Attached files
Table of Contents
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
| x | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the fiscal year ended December 31, 2010
or
| ¨ | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the transition period from to
Commission File Number: 000-51173
Targacept, Inc.
(Exact name of registrant as specified in its charter)
| Delaware | 56-2020050 | |
| (State or other jurisdiction of incorporation or organization) |
(I.R.S. Employer Identification No.) | |
| 200 East First Street, Suite 300 Winston-Salem, North Carolina |
27101 | |
| (Address of principal executive offices) | (Zip Code) | |
Registrant’s telephone number, including area code: (336) 480-2100
Securities registered pursuant to Section 12(b) of the Exchange Act:
| Title of each class |
Name of each exchange on which registered | |
| Common Stock, $0.001 par value per share | The NASDAQ Stock Market LLC (NASDAQ Global Select Market) |
Securities registered pursuant to Section 12(g) of the Exchange Act: None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. ¨ Yes x No
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. ¨ Yes x No
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes x No ¨
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Website, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§ 232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). ¨ Yes ¨ No
Indicate by check mark if disclosure of delinquent filers pursuant to Rule 405 of Regulation S-K (§ 229.405 of this chapter) is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. x
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See the definitions of “large accelerated filer,” “accelerated filer” and “smaller reporting company” in Rule 12b-2 of the Exchange Act.
| Large accelerated filer ¨ | Accelerated filer x | Non-accelerated filer ¨ | Smaller reporting company x | |||
| (Do not check if a smaller reporting company) |
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). ¨ Yes x No
The aggregate market value of the registrant’s common stock held by non-affiliates of the registrant as of June 30, 2010, was approximately $314,394,099, based on the price at which the registrant’s common stock was last sold on June 30, 2010 ($19.33).
As of February 28, 2011, the registrant had 29,021,460 shares of common stock, $0.001 par value per share, outstanding.
DOCUMENTS INCORPORATED BY REFERENCE
Specified portions of the registrant’s proxy statement for its 2011 annual meeting of stockholders, which is expected to be filed pursuant to Regulation 14A within 120 days after the end of the registrant’s fiscal year ended December 31, 2010, are incorporated by reference into Part III of this report.
Table of Contents
TARGACEPT, INC.
FORM 10-K
Table of Contents
Cautionary Note Regarding Forward-Looking Statements
This annual report includes forward-looking statements within the meaning of Section 27A of the Securities Act of 1933, as amended, which we refer to as the Securities Act, and Section 21E of the Securities Exchange Act of 1934, as amended, which we refer to as the Exchange Act. For this purpose, any statement contained in this annual report, other than statements of historical fact, regarding, among other things:
| • | the progress, scope or duration of the development of TC-5214, TC-5619, AZD3480 (TC-1734), AZD1446 (TC-6683), TC-6987, TC-6499 or any of our other product candidates or programs, such as the target indication(s) for development, the size, design, population, conduct, objective or endpoints of any clinical trial, or the timing for initiation or completion of or availability of results from any clinical trial, for submission or approval of any regulatory filing (including a new drug application for TC-5214), for meeting with regulatory authorities, or, where applicable, for an advancement decision by AstraZeneca; |
| • | the benefits that may be derived from any of our product candidates; |
| • | any payments that AstraZeneca may make to us; |
| • | our operations, financial position, revenues, costs or expenses; or |
| • | our strategies, prospects, plans, expectations or objectives |
is a forward-looking statement made under the provisions of The Private Securities Litigation Reform Act of 1995. In some cases, words such as “may,” “will,” “could,” “would,” “should,” “expect,” “intend,” “plan,” “anticipate,” “believe,” “estimate,” “predict,” “project,” “potential,” “continue,” “scheduled” or other comparable words identify forward-looking statements. Actual results, performance or experience may differ materially from those expressed or implied by forward-looking statements as a result of various important factors, including our critical accounting policies and risks and uncertainties relating, among other things, to:
| • | our dependence on the success of our collaborations with AstraZeneca; |
| • | whether the favorable results of our Phase 2b trial of TC-5214 as an adjunct treatment for major depressive disorder will be replicated in Phase 3 clinical trials; |
| • | whether TC-5214 will be eligible for treatment in the United States as a new chemical entity with a five-year statutory exclusivity period, either because we and AstraZeneca submit a new drug application for TC-5214 prior to October 1, 2012 or because the applicable statutory provision is re-authorized by the U.S. Congress; |
| • | the significant control or influence that AstraZeneca has over the development of TC-5214, AZD3480 and AZD1446, including as to the timing, scope and design of clinical trials and as to the conduct at all of further development of AZD3480 in attention deficit/hyperactivity disorder, AZD1446 in Alzheimer’s disease or TC-5619 in Alzheimer’s disease; |
| • | the conduct and results of clinical trials and non-clinical studies and assessments of TC-5214, AZD3480, AZD1446, TC-5619, TC-6987, TC-6499 or any of our other product candidates, including the performance of third parties engaged to execute them and difficulties or delays in subject enrollment and data analysis; |
| • | our ability to establish additional strategic alliances, collaborations and licensing or other arrangements on favorable terms; |
| • | our ability to protect our intellectual property; and |
| • | the timing and success of submission, acceptance and approval of regulatory filings. |
These and other risks and uncertainties are described in greater detail under the caption “Risk Factors” in Item 1A of Part I of this annual report and in other filings that we make with the Securities and Exchange
1
Table of Contents
Commission, or SEC. As a result of the risks and uncertainties, the results or events indicated by the forward-looking statements may not occur. We caution you not to place undue reliance on any forward-looking statement.
In addition, any forward-looking statement in this annual report represents our views only as of the date of this annual report and should not be relied upon as representing our views as of any subsequent date. We anticipate that subsequent events and developments may cause our views to change. Although we may elect to update these forward-looking statements publicly at some point in the future, we specifically disclaim any obligation to do so, except as required by applicable law. Our forward-looking statements do not reflect the potential impact of any future acquisitions, mergers, dispositions, joint ventures or investments we may make.
2
Table of Contents
PART I
| Item 1. | Business. |
Overview
We are a biopharmaceutical company engaged in the design, discovery and development of novel NNR Therapeutics™ for the treatment of diseases and disorders of the nervous system. Our NNR Therapeutics selectively target neuronal nicotinic receptors, which we refer to as NNRs. NNRs are found on nerve cells throughout the nervous system and serve as key regulators of nervous system activity.
We trace our scientific lineage to a research program initiated by R.J. Reynolds Tobacco Company in 1982 to study the activity and effects of nicotine, a compound that interacts non-selectively with all nicotinic receptors. Based on years of focused research in the NNR area, we believe that compounds that interact selectively with specific NNR subtypes have the potential to achieve positive medical effects by modulating their activity. We have built an extensive patent estate covering the structure or therapeutic use of small molecules designed to regulate nervous system activity by selectively affecting specific NNR subtypes.
We have multiple clinical-stage product candidates and preclinical programs in areas in which we believe there are significant medical need and commercial potential, as well as proprietary drug discovery technologies. We have entered into two significant collaborations with the global pharmaceutical company AstraZeneca to provide expertise and resources to assist in the global development and potential commercialization of many of our product candidates. One is a collaboration and license agreement focused on TC-5214 as a treatment for major depressive disorder, and we refer to that agreement in this annual report as our “TC-5214 agreement with AstraZeneca.” The other is a collaborative research and license agreement focused in cognitive disorders, and we refer to that agreement in this annual report as our “cognitive disorders agreement with AstraZeneca.” Our most advanced product candidates are described briefly below.
TC-5214
TC-5214 is a nicotinic channel modulator that is thought to derive antidepressant activity by modulating the activity of various NNR subtypes. We are co-developing TC-5214 with AstraZeneca under our TC-5214 agreement with AstraZeneca as an adjunct, or add-on, therapy for patients with major depressive disorder who do not respond adequately to initial antidepressant treatment. Phase 3 clinical trials of TC-5214 are ongoing. In addition, we and AstraZeneca initiated a Phase 2b clinical trial of TC-5214 as a “switch” monotherapy in the first quarter of 2011.
TC-5619
TC-5619 is a novel small molecule that modulates the activity of the a7 NNR. In January 2011, we announced positive top-line results from a Phase 2 clinical trial of TC-5619 in cognitive dysfunction in schizophrenia. We are currently conducting a separate Phase 2 clinical trial of TC-5619 in attention deficit/hyperactivity disorder, or ADHD, in adults and we expect results from the trial to become available by the end of the first quarter of 2011. In addition, we are conducting clinical and non-clinical studies to support the potential advancement of TC-5619 into Phase 2 clinical development in Alzheimer’s disease.
AstraZeneca has the right to license TC-5619 and to further develop and potentially commercialize TC-5619 for various conditions characterized by cognitive impairment on terms specified in our cognitive disorders agreement with AstraZeneca, as it was amended in April 2010. We expect AstraZeneca to determine whether to exercise its license right in the first half of 2011.
AZD3480 (TC-1734)
AZD3480 (TC-1734) is a novel small molecule that modulates the activity of the a4ß2 NNR and is subject to our cognitive disorders agreement with AstraZeneca. We or AstraZeneca has conducted several clinical studies
3
Table of Contents
of AZD3480 in various cognitive disorders and we are in discussions with AstraZeneca regarding potential additional development of the product candidate as a treatment for ADHD. Whether AstraZeneca will decide to conduct any additional development of AZD3480 in ADHD is uncertain in light of reservations about the adequacy of the therapeutic margin to support development across the broad ADHD patient population. We expect AstraZeneca to make its decision in the first half of 2011. In addition, we have agreed with AstraZeneca on respective roles and financial and non-financial responsibilities for an additional clinical trial of AZD3480 in Alzheimer’s disease. We have had a favorable meeting with the U.S. Food and Drug Administration, or FDA, regarding a potential development path for AZD3480 in Alzheimer’s disease and are continuing to explore the practicability of conducting an Alzheimer’s disease study in Europe.
AZD1446 (TC-6683)
AZD1446 is a novel small molecule that modulates the activity of the a4ß2 NNR and is under consideration for further development as a treatment for Alzheimer’s disease under our cognitive disorders agreement with AstraZeneca. We discovered and advanced AZD1446 as part of a now completed preclinical research collaboration conducted under the agreement. AstraZeneca has completed three of four early-stage clinical studies expected to inform its decision as to whether to conduct further clinical development of AZD1446, and we expect AstraZeneca to make its decision in the third quarter of 2011.
TC-6987
TC-6987 is a novel small molecule that modulates the activity of the a7 NNR and is in development as a treatment for inflammatory disorders. In February 2011, we announced the initiation of two Phase 2 studies planned to help guide the selection of indications for which TC-6987 is best suited for later-stage development. One of the Phase 2 studies is in asthma and the other is in Type 2 diabetes.
TC-6499
TC-6499 is a novel small molecule that modulates the activity of the a4ß2 and a3ß4 NNRs. The a3ß4 NNR is located in the gastrointestinal tract, and we believe TC-6499 may have potential as a treatment for one or more gastrointestinal disorders. In an exploratory four-week study of TC-6499 that we completed at a single site in 2011 in 24 subjects with constipation-predominant irritable bowel syndrome, TC-6499 outperformed placebo on an objective secondary efficacy outcome measure, the number of spontaneous bowel movements per week, but not on the primary efficacy outcome measure (a subjective subject rating of global symptom relief). We are currently considering possible future development plans.
Pentad™
Our drug discovery activities utilize sophisticated proprietary computer-based molecular design methodologies and extensive biological and chemical data for a library of diverse compounds developed and collected over more than 25 years. We refer to these technologies collectively as Pentad.
Role of NNRs in the Nervous System
The human nervous system is a massive communications network that sends and receives information throughout the body via billions of specialized nerve cells known as neurons. Neurons continually gather information about the body’s internal and external environment and send signals to the brain. These signals pass from one neuron to another across a gap between a communicating neuron and a receiving neuron known as a synapse. Electrical impulses of a communicating neuron are converted into chemicals called neurotransmitters that are released by the communicating neuron and bind to specialized proteins known as receptors located across the synapse on the receiving neuron to enable the signal to continue. The major neurotransmitters in the brain include dopamine, serotonin, norepinephrine, glutamate, gamma-aminobutyric acid, or GABA, and acetylcholine.
4
Table of Contents
NNRs are a class of receptors found in the nervous system that play a critical role in modulating the release of neurotransmitters to regulate nervous system activity. When the neurotransmitter acetylcholine is released from a nearby neuron, called an interneuron, and binds to an NNR on a communicating neuron, the flow of neurotransmitters from the communicating neuron to a receiving neuron is adjusted by the NNR. This action, known as neuromodulation, results in a greater release of neurotransmitters across the synapse when the nervous system is understimulated and a lesser release of neurotransmitters across the synapse when the nervous system is overstimulated. As neuromodulators, NNRs serve as the nervous system’s self-adjusting “volume knob.”
The nervous system will not operate properly if the relative levels of key neurotransmitters in the brain are not maintained in a normal balance. A disruption in this balance can cause many common nervous system diseases and disorders. We believe that compounds that target NNRs to modulate their activity have the potential to restore this balance and therefore promise as treatments for these diseases and disorders.
NNRs are comprised of five protein subunits that are arranged like staves of a barrel around a central pore. Each combination of five subunits represents an NNR subtype. There are several subtypes, each of which is identified by Greek letters. Scientific evidence has established that individual NNR subtypes have particular functions in the body that are relevant to a number of debilitating diseases and disorders.
Pfizer’s smoking cessation product Chantix, which acts on several NNR subtypes as well as other molecular targets in the body and is known outside of the United States as Champix, is currently the only product marketed in the United States that is believed to act predominantly by affecting NNRs. Beyond Chantix, many published studies have described beneficial effects of nicotine in humans and animals and the higher prevalence of diseases such as Alzheimer’s disease and Parkinson’s disease in non-smokers as compared to smokers, suggesting the therapeutic potential of compounds that interact with NNRs. However, despite their beneficial effects, these compounds have historically not been desirable as therapies because they have not been sufficiently selective. This means that these compounds interact not only with NNRs, but also with nicotinic receptors in the muscles and in groups of nerve cells known as ganglia that are associated with adverse effects such as increased heart rate, high blood pressure, irregular heartbeat, nausea, vomiting and a dangerous slowing of breathing known as respiratory depression. Based on years of focused research in the NNR area, we are developing product candidates that are designed to interact selectively with specific NNR subtypes to promote positive medical effects and limit adverse side effects.
Our Business Strategy
Our mission is to provide superior treatment options for complex diseases and disorders to improve the lives of patients by developing innovative new medicines that exploit the unique role of NNRs. To achieve our mission, our goal is to leverage our experience and expertise in the biology of NNRs and the discovery and development of novel drugs that selectively target them to become a leader in the commercialization of NNR Therapeutics for diseases and disorders where there is significant medical need and commercial potential. To achieve this goal, we are pursuing the following strategies:
| • | Continue to pursue NNR Therapeutics. We believe that drugs designed to selectively target specific NNR subtypes can have positive medical effects with limited adverse side effects. We intend to continue to use our scientific expertise and Pentad to discover compounds that selectively target specific NNR subtypes as potential treatments for diseases and disorders of the nervous system. |
| • | Collaborate selectively. We have two collaborations with AstraZeneca, one focused on TC-5214 as a treatment for major depressive disorder and one focused in cognitive disorders. We intend to selectively seek additional alliances and collaborations to assist us in furthering the development of some of our product candidates. In particular, we intend to enter into these alliances and collaborations for target indications for which our potential collaborator has particular expertise or that involve large primary care markets that must be served by large sales and marketing organizations. In entering into these alliances and collaborations, our goal will generally be to maintain co-promotion or co-commercialization rights for specialists, particularly in neurology and psychiatry, in the United |
5
Table of Contents
| States and, potentially in some cases, other markets. Under our agreements with AstraZeneca, we have the option to co-promote TC-5214 and AZD3480, as well as AZD1446 and any other licensed compounds that arose out of the preclinical research collaboration, to specified classes of physicians in the United States. |
| • | Maintain leadership position in NNR space. We have established ourselves as a leader in NNR research over more than 25 years. Our leadership position in this area is reflected in the numerous NNR-related articles and abstracts published by our scientists in prominent scientific journals, as well as our extensive patent estate. We intend to continue to invest significant resources to remain at the forefront of NNR research, build upon our NNR expertise and expand our intellectual property portfolio. We also plan to augment our own research by collaborating with commercial and academic institutions that seek access to our proprietary knowledge and compounds. |
| • | Prioritize target indications. We have identified numerous indications in which NNRs have been implicated and for which we believe that drugs that selectively target specific NNR subtypes can potentially provide a medical benefit. We prioritize our product development opportunities in an effort to apply our product pipeline to indications in which there is a significant medical need and commercial potential. |
6
Table of Contents
Our Product Development Pipeline
The following table summarizes our most advanced clinical-stage product candidates.
| Product Candidate |
Planned Target Indication(s) |
Status of Development |
Commercial Rights | |||
| TC-5214 |
Major depressive disorder (adjunct therapy, “switch” monotherapy) | Phase 3 clinical trials as an adjunct therapy and Phase 2b clinical trial as a “switch” monotherapy ongoing; | AstraZeneca | |||
| TC-5619 |
Cognitive dysfunction in schizophrenia, ADHD and Alzheimer’s disease | Phase 2 clinical trial in cognitive dysfunction in schizophrenia completed; separate Phase 2 clinical trial in ADHD in adults and additional studies to support potential Phase 2 clinical development in Alzheimer’s disease ongoing | subject to AstraZeneca’s right to license | |||
| AZD3480 (TC-1734) |
Either or both of ADHD and Alzheimer’s disease | Phase 2 clinical trial in adults with ADHD completed, with decision by AstraZeneca as to whether to advance into Phase 2b development expected in the first half of 2011; Targacept considering the practicability of conducting an additional clinical trial in Alzheimer’s disease | AstraZeneca | |||
| AZD1446 (TC-6683) |
Alzheimer’s disease | Three of four early-stage clinical trials expected to inform an AstraZeneca advancement decision completed | AstraZeneca | |||
| TC-6987 |
One or more disorders characterized by inflammation | Separate Phase 2 clinical trials in asthma and Type 2 diabetes ongoing | Targacept | |||
| TC-6499 |
One or more gastrointestinal disorders | Exploratory Phase 2a clinical trial in subjects with constipation-predominant irritable bowel syndrome completed; Targacept considering possible future development plans | Targacept | |||
Information regarding our research and development expenses for the fiscal years ended December 31, 2010, 2009 and 2008 is included under the caption “Management’s Discussion and Analysis of Financial Condition and Results of Operations” in this annual report. All of our long-lived assets are located in the United States.
7
Table of Contents
TC-5214
TC-5214 is a nicotinic channel modulator that is thought to derive antidepressant activity by modulating the activity of various NNR subtypes and is in development as a treatment for major depressive disorder. TC-5214 is one of the two enantiomers of the racemate mecamylamine hydrochloride. Enantiomers are mirror images of each other that have the same chemical but potentially different biological properties and together form a chemical mixture known as a racemate.
We are co-developing TC-5214 with AstraZeneca under our TC-5214 agreement with AstraZeneca. The initial global clinical program for TC-5214 includes development both as an adjunct, or add-on, therapy and as a “switch” monotherapy, in each case in adults with major depressive disorder who do not respond adequately to initial therapy with a medication from one of two drug classes—selective serotonin reuptake inhibitors, or SSRIs, and serotonin/norepinephrine reuptake inhibitors, or SNRIs. The Phase 3 program, which we and AstraZeneca refer to as the RENAISSANCE Program, is designed to support the planned second half of 2012 filing of a new drug application, or NDA, with the FDA for TC-5214 as an adjunct therapy for major depressive disorder. The RENAISSANCE Program includes four multi-center, double blind, parallel group clinical trials, two with a fixed dose design and two with a flexible dose design, to evaluate the efficacy and tolerability of TC-5214 as an adjunct to continued SSRI or SNRI treatment. In the fixed dose trials, each subject receiving TC-5214 receives a set dosing regimen throughout the dosing period. In the flexible dose trials, each subject receiving TC-5214 initially receives a particular dosage, which can be increased at various times during the trial at the discretion of the applicable investigator based on how the subject tolerates and responds to the then-current dosage. The primary outcome measure for each of the four trials is change from double blind baseline for TC-5214 on the Montgomery-Asberg Depression Rating Scale, or MADRS, which is a scale on which the clinician evaluates the subject’s depressed mood and other symptoms of depression and anxiety, as compared to placebo. The term “double blind” means that neither the subjects nor the investigators know which subjects receive the investigational drug and which subjects receive placebo. The RENAISSANCE Program also includes a double blind, placebo controlled long-term safety trial in which subjects receive TC-5214 or placebo for up to one year.
In addition to the RENAISSANCE Program, we and AstraZeneca are conducting multiple Phase 1 clinical trials of TC-5214, including a QTc study, which is designed to confirm that various doses of TC-5214 do not disturb the electrical activity of the heart, a renal impairment study, which is designed to evaluate the elimination of TC-5214 in subjects with impaired kidney function, and a drug-drug interaction study designed to assess the safety of TC-5214 when used together with particular drugs. We and AstraZeneca also initiated a Phase 2b clinical trial of TC-5214 as a “switch” monotherapy in February 2011.
AstraZeneca is responsible for 80% and we are responsible for 20% of the costs of the initial global clinical program, except that AstraZeneca is responsible for 100% of development costs that are required only to obtain or maintain regulatory approval in countries outside the United States and the European Union. We have the right to terminate our obligation to fund our share of the costs of the initial program once we have funded a specified amount. If we fund the specified amount and terminate our obligation to fund our share of further costs of the initial program, any future milestones and royalties payable to us under the agreement would be reduced by the amount of our unfunded share plus interest at a specified rate, subject to a maximum reduction that may be applied to any one payment.
Completed Phase 2b Clinical Trial in Major Depressive Disorder
In 2009, we completed a Phase 2b clinical trial of TC-5214 as an adjunct, or add-on, therapy in subjects with major depressive disorder who did not respond well to initial treatment with citalopram hydrobromide. Citalopram, an approved treatment for major depressive disorder marketed in the United States as Celexa, is a representative SSRI, which is the drug class most commonly prescribed for major depressive disorder.
The Phase 2b clinical trial was a two-phase study conducted at 20 sites in India and three sites in the United States. The first phase of the trial was “open label,” which means both the subjects and the investigators knew what was being administered. In the first phase, 579 subjects received initial treatment with citalopram for eight
8
Table of Contents
weeks, 20mg daily for the first four weeks and 40mg daily for the next four weeks. At the end of the eight weeks, subjects whose score on MADRS had improved less than 50 percent and was no lower than 17 and whose score on the Clinical Global Impression—Severity of Illness subscale, or CGI-S, which is a scale on which the clinician assesses how ill a subject is based on his or her total clinical experience, was no lower than 4 were considered partial or non-responders and eligible for the second phase of the trial.
The second phase of the trial was double blind and placebo controlled. In this phase, subjects continued their citalopram treatment and also received either add-on TC-5214 or add-on placebo for an additional eight weeks. The daily dosage of TC-5214 was initially 2mg and could be increased at the discretion of the investigator to 4mg and to 8mg based on how the subject tolerated and responded to the then-current dosage.
The primary outcome measure for the trial was mean change between add-on TC-5214 (TC-5214 + citalopram) and add-on placebo (placebo + citalopram) from double blind baseline as measured by the Hamilton Rating Scale for Depression-17, or HAM-D, which is another scale on which the clinician evaluates the subject’s depressed mood and other symptoms of depression and anxiety, at week 16. The magnitude of clinical response on HAM-D was 6.0 points greater for the add-on TC-5214 arm (13.75 point improvement) than for the add-on placebo arm (7.75 point improvement), and the result was highly statistically significant in favor of TC-5214 (p < 0.0001) on an intent to treat basis. The results on all of the trial’s secondary efficacy outcome measures, including MADRS, the Quick Inventory of Depressive Symptomatology – Self Reporting scale and assessments of irritability, disability, cognition, severity of illness and global improvement, were also highly statistically significant in favor of TC-5214 (p < 0.0001) on an intent to treat basis. The intent to treat dataset included 265 subjects in the second phase.
TC-5214 exhibited a favorable tolerability profile in the trial. The most frequent adverse events were headache, dizziness and constipation, and there was no clinically significant difference between the dose groups in discontinuations due to adverse events. There was one serious adverse event in the trial considered by the investigators to be related to study drug (either or both of citalopram and TC-5214), a seizure experienced by a study subject.
TC-5619
TC-5619 is a novel small molecule that modulates the activity of the a7 NNR. In a 2004 survey of 46 cognitive neuroscientists and neuropharmacologists conducted in connection with a National Institute of Mental Health initiative known as Measurement and Treatment Research to Improve Cognition in Schizophrenia, or MATRICS, a7 was selected more often than any other target as a target of interest in the development of treatments for cognitive dysfunction in schizophrenia.
We have completed a Phase 2 clinical trial of TC-5619 in cognitive dysfunction in schizophrenia. In addition, we are currently conducting a separate Phase 2 clinical trial in ADHD in adults, as well as clinical and non-clinical studies to support the potential advancement of TC-5619 into Phase 2 clinical development in Alzheimer’s disease. We expect that a decision as to whether to conduct Phase 2 clinical development of TC-5619 as a treatment for Alzheimer’s disease will be made in the future.
TC-5619 is subject to our cognitive disorders agreement with AstraZeneca as a result of a process that we initiated under the agreement in 2007 and a related election made by AstraZeneca. AstraZeneca has the right to license TC-5619 and to further develop and potentially commercialize TC-5619 for various conditions characterized by cognitive impairment on terms specified in the agreement, as it was amended in April 2010. If AstraZeneca exercises its right to license TC-5619, the agreement provides for AstraZeneca to make a $30 million payment to us and to assume responsibility for and fund all future development (except for completion of our ongoing studies) and commercialization. In that event, we would be eligible to receive additional payments of up to $212 million, if development, regulatory, first commercial sale and first detail milestone events are achieved for three indications, as well as stepped double-digit royalties on any future TC-5619 product sales. We expect AstraZeneca to determine whether to exercise its license right in the first half of 2011.
9
Table of Contents
Completed Phase 2 Trial in Cognitive Dysfunction in Schizophrenia
In January 2011, we announced positive top-line results from a Phase 2 clinical trial of TC-5619 in cognitive dysfunction in schizophrenia. The double blind, placebo controlled trial was conducted at seven sites in the United States and 12 sites in India. In the trial, 185 subjects meeting DSM-IV criteria for schizophrenia, with stable psychotic symptoms and taking a stable dose of an approved medication from the drug class known as atypical anti-psychotics (either quetiapine, marketed as Seroquel, or risperidone, marketed as Risperdal) were randomly assigned to receive either TC-5619 or placebo, together with continued treatment with the atypical antipsychotic, for 12 weeks. As planned, approximately half of the subjects were users of tobacco products. Subjects who received TC-5619 received a 1mg daily dose for the first four weeks, a 5mg daily dose for the next four weeks and a 25mg daily dose for the last four weeks.
The primary efficacy outcome measure of the trial was change from baseline on the Groton Maze Learning task of the CogState Schizophrenia Battery, on each of three measurement dates as compared to placebo. The CogState Schizophrenia Battery is a computerized battery of neuropsychiatric tests that assess specific cognitive domains, and the Groton Maze Learning task is designed to assess executive function, which is the ability to organize cognitive processes, including the ability to plan, prioritize, stop and start activities, shift from one activity to another activity and monitor one’s own behavior. The trial protocol defined a positive outcome on the Groton Maze Learning task as superiority (one-sided p-value < 0.10) for the TC-5619 dose group as compared to the placebo dose group after adjusting statistically to account for multiple comparisons.
In the trial, the results on the Groton Maze Learning task met the pre-defined success criteria (adjusted p-value = 0.054), as well as at two of the trial’s three measurement dates (at 4 weeks, unadjusted p-value = 0.018; and at 12 weeks, unadjusted p-value = 0.041), and were favorable for tobacco users as compared to non-tobacco users and for subjects at study sites in the United States as compared to subjects at study sites in India. There was no activity in non-tobacco users. Estimates of the prevalence of smoking amongst schizophrenia patients vary, with one study indicating as high as 80%. Each of the p-values noted above was derived after data log transformation, a commonly utilized technique where the data does not follow a normal distribution.
In addition, positive signals were observed in the trial on several secondary efficacy outcome measures, including Scale for Assessment of Negative Symptoms, an investigator assessment of improvement on the negative symptoms of schizophrenia, Clinical Global Impression – Global Improvement, an investigator assessment of overall response, and Subject Global Impression – Cognition scale, a patient self-assessment of cognitive change. Other secondary outcome measures of the trial, including a composite measure of the CogState Schizophrenia Battery, did not demonstrate a drug effect in the dataset that included all subjects.
TC-5619 exhibited a favorable tolerability profile in the trial. There were two serious adverse events in the trial, one in the placebo dose group and one in the TC-5619 dose group. Both were considered by the applicable investigator as not drug related.
Ongoing Phase 2 Trial in Adults with ADHD
We are currently conducting a Phase 2 clinical trial of TC-5619 in adults with ADHD. The trial is designed as a double blind, placebo controlled, parallel group study and is being conducted in the United States. In the trial, approximately 125 adult subjects are randomly assigned to one of two cohorts, TC-5619 or placebo, and dosed over a 12-week period. Subjects in the TC-5619 cohort receive 1mg doses of TC-5619 for the first four weeks, 5mg doses of TC-5619 for the next four weeks and 25mg doses of TC-5619 for the last four weeks. The primary efficacy outcome measure of the trial is change from baseline on the Conners Adult ADHD Rating Scale, a multimodal questionnaire assessment of symptoms and behaviors associated with ADHD in adults aged 18 and older, as compared to placebo. The trial also includes a number of secondary efficacy outcome measures. We expect results from the trial to become available by the end of the first quarter of 2011.
10
Table of Contents
AZD3480 (TC-1734)
AZD3480 (TC-1734) is a novel small molecule that modulates the activity of the a4ß2 NNR and is subject to our cognitive disorders agreement with AstraZeneca. We or AstraZeneca has completed Phase 2 clinical trials of AZD3480 in various indications characterized by cognitive impairment that have generated a range of efficacy results, including: (1) achievement of primary outcome measure(s) (a Phase 2 clinical trial conducted by us and AstraZeneca in adults with ADHD and our Phase 2 trial reported in 2006 in age associated memory impairment, or AAMI, a common condition characterized by gradual memory loss or other cognitive impairment that generally occurs with normal aging); (2) inconclusive (AstraZeneca’s Phase 2b trial in mild to moderate Alzheimer’s disease completed in 2008); (3) positive signals (our Phase 2a studies in AAMI and mild cognitive impairment, or MCI; and (4) failure to achieve primary outcome measures (AstraZeneca’s Phase 2b trial in cognitive dysfunction in schizophrenia completed in 2008).
We are in discussions with AstraZeneca regarding potential additional development of AZD3480 as a treatment for ADHD. Whether AstraZeneca will decide to conduct additional development of AZD3480 in ADHD is uncertain in light of reservations about the adequacy of the therapeutic margin to support development across the broad ADHD patient population. We expect AstraZeneca to make its decision in the first half of 2011.
In addition, we have agreed with AstraZeneca on respective roles and financial and non-financial responsibilities for an additional clinical trial of AZD3480 in Alzheimer’s disease. We have had a favorable meeting with the FDA regarding a potential development path for AZD3480 in Alzheimer’s disease and are continuing to explore the practicability of conducting an Alzheimer’s disease study in Europe. If an Alzheimer’s disease study proceeds, we would be responsible for funding the study but would be entitled to receive up to $5.7 million in additional payments from AstraZeneca, with the last tranche being payable to us upon first dosing in the United States and Europe.
Completed Phase 2 Trial in Adults with ADHD
In 2009, we and AstraZeneca completed a Phase 2 clinical trial of AZD3480 in adults with ADHD. The trial was a double blind, placebo controlled crossover study conducted at Fletcher Allen Health Care, an affiliate of University of Vermont College of Medicine. Subjects were non-smoking males and females between the ages of 18 and 65 who were diagnosed with ADHD based on Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, or DSM-IV, criteria and had a baseline score of at least 4 on CGI-S. Each subject received 5mg AZD3480, 50mg AZD3480 and placebo daily for two weeks, in random order, with the three dosing periods separated by three-week periods without any dosing to minimize carryover effects. As a result, each subject served as his or her own control.
The primary outcome measure for the trial was the change in total symptom score on the Conners Adult ADHD Rating Scale—Investigator Rating, or CAARS-INV, a scale that takes into account nine domains thought to encompass a range of ADHD manifestations in adults, following two weeks dosing with AZD3480 as compared to two weeks dosing with placebo. In the trial, the subjects’ symptoms of ADHD as measured by CAARS-INV improved with 50mg AZD3480, and the result was statistically significant (p < 0.01) on an intent to treat basis. Statistically significant results were also achieved at 50mg AZD3480 on some, but not all, of the secondary outcome measures in the study, including Stop Signal Reaction Time, a computerized assessment of behavioral inhibition, which is a core cognitive deficit of ADHD. AZD3480 was well tolerated in the study, and there were no serious adverse events.
Completed Phase 2b Clinical Trial in Mild to Moderate Alzheimer’s Disease
In 2008, AstraZeneca completed two Phase 2b double blind, placebo controlled, dose finding clinical trials of AZD3480, one in mild to moderate Alzheimer’s disease and one in cognitive dysfunction in schizophrenia. The trial in mild to moderate Alzheimer’s disease, known as the “Sirocco” trial, was conducted at 84 sites in Western Europe, Eastern Europe and Canada. In the Sirocco trial, 567 subjects who were between 60 and 85
11
Table of Contents
years old and diagnosed with probable Alzheimer’s disease classified as mild or moderate in severity were randomly assigned to one of three dose groups of AZD3480, to the active comparator donepezil (the most commonly prescribed drug for Alzheimer’s disease), or to placebo and dosed over a 12-week period. The primary outcome measure of the trial was change from baseline after 12 weeks on the Alzheimer’s Disease Assessment Scale-cognitive subscale, or ADAS-Cog. Some of the secondary outcome measures of the trial included the Alzheimer’s Disease Cooperative Study—Clinical Global Impression of Change, or ADCS-CGIC, which is a 7-point clinician assessment of change in behavior and the ability to function, the Mini Mental State Examination, or MMSE, which is a quantitative, 30-point cognition scale, and a computer-based test battery developed by CDR Ltd. to test cognitive function.
The results of the Sirocco trial were inconclusive. Neither the active comparator donepezil nor AZD3480 met the trial’s criteria for statistical significance on the primary outcome measure, ADAS-Cog. However, in an analysis conducted post hoc in which the most mildly impaired subjects (MMSE = 25 or 26) were excluded, the middle dose of AZD3480 tested achieved statistical significance (one-sided p-value = 0.04) and donepezil showed a strong trend (one-sided p-value = 0.065).
Subjects dosed with AZD3480 showed an improvement on ADCS-CGIC and the MMSE, two of the trial’s secondary outcome measures, at two of the three doses tested as compared to subjects dosed with placebo. Of the three AZD3480 doses evaluated, subjects in the middle dose group showed the most improvement on both measures as compared to subjects dosed with placebo, with a 0.5 point advantage on ADCS-CGIC and a 0.9 point advantage on the MMSE. Subjects dosed with donepezil also showed an improvement as compared to subjects dosed with placebo on ADCS-CGIC, with a 0.2 point advantage, and the MMSE, with a 1.0 point advantage. No improvement was shown in any domain of the CDR test battery in the pooled dataset of all subjects in the donepezil dose group or any of the AZD3480 dose groups as compared to the placebo dose group. AZD3480 exhibited an overall safety and tolerability profile comparable to placebo in the trial.
Completed Phase 2b Clinical Trial in Cognitive Dysfunction in Schizophrenia
AstraZeneca’s Phase 2b clinical trial of AZD3480 in cognitive dysfunction in schizophrenia completed in 2008, known as the “HALO” trial, was conducted at approximately 70 enrolling sites in the United States and Canada. In the trial, 445 subjects diagnosed with schizophrenia who were between 18 and 55 years old, active smokers, taking a marketed drug from the class known as atypical anti-psychotics and clinically stable were randomly assigned to one of three dose groups of AZD3480 or to placebo and dosed, together with continued treatment with the applicable atypical anti-psychotic, over a 12-week period. The primary endpoints of the trial were change from baseline after 12 weeks on scores for attention/vigilance, working memory, verbal learning, speed of processing and reasoning and problem solving as measured by a computerized test battery known as IntegNeuro. As used in this annual report, the terms “endpoint” and “outcome measure” have the same meaning. AZD3480 did not meet the HALO trial’s criteria for statistical significance on any of the primary endpoints.
Completed Phase 2 Clinical Trial in AAMI Reported in 2006
In 2006, we reported results from a double blind, placebo controlled Phase 2 clinical trial of AZD3480 in AAMI in the United States. We recruited 193 subjects between the ages of 50 and 80, who were classified with AAMI based on inclusion criteria reflecting both subjective and objective memory impairment, to participate in the trial. The trial assessed the effects of 25mg AZD3480 and 50mg AZD3480 on various aspects of cognitive function using the CDR test battery. We tested each subject at various time points prior to the first day of the 16-week dosing period to establish baseline. We tested subjects again at eight weeks and on the last day of the 16-week dosing period. The CDR test battery includes measures of attention, speed of cognitive processes and memory that assess the ability to react to stimuli, recognize words and pictures and recall words. These measures are then used to make composite assessments on five factors—power of attention, continuity of attention, working or short-term memory, episodic or long-term memory and speed of memory.
12
Table of Contents
There were three co-primary efficacy endpoints for the trial, including:
| • | power of attention—change from baseline on the power of attention factor of the CDR test battery at the end of the 16-week dosing period, as compared to placebo; |
| • | episodic memory—change from baseline on the episodic memory factor of the CDR test battery at the end of the 16-week dosing period, as compared to placebo; and |
| • | subject global impression—composite score on a cognitive performance scale comprised of three seven-point measures in which each subject rates himself or herself on attention, memory and speed of thinking at the end of the 16-week dosing period, as compared to placebo. |
On an intent to treat basis, subjects in the 50mg AZD3480 dose group showed improvement as compared to subjects in the placebo dose group on all three co-primary efficacy endpoints and subjects in the 25mg AZD3480 dose group showed improvement as compared to subjects in the placebo dose group on the power of attention endpoint. These results were statistically significant, with p-values less than 0.05.
Previously Completed Phase 2 Clinical Trials in AAMI and MCI
Prior to the Phase 2 clinical trial of AZD3480 in AAMI described above, we completed two double blind, placebo controlled, crossover design Phase 2 clinical trials of AZD3480, one in AAMI and one in MCI. In the AAMI trial, we evaluated four doses of AZD3480, 50mg, 100mg, 125mg and 150mg. In the MCI trial, we evaluated two doses of AZD3480, 50mg and 100mg. Each trial assessed the effects of AZD3480 on various aspects of cognitive function using the CDR test battery before dosing and at various time points after dosing on the first and last day of each dosing period.
In both trials, AZD3480 demonstrated positive effects at some dose levels with respect to some measures of cognition tested, but did not demonstrate positive effects as to all measures at all dose levels and placebo showed superior effects to AZD3480 as to some measures at some dose levels. The results of the AAMI trial were most favorable in the 50mg AZD3480 dose group and were less pronounced in the other dose groups. The results of the MCI trial were more favorable in the 100mg AZD3480 dose group, as the results in the 50mg AZD3480 dose group did not favor AZD3480 on any measure.
AZD1446 (TC-6683)
AZD1446 (TC-6683) is a novel small molecule that modulates the activity of the a4ß2 NNR and is under consideration for further development as a treatment for Alzheimer’s disease under our cognitive disorders agreement with AstraZeneca. We discovered and advanced AZD1446 as part of a now completed preclinical research collaboration that we and AstraZeneca conducted under the agreement. AstraZeneca is responsible for conducting and funding the development and potential future commercialization of AZD1446 and has completed three of four early-stage clinical studies expected to inform its decision as to whether to advance the product candidate, including:
| • | a trial in adults with ADHD in which AZD1446 did not improve core symptoms of ADHD, as compared to placebo, as measured by the primary outcome measure (CAARS-INV), but showed signals of a drug effect in non-nicotine using subjects (but not nicotine using subjects) at specific doses on two of five tasks of the CogState ADHD Battery, computerized tests used as secondary outcome measures to assess cognitive functions such as learning and memory (80mg of AZD1446 once daily, Groton Maze Learning Task (p = 0.019) and International Shopping List Task—Immediate Recall (p = 0.055); and 80mg of AZD1446 three times daily, International Shopping List Task—Immediate Recall (p = 0.079)—with all of such p-values statistically adjusted for multiplicity); |
| • | a four-week trial designed primarily to evaluate the safety and tolerability of AZD1446 when administered with donepezil to subjects with Alzheimer’s disease in which AZD1446 exhibited a safety |
13
Table of Contents
| and tolerability profile acceptable for further development and, as expected with a short dosing period and small number of subjects, did not show an effect on surrogate measures of cognition and global function; and |
| • | a trial designed to explore the effects of a single dose of AZD1446 in healthy volunteers with drug-induced cognitive impairment in which pro-cognitive signals were observed on various secondary outcome measures but neither AZD1446 nor the positive comparator donepezil demonstrated a statistically significant effect on an assessment of reversal of a drug-induced effect on brain waves associated with attention, which was the primary outcome measure. |
A fourth study, which has not completed, is designed to evaluate the effect of AZD1446 and donepezil on brain response in subjects with Alzheimer’s disease as assessed by electroencephalography (EEG). We expect AstraZeneca to decide whether to conduct further development of AZD1446 as a treatment for Alzheimer’s disease in the third quarter of 2011.
TC-6987
TC-6987 is a novel small molecule that modulates the activity of the a7 NNR. We have completed Phase 1 clinical development and have ongoing separate Phase 2 studies planned to help guide the selection of indications for which TC-6987 is best suited for later-stage development. One of the Phase 2 studies is in asthma and the other is in Type 2 diabetes. Both studies were designed to include a number of different efficacy measures that would show anti-inflammatory effects of TC-6987 and inform potential future development.
Ongoing Phase 2 Trial in Asthma
The Phase 2 clinical trial in asthma is a multicenter, double blind, placebo controlled, parallel group study being conducted in the United States. The study is planned to enroll approximately 90 adult subjects with asthma mild to moderate in severity. The study design provides for subjects to undergo a four-week wash-out period during which they receive a low-dose inhaled corticosteroid and cease taking their current asthma medication before being randomly assigned to one of two cohorts. Subjects then receive either placebo or TC-6987 once daily, together with the low-dose inhaled corticosteroid, for four weeks. Subjects in the TC-6987 cohort receive a 100mg dose on the first day of dosing and then a 50mg dose for the remainder of the dosing period. The study includes several efficacy outcome measures, with change in forced expiratory volume from baseline to end of dosing for subjects receiving TC-6987 as compared to placebo designated as the primary efficacy outcome measure. The study also includes assessments of safety, tolerability and pharmacokinetics of TC-6987.
Ongoing Phase 2 Trial in Type 2 Diabetes
As in the asthma study described above, the Phase 2 clinical trial in Type 2 diabetes is a multicenter double blind, placebo controlled, parallel group trial being conducted in the United States. The study is planned to enroll approximately 120 adult subjects with Type 2 diabetes. The study design includes a one-week screening period followed by a four-week washout period during which subjects cease taking their current medication for Type 2 diabetes before being randomly assigned to one of two cohorts. Subjects then receive either TC-6987 or placebo once daily for four weeks. Subjects in the TC-6987 cohort receive a 20mg dose on the first day of dosing and then a 10mg dose for the remainder of the dosing period. The study includes several efficacy outcome measures, with change in fasting plasma glucose (a metabolic measurement used to expose problems with insulin function) from baseline to end of dosing for subjects receiving TC-6987 as compared to placebo designated as the primary efficacy outcome measure. The study also includes assessments of safety, tolerability and pharmacokinetics of TC-6987.
TC-6499
TC-6499 is a novel small molecule that modulates the activity of the a4ß2 and a3ß4 NNRs. The a3ß4 NNR is located in the gastrointestinal tract and, based on observations from previous Phase 1 development of TC-6499
14
Table of Contents
in contemplation of later-stage development as a treatment for pain, we believe the product candidate may have potential as a treatment for one or more gastrointestinal disorders. In an exploratory four-week study of TC-6499 that we completed in 2011 in 24 subjects with constipation-predominant irritable bowel syndrome, TC-6499 outperformed placebo on an objective secondary efficacy outcome measure, the number of spontaneous bowel movements per week, but not on the primary efficacy outcome measure (a subjective subject rating of global symptom relief). We are currently considering possible future development plans. As previously disclosed, we are no longer developing TC-6499 as a treatment for pain.
Medical Need and Commercial Opportunity in Our Target Indications
The indications for which our most advanced product candidates are currently in development include major depressive disorder, cognitive dysfunction in schizophrenia, ADHD, Alzheimer’s disease and inflammatory disorders (currently asthma and Type 2 diabetes).
Major depressive disorder is characterized by a combination of symptoms that interfere with a person’s ability to work, sleep, study, eat and enjoy once-pleasurable activities. It is disabling and can prevent a person from functioning normally. The market research firm Decision Resources estimated that approximately 42.4 million people suffered from major depressive disorder in the world’s seven major pharmaceutical markets—the United States, France, Germany, Italy, Spain, the United Kingdom and Japan—in 2009. The Sequenced Treatment Alternatives to Relieve Depression, or STAR*D, study undertaken by the National Institute of Mental Health between 2001 and 2006 showed the inadequacy of currently available therapies for major depressive disorder. In the first phase of the STAR*D study, approximately 2,800 persons with major depressive disorder were given the representative SSRI citalopram for 12 to 14 weeks. Only about one-third of the participants became symptom free, which is referred to as achieving “remission,” and about 10-15 percent more responded, but did not reach remission.
Schizophrenia is a chronic, severe and disabling form of psychosis. In addition to symptoms such as delusions, hallucinations, the inability to disregard familiar stimuli, sometimes referred to as sensory gating, disorganized speech, grossly disorganized or catatonic behavior and prolonged loss of emotion, feeling, volition or drive, schizophrenia is often marked by impairment in cognitive functions, such as attention, vigilance, memory, and reasoning. Decision Resources estimated that there were approximately 4.6 million people with schizophrenia in the world’s seven major pharmaceutical markets in 2009. It has been estimated that up to 75% of persons with schizophrenia are cognitively impaired. There is currently no drug approved in the United States or Europe specifically for cognitive dysfunction in schizophrenia.
ADHD is a condition that develops during childhood and, if not adequately treated, can have long-term adverse effects into adolescence and adulthood. The principal characteristics of ADHD are inattention, hyperactivity and impulsivity. For an adult to be diagnosed with ADHD, the ADHD symptoms must have begun during childhood and continued throughout adulthood. Decision Resources estimated that there were approximately 23.3 million adults and 21.6 million children with ADHD in the world’s seven major pharmaceutical markets in 2009. The most commonly used treatments for ADHD are from the drug class known as stimulants. Because stimulants have potential for abuse, they are scheduled and can therefore be burdensome for patients. All of the currently available treatments for ADHD have side effects, such as increased heart rate and blood pressure, loss of appetite, insomnia and behavioral changes like irritability.
