Attached files
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
x ANNUAL REPORT UNDER SECTION 13 OR 15(d) OF THE
SECURITIES EXCHANGE ACT OF 1934
For the Fiscal Year Ended December 31, 2010
or
o TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d)
OF THE SECURITIES EXCHANGE ACT OF 1934
Commission File Number 1-33094
AMERICAN CARESOURCE HOLDINGS, INC.
(Exact name of registrant as specified in its charter)
DELAWARE | 20-0428568 | |||
(State or other jurisdiction of | (I.R.S. employer | |||
incorporation or organization) | identification no.) | |||
5429 LYNDON B. JOHNSON FREEWAY | ||||
SUITE 850 | ||||
DALLAS, TEXAS | ||||
75240 | ||||
(Address of principal executive offices) | ||||
(Zip code) |
(972) 308-6830
(Registrant’s telephone number, including area code)
Securities registered pursuant to Section 12(b) of the Exchange Act:
Title of Each Class | Name of Each Exchange on Which Registered | |
Common Stock, par value $.01 per share | The NASDAQ Capital Market |
Securities registered pursuant to Section 12(g) of the Exchange Act:
None
Indicate by checkmark if the Registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act of 1933 (the “Securities Act”). Yes o No x
Indicate by checkmark if the Registrant is not required to file reports pursuant to Section 13 or 15(d) of the Securities Exchange Act of 1934 (the “Exchange Act”). Yes o No x
Indicate by checkmark whether the Registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Exchange Act during the preceding 12 months (or for such shorter period that the Registrant was required to file such reports) and (2) has been subject to such filing requirements for the past 90 days. Yes x No o
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes o No o
Indicate by checkmark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained in this form, and will not be contained, to the best of Registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. o
Indicate by checkmark whether the Registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See the definitions of “large accelerated filer,” “accelerated filer” and “smaller reporting company” in Rule 12b-2 of the Exchange Act.
Large accelerated filer o | Non-accelerated filer o |
Accelerated filer o | Smaller Reporting Company x |
Indicate by checkmark whether the Registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes o No x
The aggregate market value of the voting and nonvoting Common Stock held by non-affiliates of the Registrant was $15,356,319, computed by reference to the price at which the Common Stock was last sold on The NASDAQ Capital Market on the last business day of the Registrant’s most recently completed second fiscal quarter (June 30, 2010).
The number of shares of the Registrant’s Common Stock, par value $.01 per share, outstanding as of March 14, 2011 was 16,922,042.
DOCUMENTS INCORPORATED BY REFERENCE
Portions of the definitive proxy statement for the annual meeting of stockholders of American CareSource Holdings, Inc. to be held on May 23, 2011 and to be filed with the Securities and Exchange Commission pursuant to Regulation 14A not later than April 30, 2011, are incorporated by reference into Part III of this Form 10-K.
AMERICAN CARESOURCE HOLDINGS, INC.
FORM 10-K
TABLE OF CONTENTS
PART I | ||
PART II | ||
PART III | ||
PART IV | ||
Index to Financial Statements | ||
Special Note Regarding Forward-Looking Statements
This annual report on Form 10-K contains forward-looking statements within the meaning of Section 27A of the Securities Act of 1933, as amended, and Section 21E of the Securities Exchange Act of 1934, as amended. These statements can be identified by forward-looking words such as “may,” “will,” “expect,” “intend”, “anticipate,” “believe,” “estimate” and “continue” or similar words and discuss the Company’s plans, objectives and expectations for future operations, including its services, contain projections of the Company’s future operating results or financial condition, and discuss its expectations with respect to the growth in health care costs in the United States, the demand for ancillary benefits management services, and the Company’s competitive advantages, or contain other “forward-looking” information.
Such forward-looking statements are based on current information, assumptions and belief of management, and are not guarantees of future performance. Substantial risks and uncertainties could cause actual results to differ materially from those indicated by such forward-looking statements, including, but not limited to, the Company’s inability to attract or maintain providers or clients or achieve its financial results, changes in national health care policy, federal or state regulation, and/or rates of reimbursement including without limitation the impact of the newly-enacted Patient Protection and Affordable Care Act, Health Care and Educational Affordability Reconciliation Act and medical loss ratio regulations, general economic conditions (including the recent economic downturns and increases in unemployment), lower than anticipated demand for ancillary services, pricing, market acceptance/preference, the Company’s ability to integrate with its clients, consolidation in the industry that may affect the Company’s key clients, changes in the business decisions by significant clients, increased competition, the Company’s inability to manage growth, implementation and performance difficulties, and other risk factors detailed from time to time in the Company’s periodic filings with the Securities and Exchange Commission, including in this annual report on Form 10-K for the year ended December 31, 2010.
Do not place undue reliance on these forward-looking statements, which speak only as of the date this document was prepared. All forward-looking statements included herein are expressly qualified in their entirety by the cautionary statements contained or referred to in this section. Except to the extent required by applicable securities laws and regulations, the Company undertakes no obligation to update or revise these forward-looking statements to reflect events or circumstances after the date of this document or to reflect the occurrence of unanticipated events.
ii
PART I
Item 1. Business.
Overview
American CareSource Holdings, Inc. (“ACS,” “Company,” the “Registrant,” “we,” “us,” or “our”) is an ancillary services company that offers cost effective access to a comprehensive national network of ancillary healthcare service providers. The Company sells its services to a number of healthcare companies including preferred provider organizations ("PPOs"), third party administrators (“TPAs”), insurance companies, large self-funded organizations and various employee groups. The Company offers payors this solution by:
• | lowering its payors’ ancillary care costs throughout our network of high quality, cost effective providers that the Company has under contract at more favorable terms than they could generally obtain on their own; |
• | providing payors with a comprehensive network of ancillary healthcare services providers that is tailored to each payor’s specific needs and is available to each payor’s covered persons for covered services; |
• | providing payors with claims management, reporting and processing and payment services; |
• | performing network/needs analysis to assess the benefits to payors of adding additional/different service providers to the payor -specific provider networks; and |
• | credentialing network service providers for inclusion in the payor -specific provider networks. |
Ancillary healthcare services encompass a broad array of services that supplement or support the care provided by hospitals and physicians and include the services listed under “-- Services and Capabilities--Ancillary care services” below.
The Company's primary focus is on direct payors. It is the Company's belief that it can best influence patient choice by working with payors who have the ability to alter benefit design in order to encourage patients to seek the most cost effective ancillary providers.
The Company's net revenue and operating results were impacted by multiple macro- and micro-economic factors in 2009 and 2010. The following macro-economic factors negatively impacted our business:
•High unemployment rates have resulted in fewer people participating in insurance programs;
• | Uncertainty surrounding the Patient Protection and Affordable Care Act and Health Care and Educational Affordability Reconciliation Act legislation; |
•Plan participants have sought to spend less money, resulting in less frequent use of our ancillary services; and
• | Payor and provider consolidation throughout the healthcare industry have reduced claims volume and may limit opportunities for growth. |
On a micro-economic basis, we have been severely impacted by the deterioration of the business of our two most significant clients. Those clients, both of which are PPO's, have seen significant declines in their number of covered lives. One client has lost payor groups due to various competitive factors, while the other client was party to a business combination, which resulted in a lengthy transition plan, reducing our business. Because we do not have a direct relationship with these organization's payors, it is difficult to competitively impact those relationships. Revenues from the two client relationships declined a combined 21% in 2010 as compared to 2009.
ACS was incorporated under the laws of the State of Delaware on November 24, 2003 as a wholly-owned subsidiary of Patient Infosystems, Inc. (“Patient Infosystems”) in order to facilitate Patient Infosystems’ acquisition of substantially all of the assets of American CareSource Corporation. American CareSource Corporation had been in operation since 1997. The predecessor company to American CareSource Corporation, Physician’s Referral Network, had been in operation since 1995. On December 23, 2005, the Company became an independent company when Patient Infosystems distributed by dividend to its stockholders substantially all of its shares of the Company. Ancillary Care Services, Inc. is a wholly owned subsidiary of the Company.
1
The Company’s principal executive offices are located at 5429 Lyndon B. Johnson Freeway, Suite 850, Dallas, TX 75240. Our Common Stock is listed on The NASDAQ Capital Market under the symbol “ANCI.” Our telephone number is (972) 308-6830. Our Internet address is www.anci-care.com.
Services and Capabilities
Ancillary care services
Ancillary healthcare services include a broad array of services that supplement or support the care provided by hospitals and physicians, including the non-hospital, non-physician services associated with surgery centers, free-standing diagnostic imaging centers, home health and infusion, supply of durable medical equipment, orthotics and prosthetics, laboratory and other services.
Ancillary healthcare services include, but are not limited to, the following categories:
· Acupuncture | · Massage Therapy |
· Cardiac Monitoring | · Occupational Therapy |
· Chiropractor | · Orthotics and Prosthetics |
· Diagnostic Imaging | · Pain Management |
· Dialysis | · Physical Therapy |
· Durable Medical Equipment | · Podiatry |
· Genetic Testing | · Rehab: Outpatient |
· Hearing Aids | · Rehab: Inpatient |
· Home Health | · Sleep |
· Hospice | · Skilled Nursing Facility |
· Implantable Devices | · Surgery Center |
· Infusion | · Transportation |
· Laboratory | · Urgent Care |
· Lithotripsy | · Vision |
· Long-term Acute Care | · Walk-in Clinics |
The Company has agreements with approximately 5,000 ancillary healthcare service providers operating in approximately 36,000 sites nationwide.
Provider Network
The Company views its ability to manage, organize and maintain its provider network and to recruit new providers as critical elements in its long-term success because its network is one of the most important reasons healthcare payors engage the Company. The Company has agreements with its network of ancillary healthcare service providers for the purpose of meeting contractual obligations to its healthcare payors to make available a comprehensive and client-specific ancillary healthcare provider network. The agreements define the scope of services to be provided to covered persons by each ancillary healthcare provider and the amounts to be charged for those services and are negotiated independently from the agreements reached with the Company’s client payors. The terms of each agreement between the Company and ancillary healthcare service providers make it clear that the Company is solely obligated to the service provider under the contract between them and do not contemplate any contractual relationship between the service providers and the Company’s payors or permit the service providers to pursue claims directly against the Company’s payors. The network is comprised of approximately 5,000 ancillary healthcare service providers that are located in 36,000 sites nationwide.
When providers initially enter the ACS provider network, the Company credentials them for inclusion in the Credentialed ACS network. The Company also re-credentials its providers on a periodic basis. From time to time, the Company reviews its provider relationships to determine whether any changes to the relationship are appropriate through sanction monitoring and other methods. The Company believes that credentialing providers represents a valuable service to both its payors and the providers in the network, who would, in the absence of such service, be forced to undergo the credentialing process with respect to each payor with whom they enter into a service relationship.
2
During 2010 and 2009, we generated revenue from ancillary healthcare services as follows:
Category | 2010 | 2009 | ||||
Dialysis | 28 | % | 27 | % | ||
Laboratory | 19 | 22 | ||||
Durable Medical Equipment | 13 | 12 | ||||
Diagnostic Imaging | 10 | 10 | ||||
Infusion | 7 | 9 | ||||
Rehab: Outpatient & Inpatient | 6 | 4 | ||||
Surgery Center | 4 | 5 | ||||
Chiropractor | 3 | 2 | ||||
Long Term Acute Care/Skilled Nursing Facilities | 2 | 4 | ||||
Orthotics and Prosthetics | 2 | 2 | ||||
Other | 6 | 3 | ||||
100 | % | 100 | % | |||
Our Model
The Company’s business model, illustrating the relationships among the persons involved, directly or indirectly, in the Company’s business and its generation of revenue and expenses is depicted below:
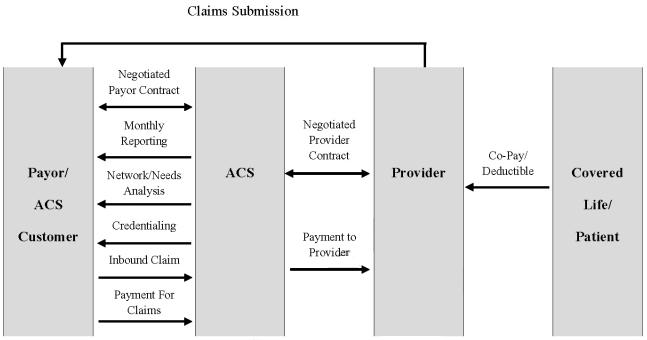
Payors route healthcare claims to us after service has been performed by participant providers in our network. We process those claims and charge the payor according to its contractual rate for the services according to our contract with the payor. In processing the claim, we are paid directly by the payor or the insurer for the service. We then pay the provider of service according to its independently-negotiated contractual rate. We assume the risk of generating positive margin, the difference between the payment we receive for the service and the amount we are obligated to pay the provider of service.
The Company may also receive a claims submission from a payor either electronically or via a paper based claim. As part of its relationship with the payors, the Company may pay an administrative fee to the payors for the modifications that may be required to the payor’s technology, systems and processes to create electronic connectivity with the Company, as well as for the aggregation of claims and the electronic transmission of those claims to us.
3
How We Deliver Services
Ancillary network analysis. The Company performs an analysis of the available claims history from each client payor and develops a specific plan to meet each payor’s needs. This analysis identifies service providers that are not already in our network. We attempt to enter into agreements with such service providers to maximize discount levels and capture a significant volume of previously out-of-network claims.
Ancillary custom network. ACS customizes its network to meet the needs of each payor. In particular, when a new payor joins and periodically for each existing payor, we review the payor’s “out-of-network” claims history through our network analysis service and develop a strategy to create a network that efficiently serves the payor’s needs. This may involve adding additional service providers for a payor or removing service providers if we determine it is beneficial for them to be excluded from the client’s network.
Ancillary network management. The Company manages ancillary service provider contracts, reimbursement and credentialing for its payors. This not only provides administrative benefits to our payors, but reduces the burden on our contracted service providers who typically must supply credentialing documentation to payors and engage in contract negotiations with separate payors.
Ancillary systems integration. The Company has created a proprietary software system that enables us to manage many different customized accounts and includes the following modules:
• | Provider network management |
• | Credentialing |
• | Data transfer management/electronic data interface |
• | Multi-level reimbursement management |
• | Posting, Explanation of Benefits, check, and e-funds processes |
• | Client service management |
• | Claims pricing |
• | Advanced data reporting |
Ancillary reporting. ACS offers a complete suite of reports to each payor on a monthly basis. These reports cover contracting efforts and capture rates, client savings, volumes by service category and complete claims and utilization reports and other information of value to the client.
Ancillary healthcare claims management. The Company can manage ancillary healthcare claims flow, both electronic and paper based, and integrate with a payor’s process electronically or through paper claims. The Company has the capability of performing a number of customized processes that may add additional value for each payor. As part of the claims management process, we manage the documentation requirements specific to each payor. In the event claims are submitted to us by a payor without the complete required documentation, we will work with the payor and/or service provider to obtain the required documentation so that the claim will be accepted by the payor. This service provides a labor cost savings to the payors and providers.
Ancillary claims collections management. The Company facilitates an expedited claims collection process by ensuring receipt of the claim by the payor, providing information to the payor required for processing the claim, tracking the status of the claim throughout the process and maintaining a team of customer service representatives to resolve any issues that might delay the collections process. The Company believes that the providers in its network are paid more effectively and efficiently than would otherwise be the case.
Ancillary data insights. The Company has developed and continues to develop an extensive database of ancillary healthcare claims history. The data provides insights into utilization and pricing across a wide variety of service categories, geographies, and service providers. The Company intends to market this data as a value added service to its payors in the design of custom networks, and the development of ancillary healthcare management programs.
4
Business Strategy
The Company’s focus is strictly on the ancillary healthcare services market, a growing market that now accounts for almost 30% of total annual healthcare spending in the United States and is estimated at $574 billion (as derived from 2006 data published by the Center for Medicare and Medicaid Services, National Health Statistics Group, U.S. Department of Commerce and Bureau of Economic Analysis and Census). Ancillary healthcare services are cost effective alternatives to physician and hospital-based services and ancillary providers offer services in 30 different categories, including those listed under “-- Services and Capabilities--Ancillary care services.” While most efforts are placed on managing outcomes and reducing healthcare costs associated with patient care in hospitals and in physician offices, the ancillary healthcare service market is an often over-looked, but very important emerging segment of the overall United States healthcare system. As more and more care is delivered in highly cost effective out-patient and ancillary care settings, the need for better organization and cost containment will only increase over the next several years.
We believe that companies who understand the nuances of the ancillary healthcare market and develop the expertise to manage this new, de-centralized system of patient care, are able to capitalize on this market opportunity. For example, contracting with ancillary healthcare service providers is difficult without a specific focus on the market. This is due to the disparate nature of ancillary healthcare services and the fact that these services are offered by a wide array of providers, ranging from small independent practitioners, regional specialty practices, national providers and within hospital systems. Since this market is so diverse, it has not been a focus of the major health plans and payors. In addition, many health plans are conflicted because their existing hospital contracts may encourage the use of the hospital systems’ more expensive in-house ancillary services. The Company believes that because it has developed a substantial network of providers, it has established a sustainable advantage in this market by becoming an aggregator of these services for health plans, and because it has been retained by substantial payors, it can offer healthcare providers a substantial number of patients who are entitled to receive services from payors. In addition, our "ancillary only" contracting focus allows us to be independent of any hospital relationships that may encourage retaining all ancillary services within the more expensive hospital setting.
Because the Company is solely focused on the nation-wide ancillary healthcare system designed specifically to help regional and mid-market payors across the country, expanding and maintaining a nation-wide, high-quality, multiple specialty ancillary provider network is a critical component of the Company’s strategy. The Company has invested to develop its ancillary service provider network both proactively, across geographical and healthcare specialties, and reactively to address specific client needs. While we have a national footprint of service providers, our intention is to focus on specific geographic markets where we can have a significant impact on a service provider’s patient load. With market strength in specific geographic areas, the Company has been able to develop favorable rates with ancillary service providers and create an attractive product offering (healthcare cost savings) to regionally-based clients in those areas.
