Attached files
| file | filename |
|---|---|
| 8-K - FORM 8-K - INFINITY PHARMACEUTICALS, INC. | d246217d8k.htm |
 Building a Sustainable, Fully Integrated
Biotechnology Company
October 2011
Exhibit 99.1 |
 Forward Looking Statements
2
•
This presentation contains forward-looking statements within the meaning of The Private Securities
Litigation Reform Act of 1995.
•
These statements involve risks and uncertainties that could cause actual results to be materially
different from historical results or from any future results expressed or implied by such
forward-looking statements.
•
Such forward-looking statements include statements regarding: the therapeutic potential of
Infinity’s Hedgehog pathway, Hsp90, PI3K and FAAH inhibitors; the potential of IPI-926
and Hedgehog pathway inhibition in addressing chondrosarcoma, pancreatic cancer and
myelofibrosis; the potential of combination therapy based on retaspimycin HCl in addressing
non-small cell lung cancer; the potential expansion of the Phase 2 trial of retaspimycin
HCl in combination with docetaxel; the commencement of Phase 1 clinical development of IPI-
145 in the second half of 2011 and Phase 2 development of IPI-940 in pain by Purdue; 2011
financial guidance (including total revenues, operating cash burn, and year-end cash and
investments balance), and the expectation that Infinity will have capital to support its current
operating plan into 2014.
•
Such forward-looking statements are subject to numerous factors, risks and uncertainties that may
cause actual events or results to differ materially from the company's current expectations.
For example, there can be no guarantee that Infinity’s strategic alliance with
Purdue/Mundipharma will continue for its expected term or that these entities will fund
Infinity’s programs as agreed, or that any product candidate Infinity is developing will
successfully complete necessary preclinical and clinical development phases. Further, there can be no
guarantee that any positive developments in Infinity’s product portfolio will result in stock
price appreciation. Infinity’s expectations could also be affected by risks and
uncertainties relating to: results of clinical trials and preclinical studies, including subsequent analysis of existing data
and new data received from ongoing and future studies; the content and timing of decisions made by the
U.S. Food and Drug Administration and other regulatory authorities, investigational review
boards at clinical trial sites, and publication review bodies; Infinity's ability to enroll
patients in its clinical trials; unplanned cash requirements and expenditures, including in connection
with business development activities; development of agents by Infinity’s competitors for
diseases in which Infinity is currently developing its product candidates; market acceptance of
any products Infinity or its partners may successfully develop; and, Infinity's ability to obtain, maintain and enforce patent and other
intellectual property protection for any product candidate it is developing.
•
These and other risks which may impact management's expectations are described in greater detail under
the caption "Risk Factors" included in Infinity's quarterly report on Form 10-Q for
the quarter ended June 30, 2011 filed with the U.S. Securities and Exchange Commission on
August 9, 2011.
•
Further, any forward-looking statements contained in this presentation speak only as of the date
hereof, and Infinity expressly disclaims any obligation to update any forward-looking
statements, whether as a result of new information, future events or otherwise.
•
All trademarks used in this presentation are the property of their respective owners.
•
Our Internet website is http://www.infi.com. We regularly use our website to post information
regarding our business, product development programs and governance. We encourage
investors to use www.infi.com, particularly the information in the section entitled “Investors/Media,”
as a source of information about Infinity. References to www.infi.com in this presentation are not
intended to, nor shall they be deemed to, incorporate information on www.infi.com into this
presentation by reference.
