Attached files
Table of Contents
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
(Mark One)
| þ | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the Fiscal Year Ended December 31, 2010
OR
| ¨ | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
Commission File Number 001-33459
Skilled Healthcare Group, Inc.
(Exact Name of Registrant as Specified in its Charter)
| Delaware | 20-3934755 | |
| (State of Incorporation) | (I.R.S. Employer Identification Number) | |
| 27442 Portola Parkway, Suite 200 Foothill Ranch, CA |
92610 | |
| (Address of Principal Executive Offices) | (Zip Code) | |
Registrant’s telephone number: (949) 282-5800
Securities registered pursuant to Section 12(b) of the Act:
| Class A Common Stock, $0.001 par value per share | New York Stock Exchange | |
| (Title of each class) | (Name of each exchange on which registered) |
Securities registered pursuant to Section 12(g) of the Act: None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ¨ No þ
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes ¨ No þ
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes þ No ¨
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes ¨ No ¨
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of registrant’s knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. ¨
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer or a smaller reporting company. See definitions of “large accelerated filer,” “accelerated filer” and “smaller reporting company” in Rule 12b-2 of the Exchange Act:
| Large accelerated filer | ¨ | Accelerated filer | þ | |||
| Non-accelerated filer | ¨ | Non-accelerated filer | ¨ | |||
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Act). Yes ¨ No þ
As of June 30, 2010, the aggregate market value of the shares of Class A common stock, par value $0.001, and Class B common stock, par value $0.001, held by non-affiliates of the registrant, computed based on the closing sale price of $6.79 per share on June 30, 2010, as reported by The New York Stock Exchange, was approximately $142.1 million. The aggregate number of shares held by non-affiliates is calculated by excluding all shares held by executive officers, directors and holders known to hold 5% or more of the voting power of the registrant’s common stock. As of February 9, 2011, there were 20,779,059 shares of the registrant’s Class A common stock issued and outstanding and 16,993,298 shares of the registrant’s Class B common stock issued and outstanding.
Documents Incorporated by Reference:
The information called for by Part III is incorporated by reference to the Definitive Proxy Statement for the 2011 Annual Meeting of Stockholders of the Registrant which will be filed with the Securities and Exchange Commission not later than April 30, 2011.
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
ANNUAL REPORT
INDEX
| Page | ||||||
| Item 1. |
1 | |||||
| Item 1A. |
23 | |||||
| Item 1B. |
41 | |||||
| Item 2. |
42 | |||||
| Item 3. |
42 | |||||
| Item 4. |
42 | |||||
| Item 5. |
43 | |||||
| Item 6. |
45 | |||||
| Item 7. |
Management’s Discussion and Analysis of Financial Condition and Results of Operations |
50 | ||||
| Item 7A. |
80 | |||||
| Item 8. |
81 | |||||
| Item 9. |
Changes in and Disagreements with Accountants on Accounting and Financial Disclosure |
81 | ||||
| Item 9A. |
82 | |||||
| Item 9B. |
84 | |||||
| Item 10. |
85 | |||||
| Item 11. |
85 | |||||
| Item 12. |
Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters |
85 | ||||
| Item 13. |
Certain Relationships and Related Transactions, and Director Independence |
85 | ||||
| Item 14. |
85 | |||||
| Item 15. |
86 | |||||
| 87 | ||||||
i
Table of Contents
PART I
| Item 1. | Business |
Overview
We are a holding company that owns subsidiaries that operate skilled nursing facilities, assisted living facilities, hospices, home health providers and a rehabilitation therapy business. We have an administrative service company that provides a full complement of administrative and consultative services that allows our facility operators and unaffiliated third-party facility operators with whom we contract to better focus on delivery of healthcare services. We currently have one such service agreement with an unaffiliated facility operator. Our operating subsidiaries focus on providing high-quality care to our patients and have a strong commitment to treating patients who require a high level of skilled nursing care and extensive rehabilitation therapy, whom we refer to as high-acuity patients. References in this report to the “Company,” “we,” “us” and “our” refer to Skilled Healthcare Group, Inc. and its wholly-owned subsidiaries, unless the context requires otherwise. As of December 31, 2010, we owned or leased 78 skilled nursing facilities and 22 assisted living facilities, together comprising 10,830 licensed beds. Our facilities, approximately 77.0% of which we owned as of December 31, 2010, are located in California, Texas, Iowa, Kansas, Missouri, Nevada and New Mexico, and are generally clustered in large urban or suburban markets. For the year ended December 31, 2010, we generated approximately 81.5% of our revenue from our skilled nursing facilities, including our integrated rehabilitation therapy services at these facilities. The remainder of our revenue was generated from our assisted living services, rehabilitation therapy services provided to third-party facilities, hospice care and home health services.
2010 Acquisitions, Developments, and Divestiture
In May 2010, we acquired substantially all of the assets of five Medicare-certified hospice companies and four Medicare-certified home health companies located in Arizona, Idaho, Montana and Nevada, referred to herein as the “Hospice/Home Health Acquisition.” The total consideration we agreed to pay in connection with the Hospice/Home Health Acquisition is approximately $63.0 million, consisting of approximately $45.3 million in cash at closing, with the remainder in the form of deferred and contingent payments payable over a three to five year period. For the year ended December 31, 2010, the Hospice/Home Health Acquisition contributed $38.6 million of our consolidated revenue. We recognized goodwill of $57.0 million from the Hospice/Home Health Acquisition, representing the commercial opportunity for the Company to expand our existing hospice operations as well as to complement to our existing core operations. We expect the recognized goodwill to be deductible for income tax purposes over the 15 years following the acquisition. All of the goodwill is included in our Hospice and Home Health reporting segment.
In July 2010, we admitted our first patients to the Fort Worth Center of Rehabilitation, our newly-constructed skilled nursing facility in Fort Worth, Texas. The center is a state-of-the-art, Leadership in Environmental and Energy Design (LEED) gold certified facility.
In September 2010, we agreed to settle the case entitled, VINNIE LAVENDER, by and through her Conservator, WANDA BAKER; WALTER SIMON; JACQUELYN VILCHINSKY vs. SKILLED HEALTHCARE GROUP, INC., et al. (and twenty-two individually-named California nursing facilities receiving administrative services from our administrative service company) which we sometimes refer to as the “Lavender Case” or the “Humboldt County Action.” As part of the settlement, we and the other defendants entered into separate settlement agreements with the plaintiffs and the Humboldt County District Attorney’s Office. The settlement was approved by the Superior Court of California, Humboldt County in November 2010.
Under the terms of the settlement agreements, we deposited a total of $50 million into escrow accounts to cover settlement payments to class members, notice and claims administration costs, reasonable attorneys’ fees and costs and certain other payments.
1
Table of Contents
The settlement agreements also institute an injunction, pursuant to which, the twenty-two defendants that operate California nursing facilities must provide specified nurse staffing levels, comply with specified state and federal laws governing staffing levels and posting requirements, and provide reports and information to a monitor. The injunction will remain in effect for a period of 24 months unless extended for additional three month periods as to those defendants that may be found in violation of the injunction. Defendants demonstrating compliance for an 18 month period may petition for early termination of the injunction. We are required to demonstrate over the term of the injunction that the costs of complying with the injunction are at least $9.6 million. The compliance costs, will include, among other things, costs attributable to (i) enhanced reporting requirements; (ii) implementing advanced staffing tracking systems; (iii) fees and expenses paid to an auditor and special master; (iv) increased labor and labor-related expenses; and (v) lost revenues attributable to admission decisions based on compliance with the terms and conditions of the injunction. To the extent the costs of complying with the injunction are less than $9.6 million, we will be required to remit any shortfall to the settlement fund. On February 14, 2011, the agreement became effective, meaning the period for any party to challenge the settlement or appeal the judgment dismissing the case has expired and settlement escrow funds may be distributed.
Pursuant to the settlement agreements, the plaintiffs and the Humboldt County District Attorney’s Office, as Intervenor on behalf of the People of the State of California, agreed to release us and the other defendants from claims related to the causes of action alleged in the Lavender Case, as further described in the settlement agreements, copies of which are filed as exhibits to this report. Neither of the settlement agreements contains an admission or concession of wrongdoing by the Company or any other defendants. For more information regarding the Lavender case and the settlement, see Note 12, Commitments and Contingencies—Litigation, in the notes to our consolidated financial statements included elsewhere in this report.
In December 2010, we sold our Westside Campus of Care skilled nursing facility and operations in Texas for $14.7 million and purchased three previously leased facilities: St. Luke Healthcare and Rehabilitation Center and Woodland Care Center, located in California, and St. Joseph Transitional Rehabilitation Center in Nevada. We recorded a net gain of $1.8 million related to these transactions.
Operations
Our services focus primarily on the medical and physical issues facing elderly patients and are provided by our skilled nursing companies, assisted living companies, integrated and third-party rehabilitation therapy business, hospice business and home health business. We have a strong commitment to treating patients who require a high level of skilled nursing care and extensive rehabilitation therapy, whom we refer to as high-acuity patients.
We have three reportable operating segments: (1) long-term care, or LTC, which includes the operation of skilled nursing facilities and assisted living facilities and is the most significant portion of our business; (2) therapy services, which includes our integrated and third-party rehabilitation therapy services; and (3) hospice and home health services, which includes our hospice and home health businesses. Our administrative and consultative services that are attributable to the reportable operating segments are allocated among the segments accordingly. For the twelve months ended December 31, 2010, the LTC operating segment generated approximately 84.7% of our revenue, with the therapy services segment and hospice and home health services segment accounting for 9.0% and 6.0% of our revenue, respectively. For additional information regarding the financial performance of our reportable operating segments, see Item 7, Management’s Discussion and Analysis of Financial Condition and Results of Operations—Revenue and Note 5, Business Segments, in the notes to our consolidated financial statements included elsewhere in this report.
Long-Term Care Services Segment
Skilled Nursing Facilities
As of December 31, 2010, our skilled nursing companies provided skilled nursing care at 78 regionally clustered facilities, having 10,830 licensed beds, in California, Texas, Iowa, Kansas, Missouri, Nevada and New Mexico. We have developed programs for, and actively market our services to high-acuity patients, who are
2
Table of Contents
typically admitted to our facilities as they recover from strokes, other neurological conditions, cardiovascular and respiratory ailments, joint replacements and other muscular or skeletal disorders. As of December 31, 2010, we employed approximately 7,537 full-time equivalent employees in our skilled nursing business.
We use interdisciplinary teams of experienced medical professionals, including therapists, to provide services prescribed by physicians. These teams include registered nurses, licensed practical nurses, certified nursing assistants and other professionals who provide individualized comprehensive nursing care 24 hours a day. Many of our skilled nursing facilities are equipped to provide specialty care, such as chemotherapy, enteral/parenteral nutrition, tracheotomy care and ventilator care. We also provide standard services to each of our skilled nursing patients, including room and board, special nutritional programs, social services, recreational activities and related healthcare and other services.
In December 2004, we introduced our Express Recovery™ program, which uses a dedicated unit within a skilled nursing facility to deliver a comprehensive rehabilitation regimen in accommodations specifically designed to serve high-acuity patients. Each Express Recovery™ unit can typically be entered without using the main facility entrance, permitting residents to bypass portions of the facility dedicated to the traditional nursing home patient. Each Express Recovery™ unit typically has 12 to 36 beds and provides skilled nursing care and rehabilitation therapy for patients recovering from conditions such as joint replacement surgery, and cardiac and respiratory ailments. Since introducing our Express Recovery™ program our skilled mix at the facilities has increased, resulting in higher reimbursement rates. Skilled mix is the average daily number of Medicare and managed care patients we serve at our skilled nursing facilities divided by the average daily number of total patients we serve at our skilled nursing facilities. As of December 31, 2010, we operated 61 Express Recovery™ units with 2,187 beds. We currently plan to expand one of our current facilities and complete the development of three additional Express Recovery™ units, adding approximately 83 beds by the end of 2011.
We have an administrative service company that provides a full complement of administrative and consultative services that allows our facility operators and unaffiliated third-party facility operators with whom we contract to better focus on delivery of healthcare services. We currently have one such service agreement with an unaffiliated facility operator. The income associated with the services our administrative service company provides is included in LTC in our segment reporting as services are performed primarily by personnel in the LTC segment. Each of our facilities operates as a distinct company to better focus on service delivery and is supported by the administrative service company for efficient delivery of non-healthcare support services.
Assisted Living Facilities
We complement our skilled nursing care business by providing assisted living services at 22 facilities with 1,264 beds as of December 31, 2010. Our assisted living companies provide residential accommodations, activities, meals, security, housekeeping and assistance in the activities of daily living to seniors who are independent or who require some support, but not the level of nursing care provided in a skilled nursing facility. Our independent living units are non-licensed independent living apartments in which residents are independent and require no support with the activities of daily living. As of December 31, 2010, we employed approximately 332 full-time equivalent employees in our assisted and independent living businesses.
Equity Investment in Pharmacy Joint Venture
We have a 50% equity interest in APS—Summit Care Pharmacy, LLC, or APS—Summit Care, which is a joint venture that serves the pharmaceutical needs of a limited number of our Texas operations, as well as a number of other unaffiliated customers. The remaining 50% equity interest in APS—Summit Care is owned by an unaffiliated third party. APS – Summit Care operates a pharmacy in Austin, Texas, through which we pay market value for prescription drugs and receive a 50% share of the net income related to the joint venture.
3
Table of Contents
Therapy Services Segment
Rehabilitation Therapy Services
As of December 31, 2010, we provided rehabilitation therapy services to a total of 172 healthcare facilities, including 68 facilities owned by us. In addition, we have contracts to manage the rehabilitation therapy services for our 10 healthcare facilities in New Mexico. We provide rehabilitation therapy services at our skilled nursing facilities as part of an integrated service offering in connection with our skilled nursing care. We believe that an integrated approach to treating high-acuity patients enhances our ability to achieve successful patient outcomes and enables us to identify and treat patients who can benefit from our rehabilitation therapy services. We believe hospitals and physician groups often refer high-acuity patients to our skilled nursing facilities because they recognize the value of an integrated approach to providing skilled nursing care and rehabilitation therapy services.
We believe that we have also established a strong reputation as a premium provider of rehabilitation therapy services to third-party skilled nursing operators in our local markets, with a recognized ability to provide these services to high-acuity patients. Our approach to providing rehabilitation therapy services for third-party operators emphasizes high-quality treatment and successful clinical outcomes. As of December 31, 2010, we employed approximately 1,032 full-time equivalent employees (primarily therapists) in our rehabilitation therapy business.
Hospice and Home Health Services Segment
Hospice Care
As a result of the Hospice/Home Health Acquisition, in May 2010 we began providing hospice services in Arizona, Nevada, Idaho, and Montana. Prior to that time we only provided hospice services in California and New Mexico. Hospice services focus on the physical, spiritual and psychosocial needs of terminally ill individuals and their families, and consist primarily of palliative and clinical care, education and counseling. As of December 31, 2010, we employed approximately 465 full-time equivalent employees in our hospice services business.
Home Health
As a result of the Hospice/Home Health Acquisition, in May 2010 we began providing home health care services in Arizona, Nevada, Idaho and Montana. We derive substantially all of the revenue from our home health business from Medicare. Our home health care services generally consist of providing some combination of the services of registered nurses, speech, occupational and physical therapists, medical social workers and certified home health aides. Home health care is often a cost-effective solution for patients, and can also increase their quality of life and allow them to receive quality medical care in the comfort and convenience of a familiar setting. As of December 31, 2010, we employed approximately 153 full-time equivalent employees in our home health business.
Our Local Referral Network
Our sales and marketing team of regionally based professionals support our facility-based personnel who are responsible for marketing our high-acuity capabilities. These marketing efforts involve developing new referral relationships and managing existing relationships within our local network. Our facility-based personnel actively call on hospitals, hospital discharge planners, primary care physicians and various community organizations as well as specialty physicians, such as orthopedic surgeons, pulmonologists, neurologists and other medical specialists who frequently treat patients who require the physical therapy or other medically complex services that we provide.
We also have established strategic alliances with medical centers in our local markets, including Baylor Health Care System in Dallas, Texas, St. Joseph’s Hospital in Orange County, California, and White Memorial in
4
Table of Contents
Los Angeles, California. We believe that forming alliances with leading medical centers will improve our ability to attract high-acuity patients to our facilities because we believe that our associations with these medical centers typically enhance our reputation for providing high-quality care. As part of these alliances, the medical centers formally evaluate and provide input with respect to our quality of care. We believe these alliances provide us with significantly greater exposure to physicians and discharge staff at these medical centers, strengthening our relationships and reputation with these valuable referral sources. These medical centers may also seek to discharge their patients more rapidly into a facility where the patient will continue to receive high-quality care.
Payment Sources
We derive revenue primarily from the Medicare and Medicaid programs, managed care payors and private pay patients. Medicaid typically covers patients who require standard room and board services and provides reimbursement rates that are generally lower than rates earned from other sources. We use skilled mix to evaluate the patient acuity mix for our skilled nursing facilities over various periods. We monitor our quality mix, which is the percentage of non-Medicaid revenue from each of our businesses, to measure the level of more attractive reimbursements that we receive across each of our business units. We believe that our focus on attracting and providing integrated care for high-acuity patients has had a positive effect on our skilled mix and quality mix.
Sources of Reimbursement
We receive a majority of our revenue from Medicare and Medicaid. The Medicare and Medicaid programs provided approximately 37.1% and 31.7%, respectively, of our revenue for the year ended December 31, 2010 and approximately 35.0% and 31.9%, respectively, of our revenue for the year ended December 31, 2009. Changes in the reimbursement rates or the system governing reimbursement for these programs directly affect our business. In addition, our rehabilitation therapy services, for which we typically receive payment from private payors, are significantly dependent on Medicare and Medicaid funding because the private payors are often reimbursed by these programs. In recent years, federal and state governments have enacted changes to these programs in response to increasing healthcare costs and budgetary constraints. See Item 1A of this report, “Risk Factors—Reductions in Medicare reimbursement rates, including annual caps that limit the amounts that can be paid for outpatient therapy services rendered to any Medicare beneficiary, or changes in the rules governing the Medicare program could have a material adverse effect on our revenue, financial condition and results of operations.” Our ability to remain certified as a Medicare and Medicaid provider depends on our ability to comply with existing and newly enacted laws or new interpretations of existing laws related to these programs.
Medicare
Medicare is a federal program that provides certain healthcare benefits to beneficiaries who are 65 years of age or older, blind, disabled or qualify for Medicare’s End Stage Renal Disease program. Medicare provides health insurance benefits in two primary parts for services that we provide:
| • | Part A. Medicare Part A is hospital insurance, which provides reimbursement for inpatient services for hospitals, skilled nursing facilities, hospices, home health and certain other healthcare providers and patients requiring daily professional skilled nursing and other rehabilitative care. Coverage in a skilled nursing facility is limited for a period of up to 100 days, if medically necessary, after the individual has qualified for Medicare coverage as a result of a three-day or longer hospital stay. Medicare pays for the first 20 days of stay in a skilled nursing facility in full and the next 80 days, to the extent above a daily coinsurance amount. Covered services include supervised nursing care, room and board, social services, pharmaceuticals and supplies as well as physical, speech and occupational therapies and other necessary services provided by nursing facilities. Medicare Part A also covers hospice care and some home health care. |
| • | Part B. Medicare Part B is supplemental medical insurance, which requires the beneficiary to pay monthly premiums, covers physician services, limited drug coverage and other outpatient services, such as physical, occupational and speech therapy services, enteral nutrition, certain medical items and X-ray services received outside of a Part A covered inpatient stay. |
5
Table of Contents
To achieve and maintain Medicare certification, a healthcare provider must meet the Centers for Medicare and Medicaid Services, or CMS, “Conditions of Participation” on an ongoing basis, as determined in periodic facility surveys conducted by the state in which the provider is located.
Medicare reimburses our skilled nursing facilities under a prospective payment system, or Prospective Pay System (PPS), for inpatient Medicare Part A covered services. Under the PPS, facilities are paid a predetermined amount per patient, per day, based on the anticipated costs of treating patients. The amount to be paid is determined by classifying each patient into a resource utilization group, or RUG, category, which is based upon each patient’s acuity level. Effective as of October 1, 2010, the RUG categories were expanded from 53 (which had been in effect since January 2006) to 66, with increased reimbursement rates for treating higher acuity patients. We believe these RUG changes more accurately pay skilled nursing facilities for the care of residents with medically complex conditions.
Medicare per diem rates for skilled nursing facilities
On August 11, 2009, CMS published its final rule on the fiscal year 2010 per diem payment rates for skilled nursing facilities. Under the final rule, CMS revised and rebased the skilled nursing facility market basket, resulting in a 2.2% market basket increase factor for fiscal year 2010. The fiscal year 2010 market basket adjustment increased aggregate payments to skilled nursing facilities nationwide by approximately $690.0 million. Additionally, in the final rule, CMS recalibrated the parity adjustment to result in a reduction in payments to skilled nursing facilities by approximately 3.3%, or $1.05 billion. CMS noted that the negative $1.05 billion adjustment described in the final rule would be partially offset by the fiscal year 2010 market basket adjustment factor of 2.2%, or $690.0 million, with a net result of a reduction in payments to skilled nursing facilities of approximately $360.0 million.
On July 22, 2010, CMS published a notice containing its fiscal year 2011 per diem payment rates for skilled nursing facilities, effective for services provided beginning October 1, 2010 through September 30, 2011. Under the notice, CMS revised and rebased the skilled nursing facility market basket, resulting in a 1.7% market basket increase factor for fiscal year 2011. The fiscal year 2011 market basket adjustment will increase aggregate payments to skilled nursing facilities nationwide by approximately $542.0 million. Skilled nursing facility payment rates are calculated using a market basket index that reflects changes in the value of goods and services relevant to nursing home care. CMS also makes a forecast error adjustment if the difference between the projected and actual market basket index exceeds 0.5%. To calculate the fiscal year 2011 payment rate, CMS looked at the most recent available data from fiscal year 2009, when the forecasted market basket index was 3.4% and the actual increase was 2.8%. As a result, the fiscal year 2011 market basket increase factor of 2.3% was decreased by 0.6%, for a net increase of 1.7%. Initially, a provision of the Patient Protection and Affordable Care Act of 2010 (the “PPACA”) delayed the implementation of the Resource Utilization Groups, Version 4 (“RUGs IV”) case-mix classification system until October 1, 2011, but the Medicare and Medicaid Extenders Act of 2010 repealed this provision and allowed RUGs IV to go into effect on October 1, 2010.
New federal health reform legislative proposals in the future may eliminate the market basket update, which elimination could lead to a reduction in payments to skilled nursing facilities. Given the substantial uncertainty surrounding federal health reform efforts, it is impossible to predict the likelihood of the elimination of the market basket update or any other proposed reductions in payments to skilled nursing facilities. Should federal health reform legislation or subsequent regulatory activities result in the reduction of payments to skilled nursing facilities, the loss of revenue associated with future changes in skilled nursing facility payments could, in the future, have an adverse impact on our financial condition or results of operations.
Medicare rates for hospice
On August 6, 2009, CMS announced a final rule increasing Medicare payments to hospices in fiscal year 2010 by 1.4%, or approximately $170.0 million. CMS said the final rule reflects a 2.1% increase in the market
6
Table of Contents
basket, offset by a 0.7% decrease in payments to hospices due to a revised phase out of the wage index budget neutrality adjustment factor, starting with a 10% reduction in fiscal year 2010 and a 15% reduction each year from fiscal year 2011 through fiscal year 2016. The fiscal year 2010 hospice payment rates were effective for care and services furnished on or after October 1, 2009 through September 30, 2010.
On July 22, 2010, CMS published a notice increasing Medicare payments to hospices in fiscal year 2011 by 1.8%, or approximately $220.0 million. CMS said the notice reflects a 2.6% increase in the market basket, offset by a 0.8% decrease in payments to hospices due to a revised phase out of the wage index budget neutrality adjustment factor, starting with a 10% reduction in fiscal year 2010 and a 15% reduction each year from fiscal year 2011 through fiscal year 2016. The fiscal year 2011 hospice payment rates are effective for care and services furnished on or after October 1, 2010 through September 30, 2011.
Medicare rates for home health services
On November 2, 2010, CMS published a final rule to update the prospective payments rates made by Medicare to home health agencies for calendar year 2011. Specifically, the rule provides for a home health market basket update, which was a 2.1% increase, minus 1% in accordance with the PPACA (for a net increase of 1.1% ), and updates the case-mix reduction percentage for calendar year 2011 to 3.79% to account for the additional increases in case-mix not due to the underlying condition of the home health patient. The final rule also contains provisions implementing further reductions in rates under the PPACA changes to the home health agency outlier policy. Prior to the enactment of the PPACA, total outlier payments could not exceed 5% of total projected or estimate home health payments in a given year. However, due to uncontrolled growth in outlier payments in a few discrete areas of the country, the PPACA implemented a change to the existing home health outlier policy through a 5% reduction to home health PPS rates, with total outlier payments not to exceed 2.5% of the total payments estimated for a given year. Home health agencies are also permanently subject to a 10% agency-level cap on outlier payments.
Recent legislative actions impacting Medicare
Beginning January 1, 2006, the Medicare Modernization Act of December 2003, or MMA, implemented a major expansion of the Medicare program through the introduction of a prescription drug benefit under Medicare Part D. Medicare beneficiaries who elect Part D coverage and are dual eligible beneficiaries, those eligible for both Medicare and Medicaid benefits are enrolled automatically in Part D and have their outpatient prescription drug costs covered by this Medicare benefit, subject to certain limitations. Most of the skilled nursing facility residents we serve whose drug costs are currently covered by state Medicaid programs are dual eligible beneficiaries. Accordingly, Medicaid is no longer a significant payor for the prescription pharmacy services provided to these residents.
Section 4541 of the Balanced Budget Act, or BBA, requires CMS to impose financial limitations or caps on outpatient physical, speech-language and occupational therapy services by all providers other than hospital outpatient departments. The law requires a combined cap for physical therapy and speech-language pathology, and a separate cap for occupational therapy, reimbursed under Part B. The combined therapy cap for calendar year 2011 for physical therapy and speech-language pathology services, combined is $1,870; for occupational therapy services, the limit is also $1,870. These caps may result in decreased demand for rehabilitation therapy services that would otherwise be reimbursable under Part B, but for the caps.
CMS, as directed by the Deficit Reduction Act of 2005, or DRA, established a process to allow exceptions to the outpatient therapy caps for certain medically necessary services provided during 2006 for patients with certain conditions or multiple complexities whose therapy is reimbursed under Medicare Part B. Congress has since extended this exception process several times, including the PPACA, which extended this exception process through December 31, 2010, and most recently, the Medicare and Medicaid Extenders Act of 2010, which extended this exception process through December 31, 2011. The majority of the residents in our skilled
7
Table of Contents
nursing facilities and patients served by our rehabilitation therapy agencies whose therapy is reimbursed under Medicare Part B have qualified for these exceptions. Following the revised expiration date for the therapy cap exception process, it is uncertain whether any further extension of the therapy cap exceptions will be included in any other federal legislation. If subsequent federal legislation fails to extend the therapy cap exceptions, the imposition of therapy caps could lead to reduced revenue for our facilities that bill for the affected therapy services and our rehabilitation company could experience reduced revenue from its third party contracts. Such reductions in revenue could adversely impact the results of our operations.
CMS, in its annual update notice, or final rule, also discusses several initiatives, including plans to: (1) continue developing an integrated system of post-acute care payments, to make payments for similar services consistent regardless of where the service is delivered; (2) encourage the increased use of health information technology to improve both quality and efficiency in the delivery of post-acute care; (3) assist beneficiaries in their need to be better informed healthcare consumers by making information about healthcare pricing and quality accessible and understandable; and (4) accelerate the progress already being made in improving quality of life for nursing home residents.
The DRA, which was expected to reduce Medicare and Medicaid payments to skilled nursing facilities by $100 million over five years (i.e., federal fiscal years 2006 to 2010), among other things, included a reduction in the amount of bad debt reimbursement for skilled nursing facilities. Medicare currently fully reimburses providers for certain unpaid Medicare beneficiary coinsurance and deductibles, also known as bad debt. Under the DRA’s revisions, for patients who are not full-benefit, dual-eligible individuals, allowable bad-debt amounts attributable to coinsurance under the Medicare program for a skilled nursing facility will be reduced to 70%. Allowable bad-debt amounts for patients who are full-benefit, dual-eligible individuals will continue to be paid at 100%. This reduction took place for Medicare cost reports beginning on or after October 1, 2005.
Also pursuant to DRA directives, CMS established a post-acute care payment reform demonstration. The goal of this initiative is to standardize patient assessment information from post-acute care settings, which includes skilled nursing facilities, long-term care hospitals, inpatient rehabilitation facilities and home health agencies, and to use this data to guide future payment policies in the Medicare program. The project will provide standardized information on patient health and functional status independent of post-acute care site of care and will examine resources and outcomes associated with treatment in each type of setting. The project is being completed in three phases: (i) Phase I, completed in December 2007, included developing a patient assessment tool, or CARE, and resource use tools, testing them in one market area, and selecting markets for further testing; (ii) Phase II began in March 2008 with data collection in the first of 11 market areas participating in the payment reform demonstration, and by November 2008, over 140 providers representing acute and post-acute care settings from around the country were actively collecting patient assessment data using the CARE tool; and (iii) pursuant to Congressional authorization in the Medicare, Medicaid and SCHIP Extension Act of 2007, beginning in fall 2009, CMS authorized the expansion of the demonstration to include an additional 66 acute and post-acute providers, with participation limited to a six-month period and without delineation of geographic markets. Although CMS is exploring the possibility of site-neutral payments for post-acute care, it remains unclear at this time how information from the project would be employed by CMS to guide future changes to payment policies for post-acute care, or how the changes would impact reimbursement rates for skilled nursing facilities.
Medicaid
Medicaid is a state-administered medical assistance program for the indigent, operated by the individual states with the financial participation of the federal government, providing health insurance coverage for certain persons in financial need, regardless of age, and that may supplement Medicare benefits for financially needy persons aged 65 and older.
Under Medicaid, most state expenditures for medical assistance are matched by the federal government. The federal medical assistance percentage, or FMAP, which is the percentage of Medicaid expenses paid by the
8
Table of Contents
federal government, ranged from 50% to 76% in fiscal year 2008, depending on the state in which the program was administered. In response to the economic downturn, Section 5001 of Division B of the American Recovery and Reinvestment Act of 2009, or ARRA, provides for a temporary increase in FMAP rates for Medicaid and certain other federal programs. The purpose of the increases to the FMAP rates was to provide fiscal relief to states and to protect and maintain state Medicaid and certain other assistance programs in a period of economic downturn, referred to as the recession adjustment period. The recession adjustment period is defined as the period beginning October 1, 2008 and ending December 31, 2010. During this recession adjustment period, each state’s FMAP rate was recalculated on a quarterly basis, based on a calculation formula set forth in Section 5001 of ARRA that increases FMAP rates based in part on unemployment levels within a state. For example, for pre-ARRA fiscal year 2009, FMAP rates ranged from 50% to 76%; by contrast, under the ARRA FMAP increases, FMAP rates for fiscal year 2009 ranged from 56% to 84%. For federal fiscal year 2009 in the states in which we currently operate, pre-ARRA FMAP rates ranged between 50% and 71%; and post-ARRA FMAP rates ranged between 62% and 79%. Thus, for federal fiscal year 2009, an additional 8% to 12% of Medicaid funds were provided by the federal government. These enhanced FMAP rates under ARRA were recalculated on a quarterly basis through December 31, 2010, and changes in a state’s unemployment rate could affect the ARRA-adjusted FMAP rates. The federal fiscal year 2011 FMAP rates in the states in which we currently operate range between 50% and 70%. Moreover, on August 10, 2010, the Education, Jobs and Medicaid Assistance Act became law and extended the enhanced FMAP rates under the ARRA through June 30, 2011. It is unclear what further FMAP enhancements, if any, will continue past June 30, 2011.
Provider taxes
To generate funds to pay for the increasing costs of the Medicaid program, many states utilize financial arrangements commonly referred to as “provider taxes.” Under provider tax arrangements, states collect taxes from healthcare providers and then use the revenue to pay the providers as a Medicaid expenditure, which allows the states to then claim additional federal matching funds on the additional reimbursements.
To curb these types of Medicaid funding arrangements by states, Congress placed restrictions on states’ use of provider taxes as a means of obtaining federal matching funds. Under the Medicaid Voluntary Contribution and Provider-Specific Tax Amendments of 1991, the federal matching funds available to a state are reduced by the total amount of healthcare related taxes that the state imposed, unless certain requirements are met. The federal matching funds are not reduced if the state taxes are broad-based and not applied specifically to Medicaid reimbursed services, and providers are at risk for the amount of tax assessed and not guaranteed to receive reimbursement for the tax assessed through the applicable state Medicaid program. Under current law, taxes imposed on providers may not exceed 5.5% of the provider’s total revenue (scheduled to increase to 6.0% in October 2011) and must be applied uniformly across all healthcare providers in the same class.
Medicaid Integrity Program
With the passage of the DRA, specifically section 6034, Congress created the Medicaid Integrity Program, or MIP, through section 1936 of the Social Security Act, or the SSA. Section 1936 of the SSA requires the Secretary of Health and Human Services, or HHS, to enter into contracts with eligible entities to perform four activities: (1) review Medicaid provider actions to detect fraud or potential fraud; (2) audit Medicaid provider claims; (3) identify overpayments; and (4) educate providers and others on payment integrity and quality of care issues. The contractors that perform these activities are known as Medicaid Integrity Contractors, or MICs.
There are three types of MICs that perform the following activities: (1) Review of Provider MICs, which analyze Medicaid claims data to identify aberrant claims and potential billing vulnerabilities, and which also provide leads to Audit of Provider and Identification of Overpayment MICs, or Audit MICs, of providers to be audited; (2) Audit MICs, which conduct post-payment audits of all types of Medicaid providers, and, where appropriate, identify overpayments to these providers; and (3) Education MICs, which develop training materials
9
Table of Contents
to conduct provider education and training on payment integrity and quality of care issues, and which highlight the value of education in preventing fraud and abuse in the Medicaid program.
Provider MIC audits began in Florida and South Carolina at the end of fiscal year 2008; audits in other jurisdictions began in fiscal year 2009. As of December 2009, MICs began actively conducting audits in over 30 states, including California, Texas, and New Mexico. Statements from CMS regarding the preliminary results of the first 500 MIC audits indicate that nearly 30% of the audits conducted have been of long-term care facilities. Unlike the Medicare Recovery Audit Contractor, or RAC, program, the MIC audits are not subject to a uniform set of federal standards, but rather are governed according to state regulations and procedures relating to Medicaid provider audits and appeals. As such, a great degree of uncertainty surrounds whether and to what extent the results of audits conducted by this new set of audit contractors will result in recoupments of alleged overpayments to our facilities. To the extent the MICs apply different or more stringent standards than other past analogous audit programs, the MIC audits could result in recoupments of alleged overpayments and could have an adverse impact on our results of operations.
In addition, Section 6411 of the PPACA expanded the RAC program, which formerly included only Medicare Part A and Part B claims, to also include Medicare Part C and Part D claims, as well as Medicaid claims effective December 31, 2010. It is uncertain at this time how the recently-expanded RAC program will interact with the MIC program. CMS has noted in a FAQ that a provider may be subject to audit by multiple oversight bodies, especially if the audits cover different programs (Medicare versus Medicaid), different audit issues (one-day stays versus post-mortem payments) or different audit periods. Moreover, in a proposed rule, published by CMS on November 10, 2010, CMS provides for States and Medicaid RACs to coordinate with other contractors and entities auditing Medicaid providers and with State and Federal law enforcement agencies.
Medicaid eligibility
The DRA limits the ability of individuals to become eligible for Medicaid by increasing from three years to five years the time period, or the look-back period, in which the transfer of assets by an individual for less than fair market value will render the individual ineligible for Medicaid benefits for nursing home care. Under the DRA, a person that transferred assets for less than fair market value during the look-back period will be ineligible for Medicaid for so long as they would have been able to fund their cost of care absent the transfer or until the transfer would no longer have been made during the look-back period. This period is referred to as the penalty period. The DRA also changes the calculation for determining when the penalty period begins and prohibits states from ignoring small asset transfers and certain other asset transfer mechanisms.
Medicaid reimbursement
Medicaid reimbursement formulas are established by each state with the approval of the federal government in accordance with federal guidelines. The Medicaid program also generally permits states to develop their own standards for the establishment of rates and varies in certain respects from state to state. The law requires each state to use a public process for establishing proposed rates whereby the methodology and justification of rates used are available for public review and comment. The states in which we operate currently use prospective cost-based reimbursement systems. Under cost-based reimbursement systems, the facility is reimbursed for the reasonable direct and indirect allowable costs it incurred in a base year in providing routine resident care services as defined by the program. The reimbursements received under a cost-based reimbursement system are updated periodically for inflation. In certain states, efficiency incentives are provided and facilities may be subject to cost ceilings. Reasonable costs normally include certain allowances for administrative and general costs, as well as the cost of capital or investment in the facility, which may be transformed into a fair rental or cost of capital charge for property and equipment. Many of the prospective payment systems under which we operate also contain an acuity measurement system, which adjusts rates based on the care needs of the resident. Retrospective cost-based systems operate similar to the pre-PPS Medicare program where skilled nursing facilities are paid on
10
Table of Contents
an interim basis for services provided, subject to adjustments based on allowable costs, which are generally submitted on an annual basis.
Managed Care
Our managed care patients consist of individuals who are insured by a third-party entity, typically called a senior Health Maintenance Organization, or senior HMO plan, or are Medicare beneficiaries who assign their Medicare benefits to a senior HMO plan.
Private Pay and Other
Private pay and other sources consist primarily of individuals or parties who directly pay for their services or are beneficiaries of the Department of Veterans Affairs or hospice beneficiaries.
Reimbursement for Specific Services
Reimbursement for Skilled Nursing Services
Skilled nursing facility revenue is primarily derived from Medicare and Medicaid reimbursement, as discussed above. Our skilled nursing companies also provide Medicaid-covered services to eligible individuals consisting of nursing care, room and board and social services. In addition, states may, at their option, cover other services such as physical, occupational and speech therapies.
Reimbursement for Assisted Living Services
Assisted living facility revenue is primarily derived from private pay residents at rates we establish based upon the services we provide and market conditions in the area of operation. In addition, Medicaid or other state-specific programs in some states where we operate supplement payments for board and care services provided in assisted living facilities.
Reimbursement for Rehabilitation Therapy Services
Our rehabilitation therapy services operations receive payment for services from affiliated and non-affiliated skilled nursing facilities and assisted living facilities that they serve. The payments are based on contracts with customers with negotiated patient per diem rates or a negotiated fee schedule based on the type of service rendered. Various federal and state laws and regulations govern reimbursement for rehabilitation therapy services to long-term care facilities and other healthcare providers participating in Medicare, Medicaid, and other federal and state healthcare programs.
The federal and state reimbursement and fraud and abuse laws and regulations are applicable to our rehabilitation therapy services operations because the services we provide to our customers, including affiliated entities, are generally paid under Medicare, Medicaid, and other federal and state healthcare programs. We could be negatively affected if we violate the laws governing our arrangements with patients or referral sources. Also, if our customers fail to comply with these laws and regulations, they could be subject to possible sanctions, including loss of licensure or eligibility to participate in reimbursement programs, as well as civil and criminal penalties, which could adversely affect our rehabilitation therapy operations, including our financial results. Our customers will also be affected by the Medicare Part B outpatient rehabilitation therapy cap discussed above.
Reimbursement for Hospice Services
For a Medicare beneficiary to qualify for the Medicare hospice benefit, two physicians must certify that, in their best judgment, the beneficiary has less than six months to live, assuming the beneficiary’s disease runs its normal course. In addition, the Medicare beneficiary must affirmatively elect hospice care and waive any rights to other Medicare benefits related to his or her terminal illness. Each benefit period, a physician must re-certify
11
Table of Contents
that the Medicare beneficiary’s life expectancy is six months or less in order for the beneficiary to continue to qualify for and to receive the Medicare hospice benefit. The first two benefit periods are measured at 90-day intervals and subsequent benefit periods are measured at 60-day intervals. There is no limit on the number of periods that a Medicare beneficiary may be re-certified. A Medicare beneficiary may revoke his or her election at any time and begin receiving traditional Medicare benefits.
Medicare reimburses for hospice care. We receive one of four predetermined daily or hourly rates based on the level of care we furnish to the beneficiary. These rates are subject to annual adjustments based on inflation and geographic wage considerations.
We are subject to two limitations on Medicare payments for hospice services. First, if inpatient days of care provided to patients at a hospice exceed 20% of the total days of hospice care provided for an annual period beginning on November 1st, then payment for days in excess of this limit are paid for at the routine home care rate. None of our hospice programs exceeded the payment limits on inpatient services for 2010 or 2009.
Second, overall payments made by Medicare to us on a per hospice program basis are also subject to a cap amount calculated by the Medicare fiscal intermediary at the end of the hospice cap period. The Medicare revenue paid to a hospice program from November 1 to October 31 may not exceed the annual aggregate cap amount. This annual aggregate cap amount is calculated by multiplying the number of first time Medicare hospice beneficiaries during the year by the Medicare per beneficiary cap amount, resulting in that hospice’s aggregate cap, which is the allowable amount of total Medicare payments that hospice can receive for that cap year. If a hospice exceeds its aggregate cap, then the hospice must repay the excess back to Medicare. The Medicare cap amount is reduced proportionately for patients who transferred in and out of our hospice services. The Medicare cap amount is adjusted annually for inflation, but is not adjusted for geographic differences in wage levels, although hospice per diem payment rates are wage indexed. Our hospice program exceeded the Medicare cap limit in 2009 by $2.1 million. In 2010 our hospice program did not exceed the Medicare cap limit. See Item 1A of this report, “Risk Factors—We are subject to a Medicare cap amount for our hospice business. Our net patient service revenue and profitability could be adversely affected by limitations on Medicare payments.”
Reimbursement for Home Health Services
Home health service revenue is primarily derived from Medicare reimbursement. Medicare pays home health agencies a predetermined base payment for the provision of home health services to Medicare beneficiaries. The payment is adjusted for the health condition and care needs of the beneficiary. The payment is also adjusted for the geographic differences in wages for home health agencies across the country. The adjustment for the health condition, or clinical characteristics, and service needs of the beneficiary is referred to as the case-mix adjustment. The home health PPS will provide home health agencies with payments for each 60-day episode of care for each beneficiary. If a beneficiary is still eligible for care after the end of the first episode, a second episode can begin. There are no limits to the number of episodes a beneficiary who remains eligible for the home health benefit can receive. While payment for each episode is adjusted to reflect the beneficiary’s health condition and needs, a special outlier provision exists to ensure appropriate payment for those beneficiaries that have the most expensive care needs. Adjusting payment to reflect the home health agency’s cost in caring for each beneficiary including the sickest, should ensure that all beneficiaries have access to home health services for which they are eligible.
Government Regulation
General
Healthcare is an area of extensive and frequent regulatory change. Our owned limited liability companies and partnerships that provide healthcare services must comply with federal, state and local laws relating to, among other things, licensure, delivery and adequacy of medical care, distribution of pharmaceuticals, equipment, personnel, operating policies, fire prevention, rate setting, building codes and environmental
12
Table of Contents
protection. Changes in the law or new interpretations of existing laws may have a significant impact on our methods and costs of doing business.
Governmental and other authorities periodically inspect our skilled nursing facilities and assisted living facilities and hospices to verify that we continue to comply with their various standards. We must pass these inspections to continue our licensing under state law, to obtain certification under the Medicare and Medicaid programs, and to continue our participation in the Veterans Administration program at some facilities. We can only participate in these third-party programs if inspections by regulatory authorities reveal that our facilities are in substantial compliance with applicable standards. In addition, regulatory authorities periodically inspect our recordkeeping and inventory control of controlled narcotics. From time to time, we, like others in the healthcare industry, may receive notices from federal and state regulatory authorities alleging that we failed to comply with applicable standards. These notices may require us to take corrective action, and may impose civil monetary penalties and other operating restrictions on us. If our facilities fail to comply with these directives or otherwise fail to comply substantially with licensure and certification laws, rules and regulations, we could lose our certification as a Medicare or Medicaid provider or lose our state licenses to operate the facilities.
Civil and Criminal Fraud and Abuse Laws and Enforcement
Federal and state healthcare fraud and abuse laws regulate both the provision of services to government program beneficiaries and the methods and requirements for submitting claims for services rendered to such beneficiaries. Under these laws, individuals and organizations can be penalized for submitting claims for services that are not provided, that have been inadequately provided, billed in an incorrect manner or other than as actually provided, not medically necessary, provided by an improper person, accompanied by an illegal inducement to utilize or refrain from utilizing a service or product, or billed or coded in a manner that does not otherwise comply with applicable governmental requirements. Penalties also may be imposed for violation of anti-kickback and patient referral laws.
Federal and state governments have a range of criminal, civil and administrative sanctions available to penalize and remediate healthcare fraud and abuse, including exclusion of the provider from participation in the Medicare and Medicaid programs, fines, criminal and civil monetary penalties and suspension of payments and, in the case of individuals, imprisonment.
We have internal policies and procedures, including a compliance program designed to facilitate compliance with and to reduce exposure for violations of these and other laws and regulations. However, because enforcement efforts presently are widespread within the industry and may vary from region to region, there can be no assurance that our internal policies and procedures will significantly reduce or eliminate exposure to civil or criminal sanctions or adverse administrative determinations.
Anti-Kickback Statute
Provisions in Title XI of the SSA, commonly referred to as the Anti-Kickback Statute, prohibit the knowing and willful offer, payment, solicitation or receipt of anything of value, directly or indirectly, in return for the referral of patients or arranging for the referral of patients, or in return for the recommendation, arrangement, purchase, lease or order of items or services that are covered by a federal healthcare program such as Medicare or Medicaid. Violation of the Anti-Kickback Statute is a felony, and sanctions for each violation include imprisonment of up to five years, criminal fines of up to $25,000, civil monetary penalties of up to $50,000 per act plus three times the amount claimed or three times the remuneration offered, and exclusion from federal healthcare programs (including Medicare and Medicaid). Many states have adopted similar prohibitions against kickbacks and other practices that are intended to induce referrals applicable to all payors.
We are required under the Medicare conditions of participation and some state licensing laws to contract with numerous healthcare providers and practitioners, including physicians, hospitals and nursing homes, and to arrange for these individuals or entities to provide services to our patients. In addition, we have contracts with other suppliers, including pharmacies, ambulance services and medical equipment companies. Some of these
13
Table of Contents
individuals or entities may refer, or be in a position to refer, patients to us, and we may refer, or be in a position to refer, patients to these individuals or entities. Certain safe harbor provisions have been created, and compliance with a safe harbor ensures that the contractual relationship will not be found in violation of the Anti-Kickback Statute. We attempt to structure these arrangements in a manner that falls within one of the safe harbors. Some of these arrangements may not ultimately satisfy the applicable safe harbor requirements, but failure to meet the safe harbor does not necessarily mean an arrangement is illegal.
We believe that our arrangements with providers, practitioners and suppliers are in compliance with the Anti-Kickback Statute and similar state laws. However, if any of our arrangements with third parties were to be challenged and found to be in violation of the Anti-Kickback Statute, we could be subject to civil and criminal penalties, and we could be excluded from participating in federal and state healthcare programs such as Medicare and Medicaid. The occurrence of any of these events could significantly harm our business and financial condition.
Stark Law
Congress has also passed a significant prohibition against certain physician referrals of patients for healthcare services, commonly known as the Stark Law. The Stark Law prohibits a physician from making referrals for particular healthcare services, referred to as to entities with which the physician (or an immediate family member of the physician) has a financial relationship if the services are payable by Medicare or Medicaid. If an arrangement is covered by the Stark Law, the requirements of a Stark Law exception must be met for the physician to be able to make referrals to the entity for designated health services and for the entity to be able to bill for these services. Although the term “designated health services” does not include long-term care services, some of the services provided at our skilled nursing facilities and other related business units are classified as designated health services, including physical, speech and occupational therapy, pharmacy and hospice services. The term “financial relationship” is defined very broadly to include most types of ownership or compensation relationships. The Stark Law also prohibits the entity receiving the referral from seeking payment from the patient or the Medicare and Medicaid programs for services rendered pursuant to a prohibited referral.
The Stark Law contains exceptions for certain physician ownership or investment interests in, and certain physician compensation arrangements with, certain entities. If a compensation arrangement or investment relationship between a physician, or immediate family member, and an entity satisfies the applicable requirements for a Stark Law exception, the Stark Law will not prohibit the physician from referring patients to the entity for designated health services. The exceptions for compensation arrangements cover employment relationships, personal services contracts and space and equipment leases, among others.
If an entity violates the Stark Law, it could be subject to civil penalties of up to $15,000 per prohibited claim and up to $100,000 for knowingly entering into certain prohibited cross-referral schemes. The entity also may be excluded from participating in federal and state healthcare programs, including Medicare and Medicaid. If the Stark Law were found to apply to our relationships with referring physicians and no exception under the Stark Law were available, we would be required to restructure these relationships or refuse to accept referrals for designated health services from these physicians. If we were found to have submitted claims to Medicare or Medicaid for services provided pursuant to a referral prohibited by the Stark Law, we would be required to repay any amounts we received from Medicare or Medicaid for those services and could be subject to civil monetary penalties. Further, we could be excluded from participating in Medicare and Medicaid and other federal and state healthcare programs. If we were required to repay any amounts to Medicare or Medicaid, subjected to fines, or excluded from the Medicare and Medicaid Programs, our business and financial condition would be harmed significantly.
As directed by the Patient Protection and Affordable Care Act (“PPACA”), on September 23, 2010, CMS released a self-referral disclosure protocol (“SRDP”) for potential or actual violations of the Stark Law. A disclosure pursuant to SRDP must include detailed and specific information, including a financial analysis setting forth the amount due and owing to the government for a violation, and the methodology used in calculating that
14
Table of Contents
amount. Under SRDP, CMS states that it may, but is not required to, reduce the amounts due and owing for a Stark Law violation, and will consider the following factors in deciding whether to grant a reduction: (1) the nature and extent of the improper or illegal practice; (2) the timeliness of the self-disclosure; (3) the cooperation in providing additional information related to the disclosure; (4) the litigation risk associated with the matter disclosed; and (5) the financial position of the disclosing party. It is difficult at present to predict how the release of the SRDP will impact those entities who disclose violations of the Stark Law.