In order to enhance its ability to recruit and manage its network of providers, the Company offers a suite of value added services specifically designed to help ancillary care service providers lower their cost of doing business by assuming the responsibility for the most complex and costly interactions with payors. The services include those listed under “-- Services and Capabilities--Ancillary care services.” The Company believes that by becoming an indispensable business partner to the ancillary healthcare service provider community, it will continue to grow its ancillary healthcare service provider network and continue to derive favorable contracting terms from these service providers.
While the Company markets its services to PPOs on an opportunistic basis, it is seeking growth from increasing its number of client payor and service provider relationships by focusing on providing in-network services for its payors and aggressively pursuing middle-market insurance companies, TPAs and direct payors. The Company continues to derive a significant amount of its net revenues from its traditional PPO relationships, but we have shifted our focus and we now aggressively target TPAs and direct payors. The Company believes that there is a large market opportunity involved in providing a highly competitive ancillary care solution to the standard service offered by the major national insurers in select regional markets across the country. The combination of our regionally specific networks of providers and the resulting contractual cost savings we are able to generate helps ACS’ payors compete more effectively against the major national insurers in their local markets.
The Company aggregates the lives of its various clients into buying power that exceeds the market power of any one of its clients individually. During 2010, the Company's contracts exposed us to 3.2 million covered lives. As a rapid aggregator of significant patient volume, the Company believes it will be able to continue to drive favorable contracting terms from the selected service providers in the ACS Network by directing patient volume to their practices and it will have the ability to negotiate exclusive contracts that will allow the Company to manage the full spectrum of a payor client’s ancillary healthcare benefit offerings. The volume of collective lives we manage allows us to obtain more favorable pricing than our clients can generally obtain on their own.
5
Sales and Marketing
The Company markets its services to PPOs on an opportunistic basis, but primarily targets direct payors such as TPAs, insurance companies, large self-funded organizations and employee groups. The Company utilizes both a new business sales organization of three senior sales professionals as well as an account management team of two professionals to contract with new payor organizations and then maximize the revenue and margin potential of each new payor. The new business sales team uses a variety of channels to reach potential clients including professional relationships, direct marketing efforts, attendance at industry-specific trade shows and conferences, and through strategic partnerships with market partners, independent brokers, and consultants. The account management team is engaged with each new payor to help manage the implementation process. In addition, an Account Manager is generally assigned to each new payor organization and is responsible for all aspects of the Company’s relationship with the entity including the expanded utilization of the Company’s services over time and the enhancement of the Company’s relationship with the payor.
The Company invests in on-going market research with its clients and maintains an informal client advisory group with a number of senior leaders in managed care organizations. From time to time, the Company meets with the advisory group to discuss changes in the marketplace and client needs. In the first quarter of 2009, the Company engaged a strategic marketing services company to conduct a “Market Pulse” which involved in-depth interviews with senior managers/decision-makers in current ACS client organizations. The purpose of the “Market Pulse” was to gain client feed-back on the Company’s optimal product messaging by market segment, differentiated “go-to-market” strategies, and new product ideas. The outcome from these sessions was used to formulate a solid base of sales, marketing and new product priorities for the next several years.
Clients
The Company’s healthcare payor clients engage the Company to manage a comprehensive array of ancillary healthcare services that they and their payors have agreed to make available to their insureds or beneficiaries or for which they have agreed to provide insurance coverage. The typical services the healthcare payors require the Company to provide include:
• | providing a comprehensive network of ancillary healthcare services providers that is available to the payor’s covered persons for covered services; |
• | providing claims management, reporting, and processing and payment services; |
• | performing network/needs analysis to assess the benefits to payors of adding additional/different service providers to the payor-specific provider networks; and |
• | credentialing network service providers for inclusion in the payor -specific provider networks. |
The terms of the agreement between the Company and the payors do not contemplate that the payors will have any relationship with the service providers and, in fact, prohibit payors from claiming directly against the service providers. The agreements between the Company and the payors provide that it is the Company’s obligation to deliver or make available the agreed-upon services. The Company is responsible irrespective of the existence or terms of any agreement the Company has with the service providers. The terms of the Company-payor agreement provide that the Company is obligated to provide or arrange for the provision of all of the services covered by such agreement and the Company is responsible for ensuring that the contractual terms are met and such services are provided (whether the services are those performed directly by the Company, such as claims management, processing and payment service, network/needs analysis and credentialing, or those performed by a service provider contracted by the Company).
The Company’s most significant payors include (i) HealthSmart (“HealthSmart”), which consists of HealthSmart and its affiliates, American Administrative Group (“AAG”), Interplan Health Group (“IHG”), Emerald Healthcare, and HealthSmart Accel Network (“Accel”), and (ii) Viant Holdings Inc. (“Viant”), consisting of Texas True Choice, Inc. and Beech Street Corporation. For the year ended December 31, 2010, ACS derived 48% of its total net revenue from HealthSmart (including its affiliates) and 27% of its total net revenue from Viant (including its affiliates). For the year ended December 31, 2009, ACS derived 47% of its total net revenue from HealthSmart and 38% of its total net revenue from Viant.
In early 2009, we entered into an amendment to our agreement with HealthSmart. The amendment extended the duration of the partnership between the Company and HealthSmart through December 31, 2012. In accordance with the amendment, we paid $1.0 million to HealthSmart for various integration services. In November 2009, HealthSmart completed a recapitalization with a private investment company and HealthSmart’s other lenders.
6
The client contract with Viant expires on May 20, 2011 and automatically renews for successive one-year periods unless either party delivers a written notice of non-renewal at least 90 days prior to expiration. Since the Company has not received written notice of non-renewal, the contract term has been automatically extended through May 20, 2012. Such contract may be terminated upon thirty (30) days’ notice in the event of a breach. In addition, in March 2010, Viant was acquired by MultiPlan, Inc., a provider of PPO network and related transaction-based solutions.
We have generated a significant portion of our net revenues from these two clients (75% in 2010 and 85% in 2009), but because of the nature of the relationships, we do not have the ability to impact the relationships these organizations have with their clients, which are direct payors. Because we have secondary relationships with these payors and cannot have a competitive impact on the payors, we have determined that it is in our best interest to pursue clients that are direct payors, primarily TPAs. We believe we can impact relationships with direct payors through various competitive avenues, such as assisting them with plan design. During 2010, of our 13 new clients, 12 were direct payors and generated approximately $5 million of revenue.
Competition
The Company faces four types of direct competitors.
• | The first group of competitors consists of larger, national health plans and insurers such as Aetna, Blue Cross/Blue Shield plans, Cigna, Humana, and United HealthCare. These larger carriers offer nation-wide, standardized products and often compete on a local level based of the cost-effectiveness of their national contracts. |
• | The second group of competitors is our own payors. Our payors have selected us based on our extensive network of service providers and cost-savings potential. However, they may choose to develop their own network instead of outsourcing ancillary management services to us in the future. |
• | The third group of competitors is more regionally-focused and consists of smaller regional PPOs, payors and community-based provider-owned networks. These regional competitors are generally managing their own home-grown network of ancillary care providers and are more likely to offer customized products and services tailored to the needs of the local community. These regional groups will often use their ownership and/or management of the full continuum of care in a local market to direct patients to the provider groups within their network. |
• | The fourth group of competitors focus on managing patients within a single ancillary specialty (e.g. dialysis, imaging or infusion), and offer comprehensive payor and provider services within their chosen ancillary category. |
Research and Development
The Company invests in its information technology infrastructure to enhance the capabilities of its databases, data retrieval tools, data exchange capabilities and claims processing engine. In addition, the Company believes that its extensive claims database of ancillary healthcare services and costs is a strategic asset. The Company’s capitalized development costs totaled approximately $402,000 and $628,000 during 2010 and 2009, respectively.
Government Regulation
The healthcare industry is extensively regulated by both the Federal and state governments. A number of states have extensive licensing and other regulatory requirements applicable to companies that provide healthcare services. Additionally, services provided to health benefit plans in certain cases are subject to the provisions of the Employee Retirement Income Security Act of 1974, as amended (“ERISA”).
Furthermore, state laws govern the confidentiality of patient information through statutes and regulations that safeguard privacy rights. The Company is subject to the Health Insurance Portability and Accountability Act of 1996 (“HIPAA”), which provides national standards for electronic health information transactions and the data elements used in such transactions. ACS and its clients may be subject to Federal and state laws and regulations that govern financial and other arrangements among healthcare providers. Furthermore, the Company and its clients may be subject to federal and state laws and regulations governing the submission of false healthcare claims to the government and private payors, mail pharmacy laws and regulations, consumer protection laws and regulations, legislation imposing benefit plan design restrictions, various licensure laws, such as managed care and third party administrator licensure laws, drug pricing legislation, and Medicare and Medicaid reimbursement regulations. Possible sanctions for violations of these laws and regulations include minimum civil penalties of between $5,000-$10,000 for each false claim and treble damages.
7
During 2010, President Obama signed the Patient Protection and Affordable Care Act (the "Affordable Care Act") and the Health Care and Educational Affordability Reconciliation Act legislating broad-based changes to the U.S. health care system. Among other things, the health reform legislation includes guaranteed coverage requirements, eliminates pre-existing condition exclusions and annual and lifetime maximum limits, restricts the extent to which policies can be rescinded, and imposes new and significant taxes on health insurers and health care benefits.
Provisions of the health reform legislation become effective at various dates over the next several years. The Department of Health and Human Services, the National Association of Insurance Commissioners, the Department of Labor and the Treasury Department have yet to issue necessary enabling regulations and guidance with respect to the health care reform legislation.
Due to the breadth and complexity of the health reform legislation, the scope of newly-issued implementing regulations and interpretive guidance, in addition to regulations and guidance yet to be issued, the phased-in nature of the implementation and possible changes to, or repeal of, the legislation by Congress, it is difficult to predict the overall impact of the health reform legislation on our business over the coming years. Possible adverse affects of the health reform legislation include reduced revenues, increased costs, exposure to expanded liability, and requirements for us to revise the ways in which we conduct business or risk of loss of business. In addition, our results of operations, our financial position, including our ability to maintain the value of our goodwill, and cash flows could be materially adversely affected.
Section 1001 of the Affordable Care Act amended Title 27 of the Public Health Service Act of 1944, as amended (the "Public Health Service Act") to add, among other things, a new Section 2718, 'Bringing Down the Cost of Health Care Coverage.' This new provision requires health insurance issuers to publicly report “the ratio of the incurred loss (or incurred claims) plus the loss adjustment expense (or change in contract reserves) to earned premiums” and account for premium revenue related to reimbursement for clinical services, activities that improve health care quality, and all other non-claims costs. The law also requires issuers to provide annual rebates to their enrollees if their medical loss ratio ("MLR") does not meet specific targets. For issuers in the large group market, the MLR must be at least 85%, and for issuers in the smaller and individual markets, the MLR must be at least 80%. The law also gives the National Association of Insurance Commissioners (“NAIC”), subject to certification of the Secretary of the Department of Health and Human Services (“HHS”), authority to develop definitions and standards by which to determine compliance with the requirements in the new § 2718(a).
On December 1, 2010, HHS published final MLR regulations, based upon the recommendations of the NAIC, implementing the new sections of the Public Health Service Act as mandated by the Affordable Care Act. The new regulations apply to issuers offering group or individual health insurance coverage. Under the MLR regulations, an issuer's MLR is calculated as the ratio of (i) incurred claims plus expenditures for activities that improve health care quality to (ii) premium revenue. The two key aspects to this calculation involve what comprises an 'incurred claim' and what qualifies as an 'expenditure for health care quality improvement.'
Incurred claims are reimbursement for clinical services, subject to specific deductions and exclusions. Specifically, incurred claims represent the total of direct paid claims, unpaid claim reserves, change in contract reserves, reserves for contingent benefits, the claim portion of lawsuits and any experience rating refunds. Prescription drug rebates received by the issuer and overpayment recoveries from providers must be deducted from incurred claims. Also, the following amounts are explicitly excluded and therefore may not be included in the calculation of incurred claims: (i) amounts paid to third party vendors for secondary network savings; (ii) amounts paid to third party vendors for network development, administrative fees, claims processing, and utilization management; or (iii) amounts paid, including amounts paid to a provider, for professional or administrative services that do not represent compensation or reimbursement for covered services provided to an enrollee. The regulation permits that some amounts “may” be included in incurred claims - market stabilization payments, state subsidies based on stop-loss methodologies, and incentive and bonus payments made to providers. The regulations themselves provide examples of specifically excluded amounts. With regard to amounts paid for network development (as noted in (ii) above), if an issuer contracts with a behavioral health, chiropractic network, or high technology radiology vendor, or a pharmacy benefit manager, and the vendor reimburses the provider at one amount but bills the issuer a higher amount to cover its network development, utilization management costs, and profits, then the amount that exceeds the reimbursement to the provider must not be included in incurred claims. With regard to administrative services (as noted in (iii) above), medical record copying costs, attorneys' fees, subrogation vendor fees, compensation to paraprofessionals, janitors, quality assurance analysts, administrative supervisors, secretaries to medical personnel and medical record clerks must not be included in incurred claims.
8
In order to properly classify what activities 'improve health care quality', the activity must be designed to improve health quality, increase the likelihood of desired health outcomes, be directed toward individual enrollees or incurred for the benefit of specific segments of enrollees, or be grounded in evidence based medicine. In addition, the activity must be primarily designed to improve health outcomes, prevent hospital readmissions, improve patient safety and reduce medical errors, implement, promote and increase wellness activities and/or enhance the use of health care data to improve quality. The regulations also contain a list of 14 expenditures that are specifically excluded from 'improvement of health care quality' activities. Among these excluded expenditures are: (1) those that are designed primarily to control or contain costs; (2) activities that can be billed or allocated by a provider for care delivery and which are, therefore, reimbursed as clinical services; (3) expenditures related to establishing or maintaining a claims adjudication system, including costs directly related to upgrades in health information technology that are designed primarily or solely to improve claims payment capabilities or to meet regulatory requirements for processing claims (for example, costs of implementing new administrative simplification standards and code sets adopted pursuant to HIPAA including the new ICD-10 requirements); (4) all retrospective and concurrent utilization review; (5) costs of developing and executing provider contracts and fees associated with establishing or managing a provider network, including fees paid to a vendor for the same reason; (6) provider credentialing; (7) marketing expenses; (8) costs associated with calculating and administering individual enrollee or employee incentives; (9) portions of prospective utilization that does not meet the definition of activities that improve health quality; and (10) any function or activity not expressly included, unless otherwise approved by and within the discretion of the Secretary.
It is possible that a portion of the fees our existing and prospective payors are contractually required to pay us and that do not qualify as 'incurred claims' may not be included as expenditures for activities that improve health care quality. Such a determination may make it more difficult for us to retain existing clients and/or add new clients, because our clients' or prospective clients' MLR may otherwise not meet the specified targets. This may reduce our net revenues and profit margins.
The Company must continually adapt to new and changing regulations in the healthcare industry. If we fail to comply with these applicable laws, we may be subject to fines, civil penalties, or criminal prosecution. If an enforcement action were to occur, our business and financial condition may be adversely affected.
Employees
As of March 14, 2011, the Company had 64 full-time employees and no part-time employees.
Item 1A. Risk Factors.
The Company’s stockholders and any potential investor in the Company’s Common Stock should carefully review and consider each of the following risk factors, as well as all other information appearing in this Annual Report on Form 10-K, relating to investment in our Common Stock. The Company’s business faces numerous risks and uncertainties, the most significant of which are described below. If any of the following risks actually occur, the business, financial condition, results of operations or cash flows of the Company could be materially adversely affected, the market price of the Company’s Common Stock could decline significantly, and a stockholder could lose all or part of an investment in the Company’s Common Stock.
The Company has a limited number of clients, two of which account for a substantial portion of its business, and failure to retain such clients or changes to these clients would have a material adverse effect on its business and results of operations. Business from these two clients has declined during the last two years, and will likely continue to decline.
Our two largest clients, HealthSmart Preferred Care, Inc. (“HealthSmart”) and Viant Holdings, Inc. (“Viant”), accounted for an aggregate of approximately 75% of our net revenue during 2010; of which 48% was derived from HealthSmart. In 2009, our two largest clients accounted for 85% of our net revenue, of which 47% was generated from HealthSmart. The loss of either one of these clients or significant declines in the level of use of our services by one or more of these clients (as would be the case, for example, if our clients decide to contract directly with ancillary healthcare service providers), without replacement by new business, would have a material adverse effect on the Company’s business and results of operations. After already declining in the year ended December 31, 2009, net revenues from our two largest clients declined $12.0 million, or 21%, for the year ended December 31, 2010, compared to the prior year.
9
The client contract with Viant expires on May 20, 2011 and automatically renews for successive one-year periods unless either party delivers a written notice of non-renewal at least 90 days prior to expiration. Since the Company has not received written notice of non-renewal, the contract term has been automatically extended through May 20, 2012. Such contract may be terminated upon thirty (30) days’ notice in the event of a breach. In addition, in March 2010, Viant was acquired by MultiPlan, Inc., a provider of PPO network and related transaction-based solutions. We expect that revenue from Viant will continue to decline as its business is integrated with its acquiror, and that even if our contract were to be renewed past May 20, 2012, it would be on a limited basis.
The client contract with HealthSmart, which was set to expire on July 31, 2009, was amended on December 31, 2008. The term was extended four years and will expire on December 31, 2012. There can be no assurance that any client will maintain its contract with us after the expiration of the then-current term or that it will renew its contract on terms favorable to us. Consequently, the Company’s failure to retain such clients could have a material adverse effect on our business and results of operations. Additionally, an adverse change in the financial condition of any of these clients, particularly HealthSmart or Viant, including an adverse change as a result of a change in governmental or private reimbursement programs, could have a material adverse effect on our business.
Proposed health care reforms could materially adversely affect our revenues, financial position and our results of operations.
