Attached files
Table of Contents
Index to Financial Statements
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
(Mark One)
| x | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the fiscal year ended December 31, 2010
OR
| ¨ | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the transition period from to
Commission File Number 001-33719
MAP PHARMACEUTICALS, INC.
(Exact name of registrant as specified in its charter)
| Delaware | 20-0507047 | |
| (State or other jurisdiction of incorporation or organization) |
(I.R.S. Employer Identification No.) |
| 2400 Bayshore Parkway, Suite 200 Mountain View, California |
94043 | |
| (Address of principal executive offices) | (Zip code) |
(650) 386-3100
(Registrant’s telephone number, including area code)
Securities registered pursuant to Section 12(b) of the Act:
| Title of Each Class |
Name of Each Exchange on Which Registered | |
| Common Stock per share $0.01 par value | The NASDAQ Global Market |
Securities registered pursuant to Section 12(g) of the Act:
None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ¨ No x
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Exchange Act. Yes ¨ No x
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes x No ¨
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes ¨ No ¨
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. x
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See definitions of “large accelerated filer,” “accelerated filer,” and “smaller reporting company” in Rule 12b-2 of the Exchange Act. (Check one):
| Large accelerated filer ¨ |
Accelerated filer x | |
| Non-accelerated filer ¨ (Do not check if a smaller reporting company) |
Smaller reporting company ¨ |
Indicate by check mark whether the registrant is a shell company (as defined by Rule 12b-2 of the Exchange Act). Yes ¨ No x
The aggregate market value of the voting and non-voting common equity stock held by non-affiliates of the registrant was $181,594,769 as of June 30, 2010, the last day of the registrant’s second fiscal quarter during its fiscal year ended December 31, 2010, based upon the closing sale price on The NASDAQ Global Market reported for such date. Shares of Common Stock held by each officer and director and by each person who may be deemed to be an affiliate have been excluded. This determination of affiliate status is not necessarily a conclusive determination for other purposes.
As of February 28, 2011, the registrant had outstanding 30,204,049 shares of Common Stock.
DOCUMENTS INCORPORATED BY REFERENCE
Portions of the registrant’s proxy statement to be filed with the Securities and Exchange Commission, or the SEC, pursuant to Regulation 14A in connection with the registrant’s 2011 Annual Meeting of Stockholders, to be filed subsequent to the date hereof, are incorporated by reference into Part III of this Annual Report on Form 10-K. Such proxy statement will be filed with the SEC not later than 120 days after the conclusion of the registrant’s fiscal year ended December 31, 2010.
Table of Contents
Index to Financial Statements
2
Table of Contents
Index to Financial Statements
PART I
| ITEM 1. | BUSINESS |
Overview
Our goal is to use our proprietary inhalation technologies to enhance the therapeutic benefits and commercial attractiveness of proven drugs in the field of neurology while minimizing risk by capitalizing on their known safety, efficacy and commercialization history. We have proprietary product candidates in development that address large market opportunities.
Our strategy is to commercialize and develop differentiated neurology product candidates that can address significant unmet medical needs and overcome limitations of existing products. Key elements of our strategy include:
| • | Obtain regulatory approval for our most advanced product candidate, LEVADEX™ orally inhaled migraine therapy, for the potential acute treatment of migraine; |
| • | Build a specialized sales force to commercialize LEVADEX to neurologists and pain specialists in the United States; |
| • | Expand the market opportunity for LEVADEX; and |
| • | Advance and expand our neurology product pipeline by leveraging our technologies and our extensive scientific expertise in aerosol science and medicine to develop additional potential product candidates offering unique features and benefits. |
Our current focus is to advance our lead product candidate, LEVADEX (MAP0004) orally inhaled migraine therapy, a proprietary orally inhaled version of dihydroergotamine mesylate, or DHE, for the potential acute treatment of migraine. We completed clinical development for LEVADEX in 2010 and we plan to submit a New Drug Application, or NDA, to the U.S. Food and Drug Administration, or FDA, in the first half of 2011. In collaboration with Allergan, Inc., we plan to commercialize LEVADEX directly to neurologists and pain specialists in the United States. We are also evaluating options to commercialize LEVADEX to primary care physicians in the United States and to physicians in markets outside the United States.
Our Lead Product Candidate
Migraine is a chronic and debilitating neurological disorder characterized by episodic attacks. Migraine attacks typically manifest themselves as moderate to severe headache pain, with associated symptoms that often include nausea and vomiting, photophobia, phonophobia, and visual disturbances or aura. They usually involve “pounding” or “throbbing” pain on one side of the head, although pain may occur on both sides. Migraines limit the normal functioning of patients, who often seek dark, quiet surroundings until the episode has passed. Most migraines last between four and 24 hours, but some last as long as three days. According to published studies, the median frequency of attack is 1.5 times per month, although approximately 25% of migraine sufferers experience one or more attacks every week.
Migraine is a major public health problem that affects up to approximately 12% of the population in the United States and approximately 15% in Europe. According to the National Headache Foundation, approximately 30 million people in the United States suffer from migraine. Migraine is more common in women, with about 18% of women affected and 6% of men. Migraine prevalence is highest during the peak productive ages of 25 to 55, which results in high costs to employers and managed care organizations.
Migraine is listed in the top 20 causes of disabling conditions and in the top four neurologic disabling conditions by the World Health Organization (WHO). Related disability from migraine is substantial, with over 90% of sufferers experiencing functional impairment with their migraine that can disrupt every aspect of day to
3
Table of Contents
Index to Financial Statements
day life, including work, school, family and social relationships. More than half of the sufferers report severe impairment or the need for bed rest as a result of their migraines, according to published surveys. The economic burden of migraine remains substantial despite existing treatments with migraine patients losing four to six work days each year due to headache. The combination of direct and indirect costs of migraine in the United States is estimated at over $20 billion annually.
In 2008, according to market data, approximately 29 million prescriptions were written for the treatment of migraine in the United States. Approximately 12 million of those prescriptions were written for acute migraine specific drugs. The majority of acute migraine specific drug prescriptions written were in the triptan class. In 2010, the triptan market in the United States totaled approximately $1.6 billion in revenues.
We have designed LEVADEX to provide faster onset and longer-lasting migraine relief than triptans, the class of drugs most often prescribed for treating migraine. LEVADEX is an easy to use, at-home therapy in development that patients self-administer using our proprietary hand-held TEMPO® inhaler. DHE currently is available as an intravenous, or IV, therapy which has been used in clinical settings for over 50 years for the safe and effective treatment of migraine, particularly forms of migraine that are severe or do not respond to triptans or other therapies. We believe LEVADEX has the potential to be suitable as a first-line therapy for some migraine patients.
In May 2009, we announced results of the efficacy portion of our Phase 3 clinical trial of LEVADEX, or FREEDOM-301. We announced that the clinical trial met its four primary endpoints, pain relief and being phonophobia, photophobia and nausea free as reported two hours after dosing. Additional endpoints showed that LEVADEX provided rapid and sustained pain relief for up to 48 hours after dosing.
Patients taking LEVADEX therapy had statistically significant improvement at two hours compared to patients on placebo for each of the primary endpoints:
| • | Pain relief: 58.7% of patients who received LEVADEX compared with 34.5% for placebo (p<0.0001); |
| • | Phonophobia free: 52.9% of patients who received LEVADEX compared with 33.8% for placebo (p<0.0001); |
| • | Photophobia free: 46.6% of patients who received LEVADEX compared with 27.2% for placebo (p<0.0001); and |
| • | Nausea free: 67.1% of patients who received LEVADEX compared with 58.7% for placebo (p=0.02). |
A total of 792 patients were included in the primary data analysis as specified in the protocol of the FREEDOM-301 study. The patient population studied had more severe migraine pain than anticipated, with 46% reporting severe pain and 54% reporting moderate pain prior to administration of the study drug.
Results from additional pre-defined analyses include:
| • | LEVADEX therapy achieved statistically significant onset of pain relief at 30 minutes after dosing (p=0.03); |
| • | While not statistically significant, 50% more of the patients receiving LEVADEX therapy than the patients receiving placebo reported pain relief at 10 minutes; |
| • | LEVADEX therapy achieved statistically significant sustained pain relief from two to 24 hours (p<0.0001), as well as two to 48 hours (p<0.0001, when unadjusted for multiplicity); |
| • | LEVADEX therapy achieved statistically significant pain freedom (pain symptom score = 0) as early as 30 minutes (p=0.002, when unadjusted for multiplicity); and |
| • | LEVADEX therapy achieved sustained pain freedom from two to 24 hours, as well as two to 48 hours (p<0.0001 for both time points, when unadjusted for multiplicity). |
4
Table of Contents
Index to Financial Statements
LEVADEX was well tolerated, with the most common adverse event reported being medication aftertaste at 6%, with 2% of patients receiving placebo also reporting medication aftertaste. The next most common adverse event was nausea at 5%, compared with 2% for placebo. Symptoms or sensitivities typically associated with commonly used triptan migraine treatments, such as chest discomfort (1%) or chest pain (0%), were rare and comparable to placebo. There were no mean decreases in lung function, as measured by spirometry, between the active and placebo groups. There were no drug-related serious adverse events reported in the trial. These data were presented in September 2009 in a late-breaking session of the 14th Congress of the International Headache Society.
In 2010, we announced that a second Phase 3 clinical trial would not be required for the LEVADEX NDA submission, completed and announced successful results from a pharmacokinetic (PK) trial in smokers, a pharmacodynamics (PD) trial evaluating pulmonary artery pressure using echocardiogram and a thorough QT trial. In addition, we completed our 12 month open-label safety extension of the Phase 3 FREEDOM 301 trial. In our clinical trials conducted for LEVADEX, no drug related serious adverse events have been reported. The LEVADEX clinical development program evaluated the efficacy, safety, PK and PD of LEVADEX in approximately 1,000 patients. We plan to submit an NDA to the FDA in the first half of 2011.
On January 28, 2011 we entered into a Collaboration Agreement and Co-Promotion Agreement with Allergan, Inc., Allergan USA, Inc. and Allergan Sales, LLC (collectively, “Allergan”) to promote LEVADEX to neurologists and pain specialists within the United States. Under the terms of these agreements, following potential FDA approval, together with Allergan, we will co-promote LEVADEX to neurologists and pain specialists in the United States. Specifically, Allergan will leverage its existing U.S. sales force dedicated to headache specialists using BOTOX® for Chronic Migraine, which will be complemented by our field sales force targeting neurologists and pain specialists. If LEVADEX receives FDA approval, profits and losses from sales of LEVADEX generated from commercialization to neurologists and pain specialists in the United States will be shared equally between us and Allergan. Following potential approval of LEVADEX for the acute treatment of migraine in adults, we and Allergan will equally share regulatory, patent and development expenses for two future LEVADEX indications. We retain all rights to commercialize LEVADEX outside the United States, subject to Allergan’s right under certain circumstances to expand the territory in which the parties will commercialize LEVADEX to neurologists and pain specialists to include Canada, and we retain all rights to commercialize LEVADEX to other physicians, including primary care physicians within the United States.
As part of the collaboration, we will be responsible for the manufacturing and distribution of LEVADEX in the United States, and for recording product revenues. The companies also have agreed, following potential approval of LEVADEX for the treatment of acute migraine in adults, to jointly develop LEVADEX for the treatment of migraine in adolescents 12 to 18 years of age and for one other additional indication. We are responsible for obtaining NDA approval, and will retain ownership of the NDA.
In February 2011, we received a $60.0 million up-front payment from Allergan and may receive up to $97 million in the form of regulatory milestones, including milestones for acceptance of filing of the LEVADEX NDA and first commercial sale associated with the initial acute migraine indication.
We may establish other partnerships with pharmaceutical companies to market LEVADEX outside the United States and to primary care physicians in the United States.
Other Product Technologies
We are exploring options to advance and expand our neurology product pipeline by leveraging our technologies and our extensive scientific expertise in aerosol science and medicine to develop additional neurological product candidates offering unique features and benefits.
Nebulized Corticosteroid Particle Technology: We have expertise in the formulation and administration of nebulized corticosteroids for the treatment of pediatric asthma. We have created novel versions of budesonide
5
Table of Contents
Index to Financial Statements
that are designed to be administered more quickly and to provide efficacy at lower doses than conventional nebulized budesonide. Conventional nebulized budesonide is an inhaled corticosteroid approved by the FDA for treating asthma in children from 12 months up to eight years of age. We have developed novel morphologies of corticosteroid particles which may allow for faster delivery and efficacy at a lower dose, which together may offer improved safety, compliance and convenience.
Combination Particle Technology: We have applied our proprietary particle formulation technologies to deliver the optimal ratio of multiple drugs in a reproducible and consistent manner. We can combine two or more drugs together into a single micron scale inhalable particle at consistent and reproducible ratios, which may improve the delivery profile and stability of the resultant combination therapy. We believe our proprietary technologies in this area have potential broad applicability for a number of combination product candidates in diverse indications via inhalation and other routes of delivery.
Stable Protein & Peptide Technology: We have also demonstrated our ability to apply our proprietary technologies to formulate and stabilize biologically active proteins and peptides. We design and incorporate our protein formulations without the need for excipients or other additives, to be stored for months at room temperature and to provide multiple doses of medicine delivered accurately without the need for needle injections.
A component of our strategy is to reduce the risk of drug development by focusing on the development of proven drugs with established safety and efficacy profiles. The compounds underlying our product candidates are well characterized and have been previously approved by the FDA or foreign agencies for other sponsors and in other dosage forms and formulations. As a result, we may seek FDA marketing approval of our product candidates under Section 505(b)(2) of the Federal Food, Drug and Cosmetic Act, or FFDCA, which, if available to us, would allow any NDA we file with the FDA to rely in part on data in the public domain or the FDA’s prior conclusions regarding the safety and effectiveness of approved compounds. This may expedite the development program for our product candidates by potentially decreasing the overall scope of work we must do ourselves.
Information About our Development Programs
LEVADEX for the Acute Treatment of Migraine
LEVADEX is our proprietary orally inhaled version of DHE that has completed Phase 3 clinical development for the acute treatment of migraine, a syndrome characterized by four symptoms: pain, nausea, phonophobia, or abnormal sensitivity to sound, and photophobia, or abnormal sensitivity to light. LEVADEX is an easy to use, non-invasive, at-home therapy in development that patients self-administer using our proprietary handheld TEMPO inhaler. DHE is available as an IV therapy which has been used in clinical settings for over 50 years for the safe and effective treatment of migraine, particularly forms of migraine that are severe or do not respond to triptans or other therapies. We believe DHE’s adoption as a first-line therapy has been limited by its invasive mode of administration and high incidence of nausea.
In May 2009, we announced results from the efficacy portion of our completed Phase 3 clinical trial of LEVADEX, or FREEDOM-301. We announced that the clinical trial met its four primary endpoints, pain relief and being nausea, phonophobia and photophobia free as reported two hours after dosing. LEVADEX was well tolerated and there were no drug-related serious adverse events reported. Symptoms and sensitivities typically associated with triptans were rare and similar to placebo. Additional analyses indicated the potential of LEVADEX to effectively treat any time during the migraine including four to eight hours after onset of migraine. In 2010, we announced that a second Phase 3 clinical trial would not be required for the LEVADEX NDA submission, completed and announced successful results from a PK trial in smokers, a PD trial evaluating pulmonary artery pressure using echocardiogram and a thorough QT trial. In addition, we completed our 12 month open-label safety extension of the Phase 3 FREEDOM 301 trial. In this trial no drug related serious adverse events were reported. The LEVADEX clinical development program evaluated the efficacy, safety, PK
6
Table of Contents
Index to Financial Statements
and PD of LEVADEX in approximately 1,000 patients. We plan to submit an NDA to the FDA in the first half of 2011. Based on these results, we believe LEVADEX has the potential to be suitable as a first-line therapy for some migraine patients.
Migraine
Background
Migraine is a chronic and debilitating neurological disorder characterized by episodic attacks. Migraine attacks typically manifest themselves as moderate to severe headache pain, with associated symptoms that often include nausea and vomiting, photophobia, phonophobia, and visual disturbances or aura. They usually involve “pounding” or “throbbing” pain on one side of the head, although pain may occur on both sides. Migraines limit the normal functioning of patients, who often seek dark, quiet surroundings until the episode has passed. Most migraines last between four and 24 hours, but some last as long as three days. According to published studies, the median frequency of attack is 1.5 times per month, although approximately 25% of migraine sufferers experience one or more attacks every week.
Prevalence
Migraine is a major public health problem that affects up to approximately 12% of the population in the United States and approximately 15% in Europe. According to the National Headache Foundation, approximately 30 million people in the United States suffer from migraine. Migraine is more common in women, with about 18% of women affected and 6% of men. Migraine prevalence is highest during the peak productive ages of 25 to 55, which results in high costs to employers and managed care organizations.
Migraine disability and economic impact
Migraine is listed in the top 20 causes of disabling conditions and in the top four neurologic disabling conditions by the World Health Organization (WHO). Related disability from migraine is substantial, with over 90% of sufferers experiencing functional impairment with their migraine that can disrupt every aspect of day to day life, including work, school, family and social relationships. More than half of sufferers report severe impairment or the need for bed rest as a result of their migraines, according to published surveys. The economic burden of migraine remains substantial despite existing treatments with migraine patients losing four to six work days each year due to headache. The combination of direct and indirect costs of migraine in the United States is estimated at over $20 billion annually.
Current treatments
There are two general categories of migraine therapies: acute and preventive. Acute therapies dominate the migraine market and are used during infrequent attacks, typically characterized as one to three attacks per month, and are designed to relieve the pain, nausea, phonophobia and photophobia symptoms of migraine. The goals of acute therapy are to stop the attack quickly and consistently, while preventing recurrence, to maintain the patient’s ability to function, to use the least amount of medication and to limit adverse side effects. Although triptans are the predominant class of drugs used to specifically target migraine, DHE is another class of acute, migraine-specific therapy.
Migraine preventative and prophylactic therapies are designed to reduce the frequency and severity of migraine attacks, to make acute migraine attacks more responsive to acute therapies and to improve the quality of life for patients. Topiramate is the market leader among preventive drugs. Other drug categories used in migraine prophylaxis include beta blockers, tricyclic antidepressants and calcium channel blockers.
7
Table of Contents
Index to Financial Statements
Prescribers of migraine therapies
Most migraine patients are first diagnosed, treated and managed by primary care physicians and internists. Referral to a neurologist or headache specialist usually occurs when the patient suffers more frequent, severe and disabling migraines. There are approximately 10,000 neurologists in the United States and they are responsible for nearly 20% of the triptan prescriptions written. About half of the neurologists account for over 90% of the triptan prescriptions written by this specialty, making a specialized sales force strategy executable.
Market size
In 2008, according to market data, approximately 29 million prescriptions were written for the treatment of migraine in the United States. Approximately 12 million of those prescriptions were written for acute migraine specific drugs. The majority of acute migraine specific drug prescriptions written were in the triptan class. In 2010, the triptan market in the United States totaled approximately $1.6 billion in revenues. The triptan with the largest market share is sumatriptan with 2010 prescriptions of approximately 6.1 million in the United States.
Limitations of Current Migraine Therapies
The type of migraine treatment prescribed depends on the frequency and severity of the headache, speed of onset and previous response to medication. In published studies, migraine sufferers often cite faster onset of pain relief and lower incidence of migraine recurrence as two key therapeutic attributes they would like from their medication. Treatment typically involves patients self-medicating with over-the-counter drugs when pain is mild and attacks are infrequent. Patients with more frequent or severe migraine or those who do not respond to simple analgesics may seek medical attention with a primary care physician initially and then with a headache clinic or neurology specialist, if needed. Once a physician has diagnosed migraine, triptans are generally prescribed. If a patient does not respond to one triptan, the physician may switch to another, as the response to various triptans is unpredictable.
Triptans have three major limitations:
| • | Slow and variable onset of action and short duration of effect: While triptans have improved the treatment of migraine, the onset of pain relief with these products tends to be relatively slow and variable due to inconsistent systemic absorption via oral and nasal routes of administration. Published studies cite that recurrence of migraine, or the recurrence within 24 hours of an effectively treated migraine, is a common reason given for dissatisfaction among migraine sufferers. |
| • | Not broadly efficacious: Approximately 30% to 40% of migraine patients do not fully respond to the first triptan prescribed. Migraine patients who do not respond to any triptan therapy have few satisfactory alternatives. Additionally, triptans have been shown to be more effective when taken early in a migraine attack; however, migraine sufferers often wait to treat or are unable to treat early and may not fully benefit from triptan therapy. |
| • | Side effects: Triptans may produce sensations of chest tightness, chest pressure and tingling, often referred to as triptan sensations. |
DHE is an acute therapy and alternative to triptans that has been used for more than 50 years to safely treat migraine. Many headache specialists consider DHE to be the standard of care in treatment of status migrainosus, which is a condition characterized by debilitating migraines that last more than 72 hours. Although DHE overcomes many of the limitations of triptans, historically it also has had its own limitations, including the following:
| • | Inconvenient and inconsistent dosing: DHE has been available predominantly for administration intravenously and nasally. Intravenous administration of DHE requires the supervision of a healthcare provider and is typically performed in a headache clinic or hospital setting, which is expensive and requires the patient to travel to one of these locations while suffering with the migraine. Absorption of DHE via the nasal pathway may lead to inconsistent dosing, and generally takes 30 to 60 minutes to |
8
Table of Contents
Index to Financial Statements
| provide significant pain relief. Nasal administration of DHE may result in unpleasant taste, and can cause congestion or irritation of the nasal membrane. |
| • | Side effects: One of the common side effects of DHE administered intravenously is nausea. Patients who receive DHE intravenously are often given an anti-nausea medication at the same time. |
Our Potential Solution: LEVADEX
Based on our Phase 3 FREEDOM-301 clinical trial, we believe that LEVADEX may provide patients with the following benefits when compared to existing migraine therapies:
| • | Rapid onset: In our Phase 3 clinical trial, LEVADEX provided significant pain relief at 30 minutes after dosing and pain relief in as early as 10 minutes for patients with severe migraine pain. |
| • | Long-lasting: In our Phase 3 clinical trial, LEVADEX provided long-lasting pain relief with low incidence of recurrence, and provided sustained pain relief through 48 hours. |
| • | Efficacy at any time after the start of migraine: Additional analyses indicated the potential of LEVADEX to effectively treat at any time during the migraine including within one hour, and after eight hours from the start of migraine. |
| • | Broadly efficacious: Based on historical DHE use, LEVADEX may provide a higher response rate and has the potential to treat patients who have not previously responded to other therapies, such as triptans. We also believe that LEVADEX has the potential to treat a broad spectrum of migraine, including migraine subpopulations that are often difficult to treat, such as menstrual migraine, morning migraine, migraine with allodynia, migraine associated with severe pain and migraine with nausea and vomiting. |
| • | Low incidence of side effects: In our Phase 3 clinical trial, LEVADEX was well tolerated, with the most common adverse event reported being medication aftertaste at 6% compared with 2% for placebo. The next most common adverse event was nausea at 5%, compared with 2% for placebo. Symptoms or sensitivities typically associated with commonly used triptan migraine treatments, such as chest discomfort or chest pain, were rare and comparable to placebo. |
| • | Convenient and consistent delivery: LEVADEX is non-injectable and designed to be easy to use, which may result in increased patient comfort and compliance. The clinical trial was performed in the home, without clinical supervision and with minimal training. In a previous trial, dose-to-dose variability was comparable to solid oral dosage forms. |
LEVADEX Clinical Development Program
We completed our LEVADEX clinical development program in 2010. Our program evaluated the efficacy, safety, PK and PD of LEVADEX in approximately 1,000 patients. In 2010, we announced that a second Phase 3 clinical trial would not be required for our NDA submission, completed and announced successful results from a PK trial in smokers, a PD trial evaluating pulmonary artery pressure via echocardiogram and a thorough QT trial. In addition, we completed our 12 month open-label safety extension of the Phase 3 FREEDOM 301 trial.
Phase 3 Clinical Program. We evaluated the safety and efficacy of LEVADEX as a potential acute treatment for migraine in a Phase 3 multi-center, randomized, double-blind, placebo-controlled or FREEDOM 301 trial followed by a 12-month open-label safety assessment. In this trial, patients were randomized to either LEVADEX or placebo during the efficacy portion of the trial.
In May 2009, we announced results of the efficacy portion of FREEDOM-301. We announced that the clinical trial met its four primary endpoints, pain relief and being nausea, phonophobia and photophobia free as reported two hours after dosing. Additional endpoints showed that LEVADEX provided rapid and sustained pain relief for up to 48 hours after dosing.
9
Table of Contents
Index to Financial Statements
Patients taking LEVADEX therapy had statistically significant improvement at two hours compared to patients on placebo for each of the primary endpoints:
| • | Pain relief: 58.7% of patients who received LEVADEX compared with 34.5% for placebo (p<0.0001); |
| • | Phonophobia free: 52.9% of patients who received LEVADEX compared with 33.8% for placebo (p<0.0001); |
| • | Photophobia free: 46.6% of patients who received LEVADEX compared with 27.2% for placebo (p<0.0001); and |
| • | Nausea free: 67.1% of patients who received LEVADEX compared with 58.7% for placebo (p=0.02). |
A total of 792 patients were included in the primary data analysis as specified in the protocol of the FREEDOM-301 study. The patient population studied had more severe migraine pain than expected, with 46% reporting severe pain and 54% reporting moderate pain prior to administration of the study drug.
Results from additional pre-defined analyses include:
| • | LEVADEX therapy achieved statistically significant onset of pain relief at 30 minutes after dosing (p=0.03); |
| • | While not statistically significant, 50% more of the patients receiving LEVADEX therapy than the patients receiving placebo reported pain relief at 10 minutes; |
| • | LEVADEX therapy achieved statistically significant sustained pain relief from two to 24 hours (p<0.0001), as well as two to 48 hours (p<0.0001, when unadjusted for multiplicity); |
| • | LEVADEX therapy achieved statistically significant pain freedom (pain symptom score = 0) as early as 30 minutes (p=0.002, when unadjusted for multiplicity); and |
| • | LEVADEX therapy achieved sustained pain freedom from two to 24 hours, as well as two to 48 hours (p<0.0001 for both time points, when unadjusted for multiplicity). |
LEVADEX was well tolerated, with the most common adverse event reported being medication aftertaste at 6%, with 2% of patients receiving placebo also reporting medication aftertaste. The next most common adverse event was nausea at 5%, compared with 2% for placebo. Symptoms or sensitivities typically associated with commonly used triptan migraine treatments, such as chest discomfort (1%) or chest pain (0%), were rare and comparable to placebo. There were no decreases in lung function, as measured by spirometry, between the active and placebo groups. There were no drug-related serious adverse events reported in the trial. These data were presented in September 2009 in a late-breaking session of the 14th Congress of the International Headache Society.
In September 2009, we announced that post-hoc analysis of data from this Phase 3 trial shows the potential of LEVADEX to be effective in treating acute migraine as well as a broad spectrum of migraine, including migraine subpopulations that are often resistant to current therapies such as triptans, migraine with moderate and severe pain, migraine with nausea and vomiting and migraine with and without aura.
In October 2009, we announced that we had completed a planned interim safety review of the open-label, long-term safety extension of FREEDOM 301. At that point, more than 400 patients had completed at least six months of treatment and over 7,800 headaches had been treated in the safety extension. No drug-related serious adverse events had been reported. The goal of the ongoing long-term safety extension was to evaluate overall safety, including pulmonary and cardiovascular safety, of LEVADEX in at least 300 patients for six months and in at least 150 patients, including migraine sufferers with asthma, for 12 months as part of a potential NDA. The interim review of the data was conducted after a pre-specified number of patients had completed six months of exposure to LEVADEX and was also reviewed by an independent Data Monitoring Committee, or DMC. The
10
Table of Contents
Index to Financial Statements
DMC is an independent group of clinical trial experts, including physicians, formed to critically review and evaluate patient safety data generated in the FREEDOM 301 trial with the objective of ensuring clinical trial patient safety, quality of the data collected and continued scientific validity of the trial design. On an ongoing basis, the DMC reviewed data from the safety extension, including results of both pulmonary lung function evaluations using measures such as DLco and FEV1 and cardiac evaluations using electrocardiograms, echocardiograms and chest X-rays.
In January 2010, we announced that the FDA had informed us that a second pivotal efficacy study would not be required for the LEVADEX NDA submission.
In July 2010, we announced results from a clinical trial comparing the PK and safety of LEVADEX and intravenous DHE in 23 smokers and 24 non-smokers. The trial was designed to measure whether systemic absorption and exposure in smokers is greater than in non-smokers. In the trial, the systemic absorption of LEVADEX was not higher and systemic exposure to DHE was not greater in smokers than in non-smokers.
In September 2010, we announced results from a PD trial evaluating pulmonary artery pressure in approximately 24 healthy volunteers using echocardiogram. The trial compared acute effects on pulmonary artery pressure of LEVADEX, DHE administered intravenously and placebo. In the trial, there was no statistically significant difference between the LEVADEX and placebo groups in the primary endpoint of pulmonary artery pressure over two hours after administration.
In September 2010, we also announced in connection with our ongoing open-label safety trial: more than 400 patients had completed at least six months of treatment and more than 200 patients had completed twelve months of treatment; all non-asthmatic patients and a subset of asthmatic patients had completed treatment; LEVADEX was well tolerated and no drug-related serious adverse events had been reported; and no clinically significant trends had been reported for LEVADEX in the evaluation of cardiovascular measurements and pulmonary function.
In November 2010, we announced results from a thorough QT trial in 54 healthy adults comparing the acute effects of a supra-therapeutic dose of LEVADEX (approximately three times the anticipated commercial dose), oral moxifloxacin (400 mg) and placebo on the cardiac QT interval as measured by electrocardiogram. Results of the trial showed that a supra-therapeutic dose of LEVADEX does not increase QTc intervals. For the supra-therapeutic dose of LEVADEX, the largest mean difference from placebo in QTc (using the individual correction method for heart rate, or QTci) was 0.08 milliseconds, and the largest one-sided 95% upper confidence bound was 2.24 milliseconds. The threshold level of regulatory concern is when the change produced by a drug has a 95% upper confidence bound that exceeds 10 milliseconds. The number of subjects with individual QTc intervals > 450 milliseconds and increases in QTc from baseline > 30 milliseconds were similar to placebo. Moxifloxacin, the positive control, produced QT prolongation consistent with previous thorough QT trials.
In December 2010, we announced completion of the LEVADEX open-label safety trial. In total, more than 475 patients completed six months treatment and more than 250 patients completed 12 months treatment. No drug-related serious adverse events were reported. We have now completed the final trial necessary to support an NDA for LEVADEX and plan to submit the NDA in the first half of 2011.
Phase 2 Clinical Trial Results. In March 2007, we announced positive results from two Phase 2 clinical trials with LEVADEX for the acute treatment for migraine.
The objective of the first Phase 2 clinical trial was to evaluate the efficacy and tolerability of three different doses of LEVADEX in adult migraine patients when self-administered at home. This Phase 2 clinical trial was a randomized, double blind, placebo-controlled trial of three doses of LEVADEX in 86 patients. The clinical trial consisted of two treatment periods. The first treatment period evaluated two doses of LEVADEX, 1.0 mg and 0.5 mg versus placebo and the second treatment period re-randomized responders in the first treatment period to
11
Table of Contents
Index to Financial Statements
evaluate a lower dose, 0.25 mg versus placebo. In the first treatment period, the 0.5 mg dose of LEVADEX showed pain relief in 32% of the patients at ten minutes (p = 0.019), pain relief in 72% of the patients at two hours, the clinical trial’s primary endpoint (p = 0.019), and sustained pain relief in 43% of the patients at 24 hours (p = 0.066) in a treatment received population. Unlike IV DHE, which is generally administered with an anti-nausea medication, LEVADEX was administered by itself and showed no statistically significant drug related increase in nausea. LEVADEX was also shown in the clinical trial to be well tolerated, with no serious adverse events reported. In the second treatment period, 35 subjects were randomized to treat a second subsequent migraine with a 0.25 mg dose versus placebo. No significant benefit was seen with this lowest dose when compared to placebo.
The objective of the second Phase 2 clinical trial was to evaluate the safety and tolerability of LEVADEX in subjects with asthma and to demonstrate that the blood levels of the drug achieved by the therapy were similar to those seen after inhalation by subjects with healthy lungs. This Phase 2 clinical trial was a randomized, double blind, placebo-controlled trial in 19 adult asthmatics. Each patient received three doses, one every week in randomized order over a 15-day period, including two 1.0 mg doses of LEVADEX and one dose of placebo. The clinical trial indicated that LEVADEX was well tolerated by subjects with compromised lung function, and that the PK of LEVADEX, or distribution of the drug in the body, was similar to that experienced by adults with healthy lungs as shown in an earlier Phase 1 clinical trial. No serious or significant drug related adverse events were reported. In addition, no clinically significant changes were observed in pulmonary function tests, heart rate, blood pressure, respiratory rate or mean IgE levels, a measure of systemic immune response, or the body’s defenses reacting to a foreign substance.
We believe that, based on our PK and receptor binding research, administration of LEVADEX via the lung may provide an opportunity to retain the efficacy attributes seen with IV DHE while minimizing the potential side effects often seen during IV DHE administration. PK data suggest that LEVADEX closely mimics the blood levels and the time to maximum drug concentration seen with effective doses of DHE administered intravenously. However, unlike IV administration of DHE, we do not expect LEVADEX to cause significant treatment related nausea which may be a factor that has limited the usage of IV DHE outside the headache clinic or hospital. In the FREEDOM 301 trial the incidence of treatment related nausea was low at 5% compared with 2% for placebo. In our Phase 1 trial comparing IV DHE to LEVADEX, the blood levels of drug were similar. However, the maximum drug concentration for inhaled DHE administered with our TEMPO inhaler was approximately 40 fold lower than that for IV DHE, which we believe in part accounts for the low incidence of drug-induced nausea observed in our clinical trials to date.
In addition, we have conducted pre-clinical animal studies to evaluate lung toxicity and coronary vascular effects of our proprietary formulation of DHE. In our six month chronic inhalation toxicity assessment of DHE, where animals were exposed to up to 1.08 mg/kg (more than 46 times the maximum potential recommended daily dose of LEVADEX, if approved) of DHE per day for six months, there was no significant respiratory tract toxicity observed. In another pre-clinical study designed to evaluate cardiovascular parameters, we observed no significant differences in coronary vascular effects comparing inhaled DHE to IV DHE.
Because DHE is well characterized and previously approved, we may seek FDA marketing approval of LEVADEX under Section 505(b)(2) of the FFDCA. Section 505(b)(2) of the FFDCA provides an alternate path to FDA approval for modifications to formulations of products previously approved by the FDA. Section 505(b)(2) permits the filing of an NDA where at least some of the information required for approval comes from clinical trials not conducted by or for the applicant and for which the applicant has not obtained a right of reference. This may expedite the development program for LEVADEX by potentially decreasing the overall scope of work we must do ourselves.
Other Potential Uses and Indications for LEVADEX
We plan to consider development of LEVADEX for use outside the United States as well as for potential additional indications beyond acute migraine.
12
Table of Contents
Index to Financial Statements
We believe there is opportunity to develop LEVADEX for potential use outside of the United States. While acute migraine is a major public health problem affecting approximately 12% of the population in the United States, it also affects approximately 15% of the population in Europe. Based on the accumulated nonclinical and clinical data to date, we believe there may be significant commercial opportunities for LEVADEX outside of the United States.
Furthermore, based on key LEVADEX attributes observed to date, including fast onset of action, long duration of effect as well as historical uses for DHE, developing additional indications for LEVADEX may represent significant opportunities. We believe LEVADEX may have the potential to treat additional migraine indications such as cluster headache, menstrual migraine, adolescent migraine, chronic migraine, chronic daily headache, medication over-use headache and status migrainosus.
Other Product Technologies
While we do not plan to make further significant direct investment in the product candidates described below, we plan to evaluate other potential product candidates which may utilize these technologies, as well as partnership opportunities for further development and commercialization of these product candidates.
Nebulized Corticosteroid Particle Technology
We have expertise in the formulation of nebulized corticosteroids for the treatment of pediatric asthma. We have created novel versions of budesonide that are designed to be administered more quickly and to provide efficacy at lower doses than conventional nebulized budesonide. Conventional nebulized budesonide is an inhaled corticosteroid approved by the FDA, for treating asthma in children from 12 months up to eight years of age. We have developed novel morphologies of corticosteroid particles which may allow for faster delivery and efficacy at a lower dose, which together may offer improved safety, compliance and convenience.
We have suspended development of Unit Dose Budesonide, our former nebulized budesonide program, after not meeting primary efficacy endpoints in a Phase 3 trial. However, we believe our technology remains applicable. We are considering options moving forward, by leveraging our experience with budesonide and our expertise in particle technology, including the development of a next generation therapy with a corticosteroid.