Alzheimer’s disease, the most common form of dementia, is a debilitating brain disorder for which there is no cure. Decision Resources estimated that there were approximately 9.7 million people with Alzheimer’s disease in the world’s seven major pharmaceutical markets in 2009. The disease progresses in stages from mild to moderate to severe and gradually destroys a person’s memory and ability to learn, reason, make judgments, communicate and carry out daily activities. Mild Alzheimer’s disease is characterized by mild forgetfulness and difficulty acquiring basic information and communicating. Patients generally exhibit the symptoms of mild Alzheimer’s disease for two to four years before progressing to the moderate stage. Moderate Alzheimer’s disease is characterized by forgetfulness, failure to recognize friends and family, disorientation regarding time
15
Table of Contents
and place and personality changes. Patients generally exhibit the symptoms of moderate Alzheimer’s disease for up to ten years before progressing to the severe stage. Severe Alzheimer’s disease is characterized by difficulty performing simple tasks and activities associated with daily living. Patients with severe Alzheimer’s disease require continuous care and generally do not survive for more than three years.
Asthma is a chronic inflammatory disorder of the lungs and airways characterized by recurring periods of wheezing, chest tightness, shortness of breath and coughing, which occurs most often at night or early in the morning. The disorder affects people of all ages, but most often starts in childhood and is one of the most common long-term diseases of childhood. Asthma attacks are triggered by various genetic and environmental factors, including family history, second-hand smoke, dust mites, air pollution and allergens. Decision Resources has estimated that there were approximately 65 million people with asthma in the world’s seven major pharmaceutical markets in 2009.
Diabetes is a chronic disease characterized by high blood sugar, either because the body does not produce enough of the blood sugar-regulating hormone insulin (Type 1 diabetes) or because the body fails to use insulin properly (Type 2 diabetes). High blood sugar, or hyperglycemia, can over time lead to serious damage to many of the body’s systems, especially the nerves and blood vessels. Symptoms of diabetes include excessive excretion of urine, thirst, constant hunger, weight loss, vision changes and fatigue. Type 2 diabetes is the most common form of diabetes and is thought to be largely the result of excess body weight and physical inactivity. According to the World Health Organization, approximately 198 million people worldwide have Type 2 diabetes, representing about 90% of all diabetics. Deaths related to complications from the disease are expected to double between 2005 and 2030.
Our Preclinical Research Programs
In addition to our clinical-stage product candidates, we focus preclinical research efforts in areas in which we believe NNRs can be exploited for medical benefit and for which we believe we can efficiently develop marketable product candidates. We have research programs targeting the design and development of (1) nicotinic channel modulators, which we believe have potential therapeutic application for a number of indications, (2) compounds that act on the a7 NNR for the treatment of disorders characterized by cytokine-mediated inflammation and (3) Parkinson’s disease. We have been awarded two grants from The Michael J. Fox Foundation for Parkinson’s Research. One of the grants is to test the potential of compounds that modulate NNRs to address abnormal involuntary movements, or dyskinesias, that are a side effect of levodopa treatment, and the other is to identify compounds that bind to specific NNRs and can be radiolabeled and used as imaging agents to better understand any relationship between those NNRs and Parkinson’s disease. Levodopa is commonly used to treat the motor deficits of Parkinson’s disease. The financial resources that we apply to and the progress that we may make in any particular preclinical program may vary from period to period and year to year.
Our Drug Discovery Technologies—Pentad
Our drug discovery activities utilize sophisticated proprietary computer-based molecular design methodologies and extensive biological and chemical data for a library of diverse compounds developed and collected over more than 25 years. We refer to these technologies collectively as Pentad. We use Pentad to predict the likelihood that novel compounds will interact with various NNRs, the degree of the interaction and the potential of these compounds to be developed as drugs based on projected pharmacokinetic profiles.
Pentad’s virtual screening facilitates more rapid identification and prioritization of compounds that may be clinically viable than we believe could be achieved using traditional laboratory synthesis and screening methods. This allows us to reduce drug development time by focusing our resources on compounds believed to have a greater likelihood of clinical success.
16
Table of Contents
Discontinued Product
As a result of increased fees charged by the FDA and declining prescriptions, we discontinued the commercialization of Inversine, which is currently our only approved product, effective as of September 30, 2009. Inversine is approved in the United States for the management of moderately severe to severe essential hypertension and uncomplicated cases of malignant hypertension, which are high blood pressure disorders. Inversine has been approved for marketing since the 1950s, and we acquired marketing rights to the product in August 2002 from Layton Bioscience, Inc., which had previously acquired the rights from Merck & Co., Inc.
Strategic Alliances and Collaborations
AstraZeneca AB – TC-5214
On December 3, 2009, we entered into a collaboration and license agreement with AstraZeneca AB for the global development and commercialization of TC-5214. The agreement became effective later in December. Pursuant to the agreement, we granted AstraZeneca an exclusive global license under patents and other technology owned or licensed by us to develop and commercialize TC-5214, as well as any other compounds of ours that meet specified structural and pharmacological criteria designed to reflect substantial similarity to TC-5214, for all fields of use except hypertension.
Payment Terms. In January 2010, AstraZeneca made a non-refundable upfront payment to us of $200 million, which was triggered upon the agreement becoming effective. The agreement provides for us to be eligible to receive up to an additional $540 million if specified development, regulatory and first commercial sale milestone events are achieved, up to an additional $500 million if specified sales-related milestones are achieved, and significant stepped double digit royalties on any future TC-5214 product sales. Under the terms of an existing license agreement, we paid $16 million to University of South Florida Research Foundation, or USFRF, based on our receipt of the upfront payment from AstraZeneca and, if we receive any milestone payments from AstraZeneca under the agreement, we would be required to pay a percentage of each such milestone payment, after deducting from the milestone payment the unexhausted portion of our projected share of the costs of the initial development program for TC-5214, as well as royalties on any future TC-5214 product sales, to USFRF. The percentage of each milestone payment, net of any deduction, that we would be required to pay would be at least 10% and could be greater in specified circumstances. Based on the terms of the license agreement with USFRF and the terms of another existing license agreement with Yale University, we expect to pay royalties at an effective worldwide rate in the low single digits and that such effective royalty rate could in some circumstances reach the mid single digits.
AstraZeneca’s obligation to pay royalties to us for TC-5214 expires on a country-by-country basis on the later of expiration of the patent rights in each country licensed by us to AstraZeneca that have a specified scope or 12 years after the first commercial sale of TC-5214 in that country. The U.S. patent rights with respect to TC-5214 licensed by us to AstraZeneca expire between 2017 and 2020 and the corresponding licensed foreign patent rights licensed by us to AstraZeneca expire between 2017 and 2019. We have also licensed to AstraZeneca pending U.S. and foreign patent applications with respect to TC-5214 that, if issued as patents, would expire between 2019 and 2030. None of the foregoing years of expiration reflect any patent term extension that may be available in a particular country. It is uncertain whether any of the pending U.S. and foreign patent applications, even if issued as a patent, would be sufficient to extend our royalty term under the agreement for TC-5214 in any particular country. Royalty rates are subject to reduction under the agreement in specified circumstances, including in any country if TC-5214 is not subject to patent protection with a specified scope in that country or if AstraZeneca licenses patent rights from any third party under circumstances in which it is more likely than not that TC-5214 would infringe the third party’s patent rights.
Development and Commercialization. The agreement provides for us and AstraZeneca to co-develop TC-5214 under the oversight of a committee comprised of representatives of each company. The initial global clinical program includes development of TC-5214 as an adjunct (or add-on) to antidepressant therapy and as a
17
Table of Contents
“switch” monotherapy, in each case in adults with major depressive disorder who do not respond adequately to initial antidepressant treatment. AstraZeneca is responsible for 80% and we are responsible for 20% of the costs of the initial program, except that AstraZeneca is responsible for 100% of development costs that are required only to obtain or maintain regulatory approval in countries outside the United States and the European Union. We have the right to terminate our obligation to fund our share of the costs of the initial program once we have funded a specified amount. If we fund the specified amount and terminate our obligation to fund our share of further costs of the initial program, any future milestones and royalties payable to us under the agreement would be reduced by the amount of our unfunded share plus interest at a specified rate, subject to a maximum reduction that may be applied to any one payment. In addition, if we and AstraZeneca mutually agree to develop TC-5214 for any indication other than major depressive disorder or in any formulation other than those contemplated by the initial program, the same cost sharing arrangement would apply, except that we would have the immediate right to terminate our obligation to fund our share of development costs for the other indication or formulation. If we terminate our obligation to fund our share of these other development costs, any future milestones and royalties payable to us under the agreement would be reduced by the amount of our unfunded share plus interest at a specified rate, subject to a maximum reduction that may be applied to any one payment, but only from and after the occurrence of a specified event to be agreed upon by both parties (e.g., receipt of regulatory approval of the applicable indication or formulation).
AstraZeneca is responsible under the agreement for executing and funding the costs of global commercialization of TC-5214, and we have retained an option to co-promote TC-5214 to a specified target physician audience in the United States. If we exercise our co-promotion option, AstraZeneca would compensate us on a per detail basis. AstraZeneca is also responsible under the agreement for the manufacture and supply of TC-5214 and has assumed our rights and obligations under our applicable agreements with third parties.
Restrictions. For a three-year period beginning with effectiveness of the agreement in December 2009, neither we nor AstraZeneca is permitted to conduct, or to grant a license to any third party to conduct, a Phase 2 or later clinical trial of a compound as an adjunct (or add-on) to antidepressant treatment for major depressive disorder, or to commercialize such a compound, subject to certain exceptions that include, among others, AstraZeneca’s right to develop and commercialize quetiapine (marketed by AstraZeneca as Seroquel XR) and other atypical antipsychotic products that meet a specified condition.
AstraZeneca has agreed under the agreement not to take specified actions with respect to acquiring control of us without our consent for a specified period. These restrictions, which cease to apply in various circumstances, do not preclude AstraZeneca from making confidential proposals that do not require us to make a public disclosure.
Termination. AstraZeneca can terminate the agreement in its entirety: within a specified period following completion of the Phase 3 development program for TC-5214 as an adjunct therapy; or if AstraZeneca determines there to be a serious safety issue regarding the continued development or commercialization of TC-5214; or if, having obtained the advice of independent patent counsel, AstraZeneca believes that the commercialization of TC-5214 is more likely than not to infringe or misappropriate intellectual property rights of third parties in the United States or any two specified major pharmaceutical markets and is unable to obtain a license on commercially reasonable terms. In addition, AstraZeneca can terminate the agreement on a major pharmaceutical market by major pharmaceutical market basis at any time beginning four years after effectiveness of the agreement, except that, if AstraZeneca terminates the agreement with respect to the United States, the agreement will terminate in its entirety. We can terminate the agreement if AstraZeneca or any of its affiliates or sublicensees challenges the validity or enforceability of any of the patent rights licensed to AstraZeneca. Either party can terminate the agreement in the event of the insolvency or uncured material breach of the other party. However, if an uncured material breach by AstraZeneca is limited to a specified major pharmaceutical market, we can terminate the agreement only with respect to that market. The rights and obligations of the parties that survive termination of the agreement, including license grants and payment obligations, vary depending on the basis for the termination.
18
Table of Contents
In addition, in the event of a change of control of us, AstraZeneca can terminate specified provisions of the agreement, including our right to participate on the committee overseeing development under the agreement and our co-promotion rights.
AstraZeneca AB – Cognitive Disorders
In December 2005, we entered into a collaborative research and license agreement with AstraZeneca AB under which we granted AstraZeneca exclusive development and worldwide commercialization rights to AZD3480 as a treatment for specified conditions characterized by cognitive impairment, including ADHD, Alzheimer’s disease, cognitive dysfunction in schizophrenia, AAMI, MCI and any other indication that is deemed a cognitive disorder under the agreement, as well as schizophrenia. The agreement became effective in January 2006.
We or AstraZeneca has conducted several clinical studies of AZD3480 in various cognitive disorders and we are in discussions with AstraZeneca regarding potential additional development of the product candidate as a treatment for ADHD. Whether AstraZeneca will decide to conduct any additional development of AZD3480 in ADHD is uncertain in light of reservations about the adequacy of the therapeutic margin to support development across the broad ADHD patient population. We expect AstraZeneca to make its decision in the first half of 2011. In addition, we are exploring the practicability of conducting an additional clinical trial of AZD3480 in Alzheimer’s disease and have agreed with AstraZeneca on respective roles and financial and non-financial responsibilities for such a study.
We and AstraZeneca also conducted a multi-year preclinical research collaboration under the agreement. The term of the research collaboration expired in January 2010. AZD1446 is the most advanced compound that arose from the research collaboration and it is under consideration for further development as a treatment for Alzheimer’s disease. AstraZeneca has completed three of four early-stage clinical studies expected to inform its decision as to whether to advance AZD1446, and we expect AstraZeneca to make its decision in the third quarter of 2011.
As a result of a process that we initiated under the agreement and a related election made by AstraZeneca, TC-5619 is also subject to the agreement. AstraZeneca has the right to license TC-5619 and to further develop and potentially commercialize TC-5619 for various conditions characterized by cognitive impairment on terms specified in the agreement, as it was amended in April 2010. We expect AstraZeneca to determine whether to exercise its license right in the first half of 2011.
Payment Terms. AstraZeneca paid us an initial fee of $10 million in February 2006, an additional $20 million in January 2007 as a result of its December 2006 determination to proceed with further development of AZD3480 and an additional $10 million in July 2009 as a result of the achievement of the objective in the Phase 2 clinical trial of AZD3480 in adults with ADHD. We are eligible to receive other payments of up to $103 million, if development, regulatory and first commercial sale milestone events for AZD3480 are achieved only for ADHD, and stepped double-digit royalties on any future AZD3480 product sales for any indication. We are also eligible to receive other payments if we proceed with another Alzheimer’s disease study of AZD3480, AstraZeneca subsequently advances AZD3480 into later-stage development for Alzheimer’s disease and development, regulatory and first commercial sale milestone events for AZD3480 are achieved for Alzheimer’s disease. The aggregate amount of contingent milestone payments that we are eligible to receive with respect to Alzheimer’s disease and ADHD is $197 million. If AZD3480 is developed under the agreement for an indication in addition to Alzheimer’s disease and ADHD, we would also be eligible to receive payments of up to $52 million for each such indication, if development, regulatory, first commercial sale and first detail milestone events are achieved. Under the terms of a sponsored research agreement and a subsequent license agreement between us and University of Kentucky Research Foundation, or UKRF, if we receive any of these payments from AstraZeneca relating to AZD3480, including royalties, we are required to pay a low single digit percentage of each such payment to UKRF.
19
Table of Contents
With respect to AZD1446, AstraZeneca has paid us $2.2 million upon the achievement of development and regulatory milestone events. We are also eligible to receive other payments of up to $73 million, if development, regulatory and first commercial sale milestone events for AZD1446 are achieved only for Alzheimer’s disease, and stepped royalties on any future AZD1446 product sales for any indication. If AZD1446 is developed under the agreement for an indication in addition to Alzheimer’s disease, we would also be eligible to receive payments of up to $35 million for each such indication, if development, regulatory, first commercial sale and first detail milestone events are achieved.
If AstraZeneca licenses TC-5619, the agreement provides for AstraZeneca to make a $30 million payment to us. In that event, we would be eligible to receive additional payments of up to $212 million, if development, regulatory and first commercial sale and first detail milestone events are achieved for three indications, as well as stepped double-digit royalties on any future TC-5619 product sales.
AstraZeneca’s obligation to pay royalties to us for each compound subject to the collaboration expires on a country-by-country basis on the later of expiration of our patent rights that provide exclusivity for that compound in that country or 12 years after the first commercial sale in that country of either that compound or any related compound that meets specified criteria. If AstraZeneca obtains a patent covering the composition of a compound that is derived within a specified period from a compound that is subject to the collaboration, the term of AstraZeneca’s patent would also be taken into account in determining the term of AstraZeneca’s obligation to pay royalties to us for that derived compound. The U.S. patent rights to the chemical genus that includes TC-5619 expire in 2019 and the U.S. patent rights to a method of using a racemic mixture that includes TC-5619 to treat schizophrenia expire in 2025. The foreign patent rights that have issued and correspond to our issued U.S. patent rights expire in 2024. We also have a pending U.S. patent application with respect to TC-5619 specifically and to a particular salt form of TC-5619 that, if issued as patents, would expire in 2028. The U.S. patent rights with respect to AZD3480 expire between 2016 and 2027. The foreign patent rights with respect to AZD3480 that have issued and correspond to our issued U.S. patent rights expire between 2017 and 2027. We also have pending U.S. and foreign patent applications with respect to AZD3480 that, if issued as patents, would expire between 2017 and 2029. In addition, we have pending U.S. and foreign patent applications with respect to AZD1446 that, if issued as patents, would expire in 2027. None of the foregoing years of expiration reflect any patent term extension that may be available in a particular country. It is uncertain whether any of the pending U.S. and foreign patent applications, even if issued as a patent, would be sufficient to extend our royalty term under the agreement for AZD3480, AZD1446 or, if licensed by AstraZeneca, TC-5619 in any particular country. Royalty rates are subject to reduction under the agreement in specified circumstances, including in any country if the licensed compound is no longer subject to adequate patent protection in that country or if AstraZeneca licenses patent rights from any third party under circumstances in which the product that we license to AstraZeneca might infringe the third party’s patent rights.
Completed Preclinical Research Collaboration. The agreement provided for a preclinical research collaboration that we and AstraZeneca conducted between January 2006 and January 2010 to discover and develop additional compounds that act on the a4ß2 NNR as treatments for conditions characterized by cognitive impairment. AstraZeneca paid us research fees based on an agreed reimbursement rate for research services rendered by us in the collaboration. AstraZeneca has exclusively licensed six of these compounds, including AZD1446, together with metabolites of these compounds and derivatives and other compounds related to these compounds that meet specified criteria, for the same indications for which AstraZeneca has development and commercialization rights for AZD3480.
Development and Commercialization Costs. AstraZeneca is responsible for the clinical development and commercialization of AZD3480, AZD1446 and any other licensed compounds that arose from the research collaboration that it elects to advance and for funding substantially all associated costs, except as described in the next sentence. If we proceed to conduct another Alzheimer’s disease study of AZD3480, we would be responsible for funding the study but would be entitled to receive up to $5.7 million in additional payments from AstraZeneca, with the last tranche being payable to us upon first dosing in the United States and Europe. We
20
Table of Contents
have the option to co-promote AZD3480, AZD1446 and any other licensed compounds that arose from the research collaboration that are selected for advancement to specified classes of specialist physicians in the United States. If we exercise our co-promotion option, AstraZeneca is required to provide training to our sales force and compensate us for our detailing efforts following regulatory approval. If AstraZeneca licenses TC-5619, it would assume responsibility for and fund all future development (except for completion of our ongoing studies) and commercialization of TC-5619.
Exclusivity Rights and Restrictions. Neither we nor AstraZeneca are permitted outside of the collaboration to develop or commercialize compounds that act on the a4ß2 NNR and meet pre-defined criteria for ADHD, Alzheimer’s disease, cognitive dysfunction in schizophrenia or other conditions characterized by cognitive impairment for which AstraZeneca has development and commercialization rights under the agreement or schizophrenia. This restriction on AstraZeneca lapses 30 months after January 2010. This restriction on us will lapse if AstraZeneca commences clinical development outside of the collaboration for a compound that acts on the a4ß2 NNR and meets pre-defined criteria.
With respect to any compound that meets pre-defined criteria for any NNR other than the a4ß2 NNR, at the time the compound has completed the preclinical testing necessary to conduct clinical development, we are entitled to offer to AstraZeneca the right to develop and commercialize it for any indication for which AstraZeneca has development and commercialization rights under the agreement. As an example, we made such an offer with respect to TC-5619, which led to AstraZeneca’s right to license TC-5619. If we do not offer this right to AstraZeneca for a compound that meets pre-defined criteria for any NNR other than the a4ß2 NNR, we are generally not permitted to develop or commercialize the compound for any indication for which AstraZeneca has development and commercialization rights under the agreement.
If we offer a compound to AstraZeneca, AstraZeneca could license the compound from us, together with metabolites of the compound and derivatives and other compounds related to the compound that meet specified criteria, on terms specified in the agreement. Alternatively, as in the case of TC-5619, AstraZeneca could negotiate a development plan with us pursuant to which we would conduct development intended to provide a pre-defined indication of efficacy. AstraZeneca could license the compound from us after we complete the additional development. For each compound licensed by AstraZeneca through this process, we are eligible to receive an exercise fee and other payments if development, regulatory, first commercial sale and first detail milestone events are achieved, as well as stepped royalties on any future product sales. If AstraZeneca elects not to license the compound, we are permitted to develop and commercialize the compound for any indication, except that, if we had offered the compound to AstraZeneca for schizophrenia, we will not be able to develop or commercialize the compound for any cognitive disorder. The agreement limits the number of compounds that we are permitted to offer to AstraZeneca through this process. We are generally not permitted to develop or commercialize compounds that meet pre-defined criteria for any NNR for any indication for which AstraZeneca has development and commercialization rights under the agreement except through this process.
We are also entitled to offer to AstraZeneca the right to develop and commercialize (1) any compound for which AstraZeneca has development and commercialization rights for specified indications under the agreement, or (2) any other compound that meets pre-defined criteria for cognitive activity, is in the same chemical family and acts on the same NNR or NNRs as any compound for which AstraZeneca has development and commercialization rights for specified indications under the agreement, for any indication for which AstraZeneca does not have development and commercialization rights under the agreement. If we do not offer this right to AstraZeneca, we are not permitted to develop or commercialize the compound.
If AstraZeneca commences clinical development outside of the collaboration of a compound that acts on any NNR other than the a7 NNR and meets other pre-defined criteria, the restriction on our right to develop and commercialize compounds that meet pre-defined criteria for any NNR, other than the a4ß2 NNR, for any indication for which AstraZeneca has development and commercialization rights under the agreement will lapse.
21
Table of Contents
If we seek a strategic collaborator to develop or commercialize compounds that act by binding to NNRs for depression, anxiety or bipolar disorder, AstraZeneca may under certain circumstances have a right of first negotiation with us. If AstraZeneca is interested in such a collaboration but we and AstraZeneca do not agree on terms, for the following three years we would only be permitted to enter into a collaboration for the applicable compounds and indications on more favorable terms than the terms offered by AstraZeneca.
Termination. AstraZeneca can terminate the agreement without cause upon 90 days notice given any time. Either we or AstraZeneca can terminate the agreement in the event of the bankruptcy or uncured material breach of the other party. However, if a breach by AstraZeneca is limited to any specific compound or specified major pharmaceutical market, we can terminate the agreement only with respect to that compound or major pharmaceutical market. If a competitor of AstraZeneca acquires control of us, AstraZeneca can terminate the agreement or specified provisions of the agreement, including our right to participate on the committee overseeing development under the agreement and our co-promotion rights.
GlaxoSmithKline
On July 27, 2007, we entered into a product development and commercialization agreement with SmithKlineBeecham Corporation and Glaxo Group Limited, which we refer to collectively as GlaxoSmithKline, that set forth the terms of an alliance designed to discover, develop and market product candidates that selectively target specified NNR subtypes in specified therapeutic focus areas. In February 2010, GlaxoSmithKline announced plans to cease discovery research in selected neuroscience areas, and, in late February 2011, we received notice of termination of the agreement from GlaxoSmithKline. By the terms of the agreement, the termination becomes effective in late May 2011.
Patents and Proprietary Rights
We actively seek to protect the proprietary technology that we consider important to our business, including chemical species, compositions and forms, their methods of use and processes for their manufacture, as well as modified forms of naturally-expressed receptors, in the United States and other jurisdictions internationally that we consider key pharmaceutical markets. We also rely upon trade secrets and contracts to protect our proprietary information.
As of February 28, 2011, our patent estate included 58 patents issued in the United States, 75 patent applications pending in the United States and approximately 600 counterpart patents and patent applications in countries other than the United States. Our issued patents and pending patent applications in the United States include composition of matter coverage on a number of different structural families of compounds. The actual protection afforded by a patent varies from country to country and depends upon many factors, including the type of patent, the scope of its coverage and the availability of legal remedies in a particular country.
22
Table of Contents
We consider the following United States patents that we own or license to be particularly important to the protection of our most advanced product candidates.
| Product Candidate |
Patent Scope |
Patent Expiration | ||
| TC-5214 |
Pharmaceutical composition of TC-5214 | January 2020 | ||
| Methods of use of TC-5214 for treatment of neuropsychiatric disorders, including depression | February 2020 | |||
| Methods of use of a class of compounds that includes TC-5214 for treatment of a nicotine-responsive psychiatric disorder, including depression | September 2017 | |||
| TC-5619 |
Composition of matter for a family of compounds that includes TC-5619 | August 2019 | ||
| Composition of matter for a racemic mixture that includes TC-5619 |
March 2019 | |||
| Methods of use of a racemic mixture that includes TC-5619 for treatment of schizophrenia | November 2025 | |||
| AZD3480 (TC-1734) |
Composition of matter for AZD3480 | July 2018 | ||
| Composition of matter for a family of compounds that includes AZD3480 | April 2016 | |||
| Methods of use of a family of compounds that includes AZD3480 for treatment and prevention of CNS disorders | February 2017 | |||
| Methods of use for AZD3480 for treatment and prevention of CNS disorders | July 2018 | |||
| Composition of matter for the preferred salt (p-hydroxybenzoate) of AZD3480 | August 2026 | |||
| TC-6987 |
Composition of matter for a family of compounds that includes TC-6987 | August 2019 | ||
| TC-6499 |
Composition of matter for TC-6499; composition of matter for a family of compounds that includes TC-6499 | February 2024 | ||
In addition to these patents, for some of these product candidates we have later-expiring patents that cover a particular form or composition, use as part of combination therapy or method of preparation or use, as well as other pending patent applications. These issued patents, including any patents that issue from the pending applications, could provide additional or a longer period of protection. We also have patent applications pending that seek equivalent or substantially comparable protection for our product candidates in jurisdictions internationally that we consider key pharmaceutical markets.
The patent expiration dates referenced above do not reflect any potential patent term extension that we may receive under The United States Drug Price Competition and Patent Term Restoration Act of 1984, known as the Hatch-Waxman Act. The Hatch-Waxman Act generally permits a patent extension term of up to five years as compensation for patent term lost during the FDA regulatory review process. Patent extension cannot extend the remaining term of a patent beyond a total of 14 years. The patent term restoration period is generally one-half of the time between the effective date of an investigational new drug application, or IND, and the submission date of an NDA plus the time between the submission date and approval date of an NDA. Only one patent applicable to an approved drug is eligible for the extension, and the extension must be applied for prior to expiration of the patent. The United States Patent and Trademark Office, in consultation with the FDA, reviews and approves applications for patent term extension.
23
Table of Contents
License Agreements
In addition to the agreements governing our collaborations with AstraZeneca, we consider the following license agreements to be important to our business as of March 11, 2011.
University of South Florida Research Foundation
Pursuant to a license agreement with USFRF, we hold an exclusive worldwide license under patents and patent applications owned by USFRF to develop and commercialize TC-5214, mecamylamine hydrochloride and other specified compounds. The licensed patent rights include issued patents covering the pharmaceutical composition of TC-5214 and methods of use of each of TC-5214, the other enantiomer of mecamylamine hydrochloride and mecamylamine hydrochloride for the treatment of various disorders, including major depressive disorder. We sublicensed rights under the licensed patents and patent applications to AstraZeneca in December 2009 pursuant to our TC-5214 agreement with AstraZeneca.
Under the license agreement with USFRF, we are obligated to pay to USFRF:
| • | an annual license fee of $50,000 until we or AstraZeneca or any future sublicensee files an NDA or foreign equivalent for use of a product subject to the license to treat a neuropsychiatric disease or disorder; |
| • | an annual fee of $20,000 to maintain our right of first refusal to acquire rights under the licensed patents and patent applications beyond the scope of our current license; |
| • | royalties on net sales of products subject to the license or, if less, a percentage of royalties that we receive from AstraZeneca or any future sublicensee; |
| • | aggregate payments of up to $200,000 based on the achievement of specified regulatory milestones; and |
| • | 10% of other amounts, including milestone payments, that we receive for a sublicense from AstraZeneca or any future sublicensee, subject to increase to a higher percentage in specified circumstances. |
The aggregate annual license fees are creditable, up to a specified amount per year, against future royalties.
We are required to use commercially reasonable efforts to develop or to market and sell one or more products subject to the license. In particular, we are required to spend a specified minimum amount on research and development of products subject to the license over each consecutive three-year period during the term of the agreement until we or a sublicensee file an NDA or foreign equivalent for use of a product subject to the license to treat a neuropsychiatric disease or disorder. If USFRF believes that we are not meeting our diligence obligation, it is entitled to terminate the agreement if we do not cure our failure within a specified cure period. If we do not agree with USFRF’s determination and specified initial dispute resolution procedures are unsuccessful, we can submit the matter to binding arbitration.
We may terminate the agreement at any time. USFRF may terminate the agreement if we fail to make a required royalty payment when due, or commit a material breach of the agreement, and do not cure the failure or breach within specified cure periods. If not earlier terminated, the agreement will terminate upon expiration of the last to expire of the licensed patent rights that includes a valid claim.
Yale University
Pursuant to an exclusive license agreement with Yale University, we hold an exclusive worldwide license to pending patent applications owned by Yale. The licensed patent applications include a pending U.S. application that, if issued in the future as a patent, could potentially cover the use of TC-5214 and mecamylamine
24
Table of Contents
hydrochloride, or other compounds classified as nicotinic antagonists, as an augmentation to other treatments for mood disorders, including major depressive disorder. We sublicensed rights under the licensed patent applications to AstraZeneca in December 2009 pursuant to our TC-5214 agreement with AstraZeneca.
Under the license agreement with Yale, we are obligated to pay to Yale:
| • | a fee of $50,000 that is conditional upon the issuance of a licensed patent in the United States that meets specified conditions; |
| • | aggregate payments of up to $1.5 million for each product subject to the license for which specified regulatory and first commercial sale milestone events are achieved; |
| • | royalties on net sales of products subject to the license, subject, following the first launch of a product subject to the license, to specified annual minimum amounts; and |
| • | a specified percentage of other amounts received from any sublicensee of the licensed patent rights, if the applicable sublicense is not combined with a license to other patent rights owned or licensed by us that cover compounds or their therapeutic use in humans or with an agreement by us to collaborate to discover, research, develop or commercialize compounds or products for therapeutic use in humans. Our sublicense to AstraZeneca under our TC-5214 agreement with AstraZeneca is combined with both a license to other patent rights and an agreement by us to co-develop TC-5214 as a treatment for major depressive disorder. Accordingly, no other amounts received from AstraZeneca under our TC-5214 agreement with AstraZeneca give rise to any payment obligation to Yale. |
We are required to use reasonable commercial efforts to develop at least one product subject to the license for commercialization in the United States. We may terminate the agreement upon 30 days notice to Yale. Yale may terminate the agreement if we fail to make a required payment when due, or commit a material breach of the agreement, and do not cure the failure or breach within a specified cure period or if we notify Yale that we are finally abandoning our research, development or marketing of, and our intent to research, develop and market, products subject to the license. If not earlier terminated, the agreement will expire upon expiration of the last to expire of the licensed patent rights that includes a valid claim.
University of Kentucky Research Foundation
Pursuant to a sponsored research agreement, UKRF agreed to assign to R.J. Reynolds Tobacco Company UKRF’s rights to inventions that resulted in patents related to AZD3480. These patents were subsequently assigned by RJR to us in August 2000, and we licensed rights under these patents to AstraZeneca pursuant to our cognitive disorders agreement with AstraZeneca. Under the sponsored research agreement and a subsequent license agreement with UKRF, we are obligated to pay royalties to UKRF based on amounts received for a license to these patents from AstraZeneca or any future licensee.
Cornerstone Therapeutics Inc.
Pursuant to an exclusive license agreement with Cornerstone Therapeutics Inc., we hold an exclusive worldwide license and sublicense under patents and patent applications owned by Cornerstone or exclusively licensed by Cornerstone from the Feinstein Institute for Medical Research. The licensed patent rights include issued patents and pending patent applications covering a library of preclinical compounds that act on the alpha7 or other nicotinic receptors, as well as the use of modulators of the a7 NNR to treat inflammatory disorders. TC-6987 modulates the activity of the a7 NNR and is currently being evaluated in Phase 2 clinical trials in asthma and Type 2 diabetes.
Under the license agreement with Cornerstone, we paid Cornerstone an upfront fee of $1.5 million and are obligated to pay to Cornerstone:
| • | payments for each compound subject to the license for which specified clinical, regulatory and sales-related milestone events are achieved, with the aggregate amount of the potential payments for a particular compound being dependent on whether and to what extent Cornerstone had exemplified and progressed the compound as of the effective date of the agreement; |
25
Table of Contents
| • | the aggregate amount of the contingent payments described in the immediately preceding bullet ranges from up to $16.1 million to up to $74.9 million, comprised of $325,000 to $1.4 million in milestones through Phase 2 clinical proof of concept, $2.8 million to $18.5 million in later-stage pre-commercialization milestones and $13.0 million to $55.0 million in sales-based milestones; to the extent the licensed patent rights cover the use of TC-6987 or any other Targacept-discovered compound, the aggregate contingent payments would be at the low point of each of the ranges; and |
| • | low single-digit royalties on net sales of products subject to the license (to the extent the licensed patent rights cover the use of TC-6987 or any other Targacept-discovered compound as a treatment for inflammatory disorders, the royalty rate would be less than 1%). |
We are required to use commercially reasonable efforts to develop at least one compound subject to the license to regulatory approval. We are also specifically required to use commercially reasonable efforts to manufacture one of two specified in-licensed compounds, in sufficient quantities and of sufficient quality to perform specified preclinical toxicology work, and, if successful, then to perform the preclinical toxicology work within a specified timeframe, subject to extension in certain circumstances.
We may terminate the agreement upon 30 days notice to Cornerstone. Cornerstone may terminate the agreement if we successfully complete the manufacturing contemplated above but do not conduct the specified preclinical toxicology work within the requisite timeframe, or if we commit a material breach of the agreement and do not cure the breach within a specified cure period. If not earlier terminated, the agreement will expire upon expiration of the period during which royalties are payable for the last product subject to the license.
Trade Secrets
In addition to patents, we rely upon unpatented trade secrets and know-how and continuing technological innovation to develop and maintain our competitive position. For example, we maintain Pentad as an unpatented trade secret. We seek to protect our proprietary information, in part, by using confidentiality agreements with our commercial partners, collaborators, employees and consultants and invention assignment agreements with our employees.
Sales and Marketing
We currently have limited sales, marketing and distribution experience with respect to pharmaceutical products and no internal sales or distribution capabilities. Our current strategy is to selectively seek alliances and collaborations for target indications for which our potential collaborator has particular expertise or that involve large primary care markets that must be served by large sales and marketing organizations. In entering into these alliances and collaborations, our goal will generally be to maintain co-promotion or co-commercialization rights in the United States and, in some cases, other markets. In order to implement this aspect of our strategy successfully, we must develop a specialized sales and marketing organization with sufficient technical expertise.
We discontinued the commercialization of Inversine, which is currently our only approved product, effective as of September 30, 2009. Inversine had been distributed by Cord Logistics, Inc., a Cardinal Health company, pursuant to an exclusive distribution agreement. We have terminated our agreement with Cord Logistics. We paid Cord Logistics approximately $31,000 in 2010, $140,000 in 2009 and $170,000 in 2008.
Manufacturing
All of our current product candidates are compounds of low molecular weight, commonly referred to as small molecules, that can be manufactured in a simple synthetic process from readily available starting materials. We expect to continue to develop product candidates that can be produced cost-effectively by third-party contract manufacturers.
26
Table of Contents
We are able to manufacture the quantities of our product candidates necessary for relatively short preclinical studies ourselves. However, we do rely and expect to continue to rely on a number of contract manufacturers to produce enough of our product candidates for use in more lengthy preclinical research. We also depend on these contract manufacturers to manufacture our product candidates in accordance with current good manufacturing practices, or cGMP, for use in clinical trials. We will ultimately depend on contract manufacturers for the manufacture of our products for commercial sale, as well as for process development. Contract manufacturers are subject to extensive governmental regulation.
Competition
Our industry is subject to rapid and intense technological change. We face, and will continue to face, worldwide competition from biotechnology, biopharmaceutical and pharmaceutical companies, research institutions, government agencies and academic institutions.
We also face substantial competition from therapies designed to target NNRs. Pfizer’s product Chantix, which is known outside of the United States as Champix, acts on several NNR subtypes as well as other molecular targets in the body. Chantix is approved as an aid for smoking cessation. In addition, we believe that several prominent pharmaceutical companies have product candidates that target NNRs in development, including as examples Roche, with a compound in Phase 2 development for Alzheimer’s disease, and Abbott Laboratories, with one compound in Phase 2 development for ADHD and a second compound in Phase 1 development for cognitive disorders. Other companies that we believe have active NNR-based programs include AstraZeneca, Eli Lilly, Sanofi-Aventis, Bristol-Myers Squibb, GlaxoSmithKline, Johnson & Johnson, Novartis, NeuroSearch A/S, Solvay, Servier, CoMentis, EnVivo Pharmaceuticals, Galantos Pharma, Proximagen, Psychogenics, AGI Therapeutics, Suven, Asmacure and Neuroderm. We expect that we will face increased competition in the future if therapies that target NNRs are further validated and if companies initiate or expand programs focused on NNRs or otherwise enter the CNS market, whether independently or by alliance or acquisition.
In addition, there are several pharmaceutical companies in the United States and globally that currently market and sell drugs for indications that we are targeting. We believe that the primary competitive products for use in indications that we are currently targeting with our most advanced product candidates include:
| • | as an adjunct treatment for major depressive disorder, the atypical antipsychotics Seroquel XR from AstraZeneca and Abilify from Bristol-Myers Squibb/Otsuka; |
| • | otherwise for major depressive disorder, SSRIs such as Prozac from Eli Lilly, Paxil/Seroxar from GlaxoSmithKline, Zoloft from Pfizer, Celexa and Lexapro from Forest Laboratories, dual uptake inhibitors such as Effexor from Wyeth and Cymbalta from Eli Lilly, and the SSRI and 5HT1A receptor partial agonist Viibryd from Clinical Data (under agreement to be acquired by Forest Laboratories); |
| • | for ADHD, stimulants such as Adderall XR and Vyanase from Shire, Concerta from Johnson & Johnson and Ritalin LA from Novartis, and Strattera, a non-stimulant acting as a norepinephrine reuptake inhibitor, from Eli Lilly; |
| • | for mild to moderate Alzheimer’s disease, acetylcholinesterase inhibitors such as Aricept from Pfizer/Eisai, Razadyne from Johnson & Johnson and Exelon from Novartis; in addition, Namenda from Forest Laboratories, which acts by regulating the neurotransmitter glutamate, is marketed for moderate to severe Alzheimer’s disease; |
| • | for asthma, long-acting beta agonist/inhaled corticosteroid combinations such as Advair from GlaxoSmithKline, Symbicort from AstraZeneca and Dulera from Merck, leukotriene inhibitors such as Singulair from Merck, Accolate from AstraZeneca and Zyflo from Cornerstone Therapeutics, antibodies such as Xolair from Novartis, long-acting beta agonists such as salmeterol and formoterol and short-acting beta agonists such as albutertol and levalbuterol; and |
27
Table of Contents
| • | for Type 2 diabetes, glucagon-like peptide-1 analogues such as Byetta from Eli Lilly and Amylin, dipeptidyl peptidase IV inhibitors such as Januvia from Merck and Onglyza from Bristol-Myers Squibb and AstraZeneca, insulin such as Lantus from Sanofi-Aventis, sulfonylureas such as Glucotrol from Pfizer, and biguanides (metformin) such as Glucophage from Bristol-Myers Squibb. |
There is currently no approved product for cognitive dysfunction in schizophrenia. There are however multiple third-party product candidates currently in clinical development for cognitive dysfunction in schizophrenia, including at least one modulator of the a7 NNR.
Many of these products have well-known brand names, are distributed by large pharmaceutical companies with substantial resources, have achieved widespread acceptance among physicians and patients and are or may become available in lower priced generic form. Furthermore, pharmaceutical, biopharmaceutical and biotechnology companies are currently developing additional treatments for the indications that we are targeting that may be approved for marketing and sale prior to any approval of our product candidates.
We expect to compete based upon, among other things, the efficacy and favorable side effect profiles of our products. Our ability to compete successfully will depend on our continued ability to attract and retain skilled and experienced scientific, clinical development and executive personnel, to identify and develop viable product candidates into products and to exploit these products commercially before others are able to develop competitive products. In addition, our ability to compete may be affected by insurers and other third-party payors favoring the use of lower priced generic products over branded products.
Regulatory Matters
Government Regulation and Product Approval
Government authorities in the United States, at the federal, state and local level, and in other countries extensively regulate, among other things, the research, development, testing, manufacture, quality control, approval, labeling, packaging, storage, record-keeping, promotion, advertising, distribution, marketing and export and import of drugs such as those we are developing. Our product candidates must be approved by the FDA through the NDA process before they may be legally marketed in the United States.
United States Drug Development Process
In the United States, the FDA regulates drugs under the Federal Food, Drug, and Cosmetic Act, or FDCA, and implementing regulations. The process of obtaining regulatory approvals and the subsequent compliance with appropriate federal, state, local and foreign laws and regulations require the expenditure of substantial time and financial resources. Failure to comply with the applicable United States requirements at any time during the product development process, the approval process or after approval may subject an applicant to administrative or judicial sanctions. These sanctions could include the FDA’s refusal to approve pending applications, withdrawal of an approval, a clinical hold, warning letters, product recalls, product seizures, total or partial suspension of production or distribution injunctions, fines, refusals of government contracts, restitution, disgorgement, or civil or criminal penalties.
The process required by the FDA before a drug may be marketed in the United States generally involves the following:
| • | completion of preclinical laboratory tests, animal studies and formulation studies conducted in accordance with good laboratory practices and other applicable regulations; |
| • | submission to the FDA of an IND, which must become effective before human clinical trials may begin; |
| • | performance of adequate and well-controlled human clinical trials conducted in accordance with the regulations and guidelines establishing good clinical practices to establish the safety and efficacy of the drug for its intended use; |
28
Table of Contents
| • | submission to the FDA of an NDA in a form and content that the FDA deems to be acceptable for filing; |
| • | satisfactory completion of an FDA inspection of the manufacturing facility or facilities at which the drug is produced to assess compliance with cGMP in order to assure that the facilities, methods and controls are adequate to preserve the drug’s identity, strength, quality and purity; and |
| • | FDA review and approval of the NDA. |
The testing and approval process requires substantial time, effort and financial resources.
Once a drug is identified for development it enters the preclinical testing stage. Preclinical tests include laboratory evaluations of chemistry, toxicity and formulation, as well as animal studies to assess the characteristics and potential effects of the drug. The results of preclinical testing are submitted to the FDA, along with other information about drug chemistry, manufacturing and controls and a proposed clinical trial protocol, as part of an IND. Long-term preclinical tests, such as animal tests of reproductive toxicity and the ability or tendency to produce cancer, may continue after the IND is submitted. The IND becomes effective 30 days after receipt by the FDA, unless within the 30-day time period the FDA places the clinical trial on a clinical hold. In such a case, the sponsor and the FDA must resolve any outstanding concerns before the clinical trial can begin. Clinical holds also may be imposed by the FDA at any time before or during studies due to safety concerns or non-compliance with applicable law or regulation.
All clinical trials must be conducted under the supervision of one or more qualified investigators in accordance with the regulations and guidelines establishing good clinical practice. These regulations include the requirement that all research subjects provide informed consent. Further, an institutional review board, or IRB, must review and approve the plan for any clinical trial before it commences at any institution. An IRB considers, among other things, whether the risks to individuals participating in the trials are minimized and reasonable in relation to the anticipated benefits. The IRB also approves the information regarding the trial and the consent form that must be provided to each trial subject or his or her legal representative and must monitor the study until completed. An IRB may impose conditions to the initiation or continued conduct of trial.
Each new clinical protocol must be submitted to the IND for FDA review and to the applicable IRBs for approval. Protocols detail, among other things, the objectives of the study, dosing procedures, subject selection and exclusion criteria, and the parameters to be used to monitor subject safety.
Clinical trials are typically conducted in three sequential phases that may overlap or be combined:
| • | Phase 1: Involves one or more clinical trials in healthy volunteers to evaluate safety, dosage tolerance, absorption, metabolism, distribution and excretion. In the case of some drugs for severe or life-threatening diseases, the initial human testing may be conducted in patients, particularly where the drug may be too inherently toxic to administer ethically to healthy volunteers; |
| • | Phase 2: Involves one or more clinical trials in a limited patient population to identify possible adverse effects and safety risks, to evaluate preliminarily the efficacy of the drug for specific targeted diseases and to determine dosage tolerance and optimal dosage; and |
| • | Phase 3: Involves one or more clinical trials to further evaluate dosage, clinical efficacy and safety in an expanded patient population at geographically dispersed study sites. These trials are intended to establish the overall risk-benefit ratio of the drug and provide, if appropriate, an adequate basis for product labeling. |
Progress reports detailing the results of clinical trials must be submitted at least annually to the FDA and safety reports must be submitted to the FDA and the investigators for serious and unexpected adverse events. Any Phase 1, Phase 2 and Phase 3 trial may not be completed successfully within any specified period, or at all. The FDA or the sponsor may suspend a clinical trial at any time on various grounds, including a finding that the
29
Table of Contents
research subjects or patients are being exposed to an unacceptable health risk. Similarly, an IRB can suspend or terminate approval of a clinical trial at its institution if the clinical trial is not being conducted in accordance with the IRB’s requirements or if the drug has been associated with unexpected serious harm to patients.
Concurrent with clinical trials, companies usually complete additional animal studies and must also develop additional information about the chemistry and physical characteristics of the drug and finalize a process for manufacturing the drug as a product in commercial quantities in accordance with cGMP requirements. The manufacturing process must be capable of consistently producing quality batches of the drug, and, among other things, the manufacturer must develop methods for testing the identity, strength, quality and purity of the final product. Additionally, appropriate packaging must be selected and tested and stability studies must be conducted to demonstrate that the product does not undergo unacceptable deterioration over its shelf life.
U.S. Review and Approval Processes
The results of product development, preclinical studies and clinical trials, along with descriptions of the manufacturing process, analytical chemistry tests, proposed labeling, and other relevant information, are submitted to the FDA as part of an NDA requesting approval to market the drug as a product. FDA approval of the NDA is required before marketing of the product may begin in the United States. The cost of preparing and submitting an NDA is substantial. Under federal law, the submission of most NDAs is additionally subject to a substantial application user fee and the manufacturer or sponsor under an approved NDA is also subject to annual product and establishment user fees. These fees are typically increased annually. A waiver or reduction of the fees may be obtained under specified limited circumstances.
In addition, under the Pediatric Research Equity Act, or PREA, an NDA or supplement to an NDA must contain data to assess the safety and effectiveness of the drug for the claimed indications in all relevant pediatric subpopulations and to support dosing and administration for each pediatric subpopulation for which the drug is safe and effective. The FDA may grant a deferral for submission of data or a full or partial waiver. Unless otherwise required by regulation, PREA does not apply to any drug for an indication for which orphan designation has been granted.
The FDA reviews all NDAs submitted to ensure that they are sufficiently complete for substantive review before it accepts them for filing. The FDA has 60 days from its receipt of an NDA to determine if it will accept the submission for a substantive review, which is referred to as accepting it for filing. The FDA may request additional information rather than accept an NDA for filing. In this event, the NDA must be resubmitted with the additional information. The resubmitted application also is subject to review before the FDA accepts it for filing. The FDA may refuse to file the NDA. If the submission is accepted for filing, the FDA begins an in-depth substantive review to determine, among other things, whether a product is safe and effective for its intended use and whether its manufacturing is cGMP-compliant to assure and preserve the product’s identity, strength, quality and purity. In that regard, the FDA will inspect the facility or facilities where the product is manufactured before approving an NDA.