The enactment of health care reforms at the federal or state level may affect certain aspects of our business, including contracting with ancillary healthcare service providers; administrative, technology or other costs; provider reimbursement methods and payment rates; premium rates; coverage determinations; mandated benefits; minimum medical expenditures; claim payments and processing; drug utilization and patient safety efforts; collection, use, disclosure, maintenance and disposal of individually identifiable health information; personal health records; consumer-driven health plans and health savings accounts and insurance market reforms; and government-sponsored programs.
During 2010, President Obama signed the Affordable Care Act and the Health Care and Educational Affordability Reconciliation Act legislating broad-based changes to the U.S. health care system. Among other things, the health reform legislation includes guaranteed coverage requirements, eliminates pre-existing condition exclusions and annual and lifetime maximum limits, restricts the extent to which policies can be rescinded, and imposes new and significant taxes on health insurers and health care benefits.
On December 1, 2010, HHS published final regulations implementing new sections of the Public Health Service Act as mandated by the Affordable Care Act. The new medical loss ratio ("MLR") regulations apply to issuers offering group or individual health insurance coverage. Under the MLR regulations, an issuer's MLR is calculated as the ratio of (i) incurred claims plus expenditures for activities that improve health care quality to (ii) premium revenue. The two key aspects to this calculation involve what comprises an 'incurred claim' and what qualifies as an 'expenditure for health care quality improvement.' It is possible that a portion of the fees our existing and prospective payors are contractually required to pay us and that do not qualify as 'incurred claims' may not be included as expenditures for activities that improve health care quality. Such a determination may make it more difficult for us to retain existing clients and/or add new clients, because our clients' or prospective clients' MLR may otherwise not meet the specified targets. This may reduce our net revenues and profit margins.
Other provisions of the health reform legislation become effective at various dates over the next several years. The Department of Health and Human Services, the National Association of Insurance Commissioners, the Department of Labor and the Treasury Department will issue necessary enabling regulations and guidance with respect to the health care reform legislation.
Due to the breadth and complexity of the health reform legislation, the scope of newly-issued implementing regulations and interpretive guidance, in addition to regulations and guidance yet to be issued, the phased-in nature of the implementation and possible changes to, or repeal of, the legislation by Congress, it is difficult to predict the overall impact of the health reform legislation on our business over the coming years. Possible adverse affects of the health reform legislation include reduced revenues, increased costs, exposure to expanded liability, and requirements for us to revise the ways in which we conduct business or risk of loss of business. In addition, our results of operations, our financial position, including our ability to maintain the value of our goodwill, and cash flows could be materially adversely affected.
10
The Company has a history of losses and has only achieved profitability in the past three years.
Although the Company achieved its third consecutive profitable year in 2010, it incurred losses in each year between its spinoff in 2003 through 2007 and has an accumulated deficit of approximately $1.0 million as of December 31, 2010. The Company will need to maintain similar levels of claims volume and revenue as it had in 2009 and 2010 in order to continue profitability. No assurances can be given that the Company will be able to continue its current operating volumes or continue to operate profitably in the future. The Company’s prospects must be considered in light of the numerous risks, expenses, delays and difficulties frequently encountered in an industry characterized by intense competition, as well as the risks inherent in the development of new programs and the commercialization of new services, particularly given its operating history through 2007.
The current financial crisis may reduce our revenue and profitability and harm our growth prospects.
Although the Company has continued to experience profitability from 2008 to 2010, its results have been impacted by the current economic crisis. First, the unemployment rate has caused fewer people to participate in insurance programs with our clients. Second, plan participants, seeking to spend less money, appear to be making less frequent use of some ancillary services. Third, the possibility exists that client and, or provider consolidation within our industry could adversely affect our business. To the extent that these trends continue, or become worse, we may receive less revenue and our profitability and growth could be adversely affected, depending on the extent of the declines. Finally, as with any business, the deterioration of the financial condition or sale or change of control of our significant clients could have a corresponding adverse effect on us.
Large competitors in the healthcare industry could choose to compete with us, reducing our margins. Some of these potential competitors may be our current clients.
Traditional health insurance companies, specialty provider networks, and specialty healthcare services companies are potential competitors of the Company. These entities include well-established companies that may have greater financial, marketing and technological resources than we have. Pricing pressure caused by competition has caused many of these companies to reduce the prices charged to clients for core services and to pass on to clients a larger portion of the formulary fees and related revenues received from service providers. Increased price competition from such companies’ entry into the market could reduce our margins and have a material adverse effect on our financial condition and results of operations. In fact, our clients could choose to establish their own network of ancillary care providers. As a result, we would not only lose the benefit of revenue from such clients, but we could face additional competition in our market.
The Company is dependent upon payments from third party payors who may reduce rates of reimbursement.
The Company’s profitability depends on payments provided by third-party payors. Competition for patients, efforts by traditional third party payors to contain or reduce healthcare costs and the increasing influence of managed care payors, such as health maintenance organizations, have resulted in reduced rates of reimbursement in recent years. If continuing, these trends could adversely affect the Company’s results of operations unless it can implement measures to offset the loss of revenues and decreased profitability. In addition, changes in reimbursement policies of private and governmental third-party payors, including policies relating to the Medicare and Medicaid programs, could reduce the amounts reimbursed to the Company’s clients for the Company’s services provided through the Company, and consequently, the amount these clients would be willing to pay for the Company’s services. Also, under the MLR regulations included in the Affordable Care Act, it is possible that a portion of the fees our existing and prospective payors are contractually required to pay us and that do not qualify as 'incurred claims' may not be included as expenditures for activities that improve health care quality. Such a determination may make it more difficult for us to retain existing clients and/or add new clients, because our clients' or prospective clients' MLR may otherwise not meet the specified targets. This may reduce our net revenues and profit margins.
The Company is dependent upon its network of qualified providers and its provider agreements may be terminated at any time.
The development of a network of qualified providers is an essential component of our business strategy. The typical form of agreement from ancillary healthcare providers provides that these agreements may be terminated at any time by either party with or without cause. If these agreements are terminated, such ancillary healthcare providers could enter into new agreements with our competitors which would have an adverse effect on our ability to continue our business as it is currently conducted.
11
For any given claim, the Company is subject to the risk of paying more to the provider than it receives from the payor.
The Company’s agreements with its payors, on the one hand, and the service providers, on the other, are negotiated separately. The Company has complete discretion in negotiating both the prices it charges its payors and the financial terms of its agreements with the providers. As a result, the Company’s profit is primarily a function of the spread between the prices it has agreed to pay the service providers and the prices the Company’s payors have agreed to pay the Company. The Company bears the pricing/margin risk because it is responsible for providing the agreed-upon services to its payors, whether or not it is able to negotiate fees and other agreement terms with service providers that result in a positive margin for the Company. For example, during 2010 and 2009, approximately 7% and 8% of claims were “loss claims” (that is, where the amount paid by the Company to the provider exceeded the amount received by the Company from the corresponding payor for that particular claim) and these loss claims, in the aggregate, comprised approximately $1.2 million in each year. There can be no assurances that the loss claim percentage will not be higher in future periods. If a higher percentage of the Company’s claims resulted in a loss, its results of operations and financial position would be adversely affected.
The Company has significantly increased in size and may not be able to effectively process the claims submitted by its providers in a timely manner.
Our size and the volume of claims has increased dramatically in the last few years. As a result, we have had to increase the size of our processing capabilities and our staff. If we are unable to effectively increase our processing speed and integrate new providers, we may be unable to process properly all claims submitted and this could have a negative impact on our relationships with clients, which in turn could lead to a loss of business.
An interruption of data processing capabilities and telecommunications could negatively impact the Company’s operating results.
Our business is dependent upon our ability to store, retrieve, process and manage data and to maintain and upgrade our data processing capabilities. An interruption of data processing capabilities for any extended length of time, loss of stored data, programming errors, other computer problems or interruptions of telephone service could have a material adverse effect on our business.
Changes in state and federal regulations could restrict our ability to conduct our business.
Numerous state and federal laws and regulations affect our business and operations. These laws and regulations include, but are not necessarily limited to:
• | Public Health Services Act, Patient Protection and Affordable Care Act and Health Care and Educational Affordability Reconciliation Act; |
• | healthcare fraud and abuse laws and regulations, which prohibit illegal referral and other payments; |
• | the Employee Retirement Income Security Act of 1974 and related regulations, which regulate many healthcare plans; |
• | mail pharmacy laws and regulations; |
• | privacy and confidentiality laws and regulations; |
• | consumer protection laws and regulations; |
• | legislation imposing benefit plan design restrictions; |
• | various licensure laws, such as managed care and third party administrator licensure laws; |
• | drug pricing legislation; |
• | Medicare and Medicaid reimbursement regulations; and |
• | Health Insurance Portability and Accountability Act of 1996. |
12
We believe we are operating our business in substantial compliance with all existing legal requirements material to the operation of our business. There are, however, significant uncertainties regarding the application of many of these legal requirements to our business, and there cannot be any assurance that a regulatory agency charged with enforcement of any of these laws or regulations will not interpret them differently or, if there is an enforcement action, that our interpretation would prevail.
If the Company fails to comply with the requirements of HIPAA, it could face sanctions and penalties.
HIPAA provides safeguards to ensure the integrity and confidentiality of health information. Violation of the standards is punishable by fines and, in the case of wrongful disclosure of individually identifiable health information, fines or imprisonment, or both. Although we intend to comply with all applicable laws and regulations regarding medical information privacy, failure to do so could have an adverse effect on our business.
Limited barriers to entry into the ancillary healthcare services market could result in greater competition.
There are limited barriers to entering our market, meaning that it is relatively easy for other companies to replicate our business model and provide the same or similar services that we currently provide. Major benefit management companies and healthcare companies not presently offering ancillary healthcare services may decide to enter the market. These companies may have greater financial, marketing and other resources than are available to us. Competition from other companies may have a material adverse effect on our financial condition and results of operations.
The Company may be unsuccessful in hiring and retaining skilled employees.
The future growth of our business depends on our ability to hire and retain skilled employees. The Company may be unable to hire and retain the skilled employees needed to succeed in our business. Qualified employees are in great demand throughout the healthcare industry. Our failure to attract and retain sufficient skilled employees may limit the rate at which our business can grow, which will result in harm to our financial performance.
An inability to adequately protect our intellectual property could harm the Company’s competitive position.
We consider our methodologies, processes and know-how to be proprietary. We seek to protect our proprietary information through confidentiality agreements with our employees, as well as our clients and contracted service providers. The Company’s policy is to have its employees enter into a confidentiality agreement at the time employment begins, with the confidentiality agreement containing provisions prohibiting the employee from disclosing our confidential information to anyone outside of the Company, requiring the employee to acknowledge, and, if requested, assist in confirming the Company’s ownership of new ideas, developments, discoveries or inventions conceived by the employee during his or her employment with the Company, and requiring the assignment by the employee to the Company of proprietary rights to such matters that are related to our business. There can be no assurance that the steps taken by the Company to protect its intellectual property will be successful. If the Company does not adequately protect its intellectual property, its competitors may be able to use its technologies and erode or negate the Company’s competitive advantage in the market.
Fluctuations in the number and types of claims processed by the Company could make it more difficult to predict the Company’s net revenues from quarter to quarter.
Monthly fluctuations in the number of claims we process and the types of claims we process will impact the quarterly and annual results of the Company. Our margins vary depending on the type of ancillary healthcare service provided, the rates associated with those services and the overall mix of these claims, each of which will impact our profitability. Consequently, it may be difficult to predict our net revenue from one quarter to another quarter.
13
Future sales of the Company’s Common Stock, or the perception that these sales may occur, could depress the price of the Company’s Common Stock.
Sales of substantial amounts of our Common Stock, or the perception in the public that such sales may occur, could cause the market price of the Company’s Common Stock to decline. This could also impair the Company’s ability to raise additional capital through the sale of equity securities. As of March 14, 2011, the Company had 16,922,042 shares of its Common Stock outstanding. The outstanding shares are either freely tradable without restriction or further registration under the Securities Act, unless the shares are held by one of our “affiliates” as such term is defined in Rule 144 of the Securities Act, or are “restricted shares” as that term is defined under the Securities Act, and may be sold from time to time pursuant to a registration statement which was declared effective on February 8, 2007 by the Securities and Exchange Commission (the “SEC”), or in reliance upon an exemption from registration available under the Securities Act. At March 14, 2011, warrants to purchase 225,000 shares of Common Stock of the Company were outstanding, and options to purchase 2,603,167 shares of Common Stock of the Company had been granted and were outstanding under the Company’s Amended and Restated 2005 Stock Option Plan and the 2009 Equity Incentive Plan. At March 14, 2011, restricted stock units (“RSUs”) relating to 85,873 shares of common stock were outstanding under our 2009 Equity Incentive Plan. In addition, an aggregate of 1,499,113 shares of the Common Stock of the Company remain available for future grants of RSUs and options to purchase shares of the Common Stock of the Company under the Company’s Amended and Restated 2005 Stock Option Plan and the 2009 Equity Incentive Plan. If all of the outstanding warrants are exercised, all options available under the Company’s Amended and Restated 2005 Stock Option Plan are issued and exercised and all RSUs are converted, there will be approximately 21,335,195 shares of Common Stock of the Company outstanding.
Some of our existing stockholders can exert control over us and may not make decisions that further the best interests of all stockholders.
As of March 14, 2011, our officers, directors and principal stockholders (greater than 5% stockholders) together control beneficially approximately 46.0% of the outstanding Common Stock of the Company. As a result, these stockholders, if they act individually or together, may exert a significant degree of influence over our management and affairs and over matters requiring stockholder approval, including the election of directors and approval of significant corporate transactions. Furthermore, the interests of this concentration of ownership may not always coincide with our interests or the interests of other stockholders and, accordingly, they could cause us to enter into transactions or agreements which we would not otherwise consider. In addition, this concentration of ownership of the Company’s Common Stock may delay or prevent a merger or acquisition resulting in a change in control of the Company and might affect the market price of our Common Stock, even when such a change in control may be in the best interest of all of our stockholders.
We are subject to the listing requirements of the Nasdaq Capital Market and there can be no assurances that we will continue to satisfy these listing requirements.
Our common stock is listed on The NASDAQ Capital Market, and we are therefore subject to continued listing requirements, including requirements with respect to the market value of publicly-held shares and minimum bid price per share, among others, and requirements relating to board and audit committee independence. If we fail to satisfy one or more of the requirements, we may be delisted from The NASDAQ Capital Market. If we are delisted from The NASDAQ Capital Market and we are not able to list our common stock on another exchange, our common stock could be quoted on the OTC Bulletin Board or on the “pink sheets”. As a result, we could face significant adverse consequences including, among others, a limited availability of market quotations for our securities and a decreased ability to issue additional securities or obtain additional financing in the future.
Item 2. Properties.
The Company occupies a total of 16,449 square feet of office space, all of which is leased. The leased space comprises our principal executive offices, which is located at 5429 Lyndon B. Johnson Freeway, Suite 850, Dallas, TX 75240, pursuant to a lease that expires on March 31, 2013. Included in the 16,449 square feet are 7,100 square feet of space added to our original lease by means of an amendment to the lease executed in February 2009. The Company does not own or lease any other real property and believes its offices are suitable to meet its current needs.
Item 3. Legal Proceedings.
None.
Item 4. Reserved.
14
PART II
Item 5. Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities.
Market Information
The Company’s Common Stock has traded on The NASDAQ Capital Market (“NASDAQ”) under the symbol ANCI since September 29, 2008. Between October 19, 2006 and September 26, 2008, our stock traded on the American Stock Exchange (“Amex”) under the symbol XSI and between December 28, 2005 and October 19, 2006, public trading of our Common Stock occurred on the OTC Bulletin Board.
The following table sets forth, for the fiscal periods indicated, the range of the high and low sales prices for our Common Stock on NASDAQ from January 1, 2009 through December 31, 2010.
High | Low | |||||
2010 | ||||||
Fourth Quarter Ended December 31 | $ | 1.62 | $ | 1.30 | ||
Third Quarter Ended September 30 | 1.69 | 1.31 | ||||
Second Quarter Ended June 30 | 2.20 | 1.55 | ||||
First Quarter Ended March 31 | 2.91 | 1.46 | ||||
2009 | ||||||
Fourth Quarter Ended December 31 | $ | 4.49 | $ | 1.95 | ||
Third Quarter Ended September 30 | 4.73 | 3.57 | ||||
Second Quarter Ended June 30 | 8.74 | 3.50 | ||||
First Quarter Ended March 31 | 8.18 | 6.40 | ||||
The closing price on NASDAQ for our Common Stock on March 14, 2011 was $1.70.
Holders
As of March 14, 2011, in accordance with the records of our transfer agent, there were 137 record holders of ACS Common Stock. The number of record holders is based on the actual number of holders registered on the books of our transfer agent and does not reflect holders of shares in “street name” or persons, partnerships, associations, corporations or other entities identified in security position listings maintained by depository trust companies.
Dividends
We have not declared cash dividends on our Common Stock. We intend to retain all earnings to finance future growth and do not anticipate that we will pay cash dividends for the foreseeable future.
Securities Authorized for Issuance Under Equity Compensation Plans
The information required to be disclosed herein is incorporated by reference to "Item 12. Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters."
Repurchases of Securities
There were no repurchases of the Common Stock of the Company by or on behalf of the Company or any affiliated purchasers during the fourth quarter of the Company’s fiscal year ended December 31, 2010.
15
Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations.
The following discussion should be read in conjunction with our consolidated financial statements, which present our results of operations for the twelve month periods ended December 31, 2010 and 2009 as well as our financial position at December 31, 2010 and 2009, contained elsewhere in this Annual Report on Form 10-K. Some of the information contained in this discussion and analysis or set forth elsewhere in this Annual Report on Form 10-K, including information with respect to our plans and strategy for our business, includes forward-looking statements that involve risks and uncertainties. You should review the “Special Note Regarding Forward Looking Statements” and “Risk Factors” sections of this Annual Report for a discussion of important factors that could cause actual results to differ materially from the results described in or implied by the forward-looking statements contained in the following discussion and analysis.
