Attached files
| file | filename |
|---|---|
| EX-23.1 - REHABCARE GROUP INC. 10K 2010 EX-23.1 - REHABCARE GROUP INC | tenk2010exhibit231.htm |
| EX-31.2 - REHABCARE GROUP INC. 10K 2010 EX-31.2 - REHABCARE GROUP INC | tenk2010exhibit312.htm |
| EX-31.1 - REHABCARE GROUP INC. 10K 2010 EX-31.1 - REHABCARE GROUP INC | tenk2010exhibit311.htm |
| EX-32.2 - REHABCARE GROUP INC. 10K 2010 EX-32.2 - REHABCARE GROUP INC | tenk2010exhibit322.htm |
| EX-21.1 - REHABCARE GROUP INC. 10K 2010 EX-21.1 - REHABCARE GROUP INC | tenk2010exhibit211.htm |
| EX-32.1 - REHABCARE GROUP INC. 10K 2010 EX-32.1 - REHABCARE GROUP INC | tenk2010exhibit321.htm |
| EX-10.10 - REHABCARE GROUP INC. 10K 2010 EX-10.10 - REHABCARE GROUP INC | tenk2010exhibit1010.htm |
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
Annual Report Pursuant to Section 13 or 15(d) of the Securities Exchange Act of 1934
for the fiscal year ended December 31, 2010
Commission file number 001-14655
RehabCare Group, Inc.
(Exact name of registrant as specified in its charter)
|
Delaware
|
51-0265872
|
||
|
(State of Incorporation)
|
(I.R.S. Employer Identification No.)
|
7733 Forsyth Boulevard, 23rd Floor, St. Louis, Missouri 63105
(Address of principal executive offices and zip code)
Registrant’s telephone number, including area code: (800) 677-1238
|
Securities registered pursuant to Section 12(b) of the Act:
|
Name of exchange on which registered:
|
|
|
Common Stock, par value $.01 per share
|
New York Stock Exchange
|
Indicate by check mark whether the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes o No x
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes o No x
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months, and (2) has been subject to such filing requirements for the past 90 days. Yes x No o
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes o No o
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. o
Indicate by a check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company (as defined in Rule 12b-2 of the Exchange Act).
Large accelerated filer o Accelerated filer x
Non-accelerated filer o Smaller reporting company o
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Act). Yes o No x
The aggregate market value of the common stock held by non-affiliates of the registrant at June 30, 2010 was approximately $527 million based on the closing price of the stock on that day. At January 31, 2011, the registrant had 24,915,796 shares of Common Stock outstanding, including unvested restricted stock.
DOCUMENTS INCORPORATED BY REFERENCE
Certain information required by Part III (Items 10, 11, 12, 13 and 14) is incorporated by reference to an amendment to this Form 10-K which will be filed not later than 120 days after the end of the fiscal year covered by this Form 10-K.
- 1 -
TABLE OF CONTENTS
|
PART I
|
|
|
Item 1.
|
Business
|
|
Item 1A.
|
Risk Factors
|
|
Item 1B.
|
Unresolved Staff Comments
|
|
Item 2.
|
Properties
|
|
Item 3.
|
Legal Proceedings
|
|
Item 4.
|
Submission of Matters to a Vote of Security Holders
|
|
PART II
|
|
|
Item 5.
|
Market for Registrant’s Common Stock, Related Stockholder Matters and Issuer Purchases of Equity Securities
|
|
Item 6.
|
Selected Financial Data
|
|
Item 7.
|
Management’s Discussion and Analysis of Financial Condition and Results of Operations
|
|
Item 7A.
|
Quantitative and Qualitative Disclosures About Market Risk
|
|
Item 8.
|
Financial Statements and Supplementary Data
|
|
Item 9.
|
Changes in and Disagreements with Accountants on Accounting and Financial Disclosure
|
|
Item 9A.
|
Controls and Procedures
|
|
Item 9B.
|
Other Information
|
|
PART III
|
|
|
Item 10.
|
Directors, Executive Officers and Corporate Governance
|
|
Item 11.
|
Executive Compensation
|
|
Item 12.
|
Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters
|
|
Item 13.
|
Certain Relationships and Related Transactions, and Director Independence
|
|
Item 14.
|
Principal Accounting Fees and Services
|
|
PART IV
|
|
|
Item 15.
|
Exhibits and Financial Statement Schedules
|
- 2 -
PART I
| ITEM 1. | BUSINESS |
The terms “RehabCare,” “our company,” “we” and “our” as used herein refer to RehabCare Group, Inc. and its subsidiaries.
Overview of Our Company
RehabCare Group, Inc., a Delaware corporation, headquartered in St. Louis, Missouri, is a leading provider of rehabilitation program management services in more than 1,250 hospitals, skilled nursing facilities, outpatient facilities and other long-term care facilities located in 42 states and Puerto Rico. We also own and operate 29 long-term acute care hospitals (“LTACHs”) and 5 rehabilitation hospitals. These hospitals provide total medical care to patients with medically complex diagnoses and to patients in need of rehabilitation.
Established in 1982, we have more than 25 years of experience helping healthcare providers grow and become more efficient while effectively and compassionately delivering rehabilitation services to patients. In partnership with healthcare providers, we provide post-acute program management, medical direction, physical therapy rehabilitation, quality assurance, compliance review, specialty programs and census development services. We believe our clients place a high value on our extensive experience in assisting them to implement clinical best practices, to address competition for patient services, and to navigate the complexities inherent in managed care contracting and government reimbursement systems. Over the years, we have diversified our program management services to include management services for inpatient rehabilitation facilities within hospitals, skilled nursing units, outpatient rehabilitation programs, home health, and skilled nursing, long-term care and assisted living facilities.
Effective November 24, 2009, we acquired all of the outstanding common stock of Triumph HealthCare Holdings, Inc. (“Triumph”) for a purchase price of approximately $541.0 million. On the acquisition date, Triumph operated 20 LTACHs in seven states. In December 2009, we acquired an LTACH in Philadelphia, Pennsylvania, and in 2010, we opened an LTACH in Houston, Texas known as The Heights. These activities expanded the number of LTACHs we own and operate to 29, making us the third largest LTACH provider in the United States.
In November 2010, we announced that we had entered into an Equity Exchange Agreement with Select Medical Corporation under which we agreed to exchange our 60-bed inpatient rehabilitation hospital in Miami for Select’s 70-bed long-term acute care hospital in northwest Indiana. This transaction closed on January 1, 2011. The Miami hospital has been classified as a discontinued operation in our accompanying consolidated financial statements.
For the year ended December 31, 2010, we had consolidated operating revenues of $1.3 billion, operating earnings of $133.6 million, net earnings attributable to RehabCare of $62.5 million and diluted earnings per share attributable to RehabCare of $2.53.
On February 7, 2011, we and Kindred Healthcare, Inc. (“Kindred”) entered into an Agreement and Plan of Merger (the “Merger Agreement”), providing for the acquisition of us by Kindred. Subject to the terms and conditions of the Merger Agreement, which has been unanimously approved by the boards of directors of the respective parties, we will be merged with and into Kindred (the “Merger”), with Kindred surviving the Merger.
- 3 -
At the effective time of the Merger, each share of our common stock outstanding immediately prior to the effective time will be converted into the right to receive 0.471 shares of Kindred common stock and $26.00 in cash, without interest. No fractional shares of Kindred common stock will be issued in the Merger, and our stockholders will receive cash in lieu of fractional shares, if any, of Kindred common stock. Each share of Kindred common stock outstanding immediately prior to the effective time will remain outstanding and will not be affected by the Merger. Upon completion of the transaction, our stockholders will own approximately 22% of Kindred’s outstanding common stock.
The consummation of the Merger is subject to certain conditions, including the adoption by our and Kindred stockholders of the Merger Agreement; clearance under the Hart-Scott-Rodino Antitrust Improvements Act of 1976, as amended; receipt of certain other licensure and regulatory approvals; receipt of the proceeds of the financing described below; and other customary closing conditions.
The Merger Agreement also contains certain termination rights and provides that (i) upon termination of the Merger Agreement under specified circumstances, including, among others, a change in the recommendation of our board of directors or termination of the Merger Agreement to enter into a written definitive agreement for a “superior proposal,” we will be required to pay Kindred a termination fee of $26 million and (ii) upon the termination of the Merger Agreement under specified circumstances, including, among others, a change in the recommendation of the board of directors of Kindred or Kindred’s failure to receive the proceeds of the financing discussed below, after all of the other conditions to closing have been met, Kindred will be required to pay us a termination fee of $62 million.
Kindred has obtained a financing commitment from JPMorgan Chase Bank, N.A., J.P. Morgan Securities LLC, Morgan Stanley Senior Funding, Inc. and Citigroup Global Markets Inc. in connection with the pending transaction. We believe these funds, in addition to existing cash balances, will be sufficient to finance the cash consideration to our stockholders and to refinance certain existing Kindred and RehabCare debt.
Industry Overview
As a provider of program management services and an operator of hospitals, our revenues and growth are affected by trends and developments in healthcare spending. According to the Centers for Medicare and Medicaid Services (“CMS”), total healthcare expenditures in the United States grew by 4.0% to approximately $2.5 trillion in 2009 or 17.6% of the United States gross domestic product.
CMS further projects that total healthcare spending in the United States will continue to grow an average of 6.3% annually from 2010 through 2019. According to these estimates, healthcare expenditures will account for approximately $4.6 trillion, or 19.6%, of the United States gross domestic product by 2020.
Demographic considerations affect long-term growth projections for healthcare spending. While we deliver therapy to adults of all ages, most of our services are delivered to persons 65 and older. According to the U.S. Census Bureau’s latest projections, there are approximately 40 million U.S. residents aged 65 or older, comprising approximately 13.0% of the total United States population. The number of U.S. residents aged 65 or older is expected to climb to approximately 55 million by 2020 and to approximately 72 million by 2030. By 2040, the number of U.S. residents 65 and older is estimated to reach approximately 81 million, or 20.0%, of the total population. Due to the increasing life expectancy of U.S. residents, the number of people aged 85 years or older is also expected to increase from 5.8 million in 2010 to 14.2 million in 2040.
- 4 -
We believe healthcare expenditures and longer life expectancy of the general population will place increased pressure on healthcare providers to find innovative, efficient means of delivering healthcare services. In particular, many of the health conditions associated with aging — such as stroke and heart attack, neurological disorders and diseases and injuries to the muscles, bones and joints — will increase the demand for rehabilitative therapy and long-term acute care. These trends, combined with the need for acute care hospitals to move their patients into the appropriate level of care on a timely basis, will encourage healthcare providers to efficiently direct patients to long-term acute care hospitals, inpatient rehabilitation facilities, skilled nursing therapy, outpatient therapy, home health and other post-acute programs.
The growth of managed care and its focus on cost control has encouraged healthcare providers to deliver quality care at the lowest cost possible. Changes in Medicare and Medicaid reimbursement rules also have driven declines in average inpatient days per admission. In many cases, patients are treated initially in a higher cost, acute-care hospital setting. After their condition has stabilized, they are either moved to a lower cost setting, such as a skilled nursing facility or subacute nursing facility, or are moved to another post-acute institution, such as an inpatient rehabilitation facility or a long-term acute care hospital. Alternatively, patients are discharged to their home and treated on a home health or outpatient basis. Thus, while hospital inpatient admissions have continued to grow, the number of average inpatient days per admission has declined.
There are approximately 4,000 general acute-care hospitals in the United States, including approximately 1,000 hospitals with inpatient rehabilitation facilities (“IRFs”). We currently provide acute rehabilitation program management services to 105 hospitals that operate inpatient rehabilitation facilities.
There are over 15,000 Medicare-certified skilled nursing facilities in the United States. We currently provide contract therapy services to 1,112 of those facilities. In addition to skilled nursing facilities, we have expanded our service offerings to deliver therapy management services in additional settings such as long-term care, home health, assisted living facilities and continuing care retirement communities.
Overview of Our Business Units
We currently operate in two business segments: program management services, which consists of two business units — hospital rehabilitation services and skilled nursing rehabilitation services — and hospitals. The following table describes the services we offer within each segment.
- 5 -
|
Business Segments
|
Description of Service
|
Benefits to Client
|
|
Program Management Services:
|
||
|
Hospital Rehabilitation Services:
|
||
|
Inpatient
Inpatient Rehabilitation Facilities:
Skilled Nursing Units (Subacute Rehabilitation):
|
High acuity rehabilitation for conditions such as stroke, orthopedic conditions and head injuries.
Lower intensity rehabilitation for medically complex patients with pulmonary conditions, stroke, cancer, heart failure, burns and wounds and other similar diagnoses.
|
Affords the client opportunities to retain and expand market share in the post-acute market by offering specialized clinical rehabilitation services to patients who might otherwise be discharged to a setting outside the client’s facility.
|
|
Outpatient
|
Outpatient therapy programs for hospital-based and satellite programs (primarily sports and work-related injuries).
|
Helps bring patients into the client’s facility by providing specialized clinical programs and helps the client compete with freestanding clinics.
|
|
Skilled Nursing Rehabilitation Services:
|
||
|
Contract Therapy
|
Rehabilitation services in freestanding skilled nursing, long-term care and assisted living facilities for neurological, orthopedic and other medical conditions.
|
Affords the client the ability to fulfill the continuing need for therapists on a full-time or part-time basis. Offers the client a better opportunity to improve the quality of their programs.
|
|
Other
|
Resident-centered consulting services and therapist and nurse staffing services for healthcare providers.
|
Provides management advisory services and solutions to healthcare providers.
|
|
Hospitals:
|
||
|
Long-Term Acute Care Hospitals (LTACHs)
Rehabilitation Hospitals
|
Provide high-level therapeutic and clinical care to patients with medically complex diagnoses generally with an average length of stay of 25 days or more.
Provide intense interdisciplinary rehabilitation services to patients on an inpatient and outpatient basis.
|
|
- 6 -
Financial information about each of our business segments is contained in Note 20, “Industry Segment Information,” to our consolidated financial statements.
The following table summarizes, by geographic region in the United States, our program management and hospital locations as of December 31, 2010.
|
Program Management Services
|
||||||||
|
Inpatient
|
||||||||
|
Rehabilitation/
|
Outpatient
|
Contract
|
||||||
|
Skilled Nursing
|
Therapy
|
Therapy
|
||||||
|
Geographic Region
|
Units
|
Programs
|
Programs
|
Hospitals
|
||||
|
Mountain Region
|
1/1
|
1
|
52
|
1
|
||||
|
North Central Region
|
37/1
|
9
|
341
|
7
|
||||
|
Northeast Region
|
14/2
|
5
|
143
|
2
|
||||
|
South Central Region
|
30/0
|
6
|
378
|
23
|
||||
|
Southeast Region
|
13/2
|
9
|
147
|
1
|
||||
|
Western Region
|
9/5
|
0
|
51
|
0
|
||||
|
Puerto Rico
|
1/0
|
0
|
0
|
0
|
||||
|
Total
|
105/11
|
30
|
1,112
|
34
|
||||
Program Management Services
Many healthcare providers partner with companies, like RehabCare, that manage either a single service line or a broad range of service lines. Partnering allows healthcare providers to take advantage of the specialized expertise of contract management companies, enabling them to concentrate on the businesses they know best, such as facility and acute-care management. Continued managed care and Medicare reimbursement controls for acute care services have driven healthcare providers to look for additional sources of revenue. As constraints on overhead and operating costs have increased and staffing has been reduced, partnering with providers of ancillary and post-acute services has become more important in order to increase patient volumes and provide services at a lower cost while maintaining high quality standards.
By partnering with contract management companies like RehabCare, healthcare facilities may be able to:
|
·
|
Improve Clinical Quality. Program managers focused on rehabilitation are able to develop and employ best practices, which benefit client facilities and their patients.
|
|
|
·
|
Increase Volumes. Through the addition of specialty services such as IRFs within acute-care hospitals, patients who were being discharged to other venues for treatment can now remain in the hospital setting. This allows hospitals to capture revenues that would otherwise be realized by another provider. Upon discharge, patients can return for outpatient care, creating added revenues for the provider. New services also help hospitals attract new patients. The addition of a managed rehabilitation program helps skilled nursing facilities attract residents by broadening their scope of services.
|
|
|
·
|
Optimize Utilization of Space. Inpatient services help hospitals optimize physical plant space to treat patients who have specific diagnoses within the particular hospital’s targeted service lines.
|
|
|
·
|
Increase Cost Control. Because of their extensive experience in the service line, contract management companies can offer pricing structures that effectively control a healthcare provider’s financial risk related to the service provided. For hospitals and other providers that utilize program managers, the result is often lower average cost than that of self-managed programs. As a result, the facility is able to increase its revenues without having to increase administrative staff or incur other fixed costs.
|
- 7 -
|
|
·
|
Establish Agreements with Managed Care Organizations. Program managers often have the ability to improve clinical care by capturing and analyzing patient information from a large number of inpatient rehabilitation and skilled nursing units, which an individual hospital could not do on its own without a substantial investment in specialized systems. Becoming part of a managed care network helps the hospital attract physicians, and in turn, attract more patients to the hospital.
|
|
|
·
|
Provide Access to Capital. Contract management companies, particularly those which have access to public markets, can in certain circumstances make capital available to their clients for adding programs and services like physical rehabilitative services or expanding existing programs when community needs dictate.
|
|
|
·
|
Obtain Reimbursement Advice. Contract management companies, like RehabCare, employ reimbursement specialists who are available to assist client facilities in interpreting complicated regulations within a given specialty — a highly valued service in the changing healthcare environment.
|
|
|
·
|
Obtain Clinical Resources and Expertise. Rehabilitation service providers have the ability to develop and implement clinical training and development programs that can provide best practices for clients.
|
|
|
·
|
Ensure Appropriate Levels of Staffing for Rehabilitation Professionals. Therapy staffing in both hospitals and skilled nursing settings presents unique challenges that can be better managed by a provider with a national recruiting presence. Program managers have the ability to more sharply focus on staffing levels in order to address the fluctuating clinical needs of the host facility.
|
Our program management services segment consists of two business units — hospital rehabilitation services (which includes inpatient acute and subacute rehabilitation programs and outpatient therapy programs) and skilled nursing rehabilitation services.
Inpatient
We have developed an effective business model in the prospective payment environment, and we are instrumental in helping our clients achieve favorable outcomes in their inpatient rehabilitation settings.
Inpatient Rehabilitation. Since 1982, our inpatient division has been a leader in operating IRFs in acute-care hospitals on a contract basis. As of December 31, 2010, we managed IRFs in 105 hospitals for patients with various diagnoses including stroke, orthopedic conditions, arthritis, spinal cord and traumatic brain injuries.
We establish IRFs in acute-care hospitals that have vacant space and unmet rehabilitation needs in their markets. We also work with hospitals that currently operate IRFs to determine the projected level of cost savings we can deliver to them by implementing our scheduling, clinical protocol and outcome systems, as well as through productivity training for existing staff. In the case of hospitals that do not operate IRFs, we review their historical and existing hospital population, as well as the demographics of the geographic region, to determine the optimal size of the proposed IRF and the potential of the new facility under our management to attract patients and generate revenues sufficient to cover anticipated expenses.
- 8 -
In the inpatient division, our relationships with hospitals are in the form of contracts for management services which are typically three to five years in duration. We are generally paid by our clients on the basis of a negotiated fee per month or fee per discharge.
An IRF within an acute-care hospital affords the hospital the ability to offer rehabilitation services to patients who might otherwise be discharged to a setting outside the hospital. An IRF within an acute-care hospital typically consists of 20 beds and is staffed with a program director, a physician or medical director, and clinical staff, which may include a psychologist, physical and occupational therapists, a speech/language pathologist, a social worker, a case manager and other appropriate support personnel.
Subacute Rehabilitation. In 1994, the inpatient division added a skilled nursing service line in response to client requests for management services and our strategic decision to broaden our inpatient services. As of December 31, 2010, we managed 11 inpatient skilled nursing units. The hospital-based skilled nursing unit enables patients to remain in a hospital setting where emergency needs can be met quickly as opposed to being sent to a freestanding skilled nursing facility. These types of units are located within the acute-care hospital and are separately licensed.
We are paid by our skilled nursing clients either based on a flat monthly fee or a negotiated fee per patient day pursuant to contracts that are typically for terms of three to five years. The hospital benefits by retaining patients who otherwise would be discharged to another setting, capturing additional revenue and utilizing idle space. A skilled nursing unit treats patients who require less intensive levels of rehabilitative care. Patients’ diagnoses typically require long-term care and cover approximately 60 clinical conditions, including stroke, post-surgical conditions, pulmonary disease, cancer, congestive heart failure, burns and wounds.
Outpatient
In 1993, we began managing outpatient therapy programs that provide therapy services to patients with work-related and sports-related illnesses and injuries. As of December 31, 2010, we managed 30 hospital-based and satellite outpatient therapy programs. An outpatient therapy program complements the hospital’s occupational medicine initiatives and allows therapy to be continued for patients discharged from inpatient rehabilitation facilities and medical/surgical beds. An outpatient therapy program also attracts patients into the hospital and is operated either on the client hospital’s campus or in satellite locations controlled by the hospital.
We believe our management of outpatient therapy programs delivers increased productivity through our scheduling, clinical protocol and outcome systems, as well as through productivity training for existing staff. We also provide our clients with expertise in compliance and quality assurance. Typically, the program is staffed with a facility director, four to six therapists, and two to four administrative and clerical staff. We are typically paid by our clients on the basis of a negotiated fee per unit of service.
Skilled Nursing Rehabilitation Services
In 1997, we added therapy management for freestanding skilled nursing facilities to our service offerings. This program affords the client the opportunity to fulfill its continuing need for therapists on a full-time or part-time basis without the need to hire and retain full-time staff. As of December 31, 2010, we managed 1,112 contract therapy programs.
- 9 -
Our typical contract therapy client has a 120 bed skilled nursing facility. We manage therapy services, including physical and occupational therapy and speech/language pathology for the skilled nursing facility and in other settings that provide services to the senior population. Our broad base of staffing service offerings — full-time and part-time — can be adjusted at each location according to the facility’s and its patients’ needs. We also provide our clients improved scheduling, clinical protocols, patient outcomes, compliance with Medicare requirements and therapist productivity through the use of handheld point of service devices by our therapists.
We are generally paid by our clients on the basis of a negotiated patient per diem rate or a negotiated fee schedule based on the type of service rendered. Typically, our contract therapy programs are led by a full-time program director who is also a therapist, and two to four full-time professionals trained in physical, occupational or speech/language therapy.
Hospitals
We entered the rehabilitation and long-term acute care hospital market in 2005 when we acquired substantially all of the operating assets of MeadowBrook Healthcare, Inc. (“MeadowBrook”), an operator of two rehabilitation hospitals and two LTACHs. These facilities treat patients who require intensive inpatient rehabilitative care and patients with medically complex diagnoses. Patient care is provided by nursing and therapy staff as directed by a physician order. Effective November 24, 2009, we acquired all of the outstanding stock of Triumph HealthCare Holdings, Inc., which operated 20 LTACHs at the time of acquisition, more than doubling the size of our hospital segment. As of December 31, 2010, we operated 29 LTACHs and five rehabilitation hospitals. We are the sole owner of 19 of these hospitals. We retain a 51% to 99% ownership in the remaining 15 jointly owned hospitals. Our hospitals are located in Texas, Oklahoma, Louisiana, Georgia, Missouri, Illinois, Ohio, Indiana, Pennsylvania, Michigan, North Dakota and Colorado. Except for two Company-owned facilities, all of these facilities are located in property leased by us under long-term leases. Our facilities range in size from 20 to 115 licensed beds. We also own a 40% equity interest in a freestanding rehabilitation hospital in Kokomo, Indiana. A rehabilitation hospital in Miami, Florida was classified as held for sale at December 31, 2010.
LTACHs serve highly complex, but relatively stable, patients. Typical diagnoses include respiratory failure, neuromuscular disorders, traumatic brain and spinal cord injuries, stroke, cardiac disorders, non-healing wounds, renal disorders and cancer. Most LTACH patients are transferred from inpatient acute medical/surgical beds. In order to remain certified as an LTACH, average length of stay for Medicare patients must be at least 25 days.
The clinical services we provide in LTACHs include: nursing care, rehabilitation therapies, pulmonology, respiratory care, cardiac and hemodynamic monitoring, ventilator weaning, dialysis services, IV antibiotic therapy, total parenteral nutrition, wound care, vacuum assisted closure, pain management and diabetes management. The majority of our LTACH patients are covered by Medicare.
Our rehabilitation hospitals provide services to patients who require intensive inpatient rehabilitative care. Inpatient rehabilitation patients typically experience significant physical disabilities due to various conditions, such as head injury, spinal cord injury, stroke, certain orthopedic problems, and neuromuscular disease. Our rehabilitation hospitals provide the medical, nursing, therapy, and ancillary services required to comply with local, state, and federal regulations, as well as accreditation standards of the Joint Commission. The outpatient services offered by our hospital division assist us in managing patients through their post-acute continuum of care. The majority of our inpatient rehabilitation facility patients are covered by Medicare.
- 10 -
In the hospital segment, we are developing joint venture relationships with acute care hospitals and physician practices whereby the joint venture owns and/or operates the LTACH or rehabilitation facility, and we provide management services to the facility, which include billing, collection, and other facility management services. This joint venture management business model provides the potential for additional profitability and significantly longer partnerships, but requires additional capital compared to our traditional contract management business.
Strategy
Our operations are guided by a defined strategy aimed at advancing the profitability and growth of our company through the delivery of high quality healthcare services to patients. The focal point of that strategy is the development of clinically integrated post acute continuums of care in geographic regions throughout the United States where we provide services in a full spectrum of post acute patient settings. We plan to execute this strategy over the long-term through acquisitions, joint ownership arrangements with market leading healthcare providers and by aggressively pursuing additional program management opportunities.
Competition
Competition in our program management business is highly fragmented and intense. We compete with large national companies and smaller regional companies that offer one or more of the same services. The fundamental challenge in this line of business is convincing our potential clients, primarily hospitals and skilled nursing facilities, that we can provide quality rehabilitation services more efficiently than they can themselves. Among our principal competitive advantages are our scale, reputation for quality, cost effectiveness, an outcomes management system, innovation, price and technology systems.
Our hospitals compete primarily with LTACHs, IRFs and skilled nursing units within acute care hospitals located in our respective markets. In addition, we face competition from other large publicly held companies such as HealthSouth Corporation, Select Medical Corporation and Kindred Healthcare, Inc.
We rely on our ability to attract, develop and retain nurses, therapists and program management personnel. We compete for these professionals with other healthcare companies, including current and potential clients, which seek to fill positions with either regular or temporary employees.
Government Regulation
Overview. The healthcare industry is required to comply with many federal, state and local laws and is subject to regulation by a number of federal, state and local governmental agencies, including those that administer the Medicare and Medicaid programs, those responsible for the licensure of healthcare providers and facilities, and those responsible for administering and approving health facility construction, new services and equipment purchasing. The healthcare industry is also affected by federal, state and local policies developed to regulate the manner in which healthcare is provided, administered and paid for nationally and locally.
Regulations in the healthcare industry are extremely complex and, in many instances, the industry does not have the benefit of significant regulatory or judicial interpretation. As a result, the healthcare industry is exposed to legislative and regulatory changes; reductions and limitations in healthcare spending by government agencies; and changes in employer healthcare policies. Moreover, our business is impacted not only by those regulations that are directly applicable to our hospitals, but also by those regulations that are applicable to our clients’ facilities.
- 11 -
If we fail to comply with the regulations applicable to our business, we could suffer civil damages or penalties, criminal penalties, and/or be excluded from contracting with providers participating in Medicare, Medicaid and other federal and state healthcare programs. Likewise, if our hospital, skilled nursing facility, or other clients fail to comply with the regulations applicable to their businesses, they also could suffer civil damages or penalties, criminal penalties and/or be excluded from participating in Medicare, Medicaid and other federal and state healthcare programs. In either event, such consequences could either directly or indirectly have an adverse impact on our business.
Facility Licensure, Medicare Certification, and Certificate of Need. Our clients and our hospitals are required to comply with state facility licensure, federal Medicare certification, and certificate of need laws in certain states that are not generally applicable to our program management business.
Generally, facility licensure and Medicare certification follow specific standards and requirements. Compliance is monitored by various mechanisms, including periodic written reports and on-site inspections by representatives of relevant government agencies. Loss of licensure or Medicare certification by a healthcare facility with which we have a contract would likely result in termination of our contract with that facility. Loss of licensure or Medicare certification in any of our hospitals would result in a material adverse impact on the revenues and profitability of the affected unit until such time as the re-certification process is completed.
A few states require that healthcare facilities obtain state permission prior to entering into contracts for the management of their services. Some states also require that healthcare facilities obtain state permission in the form of a certificate of need prior to constructing or modifying their space, purchasing high-cost medical equipment, or adding new healthcare services. If a certificate of need is required, the process may take up to 12 months or more, depending on the state. The certificate of need application may be denied if contested by a competitor or if the new facility or service is deemed unnecessary by the state reviewing agency. A certificate of need is usually issued for a specified maximum expenditure and requires implementation of the proposed improvement or new service within a specified period of time. If we or our clients are unable to obtain a certificate of need, we may not be able to implement a contract to provide therapy services or open a new hospital.
Professional Licensure and Corporate Practice. Many of the healthcare professionals employed or independently engaged by us are required to be individually licensed or certified under applicable state laws. We take reasonable steps to ensure that such healthcare professionals possess all necessary licenses and certifications, and we believe that our employees and independent contractors comply with all applicable laws.
In some states, for profit corporations are restricted from practicing rehabilitation therapy through the direct employment of therapists. To comply with the restrictions in such states, we contract to obtain therapist services from entities permitted to employ therapists.
Reimbursement. Federal and state regulations establish payment methodologies for healthcare services covered by Medicare, Medicaid and other government healthcare programs.
Medicare pays acute-care hospitals for most inpatient hospital services under a payment system known as the prospective payment system (“PPS”). Under this system, acute-care hospitals are paid a fixed amount per discharge based on the diagnosis-related group (“DRG”) to which each Medicare patient is assigned, regardless of the amount of services provided to the patient or the length of the patient’s hospital stay. The amount of reimbursement assigned to each DRG is established prospectively by the Centers for Medicare and Medicaid Services (“CMS”), an agency of the Department of Health and Human Services.
- 12 -
Under Medicare’s acute-care PPS, a hospital may keep the difference between its DRG payment and its operating costs incurred in furnishing inpatient services, but the hospital is generally at risk for any operating costs that exceed the applicable DRG payment rate. For certain Medicare beneficiaries who have unusually costly hospital stays, CMS will provide additional payments above those specified for the diagnosis-related group.