Under current performance goals, the FDA has either six or 10 months to review and act on the NDA, depending upon whether the NDA is classified by the FDA as eligible for priority (six months) or standard (10 months) review. The review process may be extended by the FDA for an additional three-month period to consider certain information or clarification regarding information already provided in the submission. The FDA may also refer NDAs for novel drug products or for drug products that present difficult questions of safety or efficacy to an advisory committee for review, evaluation and a recommendation as to whether the NDA should be approved. Advisory committees are typically comprised of clinicians and other experts in the relevant area. The FDA is not bound by the recommendation of an advisory committee, but often follows the recommendation.
The FDA approval process is lengthy and difficult and the FDA may refuse to approve an NDA if the applicable regulatory criteria are not satisfied or may require additional clinical or other data and information.
30
Table of Contents
Even if any requested additional data or information is submitted, the FDA may ultimately decide that the NDA does not satisfy the criteria for approval. Data obtained from clinical trials are not always conclusive and the FDA may interpret data differently than we or any collaborator of ours does.
NDAs receive either standard or priority review. A drug representing a significant improvement in treatment, prevention or diagnosis of disease may receive priority review. In addition, products studied for their safety and effectiveness in treating serious or life-threatening illnesses and that provide meaningful therapeutic benefit over existing treatments may receive accelerated approval and may be approved on the basis of adequate and well-controlled clinical trials establishing that the drug has an effect on a surrogate endpoint that is reasonably likely to predict clinical benefit or on the basis of an effect on a clinical endpoint other than survival or irreversible morbidity. Priority review and accelerated approval do not change the standards for approval, but may expedite the approval process.
After the FDA evaluates the NDA and the applicable manufacturing facilities, it issues an approval letter or a complete response letter. A complete response letter generally outlines the deficiencies in the submission and may require substantial additional testing or information in order for the FDA to reconsider the NDA. If and when the deficiencies have been addressed to the FDA’s satisfaction in a resubmission of the NDA, the FDA will issue an approval letter. FDA review of a resubmitted NDA can take as long as six months depending on the type of information included.
An approval letter authorizes commercial marketing of the drug with specific prescribing information for specific indications. As a condition of NDA approval, the FDA may require substantial post-approval testing and surveillance to monitor the drug’s safety or efficacy and may impose other conditions, including labeling restrictions, that can materially affect the potential market for and profitability of the drug. Once granted, product approvals may be withdrawn if compliance with regulatory standards is not maintained or problems are identified following initial marketing.
If a drug is the subject of an approved NDA, it may become a listed drug that can, in turn, be cited by potential competitors in support of approval of an abbreviated new drug application, or ANDA. An ANDA provides for marketing of a drug product that is therapeutically equivalent to a marketed listed drug. This means, among other things, that it has the same active ingredient(s), route of administration, dosage form and strength, as well as the same labeling, with certain exceptions, and the labeling must prescribe conditions of use that have been previously approved for the listed drug. If the generic drug product has a different route of administration, dosage form, or strength, the FDA must grant a suitability petition approving the difference(s) from the listed drug before the ANDA may be filed. The ANDA must also contain data and information demonstrating that the generic drug product is bioequivalent to the listed drug or, if the application is submitted pursuant to an approved suitability petition, information to show that the listed drug and the generic drug product can be expected to have the same therapeutic effect as the listed drug when administered to patients for a proposed condition of use. There is generally no requirement, other than the requirement for evidence of bioequivalence, for an ANDA applicant to conduct or submit results of preclinical tests or clinical trials to establish the safety or efficacy of its generic drug product. Drugs approved in this way are commonly referred to as generic equivalents to the listed drug, are listed as such by the FDA and can typically be substituted by pharmacists under prescriptions written for the original listed drug.
Marketing Exclusivity
Market exclusivity provisions under the FDCA also can delay the submission or the approval of certain applications. The FDCA provides a five-year period of non-patent marketing exclusivity within the United States to the first applicant to gain approval of an NDA for a new chemical entity. A drug is a new chemical entity if the FDA has not previously approved any other drug containing the same active moiety, which is the molecule or ion responsible for the action of the drug. During the exclusivity period, the FDA may not accept for review an ANDA or an NDA under Section 505(b)(2) of the FDCA submitted by another company for another version of
31
Table of Contents
such drug where the applicant does not own or have a legal right of reference to all the data required for approval. However, an application may be submitted after four years if it contains a certification of patent invalidity or non-infringement. The FDCA also provides three years of marketing exclusivity for an NDA, Section 505(b)(2) NDA or supplement to an existing NDA if new clinical investigations, other than bioavailability studies, conducted or sponsored by the applicant are deemed by the FDA to be essential to the approval of the application, for example, for new indications, dosages, or strengths of an existing drug. This three-year exclusivity covers only the conditions associated with the new clinical investigations and does not prohibit the FDA from approving ANDAs for drugs containing the original active agent. Five-year and three-year exclusivity will not delay the submission or approval of a full NDA; however, an applicant submitting a full NDA would be required to conduct or obtain a right of reference to all of the preclinical studies and adequate and well-controlled clinical trials necessary to demonstrate safety and effectiveness.
Pediatric exclusivity is another type of exclusivity in the United States. Pediatric exclusivity, if granted, provides an additional six months to an existing exclusivity or statutory delay in approval resulting from a patent certification. This six-month exclusivity, which runs from the end of other exclusivity protection or patent delay, may be granted based on the voluntary completion of a pediatric study in accordance with an FDA-issued “Written Request” for the study.
Orphan Drug Designation
Under the Orphan Drug Act, the FDA may grant orphan drug designation to a drug intended to treat a rare disease or condition, which is generally a disease or condition that either affects fewer than 200,000 individuals in the United States or affects more than 200,000 individuals in the United States but for which there is no reasonable expectation that the cost of developing and making available in the United States a drug for the disease or condition will be recovered from sales in the United States for that drug. Orphan drug designation must be requested before submitting an NDA. After the FDA grants orphan drug designation, the identity of the therapeutic agent and its potential orphan use are disclosed publicly by the FDA. Orphan drug designation does not convey any advantage in or shorten the duration of the regulatory review and approval process.
If a product that has orphan drug designation subsequently receives the first FDA approval for the disease for which it has such designation, the product is entitled to orphan product exclusivity, which means that the FDA may not approve any other applications to market the same drug for the same indication for seven years, except in very limited circumstances (such as a showing of clinical superiority to the product with orphan drug exclusivity). Orphan drug exclusivity does not prevent the FDA from approving a different drug for the same disease or condition or from approving the same drug for a different disease or condition.
The FDA also administers a clinical research grants program, whereby researchers may compete for funding to conduct clinical trials to support the approval of drugs, biologics, medical devices, and medical foods for rare diseases and conditions. A drug does not have to be designated as an orphan drug to be eligible for the grant program. An application for an orphan grant proposes one discrete clinical study to facilitate FDA approval of the product for a rare disease or condition. The study may address an unapproved new product or an unapproved new use for a product already on the market.
Post-Approval Requirements
Once an approval is granted, the FDA may withdraw the approval if compliance with regulatory standards is not maintained or if problems occur after the product reaches the market. Later discovery of previously unknown problems with a product may result in restrictions on the product or even complete withdrawal of the product from the market. After approval, some types of changes to the approved product, such as adding new indications, manufacturing changes and additional labeling claims, are subject to further FDA review and approval. Drug manufacturers and other entities involved in the manufacture and distribution of approved drugs are required to register their establishments with the FDA and certain state agencies and are subject to periodic unannounced inspections by the FDA and certain state agencies for compliance with cGMP and other laws.
32
Table of Contents
Any products manufactured or distributed by us pursuant to FDA approvals are subject to continuing regulation by the FDA, including, among other things, record-keeping requirements, reporting of adverse experiences with the drug, providing the FDA with updated safety and efficacy information, drug sampling and distribution requirements, complying with certain electronic records and signature requirements, and complying with FDA promotion and advertising requirements. The FDA strictly regulates labeling, advertising, promotion and other types of information on products on the market. Products may be promoted only for the approved indications and in accordance with the provisions of the approved label.
From time to time, legislation is drafted, introduced and passed by the U.S. Congress that could significantly change the statutory provisions governing the approval, manufacturing and marketing of products regulated by the FDA. For example, the Food and Drug Administration Amendments Act of 2007, or FDAAA, gives the FDA the authority to require post-market studies and clinical trials, labeling changes based on new safety information and compliance with a risk evaluation and mitigation strategy approved by the FDA. Failure to comply with any requirements under FDAAA may result in significant penalties. FDAAA also authorizes significant civil money penalties for the dissemination of false or misleading direct-to-consumer advertisements, allows the FDA to require companies to submit direct-to-consumer television drug advertisements for FDA review prior to public dissemination and expands the clinical trial registry so that sponsors of most clinical trials, except for Phase 1 trials, are required to submit certain clinical trial information for inclusion in the clinical trial registry data bank. In addition to the impact of new legislation, FDA regulations and guidance are often revised or reinterpreted in ways that may significantly affect our business and our product candidates.
Foreign Regulation
In addition to regulations in the United States, we are subject to a variety of foreign regulations governing clinical trials of our product candidates and commercial sales and distribution of any products. Whether or not we or any collaborator of ours obtains FDA approval for a product candidate or product, we or the collaborator must obtain approval by the comparable regulatory authorities of foreign countries before we can commence clinical trials of the product candidate or marketing of the product in those countries. The approval process varies from country to country and the time may be longer or shorter than the time required for FDA approval. The requirements governing the conduct of clinical trials, product licensing, pricing and reimbursement vary greatly from country to country.
Under European Union regulatory systems, we may submit marketing authorization applications either under a centralized or a decentralized procedure. The centralized procedure, which is compulsory for medicines produced by certain biotechnological processes and optional for those which are highly innovative, provides for the grant of a single marketing authorization that is valid for all European Union member states. For drugs without approval in any member state, the decentralized procedure provides for approval by one or more other, or concerned, member states of an assessment of an application performed by one member state, known as the reference member state. Under this procedure, an applicant submits an application, or dossier, and related materials (including a draft summary of product characteristics, draft labeling and package leaflet) to the reference member state and concerned member states. The reference member state prepares a draft assessment and drafts of the related materials within 120 days after receipt of a valid application. Within 90 days of receiving the reference member state’s assessment report, each concerned member state must decide whether to approve the assessment report and related materials. If a member state cannot approve the assessment report and related materials on the grounds of potential serious risk to public health, any disputed issues may eventually be referred to the European Commission, the decision of which would be binding on all member states.
Reimbursement
Sales of pharmaceutical products depend in significant part on the availability of third-party reimbursement. Third-party payors include government health administrative authorities, managed care providers, private health insurers and other organizations. These third-party payors are increasingly challenging the price and examining
33
Table of Contents
the cost-effectiveness of medical products and services, including prescription drugs. In addition, significant uncertainty exists as to the reimbursement status of newly approved prescription drugs and other healthcare products. We may need to conduct expensive pharmacoeconomic studies in order to demonstrate the cost-effectiveness of any of our products for which we or any collaborator of ours receives marketing approval. Our product candidates may not be considered cost-effective. It is time consuming and expensive for us or any collaborator of ours to seek reimbursement from third-party payors. Reimbursement may not be available or sufficient to allow the sale of any of our products for which we or any collaborator of ours receives marketing approval on a competitive and profitable basis.
The Medicare Prescription Drug, Improvement, and Modernization Act of 2003, or the MMA, imposes requirements for the distribution and pricing of prescription drugs for Medicare beneficiaries, and expands the prescription drug benefit under Medicare Part D. Under Part D, Medicare beneficiaries may enroll in prescription drug plans offered by private entities, which will provide coverage of outpatient prescription drugs. Part D plans include both stand-alone prescription drug benefit plans and prescription drug coverage as a supplement to Medicare Advantage plans. Unlike Medicare Part A and B, Part D coverage is not standardized. Part D prescription drug plan sponsors are not required to pay for all covered Part D drugs, and each drug plan can develop its own drug formulary that identifies which drugs it will cover and at what tier or level. However, Part D prescription drug formularies must include drugs within each therapeutic category and class of covered Part D drugs, although not necessarily all the drugs in each category or class. Any formulary used by a Part D prescription drug plan must be developed and reviewed by a pharmacy and therapeutic committee.
It is not clear what long-term effect the MMA will have on the prices paid for currently approved drugs and the pricing options for newly approved drugs. Government payment for some of the costs of prescription drugs may increase demand for any of our products for which we or any collaborator of ours receives marketing approval. However, any negotiated prices for our products covered by a Part D prescription drug plan will likely be lower than the prices we might otherwise obtain. Moreover, while the MMA applies only to drug benefits for Medicare beneficiaries, private payors often follow Medicare coverage policy and payment limitations in setting their own payment rates. Any reduction in payment that results from the MMA may result in a similar reduction in payments from non-governmental payors.
We expect that there will continue to be a number of federal and state proposals to implement governmental pricing controls and limit the growth of healthcare costs, including the cost of prescription drugs. Currently, Medicare is prohibited from negotiating directly with pharmaceutical companies for drugs. However, the U.S. Congress may consider legislation that would lift the ban on federal negotiations.
In some foreign countries, the proposed pricing for a drug must be approved before it may be lawfully marketed. The requirements governing drug pricing vary widely from country to country. For example, the European Union provides options for its member states to restrict the range of medicinal products for which their respective national health insurance systems provide reimbursement and to control the prices of medicinal products for human use. A member state may approve a specific price for the medicinal product or it may instead adopt a system of direct or indirect controls on the profitability of the company placing the medicinal product on the market. There can be no assurance that any country that has price controls or reimbursement limitations for pharmaceutical products will allow favorable reimbursement and pricing arrangements for any of our products for which we or any collaborator of ours receives marketing approval.
Employees
As of February 28, 2011, we had 132 employees, 47 of whom are Ph.D.s, M.D.s or both. Our management believes that relations with our employees are good. None of our employees is represented under a collective bargaining agreement.
34
Table of Contents
Our Corporate Information
We were incorporated in Delaware in 1997 as a wholly owned subsidiary of R.J. Reynolds Tobacco Company. In August 2000, we became an independent company when we issued and sold stock to venture capital investors. Our principal executive offices are located at 200 East First Street, Suite 300, Winston-Salem, North Carolina 27101 and our telephone number is (336) 480-2100.
Our internet address is www.targacept.com. The information contained on, or that can be accessed through, our website is not incorporated by reference into this annual report. We have included our website address as a factual reference and do not intend it as an active link to our website. Our annual reports on Form 10-K, quarterly reports on Form 10-Q and current reports on Form 8-K, and all amendments to those reports, are available to you free of charge through the Investor Relations page of our website as soon as reasonably practicable after such materials have been electronically filed with, or furnished to, the SEC.
Our trademarks and service marks include Targacept®, Pentad™, NNR Therapeutics™, TRIDMAC™ and Building Health, Restoring IndependenceSM. Other service marks, trademarks and trade names appearing in this annual report are the properties of their respective owners.
| Item 1A. | Risk Factors. |
Risks Related to Our Financial Results
We have a substantial accumulated deficit and may incur losses for future periods. We may not sustain profitability or, if we do sustain profitability, we may not grow it.
We were incorporated in 1997 and operated as a wholly owned subsidiary of R.J. Reynolds Tobacco Company until August 2000. We have a limited operating history. As of December 31, 2010, we had an accumulated deficit of $218.4 million. We had net income of $10.9 million for the year ended December 31, 2010, net loss of $39.4 million for the year ended December 31, 2009 and net loss of $25.7 million for the year ended December 31, 2008. Our net income for 2010 was due primarily to the recognition into revenue of a portion of the upfront payment that we received under our TC-5214 agreement with AstraZeneca that we entered into in December 2009. Our losses for other periods have historically resulted principally from costs incurred in connection with our research and development activities, including clinical trials, and from general and administrative expenses associated with our operations. We may incur losses for future periods as our clinical-stage and preclinical product candidates advance into later-stage development and as we progress our programs, invest in additional product opportunities and grow our business. As a result, we will need to generate significant revenues to sustain profitability.
We derived a substantial portion of our revenue for 2010, 2009 and 2008 from our strategic alliances and collaborations. We expect that a substantial portion of our operating cash flow in the next few years will depend on the following:
| • | whether and to what extent milestone events are achieved for TC-5214 under our TC-5214 agreement with AstraZeneca; |
| • | the progress of, and outcomes from, Phase 3 clinical development of TC-5214 and the amount and timing of development costs for TC-5214 payable by us; |
| • | if the outcome of Phase 3 clinical development of TC-5214 is favorable, whether we elect to exercise our co-promotion rights; |
| • | whether AstraZeneca exercises its right to license TC-5619; |
35
Table of Contents
| • | whether and to what extent AstraZeneca determines to continue clinical development of one or both of AZD3480 and AZD1446 and, if so, milestone events are achieved under our cognitive disorders agreement with AstraZeneca that we entered into in December 2005; and |
| • | whether we establish additional strategic alliances, collaborations and licensing or other arrangements, or pursue and complete any merger and acquisition transactions, on terms favorable to us. |
Sources that contributed to our revenue for any particular year may not continue. In particular, the term of the preclinical research collaboration focused in cognition that we had been conducting with AstraZeneca under our cognitive disorders agreement with AstraZeneca expired in January 2010. We had received an aggregate of $26.5 million in research fees from AstraZeneca as of December 31, 2009, and research fee revenue generated from the preclinical research collaboration represented 21% of our net operating revenues for the year ended December 31, 2009 and 45% of our net operating revenues for the year ended December 31, 2008. In addition, we do not currently have any source of product revenue.
If we or a collaborator of ours is unable to develop and commercialize one or more of our product candidates, if development is delayed or if revenue from sales of any product candidate that receives marketing approval is insufficient, we may not be profitable. Even if we are profitable for any particular period, we may not be able to sustain or grow our profitability on a quarterly or annual basis.
Our failure to obtain additional capital when needed could force us to delay, reduce or eliminate our product development programs or future commercialization efforts.
Successful drug development and commercialization requires significant amounts of capital. It is foreseeable that we will in the future require substantial additional capital in order to continue to conduct the research and development and clinical and regulatory activities necessary to bring our product candidates to market (or, where applicable for a particular product candidate, to the stage of development when a current or potential future collaborator of ours may assume responsibility under the terms of the applicable agreement for funding further development and subsequent commercialization) and to establish sales and marketing capabilities. Our future capital requirements are difficult to forecast and will depend on many factors, including:
| • | the amount of revenue that we are able to generate, which we expect will depend substantially on the outcomes of the uncertainties described in the bullets above under “We have a substantial accumulated deficit and may incur losses for future periods. We may not sustain profitability or, if we do sustain profitability, we may not grow it.”; |
| • | the progress of, and outcomes from, Phase 3 clinical development of TC-5214 and the amount and timing of development costs for TC-5214 payable by us; |
| • | the scope, progress, duration, results and costs of clinical trials, as well as non-clinical studies and assessments, of our product candidates; |
| • | the extent to which we retain development and commercialization rights or responsibilities for our product candidates that are not subject to our collaborations with AstraZeneca and incur associated development and manufacturing costs and costs to establish sales and marketing functions; |
| • | the costs, timing and outcomes of regulatory reviews or other regulatory actions; |
| • | the number and characteristics of product candidates that we pursue; |
| • | the costs of preparing, filing and prosecuting patent applications and maintaining, enforcing and defending intellectual property-related claims; |
| • | the costs of manufacturing-related services for our product candidates in clinical and late preclinical development; |
| • | the rate of technological advancements for the indications that we target; |
36
Table of Contents
| • | the costs to satisfy our obligations under existing and potential future alliances and collaborations; |
| • | the timing, receipt and amount of sales or royalties, if any, from our potential products; and |
| • | the extent and scope of our general and administrative expenses. |
In addition, we may seek additional capital due to market conditions or strategic considerations even if we believe we have sufficient funds for our current or future operating plans. To the extent that we raise additional capital through the sale of equity or convertible debt securities, the ownership interests of our stockholders may be diluted and the terms may include liquidation or other preferences that materially and adversely affect the rights of our stockholders. Debt financing, if available, may involve agreements that include covenants limiting or restricting our ability to take specific actions such as incurring additional debt, making capital expenditures or declaring dividends. If we raise additional funds through alliance, collaboration or licensing arrangements with third parties, we may have to relinquish valuable rights to our technologies or product candidates or grant licenses on terms that are not favorable to us.
Our plans provide for us to continue, either alone or with AstraZeneca or one or more potential future collaborators, to advance our product candidates through the development process. We currently expect that our existing capital resources will enable us to fund our operations at least through the end of 2013. However, our operating plan may change as a result of many factors, including those described above, and we may need additional funds sooner than planned to meet operational needs and capital requirements for product development and commercialization. Our ability to raise funds if and when needed may be materially and adversely affected by challenging U.S. and global financial markets and additional funds may not be available on terms that are acceptable to us, or at all. If adequate funds are not available on a timely basis, we may:
| • | terminate, delay or downsize clinical trials or manufacturing or other development activities for one or more of our product candidates; |
| • | delay our establishment of sales and marketing capabilities or other activities that may be necessary to commercialize our product candidates; or |
| • | terminate, delay or downsize research programs that are designed to identify new product candidates. |
Risks Related to the Development and Regulatory Approval of Our Product Candidates
Our success depends substantially on our most advanced product candidates, which are still under development. If we or a collaborator of ours is unable to bring one or more of these product candidates to market, or experience significant delays in doing so, our ability to generate product or royalty revenue and our likelihood of success will be harmed.
Our ability to generate product or royalty revenue over the next few years will depend substantially on the successful development and commercialization of our clinical-stage product candidates, including in particular: TC-5214 (which is currently in Phase 3 clinical development); TC-5619 (for which a Phase 2 clinical trial has been completed in cognitive dysfunction in schizophrenia and a separate Phase 2 clinical trial in adults with ADHD and additional studies to support potential advancement into a Phase 2 clinical trial in Alzheimer’s disease are ongoing); AZD3480 and AZD1446 (each of which is at the Phase 2 clinical development stage, with any future development by AstraZeneca uncertain); and TC-6987 (which is currently being studied in separate Phase 2 trials in asthma and Type 2 diabetes).
Any of our product candidates could be unsuccessful if it:
| • | does not demonstrate acceptable safety and efficacy in preclinical studies or clinical trials or otherwise does not meet applicable regulatory standards for approval; |
| • | does not offer therapeutic or other improvements over existing or future drugs used to treat the same condition; |
37
Table of Contents
| • | is not capable of being produced in commercial quantities at acceptable costs; or |
| • | is not accepted in the medical community and by third-party payors. |
We do not expect TC-5214 to be commercially available until at least the second half of 2013, if at all. We do not expect any of our other current product candidates to be commercially available for at least the next several years, if at all. If we or any applicable collaborator of ours is unable to make our product candidates commercially available, we will not generate substantial product revenue and we will not be successful.
If the favorable results of the completed Phase 2b clinical trial of TC-5214 as an adjunct therapy for major depressive disorder are not replicated in Phase 3 clinical trials, or if any of the other studies included in the clinical program for TC-5214 indicates that TC-5214 is not sufficiently safe, we and AstraZeneca will not obtain the regulatory approvals required to market and sell TC-5214.
Favorable results in earlier-stage clinical trials of a product candidate, such as our completed Phase 2b clinical trial of TC-5214 as an adjunct therapy for major depressive disorder, may not be replicated in later clinical trials that involve different numbers of subjects, different dosing regimens and durations, different subject populations and other differences in design or execution.
Our completed Phase 2b clinical trial of TC-5214 as an adjunct therapy for major depressive disorder was limited to subjects who did not respond adequately to the antidepressant citalopram. The ongoing Phase 3 development program for TC-5214 includes subjects who do not respond adequately to citalopram or any one of several other antidepressant therapies. It is possible that this difference in subject population, or any other difference in design between one or more of the ongoing Phase 3 clinical trials of TC-5214 and our completed Phase 2b clinical trial, will impact the likelihood that the favorable results achieved in the completed Phase 2b clinical trial will be replicated in Phase 3.
Furthermore, our completed Phase 2b clinical trial was conducted primarily in India and the ongoing Phase 3 development program is being conducted at investigative sites worldwide, including a significant number in the United States and Western Europe. Medical care in India is generally not as advanced as in the United States or Western Europe, and the treatment that subjects receive in a clinical trial in India may in some cases be their only medical treatment. As a result, clinical trial subjects in India may be less likely to discontinue participation from a clinical trial or to report adverse events experienced, either of which may impact the likelihood that the favorable results achieved in the completed Phase 2b clinical trial will be replicated. If the favorable results achieved in our completed Phase 2b clinical trial of TC-5214 are not replicated in future clinical trials, we and AstraZeneca will not obtain the regulatory approvals required to market and sell TC-5214.
In addition, the clinical program for TC-5214 includes a long-term safety study in which patients receive TC-5214 or placebo for up to one year, as well as multiple Phase 1 clinical trials—including a QTc study, which is designed to confirm that various doses of TC-5214 do not disturb the electrical activity of the heart, a renal impairment study, which is designed to evaluate the elimination of TC-5214 in subjects with impaired kidney function, and a drug-drug interaction study designed to assess the safety of TC-5214 when used together with other specified drugs. If the outcome of any of these studies indicates that TC-5214 is not sufficiently safe, we and AstraZeneca will not obtain the regulatory approvals required to market and sell TC-5214. If the outcome of any of these studies indicates that TC-5214 is not safe for certain patients or under certain circumstances, the FDA or applicable foreign regulatory authorities could limit the patient population for which TC-5214 is approved, which could materially and adversely affect its commercial potential.
If the ongoing fixed dose clinical trials included in the Phase 3 development program for TC-5214 do not result in the determination of an effective dose range for TC-5214, or if an effective dose range is determined but does not provide a sufficient safety margin, we and AstraZeneca may not obtain the regulatory approvals required to market and sell TC-5214.
Our completed Phase 2b clinical trial of TC-5214 as an adjunct therapy for major depressive disorder utilized a flexible dose design. “Flexible dose” means that each subject who received TC-5214 initially received
38
Table of Contents
a particular dosage (1mg twice per day), which could be increased (to 2mg and 4mg, in each case twice per day) at various times during the trial at the discretion of the applicable investigator based on how the subject tolerated and responded to the then-current dosage. Accordingly, the completed Phase 2b clinical trial was not designed to establish statistically the specific dosage at which TC-5214 had positive effects.
Two of the clinical trials in the Phase 3 development program for TC-5214 also utilize a flexible dose design, but two other trials in the program utilize a fixed dose design. A “fixed dose” design means that subjects in the trial receiving TC-5214 receive a set dosage regimen throughout the dosing period. Prior to initiation of the Phase 3 development program, neither we nor AstraZeneca had ever conducted a fixed dose trial of TC-5214 as an adjunct treatment for major depressive disorder. We and AstraZeneca were guided by data from the completed Phase 2b trial in selecting the dosages of TC-5214 to be evaluated in the fixed dose Phase 3 trials, but we cannot be certain that the optimum dosages were selected.
In addition, in a Phase 1 multiple rising dose clinical trial completed by AstraZeneca in healthy volunteers, the tolerability profile of TC-5214 was less favorable at the highest dose tested as compared to the other doses. If, upon completion of the fixed dose Phase 3 clinical trials, the highest dosage evaluated in the trials (4mg twice per day) is the only effective dosage, the United States Food and Drug Administration, or FDA, or foreign regulatory authorities may not determine there to be a sufficient margin of safety to support approval to market and sell TC-5214.
If, notwithstanding the favorable results of our completed Phase 2b flexible dose clinical trial of TC-5214, the fixed dose clinical trials included in the Phase 3 development program do not result in the determination of an effective dose range for TC-5214 as an adjunct treatment for major depressive disorder, or if an effective dose range is determined but does not provide a safety margin that the FDA or foreign regulatory authorities determine to be sufficient, we and AstraZeneca may not obtain the regulatory approvals required to market and sell TC-5214, even if favorable results are obtained in the flexible dose clinical trials included in the Phase 3 development program.
If we and AstraZeneca are unable to complete the Phase 3 development program for TC-5214 and submit an NDA to the FDA on or before September 30, 2012, or if other statutory conditions are not met, TC-5214 may not receive the five-year exclusivity period provided by applicable law and the ability of us and AstraZeneca to exclude third parties from marketing TC-5214 themselves would be substantially dependent on patents after three years.
The Federal Food, Drug, and Cosmetic Act, or FDCA, provides a five-year period of marketing exclusivity in the United States to the first applicant to obtain approval of a new drug application, or NDA, for a drug that qualifies as a new chemical entity. The FDA may not during this exclusivity period accept for review an abbreviated new drug application, or ANDA, or another NDA for another version of the drug in question where the applicant does not own or have a legal right of reference to all the data required for approval, except that either of these applications may be submitted after four years with a certification that applicable patents are invalid or not infringed (in which case a timely challenge to the certification would trigger a stay of the FDA’s approval of the application for a defined term). The exclusivity period runs concurrently with any patents that cover the new chemical entity, but provides exclusivity independent from and irrespective of the patents. Accordingly, a new chemical entity approved in the United States has assurance of a statutory period of marketing exclusivity in the United States whether or not the patents that cover it are sufficiently strong to withstand challenge.
TC-5214 is one of two enantiomers of a racemate previously approved by the FDA. Enantiomers are mirror images of each other that have the same chemical but potentially different biological properties, and a racemate is a chemical mixture comprised of two corresponding enantiomers. Under Section 505(u) of the FDCA, as added by the FDA Amendments Act of 2007, an NDA applicant may, if certain conditions are met, elect that a single enantiomer of a previously approved racemate not be considered the same active ingredient as the racemate and
39
Table of Contents
thereby preserve potential eligibility for the single enantiomer as a new chemical entity. The election may only be made for an NDA submitted on or before September 30, 2012, when the statutory provision that permits the election is scheduled to expire unless re-authorized by the U.S. Congress. It is uncertain whether the statutory provision will be re-authorized. If we and AstraZeneca are unable to complete the Phase 3 development program for TC-5214 in time to submit an NDA for TC-5214 on or before September 30, 2012, whether because of delays that have been experienced in subject enrollment or for any other reason, or if other statutory conditions are not met, and the statutory provision is not reauthorized, TC-5214 will not receive the five-year exclusivity period and will be limited to three years of exclusivity provided by the FDCA for certain applications. In that case, we and AstraZeneca would be substantially reliant on patent protection to provide an extended term of exclusivity in the United States. Like any patent, the patents that we own or license covering TC-5214 and those that may issue in the future are subject to being challenged, invalidated, rendered unenforceable or circumvented, any of which could limit our ability to stop third parties from marketing TC-5214 or related products themselves. If we and AstraZeneca are unable to enforce or defend patents that cover TC-5214 that we own or license and cannot stop third parties from marketing TC-5214 or related products themselves, the commercialization of TC-5214 would be materially and adversely affected and our business would suffer.
The designs, endpoints and outcomes of clinical trials that will be required to obtain regulatory approval of a drug to treat cognitive dysfunction in schizophrenia are uncertain, and we and, if AstraZeneca exercises its license right, AstraZeneca may never receive the regulatory approvals required to market and sell TC-5619 as a treatment for cognitive dysfunction in schizophrenia.
There is currently no product approved in the United States or Europe specifically for the treatment for cognitive dysfunction in schizophrenia. Accordingly, there is not a well-developed development path that, with clinical success, would be reasonably assured of receiving regulatory approval. If the FDA or any foreign regulatory authority determines that the designs or endpoints of any future clinical trials of TC-5619 as a treatment for cognitive dysfunction in schizophrenia that we or, if AstraZeneca exercises its license right, AstraZeneca conducts are not sufficient to support regulatory approval, we and, if AstraZeneca exercises its license, AstraZeneca would not receive the approval required to market and sell TC-5619 as a treatment for cognitive dysfunction in schizophrenia even if the outcomes from the trials are positive.
The positive findings in our completed Phase 2 trial of TC-5619 in cognitive dysfunction in schizophrenia may not be replicated in later clinical trials and, even if replicated, may not be sufficient to obtain required regulatory approvals.
In our completed Phase 2 trial of TC-5619 in cognitive dysfunction in schizophrenia, TC-5619 met the protocol criteria for a positive result on the primary efficacy outcome measure and positive signals were observed on some secondary efficacy outcome measures. However, TC-5619 did not demonstrate positive effects as to all of the trial’s efficacy outcome measures and all evaluation dates and the results varied by geography and by whether patients used tobacco. Moreover, the favorable findings in the trial may not be replicated in any later clinical trials of TC-5619 as a treatment of cognitive dysfunction in schizophrenia that involve a large number of subjects and a long duration of dosing. If the favorable findings in the completed Phase 2 trial are not replicated in later clinical trials of TC-5619, we and, if AstraZeneca exercises its right to license TC-5619, AstraZeneca, will not obtain the regulatory approval required to market and sell TC-5619 as a treatment for cognitive dysfunction in schizophrenia.
If AstraZeneca determines to conduct additional development of AZD3480 as a treatment for ADHD but the favorable results of the completed Phase 2 clinical trial of AZD3480 in adults with ADHD are not replicated in future clinical trials, we and AstraZeneca will not obtain the regulatory approvals required to market and sell AZD3480 as a treatment for ADHD.
Whether AstraZeneca will decide to conduct any additional development of AZD3480 as a treatment for ADHD is uncertain in light of reservations about the adequacy of the therapeutic margin to support development across the broad ADHD patient population. Even if AstraZeneca determines to advance AZD3480 in ADHD, the
40
Table of Contents
favorable results in the completed Phase 2 clinical trial of AZD3480 in adults with ADHD may not be replicated in later clinical trials. The completed Phase 2 clinical trial of AZD3480 in adults with ADHD was conducted at a single site with only 24 completed subjects and used a crossover trial design in which subjects received each treatment (5mg AZD3480, 50mg AZD3480 and placebo) and in each case for only two weeks. Because subjects received each treatment, each subject served as his or her own control. It is likely that, if there are future clinical trials of AZD3480 in adults with ADHD, they would be substantially larger, conducted at several sites and over a longer duration and use a parallel group design with placebo as a control such that each subject receives a particular dosing regimen of AZD3480 or placebo, but not both. It is possible that any of these differences or any other difference in trial design will impact the likelihood that the favorable results achieved in the completed Phase 2 clinical trial of AZD3480 in adults with ADHD would not be replicated in future clinical trials. If the favorable results achieved in the completed Phase 2 clinical trial of AZD3480 in adults with ADHD are not replicated, if future clinical trials otherwise do not establish the safety and efficacy of AZD3480 as a treatment for ADHD or if no further clinical trials of AZD3480 in ADHD are conducted, we and AstraZeneca will not obtain the regulatory approvals required to market and sell AZD3480 as a treatment for ADHD.
If AstraZeneca determines to conduct any additional development of AZD3480 as a treatment for ADHD and if the favorable results of the completed Phase 2 clinical trial of AZD3480 in adults with ADHD are not replicated in future clinical trials in children and adolescents, the commercial potential of AZD3480 would be materially and adversely affected.
If AstraZeneca determines to advance AZD3480 in ADHD, the results of the completed Phase 2 clinical trial of AZD3480 in adults with ADHD may not be predictive of results that would be obtained in any future clinical trials of AZD3480 in children or adolescents with ADHD. A drug that has positive effects in adults may not necessarily have positive effects in younger patients. Children with ADHD tend to exhibit more hyperactivity than do adults with ADHD, and it is possible that this or any other difference in the characteristics of the disorder between adults and children would cause the results of the completed Phase 2 clinical trial adults with ADHD to be not predictive of results obtained in future clinical trials in children or adolescents with ADHD, if conducted at all. Even if the favorable results in the completed Phase 2 clinical trial of AZD3480 in adults with ADHD are replicated in any future clinical trials of AZD3480 in adults with ADHD, if the results are not also replicated in any future clinical trials of AZD3480 in children or adolescents with ADHD, the FDA or applicable foreign regulatory authorities could limit the patient population for which AZD3480 is approved to adults. In that event, the commercial potential of AZD3480 would be materially and adversely affected.
If we or a collaborator of ours does not obtain the regulatory approvals required to market and sell our product candidates, our ability to generate product revenue will be materially impaired and our business will not be successful.
The preclinical laboratory testing, development, manufacturing and clinical trials of product candidates that we develop, whether independently or in collaboration with a third party, as well as their distribution, sale and marketing, are regulated by the FDA and other federal, state and local governmental and regulatory authorities in the United States and by similar agencies in other countries. We or a collaborator of ours must receive regulatory approval of each product candidate before we or the collaborator can market and sell it. We have only limited experience in pursuing regulatory approvals. Securing FDA approval requires the submission of extensive preclinical and clinical data and information about the chemistry and manufacture of, and control procedures for, each potential product. In addition, the supporting information submitted to the FDA must establish the safety and efficacy of the product candidate for each indicated use. The drug development and marketing approval process takes many years, requires the expenditure of substantial resources, is subject to delays and can vary substantially based upon the type, complexity and novelty of the product candidates involved. In addition to the time and expense involved, the process is uncertain and neither we nor any applicable collaborator of ours may ever receive the required regulatory approvals. In addition, the FDA, the U.S. Congress or foreign governmental or regulatory authorities may from time to time change approval policies or adopt new laws or regulations that could prevent or delay our receipt of required approvals. Even if we or a collaborator of ours receives regulatory
41
Table of Contents
approval to market a particular product candidate, the approval will be subject to limitations on the indicated uses for which it may be marketed and may not permit labeling claims that are necessary or desirable for its promotion.
A Phase 1 clinical trial program typically takes several months to complete, a Phase 2 clinical trial program typically takes several months to two years to complete and a Phase 3 clinical trial program typically takes one to four years to complete. Moreover, Phase 3 clinical trials may not follow successful completion of Phase 2 clinical trials directly, as additional non-clinical assessments or clinical trials may first be required. Industry sources have reported that the preparation and submission of an NDA, which is required for regulatory approval in the United States, generally takes six months to one year to complete after completion of pivotal clinical trials. However, additional clinical trials may be required by the FDA or foreign regulatory authorities following completion of pivotal clinical trials and prior to seeking approval. The Pharmaceutical Research and Manufacturers of America has reported that only one out of five product candidates that enter clinical trials will ultimately be approved by the FDA for commercial sale.
The FDA may delay, limit or deny approval of any of our product candidates for many reasons. For example:
| • | clinical trial results may indicate that the product candidate is not safe or effective; |
| • | the FDA (or any advisory committee on which the FDA relies) may interpret results of clinical trials or manufacturing or other non-clinical studies or assessments to indicate that the product candidate is not safe, effective or acceptable for commercial use, even if we or a collaborator of ours interprets the same results differently; or |
| • | the FDA may deem the processes or facilities that we, our collaborators or our third-party manufacturers propose to use in connection with the manufacture of the product candidate to be unacceptable. |
If we or a collaborator of ours obtains the requisite regulatory approval for a particular product candidate, the approval may not extend to all indications for which approval was sought, which could limit the use of the product and materially and adversely impact our revenue.
Even if the FDA approves a product candidate for marketing and sale in the United States, applicable regulatory authorities in other countries may not approve the product candidate or may subject their approval to conditions such as additional product testing or otherwise cause delays. The regulatory approval process varies among countries, but generally includes all of the risks associated with obtaining FDA approval. In addition, many countries require a separate review process prior to marketing to determine whether their respective national health insurance schemes will pay for newly approved products, as well as the price that may be charged. This process will cause delays in the marketing of any of our product candidates that receives approval and could materially and adversely impact our revenue and results of operations.
If clinical trials for our product candidates are not successful, neither we nor any applicable collaborator of ours will obtain the regulatory approvals required to market and sell them.
To obtain the requisite regulatory approvals to market and sell any of our product candidates, we or any applicable collaborator of ours must demonstrate, through extensive preclinical studies and clinical trials, that the product candidate is safe and effective in humans. The number of clinical trials required to obtain approval varies depending on the particular product candidate, the disease or condition for which it is in development and the regulations applicable to it. Preclinical studies and clinical trials are lengthy and expensive, difficult to design and implement and subject to a historically high rate of failure. The development of each of our product candidates involves significant risks at each stage of testing. A failure of one or more clinical trials of any of our product candidates could occur at any stage of testing. If we or any applicable collaborator of ours experiences
42
Table of Contents
failures in our ongoing or future clinical trials, or if we or the collaborator is not able to design clinical trials to establish the safety and efficacy of our product candidates and otherwise achieve the objectives of the trials, our product candidates may never be approved for sale or become commercially available.
We and any applicable collaborator of ours may not be able to obtain authority or approval from the FDA, applicable foreign regulatory authorities or the institutional review boards at our intended investigational sites to commence or complete our clinical trials. Before a clinical trial may commence in the United States, we or a collaborator of ours must submit an IND containing preclinical studies, chemistry, manufacturing, control and other information and a study protocol to the FDA. If the FDA does not object within 30 days after submission of the IND, then the trial may commence. If commenced, we or any applicable collaborator of ours, the FDA, applicable foreign regulatory authorities and institutional review boards may delay, suspend or terminate clinical trials of a product candidate at any time if, among other reasons, we or they believe the subjects participating in the clinical trials are being exposed to unacceptable health risks or for other reasons.
If we or any applicable collaborator of ours does not prove in clinical trials that our product candidates are safe and effective, neither we nor the collaborator will obtain marketing approvals from the FDA or applicable foreign regulatory authorities. In particular, one or more of our product candidates may not exhibit the expected medical benefits in humans, may cause harmful side effects or may have other unexpected characteristics that preclude regulatory approval for any or all indications of use or limit commercial use if approved.
Our research and preclinical programs and product candidates target diseases or disorders that are not well understood. For example, there is only limited scientific understanding of the causes of major depressive disorder, ADHD, Alzheimer’s disease and cognitive dysfunction in schizophrenia. In addition, there are no approved drugs that target NNRs to treat these diseases and disorders, and there is only limited scientific understanding of the relationships between these diseases and disorders and the neurological pathways targeted by our product candidates and research and preclinical programs. These uncertainties increase the risk that one or more of our clinical trials will not be successful.
If clinical trials for any of our product candidates are prolonged or delayed, we and any applicable collaborator of ours would experience a delay in the commercialization of the affected product candidates, which may require us to incur additional costs and delay our receipt of any revenue from potential product sales.
We cannot predict whether we or any applicable collaborator of ours will encounter problems with any completed, ongoing or planned clinical trials of our product candidates that will cause us, the collaborator or any regulatory authority to delay or suspend those clinical trials or delay the analysis of data derived from them. A number of events, including those described below, could delay the initiation or completion of any ongoing or planned clinical trial of any of our product candidates or otherwise negatively impact our ability to obtain regulatory approval for, and to market and sell, the product candidate:
| • | conditions imposed on us or any applicable collaborator of ours by the FDA or any foreign regulatory authority regarding the scope or design of the clinical trial; |
| • | delays in recruiting and enrolling subjects into the clinical trial; |
| • | delays in obtaining, or our inability to obtain, required approvals from institutional review boards, ethics committees or other reviewing entities at clinical sites selected for participation in the clinical trial; |
| • | insufficient supply or deficient quality of the product candidates or other materials necessary to conduct the clinical trial; |
| • | lower than anticipated retention rate of subjects in the clinical trial; |
| • | negative or inconclusive results from the clinical trial, or results that are inconsistent with earlier results, that necessitate additional study; |
43
Table of Contents
| • | serious and unexpected drug-related side effects experienced by subjects in the clinical trial; or |
| • | failure of third-party contractors to us or any applicable collaborator of ours to comply with regulatory requirements or otherwise meet their contractual obligations to us or the collaborator in a timely manner. |
Clinical trials require sufficient subject enrollment, which is a function of many factors—including the size of the patient population, the extent to which other clinical trials are being conducted concurrently that involve the same patient population, the number of participating clinical sites, the proximity of subjects to clinical sites, the nature of the trial protocol, the emphasis placed on ensuring a rigorous adherence to the trial protocol, the availability of effective treatments for the relevant disease and the eligibility criteria for the clinical trial. Delays in subject enrollment can result in increased costs and longer development times. The failure to enroll subjects in a clinical trial could delay the completion of the clinical trial beyond our current expectations. For example, in part due to initiatives that we and AstraZeneca implemented to assure that only patients meeting the criteria for initial and continued inclusion in the Phase 3 clinical trials of TC-5214 participate in the trials, we and AstraZeneca have experienced unexpected enrollment delays and enrollment for some of the Phase 3 clinical trials is tracking behind projections. We do not yet know whether the steps we and AstraZeneca have taken to address these enrollment delays will be successful.
In addition, the FDA or foreign regulatory authorities could require us or any applicable collaborator of ours to conduct clinical trials for any of our product candidates with a larger number of subjects than we project. We or any applicable collaborator of ours may not be able to enroll a sufficient number of subjects in a timely or cost-effective manner. Furthermore, enrolled subjects may drop out of clinical trials, which could impair the validity or statistical analysis of those clinical trials.
We do not know whether any clinical trial of any of our product candidates will begin as planned, will need to be restructured or will be completed on schedule, if at all. Delays in clinical trials may result in increased development costs for our product candidates. In addition, if our clinical trials are delayed, our competitors may be able to bring products to market before we do and the commercial viability of our product candidates could be limited.
Regulatory authorities may require more data for any of our product candidates than we currently anticipate, which could cause us to incur additional costs, extend our development timelines or delay our receipt of any revenue from potential product sales.
The FDA or applicable foreign regulatory authorities may require more preclinical or clinical data for any of our product candidates or more time to evaluate that data than we currently anticipate because drugs that act on NNRs are not a well established class of drugs, because nicotine, which interacts with all nicotinic receptors, has addictive properties and potential for abuse, because of experiences with drugs that act on NNRs that are developed or marketed by third parties or for any other reason. In particular, in February 2008, the FDA issued a public health advisory with regard to Pfizer’s aid to smoking cessation product, Chantix. In July 2009, the FDA announced that it would require each of Chantix and Zyban, which is GlaxoSmithKline’s aid to smoking cessation product, to include a boxed warning on its prescribing information. The warning makes more prominent the risk of serious mental health events, including changes in behavior, depressed mood, hostility, agitation and suicide-related events, that have been reported in some patients attempting to quit smoking while taking these drugs. The warning also states that the health benefits of quitting smoking are immediate and substantial and that the risks of the drug should be weighed against the benefits of use. Chantix acts on several NNR subtypes, as well as other molecular targets in the body. All of our product candidates currently in development affect the activity of one or more NNR subtypes.
If the FDA or any foreign regulatory authority determines that any adverse medical experiences associated with Chantix have relevance to one or more of our product candidates or that compounds that interact with NNRs may have potential for abuse, it may require us or any applicable collaborator of ours to generate more clinical data than we currently anticipate to establish that the affected product candidate is safe or does not have abuse
44
Table of Contents
potential, which could increase the cost of the development program for the affected product candidate, extend the development timeline for the affected product candidate or delay our receipt of revenue from potential product sales of the affected product candidate.
Each of our product candidates will remain subject to ongoing regulatory review even if it receives marketing approval. If we or a collaborator of ours fails to comply with continuing regulations or if patients taking our products experience adverse health effects, we or any applicable collaborator could lose the approval or the sale of the affected products could be suspended or otherwise adversely affected.