Overview
American CareSource Holdings, Inc. (“ACS,” “Company,” the “Registrant,” “we,” “us,” or “our”) is an ancillary services company that offers cost effective access to a comprehensive national network of ancillary healthcare service providers. The Company sells its services to a number of healthcare companies including preferred provider organizations ("PPOs"), third party administrators (“TPAs”), insurance companies, large self-funded organizations and various employee groups. The Company offers payors this solution by:
• | lowering its payors’ ancillary care costs throughout our network of high quality, cost effective providers that the Company has under contract at more favorable terms than they could generally obtain on their own; |
• | providing payors with a comprehensive network of ancillary healthcare services providers that is tailored to each payor’s specific needs and is available to each payor’s covered persons for covered services; |
• | providing payors with claims management, reporting and processing and payment services; |
• | performing network/needs analysis to assess the benefits to payors of adding additional/different service providers to the payor -specific provider networks; and |
• | credentialing network service providers for inclusion in the payor -specific provider networks. |
The Company’s business model, illustrating the relationships among the persons involved, directly or indirectly, in the Company’s business and its generation of revenue and expenses is depicted below:
16
Payors route healthcare claims to us after service has been performed by participant providers in our network. We process those claims and charge the payor according to its contractual rate for the services according to our contract with the payor. In processing the claim, we are paid directly by the payor or the insurer for the service. We then pay the provider of service according to its independently-negotiated contractual rate. We assume the risk of generating positive margin, the difference between the payment we receive for the service and the amount we are obligated to pay the provider of service.
The Company recognizes revenues for ancillary healthcare services when services by providers have been authorized and performed, the claim has been billed to the payor and collections from payors are reasonably assured. Cost of revenues for ancillary healthcare services consist of amounts due to providers for providing ancillary health care services, client administration fees paid to our client payors to reimburse them for routing the claims to us for processing, and the Company’s related direct labor and overhead of processing invoices, collections and payments. The Company is not liable for costs incurred by independent contract service providers until payment is received by it from the payors. The Company recognizes actual or estimated liabilities to independent contract service providers as the related revenues are recognized.
During 2010, we added thirteen new clients, which generated revenue of $5.9 million. 2010 was the second consecutive strong year in terms of sales as we generated $6.0 million from new clients in 2009. Despite the new clients, our overall net revenue was down 10% as compared to 2009 directly related to the continued declines in our two largest clients, both of which are PPOs. The Company is seeking growth in the number of client payors and service provider relationships it secures by focusing on providing in-network services for its payors and aggressively pursuing additional TPAs and other direct payors as its primary sales targets. The Company believes this strategy should increase the volume of claims the Company can process in addition to the expansion in the number of lives that are eligible to receive ancillary health care benefits. No assurances can be given that the Company can expand its service provider or payor relationships, nor that any such expansion will result in an improvement in the results of operations of the Company.
In addition, under the MLR regulations included in the Affordable Care Act, it is possible that a portion of the fees our existing and prospective payors are contractually required to pay us and that do not qualify as 'incurred claims' may not be included as expenditures for activities that improve health care quality. Such a determination may make it more difficult for us to retain existing clients and/or add new clients, because our clients' or prospective clients' MLR may otherwise not meet the specified targets. This may reduce our net revenues and profit margins..
Year Ended December 31, 2010 Compared to Year Ended December 31, 2009
Net Revenues
The Company’s net revenues are generated from ancillary healthcare service claims. Revenue is recognized when we bill our client payors for services performed and collection is reasonably assured. The Company estimates revenues using average historical collection rates. Periodically, revenues are adjusted to reflect actual cash collections so that revenues recognized accurately reflect cash collected.
The following table sets forth a comparison of our net revenues for the following years ended December 31:
Change | ||||||||||||||
($ in thousands) | 2010 | 2009 | $ | % | ||||||||||
Net Revenues | $ | 61,201 | $ | 68,226 | (7,025 | ) | (10 | )% | ||||||
The decrease in net revenue for the year ended December 31, 2010 as compared to 2009 was due primarily to a 18% and 37% decline in billed claims volume from our two significant clients, respectively.
Overall claims volume declined due to the following factors:
• | Loss of covered lives and payor groups due to the declining US economy, reduction in jobs and macroeconomic factors; |
• | Stronger presence of larger carriers in the market; |
• | Loss of key relationship with a national laboratory services provider in the third quarter of 2009; |
• | Loss of key relationship with a national laboratory services provider in the second quarter of 2010; and |
• | Transition status of one of our key accounts related to a business combination. |
17
The drop in claims volume resulted in a net $12.0 million, or 21%, decline in net revenues from our two significant clients. The decline was partially offset by the following:
• | $5.9 million of revenue generated from thirteen new clients implemented in 2010 (we refer to this revenue as incremental revenue); and |
• | A movement in the mix of provider specialties that generate revenue away from lower revenue-per-claim services, partially as a result of losing two key laboratory service providers discussed above. |
Net revenues from legacy accounts (i.e., accounts not added during 2010) declined $12.3 million, or 18%. The following tables detail the change in client accounts for the periods presented:
Net Revenue | Billed Claims Volume | |||||||||||||||||||||||||
Change | Change | |||||||||||||||||||||||||
(in thousands) | 2010 | 2009 | $ | % | 2010 | 2009 | Claims | % | ||||||||||||||||||
Client A | $ | 29,587 | $ | 32,454 | $ | (2,867 | ) | (9 | )% | 124 | 151 | (27 | ) | (18 | )% | |||||||||||
Client B | 16,715 | 25,897 | (9,182 | ) | (35 | ) | 91 | 144 | (53 | ) | (37 | ) | ||||||||||||||
Other clients | 9,695 | 9,960 | (265 | ) | (3 | ) | 86 | 78 | 8 | 10 | ||||||||||||||||
Clients implemented in 2010 | 5,899 | — | 5,899 | nm | 28 | — | 28 | nm | ||||||||||||||||||
Provision for refunds | (695 | ) | (85 | ) | (610 | ) | nm | — | — | — | nm | |||||||||||||||
Total | $ | 61,201 | $ | 68,226 | $ | (7,025 | ) | (10 | )% | 329 | 373 | (44 | ) | (12 | )% | |||||||||||
We attempt to enhance our existing client relationships through focused efforts to recruit and add ancillary service providers that will be more attractive to our clients’ base of lives and secure greater cost savings for our clients, and through programs to educate our client payors so that they may fully utilize our network.
The Company is seeking growth from increasing its number of client payor and service provider relationships by focusing on providing in-network services for its payors and aggressively pursuing middle-market insurance companies, TPAs and direct payors. The Company continues to derive a significant amount of its net revenues from its traditional PPO relationships, but we have shifted our focus and we now aggressively target TPAs and direct payors, which have accounted for a significant portion of the $5.9 million of incremental revenue in 2010. Despite the growth from new clients, we continue to see revenue declines from our two most significant clients, both of which are PPOs. Revenue from the two clients declined 9% and 35% compared to the prior year. While our new client additions in 2010 have offset some of these declines, we cannot be certain that net revenue and operating income will not continue to decline further as a result of the loss of business from our two largest clients.
The following table provides information with respect to claims processed, claims billed and the associated net revenue per claim metrics for the years ended December 31. Net revenue per claim can vary significantly depending upon factors including the types of services provided to clients’ members, the quantity of services delivered, client negotiated pricing, provider negotiated service rates, the rate of collections (which in turn depends on the client's/covered person's financial responsibility), and other factors.
2010 | 2009 | ||||||
Claims processed (in thousands) | 421 | 437 | |||||
Claims billed (in thousands) | 329 | 373 | |||||
Net revenue per billed claim | $ | 186 | $ | 183 | |||
Periodically, we pay refunds to our payors. Refunds are paid to payors for overpayments on claims, claims paid in error, and claims paid for non-covered services. Our provision for refunds is estimated based on historical data and is presented as an offset to revenue. The provision for the year ended December 31, 2010 was approximately $695,000 compared to approximately $85,000 for the year ended December 31, 2009, primarily due to refunds paid related to dialysis services and infusion services claims that had an impact of approximately $200,000. We have no direct control over the circumstances creating the need for such refunds, but we attempt to minimize our exposure through our internal processes and procedures. One such procedure is recouping amounts paid to ancillary service providers on such claims.
18
Cost of Revenues and Contribution Margin
Cost of revenues is comprised of payments to our providers, administrative fees paid to our payors for converting claims to electronic data interchange and routing them to both the Company for processing and to their payors for payment, and the fixed costs of our claims administration and ancillary service provider development organizations. Payments to providers is the largest component of our cost of revenues and it consists of our payments for ancillary care services in accordance with contracts negotiated separately with providers for specific ancillary services.
The following table sets forth a comparison of the key components of our cost of revenues, for the years ended December 31:
Change | |||||||||||||||||||||
($ in thousands) | 2010 | % of revenue | 2009 | % of revenue | $ | % | |||||||||||||||
Provider payments | $ | 45,789 | 74.8 | % | $ | 51,150 | 75.0 | % | $ | (5,361 | ) | (10 | )% | ||||||||
Administrative fees | 3,317 | 5.4 | 3,552 | 5.2 | (235 | ) | (7 | ) | |||||||||||||
Claims administration and provider development | 4,645 | 7.6 | 4,252 | 6.2 | 393 | 9 | |||||||||||||||
Total cost of revenues | $ | 53,751 | 87.8 | % | $ | 58,954 | 86.4 | % | $ | (5,203 | ) | (9 | )% | ||||||||
Provider payments. The 10% decrease in provider payments is consistent with the decline in net revenue, primarily related to our two significant clients. Provider payments as a percent of net revenues have remained consistent at 74.8% in 2010 compared to 75.0% in 2009.
Administrative fees. Administrative fees paid to clients as a percent of net revenues has increased slightly to 5.4% in 2010 compared to 5.2% in 2009.
Claims administration and provider development. Our claims administration organization consists of our operations and information technology groups. Our operations group is responsible for all aspects of the claims management and processing including billing, quality assurance and collections efforts. Our information technology group is responsible for maintaining and enhancing the technological capabilities and applications with the claims management process. Our provider development group is responsible for developing our network of ancillary healthcare service providers, which includes contracting with providers to be included in the network, credentialing new service providers and maintaining a relationship with existing providers, all for the purpose of enhancing our ancillary service provider network offering to our client payors.
The following table details the costs within the claims administration and provider development groups for the periods presented:
Claims Administration | Provider Development | Total | ||||||||||||||||||||||||||||||||||||||||||
Increase | Increase | Increase | ||||||||||||||||||||||||||||||||||||||||||
($ in thousands) | 2010 | 2009 | (Decrease) | 2010 | 2009 | (Decrease) | 2010 | 2009 | (Decrease) | |||||||||||||||||||||||||||||||||||
Total wages, incentives and benefits | $ | 2,722 | $ | 2,301 | $ | 421 | 18 | % | $ | 1,331 | $ | 1,384 | $ | (53 | ) | (4 | )% | $ | 4,053 | $ | 3,685 | $ | 368 | 10 | % | |||||||||||||||||||
Other | 126 | 29 | 97 | nm | 466 | 538 | (72 | ) | (13 | ) | 592 | 567 | 25 | 4 | ||||||||||||||||||||||||||||||
$ | 2,848 | $ | 2,330 | $ | 518 | 22 | % | $ | 1,797 | $ | 1,922 | $ | (125 | ) | (7 | )% | $ | 4,645 | $ | 4,252 | $ | 393 | 9 | % | ||||||||||||||||||||
The increase in costs during 2010 as compared to the prior year is due primarily to the expansion of our claims administration group, particularly with respect to information technology function. Wages, incentives and benefits increased as a result of the resource additions in claims administration. The increases in headcount were made to increase our information technology staff, which maintains and enhances our internal claims processing systems. Such enhancements are primarily focused on providing increased functionality, efficiencies, and accuracy within the claims processing function.
Contribution margin is calculated by dividing the difference between net revenues and total costs of revenues by net revenues. The following table sets forth a comparison of contribution margin percentage for the periods ended December 31:
2010 | 2009 | Percent Change | |||||||
Contribution margin | 12.2 | % | 13.6 | % | (1.4 | )% | |||
19
Contribution margin in 2010 was negatively impacted by an increase in claims administration and provider development costs, as a percentage of net revenue, of 1.4%. Costs related to our claims administration group increased primarily due to investment in Information Technology resources, which were utilized to maintain and enhance our internal claims processing systems. Our contribution margin percentage fluctuates over time due to changes in the prices we charge our client payors as compared to the financial terms of our provider agreements, changes in costs of claims administration and provider development, and changes in the mix of services we provide. There can be no assurances that we will be able to maintain contribution margin at current levels, either in absolute or in percentage terms.
Selling, General and Administrative Expenses
Selling, general and administrative (“SG&A”) expenses consist primarily of salaries and related benefits, travel costs, sales commissions, sales materials, other marketing related expenses, costs of corporate operations, finance and accounting, human resources and other general operating expenses of the Company. The following table sets forth a comparison of our SG&A expenses for the periods presented ending December 31:
Change | |||||||||||
($ in thousands) | 2010 | 2009 | $ | % | |||||||
Selling, general and administrative expenses | 6,190 | 7,376 | (1,186 | ) | (16 | )% | |||||
Percentage of total net revenues | 10.1 | % | 10.8 | % | |||||||
The components of SG&A expenses are as follows for the periods presented ending December 31:
Finance & Administration | Sales & Marketing | Total | |||||||||||||||||||||||||||||||||
($ in thousands) | 2010 | 2009 | Increase (Decrease) | 2010 | 2009 | Increase (Decrease) | 2010 | 2009 | Increase (Decrease) | ||||||||||||||||||||||||||
Total wages, commissions, incentives and benefits | $ | 1,327 | $ | 1,461 | $ | (134 | ) | (9 | )% | $ | 879 | $ | 1,540 | $ | (661 | ) | (43 | )% | $ | 2,206 | $ | 3,001 | $ | (795 | ) | (26 | )% | ||||||||
Professional fees (legal, accounting and consulting) | 916 | 942 | (26 | ) | (3 | ) | 215 | 187 | 28 | 15 | 1,131 | 1,129 | 2 | — | |||||||||||||||||||||
Stock-based compensation expense | 696 | 1,221 | (525 | ) | (43 | ) | — | — | — | — | 696 | 1,221 | (525 | ) | (43 | ) | |||||||||||||||||||
Other | 845 | 916 | (71 | ) | (8 | ) | 146 | 122 | 24 | 20 | 991 | 1,038 | (47 | ) | (5 | ) | |||||||||||||||||||
Allocation of shared overheads | 775 | 530 | 245 | 46 | 248 | 217 | 31 | 14 | 1,023 | 747 | 276 | 37 | |||||||||||||||||||||||
Restructuring charge | — | — | — | — | — | — | — | — | 143 | 240 | (97 | ) | (40 | ) | |||||||||||||||||||||
Total selling, general and administrative expenses | $ | 4,559 | $ | 5,070 | $ | (511 | ) | (10 | )% | $ | 1,488 | $ | 2,066 | $ | (578 | ) | (28 | )% | $ | 6,190 | $ | 7,376 | $ | (1,186 | ) | (16 | )% | ||||||||
SG&A expenses include approximately $143,000 of severance costs related to the departure of our former Chief Financial Officer in March 2010. For the year ended December 31, 2009, SG&A expenses include approximately $240,000 of severance costs related to the departure of our Vice President of Client Development. Excluding those costs, SG&A expenses were approximately $6.0 million and $7.1 million respectively, with 2010 expenses representing a 15% decline compared to the prior year. In addition, excluding the severance charges, SG&A expenses were 9.9% of net revenue for the year ended December 31, 2010 compared to 10.5% of net revenue for the year ended December 31, 2009.
Disregarding the effect of the severance charges described in the preceding paragraph, the decrease in SG&A compared to the prior year is primarily due to the following:
• | Salaries, wages and benefits decreased approximately $795,000 due primarily to the departures of our former Senior Vice President of Sales and Marketing and former Chief Financial Officer during the first quarter of 2010. Also, effective July 31, 2009, we made organizational changes, which included the reorganization of our sales and marketing and client development groups and which had the effect of reducing overall salaries, wages and benefits in 2010. In addition, charges related to our performance-based incentive plan, which is based on our operating results, declined by 71%; and |
• | A reduction in our stock-based compensation expense of approximately $525,000 related mainly to the forfeiture of non-vested equity incentive awards that had been awarded to our former Chairman of the Board of Directors, our former Chief Financial Officer, and our former Senior Vice President of Sales and Marketing. |
20
Depreciation and Amortization
The following table sets forth a comparison of depreciation and amortization for the periods ended December 31:
Change | ||||||||||||||
($ in thousands) | 2010 | 2009 | $ | % | ||||||||||
Depreciation | $ | 639 | $ | 435 | $ | 204 | 47 | % | ||||||
Amortization | 128 | 128 | — | — | ||||||||||
Total Depreciation and Amortization | $ | 767 | $ | 563 | $ | 204 | 36 | % | ||||||
Amortization of intangibles consists of $128,000 in amortization of the capitalized value of provider contracts that were acquired in the 2003 acquisition of the assets of our predecessor, American CareSource Corporation by Patient Infosystems (now CareGuide, Inc.), our former parent corporation. The provider contracts are being amortized using the straight-line method over their expected useful lives of 15 years.
The increase in depreciation expense is a direct result of an increase in capital expenditures over the past three years related mainly to software development that is being expensed over a five year period. A significant portion of our expenditures in 2010 related to the continued development of our technology infrastructure.