Many states have physician relationship and referral statutes that are similar to the Stark Law. These laws generally apply regardless of the payor. We believe that our operations are structured to comply with the Stark Law and applicable state laws with respect to physician relationships and referrals. However, any finding that we are not in compliance with these laws could require us to change our operations or could subject us to penalties. This, in turn, could significantly harm our business and financial condition.
False Claims
Federal and state laws prohibit the submission of false claims and other acts that are considered fraudulent or abusive. The submission of claims to a federal or state healthcare program for items and services that are “not provided as claimed” may lead to the imposition of civil monetary penalties, criminal fines and imprisonment, and/or exclusion from participation in state and federally-funded healthcare programs, including the Medicare and Medicaid programs. Allegations of poor quality of care can also lead to false claims suits as prosecutors allege that the provider has represented to the government healthcare program that adequate care is provided and the lack of quality care causes the service to be “not provided as claimed.”
Under the federal False Claims Act, or FCA, actions against a provider can be initiated by the federal government or by a private party on behalf of the federal government. These private parties who are often referred to as “qui tam relators” or “relators,” are entitled to share in any amounts recovered by the government. Both direct enforcement activity by the government and qui tam relator actions have increased significantly in recent years. The use of private enforcement actions against healthcare providers has increased dramatically, in part because the relators are entitled to share in a portion of any settlement or judgment. This development has increased the risk that a healthcare company will have to defend a false claims action, pay fines or settlement amounts or be excluded from the Medicare and Medicaid programs, and other federal and state healthcare programs as a result of an investigation arising out of false claims laws. Many states have enacted similar laws providing for imposition of civil and criminal penalties for the filing of fraudulent claims.
We believe that our operations comply with the FCA and similar state laws. However, if our claims practices were challenged and found to violate the applicable laws, any finding that we are not in compliance with these laws could require us to change our operations or could subject us to penalties or make us ineligible to participate in certain government funded healthcare programs, which could in turn significantly harm our business and financial condition.
Health Insurance Portability and Accountability Act of 1996
The federal Health Insurance Portability and Accountability Act of 1996, commonly known as HIPAA, created two new federal crimes: healthcare fraud and false statements relating to healthcare matters. The healthcare fraud statute prohibits knowingly and willfully executing a scheme to defraud any healthcare benefit program, including private payors. A violation of this statute is a felony and may result in fines, imprisonment or exclusion from government-sponsored programs. The false statements statute prohibits knowingly and willfully falsifying, concealing or covering up a material fact or making any materially false, fictitious or fraudulent statement in connection with the delivery of or payment for healthcare benefits, items or services. A violation of this statute is a felony and may result in fines or imprisonment as well as exclusion from participation in federal and state healthcare programs.
In addition, HIPAA established uniform standards governing the conduct of certain electronic healthcare transactions and protecting the privacy and security of certain individually identifiable health information. Three
15
Table of Contents
standards have been promulgated under HIPAA with which we currently are required to comply. First, we must comply with HIPAA’s standards for electronic transactions, which establish standards for common healthcare transactions, such as claims information, plan eligibility, payment information and the use of electronic signatures. We must also comply with the standards for the privacy of individually identifiable health information, which limit the use and disclosure of most paper and oral communications, as well as those in electronic form, regarding an individual’s past, present or future physical or mental health or condition, or relating to the provision of healthcare to the individual or payment for that healthcare, if the individual can or may be identified by such information. Finally, we must comply with HIPAA’s security standards, which require us to ensure the confidentiality, integrity and availability of all electronic protected health information that we create, receive, maintain or transmit, to protect against reasonably anticipated threats or hazards to the security of such information, and to protect such information from unauthorized use or disclosure.
The Health Information Technology for Clinical Health Act of 2009, or HITECH Act, which was signed into law on February 17, 2009, expanded the privacy and security law requirements of HIPAA by requiring HIPAA-covered entities to notify affected individuals following the discovery of a breach of unsecured protected health information, or PHI. Business associates of HIPAA-covered entities also must notify HIPAA-covered entities of any breaches. The HITECH Act now makes breach of unsecured PHI subject to self-disclosure by covered entities to affected individuals, federal officials and in some instances, the media. The HITECH Act enhances the enforcement resources dedicated to ensuring HIPAA compliance and greatly increases the penalties for noncompliance. While we maintain policies and processes designed to ensure compliance with HIPAA and the HITECH Act, from time to time violations may occur, and as a result we may be required to self-disclose breaches of unsecured PHI or other matters. The result of such self disclosure may be the imposition of civil monetary penalties and other operating restrictions on us. We believe that we are in compliance with the HIPAA standards as amended by the HITECH Act and will continue to monitor our policies and procedures in an effort to make any necessary enhancements . However, if our practices, policies and procedures are found not to comply with these standards, we could be subject to the increased criminal penalties and civil sanctions under HIPAA and the HITECH Act. For additional detail regarding the HITECH Act, see Item 1A of this report, “Risk Factors—We are subject to extensive and complex laws and government regulations. If we are not operating in compliance with these laws and regulations or if these laws and regulations change, we could be required to make significant expenditures or change our operations in order to bring our facilities and operations into compliance.”
State Privacy Laws
States also have laws that apply to the privacy of healthcare information. We must comply with these state privacy laws to the extent that they are more protective of healthcare information or provide additional protections not afforded by HIPAA. Where we are subject to these state laws, it may be necessary to modify our operations or procedures to comply with them, which may entail significant and costly changes for us. We believe that we are in material compliance with applicable state privacy and security laws. However, if we fail to comply with these laws, we could be subject to additional penalties and/or sanctions.
Federal Health Care Reform
In addition to the provisions described above affecting Medicare and Medicaid participating providers, the PPACA enacted several reforms with respect to skilled nursing facilities and hospices, including payment measures to realize significant savings of federal and state funds by deterring and prosecuting fraud and abuse in both the Medicare and Medicaid programs. While many of the provisions of the PPACA will not take effect for several years or are subject to further refinement through the promulgation of regulations, some key provisions of the PPACA are presently effective.
| • | Enhanced CMPs and Escrow Provisions. Effective March 23, 2010, the PPACA includes expanded civil monetary penalty (“CMP”) provisions applicable to all Medicare and Medicaid providers. Sections 6402 and 6408 of the PPACA provide for the imposition of CMPs of up to $50,000 and, in |
16
Table of Contents
| some cases, treble damages, for actions relating to alleged false statements to the federal government. Section 6111 of the PPACA also includes CMP provisions specific to skilled nursing facilities that in limited circumstances provide for up to a fifty percent (50%) reduction in CMPs where a facility self-reports and promptly corrects an alleged deficiency within ten (10) calendar days. In addition, the new CMP provisions specific to skilled nursing facilities provide that the Secretary of Health and Human Services may provide for the collection and placement of the CMP amount into an escrow account on the earlier of the date informal dispute resolution is completed or ninety (90) days after the imposition of the CMP. If an appeal is successful, the facility would receive a refund of the collected amounts with interest. This CMP escrow provision is a departure from prior policy, which only required remittance of CMP amounts following the final disposition of a CMP dispute. On July 12, 2010, CMS published a proposed rule implementing the PPACA’s enhanced CMP and escrow provisions. It is anticipated that the final rule implementing these provisions will be issued to take effect by July 1, 2011. To the extent our facilities are assessed significant CMPs that are collected and placed into an escrow account pending lengthy appeals, such actions could adversely affect the results of operations. |
| • | Nursing Home Transparency Requirements. In addition to expanded CMP provisions, the PPACA imposes substantial new transparency requirements for Medicare-participating nursing facilities. Existing law requires Medicare providers to disclose to CMS: (1) any person or entity that owns directly or indirectly an ownership interest of five percent (5%) or more in a provider; (2) officers and directors (if a corporation) and partners (if a partnership); and (3) holders of a mortgage, deed of trust, note or other obligation secured by the entity or the property of the entity. Section 6101 of the PPACA expands the information required to be disclosed to include: (4) the facility’s organizational structure; (5) additional information on officers, directors, trustees, and “managing employees” of the facility (including their names, titles, and start dates of services); and (6) information on any “additional disclosable party” of the facility. “Managing employee” is defined broadly as an individual (including a general manager, business manager, administrator, director, or consultant) who directly or indirectly manages, advises, or supervises any element of the practices, finances, or operations of the facility. “Additional disclosable party” of the facility is defined as any person or entity that (1) exercises operational, financial, or managerial control over the facility, or provides policies or procedures for the operations of the facility, or provides financial or cash management services to the facility; (2) leases or subleases real property to the facility, or owns a whole or partial interest equal to or exceeding five percent (5%) of the total cash value of such real property; or (3) provides management or administrative services, management or clinical consulting services, or accounting or financial services to the facility. Beginning March 23, 2010, facilities must have this information available for submission to the Secretary of Health & Human Services, the Office of the Inspector General, the state in which the facility is located, and the state long-term care ombudsman upon request. Thus, the new transparency provisions could result in the potential for greater government scrutiny and oversight of the ownership and investment structure for skilled nursing facilities, as well as more extensive disclosure of entities and individuals that comprise part of skilled nursing facilities’ ownership structure. |
| • | Suspension of Payments During Pending Fraud Investigations. The PPACA also provides the federal government with expanded authority to suspend payment if a provider is investigated for allegations or issues of fraud. Section 6402 of the PPACA provides that, beginning March 23, 2010, Medicare and Medicaid payments may be suspended pending a “credible investigation of fraud,” unless the Secretary of Health and Human Services determines that good cause exists not to suspend payments. “Credible investigation of fraud” is undefined, although the Secretary must consult with the Office of the Inspector General in determining whether a credible investigation of fraud exists. This suspension authority creates a new mechanism for the federal government to suspend both Medicare and Medicaid payments for allegations of fraud, independent of whether a state exercises its authority to suspend Medicaid payments pending a fraud investigation. To the extent the Secretary applies this suspension of payments provision to one of our facilities for allegations of fraud, such a suspension could adversely affect the results of operations. |
17
Table of Contents
| • | Overpayment Reporting and Repayment; Expanded False Claims Act Liability. The PPACA also enacted several important changes that expand potential liability under the federal False Claims Act. Effective March 23, 2010, Section 6402 of the PPACA provides that overpayments related to services provided to both Medicare and Medicaid beneficiaries must be reported and returned to the applicable payor within the later of sixty (60) days of identification of the overpayment, or the date the corresponding cost report (if applicable) is due. Any overpayment retained after the deadline is considered an “obligation” for purposes of the federal False Claims Act. This new provision substantially tightens the repayment and reporting requirements generally associated with operations of health care providers to avoid FCA exposure. To the extent we incur additional operational costs to comply with the new overpayment reporting and repayment provision, such costs may adversely affect the results of operations. |
| • | Community First Choice Option. Effective January 1, 2011, Section 2401 of the PPACA mandates that states choosing to provide home and community based services shall make them available to assist with activities of daily living, instrumental activities of daily living and health related tasks under a plan of care agreed upon by the individual and his/her representative. The PPACA then goes on to specify the models of delivery through which such services may be available and enumerates the types of services that may be covered. For states that elect to make coverage of home and community based services available as specified by the PPACA, FMAP is increased by six percentage points, and thus this Section incentivizes states to expand their home and community based services. The expansion of home and community based services has the potential to reduce the demand for the long-term care and nursing services that we provide. |
| • | Removal of Barriers to Providing Home and Community Based Services. Also effective January 1, 2011, Section 2402 of the PPACA includes additional measures related to the expansion of community and home based services. It requires the Secretary to adopt regulations that will ensure that states will develop systems that allow beneficiaries to obtain, as well as maintain, non-institutional services, and have a say in the design of their treatment. This Section also authorizes states to expand coverage of community and home based services to individuals who would not otherwise be eligible for them. |
The provisions of the PPACA discussed above are examples of recently-enacted federal health reform provisions that we believe may have a material impact on the long-term care industry generally and on our business. However, the foregoing discussion is not intended to constitute, nor does it constitute, an exhaustive review and discussion of the PPACA. It is possible that other provisions of the PPACA may be interpreted, clarified, or applied to our facilities or operations in a way that could have a material adverse impact on the results of operations.
Certificates of Need and Other Regulatory Matters
Certain states administer a certificate of need program, which applies to the incurrence of capital expenditures, the offering of certain new institutional health services, the cessation of certain services and the acquisition of major medical equipment. Such legislation also stipulates requirements for such programs, including that each program be consistent with the respective state health plan in effect pursuant to such legislation and provide for penalties to enforce program requirements. To the extent that certificates of need or other similar approvals are required for expansion of our operations, either through facility acquisitions, expansion or provision of new services or other changes, such expansion could be affected adversely by the failure or inability to obtain the necessary approvals, changes in the standards applicable to such approvals or possible delays and expenses associated with obtaining such approvals.
State Operating License Requirements
Nursing homes, pharmacies, and hospices are required to be individually licensed or certified under applicable state law and as a condition of participation under the Medicare program. In addition, healthcare
18
Table of Contents
professionals and practitioners are required to be licensed in most states. We believe that our operating companies that provide these services have all required regulatory approvals necessary for our current operations. The failure to obtain, retain or renew any required license could adversely affect our operations, including our financial results.
Rehabilitation License Requirements
Our rehabilitation therapy services operations are subject to various federal and state regulations, primarily regulations of individual practitioners. Therapists and other healthcare professionals employed by us are required to be individually licensed or certified under applicable state law. We take measures to ensure that our therapists and other healthcare professionals are properly licensed and participate in continuing education programs. The failure to obtain, retain or renew any required license or certifications by therapists or other healthcare professionals could adversely affect our operations, including our financial results.
Regulation of our Joint Venture Institutional Pharmacy
Our joint venture institutional pharmacy operations, which include medical equipment and supplies, are subject to extensive federal, state and local regulation relating to, among other things, operational requirements, reimbursement, documentation, licensure, certification and regulation of pharmacies, pharmacists, drug compounding and manufacture and controlled substances.
Institutional pharmacies are regulated under the Food, Drug and Cosmetic Act and the Prescription Drug Marketing Act, which are administered by the U.S. Food and Drug Administration. Under the Comprehensive Drug Abuse Prevention and Control Act of 1970, which is administered by the U.S. Drug Enforcement Administration, dispensers of controlled substances must register with the Drug Enforcement Administration, file reports of inventories and transactions and provide adequate security measures. Failure to comply with such requirements could result in civil or criminal penalties. The Medicare and Medicaid programs also establish certain requirements for participation of pharmacy suppliers. Our institutional pharmacy joint venture is also subject to federal and state laws that govern financial arrangements between healthcare providers, including the Anti-Kickback Statute. See Item 1 of this report, “Business—Anti-Kickback Statute.”
Competition
Our skilled nursing facilities compete primarily on a local and regional basis with many long-term care providers, from national and regional chains to smaller providers owning as few as a single nursing center. We also compete under certain circumstances with inpatient rehabilitation facilities and long-term acute care hospitals. Our ability to compete successfully varies from location to location and depends on a number of factors, including the number of competing facilities in the local market, the types of services available, our local reputation for quality care of patients, the commitment and expertise of our staff and physicians, our local service offerings and treatment programs, the cost of care in each locality, and the physical appearance, location, age and condition of our facilities.
We seek to compete effectively in each market by establishing a reputation within the local community for quality of care, attractive and comfortable facilities, and providing specialized healthcare with an emphasized focus on high-acuity patients. Programs targeting high-acuity patients, including our Express Recovery™ units, generally have a higher staffing level per patient than our other inpatient facilities and compete more directly with inpatient rehabilitation facilities and long-term acute-care hospitals. We believe that the average cost to a third-party payor for the treatment of our typical high-acuity patient is lower if that patient is treated in one of our skilled nursing facilities than if that same patient were to be treated in an inpatient rehabilitation facility or long-term acute-care hospital.
19
Table of Contents
Our other services, such as assisted living facilities, rehabilitation therapy provided to third-party facilities, hospice care and home health services, and institutional pharmacy services, also compete with local, regional, and national companies. The primary competitive factors in these businesses are similar to those for our skilled nursing facilities and include reputation, cost of services, quality of clinical services, responsiveness to patient/resident needs, location and the ability to provide support in other areas such as third-party reimbursement, information management and patient recordkeeping.
Increased competition could limit our ability to attract and retain patients, maintain or increase rates or to expand our business. Some of our competitors have greater financial and other resources than we have, may have greater brand recognition and may be more established in their respective communities than we are. Competing companies may also offer newer facilities or different programs or services than we do and may as a result be more attractive to our current patients, to potential patients and to referral sources. Some of our competitors may accept lower profit margins than we do, which could present significant price competition, particularly for managed care and private pay patients.
With respect to hospice services, while non-profit organizations continue to run approximately two-thirds of all hospice programs, for-profit companies have recently begun to occupy a larger share of the hospice market. Increasing public awareness of hospice services, the aging of the U.S. population and favorable reimbursement by Medicare, which is the primary payor for hospice services, have contributed to the recent growth in the hospice care market. As more companies enter the market to provide hospice services, we will face increasing competitive pressure.
Labor
Our most significant operating cost is labor. Our labor costs consist of salaries, wages and benefits including workers’ compensation but excluding non-cash stock-based compensation expense. We seek to manage our labor costs by improving nurse staffing retention, maintaining competitive labor rates, and reducing reliance on overtime compensation and temporary nursing agency services. We believe that we staff appropriately, focusing primarily on the acuity level and day-to-day needs of our patients and residents.
As of December 31, 2010, we had approximately 9,736 full-time equivalent employees and had eight collective bargaining agreements with unions covering approximately 418 full-time employees at eight of our facilities. Labor costs accounted for approximately 66.2%, 66.0% and 64.7% of our operating expenses (excluding impairment charges) from continuing operations for the years ended December 31, 2010, 2009 and 2008, respectively. We generally consider our relationship with our employees to be good.
Risk Management
We have developed a risk management program designed to stabilize our insurance and professional liability costs. As part of this program, we have implemented an arbitration agreement system at each of our facilities under which, upon admission, patients are requested (but not required) to execute an agreement that requires disputes to be arbitrated prior to filing a lawsuit. We believe that this program accelerates resolution of disputes and has significantly reduced our liability exposure and related costs. We have also established an incident reporting process that involves monthly follow-up with our facility administrators to monitor the progress of claims and losses. We believe that our emphasis on providing high-quality care and our attention to monitoring quality of care indicators has also helped to reduce our liability exposure and related costs.
Insurance
We maintain insurance for general and professional liability, workers’ compensation, employee benefits liability, property, casualty, directors’ and officers’ liability, inland marine, crime, boiler and machinery, automobile, employment practices liability and earthquake and flood. We believe that our insurance programs are
20
Table of Contents
adequate and where there has been a direct transfer of risk to the insurance carrier, we do not recognize a liability in our consolidated financial statements. We self-insure a significant portion of our potential liabilities for several risks, including certain types of general and professional liability, workers’ compensation, and employee benefit insurance. To the extent our insurance coverage is insufficient or unavailable to cover losses that we incur that would otherwise be insurable, or to the extent that our estimates of anticipated liabilities that we self-insure are significantly lower than the actual self-insured liabilities that we incur, our financial condition and results of operations could be materially and adversely affected.
General and Professional Liability Insurance
Effective September 1, 2008, our California-based skilled nursing facility companies purchased individual general and professional liability insurance policies with a per occurrence and annual aggregate coverage limit of $1.0 million and $3.0 million, respectively, and an unaggregated $0.1 million per claim self-insured retention. These policies are renewable for up to three years.
Effective September 1, 2008, we also had an excess liability policy with a $14.0 million per loss limit and an $18.0 million annual aggregate limit for losses arising from claims in excess of $1.1 million for our California skilled nursing facilities and in excess of $1.0 million for all of our other businesses. The policy is renewable for up to three years. We retain an unaggregated self-insured retention of $1.0 million per claim for all Texas, New Mexico and Nevada businesses, our California businesses other than skilled nursing facility companies, and our Davenport, Iowa facility. Effective January 1, 2010 all of our facilities located in Kansas, Missouri and Iowa were added to this excess policy with the same unaggregated self-insured retention of $1.0 million per claim for all of these facilities. Effective May 1, 2010 all of hospice and home health businesses located in Arizona, Idaho, Montana and Nevada that we acquired in the Hospice/Home Health Acquisition were added to this excess policy which provides $14.0 million in excess coverage in addition to the $1.0 million per claim/$3.0 million annual aggregate claims made coverage which was in place for these businesses at the time of their acquisition.
Until December 31, 2009, our Kansas and Iowa businesses were insured on an occurrence basis with a per occurrence and annual aggregate coverage limit of $1.0 million and $3.0 million, respectively. There are no applicable self-insurance retentions or deductibles under these contracts. Until December 31, 2009, our Missouri businesses were underwritten on a claims-made basis with no applicable self-insured retentions or deductibles and have a per occurrence and annual aggregate coverage limit of $1.0 million and $3.0 million, respectively.
Workers’ Compensation
We maintain workers’ compensation insurance as statutorily required. Most of our commercial workers’ compensation insurance purchased is loss sensitive in nature, except as noted below. As a result, we are responsible for adverse loss development. Additionally, we self-insure the first unaggregated $1.0 million per workers’ compensation claim for all California, New Mexico and Nevada businesses. We have elected not to carry workers’ compensation insurance in Texas and our Texas businesses may be liable for negligence claims that are asserted against them by our Texas-based employees. We have purchased guaranteed cost policies for our businesses in Kansas, Missouri, Iowa, and our recently acquired Nevada, Arizona, Idaho, and Montana based hospice and home health operations. There are no deductibles associated with these programs. We recognize a liability in our consolidated financial statements for our estimated self-insured workers’ compensation risks. Historically, our estimated liabilities have been sufficient to cover actual claims, but there can be no assurances that our current or future estimates will be sufficient.
Employee Benefit Insurance
We are self-insured for certain of our healthcare, dental and vision plans that we offer to our employees, subject to stop loss insurance with an annual $0.3 million deductible per participant, which limits our exposure to large claims. We accrue our self-insured risks costs in the period in which such costs are incurred, including an
21
Table of Contents
estimate of incurred but not reported claims. Other risks are insured and carry deductible losses of varying amounts. An increasing frequency of large claims or deterioration in overall claim experience could increase the volatility of expenses for such self-insured risks.
Environmental Matters
We are subject to a wide variety of federal, state and local environmental and occupational health and safety laws and regulations. As a healthcare provider, we face regulatory requirements in areas of air and water quality control, medical and low-level radioactive waste management and disposal, asbestos management, response to mold and lead-based paint in our facilities and employee safety.
In our role as owner and/or operator of our facilities (including our leased facilities), we also may be required to investigate and remediate hazardous substances that are located on the property, including any such substances that may have migrated off, or discharged or transported from the property. Part of our operations involves the handling, use, storage, transportation, disposal and/or discharge of hazardous, infectious, toxic, flammable and other hazardous materials, wastes, pollutants or contaminants. These activities may result in damage to individuals, property or the environment; may interrupt operations and/or increase costs; may result in legal liability, damages, injunctions or fines; may result in investigations, administrative proceedings, penalties or other governmental agency actions; and may not be covered by insurance. We believe that we are in material compliance with applicable environmental and occupational health and safety requirements. However, there can be no assurance that we will not incur environmental liabilities in the future, and such liabilities may result in material adverse consequences to our operations and financial condition.
Customers
No individual customer or client accounts for a significant portion of our revenue. We do not expect that the loss of a single customer or client would have a material adverse effect on our business, results of operations or financial condition.
Available Information
Our Annual Reports on Form 10-K, Quarterly Reports on Form 10-Q, Current Reports on Form 8-K, and amendments to reports filed pursuant to Sections 13(a) and 15(d) of the Securities Exchange Act of 1934, as amended, are filed with the U.S. Securities and Exchange Commission, or SEC. Such reports and other information filed by us with the SEC are available free of charge at the investor relations section of our website at www.skilledhealthcaregroup.com as soon as reasonably practicable after such reports are electronically filed with, or furnished to, the SEC. Copies are also available, without charge, or by writing to Skilled Healthcare Group Investor Communications, 27442 Portola Parkway, Suite 200, Foothill Ranch, CA, 92610. Reports filed with the SEC may be viewed at www.sec.gov or obtained at the SEC Public Reference Room in Washington, D.C. Information regarding the operation of the Public Reference Room may be obtained by calling the SEC at 1-800-SEC-0330. The inclusion of our website address in this annual report does not include or incorporate by reference the information on our website into this annual report.
Company History
Skilled Healthcare Group, Inc. was incorporated as SHG Holding Solutions, Inc. in Delaware in October 2005. Our predecessor company acquired Summit Care Corporation, a publicly-traded long-term care company with nursing facilities in California, Texas and Arizona, in 1998. In October 2001, our predecessor and 19 of its subsidiaries filed voluntary petitions for protection under Chapter 11 of the U.S. Bankruptcy Code and in November 2001, our remaining three companies also filed voluntary petitions for protection under Chapter 11. In August 2003, we emerged from bankruptcy, paying or restructuring all debt holders in full, paying all accrued interest expenses and issuing 5.0% of our common stock to former bondholders. In connection with our emergence from bankruptcy, we engaged in a series of transactions, including the disposition in March 2005 of our California pharmacy business, selling two institutional pharmacies in Southern California.
22
Table of Contents
In February 2007, we effected the merger of our predecessor company, which was our wholly-owned subsidiary, with and into us. We were the surviving company in the merger and changed our name from SHG Holding Solutions, Inc. to Skilled Healthcare Group, Inc. As a result of the merger, we assumed all of the rights and obligations of our predecessor company.
In June 2009, the United States Bankruptcy Court for the Central District of California granted entry of a final decree closing the aforementioned Chapter 11 cases.
| Item 1A. | Risk Factors |
Statements made by us in this report and in other reports and statements released by us that are not historical facts constitute “forward-looking statements” within the meaning of Section 21 of the Securities Exchange Act of 1934. Disclosures that use words such as we “believe,” “anticipate,” “estimate,” “intend,” “could,” “plan,” “expect,” “project” or the negative of these, as well as similar expressions, are intended to identify forward-looking statements. These forward-looking statements are necessarily estimates reflecting the best judgment of our senior management based on our current estimates, expectations, forecasts and projections, and include comments that express our current opinions about trends and factors that may impact future operating results. Such statements rely on a number of assumptions concerning future events, many of which are outside of our control, and involve known and unknown risks and uncertainties that could cause our actual results, performance or achievements, or industry results, to differ materially from any future results, performance or achievements, expressed or implied by such forward-looking statements. Any such forward-looking statements, whether made in this report or elsewhere, should be considered in the context of the various disclosures made by us about our business and other matters including, without limitation, the risk factors discussed below. We expressly disclaim any duty to update the forward-looking statements and other information contained in this report, except as required by law.
We operate in a rapidly changing environment that involves a number of risks and uncertainties. The following discussion highlights some of these risks and uncertainties, and others are discussed elsewhere in this report. These and other risks and uncertainties could materially and adversely affect our business, financial condition, prospects, operating results or cash flows. The following risk factors are not an exhaustive list of the risks and uncertainties associated with our business. New considerations may emerge or changes to the risks and uncertainties described below could occur that could materially and adversely affect our business.
Reductions in Medicare reimbursement rates, or changes in the rules governing the Medicare program could have a material adverse effect on our revenue, financial condition and results of operations.
Medicare is our largest source of revenue, accounting for 37.1% and 35.0% of our total revenue during 2010 and 2009, respectively. In addition, many private payors base their reimbursement rates on the published Medicare rates or, in the case of our rehabilitation therapy services customers, are themselves reimbursed by Medicare. Accordingly, if Medicare reimbursement rates are reduced or fail to increase as quickly as our costs, or if there are changes in the rules governing the Medicare program that are disadvantageous to our business or industry, our business and results of operations will be adversely affected.
The Medicare program and its reimbursement rates and rules are subject to frequent change. These include statutory and regulatory changes, rate adjustments (including retroactive adjustments), administrative or executive orders and government funding restrictions, all of which may materially adversely affect the rates at which Medicare reimburses us for our services. Budget pressures often lead the federal government to reduce or place limits on reimbursement rates under Medicare. Implementation of these and other types of measures has in the past and could in the future result in substantial reductions in our revenue and operating margins. Prior reductions in governmental reimbursement rates partially contributed to our bankruptcy filing under Chapter 11 of the United States Bankruptcy Code in October 2001.
23
Table of Contents
In addition, the federal government often changes the rules governing the Medicare program, including those governing reimbursement. Changes that could adversely affect our business include:
| • | administrative or legislative changes to base rates or the bases of payment; |
| • | limits on the services or types of providers for which Medicare will provide reimbursement; |
| • | the reduction or elimination of annual rate increases; or |
| • | an increase in co-payments or deductibles payable by beneficiaries. |
Given the history of frequent revisions to the Medicare program and its reimbursement rates and rules, we may not continue to receive reimbursement rates from Medicare that sufficiently compensate us for our services or, in some instances, cover our operating cots. Limits on reimbursement rates or the scope of services being reimbursed could have a material adverse effect on our revenues, financial condition and results of operations. For a more comprehensive description of recent changes in reimbursement rates provided by Medicare, see Item 1 of this report, “Business—Sources of Reimbursement—Medicare.”
We are subject to a Medicare cap amount for our hospice business. Our net patient service revenue and profitability could be adversely affected by limitations on Medicare payments.
Overall payments made by Medicare to us on a per hospice basis are subject to a cap amount. Total Medicare payments received for services rendered from November 1 through October 31 by each of our Medicare-certified programs during this period are compared to the cap amount for the relevant period. Payments in excess of the cap amount must be returned by us to Medicare. The cap amount for hospice services is calculated by multiplying the number of beneficiaries electing hospice care from October 1 through September 30 by a statutory Medicare cap amount that is indexed for inflation. The Medicare cap amount is reduced proportionately for Medicare patients who transferred into or out of our hospice programs and either received or will receive hospice services from another hospice provider. The hospice cap amount is computed on a hospice-specific basis.
Our net patient service revenue for the year ended December 31, 2009 was reduced by approximately $2.1 million as a result of our hospice programs exceeding the Medicare cap. In 2010 our hospice program did not exceed the Medicare cap limit. Our ability to comply with this limitation depends on a number of factors relating to a given hospice program, including number of admissions, average length of stay, mix in level of care and Medicare patients that transfer into and out of our hospice programs. Our revenue and profitability may be materially reduced if we are unable to comply with this and other Medicare payment limitations. We cannot assure you that additional hospice programs will not exceed the cap amount in the future or that our estimate of the Medicare cap contractual adjustment will not differ materially from the actual Medicare cap amount. Amounts that we receive in excess of the cap are required to be repaid to Medicare.
The accuracy of our estimates of the Medicare cap contractual adjustment is affected by many factors, including:
| • | the actual number of Medicare beneficiary patient admissions and discharges and the dates of occurrence of each; |
| • | changes in the average length of stay at our hospice programs; |
| • | fluctuations in admissions and discharges at our hospice programs; |
| • | possible enrollment of beneficiaries in our hospice programs who may have previously elected Medicare hospice coverage through another hospice program and whose Medicare cap amount is prorated for the days of service for the previous hospice admission; |
| • | fiscal intermediary disallowances of certain beneficiaries and changes in calculation methodology; |
24
Table of Contents
| • | uncertainty surrounding length of patient stay in various patient groups, particularly with respect to non-cancer patients; and |
| • | the need to estimate, for each fiscal year, the Medicare cap amount in advance of CMS’ determination of the actual Medicare cap for the relevant period. |
We actively monitor the Medicare cap amount and seek to implement corrective measures as necessary. We maintain what we believe are adequate allowances in the event that we exceed the Medicare cap in any give fiscal year; however, because of the many variables involved in estimating the Medicare cap contractual adjustment that are beyond our control, we cannot assure you that we will not increase or decrease our estimated contractual allowance in the future.
We expect the federal and state governments to continue their efforts to contain growth in Medicaid expenditures, which could adversely affect our revenue and profitability.
We receive a significant portion of our revenue from Medicaid, which accounted for 31.7% and 31.9% of our total revenue during 2010 and 2009, respectively. In addition, many private payors for our third-party rehabilitation therapy services are reimbursed under the Medicaid program for services that we provided to patients. Accordingly, if Medicaid reimbursement rates are reduced or fail to increase as quickly as our costs, or if there are changes in the rules governing the Medicaid program that are disadvantageous to our business or industry, our business and results of operations could be adversely affected.
Medicaid is a state-administered program financed by both state funds and matching federal funds. Medicaid spending has increased rapidly in recent years, becoming a significant component of state budgets. This, combined with slower state revenue growth, has led both the federal government and many states to institute measures aimed at controlling the growth of Medicaid spending. For example, the DRA included several measures that were expected to reduce Medicare and Medicaid payments to skilled nursing facilities by $100.0 million over five years (2006-2010). These included limiting the circumstances under which an individual may become financially eligible for nursing home services under Medicaid, which could result in fewer patients being able to afford our services. Moreover, the federal Medicaid Integrity Contractor (MIC) program is increasing the scrutiny placed on Medicaid payments, and could result in recoupments of alleged overpayments in an effort to rein in Medicaid spending; the Mid-Session Review of the presidential budget submitted for federal fiscal year 2010 included, through federal fiscal year 2014, $490.0 million in savings from improving “Medicare and Medicaid program integrity,” and another $175.0 million in Medicaid savings through implementation of coding edits to ensure “appropriate Medicaid payments.” It is uncertain what proportion of these estimated cost savings will come from recoupments against long-term care facilities. However, despite the savings projected from effectively reducing payments to Medicaid providers, we note that the Mid-Session Review of the presidential budget submitted for federal fiscal year 2010 also included an outlay of $1.5 billion for Medicaid spending through federal fiscal year 2014, with a net increase in Medicaid outlays of $48.0 billion during the same time period. In fiscal year 2010, for example, the federal share of current law Medicaid outlays is expected to be $284.0 billion, a $26.0 billion (10.1%) increase over projected fiscal year 2009 spending. Some of the projected increases in Medicaid outlays are pursuant to the American Recovery and Reinvestment Act, passed in February 2009, which contained several temporary measures expected to increase Medicaid expenditures. In order to qualify for increases in Medicaid matching funds from the federal government, states cannot implement eligibility standards, methodologies or procedures that are more restrictive than those in effect as of July 1, 2008 and, in addition, must comply with prompt pay requirements when making Medicaid payments. We can provide no assurances regarding the temporary measures’ actual effect on Medicaid claims payment in any particular state, whether these temporary measures will eventually be made permanent, or what effect, if any, they will have on our business. Despite these temporary measures and the general projected increase in overall Medicaid expenditures over the next five years, we expect continued efforts to contain Medicaid expenditures generally.
25
Table of Contents
The California Legislature initially had extended its facility specific cost based Medi-Cal long-term care reimbursement system enacted through Assembly Bill 1629 (A.B. 1629) through the 2009-2010 and 2010-2011 rate years with a growth rate of up to five percent for both years. However, due to California’s severe budget crisis in 2009, on July 24, 2009, the California Legislature passed a budget balancing proposal that eliminated this five percent growth cap by amending the then-current statute to provide that, for the 2009-2010 and 2010-2011 rate years, the weighted average Medi-Cal reimbursement rate paid to long-term care facilities shall not exceed the weighted average Medi-Cal reimbursement rate for the 2008-2009 rate year. Despite the California Legislature’s decision in 2009 to hold the growth cap flat for the 2010-2011 rate year and California’s continuing budget crisis in 2010, on October 19, 2010, the California Legislature passed a budget trailer bill that extended A.B. 1629 through the 2011-2012 rate year and ameliorated the 2009 growth cap reductions. The Legislature amended the current statute to provide that, for the 2010-2011 rate year, the weighted average Medi-Cal reimbursement rate paid to long-term care facilities shall not exceed 3.93% if the increase in the federal medical assistance percentage (FMAP) pursuant to the federal American Recovery and Reinvestment Act of 2009 (ARRA) (Public Law 111-5) is extended for the entire 2010-2011 rate year, or 3.14%, if the increase in the FMAP pursuant to the ARRA is not extended for that period of time, plus the projected cost of complying with new state or federal mandates. In addition, the budget trailer bill provided that for the 2011-2012 rate year, the weighted average Medi-Cal reimbursement rate paid to long-term care facilities shall not exceed 2.4%, plus the projected cost of complying with new state or federal mandates. Moreover, the budget trailer bill extended a change to the A.B. 1629 long-term care reimbursement system that was implemented in July of 2009 as a result of California’s 2009 budget crisis; namely, the amounts that California nursing facilities will pay to Medi-Cal in quality assurance fees for the 2009-2010 to 2011-2012, inclusive, rate years will include Medicare revenue in the calculation of the quality assurance fee that nursing facilities pay under A.B. 1629. California’s Governor signed the budget trailer bill into law on October 21, 2010. Despite its passage on October 21, 2010, these changes in reimbursement to long-term care facilities will be implemented retroactively to the beginning of the calendar quarter in which California submitted its request for federal approval to CMS. Most recently, on January 10, 2011, California Governor Jerry Brown sent the Legislature a proposed Budget for 2011-12. The Budget proposes to reduce Medi-Cal provider payments by 10%, including payments to long-term care facilities. Since a significant portion of our revenue is generated from our operation in California of nursing facilities and long-term care facilities that serve Medi-Cal beneficiaries, these Budget reductions, if approved, could adversely affect our net patient service revenue and profitability. Given that Medicaid outlays are a significant component of state budgets, we expect continuing cost containment pressures on Medicaid outlays for skilled nursing facilities in the states in which we operate. Additional states in which we operate, most notably Texas, have also proposed Medicaid spending reductions in response to state budget issues.
Recent federal government proposals could limit the states’ use of provider tax programs to generate revenue for their Medicaid expenditures, which could result in a reduction in our reimbursement rates under Medicaid.
To generate funds to pay for the increasing costs of the Medicaid program, many states utilize financial arrangements commonly referred to as “provider taxes.” Under provider tax arrangements, states collect taxes from healthcare providers and then use the revenue to pay the providers as a Medicaid expenditure, which allows the states to then claim additional federal matching funds on the additional reimbursements. Under current federal law, the maximum allowable provider tax is 5.5% of the provider’s total revenue (scheduled to increase to 6.0% in October 2011). There can be no assurance that federal law will continue to provide matching federal funds on state Medicaid expenditures funded through provider taxes, or that the current caps on provider taxes will not be reduced. Any discontinuance or reduction in federal matching of provider tax-related Medicaid expenditures could have a significant and adverse effect on states’ Medicaid expenditures, and as a result could have a material and adverse effect on our financial condition and results of operations.
Revenue we receive from Medicare and Medicaid is subject to potential retroactive reduction.
Payments we receive from Medicare and Medicaid can be retroactively adjusted after a new examination during the claims settlement process or as a result of post-payment audits. Payors may disallow our requests for
26
Table of Contents
reimbursement based on determinations that certain costs are not reimbursable because either adequate or additional documentation was not provided or because certain services were not covered or deemed to be medically necessary. Significant adjustments to our Medicare or Medicaid revenues could adversely affect our financial condition and results of operations.
Through a “demonstration project” in New York, Florida and California, mandated by the Medicare Prescription Drug Improvement and Modernization Act of 2003, and effective March 2005 through March 2008, third-party recovery audit contractors, or RACs, operating in the Medicare Integrity Program work to identify alleged Medicare overpayments based on the medical necessity of rehabilitation services that have been provided. Each RAC is paid based on a percentage of overpayments and underpayments recovered. In September 2008, CMS issued a report on the RAC demonstration in which it indicated its intent to gradually implement a “permanent” nationwide RAC program by January 1, 2010 with a number of modifications that respond to issues identified in the demonstration. On October 6, 2008, CMS announced the selection of the four new RAC contractors and a RAC expansion schedule indicating phased implementation of the permanent programs beginning on October 1, 2008. On November 4, 2008, CMS announced a stay of the program pending further notice and on February 4, 2009, CMS announced that they have lifted the stop work order and will continue with implementation. The scope of claims subject to review under the permanent RAC program includes claims up to three years old but beginning with claims from October 1, 2007 or later.
The RACs have made certain revenue recapments from our California skilled nursing facilities and third-party skilled nursing facilities to which we provide rehabilitation therapy services. As of December 31, 2010, we fully reserved all denied claims.
Health reform legislation could adversely affect our revenue and financial condition.
In recent years, there have been numerous initiatives on the federal and state levels for comprehensive reforms affecting the payment for, the availability of and reimbursement for healthcare services in the United States. These initiatives have ranged from proposals to fundamentally change federal and state healthcare reimbursement programs, including the provision of comprehensive healthcare coverage to the public under governmental funded programs, to minor modifications to existing programs. The PPACA, which was passed in 2010 and has implementation timing and costs and regulatory implications that are still uncertain in many respects, is among the most comprehensive and notable of these legislative efforts. See Item 1 of this report, “Business—Government Regulation—Federal Health Care Reform” for more information regarding the PPACA. The ultimate content or timing of any future health reform legislation, and its impact on us, is impossible to predict. If significant reforms are made to the U.S. healthcare system, those reforms may have an adverse effect on our financial condition and results of operations.
In addition, we incur considerable administrative costs in monitoring the changes made within the various reimbursement programs in which we participate determining the appropriate actions to be taken in response to those changes and implementing the required actions to meet the new requirements and minimize the repercussions of the changes to our organization, reimbursement rates and costs.
27
Table of Contents
We are subject to extensive and complex laws and government regulations. If we are not operating in compliance with these laws and regulations or if these laws and regulations change, we could be required to make significant expenditures or change our operations in order to bring our facilities and operations into compliance.
We, along with other companies in the healthcare industry, are required to comply with extensive and complex laws and regulations at the federal, state and local government levels relating to, among other things:
| • | licensure and certification; |
| • | adequacy and quality of healthcare services; |
| • | qualifications of healthcare and support personnel; |
| • | quality of medical equipment; |
| • | confidentiality, maintenance and security issues associated with medical records and claims processing; |
| • | relationships with physicians and other referral sources and recipients; |
| • | constraints on protective contractual provisions with patients and third-party payors; |
| • | operating policies and procedures; |
| • | addition of facilities and services; and |
| • | billing for services. |
Many of these laws and regulations are expansive, and we do not always have the benefit of significant regulatory or judicial interpretation of these laws and regulations. In addition, many of these laws and regulations evolve to include additional obligations and restrictions. Certain other regulatory developments, such as revisions in the building code requirements for assisted living and skilled nursing facilities, mandatory increases in scope and quality of care to be offered to residents, revisions in licensing and certification standards, and regulations restricting those we can hire could also have a material adverse effect on us. In the future, different interpretations or enforcement of these laws and regulations could subject our current or past practices to allegations of impropriety or illegality or could require us to make changes in our facilities, equipment, personnel, services, capital expenditure programs and operating expenses.
One development potentially restricting those we may hire was a decision on November 3, 2010 by the Physical Therapy Board of California (“PT Board”) to rescind their 1990 Resolution which determined that the offering of physical therapy services by a corporation, not organized as a professional corporation, was permitted by the Physical Therapy Practice Act, which is the California statute governing the provision of physical therapy within the state. This decision essentially prohibits employment of a physical therapist by any professional corporation except those owned by physical therapists and Naturopaths. In its decision, the PT Board indicates its intent to commence enforcing the opinion immediately. However, it noted that those corporations formed before November 3, 2010, as a result of the 1990 Resolution, will not be subject to discipline by the Board. We have subsidiary corporations that employ physical therapists, but are not owned by physical therapists. These corporations were formed before November 3, 2010. While the PT Board noted that it will not subject such corporations to discipline, the PT Board may take the position that these corporations will not continue to qualify for the exception from discipline if they perform certain acts, such as forming subsidiaries, entering into mergers, or even hiring new employees. Additionally, the PT Board could eventually decide that it will subject all lay corporations that employ physical therapists to discipline. If this occurs, we may have to significantly restructure the operations of our company to conform to these requirements.
28
Table of Contents
In addition, federal and state government agencies have increased and coordinated civil and criminal enforcement efforts as part of numerous ongoing investigations of healthcare companies and, in particular, skilled nursing facilities. This includes investigations of:
| • | fraud and abuse; |
| • | quality of care; |
| • | financial relationships with referral sources; and |
| • | the medical necessity of services provided. |
We are unable to predict the future course of federal, state and local regulation or legislation, including Medicare and Medicaid statutes and regulations, the intensity of federal and state enforcement actions or the extent and size of any potential sanctions, fines or penalties. Changes in the regulatory framework, our failure to obtain or renew required regulatory approvals or licenses or to comply with applicable regulatory requirements, the suspension or revocation of our licenses or our disqualification from participation in federal and state reimbursement programs, or the imposition of other enforcement sanctions, fines or penalties could have a material adverse effect upon our results of operations, financial condition and liquidity. Furthermore, should we lose licenses or certifications for a number of our facilities as a result of regulatory action or otherwise, we could be deemed to be in default under some of our agreements, including agreements governing outstanding indebtedness and the report of such issues at one of our facilities could harm our reputation for quality care and lead to a reduction in our patient referrals and ultimately our revenue and operating income. For a discussion of the material government regulations applicable to our business, see Item 1 of this report, “Business—Government Regulation.”
We face periodic reviews, audits and investigations under federal and state government programs and contracts. These audits could have adverse findings that may negatively affect our business.
As a result of our participation in the Medicare and Medicaid programs, we are subject to various governmental reviews, audits and investigations to verify our compliance with these programs and applicable laws and regulations. Managed care payors may also reserve the right to conduct audits. An adverse review, audit or investigation could result in:
| • | refunding amounts we have been paid pursuant to the Medicare or Medicaid programs or from managed care payors; |
| • | state or federal agencies imposing fines, penalties and other sanctions on us; |
| • | temporary suspension of payment for new patients to the facility; |
| • | decertification or exclusion from participation in the Medicare or Medicaid programs or one or more managed care payor networks; |
| • | damage to our reputation; |
| • | the revocation of a facility’s license; and |
| • | loss of certain rights under, or termination of, our contracts with managed care payors. |
We have in the past and will likely in the future be required to refund amounts we have been paid as a result of these reviews, audits and investigations.
Significant legal actions, which are commonplace in our industry, could subject us to increased operating costs and substantial uninsured liabilities, which would materially and adversely affect our results of operations, liquidity and financial condition.
The long-term care industry has experienced an increasing trend in the number and severity of litigation claims involving punitive damages and settlements. We believe that this trend is endemic to the industry and is a result of the increasing number of large judgments, including large punitive damage awards, against long-term
29
Table of Contents
care providers in recent years resulting in an increased awareness by plaintiffs’ lawyers of potentially large recoveries. While some states have enacted tort reform legislation that limits plaintiffs’ recoveries in some respects, should our professional liability and general liability increase significantly in the future, we may not be able to increase our revenue sufficiently to cover the cost increases, our operating income could suffer, and we may not be able to meet our obligations to repay our liabilities. For a discussion of recent litigation claims against us, including the Lavender Case, see Note 12, “Commitments and Contingencies—Litigation,” to the consolidated financial statements under Part IV, Item 15 of this report.
We also are subject from time to time to lawsuits under the federal False Claims Act and comparable state laws for submitting allegedly fraudulent or otherwise inappropriate bills for services to the Medicare and Medicaid programs. These lawsuits, which may be initiated by regulatory authorities as well as private party whistleblowers, can involve significant monetary damages, fines, attorney fees and the award of bounties to private plaintiffs who successfully bring these suits, as well as to the government programs. For a discussion of recent amendments to the False Claims Act, see Item 1 of this report, “Business—Government Regulation—False Claims.”
We could face significant financial difficulties as a result of one or more of the risks discussed above, which could cause us to seek protection under bankruptcy laws or could cause our creditors to have a receiver appointed on our behalf.
We could face significant financial difficulties if Medicare or Medicaid reimbursement rates are reduced, patient demand for our services is reduced or we incur unexpected liabilities or expenses, including in connection with legal actions, sanctions, penalties or fines. This financial difficulty could cause us to seek protection under bankruptcy laws or could cause our creditors to have a receiver appointed on our behalf.
A significant portion of our business is concentrated in certain geographical markets, and an economic downturn or changes in the laws affecting our business in those markets could have a material adverse effect on our operating results.
In 2010, we received approximately 41.9% and 23.2% of our revenue from operations in California and Texas, respectively, and in 2009, we received approximately 44.3% and 25.2% of our revenue from operations in California and Texas, respectively. Accordingly, economic conditions and changes in state healthcare spending prevailing in either of these markets could affect the ability of our patients and third-party payors to reimburse us for our services, either through a reduction of the tax base used to generate state funding of Medicaid programs, an increase in the number of indigent patients eligible for Medicaid benefits, changes in state funding levels or healthcare programs or other factors. For instance, as a result of state budget shortfalls in California, in January 2011 the state Governor proposed significant cuts in a variety of state programs, including Medi-Cal. A continued or prolonged economic downturn, significant changes in state healthcare spending, or changes in the laws affecting our business in these markets could have a material adverse effect on our financial position, results of operations and cash flows.
Failure to maintain effective internal control over our financial reporting could have an adverse effect on our ability to report our financial results on a timely and accurate basis.
We produce our consolidated financial statements in accordance with the requirements of GAAP. Effective internal control over financial reporting is necessary for us to provide reliable financial reports, to help mitigate the risk of fraud and to operate successfully. We are required by federal securities laws to document and test our internal control procedures in order to satisfy the requirements of the Sarbanes-Oxley Act of 2002, which requires annual management assessments of the effectiveness of our internal control over financial reporting. See Item 9A of this report, “Controls and Procedures.”
Testing and maintaining our internal control over financial reporting can divert our management’s attention from other matters that are important to our business. We may not be able to conclude on an ongoing basis that
30
Table of Contents
we have effective internal control over financial reporting in accordance with applicable law, or our independent registered public accounting firm may not be able or willing to issue an unqualified attestation report if we conclude that our internal control over financial reporting is not effective. If we fail to maintain effective internal control over financial reporting, or our independent registered public accounting firm is unable to provide us with an unqualified attestation report on our internal control, we could be required to take costly and time-consuming corrective measures, be required to restate the affected historical financial statements, be subjected to investigations and/or sanctions by federal and state securities regulators, and be subjected to civil lawsuits by security holders. Any of the foregoing could also cause investors to lose confidence in our reported financial information and in our company and would likely result in a decline in the market price of our stock and in our ability to raise additional financing if needed in the future.
Possible changes in the acuity mix of patients as well as payor mix and payment methodologies may significantly reduce our profitability or cause us to incur losses.
Our revenue is affected by our ability to attract a favorable patient acuity mix, and by our mix of payment sources. Changes in the type of patients we attract, as well as our payor mix among private payors, managed care companies, Medicare and Medicaid, significantly affect our profitability because not all payors reimburse us at the same rates. Particularly, if we fail to maintain our proportion of high-acuity patients or if there is any significant increase in the percentage of our population for which we receive Medicaid reimbursement, our financial position, results of operations and cash flow may be adversely affected.
