Attached files
| file | filename |
|---|---|
| EX-32 - EX-32 - CardioNet, Inc. | a2202163zex-32.htm |
| EX-31.2 - EX-31.2 - CardioNet, Inc. | a2202163zex-31_2.htm |
| EX-23.1 - EX-23.1 - CardioNet, Inc. | a2202163zex-23_1.htm |
| EX-31.1 - EX-31.1 - CardioNet, Inc. | a2202163zex-31_1.htm |
| EX-10.41 - EX-10.41 - CardioNet, Inc. | a2202163zex-10_41.htm |
| EX-10.43 - EX-10.43 - CardioNet, Inc. | a2202163zex-10_43.htm |
| EX-10.16 - EX-10.16 - CardioNet, Inc. | a2202163zex-10_16.htm |
| EX-10.39 - EX-10.39 - CardioNet, Inc. | a2202163zex-10_39.htm |
| EX-10.42 - EX-10.42 - CardioNet, Inc. | a2202163zex-10_42.htm |
| EX-10.38 - EX-10.38 - CardioNet, Inc. | a2202163zex-10_38.htm |
| EX-10.40 - EX-10.40 - CardioNet, Inc. | a2202163zex-10_40.htm |
Use these links to rapidly review the document
TABLE OF CONTENTS
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
ý |
ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
|
For the fiscal year ended December 31, 2010 |
||
OR |
||
o |
TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
|
For the transition period from N/A to N/A |
||
Commission file number: 0-10961
CardioNet, Inc.
(Exact name of registrant as specified in its charter)
| DELAWARE (State or other jurisdiction of incorporation or organization) |
94-2573850 (I.R.S. Employer Identification No.) |
|
227 Washington Street Conshohocken, Pennsylvania (Address of principal executive offices) |
19428 (Zip Code) |
(610) 729-7000
(Registrant's telephone number, including area code)
Not Applicable
(Former name, former address and former fiscal year, if changed since last report)
Securities registered pursuant to Section 12(b) of the Act:
| Title of Each Class | Name of Each Exchange on Which Registered | |
|---|---|---|
| Common Stock, $0.001 par value | NASDAQ Stock Market LLC |
Securities registered pursuant to Section 12(g) of the Act: None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes o No ý
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Exchange Act. Yes o No ý
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes ý No o
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T (§ 229.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes o No o
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of registrant's knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. o
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See the definitions of "large accelerated filer," "accelerated filer," and "smaller reporting company" in Rule 12b-2 of the Exchange Act. (Check one):
| Large accelerated filer o | Accelerated filer ý | Non-accelerated filer o (Do not check if a smaller reporting company) |
Smaller reporting company o |
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). Yes o No ý
The aggregate market value of the registrant's common stock held by non-affiliates of the registrant was $95,027,776 based on the closing sale price at which the common stock was last sold on June 30, 2010, the last business day of the registrant's most recently completed second fiscal quarter.
As of February 14, 2011, 24,256,506 shares of the registrant's common stock were outstanding.
DOCUMENTS INCORPORATED BY REFERENCE
Certain information contained in the registrant's definitive Proxy Statement for the 2011 annual meeting of stockholders is incorporated by reference into Part III of this Form 10-K.
CardioNet, Inc.
Annual Report on Form 10-K
For The Fiscal Year Ended December 31, 2010
2
CAUTIONARY STATEMENT REGARDING FORWARD-LOOKING STATEMENTS
The information in this report includes certain forward-looking statements within the meaning of the "Safe Harbor" provisions of the Private Securities Litigation Reform Act of 1995 regarding, among other things, our growth prospects, the prospects for our products and our confidence in the Company's future. These statements may be identified by words such as "expect," "anticipate," "estimate," "intend," "plan", "believe," and other words and terms of similar meaning. Such forward-looking statements are based on current expectations and involve inherent risks and uncertainties, including important factors that could delay, divert, or change any of them, and could cause actual outcomes and results to differ materially from current expectations. These factors include, among other things, the national rate set by the Centers for Medicare and Medicaid Services ("CMS") for our mobile cardiovascular telemetry service, effectiveness of our cost savings initiatives, changes to insurance coverage and reimbursement levels for our products, the success of our sales and marketing initiatives, our ability to attract and retain talented executive management and sales personnel, our ability to identify acquisition candidates, acquire them on attractive terms and integrate their operations into our business, the commercialization of new products, market factors, internal research and development initiatives, partnered research and development initiatives, competitive product development, changes in governmental regulations and legislation, the continued consolidation of payors, acceptance of our new products and services and patent protection and litigation, as well as the risks discussed in Item 1A of this report entitled "Risk Factors." We undertake no obligation to publicly update any forward-looking statement contained in this report whether as a result of new information, future events, or otherwise.
CardioNet, Inc. (the "Company," "CardioNet," "we" or "us"), a Delaware corporation, provides continuous, real-time ambulatory outpatient management solutions for monitoring relevant and timely clinical information regarding an individual's health. In September 1999, the Company began its focus on helping physicians more rapidly diagnose and more effectively manage therapy for patients with cardiovascular disease. The Company began developing its product platform in April 2000. The Company then spent seven years developing a proprietary integrated patient management platform that incorporates a wireless data transmission network, internally developed software, Food and Drug Administration (FDA) cleared algorithms and medical devices, and a 24-hour digital monitoring service center. The Company is currently focused on the diagnosis and monitoring of cardiac arrhythmias, or heart rhythm disorders, through its core Mobile Cardiac Outpatient Telemetry™ (MCOT™), event and Holter services.
In February 2002, the Company received FDA 510(k) clearance for the first and second generations of its core MCOT™ devices. MCOT™ automatically detects a patient's cardiac rhythm irregularities and transmits electrocardiogram (ECG) data to a continuously monitored information center that was opened in Conshohocken, PA in July 2002. We released our third generation of MCOT™ monitoring devices ("C3") in December 2007. The C3 generation of devices built upon our previous technology by allowing for expanded wireless transmitting capabilities and improved user interface characteristics. In April 2010, we received FDA 501(k) clearance for our next generation device, the C5, and anticipate launching C5 in 2011. The CardioNet Monitoring Center provides analysis and response for all incoming ECG data. Currently, the Company provides all cardiac arrhythmia monitoring services for MCOT™ at this location. The Company receives reimbursement for the monitoring services provided to patients from Medicare and other third-party payors. The Company was initially incorporated in California in 1994, and re-incorporated in Delaware in connection with its initial public offering in March 2008.
3
We believe that MCOT™'s continuous heartbeat-by-heartbeat monitoring is a fundamental advancement in arrhythmia monitoring. We believe our system has the potential to transform an industry that has historically relied on memory-constrained, intermittent digital or tape recorders, such as event and Holter monitors. The drawbacks of these existing technologies include the failure to provide real-time data, memory constraints, frequent inaccurate diagnoses and an inability to monitor patient compliance and interaction. We believe these drawbacks lead to suboptimal diagnostic yields, adversely impacting clinical outcomes and health care costs. In a randomized clinical trial, MCOT™ detected clinically significant arrhythmias nearly three times as often as traditional loop event monitors in patients who had previously experienced negative or inconclusive Holter monitoring.
CardioNet's MCOT™ service incorporates a lightweight patient-worn sensor attached to electrodes that capture two-channel ECG data, measuring electrical activity of the heart. The device communicates wirelessly with a compact, handheld monitor. The monitor analyzes incoming heartbeat-by-heartbeat information from the sensor on a real-time basis by applying proprietary algorithms designed to detect arrhythmias. When the monitor detects an arrhythmic event, it automatically transmits the ECG to the CardioNet Monitoring Center, even in the absence of symptoms noticed by the patient and without patient involvement. At the CardioNet Monitoring Center, which operates 24 hours a day and 7 days per week, experienced certified cardiac monitoring specialists analyze the sent data, respond to urgent events and report results in the manner prescribed by the physician. The MCOT™ devices currently store 21 days of ECG data, in contrast to 10 minutes for a typical event monitor. The MCOT™ device employs two-way wireless communications, enabling continuous transmission of patient data to the CardioNet Monitoring Center and permitting physicians to remotely adjust monitoring parameters and request previous ECG data from the memory stored in the monitor.
We completed a 300-patient randomized clinical trial in March 2007 that found that MCOT™ provided a significantly higher diagnostic yield compared to traditional loop event monitoring, including such monitoring designed to automatically detect certain arrhythmias. We are using the clinical evidence from this trial to both drive continued physician adoption of our solution and attempt to secure contracts with additional commercial payors.
Since our commercial introduction of MCOT™ in January 2003, physicians have enrolled over 400,000 patients in our MCOT™ services. Through December 31, 2010, we marketed our solution in 49 states. We have secured direct contracts with 304 commercial payors as of December 31, 2010, which we estimate that, when combined with our Medicare participation, represents more than 200 million covered lives.
The American Medical Association ("AMA") has established reimbursement rates applicable to the Category I CPT code for Mobile Cardiovascular Telemetry. These billing codes allowed for automated claims adjudication, substantially simplifying the reimbursement process for physicians and payors compared to the previous process. Reimbursement was previously obtained through non-specific billing codes which require various narratives that, in most cases, involve semi-automated or manual processing, as well as additional review by payors. The Centers for Medicare and Medicaid Services ("CMS") has established reimbursement rates that cover MCOT™. The codes and rates are contained in The Medicare Program Final Rule for the calendar year 2011.
On November 2, 2010, CMS published The Medicare Program Final Rule establishing a national rate for the MCOT™ technology (CPT Code 93229). CMS valued the CPT code at 20.14 relative value units, which was multiplied by an annually determined conversion factor to establish the amounts paid under the physician fee schedule. Using the formula and values currently in place, the Company's national rate is approximately $739 per service, effective January 1, 2011. This is a decrease of approximately 2% from the Company's current local carrier rate of $754 per service that was previously
4
established by Highmark Medicare Services ("HMS"), a contract provider for CMS, effective September 1, 2009.
On December 21, 2010, the Company completed the acquisition of Biotel Inc., and its wholly owned subsidiaries, Braemar, Inc. and Agility Centralized Research Services, Inc. The acquisition gives the Company the ability to develop, manufacture, test and market medical devices and related software to medical companies, clinics and hospitals. Additionally, the acquisition gives the Company access to established customer relationships, entry into the clinical trial service business and the ability to diversify its product and service offerings. Prior to the acquisition, Biotel Inc. common stock was traded on the Over the Counter Bulletin Board under the symbol BTEL.OB. For more information about the Company's acquisition of Biotel Inc., see Note 3 to our consolidated financial statements.
We believe that our integrated patient monitoring platform can be utilized for future applications in multiple markets beyond arrhythmia monitoring. We believe that we have growth opportunities in clinical trial monitoring, where we can leverage our FDA-cleared algorithms for uses such as specific cardiac data required in clinical trials, and in comprehensive disease management for congestive heart failure, diabetes and other diseases. We believe that our technology could also be used to create "instant telemetry beds" in hospitals, particularly in rural hospitals, step-down units or skilled nursing facilities, to help cope with acute nursing shortages by reducing the number of nurses needed to oversee ECG monitoring. In addition, the significant capital equipment costs associated with in-facility based cardiac telemetry (continuously attended ECG monitoring) could be avoided through the use of MCOT™.
Industry Overview
Overview of Cardiac Arrhythmias
A cardiac arrhythmia is categorized as a temporary or sustained abnormal heart rhythm that is caused by a disturbance in the electrical signals in the chambers of the heart. Proper transmission of electrical signals to the heart is necessary to ensure effective heart function. There are two main categories of arrhythmia: tachycardia, meaning too fast a heartbeat; and bradycardia, meaning too slow a heartbeat.
Arrhythmias affect more than four million people in the United States. According to the American Heart Association, arrhythmias result in more than 780,000 hospitalizations and contribute to approximately 480,000 deaths each year. A number of factors can contribute to arrhythmias including cardiovascular disease, high blood pressure, diabetes, smoking, excessive consumption of alcohol or caffeine, illicit drug abuse or stress. An arrhythmia may be a symptom of serious cardiovascular disease and, if left undiagnosed and untreated, can lead to stroke, other serious complications or even death. Examples of arrhythmias and their consequences include:
- •
- Atrial fibrillation. The most prevalent arrhythmia is
atrial fibrillation, an arrhythmia that affects approximately 2.2 million Americans and is characterized by a rapid, irregular quivering of the upper chambers of the heart. According to the
Framingham Study published in 2004, one in four people over the age of 40 in the United States has a lifetime risk of developing atrial fibrillation, and the incidence of atrial fibrillation increases
with age. According to the American Heart Association, approximately 15% to 20% of the estimated 700,000 strokes that occur annually in the United States are attributable to atrial fibrillation and
people with atrial fibrillation are approximately five times more likely to have a stroke.
- •
- Ventricular Tachycardia. Ventricular tachycardia is a potentially life-threatening arrhythmia initiated in the lower chambers of the heart. It can interfere with the ability of the heart to pump blood and may degenerate into ventricular fibrillation requiring CPR and defibrillation. It can occur with or without apparent heart disease.
5
- •
- Syncope. While not an arrhythmia, syncope, or fainting, many times results from an arrhythmia. It is the temporary loss of consciousness because of a sudden decline in blood flow to the brain that may be the result of tachycardia or bradycardia. Syncope accounts for 1% to 3% of emergency department visits and up to 6% of hospital admissions each year in the United States.
The ability to diagnose or rule out an arrhythmia as a symptom of a cardiac condition is important both to treat those patients with serious cardiovascular diseases as well as to identify those patients that may not require further medical attention.
Evolution of Traditional Arrhythmia Monitoring Technologies
Arrhythmias may be diagnosed either in a physician's office or other health care facility or remotely by monitoring a patient's heart rhythm. Typically, physicians will initially administer a resting ECG that monitors the electrical impulses in a patient's heart. If a physician determines that a patient needs to be monitored for a longer period of time to produce a diagnosis, the physician will typically prescribe an ambulatory cardiac monitoring device, such as a Holter monitor or an event monitor.
Some physicians own their own ambulatory cardiac monitoring devices and provide ambulatory monitoring services directly to their patients, while other physicians outsource the services to third party providers. In the wake of increasing legal and compliance requirements surrounding ambulatory cardiac monitoring, including a 2003 Medicare decision requiring 24 hour per day monitoring stations, the increasing trend is for physicians and hospitals to outsource their monitoring needs to third party providers.
If either the Holter monitor or event monitor are negative or inconclusive and the physician still suspects an arrhythmia as the cause of the symptom, the physician may decide to prescribe additional, more expensive testing or hospitalize the patient in a telemetry unit (continuously attended ECG monitoring). In-hospital telemetry is expensive and therefore is only utilized selectively and for short time periods, and the monitored data is often not reflective of real-life cardiac activity.
Holter Monitors
A Holter monitor, first used in 1961, is an ambulatory cardiac monitoring device that is generally worn by a patient for a one-day or, in rare instances, two-day period in order to record continuous ECG data. After the one- or two-day period, the magnetic or digital storage, or other medium containing the data recorded by this device, is delivered by hand, mail or internet for processing and analysis by the physician or a third party service provider. Despite the advent of newer technologies, Holter monitoring continues to be used today for patients whose suspected arrhythmia is believed to occur many times during the course of a day, in which case a Holter is often effective or adequate. However, for a patient that has an unpredictable or intermittent arrhythmia, a Holter may not provide clinically useful information due to the insufficient duration of the monitoring period. In addition, as a result of the typical one- to three-day reporting delay and the lack of real-time physician notification, patients may not receive timely diagnosis of their condition. Any artifact, or noise, in the data will not be discovered until the test is analyzed. A 2005 Frost & Sullivan study reported that Holters have been found to be effective in diagnosing arrhythmias only 10% of the time.
Event Monitors
Beginning in the 1980s, a new category of ambulatory cardiac monitoring devices called event monitors emerged, with the most common type referred to as manual-trigger loop event monitors. An event monitor records several minutes of ECG activity at a time and then begins overwriting the memory, a process referred to as memory loop recording. The memory loop event monitor continuously records and stores the previous 60 seconds of ECG signal in internal loop memory. When
6
a patient becomes symptomatic, he or she activates the monitor by pressing the record button which stores the 60 seconds of existing loop memory and an additional 30 seconds of ECG signal following patient activation. The stored data is considered one cardiac event and provides physicians a snapshot of the ECG signal recorded immediately before and during a patient's symptoms. Non-loop event monitors are kept with the patient at all times. When a patient experiences symptoms, non-loop event monitors will typically record and store 30 seconds of ECG signal immediately following activation and placement in direct contact with the patient's chest. Event monitors have limited memory, usually less than 10 minutes, and can generally store data concerning between one and six cardiac events. The patient must transmit the event data to the monitoring center, typically by phone, and then erase the memory. To the extent that the patient does not call in and transmit data concerning an event, the device will become unable to store future event data once the device event storage is full.
Event monitors offer certain advantages over Holter monitors given that they are worn over a period of up to 30 days, instead of the one- to two-day period. However, event monitors have significant shortcomings. Manual-trigger loop event monitors capture only cardiac events associated with symptoms detectable by the patient and not asymptomatic cardiac events. In our experience, only 15% to 20% of clinically significant cardiac events are symptomatic, meaning that the patient can feel them as they occur. Other drawbacks of manual-trigger loop event monitors include the limited data storage, the lack of trend data, and poor patient compliance relating to the requirement that the patient must both trigger and transmit events.
A new type of event monitoring device was introduced in 1999 called the auto-detect loop event monitor. The auto-detect loop event monitor also records using a very short memory loop and event storage capability, capturing several minutes of heart activity at a time before starting over, but incorporates basic algorithms that look at fast, slow or irregular heart rates and, in some instances, pauses to automatically detect certain asymptomatic arrhythmias. Similar to manual-trigger loop event monitors, the auto-detect loop event monitor requires the patient to call in and transmit the event by reaching the physician or a technician at a physician's office or a monitoring center and holding the cardiac event monitor up to a telephone to transmit the event data. The latest development in auto-detect loop event monitoring is referred to as auto-detect/auto-send. Auto-detect/auto-send loop event monitors have the ability to send captured event data to a monitoring center via cell phone, instead of requiring patients to manually transmit event data. Patients do not have the ability to correlate symptoms to the event via the monitor and are required to carry a diary and make contact with the monitoring center to report symptoms. These monitors still continue to suffer from limited data storage and limited algorithm capabilities. To our knowledge, randomized prospective peer reviewed clinical trials have not yet been conducted to demonstrate any improvement in diagnostic yield between the standard loop monitors and the newer auto-trigger or auto-trigger/auto-send monitors.
Shortcomings of Traditional Arrhythmia Monitoring
Despite major advances in cardiology with new therapeutic drugs, such as beta blockers and statins, and new therapeutic devices and procedures over the last several decades, there have been few advances in ambulatory monitoring. We believe that there is a significant opportunity for new arrhythmia monitoring solutions that exploit the convergence of wireless, low power microelectronic and software technologies to address the shortcomings of traditional Holter and event monitors. We believe that existing technologies have drawbacks including inability to detect asymptomatic events, failure to provide real-time data, memory constraints, frequent inaccurate diagnoses and an inability to monitor patient compliance and interaction. These drawbacks often lead to suboptimal diagnostic yields, adversely impacting clinical outcomes and health care costs.
7
MCOT™ Solution
We have developed an ambulatory, continuous and real-time arrhythmia monitoring solution that we believe represents a significant advancement over event and Holter monitoring. CardioNet's MCOT™ service incorporates a patient-worn sensor attached to leads that captures ECG data and communicates wirelessly with a compact monitor that analyzes incoming information by applying proprietary algorithms designed to detect arrhythmias and eliminate data noise. When the monitor detects an arrhythmic event, it automatically transmits the ECG data to the CardioNet Monitoring Center, where experienced certified cardiac monitoring specialists analyze the sent data, respond to urgent events and report results in the manner prescribed by the physician. The MCOT™ monitor, on average, is worn by the patient for a period of approximately 14 days. The C3 generation MCOT™ device was released in December 2007, and includes a variety of product enhancements over previous generations of CardioNet monitoring devices. Some of these enhancements include the following:
- •
- Reduction in size to allow for a lighter unit, and increased comfort to the patient;
- •
- Increased radio transmission strength from the monitoring unit to the base to allow for greater mobility within the home;
and
- •
- Improved graphical interface of the monitoring device to be more user friendly.
MCOT™ results in a high diagnostic yield of clinically significant arrhythmias, allowing for real-time detection and analysis as well as timely intervention and treatment. In a randomized 300-patient clinical study, MCOT™ detected clinically significant arrhythmias nearly three times as often as traditional loop event monitors in patients who have previously experienced negative or non-diagnostic Holter monitoring.
We believe that MCOT™ offers the following advantages to physicians, payors and patients:
- •
- Real-time, continuous
data. MCOT™ initiates real-time analysis and automatic transmissions as events occur, which allows physicians to
receive urgent notifications in a timely manner. In contrast, most event monitors require the patient to go to a phone and call in to transmit the event data, which may not happen until hours or days
after the event, or at all if the patient is not compliant.
- •
- Expanded
memory. The MCOT™ device currently stores 21 days of ECG data, considerably more than the typical 10 minutes of
memory of event monitors. Event monitors have capacity to store multiple events, but generally store only between one and six cardiac events, a subset of which may be unusable depending on degree of
data artifacts. To the extent that the patient does not call in and transmit an event, once the event monitor is full, it may become unable to capture future events. MCOT™ not only
provides 21 days of memory to prevent inadvertent loss of data, but also presents physicians with trend data for heart rate and atrial fibrillation burden.
- •
- Increased compliance through technology and reduced patient
interaction. MCOT™ works without patient interaction, automatically detecting and transmitting asymptomatic events. Event
monitors typically require the patient to call in and transmit the event by reaching the physician or a technician at a physician's office or a monitoring center and holding the event monitor up to a
telephone to transmit the event data. MCOT™ increases patient compliance by alerting the patient through the monitor of loss of communication between the sensor and monitor or that a lead
has become detached. Physicians are able to confirm the patient wore the monitor through the daily reports provided to physicians.
- •
- Reflects real-life cardiac activity. Patients using MCOT™ can continue normal activities, including activities that may trigger an arrhythmia.
8
- •
- Symptom
correlation. Patients experiencing a symptom record details of their symptom and activity data on the touch-screen of the
MCOT™ device monitor, which allows physicians to correlate the information to the underlying ECG data.
- •
- Detection of asymptomatic
events. We have developed a proprietary, FDA-cleared ECG detection algorithm that automatically identifies arrhythmic
events, even in the absence of symptoms noticed by the patient.
- •
- Minimization of data artifacts or
"noise". We have designed our algorithms to eliminate data artifacts to reduce inaccurate diagnoses and enable more efficient data
review by both physicians and the certified cardiac monitoring specialists in the CardioNet Monitoring Center. In contrast, we believe that certain of the algorithms in the auto-detect
loop event monitors rely on simplistic triggers relating to high, low and irregular heart rates and, in some cases, pauses in heart rate, and consequently result in frequent inaccurate diagnoses.
- •
- Two-way wireless capabilities for transmission, remote programming and data
retrieval. MCOT™ devices allow two-way wireless communication, compared to most event monitors that only support one-way transmissions. With
MCOT™, physicians can adjust device parameters remotely, "check in" on the patient and request ECG data from the previous 21 days.
- •
- Potential reduction in health care
costs. We have demonstrated increased diagnostic yield as compared to event monitoring, which we believe may reduce "time to diagnosis"
and reduce health care costs resulting from repeated emergency room and physician visits, additional diagnostic testing, prolonged hospitalizations for the sole purpose of arryhythmia monitoring and
unnecessary hospitalizations for drug initiation and titration, as well as expenditures resulting from stroke and other serious cardiovascular complications.
- •
- Tailored and customized to physician's needs. The prescribing physician selects patient-specific monitoring thresholds and response parameters. The physician selects the events to be monitored and the level and timing of response by the CardioNet Monitoring Center from routine daily reporting to urgent "stat" reports. Physicians can review the data by fax or internet, depending on their preferences.
In addition to MCOT™, we offer event and Holter monitoring services, positioning us as a "one-stop shop" for arrhythmia monitoring solutions. We provide cardiologists and electrophysiologists who prefer to use a single source of arrhythmia monitoring services with a full spectrum of solutions, ranging from our differentiated MCOT™ services to event and Holter monitoring.
Monitoring with MCOT™
Initiation of Service
A physician prescribing MCOT™ for his patient completes an enrollment form that describes the length of time during which the patient should be monitored, together with patient-specific monitoring thresholds and response parameters. Once the patient has been enrolled, a CardioNet representative contacts the patient to coordinate delivery and schedule a telephonic patient-education session on the use of the MCOT™ device.
Monitoring
A lightweight sensor (worn as a pendant or on a belt clip) attached to leads records two channels of ECG. The sensor constantly communicates wirelessly with the monitor, a compact handheld unit which can be tucked into a pocket or purse. The monitor analyzes incoming information from the sensor on a real-time basis by applying proprietary algorithms designed to detect arrhythmias.
9
When the monitor detects an arrhythmic event (defined by the values prescribed by the patient's physician), it transmits the ECG to the CardioNet Monitoring Center, even in the absence of symptoms noticed by the patient and without patient interaction. In instances when patients experience a symptom, they select their symptom and the contemporaneous activity level through the monitor's touch screen. Once completed, the monitor automatically transmits the event to the CardioNet Monitoring Center for review. When at home, the patient can place the monitor in a base station, which allows recharging and enables automated data transmission through the standard telephone line in the patient's home. Our monitors store 21 days of ECG data.
The monitor allows two-way wireless communications, enabling the CardioNet Monitoring Center to adjust device parameters, "check in" on the patient and pull previous ECG data, over standard telephone lines and through cellular coverage. Most other ambulatory devices on the market, such as most event monitors, only support one-way transmissions.
Central Monitoring Station/Data Transmission Network
At the CardioNet Monitoring Center in Conshohocken, PA, an Independent Diagnostic Testing Facility (IDTF) certified by Medicare, experienced certified cardiac monitoring specialists analyze the sent data, respond to urgent events and report results in the manner prescribed by the physician and monitor patient compliance. The CardioNet Monitoring Center operates 24 hours a day, 7 days per week. The data transmission is accomplished through (i) a wireless cell phone modem in the monitor or (ii) through the telephone line modem in the base station.
Physician Notification
When prescribing MCOT™, physicians will pre-prescribe the criteria for when they wish to be notified by the Monitoring Center regarding a significant arrhythmic event. The notification is based on the patient's ECG and symptoms and can occur any time, 24 hours a day, 7 days a week. Physicians can review the data in the media they prefer, choosing from fax or internet. Reports have been designed to allow rapid review of results, graphing related data and trends. The following is a summary of the types of reports we provide:
- •
- Daily Report, which includes:
- •
- Heart rate trending chart;
- •
- Charts describing the frequency and duration of atrial fibrillation (atrial fibrillation data is trended over the length
of service);
- •
- Summary of ECG activity from the prior 24 hours, including urgent ECG's;
- •
- Description of symptoms and associated activity level if reported by patient; and
- •
- Clinical indicators demonstrating trending of arrhythmias.
- •
- Urgent Report
- •
- When a patient's ECG and/or symptom meets pre-prescribed physician notification criteria, the physician is
notified immediately and provided with the relevant ECG data, along with the symptoms and activity if reported by the patient. Physicians are also allowed to revise notification criteria if
applicable.
- •
- Fetch Report
- •
- Provides ECG data from the monitor at the request of the physician for any period during the previous 21 days.
10
- •
- End of Service Summary Report
- •
- At the completion of the patient's monitoring, a report is prepared describing the length of the monitoring service and all reports that were prepared for the patient during the monitoring service.
Other Arrhythmia Monitoring Services
In addition to MCOT™, we offer event, Holter and pacemaker monitoring services.
Event Monitoring Services
The event monitor is a small portable ECG recorder about the size of a pager designed to record and store up to 540 seconds of ECG signal. Event monitors are placed on the patient in the physician's office and worn typically for 30 days. Our event monitoring services provides physicians with the flexibility to prescribe both memory loop event monitors and non-loop event monitors. In 2010, over 90% of our event monitors prescribed by physicians were memory loop event monitors. The memory loop event monitor has two to four leads that are attached to electrodes, which are placed on the patient's chest. The memory loop event monitor continuously records and stores the previous 60 seconds of ECG signal in internal loop memory. When a patient becomes symptomatic, he or she activates the monitor by pressing the record button which stores the 60 seconds of existing loop memory and an additional 30 seconds of ECG signal following patient activation. The stored data is considered one cardiac event and provides physicians a snapshot of the ECG signal recorded immediately before and during a patient's symptoms. Some of our memory loop event monitors have an internal algorithm that can automatically activate the monitor based on rate thresholds and irregular rhythms. Our non-loop event monitors are kept with the patient at all times. When a patient experiences symptoms, our non-loop event monitors will typically record and store 30 seconds of ECG signal immediately following activation and placement in direct contact with the patient's chest. Our event monitors have a capacity to store one to six cardiac events before the patient must transmit the data telephonically to one of two event monitoring centers where our trained cardiac technicians analyze the data, generate a report of the findings and return the results back to the physician. The physician then interprets the results and determines the next step for the patient. Once transmitted, the internal memory in the monitor is erased and the patient can resume activating the monitor to record further cardiac events. Our two event monitoring centers are distinct from the CardioNet Monitoring Center. We provided event monitoring services to approximately 59,655 patients in 2010.
Holter Monitoring Services
The Holter monitor is a small portable ECG recorder designed to record a continuous ECG signal for one to, in rare instances, two days. The Holter monitor has five to seven leads that are attached to electrodes, which are typically placed on the patient in the physician's office. Patients are instructed to wear the monitor continuously while they go about normal daily routine, including sleeping. During the monitoring period, the Holter monitor stores an image of the electrical impulses of every heartbeat or irregularity in either digital format on an internal compact flashcard or in analog format on a standard cassette tape located inside the monitor. Approximately 5% of our Holters are analog tape and the remaining 95% use digital flashcard technology. At the conclusion of the monitoring period, the patient returns to the physician office to have the monitor disconnected. After the patient returns home, the stored data is mailed or sent electronically through a secure web transfer to our Holter lab where our trained cardiac technicians analyze the data, generate a report of the findings and return the results back to the physician. The physician then interprets the results and determines the next step for the patient. Our Holter lab is distinct from the CardioNet Monitoring Center. We provided Holter monitoring services to approximately 56,583 patients in 2010.
11
Pacemaker Monitoring Services
Following the implantation of a pacemaker, certain physicians refer patients to us for periodic monitoring and evaluation of the device based on a pre-determined frequency set by the referring physician. The patient is provided a transmitter device that we use to telephonically transmit data to monitor the life and function of the pacemakers. For the year ended December 31, 2010, we performed approximately 15,346 pacemaker tests.
CardioNet Patient Monitoring Platform
MCOT™ is a patient monitoring platform that we believe can be leveraged for applications in multiple markets. We designed MCOT™ to connect sensors and analysis devices on the patient's body (which could include ECG, weight, blood pressure, glucose and others) to a monitoring center through the use of a wireless data transmission network. Our advanced technology allows the patient system to be housed in a small, portable, non-invasive package that requires limited patient involvement and compliance. The extended monitoring period and portability of MCOT™ enables the capture and analysis of real-life patient activity through sophisticated patient information management systems and the transmission of such data.
