risks
|
26
|
|
|
Item 4.
|
Controls and Procedures
|
26
|
|
|
PART II — OTHER INFORMATION
|
|||
|
Item 1.
|
Legal Proceedings
|
27
|
|
|
Item 1A.
|
Risk Factors
|
27
|
|
|
Item 2.
|
Unregistered Sales of Equity Securities and Use of Proceeds
|
45
|
|
|
Item 3.
|
Defaults Upon Senior Securities
|
45
|
|
|
Item 4.
|
Reserved and Removed
|
45
|
|
|
Item 5.
|
Other Information
|
45
|
|
|
Item 6.
|
Exhibits
|
46
|
|
|
SIGNATURE
|
47
|
||
|
GLOSSARY
|
48
|
||
2
PART I. — FINANCIAL INFORMATION
ITEM 1. FINANCIAL STATEMENTS
Consolidated Balance Sheets
|
September 30, 2011
|
December 31, 2010
|
|||||||
|
(Unaudited)
|
||||||||
|
Assets
|
||||||||
|
Current Assets
|
||||||||
|
Cash and cash equivalents
|
$
|
4,608,607
|
$
|
2,648,853
|
||||
|
Short-term investments
|
2,865,961
|
-
|
||||||
|
Accounts receivable – net
|
494,851
|
338,510
|
||||||
|
Other
|
123,752
|
343,417
|
||||||
|
Total Current Assets
|
8,093,171
|
3,330,780
|
||||||
|
Property and equipment, net
|
371,463
|
511,142
|
||||||
|
Goodwill
|
178,229
|
178,229
|
||||||
|
Deposits and other assets
|
32,300
|
90,848
|
||||||
|
Total Assets
|
$
|
8,675,163
|
$
|
4,110,999
|
||||
|
Liabilities and Stockholders' Equity
|
||||||||
|
Current Liabilities:
|
||||||||
|
Accounts payable
|
$
|
193,015
|
$
|
265,722
|
||||
|
Accrued liabilities
|
41,012
|
210,027
|
||||||
|
Current portion of capital lease
|
-
|
24,400
|
||||||
|
Total Current Liabilities
|
234,027
|
500,149
|
||||||
|
Long Term Liabilities:
|
||||||||
|
Accounts payable
|
2,335
|
32,335
|
||||||
|
Total Liabilities
|
236,362
|
532,484
|
||||||
|
Stockholders' Equity
|
||||||||
|
Preferred stock, $0.001 par value; 10,000,000 shares authorized,
|
||||||||
|
none issued and outstanding
|
-
|
-
|
||||||
|
Common stock, $0.001 par value; 100,000,000 shares authorized,
|
||||||||
|
28,127,644 issued and 28,209,126 outstanding
|
||||||||
|
and 23,420,189 issued and 23,338,707 outstanding
|
28,128
|
23,339
|
||||||
|
Additional paid-in capital
|
57,099,249
|
47,279,416
|
||||||
|
Accumulated deficit
|
(48,688,576
|
)
|
(43,724,240
|
)
|
||||
|
Total Stockholders' Equity
|
8,438,801
|
3,578,515
|
||||||
|
Total Liabilities and Stockholders' Equity
|
$
|
8,675,163
|
$
|
4,110,999
|
||||
See accompanying notes to unaudited consolidated financial statements
3
Consolidated Statements of Operations
(Unaudited)
|
Three months ended
September 30, |
Nine months ended
September 30, |
|||||||||||||||
|
2011
|
2010
|
2011
|
2010
|
|||||||||||||
|
Revenues:
|
||||||||||||||||
|
License revenue, net
|
$
|
-
|
$
|
-
|
$
|
-
|
$
|
2,125,000
|
||||||||
|
Laboratory revenues, net
|
293,421
|
289,898
|
972,121
|
419,825
|
||||||||||||
|
Total Revenues
|
293,421
|
289,898
|
972,121
|
2,544,825
|
||||||||||||
|
Operating Costs and Expenses:
|
||||||||||||||||
|
General and administrative
|
681,805
|
601,806
|
2,649,623
|
2,000,262
|
||||||||||||
|
Research and development
|
288,964
|
229,044
|
800,923
|
962,766
|
||||||||||||
|
Costs of laboratory services
|
260,881
|
192,176
|
805,881
|
430,001
|
||||||||||||
|
Total Operating Costs and Expenses
|
1,231,650
|
1,023,026
|
4,256,427
|
3,393,029
|
||||||||||||
|
Loss from Operations
|
(938,229
|
)
|
(733,128
|
)
|
(3,284,306
|
)
|
(848,204
|
)
|
||||||||
|
Other Income (Expense):
|
||||||||||||||||
|
Warrant expense
|
-
|
-
|
(1,491,996
|
)
|
-
|
|||||||||||
|
Change in fair value of warrant liability
|
(164,993
|
)
|
-
|
(242,464
|
)
|
-
|
||||||||||
|
Interest income
|
6,868
|
-
|
6,868
|
|||||||||||||
|
Other income (expense)
|
(1,625
|
)
|
293
|
47,562
|
7,629
|
|||||||||||
|
Total Other Income (Expense), net
|
(159,750
|
)
|
293
|
(1,680,030
|
)
|
7,629
|
||||||||||
|
Net Loss
|
$
|
(1,097,979
|
)
|
$
|
(732,835
|
)
|
$
|
(4,964,336
|
)
|
$
|
(840,575
|
)
|
||||
|
Net Loss Per Share – Basic and Dilutive
|
$
|
(0.04
|
)
|
$
|
(0.03
|
)
|
$
|
(0.18
|
)
|
$
|
(0.04
|
)
|
||||
|
Weighted average number of common shares outstanding during the period – Basic and Dilutive
|
28,089,492
|
23,003,033
|
27,075,730
|
22,095,349
|
||||||||||||
4
Consolidated Statements of Cash Flows
(Unaudited)
|
Nine months ended September 30,
|
||||||||
|
2011
|
2010
|
|||||||
|
Cash Flows From Operating Activities:
|
||||||||
|
Net loss
|
$
|
(4,964,336
|
)
|
$
|
(840,575
|
)
|
||
|
Adjustments to reconcile net loss to net cash used in operating activities:
|
||||||||
|
Recognition of stock-based compensation
|
483,424
|
324,885
|
||||||
|
Stock option modification expense
|
397,767
|
-
|
||||||
|
Stock issued for consulting fees
|
164,870
|
157,706
|
||||||
|
Stock issued as compensation
|
75,840
|
46,613
|
||||||
|
Warrant expense
|
1,491,996
|
-
|
||||||
|
Change in fair value of warrant liability
|
242,465
|
-
|
||||||
|
Unrealized loss on short term investments
|
205
|
|||||||
|
Depreciation
|
132,787
|
271,076
|
||||||
|
Provision for uncollectible accounts receivable
|
254,298
|
250,427
|
||||||
|
(Gain) loss on sale of equipment
|
5,692
|
(3,390
|
)
|
|||||
|
Gain on settlement of accounts payable
|
(62,996
|
)
|
-
|
|||||
|
Changes in operating assets and liabilities:
|
||||||||
|
Accounts receivable
|
(410,639
|
)
|
(607,225
|
)
|
||||
|
Other current assets
|
219,665
|
163
|
||||||
|
Deposits and other assets
|
58,548
|
-
|
||||||
|
Accounts payable
|
(39,711
|
)
|
(79,034
|
)
|
||||
|
Accrued liabilities
|
(169,015
|
)
|
(434
|
)
|
||||
|
Net Cash Used In Operating Activities
|
(2,119,140
|
)
|
(479,788
|
)
|
||||
|
Cash Flows From Investing Activities:
|
||||||||
|
Purchase of short term investments
|
(2,866,166
|
)
|
||||||
|
Purchase of property and equipment
|
-
|
(2,070
|
)
|
|||||
|
Proceeds from the sale of equipment
|
1,200
|
76,460
|
||||||
|
Net Cash Provided By (Used In) Investing Activities
|
(2,864,966
|
)
|
74,390
|
|||||
|
Cash Flows From Financing Activities:
|
||||||||
|
Repayments under capital lease
|
(24,400
|
)
|
(10,878
|
)
|
||||
|
Proceeds from issuance of common stock for stock option exercises
|
7,650
|
121,878
|
||||||
|
Proceeds from the issuance of common stock, net of offering costs of $539,390 and $115,276
|
6,960,610
|
884,724
|
||||||
|
Net Cash Provided By Financing Activities
|
6,943,860
|
995,724
|
||||||
|
Net increase in cash
|
1,959,754
|
590,326
|
||||||
|
Cash at beginning of period
|
2,648,853
|
2,715,044
|
||||||
|
Cash at end of period
|
$
|
4,608,607
|
$
|
3,305,370
|
||||
|
Supplemental disclosures of cash flow information :
|
||||||||
|
Cash paid for interest
|
$
|
-
|
$
|
2,784
|
||||
|
Cash paid for taxes
|
$
|
-
|
$
|
-
|
||||
|
Supplemental disclosure for non-cash item:
|
||||||||
|
Reclassification of derivative liability to additional paid in capital
|
$
|
1,734,461
|
$
|
-
|
||||
5
Notes to Consolidated Financial Statements
(Unaudited)
1. Organization
Adeona Pharmaceuticals, Inc. (the “Company” or Adeona”) is a pharmaceutical company focused on developing innovative medicines for the treatment of serious central nervous system diseases. The Company’s strategy is to license product candidates that have demonstrated a certain level of clinical efficacy and develop them to a stage that results in a significant commercial collaboration. Adeona is developing, or has partnered the development of, drug product candidates to treat multiple sclerosis, cognitive dysfunction in multiple sclerosis, fibromyalgia, amyotrophic lateral sclerosis (ALS) and Alzheimer’s disease. The Company is currently focused on the commercialization of wellZinTM, a homeopathic over-the-counter zinc acetate lozenge to reduce the duration and symptoms of the common cold. Adeona is also developing reaZinTM as a medical food for the dietary management of zinc deficiency associated with Alzheimer’s disease. Adeona also operates Adeona Clinical Laboratory, a wholly owned clinical reference laboratory that provides a broad array of chemistry and microbiology diagnostic tests.
2. Basis of Presentation
The accompanying unaudited condensed interim financial statements have been prepared in accordance with accounting principles generally accepted in the United States of America and the rules and regulations of the United States Securities and Exchange Commission for interim financial information and with the instructions to Form 10-Q and Article 10 of Regulation S-X.
The financial information as of December 31, 2010, is derived from the audited financial statements presented in the Company’s Annual Report on Form 10-K for the year ended December 31, 2010. The unaudited condensed interim financial statements should be read in conjunction with the Company’s Annual Report on Form 10-K, which contains the audited financial statements and notes thereto, together with the Management’s Discussion and Analysis, for the year ended December 31, 2010.
Certain information or footnote disclosures normally included in financial statements prepared in accordance with accounting principles generally accepted in the United States of America have been condensed or omitted, pursuant to the rules and regulations of the Securities and Exchange Commission for interim financial reporting. Accordingly, they do not include all the information and footnotes necessary for a comprehensive presentation of financial position, results of operations, or cash flows. It is management's opinion, however, that all material adjustments (consisting of normal recurring adjustments) have been made which are necessary for a fair financial statement presentation. The interim results for the period ended September 30, 2011, are not necessarily indicative of results for the full year.
The Company has eight subsidiaries, Pipex Therapeutics, Inc. (“Pipex Therapeutics”), Adeona Clinical Laboratory (formerly Hart Lab, LLC), Effective Pharmaceuticals, Inc. (“EPI”), Solovax, Inc. (“Solovax”), CD4 Biosciences, Inc. (“CD4”), Epitope Pharmaceuticals, Inc. (“Epitope”), Healthmine, Inc. (“Healthmine”) and Putney Drug Corp. (“Putney”). As of September 30, 2011, EPI, Adeona Clinical Laboratory, Healthmine and Putney are wholly owned and Pipex Therapeutics, Solovax, CD4 and Epitope are majority-owned.
3. Summary of Significant Accounting Policies
Principles of Consolidation
All significant inter-company accounts and transactions have been eliminated in consolidation.
Use of Estimates
The preparation of consolidated financial statements in conformity with United States generally accepted accounting principles requires management to make estimates and assumptions that affect the amounts reported in the consolidated financial statements and accompanying notes. Such estimates and assumptions impact, among others, the following: the amount allocated to goodwill, the estimated useful lives for intangible assets and for property and equipment, the fair value of warrants and stock options granted for services or compensation, respectively, estimates of the probability and potential magnitude of contingent liabilities and the valuation allowance for deferred tax assets due to continuing operating losses.
Making estimates requires management to exercise significant judgment. It is at least reasonably possible that the estimate of the effect of a condition, situation or set of circumstances that existed at the date of the consolidated financial statements, which management considered in formulating its estimate could change in the near term due to one or more future confirming events. Accordingly, the actual results could differ significantly from our estimates.
6
Accounts Receivable and Allowance for Doubtful Accounts
Accounts receivable are reported at realizable value, net of allowances for doubtful accounts, which is estimated and recorded in the period the related revenue is recorded. The Company estimates and reviews the collectability of its receivables based on a number of factors, including the period they have been outstanding. Historical collection and payer reimbursement experience is an integral part of the estimation process related to allowances for doubtful accounts associated with Adeona Clinical Laboratory. In addition, the Company regularly assesses the state of its billing operations in order to identify issues that may impact the collectability of these receivables or reserve estimates. Revisions to the allowances for doubtful accounts estimates are recorded as an adjustment to bad debt expense. Receivables deemed uncollectible are charged against the allowance for doubtful accounts. Recoveries of receivables previously written-off are recorded as credits to the allowance for doubtful accounts.
Revenue Recognition
The Company records revenue when all of the following have occurred: (1) persuasive evidence of an arrangement exists, (2) the service is completed without further obligation, (3) the sales price to the customer is fixed or determinable, and (4) collectability is reasonably assured. The Company recognizes milestone payments or upfront payments that have no contingencies as revenue when payment is received. The Company has two streams of revenue, license revenue and laboratory revenue.
License Revenues
The Company’s licensing agreements may contain multiple elements, such as non-refundable up-front fees, payments related to the achievement of particular milestones and royalties. Fees associated with substantive at risk performance-based milestones are recognized as revenue upon completion of the scientific or regulatory event specified in the agreement. When the Company has substantive continuing performance obligations under an arrangement, revenue is recognized over the performance period of the obligations using a time-based proportional performance approach. Under the time-based method, revenue is recognized over the arrangement’s estimated performance period based on the elapsed time compared to the total estimated performance period. Revenue recognized at any point in time is limited to the amount of non-contingent payments received or due. When the Company has no substantive continuing performance obligations under an arrangement, it recognizes revenue as the related fees become due.
Revenues from royalties on third-party sales of licensed technologies are generally recognized in accordance with the contract terms when the royalties can be reliably determined and collectibility is reasonably assured. To date, the Company has not received any royalty revenues.
Laboratory Revenues
The Company primarily recognizes revenue for services rendered upon completion of the testing process. Billing for services reimbursed by third-party payers, including Medicare and Medicaid, are recorded as revenues, net of allowances for differences between amounts billed and the estimated receipts from such payers.
The Company maintains a sales allowance to compensate for the difference in its billing practices and insurance company reimbursements. In determining this allowance, the Company looks at several factors, the most significant of which is the average difference between the amount charged and the amount reimbursed by insurance carriers over the prior 18 months, otherwise known as the yearly average adjustment amount. The actual sales allowance taken for each period is the averaged yearly average adjustment amount for these prior periods multiplied by the period’s actual gross revenues.
The Company generated reimbursements from 3 significant insurance providers for the nine months ended September 30, 2011 and 2010.
|
Customer
|
2011
|
2010
|
||||||
| A |
69
|
%
|
68
|
%
|
||||
| B |
4
|
%
|
14
|
%
|
||||
| C |
20
|
%
|
10
|
%
|
||||
Risks and Uncertainties
The Company's operations are subject to significant risk and uncertainties including financial, operational, regulatory and other risks, such as the potential risk of business failure. The recent global economic crisis has caused a general tightening in the credit markets, lower levels of liquidity, increases in the rates of default and bankruptcy, and extreme volatility in credit, equity and fixed income markets. These conditions not only limit the Company’s access to capital, but also make it difficult for the Company’s customers, the Company’s vendors and the Company to accurately forecast and plan future business activities.
7
Cash and Cash Equivalents
The Company considers all highly liquid investments with original maturities of three months or less at the time of purchase to be cash equivalents. As of September 30, 2011, and December 31, 2010, respectively, the Company had no cash equivalents.
The Company minimizes credit risk associated with cash by periodically evaluating the credit quality of its primary financial institution. The balance at times may exceed the federally insured limit of $250,000 per depositor, per bank. The Company also held cash in a money market account that is covered by the Securities Investor Protection Corporation (SIPC) for losses up to $500,000. At September 30, 2011 and December 31, 2010, the balance exceeded the federally insured limit by $2.6 million and $2.1 million, respectively.
Classification of Marketable Securities as Held to Maturity, Trading, and Available for Sale
The Company determines the appropriate classification of its investments in debt and equity securities at the time of purchase and reevaluates such determinations at each balance sheet date. Debt securities are classified as held to maturity when the Company has the positive intent and ability to hold the securities to maturity. Debt securities for which the Company does not have the intent or ability to hold to maturity are classified as available for sale. Held to maturity securities are recorded as either short-term or long-term on the balance sheet, based on contractual maturity date and are stated at amortized cost. Marketable securities that are bought and held principally for the purpose of selling them in the near term are classified as trading securities and are reported at fair value, with unrealized gains and losses recognized in earnings. Debt and marketable equity securities not classified as held to maturity or as trading, are classified as available for sale, and are carried at fair market value, with the unrealized gains and losses, net of tax, included in the determination of comprehensive income and reported in shareholders’ equity. All of the Company’s marketable securities at September 30, 2011 are classified as held to maturity.
Fair Value of Financial Instruments
The fair value accounting standards define fair value as the amount that would be received to sell an asset or paid to transfer a liability in an orderly transaction between market participants. As such, fair value is determined based upon assumptions that market participants would use in pricing an asset or liability. Fair value measurements are rated on a three-tier hierarchy as follows:
|
·
|
Level 1 inputs: Quoted prices (unadjusted) for identical assets or liabilities in active markets;
|
|
·
|
Level 2 inputs: Inputs, other than quoted prices included in Level 1 that are observable either directly or indirectly; and
|
|
·
|
Level 3 inputs: Unobservable inputs for which there is little or no market data, which require the reporting entity to develop its own assumptions.
|
In many cases, a valuation technique used to measure fair value includes inputs from multiple levels of the fair value hierarchy described above. The lowest level of significant input determines the placement of the entire fair value measurement in the hierarchy.
The carrying amounts of the Company’s short-term financial instruments approximate fair value due to the relatively short period to maturity for these instruments.
Warrant / Derivative Liabilities
Fair value accounting requires bifurcation of embedded derivative instruments such as conversion features in convertible debt or equity instruments, and measurement of their fair value for accounting purposes. In determining the appropriate fair value, the Company uses the Black-Scholes option-pricing model. In assessing the convertible debt instruments, management determines if the convertible debt host instrument is conventional convertible debt and further if there is a beneficial conversion feature requiring measurement. If the instrument is not considered conventional convertible debt, the Company will continue its evaluation process of these instruments as derivative financial instruments.
Once determined, derivative liabilities are adjusted to reflect fair value at each reporting period end, with any increase or decrease in the fair value being recorded in results of operations as an adjustment to fair value of derivatives. In addition, the fair value of freestanding derivative instruments such as warrants, are also valued using the Black-Scholes option-pricing model.
8
Net Income (Loss) per Share
Net income (loss) per share is computed by dividing net income (loss) less preferred dividends for the period by the weighted average number of common shares outstanding. Diluted income (loss) per share is computed by dividing net income (loss) less preferred dividends by the weighted average number of common shares outstanding including the effect of common share equivalents. Since the Company reported a net loss for the nine months ended September 30, 2011 and 2010, all common equivalent shares would be anti-dilutive; as such there is no separate computation for diluted loss per share. The number of options and warrants for the purchase of common stock, that were excluded from the computations of net loss per common share for the nine months ended September 30, 2011 were 2,823,281 and 3,368,738, respectively, and for the nine months ended September 30, 2010 were 2,455,759 and 1,131,078, respectively.
Research and Development Costs
The Company expenses research and development costs as incurred. Research and development expenses consist primarily of license fees, manufacturing costs, salaries, stock-based compensation and related personnel costs, fees paid to consultants and outside service providers for laboratory development, legal expenses resulting from intellectual property prosecution and other expenses relating to the design, development, testing and enhancement of the Company’s product candidates.
Share-Based Payment Arrangements
Generally, all forms of share-based payments, including stock option grants, warrants, restricted stock grants and stock appreciation rights are measured at their fair value on the awards’ grant date, based on the estimated number of awards that are ultimately expected to vest. Share-based compensation awards issued to non-employees for services rendered are recorded at either the fair value of the services rendered or the fair value of the share-based payment, whichever is more readily determinable. The expense resulting from share-based payments are recorded in cost of goods sold, research and development or general and administrative expenses in the consolidated statement of operations, depending on the nature of the services provided.