It is difficult to attract and retain qualified nurses, therapists, healthcare professionals and other key personnel, which increases our costs related to these employees and could cause us to fail to comply with state staffing requirements at one or more of our facilities.
We rely on our ability to attract and retain qualified nurses, therapists and other healthcare professionals. The market for these key personnel is highly competitive, and we could experience significant increases in our operating costs due to shortages in their availability. Like other healthcare providers, we have experienced difficulties in attracting and retaining qualified personnel, especially facility administrators, nurses, therapists, certified nurses’ aides and other important healthcare personnel. We may continue to experience increases in our labor costs, primarily due to higher wages and greater benefits required to attract and retain qualified healthcare personnel, and such increases may adversely affect our profitability.
This tight labor market and high demand for such employees contributes to the high turnover among clinical professional staff. A shortage of qualified personnel at a facility could result in significant increases in labor costs and increased reliance on overtime and expensive temporary nurse staffing agencies, and could otherwise adversely affect operations at the affected facilities. If we are unable to attract and retain qualified professionals, our ability to adequately provide services to our residents and patients may decline and our ability to grow may be constrained.
If we are unable to comply with state minimum staffing requirements at one or more of our facilities, we could be subject to fines or other sanctions.
Increased attention to the quality of care provided in skilled nursing facilities has caused several states to mandate, and other states to consider mandating, staffing laws that require minimum nursing hours of direct care per resident per day. These minimum staffing requirements further increase the gap between demand for and supply of qualified professionals, and lead to higher labor costs.
We operate a number of facilities in California, which has enacted legislation aimed at establishing minimum staffing requirements for facilities operating in that state. This legislation requires that the California Department of Public Health, or DPH, promulgate regulations requiring each skilled nursing facility to provide a minimum of 3.2 nursing hours per patient day. DPH finalized five regulations regarding nurse staffing ratios on
31
Table of Contents
January 22, 2009. Among other things, these new regulations require three 8-hour shifts for nurse-to-patient staffing, describe documentation and notice requirements, and specify procedures for obtaining a waiver from per-shift staffing requirements at skilled nursing facilities. Although DPH finalized the regulations, initial implementation of the statute authorizing the regulations is contingent on an appropriation in the annual Budget Act or another statute. Because no appropriation was made and no additional statutes were enacted, the regulations did not become operational. Therefore, DPH has announced that it will continue its current practice of determining a facility’s compliance with the 3.2 hour of nursing services per patient day measure in accordance with its internal policy and through on-site reviews conducted during periodic licensing and certification surveys and in response to complaints. If the DPH determines that a facility is out of compliance with this staffing measure, the DPH may issue a notice of deficiency, or a citation, depending on the impact on patient care. A citation carries with it the imposition of monetary fines that can range from $100 to $100,000 per citation. The issuance of either a notice of deficiency or a citation requires the facility to prepare and implement an acceptable plan of correction. The Lavender case, as described above in Item 1—Business, included allegations that certain of our California skilled nursing facilities failed to meet state-mandated minimum staffing requirements. The Lavender case resulted in a jury verdict against us and certain of our affiliated skilled nursing companies that awarded $677 million in damages. The case was ultimately settled in September 2010, pursuant to which we were required to deposit into escrow a total of $50 million to cover certain settlement costs, and we may be required to pay additional funds into the escrow to the extent that our costs of complying with the injunction issued against us as part of the settlement is less than $9.6 million. For more information regarding the Lavender case and the settlement, see Note 12, Commitments and Contingencies—Litigation, in the notes to our consolidated financial statements included elsewhere in this report.
Our ability to satisfy any minimum staffing requirements depends upon our ability to attract and retain qualified healthcare professionals, including nurses, certified nurse’s assistants and other personnel. Attracting and retaining these personnel is difficult, given existing shortages of these employees in the labor markets in which we operate. Furthermore, if states do not appropriate additional funds (through Medicaid program appropriations or otherwise) sufficient to pay for any additional operating costs resulting from minimum staffing requirements, our profitability may be materially adversely affected.
If we fail to attract patients and residents and to compete effectively with other healthcare providers, our revenue and profitability may decline and we may incur losses.
The long-term healthcare services industry is highly competitive. Our skilled nursing facilities compete primarily on a local and regional basis with many long-term care providers, from national and regional chains to smaller providers owning as few as a single nursing center. We also compete under certain circumstances with inpatient rehabilitation facilities and long-term acute care hospitals. Increased competition could limit our ability to attract and retain patients, maintain or increase rates or to expand our business. Our ability to compete successfully varies from location to location and depends on a number of factors, including the number of competing facilities in local market, the types of services available, our local reputation for quality care of patients, the commitment and expertise of our staff and physicians, our local service offerings and treatment programs, the cost of care in each locality, and the physical appearance, location, age and condition of our facilities. If we are unable to attract patients to our facilities, particularly the high-acuity patients we target for our skilled nursing facilities, then our revenue and profitability will be adversely affected. Some of our competitors may have greater brand recognition and be more established in their respective communities than we are, and may have greater financial and other resources than we have. Competing long-term care companies may also offer newer facilities or different programs or services than we do, which, combined with the foregoing factors, may result in our competitors being more attractive to our current patients, to potential patients and to referral sources. Some of our competitors may accept a lower profit margins than we do, which could present significant price competition, particularly for managed care and private pay patients.
We also encounter competition in connection with our other related healthcare services, including our rehabilitation therapy services provided to third-party facilities, assisted living facilities, hospice care, home
32
Table of Contents
health services and institutional pharmacy services. Generally, this competition is national, regional and local in nature. Many companies competing in these industries have greater financial and other resources than we have. The primary competitive factors for these other related healthcare services are similar to those for our skilled nursing and rehabilitation therapy businesses and include reputation, the cost of services, the quality of services, responsiveness to patient/resident needs and the ability to provide support in other areas such as third-party reimbursement, information management and patient recordkeeping. Furthermore, given the relatively low barriers to entry and continuing healthcare cost containment pressures, we expect that the markets we service will become increasingly competitive in the future. Increased competition in the future could limit our ability to attract and retain patients and residents, maintain or increase our fees, or expand our business.
Insurance coverage may become increasingly expensive and difficult to obtain for long-term care companies, and our self-insurance may expose us to significant losses.
It may become more difficult and costly for us to obtain coverage for patient care liabilities and certain other risks, including property and casualty insurance. Insurance carriers may require long-term care companies to significantly increase their self-insured retention levels and/or pay substantially higher premiums for reduced coverage for most insurance coverages, including workers’ compensation, employee healthcare and patient care liability.
We self-insure a significant portion of our potential liabilities for several risks, including certain types of professional and general liability, workers’ compensation and employee healthcare benefits. Due to our self-insured retentions under our professional and general liability, workers’ compensation and employee healthcare benefits programs, including our election to self insure against workers’ compensation claims in Texas, there is no limit on the maximum number of claims or amount for which we can be liable in any policy period. We base our loss estimates on actuarial analyses, which determine expected liabilities on an undiscounted basis, including incurred but not reported losses, based upon the available information on a given date. It is possible, however, for the ultimate amount of losses to exceed our estimates and our insurance limits. In the event our actual liability exceeds our estimates for any given period, our results of operations and financial condition could be materially adversely impacted.
At December 31, 2010, we had $1.9 million in accruals for self-insured medical and dental, $17.6 million in accruals for known or potential uninsured general and professional liability claims, and $16.3 million in accruals for workers’ compensation claims, based on our claims experience and an independent actuarial review. We may need to increase our accruals as a result of future actuarial reviews and claims that may develop. An adverse determination in legal proceedings, whether currently asserted or arising in the future, could have a material adverse effect on our business.
If our referral sources fail to view us as an attractive long-term care provider, our patient base would likely decrease.
We rely significantly on appropriate referrals from physicians, hospitals and other healthcare providers in the communities in which we deliver our services to attract the kinds of patients we target. Our referral sources are not obligated to refer business to us and generally also refer business to healthcare providers. We believe many of our referral sources refer business to us as a result of the types of quality of our patient service and our efforts to establish and build a relationship with them. If we lose, or fail to maintain, existing relationships with our referral resources, fail to develop new relationships or if we are perceived by our referral sources for any reason as not providing high quality patient care, our volume of referrals would likely decrease, the quality of our patient mix could suffer and our revenue and profitability could decline.
33
Table of Contents
If we do not achieve or maintain a reputation for providing high quality of care, our business may be negatively affected.
Our ability to achieve or maintain a reputation for providing high quality of care to our patients at each of our skilled nursing and assisted living facilities, or through our rehabilitation therapy and hospice businesses, is important to our ability to attract and retain patients, particularly high-acuity patients. We believe that the perception of our quality of care by a potential patient or potential patient’s family seeking to contract for our services is influenced by a variety of factors, including doctor and other healthcare professional referrals, community information and referral services, newspapers and other print and electronic media, results of patient surveys, recommendations from family and friends, and quality care statistics or rating systems compiled and published by CMS or other industry data. Through our focus on retaining high quality staffing, reviewing feedback and surveys from our patients and referral sources to highlight areas of improvement and integrating our service offerings at each of our facilities, we seek to maintain and improve on the outcomes from each of the factors listed above in order to build and maintain a strong reputation at our facilities. If any of our skilled nursing or assisted living facilities fail to achieve or maintain a reputation for providing high-quality care, or is perceived to provide a lower quality of care than comparable facilities within the same geographic area, or users of our rehabilitation therapy services perceive that they could receive higher quality services from other providers, our ability to attract and retain patients at such facility could be adversely affected. If this perception were to become widespread within the areas in which we operate, our revenue and profitability could be adversely affected.
We may be unable to reduce costs to offset decreases in our occupancy rates or other expenses completely.
We depend on implementing adequate cost management initiatives in response to fluctuations in levels of occupancy in our skilled nursing and assisted living facilities and in other sources of income in order to maintain our current cash flow and earnings levels. Fluctuation in our occupancy levels may become more common as we increase our emphasis on patients with shorter stays but higher acuities. A decline in our occupancy rates could result in decreased revenue. If we are unable to put in place corresponding reductions in costs in response to decreases in our patient census or other revenue shortfalls, our financial condition and operating results could be adversely affected.
Consolidation of managed care organizations and other third-party payors or reductions in reimbursement from these payors may adversely affect our revenue and income or cause us to incur losses.
Managed care organizations and other third-party payors have continued to consolidate in order to enhance their ability to influence the delivery of healthcare services. Consequently, the healthcare needs of a large percentage of the United States population are increasingly served by a small number of managed care organizations. These organizations generally enter into service agreements with a limited number of providers for needed services. These organizations have become an increasingly important source of revenue and referrals for us. To the extent that such organizations terminate us as a preferred provider or engage our competitors as a preferred or exclusive provider, our business could be materially adversely affected.
In addition, private third-party payors, including managed care payors, are continuing their efforts to control healthcare costs through direct contracts with healthcare providers, increased utilization reviews, or reviews of the propriety of, and charges for, services provided, and greater enrollment in managed care programs and preferred provider organizations. As these private payors increase their purchasing power, they are demanding discounted fee structures and the assumption by healthcare providers of all or a portion of the financial risk associated with the provision of care. Significant reductions in reimbursement from these sources could materially adversely affect our business and financial condition.
34
Table of Contents
Delays in reimbursement may cause liquidity problems.
If we have information systems problems or payment or other issues arise with Medicare, Medicaid or other payors, we may encounter delays in our payment cycle. For example, the ARRA extended the benefits of Medicaid’s prompt pay requirements to hospitals and nursing facilities, such that states must generally pay valid Medicaid claims within 90 days of receipt. However, the extended ARRA prompt pay requirements are set to expire on June 30, 2011 in conjunction with the temporarily enhanced FMAP rates adopted under ARRA. If the prompt pay requirements are not further extended, state budget shortfalls or other matters affecting the amount and timing of state expenditures could lead to delays in Medicaid payments.
Any significant payment timing delay could cause us to experience working capital shortages. As a result, working capital management, including prompt and diligent billing and collection, is an important factor in our consolidated results of operations and liquidity. Our working capital management procedures may not successfully mitigate the effects of any delays in our receipt of payments or reimbursements. Accordingly, such delays could have an adverse effect on our liquidity and financial condition.
Our rehabilitation and other related healthcare services are also subject to delays in reimbursement, as we act as vendors to other providers who in turn must wait for reimbursement from other third-party payors. Each of these customers is therefore subject to the same potential delays to which our nursing homes are subject, meaning any such delays would further delay the date we would receive payment for the provision of our related healthcare services. To the extent we grow and expand the rehabilitation and other complementary services that we offer to third parties, we may incur increasing delays in payment for these services, and these payment delays could have an adverse effect on our liquidity and financial condition. We may also experience delays in reimbursement related to change of ownership applications for our acquired facilities, as well as changes in fiscal intermediaries.
Our success is dependent upon retaining key personnel.
Our senior management team has extensive experience in the healthcare industry. We believe that they have been instrumental in guiding our businesses, instituting valuable performance and quality monitoring, and driving innovation. Accordingly, our future performance is substantially dependent upon the continued services of our senior management team. The loss of the services of any of these persons could have a material adverse effect upon us.
Future acquisitions may use significant resources, may be unsuccessful and could expose us to unforeseen liabilities.
We intend to selectively pursue acquisitions of skilled nursing facilities, assisted living facilities and other related healthcare operations. Acquisitions may involve significant cash expenditures, debt incurrence, operating losses and additional expenses that could have a material adverse effect on our financial position, results of operations and liquidity. Acquisitions involve numerous risks, including:
| • | difficulties integrating acquired operations, personnel and accounting and information systems, or in realizing projected efficiencies and cost savings; |
| • | diversion of management’s attention from other business concerns; |
| • | potential loss of key employees or customers of acquired companies; |
| • | entry into markets in which we may have limited or no experience; |
| • | increasing our indebtedness and limiting our ability to access additional capital when needed; |
| • | assumption of unknown material liabilities or regulatory issues of acquired companies, including failure to comply with healthcare regulations or to establish internal financial controls; and |
| • | straining of our resources, including internal controls relating to information and accounting systems, regulatory compliance, logistics and others. |
35
Table of Contents
Furthermore, certain of the foregoing risks could be exacerbated when combined with other growth measures that we may pursue.
Global economic conditions may impact our ability to obtain additional financing on commercially reasonable terms or at all and our ability to expand our business may be harmed.
Recent global market and economic conditions have been very challenging with tight credit conditions and slow or negative economic growth in most major economies generally expected to continue in 2011 and possibly beyond. Ongoing concerns about the systemic impact of potential long-term and widespread recession, energy costs, geopolitical issues, the availability and cost of credit, and the global real estate and mortgage markets have contributed to increased market volatility, uncertainty and liquidity issues for both borrowers and investors. These conditions, combined with volatile energy and food prices, unstable business and consumer confidence, and significant unemployment, have contributed to pronounced economic volatility.
As a result of these market conditions, the cost and availability of credit has been and may continue to be adversely affected by illiquid credit markets, interest rate fluctuations and wider credit spreads. Concern about the stability of the markets generally and the strength of counterparties specifically has led many lenders and institutional investors to reduce, and in some cases, cease to provide credit to businesses and consumers. These factors have led to a decrease in spending by businesses and consumers alike, and a corresponding decrease in global infrastructure spending. Continued turbulence in the U.S. and international markets and economies and prolonged declines or stagnation in business and consumer spending may adversely affect our liquidity and financial condition, and the liquidity and financial condition of our customers, including our ability to refinance maturing liabilities and access the capital markets to meet liquidity needs.
As of December 31, 2010, we had approximately $69.6 million available for additional borrowing under our senior secured credit facility. If our remaining ability to borrow under our senior secured credit facility is insufficient for our capital requirements, we will be required to seek additional sources of financing, including issuing equity, which may be dilutive to our current stockholders or incurring additional debt. Our ability to incur additional debt is subject to the restrictions in the indenture governing our 11% senior subordinated notes and our senior secured credit facility. There can be no assurance that the restrictions contained in these agreements will permit us to borrow the funds that we need to finance our operations, or that additional debt will be available to us on commercially reasonable terms or at all. Furthermore, market conditions may impede our ability to secure additional sources of financing, whether through the extension of our existing senior secured credit facility or by accessing the debt and/or equity markets. If we are unable to obtain funds sufficient to finance our capital requirements, we may have to forego opportunities to expand our business, including the acquisition or development of additional or expanded facilities.
Our substantial indebtedness could adversely affect our financial health and prevent us from fulfilling our financial obligations.
We have now and will continue to have a significant amount of indebtedness. On December 31, 2010, our total indebtedness was approximately $519.9 million.
Our substantial indebtedness could have important consequences to you. For example, it could:
| • | increase our vulnerability to adverse economic and industry conditions; |
| • | require us to dedicate a substantial portion of our cash flow from operations to payments on our indebtedness, thereby reducing the availability of our cash flow to fund working capital, capital expenditures and other general corporate purposes; |
| • | limit our flexibility in planning for, or reacting to, changes in our business and the industry in which we operate; |
| • | place us at a competitive disadvantage compared to our competitors that have less debt; |
36
Table of Contents
| • | increase the cost or limit the availability of additional financing, if needed or desired, to fund future working capital, capital expenditures and other general corporate requirements, or to carry out other aspects of our business plan; |
| • | require us to maintain debt coverage and financial ratios at specified levels, reducing our financial flexibility; and |
| • | limit our ability to make strategic acquisitions and develop new or expanded facilities. |
In addition, if we are unable to generate sufficient cash flow or otherwise obtain funds necessary to make required debt payments, or if we fail to comply with the various covenants and requirements of our 11% senior subordinated notes, our senior secured credit facility or other existing or future indebtedness, we would be in default, which could permit the holders of our 11% senior subordinated notes and the holders of our other indebtedness, including our senior secured credit facility, to accelerate the maturity of the notes or such other indebtedness, as the case may be. Any default under our 11% senior subordinated notes, our senior secured credit facility, or our other existing or future indebtedness, as well as any of the above-listed factors, could have a material adverse effect on our business, operating results, liquidity and financial condition.
Despite our substantial indebtedness, we may still be able to incur more debt. This could intensify the risks associated with this indebtedness.
The terms of the indenture governing our 11% senior subordinated notes and our senior secured credit facility contain restrictions on our ability to incur additional indebtedness. These restrictions are subject to a number of important qualifications and exceptions, and the indebtedness incurred in compliance with these exceptions could be substantial. Accordingly, we could incur significant additional indebtedness in the future. The more we become leveraged, the more we become exposed to the risks described above under “Our substantial indebtedness could adversely affect our financial health and prevent us from fulfilling our financial obligations.”
Floating rate indebtedness subjects us to interest rate risk, which could cause our debt service obligations to increase.
Borrowings under our senior secured credit facility are subject to floating rates of interest over an interest rate floor of 1.5%. If interest rates increase over the floor, our debt service obligations on our variable rate indebtedness would increase even though the amount borrowed remained the same, and our net income and cash flows would correspondingly decrease. We have entered into interest rate cap agreement with a notional amount of $70.0 million with a cap on 1 month LIBOR of 2.0% from July 2010 to December 2011. We have entered into an interest rate swap agreement with a notional amount of $70.0 million, which effectively fixes the interest rate on that portion of our borrowings under our first lien credit agreement at 6.0% from January 1, 2012 through June 30, 2013. There can be no assurance that when the interest rate cap and swap agreements expire we will be able to enter into similar replacement hedging arrangements on favorable terms or at all. As of December 31, 2010, $287.3 million of borrowings under our Senior Secured Credit Facility is not hedged and is currently subject to floating rates of interest.
Our operations are subject to environmental and occupational health and safety regulations, which could subject us to fines, penalties and increased operational costs.
We are subject to a wide variety of federal, state and local environmental and occupational health and safety laws and regulations. Regulatory requirements faced by healthcare providers such as us include those relating to air emissions, wastewater discharges, air and water quality control, occupational health and safety (such as standards regarding blood-borne pathogens and ergonomics), management and disposal of low-level radioactive medical waste, biohazards and other wastes, management of explosive or combustible gases, such as oxygen, specific regulatory requirements applicable to asbestos, lead-based paints, polychlorinated biphenyls and mold, and providing notice to employees and members of the public about our use and storage of regulated or
37
Table of Contents
hazardous materials and wastes. Failure to comply with these requirements could subject us to fines, penalties and increased operational costs. Moreover, changes in existing requirements or more stringent enforcement of them, as well as discovery of currently unknown conditions at our owned or leased facilities, could result in additional cost and potential liabilities, including liability for conducting clean-up, and there can be no guarantee that such increased expenditures would not be significant.
A portion of our workforce has unionized and our operations may be adversely affected by work stoppages, strikes or other collective actions.
As of December 31, 2010, approximately 418 of our 9,736 full time employees were represented by unions and covered by collective bargaining agreements. In addition, certain labor unions have publicly stated that they are concentrating their organizing efforts within the long-term healthcare industry. We cannot predict the effect that continued union representation or future organizational activities will have on our business or future operations. There can be no assurance that we will not experience a material work stoppage in the future.
Disasters and similar events may seriously harm our business.
Natural and man-made disasters and similar events, including terrorist attacks and acts of nature such as hurricanes, tornados, earthquakes and wildfires, may cause damage or disruption to us, our employees and our facilities, which could have an adverse impact on our patients and our business. In order to provide care for our patients, we are dependent on consistent and reliable delivery of food, pharmaceuticals, utilities and other goods to our facilities, and the availability of employees to provide services at our facilities. If the delivery of goods or the ability of employees to reach our facilities were interrupted in any material respect due to a natural disaster or other reasons, it would have a significant impact on our facilities and our business. For example, in connection with Hurricane Katrina in New Orleans, several nursing home operators unaffiliated with us have been accused of not properly caring for their residents, which has resulted in, among other things, criminal charges being filed against the proprietors of those facilities. Furthermore, the impact, or impending threat, of a natural disaster has in the past and may in the future require that we evacuate one or more facilities, which would be costly and would involve risks, including potentially fatal risks, for the patients. The impact of disasters and similar events is inherently uncertain. Such events could harm our patients and employees, severely damage or destroy one or more of our facilities, harm our business, reputation and financial performance, or otherwise cause our business to suffer in ways that we currently cannot predict.
The efficient operation of our business is dependent on our information systems.
We depend on several information technology systems for the efficient functioning of our business. The software programs supporting these systems are licensed to us by independent software developers. Our inability or the inability of these developers, to continue to maintain and upgrade these information systems and software programs could disrupt or reduce the efficiency of our operations. In addition, costs and potential problems and interruptions associated with the implementation of new or upgraded systems and technology or with maintenance or adequate support of existing systems could also disrupt or reduce the efficiency of our operations.
Risks Related to Ownership of Our Class A Common Stock
We are controlled by Onex Corporation, whose interests may conflict with yours.
Our Class A common stock has one vote per share, while our Class B common stock has ten votes per share on all matters to be voted on by our stockholders. As of December 31, 2010, Onex Corporation, its affiliates and certain of our directors and members of our senior management who are party to a voting agreement with an affiliate of Onex Corporation owned shares of common stock representing over 75.0% of the combined voting power of our outstanding common stock. Accordingly, Onex Corporation generally has the power to control the outcome of matters on which stockholders are entitled to vote. Such matters include the election and removal of
38
Table of Contents
directors, the adoption or amendment of our certificate of incorporation and bylaws, possible mergers, corporate control contests and significant transactions. Through its control of elections to our board of directors, Onex Corporation may also have the ability to appoint or replace our senior management and cause us to issue additional shares of our common stock or repurchase common stock, declare dividends or take other actions. Onex Corporation may make decisions regarding our company and business that are opposed to our other stockholders’ interests or with which they disagree. Onex Corporation may also delay or prevent a change of control of us, even if the change of control would benefit our other stockholders, which could deprive our other stockholders of the opportunity to receive a premium for their Class A common stock. The significant concentration of stock ownership and voting power may also adversely affect the trading price of our Class A common stock due to investors’ perception that conflicts of interest may exist or arise. To the extent that the interests of our public stockholders are harmed by the actions of Onex Corporation, the price of our Class A common stock may be harmed.
Additionally, Onex Corporation is in the business of making investments in companies and currently holds, and may from time to time in the future acquire, controlling interests in businesses engaged in the healthcare industries that complement or directly or indirectly compete with certain portions of our business. Further, if it pursues such acquisitions in the healthcare industry, those acquisition opportunities may not be available to us.
If our stock price is volatile, purchasers of our Class A common stock could incur substantial losses.
Our stock price has been and is likely to continue to be volatile. The stock market in general often experiences substantial volatility that is seemingly unrelated to the operating performance of particular companies. These broad market fluctuations may adversely affect the trading price of our Class A common stock. The price for our Class A common stock may be influenced by many factors, including:
| • | the depth and liquidity of the market for our Class A common stock; |
| • | developments generally affecting the healthcare industry; |
| • | investor perceptions of us and our business; |
| • | actions by institutional or other large stockholders; |
| • | strategic actions, such as acquisitions or restructurings, or the introduction of new services by us or our competitors; |
| • | new laws or regulations or new interpretations of existing laws or regulations applicable to our business; |
| • | litigation and governmental investigations; |
| • | changes in accounting standards, policies, guidance, interpretations or principles; |
| • | adverse conditions in the financial markets or general economic conditions, including those resulting from war, incidents of terrorism and responses to such events; |
| • | sales of Class B common stock by Onex, us or members of our management team; |
| • | additions or departures of key personnel; and |
| • | our results of operations, financial performance and future prospects. |
These and other factors may cause the market price and demand for our Class A common stock to fluctuate substantially, which may limit or prevent investors from readily selling their shares of Class A common stock and may otherwise negatively affect the liquidity of our Class A common stock. In addition, in the past, when the market price of a stock has been volatile, holders of that stock have sometimes instituted securities class action litigation against the company that issued the stock. If any of our stockholders brought a lawsuit against us, we could incur substantial costs defending or settling the lawsuit. Such a lawsuit could also divert the time and attention of our management from our business.
39
Table of Contents
If securities or industry analysts do not publish research or reports about our business, if they change their recommendations regarding our stock adversely or if our operating results do not meet their expectations, our stock price and trading volume could decline.
The trading market for our Class A common stock is significantly influenced by the research and reports that industry or securities analysts publish about us or our business. If one or more of these analysts cease coverage of our company or fail to publish reports on us regularly, we could lose visibility in the financial markets, which in turn could cause our stock price or trading volume to decline. Moreover, if one or more of the analysts who cover us downgrade our stock or if our operating results do not meet their expectations, our stock price could decline.
We do not intend to pay dividends on our common stock.
We do not anticipate paying any cash dividends on our common stock in the foreseeable future. We currently anticipate that we will retain all of our available cash, if any, for use as working capital and for other general purposes, including to service or repay our debt and to fund the operation and expansion of our business. Any payment of future dividends will be at the discretion of our board of directors and will depend on, among other things, our earnings, financial condition, capital requirements, level of indebtedness, statutory and contractual restrictions applying to the payment of dividends and other considerations that our board of directors deems relevant.
We are a “controlled company” within the meaning of NYSE rules and, as a result, qualify for and rely on exemptions from certain corporate governance requirements.
Onex Corporation and its affiliates continue to control a majority of the voting power of our outstanding common stock and we are a “controlled company” within the meaning of NYSE corporate governance standards. Under the NYSE rules, a company of which more than 50% of the voting power is held by another person or group of persons acting together is a “controlled company” and may elect not to comply with certain NYSE corporate governance requirements, including the requirements that:
| • | a majority of the board of directors consist of independent directors; |
| • | the nominating and corporate governance committee be entirely composed of independent directors with a written charter addressing the committee’s purpose and responsibilities; |
| • | the compensation committee be entirely composed of independent directors with a written charter addressing the committee’s purpose and responsibilities; and |
| • | there be an annual performance evaluation of the nominating and corporate governance and compensation committees. |
We elect to be treated as a controlled company and thus utilize some of these exemptions. In addition, although we currently have a board composed of a majority of independent directors and have adopted charters for our audit, corporate governance, quality and compliance and compensation committees, and intend to conduct annual performance evaluations for these committees, none of these committees are composed entirely of independent directors, except for our audit committee. Accordingly, you may not have the same protections afforded to stockholders of companies that are subject to all of NYSE corporate governance requirements.
Our amended and restated certificate of incorporation, bylaws and Delaware law contain provisions that could discourage transactions resulting in a change in control, which may negatively affect the market price of our Class A common stock.
In addition to the effect that the concentration of ownership and voting power in our significant stockholders may have, our amended and restated certificate of incorporation and our amended and restated bylaws contain
40
Table of Contents
provisions that may enable our management to resist a change in control. These provisions may discourage, delay or prevent a change in the ownership of our company or a change in our management, even if doing so might be beneficial to our stockholders. In addition, these provisions could limit the price that investors would be willing to pay in the future for shares of our Class A common stock. The provisions in our amended and restated certificate of incorporation or amended and restated bylaws include:
| • | our board of directors is authorized, without prior stockholder approval, to create and issue preferred stock, commonly referred to as “blank check” preferred stock, with rights senior to those of our Class A common stock and Class B common stock; |
| • | advance notice requirements for stockholders to nominate individuals to serve on our board of directors or to submit proposals that can be acted upon at stockholder meetings; provided, that prior to the date that the total number of outstanding shares of our Class B common stock is less than 10% of the total number of shares of common stock outstanding, which we refer to as the Transition Date, no such requirement is required for holders of at least 10% of our outstanding Class B common stock; |
| • | our board of directors is classified so not all of the members of our board of directors are elected at one time, which may make it more difficult for a person who acquires control of a majority of our outstanding voting stock to replace our directors; |
| • | following the Transition Date, stockholder action by written consent will be prohibited; |
| • | special meetings of the stockholders are permitted to be called only by the chairman of our board of directors, our chief executive officer or by a majority of our board of directors; |
| • | stockholders are not permitted to cumulate their votes for the election of directors; |
| • | newly created directorships resulting from an increase in the authorized number of directors or vacancies on our board of directors will be filled only by majority vote of the remaining directors; |
| • | our board of directors is expressly authorized to make, alter or repeal our bylaws; and |
| • | stockholders are permitted to amend our bylaws only upon receiving at least 66 2/3% of the votes entitled to be cast by holders of all outstanding shares then entitled to vote generally in the election of directors, voting together as a single class. |
After the Transition Date, we will also be subject to the provisions of Section 203 of the Delaware General Corporation Law, which may prohibit certain business combinations with stockholders owning 15% or more of our outstanding voting stock. These and other provisions in our amended and rested certificate of incorporation, amended and restated bylaws and Delaware law could discourage acquisition proposals and make it more difficult or expensive for stockholders or potential acquirers to obtain control of our board of directors or initiate actions that are opposed by our then-current board of directors, including delaying or impeding a merger, tender offer or proxy contest involving us. Any delay or prevention of a change of control transaction or changes in our board of directors could cause the market price of our Class A common stock to decline.
| Item 1B. | Unresolved Staff Comments |
Not applicable.
41
Table of Contents
| Item 2. | Properties |
As of December 31, 2010, we operated 100 long-term care facilities, 77 of which were owned and 23 of which were leased. As of December 31, 2010, our operated facilities had a total of 10,830 licensed beds.
The following table provides information by state as of December 31, 2010 regarding the skilled nursing and assisted living facilities we owned and leased.
| Owned Facilities | Leased Facilities | Total Facilities | ||||||||||||||||||||||
| Number | Licensed Beds |
Number | Licensed Beds |
Number | Licensed Beds |
|||||||||||||||||||
| California |
17 | 1,833 | 14 | 1,735 | 31 | 3,568 | ||||||||||||||||||
| Kansas |
26 | 1,422 | — | — | 26 | 1,422 | ||||||||||||||||||
| Texas |
22 | 3,203 | — | — | 22 | 3,203 | ||||||||||||||||||
| Nevada |
1 | 100 | 1 | 190 | 2 | 290 | ||||||||||||||||||
| Missouri |
7 | 1,007 | — | — | 7 | 1,007 | ||||||||||||||||||
| New Mexico |
2 | 208 | 8 | 968 | 10 | 1,176 | ||||||||||||||||||
| Iowa |
2 | 164 | — | — | 2 | 164 | ||||||||||||||||||
| Total |
77 | 7,937 | 23 | 2,893 | 100 | 10,830 | ||||||||||||||||||
| Skilled nursing |
57 | 6,939 | 21 | 2,627 | 78 | 9,566 | ||||||||||||||||||
| Assisted living |
20 | 998 | 2 | 266 | 22 | 1,264 | ||||||||||||||||||
Our executive offices are located in Foothill Ranch, California, where we lease office space, a portion of which is utilized for the administrative functions of our businesses. The term of this lease expires on June 30, 2013. We have an option to renew our lease at this location for an additional five-year term.
| Item 3. | Legal Proceedings |
For information regarding certain pending legal proceedings to which we are a party or our property is subject, see Note 12, “Commitments and Contingencies—Litigation,” to our consolidated financial statements included elsewhere in this report, which is incorporated herein by reference.
We are from time to time party to various legal actions and administrative proceedings and are subject to various claims arising in the ordinary course of business, including claims that our services have resulted in injury or death to patients of our subsidiaries and claims related to employment and commercial matters. Although we intend to vigorously defend ourselves in these matters, there can be no assurance that the outcomes of these matters will not have a material adverse effect on our results of operations and financial condition. In certain states in which we have or have had operations, insurance coverage for the risk of punitive damages arising from general and professional liability litigation may not be available due to state law public policy prohibitions. There can be no assurance that we will not be liable for punitive damages awarded in litigation arising in states for which punitive damage insurance coverage is not available.
We operate in a highly-regulated industry. As such, in the ordinary course of business, we are continuously subject to state and federal regulatory scrutiny, supervision and control. Such regulatory scrutiny often includes inquiries, investigations, examinations, audits, site visits and surveys, some of which are non-routine. In addition to being subject to direct regulatory oversight of state and federal regulatory agencies, our industry is frequently subject to the regulatory practices, which could subject us to civil, administrative or criminal fines, penalties or restitution relief, and reimbursement authorities could also seek the suspension or exclusion of the provider or individual from participation in their program. We believe that there has been, and will continue to be, an increase in governmental investigations of healthcare providers, particularly in the area of Medicare/Medicaid false claims, as well as an increase in enforcement actions resulting from these investigations. Adverse outcomes in legal proceedings or governmental investigations against us, whether currently asserted or arising in the future, could have a material adverse effect on our business and financial condition.
| Item 4. | Removed and Reserved |
42
Table of Contents
PART II
| Item 5. | Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities |
Our Class A common stock is listed on the New York Stock Exchange under the symbol “SKH.” Information with respect to sales prices and record holders of our Class A common stock is set forth below. There is no established trading market for our Class B common stock.
Market Information
The following table sets forth, for the indicated quarterly periods, the high and low sale prices of our Class A common stock as reported by the New York Stock Exchange:
| Year Ended December 31, 2010 |
High ($) | Low ($) | ||||||
| First quarter |
7.94 | 5.83 | ||||||
| Second quarter |
8.23 | 6.08 | ||||||
| Third quarter |
6.81 | 1.43 | ||||||
| Fourth quarter |
9.20 | 3.51 | ||||||
| Year Ended December 31, 2009 |
High ($) | Low ($) | ||||||
| First quarter |
10.69 | 7.60 | ||||||
| Second quarter |
11.38 | 6.40 | ||||||
| Third quarter |
9.00 | 6.53 | ||||||
| Fourth quarter |
9.36 | 6.55 | ||||||
On February 9, 2011, the closing sales price of our Class A common stock on the New York Stock Exchange was $12.39 per share. On that date, there were 9 holders of record of our Class A common stock and 30 holders of record of our Class B common stock.
Dividend Payment
We did not declare or pay cash dividends in either 2010 or 2009 on our Class A common stock or Class B common stock. We do not anticipate paying any cash dividends on our common stock in the foreseeable future. We currently anticipate that we will retain all of our available cash, if any, for use as working capital and for other general purposes, including to service or repay our debt and to fund the operation and expansion of our business.
Purchases of Equity Securities by the Issuer and Affiliated Purchasers
We did not repurchase any of our outstanding shares in the fourth quarter of 2010.
The table below sets forth information with respect to purchases of our Class A common stock made by us or on our behalf during the quarter ended December 31, 2010:
| Period |
Total Number of Shares Purchased(1) |
Average Price Paid per Share |
Total Number of Shares Purchase as Part of Publicly Announced Plans or Programs |
Maximum Dollar Value of Shares that May Yet Be Purchased Under the Plans or Programs |
||||||||||||
| October 1 - 31, 2010 |
— | $ | — | n/a | n/a | |||||||||||
| November 1 - 30, 2010 |
183 | $ | 5.25 | n/a | n/a | |||||||||||
| December 1 - 31, 2010 |
— | $ | — | n/a | n/a | |||||||||||
| Total: |
183 | $ | 5.25 | n/a | n/a | |||||||||||
| (1) | Reflects shares forfeited to us upon the vesting of restricted stock granted to participants in our 2007 Incentive |
43
Table of Contents
Award Plan, to satisfy applicable tax withholding obligations with respect to such vesting. We did not have any publicly announced plans or programs to purchase our Class A common stock in the quarter ended December 31, 2010.
Securities Authorized for Issuance Under Equity Compensation Plans
We primarily issue stock options and restricted stock under our share-based compensation plans, which are part of a broad-based, long-term retention program that is intended to attract and retain talented employees and directors, and align stockholder and employee interests.
Pursuant to our Amended and Restated Skilled Healthcare Group, Inc. 2007 Incentive Award Plan, or 2007 Plan, we grant stock-based awards, including stock options, restricted stock awards, and restricted stock units, to employees and directors. Options are granted to purchase shares of our Class A common stock at a price not less than the fair market value of our Class A common stock on the date of grant. The 2007 Plan provides for the grant of incentive and non-qualified stock options as well as stock appreciation rights, restricted stock, restricted stock units, performance units and shares, and other stock-based awards. Generally, option grants and restricted stock awards to employees vest over four years and are exercisable for up to 10 years from the grant date. The Board of Directors may terminate the 2007 Plan at any time. Only shares of our Class A common stock can be issued or transferred pursuant to awards under the 2007 Plan.
Additional information regarding our stock option plans and plan activity for fiscal 2010, 2009 and 2008 is provided in the notes to our consolidated financial statements in this annual report, see “ Note 11—Stock-Based Compensation.”
The equity compensation plan information required by this Item is set forth in Part III, Item 12 “Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters” of this report contains information concerning securities authorized for issuance under our equity compensation plans.
44
Table of Contents
Stock Performance Graph
The following graph illustrates a comparison of the total cumulative stockholder return on our Class A common stock since May 15, 2007, which is the date our Class A common stock first began trading on the New York Stock Exchange, to three indices: the S&P 500, the Hemscott Long-Term Care Index and the Morningstar Long-Term Care Index. The graph assumes an initial investment of $100 on May 15, 2007, assuming reinvestment of dividends, if any. The comparisons in the graph are required by the Securities and Exchange Commission and are not intended to forecast or be indicative of possible future performance of our Class A common stock. The following graph and related information shall not be deemed “soliciting material” or deemed to be “filed” with the Securities and Exchange Commission, nor shall such information be incorporated by reference into any SEC filing unless we specifically incorporate it by reference into the particular filing.
COMPARISON OF CUMULATIVE TOTAL RETURN ON INVESTMENT
Assuming $100 Investment on May 15, 2007 (IPO)
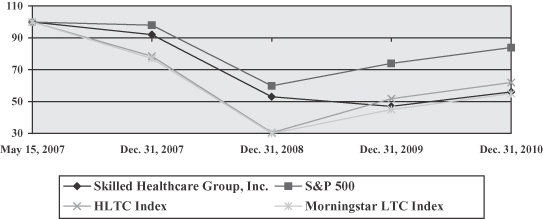
| 5/15/07 | 12/31/07 | 12/31/08 | 12/31/09 | 12/31/10 | ||||||||||||||||
| Skilled Healthcare Group, Inc. |
$ | 100.00 | $ | 92.01 | $ | 53.08 | $ | 46.86 | $ | 56.48 | ||||||||||
| S&P 500 |
100.00 | 97.81 | 60.17 | 74.28 | 83.78 | |||||||||||||||
| HLTC Index |
100.00 | 78.00 | 30.00 | 52.00 | 62.00 | |||||||||||||||
| Morningstar LTC Index |
100.00 | 77.00 | 30.00 | 45.00 | 55.00 | |||||||||||||||
| Item 6. | Selected Financial Data |
We derived the selected historical consolidated financial data below for each of the years ended December 31, 2010, 2009, and 2008, and as of December 31, 2010 and 2009, from our audited consolidated financial statements included elsewhere in this document. We derived the selected historical consolidated financial data for the years ended December 31, 2007 and 2006 and as of December 31, 2008, 2007 and 2006 from our consolidated financial statements not included in this report. Historical results are not necessarily indicative of future performance.
Our selected historical consolidated statements of operations have been recast to reflect our Ventura, California hospice business, which we closed in September 2009, as discontinued operations. Please refer to the information set forth below in conjunction with other sections of this report, including “Management’s Discussion and Analysis of Financial Condition and Results of Operations,” and our consolidated historical financial statements and related notes included elsewhere in this report.
45
Table of Contents
SELECTED CONSOLIDATED FINANCIAL DATA
| Years ended December 31, | ||||||||||||||||||||
| 2010 | 2009 | 2008 | 2007 | 2006 | ||||||||||||||||
| (in thousands, except per share data) | ||||||||||||||||||||
| Consolidated Statement of Operations Data |
||||||||||||||||||||
| Revenue |
$ | 820,238 | $ | 756,065 | $ | 729,390 | $ | 634,607 | $ | 531,657 | ||||||||||
| Expenses |
780,621 | 842,048 | 643,365 | 554,940 | 462,887 | |||||||||||||||
| Total other (expenses) income, net |
(38,186 | ) | (28,966 | ) | (33,848 | ) | (52,584 | ) | (43,384 | ) | ||||||||||
| Income (loss) from continuing operations before provision for income taxes |
1,431 | (114,949 | ) | 52,177 | 27,083 | 25,386 | ||||||||||||||
| Provision for income taxes |
2,472 | 17,842 | 18,081 | 11,801 | 10,595 | |||||||||||||||
| (Loss) income before discontinued operations and cumulative effect of a change in accounting principle |
(1,041 | ) | (132,791 | ) | 34,096 | 15,282 | 14,791 | |||||||||||||
| (Loss) income from discontinued operations, net of tax |
— | (390 | ) | — | — | — | ||||||||||||||
| Net (loss) income |
(1,041 | ) | (133,181 | ) | 34,096 | 15,282 | 14,791 | |||||||||||||
| Accretion on preferred stock |
— | — | — | (7,354 | ) | (18,406 | ) | |||||||||||||
| Net (loss) income attributable to common stockholders |
$ | (1,041 | ) | $ | (133,181 | ) | $ | 34,096 | $ | 7,928 | $ | (3,615 | ) | |||||||
| (Loss) Earnings Per Share Data: |
||||||||||||||||||||
| (Loss) earnings per common share from continuing operations, basic |
$ | (0.03 | ) | $ | (3.60 | ) | $ | 0.93 | $ | 0.29 | $ | (0.31 | ) | |||||||
| (Loss) earnings per common share from continuing operations, diluted |
$ | (0.03 | ) | $ | (3.60 | ) | $ | 0.92 | $ | 0.29 | $ | (0.31 | ) | |||||||
| Weighted-average common shares outstanding, basic |
36,988 | 36,914 | 36,573 | 27,062 | 11,638 | |||||||||||||||
| Weighted-average common shares outstanding, diluted |
36,988 | 36,914 | 36,894 | 27,715 | 11,638 | |||||||||||||||
| Other Financial Data |
||||||||||||||||||||
| Capital expenditures (excluding acquisitions) |
$ | 27,736 | $ | 41,155 | $ | 49,626 | $ | 29,398 | $ | 22,267 | ||||||||||
| Net cash provided by operating activities |
35,298 | 74,897 | 67,489 | 34,026 | 33,363 | |||||||||||||||
| Net cash used in investing activities |
(76,405 | ) | (46,168 | ) | (72,853 | ) | (123,851 | ) | (73,324 | ) | ||||||||||
| Net cash provided (used in) by financing activities |
41,771 | (27,638 | ) | 2,399 | 92,016 | 5,644 | ||||||||||||||
| EBITDA(1) |
62,552 | (60,164 | ) | 109,736 | 87,293 | 84,381 | ||||||||||||||
| EBITDA margin(1) |
7.6 | % | (8.0 | )% | 15.0 | % | 13.8 | % | 15.9 | % | ||||||||||
| Adjusted EBITDA(1) |
121,524 | 110,887 | 109,798 | 98,981 | 84,578 | |||||||||||||||
| Adjusted EBITDA margin(1) |
14.8 | % | 14.7 | % | 15.1 | % | 15.6 | % | 15.9 | % | ||||||||||
| EBITDAR(2) |
81,590 | (42,027 | ) | 127,984 | 100,147 | 94,408 | ||||||||||||||
| EBITDAR margin(2) |
9.9 | % | (5.6 | )% | 17.5 | % | 15.8 | % | 17.8 | % | ||||||||||
| Adjusted EBITDAR(2) |
140,562 | 129,024 | 128,046 | 111,835 | 94,605 | |||||||||||||||
| Adjusted EBITDAR margin(2) |
17.1 | % | 17.1 | % | 17.6 | % | 17.6 | % | 17.8 | % | ||||||||||
46
Table of Contents
| As of December 31, | ||||||||||||||||||||
| 2010 | 2009 | 2008 | 2007 | 2006 | ||||||||||||||||
| (in thousands) | ||||||||||||||||||||
| Balance Sheet Data |
||||||||||||||||||||
| Cash and cash equivalents |
$ | 4,192 | $ | 3,528 | $ | 2,047 | $ | 5,012 | $ | 2,821 | ||||||||||
| Working capital |
52,785 | 44,672 | 47,298 | 50,872 | 17,166 | |||||||||||||||
| Property and equipment, net |
387,322 | 373,211 | 346,466 | 294,281 | 230,904 | |||||||||||||||
| Total assets |
937,730 | 856,242 | 1,006,580 | 965,857 | 836,233 | |||||||||||||||
| Long-term debt (including current portion and the revolving credit facility) |
519,963 | 458,679 | 470,261 | 458,436 | 469,055 | |||||||||||||||
| Total stockholders’ equity |
277,580 | 275,422 | 404,577 | 370,056 | 238,102 | |||||||||||||||
Notes
| (1) | We define EBITDA as net (loss) income before depreciation, amortization and interest expense (net of interest income) and the provision for (benefit from) income taxes. EBITDA margin is EBITDA as a percentage of revenue. Adjusted EBITDA is EBITDA adjusted to eliminate non-core business items, which for the reported periods includes, to the extent applicable: |
| • | discontinued operations, net of tax; |
| • | the change in fair value of an interest rate hedge not qualifying for hedge accounting; |
| • | gains or losses on sale of assets; |
| • | the write-off of deferred financing costs of extinguished debt; |
| • | provision for the impairment of long-lived assets, including goodwill; |
| • | debt retirement costs; |
| • | acquisitions costs; and |
| • | certain litigation expenses. |
| (2) | We define EBITDAR as net (loss) income before depreciation, amortization, interest expense (net of interest income), the provision for (benefit from) income taxes and rent cost of revenue. EBITDAR margin is EBITDAR as a percentage of revenue. Adjusted EBITDAR is EBITDAR adjusted for the Adjusted EBITDA items (each to the extent applicable in the appropriate period listed above). |
We believe that the presentation of EBITDA, EBITDAR, Adjusted EBITDA and Adjusted EBITDAR provides useful information regarding our operational performance because they enhance the overall understanding of the financial performance and prospects for the future of our core business activities.
Specifically, we believe that a report of EBITDA, EBITDAR, Adjusted EBITDA and Adjusted EBITDAR provides consistency in our financial reporting and provides a basis for the comparison of results of core business operations between our current, past and future periods. EBITDA, EBITDAR, Adjusted EBITDA and Adjusted EBITDAR are primary indicators management uses for planning and forecasting in future periods, including trending and analyzing the core operating performance of our business from period-to-period without the effect of U.S. generally accepted accounting principles, or GAAP, expenses, revenues and gains (losses) that are unrelated to the day-to-day performance of our business. We also use EBITDA, EBITDAR, Adjusted EBITDA and Adjusted EBITDAR to benchmark the performance of our business against expected results, analyzing year-over-year trends as described below and to compare our operating performance to that of our competitors.
Management uses EBITDA, EBITDAR, Adjusted EBITDA and Adjusted EBITDAR to assess the performance of our core business operations, to prepare operating budgets and to measure our performance against those budgets on a consolidated, segment and a facility-by-facility level. We typically use Adjusted EBITDA and Adjusted EBITDAR for these purposes, on a consolidated basis (because the adjustments to
47
Table of Contents
EBITDA and EBITDAR are not generally allocable to any individual business unit) and we typically use EBITDA and EBITDAR to compare the operating performance of each skilled nursing and assisted living facility, as well as to assess the performance of our operating segments: (1) long-term care services, which include the operation of our skilled nursing and assisted living operating companies; (2) therapy services, which include our integrated and third-party rehabilitation therapy services; and (3) hospice and home health operating companies. EBITDA, EBITDAR, Adjusted EBITDA and Adjusted EBITDAR are useful in this regard because they do not include such costs as interest expense (net of interest income), income taxes, depreciation and amortization expense, rent cost of revenue (in the case of EBITDAR and Adjusted EBITDAR) and special charges, which may vary from business unit to business unit and period-to-period depending upon various factors, including the method used to finance the business, the amount of debt that we have determined to incur, whether a facility is owned or leased, the date of acquisition of a facility or business, the original purchase price of a facility or business unit or the tax law of the state in which a business unit operates. These types of charges are dependent on factors unrelated to the underlying business unit performance. As a result, we believe that the use of EBITDA, EBITDAR, Adjusted EBITDA and Adjusted EBITDAR provides a meaningful and consistent comparison of our underlying businesses and facilities between periods by eliminating certain items required by GAAP which have little or no significance to their day-to-day operations.
We also make capital allocations to each of our facilities based on expected EBITDA and EBITDAR returns and establish compensation programs and bonuses for our facility-level employees that are based upon the achievement of pre-established EBITDA and Adjusted EBITDA targets.