We have made a significant investment in infrastructure and technology over an eight year period. We have raised over $250 million in capital and spent ten years developing and deploying a proprietary integrated patient monitoring platform that incorporates a wireless data transmission network, internally developed software, FDA-cleared algorithms and medical devices, and a 24-hour digital monitoring service center. Our investment includes designing and implementing an integrated technology and service network, establishing sophisticated data services architecture in conjunction with our data partner nPhase, creating a dedicated central monitoring service center, and internally developing advanced algorithms which sense, analyze and process data.
Next Generation MCOT™ Technology Pipeline
We received FDA 510(k) clearance for our next generation platform ("C5") in April 2010. The Company expects to release its C5 generation device in 2011. The C5 features several technology enhancements including:
- •
- additional processing capabilities to operate multiple sensors;
- •
- enhanced clinical applications;
- •
- additional memory space, faster processing, and simplified software upgrades and retrieval;
- •
- waterproofing;
- •
- support for international transmission capabilities; and
- •
- advanced remote operation.
The Company expects to achieve manufacturing cost savings with the C5 versus the C3 generation devices.
Wireless Data Transmission Network
MCOT™ makes use of multiple communication networks to transmit ECG data to the technicians in the CardioNet Monitoring Center in real time. When an event meeting pre-prescribed physician notification criteria is detected by our monitor, the monitor transmits data to the CardioNet Monitoring Center over a telephone line connected to the base. The monitor transmits data to the base wirelessly within the proximity range of the base, or wirelessly over a cellular data network if the monitor is being used outside the proximity range of the base. Pursuant to our agreement with nPhase,
12
all data is sent from the monitor directly to nPhase. nPhase has both a primary and backup data center for high availability. nPhase immediately forwards the transmission to our CardioNet Monitoring Center. The CardioNet Monitoring Center is equipped with primary and backup data centers that are fully integrated with nPhase's primary and backup data centers so that data can be easily routed through a number of paths in the event of an emergency. When data is received by the CardioNet Monitoring Center, it is processed by our technicians in order of severity and time received. We have agreed with nPhase that they will be our exclusive provider of monitoring and communication services through the expiration of the agreement in September 2013 and automatically renews for successive periods for one year each, unless terminated by either party with at least 90 days advance notice to the other party. nPhase may terminate the agreement if certain conditions occur, including if we fail to maintain an agreed upon number of active cardiac monitoring devices on the nPhase network or in the event that we begin to utilize the services of a provider of monitoring and communication services other than nPhase. Pursuant to the agreement, we are required to indemnify nPhase for all claims resulting from the provision of our services.
Proprietary Software and Algorithms
We have developed a proprietary software platform which is at the core of MCOT™. In the last eight years, we have had more than 70 software releases. Key software includes:
- •
- ECG Detection Algorithm. The MCOT™ monitor
analyzes incoming information from the sensor on a real-time basis by applying proprietary algorithms which are designed to detect arrhythmias. Our original MCOT™ technology
layered internally developed algorithms on top of a commercially available algorithm. In October 2005, we received FDA 510(k) clearance for a next generation ECG detection algorithm we use in the C3,
to which several patents or patent applications relate.
- •
- SomNet. Cyclic variation of heart rate (CVHR) is reported.
SomNet uses our MCOT™ technology to automatically identify patients with CVHR patterns. By utilizing our internally developed algorithms, MCOT™ can detect CVHR episodes based
on regularity and amplitude greater than 10 bpm. Physicians are able to confirm symptoms and indicators through the daily reports provided to physicians.
- •
- CardioNet Connect. MCOT™ features separate
HIPAA compliant websites for each physician practice that allow physicians to review, edit and print patient reports. CardioNet Connect is a new generation software platform that allows integrated
access to all of our service offerings. The previous platform only allowed access to MCOT™, and none of our other service offerings. In addition, CardioNet Connect allows for
on-line patient enrollment, which we believe will increase the speed of starting patients on service.
- •
- Patient Enrollment and Management System. We maintain
demographic information for each physician practice enrolled with us which enables members of the CardioNet Monitoring Center to immediately contact a physician whose patient experiences a clinically
significant event described in predefined monitoring thresholds provided to us by the physician.
- •
- Monitoring Services Application. The monitoring services application is a software application included within the CardioNet Monitoring Center that analyzes incoming data from a patient-worn sensor on a real time basis. When the monitor detects an arrhythmic event (defined by the values prescribed by the patient's physician), it transmits the ECG data to the CardioNet Monitoring System for our review. The ECG data is reviewed by one of our monitoring specialists and a determination is made as to the "stat" nature of the data and if the physician should be notified. Our monitoring services application provides the basis for the daily, urgent and fetch reports that we send to physicians and stores 21 days of ECG data.
13
- •
- Work Order System. Our service tracks each patient from
the time MCOT™ is prescribed by their physician through the time that the patient completes MCOT™ service, returns the MCOT™ device to us and is released for
billing. We are able to schedule and track relevant events such as the date we provide patient education and service initiation to our patients and the dates that we ship and receive the
MCOT™ device to and from each patient.
- •
- Device Management System (DMS). DMS is an inventory management system that allows us to track our MCOT™ devices. The system allows us to identify where devices are based on tracking numbers assigned during shipment, and allows us to plan for patient demand and production.
Clinical Development
For the years ended December 31, 2010, 2009 and 2008, we spent $4.9 million, $5.8 million and $4.0 million, respectively, on research and development expenses. We intend to continue to develop proof of superiority of our technology through clinical data. The three primary sources of clinical data that we have used to date to illustrate the clinical value of MCOT™ include: (1) a randomized 300-patient clinical study; (2) our cumulative actual monitoring experience from our databases; and (3) other published studies.
Randomized Clinical Study
We completed a 17 center, 300-patient randomized clinical trial in March 2007 that was CardioNet sponsored. We believe this study represents the largest randomized study comparing two noninvasive arrhythmia monitoring methods.
The study was designed to evaluate patients who were suspected to have an arrhythmic cause underlying their symptoms, but who were a diagnostic challenge given that they had already had a non-diagnostic 24-hour Holter monitoring session or four hours of telemetry within 45 days prior to enrollment. Patients were randomized to either MCOT™ or to a loop event monitor for up to 30 days. Of the 300 patients who were randomized, 266 patients who completed a minimum of 25 days of monitoring were analyzed (134 patients using MCOT™ and 132 patients using loop event monitors).
Inclusion criteria included a high clinical suspicion of a malignant arrhythmia and symptoms of syncope, pre-syncope or severe palpitations occurring less frequently than once per 24 hours. Exclusion criteria included severe heart failure (as denoted by New York Heart Association Class IV), myocardial infarction (heart attack) within the prior three months, candidacy for or recent heart valve surgery, and a history of certain sustained tachycardias called ventricular tachycardia or ventricular fibrillation.
The primary endpoint was the confirmation or exclusion of a probable arrhythmic cause of the patient's symptoms, defined as "diagnosis." Study investigators classified any arrhythmias during the monitoring period as being either "clinically significant" or "clinically insignificant." "Confirmation" was based on investigators' assessment of the likelihood that a clinically significant arrhythmia caused the patient's presenting symptoms. "Exclusion" of a probable arrhythmic cause was determined if any reported symptoms were not associated with an arrhythmia. Monitoring was considered "non-diagnostic," or non-conclusive, if patients remained asymptomatic during the monitoring period with either no arrhythmia or only a clinically insignificant arrhythmia document. The study concluded that the primary endpoint was met.
Eric Prystowsky, a member of our board of directors, is the chief editor of the Journal of Cardiovascular Electrophysiology in which the study was published. Dr. Prystowsky recused himself from the journal's review of the study and a guest editor was chosen who selected the reviewers and oversaw the entire review process, which was blinded to Dr. Prystowsky.
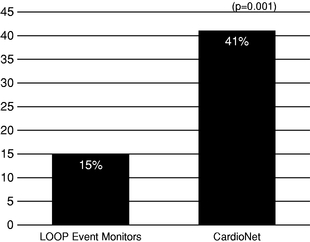
14
The following chart depicts data from the trial, indicating that MCOT™ is nearly three times more successful in detecting clinically significant arrhythmias in patients than loop event monitors:
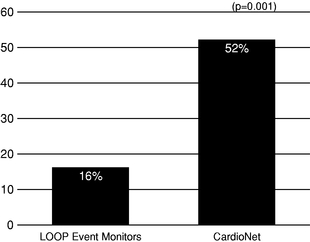
In a subgroup of patients experiencing syncope and/or pre-syncope, MCOT™ was over three times more effective than loop event monitors in diagnosing clinically significant arrhythmias, as demonstrated in the following chart:
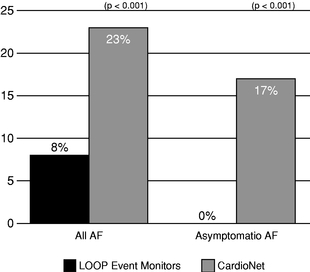
The study specifically compared the success of MCOT™ against loop event monitors in detecting patients afflicted with atrial fibrillation because of the prevalence of asymptomatic episodes that occur in cases of atrial fibrillation and the difficulty of diagnosis. Diagnosis and treatment of atrial fibrillation is important because it can lead to many other medical problems, including stroke.
15
The following chart depicts data from the trial indicating that MCOT™ demonstrated greater success in detecting atrial fibrillation than loop event monitors, especially in patients who were experiencing asymptomatic atrial fibrillation.
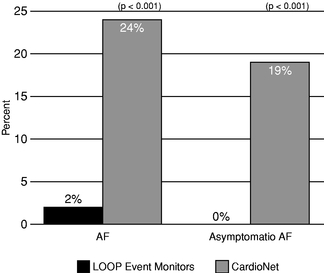
The following chart depicts data from the trial indicating the success of MCOT™ compared to loop event monitors in diagnosing atrial fibrillation in patients experiencing syncope and/or pre-syncope and who also experience asymptomatic episodes of atrial fibrillation:
CardioNet's Monitoring Experience
In January 2005, we completed a study of the first 100 patients who used CardioNet's MCOT™ service. 51% of such patients were diagnosed with clinically significant arrhythmias. 53% of patients who had previously been tested without successful diagnosis using Holter or event monitors were diagnosed with clinically significant arrhythmias by MCOT™. 34% of patients experienced a change of management by their physician as a result of their diagnosis using MCOT™. Of those, 15% were implanted with pacemakers, 6% were implanted with cardioverter- defibrillators and 12% were prescribed ablations.
16
Other Studies
MCOT™ has been cited and referenced in a total of 32 publications and abstracts, including the aforementioned 300-patient randomized clinical trial. Additional references and citations include:
- •
- "Toward a Definitive, Totally Thoracoscopic Procedure for Atrial Fibrillation." Sirak et al, The Annals of Thoracic
Surgery, Dec 2008.
- •
- "Atrial Fibrillation Detected by Mobile Cardiac Outpatient Telemetry in Cryptogenic TIA or Stroke." Tayal et al,
Neurology, Nov 2008.
- •
- "Initial Experience with Novel Mobile Cardiac Outpatient Telemetry for Children and Adolescents with Suspected
Arrhythmia." Saarel et al, Congenital Heart Disease, Jan/Feb 2008.
- •
- "Absence of Correlation Between Symptoms and Rhythm in 'Symptomatic' Atrial Fibrillation." Mehall et al, The Annals of
Thoracic Surgery, 2007.
- •
- "Utility of Mobile Cardiac Outpatient Telemetry for the Diagnosis of Palpitations, Presyncope, Syncope, and the Assessment
of Therapy Efficacy." Olson et al, Journal of Cardiovascular Electrophysiology, May 2007.
- •
- "The Importance of Mobile Cardiac Outpatient Telemetry (MCOT™) for the Detection of Cardiac Arrhythmias."
Rothman, EP Lab Digest, May 2007.
- •
- "Assessment of Rhythm and Rate Control in Patients with Atrial Fibrillation." Prystowsky, Journal of Cardiovascular
Electrophysiology, September 2006.
- •
- "Symptomatic and Asymptomatic Atrial Fibrillation in patients undergoing Radiofrequency Catheter Ablation." Vasamereddy et
al, Journal of Cardiovascular Electrophysiology, February 2006.
- •
- "Video-Assisted Bilateral Pulmonary Vein Isolation and Left Atrial Appendage Exclusion for Atrial Fibrillation." Wolf et
al, Journal Thoracic and Cardiovascular Surgery, September 2005.
- •
- "First Experience with Mobile Cardiac Outpatient Telemetry (MCOT™) System for the Diagnosis and Management of
Cardiac Arrhythmias." Joshi et al, The American Journal of Cardiology, April 2005.
- •
- "Detecting and Treating Urgent Asymptomatic Arrhythmias with Mobile Cardiac Outpatient Telemetry (MCOT™)." Sangrigoli, EP Lab Digest, May 2004.
Publications
- •
- "The Success Rate Following Maze III Procedure: A Comparison Between EKG, 24 Hours Holter, and Long-Term
Monitoring." Ad et al, Society of Thoracic Surgeons Annual Meeting, 2009.
- •
- "Totally Thoracoscopic Bipolar Radiofrequency Ablation for the Treatment of Atrial Fibrillation." Longoria et al, Society
of Thoracic Surgeons Annual Meeting, 2009.
- •
- "Surgical Correction of Atrial Fibrillation With the Procedure: Long Term Outcomes Assessed With Continuous Outpatient
Telemetry." Gammie et al, Southern Thoracic Surgical Association 55th Annual Meeting, Nov 2008.
- •
- "Cryo-Maze for Concomitant Atrial Fibrillation: Mid Term Results Using CardioNet Home Monitoring." Stevens et al, Meeting of the Pennsylvania Association of Thoracic Surgeons, Oct 2008.
Abstracts
17
- •
- "How Reliable is Asymptomatic Patient Rhythm Perception Following Maze Procedure?" Ad et al, Heart Rhythm Society Annual
Meeting, 2008.
- •
- "Utility of Noninvasive, Continuous Outpatient Cardiac Rhythm Monitoring to Diagnose Prolonged Asystole in Patients with
Seizure Disorder." Biviano et al, Heart Rhythm Society Annual Conference, 2007.
- •
- "Initial Experience with Novel Mobile Cardiac Outpatient Telemetry System for Pediatric Patients with Suspected
Arrhythmia." Saarel et al, Heart Rhythm Society Annual Conference, 2005.
- •
- "Symptomatic and Asymptomatic Atrial Fibrillation in Patients Undergoing Radiofrequency Catheter Ablation." Vasamereddy et
al, American College of Cardiology Annual Scientific Session, Mar 2005.
- •
- "Incidence of Asymptomatic Atrial Fibrillation Recurrence Post Pulmonary Vein Isolation Using a Novel Continuous Event Monitoring System." Tarakji et al, Heart Rhythm Society Annual Conference, 2005.
Business Strategy
Our goal is to expand our position as the leading provider of ambulatory, continuous and real-time outpatient monitoring services by establishing our proprietary integrated technology and service offering as the standard of care for multiple health care markets. The key elements of the business strategy by which we intend to achieve these goals include:
- •
- Leverage Monitoring Platform to New Market
Opportunities. We believe that MCOT™ is a platform that can be leveraged for applications in multiple markets. We have made
a significant investment in infrastructure and technology. Our investment includes designing and implementing an integrated technology and service network, establishing a sophisticated data services
architecture in conjunction with our data partner nPhase creating a dedicated central monitoring service center, and internally developing advanced algorithms which sense, analyze and process data.
While our initial focus has been on arrhythmia diagnosis and monitoring, we intend to expand into new market areas such as cardiac monitoring for clinical trials, including QT prolongation and
arrhythmia trials, and comprehensive disease management for congestive heart failure, diabetes and other diseases that require outpatient or ambulatory monitoring and management. We believe that our
technology could also be used to create "instant telemetry beds" in hospitals, particularly in rural hospitals, step-down units or skilled nursing facilities to help cope with acute
nursing shortages by reducing the number of nurses needed to oversee ECG monitoring and reduce capital equipment costs.
- •
- Continue to Educate the Market on the Higher Diagnostic Yield of Our
Differentiated Arrhythmia Monitoring Solution. We intend to continue to educate cardiologists and electrophysiologists on the benefits
of using MCOT™ to meet their arrhythmia monitoring needs, stressing the increased diagnostic yield and their ability to use the clinically significant data to make timely interventions and
guide more effective treatments. Physicians have responded favorably to our comprehensive and responsive service delivery model which allows predetermined notification criteria tailored to the patient
by the physician, while driving increased patient compliance and resulting in positive patient experiences.
- •
- Capitalize on Clinical Trial Results and Other Publications to Enhance Payor Relationships. At year-end 2007, we had contracts with 152 commercial payors representing over 110 million covered lives. Our efforts since year-end 2007 have resulted in an additional 152 contracts, bringing our total to 304 commercial payors and Medicare as of December 31, 2010. We estimate that this represents more than 210 million covered lives. In early 2007, we completed a
18
- •
- Position CardioNet as "One-Stop Shop" for Arrhythmia
Monitoring. We are able to offer to physicians both MCOT™ and event and Holter monitors. We believe that certain
cardiologists and electrophysiologists prefer to use a single source of arrhythmia monitoring solutions with a full spectrum of those solutions. Additionally, with the acquisition of
Biotel Inc. in December 2010, we have incorporated the direct sale of wireless event monitors to distributors, physician, clinics and research organizations.
- •
- Enhance Product Capabilities, Introduce New Products and Establish Complimentary Product Offerings through Acquisitions or Joint Ventures. We intend to grow the business through acquiring and licensing technologies and collaborating with third parties to offer new and complimentary product offerings. We believe there are opportunities to leverage these capabilities through select technology or company acquisitions, as well as collaborations that enhance our capabilities or complement our markets.
300-patient randomized clinical trial that found that MCOT™ provided a significantly higher diagnostic yield compared to traditional loop event monitoring, including technology incorporating a feature designed to automatically detect certain arrhythmias. We are using the clinical evidence from this trial, along with subsequent publications, to both drive continued physician adoption of our solution and to attempt to secure contracts with additional commercial payors.
Sales and Marketing
We market our arrhythmia monitoring solutions, including MCOT™, primarily to cardiologists and electrophysiologists, who are the physician specialists who most commonly diagnose and manage patients with arrhythmias. During 2010, we received approximately 35% of our revenue from Medicare. While we expect a significant portion of our revenue to continue to be derived from Medicare going forward, we are focused on expanding our commercial customer base.
We attend trade shows and medical conferences for organizations such as the Heart Rhythm Society, American College of Cardiology (ACC), Society of Thoracic Surgeons and the Southern Thoracic Surgical Association, as well as numerous regional ACC chapter events, and the annual Boston Atrial Fibrillation Conference to promote MCOT™ and to meet medical professionals with an interest in performing research and reporting their results in peer-reviewed medical journals and at major medical conferences. We also sponsor peer-to-peer educational opportunities and participate in targeted public relations opportunities.
Reimbursement
MCOT™
For the years ended December 31, 2010, 2009, and 2008, arrhythmia monitoring with MCOT™ involved reimbursement for services as follows:
- •
- CardioNet receives reimbursement for the technical component related to the monitoring services provided by the CardioNet
Monitoring Center, located in Conshohocken, PA. The reimbursement is either provided by the Medicare Part B carrier for Pennsylvania on behalf of the Centers for Medicare and Medicaid Services
or commercial payors. The technical component of our service is billed under the Category I CPT, Code "93229", which was approved by the AMA and CMS in October of 2008 for use effective
January 1, 2009.
- •
- Prior to receiving the CPT Code, the technical component of our MCOT™ service was billed under the non-specific billing, or CPT, Code "93799." Unlike dedicated CPT codes approved by the AMA and CMS, claims using non-specific codes sometimes required semi-automated or manual processing, as well as additional review by payors.
19
- •
- As of December 31, 2010, we had secured contracts with 304 commercial payors. We estimate that, combined with Medicare, this represents more than 210 million covered lives. We enter into contracts with commercial payors pursuant to which we receive reimbursement for our technical services. Such contracts typically provide for an initial term of between one and three years and provide for automatic renewal. Either party can typically terminate these contracts by providing between 60 to 120 days prior notice to the other party at any time following the end of the initial term of the agreement. The contracts provide for an agreed upon reimbursement rate, which in some instances is tied to the rate of reimbursement we receive from Medicare. Pursuant to these contracts, we generally agree to indemnify our commercial payors for damages arising in connection with the performance of our obligations thereunder.
We completed a 300-patient randomized clinical trial that found that MCOT™ provided a significantly higher diagnostic yield compared to traditional loop event monitoring, including technology incorporating a feature designed to automatically detect certain arrhythmias. We are using the clinical evidence from this trial to both drive continued physician adoption of our solution and attempt to secure contracts with additional commercial payors.
Other Arrhythmia Monitoring Solutions
Our other arrhythmia monitoring services, including event, Holter and pacemaker monitoring services, are reimbursed by commercial payors and government programs including Medicare. We also have direct arrangements with physicians who purchase our services and then submit claims for them directly to commercial and government payors. In some cases, patients may pay out-of-pocket on a fee for service basis. Generally our other arrhythmia monitoring services are billed using specific codes describing those services. Those codes are part of the CPT coding system which was established by the American Medical Association to describe services provided by physicians and other suppliers. The rate at which we are reimbursed by commercial payors and physicians (in those cases where physicians purchase our services) for our event, Holter and pacemaker monitoring services are negotiated between the Company and the individual commercial payor or physician. Medicare pays for our services through the Physician Fee Schedule. These reimbursement rates are determined annually by CMS and are made available to the public through publication in the Federal Register and the CMS website. Reimbursement made by physicians for purchased services is made at fair market value. The determination of fair market value is subject to interpretation under federal and state anti-kickback laws. At this time, we are not aware of any government challenge or investigations involving our arrangements with its physician customers.
Competition
Although we believe that we have a leading market share in the mobile cardiac arrhythmia monitoring industry, the market in which we operate is fragmented and characterized by a large number of smaller regional service providers. We believe that the principal competitive factors that impact the success of our cardiac monitoring solutions include some or all of the following:
- •
- quality of the algorithm used to detect symptoms;
- •
- quality of clinical data;
- •
- ease of use and reliability of cardiac monitoring solutions for patients and physicians;
- •
- technology performance, innovation, flexibility and range of application;
- •
- timeliness and clinical relevance of new product introductions;
- •
- quality and availability of customer support services;
- •
- size, experience, knowledge and training of sales and marketing staff;
20
- •
- brand recognition and reputation;
- •
- relationships with referring physicians, hospitals, managed care organizations and other third party payors;
- •
- reporting capabilities; and
- •
- perceived value.
We believe that we compete favorably based on the factors described above. However, our industry is evolving rapidly and is becoming increasingly competitive and the basis on which we compete may change over time. In addition, as companies with substantially greater resources than ours enter our market, we will face increased competition.
Intellectual Property
To protect our proprietary rights, we rely on a combination of trademark, copyright, patent, trade secret and other intellectual property laws, employment, confidentiality and invention assignment agreements with our employees and contractors, and confidentiality agreements and protective contractual provisions with our partners and other third parties.
Patents. As of February 14, 2011, we had 17 issued U.S. patents and 22 issued foreign patents relating to functionality of individual components of our MCOT™ device, operation of the total monitoring system, communication methodologies, control of data in the system, algorithms for ECG detection and analysis, and monitoring methods. We are in the process of applying for additional patents relating to various aspects of our technology, including our proprietary ECG detection algorithm. As of February 14, 2011, we had 44 U.S., foreign and international patent applications on file relating to various aspects of our technology.
Trademarks and Copyrights. As of February 14, 2011, we had 9 trademark registrations and one pending trademark application in the United States for a variety of word marks and slogans. Our trademarks are an integral part of our business and include, among others, the registered trademark CardioNet®, and the unregistered trademarks Mobile Cardiac Outpatient Telemetry™ and MCOT™. We also have a significant amount of copyright-protected materials, including among other things, software textual material.
In addition, we also seek to maintain certain intellectual property and proprietary know-how as trade secrets, and generally require our partners to execute non-disclosure agreements prior to any substantive discussions or disclosures of our technology or business plans. Our business and competitive positions are dependent in part upon our ability to protect our proprietary technology and our ability to avoid infringing the patents or proprietary rights of others.
Government Regulation
The health care industry is highly regulated, and there can be no guarantee that the regulatory environment in which we operate will not change significantly and adversely to us in the future. We believe that health care legislation, rules, regulations and interpretations will change, and we expect to modify our agreements and operations from time to time in response to changes in the health care regulatory environment.
U.S. Food and Drug Administration. The monitors and sensors that comprise part of the MCOT™ service are regulated by the FDA as a medical device under the Federal Food, Drug, and Cosmetic Act. The basic regulatory requirements that manufacturers of medical devices distributed in the U.S. must comply with are:
- •
- Premarket Notification 510(k), unless exempt, or Premarket Approval ("PMA");
21
- •
- establishment registration;
- •
- medical device listing;
- •
- quality system regulation;
- •
- labeling requirements; and
- •
- medical device reporting.
Medical devices are classified into Class I, II, and III. Regulatory control increases from Class I to Class III. The device classification regulation defines the regulatory requirements for a general device type. Most Class I devices are exempt from 510(k) requirements. Most Class II devices, including the monitors and sensors used in our MCOT™ service, require 510(k) clearance from the FDA to be marketed in the U.S. A 510(k) submission must demonstrate that the device is substantially equivalent to a device legally in commercial distribution in the United States: (1) before May 28, 1976; or (2) to a device that has been determined by the FDA to be substantially equivalent. In some instances, data from human clinical trials must also be submitted in support of a 510(k) submission. If so, this data must be collected in a manner that conforms with specific requirements in accordance with federal regulations. Changes to existing devices covered by a 510(k) which do not significantly affect safety or effectiveness can generally be made without additional 510(k) submissions. Most Class III devices are high risk devices that pose a significant risk of illness or injury or devices found not substantially equivalent to Class I and II predicate devices through the 510(k) process and require PMA. The PMA process is more involved and includes the submission of clinical data to support claims made for the device. The PMA is an actual approval of the device by the FDA.
The algorithms we use in the MCOT™ service maintain FDA 510(k) clearance as a Class II device. On October 28, 2003, the FDA issued a draft guidance document entitled: "Class II Special Controls Guidance Document: Arrhythmia Detector and Alarm." In addition to conforming to the general requirements of the Federal Food, Drug, and Cosmetic Act, including the premarket notification requirements described above, all of our 510(k) submissions address the specific issues covered in this special controls guidance document.
Failure to comply with applicable regulatory requirements can result in enforcement action by the FDA, which may include any of the following sanctions:
- •
- fines, injunctions and civil penalties;
- •
- recall or seizure of our MCOT™ devices and intellectual property;
- •
- operating restrictions, partial suspension or total shutdown of production;
- •
- withdrawal of 510(k) clearance of new components or algorithms;
- •
- withdrawal of 510(k) clearance already granted to one or more of our existing components or algorithms; and
- •
- criminal prosecution.
Health Care Fraud and Abuse. In the United States, there are state and federal anti-kickback laws that generally prohibit the payment or receipt of kickbacks, bribes or other remuneration in exchange for the referral of patients or other health care-related business. For example, the Federal Healthcare Programs' Anti-Kickback Law prohibits any person from knowingly and willfully offering, paying, soliciting or receiving remuneration, directly or indirectly, to induce or reward either the referral of an individual for an item or service, or the ordering, furnishing or arranging for an item or service, for which payment may be made under federal health care programs, such as the Medicare and Medicaid programs. Some states have anti-kickback laws which establish similar prohibitions; although these state laws may apply regardless of whether federal health care program payment is involved. Federal
22
legislation, such as the Physician Payments Sunshine Act of 2009, also has been proposed that would require disclosure to the federal government of payments to physicians. Anti-kickback laws constrain our sales, marketing and promotional activities by limiting the kinds of financial arrangements we may have with physicians, medical centers, and others in a position to purchase, recommend or refer patients for our cardiac monitoring services or other products or services we may develop and commercialize. Due to the breadth of some of these laws, it is possible that some of our current or future practices might be challenged under one or more of these laws. Furthermore, federal and state false claims laws prohibit anyone from presenting, or causing to be presented, claims for payment to third party payors that are false or fraudulent. For example, we may be subject to the federal False Claims Act if we knowingly "cause" the filing of false claims for payment by a federal health care program (including Medicaid and Medicare). Violations may result in substantial civil penalties, including treble damages, and criminal penalties, including imprisonment, fines and exclusion from participation in federal health care programs. The federal False Claims Act also contains "whistleblower" or "qui tam" provisions that allow private individuals to bring actions on behalf of the government alleging that the defendant has defrauded the government. Various states have enacted laws modeled after the federal False Claims Act, including "qui tam" provisions, and some of these laws apply to claims filed with commercial insurers. Any violations of anti-kickback and false claims laws could have a material adverse effect on our business, financial condition and results of operations.
The Patient Protection and Affordable Care Act. On March 23, 2010, the Patient Protection and Affordable Care Act was signed into law and on March 30, 2010, the Health Care and Education Reconciliation Act of 2010 was signed into law. Together, the two measures make the most sweeping and fundamental changes to the United States health care system since the creation of Medicare and Medicaid. The Health Care Reform laws include a large number of health-related provisions to take effect over the next four years, including expanding Medicaid eligibility, requiring most individuals to have health insurance, establishing new regulations on health plans, establishing health insurance exchanges, requiring manufacturers to report payments or other transfers of value made to physicians and teaching hospitals, and modifying certain payment systems to encourage more cost-effective care and a reduction of inefficiencies and waste, including through new tools to address fraud and abuse.
Health Insurance Portability and Accountability Act of 1996 (HIPAA). The Health Insurance Portability and Accountability Act was enacted by the United States Congress in 1996. Numerous state and federal laws govern the collection, dissemination, use and confidentiality of patient and other health information, including the administrative simplification provisions of HIPAA. Historically, state law has governed confidentiality issues and HIPAA preserves these laws to the extent they are more protective of a patient's privacy or provide the patient with more access to his or her health information. As a result of the implementation of the HIPAA regulations, many states are considering revisions to their existing laws and regulations that may or may not be more stringent or burdensome than the federal HIPAA provisions. HIPAA applies directly to covered entities, which include health plans, health care clearinghouses and many health care providers. The rules promulgated pursuant to HIPAA include the Standards for Privacy of Individually Identifiable Health Information, for which compliance by most entities was required by April 16, 2003, Security Standards, for which compliance by most entities was required by April 21, 2005, and the Standards for Electronic Transactions, for which compliance by most entities was required by October 16, 2003. The privacy rule, security rule, and electronic transactions rule each establish certain standards regarding health information. These rules' standard concerns are, respectively, the privacy of information when it is used and/or disclosed; confidentiality, integrity and availability of electronic health information; and the content and format of certain identified electronic health care transactions. The laws governing health care information impose civil and criminal penalties for their violation and can require substantial expenditures of financial and other resources for information technology system modifications and for implementation of operational compliance.
23
Medicare and Medicaid. Medicare is a federal program administered by the Centers for Medicare and Medicaid Services ("CMS") through fiscal intermediaries and carriers. Available to individuals age 65 or over, and certain other individuals, the Medicare program provides, among other things, health care benefits that cover, within prescribed limits, the major costs of most medically necessary care for such individuals, subject to certain deductibles and co-payments. The Medicare program has established guidelines for local and national coverage determinations and reimbursement of certain equipment, supplies and services. In general, in order to be reimbursed by Medicare, a health care item or service furnished to a Medicare beneficiary must be reasonable and necessary for the diagnosis or treatment of an illness or injury, or to improve the functioning of a malformed body part. The methodology for determining coverage status and the amount of Medicare reimbursement varies based upon, among other factors, the setting in which a Medicare beneficiary received health care items and services. Any changes in federal legislation, regulations and policy affecting Medicare coverage and reimbursement relative to our cardiac monitoring services could have an adverse effect on our performance.