Recent Accounting Pronouncements
In May 2011, the Financial Accounting Standards Board (FASB) issued guidance in regard to fair value measurement. The new guidance results in a consistent definition of fair value and common requirements for measurement of and disclosure about fair value between GAAP and International Financial Reporting Standards (IFRS). This guidance is effective for interim and annual periods beginning after December 15, 2011. The adoption of this guidance is not expected to have a material impact on the Company’s financial position or results of operations.
In September 2011, the FASB issued guidance in regard to goodwill impairment. The new guidance is intended to reduce the cost and complexity of the annual goodwill impairment test by providing entities with the option of performing a "qualitative" assessment to determine whether further impairment testing is necessary. An entity can choose to perform the qualitative assessment on none, some, or all of its reporting units. Moreover, an entity can bypass the qualitative assessment for any reporting unit in any period and proceed directly to step one of the impairment test, and then perform the qualitative assessment in any subsequent period. The new guidance is effective for annual and interim goodwill impairment tests performed for fiscal years beginning after December 15, 2011, with early adoption permitted. The adoption of this guidance is not expected to have a material impact on the Company’s financial position or results of operations.
Reclassifications
To conform prior period amounts to current year classifications, the Company has reclassified laboratory services, and research and development expenses to general and administrative expenses. These reclassifications had no impact on the Company’s previously reported results of operations or cash flows.
4. Held to Maturity Debt Securities
At September 30, 2011 and December 31, 2010, the Company held investments in marketable securities that were classified as held to maturity and consisted of corporate bonds as follows:
|
September 30, 2011
|
December 31, 2010
|
|||||||
|
Amortized cost
|
$
|
2,366,166
|
$
|
-
|
||||
|
Unrecognized holding gains
|
-
|
-
|
||||||
|
Unrecognized holding losses
|
(13,786)
|
-
|
||||||
|
Fair value
|
$
|
2,352,380
|
$
|
-
|
||||
9
Contractual maturities of held to maturity securities at September 30, 2011 are all short-term due to maturity dates of less than one year. The Company determined that these securities are all level 2 inputs in the fair value hierarchy.
5. Property and Equipment
Property and Equipment consisted of the following at September 30, 2011, and December 31, 2010.
|
September 30, 2011
|
December 31, 2010
|
|||||||
|
Leasehold improvements
|
$
|
2,070
|
$
|
864,429
|
||||
|
Manufacturing equipment
|
400,045
|
410,997
|
||||||
|
Computer and office equipment
|
160,478
|
160,478
|
||||||
|
Laboratory equipment
|
213,908
|
213,908
|
||||||
|
Total
|
776,501
|
1,649,812
|
||||||
|
Less accumulated depreciation
|
(405,038
|
)
|
(1,138,670
|
)
|
||||
|
Property and equipment, net
|
$
|
371,463
|
$
|
511,142
|
||||
The decrease in leasehold improvements during the nine months ended September 30, 2011, reflects the relocation of the Company’s headquarters within Ann Arbor, Michigan. During the nine months ended September 30, 2011, the Company sold equipment, with a net book value of $6,892, for $1,200, resulting in a loss of $5,692.
Depreciation expense for the nine months ended September 30, 2011 and 2010 was $132,787 and $271,076, respectively.
6. Stock-Based Compensation
During 2001, Pipex Therapeutics’ board of directors and stockholders adopted the 2001 Stock Incentive Plan (the “2001 Stock Plan”). This plan was assumed by Pipex in the October 2006 merger with Sheffield. As of the date of the merger, there were 1,489,353 options issued and outstanding under the 2001 plan. The total number of shares of stock with respect to which stock options and stock appreciation rights may be granted to any one employee of the Company or a subsidiary during any one-year period under the 2001 plan shall not exceed 250,000. All awards pursuant to the 2001 Stock Plan shall terminate upon the termination of the grantee’s employment for any reason. Awards include options, restricted shares, stock appreciation rights, performance shares and cash-based awards (the “Awards”). The 2001 Stock Plan contains certain anti-dilution provisions in the event of a stock split, stock dividend or other capital adjustment, as defined in the plan. The 2001 Stock Plan provides for a Committee of the Board to grant awards and to determine the exercise price, vesting term, expiration date and all other terms and conditions of the awards, including acceleration of the vesting of an award at any time. As of September 30, 2011, there were 1,320,354 options issued and outstanding under the 2001 Stock Plan.
On March 20, 2007, the Company’s board of directors approved the Company’s 2007 Stock Incentive Plan (the “2007 Stock Plan”) for the issuance of up to 2,500,000 shares of common stock to be granted through incentive stock options, nonqualified stock options, stock appreciation rights, dividend equivalent rights, restricted stock, restricted stock units and other stock-based awards to officers, other employees, directors and consultants of the Company and its subsidiaries. This plan was approved by stockholders on November 2, 2007. The exercise price of stock options under the 2007 Stock Plan is determined by the compensation committee of the Board of Directors, and may be equal to or greater than the fair market value of the Company’s common stock on the date the option is granted. The total number of shares of stock with respect to which stock options and stock appreciation rights may be granted to any one employee of the Company or a subsidiary during any one-year period under the 2001 plan shall not exceed 250,000. Options become exercisable over various periods from the date of grant, and generally expire ten years after the grant date. As of September 30, 2011, there are 1,225,427 options issued and outstanding under the 2007 Stock Plan.
On November 2, 2010, the board of directors and stockholders adopted the 2010 Stock Incentive Plan (“2010 Stock Plan”) for the issuance of up to 3,000,000 shares of common stock to be granted through incentive stock options, nonqualified stock options, stock appreciation rights, dividend equivalent rights, restricted stock, restricted stock units and other stock-based awards to officers, other employees, directors and consultants of the Company and its subsidiaries. The exercise price of stock options under the 2010 Stock Plan is determined by the compensation committee of the Board of Directors, and may be equal to or greater than the fair market value of the Company’s common stock on the date the option is granted. Options become exercisable over various periods from the date of grant, and generally expire seven years after the grant date. As of September 30, 2011, there are 277,500 options issued and outstanding under the 2010 Stock Plan.
In the event of an employee’s termination, the Company will cease to recognize compensation expense for that employee. There is no deferred compensation recorded upon initial grant date, instead, the fair value of the stock-based payment is recognized ratably over the stated vesting period.
10
The Company has applied fair value accounting for all stock-based payment awards since inception. The fair value of each option or warrant granted is estimated on the date of grant using the Black-Scholes option-pricing model. The Black-Scholes assumptions used in the nine months ended September 30, 2011 and 2010, are as follows:
|
Three Months Ended September 30,
|
Nine Months Ended September 30,
|
|||||||||||
|
2011
|
2010
|
2011
|
2010
|
|||||||||
|
Exercise price
|
$ 0.64 - $0.87
|
$ 0.80
|
$ 0.64 - $2.22
|
$ 0.80 - $0.87
|
||||||||
|
Expected dividends
|
0%
|
0%
|
0%
|
0%
|
||||||||
|
Expected volatility
|
177% - 180%
|
192%
|
177% - 188%
|
192% - 204%
|
||||||||
|
Risk free interest rates
|
1.40% - 2.17%
|
2.54%
|
1.40% - 3.58%
|
2.54% - 3.63%
|
||||||||
|
Expected life options
|
7 years
|
10 years
|
5 years - 7 years
|
10 years
|
||||||||
|
Expected forfeitures
|
0%
|
0%
|
0%
|
0%
|
||||||||
The Company records stock-based compensation based upon the stated vested provisions in the related agreements, with recognition of expense recorded on the straight line basis over the term of the related agreement. The vesting provisions for these agreements have various terms as follows:
|
·
|
immediate vesting,
|
|
|
·
|
one-half vesting immediately and the remainder over three years
|
|
|
·
|
quarterly over three years,
|
|
|
·
|
annually over three years,
|
|
|
·
|
one-third immediate vesting and remaining annually over two years,
|
|
|
·
|
one-half immediate vesting with remaining vesting over nine months; and
|
|
|
·
|
one quarter immediate vesting with the remaining over three years.
|
During the nine months ended September 30, 2011, the Company granted 377,002 options to employees and consultants having a fair value of $475,003 based upon the Black-Scholes option pricing model. During the same period of 2010, the Company granted 630,000 options to employees having a fair value of $513,750 based upon the Black-Scholes option pricing model.
On January 18, 2011, the Company amended the terms of 228,773 stock options held by a member of the Board of Directors. In connection with the modification, the Company extended the expiration date of the stock options by 5 years. The extension is considered a modification, which in substance is the issuance of a new stock option award. As a result, the Company computed the fair value of this award to be $397,767, using the Black-Scholes valuation model. The fair value was based upon the following management assumptions:
| $ | 0.09 | |||
|
Expected dividends
|
0 | % | ||
|
Expected volatility
|
187.1 | % | ||
|
Expected term
|
5 years
|
|||
|
Risk free interest rate
|
2.03 | % | ||
A summary of stock option activities as of September 30, 2011, and for the year ended December 31, 2010, is as follows:
|
Options
|
Weighted
Average
Exercise
Price
|
Weighted Average
Remaining
Contractual
Life
|
Aggregate
Intrinsic
Value
|
||||||||||||
|
Balance – December 31, 2009
|
2,561,332
|
$
|
1.26
|
||||||||||||
|
Granted
|
743,332
|
0.80
|
|||||||||||||
|
Exercised
|
( 255,954
|
)
|
0.44
|
||||||||||||
|
Forfeited or expired
|
(509,619
|
)
|
0.69
|
||||||||||||
|
Balance – December 31, 2010
|
2,539,091
|
1.32
|
|||||||||||||
|
Granted
|
377,002
|
1.50
|
|||||||||||||
|
Forfeited or expired
|
(82,812
|
)
|
0.57
|
||||||||||||
|
Exercised
|
(10,000
|
)
|
0.56
|
||||||||||||
|
Balance – September 30, 2011 - outstanding
|
2,823,281
|
$
|
1.37
|
6.14 years
|
$
|
233,777
|
|||||||||
|
Balance – September 30, 2011 – exercisable
|
2,366,688
|
$
|
1.48
|
5.77 years
|
$
|
232,827
|
|||||||||
11
The options outstanding and exercisable as of September 30, 2011, are as follows:
|
Options Outstanding
|
Options Exercisable
|
||||||||||||||||
|
Range of
Exercise
Price
|
Number
outstanding
|
Weighted
Average
Exercise
Price
|
Weighted
Average
Remaining
Contractual Life
|
Number
Exercisable
|
Weighted
Average
Exercise
Price
|
Weighted
Average
Remaining
Contractual Life
|
|||||||||||
|
$
|
0.09 - 4.57
|
2,733,282
|
$
|
1.22
|
6.24 years
|
2,276,689
|
$
|
1.30
|
5.88 years
|
||||||||
|
$
|
4.58 - 9.05
|
89,999
|
5.93
|
3.01 years
|
89,999
|
5.93
|
3.01 years
|
||||||||||
|
2,823,281
|
$
|
1.37
|
6.14 years
|
2,366,688
|
$
|
1.48
|
5.77 years
|
||||||||||
The options outstanding and exercisable as of September 30, 2010, are as follows:
|
Options Outstanding
|
Options Exercisable
|
||||||||||||||||
|
Range of
Exercise
Price
|
Number
outstanding
|
Weighted
Average
Exercise
Price
|
Weighted
Average
Remaining
Contractual Life
|
Number
Exercisable
|
Weighted
Average
Exercise
Price
|
Weighted
Average
Remaining
Contractual Life
|
|||||||||||
|
$
|
0.09 - 4.57
|
2,365,760
|
$
|
1.17
|
6.65 years
|
1,809,717
|
$
|
1.30
|
5.80 years
|
||||||||
|
$
|
4.58 - 9.05
|
89,999
|
5.93
|
4.01 years
|
89,062
|
5.93
|
3.97 years
|
||||||||||
|
2,455,759
|
$
|
1.35
|
6.55 years
|
1,898,779
|
$
|
1.52
|
5.72 years
|
||||||||||
7. Stock Purchase Warrants
On July 2, 2010, the Company entered into a Common Stock Purchase Agreement with a single investor. As part of this agreement, the Company issued warrants to purchase 60,606 shares of common stock to the placement agent, or its permitted assigns. The warrants have an exercise price of $1.32 and a life of 5 years. The warrants vested on January 1, 2011 and expire December 31, 2015. Since these warrants were granted as part of an equity raise, the Company has treated them as a direct offering cost. The result of the transaction has a $0 net effect to equity. As of September 30, 2011, 30,303 of these warrants remained outstanding.
On January 28, 2011, the Company entered into a Common Stock Purchase Agreement with three institutional investors. As part of this agreement, the Company issued warrants to purchase 1,428,572 shares of common stock. Each warrant was exercisable for thirteen months at $2.00 per share and subsequently exchanged for new warrants with substantially the same terms as the original warrants except that the expiration date was extended for two months. The original warrants had an anti-dilution price protection feature; if the Company issues securities at a price per share that is less than $2.00 per share, the warrant holders will be ratcheted down to the lower offering price. However, the Company had instituted a floor price of $1.40 per share in connection with the price protection. On April 6, 2011, the Company entered into another Common Stock Purchase Agreement that triggered the ratchet provision and re-set the price of these warrants to $1.40. Due to the re-set to the floor price, the warrant liability was marked-to-market and reclassified to additional paid in capital since it ceased to contain the provisions of a derivative liability.
The warrants were recorded as liabilities at their estimated fair value on the commitment date, which was $716,000 with subsequent changes in estimated fair value recorded as a warrant expense in the Company’s statement of operations at each subsequent reporting period. On April 6, 2011, the fair value of the warrant liability was $1,481,143, which represented an increase in fair value of $765,143. The fair value was measured using the Black Scholes valuation model, which is based, in part, upon unobservable inputs for which there is little or no market data, requiring the Company to develop its own assumptions. The assumptions used by the Company are summarized in the following table:
|
Commitment
Date
|
Remeasurement
Date
April 6, 2011
|
|||||||
|
Closing stock price
|
$
|
1.39
|
$
|
2.08
|
||||
|
Expected dividend rate
|
0
|
%
|
0
|
%
|
||||
|
Expected stock price volatility
|
117.1
|
%
|
104.6
|
%
|
||||
|
Risk free interest rate
|
0.28
|
%
|
0.29
|
%
|
||||
|
Expected life (years)
|
1.08
|
0.85
|
||||||
12
On August 10, 2011, the Company entered into an agreement to exchange the warrants issued in connection with the January 28, 2011 financing for new warrants with substantially the same terms as the original warrants except that in the new warrants the expiration date was extended by two months.
On April 6, 2011, the Company entered into a Common Stock Purchase Agreement with an institutional investor. As part of this agreement, the Company issued a warrant to purchase 844,391 shares of common stock. The warrant was initially exercisable for thirteen months at $2.0725 per share. The warrant had an anti-dilution price protection feature; that provided if the Company issues securities at a price per share that is less than $2.0725 per share, the exercise price of the warrant will be ratcheted down to the lower offering price. On July 28, 2011, the warrant was exchanged for a new warrant with substantially similar terms except that in the new warrant (i) the anti-dilution price protection was eliminated, (ii) the exercise price was lowered to $1.00, (iii) the expiration date was extended for an additional three months to August 12, 2012, and (iv) the warrant’s initial exercise date was changed to January 2012. Due to this warrant exchange, the warrant liability was marked-to-market and reclassified to additional paid in capital since it ceased to contain the provisions of a derivative liability.
The warrant is recorded as a liability at its estimated fair value on the commitment date, which was $775,995 with subsequent changes in estimated fair value recorded as a warrant expense in the Company’s statement of operations at each subsequent period. On July 28, 2011, the fair value of the warrant liability was $253,317, which represented an increase in fair value of $164,994. The fair value is measured using the Black Scholes valuation model, which is based, in part, upon unobservable inputs for which there is little or no market data, requiring the Company to develop its own assumptions. The assumptions used by the Company are summarized in the following table:
|
Commitment
Date
|
Remeasurement
Date
July 28, 2011
|
|||||||
|
Closing stock price
|
$
|
2.08
|
$
|
$0.84
|
||||
|
Expected dividend rate
|
0
|
%
|
0
|
%
|
||||
|
Expected stock price volatility
|
112.1
|
%
|
105.6
|
%
|
||||
|
Risk free interest rate
|
0.29
|
%
|
0.21
|
%
|
||||
|
Expected life (years)
|
1.08
|
1.04
|
||||||
The following table summarizes the estimated fair value of the warrant liabilities:
|
Balance at December 31, 2010
|
$
|
-
|
||
|
Warrant liability
|
1,491,996
|
|||
|
Change in fair value of warrant liability
|
242,465
|
|||
|
Reclassification to additional paid-in capital
|
(1,734,461
|
)
|
||
|
Balance at September 30, 2011
|
$
|
-
|
A summary of warrant activities as of September 30, 2011, and for the year ended December 31, 2010, is as follows:
|
Warrants
|
Weighted
Average
Exercise Price
|
|||||||
|
Balance – December 31, 2009
|
1,070,472
|
$
|
3.27
|
|||||
|
Granted
|
60,606
|
1.32
|
||||||
|
Exercised
|
-
|
-
|
||||||
|
Forfeited or expired
|
-
|
-
|
||||||
|
Balance – December 31, 2010
|
1,131,078
|
3.49
|
||||||
|
Granted
|
4,545,926
|
1.64
|
||||||
|
Forfeited or expired
|
(2,292,651
|
)
|
2.02
|
|||||
|
Exercised
|
(15,615
|
)
|
1.19
|
|||||
|
Balance – September 30, 2011 - outstanding
|
3,368,738
|
$
|
2.00
|
|||||
|
Balance – September 30, 2011 – exercisable
|
3,368,738
|
$
|
2.00
|
|||||
13
The warrants outstanding as of September 30, 2011, are as follows:
|
Range of
Exercise Price
|
Number
outstanding
|
Weighted
Average
Remaining
Contractual Life
|
||||||
|
$
|
1.00
|
844,391
|
|
0.77 years
|
||||
|
$
|
1.32
|
30,303
|
4.25 years
|
|||||
|
$
|
1.40
|
1,428,572
|
0. 58 years
|
|||||
|
$
|
2.22
|
626,809
|
4.76 years
|
|||||
|
$
|
3.30
|
61,207
|
3.67 years
|
|||||
|
$
|
3.75
|
50,000
|
4.38 years
|
|||||
|
$
|
6.36
|
327,456
|
1.11 years
|
|||||
|
3,368,738
|
1.63 years
|
|||||||
8. Stockholders’ Equity
During the nine months ended September 30, 2011, the Company issued 15,000 shares of common stock in connection with the exercise of stock options and warrants for proceeds of $7,650 and 10,615 shares of common stock related to a cashless exercise of warrants. The Company also issued 45,600 shares of common stock for employment service, having a fair value of $75,840 ($1.66 average per share) and 171,796 shares of common stock for consulting services, having a fair value of $164,870 ($0.96 average per share), based on the quoted closing trading prices.
On January 28, 2011, the Company sold 2,857,144 shares of common stock and warrants exercisable for 1,428,572 shares of common stock for $4,000,000. Direct offering costs were approximately $300,000.
On April 6, 2011, the Company sold 1,688,782 shares of common stock and a warrant exercisable for 844,391 shares of common stock for $3,500,000. Direct offering costs were approximately $250,000.
14
ITEM 2. MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL INFORMATION AND RESULTS OF OPERATIONS
The following discussion should be read in conjunction with the attached unaudited consolidated financial statements and notes thereto, and with our audited consolidated financial statements and notes thereto for the fiscal year ended December 31, 2010, found in our Annual Report on Form 10-K. In addition to historical information, the following discussion contains forward-looking statements that involve risks, uncertainties and assumptions. Where possible, we have tried to identify these forward looking statements by using words such as “anticipate,” “believe,” “intends,” “plans,” or similar expressions. Our actual results could differ materially from those anticipated by the forward-looking statements due to important factors and risks including, but not limited to, those set forth under “Risk Factors” in this 10-Q and as applicable in Part I, Item 1A of our Annual Report on Form 10-K.
Overview
We are a pharmaceutical company focused on developing innovative medicines for the treatment of serious central nervous system diseases. Our strategy is to license product candidates that have demonstrated a certain level of clinical efficacy and develop them to a stage that results in a significant commercial collaboration. We are developing, or have partnered the development of, drug product candidates to treat multiple sclerosis, cognitive dysfunction in multiple sclerosis, fibromyalgia, amyotrophic lateral sclerosis (ALS) and Alzheimer’s disease. We are currently focused on the commercialization of wellZinTM, a homeopathic over-the-counter zinc acetate lozenge to reduce the duration and symptoms of the common cold. We are also developing reaZinTM as a medical food for the dietary management of zinc deficiency associated with Alzheimer’s disease. We also operate Adeona Clinical Laboratory, a wholly owned clinical reference laboratory that provides a broad array of chemistry and microbiology diagnostic tests.