Finally, we use Adjusted EBITDA to determine compliance with our debt covenants and assess our ability to borrow additional funds and to finance or expand operations. Our senior secured credit facility uses a measure substantially similar to Adjusted EBITDA as the basis for determining compliance with our financial covenants, specifically our minimum interest coverage ratio and our maximum total leverage ratio, and for determining the interest rate of our first lien term loan. The indenture governing our 11% senior subordinated notes also uses a substantially similar measurement for determining the amount of additional debt we may incur. For example, both our senior secured credit facility and the indenture governing our 11% senior subordinated notes include adjustments to EBITDA (i) gain or losses on sale of assets and (ii) the write-off of deferred financing costs of extinguished debt, (iii) proforma adjustments for acquisitions to show a full year of EBITDA and interest expense, (iv) sponsorship fees paid to Onex which totals $0.5 million annually and (v) non-cash stock compensation. Our noncompliance with these financial covenants could lead to acceleration of amounts due under our senior secured credit facility. In addition, if we cannot satisfy certain financial covenants under the indenture for our 11% senior subordinated notes, we cannot engage in certain specified activities, such as incurring additional indebtedness or making certain payments.
Despite the importance of these measures in analyzing our underlying business, maintaining our financial requirements, designing incentive compensation and for our goal setting both on an aggregate and facility level basis, EBITDA, EBITDAR, Adjusted EBITDA and Adjusted EBITDAR are non-GAAP financial measures that have no standardized meaning defined by GAAP. Therefore, our EBITDA, EBITDAR, Adjusted EBITDA and Adjusted EBITDAR measures have limitations as analytical tools, and they should not be considered in isolation, or as a substitute for analysis of our results as reported under GAAP. Some of these limitations are:
| • | they do not reflect our cash expenditures, or future requirements, for capital expenditures or contractual commitments; |
| • | they do not reflect changes in, or cash requirements for, our working capital needs; |
| • | they do not reflect the interest expense, or the cash requirements necessary to service interest or principal payments, on our debt; |
| • | they do not reflect any income tax payments we may be required to make; |
| • | although depreciation and amortization are non-cash charges, the assets being depreciated and amortized will often have to be replaced in the future, and EBITDA and Adjusted EBITDA do not reflect any cash requirements for such replacements; |
48
Table of Contents
| • | they are not adjusted for all non-cash income or expense items that are reflected in our consolidated statements of cash flows; |
| • | they do not reflect the impact on earnings of charges resulting from certain matters we consider not to be indicative of our ongoing operations; and |
| • | other companies in our industry may calculate these measures differently than we do, which may limit their usefulness as comparative measures. |
We compensate for these limitations by using EBITDA, EBITDAR, Adjusted EBITDA and Adjusted EBITDAR only to supplement net (loss) income on a basis prepared in conformance with GAAP in order to provide a more complete understanding of the factors and trends affecting our business. We strongly encourage investors to consider net (loss) income determined under GAAP as compared to EBITDA, EBITDAR, Adjusted EBITDA and Adjusted EBITDAR, and to perform their own analysis, as appropriate.
The following table provides a reconciliation of our net (loss) income, which is the most directly comparable financial measure presented in accordance with GAAP for the periods indicated, to EBITDA, EBITDAR, Adjusted EBITDAR and Adjusted EBITDA:
| Years ended December 31, | ||||||||||||||||||||
| 2010 | 2009 | 2008 | 2007 | 2006 | ||||||||||||||||
| (in thousands) | ||||||||||||||||||||
| Net (loss) income |
(1,041 | ) | (133,181 | ) | 34,096 | 15,282 | 14,791 | |||||||||||||
| Provision for income taxes |
2,472 | 17,842 | 18,081 | 11,801 | 10,595 | |||||||||||||||
| Depreciation and amortization |
25,047 | 23,308 | 20,978 | 17,687 | 13,897 | |||||||||||||||
| Interest expense, net of interest income |
36,074 | 31,867 | 36,581 | 42,523 | 45,098 | |||||||||||||||
| EBITDA |
62,552 | (60,164 | ) | 109,736 | 87,293 | 84,381 | ||||||||||||||
| Rent cost of revenue |
19,038 | 18,137 | 18,248 | 12,854 | 10,027 | |||||||||||||||
| EBITDAR |
81,590 | (42,027 | ) | 127,984 | 100,147 | 94,408 | ||||||||||||||
| EBITDA |
62,552 | (60,164 | ) | 109,736 | 87,293 | 84,381 | ||||||||||||||
| Discontinued operations, net of tax(a) |
— | 390 | — | — | — | |||||||||||||||
| Change in fair value of interest rate hedge(b) |
— | — | — | 40 | 197 | |||||||||||||||
| (Gain) loss on sale of assets(c) |
(2,243 | ) | 61 | 62 | — | — | ||||||||||||||
| Premium on redemption of debt and write-off of deferred financing costs of extinguished debt(d) |
— | — | — | 11,648 | — | |||||||||||||||
| Goodwill impairment charge(e) |
— | 170,600 | — | — | — | |||||||||||||||
| Litigation settlement costs(f) |
53,505 | — | — | — | — | |||||||||||||||
| Debt retirement cost(g) |
7,010 | — | — | — | — | |||||||||||||||
| Acquisition costs(h) |
700 | — | — | — | — | |||||||||||||||
| Adjusted EBITDA |
121,524 | 110,887 | 109,798 | 98,981 | 84,578 | |||||||||||||||
| Rent cost of revenue |
19,038 | 18,137 | 18,248 | 12,854 | 10,027 | |||||||||||||||
| Adjusted EBITDAR |
140,562 | 129,024 | 128,046 | 111,835 | 94,605 | |||||||||||||||
Notes
| (a) | In 2009, we closed our hospice operations located in Ventura, California, and, therefore, the results of this business have been classified as discontinued operations. |
| (b) | Changes in fair value of an interest rate hedge are unrelated to our core operating activities and we believe that adjusting for these amounts allows us to focus on actual operating costs at our facilities. |
| (c) | While gains or losses on sales of assets are required under GAAP, these amounts are also not reflective of income and losses of our underlying business. |
| (d) | Write-offs for deferred financing costs are the result of distinct capital structure decisions made by our management and are unrelated to our day-to-day operations. These write-offs reflect a $7.7 million |
49
Table of Contents
| redemption premium on $70.0 million of our 11% senior subordinated notes that we redeemed in June 2007, before their scheduled maturities in 2014. |
| (e) | During the fourth quarter of 2009, we recorded a goodwill impairment charge of $170.6 million at our long-term care reporting segment. The goodwill impairment charge is a non-cash accounting adjustment to our financial statements that does not affect our cash flows or our liquidity position. The impairment charge was the result of the downturn in the expected future growth rates for governmental payors (based on patient mix and announced Medicare and Medicaid reimbursement reductions), and their effect on expected future cash flows. See “Management’s Discussion and Analysis of Financial Condition and Results of Operations—Goodwill” for a more detailed discussion of the goodwill impairment charge. |
| (f) | During the third quarter of 2010, we recorded a litigation settlement expense of $53.5 million. The $53.5 million was comprised of a $50.0 million cash settlement related to the Humboldt County Action described in Note 12, Commitments and Contingencies—Litigation and $3.0 million of related legal expenses, and $0.5 million in securities class action costs related to the Shepardson v. Skilled Healthcare Group, Inc. litigation described in Note 12, Commitments and Contingencies—Litigation, of the audited financial statements included elsewhere in this report. |
| (g) | During the second quarter of 2010, we recorded debt retirement cost of $7.0 million in conjunction with the refinancing of our senior secured credit facility due to the expensing of deferred financing fees of $6.6 million and $0.4 million of interest rate swap termination costs as the swaps were incompatible with the refinanced credit facility. |
| (h) | Hospice and home health costs of services included $0.7 million of non-recurring acquisition related costs during 2010. |
| Item 7. | Management’s Discussion and Analysis of Financial Condition and Results of Operations |
This Management’s Discussion and Analysis of Financial Condition and Results of Operations is intended to assist in understanding and assessing the trends and significant changes in our results of operations and financial condition. Historical results may not indicate future performance. Our forward-looking statements, which reflect our current views about future events, are based on assumptions and are subject to known and unknown risks and uncertainties that could cause actual results to differ materially from those contemplated by these statements. Factors that may cause differences between actual results and those contemplated by forward-looking statements include, but are not limited to, those discussed in Item 1A, “Risk Factors,” of this report on Form 10-K. This Management’s Discussion and Analysis of Financial Condition and Results of Operations should be read in conjunction with “Selected Financial Data” in Item 6 of this report on Form 10-K and our consolidated financial statements and related notes included in this report.
Certain prior year amounts have been reclassified to conform to current year presentation.
Restatement
On June 29, 2009, we restated our financial statements for the fiscal years ended December 31, 2006 through December 31, 2008, including the corresponding quarterly periods in 2007 and 2008, in our amended Form 10-K/A for the year ended December 31, 2008, and for the quarter ended March 31, 2009 in our amended Form 10-Q/A for the quarter then ended.
The restatement principally related to an understatement of accounts receivable allowance for doubtful accounts for our long-term care, or LTC, operating segment, which was caused by improper dating of accounts receivable for that segment by a former senior officer of the LTC segment, referred to as the former employee. Management conducted a review of our accounts receivable allowance for doubtful accounts related to the LTC segment after the former employee left our employment following a disciplinary meeting on unrelated matters. Management determined that the former employee had acted in a manner inconsistent with our accounting and disclosure policies and practices. As a result of its review, management recommended to the Audit Committee that a restatement was required. The Audit Committee initiated and directed a special investigation regarding the
50
Table of Contents
accounting and reporting issues raised by the former employee’s improper dating of accounts receivable. Under the oversight of the Audit Committee, internal audit personnel with the assistance of outside legal counsel and other advisors, investigated the matter and reviewed our internal controls related to accounts receivable allowance for doubtful accounts related to the LTC segment. Our investigation found no evidence that anyone else within our organization knew of or participated in the improper conduct.
Business Overview
We are a holding company with subsidiaries that operate skilled nursing facilities, assisted living facilities, hospices, home health providers and a rehabilitation therapy business. We have an administrative service company that provides a full complement of administrative and consultative services that allows our facility operators and third-party facility operators with whom we contract to better focus on delivery of healthcare services. We have one such service agreement with an unrelated facility operator. These subsidiaries focus on providing high-quality care to our patients and have a strong commitment to treating patients who require a high level of skilled nursing care and extensive rehabilitation therapy, whom we refer to as high-acuity patients. As of December 31, 2010, we owned or leased 78 skilled nursing facilities and 22 assisted living facilities, together comprising 10,830 licensed beds. Our facilities, approximately 77.0% of which we own, are located in California, Texas, Iowa, Kansas, Missouri, Nevada and New Mexico, and are generally clustered in large urban or suburban markets. For the twelve months ended December 31, 2010, we generated approximately 81.5% of our revenue from our skilled nursing facilities, including our integrated rehabilitation therapy services at these facilities. The remainder of our revenue is generated from our assisted living services, rehabilitation therapy services provided to third-party facilities, hospice care and home health services.
Our revenue was $820.2 million and $756.1 million for the years ended December 31, 2010 and 2009, respectively. To increase our revenue, we focus on acquiring existing facilities, developing new facilities, and improving our occupancy rate and our skilled mix, which is the number of Medicare and managed care patient days at our skilled nursing facilities divided by the total number of patient days at our skilled nursing facilities for any given period. Medicare and managed care payors typically provide higher reimbursement than other payors because patients in these programs typically require a greater level of care and service. Our skilled mix declined from 23.1% for 2009 to 22.7% for 2010. Our skilled mix declined primarily due to a decrease in average length of stay for our skilled patients as well as a reduction in Medicare census from lower acute-care admissions, including those from hospitals, as a result of the challenging economic environment and competitive pressures. Our skilled mix also impacts our quality mix, which is our percentage of non-Medicaid revenue. Our quality mix increased from 68.1% in 2009 to 68.3% in 2010.
We operate our business in three reportable operating segments: long-term care services, which includes the operation of skilled nursing and assisted living facilities and is the most significant portion of our business, therapy services, which includes our rehabilitation therapy, and hospice and home health services, which includes our hospice and home health businesses. The “other” category includes general and administrative items. Our reporting segments are business units that offer different services, and that are managed separately due to the nature of services provided.
Acquisitions, Developments, and Divestiture
In April 2008, we acquired the real property and assets of a 152-bed skilled nursing facility and an adjacent 34-unit assisted living facility located in Wichita, Kansas, for approximately $13.7 million. The acquisition was financed by borrowings of $13.0 million on our revolving credit facility.
In September 2008, we acquired seven assisted living facilities located in Kansas for an aggregate purchase price of $9.0 million. The acquired facilities added 208 units to our operations. The acquisition was financed by borrowings of $9.0 million on our revolving credit facility.
51
Table of Contents
In March 2009, we admitted our first patients to our newly constructed skilled nursing facility in Dallas, Texas, the Dallas Center of Rehabilitation. The opening of the Dallas Center of Rehabilitation added 136 beds to our operations.
In April 2009, we purchased a skilled nursing facility located in Des Moines, Iowa, for approximately $1.7 million in cash. This facility added 74 beds to our operations.
In April 2009, we completed construction of Vintage Park at Tonganoxie, an assisted living facility in the Kansas City market. This facility added 41 units to our operations.
In December 2009, we purchased a skilled nursing facility located in Davenport, Iowa, for approximately $2.2 million in cash. This facility added 118 beds to our operations.
In May 2010, we acquired substantially all of the assets of five Medicare-certified hospice companies and four Medicare-certified home health companies located in Arizona, Idaho, Montana and Nevada, referred to herein as the Hospice/Home Health Acquisition. See Note 17 – Acquisition, to the consolidated financial statements included elsewhere in this report for a more detailed discussion of the Hospice/Home Health Acquisition.
In July 2010, we admitted our first patients to our newly-constructed skilled nursing facility in Fort Worth, Texas, Fort Worth Center of Rehabilitation. This facility added 136 beds to our operations.
In December 2010, we sold our Westside Campus of Care skilled nursing facility and operations in Texas for $14.7 million and purchased three previously leased facilities: St. Luke Healthcare and Rehabilitation Center and Woodland Care Center, located in California, and St. Joseph Transitional Rehabilitation Center in Nevada. We recorded a net gain of $1.8 million related to these transactions.
Key Financial Performance Indicators
We manage the fiscal aspects of our business by monitoring certain key performance indicators that affect our revenue and profitability. The most important key performance indicators for our business are:
| • | Average daily number of patients—the total number of patients at our skilled nursing facilities in a period divided by the number of days in that period. |
| • | Average daily rates—revenue per patient per day for Medicare or managed care, Medicaid and private pay and other, calculated as total revenue for Medicare or managed care, Medicaid and private pay and other at our skilled nursing facilities divided by actual patient days for that revenue source for any given period. |
| • | EBITDA—net (loss) income before depreciation, amortization and interest expenses and the provision for income taxes. Additionally, Adjusted EBITDA means EBITDA as adjusted for non-core operating items. See footnote 1 under Item 6 of this report, “Selected Financial Data,” for an explanation of the adjustments and a description of our uses of, and the limitations associated with, EBITDA and Adjusted EBITDA. |
| • | EBITDAR—net (loss) income before depreciation, amortization and interest expenses (net of interest income), the provision for income taxes, and rent cost of revenue. Additionally, Adjusted EBITDAR means EBITDAR as adjusted for non-core operating items. See footnote 1 under Item 6 of this report, “Selected Financial Data,” for an explanation of the adjustments and a description of our uses of, and the limitations associated with, EBITDAR and Adjusted EBITDAR. |
| • | Number of facilities and licensed beds—the total number of skilled nursing facilities and assisted living facilities that we own or operate and the total number of licensed beds associated with our skilled nursing facilities and the total number of units associated with our assisted living facilities. |
52
Table of Contents
| • | Occupancy percentage—the average daily ratio during a measurement period of the total number of patients occupying beds in a skilled nursing facility to the number of available beds in the skilled nursing facility. During any measurement period, the number of licensed beds in a skilled nursing facility that are actually available to us may be less than the actual licensed bed capacity due to, among other things, bed de-certifications. |
| • | Percentage of facilities owned—the number of skilled nursing facilities and assisted living facilities that we own as a percentage of the total number of facilities. We believe that our success is influenced by the significant level of ownership of the facilities we operate. |
| • | Quality mix—the amount of non-Medicaid revenue from each of our business units as a percentage of total revenue. In most states, Medicaid rates are generally the lowest of all payor types. |
| • | Skilled mix—the number of Medicare and managed care patient days at our skilled nursing facilities divided by the total number of patient days at our skilled nursing facilities for any given period. |
The following tables summarize, for each of the periods indicated, our payor sources, quality mix, occupancy percentage, skilled mix, EBITDA, EBITDAR, Adjusted EBITDA and Adjusted EBITDAR and average daily rates and, at the end of the periods indicated, the number of facilities operated by us, the number of facilities that we own and lease, the total number of licensed beds and our total number of available beds:
| Year Ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Revenue from: |
||||||||||||
| Medicare |
37.1 | % | 35.0 | % | 36.6 | % | ||||||
| Managed care, private pay, and other |
31.2 | 33.1 | 32.3 | |||||||||
| Quality mix |
68.3 | 68.1 | 68.9 | |||||||||
| Medicaid |
31.7 | 31.9 | 31.1 | |||||||||
| Total |
100.0 | % | 100.0 | % | 100.0 | % | ||||||
| Occupancy statistics (skilled nursing facilities): |
||||||||||||
| Available patient days |
3,391,343 | 3,324,757 | 3,302,889 | |||||||||
| Actual patient days |
2,819,609 | 2,784,033 | 2,791,937 | |||||||||
| Occupancy percentage |
83.1 | % | 83.7 | % | 84.5 | % | ||||||
| Skilled mix |
22.7 | % | 23.1 | % | 24.2 | % | ||||||
| Average daily number of patients |
7,725 | 7,628 | 7,628 | |||||||||
| EBITDA(1) (in thousands) |
$ | 62,552 | $ | (60,164 | ) | $ | 109,736 | |||||
| Adjusted EBITDA(1) (in thousands) |
$ | 121,524 | $ | 110,887 | $ | 109,798 | ||||||
| EBITDAR(2) (in thousands) |
$ | 81,590 | $ | (42,027 | ) | $ | 127,984 | |||||
| Adjusted EBITDAR(2) (in thousands) |
$ | 140,562 | $ | 129,024 | $ | 128,046 | ||||||
| Revenue per patient day (skilled nursing facilities prior to intercompany eliminations) |
||||||||||||
| LTC only Medicare (Part A) |
$ | 515 | $ | 499 | $ | 475 | ||||||
| Medicare blended rate (Part A & B) |
$ | 578 | $ | 557 | $ | 525 | ||||||
| Managed care |
379 | 369 | 359 | |||||||||
| Medicaid |
151 | 146 | 139 | |||||||||
| Private and other |
169 | 162 | 157 | |||||||||
| Weighted-average |
$ | 237 | $ | 231 | $ | 224 | ||||||
53
Table of Contents
| As of December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Facilities: |
||||||||||||
| Skilled nursing facilities: |
||||||||||||
| Owned |
57 | 54 | 51 | |||||||||
| Leased |
21 | 24 | 24 | |||||||||
| Total skilled nursing facilities |
78 | 78 | 75 | |||||||||
| Total licensed beds |
9,566 | 9,704 | 9,373 | |||||||||
| Assisted living facilities: |
||||||||||||
| Owned |
20 | 20 | 19 | |||||||||
| Leased |
2 | 2 | 2 | |||||||||
| Total assisted living facilities |
22 | 22 | 21 | |||||||||
| Total licensed beds |
1,264 | 1,250 | 1,214 | |||||||||
| Total facilities |
100 | 100 | 96 | |||||||||
| Available beds in service (SNF only) |
9,156 | 9,280 | 8,983 | |||||||||
| Percentage of owned facilities |
77.0 | % | 74.0 | % | 72.9 | % | ||||||
| (1) | EBITDA and Adjusted EBITDA are supplemental measures of our performance that are not required by, or presented in accordance with, U.S. generally accepted accounting principles, or GAAP. We define EBITDA as net (loss) income before depreciation, amortization and interest expenses (net of interest income) and the provision for income taxes. Adjusted EBITDA means EBITDA as adjusted for non-core operating items. See reconciliation of net (loss) income to EBITDA and Adjusted EBITDA and a discussion of its uses and limitations in footnote 1 in Item 6 of this report, “Selected Financial Data.” |
| (2) | EBITDAR and Adjusted EBITDAR are supplemental measures of our performance that are not required by, or presented in accordance with, GAAP. We define EBITDAR as net (loss) income before depreciation, amortization and interest expenses (net of interest income), the provision for income taxes, and rent cost of revenue. Adjusted EBITDAR means EBITDAR as adjusted for non-core operating items. See reconciliation of net (loss) income to EBITDAR and Adjusted EBITDAR and a discussion of its uses and limitations in footnote 1 in Item 6 of this report, “Selected Financial Data.” |
54
Table of Contents
Revenue
Revenue by Service Offering
The following table shows the revenue and percentage of our total revenue generated by each of our operating segments for the periods presented (dollars in thousands):
| Year Ended December 31, | ||||||||||||||||||||||||||||||||
| 2010 | 2009 | 2008 | ||||||||||||||||||||||||||||||
| Revenue Dollars |
Revenue Percentage |
Revenue Dollars |
Revenue Percentage |
Revenue Dollars |
Revenue Percentage |
Percentage Change | ||||||||||||||||||||||||||
| 2010 vs. 2009 | 2009 vs. 2008 | |||||||||||||||||||||||||||||||
| Long-term care services: |
||||||||||||||||||||||||||||||||
| Skilled nursing facilities |
$ | 667,691 | 81.5 | % | $ | 640,080 | 84.7 | % | $ | 621,924 | 85.3 | % | 4.3 | % | 2.9 | % | ||||||||||||||||
| Assisted living facilities |
25,585 | 3.1 | 24,442 | 3.2 | 20,562 | 2.8 | 4.7 | 18.9 | ||||||||||||||||||||||||
| Administrative of third party facilities |
1,125 | 0.1 | 2,278 | 0.3 | 990 | 0.1 | (50.6 | ) | 130.1 | |||||||||||||||||||||||
| Total long-term care services |
694,401 | 84.7 | 666,800 | 88.2 | 643,476 | 88.2 | 4.1 | 3.6 | ||||||||||||||||||||||||
| Therapy services: |
||||||||||||||||||||||||||||||||
| Third-party rehabilitation therapy services |
74,118 | 9.0 | 74,723 | 9.9 | 69,931 | 9.6 | (0.8 | ) | 6.9 | |||||||||||||||||||||||
| Total therapy services |
74,118 | 9.0 | 74,723 | 9.9 | 69,931 | 9.6 | (0.8 | ) | 6.9 | |||||||||||||||||||||||
| Hospice & Home Health services: |
||||||||||||||||||||||||||||||||
| Hospice |
41,221 | 5.0 | 14,542 | 1.9 | 15,983 | 2.2 | 183.5 | (9.0 | ) | |||||||||||||||||||||||
| Home Health |
10,498 | 1.3 | — | 0.0 | — | 0.0 | 100.0 | — | ||||||||||||||||||||||||
| Total hospice & home health services |
51,719 | 6.3 | 14,542 | 1.9 | 15,983 | 2.2 | 255.7 | (9.0 | ) | |||||||||||||||||||||||
| Total |
$ | 820,238 | 100.0 | % | $ | 756,065 | 100.0 | % | $ | 729,390 | 100.0 | % | 8.5 | % | 3.7 | % | ||||||||||||||||
Sources of Revenue
The following table sets forth revenue by state in dollars and as a percentage of total revenue for the periods (dollars in thousands):
| Year Ended December 31, | ||||||||||||||||||||||||
| 2010 | 2009 | 2008 | ||||||||||||||||||||||
| Revenue Dollars |
Percentage of Revenue |
Revenue Dollars |
Percentage of Revenue |
Revenue Dollars |
Percentage of Revenue |
|||||||||||||||||||
| California |
$ | 343,984 | 41.9 | % | $ | 334,953 | 44.3 | % | $ | 325,840 | 44.7 | % | ||||||||||||
| Texas |
190,607 | 23.2 | 190,587 | 25.2 | 185,914 | 25.5 | ||||||||||||||||||
| New Mexico |
86,029 | 10.5 | 81,061 | 10.7 | 79,562 | 10.9 | ||||||||||||||||||
| Kansas |
61,657 | 7.5 | 57,864 | 7.6 | 51,331 | 7.0 | ||||||||||||||||||
| Missouri |
42,902 | 5.2 | 57,141 | 7.6 | 55,878 | 7.7 | ||||||||||||||||||
| Nevada |
48,516 | 5.9 | 30,929 | 4.1 | 30,605 | 4.2 | ||||||||||||||||||
| Montana |
22,641 | 2.8 | — | — | — | — | ||||||||||||||||||
| Iowa |
9,989 | 1.2 | 2,870 | 0.4 | — | — | ||||||||||||||||||
| Arizona |
7,928 | 1.0 | — | — | — | — | ||||||||||||||||||
| Idaho |
5,937 | 0.7 | — | — | — | — | ||||||||||||||||||
| Other |
48 | 0.1 | 660 | 0.1 | 260 | — | ||||||||||||||||||
| Total |
$ | 820,238 | 100.0 | % | $ | 756,065 | 100.0 | % | $ | 729,390 | 100.0 | % | ||||||||||||
55
Table of Contents
Long-Term Care Services Segment
Skilled Nursing Facilities. Within our skilled nursing facilities, we generate our revenue from Medicare, Medicaid, managed care providers, insurers, private pay and other sources. We believe that our skilled mix is an important indicator of our success in attracting high-acuity patients because it represents the percentage of our patients who are reimbursed by Medicare and managed care payors, for whom we generally receive higher reimbursement rates. Several of our skilled nursing facilities include our Express Recovery™ program. This program uses a dedicated unit within a skilled nursing facility to deliver a comprehensive rehabilitation and recovery regimen in accommodations specifically designed to serve high-acuity patients.
The following table sets forth our Medicare, managed care, private pay/other and Medicaid patient days as a percentage of total patient days and the level of skilled mix for our skilled nursing facilities:
| Year Ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Medicare |
15.7 | % | 16.2 | % | 17.2 | % | ||||||
| Managed care |
7.0 | 6.9 | 7.0 | |||||||||
| Skilled mix |
22.7 | 23.1 | 24.2 | |||||||||
| Private pay and other |
16.4 | 17.8 | 17.9 | |||||||||
| Medicaid |
60.9 | 59.1 | 57.9 | |||||||||
| Total |
100.0 | % | 100.0 | % | 100.0 | % | ||||||
Our skilled mix declined in 2010 primarily due to new and re-admissions staying flat coupled by a decrease in overall average length of stay. We attribute the shortened length of stays to the challenging economic environment which affects those patients wishing to avoid co-pays and as a result seeking earlier discharges as compared to historical trends. While admissions remained flat, we continued to face competitive pressures, primarily due to the continued development of new facilities and fill up of recently completed facilities in Texas located close to our existing facilities.
The following table sets forth our Medicare, managed care, private pay and Medicaid sources of revenue by percentage of total revenue and the level of quality mix for our company:
| Year Ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Medicare |
37.1 | % | 35.0 | % | 36.6 | % | ||||||
| Managed care |
9.2 | 9.4 | 9.5 | |||||||||
| Private pay and other |
22.0 | 23.7 | 22.8 | |||||||||
| Quality mix |
68.3 | 68.1 | 68.9 | |||||||||
| Medicaid |
31.7 | 31.9 | 31.1 | |||||||||
| Total |
100.0 | % | 100.0 | % | 100.0 | % | ||||||
Assisted Living Facilities. Within our assisted living facilities, which are mostly in Kansas, we generate our revenue primarily from private pay sources, with a small portion earned from Medicaid or other state-specific programs.
Therapy Services Segment
Rehabilitation Therapy. As of December 31, 2010, we provided rehabilitation therapy services to a total of 172 healthcare facilities, including 68 of our facilities, as compared to 163 facilities, including 68 of our facilities, as of December 31, 2009. In addition, we have contracts to manage the rehabilitation therapy services
56
Table of Contents
for our 10 healthcare facilities in New Mexico. The net increase of 9 facilities serviced was comprised of 20 new facilities serviced, net of 11 cancellations. Rehabilitation therapy revenue derived from servicing our own facilities is included in our revenue from skilled nursing facilities. Our rehabilitation therapy business receives payment for services from the third-party skilled nursing facilities that it serves based on negotiated patient per diem rates or a negotiated fee schedule based on the type of service rendered.
Hospice and Home Health Services Segment
Hospice. We provide hospice care in California and New Mexico and as of May 1, 2010, we provided hospice care in Arizona, Nevada, Idaho, and Montana upon the completion of the Hospice/Home Health Acquisition. We derive substantially all of the hospice business revenue from Medicare and managed care reimbursement for hospice services. Our objective is to increase the number of patients that each of our hospice programs serves, thus improving our site-level margins and leveraging our overhead.
Federal legislation imposes a Medicare payment cap on hospice service programs, as described in Item 1 of this report, “Business—Sources of Reimbursement” and Item 1A of this report “Risk Factors—We are subject to a Medicare cap amount for our hospice business. Our net patient service revenue and profitability could be adversely affected by limitations on Medicare payments.”) We are managing the Medicare cap and its impact on our hospice business by actively managing our average length-of-stay on a market-by-market basis. A key component of this strategy is to analyze each hospice program’s mix of patients and referral sources to achieve an optimal balance of the types of patients and referral sources that we serve at each of our programs. We believe this strategy will increase our net patient service revenue by reducing the possibility of experiencing a Medicare cap contractual adjustment. Developing new relationships and thereby adjusting patient mix takes time to implement and will continue to be an ongoing process.
Home Health. Effective upon our completion of the Hospice/Home Health Acquisition in May 2010, we began providing home health care services in Arizona, Nevada, Idaho and Montana. We derive substantially all of the revenue from our home health business from Medicare. Net service revenue is recorded under the PPS based on a 60-day episode payment rate that is subject to downward adjustment based on certain variables including, but not limited to: (a) an outlier payment if our patient’s care was unusually costly; (b) a low utilization adjustment (“LUPA”) if the number of visits was fewer than five; (c) a partial payment if our patient transferred to another provider or we received a patient from another provider before completing the episode; (d) a payment adjustment based upon the level of therapy services required (thresholds set at 6, 14 and 20 visits); (e) the number of episodes of care provided to a patient, regardless of whether the same home health provider provided care for the entire series of episodes; (f) changes in the base episode payments established by the Medicare program; (g) adjustments to the base episode payments for case mix and geographic wages; and (h) recoveries of overpayments.
Regulatory and other Governmental Actions Affecting Revenue
The following table summarizes the amount of revenue that we received from each of the payor classes indicated during the year indicated (dollars in thousands):
| Year Ended December 31, | ||||||||||||||||||||||||
| 2010 | 2009 | 2008 | ||||||||||||||||||||||
| Revenue Dollars |
Revenue Percentage |
Revenue Dollars |
Revenue Percentage |
Revenue Dollars |
Revenue Percentage |
|||||||||||||||||||
| Medicare |
$ | 304,413 | 37.1 | % | $ | 264,594 | 35.0 | % | $ | 267,180 | 36.6 | % | ||||||||||||
| Medicaid |
260,083 | 31.7 | 241,021 | 31.9 | 226,558 | 31.1 | ||||||||||||||||||
| Subtotal Medicare and Medicaid |
564,496 | 68.8 | 505,615 | 66.9 | 493,738 | 67.7 | ||||||||||||||||||
| Managed Care |
75,657 | 9.2 | 71,181 | 9.4 | 69,723 | 9.5 | ||||||||||||||||||
| Private pay and other |
180,085 | 22.0 | 179,269 | 23.7 | 165,929 | 22.8 | ||||||||||||||||||
| Total |
$ | 820,238 | 100.0 | % | $ | 756,065 | 100.0 | % | $ | 729,390 | 100.0 | % | ||||||||||||
57
Table of Contents
We derive a substantial portion of our revenue from government Medicare and Medicaid programs. In addition, our rehabilitation therapy services, for which we receive payment from private payors, are significantly dependent on Medicare and Medicaid funding, as those private payors are often reimbursed by these programs.
For a detailed discussion of our sources of reimbursement, see Item 1 of this report, “Business—Sources of Reimbursement.”
Primary Expense Components
Cost of Services
Cost of services in our long-term care services segment primarily includes salaries and benefits, supplies, purchased services, ancillary expenses such as the cost of pharmacy and therapy services provided to patients and residents, and operating expenses of our skilled nursing and assisted living facilities, including professional and general liability insurance.
Cost of services in our therapy services and hospice and home health services segments primarily includes salaries and benefits, supplies, purchased services, expenses for general and professional liability insurances and other operating expenses.
General and Administrative
General and administrative expenses are primarily salaries, bonuses and benefits and purchased services to operate our administrative offices. Also included in general and administrative expenses are expenses related to non-cash stock-based compensation and professional fees, including accounting, financial audit and legal fees.
Performance Based Incentive Compensation Plan. Our performance based incentive compensation plan for each of our operating segments provides for cash bonus payments that are intended to reflect the achievement of key operating measures, including quality outcomes, customer satisfaction, cash collections, efficient resource utilization and operating budget goals. We accrue bonus expense based on the ratable achievement of these operating measures.
Depreciation and Amortization
Depreciation and amortization relates to the ratable write-off of assets such as our owned buildings and equipment over their assigned useful lives as a result of wear and tear due to usage. Depreciation and amortization is computed using the straight-line method over the estimated useful lives of the assets as follows:
| Buildings and improvements |
15-40 years | |
| Leasehold improvements |
Shorter of the lease term or estimated useful life, generally 5-10 years | |
| Furniture and equipment |
3-10 years |
Rent Cost of Revenue
Rent consists of the straight-line recognition of lease amounts payable to third-party owners of skilled nursing facilities and assisted living facilities that we operate but do not own.
Critical Accounting Policies and Estimates
The preparation of our financial statements and related disclosures requires us to make judgments, estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and
58
Table of Contents
liabilities at the date of the financial statements and the reported amounts of revenue and expenses during the reporting period. On an ongoing basis, we reevaluate our judgments and estimates, including those related to doubtful accounts, income taxes and loss contingencies. We base our estimates and judgments on our historical experience, knowledge of current conditions and our belief of what could occur in the future considering available information, including assumptions that are believed to be reasonable under the circumstances. Actual results may differ from these estimates under different assumptions or conditions. By their nature, these estimates and judgments are subject to an inherent degree of uncertainty and actual results could differ materially from the amounts reported based on these policies.
The following represents a summary of our critical accounting policies, defined as those policies and estimates that we believe: (a) are the most important to the portrayal of our financial condition and results of operations and (b) require management’s most subjective or complex judgments, often as a result of the need to make estimates about the effects of matters that are inherently uncertain.
Revenue recognition
Our revenue is derived primarily from our skilled nursing facilities, which includes our integrated rehabilitation therapy services at these facilities, with the remainder generated by our other related healthcare services. These other healthcare services consist of our rehabilitation therapy services provided to third-party facilities, as well as our assisted living facilities, hospice care and home health services. We record our revenue from these governmental and managed care programs on an accrual basis as services are performed at their estimated net realizable value under these programs. Our revenue from governmental and managed care programs is subject to ongoing audit and retroactive adjustment by governmental and third-party agencies. Retroactive adjustments that are likely to result from ongoing and future audits by third-party payors are accrued on an estimated basis in the period the related services are performed. Consistent with accounting practices in the healthcare industry, we record any changes to these governmental revenue estimates in the period in which the change or adjustment becomes known based on final settlements. Because of the complexity of the laws and regulations governing Medicare and state Medicaid assistance programs, our revenue estimates may potentially change by a material amount. We record our revenue from private pay patients on an accrual basis as services are performed.
Allowance for doubtful accounts
We maintain allowances for doubtful accounts related to estimated losses resulting from nonpayment of patient accounts receivable and third-party billings and notes receivable from customers. In evaluating the collectability of accounts receivable, we consider a number of factors, including the age of the accounts, changes in collection trends, the composition of patient accounts by payor, the status of ongoing disputes with third-party payors, underlying guarantees, and general industry conditions. If the financial condition of our customers were to deteriorate, resulting in an impairment of their ability to make payments, additional allowances may be required. Our receivables from Medicare and Medicaid payor programs represent our only significant concentration of credit risk. We do not believe there to be significant credit risks associated with these governmental programs. If, at December 31, 2010, we were to recognize an increase of 10% in our allowance for doubtful accounts, our total current assets would decrease by $1.8 million, or 1.2%. There would be a corresponding increase in operating expense.
Patient liability risks
Our professional liability and general liability reserve includes amounts for patient care related claims and incurred but not reported claims. Professional liability and general liability costs for healthcare services in many states continue to be expensive and difficult to estimate, although other states have implemented tort reform that has stabilized the costs. The amount of our reserves is determined based on an estimation process that uses information obtained from both company-specific and industry data. The estimation process requires us to
59
Table of Contents
continuously monitor and evaluate the life cycle of the claims. Using data obtained from this monitoring and our assumptions about emerging trends, we, along with an independent actuary, develop information about the size of ultimate claims based on our historical experience and other available industry information. The most significant assumptions used in the estimation process include determining the trend in costs, the expected cost of claims incurred but not reported and the expected costs to settle unpaid claims. Although we believe that our reserves are adequate, it is possible that this liability will require a material adjustment in the future. For example, an adverse professional liability judgment partially contributed to our bankruptcy filing under Chapter 11 of the United States Bankruptcy Code in October 2001. If, at December 31, 2010, we were to recognize an increase of 10% in the reserve for professional liability and general liability, our total liabilities would be increased by $1.8 million, or 0.3%. There would be a corresponding increase in operating expense. We record our professional and general liability reserves on an undiscounted basis.
Impairment of long-lived assets
We periodically evaluate the carrying value of our long-lived assets other than goodwill, primarily consisting of our investments in real estate, for impairment indicators. If indicators of impairment are present, we evaluate the carrying value of the related real estate investments in relation to the future discounted cash flows of the underlying operations to assess recoverability of the assets. Measurement of the amount of the impairment, if any, may be based on independent appraisals, established market values of comparable assets or estimates of future cash flows expected. The estimates of these future cash flows are based on assumptions and projections believed by management to be reasonable and supportable. They require management’s subjective judgments and take into account assumptions about revenue and expense growth rates. These assumptions may vary by type of long-lived asset. As of December 31, 2010, none of our long-lived assets were impaired.
For property and equipment, major renovations or improvements are capitalized. Ordinary maintenance and repairs are expensed as incurred.
Goodwill
Goodwill is recorded as the difference, if any, between the aggregate consideration paid for an acquisition and the fair value of the net tangible and intangible assets acquired. The amounts and useful lives assigned to intangible assets acquired, other than goodwill, impact the amount and timing of future amortization. The value of our intangible assets, including goodwill, could be impacted by future adverse changes such as: (i) any future declines in our operating results, (ii) a decline in the valuation of healthcare provider stocks, including the valuation of our common stock or (iii) any failure to meet the performance projections included in our forecasts of future operating results.
As of December 31, 2010, goodwill in the amount of $332.7 million was recognized in our consolidated balance sheet, of which $241.7 million related to the long-term care reporting unit, $34.0 million related to the rehabilitation therapy reporting unit, $42.0 million related to the hospice reporting unit and $15.0 million related to home health reporting units. We account for goodwill in accordance with Financial Accounting Standards Board—Accounting Standards Codification (“FASB ASC”) Topic 350, “Intangibles—Goodwill and Other.”
Goodwill Impairment Testing
We compare the fair value of each reporting unit to its carrying amount on an annual basis to determine whether there is potential goodwill impairment. If the fair value of the reporting unit is less than its carrying value, an impairment loss is recorded to the extent the fair value of goodwill is less than its carrying value. We test goodwill for impairment annually at the reporting unit level on October 1 or sooner, if events or changes in circumstances indicate that the carrying amount of our reporting units, including goodwill, may exceed their fair values.
60
Table of Contents
As of September 30, 2010, our carrying value of equity exceeded our market capitalization by approximately $113 million, or 79%, which is a potential indication of impairment. However, there were a number of changes to our reimbursement rates that had recently become effective, including rate changes in several states for which we had not yet received rate letters, and Medicare’s adoption of Resource Utilization Groups, Version 4 (“RUGs IV”) and Minimum Data Service (“MDS”) 3.0, described in Management’s Discussion and Analysis of Financial Condition and Results of Operations “Sources of Revenue—Medicare”, both of which became effective October 1, 2010. We performed a goodwill impairment analysis as of September 30, 2010 and concluded that there was no impairment as of that date. On January 6, 2011, after we had issued a press release with 2011 earnings estimates which included the impact of the recent reimbursement changes, our carrying value of equity exceeded our market capitalization by approximately $68 million, or 16.2%. We updated our goodwill impairment analysis as of December 31, 2010 and concluded that there was no impairment as of that date. We assessed the fair value of each reporting unit as of December 31, 2010 for goodwill impairment based upon a combination of the discounted cash flow (income approach) and the guideline public company method along with the guideline merged and acquired company method (market approach). The income approach received a 45% weighting and the market approach received a 55% weighting.
The discounted cash flow and market approach methodologies utilized in estimating the fair value of our reporting units for purposes of goodwill impairment testing requires various assumptions about revenues, EBITDA and operating margins, growth rates, and working capital requirements. In determining those judgmental assumptions, we make a number of judgments regarding a variety of data, including—for each reporting unit—the annual budget for 2011, the longer-term business plan, economic projections, anticipated future cash flows, market data, and historical cash flow growth rates.
Below are the key assumptions used to estimate the fair value for our reporting units at the time of our December 31, 2010 goodwill impairment test using the income approach:
| Long term growth rate | Discount rate | |||||||
| Long-term care services |
2.5 | % | 10.0 | % | ||||
| Therapy services |
2.5 | % | 11.5 | % | ||||
| Hospice and home health services |
3.0 | % | 14.0 | % | ||||
Our long-term care reporting unit experienced an average annual growth rate in external revenue from 2007 to 2010 of 7.9%. However, we selected a long term growth rate of 2.5% for the discounted cash flow analysis conducted as part of the impairment analysis because the historical growth rate includes acquisitions and the 2.5% is our expected long-term growth rate from a combination of reimbursement rate increases, occupancy and skilled mix increases.
The operating expenses projected under the discounted cash flow method were based upon our historical expenses as a percentage of long-term care revenue adjusted for known efficiencies or additional costs to be incurred. Capital expenditures were based upon expected expenditures per bed, the build out of current facilities under construction, and projected acquisitions matching our revenue growth rate.
The discount rate used to present value cash flows under the discounted cash flow method is a significant assumption in the analysis. The discount rate was developed using the capital asset pricing model through which a weighted average cost of capital was derived. The discount rate was estimated using the risk free rate, market risk premium, and cost of debt prevalent as of the valuation date. In addition, for long-term care, a risk premium of 6.0% was included in order to account for the risks inherent in the cash flows. The discount rates utilized for therapy and the hospice and home health reporting units are higher due to the size and typical equity structure of these businesses, with a higher equity to debt ratio, which results in a higher discount rate as equity has a higher cost of capital than debt.
For the market approach, we compared ourselves to a peer group of other public companies. As several of our peers lease a higher percentage of their skilled nursing facilities than we do, the metric used was total
61
Table of Contents
invested capital, or TIC, divided by earnings before interest, tax, depreciation, amortization and rent, or EBITDAR. For long-term care the average TIC divided by projected 2010 and 2011 EBITDAR for the peer group, including us, was 7.0 and 6.8, respectively. For our market valuation a multiple against 2010 and 2011 EBITDAR of 7.5 and 6.5, respectively, was selected, with each year given a 50% weighting. For therapy and hospice and home health EBITDA multiples of 5.75 and 5.0, respectively, were used. A control premium of 30% was applied, based upon historical transactions, for all reporting units.
Our goodwill impairment analysis is subject to uncertainties due to uncontrollable events, including the strategic decisions made in response to economic or competitive conditions, the general economic environment, or material changes in Medicare and Medicaid reimbursement that could positively or negatively impact anticipated future operating conditions and cash flows. In addition, our goodwill impairment analysis is subject to uncertainties due to the current economic crisis, including the severity of that crisis and the time period before which the economy recovers.
Income Taxes
Income taxes are accounted for under FASB ASC Topic 740, “Income Taxes.” FASB ASC Topic 740 prescribes a recognition threshold and measurement criteria for the financial statement recognition and measurement of a tax position taken or expected to be taken in a tax return. FASB ASC Topic 740 also provides guidance on de-recognition, classification, interest and penalties, accounting in interim periods, disclosure and transition rules. As of December 31, 2010 and 2009, our accrual for unrecognized tax benefits including applicable interest and penalties was not material. As prescribed by FASB ASC Topic 740, only the amounts reasonably expected to be paid within 12 months are recorded in taxes payable, while remaining amounts after 12 months are recorded in other non-current taxes payable.
Significant judgment is required in determining our provision for income taxes. In the ordinary course of business, there are many transactions for which the ultimate tax outcome is uncertain. While we believe that our tax return positions are supportable, there are certain positions that may not be sustained upon review by tax authorities. While we believe that adequate accruals have been made for such positions, the final resolution of those matters may differ from the amounts provided for in our historical income tax provisions and accruals.
We recognize interest and penalties related to uncertain tax positions in the provision for income taxes line item of the consolidated statements of operations. As of December 31, 2010 and 2009, our accrued interest and penalties on unrecognized tax benefits was not material.
Our tax years 2007 and forward are subject to examination by the IRS and from 2006 forward, by our material state jurisdictions. The IRS is currently conducting a limited scope audit of our 2007 through 2009 tax years. With normal closures of the statute of limitations, we do not anticipate any decrease in the amount of unrecognized tax benefits within the next 12 months.
We use the liability method of accounting for income taxes as set forth in FASB ASC Topic 740. We determine deferred tax assets and liabilities at the balance sheet date based upon the difference between the financial statement and tax bases of assets and liabilities using enacted tax rates in effect for the year in which the differences are expected to affect taxable income.
Our temporary differences are primarily attributable to purchase adjustments related to intangible assets, depreciation, allowances for doubtful accounts, settlement costs, and accruals for professional and general liability expenses and compensation, which are not deductible for tax purposes until paid.
We assess the likelihood that our deferred tax assets will be recovered from future taxable income and available carryback potential and unless we believe that recovery is more likely than not, we establish a valuation allowance to reduce the deferred tax assets to the amounts expected to be realized. We make our judgments
62
Table of Contents
regarding deferred tax assets and the associated valuation allowance, based on among other things, expected future reversals of taxable temporary differences, available carryback potential, tax planning strategies and forecasts of future income. We periodically review for the requirement of a valuation allowance as necessary. As of December 31, 2010, we were in a three-year cumulative pre-tax loss position, which is considered significant negative evidence under FASB ASC Topic 740 and presumes a need for a valuation allowance. The cumulative pretax loss was attributable to a 2009 goodwill impairment charge which was non-deductible for income tax purposes and did not affect taxable income. We have a history of generating taxable earnings and will report significant taxable income in 2010. Further, as our deferred tax assets are expected to reverse in subsequent years, any deferred tax asset could be utilized to carry back against prior year income. This significant positive evidence overcomes the presumption of a need for a valuation allowance. At December 31, 2010, we retained a valuation allowance for our state loss carryforwards of $0.1 million as a result of certain restrictions regarding their utilization.
Share-Based Payments
Share-based payments are accounted for under the FASB ASC Topic 718, “Compensation—Stock Compensation,” which requires all share-based payments, including stock option grants and restricted stock awards, to be recognized in our financial statements based upon their respective grant date fair values. Under FASB ASC Topic 718, the fair value of each employee’s stock option is estimated on the date of grant using an option pricing model that meets certain requirements. We currently use the Black-Scholes option pricing model to estimate the fair value of our stock options. The Black-Scholes model meets the requirements of FASB ASC Topic 718, but the fair values generated by the model may not be indicative of the actual fair values of our equity awards as it does not consider certain factors important to those awards, such as continued employment and periodic vesting requirements as well as limited transferability. The determination of the fair value of share-based payment awards utilizing the Black-Scholes model is affected by our stock price and a number of assumptions, including expected volatility, expected life, risk-free interest rate and expected dividends. We estimated the expected volatility by examining the historical and implied volatilities of comparable publicly-traded companies due to our limited trading history and because we do not have any publicly traded options.
We estimated the expected life of the stock options as the average of the contractual term and the weighted-average vesting term of the options. The risk-free interest rate assumption is based on the implied U.S. treasury rate for the expected life of the stock option. The dividend yield assumption is based on our history and expectation of no dividend payouts. The fair value of our restricted stock awards is based on the closing market price of our Class A common stock on the date of grant. We evaluate the assumptions used to value stock awards on a quarterly basis. If factors change and we employ different assumptions, stock-based compensation expense may differ significantly from what we have recorded in the past. If there are any modifications or cancellations of the underlying unvested securities, we may be required to accelerate, increase or cancel any remaining unearned stock-based compensation expense. To the extent that we grant additional equity securities to employees, our stock-based compensation expense will be increased by the additional unearned compensation resulting from those additional grants or acquisitions.
As of December 31, 2010, there was approximately $3.6 million of total unrecognized compensation costs related to unvested stock awards, restricted stock units and performance stock awards. These costs are expected to have a weighted-average remaining recognition period of 2.0 years. As of December 31, 2010, the total compensation costs related to unvested stock option grants not yet recognized was $1.9 million. These costs are expected to have a weighted-average remaining recognition period of 2.7 years.
Accounting for Conditional Asset Retirement Obligations
In accordance with FASB ASC Topic 410, “Asset Retirement and Environmental Obligations,” we recorded a liability of $5.0 million effective December 31, 2005, substantially all of which related to estimated costs to remove asbestos that is contained within our facilities. Of this $5.0 million liability, $1.6 million was recorded as a cumulative effect of a change in accounting principle, net of tax benefit for the year ended December 31, 2005.
63
Table of Contents
We have determined that a conditional asset retirement obligation exists for asbestos remediation. Though not a current health hazard in our facilities, upon renovation, we may be required to take the appropriate remediation procedures in compliance with state law to remove the asbestos. The removal of asbestos-containing materials includes primarily floor and ceiling tiles from our pre-1980 constructed facilities. We determined the fair value of the conditional asset retirement obligation as the present value of the estimated future cost of remediation based on an estimated expected date of remediation. This computation is based on a number of assumptions which may change in the future based on the availability of new information, technology changes, changes in costs of remediation, and other factors.