The PPS for IRFs is similar to the DRG payment system used for acute-care hospital services but uses a case-mix group (“CMG”) rather than a DRG. Each patient is assigned to a CMG based on clinical characteristics and expected resource needs as a result of information reported on a patient assessment instrument which is completed upon patient admission and discharge. Under the PPS for IRFs, an IRF may keep the difference between its CMG payment and its operating costs incurred in furnishing patient services, but it is at risk for operating costs that exceed the applicable CMG payment.
To qualify for the PPS for IRFs, IRFs (such as those operated by our hospital division and managed in our hospital rehabilitation services division) must satisfy what is now known as the 60% Rule. The rule requires that 60% of patients fall within thirteen specific diagnostic categories. We continue to monitor the regulatory environment for any new rules that could affect this statute. We believe that the PPS for IRFs favors low-cost, efficient providers, and that our efficiencies gained through economies of scale and our focus on cost management in the rehabilitation field are attractive to operators in the hospital sector.
LTACHs are currently reimbursed under a prospective payment system (“LTACH-PPS”) pursuant to which Medicare classifies patients into distinct DRGs based upon specific clinical characteristics and expected resource needs. Skilled nursing facilities are also subject to a prospective payment system based on resource utilization group (“RUG”) classifications.
On March 23, 2010, the President signed the Patient Protection and Affordable Care Act (“PPACA”), commonly referred to as healthcare reform. While the bill includes numerous payment, access and participation requirements extending over the next 10 years, we are directly affected by the following Medicare provisions over the first phase of implementation:
|
1)
|
Extension of the Medicare Part B therapy cap exceptions process.
|
|
2)
|
Extension of the LTACH provisions found in MMSEA (defined below).
|
|
3)
|
Limitation on new physician owned hospitals and expansions.
|
|
4)
|
Incremental annual rate reductions for IRFs & LTACHs.
|
|
5)
|
Productivity adjustments for IRFs, LTACHs & skilled nursing facilities (“SNFs”).
|
|
6)
|
Pilot project on post-acute bundling & acute care re-admissions.
|
As of January 1, 2006, certain limits or caps on the amount of reimbursement for therapy services provided to Medicare Part B patients came into effect. Beginning January 1, 2011, the annual therapy caps are $1,870 for occupational therapy and a combined cap of $1,870 for physical and speech therapy. Prior to January 1, 2010, most of our Medicare Part B patients qualified for an automatic exception to these caps due to their clinical complexities. However, the therapy cap exception process expired on January 1, 2010. On March 2, 2010, the President signed HR 4961, a short term extension for a number of expiring provisions. Contained in this bill was a retro-active extension of the Medicare Part B therapy cap exception process from January 1, 2010 through June 30, 2010. As part of PPACA, the therapy cap exception process was extended another six months. In December 2010, the President signed a bill further extending the therapy cap exception process through December 31, 2011. Unless legislation is enacted to extend the exception process, therapy caps will return beginning on January 1, 2012.
- 13 -
The 2007 Medicare, Medicaid and SCHIP Extension Act (“MMSEA” or “2007 SCHIP Extension Act”) established a three-year moratorium, which was scheduled to end on December 31, 2010, on the establishment or classification of any new LTACH facilities, any satellite facilities and increases in bed capacity at existing LTACHs. MMSEA also provided regulatory relief for a three year period to LTACHs to ensure continued access to current long-term acute care hospital services. Specifically, until after cost reporting periods beginning on or after July 1, 2010, MMSEA prevented CMS from implementing a new payment provision for short stay outlier cases, provided that the so-called 25% Rule will not be applied to freestanding LTACHs and grandfathered LTACHs such as the one we operate in New Orleans and provided that the phase-in of the 25% Rule for admissions from hospitals co-located with an LTACH or LTACH satellite would be frozen at the 50% level. The 25% Rule limits LTACH prospective payment system paid admissions from a single referral source to 25%. Admissions beyond the 25% threshold would be paid using lower inpatient PPS rates. As part of PPACA, the MMSEA provisions noted herein were further extended through December 31, 2012.
Under PPACA, new laws were enacted effective March 23, 2010 governing physician-owned hospitals. Physician-owned hospitals are regulated under the “whole hospital” exception provision, which requires that physicians have ownership in the entire hospital and not just a department or distinct area. The whole hospital exception provision expired on December 31, 2010 for new physician owned hospitals. The new law creates a ceiling on existing ownership percentages not to exceed the levels on March 23, 2010. The new law also restricts any expansion on beds, procedural rooms or operating rooms. The Secretary of Health and Human Services (the “Secretary”) will develop new rules by February 2012 that would permit exceptions to these restrictions. We have LTACHs in Houston and Dallas which are minority owned by physicians. These hospitals were all established prior to the enactment of PPACA and therefore will continue to qualify for the whole hospital exception. Effective March of 2013, these and other existing physician owned hospitals will be subject to new disclosure and transparency requirements in order to maintain their status.
PPACA contains the following statutory annual rate reductions incremental to annual market basket adjustments (note that the 2010 payment year reductions were effective beginning April 1, 2010 while all other reductions are effective at the start of each respective rate year):
|
2010
|
2011
|
2012-2013
|
2014
|
2015-2016
|
2017-2019
|
|
|
IRF
|
0.25
|
0.25
|
0.10
|
0.30
|
0.20
|
0.75
|
|
LTACH
|
0.25
|
0.50
|
0.10
|
0.30
|
0.20
|
0.75
|
|
SNF
|
-
|
-
|
-
|
-
|
-
|
-
|
In addition, all sectors above will incur productivity adjustments as part of the annual rule making process beginning in federal rate year 2012. These calculations use a 10-year moving average statistic and as such are not expected to vary much from year to year.
Beginning by January 1, 2013, the Secretary will commission a pilot study on bundling. Bundling is the concept of making one, episodic payment for a patient to a provider for their care. It is not unlike the current Medicare Severity-DRG (MS-DRG) system currently in place since 1983 for acute care hospitals. The bundling pilot study will include the areas of post-acute care, namely IRF, LTACH, SNF and home health as well as physician services, inpatient acute care and outpatient services and will establish an episode of care spanning 3 days prior to admission into an acute care setting and 30 days post discharge from an acute care setting. Goals of the pilot are to demonstrate the ability to reduce costs while preserving or improving quality of care. Should these goals be met, the Secretary can extend the pilot to January 1, 2016.
Beginning on October 1, 2012 as part of PPACA, acute care hospitals will receive lower payments for preventable re-admissions to their hospitals. While there is no financial penalty for post-acute hospitals, such acute care re-admissions from one of our hospitals could have an adverse effect on our future referrals and admissions.
- 14 -
On July 31, 2009, CMS issued its final payment rule for skilled nursing facilities for federal rate year 2010 that included provisions that would take effect in federal rate year 2011. The final rule included a net payment rate reduction of 1.1% for skilled nursing facilities beginning on October 1, 2009 and two provisions that began on October 1, 2010: a move from the current payment system of resource utilization groups (“RUGs III”) to RUGs IV and changes to the reimbursement rules for concurrent therapy. As a result of PPACA, the start date for the conversion to RUGs IV would have been delayed until October 1, 2011. However, CMS moved forward with RUGs IV rates and the 2010 Medicare & Medicaid Extension Act signed by the President in December of 2010 included a technical correction that eliminated the delay of RUGs IV rates.
The Medicare program is administered by contractors and fiscal intermediaries. Under the authority granted by CMS, certain fiscal intermediaries have issued local coverage determinations that are intended to clarify the clinical criteria under which Medicare reimbursement is available. Certain local coverage determinations attempt to require evidence of a greater level of medical necessity for patients to receive post acute services. Those local coverage determinations have been used by fiscal intermediaries to deny admission or reimbursement for some patients in our hospital rehabilitation services and hospital divisions. Where appropriate, we and our clients will appeal such denials and many times are successful in overturning the original decision of the fiscal intermediary.
The Medicare Modernization Act of 2003 directed CMS to create a program using independent recovery audit contractors (“RACs”) to collect improper Medicare overpayments. The RAC program, which began with a demonstration pilot in three states, has now been expanded to all 50 states. We will continue to challenge and appeal any claims that we believe have been inappropriately denied.
Medicare reimbursement for outpatient rehabilitation services is based on the lesser of the provider’s actual charge for such services or the applicable Medicare physician fee schedule amount established by CMS. This reimbursement system applies regardless of whether the therapy services are furnished in a hospital outpatient department, a skilled nursing facility, an assisted living facility, a physician’s office, or the office of a therapist in private practice. The physician fee schedule is subject to change from year to year. In December 2010, the President signed a bill extending the current physician fee schedule through December 31, 2011. Failure to enact further legislation will result in a 28-30% reduction in rates beginning on January 1, 2012.
On November 2, 2010, CMS issued its final rule on an existing payment policy called the Multiple Procedure Payment Reduction for most Medicare Part B therapy services. This policy addresses one of the larger components of the procedural billing code for all therapy procedures that follow the first procedure. The final rule will result in a 25% reduction in reimbursement of practice expenses for secondary procedures when multiple therapy services are provided on the same day. This negative impact was partially offset by an 8-9% increase in practice expense relative value unit reimbursement. We estimate that the final rule will have a gross negative annual impact on operating earnings of approximately $5 to $6 million in our skilled nursing rehabilitation services (“SRS”) division based upon our 2010 Part B therapy revenue run rate. After mitigation, we believe that the net impact will be $2 to $3 million in 2011. The SRS division derives approximately one-third of its revenues from Medicare Part B. The impact on our other divisions is not expected to be material.
Health Information Practices. The Health Insurance Portability and Accountability Act of 1996, as amended, commonly known as HIPAA, was enacted to improve the efficiency and effectiveness of the healthcare system through the establishment of standards and requirements for the electronic transmission of certain health information. HIPAA regulates, among other things, the use of (i) protected health information; (ii) electronic transactions and code sets in the healthcare field; (iii) unique identifiers for patients, healthcare providers, health insurance plans, and employers; and (iv) electronic signatures. We and our program management clients are generally subject to the requirements of HIPAA. HIPAA is a very complex law that has required the careful implementation of a considerable number of policies, systems, and safeguards to better ensure our compliance with its requirements.
- 15 -
Fraud and Abuse. Various federal and state laws prohibit the knowing and willful submission of false or fraudulent claims for reimbursement, including claims to obtain payment under Medicare, Medicaid and other government healthcare programs. The federal anti-kickback statute also prohibits individuals and entities from knowingly and willfully paying, offering, receiving or soliciting money or anything else of value in order to induce the referral of patients, or to induce a person to purchase, lease, order, arrange for or recommend services or goods covered by Medicare, Medicaid, or other government healthcare programs.
The federal anti-kickback statute is susceptible to broad interpretation and potentially covers many otherwise legitimate business arrangements. Violations of the statute are punishable by criminal and civil penalties, including fines of up to $25,000 per violation, civil monetary penalties of up to $50,000 per violation, assessments of up to three times the amount of the prohibited remuneration, imprisonment, or exclusion from participation in Medicare, Medicaid, and other government healthcare programs. The Office of the Inspector General of the Department of Health and Human Services (“OIG”) has published guidelines outlining certain safe harbor arrangements that do not violate the prohibitions of the statute.
A number of states also have statutes that prohibit the same general types of conduct as that prohibited by the federal anti-kickback statute. Some states’ antifraud and anti-kickback laws apply only to goods and services covered by Medicaid. Other states’ antifraud and anti-kickback laws apply to all healthcare goods and services, regardless of whether the source of payment is governmental or private.
In recent years, federal and state government agencies have increased the level of enforcement resources and activities targeted at the healthcare industry. In addition, federal law allows individuals to bring lawsuits on behalf of the government in what are known as qui tam or “whistleblower” actions, alleging false or fraudulent Medicare or Medicaid claims and certain other violations of federal law. The use of these private enforcement actions against healthcare providers and their business is increasing, in part, because the individual filing the initial complaint is entitled to share in a portion of any settlement or judgment if successful.
Anti-Referral Laws. The federal law generally known as the Stark law provides that, if a physician or a member of a physician’s immediate family has a financial relationship with a designated healthcare service entity, the physician may not make referrals to that entity for the furnishing of designated health services covered under Medicare or Medicaid unless one of several specific exceptions applies. For purposes of the Stark law, a financial relationship with a healthcare entity includes an ownership or investment interest in that entity or a compensation relationship with that entity. Designated health services include physical and occupational therapy services, durable medical equipment, home health services, and inpatient and outpatient hospital services. CMS has promulgated regulations interpreting the Stark law and, in instances where the Stark law applies to our activities, we have instituted policies which set standards intended to prevent violations of the Stark law.
The federal government will make no payment for designated health services provided in violation of the Stark law. In addition, sanctions for violating the Stark law include civil monetary penalties of up to $15,000 per prohibited service provided and exclusion from any federal, state, or other government healthcare programs.
A number of states have statutes that prohibit the same general types of conduct as that prohibited by the federal Stark law. Some states’ Stark laws apply only to goods and services covered by Medicaid. Other states’ Stark laws apply to certain designated healthcare goods and services, regardless of whether the source of payment is a governmental or private payor.
- 16 -
Corporate Compliance Program. In recognition of the importance of achieving and maintaining regulatory compliance and establishing a culture of ethical conduct, we have a corporate compliance program that defines standards of conduct and procedures that are intended to promote compliance with applicable laws and promote proper behavior. The OIG has published guidelines for corporate compliance programs for certain types of healthcare organizations. Those guidelines encourage the following seven elements in any compliance program: (1) implementation of written standards of conduct; (2) designation of a Chief Compliance Officer with the responsibility and necessary authority to implement and enforce the compliance program, (3) regular employee education and training; (4) effective reporting lines of communication such as a “hotline;” (5) use of audits or other risk evaluation techniques; (6) disciplinary systems that consistently enforce the program standards; and (7) response and remediation systems. Our compliance program has been designed and operates to serve those seven elements.
In the recognition of the importance of compliance in our business environment, we have created a separate Compliance Committee comprised of three independent members of our board of directors. Our Chief Compliance Officer, who reports to the Compliance Committee as well as to the Chief Executive Officer, is responsible for overseeing the design, ongoing enhancement, and implementation of our compliance program. We believe these safeguards help us to conduct our operations in compliance with all applicable laws, rules, regulations, and internal company standards.
Employees
As of December 31, 2010, we had approximately 18,800 employees, approximately 9,900 of whom were full-time employees, including approximately 5,500 employees in our program management business, 3,800 employees in our hospitals and 600 employees in our corporate offices. The physicians who are the medical directors in our managed IRFs and hospitals are independent contractors and not our employees. None of our employees are subject to a collective bargaining agreement.
Non-Audit Services Performed by Independent Accountants
Pursuant to Section 10A(i)(2) of the Securities Exchange Act of 1934 and Section 202 of the Sarbanes-Oxley Act of 2002, we are responsible for disclosing to investors the non-audit services approved by our audit committee to be performed by KPMG LLP, our independent registered public accounting firm. Non-audit services are defined as services other than those provided in connection with an audit or a review of our financial statements. During the year ended December 31, 2010, we did not receive any non-audit services performed by KPMG.
Web Site Access to Reports
Our Form 10-K, Form 10-Qs, definitive proxy statements, Form 8-Ks, and any amendments to those reports are made available free of charge on our web site at www.rehabcare.com as soon as reasonably practicable after such reports are filed with the Securities and Exchange Commission.
- 17 -
| ITEM 1A. | RISK FACTORS |
Our business involves a number of risks, some of which are beyond our control. The risks and uncertainties described below are not the only ones we face. Additional risks and uncertainties that we do not currently know about, or that we currently believe to be immaterial, may also adversely affect our business.
There are risks and uncertainties associated with the proposed merger with Kindred Healthcare, Inc.
On February 7, 2011, we and Kindred Healthcare, Inc. (“Kindred”) entered into an Agreement and Plan of Merger (the “Merger Agreement”), providing for the acquisition of us by Kindred. The acquisition will be effected by the merger of us with and into Kindred (the “Merger”), with Kindred being the surviving corporation (provided that either we or Kindred may prior to the effective time of the merger elect to change the method of effecting the merger to provide for a merger of Kindred Healthcare Development, Inc. with and into us, with RehabCare Group, Inc. surviving as a wholly owned subsidiary of Kindred).
There are a number of risks and uncertainties relating to the Merger. For example, the Merger may not be consummated or may not be consummated as currently anticipated, as a result of several factors, including, but not limited to, the failure to satisfy the closing conditions set forth in the Merger Agreement. In addition, there can be no assurance that approval of our and Kindred’s stockholders and requisite regulatory approvals (including approval under the Hart-Scott-Rodino Antitrust Improvements Act of 1976, as amended) will be obtained, that the other conditions to closing of the Merger, including the obtaining of debt financing by Kindred, will be satisfied or waived or that other events will not intervene to delay or result in the termination of the Merger.
Our business could be adversely impacted as a result of uncertainty related to the Merger.
The Merger could cause disruptions in our business relationships and business generally, which could have an adverse effect on our business, financial condition, results of operations and cash flows. For example:
|
·
|
the attention of our management may be directed to transaction-related considerations and may be diverted from the day-to-day operations of our business and pursuit of our strategic initiatives;
|
|
·
|
our employees may experience uncertainty about their future roles with us, which might adversely affect our ability to retain and hire key managers and other employees; and
|
|
·
|
customers and suppliers may experience uncertainty about our future and seek alternative business relationships with third parties or seek to alter their business relationships with us.
|
Under the Merger Agreement, we are subject to certain restrictions on the conduct of our business prior to completing the Merger, which restrictions could adversely affect our ability to realize certain of our business strategies or pursue opportunities that may arise prior to the closing of the Merger.
In addition, we have incurred, and will continue to incur, significant costs, expenses and fees for professional services and other transaction costs in connection with the Merger, and we must pay many of these fees and costs regardless of whether or not we consummate the Merger.
- 18 -
Failure to complete the Merger could negatively impact our business, financial condition, results of operations or stock price.
The completion of the Merger is subject to a number of conditions and there can be no assurance that the conditions to the completion of the Merger will be satisfied or that the Merger will otherwise occur. If the Merger is not completed, we will be subject to several risks, including:
|
·
|
the current price of our common stock may reflect a market assumption that the Merger will occur, meaning that a failure to complete the Merger could result in a decline in the price of our common stock;
|
|
·
|
we may be required to pay a termination fee of $26 million if the Merger Agreement is terminated under certain circumstances, which would negatively affect our liquidity;
|
|
·
|
we expect to incur substantial transaction costs in connection with the Merger, whether or not it is completed; and
|
|
·
|
we would not realize any of the anticipated benefits of having completed the Merger.
|
Our operations may deteriorate if we are unable to attract, develop and retain our operational personnel.
Our success is dependent on attracting, developing and retaining operational personnel, especially those individuals who are responsible for administering our hospitals and operating the inpatient units, outpatient programs and contract therapy locations in our program management business. In particular, we rely significantly on our ability to attract, develop and retain qualified recruiters, area managers, program managers, regional managers and hospital administrators and operators. The available pool of individuals who meet our qualifications for these positions is limited and the competition for labor in the healthcare industry is intense. We may not be able to continue to attract and develop qualified people to fill these essential positions and we may not be able to retain them once they are employed.
Shortages of qualified therapists, nurses and other healthcare personnel could increase our operating costs and negatively impact our business.
Our operations are dependent on the efforts, abilities and experience of our management and medical support personnel, such as therapists and other allied healthcare professionals. We rely significantly on our ability to attract, develop and retain therapists, nurses and other healthcare personnel who possess the skills, experience and, as required, the licensure necessary to meet the specified requirements of our business. In some markets, the availability of nurses, therapists and other medical support personnel has become a significant operating issue to healthcare providers. Current and future shortages of such skilled labor may require us to continue to enhance wages and benefits in order to recruit and retain qualified personnel, or it may require us to hire more costly temporary personnel. We must continually evaluate, train and upgrade our employees to keep pace with clients’ and patients’ needs. If we are unable to attract and retain qualified healthcare personnel, the quality of our services may decline and we may lose customers and patients.
Unionization activities could adversely affect the profitability of our businesses.
None of our employees are subject to a collective bargaining agreement, and we are not aware of any current activities to organize our employees. We believe our relationship with our employees is good. If our employees were to unionize, we could experience an increase in labor and other costs. Furthermore, we could experience a disruption of our operations and/or higher ongoing labor costs if our employees were to engage in a strike or other work stoppage.
- 19 -
Fluctuations in census levels and patient visits may adversely affect the revenues and profitability of our businesses.
The profitability of our program management business is directly affected by the census levels, or the number of patients per unit, in the inpatient programs that we manage and the number of visits in the outpatient programs that we manage. The profitability of our hospitals business is also directly affected by the census levels at each of our hospitals. Reduction in census levels or patient visits within facilities, units or programs that we own or manage may negatively affect our revenues and profitability.
If there are changes in the rates or methods of government reimbursements of our clients for the rehabilitation services managed by us, our rehabilitation program management services clients could attempt to renegotiate our contracts with them, which may reduce our revenues and profitability.
Most of the patients cared for in our facilities are beneficiaries of government sponsored programs such as the Medicare and Medicaid programs. In an effort to control the expanding costs of the Medicare program, CMS and Congress periodically change benefits and reimbursement levels. Changes in the rates of or conditions for government reimbursement, including policies related to Medicare and Medicaid, could reduce the amounts reimbursed to our clients for rehabilitation services performed in the programs managed by us and, in turn, our clients may attempt to renegotiate the terms of our contracts.
Medicaid reimbursement is a significant revenue source for skilled nursing facilities and other long-term care facilities where contract therapy services are provided. Reductions in Medicaid reimbursement could negatively impact skilled nursing facilities and long-term care facilities which, in turn, could adversely affect the revenues, profitability and cash flows of our contract therapy business.
If we do not manage admissions in the IRFs that we manage or own in compliance with the 60% Rule, reimbursement for services rendered by us in those IRF settings will be based on less favorable rates.
IRFs are subject to the 60% Rule which now requires that 60% or more of the patients admitted to the facilities have one or more of 13 specific conditions in order to qualify for the IRF PPS. If that compliance threshold is not maintained, the IRF will be reimbursed at the lower PPS applicable to acute care hospitals. That may lead to reduced revenue in our owned IRFs and may also lead our IRF clients to attempt to renegotiate the terms of our contracts or terminate our contracts, in either case adversely affecting our revenues and profitability.
If there are changes in the rate or methods of government reimbursement for services provided by our hospitals, the revenue and profitability of those hospitals may be adversely affected.
In our hospitals business, we are directly reimbursed for a significant number of the patients we treat in those facilities through government reimbursement programs, such as Medicare. Changes in the rates of or conditions for government reimbursement could reduce the amounts reimbursed to our facilities and in turn could adversely affect the revenues and profitability of our hospitals business.
We conduct business in a heavily regulated healthcare industry and changes in regulations or violations of regulations may result in increased costs or sanctions that reduce our revenue and profitability.
The healthcare industry is subject to extensive federal and state regulation relating to, among other things:
|
·
|
facility and professional licensure;
|
|
·
|
conduct of operations;
|
|
·
|
certain clinical procedures;
|
|
·
|
addition of facilities and services, including certificates of need;
|
|
·
|
coding and billing for services; and
|
|
·
|
payment for services.
|
- 20 -
Both federal and state government agencies have increased coordinated civil and criminal enforcement efforts related to the healthcare industry. Regulations related to the healthcare industry are extremely complex and, in many instances, the industry does not have the benefit of significant regulatory or judicial interpretation of those laws. Medicare and Medicaid anti-fraud and abuse laws prohibit certain business practices and relationships related to items or services reimbursable under Medicare, Medicaid and other government healthcare programs, including the payment or receipt of remuneration to induce or arrange for referral of patients or recommendation for the provision of items or services covered by Medicare or Medicaid or any other federal or state healthcare program. Federal and state laws prohibit the submission of false or fraudulent claims, including claims to obtain reimbursement under Medicare and Medicaid. Although we have implemented a compliance program to help assure compliance with these regulations as they become effective, different interpretations or enforcement of these laws and regulations in the future could subject our current practices to allegations of impropriety or illegality or could require us to make changes in our facilities, equipment, personnel, services or the manner in which we conduct our business. If we fail to comply with government regulations, we or our clients could lose reimbursements or suffer civil or criminal penalties, which could result in cancellation of our contracts and a decrease in revenues.
Beyond these healthcare industry-specific regulatory risks, we are also subject to all of the same federal, state and local rules and regulations that apply to other publicly traded companies and large employers. We are subject to a myriad of federal, state and local laws regulating, for example, the issuance of securities, employee rights and benefits, workers compensation and safety, and many other activities attendant with our business. Failure to comply with such regulations, even if unintentional, could materially impact our financial results.
If our LTACHs fail to maintain their certification as long-term acute care hospitals, then our profitability may decline.
As of December 31, 2010, all of our 29 long-term acute care hospitals were certified by Medicare as LTACHs. If our LTACHs fail to meet or maintain the standards for certification as long-term acute care hospitals, such as average minimum length of patient stay, they will receive payments under the PPS applicable to general acute care hospitals rather than payment under the system applicable to LTACHs. Payments at rates applicable to general acute care hospitals would result in our LTACHs receiving less Medicare reimbursement than they currently receive for their patient services and our profit margins would likely decrease.
Expiration of the moratorium imposed on certain federal regulations otherwise applicable to LTACHs operated as freestanding or grandfathered “hospital in a hospital” (“HIH”) or grandfathered “satellites” may have an adverse effect on our future net operating revenues and profitability.
Medicare payments to our LTACHs are made pursuant to PPS applicable to LTACHs (“LTACH-PPS”). In addition, some LTACHs are subject to the so-called 25% Rule which requires that 25% or fewer of the patients admitted to the facility are referred from the same source. Admissions beyond the 25% threshold are paid using lower inpatient PPS rates. On May 1, 2007, CMS released a final rule extending the 25% Rule to all LTACHs, including those LTACHs that have previously operated under a statutory grandfathering exemption. We refer to such final rule as “the May 2007 final rule.”
- 21 -
Prior to the May 2007 final rule, the 25% admissions threshold was applicable only to Medicare HIH admissions from hospitals co-located with an LTACH or LTACH satellite. Under the May 2007 final rule, HIHs that admit Medicare patients from non-co-located hospitals, freestanding LTACHs and grandfathered LTACH HIHs are all subject to the Medicare admission thresholds. To the extent that any LTACH’s or LTACH satellite facility’s discharges that are admitted from an individual hospital (regardless of whether the referring hospital is co-located with the LTACH or LTACH satellite) exceed the applicable percentage threshold during a particular cost reporting period, the payment rate for those discharges would be subject to a downward payment adjustment. Cases admitted in excess of the applicable threshold would be reimbursed at inpatient PPS rates which are generally lower than LTACH-PPS rates. Cases reaching outlier status at the short term acute care hospital prior to admission to an LTACH do not count toward the threshold and would be paid under LTACH-PPS.
The 2007 SCHIP Extension Act provided regulatory relief for a three year period to LTACHs to ensure continued access to current long-term acute care hospital services. PPACA further extended the relief under the 2007 SCHIP Extension Act through 2012. Specifically, the PPACA legislation provided that the 25% Rule will not be applied to freestanding LTACHs and grandfathered LTACHs such as the one we operate in New Orleans until after cost reporting periods beginning on or after July 1, 2012.
When the moratorium period expires on December 31, 2012, the May 2007 final rule will be applied as it was originally written unless the moratorium is extended through new legislation. When the moratorium expires, it could have an adverse financial impact on our net operating revenues and profitability.
The moratorium on the Medicare certification of new LTACHs and beds in existing LTACHs could limit our ability to increase LTACH bed capacity, expand into new geographic regions, or increase services in existing areas we serve.
The 2007 SCHIP Extension Act imposed a three-year moratorium, beginning on December 29, 2007, on the establishment and classification of new LTACHs, LTACH satellite facilities and LTACH beds in existing LTACH or satellite facilities. PPACA extended this moratorium by two additional years. The moratorium does not apply to LTACHs that, before December 29, 2007, (i) began the qualifying period for payment under the LTACH-PPS, (ii) had a written agreement with an unrelated party for the construction, renovation, lease or demolition for a LTACH and had expended at least 10% of the estimated cost of the project or $2,500,000, or (iii) had obtained an approved certificate of need. The moratorium also does not apply to an increase in beds in an existing hospital or satellite facility if the LTACH is located in a state where there is only one other LTACH and the LTACH requests an increase in beds following the closure or the decrease in the number of beds of the other LTACH. We may acquire LTACHs that were in existence prior to December 29, 2007, and would not expect this moratorium to materially impact our strategy to expand by acquiring additional LTACHs if such LTACHs can be acquired at attractive valuations. This moratorium could, however, otherwise adversely affect our ability to increase LTACH bed capacity, expand into new geographic regions, or increase bed capacity in existing areas we serve.
Changes in federal or state law limiting or prohibiting certain physician referrals may preclude physicians from investing in our hospitals or referring to hospitals in which they already own an interest.
The federal self referral law, or “Stark Law,” prohibits a physician who has a financial relationship with an entity from referring his or her Medicare or Medicaid patients to that entity for certain designated health services, including inpatient and outpatient hospital services. Physicians who have a direct or indirect ownership interest in a hospital will not be prohibited from referring to the hospital because of the applicability of the “whole hospital exception” to the Stark Law. With the enactments of PPACA and the expiration of the whole hospital exception on December 31, 2010, we must now adhere to the new laws which restrict the expansion of both existing physician ownership percentages and the number of beds, procedural rooms or operating rooms. Furthermore, our existing physician owned locations in Dallas and Houston, TX will be subject to new disclosure and transparency requirements beginning in March of 2013 in order to maintain their status. There can be no assurance that new legislation or regulation further prohibiting or limiting physician referrals to physician-owned hospitals will not be successfully enacted in the future. If such federal or state laws are adopted, among other outcomes, physicians who have invested in our hospitals could be precluded from referring to, investing in or continuing to be physician owners of a hospital.
- 22 -
Our hospitals may be unable to reduce costs to offset completely any decreases in our revenues.
As of December 31, 2010, we owned and operated 29 LTACHs and five IRFs operating in 12 states. Reduced levels of occupancy in our facilities and reductions in reimbursements from Medicare, Medicaid or other payors would adversely impact our revenues and liquidity. We may be unable to put in place corresponding reductions in costs in response to declines in census or other revenue shortfalls. The inability to timely adjust our operations to address a decrease in our revenues could have a material adverse effect on our business, financial condition, results of operations and liquidity.
Our program management business operates in a highly competitive and fragmented market, and our success in that business depends on our ability to demonstrate that we can provide rehabilitation services more efficiently than our potential clients.