Product Pipeline:
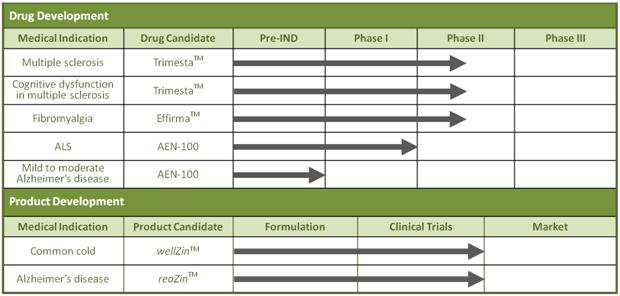
Drug Candidate Development:
|
·
|
TrimestaTM (estriol) is being developed for the treatment of relapsing-remitting multiple sclerosis in women. A randomized, double-blind, placebo-controlled clinical trial is currently underway in the United States. As of September 19, 2011, the 150th patient has been enrolled in this clinical trial, per the original protocol. The Lead Principal Investigator has also received funding to continue enrollment of an additional 10-20 patients at all 15 centers.
|
|
·
|
TrimestaTM (estriol) is being developed for the treatment of cognitive dysfunction in female multiple sclerosis patients. A randomized, double-blind, placebo-controlled Phase II clinical trial is currently screening patients for enrollment.
|
|
|
·
|
EffirmaTM (flupirtine) is being developed for the treatment of fibromyalgia. On May 6, 2010, we and Pipex Therapeutics, Inc. (Pipex), our wholly owned subsidiary, entered into a sublicense agreement with Meda AB, a multi-billion dollar international pharmaceutical company, covering all of our patents’ rights on the use of flupirtine for fibromyalgia in the United States, Canada and Japan. According to Meda’s 2010 Annual Report, flupirtine for fibromyalgia is currently in Phase II development.
|
|
·
|
AEN-100 (zinc) is being developed for the treatment of amyotrophic lateral sclerosis (ALS), or Lou Gehrig’s disease. We intend to sponsor a multi-center, double-blind, placebo-controlled clinical trial in ALS patients. It is anticipated that the clinical trial will enroll at least 60 patients and that patients will be dosed and monitored for up to 9 months.
|
|
·
|
AEN-100 (zinc) is being developed for the treatment of mild to moderate Alzheimer’s disease. We intend to conduct a randomized, double-blind, placebo-controlled clinical study in patients diagnosed with mild to moderate Alzheimer’s disease who are age 70 and over. It is anticipated that the clinical study will enroll over 100 patients and that the patients will be dosed and monitored for at least 12 months.
|
15
Product Candidate Development:
|
·
|
wellZinTM (zinc acetate lozenge) is our near-term product candidate to reduce the duration and symptoms of the common cold. On July 28, 2011, we announced that we acquired exclusive access to two sets of clinical data demonstrating, with statistical significance, the safety and efficacy of a particular oral zinc formulation in reducing the duration and severity of symptoms associated with the common cold. Based on the reduction of the duration and symptoms of the common cold demonstrated by the 13.3 mg zinc acetate formulation, we intend to commercialize wellZin, an oral zinc acetate lozenge, as a homeopathic over-the-counter (OTC) medicine.
|
|
·
|
reaZinTM (zinc cysteine) is being developed as a medical food for the dietary management of zinc deficiency associated with Alzheimer's disease. On April 14, 2011, results from a multi-center, randomized, double-blind, placebo-controlled clinical study showed that the primary outcomes of increasing serum zinc and decreasing serum free copper were effectively demonstrated in patients administered reaZin compared to placebo. In addition, on average, the cognitive function of the placebo group, declined over 6 months in comparison to patients managed with reaZin. The cognitive function trends favoring the patients managed with reaZin were observed in all three standardized cognitive tests utilized in our study and suggest that reaZin may provide an important benefit to the dietary management of zinc deficiency associated with Alzheimer’s disease.
|
Our source of liquidity as of September 30, 2011, is cash, cash equivalents and short-term investments of $7,460,782. Our projected uses of cash include funding further clinical development of our drug candidates and commercialization of our medical food candidate and homeopathic drug, working capital and other general corporate activities. We may also use our cash for the acquisition of businesses, technologies and products that will complement our existing assets.
On January 28, 2011, we entered into a Securities Purchase Agreement with institutional investors, relating to the offering and sale of 2,857,144 shares of common stock, par value $0.001 per share and warrants to purchase 1,428,572 shares of common stock. We raised gross proceeds of $4,000,000, before estimated offering expenses of approximately $300,000, which includes placement agent fees. The offering was made pursuant to t our shelf registration statement on Form S-3 (File No. 333-166750), which was declared effective by the Securities and Exchange Commission (SEC) on June 14, 2010.
On April 6, 2011, we entered into a Securities Purchase Agreement with an institutional investor, relating to the offering and sale of 1,688,782 shares of common stock, par value $0.001 per share and a warrant to purchase 844,391 shares of common stock. We raised gross proceeds of $3,500,000, before estimated offering expenses of approximately $250,000, which includes placement agent fees. The offering was made pursuant to our shelf registration statement on Form S-3 (File No. 333-166750), which was declared effective by the Securities and Exchange Commission (SEC) on June 14, 2010.
We believe that with the additional proceeds of the January and April 2011 equity financings, our cash will be sufficient to fund our planned operations for at least the next 12 months. We will need additional capital to continue the development of our product candidates and clinical programs beyond 12 months. The sale of any equity or debt securities may result in additional dilution to our stockholders, and we cannot be certain that additional financing will be available in amounts or on terms acceptable to us, if at all. If we are unable to obtain financing, we may be required to reduce the scope and timing of the planned clinical and preclinical programs, which could harm our financial condition and operating results.
Clinical Drug Development Programs
Relapsing-Remitting Multiple Sclerosis in Women
Trimesta (estriol)
Disease
Multiple sclerosis is a progressive neurological disease in which the body loses the ability to transmit messages along central nervous system nerve cells, leading to a loss of muscle control, paralysis, cognitive impairment and in some cases death. According to the National Multiple Sclerosis Society, currently, more than 2.5 million people worldwide (approximately 400,000 patients in the United States) have been diagnosed with multiple sclerosis. Young adults, ages 20 to 50, and two to three times as many women than men are predominantly diagnosed with multiple sclerosis. According to the National Multiple Sclerosis Society, approximately 85% of multiple sclerosis patients are initially diagnosed with the relapsing-remitting form, compared to 10-15% with other progressive forms.
16
There are currently 8 Food & Drug Administration (FDA)-approved therapies for the treatment of relapsing-remitting multiple sclerosis: Betaseron®, Rebif®, Avonex®, Novantrone®, Copaxone®, Tysabri®, Gylenya® and AmpyraTM. These therapies provide only a modest benefit for patients with relapsing-remitting multiple sclerosis and therefore serve to only delay progression of the disease. All of these drugs except Gylenya® and Ampyra™ require frequent (daily, weekly & monthly) injections (or infusions) on an ongoing basis and can be associated with unpleasant side effects (such as flu-like symptoms), high rates of non-compliance among users, and eventual loss of efficacy due to the appearance of resistance in approximately 30% of patients. Despite the availability of multiple FDA-approved therapies for the treatment of relapsing-remitting multiple sclerosis, the disease is highly underserved and exacts a heavy economic toll. Multiple sclerosis costs the United States more than $10.6 billion annually in medical care and lost productivity according to the Society for Neuroscience.
Background
It has been scientifically documented that pregnant women with certain autoimmune diseases experience a spontaneous reduction of disease symptoms during pregnancy, particularly in the third trimester. The PRIMS (Pregnancy In Multiple Sclerosis) study, a landmark clinical study published in the New England Journal of Medicine followed 254 women with multiple sclerosis during 269 pregnancies and for up to one year after delivery. The PRIMS study demonstrated that relapse rates were significantly reduced by 71 percent (p < 0.001) through the third trimester of pregnancy compared to pre-pregnancy-rates, and that relapse rates increased by 120 percent (p < 0.001) during the first three months after birth (post-partum) before returning to pre-pregnancy rates. It has been hypothesized that the female hormone, estriol, produced by the placenta during pregnancy, plays a role in “fetal immune privilege”, a process that prevents a mother’s immune system from attacking and rejecting her fetus. Maternal levels of estriol increase in a linear fashion through the third trimester of pregnancy until birth, whereupon they abruptly return to low circulating levels. The anti-autoimmune effects of esteriol is thought to be responsible for the therapeutic effects of pregnancy on multiple sclerosis.
Rhonda Voskuhl, M.D., Director, University of California, Los Angeles (UCLA) multiple sclerosis program, UCLA Department of Neurology, has found that pregnancy levels of estriol has potent immunomodulatory effects. She further postulated and tested in pilot clinical studies that oral doses of estriol may have a therapeutic benefit when administered to non-pregnant female multiple sclerosis patients by, in essence, mimicking the spontaneous reduction in relapse rates seen in multiple sclerosis patients during pregnancy.
Estriol has been approved and marketed for over 40 years throughout Europe and Asia for the oral treatment of post-menopausal symptoms. It has never been approved by the United States FDA for any indication.
Clinical Development
Our Trimesta (estriol) drug candidate is for the treatment of relapsing-remitting multiple sclerosis in women. An investigator-initiated, 10-patient, 22-month, single-agent, crossover clinical trial to study the therapeutic effects of 8 mg of oral Trimesta taken daily in non-pregnant female relapsing-remitting multiple sclerosis patients was completed in the United States. The total volume and number of gadolinium-enhancing lesions were measured by brain magnetic resonance imaging (an established neuroimaging measurement of disease activity in multiple sclerosis). Over the next three months of treatment with Trimesta, the median total enhancing lesion volumes decreased by 79% (p = 0.02) and the number of lesions decreased by 82% (p = 0.09). They remained decreased during the next 3 months of treatment, with lesion volumes decreased by 82% (p = 0.01), and numbers decreased by 82% (p =0.02). Following a six-month drug holiday during which the patients were not on any drug therapies, median lesion volumes and numbers returned to near baseline pretreatment levels. Trimesta therapy was reinitiated during a four-month retreatment phase of this clinical trial. The relapsing-remitting multiple sclerosis patients again demonstrated a decrease in enhancing lesion volumes of 88% (p = 0.008) and a decrease in the number of lesions by 48% (p = 0.04) compared with original baseline scores.
A Phase II randomized, double-blind, placebo-controlled clinical trial is currently underway at 15 centers in the United States. The purpose of this clinical trial is to study whether 8 mg of oral Trimesta taken daily over a 2 year period will reduce the rate of relapses in a large population of female patients with relapsing-remitting multiple sclerosis. Investigators are administering either Trimesta or matching placebo, in addition to a standard of care, glatimer acetate (Copaxone®) injections, an FDA-approved therapy for multiple sclerosis, to women between the ages of 18 to 50 who have been recently diagnosed with relapsing-remitting multiple sclerosis. The primary endpoint in this clinical trial being run under an investigator-initiated Investigational New Drug (IND) application, is relapse rates at two years. As of September 19, 2011, the 150th patient has been enrolled in this clinical trial, per the original protocol. Dr. Voskuhl has also received funding to continue enrollment of an additional 10-20 patients at all 15 centers.
With over $8 million in grant funding to date, the ongoing Trimesta clinical trial should be funded to its completion.This clinical trial previously received a $5 million grant from the National Multiple Sclerosis Society (NMSS) in partnership with the NMSS’s Southern California chapter, with support from the National Institutes of Health and $860,440 in grant funding through the American Recovery and Reinvestment Act. In November 2010, the Trimesta multiple sclerosis trial was awarded $244,480 under the Qualifying Therapeutic Discovery Project Program. In March 2011, additional grant funding of $409,426 was received from the NMSS, and in May 2011, grant funding of $1,594,553 was received from the National Institutes of Health/National Institute of Neurological Disorders and Stroke. These recent grants resulted after review of the clinical program.
17
Cognitive Dysfunction in Multiple Sclerosis
Trimesta (estriol)
Disease
According to the National Multiple Sclerosis Society and the Multiple Sclerosis Society of Canada publication, Hold that Thought! Cognition and MS, it is fairly common for people with multiple sclerosis to complain of problems remembering things, finding the right words, concentrating on a task or something they are reading, or following a conversation. These are all cognitive symptoms of multiple sclerosis. Fifty to sixty-five percent of those affected by multiple sclerosis have cognitive dysfunction. Despite the fact that most symptoms are mild to moderate, they can have a significant impact on a person’s ability to normally function. The overall cognitive dysfunction can be described as a reduction in mental “sharpness.”
The major areas of cognition that can be dysfunctional include what are termed complex attention and executive functions. Complex attention involves multitasking, the speed with which information can be processed, learning and memory, and perceptual skills; executive functions include problem solving, organizational skills, the ability to plan, and word finding. Just as the nature, frequency, and severity of multiple sclerosis-related physical problems can widely vary, not all people with multiple sclerosis will display these cognitive issues, and no two people will experience exactly the same types or severity of problems.
Background
In the investigator-initiated, 10-patient, 22-month, single-agent, crossover clinical trial conducted by Dr. Rhonda Voskuhl, a statistically significant 14% improvement from baseline in Paced Auditory Serial Addition Test (PASAT) cognitive testing scores (p = 0.04) was observed in the multiple sclerosis patients after six months of Trimesta therapy. PASAT is a routine cognitive test performed in patients with a wide variety of neuropsychological disorders such as multiple sclerosis. The PASAT scores are expressed as a mean percent change from baseline.
Clinical Development
Our
Trimesta (estriol) drug candidate is also being developed for the treatment of cognitive dysfunction in female
multiple sclerosis patients. On November 11, 2011, we announced our intention to provide financial support and Trimesta drug
supply for a randomized, double-blind, placebo-controlled Phase II clinical trial to evaluate Trimesta’s
potential neuroprotective and therapeutic effect on cognitive dysfunction in female multiple sclerosis patients. This trial
is expected to enroll 64 relapsing-remitting or secondary-progressive female multiple sclerosis patients at University of
California, Los Angeles. Patients between the ages of 18 and 50 will be randomized 1:1 into the treatment and placebo groups.
Dr. Voskuhl will administer either oral Trimesta or a matching placebo, in addition to any FDA-approved multiple sclerosis
treatment. Each patient will be dosed and monitored for one year after being enrolled. The primary endpoint in this clinical
trial being run under an investigator-initiated IND application is expected to be improvement in PASAT cognitive testing
scores versus matching placebo. Patients are currently being screened for enrollment into this trial. On November 11, 2011,
we announced that we and a private foundation have pledged to equally support this new clinical trial. The study also
received contributions from several other supporters.
Fibromyalgia
Effirma (flupirtine)
Disease
Fibromyalgia is a chronic and debilitating condition characterized by widespread pain and stiffness throughout the body, often accompanied by severe fatigue, insomnia and mood symptoms. Fibromyalgia affects an estimated 2-4% of the population worldwide, including an estimated 4 million patients in the United States. There are presently three FDA products approved for this indication in the United States – Lyrica®, Cymbalta® and Savella®. Flupirtine is differentiated from these products in that it employs a unique mode of action. Meda AB of Sweden estimates the United States market for fibromyalgia to be near $1 billion at the time of potential market launch of flupirtine.
Clinical Development
Our Effirma (flupirtine) product candidate is for the treatment of fibromyalgia. Effirma is a selective neuronal potassium channel opener that also has NMDA receptor antagonist properties. Effirma is a non-opioid, non-NSAID, non-steroidal, analgesic. Preclinical data and clinical experience suggest that Effirma should also be effective for neuropathic pain since it acts in the central nervous system via a mechanism of action distinguishable from most marketed analgesics. Effirma is especially attractive because it operates through non-opiate pain pathways, exhibits no known abuse potential, and lacks withdrawal effects. In addition, no tolerance to its antinocioceptive effects has been observed. One common link between neuroprotection, nocioception and Effirma may be the N-methyl-D-aspartic acid glutamate system, a major receptor subtype for the excitotoxic neurotransmitter, glutamate. Effirma has strong inhibitory actions on N-methyl-D-aspartic acid-mediated neurotransmission. Flupirtine was originally developed by Asta Medica (subsequently acquired by Meda AB) and has been approved and is marketed by Meda AB in Europe since 1984, as well as other countries, for the treatment of pain. It has never been approved by the FDA for any indication.
18
Meda Corporate Partnership
On May 6, 2010, we and Pipex, our wholly owned subsidiary, entered into a sublicense agreement with Meda AB, a multi-billion dollar international pharmaceutical company, pursuant to which Meda AB assumed all future development costs and may commercialize flupirtine for fibromyalgia in the United States. As consideration for such sublicense, we received an up-front payment of $2.5 million and are entitled to milestone payments of $5 million upon the FDA’s acceptance of the New Drug Application (NDA) for flupirtine for fibromyalgia and $10 million upon FDA approval of such NDA. Pursuant to the sublicense agreement, we will also receive a 7% royalty on net sales of flupirtine for fibromyalgia in the United States, Canada and Japan, with such royalties being shared equally with our licensor, McLean Hospital, a Harvard teaching hospital.
Flupirtine is approved and marketed by Meda AB and its distributors in Europe and other countries for indications other than fibromyalgia and has been prescribed to millions of patients worldwide. We believe that such substantial human experience with flupirtine should greatly assist the FDA in its evaluation of the safety of flupirtine upon review of an NDA of flupirtine for fibromyalgia. According to Meda’s 2010 Annual Report, flupirtine for fibromyalgia is currently in Phase II development.
Amyotrophic Lateral Sclerosis (ALS)
AEN-100 (zinc)
Disease
ALS, also known as Lou Gehrig’s Disease, is a devastating progressive neurodegenerative disease that affects the motor nerve cells in the brain and the spinal cord of predominantly older people of both sexes. It is estimated that as many as 30,000 Americans may have the disease at any given time. The progressive degeneration of the motor neurons in ALS eventually leads to the death of the patient. Motor neurons reach from the brain to the spinal cord and from the spinal cord to the muscles throughout the body. When motor neurons die, the ability of the brain to initiate and control muscle movement is lost. With voluntary muscle action progressively affected, patients in the later stages of the disease may become totally paralyzed. While non-invasive ventilation and gastrostomy tubes prolong life by 6-12 months, the average lifespan from time of symptom onset is 2-5 years. Currently, RILUTEK® is the only FDA-approved drug for ALS. RILUTEK is an NMDA receptor antagonist and has been shown to prolong life in patients with ALS by 3 months. Presently, there is no cure for ALS, nor is there a known cause.
Background
Clinical investigators at the PNA Center for Neurological Research cite multiple lines of scientific research that suggest a potential benefit of zinc therapy for ALS patients, including:
|
·
|
During the 1950’s, an epidemic of ALS was discovered on the island of Guam and the Trust Territories of the Pacific that revealed a form of ALS that was 100 times more prevalent than in the rest of the world.
|
|
|
o
|
Research on this cluster of ALS cases linked the neurological disease to the neurotoxin BMAA, a non-essential amino acid produced by cyanobacterium and found in large concentrations in food consumed by the people on Guam. Subsequent to the observations of a cluster of ALS cases on Guam, several groups have identified high concentrations of BMAA in the brain tissues of patients from North America and Europe with neurodegenerative diseases such as ALS.
|
|
o
|
It has been demonstrated that BMAA binds strongly to transition metal ions such as zinc, copper, and nitrogen. If BMAA crosses into the brain and enters a compartment in which glutamate is bound to zinc, the glutamate/zinc complex separates and the BMAA binds with the zinc, leaving high levels of unbound glutamate. These elevated levels of unbound glutamate are believed to be highly neurotoxic in ALS patients. Zinc is thought to serve as an endogenous antioxidant in the central nervous system and helps protect the blood-brain barrier (BBB) against oxidative stress and may prevent the neurotoxin, BMAA, from crossing into the brain.
|
|
·
|
The use of zinc therapy for ALS patients is supported in animal models of ALS. Approximately 2% of ALS diagnoses are associated with a mutation in the copper/zinc superoxide dismutase (SOD1) gene. In ALS mutant SOD1 animal models, zinc supplementation has been shown to delay death.
|
|
·
|
Genetic mutations affecting the ability of a protein known as copper/zinc superoxide dismutase (SOD1) to properly bind zinc are associated with the familial form of ALS, which shares many of the same features as the more prevalent sporadic form of ALS.
|
|
·
|
Zinc is an important modifier of glutamate toxicity, a neurotransmitter linked to cell death in ALS patients.
|
19
Clinical Development
Preparations are underway to evaluate the safety and efficacy of our proprietary drug candidate, AEN-100, a gastroretentive, sustained-release zinc-based tablet, in a multi-center, double-blind, placebo-controlled clinical trial in ALS patients intended to be conducted under an investigator-initiated IND application. We will provide the study medication and fund the clinical trial, which will be conducted by the neurology team at the PNA Center for Neurological Research.
Efforts are also underway for the manufacturing of clinical trial medication and protocol review by an Institutional Review Board. The multi-center trial is intended to take place at up to six major ALS centers in the United States. It is anticipated that the trial will enroll at least 60 ALS patients, who will continue on RILUTEK® (riluzole) as the standard of care treatment. The patients will be randomized into treatment and matching placebo groups and will receive clinical trial medications for up to 9 months with periodic monitoring. The treatment group will receive our drug candidate, AEN-100, and a commercially available copper pill.