|
    •
Clear registration paths
•
Multiple possible indications
•
Substantial market potential
•
Full U.S. commercial rights
in oncology/inflammation
INFI in 2011: Considerable Near-Term
Momentum
•
Well-financed, with capital into 2014
•
Purdue/Mundipharma alliance enables robust clinical development and approval
strategies; provides access to markets ex-US & those best served by a GP
sales force •
Compelling scientific rationale
•
Intriguing Phase 1b clinical data
•
Underserved markets
Novel
candidates in
development
•
Rigorous trials
•
Companion biomarker strategy
Active
phase
2 trials |
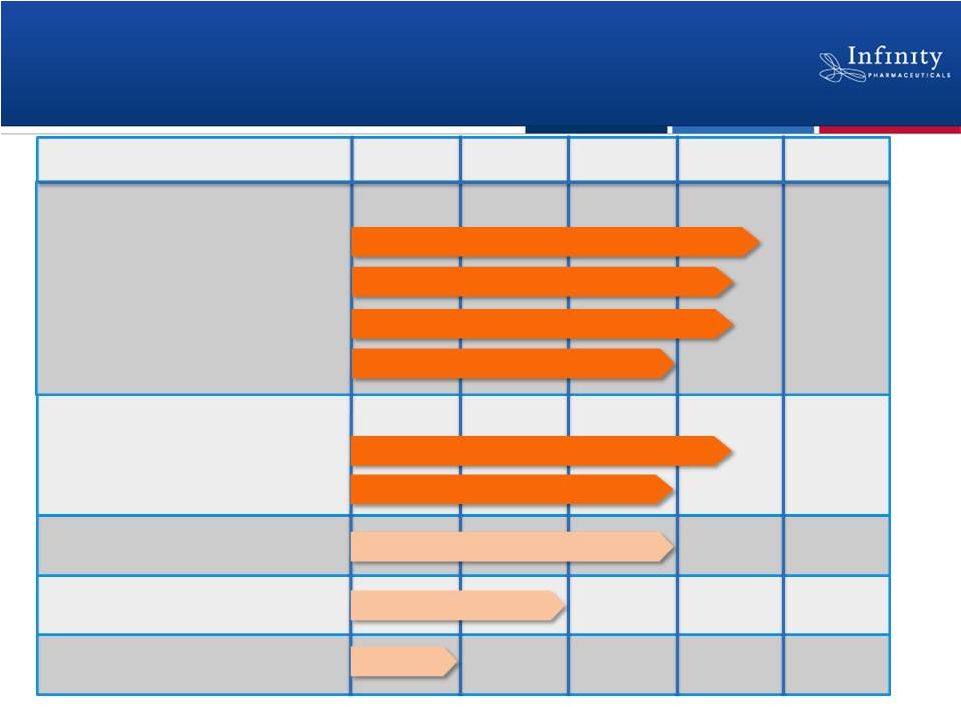 Advancing Pipeline with Broad Commercial
Potential
4
Discovery
Phase 1
Phase 2
Phase 3
Preclinical
Hedgehog: IPI-926
Hsp90: Retaspimycin HCl
FAAH: IPI-940
PI3K: IPI-145
Pancreatic Cancer
Chondrosarcoma
Solid Tumors
Non-Small Cell Lung Cancer
Discovery Programs
Myelofibrosis
Non-Small Cell Lung Cancer
Gemcitabine Combo
Docetaxel Combo
Everolimus Combo |
 IPI-926:
Addressing Difficult-to-Treat Cancers by
Targeting the Hedgehog Pathway
5 |
 IPI-926: Overview
6
•
Disrupts malignant activation of the Hedgehog pathway by inhibiting
Smoothened
–
Hedgehog pathway known to drive multiple difficult-to-treat cancers
•
Product strategy
–
Target areas of significant unmet need
–
Leverage strong scientific rationale
–
Pursue tractable clinical development path
–
Deliver commercially differentiated product |
 Large unmet need
•
~35,000 deaths /
year in the U.S. alone
•
Average survival
<6 months
•
5-year survival <5%
Resistant to therapy
•
Gemcitabine
approved Rx with
only a ~6 wk survival
benefit
•
Multiple failures in
Phase 2 and Phase 3
Treating Pancreatic Cancer Requires a
Fundamentally Novel Approach
7
Source: Xiong et. al, 2006. Drugs 66 (8): 1059-72.