Even if we or a collaborator of ours receives regulatory approval to market a particular product candidate, the approval could be conditioned on us or the collaborator conducting additional costly post-approval studies or could limit the indicated uses included in our labeling. Moreover, the product may later cause adverse medical experiences that limit or prevent its widespread use or commercial potential, force us or any applicable collaborator of ours to withdraw it from the market or impede or delay the ability of us or the collaborator to obtain regulatory approvals in additional countries. If any of our product candidates that becomes an approved product causes adverse medical experiences or becomes associated with any third-party product that is associated with adverse medical experiences such as those described above under “Regulatory authorities may require more data for any of our product candidates than we currently anticipate, which could cause us to incur additional costs, extend our development timelines or delay our receipt of any revenue from potential product sales.” for Chantix, the overall commercial success of the affected product may be negatively impacted.
In addition, if any of our product candidates becomes an approved product, the manufacturer of the product and its facilities will continue to be subject to FDA review and periodic inspections to ensure adherence to applicable regulations. After receiving marketing approval, the manufacturing, labeling, packaging, adverse event reporting, storage, advertising, promotion and recordkeeping related to the product will remain subject to extensive regulatory requirements. We or any applicable collaborator of ours may be slow to adapt, or may never adapt, to changes in existing regulatory requirements or adoption of new regulatory requirements.
The Commissioner of the FDA, who was appointed during 2009, has indicated that more enforcement actions in all areas regulated by the FDA should be expected. Although we have not received any notice that we are the subject of any such enforcement action it is possible that we may be in the future and that could have a material adverse effect on our business. If we or any applicable collaborator of ours fails to comply with the requirements of the FDA and other applicable U.S. or foreign governmental or regulatory authorities or previously unknown problems with our products or product candidates, manufacturers or manufacturing processes are discovered, we or the collaborator could be subject to administrative or judicially imposed sanctions, including:
| • | restrictions on the products, manufacturers or manufacturing processes; |
| • | warning letters; |
| • | civil or criminal penalties; |
| • | fines; |
| • | injunctions; |
| • | product seizures or detentions; |
| • | import bans; |
| • | voluntary or mandatory product recalls and publicity requirements; |
| • | suspension or withdrawal of regulatory approvals; |
| • | total or partial suspension of production; and |
| • | refusal to approve pending applications for marketing approval of new drugs or supplements to approved applications. |
45
Table of Contents
Because we have multiple compounds and are considering a variety of target indications, we may apply our finite resources to pursue a particular product candidate or indication and fail to capitalize on product candidates or indications that may be more profitable or for which there is a greater likelihood of success.
Because we have finite financial and managerial resources, we must focus on research programs and product candidates for the specific indications that we believe are the most promising. As a result, we may forego or delay pursuit of opportunities with other product candidates or other indications that later prove to have greater commercial potential. Our resource allocation decisions may cause us to fail to capitalize on viable commercial products or profitable market opportunities. Furthermore, if we do not accurately evaluate the commercial potential or target market for a particular product candidate, we may relinquish valuable rights to that product candidate through collaboration, licensing or other royalty arrangements in cases in which it would have been advantageous for us to retain sole development and commercialization rights.
We may not be successful in our efforts to identify or discover additional product candidates.
A key element of our strategy is to develop and commercialize drugs that selectively target specific NNR subtypes. A significant portion of the research that we are conducting involves new and unproven compounds. Research programs to identify new product candidates require substantial technical, financial and human resources. These research programs may initially show promise in identifying potential product candidates, yet fail to yield product candidates for clinical development for a number of reasons, including:
| • | the research methodology used may not be successful in identifying potential product candidates; or |
| • | potential product candidates may, on further study, be shown to have harmful side effects or other characteristics that indicate that they are unlikely to be effective products. |
If we are unable to develop suitable product candidates through internal research programs, we will not be able to overcome attrition inherent in drug development and generate revenue in future periods, which could result in significant harm to our financial position and materially and adversely impact our stock price. Any additional product candidates that we are able to develop through our internal research programs will require the commitment of substantial time and financial resources for further preclinical research and clinical development.
Risks Related to Our Dependence on Third Parties
The successful development and commercialization of TC-5214 depends substantially on our December 2009 collaboration with AstraZeneca.
We entered into our collaboration with AstraZeneca for TC-5214 in December 2009. We cannot predict the ultimate success of the collaboration. The collaboration involves a complex allocation of rights and responsibilities, provides for milestone payments to us if specified development, regulatory and first commercial sale milestone events are achieved and provides us with royalty-based revenue if TC-5214 is successfully commercialized. We and AstraZeneca have agreed on an initial development program for TC-5214 for major depressive disorder, but AstraZeneca has the authority to make changes to the initial program and also has decision-making authority for many other matters in our collaboration. In addition, AstraZeneca has the right to assume control of patent matters with respect to TC-5214 and has exercised its right with respect to the prosecution of some of the applicable patents.
AstraZeneca is responsible for the conduct of substantially all development of TC-5214, except for non-clinical studies that were ongoing at the time of our agreement, and has control or significant influence over the conduct and timing of development efforts with respect to TC-5214. AstraZeneca has engaged a global contract research organization to manage the initial development program of TC-5214. We have little control over the amount and timing of resources that AstraZeneca or the contract research organization with which it has contracted devotes to the development of TC-5214. If AstraZeneca (or its contract research organization) fails to
46
Table of Contents
devote sufficient financial and other resources, the development and potential commercialization of TC-5214 would be delayed. This would result in a delay in milestone payments and, if regulatory approval to market and sell TC-5214 is obtained, royalties that we could receive on any future TC-5214 product sales.
AstraZeneca has the right to terminate our TC-5214 agreement in its entirety:
| • | within a specified period following completion of the Phase 3 development program for TC-5214 as an adjunct therapy; |
| • | if AstraZeneca determines there to be a serious safety issue regarding the continued development or commercialization of TC-5214; |
| • | if, having obtained the advice of independent patent counsel, AstraZeneca believes that the commercialization of TC-5214 is more likely than not to infringe or misappropriate intellectual property rights of third parties in the United States or any two specified major pharmaceutical markets and is unable to obtain a license on commercially reasonable terms; or |
| • | for an uncured material breach of the agreement by us. |
In addition, AstraZeneca can terminate our agreement on a major pharmaceutical market by major pharmaceutical market basis at any time beginning four years after effectiveness of our agreement, except that, if AstraZeneca terminates our agreement with respect to the United States, our agreement will terminate in its entirety.
If AstraZeneca terminates our TC-5214 agreement at any time, for any reason, it would negatively impact our development of TC-5214 and materially harm our business and could accelerate our need for additional capital. In particular, we would have to fund any further clinical development and commercialization of TC-5214 on our own, seek another collaborator or licensee for clinical development and commercialization or abandon the development and commercialization of TC-5214.
If TC-5214 exhibits a similar overall therapeutic profile to AstraZeneca’s product Seroquel XR, AstraZeneca may de-emphasize the development or commercialization of TC-5214, which would materially and adversely affect the revenue that we derive based on TC-5214.
AstraZeneca’s product Seroquel XR is approved by the FDA for use, among other things, as an adjunct to antidepressant therapy for major depressive disorder. TC-5214 is in development as an adjunct to antidepressant therapy and as a “switch” monotherapy for major depressive disorder. Until the Phase 3 development program for TC-5214 is completed and regulatory approval is obtained, the overall therapeutic profile of TC-5214 and any patient population for which TC-5214 may be considered safe and effective are uncertain. AstraZeneca has control or significant influence over the conduct of future development and regulatory approval activities for TC-5214. If one or more Phase 3 clinical trials of TC-5214 indicate that its overall therapeutic profile may be similar to the overall therapeutic profile of Seroquel XR, AstraZeneca may de-emphasize or otherwise fail to devote sufficient financial and other resources to the development of TC-5214. In that event, the development and potential commercialization of TC-5214 would be delayed. This would result in a delay of milestone payments and, if regulatory approval to market and sell TC-5214 is obtained, royalties on product sales that we could receive and could result in us not receiving milestone payments or royalties at all. Even if TC-5214 is successfully developed and regulatory approvals are obtained, if AstraZeneca de-emphasizes or otherwise fails to devote sufficient financial and other resources to the commercialization of TC-5214 for any reason, the amount of royalties that we could receive on any future TC-5214 product sales would be materially and adversely affected.
If AstraZeneca exercises its right to license TC-5619 but fails to devote sufficient financial and other resources to its development, our ability to derive revenue based on TC-5619 would be materially and adversely affected.
If AstraZeneca exercises its right to license TC-5619, AstraZeneca would become generally responsible for conducting and funding substantially all future development and regulatory approval activities for TC-5619 and
47
Table of Contents
have significant control over the conduct and timing of development efforts with respect to TC-5619, including whether to conduct Phase 2 development of TC-5619 as a treatment for Alzheimer’s disease either alone or in addition to further development in either or both of cognitive dysfunction in schizophrenia and ADHD. If AstraZeneca were to fail to devote sufficient financial and other resources to the development of TC-5619, whether in favor of an internal product candidate or for any other reason, the development and potential commercialization of TC-5619 would be delayed. This would result in a delay in milestone payments and, if regulatory approval to market and sell TC-5619 is obtained, royalties that we could receive on any future TC-5619 product sales.
The successful development and commercialization of AZD3480 and AZD1446 depends substantially on our December 2005 collaboration with AstraZeneca, and AstraZeneca may decide not to conduct any further development of either or both of AZD3480 and AZD1446.
Our collaboration with AstraZeneca focused on cognitive disorders involves a complex allocation of rights, provides for milestone payments to us based on the achievement of specified development, regulatory and first commercial sale milestone events and provides us with royalty-based revenue if AZD3480, AZD1446 or another product candidate subject to the collaboration is successfully commercialized. AstraZeneca has decision-making authority for most matters in our collaboration, including, provided it meets its diligence obligations under the agreement, whether to proceed with further development and potential commercialization of any particular product candidate in the collaboration and, if so, for what indication(s). In particular, as long as AstraZeneca meets its diligence obligations under the agreement, AstraZeneca has decision-making authority with regard to whether to proceed with further development of either or both of AZD3480 in ADHD and AZD1446 in Alzheimer’s disease, although we are exploring the practicability of conducting an additional clinical trial of AZD3480 in Alzheimer’s disease and have agreed with AstraZeneca on respective roles and financial and non-financial responsibilities if we proceed to conduct such a study.
We are in discussions with AstraZeneca regarding potential additional development of AZD3480 as a treatment for ADHD. Whether AstraZeneca will decide to conduct additional development of AZD3480 in ADHD is uncertain in light of reservations about the adequacy of the therapeutic margin to support development across the broad ADHD patient population. In addition, AstraZeneca is currently considering whether to conduct further clinical development of AZD1446 as a treatment for Alzheimer’s disease. If at any time AstraZeneca decides not to conduct further development of one or both of AZD3480 or AZD1446 and its determination does not result in a failure to meet its diligence obligations under the agreement, we would not be permitted to conduct development of the affected product candidate(s) independently or with another collaborator and would not benefit from any commercial potential of the affected product candidate(s). An exception to this restriction is that we are entitled to conduct an additional clinical trial of AZD3480 in Alzheimer’s disease. Even if we proceed to conduct an additional clinical trial of AZD3480 in Alzheimer’s disease, whatever the outcome, AstraZeneca may decide not to conduct any further development of AZD3480 beyond our study, in which case we would likewise not benefit from any commercial potential of AZD3480.
If AstraZeneca decides to conduct further development of either or both of AZD3480 in ADHD and AZD1446 in Alzheimer’s disease, AstraZeneca would have significant control and we would have little control over the conduct and timing of development efforts. If AstraZeneca fails to devote sufficient financial and other resources to the development of either or both of AZD3480 and AZD1446, the development and potential commercialization of the affected product candidate(s) would be delayed. This would result in a delay in milestone payments and, if regulatory approval to market and sell AZD3480 or AZD1446 is obtained, royalties that we could receive on any future AZD3480 or AZD1446 product sales.
AstraZeneca has the right to terminate our cognitive disorders agreement in its entirety upon 90 days notice. If AstraZeneca terminates our agreement at any time, for any reason, it may negatively impact the development of AZD3480 and AZD1446. In particular, we would have to fund any further clinical development and commercialization of AZD3480 and AZD1446 on our own, seek another collaborator or licensee for clinical development and commercialization or abandon the development and commercialization of AZD3480 and AZD1446.
48
Table of Contents
We will depend on alliances and collaborations with third parties for the development and commercialization of some of our product candidates. If our alliances and collaborations are not successful, we may not be able to capitalize on the market potential of these product candidates.
In addition to our collaborations with AstraZeneca, we intend to selectively enter into alliances and collaborations for target indications for which our potential collaborator has particular expertise or that represent large primary care markets that must be served by large sales and marketing organizations. Our ability to generate revenue from our alliances and collaborations will depend on our collaborators’ abilities to establish the safety and efficacy of our product candidates, to obtain regulatory approvals and to achieve market acceptance. Strategic alliances and collaborations involving our product candidates, including our collaborations with AstraZeneca, pose many risks to us, including:
| • | collaborators have significant discretion in determining the amount and timing of efforts and resources that they will apply to these alliances and collaborations or to the development of our licensed product candidates; |
| • | collaborators may interpret clinical trial or non-clinical study results differently than we do, may pursue further development and commercialization of our product candidates for indications that we do not believe are optimal, may not pursue further development and commercialization of our product candidates at all or may elect not to continue or renew research and development programs based on preclinical or clinical trial results, changes in their strategic focus or available funding, or external factors such as an acquisition that diverts resources or creates competing priorities; |
| • | collaborators may delay clinical trials, provide insufficient funding for a clinical trial program, stop a clinical trial or abandon a product candidate, repeat or conduct new clinical trials or require a new formulation of a product candidate for clinical testing; |
| • | collaborators could independently develop, or develop with third parties, products that compete directly or indirectly with our products or product candidates if the collaborators believe that competitive products are more likely to be successfully developed or can be commercialized under terms that are more economically attractive; |
| • | collaborators with marketing and distribution rights to one or more products may not commit enough resources to their marketing and distribution; |
| • | collaborators may not properly maintain or defend our intellectual property rights or may use our proprietary information in such a way as to invite litigation that could jeopardize or invalidate our proprietary information or expose us to potential litigation; |
| • | disputes may arise between us and collaborators that result in the delay or termination of the research, development or commercialization of our product candidates, that result in costly litigation or arbitration that diverts management attention and resources or that, if resolved unfavorably to us, result in adverse financial consequences for us under the terms of the applicable agreements; and |
| • | alliances and collaborations may be terminated and, if terminated, may result in a need for a reallocation of internal funds or additional capital to pursue further development of the applicable product candidates. For example, in late February 2011, we received from GlaxoSmithKline notice of termination of our alliance agreement. |
Alliances and collaborations may not lead to development of product candidates or commercialization of products in the most efficient manner or at all.
In addition, there have been a significant number of recent business combinations among large pharmaceutical companies that have resulted in a reduced number of potential future collaborators. If a present or future collaborator of ours were to be involved in a business combination, the continued pursuit and emphasis on our product development program could be delayed, diminished or terminated.
49
Table of Contents
Our ability to establish additional alliances and collaborations may be limited by the terms of our agreements with AstraZeneca. If we do not establish additional alliances and collaborations, we may have to alter our development plans.
Our drug development programs and potential commercialization of our product candidates will require substantial additional cash to fund expenses. Our strategy includes selectively seeking alliances and collaborations to assist us in furthering development and potential commercialization of some of our product candidates. We intend to do so especially for target indications for which our potential collaborator has particular expertise or that involve large primary care markets that must be served by large sales and marketing organizations.
Under the terms of our cognitive disorders agreement with AstraZeneca, we have the right to offer to AstraZeneca the right to license any compound that meets pre-defined criteria for any NNR other than the a4ß2 NNR that we may in the future seek to exploit for any condition characterized by cognitive impairment for which AstraZeneca has development and commercialization rights under our agreement. We made such an offer with respect to TC-5619, which following a process under our agreement led to AstraZeneca’s right to license TC-5619. However, if we do not offer a compound that meets pre-defined criteria for any NNR other than the a4ß2 NNR to AstraZeneca, we are generally not permitted to develop or commercialize the compound for any of these indications. Similarly, under the terms of our TC-5214 agreement with AstraZeneca, for three years from the date the collaboration agreement became effective, we are not permitted to conduct a Phase 2 or later clinical trial, or to commercialize, a compound as an adjunct therapy for major depressive disorder. As a result, our ability to seek additional alliances and collaborations for the target indications for our two collaborations with AstraZeneca is substantially limited. In addition, AstraZeneca may under certain circumstances have a right of first negotiation under our cognitive disorders agreement with AstraZeneca for the development and commercialization of compounds that act by binding to NNRs for depression, anxiety and bipolar disorder.
We face significant competition in seeking appropriate alliances and collaborations. Alliances and collaborations are complex and time-consuming to negotiate and document. We may not be able to negotiate them on acceptable terms, or at all. If we cannot, we may have to curtail the development of a particular product candidate, reduce or delay its development program or one or more of our other development programs, delay its potential commercialization or reduce the scope of any sales or marketing activities, or increase our expenditures and undertake development or commercialization activities at our own expense. If we elect to increase our expenditures to fund development or commercialization activities on our own, we may need to obtain additional capital, which may not be available to us on acceptable terms or at all. If we do not have sufficient funds, we will not be able to bring our product candidates to market and generate product revenue.
If AstraZeneca’s contract manufacturer for TC-5214 fails to devote sufficient resources to TC-5214, or if its performance is substandard, clinical trials and product introductions of TC-5214 may be delayed or there may be a shortage of supply.
Under the terms of our TC-5214 agreement with AstraZeneca, AstraZeneca is responsible for the manufacture and supply of TC-5214 and has assumed our rights and obligations under our applicable agreements with third parties, including a supply agreement with Poli Industria Chimica, S.P.A., or Poli, and Interchem Corporation, or Interchem, for the pharmaceutical development and supply of the active ingredient form of TC-5214. The agreement with Poli and Interchem assumed by AstraZeneca provides for it to purchase its requirements for the active ingredient form of TC-5214 exclusively from Poli through Interchem during the term of the agreement, subject to specified conditions. Because of the exclusive supply relationship, if Poli breaches or fails to perform as agreed under the agreement, or if the agreement terminates for any reason, there may be a delay or interruption in manufacturing of TC-5214 that leads to a shortage of supply. If AstraZeneca were to have the right to change the manufacturer for the active ingredient form of TC-5214 and were to make the change for any reason, in addition to the risks associated with changing a contract manufacturer described below under “If the performance of our contract manufacturers or any present or future collaborator of ours with manufacturing
50
Table of Contents
responsibility for a particular product candidate is substandard, our clinical trials and product introductions may be delayed or there may be a shortage of commercial supply.,” it would be dependent on Poli to effect or facilitate a successful transfer of the manufacturing technology for TC-5214 to AstraZeneca or a replacement contract manufacturer. Such a technology transfer would require review and approval by the FDA or foreign regulatory authorities and would also likely require an inspection of the new manufacturer to assess compliance with current good manufacturing practices, or cGMP, mandated by the FDA or foreign regulatory authorities, both of which would be time-consuming and increase the likelihood of a delay or interruption in manufacture or a shortage of supply of TC-5214. Any delay or interruption in manufacture or shortage of supply of TC-5214 could delay or prevent the initiation or completion of clinical trials of TC-5214, the submission of applications for regulatory approvals of TC-5214 or the receipt of regulatory approvals for TC-5214, materially and adversely affect the commercialization of TC-5214 or result in higher costs or lost product revenue.
If third parties on which we rely for clinical trials do not perform as contractually required or as we expect, we may not be able to obtain regulatory approval for or commercialize our product candidates.
We do not have the ability to independently conduct the clinical trials required to obtain regulatory approval for our product candidates. We and applicable collaborators for our product candidates depend on independent clinical investigators and, in some cases such as the Phase 3 clinical program for TC-5214, contract research organizations and other third-party service providers to conduct the clinical trials of our product candidates and expect to continue to do so. We rely heavily on these parties for successful execution of our clinical trials, but we do not control many aspects of their activities. Nonetheless, we are responsible for confirming that each of our clinical trials is conducted in accordance with its general investigational plan and protocol. Moreover, the FDA and foreign regulatory authorities require us to comply with regulations and guidelines, commonly referred to as good clinical practice, or GCP, for conducting and recording and reporting the results of clinical trials to assure that data and reported results are credible and accurate and that the trial participants are adequately protected. Our reliance on third parties that we do not control does not relieve us of these responsibilities and requirements.
Third parties may not complete activities on schedule or may not conduct our clinical trials in accordance with regulatory requirements or the respective trial plans and protocols. These risks may be heightened for clinical trials that we conduct outside of North America and Western Europe. In particular, we have conducted trials of multiple product candidates at sites in India and we and AstraZeneca are conducting the Phase 3 clinical program for TC-5214 at sites in five continents around the world. Language barriers and the limited experience of some clinical investigators in India or other countries in conducting clinical trials in accordance with standards set forth by the FDA and applicable regulatory authorities may increase the risk of non-compliance. The failure of third parties to carry out their obligations could impair the credibility or reliability of the data generated in clinical trials of our product candidates, require a trial to be repeated and increase the overall cost of a development program, delay or prevent the development, approval and commercialization of our product candidates or result in enforcement action against us.
If the performance of our contract manufacturers or any present or future collaborator of ours with manufacturing responsibility for a particular product candidate is substandard, our clinical trials and product introductions may be delayed or there may be a shortage of commercial supply.
Our product candidates require precise, high quality manufacturing. We have limited internal manufacturing capability. We have historically manufactured our product candidates only in small quantities for early-stage preclinical testing and have contracted with third parties to manufacture, in collaboration with us, our product candidates for clinical trials. If any of our product candidates is approved by the FDA or by foreign regulatory authorities for marketing and sale, it will need to be manufactured in substantially larger, commercial quantities. Our experience in the manufacture of drugs in commercial quantities is limited to our contractual arrangements with third parties to manufacture our now discontinued product Inversine and its active ingredient.
AstraZeneca has all manufacturing responsibility for TC-5214 under our TC-5214 agreement and substantial manufacturing responsibility for AZD3480, AZD1446 and, if it licenses TC-5619, TC-5619 under our
51
Table of Contents
cognitive disorders agreement. For each of our other product candidates, we typically rely on single third-party contract manufacturers for manufacturing in drug substance form and single third-party contract manufacturers for manufacturing in a formulation for use in clinical trials. We intend to continue to rely on third-party manufacturers (or, where applicable, AstraZeneca or other current or potential future collaborators) to supply, store and distribute our product candidates for our clinical trials and to manufacture commercial supplies of any product candidate that is approved for sale. Our reliance on third-party manufacturers or collaborators will expose us to risks that could delay or prevent the initiation or completion of our clinical trials, the submission of applications for regulatory approvals, the receipt of regulatory approvals or the commercialization of our products or result in higher costs or lost product revenue. In particular, any contract manufacturer or applicable collaborator of ours could:
| • | encounter difficulties in achieving volume production, laboratory testing, quality control or quality assurance or suffer shortages of qualified personnel, any of which could result in its inability to manufacture sufficient quantities to meet clinical timelines for a particular product candidate, obtain approval to market and sell the product candidate or to commercialize the product candidate; or |
| • | fail to establish and follow cGMP or fail to document its adherence to cGMP, either of which could lead to significant delays in the availability of material for clinical study and delay or prevent filing or approval of marketing applications for our product candidates. |
In addition, any contract manufacturer could:
| • | terminate or not renew its manufacturing agreement with us or with any applicable collaborator of ours, based on its own business priorities, at a time that is costly or inconvenient; or |
| • | breach, or fail to perform as agreed under, the applicable manufacturing agreement. |
We expect to rely initially on a single contract manufacturer for any product candidate that we successfully bring to market. Changing any manufacturer that we or any applicable collaborator of ours engages for a particular product or product candidate may be difficult, as the number of potential manufacturers is limited and we or the collaborator will have to compete with third parties for access to those manufacturing facilities. cGMP manufacturing processes and procedures typically must be reviewed and approved by the FDA or foreign regulatory authorities and changing manufacturers may require re-validation of any new facility for cGMP compliance, which would likely be costly and time-consuming. We or any applicable collaborator of ours may not be able to engage replacement manufacturers on acceptable terms quickly or at all. In addition, contract manufacturers located in foreign countries may be subject to import limitations or bans. As a result, if any contract manufacturer or applicable collaborator of ours is unable, for whatever reason, to supply the contracted amounts of any product that is successfully brought to market, a shortage would result which would have a negative impact on our revenue.
Drug manufacturers are subject to ongoing periodic unannounced inspection by the FDA, the U.S. Drug Enforcement Agency and corresponding state and foreign agencies to ensure strict compliance with cGMP, other government regulations and corresponding foreign standards. While we or any applicable collaborator of ours is obligated to audit the performance of third-party contractors, we do not have control over third-party manufacturers’ compliance with these regulations and standards. Failure by us, any applicable collaborator of ours or any third-party manufacturers to comply with applicable regulations could result in sanctions being imposed on us, including fines, injunctions, civil penalties, failure of the government to grant pre-market approval of drugs, delays, suspension or withdrawal of approvals, seizures or recalls of product, operating restrictions and criminal prosecutions.
Risks Related to Our Intellectual Property
If we are unable to protect our intellectual property effectively, our competitors may develop and market similar products and the value of our technology and our ability to compete would be damaged.
Our continued success depends significantly on the ability of us or any applicable collaborator of ours to obtain and maintain meaningful intellectual property protection for our product candidates, technology and
52
Table of Contents
know-how. We generally seek to protect our compounds and technologies by, among other methods, filing U.S. and foreign patent applications related to our proprietary technology that is important to the development of our business. We file patent applications directed to our product candidates in an effort to establish intellectual property positions regarding new chemical entities and uses in the treatment of diseases and disorders.
The patent positions of companies like ours are generally uncertain and involve complex legal and factual questions. Our ability to maintain and solidify our proprietary position for our product candidates and technology will depend on the success that we or any applicable collaborator of ours has in obtaining effective patent claims and enforcing claims that are granted. We do not know whether any of our patent applications or those patent applications that we license will result in the issuance of any patents. Our issued patents and those that may issue in the future, or those licensed to us, may be challenged, invalidated, rendered unenforceable or circumvented, any of which could limit our ability to stop competitors from marketing related products. Moreover, the U.S. Supreme Court’s 2007 decision in KSR International Co. vs. Teleflex, Inc. may in some cases make it more difficult to obtain a patent, or to withstand a validity challenge to any issued patent, for pharmaceutical products that have a relationship to other pharmaceutical products, such as single enantiomers of a previously approved racemate like TC-5214, combination products or specific salt forms. In addition, the rights granted under any issued patents may not provide us with competitive advantages against competitors with similar compounds or technologies. Furthermore, our competitors may independently develop similar technologies in a manner that does not infringe our patents or other intellectual property. If we are unable to obtain, enforce or defend the patents with respect to our product candidates, our ability to commercialize our product candidates would be materially and adversely affected and our business would suffer.
Although we own or otherwise have rights to a number of patents, these patents may not effectively exclude competitors from engaging in activities that compete with us. Furthermore, the issuance of a patent is not conclusive as to its validity or enforceability, and third parties may challenge the validity or enforceability of our patents. Because patent applications in the United States and many foreign countries are confidential for a period of time after filing, and because publications of discoveries in the scientific literature often lag behind actual discoveries, we cannot be certain that we were the first to invent the inventions claimed in our issued U.S. patents or pending patent applications, or that we were the first to file for protection of the inventions set forth in the foreign patents or patent applications. It is possible that a competitor may successfully challenge our patents or that challenges will result in the elimination or narrowing of patent claims and, therefore, reduce our patent protection.
Because of the extensive time required for development, testing and regulatory review of a new drug, it is possible that any patent covering one of our product candidates may expire before the product candidate can be commercialized or remain in force for only a short period following initial commercialization. In either case, any advantages of the patent would be limited. The patent laws of various foreign countries in which we intend to compete may not protect our intellectual property to the same extent as the laws of the United States. Changes either in patent laws or in interpretations or enforcement of patent laws in the United States and other countries may diminish the value of our intellectual property or narrow the scope of our patent protection.
If we are unable to protect the confidentiality of our proprietary information and know-how, the commercial value of our technology and product candidates could be reduced.
In addition to patents, we rely on protection of trade secrets, know-how and confidential and proprietary information to maintain our competitive position. For example, we generally do not seek patent protection for the computer-based molecular design technologies that form part of Pentad and instead seek to maintain those technologies as trade secrets.
To maintain the confidentiality of trade secrets and proprietary information, we generally enter into confidentiality agreements with our employees, consultants, contractors and collaborators upon the commencement of our relationship with them. These agreements typically require that all confidential
53
Table of Contents
information developed by the individual or made known to the individual by us during the course of the individual’s relationship with us be kept confidential and not disclosed to third parties. However, we may not obtain these agreements in all circumstances, and individuals with whom we have these agreements may not comply with their terms. Even if obtained, these agreements may not provide meaningful protection for our trade secrets or other proprietary information or an adequate remedy in the event of their unauthorized use or disclosure. The loss or exposure of our trade secrets or other proprietary information could impair our competitive position.
We also typically enter into agreements with employees that provide that inventions conceived by them in the course of rendering services to us are our exclusive property and, where appropriate, we enter into similar agreements with consultants and contractors. To the extent that our employees, consultants or contractors use technology or know-how owned by others in their work for us, disputes may arise as to the rights in related inventions.
If we fail to comply with our obligations in our intellectual property licenses with third parties, we could lose license rights that are important to our business and, if we have sublicensed our license rights to a third party, the loss of the license rights may breach our obligations to our sublicensee.
We are a party to various license agreements. In particular, we license patent rights covering the pharmaceutical composition and methods of use of TC-5214 from University of South Florida Research Foundation and Yale University and have sublicensed these patent rights to AstraZeneca and we license patent rights from Cornerstone Therapeutics Inc. that cover the use of modulators of the a7 NNR to treat inflammatory disorders. We may enter into additional licenses in the future. Our existing licenses impose, and we expect future licenses will impose, various diligence, milestone payment, royalty, insurance and other obligations on us. If we fail to comply with these obligations, whether as a result of actions or inactions by AstraZeneca (with respect to TC-5214) or any other present or future collaborator of ours to which we out-license patents rights that we have in-licensed from a third party or for any other reason, the licensor may have the right to terminate the license, in which event we may not be able to market any product that is covered by the licensed patents. In addition, the failure to comply with our obligations under our license agreement with University of South Florida Research Foundation or our license agreement with Yale University could constitute a breach of our obligations under our TC-5214 agreement with AstraZeneca. A material breach by us of our TC-5214 agreement with AstraZeneca would give rise to various remedies for AstraZeneca that could have a material adverse effect on our business.
Our patent protection for any particular compound may be limited to a specific method of use or indication. If a third party were to obtain approval of a particular compound for use in another indication, we could be subject to competition arising from off-label use.
Although we generally seek the broadest patent protection available for our compounds, we or any of our applicable collaborators may not be able to obtain patent protection for the actual composition of any particular compound and may be limited to protecting a new method of use for the compound or otherwise restricted in our ability to prevent others from exploiting the compound. If we or any of our applicable collaborators are unable to obtain patent protection for the actual composition of any compound that we seek to develop and commercialize and must rely on method of use patent coverage, we would likely be unable to prevent others from manufacturing or marketing that compound for any use that is not protected by our patent rights. If a third party were to receive marketing approval of any compound for which we rely on method of use patent coverage for another use, physicians could nevertheless prescribe it for indications that are not described in the product’s labeling or approved by the FDA or foreign regulatory authorities. Even if we have patent protection for the indication for which the product is prescribed, as a practical matter, we would have little recourse as a result of this off-label use. In that event, our revenue from the commercialization of the compound would likely be materially and adversely affected.
54
Table of Contents
If a third party were to obtain approval to market and sell mecamylamine hydrochloride, TC-5214 could be subject to competition arising from off-label use.
We have licensed patent rights in the United States covering the pharmaceutical composition and methods of use of TC-5214, one of the enantiomers of mecamylamine hydrochloride. We have licensed method of use patent rights for, but do not have patent rights covering the composition of, mecamylamine hydrochloride. As a result, we may be limited in our ability to prevent others from exploiting mecamylamine, which could have a negative impact on the commercial potential of TC-5214. We believe there are at least two companies that are currently developing mecamylamine—AGI Therapeutics Ltd., which we believe is developing mecamylamine for chemotherapy-induced diarrhea, and Cary Pharmaceuticals Inc., which we believe is developing mecamylamine in a fixed dose combination with bupropion as a smoking cessation aid. In addition, mecamylamine is the active ingredient in our approved product Inversine, which we are no longer commercializing. A third party could in the future pursue marketing approval of mecamylamine for the forms of hypertension for which Inversine is approved using the abbreviated new drug application process. If any third party were to receive marketing approval for mecamylamine for any indication, physicians could prescribe it for other indications that are not described in the product’s labeling or approved by the FDA or foreign regulatory authorities. In particular, physicians could potentially prescribe mecamylamine as a treatment for major depressive disorder. In that event, if TC-5214 is in the future approved for marketing and sale by the FDA or foreign regulatory authorities, our revenue from sales of TC-5214 would likely be materially and adversely affected.
We may be involved in lawsuits to protect or enforce our patents that could be expensive and time-consuming.
We may initiate patent litigation against third parties to protect or enforce our patent rights and we may be similarly sued by third parties. We may also become subject to interference or opposition proceedings conducted in the patent and trademark offices of various countries to determine our entitlement to patents. The defense and prosecution of intellectual property suits, interference proceedings and related legal and administrative proceedings, if necessary, would be costly and divert our technical and management personnel from conducting our business. Moreover, we may not prevail in any of these suits. An adverse determination of any litigation or proceeding could put our patents at risk of being invalidated or narrowly interpreted and our patent applications at risk of not being issued and could prevent us from protecting our rights, particularly in countries where the laws may not protect such rights as fully as in the United States.
Furthermore, because of the substantial amount of discovery required in connection with intellectual property litigation, there is a risk that disclosure of some of our confidential information could be compelled and the information compromised. In addition, during the course of this kind of litigation, there could be public announcements of the results of hearings, motions or other interim proceedings or developments that, if perceived as negative by securities analysts or investors, could have a material adverse effect on the trading price of our common stock.
Claims by third parties that we infringe their proprietary rights may result in liability for damages or prevent or delay our development and commercialization efforts.
Our success depends in part on avoiding the infringement of other parties’ patents and proprietary rights. Patents may issue from patent applications of which we are unaware, and avoiding patent infringement may be difficult. We may infringe or it may be alleged that we infringe third-party patents. If a third party were to file a patent infringement suit against us, we could be forced to stop or delay research, development, manufacturing or sales of any infringing product in the country or countries covered by the patent infringed, unless we can obtain a license from the patent holder. Any necessary license may not be available on acceptable terms or at all, particularly if the third party is developing or marketing a product competitive with the infringing product. Even if we are able to obtain a license, the rights may be nonexclusive, which would give our competitors access to the same intellectual property.
55
Table of Contents
We also may be required to pay substantial damages to the patent holder in the event of an infringement. These damages could in some circumstances be triple the actual damages the patent holder incurs. If we have supplied infringing products to third parties for marketing or have licensed third parties to manufacture, use or market infringing products, we may be obligated to indemnify these third parties for any damages they may be required to pay to the patent holder and for any losses they may sustain themselves as a result.
Any successful infringement action brought against us may also materially and adversely affect marketing of the infringing product in other markets not covered by the infringement action, as well as our marketing of other products based on similar technology. Furthermore, we may suffer material adverse consequences from a successful infringement action against us even if the action is subsequently reversed on appeal, nullified through another action or resolved by settlement with the patent holder. The damages or other remedies awarded, if any, may be significant. As a result, any infringement action against us would likely delay the regulatory approval process, harm our competitive position, be very costly and require significant time and attention of our key management and technical personnel.
Risks Related to Commercialization
Even if approved for marketing and sale, our product candidates may not gain market acceptance and may fail to generate significant revenue.
The commercial success of any of our product candidates for which we may obtain marketing approval from the FDA or other regulatory authorities will depend upon their acceptance by the medical community and third-party payors as clinically useful, cost-effective and safe. Many of the product candidates that we are developing are based upon technologies or methods of treatment that are relatively new and unproven. As a result, it may be more difficult for us to achieve market acceptance of our products.
The degree of market acceptance of any drug depends on a number of factors, such as:
| • | its demonstration of efficacy and safety in clinical trials; |
| • | its superior efficacy as compared to alternative treatment methods and its side effect profile; |
| • | its cost-effectiveness and the availability of insurance or other third-party reimbursement; |
| • | its convenience and ease of administration; |
| • | the timing of its market entry relative to competitive treatments; |
| • | the extent and success of marketing and sales efforts; and |
| • | the product labeling or product insert required by the FDA or regulatory authorities in other countries. |
In addition, perceptions about the relationship or similarity between our product candidates and nicotine could limit their market potential. Our product candidates derive their medical effects by interacting with NNRs. Nicotine, which can have significantly negative health effects, also interacts with NNRs. Accordingly, our product candidates may be perceived by some to be nicotine or to be closely related to nicotine, particularly in light of the shared derivative names, “nicotine” and neuronal “nicotinic” receptors, and the fact that our company was launched originally as a research group within, and then as a subsidiary of, R.J. Reynolds Tobacco Company. This potential perception could result in a reluctance by patients to take, or by physicians to prescribe, any of our product candidates that receives marketing approval, which would affect our revenue.
We currently have limited sales, marketing and distribution experience and no internal sales or distribution capabilities. If we are unable to enter into alliances and collaborations or other arrangements with third parties to market and sell our product candidates or to develop our own internal marketing capability, or if we enter into such arrangements with third parties who do not perform well, we may not be successful in commercializing our products.
We currently have limited sales, marketing and distribution experience and no internal sales or distribution capabilities. Although we intend to focus any future internal sales and marketing resources in areas where
56
Table of Contents
specialists heavily influence our target markets, such as neurology and psychiatry, we also intend to seek to further augment our sales, marketing and distribution capabilities through arrangements with third parties such as our collaborations with AstraZeneca. In particular, our strategy includes selectively entering into strategic alliances and collaborations with respect to product candidates for indications with sales and distribution characteristics requiring a large sales force. There are risks involved with establishing our own sales force and marketing and distribution capabilities, as well as in entering into arrangements with third parties to perform these services. Developing our own sales force would be expensive and time-consuming and could delay any product launch. We may not be successful in entering into arrangements with third parties on terms that are favorable to us or at all. Also, we have little control over AstraZeneca and would have little control over such other third parties, any of which may fail to devote the necessary resources and attention to sell, market or distribute our products effectively. If we do not establish sales and distribution capabilities successfully, either on our own or in collaboration with third parties, we may not successfully commercialize our products.
Unfavorable pricing regulations, third-party reimbursement practices or healthcare reform initiatives applicable to our product candidates could limit our potential product revenue.
The regulations governing drug pricing and reimbursement vary widely from country to country. Some countries require approval of the sale price of a drug before it can be marketed and, in many of these countries, the pricing review period begins only after approval is granted. In some countries, prescription pharmaceutical pricing remains subject to continuing governmental control even after initial approval is granted. Our product candidates are currently in the development stage and we cannot yet assess the impact of price regulations. As a result, we or any applicable collaborator of ours may obtain regulatory approval for a product in a particular country, but then be subject to price regulations that delay the commercial launch of the product and may negatively impact the revenue we are able to derive from sales in that country.
Successful commercialization of any of our product candidates that is successfully developed will also depend in part on the extent to which coverage and adequate payment is available from government health administration authorities, private health insurers and other third-party payors. If we or any applicable collaborator of ours succeeds in bringing a product candidate to the market, it may not be considered cost-effective and reimbursement to the patient may not be available or sufficient to allow us or the collaborator to sell it at a satisfactory price. Because our product candidates are in the development stage, we cannot yet determine their cost-effectiveness. We may need to conduct expensive studies in order to demonstrate cost-effectiveness. Moreover, third-party payors frequently require that pharmaceutical companies provide predetermined discounts from list prices and frequently challenge the prices charged for medical products. Because our product candidates are in the development stage, we do not yet know the level of reimbursement, if any, for any product candidates that we or any applicable collaborator of ours are able to successfully develop. If the reimbursement for any of our product candidates is inadequate in light of our development and other costs, our ability to achieve or sustain profitability could be materially and adversely affected.
We believe that the efforts of governments and third-party payors to contain or reduce the cost of healthcare will continue to affect the business and financial condition of pharmaceutical and biopharmaceutical companies. In particular, the Patient Protection and Affordable Care Act, as amended by the Health Care and Education Affordability Reconciliation Act, or the Healthcare Reform Act, was enacted in 2010. This law substantially changes the way health care is financed by both governmental and private insurers. The Healthcare Reform Act contains a number of provisions that are expected to impact our business and operations, some of which in ways we cannot currently predict, including those governing enrollment in federal healthcare programs, reimbursement changes and fraud and abuse, which will impact existing government healthcare programs and will result in the development of new programs.
Additional provisions of the Healthcare Reform Act, may negatively affect our potential revenues in the future. For example, the Healthcare Reform Act imposes a non-deductible excise tax on pharmaceutical manufacturers or importers that sell branded prescription drugs to U.S. government programs, which we believe
57
Table of Contents
will increase the cost of any of our product candidates that receives regulatory approval. In addition, as part of the Healthcare Reform Act’s provisions closing a funding gap that currently exists in the Medicare Part D prescription drug program (commonly known as the “donut hole”), we will also be required to provide a 50% discount on branded prescription drugs sold to beneficiaries who fall within the donut hole.
Beyond the Healthcare Reform Act, there have been a number of legislative and regulatory proposals to change the healthcare system in the United States and other major healthcare markets proposed and adopted in recent years and there will likely continue to be proposals by legislators at both the federal and state levels, regulators and third-party payors to keep pharmaceutical costs down while expanding individual healthcare benefits. Certain of these changes could impose additional limitations on the price that we or our applicable collaborator will be able to charge for any of our product candidates that receives regulatory approval or on the amount of reimbursement available for such approved product from governmental agencies or third-party payors. For example, The American Recovery and Reinvestment Act of 2009, which became effective in February 2009, provides funding for the federal government to compare the effectiveness of different treatments for the same illness. While the specific effects that the Healthcare Reform Act, implementing regulations, the American Recovery and Reinvestment Act of 2009 or any future healthcare reform legislation or policies will have on our business is not yet known, reductions in third-party reimbursement for any of our product candidates that is successfully developed or a decision by a third-party payor to not cover any of our product candidates that is successfully developed could reduce prescriptions by physicians of the product candidate and have a material adverse effect on our potential revenue from sales of the product candidate.
If our competitors develop and market drugs that are less expensive, more effective or safer than ours, if they develop and market products faster than we do, or if they have better sales and marketing capabilities than we do, any products we are able to commercialize may not generate initial or ongoing revenue.
The development and commercialization of new drugs is highly competitive. Our business is characterized by extensive research efforts and rapid developments. We expect intense competition in our target markets as new products and advanced technologies become available. Our competitors include large pharmaceutical, biopharmaceutical, biotechnology and other companies and research institutions, many of which have greater financial, technical and other resources and personnel and more experience in research, clinical development, regulatory and drug commercialization than we have. Our competitors may:
| • | develop products that are more effective, safer, more tolerable, more convenient, less costly or otherwise more competitive than our product candidates; |
| • | obtain FDA or foreign regulatory approval for their products more rapidly than we or any applicable collaborator of ours does; |
| • | adapt more quickly to new technologies and scientific advances than we or any applicable collaborator of ours; |
| • | initiate or withstand substantial price competition more successfully than we or any applicable collaborator of ours does; |
| • | have greater success in recruiting skilled scientific workers from the limited pool of available talent than we do; |
| • | obtain more effective intellectual property protection than we have; |
| • | negotiate third-party licensing and collaboration arrangements more effectively than we do; and |
| • | take advantage of acquisition or other opportunities more readily than we do. |
Competitive products may render our product candidates obsolete or noncompetitive before we can recover our development or commercialization expenses.
58
Table of Contents
We also face substantial competition from therapies designed to target NNRs. Pfizer’s product Chantix, which is known outside of the United States as Champix, acts on several NNR subtypes as well as other molecular targets in the body. Chantix is approved as an aid for smoking cessation. In addition, we believe that several prominent pharmaceutical companies have product candidates that target NNRs in development, including as examples Roche, with a compound in Phase 2 development for Alzheimer’s disease, and Abbott Laboratories, with one compound in Phase 2 development for ADHD and a second compound in Phase 1 development for cognitive disorders. Other companies that we believe have active NNR-based programs include AstraZeneca, Eli Lilly, Sanofi-Aventis, Bristol-Myers Squibb, GlaxoSmithKline, Johnson & Johnson, Novartis, NeuroSearch A/S, Solvay, Servier, CoMentis, EnVivo Pharmaceuticals, Xytis, Galantos Pharma, Proximagen, Psychogenics, AGI Therapeutics, Suven, Asmacure and Neuroderm. We expect that we will face increased competition in the future if therapies that target NNRs are further validated and if companies initiate or expand programs focused on NNRs or otherwise enter the CNS market, whether independently or by alliance, collaboration or acquisition.
Any products that we or any applicable collaborator of ours is able to successfully develop and commercialize in the future could be subject to competition from lower priced generic drugs. The manufacturer of a generic product could challenge our patents as invalid or not infringed and subject us to expensive litigation. We do not know if we or any applicable collaborator of ours would prevail in litigation and succeed in keeping the generic product out of the market until our patent protection expires.
If we successfully develop and obtain approval for our product candidates, we will face competition based on the safety and effectiveness of our products, the timing and scope of regulatory approvals, the availability and cost of supply, marketing and sales capabilities, reimbursement coverage, price, patent position and other factors. Our competitors may develop or commercialize more effective or more affordable products, or obtain more effective patent protection, than we do. Accordingly, our competitors may commercialize products more rapidly or effectively than we do.
If approved, our product candidates will compete for a share of the existing market with numerous approved products. We believe that the primary competitive products for use in indications that we are currently targeting with our most advanced product candidates include:
| • | as an adjunct treatment for major depressive disorder, the atypical antipsychotics Seroquel XR from AstraZeneca and Abilify from Bristol-Myers Squibb/Otsuka; |
| • | otherwise for major depressive disorder, SSRIs such as Prozac from Eli Lilly, Paxil from GlaxoSmithKline, Zoloft from Pfizer, Celexa and Lexapro from Forest Laboratories, dual uptake inhibitors such as Effexor from Wyeth and Cymbalta from Eli Lilly, and the SSRI and 5HT1A receptor partial agonist Viibryd from Clinical Data (under agreement to be acquired by Forest Laboratories); |
| • | for ADHD, stimulants such as Adderall XR and Vyanase from Shire, Concerta from Johnson & Johnson and Ritalin LA from Novartis, and Strattera, a non-stimulant acting as a norepinephrine reuptake inhibitor, from Eli Lilly; |
| • | for mild to moderate Alzheimer’s disease, acetylcholinesterase inhibitors such as Aricept from Pfizer/Eisai, Razadyne from Johnson & Johnson and Exelon from Novartis; in addition, Namenda from Forest Laboratories, which acts by regulating the neurotransmitter glutamate, is marketed for moderate to severe Alzheimer’s disease; |
| • | for asthma, long-acting beta agonist/inhaled corticosteroid combinations such as Advair from GlaxoSmithKline, Symbicort from AstraZeneca and Dulera from Merck, leukotriene inhibitors such as Singulair from Merck, Accolate from AstraZeneca and Zyflo from Cornerstone Therapeutics, antibodies such as Xolair from Novartis, long-acting beta agonists such as salmeterol and formoterol and short-acting beta agonists such as albutertol and levalbuterol; and |
59
Table of Contents
| • | for Type 2 diabetes, glucagon-like peptide-1 analogues such as Byetta from Eli Lilly and Amylin, dipeptidyl peptidase IV inhibitors such as Januvia from Merck and Onglyza from Bristol-Myers Squibb and AstraZeneca, insulin such as Lantus from Sanofi-Aventis, sulfonylureas such as Glucotrol from Pfizer, and biguanides (metformin) such as Glucophage from Bristol-Myers Squibb. |
There is currently no approved product for cognitive dysfunction in schizophrenia. There are however multiple third-party product candidates currently in clinical development for cognitive dysfunction in schizophrenia, including at least one modulator of the a7 NNR.