The Medicaid program is a cooperative federal/state program that provides medical assistance benefits to qualifying low income and medically needy persons. State participation in Medicaid is optional, and each state is given discretion in developing and administering its own Medicaid program, subject to certain federal requirements pertaining to payment levels, eligibility criteria and minimum categories of services. The coverage, method and level of reimbursement varies from state to state and is subject to each state's budget restraints. Changes to the coverage, method or level of reimbursement for our services may affect future revenue negatively if reimbursement amounts are decreased or discontinued.
Both the Medicare and Medicaid programs are subject to statutory and regulatory changes, retroactive and prospective rate adjustments, administrative rulings, interpretations of policy, intermediary determinations, and government funding restrictions, all of which may materially increase or decrease the rate of program payments to health care facilities and other health care suppliers and practitioners, including those paid for our cardiac monitoring services.
Our facilities in Pennsylvania and Minnesota are enrolled as IDTFs, which is defined by CMS as an entity independent of a hospital or physician's office in which diagnostic tests are performed by licensed or certified nonphysician personnel under appropriate physician supervision. Medicare has set certain performance standards that every IDTF must meet in order to obtain or maintain their billing privileges. Specifically, an IDTF is required to: (i) operate its business in compliance with all applicable federal and state licensure and regulatory requirements for the health and safety of patients; (ii) provide complete and accurate information on its enrollment application, and report certain changes, within 30 calendar days, to the designated fee-for-service contractor on the Medicare enrollment application; (iii) maintain a physical facility on an appropriate site, that is not an office box or a commercial mail box that contains space for equipment appropriate for the services designated on the enrollment application, and both business and current medical records storage within the office setting of the IDTF; (iv) have all applicable diagnostic testing equipment, with the physical site maintaining a catalog of portable diagnostic testing equipment, including the equipments' serial numbers; (v) maintain a primary business phone under the name of the designated business, which is located at the designated site of the business, or within the home office of the mobile IDTF units; (vi) have a comprehensive liability insurance policy of at least $0.3 million per location, covering both the place of business and all customers and employees of the IDTF, and carried by a non-relative owned company; (vii) agree not to directly solicit patients and to accept only those patients referred for diagnostic testing by an attending physician, who is furnishing a consultation or treating a beneficiary for a specific medical problem and who uses the results in the management of the beneficiary's specific medical problem; (viii) answer beneficiaries' questions and respond to their complaints; (ix) openly post the Medicare standards for review by patients and the public; (x) disclose to the government any person having ownership, financial, or control interest or any other legal interest in the supplier at the
24
time of enrollment or within 30 days of a change; (xi) have its testing equipment calibrated and maintained per equipment instructions and in compliance with applicable manufacturers suggested maintenance and calibration standards; (xii) have technical staff on duty with the appropriate credentials to perform tests and produce the applicable federal or state licenses or certifications of the individuals performing these services; (xiii) have proper medical record storage and be able to retrieve medical records upon request from CMS or its fee-for-service contractor within two business days; and (xiv) permit CMS, including its agents, or its designated fee-for-service contractors, to conduct unannounced, on-site inspections to confirm the IDTFs compliance with these standards.
Environmental Regulation. We use materials and products regulated under environmental laws, primarily in manufacturing and the sterilization processes. While it is difficult to quantify, we believe the ongoing cost of compliance with environmental protection laws and regulations will not have a material impact on our business, financial position or results of operations.
Product Liability and Insurance
The design, manufacture and marketing of medical devices and services of the types we produce entail an inherent risk of product liability claims. In addition, we provide information to health care providers and payors upon which determinations affecting medical care are made, and claims may be made against us resulting from adverse medical consequences to patients resulting from the information we provide. To protect ourselves from product liability claims, we maintain professional liability and general liability insurance on a "claims made" basis. Insurance coverage under such policies is contingent upon a policy being in effect when a claim is made, regardless of when the events which caused the claim occurred. While a product liability claim has never been made against us and we believe our insurance policies are adequate in amount and coverage for our current operations, there can be no assurance that the coverage maintained by us is sufficient to cover all future claims. In addition, there can be no assurance that we will be able to obtain such insurance on commercially reasonable terms in the future.
Manufacturing
Our Chester, PA and Phoenix, AZ facilities provide space for our production and in-house depot repair operations, product upgrading, packaging, storage and shipping. We believe that our manufacturing facilities will be sufficient to meet our manufacturing needs for the foreseeable future. Our previous primary manufacturing facility located in San Diego, CA is now responsible for specifications and development under FDA guidelines.
Manufacturers (both domestic and foreign) and initial distributors of medical devices must register their facilities with the FDA. We believe our manufacturing operations are in compliance with regulations mandated by the FDA. We have been FDA-registered in San Diego since December 2001 and a California licensed medical device manufacturer since March 2002. We are subject to unannounced inspections by the FDA and we successfully completed a routine audit by the FDA in April 2006 with no significant findings noted or warnings issued. In June 2009, our San Diego and Chester facilities received ISO 13485:2003 certification, and in July 2009, we registered our Chester facility with the FDA. Additionally, our Phoenix facility received ISO 13485:2003 certification in July 2010 and became FDA-registered in October 2010. We have successfully transferred all of our manufacturing activities from San Diego to our Chester and Phoenix facilities.
25
Manufacturing of our monitors, sensors and bases is provided by a limited number of electronics manufacturing service providers. We may need to expand our manufacturing capacity for our MCOT™ monitors, sensors and bases in the future to meet market demand, and may do so by hiring and training additional skilled employees for our production group or by working with our service providers on available capacity opportunities such as increases to the personnel assigned to its CardioNet manufacturing team, adding additional manufacturing lines or expanding to a second and third shift, as necessary. We also believe that there are ample other capable suppliers available should we choose to supplement our current service providers' capabilities and capacity. Our production group provides system test and product release activities.
There are a number of critical components and sub-assemblies in the monitors, sensors and bases that compose part of our MCOT™ service. The vendors for these materials are qualified through stringent evaluation and testing of their performance. We implement a strict no change policy with our contract manufacturer to ensure that no components are changed without our approval.
The Company acquired Biotel Inc. ("Biotel") in December 2010. Biotel's manufacturing subsidiary located in Eagan, MN, Braemar, Inc., is registered with the FDA. The Eagan facility is also ISO 9001:2008 and ISO 13485:2003 certified. ISO 9001 is the quality system standard used by companies providing design, development, manufacturing, installation and servicing.
Employees
As of December 31, 2010, we employed 754 full-time employees. We consider our relationship with our employees to be good.
Seasonality
Our revenues are seasonal, as the volume of prescriptions tends to decline in the summer months due to the more limited use of our monitoring solutions as physicians and patients vacation.
Corporate Governance and Internet Address
The Company emphasizes the importance of professional business conduct and ethics through its corporate governance initiatives. The Company's Board of Directors has adopted a code of business conduct and ethics that applies to all employees, directors and officers, including the Company's principal executive officer, principal financial officer and principal accounting officer. Our corporate governance information and materials, including our Code of Business Conduct and Ethics, are posted on the corporate governance section of our website at www.cardionet.com. Our Board regularly reviews corporate governance developments and modifies these materials and practices as warranted. To the extent we make amendments to or grant waivers from our Code of Business Conduct and Ethics in the future, we intend to disclose the amendments and waivers on the corporate governance section of our website.
Available Information
We file electronically with the U.S. Securities and Exchange Commission our annual reports on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K and amendments to those reports filed or furnished pursuant to Section 13(a) or 15(d) of the Securities Exchange Act of 1934. We make available on our website at http://www.cardionet.com, free of charge, copies of these reports as soon as reasonably practicable after we electronically file such material with, or furnish it to the SEC. Further copies of these reports are located at the SEC's Public Reference Room at 100 F Street, NE, Washington, D.C. 20549. Information on the operation of the Public Reference Room can be obtained by calling the SEC at 1-800-SEC-0330. The SEC maintains a website that contains reports, proxy and information statements, and other information regarding our filings, at http://www.sec.gov.
26
Risks related to our business and industry
We have a history of net losses and future profitability is uncertain.
We incurred net losses from our inception. For the years ending December 31, 2010 and 2009, we realized net losses of $19.9 million and $20.5 million, respectively. As of December 31, 2010, we had total accumulated deficit of approximately $112.9 million. The losses in 2010 are primarily associated with the reimbursement reductions we experienced during 2009. Prior to 2009 the losses we experienced resulted from an investment in our infrastructure to support the high level of volume growth.
Although we have initiated plans to reduce our operating losses and return to profitability, we may continue to incur losses if we are not able to execute our cost reduction initiative or grow volume. If we do return to profitability, we may not be able to sustain or increase profitability on a quarterly or annual basis.
Our business is dependent upon physicians prescribing our services; if we fail to obtain those prescriptions, our revenue could fail to grow and could decrease.
The success of our business is dependent upon physicians prescribing our services. Our success in obtaining prescriptions will be directly influenced by a number of factors, including:
- •
- the ability of the physicians with whom we work to obtain sufficient reimbursement and be paid in a timely manner for the
professional services they provide in connection with the use of our arrhythmia monitoring solutions;
- •
- establish ourselves as a "one-stop shop" for arrhythmia monitoring solutions;
- •
- our ability to educate physicians regarding, and convince them of, the benefits of MCOT™ over existing
treatment methods; and
- •
- the perceived clinical efficacy of MCOT™.
If we are unable to educate physicians regarding the benefits of MCOT™ and obtain sufficient prescriptions for our services, revenue from the provision of our arrhythmia monitoring solutions could fail to grow and could decrease.
A further reduction in the published Medicare reimbursement rates could negatively impact our business and our operating results.
On November 2, 2010, the Centers for Medicare and Medicaid Services ("CMS") published The Medicare Program Final Rule establishing a national rate for the MCOT™ technology (CPT Code 93229). CMS valued the CPT code at 20.14 relative value units. Using the formula and values currently in place, the Company's national rate is approximately $739 per service, effective January 1, 2011. This is a decrease of approximately 2% from the Company's current local carrier rate of $754 per service that was previously established by Highmark Medicare Services ("HMS"), effective September 1, 2009. The decrease in the reimbursement rate for our services from the rate in existence prior to September 1, 2009 has had and will continue to have material adverse effects on our business model and operating results.
The continued decline in reimbursement rates has had a negative impact on the Company's revenue and operating results, and has presented significant challenges to the Company's current business model. Several operational initiatives have been implemented, including cost efficiency measures and a continued focus on sales volume growth. Failure to effectively execute the cost
27
efficiency and other operational and strategic initiatives may have materially adverse consequences on the Company's financial results and viability.
Reductions in the Medicare reimbursement rates applicable to the Company's services may lead to pressure from insurance carriers to reduce our commercial pricing.
After receiving the CPT code in the first quarter of 2009, the Company received pressure from several commercial payors to renegotiate reimbursement rate contracts. This pressure led to a substantial decline in our average commercial reimbursement rates in the first half of 2009. During the second half of 2009, and throughout the first half of 2010, commercial reimbursement rates stabilized. The Company experienced a decline in commercial reimbursement rates during the second half of 2010. The Company expects to experience fluctuations in its average commercial reimbursement rates due to payor mix, as well as contract negotiations for new and existing payors. Overall, we expect commercial payors to transition from commercial pricing to the national rate of approximately $739 per service over time. A decrease in commercial pricing would adversely affect our financial results.
The Company has significant outstanding accounts receivables; failure to liquidate these receivables may lead to additional bad debt expense being recorded and could have a materially adverse effect on our operating results.
The Company has implemented several strategic initiatives to collect on outstanding receivable accounts. While the Company has experienced recent improvement in days' sales outstanding (DSO) and believes that it will realize improvements in collection rates and its DSO in the foreseeable future, there is no guarantee that collection rates will improve. A failure to liquidate receivables may have a materially adverse impact on our financial results.
We and the physicians with whom we work are dependent upon reimbursement for the fees associated with our services; the absence or inadequacy of reimbursement would cause our revenue to fail to grow, or could cause our revenue to decrease.
We receive reimbursement for our services from commercial payors and from Medicare Part B carriers where the services are performed on behalf of CMS. The Medicare Part B carriers in each state change from time to time, which may result in changes to our reimbursement rates, increased administrative burden and reimbursement delays.
In addition, our prescribing physicians receive reimbursement for professional interpretation of the information provided by our products and services from commercial payors or Medicare carriers. The efficacy, safety, performance and cost-effectiveness of our products and services, on a stand-alone basis and relative to competing services, will determine the availability and level of reimbursement we and our prescribing physicians receive. Our ability to successfully contract with payors is critical to our business because physicians and their patients will select arrhythmia monitoring solutions other than ours in the event that payors refuse to adequately reimburse our technical fees and physicians' professional fees.
We may experience difficulty in obtaining reimbursement for our services from commercial payors that consider our technology to be experimental and investigational, which would adversely affect our revenue and operating results.
Many commercial payors refuse to enter into contracts to reimburse the fees associated with medical devices or services that such payors determine to be "experimental and investigational". Commercial payors typically label medical devices or services as "experimental and investigational" until such devices or services have demonstrated product superiority evidenced by a randomized clinical trial. We completed a clinical trial in March 2007 that showed that MCOT™ provided higher diagnostic
28
yield than traditional loop event monitoring. Prior to our clinical trial, MCOT™ was labeled "experimental and investigational" by several commercial payors. Since the trial was published in March 2007 we have obtained contracts with several of these commercial payors that previously labeled us experimental and investigational. We have not obtained contracts with certain remaining commercial payors, however, and these payors have informed us that they do not believe the data from this trial justifies the removal of the experimental designation. As a result, these commercial payors may refuse to reimburse the technical and professional fees associated with MCOT™.
Administration of the claims process for the many commercial payors is complex. As a result, we sometimes bill payors for services for which we have no reimbursement contract. These payors may require that we return any funds that they pay in respect to these claims.
The American Medical Association ("AMA") established reimbursement rates applicable to the Category I CPT code for Mobile Cardiovascular Telemetry. These billing codes allowed for automated claims adjudication, substantially simplifying the reimbursement process for physicians and payors compared to the previous process. Reimbursement was previously obtained through non-specific billing codes which require various narratives that, in most cases, involve semi-automated or manual processing, as well as additional review by payors. CMS has established reimbursement rates that cover MCOT™. The codes and rates are contained in The Medicare Program Final Rule for the calendar year 2011.
If commercial payors or Medicare decide not to reimburse our services or the related services provided by physicians, or the rates of such reimbursement change, or if we fail to properly administer claims, our revenue could fail to grow and could decrease.
Reimbursement by Medicare is highly regulated and subject to change; our failure to comply with applicable regulations, could decrease our revenue and may subject us to penalties or have an adverse impact on our business.
We received approximately 35% of our revenue as reimbursement from Medicare in 2010. The Medicare program is administered by CMS, which imposes extensive and detailed requirements on medical services providers, including, but not limited to, rules that govern how we structure our relationships with physicians, how and when we submit reimbursement claims, how we operate our monitoring facilities and how and where we provide our arrhythmia monitoring solutions. Our failure to comply with applicable Medicare rules could result in discontinuing our reimbursement under the Medicare payment program, our being required to return funds already paid to us, civil monetary penalties, criminal penalties and/or exclusion from the Medicare program.
In addition, reimbursement from Medicare is subject to statutory and regulatory changes, local and national coverage decisions, rate adjustments and administrative rulings, all of which could materially affect the range of services covered or the reimbursement rates paid by Medicare for use of our arrhythmia monitoring solutions. For example, on July 10, 2009, HMS announced a reduction in the Medicare reimbursement rate for our MCOT™ services to $754 per service, a reduction of approximately 33%. This new rate went into effect on September 1, 2009. The decline in reimbursement rate has had a negative impact on the Company's revenue and operating results, and has presented significant challenges to the viability of the Company's current business model.
On November 2, 2010, CMS published The Medicare Program Final Rule establishing a national rate for the MCOT™ technology (CPT Code 93229). CMS valued the CPT code at 20.14 relative value units, which was multiplied by an annually determined conversion factor to establish the amounts paid under the physician fee schedule. Using the formula and values currently in place, the Company's national rate is approximately $739 per service, effective January 1, 2011. This is a decrease of approximately 2% from the Company's current local carrier rate of $754 per service that was previously established by Highmark Medicare Services ("HMS"), a contract provider for CMS, effective
29
September 1, 2009. If the formula or values used to determine the physician fee schedule for the MCOT™ technology (CPT Code 93229) is reduced, the Company's results of operations will be negatively impacted.
CMS increased the rate of reimbursement for event services by 7%, beginning in 2011, as compared to the corresponding rate in effect in effect in 2010. This increase brought the rate or reimbursement for event services back to 2009 levels. The Holter reimbursement rate for 2011 is consistent with 2010. CMS reduced the rate of reimbursement for event services by 7%, and Holter services by 16%, for 2010 as compared to the corresponding rates in effect in 2009. Event and Holter reimbursement rates for 2009 and 2008 were consistent with 2007.
In addition, we cannot predict whether future modifications to Medicare's reimbursement policies could reduce or eliminate the amounts we receive from Medicare for the solutions we provide. In addition, Medicare's reimbursement rates can affect the rate that commercial payors are willing to pay for our products and services. Consequently, any future elimination, limitation or reduction in the reimbursement rates provided by Medicare for our arrhythmia monitoring solutions could result in a reduction in the rates we receive from commercial payors.
The national reimbursement rate set by CMS for our mobile cardiovascular telemetry service is subject to continuing change and any reductions in reimbursement levels would decrease our revenues and adversely affect our results of operations and financial condition.
Reimbursement to healthcare providers, including the Company, is subject to continuing change in policies by CMS. Reimbursement from governmental payors is subject to statutory and regulatory changes, retroactive rate adjustments and administrative rulings and other policy changes, all of which could materially decrease the range of services for which we are reimbursed or the reimbursement rates we are paid. Reimbursement under the Medicare program for our services is subject to the physician fee schedule. The fee schedule is typically updated annually.
The amounts paid under the physician fee schedule are based on geographically adjusted relative value units, or RVUs, for each procedure or service, adjusted by a budget neutrality adjustor, and multiplied by an annually determined conversion factor. Historically, the formula used to calculate the fee schedule conversion factor resulted, or would have resulted, in significant decreases in payment levels. However, in every year from 2004 through 2009, the Congress has intervened multiple times to freeze or increase the conversion factor.
On November 2, 2010, CMS published The Medicare Program Final Rule establishing a national rate for the MCOT™ technology (CPT Code 93229). CMS valued the CPT code at 20.14 relative value units, which was multiplied by an annually determined conversion factor to establish the amounts paid under the physician fee schedule. Using the formula and values currently in place, the Company's national rate is approximately $739 per service, effective January 1, 2011. This is a decrease of approximately 2% from the Company's current local carrier rate of $754 per service that was previously established by Highmark Medicare Services ("HMS"), a contract provider for CMS, effective September 1, 2009. If the formula or values used to determine the physician fee schedule for the MCOT™ technology (CPT Code 93229) is reduced, the Company's results of operations will be negatively impacted.
A reduction in sales of our services or a loss of one or more of our key commercial payors would adversely affect our business and operating results.
A small number of commercial payors represent a significant percentage of our revenue. In the year ended December 31, 2010, our top 10 commercial payors by revenue accounted for approximately 62% of our total revenue. Our agreements with these commercial payors typically allow either party to the contract to terminate the contract by providing between 60 and 120 days prior written notice to the
30
other party at any time following the end of the initial term of the contract. Our commercial payors may elect to terminate or not to renew their contracts with us for any reason and, in some instances can unilaterally change the reimbursement rates they pay. In the event any of our key commercial payors terminate their agreements with us, elect not to renew their agreements with us or enter into new agreements with us upon expiration of their current agreements on terms not as favorable as are currently provided, our business, operating results and prospects would be adversely affected.
Consolidation of commercial payors could result in payors eliminating coverage of MCOT™ services or reduced reimbursement rates for MCOT™.
The commercial payor industry is undergoing significant consolidation. When payors combine their operations, the combined company may elect to reimburse MCOT™ services at the lowest rate paid by any of the participants in the consolidation. If one of the payors participating in the consolidation does not reimburse for MCOT™ at all, the combined company may elect not to reimburse for MCOT™. Our reimbursement rates tend to be lower for larger payors. As a result, as payors consolidate, our average reimbursement rate may decline.
Several lawsuits have been brought against us and the outcome of these lawsuits is uncertain.
One lawsuit has been brought against us that allege, among other things, that we issued various materially false and misleading statements relating to the Company's projected performance that had the effect of artificially inflating the market price of our securities. We intend to vigorously defend ourselves against this lawsuit; however, no assurance can be given as to the outcome of the lawsuit. In addition, other lawsuits may be brought against us. We may be required to defend such lawsuits, thus incurring expenses which we may not be able to bear, or which we may not be successful in defending.
Our acquisition of other companies or technologies in the future could prove difficult to integrate and may disrupt our business and harm our operating results and prospects.
Acquisitions in which we may engage in the future, involve risks associated with our assumption of the liabilities of an acquired company, which may be liabilities that we were or are unaware of at the time of the acquisition, potential write-offs of acquired assets and potential loss of the acquired company's key employees or customers.
We may encounter difficulties in successfully integrating our operations, technologies, services and personnel with that of the acquired company, and our financial and management resources may be diverted from our existing operations. Offices in multiple states create a strain on our ability to effectively manage our operations and key personnel. If we elect to consolidate our facilities, we may lose key personnel unwilling to relocate to the consolidated facility, may have difficulty hiring appropriate personnel at the consolidated facility and may have difficulty providing continuity of service through the consolidation.
Physician and patient satisfaction or performance problems with an acquired business, technology, service or device could also have a material adverse effect on our reputation. Additionally, potential disputes with the seller of an acquired business or its employees, suppliers or customers and amortization expenses related to intangible assets could adversely affect our business, operating results and financial condition. If we fail to properly evaluate and execute acquisitions, our business may be disrupted and our operating results and prospects may be harmed.
On December 21, 2010, the Company completed the acquisition of Biotel Inc., and its wholly owned subsidiaries, Braemar, Inc. and Agility Centralized Research Services, Inc. The acquisition gives the Company the ability to develop, manufacture, test and market medical devices and related software to medical companies, clinics and hospitals. Inability to fully integrate this acquisition and maintain
31
customer relationships through diversified product and service offerings may disrupt our business and harm our operating results.
If we do not have enough MCOT™ monitors or sensors or experience delays in manufacturing, we may be unable to fill prescriptions in a timely manner, physicians may elect not to prescribe MCOT™, and our revenue and growth prospects could be harmed.
When a physician prescribes MCOT™ to a patient, our customer service department begins the patient hook-up process, which includes procuring a monitor, sensors and base from our distribution department and sending them to the patient. While our goal is to provide each patient with a monitor, sensors and base in a timely manner, we have experienced and may, in the future, experience delays due to the availability of monitors, primarily when converting to a new generation of monitor or in connection with the increase in prescriptions following potential acquisitions of other companies.
We may also experience shortages of monitors, sensors or bases due to manufacturing difficulties. Multiple suppliers provide the components used in our MCOT™ devices, but our facilities in Chester, PA and Phoenix, AZ are registered and approved by the FDA, as the ultimate manufacturer of MCOT™ devices. Our manufacturing operations could be disrupted by fire, earthquake or other natural disaster, a work stoppage or other labor-related disruption, failure in supply or other logistical channels, electrical outages or other reasons. If there was a disruption to our facilities in Chester or Phoenix, we would be unable to manufacture MCOT™ devices until we have restored and re-qualified our manufacturing capability or developed alternative manufacturing facilities.
Our success in obtaining future prescriptions from physicians is dependent upon our ability to promptly deliver monitors, sensors and bases to our patients, and a failure in this regard would have an adverse effect on our revenue and growth prospects.
Interruptions or delays in telecommunications systems or in the data services provided to us by nPhase or the loss of our wireless or data services could impair the delivery of MCOT™ services.
The success of MCOT™ is dependent upon our ability to store, retrieve, process and manage data and to maintain and upgrade our data processing and communication capabilities. The MCOT™ monitors rely on a third party wireless carrier to transmit data over its data network during times that the monitor is removed from its base. All data sent by our monitors via this wireless data network or via landline is routed directly to nPhase data centers and subsequently routed to our monitoring center. We are dependent upon these third parties to provide data transmission and data hosting services to us. We do not have an agreement directly with this third party wireless carrier. Although we do have an agreement with nPhase that has a termination date in September 2013, nPhase may terminate its agreement with us if certain conditions occur, including if nPhase's agreement with the third party wireless carrier terminates, in the event we fail to maintain an agreed-upon number of active cardiac monitoring devices on the nPhase network or in the event that we begin to utilize the services of a provider of monitoring and communication services other than nPhase. We have no control over the status of the agreement between nPhase and the wireless carrier. If we fail to maintain our relationships with nPhase or if we lose wireless carrier services, we would be forced to seek alternative providers of data transmission and data hosting services, which might not be available on commercially reasonable terms or at all.
As we expand our commercial activities, an increased burden will be placed upon our data processing systems and the equipment upon which they rely. Interruptions of our data networks or the data networks of nPhase for any extended length of time, loss of stored data or other computer problems could have a material adverse effect on our business, financial condition and results of operations. Frequent or persistent interruptions in our arrhythmia monitoring services could cause permanent harm to our reputation and could cause current or potential users of MCOT™ or
32
prescribing physicians to believe that our systems are unreliable, leading them to switch to our competitors. Such interruptions could result in liability, claims and litigation against us for damages or injuries resulting from the disruption in service.
Our systems are vulnerable to damage or interruption from earthquakes, floods, fires, power loss, telecommunication failures, terrorist attacks, computer viruses, break-ins, sabotage, and acts of vandalism. Despite any precautions that we may take, the occurrence of a natural disaster or other unanticipated problems could result in lengthy interruptions in these services. We do not carry business interruption insurance to protect against losses that may result from interruptions in service as a result of system failures. Moreover, the communications and information technology industries are subject to rapid and significant changes, and our ability to operate and compete is dependent in significant part on our ability to update and enhance the communication technologies used in our systems and services.
If our competitors are able to develop or market monitoring solutions that are more effective, or gain greater acceptance in the marketplace, than any solutions we develop, our commercial opportunities will be reduced or eliminated.
The market for arrhythmia monitoring solutions is evolving rapidly and becoming increasingly competitive. Our industry is highly fragmented and characterized by a small number of large providers and a large number of smaller regional service providers. These third parties compete with us in marketing to payors and prescribing physicians, recruiting and retaining qualified personnel, acquiring technology and developing solutions complementary to our programs. In addition, as companies with substantially greater resources than ours enter our market, we will face increased competition. If our competitors are better able to develop and patent arrhythmia monitoring solutions than us, or develop more effective and/or less expensive arrhythmia monitoring solutions that render our solutions obsolete or non-competitive or deploy larger or more effective marketing and sales resources than ours, our business will be harmed and our commercial opportunities will be reduced or eliminated.
If we need to raise additional funding in the future, we may be unable to raise such capital when needed, or at all, and the terms of such capital may be adverse to our stockholders.
We believe that the net proceeds from our initial public offering, together with our existing cash and cash equivalent and investment balances, will be sufficient to meet our anticipated cash requirements for the foreseeable future. However, our future funding requirements will depend on many factors, including:
- •
- the costs associated with manufacturing and building our inventory of our current and future generation monitors;
- •
- the costs of hiring additional personnel and investing in infrastructure to support future growth;
- •
- the reimbursement rates associated with our products and services;
- •
- the costs of undertaking future strategic initiatives, such as acquisitions or joint ventures;
- •
- actions taken by the FDA, CMS and other regulatory authorities affecting MCOT™ and competitive products;
33
- •
- our ability to secure contracts with additional commercial payors providing for the reimbursement of our services;
- •
- the emergence of competing technologies and products and other adverse market developments;
- •
- the costs of preparing, filing, prosecuting, maintaining and enforcing patent claims and other intellectual property
rights or defending against claims of infringement by others; and
- •
- the costs of investing in additional lines of business outside of arrhythmia monitoring solutions.
If we need to, or choose to, raise additional capital in the future, such capital may not be available on reasonable terms, or at all. If we raise additional funds by issuing equity securities, substantial dilution to existing stockholders would likely result. If we raise additional funds by incurring debt financing, the terms of the debt may involve significant cash payment obligations as well as covenants and financial ratios that may restrict our ability to operate our business.
If we or our suppliers fail to achieve or maintain regulatory approval of manufacturing facilities, our growth could be limited and our business could be harmed.
We currently assemble the monitors, sensors and bases for MCOT™ in Chester, PA and Phoenix, AZ. Monitors used for event, Holter and pacemaker services are purchased from several third parties. In order to maintain compliance with FDA and other regulatory requirements, our manufacturing facilities must be periodically re-evaluated and qualified under a quality system to ensure they meet production and quality standards. Suppliers of components of and products used to manufacture MCOT™ devices and the manufacturers of the monitors used in event, Holter and pacemaker services must also comply with FDA and foreign regulatory requirements, which often require significant resources and subject us and our suppliers to potential regulatory inspections and stoppages. We or our suppliers may not satisfy these requirements. If we or our suppliers do not maintain regulatory approval for our manufacturing operations, our business could be adversely affected.
Our dependence on a limited number of suppliers may prevent us from delivering our devices on a timely basis.
We currently rely on a limited number of suppliers of components for MCOT™ devices. If these suppliers became unable to provide components in the volumes needed or at an acceptable price, we would have to identify and qualify acceptable replacements from alternative sources of supply. Qualifying suppliers is a lengthy process. Delays or interruptions in the supply of our requirements could limit or stop our ability to provide sufficient quantities of devices on a timely basis, meet demand for our services, which could have a material adverse effect on our business, financial condition and results of operations.
We could be subject to medical liability or product liability claims which may not be covered by insurance and which would adversely affect our business and results of operations.
The design, manufacture and marketing of services of the types we provide entail an inherent risk of product liability claims. Any such claims against us may require us to incur significant defense costs, irrespective of whether such claims have merit. In addition, we provide information to health care providers and payors upon which determinations affecting medical care are made, and claims may be made against us resulting from adverse medical consequences to patients resulting from the information we provide. In addition, we may become subject to liability in the event that the monitors and sensors we use fail to correctly record or transfer patient information or if we provide incorrect information to patients or health care providers using our services. We have also agreed to indemnify nPhase for any claims resulting from the provision of our services. If we incur one or more significant claims against us, if we are required to indemnify nPhase as a result of the provision of our services, or if we are
34
required to undertake remedial actions in response to any such claims, such claims or actions would adversely affect our business and results of operations.
Our liability insurance is subject to deductibles and coverage limitations. In addition, our current insurance may not continue to be available to us on acceptable terms, if at all, and, if available, the coverages may not be adequate to protect us against any future claims. If we are unable to obtain insurance at an acceptable cost or on acceptable terms with adequate coverage or otherwise protect against any claims against us, we will be exposed to significant liabilities, which may harm our business.
If we do not obtain and maintain adequate protection for our intellectual property, the value of our technology and devices may be adversely affected.
Our business and competitive positions are dependent in part upon our ability to protect our proprietary technology. To protect our proprietary rights, we rely on a combination of trademark, copyright, patent, trade secret and other intellectual property laws, employment, confidentiality and invention assignment agreements with our employees and contractors, and confidentiality agreements and protective contractual provisions with other third parties. We attempt to protect our intellectual property position by filing trademark applications and U.S., foreign and international patent applications related to our proprietary technology, inventions and improvements that are important to the development of our business.