The determination of the asset retirement obligation is based upon a number of assumptions that incorporate our knowledge of the facilities, the asset life of the floor and ceiling tiles, the estimated time frames for periodic renovations which would involve floor and ceiling tiles, the current cost for remediation of asbestos and the current technology at hand to accomplish the remediation work. These assumptions to determine the asset retirement obligation may be imprecise or be subject to changes in the future. Any change in the assumptions can impact the value of the determined liability and impact our future earnings. If we were to experience a 10% increase in our estimated future cost of remediation, our recorded liability of $3.9 million would increase by $0.4 million.
Operating Leases
We account for operating leases in accordance with FASB ASC Topic 840, “Leases.” Accordingly, rent expense under our facilities’ and administrative offices’ operating leases is recognized on a straight-line basis over the original term of each facility’s and administrative office’s leases, inclusive of predetermined minimum rent escalations or modifications and including any lease renewal requirements.
Recent Accounting Standards
The information required by this item is incorporated herein by reference to Note 2, “Summary of Significant Accounting Policies,” to the consolidated financial statements under Part IV, Item 15 of this report.
64
Table of Contents
Results of Operations
The following table sets forth details of our revenue and earnings as a percentage of total revenue for the periods indicated:
| Year Ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Revenue |
100.0 | % | 100.0 | % | 100.0 | % | ||||||
| Expenses: |
||||||||||||
| Cost of services (exclusive of rent cost of revenue and depreciation and amortization shown below) |
80.2 | 80.0 | 79.5 | |||||||||
| Rent cost of revenue |
2.3 | 2.4 | 2.5 | |||||||||
| General and administrative |
3.1 | 3.3 | 3.4 | |||||||||
| Litigation settlement costs |
6.5 | — | — | |||||||||
| Depreciation and amortization |
3.1 | 3.1 | 2.9 | |||||||||
| Goodwill impairment charge |
— | 22.6 | — | |||||||||
| 95.2 | 111.4 | 88.3 | ||||||||||
| Other income (expenses): |
||||||||||||
| Interest expense |
(4.5 | ) | (4.4 | ) | (5.1 | ) | ||||||
| Interest income |
0.1 | 0.2 | — | |||||||||
| Equity in earnings of joint venture |
0.3 | 0.4 | 0.3 | |||||||||
| Other income |
0.3 | — | — | |||||||||
| Debt retirement costs |
(0.9 | ) | — | — | ||||||||
| Total other expenses, net |
(4.7 | ) | (3.8 | ) | (4.8 | ) | ||||||
| Income (loss) before provision for income taxes |
0.1 | (15.2 | ) | 6.9 | ||||||||
| Provision for income taxes |
0.3 | 2.4 | 2.5 | |||||||||
| Income from continuing operations |
(0.2 | ) | (17.6 | ) | 4.4 | |||||||
| Loss from discontinued operations, net of tax |
— | (0.1 | ) | — | ||||||||
| Net (loss) income |
(0.2 | )% | (17.7 | )% | 4.4 | % | ||||||
| EBITDA(1) |
7.6 | % | (8.0 | )% | 15.0 | % | ||||||
| Adjusted EBITDA(1) |
14.8 | % | 14.7 | % | 15.1 | % | ||||||
| EBITDAR(2) |
9.9 | % | (5.6 | )% | 17.5 | % | ||||||
| Adjusted EBITDAR(2) |
17.1 | % | 17.1 | % | 17.6 | % | ||||||
| (1) | See footnote 1 to Item 6 of this report, “Selected Financial Data” for a calculation of EBITDA and Adjusted EBITDA and for a description of our uses of, and the limitations associated with, EBITDA and Adjusted EBITDA. |
| (2) | See footnote 1 to Item 6 of this report, “Selected Financial Data” for a calculation of EBITDAR and Adjusted EBITDAR and for a description of our uses of, and the limitations associated with, EBITDAR and Adjusted EBITDAR. |
Year Ended December 31, 2010 Compared to Year Ended December 31, 2009
Revenue. Revenue increased $64.1 million, or 8.5%, to $820.2 million in 2010 from $756.1 million in 2009.
65
Table of Contents
Long term care services
| Year Ended December 31, | ||||||||||||||||||||||||
| 2010 | 2009 | Increase/(Decrease) | ||||||||||||||||||||||
| Revenue Dollars |
Revenue Percentage |
Revenue Dollars |
Revenue Percentage |
Dollars | Percentage | |||||||||||||||||||
| (dollars in millions) | ||||||||||||||||||||||||
| Skilled nursing facilities |
$ | 667.7 | 81.5 | % | $ | 640.1 | 84.7 | % | $ | 27.6 | 4.3 | % | ||||||||||||
| Assisted living facilities |
25.6 | 3.1 | 24.4 | 3.2 | 1.2 | 4.7 | ||||||||||||||||||
| Administrative of third party facilities |
1.1 | 0.1 | 2.3 | 0.3 | (1.2 | ) | (50.6 | ) | ||||||||||||||||
| Total long-term care services |
$ | 694.4 | 84.7 | % | $ | 666.8 | 88.2 | % | $ | 27.6 | 4.1 | % | ||||||||||||
Of the $27.6 million increase in skilled nursing facilities revenue, $13.8 million resulted primarily from the addition of acquired and newly developed facilities since the beginning of 2009, which includes the opening of the Dallas Center of Rehabilitation, Fort Worth Center of Rehabilitation, and the acquisition of two facilities in Iowa. Additionally, revenue increased $12.1 million for skilled nursing facilities operated for all of 2009 and 2010 of which $17.1 million was due to a higher weighted average per patient day rate from Medicare, Medicaid and managed care pay sources, offset by a $4.8 million decrease due to a decline in occupancy rates, which occurred primarily at our Texas facilities. Our revenue related to the administration of third party facilities decreased $1.2 million due to the reduction in number of facilities managed from four in 2009 to one in 2010. Per patient day rates were negatively impacted by the decrease in our skilled mix in 2010 as compared to 2009. We believe our skilled mix declined to 22.7% in 2010 from 23.1% in 2009 primarily due to new and re-admissions staying flat coupled by a decrease in overall average length of stay in most payor classes. While admissions remain flat, we continue to face competitive pressures, primarily due to the development of new facilities in Texas near our existing facilities. Our average daily Part A Medicare rate increased 3.2% to $515 in 2010 from $499 primarily due to the Medicare rate increase effective October 1, 2010. Our average daily Medicaid rate increased 3.4% to $151 in 2010 from $146 in 2009, primarily due to increased Medicaid rates in Texas, Nevada and Missouri. Although average daily Medicare and, in some regions, Medicaid rates increased in 2010, the increase did not fully offset the impact of flat admissions. We have experienced net reductions in Medicaid rates in California and Kansas. Revenue at our assisted living facilities increased $1.2 million, primarily as a result of having a full year of operations at our facility in Tonganoxie, Kansas, which opened in April 2009.
Therapy Services
| Year Ended December 31, | ||||||||||||||||||||||||
| 2010 | 2009 | Increase/(Decrease) | ||||||||||||||||||||||
| Revenue Dollars |
Revenue Percentage |
Revenue Dollars |
Revenue Percentage |
Dollars | Percentage | |||||||||||||||||||
| (dollars in millions) | ||||||||||||||||||||||||
| Rehabilitation therapy services to non-affiliated entities |
$ | 141.1 | 17.2 | % | $ | 141.2 | 18.7 | % | $ | (0.1 | ) | (0.08 | )% | |||||||||||
| Intersegment eliminations |
(67.0 | ) | (8.2 | ) | (66.5 | ) | (8.8 | ) | (0.5 | ) | (0.7 | ) | ||||||||||||
| Total therapy services |
$ | 74.1 | 9.0 | % | $ | 74.7 | 9.8 | % | $ | (0.6 | ) | (0.8 | )% | |||||||||||
Rehabilitation therapy services revenue stayed level as new contracts executed in 2010 offset contract lost in the fourth quarter of 2009.
66
Table of Contents
Hospice and home health services
| Year Ended December 31, | ||||||||||||||||||||||||
| 2010 | 2009 | Increase/(Decrease) | ||||||||||||||||||||||
| Revenue Dollars |
Revenue Percentage |
Revenue Dollars |
Revenue Percentage |
Dollars | Percentage | |||||||||||||||||||
| (dollars in millions) | ||||||||||||||||||||||||
| Hospice |
$ | 41.2 | 5.0 | 14.5 | 1.9 | 26.7 | 183.5 | |||||||||||||||||
| Home Health |
$ | 10.5 | 1.3 | — | 0.0 | 10.5 | 100.0 | |||||||||||||||||
| Total hospice & home health services |
$ | 51.7 | $ | 6.3 | % | $ | 14.5 | 1.9 | % | $ | 37.2 | 255.7 | % | |||||||||||
Hospice and home health revenue increased in 2010 compared to 2009, as a result of the Hospice/Home Health Acquisition.
Cost of Services Expenses. Our cost of services expenses increased $52.6 million, or 8.7%, to $657.5 million, or 80.2% of revenue, in 2010, from $604.9 million, or 80.0% of revenue, in 2009.
Long term care services
| Year Ended December 31, | ||||||||||||||||||||||||
| 2010 | 2009 | Increase/(Decrease) | ||||||||||||||||||||||
| Cost of Service Dollars (prior to intersegment eliminations) |
Revenue Percentage |
Cost of Service Dollars (prior to intersegment eliminations) |
Revenue Percentage |
Dollars | Percentage | |||||||||||||||||||
| (dollars in millions) | ||||||||||||||||||||||||
| Skilled nursing facilities |
$ | 519.3 | 77.8 | % | $ | 499.2 | 77.7 | % | $ | 20.1 | 4.0 | % | ||||||||||||
| Assisted living facilities |
18.0 | 70.3 | 17.0 | 69.7 | 1.0 | 5.9 | ||||||||||||||||||
| Regional operations support |
23.6 | n/a | 21.3 | n/a | 2.3 | 10.8 | ||||||||||||||||||
| Total long-term care services |
$ | 560.9 | 80.8 | % | $ | 537.5 | 80.6 | % | $ | 23.4 | 4.4 | % | ||||||||||||
Cost of services expenses at our skilled nursing facilities increased $20.1 million, $10.8 million of which was due to the addition of acquired and developed facilities since the beginning of 2009, which includes the opening of the Dallas Center of Rehabilitation, Fort Worth Center of Rehabilitation, and the acquisition of two facilities in Iowa, $9.3 million of the increases resulted from operating costs increasing at facilities acquired or developed prior to January 1, 2009 by $4.70 per patient day, or 2.7%, to $183.1 per patient day in the year ended December 31, 2010 from $178 per patient day in the year ended December 31, 2009. The $9.3 million increase in operating costs resulted from a $5.1 million increase in labor costs, which represented an increase of $2.6, or 2.6%, on a per patient day basis. Additionally, the increase in operating costs resulted from a $3.2 million increase in taxes and licenses and a $1.2 million increase in expenses related to rehab/ancillaries. Cost of services expenses at our assisted living facilities increased $1.0 million, primarily due to our newly developed facility in Tonganoxie, Kansas, which opened in April 2009. In the next twelve months, we expect our cost of services expense to increase as we comply with the terms of the injunction related to the Humboldt County Action described in Note 12, Commitments and Contingencies—Litigation to our audited financial statements.
67
Table of Contents
Therapy Services
| Year Ended December 31, | ||||||||||||||||||||||||||||||||
| 2010 | 2009 | Increase/(Decrease) | ||||||||||||||||||||||||||||||
| Revenue Dollars (prior to intersegment eliminations) |
Cost of Service Dollars (prior to intersegment eliminations) |
Revenue Percentage |
Revenue Dollars (prior to intersegment eliminations) |
Cost of Service Dollars (prior to intersegment eliminations) |
Revenue Percentage |
Dollars | Percentage | |||||||||||||||||||||||||
| (dollars in millions) | ||||||||||||||||||||||||||||||||
| Rehabilitation therapy services to non-affiliated entities |
$ | 141.1 | $ | 121.9 | 86.4 | % | $ | 141.2 | $ | 120.5 | 85.3 | % | $ | 1.4 | 1.2 | % | ||||||||||||||||
| Total therapy services |
$ | 141.1 | $ | 121.9 | 86.4 | % | $ | 141.2 | $ | 120.5 | 85.3 | % | $ | 1.4 | 1.2 | % | ||||||||||||||||
Rehabilitation therapy costs as a percentage of revenue increased primarily because of flat revenue rates and salary, wages, and benefits increased as a percentage of total costs due to a decrease in third party facility contracts, as described under “Sources of Revenue—Ancillary Service Segment—Rehabilitation Therapy.”
Hospice and home health services
| Year Ended December 31, | ||||||||||||||||||||||||
| 2010 | 2009 | Increase/(Decrease) | ||||||||||||||||||||||
| Cost of Service Dollars |
Revenue Percentage |
Cost of Service Dollars |
Revenue Percentage |
Dollars | Percentage | |||||||||||||||||||
| (dollars in millions) | ||||||||||||||||||||||||
| Hospice |
$ | 33.4 | 81.1 | % | 15.9 | 109.7 | % | $ | 17.5 | 110.1 | % | |||||||||||||
| Home Health |
9.1 | 86.7 | — | — | 9.1 | 100.0 | ||||||||||||||||||
| Total hospice & home health services |
$ | 42.5 | 82.2 | % | $ | 15.9 | 109.7 | % | $ | 26.6 | 167.3 | % | ||||||||||||
The increase in hospice cost of services was the result of the Hospice/Home Health Acquisition. Cost of services expense in our hospice business was challenged by labor inefficiencies in our California operations in 2009, which have since been remediated in 2010. Hospice and home health costs of services included $0.7 million of acquisition related costs in the year ended December 31, 2010.
Rent cost of revenue. Rent cost of revenue increased by $0.9 million, or 5.0%, to $19.0 million, or 2.3% of revenue, in 2010 from $18.1 million, or 2.4% of revenue, in 2009.
General and Administrative Services Expenses. Our general and administrative services expenses increased $0.4 million, or 1.6%, to $25.5 million, or 3.1% of revenue, in 2010 from $25.1 million, or 3.3% of revenue, in 2009. The increase in our general and administrative expenses was primarily the result of an increase in compensation costs.
Litigation Settlement Expense. Litigation settlement expense totaled $53.5 million for the year ended 2010 with no comparable amount for the year ended 2009. This was comprised of a $50.0 million cash settlement related to the Humboldt County Action described in Note 12, Commitments and Contingencies—Litigation, to our audited financial statements included elsewhere in this report, $3.0 million of related legal expenses, and $0.5 million in securities class action costs related to the Shepardson v. Skilled Healthcare Group, Inc. action described in Note 12.
Depreciation and Amortization. Depreciation and amortization increased by $1.7 million, or 7.3%, to $25.0 million in 2010 from $23.3 million in 2009. This increase primarily resulted from increased depreciation and
68
Table of Contents
amortization related to the opening of our developed skilled nursing facilities in Dallas and Fort Worth as well as other new assets placed in service during 2009 and 2010.
Interest Expense. Interest expense increased by $4.0 million, or 12.1%, to $37.0 million in 2010 from $33.0 million in 2009. The increase in our interest expense was primarily due to an increase in the average interest rate on our debt from 5.9% in 2009 to 6.3% in 2010, which resulted in additional interest expense of $2.2 million. The increase in our cost of borrowing was due to the refinancing of our senior secured credit facility in April 2010. Average debt outstanding increased by $29.9 million, from $473.3 million in 2009 to $503.2 million in 2010 which resulted in additional interest expense of $1.8 million. The increase in average debt outstanding was primarily due to borrowings used to finance the Hospice/Home Health Acquisition and settlement costs. The all in rate for the full year ended December 31, 2010 was 7.4%, as compared to 7.0% in 2009.
Interest Income. Interest income decreased by $0.2 million to $0.9 million in 2010 from $1.1 million in 2009 due to a decrease in outstanding notes receivable.
Equity in Earnings of Joint Venture. Equity earnings of our joint venture decreased by $0.2 million, or 7.1% to $2.6 million, or 0.3% of revenue, in 2010 from $2.8 million, or 0.4% of revenue, in 2009. These earnings relate primarily to our pharmacy joint venture.
Debt Retirement Cost. Debt retirement cost was $7.0 million for the year ended 2010 with no comparable amount for the year ended 2009 due to the expensing of deferred financing fees of $6.6 million and $0.4 million of interest rate swap termination costs as the swap was incompatible with the refinanced senior secured credit facility.
Provision for Income Taxes. Our provision for income taxes in 2010 was $2.5 million, or 172.7% of pre-tax income from continuing operations, as compared to $17.8 million, or 15.5% of pre-tax loss from continuing operations in 2009. The effective tax rate of 172.7% for 2010 was not meaningful due to the low level of pre-tax earnings from operations.
EBITDA. EBITDA increased by $122.7 million to $62.5 million in 2010 from a loss of $60.2 million in 2009. The $122.7 million increase was primarily related to the decrease of $170.6 million non-cash impairment charge in 2009 partially offset by the $53.5 million litigation settlement expense in 2010, all discussed above.
Loss from Continuing Operations. Loss from continuing operations decreased by $131.7 million to a loss of $1.0 million in 2010 from a loss from continuing operations of $132.8 million in 2009. The $131.7 million decrease was related primarily to the decrease of $170.6 million goodwill impairment expense in 2009, $64.1 million increase in revenue, offset by the $53.5 million litigation settlement expense in 2010 and $52.6 million increase in cost of services, all discussed above.
Year Ended December 31, 2009 Compared to Year Ended December 31, 2008
Revenue. Revenue increased $26.7 million, or 3.7%, to $756.1 million in 2009 from $729.4 million in 2008.
Long term care services
| Year Ended December 31, | ||||||||||||||||||||||||
| 2009 | 2008 | Increase/(Decrease) | ||||||||||||||||||||||
| Revenue Dollars |
Revenue Percentage |
Revenue Dollars |
Revenue Percentage |
Dollars | Percentage | |||||||||||||||||||
| (dollars in millions) | ||||||||||||||||||||||||
| Skilled nursing facilities |
$ | 640.1 | 84.7 | % | $ | 621.9 | 85.3 | % | $ | 18.2 | 2.9 | % | ||||||||||||
| Assisted living facilities |
24.4 | 3.2 | 20.6 | 2.8 | 3.8 | 18.9 | ||||||||||||||||||
| Administrative of third party facilities |
2.3 | 0.3 | 0.9 | 0.1 | 1.4 | 130.1 | ||||||||||||||||||
| Total long-term care services |
$ | 666.8 | 88.2 | % | $ | 643.4 | 88.2 | % | $ | 23.4 | 3.6 | % | ||||||||||||
69
Table of Contents
The increase in skilled nursing facilities revenue resulted primarily from a $10.2 million increase due to the addition of acquired and developed facilities since the beginning of 2008, including the acquisition of a Kansas facility in April 2008, the opening of the Dallas Center of Rehabilitation, and the acquisition of two facilities in Iowa. Additionally, for skilled nursing facilities operated for all of 2008 and 2009, revenue increased $32.2 million due to higher rates from Medicare, Medicaid and managed care pay sources, offset by a $24.2 million decrease due to a decline in occupancy rates. Our revenue related to the administration of third party facilities increased $1.3 million. Occupancy and per patient day rates were both negatively impacted by the decrease in our skilled mix in 2009 as compared to 2008. We believe our skilled mix declined to 23.1% in 2009 from 24.2% in 2008 primarily due to a decrease in average length of stay for our skilled patients as well as a reduction in Medicare census from lower acute-care admissions, including those from hospitals, as a result of the challenging economic environment and competitive pressures, primarily due to the development of new facilities in Texas near our existing facilities. Our average daily Part A Medicare rate increased 5.1% to $499 in 2009 from $475 in 2008 as a result of market basket increases provided under the Medicare program in October 2008, as well as a higher patient acuity mix from the expansion of our Express Recovery™ unit services. Our average daily Medicaid rate increased 5.0% to $146 in 2009 from $139 per day in 2008, primarily due to increased Medicaid rates in Texas, California and Missouri. We incurred a Medicare rate decrease of 1.1% as of October 1, 2009, which will negatively impact per patient day rates in 2010 as compared to 2009. We have also experienced Medicaid rate reductions in certain states. The $3.8 million increase in assisted living facilities revenue is primarily attributed to the acquisition of the Kansas assisted living facilities in September 2008.
Therapy services
| Year Ended December 31, | ||||||||||||||||||||||||
| 2009 | 2008 | Increase/(Decrease) | ||||||||||||||||||||||
| Revenue Dollars |
Revenue Percentage |
Revenue Dollars |
Revenue Percentage |
Dollars | Percentage | |||||||||||||||||||
| (dollars in millions) | ||||||||||||||||||||||||
| Rehabilitation therapy services to non-affiliated entities |
$ | 141.2 | 18.7 | % | $ | 135.1 | 18.5 | % | $ | 6.1 | 4.5 | % | ||||||||||||
| Intersegment eliminations |
$ | (66.5 | ) | (8.8 | ) | $ | (65.2 | ) | (8.9 | ) | $ | (1.3 | ) | (2.1 | ) | |||||||||
| Total therapy services |
$ | 74.7 | 9.9 | % | $ | 69.9 | 9.6 | % | $ | 4.8 | 6.6 | % | ||||||||||||
The increase in rehabilitation therapy services revenue resulted primarily from an increase in therapy services under existing third-party facility contracts due to higher rates, increased census and improved Medicare Part A RUG distribution. As discussed above under “Revenue—Therapy Services Segment,” we cancelled 35 rehabilitation therapy services contracts during the year ended December 31, 2009. The margins on the cancelled contracts were significantly below the overall margin of the therapy business.
Hospice and home health services
| Year Ended December 31, | ||||||||||||||||||||||||
| 2009 | 2008 | Increase/(Decrease) | ||||||||||||||||||||||
| Revenue Dollars |
Revenue Percentage |
Revenue Dollars |
Revenue Percentage |
Dollars | Percentage | |||||||||||||||||||
| (dollars in millions) | ||||||||||||||||||||||||
| Hospice |
$ | 14.5 | 1.9 | 15.9 | 2.2 | (1.4 | ) | (9.0 | ) | |||||||||||||||
| Home Health |
$ | — | — | — | — | — | — | |||||||||||||||||
| Total hospice & home health services |
$ | 14.5 | $ | 1.9 | % | $ | 15.9 | 2.2 | % | $ | (1.4 | ) | (9.0 | )% | ||||||||||
Hospice revenue decreased primarily as a result of a Medicare cap contractual adjustment in 2009.
70
Table of Contents
Cost of Services Expenses. Our cost of services expenses increased $25.3 million, or 4.4%, to $604.9 million, or 80.0% of revenue, in 2009, from $579.6 million, or 79.5% of revenue, in 2008.
Long term care services
| Year Ended December 31, | ||||||||||||||||||||||||
| 2009 | 2008 | Increase/(Decrease) | ||||||||||||||||||||||
| Cost of Service Dollars (prior to intersegment eliminations) |
Revenue Percentage |
Cost of Service Dollars (prior to intersegment eliminations) |
Revenue Percentage |
Dollars | Percentage | |||||||||||||||||||
| (dollars in millions) | ||||||||||||||||||||||||
| Skilled nursing facilities |
$ | 499.2 | 78.0 | % | $ | 485.9 | 78.1 | % | $ | 13.3 | 2.7 | % | ||||||||||||
| Assisted living facilities |
17.0 | 69.7 | 13.9 | 67.5 | 3.1 | 22.3 | ||||||||||||||||||
| Regional operations support |
21.3 | n/a | 16.2 | n/a | 5.1 | 31.5 | ||||||||||||||||||
| Total long-term care services |
$ | 537.5 | 80.6 | % | $ | 516.0 | 80.2 | % | $ | 21.5 | 4.2 | % | ||||||||||||
Cost of services expenses at our skilled nursing facilities increased $10.1 million due to the acquisition of a Kansas facility in April 2008, the opening of the Dallas Center of Rehabilitation and acquisition of the Rehabilitation Center of Des Moines and St. Mary Healthcare and Rehabilitation Center, and $3.0 million resulted from operating costs increasing at facilities acquired or developed prior to January 1, 2008 by $4 per patient day, or 2.3%, to $179 per patient day in 2009 from $175 per patient day in 2008. The $3.0 million increase in operating costs resulted from a $9.3 million increase in labor costs, or 5.4%, on a per patient day basis, as the fixed labor costs increased as a percent of total labor costs due to the decline in census and also due to slight labor rate increases. These labor cost increases were offset by a $3.4 million decrease in ancillary costs and a $2.9 million decrease in other expenses such as food, therapy, and other purchased services primarily due to the decreased census. Cost of services expenses at our assisted living facilities increased primarily due to the acquisition of seven assisted living facilities in September 2008.
Therapy services
| Year Ended December 31, | ||||||||||||||||||||||||||||||||
| 2009 | 2008 | Increase/(Decrease) | ||||||||||||||||||||||||||||||
| Revenue Dollars (prior to intersegment eliminations) |
Cost of Service Dollars (prior to intersegment eliminations) |
Revenue Percentage |
Revenue Dollars (prior to intersegment eliminations) |
Cost of Service Dollars (prior to intersegment eliminations) |
Revenue Percentage |
Dollars | Percentage | |||||||||||||||||||||||||
| (dollars in millions) | ||||||||||||||||||||||||||||||||
| Rehabilitation therapy services to non-affiliated entities |
$ | 141.2 | $ | 120.5 | 85.3 | % | $ | 135.1 | $ | 117.5 | 87.0 | % | $ | 3.0 | 2.6 | % | ||||||||||||||||
| Total therapy services |
$ | 141.2 | $ | 120.5 | 85.3 | % | $ | 135.1 | $ | 117.5 | 87.0 | % | $ | 3.0 | 2.6 | % | ||||||||||||||||
The decrease in rehabilitation therapy costs as a percentage of revenue was primarily due to increased labor productivity as well as lower bad debt expense in 2009 as compared to 2008. Cost of services expenses related to our hospice services were 96.6% of total hospice revenue excluding the 2009 cap overage of $2.1 million from revenue, resulting in revenue of $20.3 million in 2009, as compared to 94.0% of total hospice revenue of $19.9 million in 2008.
71
Table of Contents
Hospice and home health services
| Year Ended December 31, | ||||||||||||||||||||||||
| 2009 | 2008 | Increase/(Decrease) | ||||||||||||||||||||||
| Cost of Service Dollars |
Revenue Percentage |
Cost of Service Dollars |
Revenue Percentage |
Dollars | Percentage | |||||||||||||||||||
| (dollars in millions) | ||||||||||||||||||||||||
| Hospice |
$ | 15.9 | 109.7 | % | 14.8 | 93.1 | % | $ | 1.1 | 7.4 | % | |||||||||||||
| Home Health |
— | — | — | — | — | — | ||||||||||||||||||
| Total hospice & home health services |
$ | 15.9 | 109.7 | % | $ | 14.8 | 93.1 | % | $ | 1.1 | 7.4 | % | ||||||||||||
Cost of services expense in our hospice business was challenged by labor inefficiencies in our California operations, which have since been remediated.
Rent cost of revenue. Rent cost of revenue decreased by $0.1 million, or 0.5%, to $18.1 million, or 2.4% of revenue, in 2009 from $18.2 million, or 2.5% of revenue, in 2008.
General and Administrative Services Expenses. Our general and administrative services expenses increased $0.6 million, or 2.4%, to $25.1 million, or 3.3% of revenue, in 2009 from $24.5 million, or 3.3% of revenue, in 2008. The increase in our general and administrative expenses was primarily the result of $0.9 million of expense incurred related to the restatement of our financial results.
Depreciation and Amortization. Depreciation and amortization increased by $2.3 million, or 11.0%, to $23.3 million in 2009 from $21.0 million in 2008. This increase primarily resulted from increased depreciation and amortization related to the opening of the Dallas Center of Rehabilitation skilled nursing facility as well as new assets placed in service during 2008 and 2009. We expect that depreciation costs will continue to increase as we place additional Express Recovery™ units in service in 2010 as well as from a full year of depreciation recorded for assets placed in service during 2009.
Goodwill Impairment Charge. We recorded a goodwill impairment charge of $170.6 million in 2009. There was no goodwill impairment charge recorded in 2008. See “Management’s Discussion and Analysis of Financial Condition and Results of Operations—Goodwill” for a more detailed discussion of the goodwill impairment charge.
Interest Expense. Interest expense decreased by $4.3 million, or 11.5%, to $33.0 million in 2009 from $37.3 million in 2008. The decrease in our interest expense was primarily due to a decrease in the average interest rate on our debt from 7.2% in 2008 to 5.9% in 2009, which resulted in $6.1 million of savings. Average debt outstanding increased by $0.4 million, from $472.9 million in 2008 to $473.3 million in 2009. The impact of the lower average interest rate was partially offset by a $1.6 million increase in the amortization of deferred financing fees as a result of amounts paid to extend the maturity date of our revolving credit facility in April 2009. The all in rate for the full year ended December 31, 2009 was 7.0%, as compared to 7.9% in 2008.
Interest Income. Interest income increased by $0.4 million to $1.1 million in 2009 from $0.7 million in 2008 due to an increase in outstanding notes receivable balances.
Equity in Earnings of Joint Venture. Equity earnings of our joint venture increased by $0.3 million, or 12.0% to $2.8 million, or 0.4% of revenue, in 2009 from $2.5 million, or 0.3% of revenue, in 2008. These earnings relate primarily to our pharmacy joint venture.
Provision for Income Taxes. Our provision for income taxes in 2009 was $17.8 million, or (15.5)% of pre-tax loss from continuing operations, as compared to $18.1 million and 34.7% of pre-tax earnings from continuing operations in 2008. The change in the effective tax rate for 2009 was primarily due to a $170.6
72
Table of Contents
million impairment charge for goodwill which was not deductible for tax purposes. Absent this charge, our effective tax rate for 2009 would have been 32.1%.
EBITDA. EBITDA decreased by $169.9 million to a loss of $60.2 million in 2009 from $109.7 million in 2008. The $169.9 million decrease was primarily related to the $170.6 million non-cash impairment charge, $25.0 million increase in cost of services expenses, and $0.6 million increase in general and administrative service expenses, partially offset by the $26.5 million increase in revenue and $0.1 million decrease in rent cost of revenue for the period, all discussed above.
Loss from Continuing Operations. Income from continuing operations decreased by $166.9 million to a loss of $132.8 million in 2009 from income of $34.1 million in 2008. The $166.9 million decrease was related primarily to the $170.6 million non cash impairment charge, partially offset by the $0.4 million increase in interest income, the $4.3 million decrease in interest expense, and the $0.2 million decrease in income tax expense, all discussed above.
73
Table of Contents
Quarterly Data
The following is a summary of our unaudited quarterly results from operations for each of the years ended December 31, 2010 and 2009.
| Three Months Ended, | ||||||||||||||||||||||||||||||||
| December 31, 2010 |
September 30, 2010 |
June 30, 2010 |
March 31, 2010 |
December 31, 2009 |
September 30, 2009 |
June 30, 2009 |
March 31, 2009 |
|||||||||||||||||||||||||
| (In thousands, except per share data) | ||||||||||||||||||||||||||||||||
| Consolidated Statement of Operations Data |
||||||||||||||||||||||||||||||||
| Revenue |
$ | 220,749 | $ | 209,199 | $ | 200,971 | $ | 189,319 | $ | 188,390 | $ | 187,447 | $ | 192,154 | $ | 188,074 | ||||||||||||||||
| Expenses: |
||||||||||||||||||||||||||||||||
| Cost of services (exclusive of rent cost of revenue and depreciation and amortization shown below) |
175,224 | 168,579 | 162,007 | 151,705 | 151,718 | 151,539 | 152,879 | 148,777 | ||||||||||||||||||||||||
| Rent cost of revenue |
4,829 | 4,796 | 4,832 | 4,581 | 4,569 | 4,509 | 4,544 | 4,515 | ||||||||||||||||||||||||
| General and administrative |
7,037 | 6,016 | 6,112 | 6,351 | 5,684 | 6,343 | 6,823 | 6,240 | ||||||||||||||||||||||||
| Litigation settlement costs |
— | 53,505 | — | — | ||||||||||||||||||||||||||||
| Depreciation and amortization |
6,806 | 6,305 | 5,992 | 5,944 | 5,950 | 6,014 | 5,867 | 5,477 | ||||||||||||||||||||||||
| Goodwill impairment charge |
— | — | — | — | 170,600 | — | — | — | ||||||||||||||||||||||||
| 193,896 | 239,201 | 178,943 | 168,581 | 338,521 | 168,405 | 170,113 | 165,009 | |||||||||||||||||||||||||
| Other income (expenses): |
||||||||||||||||||||||||||||||||
| Interest expense |
(10,487 | ) | (10,086 | ) | (9,164 | ) | (7,284 | ) | (8,265 | ) | (8,417 | ) | (8,241 | ) | (8,090 | ) | ||||||||||||||||
| Interest income |
263 | 260 | 196 | 228 | 250 | 285 | 420 | 191 | ||||||||||||||||||||||||
| Equity in earnings of joint venture |
345 | 746 | 678 | 797 | 521 | 746 | 751 | 733 | ||||||||||||||||||||||||
| Other income (expense) |
1,744 | 9 | 583 | (4 | ) | 151 | 59 | — | (60 | ) | ||||||||||||||||||||||
| Debt retirement costs |
— | — | (7,010 | ) | ||||||||||||||||||||||||||||
| Total other expenses, net |
(8,135 | ) | (9,071 | ) | (14,717 | ) | (6,263 | ) | (7,343 | ) | (7,327 | ) | (7,070 | ) | (7,226 | ) | ||||||||||||||||
| (Loss) income from continuing operations before provision for income taxes |
18,718 | (39,073 | ) | 7,311 | 14,475 | (157,474 | ) | 11,715 | 14,971 | 15,839 | ||||||||||||||||||||||
| Provision for income taxes |
7,878 | (13,766 | ) | 2,766 | 5,594 | 3,841 | 2,420 | 5,797 | 5,784 | |||||||||||||||||||||||
| (Loss) income from continuing operations |
10,840 | (25,307 | ) | 4,545 | 8,881 | (161,315 | ) | 9,295 | 9,174 | 10,055 | ||||||||||||||||||||||
| Loss from discontinued operations, net of tax |
— | — | — | — | — | (243 | ) | (95 | ) | (52 | ) | |||||||||||||||||||||
| Net (loss) income |
$ | 10,840 | $ | (25,307 | ) | $ | 4,545 | $ | 8,881 | $ | (161,315 | ) | $ | 9,052 | $ | 9,079 | $ | 10,003 | ||||||||||||||
| Earnings (loss) per share, basic: |
||||||||||||||||||||||||||||||||
| Earnings (loss) per common share from continuing operations |
$ | 0.29 | $ | (0.68 | ) | $ | 0.12 | $ | 0.24 | $ | (4.37 | ) | $ | 0.25 | $ | 0.25 | $ | 0.27 | ||||||||||||||
| Loss per common share from discontinued operations |
— | — | — | — | — | (0.01 | ) | — | — | |||||||||||||||||||||||
| Earnings (loss) per share |
$ | 0.29 | $ | (0.68 | ) | $ | 0.12 | $ | 0.24 | $ | (4.37 | ) | $ | 0.24 | $ | 0.25 | $ | 0.27 | ||||||||||||||
| Earnings (loss) per share, diluted: |
||||||||||||||||||||||||||||||||
| Earnings (loss) per common share from continuing operations |
$ | 0.29 | $ | (0.68 | ) | $ | 0.12 | $ | 0.24 | $ | (4.37 | ) | $ | 0.25 | $ | 0.25 | $ | 0.27 | ||||||||||||||
| Loss per common share from discontinued operations |
— | — | — | — | — | (0.01 | ) | — | — | |||||||||||||||||||||||
| Earnings (loss) per share |
$ | 0.29 | $ | (0.68 | ) | $ | 0.12 | $ | 0.24 | $ | (4.37 | ) | $ | 0.24 | $ | 0.25 | $ | 0.27 | ||||||||||||||
| Weighted-average common shares outstanding, basic |
37,010 | 36,997 | 36,983 | 36,962 | 36,943 | 36,927 | 36,904 | 36,881 | ||||||||||||||||||||||||
| Weighted-average common shares outstanding, diluted |
37,150 | 36,997 | 37,084 | 37,037 | 36,943 | 36,950 | 36,928 | 36,911 | ||||||||||||||||||||||||
74
Table of Contents
Liquidity and Capital Resources
The following table presents selected data from our consolidated statements of cash flows (in thousands):
| Twelve Months Ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Cash Flows from Continuing Operations |
||||||||||||
| Net cash provided by operating activities |
$ | 35,298 | $ | 74,897 | $ | 67,489 | ||||||
| Net cash used in investing activities |
(76,405 | ) | (46,168 | ) | (72,853 | ) | ||||||
| Net cash provided by (used in) financing activities |
41,771 | (27,638 | ) | 2,399 | ||||||||
| Cash flows from discontinued operations |
— | 390 | — | |||||||||
| Net increase (decrease) in cash and equivalents |
664 | 1,481 | (2,965 | ) | ||||||||
| Cash and cash equivalents at beginning of period |
3,528 | 2,047 | 5,012 | |||||||||
| Cash and cash equivalents at end of period |
$ | 4,192 | $ | 3,528 | $ | 2,047 | ||||||
Years Ended December 31, 2010 and 2009
Net cash provided by operating activities primarily consists of net loss (income) adjusted for certain non-cash items including depreciation and amortization, provision for doubtful accounts, stock-based compensation, and write-off of deferred financing costs, as well as the effect of changes in working capital and other activities. Cash provided by operating activities for the year ended December 31, 2010 was $35.3 million and consisted of net loss of $1.0 million, adjustments for non-cash items of $46.8 million and $10.5 million used by working capital and other activities. Working capital and other activities primarily consisted of an increase in accounts receivable of $14.5 million, $8.1 million increase in other current and non-current assets, and decrease in insurance liability risks of $4.4 million offset by a $4.8 million increase of payments in notes receivable, increase in accounts payable and accrued liabilities of $1.7 million, increase in employee compensation and benefits of $9.2 million and $0.8 million increase in other long-term liabilities. The increase in accounts receivable was due primarily to an increase in revenue for the year ended December 31, 2010, as compared to the year ended December 31, 2009. Days sales outstanding (“DSO”) decreased from 47.0 for the three months ended December 31, 2009 to 41.2 for the three months ended December 31, 2010. The reduction in DSO offset the increase in sales, resulting in the net $14.5 million increase in accounts receivable. The aforementioned legal settlement expense negatively impacted cash flows from operations of $35.3 million by $53.5 million for the year ended December 31, 2010, as compared to cash flows from operations of $74.9 million in 2009.
Investing activities used $76.4 million in 2010, as compared to $46.2 million in 2009. The primary use of funds in 2010 consisted of $45.4 million of cash consideration paid for the Hospice/Home Health Acquisition in May 2010, $18.0 million cash paid for the purchase of previously leased facilities, capital expenditures of $27.7 million, offset by the cash proceeds of $14.7 million received from our sale of the Westside Campus Care in December 2010. The capital expenditures consisted of $7.9 million for construction of new healthcare facilities, $5.6 million for expansion of our Express Recovery™ unit program and $14.3 million of routine capital expenditures.
Net cash provided by financing activities was $41.8 million in 2010, as compared to net cash used in financing activities of $27.6 million in 2009. In 2010, net cash provided by financing activities primarily reflects net repayment of borrowings under our line of credit of $46.0 million and repayment of long-term debt of $259.3 million, offset by the $357.3 million of proceeds from issuance of long-term debt and additions to deferred financing fees of $10.2 million, associated with the refinancing of our senior secured credit facility in April 2010.
Years Ended December 31, 2009 and 2008
Net cash provided by operating activities primarily consists of net loss (income) adjusted for certain non-cash items including depreciation and amortization, provision for doubtful accounts, stock-based compensation, and goodwill impairment charge, as well as the effect of changes in working capital and other
75
Table of Contents
activities. Cash provided by operating activities for the year ended December 31, 2009 was $74.9 million and consisted of net loss of $133.2 million, adjustments for non-cash items of $215.2 million and $7.2 million used by working capital and other activities. Working capital and other activities primarily consisted of an increase in accounts receivable of $15.8 million, decrease in accounts payable and accrued liabilities of $2.2 million, decrease in employee compensation and benefits of $1.6 million, and decrease in insurance liability risks of $3.9 million offset by a $5.5 million increase of payments in notes receivable, $9.8 million decrease in other current and non-current assets and $1.2 million increase in other long-term liabilities. The increase in accounts receivable offset by collections was due primarily to an increase in revenue for the year ended December 31, 2009, as compared to the year ended December 31, 2008. Days sales outstanding decreased slightly from 49.9 for the three months ended December 31, 2008 to 47.0 for the three months ended December 31, 2009. The reduction in accounts payable and accrued liabilities was primarily due to decreases in accrued interest payable and income taxes payable.
Investing activities used $46.2 million in 2009, as compared to $72.9 million in 2008. The primary use of funds in 2009 was $5.0 million used to acquire healthcare facilities and $41.2 million for capital expenditures. The capital expenditures consisted of $12.2 million for construction of new healthcare facilities for the completion of the Dallas Center of Rehabilitation and Vintage Park at Tonganoxie and for the construction costs to date for Fort Worth Center of Rehabilitation, $8.7 million for expansion of our Express Recovery™ unit program and $20.3 million of routine capital expenditures.
Net cash used in financing activities was $27.6 million in 2009, as compared to net cash provided by financing activities of $2.4 million in 2008. In 2009, net cash used in financing activities reflected $9.0 million of net repayments under our line of credit, $10.7 million of scheduled debt repayments and a $7.9 million increase in deferred financing fees.
Principal Debt Obligations
Our primary sources of liquidity are our cash on hand, our cash flows from operations and our senior secured credit facility, which is subject to the satisfaction of certain financial covenants therein. Our primary liquidity requirements are for debt service on our first lien senior secured credit facility and our 11% senior subordinated notes, capital expenditures and working capital.
We are significantly leveraged. As of December 31, 2010, we had $519.9 million in aggregate indebtedness outstanding, consisting of $129.7 million principal amount of our 11% senior subordinated notes (net of the unamortized portion of the original issue discount of $0.3 million), a $354.9 million first lien senior secured term loan (net of the unamortized portion of the original issue discount of $2.4 million), $26.0 million outstanding under our $100.0 million revolving credit facility, and other debt of approximately $9.3 million. Furthermore, we had $4.4 million in outstanding letters of credit against our $100.0 million revolving credit facility, leaving approximately $69.6 million of additional borrowing capacity under our amended senior secured credit facility as of December 31, 2010. For 2010, 2009, and 2008, our interest expense, net of interest income, was $36.1 million, $31.9 million, and $36.6 million, respectively. For 2010, 2009, and 2008, we capitalized $0.3 million, $0.4 million, and $0.8 million, respectively, of interest expense related to new facilities that we are developing.
If our remaining ability to borrow under our revolving credit facility is insufficient for our capital requirements, we will be required to seek additional sources of financing, including issuing equity, which may be dilutive to our current stockholders, or incurring additional debt. Our ability to incur additional debt is subject to the restrictions in the indenture governing our 11% senior subordinated notes and our senior secured credit facility. We cannot assure you that the restrictions contained in these agreements will permit us to borrow the funds that we need to finance our operations, or that additional debt will be available to us on commercially reasonable terms or at all. If we are unable to obtain funds sufficient to finance our capital requirements, we may have to forego opportunities to expand our business, including the acquisition of additional facilities. See Item 1A of this report, “Risk Factors—Global economic conditions may impact our ability to obtain additional financing on commercially reasonable terms or at all and our ability to expand our business may be harmed.”
76
Table of Contents
Term Loan and Revolving Loan
On April 9, 2010, we entered into an up to $360.0 million term loan and a $100.0 million revolving credit facility (the “Restated Credit Agreement”) that replaced the senior secured term loan and revolving credit facility that were set to mature in June 2012. The new revolving credit facility was undrawn at closing. We refer to the senior secured term loan and revolving credit facility provided under the Restated Credit Agreement as our “senior secured credit facility.”
The term loan requires principal payments of 0.25% of the original principal amount, or $0.9 million on the last business day of each of March, June, September and December, commencing on June 30, 2010, with the balance due April 9, 2016. Amounts borrowed under the term loan may be prepaid at any time without penalty except for breakage costs. Commitments under the revolving loan terminate on April 9, 2015. However, if any of our 11% senior subordinated notes remain outstanding on October 14, 2013, then the maturity date of the term loan and revolving loan will be October 14, 2013. Amounts borrowed pursuant to the Restated Credit Agreement are secured by substantially all of our assets.
Under the Restated Credit Agreement, we must maintain compliance with specified financial covenants measured on a quarterly basis, including a minimum fixed charge coverage ratio (with a range of 1.5:1 to 2:1 as set forth in further detail in the Restated Credit Agreement) as well as a maximum leverage ratio (with a range of 5.5:1 to 4:1 as set forth in further detail in the Restated Credit Agreement). The Restated Credit Agreement also includes certain additional affirmative and negative covenants, including limitations on the incurrence of additional indebtedness, liens, investments in other businesses and capital expenditures. Also under the Restated Credit Agreement, subject to certain exceptions and minimum thresholds, we are required to apply all of the proceeds from any issuance of debt, half of the proceeds from any issuance of equity, half (or one quarter if our Consolidated Leverage Ratio, as defined in the Restated Credit Agreement, for such fiscal year is less than 3:1) of our annual Consolidated Excess Cash Flow, as defined in the Restated Credit Agreement, and, subject to permitted reinvestments, all amounts received in connection with any sale of our assets and casualty insurance and condemnation or eminent domain proceedings, in each case to repay the outstanding amounts under the Restated Credit Agreement.
Loans outstanding under the Restated Credit Agreement bear interest, at our election, either at the prime rate plus an initial margin of 2.75% or the London Interbank Offered Rate (“LIBOR”) plus an initial margin of 3.75%. Under the terms of the Restated Credit Agreement there is a LIBOR floor of 1.50%. We have a 0.5% commitment fee on the unused portion of the revolving line of credit. The interest rate margin on the loans can be reduced by 0.25% based on our Consolidated Leverage Ratio, as defined in the Restated Credit Agreement, for the applicable four-quarter period. Furthermore, we have the right to increase our borrowings under the term loan and/or the revolving loan up to an aggregate amount of $150.0 million provided that we are in compliance with the Restated Credit Agreement, that the additional debt would not cause any covenant violation of the Restated Credit Agreement, and that existing or new lenders within the Restated Credit Agreement or new lenders agree to increase their commitments. We believe that we were in compliance with our debt covenants as of December 31, 2010.
In addition, we expensed deferred financing fees related to the Restated Credit Agreement in the amount of $6.6 million in April 2010. In conjunction with the closing of the refinancing, we terminated our existing interest rate swap agreements as they were incompatible with the new financing due to the existence of the LIBOR floor. The termination of the interest rate swap agreements cost $0.4 million.
Senior Subordinated Notes
Our 11% senior subordinated notes were issued in December 2005 in the aggregate principal amount of $200.0 million, with an interest rate of 11.0% per annum. The 11% senior subordinated notes were issued at a discount of $1.3 million. Interest is payable semiannually in January and July of each year. The 11% senior subordinated notes mature on January 15, 2014. The 11% senior subordinated notes are unsecured senior
77
Table of Contents
subordinated obligations and rank junior to all of our existing and future senior indebtedness, including indebtedness under our senior secured credit facility. The 11% senior subordinated notes are guaranteed on a senior subordinated basis by certain of our current and future subsidiaries. There was $130.0 million aggregate principal amount of our 11% senior subordinated notes outstanding as of December 31, 2010.
As of January 15, 2011, we are entitled to redeem all or a portion of the remaining $130.0 million aggregate principal amount of our 11% senior subordinated notes upon not less than 30 nor more than 60 days notice, at redemption prices (expressed in percentages of principal amount on the redemption date), plus accrued interest to the redemption date if redeemed during the 12-month period commencing on January 15, 2011 and 2012 and thereafter of 102.75% and 100.00%, respectively.
Capital Expenditures
We intend to invest in the maintenance and general upkeep of our facilities on an ongoing basis. We also expect to perform renovations of our existing facilities every five to ten years to remain competitive. Combined, we expect that these activities will amount to approximately $1,500 per bed, or approximately $14.0 million in capital expenditures in 2011 on our existing facilities. In addition, we are continuing with the expansion of our Express Recovery™ units. These units cost, on average, between $0.4 million and $0.6 million each. We completed four Express Recovery™ units in 2010. We are in the process of developing an additional three Express Recovery™ units in 2011.
In the second quarter of 2010, we completed a 136-bed skilled nursing facility in downtown Forth Worth, Texas. We may also invest in expansions of our existing facilities and the acquisition or development of new facilities. We anticipate that we will have capital expenditures in 2011 of approximately $21 million. We will continue to assess our capital spending plans on an ongoing basis.
Liquidity
Based upon our current level of operations, we believe that cash generated from operations, cash on hand and borrowings available to us will be adequate to meet our anticipated debt service requirements, capital expenditures and working capital needs for at least the next 12 months. There can be no assurance, however, that our business will generate sufficient cash flow from operations or that future borrowings will be available under our senior secured credit facility, or otherwise, to enable us to grow our business, service our indebtedness, including our amended senior secured credit agreement and our 11% senior subordinated notes, or make anticipated capital expenditures. One element of our business strategy is to selectively pursue acquisitions and strategic alliances. Any acquisitions or strategic alliances may result in our incurrence or assumption of additional indebtedness. We assess our capital needs on an ongoing basis and may seek additional financing through a variety of methods including through an extension of our senior secured credit facility or by accessing available debt and/or equity markets, as we deem necessary to fund our capital expenditures and potential acquisitions or for other purposes. Our future operating performance, ability to service or refinance our 11% senior subordinated notes and ability to service and extend or refinance our senior secured credit facility will be subject to future economic conditions and to financial, business and other factors, many of which are beyond our control.
In June 2010 we entered into an interest rate cap agreement and an interest rate swap agreement as required by our senior secured credit facility. The interest rate cap agreement is for a notional amount of $70.0 million with a cap rate on 1 month LIBOR of 2.0% from July 2010 to December 2011. The interest rate swap agreement is for a notional amount of $70.0 million with an interest rate of 2.3% from January 2012 to June 2013. We paid $0.1 million for the interest rate cap and the interest rate swap had no value at inception. Under the terms of the interest rate swap agreement, we will be required to pay a fixed per annum interest rate of 2.3%, plus a 3.75% margin, or 6.0% in total. In exchange for the payment of the fixed interest rate amounts, we will receive floating interest rate amounts equal to the one-month LIBOR rate in effect on the effective date of the interest rate swap
78
Table of Contents
agreement and the subsequent reset dates, which are the monthly anniversaries of the effective date. The effect of the swap agreement is to convert $70.0 million of variable interest rate debt into fixed rate debt, with an effective per annum interest rate of 6.0%.