The planned co-primary endpoints are: 1) determining the safety of AEN-100 given to patients once daily with ALS by assessing adverse events and measuring zinc and copper levels every three months; and 2) determining the efficacy of AEN-100 by assessing the rate of disease progression as measured by the ALSFRS-R, a revised ALS functional rating scale that incorporates assessments of respiratory function.
The planned secondary endpoints are: 1) measuring levels of beta-methylamino-L-alanine (BMAA) in blood and urine to determine if there is a decline in these levels over the course of treatment; 2) following disease progression as measured by Forced Vital Capacity (FVC), a measurement of lung function that has been shown to correlate with disease survival; and 3) following progression of muscle weakness through quantitative strength measurements using hand-held dynamometry.
Currently the clinical investigators at the PNA Center for Neurological Research are conducting a Phase I/II open label study under an IND application of zinc therapy in ALS patients to determine the safety of zinc in conjunction with low doses of copper. To date, no safety issues related to zinc therapy have been observed in the ALS patients. Principal investigators from the PNA Center for Neurological Research will be presenting the final results from this open-label study at the 22nd International Symposium on ALS/MND in Sydney, Australia being held from November 30 to December 2, 2011. As the findings from this study are the basis for our planned clinical trial, we intend to disclose the results concurrent with the presentation at the international symposium.
Mild to Moderate Alzheimer’s Disease
AEN-100 (zinc)
Disease
Alzheimer's is a progressive neurodegenerative disease in which affected nerve cells in the brain die, making it increasingly difficult for the brain's memory and learning areas to properly function. A person with Alzheimer's disease has problems with memory, judgment and thinking, making it hard for the person to work or take part in normal day-to-day activities. The death of the nerve cells occurs gradually over a period of years. According to the Alzheimer’s Association, it is estimated that over 5 million Americans today have Alzheimer’s disease and that America spends $183 billion caring for people with Alzheimer’s and other dementias. Revised guidelines have recently been published for diagnosing Alzheimer’s disease that could double the population size. We believe that dysfunction of proper zinc and copper handling in the brain is implicated in Alzheimer’s disease.
Clinical Development
We announced the top-line results in April 2011 from a randomized, double-blind, placebo-controlled clinical study evaluating reaZin in Alzheimer’s patients. This study met its primary endpoint of increasing serum zinc and reducing free copper in serum. Secondary endpoints showed trends that cognitive function (as measured by three standardized cognitive tests) of the patients managed with reaZin on average, remained relatively stable over six months compared to the placebo group, which showed deterioration on average. We conducted further analyses to determine if certain subgroups in the patient sample benefitted from reaZin more than others. After analyzing a number of independent variables associated with the patients enrolled in the clinical study on a post-hoc basis, the strongest relationship was found to be between age and cognitive outcomes. Patients in the study ranged from 52 to 86 years of age. Patients in the placebo group, on average, showed age-related cognitive decline – the older the patient, the greater the rate of cognitive decline. In contrast, patients in the reaZin treatment group, on average, showed cognitive stabilization, independent of their age. Therefore, the older the reaZin treatment patient, the greater the amount of cognitive benefit compared to the placebo patients of the same age.
20
These observations were supported by a post-hoc age-related subgroup analysis that showed dosing-compliant patients age 70 and over (approximately the oldest three quartiles of the patients evaluable at the end of the study) demonstrated statistically significant improvements in two of the three cognitive scoring measurements in the reaZin treatment group compared to the placebo group. As presented below, in this subgroup, two of the three standard cognitive measures reached statistical significance (p < 0.05) as determined by the p-values (the average changes in cognitive scores from baseline to 6 months in the treatment group compared to the placebo group). The p-values were as follows:
|
·
|
ADAS-Cog - Alzheimer's Disease Assessment Scale - Cognitive Subscale p-value: 0.037
|
|
|
·
|
CDR-SOB - Clinical Dementia Rating Scale - Sum of Boxes p-value: 0.032
|
|
|
·
|
MMSE - Mini Mental State Examination p-value: 0.067
|
Based upon the apparent cognitive benefit observed in older patients who were managed with reaZin (our medical food) in comparison to patients who received the matching placebo, we are preparing a larger clinical study protocol to evaluate patients diagnosed with mild to moderate Alzheimer’s disease who are age 70 and over. It is anticipated that the clinical study will enroll over 100 patients and that the evaluation period will be at least 12 months. The intention is to develop our proprietary AEN-100, a zinc-based tablet, as a drug and to conduct this new clinical study under an IND application to be filed with the FDA.
Product Development Programs
Common Cold
wellZin (zinc acetate lozenge)
Disease
According to the “Zinc for the Common Cold Review” prepared by The Cochrane Collaboration® and published in 2011, the common cold is one of the most widespread illnesses, with adults having two to four episodes annually. In the United States, the common cold leads to 75 to 100 million physician visits annually at a conservative cost estimate of $7.7 billion per year. Americans spend $2.9 billion on over-the-counter drugs and another $400 million on prescription medicines for symptomatic relief. More than one-third of patients who saw a doctor received an antibiotic prescription, which has implications for antibiotic resistance from overuse of such drugs. An estimated 22 to 189 million school days are missed annually due to the common cold. As a result, parents missed 126 million workdays to stay home to care for their children. When added to the 150 million work days missed by employees suffering from a cold, the total economic impact of cold-related work loss exceeds $20 billion per year. This accounts for 40% of time lost from work. The complications of the common cold include otitis media, sinusitis and exacerbations of reactive airway diseases. Rhinoviruses are the most frequent cause and may account for nearly 80% of common colds during autumn.
Product Development
We are currently focused on the commercialization of wellZinTM, our oral zinc acetate lozenge intended to reduce the duration and symptoms of the common cold when taken within 24 hours of symptom onset. Plans for manufacturing, packaging and marketing of wellZin are currently underway. On November 4, 2011, we executed an agreement with F&F Foods of Chicago, Illinois, to provide commercial-scale manufacturing of wellZin. wellZin is intended to be marketed as a homeopathic OTC medicine for adults in the United States.
Our proprietary wellZin contains 13.3 mg of zinc acetate based on clinical findings from two independent, randomized, double-blind, placebo-controlled studies conducted by Ananda S. Prasad, M.D., Ph.D. Pursuant to the agreement with Dr. Prasad, a Distinguished Professor of Internal Medicine at Wayne State University School of Medicine, an Adeona Scientific Advisory Board member, we acquired exclusive access to these two sets of clinical data demonstrating, the safety and efficacy of a particular oral zinc formulation in reducing the duration and severity of symptoms associated with the common cold as summarized by the following:
|
·
|
A randomized, double-blind, placebo-controlled study of 50 participants demonstrated that compared to the placebo group, the zinc lozenge group (13.3 mg of zinc acetate) had a mean overall reduction of the following ( JID , 2008; 197:795-802):
|
|||
|
o
|
Duration of the cold (4.0 versus 7.1 days; P-value < 0.0001)
|
|||
|
o
|
Cough (2.1 versus 5.0 days; P-value < 0.0001)
|
|||
|
o
|
Nasal discharge (3.0 versus 4.5 days; P-value < 0.02)
|
|||
|
·
|
A randomized, double-blind, placebo-controlled study of 48 participants demonstrated that compared to the placebo group, the zinc lozenge group (12.8 mg of zinc acetate) had a mean overall reduction of the following (Ann Intern Med, 2000; 133:245-252):
|
|||
|
o
|
Duration of the cold (4.5 versus 8.1 days; P-value < 0.01)
|
|||
|
o
|
Cough (3.1 versus 6.3 days; P-value < 0.001)
|
|||
|
o
|
Nasal discharge (4.1 versus 5.8 days; P-value < 0.025)
|
|||
21
Both of the clinical studies demonstrated that these zinc lozenges were well-tolerated by the treatment participants and that the zinc and placebo groups did not significantly differ in the incidences of adverse effects. Clinical data from Dr. Prasad’s two studies are included in the “Zinc for the Common Cold Review” (“Cochrane Review”) prepared by The Cochrane Collaboration® and published in 2011. In the Cochrane Review, the authors included 15 studies that enrolled a combined 1,360 participants and concluded that zinc administered within 24 hours of onset of symptoms reduces the duration and severity of the common cold in healthy people.
Zinc Deficiency Associated with Alzheimer’s Disease
reaZin (zinc cysteine)
Product Development
Our reaZin (zinc cysteine) product candidate is being developed as a medical food to be sold by prescription only for the dietary management of zinc deficiency associated with Alzheimer’s disease. reaZin is a proprietary, once-daily, gastroretentive, sustained-release, oral tablet formulation of zinc and cysteine. All constituents included in reaZin are believed to have Generally Recognized as Safe (GRAS) status according to FDA standards. reaZin was invented and developed by us to achieve the convenience of once-daily dosing, high bioavailability (the quantity or fraction of the ingested dose that is absorbed) and to minimize gastrointestinal side effects of oral zinc therapy.
Our clinical study evaluating reaZin was divided into two parts. Part 1 was a 13-patient, three-arm, single-dose, comparator study in Alzheimer's disease patients that compared the tolerability and bioavailability of oral reaZin to Galzin® (the only FDA-approved zinc preparation) and placebo. On April 14, 2010, we announced results from Part 1 of the study demonstrated a superior serum zinc bioavailability and a substantially lower incidence of adverse effects in Alzheimer's disease patients in favor of reaZin compared to Galzin.
On April 14, 2011, top-line results from Part 2 of the clinical study (a controlled, randomized, double-blind, placebo-controlled clinical study at 2 centers in the United States) were presented at the 63rd Annual Meeting of the American Academy of Neurology. Findings from 42 of 57 subjects were evaluable at the end of the study (21 subjects in the reaZin group and 21 subjects in the placebo group). The primary outcomes of the study were effectively demonstrated as the patients administered reaZin showed significant reductions in serum free copper levels and elevations in serum zinc levels over the placebo group, resulting in a statistically significant change in the free copper to zinc ratio of p < 0.0006 (the primary endpoint). In addition, the cognitive function of the placebo group, on average, declined over 6 months in comparison to patients managed with reaZin . The cognitive function trends favoring the patients managed with reaZin were observed in all three standardized cognitive tests utilized in our study and suggest that reaZin may provide benefit to the dietary management of zinc deficiency associated with Alzheimer’s disease.
Based on results from this clinical study, we intend to commercialize reaZin as a medical food to be sold by prescription only for the dietary management of zinc deficiency associated with Alzheimer’s disease. On April 20, 2011, we announced that we had executed an agreement with TG United, Inc. of Brooksville, Florida, to provide commercial-scale manufacturing for reaZin.
In November 2010, we were awarded a grant in the amount of $244,480 under the Qualifying Therapeutic Discovery Project Program to support our Alzheimer’s disease program.
Critical Accounting Policies
In December 2001, the SEC requested that all registrants discuss their most “critical accounting policies” in management’s discussion and analysis of financial condition and results of operations. The SEC indicated that a “critical accounting policy” is one which is both important to the portrayal of the company’s financial condition and results and requires management’s most difficult, subjective or complex judgments, often as a result of the need to make estimates about the effect of matters that are inherently uncertain. We believe that the following discussion regarding research and development expenses, general and administrative expenses and non-cash compensation expense involve our most critical accounting policies.
Accounts Receivable and Allowance for Doubtful Accounts
Accounts receivable are reported at realizable value, net of allowances for doubtful accounts, which is estimated and recorded in the period the related revenue is recorded. We estimate and review the collectability of our receivables based on a number of factors, including the period they have been outstanding. Historical collection and payer reimbursement experience is an integral part of the estimation process related to allowances for doubtful accounts associated with Adeona Clinical Laboratory. In addition, we regularly assess the state of our billing operations in order to identify issues, which may impact the collectability of these receivables or reserve estimates. Revisions to the allowances for doubtful accounts estimates are recorded as an adjustment to bad debt expense. Receivables deemed uncollectible are charged against the allowance for doubtful accounts. Recoveries of receivables previously written-off are recorded as credits to the allowance for doubtful accounts.
22
Revenue Recognition
We record revenue when all of the following have occurred: (1) persuasive evidence of an arrangement exists, (2) the service is completed without further obligation, (3) the sales price to the customer is fixed or determinable, and (4) collectability is reasonably assured. We recognize milestone payments or upfront payments that have no contingencies as revenue when payment is received. During the nine months ended September 30, 2011 our sole revenue was laboratory revenue and for the nine months ended September 30, 2010, our stream of revenue was license and laboratory revenues.
License Revenues
Our licensing agreements may contain multiple elements, such as non-refundable up-front fees, payments related to the achievement of particular milestones and royalties. Fees associated with substantive at risk performance-based milestones are recognized as revenue upon completion of the scientific or regulatory event specified in the agreement. When we have substantive continuing performance obligations under an arrangement, revenue is recognized over the performance period of the obligations using a time-based proportional performance approach. Under the time-based method, revenue is recognized over the arrangement’s estimated performance period based on the elapsed time compared to the total estimated performance period. Revenue recognized at any point in time is limited to the amount of non-contingent payments received or due. When we have no substantive continuing performance obligations under an arrangement, it recognizes revenue as the related fees become due.
Revenues from royalties on third-party sales of licensed technologies are generally recognized in accordance with the contract terms when the royalties can be reliably determined and collectibility is reasonably assured. To date, we have not received any royalty revenues.
Laboratory Revenues
We primarily recognize revenue for services rendered upon completion of the testing process. Billing for services reimbursed by third-party payers, including Medicare and Medicaid, are recorded as revenues, net of allowances for differences between amounts billed and the estimated receipts from such payers.
We maintain a sales allowance to compensate for the difference in our billing practices and insurance company reimbursements. In determining this allowance, we look at several factors, the most significant of which is the average difference between the amount charged and the amount reimbursed by insurance carriers over the prior 18 months, otherwise known as the yearly average adjustment amount. The allowance taken is the averaged yearly average adjustment amount for these prior periods and multiplied by the period’s actual gross sales to determine the actual sales allowance for each period.
Warrant / Derivative Liabilities
Fair value accounting requires bifurcation of embedded derivative instruments such as conversion features in convertible debt or equity instruments, and measurement of their fair value for accounting purposes. In determining the appropriate fair value, we use the Black-Scholes option-pricing model. In assessing the convertible debt instruments, management determines if the convertible debt host instrument is conventional convertible debt and further if there is a beneficial conversion feature requiring measurement. If the instrument is not considered conventional convertible debt, we will continue its evaluation process of these instruments as derivative financial instruments.
Once determined, derivative liabilities are adjusted to reflect fair value at each reporting period end, with any increase or decrease in the fair value being recorded in results of operations as an adjustment to fair value of derivatives. In addition, the fair value of freestanding derivative instruments such as warrants, are also valued using the Black-Scholes option-pricing model.
Research and Development Expenses
We expense research and development costs as incurred. Research and development expenses consist primarily of license fees, manufacturing costs, salaries, stock-based compensation and related personnel costs, fees paid to consultants and outside service providers for laboratory development, legal expenses resulting from intellectual property prosecution and other expenses relating to the design, development, testing and enhancement of our product candidates.
Share-Based Payment Arrangements
Generally, all forms of share-based payments, including stock option grants, warrants, restricted stock grants and stock appreciation rights are measured at their fair value on the awards’ grant date, based on the estimated number of awards that are ultimately expected to vest. Share-based compensation awards issued to non-employees for services rendered are recorded at either the fair value of the services rendered or the fair value of the share-based payment, whichever is more readily determinable. The expense resulting from share-based payments are recorded in cost of goods sold, research and development or general and administrative expenses in the consolidated statement of operations, depending on the nature of the services provided.
23
Results of Operations
Three Months Ended September 30, 2011 and 2010
Revenues,net. Total net revenues for the three months ended September 30, 2011 and 2010 were $293,421 and $289,898, respectively. Revenues consisted of laboratory revenues from Adeona Clinical Laboratory. The slight increase in laboratory revenues for the three months ended September 30, 2011, reflects an increase in the client base and the expansion of in-house diagnostic testing services to include a full array of microbiology testing at Adeona Clinical Laboratory.
General and Administrative Expenses. General and administrative expenses increased to $681,805 for the three months ended September 30, 2011, from $601,806 for the three months ended September 30, 2010. This increase of 13% is primarily the result of increased salary expense and consultant fees. The non-cash charge relating to stock-based compensation expense was $50,509 for the three months ended September 30, 2011, compared to $68,493 for the three months ended September 30, 2010.
Research and Development Expenses. Research and development expenses increased to $288,964 for the three months ended September 30, 2011, from $229,044 for the three months ended September 30, 2010. This increase of approximately 26% is primarily the result of increased costs associated with our new clinical programs and the development costs associated with the commercialization of wellZin. Research and development expenses also include a non-cash charge relating to stock-based compensation expense of $5,749 for the three months ended September 30, 2011, compared to $19,817 for the three months ended September 30, 2010.
Costs of Laboratory Services. Costs of laboratory services increased to $260,881 for the three months ended September 30, 2011, from $192,176 for the three months ended September 30, 2010. This increase of approximately 36% is primarily the result of increased costs associated with the increased client base and expansion of in-house diagnostic testing services to include a full array of microbiology testing at Adeona Clinical Laboratory, including salary and supply costs.
Total Other Income (Expense), net. Total net other expense was $159,750 for the three months ended September 30, 2011, compared to $293 of other income for the three months ended September 30, 2010. Total net other expense for the three months ended September 30, 2011, includes $164,993 relating to the estimated fair value of the warrants associated with the January 2011 and April 2011 financings, adjusted for the change in their fair value at September 30, 2011. Other income for the three months ended September 30, 2011 included $6,868 of interest income from our short-term investments.
Net Loss. Our net loss was $1,097,979, or $0.04 per common share for the three months ended September 30, 2011, compared to net loss of $732,835, or $0.03 per common share for the three months ended September 30, 2010.
Nine Months Ended September 30, 2011 and 2010
Revenues, net. Total net revenues for the nine months ended September 30, 2011 and 2010 were $972,121 and $2,544,825, respectively. Revenues consisted of $972,121 of laboratory revenues for the nine months ended September 30, 2011 and $2,125,000 from the flupirtine sublicense fee with Meda and $419,825 of laboratory revenues from Adeona Clinical Laboratory for the nine months ended September 30, 2010. The increase in laboratory revenues for the nine months ended September 30, 2011, reflects an approximate 132% increase in laboratory revenues from the nine months ended September 30, 2010. This significant change in laboratory revenue resulted from an increase in the client base and the expansion of in-house diagnostic testing services to include a full array of microbiology testing at Adeona Clinical Laboratory.
General and Administrative Expenses. General and administrative expenses increased to $2,649,623 for the nine months ended September 30, 2011, from $2,000,262 for the nine months ended September 30, 2010. This increase of 32% is primarily the result of the increase in stock-based compensation expense for the nine months ended September 30, 2011. The non-cash charge relating to share-based compensation expense was $860,833 for the nine months ended September 30, 2011, compared to $252,100 for the nine months ended September 30, 2010. The stock-based compensation for the nine months ended September 30, 2011 includes a one-time charge of $397,767 relating to the modification of certain stock options, prior to expiration, held by a member of the Board of Directors.
Research and Development Expenses. Research and development expenses decreased to $800,923 for the nine months ended September 30, 2011, from $962,766 for the nine months ended September 30, 2010. This decrease of 17% is primarily the result of decreased costs associated with the discontinuation in prior periods of some of our clinical programs. Research and development expenses also include a non-cash charge relating to share-based compensation expense of $20,358 for the nine months ended September 30, 2011, compared to $72,785 for the nine months ended September 30, 2010.
24
Costs of Laboratory Services. Costs of laboratory services increased to $805,881 for the nine months ended September 30, 2011, from $430,001 for the nine months ended September 30, 2010. This increase of approximately 87% is primarily the result of increased costs associated with the increased client base and expansion of in-house diagnostic testing services to include a full array of microbiology testing at Adeona Clinical Laboratory, including salary and supply costs.
Total Other Income (Expense), net. Total net other expense was $1,680,030 for the nine months ended September 30, 2011, compared to other income of $7,629 for the nine months ended September 30, 2010. Total net other expense for the nine months ended September 30, 2011, includes $1,734,460 relating to the estimated fair value of the warrants associated with the January 2011 and April 2011 financings, adjusted for the change in their fair value at September 30, 2011. Other income for the nine months ended September 30, 2011 included $62,996 relating to the settlement of accounts payable previously accrued in prior periods and $6,868 of interest income from our short-term investments.
Net Loss. Our net loss was $4,964,336, or $0.18 per common share for the nine months ended September 30, 2011, compared to a net loss of $840,575, or $0.04 per common share for the nine months ended September 30, 2010.
Liquidity and Capital Resources
We have financed our operations since inception primarily through proceeds from equity financings and various private financings, primarily involving private sales of our common stock and other equity securities, corporate partnering license fees and from the proceeds from the sale of our common stock under our registration statement on Form S-3, laboratory testing revenues and miscellaneous equipment sales.