We may have substantial exposure to product liability claims and may not have adequate insurance to pay them.
We face an inherent business risk of exposure to product liability claims if the use of our products is alleged to have resulted in harm to others. This risk exists for product candidates in clinical trials, whether or not the product candidate is subsequently approved for commercial sale, as well as for products in commercial distribution. Any product liability claim arising in the future against us or any third party that we have agreed to indemnify, regardless of its merit or eventual adjudication, could be costly and significantly divert management’s attention from conducting our business or materially and adversely affect our reputation and the demand for our products.
We have secured product liability insurance coverage in amounts that we believe to be appropriate for our current operations. Our current insurance coverage may not reimburse us or may not be sufficient to reimburse us for any expenses or losses we may incur. We expect that we will expand our coverage with respect to any products for which we obtain marketing approval. However, additional insurance may not be available to cover our potential liabilities fully or may be prohibitively expensive. In addition, some potential product liability claims may be excluded from coverage under the terms of the policy. Our inability to obtain adequate insurance coverage at an acceptable cost could prevent or impede the commercialization of our product candidates.
Our business activities involve hazardous materials, which could subject us to significant liability.
Our research and development activities involve, and any future manufacturing processes that we conduct may involve, the use of hazardous materials, including hazardous chemicals and radioactive materials. Accordingly, we are subject to federal, state and local laws and regulations governing the use, manufacture, storage, handling and disposal of these materials. We incur significant costs in our efforts to comply with these laws and regulations, but our efforts may not ensure compliance in all cases. Moreover, despite precautionary procedures that we implement, we cannot eliminate the risk of accidental contamination or injury from these materials. In the event of an accident or environmental discharge, we may be held liable for any resulting damages. We do not carry insurance specifically for the risk of contamination or injury from hazardous materials.
If any promotional activities that we undertake fail to comply with the regulations and guidelines of the FDA and applicable foreign regulatory authorities, we may be subject to warnings or enforcement actions that could harm our business.
Physicians may prescribe drugs for uses that are not described in the product’s labeling or for uses that differ from those tested in clinical studies and approved by the FDA or similar regulatory authorities in other countries. Regulatory authorities generally do not regulate the behavior of physicians in their choice of treatments. Regulatory authorities do, however, restrict communications on the subject of off-label use. Companies cannot actively promote approved drugs for off-label uses but may in some jurisdictions and under specified conditions disseminate articles published in peer-reviewed journals that discuss off-label uses of approved products to physicians. To the extent allowed, we may in the future disseminate peer-reviewed articles on our products to physicians. If we undertake any promotional activities in the future for any product candidate for which we receive regulatory approval and our activities fail to comply with these regulations or guidelines, we may be subject to warnings from, or enforcement action by, these authorities.
60
Table of Contents
Risks Related to Employees and Managing Growth
If we lose our key personnel or are unable to attract and retain additional skilled personnel, we may be unable to successfully develop and commercialize our product candidates or effectively compete in our industry.
Our performance depends substantially on the performance of our senior management and key scientific, technical and managerial personnel, including our Chief Executive Officer and President, J. Donald deBethizy, and our Senior Vice President, Clinical Development and Regulatory Affairs and Chief Medical Officer, Geoffrey C. Dunbar. Our executive officers, including these individuals, can terminate their employment with us at any time. The loss of the services of any of our executive officers may significantly delay or prevent the achievement of product research and development and other business objectives. We also rely on consultants and advisors from time to time to assist us in formulating our research and development strategy. All of our consultants and advisors are either self-employed or employed by other organizations, and they may have other commitments, including consulting or advisory contracts with other organizations, that may affect their ability to contribute to us.
Our ability to operate successfully and manage our potential future growth will depend on our ability to identify, recruit and retain additional qualified scientific, technical, financial and managerial personnel. We face intense competition for skilled executives in our industry. We may not be able to continue to attract and retain personnel with the advanced qualifications necessary for the growth of our business.
We may encounter difficulties in managing our growth, which could have a material adverse effect on our business.
The number of our employees and the scope of our operations have grown over the last several years. Any continued growth could place a significant strain on our managerial, operational and financial resources. To manage our growth, we must continue to implement and improve our managerial, operational and financial systems and controls and reporting processes and procedures. We may not be able to manage our growth effectively. Moreover, if our existing systems and internal controls over financial reporting are not implemented properly or are not adequate, we could be exposed to an increased risk of incurring financial or accounting irregularities or fraud, which would cause our stock price to suffer.
Risks Related to Our Common Stock
The market price of our common stock may be highly volatile.
We expect that the trading price of our common stock is likely to be highly volatile in response to factors that are beyond our control. The stock market in general has experienced extreme price and volume fluctuations. The market prices of securities of pharmaceutical, biopharmaceutical and biotechnology companies have been extremely volatile and have experienced fluctuations that have often been unrelated or disproportionate to operating performance. These broad market fluctuations could result in extreme fluctuations in the price of our common stock, which could cause a decline in the value of shares held by any stockholder.
If our operating results fluctuate significantly, our stock price may decline.
Our operating results are likely to fluctuate significantly from quarter to quarter and year to year. These fluctuations could cause our stock price to decline. Some of the factors that could cause our operating results to fluctuate include:
| • | whether and to what extent milestone events are achieved for TC-5214 under our TC-5214 agreement with AstraZeneca; |
| • | the outcomes from Phase 3 clinical development of TC-5214; |
61
Table of Contents
| • | whether AstraZeneca exercises its right to license TC-5619; |
| • | whether and to what extent AstraZeneca determines to continue clinical development of one or both of AZD3480 or AZD1446 and, if so, milestone events are achieved under our cognitive disorders agreement with AstraZeneca; |
| • | whether we proceed with an additional clinical trial of AZD3480 in Alzheimer’s disease; |
| • | the scope, progress, duration, results and cost of clinical trials, as well as non-clinical studies and assessments, of our other product candidates and programs; |
| • | our inability, or the inability of AstraZeneca or any potential future collaborator, to successfully complete clinical trials or non-clinical studies and assessments in a timely manner or at all, resulting in a delay in receiving, or a failure to receive, the required regulatory approvals to commercialize our product candidates; |
| • | the extent to which we retain development and commercialization rights or responsibilities for our product candidates that are not subject to either of our collaborations with AstraZeneca and incur associated development and manufacturing costs and costs to establish sales and marketing functions; |
| • | our ability to establish strategic alliances, collaborations and licensing or other arrangements on terms favorable to us; |
| • | whether we pursue and complete any in-licensing, merger and acquisition and other business combination or corporate partnering opportunities and, if so, the terms of any transaction; |
| • | the cost, timing and outcomes of regulatory approvals or other regulatory actions; |
| • | the number and characteristics of product candidates that we pursue; |
| • | general and industry-specific economic conditions that may affect the research and development expenditures of AstraZeneca or any of our potential future collaborators; |
| • | the expiration or termination of agreements with AstraZeneca or any potential future collaborator, or the execution of new agreements; and |
| • | general conditions in the pharmaceutical, biopharmaceutical or biotechnology industries or in the U.S. or global credit or financial markets. |
Due to fluctuations in our operating results, a period-to-period comparison of our results of operations may not be a good indication of our future performance. For any particular quarter or quarters, our operating results could be below the expectations of securities analysts or investors and our stock price could decline.
If our stockholders sell a substantial number of shares of our common stock in the public market, our stock price may decline.
Our current trading volumes are modest, and sales of a substantial number of shares of our common stock in the public market could cause the market price to decline. Such sales also might make it more difficult for us to sell equity securities in the future at a time and at a price that we deem appropriate. If there are more shares of our common stock offered for sale than buyers are willing to purchase, the market price of our common stock may decline to a market price at which buyers are willing to purchase the offered shares and sellers remain willing to sell the shares. The number of shares of our common stock owned by our stockholders and available for sale in the public market is limited only to the extent provided under applicable federal securities laws. In addition, we may, in the future, issue additional shares of our common stock as compensation to our employees, directors or consultants, in connection with strategic alliances, collaborations, acquisitions or other transactions or to raise capital. Accordingly, sales of a substantial number of shares of our common stock in the public market could occur at any time.
62
Table of Contents
Concentration of ownership among our existing executive officers, directors and principal stockholders may prevent new investors from influencing significant corporate decisions.
Our executive officers, directors and 10% or greater stockholders beneficially own or control approximately 42% of the outstanding shares of our common stock, based on the shares outstanding as of February 28, 2011. Accordingly, our executive officers and directors and these principal stockholders have substantial control over the outcome of corporate actions requiring stockholder approval, including the election of directors, any merger, consolidation or sale of all or substantially all of our assets or any other significant corporate transactions, as well as our management and affairs. The concentration of ownership may also delay or prevent a change of control of us at a premium price if these stockholders oppose it, even if it would benefit our other stockholders.
Provisions of our collaboration agreements with AstraZeneca and provisions of our charter, bylaws and Delaware law may discourage or make an acquisition of us or a change in our management more difficult.
Under each of our TC-5214 agreement with AstraZeneca and our cognitive disorders agreement with AstraZeneca, AstraZeneca may elect to terminate certain aspects of the agreement if there were to be a change of control of us, as defined in the applicable agreement. In particular, AstraZeneca may elect to terminate our co-promotion rights under each agreement. These rights of AstraZeneca could discourage, delay or prevent a merger, acquisition or other change of control of us involving a third party that stockholders may consider favorable, including transactions in which stockholders might otherwise receive a premium for their shares. These rights also could limit the price that investors might be willing to pay in the future for shares of our common stock, thereby depressing the market price of our common stock. Stockholders who wish to participate in these transactions may not have the opportunity to do so.
Provisions of our certificate of incorporation and bylaws could have a similar deterrent effect and could also prevent or frustrate attempts by our stockholders to replace or remove our management. These provisions:
| • | allow the authorized number of directors to be changed only by resolution of our board of directors; |
| • | establish a classified board of directors, providing that not all members of the board be elected at one time; |
| • | authorize our board of directors to issue without stockholder approval blank check preferred stock that, if issued, could operate as a “poison pill” to dilute the stock ownership of a potential hostile acquirer or otherwise to prevent an acquisition that is not approved by our board of directors; |
| • | require that stockholder actions must be effected at a duly called stockholder meeting and prohibit stockholder action by written consent; |
| • | establish advance notice requirements for stockholder nominations to our board of directors or for stockholder proposals that can be acted on at stockholder meetings; |
| • | limit who may call stockholder meetings; and |
| • | require the approval of the holders of 66 2/3% of the outstanding shares of our capital stock entitled to vote in order for the stockholders to amend certain provisions of our certificate of incorporation and bylaws. |
In addition, because we are incorporated in Delaware, we are governed by the provisions of Section 203 of the Delaware General Corporation Law, which may, unless certain criteria are met, prohibit large stockholders, in particular those owning 15% or more of our outstanding voting stock, from merging or combining with us for a prescribed period of time.
| Item 1B. | Unresolved Staff Comments. |
None.
63
Table of Contents
| Item 2. | Properties. |
We lease approximately 79,000 square feet of laboratory and office space located in the Piedmont Triad Research Park in Winston-Salem, North Carolina. The term of our lease expires July 31, 2012, and we have a renewal option for an additional five-year term at a rental rate to be mutually determined between us and the landlord. The current monthly payment under our lease is approximately $208,000. We believe our laboratory and office space is suitable for its intended purpose.
| Item 3. | Legal Proceedings. |
We are not currently a party to any material pending legal proceedings or aware of any contemplated proceeding against us by any governmental authority.
| Item 4. | (Removed and Reserved). |
64
Table of Contents
PART II
| Item 5. | Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities. |
Market Information
Our common stock currently trades on the NASDAQ Global Select Market under the symbol “TRGT.” The following table sets forth, for the periods indicated, the high and low sales prices for our common stock:
| Common Stock | ||||||||||
| High | Low | |||||||||
| 2009: |
||||||||||
| First Quarter | $ | 3.94 | $ | 2.00 | ||||||
| Second Quarter | $ | 4.17 | $ | 2.26 | ||||||
| Third Quarter | $ | 21.84 | $ | 2.00 | ||||||
| Fourth Quarter | $ | 24.50 | $ | 17.59 | ||||||
| 2010: | ||||||||||
| First Quarter | $ | 21.35 | $ | 18.29 | ||||||
| Second Quarter | $ | 25.00 | $ | 19.25 | ||||||
| Third Quarter | $ | 23.59 | $ | 17.80 | ||||||
| Fourth Quarter | $ | 27.65 | $ | 20.50 | ||||||
Comparative Stock Performance Graph
The following graph and related information shall not be deemed “soliciting material” or to be “filed” with the SEC or subject to Regulation 14A or 14C, other than as provided in Item 201 of Regulation S-K, or to the liabilities of Section 18 of the Exchange Act, nor shall such information be incorporated by reference into any future filing under the Securities Act or the Exchange Act, except to the extent that we specifically incorporate it by reference into such a filing.
65
Table of Contents
The following graph compares the cumulative total stockholder return for our common stock with the cumulative total stockholder return of the NASDAQ Composite Index and the NASDAQ Biotechnology Index. The comparison assumes the investment of $100.00 on April 12, 2006 (the date our common stock was first publicly traded) in each of our common stock, the NASDAQ Composite Index and the NASDAQ Biotechnology Index and the reinvestment of any dividends. We have not paid any dividends on our common stock and do not include dividends in the representation of our performance. The performance shown for any prior period does not predict the performance to be expected for the current period or any future period.
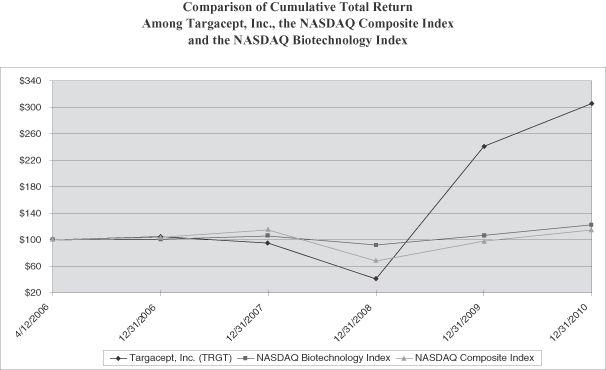
| Cumulative Total Return | ||||||||||||||||||||||||
| 4/12/06 | 12/31/06 | 12/31/07 | 12/30/08 | 12/30/09 | 12/31/10 | |||||||||||||||||||
| Targacept, Inc. |
100 | 105 | 95 | 41 | 241 | 306 | ||||||||||||||||||
| NASDAQ Biotechnology Index |
100 | 101 | 106 | 92 | 107 | 123 | ||||||||||||||||||
| NASDAQ Composite Index |
100 | 104 | 115 | 68 | 98 | 115 | ||||||||||||||||||
Stockholders
As of February 28, 2011, there were approximately 57 holders of record of our common stock. Because many of our shares are held by brokers or other nominees on behalf of beneficial owners, we are unable to determine precisely the total number of beneficial owners represented by the holders of record. As of February 28, 2011, we estimate the total number of beneficial owners of our common stock whose shares are held by brokers or other nominees on their behalf to be approximately 3,075.
Dividends
We have never declared or paid cash dividends on any of our shares of capital stock. We currently intend to retain future earnings, if any, to finance the expansion and growth of our business and do not anticipate paying any cash dividends in the foreseeable future. Any future determination to pay dividends will be at the discretion
66
Table of Contents
of our board of directors and will depend on our financial condition, results of operations, capital requirements and other factors that our board of directors deems relevant. In addition, the terms of any future debt or credit facility may preclude us from paying dividends.
Calculation of Aggregate Market Value of Non-Affiliate Shares
For purposes of calculating the aggregate market value of shares of our common stock held by non-affiliates as set forth on the cover page of this annual report, we have assumed that all outstanding shares are held by non-affiliates, except for shares held by our executive officers, directors and stockholders that hold at least 10% of our outstanding common stock as of the determination date. This assumption is not intended to constitute an admission that all executive officers, directors and 10% or greater stockholders are, in fact, our affiliates or that there are not other persons who may be deemed to be our affiliates.
Unregistered Sales of Securities; Use of Proceeds from Registered Securities; Issuer Purchases of Equity Securities
None.
67
Table of Contents
| Item 6. | Selected Financial Data. |
You should read the following selected financial data together with our financial statements and the related notes included in this annual report and the “Management’s Discussion and Analysis of Financial Condition and Results of Operations” section of this annual report. The selected financial data in this section are not intended to replace our financial statements.
We derived the statements of operations data for the years ended December 31, 2010, 2009, and 2008 and the balance sheet data as of December 31, 2010 and 2009 from our audited financial statements included in this annual report. We derived the statements of operations data for the years ended December 31, 2007 and 2006 and the balance sheet data as of December 31, 2008, 2007, and 2006 from our audited financial statements not included in this report. Our historical results for any prior period are not necessarily indicative of the results to be expected for any future period. You should read the notes to our financial statements for an explanation of the method used to determine the number of shares used in computing basic and diluted net loss per share.
| Year Ended December 31, | ||||||||||||||||||||
| 2010 | 2009 | 2008 | 2007 | 2006 | ||||||||||||||||
| (in thousands, except share and per share data) | ||||||||||||||||||||
| Statement of Operations Data: |
||||||||||||||||||||
| Net operating revenues |
$ | 85,713 | $ | 25,062 | $ | 20,085 | $ | 11,576 | $ | 27,537 | ||||||||||
| Operating expenses: |
||||||||||||||||||||
| Research and development |
64,546 | 40,179 | 40,981 | 34,620 | 21,788 | |||||||||||||||
| General and administrative |
8,052 | 8,167 | 6,499 | 8,013 | 5,696 | |||||||||||||||
| License fees and royalties |
— | 16,350 | — | — | — | |||||||||||||||
| Cost of product sales |
— | 691 | 749 | 715 | 457 | |||||||||||||||
| Total operating expenses |
72,598 | 65,387 | 48,229 | 43,348 | 27,941 | |||||||||||||||
| Income (loss) from operations |
13,115 | (40,325 | ) | (28,144 | ) | (31,772 | ) | (404 | ) | |||||||||||
| Interest and dividend income |
1,463 | 1,050 | 2,734 | 3,837 | 2,584 | |||||||||||||||
| Interest expense |
(153 | ) | (217 | ) | (251 | ) | (138 | ) | (83 | ) | ||||||||||
| Income (loss) before income taxes |
14,425 | (39,492 | ) | (25,661 | ) | (28,073 | ) | 2,097 | ||||||||||||
| Income tax (expense) benefit |
(3,526 | ) | 88 | — | — | — | ||||||||||||||
| Preferred stock accretion |
— | — | — | — | (3,333 | ) | ||||||||||||||
| Net income (loss) attributable to common stockholders |
$ | 10,899 | $ | (39,404 | ) | $ | (25,661 | ) | $ | (28,073 | ) | $ | (1,236 | ) | ||||||
| Basic net income (loss) attributable to common stockholders per share |
$ | 0.38 | $ | (1.54 | ) | $ | (1.04 | ) | $ | (1.42 | ) | $ | (0.09 | ) | ||||||
| Diluted net income (loss) attributable to common stockholders per share |
$ | 0.36 | $ | (1.54 | ) | $ | (1.04 | ) | $ | (1.42 | ) | $ | (0.09 | ) | ||||||
| Weighted average common shares outstanding—basic |
28,543,408 | 25,636,419 | 24,664,169 | 19,720,732 | 13,595,523 | |||||||||||||||
| Weighted average common shares outstanding—diluted |
30,150,324 | 25,636,419 | 24,664,169 | 19,720,732 | 13,595,523 | |||||||||||||||
| As of December 31, | ||||||||||||||||||||
| 2010 | 2009 | 2008 | 2007 | 2006 | ||||||||||||||||
| (in thousands) | ||||||||||||||||||||
| Balance Sheet Data: |
||||||||||||||||||||
| Cash, cash equivalents and investments |
$ | 252,509 | $ | 111,066 | $ | 88,363 | $ | 87,040 | $ | 54,190 | ||||||||||
| Working capital |
119,422 | 213,269 | 78,174 | 77,217 | 69,903 | |||||||||||||||
| Total assets |
262,787 | 319,379 | 98,551 | 98,965 | 81,368 | |||||||||||||||
| Long-term debt, net of current portion |
1,349 | 1,966 | 3,408 | 1,686 | 816 | |||||||||||||||
| Accumulated deficit |
(218,401 | ) | (229,300 | ) | (189,896 | ) | (164,235 | ) | (136,162 | ) | ||||||||||
| Total stockholders’ equity |
91,847 | 68,991 | 57,373 | 51,584 | 64,999 | |||||||||||||||
68
Table of Contents
| Item 7. | Management’s Discussion and Analysis of Financial Condition and Results of Operations. |
You should read the following discussion and analysis of our financial condition and results of operations together with our financial statements and the related notes included in this annual report. In addition to historical information, the following discussion contains forward-looking statements that involve risks, uncertainties and assumptions. Our actual results, performance or experience could differ materially from those indicated by any forward-looking statement due to various important factors, risks and uncertainties, including, but not limited to, those set forth under “Cautionary Note Regarding Forward-Looking Statements,” which precedes Part I of this annual report, and under “Risk Factors” in Item 1A of Part I of this annual report.
Overview
Background
We are a biopharmaceutical company engaged in the design, discovery and development of novel NNR Therapeutics for the treatment of diseases and disorders of the nervous system. Our NNR Therapeutics selectively target a class of receptors known as neuronal nicotinic receptors, which we refer to as NNRs. NNRs are found on nerve cells throughout the nervous system and serve as key regulators of nervous system activity. Our most advanced product candidates are TC-5214, TC-5619, AZD3480 (TC-1734), AZD1446 (TC-6683) and TC-6987, and they are discussed under the caption “Business” in Item 1 of Part I of this annual report.
We have two collaboration agreements with AstraZeneca, one that we entered into in December 2009 for the global development and commercialization of TC-5214 as a treatment for major depressive disorder and refer to in this annual report as our “TC-5214 agreement with AstraZeneca” and the other focused in cognitive disorders that we entered into in December 2005 and refer to in this annual report as our “cognitive disorders agreement with AstraZeneca.”
Under our TC-5214 agreement with AstraZeneca, we and AstraZeneca have jointly designed an initial program that includes development of TC-5214 as an adjunct therapy and as a “switch” monotherapy, in each case in patients with major depressive disorder, or MDD, who do not respond adequately to initial antidepressant treatment. AstraZeneca is responsible for 80% and we are responsible for 20% of the cost of the initial program, except that AstraZeneca is responsible for 100% of development costs that are required only to obtain or maintain regulatory approval in countries outside the United States and the European Union. We have the right to terminate our obligation to fund our share of the costs of the initial program once we have funded a specified amount. In addition, for each of us and AstraZeneca, costs that were not contemplated at execution to be part of the initial program may in some cases be excluded from the cost-sharing arrangement. If we fund the specified amount and terminate our obligation to fund our share of further costs of the initial program, any future milestones and royalties payable to us under the agreement would be reduced by the amount of our unfunded share plus interest at a specified rate, subject to a maximum reduction that may be applied to any one payment. AstraZeneca is responsible for executing and funding the costs of global commercialization of TC-5214.
Under our cognitive disorders agreement with AstraZeneca:
| • | AstraZeneca has an exclusive license to AZD3480, AZD1446 and earlier-stage compounds that arose from the preclinical research collaboration conducted under the agreement; |
| • | we conducted and funded the development of TC-5619 to date; AstraZeneca has the right to license TC-5619 and, if it exercises its right, would assume responsibility for and fund all future development (except for completion of our ongoing studies) and commercialization of TC-5619; |
| • | except as discussed in the next bullet, AstraZeneca is responsible for substantially all future development costs for AZD3480, AZD1446 and each other compound arising from the preclinical research collaboration described below that it elects to advance; |
| • | we are exploring the practicability of conducting an additional clinical trial of AZD3480 in Alzheimer’s disease and have agreed with AstraZeneca on respective roles and financial and |
69
Table of Contents
| non-financial responsibilities for such a study; we have received $500,000 and, if an Alzheimer’s disease study proceeds, we would be responsible for funding the study but would be entitled to receive up to $5.7 million in additional payments from AstraZeneca, with the last tranche being payable upon first dosing in the United States and Europe; and |
| • | from January 2006 to January 2010, we and AstraZeneca conducted a preclinical research collaboration under the agreement to discover and develop compounds that act on the a4ß2 NNR as treatments for conditions characterized by cognitive impairment; AstraZeneca paid us research fees, based on a reimbursement rate specified under the agreement, for services rendered in the preclinical research collaboration. |
In addition to our two collaboration agreements with AstraZeneca, we entered into a product development and commercialization agreement with GlaxoSmithKline in July 2007 that was designed to discover, develop and market product candidates that selectively target specified NNR subtypes in five therapeutic focus areas. In late February 2011, we received notice of termination of the agreement from GlaxoSmithKline. By the terms of the agreement, the termination becomes effective in late May 2011.
We trace our scientific lineage to a research program initiated by R.J. Reynolds Tobacco Company in 1982 to study the activity and effects of nicotine in the body. We were incorporated in 1997 as a wholly owned subsidiary of RJR. In August 2000, we became an independent company when we issued and sold stock to venture capital investors. Since our inception, we have had limited revenue from product sales and have funded our operations principally through the sale of equity securities, revenue from collaboration agreements, grants and equipment and building lease incentive financing. We have devoted substantially all of our resources to the discovery and development of our product candidates and technologies, including the design, conduct and management of preclinical and clinical studies and related manufacturing, regulatory and clinical affairs, as well as intellectual property prosecution.
We generated net income for the year ended December 31, 2010, and for three quarterly periods within the year, due primarily to recognition into revenue of a portion of the upfront payment received under our TC-5214 agreement with AstraZeneca. We also generated net income for two other quarterly periods since inception, in each case due primarily to the achievement in each period of a single milestone event related to AZD3480 under our cognitive disorders agreement with AstraZeneca. Except for these periods, we have never been profitable and may incur losses in future periods as our clinical-stage and preclinical product candidates advance into later-stage development and as we progress our programs, invest in additional product opportunities and grow our business. As of December 31, 2010, we had an accumulated deficit of $218.4 million. Clinical trials and preclinical studies are time-consuming, expensive and may never yield a product that will generate revenue.
As a clinical-stage company, our revenues, expenses and results of operations are likely to fluctuate significantly from quarter to quarter and year to year. We believe that period-to-period comparisons of our results of operations should not be relied upon as indicative of our future performance.
Revenue
In January 2010, we received a $200.0 million upfront payment under our TC-5214 agreement with AstraZeneca, which we recorded as deferred revenue and are recognizing into revenue on a straight-line basis over the estimated development period for TC-5214 to submission of an NDA to the FDA. As of December 31, 2010, we had $127.0 million of the upfront payment remaining to be recognized into revenue. We are eligible under our TC-5214 agreement with AstraZeneca to receive additional payments of over $1.0 billion if development, regulatory, first commercial sale and specified sales related milestone events for TC-5214 are achieved and stepped double-digit royalties on any future TC-5214 product sales.
Pursuant to an April 2010 amendment to our cognitive disorders agreement with AstraZeneca related to an expansion of the development program for TC-5619, we received an $11.0 million payment in May 2010, which
70
Table of Contents
we recorded as deferred revenue and are recognizing into revenue on a straight-line basis over the estimated period of our research and development obligations related to TC-5619. Pursuant to a September 2010 amendment to our cognitive disorders agreement with AstraZeneca related to a potential additional clinical trial of AZD3480 in Alzheimer’s disease, we received an additional $500,000 payment in October 2010, which we recorded as deferred revenue and are recognizing into revenue on a straight-line basis over the estimated period of our obligations with respect to the potential study.
As of December 31, 2010, we had received $82.6 million in aggregate upfront fees and milestone payments under our cognitive disorders agreement with AstraZeneca and recognized an additional $26.5 million in collaboration research and development revenue for research services that we provided in the preclinical research collaboration conducted under that agreement. We deferred recognition of an aggregate of $21.5 million of the amounts received under our cognitive disorders agreement with AstraZeneca and are recognizing these deferred amounts into revenue over the periods discussed in Note 12 to our audited financial statements for the year ended December 31, 2010 included in this annual report. As of December 31, 2010, we had $7.0 million of amounts received under our cognitive disorders agreement with AstraZeneca remaining to be recognized into revenue.
As of December 31, 2010, we had also received $45.0 million in aggregate payments under our alliance agreement with GlaxoSmithKline, of which we initially deferred recognition of $29.5 million that we were recognizing into revenue over the period discussed in Note 12 to our audited financial statements for the year ended December 31, 2010 included in this annual report. As a result of our receipt in late February 2011 of notice of termination of the agreement, we expect to recognize the remaining $18.4 million into revenue in the first quarter of 2011.
Under our cognitive disorders agreement with AstraZeneca, we are eligible to receive other payments of up to $103.0 million, if development, regulatory and first commercial sale milestone events for AZD3480 are achieved only for ADHD, up to $145.0 million if we proceed with another Alzheimer’s disease study of AZD3480, AstraZeneca subsequently advances AZD3480 into later-stage development for Alzheimer’s disease and development, regulatory and first commercial sale milestone events are achieved for Alzheimer’s disease, and up to $197.0 million if both ADHD and Alzheimer’s disease are successfully pursued. If AZD3480 is developed for an indication in addition to Alzheimer’s disease and ADHD, we would also be eligible to receive payments of up to $52.0 million for each such indication, if development, regulatory, first commercial sale and first detail milestone events are achieved. We are also eligible to receive stepped double-digit royalties on any future AZD3480 product sales for any indication.
With regard to AZD1446, we are eligible under our cognitive disorders agreement with AstraZeneca to receive payments of up to $73.0 million, if development, regulatory and first commercial sale milestones are achieved only for Alzheimer’s disease, as well as stepped royalties on any future AZD1446 product sales for any indication. If AZD1446 is developed under the agreement for an indication in addition to Alzheimer’s disease, we would also be eligible to receive payments of up to $35.0 million for each such indication, if development, regulatory, first commercial sale and first detail milestone events are achieved.
In addition, if AstraZeneca licenses TC-5619, our cognitive disorders agreement with AstraZeneca provides for AstraZeneca to make a $30.0 million payment to us and to assume responsibility for and fund all future development (except for completion of our ongoing studies) and commercialization. In that event, we would be eligible to receive additional payments of up to $212.0 million, if development, regulatory, first commercial sale and first detail milestones are achieved for three indications, as well as stepped double-digit royalties on any future TC-5619 product sales.
Our TC-5214 agreement with AstraZeneca can be terminated by AstraZeneca in whole or in part at various times and under various circumstances as discussed above under the caption “Business—Strategic Alliances and Collaborations—AstraZeneca AB—TC-5214—Termination” in Item 1 of Part I of this annual report. Our cognitive disorders agreement with AstraZeneca can be terminated by AstraZeneca for an uncured material breach by us or upon 90 days notice given at any time.
71
Table of Contents
We acquired rights to Inversine, which is our only product to have been approved by the FDA for marketing, in August 2002. Effective September 30, 2009, we discontinued Inversine. Sales of Inversine generated net revenue of $473,000 and $718,000 for the years ended December 31, 2009 and 2008, respectively.
From time to time we seek and are awarded grants or work to be performed under grants awarded to third-party collaborators from which we derive revenue. As of December 31, 2010 we have been awarded two grants from The Michael J. Fox Foundation for Parkinson’s Research, or MJFF. One of the grants is to fund preclinical research involving the use of compounds that modulate NNRs to address Levodopa-induced abnormal involuntary movements, known as dyskinesias, and we have received aggregate payments of $641,000 from MJFF since August 2009 in connection with this grant. The other grant is to fund research to identify NNR-related biomarkers relevant to Parkinson’s disease, and we have received an aggregate of $304,000 from MJFF in connection with this grant. In addition, as of December 31, 2010, we are a named subcontractor under a grant awarded to The California Institute of Technology by the National Institute on Drug Abuse, or NIDA, part of the National Institutes of Health, to fund research on innovative NNR-based approaches to the development of therapies for smoking cessation. Funding for awards under federal grant programs is subject to the availability of funds as determined annually in the federal appropriations process.
Research and Development Expenses
Since our inception, we have focused our activities on our drug discovery and development programs. We record research and development expenses as they are incurred. Research and development expenses represented approximately 89%, 61% and 85% of our total operating expenses for the years ended December 31, 2010, 2009, and 2008, respectively. For 2009, license fees of $16.4 million, which are not included in research and development expenses, represented 25% of our total operating expenses. There was no license fees expense for the 2010 and 2008 periods.
Research and development expenses include costs associated with:
| • | the employment of personnel involved in our drug discovery, research and development activities; |
| • | research and development facilities, equipment and supplies; |
| • | clinical trials, including fees paid to contract research organizations to monitor and oversee some of our trials; |
| • | the conduct of research activities under the preclinical research collaboration that we conducted with AstraZeneca from January 2006 to January 2010; |
| • | the screening, identification and optimization of product candidates; |
| • | formulation and chemical development; |
| • | production of clinical trial materials, including fees paid to contract manufacturers; |
| • | preclinical animal studies, including the costs to engage third-party research organizations; |
| • | quality assurance activities; |
| • | compliance with FDA regulatory requirements; |
| • | consulting, license and sponsored research fees paid to third parties; |
| • | the development and enhancement of our drug discovery technologies that we refer to as Pentad; |
| • | depreciation of capital assets used to develop our products; and |
| • | stock options granted to personnel in research and development functions. |
In particular, research and development expenses include 20% of the costs of the initial development program for TC-5214, as provided in our TC-5214 agreement with AstraZeneca.
72
Table of Contents
We utilize our research and development personnel and infrastructure resources across several programs. We currently have clinical, preclinical and discovery-stage programs, and many of our costs are not specifically attributable to a single program. Instead, these costs are directed to broadly applicable research efforts. Accordingly, we cannot state precisely our total costs incurred on a program-by-program basis.
We have not received FDA or foreign regulatory marketing approval for any of our product candidates that are in development. Our current and future expenditures on preclinical and clinical development programs are subject to numerous uncertainties in timing and cost to completion. We or a collaborator of ours tests compounds in numerous preclinical studies for safety, toxicology and efficacy. We or a collaborator of ours then conducts clinical trials for those product candidates that are determined to be the most promising. If we do not establish an alliance or collaboration in which our collaborator assumes responsibility for funding the development of a particular product candidate, we fund these trials ourselves. As we or a collaborator of ours obtains results from clinical trials, we or the collaborator may elect to discontinue or delay trials for some product candidates in order to focus resources on more promising product candidates. Completion of clinical trials by us or a collaborator of ours may take several years or more, and the length of time generally varies substantially according to the type, complexity, novelty and intended use of a product candidate. The cost of clinical trials for a particular product candidate may vary significantly as a result of a variety of factors, including:
| • | the number of subjects who participate in the trials; |
| • | the number and locations of sites included in the trials; |
| • | the length of time required to enroll trial subjects; |
| • | the therapeutic areas being investigated; |
| • | the duration of the trials and subject follow-up; |
| • | the costs of producing supplies of the product candidate needed for trials and regulatory submissions; |
| • | the efficacy and safety profile of the product candidate; and |
| • | the costs and timing of, and the ability to secure, regulatory approvals. |
In addition, our strategy includes entering into alliances and collaborations with third parties to participate in the development and commercialization of some of our product candidates. Where a third party has responsibility for or authority over any or all of the non-clinical or clinical development of a particular product candidate, the estimated completion date may be largely under control of that third party and not under our control. We cannot forecast with any degree of certainty whether AstraZeneca will exercise its option to license TC-5619, whether any of our product candidates will be subject to future alliances or collaborations or how any such arrangements would affect our development plans or capital requirements. Because of this uncertainty, and because of the numerous uncertainties related to clinical trials and related activities as described above, we are unable to determine the duration and completion costs of our research and development programs or whether or when we will generate revenue from the commercialization and sale of any of our product candidates in development.
General and Administrative Expenses
General and administrative expenses consist principally of salaries and other related costs for personnel in executive, finance, business development, legal and human resource functions. Other general and administrative expenses include expenses associated with stock options granted to personnel in those functions, depreciation and other facility costs not otherwise included in research and development expenses, patent-related costs, insurance costs and professional fees for consulting, legal, accounting and public and investor relations services.
License Fees
License fees consist of amounts that we become required to pay to third parties from which we license or otherwise acquire intellectual property rights, such as University of South Florida Research Foundation, or USFRF, with respect to TC-5214 and University of Kentucky Research Foundation, or UKRF, with respect to
73
Table of Contents
AZD3480. Under the terms of a license agreement with USFRF, if we receive any milestone payments under our TC-5214 agreement with AstraZeneca, we would be required to pay a percentage of each such milestone payment, after deducting from the milestone payment the unexhausted portion of our projected share of the costs of the initial development program for TC-5214, as well as royalties on any future TC-5214 product sales, to USFRF. The percentage of each milestone payment, net of any deduction, that we would be required to pay would be at least 10% and could be greater in specified circumstances. Based on the terms of the license agreement with USFRF and the terms of another license agreement with Yale University, we expect to pay royalties at an effective worldwide rate in the low single digits and that such effective royalty rate could in some circumstances reach the mid single digits. Under the terms of a sponsored research agreement and a subsequent license agreement with UKRF, if we receive any qualifying milestone or royalty payments from AstraZeneca relating to AZD3480, we are required to pay a low single digit percentage of each such payment to UKRF.
The amount and timing of our payment obligations to USFRF depend on whether and when milestone events under our TC-5214 agreement with AstraZeneca are achieved and we receive the corresponding payments from AstraZeneca and whether and when regulatory approval for TC-5214 is obtained and product sales are generated. Likewise, the amount and timing of our payment obligations to UKRF depend on whether and when milestone events for AZD3480 under our cognitive disorders agreement with AstraZeneca are achieved and we receive the corresponding payments from AstraZeneca and whether and when regulatory approval for AZD3480 is obtained and product sales are generated. Accordingly, we cannot forecast with any degree of certainty whether or to what extent we will incur license fee and royalty expense in future periods.
Income Taxes
We incurred net operating losses through December 31, 2009 and have not paid federal, state or foreign income taxes for any period through December 31, 2009. For the year ended December 31, 2010, we recognized $3.5 million of income tax expense, primarily as a result of the application of Accounting Standards Codification Topic 740, Income Taxes, or ASC 740, to stock-based compensation. Exercises of stock options during the year ended December 31, 2010 resulted in tax deductions for stock-based compensation in excess of expense recorded for the stock options under U.S. generally accepted accounting principles, or GAAP, resulting in an income tax benefit of $3.5 million. We recognized the income tax benefit related to the excess tax deductions as an increase to capital in excess of par value, which based on ASC 740 resulted in an offsetting charge in the same amount to income tax expense.
As of December 31, 2010, we had net operating loss carryforwards of $39.0 million for federal income tax purposes and $76.2 million for state income tax purposes. We also had research and development income tax credit carryforwards of $9.6 million for federal income tax purposes and $1.0 million for state income tax purposes as of December 31, 2010. The federal net operating loss carryforwards begin to expire in 2021. The state net operating loss carryforwards begin to expire in 2016. The federal and state research and development tax credits begin to expire in 2021. As a result of various factors, including the subjectivity of measurements used in the calculation of particular tax positions taken or that may in the future be taken in our tax returns, it is uncertain whether or to what extent we will be eligible to use the tax credits.
Utilization of the net operating loss carryforwards and credits may be subject to a substantial annual limitation due to ownership change limitations provided by Section 382 of the Internal Revenue Code of 1986, as amended, and similar state provisions. When an ownership change, as defined by Section 382, occurs, an annual limitation is imposed on a company’s use of net operating loss and credit carryforwards attributable to periods before the change. A series of stock issuances occurring prior to our initial public offering gave rise to such an ownership change. As a result, an annual limitation is imposed on our use of net operating loss and credit carryforwards that are attributable to periods before the change. In addition, a portion of the net operating loss carryforwards described above may potentially not be usable by us if we experience further ownership changes in the future. For financial reporting purposes, we have recorded a valuation allowance to fully offset the deferred tax assets related to the carryforwards and the tax credits because it is uncertain whether we will be eligible to use or realize any benefit from them.
74
Table of Contents
Fair Value
The carrying amounts of our cash and cash equivalents, investments in marketable securities, accounts receivable, accounts payable and accrued expenses are considered to be representative of their respective fair values due to their short-term natures and, in the case of short-term investments, their market interest rates. Likewise, the carrying amounts of our long-term debts are considered to be representative of their fair value due to their market interest rates. Cash that we do not expect to use to fund our short-term liquidity requirements is invested in U.S. Treasury notes and bonds, U.S. and state agency-backed certificates, corporate debt securities that are rated at least A quality or equivalent and certificates of deposits. Our investments in marketable securities of $86.7 million at December 31, 2010 are recorded at quoted market prices.
Our intangible assets consist of rights assigned to us from Layton Bioscience, Inc., including licensed patent rights and rights related to the Inversine trademark and product technology. Our original assigned value of the Inversine trademark and product technology intangible asset was $346,000. During the fourth quarter of 2008, as part of our processes for preparation of our financial statements, we performed an impairment analysis of the Inversine trademark and product technology intangible asset. As of the date of the analysis, we had recognized a net loss on sales of Inversine for each of 2008 and 2007 and did not expect to recognize net income from sales of Inversine in future periods. The history of losses on sales of Inversine and the forecast for future periods indicated the carrying value of the intangible asset may not have been recoverable. Using a discounted cash flow model that was based on estimated future net product sales and cost of product sales and considered assumptions such as, among other things, estimated future product sales volumes and estimated future sales price increases, we determined that the Inversine trademark and product technology had no fair value. As a result, we recorded an impairment charge for the full amount of the unamortized balance of the Inversine trademark and product technology intangible asset as of the valuation date, or $220,000, to research and development expenses in the fourth quarter of 2008. The impairment charge has no effect on our prospective amortization of the licensed patent rights intangible asset to research and development expenses on a straight-line basis over the remaining useful life of the patents.
Critical Accounting Policies and Estimates
Our management’s discussion and analysis of our financial condition and results of operations are based on our audited financial statements, which have been prepared in accordance with GAAP. The preparation of these financial statements requires us to make estimates and judgments that affect the reported amounts of assets, liabilities, revenues and expenses. On an ongoing basis, we evaluate these estimates and judgments. We base our estimates on historical experience and on various assumptions that we believe to be reasonable under the circumstances. These estimates and assumptions form the basis for making judgments about the carrying values of assets and liabilities and the recording of revenues and expenses that are not readily apparent from other sources. Actual results and experiences may differ materially from these estimates. In addition, our reported financial condition and results of operations could vary if new accounting standards are enacted that are applicable to our business.
Our significant accounting policies are described in Note 2 to our audited financial statements for the year ended December 31, 2010 included in this annual report. We believe that our accounting policies relating to revenue recognition, accrued expenses and stock-based compensation are the most critical to understanding and evaluating our reported financial results. We have identified these policies as critical because they both are important to the presentation of our financial condition and results of operations and require us to make judgments and estimates on matters that are inherently uncertain and may change in future periods. For more information regarding these policies, you should refer to Note 2 to our audited financial statements included in this annual report.
Revenue Recognition
We have historically derived a substantial portion of our revenues from our strategic alliances and collaborations and expect that we will continue to derive a substantial portion of our revenues from our collaborations with AstraZeneca over at least the next several years.
75
Table of Contents
Our collaboration and alliance agreements contain multiple elements, including: upfront fees, which may include initial payments upon commencement of the contractual relationship, payment representing a common stock purchase premium or payment to secure a right for a future license; research fees for ongoing research and development; payments associated with the achievement of discovery, development, regulatory and commercial milestone events; and rights to receive royalties based on specified percentages of any net product sales. In determining the accounting for collaboration and alliance agreements, we first determine whether the agreement involves a single unit of accounting or separate units of accounting for revenue recognition purposes by evaluating each deliverable under the terms of the agreement. If a deliverable has value on a stand-alone basis and there is objective and reliable evidence of that fair value, we treat the deliverable as a separate unit of accounting. If an agreement does not have multiple deliverables that meet these criteria, we consider the agreement to have one unit of accounting. If an agreement involves separate units of accounting, we then determine how to allocate amounts received under the agreement among the separate units, based on the respective fair value of each unit and the revenue recognition applicable to each unit. If an agreement involves a single unit of accounting, we determine the revenue recognition applicable to the entire agreement.
We defer recognition of non-refundable upfront fees and recognize them into revenue on a straight-line basis over the estimated period of our substantive performance obligations. If we do not have substantive performance obligations, we recognize non-refundable upfront fees into revenue over the estimated development period for the applicable licensed product candidate(s). The period over which we recognize the revenue may be adjusted from time to time to take into account any delays or acceleration in the development of the applicable product candidate or any extension or shortening of the applicable performance period. Any such delay or acceleration in the development of a product candidate, or extension or shortening of a performance period, could result in further deferral of revenue or acceleration in the recognition of deferred revenue. As of December 31, 2010, all amounts that we have received from AstraZeneca and GlaxoSmithKline are non-refundable.
We recognize collaboration research and development revenue from research services performed under our collaboration agreements as research is performed and related expenses are incurred.
We recognize revenue for non-refundable payments that are based on the achievement of discovery, development, regulatory and commercial milestone events upon achievement of the milestone event if all of the following conditions are met:
| • | achievement of the milestone event was not reasonably assured at the inception of the arrangement; |
| • | substantive effort is involved to achieve the milestone event; and |
| • | the amount of the milestone payment appears reasonable in relation to the effort expended, the other milestone payments in the arrangement and the related risk associated with achievement of the milestone event. |
If any of these conditions are not met, we defer recognition of the payment and recognize the payment on a straight-line basis as discussed above.
To the extent we are reimbursed under a collaboration or alliance agreement for specific research and development costs, such as third-party manufacturing costs for drug material, we reflect these reimbursable amounts as a component of collaboration research and development revenue and the costs associated with these reimbursable amounts as a component of research and development expenses.
Under our TC-5214 agreement with AstraZeneca, we received an upfront payment of $200.0 million. We recorded such amount as deferred revenue and commenced in December 2009 recognizing the payment ratably over the estimated development period for TC-5214 to submission of an NDA to the FDA.