Multiple Failures in Pancreatic Cancer
Single Agents
•
Topotecan
•
Irinotecan
•
Cisplatin
•
Oxaliplatin
•
Ifosfamide
•
Epirubicin
•
Docetaxel
•
Paclitaxel
•
Capeticabine
•
Pemetrexed
Combinations with Gemcitabine (Gem)
•
Gem + Fluorouracil
•
Gem + Cisplatin
•
Gem + Irinotecan
•
Gem + Oxaliplatin
•
Gem + Exatecan
•
Gem + Epirubicin
•
Gem + Carboplatin
•
Gem + Mitomycin
•
Gem + Docetaxel
•
Gem + Capeticabine
•
Gem + Pemetrexed
•
Gem + Tegafur/Uracil
•
Gem + Fluorouracil +
Leucovorin
•
Gem + Fluorouracil +
Cisplatin
•
Gem + Fluorouracil +
Tegafur/Uracil
•
Gem + Fluorouracil +
Cisplatin + Epirubicin |
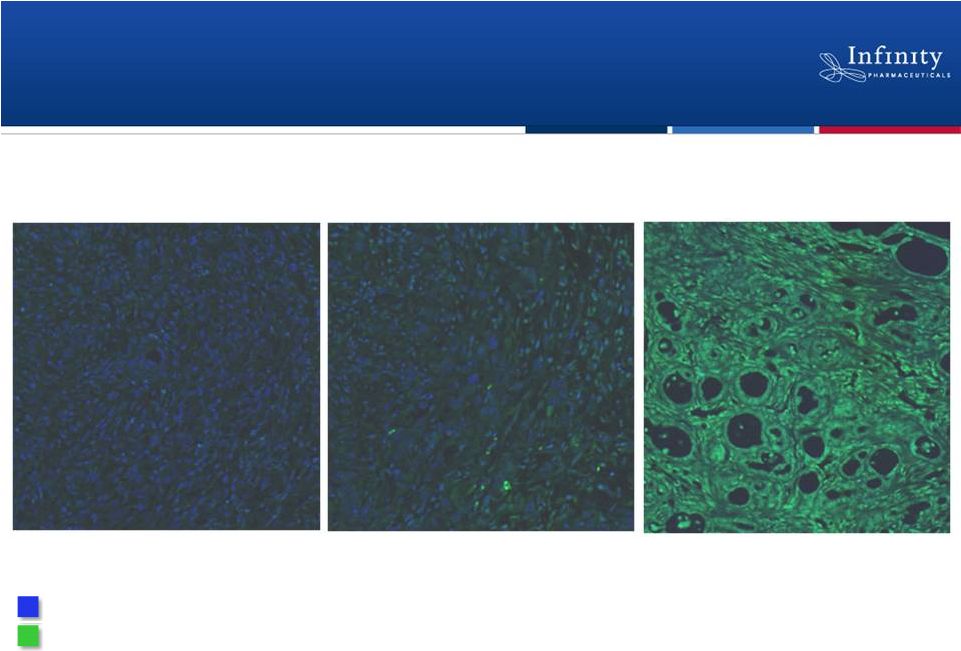 IPI-926 Enhances Delivery of Gemcitabine
to Tumor
8
Vehicle
Gemcitabine alone
IPI-926 +
gemcitabine
Current standard of care
in pancreatic cancer
Tumor cell nuclei
Fluorescent contrast agent
IPI-926 + gemcitabine doubles median survival in a mouse model of pancreatic
cancer (Olive et al. 2009, Science 324: 1457-61.)