Other Factors Affecting Liquidity and Capital Resources
Medical and Professional Malpractice and Workers’ Compensation Insurance. Skilled nursing facilities, like physicians, hospitals and other healthcare providers, are subject to a significant number of legal actions alleging malpractice, product liability or related legal theories. Many of these actions involve large claims and significant defense costs. To protect ourselves from the cost of these claims, we maintain professional liability and general liability as well as workers’ compensation insurance in amounts and with deductibles that we believe to be sufficient for our operations. Historically, unfavorable pricing and availability trends emerged in the professional liability and workers’ compensation insurance market and the insurance market in general that caused the cost of these liability coverages to generally increase dramatically. Many insurance underwriters became more selective in the insurance limits and types of coverage they would provide as a result of rising settlement costs and the significant failures of some nationally known insurance underwriters. As a result, we experienced substantial changes in our professional insurance program beginning in 2001. Specifically, we were required to assume substantial self-insured retentions for our professional liability claims. A self-insured retention is a minimum amount of damages and expenses (including legal fees) that we must pay for each claim. We use actuarial methods to estimate the value of the losses that may occur within this self-insured retention level and we are required under our workers’ compensation insurance agreements to post a letter of credit or set aside cash in trust funds to securitize the estimated losses that we may incur. Because of the high retention levels, we cannot predict with certainty the actual amount of the losses we will assume and pay.
We estimate our self-insured general and professional liability reserves on a quarterly basis and our self-insured workers’ compensation reserve on a semiannual basis, based upon actuarial analyses using the most recent trends of claims, settlements and other relevant data from our own and our industry’s loss history. Based upon these analyses, at December 31, 2010, we had reserved $17.6 million for known or unknown or potential self-insured general and professional liability claims and $16.4 million for self-insured workers’ compensation claims. We have estimated that we may incur approximately $4.0 million for self-insured general and professional liability claims and $4.5 million for self-insured workers’ compensation claims for a total of $8.5 million to be payable within 12 months; however, there are no set payment schedules and there can be no assurance that the payment amount in 2011 will not be significantly larger or smaller. To the extent that subsequent claims information varies from loss estimates, the liabilities will be adjusted to reflect current loss data. There can be no assurance that in the future general and professional liability or workers’ compensation insurance will be available at a reasonable price and that we will not have to further increase our levels of self-insurance. For a detailed discussion of our professional and general liability and workers’ compensation reserve, see Item 1 of this report, “Business—Insurance.”
Inflation. We derive a substantial portion of our revenue from the Medicare program. We also derive revenue from state Medicaid and similar reimbursement programs. Payments under these programs generally provide for reimbursement levels that are adjusted for inflation annually based upon the state’s fiscal year for the Medicaid programs and in each October for the Medicare program. However, there can be no assurance that these adjustments will continue in the future and, if received, will reflect the actual increase in our costs for providing healthcare services.
Labor and supply expenses make up a substantial portion of our operating expenses. Those expenses can be subject to increase in periods of rising inflation and when labor shortages occur in the marketplace. To date, we have generally been able to implement cost control measures or obtain increases in reimbursement sufficient to offset increases in these expenses. We cannot assure you that we will be successful in offsetting future cost increases.
79
Table of Contents
Global Market and Economic Conditions. Global market and economic conditions over the past two years have been very challenging with tight credit conditions and slow or negative economic growth in most major economies generally expected to continue in 2011 and possibly beyond. As a result of these market conditions, the cost and availability of credit has been and may continue to be adversely affected by illiquid credit markets and wider credit spreads. Concern about the stability of the markets generally and the strength of counterparties specifically has led many lenders and institutional investors to reduce, and in some cases, cease to provide credit to borrowers. These factors have led to a decrease in spending by businesses and consumers alike, and a corresponding decrease in global infrastructure spending. Continued turbulence in the U.S. and international markets and economies and prolonged declines or stagnation in business and consumer spending may adversely affect our liquidity and financial condition. Although we were able to refinance our senior secured credit facility in 2010 (see—“Principal Debt Obligations” above), if these market conditions continue, they may impact our ability in the future to timely replace maturing liabilities, access the capital markets to meet liquidity needs, and service or refinance our 11% senior subordinated notes and our senior secured credit facility, resulting in an adverse effect on our financial condition, including liquidity, capital resources and results of operations.
Off Balance Sheet Arrangements
We had outstanding letters of credit of $4.4 million under our senior secured credit facility as of December 31, 2010.
Contractual Obligations
The following table sets forth our contractual obligations as of December 31, 2010 (in thousands):
| Total | Less Than 1 Yr. |
1-3 Yrs. | 3-5 Yrs. | More than 5 Yrs. |
||||||||||||||||
| Long-term debt obligations |
||||||||||||||||||||
| 11% senior subordinated notes |
$ | 201,500 | $ | 14,300 | $ | 28,600 | $ | 158,600 | $ | — | ||||||||||
| Senior secured credit facility(1)(2) |
504,682 | 23,629 | 49,040 | 85,185 | 346,829 | |||||||||||||||
| Other long-term debt obligations |
10,899 | 2,682 | 5,005 | 2,545 | 667 | |||||||||||||||
| Operating lease obligations(3) |
108,452 | 17,803 | 30,120 | 22,607 | 37,922 | |||||||||||||||
| $ | 825,533 | $ | 58,414 | $ | 112,765 | $ | 268,937 | $ | 385,418 | |||||||||||
| (1) | Based on implied forward one-month LIBOR rates in the yield curve as of December 31, 2010. |
| (2) | If the 11% senior subordinated notes remain outstanding on October 14, 2013, then the maturity date of the senior secured credit facility will be October 14, 2013. |
| (3) | We lease some of our facilities under noncancelable operating leases. The leases generally provide for our payment of property taxes, insurance and repairs, and have rent escalation clauses, principally based upon the Consumer Price Index or other fixed annual adjustments. The amounts shown reflect the future minimum rental payments under these leases. |
| Item 7A. | Quantitative and Qualitative Disclosures About Market Risk |
In the normal course of business, our operations are exposed to risks associated with fluctuations in interest rates. To the extent these interest rates increase, our interest expense will increase, which will make our interest payments and funding our other fixed costs more expensive, and our available cash flow may be adversely affected. We routinely monitor our risks associated with fluctuations in interest rates and consider the use of derivative financial instruments to hedge these exposures. We do not enter into derivative financial instruments for trading or speculative purposes nor do we enter into energy or commodity contracts.
Interest Rate Exposure—Interest Rate Risk Management
We use our senior secured credit facility and 11% senior subordinated notes to finance our operations. Our senior secured credit facility agreement exposes us to variability in interest payments due to changes in interest rates. We entered into an interest rate Cap agreement and an interest rate swap agreement on June 30, 2010 in order to
80
Table of Contents
manage fluctuations in cash flows resulting from interest rate risk. The interest rate cap agreement is for a notional amount of $70.0 million with a cap rate on 1 month LIBOR of 2.0% from July 2010 to December 2011. The interest rate swap agreement is for a notional amount of $70.0 million with an interest rate of 2.3% from January 2012 to June 2013.
The table below presents the principal amounts, weighted-average interest rates and fair values by year of expected maturity to evaluate our expected cash flows and sensitivity to interest rate changes (dollars in thousands):
| Twelve Months Ending December 31,(3) | ||||||||||||||||||||||||||||||||
| 2011 | 2012 | 2013 | 2014 | 2015 | Thereafter | Total | Fair Value | |||||||||||||||||||||||||
| Fixed-rate debt(1) |
$ | 2,142 | $ | 2,150 | $ | 2,160 | $ | 132,170 | (4) | $ | 180 | $ | 609 | $ | 139,410 | $ | 142,934 | |||||||||||||||
| Average interest rate |
6.0 | % | 6.0 | % | 6.0 | % | 10.9 | % | 6.0 | % | 6.0 | % | ||||||||||||||||||||
| Variable-rate debt(2) |
$ | 3,600 | $ | 3,600 | $ | 3,600 | $ | 3,600 | $ | 29,600 | $ | 339,300 | $ | 383,300 | $ | 376,154 | ||||||||||||||||
| Average interest rate(3) |
5.3 | % | 5.3 | % | 5.9 | % | 6.9 | % | 7.6 | % | 8.0 | % | ||||||||||||||||||||
| (1) | Excludes unamortized original issue discount of $0.3 million on our 11.0% senior subordinated notes. |
| (2) | Excludes unamortized original issue discount of $2.4 million on our first lien senior secured term loan debt. |
| (3) | Based on implied forward three-month LIBOR rates in the yield curve as of December 31, 2010. |
| (4) | If the 11% senior subordinated notes remain outstanding on October 14, 2013, then the maturity date of the senior secured credit facility will be October 14, 2013. |
For 2010, the loss recognized from converting from floating rate (one-month LIBOR) to fixed rate for a portion of the interest payments under our long-term debt obligations was approximately $0.4 million. At December 31, 2010, an unrealized loss of $0.2 million (net of income tax) is included in accumulated other comprehensive income. Below is a table listing the interest expense exposure detail and the fair value of the interest rate swap agreement as of December 31, 2010 (dollars in thousands):
| Loan |
Transaction Type |
Notional Amount |
Trade Date |
Effective Date |
Maturity/ Termination Date |
Year
Ended December 31, 2010 |
Fair
Value (Pre-tax) |
|||||||||||||||||||||
| First Lien |
Swap | $ | 145,000 | 12/07/09 | 12/31/09 | 4/9/10 | $ | (148 | ) | $ | — | |||||||||||||||||
| First Lien |
Swap | $ | 100,000 | 12/07/09 | 01/31/10 | 4/9/10 | $ | (116 | ) | $ | — | |||||||||||||||||
| First Lien |
Cap | $ | 70,000 | 6/30/2010 | 7/2/10 | 12/31/11 | $ | (106 | ) | $ | — | |||||||||||||||||
| First Lien |
Swap | $ | 70,000 | 6/30/2010 | 1/1/12 | 6/30/2013 | $ | — | $ | (316 | ) | |||||||||||||||||
| $ | (370 | ) | $ | (316 | ) | |||||||||||||||||||||||
The fair value of interest rate hedge agreements designated as hedging instruments against the variability of cash flows associated with floating-rate, long-term debt obligations are reported in accumulated other comprehensive income. These amounts subsequently are reclassified into interest expense as a yield adjustment in the same period in which the related interest on the floating-rate debt obligation affects earnings. We evaluate the effectiveness of the cash flow hedge, in accordance with FASB ASC Topic 815, “Derivatives and Hedging,” on a quarterly basis. Should the hedge become ineffective, the change in fair value would be recognized in our consolidated statements of operations. Should the counterparty’s credit rating deteriorate to the point at which it would be likely that the counterparty would default, the hedge would then be ineffective.
| Item 8. | Financial Statements and Supplementary Data |
The information required by this item is incorporated herein by reference to the financial statements set forth in Item 15 of this report, “Exhibits and Financial Statement Schedules—Consolidated Financial Statements and Supplementary Data.”
| Item 9. | Changes in and Disagreements with Accountants on Accounting and Financial Disclosure |
None.
81
Table of Contents
| Item 9A. | Controls and Procedures |
Evaluation of Disclosure Controls and Procedures
As required by Rules 13a-15 and 15d-15 under the Securities Exchange Act of 1934, as amended (the “Exchange Act”), management has evaluated, with the participation of our Chief Executive Officer and Chief Financial Officer, the effectiveness of our disclosure controls and procedures as of the end of the period covered by this report.
Disclosure controls and procedures, as defined by Rules 13a-15(e) and 15d-15(e) of the Exchange Act, refer to controls and other procedures designed to ensure that information required to be disclosed in the reports we file or submit under the Exchange Act is recorded, processed, summarized and reported, within the time periods specified in the rules and forms of the Securities and Exchange Commission. Disclosure controls and procedures include, without limitation, controls and procedures designed to ensure that information required to be disclosed by us in our reports that we file or submit under the Exchange Act is accumulated and communicated to management, including our Chief Executive Officer and Chief Financial Officer, as appropriate to allow timely decisions regarding our required disclosure. In designing and evaluating our disclosure controls and procedures, management recognizes that any controls and procedures, no matter how well designed and operated, can provide only reasonable assurance of achieving the desired control objectives, and management was required to apply its judgment in evaluating and implementing possible controls and procedures.
Based upon our evaluation, our Chief Executive Officer and Chief Financial Officer have concluded that, as of December 31, 2010, the end of the period covered by this report, the disclosure controls and procedures were effective at a reasonable assurance level to provide information required to be disclosed in the reports we file and submit under the Exchange Act is recorded, processed, summarized and reported as and when required.
Management’s Report on Internal Control over Financial Reporting
Management is responsible for establishing and maintaining adequate internal control over financial reporting as defined in Rule 13a-15(f) under the Exchange Act.
Internal control over financial reporting refers to a process designed by, or under the supervision of, our Chief Executive Officer and Chief Financial Officer and effected by our board of directors, management and other personnel, to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles and includes those policies and procedures that:
| • | pertain to the maintenance of records that in reasonable detail accurately and fairly reflect the transactions and dispositions of our assets; |
| • | provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that our receipts and expenditures are being made only in accordance with authorizations of our management and members of our board of directors; and |
| • | provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of our assets that could have a material effect on our financial statements. |
Internal control over financial reporting cannot provide absolute assurance of achieving financial reporting objectives because of its inherent limitations. Internal control over financial reporting is a process that involves human diligence and compliance and is subject to lapses in judgment and breakdowns resulting from human failures. Internal control over financial reporting also can be circumvented by collusion or improper override. Because of such limitations, there is a risk that material misstatements may not be prevented or detected on a timely basis by internal control over financial reporting. However, these inherent limitations are known features of the financial reporting process, and it is possible to design into the process safeguards to reduce, though not eliminate, this risk.
82
Table of Contents
Management conducted the above-referenced assessment of the effectiveness of our internal control over financial reporting as of December 31, 2010 using the framework set forth in the report entitled, “Internal Control—Integrated Framework,” issued by the Committee of Sponsoring Organizations of the Treadway Commission, or the COSO Report. Based on management’s evaluation and the criteria set forth in the COSO Report, management concluded that our internal control over financial reporting was effective as of December 31, 2010.
The effectiveness of our internal control over financial reporting as of December 31, 2010 has been audited by Ernst & Young LLP, our independent registered public accounting firm. Ernst & Young’s attestation report of our internal control over financial reporting is included in this item under “Report of Independent Registered Public Accounting Firm” and expresses an unqualified opinion on the effectiveness of our internal control over financial reporting as of December 31, 2010.
Changes in Internal Control Over Financial Reporting
Management determined that, as of December 31, 2010, there were no changes in our internal control over financial reporting that occurred during the last fiscal quarter then ended that has materially affected, or is reasonably likely to materially affect, our internal control over financial reporting.
83
Table of Contents
Report of Independent Registered Public Accounting Firm
The Board of Directors and Stockholders
Skilled Healthcare Group, Inc.
We have audited Skilled Healthcare Group, Inc.’s (the Company’s) internal control over financial reporting as of December 31, 2010, based on criteria established in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (the COSO criteria). The Company’s management is responsible for maintaining effective internal control over financial reporting, and for its assessment of the effectiveness of internal control over financial reporting included in the accompanying Management’s Report on Internal Control over Financial Reporting. Our responsibility is to express an opinion on the Company’s internal control over financial reporting based on our audit.
We conducted our audit in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects. Our audit included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, testing and evaluating the design and operating effectiveness of internal control based on the assessed risk, and performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
In our opinion, the Company maintained, in all material respects, effective internal control over financial reporting as of December 31, 2010, based on the COSO criteria.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), the consolidated balance sheets of Skilled Healthcare Group, Inc. as of December 31, 2010 and 2009 and the related consolidated statements of operations, stockholders’ equity and cash flows for each of the three years in the period ended December 31, 2010 of Skilled Healthcare Group, Inc. and our report dated February 14, 2011 expressed an unqualified opinion thereon.
/s/ Ernst & Young LLP
Irvine, California
February 14, 2011
| Item 9B. | Other Information |
Not applicable.
84
Table of Contents
PART III
| Item 10. | Directors, Executive Officers and Corporate Governance |
The information to be included in the sections entitled, “Election of Directors” and “Our Executive Officers,” respectively, in the Definitive Proxy Statement for the Annual Meeting of Stockholders to be filed by us with the Securities and Exchange Commission no later than 120 days after December 31, 2010 (the “2011 Proxy Statement”) is incorporated herein by reference.
The information to be included in the section entitled “Section 16(a) Beneficial Ownership Reporting Compliance” in the 2011 Proxy Statement is incorporated herein by reference.
The information to be included in the section entitled “Code of Business Conduct and Ethics” in the 2011 Proxy Statement is incorporated herein by reference.
We have filed, as exhibits to this annual report, the certifications of our Principal Executive Officer and Principal Financial Officer required pursuant to Section 302 of the Sarbanes-Oxley Act of 2002.
| Item 11. | Executive Compensation |
The information to be included in the sections entitled “Executive Compensation” and “Directors’ Compensation” in the 2011 Proxy Statement is incorporated herein by reference.
| Item 12. | Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters |
The information to be included in the section entitled “Security Ownership of Certain Beneficial Owners and Management” in the 2011 Proxy Statement is incorporated herein by reference.
| Item 13. | Certain Relationships and Related Transactions, and Director Independence |
The information to be included in the sections entitled “Certain Relationships and Related Transactions,” “Board Independence,” and “Compensation Committee Interlocks and Insider Participation” in the 2011 Proxy Statement is incorporated herein by reference.
| Item 14. | Principal Accountant Fees and Services |
The information to be included in the section entitled “Independent Registered Public Accountants” in the 2011 Proxy Statement is incorporated herein by reference.
85
Table of Contents
| Item 15. | Exhibits and Financial Statement Schedules |
| (a) | 1. Consolidated Financial Statements and Supplementary Data: |
The following consolidated financial statements, and notes thereto, and the related Report of our Independent Registered Public Accounting Firm, are filed as part of this Form 10-K:
| Page Number |
||||
| F-1 | ||||
| F-2 | ||||
| F-3 | ||||
| F-4 | ||||
| F-5 | ||||
| F-7 | ||||
| 2. | Financial Statement Schedule: |
The following financial statement schedule is filed as part of this Form 10-K:
| Page Number |
||||
| S-1 | ||||
All other schedules have been omitted for the reason that the required information is presented in financial statements or notes thereto, the amounts involved are not significant or the schedules are not applicable.
| (b) | Item 601 Exhibits |
Reference is hereby made to Item 15 of this report, “Exhibits and Financial Statement Schedules—Exhibits.”
86
Table of Contents
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, as amended, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
| SKILLED HEALTHCARE GROUP, INC. | ||||||
| By | /S/ BOYD HENDRICKSON | |||||
| Boyd Hendrickson | ||||||
| Chairman of the Board, | ||||||
| Chief Executive Officer and Director | ||||||
Date: February 14, 2011
Pursuant to the requirements of the Securities Exchange Act of 1934, as amended, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the date indicated.
| Date: February 14, 2011 | By | /S/ BOYD HENDRICKSON | ||||||
| Boyd Hendrickson | ||||||||
| Chairman of the Board, | ||||||||
| Chief Executive Officer and Director | ||||||||
| Date: February 14, 2011 | By | /S/ JOSE LYNCH | ||||||
| Jose Lynch | ||||||||
| President, Chief Operating Officer and Director | ||||||||
| Date: February 14, 2011 | By | /S/ DEVASIS GHOSE | ||||||
| Devasis Ghose | ||||||||
| Executive Vice President, Treasurer and Chief Financial Officer | ||||||||
| (Principal Financial Officer) | ||||||||
| Date: February 14, 2011 | By | /S/ CHRISTOPHER N. FELFE | ||||||
| Christopher N. Felfe | ||||||||
| Senior Vice President of Finance and Chief Accounting Officer | ||||||||
| (Principal Accounting Officer) | ||||||||
| Date: February 14, 2011 | By | /S/ ROBERT M. LE BLANC | ||||||
| Robert M. Le Blanc Lead Director | ||||||||
| Date: February 14, 2011 | By | /S/ MICHAEL BOXER | ||||||
| Michael Boxer Director | ||||||||
| Date: February 14, 2011 | By | /S/ M. BERNARD PUCKETT | ||||||
| M. Bernard Puckett Director | ||||||||
| Date: February 14, 2011 | By | /S/ LINDA ROSENSTOCK | ||||||
| Linda Rosenstock Director | ||||||||
| Date: February 14, 2011 | By | /S/ GLENN SCHAFER | ||||||
| Glenn Schafer Director | ||||||||
87
Table of Contents
| Date: February 14, 2011 | By | /S/ WILLIAM SCOTT | ||||||
| William Scott Director | ||||||||
| Date: February 14, 2011 | By | /S/ MICHAEL D. STEPHENS | ||||||
| Michael D. Stephens Director | ||||||||
88
Table of Contents
| 3. | Exhibits: A list of the exhibits filed or furnished with this Form 10-K is set forth on the Index of Exhibit immediately following the signature page to this Form 10-K and is incorporated herein by reference. |
INDEX OF EXHIBITS
| Number |
Description | |
| 2.1 | Asset Purchase Agreement, dated as of May 1, 2010 by and between Home and Hospice Care Investments, LLC and each of the other parties thereto (filed as Exhibit 2.1 to our Form 10-Q for the quarter ended March 31, 2010, and incorporated herein by reference). | |
| 2.2 | Joinder Agreement and Amendment No. 1, dated as of May 21, 2010, to Asset Purchase Agreement by and between Home and Hospice Care Investments, LLC and each of the other parties thereto (filed as Exhibit 2.1 to our Current Report on Form 8-K dated May 26, 2010 and incorporated herein by reference). | |
| 3.1 | Amended and Restated Certificate of Incorporation of Skilled Healthcare Group, Inc. (filed as Exhibit 3.2 to our Form 10-Q for the quarter ended June 30, 2007, and incorporated herein by reference). | |
| 3.2 | Amended and Restated By-Laws of Skilled Healthcare Group, Inc. (filed as Exhibit 3.4 to our Registration Statement on Form S-1/A, No. 333-137897, filed on April 27, 2007, and incorporated herein by reference). | |
| 4.1 | Indenture, dated as of December 27, 2005, by and among SHG Acquisition Corp., Wells Fargo Bank, N.A. and certain subsidiaries of Skilled Healthcare Group, Inc. (filed as Exhibit 4.2 to our Registration Statement on Form S-1, No. 333-137897, filed on October 10, 2006, and incorporated herein by reference). | |
| 4.2 | Investor Stockholders’ Agreement, dated as of December 27, 2005, among SHG Holding Solutions, Inc., Onex Partners LP and the stockholders listed on the signature pages thereto (filed as Exhibit 4.4 to our Registration Statement on Form S-1, No. 333-137897, filed on October 10, 2006, and incorporated herein by reference). | |
| 4.3 | Registration Agreement dated as of December 27, 2005, among SHG Holding Solutions, Inc. and the persons listed thereon (filed as Exhibit 4.5 to our Registration Statement on Form S-1, No. 333-137897, filed on October 10, 2006, and incorporated herein by reference). | |
| 4.4 | Form of specimen certificate for Skilled Healthcare Group, Inc.’s Class A common stock (filed as Exhibit 4.1 to our Registration Statement on Form S-1/A, No. 333-137897, filed on April 27, 2007, and incorporated herein by reference). | |
| 4.5 | Form of 11% Senior Subordinated Notes due 2014 (included in the Indenture referenced in Exhibit 4.1 above). | |
| 10.1* | Skilled Healthcare Group, Inc. Restricted Stock Plan (filed as Exhibit 10.1 to our Registration Statement on Form S-1, No. 333-137897, filed on October 10, 2006 and incorporated herein by reference). | |
| 10.3* | Employment Agreement, dated April 30, 2005, by and between Skilled Healthcare Group, Inc. and Boyd Hendrickson (filed as Exhibit 10.5 to our Registration Statement on Form S-1, No. 333-137897, filed on October 10, 2006 and incorporated herein by reference). | |
| 10.4* | Employment Agreement, dated December 27, 2005, by and between Skilled Healthcare Group, Inc. and Jose Lynch (filed as Exhibit 10.6 to our Registration Statement on Form S-1, No. 333-137897, filed on October 10, 2006 and incorporated herein by reference). | |
| 10.5* | Employment Agreement, dated December 27, 2005, by and between Skilled Healthcare Group, Inc. and Roland G. Rapp (filed as Exhibit 10.8 to our Registration Statement on Form S-1, No. 333-137897, filed on October 10, 2006 and incorporated herein by reference). | |
89
Table of Contents
| Number |
Description | |
| 10.6 | Lease, dated as of August 26, 2002, by and between CT Foothill 10/241, LLC, and Fountain View, Inc., and amendments thereto (filed as Exhibit 10.13 to our Registration Statement on Form S-1, No. 333-137897, filed on October 10, 2006 and incorporated herein by reference). | |
| 10.7* | Form of Indemnification Agreement with Skilled Healthcare Group’s directors, executive officers, and certain employees (filed as Exhibit 10.10 to our Registration Statement on Form S-1/A, No. 333-137897, filed on April 27, 2007, and incorporated herein by reference). | |
| 10.9* | Employment Agreement, dated as of November 30, 2007, by and between Skilled Healthcare LLC and Devasis Ghose (filed as Exhibit 10.1 to our Form 8-K dated November 30, 2007, and incorporated herein by reference). | |
| 10.10* | Amended and Restated Skilled Healthcare Group, Inc. 2007 Incentive Award Plan (filed as Appendix A to our Definitive Proxy Statement filed on April 7, 2008, and incorporated herein by reference). | |
| 10.11 | Amendment and Restatement Agreement, dated as of April 9, 2010, by and among us, the subsidiary guarantors on the signature pages thereto, the lenders listed on the signature pages thereto and Credit Suisse AG, as Administrative Agent for the lenders and as Collateral Agent for the lenders, including the Third Amended and Restated Credit Agreement by and among us, the lenders party thereto and Credit Suisse AG, as Administrative Agent for the lenders and Collateral Agent for the lenders attached as Exhibit A to such Amendment and Restatement Agreement (filed as Exhibit 10.1 to our Quarterly Report on Form 10-Q filed on August 5, 2010 and incorporated herein by reference). | |
| 10.12 | Form of Restricted Stock Award Agreement (revised April 2010) (filed as Exhibit 10.2 to our Form 10-Q filed on May 4 2010 and incorporated herein by reference) | |
| 10.13 | Class Settlement Agreement and Release, dated as of September 7, 2010 (filed as Exhibit 10.1 to our Current Report on Form 8-K filed on September 8, 2010 and incorporated herein by reference). | |
| 10.14 | Settlement Agreement and Release with The People of the State of California, by and through Intervenor, the Humboldt County District Attorney’s Office, dated as of September 7, 2010 (filed as Exhibit 10.2 to our Current Report on Form 8-K filed on September 8, 2010 and incorporated herein by reference) | |
| 10.15* | Employment Agreement, dated as of May 1, 2010, by and between Skilled Healthcare Group, Inc. and Douglas Shane Peck (filed as Exhibit 10.2 to our Quarterly Report on Form 10-Q, filed on August 5, 2010, and incorporated herein by reference) | |
| 10.16 | Stipulation and Order (Case No. DR060264), Superior Court of California, Humboldt County, dated July 15, 2010 (filed as Exhibit 10.1 to our Current Report on Form 8-K filed on July 15, 2010 and incorporated herein by reference) | |
| 10.17* | Employment Agreement, dated as of April 1, 2010 by and between Skilled Healthcare, LLC and Matthew Moore, as amended on November 5, 2010 | |
| 21 | Subsidiaries of the Registrant. | |
| 23.1 | Consent of Independent Registered Public Accounting Firm. | |
| 31.1 | Certification of Principal Executive Officer pursuant to Section 302 of the Sarbanes-Oxley Act of 2002. | |
| 31.2 | Certification of Principal Financial Officer pursuant to Section 302 of the Sarbanes-Oxley Act of 2002. | |
| 32** | Certification pursuant to 18 U.S.C. Section 1350, as adopted pursuant to Section 906 of the Sarbanes-Oxley Act of 2002. | |
90
Table of Contents
| * | Management contract or compensatory plan or arrangement. |
| ** | Furnished herewith and not “filed” for purposes of Section 18 of the Securities Exchange Act of 1934, as amended. |
91
Table of Contents
Report of Independent Registered Public Accounting Firm
The Board of Directors and Stockholders
Skilled Healthcare Group, Inc.
We have audited the accompanying consolidated balance sheets of Skilled Healthcare Group, Inc. (the “Company”) as of December 31, 2010 and 2009, and the related consolidated statements of operations, stockholders’ equity, and cash flows for each of the three years in the period ended December 31, 2010. Our audits also included the financial schedule listed in the Index at Item 15(a)(2). These financial statements and schedule are the responsibility of the Company’s management. Our responsibility is to express an opinion on these financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements. An audit also includes assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the financial statements referred to above present fairly, in all material respects, the consolidated financial position of the Company at December 31, 2010 and 2009, and the consolidated results of its operations and its cash flows for each of the three years in the period ended December 31, 2010, in conformity with U.S. generally accepted accounting principles. Also, in our opinion, the related financial statement schedule, when considered in relation to the basic financial statements taken as a whole, presents fairly in all material respects the information set forth therein.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), the Company’s internal control over financial reporting as of December 31, 2010, based on criteria established in Internal Control-Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission and our report dated February 14, 2011 expressed an unqualified opinion thereon.
/s/ Ernst & Young LLP
Irvine, California
February 14, 2011
F-1
Table of Contents
Skilled Healthcare Group, Inc.
Consolidated Balance Sheets
(In thousands, except per share data)
| December 31, | ||||||||
| 2010 | 2009 | |||||||
| ASSETS |
||||||||
| Current assets: |
||||||||
| Cash and cash equivalents |
$ | 4,192 | $ | 3,528 | ||||
| Accounts receivable, less allowance for doubtful accounts of $17,710 and $21,318 at December 31, 2010 and December 31, 2009, respectively |
98,777 | 96,610 | ||||||
| Deferred income taxes |
20,419 | 15,003 | ||||||
| Prepaid expenses |
9,618 | 8,159 | ||||||
| Other current assets |
15,819 | 8,303 | ||||||
| Total current assets |
148,825 | 131,603 | ||||||
| Property and equipment, less accumulated depreciation of $76,017 and $59,448 at December 31, 2010 and December 31, 2009, respectively |
387,322 | 373,211 | ||||||
| Other assets: |
||||||||
| Notes receivable |
5,877 | 8,060 | ||||||
| Deferred financing costs, net |
13,165 | 13,425 | ||||||
| Goodwill |
332,724 | 279,362 | ||||||
| Intangible assets, less accumulated amortization of $15,646 and $14,413 at December 31, 2010 and December 31, 2009, respectively |
25,341 | 26,297 | ||||||
| Other assets |
24,476 | 24,284 | ||||||
| Total other assets |
401,583 | 351,428 | ||||||
| Total assets |
$ | 937,730 | $ | 856,242 | ||||
| LIABILITIES AND STOCKHOLDERS’ EQUITY |
||||||||
| Current liabilities: |
||||||||
| Accounts payable and accrued liabilities |
$ | 50,898 | $ | 49,355 | ||||
| Employee compensation and benefits |
39,400 | 29,753 | ||||||
| Current portion of long-term debt and capital leases |
5,742 | 7,823 | ||||||
| Total current liabilities |
96,040 | 86,931 | ||||||
| Long-term liabilities: |
||||||||
| Insurance liability risks |
25,474 | 27,407 | ||||||
| Deferred income taxes |
8,431 | 3,200 | ||||||
| Other long-term liabilities |
15,984 | 12,426 | ||||||
| Long-term debt and capital leases, less current portion |
514,221 | 450,856 | ||||||
| Total liabilities |
660,150 | 580,820 | ||||||
| Stockholders’ equity: |
||||||||
| Class A common stock, 175,000 shares authorized, $0.001 par value per share; 20,780 and 20,334 issued and outstanding at December 31, 2010 and December 31, 2009, respectively |
21 | 20 | ||||||
| Class B common stock, 30,000 shares authorized, $0.001 par value per share; 16,994 and 17,001 issued and outstanding at December 31, 2010 and December 31, 2009, respectively |
17 | 17 | ||||||
| Additional paid-in-capital |
368,582 | 365,126 | ||||||
| Accumulated deficit |
(90,822 | ) | (89,781 | ) | ||||
| Accumulated other comprehensive (loss) income |
(218 | ) | 40 | |||||
| Total stockholders’ equity |
277,580 | 275,422 | ||||||
| Total liabilities and stockholders’ equity |
$ | 937,730 | $ | 856,242 | ||||
The accompanying notes are an integral part of these consolidated financial statements.
F-2
Table of Contents
Skilled Healthcare Group, Inc.
Consolidated Statements of Operations
(In thousands, except per share data)
| Year Ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Revenue |
$ | 820,238 | $ | 756,065 | $ | 729,390 | ||||||
| Expenses: |
||||||||||||
| Cost of services (exclusive of rent cost of revenue and depreciation and amortization shown below) |
657,515 | 604,913 | 579,625 | |||||||||
| Rent cost of revenue |
19,038 | 18,137 | 18,248 | |||||||||
| General and administrative |
25,516 | 25,090 | 24,514 | |||||||||
| Litigation settlement costs |
53,505 | — | — | |||||||||
| Depreciation and amortization |
25,047 | 23,308 | 20,978 | |||||||||
| Goodwill impairment charge |
— | 170,600 | — | |||||||||
| 780,621 | 842,048 | 643,365 | ||||||||||
| Other income (expenses): |
||||||||||||
| Interest expense |
(37,021 | ) | (33,013 | ) | (37,261 | ) | ||||||
| Interest income |
947 | 1,146 | 680 | |||||||||
| Equity in earnings of joint venture |
2,566 | 2,751 | 2,487 | |||||||||
| Other income |
2,332 | 150 | 246 | |||||||||
| Debt retirement costs |
(7,010 | ) | — | — | ||||||||
| Total other (expenses) income, net |
(38,186 | ) | (28,966 | ) | (33,848 | ) | ||||||
| Income (loss) from continuing operations before provision for income taxes |
1,431 | (114,949 | ) | 52,177 | ||||||||
| Provision for income taxes |
2,472 | 17,842 | 18,081 | |||||||||
| (Loss) income from continuing operations |
(1,041 | ) | (132,791 | ) | 34,096 | |||||||
| Loss from discontinued operations, net of tax |
— | (390 | ) | — | ||||||||
| Net (loss) income |
$ | (1,041 | ) | $ | (133,181 | ) | $ | 34,096 | ||||
| (Loss) earnings per share, basic: |
||||||||||||
| (Loss) earnings per common share from continuing operations |
$ | (0.03 | ) | $ | (3.60 | ) | $ | 0.93 | ||||
| Loss per common share from discontinued operations |
— | (0.01 | ) | — | ||||||||
| (Loss) earnings per share |
$ | (0.03 | ) | $ | (3.61 | ) | $ | 0.93 | ||||
| (Loss) earnings per share, diluted: |
||||||||||||
| (Loss) earnings per common share from continuing operations |
$ | (0.03 | ) | $ | (3.60 | ) | $ | 0.92 | ||||
| Loss per common share from discontinued operations |
— | (0.01 | ) | — | ||||||||
| (Loss) earnings per share |
$ | (0.03 | ) | $ | (3.61 | ) | $ | 0.92 | ||||
| Weighted-average common shares outstanding, basic |
36,988 | 36,914 | 36,573 | |||||||||
| Weighted-average common shares outstanding, diluted |
36,988 | 36,914 | 36,894 | |||||||||
The accompanying notes are an integral part of these consolidated financial statements.
F-3
Table of Contents
Skilled Healthcare Group, Inc.
Consolidated Statements of Stockholders’ Equity
(In Thousands)
| Class A Common Stock |
Class B Common Stock |
Additional Paid-In Capital |
(Accumulated Deficit) Retained Earnings |
Other Comprehensive (Loss) income |
Total | |||||||||||||||||||||||||||
| Shares | Amount | Shares | Amount | |||||||||||||||||||||||||||||
| Balance at December 31, 2007 |
19,261 | $ | 19 | 17,696 | $ | 18 | $ | 361,468 | $ | 9,304 | $ (753) | $ | 370,056 | |||||||||||||||||||
| Net income |
— | — | — | — | — | 34,096 | — | 34,096 | ||||||||||||||||||||||||
| Conversion of class B common stock into class A common stock |
625 | 1 | (625 | ) | (1 | ) | — | — | — | — | ||||||||||||||||||||||
| Issuance of restricted stock |
309 | — | — | — | — | — | — | — | ||||||||||||||||||||||||
| Forfeiture of restricted stock |
(2 | ) | — | (44 | ) | — | — | — | — | — | ||||||||||||||||||||||
| Stock-based compensation |
— | — | — | — | 1,558 | — | — | 1,558 | ||||||||||||||||||||||||
| Restricted stock traded to pay tax |
(4 | ) | — | — | — | (67 | ) | — | — | (67 | ) | |||||||||||||||||||||
| Excess tax benefits from stock-based payment arrangements |
— | — | — | — | 23 | — | — | 23 | ||||||||||||||||||||||||
| Unrealized loss on interest rate swap, net of tax |
— | — | — | — | — | — | (1,089 | ) | (1,089 | ) | ||||||||||||||||||||||
| Balance at December 31, 2008 |
20,189 | 20 | 17,027 | 17 | 362,982 | 43,400 | (1,842 | ) | 404,577 | |||||||||||||||||||||||
| Net loss |
— | — | — | — | — | (133,181 | ) | — | (133,181 | ) | ||||||||||||||||||||||
| Conversion of class B common stock into class A common stock |
26 | — | (26 | ) | — | — | — | — | — | |||||||||||||||||||||||
| Issuance of restricted stock |
176 | — | — | — | — | — | — | — | ||||||||||||||||||||||||
| Forfeiture of restricted stock |
(45 | ) | — | — | — | — | — | — | — | |||||||||||||||||||||||
| Stock-based compensation |
— | — | — | — | 2,268 | — | — | 2,268 | ||||||||||||||||||||||||
| Restricted stock traded to pay tax |
(12 | ) | — | — | — | (101 | ) | — | — | (101 | ) | |||||||||||||||||||||
| Tax impact from stock-based payment arrangements |
— | — | — | — | (23 | ) | — | — | (23 | ) | ||||||||||||||||||||||
| Unrealized gain on interest rate swap, net of tax. |
— | — | — | — | — | — | 1,882 | 1,882 | ||||||||||||||||||||||||
| Balance at December 31, 2009 |
20,334 | 20 | 17,001 | 17 | 365,126 | (89,781 | ) | 40 | 275,422 | |||||||||||||||||||||||
| Net loss |
— | — | — | — | — | (1,041 | ) | — | (1,041 | ) | ||||||||||||||||||||||
| Conversion of class B common stock into class A common stock |
7 | — | (7 | ) | — | — | — | — | — | |||||||||||||||||||||||
| Issuance of restricted stock |
549 | 1 | — | — | — | — | — | 1 | ||||||||||||||||||||||||
| Forfeiture of restricted stock |
(94 | ) | — | — | — | — | — | — | — | |||||||||||||||||||||||
| Stock-based compensation |
— | — | — | — | 3,549 | — | — | 3,549 | ||||||||||||||||||||||||
| Restricted stock traded to pay tax |
(16 | ) | — | — | — | (93 | ) | — | — | (93 | ) | |||||||||||||||||||||
| Unrealized loss on interest rate swap, net of tax |
— | — | — | — | — | — | (258 | ) | (258 | ) | ||||||||||||||||||||||
| Balance at December 31, 2010 |
20,780 | $ | 21 | 16,994 | $ | 17 | $ | 368,582 | $ | (90,822 | ) | $ | (218 | ) | $ | 277,580 | ||||||||||||||||
The accompanying notes are an integral part of these consolidated financial statements.
F-4
Table of Contents
Skilled Healthcare Group, Inc.
Consolidated Statements of Cash Flows
(In Thousands)
| Year Ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Cash Flows from Operating Activities |
||||||||||||
| Net (loss) income from continuing operations |
$ | (1,041 | ) | $ | (132,791 | ) | $ | 34,096 | ||||
| Net loss from discontinued operations |
— | (390 | ) | — | ||||||||
| Net (loss) income |
(1,041 | ) | (133,181 | ) | 34,096 | |||||||
| Adjustments to reconcile net (loss) income to net cash provided by operating activities: |
||||||||||||
| Depreciation and amortization |
25,047 | 23,308 | 20,978 | |||||||||
| Provision for doubtful accounts |
9,617 | 11,039 | 15,171 | |||||||||
| Non-cash stock-based compensation |
3,549 | 2,268 | 1,558 | |||||||||
| Excess tax benefits from stock-based payment arrangements |
— | — | (23 | ) | ||||||||
| (Gain) loss on disposal of asset |
(2,243 | ) | 61 | 62 | ||||||||
| Amortization of deferred financing costs |
3,892 | 4,711 | 3,068 | |||||||||
| Tax benefit from reversal of accrual for uncertain tax positions |
— | (2,828 | ) | (1,444 | ) | |||||||
| Deferred income taxes |
(54 | ) | 5,966 | (2,630 | ) | |||||||
| Write-off of deferred financing costs |
6,574 | — | — | |||||||||
| Goodwill impairment charge |
— | 170,600 | — | |||||||||
| Amortization of discount on debt |
465 | 107 | 107 | |||||||||
| Changes in operating assets and liabilities: |
||||||||||||
| Accounts receivable |
(14,508 | ) | (15,836 | ) | (15,668 | ) | ||||||
| Payments on notes receivable |
4,846 | 5,464 | 4,476 | |||||||||
| Other current and non-current assets |
(8,172 | ) | 9,771 | 2,109 | ||||||||
| Accounts payable and accrued liabilities |
1,696 | (2,212 | ) | 923 | ||||||||
| Employee compensation and benefits |
9,181 | (1,597 | ) | 355 | ||||||||
| Insurance liability risks |
(4,390 | ) | (3,934 | ) | (490 | ) | ||||||
| Other long-term liabilities |
839 | 1,190 | 4,841 | |||||||||
| Net cash provided by operating activities |
35,298 | 74,897 | 67,489 | |||||||||
| Cash Flows from Investing Activities |
||||||||||||
| Acquistion of healthcare facilities and businesses |
(45,380 | ) | (5,013 | ) | (23,360 | ) | ||||||
| Proceeds from disposal of property and equipment |
— | — | 133 | |||||||||
| Additions to property and equipment |
(27,736 | ) | (41,155 | ) | (49,626 | ) | ||||||
| Proceeds from divestitures |
14,746 | — | — | |||||||||
| Cash paid for purchase of previously leased facilities |
(18,035 | ) | — | — | ||||||||
| Net cash used in investing activities |
(76,405 | ) | (46,168 | ) | (72,853 | ) | ||||||
| Cash Flows from Financing Activities |
||||||||||||
| Borrowings under line of credit |
174,500 | 80,000 | 81,000 | |||||||||
| Repayments under line of credit |
(220,500 | ) | (89,000 | ) | (68,000 | ) | ||||||
| Repayments of long-term debt and capital leases |
(259,322 | ) | (10,686 | ) | (9,241 | ) | ||||||
| Issuance of debt |
357,300 | — | — | |||||||||
| Fees paid for early extinguishment of debt |
— | (7,952 | ) | (1,383 | ) | |||||||
| Additions to deferred financing costs |
(10,207 | ) | — | 23 | ||||||||
| Net cash provided (used in) by financing activities |
41,771 | (27,638 | ) | 2,399 | ||||||||
| Cash flows from discontinued operations |
— | 390 | — | |||||||||
| Increase (decrease) in cash and cash equivalents |
664 | 1,481 | (2,965 | ) | ||||||||
| Cash and cash equivalents at beginning of period |
3,528 | 2,047 | 5,012 | |||||||||
| Cash and cash equivalents at end of period |
$ | 4,192 | $ | 3,528 | $ | 2,047 | ||||||
The accompanying notes are an integral part of these consolidated financial statements.
F-5
Table of Contents
| Year Ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Supplemental cash flow information |
||||||||||||
| Cash paid for: |
||||||||||||
| Interest expense, net of capitalized interest |
$ | 29,960 | $ | 30,143 | $ | 34,938 | ||||||
| Income taxes, net |
$ | 10,081 | $ | 15,667 | $ | 20,909 | ||||||
| Non-cash activities: |
||||||||||||
| Conversion of accounts receivable into notes receivable, net |
$ | 4,038 | $ | 11,158 | $ | 3,289 | ||||||
| Liabilities issued as purchase consideration for purchase of business |
$ | 15,030 | $ | — | $ | — | ||||||
| Insurance premium financed |
$ | 1,100 | $ | 7,970 | $ | 7,959 | ||||||
The accompanying notes are an integral part of these consolidated financial statements.
F-6
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
1. Description of Business
Current Business
Skilled Healthcare Group, Inc. (“Skilled”) is a holding company that owns subsidiaries which operate long-term care facilities and provide a wide range of post-acute care services, with a strategic emphasis on sub-acute specialty medical care. Skilled and its consolidated wholly-owned companies are collectively referred to as the “Company.” As of December 31, 2010, the Company operated facilities in California, Iowa, Kansas, Missouri, Nevada, New Mexico and Texas, including 78 skilled nursing facilities (“SNFs”), which offer sub-acute care and rehabilitative and specialty healthcare skilled nursing care, and 22 assisted living facilities (“ALFs”), which provide room and board and social services. In addition, the Company provides a variety of ancillary services such as physical, occupational and speech therapy in Company-operated facilities and unaffiliated facilities. Furthermore, as of December 31, 2010, the Company provided hospice care in the Arizona, California, Idaho, Montana, Nevada and New Mexico markets. Additionally, the Company operates home health agencies in Nevada, Arizona, Idaho, and Montana. The Company also has an administrative service company that provides a full complement of administrative and consultative services that allows its facility operators, that unrelated facility operator with whom the Company contracts, and the Company’s ancillary healthcare operators to better focus on delivery of healthcare services. The Company is also a member in a joint venture located in Texas that provides institutional pharmacy services, which currently serves eight of the Company’s SNFs and other facilities unaffiliated with the Company.
Company History
Skilled was incorporated as SHG Holding Solutions, Inc. in Delaware in October 2005. The Company’s predecessor company acquired Summit Care, a publicly traded long-term care company with nursing facilities in California, Texas and Arizona, in 1998. On October 2, 2001, the Company’s predecessor and 19 of its subsidiaries filed voluntary petitions for protection under Chapter 11 of the U.S. Bankruptcy Code and on November 28, 2001, the Company’s remaining three companies also filed voluntary petitions for protection under Chapter 11. In August 2003, the Company emerged from bankruptcy, paying or restructuring all debt holders in full, paying all accrued interest expenses and issuing 5.0% of the Company’s common stock to former bondholders. In connection with the Company’s emergence from bankruptcy, the Company engaged in a series of transactions, including the disposition of the Company’s California pharmacy business, selling two institutional pharmacies in Southern California. On June 30, 2009, the United States Bankruptcy Court for the Central District of California granted entry of a final decree closing the aforementioned Chapter 11 cases.
The Onex Transaction
In October 2005, Skilled (known as SHG Holding Solutions, Inc. at that time) entered into an agreement and plan of merger (the “Agreement”) with its predecessor company known then as Skilled Healthcare Group, Inc. (“SHG”), which was the entity that owned the subsidiaries that then operated Skilled’s business, SHG Acquisition Corp. (“Acquisition”) and SHG’s former sponsor, Heritage Fund II LP and related investors (“Heritage”). Skilled and Acquisition were formed by Onex Partners LP, Onex American Holdings II LLC and Onex U.S. Principals LP (“Onex”) and certain of their associates (collectively the “Sponsors”) for purposes of acquiring SHG. The merger was completed effective December 27, 2005 (the “Onex Transaction”). Under the Agreement, Acquisition acquired substantially all of the outstanding shares of SHG through a merger with SHG, with SHG being the surviving corporation. The Onex Transaction was accounted for using the purchase method of accounting and, accordingly, all assets and liabilities of SHG and its consolidated subsidiaries were recorded at their fair values as of the date of the acquisition. The Company refers to the transactions contemplated by the merger agreement, the equity contributions, the financings and use of proceeds of the financings, collectively, as the Transactions.
F-7
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Acquisitions, Developments, and Divestitures
Effective May 1, 2010, the Company acquired substantially all of the assets of five Medicare-certified hospice companies and four Medicare-certified home health companies located in Arizona, Idaho, Montana and Nevada, referred to herein as the Hospice/Home Health Acquisition. See Note 17—Acquisition, for a more detailed discussion of the Hospice/Home Health Acquisition.
The Company admitted its first patients in July 2010 to its newly constructed skilled nursing facility in Fort Worth, Texas, called the Fort Worth Center of Rehabilitation, which has received its state license as well as Medicaid and Medicare certification.
On September 7, 2010, the Company reached an agreement to settle the case entitled, VINNIE LAVENDER, by and through her Conservator, WANDA BAKER; WALTER SIMON; JACQUELYN VILCHINSKY vs. SKILLED HEALTHCARE GROUP, INC., et al. (and twenty-two individually named California nursing facilities receiving administrative services from Skilled Healthcare, LLC), see Note 12, which is referred to herein as the “Lavender Case” or the “Humboldt County Action.” As part of the settlement, the Company and other defendants entered into separate settlement agreements with the plaintiffs and the Humboldt County District Attorney’s Office, each dated as of September 7, 2010. The settlement was approved by the Superior Court of California, Humboldt County on November 30, 2010.
Under the terms of the settlement agreements, the Company deposited a total of $50 million into escrow accounts to cover settlement payments to class members, notice and claims administration costs, reasonable attorneys’ fees and costs and certain other payments.
The settlement agreements also institute an injunction, pursuant to which the twenty-two defendants that operate California nursing facilities must provide specified nurse staffing levels, comply with specified state and federal laws governing staffing levels and posting requirements, and provide reports and information to a monitor. The injunction will remain in effect for a period of 24 months unless extended for additional three month periods as to those defendants that may be found in violation. Defendants demonstrating compliance for an 18 month period may petition for early termination of the injunction. The Company is required to demonstrate that the costs of the injunction are at least $9.6 million over the term of the injunction. The injunction costs include, among other things, costs attributable to (i) enhanced reporting requirements; (ii) implementing advanced staffing tracking systems; (iii) fees and expenses paid to an auditor and special master; (iv) increased labor and labor related expenses; and (v) lost revenues attributable to admission decisions based on compliance with the terms and conditions of the injunction. To the extent the costs of complying with the injunction are less than $9.6 million, the Company will be required to remit any shortfall to the settlement fund.