As of February 14, 2011, we had 17 issued U.S. patents, 22 foreign patents and 44 pending U.S. and international patent applications relating to various aspects of our MCOT™ service. We also had 9 trademark registrations in the United States for a variety of word marks and slogans. We do not believe that any single patent, trademark or other intellectual property right of ours, or combination of our intellectual property rights, is likely to prevent others from competing with us using a similar business model. There are many issued patents and patent applications held by others in our industry and the electronics field. Our competitors may independently develop technologies that are substantially similar or superior to our technologies, or design around our patents or other intellectual property to avoid infringement. In addition, we may not apply for a patent relating to products or processes that are patentable, we may fail to receive any patent for which we apply or have applied, and any patent owned by us or issued to us could be circumvented, challenged, invalidated, or held to be unenforceable, or rights granted thereunder may not adequately protect our technology or provide a competitive advantage to us. For example, with respect to one of our U.S. patents, we have a corresponding foreign patent, the claims of which were amended substantially more so than in the United States, to overcome art that was of record in the U.S. patent. If a third-party challenges the validity of any patents or proprietary rights of ours, we may become involved in intellectual property disputes and litigation that would be costly and time-consuming.
Although third parties may infringe on our patents and other intellectual property rights, we may not be aware of any such infringement, or we may be aware of potential infringement but elect not to seek to prevent such infringement or pursue any claim of infringement, and the third party may continue its potentially infringing activities. Any decision whether or not to take further action in response to potential infringement of our patent or other intellectual property rights may be based on any one or more of a variety of factors, such as the potential costs and benefits of taking such action, and business and legal issues and circumstances. Litigation of claims of infringement of a patent or other intellectual property rights may be costly and time-consuming and divert the attention of key company personnel, and may not be successful or result in any significant recovery of compensation for any infringement or enjoining of any infringing activity. Litigation or licensing discussions may also involve or lead to counterclaims that could be brought by a potential infringer to challenge the validity or enforceability of our patents and other intellectual property.
35
To protect our trade secrets and other proprietary information, we generally require our employees, consultants, contractors and outside collaborators to enter into written nondisclosure agreements. These agreements, however, may not provide adequate protection to prevent any unauthorized use, misappropriation or disclosure of our trade secrets, know-how or other proprietary information. These agreements may be breached, and we may not become aware of, or have adequate remedies in the event of, any such breach. Also, others may independently develop the same or substantially equivalent proprietary information and techniques or otherwise gain access to our trade secrets.
Our ability to market our services may be impaired by the intellectual property rights of third parties.
Our success is dependent in part upon our ability to avoid infringing the patents or proprietary rights of others. Our industry and the electronics field are characterized by a large number of patents, patent filings and frequent litigation based on allegations of patent infringement. Competitors may have filed applications for or have been issued patents and may obtain additional patents and proprietary rights related to devices, services or processes that we compete with or are similar to ours. We may not be aware of all of the patents or patent applications potentially adverse to our interests that may have been or may later be issued to or filed by others.
U.S. patent applications may be kept confidential while pending in the Patent and Trademark Office. If other companies have or obtain patents relating to our products or services, we may be required to obtain licenses to those patents or to develop or obtain alternative technology. We may not be able to obtain any such licenses on acceptable terms, or at all. Any failure to obtain such licenses could impair or foreclose our ability to make, use, market or sell our products and services.
Based on the litigious nature of our industry and the electronics field and the fact that we may pose a competitive threat to some companies who own or control various patents, it is always possible that one or more third parties may assert a patent infringement claim seeking damages and to enjoin the manufacture, use, sale and marketing of our products and services. If a third- party asserts that we have infringed on its patent or proprietary rights, we may become involved in intellectual property disputes and litigation that would be costly and time-consuming and could impair or foreclose our ability to make, use, market or sell our products and services.
Lawsuits may have already been filed against us without our knowledge. Additionally, we may receive notices from other third parties suggesting or asserting that we are infringing their patents and inviting us to license such patents. We do not believe that we are infringing on any other party's patents or that a license to any such patents is necessary. Should litigation over such patents arise, we intend to vigorously defend against any allegation of infringement.
If we are found to infringe on the patent or intellectual property rights of others, we may be required to pay damages, stop the infringing activity or obtain licenses or rights to the patents or other intellectual property in order to use, manufacture, market or sell our products and services. Any required license may not be available to us on acceptable terms or at all. If we succeed in obtaining such licenses, payments under such licenses would reduce any earnings from our products. In addition, licenses may be non-exclusive and, accordingly, our competitors may have access to the same technology as that which may be licensed to us. If we fail to obtain a required license or are unable to alter the design of our product candidates to make a license unnecessary, we may be unable to manufacture, use, market or sell our products and services, which could significantly affect our ability to achieve, sustain or grow our commercial business.
Moreover, regardless of the outcome, patent litigation against or by us could significantly disrupt our business, divert our management's attention and consume our financial resources. We cannot predict if or when any third party will file suit for patent or other intellectual property infringement.
36
Our business operations could be significantly disrupted if we fail to properly integrate our management team.
Our Chief Executive Officer and Senior Vice President of Business Operations recently joined CardioNet within the last year in their current capacities and are being integrated into our management team. They will have significant responsibility for our operations and success, but have only limited experience with our business. If they do not smoothly and rapidly develop knowledge of our business and integrate with our existing management, our business operations could be significantly disrupted.
If we fail to obtain and maintain necessary FDA clearances, our business will be adversely affected.
The monitors, sensors and bases that we manufacture and use as part of our MCOT™ service are classified as medical devices and are subject to extensive regulation by the FDA. Further, we maintain establishment registration with the FDA as a distributor of medical devices. FDA regulations govern manufacturing, labeling, promotion, distribution, importing, exporting, shipping and sale of these devices.
Our MCOT™ devices, including our C3 monitor, and our arrhythmia detection algorithms have "510(k) clearance" status from the FDA. Modifications to our MCOT™ devices, such as our C5 device development, or our algorithms that could significantly affect safety or effectiveness, or that could constitute a significant change in intended use, would require a new clearance from the FDA. If in the future we make changes to our MCOT™ devices or our algorithms, the FDA could determine that such modifications require new FDA clearance, and we may not be able to obtain such FDA clearances in a timely fashion or at all.
We are subject to continuing regulation by the FDA, including quality regulations applicable to the manufacture of our MCOT™ devices and various reporting regulations and regulations that govern the promotion and advertising of medical devices. The FDA could find that we have failed to comply with one of these requirements, which could result in a wide variety of enforcement actions, ranging from a warning letter to one or more severe sanctions, including the following:
- •
- fines, injunctions and civil penalties;
- •
- recall or seizure of MCOT™ devices;
- •
- operating restrictions, partial suspension or total shutdown of production;
- •
- refusal to grant 510(k) clearance of new components or algorithms;
- •
- withdrawing 510(k) clearance already granted to one or more of our existing components or algorithms; and
- •
- criminal prosecution.
Any of these enforcement actions could be costly and significantly harm our business, financial condition and results of operations.
Enforcement of federal and state laws regarding privacy and security of patient information may adversely affect our business, financial condition or operations.
The use and disclosure of certain health care information by health care providers and their business associates have come under increasing public scrutiny. Recent federal standards under the Health Insurance Portability and Accountability Act of 1996, or HIPAA, establish rules concerning how individually-identifiable health information may be used, disclosed and protected. Historically, state law has governed confidentiality issues, and HIPAA preserves these laws to the extent they are more protective of a patient's privacy or provide the patient with more access to his or her health information. As a result of the implementation of the HIPAA regulations, many states are considering revisions to their existing laws and regulations that may or may not be more stringent or burdensome
37
than the federal HIPAA provisions. We must operate our business in a manner that complies with all applicable laws, both federal and state, and that does not jeopardize the ability of our customers to comply with all applicable laws. We believe that our operations are consistent with these legal standards. Nevertheless, these laws and regulations present risks for health care providers and their business associates that provide services to patients in multiple states. Because these laws and regulations are recent, and few have been interpreted by government regulators or courts, our interpretations of these laws and regulations may be incorrect. If a challenge to our activities is successful, it could have an adverse effect on our operations, may require us to forego relationships with customers in certain states and may restrict the territory available to us to expand our business. In addition, even if our interpretations of HIPAA and other federal and state laws and regulations are correct, we could be held liable for unauthorized uses or disclosures of patient information as a result of inadequate systems and controls to protect this information or as a result of the theft of information by unauthorized computer programmers who penetrate our network security. Enforcement of these laws against us could have a material adverse effect on our business, financial condition and results of operations.
We may be subject, directly or indirectly, to federal and state health care fraud and abuse laws and regulations and, if we are unable to fully comply with such laws, could face substantial penalties.
Our operations may be directly or indirectly affected by various broad state and federal health care fraud and abuse laws, including the Federal Healthcare Programs' Anti-Kickback Statute, which prohibits any person from knowingly and willfully offering, paying, soliciting or receiving remuneration, directly or indirectly, to induce or reward either the referral of an individual for an item or service, or the ordering, furnishing or arranging for an item or service, for which payment may be made under federal health care programs, such as the Medicare and Medicaid programs. For some of our services, we directly bill physicians for our services, who in turn bill payors. Although we believe such payments to be proper and in compliance with laws and regulations, we may be subject to claims that we are in violation of these laws and regulations. If our past or present operations are found to be in violation of these laws, we or our officers may be subject to civil or criminal penalties, including large monetary penalties, damages, fines, imprisonment and exclusion from Medicare and Medicaid program participation. If enforcement action were to occur, our business and results of operations could be adversely affected.
The operation of our call centers and monitoring facilities is subject to rules and regulations governing IDTFs and state licensure requirements; failure to comply with these rules could prevent us from receiving reimbursement from Medicare and some commercial payors.
We have call centers and monitoring facilities in Pennsylvania and Minnesota that analyze the data obtained from arrhythmia monitors and report the results to physicians. In order for us to receive reimbursement from Medicare and some commercial payors, we must have a call center certified as an IDTF. Certification as an IDTF requires that we follow strict regulations governing how the center operates, such as requirements regarding the experience and certifications of the technicians who review data transmitted from our monitors. These rules and regulations vary from location to location and are subject to change. If they change, we may have to change the operating procedures at our monitoring facilities and call centers, which could increase our costs significantly. If we fail to obtain and maintain IDTF certification, our services may no longer be reimbursed by Medicare and some commercial payors, which could have a material adverse impact on our business.
We may be subject to federal and state false claims laws which impose substantial penalties.
Many of the physicians and patients who use our services file claims for reimbursement with government programs such as Medicare and Medicaid. As a result, we may be subject to the federal
38
False Claims Act if we knowingly "cause" the filing of false claims. Violations may result in substantial civil penalties, including treble damages. The federal False Claims Act also contains "whistleblower" or "qui tam" provisions that allow private individuals to bring actions on behalf of the government alleging that the defendant has defrauded the government. In recent years, the number of suits brought in the medical industry by private individuals has increased dramatically. Various states have enacted laws modeled after the federal False Claims Act, including "qui tam" provisions, and some of these laws apply to claims filed with commercial insurers.
We are unable to predict whether we could be subject to actions under the federal False Claims Act, or the impact of such actions. However, the costs of defending claims under the False Claims Act, as well as sanctions imposed under the False Claims Act, could significantly affect our financial performance.
Changes in the regulatory environment may constrain or require us to restructure our operations, which may harm our revenue and operating results.
Health care laws and regulations change frequently and may change significantly in the future. We may not be able to adapt our operations to address every new regulation, and new regulations may adversely affect our business. We cannot provide assurance that a review of our business by courts or regulatory authorities would not result in a determination that adversely affects our revenue and operating results, or that the health care regulatory environment will not change in a way that restricts our operations. In addition, as a result of the focus on health care reform, there is risk that Congress may implement changes in laws and regulations governing health care service providers, including measures to control costs, or reductions in reimbursement levels, which may adversely affect our business and results of operations.
Changes in the health care industry or tort reform could reduce the number of arrhythmia monitoring solutions ordered by physicians, which could result in a decline in the demand for our solutions, pricing pressure and decreased revenue.
Changes in the health care industry directed at controlling health care costs or perceived over-utilization of arrhythmia monitoring solutions could reduce the volume of solutions ordered by physicians. If more health care cost controls are broadly instituted throughout the health care industry, the volume of cardiac monitoring solutions could decrease, resulting in pricing pressure and declining demand for our services, which could harm our operating results. In addition, it has been suggested that some physicians order arrhythmia monitoring solutions even when the services may have limited clinical utility in large part to establish a record for defense in the event of a claim of medical malpractice against the physician. Legal changes making it more difficult to bring medical malpractice cases, known as tort reform, could reduce the amount of our services prescribed as physicians respond to reduced risks of litigation, which could harm our operating results.
Legislation and policy changes reforming the United States healthcare system may have a material adverse effect on our operating results and financial condition.
On March 23, 2010, the Patient Protection and Affordable Care Act was signed into law and on March 30, 2010, the Health Care and Education Reconciliation Act of 2010 was signed into law. Together, the two measures make the most sweeping and fundamental changes to the United States health care system since the creation of Medicare and Medicaid. The Health Care Reform laws include a large number of health-related provisions to take effect over the next four years, including expanding Medicaid eligibility, requiring most individuals to have health insurance, establishing new regulations on health plans, establishing health insurance exchanges, requiring manufacturers to report payments or other transfers of value made to physicians and teaching hospitals, and modifying certain payment
39
systems to encourage more cost-effective care and a reduction of inefficiencies and waste, including through new tools to address fraud and abuse.
In addition, various healthcare reform proposals have also emerged at the state level. We cannot predict the effect that newly enacted laws or any future legislation or regulation will have on us. However, the implementation of new legislation and regulation may lower reimbursements for our products, reduce medical procedure volumes and adversely affect our business, possibly materially. The enacted excise tax may materially and adversely affect our operating expenses and results of operations.
A write-off of the value of our goodwill or intangible assets could adversely affect our results of operations.
As of December 31, 2010, we had $49.4 million of goodwill and $3.8 million of net intangible assets, most of which resulted from the acquisition of PDSHeart in 2007 and Biotel Inc. in 2010. Current accounting rules require that goodwill and certain intangible assets be assessed for impairment using fair value measurement techniques. If the carrying amount of a reporting unit exceeds its fair value, then a goodwill impairment test is performed to measure the amount of the impairment loss, if any. The goodwill impairment test compares the implied fair value of the reporting unit's goodwill with the carrying amount of that goodwill. Determining the fair value of the implied goodwill is judgmental in nature and often involves the use of significant estimates and assumptions. Any determination requiring the write-off of a significant portion of goodwill or intangible assets could have a material adverse effect on our financial condition and results of operations.
We have a concentration of risk related to the accounts receivable from one customer. Failure to fully collect outstanding balances from this customer, or a combination of other customers, may adversely affect our results of operations.
As of December 31, 2010, we have balances owed to us from one customer representing approximately 14% of our total gross accounts receivable. We maintain an allowance for doubtful accounts based on the aging of outstanding receivables, as well as for any specific instances we become aware of that may preclude us from reasonably assuring collection on outstanding balances. Determining the allowance for doubtful accounts is judgmental in nature and often involves the use of significant estimates. A determination that requires a change in our estimates could have a materially adverse effect on our financial condition and operating results.
Tax requirements and audits could impact our results of operations.
We are subject to the tax laws of various jurisdictions. Our results of operations could be materially affected with a change in tax law or in the interpretation of tax law. This also includes the risk of changes in tax rates and the risk of failure to comply with procedures required by the taxing authorities. Failure to manage our tax strategies could lead to an additional tax charge. Any material disagreement with taxing authorities could result in cash expenditures and adversely affect our results of operations and financial condition.
Our annual operating results and stock price may be volatile or may decline regardless of our operating performance.
The market price for our common stock has been and is likely to continue to be volatile and may fluctuate significantly in response to a number of factors, most of which we cannot control, including:
- •
- changes in reimbursement rates or policies by payors;
- •
- adoption of our services by physicians;
- •
- changes in Medicare rules or regulations;
40
- •
- the development of increased competition for arrhythmia monitoring solutions;
- •
- price and volume fluctuations in the overall stock market;
- •
- changes in operating performance and stock market valuations of other early stage companies generally;
- •
- the seasonal nature of our revenue, which have typically been moderately lower during summer months, which we believe may
be due to physician and patient vacation schedules and patient reluctance to initiate cardiac monitoring during months when patients are more likely to be more active;
- •
- changes in the competitive landscape of the market for our services, including technological innovations by our
competitors and new entrants to the market;
- •
- the financial projections we may provide to the public, any changes in these projections or our failure to meet these
projections;
- •
- changes in financial estimates by any securities analysts who follow our common stock, our failure to meet these estimates
or failure of those analysts to initiate or maintain coverage of our common stock;
- •
- ratings downgrades by any securities analysts who follow our common stock;
- •
- the public's response to press releases or other public announcements by us or third parties, including our filings with
the SEC and announcements relating to payor reimbursement decisions, product development, litigation and intellectual property impacting us or our business;
- •
- market conditions or trends in our industry or the economy as a whole;
- •
- the development and sustainability of an active trading market for our common stock;
- •
- future sales of our common stock by our officers, directors and significant stockholders;
- •
- other events or factors, including those resulting from war, incidents of terrorism, natural disasters or responses to
these events; and
- •
- changes in accounting principles.
In addition, the stock markets, and in particular the Nasdaq Global Market, have experienced extreme price and volume fluctuations that have affected and continue to affect the market prices of equity securities of many health care companies. Stock prices of many health care companies have fluctuated in a manner unrelated or disproportionate to the operating performance of those companies. In the past, stockholders have instituted securities class action litigation following periods of market volatility. If we were involved in securities litigation we could incur substantial costs, and our resources and the attention of management could be diverted from our business.
Future sales of our common stock may depress our stock price.
Sales of a substantial number of shares of our common stock in the public market could occur at any time. These sales, or the perception in the market that the holders of a large number of shares intend to sell shares, could reduce the market price of our common stock. As of December 31, 2010, we had 24,251,170 outstanding shares of vested common stock. In addition, we have outstanding 2,102,376 options and restricted stock units (RSU's) to purchase shares of our common stock that will become exercisable over the next four years. If exercised, these options and RSU's would result in additional shares becoming available for sale upon expiration of the lock-up agreements.
41
Anti-takeover provisions in our charter documents and Delaware law might deter acquisition bids for us that our stockholders might consider favorable.
Our amended and restated certificate of incorporation and bylaws contain provisions that may make the acquisition of our Company more difficult without the approval of our Board of Directors. These provisions:
- •
- establish a classified board of directors so that not all members of our board are elected at one time;
- •
- authorize the issuance of undesignated preferred stock, the terms of which may be established and shares of which may be
issued without stockholder approval, and which may include rights superior to the rights of the holders of common stock;
- •
- prohibit stockholder action by written consent, which requires all stockholder actions to be taken at a meeting of our
stockholders;
- •
- provide that the board of directors is expressly authorized to make, alter, or repeal our bylaws; and
- •
- establish advance notice requirements for nominations for elections to our board or for proposing matters that can be acted upon by stockholders at stockholder meetings.
In addition, because we are incorporated in Delaware, we are subject to Section 203 of the Delaware General Corporation Law which, subject to certain exceptions, prohibits stockholders owning in excess of 15% of our outstanding voting stock from merging or combining with us. These anti-takeover provisions and other provisions under Delaware law could discourage, delay or prevent a transaction involving a change of control of our Company, even if doing so would benefit our stockholders. These provisions could also discourage proxy contests and make it more difficult for our stockholders to elect directors of their choosing and cause us to take other corporate actions such stockholders desire.
If securities or industry analysts publish inaccurate or unfavorable research about our business, our stock price and trading volume could decline.
The trading market for our common stock will depend in part on the research and reports that securities or industry analysts publish about us or our business. If one or more of the analysts who covers us downgrades our stock or publishes inaccurate or unfavorable research about our business, our stock price would likely decline. If one or more of these analysts ceases coverage of us or fails to publish reports on us regularly, demand for our stock could decrease, which could cause our stock price and trading volume to decline.
We do not expect to pay any cash dividends for the foreseeable future.
The continued expansion of our business may require substantial funding. Accordingly, we do not anticipate that we will pay any cash dividends on shares of our common stock for the foreseeable future. Even if we were not prohibited from paying dividends, any determination to do so in the future would be at the discretion of our Board of Directors and will depend upon our results of operations, financial condition, contractual restrictions, restrictions imposed by applicable law and other factors our Board of Directors deems relevant. Accordingly, realization of a gain on your investment will depend on the appreciation of the price of our common stock, which may never occur. Investors seeking cash dividends in the foreseeable future should not purchase our common stock.
42
General economic conditions, which are largely out of our control, may adversely affect the Company's financial condition and results of operations.
The Company's operations may be affected by changes in general economic conditions. Recessionary economic cycles, higher interest rates, inflation, higher levels of unemployment, changes in the laws or industry regulations or other economic factors may adversely affect the demand for the Company's products. Additionally, these economic factors and changes in laws and regulations may adversely affect the Company's financial condition and results of operations.
Economic conditions may materially and adversely affect our investment portfolio.
We have invested our excess cash in money market funds and corporate debt securities issued by banks and corporations. The interest paid on these types of investments and the value of certain securities may decline due to general market conditions, such as the recent volatility in credit markets and the national and global financial crisis. If there is continued and expanded disruption in the credit markets, our investment portfolio could be adversely affected. There is no assurance that the financial or credit markets will improve in the near term, or that the national and worldwide economic conditions will not worsen.
The illiquid capital markets may have an impact on our business and financial condition in ways that we currently cannot predict.
The continued credit crisis, reduction in confidence and related turmoil in the global financial system may have an impact on our business and our financial condition. The global financial and credit markets continue to experience declines or slow growth and there continues to be diminished liquidity and credit availability. Due to the recent tightening of credit markets and concerns regarding the availability of credit, patients and payors may not have access to sufficient cash or short-term credit to obtain MCOT™ or other services provided by the Company. We believe that we could be negatively impacted if these conditions continue for a sustained period of time, or if there is further deterioration in financial markets and major economies. Delays of this nature would adversely affect our service revenue, and therefore harm our business and results of operations.
We operate in an intensely competitive industry, and our failure to respond quickly to technological developments and incorporate new features into our products could harm our ability to compete.
We operate in an intensely competitive industry that experiences rapid technological developments, changes in industry standards, changes in patient requirements, and frequent new product introductions and improvements. If we are unable to respond quickly and successfully to these developments, we may lose our competitive position, and our products or technologies may become uncompetitive or obsolete. To compete successfully, we must maintain a successful research and development effort, develop new products and production processes, and improve our existing products and processes at the same pace or ahead of our competitors. Our research and development efforts are aimed at solving increasingly complex problems, as well as creating new technologies, and we do not expect that all of our projects will be successful. If our research and development efforts are unsuccessful, our future results of operations could be materially harmed.
43
Item 1B. Unresolved Staff Comments
None.
We lease approximately 55,000 square feet of space for our headquarters and service center in Conshohocken, PA under an agreement that expires in December 2013. We also lease approximately 20,000 square feet of space for our San Diego, CA facility under an agreement that expires in August 2011, which is dedicated to research and development, various IT functions, and engineering activities. The balance of the floor space is dedicated to office space. We leased approximately 10,000 square feet of space for our distribution operation in Chester, PA, under an agreement that expires in October 2012. Additionally, we leased approximately 10,800 square feet of space for our distribution operation in Phoenix, AZ, under an agreement that expires in April 2015. We also have service operations in our leased premises located in Edina, MN, consisting of approximately 2,030 square feet of space under an agreement that expires in February 2015. We believe that our existing facilities are adequate to meet our current needs, and that suitable additional alternative spaces will be available in the future on commercially reasonable terms.
The Company acquired Biotel Inc. in December 2010. The acquisition added three leased facilities dedicated to production, engineering, administration and service operations. Leased facility transactions are operated through the wholly owned subsidiaries of Biotel Inc., Braemar, Inc. and Agility Centralized Research Services, Inc. Braemar, Inc. leases approximately 17,300 square feet of space in Eagan, MN under an agreement that expires in August 2011. Additionally, Braemar, Inc. leases approximately 2,900 square feet of space in Columbia, SC under an agreement that expires in April 2011. Agility Centralized Research Services, Inc. leases approximately 1,225 square feet of space in Bannockburn, IL under an agreement that expires in April 2013. No amendments to the existing lease agreements have been made since the date of acquisition. The Company anticipates renewing the lease agreements that are currently scheduled to expire in 2011.
On March 5, 2010, West Palm Beach Police Pension Fund filed a putative class action complaint in California Superior Court, San Diego County asserting claims for violations of Sections 11, 12 and 15 of the Securities Act of 1933, as amended, against CardioNet, nine current and former officers and directors of CardioNet and six underwriters of CardioNet's intial public offering (IPO) consummated March 25, 2008 and/or Secondary Offering on August 6, 2008 (together with the IPO, the "Offerings"). The complaint filed March 5, 2010 also asserted claims for alleged violations of Sections 25401 and 25501 of the California Corporations Code against defendants James M. Sweeney and Fred Middleton. The plaintiff seeks to bring claims on behalf of all those who acquired the common stock of CardioNet pursuant and/or traceable to the Company's IPO and/or Secondary Offering. On March 10, 2010, plaintiff filed an Amended Complaint that deleted the claims for violations of the California Corporations Code. The claims are based on purported misrepresentations and omissions in the Registration Statements for the Offerings relating to alleged business decisions made by CardioNet that were supposedly not disclosed to investors and alleged misstatements concerning CardioNet's business. On April 5, 2010, all defendants removed the case to the Southern District of California, where it is pending. On April 7, 2010, defendants filed a Motion to Transfer the case to the Eastern District of Pennsylvania, which Motion to Transfer is noticed for hearing on June 28, 2010. On April 23, 2010, the plaintiff moved to remand the case to state court. On May 28, 2010, defendants filed their opposition to the Motion to Remand, and plaintiff filed its opposition to the Motion to Transfer. On June 14, 2010, plaintiff filed its reply in support of the Motion to Remand, and on June 18, 2010, defendants' reply in support of the Motion to Transfer was filed. Consistent with the accounting for contingent liabilities, no accrual has been recorded in the financial statements. The Company believes that the claims are without merit and intends to defend the litigation vigorously.
44
On April 2, 2009 CardioNet entered into a Merger Agreement (the "2009 Merger Agreement") to acquire Biotel Inc. ("Biotel") for $14.0 million. On July 14, 2009, CardioNet exercised its contractual right to terminate the Merger Agreement due to Biotel's breach of certain covenants in the agreement. On or about July 16, 2009, Biotel subsequently commenced litigation against CardioNet, alleging that CardioNet had breached and improperly terminated the Merger Agreement. Biotel sought specific performance and damages in an amount in excess of $10.0 million. CardioNet counterclaimed under the terms of the Merger Agreement for its termination fee and associated expenses of $1.4 million. In conjunction with CardioNet's 2010 Merger Agreement to acquire Biotel, a Settlement Agreement was entered into that resolved the CardioNet-Biotel litigation and resulted in the dismissal and mutual release of all claims arising out of, in connection with, or related to the 2009 Merger Agreement, including the claims in the litigation.
On September 25, 2009, LifeWatch Services, Inc., and Card Guard Scientific Survival, Ltd., the licensee and owner, respectively, of U.S. Patent Nos. 7,542,878 B2 ("the '878 Patent") and 5,730,143 ("the '143 Patent") commenced an action LifeWatch Patent Matter against CardioNet's wholly owned subsidiary, Braemar Inc. ("Braemar"), and one of its customers, eCardio Diagnostics, LLC ("eCardio"), in Federal District Court for the Northern District of Illinois, File No. 09-CV-6001, alleging that Braemar and eCardio had infringed the '878 and '143 Patents. The Supply Agreement between Braemar and eCardio provides that Braemar will hold eCardio harmless from any liability it incurs in connection with a claim that Braemar's products violate the intellectual property rights or infringe upon any patent of a third party. Braemar and eCardio have denied the allegations. Since the action was commenced, the Plaintiffs have dismissed their claims relating to alleged infringement of the '878 Patent, Card Guard dropped out of the action, and LifeWatch has continued to pursue its claims relating to the alleged infringement of the '143 Patent. The '143 Patent has been in reexamination proceedings since February 19, 2010. On February 1, 2011, the U.S. Patent Office indicated that the claims as amended during the reexamination will be issued. The Company believes that LifeWatch's claims under the original '143 Patent and under the soon-to-issue amended patent are without merit and intends to defend the litigation vigorously. Consistent with the accounting for contingent liabilities, no accrual has been recorded in the financial statements. The Company believes that the claims are without merit and intends to defend the litigation vigorously.
45
Item 5. Market for Registrant's Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities
Market Information for Common Stock
Our common stock has been traded on the Nasdaq Global Market under the symbol "BEAT" since March 19, 2008. Prior to that time, there was no public market for the common stock. The following table sets forth the range of high and low sale prices of our common stock for the periods indicated.
2010
Quarter Ended
|
High | Low | |||||
|---|---|---|---|---|---|---|---|
December 31, 2010 |
$ | 5.83 | $ | 4.01 | |||
September 30, 2010 |
5.16 | 4.20 | |||||
June 30, 2010 |
9.98 | 5.48 | |||||
March 31, 2010 |
7.72 | 5.48 | |||||
2009
Quarter Ended
|
High | Low | |||||
|---|---|---|---|---|---|---|---|
December 31, 2009 |
$ | 7.29 | $ | 4.36 | |||
September 30, 2009 |
9.57 | 5.87 | |||||
June 30, 2009 |
27.45 | 15.01 | |||||
March 31, 2009 |
29.37 | 20.49 | |||||
As of February 14, 2011, there were 24,256,506 shares of our common stock outstanding. Also as of that date, we had approximately 73 holders of record, including multiple beneficial holders at depositories, banks and brokers included as a single holder in the single "street" name of each respective depository, bank or broker.
Share Repurchases
We did not repurchase any of our equity securities during 2010 or 2009.
Dividends
We have never declared or paid any cash dividends on our capital stock. We currently intend to retain all available funds and any future earnings to support our operations and finance the growth and development of our business. We do not intend to pay cash dividends on our common stock for the foreseeable future. Any future determination related to dividend policy will be made at the discretion of our Board of Directors.
46
Stock Performance Graph
The graph below compares the total stockholder return of an investment of $100 on March 19, 2008 (the first day of trading of our common stock on the Nasdaq Stock Exchange) through December 31, 2010 for (i) our common stock (ii) The Nasdaq Health Care Index and (iii) The Russell 2000 Index. Each of the three measures of cumulative total return assumes reinvestment of dividends, if any. The stock price performance show on the graph below is based on historical data and is not indicative of future stock price performance.