Other Income
The following table sets forth a comparison of the components of other income for the periods ended December 31:
Change | ||||||||||||||
($ in thousands) | 2010 | 2009 | $ | % | ||||||||||
Interest income | $ | 86 | $ | 130 | $ | (44 | ) | (34 | )% | |||||
Unrealized gain on warrant derivative | 18 | 324 | (306 | ) | (94 | ) | ||||||||
Total other income | $ | 104 | $ | 454 | $ | (350 | ) | (77 | )% | |||||
As of December 31, 2009, we had unrealized gains of approximately $324,000, related to warrants accounted for under the liability method. We use a two-step process for evaluating whether our equity-linked financial instruments or embedded features are indexed to our own stock. Warrants to purchase 109,095 shares of common stock issued by the Company contain a strike price adjustment feature, which results in the instruments no longer being considered indexed to the Company’s own stock and required the Company to record these warrants under the liability accounting method. Accordingly, on January 1, 2009, we adopted current accounting guidance that changed the current classification (from equity to liability) and the related accounting for these warrants. As of that date, we reclassified the warrants, based on a fair value of $3.43 per warrant, as calculated using the Black–Scholes–Merton valuation model. No liability related to the stock warrants is included as a warrant derivative liability in our consolidated balance sheet as of December 31, 2010 due to the short remaining life of the stock warrants and an exercise price of $5.50. The valuation of the stock warrants is discussed further in Item 15, Exhibits and Financial Statement Schedules, Note 11. The unrealized gain on the warrant derivative reflects the change in fair value of the warrants.
Income Tax Provision
For the year ended December 31, 2010, we recorded an income tax provision of approximately $111,000, while for the year ended December 31, 2009, we recorded an income tax benefit of approximately $533,000.
Liquidity and Capital Resources
As of December 31, 2010, the Company had a working capital surplus of $12.6 million compared to $11.1 million at December 31, 2009. In addition, our cash and cash equivalents balance increased to $14.5 million as of December 31, 2010 compared to $11.9 million at December 31, 2009. The increase is primarily the result of net cash provided by operating activities of approximately $3.2 million. That increase was offset by capital expenditures of approximately $702,000 during 2010.
21
During 2010, operating activities provided net cash of approximately $3.2 million, the primary components of which were net income of approximately $486,000, adjusted for non-cash charges of share-based compensation expense of approximately $871,000, depreciation and amortization of approximately $767,000, a unrealized gain on our warrant derivative of approximately $18,000, amortization of the amendment of our client agreement with one of our significant clients of approximately $250,000, amortization of the warrant costs of approximately $200,000, a deferred income tax provision of approximately $47,000, as well as, a net cash inflow from operating assets and liabilities of approximately $586,000. The net cash inflow from operating assets and liabilities was primarily due to the timing of payments made to us by our clients and the timing of provider payments made related to cash received from claims prior to December 31, 2010.
Investing activities during 2010 were comprised of investments in software development costs of approximately $402,000 and in property and equipment of approximately $300,000. The software development costs relate primarily to enhancements of our internal billing system, while the increase in property and equipment relates primarily to investments in computer equipment.
Financing activities during 2010 generated cash of approximately $157,000 related to the cash exercise of Series B warrants to purchase approximately 320,000 shares of common stock. The exercise price of the warrants was $0.49 per share.
Historically, we have relied on external sources of capital, including indebtedness or issuance of equity securities, and during the past three years, earnings, to fund our operations. We believe our current cash balance of $14.5 million as of December 31, 2010 and expected future cash flows from operations will be sufficient to meet our anticipated cash needs for working capital, capital expenditures and other activities through at least the next twelve months. If operating cash flows are not sufficient to meet our needs, we believe that credit or access to capital through issuance of equity would be available to us. However, as a result of the tightening in the credit markets, low level of liquidity in many financial markets and extreme volatility in fixed income, credit, currency and equity markets, there cannot be assurances that, if necessary, we would be successful in obtaining sufficient capital financing on commercially reasonable terms or at all. We do not have any lines of credit, credit facilities or outstanding bank indebtedness as of December 31, 2010.
Inflation
Inflation did not have a significant impact on the Company’s costs during the years ended December 31, 2010 and December 31, 2009, respectively. The Company continues to monitor the impact of inflation in order to minimize its effects through pricing strategies, productivity improvements and cost reductions.
Off-Balance Sheet Arrangements
The Company did not have any off-balance sheet arrangements at December 31, 2010 or December 31, 2009 or for the periods then ended.
Critical Accounting Policies
Critical accounting policies are those that require application of management’s most difficult, subjective or complex judgments, often as a result of the need to make estimates about the effect of matters that are inherently uncertain and may change in subsequent periods.
The Company’s significant accounting policies are described in the Notes to the Consolidated Financial Statements located elsewhere in this Annual Report on Form 10-K. Not all of these significant accounting policies require management to make difficult, subjective or complex judgments or estimates. However, the following accounting policies are deemed to be critical by our management:
Intangible Assets.
Intangible assets consist of provider contracts and internally developed claims payment and billing software. The software has been fully amortized using the straight-line method over its expected useful life of 5 years. The provider contracts are being amortized using the straight-line method over its expected useful life of 15 years. Our experience to date is that we have approximately 2-4% annual turnover or attrition of provider contracts. The provider contracts are being accounted for on a pooled basis and the actual cancellation rates of provider contracts that were acquired will be monitored for potential impairment or amortization adjustment, if warranted. As of December 31, 2010, there is no impairment of this intangible asset. The cost of adding additional providers is considered an ongoing operating expense.
22
Revenue recognition.
The Company recognizes revenue on the services that it provides, which includes (i) providing payor clients with a comprehensive network of ancillary healthcare providers, (ii) providing claims management, reporting, processing and payment services, (iii) providing network/need analysis to assess the benefits to payor clients of adding what additional/different service providers to the client-specific provider networks and (iv) providing credentialing of network services providers for inclusion in the client payor-specific provider networks. Revenue is recognized when services are delivered, which occurs after processed claims are billed to the client payors and collections are reasonably assured. The Company estimates revenues and costs of revenues using average historical collection rates and average historical margins earned on claims. Periodically, revenues are adjusted to reflect actual cash collections so that revenues recognized accurately reflect cash collected.
The Company determines whether it is acting as a principal or agent in the fulfillment of the services rendered. After careful evaluation of the key gross and net revenue recognition indicators, the Company acknowledges that while the determination of gross versus net reporting is highly judgmental in nature, the Company has concluded that its circumstances are most consistent with those key indicators that support gross revenue reporting.
Following are the key indicators that support the Company’s conclusion that it acts as a principal when settling claims for service providers through its contracted service provider network:
• | The Company is the primary obligor in the arrangement. The Company has assessed its role as primary obligor as a strong indicator of gross reporting. The Company believes that it is the primary obligor in its transactions because it is responsible for providing the services desired by its client payors. The Company has distinct, separately negotiated contractual relationships with its client payors and with the ancillary health care providers in its networks. The Company does not negotiate “on behalf of” its client payors and does not hold itself out as the agent of the client payors when negotiating the terms of the Company’s ancillary healthcare service provider agreements. The Company’s agreements contractually prohibit client payors and service providers to enter into direct contractual relationships with one another. The client payors have no control over the terms of the Company’s agreements with the service providers. In executing transactions, the Company assumes key performance-related risks. The client payors hold the Company responsible for fulfillment, as the provider, of all of the services the client payors are entitled to under their contracts; client payors do not look to the service providers for fulfillment. In addition, the Company bears the pricing/margin risk as the principal in the transactions. Because the contracts with the client payors and service providers are separately negotiated, the Company has complete discretion in negotiating both the prices it charges its client payors and the financial terms of its agreements with the service providers. Since the Company’s profit is the spread between the amounts received from the client payors and the amount paid to the service providers, it bears significant pricing/margin risk. There is no guaranteed mark-up payable to the Company on the amount the Company has contracted. Thus, the Company bears the risk that amounts paid to the service provider will be greater than the amounts received from the client payors, resulting in a loss or negative claim. |
• | The Company has latitude in establishing pricing. As stated above, the Company has complete latitude in negotiating the price to be paid to the Company by each client payor and the price to be paid to each contracted service provider. This type of pricing latitude indicates that the Company has the risks and rewards normally attributed to a principal in the transactions. |
• | The Company changes the product or performs part of the services. The Company provides the benefits associated with the relationships it builds with the client payors and the services providers. While the parties could deal with each other directly, the client payors would not have the benefit of the Company’s experience and expertise in assembling a comprehensive network of service providers, in claims management, reporting and processing and payment services, in performing network/needs analysis to assess the benefits to client payors of adding additional/different service providers to the client payor-specific provider networks, and in credentialing network service providers. |
• | The Company has complete discretion in supplier selection. One of the key factors considered by client payors who engage the Company is to have the Company undertake the responsibility for identifying, qualifying, contracting with and managing the relationships with the ancillary healthcare service providers. As part of the contractual arrangement between the Company and its client payors, the payors identify their obligations to their respective covered persons and then work with the Company to determine the types of ancillary healthcare services required in order for the payors to meet their obligations. The Company may select the providers and contract with them to provide services at its discretion. |
23
• | The Company is involved in the determination of product or service specifications. The Company works with its client payors to determine the types of ancillary healthcare services required in order for the payors to meet their obligations to their respective covered persons. In some respects, the Company is customizing the product through its efforts and ability to assemble a comprehensive network of providers for its payors that is tailored to each payor’s specific needs. In addition, as part of its claims processing and payment services, the Company works with the client payors, on the one hand, and the providers, on the other, to set claims review, management and payment specifications. |
• | The supplier (and not the Company) has credit risk. The Company believes it has some level of credit risk, but that risk is mitigated because the Company does not remit payment to providers unless and until it has received payment from the relevant client payors following the Company’s processing of a claim. |
• | The amount that the Company earns is not fixed. The Company does not earn a fixed amount per transaction nor does it realize a per-person per-month charge for its services. |
The Company has evaluated the other indicators of gross and net revenue recognition, including whether or not the Company has general inventory risk. The Company does not have any general inventory risk, as its business is not related to the manufacture, purchase or delivery of goods and it does not purchase in advance any of the services to be provided by the ancillary healthcare service providers. While the absence of this risk would be one indicator in support of net revenue reporting, as described in detail above, the Company has carefully evaluated all of the key gross and net revenue recognition indicators and has concluded that its circumstances are most consistent with those key indicators that support gross revenue reporting.
The Company records a provision for refunds on a periodic basis. Refunds are paid to payors for overpayments on claims, claims paid in error, and claims paid for non-covered services. In some instances, we will recoup payment made to the ancillary service provider if the claim has been fully resolved. An evaluation is performed periodically and is based on historical data. We present revenue net of the provision for refunds on the consolidated income statement.
Pending Accounting Pronouncements
None.
Item 8. Financial Statement and Supplementary Data.
The Company’s financial statement and supplementary data required to be filed pursuant to this Item 8 are located at the end of this Annual Report on Form 10-K, beginning on page F-1.
Item 9. Changes in and Disagreements with Accountants on Accounting and Financial Disclosure.
None.
Item 9A. Controls and Procedures.
Evaluation of Disclosure Controls and Procedures
Our management, with the participation of our Chief Executive Officer and Chief Financial Officer, has evaluated the effectiveness of our disclosure controls and procedures as of December 31, 2010. Based upon this evaluation, our Chief Executive Officer and Chief Financial Officer concluded that our disclosure controls and procedures (as defined in Rules 13a-15(e) and 15(d)-15(e) under the Exchange Act) are effective to ensure that information required to the disclosed by us in reports we file or submit under the Exchange Act is recorded, processed, summarized and reported within the time periods specified in the SEC’s rules and forms, and is accumulated and communicated to our management, including our Chief Executive Officer and Chief Financial Officer, as appropriate to allow timely decisions regarding required disclosures.
24
Management’s Annual Report on Internal Control over Financial Reporting
The management of the Company is responsible for establishing and maintaining adequate internal control over financial reporting by the Company. “Internal control over financial reporting“ is defined in Rule 13a-15(f) and Rule 15d-15(f) under the Exchange Act, as amended, as a process designed by, or under the supervision of, the Company’s principal executive and principal financial officers, or persons performing similar functions, and effected by the Company’s Board of Directors, management and other personnel to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles and includes those policies and procedures that:
• | Pertain to the maintenance of records that in reasonable detail accurately and fairly reflect the transactions and dispositions of the assets of the Company; |
• | Provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the issuer are being made only in accordance with authorizations of management and directors of the Company; and |
• | Provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use or disposition of the Company’s assets that could have a material effect on the financial statements. |
Internal control over financial reporting has inherent limitations and may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risks that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Management assessed the effectiveness of the Company’s internal control over financial reporting as of December 31, 2010. In making this assessment, management used the criteria set forth by the Committee of Sponsoring Organizations of the Treadway Commission (COSO) in Internal Control – Integrated Framework. Management reviewed the results of its assessment with the Audit Committee of the Company’s Board of Directors. Based on this assessment, management believes that, as of December 31, 2010, the Company has maintained effective internal control over financial reporting.
This Annual Report does not include an attestation report of the Company’s registered public accounting firm regarding internal control over financial reporting. Management’s report was not subject to attestation by the Company’s registered public accounting firm pursuant to rules of the Securities and Exchange Commission that permit the Company to provide only management’s report in this Annual Report.
Changes in Internal Control over Financial Reporting
Our management, with the participation of our Chief Executive Officer and Chief Financial Officer, has concluded there were no changes in the Company’s internal controls over financial reporting (as defined in Rules 13a-15(f) and 15d-15(f) under the Exchange Act) that occurred during the Company's last fiscal quarter that have materially affected the Company’s internal controls over financial reporting or are reasonably likely to materially affect internal controls over financial reporting, including any corrective actions with regard to significant deficiencies and material weaknesses.
Item 9B. Other Information
Not applicable
25
PART III
Item 10. Directors, Executive Officers and Corporate Governance
The information required by this Item 10 is incorporated herein by reference to the applicable information contained in the definitive proxy statement for our annual meeting of stockholders to be held on or about May 23, 2011, which will be filed with the SEC pursuant to Regulation 14A not later than 120 days after the Company’s fiscal year ended December 31, 2010.
Item 11. Executive Compensation
The information required by this Item 11 is incorporated herein by reference to the applicable information contained in the definitive proxy statement for our annual meeting of stockholders to be held on or about May 23, 2011, which will be filed with the SEC pursuant to Regulation 14A not later than 120 days after the Company’s fiscal year ended December 31, 2010.
Item 12. Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters
The following table provides information with respect to the equity securities that are authorized for issuance under our equity compensation plans as of December 31, 2010:
Equity Compensation Plan Information at December 31, 2010 | |||||||
Plan Category | Number of securities to be issued upon exercise of outstanding options, warrants and rights (Column (a)) | Weighted-average exercise price of outstanding options, warrants and rights | Number of securities remaining available for future issuance under equity compensation plans, excluding securities reflected in column (a) | ||||
Equity compensation plans approved by security holders | 3,009,991 | $ | 2.25 | 1,502,813 | |||
Equity compensation plans not approved by security holders | — | — | — | ||||
Total | 3,009,991 | $ | 2.25 | 1,502,813 | |||
In addition, warrants to purchase 324,651 shares of Common Stock of the Company were issued and outstanding as of December 31, 2010, as shown in the table below. These warrants had been granted as part of compensation to the placement agent in connection with a March 2006 private placement of the Company’s Common Stock and to a client of the Company as partial compensation for services performed.
Shares of Common Stock issuable under outstanding warrants | Weighted-average exercise price of outstanding warrants | ||||
Series C (1) | 99,651 | $ | 5.50 | ||
Series D (2) | 225,000 | $ | 1.84 | ||
Total Warrants Outstanding | 324,651 | $ | 2.96 | ||
(1) | Service warrants were granted as part of the compensation to Laidlaw and Company in connection with the Company’s March 2006 private placement. |
(2) | These warrants were granted on May 21, 2007 to Corporate Health Plans of America, Inc., an affiliate of the Company’s client, Texas True Choice, Inc. (“Texas True Choice”), as partial compensation to Texas True Choice for services to be performed by it pursuant to an ancillary care services network access agreement between the Company and Texas True Choice. |
The other information required by this Item 12 is incorporated herein by reference to the applicable information contained in the definitive proxy statement for our annual meeting of stockholders to be held on or about May 23, 2011, which will be filed with the SEC pursuant to Regulation 14A not later than 120 days after the Company’s fiscal year ended December 31, 2010.
26
Item 13. Certain Relationships and Related Transactions, and Director Independence
The information required by this Item 13 is incorporated herein by reference to the applicable information contained in the definitive proxy statement for our annual meeting of stockholders to be held on or about May 23, 2011, which will be filed with the SEC pursuant to Regulation 14A not later than 120 days after the Company’s fiscal year ended December 31, 2010.
Item 14. Principal Accounting Fees and Services
The information required by this Item 14 is incorporated herein by reference to the applicable information contained in the definitive proxy statement for our annual meeting of stockholders to be held on or about May 23, 2011, which will be filed with the SEC pursuant to Regulation 14A not later than 120 days after the Company’s fiscal year ended December 31, 2010.
PART IV
Item 15. Exhibits and Financial Statement Schedules
(a) The following documents are filed as part of this Annual Report on Form 10-K:
(1) Financial Statements
The following financial statements are set forth in Item 8 hereof:
Document | Pages |
(2) Financial Statement Schedules
None.
(3) Exhibits
Reference is made to the Exhibit Index following this Annual Report on Form 10-K.
27
Report of Independent Registered Public Accounting Firm
To the Board of Directors and Stockholders
American CareSource Holdings, Inc.
We have audited the accompanying consolidated balance sheets of American CareSource Holdings, Inc. and subsidiary as of December 31, 2010 and 2009, and the related consolidated statements of income, stockholders’ equity, and cash flows for the years then ended. These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on these financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. The Company is not required to have, nor were we engaged to perform an audit of its internal control over financial reporting. Our audit included consideration of internal control over financial reporting as a basis for designing audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no such opinion. An audit also includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements, assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the financial position of American CareSource Holdings, Inc. and subsidiary as of December 31, 2010 and 2009, and the results of their operations and their cash flows for the years then ended, in conformity with U.S. generally accepted accounting principles.
/s/ McGladrey & Pullen, LLP
Des Moines, Iowa
March 18, 2011
F-1
AMERICAN CARESOURCE HOLDINGS, INC.