Pursuant to the settlement agreements, the plaintiffs and the Humboldt County District Attorney’s Office, as Intervenor on behalf of the People of the State of California, agreed to release the Company and the other defendants from claims related to the causes of action alleged in the Lavender Case, as further described in the settlement agreements, which are filed as exhibits to the Company’s Annual Report on Form 10-K for the fiscal year ended December 31, 2010. Neither of the settlement agreements contains an admission or concession of wrongdoing by the Company or any other defendants. See Note 12, Commitments and Contingencies—Litigation, for more information.
In December 2010, the Company sold its Westside Campus of Care skilled nursing facility and operations in Texas for $14.7 million and purchased three previously leased facilities: St. Luke Healthcare and Rehabilitation Center and Woodland Care Center, located in California, and St. Joseph Transitional Rehabilitation Center in Nevada. A net gain of $1.8 million was recorded related to these transactions.
F-8
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
2. Summary of Significant Accounting Policies
Basis of Presentation
The consolidated financial statements of the Company include the accounts of the Company and the Company’s wholly-owned companies. All significant intercompany transactions have been eliminated in consolidation.
Estimates and Assumptions
The preparation of consolidated financial statements in conformity with U.S. generally accepted accounting principles (“GAAP”) requires management to consolidate company financial information and make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenue and expenses during the reporting period. The most significant estimates in the Company’s consolidated financial statements relate to revenue, allowance for doubtful accounts, self-insured liability risks, income taxes, and impairment of long-lived assets and goodwill. Actual results could differ from those estimates.
Reclassifications
Certain prior year amounts have been reclassified to conform to current year presentation, including payments on notes receivable in the consolidated statements of cash flows and total assets by segment. Certain reimbursable room and board costs within the Company’s hospice reporting unit were reclassified from revenue to cost of service in the amount of $3.7 million and $ 3.9 million for the year ended December 31, 2009 and 2008 because they are more appropriately deemed to be pass-through costs.
Revenue and Accounts Receivables
Revenue and accounts receivable are recorded on an accrual basis as services are performed at their estimated net realizable value. The Company derives a majority of its revenue from funds under federal Medicare and state Medicaid assistance programs, the continuation of which are dependent upon governmental policies and are subject to audit risk and potential recoupment.
The following table summarizes how the Company’s revenue is derived from services provided to patients by payor classes (dollars in thousands):
| Year Ended December 31, | ||||||||||||||||||||||||
| 2010 | 2009 | 2008 | ||||||||||||||||||||||
| Revenue Dollars |
Revenue Percentage |
Revenue Dollars |
Revenue Percentage |
Revenue Dollars |
Revenue Percentage |
|||||||||||||||||||
| Medicare |
$ | 304,413 | 37.1 | % | $ | 264,594 | 35.0 | % | $ | 267,180 | 36.6 | % | ||||||||||||
| Medicaid |
260,083 | 31.7 | 241,021 | 31.9 | 226,558 | 31.1 | ||||||||||||||||||
| Subtotal Medicare and Medicaid |
564,496 | 68.8 | 505,615 | 66.9 | 493,738 | 67.7 | ||||||||||||||||||
| Managed Care |
75,657 | 9.2 | 71,181 | 9.4 | 69,723 | 9.5 | ||||||||||||||||||
| Private pay and other |
180,085 | 22.0 | 179,269 | 23.7 | 165,929 | 22.8 | ||||||||||||||||||
| Total |
$ | 820,238 | 100.0 | % | $ | 756,065 | 100.0 | % | $ | 729,390 | 100.0 | % | ||||||||||||
F-9
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
The following table sets forth revenue by state and revenue by state as a percentage of total revenue for the periods (dollars in thousands):
| Year Ended December 31, | ||||||||||||||||||||||||
| 2010 | 2009 | 2008 | ||||||||||||||||||||||
| Revenue Dollars |
Percentage of Revenue |
Revenue Dollars |
Percentage of Revenue |
Revenue Dollars |
Percentage of Revenue |
|||||||||||||||||||
| California |
$ | 343,984 | 41.9 | % | $ | 334,953 | 44.3 | % | $ | 325,840 | 44.7 | % | ||||||||||||
| Texas |
190,607 | 23.2 | 190,587 | 25.2 | 185,914 | 25.5 | ||||||||||||||||||
| New Mexico |
86,029 | 10.5 | 81,061 | 10.7 | 79,562 | 10.9 | ||||||||||||||||||
| Kansas |
61,657 | 7.5 | 57,864 | 7.6 | 51,331 | 7.0 | ||||||||||||||||||
| Missouri |
42,902 | 5.2 | 57,141 | 7.6 | 55,878 | 7.7 | ||||||||||||||||||
| Nevada |
48,516 | 5.9 | 30,929 | 4.1 | 30,605 | 4.2 | ||||||||||||||||||
| Montana |
22,641 | 2.8 | — | — | — | — | ||||||||||||||||||
| Iowa |
9,989 | 1.2 | 2,870 | 0.4 | — | — | ||||||||||||||||||
| Arizona |
7,928 | 1.0 | — | — | — | — | ||||||||||||||||||
| Idaho |
5,937 | 0.7 | — | — | — | — | ||||||||||||||||||
| Other |
48 | 0.1 | 660 | 0.1 | 260 | — | ||||||||||||||||||
| Total |
$ | 820,238 | 100.0 | % | $ | 756,065 | 100.0 | % | $ | 729,390 | 100.0 | % | ||||||||||||
The Company’s accounts receivable is derived from services provided to patients in the following payor classes for the years ended December 31 (in thousands):
| Year Ended December 31, | ||||||||
| 2010 | 2009 | |||||||
| Medicare |
$ | 30,578 | $ | 22,620 | ||||
| Medicaid |
25,219 | 29,259 | ||||||
| Subtotal Medicare and Medicaid |
55,797 | 51,879 | ||||||
| Managed care |
23,257 | 23,835 | ||||||
| Private pay and other |
37,433 | 42,214 | ||||||
| Total accounts receivable |
116,487 | 117,928 | ||||||
| Allowance for doubtful accounts |
(17,710 | ) | (21,318 | ) | ||||
| Accounts receivable, net |
$ | 98,777 | $ | 96,610 | ||||
The Company estimates bad debt expense and the allowance for doubtful accounts based on historical experience.
In 2010, the Company converted $4.0 million of accounts receivable to notes receivable for certain of its rehabilitation business customers. As of December 31, 2010 and 2009, notes receivable were approximately $9.9 million and $124 million, of which $4.0 million and $4.4 million as of December 31, 2010 and 2009, respectively, were reflected as current assets with the remaining balances reflected as long-term assets. Interest rates on these notes approximate market rates as of the dates of the notes.
As of December 31, 2010, three Hallmark Rehabilitation business customers owed $9.5 million, or 96% of the total notes receivable balance. These notes receivable, as well as the trade receivables from the customers, are guaranteed both by the assets of the customers as well as personally by the principal owners of the customers. Additionally, as of December 31, 2010, these three customers represented 57% of the accounts receivable for the
F-10
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Company’s rehabilitation therapy services company and approximately 60% of the rehabilitation therapy services company external revenue for 2010. The remaining notes receivable of $0.4 million, or 4% of the notes receivable balance, are primarily past due accounts receivable converted to notes receivable. The notes receivable balance is stated net of an allowance for uncollectibility of approximately $0.2 million and $0.6 million at December 31, 2009, respectively.
Hospice net patient service revenue is reported at the estimated net realizable amounts (exclusive of the provision for uncollectible accounts) from Medicare, Medicaid, commercial insurance and managed care payors, patients and others for services rendered to patients. To determine net patient service revenue, management adjusts gross patient service revenue for estimated contractual adjustments based on historical experience and estimated Medicare cap limits. Net patient service revenue is recognized in the month in which services are delivered.
The Company’s hospice program exceeded the Medicare cap limit in 2009 by $2.1 million. In 2010, the Company’s hospice program did not exceed the Medicare cap limit.
Risks and Uncertainties
Laws and regulations governing the Medicare and Medicaid programs are complex and subject to interpretation. The Company believes that it is in substantial compliance with all applicable laws and regulations. Compliance with such laws and regulations is subject to ongoing and future government review and interpretation, including processing claims at lower amounts upon audit as well as significant regulatory action including revenue adjustments, fines, penalties, and exclusion from the Medicare and Medicaid programs.
Provider Medicaid Integrity Contractors (MIC) audits began in Florida and South Carolina at the end of fiscal year 2008; audits in other jurisdictions began in fiscal year 2009. As of December 2009, MICs began actively conducting audits in over 30 states, including California, Texas, and New Mexico. Statements from CMS regarding the preliminary results of the first 500 MIC audits indicate that nearly 30% of the audits conducted have been of long-term care facilities. Unlike the Medicare Recovery Audit Contractor, or RAC, program, the MIC audits are not subject to a uniform set of federal standards, but rather are governed according to state regulations and procedures relating to Medicaid provider audits and appeals. As such, a great degree of uncertainty surrounds whether and to what extent the results of audits conducted by this new set of audit contractors will result in recoupments of alleged overpayments to our facilities. To the extent the MICs apply different or more stringent standards than other past analogous audit programs, the MIC audits could result in recoupments of alleged overpayments and could have an adverse impact on the Company’s results of operations. There are no ongoing MIC audits as of December 31, 2010.
In addition, Section 6411 of the Patient Protection and Affordable Care Act (PPACA) expanded the RAC program, which formerly included only Medicare Part A and Part B claims, to also include Medicare Part C and Part D claims, as well as Medicaid claims effective December 31, 2010. It is uncertain at this time how the recently-expanded RAC program will interact with the MIC program. CMS has noted in a FAQ that a provider may be subject to audit by multiple oversight bodies, especially if the audits cover different programs (Medicare versus Medicaid), different audit issues (one-day stays versus post-mortem payments) or different audit periods. Moreover, in a proposed rule, published by CMS on November 10, 2010, CMS provides for States and Medicaid RACs to coordinate with other contractors and entities auditing Medicaid providers and with State and Federal law enforcement agencies.
The RACs have made certain revenue recoupments from the Company’s California skilled nursing facilities and third-party skilled nursing facilities to which the Company provides rehabilitation therapy services. As of December 31, 2010, the Company has fully reserved all denied claims.
F-11
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Concentration of Credit Risk
The Company has significant accounts receivable balances whose collectability is dependent on the availability of funds from certain governmental programs, primarily Medicare and Medicaid. These receivables represent the only significant concentration of credit risk for the Company. The Company does not believe there is significant credit risk associated with these governmental programs. The Company believes that an adequate allowance has been recorded for the possibility of these receivables proving uncollectible, and continually monitors and adjusts these allowances as necessary.
Cash and Cash Equivalents
Cash and cash equivalents consist of cash and short-term investments with original maturities of three months or less. At December 31, 2010, the Company had aggregate cash of $4.2 million. This available cash is held in accounts at commercial banking institutions. The Company has periodically invested in AAA money market funds. To date, the Company has not experienced any loss or access to its invested cash or cash equivalents; however, the Company can provide no assurances that access to its invested cash or cash equivalents will not be impacted by adverse conditions in the financial markets.
Capitalized Interest
Interest costs capitalized on construction projects were $0.3 million and $0.4 million for the years ended December 31, 2010 and 2009, respectively.
Property and Equipment
Upon the consummation of the Onex Transaction all property and equipment were stated at fair value. Property and equipment acquired subsequent to the Onex Transaction were recorded at cost or at fair value if acquired as part of a business combination. Major renovations or improvements are capitalized, whereas ordinary maintenance and repairs are expensed as incurred. Depreciation and amortization is computed using the straight-line method over the estimated useful lives of the assets as follows:
| Buildings and improvements |
15-40 years | |
| Leasehold improvements |
Shorter of the lease term or estimated useful life, generally 5-10 years | |
| Furniture and equipment |
3-10 years |
Depreciation and amortization of property and equipment under capital leases is included in depreciation and amortization expense. For leasehold improvements, where the Company has acquired the right of first refusal to purchase or to renew the lease, amortization is based on the lesser of the estimated useful lives or the period covered by the right. Depreciation expense was $21.4 million, $19.4 million, and $16.8 million in 2010, 2009, and 2008, respectively.
Goodwill and Intangible Assets
Goodwill was approximately $332.7 million and $279.4 million as of December 31, 2010 and 2009 respectively. The Company accounts for goodwill in accordance with FASB ASC Topic 350, “Intangibles – Goodwill and Other.”
F-12
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Determination of Reporting Units
The Company considers the following businesses to be reporting units for the purpose of testing goodwill for impairment under FASB ASC Topic 350:
- Long-term care services, which includes the operation of skilled nursing and assisted living facilities and is the most significant portion of the Company’s business;
- Rehabilitation therapy, which provides physical, occupational and speech therapy in Company-owned facilities and unaffiliated facilities; and
- Hospice care, which was established in 2004 and currently provides hospice care in Arizona, California, Idaho, Nevada , New Mexico, and Montana.
- Home health care, which was established in 2010 and currently provides home health services care in Arizona, Idaho, Nevada, and Montana.
The goodwill that resulted from the Onex Transaction as of December 27, 2005 was allocated to the long-term care services reporting unit and the rehabilitation therapy reporting unit based on the relative fair value of the assets on the date of the Onex Transaction. No goodwill was allocated to the hospice care reporting unit due to the start-up nature of the business at the time and cumulative net losses before depreciation, amortization, interest expense (net) and provision for (benefit from) income taxes attributable to that segment. In addition, no synergies were expected to arise as a result of the Onex Transaction which might have provided a different basis for allocation of goodwill to reporting units. Subsequent to the Onex Transaction, goodwill has been allocated to each reporting unit at the time of a business acquisition and is adjusted upon finalization of the purchase price of an acquisition. The Hospice/Home Health Acquisition generated $57 million of goodwill that was recorded as an asset of the hospice and home health services segment.
As of December 31, 2010, $241.7 million related to the long-term care reporting unit, $34.0 million related to the rehabilitation therapy reporting unit, $57 related to the hospice and home health reporting unit.
Goodwill Impairment Testing
We compare the fair value of each reporting unit to its carrying amount on an annual basis to determine whether there is potential goodwill impairment. If the fair value of the reporting unit is less than its carrying value, an impairment loss is recorded to the extent the fair value of goodwill is less than its carrying value. We test goodwill for impairment annually at the reporting unit level on October 1 or sooner, if events or changes in circumstances indicate that the carrying amount of our reporting units, including goodwill, may exceed their fair values.
As of September 30, 2010, carrying value of equity exceeded the Company’s market capitalization by approximately $113 million, or 79%, which is a potential indication of impairment. However, there were a number of changes to our reimbursement rates that had recently become effective, including rate changes in several states for which we had not yet received rate letters, and Medicare’s adoption of Resource Utilization Groups, Version 4 (“RUGs IV”) and Minimum Data Service (“MDS”) 3.0, described in Management’s Discussion and Analysis of Financial Condition and Results of Operations “Sources of Revenue—Medicare”, both of which became effective October 1, 2010. A goodwill impairment analysis was performed as of September 30, 2010 and it was concluded that there was no impairment analysis as of that date. On January 6, 2011, after a press release with revised 2010 earnings estimates and 2011 earnings estimates had been issued, which included the impact of the recent reimbursement changes, carrying value was exceeded by the Company’s market capitalization by approximately $68 million, or 16.2%. The goodwill impairment analysis was updated as of December 31, 2010 and it was concluded that there was no impairment as of that date.
F-13
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Deferred Financing Costs
Deferred financing costs substantially relate to the 11% Senior Subordinated Notes due 2014 (the “2014 Notes”), and the senior secured credit facility Agreement (Note 6) and are being amortized over the maturity periods using an effective-interest method for the 2014 Notes and the term debt component of the senior secured credit facility and the straight-line method for the revolving debt component of the senior secured credit facility. At December 31, 2010 and 2009, deferred financing costs, net of amortization, were approximately $13.2 million, and $13.4 million, respectively.
Income Taxes
The Company uses the liability method of accounting for income taxes as set forth in FASB ASC Topic 740, “Income Taxes.” Under the liability method, deferred taxes are determined based on the differences between the financial statement and tax bases of assets and liabilities using currently enacted tax rates. A valuation allowance is established for deferred tax assets unless their realization is considered more likely than not.
FASB ASC Topic 740 prescribes a recognition threshold and measurement attribute for the financial statement recognition and measurement of a tax position taken or expected to be taken in a tax return. FASB ASC Topic 740 also provides guidance on de-recognition, classification, interest and penalties, accounting in interim periods, disclosure and transition.
Impairment of Long-Lived Assets
As of December 31, 2010 and 2009, none of the Company’s long-lived assets were impaired. The Company periodically evaluates the carrying value of long-lived assets other than goodwill in relation to the future undiscounted cash flows of the underlying businesses to assess recoverability of the assets. If the estimated undiscounted future cash flows are less than the carrying amount, an impairment loss, which is determined based on the difference between the fair value and the carrying value of the assets, would be recognized.
Interest Rate Hedges
The Company uses its senior secured credit facility and the 2014 Notes to finance its operations. The Company’s senior secured credit facility exposes the Company to variability in interest payments due to changes in interest rates. The Company entered into an interest rate hedge transaction agreement on June 30, 2010 in order to manage fluctuations in cash flows resulting from interest rate risk. The interest rate cap agreement is for a notional amount of $70.0 million with a cap rate on 1 month LIBOR of 2.0% from July 2010 to December 2011. The interest rate swap agreement is for a notional amount of $70.0 million with an interest rate of 2.3% from January 2012 to June 2013.
Interests in joint ventures
Joint ventures are entities over which the Company has significant influence but not control, generally achieved by a shareholding of 50% of the voting rights. The equity method is used to account for investments in joint ventures and investments are initially recognized at cost.
Stock Options and Equity Related Charges
FASB ASC Topic 718, “Compensation—Stock Compensation,” requires measurement and recognition of compensation expense for all share-based payment awards made to employees and directors. Under FASB ASC
F-14
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Topic 718, the fair value of share-based payment awards is estimated at grant date using an option pricing model and the portion that is ultimately expected to vest is recognized as compensation cost over the requisite service period.
Asset Retirement Obligations
FASB ASC Topic 410, “Asset Retirement and Environmental Obligations,” requires that either a liability be recognized for the fair value of a legal obligation to perform asset-retirement activities that are conditioned on the occurrence of a future event if the amount can be reasonably estimated, or where it cannot, that disclosure of the liability exists, but has not been recognized, and the reasons why a reasonable estimate cannot be made.
The Company determined that a conditional asset retirement obligation exists for asbestos remediation. Though not a current health hazard in its facilities, upon renovation the Company may be required to take the appropriate remediation procedures in compliance with state law to remove the asbestos. The removal of asbestos-containing materials includes primarily floor and ceiling tiles from the Company’s pre-1980 constructed facilities. The fair value of the conditional asset retirement obligation was determined as the present value of the estimated future cost of remediation based on an estimated expected date of remediation. This computation is based on a number of assumptions which may change in the future based on the availability of new information, technology changes, changes in costs of remediation, and other factors. Any change in the assumptions can impact the value of the determined liability and will be recognized as a change in estimate in the period identified.
As of December 31, 2010 and 2009, the asset retirement obligations were $3.9 million and $5.5 million, respectively, which are classified as other long-term liabilities.
Operating Leases
The Company accounts for operating leases in accordance with FASB ASC Topic 840, “Leases.” Accordingly, rent expense under the Company’s facilities’ and administrative offices’ operating leases is recognized on a straight-line basis over the original term of each lease, inclusive of predetermined minimum rent escalations or modifications and including any lease renewal options.
(Loss) earnings per Share
The Company computes (loss) earnings per share of Class A common stock and Class B common stock in accordance with FASB ASC Topic 260, “Earnings per Share,” using the two-class method. The Company’s Class A common stock and Class B common stock are identical in all respects, except with respect to voting rights and except that each share of Class B common stock is convertible into one share of Class A common stock under certain circumstances. Net (loss) income is allocated on a proportionate basis to each class of common stock in the determination of (loss) earnings per share.
Basic (loss) earnings per share were computed by dividing net (loss) income by the weighted-average number of outstanding shares for the period. Dilutive (loss) earnings per share is computed by dividing net (loss) income plus the effect of assumed conversions (if applicable) by the weighted-average number of outstanding shares after giving effect to all potential dilutive common stock, including options, warrants, common stock subject to repurchase and convertible preferred stock, if any.
F-15
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
The following table sets forth the computation of basic and diluted (loss) earnings per share of Class A common stock and Class B common stock (dollars in thousands, except per share data):
| December 31, 2010 | December 31, 2009 | December 31, 2008 | ||||||||||||||||||||||||||||||||||
| Class A | Class B | Total | Class A | Class B | Total | Class A | Class B | Total | ||||||||||||||||||||||||||||
| (Loss) earnings per share, basic |
||||||||||||||||||||||||||||||||||||
| Numerator: |
||||||||||||||||||||||||||||||||||||
| Allocation of net (loss) income from continuing operations |
$ | (563 | ) | $ | (478 | ) | $ | (1,041 | ) | $ | (71,597 | ) | $(61,194) | $ | (132,791 | ) | $ | 18,093 | $ | 16,003 | $ | 34,096 | ||||||||||||||
| Allocation of loss from discontinued operations |
— | — | — | (210 | ) | (180 | ) | (390 | ) | — | — | — | ||||||||||||||||||||||||
| Allocation of net (loss) income |
$ | (563 | ) | $ | (478 | ) | $ | (1,041 | ) | $ | (71,807 | ) | $(61,374) | $ | (133,181 | ) | $ | 18,093 | $ | 16,003 | $ | 34,096 | ||||||||||||||
| (Loss) earnings per share, diluted |
||||||||||||||||||||||||||||||||||||
| Numerator: |
||||||||||||||||||||||||||||||||||||
| Allocation of net (loss) income from continuing operations |
$ | (563 | ) | $ | (478 | ) | $ | (1,041 | ) | $ | (71,597 | ) | $(61,194) | $ | (132,791 | ) | $ | 17,971 | $ | 16,125 | $ | 34,096 | ||||||||||||||
| Allocation of loss from discontinued operations |
— | — | — | (210 | ) | (180 | ) | (390 | ) | — | — | — | ||||||||||||||||||||||||
| Allocation of net (loss) income |
$ | (563 | ) | $ | (478 | ) | $ | (1,041 | ) | $ | (71,807 | ) | $(61,374) | $ | (133,181 | ) | $ | 17,971 | $ | 16,125 | $ | 34,096 | ||||||||||||||
| Denominator for basic and diluted (loss) earnings per share: |
||||||||||||||||||||||||||||||||||||
| Weighted-average common shares outstanding, basic |
19,988 | 17,000 | 36,988 | 19,903 | 17,011 | 36,914 | 19,407 | 17,166 | 36,573 | |||||||||||||||||||||||||||
| Plus: incremental shares related to dilutive effect of stock options and restricted stock, if applicable |
— | — | — | — | — | — | 39 | 282 | 321 | |||||||||||||||||||||||||||
| Adjusted weighted-average common shares outstanding, diluted |
19,988 | 17,000 | 36,988 | 19,903 | 17,011 | 36,914 | 19,446 | 17,448 | 36,894 | |||||||||||||||||||||||||||
| (Loss) earnings per share, basic: |
||||||||||||||||||||||||||||||||||||
| (Loss) earnings per common share from continuing operations |
$ | (0.03 | ) | $ | (0.03 | ) | $ | (0.03 | ) | $ | (3.60 | ) | $ | (3.60 | ) | $ | (3.60 | ) | $ | 0.93 $ | 0.93 | $ | 0.93 | |||||||||||||
| Loss per common share from discontinued operations |
— | — | — | (0.01 | ) | (0.01 | ) | (0.01 | ) | — | — | — | ||||||||||||||||||||||||
| (Loss) earnings per share |
$ | (0.03 | ) | $ | (0.03 | ) | $ | (0.03 | ) | $ | (3.61 | ) | $ | (3.61 | ) | $ | (3.61 | ) | $ | 0.93 $ | 0.93 | $ | 0.93 | |||||||||||||
| (Loss) earnings per share, diluted: |
||||||||||||||||||||||||||||||||||||
| (Loss) earnings per common share from continuing operations |
$ | (0.03 | ) | $ | (0.03 | ) | $ | (0.03 | ) | $ | (3.60 | ) | $ | (3.60 | ) | $ | (3.60 | ) | $ | 0.92 $ | 0.92 | $ | 0.92 | |||||||||||||
| Loss per common share from discontinued operations |
— | — | — | (0.01 | ) | (0.01 | ) | (0.01 | ) | — | — | — | ||||||||||||||||||||||||
| (Loss) earnings per share |
$ | (0.03 | ) | $ | (0.03 | ) | $ | (0.03 | ) | $ | (3.61 | ) | $ | (3.61 | ) | $ | (3.61 | ) | $ | 0.92 $ | 0.92 | $ | 0.92 | |||||||||||||
The following were excluded from the weighted-average diluted shares computation for 2010, 2009, and 2008 (shares in thousands):
| Year Ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Options to purchase common shares |
590 | 536 | 103 | |||||||||
| Non-vested restricted stock and restricted stock units |
3 | 55 | (1) | — | ||||||||
| Total excluded |
593 | 591 | 103 | |||||||||
| (1) | Amount includes two shares for Class B shares |
F-16
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Accumulated Other Comprehensive (Loss) Income
Accumulated other comprehensive (loss) income consists of two components, net (loss) income and other comprehensive (loss) income. Other comprehensive (loss) income refers to revenue, expenses, gains, and losses that, under GAAP, are recorded as an element of stockholders’ equity but are excluded from net (loss) income. Currently, the Company’s other comprehensive (loss) income consists of deferred gains and losses on the Company’s interest rate hedge transactions accounted for as a cash flow hedge.
The following table summarizes activity in other comprehensive income related to the Company’s interest rate hedge transactions, net of taxes, held by the Company (in thousands):
| 2010 | 2009 | 2008 | ||||||||||
| Net unrealized (loss) income, net of tax (benefit) expense of $(122) in 2010, $1,190 in 2009, and ($690) in 2008 |
$ | (258 | ) | $ | 1,882 | $ | (1,089 | ) | ||||
Recent Accounting Pronouncements
There are no recent accounting pronouncements that have a material effect on the Company’s financial statements.
3. Fair Value of Financial Instruments
The following methods and assumptions were used by the Company in estimating fair value of each class of financial instruments for which it is practicable to estimate this value:
Cash and Cash Equivalents
The carrying amounts approximate fair value because of the short maturity of these instruments.
Interest Rate Swaps and Contingent Consideration
The carrying amounts approximate the fair value for the Company’s interest rate swaps based on an estimate obtained from a broker.
The following table summarizes the valuation of the Company’s interest rate swaps as of December 31, 2010 by the FASB ASC Topic 820, “Fair Value Measurement and Disclosures,” fair value hierarchy (in thousands):
| Level 1 | Level 2 | Level 3 | Total | |||||||||||||
| Interest rate hedges |
$ | — | $ | (316 | ) | $ | — | $ | (316 | ) | ||||||
| Contingent Consideration—acquisition |
$ | — | $ | — | $ | 5,350 | $ | 5,350 | ||||||||
In June 2010, the Company entered into an interest rate cap agreement and an interest rate swap agreement in order to manage fluctuations in cash flows resulting from interest rate risk. The interest rate cap agreement is for a notional amount of $70.0 million with a cap rate on 1 month LIBOR of 2.0% from July 2010 to December 2011. The interest rate swap agreement is for a notional amount of $70.0 million with an interest rate of 2.3% from January 2012 to June 2013. The Company continues to assess its exposure to interest rate risk on an ongoing basis.
F-17
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
The interest rate swap is required to be measured at fair value on a recurring basis. The fair value of the interest rate swap contract is determined by calculating the value of the discounted cash flows of the difference between the fixed interest rate of the interest rate swap and the counterparty’s forward LIBOR curve, which is the input used in the valuation. The forward LIBOR curve is readily available in public markets or can be derived from information available in publicly quoted markets. Therefore, the Company has categorized the interest rate swap as Level 2. The Company obtained the counterparty’s calculation of the valuation of the interest rate swap as well as a forward LIBOR curve from another investment bank and recalculated the valuation of the interest rate swap, which agreed with the counterparty’s calculation.
The fair value of the interest rate swap agreement designated as a hedging instrument against the variability of cash flows associated with floating-rate, long-term debt obligations is reported in accumulated other comprehensive income. These amounts subsequently are reclassified into interest expense as a yield adjustment in the same period in which the related interest on the floating-rate debt obligation affects earnings. The Company evaluates the effectiveness of the cash flow hedge, in accordance with FASB ASC Topic 815, “Derivatives and Hedging,” on a quarterly basis. The change in fair value is recorded as a component of other comprehensive income. Should the hedge become ineffective, the change in fair value would be recognized in the consolidated statements of operations.
For the year ended December 31, 2010, the total net loss recorded through OCI from converting from floating rate (one-month LIBOR) to fixed rate for a portion of the interest payments under our long-term debt obligations was approximately $0.3 million.
On May 1, 2010, the Company acquired substantially all of the assets of five Medicare-certified hospice companies and four Medicare-certified home health companies located in Arizona, Idaho, Montana and Nevada (the“ Hospice/Home Health Acquisition”), described in Note 17—Acquisition. As part of the purchase agreement, the purchase consideration included cash, promissory notes, contingent consideration, and deferred cash payments. The contingent consideration arrangement requires the Company to pay contingent payments should the acquired operations achieve certain financial targets based on EBITDA, as defined in the acquisition agreement. The purchase price included in the initial closing price may be adjusted upwards by $7.0 million over an earnout period of 5 years. We estimated the fair value of the contingent consideration using a probability-weighted discounted cash flow model. This fair value measurement is based on significant inputs not observable in the market and thus represents a Level 3 measurement. The contingent consideration was recorded at the date of acquisition in the amount of $4.9 million. As of December 31, 2010 the contingent consideration had a fair value of $5.4 million. This is included in other non-current liabilities on the Company’s consolidated balance sheet. The change in fair value of $0.4 million from the contingent consideration was recorded within depreciation and amortization expense.
Below is a table listing the Level 3 rollforward as of December 31, 2010 (in thousands):
| Level 3 Rollforward |
||||
| Value at January 1, 2010 |
$ | — | ||
| Value at acquisition date |
4,930 | |||
| Change in fair value |
420 | |||
| Value at December 31, 2010 |
5,350 | |||
F-18
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Below is a table listing the fair value of the interest rate swap as of December 31, 2010 and December 31, 2009 (in thousands):
| December 31, 2010 | December 31, 2009 | |||||||
| Derivatives designated as hedging instruments under ASC Topic 815 |
Balance Sheet Location | Fair Value (Pre-tax) |
Balance Sheet Location | Fair Value (Pre-tax) | ||||
| Interest rate swap |
Accounts payable and accrued liabilities |
$(316) | Accounts payable and accrued liabilities |
$65 | ||||
Below is a table listing the amount of gain (loss) recognized before income tax in other comprehensive income (“OCI”) on the interest rate swap for the years ending December 31, 2010, 2009, and 2008 (in thousands):
| Derivatives in ASC Topic 815 Cash Flow Hedging Relationships |
Amount of Gain
(Loss) Recognized in OCI on Derivative (Effective Portion) |
|||||||||||
| Year Ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Interest rate swap |
$ | (379 | ) | $ | 3,072 | $ | (1,779 | ) | ||||
Below is a table listing the amount of gain (loss) reclassified from accumulated OCI into income (effective portion) for the year ending December 31, 2010, 2009, and 2008 (in thousands):
| Location of Gain (Loss) Reclassified from Accumulated OCI into Income (Effective Portion) |
Amount of Gain
(Loss) Reclassified from Accumulated OCI into Income (Effective Portion) |
|||||||||||
| Year Ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Interest (expense) income |
$ | (264 | ) | $ | (3,430 | ) | $ | (1,184 | ) | |||
Long-Term Debt
The carrying value of the Company’s long-term debt is considered to approximate the fair value of such debt for all periods presented based upon the interest rates that the Company believes it can currently obtain for similar debt.
F-19
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
4. Intangible Assets
Identified intangible assets are amortized over their useful lives except for trade names and certain other long-lived intangibles, which have an indefinite life. Amortization expense was approximately $3.2 million, $3.9 million and $4.2 million in 2010, 2009 and 2008, respectively. Amortization of the Company’s intangible assets at December 31, 2010 is expected to be approximately $1.0 million, $0.2 million, $0.2 million, $0.2 million and $0.2 million in 2011, 2012, 2013, 2014, and 2015 respectively. Identified intangible asset balances by major class at December 31, 2010 and 2009, are as follows (dollars in thousands):
| Cost | Life (in years) |
Accumulated Amortization |
Net Balance | |||||||||||||
| Intangible assets subject to amortization: |
||||||||||||||||
| Covenants not-to-compete |
$ | 2,987 | 5.0 | $ | (2,945 | ) | $ | 42 | ||||||||
| Managed care contracts |
10,920 | 4.8 | (10,180 | ) | 740 | |||||||||||
| Leasehold interests |
4,318 | 14.5 | (2,521 | ) | 1,797 | |||||||||||
| Total |
$ | 18,225 | 7.1 | $ | (15,646 | ) | 2,579 | |||||||||
| Intangible assets not subject to amortization: |
||||||||||||||||
| Trade names |
17,130 | |||||||||||||||
| Other long-lived intangibles |
5,632 | |||||||||||||||
| Balance at December 31, 2010 |
$ | 25,341 | ||||||||||||||
| Cost | Life (in years) |
Accumulated Amortization |
Net Balance | |||||||||||||
| Intangible assets subject to amortization: |
||||||||||||||||
| Covenants not-to-compete |
$ | 2,987 | 5.0 | $ | (2,892 | ) | $ | 95 | ||||||||
| Managed care contracts |
10,920 | 4.8 | (7,897 | ) | 3,023 | |||||||||||
| Leasehold interests |
9,180 | 11.3 | (3,624 | ) | 5,556 | |||||||||||
| Total |
$ | 23,087 | 7.4 | $ | (14,413 | ) | 8,674 | |||||||||
| Intangible assets not subject to amortization: |
||||||||||||||||
| Trade names |
17,130 | |||||||||||||||
| Other long-lived intangibles |
493 | |||||||||||||||
| Balance at December 31, 2009 |
$ | 26,297 | ||||||||||||||
5. Business Segments
The Company has three reportable operating segments—LTC, which includes the operation of SNFs and ALFs and is the most significant portion of the Company’s business, therapy services, which includes the Company’s rehabilitation therapy, and hospice and home health services, which includes the Company’s hospice and home health businesses. The “other” category in the table below includes general and administrative items. The Company’s reporting segments are business units that offer different services, and that are managed differently due to the nature of the services provided.
At December 31, 2010, LTC services are provided by 78 wholly-owned SNF operating companies that offer post-acute, rehabilitative and specialty skilled nursing care, as well as 22 wholly-owned ALF operating companies that provide room and board and social services. Therapy services include rehabilitative services such as physical, occupational and speech therapy provided in the Company’s facilities and in unaffiliated facilities by its wholly-owned operating company, Hallmark Rehabilitation GP, LLC.
F-20
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
The Company evaluates performance and allocates capital resources to each segment based on an operating model that is designed to maximize the quality of care provided and profitability. Accordingly, earnings from continuing operations before net interest, tax, depreciation and amortization (“EBITDA”) and rent cost of revenue (“EBITDAR”) is used as the primary measure of each segment’s operating results because it does not include such costs as interest expense, income taxes, depreciation, amortization and rent cost of revenue which may vary from segment to segment depending upon various factors, including the method used to finance the original purchase of a segment or the tax law of the states in which a segment operates. By excluding these items, the Company is better able to evaluate operating performance of the segment by focusing on more controllable measures. General and administrative expenses are not allocated to any segment for purposes of determining segment profit or loss, and are included in the “other” category in the selected segment financial data that follows. The accounting policies of the reporting segments are the same as those described in the “Summary of Significant Accounting Policies” in Note 2. Intersegment sales and transfers are recorded at cost plus standard mark-up; intersegment transactions have been eliminated in consolidation.
F-21
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
The following table sets forth selected financial data consolidated by business segment (in thousands):
| Long-term Care Services |
Therapy Services |
Hospice & Home Health Services |
Other | Elimination | Total | |||||||||||||||||||
| Year ended December 31, 2010 |
||||||||||||||||||||||||
| Revenue from external customers |
$ | 694,401 | $ | 74,118 | $ | 51,719 | $ | — | $ | — | $ | 820,238 | ||||||||||||
| Intersegment revenue |
1,414 | 67,005 | — | — | (68,419 | ) | — | |||||||||||||||||
| Total revenue |
$ | 695,815 | $ | 141,123 | $ | 51,719 | $ | — | $ | (68,419 | ) | $ | 820,238 | |||||||||||
| Operating income (loss) |
$ | 40,110 | $ | 18,619 | $ | 8,040 | $ | (27,152 | ) | $ | — | $ | 39,617 | |||||||||||
| Interest expense, net of interest income |
(36,074 | ) | ||||||||||||||||||||||
| Other expense |
2,332 | |||||||||||||||||||||||
| Equity in earnings of joint venture |
2,566 | |||||||||||||||||||||||
| Debt retirement costs |
(7,010 | ) | ||||||||||||||||||||||
| Income before provision for income taxes |
1,431 | |||||||||||||||||||||||
| Income tax expense |
2,472 | |||||||||||||||||||||||
| Net loss from continuing operations |
$ | (1,041 | ) | |||||||||||||||||||||
| Depreciation and amortization |
$ | 22,875 | $ | 360 | $ | 785 | $ | 1,027 | $ | — | $ | 25,047 | ||||||||||||
| Segment capital expenditures |
$ | 26,243 | $ | 728 | $ | 283 | $ | 482 | $ | — | $ | 27,736 | ||||||||||||
| EBITDA(1) |
$ | 58,627 | $ | 18,978 | $ | 8,827 | $ | (23,880 | ) | $ | — | $ | 62,552 | |||||||||||
| EBITDAR(2) |
$ | 77,109 | $ | 19,177 | $ | 9,671 | $ | (23,791 | ) | $ | (578 | ) | $ | 81,590 | ||||||||||
| Year ended December 31, 2009 |
||||||||||||||||||||||||
| Revenue from external customers |
$ | 666,800 | $ | 74,088 | $ | 15,177 | $ | — | $ | — | $ | 756,065 | ||||||||||||
| Intersegment revenue |
3,034 | 66,518 | — | — | (69,552 | ) | — | |||||||||||||||||
| Total revenue |
$ | 669,834 | $ | 140,606 | $ | 15,177 | $ | — | $ | (69,552 | ) | $ | 756,065 | |||||||||||
| Operating (loss) income |
$ | (78,063 | ) | $ | 20,734 | $ | (2,243 | ) | $ | (26,411 | ) | $ | — | $ | (85,983 | ) | ||||||||
| Interest expense, net of interest income |
(31,867 | ) | ||||||||||||||||||||||
| Other expense |
150 | |||||||||||||||||||||||
| Equity in earnings of joint venture |
2,751 | |||||||||||||||||||||||
| Loss before provision for income taxes |
(114,949 | ) | ||||||||||||||||||||||
| Income tax expense |
17,842 | |||||||||||||||||||||||
| Net loss from continuing operations |
$ | (132,791 | ) | |||||||||||||||||||||
| Depreciation and amortization |
$ | 21,491 | $ | 326 | $ | 264 | $ | 1,227 | $ | — | $ | 23,308 | ||||||||||||
| Segment capital expenditures |
$ | 40,013 | $ | 110 | $ | 199 | $ | 833 | $ | — | $ | 41,155 | ||||||||||||
| EBITDA(1) |
$ | (56,633 | ) | $ | 20,857 | $ | (1,603 | ) | $ | (22,785 | ) | $ | — | $ | (60,164 | ) | ||||||||
| EBITDAR(2) |
$ | (38,381 | ) | $ | 21,001 | $ | (1,380 | ) | $ | (22,691 | ) | $ | (576 | ) | $ | (42,027 | ) | |||||||
| Year ended December 31, 2008 |
||||||||||||||||||||||||
| Revenue from external customers |
$ | 643,476 | $ | 69,931 | $ | 15,983 | $ | — | $ | — | $ | 729,390 | ||||||||||||
| Intersegment revenue |
4,031 | 65,174 | — | — | (69,205 | ) | — | |||||||||||||||||
| Total revenue |
$ | 647,507 | $ | 135,105 | $ | 15,983 | $ | — | $ | (69,205 | ) | $ | 729,390 | |||||||||||
| Operating income |
$ | 93,707 | $ | 16,999 | $ | 954 | $ | (25,635 | ) | $ | — | $ | 86,025 | |||||||||||
| Interest expense, net of interest income |
(36,581 | ) | ||||||||||||||||||||||
| Other income |
246 | |||||||||||||||||||||||
| Equity in earnings of joint venture |
2,487 | |||||||||||||||||||||||
| Income before provision for income taxes |
52,177 | |||||||||||||||||||||||
| Income tax expense |
18,081 | |||||||||||||||||||||||
| Net income from continuing operations |
$ | 34,096 | ||||||||||||||||||||||
| Depreciation and amortization |
$ | 8,894 | $ | 307 | $ | 152 | $ | 11,625 | $ | — | $ | 20,978 | ||||||||||||
| Segment capital expenditures |
$ | 46,062 | $ | 505 | $ | 911 | $ | 2,148 | $ | — | $ | 49,626 | ||||||||||||
| EBITDA(1) |
$ | 113,122 | $ | 17,307 | $ | 1,295 | $ | (21,988 | ) | $ | — | $ | 109,736 | |||||||||||
| EBITDAR(2) |
$ | 131,399 | $ | 17,562 | $ | 1,457 | $ | (21,866 | ) | $ | (568 | ) | $ | 127,984 | ||||||||||
F-22
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
The following table presents the segment assets by business segments (in thousands):
| Long-term Care Services |
Therapy Services |
Hospice & Home Health Services |
Other | Total | ||||||||||||||||
| December 31, 2010: |
||||||||||||||||||||
| Segment total assets |
$ | 711,108 | $ | 81,863 | $ | 76,950 | $ | 67,809 | $ | 937,730 | ||||||||||
| Goodwill and intangibles included in total assets |
$ | 244,760 | $ | 50,993 | $ | 62,312 | $ | — | $ | 358,065 | ||||||||||
| December 31, 2009: |
||||||||||||||||||||
| Segment total assets |
$ | 715,588 | $ | 87,983 | $ | 3,975 | $ | 48,696 | $ | 856,242 | ||||||||||
| Goodwill and intangibles included in total assets |
$ | 254,536 | $ | 50,993 | $ | 130 | $ | — | $ | 305,659 | ||||||||||
| (1) | EBITDA is defined as net (loss) income before depreciation, amortization and interest expense (net of interest income) and the provision for income taxes. EBITDA margin is EBITDA as a percentage of revenue. The Company prepares Adjusted EBITDA by adjusting EBITDA to eliminate non-core business items, which for the reported periods includes, to the extent applicable: |
| • | discontinued operations, net of tax; |
| • | gains or losses on sale of assets |
| • | the write-off of deferred financing costs of extinguished debt; |
| • | provision for the impairment of long-lived assets, including goodwill |
| • | certain litigation expenses; and |
| • | acquisition costs. |
| (2) | EBITDAR is defined as net (loss) income before depreciation, amortization and interest expense (net of interest income), the provision for income taxes and rent cost of revenue. EBITDAR margin is EBITDAR as a percentage of revenue. |
The Company believes that the presentation of EBITDA, EBITDAR, Adjusted EBITDA, and Adjusted EBITDAR provides useful information regarding its operational performance because it enhances the overall understanding of the financial performance and prospects for the future of core business activities.
Specifically, the Company believes that a report of EBITDA, EBITDAR, Adjusted EBITDA, and Adjusted EBITDAR provides consistency in its financial reporting and provides a basis for the comparison of results of core business operations between current, past, and future periods. EBITDA, EBITDAR, Adjusted EBITDA, and Adjusted EBITDAR are primary indicators management uses for planning and forecasting in future periods, including trending and analyzing the core operating performance of business from period-to-period without the effect of accounting principles generally accepted in the United States of America, or GAAP, expenses, revenues and gains that are unrelated to the day-to-day performance of its business. The Company also uses EBITDA, EBITDAR, Adjusted EBITDA, and Adjusted EBITDAR to prepare operating budgets, to measure its performance against those budgets on a consolidated segment and a facility-by-facility level, analyzing year-over-year trends as described below and to compare its operating performance to that of its competitors.
The Company typically uses Adjusted EBITDA and Adjusted EBITDAR for these purposes at the administrative level (because the adjustments to EBITDA and EBITDAR are not generally allocable to any individual business unit) and the Company typically uses EBITDA and EBITDAR to compare the operating performance of each of the Company’s businesses, as well as to assess the performance of operating segments: long-term care services, which include the operation of skilled nursing and assisted living facilities; and ancillary services, which include rehabilitation therapy and hospice businesses. EBITDA, EBITDAR, Adjusted EBITDA,
F-23
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
and Adjusted EBITDAR are useful in this regard because they do not include such costs as interest expense (net of interest income), income taxes, depreciation and amortization expense, rent cost of revenue and special charges, which may vary from business unit to business unit and period-to-period depending upon various factors, including the method used to finance the business, the amount of debt that the Company has determined to incur, whether a facility is owned or leased, the date of acquisition of a facility or business, the original purchase price of a facility or business unit or the tax law of the state in which a business unit operates. These types of charges are dependent on factors unrelated to the underlying business. As a result, the Company believes that the use of EBITDA, EBITDAR, Adjusted EBITDA, and Adjusted EBITDAR provides a meaningful and consistent comparison of its underlying business between periods by eliminating certain items required by GAAP which have little or no significance in day-to-day operations.
The Company also makes capital allocations to each of its facilities based on expected EBITDA returns and establishes compensation programs and bonuses for facility-level employees that are based upon the achievement of pre-established EBITDA and Adjusted EBITDA targets.
Finally, the Company uses Adjusted EBITDA to determine compliance with debt covenants and assess its ability to borrow additional funds and to finance or expand operations. The senior secured credit facility agreement uses a measure substantially similar to Adjusted EBITDA as the basis for determining compliance with financial covenants, specifically minimum interest coverage ratio and maximum total leverage ratio, and for determining the interest rate of the first lien term loan. The indenture governing the 11% senior subordinated notes also uses a substantially similar measurement for determining the amount of additional debt the Company may incur. For example, both the senior secured credit facility and the indenture governing the 11% senior subordinated notes include adjustments for (i) gain or losses on disposal of assets, (ii) the write-off of deferred financing costs of extinguished debt, (iii) proforma adjustments for acquisitions to show a full year of EBITDA and interest expense, (iv) sponsorship fees paid to Onex which totals $0.5 million annually and (v) non-cash stock compensation. Non-compliance with these financial covenants could lead to acceleration of amounts due under the senior secured credit facility. In addition, if the Company cannot satisfy certain financial covenants under the indenture for the 11% senior subordinated notes, the Company cannot engage in certain specified activities, such as incurring additional indebtedness or making certain payments.
Despite the importance of these measures in analyzing underlying business, maintaining financial requirements, designing incentive compensation and for goal setting both on an aggregate and facility level basis, EBITDA, EBITDAR, Adjusted EBITDA, and Adjusted EBITDAR are non-GAAP financial measures that have no standardized meaning defined by GAAP. Therefore, EBITDA, EBITDAR, Adjusted EBITDA, and Adjusted EBITDAR measures have limitations as analytical tools, and they should not be considered in isolation, or as a substitute for analysis of results as reported under GAAP. Some of these limitations are:
| • | they do not reflect the Company’s cash expenditures, or future requirements, for capital expenditures or contractual commitments; |
| • | they do not reflect changes in, or cash requirements for, working capital needs; |
| • | they do not reflect the interest expense, or the cash requirements necessary to service interest or principal payments, on debt; |
| • | they do not reflect any income tax payments the Company may be required to make; |
| • | although depreciation and amortization are non-cash charges, the assets being depreciated and amortized will often have to be replaced in the future, and EBITDA, EBITDAR, Adjusted EBITDA, and Adjusted EBITDAR do not reflect any cash requirements for such replacements; |
| • | they are not adjusted for all non-cash income or expense items that are reflected in consolidated statements of cash flows; |
F-24
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
| • | they do not reflect the impact on earnings of charges resulting from certain matters the Company does consider not to be indicative of ongoing operations; and |
| • | other companies in the Company’s industry may calculate these measures differently than the Company does, which may limit their usefulness as comparative measures. |
The Company compensates for these limitations by using them only to supplement net (loss) income on a basis prepared in conformance with GAAP in order to provide a more complete understanding of the factors and trends affecting its business. The Company strongly encourages investors to consider net (loss) income determined under GAAP as compared to EBITDA, EBITDAR, Adjusted EBITDA, and Adjusted EBITDAR and to perform their own analysis, as appropriate.