Our cash, cash equivalents and short-term investments totaled $7,474,568 as of September 30, 2011, an increase of $4,825,715 from December 31, 2010. During the nine months ended September 30, 2011, the primary sources of cash were net proceeds from the issuances of common stock to institutional investors of $6,960,610 and stock option exercises of $7,650. The primary use of cash during the nine months ended September 30, 2011 was for working capital requirements. Our cash, cash equivalents and short-term investments at October 31, 2011 was approximately $7.2 million.
Our continued operations will primarily depend on whether we are able to generate revenues and profits through partnerships, joint ventures or sales of diagnostic clinical laboratory services and/or raise additional funds through various potential sources, such as license fees from a potential corporate partner, equity and debt financing. Such additional funds may not become available on acceptable terms and there can be no assurance that any additional funding that we do obtain will be sufficient to meet our needs in the long term. We will continue to fund operations from cash on hand and through the similar sources of capital previously described. We can give no assurances that any additional capital that we are able to obtain will be sufficient to meet our needs.
Current and Future Financing Needs
We have incurred an accumulated deficit of approximately $48.7 million as of September 30, 2011. With the exception of the quarter ended June 30, 2010, we have incurred negative cash flow from operations since we started our business. We have spent, and expect to continue to spend, substantial amounts in connection with implementing our business strategy, including our planned product development efforts, our clinical trials, and our research and discovery efforts.
Based on our current plans, we believe that our cash will be sufficient to enable us to meet our planned operating needs for at least the next 12 months.
However, the actual amount of funds we will need to operate is subject to many factors, some of which are beyond our control. These factors include the following:
|
·
|
the progress of our research activities;
|
|
|
·
|
the number and scope of our research programs;
|
|
|
·
|
the progress of our preclinical and clinical development activities;
|
|
|
·
|
the progress of the development efforts of parties with whom we have entered into research and development agreements;
|
|
|
·
|
costs associated with additional clinical trials of our drug candidates;
|
|
|
|
·
|
our ability to maintain current research and development licensing arrangements and to establish new research and development and licensing arrangements;
|
|
·
|
our ability to achieve our milestones under licensing arrangements;
|
|
|
·
|
the costs involved in prosecuting and enforcing patent claims and other intellectual property rights;
|
|
|
·
|
the costs and timing of regulatory approvals;
|
|
|
·
|
marketing costs associated with our near-term product candidates, clinical laboratory diagnostic and microbiology services business; and
|
|
|
·
|
profitability of our near-term product candidates and clinical laboratory diagnostic and microbiology services business.
|
We have based our estimate on assumptions that may prove to be wrong. We may need to obtain additional funds sooner or in greater amounts than we currently anticipate. Potential sources of financing include strategic relationships, public or private sales of our shares or debt and other sources. We may seek to access the public or private equity markets when conditions are favorable due to our long-term capital requirements. We do not have any committed sources of financing at this time, and it is uncertain whether additional funding will be available when we need it on terms that will be acceptable to us, or at all. If we raise funds by selling additional shares of common stock or other securities convertible into common stock, the ownership interest of our existing stockholders will be diluted. If we are not able to obtain financing when needed, we may be unable to carry out our business plan. As a result, we may have to significantly limit our operations and our business, financial condition and results of operations would be materially harmed.
25
ITEM 3. QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK.
Not applicable.
ITEM 4. CONTROLS AND PROCEDURES
(a) Evaluation of disclosure controls and procedures
Pursuant to Rule 13a-15(b) under the Securities Exchange Act of 1934 (“Exchange Act”), the Company carried out an evaluation, with the participation of the Company’s management, including the Company’s Chief Executive Officer (“CEO”), who also serves as our principal financial and accounting officer, of the effectiveness of the Company’s disclosure controls and procedures (as defined under Rule 13a-15(e) under the Exchange Act) as of the end of the period covered by this report. Based upon that evaluation, the Company’s CEO concluded that the Company’s disclosure controls and procedures are effective as of September 30, 2011 to ensure that information required to be disclosed by the Company in the reports that the Company files or submits under the Exchange Act, is recorded, processed, summarized and reported, within the time periods specified in the SEC’s rules and forms, and that such information is accumulated and communicated to the Company’s management, including the Company’s CEO, as appropriate, to allow timely decisions regarding required disclosure.
(b) Changes in Internal Control over Financial Reporting
There has been no change in our internal control over financial reporting (as defined in Rules 13a-15(f) and 15d-15(f) of the Exchange Act) that occurred during our fiscal quarter ended September 30, 2011, that has materially affected, or is reasonably likely to materially affect, our internal control over financial reporting.
26
PART II—OTHER INFORMATION
ITEM 1. LEGAL PROCEEDINGS
None.
ITEM 1A. RISK FACTORS
An investment in our securities is highly speculative and involves a high degree of risk. Therefore, in evaluating us and our business you should carefully consider the risks set forth below, which are only a few of the risks associated with our business and our common stock. You should be in a position to risk the loss of your entire investment.
RISKS RELATING TO OUR BUSINESS
We currently have very minimal revenues and expect we will need to raise additional capital to operate our business.
With the exception of the quarter ended June 30, 2010, we have experienced significant losses since inception and have a significant accumulated deficit. We expect to incur additional operating losses in the future and therefore our cumulative losses to increase. To date, other than the licensing fee we received from Meda AB for the development of and commercialization of Effirma (flupirtine) for fibromyalgia in the United States, Canada and Japan and laboratory revenues from Adeona Clinical Laboratory, we have generated very minimal revenues. As of September 30, 2011, our accumulated deficit totaled approximately $48.7 million on a consolidated basis. Until such time as we receive approval from the FDA and other regulatory authorities for our prescription drug product candidates, we will not be permitted to sell our drugs and therefore will not have product revenues from the sale of drug products. For the foreseeable future we will have to fund all of our operations and capital expenditures from equity and debt offerings, cash on hand, licensing fees, homeopathic product revenues, laboratory revenues and grants. If the upfront licensing fee we received together with the proceeds from our recent financings, potential wellZin revenues and laboratory revenues are not sufficient to sustain our operations, we will need to seek additional sources of financing and such additional financing may not be available on favorable terms, if at all. If we do not succeed in raising additional funds on acceptable terms, we may be unable to complete planned preclinical and clinical trials or obtain approval of our product candidates from the FDA and other regulatory authorities. In addition, we could be forced to discontinue product development, forego sales and marketing efforts, and forego licensing in attractive business opportunities. Any additional sources of financing will likely involve the issuance of our equity or debt securities, which will have a dilutive effect on our stockholders.
We have not been able to sustain profitability.
Other than with respect to the quarter ended June 30, 2010, we have a history of losses and we have incurred and continue to incur substantial losses and negative operating cash flow. Even if we succeed in developing and commercializing one or more of our product candidates, we may still incur substantial losses for the foreseeable future and may not sustain profitability. We also expect to continue to incur significant operating and capital expenditures and anticipate that our expenses will substantially increase in the foreseeable future as we do the following:
|
·
|
continue to undertake preclinical development and clinical trials for our product candidates;
|
|
·
|
seek regulatory approvals for our product candidates;
|
|
·
|
develop our product candidates for commercialization;
|
|
·
|
implement additional internal systems and infrastructure;
|
|
·
|
lease additional or alternative office facilities; and
|
|
·
|
hire additional personnel, including members of our management team.
|
We may experience negative cash flow for the foreseeable future as we fund our technology development with capital expenditures. As a result, we will need to generate significant revenues in order to achieve and maintain profitability. We may not be able to generate these revenues or achieve profitability in the future. Our failure to achieve or maintain profitability could negatively impact the value of our common stock and underlying securities.
Our research and development efforts may not succeed in developing commercially successful products and technologies, which may limit our ability to achieve profitability.
We must continue to explore opportunities that may lead to new products and technologies. To accomplish this, we must commit substantial efforts, funds, and other resources to research and development. A high rate of failure is inherent in the research and development of new products and technologies. Any such expenditures that we make will be made without any assurance that our efforts will be successful. Failure can occur at any point in the process, including after significant funds have been invested.
27
Regardless of whether our clinical trials are deemed to be successful, promising new product candidates may fail to reach the market or may only have limited commercial success because of efficacy or safety concerns, failure to achieve positive clinical outcomes, inability to obtain necessary regulatory approvals or satisfy regulatory criteria, limited scope of approved uses, excessive costs to manufacture, the failure to establish or maintain intellectual property rights, or infringement of the intellectual property rights of others. Even if we successfully develop new products or enhancements, they may be quickly rendered obsolete by changing customer preferences, changing industry standards, or competitors' innovations. Innovations may not be quickly accepted in the marketplace because of, among other things, entrenched patterns of clinical practice or uncertainty over third-party reimbursement. We cannot state with certainty when or whether any of our products under development will be launched, whether we will be able to develop, license, or otherwise acquire drug candidates or products, or whether any products will be commercially successful. Failure to launch successful new products or new indications for existing products may cause our products to become obsolete, which may limit our ability to achieve profitability.
We have a limited operating history on which investors can base an investment decision.
We have not yet demonstrated our ability to perform the functions necessary for the successful commercialization of any of our product candidates. The successful commercialization of our product candidates will require us to perform a variety of functions, including:
|
·
|
continuing to undertake preclinical development and clinical trials;
|
|
|
·
|
participating in regulatory approval processes;
|
|
|
·
|
formulating and manufacturing products; and
|
|
|
·
|
conducting sales and marketing activities.
|
Our operations have been limited to organizing and staffing our company, acquiring, developing, and securing our proprietary technology, and undertaking preclinical trials and Phase I/II, Phase II and Phase III clinical trials of our principal product candidates. These operations provide a limited basis for you to assess our ability to commercialize our product candidates and the advisability of investing in our securities.
We have limited experience in commercializing medical food and homeopathic OTC drug products and therefore we may not be effective in developing and commercializing products.
We have no experience in marketing a medical food such as reaZin, nor can we provide any assurance that the results of our reaZin clinical study will be perceived as demonstrating sufficient clinical benefit to permit us to be accepted by the market, obtain reimbursement from health insurance payers or profitably market such medical food with or without health insurance reimbursement. Even if we are able to successfully manufacture reaZin and establish distribution channels, there can be no assurance that reaZin will receive market acceptance.
We have no experience in marketing a homeopathic OTC drug product such as wellZin, nor can we provide any assurance that clinical data we acquired in July 2011 will be perceived as demonstrating sufficient clinical benefit to permit us to be accepted by the market or profitably market such a homeopathic drug product. Even if we are able to successfully manufacture wellZin or have it manufactured for us and establish distribution channels, there can be no assurance that wellZin will receive market acceptance.
We may not generate additional revenue from our relationships with our corporate collaborators.
On May 6, 2010, we and Pipex, our wholly owned subsidiary, entered into a sublicense agreement with Meda AB whereby we may receive milestone payments totaling $17.5 million (including an upfront payment of $2.5 million that has already been received), plus royalties on our flupirtine program. There can be no assurance that Meda AB will successfully develop flupirtine for fibromyalgia in the United States, Canada or Japan that would allow us to receive such additional $15 million in milestone payments and royalties on sales in connection with such agreement. The successful achievement of the various milestones set forth in the sublicense agreement is not within our control and we will be dependent upon Meda AB for achievement of such milestones. According to Meda’s 2010 Annual Report, flupirtine for fibromyalgia is currently in Phase II development.
28
We may not be able to generate any significant revenue from copper and zinc status tests or any other tests we may develop.
We have committed significant research and development resources to the development of copper and zinc status tests. Although there may be a large potential market for such testing, there is no guarantee that we will successfully generate significant revenues from this or any other tests for any use. In November 2009, we launched a copper and zinc status test panel through Adeona Clinical Laboratory, our CLIA-certified reference laboratory.
However, sales of our zinc and copper status test panel have generated only very limited revenue and there is no guarantee that we will be able to successfully market this test panel or other diagnostic tests. If we are not able to successfully market or sell our diagnostic tests we may develop for any reason, we will not generate any revenue from the sale of such tests. Even if we are able to develop diagnostic or other tests for sale in the marketplace, a number of factors could impact our ability to generate any significant revenue from the sale of such tests, including the following:
|
|
|
·
|
reliance on our Adeona Clinical Laboratory operations, which are subject to routine governmental oversight and inspections for continued operation pursuant to CLIA and other regulations;
|
|
|
|
·
|
our ability to establish and maintain adequate infrastructure to support the commercial launch and sale of our diagnostic tests through our Adeona Clinical Laboratory subsidiary, including establishing adequate laboratory space, information technology infrastructure, sample collection and tracking systems and electronic ordering and reporting systems and other infrastructure and hiring adequate laboratory and other personnel;
|
|
|
|
·
|
the availability of adequate study samples for validation studies for any diagnostic tests we develop, the success of such validation studies and our ability to publish study results in peer-reviewed journals;
|
|
|
|
·
|
the availability of alternative and competing tests or products and technological innovations or other advances in medicine that cause our technologies to be less competitive;
|
|
|
|
·
|
compliance with federal, state and foreign regulations governing laboratory testing and the sale and marketing of diagnostic or other tests, including copper and zinc status tests;
|
|
|
|
·
|
the accuracy rates of such tests, including rates of false-negatives and/or false-positives;
|
|
|
|
·
|
concerns regarding the safety effectiveness or clinical utility of our tests;
|
|
|
|
·
|
changes in the regulatory environment affecting health care and health care providers, including changes in laws regulating laboratory testing and/or device manufacturers and any laws regulating diagnostic testing;
|
|
|
|
·
|
the extent and success of our sales and marketing efforts and ability to drive adoption of our diagnostic tests;
|
|
|
|
·
|
coverage and reimbursement levels by government payers and private insurers;
|
|
|
|
·
|
the level of physician and customer adoption of any diagnostic tests we develop;
|
|
|
|
·
|
pricing pressures and changes in third-party payer reimbursement policies;
|
|
|
|
·
|
general changes or developments in the market for Alzheimer’s disease diagnostics or diagnostics in general;
|
|
|
|
·
|
ethical and legal issues concerning the appropriate use of the information resulting from Alzheimer’s disease diagnostic tests or other tests;
|
|
|
|
·
|
our ability to promote and protect our products and technology; and
|
|
|
|
·
|
intellectual property rights held by others or others infringing our intellectual property rights.
|
29
We are dependent on a limited number of customers, the loss of any of which would have a material adverse effect upon our revenue.
During the nine months ended September 30, 2011 we generated revenues from three significant insurance providers, which accounted for 69%, 4% and 20% of our revenue for such nine month period. During the nine months ended September 30, 2010, we generated revenues from the same significant insurance providers, which accounted for 68%, 14% and 10% of our revenues for such nine month period. The loss of revenue from these insurance providers could have an immediate significant adverse effect upon our revenue and results of operations.
We have experienced several management changes.
We have had significant changes in management in the past three years. Effective June 26, 2009, Max Lyon was appointed our Chief Executive Officer and President, while Steve Kanzer remained as Chairman of our Board. Effective February 6, 2010, James S. Kuo, M.D., M.B.A., was appointed as Chairman of our Board, Chief Executive Officer and President and Mr. Lyon resigned from his position as Chief Executive Officer, President and director. Effective October 31, 2011, Jeff Lucero Riley was appointed as independent, non-executive Chairman of our Board; Dr. Kuo remains as Chief Executive Officer, President and a member of the Board. Changes in our key positions, as well as additions of new personnel and departures of existing personnel, can be disruptive, might lead to additional departures of existing personnel and could have a material adverse effect on our business, operating results, financial results and internal controls over financial reporting.
We only acquired our CLIA-certified reference laboratory in July of 2009 and have limited experience operating a diagnostic and microbiology testing laboratory. Our ability to successfully develop and commercialize diagnostic and microbiology tests will depend on our ability to successfully operate our CLIA-certified reference laboratory and obtain and maintain required regulatory certifications.
We acquired Adeona Clinical Laboratory, our CLIA-licensed clinical reference laboratory located in Bolingbrook, IL, in July of 2009. Because there is substantial distance between Adeona Clinical Laboratory and our corporate headquarters in Ann Arbor, Michigan, we may have logistical and operational challenges in effectively managing and operating Adeona Clinical Laboratory. In November of 2009, we launched a panel of copper and zinc status tests through Adeona Clinical Laboratory. If we are unable to successfully commercialize our serum based copper and zinc diagnostic test panels through Adeona Clinical Laboratory, we may not be able to achieve significant revenues and profitability with respect to such activities. Our ability to successfully develop and commercialize diagnostic tests and microbiology testing will depend on our ability to successfully operate Adeona Clinical Laboratory and obtain and maintain required regulatory approvals.
30
As a clinical reference laboratory, Adeona Clinical Laboratory is subject to CLIA regulations, which are designed to ensure the quality and reliability of clinical laboratories by mandating specific standards in the areas of personnel qualifications, administration and participation in various areas, including proficiency testing, patient test management, quality control, quality assurance and inspections. The sanction for failure to comply with CLIA requirements may be suspension, revocation or limitation of a laboratory’s CLIA certificate, which is necessary to conduct business, as well as significant fines and/or criminal penalties. Adeona Clinical Laboratory is also subject to regulation of laboratory operations under state clinical laboratory laws. State clinical laboratory laws may require that laboratories and/or laboratory personnel meet certain qualifications, specify certain quality controls and require maintenance of certain records. Certain states, including California, Maryland, New York, Pennsylvania and Rhode Island, require that you obtain licenses to test specimens from patients residing in those states and additional states may require similar licenses in the future. If we are unable to obtain licenses from these states or there is delay in obtaining such licenses, we will not be able to process any samples from patients located in those states until we have obtained the requisite licenses. Potential sanctions for violation of these statutes and regulations include significant fines and the suspension or loss of various licenses, certificates and authorizations, which could adversely affect our business and results of operations.
We may not obtain the necessary United States or worldwide regulatory approvals to commercialize our product candidate(s).
We will need FDA approval to commercialize our prescription drug product candidates in the United States and approvals from equivalent regulatory authorities in foreign jurisdictions to commercialize our prescription drug product candidates in those jurisdictions. In order to obtain FDA approval for marketing any of these product candidates, we must submit to the FDA an NDA, demonstrating that the product candidate is safe for humans and effective for its intended use and that the product candidate can be consistently manufactured and is stable. This demonstration requires significant research and animal tests, which are referred to as “preclinical studies,” human tests, which are referred to as “clinical trials” as well as the ability to manufacture the product candidate, referred to as “chemistry, manufacturing, and controls” or “CMC.” We will also need to file additional IND applications and protocols in order to initiate clinical testing of our drug candidates in new therapeutic indications and delays in obtaining required FDA and institutional review board approvals to commence such studies will delay our initiation of such planned additional studies.
Satisfying the FDA’s regulatory requirements typically takes many years, depending on the type, complexity, and novelty of the product candidate, and requires substantial resources for research development, and testing. We cannot predict whether our research and clinical approaches will result in drugs that the FDA considers safe for humans and effective for indicated uses. The FDA has substantial discretion in the drug approval process and may require us to conduct additional preclinical and clinical testing or to perform post-marketing studies.
The approval process may also be delayed by changes in government regulation, future legislation or administrative action, or changes in FDA policy that occur prior to or during our regulatory review. Delays in obtaining regulatory approvals may do the following:
|
·
|
delay commercialization of, and our ability to derive product revenues from, our product candidates;
|
|
|
·
|
impose costly procedures on us; and
|
|
|
·
|
diminish any competitive advantages that we may otherwise enjoy.
|
The on-going and future development and commercialization of Effirma (flupirtine) for fibromyalgia is the responsibility of Meda AB and no assurance can be given that Meda will gain the FDA’s acceptance of the NDA or obtain NDA approval from the FDA of flupirtine for fibromyalgia.
Even if we comply with all FDA requests, the FDA may ultimately reject one or more of our NDAs. We cannot be sure that we will ever obtain regulatory clearance for our product candidates. Failure to obtain FDA approval of any of our product candidates will severely undermine our business by reducing our number of salable products and, therefore, corresponding product revenues.
In foreign jurisdictions, we must receive approval from the appropriate regulatory authorities before we can commercialize our drugs. Foreign regulatory approval processes generally include all of the risks associated with the FDA approval procedures described above. We cannot assure you that we will receive the approvals necessary to commercialize our product candidate for sale outside the United States.
Our diagnostic and microbiology tests are subject to changes in CLIA, FDA and other regulatory requirements.
We initially plan to develop assays and commercialize our tests in the form of laboratory developed tests (LDTs) through Adeona Clinical Laboratory, our CLIA-certified laboratory. Although LDT testing is currently solely under the purview of CMS and state agencies who oversee LDTs, the FDA and the United States Department of Health and Human Services have been reviewing their approach to regulation in the area of LDTs, and the laws and regulations may undergo change in the near future. The FDA has indicated that it does intend to regulate some LDTs as medical devices under the Federal Food, Drug, and Cosmetic Act. Although we have no current plans in our LDT strategy to utilize analyte specific reagents (ASRs) or In Vitro Diagnostic Multivariate Index Assay (IVDMIAs), which have been the focus of recent regulatory actions by the FDA, we cannot predict the extent of the FDA’s future regulation and policies with respect to LDTs. Concurrently with our LDT commercialization activities, we may conduct the development, validation, and other activities necessary to file submissions with the FDA seeking approval for selected diagnostic tests. If we are required to obtain FDA authorization to market a laboratory test as a device, that will substantially delay the marketing of the test and increase the costs of entering the market. In addition, devices are subject to various other regulatory requirements, such as the need to comply with the Quality System regulation and to comply with various FDA reporting requirements. If we are unable to successfully launch any diagnostic tests as LDTs or if we are otherwise required to obtain FDA premarket clearance or approval prior to commercializing any diagnostic tests or maintain Adeona Clinical Laboratory’s CLIA-certified laboratory status, our ability to generate revenue from the sale of such tests may be delayed and we may never be able to generate significant revenues from sales of diagnostic products.