CONSOLIDATED STATEMENTS OF INCOME
For the years ended December 31
(amounts in thousands, except per share data)
2010 | 2009 | ||||||
Net revenues | $ | 61,201 | $ | 68,226 | |||
Cost of revenues: | |||||||
Provider payments | 45,789 | 51,150 | |||||
Administrative fees | 3,317 | 3,552 | |||||
Claims administration and provider development | 4,645 | 4,252 | |||||
Total cost of revenues | 53,751 | 58,954 | |||||
Contribution margin | 7,450 | 9,272 | |||||
Selling, general and administrative expenses | 6,190 | 7,376 | |||||
Depreciation and amortization | 767 | 563 | |||||
Total operating expenses | 6,957 | 7,939 | |||||
Operating income | 493 | 1,333 | |||||
Other income: | |||||||
Interest income | 86 | 130 | |||||
Unrealized gain on warrant derivative | 18 | 324 | |||||
Total other income | 104 | 454 | |||||
Income before income taxes | 597 | 1,787 | |||||
Income tax provision (benefit) | 111 | (533 | ) | ||||
Net income | $ | 486 | $ | 2,320 | |||
Earnings per common share: | |||||||
Basic | $ | 0.03 | $ | 0.15 | |||
Diluted | $ | 0.03 | $ | 0.11 | |||
Basic weighted average common shares outstanding | 16,550 | 15,469 | |||||
Diluted weighted average common shares outstanding | 17,176 | 17,764 | |||||
See accompanying notes.
F-2
AMERICAN CARESOURCE HOLDINGS, INC.
CONSOLIDATED BALANCE SHEETS
December 31
(amounts in thousands except per share amounts)
2010 | 2009 | ||||||
ASSETS | |||||||
Current assets: | |||||||
Cash and cash equivalents | $ | 14,512 | $ | 11,868 | |||
Accounts receivable, net | 5,510 | 7,355 | |||||
Prepaid expenses and other current assets | 532 | 822 | |||||
Deferred income taxes | 237 | 576 | |||||
Total current assets | 20,791 | 20,621 | |||||
Property and equipment, net | 1,824 | 1,762 | |||||
Other assets: | |||||||
Deferred income taxes | 609 | 317 | |||||
Other assets | 340 | 657 | |||||
Intangible assets, net | 1,025 | 1,153 | |||||
Goodwill | 4,361 | 4,361 | |||||
$ | 28,950 | $ | 28,871 | ||||
LIABILITIES AND SHAREHOLDERS’ EQUITY | |||||||
Current liabilities: | |||||||
Due to service providers | $ | 6,718 | $ | 7,702 | |||
Accounts payable and accrued liabilities | 1,446 | 1,861 | |||||
Total current liabilities | 8,164 | 9,563 | |||||
Warrant derivative liability | — | 18 | |||||
Commitments and contingencies | |||||||
Shareholders’ equity: | |||||||
Preferred stock, $0.01 par value; 10,000 shares authorized none issued | — | — | |||||
Common stock, $0.01 par value; 40,000 shares authorized; 16,922 and 15,642 shares issued and outstanding in 2010 and 2009, respectively | 169 | 156 | |||||
Additional paid-in capital | 21,602 | 20,605 | |||||
Accumulated deficit | (985 | ) | (1,471 | ) | |||
Total shareholders’ equity | 20,786 | 19,290 | |||||
$ | 28,950 | $ | 28,871 | ||||
See accompanying notes.
F-3
AMERICAN CARESOURCE HOLDINGS, INC.
CONSOLIDATED STATEMENT OF STOCKHOLDERS’ EQUITY
For the years ended December 31, 2010 and 2009
(amounts in thousands)
Common Stock | |||||||||||||||||||
Shares | Amount | Additional Paid-in Capital | Accumulated Deficit | Total Stockholders’ Equity | |||||||||||||||
Balance at December 31, 2008 | 15,407 | $ | 154 | $ | 19,046 | $ | (3,733 | ) | $ | 15,467 | |||||||||
Cumulative effect of change in accounting principle – January 1, 2009 reclassification of embedded feature of equity-linked financial instrument to warrant derivative liability | — | — | (316 | ) | (58 | ) | (374 | ) | |||||||||||
Net income | — | — | — | 2,320 | 2,320 | ||||||||||||||
Stock-based compensation expense | — | — | 1,495 | — | 1,495 | ||||||||||||||
Issuance of common stock upon exercise of stock options and restricted stock units, net of tax withholdings | 20 | — | (12 | ) | — | (12 | ) | ||||||||||||
Issuance of common stock upon exercise of stock warrants | 215 | 2 | 81 | — | 83 | ||||||||||||||
Issuance of common stock warrants for payment of client management fees | — | — | 311 | — | 311 | ||||||||||||||
Balance at December 31, 2009 | 15,642 | $ | 156 | $ | 20,605 | $ | (1,471 | ) | $ | 19,290 | |||||||||
Net income | — | — | — | 486 | 486 | ||||||||||||||
Stock-based compensation expense | — | — | 871 | — | 871 | ||||||||||||||
Issuance of common stock upon exercise of restricted stock units, net of tax withholdings | 23 | 1 | (19 | ) | — | (18 | ) | ||||||||||||
Issuance of common stock upon exercise of stock warrants | 1,257 | 12 | 145 | — | 157 | ||||||||||||||
Balance at December 31, 2010 | 16,922 | $ | 169 | $ | 21,602 | $ | (985 | ) | $ | 20,786 | |||||||||
See accompanying notes.
F-4
AMERICAN CARESOURCE HOLDINGS, INC.
CONSOLIDATED STATEMENTS OF CASH FLOWS
For the years ended December 31
(amounts in thousands)
2010 | 2009 | |||||||
Cash flows from operating activities: | ||||||||
Net income | $ | 486 | $ | 2,320 | ||||
Adjustments to reconcile net income to net cash provided by operations: | ||||||||
Stock-based compensation expense | 871 | 1,495 | ||||||
Depreciation and amortization | 767 | 563 | ||||||
Unrealized gain on warrant derivative | (18 | ) | (324 | ) | ||||
Amortization of long-term client agreement | 250 | 250 | ||||||
Client administration fee expense related to warrants | 200 | 156 | ||||||
Deferred income tax provision (benefit) | 47 | (643 | ) | |||||
Changes in operating assets and liabilities: | ||||||||
Accounts receivable | 1,845 | (1,567 | ) | |||||
Prepaid expenses and other assets | 157 | (212 | ) | |||||
Accounts payable and accrued liabilities | (432 | ) | (1,221 | ) | ||||
Due to service providers | (984 | ) | 1,738 | |||||
Net cash provided by operating activities | 3,189 | 2,555 | ||||||
Cash flows from investing activities: | ||||||||
Investments in software development costs | (402 | ) | (628 | ) | ||||
Additions to property and equipment | (300 | ) | (653 | ) | ||||
Net cash used in investing activities | (702 | ) | (1,281 | ) | ||||
Cash flows from financing activities: | ||||||||
Proceeds from exercise of equity warrants | 157 | 13 | ||||||
Proceeds from exercise of equity incentive awards | — | 3 | ||||||
Net cash provided by financing activities | 157 | 16 | ||||||
Net increase in cash and cash equivalents | 2,644 | 1,290 | ||||||
Cash and cash equivalents at beginning of period | 11,868 | 10,578 | ||||||
Cash and cash equivalents at end of period | $ | 14,512 | $ | 11,868 | ||||
Supplemental cash flow information: | ||||||||
Cash paid for taxes, net of refunds received | $ | 103 | $ | 90 | ||||
Supplemental non-cash financing activity: | ||||||||
Warrants issued as payment of client management fees | $ | — | $ | 311 | ||||
Warrant exercise in accrued liabilities | — | 38 | ||||||
Warrant derivative liability transferred to equity upon exercise | — | 32 | ||||||
Income tax withholdings on exercise of equity incentives | 19 | — | ||||||
See accompanying notes.
F-5
AMERICAN CARESOURCE HOLDINGS, INC.
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
December 31, 2010
(Tables in thousands, except per share amounts)
1. Summary of Significant Accounting Policies
American CareSource Holdings, Inc. (“ACS,” “Company,” the “Registrant,” “we,” “us,” or “our”) is an ancillary services company that offers cost effective access to a comprehensive national network of ancillary healthcare service providers. The Company sells its services to a number of healthcare companies including preferred provider organizations ("PPOs"), third party administrators (“TPAs”), insurance companies, large self-funded organizations and various employee groups. The Company offers payors this solution by:
• | lowering its payors’ ancillary care costs throughout our network of high quality, cost effective providers that the Company has under contract at more favorable terms than they could generally obtain on their own; |
• | providing payors with a comprehensive network of ancillary healthcare services providers that is tailored to each payor’s specific needs and is available to each payor’s covered persons for covered services; |
• | providing payors with claims management, reporting and processing and payment services; |
• | performing network/needs analysis to assess the benefits to payors of adding additional/different service providers to the payor -specific provider networks; and |
• | credentialing network service providers for inclusion in the payor -specific provider networks. |
Basis of Presentation
The consolidated financial statements include the accounts of the Company and its one wholly-owned subsidiary, Ancillary Care Services, Inc. All material intercompany accounts and transactions are eliminated in consolidation. Certain prior year amounts have been reclassified within the consolidated statement of income, consolidated balance sheet, and statement of cash flow to conform to the current year presentation.
Cash and Cash Equivalents
The Company considers all highly-liquid investments with original maturities of three months or less to be cash equivalents. Cash and cash equivalents include amounts in deposit accounts in excess of federally insured limits of $250,000. The Company has not experienced any losses in such accounts.
Revenue Recognition
The Company recognizes revenue on the services that it provides, which includes (i) providing payor clients with a comprehensive network of ancillary healthcare providers, (ii) providing claims management, reporting, processing and payment services, (iii) providing network/need analysis to assess the benefits to payor clients of adding what additional/different service providers to the client-specific provider networks and (iv) providing credentialing of network services providers for inclusion in the client payor-specific provider networks. Revenue is recognized when services are delivered, which occurs after processed claims are billed to the client payors and collections are reasonably assured. The Company estimates revenues and costs of revenues using average historical collection rates and average historical margins earned on claims. Periodically, revenues are adjusted to reflect actual cash collections so that revenues recognized accurately reflect cash collected.
The Company determines whether it is acting as a principal or agent in the fulfillment of the services rendered. After careful evaluation of the key gross and net revenue recognition indicators, the Company acknowledges that while the determination of gross versus net reporting is highly judgmental in nature, the Company has concluded that its circumstances are most consistent with those key indicators that support gross revenue reporting.
Following are the key indicators that support the Company’s conclusion that it acts as a principal when settling claims for service providers through its contracted service provider network:
F-6
• | The Company is the primary obligor in the arrangement. The Company has assessed its role as primary obligor as a strong indicator of gross reporting. The Company believes that it is the primary obligor in its transactions because it is responsible for providing the services desired by its client payors. The Company has distinct, separately negotiated contractual relationships with its client payors and with the ancillary health care providers in its networks. The Company does not negotiate “on behalf of” its client payors and does not hold itself out as the agent of the client payors when negotiating the terms of the Company’s ancillary healthcare service provider agreements. The Company’s agreements contractually prohibit client payors and service providers to enter into direct contractual relationships with one another. The client payors have no control over the terms of the Company’s agreements with the service providers. In executing transactions, the Company assumes key performance-related risks. The client payors hold the Company responsible for fulfillment, as the provider, of all of the services the client payors are entitled to under their contracts; client payors do not look to the service providers for fulfillment. In addition, the Company bears the pricing/margin risk as the principal in the transactions. Because the contracts with the client payors and service providers are separately negotiated, the Company has complete discretion in negotiating both the prices it charges its client payors and the financial terms of its agreements with the service providers. Since the Company’s profit is the spread between the amounts received from the client payors and the amount paid to the service providers, it bears significant pricing/margin risk. There is no guaranteed mark-up payable to the Company on the amount the Company has contracted. Thus, the Company bears the risk that amounts paid to the service provider will be greater than the amounts received from the client payors, resulting in a loss or negative claim. |
• | The Company has latitude in establishing pricing. As stated above, the Company has complete latitude in negotiating the price to be paid to the Company by each client payor and the price to be paid to each contracted service provider. This type of pricing latitude indicates that the Company has the risks and rewards normally attributed to a principal in the transactions. |
• | The Company changes the product or performs part of the services. The Company provides the benefits associated with the relationships it builds with the client payors and the services providers. While the parties could deal with each other directly, the client payors would not have the benefit of the Company’s experience and expertise in assembling a comprehensive network of service providers, in claims management, reporting and processing and payment services, in performing network/needs analysis to assess the benefits to client payors of adding additional/different service providers to the client payor-specific provider networks, and in credentialing network service providers. |
• | The Company has discretion in supplier selection. The Company has complete discretion in supplier selection. One of the key factors considered by client payors who engage the Company is to have the Company undertake the responsibility for identifying, qualifying, contracting with and managing the relationships with the ancillary healthcare service providers. As part of the contractual arrangement between the Company and its client payors, the payors identify their obligations to their respective covered persons and then work with the Company to determine the types of ancillary healthcare services required in order for the payors to meet their obligations. The Company may select the providers and contract with them to provide services at its discretion. |
• | The Company is involved in the determination of product or service specifications. The Company works with its client payors to determine the types of ancillary healthcare services required in order for the payors to meet their obligations to their respective covered persons. In some respects, the Company is customizing the product through its efforts and ability to assemble a comprehensive network of providers for its payors that is tailored to each payor’s specific needs. In addition, as part of its claims processing and payment services, the Company works with the client payors, on the one hand, and the providers, on the other, to set claims review, management and payment specifications. |
• | The supplier (and not the Company) has credit risk. The Company believes it has some level of credit risk, but that risk is mitigated because the Company does not remit payment to providers unless and until it has received payment from the relevant client payors following the Company’s processing of a claim. |
• | The amount that the Company earns is not fixed. The Company does not earn a fixed amount per transaction nor does it realize a per-person per-month charge for its services. |
The Company has evaluated the other indicators of gross and net revenue recognition, including whether or not the Company has general inventory risk. The Company does not have any general inventory risk, as its business is not related to the manufacture, purchase or delivery of goods and it does not purchase in advance any of the services to be provided by the ancillary healthcare service providers. While the absence of this risk would be one indicator in support of net revenue reporting, as described in detail above, the Company has carefully evaluated all of the key gross and net revenue recognition indicators and has concluded that its circumstances are most consistent with those key indicators that support gross revenue reporting.
F-7
If the Company were to report its revenues net of provider payments rather than on a gross reporting basis, for the years ended December 31, 2010 and December 31, 2009, its net revenues would have been $15.4 million and $17.1 million, respectively.
The Company records a provision for refunds on a periodic basis. Refunds are paid to payors for overpayments on claims, claims paid in error, and claims paid for non-covered services. In some instances, we will recoup payment made to the ancillary service provider if the claim has been fully resolved. The evaluation is performed periodically and is based on historical data. We present revenue net of the provision for refunds on the consolidated income statement.
Provider Payments
Payments to providers is the largest component of our cost of revenues and it consists of our payments for ancillary care services in accordance with contracts negotiated separately with providers for specific ancillary services.
Use of Estimates
The preparation of the financial statements in conformity with accounting principles generally accepted in the United States requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenues and expenses during the reporting period. Actual amounts could differ from those estimates.
Property and Equipment
Property and equipment are recorded at original cost and increased by the cost of any significant improvements subsequent to purchase. The Company expenses repairs and maintenance as incurred. Depreciation and amortization is calculated using the straight-line method over the shorter of the asset’s estimated useful life or the term of the lease in the case of leasehold improvements. The Company capitalizes costs associated with software developed for internal use. During 2010 and 2009, we capitalized approximately $402,000 and $628,000 of internally developed software costs, respectively. Internally developed software is being amortized over a useful life of 5-years.
Research and Development
Research and development costs are expensed as incurred.
Income Taxes
Income taxes are accounted for under the asset and liability method. Deferred taxes arise because of different treatment between financial statement accounting and tax accounting, known as “temporary differences”. The Company records the tax effect of these temporary differences as “deferred tax assets” (generally items that can be used as a tax deduction of credit in the future periods) and “deferred tax liabilities” (generally items that we received a tax deduction for, which have not yet been recorded in the income statement). The deferred tax assets and liabilities are measured using enacted tax rules and laws that are expected to be in effect when the temporary differences are expected to be recovered or settled. A valuation allowance would be established to reduce deferred tax assets if it is more likely than not that a deferred tax assets will not be realized.
Stock Compensation
The Company records all stock-based payments to employees in the consolidated financial statements based on their estimated fair values as of the measurement date of the respective awards. Additional information about the Company’s share-based payment plan is presented in Note 8.
Segment and Related Information
The Company uses the “management approach” for reporting information about segments in our annual and interim financial statements. The management approach is based on the way the chief operating decision-maker organizes segments within a company for making operating decisions and assessing performance. Reportable segments are based on products and services, geography, legal structure, management structure and any other manner in which management disaggregates a company. Based on the “management approach” model, the Company determined that our business is comprised of a single operating segment.
F-8
Fair Value of Financial Instruments
The Company’s financial instruments consist primarily of cash and cash equivalents, accounts receivable, accounts payable and accrued expenses. The fair value of instruments is determined by reference to various market data and other valuation techniques, as appropriate. Unless otherwise disclosed, the fair value of short-term financial instruments approximates their recorded values due to the short-term nature of the instruments.
Recently Adopted Accounting Pronouncements
In January 2010, the Financial Accounting Standards Board (“FASB”) issued Accounting Standards Update No. 2010-06, Improving Disclosures about Fair Value Measurements ("the Update). The Update provides amendments to FASB ASC 820-10 that requires entities to disclose separately the amounts of significant transfers in and out of Level 1 and Level 2 fair value measurements and describe the reasons for the transfers. In addition, the Update requires entities to present separately information about purchases, sales, issuances, and settlements in the reconciliation for fair value measurements using significant unobservable inputs (Level 3). The disclosures related to Level 1 and Level 2 fair value measurements became effective for us in 2010 and the disclosures related to Level 3 fair value measurements are effective for us in 2011. The Update requires new disclosures only, and will have no impact on our consolidated financial position, results of operations, or cash flows.