Competition for our program management business is highly fragmented and intense. Hospitals, skilled nursing facilities and other long-term care facilities that do not choose to outsource the management of their physical rehabilitation services are the primary competitors of our program management business. The fundamental challenge in our program management business is demonstrating to potential clients, primarily hospitals, skilled nursing facilities and other long-term care facilities, that we can provide rehabilitation services more efficiently than they can themselves. The programs we manage are in highly competitive markets and compete for patients with hospitals, skilled nursing facilities and long-term care facilities, as well as other larger companies such as HealthSouth Corporation, Kindred Healthcare, Inc. and Select Medical Corporation. Some of these competitors may be better capitalized, have greater name recognition, longer operating histories and their managers may have stronger relationships with physicians in the communities that they serve. All of these factors could give our competitors an advantage over us.
Competition may restrict our future growth by limiting our ability to make acquisitions or enter into joint ownership agreements at reasonable valuations.
We have historically faced competition in acquiring companies or entering into joint ownership agreements with partners in facilities complementary to our lines of business. Our competitors may acquire or seek to acquire many of the companies that would be suitable candidates for acquisition by us or enter into or seek to enter into joint ownership agreements with entities that would be suitable partners for us. This could limit our ability to grow by either acquisitions or joint ownership agreements, or make the cost of acquisitions or joint ownership arrangements higher and less attractive to us.
We may face difficulties integrating acquisitions into our operations, and our acquisitions may be unsuccessful, involve significant cash expenditures or expose us to unforeseen liabilities. Our joint ownership arrangements may be subject to similar difficulties, require significant cash expenditures or expose us to unforeseen liabilities.
We expect to continue pursuing acquisitions and joint ownership arrangements, each of which involve numerous risks, including:
- 23 -
|
·
|
difficulties integrating acquired personnel and distinct cultures into our business;
|
|
·
|
disagreements with our joint ownership partners;
|
|
·
|
incomplete due diligence or misunderstanding as to the target company’s future prospects;
|
|
·
|
diversion of management attention and capital resources from existing operations;
|
|
·
|
short-term (or longer lasting) dilution in the value of our shares;
|
|
·
|
over-paying for an acquired company or joint ownership entity due to incorrect analysis or because of competition from other companies for the same target;
|
|
·
|
inability to achieve forecasted revenues, cost savings or other synergies;
|
|
·
|
potential loss of key employees, customers or relationships; and
|
|
·
|
assumption of liabilities and exposure to unforeseen liabilities of acquired or joint ownership companies, including liabilities for failure to comply with healthcare regulations.
|
These acquisitions and joint ownership arrangements may also result in significant cash expenditures, incurrence of debt, impairment of goodwill and other intangible assets, and other expenses that could have a material adverse effect on our financial condition and results of operations.
Significant legal actions could subject us to substantial uninsured liabilities.
In recent years, healthcare providers have become subject to an increasing number of legal actions alleging malpractice, product liability, fraud, labor violations or related legal theories. Many of these actions involve complex claims that can be extraordinarily broad given the scope of our operations. They may also entail significant defense costs. To protect us from the cost of these claims, we maintain professional malpractice liability insurance, general liability insurance and employment practices liability coverage in amounts and with deductibles that we believe are appropriate for our operations. However, our insurance coverage may not cover all claims against us or continue to be available to us at a reasonable cost. If we are unable to maintain adequate insurance coverage, we may be exposed to substantial liabilities.
Our success depends on retention of our key officers.
Our future success depends in significant part on the continued service of our key officers. Competition for these individuals is intense and there can be no assurance that we will retain our key officers or that we can attract or retain other highly qualified executives in the future. The loss of any of our key officers could have a material adverse effect on our business, financial condition, results of operations and/or prospects.
We may have future capital needs and any future issuances of equity securities may result in dilution of the value of our common stock.
We anticipate that the amounts generated internally, together with amounts available under our credit facility, will be sufficient to implement our business plan for the foreseeable future, subject to additional needs that may arise if unexpected events occur or if a substantial acquisition or other growth opportunity becomes available. We may obtain additional capital through the public or private sale of debt or equity securities. If we sell equity securities, the value of our common stock could experience dilution. Furthermore, these securities could have rights, preferences and privileges more favorable than those of the common stock. We cannot be assured that additional capital will be available, or available on terms favorable to us. If capital is not available, we may not be able to fund internal or external business expansion or respond to competitive pressures.
- 24 -
We have incurred substantial indebtedness to grow our business and we may be unable to service or refinance this debt, which could have negative consequences on our business in the future and may place us at a competitive disadvantage in our industry.
As of December 31, 2010, we had total outstanding indebtedness of $398.5 million and total consolidated stockholders’ equity of $500.1 million. This high level of debt could have negative consequences. For example, it could:
|
·
|
result in our inability to comply with the financial and other restrictive covenants in our credit facilities;
|
|
·
|
increase our vulnerability to adverse industry and general economic conditions;
|
|
·
|
require us to dedicate a substantial portion of our cash flow from operations to make payments on our debt, thereby reducing the availability of our cash flow for working capital, capital investments and other business activities;
|
|
·
|
limit our ability to obtain additional financing to fund future working capital, capital investments and other business activities;
|
|
·
|
limit our ability to refinance our indebtedness on terms that are commercially reasonable, or at all;
|
|
·
|
expose us to the risk of interest rate fluctuations to the extent we pay interest at variable rates on the debt;
|
|
·
|
limit our flexibility to plan for, and react to, changes in our business and our industry; and
|
|
·
|
place us at a competitive disadvantage relative to our less leveraged competitors.
|
Our senior credit facilities contain restrictions that may limit our ability to pursue our business strategies.
Our senior credit facilities contain a number of covenants that impose significant operating and financial restrictions on us and may limit our ability to engage in acts that may be in our long-term best interests. These covenants restrict, among other things, our ability to:
|
·
|
incur or guarantee additional debt or issue certain preferred stock;
|
|
·
|
pay dividends or make distributions on our capital stock or certain subordinated debt or redeem, repurchase or retire our capital stock or certain subordinated debt;
|
|
·
|
make certain investments;
|
|
·
|
create liens on our or our subsidiaries’ assets;
|
|
·
|
make distributions from our joint ventures;
|
|
·
|
enter into transactions with affiliates;
|
|
·
|
merge or consolidate with another person or sell or otherwise dispose of all or substantially all of our assets;
|
|
·
|
enter into sales leaseback transactions;
|
|
·
|
sell assets, including capital stock of our subsidiaries;
|
|
·
|
alter the business that we conduct; and
|
|
·
|
change our fiscal year.
|
In addition, we are required to maintain a total leverage ratio, a senior leverage ratio and a fixed charge coverage ratio which become more restrictive over time. A breach of any covenant contained in the senior credit facilities could result in a default under those agreements. If any such default occurs, the lenders under the senior credit facilities may elect (after the expiration of any applicable notice or grace periods) to declare all outstanding borrowings, together with accrued and unpaid interest and other amounts payable thereunder, to be immediately due and payable. The lenders under the senior credit facilities will also have the right upon an event of default thereunder to terminate any commitments they have to provide further borrowings. If the debt under the senior credit facilities were to be accelerated, our assets may not be sufficient to repay in full that debt or any other debt that may become due as a result of that acceleration.
- 25 -
Uncertainty in the financial markets could limit the availability and terms of debt financing sources to fund the capital and liquidity requirements of our business.
One of the primary risks relating to current market conditions is the possibility that the lenders under our credit agreement will be unable to provide liquidity when needed. While we are not aware of any specific risks involving our counterparties, there can be no assurance that all of the lenders to our credit agreement will fulfill their commitments if we need to make additional draws against our revolving credit facility. In addition, a rapid increase in interest rates and/or a decline in our operating performance could impair our ability to comply with the financial covenants contained in our credit facility. A default due to the violation of these covenants could require us to immediately repay all amounts then outstanding under the credit facility. If we anticipate a potential covenant violation, we would seek relief from our lenders; however, such relief might not be granted or might be granted on terms less favorable than those in our existing credit agreement. As of December 31, 2010, we were in compliance with all debt covenants.
We depend on the proper functioning and availability of our information systems.
We are dependent on the proper functioning and availability of our information systems in operating our business. Our information systems are protected through physical and software safeguards. However, they are still vulnerable to facility infrastructure failure, fire, storm, flood, power loss, telecommunications failures, physical or software break-ins and similar events. Our business interruption insurance may be inadequate to protect us in the event of a catastrophe. We also retain confidential patient information in our database. It is critical that our facilities and infrastructure remain secure and are perceived by clients as secure. A material security breach could damage our reputation or result in liability to us. Despite the implementation of security measures, we may be vulnerable to losses associated with the improper functioning or unavailability of our information systems. From time to time, we may also modify our information systems to take advantage of new technologies. Such modifications may cause temporary disruptions to the operations of our business, which could have a material adverse effect on our results from operations in the periods affected.
Natural disasters, pandemics and other unexpected events, including earthquakes, hurricanes, fires and floods, could severely damage or interrupt our systems and operations and result in a material adverse effect on our business, financial condition and/or results of operations.
Natural disasters such as fire, flood, earthquake, hurricane and tornado and other events such as pandemic, power loss, computer virus, telecommunications failure, break-in or similar event could severely damage or interrupt our systems and operations, result in loss of data and/or delay or impair our ability to service our clients and patients. We have in place a disaster recovery plan that is intended to provide us with the ability to restore critical information systems; however, we do not have full redundancy for all of our information systems in the event of a natural disaster. There can be no assurance that our disaster recovery plan will prevent damage or interruption of our systems and operations if a natural disaster were to occur. Any such disaster or similar event could have a material adverse effect on our business, financial condition and/or results of operations.
- 26 -
Changes in federal and state income tax laws and regulations or adverse decisions by regulatory taxing authorities could cause a material adverse effect on our results of operations.
United States generally accepted accounting principles require financial statement recognition of a tax position taken or expected to be taken in a tax return, if that position is more likely than not of being sustained upon examination, based on the technical merits of the position. Management believes its estimates and judgments related to its uncertain tax positions are reasonable. Nevertheless, the ultimate resolution of our tax matters could differ from management’s estimates and such differences could be material. See Note 14 to our accompanying consolidated financial statements for additional information regarding our uncertain tax positions.
We are exposed to the credit risk of our payors which in the future may cause us to make larger allowances for doubtful accounts or incur bad debt write-offs.
Due to deteriorating economic conditions or other factors, commercial payors and customers may default on their payments to us and individual patients may default on co-payments and deductibles for which they are responsible under the terms of either commercial insurance programs or Medicare. Although we review the credit risk of our commercial payors and customers regularly, such risks will nevertheless arise from events or circumstances that are difficult to anticipate or control, such as a general economic downturn. If our payors default on their payments to us in the future, we may have to make larger allowances for doubtful accounts or incur bad debt write-offs, both of which may have an adverse impact on our profitability and cash flow.
Different interpretations of accounting principles could result in material changes to our reported results and financial condition.
U. S. generally accepted accounting principles (“GAAP”) are complex, continually evolving and may be subject to varied interpretation by third parties, including the SEC. Such varied interpretations could result from differing views related to specific facts and circumstances. Differences in interpretation of GAAP could result in material changes to our reported results and financial condition.
If we are found to have violated laws protecting the confidentiality of patient health information, we could be subject to civil or criminal penalties, which could increase our liabilities and harm our reputation or our business.
There are a number of federal and state laws protecting the confidentiality of certain patient health information, including patient records, and restricting the use and disclosure of that protected information. In particular, the U.S. Department of Health and Human Services promulgated patient privacy rules under the Health Insurance Portability and Accountability Act of 1996, as amended, or HIPAA. These privacy rules protect medical records and other personal health information by limiting their use and disclosure, giving individuals the right to access, amend and seek accounting of their own health information and limiting most use and disclosures of health information to the minimum amount reasonably necessary to accomplish the intended purpose. If we are found to be in violation of the privacy rules under HIPAA, we could be subject to civil or criminal penalties, which could increase our liabilities, harm our reputation and have a material adverse effect on our business, financial condition and results of operations.
| ITEM 1B. | UNRESOLVED STAFF COMMENTS |
None.
- 27 -
| ITEM 2. | PROPERTIES |
We currently lease approximately 71,000 square feet of executive office space in St. Louis, Missouri under a long-term lease which expires in September 2017 and includes options for us to renew the lease for an additional ten year period beyond the expiration date. In addition to the monthly rental cost, we are also responsible for a share of certain other facility charges and specified increases in operating costs.
We continue to operate Triumph’s headquarters, which are located in an 86,000 square foot medical office building in Houston, Texas. We own a controlling interest in the building and approximately 45,000 square feet of office space is leased out to physicians and other healthcare service providers.
Our hospitals generally lease the facilities that support their operations typically under long-term non-cancellable operating leases and our hospital facility leases represent the largest portion of our rent expense. As of December 31, 2010, 32 of our hospitals leased the facilities that support their operations and two hospitals owned their facilities. Our hospital leases generally have initial terms of 12 to 20 years, and most of our leases contain one or more options to extend the lease term for up to five additional years for each option. Our hospitals are generally responsible for property taxes, property and casualty insurance and routine maintenance expenses. Other than our principal executive offices and hospital facilities, none of our other properties are considered materially important.
Our principal executive offices, hospitals, and other properties are suitable for their respective uses and are, in general, adequate for our present needs. Our properties are subject to various federal, state, and local statutes and ordinances regulating their operation. Management does not believe compliance with such statutes and ordinances will materially affect our business, financial position, results of operations, or cash flows.
| ITEM 3. | LEGAL PROCEEDINGS |
On February 10, 2011, a purported class action complaint relating to Kindred’s proposed acquisition of us was filed in the Circuit Court of St. Louis County, Missouri, against us and certain of our directors and officers, as well as Kindred, by Arthur I. Murray, Jr., individually and on behalf of all of our stockholders, excluding the defendants and their affiliates. The complaint alleges, among other allegations, that the consideration our stockholders will receive in connection with the proposed transaction is inadequate and that the individual director and officer defendants breached their fiduciary duties to our stockholders in approving the Merger Agreement. The complaint further alleges that the individual director and officer defendants were aided and abetted in such breaches by us and Kindred. The complaint seeks various forms of relief, including injunctive relief that would, if granted, prevent the Merger from being consummated in accordance with the agreed-upon terms. The case is styled Arthur I. Murray, Jr. v. RehabCare Group, Inc., et al. (No. I.I.S.L. – CC00566, Circuit Court, St. Louis Co., MO). Another purported class action complaint, styled Norfolk County Retirement System v. Harry E. Rich, et al. (C.A. No. 6197 (DE (Wilmington) Court of Chancery) and filed on February 15, 2011, asserts substantially identical claims and seeks similar relief against us, certain of our directors and officers and Kindred, on behalf of all of our stockholders, excluding the defendants and their affiliates. We believe that these complaints are without merit and intend to defend them vigorously.
- 28 -
In the ordinary course of our business, we are a party to a number of other claims and lawsuits, as both plaintiff and defendant, which we regard as immaterial. From time to time, and depending upon the particular facts and circumstances, we may be subject to indemnification obligations under our various contracts. We do not believe that any liability resulting from such matters, after taking into consideration our insurance coverage and amounts already provided for, will have a material effect on our consolidated financial position or overall liquidity; however, such matters, or the expense of prosecuting or defending them, could have a material effect on cash flows and results of operations in a particular quarter or fiscal year as they develop or as new issues are identified.
| ITEM 4. | SUBMISSION OF MATTERS TO A VOTE OF SECURITY HOLDERS |
Not applicable.
- 29 -
PART II
|
|
ITEM 5.
|
MARKET FOR THE REGISTRANT’S COMMON STOCK, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES
|
Our common stock is listed and traded on the New York Stock Exchange under the symbol “RHB.” The following graph compares the cumulative total stockholder returns, assuming the reinvestment of dividends, of our common stock on an indexed basis with the New York Stock Exchange (“NYSE”) Market Index and the Dow Jones U.S. Health Care Providers Index for the five year period ended December 31, 2010. The graph assumes an investment of $100 made in our common stock and each index on January 1, 2006. We did not pay any dividends during the period reflected in the graph. The Company does not anticipate paying cash dividends in the foreseeable future. Our common stock price performance shown below should not be viewed as being indicative of future performance.
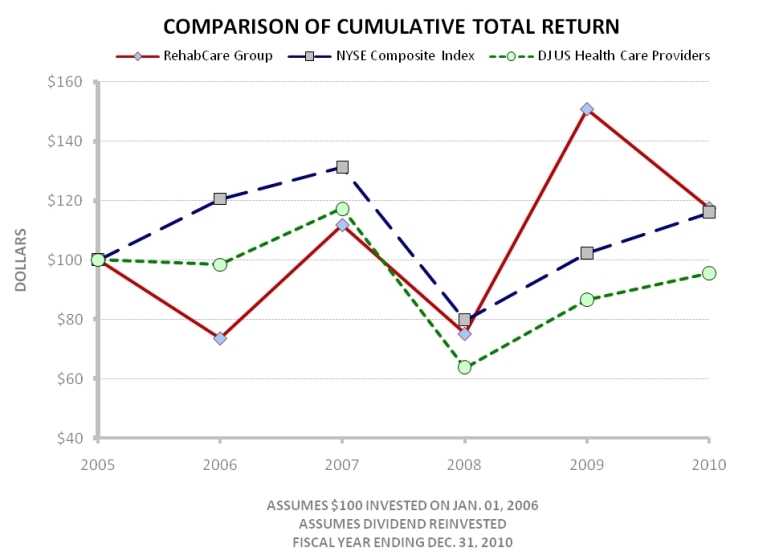
|
1/1/2006
|
12/31/2006
|
12/31/2007
|
12/31/2008
|
12/31/2009
|
12/31/2010
|
||||||
|
RehabCare Group
|
$100.00
|
$73.51
|
$111.68
|
$75.05
|
$150.64
|
$117.33
|
|||||
|
NYSE Market Index
|
$100.00
|
$120.47
|
$131.15
|
$79.67
|
$102.20
|
$115.88
|
|||||
|
Health Care Providers
|
$100.00
|
$98.43
|
$117.33
|
$63.74
|
$86.58
|
$95.51
|
- 30 -
As of January 31, 2011, there were 520 shareholders of record of the Company’s common stock and an estimated 7,900 persons or entities holding common stock in nominee name. The following table sets forth the high and low sales price per share of our common stock, as reported on the New York Stock Exchange, for the periods indicated. The stock price information is based on published financial sources.
|
Calendar Quarter
|
1st
|
2nd
|
3rd
|
4th
|
|||||
|
2010
|
High
|
$ |
34.19
|
$ |
31.52
|
$ |
22.21
|
$ |
23.77
|
|
Low
|
25.10
|
21.78
|
16.25
|
18.89
|
|||||
|
2009
|
High
|
$ |
18.75
|
$ |
23.93
|
$ |
25.65
|
$ |
31.29
|
|
Low
|
12.45
|
16.04
|
20.63
|
18.75
|
|||||
We did not purchase any of our equity securities during 2009 or 2010.
See Part III, Item 12, “Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters,” for information regarding common stock authorized for issuance under equity compensation plans.
| ITEM 6. | SELECTED FINANCIAL DATA |
The following table presents selected financial data for the periods indicated for our continuing operations only. See Item 7, “Management’s Discussion and Analysis of Financial Condition and Results of Operations,” and the notes to our accompanying consolidated financial statements for additional information regarding the financial data presented under this item.
- 31 -
|
SIX-YEAR FINANCIAL SUMMARY
|
|||||||||||||||||||||||
|
Dollars in thousands, except per share data
|
|||||||||||||||||||||||
|
(Year ended December 31,)
|
2010
|
2009
|
2008
|
2007
|
2006
|
2005
|
|||||||||||||||||
|
Consolidated statement of earnings data:
|
|||||||||||||||||||||||
|
Operating revenues
|
$
|
1,329,443
|
$
|
848,612
|
$
|
714,030
|
$
|
675,600
|
$
|
585,923
|
$
|
438,048
|
|||||||||||
|
Operating earnings
|
133,559
|
40,920
|
28,299
|
24,861
|
19,758
|
32,489
|
|||||||||||||||||
|
Amounts attributable to RehabCare: (2)
|
|||||||||||||||||||||||
|
Earnings (loss) from continuing operations
|
$
|
61,213
|
$
|
21,590
|
$
|
16,711
|
$
|
11,402
|
$
|
6,500
|
$
|
(17,447)
|
|||||||||||
|
Basic EPS from continuing operations
|
$
|
2.53
|
$
|
1.17
|
$
|
0.95
|
$
|
0.66
|
$
|
0.38
|
$
|
(1.04)
|
|||||||||||
|
Diluted EPS from continuing operations
|
$
|
2.48
|
$
|
1.14
|
$
|
0.94
|
$
|
0.65
|
$
|
0.38
|
$
|
(1.04)
|
|||||||||||
|
Weighted average shares outstanding (000s):
|
|||||||||||||||||||||||
|
Basic
|
24,231
|
18,481
|
17,583
|
17,226
|
17,008
|
16,751
|
|||||||||||||||||
|
Diluted
|
24,706
|
18,862
|
17,798
|
17,459
|
17,243
|
16,751
|
|||||||||||||||||
|
Consolidated balance sheet data:
|
|||||||||||||||||||||||
|
Working capital
|
$
|
117,613
|
$
|
110,882
|
$
|
97,284
|
$
|
80,285
|
$
|
85,982
|
$
|
60,664
|
|||||||||||
|
Total assets
|
1,126,569
|
1,109,980
|
438,406
|
408,560
|
428,296
|
272,925
|
|||||||||||||||||
|
Total liabilities
|
605,586
|
650,360
|
160,606
|
163,271
|
217,431
|
74,677
|
|||||||||||||||||
|
Total equity
|
520,983
|
459,620
|
277,800
|
245,289
|
210,865
|
198,248
|
|||||||||||||||||
|
Financial statistics:
|
|||||||||||||||||||||||
|
Operating margin
|
10.0%
|
4.8%
|
4.0%
|
3.7%
|
3.4%
|
7.4%
|
|||||||||||||||||
|
Net margin (2)
|
4.6%
|
2.5%
|
2.3%
|
1.7%
|
1.1%
|
(4.0)%
|
|||||||||||||||||
|
Current ratio
|
1.7:1
|
1.7:1
|
2.1:1
|
1.9:1
|
1.9:1
|
1.9:1
|
|||||||||||||||||
|
Diluted EPS growth rate (2)
|
117.5%
|
21.3%
|
44.6%
|
71.1%
|
136.5%
|
(176.5)%
|
|||||||||||||||||
|
Return on equity (1) (2)
|
12.5%
|
5.9%
|
6.4%
|
5.0%
|
3.2%
|
(8.6)%
|
|||||||||||||||||
|
Operating statistics:
|
|||||||||||||||||||||||
|
Hospitals:
|
|||||||||||||||||||||||
|
Number of hospitals at end of year (3)
|
34
|
33
|
10
|
7
|
6
|
4
|
|||||||||||||||||
|
Number of patient discharges (3)
|
17,984
|
7,054
|
4,620
|
3,946
|
2,640
|
732
|
|||||||||||||||||
|
Program management:
|
|||||||||||||||||||||||
|
Inpatient units:
|
|||||||||||||||||||||||
|
Average number of programs
|
116
|
121
|
122
|
127
|
137
|
145
|
|||||||||||||||||
|
Average admissions per program
|
396
|
393
|
377
|
363
|
360
|
372
|
|||||||||||||||||
|
Outpatient programs:
|
|||||||||||||||||||||||
|
Average number of locations
|
31
|
35
|
33
|
35
|
41
|
42
|
|||||||||||||||||
|
Patient visits (000s)
|
1,078
|
1,264
|
983
|
1,006
|
1,130
|
1,146
|
|||||||||||||||||
|
Contract therapy:
|
|||||||||||||||||||||||
|
Average number of locations (4)
|
1,135
|
1,088
|
1,066
|
1,125
|
1,018
|
749
|
|
(1)
|
Based on average of beginning and ending equity.
|
|
(2)
|
The results for 2005 include after tax losses on our equity investment in InteliStaf Holdings, Inc. of $36.5 million or $2.18 per diluted share.
|
|
(3)
|
We entered the freestanding hospitals business on August 1, 2005 with the acquisition of substantially all of the operating assets of MeadowBrook Healthcare, Inc. Effective November 24, 2009, we acquired Triumph HealthCare Holdings, Inc., which added 20 long-term acute care hospitals to our portfolio of hospitals.
|
|
(4)
|
Effective July 1, 2006, we acquired Symphony Health Services, LLC and its RehabWorks business, which added 470 contract therapy locations.
|
- 32 -
|
ITEM 7.
|
MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS
|
Overview
We operate in the following two business segments, which are managed separately based on fundamental differences in operations: program management services and hospitals. Program management services include hospital rehabilitation services (including inpatient acute and subacute rehabilitation and outpatient therapy programs) and skilled nursing rehabilitation services (including contract therapy in skilled nursing facilities, resident-centered management consulting services and staffing services for therapists and nurses). Our hospitals segment owns and operates 29 long-term acute care hospitals (LTACHs) and 5 inpatient rehabilitation hospitals.
|
Year Ended December 31,
|
|||||||||
|
2010
|
2009
|
2008
|
|||||||
|
(in thousands)
|
|||||||||
|
Revenues:
|
|||||||||
|
Program management:
|
|||||||||
|
Skilled nursing rehabilitation services
|
$
|
516,278
|
$
|
496,250
|
$
|
457,229
|
|||
|
Hospital rehabilitation services
|
180,009
|
178,168
|
165,658
|
||||||
|
Program management total
|
696,287
|
674,418
|
622,887
|
||||||
|
Hospitals
|
633,156
|
174,194
|
91,143
|
||||||
|
Total
|
$
|
1,329,443
|
$
|
848,612
|
$
|
714,030
|
|||
|
Operating Earnings (Loss):
|
|||||||||
|
Program management:
|
|||||||||
|
Skilled nursing rehabilitation services
|
$
|
39,184
|
$
|
37,753
|
$
|
25,544
|
|||
|
Hospital rehabilitation services
|
32,925
|
29,487
|
21,997
|
||||||
|
Program management total
|
72,109
|
67,240
|
47,541
|
||||||
|
Hospitals (1)
|
61,450
|
(26,066
|
)
|
(18,511
|
)
|
||||
|
Unallocated corporate expenses (2)
|
—
|
(254
|
)
|
(731
|
)
|
||||
|
Total
|
$
|
133,559
|
$
|
40,920
|
$
|
28,299
|
|||
|
|
(1)
|
The 2009 operating earnings of hospitals include $7.2 million of acquisition-related expenses for costs directly related to the acquisition of Triumph including fees for legal, accounting, advisory and other outside services.
|
|
|
(2)
|
Represents general corporate overhead costs associated with Phase 2 Consulting, Inc., which was sold on June 1, 2009.
|
Effective November 24, 2009, we acquired all of the outstanding common stock of Triumph HealthCare Holdings, Inc. (“Triumph”) for a purchase price of approximately $541.0 million. On the acquisition date, Triumph operated 20 LTACHs in seven states. Triumph’s results of operations have been included in our financial statements prospectively beginning after the date of acquisition. In 2009, we also acquired LTACHs in Dallas, Texas and Philadelphia, Pennsylvania and opened a majority-owned LTACH in Peoria, Illinois. In 2010, we opened an LTACH in Houston, Texas. These activities expanded the number of LTACHs we own and operate to 29, making us the third largest LTACH provider in the United States.
- 33 -
In November 2010, we announced that we had entered into an Equity Exchange Agreement with Select Medical Corporation under which we agreed to exchange our 60-bed inpatient rehabilitation hospital in Miami (the “Miami hospital”) for Select’s 70-bed long-term acute care hospital in northwest Indiana. This transaction closed on January 1, 2011. The Miami hospital has been classified as a discontinued operation pursuant to U.S. generally accepted accounting principles (“GAAP”). Prior year comparative amounts throughout Management’s Discussion and Analysis of Financial Condition and Results of Operations have been adjusted to reflect the treatment of the Miami hospital as a discontinued operation.
Effective June 1, 2009, we completed the sale of all the outstanding common stock of Phase 2 Consulting, Inc. (“Phase 2”) to Premier, Inc. for approximately $5.5 million. Phase 2 provides management and economic consulting services to the healthcare industry and had been a subsidiary of ours since it was acquired in 2004. This transaction allows our management to focus on its core businesses. Phase 2 has been classified as a discontinued operation pursuant to GAAP.
Sources of Revenue
In our program management segment, we derive the majority of our revenues from fees paid directly by healthcare providers rather than through payment or reimbursement by government or other third-party payors. A portion of our revenues in this segment are derived from our direct bill contract therapy rehab agencies. Our inpatient and outpatient therapy programs are typically provided through agreements with hospital clients with three to five-year terms. Our contract therapy services are typically provided under one to two year agreements primarily with skilled nursing facilities.
In our hospital segment, we derive nearly all of our revenues from fees for patient care services, which are usually paid for or reimbursed by Medicare, Medicaid or third party managed care programs. Our hospital segment accounted for 47.6% of our consolidated operating revenues in 2010. The following table identifies the primary payer sources and relative mix of our hospital segment’s net operating revenues for the periods stated:
|
Year Ended December 31,
|
|||||||||
|
2010
|
2009
|
2008
|
|||||||
|
Medicare
|
69.5
|
%
|
69.1
|
%
|
75.9
|
%
|
|||
|
Medicaid
|
1.2
|
2.1
|
0.7
|
||||||
|
Other third party payors
|
28.8
|
27.9
|
22.3
|
||||||
|
Self-pay
|
0.1
|
0.1
|
0.5
|
||||||
|
Total net patient revenue
|
99.6
|
99.2
|
99.4
|
||||||
|
Other revenue
|
0.4
|
0.8
|
0.6
|
||||||
|
100.0
|
%
|
100.0
|
%
|
100.0
|
%
|
||||
Triumph’s results of operations have been included in our hospital segment’s results prospectively beginning after the November 2009 date of acquisition. The decrease in the percent of net revenues attributable to Medicare from 2008 to 2010 reflects an increase in revenues attributable to managed Medicare and private fee-for-service plans that are included in “other third party payors” category in the table above. As part of the Balanced Budget Act of 1997, Congress created a program of private, managed healthcare coverage for Medicare beneficiaries. This program has been referred to as Medicare Part C, Medicare+Choice or Medicare Advantage. While we expect our payor mix will remain heavily weighted towards traditional Medicare, we could continue to see a shift of traditional Medicare patients into managed Medicare and private fee-for-service plans.