|
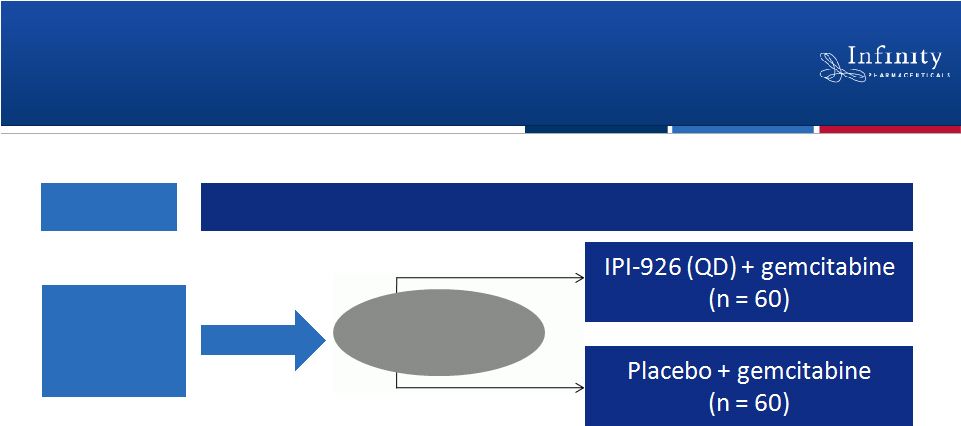 Rapid Translation of Preclinical Insights to
Randomized Phase 2 Clinical Trial
9
•
Primary endpoint is overall survival
–
Secondary endpoints include progression free survival, time to progression,
overall response rate
•
Rigorous design to mitigate Phase 3 risk
•
Enrollment
completed
October
17 ,
ahead
of
schedule
Dose
Escalation
MTD
Phase 1b
Phase 2
th
1:1
Randomization |
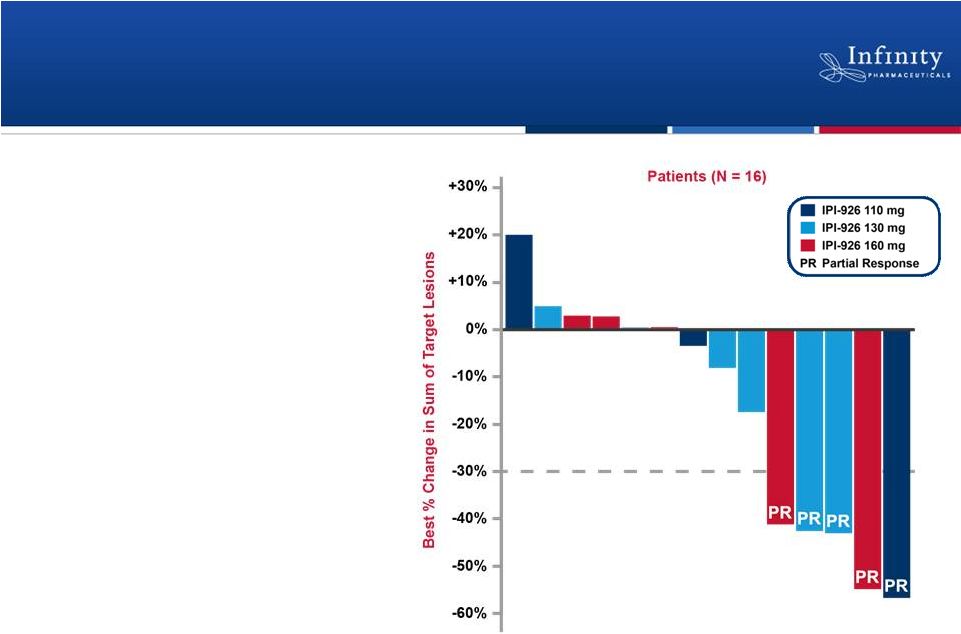 Encouraging Activity and Tolerability Observed
in Phase 1b
•
IPI-926 + gemcitabine
led to a 31% response
rate
–
Overall response rate to
gemcitabine is historically
<10%*
•
Favorable PK and safety
profile
–
No interaction between IPI-
926 and gemcitabine
–
Most common AEs were
fatigue and nausea
–
Combination did not reveal
unique or more severe AEs
10
Stephenson et al., ASCO 2011.