Comparison of Cumulative Total Return
Among CardioNet, Inc., The NASDAQ Health Care Index
and The Russell 2000 Index
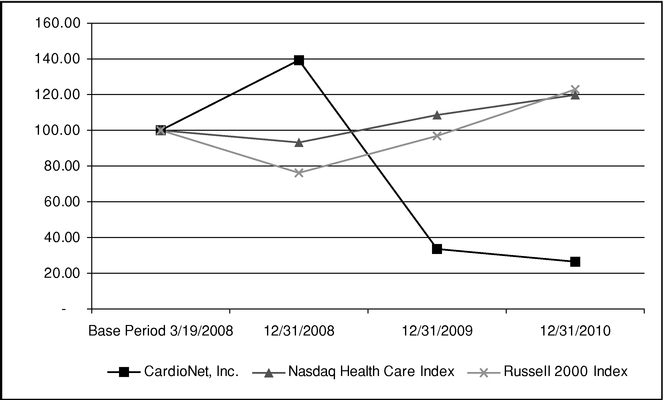
Company/Index
|
Base Period 3/19/2008 |
12/31/2008 | 12/31/2009 | 12/31/2010 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
CardioNet, Inc. |
$ | 100.00 | $ | 139.27 | $ | 33.56 | $ | 26.44 | |||||
Nasdaq Health Care Index |
100.00 | 93.19 | 108.59 | 119.81 | |||||||||
Russell 2000 Index |
100.00 | 76.17 | 96.87 | 122.89 | |||||||||
The foregoing graph and chart shall not be deemed incorporated by reference by any general statement incorporating by reference this Annual Report on Form 10-K into any filing under the Securities Act of 1933, as amended, or under the Securities Exchange Act of 1934, as amended, except to the extent we specifically incorporate this information by reference, and shall not otherwise be deemed filed under those acts.
47
Item 6. Selected Financial Data
The selected financial data set forth below are derived from our consolidated financial statements. The statement of operations for the years ended December 31, 2010, 2009 and 2008, and the balance sheet data at December 31, 2010 and 2009 are derived from our audited consolidated financial statements included elsewhere in this report. The statement of operations data for the years ended December 31, 2007 and 2006 and the balance sheet data at December 2008, 2007 and 2006 are derived from our audited consolidated financial statements which are not included herein.
The following selected financial data should be read in conjunction with the Consolidated Financial Statements and related notes thereto in Item 8 and "Management's Discussion and Analysis of Financial Condition and Results of Operation" in Item 7 of this report.
| |
Year ended December 31, | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |
2010 | 2009 | 2008 | 2007 | 2006 | ||||||||||||
| |
in thousands, except per share data |
||||||||||||||||
Statement of Operations Data: |
|||||||||||||||||
Revenues: |
|||||||||||||||||
Net patient revenues |
$ | 119,924 | $ | 140,233 | $ | 119,764 | $ | 72,357 | $ | 33,019 | |||||||
Other revenues |
— | 388 | 690 | 635 | 904 | ||||||||||||
Total revenues |
119,924 | 140,621 | 120,454 | 72,992 | 33,923 | ||||||||||||
Cost of revenues |
47,492 | 48,688 | 39,913 | 25,526 | 12,701 | ||||||||||||
Gross profit |
72,432 | 91,933 | 80,541 | 47,466 | 21,222 | ||||||||||||
Operating expenses: |
|||||||||||||||||
General and administrative |
34,657 | 39,153 | 27,607 | 19,397 | 11,436 | ||||||||||||
Sales and marketing |
29,338 | 34,656 | 21,111 | 15,968 | 6,448 | ||||||||||||
Bad debt expense |
18,578 | 19,982 | 13,253 | 8,077 | 4,195 | ||||||||||||
Research and development |
4,897 | 5,810 | 3,999 | 3,782 | 3,631 | ||||||||||||
Integration, restructuring and other charges |
4,654 | 12,981 | 4,880 | — | — | ||||||||||||
Total operating expenses |
92,124 | 112,582 | 70,850 | 47,224 | 25,710 | ||||||||||||
(Loss) income from operations |
(19,692 | ) | (20,649 | ) | 9,691 | 242 | (4,488 | ) | |||||||||
Other income (expense): |
|||||||||||||||||
Interest income |
97 | 190 | 1,167 | 1,621 | 114 | ||||||||||||
Interest expense |
(3 | ) | (12 | ) | (170 | ) | (2,221 | ) | (3,271 | ) | |||||||
Total other income (expense) |
94 | 178 | 997 | (600 | ) | (3,157 | ) | ||||||||||
(Loss) income before provision from income taxes |
$ | (19,598 | ) | $ | (20,471 | ) | $ | 10,688 | $ | (358 | ) | $ | (7,645 | ) | |||
Provision for income taxes |
262 | 5 | 1,483 | — | — | ||||||||||||
Net (loss) income |
$ | (19,860 | ) | $ | (20,476 | ) | $ | 9,205 | $ | (358 | ) | $ | (7,645 | ) | |||
Dividends on and accretion of mandatorily redeemable convertible preferred stock |
— | — | (2,597 | ) | (8,346 | ) | — | ||||||||||
Net (loss) income applicable to common shares |
$ | (19,860 | ) | $ | (20,476 | ) | $ | 6,608 | $ | (8,704 | ) | $ | (7,645 | ) | |||
Net (loss) income per common share: |
|||||||||||||||||
Basic |
$ | (0.82 | ) | $ | (0.86 | ) | $ | 0.36 | $ | (2.89 | ) | $ | (2.63 | ) | |||
Diluted |
$ | (0.82 | ) | $ | (0.86 | ) | $ | 0.29 | $ | (2.89 | ) | $ | (2.63 | ) | |||
Shares used to compute net (loss) income per share: |
|||||||||||||||||
Basic |
24,109,085 | 23,771,368 | 18,348,594 | 3,011,699 | 2,908,360 | ||||||||||||
Diluted |
24,109,085 | 23,771,368 | 22,658,813 | 3,011,699 | 2,908,360 | ||||||||||||
48
| |
As of December 31, | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |
2010 | 2009 | 2008 | 2007 | 2006 | |||||||||||
| |
in thousands |
|||||||||||||||
Balance Sheet Data: |
||||||||||||||||
Cash and cash equivalents |
$ | 18,705 | $ | 49,152 | $ | 58,171 | $ | 18,091 | $ | 3,909 | ||||||
Working capital |
60,634 | 75,383 | 84,003 | 29,375 | (18,713 | ) | ||||||||||
Total assets |
156,692 | 168,322 | 165,773 | 103,040 | 17,170 | |||||||||||
Total debt |
— | — | 72 | 2,743 | 29,488 | |||||||||||
Total mandatorily redeemable convertible preferred stock |
— | — | — | 115,302 | — | |||||||||||
Total shareholders' equity |
134,928 | 149,353 | 150,117 | (26,865 | ) | (19,857 | ) | |||||||||
Item 7. Management's Discussion and Analysis of Financial Condition and Results of Operation
You should read the following discussion and analysis of our financial condition and results of our operations in conjunction with our consolidated financial statements and the related notes to those statements included elsewhere in this report. This discussion contains forward-looking statements reflecting our current expectations that involve risks and uncertainties. Our actual results and the timing of events may differ materially from those contained in these forward-looking statements due to a number of factors, including those discussed in the section entitled "Risk Factors," and elsewhere in this prospectus. We are on a calendar year end, and except where otherwise indicated below, "2010" refers to the year ended December 31, 2010, "2009" refers to the year ended December 31, 2009 and "2008" refers to the year ended December 31, 2008.
Overview
Company Background
CardioNet is a leading provider of ambulatory, continuous, real-time outpatient management solutions for monitoring relevant and timely clinical information regarding an individual's health. The Company's efforts have initially been focused on the diagnosis and monitoring of cardiac arrhythmias, or heart rhythm disorders, with a solution that it markets as Mobile Cardiac Outpatient Telemetry™ (MCOT™). The Company actively began developing its product platform in April 2000, and since that time, has devoted substantial resources in advancing its patient monitoring solutions. The platform successfully integrates a wireless data transmission network, internally developed software, FDA-cleared algorithms and medical devices, and a 24-hour monitoring service center.
The Company's Conshohocken location has been an approved Independent Diagnostic Testing Facility ("IDTF") by Medicare since it received 510(k) clearance for the first and second generation of our core MCOT™ devices in 2002. The CardioNet Monitoring Center commenced operations in Conshohocken, Pennsylvania in 2002, concurrent with its first FDA approval, and all of the Company's MCOT™ arrhythmia monitoring activities are currently conducted at that location. The Company received FDA 510(k) clearance for the proprietary algorithm included in its third generation product, or C3, in October 2005. Subsequently in November 2006, the Company received FDA 510(k) clearance for its C3 system which it has incorporated as part of its monitoring solution. The Company received FDA 510(k) clearance for its next generation platform in April 2010 and expects the product launch to occur in early 2011. The Company continues to pursue innovation of new and existing medical solutions through investments in research and development.
On August 6, 2008, an underwritten secondary public offering of shares of common stock held by certain of the Company's existing stockholders was completed. The Company did not issue any shares and received no proceeds in connection with such offering.
49
On March 25, 2008, the Company completed its initial public offering generating net proceeds to the Company of approximately $46.7 million, after deducting underwriter commissions and offering expenses. Upon the closing of the Company's initial public offering, all outstanding shares of the Company's mandatorily redeemable convertible preferred stock and convertible preferred stock converted into shares of common stock. At December 31, 2010, the Company had no shares of preferred stock outstanding.
In March 2007, the Company acquired all of the outstanding capital stock of PDSHeart. The acquisition of PDSHeart provided event, Holter and Pacemaker monitoring product lines to compliment the Company's MCOT™ solution. In addition, the acquisition supplied the Company with existing sales channels and relationships in geographic areas that had not been penetrated prior to the acquisition.
In December 2010, the Company completed the acquisition of Biotel Inc., and its wholly owned subsidiaries, Braemar, Inc. and Agility Centralized Research Services, Inc. The acquisition gives the Company the ability to develop, manufacture, test and market medical devices and related software to medical companies, clinics and hospitals. Additionally, the acquisition also gave the Company access to established customer relationships, entry into the clinical trial service business and the ability to diversify its product and service offerings. The opening balance sheet and purchase price allocation have been reflected in the consolidated financial statements as of December 31, 2010. However, due to the timing of the acquisition, the results of operations for Biotel for the period December 21, 2010, the date of acquisition, through December 31, 2010 were not material.
Medical Industry Trends
Based on recent business journal articles, several trends have emerged in the medical services industry during 2010. Physicians, clinics and hospitals have experienced a lower level of patient visits, and performed fewer elective procedures. The downward trend in census is being attributed to weak economic conditions, as well as changes in insurance coverage. Patients are delaying doctor visits and deferring elective medical treatments that are not perceived to be critical to patients' immediate health. The Company believes this overall economic trend has impacted its volume, contributing to three consecutive quarters of modest volume declines. This trend has appeared to reverse somewhat in the fourth quarter of 2010, as we experienced an increase in volume compared to the third quarter of 2010.
nPhase Supplier Agreement
The Company established a relationship with nPhase, formerly Qualcomm Inc., in May 2003. nPhase is the sole provider of wireless cellular data connectivity solutions and data hosting and queuing services for the Company's monitoring network. The Company has no fixed or minimum financial commitment as it relates to network usage or volume activity. However, if the Company fails to maintain an agreed-upon number of active cardiac monitoring devices on the nPhase network or it utilizes the monitoring and communications services of a provider other than nPhase, the Company may be subject to penalties and nPhase has the right to terminate its relationship with the Company.
Reimbursement
In October 2008, the Centers for Medicare and Medicaid Services ("CMS") established reimbursement rates that cover MCOT™ services. The reimbursement rates applicable to the Category I CPT codes (93228 and 93229) established by the American Medical Association ("AMA") for MCOT™ became effective on January 1, 2009. Highmark Medicare Services ("HMS") was responsible for setting the reimbursement rate on behalf of CMS for code 93229, which is the code for the technical component of our services. The new billing codes allow for automated claims adjudication, substantially simplifying the reimbursement process for physicians and payors compared to
50
the previous process. Reimbursement prior to the use of the new CPT codes was obtained through non-specific billing codes which require various narratives that, in most cases, involve semi-automated or manual processing, as well as additional review by payors.
After receiving the CPT code in the first quarter of 2009, the Company received pressure from several commercial payors to renegotiate reimbursement rate contracts. This pressure led to a substantial decline in our average commercial reimbursement rates in the first half of 2009. During the second half of 2009, and throughout the first half of 2010, we have seen commercial reimbursement rates stabilize. The Company experienced a decline in commercial reimbursement rates during the second half of 2010. The Company expects to experience fluctuations in its average commercial reimbursement rates due to payor mix, as well as contract negotiations for new and existing payors. Overall, we expect the average commercial reimbursement rates to remain stable or decline over time.
On July 10, 2009, HMS announced a reduction in the reimbursement rate for our MCOT™ services to $754 per service, a reduction of approximately 33%. This new rate went into effect on September 1, 2009. The decline in reimbursement rate has had a negative impact on the Company's revenue and operating results, and presented significant challenges to the viability of the Company's current business model. The Company estimates that the rate reduction caused a reduction in revenue for the four months ended December 31, 2009 and the year ended December 31, 2010, of approximately $6.3 million and $25.4 million, respectively. Several strategic initiatives have been implemented, including cost reduction initiatives, process improvement and facility consolidation in an effort to improve the Company's operating performance given the reduced reimbursement rate.
On November 2, 2010, CMS published The Medicare Program Final Rule establishing a national rate for the MCOT™ technology (CPT Code 93229). CMS valued the CPT code at 20.14 relative value units, which was multiplied by an annually determined conversion factor to establish the amounts paid under the physician fee schedule. Using the formula and values currently in place, the Company's national rate is approximately $739 per service, effective January 1, 2011. This is a decrease of approximately 2% from the Company's current local carrier rate of $754 per service that was previously established by Highmark Medicare Services ("HMS"), a contract provider for CMS, effective September 1, 2009 .
We have successfully secured contracts with many national and regional commercial payors. As of December 31, 2010, we have 304 MCOT™ contracts with commercial payors, compared to 245 at December 31, 2009. The current estimated total of over 210 million covered lives for Medicare and commercial lives for which we had reimbursement contracts as of December 31, 2010 represents approximately 79% of the total covered lives in the United States. The MCOT™ contracts also cover event, Holter and Pacemaker service pricing. In addition, as of December 31, 2010, there were approximately 173 contracts with commercial payors that pertained only to event, Holter and Pacemaker service pricing, and did not cover MCOT™. The majority of the remaining covered lives are insured by a relatively small number of large commercial insurance companies that deemed MCOT™ to be experimental in nature and do not currently reimburse us for services provided to their beneficiaries.
Restructuring and Other Activities
During the first quarter of 2010, the Company undertook an initiative to streamline its sales and service organizations and reduce support costs Company-wide. It also initiated plans to close its event monitoring facility in Georgia and consolidate it with the Company's monitoring facilities in Pennsylvania and Minnesota. The Company realized cost efficiencies by undertaking these initiatives. The Company incurred restructuring expenses of $3.5 million for the year ended December 31, 2010, and does not expect to incur additional charges related to this restructuring plan. The activities were substantially complete as of December 31, 2010.
51
Critical Accounting Policies and Estimates
The discussion and analysis of our financial condition and results of operations are based on our financial statements, which we have prepared in accordance with generally accepted accounting principles. The preparation of these financial statements requires us to make estimates and assumptions that affect the reported amount of assets and liabilities, revenues and expenses, and related disclosures. We base our estimates and judgments on historical experience and on various other factors that we believe to be reasonable under the circumstances; however, actual results may differ from these estimates. We review our estimates and judgments on an ongoing basis.
We believe that the following accounting policies and estimates are most critical to a full understanding and evaluation of our reported financial results. Our significant accounting policies are more fully described in Note 2 to our consolidated financial statements.
Revenue Recognition
The Company recognizes revenue primarily from patient monitoring services, derived from its MCOT™, event, Holter and pacemaker services. The Company receives a significant portion of its revenue reimbursement from third party commercial insurance organizations and governmental entities. It also receives reimbursement directly from patients through co-pay and self-pay arrangements.
Revenue from the Medicare program is based on reimbursement rates set by governmental authorities and revenue from contracted commercial payors is recorded at the negotiated contractual rate. Revenue from non-contracted commercial payors is recorded at net realizable value based on historical payment patterns. Billings for services reimbursed by contract third party payors, including Medicare, are recorded as revenues net of allowances for differences between amounts billed and the estimated receipts from such payors. Adjustments to the estimated receipts, based on final settlement with the third party payors, are recorded upon settlement. If the Company does not have consistent historical information regarding collectability from a given payor, revenue is recognized when cash is received. Unearned amounts are appropriately deferred until service is performed.
Effective September 1, 2009, the Medicare reimbursement rate for MCOT™ services was reduced by 33%. For the years ended December 31, 2010, 2009 and 2008, the Medicare revenue as a percentage of the Company's total revenue was 35%, 36% and 33%, respectively. Effective January 1, 2011, the Medicare reimbursement rate for MCOT™ services was reduced another 2% to $739.
Other revenue in 2009 and 2008 consisted mainly of information technology services provided to an affiliate of a stockholder, is recognized at the contractually established rate and is recognized at the time service is provided.
Accounts Receivable
Accounts receivable are recorded at the time revenue is recognized, net of contractual allowances and are presented on the balance sheet net of allowance for doubtful accounts. The Company performs analyses to evaluate the net realizable value of accounts receivable as of the balance sheet date. Specifically, the Company considers historical realization data, accounts receivable aging trends, other operating trends and relevant business conditions. Because of continuing changes in the health care industry and third party reimbursement, it is possible that our estimates could change, which could have a material impact on our operations and cash flows.
The Company realized improvements in its billing procedures and cash collections activity during 2010 and experienced a corresponding decline in its days sales outstanding. The Company believes that it can realize additional improvement in its billing and collection processes, and engaged a third party consultant that is a specialist with significant experience in medical claims reimbursement to assist. The first phase of the project included a review of all outstanding receivables. This review was substantially
52
complete by the end of the fourth quarter of 2010, and did not result in material adjustments to the estimate of allowances for doubtful accounts. The second phase of the project, expected to be completed in the first half of 2011, will include an internal review of the recommendations for changes in the Company's patient intake, billing and reimbursement practices and processes.
During the third quarter of 2010, Highmark Medical Services conducted a prepayment review of the Company's Medicare claims. This review involved an evaluation of medical records and application of clinical judgment by Highmark about whether a service is covered, and is reasonable and necessary. As a result of this review, reimbursement payments to the Company were temporarily suspended in the third quarter of 2010. Effective October 25, 2010, Highmark completed the prepayment review and the Company's cash collections resumed for its Medicare claims during November 2010. As of December 31, 2010, substantially all of the outstanding receivables related to the prepayment review were collected.
The ultimate collection of accounts receivable may not be known for several months after services have been provided and billed. The Company records bad debt expense based on the aging of the receivable using historical Company-specific data. The percentages and amounts used to record bad debt expense and the allowance for doubtful accounts are supported by various methods and analyses, including current and historical cash collections, and the aging of specific receivables. The Company will write-off receivables when the likelihood for collection is remote, the receivables have been fully reserved, and when the Company believes collection efforts have been fully exhausted and it does not intend to devote additional resources in attempting to collect. Prior to the third quarter of 2010, the Company performed an annual accounts receivable write-off in the fourth quarter. Beginning in the third quarter of 2010, the Company has determined it will evaluate outstanding receivables and perform write-offs quarterly going forward. The Company wrote off $29.2 million and $12.0 million of receivables for the years ended December 31, 2010 and 2009, respectively. The impact was a reduction of gross receivables and a reduction in the allowance for doubtful accounts. Additionally, the Company recorded bad debt expense of $18.6 million and $20.0 million for the years ended December 31, 2010 and 2009, respectively. Based on collection experience in 2010 and 2009, the Company recorded additional bad debt expense of $11.7 million and $9.1 million, in 2010 and 2009 respectively, related to prior years' accounts receivable.
Stock Based Compensation
ASC 718, Compensation—Stock Compensation, addresses the accounting for share-based payment transactions in which an enterprise receives employee services in exchange for (a) equity instruments of the enterprise or (b) liabilities that are based on the fair value of the enterprise's equity instruments or that may be settled by the issuance of such equity instruments. ASC 718 requires that an entity measure the cost of equity-based service awards based on the grant-date fair value of the award and recognize the cost of such awards over the period during which the employee is required to provide service in exchange for the award (the vesting period). ASC 718 requires that an entity measure the cost of liability-based service awards based on current fair value that is re-measured subsequently at each reporting date through the settlement date. The Company accounts for equity awards issued to non-employees in accordance with ASC 505-50, Equity-Based Payments to Non-Employees.
We estimate the fair value of our share-based awards to employees and directors using the Black-Scholes option valuation model. The Black-Scholes option valuation model requires the use of certain subjective assumptions. The most significant of these assumptions are our estimates of the expected volatility of the market price of our stock and the expected term of the award. We base our estimates of expected volatility on a group of similar entities whose stock prices are publicly available. The expected term represents the period of time that stock-based awards granted are expected to be outstanding. Other assumptions used in the Black-Scholes option valuation model include the risk-free interest rate and expected dividend yield. The risk-free interest rate for periods pertaining to the
53
contractual life of each option is based on the U.S. Treasury yield of a similar duration in effect at the time of grant. We have never paid, and do not expect to pay, dividends in the foreseeable future. The fair value of our stock-based awards was estimated at the date of grant using the following assumptions:
| |
Year Ended December 31, | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| |
2010 | 2009 | 2008 | |||||||
Expected volatility |
65.0 | % | 54.0 | % | 50.0 | % | ||||
Expected term (in years) |
6.25 | 6.25 | 6.25 | |||||||
Weighted-average risk-free interest rate |
2.29 | % | 2.23 | % | 2.60 | % | ||||
Expected dividends |
0.0 | % | 0.0 | % | 0.0 | % | ||||
Weighted-average grant date fair value per share |
$ | 3.95 | $ | 10.26 | $ | 12.17 | ||||
ASC 718 requires forfeitures to be estimated at the time of grant and revised, if necessary, in subsequent periods if actual forfeitures differ from estimates. Forfeitures are estimated based on our historical experience and separate groups of employees that have similar historical forfeiture behavior are separately considered for expense recognition.
In the absence of a public trading market for our common stock prior to our initial public offering on March 18, 2008 and for the year-to-date period ended March 18, 2008, the day prior to our initial public offering, was determined by our Board of Directors in good faith based upon consideration of a number of objective and subjective factors. The approach we used was consistent with the methods outlined in the AICPA Practice Aid, Valuation of Privately-Held-Company Equity Securities Issued as Compensation. Based on our assessment, we concluded that the fair value of our common stock ranged from $13.38 to $18.30 per share for the periods prior to our initial public offering.
Goodwill and Acquired Intangible Assets
The Company considers its business to be one reporting unit for the purpose of performing its goodwill impairment analysis. Goodwill is reviewed for impairment annually, or when events arise that could indicate that impairment exists. To determine whether impairment exists, the Company estimates the fair value of the reporting unit using an income approach, generally a discounted cash flow methodology that includes assumptions for, among other things, forecasted income, cash flow, growth rates, income tax rates, expected tax benefits and long-term discount rates, all of which require significant judgment. The Company also considers comparable market data to assist in determining the fair value of its reporting unit. There are inherent uncertainties related to these factors and the judgment applied in the analysis. The Company believes that the combination of an income and a market approach provides a reasonable basis to estimate the fair value of the reporting unit. If the estimated fair value of the reporting unit is less than its carrying value, impairment may exist and additional analysis will be undertaken to determine the amount of impairment.
In accordance with ASC 350-20-35, Intangibles—Goodwill and Other, and based on the results of the analyses performed, no impairment loss has been recorded for the years ended December 31, 2010 or 2009. Acquired intangible assets consist of trade names, customer relationships, proprietary technology and signed backlog. The Company amortizes acquired intangible assets over their estimated useful lives on a straight-line basis.
Statements of Operations Overview
Revenue
Our principal source of revenue is patient revenue from cardiac monitoring services. The amount of revenue generated is based on the number of patients enrolled through physician prescriptions and the rates reimbursed to us by commercial payors, patients and Medicare. Reimbursement rates are set by a contract reimbursement provider, Highmark Medicare Services ("HMS"), on behalf of the Centers
54
for Medicare and Medicaid Services ("CMS") on a case rate basis for the Medicare program. Rates are also set through negotiations with commercial payors who may pay either a case rate or a daily monitoring rate. From 2002 through September 2009, our average case rate for monitoring Medicare patients remained relatively stable. Effective September 1, 2009, our Medicare reimbursement rate for our MCOT™ services was reduced by 33% from $1,123 to $754. During 2010, we achieved a national price set by CMS that became effective January 1, 2011. On that date, our Medicare reimbursement rate declined another 2% from $754 to $739. We do not believe the decision to reduce our rate in 2009, nor the national pricing level we began receiving effective January 1, 2011, appropriately reflect the value provided and cost incurred to provide the service. We will continue to work with CMS to establish a reimbursement rate that we believe appropriately reflects the value MCOT™ provides. Overall, we experienced a decline in commercial pricing in the first half of 2009 as many of the larger payors brought their prices to be more in line with the previous Medicare price of $1,123. Commercial prices stabilized in the latter half of 2009 and the first half of 2010. In the second half of 2010, we experienced a decline in commercial pricing as a result of certain non-contracted commercial payors no longer reimbursing us for our services.
We expect pricing to decline over time in a manner consistent with the introduction and penetration of a premium priced service due to competition and the introduction of new technologies. Since our MCOT™ services are relatively new and the reimbursement status is evolving, our revenues are subject to fluctuations due to increases or decreases in rates and decisions by payors regarding reimbursement.
For the event, Holter and pacemaker monitoring market, we expect the price to remain constant or decline as the new generation technology gains wider acceptance in the market. The established 2007 Medicare rates were relatively stable through 2009 for our event and Holter monitoring services. Rates for both event and Holter declined slightly in 2010. We expect reimbursement rates for event and Holter monitoring services to remain stable or increase slightly in 2011.
We believe MCOT™ revenue will increase as a percentage of revenue going forward as we emphasize this service, continue our geographic expansion and achieve greater market penetration in existing markets. We expect that the event, Holter and pacemaker monitoring services revenues will remain constant or decline in absolute terms as the old technology is replaced and therefore, decrease as a percentage of revenue going forward. Our revenues are seasonal, as the volume of prescriptions tends to slow down in the summer months due to the more limited use of our monitoring solutions as physicians and patients vacation.
Gross Profit
Gross profit consists of revenue less the cost of revenue. Cost of revenue includes:
- •
- salaries and benefits for personnel providing various services and customer support to physicians and patients including
patient enrollment and education, monitoring services, distribution services (scheduling, packaging and delivery of the monitors and sensors to the patients), device repair and maintenance, and
quality assurance;
- •
- cost of patient-related services provided by third-party subcontractors including device transportation to and from the
patient, cellular airtime charges related to transmission of ECGs to the CardioNet Monitoring Center and cost for in-home customer hook-ups when necessary;
- •
- consumable supplies sent to patients along with the durable components of MCOT™ devices; and
- •
- depreciation on our medical devices.
55
For the year ended December 31, 2010, our gross profit margin was 60.4%. We expect multiple factors to influence our gross profit margins in the foreseeable future. First, should reimbursement rates decline this would have an adverse affect on our gross profit margin. In the past, we have seen commercial payors migrate down toward the Medicare rate over time. Second, we expect to continue to achieve efficiencies in cost of revenues through process improvements, as well as from a reduction in the cost of our devices. These factors will have a favorable impact on our gross profit margins. While these factors are offsetting, it is difficult to predict how quickly they will influence our gross profit margins.
Sales and Marketing
Sales and marketing expense consists primarily of salaries and benefits related to account executives, marketing personnel and contracting personnel, account executive commissions, travel and other reimbursable expenses, and marketing programs such as trade shows and marketing campaigns.
In 2010, we rationalized the sales force by consolidating low volume and underperforming territories. We also consolidated our specialty account executives into our sales force. As a result, we still maintain the same geographic coverage in 49 states. We also increased our marketing activities to better support the reduction in total number of account executives.
Research and Development
Research and development expense consists primarily of salaries and benefits of personnel and the cost of subcontractors who work on the development of the hardware and software for our next generation monitors and enhance the hardware and software of our existing monitors. Expenses related to clinical trials are also included in research and development expenses.
General and Administrative
General and administrative expense consists primarily of salaries and benefits related to general and administrative personnel, stock-based compensation, professional fees primarily related to legal and audit fees, facilities expenses and the related overhead.
Income Taxes
The Company had approximately $1.6 million in taxes receivable as of December 31, 2010 related to overpayments in 2009. We made estimated payments in the second quarter of 2009 based on projected pre-tax income for the full fiscal year 2009. In the third quarter of 2009, our projections changed to an anticipated pre-tax loss. We have determined to either take a refund of certain of the 2009 overpayments, or apply the overpayment to current or future taxes owed depending on the taxing authority. At the end of 2010, we had gross deferred tax assets totaling approximately $44.3 million, consisting primarily of federal and state net operating loss and credit carryforwards. The pre-tax loss resulted in an effective tax rate of (1.34)% for 2010. The Company has $74.3 million of federal net operating loss carryforwards remaining for use in future periods.
Integration, Restructuring and Other Charges
During the first quarter of 2010, the Company undertook an initiative to streamline its sales and service organizations and reduce support costs company-wide. It also initiated plans to close its event monitoring facility in Georgia and consolidate it with the Company's monitoring facilities in Pennsylvania and Minnesota. The Company realized cost efficiencies by undertaking these initiatives.
The restructuring plan involved the elimination of approximately 100 positions. The restructuring activities were substantially complete as of December 31, 2010. The Company incurred restructuring
56
expenses of $3.5 million for the year ended December 31, 2010, and does not expect to incur additional charges related to this restructuring plan.
The Company incurred other charges of $1.1 million for the year ended December 31, 2010, including legal costs related to the Company's defense of class-action and Biotel lawsuits. Additional information regarding legal proceedings can be found in Note 15 to our consolidated financial statements.
Results of Operations
Years Ended December 31, 2010 and 2009
Revenue. Total revenue for the year ended December 31, 2010 decreased to $119.9 million from $140.6 million for the year ended December 31, 2009, a decrease of $20.7 million, or 14.7%. MCOT™ revenue decreased $19.0 million due to a decrease in MCOT™ reimbursement rates totaling $25.4 million. The decrease in reimbursement rates was offset by an increase in volume in 2010 compared to 2009, or $4.7 million. Additionally, there was a decrease in event, Holter and other revenue of $1.7 million for the year ended December 31, 2010 compared to the year ended December 31, 2009, due to both volume and price declines.
Gross Profit. Gross profit decreased to $72.4 million for the year ended December 31, 2010 from $91.9 million for the year ended December 31, 2009. The decrease of $19.5 million was due to a decrease in revenue offset by $3.8 million of lower cost of sales resulting from our Company-wide cost reduction initiatives for the year ended December 31, 2010 compared to the year ended December 31, 2009. Gross profit as a percentage of revenue declined to 60.4% for the year ended December 31, 2010 compared to 65.4% for the year ended December 31, 2009 due to pricing pressures, partially offset by operational efficiencies.
General and Administrative Expense. General and administrative expense was $34.6 million for the year ended December 31, 2010 compared to $39.1 million for the year ended December 31, 2009. The decrease of $4.5 million, or 11.5%, was due primarily to our cost reduction efforts resulting in a decrease in stock compensation expense of $2.2 million, professional fees of $0.7 million, payroll costs of $1.1 million and other costs of $0.5 million. As a percent of total revenues, general and administrative expense was 28.9% for the year ended December 31, 2010 compared to 27.8% for the year ended December 31, 2009.
Sales and Marketing Expense. Sales and marketing expense was $29.3 million for the year ended December 31, 2010 compared to $34.7 million for the year ended December 31, 2009. The decrease of $5.4 million, or 15.3%, was due to lower payroll, travel and stock based compensation costs primarily resulting from Company-wide cost reduction efforts in 2010. As a percentage of total revenues, sales and marketing expense was 24.5% for the year ended December 31, 2010 compared to 24.6% for the year ended December 31, 2009.