MAP0005 — Combination Particle Technology
We believe MAP0005 serves as a proof of concept for the robust, specific delivery of two therapeutic agents that could benefit from targeted receptor delivery in a fixed ratio within a single particle. We intend to opportunistically evaluate the application of this technology to additional product candidates because we believe our proprietary technologies in this area have potential broad applicability for a number of combination product candidates in diverse indications via inhalation and other routes of delivery. MAP0005, our proprietary combination of an inhaled corticosteroid and a long-acting beta-agonist, or LABA, for the potential treatment of asthma and chronic obstructive pulmonary disease, or COPD, utilizes our proprietary particle formulation technologies to administer the optimal ratio of multiple drugs in a reproducible and consistent manner. We combine two or more drugs together into a single micron scale inhalable particle at a pre-defined consistent and reproducible ratio, which may improve the delivery profile and stability of the resultant combination therapy. In April 2008, we announced positive results from a Phase 2a clinical trial evaluating MAP0005 for the potential treatment of asthma and COPD. We believe this approach, as compared to current ICS/LABA combinations, may allow the optimal ratio of each drug to the lung to reach the relevant receptors at the cellular level in the lung in a more reproducible and consistent manner, reducing the amount of drug delivered systemically and potentially improving the side effect profile, while improving therapeutic efficacy.
MAP0001 — Stable Protein and Peptide Particle Technology
We believe MAP0001 serves as proof of concept for the ability to formulate and stabilize biologically-active proteins and peptides and deliver them to the lung. We design and incorporate our protein formulations
13
Table of Contents
Index to Financial Statements
without the need for excipients or other additives, to be stored for months at room temperature and to provide multiple doses of medicine delivered accurately without the need for invasive needle injections. We intend to opportunistically evaluate the application of this technology to additional product candidates. We are demonstrating this capability with MAP0001, our proprietary formulation of insulin for the potential treatment of Type 1 and Type 2 diabetes via pulmonary delivery using our proprietary TEMPO inhaler. In a Phase 1a clinical trial conducted in Australia, MAP0001 was biologically active and achieved maximum therapeutic blood levels as quickly as Novorapid subcutaneous injection, a widely used injectable insulin.
We have not filed an IND with the FDA for MAP0005 or MAP0001 because our clinical trials were not conducted in the United States.
Our Technology
Our aerosol delivery and pharmacological profiling technology combines our knowledge of aerosol science and medicine, and enables us to create inhaled drug products with potentially enhanced pharmacological profiles relative to the parent drugs, thereby improving their efficacy and safety. Starting with the bulk drug substance, we develop particles with physical and chemical characteristics that are well suited for the aerosol delivery of the product candidate. The particle engineering allows more of our drug to reach the areas of the respiratory tract to treat disease and reduces the amount of drug that is deposited in the back of the throat where it can cause local and systemic side effects. We then formulate the drug particles into a delivery medium and package them into the aerosol delivery system that is best suited for the formulation and dosing regimen in order to maximize patient compliance. Our expertise in aerosol formulation science and pulmonary medicine allows us to select excipients, if any, already in wide use and regarded as safe, that result in favorable safety characteristics and allow flexibility in delivery format. The resulting drug products can be as consistent and efficient as alternative, often more invasive dosing formats, such as injection, but with the advantages of fast onset, high degree of intake at the target organs, and lower or controlled systemic exposure. The convenience, consistency and efficiency of inhaled administration in combination with the characteristics of our product candidates can offer meaningful therapeutic benefits when compared to existing drugs, increasing the probability of the successful adoption of our product candidates.
We apply our proprietary technologies to optimize drugs for two general types of therapeutic applications:
| • | Pulmonary delivery as a non-invasive method of quickly and safely administering systemic drugs. Administration of drugs via the respiratory tract is a non-invasive method of delivering drugs efficiently to the systemic circulation, with rapid onset of action, bypassing the gastrointestinal tract where many drugs are extensively metabolized after oral administration, and with rapid onset of action. The drug, or combination of drugs, can reach the intended site of action as quickly as intravenously administered drugs and more quickly than oral, dermal, sublingual or even alternative injection routes, such as subcutaneous or intramuscular. We can apply our technology to small or large molecules, including peptides and proteins. |
| • | Delivery of drugs to treat respiratory diseases locally. Diseases such as asthma, COPD and some respiratory tract infections have been treated by pulmonary drug delivery for many years in order to target therapeutic effect to the lung and reduce systemic drug exposure and related side effects. Our technology is designed to improve the therapeutic efficacy and safety of known drugs for these applications, by efficiently delivering customized drug particles to those areas in the lung where drug is required and minimizing the drug exposure to other areas of the respiratory tract and body. In addition, our technologies have the potential to broaden the types of respiratory illnesses that can effectively be targeted and treated safely via pulmonary delivery. |
Aerosol Delivery and Pharmacological Profiling Technology
Our proprietary technologies include particle creation and formulation technologies, which can be applied to small or large molecules, including peptides and proteins. Our technologies also include the development and
14
Table of Contents
Index to Financial Statements
manufacturing of aerosol delivery platforms, including our TEMPO inhaler. The TEMPO inhaler is a proprietary, next generation pressurized metered dose inhaler, or MDI, that dispenses drug automatically when the patient inhales and has high consistency and efficiency compared to other inhalers. Our technologies are covered by over 15 issued U.S. patents and over 25 U.S. patent applications that we own or have licensed, as well as their foreign counterparts.
Particle Creation and Formulation
We control the characteristics of our drug particles by using technology and expertise in aerosol physics, particle science and formulation, and in safety toxicology and pharmacology. We can consistently generate drug-containing aerosols with the optimal particle or droplet sizes for the therapeutic indication. Particles that are too large tend to be deposited in the throat, while medium sized particles are more efficiently delivered to the large bronchial tubes and small particles are more efficiently delivered to the alveoli, the small sacks that make up most of the absorptive surface area of the lung. We can formulate product candidates in propellants without additional excipients, or with small amounts of excipients previously shown to be safe. We can also combine drugs by producing small, inhalable particles composed of one drug which is reproducibly intermingled or coated with multiple drugs in fixed ratios.
One of our key technologies is the generation of particles by supercritical fluid, or SCF, crystallization. SCF gives us the ability to create very small particles ranging from 100 nanometers to 10 microns in diameter with highly precise particle size distributions. The particles have uniform surfaces with few discontinuities or irregularities that provide enhanced aerosol performance. They are also stable for long storage periods without refrigeration, and require minimal or no excipients that can increase the potential for local toxicity or inflammatory response.
In addition to particle generation, we have extensive expertise in formulating aerosol drugs, especially for nebulized and MDI delivery formats. A key feature of this expertise is our know-how in formulating aerosolized drugs with appropriate excipients. We have expertise in formulation screening, assay development, aerosol performance testing and clinical performance simulation, long-term stability testing, large volume non-clinical testing and generation and release of pre-clinical and clinical supplies through to human clinical proof of concept.
We believe that the combination of these various particle creation and formulation technologies is a key component of our competitive advantage.
TEMPO Inhaler Platform
We designed our proprietary TEMPO inhaler to enable accurate and reproducible pulmonary delivery of the drug particles we develop. Our TEMPO inhaler is an innovative next generation MDI. The TEMPO inhaler incorporates the size, ease of use and convenience advantages associated with standard MDIs, and is designed to overcome their greatest limitations: inconsistent dosing, drug delivery inefficiency and the need for patients to synchronize a breath with manual triggering of the inhaler, which is particularly difficult for certain patient populations. Even the more recently introduced breath-actuated MDIs exhibit the inconsistent dosing and drug delivery inefficiency of older MDIs.
The TEMPO inhaler is designed to offer a number of key competitive advantages compared to standard MDIs. These advantages include:
| • | Automatic, optimal release of therapy: Our triggering technology is tuned for each particular drug so that drug release is synchronized to the optimal point in the breathing cycle to allow the released drug to reach the targeted area of the respiratory tract. For example, data from a scintigraphy study showed that the TEMPO inhaler deposited 75% less of a corticosteroid in the mouth and throat and delivered three times as much drug to the lungs as a conventional MDI. |
15
Table of Contents
Index to Financial Statements
| • | Plume speed control: Conventional MDIs spray plumes of drug at speeds of up to 50 miles per hour, causing much of the drug to hit the back of the throat. By contrast, our TEMPO inhaler controls and slows down the drug plume to match the speed of the patient’s inhaled breath, so more of the drug is entrained in the inhaled air and carried into the lungs. |
| • | Dose consistency: Results from the TEMPO inhaler performance data along with results from our clinical trials indicate that the TEMPO inhaler’s dose-to-dose consistency is comparable to IV dosing. The TEMPO inhaler also includes a dose counter to display how many doses remain available for use. The dose counter can prevent dispensing of additional doses after a maximum number of doses have been delivered. |
| • | Convenient, multiple dose use: The TEMPO inhaler does not use electronics or batteries and can conveniently contain multiple doses. It can include up to a month’s supply depending on the drug, in a small, handheld inhaler approximately the same size as a conventional MDI and it may be used with small molecule drugs and biologics. |
We have conducted clinical trials with three clinical product candidates which utilize our TEMPO inhaler: LEVADEX for the potential treatment of migraine, MAP0005 for the potential treatment of asthma and COPD and MAP0001 for the potential treatment of diabetes.
Our Strategy
Key elements of our strategy include:
| • | Obtain regulatory approval for our most advanced product candidate LEVADEX: LEVADEX has completed Phase 3 clinical development and we plan to submit an NDA with the FDA for the acute treatment of migraine in the first half of 2011. We believe the risk of clinical trial failure may be lower than traditional new chemical entities because we are evaluating drugs that have been previously reviewed and approved by the FDA and have a known safety and efficacy profile. |
| • | Build a specialized sales force to commercialize LEVADEX to neurologists and pain specialists in the United States: Our goal is to build a sales force in the United States to market and sell our products, if approved, to neurologists and pain specialists. |
| • | Expand the market opportunity for LEVADEX: In order to expand the commercial opportunity for LEVADEX, we may develop additional follow-on indications for LEVADEX and develop partnerships with pharmaceutical companies to market and sell to primary care physicians. Outside the United States, we may establish commercial partnerships for all of our product candidates in order to accelerate development and regulatory approvals in those countries and further broaden their commercial potential. |
| • | Advance and expand our neurology product pipeline, by leveraging our technologies and our extensive scientific expertise in aerosol science and medicine to develop additional potential product candidates offering unique features and benefits: We intend to focus our pipeline development initially on products with established safety and efficacy records, but whose market potential has been limited by safety, relative efficacy and patient compliance. We believe that we can overcome these limitations by leveraging our technologies. These technologies underpin our competitive advantage in developing multiple, high-value products with clearly defined patient benefits. In addition, we may in-license additional product candidates to be marketed to the same neurology channel. |
Collaborations and License Agreements
Allergan
On January 28, 2011, we entered into a Collaboration Agreement (the “Collaboration Agreement”) and a Co-Promotion Agreement (the “Co-Promotion Agreement,” and together with the Collaboration Agreement, the “Allergan Agreements”) with Allergan, Inc., Allergan USA, Inc. and Allergan Sales, LLC (collectively,
16
Table of Contents
Index to Financial Statements
“Allergan”). Pursuant to the terms of the Allergan Agreements, we have granted Allergan a co-exclusive license to market and promote LEVADEX to neurologists and pain specialists in the United States in collaboration with us.
Under the Allergan Agreements, we retain the right to market and promote LEVADEX to other physicians within the United States. We also retain all rights to LEVADEX in all other countries, subject to Allergan’s right under certain circumstances to expand the territory to include Canada. Allergan and we will each provide sales representatives and other sales support for such marketing and promotional efforts. The Allergan Agreements specify minimum annual sales detail requirements to be provided by each party, and establish maximum annual amounts of detailing costs that each party will be obligated to incur pursuant to a commercialization plan.
The parties will collaborate in the development of LEVADEX for the treatment of migraine in adolescents 12 to 18 years of age, and for at least one other indication. We may develop LEVADEX for certain other indications independently of the collaboration if Allergan does not agree to develop LEVADEX for such indications pursuant to the Allergan Agreements. We will be responsible for manufacturing and supplying LEVADEX, and for distributing the product and recording product revenues from sales of LEVADEX resulting from the parties’ collaboration.
The parties will share profits and losses resulting from the collaboration equally. We will be solely responsible for payment of all remaining costs of obtaining regulatory approval of LEVADEX for the acute treatment of migraine in adults, except that if the FDA notifies us that additional development or manufacturing activities costing in excess of a certain threshold amount will be required for such regulatory approval, the parties will share any such excess costs. The parties generally will share equally all other costs of developing LEVADEX under the Allergan Agreements, except that neither party shall be obligated for more than a certain threshold amount in a given year, or for more than a certain threshold amount in the aggregate, for development or manufacturing costs or expenses incurred by us for such activities.
Under the terms of the Allergan Agreements, Allergan has paid us an upfront payment of $60.0 million. We may also receive up to an additional $97 million in the form of regulatory milestones, which includes milestones for acceptance of filing of the LEVADEX NDA and first commercial sale associated with the initial acute migraine indication.
The Collaboration Agreement may be terminated (i) by Allergan, at will, after first commercial sale of LEVADEX in the United States, upon 180 days’ prior written notice, (ii) by Allergan, upon written notice to us, if we receive a complete response letter or equivalent communication from the FDA, that Allergan determines will extend potential approval beyond a certain date or requires a certain minimum level of additional investment, (iii) by us, upon written notice to Allergan, if Allergan commercializes a competing product in the United States (or, if the territory of the Allergan Agreements is expanded, Canada) and (iv) by us, upon written notice to Allergan, if Allergan challenges or opposes patent rights licensed to Allergan pursuant to the Collaboration Agreement. Additionally, either party may terminate the Collaboration Agreement in the event of an uncured material breach. The Co-Promotion Agreement will terminate upon termination of the Collaboration Agreement.
Nektar Therapeutics
We entered into a license agreement with Nektar Therapeutics UK Limited, or Nektar, in June 2004, and amended the agreement in August 2006 and October 2007. Under the agreement, Nektar granted us a worldwide, exclusive license, with a right to sublicense, under Nektar patents and know-how to develop and commercialize any formulation of a form of dihydroergotamine for administration by inhalation using a delivery platform. The Nektar patents licensed to us include two types of patent claims: compound-limited claims and compound-inclusive claims. Compound-limited claims are Nektar patent claims that claim a form of dihydroergotamine, or formulations or methods of manufacture or methods of use of dihydroergotamine, and our license to these claims
17
Table of Contents
Index to Financial Statements
is fully-paid up and royalty free and will survive expiration or any termination of the agreement. Compound-inclusive claims are Nektar patent claims that are not compound-limited claims and our license to these claims is royalty-bearing.
Our obligation to pay royalties to Nektar is based on net sales of products, and will continue, on a country-by-country basis, until the longer of expiration of Nektar patents covering the product, ten years after the first commercial sale of the product, or the date that Nektar’s know-how becomes known to the general public. In addition, we are required to make future payments based upon achievement of certain product development milestones. As of December 31, 2010, when and if certain milestones are achieved we may be obligated to pay Nektar up to $5.0 million in total future development milestone payments with respect to our LEVADEX product candidate.
Under the agreement, we granted Nektar a worldwide, nonexclusive, royalty-free license under our patents and know-how solely to the extent useful or necessary for Nektar to fulfill its obligations under the agreement.
Either party may terminate the agreement upon a material, uncured default of the other party. We may terminate the agreement, with or without cause, at any time upon six months’ written notice.
Exemplar Pharmaceuticals
In April 2006 we entered into a manufacturing and supply agreement with Exemplar Pharmaceuticals, LLC, or Exemplar, formerly known as Xemplar Pharmaceuticals, LLC, for the manufacture and supply by Exemplar to us of our clinical and commercial requirements of pressurized metered dose aerosol canisters containing placebo or active ingredient that is to be housed within a fully-assembled TEMPO inhaler and packaged for clinical and commercial use.
Exemplar agreed to convert its manufacturing facility into a Good Manufacturing Practices, or GMP, contract manufacturing facility suitable for the commercial production of the product prior to or when Exemplar obtains the approvals necessary to manufacture these products in compliance with the manufacturing agreement.
We have agreed that, from the date the first NDA is submitted for a product and for a certain period thereafter Exemplar will manufacture and supply from its manufacturing facility all such filled canisters as we require to support development and commercialization. If Exemplar fails to supply on time under certain circumstances, we have the right to immediately terminate the manufacturing agreement by written notice and to manufacture the product ourselves or purchase it from a third party.
Either party may terminate the agreement upon a material, uncured breach or default by the other party. We may terminate the agreement upon 60 days written notice upon our reasonable determination that Exemplar does not have the capability to manufacture the product in accordance with the warranty or in sufficient quantities.
Intellectual Property
We protect our technology through the use of patents, trade secrets and proprietary know-how. We own or in-license six issued U.S. patents, and 14 U.S. patent applications, as well as their foreign counterparts, which relate to our most advanced product candidate LEVADEX. The patents and patent applications that may issue that we own or in-license, which we rely on for LEVADEX, expire between 2017 and 2030. Our patent and patent applications relating to LEVADEX include claims covering:
| • | TEMPO inhaler devices and components; |
| • | various formulations of the LEVADEX active ingredient; |
| • | the processing of the LEVADEX active ingredient; |
18
Table of Contents
Index to Financial Statements
| • | stabilization of the formulation; |
| • | pharmacokinetics of the active ingredient delivered by the inhalation system; and |
| • | the treatment of migraine via delivery of the formulation to the lung. |
Our commercial success will depend in part on obtaining and maintaining patent protection and trade secret protection of our product candidates, and the methods used to manufacture them, as well as successfully defending these patents against third-party challenges. Our ability to protect our product candidates from unauthorized making, using, selling, offering to sell or importation by third parties is dependent upon the extent to which we have rights under valid and enforceable patents or trade secrets that cover these activities. We have rights to several third-party proprietary processing and manufacturing technologies related to our product candidates. See “Collaborations and License Agreements.” We rely on such third parties to protect the intellectual property we license, and we do not and have not had any control over the filing or prosecution of patent applications. We cannot be certain that such prosecution efforts have been or will be conducted in compliance with applicable laws and regulations or will result in valid and enforceable patents. Our enforcement of these licensed patents or defense of any claims asserting the invalidity of these patents would also be subject to the cooperation of the third parties.
Manufacturing
All of our manufacturing processes, which comply with current good manufacturing practices, or cGMP, are outsourced to third parties with oversight by our internal managers. We have limited cGMP manufacturing capacity in house. We rely on third-party manufacturers to produce sufficient quantities of drug product for use in clinical trials. We intend to continue this practice for any future clinical trials and large-scale commercialization of LEVADEX and for any other potential products for which we retain significant development and commercialization rights.
The drug substance of LEVADEX has been manufactured by a contract manufacturing organization, or CMO, located in Europe. Our CMO has extensive experience manufacturing bulk drug under cGMP and has the capacity to manufacture at commercial scale. We are exclusive licensees of the manufacturing process for production of LEVADEX final drug substance. Under our worldwide license from Nektar, we have enabled another CMO to manufacture clinical and commercial supply of the final drug substance to be used in the development and commercialization of LEVADEX. The TEMPO inhaler is manufactured by third-party CMOs. The plastic inhaler component manufacture and assembly, valve manufacture and canister fill are each performed by specific third-party CMOs.
Competition
The pharmaceutical industry is highly competitive, with a number of established, large pharmaceutical companies, as well as many smaller companies. Many of these companies have greater financial resources, marketing capabilities and experience in obtaining regulatory approvals for product candidates. There are many pharmaceutical companies, biotechnology companies, public and private universities, government agencies and research organizations actively engaged in research and development of products which may target the same markets as our product candidates. We expect any future products we develop to compete on the basis of, among other things, product efficacy and safety, time to market, price, extent of adverse side effects experienced and convenience of administration and drug delivery. One or more of our competitors may develop products based upon the principles underlying our proprietary technologies earlier than us, obtain approvals for such products from the FDA more rapidly than us or develop alternative products or therapies that are safer, more effective and/ or more cost effective than any future products developed by us. We also expect to face competition in our efforts to identify appropriate collaborators or partners to help commercialize our product candidates in our target commercial areas.
19
Table of Contents
Index to Financial Statements
If approved for the acute treatment of migraine, we anticipate that LEVADEX would compete against other marketed migraine therapies and companies and may compete with products currently under development by large and small companies. In 2008, according to market data, approximately 29 million prescriptions were written for the treatment of migraine in the United States. Approximately 12 million of those prescriptions were written for acute migraine specific drugs. The majority of marketed prescription products for the treatment of migraine are in the triptan class. In 2010, the triptan market in the United States totaled approximately $1.6 billion in revenues. The triptan with the largest market share is sumatriptan with 2010 prescriptions of approximately 6.1 million in the United States. There are at least six other branded triptan therapies being sold by pharmaceutical companies. Alternative formulations of triptans are available that may have faster onset of action than solid oral dosage forms. In April 2008, GlaxoSmithKline’s Treximet, a combination oral formulation of sumatriptan and naproxen sodium, was approved by the FDA for the treatment of acute migraine. In July 2009, Zogenix, Inc’s Sumavel DosePro needle-free sumatriptan was approved by the FDA for the treatment of acute migraine and cluster headache. Alternative formulations of DHE include Migranal, which is nasally delivered and which may become generically available prior to any commercial introduction of LEVADEX. In addition to marketed migraine therapies, there are product candidates under development by large pharmaceutical companies such as Merck & Co., Inc. and other smaller companies. In October 2010, Allergan’s BOTOX injectable onabotulinumtoxinA was approved by the FDA for the treatment of chronic migraine, a different indication than acute migraine.
We will also face competition from generic sumatriptan, the active ingredient in Imitrex. Although we believe generic sumatriptan could not be substituted for LEVADEX, a generic version of sumatriptan may be more quickly adopted by health insurers and patients than LEVADEX. Financial pressure to use generic products and uncertainty of reimbursement for single source alternatives, such as LEVADEX, may encourage the use of a generic product over LEVADEX.
Government Regulation Federal Food, Drug and Cosmetic Act
Prescription drug products are subject to extensive pre- and post-market regulation by the FDA, including regulations that govern the testing, manufacturing, safety, efficacy, labeling, storage, record keeping, advertising, and promotion of such products under the Federal Food, Drug and Cosmetic Act, or FFDCA, and its implementing regulations, and by comparable agencies and laws in foreign countries. Failure to comply with applicable FDA or other requirements may result in civil or criminal penalties, recall or seizure of products, partial or total suspension of production or withdrawal of the product from the market. FDA approval is required before any new unapproved drug or dosage form, including a new use of a previously approved drug, can be marketed in the United States. All applications for FDA approval must contain, among other things, information relating to safety and efficacy, pharmaceutical formulation, stability, manufacturing, processing, packaging, labeling and quality control.
New Drug Applications
A new drug approval by the FDA is generally required before a drug may be marketed in the United States. This process generally involves:
| • | completion of pre-clinical laboratory and animal testing in compliance with the FDA’s Good Laboratory Practice, or GLP, regulations; |
| • | submission to the FDA of an IND application for human clinical testing which must become effective before human clinical trials may begin in the United States; |
| • | performance of adequate and well-controlled human clinical trials to establish the safety and efficacy of the proposed drug product for each intended use; |
| • | satisfactory completion of an FDA pre-approval inspection of the facility or facilities at which the product is manufactured to assess compliance with the FDA’s cGMP regulations; and |
| • | submission to and approval by the FDA of an NDA application. |
20
Table of Contents
Index to Financial Statements
The pre-clinical and clinical testing and approval process requires substantial time, effort and financial resources, and we cannot be certain that any approvals for our product candidates will be granted on a timely basis, if at all. Pre-clinical tests include laboratory evaluation of product chemistry, formulation and stability, as well as studies to evaluate toxicity in animals. The results of pre-clinical tests, together with manufacturing information and analytical data, are submitted as part of an IND application to the FDA. The IND automatically becomes effective 30 days after receipt by the FDA, unless the FDA, within the 30 day time period, raises concerns or questions about the conduct of the clinical trial, including concerns that human research subjects will be exposed to unreasonable health risks. In such a case, the IND sponsor and the FDA must resolve any outstanding concerns before the clinical trial can begin. Our submission of an IND may not result in FDA authorization to commence a clinical trial. A separate submission to an existing IND must also be made for each successive clinical trial conducted during product development. Further, an independent institutional review board, or IRB, covering each medical center proposing to conduct the clinical trial must review and approve the plan for any clinical trial before it commences at that center and it must monitor the clinical trial until completed. The FDA, the IRB or the sponsor may suspend a clinical trial at any time on various grounds, including a finding that the subjects or patients are being exposed to an unacceptable health risk. As a separate amendment to an IND, a sponsor may submit a request for a SPA from the FDA. Under the SPA procedure, a sponsor may seek the FDA’s agreement on the design and size of a clinical trial intended to form the primary basis of an efficacy claim. If the FDA agrees in writing, its agreement may not be changed after the clinical trial begins, except in limited circumstances, such as when a substantial scientific issue essential to determining the safety and effectiveness of a product candidate is identified after a Phase 3 clinical trial is commenced. If the outcome of the clinical trial is successful, the sponsor will ordinarily be able to rely on it as the primary basis for approval with respect to effectiveness. Clinical testing also must satisfy extensive Good Clinical Practice, or GCP, regulations, including regulations for informed consent.
For purposes of an NDA submission and approval, human clinical trials are typically conducted in the following three sequential phases, which may overlap:
| • | Phase 1: Clinical trials are initially conducted in a limited population to test the product candidate for safety, dose tolerance, absorption, metabolism, distribution and excretion in healthy humans or, on occasion, in patients, such as cancer patients. |
| • | Phase 2: Clinical trials are generally conducted in a limited patient population to identify possible adverse effects and safety risks, to determine the efficacy of the product for specific targeted indications and to determine dose tolerance and optimal dosage. Multiple Phase 2 clinical trials may be conducted by the sponsor to obtain information prior to beginning larger and more extensive Phase 3 clinical trials. In some cases, a sponsor may decide to run what is referred to as a “Phase 2b” evaluation, which is a second, confirmatory Phase 2 clinical trial that could, if positive and accepted by the FDA, serve as a pivotal trial in the approval of a product candidate. |
| • | Phase 3: These are commonly referred to as pivotal clinical trials. When Phase 2 evaluations demonstrate that a dose range of the product is effective and has an acceptable safety profile, Phase 3 clinical trials are undertaken in large patient populations to further evaluate dosage, to provide substantial evidence of clinical efficacy and to further test for safety in an expanded and diverse patient population at multiple, geographically-dispersed clinical trial sites. |
| • | Phase 4: These are clinical trials conducted after a drug has been approved. In some cases, the FDA may condition approval of an NDA for a product candidate on the sponsor’s agreement to conduct additional clinical trials to further assess the drug’s safety and effectiveness after NDA approval. Such post approval trials are typically referred to as Phase 4 clinical trials. |
The results of product development, pre-clinical studies and clinical trials are submitted to the FDA as part of an NDA. NDAs must also contain extensive manufacturing information. Once the submission has been accepted for filing, by law the FDA has 180 days to review the application and respond to the applicant. Under the Prescription Drug User Fee Act, or PDUFA, the FDA agrees to specific goals for NDA review time through a
21
Table of Contents
Index to Financial Statements
two-tiered classification system, Standard Review and Priority Review. Standard Review is applied to a drug that offers at most only minor improvement over existing marketed therapies. Standard Review NDAs have a goal of being completed within a 10-month timeframe. A Priority Review designation is given to drugs that offer major advances in treatment, or provide a treatment where no adequate therapy exists. A Priority Review means that the time it takes the FDA to review an NDA is reduced such that the goal for completing a Priority Review initial review cycle is six months. It is likely that our product candidates will be granted a Standard Review. The review process is often significantly extended by FDA requests for additional information or clarification. The FDA may refer the application to an advisory committee for review, evaluation and recommendation as to whether the application should be approved. The FDA is not bound by the recommendation of an advisory committee, but it generally follows such recommendations.
The FDA may deny approval of an NDA if the applicable regulatory criteria are not satisfied, or it may require additional clinical data and/or an additional pivotal Phase 3 clinical trial. Even if such data are submitted, the FDA may ultimately decide that the NDA does not satisfy the criteria for approval. Data from clinical trials are not always conclusive and FDA may interpret data differently than we do. Once issued, the FDA may withdraw product approval if ongoing regulatory requirements are not met or if safety problems occur after the product reaches the market. In addition, the FDA may require testing, including Phase 4 clinical trials and surveillance programs, to monitor the effect of approved products that have been commercialized, and the FDA has the power to prevent or limit further marketing of a product based on the results of these postmarketing programs. Drugs may be marketed only for approved indications and in accordance with the provisions of the approved label. Further, if there are any modifications to the drug, including changes in indications, labeling or manufacturing processes or facilities, we may be required to submit and obtain FDA approval of a new or supplemental NDA, which may require us to develop additional data or conduct additional pre-clinical studies and clinical trials.
Section 505(b)(2) New Drug Applications
As an alternate path to FDA approval for modifications to formulations of products previously approved by the FDA, an applicant may file an NDA under Section 505(b)(2) of the FFDCA. Section 505(b)(2) was enacted as part of the Drug Price Competition and Patent Term Restoration Act of 1984, also known as the Hatch-Waxman Act, and permits the filing of an NDA where at least some of the information required for approval comes from clinical trials not conducted by or for the applicant and for which the applicant has not obtained a right of reference. The Hatch-Waxman Act permits the applicant to rely upon the FDA’s findings of safety and effectiveness based on certain pre-clinical or clinical trials conducted for an approved product. The FDA may also require companies to perform additional clinical trials or measurements to support the change from the approved product. The FDA may then approve the new product candidate for all or some of the label indications for which the referenced product has been approved, as well as for any new indication sought by the Section 505(b)(2) applicant.
To the extent that a Section 505(b)(2) NDA relies on clinical trials conducted for a previously approved drug product, the applicant is required to certify to the FDA concerning any patents listed for the approved product in the Orange Book. Specifically, the applicant must certify for each listed patent that (1) the required patent information has not been filed; (2) the listed patent has expired; (3) the listed patent has not expired, but will expire on a particular date and approval is sought after patent expiration; or (4) the listed patent is invalid, unenforceable or will not be infringed by the new product. A certification that the new product will not infringe the already approved product’s listed patent or that such patent is invalid is known as a Paragraph IV certification. If the applicant does not challenge the listed patents through a Paragraph IV certification, the Section 505(b)(2) NDA application will not be approved until all the listed patents claiming the referenced product have expired. The Section 505(b)(2) NDA application also will not be accepted or approved until any non-patent exclusivity, such as exclusivity for obtaining approval of a New Chemical Entity, listed in the Orange Book for the referenced product, has expired.
22
Table of Contents
Index to Financial Statements
If the 505(b)(2) NDA applicant has provided a Paragraph IV certification to the FDA, the applicant must also send notice of the Paragraph IV certification to the referenced NDA and patent holders once the 505(b)(2) NDA has been accepted for filing by the FDA. The NDA and patent holders may then initiate a legal challenge to the Paragraph IV certification. Under the FFDCA, the filing of a patent infringement lawsuit within 45 days of their receipt of a Paragraph IV certification automatically prevents the FDA from approving the Section 505(b)(2) NDA for 30 months, or until a court decides that the patent is invalid, unenforceable or not infringed, whichever is earlier. The court also has the ability to shorten or lengthen the 30 month stay if either party is found not to be reasonably cooperating in expediting the litigation. Thus, the Section 505(b)(2) applicant may invest a significant amount of time and expense in the development of its product only to be subject to significant delay and patent litigation before its product may be commercialized. Alternatively, if the listed patent holder does not file a patent infringement lawsuit within the required 45 day period, the applicant’s NDA will not be subject to the 30 month stay.
DEA Regulation
Our research and development processes involve the controlled use of hazardous materials, including chemicals. Some of these hazardous materials are considered to be controlled substances and are subject to regulation by the U.S. Drug Enforcement Agency, or the DEA. Controlled substances are those drugs that appear on one of five schedules promulgated and administered by the DEA under the Controlled Substances Act, or CSA. The CSA governs, among other things, the distribution, recordkeeping, handling, security and disposal of controlled substances. We must be registered by the DEA in order to engage in these activities, and are subject to periodic and ongoing inspections by the DEA and similar state drug enforcement authorities to assess ongoing compliance with the DEA’s regulations. Any failure to comply with these regulations could lead to a variety of sanctions, including the revocation, or a denial of renewal, of the DEA registration, injunctions or civil or criminal penalties.
International Regulation
In addition to regulations in the United States, we will be subject to a variety of foreign regulations governing clinical trials and commercial sales and distribution of any future products. Whether or not we obtain FDA approval for a product, we must obtain approval by the comparable regulatory authorities of foreign countries before we can commence clinical trials or marketing of the product in those countries. The approval process varies from country to country, and the time may be longer or shorter than that required for FDA approval. The requirements governing the conduct of clinical trials, product licensing, pricing and reimbursement vary greatly from country to country.
For example, under European Union regulatory systems, marketing authorizations may be submitted either under a centralized or mutual recognition procedure. The centralized procedure provides for the grant of a single marketing authorization that is valid for all European Union member states. The mutual recognition procedure provides for mutual recognition of national approval decisions. Under this procedure, the holder of a national marketing authorization may submit an application to the remaining member states. Within 90 days of receiving the applications and assessment report, each member state must decide whether to recognize approval.
In addition to regulations in Europe and the United States, we will be subject to a variety of foreign regulations governing clinical trials and commercial distribution of any future products.
Third-Party Payor Coverage and Reimbursement
Although none of our product candidates has been commercialized for any indication, if they are approved for marketing, commercial success of our product candidates will depend, in part, upon the availability of coverage and reimbursement from third-party payors at the federal, state and private levels. Government payor
23
Table of Contents
Index to Financial Statements
programs, including Medicare and Medicaid, private health care insurance companies and managed care plans have attempted to control costs by limiting coverage and the amount of reimbursement for particular procedures or drug treatments. The United States Congress and state legislatures from time to time propose and adopt initiatives aimed at cost containment. Ongoing federal and state government initiatives directed at lowering the total cost of health care will likely continue to focus on health care reform, the cost of prescription pharmaceuticals and on the reform of the Medicare and Medicaid payment systems. Examples of how limits on drug coverage and reimbursement in the United States may cause reduced payments for drugs in the future include:
| • | changing Medicare reimbursement methodologies; |
| • | fluctuating decisions on which drugs to include in formularies; |
| • | revising drug rebate calculations under the Medicaid program; and |
| • | reforming drug importation laws. |
Some third-party payors also require pre-approval of coverage for new or innovative platforms or drug therapies before they will reimburse health care providers that use such therapies. While we cannot predict whether any proposed cost-containment measures will be adopted or otherwise implemented in the future, the announcement or adoption of these proposals could have a material adverse effect on our ability to obtain adequate prices for our product candidates and operate profitably.
Manufacturing Requirements
We and our third-party manufacturers must comply with applicable FDA regulations relating to FDA’s cGMP regulations. The cGMP regulations include requirements relating to organization of personnel, buildings and facilities, equipment, control of components and drug product containers and closures, production and process controls, packaging and labeling controls, holding and distribution, laboratory controls, records and reports, and returned or salvaged products. The manufacturing facilities for our products must meet cGMP requirements to the satisfaction of the FDA pursuant to a pre-approval inspection before we can use them to manufacture our products. We and our third-party manufacturers are also subject to periodic inspections of facilities by the FDA and other authorities, including procedures and operations used in the testing and manufacture of our products to assess our compliance with applicable regulations. Failure to comply with statutory and regulatory requirements subjects a manufacturer to possible legal or regulatory action, including warning letters, the seizure or recall of products, injunctions, consent decrees placing significant restrictions on or suspending manufacturing operations and civil and criminal penalties. Adverse experiences with the product must be reported to the FDA and could result in the imposition of market restrictions through labeling changes or in product removal. Product approvals may be withdrawn if compliance with regulatory requirements is not maintained or if problems concerning safety or efficacy of the product occur following approval.
Other Regulatory Requirements
With respect to post-market product advertising and promotion, the FDA imposes a number of complex regulations on entities that advertise and promote pharmaceuticals, which include, among other things, standards for direct-to-consumer advertising, off-label promotion, industry-sponsored scientific and educational activities and promotional activities involving the Internet. The FDA has very broad enforcement authority under the FFDCA, and failure to abide by these regulations can result in penalties, including the issuance of a warning letter directing entities to correct deviations from FDA standards, a requirement that future advertising and promotional materials be pre-cleared by the FDA and state and federal civil and criminal investigations and prosecutions. We are also subject to various laws and regulations regarding laboratory practices, the experimental use of animals and the use and disposal of hazardous or potentially hazardous substances in connection with our research. In each of these areas, as above, the FDA has broad regulatory and enforcement powers, including the ability to levy fines and civil penalties, suspend or delay issuance of approvals, seize or recall products and withdraw approvals, any one or more of which could have a material adverse effect on us.
24
Table of Contents
Index to Financial Statements
Employees
As of December 31, 2010, we had 100 full-time employees. Of the full-time employees, 73 were engaged in product development and clinical activities, and 27 were engaged in sales, general and administrative activities. We plan to continue to expand our product development programs. To support this growth, we will need to expand managerial, operations, development, regulatory, sales, marketing, finance and other functions. None of our employees are represented by a labor union, and we consider our employee relations to be good.