- 34 -
Results of Operations
The following table sets forth the percentage that selected items in the consolidated statements of earnings bear to operating revenues for the years ended December 31, 2010, 2009 and 2008:
|
Year Ended December 31,
|
|||||||||
|
2010
|
2009
|
2008
|
|||||||
|
Operating revenues
|
100.0
|
%
|
100.0
|
%
|
100.0
|
%
|
|||
|
Cost and expenses:
|
|||||||||
|
Operating
|
79.5
|
80.7
|
81.1
|
||||||
|
Selling, general and administrative
|
8.2
|
12.6
|
12.9
|
||||||
|
Depreciation and amortization
|
2.3
|
1.9
|
2.0
|
||||||
|
Operating earnings
|
10.0
|
4.8
|
4.0
|
||||||
|
Interest expense
|
(2.5
|
)
|
(0.7
|
)
|
(0.6
|
)
|
|||
|
Equity in net income of affiliate
|
0.1
|
0.1
|
0.1
|
||||||
|
Earnings from continuing operations before income taxes
|
7.6
|
4.2
|
3.5
|
||||||
|
Income taxes
|
2.7
|
1.9
|
1.4
|
||||||
|
Earnings from continuing operations, net of tax
|
4.9
|
2.3
|
2.1
|
||||||
|
Gain from discontinued operations, net of tax
|
0.1
|
0.2
|
0.2
|
||||||
|
Net earnings
|
5.0
|
2.5
|
2.3
|
||||||
|
Net (income) loss attributable to noncontrolling interests
|
(0.3
|
)
|
0.2
|
0.3
|
|||||
|
Net earnings attributable to RehabCare
|
4.7
|
%
|
2.7
|
%
|
2.6
|
%
|
|||
Twelve Months Ended December 31, 2010 Compared to Twelve Months Ended December 31, 2009
|
Revenues
|
||||||||
|
2010
|
2009
|
% Change
|
||||||
|
(dollars in thousands)
|
||||||||
|
Skilled nursing rehabilitation services
|
$
|
516,278
|
$
|
496,250
|
4.0
|
%
|
||
|
Hospital rehabilitation services
|
180,009
|
178,168
|
1.0
|
|||||
|
Hospitals
|
633,156
|
174,194
|
263.5
|
|||||
|
Consolidated revenues
|
$
|
1,329,443
|
$
|
848,612
|
56.7
|
%
|
||
Consolidated operating revenues increased from $848.6 million in 2009 to over $1.3 billion in 2010. The revenue increase primarily reflects the continued growth of our hospital and skilled nursing rehabilitation services. The 2010 growth in our hospital business is primarily due to the acquisition of Triumph on November 24, 2009 but also reflects same store revenue growth. Revenues for hospital rehabilitation services increased slightly in 2010.
Skilled Nursing Rehabilitation Services (SRS). SRS operating revenues increased $20.0 million or 4.0% from 2009 to 2010. The average number of contract therapy locations operated in 2010 grew 4.3% compared to 2009. Same store contract therapy revenues increased by 2.2% while minutes of service decreased by 0.1% in 2010 as compared to 2009. Same store revenues grew by 8.8% in 2009 as compared to 2008. The reduction in our same store revenue growth rate primarily reflects both pricing pressure resulting from a market basket decrease for skilled nursing facilities as per CMS’s final rule for rate year 2010, which was effective beginning on October 1, 2009, and a reduction in Medicare Part B therapy minutes delivered resulting from the elimination of the Part B therapy cap exception process during the months of January and February 2010. We also believe the higher same store revenue growth rate in the prior year reflected the continued development and implementation of clinical programs designed to achieve optimal outcomes, and there is currently less of an opportunity for incremental growth from such programs.
- 35 -
Hospital Rehabilitation Services (HRS). HRS operating revenues increased $1.8 million or 1.0% from 2009 to 2010 as inpatient revenue declined by 1.3% and outpatient revenue increased by 7.6%. The decline in inpatient revenue in 2010 was primarily due to a 4.1% decline in the average number of inpatient programs operated, partially offset by a 2.9% increase in average revenue per program. The increase in average revenue per program reflects same store inpatient rehabilitation facility (“IRF”) revenue and discharge growth of 3.7% and 3.8%, respectively, compared to 2009. HRS operated 105 IRF programs as of December 31, 2010 compared to 106 as of December 31, 2009. The increase in outpatient revenue in 2010 reflects a 23.2% increase in average revenue per program due to a 9.3% increase in outpatient same store revenues, a 7.6% increase in same store outpatient units of service and a significant change in contract mix. The average number of outpatient units operated declined by 12.7% in 2010.
Hospitals. Hospitals segment revenues increased $459.0 million or 263.5% from 2009 to 2010. Triumph, including the impact of new locations in Philadelphia and Houston Heights, contributed incremental revenues of $413.0 million in 2010. The increase in revenues in 2010 also reflects the June 2009 acquisition of an LTACH in Dallas, Texas and the August 2009 opening of an LTACH in Peoria, Illinois, which became certified as an LTACH effective May 1, 2010. Same store revenues increased by $12.7 million or 10.1% in 2010 reflecting a 3.1% increase in same store patient discharges and a 7.9% increase in same store revenue per patient day primarily attributable to improved case management.
|
Cost and Expenses
|
||||||||||||||
|
% of
|
% of
|
|||||||||||||
|
2010
|
Revenue
|
2009
|
Revenue
|
|||||||||||
|
(dollars in thousands)
|
||||||||||||||
|
Consolidated costs and expenses:
|
||||||||||||||
|
Operating expenses
|
$
|
1,056,671
|
79.5
|
%
|
$
|
684,312
|
80.7
|
%
|
||||||
|
Selling, general and administrative
|
108,618
|
8.2
|
107,130
|
12.6
|
||||||||||
|
Depreciation and amortization
|
30,595
|
2.3
|
16,250
|
1.9
|
||||||||||
|
Total costs and expenses
|
$
|
1,195,884
|
90.0
|
%
|
$
|
807,692
|
95.2
|
%
|
||||||
Operating expenses decreased as a percentage of revenues as a result of improved operating performance by our hospitals segment, particularly our legacy hospitals. Triumph also contributed to the hospital segment’s improvement in 2010. This impact was partially offset by an increase in SRS’s and HRS’s operating expenses as explained below. The decrease in selling, general and administrative expenses as a percentage of revenues reflects the increase in consolidated revenues, resulting in improved fixed overhead leverage, combined with the cost savings achieved by corporate and division realignment activities completed in 2009 and a reduction in corporate senior management incentive costs incurred in 2010. Selling, general and administrative expenses for 2009 also included approximately $7.2 million of external costs associated with the Triumph acquisition.
Our provision for doubtful accounts is included in operating expenses. On a consolidated basis, the provision for doubtful accounts increased by $2.6 million from $7.5 million in 2009 to $10.1 million in 2010. Triumph, which was acquired in November 2009, recorded provisions for doubtful accounts of $3.6 million and $0.3 million in 2010 and 2009, respectively.
- 36 -
|
% of
|
% of
|
|||||||||||||
|
Unit
|
Unit
|
|||||||||||||
|
2010
|
Revenue
|
2009
|
Revenue
|
|||||||||||
|
(dollars in thousands)
|
||||||||||||||
|
Skilled Nursing Rehabilitation Services:
|
||||||||||||||
|
Operating expenses
|
$
|
423,399
|
82.0
|
%
|
$
|
402,461
|
81.1
|
%
|
||||||
|
Selling, general and administrative
|
48,172
|
9.3
|
49,753
|
10.0
|
||||||||||
|
Depreciation and amortization
|
5,523
|
1.1
|
6,283
|
1.3
|
||||||||||
|
Total costs and expenses
|
$
|
477,094
|
92.4
|
%
|
$
|
458,497
|
92.4
|
%
|
||||||
|
Hospital Rehabilitation Services:
|
||||||||||||||
|
Operating expenses
|
$
|
127,550
|
70.9
|
%
|
$
|
124,758
|
70.0
|
%
|
||||||
|
Selling, general and administrative
|
17,312
|
9.6
|
21,500
|
12.1
|
||||||||||
|
Depreciation and amortization
|
2,222
|
1.2
|
2,423
|
1.3
|
||||||||||
|
Total costs and expenses
|
$
|
147,084
|
81.7
|
%
|
$
|
148,681
|
83.4
|
%
|
||||||
|
Hospitals:
|
||||||||||||||
|
Operating expenses
|
$
|
505,722
|
79.9
|
%
|
$
|
157,093
|
90.2
|
%
|
||||||
|
Selling, general and administrative
|
43,134
|
6.8
|
35,623
|
20.5
|
||||||||||
|
Depreciation and amortization
|
22,850
|
3.6
|
7,544
|
4.3
|
||||||||||
|
Total costs and expenses
|
$
|
571,706
|
90.3
|
%
|
$
|
200,260
|
115.0
|
%
|
||||||
Skilled Nursing Rehabilitation Services (SRS). Total SRS costs and expenses as a percentage of unit revenue remained flat in 2010 compared to 2009. Direct operating expenses increased as a percentage of unit revenue as a 3.9% increase in contract therapy labor and benefit costs per minute of service more than offset increases in average contract therapy revenue per minute. The increase in labor costs is primarily the result of lower therapist productivity in 2010 which we believe was negatively impacted by the rollout of our new point of service technologies to approximately 60% of our units, the transition to Minimum Data Set (MDS) 3.0 and a shift away from concurrent therapy to therapy in individual settings. This shift to therapy in individual settings began in September 2010 in anticipation of reimbursement rule changes on concurrent therapy that went into effect on October 1, 2010. Selling, general and administrative expenses as a percentage of unit revenue declined in 2010 primarily as a result of improvements in fixed overhead leverage combined with lower corporate and division management incentive costs. Depreciation and amortization expense decreased as certain fixed assets and intangible assets became fully amortized in 2010 and 2009. As a result of these factors combined with higher revenues, SRS’s operating earnings increased by approximately $1.4 million from $37.8 million in 2009 to $39.2 million in 2010.
Hospital Rehabilitation Services (HRS). Total HRS costs and expenses as a percentage of unit revenue decreased in 2010 compared to 2009 primarily due to a decrease in selling, general and administrative expenses. Operating expenses increased as a percentage of unit revenue in 2010 primarily due to a change in our outpatient contract mix. Selling, general and administrative expenses decreased primarily as a result of improvements in fixed overhead leverage combined with cost savings from corporate and division realignment activities that were completed in 2009 and a reduction in corporate senior management incentive costs. Depreciation and amortization expense decreased as certain fixed assets became fully amortized in 2009. HRS’s operating earnings increased from $29.5 million in 2009 to $32.9 million in 2010.
- 37 -
Hospitals. Total hospital segment costs and expenses as a percentage of unit revenue declined from 2009 to 2010 reflecting the incremental profit contributed by the Triumph hospitals, improved operating performance by our legacy hospitals and improved leverage of selling, general and administrative expenses and other operating expenses. Combined start-up and ramp-up losses decreased from $4.8 million in 2009 to $1.6 million in 2010. The 2009 losses primarily related to the ramp-up of our LTACH in Kansas City, Missouri and start-up of our LTACH in Peoria, Illinois while the 2010 losses relate entirely to the start-up and ramp-up of our LTACH in Peoria, Illinois. Additionally, the Dallas LTAC Hospital, which was acquired on June 30, 2009, improved its operating earnings by approximately $6.9 million from 2009 to 2010. Selling, general and administrative expenses decreased from the prior year largely due to improvements in fixed overhead leverage combined with a $9.9 million decrease in merger, acquisition and joint venture development expenses. Depreciation and amortization expense increased from 2009 to 2010 primarily due to depreciation and amortization associated with Triumph but declined as a percentage of revenue. The hospital segment generated operating earnings of $61.5 million in 2010 compared to an operating loss of $26.1 million in 2009. The Triumph hospitals contributed operating earnings of $64.1 million and $3.7 million in 2010 and 2009, respectively.
Non-operating Items
Interest expense increased from $5.5 million in 2009 to $33.2 million in 2010 primarily due to the net increase in borrowings which occurred in connection with funding the November 24, 2009 acquisition of Triumph. The balances outstanding on all forms of indebtedness were $398.5 million and $464.2 million at December 31, 2010 and 2009, respectively. These balances exclude unamortized original issue discounts. Interest expense includes interest incurred on all borrowings, amortization of deferred loan origination fees, amortization of original issue discounts, commitment fees paid on the unused portion of our line of credit and fees paid on outstanding letters of credit.
Earnings from continuing operations before income taxes increased to $101.4 million in 2010 from $35.9 million in 2009. The provision for income taxes was $36.6 million in 2010 and $16.3 million in 2009. The provision for income taxes as a percentage of income before taxes less net earnings attributable to noncontrolling interests was 37.4% in 2010 and 43.0% in 2009. The decrease in the effective tax rate reflects a lower overall weighted average statutory state tax rate resulting from the Triumph acquisition and a smaller unfavorable effective tax rate impact of permanent tax differences due to increased taxable income. In addition, during the second quarter of 2010, we recognized a $0.8 million tax benefit for the combined impact of the reversal of a contingency reserve due to a favorable ruling received from the Internal Revenue Service and the benefit of tax credits identified during the quarter. Finally, the higher effective tax rate in 2009 reflects the fact that certain acquisition-related expenses incurred in connection with the Triumph transaction were not deductible for tax purposes.
We recorded income from discontinued operations, net of tax, of approximately $1.2 million in 2010 and $1.4 million in 2009. Such income primarily relates to the operations of our Miami hospital, which was classified as held for sale as of December 31, 2010. Income from discontinued operations in 2009 is net of a $0.7 million after tax loss on the sale of Phase 2.
Net earnings (losses) attributable to noncontrolling interests in consolidated subsidiaries were $3.7 million and $(2.0) million in 2010 and 2009, respectively. Nearly all of our consolidated subsidiaries with a noncontrolling interest were profitable in 2010. The net losses in 2009 primarily relate to the recognition of the noncontrolling interests’ share of the losses incurred by our hospitals in Peoria, Kansas City and Dallas.
Net earnings attributable to RehabCare were $62.5 million in 2010 compared to $23.0 million in 2009. Diluted earnings per share attributable to RehabCare were $2.53 in 2010 compared to $1.22 in 2009.
- 38 -
Twelve Months Ended December 31, 2009 Compared to Twelve Months Ended December 31, 2008
|
Revenues
|
|||||||||
|
2009
|
2008
|
% Change
|
|||||||
|
(dollars in thousands)
|
|||||||||
|
Skilled nursing rehabilitation services
|
$
|
496,250
|
$
|
457,229
|
8.5
|
%
|
|||
|
Hospital rehabilitation services
|
178,168
|
165,658
|
7.6
|
||||||
|
Hospitals
|
174,194
|
91,143
|
91.1
|
||||||
|
Consolidated revenues
|
$
|
848,612
|
$
|
714,030
|
18.8
|
%
|
|||
Consolidated operating revenues increased from $714.0 million in 2008 to $848.6 million in 2009 due to growth in each of our business units.
Skilled Nursing Rehabilitation Services (SRS). SRS operating revenues increased $39.0 million or 8.5% from 2008 to 2009. Same store contract therapy revenues grew 8.8% reflecting a 5.7% increase in same store minutes of service. Higher average daily census, improved therapist productivity, a market basket adjustment for skilled nursing facilities which became effective October 1, 2008 and the continued development and implementation of clinical programs contributed to the growth in same store revenues. The average number of contract therapy locations operated during 2009 grew 2.1% compared to 2008.
Hospital Rehabilitation Services (HRS). HRS operating revenues increased 7.6% in 2009 as inpatient revenue increased 6.6% and outpatient revenue increased 10.4%. Inpatient average revenue per program increased 7.7% in 2009 reflecting a favorable change in the division’s contract mix which included a 2.7% increase in the average number of inpatient rehabilitation facility programs operated in 2009. In addition, same store revenues for inpatient rehabilitation facilities grew 2.4% and same store discharges increased 1.2% compared to 2008. The increase in outpatient revenue in 2009 reflects a 6.7% increase in the average number of units operated and a 7.4% increase in same store revenues.
Hospitals. Hospitals segment revenues increased $83.1 million or 91.1% from 2008 to 2009. The acquisition of Triumph contributed incremental revenues of $39.7 million in 2009. The increase in revenues in 2009 also reflects the June 2009 acquisition of an LTACH in Dallas, the June 2008 acquisition of The Specialty Hospital in Rome, Georgia, the November 2008 opening of a rehabilitation hospital in St. Louis, Missouri and the December 2008 certification of an LTACH in Kansas City, Missouri. Same store revenues increased by $9.4 million or 11.4% in 2009 as compared to 2008. One LTACH hospital contributed $5.4 million to the same store revenue growth primarily as a result of an increase in patient census.
|
Cost and Expenses
|
||||||||||||||
|
% of
|
% of
|
|||||||||||||
|
2009
|
Revenue
|
2008
|
Revenue
|
|||||||||||
|
(dollars in thousands)
|
||||||||||||||
|
Consolidated costs and expenses:
|
||||||||||||||
|
Operating expenses
|
$
|
684,312
|
80.7
|
%
|
$
|
579,179
|
81.1
|
%
|
||||||
|
Selling, general and administrative
|
107,130
|
12.6
|
92,177
|
12.9
|
||||||||||
|
Depreciation and amortization
|
16,250
|
1.9
|
14,375
|
2.0
|
||||||||||
|
Total costs and expenses
|
$
|
807,692
|
95.2
|
%
|
$
|
685,731
|
96.0
|
%
|
||||||
- 39 -
Operating expenses as a percentage of revenues decreased primarily due to improved operating performances by all of our businesses. The decrease in selling, general and administrative expenses as a percentage of revenues reflects the increase in revenues combined with the cost savings achieved by eliminating approximately 60 corporate and division support positions in the second half of 2008. These cost savings were more than offset by, an increase in both long-term and short-term management incentives, reflecting our improved overall performance , and an increase in selling, general and administrative expenses incurred by our hospital segment including approximately $7.2 million of external costs associated with the Triumph acquisition.
Our provision for doubtful accounts is included in operating expenses. On a consolidated basis, the provision for doubtful accounts decreased by $1.1 million from $8.6 million in 2008 to $7.5 million in 2009. Our HRS business decreased its provision by $1.2 million in 2009. HRS recorded a $1.2 million specific provision in 2008 related to our trade and note receivables due from Signature Healthcare Foundation. This specific provision was a result of Signature’s deteriorating financial condition during 2008. In February 2009, we terminated our staffing agreement with Signature and took possession of Signature’s operating assets in full satisfaction of our receivables from Signature.
|
% of
|
% of
|
|||||||||||||
|
Unit
|
Unit
|
|||||||||||||
|
2009
|
Revenue
|
2008
|
Revenue
|
|||||||||||
|
(dollars in thousands)
|
||||||||||||||
|
Skilled Nursing Rehabilitation Services:
|
||||||||||||||
|
Operating expenses
|
$
|
402,461
|
81.1
|
%
|
$
|
373,939
|
81.8
|
%
|
||||||
|
Selling, general and administrative
|
49,753
|
10.0
|
50,911
|
11.1
|
||||||||||
|
Depreciation and amortization
|
6,283
|
1.3
|
6,835
|
1.5
|
||||||||||
|
Total costs and expenses
|
$
|
458,497
|
92.4
|
%
|
$
|
431,685
|
94.4
|
%
|
||||||
|
Hospital Rehabilitation Services:
|
||||||||||||||
|
Operating expenses
|
$
|
124,758
|
70.0
|
%
|
$
|
118,291
|
71.4
|
%
|
||||||
|
Selling, general and administrative
|
21,500
|
12.1
|
22,729
|
13.7
|
||||||||||
|
Depreciation and amortization
|
2,423
|
1.3
|
2,641
|
1.6
|
||||||||||
|
Total costs and expenses
|
$
|
148,681
|
83.4
|
%
|
$
|
143,661
|
86.7
|
%
|
||||||
|
Hospitals:
|
||||||||||||||
|
Operating expenses
|
$
|
157,093
|
90.2
|
%
|
$
|
86,949
|
95.4
|
%
|
||||||
|
Selling, general and administrative
|
35,623
|
20.5
|
17,806
|
19.5
|
||||||||||
|
Depreciation and amortization
|
7,544
|
4.3
|
4,899
|
5.4
|
||||||||||
|
Total costs and expenses
|
$
|
200,260
|
115.0
|
%
|
$
|
109,654
|
120.3
|
%
|
||||||
Skilled Nursing Rehabilitation Services (SRS). Total SRS costs and expenses as a percentage of unit revenue decreased in 2009 compared to 2008 primarily due to an increase in therapist productivity and a decrease in selling, general and administrative expenses. Operating expenses declined as a percentage of unit revenue primarily due to a reduction in labor and benefit costs as a percentage of revenue. This was driven by therapist productivity improvements and lower contract labor usage in 2009 which more than offset the impact of wage rate and benefit cost increases. Improved therapist retention and a reduction in the time to fill permanent positions may have contributed to the decreased use of contract labor. Selling, general and administrative expenses decreased primarily due to the cost savings achieved from the division and corporate realignment activities that were completed in the second half of 2008. Depreciation and amortization expense decreased primarily due to lower depreciation associated with capitalized software which became fully depreciated in 2008. As a result of these factors combined with higher revenues, SRS’s operating earnings increased by approximately $12.3 million from $25.5 million in 2008 to $37.8 million in 2009.
- 40 -
Hospital Rehabilitation Services (HRS). Total HRS costs and expenses as a percentage of unit revenue decreased in 2009 compared to 2008 primarily due to improved operating performance and a decrease in selling, general and administrative expenses. Operating expenses decreased as a percentage of unit revenue in 2009 reflecting a favorable change in the division’s contract mix, which included an additional 2.9 IRF programs on average in 2009 as compared to 2008 as well as a lower provision for doubtful accounts primarily due the charge taken in 2008 for receivables from Signature. While the average number of IRF programs increased from 2008 to 2009, the actual number of IRF programs declined from 113 at the beginning of 2009 to 106 as of December 31, 2009. Selling, general and administrative expenses decreased primarily as a result of corporate and division realignment activities during late 2008 and early 2009, respectively. Depreciation and amortization expense decreased primarily due to lower depreciation associated with capitalized software which became fully depreciated in 2008. HRS’s operating earnings increased from $22.0 million in 2008 to $29.5 million in 2009.
Hospitals. Total hospital segment costs and expenses as a percentage of unit revenue decreased from 2008 to 2009. Operating expenses decreased as a percentage of unit revenue in 2009 primarily as a result of improved operating performance by our legacy LTACHs in 2009. In addition, Triumph’s hospitals generated operating profit of $3.7 million or 9.3% of revenue during the 37 days we owned Triumph in 2009. Combined start-up and ramp-up losses declined from $5.8 million in 2008 to $4.8 million in 2009. The 2009 losses relate primarily to the start-up of our LTACH in Peoria, Illinois and the ramp-up of our LTACH in Kansas City. We define the ramp-up phase for an LTACH as the period during which the hospital attempts to build its patient census following the receipt of its LTACH Medicare provider number. Selling, general and administrative expenses increased from the prior year largely due to costs incurred for acquisition and joint venture development activities and an investment in back office resources to support the growth of the business. In 2009, we incurred $7.2 million of acquisition-related expenses for outside costs directly related to the acquisition of Triumph and another $3.5 million of expenses for outside services related to other acquisition-related activities. In 2008, we incurred $1.8 million of expense related to outside services for canceled acquisitions and joint venture development projects. On January 1, 2009, we adopted a new accounting standard for business combinations which requires us to expense all acquisition-related costs. Prior to January 1, 2009, outside service costs incurred for consummated transactions were capitalized as a component of the acquisition cost and only costs related to canceled transactions were expensed. Depreciation and amortization expense increased from 2008 to 2009 primarily due to depreciation and amortization associated with Triumph and our other new facilities. As a result of these factors, the hospital segment incurred operating losses of $26.1 million in 2009 and $18.5 million in 2008.
Non-operating Items
Interest expense increased from $3.9 million in 2008 to $5.5 million in 2009 primarily due to the net increase in borrowings which occurred in connection with funding the November 24, 2009 acquisition of Triumph. The balances outstanding on all forms of indebtedness were $464.2 million and $57.0 million at December 31, 2009 and 2008, respectively. Interest expense includes interest incurred on all our borrowings, amortization of deferred loan origination fees, amortization of original issue discounts, commitment fees paid on the unused portion of our line of credit and fees paid on outstanding letters of credit.
Earnings from continuing operations before income taxes increased to $35.9 million in 2009 from $25.0 million in 2008. The provision for income taxes was $16.3 million in 2009 compared to $10.3 million in 2008. The provision for income taxes as a percentage of income before taxes less net earnings attributable to noncontrolling interests was 43.0% in 2009 and 38.2% in 2008. The increase in the effective tax rate in 2009 reflects the fact that certain acquisition-related expenses incurred in connection with the Triumph transaction were not deductible for tax purposes.
- 41 -
We recorded income from discontinued operations, net of tax, of approximately $1.4 million in 2009 and $2.0 million in 2008. Such income primarily relates to our Miami hospital, which was classified as held for sale as of December 31, 2010. Discontinued operations also include Phase 2, which was sold in the second quarter of 2009, and a rehabilitation hospital located in Midland, Texas, which was sold in the third quarter of 2008. The Company incurred an after tax loss of approximately $0.7 million on the sale of Phase 2 in 2009.
Net losses attributable to noncontrolling interests in consolidated subsidiaries were $2.0 million in both 2009 and 2008. The 2009 losses primarily relate to our hospitals in Peoria, Dallas and Kansas City while the 2008 losses primarily relate to our hospitals in Kansas City and St. Louis.
Net earnings attributable to RehabCare were $23.0 million in 2009 compared to $18.7 million in 2008. Diluted earnings per share attributable to RehabCare were $1.22 in 2009 compared to $1.05 in 2008.
Liquidity and Capital Resources
As of December 31, 2010, we had $23.2 million in cash and cash equivalents, and a current ratio, the amount of current assets divided by current liabilities, of 1.7 to 1. Net working capital increased by $6.7 million to $117.6 million at December 31, 2010 as compared to $110.9 million at December 31, 2009. Net accounts receivable were $222.2 million at December 31, 2010, compared to $199.4 million at December 31, 2009. The increase in net accounts receivable occurred primarily in our hospital segment and is primarily attributable to the increase in revenues. In addition, our Peoria hospital recently received its LTACH provider number and has retroactively billed Medicare back to May 1, 2010. Including Triumph, the number of days sales outstanding (“DSO”) in net receivables was 61.9, 60.2 and 66.0 at December 31, 2010, 2009 and 2008, respectively.
We generated cash from operations of $103.8 million, $48.1 million and $48.7 million in the years ended December 31, 2010, 2009 and 2008, respectively. Capital expenditures were $30.6 million, $13.2 million and $18.5 million in the years ended December 31, 2010, 2009 and 2008, respectively. Our capital expenditures primarily relate to the construction of new hospitals, investments in information technology systems, equipment additions and replacements and various other capital improvements. Over the next few years, we plan to continue to invest in information technology systems and the development and renovation of hospitals. As noted earlier, Triumph’s results of operations have been included in our financial statements prospectively beginning after the date of acquisition.
We have historically financed our operations with funds generated from operating activities and borrowings under credit facilities and long-term debt instruments. We believe our cash on hand, cash generated from operations and availability under our credit facility will be sufficient to meet our future working capital, capital expenditures, internal and external business expansion, and debt service requirements.
On November 24, 2009, we entered into a Credit Agreement (as defined in Note 9 to our accompanying consolidated financial statements). The Credit Agreement provides for a five-year revolving credit facility of $125 million and a swingline subfacility of up to $25 million. At December 31, 2010, the balance outstanding under the revolving credit facility was $1.4 million. As of December 31, 2010, we had $11.8 million in letters of credit issued to insurance carriers as collateral for reimbursement of claims. The letters of credit reduce the amount we may borrow under the revolving credit facility. As of December 31, 2010, after consideration of the effects of restrictive covenants, the available borrowing capacity under the line of credit was approximately $111.8 million.
- 42 -
The Credit Agreement also provided for a six-year $450 million term loan facility. At December 31, 2010, the balance outstanding under the term loan was $385.5 million. The term loan facility requires quarterly installments of $1,125,000 with the balance payable upon the final maturity. In addition, we are required to make mandatory principal prepayments equal to a portion of our consolidated excess cash flow (as defined in the Credit Agreement) when our consolidated leverage ratio reaches certain levels.
The Credit Agreement contains certain restrictive covenants that, among other things, limit the incurrence of additional indebtedness, investments, dividends, transactions with affiliates, asset sales, acquisitions, mergers and consolidations, liens and encumbrances and other matters customarily restricted in similar credit facilities. In addition, we are required to maintain on a consolidated basis a maximum ratio of total funded debt to earnings before interest, taxes, depreciation and amortization (“EBITDA” as defined in the Credit Agreement), a maximum ratio of senior funded debt to EBITDA and a minimum ratio of adjusted earnings before interest, taxes, depreciation, amortization, rent and operating lease expense (“Adjusted EBITDAR” as defined in the Credit Agreement) to fixed charges. As of December 31, 2010, we were in compliance with all debt covenants. If we anticipate a potential covenant violation, we would seek relief from our lenders; however, such relief might not be granted or might be granted on terms less favorable than those in our existing Credit Agreement.
In 2009, we issued 6,210,000 shares of our common stock in a public equity offering which resulted in net proceeds, after underwriting fees and other direct costs, of approximately $140.2 million. We used the net proceeds from the public equity offering along with the proceeds from our term loan facility to pay for the majority of the consideration used to acquire Triumph.
Inflation
Although inflation has abated during the last several years, the rate of inflation in healthcare related services continued to exceed the rate experienced by the economy as a whole. Our management contracts often provide for an annual increase in the fees paid to us by our clients based on increases in various inflation indices.
Effect of Recent Accounting Pronouncements
See Note 1 to the consolidated financial statements in Item 8 for a full description of recent accounting pronouncements, including the expected dates of adoption and estimated effects on results of operations and financial condition, which is incorporated herein by reference.