76
Table of Contents
We have received various payments under our cognitive disorders agreement with AstraZeneca as discussed below.
| • | We received an initial fee of $10.0 million in February 2006. Based on the agreement terms and consideration of fair value, we allocated $5.0 million of the initial fee to the preclinical research collaboration. Upon effectiveness of the agreement in January 2006, we commenced recognizing the $5.0 million as revenue over the planned four-year term of the research collaboration. We deferred recognition of the remaining $5.0 million of the initial fee, which we allocated to the AZD3480 license grants, until AstraZeneca made its determination in December 2006 to proceed with further development of AZD3480. Beginning in January 2007, we commenced recognizing the previously deferred $5.0 million of the initial fee ratably over the expected remaining development period for AZD3480. |
| • | We received a $2.0 million payment from AstraZeneca in November 2007 to secure the right to license TC-5619 following our completion of an agreed development plan. Beginning in November 2007, we commenced recognizing the $2.0 million payment ratably over the estimated period of our research and development obligations for TC-5619. |
| • | We received an $11.0 million payment from AstraZeneca in May 2010 in connection with an amendment to the agreement to modify the terms applicable to TC-5619. In conjunction with the amendment, we and AstraZeneca agreed to an expanded development program for TC-5619 and AstraZeneca maintained its option to license TC-5619. Beginning in May 2010, we commenced recognizing the $11.0 million payment ratably over the estimated period of our research and development obligations for TC-5619. |
| • | We received a $500,000 payment from AstraZeneca in October 2010 in connection with an amendment to the agreement to provide for a potential additional clinical trial of AZD3480 in Alzheimer’s disease. Beginning in October 2010, we commenced recognizing the $500,000 payment ratably over the estimated period of our performance obligations with respect to the potential study. |
| • | We received cumulative research fees of $26.5 million since inception of the agreement. We recognized all of these fees as the research was performed and related expenses were incurred. |
| • | We received payments from AstraZeneca upon achievement of milestone events related to the development of product candidates in the aggregate amount of $34.6 million since inception of the agreement. We recognized the full amount of each payment as revenue upon achievement of the corresponding milestone event because the event met each of the conditions required for immediate recognition under our revenue recognition policy. |
We have also received various payments under our alliance agreement and related stock purchase agreement with GlaxoSmithKline.
| • | GlaxoSmithKline made an initial payment to us of $20.0 million and purchased 1,275,502 shares of our common stock for an aggregate purchase price of $15.0 million, which resulted in an aggregate deemed premium of $3.5 million based on the closing price of our common stock on the trading day immediately preceding the date that the alliance was announced. In July 2007, we commenced recognizing the initial payment and deemed premium as revenue on a straight-line basis over the estimated period of our research and early development performance obligations under the agreement. |
| • | In December 2007, we initiated a Phase 1 clinical trial of a product candidate that had been in development for pain, triggering a $6.0 million milestone payment to us from GlaxoSmithKline. We determined the milestone payment did not meet all of the conditions required for immediate revenue recognition. Specifically, based on the status of development of the applicable product candidate as of the inception of the agreement, we determined that achievement of the milestone event was reasonably assured. Consequently, we recorded the $6.0 million payment as deferred revenue and, in December 2007, commenced recognizing such amount on a straight-line basis over the estimated period of our research and early development performance obligations under the agreement. |
77
Table of Contents
| • | We received cumulative payments of $4.0 million from GlaxoSmithKline upon achievement of milestone events under the alliance agreement since inception of the agreement. We recognized the full amount of each payment as revenue upon achievement of the milestone event because the event met each of the conditions required for immediate recognition under our revenue recognition policy. |
As a result of our receipt in late February 2011 of notice of termination of the alliance agreement, we expect to recognize into revenue in the first quarter of 2011 $18.4 million in deferred amounts received under the alliance agreement and remaining to be recognized as of December 31, 2010.
Accrued Expenses
In the normal course of our business, we contract with research institutions and contract research organizations that conduct or manage clinical trials or other research and development activities on our behalf and with contract manufacturers that produce drug substance or drug product for us. The financial terms of these agreements are subject to negotiation, vary among agreements and may result in uneven payment flows. Payments under these agreements depend on the performance of services or the achievement of specified events, such as the production of drug substance or drug product, the recruitment of clinical trial subjects, the completion of portions of a non-clinical study or clinical trial or similar conditions.
As part of the process of preparing financial statements, we are required to estimate accrued expenses with the objective of matching the recording of expenses in our financial statements to the actual services received and efforts expended. This process involves reviewing open contracts and purchase orders, communicating with our applicable personnel to identify services that have been performed on our behalf, estimating level of services performed and the associated cost incurred for the services when we have not yet been invoiced or otherwise notified of actual cost and reviewing invoices received that have not yet become due and payable. We make estimates of our accrued expenses as of each balance sheet date in our financial statements based on facts and circumstances known to us. We periodically confirm the accuracy of our estimates with the service providers and make adjustments if necessary. If we do not identify costs that we have begun to incur or if we underestimate or overestimate the level of services performed or the costs of these services, our actual expenses could differ from our estimates. Examples of estimated accrued expenses include:
| • | fees for services performed by contract research organizations in connection with clinical trials and non-clinical studies; |
| • | fees for services performed by clinical trial sites in connection with clinical trials; |
| • | fees for services performed by contract manufacturers in connection with the production of clinical trial materials; and |
| • | professional service fees. |
Stock-Based Compensation
We record the grant date fair value of stock options issued to employees and non-employee directors as stock-based compensation expense over the requisite service periods, which are typically the vesting periods. We currently use the Black-Scholes-Merton formula to estimate grant date fair value and expect to continue to use this valuation model in the future. The Black-Scholes-Merton formula requires us to make various assumptions, including among others the expected term of the award and expected volatility of our common stock. We recorded stock-based compensation expense related to stock options granted to employees and directors of $4.9 million for the year ended December 31, 2010, $2.5 million for the year ended December 31, 2009 and $2.1 million for the year ended December 31, 2008. As of December 31, 2010, we had $11.0 million in total unrecognized compensation cost related to non-vested stock-based compensation arrangements, which we expect to record over a weighted average period of 2.6 years.
78
Table of Contents
Results of Operations
Years ended December 31, 2010 and December 31, 2009
Net Operating Revenues
| Year ended December 31, |
||||||||||||
| 2010 | 2009 | Change | ||||||||||
| (in thousands) | ||||||||||||
| Operating revenues: |
||||||||||||
| Milestones and license fees from collaborations |
$ | 83,380 | $ | 18,934 | $ | 64,446 | ||||||
| Collaboration research and development |
— | 5,246 | (5,246 | ) | ||||||||
| Product sales, net |
— | 473 | (473 | ) | ||||||||
| Grant revenue |
2,333 | 409 | 1,924 | |||||||||
| Net operating revenues |
$ | 85,713 | $ | 25,062 | $ | 60,651 | ||||||
Net operating revenues for the year ended December 31, 2010 increased by $60.7 million as compared to the year ended December 31, 2009. The higher net operating revenues were primarily attributable to increases of $64.4 million in milestones and license fees from collaborations revenue and $1.9 million in grant revenue, partially offset by a decrease of $5.2 million in collaboration research and development revenue. The increase in milestones and license fees from collaborations revenue was principally due to recognition of $72.6 million of the $200.0 million upfront payment received under our TC-5214 agreement with AstraZeneca and $6.3 million of the $11.0 million payment received under the April 2010 amendment to our cognitive disorders agreement with AstraZeneca, partially offset by the achievement for 2009 of a milestone event under the cognitive disorders agreement for which we received $10.0 million, decreases of $2.5 million in aggregate payments received from GlaxoSmithKline upon achievement of milestone events under our alliance agreement and $1.1 million in license fees derived from the cognitive disorders agreement as a result of the expiration of the term of the preclinical research collaboration in January 2010.
The increase in grant revenue was primarily attributable to $1.5 million received under the U.S. government’s Qualifying Therapeutic Discovery Project tax credit program. The decrease in collaboration research and development revenue resulted from the completion of the preclinical research collaboration under the cognitive disorders agreement with AstraZeneca.
In future periods, we are eligible to receive additional license fees and milestone payments under our agreements with AstraZeneca. The amount of license fees and milestone fees will depend on the timing and achievement of the discovery, development, regulatory and commercial milestone events and whether AstraZeneca exercises its right to license TC-5619. It is uncertain whether we will achieve any particular milestone event in 2011, in any future period or at all. We expect that the amount of our milestone-based revenue may vary from period to period.
Net product sales for the year ended December 31, 2010 decreased by $473,000 as compared to the year ended December 31, 2009 as a result of our discontinuation of Inversine effective as of September 30, 2009.
Research and Development Expenses
| Year ended December 31, |
||||||||||||
| 2010 | 2009 | Change | ||||||||||
| (in thousands) | ||||||||||||
| Research and development expenses |
$ | 64,546 | $ | 40,179 | $ | 24,367 | ||||||
79
Table of Contents
Research and development expenses for the year ended December 31, 2010 increased by $24.4 million as compared to the year ended December 31, 2009. The higher research and development expenses were principally attributable to:
| • | an increase of $17.3 million in costs incurred for third-party research and development services in connection with our clinical-stage product candidates, including costs for clinical trial activities, formulation activities, production of clinical trial materials and pharmacology, toxicology and other non-clinical studies, to $27.6 million for 2010, from $10.3 million for 2009; this increase was principally due to our cost-sharing obligations with respect to ongoing Phase 3 clinical development of TC-5214, the conduct of Phase 2 clinical development of TC-5619 for two indications and the conduct of multiple Phase 1 clinical trials of TC-6987; |
| • | an increase of $2.5 million in stock-based compensation, salary and other compensation-related expenses for research and development activities to $17.0 million for 2010, from $14.5 million for 2009; the largest component of this increase was stock-based compensation expense and was primarily due to a significantly higher fair value calculated for stock options granted during 2010 as compared to the fair value calculated for prior stock option grants; |
| • | an increase of $3.0 million in other research and development expenses, including infrastructure costs, to $13.8 million for 2010, from $10.8 million for 2009; this increase was primarily due to increases in the number of employees and depreciable equipment utilized in our research and development functions; and |
| • | a $1.5 million upfront payment that we made to Cornerstone Therapeutics Inc. during 2010 under an exclusive license agreement. |
Costs incurred for third-party research and development services in connection with our preclinical programs were $4.6 million for each of the years ended December 31, 2010 and 2009.
The costs that we incurred for the years ended December 31, 2010 and 2009 for third-party services in connection with research and development of clinical-stage product candidates are shown in the table below:
| Year ended December 31, |
||||||||||||
| 2010 | 2009 | Change | ||||||||||
| (in thousands) | ||||||||||||
| TC-5214 |
$ | 10,771 | $ | 5,527 | $ | 5,244 | ||||||
| TC-5619 |
10,483 | 2,585 | 7,898 | |||||||||
| TC-6987 |
5,534 | 1,752 | 3,782 | |||||||||
| TC-6499 |
798 | 210 | 588 | |||||||||
| AZD3480 |
35 | 217 | (182 | ) | ||||||||
| AZD1446 |
— | — | — | |||||||||
| $ | 27,621 | $ | 10,291 | $ | 17,330 | |||||||
We expect our research and development expenses for the year ending December 31, 2011 to increase, with the largest component anticipated to result from our obligation under our TC-5214 agreement with AstraZeneca to fund a portion of the costs of the initial development program for TC-5214.
General and Administrative Expenses
| Year ended December 31, |
||||||||||||
| 2010 | 2009 | Change | ||||||||||
| (in thousands) | ||||||||||||
| General and administrative expenses |
$ | 8,052 | $ | 8,167 | $ | (115 | ) | |||||
80
Table of Contents
General and administrative expenses for the year ended December 31, 2010 decreased by $115,000 as compared to the year ended December 31, 2009. The change reflected a decrease of $839,000 in employee compensation and related expenses to $2.9 million for 2010, from $3.7 million for 2009, arising primarily from lower incentive compensation expenses, and a decrease of $344,000 in infrastructure costs to $3.0 million for 2010, from $3.3 million for 2009. These decreases were substantially offset by an increase of $1.1 million in stock-based compensation for general and administrative personnel to $2.2 million for 2010, from $1.1 million for 2009, primarily due to a significantly higher fair value calculated for stock options granted during 2010 as compared to the fair value calculated for prior stock option grants.
License Fees
| Year ended December 31, |
||||||||||||
| 2010 | 2009 | Change | ||||||||||
| (in thousands) | ||||||||||||
| License fees |
$ | — | $ | 16,350 | $ | (16,350 | ) | |||||
License fees for the year ended December 31, 2010 decreased by $16.4 million as compared to the year ended December 31, 2009. License fees for 2009 reflected $16.0 million payable to USFRF based on our receipt of the $200.0 million upfront payment under our TC-5214 agreement with AstraZeneca and $350,000 paid to UKRF based on the $10.0 million milestone payment received under our cognitive disorders agreement with AstraZeneca based on the achievement of the objective in the completed Phase 2 clinical trial of AZD3480 in adults with ADHD.
Cost of Product Sales
| Year ended December 31, |
||||||||||||
| 2010 | 2009 | Change | ||||||||||
| (in thousands) | ||||||||||||
| Cost of product sales |
$ | — | $ | 691 | $ | (691 | ) | |||||
Our cost of product sales are those costs related directly to the sale of Inversine. Cost of product sales for the year ended December 31, 2010 decreased by $691,000 as compared to the year ended December 31, 2009 as a result of our discontinuation of Inversine effective as of September 30, 2009.
Interest Income and Interest Expense
| Year ended December 31, |
||||||||||||
| 2010 | 2009 | Change | ||||||||||
| (in thousands) | ||||||||||||
| Interest income |
$ | 1,463 | $ | 1,050 | $ | 413 | ||||||
| Interest expense |
153 | 217 | (64 | ) | ||||||||
Interest income for the year ended December 31, 2010 increased by $413,000 as compared to the year ended December 31, 2009. The increase was primarily attributable to significantly increased cash and investment balances, partially offset by lower short-term interest rates.
Interest expense for the year ended December 31, 2010 decreased by $64,000 as compared to the year ended December 31, 2009. The decrease was attributable to lower average interest rates and principal balances under loan facilities used to finance equipment, furnishings, software and other fixed assets.
81
Table of Contents
Years ended December 31, 2009 and December 31, 2008
Net Operating Revenues
| Year ended December 31, |
||||||||||||
| 2009 | 2008 | Change | ||||||||||
| (in thousands) | ||||||||||||
| Operating revenues: |
||||||||||||
| Collaboration research and development |
$ | 5,246 | $ | 8,967 | $ | (3,721 | ) | |||||
| Milestones and license fees from collaborations |
18,934 | 10,179 | 8,755 | |||||||||
| Product sales, net |
473 | 718 | (245 | ) | ||||||||
| Grant revenue |
409 | 221 | 188 | |||||||||
| Net operating revenues |
$ | 25,062 | $ | 20,085 | $ | 4,977 | ||||||
Net operating revenues for the year ended December 31, 2009 increased by $5.0 million as compared to the year ended December 31, 2008. The higher net operating revenues were primarily attributable to an increase of $8.8 million in milestones and license fees from collaborations, partially offset by a decrease of $3.7 million in collaboration research and development revenue. The increase in milestones and license fees from collaborations was principally attributable to the $10.0 million payment received under our cognitive disorders agreement with AstraZeneca based on the achievement of the objective in the completed Phase 2 clinical trial of AZD3480 in adults with ADHD and recognition of $398,000 of the upfront payment received under our TC-5214 agreement with AstraZeneca. These increases were partially offset by a decrease of $1.0 million in payments received based on the achievement of preclinical milestone events under our cognitive disorders agreement with AstraZeneca and our alliance agreement with GlaxoSmithKline and our recognition of less deferred license fee revenue for 2009 as a result of an extension of the estimated remaining development period for AZD3480 and an extension of the estimated period of our research and development obligations for TC-5619.
The decrease in collaboration research and development revenue for the year ended December 31, 2009 reflected reduced services rendered by us in our preclinical research collaboration with AstraZeneca as a result of progress that had previously been made toward meeting the objectives of the research plan. All of our collaboration research and development revenue for 2009 and 2008 was derived from our preclinical research collaboration with AstraZeneca. The preclinical research collaboration expired in January 2010.
Net product sales for the year ended December 31, 2009 decreased by $245,000 as compared to the year ended December 31, 2008 primarily as a result of our discontinuation of Inversine effective as of September 30, 2009. Grant revenue for the year ended December 31, 2009 increased by $188,000 as compared to the year ended December 31, 2008. The higher grant revenue was primarily due to recognition of $147,000 of the amounts awarded by MJFF.
Research and Development Expenses
| Year ended December 31, |
||||||||||||
| 2009 | 2008 | Change | ||||||||||
| (in thousands) | ||||||||||||
| Research and development expenses |
$ | 40,179 | $ | 40,981 | $ | (802 | ) | |||||
Research and development expenses for the year ended December 31, 2009 decreased by $802,000 as compared to the year ended December 31, 2008. The lower research and development expenses were primarily attributable to a decrease of $908,000 in costs incurred for third-party research and development services in connection with our clinical-stage product candidates, including costs for clinical trial activities, formulation activities, production of clinical trial materials and pharmacology, toxicology and other non-clinical studies, to
82
Table of Contents
$10.3 million for 2009, from $11.2 million for 2008. This decrease in third-party research and development costs for our clinical-stage product candidates was partially offset by an increase of $310,000 in costs incurred for third-party research and development services in connection with our preclinical programs.
The costs that we incurred for the years ended December 31, 2009 and 2008 for third-party services in connection with research and development of clinical-stage product candidates are shown in the table below:
| Year ended December 31, |
||||||||||||
| 2009 | 2008 | Change | ||||||||||
| (in thousands) | ||||||||||||
| TC-5214 |
$ | 5,527 | $ | 4,826 | $ | 701 | ||||||
| TC-5619 |
2,585 | 3,151 | (566 | ) | ||||||||
| TC-6987 |
1,752 | 78 | 1,674 | |||||||||
| TC-6499 |
210 | 2,291 | (2,081 | ) | ||||||||
| AZD3480 |
217 | 322 | (105 | ) | ||||||||
| AZD1446 |
— | — | — | |||||||||
| $ | 10,291 | $ | 10,668 | $ | (377 | ) | ||||||
The table above does not include costs incurred for TC-2216, a compound that we are not currently progressing. For the years ended December 31, 2009 and 2008, we incurred $11,000 and $549,000, respectively, in expenses for third-party research and development services in connection with TC-2216.
General and Administrative Expenses
| Year ended December 31, |
||||||||||||
| 2009 | 2008 | Change | ||||||||||
| (in thousands) | ||||||||||||
| General and administrative expenses |
$ | 8,167 | $ | 6,499 | $ | 1,668 | ||||||
General and administrative expenses for the year ended December 31, 2009 increased by $1.7 million as compared to the year ended December 31, 2008. The higher general and administrative expenses were principally attributable to increased employee compensation and related expenses, primarily as a result of special bonuses paid to employees in December 2009, and increased legal and professional fees associated with our TC-5214 agreement with AstraZeneca.
License Fees
| Year ended December 31, |
||||||||||||
| 2009 | 2008 | Change | ||||||||||
| (in thousands) | ||||||||||||
| License fees and royalties |
$ | 16,350 | — | $ | 16,350 | |||||||
License fees for the year ended December 31, 2009 increased by $16.4 million as compared to the year ended December 31, 2008. License fees for 2009 reflected $16.0 million payable to USFRF based on our receipt of the $200.0 million upfront payment under our TC-5214 agreement with AstraZeneca and $350,000 paid to UKRF based on the $10.0 million milestone payment received under our cognitive disorders agreement with AstraZeneca.
83
Table of Contents
Cost of Product Sales
| Year ended December 31, |
||||||||||||
| 2009 | 2008 | Change | ||||||||||
| (in thousands) | ||||||||||||
| Cost of product sales |
$ | 691 | $ | 749 | $ | (58 | ) | |||||
Our cost of product sales are those costs related directly to the sale of Inversine. Cost of product sales for the year ended December 31, 2009 decreased by $58,000 as compared to the year ended December 31, 2008. The decrease was primarily attributable to our discontinuation of Inversine effective as of September 30, 2009.
Interest Income and Interest Expense
| Year ended December 31, |
||||||||||||
| 2009 | 2008 | Change | ||||||||||
| (in thousands) | ||||||||||||
| Interest income |
$ | 1,050 | $ | 2,734 | $ | (1,684 | ) | |||||
| Interest expense |
217 | 251 | (34 | ) | ||||||||
Interest income for the year ended December 31, 2009 decreased by $1.7 million as compared to the year ended December 31, 2008. The decrease was primarily attributable to lower short-term interest rates.
Interest expense for the year ended December 31, 2009 decreased by $34,000 as compared to the year ended December 31, 2008. The decrease was attributable to lower average principal balances under loan facilities used to finance equipment, furnishings, software and other fixed assets.
Liquidity and Capital Resources
Sources of Liquidity
We have historically financed our operations and internal growth primarily through public and private offerings of our securities, payments under collaborations and alliances, including upfront fees received, payments received for research and development services and payments received upon achievement of milestone events, equipment and building lease incentive financing, government grants and interest income. We discontinued our only approved product, Inversine, effective as of September 30, 2009. The net contribution from Inversine sales has not historically been a significant source of cash.
Our cash, cash equivalents and investments were $252.5 million as of December 31, 2010 and $111.1 million as of December 31, 2009. As of December 31, 2010, we had $147.3 million of cash in bank depository accounts and institutional money market funds at Branch Banking and Trust Company, RBC Bank and Wells Fargo & Company. Substantially all of our remaining cash, cash equivalents and investments, which we do not expect to use to fund our short-term liquidity requirements, was invested as of December 31, 2010 in U.S. Treasury notes and bonds, U.S. and state agency-backed certificates, corporate debt securities that are rated at least A quality or equivalent and certificates of deposit.
Strategic Alliances and Collaborations
In May 2010, we received an $11.0 million payment from AstraZeneca in connection with a separate amendment to our cognitive disorders agreement with AstraZeneca to modify the terms applicable to TC-5619. In July 2009, we received a $10.0 million payment from AstraZeneca as a result of the achievement of the objective in the completed Phase 2 trial of AZD3480 in adults with ADHD, a milestone event under an amendment to our cognitive disorders agreement. From 2008 through 2010, we received cumulative payments of
84
Table of Contents
$2.6 million from AstraZeneca upon achievement of milestone events under our cognitive disorders agreement related to the development of AZD1446 and other product candidates arising under the preclinical research collaboration conducted under the agreement. As of December 31, 2010, we had received $56.1 million in aggregate upfront fees and milestone payments under our cognitive disorders agreement with AstraZeneca and had recognized an additional $26.5 million in collaboration research and development revenue for research services that we provided in the preclinical research collaboration.
In December 2009, we entered into our TC-5214 agreement with AstraZeneca for the global development and commercialization of TC-5214. We received a $200.0 million upfront payment from AstraZeneca in January 2010. Under the terms of an existing license agreement, we paid $16.0 million to USFRF in January 2010 based on our receipt of the upfront payment from AstraZeneca.
In July 2007, we entered into a product development and commercialization agreement and related stock purchase agreement with GlaxoSmithKline. As of December 31, 2010, we had received $45.0 million in aggregate payments from GlaxoSmithKline under the agreements. We received notice of termination of the product development and commercialization agreement from GlaxoSmithKline in late February 2011, and the agreement will no longer be a potential source of future funds.
As discussed above under the caption “—Overview—Revenue,” we are eligible to receive substantial additional payments from AstraZeneca, contingent on the achievement of specified milestone events related to TC-5214, AZD3480, AZD1446, and, if AstraZeneca licenses TC-5619, TC-5619. There is no assurance that we will achieve any particular milestone event in 2011, in any future period or at all.
Stock Offerings
In October 2009 and January 2008, we completed public offerings of our common stock. The October 2009 offering consisted of 2.2 million shares at a price of $21.00 per share and, after deducting underwriting discounts and commissions and offering expenses payable by us, our net proceeds from the offering were $44.4 million. The January 2008 offering consisted of 4.4 million shares at a price of $7.07 per share and, after deducting underwriting discounts and commissions and offering expenses payable by us, our net proceeds from the offering were $29.1 million. Taken together with our initial public offering in April 2006, we have derived aggregate net proceeds of $114.3 million from public offerings of our common stock. We have also derived aggregate net proceeds of $121.8 million from private placements of convertible preferred stock, all of which occurred prior to our initial public offering.
In October 2009, we received written notice from a stockholder that the stockholder had violated Section 16(b) of the Exchange Act as a result of certain purchases and sales of shares of our common stock made by the stockholder within a period of less than six months that generated “short-swing” profits under Section 16(b). Later in October 2009, the stockholder made a $724,000 payment to us in disgorgement of the short-swing profits.
Loan Financing
In July 2010, we entered into a loan agreement with a bank that provides aggregate borrowing capacity of $4.0 million to be provided in up to three individual term loans that we may take at any time on or prior to June 30, 2011 to fund the purchase of equipment, furnishings, software and other fixed assets. In September 2010, we borrowed $1.2 million under this loan facility at a fixed interest rate of 3.4% per annum. We were obligated only to pay interest through the remainder of 2010. Beginning January 1, 2011 and continuing through the maturity date of December 1, 2014, the loan is repayable in equal monthly installments of $28,000. We granted to the bank a first priority security interest in the assets acquired with the proceeds of the loan. Any future loan under the facility would, at our discretion on a loan-by-loan basis, bear interest at either a variable rate equal to the thirty-day LIBOR plus 2.15%, adjusted monthly on the first day of each month, or a fixed rate
85
Table of Contents
equal to the bank’s fixed rate cost of funds index corresponding to the term of the loan plus 2.15%. Any loan that we take during the first half of 2011 would be interest only through June 30, 2011 and then would be re-payable in equal monthly installments of principal and interest over the next 48 months.
In March 2008, we entered into a loan agreement with a bank that provided borrowing capacity of $5.3 million to fund the purchase of equipment, furnishings, software and other fixed assets and enabled the refinancing of a previous loan facility that we had with R.J. Reynolds Tobacco Holdings, Inc., or RJRT. We borrowed $4.8 million upon entering into the loan agreement and borrowed the remaining $489,000 in September 2008. Pursuant to the loan agreement, we granted a first priority security interest in favor of the bank in the assets acquired with the proceeds of the loan facility. The March 2008 loan bears interest at a fixed rate of 5.231% per annum and is repayable in equal monthly installments of $112,000 beginning April 1, 2008 and continuing through the maturity date of March 1, 2012. We used $1.7 million of the proceeds from the March 2008 loan to pay and satisfy in full the principal and interest outstanding on two of the tranches under the loan facility with RJRT and granted a first priority security interest in favor of the bank in assets previously acquired with the proceeds of those tranches. The September 2008 loan bears interest at a fixed rate of 6.131% per annum and is repayable in equal monthly installments of $11,000 beginning October 1, 2008 and continuing through the maturity date of September 1, 2012. As of December 31, 2010, the outstanding principal balance under the loan facility was $1.8 million. There is no additional borrowing capacity remaining available to us under the loan agreement.
In April 2002, we received a $500,000 loan from the City of Winston-Salem. Under the terms of the loan, there was no interest accrual or payment due until the fifth anniversary of the loan. Following expiration of the five-year grace period in April 2007, the outstanding principal balance of the loan began to bear interest at an annual interest rate of 5% and became payable in 60 equal monthly installments of $9,000. In December 2010, we repaid in full the $135,000 that remained outstanding under the loan.
Cash Flows
| Year ended December 31, |
||||||||||||
| 2010 | 2009 | Change | ||||||||||
| (in thousands) | ||||||||||||
| Net cash provided by (used in) operating activities |
$ | 138,298 | $ | (24,271 | ) | $ | 162,569 | |||||
| Net cash (used in) provided by investing activities |
(62,799 | ) | 9,800 | (72,599 | ) | |||||||
| Net cash provided by financing activities |
6,446 | 47,178 | (40,732 | ) | ||||||||
| Net increase in cash and cash equivalents |
$ | 81,945 | $ | 32,707 | ||||||||
| Year ended December 31, |
||||||||||||
| 2009 | 2008 | Change | ||||||||||
| (in thousands) | ||||||||||||
| Net cash used in operating activities |
$ | (24,271 | ) | $ | (28,261 | ) | $ | 3,990 | ||||
| Net cash provided by (used in) investing activities |
9,800 | (5,519 | ) | 15,319 | ||||||||
| Net cash provided by financing activities |
47,178 | 31,579 | 15,599 | |||||||||
| Net increase (decrease) in cash and cash equivalents |
$ | 32,707 | $ | (2,201 | ) | |||||||
Net cash provided by operating activities for the year ended December 31, 2010 was $138.3 million and net cash used in operating activities for the year ended December 31, 2009 was $24.3 million, a difference of $162.6 million.
For 2010, net cash provided by operating activities was principally the result of our receipt of:
| • | the $200.0 million upfront payment under our TC-5214 agreement with AstraZeneca in January 2010; |
| • | the $11.0 million payment under an amendment to our cognitive disorders agreement with AstraZeneca to modify the terms applicable to TC-5619 in April 2010; |
86
Table of Contents
| • | $1.5 million in payments for research services under our preclinical research collaboration with AstraZeneca, which ended in January 2010; |
| • | the $1.5 million grant under the U.S. government’s Qualifying Therapeutic Discovery Project tax credit program; and |
| • | $1.3 million in interest income. |
These cash inflows were partially offset by:
| • | our payments in January 2010 of $16.0 million to USFRF based on our receipt of the $200.0 million upfront payment under our TC-5214 agreement with AstraZeneca; |
| • | our payment of $1.5 million to Cornerstone Therapeutics Inc. under an exclusive worldwide license agreement in August 2010; and |
| • | aggregate payments of $58.7 million for routine operating activities, including third-party research and development services in connection with clinical-stage product candidates and preclinical programs and personnel and infrastructure costs. |
We expect payments for operating activities for the year ending December 31, 2011 to increase, with the largest component anticipated to result from our obligation under our TC-5214 agreement with AstraZeneca to fund a portion of the costs of the initial development program for TC-5214.
For 2009, net cash used in operating activities was principally the result of aggregate payments of $44.2 million for routine operating activities, including third-party research and development services in connection with clinical-stage product candidates and preclinical programs and personnel and infrastructure costs, and was partially offset by our receipt of:
| • | the $10.0 million payment from AstraZeneca in July 2009; |
| • | $5.5 million in payments for research services under our preclinical research collaboration with AstraZeneca; |
| • | $2.5 million in aggregate payments from GlaxoSmithKline upon achievement of milestone events under our alliance agreement; and |
| • | $1.0 million in interest income. |
Net cash used in operating activities for the year ended December 31, 2009 of $24.3 million decreased by $4.0 million as compared to net cash used in operating activities for the year ended December 31, 2008 of $28.3 million.
For 2008, net cash used in operating activities was principally the result of aggregate payments of $46.3 million made for routine operating activities, including third-party research and development services in connection with clinical-stage product candidates and preclinical programs and personnel and infrastructure costs, and was partially offset by our receipt of:
| • | $11.1 million in payments for research services under our preclinical research collaboration with AstraZeneca; |
| • | $2.7 million in interest income; |
| • | $2.2 million in aggregate payments upon achievement of milestone events under our cognitive disorders agreement with AstraZeneca related to the development of product candidates arising under the preclinical research collaboration; and |
| • | $1.5 million in aggregate payments from GlaxoSmithKline upon achievement of milestone events under our alliance agreement. |
87
Table of Contents
Net cash used in investing activities for the year ended December 31, 2010 was $62.8 million and net cash provided by investing activities for the year ended December 31, 2009 was $9.8 million, a difference of $72.6 million. Net cash provided by investing activities for the year ended December 31, 2009 changed by $15.3 million as compared to net cash used in operating activities of $5.5 million for the year ended December 31, 2008. Cash provided by or used in investing activities primarily reflects the portion of our cash that we allocate to, and the timing of purchases and maturities of, our investments in marketable securities. A transfer of funds from an investment in marketable securities to cash generates cash provided by investing activities, while a transfer of funds from cash or a cash equivalent to investments in marketable securities generates cash used in investing activities. Our net purchases of investments in marketable securities for 2010 were $59.5 million and occurred primarily as a result of our receipt of the upfront payment under our TC-5214 agreement with AstraZeneca. Our net sales of investments in marketable securities for 2009 were $10.0 million. During 2009, we re-allocated substantial funds from certificates of deposit to bank depository accounts and institutional money market funds as the certificates of deposit came due in order to yield more favorable interest rates and provide increased liquidity. Our net purchases of investments in marketable securities for 2008 were $3.5 million. Additionally, we purchased $3.3 million of property and equipment during 2010, an increase of $3.1 million from $200,000 during 2009. The $200,000 of property and equipment purchases during 2009 reflected a decrease of $1.9 million from $2.1 million for 2008. Purchases of property and equipment for 2010 were primarily to expand our internal research and development capacity.
Net cash provided by financing activities for the year ended December 31, 2010 decreased by $40.7 million as compared to the year ended December 31, 2009. The decrease was primarily attributable to net proceeds of $44.4 million in October 2009 from a common stock offering and the receipt in October 2009 of $724,000 from a stockholder for disgorgement of “short-swing” profits under Section 16(b) of the Exchange Act, partially offset by the income tax effect of tax deductions for stock-based compensation in excess of expense recorded for stock options under GAAP of $3.5 million for the year ended 2010 and a decrease in net borrowings under our loan facilities of $1.0 million. Net cash provided by financing activities for the year ended December 31, 2009 increased by $15.6 as compared to the year ended December 31, 2008. Cash provided by financing activities for the year ended December 31, 2008 reflected proceeds of $29.1 million from a common stock offering in January 2008 and net borrowings under our loan facilities of $2.2 million.
Funding Requirements
As of December 31, 2010, we had an accumulated deficit of $218.4 million. We may incur operating losses or require additional capital in future periods as our clinical-stage and preclinical product candidates advance into later-stage development and as we progress our programs, invest in additional product opportunities and grow our business. However, we may generate operating income for any particular reporting period as a result of the recognition into revenue of amounts previously received under our agreements with AstraZeneca and GlaxoSmithKline, including in particular our TC-5214 agreement with AstraZeneca, the timing of milestone events that may be achieved under our agreements with AstraZeneca and the timing of costs incurred related to development of our clinical-stage and preclinical product candidates. Our future capital requirements are difficult to forecast and will depend on many factors, including:
| • | whether and to what extent milestone events are achieved for TC-5214 under our TC-5214 agreement with AstraZeneca and for AZD3480 and AZD1446 under our cognitive disorders agreement with AstraZeneca; |
| • | the progress of, and outcomes from, Phase 3 clinical development of TC-5214 and the amount and timing of development costs for TC-5214 payable by us; |
| • | whether AstraZeneca exercises its right to license TC-5619; |
| • | the scope, progress, duration, results and cost of clinical trials, as well as non-clinical studies and assessments, of our other product candidates; |
| • | the impact of the termination of our alliance agreement with GlaxoSmithKline; |
88
Table of Contents
| • | the extent to which we retain development and commercialization rights or responsibilities for our product candidates that are not subject to our collaborations with AstraZeneca and incur associated development costs, manufacturing costs or costs to establish sales and marketing functions; |
| • | whether we establish strategic alliances, collaborations and licensing or other arrangements on terms favorable to us; |
| • | the costs, timing and outcomes of regulatory reviews or other regulatory actions; |
| • | the number and characteristics of product candidates that we pursue; |
| • | the costs of preparing, filing and prosecuting patent applications and maintaining, enforcing and defending patents and other intellectual property rights; |
| • | the costs of manufacturing-related services for our product candidates in clinical and late preclinical development; |
| • | the rate of technological advancements for the indications that we target; |
| • | the costs to satisfy our obligations under existing and potential future alliances and collaborations; |
| • | the timing, receipt and amount of sales or royalties, if any, from our potential products; and |
| • | the extent and scope of our general and administrative expenses. |
Our existing capital resources may not be sufficient to enable us to fund the completion of the development of any of our product candidates. We currently expect our existing capital resources to be sufficient to fund our operations at least through the end of 2013, without taking into account any amounts that we would be entitled to receive if milestone events are achieved under either of our collaboration agreements with AstraZeneca. However, our operating plan may change as a result of many factors, including those described above, and we may need additional funds sooner than planned to meet operational needs and capital requirements for product development.
To the extent our capital resources are insufficient to meet future capital requirements, we may need to finance future cash needs through alliances, collaborations or licensing or other arrangements, public or private equity or debt offerings or other financings. The global credit and financial markets continue to be negatively impacted by the recessionary environment. This, coupled with other factors, may limit our access to additional equity or debt financing in the future on acceptable terms or at all. Also, additional strategic alliances, collaborations or licensing or other arrangements may not be available on acceptable terms or at all. If adequate funds are not available, we may be required to delay, reduce the scope of or eliminate our research and development programs or obtain funds through arrangements with collaborators or others that may require us to relinquish rights to certain product candidates that we might otherwise seek to develop or commercialize independently. Additionally, any future equity funding may dilute the ownership of our stockholders.
We cannot accurately determine the completion dates and related costs of our research and development programs due to inherent uncertainties in outcomes of clinical trials and regulatory approvals of our product candidates. We cannot be certain that we will be able to successfully complete our research and development projects or establish strategic alliances, collaborations or licensing or other arrangements for our product candidates. Our failure, or the failure of any of our licensees or collaborators, to complete research and development programs for our product candidates could have a material adverse effect on our financial position or results of operations.
To date, inflation has not had a material effect on our business.
89
Table of Contents
Contractual Obligations
The following table summarizes our fixed contractual obligations as of December 31, 2010:
| Payments Due by Period | ||||||||||||||||||||
| Contractual Obligation |
Total | Less Than 1 Year |
1 - 3 Years |
3 - 5 Years |
More Than 5 Years |
|||||||||||||||
| (in thousands) | ||||||||||||||||||||
| Long-term debt obligations |
$ | 3,215 | $ | 1,812 | $ | 1,095 | $ | 308 | $ | — | ||||||||||
| Operating lease obligations |
4,076 | 2,531 | 1,518 | 27 | — | |||||||||||||||
| Purchase obligations |
22,222 | 21,642 | 517 | 49 | 14 | |||||||||||||||
| $ | 29,513 | $ | 25,985 | $ | 3,130 | $ | 384 | $ | 14 | |||||||||||
The amounts of license fee obligations for all periods reflected in the above table exclude contingent license and royalty payments and other contingent payments payable upon achievement of specified development, regulatory, commercial or other milestone events under our license agreements with USFRF, Yale University, UKRF or Cornerstone Therapeutics Inc. The amounts of purchase obligations reflected in the above table include obligations to purchase drug product or drug substance, to compensate clinical investigators, clinical trial sites and contract research organizations contingent on the performance of services in connection with clinical trials and to compensate contract research organizations contingent on the performance of non-clinical research and development services, but do not include our share of the anticipated development costs for TC-5214. The amounts of purchase obligations also include contractual obligations for insurance and other general and administrative expenses. The amounts of long-term debt obligations for all periods reflected in the above table include principal and interest payments on loan facilities outstanding at December 31, 2010 and exclude payments on amounts available under loan facilities at December 31, 2010.
Off-Balance Sheet Arrangements
We do not have any off-balance sheet arrangements.
Recent Accounting Pronouncements
In April 2010, the Financial Accounting Standards Board, or FASB, issued Accounting Standards Update No. 2010-17, Milestone Method of Revenue Recognition, or ASU 2010-17. ASU 2010-17 defines a milestone event and permits an entity to make an accounting policy election to recognize a payment that is contingent upon achievement of a substantive milestone in its entirety in the period in which the milestone is achieved. ASU 2010-17 is effective for fiscal years beginning on or after June 15, 2010, and for interim periods within those years, and may be applied prospectively to milestones achieved after the adoption date or retrospectively for all periods presented. Early adoption is permitted. We do not expect ASU 2010-17 to have a material impact on our financial results.
In October 2009, the FASB issued Accounting Standards Update No. 2009-13, Revenue Recognition (Topic 605): Multiple-Deliverable Revenue Arrangements—a consensus of the FASB Emerging Issues Task Force, or ASU 2009-13. ASU 2009-13 addresses the units of accounting for arrangements involving multiple deliverables and how arrangement consideration should be allocated to the separate units of accounting, when applicable. ASU 2009-13 eliminates the criterion in prior accounting guidance that objective and reliable evidence of the fair value of any undelivered items must exist for the delivered items to be considered a separate unit or separate units of accounting. ASU 2009-13 is effective for financial statements issued for fiscal years beginning after June 15, 2010 and can be applied either prospectively or retrospectively for all periods presented. We do not plan to apply ASU 2009-13 retrospectively and, therefore, do not expect ASU 2009-13 to impact the accounting treatment for our current strategic alliance and collaboration agreements. The impact of ASU 2009-13 on the accounting treatment for any future strategic alliance or collaboration agreement, or for any amendment to a current agreement, is not yet determinable.
90
Table of Contents
| Item 7A. | Quantitative and Qualitative Disclosures About Market Risk. |
The primary objective of our investment activities is to preserve our capital and meet our liquidity needs to fund operations. We also seek to generate competitive rates of return from our investments without assuming significant risk. To achieve our objectives, we maintain a portfolio of cash equivalents and investments in a variety of securities that are of high credit quality based on ratings from commonly relied upon rating agencies. As of December 31, 2010, we had cash, cash equivalents and investments in marketable securities of $252.5 million. Our investments may be subject to interest rate risk and could fall in value if market interest rates increase. However, because our cash equivalents are invested in accounts with market interest rates and are short term in nature and our investments in marketable securities are traded in active markets, we believe that our exposure to interest rate risk is not significant and estimate that an immediate and uniform 10% increase in market interest rates from levels as of December 31, 2010 would not have a material impact on the total fair value of our portfolio.
We contract for the conduct of some of our clinical trials and other research and development and manufacturing activities with contract research organizations, clinical trial sites and contract manufacturers in Europe and India. We may be subject to exposure to fluctuations in foreign currency exchange rates in connection with these agreements. If the average Euro/U.S. dollar or Indian Rupee/U.S. dollar exchange rate were to strengthen or weaken by 10% against the corresponding exchange rate as of December 31, 2010, we estimate that the impact on our financial position, results of operations and cash flows would not be material. We do not hedge our foreign currency exposures.
We have not used derivative financial instruments for speculation or trading purposes.
91
Table of Contents
| Item 8. | Financial Statements and Supplementary Data. |
INDEX TO THE FINANCIAL STATEMENTS
TARGACEPT, INC.
| 93 | ||||
| 94 | ||||
| 95 | ||||
| 96 | ||||
| 97 | ||||
| 98 | ||||
92
Table of Contents
Report of Independent Registered Public Accounting Firm
The Board of Directors and Stockholders of
Targacept, Inc.
We have audited the accompanying balance sheets of Targacept, Inc. as of December 31, 2010 and 2009, and the related statements of operations, stockholders’ equity and cash flows for each of the three years in the period ended December 31, 2010. These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on these financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements. An audit also includes assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the financial statements referred to above present fairly, in all material respects, the financial position of Targacept, Inc. at December 31, 2010 and 2009, and the results of its operations and its cash flows for each of the three years in the period ended December 31, 2010, in conformity with U.S. generally accepted accounting principles.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), Targacept, Inc.’s internal control over financial reporting as of December 31, 2010, based on criteria established in Internal Control-Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission and our report dated March 11, 2011 expressed an unqualified opinion thereon.
/s/ Ernst & Young LLP
Raleigh, North Carolina
March 11, 2011
93
Table of Contents
BALANCE SHEETS
(in thousands, except share and par value amounts)
| December 31, | ||||||||
| 2010 | 2009 | |||||||
| ASSETS |
||||||||
| Current assets: |
||||||||
| Cash and cash equivalents |
$ | 165,854 | $ | 83,909 | ||||
| Investments in marketable securities—short term |
48,168 | 27,157 | ||||||
| Receivables from collaborations |
838 | 201,801 | ||||||
| Prepaid expenses |
3,219 | 1,562 | ||||||
| Total current assets |
218,079 | 314,429 | ||||||
| Investments in marketable securities—long term |
38,487 | — | ||||||
| Property and equipment, net |
6,072 | 4,783 | ||||||
| Intangible assets |
149 | 167 | ||||||
| Total assets |
$ | 262,787 | $ | 319,379 | ||||
| LIABILITIES AND STOCKHOLDERS’ EQUITY |
||||||||
| Current liabilities: |
||||||||
| Accounts payable |
$ | 4,721 | $ | 1,275 | ||||
| License fee payable |
— | 16,000 | ||||||
| Accrued expenses |
10,516 | 5,267 | ||||||
| Current portion of long-term debt |
1,710 | 1,442 | ||||||
| Current portion of deferred revenue |
81,710 | 77,243 | ||||||
| Total current liabilities |
98,657 | 101,227 | ||||||
| Long-term debt, net of current portion |
1,349 | 1,966 | ||||||
| Deferred revenue, net of current portion |
70,934 | 147,195 | ||||||
| Total liabilities |
170,940 | 250,388 | ||||||
| Commitments and contingencies |
||||||||
| Stockholders’ equity: |
||||||||
| Common stock, $0.001 par value, 100,000,000 shares authorized ; 28,870,691 and 28,226,829 shares issued and outstanding at December 31, 2010 and December 31 2009, respectively |
29 | 28 | ||||||
| Preferred stock, $0.001 par value, 5,000,000 shares authorized; 0 shares issued and outstanding at December 31, 2010 and 2009 |
— | — | ||||||
| Capital in excess of par value |
309,994 | 298,263 | ||||||
| Accumulated other comprehensive income |
225 | — | ||||||
| Accumulated deficit |
(218,401 | ) | (229,300 | ) | ||||
| Total stockholders’ equity |
91,847 | 68,991 | ||||||
| Total liabilities and stockholders’ equity |
$ | 262,787 | $ | 319,379 | ||||
See accompanying notes.
94
Table of Contents
STATEMENTS OF OPERATIONS
(in thousands, except share and per share amounts)
| Year ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Operating revenues: |
||||||||||||
| Milestones and license fees from collaborations |
$ | 83,380 | $ | 18,934 | $ | 10,179 | ||||||
| Collaboration research and development |
— | 5,246 | 8,967 | |||||||||
| Product sales, net |
— | 473 | 718 | |||||||||
| Grant revenue |
2,333 | 409 | 221 | |||||||||
| Net operating revenues |
85,713 | 25,062 | 20,085 | |||||||||
| Operating expenses: |
||||||||||||
| Research and development (including stock-based compensation of $2,768, $1,353 and $1,130 in 2010, 2009 and 2008, respectively) |
64,546 | 40,179 | 40,981 | |||||||||
| General and administrative (including stock-based compensation of $2,169, $1,101 and $935 in 2010, 2009 and 2008, respectively) |
8,052 | 8,167 | 6,499 | |||||||||
| License fees |
— | 16,350 | — | |||||||||
| Cost of product sales |
— | 691 | 749 | |||||||||
| Total operating expenses |
72,598 | 65,387 | 48,229 | |||||||||
| Income (loss) from operations |
13,115 | (40,325 | ) | (28,144 | ) | |||||||
| Other income (expense): |
||||||||||||
| Interest income |
1,463 | 1,050 | 2,734 | |||||||||
| Interest expense |
(153 | ) | (217 | ) | (251 | ) | ||||||
| Total other income (expense) |
1,310 | 833 | 2,483 | |||||||||
| Income (loss) before income taxes |
14,425 | (39,492 | ) | (25,661 | ) | |||||||
| Income tax (expense) benefit |
(3,526 | ) | 88 | — | ||||||||
| Net income (loss) |
$ | 10,899 | $ | (39,404 | ) | $ | (25,661 | ) | ||||
| Basic net income (loss) per share |
$ | 0.38 | $ | (1.54 | ) | $ | (1.04 | ) | ||||
| Diluted net income (loss) per share |
$ | 0.36 | $ | (1.54 | ) | $ | (1.04 | ) | ||||
| Weighted average common shares outstanding—basic |
28,543,408 | 25,636,419 | 24,664,169 | |||||||||
| Weighted average common shares outstanding—diluted |
30,150,324 | 25,636,419 | 24,664,169 | |||||||||
See accompanying notes.