Available Information
We file electronically with the Securities and Exchange Commission, or SEC, our annual reports on Form 10-K, quarterly reports on Form 10-Q and current reports on Form 8-K pursuant to Section 13(a) or 15(d) of the Securities Exchange Act of 1934. The public may read or copy any materials we file with the SEC at the SEC’s Public Reference Room at 100 F Street, NE, Washington, DC 20549. The public may obtain information on the operation of the Public Reference Room by calling the SEC at 1-800-SEC-0330. The SEC maintains an Internet site that contains reports, proxy and information statements, and other information regarding issuers that file electronically with the SEC. The address of that site is http://www.sec.gov.
We incorporated in the state of Delaware, were originally formed as a limited liability company on July 3, 2003 and converted to a corporation on December 11, 2003. Our principal executive offices are located at 2400 Bayshore Parkway, Suite 200, Mountain View, California, 94043. Our telephone number is (650) 386-3100, and our web site address is www.mappharma.com. Our annual reports on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K and amendments to those reports are available free of charge on our web site as soon as reasonably practicable after such reports are filed with or furnished to the SEC. Our Code of Business Conduct and Ethics can also be found on our website.
Financial Information
See Item 6, Selected Financial Data and Item 7, Management’s Discussion and Analysis of Financial Condition and Results of Operations.
25
Table of Contents
Index to Financial Statements
| ITEM 1A. | RISK FACTORS |
Certain factors may have a material adverse effect on our business, financial condition and results of operations, and you should carefully consider them. Accordingly, in evaluating our business, we encourage you to consider the following discussion of risk factors, in its entirety, in addition to other information contained in this report as well as our other public filings with the Securities and Exchange Commission.
Risks Relating to Our Financial Position and Need for Additional Capital
We have a history of net losses. Currently, we have no products approved for commercial sale, and to date we have not generated any product revenue. As a result, we may continue to incur substantial and increasing net losses for the foreseeable future, and we may never achieve or maintain profitability.
We are not profitable and do not expect to be profitable on a sustained basis in the foreseeable future. We have incurred significant net losses and negative cash flow in each year since our inception, including net losses of approximately $54.7 million, $9.0 million and $72.9 million for the years ended December 31, 2010, 2009 and 2008, respectively. As of December 31, 2010, we had a deficit accumulated during development stage of approximately $239.6 million. We have devoted most of our financial resources to research and development, including our pre-clinical development activities, clinical trials and manufacturing-related activities. We have not obtained regulatory approval for, or commercialized any product candidate and have therefore not generated any product revenues. In that regard, we expect to incur additional expenses as we prepare and pursue our new drug application, or NDA, for LEVADEX, our most advanced product candidate, with the U.S. Food and Drug Administration, or the FDA. In addition, if we are required by the FDA to perform studies in addition to those we have conducted, our expenses will increase beyond expectations and the timing of any potential product approval may be delayed. We also expect an increase in our expenses associated with our manufacturing work and with preparing for commercialization. In addition, we expect to continue to incur costs to support operations as a public company. As a result, we may continue to incur substantial net losses and negative cash flow for the foreseeable future. These losses and negative cash flows have had, and will continue to have, an adverse effect on our stockholders’ equity and working capital.
Because of the numerous risks and uncertainties associated with pharmaceutical product development, we are unable to accurately predict the timing or amount of substantial expenses or when, or if, we will be able to achieve or maintain profitability. We have financed our operations primarily through the sale of equity securities, collaboration payments and debt financings. The size of our future net losses will depend, in part, on the rate of growth of our expenses and the rate of growth, if any, of our revenues. Revenues from potential strategic partnerships are uncertain because we may not enter into any additional strategic partnerships. On January 28, 2011, we entered into a collaboration agreement with Allergan, Inc., or Allergan, pursuant to which Allergan will co-promote LEVADEX with us in the United States to neurologists and pain specialists. In addition to the $60 million upfront payment already received from Allergan, we are eligible to receive additional payments upon achievement of regulatory milestones and first commercial sale. If we do not meet these milestones, we will not receive additional payments and, under certain circumstances, Allergan may terminate our collaboration. On July 8, 2009, we received a notice of termination of our license agreement with AstraZeneca AB, or the AstraZeneca Agreement, related to our Unit Dose Budesonide, or UDB, product candidate. Under the AstraZeneca Agreement, AstraZeneca had agreed to fund our remaining development activities for UDB and to reimburse us for costs we incur with respect to future development activities conducted for the U.S. registration of our UDB product candidate, subject to the terms and conditions of the AstraZeneca Agreement. Following the termination of the AstraZeneca Agreement, we suspended development of UDB. If we are unable to develop and commercialize our other product candidates, including pursuant to strategic partnerships, or if sales revenue from any product candidate that receives marketing approval is insufficient, we will not achieve profitability. Even if we do achieve profitability, we may not be able to sustain or increase profitability.
26
Table of Contents
Index to Financial Statements
We have a limited operating history, and we expect a number of factors to cause our operating results to fluctuate on a quarterly and annual basis, which may make it difficult to predict our future performance.
Our operations to date have been primarily limited to organizing and staffing our company, developing our technology and undertaking pre-clinical studies, clinical trials and manufacturing-related activities of our product candidates. We have not yet obtained regulatory approvals for any of our product candidates. Consequently, any predictions you make about our future success or viability may not be as accurate as they could be if we had a longer operating history. Specifically, our financial condition and operating results have varied significantly in the past and will continue to fluctuate from quarter-to-quarter and year-to-year in the future due to a variety of factors, many of which are beyond our control. Factors relating to our business that may contribute to these fluctuations include the following factors, among others:
| • | our ability to obtain additional funding to develop our product candidates; |
| • | the need to obtain regulatory approval of our most advanced product candidate, LEVADEX for the potential treatment of migraine; |
| • | potential risks related to any collaborations we may enter into for our product candidates, including our current collaboration with Allergan for LEVADEX; |
| • | delays in the commencement, enrollment and completion of clinical testing, as well as the analysis and reporting of results from such clinical testing; |
| • | the success of clinical trials of our LEVADEX product candidate or future product candidates; |
| • | any delays in regulatory review and approval of product candidates in development, including any requirements to perform additional preclinical or clinical trials; |
| • | our ability to receive regulatory approval or commercialize our product candidates; |
| • | our ability to rely on Section 505(b)(2) of the Federal Food, Drug and Cosmetic Act, or FFDCA, to seek FDA marketing approval of our product candidates; |
| • | market acceptance and rate of market adoption of our product candidates for which we obtain regulatory approval; |
| • | our ability, and our partners’ ability, to establish an effective sales and marketing infrastructure; |
| • | competition from existing products or new products that may emerge; |
| • | the impact of competition, including generics, in the migraine market on our ability to commercialize LEVADEX; |
| • | the ability of patients to obtain coverage of or sufficient reimbursement for our products; |
| • | the ability to receive regulatory approval or commercialize our products outside of the United States; |
| • | potential side effects of our future products that could delay or prevent commercialization or cause an approved drug to be taken off the market; |
| • | regulatory difficulties relating to products that have already received regulatory approval; |
| • | guidelines and recommendations of therapies published by various organizations; |
| • | potential product liability claims; |
| • | potential liabilities associated with hazardous materials; |
| • | our ability to maintain adequate insurance policies; |
| • | our dependency on third-party manufacturers to supply or manufacture our products; |
| • | our ability to establish or maintain collaborations, licensing or other arrangements; |
27
Table of Contents
Index to Financial Statements
| • | our ability, our partners’ abilities, and third parties’ abilities to protect and assert intellectual property rights; |
| • | costs related to and outcomes of potential intellectual property litigation; |
| • | compliance with obligations under intellectual property licenses with third parties; |
| • | our ability to adequately support future growth; and |
| • | our ability to attract and retain key personnel to manage our business effectively. |
Due to the various factors mentioned above, and others, the results of any prior quarterly or annual periods should not be relied upon as indications of our future operating performance.
We will need substantial additional funding and if we are unable to raise capital when needed, we would be forced to delay, reduce or eliminate our product development programs.
Developing biopharmaceutical products, including conducting pre-clinical studies and clinical trials and establishing manufacturing capabilities, is expensive. While we have completed our clinical development program for LEVADEX for the treatment of acute migraine in adults, we expect to have continued expenses in connection with our ongoing activities, particularly as we focus on and proceed with our NDA submission for LEVADEX, our most advanced product candidate. In addition, our expenses could increase beyond expectations if the FDA requires that we perform additional studies to those that we have conducted, in which case the timing of any potential product approval may be delayed. We believe that our existing cash and cash equivalents, together with the upfront payment of $60.0 million we received in February 2011 pursuant to the collaboration agreement with Allergan, will be sufficient to fund our projected operating requirements for at least 12 months. We will need substantial additional capital in the future in order to commercialize LEVADEX and to fund the development and commercialization of future product candidates. Until we can generate a sufficient amount of product revenue, if ever, we expect to finance future cash needs through public or private equity offerings, debt financings or corporate collaboration and licensing arrangements, including our collaboration with Allergan. Such funding, if needed, may not be available on favorable terms, if at all. In the event we are unable to obtain additional capital, we may delay or reduce the scope of our current research and development programs and other expenses.
If adequate funds are not available, we may be required to delay, reduce the scope of or eliminate one or more of our research or development programs or our commercialization efforts. To the extent that we raise additional funds by issuing equity securities, our stockholders may experience additional significant dilution, and debt financing, if available, may involve restrictive covenants. To the extent that we raise additional funds through collaboration and licensing arrangements, it may be necessary to relinquish some rights to our technologies or our product candidates or to grant licenses on terms that may not be favorable to us. We may seek to access the public or private capital markets whenever conditions are favorable, even if we do not have an immediate need for additional capital at that time.
Our forecast of the period of time through which our financial resources will be adequate to support our operations is a forward-looking statement and involves risks and uncertainties, and actual results could vary as a result of a number of factors, including the factors discussed elsewhere in this “Risk Factors” section. We have based this estimate on assumptions that may prove to be wrong, and we could utilize our available capital resources sooner than we currently expect. Our future funding requirements will depend on many factors, including, but not limited to:
| • | the scope, rate of progress and cost of our clinical trials and other research and development activities; |
| • | the costs and timing of regulatory approval including any potential delays that may occur; |
| • | the costs of filing, prosecuting, defending and enforcing any patent claims and other intellectual property rights; |
28
Table of Contents
Index to Financial Statements
| • | the effect of competing technological and market developments; |
| • | the terms and timing of any collaboration, licensing or other arrangements that we may establish, including our current collaboration agreement with Allergan;. |
| • | the cost and timing of commercial-scale manufacturing and distribution activities; |
| • | the costs of establishing sales, marketing and distribution capabilities for any product candidates for which we may receive regulatory approval; and |
| • | rate of market adoption of our product candidates for which we obtain regulatory approval. |
Risks Relating to the Development, Regulatory Approval and Commercialization of Our Product Candidates
We are largely dependent on the success of one product candidate, and we cannot be certain that this product candidate will receive regulatory approval.
We have invested a significant portion of our efforts and financial resources in the development of LEVADEX and UDB. In February 2009, we announced top-line results from our first Phase 3 trial of UDB, indicating that the trial did not meet its co-primary endpoints in either dose evaluated when compared to placebo. In July 2009, we announced that we were suspending development of UDB, after our partner AstraZeneca terminated our license agreement. We are now largely dependent on the success of one product candidate, LEVADEX, for which we have completed a Phase 3 clinical development program. Our ability to generate product revenue, which we do not expect will occur for some time, if ever, will depend heavily on the successful regulatory approval and commercialization of this product candidate. We may have inadequate financial or other resources to advance LEVADEX through the NDA process, depending on the requirements of the FDA. In May 2009, we announced top-line results from the efficacy portion of our first Phase 3 trial of LEVADEX, indicating that the trial met all its co-primary endpoints when LEVADEX was compared to placebo. A long-term safety extension of the trial has also been completed and no drug-related serious adverse events were reported in the trial. Although we had planned to initiate a second Phase 3 efficacy study in the first quarter of 2010, we have been informed by the FDA that a second pivotal efficacy study is not required for submission of our NDA if the topline efficacy results we submitted in 2009 are confirmed during the NDA review. We have completed a pharmacokinetics trial in 23 adult smokers comparing them to 24 adult non-smokers. The trial was designed to measure whether the systemic absorption of LEVADEX is higher and exposure to dihydroergotamine mesylate, or DHE, is greater in smokers than in non-smokers. In the trial, the systemic absorption of LEVADEX was not higher and systemic exposure to DHE was not greater in smokers than in non-smokers. We also have completed a pharmacodynamics trial evaluating pulmonary artery pressure in approximately 24 healthy volunteers using echocardiograms. The trial compared the acute effects on pulmonary artery pressure of LEVADEX, DHE administered intravenously and placebo. In the trial, there was no statistically significant difference between the LEVADEX and placebo groups in the primary endpoint of pulmonary artery pressure over two hours after administration. In addition we have completed a thorough QT trial in which LEVADEX had no effect on QT interval as measured by electrocardiograms. Our clinical development program for LEVADEX may not lead to regulatory approval from the FDA and similar foreign regulatory agencies if we fail to demonstrate that the product candidate is safe and effective, and we may therefore fail to commercialize LEVADEX. Any failure to obtain regulatory approval of LEVADEX would have a material and adverse impact on our business.
With the suspension of development for our UDB product candidate, LEVADEX is our only current late stage product candidate. Our drug development efforts may not produce any other proprietary product candidates. We cannot be certain that we will be able to acquire or in-license other product candidates or develop other product candidates. . Our failure to develop product candidates will limit our ability to generate additional revenue.
We currently have no approved drug products for sale and we cannot guarantee that we will ever have marketable drug products. The research, testing, manufacturing, labeling, approval, selling, marketing and
29
Table of Contents
Index to Financial Statements
distribution of drug products are subject to extensive regulation by the FDA and other regulatory authorities in the United States and other countries, with regulations differing from country to country. We are not permitted to market our product candidates in the United States until we receive approval of an NDA from the FDA for each product candidate. We have not submitted an NDA or received marketing approval for any of our product candidates in any country. Obtaining approval of an NDA is a lengthy, expensive and uncertain process. Markets outside of the United States also have requirements for approval of drug candidates which we must comply with prior to marketing.
We have entered into a collaboration arrangement with Allergan, pursuant to which Allergan will commercialize LEVADEX, with us, to neurologists and pain specialists in the United States, following regulatory approval of LEVADEX. We may not fully realize the potential benefits of our collaboration with Allergan which may lead to an inability to obtain significant sales within the neurology and pain specialist segment of the migraine market and we may not be able to commercialize LEVADEX to primary care physicians.
We have entered into a collaboration agreement targeting the neurology and pain specialist segment of the United States market. We believe that adoption of LEVADEX by neurologists and pain specialists, who regularly treat migraine patients, will help to lead to broader adoption in the United States market. Our dependence on Allergan to help us to commercialize LEVADEX in this market segment and Allergan’s performance under our collaboration agreement may not lead to physician uptake in this market and we may not be able to successfully commercialize LEVADEX in the specialty market. While we believe that neurologists and pain specialists, because they treat migraine patients, may be early adopters of LEVADEX and drive market adoption in the primary physician segment of the market, our ability to enter into a partnership targeting the primary physician market may have an effect on the overall sales of LEVADEX. If we are unable to enter into a commercial partnership targeting primary care physicians, we may be unable to commercialize LEVADEX to primary care physicians on our own, and we may not realize significant revenues from product sales relating to that segment. Our profits from the collaboration are shared equally with Allergan and this can limit overall profits and financial performance of the Company.
We may enter into additional collaborations with third parties to develop and commercialize our product candidates, including LEVADEX. These collaborations may place the development and commercialization of our product candidates outside our control, may require us to relinquish important rights or may otherwise be on terms unfavorable to us.
We may enter into additional collaborations with third parties to develop and commercialize our product candidates, including LEVADEX. For example, we may enter into a collaboration with a third party in the Unites States to commercialize LEVADEX to primary care physicians and/or to develop and commercialize LEVADEX outside the United States. Our dependence on current and future partners for development and commercialization of our product candidates will subject us to a number of risks, including:
| • | we may not be able to control the amount and timing of resources that our partners may devote to the development or commercialization of product candidates or to their marketing and distribution; |
| • | partners may delay clinical trials, provide insufficient funding for a clinical trial program, stop a clinical trial or abandon a product candidate, repeat or conduct new clinical trials or require a new formulation of a product candidate for clinical testing; |
| • | disputes may arise between us and our partners that result in the delay or termination of the research, development or commercialization of our product candidates or that result in costly litigation or arbitration that diverts management’s attention and resources; |
| • | partners may experience financial difficulties; |
| • | partners may not properly maintain or defend our intellectual property rights, or may use our proprietary information, in such a way as to invite litigation that could jeopardize or invalidate our intellectual property rights or proprietary information or expose us to potential litigation; |
30
Table of Contents
Index to Financial Statements
| • | business combinations or significant changes in a partner’s business strategy may adversely affect a partner’s willingness or ability to meet its obligations under any arrangement; |
| • | a partner could independently move forward with a competing product candidate developed either independently or in collaboration with others, including our competitors; and |
| • | the collaborations with our partners may be terminated or allowed to expire, which would delay the development and may increase the cost of developing our product candidates. |
Delays in the commencement, enrollment and completion of clinical testing could result in increased costs to us and delay or limit our ability to obtain regulatory approval for our product candidates.
Delays in the commencement, enrollment and completion of clinical testing could significantly affect our product development costs. While we have completed clinical development for our LEVADEX product candidate, we may be requested by the FDA to conduct additional clinical trials. In addition we will need to conduct clinical trials for future product candidates. The commencement and completion of clinical trials requires us to identify and maintain a sufficient number of trial sites, many of which may already be engaged in other clinical trial programs for the same indication as our product candidates or may be required to withdraw from our clinical trial as a result of changing standards of care or may become ineligible to participate in clinical studies. The commencement, enrollment and completion of clinical trials can be delayed for a variety of other reasons, including delays related to:
| • | reaching agreements on acceptable terms with prospective contract research organizations, or CROs, and trial sites, the terms of which can be subject to extensive negotiation and may vary significantly among different CROs and trial sites; |
| • | obtaining regulatory approval to commence a clinical trial; |
| • | obtaining institutional review board, or IRB, approval to conduct a clinical trial at numerous prospective sites; |
| • | recruiting and enrolling patients to participate in clinical trials for a variety of reasons, including meeting the enrollment criteria for our study and competition from other clinical trial programs for the same indication as our product candidates; |
| • | retaining patients who have initiated a clinical trial but may be prone to withdraw due to the treatment protocol, lack of efficacy, personal issues or side effects from the therapy or who are lost to further follow-up; |
| • | maintaining and supplying clinical trial material on a timely basis; and |
| • | collecting, analyzing and reporting final data from the clinical trials. |
In addition, a clinical trial may be suspended or terminated by us, the FDA or other regulatory authorities due to a number of factors, including:
| • | failure to conduct the clinical trial in accordance with regulatory requirements or our clinical protocols; |
| • | inspection of the clinical trial operations or trial sites by the FDA or other regulatory authorities resulting in the imposition of a clinical hold; |
| • | unforeseen safety issues or any determination that a trial presents unacceptable health risks; and |
| • | lack of adequate funding to continue the clinical trial, including the incurrence of unforeseen costs due to enrollment delays, requirements to conduct additional trials and studies and increased expenses associated with the services of our CROs and other third parties. |
We have completed a Phase 3 clinical program to support our NDA for LEVADEX. In October 2009, we submitted our topline efficacy results for the double-blind efficacy portion of our pivotal Phase 3 study. We also
31
Table of Contents
Index to Financial Statements
have completed the long-term safety extension of our pivotal Phase 3 trial, a pharmacokinetics trial in healthy adult smokers and non-smokers, a pharmacodynamics trial measuring pulmonary artery pressure in healthy adults and a thorough QT trial in support of our NDA for LEVADEX. FDA communicated its agreement with the design, execution, and analyses for our pivotal Phase 3 trial, which we submitted to the FDA under the Special Protocol Assessment, or SPA, process and modified as suggested by FDA. Under a SPA, the FDA agrees to not later alter its position with respect to adequacy of the design, execution, or analyses of the clinical trial intended to form the primary basis of an effectiveness claim in an NDA, without the sponsor’s agreement unless the FDA identifies a substantial scientific issue essential to determining the safety or efficacy of the drug after testing begins. In March 2010, we held a pre-NDA meeting with the FDA to discuss the clinical portion of our anticipated NDA filing. The FDA’s minutes of that meeting state that, while the FDA did not have a record of a formal SPA, the FDA concurred with the selection of our co-primary endpoints and confirmed that a second pivotal efficacy study was not necessary if topline efficacy results were confirmed during the NDA review. We believe that our prior written correspondence and interactions with the FDA under the SPA process constitute an SPA with the agency. The FDA may take a different view and could request additional safety and efficacy studies without having to identify a substantial scientific issue with our Phase 3 trial that is essential to determining the safety and efficacy of LEVADEX. If we are required to conduct additional clinical trials or other testing of our LEVADEX product candidate beyond those that we currently contemplate, we may be delayed in obtaining, or may not be able to obtain, marketing approval for this product candidate. We may not be able to obtain approval for indications that are as broad as intended or we may obtain approval for indications different than those indications for which we seek approval. Furthermore we may not be able to obtain approval for any of our other product candidates.
Additionally, changes in regulatory requirements and guidance may occur and we may need to amend clinical trial protocols to reflect these changes with appropriate regulatory authorities. Amendments may require us to resubmit our clinical trial protocols to IRBs for re-examination, which may impact the costs, timing or successful completion of a clinical trial. If we experience delays in the completion of, or if we terminate, our clinical trials, the commercial prospects for our product candidates will be harmed, and our ability to generate product revenues will be delayed. In addition, many of the factors that cause, or lead to, a delay in the commencement or completion of clinical trials may also ultimately lead to the denial of regulatory approval of a product candidate. Even if we are able to ultimately commercialize our product candidates, other therapies for the same or similar indications may have been introduced to the market and established a competitive advantage.
Because the results of prior clinical trials are not necessarily predictive of future results, LEVADEX or any other product candidate advanced into clinical trials may not have favorable results in subsequent clinical trials or receive regulatory approval.
Success in pre-clinical studies and clinical trials does not ensure that subsequent clinical trials will generate adequate data to demonstrate the efficacy and safety of the investigational drug. A number of companies in the pharmaceutical industry, including those with greater resources and experience, have suffered significant setbacks in Phase 3 clinical trials, even after seeing promising results in prior clinical trials.
The data collected from our clinical trials may not be adequate to support regulatory approval of LEVADEX or any of our other product candidates. In May 2009, we announced top-line results from the efficacy portion of our Phase 3 trial of LEVADEX, indicating that the trial met all four of its co-primary endpoints when LEVADEX was compared to placebo. We have completed a long-term safety extension of this Phase 3 trial, and no drug-related serious adverse events were reported in the trial. In July 2010, we announced that in a pharmacokinetics trial of LEVADEX, systemic absorption of LEVADEX was not higher and systemic exposure to DHE was not greater in smokers than in non-smokers. In September 2010, we reported results from a pharmacodynamics trial comparing the acute effects on pulmonary artery pressure of LEVADEX, DHE administered intravenously and placebo. In the trial, there was no statistically significant difference between the LEVADEX and placebo groups in the primary endpoint of pulmonary artery pressure over two hours after administration. In November 2010, we announced that in a thorough QT trial, a supra-therapeutic dose of
32
Table of Contents
Index to Financial Statements
LEVADEX did not cause an increase in the QTc interval. Even if we obtain regulatory approval of a product candidate, the FDA may require continuing evaluation and study of our product through clinical trials as a condition of any approval. Despite the results reported in prior clinical trials for our product candidates, we do not know whether subsequent clinical trials we may conduct will demonstrate adequate efficacy and safety to result in regulatory approval to market our product candidates. For example, after receiving positive data from a previous Phase 2 trial, in February 2009 we announced top-line results from our Phase 3 trial of UDB, indicating that the trial did not meet its co-primary endpoints in either dose evaluated when compared to placebo.
If clinical trials of our LEVADEX product candidate or future product candidates do not produce results necessary to support regulatory approval in the United States or elsewhere or show undesirable side effects, we will be unable to commercialize these products.
To receive regulatory approval for the commercial sale of LEVADEX or any other product candidates, we must conduct adequate and well-controlled clinical trials to demonstrate efficacy and safety in humans. Clinical testing is expensive, takes many years and has an uncertain outcome. Clinical failure can occur at any stage of the testing. Our clinical trials may produce negative or inconclusive results. In such cases, we may decide, or regulators may require us, to conduct additional clinical and/or non-clinical testing, or we may decide not to pursue further development of a product candidate, such as the case of our UDB product candidate, where top-line results of our Phase 3 clinical trial indicated that the trial failed to meet the primary endpoints. Subsequently we suspended development of UDB. In addition, the results of our clinical trials may show that our product candidates may cause undesirable side effects, which could interrupt, delay or halt clinical trials, resulting in our inability to obtain regulatory approval by the FDA and other regulatory authorities.
In light of widely publicized events concerning the safety risk of certain drug products, regulatory authorities, members of Congress, the Government Accounting Office, medical professionals and the general public have raised concerns about potential drug safety issues. These events have resulted in the withdrawal of drug products, revisions to drug labeling that further limit use of the drug products and establishment of risk management programs that may, for instance, restrict distribution of drug products. The increased attention to drug safety issues may result in a more cautious approach by the FDA to clinical trials and regulatory approval. Data from clinical trials may receive greater scrutiny with respect to safety, which may make the FDA or other regulatory authorities more likely to terminate clinical trials before completion, or require longer or additional clinical trials that may result in substantial additional expense and a delay or failure in obtaining approval or approval for a more limited indication than originally sought.
Our failure to adequately demonstrate the efficacy and safety of LEVADEX or any other product candidates would prevent regulatory approval and, ultimately, the commercialization of that product candidate.
All of our product candidates in development require regulatory review and approval prior to commercialization. Any delay in the regulatory review or approval of any of our product candidates in development will harm our business.
All of our product candidates in development require regulatory review and approval prior to commercialization, including review of pre-clinical data, clinical data and inspection of manufacturing facilities and processes. Any delays in the regulatory review or approval of our product candidates in development would delay market launch, increase our cash requirements and result in additional operating losses.
The process of obtaining FDA and other required regulatory approvals, including foreign approvals, often takes many years and can vary substantially based upon the type, complexity and novelty of the products involved. Furthermore, this approval process is extremely complex, expensive and uncertain. We or our partners may not be able to maintain our proposed schedules for the submission of any NDA in the United States or any marketing approval application or other foreign applications for any of our products. If we or our partners submit
33
Table of Contents
Index to Financial Statements
any NDA, including any amended NDA or supplemental NDA, to the FDA seeking marketing approval for any of our product candidates, the FDA must decide whether to either accept or reject the submission for filing. We cannot be certain that any of these submissions will be accepted for filing and reviewed by the FDA, or that our marketing approval application submissions to any other regulatory authorities will be accepted for filing and review by those authorities. We cannot be certain that we or our partners will be able to respond to any regulatory requests during the review period in a timely manner without delaying potential regulatory action. We also cannot be certain that any of our product candidates will receive favorable recommendation from any FDA advisory committee or foreign regulatory bodies or be approved for marketing by the FDA or foreign regulatory authorities. In addition, delays in approvals or rejections of marketing applications may be based upon many factors, including regulatory requests for additional analyses, reports, data and/or studies, regulatory questions regarding data and results, changes in regulatory policy during the period of product development and/or the emergence of new information regarding our products or other products.
Data obtained from pre-clinical studies and clinical trials are subject to different interpretations, which could delay, limit or prevent regulatory review or approval of any of our products. In addition, as a routine part of the evaluation of any potential drug, clinical studies are generally conducted to assess the potential for drug-drug interactions that could impact potential product safety. At this point in time, we have not been requested to perform drug-drug interaction studies, but any such requirement may delay any potential product approval and will increase our expenses associated with our clinical programs. Furthermore, regulatory attitudes towards the data and results required to demonstrate safety and efficacy can change over time and can be affected by many factors, such as the emergence of new information, including on other products, changing policies and agency funding, staffing and leadership. We cannot be sure whether future changes to the regulatory environment will be favorable or unfavorable to our business prospects.
In addition, the environment in which our regulatory submissions may be reviewed changes over time. For example, average review times at the FDA for marketing approval applications have fluctuated over the last ten years, and we cannot predict the review time for any of our submissions with any regulatory authorities. In addition, review times can be affected by a variety of factors, including budget and funding levels and statutory, regulatory and policy changes.
We may not be able to rely on Section 505(b)(2) of the Federal Food, Drug and Cosmetic Act, which could result in a longer development program and more costly trials than we anticipate.
We may not be able to seek FDA marketing approval of our product candidates under Section 505(b)(2) of the FFDCA. Section 505(b)(2), if applicable to us, would allow an NDA we file with the FDA to rely in part on data in the public domain or the FDA’s prior conclusions regarding the safety and effectiveness of approved compounds, which could expedite the development program for our product candidates by potentially decreasing the overall scope of work we must do ourselves. If we are unable to rely on Section 505(b)(2), the development program for our product candidates would be longer than we expect, and we would also have to conduct more costly trials than we anticipate.
If any of our product candidates for which we or our partners receive regulatory approval do not achieve broad market acceptance, the revenues that we generate from their sales will be limited.
The commercial success of our product candidates for which we or our partners obtain marketing approval from the FDA or other regulatory authorities will depend upon the acceptance of these products among physicians, the medical community, patients, and coverage and reimbursement of them by third-party payors, including government payors. The degree of market acceptance of any of our approved products will depend on a number of factors, including:
| • | a product’s FDA-approved labeling as well as limitations or warnings contained in the labeling; |
| • | changes in the standard of care for the targeted indications for any of our product candidates, which could reduce the marketing impact of any claims that we could make following FDA approval; |
34
Table of Contents
Index to Financial Statements
| • | limitations inherent in the approved indication and product labeling for any of our product candidates compared to more commonly understood or addressed medical conditions; |
| • | lower demonstrated efficacy and a less favorable safety or tolerability profile compared to other products; |
| • | device-related difficulties associated with our TEMPO inhaler; |
| • | prevalence and severity of adverse effects; |
| • | ineffective marketing and distribution efforts; |
| • | lack of availability of reimbursement from managed care plans and other third-party payors; |
| • | lack of cost-effectiveness; |
| • | timing of market introduction and perceived effectiveness of competitive products; |
| • | availability of alternative therapies, including generics, at similar or lower costs; |
| • | patients’ potential preferences to take oral medications over inhaled medications; and |
| • | potential product liability claims. |
Our and our partners’ ability to effectively promote and sell our product candidates in the marketplace will also depend on pricing and cost effectiveness, including our and our partners’ ability to manufacture a product at a competitive price. We will also need to demonstrate acceptable evidence of safety and efficacy and may need to demonstrate relative convenience and ease of administration. Inhaled versions of certain previously approved drugs have suffered commercial failure, including recently inhaled insulin. If our product candidates are approved but do not achieve an adequate level of acceptance by physicians, health care payors and patients, we may not generate sufficient revenue from these products, and we may not become or remain profitable. In addition, our and our partners’ efforts to educate the medical community and third-party payors on the benefits of our product candidates may require significant resources and may never be successful. If our approved drugs fail to achieve market acceptance, we will not be able to generate significant revenue, if any.
We have never marketed a drug before, and if we are unable to establish, or access an effective and specialized sales force and marketing infrastructure, we will not be able to commercialize our product candidates successfully.
We plan to market or co-promote our products where appropriate and build our own specialized sales force in the United States. We currently do not have significant internal sales, distribution and marketing capabilities. For example, in order to commercialize LEVADEX, we intend to develop a specialized sales force and marketing capabilities in the United States directed at high prescribers including specialists such as neurologists and pain specialists. We have entered into a collaboration with Allergan pursuant to which we will co-promote LEVADEX to neurologists and pain specialists in the United States, following potential FDA approval of LEVADEX. The development of a sales and marketing infrastructure for our domestic operations will require substantial resources, will be expensive and time consuming and could negatively impact our commercialization efforts, including delay of any product launch. Many of these costs will be incurred in advance of notice to us that any of our product candidates has been approved. In addition, we may not be able to hire a specialized sales force in the United States that is sufficient in size or has adequate expertise in the medical markets that we intend to target, including neurology. If we are unable to establish our specialized sales force and marketing capability for our most advanced product candidate, we may not be able to generate any product revenue, may generate increased expenses and may never become profitable.
We expect intense competition with respect to our existing and future product candidates.
The pharmaceutical industry is highly competitive, with a number of established, large pharmaceutical companies, as well as many smaller companies. Many of these companies have greater financial resources,
35
Table of Contents
Index to Financial Statements
marketing capabilities and experience in obtaining regulatory approvals for product candidates. There are many pharmaceutical companies, biotechnology companies, public and private universities, government agencies and research organizations actively engaged in research and development of products which may target the same indications as our product candidates. We expect any future products we develop to compete on the basis of, among other things, product efficacy and safety, time to market, price, extent of adverse side effects and convenience of treatment procedures. One or more of our competitors may develop products based upon the principles underlying our proprietary technologies earlier than us, obtain approvals for such products from the FDA more rapidly than us or develop alternative products or therapies that are safer, more effective and/or more cost effective than any products developed by us.
Competitors may seek to develop alternative formulations of our product candidates that address our targeted indications. The commercial opportunity for our product candidates could be significantly harmed if competitors are able to develop alternative formulations outside the scope of our products. Compared to us, many of our potential competitors have substantially greater:
| • | capital resources; |
| • | research and development resources, including personnel and technology; |
| • | clinical trial experience; |
| • | regulatory experience; |
| • | expertise in prosecution of intellectual property rights; |
| • | manufacturing and distribution experience; and |
| • | sales and marketing resources and experience. |
As a result of these factors, our competitors may obtain regulatory approval of their products more rapidly than we are able to or may obtain patent protection or other intellectual property rights that limit our ability to develop or commercialize our product candidates. Our competitors may also develop drugs that are more effective, useful and less costly than ours and may also be more successful than us in manufacturing and marketing their products.
The migraine market is extremely competitive which may negatively impact our ability to commercialize LEVADEX.
If approved for the treatment of acute migraine, we anticipate that LEVADEX would compete against other marketed migraine therapies and may compete with products currently under development by both large and small companies. The majority of marketed prescription products for the treatment of migraine are in the triptan class. In 2010, the triptan market in the United States totaled approximately $1.6 billion in revenue. The triptan with the largest market share is sumatriptan with 2010 prescriptions of approximately 6.1 million in the United States. There are at least six other branded triptan therapies being sold by pharmaceutical companies. Alternative formulations of triptans are available that may have faster onset of action than solid oral dosage forms. In April 2008, GlaxoSmithKline’s Treximet, a combination oral formulation of sumatriptan and naproxen sodium, was approved by the FDA for the acute treatment of migraine. In July 2009, Zogenix, Inc’s Sumavel DosePro needle-free sumatriptan was approved by the FDA for the treatment of acute migraine and cluster headache. Alternative formulations of dihydroergotamine, or DHE, include Migranal, which is nasally delivered, and which may become generically available prior to any commercial introduction of LEVADEX. In addition to the marketed migraine therapeutics, there are product candidates under development by large pharmaceutical companies, such as Merck & Co., Inc., and other smaller companies, that could potentially be used to treat acute migraine and compete with LEVADEX. In October 2010, Allergan, Inc.’s BOTOX botulinum toxin was approved by the FDA for the treatment of chronic migraine, a different indication than acute migraine.
36
Table of Contents
Index to Financial Statements
We would also face competition from generic sumatriptan, the active ingredient in Imitrex. The FDA has approved generic versions of sumatriptan. Although we believe generic sumatriptan could not be substituted for LEVADEX, generic sumatriptan may be more quickly adopted by health insurers and patients than LEVADEX. Financial pressure to use generic products and uncertainty of reimbursement for single source alternatives, such as LEVADEX, may encourage the use of a generic product over LEVADEX.
If our patients are unable to obtain coverage of or sufficient reimbursement for our products, it is unlikely that our products will be widely used.
Successful sales of our products depend on the availability of adequate coverage and reimbursement from third-party payors. Healthcare providers that purchase medicine or medical products for treatment of their patients generally rely on third-party payors to reimburse all or part of the costs and fees associated with the products. Adequate coverage and reimbursement from governmental payors, such as Medicare and Medicaid, and commercial payors is critical to new product acceptance. Patients are unlikely to use our products if they do not receive reimbursement adequate to cover the cost of our products.
In addition, the market for our future products will depend significantly on access to third-party payors’ drug formularies, or lists of medications for which third-party payors provide coverage and reimbursement. Industry competition to be included in such formularies results in downward pricing pressures on pharmaceutical companies. Third-party payors may refuse to include a particular branded drug in their formularies when a generic drug for the same or similar indication is available.