The following table provides a reconciliation from net (loss) income which is the most directly comparable financial measure presented in accordance with GAAP for the periods indicated (in thousands):
| Year Ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Reconciliation from net (loss) income to EBITDA, EBITDAR, Adjusted EBITDA and Adjusted EBITDAR (in thousands): |
||||||||||||
| Net (loss) income |
$ | (1,041 | ) | $ | (133,181 | ) | $ | 34,096 | ||||
| Interest expense, net of interest income |
36,074 | 31,867 | 36,581 | |||||||||
| Provision for income taxes |
2,472 | 17,842 | 18,081 | |||||||||
| Depreciation and amortization expense |
25,047 | 23,308 | 20,978 | |||||||||
| EBITDA |
62,552 | (60,164 | ) | 109,736 | ||||||||
| Rent cost of revenue |
19,038 | 18,137 | 18,248 | |||||||||
| EBITDAR |
81,590 | (42,027 | ) | 127,984 | ||||||||
| EBITDA |
62,552 | (60,164 | ) | 109,736 | ||||||||
| Discontinued operations(a) |
— | 390 | — | |||||||||
| Loss (gain) on sale of assets(b) |
(2,243 | ) | 61 | 62 | ||||||||
| Debt retirement costs(c) |
7,010 | — | — | |||||||||
| Goodwill impairment charge(d) |
— | 170,600 | — | |||||||||
| Litigation settlement costs(e) |
53,505 | — | — | |||||||||
| Acquisition costs(f) |
700 | — | — | |||||||||
| Adjusted EBITDA |
121,524 | 110,887 | 109,798 | |||||||||
| Rent cost of revenue |
19,038 | 18,137 | 18,248 | |||||||||
| Adjusted EBITDAR |
$ | 140,562 | $ | 129,024 | $ | 128,046 | ||||||
Notes
| (a) | In 2009, the Company closed its hospice operations located in Ventura, California, and, therefore, the results of this business have been classified as discontinued operations. |
| (b) | While gains or losses on sales of assets are required under GAAP, these amounts are also not reflective of income and losses of the Company’s underlying business. |
| (c) | During the second quarter of 2010, the Company expensed deferred financing fees in the amount of $6.6 million. In conjunction with the closing of the refinancing, the Company terminated its then existing swap agreements as they were incompatible with the new financing due to the existence of the LIBOR floor. The termination of the swap agreements cost $0.4 million, which was recorded as debt retirement costs. |
F-25
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
| (d) | During the fourth quarter of 2009, the Company recorded a goodwill impairment charge of $170.6 million at its long-term care reporting unit. The goodwill impairment charge is a non-cash accounting adjustment to the Company’s financial statements that does not affect its cash flows, or its liquidity position and is not expected to have any impact on its business. The impairment charge is the result of the downturn in the expected future growth rates for governmental payors (based on patient mix and announced Medicare and Medicaid reimbursement reductions), and their effect on expected future cash flows. See “Management’s Discussion and Analysis of Financial Condition and Results of Operations—Goodwill” for a more detailed discussion of the goodwill impairment charge. |
| (e) | During the third quarter of 2010, the Company recorded a litigation settlement expense of $53.5 million. The $53.5 million was comprised of a $50.0 million cash settlement related to the Humboldt County Action and $3.0 million of related legal expenses, and $0.5 million in securities class action costs related to the Shepardson v. Skilled Healthcare Group, Inc. litigation described in Note 12, Commitments and Contingencies—Litigation. |
| (f) | Hospice and home health costs of services included $0.7 million of non-recurring acquisition related costs during 2010. |
6. Debt
The Company’s long-term debt as of December 31, 2010 and 2009 is summarized as follows (in thousands):
| 2010 | 2009 | |||||||
| Revolving Credit Facility, interest rate comprised of LIBOR (subject to a 1.50% floor) plus 3.75%, or 5.25% at December 31, 2010, and LIBOR plus 2.75%, or 2.99% at December 31, 2009; collateralized by substantially all assets of the Company; December 31, 2010 amount due 2015, December 31, 2009 amount due 2012 |
$ | 26,000 | $ | 61,000 | ||||
| Revolving Credit Facility, interest rate based on prime plus 1.75%, or 5.00% at December 31, 2009) collateralized by substantially all assets of the Company, due 2012 |
— | 11,000 | ||||||
| Term Loan, interest rate based on LIBOR (subject to a 1.50% floor) plus 3.75%, or 5.25% at December 31, 2010, and LIBOR plus 2.00%, or 2.28% at December 31, 2009; collateralized by substantially all assets of the Company; December 31, 2010 amount due 2016, December 31, 2009 amount due 2012 |
354,935 | 100,000 | ||||||
| Term Loan, interest rate swapped at 2.58% through December 31, 2010 as of December 31, 2009; collateralized by substantially all assets of the Company; amount due 2012 |
— | 145,000 | ||||||
| Term Loan, interest rate based on LIBOR plus 2.00%, or 2.25% at December 31, 2009; collateralized by substantially all assets of the Company; amount due 2012 |
— | 3,300 | ||||||
| 2014 Senior Subordinated Notes, interest rate 11.0%, with an original issue discount of $331 and $438 at December 31, 2010 and December 31, 2009, respectively, interest payable semiannually, principal due 2014 |
129,669 | 129,562 | ||||||
| Notes payable, interest rate fixed at 6.5%, payable in monthly installments, collateralized by a first priority deed of trust, due December 2018 |
1,411 | 1,544 | ||||||
| Insurance premium financing |
— | 5,071 | ||||||
| Hospice/Home Health Acquisition note, interest rate fixed at 6.00%, payable in annual installments, due 2014 |
7,948 | — | ||||||
| Present value of capital lease obligations at effective interest rates, collateralized by property and equipment |
— | 2,202 | ||||||
| Total long-term debt and capital leases |
519,963 | 458,679 | ||||||
| Less amounts due within one year |
(5,742 | ) | (7,823 | ) | ||||
| Long-term debt and capital leases, net of current portion |
$ | 514,221 | $ | 450,856 | ||||
F-26
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Term Loan and Revolving Loan
On April 9, 2010, the Company entered into an up to $360.0 million senior secured term loan and a $100.0 million revolving credit facility (“Restated Credit Agreement”) that amended and restated the senior secured term loan and revolving credit facility that were set to mature in June 2012. As of December 31, 2010, there was $26.0 million outstanding on the revolving credit facility. The credit arrangements provided under the Restated Credit Agreement are sometimes collectively referred to herein as the Company’s senior secured credit facility.
The term loan requires principal payments of 0.25% of the original principal amount issued on the last business day of each of March, June, September and December, commencing on June 30, 2010, with the balance due April 9, 2016. Amounts borrowed under the term loan may be prepaid at any time without penalty except for LIBOR breakage costs. Commitments under the revolving loan terminate on April 9, 2015. However, if any of the 2014 Senior Subordinated Notes remain outstanding on October 14, 2013, then the maturity date of the term loan and revolving loan will be October 14, 2013. Amounts borrowed pursuant to the Restated Credit Agreement are secured by substantially all of the Company’s assets.
Under the Restated Credit Agreement, the Company must maintain compliance with specified financial covenants measured on a quarterly basis. The Restated Credit Agreement also includes certain additional affirmative and negative covenants, including limitations on the incurrence of additional indebtedness, liens, investments in other businesses and capital expenditures. Also under the Restated Credit Agreement, subject to certain exceptions and minimum thresholds, the Company is required to apply all of the proceeds from any issuance of debt, as much as half of the proceeds from any issuance of equity, half of the Company’s annual Consolidated Excess Cash Flow, as defined in the Restated Credit Agreement, and amounts received in connection with any sale of the Company’s assets to repay the outstanding amounts under the Restated Credit Agreement.
Loans outstanding under the Restated Credit Agreement bear interest, at the Company’s election, either at the prime rate plus an initial margin of 2.75% or the London Interbank Offered Rate (“LIBOR”) plus an initial margin of 3.75%. Under the terms of the Restated Credit Agreement there is a LIBOR floor of 1.50%. The Company has a 0.5% commitment fee on the unused portion of the revolving line of credit. The Company has the right to increase its borrowings under the senior secured credit facility up to an aggregate amount of $150 million provided that the Company is in compliance with the Restated Credit Agreement, that the additional debt would not cause any covenant violation of the Restated Credit Agreement, and that existing or new lenders within the Restated Credit Agreement or new lenders agree to increase their commitments. To reduce the risk related to interest rate fluctuations, the Restated Credit Agreement required the Company to enter into an interest rate swap, cap or similar agreement to effectively fix or cap the interest rate on 40% of its funded long-term debt. The Company entered into two interest rate hedge transactions, as described in Note 3—Fair Value of Financial Instruments, in order to comply with this requirement.
In addition, the Company expensed deferred financing fees in the amount of $6.6 million. In conjunction with the closing of the refinancing, the Company terminated its then existing swap agreements as they were incompatible with the new financing due to the existence of the LIBOR floor. The termination of the swap agreements cost $0.4 million, which was recorded as debt retirement costs.
The Company issued $10.0 million of notes as part of the purchase consideration for the Hospice/Home Health Acquisition. The note bears interest at 6.0% with $2.0 million of principal due annually beginning November 1, 2010. The $10.0 million of notes are payable to the selling entities, of which the Company’s President and Chief Operating Officer of Home and Hospice Care Investments, LLC and the Company’s Regional Vice President of Hospice/Home Health are significant shareholders.
F-27
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Senior Subordinated Notes
The 2014 Notes were issued in December 2005 in the aggregate principal amount of $200.0 million, with an interest rate of 11.0% and a discount of $1.3 million. Interest is payable semiannually in January and July of each year. The 2014 Notes mature on January 15, 2014. The 2014 Notes are unsecured senior subordinated obligations and rank junior to all of the Company’s existing and future senior indebtedness, including indebtedness under the Restated Credit Agreement. The 2014 Notes are guaranteed on a senior subordinated basis by certain of the Company’s current and future companies Note 12—Commitment and Contingencies.
On and after January 15, 2011, the Company is entitled to redeem all or a portion of the 2014 Notes upon not less than 30 nor more than 60 days notice, at redemption prices (expressed in percentages of principal amount on the redemption date), plus accrued interest to the redemption date if redeemed during the 12-month period commencing on January 15, 2011 and 2012 and thereafter of 102.75% and 100.00%, respectively.
Debt Covenants
The Company must maintain compliance with certain financial covenants measured on a quarterly basis, including an interest coverage minimum ratio as well as a total leverage maximum ratio.
The covenants also include certain limitations, including the incurrence of additional indebtedness, liens, investments in other businesses, annual capital expenditures and, in the case of the 2014 Notes, issuance of preferred stock. Furthermore, the Company must permanently reduce the principal amount of debt outstanding by applying the proceeds from any asset sale, insurance or condemnation payments, additional indebtedness or equity securities issuances, and 25% to 50% of excess cash flows from operations based on the leverage ratio then in effect. The Company believes that it was in compliance with its debt covenants at December 31, 2010.
Scheduled Maturities of Long-Term Debt
The scheduled maturities of long-term debt as of December 31, 2010 are as follows (in thousands):
| Long-Term Debt |
||||
| 2011 |
$ | 5,742 | ||
| 2012 |
5,750 | |||
| 2013 |
5,760 | |||
| 2014 |
135,770 | |||
| 2015 |
29,780 | |||
| Thereafter |
337,604 | |||
| 520,406 | ||||
| Less original issue discount at December 31, 2010 |
441 | |||
| $ | 519,963 | |||
F-28
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
7. Other Current Assets and Other Assets
Other current assets consisted of the following at December 31 (in thousands):
| December 31, 2010 | December 31, 2009 | |||||||
| Current portion of notes receivable, net |
$ | 3,824 | $ | 3,762 | ||||
| Supplies inventory |
2,809 | 2,788 | ||||||
| Income tax refund receivable |
9,074 | 1,597 | ||||||
| Other current assets |
112 | 156 | ||||||
| $ | 15,819 | $ | 8,303 | |||||
Other assets consisted of the following at December 31 (in thousands):
| December 31, 2010 | December 31, 2009 | |||||||
| Equity investment in joint ventures |
$ | 5,379 | $ | 5,041 | ||||
| Restricted cash |
14,502 | 14,610 | ||||||
| Deposits and other assets |
4,595 | 4,633 | ||||||
| $ | 24,476 | $ | 24,284 | |||||
Equity Investment in Pharmacy Joint Venture
The Company has an investment in a joint venture which serves its pharmaceutical needs for a limited number of its Texas operations (the “APS—Summit Care Pharmacy”). APS—Summit Care Pharmacy, a limited liability company, was formed in 1995, and is owned 50% by the Company and 50% by APS Acquisition, LLC. APS—Summit Care Pharmacy operates a pharmacy in Austin, Texas, and the Company pays market value for prescription drugs and receives a 50% share of the net income related to this joint venture. Based on the Company’s lack of any controlling influence, the Company’s investment in APS—Summit Care Pharmacy is accounted for using the equity method of accounting.
Restricted Cash
In August 2003, SHG formed Fountain View Reinsurance, Ltd. (the “Captive”), a wholly-owned offshore captive insurance company, for the purpose of insuring its workers’ compensation liability in California. In connection with the formation of the Captive, the Company funds its estimated losses and is required to maintain certain levels of cash reserves on hand for claims related to occurrences prior to September 1, 2005. As the use of these funds is restricted, the funds are classified as restricted cash in the Company’s consolidated balance sheets. Additionally, restricted cash includes amounts on deposit at the Company’s workers’ compensation third-party claims administrator.
Deposits
In the normal course of business the Company is required to post security deposits with respect to its leased properties and to many of the vendors with which it conducts business.
F-29
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
8. Property and Equipment
Property and equipment consisted of the following at December 31 (in thousands):
| 2010 | 2009 | |||||||
| Land and land improvements |
$ | 66,753 | $ | 59,448 | ||||
| Buildings and leasehold improvements |
321,726 | 288,921 | ||||||
| Furniture and equipment |
70,812 | 61,717 | ||||||
| Construction in progress |
4,048 | 22,573 | ||||||
| 463,339 | 432,659 | |||||||
| Less accumulated depreciation |
(76,017 | ) | (59,448 | ) | ||||
| $ | 387,322 | $ | 373,211 | |||||
9. Income Taxes
The income tax expense from continuing operations consisted of the following for the years ended December 31 (in thousands):
| 2010 | 2009 | 2008 | ||||||||||
| Federal: |
||||||||||||
| Current |
$ | 1,817 | $ | 10,311 | $ | 17,879 | ||||||
| Deferred |
1,681 | 6,550 | (1,192 | ) | ||||||||
| State: |
||||||||||||
| Current |
778 | 1,548 | 2,820 | |||||||||
| Deferred |
(1,804 | ) | (567 | ) | (1,426 | ) | ||||||
| $ | 2,472 | $ | 17,842 | $ | 18,081 | |||||||
The income tax (benefit) expense applicable to continuing and discontinued operations is as follows for the years ended December 31 (in thousands):
| 2010 | 2009 | 2008 | ||||||||||
| Income tax expense on continuing operations |
$ | 2,472 | $ | 17,842 | $ | 18,081 | ||||||
| Income benefit on discontinued operations |
— | (247 | ) | — | ||||||||
| $ | 2,472 | $ | 17,595 | $ | 18,081 | |||||||
A reconciliation of the income tax expense on income computed at statutory rates to the Company’s actual effective tax rate is summarized as follows for the years ended December 31 (in thousands):
| 2010 | 2009 | 2008 | ||||||||||
| Federal rate (35%) |
$ | 501 | $ | (40,232 | ) | $ | 18,262 | |||||
| State taxes, net of federal tax benefit |
(666 | ) | 1,277 | 906 | ||||||||
| Uncertain tax positions and related interest |
(9 | ) | (2,828 | ) | (1,350 | ) | ||||||
| Goodwill |
1,288 | 59,710 | — | |||||||||
| Lavender Class Action Settlement |
1,748 | — | — | |||||||||
| Other, net |
(390 | ) | (85 | ) | 263 | |||||||
| $ | 2,472 | $ | 17,842 | $ | 18,081 | |||||||
F-30
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Deferred income taxes result from temporary differences between the tax basis of assets and liabilities for financial reporting purposes and the amounts used for income tax purposes. The Company’s temporary differences are primarily attributable to purchase adjustments related to intangible assets, depreciation, allowances for doubtful accounts, settlement costs and accruals for professional and general liability expenses and compensation which are not deductible for tax purposes until paid.
In assessing the realizability of deferred tax assets, management considers whether it is more likely than not that some portion or all of the deferred tax assets will not be realized. The ultimate realization of deferred tax assets is primarily dependent upon the Company generating sufficient operating income during the periods in which temporary differences become deductible. At December 31, 2010 and 2009, a valuation allowance of $0.1 million has been recognized against the Company’s state tax loss carryforwards as a result of certain restrictions regarding their utilization. At December 31, 2010, the Company has $3.8 million of enterprise zone tax credits for California income tax purposes which do not expire.
Significant components of the Company’s deferred income tax assets and liabilities at December 31 are as follows (in thousands):
| 2010 | 2009 | |||||||||||||||
| Current | Non- Current |
Current | Non- Current |
|||||||||||||
| Deferred income tax assets: |
||||||||||||||||
| Vacation and other accrued expenses |
$ | 5,945 | $ | 6,583 | $ | 4,762 | $ | 4,280 | ||||||||
| Allowance for doubtful accounts |
6,468 | — | 8,317 | — | ||||||||||||
| Professional liability accrual |
1,645 | 5,527 | 2,425 | 7,199 | ||||||||||||
| Rent accrual |
94 | 2,505 | 239 | 2,675 | ||||||||||||
| Asset retirement obligation, net |
— | 1,217 | — | 1,539 | ||||||||||||
| CA EZ credit carryforward |
— | 3,812 | — | 2,322 | ||||||||||||
| Lavender Class Action Settlement |
8,874 | — | — | — | ||||||||||||
| Other |
661 | 198 | 2,180 | — | ||||||||||||
| Total deferred income tax assets |
23,687 | 19,842 | 17,923 | 18,015 | ||||||||||||
| Deferred income tax liabilities: |
||||||||||||||||
| Intangible assets |
— | (11,826 | ) | — | (11,447 | ) | ||||||||||
| Fixed assets |
— | (14,266 | ) | — | (9,128 | ) | ||||||||||
| Prepaid Expenses |
(3,268 | ) | — | (2,920 | ) | — | ||||||||||
| Other |
— | (2,125 | ) | — | (583 | ) | ||||||||||
| Total deferred income tax liabilities |
(3,268 | ) | (28,217 | ) | (2,920 | ) | (21,158 | ) | ||||||||
| Net deferred income tax assets |
20,419 | (8,375 | ) | 15,003 | (3,143 | ) | ||||||||||
| Valuation allowance |
— | (56 | ) | — | (57 | ) | ||||||||||
| Net deferred income tax assets (liabilities) |
$ | 20,419 | $ | (8,431 | ) | $ | 15,003 | $ | (3,200 | ) | ||||||
Significant judgment is required in determining the Company’s provision for income taxes. In the ordinary course of business, there are many transactions for which the ultimate tax outcome is uncertain. While the Company believes that its tax return positions are supportable, there are certain positions that may not be sustained upon review by tax authorities. While the Company believes that adequate accruals have been made for such positions, the final resolution of those matters may be materially different than the amounts provided for in the Company’s historical income tax provisions and accruals.
F-31
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
FASB ASC Topic 740, “Income Taxes,” prescribes a minimum probability threshold that a tax position must meet before a financial statement benefit is recognized. The minimum threshold is defined in FASB ASC Topic 740 as a tax position that is more likely than not to be sustained upon examination by the applicable taxing authority, including resolution of any related appeals or litigation processes, based on the technical merits of the position.
A reconciliation of the beginning and ending amount of unrecognized tax benefits is as follows for 2010, 2009 and 2008 (in thousands):
| 2010 | 2009 | 2008 | ||||||||||
| Balance at January 1 |
$ | 94 | $ | 2,827 | $ | 11,027 | ||||||
| Additions based on tax positions related to the current year |
— | — | — | |||||||||
| Additions for tax positions of prior years |
— | — | — | |||||||||
| Reductions for tax positions of prior years |
— | — | — | |||||||||
| Settlements |
— | — | — | |||||||||
| Reductions for lapses of statutes |
(76 | ) | (2,733 | ) | (8,200 | ) | ||||||
| Balance at December 31, |
$ | 18 | $ | 94 | $ | 2,827 | ||||||
At December 31, 2010, the total amount of unrecognized tax benefit was $18 thousand, which will result in a benefit to the provision for income taxes in 2011 and subsequent years, if recognized.
The Company recognizes interest and penalties related to uncertain tax positions in the provision for income taxes line item of the consolidated statements of operations. As of December 31, 2010 and 2009, our accrued interest and penalties on unrecognized tax benefits was not material.
The Company is subject to taxation in the United States and in various state jurisdictions. The Company’s tax years 2007 and forward are subject to examination by the United States Internal Revenue Service and from 2006 forward by the Company’s material state jurisdictions. The Internal Revenue Service is currently conducting a limited scope audit of our 2007 through 2009 tax years.
10. Stockholders’ Equity
The Company did not declare or pay cash dividends in either 2010 or 2009. The Company does not anticipate paying any cash dividends on our common stock in the foreseeable future. The Company currently anticipates that it will retain all available cash, if any, for use as working capital and for other general purposes, including to service or repay the debt and to fund the operation and expansion of their business. Any payment of future dividends will be at the discretion of the board of directors and will depend on, among other things, the Company’s earnings, financial condition, capital requirements, level of indebtedness, statutory and contractual restrictions applying to the payment of dividends and other considerations that the board of directors deems relevant.
Holders of the Company’s Class A common stock are entitled to a voting power of one vote per share and holders of the Company’s Class B common stock are entitled to a voting power of ten votes per share. Mandatory and optional conversion of the class B common stock into Class A common stock exists on a one-for-one basis under certain circumstances.
F-32
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
11. Stock-Based Compensation
2005 Restricted Stock Plan
In December 2005, the Company’s board of directors adopted a restricted stock plan with respect to Skilled’s Class B common stock (the “Restricted Stock Plan”). The Restricted Stock Plan provided for awards of restricted stock to the Company’s officers and other key employees. Such grants of restricted stock were required to be evidenced by restricted stock agreements and were subject to the vesting and other requirements as determined at the time of grant by a committee appointed by the board of directors. Restricted shares of each initial participant vested (i) 25% on the date of grant and (ii) 25% on each of the first three anniversaries of the date of grant, unless such initial participant ceases to be an employee of or consultant to Skilled or any of its companies on the relevant anniversary date. As of December 31, 2010, the aggregate number of shares of Class B stock issued under the Restricted Stock Plan was 1.3 million, net of forfeitures, all of which have fully vested. No additional shares of common stock are available for issuance under this plan.
2007 Incentive Award Plan
In April 2007, Skilled’s board of directors adopted the Skilled Healthcare Group, Inc. 2007 Incentive Award Plan (the “2007 Plan”) that provides for cash-based and equity-based awards to the Company’s directors, officers, and other key employees. In May 2008, the stockholders of the Company approved the 2007 Plan increasing the number of shares of the Company’s Class A common stock that may be issued under the 2007 Plan by 1.5 million shares to a total of 2.6 million shares. The 2007 Plan became effective immediately upon stockholder approval.
Restricted stock awards granted under the 2007 Plan are subject to vesting and other requirements as determined at the time of award by a committee appointed by the board of directors. The restricted awards granted to non-employee directors are generally subject to a one-year vesting requirement. The restricted common shares awarded to executive officers and other key employees generally vest 25% on the first four anniversary dates of the award. In addition to restricted common shares, the Company also awards restricted stock units to certain directors. The restricted stock units have rights similar to the rights of restricted vested common shares and the non-employee director will ultimately receive one common share for each restricted stock unit. The fair value of the restricted common shares and restricted stock units is based on the award date market value of the common shares and is amortized over the vesting period on a ratable basis.
Under the 2007 Plan, incentive and nonqualified stock options may be granted to eligible participants for the right to purchase common stock at a specified price which may not be less than the fair market value on the date of the grant. Based on the terms of individual option grants, options granted under the 2007 Plan generally expire 10 years after the grant date and generally become exercisable over a period of four years, with annual vesting, based on continued employment. In 2010, 2009, and 2008, the Company granted 0.5 million, 0.3 million, and 0.1 million options, respectively, to purchase shares of Class A common stock.
In November 2008, the Company began granting performance based restricted Class A common shares and stock options to executive officers. In 2008, the senior management performance program provided for performance awards comprised of up to 50% stock options and up to 50% restricted stock, which structure generally reflected a combination of the equity vehicles used by its peer group. The stock options vest ratably over a four-year period. The performance-vested restricted stock fair value is estimated utilizing the Black Scholes method to estimate the fair value of the award and is recognized as compensation expense based on the most probable outcome of the performance condition which is evaluated quarterly using the Company’s plan and actual results. As of December 31, 2010, there were 0.4 million non-vested performance based restricted stock awards outstanding.
F-33
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
As of December 31, 2010, the aggregate number of Class A common shares and restricted stock units issued under the 2007 plan was 0.8 million.
During the year ended December 31, 2010, the following restricted stock awards, restricted stock units and performance stock awards occurred under the Company’s existing plans (number of shares in thousands):
| Number of Shares |
Weighted- Average Grant Date Fair Value |
|||||||
| Non-vested balance at January 1, 2010 |
440 | $ | 10.48 | |||||
| Granted |
234 | 5.86 | ||||||
| Vested |
(80 | ) | 11.61 | |||||
| Forfeited |
(85 | ) | 8.77 | |||||
| Non-vested balance at December 31, 2010 |
509 | $ | 8.46 | |||||
As of December 31, 2010, there was approximately $3.6 million of total unrecognized compensation costs related to restricted stock awards, restricted stock units and performance stock awards. These costs have a weighted-average remaining recognition period of 2.0 years. The total fair value of shares vested during the years ended December 31, 2010, 2009, and 2008 was $0.4 million, $0.7 million, and $0.7 million, respectively.
The fair value of the stock option grants for the year ended December 31, 2010, 2009 and 2008 under FASB ASC Topic 718, “Compensation—Stock Compensation,” was estimated on the date of the grants using the Black-Scholes option pricing model with the following assumptions and resulting fair value amounts:
| Year Ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Risk-free interest rate |
2.57 | % | 2.62 | % | 3.23 | % | ||||||
| Expected life |
6.25 years | 6.25 years | 6.25 years | |||||||||
| Dividend yield |
0 | % | 0 | % | 0 | % | ||||||
| Volatility |
44.18 | % | 54.3 | % | 40.6 | % | ||||||
| Weighted-average fair value |
$ | 2.81 | $ | 5.49 | $ | 5.89 | ||||||
The Company estimated the expected volatility by examining the historical and implied volatilities of comparable publicly traded companies due to the Company’s limited trading history and because the Company does not have any publicly traded options.
There were no options exercised during the years 2010, 2009, and 2008. As of December 31, 2010, there was $1.9 million of unrecognized compensation cost related to outstanding stock options, net of forecasted forfeitures. This amount is expected to be recognized over a weighted-average period of 2.7 years. To the extent the forfeiture rate is different than the Company has anticipated, stock-based compensation related to these awards will be different from the Company’s expectations. Upon option exercise, the Company will issue new shares of Class A common stock.
F-34
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
The following table summarizes stock option activity during the year ended December 31, 2010 under the 2007 Stock Incentive Plan (number of shares in thousands):
| Number of Shares |
Weighted- Average Exercise Price |
Weighted- Average Remaining Contractual Term (in years) |
Aggregate Intrinsic Value |
|||||||||||||
| Outstanding at January 1, 2010 |
576 | $ | 12.07 | |||||||||||||
| Granted |
531 | $ | 6.06 | |||||||||||||
| Exercised |
— | $ | — | |||||||||||||
| Forfeited or cancelled |
(109 | ) | $ | 10.78 | ||||||||||||
| Outstanding at December 31, 2010 |
998 | $ | 9.01 | 8.28 | $ | — | ||||||||||
| Fully vested and expected to vest at December 31, 2010 (assuming a 5% forfeiture rate) |
949 | $ | 9.13 | 8.24 | $ | — | ||||||||||
| Exercisable at December 31, 2010 |
241 | $ | 13.56 | 6.83 | $ | — | ||||||||||
Aggregate intrinsic value represents the value of the Company’s closing stock price on the last trading day of the fiscal period in excess of the exercise price, multiplied by the number of options outstanding or exercisable.
Equity related to stock option grants and stock awards included in general and administrative expenses in the Company’s consolidated statements of operations was $2.3 million, $1.3 million, and $1.0 million, for 2010, 2009, and 2008, respectively. The amount in cost of services was $1.2 and $1.0 million in 2010 and 2009, respectively. There was no amount of stock compensation recorded in cost of services for 2008. The total income tax benefit recognized in the income statement for share-based compensation arrangements was $1.4 million, $0.9 million, and $0.6 million for 2010, 2009 and 2008, respectively.
12. Commitments and Contingencies
Leases
The Company leases certain of its facilities under non-cancelable operating leases. The leases generally provide for payment of property taxes, insurance and repairs, and have rent escalation clauses, principally based upon the Consumer Price Index or other fixed annual adjustments.
The future minimum rental payments under non-cancelable operating leases that have initial or remaining lease terms in excess of one year as of December 31, 2010 are as follows (in thousands):
| 2011 |
$ | 17,803 | ||
| 2012 |
16,932 | |||
| 2013 |
13,188 | |||
| 2014 |
12,616 | |||
| 2015 |
9,991 | |||
| Thereafter |
37,922 | |||
| $ | 108,452 | |||
F-35
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Litigation
Lavender, et al. vs. Skilled Healthcare Group, Inc., et al. (and twenty-two individually-named California nursing facilities receiving administrative services from Skilled Healthcare, LLC)
On May 4, 2006, three plaintiffs filed a complaint against the Company in the Superior Court of California, Humboldt County, entitled VINNIE LAVENDER, by and through her Conservator, WANDA BAKER; WALTER SIMON; JACQUELYN VILCHINSKY vs. SKILLED HEALTHCARE GROUP, INC., et al. (and twenty-two individually-named California nursing facilities receiving administrative services from Skilled Healthcare, LLC) (the “Lavender Case” or “Humboldt County Action”). The complaint alleged, among other things, that certain California-based facilities operated by the Company’s wholly-owned operating companies failed to provide an adequate number of qualified personnel to care for their residents and misrepresented the quality of care provided in their facilities.
Trial in this matter commenced November 30, 2009. On July 6, 2010, the jury returned a verdict in the liability, statutory damages and restitution damages phase of the trial, awarding $677 million in compensatory damages against the twenty-two defendant facilities, with Skilled and Skilled Healthcare LLC also liable as agents. On August 6, 2010, the Company filed a motion for mistrial or new trial based upon juror misconduct. On August 27, 2010, the Humboldt Court denied the motion for mistrial or new trial based on juror misconduct. On August 13, 2010, the Company filed motions for judgment not withstanding the verdict and for new trial on all grounds other than juror misconduct. On August 26, 2010, the Humboldt Court entered an order for permanent injunction against the Company and all other defendants. Also on August 27, 2010, the Company filed a notice of appeal of the Humboldt Court’s August 26, 2010 order for permanent injunction. Because no final judgment had been entered, the Company did not file a notice of appeal of the Humboldt Court’s denial of the motion for mistrial or new trial based on juror misconduct.
On September 7, 2010, the Company reached agreement to settle the Humboldt County Action. As part of the settlement, the Company and other defendants entered into separate settlement agreements with the plaintiffs and the Humboldt County District Attorney’s Office, each dated as of September 7, 2010. The settlement was approved by the Superior Court of California, Humboldt County on November 30, 2010.
Under the terms of the settlement agreements, the Company deposited a total of $50.0 million into escrow accounts to cover settlement payments to class members, notice and claims administration costs, reasonable attorneys’ fees and costs and certain other payments.
The settlement agreements also instituted an injunction, pursuant to which the twenty-two defendants that operate California nursing facilities must provide specified nurse staffing levels, comply with specified state and federal laws governing staffing levels and posting requirements, and provide reports and information to a monitor. The injunction will remain in effect for a period of twenty-four months unless extended for additional three-month periods as to those defendants that may be found in violation. Defendants demonstrating compliance for an eighteen-month period may petition for early termination of the injunction. The Company is required to demonstrate over the term of the injunction that the costs of the injunction are at least $9.6 million. The injunction costs include, among other things, costs attributable to (i) enhanced reporting requirements; (ii) implementing advanced staffing tracking systems; (iii) fees and expenses paid to an auditor and special master; (iv) increased labor and labor related expenses; and (v) lost revenues attributable to admission decisions based on compliance with the terms and conditions of the injunction. To the extent the costs of complying with the injunction are less than $9.6 million, the Company will be required to remit any shortfall to the settlement fund.
F-36
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Pursuant to the settlement agreements, the plaintiffs and the Humboldt County District Attorney’s Office, as Intervenor on behalf of the People of the State of California, have agreed to release the Company and the other defendants from claims related to the causes of action alleged in the Lavender Case, as further described in the settlement agreements, which are filed as exhibits to the Company’s Annual Report on Form 10-K for the year ended December 31, 2010. Neither of the settlement agreements contains an admission or concession of wrongdoing by the Company or any other defendants. As described above, the settlement was approved by the Superior Court of California, Humboldt County on November 30, 2010. The Company continues to pursue its claim for insurance coverage.
Shepardson v. Skilled Healthcare Group, Inc.
On July 24, 2009, a purported class action complaint captioned Shepardson v. Skilled Healthcare Group, Inc., et al. was filed in the U.S. District Court for the Central District of California against the Company, its Chairman and Chief Executive Officer, its current Chief Financial Officer, its former Chief Financial Officer, and investment banks that underwrote the Company’s initial public offering, on behalf of two classes of purchasers of its securities. On November 10, 2009, the District Court appointed lead plaintiffs and co-lead counsel, re-captioned the action “In re Skilled Healthcare Group Inc. Securities Litigation,” and ordered that lead plaintiffs file an amended class action complaint.
An amended class action complaint was filed on January 12, 2010 on behalf of purchasers of the Company’s Class A common stock pursuant or traceable to the Company’s initial public offering and purchasers between May 14, 2007 and June 9, 2009, inclusive, against the Company, its Chairman and Chief Executive Officer, its President, its current Chief Financial Officer, its former Chief Financial Officer, its largest stockholder and related entities, and a director affiliated with that stockholder. The amended class action complaint sought an unspecified amount of damages (including rescissory damages), and asserted claims under the federal securities laws relating to the Company’s June 9, 2009 announcement that it would restate its financial statements for the period from January 1, 2006 to March 31, 2009, and that the restatement was likely to require cumulative charges against after-tax earnings in the aggregate amount of between $8.0 million and $9.0 million over the affected periods. The complaint also alleged that the Company’s registration statement and prospectus, financial statements, and public statements about its results of operations contained material false and misleading statements. Defendants moved to dismiss the amended class action complaint on March 15, 2010. In September 2010, the parties reached a settlement in the amount of $3.0 million. The Company contributed the portion of its $1.0 million insurance retention that it had not incurred in legal fees ($0.5 million), and its insurance carriers contributed the balance of the $3.0 million. The District Court entered an order granting final approval of the settlement in January 2011.
BMFEA Matter
On April 15, 2009, two of Skilled Healthcare Group’s wholly-owned companies, Eureka Healthcare and Rehabilitation Center, LLC, which operates Eureka Healthcare and Rehabilitation Center (the “Facility”), and Skilled Healthcare, LLC, the Administrative Services provider for the Facility, were served with a search warrant that relates to an investigation of the Facility by the California Attorney General’s Bureau of Medi-Cal Fraud & Elder Abuse (“BMFEA”). The search warrant related to, among other things, records, property and information regarding certain enumerated patients of the Facility and covered the period from January 1, 2007 through the date of the search. The Facility represents less than 1% of the Company’s revenue and less than 0.3% of its Adjusted EBITDA based on full year 2009 and 2008. Nevertheless, although the Company is unable to assess the potential exposure, any fines or penalties that may result from the BMFEA’s investigation could be significant. The Company is committed to working cooperatively with the BMFEA on this matter.
F-37
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Insurance
The Company maintains insurance for workers’ compensation, general and professional liability, employee benefits liability, property, casualty, directors’ and officers’ liability, inland marine, crime, boiler and machinery, automobile, employment practices liability and earthquake and flood. The Company believes that its insurance programs are adequate and where there has been a direct transfer of risk to the insurance carrier, the Company does not recognize a liability in the consolidated financial statements. The Company reduced its workers’ compensation and general and professional liability related to prior policy years by $3.5 million, $3.3 million, and $4.1 million in the years ended December 31, 2010, 2009, and 2008, respectively.
Workers’ Compensation. The Company has maintained workers’ compensation insurance as statutorily required. Most of its commercial workers’ compensation insurance purchased is loss sensitive in nature, except as noted below. As a result, the Company is responsible for adverse loss development. Additionally, the Company self-insures the first unaggregated $1.0 million per workers’ compensation claim for all California, New Mexico and Nevada businesses. The Company has elected not to carry workers’ compensation insurance in Texas and it may be liable for negligence claims that are asserted against it by its Texas-based employees. The Company has purchased guaranteed cost policies for Kansas, Missouri, Iowa, and its recently acquired Nevada, Arizona, Idaho, and Montana based hospice and home health operations. There are no deductibles associated with these programs. The Company recognizes a liability in its consolidated financial statements for its estimated self-insured workers’ compensation risks. Historically, estimated liabilities have been sufficient to cover actual claims.
General and Professional Liability. The Company’s skilled nursing and assisted living services subject it to certain liability risks. Malpractice claims may be asserted against the Company if its services are alleged to have resulted in patient injury or other adverse effects, the risk of which may be greater for higher-acuity patients, such as those receiving specialty and sub-acute services, than for traditional LTC patients. The Company has from time to time been subject to malpractice claims and other litigation in the ordinary course of business.
Effective September 1, 2008, California-based skilled nursing facility companies purchased individual general and professional liability insurance policies with a per occurrence and annual aggregate coverage limit of $1.0 million and $3.0 million, respectively, and an unaggregated $0.1 million per claim self-insured retention. These policies are renewable for up to three years.
Until December 31, 2009, the Company’s Kansas and Iowa businesses were insured on an occurrence basis with a per occurrence and annual aggregate coverage limit of $1.0 million and $3.0 million, respectively. There are no applicable self-insurance retentions or deductibles under these contracts. Until December 31, 2009, the Company’s Missouri businesses were underwritten on a claims-made basis with no applicable self-insured retentions or deductibles and have a per occurrence and annual aggregate coverage limit of $1.0 million and $3.0 million, respectively.
Effective September 1, 2008, the Company also had an excess liability policy with a $14.0 million per loss limit and an $18.0 million annual aggregate limit for losses arising from claims in excess of $1.1 million for the California skilled nursing facilities and in excess of $1.0 million for all other businesses. The policy is renewable for up to three years. The Company retains an unaggregated self-insured retention of $1.0 million per claim for all Texas, New Mexico and Nevada businesses, its California businesses other than skilled nursing facility companies, and its Davenport, Iowa facility. Effective January 1, 2010 all of the facilities located in Kansas, Missouri and Iowa were added to this excess policy with the same unaggregated self-insured retention of $1.0 million per claim for all of these facilities. Effective May 1, 2010 all of the acquired hospice and home health businesses located in Arizona, Idaho, Montana and Nevada were added to this excess policy which provides
F-38
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
$14.0 million in excess coverage in addition to the $1.0 million per claim/$3.0 million annual aggregate claims made coverage which was in place for these businesses at the time of their acquisition.
Employee Medical Insurance. Medical preferred provider option programs are offered as a component of the Company’s employee benefits. The Company retains a self-insured amount up to a contractual stop loss amount of $0.3 million per claim on its preferred provider organization plan and all other employee medical plans are guaranteed cost plans for the Company.
A summary of the liabilities related to insurance risks are as follows (in thousands):
| As of December 31, 2010 | As of December 31, 2009 | |||||||||||||||||||||||||||||||
| General
and Professional Liability |
Employee Medical |
Workers’ Compensation |
Total | General
and Professional Liability |
Employee Medical |
Workers’ Compensation |
Total | |||||||||||||||||||||||||
| Current |
$ | 4,037 | (1) | $ | 1,965 | (2) | $ | 4,484 | (2) | $ | 10,486 | $ | 6,960 | (1) | $ | 1,784 | (2) | $ | 4,198 | (2) | $ | 12,942 | ||||||||||
| Non-current |
13,564 | — | 11,910 | 25,474 | 16,660 | — | 10,747 | 27,407 | ||||||||||||||||||||||||
| $ | 17,601 | $ | 1,965 | $ | 16,394 | $ | 35,960 | $ | 23,620 | $ | 1,784 | $ | 14,945 | $ | 40,349 | |||||||||||||||||
| (1) | Included in accounts payable and accrued liabilities. |
| (2) | Included in employee compensation and benefits. |
Hallmark Indemnification
Hallmark Rehabilitation GPLLC (“Hallmark”), the Company’s wholly-owned rehabilitation services company, provides physical, occupational and speech therapy services to various unaffiliated skilled nursing facilities. These unaffiliated skilled nursing facilities are reimbursed for these services from the Medicare Program and other third-party payors. Hallmark has indemnified these unaffiliated skilled nursing facilities from a portion of certain disallowances of these services. Additionally, to the extent a RAC is successful in making a claim for recoupment of revenue from any of these skilled nursing facilities, the Company will typically be required to indemnify them for its charges associated with this loss. RAC recoupment risk is described in Note 2—Summary of Significant Accounting Policies.
Financial Guarantees
Substantially all of the companies that comprise the Company guarantee the 2014 Notes and the Company’s senior secured credit facility. Financial guarantees are described in more detail in Note 6—Debt. The guarantees provided by the companies are full and unconditional and joint and several. Other companies of the Company that are not guarantors are considered minor.
Purchase Commitment
As of December 31, 2010, the Company had no outstanding purchase commitments.
13. Discontinued Operations
In accordance with FASB ASC Topic 205, “Presentation of Financial Statements,” and FASB ASC Topic 360, “Property, Plant and Equipment,” the results of operations of disposed assets and the losses related to the abandonment have been classified as discontinued operations for all periods presented in the accompanying consolidated income statements as the operations and cash flows have been eliminated from the Company’s ongoing operations.
F-39
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
During 2009, the Company noted that its hospice business based in Ventura, CA, was not meeting expectations. The Company closed the operations on September 30, 2009 and recorded a net loss of $0.4 million, which includes the write-off of the $0.2 million intangible asset associated with the hospice business based in Ventura, California. Patients for the hospice business based in Ventura, California, were transferred to other local hospice businesses.
A summary of the discontinued operations for the periods presented is as follows (in thousands):
| Year Ended December 31, | ||||||||||||
| 2010 | 2009 | 2008 | ||||||||||
| Net operating revenues |
$ | — | $ | 635 | $ | — | ||||||
| Loss from discontinued operations before income tax |
— | (637 | ) | — | ||||||||
| Tax benefit |
— | (247 | ) | — | ||||||||
| Loss from discontinued operations |
$ | — | $ | (390 | ) | $ | — | |||||
14. Material Transactions with Related Parties
Agreement with Onex Partners Manager LP
Upon completion of the Transactions, the Company entered into an agreement with Onex Partners Manager LP, or Onex Manager, a wholly-owned subsidiary of Onex Corporation. In exchange for providing the Company with corporate finance and strategic planning consulting services, the Company pays Onex Manager an annual fee of $0.5 million.
15. Defined Contribution Plan
The Company sponsors a defined contribution plan covering substantially all employees who meet certain eligibility requirements. In 2008, the Company recorded $0.6 million, of matching contributions, which were funded in February 2009. The Company did not match employee contributions for the defined contribution plan in 2010 and 2009
F-40
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
16. Quarterly Financial Information (Unaudited)
The following table summarizes unaudited quarterly financial data for the years ended December 31, 2010 and 2009 (dollars in thousands, except share and per share data):
| Three Months Ended, | ||||||||||||||||
| December 31 | September 30 | June 30 | March 31 | |||||||||||||
| 2010 |
||||||||||||||||
| Revenue |
$ | 220,749 | $ | 209,199 | $ | 200,971 | $ | 189,319 | ||||||||
| Total expense |
193,896 | 239,201 | 178,943 | 168,581 | ||||||||||||
| Other expenses, net of other income |
(8,135 | ) | (9,071 | ) | (14,717 | ) | (6,263 | ) | ||||||||
| Income (loss) from continuing operations before provision for income taxes |
18,718 | (39,073 | ) | 7,311 | 14,475 | |||||||||||
| Provision (benefit) for income taxes |
7,878 | (13,766 | ) | 2,766 | 5,594 | |||||||||||
| Income (loss) income from continuing operations |
10,840 | (25,307 | ) | 4,545 | 8,881 | |||||||||||
| Net income (loss) |
$ | 10,840 | $ | (25,307 | ) | $ | 4,545 | $ | 8,881 | |||||||
| Earnings (loss) per share, basic: |
||||||||||||||||
| Earnings (loss) earnings per share |
$ | 0.29 | $ | (0.68 | ) | $ | 0.12 | $ | 0.24 | |||||||
| Earnings (loss) earnings per share, diluted: |
||||||||||||||||
| (Loss) earnings per share |
$ | 0.29 | $ | (0.68 | ) | $ | 0.12 | $ | 0.24 | |||||||
| Weighted-average common shares outstanding, basic |
37,010 | 36,997 | 36,983 | 36,962 | ||||||||||||
| Weighted-average common shares outstanding, diluted |
37,150 | 36,997 | 37,084 | 37,037 | ||||||||||||
| Three Months Ended, | ||||||||||||||||
| December 31 | September 30 | June 30 | March 31 | |||||||||||||
| 2009 |
||||||||||||||||
| Revenue |
$ | 188,390 | $ | 187,447 | $ | 192,154 | $ | 188,074 | ||||||||
| Total expense |
338,521 | 168,405 | 170,113 | 165,009 | ||||||||||||
| Other expenses, net of other income |
(7,343 | ) | (7,327 | ) | (7,070 | ) | (7,226 | ) | ||||||||
| (Loss) income from continuing operations before provision for income taxes |
(157,474 | ) | 11,715 | 14,971 | 15,839 | |||||||||||
| Provision for income taxes |
3,841 | 2,420 | 5,797 | 5,784 | ||||||||||||
| (Loss) income from continuing operations |
(161,315 | ) | 9,295 | 9,174 | 10,055 | |||||||||||
| Loss from discontinued operations, net of tax |
— | (243 | ) | (95 | ) | (52 | ) | |||||||||
| Net (loss) income |
$ | (161,315 | ) | $ | 9,052 | $ | 9,079 | $ | 10,003 | |||||||
| (Loss) earnings per share, basic: |
||||||||||||||||
| (Loss) earnings per common share from continuing operations |
$ | (4.37 | ) | $ | 0.25 | $ | 0.25 | $ | 0.27 | |||||||
| Loss per common share from discontinued operations |
— | (0.01 | ) | — | — | |||||||||||
| (Loss) earnings per share |
$ | (4.37 | ) | $ | 0.24 | $ | 0.25 | $ | 0.27 | |||||||
| (Loss) earnings per share, diluted: |
||||||||||||||||
| (Loss) earnings per common share from continuing operations |
$ | (4.37 | ) | $ | 0.25 | $ | 0.25 | $ | 0.27 | |||||||
| Loss per common share from discontinued operations |
— | (0.01 | ) | — | — | |||||||||||
| (Loss) earnings per share |
$ | (4.37 | ) | $ | 0.24 | $ | 0.25 | $ | 0.27 | |||||||
| Weighted-average common shares outstanding, basic |
36,943 | 36,927 | 36,904 | 36,881 | ||||||||||||
| Weighted-average common shares outstanding, diluted |
36,943 | 36,950 | 36,928 | 36,911 | ||||||||||||
F-41
Table of Contents
SKILLED HEALTHCARE GROUP, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Earnings per basic and diluted share are computed independently for each of the quarters presented based upon basic and diluted shares outstanding per quarter and therefore may not sum to the totals for the year.
17. Acquisitions
Effective May 1, 2010, the Company acquired substantially all of the assets of five Medicare-certified hospice companies and four Medicare-certified home health companies located in Arizona, Idaho, Montana and Nevada, referred to herein as the Hospice/Home Health Acquisition. The total consideration payable by the Company in connection with acquisition transactions is approximately $63.0 million, consisting of approximately $45.3 million in cash at closing, with the remainder in the form of deferred and contingent payments payable over a three to five year period. For the twelve months ended December 31, 2010, the Hospice/Home Health Acquisition contributed revenue of $38.6 million. The goodwill of $57.0 million arising from the acquisition represents the commercial opportunity for the Company to expand the existing Hospice operations as well as to complement the Company’s existing core operations and is expected to be deductible for income tax purposes over the 15 years following the completion of the acquisition. All of the goodwill is included in the Company’s hospice and home health services segment.
The assets of Hospice/Home Health Acquisition were recorded at estimated fair value as of the date of acquisition under the purchase method of accounting. The following table summarizes the allocation of the purchase price to the fair value of assets acquired at the date of acquisition (dollars in thousands):
| Depreciable fixed assets, Net |
$ | 591 | ||
| Licenses |
5,140 | |||
| Goodwill |
57,042 | |||
| Total assets acquired |
$ | 62,773 | ||
The purchase consideration is equal to the sum of the cash paid and the fair value of the deferred payments, the promissory notes, and the contingent consideration. As part of the purchase price, annual aggregate deferred cash payments of $1.0 million are to be made over a 3-year period starting May 1, 2011. The promissory notes bear interest at 6.00% with $2.0 million of principal payments due annually beginning November 1, 2010. The contingent consideration arrangement requires the Company to pay contingent payments up to $7 million over a 5 year period should the acquired operations achieve certain financial targets based on EBITDA, as defined in the acquisition agreement. The notes payable, the deferred payments and the contingent consideration are payable to the selling entities, of which the Company’s President and Chief Operating Officer of Home and Hospice Care Investments, LLC and the Company’s Regional Vice President of Hospice/Home Health are significant shareholders. We estimated the fair value of the contingent consideration using a probability-weighted discounted cash flow model. This fair value measurement is based on significant input not observable in the market and thus represents a Level 3 measurement as defined in Note 3-Fair Value Measurements. The following table summarizes the allocation of the total purchase consideration at the date of acquisition (dollars in thousands):
| Cash |
$ | 45,380 | ||
| Deferred cash payments |
2,537 | |||
| Promissory note |
9,926 | |||
| Contigent Consideration |
4,930 | |||
| Total purchase consideration |
$ | 62,773 | ||
F-42
Table of Contents
| (a) | 2. Financial Statement Schedule: |
SKILLED HEALTHCARE GROUP, INC.
SCHEDULE II—VALUATION ACCOUNTS
(in thousands)
| Balance at Beginning of Period |
Charged to Costs and Expenses |
Deductions(1) | Transfers
to Notes Receivable |
Balance at End of Period |
||||||||||||||||
| Accounts receivable allowances |
||||||||||||||||||||
| Year Ended December 31, 2010 |
$ | 21,318 | $ | 9,617 | $ | (13,050 | ) | $ | (175 | ) | $ | 17,710 | ||||||||
| Year Ended December 31, 2009 |
$ | 26,593 | $ | 11,039 | $ | (15,721 | ) | $ | (593 | ) | $ | 21,318 | ||||||||
| Year Ended December 31, 2008 |
$ | 16,890 | $ | 15,171 | $ | (5,468 | ) | $ | — | $ | 26,593 | |||||||||
| Notes receivable allowances |
||||||||||||||||||||
| Year Ended December 31, 2010 |
$ | 593 | $ | — | $ | (418 | ) | $ | 175 | $ | 175 | |||||||||
| Year Ended December 31, 2009 |
$ | — | $ | — | $ | — | $ | 593 | $ | 593 | ||||||||||
| Year Ended December 31, 2008 |
$ | — | $ | — | $ | — | $ | — | $ | — | ||||||||||
| (1) | Uncollectible accounts written off, net of recoveries |
S-1