95
Table of Contents
STATEMENTS OF STOCKHOLDERS’ EQUITY
(in thousands, except share amounts)
| Common Stock | Capital in Excess of Par Value |
Accumulated Other Comprehensive Income |
Accumulated Deficit |
Total Stockholders’ Equity |
||||||||||||||||||||
| Shares | Amount | |||||||||||||||||||||||
| Balances at December 31, 2007 |
20,503,419 | $ | 20 | $ | 215,799 | $ | — | $ | (164,235 | ) | $ | 51,584 | ||||||||||||
| Issuance of common stock related to exercise of stock options |
90,954 | — | 271 | — | — | 271 | ||||||||||||||||||
| Stock-based compensation |
— | — | 2,065 | — | — | 2,065 | ||||||||||||||||||
| Net proceeds from public stock offering |
4,370,000 | 5 | 29,109 | — | — | 29,114 | ||||||||||||||||||
| Net loss and comprehensive loss |
— | — | — | — | (25,661 | ) | (25,661 | ) | ||||||||||||||||
| Balances at December 31, 2008 |
24,964,373 | 25 | 247,244 | — | (189,896 | ) | 57,373 | |||||||||||||||||
| Issuance of common stock related to exercise of stock options |
1,062,456 | 1 | 3,353 | — | — | 3,354 | ||||||||||||||||||
| Stock-based compensation |
— | — | 2,454 | — | — | 2,454 | ||||||||||||||||||
| Net proceeds from public stock offering |
2,200,000 | 2 | 44,447 | — | — | 44,449 | ||||||||||||||||||
| Stockholder short swing profit payment |
— | — | 724 | — | — | 724 | ||||||||||||||||||
| Excess tax deductions from stock-based compensation |
— | — | 41 | — | — | 41 | ||||||||||||||||||
| Net loss and comprehensive loss |
— | — | — | — | (39,404 | ) | (39,404 | ) | ||||||||||||||||
| Balances at December 31, 2009 |
28,226,829 | 28 | 298,263 | — | (229,300 | ) | 68,991 | |||||||||||||||||
| Issuance of common stock related to exercise of stock options |
643,862 | 1 | 3,291 | — | — | 3,292 | ||||||||||||||||||
| Stock-based compensation |
— | — | 4,937 | — | — | 4,937 | ||||||||||||||||||
| Excess tax deductions from stock-based compensation |
— | — | 3,503 | — | — | 3,503 | ||||||||||||||||||
| Net change in unrealized holding gain on available for sale marketable securities |
— | — | — | 225 | — | 225 | ||||||||||||||||||
| Net income |
— | — | — | — | 10,899 | 10,899 | ||||||||||||||||||
| Comprehensive income |
— | — | — | — | — | 11,124 | ||||||||||||||||||
| Balances at December 31, 2010 |
28,870,691 | $ | 29 | $ | 309,994 | $ | 225 | $ | (218,401 | ) | $ | 91,847 | ||||||||||||
See accompanying notes.
96
Table of Contents
STATEMENTS OF CASH FLOWS
(in thousands)
| Year ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Operating activities |
||||||||||||
| Net income (loss) |
$ | 10,899 | $ | (39,404 | ) | $ | (25,661 | ) | ||||
| Adjustments to reconcile net income (loss) to net cash provided by (used in) operating activities: |
||||||||||||
| Recognition of deferred revenue |
(83,767 | ) | (6,383 | ) | (6,479 | ) | ||||||
| Amortization of premium on marketable securities, net |
416 | — | — | |||||||||
| Depreciation and amortization |
1,997 | 1,835 | 1,800 | |||||||||
| Stock-based compensation expense |
4,937 | 2,454 | 2,065 | |||||||||
| Impairment of intangible asset |
— | — | 220 | |||||||||
| Excess tax benefits from stock-based compensation |
(3,503 | ) | (41 | ) | — | |||||||
| Changes in operating assets and liabilities: |
||||||||||||
| Receivables from collaborations(1) |
200,963 | 272 | 2,125 | |||||||||
| Prepaid expenses, inventories and accrued interest receivable |
(1,815 | ) | (28 | ) | (413 | ) | ||||||
| Accounts payable, license fees payable and accrued expenses |
(3,802 | ) | 16,551 | (1,918 | ) | |||||||
| Deferred revenue(1) |
11,973 | 473 | — | |||||||||
| Net cash provided by (used in) operating activities |
138,298 | (24,271 | ) | (28,261 | ) | |||||||
| Investing activities |
||||||||||||
| Purchase of investments in marketable securities |
(144,012 | ) | (31,000 | ) | (104,800 | ) | ||||||
| Proceeds from sale of investments in marketable securities |
84,481 | 41,000 | 101,334 | |||||||||
| Purchase of property and equipment |
(3,311 | ) | (200 | ) | (2,053 | ) | ||||||
| Proceeds from sale of property and equipment |
43 | — | — | |||||||||
| Net cash (used in) provided by investing activities |
(62,799 | ) | 9,800 | (5,519 | ) | |||||||
| Financing activities |
||||||||||||
| Proceeds from issuance of long-term debt |
1,228 | — | 5,300 | |||||||||
| Principal payments on long-term debt |
(1,577 | ) | (1,390 | ) | (3,106 | ) | ||||||
| Proceeds from issuance of common stock, net |
3,292 | 48,527 | 29,385 | |||||||||
| Excess tax benefits from stock-based compensation |
3,503 | 41 | — | |||||||||
| Net cash provided by financing activities |
6,446 | 47,178 | 31,579 | |||||||||
| Net increase (decrease) in cash and cash equivalents |
81,945 | 32,707 | (2,201 | ) | ||||||||
| Cash and cash equivalents at beginning of year |
83,909 | 51,202 | 53,403 | |||||||||
| Cash and cash equivalents at end of year |
$ | 165,854 | $ | 83,909 | $ | 51,202 | ||||||
| (1) | 2009 amount does not include a $200,000 non-cash item related to the Company’s December 2009 collaboration and license agreement with AstraZeneca AB (see Note 12). |
See accompanying notes.
97
Table of Contents
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2010
1. The Company and Nature of Operations
Targacept, Inc., or the Company, is a Delaware corporation formed on March 7, 1997. The Company is a biopharmaceutical company engaged in the design, discovery and development of novel NNR Therapeutics™ for the treatment of diseases and disorders of the nervous system. The Company’s NNR Therapeutics selectively target neuronal nicotinic receptors, which it refers to as NNRs. Its facilities are located in Winston-Salem, North Carolina.
2. Summary of Significant Accounting Policies
Use of Estimates and Reclassifications
The preparation of financial statements in conformity with U.S. generally accepted accounting principles, or GAAP, requires management to make estimates and assumptions that affect the amounts of assets, liabilities, revenues and expenses reported in the financial statements and accompanying notes. Actual results could differ from these estimates.
Certain reclassifications have been made to the financial statements for the years ended December 31, 2009 and 2008 to conform to the presentation in the financial statements for the year ended December 31, 2010. These reclassifications had no impact on previously reported net loss or stockholders’ equity.
Cash and Cash Equivalents
The Company considers cash equivalents to be those investments which are highly liquid, readily convertible to cash and mature within three months from the date of purchase.
Investments in Marketable Securities
Consistent with its investment policy, the Company invests its cash expected to fund its short-term liquidity requirements with prominent financial institutions in bank depository accounts and institutional money market funds and the Company invests the remainder of its cash in U.S. Treasury notes and bonds, U.S. and state agency-backed certificates and corporate debt securities that are rated at least A quality or equivalent and certificates of deposit.
The Company determines the appropriate classification of marketable securities at the time of purchase and reevaluates the classification as of each balance sheet date. All marketable securities owned during 2010 and 2009 were classified as available for sale. The cost of securities sold is based on the specific identification method. Investments in marketable securities are recorded as of each balance sheet date at fair value, with unrealized gains and, to the extent deemed temporary, unrealized losses included in stockholders’ equity. Interest and dividend income on investments in marketable securities, accretion of discounts and amortization of premiums and realized gains and losses are included in interest income in the statement of operations.
An investment in marketable securities is considered to be impaired when a decline in fair value below its cost basis is determined to be other than temporary. The Company evaluates whether a decline in fair value of an investment in marketable securities below its cost basis is other than temporary using available evidence. In the event that the cost basis of the investment exceeds its fair value, the Company evaluates, among other factors, the amount and duration of the period that the fair value is less than the cost basis, the financial health of and business outlook for the issuer, including industry and sector performance, and operational and financing cash flow factors, overall market conditions and trends, the Company’s intent to sell the investment and whether it is
98
Table of Contents
TARGACEPT, INC.
NOTES TO FINANCIAL STATEMENTS—(continued)
DECEMBER 31, 2010
2. Summary of Significant Accounting Policies—(continued)
more likely than not the Company would be required to sell the investment before its anticipated recovery. If a decline in fair value is determined to be other than temporary, the Company records an impairment charge in the statement of operations and establishes a new cost basis in the investment.
Receivables from Collaborations
Substantially all of the Company’s collaboration revenue is related to the collaboration and alliance agreements discussed in Note 12. A substantial majority of the Company’s receivables from collaborations at December 31, 2010 and 2009 are related to the Company’s collaboration agreement with AstraZeneca AB entered into in December 2009.
During 2010, 2009, and 2008, the Company recognized revenue of $83,380,000, $24,180,000, and $19,146,000, respectively, or 97%, 96% and 95% of net operating revenues, respectively, from the collaboration and alliance agreements discussed in Note 12.
Product Sales
Effective as of September 30, 2009, the Company discontinued commercialization of its only marketed product, Inversine. Cost of product sales for each of the years ended December 31, 2009 and 2008 includes materials and manufacturing costs, applied by the weighted average method, FDA fees and other fees associated with the manufacture and selling of Inversine. As a result of the discontinuation of Inversine, the Company recorded aggregate charges of $77,000 related to the impairment of its remaining raw materials and finished goods inventory to cost of product sales for the year ended December 31, 2009. The discontinuation of Inversine did not have a material impact on the Company’s cash flows or results of operations for any of the periods presented.
During 2009 and 2008, cost of product sales included of shipping and handling costs of $183,000 and $204,000, respectively.
Long-lived Assets
Property and equipment consists primarily of laboratory equipment, office furniture and fixtures and leasehold improvements and is recorded at cost. Depreciation is computed using the straight-line method over the estimated useful lives of the assets ranging from 3-10 years. Laboratory equipment is typically depreciated over 3-5 years, office furniture and fixtures are typically depreciated over 5-10 years, and leasehold improvements are typically amortized over the lesser of the asset life or the lease term.
The Company capitalizes the costs of intellectual property acquired or licensed from external sources as intangible assets if, at the time of acquisition, the intellectual property has reached technological feasibility. Intellectual property acquired or licensed from external sources that has not reached technological feasibility at the time of acquisition or that has no expected future use is charged to research and development expense as incurred. The Company records all other charges related to the filing, prosecution and maintenance of patents to expense as incurred.
The Company assesses the net realizable value of its long-lived assets and evaluates these assets for impairment whenever events or changes in business circumstances indicate that the carrying amount of an asset
99
Table of Contents
TARGACEPT, INC.
NOTES TO FINANCIAL STATEMENTS—(continued)
DECEMBER 31, 2010
2. Summary of Significant Accounting Policies—(continued)
may not be recoverable. An impairment charge would be recognized when estimated undiscounted future cash flows expected to result from the use of the asset and its eventual disposition are less than its carrying amount. An impairment charge, if recognized, would be based on the excess of the carrying value of the impaired asset over its estimated fair value.
Research and Development Expense
Research and development costs are expensed as incurred and include direct costs incurred to third parties related to the Company’s clinical and preclinical product candidates, salaries of, and stock-based compensation for, personnel involved in research and development activities, contractor fees, administrative expenses and allocations of research-related overhead costs. Administrative expenses and research-related overhead costs included in research and development expense consist of allocations of facility and equipment lease charges, depreciation and amortization of assets, and insurance, legal and supply costs that are directly related to research and development activities. The Company directly reduces research and development expenses for amounts reimbursed pursuant to the cost-sharing agreements described in Note 12.
Accrued Expenses
The Company records accruals based on estimates of the services received, efforts expended and amounts owed pursuant to contracts with clinical trial sites, contract research organizations and other service providers. In the normal course of business, the Company contracts with third parties to perform various clinical trial and other research and development activities in the ongoing development of potential products. The financial terms of these agreements are subject to negotiation, vary from contract to contract and may result in uneven payment flows. Payments under these agreements depend on the performance of services or the achievement of specified events, such as the production of drug substance or drug product, the recruitment of clinical trial subjects, the completion of portions of a non-clinical study or clinical trial or similar conditions. The objective of the Company’s accrual policy is to match the recording of expenses in its financial statements to the actual services received and efforts expended. As such, expense accruals are recognized based on the Company’s estimate of the degree of completion of the event or events specified in a particular contract as giving rise to a payment.
Credit Risk
Financial instruments that potentially subject the Company to credit risk consist principally of cash, investments in marketable securities and receivables from collaborations. The Company has established guidelines for investment of its cash that are designed to emphasize safety, liquidity and preservation of capital. The Company places its cash and cash equivalents with prominent financial institutions. At December 31, 2010 and 2009, the Company had deposits in excess of federally insured limits of $160,932,000 and $110,159,000, respectively.
Revenue Recognition
The Company uses the revenue recognition guidance established by Financial Accounting Standards Board, or FASB, Accounting Standards Codification, or ASC, Topic 605, Revenue Recognition, or ASC 605. In determining the accounting for collaboration and alliance agreements, the Company follows the provisions of ASC 605, Subtopic 25, Multiple Element Arrangements, or ASC 605-25. ASC 605-25 provides guidance on whether an arrangement that involves multiple revenue-generating activities or deliverables should be divided
100
Table of Contents
TARGACEPT, INC.
NOTES TO FINANCIAL STATEMENTS—(continued)
DECEMBER 31, 2010
2. Summary of Significant Accounting Policies—(continued)
into separate units of accounting for revenue recognition purposes and, if division is required, how the arrangement consideration should be allocated among the separate units of accounting. If the arrangement constitutes separate units of accounting according to the separation criteria of ASC 605-25, a revenue recognition policy must be determined for each unit. If the arrangement constitutes a single unit of accounting, the revenue recognition policy must be determined for the entire arrangement.
Collaboration research and development revenue is earned and recognized as research is performed and related expenses are incurred. Non-refundable upfront fees, which may include, for example, an initial payment upon effectiveness of the contractual relationship, payment representing a common stock purchase premium or payment to secure a right for a future license, are recorded as deferred revenue and recognized into revenue as milestones and license fees from collaborations on a straight-line basis over the estimated period of the Company’s substantive performance obligations. If the Company does not have substantive performance obligations, it recognizes non-refundable upfront fees into revenue over the estimated development period for the applicable licensed product candidate(s).
Revenue for non-refundable payments based on the achievement of collaboration milestones is recognized as revenue when the milestone events are achieved if all of the following conditions are met: (1) achievement of the milestone event was not reasonably assured at the inception of the arrangement; (2) substantive effort is involved to achieve the milestone event; and (3) the amount of the milestone payment appears reasonable in relation to the effort expended, the other milestone payments in the arrangement and the related risk associated with achievement of the milestone event. If any of these conditions is not met, the milestone payment is deferred and recognized on a straight-line basis over a period determined as discussed above.
Research and development costs that are reimbursable under collaboration agreements are recorded in accordance with ASC 605, Subtopic 45, Principal Agent Considerations. Amounts reimbursed under a cost sharing arrangement are reflected as a reduction of research and development expense.
Product sales revenue is recognized when goods are shipped, at which point title has passed, net of allowances for returns and discounts. Grant payments received prior to the Company’s performance of work required by the terms of the award are recorded as deferred revenue and recognized as grant revenue as the Company performs the work and incurs reimbursable costs in accordance with the objectives of the award.
Income Taxes
The Company uses the liability method in accounting for income taxes as required by ASC Topic 740, Income Taxes, or ASC 740. Under ASC 740, deferred tax assets and liabilities are recorded for operating loss and tax credit carryforwards and for the future tax consequences attributable to the differences between the financial statement carrying amounts of existing assets and liabilities and their respective tax bases. Deferred tax assets and liabilities are measured using enacted tax rates expected to apply to taxable income in the years in which those temporary differences are expected to be recovered or settled. The effect of a change in tax rates on deferred tax assets and liabilities is recognized in the results of operations in the period that includes the enactment date. A valuation allowance is recorded to reduce the carrying amounts of deferred tax assets unless it is more likely than not that these assets will be realized. ASC 740 prescribes a recognition threshold and measurement attribute for the financial statement recognition and measurement of a tax position taken or expected to be taken in a tax return. ASC 740 also provides guidance on de-recognition, classification, interest
101
Table of Contents
TARGACEPT, INC.
NOTES TO FINANCIAL STATEMENTS—(continued)
DECEMBER 31, 2010
2. Summary of Significant Accounting Policies—(continued)
and penalties, accounting in interim periods, disclosures and transition. The Company’s policy is to classify any interest recognized in accordance with ASC 740 as interest expense and to classify any penalties recognized in accordance with ASC 740 as an expense other than income tax expense.
Net Income (Loss) Per Share
The Company computes net income (loss) per share in accordance with ASC Topic 260, Earnings Per Share, or ASC 260. Under the provisions of ASC 260, basic net income (loss) per share, or Basic EPS, is computed by dividing net income (loss) by the weighted average number of common shares outstanding. Diluted net income (loss) per share, or Diluted EPS, is computed by dividing net income (loss) by the weighted average number of common shares and dilutive common share equivalents outstanding. The calculations of Basic EPS and Diluted EPS are set forth in the table below (in thousands, except share and per share amounts):
| Year Ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Basic: |
||||||||||||
| Net income (loss) |
$ | 10,899 | $ | (39,404 | ) | $ | (25,661 | ) | ||||
| Weighted average common shares—basic |
28,543,408 | 25,636,419 | 24,664,169 | |||||||||
| Basic EPS |
$ | 0.38 | $ | (1.54 | ) | $ | (1.04 | ) | ||||
| Diluted: |
||||||||||||
| Net income (loss) |
$ | 10,899 | $ | (39,404 | ) | $ | (25,661 | ) | ||||
| Weighted average common shares—basic |
28,543,408 | 25,636,419 | 24,664,169 | |||||||||
| Common share equivalents |
1,606,916 | — | — | |||||||||
| Weighted average common shares—diluted |
30,150,324 | 25,636,419 | 24,664,169 | |||||||||
| Diluted EPS |
$ | 0.36 | $ | (1.54 | ) | $ | (1.04 | ) | ||||
Common share equivalents consist of the incremental common shares issuable upon the exercise of stock options. For each of the years ended December 31, 2009 and 2008, the Company excluded all common share equivalents from the calculation of Diluted EPS because their effect was anti-dilutive. As a result, Diluted EPS is identical to Basic EPS for those years. For each of the years ended December 31, 2009 and 2008, shares subject to outstanding stock options may have been included in the calculation of common share equivalents using the treasury stock method if the Company had been in a net income position. Shares subject to outstanding stock options that were anti-dilutive and consequently not included in the calculation of common share equivalents totaled 850,683, 3,648,268, and 3,123,249 for the years ended December 31, 2010, 2009, and 2008, respectively, calculated on a weighted-average basis.
Public Offerings of Common Stock
On January 23, 2008, the Company completed a public offering of 4,370,000 shares of its common stock at a price of $7.07 per share. The Company’s net proceeds from the offering, after deducting underwriters’ discounts and commissions and offering expenses payable by the Company, were $29,114,000.
102
Table of Contents
TARGACEPT, INC.
NOTES TO FINANCIAL STATEMENTS—(continued)
DECEMBER 31, 2010
2. Summary of Significant Accounting Policies—(continued)
On October 13, 2009, the Company completed a public offering of 2,200,000 shares of its common stock. The offering was priced to the public at $21.00 per share. The Company’s net proceeds from the offering, after deducting underwriters’ discounts and commissions and offering expenses payable by the Company, were $44,449,000.
In October 2009, the Company was notified by one of its stockholders that the stockholder had generated short swing profits under the provisions of Section 16(b) of the Exchange Act on its purchases and sales of shares of the Company’s common stock. The amount of realized profit under Section 16(b) was calculated to be $724,000, and the stockholder made a payment to the Company in that amount later in October.
Stock-Based Compensation
The Company has two stock-based incentive plans, the 2000 Equity Incentive Plan of Targacept, Inc., as amended and restated through March 15, 2006, or the 2000 Plan, and the Targacept, Inc. 2006 Stock Incentive Plan, as amended and restated through November 28, 2007 and further amended effective June 10, 2009, or the 2006 Plan. The 2000 Plan and the 2006 Plan, or the Plans, are described more fully in Note 9.
The Company records stock-based compensation under the fair value recognition provisions of ASC Topic 718, Compensation—Stock Compensation, or ASC 718. Under ASC 718, the Company calculates the fair value of each option grant using the Black-Scholes-Merton valuation formula. The fair value of each grant is recorded as expense on a straight-line basis over the option’s vesting period.
ASC 718 also requires the benefits of tax deductions in excess of recognized compensation expense to be reported as a financing cash flow, rather than as an operating cash flow. This requirement reduces net operating cash flows and increases net financing cash flows for periods after adoption. The Company recognized $3,503,000 and $41,000 in excess tax deductions for the years ended December 31, 2010 and 2009, respectively. The Company cannot estimate the future effect of excess tax deductions or shortfalls on cash flows because they depend on, among other things, when employees exercise stock options and the tax deductions available to the Company at those times. No financing or operating cash flows have been recognized in periods prior to 2009 for excess tax deductions because of cumulative net operating losses generated since inception and because the related deferred tax assets are offset by a valuation allowance.
Non-refundable Advance Payments
The Company defers and capitalizes non-refundable advance payments for goods or services to be received in the future for use in research and development activities. The Company then charges the advance payments to expense ratably as the goods are delivered or the services are rendered in accordance with ASC Subtopic 730-20, Research and Development Arrangements, or ASC 730-20. If the Company’s expectations change such that it does not expect it will need the goods to be delivered or the services to be rendered, it will charge the remaining balance of capitalized non-refundable advance payments to expense.
Fair Value
The carrying amounts of cash and cash equivalents, investments in marketable securities, receivables from collaborations, accounts payable and accrued expenses are considered to be representative of their respective fair
103
Table of Contents
TARGACEPT, INC.
NOTES TO FINANCIAL STATEMENTS—(continued)
DECEMBER 31, 2010
2. Summary of Significant Accounting Policies—(continued)
values due to their short-term natures and, in the case of investments in marketable securities, their market interest rates. Likewise, the carrying amounts of the Company’s long-term debts are considered to be representative of their fair value due to their respective market interest rates.
The Company follows ASC Topic 820, Fair Value Measurements and Disclosures, or ASC 820, for application to financial assets. ASC 820 defines fair value, provides a consistent framework for measuring fair value under GAAP and requires fair value financial statement disclosures. ASC 820 applies only to measurement and disclosure of financial assets that are required or permitted to be measured and reported at fair value under other ASC topics (except for standards that relate to share-based payments such as ASC Topic 718, Compensation—Stock Compensation).
The valuation techniques of ASC 820 are based on both observable and unobservable inputs. Observable inputs reflect readily obtainable data from independent sources, and unobservable inputs reflect the Company’s market assumptions. ASC 820 classifies these inputs into the following hierarchy:
Level 1 Inputs—quoted prices (unadjusted) in active markets for identical assets that the reporting entity has the ability to access at the measurement date;
Level 2 Inputs—inputs other than quoted prices included within Level 1 that are observable for the asset, either directly or indirectly; and
Level 3 Inputs—unobservable inputs for the assets.
The following tables present the Company’s investments in marketable securities that are measured at fair value on a recurring basis as of December 31, 2010 and 2009, respectively:
| December 31, 2010 |
Quoted Prices in Active Markets (Level 1) |
Significant Other Observable Inputs (Level 2) |
Significant Unobservable Inputs (Level 3) |
|||||||||
| (in thousands) | ||||||||||||
| U.S. Treasury and U.S. government and state government agency-backed securities |
$ | 47,463 | $ | — | $ | — | ||||||
| Corporate debt securities |
41,874 | — | — | |||||||||
| Certificates of deposit |
13,000 | — | — | |||||||||
| Accrued interest |
314 | — | — | |||||||||
| Total cash equivalents and marketable securities |
$ | 102,651 | $ | — | $ | — | ||||||
| December 31, 2009 |
Quoted Prices in Active Markets (Level 1) |
Significant Other Observable Inputs (Level 2) |
Significant Unobservable Inputs (Level 3) |
|||||||||
| (in thousands) | ||||||||||||
| Certificates of deposit |
$ | 27,000 | $ | — | $ | — | ||||||
| Accrued interest |
157 | — | — | |||||||||
| Total cash equivalents and marketable securities |
$ | 27,157 | $ | — | $ | — | ||||||
104
Table of Contents
TARGACEPT, INC.
NOTES TO FINANCIAL STATEMENTS—(continued)
DECEMBER 31, 2010
2. Summary of Significant Accounting Policies—(continued)
The Company valued non-financial assets as of December 31, 2008, such as intangible assets measured at fair value, for an impairment assessment using other accounting standards in accordance with Section 15, Scope and Scope Exceptions, of ASC 820, Subtopic 10, Overall (see Note 5).
Comprehensive Income (Loss)
Comprehensive income (loss) is comprised of net income (loss) and net other comprehensive income. Net other comprehensive income includes unrealized gain and loss on the Company’s available-for-sale securities, which are excluded from net income (loss). The following is a reconciliation of net income (loss) to comprehensive income (loss) for the years presented.
| Year Ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| (in thousands) | ||||||||||||
| Net income (loss) |
$ | 10,899 | $ | (39,404 | ) | $ | (25,661 | ) | ||||
| Unrealized gain on marketable securities, net |
225 | — | — | |||||||||
| Comprehensive income (loss) |
$ | 11,124 | $ | (39,404 | ) | $ | (25,661 | ) | ||||
Recent Accounting Pronouncements
In April 2010, the FASB issued Accounting Standards Update No. 2010-17, Milestone Method of Revenue Recognition, or ASU 2010-17. ASU 2010-17 defines a milestone event and permits an entity to make an accounting policy election to recognize a payment that is contingent upon achievement of a substantive milestone in its entirety in the period in which the milestone is achieved. ASU 2010-17 is effective for fiscal years beginning on or after June 15, 2010, and for interim periods within those years, and may be applied prospectively to milestones achieved after the adoption date or retrospectively for all periods presented. Early adoption is permitted. The Company does not expect ASU 2010-17 to have a material impact on its financial results.
In October 2009, the FASB issued Accounting Standards Update No. 2009-13, Revenue Recognition (Topic 605): Multiple-Deliverable Revenue Arrangements—a consensus of the FASB Emerging Issues Task Force, or ASU 2009-13. ASU 2009-13 addresses the units of accounting for arrangements involving multiple deliverables and how arrangement consideration should be allocated to the separate units of accounting, when applicable. ASU 2009-13 eliminates the criterion in prior accounting guidance that objective and reliable evidence of the fair value of any undelivered items must exist for the delivered items to be considered a separate unit or separate units of accounting. ASU 2009-13 is effective for financial statements issued for fiscal years beginning after June 15, 2010 and can be applied either prospectively or retrospectively for all periods presented. The Company does not plan to apply ASU 2009-13 retrospectively and, therefore, does not expect ASU 2009-13 to impact the accounting treatment for its current strategic alliance and collaboration agreements. The impact of ASU 2009-13 on the accounting treatment for any future strategic alliance or collaboration agreement, or for any amendment to a current agreement, is not yet determinable.
105
Table of Contents
TARGACEPT, INC.
NOTES TO FINANCIAL STATEMENTS—(continued)
DECEMBER 31, 2010
3. Investments in Marketable Securities
The following is a reconciliation of amortized cost to fair value of available-for-sale marketable securities held at December 31, 2010:
| December 31, 2010 |
Amortized Cost |
Gross Unrealized Gains |
Gross Unrealized Losses |
Fair Value | ||||||||||||
| (in thousands) | ||||||||||||||||
| Security type |
||||||||||||||||
| Cash Equivalents |
||||||||||||||||
| U.S.Treasury and U.S. government and state government agency-backed securities |
$ | 11,998 | $ | 1 | $ | — | $ | 11,999 | ||||||||
| Corporate debt securities |
3,999 | — | (2 | ) | 3,997 | |||||||||||
| Marketable Securities—Short term |
||||||||||||||||
| U.S. Treasury and U.S. government and state government agency-backed securities |
14,698 | 2 | — | 14,700 | ||||||||||||
| Corporate debt securities |
20,391 | 18 | — | 20,409 | ||||||||||||
| Certificates of deposit |
13,000 | — | — | 13,000 | ||||||||||||
| Accrued interest |
59 | — | — | 59 | ||||||||||||
| Marketable Securities—Long term |
||||||||||||||||
| U.S. Treasury and U.S. government and state government agency-backed securities |
20,689 | 84 | (9 | ) | 20,764 | |||||||||||
| Corporate debt securities—long term |
17,337 | 149 | (18 | ) | 17,468 | |||||||||||
| Accrued interest |
255 | — | — | 255 | ||||||||||||
| Total available-for-sale marketable securities |
$ | 102,426 | $ | 254 | $ | (29 | ) | $ | 102,651 | |||||||
As of December 31, 2010, the Company held investments in marketable securities with unrealized gains of $254,000 and unrealized losses of $29,000. For investments in an unrealized loss position, the duration of the loss was less than 12 months. None of these investments is considered to be other-than-temporarily impaired.
As of December 31, 2010, the Company’s investments in marketable securities including those classified on its balance sheet as cash equivalents, reach maturity between January 12, 2011 and November 15, 2013, with a weighted average maturity date of approximately October 31, 2011.
As of December 31, 2009, the Company’s investments in marketable securities consisted of certificates of deposit of $27,000,000 and accrued interest of $157,000 for which amortized cost approximated fair value.
4. Property and Equipment
As of the respective dates shown, property and equipment consisted of the following:
| December 31, | ||||||||
| 2010 | 2009 | |||||||
| (in thousands) | ||||||||
| Laboratory equipment |
$ | 12,133 | $ | 10,371 | ||||
| Office furniture and fixtures |
4,640 | 3,328 | ||||||
| Leasehold improvements |
1,175 | 1,133 | ||||||
| 17,948 | 14,832 | |||||||
| Less: accumulated depreciation |
(11,876 | ) | (10,049 | ) | ||||
| Property and equipment, net |
$ | 6,072 | $ | 4,783 | ||||
106
Table of Contents
TARGACEPT, INC.
NOTES TO FINANCIAL STATEMENTS—(continued)
DECEMBER 31, 2009
4. Property and Equipment—(continued)
The Company recorded $1,979,000, $1,818,000, and $1,767,000 of depreciation expense for the years ended December 31, 2010, 2009 and 2008, respectively.
5. Intangible Assets
As of the respective dates shown, intangible assets consisted of the following:
| December 31, | ||||||||
| 2010 | 2009 | |||||||
| (in thousands) | ||||||||
| Patents |
$ | 296 | $ | 296 | ||||
| Less: accumulated amortization |
(147 | ) | (129 | ) | ||||
| Total |
$ | 149 | $ | 167 | ||||
Intangible assets consist of licensed patent rights assigned to the Company by Layton Bioscience, Inc. in 2002, which had an original value to the Company of $296,000.
The 2002 assignment by Layton Bioscience also included rights related to the Inversine trademark and product technology, an intangible asset that had an original value to the Company of $346,000. During the fourth quarter of 2008, as part of its processes for preparation of its financial statements, the Company performed an impairment analysis of its intangible assets. As of the date of the analysis, the Company had recognized a net loss on sales of Inversine in each of 2008 and 2007 and did not expect to recognize net income from sales of Inversine in future periods. The history of losses on sales of Inversine and the forecast for future periods indicated the carrying value of the Inversine trademark and product technology intangible asset may not have been recoverable. Using a discounted cash flow model that is based on estimated future net product sales and cost of product sales and considers assumptions such as, among other things, estimated future product sales volumes and estimated future sales price increases, the Company estimated the fair value of the Inversine trademark and product technology intangible asset and determined that it had no fair value. As a result, the Company recorded an impairment charge for the full amount of the unamortized balance of the Inversine trademark and product technology intangible asset as of the valuation date, or $220,000, to research and development expense in the fourth quarter of 2008.
The impairment charge had no effect on the Company’s prospective amortization of $17,000 each year of the licensed patent rights intangible asset to research and development expense on a straight-line basis over the remaining useful life of the patents, a period of 17 years from the date of acquisition.
6. Accrued Expenses
As of the respective dates shown, accrued expenses consisted of the following:
| December 31, | ||||||||
| 2010 | 2009 | |||||||
| (in thousands) | ||||||||
| Clinical trial and preclinical study costs |
$ | 8,326 | $ | 2,551 | ||||
| Employee compensation |
2,032 | 2,447 | ||||||
| Other |
158 | 269 | ||||||
| Total |
$ | 10,516 | $ | 5,267 | ||||
107
Table of Contents
TARGACEPT, INC.
NOTES TO FINANCIAL STATEMENTS—(continued)
DECEMBER 31, 2010
7. Long-term Debt
In July 2010, the Company entered into a loan agreement with a bank that provides aggregate borrowing capacity of $4,000,000 to be provided in up to three individual term loans that the Company may take at any time on or prior to June 30, 2011 to fund the purchase of equipment, furnishings, software and other fixed assets. The Company borrowed $1,228,000 under the loan agreement in September 2010. The Company’s September 2010 borrowing bears interest at a fixed rate of 3.40% per annum and is repayable in equal monthly installments of $28,000 beginning January 1, 2011 through the maturity date of December 1, 2014. Any future borrowing under the loan agreement would bear interest, at the Company’s discretion on a loan-by-loan basis, at either a variable rate equal to the thirty-day LIBOR plus 2.15%, adjusted monthly on the first day of each month, or a fixed rate equal to the bank’s fixed rate cost of funds index corresponding to the term of the loan plus 2.15%. Also, any future borrowing would be interest only through June 30, 2011 and then would be re-payable in equal monthly installments of principal and interest over the next 48 months. Pursuant to the loan agreement, the Company granted a first priority security interest in favor of the bank in the assets acquired with the proceeds of the loan facility.
In March 2008, the Company entered into a loan agreement with a bank that provided borrowing capacity of $5,300,000 to fund the purchase of equipment, furnishings, software and other fixed assets and enable the refinancing of an existing loan facility with another lender. The Company borrowed $4,811,000 upon entering into the loan agreement and borrowed the remaining $489,000 in September 2008. The Company’s March 2008 borrowing bears interest at a fixed rate of 5.231% per annum and is repayable in equal monthly installments of $112,000 beginning April 1, 2008 through the maturity date of March 1, 2012. The Company used $1,679,000 of the proceeds from the March 2008 borrowing to pay and satisfy in full the principal and interest outstanding on two tranches of the existing loan facility with another lender and granted a first priority security interest in favor of the bank in assets previously acquired with the proceeds of those tranches. The Company’s September 2008 borrowing bears interest at a fixed rate of 6.131% per annum and is repayable in equal monthly installments of $11,000 beginning October 1, 2008 through the maturity date of September 1, 2012.
During 2002, the Company borrowed $500,000 from the City of Winston-Salem. No payments were due on the City of Winston-Salem note until April 2007, when the Company began making monthly payments of $9,000 on the loan based on an interest rate of 5%. The note payable to the City of Winston-Salem was scheduled to mature on April 19, 2012. In December 2010, the Company repaid the remaining $135,000 balance of the note payable.
The Company paid $156,000, $223,000 and $244,000 in interest under notes payable during the years ended December 31, 2010, 2009 and 2008, respectively. Maturities of long-term debt were as follows at December 31, 2010 (in thousands):
| 2011 |
$ | 1,710 | ||
| 2012 |
728 | |||
| 2013 |
319 | |||
| 2014 and thereafter |
302 | |||
| $ | 3,059 | |||
8. Income Taxes
For the year ended December 31, 2010, the Company recognized $3,526,000 of income tax expense primarily as a result of the application of ASC 740 to stock-based compensation. Exercises of stock options during year ended December 31, 2010 resulted in tax deductions for stock-based compensation in excess of
108
Table of Contents
TARGACEPT, INC.
NOTES TO FINANCIAL STATEMENTS—(continued)
DECEMBER 31, 2009
8. Income Taxes—(continued)
expense recorded for the stock options under GAAP, resulting in an income tax benefit of $3,503,000. The Company recognized the income tax benefit related to the excess tax deductions as an increase to capital in excess of par value, which based on ASC 740 resulted in an offsetting charge in the same amount to income tax expense.
For the year ended December 31, 2009, the Company recognized an $88,000 income tax benefit primarily as a result of elections to forgo certain “bonus depreciation” deductions for federal income tax purposes in exchange for refundable research and development tax credits under the Housing Assistance Tax Act of 2008, as extended by the American Recovery and Reinvestment Act of 2009. For the year ended December 31, 2008, there was no net income tax expense (benefit) for federal or state income taxes because the Company incurred net operating losses. The Company has incurred cumulative net operating losses since inception. For the years shown, components of the Company’s income tax expense (benefit) were as follows:
| Year Ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| (in thousands) | ||||||||||||
| Current: |
||||||||||||
| Federal |
$ | 3,086 | $ | (96 | ) | $ | — | |||||
| State |
440 | 8 | — | |||||||||
| Net current income tax expense (benefit) |
3,526 | (88 | ) | — | ||||||||
| Deferred: |
||||||||||||
| Federal |
(1,519 | ) | 13,230 | 9,462 | ||||||||
| State |
1,321 | 2,951 | 1,112 | |||||||||
| Valuation allowance |
198 | (16,181 | ) | (10,574 | ) | |||||||
| Net deferred income tax expense (benefit) |
— | — | — | |||||||||
| Net income tax expense (benefit) |
$ | 3,526 | $ | (88 | ) | $ | — | |||||
The Company’s effective tax rate differs from the federal income tax rate for the following reasons:
| Year Ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Expected federal income tax benefit/expense at statutory rate |
35 | % | 35 | % | 34 | % | ||||||
| Increase (decrease) resulting from: |
||||||||||||
| Research and development credits |
(12 | ) | 5 | 4 | ||||||||
| Stock-based compensation |
4 | (1 | ) | (1 | ) | |||||||
| State income tax expense, net of federal benefit |
3 | 4 | 4 | |||||||||
| Qualifying Therapeutic Drug Project grant |
(3 | ) | — | — | ||||||||
| Change in unrecognized tax benefit reserves |
(3 | ) | — | — | ||||||||
| Change in valuation allowance |
(1 | ) | (41 | ) | (41 | ) | ||||||
| Other |
1 | (2 | ) | — | ||||||||
| 24 | % | — | % | — | % | |||||||
At December 31, 2010, 2009 and 2008, the Company had net operating loss carryforwards for federal income tax purposes of $39,011,000, $152,839,000 and $113,648,000, respectively, and for state income tax
109
Table of Contents
TARGACEPT, INC.
NOTES TO FINANCIAL STATEMENTS—(continued)
DECEMBER 31, 2009
8. Income Taxes—(continued)
purposes of $76,178,000, $135,789,000 and $113,493,000, respectively. At December 31, 2010, 2009 and 2008, the Company had research and development income tax credits for federal income tax purposes of $9,556,000, $7,340,000 and $6,118,000, respectively. The Company had research and development income tax credits for state income tax purposes of $1,021,000 and $595,000 at December 31, 2010 and 2009, respectively. The federal net operating loss carryforwards begin to expire in 2021. The state net operating loss carryforwards begin to expire in 2016. The federal and state research and development tax credits begin to expire in 2021.
Utilization of the net operating loss carryforwards and credits may be subject to a substantial annual limitation due to ownership change limitations provided by Section 382 of the Internal Revenue Code of 1986, as amended, and similar state provisions. A series of stock issuances occurring prior to the Company’s initial public offering gave rise to such an ownership change. As a result, an annual limitation is imposed on the Company’s use of net operating loss and credit carryforwards attributable to periods before the change.
Deferred income taxes reflect the net tax effects of temporary differences between the carrying amount of assets and liabilities for financial reporting purposes and the amounts used for income tax purposes. The Company’s net deferred tax assets relate principally to its recognition of deferred license fees from collaborations, research and development tax credits and net operating loss carryforwards. A valuation allowance has been recognized to offset the deferred tax assets. If and when recognized, the tax benefit for those items will be reflected in the period in which the benefit is recorded as a reduction of income tax expense. However, in the event the Company has excess tax deductions related to the exercise of stock options, the tax benefit will be reflected as an increase to capital in excess of par value. The utilization of the loss carryforwards to reduce future income taxes will depend on the Company’s ability to generate sufficient taxable income prior to the expiration of the net operating loss carryforwards. For the year ended December 31, 2010, the valuation allowance decreased $198,000. For the years ended December 31, 2009 and 2008, the valuation allowance increased $16,181,000 and $10,574,000, respectively.
As of the respective dates shown, significant components of the Company’s deferred tax assets (liabilities) were as follows:
| December 31, | ||||||||
| 2010 | 2009 | |||||||
| (in thousands) | ||||||||
| Deferred tax assets: |
||||||||
| Collaboration revenue |
$ | 55,857 | $ | 9,296 | ||||
| Research and development tax credit |
8,443 | 6,346 | ||||||
| Net operating loss carryforward |
7,463 | 50,750 | ||||||
| Patents |
2,125 | 1,704 | ||||||
| Stock-based compensation |
1,903 | 1,317 | ||||||
| Accrued royalties |
— | 6,068 | ||||||
| Other |
35 | — | ||||||
| Total gross deferred tax assets |
75,826 | 75,481 | ||||||
| Valuation allowance |
(75,114 | ) | (75,311 | ) | ||||
| Net deferred tax asset |
712 | 170 | ||||||
| Deferred tax liabilities |
||||||||
| Equipment and other |
(712 | ) | (170 | ) | ||||
| Net deferred tax asset |
$ | — | $ | — | ||||
110
Table of Contents
TARGACEPT, INC.
NOTES TO FINANCIAL STATEMENTS—(continued)
DECEMBER 31, 2009
8. Income Taxes—(continued)
For the year ended December 31, 2009, stock option exercises resulted in $5,714,000 in excess tax deductions. The benefit of these excess tax deductions had not begun to be realized as of December 31, 2010 because the Company has incurred cumulative net operating losses. Accordingly, the tax benefit will not be recognized as an increase to capital in excess of par value until the excess deductions reduce income taxes payable.
The Company follows the provisions ASC 740, which prescribes a threshold and measurement attribute for the financial statement recognition and measurement of a tax position taken or expected to be taken in a tax return and also provides guidance on de-recognition, classification, interest and penalties, accounting in interim periods and disclosures. There was no cumulative effect adjustment upon adoption.
A reconciliation of beginning and ending unrecognized tax benefits is as follows (in thousands):
| Balance at January 1, 2008 |
$ | 942 | ||
| Additions based on tax positions related to the current year |
278 | |||
| Balance at December 31, 2008 |
1,220 | |||
| Additions based on tax positions related to the current year |
532 | |||
| Additions based on tax positions related to prior years |
134 | |||
| Balance at December 31, 2009 |
1,886 | |||
| Decreases based on tax positions related to prior years |
(412 | ) | ||
| Balance at December 31, 2010 |
$ | 1,474 | ||
None of the unrecognized tax benefits would, if recognized, affect the effective tax rate because the Company has recorded a valuation allowance to fully offset federal and state deferred tax assets. The Company has no tax positions for which it is reasonably possible that the total amount of unrecognized tax benefits will significantly increase or decrease during 2011. No interest or penalties with respect to unrecognized tax positions are recognized in the statement of operations for any of the years ended December 31, 2010, 2009 or 2008.
Because the Company has incurred cumulative net operating losses since inception, all tax years remain open to examination by U.S. federal, North Carolina and Massachusetts tax authorities. An examination of the Company’s 2006 federal income tax return was completed in 2009 with no adjustments. The Company’s 2009, 2008, 2007 and 2006 North Carolina income tax returns are under examination.
In November 2010, the Internal Revenue Service notified the Company that it had approved cumulative grants of $1,467,000 to the Company under the Qualifying Therapeutic Discovery Project tax credit program enacted as part of the Patient Protection and Affordable Care Act of 2010. In the fourth quarter of 2010, the Company recorded the cumulative grants as grant revenue in its financial statements.
9. Stock-Based Incentive Plans
The 2000 Plan became effective in August 2000. The 2006 Plan became effective in April 2006 and is the successor equity incentive program to the 2000 Plan. All shares previously reserved under the 2000 Plan and not subject to outstanding awards under the 2000 Plan are now reserved for grant under the 2006 Plan. As of December 31, 2010, the number of shares authorized for issuance under the Plans was 7,282,078, of which 2,261,896 shares remained available for grant.
Awards may be made with respect to the 2006 Plan, or may have been made with respect to both Plans, to participants under the Plans in the form of incentive and nonqualified stock options, restricted stock, stock
111
Table of Contents
TARGACEPT, INC.
NOTES TO FINANCIAL STATEMENTS—(continued)
DECEMBER 31, 2009
9. Stock-Based Incentive Plans—(continued)
appreciation rights, stock awards, and performance awards. Eligible participants under the Plans include employees, directors and certain independent contractors, consultants or advisors of the Company or a related corporation. Awards made under the Plans have vesting periods that are determined at the discretion of the administrator and range from 0 to 5 years and most commonly have 10-year contractual terms or, in some cases, shorter terms designed to comply with Section 409A of the Internal Revenue Code. The exercise price of incentive options granted under the Plans may not be less than 100% of the fair market value of the common stock on the date of grant, as determined by the administrator.
Under ASC 718, the Company recognizes the grant date fair value of stock options issued to employees and non-employee directors over the requisite service periods, which are typically the vesting periods. The Company uses the Black-Scholes-Merton formula to estimate the fair value of its stock-based payments. The volatility assumption used in the Black-Scholes-Merton formula is based on the calculated historical volatility of twelve to sixteen benchmark companies in the Company’s industry that have been identified as comparable public entities. The expected term for stock options granted during 2010, 2009 and 2008 is based on historical analysis. The risk-free rate for periods within the contractual life of the option is based on the U.S. Treasury yield curve in effect at the time of grant.
The following table illustrates the weighted average assumptions for the Black-Scholes-Merton model used in determining the fair value of stock options granted as of the respective dates shown:
| Year ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Dividend yield |
— | — | — | |||||||||
| Risk-free interest rate |
2.9 | % | 2.0 | % | 3.4 | % | ||||||
| Volatility |
0.7 | 0.7 | 0.7 | |||||||||
| Expected term |
6.27 years | 6.72 years | 6.43 years | |||||||||
A summary of option activity and changes during each of the years ended December 31, 2010, 2009 and 2008 appears below:
| Shares Subject to Options |
Weighted Average Exercise Price Per Share |
Weighted Average Remaining Contractual Term |
Aggregate Intrinsic Value |
|||||||||||||
| (in thousands) | ||||||||||||||||
| Outstanding at December 31, 2007 |
3,125,161 | $ | 5.11 | |||||||||||||
| Granted |
106,485 | 6.71 | ||||||||||||||
| Forfeited |
(21,595 | ) | 6.73 | |||||||||||||
| Exercised |
(90,954 | ) | 2.98 | |||||||||||||
| Outstanding at December 31, 2008 |
3,119,097 | 5.21 | ||||||||||||||
| Granted |
779,400 | 3.06 | ||||||||||||||
| Forfeited |
(12,229 | ) | 4.30 | |||||||||||||
| Exercised |
(1,062,456 | ) | 3.16 | |||||||||||||
| Outstanding at December 31, 2009 |
2,823,812 | 5.40 | ||||||||||||||
| Granted |
941,532 | 20.88 | ||||||||||||||
| Forfeited |
(21,867 | ) | 17.63 | |||||||||||||
| Exercised |
(643,862 | ) | 5.12 | |||||||||||||
| Outstanding at December 31, 2010 |
3,099,615 | $ | 10.07 | 7.11 years | $ | 50,931 | ||||||||||
| Vested and exercisableat December 31, 2010 |
1,933,244 | $ | 7.38 | 6.20 years | $ | 36,971 | ||||||||||
112
Table of Contents
TARGACEPT, INC.