Commitments and Contractual Obligations
The following table summarizes our scheduled contractual commitments as of December 31, 2010 (in thousands):
- 43 -
|
Less than
|
2-3
|
4-5
|
More than
|
|||||||||||||||
|
Total
|
1 year
|
years
|
years
|
5 years
|
Other
|
|||||||||||||
|
Operating leases (1)
|
$
|
483,600
|
$
|
32,154
|
$
|
73,601
|
$
|
73,469
|
$
|
304,376
|
$
|
—
|
||||||
|
Purchase obligations (2)
|
3,620
|
1,158
|
2,462
|
—
|
—
|
—
|
||||||||||||
|
Long-term debt including capital lease obligations (3)
|
398,479
|
9,116
|
13,405
|
375,958
|
—
|
—
|
||||||||||||
|
Interest on long-term debt (4)
|
111,690
|
23,737
|
45,787
|
42,166
|
—
|
—
|
||||||||||||
|
Unrecognized tax benefits (5)
|
1,532
|
—
|
—
|
—
|
—
|
1,532
|
||||||||||||
|
Other long-term liabilities (6)
|
3,958
|
—
|
—
|
—
|
—
|
3,958
|
||||||||||||
|
Total
|
$
|
1,002,879
|
$
|
66,165
|
$
|
135,255
|
$
|
491,593
|
$
|
304,376
|
$
|
5,490
|
||||||
|
(1)
|
We lease many of our facilities under non-cancelable operating leases in the normal course of business. Some lease agreements provide us with the option to renew the lease. Our future operating lease obligations would change if we exercised these renewal options and if we entered into additional operating lease agreements. For more information, see Note 13 to our accompanying consolidated financial statements.
|
|
(2)
|
Purchase obligations include agreements to purchase goods or services that are enforceable and legally binding on us and that specify all significant terms. Purchase obligations exclude agreements that are cancelable without penalty.
|
|
(3)
|
The amount of long-term debt reported on our consolidated balance sheet at December 31, 2010 includes unamortized original issue discounts of approximately $7,591,000.
|
|
(4)
|
Interest on our variable rate debt is estimated using the rate in effect as of December 31, 2010. This line also includes interest related to capital lease obligations, but excludes the amortization of original issue discounts and the amortization of deferred loan fees.
|
|
(5)
|
Represents our total liability for unrecognized tax benefits based on the guidance in the Financial Accounting Standards Board’s Accounting Standards Codification Topic 740, “Income Taxes.” There is a high degree of uncertainty regarding the timing of future cash outflows associated with these liabilities, which involve various taxing authorities. As a result, we are unable to predict the timing of payments against this obligation.
|
|
(6)
|
We maintain a nonqualified deferred compensation plan for certain employees. Under the plan, participants may defer up to 70% of their salary and cash incentive compensation. The amounts are held in trust in investments designated by participants but remain our property until distribution. Because most distributions of funds are tied to the termination of employment or retirement of participants, we are not able to predict the timing of payments against this obligation. At December 31, 2010, we owned trust assets with a value approximately equal to the total amount of this obligation.
|
Critical Accounting Policies and Estimates
The preparation of our consolidated financial statements in conformity with accounting principles generally accepted in the United States of America requires us to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenues and expenses during the reporting period. Our estimates, judgments and assumptions are continually evaluated based on available information and experience. Because of the use of estimates inherent in the financial reporting process, actual results could differ from those estimates. Management has discussed and will continue to discuss its critical accounting policies with the audit committee of our board of directors.
- 44 -
Certain of our accounting policies require higher degrees of judgment than others in their application. These include accounting for business combinations, estimating the allowance for doubtful accounts, estimating contractual allowances, impairment of goodwill and other intangible assets, and establishing accruals for known and incurred but not reported health, workers compensation and professional liability claims. In addition, Note 1 to the consolidated financial statements includes further discussion of our significant accounting policies.
Management believes the following critical accounting policies affect our more significant judgments and estimates used in the preparation of our consolidated financial statements.
Business Combinations. We allocate the purchase price of acquired companies to the tangible assets acquired, intangible assets acquired and liabilities assumed based on their estimated fair values. The excess of the purchase price over these fair values is recorded as goodwill. We engage independent third-party appraisal firms to assist us in determining the fair values of assets acquired and liabilities assumed. Such valuations require management to make significant estimates and assumptions, especially with respect to intangible assets. The significant purchased intangible assets recorded by RehabCare include customer contracts, trade names and Medicare provider numbers. Critical estimates in valuing these intangible assets include but are not limited to discount rates, the asset’s remaining economic life and future expected cash flows generated by the assets. Management's estimates of fair value are based upon assumptions believed to be reasonable, but which are inherently uncertain and unpredictable and, as a result, actual results may differ from estimates.
Allowance for Doubtful Accounts. We make estimates of the collectability of our accounts receivable balances. We determine an allowance for doubtful accounts based upon an analysis of the collectability of specific accounts, historical experience and the aging of the accounts receivable. We specifically analyze customers with historical poor payment history and customer creditworthiness when evaluating the adequacy of the allowance for doubtful accounts. In our hospitals segment, the primary collection risks relate to the amounts for which the patient is responsible (deductibles and co-payments). Our accounts receivable balance as of December 31, 2010 was $222.2 million, net of allowance for doubtful accounts of $24.3 million. Our estimates of collectability require significant judgment. If our customers’ ability to make payments to us were to deteriorate beyond the levels estimated, additional allowances may be required. We continually evaluate the adequacy of our allowance for doubtful accounts and make adjustments in the periods any excess or shortfall is identified.
Contractual Allowances. Our hospitals recognize net patient revenue in the reporting period in which the services are performed based on our current billing rates, less actual adjustments and estimated discounts for contractual allowances. An individual patient’s bill is subject to adjustment on a patient-by-patient basis in the ordinary course of business by the payors following their review of each particular bill. We estimate the discounts for contractual allowances using the balance sheet approach on an individual hospital basis. Patient accounts receivable detail is analyzed to determine expected reimbursement for each patient. Expected reimbursement is summarized by payor classification and reconciled to the balance sheet. A secondary review is completed at the consolidated hospitals level to validate calculations. Estimates are regularly reviewed for accuracy by taking into consideration Medicare reimbursement rules and known changes to contract terms, laws and regulations and payment history. If such information indicates that our allowances are overstated or understated, we reduce or provide for additional allowances as appropriate in the period in which we make such a determination.
- 45 -
Laws and regulations governing Medicare and Medicaid programs are complex and subject to interpretation. As a result, there is at least a reasonable possibility that recorded estimates will change by a material amount. The estimated reimbursement amounts are adjusted in subsequent periods as cost reports are prepared and filed and as final settlements are determined. We did not record any significant adjustments for prior year Medicare or Medicaid cost reports in 2010, 2009 or 2008. We are not aware of any material claims, disputes, or unsettled matters with third-party payors.
Goodwill and Other Intangible Assets. The cost of acquired companies is allocated first to their identifiable assets, both tangible and intangible, based on estimated fair values. Costs allocated to identifiable intangible assets with finite lives are generally amortized on a straight-line basis over the remaining estimated useful lives of the assets. The excess of the purchase price over the fair value of identifiable assets acquired, net of liabilities assumed, is recorded as goodwill.
Under GAAP, goodwill and identifiable intangible assets with indefinite lives are not amortized but must be reviewed at least annually for impairment. If the impairment test indicates that the carrying value of an intangible asset exceeds its fair value, then an impairment loss should be recognized in the consolidated statement of earnings in an amount equal to the excess carrying value. No impairments of identifiable intangible assets with indefinite-lives were identified during the three years ended December 31, 2010.
As required by GAAP, we evaluate goodwill for impairment annually and whenever events or changes in circumstances indicate the carrying value of the goodwill may not be recoverable. Goodwill impairment is determined using a two-step process. The first step is to identify if a potential impairment exists by comparing the fair value of each reporting unit to its carrying amount. If the fair value of a reporting unit exceeds its carrying amount, goodwill of that reporting unit is not considered to have a potential impairment and the second step of the impairment test is not necessary. However, if the carrying amount of a reporting unit exceeds its fair value, the second step is performed to determine the implied fair value of a reporting unit’s goodwill, by comparing the reporting unit’s fair value to the allocated fair values of all assets and liabilities, including any unrecognized intangible assets, as if the reporting unit had been acquired in a business combination. If the carrying amount of goodwill exceeds its implied fair value, an impairment is recognized in an amount equal to that excess.
Reporting units are defined as an operating segment or one level below an operating segment. Our primary reporting units are our skilled nursing rehabilitation services, hospital rehabilitation services and hospital businesses. We calculated the fair value of each reporting unit based on a discounted cash flow analysis which requires us to make assumptions and estimates about future cash flows and discount rates. These assumptions are often subjective and can be affected by a variety of factors, including external factors such as economic trends and government regulations, and internal factors such as changes in our forecasts or in our business strategies. We believe the assumptions used in our impairment analysis are reasonable and appropriate; however, different assumptions and estimates could affect the results of our impairment analysis and in turn result in an impairment charge. We could be required to evaluate the recoverability of goodwill prior to the annual assessment if we experience disruptions to the business, unexpected significant declines in operating results, a divestiture of a significant component of our business, significant declines in market capitalization or other triggering events. In addition, as our business or the way we manage our business changes, our reporting units may also change. These types of events and the resulting analyses could result in goodwill impairment charges in the future which could materially impact our reported earnings in the periods such charges occur.
At December 31, 2010, unamortized goodwill related to our skilled nursing rehabilitation services, hospital rehabilitation services and hospitals businesses was $79.4 million, $39.7 million and $440.7 million, respectively. We have not recorded any goodwill impairments during the three years ended December 31, 2010. Our most recent impairment test was performed as of December 31, 2010. A 10% decrease in the calculated fair value of each of our reporting units as of December 31, 2010 would not have resulted in a potential goodwill impairment. However, for our hospitals reporting unit, a 15% decrease in the fair value of the reporting unit would have resulted in a potential goodwill impairment. The amount of impairment loss, if any, would be determined during the second step of the impairment test.
- 46 -
Health, Workers Compensation, and Professional Liability Insurance Accruals. We maintain an accrual for our health, workers compensation and professional liability claim costs that are partially self-insured and are classified in accrued salaries and wages (health insurance) and accrued expenses (workers compensation and professional liability) in our consolidated balance sheets. At December 31, 2010, the combined amount of these accruals was approximately $23.1 million. We determine the adequacy of these accruals by periodically evaluating our historical experience and trends related to health, workers compensation, and professional liability claims and payments, based on actuarial computations and industry experience and trends. In analyzing the accruals, we also consider the nature and severity of the claims, analyses provided by third party claims administrators, as well as current legal, economic and regulatory factors. If such information indicates that our accruals are overstated or understated, we reduce or provide for additional accruals as appropriate in the period in which we make such a determination. The ultimate cost of these claims may be greater than or less than the established accruals. While we believe that the recorded amounts are appropriate, there can be no assurances that changes to management’s estimates will not occur due to limitations inherent in the estimation process.
We are subject to various claims and legal actions in the ordinary course of our business. Some of these matters include professional liability and employee-related matters. Our hospital and healthcare facility clients may also become subject to claims, governmental inquiries and investigations and legal actions to which we may become a party relating to services provided by our professionals. From time to time, and depending upon the particular facts and circumstances, we may be subject to indemnification obligations under our contracts with our hospital and healthcare facility clients relating to these matters. Although we are currently not aware of any such pending or threatened litigation that we believe is reasonably likely to have a material adverse effect on us, if we become aware of such claims against us, we will evaluate the probability of an adverse outcome and provide accruals for such contingencies as necessary.
Forward-Looking Statements
This annual report contains historical information, as well as forward-looking statements that involve known and unknown risks and relate to future events, our future financial performance or our projected business results. In some cases, forward-looking statements can be identified by terminology such as “may,” “will,” “should,” “expects,” “plans,” “anticipates,” “believes,” “estimates,” “predicts,” “targets,” “potential,” or “continue” or the negative of these terms or other comparable terminology. These statements are made on the basis of our views and assumptions as of the time the statements are made and we undertake no obligation to update these statements. We caution investors that any such forward-looking statements we make are not guarantees of future performance and that actual results may differ materially from anticipated results or expectations expressed in our forward-looking statements as a result of a variety of factors. While it is impossible to identify all such factors, some of the factors that could impact our business and cause actual results to differ materially from forward-looking statements are discussed in Item 1A, “Risk Factors.”
| ITEM 7A. | QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK |
The Company’s primary market risk exposure consists of changes in interest rates on certain borrowings that bear interest at floating rates. Interest rate changes on variable rate debt impact our interest expense and cash flows, but do not impact the fair value of the underlying debt instruments. Borrowings under our revolving credit facility bear interest at our option at either a base rate or the London Interbank Offering Rate (“LIBOR”) for one, two, three or six month interest periods, or a nine or twelve month period if available, plus an applicable margin percentage. The base rate is the greater of the federal funds rate plus one-half of 1%, Bank of America N.A.’s prime rate or one month LIBOR plus 1%. The applicable margin percentage is based upon our consolidated total leverage ratio. As of December 31, 2010, the balance outstanding under the revolving credit facility was $1.4 million and the interest rate on such borrowings was 5.75%. A 100 basis point increase in the interest rate charged on the revolving credit facility would result in additional interest expense of approximately $14,000 on an annualized basis.
- 47 -
Borrowings under our term loan facility bear interest at our option at either the base rate plus 300 basis points or LIBOR plus 400 basis points with a LIBOR floor of 200 basis points. As of December 31, 2010, the balance outstanding against the term loan facility was $385.5 million. At December 31, 2010, the term loan facility was subject to a one-month LIBOR contract and the one-month LIBOR rate was 0.26% resulting in an all-in interest rate of 6.0% due to the 2.0% LIBOR floor and the 400 basis point margin. Based on the $385.5 million of term loan debt outstanding at December 31, 2010, a 100 basis point increase in the one-month LIBOR rate would result in no additional interest expense (as a result of the LIBOR floor). A 200 basis point increase in the LIBOR rate would result in additional interest expense of approximately $1.0 million on an annualized basis.
At December 31, 2010, we were not a party to any derivative financial instruments.
- 48 -
| ITEM 8. | FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA |
|
Report of Independent Registered Public Accounting Firm
|
50
|
|
Consolidated Balance Sheets as of December 31, 2010 and 2009
|
52
|
|
Consolidated Statements of Earnings for the years
|
|
|
ended December 31, 2010, 2009 and 2008
|
53
|
|
Consolidated Statements of Comprehensive Income for the years
|
|
|
ended December 31, 2010, 2009 and 2008
|
54
|
|
Consolidated Statements of Changes in Equity for the years
|
|
|
ended December 31, 2010, 2009 and 2008
|
55
|
|
Consolidated Statements of Cash Flows for the years
|
|
|
ended December 31, 2010, 2009 and 2008
|
56
|
|
Notes to the Consolidated Financial Statements
|
57
|
- 49 -
Report of Independent Registered Public Accounting Firm
The Board of Directors and Stockholders
RehabCare Group, Inc.:
We have audited the accompanying consolidated balance sheets of RehabCare Group, Inc. (the Company) as of December 31, 2010 and 2009, and the related consolidated statements of earnings, comprehensive income, changes in equity, and cash flows for each of the years in the three-year period ended December 31, 2010. We also have audited the Company’s internal control over financial reporting as of December 31, 2010, based on criteria established in Internal Control – Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO). The Company’s management is responsible for these consolidated financial statements, for maintaining effective internal control over financial reporting, and for its assessment of the effectiveness of internal control over financial reporting, included in the accompanying “Management’s Report on Internal Control over Financial Reporting”. Our responsibility is to express an opinion on these consolidated financial statements and an opinion on the Company’s internal control over financial reporting based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audits to obtain reasonable assurance about whether the financial statements are free of material misstatement and whether effective internal control over financial reporting was maintained in all material respects. Our audits of the consolidated financial statements included examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements, assessing the accounting principles used and significant estimates made by management, and evaluating the overall financial statement presentation. Our audit of internal control over financial reporting included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, and testing and evaluating the design and operating effectiveness of internal control based on the assessed risk. Our audits also included performing such other procedures as we considered necessary in the circumstances. We believe that our audits provide a reasonable basis for our opinions.
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
- 50 -
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the financial position of RehabCare Group, Inc. as of December 31, 2010 and 2009, and the results of its operations and its cash flows for each of the years in the three-year period ended December 31, 2010, in conformity with U.S. generally accepted accounting principles. Also in our opinion, the Company maintained, in all material respects, effective internal control over financial reporting as of December 31, 2010, based on criteria established in Internal Control – Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission.
The Company adopted FASB Financial Accounting Standard No. 141(R), Business Combinations (included in FASB ASC Topic 805, Business Combinations), as of January 1, 2009.

St. Louis, Missouri
February 28, 2011
- 51 -
REHABCARE GROUP, INC.
Consolidated Balance Sheets
(dollars in thousands, except per share data)
|
December 31,
|
|||||||
|
Assets
|
2010
|
2009
|
|||||
|
Current assets:
|
|||||||
|
Cash and cash equivalents
|
$
|
23,205
|
$
|
24,690
|
|||
|
Accounts receivable, net of allowance for doubtful accounts of $24,273 and $24,729, respectively
|
222,179
|
199,447
|
|||||
|
Deferred tax assets
|
21,034
|
21,249
|
|||||
|
Other current assets
|
14,559
|
17,116
|
|||||
|
Total current assets
|
280,977
|
262,502
|
|||||
|
Marketable securities, trading
|
3,965
|
3,314
|
|||||
|
Property and equipment, net
|
119,591
|
111,814
|
|||||
|
Goodwill
|
559,866
|
568,492
|
|||||
|
Intangible assets, net
|
127,227
|
135,406
|
|||||
|
Assets held for sale
|
10,407
|
—
|
|||||
|
Investment in unconsolidated affiliate
|
4,913
|
4,761
|
|||||
|
Other
|
19,623
|
23,691
|
|||||
|
Total assets
|
$
|
1,126,569
|
$
|
1,109,980
|
|||
|
Liabilities and Equity
|
|||||||
|
Current liabilities:
|
|||||||
|
Current portion of long-term debt
|
$
|
9,116
|
$
|
7,507
|
|||
|
Accounts payable
|
16,440
|
14,615
|
|||||
|
Accrued salaries and wages
|
78,863
|
80,138
|
|||||
|
Income taxes payable
|
2,906
|
97
|
|||||
|
Accrued expenses
|
56,039
|
49,263
|
|||||
|
Total current liabilities
|
163,364
|
151,620
|
|||||
|
Long-term debt, less current portion
|
381,772
|
447,760
|
|||||
|
Deferred compensation
|
3,958
|
3,352
|
|||||
|
Deferred tax liabilities
|
54,755
|
45,605
|
|||||
|
Other
|
1,737
|
2,023
|
|||||
|
Total liabilities
|
605,586
|
650,360
|
|||||
|
Stockholders’ equity:
|
|||||||
|
Preferred stock, $.10 par value; authorized 10,000,000 shares, none issued and outstanding
|
—
|
—
|
|||||
|
Common stock, $.01 par value; authorized 60,000,000 shares, issued 28,304,789 shares and 28,036,014 shares as of December 31, 2010 and 2009, respectively
|
283
|
280
|
|||||
|
Additional paid-in capital
|
292,078
|
291,771
|
|||||
|
Retained earnings
|
262,441
|
199,991
|
|||||
|
Less common stock held in treasury at cost; 4,002,898 shares as of December 31, 2010 and 2009
|
(54,704
|
)
|
(54,704
|
)
|
|||
|
Total stockholders’ equity
|
500,098
|
437,338
|
|||||
|
Noncontrolling interests
|
20,885
|
22,282
|
|||||
|
Total equity
|
520,983
|
459,620
|
|||||
|
Total liabilities and equity
|
$
|
1,126,569
|
$
|
1,109,980
|
|||
See accompanying notes to consolidated financial statements.
- 52 -
REHABCARE GROUP, INC.
Consolidated Statements of Earnings
(in thousands, except per share data)
|
Year Ended December 31,
|
||||||||||||
|
2010
|
2009
|
2008
|
||||||||||
|
Operating revenues
|
$
|
1,329,443
|
$
|
848,612
|
$
|
714,030
|
||||||
|
Costs and expenses:
|
||||||||||||
|
Operating
|
1,056,671
|
684,312
|
579,179
|
|||||||||
|
Selling, general and administrative
|
108,618
|
107,130
|
92,177
|
|||||||||
|
Depreciation and amortization
|
30,595
|
16,250
|
14,375
|
|||||||||
|
Total costs and expenses
|
1,195,884
|
807,692
|
685,731
|
|||||||||
|
Operating earnings
|
133,559
|
40,920
|
28,299
|
|||||||||
|
Interest income
|
98
|
98
|
143
|
|||||||||
|
Interest expense
|
(33,167
|
)
|
(5,546
|
)
|
(3,897
|
)
|
||||||
|
Other income
|
319
|
12
|
21
|
|||||||||
|
Equity in net income of affiliate
|
640
|
431
|
471
|
|||||||||
|
Earnings from continuing operations before income taxes
|
101,449
|
35,915
|
25,037
|
|||||||||
|
Income taxes
|
36,559
|
16,291
|
10,312
|
|||||||||
|
Earnings from continuing operations, net of tax
|
64,890
|
19,624
|
14,725
|
|||||||||
|
Gain from discontinued operations, net of tax
|
1,237
|
1,365
|
1,994
|
|||||||||
|
Net earnings
|
66,127
|
20,989
|
16,719
|
|||||||||
|
Net (earnings) loss attributable to noncontrolling interests
|
(3,677
|
)
|
1,966
|
1,986
|
||||||||
|
Net earnings attributable to RehabCare
|
$
|
62,450
|
$
|
22,955
|
$
|
18,705
|
||||||
|
Amounts attributable to RehabCare stockholders:
|
||||||||||||
|
Earnings from continuing operations, net of tax
|
$
|
61,213
|
$
|
21,590
|
$
|
16,711
|
||||||
|
Gain from discontinued operations, net of tax
|
1,237
|
1,365
|
1,994
|
|||||||||
|
Net earnings
|
$
|
62,450
|
$
|
22,955
|
$
|
18,705
|
||||||
|
Basic earnings per share attributable to RehabCare:
|
||||||||||||
|
Earnings from continuing operations, net of tax
|
$
|
2.53
|
$
|
1.17
|
$
|
0.95
|
||||||
|
Gain from discontinued operations, net of tax
|
0.05
|
0.07
|
0.11
|
|||||||||
|
Net earnings
|
$
|
2.58
|
$
|
1.24
|
$
|
1.06
|
||||||
|
Diluted earnings per share attributable to RehabCare:
|
||||||||||||
|
Earnings from continuing operations, net of tax
|
$
|
2.48
|
$
|
1.14
|
$
|
0.94
|
||||||
|
Gain from discontinued operations, net of tax
|
0.05
|
0.08
|
0.11
|
|||||||||
|
Net earnings
|
$
|
2.53
|
$
|
1.22
|
$
|
1.05
|
||||||
See accompanying notes to consolidated financial statements.
- 53 -
REHABCARE GROUP, INC.
Consolidated Statements of Comprehensive Income
(in thousands)
|
Year Ended December 31,
|
||||||||||
|
2010
|
2009
|
2008
|
||||||||
|
Net earnings
|
$
|
66,127
|
$
|
20,989
|
$
|
16,719
|
||||
|
Other comprehensive income (loss), net of tax:
|
||||||||||
|
Changes in the fair value of derivative designated as a cash flow hedge, net of income tax expense (benefit) of $0, $267 and $(226), respectively
|
—
|
424
|
(358
|
)
|
||||||
|
Total other comprehensive income (loss), net of tax
|
—
|
424
|
(358
|
)
|
||||||
|
Comprehensive income
|
66,127
|
21,413
|
16,361
|
|||||||
|
Comprehensive (income) loss attributable to noncontrolling interests
|
(3,677
|
)
|
1,966
|
1,986
|
||||||
|
Comprehensive income attributable to RehabCare
|
$
|
62,450
|
$
|
23,379
|
$
|
18,347
|
||||
See accompanying notes to consolidated financial statements.
- 54 -
REHABCARE GROUP, INC.
Consolidated Statements of Changes in Equity
(in thousands)
|
Amounts Attributable to RehabCare Stockholders
|
|||||||||||||||||||||
|
Accumulated
|
|||||||||||||||||||||
|
Additional
|
other
|
Non-
|
|||||||||||||||||||
|
Common
|
paid-in
|
Retained
|
Treasury
|
comprehensive
|
controlling
|
Total
|
|||||||||||||||
|
stock
|
capital
|
earnings
|
stock
|
earnings (loss)
|
interests
|
equity
|
|||||||||||||||
|
Balance, December 31, 2007
|
$
|
215
|
$
|
140,246
|
$
|
158,331
|
$
|
(54,704
|
)
|
$
|
(66
|
)
|
$
|
1,267
|
$
|
245,289
|
|||||
|
Net earnings (loss)
|
—
|
—
|
18,705
|
—
|
—
|
(1,986
|
)
|
16,719
|
|||||||||||||
|
Changes in the fair value of derivative, net of tax
|
—
|
—
|
—
|
—
|
(358
|
)
|
—
|
(358
|
)
|
||||||||||||
|
Stock-based compensation
|
—
|
3,195
|
—
|
—
|
—
|
—
|
3,195
|
||||||||||||||
|
Activity under stock plans
|
2
|
2,206
|
—
|
—
|
—
|
—
|
2,208
|
||||||||||||||
|
Contributions made by noncontrolling interests
|
—
|
—
|
—
|
—
|
—
|
10,747
|
10,747
|
||||||||||||||
|
Balance, December 31, 2008
|
217
|
145,647
|
177,036
|
(54,704
|
)
|
(424
|
)
|
10,028
|
277,800
|
||||||||||||
|
Net earnings (loss)
|
—
|
—
|
22,955
|
—
|
—
|
(1,966
|
)
|
20,989
|
|||||||||||||
|
Changes in the fair value of derivative, net of tax
|
—
|
—
|
—
|
—
|
424
|
—
|
424
|
||||||||||||||
|
Sale of common stock
|
62
|
140,187
|
—
|
—
|
—
|
—
|
140,249
|
||||||||||||||
|
Stock-based compensation
|
—
|
4,662
|
—
|
—
|
—
|
—
|
4,662
|
||||||||||||||
|
Activity under stock plans
|
1
|
1,275
|
—
|
—
|
—
|
—
|
1,276
|
||||||||||||||
|
Business combinations
|
—
|
—
|
—
|
—
|
—
|
11,591
|
11,591
|
||||||||||||||
|
Contributions made by noncontrolling interests
|
—
|
—
|
—
|
—
|
—
|
4,423
|
4,423
|
||||||||||||||
|
Distributions to noncontrolling interests
|
—
|
—
|
—
|
—
|
—
|
(1,794
|
)
|
(1,794
|
)
|
||||||||||||
|
Balance, December 31, 2009
|
280
|
291,771
|
199,991
|
(54,704
|
)
|
—
|
22,282
|
459,620
|
|||||||||||||
|
Net earnings
|
—
|
—
|
62,450
|
—
|
—
|
3,677
|
66,127
|
||||||||||||||
|
Stock-based compensation
|
—
|
3,940
|
—
|
—
|
—
|
—
|
3,940
|
||||||||||||||
|
Activity under stock plans
|
3
|
3,698
|
—
|
—
|
—
|
—
|
3,701
|
||||||||||||||
|
Contributions made by noncontrolling interests
|
—
|
—
|
—
|
—
|
—
|
2,354
|
2,354
|
||||||||||||||
|
Distributions to noncontrolling interests
|
—
|
—
|
—
|
—
|
—
|
(2,728
|
)
|
(2,728
|
)
|
||||||||||||
|
Purchase of noncontrolling interests in subsidiaries
|
—
|
(7,331
|
)
|
—
|
—
|
—
|
(4,700
|
)
|
(12,031
|
)
|
|||||||||||
|
Balance, December 31, 2010
|
$
|
283
|
$
|
292,078
|
$
|
262,441
|
$
|
(54,704
|
)
|
$
|
—
|
$
|
20,885
|
$
|
520,983
|
||||||
See accompanying notes to consolidated financial statements.
- 55 -
REHABCARE GROUP, INC.
Consolidated Statements of Cash Flows
(in thousands)
|
Year Ended December 31,
|
|||||||||||||
|
2010
|
2009
|
2008
|
|||||||||||
|
Cash flows from operating activities:
|
|||||||||||||
|
Net earnings
|
$
|
66,127
|
$
|
20,989
|
$
|
16,719
|
|||||||
|
Reconciliation to net cash provided by operating activities:
|
|||||||||||||
|
Depreciation and amortization
|
30,808
|
16,522
|
14,886
|
||||||||||
|
Provision for doubtful accounts
|
10,209
|
7,794
|
10,178
|
||||||||||
|
Equity in net income of affiliate
|
(640
|
)
|
(431
|
)
|
(471
|
)
|
|||||||
|
Stock-based compensation
|
3,940
|
4,662
|
3,195
|
||||||||||
|
Income tax benefit related to stock options exercised
|
1,890
|
916
|
812
|
||||||||||
|
Excess tax benefit related to stock options exercised
|
(962
|
)
|
(405
|
)
|
(564
|
)
|
|||||||
|
Loss (gain) on disposal of discontinued operation
|
—
|
1,188
|
(321
|
)
|
|||||||||
|
Gain on disposal of property and equipment
|
(319
|
)
|
(12
|
)
|
(21
|
)
|
|||||||
|
Changes in assets and liabilities:
|
|||||||||||||
|
Accounts receivable, net
|
(32,941
|
)
|
(5,837
|
)
|
(11,318
|
)
|
|||||||
|
Other current assets
|
2,413
|
(6,821
|
)
|
846
|
|||||||||
|
Accounts payable
|
1,825
|
(3,478
|
)
|
2,328
|
|||||||||
|
Accrued salaries and wages
|
(1,070
|
)
|
5,715
|
4,952
|
|||||||||
|
Income taxes payable and deferred taxes
|
10,643
|
477
|
4,456
|
||||||||||
|
Accrued expenses
|
6,776
|
6,212
|
2,629
|
||||||||||
|
Other assets and other liabilities
|
5,139
|
599
|
352
|
||||||||||
|
Net cash provided by operating activities
|
103,838
|
48,090
|
48,658
|
||||||||||
|
Cash flows from investing activities:
|
|||||||||||||
|
Additions to property and equipment
|
(30,579
|
)
|
(13,215
|
)
|
(18,502
|
)
|
|||||||
|
Purchase of marketable securities
|
(783
|
)
|
(476
|
)
|
(509
|
)
|
|||||||
|
Proceeds from sale/maturities of marketable securities
|
506
|
607
|
546
|
||||||||||
|
Proceeds from disposition of business
|
—
|
5,043
|
7,193
|
||||||||||
|
Purchase of businesses, net of cash acquired
|
—
|
(549,783
|
)
|
(8,408
|
)
|
||||||||
|
Other, net
|
(125
|
)
|
(27
|
)
|
(406
|
)
|
|||||||
|
Net cash used in investing activities
|
(30,981
|
)
|
(557,851
|
)
|
(20,086
|
)
|
|||||||
|
Cash flows from financing activities:
|
|||||||||||||
|
Net change in revolving credit facility
|
1,400
|
(57,000
|
)
|
(11,500
|
)
|
||||||||
|
Proceeds from the issuance of long-term debt
|
—
|
450,000
|
—
|
||||||||||
|
Debt issuance costs
|
—
|
(28,448
|
)
|
—
|
|||||||||
|
Principal payments on long-term debt
|
(67,080
|
)
|
(1,749
|
)
|
(6,000
|
)
|
|||||||
|
Net proceeds from the sale of common stock
|
—
|
140,249
|
—
|
||||||||||
|
Cash contributed by noncontrolling interests
|
2,354
|
4,423
|
3,663
|
||||||||||
|
Cash distributed to noncontrolling interests
|
(2,728
|
)
|
(1,794
|
)
|
—
|
||||||||
|
Purchase of noncontrolling interests in subsidiaries
|
(12,031
|
)
|
—
|
—
|
|||||||||
|
Activity under stock plans
|
2,781
|
992
|
1,809
|
||||||||||
|
Excess tax benefit related to stock options exercised
|
962
|
405
|
564
|
||||||||||
|
Net cash provided by (used in) financing activities
|
(74,342
|
)
|
507,078
|
(11,464
|
)
|
||||||||
|
Net (decrease) increase in cash and cash equivalents
|
(1,485
|
)
|
(2,683
|
)
|
17,108
|
||||||||
|
Cash and cash equivalents at beginning of year
|
24,690
|
27,373
|
10,265
|
||||||||||
|
Cash and cash equivalents at end of year
|
$
|
23,205
|
$
|
24,690
|
$
|
27,373
|
|||||||
See accompanying notes to consolidated financial statements.