31
If the medical relevance of copper and zinc in Alzheimer’s disease is not demonstrated or is not recognized by others, we may have less demand for our products and services and may have less opportunity to enter into diagnostic product development and commercialization collaborations with others.
Some of the products we have developed and additional products that we hope to develop involve new and unproven approaches or involve applications in markets that we are only beginning to explore. They are based on the assumption that information about the roles of copper and zinc in the progression and development of neurodegenerative diseases such as Alzheimer’s disease and dementia may help scientists and clinicians better understand and treat conditions or complex disease processes. We cannot be certain that this type of information will play a key role in the development of therapeutics, diagnostics or other products in the future, or that any of our findings would be accepted by clinicians, researchers or by any other potential market or industry partner or customer. If we are unable to generate additional valuable information and data about the usefulness of copper and zinc status testing, the demand for our products, applications, and services will be reduced and our business will be harmed.
We may not be able to retain rights licensed to us by others to commercialize key products and may not be able to establish or maintain the relationships we need to develop, manufacture, and market our products.
In addition to our own patent applications, we also currently rely on licensing agreements with third party patent holders/licensors for our products. Pipex, our wholly owned subsidiary, has an exclusive license agreement with the McLean Hospital relating to the use of flupirtine to treat fibromyalgia which was recently sublicensed to Meda AB and an exclusive license agreement with the Regents of the University of California relating to our Trimesta technology. Each of these agreements requires us or our sublicensee to use our best efforts to commercialize each of the technologies as well as meet certain diligence requirements and timelines in order to keep the license agreement in effect. In the event we or our sublicensee are not able to meet our diligence requirements, we may not be able to retain the rights granted under our agreements or renegotiate our arrangement with these institutions on reasonable terms, or at all. Furthermore, we currently have very limited product development capabilities, and limited marketing or sales capabilities. For us to research, develop, and test our product candidates, we would need to contract with outside researchers, in most cases those parties that did the original research and from whom we have licensed the technologies.
We can give no assurances that any of our issued patents licensed to us or any of our other patent applications will provide us with significant proprietary protection or be of commercial benefit to us. Furthermore, the issuance of a patent is not conclusive as to its validity or enforceability, nor does the issuance of a patent provide the patent holder with freedom to operate without infringing the patent rights of others.
Developments by competitors may render our products or technologies obsolete or non-competitive.
Companies that currently sell or are developing both generic and proprietary pharmaceutical compounds to treat central nervous system diseases include: Pfizer, GlaxoSmithKline Pharmaceuticals, Merck & Co., Eli Lilly & Co., Biogen Idec, Forest Laboratories, Novartis, Teva Pharmaceuticals, Prana Biotechnology, Merz & Co., Alcon and Bausch and Lomb. Companies that currently sell or are developing homeopathic OTC drugs to reduce the duration and severity of symptoms caused by the common cold include: ProPhase Labs, Inc. and Matrixx Initiatives, Inc. Many of our competitors have significant financial and human resources. In addition, academic research centers may develop technologies that compete with our Trimesta, modified release zinc preparations (reaZin and AEN-100), wellZin and flupirtine technologies. Should clinicians or regulatory authorities view these therapeutic regiments as more effective than our products, this might delay or prevent us from obtaining regulatory approval for our products, or it might prevent us from obtaining favorable reimbursement rates from payers, such as Medicare, Medicaid and private insurers.
No assurance can be given that our once daily reaZin, a medical food for the dietary management of zinc deficiency associated with Alzheimer’s disease, or our wellZin , a homeopathic OTC zinc acetate lozenge to reduce the duration and symptoms of the common cold, will be viewed as more effective than current zinc therapies or any newly developed therapies or demonstrate sufficient clinical benefit to gain market acceptance.
32
Competitors could develop and/or gain FDA approval of our products for a different indication.
Since we do not have composition of matter patent claims for flupirtine and estriol, others may obtain approvals for other uses of these products that are not covered by our issued or pending patents. For example, the active ingredients in both Effirma (flurpirtine) and Trimesta (estriol) have been approved for marketing in overseas countries for different uses and an oral immediate release form of zinc is approved in the Unites States and Europe for the treatment of Wilson’s disease. Other companies, including the original developers or licensees or affiliates may seek to develop Effirma or Trimesta or their respective active ingredient(s) for other uses in the United States or any country we are seeking approval for. We cannot provide any assurances that any other company may obtain FDA approval for products that contain flupirtine or estriol in various formulations or delivery systems that might adversely affect our ability or the ability of our sublicensee to develop and market these products in the United States. We are aware that other companies have intellectual property protection using the active ingredients and have conducted clinical trials of flupirtine, estriol and zinc for different applications than what we are developing. Many of these companies may have more resources than us. Should a competitor obtain FDA approval for its product for any indication prior to us, we might be precluded under the Hatch-Waxman Act to obtain approval for our product candidates for a period of five years. We cannot provide any assurances that our products will be FDA approved prior to our competitors.
If the FDA approves other products containing our active ingredients to treat indications other than those covered by our issued or pending patent applications, physicians may elect to prescribe a competitor’s products to treat the diseases for which we are developing—this is commonly referred to as “off-label” use. While under FDA regulations a competitor is not allowed to promote off-label uses of its product, the FDA does not regulate the practice of medicine and, as a result, cannot direct physicians as to which source it should use for these products they prescribe to their patients. Consequently, we might be limited in our ability to prevent off-label use of a competitor’s product to treat the diseases we are developing, even if we have issued patents for that indication. If we are not able to obtain and enforce these patents, a competitor could use our products for a treatment or use not covered by any of our patents. We cannot provide any assurances that a competitor will not obtain FDA approval for a product that contains the same active ingredients as our products.
None of our drug candidates or our reaZin medical food product candidate contain the patented ingredient zinc-monocysteine and is instead the subject of pending United States and international patent applications initially filed in January 2006 (see. United States Ser. No 11/621,962), which may not provide substantial protection from competitive products until such pending patents issue, if at all. As a medical food, no regulatory protection is afforded through FDA regulations to prevent others from marketing similar products. Similarly, the CopperProof Test Panel offered by our Adeona Clinical Laboratory subsidiary is the subject of pending patent applications that are expected to require a substantial amount of time to issue in order to provide protection from potential competitors.
We rely primarily on method patents and patent applications and various regulatory exclusivities to protect the development of our technologies, and our ability to compete may decrease or be eliminated if we are not able to protect our proprietary technology.
Our competitiveness may be adversely affected if we are unable to protect our proprietary technologies. We do not have composition of matter patents for Trimesta or Effirma, or their respective active ingredients estriol and flupirtine. We rely on issued patent and pending patent applications for use of Trimesta to treat multiple sclerosis (issued United States Patent No. 6,936,599) and various other therapeutic indications, which have been exclusively licensed to us. We have exclusively licensed an issued patent for the treatment of fibromyalgia with flupirtine, which we have sublicensed to Meda AB.
Our reaZin medical food and AEN-100 drug candidate (gastroretentive, sustained-release zinc-based tablets) are the subject of United States and international pending patent applications, such as published United States patent application Ser. No. 11/621,962 and corresponding international applications that claim priority to January 10, 2006 as well as additional unpublished patent applications. On October 26, 2011, we received a final rejection letter with regard to United States patent application Ser. No. 11/621,962 We have several options to consider with regard to this patent including filing: a response, a Notice of Appeal, or a Request for Continued Examination. We expect to take further action by January 26, 2012.
Our oral zinc lozenge, wellZin, is currently not covered by any issued or pending patents. No assurance can be given that others will not develop and market competing products.
The patent positions of pharmaceutical companies are uncertain and may involve complex legal and factual questions. We may incur significant expense in protecting our intellectual property and defending or assessing claims with respect to intellectual property owned by others. Any patent or other infringement litigation by or against us could cause us to incur significant expense and divert the attention of our management.
We may also rely on the United States Drug Price Competition and Patent Term Restoration Act, commonly known as the “Hatch-Waxman Amendments,” to protect some of our current product candidates, specifically Trimesta and other future product candidates we may develop. Once a drug containing a new molecule is approved by the FDA, the FDA cannot accept an abbreviated NDA for a generic drug containing that molecule for five years, although the FDA may accept and approve a drug containing the molecule pursuant to an NDA supported by independent clinical data. Recent amendments have been proposed that would narrow the scope of Hatch-Waxman exclusivity and permit generic drugs to compete with our drug.
33
Others may file patent applications or obtain patents on similar technologies or compounds that compete with our products. We cannot predict how broad the claims in any such patents or applications will be, and whether they will be allowed. Once claims have been issued, we cannot predict how they will be construed or enforced. We may infringe intellectual property rights of others without being aware of it. If another party claims we are infringing their technology, we could have to defend an expensive and time consuming lawsuit, pay a large sum if we are found to be infringing, or be prohibited from selling or licensing our products unless we obtain a license or redesign our product, which may not be possible.
We also rely on trade secrets and proprietary know-how to develop and maintain our competitive position. Some of our current or former employees, consultants, scientific advisors, current or prospective corporate collaborators, may unintentionally or willfully disclose our confidential information to competitors or use our proprietary technology for their own benefit. Furthermore, enforcing a claim alleging the infringement of our trade secrets would be expensive and difficult to prove, making the outcome uncertain. Our competitors may also independently develop similar knowledge, methods, and know-how or gain access to our proprietary information through some other means.
We may fail to retain or recruit necessary personnel, and we may be unable to secure the services of consultants.
As of September 30, 2011, we had 15 employees. We have also engaged regulatory consultants to advise us on our dealings with the FDA and other foreign regulatory authorities. Our future performance will depend in part on our ability to successfully integrate newly hired officers into our management team and our ability to develop an effective working relationship among senior management.
Certain of our directors Jeffrey Kraws, Jeffrey Wolf, Steve Kanzer, and Jeff Riley, scientific advisors, and consultants serve as officers, directors, scientific advisors, or consultants of other biopharmaceutical or biotechnology companies that might be developing competitive products to ours. Other than corporate opportunities, none of our directors are obligated under any agreement or understanding with us to make any additional products or technologies available to us. Similarly, we can give no assurances, and we do not expect and stockholders should not expect, that any biomedical or pharmaceutical product or technology identified by any of our directors or affiliates in the future would be made available to us other than corporate opportunities. We can give no assurances that any such other companies will not have interests that are in conflict with our interests.
Losing key personnel or failing to recruit necessary additional personnel would impede our ability to attain our development objectives. David A. Newsome, M.D., our former Senior Vice President of Research and Development recently passed away. There is intense competition for qualified personnel in the drug-development field, and we may not be able to attract and retain the qualified personnel we would need to develop our business.
We rely on independent organizations, advisors, and consultants to perform certain services for us, including handling substantially all aspects of regulatory approval, clinical management, manufacturing, marketing, and sales. We expect that this will continue to be the case. Such services may not always be available to us on a timely basis when we need them.
We may experience difficulties in obtaining sufficient quantities of our products or other compounds.
In order to successfully commercialize our product candidates, we and our sublicensees must be able to manufacture our products in commercial quantities, in compliance with regulatory requirements, at acceptable costs, and in a timely manner. Manufacture of the types of biopharmaceutical products that we propose to develop present various risks.
For manufacturing and nonclinical information for Trimesta (estriol), we previously relied upon an agreement with Organon, a division of Schering-Plough, for access to clinical, nonclinical, stability and drug supply relating to estriol, the active ingredient in Trimesta, which is currently used in the clinical trial for relapsing-remitting multiple sclerosis. Organon informed us of its decision to discontinue supply of estriol tablets beyond that required to satisfy our planned needs of the ongoing clinical trial for relapsing-remitting multiple sclerosis. We believe our current supply of estirol is sufficient for the ongoing clinical trial for relapsing-remitting multiple sclerosis. In addition, we have identified and contracted an alternative supplier of estriol and an alternative manufacturer of Trimesta tablets for our recently announced clinical trial for cognitive dysfunction in multiple sclerosis.
Our plans to launch reaZin as a medical food for the dietary management of zinc deficiency in Alzheimer’s disease and clinical testing of AEN-100 will depend upon the successful cGMP manufacture, quality control and acceptable results of stability studies. In April 2011, we engaged TG United, Inc. of Brooksville, Florida, a third party contract manufacturer, to provide commercial-scale manufacturing for reaZin. There can be no assurance that TG United, Inc. will be able to manufacture reaZin in such quantities on a timely basis as we require.
34
Our plans to launch wellZin, our zinc acetate lozenge as a homeopathic OTC medicine to reduce the duration and symptoms of the common cold will depend on the successful cGMP manufacture and quality control of wellZin. On November 4, 2011, we executed an agreement with F&F Foods of Chicago, Illinois, to provide commercial-scale manufacturing of wellZin. There can be no assurance that F&F Foods will be able to manufacture wellZin in such quantities on a timely basis as we require.
Historically, our manufacturing has been handled by contract manufacturers and compounding pharmacies. We can give no assurances that we will be able to continue to use our current manufacturer or be able to establish another relationship with a manufacturer quickly enough so as not to disrupt commercialization of any of our products, or that commercial quantities of any of our products, if approved for marketing, will be available from contract manufacturers at acceptable costs.
In addition, any contract manufacturer that we select to manufacture our product candidates might fail to maintain a current “good manufacturing practices” (cGMP) manufacturing facility or fail to comply with other potentially applicable requirements, such as Hazard Analysis and Risk-Based Preventive Controls requirements under the Federal Food, Drug, and Cosmetic Act, as amended by the FDA Food Safety Modernization Act. Failure of a manufacturer to maintain cGMP or to comply with other potentially applicable requirements could subject us to penalties, restrictions, and/or prohibitions affecting our ability to further manufacture and distribute our products.
The cost of manufacturing certain product candidates may make them prohibitively expensive. In order to successfully commercialize our product candidates we may be required to reduce the costs of production, and we may find that we are unable to do so. We may be unable to obtain, or may be required to pay high prices for compounds manufactured or sold by others that we need for comparison purposes in clinical trials and studies for our product candidates.
The manufacture of our products is a highly exacting process, and if we or one of our materials suppliers encounter problems manufacturing our products, our business could suffer.
The FDA and foreign regulators require manufacturers to register manufacturing facilities. The FDA and foreign regulators also inspect these facilities to confirm compliance with cGMP or similar requirements that the FDA or foreign regulators establish. We, or our materials suppliers, may face manufacturing or quality control problems causing product production and shipment delays or a situation where we or the supplier may not be able to maintain compliance with the FDA’s cGMP requirements, or those of foreign regulators, necessary to continue manufacturing our products. Any failure to comply with cGMP requirements or other FDA or foreign regulatory requirements could adversely affect our clinical research activities and our ability to market and develop our products.
Although medical foods and homeopathic OTC drugs do not require pre-market approval by the FDA, manufacturers of medical foods and homeopathic OTC drugs must meet applicable regulatory criteria, be registered with the FDA and are subject to inspection by the FDA. If the outcome of any inspection is negative or the manufacturer or we fail to comply with any regulatory requirements, we could be subject to penalties, restrictions and/or prohibitions affecting on our ability to further manufacture and distribute our products.
If our laboratory facilities are damaged, our business would be seriously harmed.
Our only laboratory facility for copper and zinc testing products and general reference lab services is located in Bolingbrook, IL. Damage to our facility due to war, fire, natural disaster, power loss, communications failure, terrorism, unauthorized entry, or other events could prevent us from conducting our business for an indefinite period, could result in a loss of important data or cause us to cease development and production of our products. We cannot be certain that our limited insurance to protect against business interruption would be adequate or would continue to be available to us on commercially reasonable terms, or at all.
If the parties we depend on for supplying our drug substance raw materials and certain manufacturing-related services do not timely supply these products and services, it may delay or impair our ability to develop, manufacture and market our products.
We rely on suppliers for our drug substance raw materials and third parties for certain manufacturing-related services to produce material that meets appropriate content, quality and stability standards and use in clinical trials of our products and, after approval, for commercial distribution. To succeed, clinical trials require adequate supplies of drug substance and drug product, which may be difficult or uneconomical to procure or manufacture. We and our suppliers and vendors may not be able to (i) produce our drug substance or drug product to appropriate standards for use in clinical studies, (ii) perform under any definitive manufacturing, supply or service agreements with us or (iii) remain in business for a sufficient time to successfully produce and market our product candidates. If we do not maintain important manufacturing and service relationships, we may fail to find a replacement supplier or required vendor or develop our own manufacturing capabilities which could delay or impair our ability to obtain regulatory approval for our products and substantially increase our costs or deplete profit margins, if any. If we do find replacement manufacturers and vendors, we may not be able to enter into agreements with them on terms and conditions favorable to us and, there could be a substantial delay before a new facility could be qualified and registered with the FDA and foreign regulatory authorities.
35
Clinical trials are very expensive, time-consuming, and difficult to design and implement.
Human clinical trials are very expensive and difficult to design and implement, in part because they are subject to rigorous regulatory requirements. The clinical trial process is also time-consuming. We estimate that clinical trials of our product candidates would take at least several years to complete. Furthermore, failure can occur at any stage of the trials, and we could encounter problems that cause us to abandon or repeat clinical trials. Commencement and completion of clinical trials may be delayed by several factors, including:
|
·
|
obtaining an IND application with the FDA to commence clinical trials;
|
|
|
·
|
identification of, and acceptable arrangements with, one or more clinical sites;
|
|
|
·
|
obtaining IRB approval to commence clinical trials;
|
|
|
·
|
unforeseen safety issues;
|
|
|
·
|
determination of dosing;
|
|
|
·
|
lack of effectiveness during clinical trials;
|
|
|
·
|
slower than expected rates of patient recruitment;
|
|
|
·
|
inability to monitor patients adequately during or after treatment;
|
|
|
·
|
inability or unwillingness of medical investigators to follow our clinical protocols; and
|
|
|
·
|
unwillingness of the FDA or IRBs to permit the clinical trials to be initiated.
|
In addition, we, IRBs or the FDA may suspend our clinical trials at any time if it appears that we are exposing participants to unacceptable health risks or if IRBs or the FDA finds deficiencies in our submissions or conduct of our trials.
The results of our clinical trials may not support our product candidate claims and the results of preclinical studies and completed clinical trials are not necessarily predictive of future results.
To date, long-term safety and efficacy have not yet been demonstrated in clinical trials for any of our diagnostic product candidates. Favorable results in our early studies or trials may not be repeated in later studies or trials. Even if our clinical trials are initiated and completed as planned, we cannot be certain that the results will support our product candidate claims. Success in preclinical testing and Phase II clinical trials does not ensure that later Phase II or Phase III clinical trials will be successful. We cannot be sure that the results of later clinical trials would replicate the results of prior clinical trials and preclinical testing. In particular, the limited results that we have obtained for our diagnostic tests may not predict results from studies in larger numbers of subjects drawn from more diverse populations over a longer period of time. Clinical trials may fail to demonstrate that our product candidates are safe for humans and effective for indicated uses. Any such failure could cause us or our sublicensee to abandon a product candidate and might delay development of other product candidates. Preclinical and clinical results are frequently susceptible to varying interpretations that may delay, limit or prevent regulatory approvals or commercialization. Any delay in, or termination of, our clinical trials would delay our obtaining FDA approval for the affected product candidate and, ultimately, our ability to commercialize that product candidate.
Physicians and patients may not accept and use our technologies.
Even if our products demonstrate sufficient clinical benefit and the FDA approves our drug product candidates, physicians and patients may not accept and use them. Acceptance and use of our products will depend upon a number of factors, including the following:
|
·
|
the perception of members of the health care community, including physicians, regarding the safety and effectiveness of our product candidates;
|
|
|
·
|
the cost-effectiveness of our product relative to competing products;
|
|
|
·
|
availability of reimbursement for our products from government or other healthcare payers; and
|
|
|
·
|
the effectiveness of marketing and distribution efforts by us and our licensees and distributors, if any.
|
Because we expect sales of our clinical laboratory services and current product candidates (when required, if approved), to generate substantially all of our revenues for the foreseeable future, the failure of any of these drugs to find market acceptance would harm our business and could require us to seek additional financing.
We depend on third parties, including researchers and sublicensees, who are not under our control.