*Moore, et al. J Clin Oncol 25:1960-6.; Seitz et al. Oncology
18:43-7. |
 Myelofibrosis: Phase 2 Trial
•
Hedgehog pathway plays a key role in pathogenic fibrosis
–
Significant need exists for novel treatment options that can directly target the
malignant fibrosis underlying this disease
•
No current treatments for underlying disease
–
Agents in development reduce spleen size, address symptoms
•
Phase 2 trial initiated October 2011
–
Design: Single-arm, single-agent, exploratory trial in up to
45 patients with myelofibrosis
–
Dose: 160 mg IPI-926 administered orally once daily
–
Primary endpoint: Hematologic response rate
11 |
 Chondrosarcoma: First and Only
Randomized Trial in this Patient Population
•
Significant unmet need
–
Chondrosarcoma is highly resistant to chemotherapy
and radiotherapy
–
Therapeutic standard is surgery
–
No effective treatments and no established standard of care for
patients with metastatic or locally advanced, inoperable disease
12
•
Preclinical data suggests inhibiting the Hedgehog pathway
reduces tumor volume and leads to calcification
•
IPI-926 granted Orphan Drug Designation by FDA and EMA
in this indication |
 Rigorous Phase 2 Trial Under Way
•
Global trial at approximately 50 sites
•
Randomized, double-blind, single-agent, placebo controlled study in
metastatic or locally advanced, inoperable chondrosarcoma
–
Trial design reviewed with FDA and EMA prior to study
•
Primary endpoint is progression free survival
–
Secondary endpoints include time to progression, overall survival, overall
response rate and response duration
13
2:1
Randomization
Progression -
crossover to IPI-926
~140
Patients
IPI-926 (QD)
Placebo |
 Retaspimycin HCl (IPI-504)