- 56 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements
December 31, 2010, 2009 and 2008
| (1) | Overview of Company and Summary of Significant Accounting Policies |
Overview of Company
RehabCare Group, Inc. (“the Company”) is a leading provider of program management services for inpatient rehabilitation and skilled nursing units, outpatient therapy programs and contract therapy services in conjunction with more than 1,250 hospitals, skilled nursing facilities, outpatient facilities and other long-term care facilities throughout the United States. RehabCare also operates five rehabilitation hospitals and 29 long term acute care hospitals, which provide specialized acute care for medically complex patients.
Effective November 24, 2009, the Company acquired all of the outstanding common stock of Triumph HealthCare Holdings, Inc. (“Triumph”). On the acquisition date, Triumph operated 20 LTACHs in seven states. Triumph’s results of operations have been included in the Company’s financial statements prospectively beginning after the date of acquisition. As a result of the acquisition of Triumph, the Company believes it is now the third largest LTACH provider in the United States.
Basis of Presentation and Principles of Consolidation
The accompanying consolidated financial statements of the Company and its subsidiaries were prepared in accordance with generally accepted accounting principles in the United States of America (“GAAP”) and include the accounts of the Company and all of its wholly owned subsidiaries, majority-owned subsidiaries over which the Company exercises control and, when applicable, entities for which the Company has a controlling financial interest. All significant intercompany balances and transactions have been eliminated in consolidation.
The Company uses the equity method to account for its investments in entities that the Company does not control but has the ability to exercise significant influence over the entity’s operating and financial policies.
Certain prior year amounts have been reclassified to conform to current year presentation. Such reclassifications primarily relate to the Company’s 60-bed inpatient rehabilitation hospital in Miami, Florida (the “Miami hospital”), which has been classified as held for sale as of December 31, 2010. The Company reclassified its consolidated statements of earnings for the years ended December 31, 2009 and 2008 to show the results of operations for the Miami hospital as discontinued operations.
Cash Equivalents and Marketable Securities
Cash in excess of daily requirements is invested in short-term investments with original maturities of three months or less. Such investments are deemed to be cash equivalents for purposes of the consolidated statements of cash flows.
The Company classifies its debt and equity securities into one of three categories: held-to-maturity, trading, or available-for-sale. Management determines the appropriate classification of its investments at the time of purchase and reevaluates such determination at each balance sheet date. Investments at December 31, 2010 and 2009 consist of noncurrent marketable equity and debt securities. All noncurrent marketable securities are classified as trading, with all investment income, including unrealized gains or losses recognized in the consolidated statements of earnings. Noncurrent marketable securities include assets held in trust for the Company’s deferred compensation plan that are not available for operating purposes.
- 57 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
Accounts Receivable and Credit Risk
The Company’s program management services segment provides services to a geographically diverse clientele of healthcare providers throughout the United States. The Company performs ongoing credit evaluations of its clientele and does not require collateral. The Company’s hospital segment is reimbursed for its services primarily by Medicare and other third party payors. As such, the hospital segment’s primary collection risks relate to the amounts for which the patient is responsible (such as deductibles and co-payments).
An allowance for doubtful accounts is maintained at a level which management believes is sufficient to cover anticipated credit losses. The Company determines its allowance for doubtful accounts based upon an analysis of the collectability of specific accounts, historical experience and the aging of the accounts receivable. The Company specifically analyzes customers with historical poor payment history and customer creditworthiness when evaluating the adequacy of the allowance for doubtful accounts. The Company continually evaluates the adequacy of its allowance for doubtful accounts and makes adjustments in the periods any excess or shortfall is identified. Accounts are written off after all collection efforts (internal and external) have been exhausted.
At December 31, 2010, the Company’s hospital segment accounted for $106.2 million or 47.8% of the Company’s total net accounts receivable and $7.5 million or 30.7% of the Company’s total allowance for doubtful accounts. A significant portion of Triumph’s business is concentrated in Houston, Texas. Because the hospital segment is primarily reimbursed by Medicare and other third party payors, the Company believes concentrations by type of payor are more meaningful than geographic concentrations. The following table identifies the sources and relative mix of the hospital segment’s net accounts receivable as of the dates stated:
|
As of December 31,
|
||||||
|
Hospital segment
|
2010
|
2009
|
||||
|
Medicare
|
62.9
|
%
|
58.7
|
%
|
||
|
Medicaid
|
2.3
|
2.8
|
||||
|
Other third party payors
|
32.4
|
36.8
|
||||
|
Self-pay
|
2.4
|
1.6
|
||||
|
Total net patient accounts receivable
|
100.0
|
99.9
|
||||
|
Other receivables
|
—
|
0.1
|
||||
|
Total net accounts receivable
|
100.0
|
%
|
100.0
|
%
|
||
During the years ended December 31, 2010, 2009, and 2008, approximately 69.5%, 69.1%, and 75.9%, respectively, of the hospital segment’s net operating revenues related to patients participating in the Medicare program. Because Medicare traditionally pays claims faster than other third-party payors, the hospital segment’s percentage of accounts receivable from Medicare is less than its percentage of net operating revenues from Medicare. While revenues and accounts receivable from the Medicare program are significant to the Company’s operations, the Company does not believe there are significant credit risks associated with these receivables.
- 58 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
Derivative Instruments and Hedging Activities
GAAP requires that every derivative instrument be recorded in the balance sheet as either an asset or a liability measured at its fair value. In December 2007, the Company entered into an interest rate swap agreement to reduce the Company’s exposure to changes in interest rates on certain borrowings that bear interest at floating rates. The swap agreement expired in December 2009. This swap agreement was designated as a cash flow hedge. Therefore, the unrealized gains and losses resulting from the change in fair value of the swap contract were reflected in other comprehensive income. Realized gains and losses were reclassified to interest expense in the period in which the related interest payments being hedged were made. The Company formally documented its hedging relationships, including identification of the hedging instruments and hedged items, as well as the Company’s risk management objectives and strategies for undertaking each hedge transaction.
Property and Equipment
Property and equipment are initially recorded at cost. Depreciation and amortization of property and equipment are computed using the straight-line method over the estimated useful lives of the related assets, principally: equipment – three to seven years; buildings – 39 years; and leasehold improvements – life of asset or life of lease, whichever is less. Upon retirement or disposition, the cost and related accumulated depreciation are removed from the accounts and any gain or loss is included in the results of operations. Repairs and maintenance are expensed as incurred.
Goodwill and Other Intangible Assets
Under GAAP, the cost of acquired companies is allocated first to their identifiable assets, both tangible and intangible, based on estimated fair values. The excess of the purchase price over the fair value of identifiable assets acquired, net of liabilities assumed, is recorded as goodwill. Goodwill and intangible assets with indefinite lives are not amortized to expense, but instead tested for impairment at least annually and any related losses recognized in earnings when identified. See Note 7, “Goodwill and Other Intangible Assets,” for further discussion. Other identifiable intangible assets with a finite life are amortized on a straight-line basis over their estimated lives.
Long-Lived Assets
The Company reviews identified intangible and other long-lived assets for impairment whenever events or changes in circumstances indicate that the carrying value of the asset may not be recoverable. If such events or changes in circumstances are present, an impairment loss would be recognized if the sum of the expected future net cash flows was less than the carrying amount of the asset.
Disclosure About Fair Value of Financial Instruments
At December 31, 2010, the Company’s financial instruments consist of cash equivalents, accounts receivable, marketable securities, accounts payable and long-term debt. The carrying values of cash equivalents, accounts receivable and accounts payable approximate fair value due to their relatively short-term nature. The carrying values of long-term debt were $390.9 million and $455.3 million at December 31, 2010 and 2009, respectively. The fair values of long-term debt were $398.7 million and $464.2 million at December 31, 2010 and 2009, respectively, and are based on the interest rates offered for borrowings with comparable maturities. The Company’s marketable securities (which had carrying values of $4.0 million and $3.3 million at December 31, 2010 and 2009, respectively) are recorded at fair value. See Note 18, “Fair Value Measurements,” for additional information.
- 59 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
Revenue Recognition
In the Company’s program management services segment, the Company derives a significant majority of its revenues from fees paid directly by healthcare providers (i.e., acute care hospitals and skilled nursing facilities) rather than through payment or reimbursement by government or other third-party payors. Revenues are generally recognized as services are provided to patients based on the contractually agreed upon rate per unit of service, rate per patient discharge, a negotiated patient per diem rate, or a negotiated fee schedule based on the type of service rendered. The Company’s inpatient business also accrues revenues at the end of each period for services provided to patients that have not been discharged by the period end based on the number of patient days completed as a percentage of the average length of stay for the facility under contract.
The Company’s hospitals segment derives substantially all of its revenues from fees for patient care services, which are usually reimbursed by Medicare, Medicaid or third party managed care programs. The Company’s hospitals recognize net patient revenues in the reporting period in which the services are performed based on our current gross billing rates, less actual adjustments and estimated discounts for contractual allowances. These allowances are principally required for patients covered by Medicare, Medicaid, managed care health plans and other third-party payors. Laws governing the Medicare and Medicaid programs are complex and subject to interpretation. All healthcare providers participating in the Medicare and Medicaid programs are required to meet certain financial reporting requirements. Federal regulations require submission of annual cost reports covering medical costs and expenses associated with the services provided by each facility to program beneficiaries. Annual cost reports required under the Medicare and Medicaid programs are subject to routine audits, which may result in adjustments to the amounts ultimately determined to be due to the Company under these reimbursement programs. We did not record any significant adjustments for prior year Medicare or Medicaid cost reports in 2010, 2009 or 2008.
In estimating the discounts for contractual allowances, the Company reduces its gross patient receivables to the estimated amount that will be recovered for the service rendered based upon previously agreed to rates with the payor. These estimates are regularly reviewed for accuracy by taking into consideration Medicare reimbursement rules and known changes to payor contract terms, laws and regulations and payment history. If such information indicates that the Company’s allowances are overstated or understated, the Company reduces or provides for additional allowances as appropriate in the period in which such a determination is made.
Health, Workers Compensation and Professional Liability Insurance Accruals
The Company maintains an accrual for health, workers compensation and professional liability claim costs that are partially self-insured and are classified in accrued salaries and wages (health insurance) and accrued expenses (workers compensation and professional liability). The Company determines the adequacy of these accruals by periodically evaluating historical experience and trends related to claims and payments based on actuarial computations and industry experiences and trends. At December 31, 2010, the balances for accrued health, workers compensation and professional liability were $7.1 million, $8.7 million and $7.3 million, respectively. At December 31, 2009, the balances for accrued health, workers compensation and professional liability were $8.0 million, $5.3 million and $7.8 million, respectively.
- 60 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
Income Taxes
Deferred tax assets and liabilities are recognized for temporary differences between the financial statement carrying amounts of existing assets and liabilities and their respective tax bases and operating loss and tax credit carryforwards. Deferred tax assets and liabilities are measured using enacted tax rates in effect for the year in which those differences are expected to be recovered or settled.
Treasury Stock
The purchase of the Company’s common stock is recorded at cost. Upon subsequent reissuance, the treasury stock account is reduced by the average cost basis of such stock.
Use of Estimates
The preparation of financial statements in conformity with GAAP requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the consolidated financial statements. Estimates also affect the reported amounts of revenues and expenses during the period. Actual results may differ from those estimates.
Recently Issued Accounting Pronouncements
In October 2009, the FASB issued ASU 2009-13, “Multiple-Deliverable Revenue Arrangements.” ASU 2009-13 requires entities to allocate revenue in an arrangement using estimated selling prices of the delivered goods and services based on a selling price hierarchy. The amendments eliminate the residual method of revenue allocation and require revenue to be allocated using the relative selling price method. ASU 2009-13 should be applied on a prospective basis for revenue arrangements entered into or materially modified in fiscal years beginning on or after June 15, 2010, with early adoption permitted. The Company will adopt ASU 2009-13 effective January 1, 2011. The Company does not expect adoption of ASU 2009-13 to have a material impact on the Company’s consolidated financial position or results of operations.
In December 2009, the FASB issued ASU 2009-17, “Improvements to Financial Reporting by Enterprises Involved with Variable Interest Entities,” which amends the related subsections of the Codification to require ongoing reassessments of whether an enterprise is the primary beneficiary of a variable interest entity. In addition, the new standard amends the pre-existing guidance for determining whether an entity is a variable interest entity and for identifying the primary beneficiary of a variable interest entity. The Company adopted ASU 2009-17 effective January 1, 2010. The Company’s adoption of ASU 2009-17 did not have a material impact on the Company’s financial position or results of operations.
In August 2010, the FASB issued ASU 2010-24, “Presentation of Insurance Claims and Related Insurance Recoveries,” which addresses the current diversity in practice related to the accounting by health care entities for medical malpractice claims and similar liabilities and their related anticipated insurance recoveries. Many health care entities, including the Company, have netted anticipated insurance recoveries against the related accrued liability. ASU 2010-24 clarifies that a health care entity should not net insurance recoveries against the related claim liability and the amount of the claim liability should be determined without consideration of insurance recoveries. ASU 2010-24 is effective for fiscal years, and interim periods within those years, beginning after December 15, 2010. The Company will adopt ASU 2010-24 effective January 1, 2011. The Company believes ASU 2010-24 will not have a material impact on the Company’s consolidated financial position or results of operations.
- 61 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
In December 2010, the FASB issued ASU 2010-29, “Disclosure of Supplementary Pro Forma Information for Business Combinations,” which addresses the current diversity in practice related to the disclosure of pro forma information for business combinations. In practice, some preparers, including the Company, have presented the pro forma information in their comparative financial statements as if the business combination that occurred in the current reporting period had occurred as of the beginning of each of the current and prior annual reporting periods. ASU 2010-29 clarifies that an entity should disclose revenue and earnings of the combined entity as though the business combination that occurred during the current year had occurred as of the beginning of the comparable prior annual reporting period only. The amendments in ASU 2010-29 are effective prospectively for business combinations which occur on or after the beginning of the first fiscal year which begins on or after December 15, 2010. The Company will adopt ASU 2010-29 effective January 1, 2011. The Company’s adoption of ASU 2010-29 will have no impact on the Company’s consolidated financial position or results of operations.
| (2) | Stock-Based Compensation |
GAAP requires the recognition of compensation expense for all share-based compensation awarded to employees, net of estimated forfeitures, using a fair-value-based method. The grant-date fair value of each award is amortized to expense over the award’s vesting period. Compensation expense associated with share-based awards is included in selling, general and administrative expense in the accompanying consolidated statements of earnings. Total pre-tax compensation expense and its related income tax benefit were as follows (in thousands of dollars):
|
Year Ended December 31,
|
|||||||||
|
2010
|
2009
|
2008
|
|||||||
|
Share-based compensation expense
|
$
|
3,940
|
$
|
4,662
|
$
|
3,195
|
|||
|
Income tax benefit
|
1,483
|
1,802
|
1,235
|
||||||
The Company has various incentive plans that provide long-term incentive and retention awards. These awards include stock options and restricted stock awards. At December 31, 2010, a total of 2,181,606 shares were available for future issuance under the plans. The Company generally issues new shares of common stock to satisfy stock option exercises and restricted stock award vestings.
Stock Options
Stock options may be granted for a term not to exceed 10 years and must be granted within 5 years from the adoption of the current equity incentive plan. All of the unvested stock options currently outstanding became fully exercisable after four years from date of grant. The fair value of each option award is estimated on the date of grant using a Black-Scholes-Merton option valuation model. Estimates of fair value may not equal the value ultimately realized by those who receive equity awards. No options were granted in 2010, 2009 or 2008.
- 62 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
The following table provides a summary of stock options outstanding as of December 31, 2010 and changes during the year then ended:
|
Weighted-
|
Weighted-Average
|
Aggregate
|
||||||
|
Average
|
Remaining
|
Intrinsic
|
||||||
|
Exercise
|
Contractual
|
Value
|
||||||
|
Stock Options
|
Shares
|
Price
|
Life (yrs)
|
(millions)
|
||||
|
Outstanding at January 1, 2010
|
870,829
|
$25.11
|
||||||
|
Granted
|
—
|
—
|
||||||
|
Exercised
|
(161,162
|
)
|
22.68
|
|||||
|
Forfeited or expired
|
(104,799
|
)
|
33.28
|
|||||
|
Outstanding at December 31, 2010
|
604,868
|
$24.33
|
3.1
|
$1.2
|
||||
|
Exercisable at December 31, 2010
|
604,868
|
$24.33
|
3.1
|
$1.2
|
The total intrinsic values of options exercised during the years ended December 31, 2010, 2009 and 2008 were approximately $1.2 million, $0.9 million and $1.4 million, respectively.
A summary of the status of the Company’s nonvested stock options as of December 31, 2010 and changes during the year ended December 31, 2010 is presented below:
|
Weighted-
|
|||||
|
Average
|
|||||
|
Grant-Date
|
|||||
|
Nonvested Stock Options
|
Shares
|
Fair Value
|
|||
|
Nonvested at January 1, 2010
|
7,500
|
$7.78
|
|||
|
Granted
|
—
|
—
|
|||
|
Vested
|
(7,500
|
)
|
7.78
|
||
|
Forfeited
|
—
|
—
|
|||
|
Nonvested at December 31, 2010
|
—
|
$ —
|
As of December 31, 2010, all options outstanding were fully vested, and therefore, there was no unrecognized compensation cost related to nonvested options.
Restricted Stock Awards
In 2006, the Company began issuing restricted stock awards to attract and retain key Company executives. Nearly all of the awards will vest and be transferred to the participant at the end of a three-year restriction period provided that the participant has been an employee of the Company continuously throughout the restriction period. In 2007, the Company also began issuing restricted stock awards to its nonemployee directors. Such awards generally vest each quarter over the first four quarters following the date of grant. All unvested restricted stock awards will immediately vest upon a change in control of the Company as defined in the restricted stock award agreement.
- 63 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
The Company’s restricted stock awards have been classified as equity awards under GAAP. New shares of common stock are issued to satisfy restricted stock award vestings. The Company generally receives a tax deduction for each restricted stock award equal to the fair market value of the restricted stock award on the award’s vesting date. Upon vesting, the Company may withhold shares with value equivalent to the minimum statutory withholding tax obligation and then remit cash to the appropriate taxing authorities. The shares withheld are effectively share repurchases by the Company as they reduce the number of shares that would have otherwise been issued as a result of the vesting.
The following table provides a summary of the status of the Company’s nonvested restricted stock awards as of December 31, 2010 and the changes during the year ended December 31, 2010:
|
Weighted-
|
|||||
|
Average
|
|||||
|
Grant-Date
|
|||||
|
Nonvested Restricted Stock Awards
|
Shares
|
Fair Value
|
|||
|
Nonvested at January 1, 2010
|
629,733
|
$16.81
|
|||
|
Granted
|
200,383
|
27.51
|
|||
|
Vested
|
(142,259
|
)
|
16.68
|
||
|
Forfeited
|
(72,440
|
)
|
18.67
|
||
|
Nonvested at December 31, 2010
|
615,417
|
$20.11
|
|||
The weighted-average grant-date fair value of restricted stock granted during the years ended December 31, 2010, 2009 and 2008 was $27.51, $14.80 and $21.71, respectively. The total fair value of shares vested during the years ended December 31, 2010, 2009 and 2008 was approximately $3.8 million, $1.5 million and $0.6 million, respectively. As of December 31, 2010, there was approximately $3.1 million of unrecognized compensation cost related to nonvested restricted stock awards. Such cost is expected to be recognized over a weighted-average period of approximately 1.8 years.
| (3) | Marketable Securities |
Noncurrent marketable securities at December 31, 2010 and 2009 consist primarily of marketable equity securities, including mutual funds ($2.5 million and $1.9 million at December 31, 2010 and 2009, respectively), corporate and government bonds ($0.8 million at December 31, 2010 and 2009) and money market securities ($0.7 million and $0.6 million at December 31, 2010 and 2009, respectively) held in trust under the Company’s deferred compensation plan.
| (4) | Allowance for Doubtful Accounts |
Accounts receivable is reported net of the allowance for doubtful accounts. Activity in the allowance for doubtful accounts is as follows (in thousands):
- 64 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
|
Year Ended December 31,
|
||||||||||
|
2010
|
2009
|
2008
|
||||||||
|
Balance at beginning of year
|
$
|
24,729
|
$
|
19,480
|
$
|
16,266
|
||||
|
Provisions for doubtful accounts
|
10,209
|
7,794
|
9,643
|
|||||||
|
Acquisitions
|
—
|
8,201
|
17
|
|||||||
|
Disposition
|
—
|
(41
|
)
|
—
|
||||||
|
Accounts written off, net of recoveries
|
(10,665
|
)
|
(10,705
|
)
|
(6,446
|
)
|
||||
|
Balance at end of year
|
$
|
24,273
|
$
|
24,729
|
$
|
19,480
|
||||
In 2008, the Company also recorded a $535,000 provision for doubtful accounts related to a note receivable.
| (5) | Property and Equipment |
Property and equipment, at cost, consist of the following (in thousands):
|
December 31,
|
|||||||
|
2010
|
2009
|
||||||
|
Equipment
|
$
|
105,539
|
$
|
88,808
|
|||
|
Land
|
6,043
|
6,043
|
|||||
|
Buildings and leasehold improvements
|
68,404
|
60,328
|
|||||
|
Buildings and equipment under capital lease obligations
|
11,243
|
11,243
|
|||||
|
191,229
|
166,422
|
||||||
|
Less accumulated depreciation
|
71,638
|
54,608
|
|||||
|
$
|
119,591
|
$
|
111,814
|
||||
Depreciation expense incurred by continuing operations was approximately $21.7 million, $11.1 million and $10.0 million for the years ended December 31, 2010, 2009 and 2008, respectively. These amounts include amortization of assets recorded under capital leases.
| (6) | Business Combinations |
Effective November 24, 2009, the Company acquired all of the outstanding common stock of Triumph HealthCare Holdings, Inc. (“Triumph”) for a total purchase price of approximately $541.0 million, which includes a favorable purchase price adjustment of $3.3 million based on acquired working capital levels. The seller originally disputed the Company’s calculation of the adjustment for acquired working capital levels. The dispute was settled in the fourth quarter of 2010 with both parties agreeing to the final purchase price adjustment of $3.3 million. At the acquisition date, Triumph operated 20 long-term acute care hospitals (“LTACHs”) in seven states. In connection with this transaction, the Company recorded acquisition-related expenses of approximately $0.1 million and $7.2 million in the years ended December 31, 2010 and 2009, respectively. Acquisition-related expenses are included in selling, general and administrative expenses in the Company’s consolidated statements of earnings.
- 65 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
Triumph’s results of operations have been included in the Company’s consolidated financial statements prospectively beginning after the date of acquisition. The Company’s statements of earnings for 2010 and 2009 include operating revenues of approximately $452.7 million and $39.7 million, respectively, and operating earnings of approximately $64.1 million and $3.7 million, respectively, related to Triumph’s hospitals. The following pro forma information assumes the Triumph acquisition had occurred at the beginning of each period presented. Such results have been prepared by adjusting the historical Company results to include Triumph’s results of operations, amortization of acquired finite-lived intangibles and incremental interest related to acquisition debt. The pro forma results do not include any cost savings that may result from the combination of the Company’s and Triumph’s operations. The pro forma results may not necessarily reflect the consolidated operations that would have existed had the acquisition been completed at the beginning of such periods nor are they necessarily indicative of future results. Amounts are in thousands of dollars, except per share data.
|
Year ended
|
Year ended
|
||||||||||||||||
|
December 31, 2009
|
December 31, 2008
|
||||||||||||||||
|
As Reported
|
Pro Forma
|
As Reported
|
Pro Forma
|
||||||||||||||
|
Operating revenues
|
$
|
848,612
|
$
|
1,239,960
|
$
|
714,030
|
$
|
1,137,756
|
|||||||||
|
Net earnings from continuing operations attributable to RehabCare
|
$
|
21,590
|
$
|
43,520
|
$
|
16,711
|
$
|
32,287
|
|||||||||
|
Diluted earnings per share from continuing operations attributable to RehabCare
|
$
|
1.14
|
$
|
1.79
|
$
|
0.94
|
$
|
1.34
|
|||||||||
| (7) | Goodwill and Other Intangible Assets |
In accordance with GAAP, the Company performs an annual test of impairment for goodwill and other indefinite lived intangible assets. The impairment analysis is performed more frequently if events or changes in circumstances indicate that the carrying amount of such assets may exceed fair value.
Intangible assets with indefinite lives are not amortized but must be reviewed for impairment annually and whenever events or changes in circumstances indicate that the asset might be impaired. If the impairment test indicates that the carrying value of an intangible asset exceeds its fair value, then an impairment loss should be recognized in the consolidated statement of earnings in an amount equal to the excess carrying value. The Company performed a test for impairment for goodwill and other indefinite lived intangible assets as of December 31, 2010, 2009 and 2008. Based upon the results of the tests performed, no impairment of goodwill or other intangible assets with indefinite useful lives was identified during the three years ended December 31, 2010.
In March 2007, the Company and St. Luke’s Episcopal-Presbyterian Hospitals (“St. Luke’s Hospitals”) formed a jointly-owned entity, St. Luke’s Rehabilitation Hospital, LLC, which began developing a new 35-bed rehabilitation hospital facility in St. Louis, Missouri. In December 2008, St. Luke’s Rehabilitation Hospital completed construction of the new facility and acquired the assets of St. Luke’s Hospitals’ existing 16-bed inpatient rehabilitation facility (“IRF”) in exchange for St. Luke’s Hospitals’ minority interest in the new entity. The operations of the existing IRF were relocated to the new 35-bed hospital facility. The Company maintains a controlling ownership interest in St. Luke’s Rehabilitation Hospital, LLC. This transaction did not qualify as the purchase of a “business” based on the guidance in GAAP. As a result, the cost of the assets acquired from St. Luke’s Hospitals were allocated to the individual assets acquired based on their relative fair values and no goodwill arose from the transaction.
- 66 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
At December 31, 2010 and 2009, the Company had the following intangible asset balances (in thousands of dollars):
|
December 31, 2010
|
December 31, 2009
|
||||||||||||||||
|
Gross
|
Gross
|
||||||||||||||||
|
Carrying
|
Accumulated
|
Carrying
|
Accumulated
|
||||||||||||||
|
Amount
|
Amortization
|
Amount
|
Amortization
|
||||||||||||||
|
Amortizing Intangible Assets:
|
|||||||||||||||||
|
Noncompete agreements
|
$
|
4,710
|
$
|
(3,078
|
)
|
$
|
4,710
|
$
|
(1,566
|
)
|
|||||||
|
Customer contracts and relationships
|
23,096
|
(14,848
|
)
|
23,096
|
(12,577
|
)
|
|||||||||||
|
Trade names
|
40,083
|
(5,529
|
)
|
40,083
|
(2,792
|
)
|
|||||||||||
|
Medicare exemption
|
454
|
(454
|
)
|
454
|
(340
|
)
|
|||||||||||
|
Market access assets
|
5,720
|
(596
|
)
|
5,720
|
(310
|
)
|
|||||||||||
|
Certificates of need
|
9,442
|
(1,130
|
)
|
9,442
|
(152
|
)
|
|||||||||||
|
Lease arrangements
|
1,305
|
(578
|
)
|
1,305
|
(297
|
)
|
|||||||||||
|
Total
|
$
|
84,810
|
$
|
(26,213
|
)
|
$
|
84,810
|
$
|
(18,034
|
)
|
|||||||
|
Non-amortizing Intangible Assets:
|
|||||||||||||||||
|
Trade names
|
$
|
410
|
$
|
410
|
|||||||||||||
|
Medicare provider numbers
|
68,220
|
68,220
|
|||||||||||||||
|
$
|
68,630
|
$
|
68,630
|
||||||||||||||
The market access assets were acquired in the transaction with St. Luke’s Hospitals noted above. The assets were valued using a discounted cash flows analysis under the income approach. The estimated value of the market access assets is attributable to the Company’s ability to gain access to and penetrate the former facility’s historical patient market.
Certain customer contracts and lease arrangements have contractual provisions that enable renewal or extension of the asset's contractual life. Costs incurred to renew or extend the term of a recognized intangible asset are expensed in the period incurred.
Amortizing intangible assets have the following weighted average useful lives as of December 31, 2010: noncompete agreements – 3.8 years; contractual customer relationships – 5.3 years; amortizing trade names – 13.8 years; market access assets – 17.9 years; certificates of need – 8.9 years; and lease arrangements – 6.2 years.
Amortization expense incurred by continuing operations was approximately $8.2 million, $4.3 million and $3.7 million for the years ended December 31, 2010, 2009 and 2008, respectively. Estimated annual amortization expense for the next 5 years is: 2011 – $6.5 million; 2012 – 5.6 million; 2013 – $5.4 million; 2014 – $5.4 million and 2015 – $5.2 million.