All third-party payors, whether governmental or commercial, whether inside the United States or outside, are developing increasingly sophisticated methods for controlling healthcare costs. In addition, in the United States, no uniform policy of coverage and reimbursement for medical technology exists among all these payors. Therefore, coverage of and reimbursement for medical products can differ significantly from payor to payor.
Further, we believe that future coverage and reimbursement may be subject to increased restrictions both in the United States and in international markets, pursuant to currently proposed healthcare reforms or otherwise. Third-party coverage and reimbursement for our products may not be available or adequate in either the United States or international markets, limiting our ability to sell our products on a profitable basis.
Even if our product candidates receive regulatory approval in the United States, we or our partners may never receive approval or commercialize our products outside of the United States.
In order to market and commercialize any products outside of the United States, we and our partners must establish and comply with numerous and varying regulatory requirements of other countries regarding safety and efficacy. Approval procedures vary among countries and can involve additional pre-clinical studies and clinical trials and additional administrative review periods. For example, European regulatory authorities generally require clinical testing comparing the efficacy of the new drug to an existing drug prior to granting approval. The time required to obtain approval in other countries might differ from that required to obtain FDA approval. The regulatory approval process in other countries may include all of the risks detailed above regarding FDA approval in the United States, as well as other risks. Regulatory approval in one country does not ensure regulatory approval in another, but a failure or delay in obtaining regulatory approval in one country may have a negative effect on the regulatory process in other countries. Failure to obtain regulatory approval in other countries or any delay or setback in obtaining such approval could have the same adverse effects detailed above regarding FDA approval in the United States. As described above, such effects include the risks that our product candidates may not be approved for all indications requested, which could limit the uses of our product candidates and have an adverse effect on product sales and potential royalties, and that such approval may be subject to limitations on the indicated uses for which the product may be marketed or require costly, post-marketing follow-up studies.
37
Table of Contents
Index to Financial Statements
Our product candidates may have undesirable side effects and cause our approved drugs to be taken off the market.
If our most advanced product candidate, LEVADEX, or any other product candidate, receives marketing approval and we or others later identify undesirable side effects caused by such products:
| • | regulatory authorities may require the addition of labeling statements, specific warnings, contraindications or field alerts to physicians and pharmacies; |
| • | regulatory authorities may withdraw their approval of the product and require us to take our approved drug off the market; |
| • | we may be required to change the way the product is administered, conduct additional clinical trials, change the labeling of the product or conduct a Risk Evaluation and Mitigation Strategies, or REMS, program; |
| • | we may have limitations on how we promote our drugs; |
| • | sales of products may decrease significantly; |
| • | we may be subject to litigation or product liability claims; and |
| • | our reputation may suffer. |
Any of these events could prevent us from achieving or maintaining market acceptance of the affected product or could substantially increase our commercialization costs and expenses, which in turn could delay or prevent us from generating significant revenues from its sale.
Even if our product candidates receive regulatory approval, we and our partners may still face future development and regulatory difficulties.
Even if U.S. regulatory approval is obtained, the FDA may still impose significant restrictions on a product’s indicated uses or marketing or impose ongoing requirements for potentially costly post-approval studies. Given the number of recent high profile adverse safety events with certain drug products, the FDA may require, as a condition of approval, costly risk management programs which may include safety surveillance, restricted distribution and use, patient education, enhanced labeling, special packaging or labeling, expedited reporting of certain adverse events, pre-approval of promotional materials and restrictions on direct-to-consumer advertising. In addition, the FDA could condition any approval of LEVADEX on our implementation of a post-approval risk management plan. Furthermore, heightened Congressional scrutiny on the adequacy of the FDA’s drug approval process and the agency’s efforts to assure the safety of marketed drugs has resulted in the proposal of new legislation addressing drug safety issues. Any new legislation could result in delays or increased costs during the period of product development, clinical trials and regulatory review and approval, as well as increased costs to assure compliance with any new post-approval regulatory requirements. Any of these restrictions or requirements could force us to conduct costly studies or increase the time for us to become profitable. For example, any labeling approved for LEVADEX or any other product candidates may include a restriction on the term of its use, such as a black box warning, or it may not include one or more of our intended indications. The FDA historically has required that labeling for products containing DHE include a contraindication for use in women who are, or who may become, pregnant. Although we believe that this contraindication is not applicable to our formulation of DHE, the FDA may disagree and require the LEVADEX labeling to carry this contraindication.
Our product candidates will also be subject to ongoing FDA requirements for the current Good Manufacturing Practices, or cGMP, labeling, packaging, storage, advertising, promotion, record-keeping and submission of safety and other post-market information on the drug. In addition, approved products, manufacturers and manufacturers’ facilities are subject to continual review and periodic inspections. If a regulatory agency discovers previously unknown problems with a product, such as adverse events of
38
Table of Contents
Index to Financial Statements
unanticipated severity or frequency, or problems with the facility where the product is manufactured, a regulatory agency may impose restrictions on that product or us, including requesting withdrawal of the product from the market. If our product candidates fail to comply with applicable regulatory requirements, or fail to be made in compliance with applicable regulatory requirements such as cGMP, a regulatory agency may:
| • | issue warning letters or untitled letters identifying violations; |
| • | require us to enter into a consent decree, which can include imposition of various fines, reimbursements for inspection costs, required due dates for specific actions and penalties for noncompliance; |
| • | impose other civil or criminal penalties; |
| • | suspend regulatory approval; |
| • | suspend any ongoing clinical trials; |
| • | refuse to approve pending applications or supplements to approved applications filed by us; |
| • | impose restrictions on operations, including costly new manufacturing requirements; or |
| • | seize or detain products or require a product recall. |
We or our potential partners will need to obtain FDA approval of the proposed product names for our product candidates and any failure or delay associated with such approval may adversely impact our business.
Any name we or our potential partners intend to use for our product candidates will require approval from the FDA regardless of whether we or our partners have secured a formal trademark registration from the U.S. Patent and Trademark Office. The FDA typically conducts a rigorous review of proposed product names, including an evaluation of potential for confusion with other product names. The FDA may also object to a product name if it believes the name inappropriately implies medical claims. If the FDA objects to our product names, we may be required to adopt an alternative name for our product candidates. If we or our partners adopt an alternative name, we or our partners would lose the benefit of our existing trademark applications and may be required to expend significant additional resources in an effort to identify a suitable product name that would qualify under applicable trademark laws, not infringe the existing rights of third parties and be acceptable to the FDA. We or our partners may be unable to build a successful brand identity for a new trademark in a timely manner or at all, which would limit our ability to commercialize our product candidates.
Guidelines and recommendations published by various organizations may affect the use of our products.
Government agencies issue regulations and guidelines directly applicable to us and to our products. In addition, professional societies, practice management groups, private health/science foundations and organizations involved in various diseases from time to time publish guidelines or recommendations to the medical and patient communities. These various sorts of recommendations may relate to such matters as product usage, dosage, route of administration and use of related or competing therapies. Changes to this recommendation or other guidelines advocating alternative therapies could result in decreased use of our products, which may adversely affect our results of operations.
We face potential product liability exposure and, if successful claims are brought against us, we may incur substantial liability for a product candidate and may have to limit its commercialization.
The use of our product candidates in clinical trials and the sale of any products for which we obtain marketing approval, if at all, expose us to the risk of product liability claims. Product liability claims might be brought against us by consumers, health care providers or others using, administering or selling our products. If we cannot successfully defend ourselves against these claims, we will incur substantial liabilities. Regardless of merit or eventual outcome, liability claims may result in:
| • | withdrawal of clinical trial participants; |
| • | termination of clinical trial sites or entire trial programs; |
39
Table of Contents
Index to Financial Statements
| • | costs of related litigation; |
| • | substantial monetary awards to patients or other claimants; |
| • | decreased demand for our product candidates; |
| • | impairment of our business reputation; |
| • | loss of revenues; and |
| • | the inability to commercialize our product candidates. |
We have obtained limited product liability insurance coverage for our clinical trials domestically and in selected foreign countries where we conduct clinical trials. However, our insurance coverage may not reimburse us or may not be sufficient to reimburse us for any expenses or losses we may suffer. Moreover, insurance coverage is becoming increasingly expensive and, in the future, we may not be able to maintain insurance coverage at a reasonable cost or in sufficient amounts to protect us against losses due to liability. We intend to expand our insurance coverage to include the sale of commercial products if we obtain marketing approval for our product candidates in development, but we may be unable to obtain commercially reasonable product liability insurance for any products approved for marketing. On occasion, large judgments have been awarded in class action lawsuits based on drugs that had unanticipated side effects. A successful product liability claim or series of claims brought against us could cause our stock price to fall and, if judgments exceed our insurance coverage, could decrease our cash and adversely affect our business.
Our operations involve hazardous materials, which could subject us to significant liabilities.
Our research and development processes involve the controlled use of hazardous materials, including chemicals. Our operations produce hazardous waste products. We cannot eliminate the risk of accidental contamination or discharge or injury from these materials. Federal, state and local laws and regulations govern the use, manufacture, storage, handling and disposal of these materials. We could be subject to civil damages in the event of an improper or unauthorized release of, or exposure of individuals, including employees, to hazardous materials. In addition, claimants may sue us for injury or contamination that results from our use of these materials and our liability may exceed our total assets. We maintain limited insurance for the use of hazardous materials which may not be adequate to cover any claims. Compliance with environmental and other laws and regulations may be expensive and current or future regulations may impair our research, development or production efforts.
Our insurance policies are expensive and protect us only from some business risks, which will leave us exposed to significant uninsured liabilities.
We do not carry insurance for all categories of risk that our business may encounter. For example, we do not carry earthquake insurance. In the event of a major earthquake in our region, our business could suffer significant and uninsured damage and loss. Some of the policies we currently maintain include general liability, property, auto, workers’ compensation, products liability and directors’ and officers’ insurance policies. Our insurance is expensive and we do not know if we will be able to maintain existing insurance with adequate levels of coverage. Any significant uninsured liability may require us to pay substantial amounts, which would adversely affect our cash position and results of operations.
40
Table of Contents
Index to Financial Statements
Risks Related to Our Dependence on Third Parties
We have no experience manufacturing large clinical-scale or commercial-scale pharmaceutical products and we do not own or operate a manufacturing facility. As a result, we are dependent on numerous third parties for the manufacture of our product candidates and our supply chain, and if we experience problems with any of these suppliers the manufacturing of our products could be delayed.
We do not own or operate manufacturing facilities for clinical or commercial manufacture of our product candidates, which includes drug substance and drug packaging, including the components of the TEMPO inhaler, the device used to administer certain of our drug candidates, including LEVADEX. We have limited personnel with experience in drug manufacturing and we lack the capabilities to manufacture any of our product candidates on a clinical or commercial scale. We currently outsource all manufacturing and packaging of our pre-clinical and clinical product candidates to third parties. In addition, we do not currently have all necessary agreements with third-party manufacturers for the long-term commercial supply of our product candidates. We may be unable to enter agreements for commercial supply with all third-party manufacturers, or may be unable to do so on acceptable terms. Even if we enter into these agreements or, for those agreements that we have already entered into, the various manufacturers of each product candidate will likely be single source suppliers to us for a significant period of time. We may not be able to establish additional sources of supply for our products prior to commercialization. Such suppliers are subject to regulatory requirements covering manufacturing, testing, quality control and record keeping relating to our product candidates, and are subject to pre-approval and ongoing inspections by the regulatory agencies. Failure by any of our suppliers to comply with applicable regulations may result in long delays and interruptions to our manufacturing capacity while we seek to secure another supplier that meets all regulatory requirements.
Reliance on third-party manufacturers entails risks to which we would not be subject if we manufactured the product candidates ourselves, including:
| • | reliance on the third parties for regulatory compliance, quality assurance and hazardous materials handling; |
| • | the possible breach of the manufacturing and quality agreements by the third parties because of factors beyond our control; and |
| • | the possibility of termination or nonrenewal of the agreements by the third parties because of our breach of the manufacturing agreement or based on their own business priorities. |
Any of these factors could cause the delay or suspension of initiation or completion of clinical trials, regulatory submissions, required approvals or commercialization of our products, cause us to incur higher costs and could prevent us from commercializing our product candidates successfully. Furthermore, if our contract manufacturers fail to deliver the required commercial quantities of finished product on a timely basis and at commercially reasonable prices and we are unable to find one or more replacement manufacturers capable of production at a substantially equivalent cost, in substantially equivalent volumes and quality and on a timely basis, we would likely be unable to meet demand for our products and we would lose potential revenue. It may take a significant period of time to establish an alternative source of supply for our product candidates and to have any such new source approved by the FDA.
If we are unable to establish additional marketing, sales and distribution collaborations with third parties, we may not be able to commercialize LEVADEX successfully.
We have a collaboration agreement with Allergan to commercialize LEVADEX to neurologists and pain specialists in the United States. We may establish additional marketing, sales and distribution collaborations with third parties where appropriate. For example, if we choose to expand the marketing and sales of LEVADEX to primary care physicians beyond neurologists and pain specialists, we may establish partnerships with other companies to maximize the potential of the commercialization opportunity. Outside the United States, we may
41
Table of Contents
Index to Financial Statements
establish commercial partnerships for LEVADEX in order to effectively reach target markets in order to maximize its commercial opportunities. We also expect to face competition in our efforts to identify appropriate collaborators or partners to help commercialize LEVADEX to primary care physicians or outside the Unites States. If we are unable to establish adequate marketing, sales and distribution collaborations to target primary care physicians, specialists and other large groups of prescribing physicians within and outside the United States, then we may not be able to achieve the full commercial opportunity for LEVADEX.
We may not be successful in maintaining or establishing collaborations, which could adversely affect our ability to develop and commercialize certain of our product candidates.
We may not be able to establish or maintain collaborations around our product candidates, which may adversely affect our ability to develop and commercialize our product candidates. We have entered into a collaboration agreement and co-promotion agreement with Allergan pursuant to which Allergan will co-promote LEVADEX to neurologists and pain specialists in the United States, following potential FDA product approval, and will share expenses relating to the commercialization of LEVADEX. Under certain circumstances, Allergan has the right to terminate these agreements. If Allergan terminates our agreement, we would not receive milestones due after the termination date, and we would be responsible for commercialization expenses previously covered by Allergan. Also in the event of a termination by Allergan, we may have difficulty commercializing LEVADEX to neurologists and pain specialists, as we have no experience marketing pharmaceutical products on our own. In July 2009, we received a notice of termination of our AstraZeneca Agreement related to our UDB product candidate. Our AstraZeneca Agreement provided that AstraZeneca could terminate the agreement in the event that the primary endpoints of our Phase 3 clinical trial of UDB were not met. Following the termination of the AstraZeneca Agreement, we suspended development of UDB. In addition, our earlier stage product portfolio includes next generation budesonide, MAP0005 and MAP0001. We have no current intention to further develop either of these earlier stage product candidates independently. Developing pharmaceutical products, conducting clinical trials, establishing manufacturing capabilities and marketing approved products is expensive. Consequently, we may establish partnerships for further development and commercialization of these two product candidates. We expect to face competition in seeking appropriate partners. Moreover, collaboration arrangements are complex and time consuming to negotiate, document and implement and they may require substantial resources to maintain. We may not be successful in our efforts to establish and implement collaborations or other alternative arrangements, if any. The terms of any collaboration or other arrangement that we establish may not be favorable to us. In addition, any collaboration that we enter into may not be successful. If we seek partners to help develop next generation budesonide, MAP0005 and MAP0001, but are unable to reach agreements with suitable partners, we may fail to commercialize such products.
Risks Relating to Our Intellectual Property
It is difficult and costly to protect our proprietary rights, and we may not be able to ensure their protection.
Our commercial success will depend in part on obtaining and maintaining patent protection and trade secret protection of our product candidates and the methods used to manufacture them, as well as successfully defending these patents against third-party challenges. Our ability to stop third parties from making, using, selling, offering to sell or importing our products is dependent upon the extent to which we have rights under valid and enforceable patents or trade secrets that cover these activities.
We license certain intellectual property from third parties that covers our product candidates. We rely on certain of these third parties to file, prosecute and maintain patent applications and otherwise protect the intellectual property to which we have a license, and we have not had and do not have primary control over these activities for certain of these patents or patent applications and other intellectual property rights. We cannot be certain that such activities by third parties have been or will be conducted in compliance with applicable laws and regulations or will result in valid and enforceable patents and other intellectual property rights. Our enforcement
42
Table of Contents
Index to Financial Statements
of certain of these licensed patents or defense of any claims asserting the invalidity of these patents would also be subject to the cooperation of the third parties.
The patent positions of pharmaceutical and biopharmaceutical companies can be highly uncertain and involve complex legal and factual questions for which important legal principles remain unresolved. No consistent policy regarding the breadth of claims allowed in biopharmaceutical patents has emerged to date in the United States. The biopharmaceutical patent situation outside the United States is even more uncertain. Changes in either the patent laws or in interpretations of patent laws in the United States and other countries may diminish the value of our intellectual property. Accordingly, we cannot predict the breadth of claims that may be allowed or enforced in the patents we own or to which we have a license from a third-party. Further, if any of our patents are deemed invalid and unforceable, it could impact our ability to commercialize or license our technology.
The degree of future protection for our proprietary rights is uncertain because legal means afford only limited protection and may not adequately protect our rights or permit us to gain or keep our competitive advantage. For example:
| • | others may be able to make compositions or formulations that are similar to our product candidates but that are not covered by the claims of our patents; |
| • | we might not have been the first to make the inventions covered by our issued patents or pending patent applications; |
| • | we might not have been the first to file patent applications for these inventions; |
| • | others may independently develop similar or alternative technologies or duplicate any of our technologies; |
| • | it is possible that our pending patent applications will not result in issued patents; |
| • | our issued patents may not provide us with any competitive advantages, or may be held invalid or unenforceable as a result of legal challenges by third parties; |
| • | we may not develop additional proprietary technologies that are patentable; or |
| • | the patents of others may have an adverse effect on our business. |
We also may rely on trade secrets to protect our technology, especially where we do not believe patent protection is appropriate or obtainable. However, trade secrets are difficult to protect. Although we use reasonable efforts to protect our trade secrets, our employees, consultants, contractors, outside scientific collaborators and other advisors may unintentionally or willfully disclose our information to competitors. Enforcing a claim that a third party illegally obtained and is using any of our trade secrets is expensive and time consuming, and the outcome is unpredictable. In addition, courts outside the United States are sometimes less willing to protect trade secrets. Moreover, our competitors may independently develop equivalent knowledge, methods and know-how.
We may incur substantial costs as a result of litigation or other proceedings relating to patent and other intellectual property rights and we may be unable to protect our rights to, or use, our technology.
If we or our partners choose to go to court to stop someone else from using the inventions claimed in our patents, that individual or company has the right to ask the court to rule that these patents are invalid and/or should not be enforced against that third party. These lawsuits are expensive and would consume time and other resources even if we were successful in stopping the infringement of these patents. In addition, there is a risk that the court will decide that these patents are not valid and that we do not have the right to stop a third party from using the inventions. There is also the risk that, even if the validity of these patents is upheld, the court will refuse to prevent the other party’s activities on the ground that such other party’s activities do not infringe our rights to these patents. In addition, the U.S. Supreme Court has recently invalidated some tests used by the U.S.
43
Table of Contents
Index to Financial Statements
Patent and Trademark Office in granting patents over the past 20 years. As a consequence, several issued patents may be found to contain invalid claims according to the newly revised standards. Some of our own or in-licensed patents may be subject to challenge and subsequent invalidation in a re-examination proceeding before the U.S. Patent and Trademark Office or during litigation under the revised criteria which make it more difficult to obtain patents.
Furthermore, a third party may claim that we or our manufacturing or commercialization partners are using inventions covered by the third party’s patent rights and may go to court to stop us from engaging in our normal operations and activities, including making or selling our product candidates. These lawsuits are costly and could affect our results of operations and divert the attention of managerial and technical personnel. We are aware that claims in patents owned by others may relate to our business and technologies. If we are sued for patent infringement, we would need to demonstrate that our products or methods of use either do not infringe the patent claims of the relevant patent and/or that the patent claims are invalid, and we may not be able to do this. Proving invalidity, in particular, is difficult since it requires a showing of clear and convincing evidence to overcome the presumption of validity enjoyed by issued patents. If we are sued for patent infringement, there is a risk that a court would order us or our partners to stop the activities covered by the patents. In addition, there is a risk that a court will order us or our partners to pay the other party damages for having violated the other party’s patent rights. We have agreed to indemnify certain of our commercial partners against certain patent infringement claims brought by third parties. The biotechnology industry has produced a proliferation of patents, and it is not always clear to industry participants, including us, which patents cover various types of products or methods of use. The coverage of patents is subject to interpretation by the courts, and the interpretation is not always uniform.
Because some patent applications in the United States may be maintained in secrecy until the patents are issued, because patent applications in the United States and many foreign jurisdictions are typically not published until eighteen months after filing and because publications in the scientific literature often lag behind actual discoveries, we cannot be certain that others have not filed patent applications for technology covered by our issued patents or our pending applications, or that we were the first to invent the technology. Our competitors may have filed, and may in the future file, patent applications covering technology similar to ours. Any such patent application may have priority over our patent applications or patents, which could further require us to obtain rights to issued patents by others covering such technologies. If another party has filed a U.S. patent application on inventions similar to ours, we may have to participate in an interference proceeding declared by the U.S. Patent and Trademark Office to determine priority of invention in the United States. The costs of these proceedings could be substantial, and it is possible that such efforts would be unsuccessful if, unbeknownst to us, the other party had independently arrived at the same or similar invention prior to our own invention, resulting in a loss of our U.S. patent position with respect to such inventions.
Some of our competitors may be able to sustain the costs of complex patent litigation more effectively than we can because they have substantially greater resources. In addition, any uncertainties resulting from the initiation and continuation of any litigation could have a material adverse effect on our ability to raise the funds necessary to continue our operations.
If we fail to comply with our obligations in our intellectual property licenses with third parties, we could lose license rights that are important to our business.
We are a party to a license agreement with Nektar Therapeutics UK Limited, pursuant to which we license key intellectual property, including intellectual property relating to our most advanced product candidate. These existing licenses impose various diligence, milestone payment, royalty, insurance and other obligations on us. If we fail to comply with these obligations, the licensors may have the right to terminate the license, in which event we might not be able to develop or market any product that is covered by the licensed patents. If we lose such license rights that are important to our product candidate, our business may be materially adversely affected. We may enter into additional licenses in the future and if we fail to comply with obligations under those agreements, we could suffer similar consequences.
44
Table of Contents
Index to Financial Statements
We may be subject to claims that our employees have wrongfully used or disclosed alleged trade secrets of their former employers.
As is common in the biotechnology and pharmaceutical industries, we employ individuals who were previously employed at other biotechnology or pharmaceutical companies, including our competitors or potential competitors. Although no claims against us are currently pending, we may be subject to claims that these employees or we have inadvertently or otherwise used or disclosed trade secrets or other proprietary information of their former employers. Litigation may be necessary to defend against these claims. Even if we are successful in defending against these claims, litigation could result in substantial costs and be a distraction to management.
Risks Related to Employee Matters and Managing Growth
We may need to increase the size of our company, and we may experience difficulties in managing growth.
As of December 31, 2010, we had 100 full-time employees. We may need to expand our managerial, operational, administrative and other resources in order to manage and fund our operations, continue our development activities and commercialize our product candidates. To support this growth, we may hire additional employees within the next 12 months. Our management, personnel, systems and facilities currently in place may not be adequate to support this future growth. Our need to effectively manage our operations, growth and various projects requires that we:
| • | manage our development program for LEVADEX, including manufacturing and regulatory activities in support of an NDA submission to the FDA, and potential approval from the FDA; |
| • | begin activities related to commercialization as we prepare for a potential product launch of LEVADEX; and |
| • | continue to improve our operational, financial and management controls, reporting systems and procedures. |
We may be unable to successfully implement these tasks on a larger scale and, accordingly, may not achieve our development and commercialization goals.
We may not be able to manage our business effectively if we are unable to attract and retain key personnel.
We may not be able to attract or retain qualified management, scientific and clinical personnel in the future due to competition for qualified personnel among biotechnology, pharmaceutical and other businesses, particularly in the Silicon Valley region of California. If we are not able to attract and retain necessary personnel to accomplish our business objectives, we may experience constraints that will significantly impede the achievement of our development objectives, our ability to raise additional capital and our ability to implement our business strategy.
Our industry has experienced a high rate of turnover of management personnel in recent years. We are highly dependent on the development, regulatory, commercialization and product acquisition expertise of our senior management, particularly Timothy S. Nelson, our President and Chief Executive Officer, and Thomas A. Armer, our co-founder and Chief Scientific Officer. If we lose one or more of these key employees, our ability to implement our business strategy successfully could be seriously harmed. Replacing key employees may be difficult and may take an extended period of time because of the limited number of individuals in our industry with the breadth of skills and experience required to develop, obtain regulatory approval of and commercialize products successfully. Competition to hire from this limited pool is intense, and we may be unable to hire, train, retain or motivate these additional key personnel.
In addition, we have scientific and clinical advisors who assist us in our product development and clinical strategies. These advisors are not our employees and may have commitments to, or consulting or advisory
45
Table of Contents
Index to Financial Statements
contracts with, other entities that may limit their availability to us, or may have arrangements with other companies to assist in the development of products that may compete with ours. Because our business depends on certain key personnel and advisors, the loss of such personnel and advisors could weaken our management team and we may experience difficulty in attracting and retaining qualified personnel and advisors.
Risks Relating to Owning Our Common Stock
Our share price may be volatile which may cause the value of our common stock to decline and subject us to securities class action litigation.
The market price of shares of our common stock could be subject to wide fluctuations in response to many risk factors listed in this section, and others beyond our control, including:
| • | actual or anticipated fluctuations in our financial condition and operating results; |
| • | status and/or results of our clinical trials; |
| • | results of clinical trials of our competitors’ products; |
| • | regulatory actions with respect to our products or our competitors’ products; |
| • | actions and decisions by our collaborators or partners; |
| • | our growth rate and actual or anticipated changes in our growth rate relative to our competitors; |
| • | actual or anticipated fluctuations in our competitors’ operating results or changes in their growth rate; |
| • | competition from existing products, new products or generics that may emerge; |
| • | issuance of new or updated research or reports by securities analysts; |
| • | fluctuations in the valuation of companies perceived by investors to be comparable to us; |
| • | share price and volume fluctuations attributable to inconsistent trading volume levels of our shares; |
| • | market conditions for biopharmaceutical stocks in general; and |
| • | general economic and market conditions. |
If securities or industry analysts do not publish research or reports about our business, or publish negative reports about our business, our stock price and trading volume could decline.
The trading market for our common stock depends on the research and reports that securities or industry analysts publish about us or our business. We do not have any control over these analysts. If one or more of the analysts who cover us downgrade our stock or change their opinion of our stock, our stock price would likely decline. If one or more of these analysts cease coverage of our company or fail to regularly publish reports on us, we could lose visibility in the financial markets, which could cause our stock price or trading volume to decline.
Future sales of our common stock may cause our stock price to decline.
Persons who were our stockholders prior to the sale of shares in our IPO continue to hold a substantial number of shares of our common stock that they are now able to sell in the public market. Significant portions of these shares are held by a small number of stockholders. Sales by our current stockholders of a substantial number of shares, or the expectation that such sales may occur, could significantly reduce the market price of our common stock. Moreover, the holders of a substantial number of shares of common stock may have rights, subject to certain conditions, to require us to file registration statements to permit the resale of their shares in the public market or to include their shares in registration statements that we may file for ourselves or other stockholders.
46
Table of Contents
Index to Financial Statements
We have also registered or plan to register all common stock that we may issue under our employee benefits plans. As a result, these shares can be freely sold in the public market upon issuance, subject to restrictions under the securities laws. In addition, our directors and executive officers may establish programmed selling plans under Rule 10b5-1 of the Exchange Act for the purpose of effecting sales of our common stock. If any of these events cause a large number of our shares to be sold in the public market, the sales could reduce the trading price of our common stock and impede our ability to raise future capital.
We will continue to incur significant increased costs as a result of operating as a public company.
As a public company, we will continue to incur significant legal, accounting and other expenses to comply with the laws and regulations affecting public companies, including the provisions of the Sarbanes-Oxley Act of 2002 and rules adopted by the Securities and Exchange Commission and by the NASDAQ Global Market. In addition, any changes in such regulations will result in increased costs to us as we respond to these requirements. For example, we must use certain required internal controls and disclosure controls and procedures, as required by Section 404 of the Sarbanes-Oxley Act of 2002. Our testing, or the subsequent testing by our independent registered public accounting firm, may reveal deficiencies in our internal controls over financial reporting that are deemed to be material weaknesses. Our compliance with Section 404 will require that we incur substantial accounting expense and expend significant management efforts. In addition, we will continue to bear all of the internal and external costs of preparing and distributing periodic public reports in compliance with our obligations under the securities laws.
Changing laws, regulations and standards relating to corporate governance and public disclosure, including the Sarbanes-Oxley Act of 2002 and related regulations implemented by the Securities and Exchange Commission and The NASDAQ Global Market, are creating uncertainty for public companies, increasing legal and financial compliance costs and making some activities more time consuming. We are currently evaluating and monitoring developments with respect to new and proposed rules and cannot predict or estimate the amount of additional costs we may incur or the timing of such costs. These laws, regulations and standards are subject to varying interpretations, in many cases due to their lack of specificity, and, as a result, their application in practice may evolve over time as new guidance is provided by regulatory and governing bodies. This could result in continuing uncertainty regarding compliance matters and higher costs necessitated by ongoing revisions to disclosure and governance practices. We will continue to invest resources to comply with evolving laws, regulations and standards, and this investment may result in increased general and administrative expenses and a diversion of management’s time and attention from potentially revenue-generating activities to compliance activities. If our efforts to comply with new laws, regulations and standards differ from the activities intended by regulatory or governing bodies due to ambiguities related to practice, regulatory authorities may initiate legal proceedings against us and our business may be harmed.
Anti-takeover provisions in our charter documents and under Delaware law could make an acquisition of us, which may be beneficial to our stockholders, more difficult and may prevent attempts by our stockholders to replace or remove our current management.
Provisions in our amended and restated certificate of incorporation and our bylaws may delay or prevent an acquisition of us. In addition, these provisions may frustrate or prevent any attempts by our stockholders to replace or remove our current management by making it more difficult for stockholders to replace members of our board of directors, who are responsible for appointing the members of our management team. In addition, because we are incorporated in Delaware, we are governed by the provisions of Section 203 of the Delaware General Corporation Law, which prohibits, with some exceptions, stockholders owning in excess of 15% of our outstanding voting stock from merging or combining with us. Finally, our charter documents establish advanced notice requirements for nominations for election to our board of directors and for proposing matters that can be acted upon at stockholder meetings. Although we believe these provisions together provide for an opportunity to receive higher bids by requiring potential acquirers to negotiate with our board of directors, they would apply even if the offer may be considered beneficial by some stockholders.
47
Table of Contents
Index to Financial Statements
We have never paid dividends on our common stock, and because we do not anticipate paying any cash dividends in the foreseeable future, capital appreciation, if any, of our common stock will be your sole source of gain on an investment in our stock.
We have never paid cash dividends on our common stock and we currently intend to retain our cash and future earnings, if any, to fund the development and growth of our business. We do not anticipate paying any cash dividends on our common stock in the foreseeable future. As a result, capital appreciation, if any, of our common stock will be your sole source of gain for the foreseeable future.
We may become involved in securities class action litigation that could divert management’s attention and harm our business.
The stock markets have from time to time experienced significant price and volume fluctuations that have affected the market prices for the common stock of biotechnology and biopharmaceutical companies. These broad market fluctuations may cause the market price of our common stock to decline. In the past, securities class action litigation has often been brought against a company following a decline in the market price of its securities. This risk is especially relevant for us because biotechnology and biopharmaceutical companies have experienced significant stock price volatility in recent years. We may become involved in this type of litigation in the future. Litigation often is expensive and diverts management’s attention and resources, which could adversely affect our business.
| ITEM 2. | PROPERTIES |
The following chart indicates the facilities that we lease, the location and size of each such facility and their designated use.
| Location |
Approximate Square Feet |
Operation | Expiration | |||
| Mountain View, CA |
43,000 | Office and Laboratory | Lease expires June 2012 (with an option to renew for an additional three to five years) |
We believe that the facilities that we currently lease are suitable and adequate for our needs for the immediate future and that, should it be needed, additional space can be leased to accommodate any future growth.
| ITEM 3. | LEGAL PROCEEDINGS |
We are not a party to any material legal proceeding.
| ITEM 4. | (REMOVED AND RESERVED) |
48
Table of Contents
Index to Financial Statements
PART II
| ITEM 5. | MARKET FOR REGISTRANT’S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES |
Our common stock has been listed on The NASDAQ Global Market under the symbol “MAPP” since October 5, 2007. Prior to that time, there was no public market for our stock. The following table sets forth the high and low intra-day sales prices per share for our common stock on The NASDAQ Global Market for the indicated periods.
| Year Ended December 31, 2010: |
High | Low | ||||||
| First Quarter |
$ | 17.83 | $ | 9.34 | ||||
| Second Quarter |
$ | 18.97 | $ | 11.32 | ||||
| Third Quarter |
$ | 15.49 | $ | 10.61 | ||||
| Fourth Quarter |
$ | 16.98 | $ | 13.95 | ||||
| Year Ended December 31, 2009: |
||||||||
| First Quarter |
$ | 13.08 | $ | 1.57 | ||||
| Second Quarter |
$ | 13.85 | $ | 2.00 | ||||
| Third Quarter |
$ | 12.52 | $ | 8.54 | ||||
| Fourth Quarter |
$ | 10.85 | $ | 7.86 | ||||
Holders of Record
As of February 28, 2011, there were approximately 59 stockholders of record of our common stock.
Dividend Policy
We have never declared or paid any cash dividend on our common stock and have no present plans to do so. We currently intend to retain any future earnings and do not expect to pay any dividends in the foreseeable future.
49
Table of Contents
Index to Financial Statements
Performance Graph
This performance graph shall not be deemed “soliciting material” or to be “filed” with the SEC, for purposes of Section 18 of the Securities Exchange Act of 1934, as amended, or the Exchange Act, or otherwise subject to the liabilities under that Section, and shall not be deemed to be incorporated by reference into any filing of MAP Pharmaceuticals, Inc. under the Securities Act of 1933, as amended, or the Exchange Act.
The following graph shows a comparison from October 5, 2007 (the date our common stock commenced trading on The NASDAQ Global Market) through December 31, 2010 of cumulative total return for our common stock, the NASDAQ Composite Index and the NASDAQ Biotechnology Index. Such returns are based on historical results and are not intended to suggest future performance. Data for the NASDAQ Composite Index and the NASDAQ Biotechnology Index assume reinvestment of dividends.
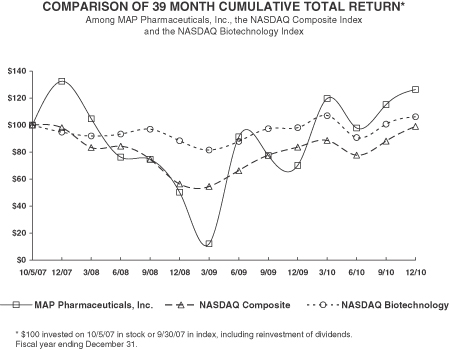
| 10/5/07 | 12/31/07 | 3/31/08 | 6/30/08 | 9/30/08 | 12/31/08 | 3/31/09 | 6/30/09 | 9/30/09 | ||||||||||||||||||||||||||||
| MAP Pharmaceuticals, Inc. |
100.00 | 131.16 | 104.64 | 77.38 | 75.81 | 52.28 | 15.73 | 91.54 | 78.35 | |||||||||||||||||||||||||||
| NASDAQ Composite |
100.00 | 98.26 | 84.10 | 85.03 | 75.76 | 58.15 | 56.46 | 67.87 | 78.61 | |||||||||||||||||||||||||||
| NASDAQ Biotechnology |
100.00 | 95.09 | 92.29 | 93.59 | 97.13 | 88.86 | 82.34 | 88.56 | 97.47 | |||||||||||||||||||||||||||
| 12/31/09 | 3/31/10 | 6/30/10 | 9/30/10 | 12/31/10 | ||||||||||||||||
| MAP Pharmaceuticals, Inc. |
71.39 | 119.03 | 98.05 | 114.61 | 125.39 | |||||||||||||||
| NASDAQ Composite |
84.43 | 89.21 | 78.61 | 88.66 | 99.25 | |||||||||||||||
| NASDAQ Biotechnology |
98.22 | 106.98 | 91.12 | 100.79 | 105.89 | |||||||||||||||
50
Table of Contents
Index to Financial Statements
Recent Sales of Unregistered Securities
None
Use of Proceeds from the Sale of Registered Securities
Our initial public offering of common stock was effected through a Registration Statement on Form S-1 (File No. 333-143823), or the Registration Statement, that was declared effective by the SEC on October 4, 2007, which registered an aggregate of 5,750,000 shares of our common stock. In October 2007, we sold 5,750,000 shares of common stock at an initial public offering price of $12.00 per share, for aggregate gross proceeds of $69.0 million, managed by Merrill Lynch & Co., Morgan Stanley & Co. and Deutsche Bank Securities. We paid $4.8 million in underwriting discount and commissions to the underwriters, and we incurred an additional $2.0 million of other expenses related to the offering during the fiscal year ended December 31, 2007. The net offering proceeds to us, after deducting underwriting discounts paid by us and offering costs, were $62.1 million. None of the expenses were paid, directly or indirectly, to directors, officers or persons owning 10% or more of our common stock, or to our affiliates.