Targeting Non-Small Cell Lung Cancer Through
Hsp90 Inhibition
14 |
 Function of Hsp90
•
“Chaperone”
protein necessary for stability
and
function
of
certain
‘client’
proteins,
including oncoproteins
Retaspimycin HCl (IPI-504)
•
Highly potent, selective, water
soluble Hsp90 inhibitor
Program strategy; determine optimal:
Dose and schedule
Combination agents
Indications
Current status: Two clinical trials in NSCLC
15
Heat Shock Protein 90 (Hsp90):
An Important Cancer Target |
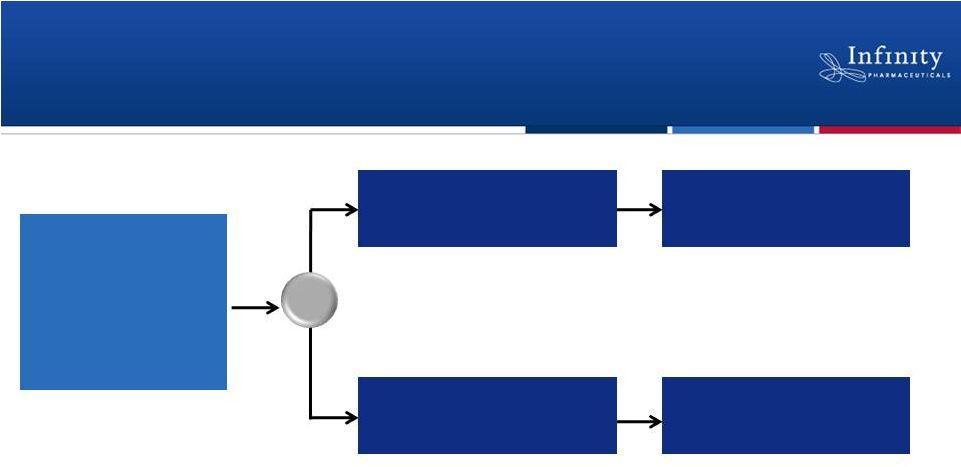
 Retaspimycin HCl: Potential Breakthrough
Approach to NSCLC
Pursuing multiple development paths as combination therapy
16
•
Based on clinical data from
Phase 1b study
•
Randomized, double-blind, placebo-
controlled Phase 2
•
Biomarker exploration
Combination with
Everolimus in
Patients with a
KRAS Mutation
•
Based on preclinical data in well-
defined patient population
•
Phase 1b/2 exploratory study
Combination with
Docetaxel in
Patients with a
Smoking History |
 Phase 1b Trial: Clinically Active in
Combination with Docetaxel
17
Compelling Phase 1b data
•
Partial response seen in 6
patients (ORR = 26%)
1
•
Stable disease seen in 7
patients
1
Riely et al., ASCO 2011. |
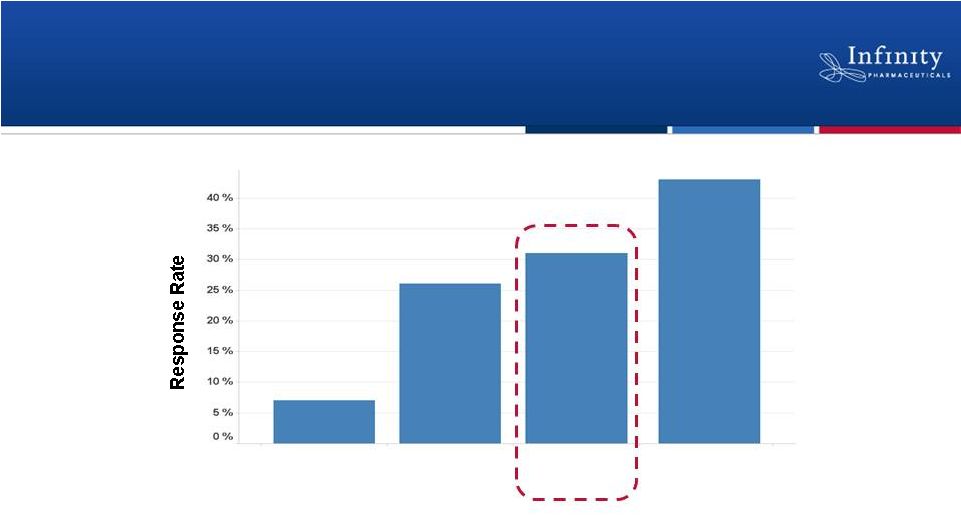 Responses Observed in Patients with
Historically Poor Prognoses
•
In exploratory analyses, patients with the highest response rates fell into
overlapping categories:
–
Current or former smokers (ORR = 33%)
–
Those with squamous cell carcinoma (ORR = 43%)
18
Historical 2
nd
Line
Docetaxel
NSCLC
Patients in
Trial
N=23
Smokers
N=18
Squamous
Cell
Carcinoma
N=7
Patient Populations
Retaspimycin HCl plus Docetaxel
Overall Response Rate
Riely et al., ASCO 2011. |