Bad Debt Expense. Bad debt expense was $18.6 million for the year ended December 31, 2010 compared to $20.0 million for the year ended December 31, 2009. The decrease of $1.4 million, or 7.0%, was due to lower gross receivable balances moving into older aging brackets with higher reserve percentages, which was primarily a result of improved cash collections during 2010. The bad debt expense we recorded was based upon an evaluation of our historical collection experience and a review of outstanding accounts receivable, by age, for our various payor classes. HMS' prepayment review did not have an impact on the bad debt expense for the year ended December 31, 2010. As a percentage of total revenues, bad debt expense was 15.5% for the year ended December 31, 2010 compared to 14.2% for the year ended December 31, 2009.
57
Research and Development Expense. Research and development expense was $4.9 million for the year ended December 31, 2010 compared to $5.8 million for the year ended December 31, 2009. The decrease of $0.9 million, or 15.7%, was largely due to lower consulting costs. As a percent of total revenue, research and development expense was 4.1% for the year ended December 31, 2010 compared to 4.1% for the year ended December 31, 2009.
Integration, Restructuring and Other Charges. The Company incurred restructuring costs of $3.5 million and other charges of $1.1 million for the year ended December 31, 2010. The restructuring costs included $2.1 million of severance and employee related costs and $1.4 million of other charges related to the 2010 restructuring plan. The 2010 restructuring plan included the consolidation of the Company's sales and service organizations, the closure of the Company's event monitoring facility in Georgia and consolidation with its monitoring facilities in Pennsylvania and Minnesota, and an overall reduction of administrative costs company-wide. Integration, restructuring and other charges were 3.9% of total revenues for the year ended December 31, 2010. The other charges related to legal costs and other miscellaneous items.
Integration, restructuring and other charges were $13.0 million for the year ended December 31, 2009. The Company incurred a one-time charge of $9.8 million related to the cancellation of unvested stock options held by certain of the Company's executive officers, severance expenses of $2.1 million related to the departure of certain executives, including the Company's former Chief Executive Officer, in the first quarter of 2009 and $1.2 million of costs associated with the 2009 restructuring plan activities that were initiated in the third quarter of 2009. These costs were offset slightly by a realized gain of $0.2 million from insurance proceeds related to the Conshohocken fire in 2008. Integration, restructuring and other charges were 9.2% of total revenues for the year ended December 31, 2009.
Other Income. Net interest income was $0.1 million for the year ended December 31, 2010, a decrease of $0.1 million, or 47.2% from $0.2 million for the year ended December 31, 2009. The Company had additional interest income and realized gains on available-for-sale investments, all of which were primarily offset by amortization of bond premiums during 2010.
Income Taxes. The Company's effective tax rate was (1.34)% for the year ended December 31, 2010, compared to an effective tax rate of zero for the year ended December 31, 2009. The tax expense resulted from certain state taxes that are based on gross receipts rather than income. Additionally, the Company recognized tax expense related to the reconciliation of its prior year provision to tax return filed during 2010.
Net Loss. The Company incurred a net loss of $19.9 million for the year ended December 31, 2010 compared to a net loss of $20.5 million for the year ended December 31, 2009.
Years Ended December 31, 2009 and 2008
Revenue. Total revenue for the year ended December 31, 2009 increased to $140.6 million from $120.5 million for the year ended December 31, 2008, an increase of $20.1 million, or 16.7%. MCOT™ revenue increased $24.7 million due to an increase in sales volume, partially offset by a decrease in MCOT™ reimbursement rates. The net increase in MCOT™ revenue was offset by a decrease in PDSHeart and other revenue of $4.6 million resulting from a reduction of volume.
Gross Profit. Gross profit increased to $91.9 million for the year ended December 31, 2009, or 65.4% of revenue, from $80.5 million for the year ended December 31, 2008, or 66.9% of revenue. The increase of $11.4 million, or 14.1%, was due to increased volume from MCOT™ services, offset by an increase of $5.3 million of payroll expense due to higher headcount, increased depreciation expense of $2.0 million related to additional devices being in service in the 2009 period compared to the 2008 period and an increase in other costs of $1.4 million. As a percentage of revenue gross margin declined 1.5%. This decline was largely a result of the reduction in reimbursement rates the Company
58
experienced in 2009. The impact of the reduction in rates was partially offset by efficiencies gained in the Company's operations a result of the 2009 restructuring plan.
General and Administrative Expense. General and administrative expense increased to $39.1 million for the year ended December 31, 2009 from $27.6 million for the year ended December 31, 2008. This increase of $11.5 million, or 41.8%, was primarily due to an increase in stock compensation expense of $4.2 million, increase in payroll expense largely resulting from the investment in the customer care organization of $2.6 million, increase in legal fees of $1.6 million and $3.1 million of other increased expenses resulting from depreciation, professional fees and rent expense. As a percentage of total revenue, general and administrative expense was 27.8% for the year ended December 31, 2009 compared to 22.9% for the year ended December 31, 2008.
Sales and Marketing Expense. Sales and marketing expense was $34.7 million for the year ended December 31, 2009 compared to $21.1 million for the year ended December 31, 2008. The increase of $13.6 million, or 64.2%, was due to the growth of the sales force and sales operations infrastructure. As a percent of total revenue, sales and marketing expense was 24.6% for the year ended December 31, 2009 compared to 17.5% for the year ended December 31, 2008.
Bad Debt Expense. Bad debt expense was $20.0 million for the year ended December 31, 2009 compared to $13.3 million for the year ended December 31, 2008. The increase of $6.7 million, or 50.8%, was due to several operational challenges the Company experienced in the first half of 2009 and the implementation of a new CPT code. Operational challenges included billing and collections inefficiencies, which led to a longer billing cycle, declined cash collections and receivables that aged to a point that became uncollectible due to the passage of time. Additionally, the implementation of the Category I CPT code 93229 established by the American Medical Association for Mobile Cardiovascular Telemetry occurred in the same time frame as the impact from the operational challenges. The implementation of the CPT code caused an already complicated reimbursement environment with insurance carriers to become more complex. The various challenges experienced from working with payors during the implementation of the CPT code took longer than anticipated to resolve. Ultimately, due to the operational challenges and implementation of the CPT code, a large portion of receivables remained outstanding compared to the prior year, and were deemed uncollectible as they aged. As a percentage of total revenues, bad debt expense was 14.2% for the year ended December 31, 2009 compared to 11.0% for the year ended December 31, 2008.
Research and Development Expense. Research and development expense was $5.8 million for the year ended December 31, 2009 compared to $4.0 million for the year ended December 31, 2008. The increase of $1.8 million, or 45.3%, was due primarily to an increase in payroll expense and consulting fees as the Company builds its next generation device. As a percent of total revenue, research and development expense increased to 4.1% for the year ended December 31, 2009 from 3.3% for the year ended December 31, 2008.
Integration, Restructuring and Other Charges. Integration, restructuring and other charges were $13.0 million, or 9.2% of revenue, for the year ended December 31, 2009. The amount is comprised primarily of a one-time charge of $9.8 million related to the cancellation of unvested stock options held by certain of the Company's executive officers, severance expenses of $2.1 million related to the departure of certain executives, including the Company's former Chief Executive Officer, in the first quarter of 2009 and $1.2 million of costs associated with the 2009 restructuring plan activities that were initiated in the third quarter of 2009. The 2009 restructuring plan included the consolidation and closure of the Company's event monitoring facility in Florida with its event monitoring facility in Georgia, the shift of the majority of the Company's manufacturing activities to its Chester, PA facility, and an overall reduction of support costs company-wide. These costs were offset slightly by a realized gain of $0.2 million in 2009 from insurance proceeds related to a fire at our Conshohocken facility in August 2008.
59
For the year ended December 31, 2008, integration, restructuring and other charges were $4.9 million. Integration charges relating to the PDSHeart acquisition were $1.0 million for the year ended December 31, 2008, and restructuring charges relating to consolidating our Finance and Human Resources functions in Pennsylvania were $1.0 million. Secondary offering costs were $0.9 million, costs related to the resolution of intellectual property litigation were $1.0 million and other nonrecurring charges related to the departure of certain directors were $1.1 million for the year ended December 31, 2008. These costs were offset slightly by a realized gain of $0.1 million in 2008 from insurance proceeds related to the Conshohocken fire in 2008.
Other Income. Net interest income was $0.2 million for the year ended December 31, 2009, a decrease of $0.8 million, or 82.1% from $1.0 million for the year ended December 31, 2008. The decrease was primarily due to lower short term interest rates and a lower average cash balance in 2009 compared to 2008.
Income Taxes. The Company's effective tax rate was zero for the year ended December 31, 2009, compared to an effective tax rate of 13.9% for the year ended December 31, 2008. The decrease in the effective tax rate is due primarily to the pre-tax loss incurred for the year ended December 31, 2009, compared to pre-tax income for the year ended December 31, 2008.
Net (Loss) Income. The Company incurred a net loss of $20.5 million for the year ended December 31, 2009, a decline from net income of $6.6 million for the year ended December 31, 2008.
Liquidity and Capital Resources
As of December 31, 2010, our principal source of liquidity was cash and cash equivalents of $18.7 million, available-for-sale investments of $26.8 million and net accounts receivable of $28.0 million. The Company has no short or long-term debt and does not anticipate needing to secure financing from external sources for cash to operate the business. The Company had working capital of $60.6 million as of December 31, 2010. We believe that our existing cash and cash equivalents balances will be sufficient to meet our anticipated cash requirements for the foreseeable future.
The Company generated $10.4 million of cash from operations for the year ended December 31, 2010, primarily through revenue and improved cash collection efforts. Cash was used primarily to fund the Company's net working capital cash flow requirements of $13.3 million. The Company's working capital requirements were driven primarily by a decrease in accounts payable as the Company had less outstanding payables for capital expenditures compared to 2009. In addition, we experienced a reduction in accrued payroll and restructuring as a significant portion of activities initiated by the 2009 restructuring plan were completed during 2010. Additionally, the Company had $15.6 million of non-cash items related to depreciation and stock compensation expense during the twelve month period.
The Company used $5.2 million for the investment in medical devices for use in its ongoing operations for the year ended December 31, 2010. In addition, the Company used $36.9 million for the purchase of available-for-sale securities for the year ended December 31, 2010. The Company believes that the available-for-sale investments can be converted to cash in a short period of time, if needed, as all of our securities will mature within one year.
Prior to the completion of our initial public offering, our operations were financed primarily through the private placement of equity securities and both long-term and short-term debt financings. We completed a financing involving shares of our mandatorily redeemable convertible preferred stock in March 2007, in which we received net proceeds of approximately $102.1 million. We completed our initial public offering in March 2008, in which we received net proceeds, after underwriting discounts and offering expenses, of approximately $46.7 million. As a result of the public offering, all outstanding mandatorily redeemable convertible preferred stock was converted to common stock. From the time of
60
the public offering through December 31, 2010, we have not used the proceeds other than to repay outstanding debt and make certain contingent payments triggered by the public offering. The remainder of the funds have been invested primarily in available-for-sale investments.
If the Company determines that it needs to raise additional capital, such capital may not be available on reasonable terms, or at all. If the Company raises additional funds by issuing equity securities, its existing stockholders' ownership will be diluted. If the Company raises additional funds by incurring debt financing, the terms of the debt may involve significant cash payment obligations as well as covenants and specific financial ratios that may restrict its ability to operate the business.
Contractual Obligations and Commitments
The following table describes our long-term contractual obligations and commitments as of December 31, 2010:
| |
(in thousands) Payments due by period |
|||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
Contractual obligations
|
Total | 2011 | 2012 | 2013 | 2014 | 2015 | Beyond | |||||||||||||||
Operating lease obligations |
6,835 | 2,538 | 2,076 | 1,997 | 177 | 47 | — | |||||||||||||||
Total |
$ | 6,835 | $ | 2,538 | $ | 2,076 | $ | 1,997 | $ | 177 | 47 | $ | — | |||||||||
As of December 31, 2010, the Company is bound under eight facility leases, and several office equipment leases that are included in the table above. From time to time, we may enter into contracts or purchase orders with third parties under which we may be required to make payments. Our payment obligations under certain agreements will depend on, among other things, the progress of our development programs. Therefore, we are unable at this time to estimate with certainty the potential future costs we will incur under these agreements or purchase orders.
Recent Accounting Pronouncements
In January 2010, the FASB issued Accounting Standards Update (ASU) No. 2010-06, Fair Value Measurements and Disclosures (Topic 820): Improving Disclosures about Fair Value Measurements. The guidance requires entities to disclose significant transfers in and out of fair value hierarchy levels and the reasons for the transfers. Additionally, the guidance clarifies that a reporting entity should provide fair value measurements for each class of assets and liabilities and disclose the inputs and valuation techniques used for fair value measurements using significant other observable inputs (Level 2) and significant unobservable inputs (Level 3). Level 3 reconciliations should present separately information about purchases, sales, issuances and settlements. To date, the Company has not had any assets or liabilities that transferred in or out of fair value hierarchy levels. This guidance is effective for interim and annual periods beginning after December 15, 2009, except for the disclosures about purchases, sales, issuances and settlements in the Level 3 reconciliations, which is effective for fiscal years beginning after December 15, 2010. This guidance did not have an impact on the Company's results of operations or financial position. The Company adopted this guidance effective December 31, 2009. The Company believes the enhanced Level 3 disclosures will not have an impact on the Company's results of operations or financial position.
In February 2010, the FASB issued ASU No. 2010-09, Subsequent Events (Topic 855). The guidance requires an SEC filer to evaluate subsequent events through the date the financial statements are issued but no longer requires an SEC filer to disclose the date through which the subsequent event evaluation occurred. The guidance became effective for the Company upon issuance and had no impact on the Company's results of operations or financial position.
61
In December 2010, the FASB issued ASU No. 2010-29, Intangibles—Goodwill and Other (Topic 350). The guidance requires entities that have recognized goodwill and have one or more reporting unit whose carrying amount for purposes of performing Step 1 of the goodwill impairment test is zero or negative to perform Step 2 of the goodwill impairment test if it is more likely than not that a goodwill impairment exists. In determining whether it is more likely than not that goodwill impairment exists, an entity should consider whether there are any adverse qualitative factors indicating that impairment may exist. The qualitative factors are consistent with the existing guidance defined in ASC 350-20-35-30, Intangibles—Goodwill and Other, which requires that goodwill of a reporting unit be tested for impairment between annual tests if an event occurs or circumstances change that would more likely than not reduce the fair value of a reporting unit below its carrying amount. The amendments are effective for fiscal years beginning after December 15, 2010. The Company does not believe the adoption of ASU No. 2010-28 will have an impact on the Company's results of operations or financial position.
In December 2010, the FASB issued ASU No. 2010-29, Business Combinations (Topic 805): Disclosing of Supplementary Pro Forma Information for Business Combinations. The guidance affects any public entity as defined by ASC 805, Business Combination, which enters into business combinations that are material on an individual or aggregate basis. The comparative financial statements should present and disclose revenue and earnings of the combined entity as though the business combination(s) that occurred during the current year had occurred as of the beginning of the comparable prior annual reporting period only. The amendments also expand the supplemental pro forma disclosures to include a description of the nature and amount of material, nonrecurring pro forma adjustments directly attributable to the business combination included in the reported pro forma revenue and earnings. The amendments are effective prospectively for business combinations for which the acquisition date is on or after the beginning of the first annual reporting period beginning on or after December 15, 2010. The Company does not believe the adoption of ASU No. 2010-29 will have an impact on the Company's results of operations or financial position.
Off-Balance Sheet Arrangements
As of December 31, 2010 and 2009, we did not have any relationships with unconsolidated entities or financial partnerships, such as entities referred to as structured finance or special purpose entities, which would have been established for the purpose of facilitating off-balance sheet arrangements or other contractually narrow or limited purposes.
Item 7A. Quantitative and Qualitative Disclosures About Market Risk
Our cash and cash equivalents as of December 31, 2010 were $18.7 million, and consisted primarily of cash and money market funds with maturities of less than 90 days. We also invest our excess funds, which were $26.8 million as of December 31, 2010, in available-for-sale securities. The Company earned approximately $0.5 million in interest during 2010. A decrease in interest rates of 100 basis points would not have a material impact on the Company's financial results. The primary objective of our investment activities is to preserve our capital for the purpose of funding operations while, at the same time, maximizing the income we receive from our investments without significantly increasing risk. To achieve this objective, our investment policy allows us to maintain a portfolio of cash equivalents and short term investments in a variety of securities including money market funds and corporate debt securities. Due to the short term nature of our investments, we believe we have no material exposure to interest rate risk.
62
Item 8. Financial Statements and Supplementary Data
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
The
Board of Directors and Shareholders
CardioNet, Inc.
We have audited the accompanying consolidated balance sheets of CardioNet, Inc. as of December 31, 2010 and 2009, and the related consolidated statements of operations, cash flows, and redeemable convertible preferred stock and shareholders' equity for each of the three years in the period ended December 31, 2010. Our audits also included the financial statement schedule listed at Item 15(a). These financial statements and schedule are the responsibility of the Company's management. Our responsibility is to express an opinion on these financial statements and schedule based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements. An audit also includes assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the financial statements referred to above present fairly, in all material respects, the consolidated financial position of CardioNet, Inc. at December 31, 2010 and 2009, and the consolidated results of its operations and its cash flows for each of the three years in the period ended December 31, 2010, in conformity with U.S. generally accepted accounting principles. Also, in our opinion, the related financial statement schedule, when considered in relation to the basic financial statements taken as a whole, presents fairly in all material respects the information set forth therein.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), CardioNet, Inc.'s internal control over financial reporting as of December 31, 2010, based on criteria established in "Internal Control—Integrated Framework" issued by the Committee of Sponsoring Organizations of the Treadway Commission and our report dated February 25, 2011 expressed an unqualified opinion thereon.
/s/ ERNST & YOUNG LLP
Philadelphia,
Pennsylvania
February 25, 2011
63
CARDIONET, INC.
CONSOLIDATED BALANCE SHEETS
(In thousands, except shares and per share amounts.)
| |
December 31, | |||||||
|---|---|---|---|---|---|---|---|---|
| |
2010 | 2009 | ||||||
Assets |
||||||||
Current assets: |
||||||||
Cash and cash equivalents |
$ | 18,705 | $ | 49,152 | ||||
Short-term available-for-sale investments |
26,779 | — | ||||||
Accounts receivable, net of allowance for doubtful accounts of $11,779 and $22,396 at December 31, 2010 and 2009, respectively |
24,978 | 40,885 | ||||||
Other receivables |
3,041 | — | ||||||
Inventory |
1,461 | — | ||||||
Prepaid expenses and other current assets |
3,086 | 2,818 | ||||||
Total current assets |
78,050 | 92,855 | ||||||
Property and equipment, net |
22,000 | 28,243 | ||||||
Intangible assets, net |
3,764 | 939 | ||||||
Goodwill |
49,362 | 45,999 | ||||||
Other assets |
3,516 | 286 | ||||||
Total assets |
$ | 156,692 | $ | 168,322 | ||||
Liabilities and shareholders' equity |
||||||||
Current liabilities: |
||||||||
Accounts payable |
$ | 7,127 | $ | 7,160 | ||||
Accrued expenses |
9,881 | 9,919 | ||||||
Deferred revenue |
408 | 393 | ||||||
Total current liabilities |
17,416 | 17,472 | ||||||
Deferred tax liability |
3,191 | — | ||||||
Deferred rent |
1,157 | 1,497 | ||||||
Total liabilities |
21,764 | 18,969 | ||||||
Shareholders' equity |
||||||||
Common stock—$.001 par value as of December 31, 2010 and 2009; 200,000,000 shares authorized as of December 31, 2010 and 2009; 24,251,170 and 23,965,405 shares issued and outstanding at December 31, 2010 and 2009, respectively |
24 | 24 | ||||||
Paid-in capital |
247,747 | 242,320 | ||||||
Accumulated other comprehensive income |
8 | — | ||||||
Accumulated deficit |
(112,851 | ) | (92,991 | ) | ||||
Total shareholders' equity |
134,928 | 149,353 | ||||||
Total liabilities and shareholders' equity |
$ | 156,692 | $ | 168,322 | ||||
See accompanying notes.
64
CARDIONET, INC.
CONSOLIDATED STATEMENTS OF OPERATIONS
(In thousands, except shares and per share amounts.)
| |
Year Ended December 31, | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |
2010 | 2009 | 2008 | |||||||||
Revenues: |
||||||||||||
Net patient service revenues |
$ | 119,924 | $ | 140,233 | $ | 119,764 | ||||||
Other revenues |
— | 388 | 690 | |||||||||
Total revenues |
119,924 | 140,621 | 120,454 | |||||||||
Cost of revenue |
47,492 | 48,688 | 39,913 | |||||||||
Gross profit |
72,432 | 91,933 | 80,541 | |||||||||
Operating expenses: |
||||||||||||
General and administrative |
34,657 | 39,153 | 27,607 | |||||||||
Sales and marketing |
29,338 | 34,656 | 21,111 | |||||||||
Bad debt expense |
18,578 | 19,982 | 13,253 | |||||||||
Research and development |
4,897 | 5,810 | 3,999 | |||||||||
Integration, restructuring and other charges |
4,654 | 12,981 | 4,880 | |||||||||
Total operating expenses |
92,124 | 112,582 | 70,850 | |||||||||
(Loss) income from operations |
(19,692 | ) | (20,649 | ) | 9,691 | |||||||
Other income (expense): |
||||||||||||
Interest income |
97 | 190 | 1,167 | |||||||||
Interest expense |
(3 | ) | (12 | ) | (170 | ) | ||||||
Total other income |
94 | 178 | 997 | |||||||||
(Loss) income before income taxes |
(19,598 | ) | (20,471 | ) | 10,688 | |||||||
Provision for income taxes |
262 | 5 | 1,483 | |||||||||
Net (loss) income |
(19,860 | ) | (20,476 | ) | 9,205 | |||||||
Dividends on and accretion of mandatorily redeemable convertible preferred stock |
— | — | (2,597 | ) | ||||||||
Net (loss) income available to common shareholders |
$ | (19,860 | ) | $ | (20,476 | ) | $ | 6,608 | ||||
Net (loss) income per common share: |
||||||||||||
Basic |
$ | (0.82 | ) | $ | (0.86 | ) | $ | 0.36 | ||||
Diluted |
$ | (0.82 | ) | $ | (0.86 | ) | $ | 0.29 | ||||
Weighted average number of common shares outstanding: |
||||||||||||
Basic |
24,109,085 | 23,771,368 | 18,348,594 | |||||||||
Diluted |
24,109,085 | 23,771,368 | 22,658,813 | |||||||||
See accompanying notes.
65
CARDIONET, INC.
CONSOLIDATED STATEMENTS OF CASH FLOWS
(In thousands, except shares and per share amounts.)
| |
Year Ended December 31, | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| |
2010 | 2009 | 2008 | ||||||||
Operating activities |
|||||||||||
Net (loss) income |
$ | (19,860 | ) | $ | (20,476 | ) | $ | 9,205 | |||
Adjustments to reconcile net (loss) income to net cash provided by operating activities: |
|||||||||||
Depreciation |
11,696 | 10,053 | 7,709 | ||||||||
Loss on the disposal of property & equipment |
807 | 408 | 423 | ||||||||
(Decrease) increase in deferred rent |
(340 | ) | 532 | 86 | |||||||
Provision for doubtful accounts |
18,578 | 19,982 | 13,253 | ||||||||
Stock-based compensation |
3,945 | 16,625 | 3,392 | ||||||||
Amortization of intangibles |
375 | 884 | 984 | ||||||||
Amortization of investment premium |
421 | — | — | ||||||||
Changes in operating assets and liabilities: |
|||||||||||
Accounts receivable |
(3,062 | ) | (21,436 | ) | (29,687 | ) | |||||
Prepaid expenses and other current assets |
— | (1,759 | ) | (772 | ) | ||||||
Other assets |
(2,043 | ) | 238 | 2,077 | |||||||
Accounts payable |
(1,182 | ) | 3,322 | (134 | ) | ||||||
Accrued and other liabilities |
1,027 | (469 | ) | 3,772 | |||||||
Net cash provided by operating activities |
10,362 | 7,904 | 10,308 | ||||||||
Investing activities |
|||||||||||
Purchases of property and equipment |
(5,247 | ) | (19,938 | ) | (11,804 | ) | |||||
Purchases of short-term available-for-sale investments |
(36,942 | ) | — | — | |||||||
Sale or maturity of short-term available-for-sale investments |
9,750 | — | — | ||||||||
Acquisition of business, net of cash acquired |
(9,852 | ) | — | (4,836 | ) | ||||||
Net cash used in investing activities |
(42,291 | ) | (19,938 | ) | (16,640 | ) | |||||
Financing activities |
|||||||||||
Proceeds from issuance of common stock |
10 | 36 | 46,475 | ||||||||
Proceeds from the exercise of employee stock options and employee stock purchase plan contributions |
1,472 | 3,051 | 2,539 | ||||||||
Proceeds from issuance of debt |
— | — | 500 | ||||||||
Repayment of debt |
— | (72 | ) | (3,171 | ) | ||||||
Payments received on shareholder notes |
— | — | 69 | ||||||||
Net cash provided by financing activities |
1,482 | 3,015 | 46,412 | ||||||||
Net (decrease) increase in cash and cash equivalents |
(30,447 | ) | (9,019 | ) | 40,080 | ||||||
Cash and cash equivalents—beginning of period |
49,152 | 58,171 | 18,091 | ||||||||
Cash and cash equivalents—end of period |
$ | 18,705 | $ | 49,152 | $ | 58,171 | |||||
Supplemental disclosure of cash flow information |
|||||||||||
Cash paid for interest |
$ | 3 | $ | 12 | $ | 386 | |||||
Cash paid for taxes |
$ | 692 | $ | 6,218 | — | ||||||
Supplemental disclosure for noncash financing activities |
|||||||||||
Noncash dividends paid on mandatorily redeemable convertible preferred stock |
— | — | 2,597 | ||||||||
Mandatorily redeemable convertible preferred stock converted to common stock related to the initial public offering |
— | — | 117,899 | ||||||||
Convertible preferred stock converted to common stock in connection with the initial public offering |
— | — | 53,456 | ||||||||
See accompanying notes.
66
CARDIONET, INC.
CONSOLIDATED STATEMENTS OF REDEEMABLE CONVERTIBLE PREFERRED STOCK
AND SHAREHOLDERS' EQUITY
(In thousands, except share amounts.)
| |
Redeemable Convertible Preferred Stock |
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |
Shareholders' Equity | |||||||||||||||||||||||||||||||||
| |
Mandatorily Redeemable Convertible Preferred Stock |
|||||||||||||||||||||||||||||||||
| |
Convertible Preferred Stock |
|
|
|
|
|
|
|||||||||||||||||||||||||||
| |
Common Stock | |
Accumulated Other Comprehensive Income |
|
|
|||||||||||||||||||||||||||||
| |
Paid-in Capital |
Accumulated Deficit |
Total Shareholders' Equity |
|||||||||||||||||||||||||||||||
| |
Shares | Amount | Shares | Amount | Shares | Amount | ||||||||||||||||||||||||||||
Balance, December 31, 2007 |
114,839 | 115,302 | 17,670,106 | 53,456 | 3,130,054 | 1,399 | — | — | (81,720 | ) | (26,865 | ) | ||||||||||||||||||||||
Issuance/vesting of common stock |
— | — | — | — | 61,551 | — | 69 | — | — | 69 | ||||||||||||||||||||||||
Exercise of stock options and purchase of shares related to the employee stock purchase plan |
— | — | — | — | 474,989 | 1 | 2,538 | — | — | 2,539 | ||||||||||||||||||||||||
Stock based compensation |
— | — | — | — | — | — | 3,392 | — | — | 3,392 | ||||||||||||||||||||||||
Dividend on and accretion of MRCPS |
— | 2,597 | — | — | — | — | (2,597 | ) | — | — | (2,597 | ) | ||||||||||||||||||||||
Conversion of MRCPS to common stock |
(114,839 | ) | (117,899 | ) | — | — | 7,680,902 | 8 | 117,891 | — | — | 117,899 | ||||||||||||||||||||||
Conversion of Convertible Preferred Stock |
— | — | (17,670,106 | ) | (53,456 | ) | 8,835,042 | (1,387 | ) | 54,843 | — | — | — | |||||||||||||||||||||
Proceeds from IPO (net of underwriter commissions) |
— | — | — | — | 3,000,000 | 3 | 46,472 | — | — | 46,475 | ||||||||||||||||||||||||
Exercise of warrants |
— | — | — | — | 294,599 | — | — | — | — | — | ||||||||||||||||||||||||
Net income |
— | — | — | — | — | — | — | 9,205 | 9,205 | |||||||||||||||||||||||||
Balance, December 31, 2008 |
— | — | — | — | 23,477,137 | 24 | 222,608 | — | (72,515 | ) | 150,117 | |||||||||||||||||||||||
Issuance/vesting of common stock |
— | — | — | — | 129,618 | — | 1,026 | — | — | 1,026 | ||||||||||||||||||||||||
Exercise of stock options and purchase of shares related to the employee stock purchase plan |
— | — | — | — | 353,124 | — | 3,051 | — | — | 3,051 | ||||||||||||||||||||||||
Stock based compensation |
— | — | — | — | — | — | 15,635 | — | — | 15,635 | ||||||||||||||||||||||||
Exercise of warrants |
— | — | — | — | 5,526 | — | — | — | — | — | ||||||||||||||||||||||||
Net loss |
— | — | — | — | — | — | — | — | (20,476 | ) | (20,476 | ) | ||||||||||||||||||||||
Balance December 31, 2009 |
— | — | — | — | 23,965,405 | 24 | 242,320 | — | (92,991 | ) | 149,353 | |||||||||||||||||||||||
Issuance/vesting of common stock |
— | — | — | — | 22,083 | — | 1,422 | — | — | 1,422 | ||||||||||||||||||||||||
Exercise of stock options and purchase of shares related to the employee stock purchase plan |
— | — | — | — | 263,682 | — | 1,472 | — | — | 1,472 | ||||||||||||||||||||||||
Stock based compensation |
— | — | — | — | — | — | 2,533 | — | — | 2,533 | ||||||||||||||||||||||||
Comprehensive loss: |
||||||||||||||||||||||||||||||||||
Net loss |
— | — | — | — | — | — | — | — | (19,860 | ) | (19,860 | ) | ||||||||||||||||||||||
Changes in unrealized gain on available-for-sale investments |
— | — | — | — | — | — | — | 8 | — | 8 | ||||||||||||||||||||||||
Total comprehensive loss |
— | — | — | — | — | — | — | — | — | (19,852 | ) | |||||||||||||||||||||||
Balance December 31, 2010 |
— | $ | — | — | $ | — | 24,251,170 | $ | 24 | $ | 247,747 | $ | 8 | $ | (112,851 | ) | $ | 134,928 | ||||||||||||||||
See accompanying notes.
67
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Years Ended December 31, 2010, 2009 and 2008
(In thousands,
except shares and per share amounts.)
1. Organization and Description of Business
CardioNet is a leading provider of ambulatory, continuous, real-time outpatient management solutions for monitoring relevant and timely clinical information regarding an individual's health. The Company's efforts have initially been focused on the diagnosis and monitoring of cardiac arrhythmias, or heart rhythm disorders, with a solution that it markets as Mobile Cardiac Outpatient Telemetry™ (MCOT™). The Company actively began developing its product platform in April 2000, and since that time, has devoted substantial resources in advancing its patient monitoring solutions. The platform successfully integrates a wireless data transmission network, internally developed software, FDA-cleared algorithms and medical devices, and a 24-hour monitoring service center.