In August 2009, we completed a follow-on public offering in which we sold and issued 3,500,000 shares of our common stock at a price of $9.70 per share. We raised a total of $34.0 million in gross proceeds or approximately $31.6 million in net proceeds after deducting expenses and underwriters’ discounts and commissions. The offering was made pursuant to a shelf registration statement on Form S-3 that we filed with the Securities and Exchange Commission on February 13, 2009, as amended on April 16, 2009, which became effective on May 5, 2009 (File No. 333-157339).
On November 11, 2009, we entered into a $60.0 million Common Stock Purchase Agreement, or the Purchase Agreement, with Azimuth Opportunity Ltd., or Azimuth, which provides us with what is sometimes termed an equity line of credit arrangement. In January 2010, we accessed our equity line of credit and sold 1,527,695 shares of common stock at a price of approximately $13.70 per share less a discount of approximately 4.5% per share for a net price of approximately $13.09 per share. The total purchase price for all these shares was $20.0 million or approximately $19.7 million after deducting offering expenses. The shares of common stock sold to Azimuth pursuant to the Purchase Agreement in this offering were registered on our effective Registration Statement on Form S-3 (File No. 333-157339).
In October 2010, we completed an equity offering in which we sold a total of 3,450,000 shares of common stock at an offering price of $14.50 per share. We raised a total of $50.0 million in gross proceeds, or approximately $47.0 million in net proceeds after deducting underwriting discounts, commissions and offering expenses. The offering was made pursuant to a shelf registration statement on Form S-3 that we filed with the Securities and Exchange Commission on February 12, 2010, as amended on March 9, 2010, which became effective on April 16, 2010 (File No. 333-164894).
We have applied the net proceeds from the equity offerings to our working capital for general corporate purposes. Cash in excess of immediate requirements is invested in accordance with our investment policy primarily with a view to capital preservation and liquidity.
51
Table of Contents
Index to Financial Statements
| ITEM 6. | SELECTED FINANCIAL DATA |
You should read the following selected consolidated financial data in conjunction with “Management’s Discussion and Analysis of Financial Condition and Results of Operations” and our consolidated financial statements and the related notes appearing elsewhere in this Annual Report on Form 10-K.
We were incorporated in July 2003. The consolidated statements of operations data for the years ended December 31, 2010, 2009, 2008 and for the period from July 3, 2003 (date of inception) through December 31, 2010, and the consolidated balance sheet data as of December 31, 2010 and 2009, are derived from our audited consolidated financial statements appearing elsewhere in this Annual Report on Form 10-K. The consolidated statements of operations data for the years ended December 31, 2007 and 2006, and the consolidated balance sheet data as of December 31, 2008, 2007 and 2006, are derived from our audited consolidated financial statements that are not included in this Annual Report on Form 10-K. The historical results are not necessarily indicative of the results to be expected in any future period. Our consolidated financial statements reflect a 1-for-1.77 reverse stock split of our common stock and preferred stock effected on October 4, 2007.
| Year Ended December 31, | Period from July 3, 2003 (Date of Inception) to December 31, 2010 |
|||||||||||||||||||||||
| 2010 | 2009 | 2008 | 2007 | 2006 | ||||||||||||||||||||
| (in thousands, except per share data) | ||||||||||||||||||||||||
| Consolidated Statement of Operations Data: |
||||||||||||||||||||||||
| Collaboration revenue |
$ | — | $ | 54,166 | $ | — | $ | — | $ | — | $ | 54,166 | ||||||||||||
| Operating expenses |
||||||||||||||||||||||||
| Research and development |
37,775 | 47,996 | 59,277 | 31,362 | 22,268 | 217,469 | ||||||||||||||||||
| Sales, general and administrative |
15,713 | 13,139 | 13,417 | 9,567 | 4,128 | 62,914 | ||||||||||||||||||
| Total operating expenses |
53,488 | 61,135 | 72,694 | 40,929 | 26,396 | 280,383 | ||||||||||||||||||
| Loss from operations |
(53,488 | ) | (6,969 | ) | (72,694 | ) | (40,929 | ) | (26,396 | ) | (226,217 | ) | ||||||||||||
| Interest income |
37 | 119 | 2,103 | 2,775 | 905 | 6,405 | ||||||||||||||||||
| Interest expense |
(1,242 | ) | (2,118 | ) | (2,056 | ) | (1,343 | ) | (235 | ) | (6,993 | ) | ||||||||||||
| Other income (expense), net |
20 | (29 | ) | (281 | ) | (563 | ) | (83 | ) | (742 | ) | |||||||||||||
| Net loss |
$ | (54,673 | ) | $ | (8,997 | ) | $ | (72,928 | ) | $ | (40,060 | ) | $ | (25,809 | ) | $ | (227,547 | ) | ||||||
| Net loss attributed to common stockholders |
$ | (54,673 | ) | $ | (8,997 | ) | $ | (72,928 | ) | $ | (45,635 | ) | $ | (30,538 | ) | $ | (241,472 | ) | ||||||
| Net loss per share attributed to common stockholders — basic and diluted |
$ | (2.01 | ) | $ | (0.41 | ) | $ | (3.58 | ) | $ | (8.28 | ) | $ | (43.11 | ) | |||||||||
| Weighted average shares outstanding used in calculating net loss per share attributed to common stockholders — basic and diluted |
27,261 | 22,195 | 20,350 | 5,510 | 708 | |||||||||||||||||||
| As of Year Ended December 31, | ||||||||||||||||||||
| 2010 | 2009 | 2008 | 2007 | 2006 | ||||||||||||||||
| (in thousands) | ||||||||||||||||||||
| Balance Sheet Data: |
||||||||||||||||||||
| Cash, cash equivalents and short-term investments |
$ | 76,007 | $ | 65,776 | $ | 44,710 | $ | 94,990 | $ | 17,746 | ||||||||||
| Working capital |
56,630 | 44,629 | 22,091 | 83,337 | 13,258 | |||||||||||||||
| Total assets |
82,794 | 70,996 | 50,860 | 100,695 | 21,625 | |||||||||||||||
| Long-term debt, net of current portion |
— | 7,337 | 14,229 | 6,357 | 10,061 | |||||||||||||||
| Redeemable convertible preferred stock warrant liability |
— | — | — | — | 411 | |||||||||||||||
| Redeemable convertible preferred stock |
— | — | — | — | 64,898 | |||||||||||||||
| Deficit accumulated during the development stage |
(239,564 | ) | (184,891 | ) | (175,894 | ) | (102,966 | ) | (58,686 | ) | ||||||||||
| Total stockholders’ equity (deficit) |
62,656 | 41,802 | 13,147 | 81,606 | (58,676 | ) | ||||||||||||||
52
Table of Contents
Index to Financial Statements
| ITEM 7. | MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS |
You should read the following discussion and analysis together with “Item 6 — Selected Financial Data” and the financial statements and the related notes to those statements included elsewhere in this Annual Report on Form 10-K. This discussion contains forward-looking statements that involve risks and uncertainties. As a result of many factors, such as those set forth under “Risk Factors” and elsewhere in this Annual Report on Form 10-K, our actual results may differ materially from those anticipated in these forward-looking statements.
Overview
Our goal is to use our proprietary inhalation technologies to enhance the therapeutic benefits and commercial attractiveness of proven drugs in the field of neurology while minimizing risk by capitalizing on their known safety, efficacy and commercialization history. We have proprietary product candidates in development that address large market opportunities.
Our strategy is to commercialize and develop differentiated neurology product candidates that can address significant unmet medical needs and overcome limitations of existing products. Key elements of our strategy include:
| • | Obtain regulatory approval for our most advanced product candidate, LEVADEXTM orally inhaled migraine therapy, for the potential acute treatment of migraine; |
| • | Build a specialized sales force to commercialize LEVADEX to neurologists and pain specialists in the United States; |
| • | Expand the market opportunity for LEVADEX; and |
| • | Advance and expand our neurology product pipeline by leveraging our technologies and our extensive scientific expertise in aerosol science and medicine to develop additional potential product candidates offering unique features and benefits. |
Our current focus is to advance our lead product candidate, LEVADEX (MAP0004) orally inhaled migraine therapy, a proprietary orally inhaled version of dihydroergotamine mesylate, or DHE, for the potential acute treatment of migraine. We completed clinical development for LEVADEX in 2010 and we plan to submit a New Drug Application, or NDA, to the U.S. Food and Drug Administration, or FDA, in the first half of 2011. In collaboration with Allergan, Inc., we plan to commercialize LEVADEX directly to neurologists and pain specialists in the United States. We are also evaluating options to commercialize LEVADEX to primary care physicians in the United States and to physicians in markets outside the United States.
Our Lead Product Candidate
Migraine is a chronic and debilitating neurological disorder characterized by episodic attacks. Migraine attacks typically manifest themselves as moderate to severe headache pain, with associated symptoms that often include nausea and vomiting, photophobia, phonophobia, and visual disturbances or aura. They usually involve “pounding” or “throbbing” pain on one side of the head, although pain may occur on both sides. Migraines limit the normal functioning of patients, who often seek dark, quiet surroundings until the episode has passed. Most migraines last between four and 24 hours, but some last as long as three days. According to published studies, the median frequency of attack is 1.5 times per month, although approximately 25% of migraine sufferers experience one or more attacks every week.
Migraine is a major public health problem that affects up to approximately 12% of the population in the United States and approximately 15% in Europe. According to the National Headache Foundation, approximately 30 million people in the United States suffer from migraine. Migraine is more common in women, with about 18% of women affected and 6% of men. Migraine prevalence is highest during the peak productive ages of 25 to 55, which results in high costs to employers and managed care organizations.
53
Table of Contents
Index to Financial Statements
Migraine is listed in the top 20 causes of disabling conditions and in the top four neurologic disabling conditions by the World Health Organization (WHO). Related disability from migraine is substantial, with over 90% of sufferers experiencing functional impairment with their migraine that can disrupt every aspect of day to day life, including work, school, family and social relationships. More than half of the sufferers report severe impairment or the need for bed rest as a result of their migraines, according to published surveys. The economic burden of migraine remains substantial despite existing treatments with migraine patients losing four to six work days each year due to headache. The combination of direct and indirect costs of migraine in the United States is estimated at over $20 billion annually.
In 2008, according to market data, approximately 29 million prescriptions were written for the treatment of migraine in the United States. Approximately 12 million of those prescriptions were written for acute migraine specific drugs. The majority of acute migraine specific drug prescriptions written were in the triptan class. In 2010, the triptan market in the United States totaled approximately $1.6 billion in revenues.
We have designed LEVADEX to provide faster onset and longer-lasting migraine relief than triptans, the class of drugs most often prescribed for treating migraine. LEVADEX is an easy to use, at-home therapy in development that patients self-administer using our proprietary hand-held TEMPO® inhaler. DHE currently is available as an intravenous, or IV, therapy which has been used in clinical settings for over 50 years for the safe and effective treatment of migraine, particularly forms of migraine that are severe or do not respond to triptans or other therapies. We believe LEVADEX has the potential to be suitable as a first-line therapy for some migraine patients.
In May 2009, we announced results of the efficacy portion of our Phase 3 clinical trial of LEVADEX, or FREEDOM-301. We announced that the clinical trial met its four primary endpoints, pain relief and being phonophobia, photophobia and nausea free as reported two hours after dosing. Additional endpoints showed that LEVADEX provided rapid and sustained pain relief for up to 48 hours after dosing.
Patients taking LEVADEX therapy had statistically significant improvement at two hours compared to patients on placebo for each of the primary endpoints:
| • | Pain relief: 58.7% of patients who received LEVADEX compared with 34.5% for placebo (p<0.0001); |
| • | Phonophobia free: 52.9% of patients who received LEVADEX compared with 33.8% for placebo (p<0.0001); |
| • | Photophobia free: 46.6% of patients who received LEVADEX compared with 27.2% for placebo (p<0.0001); and |
| • | Nausea free: 67.1% of patients who received LEVADEX compared with 58.7% for placebo (p=0.02). |
A total of 792 patients were included in the primary data analysis as specified in the protocol of the FREEDOM-301 study. The patient population studied had more severe migraine pain than anticipated, with 46% reporting severe pain and 54% reporting moderate pain prior to administration of the study drug.
Results from additional pre-defined analyses include:
| • | LEVADEX therapy achieved statistically significant onset of pain relief at 30 minutes after dosing (p=0.03); |
| • | While not statistically significant, 50% more of the patients receiving LEVADEX therapy than the patients receiving placebo reported pain relief at 10 minutes; |
| • | LEVADEX therapy achieved statistically significant sustained pain relief from two to 24 hours (p<0.0001), as well as two to 48 hours (p<0.0001, when unadjusted for multiplicity); |
54
Table of Contents
Index to Financial Statements
| • | LEVADEX therapy achieved statistically significant pain freedom (pain symptom score = 0) as early as 30 minutes (p=0.002, when unadjusted for multiplicity); and |
| • | LEVADEX therapy achieved sustained pain freedom from two to 24 hours, as well as two to 48 hours (p<0.0001 for both time points, when unadjusted for multiplicity). |
LEVADEX was well tolerated, with the most common adverse event reported being medication aftertaste at 6%, with 2% of patients receiving placebo also reporting medication aftertaste. The next most common adverse event was nausea at 5%, compared with 2% for placebo. Symptoms or sensitivities typically associated with commonly used triptan migraine treatments, such as chest discomfort (1%) or chest pain (0%), were rare and comparable to placebo. There were no mean decreases in lung function, as measured by spirometry, between the active and placebo groups. There were no drug-related serious adverse events reported in the trial. These data were presented in September 2009 in a late-breaking session of the 14th Congress of the International Headache Society.
In 2010, we announced that a second Phase 3 clinical trial would not be required for the LEVADEX NDA submission, completed and announced successful results from a pharmacokinetic (PK) trial in smokers, a pharmacodynamics (PD) trial evaluating pulmonary artery pressure using echocardiogram and a thorough QT trial. In addition, we completed our 12 month open-label safety extension of the Phase 3 FREEDOM 301 trial. In our clinical trials conducted for LEVADEX, no drug related serious adverse events have been reported. The LEVADEX clinical development program evaluated the efficacy, safety, PK and PD of LEVADEX in approximately 1,000 patients. We plan to submit an NDA to the FDA in the first half of 2011.
On January 28, 2011 we entered into a Collaboration Agreement and Co-Promotion Agreement with Allergan, Inc., Allergan USA, Inc. and Allergan Sales, LLC (collectively, “Allergan”) to promote LEVADEX to neurologists and pain specialists within the United States. Under the terms of these agreements, following potential FDA approval, together with Allergan, we will co-promote LEVADEX to neurologists and pain specialists in the United States. Specifically, Allergan will leverage its existing U.S. sales force dedicated to headache specialists using BOTOX® for Chronic Migraine, which will be complemented by our field sales force targeting neurologists and pain specialists. If LEVADEX receives FDA approval, profits and losses from sales of LEVADEX generated from commercialization to neurologists and pain specialists in the United States will be shared equally between us and Allergan. Following potential approval of LEVADEX for the acute treatment of migraine in adults, we and Allergan will equally share regulatory, patent and development expenses for two future LEVADEX indications. We retain all rights to commercialize LEVADEX outside the United States, subject to Allergan’s right under certain circumstances to expand the territory in which the parties will commercialize LEVADEX to neurologists and pain specialists to include Canada, and we retain all rights to commercialize LEVADEX to other physicians, including primary care physicians within the United States.
As part of the collaboration, we will be responsible for the manufacturing and distribution of LEVADEX in the United States, and for recording product revenues. The companies also have agreed, following potential approval of LEVADEX for the treatment of acute migraine in adults, to jointly develop LEVADEX for the treatment of migraine in adolescents 12 to 18 years of age and for one other additional indication. We are responsible for obtaining NDA approval, and will retain ownership of the NDA.
In February 2011, we received a $60.0 million up-front payment from Allergan and may receive up to $97 million in the form of regulatory milestones, including milestones for acceptance of filing of the LEVADEX NDA and first commercial sale associated with the initial acute migraine indication.
We may establish other partnerships with pharmaceutical companies to market LEVADEX outside the United States and to primary care physicians in the United States.
55
Table of Contents
Index to Financial Statements
Other Product Technologies
We are exploring options to advance and expand our neurology product pipeline by leveraging our technologies and our extensive scientific expertise in aerosol science and medicine to develop additional neurological product candidates offering unique features and benefits.
Nebulized Corticosteroid Particle Technology: We have expertise in the formulation and administration of nebulized corticosteroids for the treatment of pediatric asthma. We have created novel versions of budesonide that are designed to be administered more quickly and to provide efficacy at lower doses than conventional nebulized budesonide. Conventional nebulized budesonide is an inhaled corticosteroid approved by the FDA for treating asthma in children from 12 months up to eight years of age. We have developed novel morphologies of corticosteroid particles which may allow for faster delivery and efficacy at a lower dose, which together may offer improved safety, compliance and convenience.
Combination Particle Technology: We have applied our proprietary particle formulation technologies to deliver the optimal ratio of multiple drugs in a reproducible and consistent manner. We can combine two or more drugs together into a single micron scale inhalable particle at consistent and reproducible ratios, which may improve the delivery profile and stability of the resultant combination therapy. We believe our proprietary technologies in this area have potential broad applicability for a number of combination product candidates in diverse indications via inhalation and other routes of delivery.
Stable Protein & Peptide Technology: We have also demonstrated our ability to apply our proprietary technologies to formulate and stabilize biologically active proteins and peptides. We design and incorporate our protein formulations without the need for excipients or other additives, to be stored for months at room temperature and to provide multiple doses of medicine delivered accurately without the need for needle injections.
A component of our strategy is to reduce the risk of drug development by focusing on the development of proven drugs with established safety and efficacy profiles. The compounds underlying our product candidates are well characterized and have been previously approved by the FDA or foreign agencies for other sponsors and in other dosage forms and formulations. As a result, we may seek FDA marketing approval of our product candidates under Section 505(b)(2) of the Federal Food, Drug and Cosmetic Act, or FFDCA, which, if available to us, would allow any NDA we file with the FDA to rely in part on data in the public domain or the FDA’s prior conclusions regarding the safety and effectiveness of approved compounds. This may expedite the development program for our product candidates by potentially decreasing the overall scope of work we must do ourselves.
Allergan Collaboration
On January 28, 2011, we entered into a Collaboration Agreement (the “Collaboration Agreement”) and a Co-Promotion Agreement (the “Co-Promotion Agreement,” and together with the Collaboration Agreement, the “Allergan Agreements”) with Allergan, Inc., Allergan USA, Inc. and Allergan Sales, LLC (collectively, “Allergan”). Pursuant to the terms of the Allergan Agreements, we have granted Allergan a co-exclusive license to market and promote LEVADEX, our proprietary novel migraine therapy for delivery by inhalation, to neurologists and pain specialists in the United States in collaboration with us. Under the Allergan Agreements, we retain the right to market and promote LEVADEX to other physicians within the United States and also retain all rights to LEVADEX in all other countries, subject to Allergan’s right under certain circumstances to expand the territory in which the parties will market and promote LEVADEX to neurologists and pain specialists to include Canada. We and Allergan will each provide sales representatives and other sales support for such marketing and promotional efforts. The Allergan Agreements specify minimum annual sales detail requirements to be provided by each party, and establish maximum annual amounts of detailing costs that each party will be obligated to incur pursuant to a commercialization plan. The parties will collaborate in the development of LEVADEX for the treatment of migraine in adolescents 12 to 18 years of age, and for at least one other
56
Table of Contents
Index to Financial Statements
indication. We may develop LEVADEX for certain other indications independently of the collaboration if Allergan does not agree to develop LEVADEX for such indications pursuant to the Allergan Agreements. We will be responsible for manufacturing and supplying LEVADEX, and for distributing the product and recording product revenues from sales of LEVADEX resulting from the parties’ collaboration. The parties will share profits and losses resulting from the collaboration equally. We will be solely responsible for payment of all remaining costs of obtaining regulatory approval of LEVADEX for the treatment of acute migraine in adults, except that if the FDA notifies us that additional development or manufacturing activities costing in excess of a certain threshold amount will be required for such regulatory approval, the parties will share any such excess costs. The parties generally will share equally all other costs of developing LEVADEX under the Allergan Agreements, except that neither party shall be obligated for more than a certain threshold amount in a given year, or for more than a certain threshold amount in the aggregate, for development or manufacturing costs or expenses incurred by us for such activities.
In February 2011, we received an upfront payment of $60.0 million from Allergan. Under the terms of Collaboration Agreement, we may also receive up to an additional $97 million in the form of regulatory milestones, including milestones for acceptance of filing of the LEVADEX NDA and first commercial sale associated with the initial acute migraine indication.
Critical Accounting Policies and Significant Judgments and Estimates
Our management’s discussion and analysis of our financial condition and results of operations are based on our financial statements, which have been prepared in accordance with accounting principles generally accepted in the United States. The preparation of these financial statements requires us to make estimates and assumptions that affect the reported amounts of assets and liabilities and the disclosure of contingent assets and liabilities at the date of the financial statements as well as the reported revenues and expenses during the reporting periods. We evaluate our estimates and judgments on an ongoing basis. Actual results may differ materially from these estimates under different assumptions or conditions.
While our significant accounting policies are more fully described in “Note 2 Summary of Significant Accounting Policies” in Part II, Item 8 of this Form 10-K, we believe the following accounting policies are critical to the process of making significant judgments and estimates in the preparation of our financial statements.
Revenue Recognition
We recognize revenue in accordance with Accounting Standards Codification, or ASC 605, Revenue Recognition, which requires that certain criteria must be met before revenue can be recognized: persuasive evidence of an arrangement exists; delivery has occurred or services have been rendered; the fee is fixed or determinable; and collectability is reasonably assured. Determination of whether persuasive evidence of an arrangement exists and whether delivery has occurred or services have been rendered are based on management’s judgments regarding the fixed nature of the fee charged for research performed and milestones met, and the collectability of those fees. Should changes in conditions cause management to determine these criteria are not met for certain future transactions, revenue recognized for any reporting period could be adversely affected.
Collaboration revenue, which is earned under agreements with third parties for research and development activities, may include nonrefundable license fees, cost reimbursements and contingent milestones and royalties. Our revenue arrangements with multiple elements are evaluated in accordance with ASC 605-25 Revenue Recognition — Multiple-Element Arrangements, and are divided into separate units of accounting if certain criteria are met, including whether the delivered element has stand-alone value and whether there is verifiable objective and reliable evidence of the fair value of the undelivered items. The consideration we receive is allocated among the separate units based on their respective fair values, and the applicable revenue recognition criteria are applied to each of the separate units.
57
Table of Contents
Index to Financial Statements
Upfront payments received upon execution of collaborative agreements are recorded as deferred revenue and recognized as collaboration revenue over the research and development period pursuant to the agreement. Such period generally represents the research and development period set forth in the agreement between our third party collaborator and us. The research and development period is estimated at the inception of the arrangement and is periodically reevaluated. Reevaluation of the research and development period may shorten or lengthen the period during which the deferred revenue is recognized. We evaluate the appropriate period based on research progress attained and reevaluate the period when significant changes occur. If the collaboration agreement is terminated, all the remaining unamortized deferred revenue will be recognized as collaboration revenue on the date of termination.
Cost reimbursements are based upon negotiated rates for our full time employee equivalents, or FTE, and actual out-of-pocket costs. They are recognized as collaboration revenue as the related research and development services are performed. The cost reimbursements are generally based on qualified expenses as defined in the collaborative agreement. FTE rates are intended to approximate our anticipated cost.
We recognize milestone payments as revenue upon achievement of the milestone provided the milestone payment is nonrefundable, substantive effort and risk is involved in achieving the milestone and the amount of the milestone is reasonable in relation to the effort expended or risk associated with the achievement of the milestone. If these conditions are not met, we defer the milestone payment and recognize it as revenue over the estimated period of performance under the contract as we complete our performance obligations.
Pre-clinical Study and Clinical Trial Accruals
We estimate our pre-clinical study and clinical trial expenses based on the services received pursuant to contracts with several research institutions and contract research organizations that conduct and manage pre-clinical studies and clinical trials on our behalf. The financial terms of these agreements vary from contract to contract and may result in uneven expenses and payment flows. Pre-clinical study and clinical trial expenses include the following:
| • | fees paid to contract research organizations, or CROs, in connection with pre-clinical studies; |
| • | fees paid to CROs and investigative sites in connection with clinical trials; and |
| • | fees paid to contract manufacturers and service providers in connection with the production and testing of active pharmaceutical ingredients and drug materials for use in pre-clinical studies and clinical trials. |
Payments under some of these contracts depend on factors such as the milestones accomplished, successful enrollment of certain number of patients, site initiation and completion of clinical trial milestones. In accruing services fees, we estimate the time period over which services will be performed and the level of effort to be expended in each period. We monitor patient enrollment levels and related activities to the extent possible through internal reviews, correspondence and status meetings with CROs and review of contractual terms. Our estimates are dependent on the timeliness and accuracy of data provided by our CROs and other vendors.
Stock-Based Compensation
Effective January 1, 2006, we adopted ASC 718 Compensation — Stock Compensation, or ASC 718, which requires the recognition of compensation expense using a fair-value based method for costs related to all stock-based payments. ASC 718 requires companies to estimate the fair value of the stock-based payment awards on the date of grant using an option-pricing model.
For stock option grants and shares from the Employee Stock Purchase Plan, or ESPP, we selected the Black-Scholes valuation model as the most appropriate valuation method. The fair value of these stock options grants
58
Table of Contents
Index to Financial Statements
and shares from the ESPP is estimated as of the date of grant using the Black-Scholes valuation model. The risk-free interest rate assumption was based on U.S. Treasury instruments with a term that is consistent with the expected term of our stock options or shares from the ESPP. The expected stock price volatility of stock options was determined by examining the historical volatilities for industry peers and using an average of the historical volatilities of our industry peers as we did not have sufficient trading history for our common stock. Industry peers consist of several public companies in the biopharmaceutical industry similar to us in size, stage of life-cycle and financial leverage. We will continue to analyze the expected stock price volatility of stock options as more historical data for our common stock becomes available. Effective on January 1, 2010, the expected stock price volatility for shares from the ESPP is determined based on our own historical volatilities. The expected term of stock options represents the weighted average period the stock options are expected to remain outstanding. It was calculated based on the historical experience that we have had with stock option grants as well as the expected term of industry peers, as we did not have sufficient historical information to develop reasonable expectations about future exercise patterns and post-vesting employment termination behavior for the full term of our stock options. We will continue to analyze the expected term of stock options as more historical data for our common stock becomes available. The expected term for shares from the ESPP is determined based on the length of offering periods for the ESPP. The expected dividend yield of 0% is based on our history and expectation of dividend payouts. We do not anticipate paying any dividends in the near future. We have not paid any dividends, other than a cumulative dividend on our preferred stock paid in connection with our initial public offering, or IPO, in 2007, pursuant to the terms of our certificate of incorporation. Stock-based compensation expense is determined based on when awards are ultimately expected to vest, and it has been reduced for estimated forfeitures. ASC 718 requires forfeitures to be estimated at the time of grant and revised, if necessary, in subsequent periods if actual forfeitures differ from those estimates. Forfeitures were estimated based on our historical experience.
For performance-based restricted stock units, or RSUs, the fair value was determined using the stock price of our common stock on the date of the grant. A probability assessment that performance goals will be achieved is made quarterly. The compensation expense is recognized over the vesting period, and is adjusted periodically for forfeiture rate and any changes to our probability assessment of the number of performance-based RSUs expected to vest as a result of our achievement of the performance goals.
Net Operating Loss Carryforwards
At December 31, 2010, we had federal and state net operating loss carryforwards of approximately $214.6 million and $204.4 million, respectively. The net operating loss carryforwards expire between 2014 and 2030, if not utilized. We have established a full valuation allowance against our deferred tax assets due to our history of losses and the uncertainty of future taxable income. The valuation allowance increased by $23.3 million, $6.4 million and $31.6 million during the years ended December 31, 2010, 2009 and 2008, respectively.
As of December 31, 2010, we also had federal and state research and development tax credit carryforwards of approximately $7.4 million and $4.3 million, respectively. If not utilized, the federal carryforwards will expire beginning in 2024. The state credits can be carried forward indefinitely. The Tax Reform Act of 1986 limits the use of net operating loss carryforwards in certain situations where changes occur in the stock ownership of a company. In the event we have a change in ownership, utilization of the carryforwards could be limited.
We adopted ASC 740-10, Accounting for Uncertainty in Income Taxes, on January 1, 2007. As of December 31, 2010, we had no unrecognized tax benefits As of December 31, 2010 we have not recorded any interest or penalties under this pronouncement.
59
Table of Contents
Index to Financial Statements
Financial Overview
Collaboration Revenue
We recognize revenues from collaborative research and development activities. Collaboration revenue, which is earned under agreements with third parties for research and development activities, may include nonrefundable upfront payments, cost reimbursements and milestone payments.
Research and Development Expenses
Research and development costs include, but are not limited to: (i) expenses incurred under agreements with contract research organizations and investigative sites, which conduct our clinical trials and a substantial portion of our pre-clinical studies; (ii) milestone payments paid to our collaborative partners who work on our processing and supply of clinical trial material; (iii) the cost of manufacturing and supplying clinical trial materials; (iv) payments to contract service organizations, as well as consultants; (v) employee-related expenses, which include salaries and benefits; (vi) facilities, depreciation and other allocated expenses, which include direct and allocated expenses for rent and maintenance of facilities and equipment, depreciation of leasehold improvements and equipment and laboratory and other supplies; and (vii) stock-based compensation expense. All research and development expenses are expensed as incurred.
Conducting a significant amount of research and development is central to our business model. Through December 31, 2010, we had incurred approximately $217.5 million in research and development expenses since our inception in 2003. Product candidates in later-stage clinical development generally have higher development costs than those in earlier stages of development, primarily due to the significantly increased size and duration of later-stage clinical trials. We plan to incur substantial research and development expenses for the foreseeable future in order to complete development of our most advanced product candidate, LEVADEX, and to conduct earlier-stage research and development projects. Pursuant to the AstraZeneca Agreement, AstraZeneca reimbursed our development costs related to the UDB program beginning on the effective date of February 2, 2009. The agreement was terminated on July 8, 2009, and we suspended development of UDB in the third quarter of 2009.
The following table summarizes the percentages of our research and development expenses related to our LEVADEX program, our UDB program, which has been suspended, and other earlier stage projects for the years ended December 31, 2010, 2009 and 2008, respectively. The percentages summarized in the following table reflect costs directly attributable to each development candidate, which are tracked on a project basis. A portion of our internal costs, including indirect costs relating to our product candidates, is not tracked on a project basis and has been allocated based on management estimates.
|
Year Ended December 31, |
Period from July 3, 2003 (Date of Inception) through December 31, 2010 |
|||||||||||||||
| 2010 | 2009 | 2008 | ||||||||||||||
| Our product candidates: |
||||||||||||||||
| LEVADEX |
91 | % | 62 | % | 44 | % | 58 | % | ||||||||
| UDB (suspended) |
— | 25 | % | 50 | % | 33 | % | |||||||||
| Other projects |
9 | % | 13 | % | 6 | % | 9 | % | ||||||||
| Total |
100 | % | 100 | % | 100 | % | 100 | % | ||||||||
The process of conducting pre-clinical studies and clinical trials necessary to obtain FDA approval is costly and time consuming. The probability of success for each product candidate and clinical trial may be affected by a variety of factors, including, among other things, the quality of the product candidate’s early clinical data, investment in the program, competition, manufacturing capabilities and commercial viability. As a result of the
60
Table of Contents
Index to Financial Statements
uncertainties discussed above, uncertainty associated with clinical trial enrollment and risks inherent in the development process, we are unable to determine the duration and completion costs of current or future clinical stages of our product candidates or when, or to what extent, we will generate revenues from the commercialization and sale of any of our product candidates. Development timelines, probability of success and development costs vary widely. We are currently focused on developing our most advanced product candidate, LEVADEX. We will need substantial additional capital in the future in order to commercialize LEVADEX and to fund the development and commercialization of future product candidates. However, we may receive additional capital from the Collaboration Agreement with Allergan.
Sales, General and Administrative Expenses
Sales, general and administrative expenses consist primarily of compensation for executive, finance, marketing, legal and administrative personnel, including stock-based compensation. Other sales, general and administrative expenses include facility costs not otherwise included in research and development expenses, legal and accounting services, other professional services, the cost of market research activities and consulting fees. Through December 31, 2010, we incurred approximately $62.9 million in sales, general and administrative expenses since our inception in 2003.
Results of Operations
Comparison of Years Ended December 31, 2010 and 2009
| Year Ended December 31, |
Increase/ (Decrease) |
% Increase/ (Decrease) |
||||||||||||||
| 2010 | 2009 | |||||||||||||||
| (in thousands, except percentages) | ||||||||||||||||
| Collaboration revenue |
$ | — | $ | 54,166 | $ | (54,166 | ) | (100 | )% | |||||||
Collaboration Revenue. Revenues for the year ended December 31, 2010 were $0, compared to $54.2 million for the year ended December 31, 2009. Total collaboration revenue recognized under the AstraZeneca Agreement was $54.2 million for the year ended December 31, 2009 and consists of a $40.0 million upfront payment and $14.2 million from reimbursement of qualified development expenses. The AstraZeneca Agreement was terminated in July 2009.
| Year Ended December 31, |
$ Increase/ (Decrease) |
% Increase/ (Decrease) |
||||||||||||||
| 2010 | 2009 | |||||||||||||||
| (in thousands, except percentages) | ||||||||||||||||
| Research and development expenses |
$ | 37,775 | $ | 47,996 | $ | (10,221 | ) | (21 | )% | |||||||
| Sales, general and administrative expenses |
15,713 | 13,139 | 2,574 | 20 | % | |||||||||||
| Interest income |
(37 | ) | (119 | ) | (82 | ) | (69 | )% | ||||||||
| Interest expense |
1,242 | 2,118 | (876 | ) | (41 | )% | ||||||||||
| Other (income) expense, net |
(20 | ) | 29 | 49 | * | |||||||||||
| * | Percentage is not meaningful. |
Research and Development Expenses. The decrease in research and development expenses was due primarily to a decrease of $8.8 million in clinical and other project expenses to support the UDB Phase 3 clinical program, which was suspended in the third quarter of 2009, and a decrease of $3.5 million in clinical and other project expenses to support the LEVADEX Phase 3 clinical program. We completed clinical development for LEVADEX in 2010 and we plan to submit an NDA to the FDA in the first half of 2011. The decrease in research and development expenses was partially offset by an increase of $2.1 million in personnel related expenses, including stock-based compensation.
61
Table of Contents
Index to Financial Statements
Sales, General and Administrative Expenses. The increase in sales, general and administrative expenses was due primarily to an increase of $1.3 million in personnel related expenses, including stock-based compensation, an increase of $0.6 million in professional services and LEVADEX related marketing activities and an increase of $0.5 million in other expenses.
Interest Income. The decrease in interest income was due primarily to a decrease in market interest rates in the year ended December 31, 2010 as compared to 2009. We expect our interest income to fluctuate in the future with changes in average investment balances and market interest rates.
Interest Expense. The decrease in interest expense was due primarily to lower debt balances related to the 2008 Working Capital Loan. We expect our interest expense to fluctuate in the future with average debt balances.
Comparison of Years Ended December 31, 2009 and 2008
| Year Ended December 31, |
$ Increase/ (Decrease) |
% Increase/ (Decrease) |
||||||||||||||
| 2009 | 2008 | |||||||||||||||
| (in thousands, except percentages) | ||||||||||||||||
| Collaboration revenue |
$ | 54,166 | $ | — | $ | 54,166 | N/A | |||||||||
Collaboration Revenue. Revenues for the year ended December 31, 2009 were $54.2 million, compared to $0 for the year ended December 31, 2008. Total collaboration revenue recognized under the AstraZeneca Agreement was $54.2 million for the year ended December 31, 2009 and consists of a $40.0 million upfront payment and $14.2 million from reimbursement of qualified development expenses. The $40.0 million upfront payment initially was recognized as collaboration revenue on a straight-line basis over the term of our research and development period with respect to UDB. The AstraZeneca Agreement was terminated in July 2009, and we suspended development of UDB in the third quarter of 2009. Effective on the date of termination, the remaining unamortized deferred revenue of $33.1 million was recognized as collaboration revenue in the third quarter of 2009.
| Year Ended December 31, |
$ Increase/ (Decrease) |
% Increase/ (Decrease) |
||||||||||||||
| 2009 | 2008 | |||||||||||||||
| (in thousands, except percentages) | ||||||||||||||||
| Research and development expenses |
$ | 47,996 | $ | 59,277 | $ | (11,281 | ) | (19 | )% | |||||||
| Sales, general and administrative expenses |
13,139 | 13,417 | (278 | ) | (2 | )% | ||||||||||
| Interest income |
(119 | ) | (2,103 | ) | (1,984 | ) | (94 | )% | ||||||||
| Interest expense |
2,118 | 2,056 | 62 | 3 | % | |||||||||||
| Other expense, net |
29 | 281 | (252 | ) | (90 | )% | ||||||||||
Research and Development Expenses. The decrease in research and development expenses for the year ended December 31, 2009 was driven primarily by a decrease of $15.8 million in clinical and other related expenses to support the UDB Phase 3 clinical program as a result of suspending the development of our UDB product candidate in the third quarter of 2009, partially offset by an increase of $2.2 million in clinical and other related expenses to support the LEVADEX Phase 3 clinical program and by an increase of $0.8 million in personnel related expenses.