2. Concentration of Credit Risk
The Company has two client payor relationships that individually comprise a significant portion of our net revenue. The following is a summary of the approximate amounts of the Company’s net revenue and accounts receivable contributed by each of these clients as of and for the years ended December 31:
2010 | 2009 | |||||||||||||||||||||
Accounts Receivable | Revenue | % of Total Revenue | Accounts Receivable | Revenue | % of Total Revenue | |||||||||||||||||
Client A | $ | 2,448 | $ | 29,587 | 48 | % | $ | 3,040 | $ | 32,454 | 47 | % | ||||||||||
Client B | 1,399 | 16,715 | 27 | 3,552 | 25,897 | 38 | ||||||||||||||||
All Others | 2,026 | 15,594 | 26 | 1,040 | 9,960 | 15 | ||||||||||||||||
Allowance for Uncollectable Receivables/Provision for refunds | (363 | ) | (695 | ) | (1 | ) | (277 | ) | (85 | ) | — | |||||||||||
$ | 5,510 | $ | 61,201 | 100 | % | $ | 7,355 | $ | 68,226 | 100 | % | |||||||||||
Client A includes five entities and Client B includes two entities, which are aggregated for this presentation.
3. Allowance for Uncollectable Receivables
The Company maintains an allowance for uncollectable receivables which primarily relates to payor refunds. Refunds are paid to payors for overpayments on claims, claims paid in error, and claims paid for non-covered services. In some instances, we will recoup payment made to the ancillary service provider if the claim has been fully resolved. Co-payments, deductibles and co-insurance payments can also impact the collectability of claims. While the Company is able to process a claim and estimate the cash it will receive from the payor for that claim, the presence of co-pays, deductibles and co-insurance payments can affect the ultimate collectability of the claim. The Company records an allowance against revenue to better estimate collectability. The evaluation is performed periodically and is based on historical data. Provisions for refunds recorded to the allowance were approximately $695,000 for the year ended December 31, 2010 compared to approximately $85,000 for the year ended December 31, 2009. The allowance was approximately $363,000 for the year ended December 31, 2010 compared to approximately $277,000 for the year ended December 31, 2009.
F-9
4. Property and Equipment
Property and equipment, net consists of the following:
Useful Lives (years) | 2010 | 2009 | ||||||||
Software – internally developed | 5 | $ | 1,566 | $ | 1,164 | |||||
Software – purchased | 3-5 | 576 | 434 | |||||||
Computer equipment | 3-5 | 465 | 428 | |||||||
Furniture and fixtures | 5 | 356 | 356 | |||||||
Leasehold improvements | 7 | 205 | 205 | |||||||
3,168 | 2,587 | |||||||||
Accumulated depreciation and amortization | (1,344 | ) | (825 | ) | ||||||
Property and equipment, net | $ | 1,824 | $ | 1,762 | ||||||
The Company recognized depreciation expense of approximately $639,000 and $435,000 during 2010 and 2009, respectively. The depreciation amounts include approximately $260,000 and $163,000 of amortization of internally developed software during 2010 and 2009, respectively.
The Company capitalizes costs associated with internally developed software, developed for internal use only, during the application development stage. Application development stage costs generally include costs associated with internal-use software configuration, coding, installation and testing. Costs of significant upgrades and enhancements that result in additional functionality also are capitalized, whereas costs incurred for maintenance and minor upgrades and enhancements are expensed as incurred. Capitalized costs include external direct costs of materials and services utilized in developing or obtaining internal-use software and payroll and payroll-related expenses for employees who are directly associated with and devote time to the internal-use software project. Capitalization of such costs begins when the preliminary project stage is complete and ceases no later than the point at which the project is substantially complete and ready for its intended purpose. Capitalized costs are amortized using the straight-line method over the useful life of the software, which is typically five years.
During the years ended December 31, 2010 and December 31, 2009, the Company capitalized costs related to enhancements to its internal information technology claims management applications. The applications were originally developed in 2005 and from time to time, the Company will enhance the functionality and reporting capabilities of the applications. The enhancements are typically developed by the Company's internal information technology group. Periodically, third-party consultants will be utilized to perform the development. For internal resources, the Company capitalizes salary and related benefits, while it capitalizes the cost of external consultants.
5. Income Taxes
Income tax provision (benefit) for the years ended December 31 differed from the U.S. federal income tax rate of 34% approximately in the amounts indicated as a result of the following:
2010 | 2009 | |||||||
Computed “expected” tax provision | $ | 203 | $ | 608 | ||||
Change in the valuation allowance for deferred tax assets | — | (1,199 | ) | |||||
Change in fair value of warrant derivative liability | (6 | ) | (113 | ) | ||||
State taxes | 54 | 80 | ||||||
Return to provision adjustment | (167 | ) | — | |||||
Other | 27 | 91 | ||||||
Total income tax provision (benefit) | $ | 111 | $ | (533 | ) | |||
Differences between financial accounting principles and tax laws cause differences between the bases of certain assets and liabilities for financial reporting purposes and tax purposes.
F-10
The tax effects of these differences, to the extent they are temporary, are recorded as deferred tax assets and liabilities and consisted of the following components:
2010 | 2009 | |||||||
Deferred tax assets: | ||||||||
Operating loss carryforward | $ | 101 | $ | 196 | ||||
Accounts receivable allowance | 69 | 55 | ||||||
Warrants | 179 | 229 | ||||||
Texas tax credit carryforward | 238 | 244 | ||||||
Stock option compensation | 1,140 | 911 | ||||||
Accrued expenses | 203 | 147 | ||||||
Alternative Minimum Tax credit carryforwards | 16 | 39 | ||||||
Total deferred tax assets | 1,946 | 1,821 | ||||||
Deferred tax liabilities: | ||||||||
Goodwill | (563 | ) | (442 | ) | ||||
Property and equipment | (496 | ) | (456 | ) | ||||
Prepaid expense | (41 | ) | (30 | ) | ||||
Total deferred tax liabilities | (1,100 | ) | (928 | ) | ||||
Net deferred tax assets | $ | 846 | $ | 893 | ||||
As of December 31, 2009, based on the operating results achieved in 2008 and 2009, the Company determined that it was more likely than not that it would utilize its existing deferred tax assets. Thus, the existing valuation allowance of $1.2 million was eliminated during the year ended December 31, 2009.
As of December 31, 2010, the net operating loss carryforward was approximately $5.7 million which expires in 2025 through 2030. Included in the net operating loss carryforward is approximately $5.4 million which relates to the excess tax benefits for stock options and warrants exercised which will result in a credit into additional paid-in capital of approximately $1.9 million when the associated tax deduction results in a reduction in income taxes payable.
The income tax expense (benefit) shown on the statement of operations for the years ended December 31, 2010 and 2009 consisted of the following:
2010 | 2009 | |||||||
Current | $ | 64 | $ | 110 | ||||
Deferred | 47 | (643 | ) | |||||
$ | 111 | $ | (533 | ) | ||||
The Company has evaluated the accounting guidance for uncertainty in income taxes. Management has evaluated their material tax positions and determined no income tax effects with respect to the financial statements. The Company has identified the United States and Texas as major tax jurisdictions and is no longer subject to federal or state income tax examinations by tax authorities for years before 2006. The Company has been notified of a pending examination by tax authorities for its U.S. federal return for the year ended 2009.
6. Goodwill and Intangible Assets
Goodwill is evaluated for impairment annually as of December or more frequently if impairment indicators arise. An impairment loss is recognized to the extent that the carrying amount exceeds the asset’s fair value. As of December 31, 2010 and 2009, we have determined that no impairment of goodwill exists.
Intangible assets consist of provider contracts and claims payment and billing software. The software has been fully amortized using the straight-line method over its expected useful life of 5 years. The provider contracts are being amortized using the straight-line method over their expected useful lives of 15 years. Our experience to date is that we have approximately 2-4% annual turnover or attrition of provider contracts. The provider contracts are being accounted for on a pooled basis and the actual cancellation rates of provider contracts that were acquired are monitored for potential impairment or amortization adjustment, if warranted. As of December 31, 2010 and 2009, there were no indicators of impairment of the intangible assets. The cost of adding additional providers is considered an ongoing operating expense.
F-11
The following is a summary of our intangible assets as of December 31 for the years presented:
2010 | 2009 | |||||||
Provider contracts | $ | 1,921 | $ | 1,921 | ||||
Software | 428 | 428 | ||||||
2,349 | 2,349 | |||||||
Accumulated amortization | (1,324 | ) | (1,196 | ) | ||||
Intangibles, net | $ | 1,025 | $ | 1,153 | ||||
Amortization expense was approximately $128,000 for each of the years ended December 31, 2010 and 2009. Amortization expense is estimated at $128,000 per year through 2018.
7. Commitments and Contingencies
The Company leases certain equipment and office space under non-cancelable lease agreements, which expire at various dates through April 2013.
At December 31, 2010 minimum annual lease payments for operating leases are approximately as follows:
Operating Leases | |||
2011 | $ | 434 | |
2012 | 412 | ||
2013 | 104 | ||
Total minimum lease payments | $ | 950 | |
Expense related to operating leases was approximately $363,000 and $342,000 for the years ended December 31, 2010 and 2009, respectively.
8. Stock-Based Compensation
Stock Options
American CareSource Holdings, Inc. has an Employee Stock Option Plan (the “Stock Option Plan”) for the benefit of certain employees, non-employee directors, and key advisors. On May 16, 2005, the stockholders approved the 2005 Stock Option Plan which (i) authorized options to purchase 2,249,329 shares and (ii) established the class of eligible participants to include employees, nominees to the Board of Directors of American CareSource Holdings and consultants engaged by American CareSource Holdings, limited to 50,000 the number of shares of Common Stock underlying the one-time grant of a Non-Qualified Option to which non-employee directors or non-employee nominees of the Board of Directors may be entitled. The Company filed a registration statement on Form S-8 registering the issuance of 2,249,329 of the Stock Option Plan shares on April 7, 2006. Stock options granted under the Stock Option Plan may be of two types: (1) incentive stock options and (2) nonqualified stock options. The option price of such grants shall be determined by a Committee of the Board of Directors (the “Committee”), but shall not be less than the estimated fair value of the common stock at the date the option is granted. The Committee shall fix the terms of the grants with no option term lasting longer than ten years. The ability to exercise such options shall be determined by the Committee when the options are granted.
On May 24, 2007, the Company amended the Stock Option Plan to increase the maximum number of shares of Common Stock that may be issued pursuant to the Stock Option Plan. The American CareSource Holdings, Inc. Amended and Restated 2005 Stock Option Plan (the “Amended and Restated Plan”) increased the shares available for issue under the Stock Option Plan by 1,000,000 shares to a total of 3,249,329 shares. The Company filed a registration statement on Form S-8 registering the issuance of the additional shares on June 14, 2007.
In November 2008, the Company again amended the Plan to increase the number of shares under the plan by 500,000 to a total of 3,749,329 shares, which amendment was approved by the stockholders of the Company on May 19, 2009. The Company filed a registration statement on Form S-8 registering the issuance of the additional shares on May 21, 2009.
F-12
On May 19, 2009, the stockholders of the Company approved the 2009 Equity Incentive Plan (the “2009 Plan”). The purpose of the 2009 Plan is (a) to allow selected employees and officers of the Company to acquire and increase equity ownership in the Company, which will strengthen their commitment to the success of the Company, and to attract new employees, officers and consultants, (b) to provide annual cash incentive compensation opportunities that are competitive with other peer corporations, (c) to optimize the profitability and growth of the Company through incentives that are consistent with the Company’s goals, (d) to provide grantees an incentive for individual excellence, (e) to promote teamwork and (f) to attract and retain highly-qualified persons to serve as non-employee directors. The Company filed a registration statement on Form S-8 registering the issuance of the 1,500,000 shares of the 2009 Plan on May 21, 2009. The 2009 Plan allows for awards of non-qualified options, stock appreciation rights, restricted shares, performance units/shares, deferred stock, dividend equivalents and other stock-based awards. The term of the 2009 Plan is ten years and all non-qualified options will be valued at not less than 100% of the market value of the Company’s stock on the date of grant.
Shares of common stock reserved for future grants under the Stock Option Plan and the 2009 Plan (the “Plans”) were 1,502,813 and 1,590,178 at December 31, 2010 and 2009, respectively.
Compensation expense related to all equity awards, including non-qualified stock options and restricted stock units, that has been charged against income for the years ended December 31, 2010 and 2009 was approximately $871,000 and $1.5 million, respectively.
The awards granted to employees and non-employee directors become exercisable over periods of one to five years. The fair value of each option award granted is estimated on the date of grant using the Black-Scholes-Merton valuation model that uses the assumptions noted in the following table. Volatility is calculated using an analysis of historical volatility. The Company believes that the historical volatility of the Company’s stock is the best method for estimating future volatility. The expected lives of options are determined based on the Company’s historical share option exercise experience. The Company believes the historical experience method is the best estimate of future exercise patterns currently available. The risk-free interest rates are determined using the implied yield currently available for zero-coupon U.S. government issues with a remaining term equal to the expected life of the options. The expected dividend yields are based on the approved annual dividend rate in effect and current market price of the underlying common stock at the time of grant.
2010 | 2009 | |||||||
Weighted average grant date fair value | $ | 1.04 | $ | 3.87 | ||||
Weighted average assumptions used | ||||||||
Expected volatility | 69.3 | % | 69.8 | % | ||||
Expected lives (years) | 6.3 | 6.4 | ||||||
Risk free interest rate | 2.6 | % | 2.6 | % | ||||
Forfeiture rate | 20.5 | % | 24.3 | % | ||||
Dividend rate | — | — | ||||||
A summary of stock option activity is as follows:
Options (thousands) | Weighted-Average Exercise Price | |||||
Outstanding at December 31, 2008 | 2,355 | $ | 3.25 | |||
Granted | 450 | $ | 5.96 | |||
Forfeited | (167 | ) | $ | 3.68 | ||
Cancelled | (130 | ) | $ | 7.02 | ||
Exercised | (20 | ) | $ | 2.47 | ||
Outstanding at December 31, 2009 | 2,488 | $ | 3.52 | |||
Granted | 964 | $ | 1.70 | |||
Forfeited | (479 | ) | $ | 5.25 | ||
Cancelled | (374 | ) | $ | 5.47 | ||
Outstanding at December 31, 2010 | 2,599 | $ | 2.24 | |||
Exercisable at December 31, 2010 | 1,434 | $ | 2.11 | |||
As of December 31, 2010, the weighted average remaining contractual life of the options outstanding was 7.4 years and the weighted average remaining contractual life of the outstanding exercisable options was 6.1 years.
F-13
The following table summarizes information concerning outstanding and exercisable options at December 31, 2010:
(in thousands) | Options Outstanding | Options Exercisable | |||||||||||||||
Range of Exercise Price | Number Outstanding | Weighted Average Outstanding Contractual Life | Weighted Average Exercise Price | Number Exercisable | Weighted Average Exercise Price | ||||||||||||
Under $1.00 | 438 | 4.4 | $ | 0.34 | 438 | $ | 0.34 | ||||||||||
$1.00 - $2.00 | 976 | 8.3 | $ | 1.64 | 450 | $ | 1.81 | ||||||||||
$2.01 - $3.00 | 622 | 8.3 | $ | 2.28 | 213 | $ | 2.60 | ||||||||||
$3.01 - $4.00 | 180 | 7.2 | $ | 3.29 | 124 | $ | 3.29 | ||||||||||
$4.01 - $5.00 | 208 | 7.4 | $ | 4.17 | 114 | $ | 4.18 | ||||||||||
$5.01 - $6.00 | 50 | 5.1 | $ | 5.60 | 50 | $ | 5.60 | ||||||||||
$6.01 - $7.00 | 7 | 7.9 | $ | 7.00 | 4 | $ | 7.00 | ||||||||||
Greater than $7.01 | 118 | 8.1 | $ | 7.33 | 41 | $ | 7.50 | ||||||||||
The total intrinsic value of options outstanding at December 31, 2010 and 2009 was approximately $465,000 and $1.1 million, respectively. The total intrinsic value of the options that are exercisable at December 31, 2010 and 2009 was approximately $462,000 and $1.1 million, respectively. The total intrinsic value of options exercised during the year ended December 31, 2009 was approximately $82,000. No options were exercised during the year ended December 31, 2010.
Compensation expense related to non-qualified stock options charged to operations during 2010 was approximately $599,000. As of December 31, 2010, there was approximately $1.6 million of total unrecognized compensation cost related to non-vested non-qualified stock options granted under the plan. The cost is expected to be recognized over a weighted average period of 3.5 years.
Restricted Stock Units
Under the 2009 Plan, the Company issued restricted stock units (“RSUs”) to certain employees and the Board of Directors during the twelve months ended December 31, 2009. As RSUs vest, they are convertible into shares of the Company’s common stock. The RSUs are valued at the market price of the Company’s stock on the measurement date, which is the date of grant. Compensation expense is recognized ratably over the vesting period. Our future estimated forfeiture rate on RSUs is 0% as the RSUs have been awarded primarily to members of our Board of Directors and members of senior management of the Company. No RSUs were issued during the twelve months ended December 31, 2010.
A summary of RSU activity is as follows:
RSUs | Weighted-Average Grant Date Fair Value | |||||
Outstanding at December 31, 2008 | — | $ | — | |||
Granted | 154 | $ | 7.00 | |||
Forfeited | (4 | ) | $ | 7.02 | ||
Converted to common stock | (10 | ) | $ | 7.02 | ||
Outstanding at December 31, 2009 | 140 | $ | 6.99 | |||
Forfeited | (23 | ) | $ | 6.68 | ||
Converted to common stock | (31 | ) | $ | 7.02 | ||
Outstanding at December 31, 2010 | 86 | $ | 7.07 | |||
Vested and convertible to common stock at December 31, 2010 | 37 | $ | 7.04 | |||
Compensation expense related to RSUs charged to operations during 2010 was approximately $272,000. As of December 31, 2010, there was approximately $307,000 of total unrecognized compensation cost related to non-vested RSUs granted under the plan. The cost is expected to be recognized over a weighted average period of 2.9 years.