The changes in the carrying amount of goodwill for the years ended December 31, 2010 and 2009 are as follows (in thousands):
- 67 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
|
Healthcare Management
|
|||||||||||||||||||
|
SRS (a)
|
HRS (b)
|
Hospitals
|
Consulting (c)
|
Total
|
|||||||||||||||
|
Balance at December 31, 2008
|
$ |
79,419
|
$ |
39,715
|
$ |
48,087
|
$ |
4,144
|
$
|
171,365
|
|||||||||
|
Acquisitions
|
—
|
—
|
401,271
|
—
|
401,271
|
||||||||||||||
|
Dispositions
|
—
|
—
|
—
|
(4,144
|
)
|
(4,144
|
)
|
||||||||||||
|
Balance at December 31, 2009
|
|
79,419
|
|
39,715
|
|
449,358
|
|
—
|
568,492
|
||||||||||
|
Assets held for sale
|
—
|
—
|
(8,626
|
)
|
—
|
(8,626
|
)
|
||||||||||||
|
Balance at December 31, 2010
|
$
|
79,419
|
$
|
39,715
|
$
|
440,732
|
$
|
—
|
$
|
559,866
|
|||||||||
|
|
(a)
|
Skilled Nursing Rehabilitation Services (SRS).
|
|
|
(b)
|
Hospital Rehabilitation Services (HRS).
|
|
|
(c)
|
The healthcare management consulting segment consists of Phase 2 Consulting, Inc., which was sold effective June 1, 2009.
|
| (8) | Assets Held for Sale and Discontinued Operations |
On November 3, 2010, the Company announced that it had entered into an Equity Exchange Agreement with Select Medical Corporation under which the Company agreed to exchange its 60-bed inpatient rehabilitation hospital in Miami (the “Miami hospital”) for Select’s 70-bed long-term acute care hospital in northwest Indiana (the “Northwest Indiana LTACH”). This transaction closed on January 1, 2011. At closing, Select also paid the Company cash consideration of approximately $2.0 million. The total value of the transaction has been estimated at approximately $15.0 million. The assets of the Northwest Indiana LTACH were valued using a discounted cash flows analysis under the income approach. The Company expects to recognize a gain on the sale of the Miami hospital of approximately $5.0 million in the first quarter of 2011.
In accordance with the requirements of GAAP, the assets and liabilities of the Miami hospital have been reported on the December 31, 2010 consolidated balance sheet as assets and liabilities held for sale. Summarized below are the carrying amounts of the major classes of these assets and liabilities at December 31, 2010 (in thousands):
|
Assets:
|
||||
|
Current deferred tax assets
|
$
|
43
|
||
|
Other current assets
|
144
|
|||
|
Property and equipment, net
|
1,165
|
|||
|
Goodwill
|
8,626
|
|||
|
Other assets
|
429
|
|||
|
Total assets held for sale
|
$
|
10,407
|
||
|
Liabilities:
|
||||
|
Accrued vacation
|
$
|
205
|
||
|
Total liabilities held for sale
|
$
|
205
|
||
The Miami hospital has been classified as a discontinued operation pursuant to GAAP. The operating results for this discontinued operation are shown in the following table (in thousands). No interest expense has been allocated.
- 68 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
|
2010
|
2009
|
2008
|
|||||||||||
|
Operating revenues
|
$
|
19,627
|
$
|
20,815
|
$
|
21,382
|
|||||||
|
Costs and expenses
|
17,632
|
17,261
|
16,774
|
||||||||||
|
Operating gain from discontinued operations
|
1,995
|
3,554
|
4,608
|
||||||||||
|
Income tax expense
|
(758
|
)
|
(1,350
|
)
|
(1,751
|
)
|
|||||||
|
Gain from discontinued operations
|
$
|
1,237
|
$
|
2,204
|
$
|
2,857
|
|||||||
Effective June 1, 2009, the Company completed the sale of all the outstanding common stock of Phase 2 Consulting, Inc. (“Phase 2”) to Premier, Inc. for approximately $5.5 million. This transaction allows the Company’s management to focus on its core businesses. Phase 2 provides management and economic consulting services to the healthcare industry and had been a subsidiary of the Company since it was acquired in 2004. In connection with this transaction, the Company recognized a pre-tax loss related to the disposal of the Phase 2 business of approximately $1.2 million in 2009.
Phase 2 has been classified as a discontinued operation pursuant to GAAP. The operating results for this discontinued operation are shown in the following table (in thousands). No interest expense has been allocated.
|
2010
|
2009
|
2008
|
|||||||||||
|
Operating revenues
|
$
|
—
|
$
|
2,833
|
$
|
9,563
|
|||||||
|
Costs and expenses
|
—
|
3,064
|
9,789
|
||||||||||
|
Operating loss from discontinued operations
|
—
|
(231
|
)
|
(226
|
)
|
||||||||
|
Loss on disposal of assets of discontinued operations
|
—
|
(1,188
|
)
|
—
|
|||||||||
|
Income tax benefit
|
—
|
553
|
88
|
||||||||||
|
Loss from discontinued operations
|
$
|
—
|
$
|
(866
|
)
|
$
|
(138
|
)
|
|||||
Effective August 30, 2008, the Company completed the sale of equipment, goodwill, other intangible assets and certain related assets associated with an inpatient rehabilitation hospital located in Midland, Texas (the “Midland hospital”) to HealthSouth Corporation for approximately $7.2 million less direct selling costs. This transaction was the result of a strategic review of the Midland-Odessa market. The Midland hospital has been classified as a discontinued operation pursuant to GAAP. The operating results for this discontinued operation are shown in the following table (in thousands). No interest expense has been allocated.
|
2010
|
2009
|
2008
|
|||||||||||
|
Operating revenues
|
$
|
—
|
$
|
—
|
$
|
3,962
|
|||||||
|
Costs and expenses
|
—
|
(44
|
)
|
5,471
|
|||||||||
|
Operating gain (loss) from discontinued operations
|
—
|
44
|
(1,509
|
)
|
|||||||||
|
Gain on disposal of assets of discontinued operations
|
—
|
—
|
321
|
||||||||||
|
Income tax (expense) benefit
|
—
|
(17
|
)
|
463
|
|||||||||
|
Gain (loss) from discontinued operations
|
$
|
—
|
$
|
27
|
$
|
(725
|
)
|
||||||
- 69 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
| (9) | Long-Term Debt |
On November 24, 2009, the Company entered into an Amended and Restated Credit Agreement (the “Credit Agreement”) with Bank of America, N.A., as administrative agent and collateral agent, and Banc of America Securities LLC, RBC Capital Markets and BNP Paribas Securities Corp., as joint lead arrangers. The Credit Agreement provides for a six-year $450 million term loan facility, a five-year revolving credit facility of $125 million and a swingline subfacility of up to $25 million. The Company used the proceeds of the term loan facility and approximately $22 million in borrowings under the revolving credit facility to pay a portion of the consideration for its acquisition of Triumph.
The Credit Agreement contains certain restrictive covenants that, among other things, limit the incurrence of additional indebtedness, investments, dividends, transactions with affiliates, asset sales, acquisitions, mergers and consolidations, liens and encumbrances and other matters customarily restricted in similar credit facilities. In addition, the Company is required to maintain a maximum ratio of total funded debt to earnings before interest, taxes, depreciation and amortization ((“EBITDA”) as defined in the Credit Agreement), a maximum ratio of senior funded debt to EBITDA and a minimum ratio of adjusted earnings before interest, taxes, depreciation, amortization, rent and operating leases ((“Adjusted EBITDAR) as defined in the Credit Agreement) to fixed charges. As of December 31, 2010, the Company was in compliance with all debt covenants. The annual commitment fees, letter of credit fees and interest rates to be charged on the outstanding principal balances in connection with the revolving credit facility are variable based upon the Company’s consolidated leverage ratios.
As of December 31, 2010, the balance outstanding under the revolving credit facility was $1.4 million. At that date, the Company had approximately $11.8 million in letters of credit outstanding to its insurance carriers as collateral for reimbursement of claims. The letters of credit reduce the amount the Company may borrow under its revolving credit facility. As of December 31, 2010, after consideration of the effects of restrictive covenants, the available borrowing capacity under the revolving credit facility was approximately $111.8 million.
The term loan facility requires quarterly installments of $1,125,000 with the balance payable upon the final maturity. In addition, the Company is required to make mandatory principal prepayments equal to a portion of its consolidated excess cash flow (as defined in the Credit Agreement) when its consolidated leverage ratio reaches certain levels. At December 31, 2010, the balance outstanding under the term loan was $385.5 million, which excludes unamortized original issue discounts of $7.6 million.
As of December 31, 2010 and 2009, long-term borrowings, including the current portion of long-term debt, were as follows (dollars in thousands unless otherwise noted):
- 70 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
|
December 31,
|
|||||||
|
2010
|
2009
|
||||||
|
Borrowings under $125 million revolving credit facility; maturity date of November 24, 2014
|
$
|
1,400
|
$
|
—
|
|||
|
Term loan facility; payable in quarterly installments of $1,125 with remaining balance due on November 24, 2015; net of unamortized original issue discount of $7,591 and $8,892 at December 31, 2010 and 2009, respectively
|
377,909
|
441,108
|
|||||
|
Note payable to bank; bearing interest at LIBOR plus 4%; payable in monthly installments through November 2015 and $3.5 million due in December 2015
|
4,650
|
—
|
|||||
|
Note payable to bank; bearing interest at prime plus 1%, but not less than 5% nor greater than 7.5%; refinanced in December 2010
|
—
|
4,528
|
|||||
|
Capital lease obligations
|
6,929
|
9,631
|
|||||
|
390,888
|
455,267
|
||||||
|
Less: current portion
|
(9,116
|
)
|
(7,507
|
)
|
|||
|
$
|
381,772
|
$
|
447,760
|
||||
The Credit Agreement is collateralized by substantially all of the Company’s assets. Borrowings under the $125 million revolving credit facility bear interest at the Company’s option at either a base rate or the London Interbank Offering Rate (“LIBOR”) for one, two, three or six month interest periods, or a nine or twelve month period if available, plus an applicable margin percentage. The base rate is the greater of the federal funds rate plus one-half of 1%, Bank of America N.A.’s prime rate and one month LIBOR plus 1%. The interest rate on the borrowings under the revolving credit facility was 5.75% at December 31, 2010.
Borrowings under the term loan facility bear interest at either the base rate plus 300 basis points or LIBOR plus 400 basis points with a LIBOR floor of 200 basis points. The interest rate under the term loan facility was 6.0% at December 31, 2010.
Certain of the Company’s leases that meet the lease capitalization criteria in accordance with FASB ASC 840-30 have been recorded as an asset and liability at the lower of fair value or the net present value of the aggregate future minimum lease payments at the inception of the lease. Interest rates used in computing the net present value of the lease payments ranged from 6.5% to 10.7% and were generally based on the lessee’s incremental borrowing rate at the inception of the lease.
The Company’s long-term debt is scheduled to mature as follows. The maturities below exclude the impact of the term loan’s unamortized original issue discount of $7,591,000 at December 31, 2010. Amounts are in thousands.
- 71 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
|
2011
|
$
|
9,116
|
||
|
2012
|
8,024
|
|||
|
2013
|
5,381
|
|||
|
2014
|
4,738
|
|||
|
2015
|
371,220
|
|||
|
Thereafter
|
—
|
|||
|
Total
|
$
|
398,479
|
Interest paid for 2010, 2009 and 2008 was $28.7 million, $4.8 million and $4.4 million, respectively. Included in the interest paid amounts are commitment fees on the unused portion of the revolving credit facility of $0.6 million, $0.3 million and $0.3 million for 2010, 2009 and 2008, respectively.
| (10) | Stockholders’ Equity |
In November 2009, the Company issued 6,210,000 shares of common stock, par value of $0.01 in a public equity offering which resulted in net proceeds, after underwriting fees and other direct costs, of approximately $140.2 million. The net proceeds from the public equity offering were used in the acquisition of Triumph HealthCare.
As a result of activity under its equity compensation plans, the Company issued 268,775, 168,470, and 190,550 shares of common stock in 2010, 2009 and 2008, respectively.
Pursuant to a rights agreement, dated as of August 28, 2002, by and between the Company and Computershare Trust Company, N.A., as Rights Agent (the “Rights Agent”), the Company distributed one preferred share purchase right for each outstanding share of the Company’s common stock. On April 1, 2010, the Company and the Rights Agent entered into an amendment to the rights agreement. Pursuant to the amendment, the final expiration date of the rights was changed from October 1, 2012 to April 1, 2010. As a result of the amendment, effective April 1, 2010, the rights are no longer outstanding and are not exercisable.
| (11) | Earnings per Share |
Basic earnings per share excludes dilution and is computed by dividing income available to RehabCare common stockholders by the weighted average common shares outstanding for the period. Diluted earnings per share reflects the potential dilution that could occur if securities or other contracts to issue common stock were exercised and converted into common stock or resulted in the issuance of common stock that then shared in the earnings of the entity (as calculated utilizing the treasury stock method). These potential shares include dilutive stock options and unvested restricted stock awards.
The following table sets forth the computation of basic and diluted earnings (loss) per share attributable to RehabCare stockholders (in thousands, except per share data). The net earnings amounts presented below exclude income and losses attributable to noncontrolling interests in consolidated subsidiaries.
- 72 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
|
Year Ended December 31,
|
||||||||||||
|
2010
|
2009
|
2008
|
||||||||||
|
Numerator:
|
||||||||||||
|
Earnings from continuing operations, net of tax
|
$
|
61,213
|
$
|
21,590
|
$
|
16,711
|
||||||
|
Gain from discontinued operations, net of tax
|
1,237
|
1,365
|
1,994
|
|||||||||
|
Net earnings
|
$
|
62,450
|
$
|
22,955
|
$
|
18,705
|
||||||
|
Denominator:
|
||||||||||||
|
Basic weighted average common shares outstanding
|
24,231
|
18,481
|
17,583
|
|||||||||
|
Effect of dilutive securities:
|
||||||||||||
|
stock options and restricted stock awards
|
475
|
381
|
215
|
|||||||||
|
Diluted weighted average common shares outstanding
|
24,706
|
18,862
|
17,798
|
|||||||||
|
Basic earnings per common share:
|
||||||||||||
|
Earnings from continuing operations, net of tax
|
$
|
2.53
|
$
|
1.17
|
$
|
0.95
|
||||||
|
Gain from discontinued operations, net of tax
|
0.05
|
0.07
|
0.11
|
|||||||||
|
Net earnings
|
$
|
2.58
|
$
|
1.24
|
$
|
1.06
|
||||||
|
Diluted earnings per common share:
|
||||||||||||
|
Earnings from continuing operations, net of tax
|
$
|
2.48
|
$
|
1.14
|
$
|
0.94
|
||||||
|
Gain from discontinued operations, net of tax
|
0.05
|
0.08
|
0.11
|
|||||||||
|
Net earnings
|
$
|
2.53
|
$
|
1.22
|
$
|
1.05
|
||||||
For fiscal 2010, 2009 and 2008, outstanding stock options totaling approximately 179,000, 710,000 and 912,000 potential shares, respectively, were excluded from the calculation of diluted earnings per share because their effect would have been anti-dilutive.
| (12) | Employee Benefits |
The Company has an Employee Savings Plan, which is a defined contribution plan qualified under Section 401(k) of the Internal Revenue Code, for the benefit of its eligible employees. All employees who are at least 21 years of age are immediately eligible to participate in the plan. Each participant may contribute from 2% to 20% of his or her annual compensation to the plan subject to limitations on the highly compensated employees to ensure the plan is nondiscriminatory. Contributions made by the Company to the Employee Savings Plan are at rates of up to 50% of the first 4% of employee contributions. Expense in connection with the Employee Savings Plan for 2010, 2009 and 2008 totaled $4.1 million, $4.0 million and $3.9 million, respectively.
In connection with the acquisition of Triumph on November 24, 2009, the Company added the Triumph 401(k) Plan to its portfolio of employee benefit plans. Substantially all full-time Triumph employees are eligible to participate in the plan. Matching contributions under the plan are equal to 25% of the participant contributions up to 6% of their salary. The Company’s matching contributions in connection with the Triumph 401(k) Plan were approximately $0.5 million in 2010 and $62,000 in 2009.
- 73 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
The Company maintains nonqualified deferred compensation plans for certain employees. Due to changes in the Internal Revenue Code impacting deferred compensation arrangements, the Company froze its plan, which became ineligible to receive future deferrals, on December 31, 2004. To ensure compliance with Internal Revenue Code section 409A, a new plan was developed and implemented on July 1, 2005. Under the 2005 plan, participants may defer up to 70% of their base salary and up to 70% of their cash incentive compensation. Amounts for both plans are held by a trust in investments that are designated by participants but remain the property of the Company until distribution. At December 31, 2010 and 2009, approximately $4.0 million and $3.4 million, respectively, were payable under the nonqualified deferred compensation plans and approximated the value of the trust assets owned by the Company.
| (13) | Commitments |
The Company is obligated under non-cancelable operating leases for the facilities that support the Company’s hospitals, the Company’s administrative functions and other operations. The Company’s hospital facility leases represent the largest portion of rent expense and such leases generally have initial terms of 12 to 20 years with one or more renewal options. Contingent rents are included in rent expense in the year incurred. Future minimum lease payments at December 31, 2010 for those operating leases having an initial or remaining non-cancelable lease term in excess of one year are as follows (amounts in thousands):
|
2011
|
$
|
32,154
|
||
|
2012
|
36,092
|
|||
|
2013
|
37,509
|
|||
|
2014
|
37,932
|
|||
|
2015
|
35,537
|
|||
|
Thereafter
|
304,376
|
|||
|
Total
|
$
|
483,600
|
Rent expense for 2010, 2009 and 2008 was approximately $49.2 million, $18.8 million and $11.2 million, respectively. As of December 31, 2010, the Company expected to receive future minimum rentals of approximately $0.3 million under noncancelable subleases having a remaining term in excess of one year.
Triumph’s headquarters are located in a medical office building in Houston, Texas. Triumph owns a controlling interest in the building and leases out the remaining office space to physicians and other healthcare service providers. As of December 31, 2010, the building had a carrying value of approximately $6.7 million and the Company expected to receive future minimum rentals under noncancelable leases of approximately $1.1 million.
Certain of the Company’s hospitals lease facilities and/or equipment under leases that are classified as capital leases. Lease commitments under capital leases at December 31, 2010 are as follows (amounts in thousands):
- 74 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
|
2011
|
$
|
3,533
|
||
|
2012
|
3,533
|
|||
|
2013
|
658
|
|||
|
2014
|
5
|
|||
|
2015
|
—
|
|||
|
Thereafter
|
—
|
|||
|
Total minimum lease payments
|
7,729
|
|||
|
Less: interest portion
|
(800
|
)
|
||
|
Total obligations under capital leases
|
$
|
6,929
|
||
The Company was not a party to any material open construction contracts as of December 31, 2010.
| (14) | Income Taxes |
The components of income tax expense (benefit), excluding discontinued operations, are as follows (in thousands):
|
Year Ended December 31,
|
|||||||||||
|
2010
|
2009
|
2008
|
|||||||||
|
Federal – current
|
$
|
25,032
|
$
|
12,123
|
$
|
6,112
|
|||||
|
Federal – deferred
|
7,699
|
1,914
|
2,867
|
||||||||
|
State
|
3,828
|
2,254
|
1,333
|
||||||||
|
$
|
36,559
|
$
|
16,291
|
$
|
10,312
|
||||||
A reconciliation between expected income taxes, computed by applying the statutory Federal income tax rate of 35% to earnings from continuing operations before income taxes, and actual income tax is as follows (in thousands):
|
Year Ended December 31,
|
|||||||||||
|
2010
|
2009
|
2008
|
|||||||||
|
Expected income taxes
|
$
|
35,507
|
$
|
12,570
|
$
|
8,763
|
|||||
|
State income taxes, net of federal income tax benefit
|
2,644
|
1,527
|
844
|
||||||||
|
Tax effect of (earnings)/losses attributable to noncontrolling interests not (taxable)/deductible by the Company
|
(1,287
|
)
|
688
|
695
|
|||||||
|
Tax effect of nondeductible acquisition-related expenses
|
—
|
1,347
|
—
|
||||||||
|
Other, net
|
(305
|
)
|
159
|
10
|
|||||||
|
$
|
36,559
|
$
|
16,291
|
$
|
10,312
|
||||||
The tax effects of temporary differences that give rise to the deferred tax assets and liabilities are as follows (in thousands):
- 75 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
|
December 31,
|
|||||||
|
2010
|
2009
|
||||||
|
Deferred tax assets:
|
|||||||
|
Allowance for doubtful accounts
|
$
|
6,922
|
$
|
7,588
|
|||
|
Accrued insurance, vacation, bonus and deferred compensation
|
17,234
|
12,563
|
|||||
|
Net operating loss carryforward/capital loss carryforward
|
1,477
|
1,697
|
|||||
|
Stock based compensation
|
3,595
|
3,081
|
|||||
|
Accrued expenses
|
4,146
|
4,081
|
|||||
|
Other
|
2,486
|
2,435
|
|||||
|
Total gross deferred tax assets
|
35,860
|
31,445
|
|||||
|
Valuation allowance
|
(106
|
)
|
(74
|
)
|
|||
|
Net deferred tax assets
|
35,754
|
31,371
|
|||||
|
Deferred tax liabilities:
|
|||||||
|
Acquired goodwill and intangibles
|
52,023
|
47,402
|
|||||
|
Depreciation and amortization
|
10,047
|
5,229
|
|||||
|
481(a) adjustment for accrued bonus
|
3,690
|
—
|
|||||
|
Prepaid expenses
|
2,270
|
2,438
|
|||||
|
Other
|
1,445
|
658
|
|||||
|
Total deferred tax liabilities
|
69,475
|
55,727
|
|||||
|
$
|
(33,721
|
)
|
$
|
(24,356
|
)
|
||
In connection with the acquisition of Triumph, the Company acquired gross net operating loss carryforwards of approximately $6.6 million. Section 382 of the Internal Revenue Code restricts the utilization of net operating losses and other carryover tax attributes upon the occurrence of an ownership change such as the Company’s acquisition of Triumph. Accordingly, utilization of the acquired Triumph net operating loss carryforwards will be limited to approximately $0.7 million per tax year. Based on this limitation and the expiration of the carryforwards in 2016, the Company estimates approximately $2.2 million of the acquired net operating loss carryforwards will expire unused. At the date of acquisition, the Company recorded the acquired net operating loss carryforwards at their estimated net realizable value, net of the section 382 limitation. At December 31, 2010, the remaining unused net operating loss carryforwards, net of the section 382 limitation, were approximately $3.6 million and the tax effect of these carryforwards was approximately $1.3 million.
At December 31, 2010, the Company also had state net operating loss carryforwards and federal capital loss carryforwards which resulted in a deferred tax asset of approximately $0.1 million. These carryforwards expire on various dates between 2011 and 2026.
The Company is required to establish a valuation allowance for deferred tax assets if, based on the weight of available evidence, it is more likely than not that some portion or all of the deferred tax assets will not be realized. The ultimate realization of deferred tax assets is dependent upon the generation of future taxable income during the periods in which those temporary differences become deductible. Management considers the scheduled reversal of deferred tax liabilities, projected future taxable income and tax planning strategies in making this assessment. After consideration of all evidence, both positive and negative, management concluded that it was more likely than not that the Company will not realize a portion of its deferred tax assets and that valuation allowances of approximately $0.1 million were necessary as of both December 31, 2010 and 2009. For the years ended December 31, 2010, 2009, and 2008, the net increases (decreases) in the valuation allowance were $0.0 million, $0.0 million, and $0.3 million, respectively.
- 76 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
The following table provides a reconciliation of the beginning and ending amount of unrecognized tax benefits for the years ended December 31, 2010 and 2009 (in thousands):
|
2010
|
2009
|
|||||||
|
Balance at beginning of year
|
$
|
1,647
|
$
|
448
|
||||
|
Liability assumed in acquisition of Triumph
|
—
|
133
|
||||||
|
Increase as a result of tax positions taken in prior years, including interest
|
71
|
510
|
||||||
|
Increase as a result of tax positions taken in the current year
|
298
|
710
|
||||||
|
Decrease due to IRS approval of accounting method change
|
(484
|
)
|
—
|
|||||
|
Lapse of applicable statute of limitations
|
—
|
(154
|
)
|
|||||
|
Balance at end of year
|
$
|
1,532
|
$
|
1,647
|
As of December 31, 2010, the Company had approximately $1.0 million of unrecognized tax benefits that, if recognized, would favorably affect the Company’s effective income tax rate. The Company currently does not expect any significant changes to unrecognized tax positions within the next twelve months.
The Company’s practice is to recognize interest related to unrecognized tax benefits as a component of interest expense and penalties related to unrecognized tax benefits as a component of selling, general and administrative expenses.
RehabCare and its subsidiaries file income tax returns for U.S. federal income taxes and various state income taxes. The Company is no longer subject to U.S. federal income tax examination for years prior to 2007. The IRS completed its examination of the Company’s 2006 federal income tax return in 2009.
Income taxes paid by the Company for 2010, 2009 and 2008 were $24.8 million, $15.8 million and $6.7 million, respectively.
| (15) | Investment in Unconsolidated Affiliate |
The Company maintains a 40% equity interest in Howard Regional Specialty Care, LLC (“HRSC”), which operates a freestanding rehabilitation hospital in Kokomo, Indiana. The Company uses the equity method to account for its investment in HRSC. The Company’s initial investment in HRSC exceeded the Company’s share of the book value of HRSC’s stockholders’ equity by approximately $3.5 million. This excess is being accounted for as equity method goodwill. The carrying value of the Company’s investment in HRSC was approximately $4.9 million and $4.8 million at December 31, 2010 and 2009, respectively.
| (16) | Severance Costs |
In the fourth quarter of 2009, the Company eliminated 13 corporate positions in an effort to reduce corporate overhead and eliminate redundancies created by the acquisition of Triumph. In connection with these efforts, the Company recognized a pre-tax charge of approximately $0.9 million for employee severance costs including costs incurred under pre-existing severance plans. This charge is reflected on the selling, general and administrative expense line of the Company’s consolidated statement of earnings for 2009. The following table provides a roll-forward of the liability for accrued severance costs from January 1, 2009 through December 31, 2010 (amounts in thousands):
- 77 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
|
Balance, January 1, 2009
|
$
|
—
|
|||
|
Accrual for severance costs
|
862
|
||||
|
Payments
|
(105
|
)
|
|||
|
Balance, December 31, 2009
|
$
|
757
|
|||
|
Payments
|
(757
|
)
|
|||
|
Balance, December 31, 2010
|
$
|
—
|
|||
| (17) | Related Party Transactions |
The Company purchased air transportation services from 55JS Limited, Co. at an approximate cost of $759,000, $735,000 and $510,000 for the years ended December 31, 2010, 2009 and 2008, respectively. 55JS Limited, Co. is owned by the Company’s President and Chief Executive Officer, John Short. The air transportation services are billed to the Company for hourly usage of the 55JS Limited, Co. plane for Company business at rates which approximate market rates for similar transportation services.
| (18) | Fair Value Measurements |
GAAP defines fair value as the price that would be received to sell an asset or paid to transfer a liability in an orderly transaction between market participants at the measurement date. The following disclosures provide information about the extent to which fair value is used to measure recognized assets and liabilities, the inputs used to develop the measurements and the effect of certain of the measurements on earnings for the period.
The Company uses a three-level fair value hierarchy that categorizes assets and liabilities measured at fair value based on the observability of the inputs utilized in the valuation: Level 1 - inputs are quoted prices in active markets for the identical assets or liabilities; Level 2 - inputs other than quoted prices that are directly or indirectly observable through market-corroborated inputs; and Level 3 - inputs are unobservable, or observable but cannot be market-corroborated, requiring the Company to make assumptions about pricing by market participants. The following tables set forth information for the Company’s financial assets and liabilities that are measured at fair value on a recurring basis (amounts in thousands):
|
December 31, 2010
|
||||||||||||||||
|
Carrying
|
Fair Value Measurements
|
|||||||||||||||
|
Value
|
Level 1
|
Level 2
|
Level 3
|
|||||||||||||
|
Trading securities
|
$
|
3,965
|
$
|
3,965
|
$
|
—
|
$
|
—
|
||||||||
- 78 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
|
December 31, 2009
|
||||||||||||||||
|
Carrying
|
Fair Value Measurements
|
|||||||||||||||
|
Value
|
Level 1
|
Level 2
|
Level 3
|
|||||||||||||
|
Trading securities
|
$
|
3,314
|
$
|
3,314
|
$
|
—
|
$
|
—
|
||||||||
The Company’s nonfinancial assets and liabilities (including property and equipment, goodwill and other intangible assets) are not measured at fair value on a recurring basis; however, they are subject to fair value adjustments in certain circumstances, such as when there is evidence that impairment may exist. No impairment related to these assets was identified in 2010.
| (19) | Noncontrolling Interests |
Nine of Triumph’s LTACHs in Houston are jointly owned under three limited partnerships and the noncontrolling interests in these partnerships ranged from 12.9% to 14.9% as of December 31, 2009. The noncontrolling interests in these partnerships were primarily owned by individual physicians located in the Houston area, and certain of these physicians and one other limited partner expressed interest in selling all or part of their limited partnership interests to the Company following the Company’s acquisition of Triumph. In 2010, the Company offered each limited partner an opportunity to retain all, sell 50% or sell 100% of their limited partnership interests for a fixed purchase price in cash. As of December 31, 2010, the Company entered into agreements with 113 limited partners to purchase all or 50% of their limited partnership interests for combined cash consideration totaling approximately $12.0 million. In accordance with GAAP, these payments have been accounted for as equity transactions. As of December 31, 2010, the noncontrolling interests in these three limited partnerships ranged from 1.2% to 8.6%.
The following table discloses the effects on the Company’s equity for the year ended December 31, 2010 of all changes in the Company’s ownership interest in consolidated subsidiaries including the changes noted in the paragraph above (amounts in thousands):
|
Decrease in Company’s additional paid-in capital for purchase of noncontrolling interests in subsidiaries
|
$
|
7,331
|
|||
|
Decrease in carrying value of noncontrolling interests for purchase of noncontrolling interests in subsidiaries
|
4,700
|
||||
|
Total cash consideration paid in exchange for purchase of noncontrolling interests
|
$
|
12,031
|
|||
| (20) | Industry Segment Information |
The Company operates in the following two reportable business segments, which are managed separately based on fundamental differences in operations: program management services and hospitals. Program management services include hospital rehabilitation services (including inpatient acute and subacute rehabilitation and outpatient therapy programs) and skilled nursing rehabilitation services (including contract therapy in skilled nursing facilities, resident-centered management consulting services and staffing services for therapists and nurses). The Company’s hospitals segment owns and operates 29 long-term acute care hospitals and five inpatient rehabilitation hospitals.