During the third quarter of 2009, we suspended the development of our UDB product candidate. As a result, for the year ended December 31, 2009, we recorded wind-down costs and writedown of fixed assets charges of approximately $2.8 million.
Sales, General and Administrative Expenses. The decrease in sales, general and administrative expenses for the year ended December 31, 2009 was related primarily to a decrease of $1.1 million in professional services, partially offset by an increase of $0.7 million in stock-based compensation and an increase of $0.4 million in personnel related expenses.
62
Table of Contents
Index to Financial Statements
Interest Income. Interest income decreased due primarily to a decrease in market interest rates and, to a lesser extent, a decrease in the 12-month average cash, cash equivalents and short-term investment balances. We expect our interest income to fluctuate in the future due to changes in market interest rates and average cash, cash equivalents and short-term investment balances.
Interest Expense. Interest expense for the year ended December 31, 2009 was similar to the year ended December 31, 2008.
Other Expense, Net. For the year ended December 31, 2009 compared to the year ended December 31, 2008, other expense decreased due primarily to the fact that in the second quarter of 2008, we incurred a debt issuance cost of $394,000 upon the retirement of the 2006 Working Capital Loan and commencement of the 2008 Working Capital Loan. We did not incur such expenses for the year ended December 31, 2009.
Liquidity and Capital Resources
Liquidity
We have incurred losses since our inception in July 2003 and as of December 31, 2010 we had an accumulated deficit of $239.6 million. We will continue to incur losses until we generate sufficient revenue to offset our expenses, and we anticipate that we may continue to incur net losses for at least the next several years. We expect to incur increased research and development and sales, general and administrative expenses related to our development and potential commercialization of LEVADEX and, as a result, we will need to generate significant net product sales, royalty and other revenues to achieve profitability.
We have financed our operations through equity financing, debt financing, the issuance of convertible notes and collaboration payments, as follows:
Equity
| • | Prior to our IPO in October 2007, we received net proceeds of $106.7 million from the issuance of convertible notes and convertible preferred stock; |
| • | With the completion of our IPO, we received net proceeds of $62.1 million after deducting expenses and underwriters’ discounts and commissions; |
| • | In August 2009, we completed a follow-on public offering in which we sold and issued 3,500,000 shares of our common stock at a price of $9.70 per share. We raised a total of $34.0 million in gross proceeds or approximately $31.6 million in net proceeds after deducting expenses and underwriters’ discounts and commissions; |
| • | In January 2010, we accessed our equity line of credit with Azimuth and sold 1,527,695 shares of common stock at a price of approximately $13.70 per share, less a discount of approximately 4.5% per share, for a net price of approximately $13.09 per share. The total purchase price for these shares was $20.0 million or approximately $19.7 million after deducting the offering expenses; |
| • | In October 2010, we completed an equity offering in which we sold a total of 3,450,000 shares of common stock at an offering price of $14.50 per share. We raised a total of $50.0 million in gross proceeds, or approximately $47.0 million in net proceeds after deducting underwriting discounts and commissions and offering expenses. |
Debt
| • | In September 2006, we entered into a loan facility agreement and borrowed $10.0 million to finance working capital and a $1.0 million loan facility to finance equipment purchases; |
| • | In May 2008, we entered into an agreement to borrow $20.0 million in order to repay the earlier working capital loan and to support general corporate purposes; |
63
Table of Contents
Index to Financial Statements
Collaboration
| • | In 2009, we received $54.2 million in an upfront payment and reimbursement of qualified development expenses pursuant to our now terminated collaboration agreement with AstraZeneca; and |
| • | In February 2011, we received $60.0 million in an upfront payment pursuant to the Collaboration Agreement with Allergan. |
As of December 31, 2010, we had approximately $76.0 million in cash and cash equivalents, which does not reflect the upfront payment of $60.0 million we received in February 2011 pursuant to the Collaboration Agreement with Allergan. Our cash and cash equivalents are held primarily in money market funds. Cash in excess of immediate requirements is invested in accordance with our investment policy with a view toward capital preservation and liquidity.
Cash Flows
This data should be read in conjunction with our Consolidated Statements of Cash Flows.
| December 31, | ||||||||
| 2010 | 2009 | |||||||
| (in thousands) | ||||||||
| Cash and cash equivalents |
$ | 76,007 | $ | 65,776 | ||||
| Working capital |
56,630 | 44,629 | ||||||
| Stockholders’ equity |
62,656 | 41,802 | ||||||
A summary of our cash flows is as follows:
| Year Ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| (in thousands) | ||||||||||||
| Cash provided by (used in): |
||||||||||||
| Operating activities |
$ | (49,363 | ) | $ | (4,008 | ) | $ | (59,473 | ) | |||
| Investing activities |
(2,080 | ) | 11,424 | 31,546 | ||||||||
| Financing activities |
61,674 | 26,433 | 10,738 | |||||||||
Net cash used in operating activities. We used $49.4 million of cash for operating activities for the year ended December 31, 2010, compared to cash usage of $4.0 million for the year ended December 31, 2009. The increase of cash used for operating activities for the year ended December 31, 2010 as compared to the year ended December 31, 2009 was driven primarily by a net loss of $54.7 million and a decrease in accrued liabilities of $2.1 million as a result of paying down expenses related to the LEVADEX Phase 3 clinical program and the UDB program, which was suspended in the third quarter of 2009, partially offset by stock-based compensation of $6.6 million. The decrease of cash used for operating activities for the year ended December 31, 2009 as compared to the year ended December 31, 2008 was due primarily to the decreased loss, as a result of revenue recognition of $54.2 million from the AstraZeneca Agreement, which was terminated in July 2009, together with a decrease in accrued liabilities of $3.9 million as a result of suspending the development of our UDB product candidate in the third quarter of 2009. Net cash used for operating activities for the year ended December 31, 2008 was driven primarily to a net loss of $72.9 million resulting from the operating expenses related to our clinical development programs and an increase in headcount across all departments.
Net cash provided by (used in) investing activities. We used $2.1 million of cash for investing activities for the year ended December 31, 2010, compared to receiving cash of $11.4 million for the year ended December 31, 2009. Net cash used in investing activities for the year ended December 31, 2010 was due primarily to purchase of property and equipment. Net cash provided by investing activities for the year ended December 31, 2009 was
64
Table of Contents
Index to Financial Statements
due primarily to sales and maturities of our short-term investments of $12.7 million. Net cash provided by investing activities for 2008 was related primarily to investment activity, with more maturities than purchases of investments.
Net cash provided by financing activities. We received $61.7 million of cash from financing activities for the year ended December 31, 2010 compared to receiving cash of $26.4 million for the year ended December 31, 2009. Net cash provided by financing activities for the year ended December 31, 2010 was due primarily to the net proceeds of approximately $47.0 million from the issuance of our common stock from the equity offering we completed in October 2010, the net proceeds of approximately $19.7 million from the issuance of our common stock from the drawdown of the equity line of credit with Azimuth completed in January 2010 and the proceeds of $2.3 million from sales of shares through equity plans, partially offset by the repayment of $7.3 million for the 2008 Working Capital Loan. Net cash provided by financing activities for the year ended December 31, 2009 was due primarily to the net proceeds of $31.6 million from our follow-on public offering and the proceeds of $1.2 million from sales of shares through equity plans, partially offset by the repayment of $6.3 million for the 2008 Working Capital Loan. Net cash provided by financing activities in 2008 was primarily attributable to the issuance of $20.0 million in debt in May 2008 and the proceeds of $0.7 million from sales of shares through equity plans, offset by the repayment of $1.7 million for the 2008 Working Capital Loan and the repayment of $8.3 million for an earlier working capital loan which was fully paid in May 2008.
Equity Line of Credit
On November 11, 2009, we entered into a Common Stock Purchase Agreement, or the Purchase Agreement, with Azimuth, which provides us with what is sometimes termed an equity line of credit arrangement. Upon the terms and subject to the conditions set forth in the Purchase Agreement, Azimuth is committed to purchase up to $60.0 million worth of shares of our common stock over the 24-month term of the Purchase Agreement; provided, however, in no event may we sell under the Purchase Agreement more than such number of shares of common stock which is equal to one share less than 20% of our outstanding shares of common stock on the effective date of the Purchase Agreement. From time to time over the term of the Purchase Agreement, and at our sole discretion, we may present Azimuth with draw down notices requiring Azimuth to purchase a specified dollar amount of shares of our common stock, based on the price per share over ten consecutive trading days or such other period mutually agreed upon by Azimuth and us, with each draw down subject to limitations based on the price of our common stock and a maximum limit of 2.5% of our market capitalization at the time of such draw down, or such other limit of our market capitalization as mutually agreed upon by Azimuth and us.
In January 2010 we accessed our equity line of credit and sold 1,527,695 shares of common stock at a price of approximately $13.70 per share less a discount of approximately 4.5% per share for a net price of approximately $13.09 per share. The total purchase price for all these shares was $20.0 million or approximately $19.7 million after deducting offering expenses.
Contractual Obligations
The following table summarizes our contractual obligations as of December 31, 2010:
| Year Ended December 31, | ||||||||||||||||
| 2011 | 2012 | Thereafter | Total | |||||||||||||
| (In thousands) | ||||||||||||||||
| Contractual Obligations: |
||||||||||||||||
| Debt(1) |
$ | 7,952 | $ | — | $ | — | $ | 7,952 | ||||||||
| Operating lease obligation(2) |
1,357 | 700 | — | 2,057 | ||||||||||||
| Total |
$ | 9,309 | $ | 700 | $ | — | $ | 10,009 | ||||||||
| (1) | In May 2008, we entered into an agreement to borrow $20.0 million, or the 2008 Working Capital Loan, in order to repay an earlier working capital loan and to support general corporate purposes. The amounts in the |
65
Table of Contents
Index to Financial Statements
| table above include interest and principal repayments on the loan. As of December 31, 2010, we were in compliance with the loan covenants. Please see “Note 5. Debt” in Part II, Item 8 of this Form 10-K for additional information. |
| (2) | The amounts in the table above include the minimum rental payments for our laboratory and office facilities in Mountain View, California. Please see “Note 6. Commitments and Contingencies” in Part II, Item 8 of this Form 10-K for additional information. |
The table above reflects only payment obligations that are fixed and determinable. Milestone payments and royalty payments under our license, supply and service agreements are not included in the table above because we cannot, at this time, determine when or if the related milestones will be achieved or the events triggering the commencement of payment obligations will occur. Amounts and an estimate of significant payments related to licensing and other arrangements not included in the contractual obligations table above are as follows:
Agreement with Nektar Under our June 2004 agreement, as amended, with Nektar Therapeutics UK Limited, or the Nektar Agreement, we were granted a worldwide, exclusive license, with a right to sublicense, under Nektar patents and know-how, to develop and commercialize any formulation of a form of dihydroergotamine for administration by inhalation using a device. We also agreed to pay royalties at specified rates based on net sales. As of December 31, 2010, we are required to make future nonrefundable milestone payments of up to $5.0 million related to products currently being developed under the Nektar Agreement, when and if certain regulatory and commercial milestones are met. We paid $0 for the years ended December 31, 2010, 2009 and 2008, respectively. We paid $2.6 million for the cumulative period from July 3, 2003 (date of inception) to December 31, 2010. Either party may terminate the Nektar Agreement upon a material, uncured default of the other party. We may terminate the Nektar Agreement, with or without cause, at any time upon six months’ prior written notice.
Agreement with Allergan Under the Collaboration Agreement with Allergan effective January 28, 2011, we will be responsible for manufacturing and supplying LEVADEX, and for distributing the product and recording product revenues from sales of LEVADEX resulting from the parties’ collaboration. The parties will share profits and losses resulting from the collaboration equally. We will be solely responsible for payment of all remaining costs of obtaining regulatory approval of LEVADEX for the treatment of acute migraine in adults, except that if the FDA notifies us that additional development or manufacturing activities costing in excess of a certain threshold amount will be required for such regulatory approval, the parties will share any such excess costs. The parties generally will share equally all other costs of developing LEVADEX under the Allergan Agreements, except that neither party shall be obligated for more than a certain threshold amount in a given year, or for more than a certain threshold amount in the aggregate, for development or manufacturing costs or expenses incurred by us for such activities. We have agreed to indemnify Allergan against any losses incurred in connection with, among other things, any negligence, recklessness or wrongful intentional acts by us, any breach by us of the Allergan Agreements, the development and commercialization of LEVADEX actually conducted by or for us or our affiliates or sublicensees, allegations that the manufacture, use or commercialization of LEVADEX infringes third party intellectual property rights, or allegations that personal injury or death or property damage was caused by a defect in LEVADEX manufactured by or for us. The Collaboration Agreement may be terminated (i) by Allergan, at will, after first commercial sale of LEVADEX in the United States, upon 180 days’ prior written notice, (ii) by Allergan, upon written notice to us, if we receive a complete response letter or equivalent communication from the FDA, that Allergan determines will extend potential approval beyond a certain date or requires a certain minimum level of additional investment, (iii) by us, upon written notice to Allergan, if Allergan commercializes a competing product in the United States (or, if the territory of the Allergan Agreements is expanded, Canada) and (iv) by us, upon written notice to Allergan, if Allergan challenges or opposes patent rights licensed to Allergan pursuant to the Collaboration Agreement. Additionally, either party may terminate the Collaboration Agreement in the event of an uncured material breach. The Co-Promotion Agreement will terminate upon termination of the Collaboration Agreement.
66
Table of Contents
Index to Financial Statements
Operating Capital and Capital Expenditure Requirements
Our future capital requirements will depend on many forward looking factors and are not limited to the following:
| • | the initiation, progress, timing and completion of clinical trials for our product candidates and potential product candidates; |
| • | the outcome, timing and cost of regulatory approvals and the regulatory approval process; |
| • | delays that may be caused by changing regulatory requirements; |
| • | the number of product candidates that we pursue; |
| • | the costs involved in filing and prosecuting patent applications and enforcing and defending patent claims; |
| • | the timing and terms of future in-licensing and out-licensing transactions; |
| • | the cost and timing of establishing commercial infrastructure including sales, marketing, manufacturing and distribution capabilities; |
| • | the cost of procuring clinical and commercial supplies of our product candidates; |
| • | the cost of maintaining adequate working capital; |
| • | the extent to which we acquire or invest in businesses, products or technologies; and |
| • | the possible costs of litigation. |
We believe that our existing cash and cash equivalents, together with the upfront payment of $60.0 million we received in February 2011 pursuant to the Collaboration Agreement with Allergan, will be sufficient to fund our projected operating requirements for at least 12 months. We will need substantial additional capital in the future in order to complete the development and commercialization of LEVADEX and to fund the development and commercialization of any future product candidates. Until we can generate a sufficient amount of product revenue, if ever, we expect to finance future cash needs through public or private equity offerings, debt financings or corporate collaboration and licensing arrangements. Such funding, if needed, may not be available on favorable terms, if at all. In the event we are unable to obtain additional capital, we may delay or reduce the scope of our current research and development programs and other expenses.
If adequate funds are not available, we may be required to delay, reduce the scope of or eliminate one or more of our research or development programs or our commercialization efforts. To the extent that we raise additional funds by issuing equity securities, our stockholders may experience additional significant dilution, and debt financing, if available, may involve restrictive covenants. To the extent that we raise additional funds through collaboration and licensing arrangements, it may be necessary to relinquish some rights to our technologies or our product candidates or grant licenses on terms that may not be favorable to us. We may seek to access the public or private capital markets whenever conditions are favorable, even if we do not have an immediate need for additional capital at that time.
Recent Accounting Pronouncements
On April 29, 2010, the Financial Accounting Standards Board, or FASB, issued Accounting Standards Update, or ASU, No. 2010-17, Revenue Recognition — Milestone Method (Topic 605): Milestone Method of Revenue Recognition (a consensus of the FASB Emerging Issues Task Force). It establishes a revenue recognition model for contingent consideration that is payable upon the achievement of an uncertain future event, referred to as a milestone. The scope of ASU 2010-17 is limited to research or development arrangements and requires an entity to record the milestone payment in its entirety in the period received if the milestone meets all the necessary criteria to be considered substantive. ASU 2010-17 is effective for fiscal years (and interim periods
67
Table of Contents
Index to Financial Statements
within those fiscal years) beginning on or after June 15, 2010. Early adoption is permitted. Entities can apply this guidance prospectively to milestones achieved after adoption. However, retrospective application to all prior periods is also permitted. We will adopt ASU 2010-17 in the first quarter of fiscal year 2011. We do not believe that the adoption of ASU 2010-17 will have a material impact on our consolidated financial statements.
In October 2009, the FASB ratified Revenue Arrangements with Multiple Deliverables issued as ASU 2009-13. ASU 2009-13 updates the existing multiple-element arrangements guidance currently included in ASC 605-25, Revenue Recognition — Multiple-Element Arrangements. The revised guidance provides for two significant changes to the existing multiple-element arrangements guidance. The first relates to the determination of when the individual deliverables included in a multiple-element arrangement may be treated as separate units of accounting. This change is significant as it will likely result in the requirement to separate more deliverables within an arrangement, ultimately leading to less revenue deferral. The second change modifies the manner in which the transaction consideration is allocated across the separately identifiable deliverables. These changes are likely to result in earlier recognition of revenue for multiple-element arrangements than under previous guidance. ASU 2009-13 also significantly expands the disclosures required for multiple-element revenue arrangements. The revised multiple-element arrangements guidance will be effective for the first annual reporting period beginning on or after June 15, 2010, and may be applied retrospectively for all periods presented or prospectively to arrangements entered into or modified after the adoption date. Early adoption is permitted provided that the revised guidance is retroactively applied to the beginning of the year of adoption. If the guidance is adopted prospectively, certain transitional disclosures are required for each reporting period in the initial year of adoption. We will adopt the new pronouncement in the first quarter of fiscal year 2011. We do not believe that the adoption of ASU 2009-13 will have a material impact on our consolidated financial statements.
Off-Balance Sheet Arrangements
Since our inception, we have not engaged in any off-balance sheet arrangements, including the use of structured finance, special purpose entities or variable interest entities.
| ITEM 7A. | QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK |
Our exposure to market risk is confined to our cash and cash equivalents. We consider all highly liquid investments purchased with an original maturity of less than or equal to ninety days to be cash equivalents. The goals of our investment policy are preservation of capital, fulfillment of liquidity needs and capturing a market rate of return based on our investment policy parameters and market conditions. We also seek to maximize income from our investments without assuming significant risk. To achieve our goals, we maintain a portfolio of investments in securities of high credit quality.
Our primary exposure to market risk is interest rate related, which is affected by changes in the general level of U.S. interest rates. We currently do not hedge interest rate exposure. Because of the very short term maturity nature of our investments, we do not believe that an increase in market rates would have any material negative impact on the value of our investment portfolio. We do not have any foreign currency or other derivative financial instruments.
68
Table of Contents
Index to Financial Statements
| ITEM 8. | FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA |
MAP PHARMACEUTICALS, INC.
(a development stage enterprise)
INDEX TO CONSOLIDATED FINANCIAL STATEMENTS
| Page | ||||
| 70 | ||||
| 71 | ||||
| 72 | ||||
| 73 | ||||
| 75 | ||||
| 76 | ||||
69
Table of Contents
Index to Financial Statements
Report of Independent Registered Public Accounting Firm
To Board of Directors and Stockholders of MAP Pharmaceuticals, Inc
In our opinion, the consolidated financial statements listed in the accompanying index present fairly, in all material respects, the financial position of MAP Pharmaceuticals, Inc. and its subsidiaries (a development stage enterprise) at December 31, 2010 and 2009, and the results of their operations and their cash flows for each of the three years in the period ended December 31, 2010, and cumulatively, for the period from July 3, 2003 (date of inception) to December 31, 2010 in conformity with accounting principles generally accepted in the United States of America. Also in our opinion, the Company maintained, in all material respects, effective internal control over financial reporting as of December 31, 2010, based on criteria established in Internal Control — Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO). The Company’s management is responsible for these financial statements, for maintaining effective internal control over financial reporting and for its assessment of the effectiveness of internal control over financial reporting, included in Management’s Report on Internal Control Over Financial Reporting appearing under Item 9A. Our responsibility is to express opinions on these financial statements, and on the Company’s internal control over financial reporting based on our integrated audits. We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audits to obtain reasonable assurance about whether the financial statements are free of material misstatement and whether effective internal control over financial reporting was maintained in all material respects. Our audits of the financial statements included examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements, assessing the accounting principles used and significant estimates made by management, and evaluating the overall financial statement presentation. Our audit of internal control over financial reporting included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, and testing and evaluating the design and operating effectiveness of internal control based on the assessed risk. Our audits also included performing such other procedures as we considered necessary in the circumstances. We believe that our audits provide a reasonable basis for our opinions.
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (i) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (ii) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (iii) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
/s/ PricewaterhouseCoopers LLP
San Jose, California
March 4, 2011
70
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
(a development stage enterprise)
(In thousands, except share and per share data)
| December 31, | ||||||||
| 2010 | 2009 | |||||||
| ASSETS |
||||||||
| Current assets: |
||||||||
| Cash and cash equivalents |
$ | 76,007 | $ | 65,776 | ||||
| Prepaid expenses and other current assets |
644 | 620 | ||||||
| Total current assets |
76,651 | 66,396 | ||||||
| Property and equipment, net |
5,803 | 4,164 | ||||||
| Other assets |
30 | 126 | ||||||
| Restricted investment |
310 | 310 | ||||||
| Total assets |
$ | 82,794 | $ | 70,996 | ||||
| LIABILITIES AND STOCKHOLDERS’ EQUITY |
||||||||
| Current liabilities: |
||||||||
| Accounts payable |
$ | 2,998 | $ | 2,916 | ||||
| Accrued liabilities |
9,442 | 11,568 | ||||||
| Current portion of long-term debt |
7,581 | 7,283 | ||||||
| Total current liabilities |
20,021 | 21,767 | ||||||
| Long-term debt, net of current |
— | 7,337 | ||||||
| Other liabilities |
117 | 90 | ||||||
| Total liabilities |
20,138 | 29,194 | ||||||
| Commitments and contingencies (Note 6) |
||||||||
| Stockholders’ equity: |
||||||||
| Preferred stock: $0.01 par value; issuable in series; 5,000,000 shares authorized; none issued or outstanding |
— | — | ||||||
| Common stock: $0.01 par value, 100,000,000 shares authorized; 30,189,650 and 24,696,666 shares issued and outstanding at December 31, 2010 and 2009, respectively |
296 | 241 | ||||||
| Additional paid-in capital |
301,924 | 226,452 | ||||||
| Deficit accumulated during the development stage |
(239,564 | ) | (184,891 | ) | ||||
| Total stockholders’ equity |
62,656 | 41,802 | ||||||
| Total liabilities and stockholders’ equity |
$ | 82,794 | $ | 70,996 | ||||
The accompanying notes are an integral part of these consolidated financial statements.
71
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
(a development stage enterprise)
CONSOLIDATED STATEMENTS OF OPERATIONS
(In thousands, except per share data)
|
Years Ended December 31, |
Cumulative Period from July 3, 2003 (Date of Inception) to December 31, 2010 |
|||||||||||||||
| 2010 | 2009 | 2008 | ||||||||||||||
| Collaboration revenue |
$ | — | $ | 54,166 | $ | — | $ | 54,166 | ||||||||
| Operating expenses: |
||||||||||||||||
| Research and development |
37,775 | 47,996 | 59,277 | 217,469 | ||||||||||||
| Sales, general and administrative |
15,713 | 13,139 | 13,417 | 62,914 | ||||||||||||
| Total operating expenses |
53,488 | 61,135 | 72,694 | 280,383 | ||||||||||||
| Loss from operations |
(53,488 | ) | (6,969 | ) | (72,694 | ) | (226,217 | ) | ||||||||
| Interest income |
37 | 119 | 2,103 | 6,405 | ||||||||||||
| Interest expense |
(1,242 | ) | (2,118 | ) | (2,056 | ) | (6,993 | ) | ||||||||
| Other income (expense), net |
20 | (29 | ) | (281 | ) | (742 | ) | |||||||||
| Net loss |
(54,673 | ) | (8,997 | ) | (72,928 | ) | (227,547 | ) | ||||||||
| Cumulative stock dividend attributed to preferred stockholders |
— | — | — | (13,925 | ) | |||||||||||
| Net loss attributed to common stockholders |
$ | (54,673 | ) | $ | (8,997 | ) | $ | (72,928 | ) | $ | (241,472 | ) | ||||
| Net loss per share attributed to common stockholders —basic and diluted |
$ | (2.01 | ) | $ | (0.41 | ) | $ | (3.58 | ) | |||||||
| Weighted average shares outstanding used in calculating net loss per share attributed to common stockholders — basic and diluted |
27,261 | 22,195 | 20,350 | |||||||||||||
The accompanying notes are an integral part of these consolidated financial statements.
72
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
(a development stage enterprise)
CONSOLIDATED STATEMENTS OF STOCKHOLDERS’ EQUITY (DEFICIT)
(In thousands, except share and per share data)
|
Common Stock |
Additional Paid-In Capital |
Accumulated Other Comprehensive Income |
Deficit Accumulated During the Development Stage |
Total Stockholders’ Equity (Deficit) |
||||||||||||||||||||
| Shares | Amount | |||||||||||||||||||||||
| Issuance of common stock to founders in December 2003 at $0.001 per share |
610,164 | $ | 1 | $ | — | $ | — | $ | — | $ | 1 | |||||||||||||
| Balances at December 31, 2003 |
610,164 | 1 | — | — | — | 1 | ||||||||||||||||||
| Issuance of restricted common stock at $0.25 per share in August 2004 for services |
208,270 | 2 | 49 | — | — | 51 | ||||||||||||||||||
| Accretion of cumulative dividend on redeemable convertible preferred stock |
— | — | (49 | ) | — | (970 | ) | (1,019 | ) | |||||||||||||||
| Net loss |
— | — | — | — | (8,831 | ) | (8,831 | ) | ||||||||||||||||
| Balances at December 31, 2004 |
818,434 | 3 | — | — | (9,801 | ) | (9,798 | ) | ||||||||||||||||
| Stock-based compensation |
— | — | 82 | — | — | 82 | ||||||||||||||||||
| Accretion of cumulative dividend on redeemable convertible preferred stock |
— | — | (82 | ) | — | (2,519 | ) | (2,601 | ) | |||||||||||||||
| Net loss |
— | — | — | — | (16,249 | ) | (16,249 | ) | ||||||||||||||||
| Balances at December 31, 2005 |
818,434 | 3 | — | — | (28,569 | ) | (28,566 | ) | ||||||||||||||||
| Issuance of common stock in conjunction with exercise of stock options |
2,400 | — | 2 | — | — | 2 | ||||||||||||||||||
| Employee stock-based compensation expense recognized under ASC 718 |
— | — | 279 | — | — | 279 | ||||||||||||||||||
| Stock-based compensation expense from vesting of service award |
— | — | 140 | — | — | 140 | ||||||||||||||||||
| Accretion of cumulative dividend on redeemable convertible preferred stock |
— | — | (421 | ) | — | (4,308 | ) | (4,729 | ) | |||||||||||||||
| Components of other comprehensive loss: |
||||||||||||||||||||||||
| Change in unrealized gain on marketable securities |
— | — | — | 6 | — | 6 | ||||||||||||||||||
| Net loss |
— | — | — | — | (25,809 | ) | (25,809 | ) | ||||||||||||||||
| Total comprehensive loss |
(25,803 | ) | ||||||||||||||||||||||
| Balances at December 31, 2006 |
820,834 | 3 | — | 6 | (58,686 | ) | (58,677 | ) | ||||||||||||||||
| Conversion of redeemable convertible preferred stock to common stock at initial public offering |
12,634,845 | 126 | 106,601 | 106,727 | ||||||||||||||||||||
| Issuance of redeemable convertible preferred stock dividend in common stock at initial public offering |
928,314 | 9 | 13,916 | — | — | 13,925 | ||||||||||||||||||
| Conversion of warrants from warrants for preferred stock to warrants for common stock |
— | — | 948 | — | — | 948 | ||||||||||||||||||
| Elimination of fractional shares resulting from reverse stock split |
— | — | 6 | — | (6 | ) | — | |||||||||||||||||
| Issuance of common stock from initial public offering, net of issuance costs |
5,750,000 | 58 | 62,063 | — | — | 62,121 | ||||||||||||||||||
| Issuance of common stock in conjunction with exercise of stock options |
94,369 | 1 | 61 | — | — | 62 | ||||||||||||||||||
| Employee stock-based compensation expense recognized under ASC 718 |
— | — | 1,711 | — | — | 1,711 | ||||||||||||||||||
| Stock-based compensation for non-employee services |
— | — | 249 | — | — | 249 | ||||||||||||||||||
| Accretion of cumulative dividend on redeemable convertible preferred stock |
— | — | (1,361 | ) | — | (4,214 | ) | (5,575 | ) | |||||||||||||||
| Components of other comprehensive loss: |
||||||||||||||||||||||||
| Change in unrealized gain on marketable securities |
— | — | — | 175 | — | 175 | ||||||||||||||||||
| Net loss |
— | — | — | — | (40,060 | ) | (40,060 | ) | ||||||||||||||||
| Total comprehensive loss |
(39,885 | ) | ||||||||||||||||||||||
| Balances at December 31, 2007 |
20,228,362 | 197 | 184,194 | 181 | (102,966 | ) | 81,606 | |||||||||||||||||
73
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
(a development stage enterprise)
CONSOLIDATED STATEMENTS OF STOCKHOLDERS’ EQUITY (DEFICIT)—(Continued)
(In thousands, except share and per share data)
|
Common Stock |
Additional Paid-In Capital |
Accumulated Other Comprehensive Income |
Deficit Accumulated During the Development Stage |
Total Stockholders’ Equity (Deficit) |
||||||||||||||||||||
| Shares | Amount | |||||||||||||||||||||||
| Issuance of common stock in conjunction with exercise of stock options and purchase under employee stock purchase plan |
318,088 | 3 | 719 | — | — | 722 | ||||||||||||||||||
| Employee stock-based compensation expense recognized under ASC 718 |
— | — | 3,359 | — | — | 3,359 | ||||||||||||||||||
| Stock-based compensation for non-employee services |
— | — | 534 | — | — | 534 | ||||||||||||||||||
| Adjustment to issuance cost related to IPO |
— | — | (9 | ) | — | — | (9 | ) | ||||||||||||||||
| Components of other comprehensive loss: |
||||||||||||||||||||||||
| Change in unrealized loss on marketable securities |
— | — | — | (137 | ) | — | (137 | ) | ||||||||||||||||
| Net loss |
— | — | — | — | (72,928 | ) | (72,928 | ) | ||||||||||||||||
| Total comprehensive loss |
(73,065 | ) | ||||||||||||||||||||||
| Balances at December 31, 2008 |
20,546,450 | 200 | 188,797 | 44 | (175,894 | ) | 13,147 | |||||||||||||||||
| Issuance of common stock in conjunction with exercise of stock options and purchase under employee stock purchase plan |
644,399 | 6 | 1,156 | — | — | 1,162 | ||||||||||||||||||
| Employee stock-based compensation expense recognized under ASC 718 |
— | — | 4,835 | — | — | 4,835 | ||||||||||||||||||
| Stock-based compensation for non-employee services |
— | — | 80 | — | — | 80 | ||||||||||||||||||
| Issuance of common stock from follow-on public offering, net of issuance costs |
3,500,000 | 35 | 31,584 | — | — | 31,619 | ||||||||||||||||||
| Issuance of common stock from warrant exercise |
5,817 | — | — | — | — | — | ||||||||||||||||||
| Components of other comprehensive loss: |
||||||||||||||||||||||||
| Change in unrealized loss on marketable securities |
— | — | — | (44 | ) | — | (44 | ) | ||||||||||||||||
| Net loss |
— | — | — | — | (8,997 | ) | (8,997 | ) | ||||||||||||||||
| Total comprehensive loss |
(9,041 | ) | ||||||||||||||||||||||
| Balances at December 31, 2009 |
24,696,666 | 241 | 226,452 | — | (184,891 | ) | 41,802 | |||||||||||||||||
| Issuance of common stock in conjunction with exercise of stock options and purchase under employee stock purchase plan |
502,994 | 5 | 2,268 | — | — | 2,273 | ||||||||||||||||||
| Employee stock-based compensation expense recognized under ASC 718 |
— | — | 6,572 | — | — | 6,572 | ||||||||||||||||||
| Issuance of common stock from equity offering, net of issuance costs |
3,450,000 | 35 | 46,994 | — | — | 47,029 | ||||||||||||||||||
| Issuance of common stock from drawing down of Azimuth equity line of credit, net of issuance costs |
1,527,695 | 15 | 19,638 | — | — | 19,653 | ||||||||||||||||||
| Issuance of common stock from warrant exercise |
12,295 | — | — | — | — | — | ||||||||||||||||||
| Components of other comprehensive loss: |
||||||||||||||||||||||||
| Net loss |
— | — | — | — | (54,673 | ) | (54,673 | ) | ||||||||||||||||
| Total comprehensive loss |
(54,673 | ) | ||||||||||||||||||||||
| Balances at December 31, 2010 |
30,189,650 | $ | 296 | $ | 301,924 | $ | — | $ | (239,564 | ) | $ | 62,656 | ||||||||||||
The accompanying notes are an integral part of these consolidated financial statements.