F-14
9. Stock Warrants
In January 2005, the Company issued Series A warrants to purchase 1,096,491 shares of common stock to two directors of the Company in exchange for a guarantee of the Company’s $3.0 million line of credit. In addition, in August 2005, we issued Series B warrants to purchase 641,059 shares of common stock to two directors and a stockholder of the Company to increase the associated line of credit. The total number of warrants issued in exchange for the guarantee of debt was 1,737,550. Under the Black-Scholes Merton value method, the warrants were valued at approximately $377,000 as of the dates of the grants using the fair value method. The exercise price of these warrants ranges from $0.40 - $0.49. These deferred debt issuance costs were amortized to expense over the life of the guarantee.
On January 22, 2010, the Company issued 727,498 shares of common stock in connection with the cashless exercise of the remaining Series A warrants. The exercise price of the warrants was $0.40 per share.
On August 15, 2010, the Company issued 530,198 shares of common stock in connection with the exercise of the remaining Series B warrants, whereby 320,248 shares were issued by utilizing a cash exercise and 209,950 shares were issued under a cashless exercise. The exercise price of the warrants was $0.49 per share. Total proceeds from the cash exercise were approximately $157,000.
The Company also issued warrants to purchase up to 159,952 shares of common stock with an exercise price of $5.50, in connection with the Private Placement financing completed in March 2006, to Laidlaw as part of their compensation for the financing. The warrants were valued at approximately $464,000 as of the date of the grant using the Black-Scholes Merton fair value method. In September 2008, additional accounting guidance was issued relating to determining whether an instrument (or embedded feature) is indexed to entity’s own stock. The guidance mandates a two-step process for evaluating whether an equity-linked financial instrument or embedded feature is indexed to the entity’s own stock. Warrants to purchase 109,095 shares of common stock issued by the Company contain a strike price adjustment feature, which upon adoption, resulted in the instruments no longer being considered indexed to the Company’s own stock. Accordingly, adoption changed the classification (from equity to liability) and the related accounting for these warrants outstanding as of January 1, 2009. As of that date, we reclassified the warrants, based on a fair value of $3.43 per warrant, as calculated using the Black–Scholes–Merton valuation model. During 2009, the liability was adjusted for warrants exercised and the change in fair value of the remaining outstanding warrants. As of December 31, 2010, no liability is included as a warrant derivative liability as the outstanding warrants are valued at $0, as calculated using the Black-Scholes-Merton valuation model. During 2010, we recorded an unrealized gain of approximately $18,000 related to the change in fair value of the warrants. As of December 31, 2010, warrants to purchase 99,651 shares of common stock remained outstanding. The outstanding warrants expired on February 17, 2011.
On July 2, 2007, the Company announced that it had signed an Ancillary Care Services Network Access Agreement (the “Ancillary Care Services Agreement”) effective as of May 21, 2007 (the “Effective Date”) with a new client, Texas True Choice, Inc. (“Texas True Choice”), a Texas-based preferred provider organization network, and certain subsidiaries of Texas True Choice. As partial compensation to Texas True Choice under the Ancillary Care Services Agreement, the Company issued to Corporate Health Plans of America, Inc., an affiliate of Texas True Choice, warrants to purchase a total of 225,000 shares of the Company’s common stock at an exercise price of $1.84, the closing price of the common stock of the Company as reported on the American Stock Exchange on the Effective Date. The Company valued the warrants when various measurement dates had been reached under the agreement. Utilizing the Black-Scholes Merton valuation method, 112,500 warrants were valued at $0.94 in 2007, 56,250 warrants were valued at $2.87 at June 2008 and the remaining 56,250 were valued at $5.53 in June 2009.
These warrants vested 25% on the Effective Date, an additional 25% on each anniversary date of the Effective Date, and have an expiration date of May 20, 2012. As of December 31, 2010, all warrants to purchase shares of the Company's common stock were fully vested. The Company recorded the value of warrants as deferred costs upon vesting and is amortizing the deferred costs as administrative fees over the related contract term. As of December 31, 2010, the total unrecognized cost related to the warrants of approximately $67,000 was included as Prepaid and Other Current Assets. The weighted average remaining contractual life of the warrants is 1.5 years.
F-15
A summary of stock warrant activity is as follows:
Outstanding Warrants (thousands) | Weighted-Average Exercise Price | ||||
Outstanding at December 31, 2008 | 2,066 | $ | 0.85 | ||
Exercised | (239 | ) | $ | 0.60 | |
Outstanding at December 31, 2009 | 1,827 | $ | 0.89 | ||
Exercised | (1,502 | ) | $ | 0.44 | |
Outstanding at December 31, 2010 | 325 | $ | 2.96 | ||
Vested at December 31, 2010 | 325 | $ | 2.96 | ||
For the warrant derivative liability, the assumptions used in the Black-Scholes-Merton valuation model were as follows:
December 31 | December 31, | |||||
2010 | 2009 | |||||
Exercise price | $ | 5.50 | $ | 5.50 | ||
Expected volatility | 38.7 | % | 68.9 | % | ||
Expected life (years) | 0.21 | 1.17 | ||||
Risk free interest rate | 0.1 | % | 0.6 | % | ||
Forfeiture rate | — | — | ||||
Dividend rate | — | — | ||||
The following table reflects the activity for the warrant derivative liability:
Initial recognition of warrant derivative as of January 1, 2009 | $ | 374 | |
Sales of warrant derivative | (32 | ) | |
Unrealized gains related to the change in fair value | (324 | ) | |
Fair value as of December 31, 2009 | $ | 18 | |
Unrealized gains related to the change in fair value | (18 | ) | |
Fair value as of December 31, 2010 | $ | — | |
F-16
10. Earnings per Share
Basic earnings per share is computed by dividing net income by the weighted average number of shares of common stock outstanding during the year. Diluted earnings per share reflects the potential dilution that could occur if options, warrants and restricted stock units to purchase common stock were exercised or converted. For purposes of this calculation, outstanding stock options, stock warrants and restricted stock units are considered common stock equivalents using the treasury stock method, and are the only such equivalents outstanding.
For the year ended December 31, 2010, options to purchase approximately 2.0 million shares of commons stock, warrants to purchase approximately 325,000 shares of common stock, and approximately 49,000 unvested restricted stock units were excluded from the calculation as their impact would be anti-dilutive.
Basic earnings and diluted earnings per share data were computed as follows:
2010 | 2009 | |||||
Numerator: | ||||||
Net income for basic earnings per share | $ | 486 | $ | 2,320 | ||
Less: | ||||||
Change in fair value of warrant derivative liability | 18 | 324 | ||||
Net income for diluted earnings per share | $ | 468 | $ | 1,996 | ||
Denominator: | ||||||
Weighted-average basic common shares outstanding | 16,550 | 15,469 | ||||
Assumed conversion of dilutive securities: | ||||||
Stock options | 271 | 691 | ||||
Warrants | 355 | 1,602 | ||||
Restricted stock units | — | 2 | ||||
Potentially dilutive common shares | 626 | 2,295 | ||||
Denominator for diluted earnings per share – Adjusted weighted-average shares | 17,176 | 17,764 | ||||
Earnings per common share: | ||||||
Basic | $ | 0.03 | $ | 0.15 | ||
Diluted | $ | 0.03 | $ | 0.11 | ||
11. Significant Client Agreements
On December 31, 2008, we entered into an amendment (the “Amendment”) to our Provider Service Agreement with one of our significant clients. The purpose of the Amendment is, among other things, to facilitate and accelerate the integration into the Company’s business model of one of the client’s affiliates, adjust the administrative fees outlined in the previous amendment, define and clarify the exclusivity and levels of cooperation contemplated by the previous amendments, and extend the partnership between the Company and the client and the duration of their Provider Service Agreement to December 31, 2012. Under a strategic contracting plan that the Amendment requires the parties to develop, the Company will be the exclusive outsourced ancillary contracting and network management provider for the client’s group health clients and any third party administrators.
As part of the Amendment, the Company agreed to pay to the client $1.0 million for costs incurred in connection with the integration of and access to the Company’s network by members of the affiliate’s network, including, but not limited to, costs associated with salaries, benefits, and third party contracts. The payment was made in April 2009. The Company will continue to pay an administrative fee to the client designed to reimburse and compensate for the work that it is required to perform to support the Company’s program. The Company has recognized the $1.0 million fee as a prepaid expense which is being amortized over the term of the agreement. During 2010, we recorded amortization related to the agreement of $250,000. At December 31, 2010, $250,000 was classified as a current asset on the consolidated balance sheet representing the amount to be amortized during the subsequent twelve-month period. The remaining $250,000 balance was classified as a long-term other asset at December 31, 2010.
F-17
During the year ended December 31, 2010, one of our significant clients, accounting for 27% of our net revenues during 2010, merged with a large supplier of independent, network-based cost management solutions. The contract with the client expires on May 21, 2011 and will automatically renew for successive one-year terms unless either party delivers written notice of non-renewal at least ninety days prior to expiration. Since the Company has not received written notice of non-renewal, the contract term has been automatically extended through May 20, 2012. Such contract may be terminated upon thirty (30) days’ notice in the event of a breach.
During the year ended December 31, 2010, an ancillary service provider terminated its agreement with the Company to provide laboratory services in Texas to clients of the Company on an “as needed” basis. Services provided by the provider accounted for approximately 3% of the Company’s net revenues in 2010 compared to 5% in 2009.
During the year ended December 31, 2009, an ancillary service provider terminated its agreement with the Company to provide laboratory services to clients of the Company. Services provided by the provider accounted for approximately 5% of the Company's net revenues in 2009.
12. Employee Benefit Plans
We provide a defined contribution plan for our employees meeting minimum service requirements. Employees can contribute up to 100% of their current compensation to the plan subject to certain statutory limitations. We contribute up to a maximum of 3.5% of an employee’s compensation and plan participants are fully-vested in the Company’s contributions immediately. We made contributions to the plan and charged operations approximately $123,000 and $121,000 during the years ended December 31, 2010 and 2009.
13. Quarterly Financial Information (unaudited)
The following table contains selected financial information from unaudited statements of operations for each quarter of 2010 and 2009.
Quarters Ended | ||||||||||||||||||||||||||||||||
2010 | 2009 | |||||||||||||||||||||||||||||||
Dec. 31 | Sept. 30 | June 30 | Mar. 31 | Dec. 31 | Sept. 30 | June 30 | Mar. 31 | |||||||||||||||||||||||||
Net revenues | $ | 16,109 | $ | 14,763 | $ | 15,958 | $ | 14,371 | $ | 16,801 | $ | 18,235 | $ | 17,135 | $ | 16,055 | ||||||||||||||||
Contribution margin | 1,678 | 1,706 | 2,098 | 1,968 | 2,459 | 2,294 | 2,283 | 2,236 | ||||||||||||||||||||||||
Contribution margin % | 10.4 | 11.6 | 13.1 | 13.7 | 14.6 | 12.6 | 13.3 | 13.9 | ||||||||||||||||||||||||
Income before income taxes | 33 | 87 | 450 | 27 | 770 | 168 | 547 | 302 | ||||||||||||||||||||||||
Net income | 142 | 44 | 299 | 1 | 1,360 | 147 | 534 | 279 | ||||||||||||||||||||||||
Earnings per diluted share | 0.01 | 0.00 | 0.02 | 0.00 | 0.07 | 0.01 | 0.01 | 0.02 | ||||||||||||||||||||||||
Shares used in computing diluted earnings per share | 17,193 | 17,124 | 17,120 | 16,203 | 17,140 | 17,573 | 18,055 | 18,287 | ||||||||||||||||||||||||
F-18
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the Registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
AMERICAN CARESOURCE HOLDINGS, INC.
By: /s/ David S. Boone | March 18, 2011 | |
David S. Boone Chief Executive Officer Director (Principal Executive Officer) | Date |
Pursuant to the requirements the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the Registrant and in the capacities and on the dates indicated.
By: /s/ Kenneth S. George | March 18, 2011 | |
Kenneth S. George Chairman of the Board of Directors | Date |
By: /s/ David S. Boone | March 18, 2011 | |
David S. Boone Chief Executive Officer Director (Principal Executive Officer) | Date |
By: /s/ Matthew D. Thompson | March 18, 2011 | |
Matthew D. Thompson Chief Financial Officer (Principal Financial Officer and Principal Accounting Officer) | Date |
By: /s/ William J. Simpson, Jr. | March 18, 2011 | |
William J. Simpson, Jr. Chief Operating Officer Director | Date |
By: /s/ Sam S. Abbasi | March 18, 2011 | |
Sam S. Abbasi Director | Date |
By: /s/ Edward B. Berger | March 18, 2011 | |
Edward B. Berger Director | Date |
By: /s/ John N. Hatsopoulos | March 18, 2011 | |
John N. Hatsopoulos Director | Date |
By: /s/ Derace L. Schaffer | March 18, 2011 | |
Derace L. Schaffer Director | Date |
By: /s/ John Pappajohn | March 18, 2011 | |
John Pappajohn Director | Date |
By: /s/ John W. Colloton | March 18, 2011 | |
John W. Colloton Director | Date |
EXHIBIT INDEX
Exhibit # | Description of Exhibits |
3.1** | Certificate of Incorporation of American CareSource Holdings, Inc., as amended |
3.2(1) | By-Laws |
4.1(2) | Specimen Stock Certificate |
4.2(3) | Amended and Restated 2005 Stock Option Plan |
4.3 (4) | 2009 Equity Incentive Plan |
10.02(2), * | Employment Agreement dated May 1, 2005 between American CareSource Holdings, Inc. and David Boone |
10.06(5), * | Employment Agreement dated October 12, 2007 between American CareSource Holdings, Inc. and Steven J. Armond |
10.08(6), * | Employment Letter dated January 29, 2008 between American CareSource Holdings, Inc. and Cornelia Outten |
10.09(6), * | Employment Letter dated March 6, 2008 between American CareSource Holdings, Inc. and Rost Ginevich |
10.10(7) | Form of Registration Rights Agreement used in March 2006 private placement |
10.11(7) | Form of Subscription Agreement used in March 2006 private placement |
10.17(8) | Lease dated June 14, 2006, between American CareSource Holdings, Inc. and TR LBJ Campus Partners, L.P. |
10.18(9) | First Amendment to Office Lease, dated December 1, 2008, between American CareSource Holdings, Inc. and TR LBJ Campus Partners, L.P. |
10.19(10), *** | Provider Services Agreement, dated as of August 1, 2002, by and among the Company, HealthSmart Holdings, Inc. and HealthSmart Preferred Care II, L.P, and Amendment No. 1, 2, 3 and 4 thereto, dated September 1, 2005, January 1, 2007, July 31, 2007 and December 20, 2008, respectively. |
10.20(9), * | Employment Letter dated November 10, 2008 between American CareSource Holdings, Inc. and James T. Robinson. |
10.21(10), *** | Ancillary Care Services Network Access Agreement, dated as of July 2, 2007, by and between the Company and Texas True Choice, Inc. and its subsidiaries and Amendment dated December 31, 2009. |
10.22(11), * | Letter Agreement dated December 24, 2009 by and between American CareSource Holdings, Inc. and James T. Robinson. |
10.23(11), * | Letter Agreement dated November 4, 2009 by and between American CareSource Holdings, Inc. and Steven J. Armond. |
14.1(7) | Code of Ethics |
21.1** | Subsidiaries |
23.1** | Consent of McGladrey & Pullen LLP |
31.1** | Certification of the Chief Executive Officer pursuant to Section 302 of the Sarbanes-Oxley Act of 2002. |
31.2** | Certification of the Chief Financial Officer pursuant to Section 302 of the Sarbanes-Oxley Act of 2002. |
32.1** | Certification pursuant to Section 906 of the Sarbanes-Oxley Act of 2002. |
* Designates a management contract or compensatory plan or arrangement required to be filed as an exhibit to this report pursuant to Item 15(a)(3) of this report.
** Filed herewith
*** Certain confidential portions of this exhibit have been omitted and filed separately with the Securities and Exchange Commission pursuant to a request for confidential treatment under Rule 24b-2 of the Securities Exchange Act of 1934.
(1) | Previously filed with the Securities and Exchange Commission as an exhibit to Amendment No. 1 to the Form SB-2 filed May 13, 2005 and incorporated herein by reference. |
(2) | Previously filed with the Securities and Exchange Commission as an exhibit to Amendment No. 5 to the Form SB-2 filed August 12, 2005 and incorporated herein by reference. |
(3) | Previously filed with the Securities and Exchange Commission as Exhibit B to the Proxy Statement for the 2009 Annual Meeting of Stockholders filed on April 20, 2009 and incorporated herein by reference. |
(4) | Previously filed with the Securities and Exchange Commission as Exhibit A to the Proxy Statement for the 2009 Annual Meeting of Stockholders filed on April 20, 2009 and incorporated herein by reference. |
(5) | Previously filed with the Securities and Exchange Commission as an exhibit to the Form 10-QSB filed November 13, 2007 and incorporated herein by reference. |
(6) | Previously filed with the Securities and Exchange Commission as an exhibit to the Form 10-K filed March 31, 2008 and incorporated herein by reference. |
(7) | Previously filed with the Securities and Exchange Commission as an exhibit to the Form 10-KSB filed March 31, 2006 and incorporated herein by reference. |
(8) | Previously filed with the Securities and Exchange Commission as an exhibit to the Form 10-QSB filed August 11, 2006 and incorporated herein by reference. |
(9) | Previously filed with the Securities and Exchange Commission as an exhibit to the Form 10-K filed March 31, 2009 and incorporated herein by reference. |
(10) | Previously filed with the Securities and Exchange Commission as an exhibit to the Form 10-Q filed November 12, 2010 and incorporated herein by reference. |
(11) | Previously filed with the Securities and Exchange Commission as an exhibit to the Form 10-K filed March, 26, 2010 and incorporated herein by reference. |