Since we have in-licensed some of our product candidates and have sublicensed a product candidate, we depend upon our sublicensee and independent investigators and scientific collaborators, such as universities and medical institutions or private physician scientists, to conduct our preclinical and clinical trials under agreements with us. These collaborators are not our employees and we cannot control the amount or timing of resources that they devote to our programs or the timing of their procurement of clinical-trial data or their compliance with applicable regulatory guidelines. Should any of these scientific inventors/advisors or those of our sublicensee become disabled or die unexpectedly, or should they fail to comply with applicable regulatory guidelines, we or our sublicensee may be forced to scale back or terminate development of that program. They may not assign as great a priority to our programs or pursue them as diligently as we would if we were undertaking those programs ourselves. Failing to devote sufficient time and resources to our drug-development programs, or substandard performance and failure to comply with regulatory guidelines, could result in delay of any FDA applications and our commercialization of the drug candidate involved.
These collaborators may also have relationships with other commercial entities, some of which may compete with us. Our collaborators assisting our competitors at our expense could harm our competitive position. For example, we are highly dependent on scientific collaborators for our Trimesta development program. Specifically, all of the clinical trials have been conducted under physician-sponsored investigational new drug applications (INDs), not corporate-sponsored INDs. Generally, we have experienced difficulty in collecting data generated from these physician-sponsored clinical trials for our programs. We cannot provide any assurances that we will not experience any additional delays in the future.
36
We are also highly dependent on government and private grants to fund certain of our clinical trials for our product candidates. For example, Trimesta (estriol) has received grants totaling over $8 million, predominantly from the Southern California Chapter of the National Multiple Sclerosis Society and the National Institutes of Health which funds a majority of the ongoing 150 patient clinical trial in relapsing-remitting multiple sclerosis for women. Although we believe that the grant funding received to date is sufficient to complete the current clinical trial based upon current cost estimates, if we experience any additional unanticipated costs or require further clinical trials, and our scientific collaborator is unable to maintain or receive additional grants, we might be forced to scale back or terminate the development of this product candidate. We will also need to cross reference our IND with the inventor/IND holder for this program should we elect to file our own corporate IND for our Trimesta (estriol) program. The on-going and future development and commercialization of Effirma (flupirtine) for fibromyalgia is the responsibility of Meda AB and no assurance can be given that Meda will gain the FDA’s acceptance of the NDA or obtain NDA approval from the FDA of flupirtine for fibromyalgia.
We have no experience selling, marketing, or distributing products and do not have the capability to do so.
We currently have no sales, marketing, or distribution capabilities. We do not anticipate having significant resources in the foreseeable future to allocate to selling and marketing our proposed products. Our success will depend, in part, on whether we are able to enter into and maintain collaborative relationships with a pharmaceutical or a biotechnology company charged with marketing one or more of our products. We may not be able to establish or maintain such collaborative arrangements or to commercialize our products in foreign territories, and even if we do, our collaborators may not have effective sales forces.
If we do not, or are unable to, enter into collaborative arrangements to sell and market our proposed products, we will need to devote significant capital, management resources, and time to establishing and developing an in-house marketing and sales force with technical expertise. We may be unsuccessful in doing so.
If we fail to maintain positive relationships with particular individuals, we may be unable to successfully develop our product candidates, conduct clinical trials, and obtain financing.
If we fail to maintain positive relationships with members of our management team or if these individuals decrease their contributions to our company, our business could be adversely impacted. We do not carry key employee insurance policies for any of our key employees.
We also rely greatly on employing and retaining other highly trained and experienced senior management and scientific personnel. The competition for these and other qualified personnel in the biotechnology field is intense. If we are not able to attract and retain qualified scientific, technical, and managerial personnel, we probably will be unable to achieve our business objectives.
We may not be able to compete successfully for market share against other drug companies.
The markets for our product candidates are characterized by intense competition and rapid technological advances. If our prescription drug product candidates receive FDA approval, they will compete with existing and future drugs and therapies developed, manufactured, and marketed by others. Our medical food product and our homeopathic OTC drug will also compete with existing and future comparable products. Competing products may have greater market acceptance and/or provide greater therapeutic convenience or clinical or other benefits for a specific indication than our products, or may offer comparable performance at a lower cost. If our products fail to capture and maintain market share, we may not achieve sufficient product revenues and our business will suffer.
We will compete against fully integrated pharmaceutical companies and smaller companies that are collaborating with larger pharmaceutical companies, academic institutions, government agencies, or other public and private research organizations. Many of these competitors have therapies to treat central nervous system diseases already approved or in development. In addition, many of these competitors, either alone or together with their collaborative partners, operate larger research and development programs than we do, have substantially greater financial resources than we do, and have significantly greater experience in the following areas:
|
·
|
developing drugs;
|
|
|
·
|
undertaking preclinical testing and human clinical trials;
|
|
|
·
|
obtaining FDA and other regulatory approvals of drugs;
|
|
|
·
|
formulating and manufacturing drugs; and
|
|
|
·
|
launching, marketing and selling drugs.
|
37
We may incur substantial costs as a result of litigation or other proceedings relating to patent and other intellectual property rights, as well as costs associated with lawsuits.
If any other person files patent applications, or is issued patents, claiming technology also claimed by us in pending applications, we may be required to participate in interference proceedings in the United States Patent and Trademark Office to determine priority of invention. We, or our licensors, may also need to participate in interference proceedings involving our issued patents and pending applications of another entity.
We cannot guarantee that the practice of our technologies will not conflict with the rights of others. In some foreign jurisdictions, we could become involved in opposition proceedings, either by opposing the validity of another’s foreign patent or by persons opposing the validity of our foreign patents.
We may also face frivolous litigation or lawsuits from various competitors or from litigious securities attorneys. The cost to us of any litigation or other proceeding relating to these areas, even if deemed frivolous or resolved in our favor, could be substantial and could distract management from our business. Uncertainties resulting from initiation and continuation of any litigation could have a material adverse effect on our ability to continue our operations.
If we infringe the rights of others we could be prevented from selling products or forced to pay damages.
If our products, methods, processes, and other technologies are found to infringe the proprietary rights of other parties, we could be required to pay damages, or we may be required to cease using the technology or to license rights from the prevailing party. Any prevailing party may be unwilling to offer us a license on commercially acceptable terms.
Our products, if approved, may not be commercially viable due to change in health care practice and third party reimbursement limitations
Recent initiatives to reduce the federal deficit and to change health care delivery are increasing cost-containment efforts. We anticipate that Congress, state legislatures and the private sector will continue to review and assess alternative benefits, controls on health care spending through limitations on the growth of private health insurance premiums and Medicare and Medicaid spending, price controls on pharmaceuticals, and other fundamental changes to the health care delivery system. Any changes of this type could negatively impact the commercial viability of our products, if approved. Our ability to successfully commercialize our product candidates, if they are approved, will depend in part on the extent to which appropriate reimbursement codes and authorized cost reimbursement levels of these products and related treatment are obtained from governmental authorities, private health insurers and other organizations, such as health maintenance organizations. In the absence of national Medicare coverage determination, local contractors that administer the Medicare program may make their own coverage decisions. Any of our product candidates, if approved and when commercially available, may not be included within the then current Medicare coverage determination or the coverage determination of state Medicaid programs, private insurance companies or other health care providers. In addition, third-party payers are increasingly challenging the necessity and prices charged for medical products, treatments and services.
Our medical food product and our homeopathic OTC drug may not be eligible for third-party reimbursement.
We do not currently have product liability or malpractice insurance and may not be able to obtain adequate insurance coverage against product liability claims.
Our business exposes us to potential product liability and other types of claims and our exposure will increase as we prepare to commercialize wellZin, our zinc acetate lozenge to reduce the duration and symptoms of the common cold. We do not currently have any product liability or malpractice insurance that would cover us against any product liability, or malpractice claims. Any such claim would have to be paid out of our cash reserves, which would have a detrimental effect on our financial condition. Even if it is available, product liability insurance for the pharmaceutical and biotechnology industry generally is expensive. Adequate insurance coverage may not be available at a reasonable cost. We cannot assure you that we can or will be able to obtain product liability or malpractice insurance policies on commercially acceptable terms, or at all.
38
RISKS RELATING TO OUR STOCK
We will seek to raise additional funds in the future, which may be dilutive to stockholders or impose operational restrictions.
We expect to seek to raise additional capital in the future to help fund development of our proposed products. If we raise additional capital through the issuance of equity (as we recently have) or of debt securities, the percentage ownership of our current stockholders will be reduced. We may also enter into strategic transactions, issue equity as part of license issue fees to our licensors, compensate consultants or settle outstanding payables using equity that may be dilutive. Our stockholders may experience additional dilution in net book value per share and any additional equity securities may have rights, preferences and privileges senior to those of the holders of our common stock. If we cannot raise additional funds, we will have to delay development activities of our products candidates.
We are substantially controlled by our current officers, directors, and principal stockholders.
Currently, our directors, executive officer, and principal stockholders beneficially own a substantial number of shares of our common stock. As a result, they will be able to exert substantial influence over the election of our board of directors and the vote on issues submitted to our stockholders. Our executive officer, directors and principal stockholders beneficially owned approximately 12.1 million shares of our common stock, including the stock options and warrants exercisable within 60 days of September 30, 2011. Because our common stock has from time to time been “thinly traded”, the sale of these shares by our executive officer, directors and principal stockholders could have an adverse effect on the market for our stock and our share price.
Our shares of common stock are from time to time thinly traded, so stockholders may be unable to sell at or near ask prices or at all if they need to sell shares to raise money or otherwise desire to liquidate their shares.
Our common stock has from time to time been “thinly-traded,” meaning that the number of persons interested in purchasing our common stock at or near ask prices at any given time may be relatively small or non-existent. This situation is attributable to a number of factors, including the fact that we are a small company that is relatively unknown to stock analysts, stock brokers, institutional investors and others in the investment community that generate or influence sales volume, and that even if we came to the attention of such persons, they tend to be risk-averse and would be reluctant to follow an unproven company such as ours or purchase or recommend the purchase of our shares until such time as we became more seasoned and viable. As a consequence, there may be periods of several days or more when trading activity in our shares is minimal or non-existent, as compared to a seasoned issuer which has a large and steady volume of trading activity that will generally support continuous sales without an adverse effect on share price. We cannot give stockholders any assurance that a broader or more active public trading market for our common shares will develop or be sustained, or that current trading levels will be sustained.
Our compliance with the Sarbanes-Oxley Act and SEC rules concerning internal controls may be time consuming, difficult and costly.
Although individual members of our management team have experience as officers of publicly traded companies, much of that experience came prior to the adoption of the Sarbanes-Oxley Act of 2002. It may be time consuming, difficult and costly for us to develop and implement the internal controls and reporting procedures required by Sarbanes-Oxley. We may need to hire additional financial reporting, internal controls and other finance staff in order to develop and implement appropriate internal controls and reporting procedures. If we are unable to comply with Sarbanes-Oxley’s internal controls requirements, we may not be able to obtain the independent accountant certifications that Sarbanes-Oxley Act requires publicly traded companies to obtain.
We cannot assure you that the common stock will be liquid or that it will remain listed on the NYSE Amex.
We cannot assure you that we will be able to maintain the continued listing standards of the NYSE Amex (formerly the American Stock Exchange) or NYSE Alternext US. The NYSE Amex requires companies to meet certain continued listing criteria including certain minimum stockholders' equity and equity prices per share as outlined in the Exchange Company Guide. We may not be able to maintain such minimum stockholders' equity or prices per share or may be required to effect a reverse stock split to maintain such minimum prices and/or issue additional equity securities in exchange for cash or other assets, if available, to maintain certain minimum stockholders' equity required by the NYSE Amex. If we are delisted from the Exchange then our common stock will trade, if at all, only on the over-the-counter market, such as the OTC Bulletin Board securities market, and then only if one or more registered broker-dealer market makers comply with quotation requirements. In addition, delisting of our common stock could depress our stock price, substantially limit liquidity of our common stock and materially adversely affect our ability to raise capital on terms acceptable to us, or at all. Delisting from the Exchange could also have other negative results, including the potential loss of confidence by suppliers and employees, the loss of institutional investor interest and fewer business development opportunities. In order to remain listed on NYSE Amex, we are required to maintain a minimum stockholders’ equity of $6 million.
There may be issuances of shares of preferred stock in the future.
Although we currently do not have preferred shares outstanding, the board of directors could authorize the issuance of a series of preferred stock that would grant holders preferred rights to our assets upon liquidation, the right to receive dividends before dividends would be declared to common stockholders, and the right to the redemption of such shares, possibly together with a premium, prior to the redemption of the common stock. To the extent that we do issue preferred stock, the rights of holders of common stock could be impaired thereby, including without limitation, with respect to liquidation.
39
We have never paid dividends.
We have never paid cash dividends on our common stock and do not anticipate paying any for the foreseeable future.
RISKS RELATED TO OUR INDUSTRY
We are subject to government regulation, compliance with which can be costly and difficult.
In the United States, the formulation, manufacturing, packaging, storing, labeling, promotion, advertising, distribution and sale of our products are subject to regulation by various governmental agencies, including (1) the Food and Drug Administration, or FDA, (2) the Federal Trade Commission, or FTC, (3) the Consumer Product Safety Commission, or CPSC, (4) the United States Department of Agriculture, or USDA. Our proposed activities may also be regulated by various agencies of the states, localities and foreign countries in which our proposed products may be manufactured, distributed and sold. The FDA, in particular, regulates the formulation, manufacture and labeling of over-the-counter, or OTC drugs, prescription drugs, medical foods, conventional foods, homeopathic OTC drugs, dietary supplements, and cosmetics such as those that we intend to distribute. FDA regulations require us and our suppliers to meet relevant current good manufacturing practice, or cGMP, regulations for the preparation, packing, labeling, and storage of all drugs and foods.
Any products manufactured or distributed by us pursuant to FDA approvals are subject to pervasive and continuing FDA regulation, including record-keeping requirements, reporting of adverse experiences, submitting periodic reports, drug sampling and distribution requirements, manufacturing or labeling changes, record-keeping requirements, and compliance with FDA promotion and advertising requirements. Drug manufacturers and their subcontractors are required to register their facilities with the FDA and state agencies, and are subject to periodic unannounced inspections for GMP compliance, imposing procedural and documentation requirements upon us and third-party manufacturers. Failure to comply with these regulations could result, among other things, in suspension of regulatory approval, recalls, suspension of production or injunctions, seizures, or civil or criminal sanctions. We cannot be certain that we or our present or future subcontractors will be able to comply with these regulations.
The FDA regulates prescription drug labeling and promotion activities. The FDA actively enforces regulations prohibiting the marketing of products for unapproved uses. The FDA permits the promotion of drugs for unapproved uses in certain circumstances, subject to stringent requirements. We and our product candidates are subject to a variety of state laws and regulations which may hinder our ability to market our products. Whether or not FDA approval has been obtained, approval by foreign regulatory authorities must be obtained prior to commencing clinical trials, and sales and marketing efforts in those countries. These approval procedures vary in complexity from country to country, and the processes may be longer or shorter than that required for FDA approval. We may incur significant costs to comply with these laws and regulations now or in the future.
We may seek to market some of our proposed products as medical foods for the dietary management of certain diseases. Medical foods are defined in section 5(b) of the Orphan Drug Act (21 U.S.C. 360ee (b) (3)) as "a food which is formulated to be consumed or administered enterally under the supervision of a physician and which is intended for the specific dietary management of a disease or condition for which distinctive nutritional requirements, based on recognized scientific principles, are established by medical evaluation." We believe our product may qualify as a medical food provided we are able to generate, and have published, sufficient clinical data to support such claims. Medical foods are required to be utilized under a medical doctor’s supervision and as such, our distribution channels may be limited and/or complicated.
Some of the products marketed by us are considered medical foods and will be labeled as such. Within the United States, this category of products is subject to the Federal Food, Drug, and Cosmetic Act (FFDC Act) and pertinent amendments thereto. The ingredients added to medical foods must either be FDA-approved food additives or generally recognized as safe (GRAS) by qualified experts. reaZin is comprised of zinc (a GRAS ingredient) and cysteine (an amino acid that also has GRAS status). While many chelated zinc products are currently on the market and are generally not considered to contain unapproved food additives or non-GRAS substances, we cannot provide any assurance that reaZin will be similarly considered by the FDA.
Furthermore, in the last few years, the FDA has issued several warning letters to companies marketing medical foods, questioning the basis upon which the products qualified as a medical food and objecting to certain claims made for the products. Because there is little guidance on what constitutes a medical food, and given the current regulatory climate for these products, we cannot provide any assurance that FDA would agree with the positioning of our products as medical foods.
We intend to develop our zinc candidate, AEN-100, as a drug and intend to file an IND with the FDA in order to conduct necessary clinical trials to support new medical claims and ultimately file one or more NDA with respect to such products which would subject us to time, expense and uncertainty associated with achieving approval of such NDA by the FDA.
40
It is anticipated that the marketing of wellZin, a homeopathic OTC drug, will involve claims that this product assists in reducing the duration and symptoms of the common cold. Under FDA and FTC rules, we are required to obtain scientific data to support any claims we make concerning our products. Although we have scientic data to support our intended product claims, we cannot be certain that these scientific data will be deemed acceptable to the FDA, FTC or other regulatory bodies. If any regulatory body requests supporting information and we are unable to provide support that is acceptable, either the FDA or FTC could force us to stop making the claims in question or restrict us from selling the affected products. Further, because there is no premarket review or approval of homeopathic OTC drug products, we cannot provide any assurance that the FDA would agree with the positioning of any of our products as a homeopathic OTC drug.
The FTC, which exercises jurisdiction over the advertising of our proposed homeopathic OTC, medical food and lab test products, has in the past several years instituted enforcement actions against several dietary supplement and food companies for false and misleading advertising related to health. These enforcement actions have resulted in consent decrees and monetary payments by the companies involved. In addition, the FTC has recently updated its guides on the use of testimonials and endorsements in advertising. As a result, the FTC appears to have increased its scrutiny of the use of testimonials, which we could utilize, as well as the role of expert endorsers and product clinical studies. It is unclear whether the FTC will subject our advertisements to increased surveillance to ensure compliance with the principles set forth in its newly revised endorsements/testimonial advertising guidances.
The FDA, comparable foreign regulators and state and local pharmacy regulators impose substantial requirements upon clinical development, manufacture and marketing of pharmaceutical products. These and other entities regulate research and development and the testing, manufacture, quality control, safety, effectiveness, labeling, storage, record keeping, approval, advertising, and promotion of our products. The drug approval process required by the FDA under the Food, Drug, and Cosmetic Act generally involves:
|
·
|
preclinical laboratory and animal tests;
|
|
|
·
|
submission of an IND, prior to commencing human clinical trials;
|
|
|
·
|
adequate and well-controlled human clinical trials to establish safety and efficacy for intended use;
|
|
|
·
|
submission to the FDA of a NDA; and
|
|
|
·
|
FDA review and approval of a NDA.
|
The testing and approval process requires substantial time, effort, and financial resources, and we cannot be certain that any approval will be granted on a timely basis, if at all.
Preclinical tests include laboratory evaluation of the product candidate, its chemistry, formulation and stability, and animal studies to assess potential safety and efficacy. Certain preclinical tests must be conducted in compliance with good laboratory practice regulations. Violations of these regulations can, in some cases, lead to invalidation of the studies, requiring them to be replicated. In some cases, long-term preclinical studies are conducted concurrently with clinical studies.
We will submit the preclinical test results, together with manufacturing information and analytical data, to the FDA as part of an IND, which must become effective before we begin human clinical trials. The IND automatically becomes effective 30 days after filing, unless the FDA raises questions about conduct of the trials outlined in the IND and imposes a clinical hold, in which case, the IND sponsor and FDA must resolve the matters before clinical trials can begin. It is possible that our submission may not result in FDA authorization to commence clinical trials.
Clinical trials must be supervised by a qualified investigator in accordance with good clinical practice regulations, which include informed consent requirements. An independent Institutional Review Board (“IRB”) at each medical center reviews and approves and monitors the study, and is periodically informed of the study’s progress, adverse events and changes in research. Progress reports are submitted annually to the FDA and more frequently if adverse events occur.
Human clinical trials of drug candidates typically have three sequential phases that may overlap:
Phase I: The drug is initially tested in healthy human subjects or patients for safety, dosage tolerance, absorption, metabolism, distribution, and excretion.
Phase II: The drug is studied in a limited patient population to identify possible adverse effects and safety risks, determine efficacy for specific diseases and establish dosage tolerance and optimal dosage.
Phase III: When phase II evaluations demonstrate that a dosage range is effective with an acceptable safety profile, Phase III trials to further evaluate dosage, clinical efficacy and safety, are undertaken in an expanded patient population, often at geographically dispersed sites.
41
We cannot be certain that we will successfully complete Phase I, Phase II, or Phase III testing of our product candidates within any specific time period, if at all. Furthermore, the FDA, an IRB or the IND sponsor may suspend clinical trials at any time on various grounds, including a finding that subjects or patients are exposed to unacceptable health risk. Concurrent with these trials and studies, we also develop chemistry and physical characteristics data and finalize a manufacturing process in accordance with good manufacturing practice (“GMP”) requirements. The manufacturing process must conform to consistency and quality standards, and we must develop methods for testing the quality, purity, and potency of the final products. Appropriate packaging is selected and tested, and chemistry stability studies are conducted to demonstrate that the product does not undergo unacceptable deterioration over its shelf-life. Results of the foregoing are submitted to the FDA as part of a NDA for marketing and commercial shipment approval. The FDA reviews each NDA submitted and may request additional information.