74
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
(a development stage enterprise)
CONSOLIDATED STATEMENTS OF CASH FLOWS
(In thousands)
|
Years Ended December 31, |
Cumulative Period from July 3, 2003 (Date of Inception) to December 31, 2010 |
|||||||||||||||
| 2010 | 2009 | 2008 | ||||||||||||||
| Cash flows from operating activities: |
||||||||||||||||
| Net loss |
$ | (54,673 | ) | $ | (8,997 | ) | $ | (72,928 | ) | $ | (227,547 | ) | ||||
| Adjustments to reconcile net loss to net cash used in operating activities: |
||||||||||||||||
| Depreciation and amortization |
1,222 | 1,476 | 1,275 | 5,878 | ||||||||||||
| Accretion of investment discounts, net |
— | (1 | ) | (696 | ) | (1,595 | ) | |||||||||
| Amortization of debt issuance costs |
— | — | 102 | 210 | ||||||||||||
| Accretion of debt payment premium |
244 | 391 | 300 | 935 | ||||||||||||
| Change in carrying value of warrant liability |
— | — | — | 621 | ||||||||||||
| Issuance of common stock in exchange for services |
— | — | — | 51 | ||||||||||||
| Stock-based compensation |
6,572 | 4,915 | 3,893 | 17,841 | ||||||||||||
| Loss on disposal and other non-cash items |
309 | 683 | 16 | 1,376 | ||||||||||||
| Changes in operating assets and liabilities: |
||||||||||||||||
| Prepaid expenses and other current assets |
(24 | ) | 185 | 274 | (869 | ) | ||||||||||
| Other assets |
96 | (51 | ) | 67 | 110 | |||||||||||
| Accounts payable |
(1,008 | ) | 1,285 | 341 | 1,879 | |||||||||||
| Accrued liabilities |
(2,128 | ) | (3,924 | ) | 7,823 | 9,362 | ||||||||||
| Other liabilities |
27 | 30 | 60 | 117 | ||||||||||||
| Net cash used in operating activities |
(49,363 | ) | (4,008 | ) | (59,473 | ) | (191,631 | ) | ||||||||
| Cash flows from investing activities: |
||||||||||||||||
| Purchase of intangible assets and in-process research and development |
— | — | — | (412 | ) | |||||||||||
| Purchase of property and equipment |
(2,080 | ) | (1,316 | ) | (2,115 | ) | (11,521 | ) | ||||||||
| Purchase of short-term investments |
— | — | (55,642 | ) | (169,497 | ) | ||||||||||
| Sales and maturities of short-term investments |
— | 12,740 | 89,292 | 171,411 | ||||||||||||
| Sales (Purchase) of restricted investment |
— | — | 11 | (310 | ) | |||||||||||
| Net cash provided by (used in) investing activities |
(2,080 | ) | 11,424 | 31,546 | (10,329 | ) | ||||||||||
| Cash flows from financing activities: |
||||||||||||||||
| Proceeds from issuance of convertible notes payable |
— | — | — | 4,300 | ||||||||||||
| Proceeds from issuance of debt |
— | — | 20,000 | 31,006 | ||||||||||||
| Proceeds from sales of shares through equity plans |
2,273 | 1,162 | 722 | 4,222 | ||||||||||||
| Repayment of debt |
(7,283 | ) | (6,348 | ) | (9,975 | ) | (24,460 | ) | ||||||||
| Proceeds from issuance of common stock in IPO, net of issuance costs(1) |
— | — | (9 | ) | 62,168 | |||||||||||
| Proceeds from issuance of common stock in follow-on public offering, net of issuance costs |
— | 31,619 | — | 31,619 | ||||||||||||
| Proceeds from issuance of common stock resulting from drawdown of equity line of credit, net of issuance costs |
19,653 | — | — | 19,653 | ||||||||||||
| Proceeds from issuance of common stock in equity offering, net of issuance costs(2) |
47,031 | — | — | 47,031 | ||||||||||||
| Proceeds from issuance of convertible preferred stock, net of issuance costs |
— | — | — | 102,428 | ||||||||||||
| Net cash provided by financing activities |
61,674 | 26,433 | 10,738 | 277,967 | ||||||||||||
| Net increase (decrease) in cash and cash equivalents |
10,231 | 33,849 | (17,189 | ) | 76,007 | |||||||||||
| Cash and cash equivalents at beginning of period |
65,776 | 31,927 | 49,116 | — | ||||||||||||
| Cash and cash equivalents at end of period |
$ | 76,007 | $ | 65,776 | $ | 31,927 | $ | 76,007 | ||||||||
| Supplemental disclosures of cash flow information |
||||||||||||||||
| Cash paid for interest |
$ | 998 | $ | 1,727 | $ | 1,658 | $ | 5,747 | ||||||||
| Supplemental disclosure of non-cash investing and financing activities |
||||||||||||||||
| Purchase of property and equipment through accounts payable |
$ | 1,090 | $ | — | $ | — | $ | 1,090 | ||||||||
| Conversion of notes payable to convertible preferred stock |
$ | — | $ | — | $ | — | $ | 4,300 | ||||||||
| Issuance of convertible preferred stock warrants |
$ | — | $ | — | $ | — | $ | 327 | ||||||||
| Accretion of cumulative dividends on redeemable convertible preferred stock |
$ | — | $ | — | $ | — | $ | 13,925 | ||||||||
| Conversion of redeemable convertible preferred stock to common stock upon IPO |
$ | — | $ | — | $ | — | $ | 106,727 | ||||||||
| Reclassification of preferred warrants to common warrants |
$ | — | $ | — | $ | — | $ | 948 | ||||||||
| Issuance of common stock to preferred stockholders as cumulative dividend |
$ | — | $ | — | $ | — | $ | 13,925 | ||||||||
| (1) | The difference between $62,168,000 and $62,109,000 in Note 8 is $59,000 in offering costs accrued and not yet paid at December 31, 2007. |
| (2) | The difference between $47,031,000 and $47,029,000 in Consolidated Statements of Stockholders’ Equity is $2,000 in offering costs accrued and not yet paid at December 31, 2010. |
The accompanying notes are an integral part of these consolidated financial statements.
75
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
(a development stage enterprise)
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
| NOTE 1. | THE COMPANY |
Nature of Operation
MAP Pharmaceuticals, Inc., incorporated in the state of Delaware, originally was formed as a limited liability company on July 3, 2003 and converted to a corporation on December 11, 2003. Our goal is to use proprietary inhalation technologies to enhance the therapeutic benefits and commercial attractiveness of proven drugs while minimizing risk by capitalizing on their known safety, efficacy and commercialization history. Our current focus is to advance the development of our Phase 3 product candidate, LEVADEX™, formerly known as MAP0004, a proprietary orally inhaled version of dihydroergotamine for the potential treatment of migraine. We are in the development stage and since inception have devoted substantially all of our efforts to research and development, raising capital and recruiting personnel.
We have incurred losses and negative cash flow since our inception in July 2003. We will continue to incur losses until we generate sufficient revenue to offset our expenses, and we anticipate that we may continue to incur net losses for the next several years. We will need substantial additional capital in the future in order to complete the development and potential commercialization of LEVADEX and to fund the development and commercialization of any future product candidates. Prior to achieving profitable operations, we intend to continue to fund operations through public or private financings, strategic partnerships or other arrangements. Such funding, if needed, may not be available on favorable terms, if at all. In the event we are unable to obtain additional capital, we may delay or reduce the scope of our current research and development programs and other expenses.
Reverse Stock Split
We initiated a 1-for-1.77 reverse stock split effective October 4, 2007. All shares and per share amounts in the consolidated financial statements and notes have been retroactively adjusted to give effect to the reverse stock split.
| NOTE 2. | SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES |
Use of Estimates
The preparation of the accompanying consolidated financial statements in conformity with accounting principles generally accepted in the United States requires management to make certain estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the financial statements and reported amounts of revenues and expenses during the reporting period. Actual results could differ from those estimates.
Principles of Consolidation
The consolidated financial statements include our accounts and those of our wholly-owned subsidiaries. All intercompany accounts and transactions have been eliminated.
Revenue Recognition
We recognize revenue in accordance with Accounting Standards Codification, or ASC 605, Revenue Recognition, which requires that certain criteria must be met before revenue can be recognized: persuasive evidence of an arrangement exists; delivery has occurred or services have been rendered; the fee is fixed or
76
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
determinable; and collectability is reasonably assured. Determination of whether persuasive evidence of an arrangement exists and whether delivery has occurred or services have been rendered are based on management’s judgments regarding the fixed nature of the fee charged for research performed and milestones met, and the collectability of those fees. Should changes in conditions cause management to determine these criteria are not met for certain future transactions, revenue recognized for any reporting period could be adversely affected.
Collaboration revenue, which is earned under agreements with third parties for research and development activities, may include nonrefundable license fees, cost reimbursements and contingent milestones and royalties. Our revenue arrangements with multiple elements are evaluated in accordance with ASC 605-25 Revenue Recognition — Multiple-Element Arrangements, and are divided into separate units of accounting if certain criteria are met, including whether the delivered element has stand-alone value and whether there is verifiable objective and reliable evidence of the fair value of the undelivered items. The consideration we receive is allocated among the separate units based on their respective fair values, and the applicable revenue recognition criteria are applied to each of the separate units.
Upfront payments received upon execution of collaborative agreements are recorded as deferred revenue and recognized as collaboration revenue over the research and development period pursuant to the agreement. Such period generally represents the research and development period set forth in the agreement between our third party collaborator and us. The research and development period is estimated at the inception of the arrangement and is periodically reevaluated. Reevaluation of the research and development period may shorten or lengthen the period during which the deferred revenue is recognized. We evaluate the appropriate period based on research progress attained and reevaluate the period when significant changes occur. If the collaboration agreement is terminated, all the remaining unamortized deferred revenue will be recognized as collaboration revenue on the date of termination.
Cost reimbursements are based upon negotiated rates for our full time employee equivalents, or FTE, and actual out-of-pocket costs. They are recognized as collaboration revenue as the related research and development services are performed. The cost reimbursements are generally based on qualified expenses as defined in the collaborative agreement. FTE rates are intended to approximate our anticipated cost.
We recognize milestone payments as revenue upon achievement of the milestone provided the milestone payment is nonrefundable, substantive effort and risk is involved in achieving the milestone and the amount of the milestone is reasonable in relation to the effort expended or risk associated with the achievement of the milestone. If these conditions are not met, we defer the milestone payment and recognize it as revenue over the estimated period of performance under the contract as we complete our performance obligations.
Pre-clinical Study and Clinical Trial Accruals
We estimate our pre-clinical study and clinical trial expenses based on the services received pursuant to contracts with several research institutions and contract research organizations that conduct and manage pre-clinical studies and clinical trials on our behalf. The financial terms of these agreements vary from contract to contract and may result in uneven expenses and payment flows. Pre-clinical study and clinical trial expenses include the following:
| • | fees paid to contract research organizations, or CROs, in connection with pre-clinical studies; |
| • | fees paid to CROs and investigative sites in connection with clinical trials; and |
| • | fees paid to contract manufacturers and service providers in connection with the production and testing of active pharmaceutical ingredients and drug materials for use in pre-clinical studies and clinical trials. |
77
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
Payments under some of these contracts depend on factors such as the milestones accomplished, successful enrollment of certain number of patients, site initiation and completion of clinical trial milestones. In accruing services fees, we estimate the time period over which services will be performed and the level of effort to be expended in each period. We monitor patient enrollment levels and related activities to the extent possible through internal reviews, correspondence and status meetings with CROs and review of contractual terms. Our estimates are dependent on the timeliness and accuracy of data provided by our CROs and other vendors.
Cash and Cash Equivalents
We consider all highly liquid investments purchased with an original maturity of less than or equal to ninety days to be cash equivalents. Cash and cash equivalents primarily consist of money market funds.
Concentration of Credit Risk and Other Risks and Uncertainties
We invest cash that is not currently being used for operational purposes in accordance with our investment policy. The policy allows for the purchase of debt securities such as those issued by the U.S. government and its agencies and corporations, subject to certain concentration limits. We also strive to limit risk by specifying a minimum credit quality of A1/P1 for commercial paper and AAA for other investments. The maximum maturity for these securities does not exceed 12 months. We believe our established guidelines for investment of our excess cash maintains safety and liquidity through our policies on diversification and investment maturity. Our cash and cash equivalent balances can be in excess of federally insured amounts.
Our product candidates require approval from the U.S. Food and Drug Administration or other international regulatory agencies prior to commencing commercial sales. There can be no assurance that our product candidates will receive any of these required approvals. If we are denied such approvals or such approvals are delayed, our results of operations, financial position and future cash flows may be materially adversely affected.
Property and Equipment, Net
Property and equipment are stated at cost, subject to adjustments for impairment, less accumulated depreciation and amortization. Depreciation and amortization are provided on a straight-line basis over the following estimated useful lives:
| Laboratory equipment |
3-5 years | |
| Office furniture and fixtures |
7 years | |
| Computer equipment and software |
3 years | |
| Leasehold improvements |
Shorter of useful life or remaining lease term |
Upon sale or retirement of assets, the cost and related accumulated depreciation are removed from the consolidated balance sheet and the resulting gain or loss is recorded in other income (expense). Maintenance and repairs are charged to expense as incurred, and improvements and betterments are capitalized.
Restricted Investment
Restricted investment represents collateral held at a financial institution for a letter of credit related to our facility lease.
Research and Development Costs
Research and development costs include, but are not limited to: (i) expenses incurred under agreements with contract research organizations and investigative sites, which conduct our clinical trials and a substantial portion
78
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
of our pre-clinical studies; (ii) milestone payments paid to our collaborative partners who work on our processing and supply of clinical trial material; (iii) the cost of manufacturing and supplying clinical trial materials; (iv) payments to contract service organizations, as well as consultants; (v) employee-related expenses, which include salaries and benefits; (vi) facilities, depreciation and other allocated expenses, which include direct and allocated expenses for rent and maintenance of facilities and equipment, depreciation of leasehold improvements and equipment and laboratory and other supplies; and (vii) stock-based compensation expense. All research and development expenses are expensed as incurred.
During the third quarter of 2009, we suspended the development of our UDB product candidate. As a result, for the year ended December 31, 2009, we recorded wind-down costs and write-down of fixed assets charges of approximately $2.8 million, which are included in the research and development expenses for the year ended December 31, 2009.
Income Taxes
We account for income taxes under the asset and liability method, which requires, among other things, that deferred income taxes be provided for temporary differences between the tax bases of our assets and liabilities and their financial statement reported amounts. In addition, deferred tax assets are recorded for the future benefit of utilizing net operating losses and research and development credit carryforwards. A valuation allowance is provided against deferred tax assets unless it is more likely than not that they will be realized.
Stock-Based Compensation
Effective January 1, 2006, we adopted ASC 718 Compensation — Stock Compensation, using the prospective transition method, which requires the measurement and recognition of compensation expense for all stock-based payment awards granted, modified and settled to our employees and directors after January 1, 2006. Our financial statements reflect the impact of ASC 718. We chose the “straight-line” attribution method for allocating compensation costs and recognized the fair value of each stock option on a straight-line basis over the requisite service period.
For the performance-based restricted stock units, or RSUs, the fair value was determined using the stock price of our common stock on the date of the grant. A probability assessment that performance goals will be achieved is made quarterly. The compensation expense is recognized over the vesting period, and is adjusted periodically for forfeiture rate and any changes to our probability assessment of the number of performance-based RSUs expected to vest as a result of our achievement of the performance goals.
We account for equity instruments issued to non-employees in accordance with ASC 505-50 Accounting for Equity Instruments That Are Issued to Other Than Employees for Acquiring, or in Conjunction with Selling, Goods or Services. Equity instruments issued to non-employees are recorded at their fair value on the measurement date and are subject to periodic adjustment as the underlying equity instruments vest.
Net Loss per Share
Basic net loss per share is computed by dividing net loss attributed to common stockholders by the weighted average number of common shares outstanding during the period. Our potential dilutive shares, which include outstanding common stock options, common stock issuable pursuant to ESPP, warrants to purchase common stock and performance-based RSUs, have not been included in the computation of diluted net loss per share for all the periods as the result would be anti-dilutive. Such potentially dilutive shares are excluded when the effect would be to reduce a net loss per share.
79
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
The numerator and denominator used in the calculation of basic and diluted net loss per share were as follows (in thousands, except share and per share amounts):
| Year Ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Historical net loss per share: |
||||||||||||
| Numerator |
||||||||||||
| Net loss attributed to common stockholders |
$ | (54,673 | ) | $ | (8,997 | ) | $ | (72,928 | ) | |||
| Denominator |
||||||||||||
| Weighted-average common shares outstanding |
27,260,955 | 22,194,686 | 20,360,491 | |||||||||
| Less: Weighted average shares subject to repurchase |
— | — | (10,124 | ) | ||||||||
| Denominator for basic and diluted net loss per share |
27,260,955 | 22,194,686 | 20,350,367 | |||||||||
| Basic and diluted net loss per share |
$ | (2.01 | ) | $ | (0.41 | ) | $ | (3.58 | ) | |||
The following outstanding common stock options, common stock issuable pursuant to ESPP, warrants to purchase common stock and performance-based RSUs were excluded from the computation of diluted net loss per share for the periods presented because including them would have had an anti-dilutive effect:
| Years Ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Options to purchase common stock |
4,071,903 | 3,628,845 | 3,178,837 | |||||||||
| Common stock issuable pursuant to ESPP |
8,886 | 10,545 | 24,423 | |||||||||
| Warrants to purchase common stock |
26,903 | 51,571 | 73,989 | |||||||||
| Performance-based RSUs |
98,000 | — | — | |||||||||
Operating Leases
We lease office and laboratory facilities under operating leases. Lease agreements may include rent escalation clauses and tenant improvement allowances. We recognize scheduled rent increases on a straight-line basis over the lease term beginning with the date we take possession of the leased space. Differences between rental expense and actual rental payments are recorded as deferred rent liabilities included in “Other liabilities” on the consolidated balance sheets.
Business Segments
We operate in one segment. Management uses one measure of profitability and does not segment its business for internal reporting.
Recent Accounting Pronouncements
On April 29, 2010, FASB issued Accounting Standards Update No. 2010-17, Revenue Recognition — Milestone Method (Topic 605): Milestone Method of Revenue Recognition (a consensus of the FASB Emerging Issues Task Force). It establishes a revenue recognition model for contingent consideration that is payable upon the achievement of an uncertain future event, referred to as a milestone. The scope of ASU 2010-17 is limited to research or development arrangements and requires an entity to record the milestone payment in its entirety in the period received if the milestone meets all the necessary criteria to be considered substantive. ASU 2010-17 is effective for fiscal years (and interim periods within those fiscal years) beginning on or after June 15, 2010. Early
80
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
adoption is permitted. Entities can apply this guidance prospectively to milestones achieved after adoption. However, retrospective application to all prior periods is also permitted. We will adopt ASU 2010-17 in the first quarter of fiscal year 2011. We do not believe that the adoption of ASU 2010-17 will have a material impact on our consolidated financial statements.
In October 2009, the FASB ratified Revenue Arrangements with Multiple Deliverables issued as ASU 2009-13. ASU 2009-13 updates the existing multiple-element arrangements guidance currently included in ASC 605-25, Revenue Recognition — Multiple-Element Arrangements. The revised guidance provides for two significant changes to the existing multiple-element arrangements guidance. The first relates to the determination of when the individual deliverables included in a multiple-element arrangement may be treated as separate units of accounting. This change is significant as it will likely result in the requirement to separate more deliverables within an arrangement, ultimately leading to less revenue deferral. The second change modifies the manner in which the transaction consideration is allocated across the separately identifiable deliverables. These changes are likely to result in earlier recognition of revenue for multiple-element arrangements than under previous guidance. ASU 2009-13 also significantly expands the disclosures required for multiple-element revenue arrangements. The revised multiple-element arrangements guidance will be effective for the first annual reporting period beginning on or after June 15, 2010, and may be applied retrospectively for all periods presented or prospectively to arrangements entered into or modified after the adoption date. Early adoption is permitted provided that the revised guidance is retroactively applied to the beginning of the year of adoption. If the guidance is adopted prospectively, certain transitional disclosures are required for each reporting period in the initial year of adoption. We will adopt the new pronouncement in the first quarter of fiscal year 2011. We do not believe that the adoption of ASU 2009-13 will have a material impact on our consolidated financial statements.
| NOTE 3. | FAIR VALUE MEASUREMENTS |
On January 1, 2008, we adopted ASC 820, Fair Value Measurements, as it relates to financial assets and financial liabilities. ASC 820 defines fair value, establishes a framework for measuring fair value in GAAP and expands disclosures about fair value measurements.
ASC 820 defines fair value as the price that would be received to sell an asset or paid to transfer a liability in an orderly transaction between market participants at the measurement date. This standard is now the single source in GAAP for the definition of fair value, except for the fair value of leased property as defined in ASC 840 Accounting for Leases, which establishes a fair value hierarchy that distinguishes between (1) market participant assumptions developed based on market data obtained from independent sources (observable inputs) and (2) an entity’s own assumptions about market participant assumptions developed based on the best information available in the circumstances (unobservable inputs). The fair value hierarchy consists of three broad levels, which gives the highest priority to unadjusted quoted prices in active markets for identical assets or liabilities (Level 1) and the lowest priority to unobservable inputs (Level 3). The three levels of the fair value hierarchy under ASC 820 are described below:
| • | Level 1: Quoted prices (unadjusted) in active markets that are accessible at the measurement date for assets or liabilities. The fair value hierarchy gives the highest priority to Level 1 inputs. |
| • | Level 2: Directly or indirectly observable inputs as of the reporting date through correlation with market data, including quoted prices for similar assets and liabilities in active markets and quoted prices in markets that are not active. Level 2 also includes assets and liabilities that are valued using models or other pricing methodologies that do not require significant judgment since the input assumptions used in the models, such as interest rates and volatility factors, are corroborated by readily observable data from actively quoted markets for substantially the full term of the financial instrument. |
81
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
| • | Level 3: Unobservable inputs that are supported by little or no market activity and reflect the use of significant management judgment. These values are generally determined using pricing models for which the assumptions utilize management’s estimates of market participant assumptions. |
In determining fair value, we utilize valuation techniques that maximize the use of observable inputs and minimize the use of unobservable inputs to the extent possible, as well as consider counterparty credit risk in our assessment of fair value.
The following is a summary of our cash, cash equivalents and restricted investment as of December 31, 2010 and 2009, respectively (in thousands):
| Amortized Cost |
As of December 31, 2010 | |||||||||||
| Unrealized
Gain (Loss) |
Estimated
Fair Value |
|||||||||||
| Cash |
$ | 2,327 | $ | — | $ | 2,327 | ||||||
| Certificates of deposit |
310 | — | 310 | |||||||||
| Money market funds |
73,680 | — | 73,680 | |||||||||
| $ | 76,317 | $ | — | $ | 76,317 | |||||||
| Reported as: |
||||||||||||
| Cash and cash equivalents |
$ | 76,007 | ||||||||||
| Restricted investment |
310 | |||||||||||
| $ | 76,317 | |||||||||||
| Amortized Cost |
As of December 31, 2009 | |||||||||||
| Unrealized
Gain (Loss) |
Estimated
Fair Value |
|||||||||||
| Cash |
$ | 4,620 | $ | — | $ | 4,620 | ||||||
| Certificates of deposit |
310 | — | 310 | |||||||||
| Money market funds |
61,156 | — | 61,156 | |||||||||
| $ | 66,086 | $ | — | $ | 66,086 | |||||||
| Reported as: |
||||||||||||
| Cash and cash equivalents |
$ | 65,776 | ||||||||||
| Restricted investment |
310 | |||||||||||
| $ | 66,086 | |||||||||||
Our investment instruments are classified within Level 1 or Level 2 of the fair value hierarchy because they are valued using quoted market prices, broker or dealer quotations, or alternative pricing sources with reasonable levels of price transparency. The types of instruments that are generally classified within Level 1 of the fair value hierarchy include money market securities. The types of investments that are generally classified within Level 2 of the fair value hierarchy include U.S. government and agency securities, corporate debt securities and certificates of deposit.
82
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
As of December 31, 2010 and 2009, financial assets measured and recognized at fair value on a recurring basis and classified under the appropriate level of the fair value hierarchy as described above were as follows, respectively (in thousands):
| As of December 31, 2010 |
Level 1 | Level 2 | Level 3 | Total | ||||||||||||
| Certificates of deposit |
$ | — | $ | 310 | $ | — | $ | 310 | ||||||||
| Money market funds |
73,680 | — | — | 73,680 | ||||||||||||
| Total |
$ | 73,680 | $ | 310 | $ | — | $ | 73,990 | ||||||||
| As of December 31, 2009 |
Level 1 | Level 2 | Level 3 | Total | ||||||||||||
| Certificates of deposit |
$ | — | $ | 310 | $ | — | $ | 310 | ||||||||
| Money market funds |
61,156 | — | — | 61,156 | ||||||||||||
| Total |
$ | 61,156 | $ | 310 | $ | — | $ | 61,466 | ||||||||
Our investments in money market funds are measured at fair value on a recurring basis. Our money market funds comply with Rule 2a-7 of the Investment Company Act of 1940 and are required to be priced and have a fair value of $1.00 net asset value per share. These money market funds are actively traded and reported daily through a variety of sources. Due to the structure and valuation required by the Investment Company Act of 1940 regarding Rule 2a-7 funds, the fair value of the money market fund investments is classified as Level 1.
The fair value of the certificates of deposit is classified as Level 2 due to the nature of a contractual restriction in our lease agreement which limits our ability to liquidate the investment.
The carrying amount for our debt reported in the consolidated balance sheet as of December 31, 2010 was $7.6 million. Using a discounted cash flow technique that incorporates a market interest rate, we have determined the fair value of our debt to be $7.5 million at December 31, 2010.
| NOTE 4. | BALANCE SHEET COMPONENTS |
Property and Equipment, Net
Property and equipment, net consist of the following (in thousands):
| December 31, | ||||||||
| 2010 | 2009 | |||||||
| Laboratory equipment |
$ | 4,770 | $ | 5,005 | ||||
| Office furniture and fixtures |
609 | 611 | ||||||
| Computer equipment and software |
1,086 | 955 | ||||||
| Leasehold improvements |
637 | 582 | ||||||
| Construction-in-progress |
3,503 | 939 | ||||||
| 10,605 | 8,092 | |||||||
| Less: Accumulated depreciation and amortization |
(4,802 | ) | (3,928 | ) | ||||
| $ | 5,803 | $ | 4,164 | |||||
The increase in the construction-in-process balance as of December 31, 2010 as compared to December 31, 2009 was primarily due to the purchase of equipment as part of the LEVADEX program.
83
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
Depreciation and amortization expense was approximately $1.2 million, $1.5 million and $1.3 million and $5.9 million for the years ended December 31, 2010, 2009, 2008, and for the cumulative period from July 3, 2003 (date of inception) to December 31, 2010, respectively.
Accrued Liabilities
Accrued liabilities consist of the following (in thousands):
| December 31, | ||||||||
| 2010 | 2009 | |||||||
| Clinical trial related |
$ | 4,363 | $ | 7,573 | ||||
| Payroll and related expenses |
3,993 | 2,932 | ||||||
| Professional services |
998 | 905 | ||||||
| Other |
88 | 158 | ||||||
| $ | 9,442 | $ | 11,568 | |||||
| NOTE 5. | DEBT |
In September 2006, we entered into a $3.0 million loan facility agreement for the purpose of financing equipment purchases, or the Equipment Loan, and borrowed $1.0 million under this facility. The Equipment Loan bore interest at an annual interest rate of 9.5% and was fully paid as of September 30, 2009.
In May 2008, we entered into the 2008 Working Capital Loan, for $20.0 million, in order to repay an earlier working capital loan and to support general corporate purposes. The 2008 Working Capital Loan bears interest at an annual rate of 9.95%, with an effective rate of approximately 12% after factoring in a $1.0 million payment due at the termination of this agreement. The 2008 Working Capital Loan had interest-only payments up to and including January 2009, matures in October 2011, and includes customary loan covenants. As of December 31, 2010, we were in compliance with these loan covenants.
The 2008 Working Capital Loan amounts are collateralized by all of our assets, excluding intellectual property.
Our debt consisted of the following (in thousands):
| December 31, 2010 |
December 31, 2009 |
|||||||
| Principal amount |
$ | 6,646 | $ | 13,929 | ||||
| Plus: premium, based on imputed interest rate of 12% |
935 | 691 | ||||||
| 7,581 | 14,620 | |||||||
| Less: current portion of debt |
7,581 | 7,283 | ||||||
| Long-term portion |
$ | — | $ | 7,337 | ||||
As of December 31, 2010, debt payments, which include interest and principal, are as follows (in thousands):
| Year ending December 31, |
Amount | |||
| 2011 |
$ | 7,952 | ||
| Total debt payments |
$ | 7,952 | ||
84
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
| NOTE 6. | COMMITMENTS AND CONTINGENCIES |
Operating Leases
In June 2004, we entered into a lease agreement for laboratory and office facilities in Mountain View, California, or the Lease, and in August 2006 we amended the Lease to include additional square footage within the same building. The Lease was to expire in June 2008. In March 2008, we entered into another amendment to the Lease, or the March 2008 Amendment, to extend the term of the Lease until June 2012, and to include additional square footage and options to lease additional square footage. In September 2008, we amended and restated the Lease, providing for expanded square footage and certain renewal options. Under the Lease, we pay operating costs, including property taxes, insurance and maintenance, in addition to monthly rent. Rent is subject to an annual increase for the duration of the Lease, which we recognize on a straight-line basis. The annual lease payments for the space under the amended and restated Lease were effective on July 1, 2008.
Rent expense was approximately $1.3 million, $1.1 million, $1.0 million and $5.8 million for the years ended December 31, 2010, 2009, 2008 and for the cumulative period from July 3, 2003, (date of inception) to December 31, 2010, respectively.
As of December 31, 2010, future minimum lease payments are as follows (in thousands):
| Year ending December 31, |
Amount | |||
| 2011 |
$ | 1,357 | ||
| 2012 |
700 | |||
| Total minimum lease payments |
$ | 2,057 | ||
In accordance with the terms of the Lease, we are obligated to maintain an irrevocable letter of credit from a bank as a security deposit. As collateral for the letter of credit, we are required to maintain a bank deposit account of $0.3 million, which is shown as a restricted investment on our consolidated balance sheets at December 31, 2010 and 2009.
Contingencies
We are subject to claims and assessments from time to time in the ordinary course of business. We do not believe that any such matters, individually or in the aggregate, will have a material adverse effect on our financial condition or results of operation.
Indemnification
In the normal course of business, we enter into contracts and agreements that contain a variety of representations and warranties and provide for indemnification. Our exposure under these agreements is unknown because it involves claims that may be made against us in the future, but have not yet been made. To date, we have not paid any claims or been required to defend any action related to our indemnification obligations. However, we may record charges in the future as a result of these indemnification obligations.
In accordance with our certificate of incorporation and bylaws, we have indemnification obligations to our officers and directors for certain events or occurrences, subject to certain limits, while they are serving at our request in their respective capacities. There have been no claims to date and we have a director and officer insurance policy that enables us to recover a portion of any amounts paid for future potential claims.
85
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
| NOTE 7. | LICENSE AND SUPPLY AGREEMENTS |
Agreement with Nektar
Under our June 2004 agreement, as amended, with Nektar Therapeutics UK Limited, or the Nektar Agreement, we were granted a worldwide, exclusive license, with a right to sublicense, under Nektar patents and know-how, to develop and commercialize any formulation of a form of dihydroergotamine for administration by inhalation using a device. We also agreed to pay royalties at specified rates based on net sales. As of December 31, 2010, we are required to make future nonrefundable milestone payments of up to $5.0 million related to products currently being developed under the Nektar Agreement, when and if certain regulatory and commercial milestones are met. We paid $0 for the years ended December 31, 2010, 2009 and 2008, respectively. We paid $2.6 million for the cumulative period from July 3, 2003 (date of inception) to December 31, 2010. Either party may terminate the Nektar Agreement upon a material, uncured default of the other party. We may terminate the Nektar Agreement, with or without cause, at any time upon six months’ prior written notice.
Agreement with Elan
Under the April 2004 agreement, as amended, with Elan Pharma International Limited, or the Elan Agreement, Elan granted to us a worldwide, exclusive, sub-licensable license under certain of Elan’s intellectual property rights related to our UDB product candidate. We paid $0, $0 and $0.8 million for the years ended December 31, 2010, 2009 and 2008, respectively. We paid $4.0 million for the cumulative period from July 3, 2003 (date of inception) to the date of termination in August 2010. We also entered into a services agreement with Elan Drug Delivery International in February 2005, amended subsequently, which describes the terms and conditions for clinical and commercial supply of product intermediate for our UDB product candidate. In August 2010, our agreement with Elan Pharma International Limited terminated as a result of our election not to extend the agreement. Our agreement with Elan Drug Delivery International also was terminated in August 2010.
We currently are not developing any product candidates requiring the technology licensed in the Elan Agreement. The termination of the Elan Agreement did not have a material impact on our consolidated financial statements.
Agreement with AstraZeneca
In December 2008, we entered into an agreement with AstraZeneca AB, or AstraZeneca Agreement, which became effective in February 2009. Pursuant to the terms of the agreement, we licensed to AstraZeneca global rights to develop and commercialize our proprietary nebulized formulation of UDB, our next generation UDB therapy and certain combination nebulization therapies for the potential treatment of asthma in children. The AstraZeneca Agreement was terminated in July 2009.
In February 2009, under the terms of the AstraZeneca Agreement, AstraZeneca paid us a nonrefundable upfront cash payment of $40.0 million. On February 23, 2009, we announced top-line results of our initial Phase 3 clinical trial of UDB for the potential treatment of children with asthma. We announced that the clinical trial did not meet its co-primary endpoints, asthma control as assessed by changes from baseline in nighttime and daytime composite symptom scores, in either of the doses evaluated when compared with placebo.
On July 8, 2009, we received notice from AstraZeneca of the termination of the AstraZeneca Agreement. Effective on the date of termination, all rights licensed to AstraZeneca in the AstraZeneca Agreement reverted back to us. We were jointly developing UDB with AstraZeneca, and were responsible for executing the development plan. In the third quarter of 2009 we suspended development of our UDB product candidate.
86
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
Total collaboration revenue recognized under the AstraZeneca Agreement was $54.2 million for the year ended December 31, 2009 and consists of a $40 million upfront payment and $14.2 million from reimbursement of qualified development expenses. We received $54.2 million in cash for the cumulative period from July 3, 2003 (date of inception) to December 31, 2009.
| NOTE 8. | STOCKHOLDERS’ EQUITY |
Preferred Stock
Our Certificate of Incorporation, as amended and restated in October 2007 in connection with the closing of our IPO, authorizes us to issue 5,000,000 shares of $0.01 par value preferred stock. As of December 31, 2010 and 2009, there were no shares of preferred stock issued or outstanding.
Common Stock
In October 2007, we completed our IPO of 5,750,000 shares of common stock at a public offering price of $12.00 per share. The aggregate net cash proceeds from the IPO were approximately $62.1 million, after deducting the underwriting discount and commissions and other offering expenses. In connection with the IPO, all outstanding redeemable convertible preferred stock converted into common stock, warrants to purchase convertible preferred stock converted into warrants to purchase common stock, and redeemable convertible preferred stock warrant liability was reclassified to equity.
In August 2009, we completed a follow-on public offering in which we sold and issued 3,500,000 shares of our common stock at a per share price of $9.70. We raised a total of $34.0 million in gross proceeds or approximately $31.6 million in net proceeds after deducting expenses and underwriters’ discounts and commissions.
On November 11, 2009, we entered into a Common Stock Purchase Agreement, or the Purchase Agreement, with Azimuth Opportunity Ltd., or Azimuth, which provides us with what is sometimes termed an equity line of credit arrangement. Upon the terms and subject to the conditions set forth in the Purchase Agreement, Azimuth committed to purchase up to $60.0 million worth of shares of our common stock over the 24-month term of the Purchase Agreement; provided, however, in no event may we sell under the Purchase Agreement more than such number of shares of common stock which is equal to one share less than 20% of our outstanding shares of common stock on the effective date of the Purchase Agreement. From time to time over the term of the Purchase Agreement, and at our sole discretion, we may present Azimuth with draw down notices requiring Azimuth to purchase a specified dollar amount of shares of our common stock, based on the price per share over ten consecutive trading days or such other period mutually agreed upon by Azimuth and us, with each draw down subject to limitations based on the price of our common stock and a maximum limit of 2.5% of our market capitalization at the time of such draw down, or such other limit as mutually agreed upon by Azimuth and us. In January 2010 we accessed our equity line of credit and sold 1,527,695 shares of common stock at a price of approximately $13.70 per share less a discount of approximately 4.5% per share for a net price of approximately $13.09 per share. The total purchase price for all these shares was $20.0 million or approximately $19.7 million after deducting the offering expenses.
In October 2010, we completed an equity offering in which we sold a total of 3,450,000 shares of common stock at an offering price of $14.50 per share. We raised a total of $50.0 million in gross proceeds, or approximately $47.0 million in net proceeds after deducting underwriting discounts, commissions and offering expenses.
87
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
Warrants
We issued warrants to purchase 73,989 shares of common stock to selected lenders in connection with an earlier working capital loan which was fully paid in May 2008 and the Equipment Loan which was fully paid in September 2009. The warrants are exercisable at a price of $7.43 per share and expire in September 2013. In October 2009 and March 2010, warrants to purchase 22,418 shares and 24,668 shares were exercised, respectively, resulting in a net issuance of 5,817 shares and 12,295 shares, respectively. As of December 31, 2010, warrants to purchase the remaining 26,903 shares of common stock were outstanding.
Equity Plans
2005 Equity Incentive Plan
In 2005, we adopted the 2005 Equity Incentive Plan, or 2005 Plan, as amended in February 2006, which provides for the grant of stock options to employees and consultants of the Company. Stock options granted under the 2005 Plan may be either incentive stock options, or ISOs, or nonqualified stock options, or NSOs. ISOs may be granted only to employees. NSOs may be granted to employees, consultants and directors. Stock options under the 2005 Plan may be granted with a term of up to ten years and at prices no less than fair market value as determined by the Board of Directors. To date, stock options granted generally vest over four years and vest at a rate of 25% upon the first anniversary of the vesting commencement date and 1/48th per month thereafter. Subsequent to the IPO in October 2007, no further stock options were granted under the 2005 Plan. Upon the completion of the IPO, 394,580 shares of common stock remained available for issuance under the 2005 Plan and were made available for future grant under the 2007 Equity Award Plan.
2007 Equity Award Plan
In September 2007, we adopted the 2007 Equity Award Plan, or 2007 Plan, which became effective upon the completion of the IPO. The remaining common stock available for issuance under the 2005 Plan was made available for future grant under the 2007 Plan. Outstanding options under the 2005 Plan that expire or are canceled without having been exercised in full or are repurchased or forfeited will be available for future issuance under the 2007 Plan. Under the 2007 plan, with the approval of the Compensation Committee of the Board of Directors, we may grant restricted stock, RSU, stock appreciation rights and new shares of common stock upon exercise of stock options.
Stock options granted under the 2007 Plan may be either ISOs or NSOs. ISOs may be granted only to employees. NSOs may be granted to employees, consultants and directors. Stock options under the 2007 Plan may be granted with a term of up to ten years and at prices no less than the fair market value of our common stock on the date of grant. To date, stock options granted generally vest over four years and vest at a rate of 25% upon the first anniversary of the vesting commencement date and 1/48th per month thereafter.