NOTES TO FINANCIAL STATEMENTS—(continued)
DECEMBER 31, 2009
9. Stock-Based Incentive Plans—(continued)
The weighted average grant date fair value of options granted during the years ended December 31, 2010, 2009, and 2008 was $13.46, $2.03, and $4.38, respectively. The total intrinsic value of options exercised during the years ended December 31, 2010, 2009, and 2008 was $11,527,000, $16,833,000, and $489,000, respectively.
A summary of the status of non-vested stock options granted under the 2006 Plan as of December 31, 2010 and changes during the year ended December 31, 2010 appears below:
| Shares Subject to Options |
Weighted Average Grant-Date Fair Value Per Share |
|||||||
| Non-vested at January 1, 2010 |
936,326 | $ | 3.14 | |||||
| Granted |
941,532 | 13.46 | ||||||
| Vested |
(690,166 | ) | 6.37 | |||||
| Forfeited |
(21,321 | ) | 11.43 | |||||
| Non-vested at December 31, 2010 |
1,166,371 | $ | 9.41 | |||||
As of December 31, 2010, there was $10,972,000 of total unrecognized compensation expense related to non-vested stock-based compensation arrangements granted under the Plans, before considering estimated forfeitures. That cost is expected to be recorded over a weighted average period of 2.62 years. The total fair value of shares subject to stock-based compensation arrangements granted under the Plans that vested during the years ended December 31, 2010, 2009, and 2008 was $4,396,000, $2,338,000 and $2,217,000, respectively.
The Company had 3,099,615 and 2,823,812 shares of common stock reserved for future issuance upon the exercise of outstanding stock options at December 31, 2010 and 2009, respectively.
10. Commitments and Contingencies
Office Lease
On March 1, 2002, the Company entered into an agreement with Wake Forest University Health Sciences to lease an office and research facility in Winston-Salem, North Carolina with an initial term that extended through July 31, 2007. The lease contained a renewal option for up to one additional five-year term, with a rental rate for the renewal term similar to the initial term. From 2005 to 2010, the terms of the lease were amended to, among other things, increase the rental space and include a second renewal term, exercisable at the Company’s option, at the then-existing market rate for similar space in the Piedmont Triad in North Carolina. The Company exercised its first renewal option in January 2007 and, as a result, the lease extends until July 31, 2012.
Rent expense incurred by the Company under the office lease and other operating leases was $2,003,000 for the year ended December 31, 2010 and $2,148,000 for each of the years ended December 31, 2009 and 2008.
The following table illustrates expected future lease payments under operating leases (in thousands):
| 2011 |
$ | 2,531 | ||
| 2012 |
1,489 | |||
| 2013 |
29 | |||
| 2014 and thereafter |
27 | |||
| $ | 4,076 | |||
113
Table of Contents
TARGACEPT, INC.
NOTES TO FINANCIAL STATEMENTS—(continued)
DECEMBER 31, 2009
10. Commitments and Contingencies—(continued)
Employment Arrangements
The Company has entered into employment agreements with some of its executive officers. Under the agreements, if the Company terminates the employment of the executive officer other than for just cause or if the executive officer terminates his employment for good reason, in each case as that term is defined in the agreement, the executive officer is entitled, among other things, to receive severance equal to his current base salary for nine to twelve months following termination or, if shorter, until he secures other employment. The executive officer would also be entitled to continuation of the health and life insurance benefits coverage provided to him as of the date of termination for the period during which he receives severance.
11. Retirement Savings Plan
The Company has a 401(k) retirement plan in which all of its employees are eligible to participate. The Company contributed $487,000, $666,000, and $558,000 to the plan for the years ended December 31, 2010, 2009 and 2008, respectively. The Company matched employee contributions to the plan, on a per employee basis, up to 4% of each employee’s wages for the year ended December 31, 2010. During 2009 and 2008 the Company matched employee contributions to the plan, on a per employee basis, up to 6% of each employee’s wages.
12. Strategic Alliance and Collaboration Agreements
AstraZeneca AB
Cognitive Disorders
In December 2005, the Company entered into a collaborative research and license agreement with AstraZeneca AB under which the Company granted AstraZeneca exclusive development and worldwide commercialization rights to the Company’s product candidate known as AZD3480 (TC-1734) as a treatment for specified conditions characterized by cognitive impairment, including attention deficit/hyperactivity disorder, or ADHD. The Company is eligible to receive license fees and milestone payments under the agreement. The amount of license fees and milestone payments depends on the timing and achievement of development, regulatory, first commercial sale and first detail milestone events.
AstraZeneca paid the Company an initial fee of $10,000,000 in February 2006. Based on the agreement terms, the Company allocated $5,000,000 of the initial fee to the research collaboration, which the Company recognized as revenue on a straight-line basis over the four-year term of the research collaboration. The Company deferred recognition of the remaining $5,000,000 of the initial fee, which was allocated to the AZD3480 license grants, until December 2006, when AstraZeneca made a determination to proceed with further development of AZD3480. As a result, in the first quarter of 2007, the Company began recognizing the $5,000,000 of the initial fee that it had previously deferred as revenue on a straight-line basis over the estimated five-year development period for AZD3480. In July 2009, based on feedback received from AstraZeneca regarding its development plans for AZD3480 for ADHD, the Company extended its estimate of the development period for AZD3480 to continue through 2013 and began recognizing the part of the $5,000,000 portion of the initial fee not yet recognized as of April 1, 2009 as revenue on a straight-line basis over the remaining estimated development period. The Company recognized $683,000, $1,934,000, and $2,250,000 of the initial fee as revenue for the years ended December 31, 2010, 2009, and 2008, respectively.
Under the agreement, the Company is also eligible to receive (1) additional payments of up to $103,000,000 if development, regulatory, and first commercial sale milestone events for AZD3480 are achieved only for
114
Table of Contents
TARGACEPT, INC.
NOTES TO FINANCIAL STATEMENTS—(continued)
DECEMBER 31, 2010
12. Strategic Alliance and Collaboration Agreements—(continued)
ADHD, (2) other payments if development, regulatory, first commercial sale and first detail milestone events for AZD3480 are achieved for any other target indication under the agreement and (3) if regulatory approval is achieved for AZD3480 for any particular indication, stepped double-digit royalties on any sales of AZD3480 for that indication or any other indication. Under the terms of a sponsored research agreement and a subsequent license agreement between the Company and University of Kentucky Research Foundation, or UKRF, if the Company receives any of these payments from AstraZeneca related to AZD3480, including royalties, the Company is required to pay a low-single digit percentage of each such payment to UKRF.
The Company is exploring the practicability of conducting an additional clinical trial of AZD3480 in Alzheimer’s disease. In September 2010, the Company and AstraZeneca amended the agreement to enable the Company potentially to conduct such a trial and to provide for respective roles and responsibilities and associated financial terms. Under the amendment, the Company received $500,000 from AstraZeneca in October 2010 and is eligible to receive additional payments of up to $5,700,000 in the aggregate.
With respect to AZD1446, the most advanced product candidate that arose out of the parties’ preclinical research collaboration described below, the Company is also eligible to receive payments of up to $73,000,000, if development, regulatory, first commercial sale and first detail milestone events for AZD1446 are achieved for a single indication under the agreement, and, if regulatory approval is achieved for AZD1446 for any particular indication, stepped royalties on any sales of AZD1446 for that indication or any other indication.
The Company would recognize any revenue based on the achievement of any milestone event under the agreement upon achievement of the milestone event if the Company determines that the revenue satisfies the requirements for immediate recognition under its revenue recognition policy (see Note 2).
The Company and AstraZeneca conducted a multi-year preclinical research collaboration under the agreement. The term of the research collaboration expired in January 2010 and, as a result, the Company did not recognize any collaboration research and development revenue for the year ended December 31, 2010. While the research collaboration was ongoing, the Company was eligible to receive payments from AstraZeneca for research services performed. The Company recognized collaboration research and development revenue as the research was performed and related expenses were incurred. The Company recognized collaboration research and development revenue of $5,246,000 and $8,921,000 for the years ended December 31, 2009 and 2008, respectively. The Company recognized additional collaboration research and development revenue of $46,000 for the year ended December 31, 2008 for clinical trial material purchased by AstraZeneca from the Company and other research and development costs reimbursable under the collaboration.
In October 2007, the Company provided notice under the agreement offering AstraZeneca the right to license its product candidate TC-5619 for specified conditions characterized by cognitive impairment. Based on a subsequent election by AstraZeneca made under the terms of the agreement, AstraZeneca paid the Company $2,000,000 and the Company agreed to develop TC-5619 independently through completion of Phase 1 clinical development and a Phase 2 clinical proof of concept clinical trial in accordance with a mutually acceptable development plan, following which AstraZeneca would have the right to license TC-5619 on terms specified in the agreement, as it was amended in April 2010 as described below. The Company is recognizing the $2,000,000 payment as revenue on a straight-line basis over the estimated period of the Company’s research and development obligations for TC-5619. Accordingly, the Company recognized $278,000, $596,000 and $923,000 of the payment as revenue for the years ended December 31, 2010, 2009 and 2008, respectively.
115
Table of Contents
TARGACEPT, INC.
NOTES TO FINANCIAL STATEMENTS—(continued)
DECEMBER 31, 2009
12. Strategic Alliance and Collaboration Agreements—(continued)
In April 2010, the Company and AstraZeneca amended the agreement to modify the terms applicable to TC-5619. In conjunction with the amendment, the Company and AstraZeneca agreed to an expanded development program for TC-5619 and the Company received a payment of $11,000,000 to maintain AstraZeneca’s option to license TC-5619. The Company recorded the $11,000,000 payment as deferred revenue and is recognizing it as revenue on a straight-line basis over the estimated period of the Company’s research and development obligations for TC-5619. The Company recognized $6,286,000 of the payment as revenue for the year ended December 31, 2010.
As part of the expanded TC-5619 development program, the Company had two Phase 2 clinical proof of concept trials ongoing as of December 31, 2010, one in cognitive dysfunction in schizophrenia, or CDS, and one in adults with ADHD. The Company is also conducting specified clinical and non-clinical studies to support the potential advancement of TC-5619 into Phase 2 clinical development for Alzheimer’s disease. Under the agreement, AstraZeneca has an option for an exclusive license to TC-5619 for various cognitive disorders. If TC-5619 has been licensed by AstraZeneca or remains subject to AstraZeneca’s license option, any future Phase 2 clinical development for Alzheimer’s disease will be funded by AstraZeneca.
In January 2011, the Company announced positive top-line results from the CDS trial. If AstraZeneca exercises its option, it would pay the Company an exercise fee of $30,000,000 and assume responsibility for and fund all future development (except for completion of the Company’s ongoing studies) and commercialization for TC-5619. In that event, the Company would be eligible to receive additional payments of up to $212,000,000, if development, regulatory, first commercial sale and first detail milestone events for TC-5619 are achieved in three indications, and stepped double-digit royalties on any future TC-5619 product sales for any indication. If AstraZeneca does not exercise its option, the Company would retain all of its rights in TC-5619.
The Company has also received payments under the agreement that it recognized in full as revenue upon achievement of the corresponding milestone event because the event met each of the conditions required for immediate recognition under its revenue recognition policy (see Note 2). In particular, the Company received a $10,000,000 payment from AstraZeneca in July 2009 based on achievement of the objective in a completed Phase 2 clinical trial of AZD3480 in adults with ADHD, a milestone event under an amendment to the agreement. The Company made a payment of $350,000 to UKRF in December 2009 as a result of the $10,000,000 payment received from AstraZeneca. The Company has also received cumulative payments from AstraZeneca of $2,600,000 based on the achievement of milestone events related to the development of product candidates arising under the parties’ completed preclinical research collaboration, including AZD1446.
AstraZeneca has paid the Company an aggregate of $82,620,000 under the agreement since its inception.
TC-5214
In December 2009, the Company entered into a collaboration and license agreement with AstraZeneca AB for the global development and commercialization of TC-5214. Under the agreement, AstraZeneca made an upfront payment to the Company of $200,000,000 and the Company is eligible to receive cumulative payments of up to an additional $540,000,000 if specified development, regulatory and first commercial sale milestone events for TC-5214 are achieved, cumulative payments of up to an additional $500,000,000 if specified sales related milestone events for TC-5214 are achieved and significant stepped double-digit royalties on net sales of TC-5214 worldwide. The Company recorded the upfront payment made by AstraZeneca as deferred revenue and is recognizing the payment as revenue on a straight-line basis over the estimated period of the Company’s
116
Table of Contents
TARGACEPT, INC.
NOTES TO FINANCIAL STATEMENTS—(continued)
DECEMBER 31, 2010
12. Strategic Alliance and Collaboration Agreements—(continued)
substantive performance obligations under the agreement, or approximately 33 months. The Company recognized $72,565,000 and $398,000 of the upfront payment as revenue for the years ended December 31, 2010 and 2009, respectively. The Company would recognize as revenue the full amount of each payment received based on the achievement of milestone events under the agreement upon its achievement if the Company determines that the revenue satisfies the requirements for immediate recognition under its revenue recognition policy (see Note 2).
The Company and AstraZeneca have jointly designed a program for the global development of TC-5214. The initial program includes development of TC-5214 as an adjunct therapy and as a “switch” monotherapy, in each case in patients with major depressive disorder who do not respond adequately to initial antidepressant treatment. AstraZeneca is responsible for 80% and the Company is responsible for 20% of the costs of the initial program, except that AstraZeneca is responsible for 100% of development costs that are required only to obtain or maintain regulatory approval in countries outside the United States and the European Union. The Company has the right to terminate its obligation to fund its share of the costs of the initial program once it has funded a specified amount. In addition, for each of the Company and AstraZeneca, costs that were not contemplated at execution to be part of the initial program may in some cases be excluded from the cost-sharing arrangement. If the Company funds the specified amount and terminates its obligation to fund its share of further costs of the initial program, any future milestones and royalties payable to the Company under this agreement would be reduced by the amount of the Company’s unfunded share plus interest at a specified rate, subject to a maximum reduction that may be applied to any one payment. In addition, if the Company and AstraZeneca mutually agree to develop TC-5214 for any indication other than major depressive disorder or in any formulation other than those contemplated by the initial program, the same cost-sharing arrangement would apply, except that the Company would have the immediate right to terminate its obligation to fund its share of development costs for the other indication or formulation. If the Company terminates its obligation to fund its share of these other development costs, any future milestones and royalties payable to the Company under this agreement would be reduced by the amount of the Company’s unfunded share plus interest at a specified rate, subject to a maximum reduction that may be applied to any one payment, but only from and after the occurrence of a specified event to be agreed upon by the parties.
The Company’s portion of the costs of the initial program for the year ended December 31, 2010 was $10,771,000. AstraZeneca’s allocable portion of the initial program costs paid by the Company for the year ended December 31, 2010 was $2,023,000, which is reflected in the Company’s financial statements as a reduction to research and development expense.
AstraZeneca is responsible under the agreement for executing and funding the costs of global commercialization of TC-5214. The Company has retained an option to co-promote TC-5214 to a specified target physician audience in the United States. If the Company exercises its co-promotion option, AstraZeneca would compensate the Company on a per detail basis. AstraZeneca is also responsible under the agreement for the manufacture and supply of TC-5214.
Under the terms of an existing license agreement, the Company paid $16,000,000 to University of South Florida Research Foundation, or USFRF, in February 2010 based on the Company’s receipt of the upfront payment from AstraZeneca and would be required to pay to USFRF a percentage of each milestone payment that may be received from AstraZeneca, after deducting from the milestone payment the unexhausted portion of the Company’s projected share of the costs of the initial development program for TC-5214, as well as royalties on
117
Table of Contents
TARGACEPT, INC.
NOTES TO FINANCIAL STATEMENTS—(continued)
DECEMBER 31, 2010
12. Strategic Alliance and Collaboration Agreements—(continued)
any future TC-5214 product sales. The percentage of each milestone payment, net of any deduction, that the Company would be required to pay would be at least 10% and could be greater in specified circumstances. Based on the terms of the license agreement with USFRF and the terms of another existing license agreement with Yale University, the Company expects to pay royalties at an effective worldwide rate in the low single digits and that the effective royalty rate could in some circumstances reach the mid single digits.
GlaxoSmithKline
On July 27, 2007, the Company entered into a product development and commercialization agreement with SmithKline Beecham Corporation, doing business as GlaxoSmithKline, and Glaxo Group Limited, which are referred to together as GlaxoSmithKline, that sets forth the terms of an alliance designed to discover, develop and market product candidates that selectively target specified NNR subtypes in five therapeutic focus areas: pain, smoking cessation, addiction, obesity and Parkinson’s disease.
Under the agreement and a related stock purchase agreement, GlaxoSmithKline made an initial payment to the Company of $20,000,000 and purchased 1,275,502 shares of the Company’s common stock for an aggregate purchase price of $15,000,000 on July 27, 2007. The purchase price paid by GlaxoSmithKline reflected an aggregate deemed premium of $3,521,000, based on the closing price of the Company’s common stock on the trading day immediately preceding the date that agreements were signed and announced. The Company deferred recognition of both the initial payment made by GlaxoSmithKline and the deemed premium paid for the shares of the Company’s common stock purchased by GlaxoSmithKline and is recognizing both amounts into revenue on a straight-line basis over the estimated nine-year period of the Company’s research and early development obligations under the agreement. The Company recognized $2,613,000 of the initial payment and deemed premium as revenue for each of the years ended December 31, 2010, 2009, and 2008.
In December 2007, the Company received a $6,000,000 payment from GlaxoSmithKline upon the achievement of a specified milestone event under the agreement. The Company determined the payment did not meet each of the conditions of its revenue recognition policy (see Note 2) required for recognition of the full amount into revenue upon achievement of the milestone. Specifically, based on the progress of this product candidate as of inception of the agreement, achievement of this milestone was reasonably assured within the meaning of the Company’s revenue recognition policy. Accordingly, the Company recorded the payment as deferred revenue and is recognizing it into revenue on a straight-line basis over the estimated period of the Company’s research and early development obligations under the agreement. The Company recognized $692,000 of the payment as revenue for each of the years ended December 31, 2010, 2009 and 2008.
Beyond the $6,000,000 payment discussed above, the Company has received an aggregate of $4,000,000 in payments from GlaxoSmithKline for achievement of various milestone events under the agreement related to progress in the Company’s preclinical programs, including $2,500,000 for the year ended December 31, 2009. The Company immediately recognized the full amount of each payment as revenue upon achievement of the corresponding milestone event because each event met each of the conditions required for immediate recognition under its revenue recognition policy (see Note 2).
13. Subsequent Event
In late February 2011, the Company received notice of termination of its product development and commercialization agreement from GlaxoSmithKline. By the terms of the agreement, the termination becomes effective in late May 2011. As a result of the termination, the Company expects to recognize into revenue in the
118
Table of Contents
TARGACEPT, INC.
NOTES TO FINANCIAL STATEMENTS—(continued)
DECEMBER 31, 2010
13. Subsequent Event —(continued)
first quarter of 2011 $18,421,000 in deferred amounts received under the agreement and remaining to be recognized as of December 31, 2010. The Company recognized $3,305,000 of the deferred amounts received under the agreement for each of 2010, 2009 and 2008.
14. Selected Quarterly Financial Data (unaudited)
| 2010 Quarter | ||||||||||||||||
| First | Second | Third | Fourth | |||||||||||||
| (in thousands, except share and per share amounts) | ||||||||||||||||
| Net operating revenues |
$ | 19,518 | $ | 20,902 | $ | 21,798 | $ | 23,495 | ||||||||
| Income (loss) from operations |
7,089 | 4,966 | 2,417 | (1,357 | ) | |||||||||||
| Income tax expense |
(626 | ) | (1,512 | ) | (257 | ) | (1,131 | ) | ||||||||
| Net income (loss) |
6,795 | 3,782 | 2,486 | (2,164 | ) | |||||||||||
| Basic net income (loss) per share(1) |
$ | 0.24 | $ | 0.13 | $ | 0.09 | $ | (0.08 | ) | |||||||
| Diluted net income (loss) per share |
$ | 0.23 | $ | 0.13 | $ | 0.08 | $ | (0.08 | ) | |||||||
| Weighted average common shares outstanding—basic |
28,311,452 | 28,509,619 | 28,622,187 | 28,724,965 | ||||||||||||
| Weighted average common shares outstanding—diluted |
29,172,218 | 30,152,309 | 30,173,406 | 28,724,965 | ||||||||||||
| 2009 Quarter | ||||||||||||||||
| First | Second | Third | Fourth | |||||||||||||
| (in thousands, except share and per share amounts) | ||||||||||||||||
| Net operating revenues |
$ | 6,141 | $ | 2,830 | $ | 12,663 | $ | 3,428 | ||||||||
| (Loss) income from operations |
(5,052 | ) | (9,855 | ) | 1,204 | (26,622 | ) | |||||||||
| Income tax benefit |
73 | — | 10 | 5 | ||||||||||||
| Net (loss) income |
(4,677 | ) | (9,654 | ) | 1,334 | (26,407 | ) | |||||||||
| Basic net (loss) income per share(1)(2) |
$ | (0.19 | ) | $ | (0.39 | ) | $ | 0.05 | $ | (0.96 | ) | |||||
| Diluted net (loss) income per share |
$ | (0.19 | ) | $ | (0.39 | ) | $ | 0.05 | $ | (0.96 | ) | |||||
| Weighted average common shares outstanding—basic(2) |
24,964,909 | 24,966,347 | 25,126,823 | 27,465,714 | ||||||||||||
| Weighted average common shares outstanding—diluted(2) |
24,964,909 | 24,966,347 | 26,943,535 | 27,465,714 | ||||||||||||
| (1) | Per common share amounts for the quarters and full years have been calculated separately. Accordingly, the sum of quarterly amounts may not equal the annual amount because of differences in the weighted average common shares outstanding during each period, principally due to the effect of share issuances by the Company during the year. |
| (2) | Diluted weighted average common shares outstanding are identical to basic weighted average common shares outstanding and Diluted EPS is identical to Basic EPS for the fourth quarter of 2010 and for the first, second and fourth quarters of 2009 because common share equivalents are excluded from the calculations of diluted weighted average common shares outstanding for those quarters, as their effect is antidilutive. |
119
Table of Contents
| Item 9. | Changes in and Disagreements with Accountants on Accounting and Financial Disclosure. |
None.
| Item 9A. | Controls and Procedures. |
(a) Evaluation of Disclosure Controls and Procedures. Our management, with the participation of our chief executive officer and chief financial officer, evaluated the effectiveness of our disclosure controls and procedures in accordance with Rule 13a-15(b) under the Exchange Act as of the end of the period covered by this annual report. In designing and evaluating our disclosure controls and procedures, our management recognized that any controls and procedures, no matter how well designed and operated, can provide only reasonable assurance of achieving their objectives, and our management necessarily applied its judgment in evaluating the cost-benefit relationship of possible controls and procedures. Based on the evaluation of our disclosure controls and procedures as of the end of the period covered by this annual report, our chief executive officer and chief financial officer concluded that, as of such date, our disclosure controls and procedures were effective to provide reasonable assurance that information required to be disclosed by us in the reports that we file or submit under the Exchange Act is (a) accumulated and communicated to our management, including our chief executive officer and chief financial officer, as appropriate to allow timely decisions regarding required disclosure and (b) recorded, processed, summarized and reported within the time periods specified in the SEC’s rules and forms.
(b) Management’s Report on Internal Control Over Financial Reporting. Our management is responsible for establishing and maintaining adequate internal control over financial reporting. Internal control over financial reporting is defined in Rule 13a-15(f) or Rule 15d-15(f) promulgated under the Exchange Act as a process designed by, or under the supervision of, the principal executive and principal financial officers and effected by the board of directors, management and other personnel to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles and includes those policies and procedures that:
| • | pertain to the maintenance of records that in reasonable detail accurately and fairly reflect the transactions and dispositions of our assets; |
| • | provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that our receipts and expenditures are being made only in accordance with authorizations of our management and directors; and |
| • | provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use or disposition of our assets that could have a material effect on the financial statements. |
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions or that the degree of compliance with the policies or procedures may lessen. Our management, including our chief executive officer and chief financial officer, assessed the effectiveness of our internal control over financial reporting as of December 31, 2010 using the criteria established in a report entitled “Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission” and in accordance with the interpretive guidance issued by the SEC in Release No. 34-55929. Based on its assessment, our management concluded that, as of December 31, 2010, our internal control over financial reporting was effective.
Our independent registered public accounting firm has issued an audit report on the effectiveness of our internal control over financial reporting as of December 31, 2010. The report appears below.
120
Table of Contents
Report of Independent Registered Public Accounting Firm
The Board of Directors and Stockholders of
Targacept, Inc.
We have audited Targacept, Inc.’s internal control over financial reporting as of December 31, 2010, based on criteria established in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (the COSO criteria). Targacept, Inc.’s management is responsible for maintaining effective internal control over financial reporting, and for its assessment of the effectiveness of internal control over financial reporting included in the accompanying Management’s Report on Internal Control Over Financial Reporting. Our responsibility is to express an opinion on the Company’s internal control over financial reporting based on our audit.
We conducted our audit in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects. Our audit included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, testing and evaluating the design and operating effectiveness of internal control based on the assessed risk, and performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
In our opinion, Targacept, Inc. maintained, in all material respects, effective internal control over financial reporting as of December 31, 2010, based on the COSO criteria.
We have also audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), the balance sheets of Targacept, Inc. as of December 31, 2010 and 2009, and the related statements of operations, stockholders’ equity and cash flows for each of the three years in the period ended December 31, 2010 and our report dated March 11, 2011 expressed an unqualified opinion thereon.
/s/ Ernst & Young LLP
Raleigh, North Carolina
March 11, 2011
121
Table of Contents
(c) Changes in Internal Controls. No change in our internal control over financial reporting (as defined in Rule 13a-15(f) under the Exchange Act) occurred during the quarter ended December 31, 2010 that has materially affected, or is reasonably likely to materially affect, our internal control over financial reporting.
| Item 9B. | Other Information. |
None.
122
Table of Contents
PART III
| Item 10. | Directors, Executive Officers and Corporate Governance. |
Information called for by this Item may be found in our definitive Proxy Statement in connection with our 2011 Annual Meeting of Stockholders to be filed with the SEC under the captions “Board of Directors and Management,” “Corporate Governance” and “Section 16(a) Beneficial Ownership Reporting Compliance” and is incorporated by reference in this Item 10.
Code of Business Conduct and Ethics
We have adopted a code of business conduct and ethics that applies to all of our directors and officers and other employees, including our principal executive officer, principal financial officer and principal accounting officer. This code is publicly available on our website at www.targacept.com. To the extent permissible under applicable law, the rules of the SEC or NASDAQ listing standards, we intend to post on our website any amendment to the code of business conduct and ethics, or any grant of a waiver from a provision of the code of business conduct and ethics, that requires disclosure under applicable law, the rules of the SEC or NASDAQ listing standards.
| Item 11. | Executive Compensation. |
Information called for by this Item may be found in our definitive Proxy Statement in connection with our 2011 Annual Meeting of Stockholders to be filed with the SEC under the captions “Executive Compensation” and “Corporate Governance” and is incorporated by reference in this Item 11.
| Item 12. | Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters. |
Information called for by this Item may be found in our definitive Proxy Statement in connection with our 2011 Annual Meeting of Stockholders to be filed with the SEC under the captions “Security Ownership of Certain Beneficial Owners and Management” and “Equity Compensation Plan Information” and is incorporated by reference in this Item 12.
| Item 13. | Certain Relationships and Related Transactions, and Director Independence. |
Information called for by this Item may be found in our definitive Proxy Statement in connection with our 2011 Annual Meeting of Stockholders to be filed with the SEC under the captions “Certain Relationships and Related Person Transactions” and “Corporate Governance” and is incorporated by reference in this Item 13.
| Item 14. | Principal Accounting Fees and Services. |
Information called for by this Item may be found in our definitive Proxy Statement in connection with our 2011 Annual Meeting of Stockholders to be filed with the SEC under the caption “Independent Registered Public Accounting Firm Fee Information and Audit Committee Pre-Approval Policy” and is incorporated by reference in this Item 14.
123
Table of Contents
PART IV
| Item 15. | Exhibits, Financial Statement Schedules. |
(a)(1) Financial Statements. For a list of the financial statements included in this annual report, see “Index to the Financial Statements” on page 92.
(a)(2) Financial Statement Schedules. All schedules are omitted because they are not applicable or because the required information is shown under Item 8, “Financial Statements and Supplementary Data.”
(a)(3) Exhibits. The list of exhibits filed as a part of this annual report is set forth on the Exhibit Index immediately preceding such exhibits and is incorporated by reference in this Item 15(a)(3).
(b) Exhibits. See Exhibit Index.
(c) Separate Financial Statements and Schedules. None.
124
Table of Contents
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
| Date: March 11, 2011 | Targacept, Inc. | |||||
| By: | /S/ J. DONALD DEBETHIZY | |||||
| J. Donald deBethizy | ||||||
| Chief Executive Officer and President | ||||||
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated. Each person whose signature appears below hereby constitutes and appoints J. Donald deBethizy, Alan A. Musso and Peter A. Zorn, and each of them singly (with full power to each of them to act alone), as such person’s true and lawful attorneys-in-fact and agents, with full power of substitution and re-substitution, to sign any and all amendments to this Annual Report on Form 10-K and to file the same, with all exhibits thereto and other documents in connection therewith, with the Securities and Exchange Commission, granting unto said attorneys-in-fact and agents, and each of them, full power and authority to do and perform each and every act and thing requisite or necessary to be done, as fully to all intents and purposes as such person might or could do in person, hereby ratifying and confirming all that said attorneys-in-fact and agents, or any of them or any of their substitute or substitutes, may lawfully do or cause to be done by virtue hereof.
| Signature |
Title |
Date | ||
| /S/ J. DONALD DEBETHIZY J. Donald deBethizy |
Chief Executive Officer, President and Director (principal executive officer) | March 11, 2011 | ||
| /S/ ALAN A. MUSSO Alan A. Musso |
Senior Vice President, Chief Financial Officer and Treasurer (principal financial officer and principal accounting officer) |
March 11, 2011 | ||
| /S/ MARK SKALETSKY Mark Skaletsky |
Chairman of the Board of Directors | March 11, 2011 | ||
| /S/ M. JAMES BARRETT M. James Barrett |
Director | March 11, 2011 | ||
| /S/ CHARLES A. BLIXT Charles A. Blixt |
Director | March 11, 2011 | ||
| /S/ JULIA R. BROWN Julia R. Brown |
Director | March 11, 2011 | ||
| /S/ G. STEVEN BURRILL G. Steven Burrill |
Director | March 11, 2011 | ||
| /S/ ERROL B. DE SOUZA Errol B. De Souza |
Director | March 11, 2011 | ||
| /S/ ALAN W. DUNTON Alan W. Dunton |
Director | March 11, 2011 | ||
| /S/ JOHN P. RICHARD John P. Richard |
Director | March 11, 2011 | ||
| /S/ RALPH SNYDERMAN Ralph Snyderman |
Director | March 11, 2011 | ||
125
Table of Contents
| Exhibit |
Description | |
| 3.1 | Fourth Amended and Restated Certificate of Incorporation of the Company (incorporated by reference to Exhibit 4.1 to the Company’s Registration Statement on Form S-8, as filed with the SEC on May 8, 2006 (Registration No. 333-133881)) | |
| 3.2 | Bylaws of the Company, as amended and restated January 9, 2009 and further amended effective as of August 6, 2009 (incorporated by reference to Exhibit 3.1 to the Company’s Current Report on Form 8-K, as filed with the SEC on August 11, 2009) | |
| 4.1 | Specimen common stock certificate (incorporated by reference to Exhibit 4.1 to Amendment No. 3 to the Company’s Registration Statement on Form S-1, as filed with the SEC on March 16, 2006 (Registration No. 333-131050)) | |
| 4.2(a) | Third Amended and Restated Investor Rights Agreement, dated as of May 12, 2004, by and among the Company and certain stockholders of the Company (incorporated by reference to Exhibit 4.2(a) to the Company’s Registration Statement on Form S-1, as filed with the SEC on January 17, 2006 (Registration No. 333-131050)) | |
| 4.2(b) | Amendment No. 1, dated December 6, 2004, to Third Amended and Restated Investor Rights Agreement, dated May 12, 2004 (incorporated by reference to Exhibit 4.2(b) to the Company’s Registration Statement on Form S-1, as filed with the SEC on January 17, 2006 (Registration No. 333-131050)) | |
| 4.2(c) | Amendment No. 2, dated March 16, 2006, to Third Amended and Restated Investor Rights Agreement, dated May 12, 2004 (incorporated by reference to Exhibit 4.2(c) to Amendment No. 4 to the Company’s Registration Statement on Form S-1, as filed with the SEC on March 24, 2006 (Registration No. 333-131050)) | |
| 10.1* | Form of Indemnification Agreement between the Company and each of its directors and officers (incorporated by reference to Exhibit 10.1 to Amendment No. 3 to the Company’s Registration Statement on Form S-1, as filed with the SEC on March 16, 2006 (Registration No. 333-131050)) | |
| 10.2(a) | Lease, effective August 1, 2002, by and between the Company and Wake Forest University Health Sciences (incorporated by reference to Exhibit 10.2(a) to the Company’s Registration Statement on Form S-1, as filed with the SEC on January 17, 2006 (Registration No. 333-131050)) | |
| 10.2(b) | First Lease Amendment, effective as of January 1, 2005, to Lease effective August 1, 2002, by and between the Company and Wake Forest University Health Sciences (incorporated by reference to Exhibit 10.2(b) to the Company’s Registration Statement on Form S-1, as filed with the SEC on January 17, 2006 (Registration No. 333-131050)) | |
| 10.2(c) | Second Lease Amendment, executed June 30, 2006 effective as of March 31, 2006, to Lease effective August 1, 2002, by and between the Company and Wake Forest University Health Sciences (incorporated by reference to Exhibit 10.2 to the Company’s Quarterly Report on Form 10-Q for the Quarter Ended June 30, 2006) | |
| 10.2(d)+ | Third Lease Amendment, dated January 22, 2007 effective January 1, 2007, to Lease, effective August 1, 2002, by and between the Company and Wake Forest University Health Sciences (incorporated by reference to Exhibit 10.2(d) to the Company’s Annual Report on Form 10-K for the Year Ended December 31, 2006) | |
| 10.2(e) | Fourth Lease Amendment, dated September 18, 2007 effective August 1, 2007, to Lease, effective August 1, 2002, by and between the Company and Wake Forest University Health Sciences (incorporated by reference to Exhibit 10.2(e) to the Company’s Annual Report on Form 10-K for the Year Ended December 31, 2009) | |
126
Table of Contents
| Exhibit |
Description | |
| 10.2(f) | Fifth Lease Amendment, executed January 20, 2010 effective October 1, 2009, to Lease, effective August 1, 2002, by and between the Company and Wake Forest University Health Sciences (incorporated by reference to Exhibit 10.2(f) to the Company’s Annual Report on Form 10-K for the Year Ended December 31, 2009) | |
| 10.2(g) | Sixth Lease Amendment, effective June 30, 2010, to Lease, effective August 1, 2002, by and between the Company and Wake Forest University Health Sciences (incorporated by reference to Exhibit 10.2 to the Company’s Quarterly Report on Form 10-Q for the Quarter Ended June 30, 2010) | |
| 10.3(a)* | Amended and Restated Targacept, Inc. 2000 Equity Incentive Plan (incorporated by reference to Exhibit 99 to the Company’s Registration Statement on Form S-8, as filed with the SEC on May 8, 2006 (Registration No. 333-133882)) | |
| 10.3(b)* | Form of Incentive Stock Option Agreement under Targacept, Inc. 2000 Equity Incentive Plan (incorporated by reference to Exhibit 10.5(b) to the Company’s Registration Statement on Form S-1, as filed with the SEC on January 17, 2006 (Registration No. 333-131050)) | |
| 10.3(c)* | Form of Non-employee Director Nonqualified Stock Option Agreement under Targacept, Inc. 2000 Equity Incentive Plan (incorporated by reference to Exhibit 10.5(c) to the Company’s Registration Statement on Form S-1, as filed with the SEC on January 17, 2006 (Registration No. 333-131050)) | |
| 10.3(d)* | Form of Restricted Stock Award Agreement under Targacept, Inc. 2000 Equity Incentive Plan (incorporated by reference to Exhibit 10.5(d) to the Company’s Registration Statement on Form S-1, as filed with the SEC on January 17, 2006 (Registration No. 333-131050)) | |
| 10.4(a)* | Targacept, Inc. 2006 Stock Incentive Plan, as amended and restated through March 9, 2011 | |
| 10.4(b)* | Form of Incentive Stock Option Agreement under Targacept, Inc. 2006 Stock Incentive Plan (incorporated by reference to Exhibit 10.6(a) to Amendment No. 3 to the Company’s Registration Statement on Form S-1, as filed with the SEC on March 16, 2006 (Registration No. 333-131050)) | |
| 10.4(c)* | Form of Nonqualified Stock Option Agreement under Targacept, Inc. 2006 Stock Incentive Plan (incorporated by reference to Exhibit 10.6(b) to Amendment No. 3 to the Company’s Registration Statement on Form S-1, as filed with the SEC on March 16, 2006 (Registration No. 333-131050)) | |
| 10.4(d)* | Form of Non-employee Director Nonqualified Stock Option Agreement under Targacept, Inc. 2006 Stock Incentive Plan (incorporated by reference to Exhibit 10.6(c) to Amendment No. 3 to the Company’s Registration Statement on Form S-1, as filed with the SEC on March 16, 2006 (Registration No. 333-131050)) | |
| 10.4(e)* | Form of Restricted Stock Award Agreement under Targacept, Inc. 2006 Stock Incentive Plan (incorporated by reference to Exhibit 10.6(d) to Amendment No. 3 to the Company’s Registration Statement on Form S-1, as filed with the SEC on March 16, 2006 (Registration No. 333-131050)) | |
| 10.5(a)* | Employment Agreement, dated as of August 22, 2000, by and between the Company and J. Donald deBethizy (incorporated by reference to Exhibit 10.7 to the Company’s Registration Statement on Form S-1, as filed with the SEC on January 17, 2006 (Registration No. 333-131050)) | |
| 10.5(b)* | Amendment No. 1, dated March 13, 2008, to Employment Agreement, dated as of August 22, 2000, by and between the Company and J. Donald deBethizy (incorporated by reference to Exhibit 10.2 to the Company’s Quarterly Report on Form 10-Q for the Quarter Ended March 31, 2008) | |
| 10.6(a)* | Employment Agreement, dated as of August 22, 2000, by and between the Company and Merouane Bencherif (incorporated by reference to Exhibit 10.8 to the Company’s Registration Statement on Form S-1, as filed with the SEC on January 17, 2006 (Registration No. 333-131050)) | |
127
Table of Contents
| Exhibit |
Description | |
| 10.6(b)* | Amendment No. 1, dated March 13, 2008, to Employment Agreement, dated as of August 22, 2000, by and between the Company and Merouane Bencherif (incorporated by reference to Exhibit 10.3 to the Company’s Quarterly Report on Form 10-Q for the Quarter Ended March 31, 2008) | |
| 10.7(a)* | Employment Agreement, dated as of August 22, 2000, by and between the Company and William S. Caldwell (incorporated by reference to Exhibit 10.9 to the Company’s Registration Statement on Form S-1, as filed with the SEC on January 17, 2006 (Registration No. 333-131050)) | |
| 10.7(b)* | Amendment No. 1, dated March 13, 2008, to Employment Agreement, dated as of August 22, 2000, by and between the Company and William S. Caldwell (incorporated by reference to Exhibit 10.5 to the Company’s Quarterly Report on Form 10-Q for the Quarter Ended March 31, 2008) | |
| 10.8(a)* | Employment Agreement, dated as of April 24, 2001, by and between the Company and Geoffrey C. Dunbar (incorporated by reference to Exhibit 10.10 to the Company’s Registration Statement on Form S-1, as filed with the SEC on January 17, 2006 (Registration No. 333-131050)) | |
| 10.8(b)* | Amendment No. 1, dated March 13, 2008, to Employment Agreement, dated as of April 24, 2001, by and between the Company and Geoffrey C. Dunbar (incorporated by reference to Exhibit 10.6 to the Company’s Quarterly Report on Form 10-Q for the Quarter Ended March 31, 2008) | |
| 10.9(a)* | Employment Agreement, dated as of February 8, 2002, by and between the Company and Alan A. Musso (incorporated by reference to Exhibit 10.11 to the Company’s Registration Statement on Form S-1, as filed with the SEC on January 17, 2006 (Registration No. 333-131050)) | |
| 10.9(b)* | Amendment No. 1, dated March 13, 2008, to Employment Agreement, dated as of February 8, 2002, by and between the Company and Alan A. Musso (incorporated by reference to Exhibit 10.7 to the Company’s Quarterly Report on Form 10-Q for the Quarter Ended March 31, 2008) | |
| 10.10(a)* | Employment Agreement, dated as of September 1, 2003, by and between the Company and Jeffrey P. Brennan (incorporated by reference to Exhibit 10.12 to the Company’s Registration Statement on Form S-1, as filed with the SEC on January 17, 2006 (Registration No. 333-131050)) | |
| 10.10(b)* | Amendment No. 1, dated December 3, 2007, to Employment Agreement, dated as of September 1, 2003, by and between the Company and Jeffrey P. Brennan (incorporated by reference to Exhibit 10.12(b) to the Company’s Annual Report on Form 10-K for the Year Ended December 31, 2007) | |
| 10.10(c)* | Amendment No. 2, dated March 13, 2008, to Employment Agreement, dated as of September 1, 2003, by and between the Company and Jeffrey P. Brennan (incorporated by reference to Exhibit 10.4 to the Company’s Quarterly Report on Form 10-Q for the Quarter Ended March 31, 2008) | |
| 10.11* | Employment Agreement, dated as of March 13, 2008, by and between the Company and Peter A. Zorn (incorporated by reference to Exhibit 10.8 to the Company’s Quarterly Report on Form 10-Q for the Quarter Ended March 31, 2008) | |
| 10.12(a)+ | Amended and Restated License Agreement, dated as of March 9, 2004, by and between the Company and University of South Florida Research Foundation, Inc. (incorporated by reference to Exhibit 10.16 to the Company’s Registration Statement on Form S-1, as filed with the SEC on January 17, 2006 (Registration No. 333-131050)) | |
| 10.12(b)+ | Amendment No. 1, effective September 21, 2009, to Amended and Restated License Agreement dated March 9, 2004, by and between the Company and University of South Florida Research Foundation, Inc. (incorporated by reference to Exhibit 10.2 to the Company’s Quarterly Report on Form 10-Q for the Quarter Ended September 30, 2009) | |
128
Table of Contents
| Exhibit |
Description | |
| 10.13(a)+ | License Agreement, dated May 26, 1999, by and between the Company and University of Kentucky Research Foundation (incorporated by reference to Exhibit 10.18(a) to the Company’s Registration Statement on Form S-1, as filed with the SEC on January 17, 2006 (Registration No. 333-131050)) | |
| 10.13(b)+ | Amendment No. 1, dated August 16, 2005, to License Agreement, dated May 26, 1999, by and between the Company and University of Kentucky Research Foundation (incorporated by reference to Exhibit 10.18(b) to Amendment No. 5 to the Company’s Registration Statement on Form S-1, as filed with the SEC on April 6, 2006 (Registration No. 333-131050)) | |
| 10.14(a)+ | Collaborative Research and License Agreement, dated as of December 27, 2005, by and between the Company and AstraZeneca AB (incorporated by reference to Exhibit 10.1 to the Company’s Quarterly Report on Form 10-Q for the Quarter Ended March 31, 2006) | |
| 10.14(b) | Amendment No. 1 dated November 10, 2006 to Collaborative Research and License Agreement between the Company and AstraZeneca AB dated December 27, 2005 (incorporated by reference to Exhibit 10.1 to the Company’s Quarterly Report on Form 10-Q for the Quarter Ended September 30, 2006) | |
| 10.14(c)+ | Amendment No. 2 dated July 8, 2009 to Collaborative Research and License Agreement between the Company and AstraZeneca AB dated December 27, 2005 (incorporated by reference to Exhibit 10.1 to the Company’s Quarterly Report on Form 10-Q for the Quarter Ended September 30, 2009) | |
| 10.14(d)+ | Amendment No. 3, effective as of April 30, 2010, to Collaborative Research and License Agreement between the Company and AstraZeneca AB dated December 27, 2005 (incorporated by reference to Exhibit 10.1 to the Company’s Quarterly Report on Form 10-Q for the Quarter Ended June 30, 2010) | |
| 10.14(e)+ | Amendment No. 4, effective as of September 28, 2010, to Collaborative Research and License Agreement between the Company and AstraZeneca AB dated December 27, 2005 (incorporated by reference to Exhibit 10.1 to the Company’s Quarterly Report on Form 10-Q for the Quarter Ended September 30, 2010) | |
| 10.15+ | Exclusive License Agreement, dated January 22, 2007, by and between the Company and Yale University (incorporated by reference to Exhibit 10.20 to the Company’s Annual Report on Form 10-K for the Year Ended December 31, 2006) | |
| 10.16+ | Product Development and Commercialization Agreement, dated July 27, 2007, by and between the Company, on the one hand, and SmithKline Beecham Corporation, doing business as GlaxoSmithKline, and Glaxo Group Limited, on the other hand (incorporated by reference to Exhibit 10.1 to the Company’s Quarterly Report on Form 10-Q for the Quarter Ended September 30, 2007) | |
| 10.17+ | Collaboration and License Agreement, dated as of December 3, 2009, by and between the Company and AstraZeneca AB (incorporated by reference to Exhibit 10.20 to the Company’s Annual Report on Form 10-K for the Year Ended December 31, 2009) | |
| 10.18^ | Exclusive License Agreement, effective August 3, 2010, between the Company and Cornerstone Therapeutics Inc. | |
| 10.19* | Description of Annual Cash Incentive Program | |
| 10.20* | Description of Non-Employee Director Compensation Program (incorporated by reference to Exhibit 10.22 to the Company’s Annual Report on Form 10-K for the Year Ended December 31, 2009) | |
129
Table of Contents
| Exhibit |
Description | |
| 23.1 | Consent of Ernst & Young LLP | |
| 24.1 | Power of Attorney (included on signature page) | |
| 31.1 | Certification of the Chief Executive Officer pursuant to Rule 13a-14(a) and 15d-14(a) of the Securities Exchange Act of 1934, as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 | |
| 31.2 | Certification of the Chief Financial Officer pursuant to Rule 13a-14(a) and 15d-14(a) of the Securities Exchange Act of 1934, as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 | |
| 32.1 | Certification of the Chief Executive Officer pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 | |
| 32.2 | Certification of the Chief Financial Officer pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 | |
| + | Confidential treatment has been granted with respect to certain portions of this Exhibit, which portions have been omitted and filed separately with the SEC as part of an application for confidential treatment. |
| ^ | Portions of this Exhibit have been omitted and filed separately with the Securities and Exchange Commission as part of an application for confidential treatment pursuant to the Exchange Act. |
| * | Denotes management compensation plan or contract |
Our SEC file number for documents filed with the SEC pursuant to the Securities Exchange Act of 1934, as amended, is 000-51173.
130