The Company has been approved as an Independent Diagnostic Testing Facility ("IDTF") for Medicare since it received 510(k) clearance for the first and second generation of our core MCOT™ devices in 2002. The Company received FDA 510(k) clearance for the proprietary algorithm included in its third generation product, or C3, in October 2005. Subsequently in November 2006, the Company received FDA 510(k) clearance for its C3 system which it has incorporated as part of its monitoring solution. The Company continues to pursue innovation of new and existing medical solutions through investments in research and development. The CardioNet Monitoring Center commenced operations in Conshohocken, PA in 2002, concurrent with its first FDA approval, and all of the Company's MCOT™ arrhythmia monitoring activities are currently conducted at that location. The Company received FDA 510(k) clearance for its next generation platform, known as C5, in April 2010 and expects the product launch to occur in early 2011. The Company continues to pursue innovation of new and existing medical solutions through investments in research and development.
In October 2008, the Centers for Medicare and Medicaid Services ("CMS") established reimbursement rates that cover MCOT™ services. The reimbursement rates are applicable to the Category I CPT codes (93228 and 93229) established by the American Medical Association ("AMA") for MCOT™ and became effective on January 1, 2009. Highmark Medicare Services ("HMS") is responsible for setting the reimbursement rate on behalf of CMS for code 93229, which is the code for the technical component of our services. These billing codes allow for automated claims adjudication, substantially simplifying the reimbursement process for physicians and payors compared to the previous process. Reimbursement prior to the use of the new CPT codes was obtained through non-specific billing codes which require various narratives that, in most cases, involve semi-automated or manual processing, as well as additional review by payors.
On August 6, 2008, an underwritten secondary public offering of shares of common stock held by certain of the Company's existing stockholders was completed. The Company did not issue any shares and received no proceeds in connection with such offering.
On March 25, 2008, the Company completed its initial public offering generating net proceeds to the Company of approximately $46.7 million, after deducting underwriter commissions and offering expenses. Upon the closing of the Company's initial public offering, all outstanding shares of the Company's mandatorily redeemable convertible preferred stock and convertible preferred stock converted into shares of common stock. At December 31, 2008, the Company had no shares of preferred stock outstanding.
68
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
1. Organization and Description of Business (Continued)
On February 25, 2008, the Board of Directors of the Company, subject to stockholder approval, approved a reverse stock split of the Company's common stock at a ratio of one share for every two shares previously held. On March 5, 2008, the stockholders of the Company approved the reverse stock split and the reverse stock split became effective. All common stock share and per-share data included in these consolidated financial statements reflect the reverse stock split.
In March 2007, the Company acquired all of the outstanding capital stock of PDSHeart. The acquisition of PDSHeart provided three additional product lines to compliment MCOT™: event, Holter and pacemaker monitoring solutions. In addition, the acquisition supplied the Company with existing sales channels and relationships in geographic areas that were previously had not been penetrated prior to the acquisition.
In December 2010, the Company completed the acquisition of Biotel Inc., and its wholly owned subsidiaries, Braemar, Inc. and Agility Centralized Research Services, Inc. The acquisition gives the Company the ability to develop, manufacture, test and market medical devices and related software to medical companies, clinics and hospitals. Additionally, the acquisition also gave the Company access to established customer relationships, entry into the clinical trial service business and the ability to diversify its product and service offerings. The opening balance sheet and purchase price allocation have been reflected in the consolidated financial statements as of December 31, 2010. However, due to the timing of the acquisition, the results of operations for Biotel for the period December 21, 2010, the date of acquisition, through December 31, 2010 were not material.
2. Summary of Significant Accounting Policies
Principals of Consolidation
The accompanying consolidated financial statements include the accounts of the Company and its wholly owned subsidiaries. All significant intercompany transactions and balances have been eliminated in consolidation.
Use of Estimates
The preparation of financial statements in conformity with accounting principles generally accepted in the United States requires that management make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosures of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenue and expenses during the reporting period. Actual results may differ from those estimates.
Business Combinations
In December 2010, we completed the acquisition of Biotel, Inc., and we may pursue additional acquisitions in the future. Business combinations are accounted for in accordance with the provisions of ASC 805, Business Combination. We are required to allocate the purchase price of acquired companies to the tangible and intangible assets we acquired and liabilities we assumed based on their estimated fair values. This valuation requires management to make significant estimates and assumptions,
69
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
2. Summary of Significant Accounting Policies (Continued)
especially with respect to long-lived and intangible assets. Critical estimates in valuing certain of the intangible assets include, but are not limited to, future expected cash flows from customer contracts, customer relationships, proprietary technology and discount rates. Our estimates of fair value are based upon assumptions we believe to be reasonable, but which are inherently uncertain and unpredictable. Assumptions may be incomplete or inaccurate, and unanticipated events and circumstances may occur. Other estimates associated with the accounting for acquisitions may change as additional information becomes available regarding the assets we acquired and liabilities we assumed. For a discussion of how we allocated the purchase price of Biotel, see Note 3.
Fair Value of Financial Instruments
The Company's financial instruments consist mainly of cash and cash equivalent, available-for-sale investments, accounts receivable, other current assets, accounts payable, deferred revenue and other current liabilities. The carrying value of these financial instruments approximates their fair value because of their short-term nature. The fair value of financial instruments is defined as the amount at which the instrument could be exchanged in a current transaction between willing parties.
Cash and Cash Equivalents
Cash and cash equivalents are held in U.S. financial institutions or in custodial accounts with U.S. financial institutions. Cash equivalents are defined as liquid investments and money market funds with maturity from date of purchase of 90 days or less that are readily convertible into cash and have insignificant interest rate risk.
Available-for-Sale Investments
Marketable securities that do not meet the definition of cash and cash equivalents are classified as available-for-sale. Available-for-sale securities are carried at fair value, based on quoted market prices and observable inputs, with unrealized gains and losses, reported as a separate component of stockholders' equity. We classify securities as current or non-current assets on the consolidated balance sheet based on maturity dates. The amortized cost of debt securities is adjusted for amortization of premiums and accretions of discounts to maturity. Amortization of debt premiums and accretion of debt discounts are recorded in other income and expense. Realized gains and losses, and declines in value, that are considered to be other-than-temporary, are recorded in other income and expense. The cost of securities sold is based on specific identification.
Accounts Receivable and Allowance for Bad Debt
Accounts receivable are recorded at the time revenue is recognized, net of contractual allowances and are presented on the balance sheet net of allowance for doubtful accounts. The Company performs analyses to evaluate the net realizable value of accounts receivable as of the balance sheet date. Specifically, the Company considers historical realization data, accounts receivable aging trends, other operating trends and relevant business conditions. Because of continuing changes in the health care
70
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
2. Summary of Significant Accounting Policies (Continued)
industry and third party reimbursement, it is possible that our estimates could change, which could have a material impact on our operations and cash flows.
The Company realized improvements in its billing procedures and cash collections activity during 2010 and experienced a corresponding decline in its days sales outstanding. The Company believes that it can realize additional improvement in its billing and collection processes, and has engaged a third party consultant that is a specialist with significant experience in medical claims reimbursement to assist. The first phase of the project will include a review of all outstanding receivables. The Company cannot reasonably determine as of the balance sheet date what impact, if any, this review will have on the financial statements. This review was substantially complete by the end of the fourth quarter of 2010. The second phase of the project, expected to be completed in the first half of 2011, will include an internal review of the recommendations for changes in the Company's patient intake, billing and reimbursement practices and processes.
During the third quarter of 2010, Highmark Medical Services conducted a prepayment review of the Company's Medicare claims. This review involved an evaluation of medical records and application of clinical judgment by Highmark about whether a service is covered, and is reasonable and necessary. As a result of this review, reimbursement payments to the Company were temporarily suspended in the third quarter of 2010. Effective October 25, 2010, Highmark completed the prepayment review and the Company's cash collections resumed for its Medicare claims during November 2010. As of December 31, 2010, substantially all of the outstanding receivables related to the prepayment review were collected.
The ultimate collection of accounts receivable may not be known for several months after services have been provided and billed. The Company records bad debt expense based on the aging of the receivable using historical Company-specific data. The percentages and amounts used to record bad debt expense and the allowance for doubtful accounts are supported by various methods and analyses, including current and historical cash collections, and the aging of specific receivables. The Company will write-off receivables when the likelihood for collection is remote, the receivables have been fully reserved, and when the Company believes collection efforts have been fully exhausted and it does not intend to devote additional resources in attempting to collect. Prior to the third quarter of 2010, the Company performed an annual accounts receivable write-off in the fourth quarter. Beginning in the third quarter of 2010, the Company has determined it will evaluate outstanding receivables and perform write-offs quarterly going forward. The Company wrote off $29,195 and $12,012 of receivables for the years ended December 31, 2010 and 2009, respectively. The impact was a reduction of gross receivables and a reduction in the allowance for doubtful accounts. Additionally, the Company recorded bad debt expense of $18,578 and $19,982 for the years ended December 31, 2010 and 2009, respectively. Based on collection experience in 2010 and 2009, the Company recorded additional bad debt expense of $11,669 and $9,112, in 2010 and 2009 respectively, related to prior years' accounts receivable.
Concentrations of Credit Risk
Financial instruments that potentially subject the Company to concentrations of credit risk consist primarily of cash, cash equivalents, short-term available-for-sale investments and accounts receivable.
71
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
2. Summary of Significant Accounting Policies (Continued)
The Company maintains its cash and cash equivalents with high quality financial institutions to mitigate this risk. The Company has established guidelines to limit exposure to credit risk by placing investments with high quality financial institutions, diversifying our investment portfolio and placing investments with maturities that maintain safety and liquidity. The Company performs ongoing credit evaluations of its customers and generally does not require collateral. The Company records an allowance for doubtful accounts in accordance with the procedures described above. Past-due amounts are written off against the allowance for doubtful accounts when collections are believed to be unlikely and all collection efforts have ceased.
At December 31, 2010, 2009 and 2008, one customer accounted for 18%, 20% and 23%, respectively, of our net accounts receivable.
Inventory
Inventory is valued at the lower of cost (using the average and first-in, first-out cost methods) or market (net realizable value or replacement cost). Company management periodically reviews inventory for specific future usage, and estimates of impairment of individual inventory items are recorded to reduce inventory to the lower of cost or market.
Property and Equipment
Property and equipment is recorded at cost. Depreciation is provided over the estimated useful life of each class of depreciable assets (generally 2-5 years), and is computed using the straight-line method. Leasehold improvements are amortized over the shorter of the estimated asset life or term of the lease. Repairs and maintenance costs are charged to expense as incurred.
Impairment of Long-Lived Assets
The Company periodically evaluates the recoverability of the carrying value of its long-lived assets based on the criteria established in ASC 360, Property, Plant & Equipment. The Company considers historical performance and anticipated future results in its evaluation of potential impairment. Accordingly, when indicators of impairment are present, the Company evaluates the carrying value of these assets in relation to the operating performance of the business and the undiscounted cash flows expected to result from the use of these assets. Impairment losses are recognized when the sum of the expected future cash flows is less than the assets' carrying value. No impairment losses have been recognized for the years ended December 31, 2010 or 2009.
Goodwill and Acquired Intangible Assets
The Company considers its business to be one reporting unit for purposes of performing its goodwill impairment analysis. Goodwill is reviewed for impairment annually, or when events arise that could indicate that impairment exists. To determine whether impairment exists, the Company estimates the fair value of the reporting unit using an income approach, generally a discounted cash flow methodology that includes assumptions for, among other things, forecasted income, cash flow, growth rates, income tax rates, expected tax benefits and long-term discount rates, all of which require
72
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
2. Summary of Significant Accounting Policies (Continued)
significant judgments. The Company also considers comparable market data to assist in determining the fair value of its reporting unit. There are inherent uncertainties related to these factors and the judgment applied in the analysis. The Company believes that the combination of an income and a market approach provides a reasonable basis to estimate the fair value of the reporting unit. If the estimated fair value of the reporting unit is less than its carrying value, impairment may exist and additional analysis will be undertaken to determine the amount of impairment.
In accordance with ASC 350-20-35, Intangibles—Goodwill and Other, and based on the results of the analyses performed, no impairment loss has been recorded for the years ended December 31, 2010 or 2009. Acquired intangible assets consist of trade names, customer relationships, proprietary technology and signed backlog. The Company amortizes acquired intangible assets over their estimated useful lives on a straight-line basis.
Revenue Recognition
The Company recognizes revenue primarily from patient monitoring services, derived from its MCOT™, event, Holter and pacemaker services. The Company receives a significant portion of its revenue reimbursement from third party commercial insurance organizations and governmental entities. It also receives reimbursement directly from patients through co-pay and self-pay arrangements.
Revenue from the Medicare program is based on reimbursement rates set by governmental authorities and revenue from contracted commercial payors is recorded at the negotiated contractual rate. Revenue from non-contracted commercial payors is recorded at net realizable value based on historical payment patterns.
Billings for services reimbursed by contract third party payors, including Medicare, are recorded as revenue net of allowances for differences between amounts billed and the estimated receipts from such payors. Adjustments to the estimated receipts, based on final settlement with the third party payors, are recorded upon settlement. If the Company does not have consistent historical information regarding collectability from a given payor, revenue is recognized when cash is received. Unearned amounts are appropriately deferred until service is performed.
Effective September 1, 2009, the Medicare reimbursement rate for MCOT™ services was reduced by 33%. For the years ended December 31, 2010, 2009 and 2008, the Medicare revenue as a percentage of the Company's total revenue was 35%, 36% and 33%, respectively.
Other revenue, consisting mainly of information technology services provided to an affiliate of a stockholder, is recognized at the contractually established rate and is recognized at the time service is provided.
Advertising Costs
Advertising costs are charged to expense as incurred. For the years ended December 31, 2010, 2009 and 2008, the Company incurred advertising costs of $823, $628, $452, respectively.
73
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
2. Summary of Significant Accounting Policies (Continued)
Research and Development Costs
Research and development costs are charged to expense as incurred.
Net (Loss) Income
The Company computes net (loss) income per share in accordance with ASC 260, Earnings Per Share. In accordance with this guidance, basic net (loss) income per share is computed by dividing net loss per share available to common stockholders by the weighted average number of common shares outstanding for the period, and excludes the effects of any potentially dilutive securities. Diluted earnings per share, if presented, would include the dilution that would occur upon the exercise or conversion of all potentially dilutive securities into common stock using the treasury stock or if converted methods, as applicable.
The following summarizes the potential outstanding common stock of the Company as of the end of each period:
| |
December 31, 2010 |
December 31, 2009 |
December 31, 2008 |
|||||||
|---|---|---|---|---|---|---|---|---|---|---|
Series B warrants |
— | — | 6,250 | |||||||
Employee stock purchase plan estimated share options outstanding |
40,208 | 58,095 | 9,889 | |||||||
Common stock options and restricted stock units ("RSU's") outstanding |
2,102,376 | 1,575,645 | 1,635,205 | |||||||
Common stock options available for grant |
1,649,723 | 1,132,135 | 340,935 | |||||||
Common stock held by certain employees and unvested |
— | 9,583 | 41,718 | |||||||
Common stock |
24,251,170 | 23,965,405 | 23,477,137 | |||||||
Total |
28,043,477 | 26,740,863 | 25,511,134 | |||||||
Basic net (loss) income per share is computed by dividing net loss by the weighted average number of fully vested common shares outstanding during the period. Diluted net income per share is computed by giving effect to all potential dilutive common shares, including stock options, warrants and convertible preferred stock.
74
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
2. Summary of Significant Accounting Policies (Continued)
The following table presents the calculation of historical basic and diluted net (loss) income per share:
| |
Year Ended December 31, | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| |
2010 | 2009 | 2008 | ||||||||
| |
(in thousands, except per share amounts) |
||||||||||
Numerator: |
|||||||||||
Net (loss) income applicable to common stockholders |
$ | (19,860 | ) | $ | (20,476 | ) | $ | 6,608 | |||
Denominator: |
|||||||||||
Weighted average common shares outstanding—Basic |
24,109,085 | 23,771,368 | 18,348,594 | ||||||||
Dilutive effect of the Company's employee stock compensation plans |
— | — | 4,310,219 | ||||||||
Weighted average shares used in computing diluted net loss per share |
24,109,085 | 23,771,368 | 22,658,813 | ||||||||
Basic net (loss) income per share |
$ | (0.82 | ) | $ | (0.86 | ) | $ | 0.36 | |||
Diluted net (loss) income per share |
$ | (0.82 | ) | $ | (0.86 | ) | $ | 0.29 | |||
If the outstanding options and unvested stock were exercised or converted into common stock, the result would be anti-dilutive for the years ended December 31, 2010 and 2009. Accordingly, basic and diluted net loss attributable to common stockholders per share are identical for these periods presented in the accompanying consolidated statements of operations.
Comprehensive (Loss) Income
Comprehensive loss consists of net (loss) income for the period plus all changes to stockholders' equity that are not reflected in the consolidated statement of operations. The following summarizes the components of the Company's comprehensive (loss) income:
| |
Year Ended December 31, | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| |
2010 | 2009 | 2008 | ||||||||
Net (loss) income applicable to common stockholders |
$ | (19,860 | ) | $ | (20,476 | ) | $ | 6,608 | |||
Other comprehensive income: |
|||||||||||
Unrealized gain on securities |
8 | — | — | ||||||||
Total comprehensive (loss) income |
(19,852 | ) | (20,476 | ) | 6,608 | ||||||
Stock-Based Compensation
ASC 718, Compensation—Stock Compensation, addresses the accounting for share-based payment transactions in which an enterprise receives employee services in exchange for (a) equity instruments of the enterprise or (b) liabilities that are based on the fair value of the enterprise's equity instruments or
75
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
2. Summary of Significant Accounting Policies (Continued)
that may be settled by the issuance of such equity instruments. ASC 718 requires that an entity measure the cost of equity-based service awards based on the grant-date fair value of the award and recognize the cost of such awards over the period during which the employee is required to provide service in exchange for the award (the vesting period). ASC 718 requires that an entity measure the cost of liability-based service awards based on current fair value that is re-measured subsequently at each reporting date through the settlement date. The Company accounts for equity awards issued to non-employees in accordance with ASC 505-50, Equity-Based Payments to Non-Employees.
Income Taxes
The Company accounts for income taxes under the liability method, as described in ASC 740, Income Taxes. Deferred income taxes are recognized for the tax consequences of temporary differences between the tax and financial statement reporting bases of assets and liabilities. A valuation allowance for net deferred tax assets is provided unless realizability is judged by us to be more likely than not.
Certain Significant Risks and Uncertainties
Financial instruments that potentially subject the Company to concentrations of credit risk consist primarily of cash, cash equivalents, short-term available-for-sale investments and accounts receivable balances. Cash and cash equivalents consist primarily of cash in bank accounts, as well as money market funds. Short-term available-for-sale investments consist of investments with high quality financial institutions. The Company diversifies its investment portfolio and places investments with maturities that maintain safety and liquidity.
Accounts receivable consist of amounts due to the Company from its normal business activities. The Company performs ongoing credit evaluations of its customers' financial condition and if applicable maintains an allowance for potential credit losses.
Segment information
ASC 280, Segment Reporting, establishes standards for reporting information relating to operating segments. An operating segment is identified as a component of a business that has discrete financial information available, and one that the chief operating decision maker must decide the level of resource allocation directed to the segment. In addition, the guidance indicates certain quantitative thresholds for segment reporting. The Company considers its operations and manages its business as one operating segment.
Recent Accounting Pronouncements
In January 2010, the FASB issued Accounting Standards Update (ASU) No. 2010-06, Fair Value Measurements and Disclosures (Topic 820): Improving Disclosures about Fair Value Measurements. The guidance requires entities to disclose significant transfers in and out of fair value hierarchy levels and the reasons for the transfers. Additionally, the guidance clarifies that a reporting entity should provide fair value measurements for each class of assets and liabilities and disclose the inputs and valuation techniques used for fair value measurements using significant other observable inputs (Level 2) and
76
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
2. Summary of Significant Accounting Policies (Continued)
significant unobservable inputs (Level 3). Level 3 reconciliations should present separately information about purchases, sales, issuances and settlements. To date, the Company has not had any assets or liabilities that transferred in or out of fair value hierarchy levels. This guidance is effective for interim and annual periods beginning after December 15, 2009, except for the disclosures about purchases, sales, issuances and settlements in the Level 3 reconciliations, which is effective for fiscal years beginning after December 15, 2010. This guidance did not have an impact on the Company's results of operations or financial position. The Company adopted this guidance effective December 31, 2009. The Company believes the enhanced Level 3 disclosures will not have an impact on the Company's results of operations or financial position.
In February 2010, the FASB issued ASU No. 2010-09, Subsequent Events (Topic 855). The guidance requires an SEC filer to evaluate subsequent events through the date the financial statements are issued but no longer requires an SEC filer to disclose the date through which the subsequent event evaluation occurred. The guidance became effective for the Company upon issuance and had no impact on the Company's results of operations or financial position.
In December 2010, the FASB issued ASU No. 2010-29, Intangibles—Goodwill and Other (Topic 350). The guidance requires entities that have recognized goodwill and have one or more reporting unit whose carrying amount for purposes of performing Step 1 of the goodwill impairment test is zero or negative to perform Step 2 of the goodwill impairment test if it is more likely than not that a goodwill impairment exists. In determining whether it is more likely than not that goodwill impairment exists, an entity should consider whether there are any adverse qualitative factors indicating that impairment may exist. The qualitative factors are consistent with the existing guidance defined in ASC 350-20-35-30, Intangibles—Goodwill and Other, which requires that goodwill of a reporting unit be tested for impairment between annual tests if an event occurs or circumstances change that would more likely than not reduce the fair value of a reporting unit below its carrying amount. The amendments are effective for fiscal years beginning after December 15, 2010. The Company does not believe the adoption of ASU No. 2010-28 will have an impact on the Company's results of operations or financial position.
In December 2010, the FASB issued ASU No. 2010-29, Business Combinations (Topic 805): Disclosing of Supplementary Pro Forma Information for Business Combinations. The guidance affects any public entity as defined by ASC 805, Business Combination, which enters into business combinations that are material on an individual or aggregate basis. The comparative financial statements should present and disclose revenue and earnings of the combined entity as though the business combination(s) that occurred during the current year had occurred as of the beginning of the comparable prior annual reporting period only. The amendments also expand the supplemental pro forma disclosures to include a description of the nature and amount of material, nonrecurring pro forma adjustments directly attributable to the business combination included in the reported pro forma revenue and earnings. The amendments are effective prospectively for business combinations for which the acquisition date is on or after the beginning of the first annual reporting period beginning on or after December 15, 2010. The Company does not believe the adoption of ASU No. 2010-29 will have an impact on the Company's results of operations or financial position.
77
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
3. Business Combination
On December 21, 2010, the Company acquired all of the outstanding common stock, as defined in the Merger Agreement among the Company, Biotel Inc. and Garden Merger Sub, Inc. (the "2010 Merger Agreement"), of Biotel Inc., and its wholly owned subsidiaries, Braemar, Inc. and Agility Centralized Research Services, Inc. (referred to herein as "Biotel," "Braemar," and "Agility," respectively). The Company paid an aggregate cash purchase price of $11,624. The acquisition has been included within the consolidated results of operations and financial condition from the date of the acquisition. The acquisition gives the Company the ability to develop, manufacture, test and market medical devices and related software to medical companies, clinics and hospitals. The acquisition also gave the Company access to established customer relationships, entry into the clinical trial service business and the ability to diversity its product and service offerings.
Biotel designs, manufactures and services non-invasive diagnostic cardiology devices for original equipment manufacturers, and provides electrocardiogram ("ECG") data and management services for clinical trials. Braemar develops and manufactures 24- and 48-hour Holter recorders, 30-day ECG event recorders, and other non-invasive custom medical devices. Additionally, Braemar sells maintenance services and sells Holter recorders and event recorders manufactured by Braemar, diagnostic Holter software provided by others, and related supplies to clinics and hospitals. Agility provides 24-hour/7-day ECG data and management services to the medical device and pharmaceutical industries, contract research organizations, and academic research organizations for cardiac safety and therapeutic evaluation purposes within clinical trials.
The Biotel acquisition purchase consideration of $11,624 has been allocated to assets acquired and liabilities assumed based on estimated fair values at the date of acquisition as follows:
Fair value of assets acquired: |
||||||
Cash and cash equivalents |
$ | 1,649 | ||||
Accounts receivable |
2,772 | |||||
Inventory |
1,461 | |||||
Prepaid expenses and other current assets |
261 | |||||
Property and equipment |
1,013 | |||||
Goodwill |
3,363 | |||||
Intangible assets |
3,200 | |||||
Other assets |
1,195 | |||||
Total assets acquired |
14,914 | |||||
Liabilities assumed: |
||||||
Accounts payable |
1,149 | |||||
Accrued expenses |
641 | |||||
Other liabilities |
1,500 | |||||
Total liabilities assumed |
3,290 | |||||
Net assets acquired |
$ | 11,624 | ||||
78
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
3. Business Combination (Continued)
The intangible assets with definite lives are being amortized on a straight-line basis over lives ranging from one to ten years. The depreciable tax basis in acquired goodwill as of the acquisition date is $314.
The results of operations for Biotel for the year-to-date period ended December 20, 2010, and for the years ended December 31, 2009 and 2008, were not material to the Company's consolidated results of operations. The results of operations for Biotel for the period December 21, 2010, the date of acquisition, through December 31, 2010 were not material. As such, the results of operations from Biotel for this 10 day period are not included in the Company's consolidated results of operations.
4. Available-for-Sales Investments
We invest our excess funds in securities issued by the United States government, corporations, banks, municipalities, financial holding companies and in money market funds comprised of these same types of securities. Our cash and cash equivalents and available-for-sale investments are placed with high credit quality financial institutions. Additionally, we diversify our investment portfolio in order to maintain safety and liquidity. We do not hold mortgage-backed securities. As of December 31, 2010, all of our investments will mature within one year. These investments are recorded at fair value, based on quoted market prices, with unrealized gains and losses reported as a separate component of stockholders' equity. At December 31, 2009, the Company had no investments classified as available-for-sale investments.
Investments have been classified as available-for-sale investments. At December 31, 2010, available-for-sale investments are detailed as follows:
| |
Amortized Cost |
Gross Unrealized Gains |
Gross Unrealized Losses |
Estimated Fair Value |
|||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
Short-term investments: |
|||||||||||||||
Corporate debt securities |
$ | 13,132 | $ | 2 | $ | (5 | ) | $ | 13,129 | ||||||
U.S. Treasury and agency debt securities |
13,639 | 11 | — | 13,650 | |||||||||||
Total |
$ | 26,771 | $ | 13 | $ | (5 | ) | $ | 26,779 | ||||||
Net unrealized gains on available-for-sale investments are included as a component of stockholders' equity and comprehensive loss until realized from a sale or other-than-temporary impairment. The Company recorded net unrealized gains for the years ended December 31, 2010, 2009 and 2008 of $8, $0 and $0, respectively. Realized gains and losses from the sale of securities are determined on a specific identification basis. Purchases and sales of investments are recorded on their trade dates. The Company recorded realized gains for the years ended December 31, 2010, 2009 and 2008 of $2, $0 and $0, respectively. Dividend and interest income are recognized when earned. Interest income for the year ended December 31, 2010 was $510, which was partially offset by $421 related to amortization of investment premiums.
At December 31, 2010, the Company had 13 corporate debt securities and eight U.S. Treasury and agency debt securities in its available-for-sale investment balance, of which 10 securities were in an
79
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
4. Available-for-Sales Investments (Continued)
unrealized loss position totaling $5. The aggregate related fair value of available-for-sale investments with unrealized losses is $10,342 at December 31, 2010. Based on the Company's intent to hold these investments for a reasonable period of time sufficient for a forecasted recovery of fair value, the Company does not consider these investments to be other-than-temporarily impaired at December 31, 2010.
5. Fair Value Measurements
ASC 820 defines fair value as an exit price that would be received from the sale of an asset or paid to transfer a liability in the principal or most advantageous market for the asset or liability in an orderly transaction between market participants on the measurement date. ASC 820 establishes a three-level hierarchy for disclosure that is based on the extent and level of judgment used to estimate the fair value of assets and liabilities.
- •
- Level 1—Valuations based on quoted prices for identical assets or liabilities in active markets at the
measurement date. Since valuations are based on quoted prices that are readily and regularly available in an active market, valuation of these products does not entail a significant degree of
judgment. Our Level 1 assets consist of cash and money market funds, as well as U.S. Treasury and agency debt securities.
- •
- Level 2—Valuations based on quoted prices for similar assets and liabilities in active markets; quoted
prices for identical or similar assets and liabilities in markets that are not active; or other inputs that are observable or can be corroborated by observable market data, such as alternative pricing
sources with reasonable levels of price transparency. Our Level 2 assets consist of fixed income securities such as corporate debt securities including commercial paper and corporate bonds.
- •
- Level 3—Valuations based on inputs that are unobservable and significant to the overall fair value measurement. We have not measured the fair value of any of our assets using Level 3 inputs.
In January 2010, the FASB updated the disclosure requirements for fair value measurements. The updated guidance requires companies to disclose separately the investments that transfer in and out of Levels 1 and 2 and the reason for those transfers. Additionally, in the reconciliation for fair value measurements using significant unobservable inputs (Level 3), companies should present separately information about purchases, sales, issuances and settlements.
In accordance with the new guidance, the Company is required to disclose transfers between category levels, as well as certain other disclosures related to Level 3 investments. No transfers were made into or out of the different category levels, nor did the Company categorize any of its investments as Level 3 as of December 31, 2010. We will continue to review our fair value inputs on a quarterly basis. The updated guidance is effective for the reporting periods beginning after December 15, 2009, except for the disclosures about purchases, sales, issuances and settlements in the Level 3 reconciliations, which is effective for fiscal years beginning after December 15, 2010.
80
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
5. Fair Value Measurements (Continued)
The fair value of our financial assets subject to the disclosure requirements of ASC 820 was determined using the following levels of inputs at December 31, 2010:
Fair Value Measurements at December 31, 2010
| |
Level 1 | Level 2 | Level 3 | Total | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
Assets: |
|||||||||||||||
Cash |
$ | 12,681 | $ | — | $ | — | $ | 12,681 | |||||||
Money market funds |
5,024 | — | — | 5,024 | |||||||||||
Corporate debt securities |
— | 14,129 | — | 14,129 | |||||||||||
U.S. Treasury and agency debt securities |
13,650 | — | — | 13,650 | |||||||||||
Total |
$ | 31,355 | $ | 14,129 | $ | — | $ | 45,484 | |||||||
6. Inventory
Inventory consists of the following:
| |
December 31, | ||||||
|---|---|---|---|---|---|---|---|
| |
2010 | 2009 | |||||
Raw materials and supplies |
$ | 1,218 | $ | — | |||
Finished goods |
243 | — | |||||
Total inventories |
$ | 1,461 | $ | — | |||
Inventories, which include purchased parts, materials, direct labor and applied manufacturing overhead, are stated at the lower of cost or net realizable value, with cost determined by use of the first-in, first-out method.