88
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
Option activity for fiscal year 2010 was as follows:
| Outstanding Options | ||||||||||||
| Number of Shares |
Weighted Average Exercise Price |
Aggregate Intrinsic Value |
||||||||||
| (In thousands) | ||||||||||||
| Balances, at December 31, 2009 |
3,628,845 | $ | 7.30 | |||||||||
| Options granted |
962,781 | $ | 15.91 | |||||||||
| Options exercised |
(427,944 | ) | $ | 3.61 | $ | 4,614 | (1) | |||||
| Options forfeited |
(84,318 | ) | $ | 10.72 | ||||||||
| Options expired |
(7,461 | ) | $ | 13.21 | ||||||||
| Balances, at December 31, 2010 |
4,071,903 | $ | 9.64 | $ | 28,911 | (2) | ||||||
| (1) | Amounts represent the difference between the exercise price and market price of MAP Pharmaceuticals’ stock at the time of exercise. |
| (2) | Amount represents the difference between the exercise price and $16.74, the closing price of MAP Pharmaceuticals’ stock on December 31, 2010, as reported on The NASDAQ Global Market, for all in-the-money options outstanding. |
The following table summarizes options outstanding at December 31, 2010:
| Options Outstanding at December 31, 2010 |
Options Exercisable and Vested at December 31, 2010 |
|||||||||||||||
| Exercise Price |
Number of Options |
Weighted Average Remaining Contractual Life (Years) |
Number of Options |
Weighted Average Exercise Price |
||||||||||||
| $0.64 - $2.82 |
654,413 | 5.0 | 644,183 | $ | 0.71 | |||||||||||
| $3.18 - $6.39 |
654,917 | 6.5 | 589,160 | $ | 5.18 | |||||||||||
| $7.41 - $9.44 |
287,777 | 8.2 | 123,239 | $ | 9.01 | |||||||||||
| $10.08 - $11.15 |
806,037 | 8.2 | 341,060 | $ | 10.38 | |||||||||||
| $12.19 - $13.75 |
749,488 | 7.1 | 557,585 | $ | 12.84 | |||||||||||
| $14.06 - $16.75 |
919,271 | 9.0 | 37,500 | $ | 14.86 | |||||||||||
| 4,071,903 | 7.4 | 2,292,727 | $ | 6.92 | ||||||||||||
The following table summarizes options outstanding that have vested and are expected to vest based on options outstanding as of December 31, 2010:
| Number of Shares |
Weighted Average Exercise Price |
Aggregate Intrinsic Value(1) |
Weighted Average Remaining Contractual Life |
|||||||||||||
| (In thousands) | (In years) | |||||||||||||||
| Vested |
2,292,727 | $ | 6.92 | $ | 22,507 | 6.6 | ||||||||||
| Vested and expected to vest(2) |
3,971,648 | $ | 9.48 | $ | 28,832 | 7.4 | ||||||||||
| (1) | Amounts represent the difference between the exercise price and $16.74, the closing price of MAP Pharmaceuticals’ stock on December 31, 2010, as reported on The NASDAQ Global Market, for all in-the-money options outstanding. |
| (2) | Options outstanding that have vested and expected to vest are net of estimated future option forfeitures in accordance with the provisions of ASC 718. |
89
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
The weighted average grant-date fair value of options granted was $8.59 in 2010, $5.02 in 2009 and $6.75 in 2008.
The total fair value of options granted to employees that vested during the years ended December 31, 2010, 2009 and 2008 was approximately $5.0 million, $4.9 million and $5.4 million, respectively.
Performance-Based RSUs: On February 2, 2010, the Compensation Committee of the Board of Directors approved awards of 98,000 performance-based RSUs from the 2007 Plan to certain of our employees. These awards will convert into shares of our common stock upon vesting at the end of the performance periods, if specific performance goals set by the Compensation Committee are achieved. No performance-based RSUs will vest if the performance goals are not met. Each vested performance-based RSU will convert into one share of our common stock on the vesting dates. The fair value of the performance-based RSUs was determined using the stock price of our common stock on the date of the grant which was $16.19. A probability assessment that performance goals will be achieved is made quarterly. The compensation expense is recognized over the vesting period, and is adjusted periodically for any changes to our probability assessment of the number of performance-based RSUs expected to vest as a result of our achievement of the performance goals. For the year ended December 31, 2010, we recorded compensation expense of $675,000 related to performance-based RSUs. As of December 31, 2010, there were unrecognized compensation costs of approximately $707,000, net of estimated forfeitures, related to the performance-based RSUs. As of December 31, 2010, 98,000 performance-based RSUs were unvested.
As of December 31, 2010, 1,859,519 shares of common stock were available for future grant under the 2007 Plan. In December 2010, the Board of Directors authorized increasing the number of shares under the 2007 Equity Award Plan by one million shares, effective January 1, 2011
Employee Stock Purchase Plan
Upon the effectiveness of the IPO in October 2007, we adopted the Employee Stock Purchase Plan, or Purchase Plan. We reserved a total of 500,000 shares of common stock for issuance under the Purchase Plan. The Purchase Plan permits eligible employees to purchase common stock at a discount through payroll deductions during defined offering periods. The price at which the stock is purchased is equal to the lower of 85% of the fair market value of the common stock at the beginning or end of a purchase period.
As of December 31, 2010, 492,680 shares of common stock were available for future grant and 427,320 shares of common stock have been issued under the employee stock purchase plan. In December 2010, the Board of Directors authorized increasing the number of shares under the Employee Stock Purchase Plan by 215,000 shares, effective January 1, 2011.
Other Information Related to Equity Plans
Issuance of shares: Upon exercise of stock options, vesting of performance-based RSUs at the end of the performance periods and purchases of shares under the ESPP, we will issue common stock.
We received $2.3 million, $1.2 million, and $0.7 million in cash from sales of shares through our equity plans for the years ended December 31, 2010, 2009 and 2008, respectively, and $4.2 million for the cumulative period from July 3, 2003 (date of inception) through December 31, 2010.
90
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
Stock-Based Compensation for Employees
The following table summarizes the stock-based compensation expense for stock options, shares from the ESPP and performance-based RSUs that we recorded in the statements of operations in accordance with ASC 718 for the years ended December 31, 2010, 2009 and 2008, respectively (in thousands):
| Years Ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Research and development |
$ | 2,975 | $ | 1,955 | $ | 1,152 | ||||||
| Sales, general and administrative |
3,597 | 2,880 | 2,207 | |||||||||
| $ | 6,572 | $ | 4,835 | $ | 3,359 | |||||||
We used the following assumptions to estimate the fair value of options granted under our stock option plans for the years ended December 31, 2010, 2009 and 2008:
| Years Ended December 31, | ||||||
| 2010 | 2009 | 2008 | ||||
| Risk-free interest rate |
1.08%-2.45% | 1.62%-2.52% | 1.75%-3.60% | |||
| Expected volatility |
62%-75% | 62%-65% | 63%-65% | |||
| Expected term (in years) |
5 | 5 | 5.5 | |||
| Expected dividend yield |
— | — | — | |||
We used the following assumptions to estimate the fair value of shares purchased under our ESPP for the years ended December 31, 2010, 2009 and 2008:
| Years Ended December 31, | ||||||
| 2010 | 2009 | 2008 | ||||
| Risk-free interest rate |
0.14%-0.24% | 0.14%-0.30% | 0.27%-2.91% | |||
| Expected volatility |
38%-76% | 76%-99% | 81%-99% | |||
| Expected term (in years) |
0.5 | 0.5 | 0.5 – 0.6 | |||
| Expected dividend yield |
— | — | — | |||
We selected the Black-Scholes valuation model as the most appropriate valuation method for stock option grants and shares from the ESPP. The fair value of the stock option grants and shares from the ESPP is estimated as of the date of grant using the Black-Scholes valuation model.
Risk-Free Interest Rate: The risk-free interest rate assumption was based on U.S. Treasury instruments with a term that is consistent with the expected term of our stock options or shares from the ESPP.
Expected Volatility: The expected stock price volatility of stock options was determined by examining the historical volatilities for industry peers and using an average of the historical volatilities of our industry peers as we did not have sufficient trading history for our common stock. Industry peers consist of several public companies in the biopharmaceutical industry similar to us in size, stage of life-cycle and financial leverage. We will continue to analyze the expected stock price volatility of stock options as more historical data for our common stock becomes available. Effective on January 1, 2010, the expected stock price volatility for shares from the ESPP is determined based on our own historical volatilities.
Expected Term: The expected term of stock options represents the weighted average period the stock options are expected to remain outstanding. It was calculated based on the historical experience that we have had
91
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
with stock option grants as well as the expected term of industry peers, as we did not have sufficient historical information to develop reasonable expectations about future exercise patterns and post-vesting employment termination behavior for the full term of our stock options. We will continue to analyze the expected term of stock options as more historical data for our common stock becomes available. The expected term for shares from the ESPP is determined based on the length of offering periods for the ESPP.
Expected Dividend Yield: The expected dividend yield of 0% is based on our history and expectation of dividend payouts. We do not anticipate paying any dividends in the near future. We have not paid any dividends, other than a cumulative dividend on our preferred stock paid in connection with our initial public offering in 2007, pursuant to the terms of our certificate of incorporation.
Forfeitures: Forfeitures are determined based on when awards are ultimately expected to vest. ASC 718 requires forfeitures to be estimated at the time of grant and revised, if necessary, in subsequent periods if actual forfeitures differ from those estimates. Forfeitures were estimated based on our historical experience.
As of December 31, 2010, there were unrecognized compensation costs of approximately $6.2 million related to non-vested stock option awards granted after January 1, 2006 that will be recognized on a straight-line basis over the weighted average remaining period of 2.0 years.
Stock-Based Compensation for Non-Employees
Stock-based compensation expense related to stock options granted to non-employees is recognized as the stock options are earned. Management believes that the fair value of the stock options is more reliably measurable than the fair value of the service received. The fair value of stock options granted to non-employees is calculated at each grant date and remeasured at each reporting date. The stock-based compensation expense will fluctuate as the price of our common stock fluctuates. We recorded stock-based compensation expense for non-employees of $0, $0.1 million and $0.5 million for the years ended December 31, 2010, 2009 and 2008, respectively and $0.9 million for the cumulative period from July 3, 2003 (date of inception) through December 31, 2010.
| NOTE 9. | LONG-TERM INCENTIVE PLAN |
In March 2004, our Board of Directors adopted the 2004 Long-Term Incentive Plan, or Incentive Plan, which provides cash-based and equity-based incentives to eligible persons, including employees, non-employee directors, and consultants, advisors or independent contractors designated by the Compensation Committee of the Board of Directors. Cash and equity-based awards are generally based upon the attainment of performance goals over a particular period. The Board of Directors may specify a vesting period for cash and equity awards that may be longer than the performance period. The expense related to the cash and equity awards will be recognized over the performance period or the vesting period, whichever is longer, on a straight line basis. The Incentive Plan shall terminate on February 1, 2014, unless sooner terminated by the Board of Directors. As of December 31, 2010, no incentives under this plan remained available for grant.
| NOTE 10. | EMPLOYEE BENEFIT PLAN |
In January 2005, we implemented a 401(k) Plan covering certain employees. Eligible employees may make pre-tax salary deferral contributions up to a specified maximum. Since the inception of the plan we have not made any company contributions to this plan.
92
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
| NOTE 11. | INCOME TAXES |
We have not recorded any income tax expense for the periods ended December 31, 2010, 2009 and 2008 due to our history of operating losses.
The reconciliation of income tax expenses (benefit) at the statutory federal income tax rate of 34% to net income tax expenses (benefit) for the years ended December 31, 2010, 2009 and 2008 is as follows (in thousands):
| Years Ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| U.S. federal taxes (benefit) at statutory rate |
$ | (18,682 | ) | $ | (3,058 | ) | $ | (24,795 | ) | |||
| Stock compensation expense |
(567 | ) | (96 | ) | 264 | |||||||
| Others |
23 | 19 | 26 | |||||||||
| Net operating loss not used |
19,226 | 3,135 | 24,505 | |||||||||
| $ | — | $ | — | $ | — | |||||||
The tax effects of temporary differences and carry forwards that give rise to significant portions of the deferred tax assets are as follows:
| December 31, | ||||||||
| 2010 | 2009 | |||||||
| Deferred tax assets |
||||||||
| Net operating loss carryforwards |
$ | 84,875 | $ | 64,343 | ||||
| Tax credit carryforwards |
10,207 | 9,057 | ||||||
| Capitalized intangibles |
93 | 70 | ||||||
| Accruals and reserves |
4,243 | 2,626 | ||||||
| Total deferred tax assets |
99,418 | 76,096 | ||||||
| Less: Valuation allowance |
(99,418 | ) | (76,096 | ) | ||||
| Net deferred tax assets |
$ | — | $ | — | ||||
The valuation allowance increased by $23.3 million, $6.4 million and $31.6 million during the years ended December 31, 2010, 2009 and 2008, respectively.
At December 31, 2010, we had net operating loss carry forwards of approximately $214.6 million and $204.4 million available to reduce future taxable income, if any, for Federal and California state income tax purposes, respectively. The net operating loss carry forwards expire between 2014 and 2030, and valuation allowances have been provided.
We also had federal and state research and development credit carry forwards of approximately $7.4 million and $4.3 million, respectively, at December 31, 2010. The federal credits will expire starting in 2024 if not utilized. The California credits have no expiration date.
Pursuant to ASC 718, the benefit of stock options will only be recorded to equity when they reduce cash taxes payable. As of December 31, 2010, the portion of the federal and state net operating loss related to stock options is approximately $6.6 million.
93
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
Utilization of the net operating loss carry forward may be subject to an annual limitation due to the ownership percentage change limitations provided by the Internal Revenue Code of 1986 and similar state provisions. The annual limitations may result in the expiration of the net operating loss before utilization.
We adopted ASC 740-10 on January 1, 2007. As of December 31, 2010, we had no unrecognized tax benefits. As of December 31, 2010, we have not recorded any interest or penalties under this pronouncement.
We file U.S. and state income tax returns with varying statutes of limitations. The tax years 2004 and forward remain open to examination due to the carryover of unused net operating losses or tax credits.
| NOTE 12. | SUBSEQUENT EVENTS |
On January 28, 2011, we entered into a Collaboration Agreement (the “Collaboration Agreement”) and a Co-Promotion Agreement (the “Co-Promotion Agreement,” and together with the Collaboration Agreement, the “Allergan Agreements”) with Allergan, Inc., Allergan USA, Inc. and Allergan Sales, LLC (collectively, “Allergan”). Pursuant to the terms of the Allergan Agreements, we have granted Allergan a co-exclusive license to market and promote LEVADEX™, our proprietary novel migraine therapy for delivery by inhalation, to neurologists and pain specialists in the United States in collaboration with us.
Under the Allergan Agreements, we retain the right to market and promote LEVADEX to other physicians within the United States and also retain all rights to LEVADEX in all other countries, subject to Allergan’s right under certain circumstances to expand the territory in which the parties will market and promote LEVADEX to neurologists and pain specialists to include Canada. We and Allergan will each provide sales representatives and other sales support for such marketing and promotional efforts. The Allergan Agreements specify minimum annual sales detail requirements to be provided by each party, and establish maximum annual amounts of detailing costs that each party will be obligated to incur pursuant to a commercialization plan.
The parties will collaborate in the development of LEVADEX for the treatment of migraine in adolescents 12 to 18 years of age, and for at least one other indication. We may develop LEVADEX for certain other indications independently of the collaboration if Allergan does not agree to develop LEVADEX for such indications pursuant to the Allergan Agreements. We will be responsible for manufacturing and supplying LEVADEX, and for distributing the product and recording product revenues from sales of LEVADEX resulting from the parties’ collaboration.
The parties will share profits and losses resulting from the collaboration equally. We will be solely responsible for payment of all remaining costs of obtaining regulatory approval of LEVADEX for the treatment of acute migraine in adults, except that if the FDA notifies us that additional development or manufacturing activities costing in excess of a certain threshold amount will be required for such regulatory approval, the parties will share any such excess costs. The parties generally will share equally all other costs of developing LEVADEX under the Allergan Agreements, except that neither party shall be obligated for more than a certain threshold amount in a given year, or for more than a certain threshold amount in the aggregate, for development or manufacturing costs or expenses incurred by us for such activities.
The Collaboration Agreement may be terminated (i) by Allergan, at will, after first commercial sale of LEVADEX in the United States, upon 180 days’ prior written notice, (ii) by Allergan, upon written notice to us, if we receive a complete response letter or equivalent communication from the FDA, that Allergan determines will extend potential approval beyond a certain date or requires a certain minimum level of additional investment, (iii) by us, upon written notice to Allergan, if Allergan commercializes a competing product in the
94
Table of Contents
Index to Financial Statements
MAP PHARMACEUTICALS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS—(Continued)
United States (or, if the territory of the Allergan Agreements is expanded, Canada) and (iv) by us, upon written notice to Allergan, if Allergan challenges or opposes patent rights licensed to Allergan pursuant to the Collaboration Agreement. Additionally, either party may terminate the Collaboration Agreement in the event of an uncured material breach. The Co-Promotion Agreement will terminate upon termination of the Collaboration Agreement.
In February 2011, Allergan paid us an upfront payment of $60.0 million. Under the terms of agreement, we may also receive up to an additional $97 million in the form of regulatory milestones, which includes milestones for acceptance of filing of the LEVADEX NDA and first commercial sale associated with the initial acute migraine indication.
| NOTE 13. | UNAUDITED SELECTED QUARTERLY FINANCIAL DATA (in thousands, except per share amounts) |
The following tables summarize the unaudited quarterly financial data for the last two fiscal years:
| Fiscal 2010 Quarter Ended | ||||||||||||||||
| March 31 | June 30 | September 30 | December 31 | |||||||||||||
| Loss from operations |
$ | (13,667 | ) | $ | (12,152 | ) | $ | (13,930 | ) | $ | (13,739 | ) | ||||
| Net loss attributable to common stockholders |
$ | (14,058 | ) | $ | (12,489 | ) | $ | (14,178 | ) | $ | (13,948 | ) | ||||
| Basic and diluted net loss per common share |
$ | (0.54 | ) | $ | (0.47 | ) | $ | (0.53 | ) | $ | (0.46 | ) | ||||
| Weighted average common shares used in computing basic and diluted net loss per common share |
25,852 | 26,480 | 26,629 | 30,043 | (1) | |||||||||||
| Fiscal 2009 Quarter Ended | ||||||||||||||||
| March 31 | June 30 | September 30(2) | December 31 | |||||||||||||
| Collaboration revenue |
$ | 7,484 | $ | 8,645 | $ | 35,273 | $ | 2,764 | ||||||||
| Income (loss) from operations |
$ | (9,399 | ) | $ | (4,420 | ) | $ | 19,764 | $ | (12,914 | ) | |||||
| Net income (loss) attributable to common stockholders |
$ | (9,920 | ) | $ | (4,969 | ) | $ | 19,259 | $ | (13,367 | ) | |||||
| Net income (loss) per common share: |
||||||||||||||||
| Basic |
$ | (0.48 | ) | $ | (0.24 | ) | $ | 0.84 | $ | (0.54 | ) | |||||
| Diluted |
$ | (0.48 | ) | $ | (0.24 | ) | $ | 0.80 | $ | (0.54 | ) | |||||
| Weighted average common shares used in computing net income (loss) per common share: |
||||||||||||||||
| Basic |
20,584 | 20,699 | 22,861 | 24,583 | ||||||||||||
| Diluted |
20,584 | 20,699 | 24,054 | 24,583 | ||||||||||||
| (1) | Weighted average common shares used in computing basic and diluted net loss per common share for the fourth quarter of 2010 includes the effect of the equity offering completed in October 2010, in which we sold a total of 3,450,000 shares of common stock at an offering price of $14.50 per share. |
| (2) | Net income includes the effect of $33.1 million remaining from an upfront payment recognized as collaboration revenue in the third quarter of 2009 in connection with the termination of the AstraZeneca Agreement. |
95
Table of Contents
Index to Financial Statements
| ITEM 9. | CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE |
None
| ITEM 9A. | CONTROLS AND PROCEDURES |
Evaluation of disclosure controls and procedures. Our management evaluated, with the participation of our Chief Executive Officer and our Chief Financial Officer, the effectiveness of our disclosure controls and procedures as of the end of the period covered by this Annual Report on Form 10-K. Based on this evaluation, our Chief Executive Officer and our Chief Financial Officer have concluded that our disclosure controls and procedures are effective to ensure that information we are required to disclose in reports that we file or submit under the Securities Exchange Act of 1934 is recorded, processed, summarized and reported within the time periods specified in Securities and Exchange Commission rules and forms.
Management’s annual report on internal control over financial reporting. We are responsible for establishing and maintaining adequate internal control over our financial reporting. We have assessed the effectiveness of internal control over financial reporting as of December 31, 2010. Our assessment was based on criteria set forth by the Committee of Sponsoring Organizations of the Treadway Commission, or COSO, in Internal Control-Integrated Framework.
Our internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. Our internal control over financial reporting includes those policies and procedures that:
| (1) | pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect our transactions and dispositions of our assets; |
| (2) | provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that our receipts and expenditures are being made only in accordance with authorizations of our management and board of directors; and |
| (3) | provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use or disposition of our assets that could have a material effect on the financial statements. |
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Based on using the COSO criteria, we believe our internal control over financial reporting as of December 31, 2010 was effective.
The effectiveness of our internal control over financial reporting as of December 31, 2010 has been audited by PricewaterhouseCoopers LLP, an independent registered public accounting firm, as stated in their report which appears in Item 8 of this Annual Report on Form 10-K.
Changes in internal control over financial reporting. There was no change in our internal control over financial reporting that occurred during the quarter ended December 31, 2010 that has materially affected, or is reasonably likely to materially affect, our internal control over financial reporting.
| ITEM 9B. | OTHER INFORMATION |
None
96
Table of Contents
Index to Financial Statements
PART III
| ITEM 10. | DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE |
The information required by this item is incorporated by reference to MAP Pharmaceuticals, Inc. Proxy Statement for its 2011 Annual Meeting of Stockholders to be filed with the SEC within 120 days after the end of the fiscal year ended December 31, 2010.
| ITEM 11. | EXECUTIVE COMPENSATION |
The information required by this item is incorporated by reference to MAP Pharmaceuticals, Inc. Proxy Statement for its 2011 Annual Meeting of Stockholders to be filed with the SEC within 120 days after the end of the fiscal year ended December 31, 2010.
| ITEM 12. | SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS |
The information required by this item is incorporated by reference to MAP Pharmaceuticals, Inc. Proxy Statement for its 2011 Annual Meeting of Stockholders to be filed with the SEC within 120 days after the end of the fiscal year ended December 31, 2010.
| ITEM 13. | CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE |
The information required by this item is incorporated by reference to MAP Pharmaceuticals, Inc. Proxy Statement for its 2011 Annual Meeting of Stockholders to be filed with the SEC within 120 days after the end of the fiscal year ended December 31, 2010.
| ITEM 14. | PRINCIPAL ACCOUNTANT FEES AND SERVICES |
The information required by this item is incorporated by reference to MAP Pharmaceuticals, Inc. Proxy Statement for its 2011 Annual Meeting of Stockholders to be filed with the SEC within 120 days after the end of the fiscal year ended December 31, 2010.
97
Table of Contents
Index to Financial Statements
PART IV
| ITEM 15. | EXHIBITS AND FINANCIAL STATEMENT SCHEDULES |
(a) We have filed the following documents as part of this Form 10-K:
(1) Consolidated Financial Statements
| 70 | ||||
| Financial Statements |
||||
| 71 | ||||
| 72 | ||||
| 73 | ||||
| 75 | ||||
| 76 |
(2) Financial Statement Schedules
All financial statement schedules have been omitted because they are not required, not applicable, or the required information is otherwise included.
(3) Exhibits.
A list of exhibits filed with this report or incorporated herein by reference is found in the Exhibit Index immediately following the signature page of this report.
(b) Exhibits:
See Item 15(a)(3) above.
(c) Financial Schedules:
See Item 15(a)(2) above.
98
Table of Contents
Index to Financial Statements
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the Registrant has duly caused this Annual Report on Form 10-K to be signed on its behalf by the undersigned, thereunto duly authorized, on March 4, 2011.
| MAP PHARMACEUTICALS, INC. | ||
| By: | /S/ TIMOTHY S. NELSON | |
| Timothy S. Nelson President and Chief Executive Officer | ||
POWER OF ATTORNEY
KNOW ALL MEN BY THESE PRESENTS, that each person whose signature appears below constitutes and appoints Timothy S. Nelson and Christopher Y. Chai, jointly and severally, his or her attorney-in-fact, with the power of substitution, for him or her in any and all capacities, to sign any amendments to this Annual Report on Form 10-K and to file the same, with exhibits thereto and other documents in connection therewith, with the Securities and Exchange Commission, hereby ratifying and confirming all that each of said attorneys-in-fact, or his or her substitute or substitutes, may do or cause to be done by virtue hereof.
Pursuant to the requirements of the Securities Exchange Act of 1934, this Annual Report on Form 10-K has been signed below by the following persons on behalf of the Registrant and in the capacities and on the dates indicated.
| Signature |
Title |
Date | ||
| /S/ TIMOTHY S. NELSON Timothy S. Nelson |
President and Chief Executive Officer, Director (Principal Executive Officer) |
March 4, 2011 | ||
| /S/ CHRISTOPHER Y. CHAI Christopher Y. Chai |
Senior Vice President and Chief Financial Officer (Principal Financial and Accounting Officer) |
March 4, 2011 | ||
| /S/ SCOTT R. WARD Scott R. Ward |
Chairman of the Board of Directors |
March 4, 2011 | ||
| /S/ THOMAS A. ARMER, PH. D. Thomas A. Armer, Ph. D. |
Director |
March 4, 2011 | ||
| /S/ JOHN G. FREUND, M.D. John G. Freund, M.D. |
Director |
March 4, 2011 | ||
| /S/ CARL S. GOLDFISCHER, M.D. Carl S. Goldfischer, M.D. |
Director |
March 4, 2011 | ||
| /S/ GERRI A. HENWOOD Gerri A. Henwood |
Director |
March 4 2011 | ||
| /S/ BERNARD J. KELLEY Bernard J. Kelley |
Director |
March 4, 2011 | ||
99
Table of Contents
Index to Financial Statements
| Signature |
Title |
Date | ||
| /S/ MATTHEW V. MCPHERRON Matthew V. McPherron |
Director |
March 4, 2011 | ||
| /S/ H. WARD WOLFF H. Ward Wolff |
Director |
March 4, 2011 | ||
100
Table of Contents
Index to Financial Statements
| Exhibit No. |
Description | |
| 3.1 | Amended and Restated Certificate of Incorporation of the Registrant (filed as Exhibit 3.1 to the Registrant’s Quarterly Report on Form 10-Q for the quarter ended September 30, 2007 and incorporated herein by reference). | |
| 3.2 | Amended and Restated Bylaws of the Registrant (filed as Exhibit 3.2 to the Registrant’s Quarterly Report on Form 10-Q for the quarter ended September 30, 2007 and incorporated herein by reference). | |
| 4.1 | Specimen Stock Certificate (filed as Exhibit 4.1 to the Registrant’s Registration Statement on Form S-1-A (File No. 333-143823), filed on September 20, 2007, and incorporated herein by reference). | |
| 4.2 | Third Amended and Restated Registration Rights Agreement dated March 21, 2007 (filed as Exhibit 4.2 to the Registrant’s Registration Statement on Form S-1 (File No. 333-143823), filed on June 18, 2007, and incorporated herein by reference). | |
| 4.3 | Warrant to purchase shares of Series C Preferred Stock issued to Horizon Technology Funding Company II LLC dated September 14, 2006 (filed as Exhibit 10.18 to the Registrant’s Registration Statement on Form S-1 (File No. 333-143823), filed on June 18, 2007, and incorporated herein by reference). | |
| 10.1# | MAP Pharmaceuticals, Inc. 2004 Long-Term Equity Incentive Plan (filed as Exhibit 10.1 to the Registrant’s Registration Statement on Form S-1 (File No. 333-143823), filed on June 18, 2007, and incorporated herein by reference). | |
| 10.2# | MAP Pharmaceuticals, Inc. Amended and Restated 2005 Equity Incentive Plan and forms of agreements relating thereto (filed as Exhibit 10.2 to the Registrant’s Registration Statement on Form S-1 (File No. 333-143823), filed on June 18, 2007, and incorporated herein by reference). | |
| 10.3# | MAP Pharmaceuticals, Inc. 2007 Equity Award Plan and forms of agreements relating thereto (filed as Exhibit 10.3 to the Registrant’s Registration Statement on Form S-1/A (File No. 333-143823), filed on September 20, 2007, and incorporated herein by reference). | |
| 10.4# | MAP Pharmaceuticals, Inc. Employee Stock Purchase Plan (filed as Exhibit 10.30 to the Registrant’s Registration Statement on Form S-1/A (File No. 333-143823), filed on September 20, 2007, and incorporated herein by reference). | |
| 10.5# | Form of Indemnification Agreement by and between the Registrant and each of its directors and executive officers (filed as Exhibit 10.4 to the Registrant’s Registration Statement on Form S-1/A (File No. 333-143823), filed on July 30, 2007, and incorporated herein by reference). | |
| 10.6# | Employment Agreement dated March 20, 2005, between Timothy S. Nelson and the Registrant (filed as Exhibit 10.5 to the Registrant’s Registration Statement on Form S-1 (File No. 333-143823), filed on June 18, 2007, and incorporated herein by reference). | |
| 10.7# | Amendment to Employment Agreement dated July 22, 2005, between Timothy S. Nelson and the Registrant (filed as Exhibit 10.6 to the Registrant’s Registration Statement on Form S-1 (File No. 333-143823), filed on June 18, 2007, and incorporated herein by reference). | |
| 10.8# | Employment Agreement dated April 14, 2008, between Thomas A. Armer and the Registrant (filed as Exhibit 10.1 to the Registrant’s Quarterly Report on Form 10-Q (File No. 001-33719), filed on May 14, 2008, and incorporated herein by reference). | |
| 10.9# | Restricted Stock Agreement dated August 12, 2004, between Thomas A. Armer and the Registrant (filed as Exhibit 10.8 to the Registrant’s Registration Statement on Form S-1 (File No. 333-143823), filed on June 18, 2007, and incorporated herein by reference). | |
101
Table of Contents
Index to Financial Statements
| Exhibit No. |
Description | |
| 10.10# | Offer Letter dated September 14, 2006, between Christopher Y. Chai and the Registrant (filed as Exhibit 10.9 to the Registrant’s Registration Statement on Form S-1 (File No. 333-143823), filed on June 18, 2007, and incorporated herein by reference). | |
| 10.11# | Amended and Restated Offer Letter dated September 11, 2007, between Anastasios Gianakakos and the Registrant (filed as Exhibit 10.10 to the Registrant’s Registration Statement on Form S-1 (File No. 333-143823), filed on June 18, 2007, and incorporated herein by reference). | |
| 10.12# | Form of Change in Control Agreement between the executive officers of the Registrant and the Registrant (filed as Exhibit 10.12 to the Registrant’s Registration Statement on Form S-1/A (File No. 333-143823), filed on September 20, 2007, and incorporated herein by reference). | |
| 10.13 | Lease Agreement between the Registrant and ARE-2425/2400/2450 Garcia Bayshore, LLC dated June 10, 2004 (filed as Exhibit 10.13 to the Registrant’s Registration Statement on Form S-1 (File No. 333-143823), filed on June 18, 2007, and incorporated herein by reference). | |
| 10.14 | First Amendment to Lease Agreement between the Registrant and ARE-2425/2400/2450 Garcia Bayshore, LLC dated August 2, 2004 (filed as Exhibit 10.14 to the Registrant’s Registration Statement on Form S-1 (File No. 333-143823), filed on June 18, 2007, and incorporated herein by reference). | |
| 10.15 | Second Amendment to Lease Agreement between the Registrant and ARE-2425/2400/2450 Garcia Bayshore, LLC dated July 26, 2006 (filed as Exhibit 10.15 to the Registrant’s Registration Statement on Form S-1 (File No. 333-143823), filed on June 18, 2007, and incorporated herein by reference). | |
| 10.16† | Research and Development, License and Supply Agreement between the Registrant and Eiffel Technologies Limited dated September 22, 2005 (filed as Exhibit 10.25 to the Registrant’s Registration Statement on Form S-1 (File No. 333-143823), filed on June 18, 2007, and incorporated herein by reference). | |
| 10.17† | Restated and Amended License Agreement between Nektar Therapeutics and the Registrant dated August 7, 2006 (filed as Exhibit 10.27 to the Registrant’s Registration Statement on Form S-1 (File No. 333-143823), filed on June 18, 2007, and incorporated herein by reference). | |
| 10.18† | Manufacturing and Supply Agreement between Xemplar Pharmaceuticals, LLC and the Registrant dated April 26, 2006 (filed as Exhibit 10.28 to the Registrant’s Registration Statement on Form S-1 (File No. 333-143823), filed on June 18, 2007, and incorporated herein by reference). | |
| 10.19* | Amendment to Restated and Amended License Agreement between Nektar Therapeutics UK Limited and the Registrant dated October 8, 2007 (filed as Exhibit 10.1 to Registrant’s Quarterly Report on Form 10-Q for the quarter ended September 30, 2007 and incorporated herein by reference). | |
| 10.20 | Third Amendment to Lease Agreement between the Registrant and ARE-2425/2400/2450 Garcia Bayshore, LLC dated November 30, 2007 (filed as Exhibit 10.27 to the Registrant’s Annual Report on Form 10-K filed on March 20, 2008, and incorporated herein by reference). | |
| 10.21 | Loan and Security Agreement by and among the Registrant, Oxford Finance Corporation and Silicon Valley Bank dated May 2, 2007 (filed as Exhibit 10.1 to the Registrant’s Current Report on Form 8-K filed on May 7, 2008, and incorporated herein by reference). | |
| 10.22† | Fourth Amendment to Lease Agreement between the Registrant and ARE-2425/2400/2450 Garcia Bayshore, LLC dated March 26, 2008 (filed as Exhibit 10.2 to the Registrant’s Quarterly Report on Form 10-Q filed on May 14, 2008, and incorporated herein by reference). | |
102
Table of Contents
Index to Financial Statements
| Exhibit No. |
Description | |
| 10.23† | Transfer and Assignment Agreement dated June 19, 2008 between Telesso Technologies Limited and the Registrant (filed as Exhibit 10.2 to the Registrant’s Quarterly Report on Form 10-Q filed on August 13, 2008, and incorporated herein by reference). | |
| 10.24† | Amended and Restated Fourth Amendment to Lease Agreement between the Registrant and ARE-2425/2400/2450 Garcia Bayshore, LLC dated July 15, 2008 (filed as Exhibit 10.1 to the Registrant’s Quarterly Report on Form 10-Q filed on November 13, 2008, and incorporated herein by reference). | |
| 10.25# | Severance Agreement dated March 19, 2009, between Timothy S. Nelson and the Registrant (filed as Exhibit 10.1 to the Registrant’s Quarterly Report on Form 10-Q filed on May 8, 2009, and incorporated herein by reference). | |
| 10.26 | Common Stock Purchase Agreement dated November 11, 2009, between Azimuth Opportunity Ltd and the Registrant (filed as Exhibit 10.1 to the Registrant’s Current Report on Form 8-K filed on November 12, 2009, and incorporated herein by reference). | |
| 10.27# | Form of RSU grant agreement relating to MAP Pharmaceuticals, Inc. 2007 Equity Award Plan (filed as Exhibit 10.39 to the Registrant’s Annual Report on Form 10-K filed on March 5, 2010, and incorporated herein by reference). | |
| 10.28# | Offer Letter dated July 5, 2007, between Charlene Friedman and the Registrant (filed as Exhibit 10.37 to the Registrant’s Annual Report on Form 10-K filed on March 12, 2009, and incorporated herein by reference). | |
| 10.29# | Offer Letter dated June 18, 2008, between Donald Kellerman and the Registrant. | |
| 10.30* | Collaboration Agreement by and among MAP Pharmaceuticals, Inc., Allergan Sales, LLC, Allergan USA, Inc. and Allergan, Inc. dated January 28, 2011 (filed as Exhibit 10.1 to the Registrant’s Current Report on Form 8-K/A filed on February 16, 2011, and incorporated herein by reference). | |
| 10.31* | Co-Promotion Agreement by and between MAP Pharmaceuticals, Inc., Allergan USA, Inc., dated January 28, 2011 (filed as Exhibit 10.2 to the Registrant’s Current Report on Form 8-K/A filed on February 16, 2011, and incorporated herein by reference). | |
| 23.1 | Consent of Independent Registered Public Accounting Firm. | |
| 31.1 | Certification of Principal Executive Officer Required Under Rules 13a-14(a) or 15d-14(a) of the Securities Exchange Act of 1934, as amended. | |
| 31.2 | Certification of Principal Financial Officer Required Under Rules 13a-14(a) or 15d-14(a) of the Securities Exchange Act of 1934, as amended. | |
| 32.1 | Certification of Principal Executive Officer and Principal Financial Officer Required Under Rule 13a-14(b) of the Securities Exchange Act of 1934, as amended, and 18 U.S.C. §1350. | |
| # | Indicates management contract or compensatory plan. |
| † | Confidential treatment has been granted as to certain portions, which portions have been omitted and filed separately with the Securities and Exchange Commission. |
| * | Confidential treatment requested for certain portions. |
103