 Phase 1b Trial: Favorable Safety Profile
•
All toxicities were manageable
•
No unexpected or overlapping toxicities seen
•
GI toxicities were primarily Grade 1 or Grade 2
•
No significant ocular toxicities were observed
•
No dose reductions or discontinuations in response to liver
function tests
19
Riely et al., ASCO 2011. |
 Phase 2 Trial Ongoing in NSCLC
20
~200 smokers w/
2
nd
-
or 3
rd
-line
NSCLC
(docetaxel naïve)
•
1°
Endpoint:
OS
•
2°
Endpoints:
PFS,
ORR,
Safety
•
Exploratory:
Biomarkers,
PG
markers
Follow-up for OS
Follow-up for OS
Docetaxel (q3w) +
Retaspimycin HCl (weekly)
(N=100)
Docetaxel (q3w) +
placebo (weekly)
(N=100)
•
Dosing Schedule
–
Retaspimycin
HCl:
450
mg/m
2
IV QW
–
Docetaxel:
75
mg/m
2
IV
Q3W
R |
 Phase 1b/2 Trial Ongoing in NSCLC Patients
with mKRAS
•
Encouraging preclinical rationale
–
Retaspimycin HCl plus an mTOR inhibitor resulted in synergistic
activity and substantial tumor regression in a mouse model
•
Exploratory Phase 1b/2 trial underway in up to 45 patients with a
KRAS mutation
–
Phase 1b: Dose-escalation study to determined recommended dose
combination
–
Phase 2: Will evaluate safety and clinical activity; may be expanded
based on overall response rate
21 |
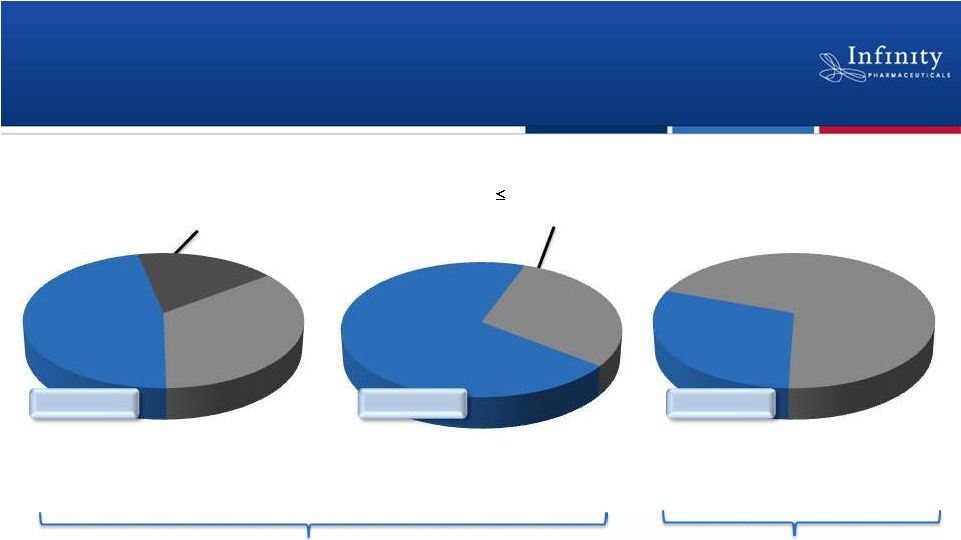 % NSCLC Patients
by Cell Type (2009)
% Stage IIIb/IV NSCLC Patients
by Smoking Status (2009)
NSCLC: Significant Commercial Opportunity
% NSCLC Patients
by Mutation Status (2009)
22
Squamous
Cell
Carcinoma
35%
Adenocarcinoma
47%
Large Cell
Carcinoma
18%
> 15 pack years
70%
Non-smokers &
15 pack years
30%
KRAS
30%
Non-KRAS
70%
Sources:
Decision
Resources
NSCLC
Pharmacor
Report,
June
2009;
Cancer.
2010
February
1;
116(3):
670–675.
doi:
10.1002/cncr.24813.