81
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
7. Property and Equipment
Property and equipment consists of the following:
| |
|
December 31, | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| |
Estimated Useful Life (Years) |
|||||||||
| |
2010 | 2009 | ||||||||
Cardiac monitoring devices and device parts and components |
3 - 5 | $ | 44,529 | $ | 54,246 | |||||
Computers and purchased software |
3 - 5 | 10,336 | 9,284 | |||||||
Equipment, tools and molds |
3 | 5,180 | 1,540 | |||||||
Furniture and fixtures |
3 | 2,819 | 2,712 | |||||||
Leasehold improvements |
Life of lease | 4,759 | 4,707 | |||||||
Total property and equipment, at cost |
67,623 | 72,489 | ||||||||
Less accumulated depreciation |
(45,623 | ) | (44,246 | ) | ||||||
Total property and equipment, net |
$ | 22,000 | $ | 28,243 | ||||||
Depreciation expense associated with property and equipment was $11,696, $10,053 and $7,709, for the years ended December 31, 2010, 2009 and 2008, respectively.
8. Goodwill and Intangible Assets
The carrying amount of goodwill was recognized at the time of the Biotel and PDSHeart acquisitions, adjusted for contingent payments to former shareholders. The carrying amount of goodwill as of December 31, 2010 and 2009 was $49,362 and $45,999, respectively.
The gross carrying amounts and accumulated amortization of the Company's intangible assets as of December 31, 2010 and 2009 are as follows:
| |
|
December 31, | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| |
Estimated Useful Life (Years) |
|||||||||
| |
2010 | 2009 | ||||||||
Trade name |
3 | $ | — | $ | 1,810 | |||||
Customer relationships |
6 - 10 | 2,551 | 1,551 | |||||||
Proprietary Technology |
5 | 800 | — | |||||||
Signed Backlog |
1 | 700 | — | |||||||
Total intangible assets, gross |
4,051 | 3,361 | ||||||||
Trade name accumulated amortization |
— | 1,694 | ||||||||
Customer relationships accumulated amortization |
987 | 728 | ||||||||
Total accumulated amortization |
987 | 2,422 | ||||||||
Indefinite-lived trade name |
700 | — | ||||||||
Total intangible assets, net |
$ | 3,764 | $ | 939 | ||||||
82
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
8. Goodwill and Intangible Assets (Continued)
The estimated amortization expense for the next five years is summarized as follows at December 31, 2010:
2011 |
1,219 | ||||
2012 |
519 | ||||
2013 |
307 | ||||
2014 |
260 | ||||
2015 |
260 | ||||
Total |
$ | 2,564 | |||
Amortization expense for the years ending December 31, 2010, 2009 and 2008 was $375, $884 and $984, respectively.
9. Accrued Expenses
Accrued expenses consisted of the following:
| |
December 31, | |||||||
|---|---|---|---|---|---|---|---|---|
| |
2010 | 2009 | ||||||
Accrued purchases |
$ | 538 | $ | 672 | ||||
Accrued compensation |
6,470 | 7,281 | ||||||
Accrued professional fees |
834 | 722 | ||||||
2010 restructuring costs |
463 | — | ||||||
2009 restructuring costs |
— | 217 | ||||||
Other |
1,576 | 1,027 | ||||||
Total |
$ | 9,881 | $ | 9,919 | ||||
10. Integration, Restructuring and Other Charges
2010 Integration, Restructuring and Other Charges
For the year ended December 31, 2010, we incurred expenses related to restructuring, integration and other activities. A summary of these expenses is as follows:
2010 restructuring |
$ | 3,523 | |||
Other charges |
1,131 | ||||
Total |
$ | 4,654 | |||
83
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
10. Integration, Restructuring and Other Charges (Continued)
2010 Restructuring
During the first quarter of 2010, the Company undertook an initiative to streamline its sales and service organizations and reduce support costs company-wide. It also initiated plans to close its event monitoring facility in Georgia and consolidate it with the Company's monitoring facilities in Pennsylvania and Minnesota. The Company realized cost efficiencies by undertaking these initiatives.
The restructuring plan involved the elimination of approximately 100 positions. The restructuring activities are substantially complete as of December 31, 2010. The Company incurred restructuring expenses of $3,523 for the year ended December 31, 2010, and does not expect to incur additional charges related to this restructuring plan.
A summary of the reserve activity related to the 2010 restructuring plan as of December 31, 2010 is as follows:
| |
Initial Reserve Recorded |
Payments through December 31, 2010 |
Balance as of December 31, 2010 |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
Severance and employee related costs |
$ | 2,140 | $ | 1,677 | $ | 463 | |||||
Other exit activity costs |
1,383 | 1,383 | — | ||||||||
Total |
$ | 3,523 | $ | 3,060 | $ | 463 | |||||
The Company accounts for expenses associated with exit or disposal activities in accordance with ASC 420, Exit or Disposal Cost Obligations, and records the expenses in Integration, restructuring and other charges in its statement of operations, and records the related accrual in the Accrued liabilities line of its balance sheet.
Other Charges
The Company incurred other charges of $1,131 for the year ended December 31, 2010, including legal costs related to the Company's defense of class-action and Biotel lawsuits. Additional information regarding legal proceedings can be found in Note 15.
2009 Integration, Restructuring and Other Charges
For the year ended December 31, 2009, we incurred expenses related to restructuring, integration and other activities. A summary of these expenses is as follows:
2009 restructuring |
$ | 1,153 | |||
Costs associated with option cancellation |
9,818 | ||||
PDSHeart integration |
(143 | ) | |||
Conshohocken fire |
(181 | ) | |||
Other costs |
2,334 | ||||
Total |
$ | 12,981 | |||
84
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
10. Integration, Restructuring and Other Charges (Continued)
2009 Restructuring
During the third quarter of 2009, the Company undertook an initiative to reduce support costs company-wide and initiated plans to move the majority of its manufacturing activities from San Diego to its facility in Chester, PA. The Company achieved a reduction in shipping and administrative costs by combining its manufacturing facilities into one location. Prior to the restructuring, devices were shipped to and from the San Diego location for production and maintenance before being deployed out of the Company's distribution facility in Pennsylvania.
Also during the third quarter of 2009, the Company closed its event monitoring facility in Florida and consolidated it with the Company's event monitoring facility in Georgia. The Company realized cost efficiencies by consolidating its event monitoring centers in the southeastern United States and by eliminating duplicative administrative costs.
The restructuring plan involved the elimination of approximately 80 positions and the relocation of 15 employees. The restructuring was substantially completed as of December 31, 2009. The Company incurred restructuring expenses of $1,153 for the year ended December 31, 2009.
A summary of the reserve activity related to the 2009 restructuring plan as of December 31, 2009 is as follows:
| |
Initial Reserve Recorded |
Payments through December 31, 2009 |
Balance as of December 31, 2009 |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
Severance and employee related costs |
$ | 1,014 | $ | 797 | $ | 217 | |||||
Other exit activity costs |
139 | 139 | — | ||||||||
Total |
$ | 1,153 | $ | 936 | $ | 217 | |||||
The remaining accrual as of December 31, 2009 was paid in 2010.
The Company accounts for expenses associated with exit or disposal activities in accordance with ASC 420, Exit or Disposal Cost Obligations, and records the expenses in the Integration, restructuring and other charges line in its statement of operations, and records the related accrual in the Accrued expenses line in its balance sheet.
Option Cancellation
On December 1, 2009, certain executive officers cancelled a portion of their remaining unvested stock options as of that date. No consideration was given in exchange for the cancellation, and no new options were granted. The Company incurred a one-time charge of $9,818 to recognize the remaining unamortized expense associated with the cancelled options. The Company has recognized this charge in accordance with the guidance in ASC 718, Compensation—Stock Compensation. This charge was recorded in the Integration, restructuring and other charges line in its statement of operations.
85
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
10. Integration, Restructuring and Other Charges (Continued)
Conshohocken Fire
In August 2008, the Company's corporate headquarters were affected by a fire at an adjacent construction site. The fire caused water and electrical damage in one corner of the Company's building. The Company's patient monitoring services were not interrupted. Costs of $485 were incurred through December 31, 2008, including $220 of newly acquired fixed assets that have been capitalized as of the balance sheet date, $53 of fixed asset impairments, and $212 of out of pocket costs.
The Company's insurance policy covers all out of pocket costs and damaged fixed assets at replacement value, and as such, the Company does not expect to incur a loss as a result of the fire damage. During 2009, we received a final insurance settlement for the assets damaged in the fire. A gain of $181 was realized as a result of the final settlement.
Other Costs
In January 2009, the Company incurred costs related to the departure of certain executive officers, including the former Chief Executive Officer. The costs include primarily severance and benefit payments. The expenses are included in the Integration, restructuring and other charges line in its statement of operations, and unpaid amounts are included in the Accrued expenses line in the balance sheet as accrued compensation.
2008 Integration, Restructuring and Other Charges
For the year ended December 31, 2008, we incurred expenses related to restructuring, integration and other activities. A summary of these expenses is as follows:
PDSHeart integration |
$ | 977 | |||
San Diego restructuring |
976 | ||||
Legal settlement |
950 | ||||
Secondary offering expenses |
942 | ||||
Conshohocken fire |
(85 | ) | |||
Other |
1,120 | ||||
Total |
$ | 4,880 | |||
PDSHeart Integration
In connection with the acquisition of PDSHeart, the Company completed exit activities to eliminate redundant operational and administrative positions. The exit plan included the closure of a facility and the elimination of approximately 35 positions in the areas of sales, finance, service and management. In connection with the plan, the Company established reserves of $510 that were included in the purchase price allocation. As of December 31, 2008, all of the positions had been eliminated and the Company vacated the facility. The reserve is included in accrued liabilities in the accompanying consolidated balance sheets.
86
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
10. Integration, Restructuring and Other Charges (Continued)
A summary of the reserve activity related to the PDSHeart acquisition-related integration plan as of December 31, 2008 is as follows (in thousands):
| |
Initial Reserves Recorded in Purchase Accounting |
Payments/Adjustments through December 31, 2008 |
Balance as of December 31, 2008 |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
Severance and employee related costs |
$ | 366 | $ | 366 | $ | — | |||||
Rent abandonment |
$ | 144 | $ | 76 | $ | 68 | |||||
Total |
$ | 510 | $ | 442 | $ | 68 | |||||
The remaining accrual as of December 31, 2008 was paid in 2009.
Additionally, the Company incurred expenses of $977 for the year ended December 31, 2008 to integrate these functions, and incurred no additional costs in 2009. Post-acquisition integration costs included severance and employee related costs, IT costs, and other administrative costs to complete the integration activities. These costs were expensed as incurred and are included in Integration, restructuring, and other charges.
San Diego Restructuring
During the first quarter of 2008, the Company initiated plans to consolidate its Finance and Human Resource functions in Pennsylvania. This plan involved the elimination of 7 positions in San Diego. The Company incurred expenses of $976 for the year ended December 31, 2008 to consolidate these functions. The integration was substantially completed as of December 31, 2008. These costs were expensed as incurred.
A summary of the reserve activity related to the San Diego restructuring plan as of December 31, 2008 is as follows:
| |
Initial Reserve Recorded |
Payments through December 31, 2008 |
Additional reserves through December 31, 2008 |
Balance as of December 31, 2008 |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
Severance and employee related costs |
$ | 662 | 388 | 501 | 775 | ||||||||
The remaining accrual as of December 31, 2008 was paid in 2009.
Conshohocken Fire
In August 2008, the Company's corporate headquarters were affected by a fire at an adjacent construction site. The fire caused water and electrical damage in one corner of the Company's building. The Company's patient monitoring services were not interrupted. Costs of $485 were incurred through
87
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
10. Integration, Restructuring and Other Charges (Continued)
December 31, 2008, including $220 of newly acquired fixed assets that have been capitalized as of the balance sheet date, $53 of fixed asset impairments, and $212 of out of pocket costs.
The Company's insurance policy covers all out of pocket costs and damaged fixed assets at replacement value, and as such, the Company does not expect to incur a loss as a result of the fire damage. As of December 31, 2008, the Company recognized a gain of $85 for insurance proceeds received to date in excess of accrued costs. We received a final insurance settlement to cover the replacement cost of damaged assets in 2009.
Legal Settlement and Secondary Offering Expenses
In May 2008, the Company settled an intellectual property dispute with LifeWatch Corp., where both sides agreed to dismiss all claims pending in the lawsuit. We incurred legal fees of $950 for the year ended December 31, 2008.
On August 6, 2008, we offered shares of our common stock through a secondary offering. We incurred expenses of $942 in connection with the offering. The secondary offering is more fully discussed in Note 1.
11. Shareholders' Equity
Common Stock
As of December 31, 2010 and 2009, the Company was authorized to issue 200,000,000 shares of common stock. As of December 31, 2010 and 2009, the Company had 24,251,170 and 23,965,405 shares outstanding, respectively. In March 2008, the Company completed its initial public offering in which we sold and issued 3,000,000 shares of common stock at an issue price of $18.00 per share. The Company raised proceeds of $46,700, net of underwriting and offering costs.
Preferred Stock
The Company maintains an unregistered blank check preferred stock class. As of December 31, 2010 and 2009, there are no shares authorized and outstanding.
Stock Based Compensation
2008 Equity Incentive Plan
The Company's 2008 Equity Incentive Plan (the 2008 Option Plan) became effective on March 18, 2008. The Plan permits the Company's Board of Directors to grant incentive stock options to employees of the Company and non-qualified stock options, restricted stock, performance stock and other stock-based incentive awards to officers, directors, employees and consultants of the Company. On that date, the Company began granting options to purchase shares of common stock to employees, executives, directors and consultants. Under the terms of the 2008 Option Plan, all available shares in the 2003 Option Plan's share reserve automatically roll into the 2008 Option Plan. Any cancellations or forfeitures of granted options under the 2003 Option Plan also automatically roll into the 2008 Option
88
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
11. Shareholders' Equity (Continued)
Plan. Beginning on January 1, 2009, and each year thereafter, the number of options available to be granted under the plan will increase by the lesser of 4% of the total number of common shares outstanding or 1,500,000 shares.
The restrictions on restricted stock units issued under the plan lapse as follows: one third on the date of grant, one third on the first anniversary of the date of grant, and one third on the second anniversary of the date of grant. The restrictions on certain other restricted stock units issued under the plan lapse in full on the third anniversary of the date of grant. Options granted to certain officers of the Company in combination with restricted stock units, described above, under the Plan vest in three equal installments beginning on the third anniversary from the date of grant.
Options granted under the 2008 Option Plan have exercise prices not less than the fair market value at the date of grant and have an expiration date of no greater than ten years from the date of grant. There is no vesting schedule provided in the 2008 Option Plan, and vesting is determined by the Board of Directors on the date of grant. However, the Company's practice is to follow a four year vesting schedule such that 25% of the granted options vest on the anniversary date of grant, and the remaining options granted vest ratably over 36 months thereafter. No options have been granted with vesting schedules that differ from Company practice.
2008 Non-employee Directors' Stock Option Plan
The Company's 2008 Non-employee Directors' Stock Option Plan (the Directors' Plan) became effective March 18, 2008. Beginning on that date, all directors elected for the first time to the Board of Directors receive a fixed number of options. On the date of the annual meeting, and when directors are elected to a committee or a chair position of a committee, they will also receive a grant equal to a fixed number of options per the Directors' Plan. Options granted under the Directors' Plan have exercise prices not less than the fair market value at the date of grant, and have an expiration date of no greater than ten years from the date of grant. Initial and committee chair grants vest 33% on the first anniversary date of grant, and the balance vests ratably over 24 months. Annual grants vest ratably over 12 months from the date of grant.
2003 Equity Incentive Plan
As of March 18, 2008 the Company no longer granted options to purchase shares of common stock to employees, executives, directors and consultants under the Company's 2003 Equity Incentive Plan (the 2003 Option Plan). Options granted under the 2003 Option Plan have exercise prices not less than the fair market value at date of grant for incentive stock options and not less than 85% of the fair market value at the date of grant for non-statutory options. The options generally expire ten years from the date of grant and generally vest 25% twelve months from the date of grant, and ratably over the next 36 months thereafter.
The 2003 Option Plan allows for employees to early exercise options on the first anniversary date of employment, regardless of the vested status of granted options. If an employee terminates prior to fully vesting in options that have been early exercised, the Company repurchases the common stock associated with unvested options at the original exercise price.
89
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
11. Shareholders' Equity (Continued)
Option activity under all stock option plans is summarized as follows for the years ended December 31, 2010, 2009 and 2008:
| |
|
Options Outstanding | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| |
Shares Available for Grant |
Number of Shares |
Weighted Average Exercise Price |
|||||||
Balance—December 31, 2007 |
617,518 | 1,641,614 | $ | 6.38 | ||||||
Additional shares authorized for grant |
142,500 | — | — | |||||||
Granted |
(793,217 | ) | 793,217 | $ | 22.11 | |||||
Cancelled/forfeited |
374,134 | (374,134 | ) | $ | 7.31 | |||||
Exercised |
— | (425,492 | ) | $ | 4.22 | |||||
Balance—December 31, 2008 |
340,935 | 1,635,205 | $ | 13.67 | ||||||
Additional shares authorized for grant |
1,024,921 | — | — | |||||||
Granted |
(1,569,276 | ) | 1,569,276 | $ | 10.26 | |||||
Cancelled/forfeited |
1,335,555 | (1,335,555 | ) | $ | 20.37 | |||||
Exercised |
— | (293,281 | ) | $ | 8.21 | |||||
Balance—December 31, 2009 |
1,132,135 | 1,575,645 | $ | 15.21 | ||||||
Additional shares authorized for grant |
1,194,094 | — | — | |||||||
Granted |
(1,034,663 | ) | 1,034,663 | $ | 6.70 | |||||
Cancelled/forfeited |
358,157 | (358,157 | ) | $ | 14.44 | |||||
Exercised |
— | (149,775 | ) | $ | 8.21 | |||||
Balance—December 31, 2010 |
1,649,723 | 2,102,376 | $ | 12.18 | ||||||
A summary of total outstanding stock options as of December 31, 2010 is as follows:
| |
Options Outstanding | Options Exercisable | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
Range of Exercise Price
|
Number Outstanding |
Weighted- Average Remaining Contractual Life (in years) |
Weighted- Average Exercise Price |
Number Exercisable |
Weighted- Average Remaining Contractual Life (in years) |
Weighted- Average Exercise Price |
|||||||||||||
$ 0.70 - $ 7.50 |
893,366 | 8.96 | $ | 6.06 | 158,126 | 6.58 | $ | 5.93 | |||||||||||
$ 7.51 - $15.00 |
138,545 | 8.40 | 9.33 | 65,300 | 7.75 | 9.69 | |||||||||||||
$15.01 - $22.50 |
342,458 | 8.15 | 18.87 | 357,958 | 8.15 | 18.87 | |||||||||||||
$22.51 - $31.18 |
215,502 | 7.59 | 29.24 | 207,170 | 7.59 | 29.17 | |||||||||||||
$ 0.70 - $31.18 |
1,589,871 | 8.55 | 12.18 | 788,554 | 7.65 | 18.22 | |||||||||||||
90
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
11. Shareholders' Equity (Continued)
In addition, a summary of total outstanding RSU's as of December 31, 2010 is as follows:
Range of Grant Price
|
RSU's Outstanding |
|||
|---|---|---|---|---|
$ 4.24 - $ 6.75 |
90,000 | |||
$ 6.76 - $ 7.75 |
273,000 | |||
$ 7.76 - $17.75 |
90,715 | |||
$17.76 - $26.49 |
55,776 | |||
$ 4.24 - $26.49 |
509,491 | |||
The table below summarizes certain additional information with respect to our options:
(In thousands)
|
2010 | 2009 | 2008 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
Aggregate intrinsic value of options outstanding at year-end |
$ | 141 | $ | 182 | $ | 18,802 | ||||
Aggregate intrinsic value of options exercisable at year-end |
87 | 156 | 18,660 | |||||||
Aggregate market value of unvested stock awards at year-end |
15,751 | 16,475 | 19,230 | |||||||
Aggregate intrinsic value of options exercised during the year |
151 | 3,892 | 8,771 | |||||||
Aggregate market value of stock awards vested during the year |
8,936 | 5,624 | 4,254 | |||||||
The Company estimated the fair value of its common stock for the period from January 1, 2008 to March 17, 2008, the day prior to our initial public offering. In the absence of a public trading market, our stock price was determined by our Board of Directors in good faith based upon consideration of a number of objective and subjective factors. The approach we used was consistent with the methods outlined in the AICPA Practice Aid, Valuation of Privately-Held-Company Equity Securities Issued as Compensation. Based on our assessment, we concluded that the fair value of our common stock ranged from $13.38 to $18.30 per share for the periods prior to our initial public offering.
Valuation models require the input of highly subjective assumptions. Prior to the Company's initial public offering, its common stock had characteristics significantly different from that of publicly traded common stock. Because changes in the subjective input assumptions could have materially affected the fair value estimate, in management's opinion, the models employed prior to the initial public offering do not necessarily provide a reliable single measure of the fair value of our common stock.
As of December 31, 2010, 2009 and 2008, the Company has reserved shares of common stock for issuance as follows:
| |
December 31, | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| |
2010 | 2009 | 2008 | |||||||
Exercise of options available and grants of awards under equity plans |
3,752,099 | 2,707,780 | 1,976,140 | |||||||
Conversion of preferred stock issuable under outstanding preferred stock warrant |
— | — | 6,250 | |||||||
|
3,752,099 | 2,707,780 | 1,982,390 | |||||||
91
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
11. Shareholders' Equity (Continued)
The Company's income before income taxes for the years ended December 31, 2010, 2009 and 2008 was $3,945, $16,625 and $3,392 lower, respectively, and the Company's after-tax net loss or income for years ended December 31, 2010, 2009 and 2008 was $3,892, $16,625 and $2,891 lower, respectively, as a result of stock- based compensation expense incurred. The impact of stock-based compensation expense was $(0.16) and $(0.70) on the basic and diluted earnings per share for the years ended December 31, 2010 and 2009, respectively. For the year ended December 31, 2008, the impact of stock-based compensation expense was $(0.16) and $(0.13) on the basic and diluted earnings per share, respectively.
Total cash received from the exercise of stock options for the year ended December 31, 2010 and 2009 was $665 and $1,935, respectively. The tax benefit realized from the exercise of nonqualified stock options for the year ended December 31, 2009 was $357. The tax benefit was fully reserved for through a tax valuation allowance.
We estimate the fair value of our share-based awards to employees and directors using the Black-Scholes option valuation model. The Black-Scholes option valuation model requires the use of certain subjective assumptions. The most significant of these assumptions are our estimates of the expected volatility of the market price of our stock and the expected term of the award. We base our estimates of expected volatility on a group of similar entities whose stock prices are publicly available. The expected term represents the period of time that stock-based awards granted are expected to be outstanding. Other assumptions used in the Black-Scholes option valuation model include the risk-free interest rate and expected dividend yield. The risk-free interest rate for periods pertaining to the contractual life of each option is based on the U.S. Treasury yield of a similar duration in effect at the time of grant. We have never paid, and do not expect to pay, dividends in the foreseeable future.
The fair value of our stock-based awards was estimated at the date of grant using the following weighted average assumptions:
| |
Year Ended December 31, | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| |
2010 | 2009 | 2008 | |||||||
Expected volatility |
65.0 | % | 54.0 | % | 50.0 | % | ||||
Expected term (in years) |
6.25 | 6.25 | 6.25 | |||||||
Weighted-average risk-free interest rate |
2.29 | % | 2.23 | % | 2.60 | % | ||||
Expected dividends |
0.0 | % | 0.0 | % | 0.0 | % | ||||
Weighted-average grant date fair value per share |
$ | 3.95 | $ | 10.26 | $ | 12.17 | ||||
Based on the Company's historical experience of options that cancel before becoming fully vested, the Company has assumed an annualized forfeiture rate of 15% for all options. Under the true-up provision of ASC 718, the Company will record additional expense if the actual forfeiture rate is lower than estimated, and will record a recovery of prior expense if the actual forfeiture rate is higher than estimated.
92
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
11. Shareholders' Equity (Continued)
Based on the above assumptions, the per share weighted average fair value of the options granted under the stock option plan for the years ended December 31, 2010, 2009 and 2008 was $3.95, $10.26 and $12.17, respectively.
Total compensation cost of options granted but not yet vested at December 31, 2010, 2009 and 2008 was approximately $5,047, $4,397 and $8,970, respectively. At December 31, 2010, 2009 and 2008, the weighted average remaining periods over which the above amounts are expected to be recognized are 3.09 years, 2.06 years and 2.08 years, respectively. At December 31, 2010, 1,649,723 shares remained available for future grant under the Plan.
A summary of the status of our unvested stock options as of the respective balance sheet dates, and changes during years, is presented below:
| |
Number of Shares |
Weighted- Average Grant-Date Fair Value (per share) |
|||||
|---|---|---|---|---|---|---|---|
Unvested shares at December 31, 2008 |
1,212,638 | $ | 15.86 | ||||
Granted |
1,569,276 | $ | 10.26 | ||||
Vested |
(275,967 | ) | $ | 6.25 | |||
Cancelled/forfeited |
(1,335,555 | ) | $ | 10.53 | |||
Unvested shares at December 31, 2009 |
1,170,392 | $ | 14.08 | ||||
Granted |
1,034,663 | $ | 6.70 | ||||
Vested |
(252,378 | ) | $ | 8.21 | |||
Cancelled/forfeited |
(358,157 | ) | $ | 14.44 | |||
Unvested shares at December 31, 2010 |
1,594,520 | $ | 9.88 | ||||
Option Acceleration
On December 1, 2009, the Company accelerated the vesting of certain employees' unvested options that were deeply out-of-the-money. The acceleration was done because the Company believed that there was no longer a compensation incentive tied to Company performance, given the exercise price of the options that were accelerated. Consistent with ASC 718, the Company will continue to expense the accelerated options over the remaining service period. The Company does not have a static policy threshold to use for determining whether an option is "deeply out-of-the-money." Rather, the Company believes that the determination should be made in light of current market conditions, probability of stock price recovery within the remaining service period, and historical volatility of the Company's stock price. For the purposes of this option acceleration, the Company determined that options that were out-of-the-money by 30% or more were deeply out-of-the-money. As a result of the option acceleration, approximately 309,000 previously unvested shares became fully vested on December 1, 2009. The Company incurred an expense associated with the options that were accelerated in the amount of $1,269 and $75 for the years ended December 31, 2010 and 2009, respectively, which has
93
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
11. Shareholders' Equity (Continued)
been recorded in the General and administrative line of the consolidated statement of operations. The weighted average exercise price of the accelerated options is $19.87, and the average remaining service period is 2.15 years.
In connection with certain restructuring activities, we terminated certain employees at our San Diego location. In addition, a director stepped down from the Board of Directors in the second quarter of 2008. In accordance with their severance agreements, we accelerated all previously unvested stock options. For the year ended December 31, 2008, we incurred additional expenses of $767 related to the acceleration of previously unvested stock options.
Option Cancellation
On December 1, 2009, certain executive officers of the Company cancelled approximately 707,000 of their unvested outstanding options. No consideration was given in exchange for the cancellation, and no new options were granted. The Company has recognized this charge in accordance with the guidance in ASC 718, Compensation—Stock Compensation. This charge was recorded in the Integration, restructuring and other charges line in the statement of operations. The weighted average exercise price of the cancelled options was 26.85 and the average service period remaining at the time of the cancellation was 3.02 years. The Company incurred a one-time charge of $9,818 to recognize the remaining unamortized expense associated with the cancelled options. The impact on basic and diluted earnings per share for the year ended December 31, 2009 was $(0.41).
Employee Stock Purchase Plan
In July 2008, the Company made available an employee stock purchase plan in which substantially all of the Company's full-time employees became eligible to participate effective March 18, 2008. Under the plan, employees may contribute through payroll deductions up to 15% of their compensation toward the purchase of the Company's common stock, or $21, whichever is lower. The price per share is equal to the lower of 85% of the fair market price on the first day of the offering period, or 85% of the fair market price on the day of purchase. Proceeds received from the issuance of shares are credited to stockholders' equity in the period that the shares are issued. Under the terms of the plan, a total of 238,000 shares of common stock have been reserved for issuance to employees. In January 2010, the number of shares available for grant was increased by 239,750, per the ESPP plan documents. On March 17, 2010 and September 17, 2010, 83,659 shares and 77,440 shares, respectively, were purchased in accordance with the Employee Stock Purchase Plan (ESPP). Net proceeds to the Company from the issuance of shares of common stock under the ESPP for the year ended December 31, 2010 were $0.8 million. At December 31, 2010, approximately 381,144 shares remain available for purchase under the ESPP. For the years ended December 31, 2010, 2009 and 2008, the Company incurred ESPP expenses of $202, $614, $396, respectively.
12. Income Taxes
The Company has net deferred income tax assets totaling $41,113 at December 31, 2010, consisting primarily of federal and state net operating loss and credit carryforwards. Due to uncertainty regarding
94
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
12. Income Taxes (Continued)
the ultimate realization of these net operating loss and credit carryforwards and other deferred income tax assets, we have established a full valuation allowance for these assets and will recognize the benefits only as reassessment indicates the benefits are realizable. The determination of the required valuation allowance against net deferred tax assets was made without taking into account the deferred tax liabilities created from the book and tax differences on indefinite-lived assets.
The Company's effective tax rate for 2010 of (1.34)% primarily relates to certain state taxes based on gross receipts or modified gross receipts calculations properly included as income taxes. The Company recently performed an analysis to determine the extent to which it can use its net operating loss carryforwards in future periods, subject to certain limitations imposed by the Internal Revenue Code. The Company concluded that because of the Company's limited history of reporting a net profit, it cannot predict that the benefits of the net operating loss carryfowards will be realized in future periods, and therefore the Company continues to provide a full valuation allowance for deferred tax assets. The Company will perform a similar analysis during 2011 to reassess the estimated future realizability of net operating loss carryforwards.
Deferred taxes result from temporary differences between the carrying amounts of assets and liabilities used for financial reporting purposes and the amounts used for income tax purposes. The significant components of the Company's deferred tax assets and liabilities are as follows:
| |
December 31, | |||||||
|---|---|---|---|---|---|---|---|---|
| |
2010 | 2009 | ||||||
Deferred tax assets: |
||||||||
Net operating loss carryforwards |
$ | 30,142 | $ | 16,348 | ||||
Research & development and AMT credit carryforwards |
3,716 | 2,646 | ||||||
Stock option grants |
3,419 | 2,042 | ||||||
Allowance for doubtful accounts |
4,674 | 8,482 | ||||||
Property, plant and equipment |
— | 179 | ||||||
Goodwill and acquired intangibles |
458 | 433 | ||||||
Other, net |
1,938 | 2,738 | ||||||
Total deferred tax assets |
44,347 | 32,868 | ||||||
Less valuation allowance |
(41,369 | ) | (32,827 | ) | ||||
Net deferred tax assets |
$ | 2,978 | $ | 41 | ||||
Deferred tax liabilities: |
||||||||
Property, plant and equipment |
(2,061 | ) | — | |||||
Identified intangible assets |
(875 | ) | — | |||||
Indefinite lived intangible assets |
(256 | ) | — | |||||
Prepaid insurance |
(42 | ) | (41 | ) | ||||
Total deferred tax liabilities |
$ | (3,234 | ) | $ | (41 | ) | ||
Net deferred tax asset (liability) |
$ | (256 | ) | — | ||||
95
CARDIONET, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
Years Ended December 31, 2010, 2009 and 2008
(In thousands, except shares and per share amounts.)
12. Income Taxes (Continued)