Once the FDA accepts the NDA for filing, it begins its in-depth review. The FDA has substantial discretion in the approval process and may disagree with our interpretation of the data submitted. The process may be significantly extended by requests for additional information or clarification regarding information already provided. As part of this review, the FDA may refer the application to an appropriate advisory committee, typically a panel of clinicians. Manufacturing establishments often are inspected prior to NDA approval to assure compliance with GMPs and with manufacturing commitments made in the application.
Submission of a NDA with clinical data requires payment of a fee. In return, the FDA assigns a goal of ten months for issuing its “complete response,” in which the FDA may approve or deny the NDA, or require additional clinical data. Even if these data are submitted, the FDA may ultimately decide the NDA does not satisfy approval criteria. If the FDA approves the NDA, the product becomes available for physicians prescription. Product approval may be withdrawn if regulatory compliance is not maintained or safety problems occur. The FDA may require post-marketing studies, also known as phase IV studies, as a condition of approval, and requires surveillance programs to monitor approved products that have been commercialized. The agency has the power to require changes in labeling or prohibit further marketing based on the results of post-marketing surveillance.
Satisfaction of these and other regulatory requirements typically takes several years, and the actual time required may vary substantially based upon the type, complexity and novelty of the product. Government regulation may delay or prevent marketing of potential products for a considerable period of time and impose costly procedures on our activities. We cannot be certain that the FDA or other regulatory agencies will approve any of our products on a timely basis, if at all. Success in preclinical or early-stage clinical trials does not assure success in later-stage clinical trials. Data obtained from preclinical and clinical activities are not always conclusive and may be susceptible to varying interpretations that could delay, limit or prevent regulatory approval. Even if a product receives regulatory approval, the approval may be significantly limited to specific indications or uses.
Even after regulatory approval is obtained, later discovery of previously unknown problems with a product may result in restrictions on the product or even complete withdrawal of the product from the market. Delays in obtaining, or failures to obtain regulatory approvals would have a material adverse effect on our business.
The FDA’s policies may change, and additional government regulations may be enacted which could prevent or delay regulatory approval of our potential products. Increased attention to the containment of health care costs worldwide could result in new government regulations materially adverse to our business. We cannot predict the likelihood, nature or extent of adverse governmental regulation that might arise from future legislative or administrative action, either in the United States or abroad.
Failure to adhere to the quality control and other regulatory requirements could result in additional expense to us or the suspension of such certification necessary to perform clinical testing.
We are subject to numerous federal, state and local laws relating to safe working conditions, manufacturing practices, environmental protection, fire hazard control, and disposal of hazardous or potentially hazardous substances. We may incur significant costs to comply with these laws and regulations. The regulatory framework under which we operate will inevitably change in light of scientific, economic, demographic and policy developments and such changes may have a material adverse effect on our business.
Clinical laboratories in the United States are subject to regulation under the Clinical Laboratory Improvements Act of 1988 (“CLIA”) as well as corresponding state regulations. Failure to adhere to the quality control and other regulatory requirements of CLIA could result in the suspension of such certification necessary to perform clinical testing and generate revenues.
Changes in the health care regulatory environment may adversely affect our business.
The Patient Protection and Affordable Care Act and the Health Care and Education Reconciliation Act of 2010 were signed into law on March 23, 2010 and March 30, 2010, respectively. A number of the provisions of those laws require further rulemaking action by governmental agencies to implement. The laws change access to health care products and services and create new fees for the pharmaceutical and medical device industries. Future rulemaking could increase rebates, reduce prices or the rate of price increases for health care products and services, or require additional reporting and disclosure. We cannot predict the timing or impact of any future rulemaking.
42
Failure to comply with requirements of the European Union can be costly and time consuming.
Prior regulatory approval for human healthy volunteer studies (Phase I studies) is required in member states of the European Union (E.U.). Summary data from successful Phase I studies are submitted to regulatory authorities in member states to support applications for Phase II studies. E.U. authorities typically have one to three months (which often may be extended in their discretion) to raise objections to the proposed study. One or more independent ethics committees (similar to United States IRBs) review relevant ethical issues.
For E.U. marketing approval, we submit to the relevant authority for review a dossier, or MAA (Market Authorization Application), providing information on the quality of the chemistry, manufacturing and pharmaceutical aspects of the product as well as non-clinical and clinical data.
Approval can take several months to several years, and can be denied, depending on whether additional studies or clinical trials are requested (which may delay marketing approval and involve unbudgeted costs) or regulatory authorities conduct facilities (including clinical investigation site) inspections and review manufacturing procedures, operating systems and personnel qualifications. In many cases, each drug manufacturing facility must be approved, and further inspections may occur over the product’s life.
The regulatory agency may require post-marketing surveillance to monitor for adverse effects or other studies. Further clinical studies are usually necessary for approval of additional indications. The terms of any approval, including labeling content, may be more restrictive than expected and could affect the marketability of a product.
Failure to comply with these ongoing requirements can result in suspension of regulatory approval and civil and criminal sanctions. European renewals may require additional data, resulting in a license being withdrawn. E.U. regulators have the authority to revoke, suspend or withdraw approvals, prevent companies and individuals from participating in the drug approval process, request recalls, seize violative products, obtain injunctions to close non-compliant manufacturing plants and stop shipments of violative products.
We are subject to pricing controls that may not result in favorable arrangements for our products.
Pricing for products under approval applications is also subject to regulation. Requirements vary widely between countries and can be implemented disparately intra-nationally. The E.U. generally provides options for member states to control pricing of medicinal products for human use, ranging from specific price-setting to systems of direct or indirect controls on the producer’s profitability. U.K. regulation, for example, generally provides controls on overall profits derived from sales to the U.K. National Health Service that are based on profitability targets or a function of capital employed in servicing the National Health Service market. Italy generally utilizes a price monitoring system based on the European average price over the reference markets of France, Spain, Germany and the U.K. Italy typically establishes price within a therapeutic class based on the lowest price for a medicine belonging to that category. Spain generally establishes selling price based on prime cost plus a profit margin within a range established yearly by the Spanish Commission for Economic Affairs.
There can be no assurance that price controls or reimbursement limitations will result in favorable arrangements for our products.
43
If we are not able to receive third-party reimbursements we may not be able to sell products at competitive prices.
In the United States, the E.U. and elsewhere, pharmaceutical sales are dependent in part on the availability and adequacy of reimbursement from third party payers such as governments and private insurance plans. Third party payers are increasingly challenging established prices, and new products that are more expensive than existing treatments may have difficulty finding ready acceptance unless there is a clear therapeutic benefit.
In the United States, consumer willingness to choose a self-administered outpatient prescription drug over a different drug or other form of treatment often depends on the manufacturer’s success in placing the product on a health plan formulary or drug list, which results in lower out-of-pocket costs. Favorable formulary placement typically requires the product to be less expensive than what the health plan determines to be therapeutically equivalent products, and often requires manufacturers to offer rebates. Federal law also requires manufacturers to pay rebates to state Medicaid programs in order to have their products reimbursed by Medicaid. Medicare, which covers most Americans over age 65 and the disabled, adopted an insurance regime that offers eligible beneficiaries limited coverage for outpatient prescription drugs that became effective January 1, 2006. The prescription drugs that are covered under this insurance are specified on a formulary published by Medicare. As part of these changes, Medicare has adopted new payment formulas for prescription drugs administered by providers, such as hospitals or physicians that are generally expected to lower reimbursement.
The E.U. generally provides options for member states to restrict the range of medicinal products for which their national health insurance systems provide reimbursement. Member states can opt for a “positive” or “negative” list, with the former listing all covered medicinal products and the latter designating those excluded from coverage. The E.U., the U.K. and Spain have negative lists, while France uses a positive list. Canadian provinces establish their own reimbursement measures. In some countries, products may also be subject to clinical and cost effectiveness reviews by health technology assessment bodies. Negative determinations in relation to our products could affect prescribing practices. In the U.K., the National Institute for Clinical Excellence (“NICE”) provides such guidance to the National Health Service, and doctors are expected to take it into account when choosing drugs to prescribe. Health authorities may withhold funding from drugs not given a positive recommendation by NICE. A negative determination by NICE may mean fewer prescriptions. Although NICE considers drugs with orphan status, there is a degree of tension on the application of standard cost assessment for orphan drugs, which are often priced higher to compensate for a limited market. It is unclear whether NICE will adopt a more relaxed approach toward the assessment of orphan drugs.
We cannot assure you that any of our products will be considered cost effective, or that reimbursement will be available or sufficient to allow us to sell them competitively and profitably. Our medical food product and our homeopathic OTC drug may not be eligible for third-party reimbursement.
There is no certainty that our medical food products will be reimbursed by private insurance, government programs such as Medicaid and Medicare and workers compensation insurers. If these entities do not reimburse for the costs of such products, this could have a material adverse effect on our business and results of operations.
Inasmuch as medical foods are distinguished by the FDA and other organizations from prescription drugs and exempt from certain regulations that apply to prescription drugs, it is possible that private insurance, government programs such as Medicaid and Medicare and workers compensation insurers will not reimburse costs incurred for medical foods in the same manner as prescription drugs. There is no certainty that we will be able to maintain the necessary requirements for insurance reimbursement of our medical food products. If our physician clients do not continue to be reimbursed for dispensing our medical food products, they may choose not to purchase them and our business and results of operations may be adversely affected.
It is unlikely that our homeopathic OTC drug products will be reimbursed by private insurance, government programs such as Medicaid and Medicare and workers compensation insurers. If these entities do not reimburse for the costs of such products, this could have a material adverse effect on our business and results of operations.
Inasmuch as homeopathic OTC drug products are distinguished by the FDA and other organizations from prescription drugs and exempt from certain regulations that apply to prescription drugs, it is likely that private insurance, government programs such as Medicaid and Medicare and workers compensation insurers will not reimburse costs incurred for homeopathic OTC drugs.
We could be subject to challenges under fraud and abuse laws.
The United States federal Medicare/Medicaid anti-kickback law and similar state laws prohibit remuneration intended to induce physicians or others either to refer patients, or to acquire or arrange for or recommend the acquisition of health care products or services. While the federal law applies only to referrals, products or services receiving federal reimbursement, state laws often apply regardless of whether federal funds are involved. Other federal and state laws prohibit anyone from presenting or causing to be presented false or fraudulent payment claims. Recent federal and state enforcement actions under these statutes have targeted sales and marketing activities of prescription drug manufacturers. As we begin to market our products to health care providers, the relationships we form, such as compensating physicians for speaking or consulting services, providing financial support for continuing medical education or research programs, and assisting customers with third-party reimbursement claims, could be challenged under these laws and lead to civil or criminal penalties, including the exclusion of our products from federally-funded reimbursement. Even an unsuccessful challenge could cause adverse publicity and be costly to respond to, and thus could have a material adverse effect on our business, results of operations and financial condition. We intend to consult counsel concerning the potential application of these and other laws to our business and to our sales, marketing and other activities to comply with them. Given their broad reach and the increasing attention given them by law enforcement authorities, however, we cannot assure you that some of our activities will not be challenged.
44
We do not have a guarantee of patent restoration and marketing exclusivity of the ingredients for our drugs even if we are granted FDA approval of our products.
The United States Drug Price Competition and Patent Term Restoration Act of 1984 (Hatch-Waxman) permits the FDA to approve Abbreviated New Drug Applications (“ANDAs”) for generic versions of innovator drugs, as well as NDAs with less original clinical data, and provides patent restoration and exclusivity protections to innovator drug manufacturers. The ANDA process permits competitor companies to obtain marketing approval for drugs with the same active ingredient and for the same uses as innovator drugs, but does not require the conduct and submission of clinical studies demonstrating safety and efficacy. As a result, a competitor could copy any of our drugs and only need to submit data demonstrating that the copy is bioequivalent to gain marketing approval from the FDA. Hatch-Waxman requires a competitor that submits an ANDA, or otherwise relies on safety and efficacy data for one of our drugs, to notify us and/or our business partners of potential infringement of our patent rights. We and/or our business partners may sue the company for patent infringement, which would result in a 30-month stay of approval of the competitor’s application. The discovery, trial and appeals process in such suits can take several years. If the litigation is resolved in favor of the generic applicant or the challenged patent expires during the 30-month period, the stay is lifted and the FDA may approve the application. Hatch-Waxman also allows competitors to market copies of innovator products by submitting significantly less clinical data outside the ANDA context. Such applications, known as “505(b)(2) NDAs” or “paper NDAs,” may rely on clinical investigations not conducted by or for the applicant and for which the applicant has not obtained a right of reference or use and are subject to the ANDA notification procedures described above.
The law also permits restoration of a portion of a product’s patent term that is lost during clinical development and NDA review, and provides statutory protection, known as exclusivity, against FDA approval or acceptance of certain competitor applications. Restoration can return up to five years of patent term for a patent covering a new product or its use to compensate for time lost during product development and regulatory review. The restoration period is generally one-half the time between the effective date of an IND and submission of an NDA, plus the time between NDA submission and its approval (subject to the five-year limit), and no extension can extend total patent life beyond 14 years after the drug approval date. Applications for patent term extension are subject to United States Patent and Trademark Office (“USPTO”) approval, in conjunction with FDA. Approval of these applications takes at least nine months, and there can be no guarantee that it will be given at all.
Hatch-Waxman also provides for differing periods of statutory protection for new drugs approved under an NDA. Among the types of exclusivity are those for a “new molecular entity” and those for a new formulation or indication for a previously-approved drug. If granted, marketing exclusivity for the types of products that we are developing, which include only drugs with innovative changes to previously-approved products using the same active ingredient, would prohibit the FDA from approving an ANDA or 505(b)(2) NDA relying on our safety and efficacy data for three years. This three-year exclusivity, however, covers only the innovation associated with the original NDA. It does not prohibit the FDA from approving applications for drugs with the same active ingredient but without our new innovative change. These marketing exclusivity protections do not prohibit the FDA from approving a full NDA, even if it contains the innovative change.
ITEM 2. UNREGISTERED SALES OF EQUITY SECURITIES AND USE OF PROCEEDS
On July 28, 2011, we exchanged the warrant issued in connection with the April 6, 2011 financing for a new warrant with substantially the same terms as the original warrant. We exchanged our warrant with existing security holders and no remuneration or commission was paid in reliance on Section 3(a)(9) of the Securities Act of 1933.
On August 2, 2011, we issued 130,000 restricted shares of our common stock in consideration of financial advisory services to be provided. The issuance qualified for exemption on section 4(2) of the Securities Act of 1933 since the issuance did not involve a public offering because it was made to an insubstantial number of persons and because of the manner in which it was made. There was no general solicitation or advertising by us. Based on an analysis of the above factors, we have met the requirements to qualify for exemption under section 4(2) of the Securities Act of 1933 for this issuance.
On August 10, 2011, we entered into an agreement to exchange the warrants issued in connection with the January 28, 2011 financing for new warrants. We exchanged our warrant with existing security holders and no remuneration or commission was paid in reliance on Section 3(a)(9) of the Securities Act of 1933.
ITEM 3. DEFAULTS UPON SENIOR SECURITIES
None.
ITEM 4. RESERVED AND REMOVED
ITEM 5. OTHER INFORMATION
None.
45
ITEM 6. EXHIBITS
|
4.1
|
Form of Warrant issued in exchange of the warrant issued in connection with the April 6, 2011 financing 1
|
|
4.2
|
Form of Warrant issued in exchange of the warrant issued in connection with the January 28, 2011 financing 1
|
|
10.1
|
Exchange Agreement entered into in exchange for the warrant issued in connection with the April 6, 2011 financing 1
|
|
10.2
|
Exchange Agreement entered into in exchange for the warrant issued in connection with the January 28, 2011 financing 1
|
|
31.1
|
Certification of Principal Executive Officer pursuant to Rule 13a-14(a)/15d-14(a) *
|
|
31.2
|
Certification of Principal Financial Officer pursuant to Rule 13a-14(a)/15d-14(a) *
|
|
32.1
|
Certification pursuant to Section 1350 of the Sarbanes-Oxley Act of 2002 *
|
|
*
|
Filed herewith
|
|
1
|
Incorporated by reference to Registrant’s Quarterly Report on Form 10-Q for the quarter ended June 30, 2011, filed with the Securities and Exchange Commission on August 15, 2011.
|
46
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned.
|
ADEONA PHARMACEUTICALS, INC.
|
|||
|
By:
|
/s/ James S. Kuo
|
||
|
James S. Kuo, M.D., M.B.A.
|
|||
|
President and Chief Executive Officer
|
|||
|
(Principal Executive Officer and Principal
|
|||
|
Financial Officer)
|
|||
|
Date: November 14, 2011
|
|||
47
GLOSSARY
|
Term
|
Definition
|
|
|
Adverse Event
|
Any adverse change in health or “side-effect” that occurs in a person participating in a clinical trial, from the time they consent to joining the trial until a pre-specified period of time after their treatment has been completed.
|
|
|
Bioavailability
|
The quantity or fraction of the ingested dose that is absorbed by the body.
|
|
|
AEN-100 (zinc)
|
Adeona’s proprietary, once-daily, gastroretentive, sustained-release oral tablet formulation of zinc acetate.
|
|
|
Clinical Study/Trial
|
A research study that is conducted to find out if a treatment or procedure is safe and/or effective in humans.
|
|
|
Controlled Clinical Trial
|
A clinical study that compares patients receiving a specific treatment to patients receiving an alternate treatment for the condition of interest. The alternate treatment may be another active treatment, standard of care for the condition and/or a placebo (inactive) treatment.
|
|
|
Double-blinded Study/Trial
|
Both the participant and the researcher are unaware of who is receiving the active treatment or the placebo.
|
|
|
Effirma (flupirtine)
|
Proposed tradename of Adeona’s centrally-acting investigational oral drug for the treatment of fibromyalgia syndrome
|
|
|
FDA – Food & Drug Administration
|
The United States government agency that ensures that medicines, medical devices, medical foods and radiation-emitting consumer products are safe and effective. Authorized by Congress to enforce the Federal Food, Drug, and Cosmetic Act and several other public health laws, the agency monitors the manufacture, import, transport, storage, and sale of $1 trillion worth of goods annually.
|
|
|
Gastroretentive
|
Medications designed to be retained in the upper gastrointestinal system.
|
|
|
GMP – Good Manufacturing Practice
|
Regulations that require that manufacturers, processors, and packagers of drugs, medical devices, some food, and blood take proactive steps to ensure that their products are consistently produced, pure, and stable. GMP regulations require a quality approach to manufacturing, enabling companies to minimize or eliminate instances of contamination, mix-ups, and errors.
|
|
|
GRAS – Generally Recognized As Safe
|
If the use of a substance in food is generally recognized as safe (GRAS) by qualified experts, then that use is exempted from the premarket approval requirements that apply to food additives under the Federal Food, Drug, and Cosmetic Act (FFDCA).
|
|
|
IND – Investigational New Drug
|
An application submitted to the FDA for a new drug or biologic that, if allowed, will be used in a clinical trial.
|
|
|
Open-label Clinical Study/Trial
|
A trial in which both the treating physician and the patient know they are receiving the experimental treatment.
|
|
|
Phase I Clinical Trial
|
A Phase I trial represents an initial study in a small group of patients to primarily test for safety.
|
|
|
Phase II Clinical Trial
|
A Phase II trial represents a study in a larger number of patients to assess the safety and efficacy of a product.
|
|
|
Phase III Clinical Trial
|
Phase III trials are initiated to establish safety and efficacy in an expanded patient population and at multiple clinical trial sites and are generally larger than trials in earlier phases of development.
|
|
|
Placebo
|
An inactive pill or liquid. Many studies compare an active drug to a placebo to determine whether any changes seen during the study can be attributed to the active drug.
|
48
|
Principal Investigator
|
This is the study director who is ultimately responsible for the conduct of the study.
|
|
|
Prospective Clinical Study/Trial
|
A clinical study/trial in which participants are identified and then followed throughout the study going forward in time.
|
|
|
Protocol
|
A clinical study/trial’s plan — includes the schedule of tests, requirements for participation, procedures, and medications.
|
|
|
Randomized Study/Trial
|
Participants in a study are assigned by chance to either one or more of the active treatment group(s) or the placebo group.
|
|
|
reaZinTM (zinc cysteine)
|
Tradename of Adeona’s oral medical food product containing zinc and cysteine, available only by prescription, that is being developed for the dietary management of zinc deficiency associated with Alzheimer's disease.
|
|
|
Single-blinded Study/Trial
|
One party, either the participant or the researcher, does not know if the participant is taking the active treatment or the placebo.
|
|
|
Study/Trial Coordinator
|
Staff member who is often the primary contact for research participants and coordinates their care and evaluations throughout the study.
|
|
|
Trimesta (estriol)
|
Proposed tradename of Adeona’s investigational oral drug for the treatment of relapsing- remitting multiple sclerosis.
|
|
|
wellZinTM (oral zinc acetate lozenge)
|
Tradename of Adeona’s oral zinc acetate lozenge being developed to reduce the duration and symptoms of the common cold.
|
49