Estimates based upon G7 regions (US, UK, IT, DE, ES, FR, JP)
Phase 1b/2 trial of
retaspimycin HCl +
everolimus
Phase 2 trial of retaspimycin HCl + docetaxel
~145,000
~182,000
~125,000 |
 IPI-926 and Retaspimycin HCl:
Development Summary
IPI-926
•
Opportunity to deliver commercially differentiated product for broad
range of difficult-to-treat cancers
•
Phase 2 clinical trial program underway
–
Enrollment completed in pancreatic cancer
–
Enrollment ongoing in myelofibrosis and chondrosarcoma
Retaspimycin HCl
•
Combination therapy based on retaspimycin HCl may provide important
therapeutic benefit in NSCLC
•
Two trials underway
–
Phase 2 trial in combination with docetaxel in smokers
–
Phase 1b/2 trial in combination with everolimus in patients
with KRAS mutation
23 |
 Additional Pipeline Opportunities |
 IPI-145: Novel PI3K Inhibitor Rapidly
Advancing to the Clinic
25
•
IPI-145 is a potent, oral inhibitor of PI3K
and
PI3K
–
PI3K plays a role in hematologic
malignancies and inflammatory conditions
•
Compelling
human
proof-of-concept
of
PI3K
inhibition in heme malignancies
–
IPI-145 is 10-
to 30-fold more potent inhibitor of
PI3K
than PI3K
inhibitor with reported data
•
Data
suggest
inhibition
of
PI3K
is
important,
particularly in inflammation
–
IPI-145 has shown compelling preclinical activity in
several models of inflammation
•
Phase 1 development expected to begin in 2H
2011 |
 •
IPI-940 inhibits FAAH and is designed to potentiate the effect
of anandamide
•
Encouraging data from Phase 1 trial in healthy volunteers
•
Purdue and Mundipharma exercised rights for
worldwide development and commercialization
IPI-940: Phase 2-Ready FAAH Inhibitor
26
–
Constitutively active FAAH degrades anandamide, the body’s
natural source of pain relief
–
Marked FAAH inhibition and increased anandamide levels
–
No observed dose-limiting toxicities
–
Purdue expected to begin Phase 2 development in pain
|
 Strong Financial Foundation to
Reach Key Inflection Points
27 |
 Strategic Alliances Provide Funding and
Access to Global Markets
28
Hedgehog, PI3K and early discovery
•
R&D funding from Mundipharma
•
INFI to develop and register product candidates globally
•
INFI to commercialize products in the U.S.
•
Access to ex-US markets: Mundipharma to commercialize
products ex-U.S.
•
INFI entitled to royalty of 10% to 20% on ex-U.S. sales
FAAH
•
Purdue and Mundipharma responsible for global development
and commercialization
•
Access to GP sales force: Purdue and Mundipharma
responsible for global commercialization
•
INFI entitled to royalty of 10% to 20% on global sales
|
 Financial Strength to Drive Value Creation
29
$152.5M
Committed R&D Funding
Remaining in 2011 and 2012
(as of 6/30/11)
$50M
Line
of
Credit
1
(Balloon note at prime, matures 2019)
Cash and Investments
(as of 6/30/10)
Current and Committed Capital
$285 Million
1
Line of credit may be drawn for any corporate purpose.
~$82M
0
50
100
150
200
250
300 |
 2011 Financial Guidance:
Cash Runway into 2014
•
Projected
2011
revenue
of
$90M
-
$95M
•
Projected
2011
operating
cash
burn
of
$30M
-
$40M
•
Anticipate year-end cash and investments balance of
$110M -
$120M
–
Based on current operating plan; excludes $110M R&D funding
commitment from Mundipharma for 2012
•
Approximately 26.6 million shares outstanding
30 |
    INFI
in 2011: Considerable Near-Term Momentum
•
Well-financed, with capital into 2014
•
Purdue/Mundipharma alliance enables robust clinical development and approval
strategies; provides access to markets ex-US & those best served by a GP
sales force •
Compelling scientific rationale
•
Intriguing Phase 1b clinical data
•
Underserved markets
Novel
candidates in
development
•
Rigorous trials
•
Companion biomarker strategy
Active
phase
2 trials
•
Clear registration paths
•
Multiple possible indications
•
Substantial market potential
•
Full U.S. commercial rights
in oncology/inflammation |
 Building a Sustainable, Fully Integrated
Biotechnology Company
October 2011 |