- 79 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
Virtually all of the Company’s services are provided in the United States. Summarized information about the Company’s operations in each industry segment is as follows (in thousands).
|
Operating Revenues
|
Operating Earnings (Loss)
|
||||||||||||||||||
|
2010
|
2009
|
2008
|
2010
|
2009
|
2008
|
||||||||||||||
|
Program management:
|
|||||||||||||||||||
|
Skilled nursing rehabilitation services
|
$
|
516,278
|
$
|
496,250
|
$
|
457,229
|
$
|
39,184
|
$
|
37,753
|
$
|
25,544
|
|||||||
|
Hospital rehabilitation services
|
180,009
|
178,168
|
165,658
|
32,925
|
29,487
|
21,997
|
|||||||||||||
|
Program management total
|
696,287
|
674,418
|
622,887
|
72,109
|
67,240
|
47,541
|
|||||||||||||
|
Hospitals
|
633,156
|
174,194
|
91,143
|
61,450
|
(26,066
|
)
|
(18,511
|
)
|
|||||||||||
|
Unallocated corporate expenses (1)
|
N/A
|
N/A
|
N/A
|
—
|
(254
|
)
|
(731
|
)
|
|||||||||||
|
Total
|
$
|
1,329,443
|
$
|
848,612
|
$
|
714,030
|
$
|
133,559
|
$
|
40,920
|
$
|
28,299
|
|||||||
|
Depreciation and Amortization
|
Capital Expenditures
|
||||||||||||||||||
|
2010
|
2009
|
2008
|
2010
|
2009
|
2008
|
||||||||||||||
|
Program management:
|
|||||||||||||||||||
|
Skilled nursing rehabilitation services
|
$
|
5,523
|
$
|
6,283
|
$
|
6,835
|
$
|
6,446
|
$
|
2,422
|
$
|
3,824
|
|||||||
|
Hospital rehabilitation services
|
2,222
|
2,423
|
2,641
|
894
|
1,328
|
1,032
|
|||||||||||||
|
Program management total
|
7,745
|
8,706
|
9,476
|
7,340
|
3,750
|
4,856
|
|||||||||||||
|
Hospitals
|
22,850
|
7,544
|
4,899
|
23,239
|
9,465
|
13,604
|
|||||||||||||
|
Healthcare management consulting (2)
|
N/A
|
N/A
|
N/A
|
—
|
—
|
42
|
|||||||||||||
|
Total
|
$
|
30,595
|
$
|
16,250
|
$
|
14,375
|
$
|
30,579
|
$
|
13,215
|
$
|
18,502
|
|||||||
|
Total Assets
|
|||||||||||
|
as of December 31,
|
|||||||||||
|
2010
|
2009
|
2008
|
|||||||||
|
Program management:
|
|||||||||||
|
Skilled nursing rehabilitation services
|
$
|
196,264
|
$
|
187,744
|
$
|
198,236
|
|||||
|
Hospital rehabilitation services
|
117,548
|
127,212
|
115,044
|
||||||||
|
Program management total
|
313,812
|
314,956
|
313,280
|
||||||||
|
Hospitals (3)
|
812,757
|
795,024
|
118,267
|
||||||||
|
Healthcare management consulting
|
—
|
—
|
6,859
|
||||||||
|
Total
|
$
|
1,126,569
|
$
|
1,109,980
|
$
|
438,406
|
|||||
|
|
(1)
|
Represents general corporate overhead expenses associated with Phase 2 Consulting, Inc., which was sold effective June 1, 2009. All other costs and expenses associated with Phase 2 have been reported in discontinued operations.
|
- 80 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
|
|
(2)
|
The healthcare management consulting segment consists of Phase 2 Consulting, Inc., which was sold effective June 1, 2009. Depreciation and amortization expense associated with Phase 2 has been reported in discontinued operations.
|
|
|
(3)
|
Hospitals segment total assets include the carrying value of the Company’s investment in HRSC.
|
| (21) | Quarterly Financial Information (Unaudited) |
The following tables present the Company’s quarterly financial data. Consistent with Note 1, the Company reclassified certain prior year amounts to conform to the current year presentation.
|
Quarter Ended
|
||||||||||||||||
|
2010
|
December 31
|
September 30
|
June 30
|
March 31
|
||||||||||||
|
(in thousands, except per share data)
|
||||||||||||||||
|
Operating revenues
|
$
|
339,344
|
$
|
337,481
|
$
|
330,664
|
$
|
321,954
|
||||||||
|
Operating earnings
|
36,113
|
33,730
|
32,151
|
31,565
|
||||||||||||
|
Earnings from continuing operations, net of tax
|
18,630
|
16,237
|
15,758
|
14,265
|
||||||||||||
|
Gain (loss) from discontinued operations, net of tax
|
673
|
541
|
(541
|
)
|
564
|
|||||||||||
|
Net earnings
|
19,303
|
16,778
|
15,217
|
14,829
|
||||||||||||
|
Net earnings attributable to RehabCare
|
17,053
|
15,699
|
14,705
|
14,993
|
||||||||||||
|
Net earnings per share attributable to RehabCare:
|
||||||||||||||||
|
Basic
|
0.70
|
0.65
|
0.61
|
0.62
|
||||||||||||
|
Diluted
|
0.69
|
0.64
|
0.59
|
0.61
|
||||||||||||
|
Quarter Ended
|
||||||||||||||||
|
2009
|
December 31
|
September 30
|
June 30
|
March 31
|
||||||||||||
|
(in thousands, except per share data)
|
||||||||||||||||
|
Operating revenues
|
$
|
249,807
|
$
|
203,264
|
$
|
199,596
|
$
|
195,945
|
||||||||
|
Operating earnings (1)
|
6,470
|
10,087
|
11,597
|
12,766
|
||||||||||||
|
Earnings from continuing operations, net of tax
|
46
|
5,462
|
6,664
|
7,452
|
||||||||||||
|
Gain (loss) from discontinued operations, net of tax
|
257
|
228
|
(116
|
)
|
996
|
|||||||||||
|
Net earnings
|
303
|
5,690
|
6,548
|
8,448
|
||||||||||||
|
Net earnings attributable to RehabCare
|
655
|
6,757
|
6,883
|
8,660
|
||||||||||||
|
Net earnings per share attributable to RehabCare:
|
||||||||||||||||
|
Basic
|
0.03
|
0.38
|
0.39
|
0.49
|
||||||||||||
|
Diluted
|
0.03
|
0.37
|
0.38
|
0.48
|
||||||||||||
- 81 -
REHABCARE GROUP, INC.
Notes to Consolidated Financial Statements (Continued)
December 31, 2010, 2009 and 2008
|
|
(1)
|
Operating earnings for the quarter ended December 31, 2009 include $7.2 million of acquisition-related expenses for costs directly related to the acquisition of Triumph including fees for legal, accounting, advisory and other outside services.
|
| (22) | Contingencies |
The Company is currently not a party to any material pending legal proceedings.
In the ordinary course of our business, the Company is a party to a number of claims and lawsuits, as both plaintiff and defendant, which the Company regards as immaterial. From time to time, and depending upon the particular facts and circumstances, the Company may be subject to indemnification obligations under its various contracts. The Company does not believe that any liability resulting from such matters, after taking into consideration the Company’s insurance coverage and amounts already provided for, will have a material effect on the Company’s consolidated financial position or overall liquidity; however, such matters, or the expense of prosecuting or defending them, could have a material effect on cash flows and results of operations in a particular quarter or fiscal year as they develop or as new issues are identified.
| (23) | Subsequent Events |
On February 7, 2011, the Company and Kindred Healthcare, Inc. (“Kindred”) entered into an Agreement and Plan of Merger (the “Merger Agreement”), providing for the acquisition of the Company by Kindred. Subject to the terms and conditions of the Merger Agreement, which has been unanimously approved by the boards of directors of the respective parties, the Company will be merged with and into Kindred (the “Merger”), with Kindred surviving the Merger.
At the effective time of the Merger, each share of RehabCare common stock outstanding immediately prior to the effective time will be converted into the right to receive 0.471 shares of Kindred common stock and $26.00 in cash, without interest. No fractional shares of Kindred common stock will be issued in the Merger, and the Company’s stockholders will receive cash in lieu of fractional shares, if any, of Kindred common stock. Each share of Kindred common stock outstanding immediately prior to the effective time will remain outstanding and will not be affected by the Merger. Upon completion of the transaction, the Company’s stockholders will own approximately 22% of Kindred’s outstanding common stock.
The consummation of the Merger is subject to certain conditions, including the adoption by the Company and Kindred stockholders of the Merger Agreement; clearance under the Hart-Scott-Rodino Antitrust Improvements Act of 1976, as amended; receipt of certain other licensure and regulatory approvals; receipt of the proceeds of the financing described below; and other customary closing conditions.
- 82 -
The Merger Agreement also contains certain termination rights and provides that (i) upon termination of the Merger Agreement under specified circumstances, including, among others, a change in the recommendation of the board of directors of the Company or termination of the Merger Agreement to enter into a written definitive agreement for a “superior proposal,” the Company will be required to pay Kindred a termination fee of $26 million and (ii) upon the termination of the Merger Agreement under specified circumstances, including, among others, a change in the recommendation of the board of directors of Kindred or Kindred’s failure to receive adequate financing after all of the other conditions to closing have been met, Kindred will be required to pay the Company a termination fee of $62 million.
- 83 -
| ITEM 9. | CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS |
| ON ACCOUNTING AND FINANCIAL DISCLOSURE |
Not applicable.
| ITEM 9A. | CONTROLS AND PROCEDURES |
Evaluation of Controls and Procedures
Under the supervision and with the participation of our management, including the Chief Executive Officer and Chief Financial Officer, we conducted an evaluation of the effectiveness of the Company’s disclosure controls and procedures, as defined in Rules 13a-15(e) and 15d-15(e) of the Securities and Exchange Act of 1934. Based on that evaluation, the Chief Executive Officer and Chief Financial Officer have concluded that the Company’s disclosure controls and procedures as of December 31, 2010 were effective to ensure that information required to be disclosed by the Company in reports that it files or submits under the Securities Exchange Act of 1934 is recorded, processed, summarized and reported within the time periods specified in Securities and Exchange Commission’s rules and forms.
There have been no changes in the Company’s internal control over financial reporting during the fourth quarter of 2010 that have materially affected, or are reasonably likely to materially affect, the Company’s internal control over financial reporting.
Management’s Report on Internal Control Over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over financial reporting, as defined in Rule 13a-15(f) under the Securities Exchange Act of 1934. Under the supervision and with the participation of our management, including the Chief Executive Officer and the Chief Financial Officer, we conducted an evaluation of the effectiveness of our internal control over financial reporting as of December 31, 2010. All internal control systems have inherent limitations, including the possibility of circumvention and overriding the control. Accordingly, even effective internal control can provide only reasonable assurance as to the reliability of financial statement preparation and presentation. Further, because of changes in conditions, the effectiveness of internal control may vary over time.
In making its evaluation, our management used the criteria set forth by the Committee of Sponsoring Organizations of the Treadway Commission (“COSO”) in Internal Control-Integrated Framework. Based upon this evaluation, our management has concluded that our internal control over financial reporting as of December 31, 2010 is effective.
Our independent registered public accounting firm, KPMG LLP, has audited the effectiveness of our internal control over financial reporting, as stated in its report which is included herein.
| ITEM 9B. | OTHER INFORMATION |
Not applicable.
- 84 -
PART III
| ITEM 10. | DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE |
The following information is included in an amendment to this Annual Report on Form 10-K to be filed within 120 days after the Company’s fiscal year end of December 31, 2010 and is incorporated herein by reference:
|
|
·
|
Information regarding directors of the Company.
|
|
|
·
|
Information regarding the Company’s audit committee and designated "audit committee financial experts."
|
|
|
·
|
Information regarding Section 16(a) beneficial ownership reporting compliance.
|
The Company has adopted a Code of Ethics that applies to its principal executive officer, principal financial officer, principal accounting officer or controller, or persons performing similar functions. The Code of Ethics is available through the Company’s web site at www.rehabcare.com.
The following table sets forth the name, age and position of each of our executive officers as of December 31, 2010. There is no family relationship between any of the following individuals.
|
Name
|
Age
|
Position
|
||
|
John H. Short, Ph.D.
|
66
|
President and Chief Executive Officer
|
||
|
Jay W. Shreiner
|
60
|
Executive Vice President, Chief Financial Officer
|
||
|
Patricia S. Williams
|
43
|
Senior Vice President, General Counsel and Secretary
|
||
|
Patricia M. Henry
|
58
|
Executive Vice President, Operations
|
||
|
Mary Pat Welc
|
56
|
Senior Vice President, Operations
|
||
|
Brock Hardaway
|
44
|
Executive Vice President, Operations
|
||
|
James F. Martin
|
60
|
Senior Vice President, Chief Human Resources Officer
|
||
|
Jeff A. Zadoks
|
45
|
Senior Vice President, Chief Accounting Officer
|
||
|
Samuel W. Duggan II
|
47
|
Vice President, Treasurer
|
The following paragraphs contain biographical information about our executive officers.
John H. Short, Ph.D. has been President and Chief Executive Officer since May 2004, having served as Interim President and Chief Executive Officer since June 2003 and a director of the company since 1991. Prior to May 2004, Dr. Short was the managing partner of Phase 2 Consulting, Inc., a healthcare management consulting firm, for more than 18 years.
Jay W. Shreiner has been Chief Financial Officer of the Company since joining the Company in March 2006. Prior to joining the Company, Mr. Shreiner was Chief Financial Officer for several private companies within Austin Ventures’ portfolio of companies.
- 85 -
Patricia S. Williams has been Senior Vice President, General Counsel and Secretary since joining the Company in November 2007. Prior to joining the Company, Ms. Williams was Vice President, General Counsel and Corporate Secretary for Thermadyne Holdings Corporation, a multi-national, publicly-traded company engaged in the design, manufacture, and sale of cutting and welding equipment.
Patricia M. Henry has been Executive Vice President, Operations since September 2004, having served most recently as President of our contract therapy division since November 2001. Ms. Henry joined the Company in October 1998.
Mary Pat Welc has been Senior Vice President, Operations since 2003. Prior to that, Ms. Welc served as Regional Vice President of Operations. Ms. Welc joined the Company in 1996.
Brock Hardaway has been Executive Vice President, Operations since May 2010. Prior to that, Mr. Hardaway served as President and Chief Operating Officer of Triumph HealthCare. Mr. Hardaway joined Triumph in 2005.
James F. Martin has been Senior Vice President, Chief Human Resources Officer since December 2007, having served most recently as the Vice President, Human Resources since joining the Company in March 2005. Prior to joining the Company, Mr. Martin was Vice-President, Human Resources at Bankers Life & Casualty Company, a division of Conseco.
Jeff A. Zadoks has been Senior Vice President and Chief Accounting Officer since February 2010. Mr. Zadoks has also served as Vice President and Corporate Controller since joining the Company in December 2003. Prior to joining the Company, Mr. Zadoks was Corporate Controller of MEMC Electronic Materials, Inc.
Samuel W. Duggan II has been Vice President and Treasurer since joining the Company in January 2009. Prior to joining the Company, Mr. Duggan was Vice President, Investor Relations and Treasurer for Kellwood Company from June 2007 to December 2008. He also served as Kellwood’s Vice President, Treasury Services and Vice President, Shared Services from 2005 to 2007.
Section 303A.12(a) of the NYSE Listed Company Manual requires the chief executive officer (“CEO”) of each listed company to certify to the NYSE each year that he or she is not aware of any violation by the listed company of any of the NYSE’s corporate governance rules. The CEO of RehabCare submitted the required certification without qualification to the NYSE on May 5, 2010.
|
ITEM 11.
|
EXECUTIVE COMPENSATION
|
Information regarding executive compensation is included in an amendment to this Form 10-K which will be filed not later than 120 days after the end of the fiscal year covered by this Form 10-K and is incorporated herein by reference.
| ITEM 12. | SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND |
| MANAGEMENT AND RELATED STOCKHOLDER MATTERS |
Information regarding security ownership of certain beneficial owners and management is included in an amendment to this Form 10-K which will be filed not later than 120 days after the end of the fiscal year covered by this Form 10-K and is incorporated herein by reference.
- 86 -
The following table provides information as of fiscal year ended December 31, 2010 with respect to the shares of common stock that may be issued under our existing equity compensation plans:
|
Plan category
|
Number of
securities to
be issued
upon
exercise of
outstanding
options,
warrants and
rights
(a)
|
Weighted-average
exercise price of
outstanding
options, warrants
and rights
(b)
|
Number of securities
remaining available
for future issuance
under equity
compensation plans
(excluding securities
reflected in column (a))
(c)
|
|
|
Equity compensation plans approved by security holders
|
604,868
|
$24.33
|
2,181,606
|
(1)
|
|
Equity compensation plans not approved by security holders
|
-
|
-
|
-
|
|
|
Total
|
604,868
|
$24.33
|
2,181,606
|
|
|
|
(1)
|
Represents the number of shares of common stock available for future issuance under the Company’s 2006 Equity Incentive Plan. Permissible awards under the Company’s plan include stock options, stock appreciation rights, restricted stock, stock units and other equity-based awards.
|
|
ITEM 13.
|
CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE
|
Information regarding certain relationships and related transactions is included in an amendment to this Form 10-K which will be filed not later than 120 days after the end of the fiscal year covered by this Form 10-K and is incorporated herein by reference.
| ITEM 14. | PRINCIPAL ACCOUNTANT FEES AND SERVICES |
Information regarding principal accountant fees and services is included in an amendment to this Form 10-K which will be filed not later than 120 days after the end of the fiscal year covered by this Form 10-K and is incorporated herein by reference.
- 87 -
PART IV
|
ITEM 15.
|
EXHIBITS AND FINANCIAL STATEMENT SCHEDULES
|
|
(a)
|
The following documents are filed as part of this Annual Report on Form 10-K:
|
||
|
(1)
|
Financial Statements:
|
||
|
Report of Independent Registered Public Accounting Firm
|
|||
|
Consolidated Balance Sheets as of December 31, 2010 and 2009
|
|||
|
Consolidated Statements of Earnings for the years ended December 31, 2010, 2009 and 2008
|
|||
|
Consolidated Statements of Comprehensive Income for the years ended December 31, 2010, 2009 and 2008
|
|||
|
Consolidated Statements of Changes in Equity for the years ended December 31, 2010, 2009 and 2008
|
|||
|
Consolidated Statements of Cash Flows for the years ended December 31, 2010, 2009 and 2008
|
|||
|
Notes to Consolidated Financial Statements
|
|||
|
(2)
|
Financial Statement Schedules:
|
||
|
None
|
|||
|
(3)
|
Exhibits:
|
||
|
See Exhibit Index on page 90 of this Annual Report on Form 10-K.
|
|||
- 88 -
|
|
SIGNATURES
|
Pursuant to the requirements of Section 13 of the Securities Exchange Act of 1934, the Registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
Dated: February 28, 2011
| REHABCARE GROUP, INC. | ||
| (Registrant) | ||
|
By:
|
/s/ John H. Short
|
|
|
John H. Short
|
||
|
President and Chief Executive Officer
|
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the Registrant and in the capacities and on the date indicated.
|
Signature
|
Title
|
Dated
|
||
|
/s/ John H. Short
|
President, Chief Executive
|
February 28, 2011
|
||
|
John H. Short
|
Officer and Director
|
|||
|
(Principal Executive Officer)
|
||||
|
/s/ Jay W. Shreiner
|
Executive Vice President and
|
February 28, 2011
|
||
|
Jay W. Shreiner
|
Chief Financial Officer
|
|||
|
(Principal Financial Officer)
|
||||
|
/s/ Jeff A. Zadoks
|
Senior Vice President and
|
February 28, 2011
|
||
|
Jeff A. Zadoks
|
Chief Accounting Officer
|
|||
|
(Principal Accounting Officer)
|
||||
|
/s/ Colleen Conway-Welch
|
Director
|
February 28, 2011
|
||
|
Colleen Conway-Welch
|
||||
|
/s/ Christopher T. Hjelm
|
Director
|
February 28, 2011
|
||
|
Christopher T. Hjelm
|
||||
|
/s/ Anthony S. Piszel
|
Director
|
February 28, 2011
|
||
|
Anthony S. Piszel
|
||||
|
/s/ Suzan L. Rayner
|
Director
|
February 28, 2011
|
||
|
Suzan L. Rayner
|
||||
|
/s/ Harry E. Rich
|
Director
|
February 28, 2011
|
||
|
Harry E. Rich
|
||||
|
/s/ Larry Warren
|
Director
|
February 28, 2011
|
||
|
Larry Warren
|
||||
|
/s/ Theodore M. Wight
|
Director
|
February 28, 2011
|
||
|
Theodore M. Wight
|
- 89 -
EXHIBIT INDEX
|
2.1
|
Agreement and Plan of Merger, dated November 3, 2009, between the Registrant, RehabCare Group East, Inc., RehabCare Hospital Holdings, L.L.C., RehabCare Merger Sub Corporation, Triumph HealthCare Holdings, Inc. and TA Associates, Inc. (filed as Exhibit 99.2 to the Registrant’s Current Report on Form 8-K dated November 3, 2009 and incorporated herein by reference)
|
|
2.2
|
Agreement and Plan of Merger, dated February 7, 2011, between the Registrant and Kindred Healthcare, Inc. and Kindred Healthcare Development, Inc. (filed as Exhibit 2.1 to the Registrant’s Current Report on Form 8-K dated February 8, 2011 and incorporated herein by reference)
|
|
3.1
|
Restated Certificate of Incorporation (filed as Exhibit 3.1 to the Registrant’s Registration Statement on Form S-1, dated May 9, 1991 [Registration No. 33-40467], and incorporated herein by reference)
|
|
3.2
|
Certificate of Amendment of Certificate of Incorporation (filed as Exhibit 3.1 to the Registrant’s Quarterly Report on Form 10-Q for the quarter ended May 31, 1995 and incorporated herein by reference)
|
|
3.3
|
Amended and Restated Bylaws, dated October 30, 2007 (filed as Exhibit 3.1 to the Registrant’s Current Report on Form 8-K dated October 31, 2007 and incorporated herein by reference)
|
|
10.1
|
1987 Incentive Stock Option and 1987 Nonstatutory Stock Option Plans (filed as Exhibit 10.1 to the Registrant’s Registration Statement on Form S-1, dated May 9, 1991 [Registration No. 33-40467] and incorporated herein by reference) *
|
|
10.2
|
Form of Stock Option Agreement for 1987 Incentive Stock Option and 1987 Nonstatutory Stock Option Plans (filed as Exhibit 10.2 to the Registrant’s Registration Statement on Form S-1, dated May 9, 1991 [Registration No. 33-40467] and incorporated herein by reference) *
|
|
10.3
|
Termination Compensation Agreement, dated December 11, 2007 by and between RehabCare Group, Inc. and John H. Short, Ph.D. (filed as Exhibit 10.1 to Registrant’s Annual Report on Form 8-K dated December 12, 2007 and incorporated herein by reference) *
|
|
10.4
|
Amendment to Termination Compensation Agreement, dated December 11, 2007 by and between RehabCare Group, Inc. and John H. Short, Ph.D. (filed as Exhibit 10.1 to Registrant’s Current Report on Form 8-K dated December 12, 2008 and incorporated herein by reference) *
|
|
10.5
|
Letter agreement, dated February 7, 2011, by and between RehabCare Group, Inc. and John H. Short, Ph.D. (filed as Exhibit 10.1 to the Registrant’s Current Report on Form 8-K dated February 8, 2011 and incorporated herein by reference)*
|
|
10.6
|
Termination Compensation Agreement dated December 8, 2008 by and between RehabCare Group, Inc. and Jay W. Shreiner (filed as Exhibit 10.2 to Registrant’s Current Report on Form 8-K dated December 12, 2008 and incorporated herein by reference) *
|
- 90 -
|
10.7
|
Termination Compensation Agreement dated December 8, 2008 by and between RehabCare Group, Inc. and Patricia M. Henry (filed as Exhibit 10.3 to Registrant’s Current Report on Form 8-K dated December 12, 2008 and incorporated herein by reference) *
|
|
10.8
|
Form of Change in Control Termination Agreement dated December 8, 2008 by and between RehabCare Group, Inc. and Mary Patricia Welc (filed as Exhibit 10.4 to Registrant’s Current Report on Form 8-K dated December 12, 2008 and incorporated herein by reference) *
|
|
10.9
|
Change in Control Termination Agreement dated November 12, 2007 by and between RehabCare Group, Inc. and Patricia S. Williams (filed as Exhibit 10.6 to Registrant’s Annual Report on Form 10-K for the year ended December 31, 2007 and incorporated herein by reference) *
|
|
10.10
|
Termination Compensation Agreement dated November 3, 2009 by and between RehabCare Group, Inc. and William “Brock” Hardaway (filed herewith) *
|
|
10.11
|
Form of Termination Compensation Agreement dated March 10, 2006 by and between RehabCare Group, Inc. and other executive officers who are not named executive officers (filed as Exhibit 10.5 to Registrant’s Annual Report on Form 10-K for the year ended December 31, 2005 and incorporated herein by reference) *
|
|
10.12
|
RehabCare Severance Plan for Company Senior Vice Presidents effective January 1, 2009 (filed as Exhibit 10.5 to Registrant’s Current Report on Form 8-K dated December 12, 2008 and incorporated herein by reference) *
|
|
10.13
|
RehabCare Severance Plan for Company Vice Presidents effective January 1, 2009 (filed as Exhibit 10.6 to Registrant’s Current Report on Form 8-K dated December 12, 2008 and incorporated herein by reference) *
|
|
10.14
|
RehabCare Executive Deferred Compensation Plan (filed as Exhibit 10.12 to the Registrant’s Report on Form 10-K, dated May 27, 1994 and incorporated herein by reference) *
|
|
10.15
|
RehabCare Executive Deferred Compensation Plan as amended and restated effective January 1, 2009 (filed as Exhibit 10.7 to Registrant’s Current Report on Form 8-K dated December 12, 2008 and incorporated herein by reference) *
|
|
10.16
|
RehabCare Directors’ Stock Option Plan (filed as Appendix A to Registrant’s definitive Proxy Statement for the 1994 Annual Meeting of Stockholders and incorporated herein by reference) *
|
|
10.17
|
Second Amended and Restated 1996 Long-Term Performance Plan (filed as Appendix B to Registrant’s definitive Proxy Statement for the 2004 Annual Meeting of Stockholders and incorporated herein by reference) *
|
- 91 -
|
10.18
|
Form of Stock Option Agreement for the Second Amended and Restated 1996 Long-Term Performance Plan (filed as Exhibit 10.10 to the Registrant’s Annual Report on Form 10-K for the year ended December 31, 2005 and incorporated herein by reference) *
|
|
10.19
|
Form of Restricted Stock Agreement for the Second Amended and Restated 1996 Long-Term Performance Plan (filed as Exhibit 10.11 to the Registrant’s Annual Report on Form 10-K for the year ended December 31, 2005 and incorporated herein by reference) *
|
|
10.20
|
RehabCare Group, Inc. 2006 Equity Incentive Plan (filed as Appendix A to the Registrant’s Definitive Proxy Statement for the 2006 Annual Meeting of Shareholders and incorporated herein by reference) *
|
|
10.21
|
RehabCare Group, Inc. 2006 Equity Incentive Plan, as amended and restated effective May 4, 2010 (filed as Appendix A to the Registrant’s Definitive Proxy Statement for the 2010 Annual Meeting of Shareholders and incorporated herein by reference)*
|
|
10.22
|
Amended and Restated Credit Agreement, dated November 24, 2009, by and among RehabCare Group, Inc., as borrower, certain subsidiaries and affiliates of the borrower, as guarantors, and Bank of America, N.A., as administrative agent and collateral agent, and Banc of America Securities LLC, RBC Capital Markets and BNP Paribas Securities Corp., as joint lead arrangers (filed as Exhibit 10.1 to the Registrant’s Current Report on Form 8-K dated November 24, 2009 and incorporated herein by reference)
|
|
10.23
|
Pledge Agreement, dated as of November 24, 2009, by and among RehabCare Group, Inc. and subsidiaries, as pledgors, and Bank of America, N.A., as collateral agent (filed as Exhibit 10.1 to the Registrant’s Current Report on Form 8-K dated November 24, 2009 and incorporated herein by reference)
|
|
10.24
|
Security Agreement, dated as of November 24, 2009, by and among RehabCare Group, Inc. and subsidiaries, as grantors, and Bank of America, N.A., as collateral agent (filed as Exhibit 10.1 to the Registrant’s Current Report on Form 8-K dated November 24, 2009 and incorporated herein by reference)
|
|
10.25
|
Non-Continuous Aircraft Dry Lease Agreement by and between 55JS Limited, Co. and RehabCare Group, Inc. (filed as Exhibit 10.1 to Registrant’s Current Report on Form 8-K dated September 7, 2006 and incorporated herein by reference)
|
|
10.26
|
Asset Purchase Agreement dated June 8, 2005 by and among RehabCare Group East, Inc., a wholly owned subsidiary of Registrant, MeadowBrook HealthCare, Inc., MeadowBrook Specialty Hospital of Tulsa LLC, Lafayette Rehab Associate Limited Partnership, Clear Lake Rehabilitation Hospital, Inc. and South Dade Rehab Associates Limited Partnership (filed as Exhibit 10.1 to Registrant’s Current Report on Form 8-K dated August 4, 2005 and incorporated herein by reference)
|
|
10.27
|
Purchase and Sale Agreement, dated May 3, 2006, by and among LUK-Symphony Management, LLC, Symphony Health Services, LLC and RehabCare Group, Inc. (filed as exhibit 10.1 to the Registrant’s Current Report on Form 8-K dated May 8, 2006 and incorporated herein by reference)
|
- 92 -
|
21.1
|
Subsidiaries of the Registrant (filed herewith)
|
|
23.1
|
Consent of KPMG LLP (filed herewith)
|
|
31.1
|
Certification by Chief Executive Officer in accordance with Rule 13a-14(a) under the Securities Exchange Act of 1934, as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 (filed herewith)
|
|
31.2
|
Certification by Chief Financial Officer in accordance with Rule 13a-14(a) under the Securities Exchange Act of 1934, as adopted pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 (filed herewith)
|
|
32.1
|
Certification by Chief Executive Officer in accordance with 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 (filed herewith)
|
|
32.2
|
Certification by Chief Financial Officer in accordance with 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 (filed herewith)
|
_________________________
* Management contract or compensatory plan or arrangement.
- 93 -