Attached files
| file | filename |
|---|---|
| EX-31 - EXHIBIT 31 - Alliance HealthCare Services, Inc | a2196739zex-31.htm |
| EX-32 - EXHIBIT 32 - Alliance HealthCare Services, Inc | a2196739zex-32.htm |
| EX-23.1 - EXHIBIT 23.1 - Alliance HealthCare Services, Inc | a2196739zex-23_1.htm |
| EX-10.35 - EXHIBIT 10.35 - Alliance HealthCare Services, Inc | a2196739zex-10_35.htm |
| EX-10.36 - EXHIBIT 10.36 - Alliance HealthCare Services, Inc | a2196739zex-10_36.htm |
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF
THE SECURITIES EXCHANGE ACT OF 1934
For the fiscal year ended December 31, 2009
Commission File Number 1-16609
ALLIANCE HEALTHCARE SERVICES, INC.
(Exact name of registrant as specified in its charter)
| DELAWARE (State or other jurisdiction of incorporation or organization) |
33-0239910 (IRS Employer Identification Number) |
100 Bayview Circle, Suite 400, Newport Beach, California 92660
(Address of principal executive office) (Zip Code)
Registrant's telephone number, including area code: (949) 242-5300
Securities registered pursuant to Section 12(b) of the Act:
| Title of Each Class | Name of Each Exchange on Which Registered | |
|---|---|---|
| Common Stock, Par Value $0.01 | New York Stock Exchange |
Securities registered pursuant to Section 12(g) of the Act: None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes o No ý
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes o No ý
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes ý No o
Indicate by check mark whether the registrant has submitted electronically and posted on its corporate Web site, if any, every Interactive Data File required to be submitted and posted pursuant to Rule 405 of Regulation S-T during the preceding 12 months (or for such shorter period that the registrant was required to submit and post such files). Yes o No o
Indicate by check mark if disclosure of delinquent filers pursuant to Item 405 of Regulation S-K is not contained herein, and will not be contained, to the best of registrant's knowledge, in definitive proxy or information statements incorporated by reference in Part III of this Form 10-K or any amendment to this Form 10-K. o
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, or a smaller reporting company. See the definitions of "large accelerated filer," "accelerated filer" and "smaller reporting company" in Rule 12b-2 of the Exchange Act.
| Large accelerated filer o | Accelerated filer ý | Non-accelerated filer o (Do not check if a smaller reporting company) |
Smaller reporting company o |
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Act). Yes o No ý
The aggregate market value of the voting and non-voting common equity held by non-affiliates of the registrant as of June 30, 2009, based upon the closing price of the Common Stock as reported by the New York Stock Exchange on such date, was $191.0 million.
The number of shares outstanding of Common Stock, par value $0.01, as of March 9, 2010 was 52,755,014 shares.
Documents Incorporated by Reference
The registrant's definitive proxy statement for the Annual Meeting of Stockholders, to be filed within 120 days of December 31, 2009 is incorporated by reference into Part III of this Form 10-K to the extent stated herein.
General
We are a leading national provider of outpatient diagnostic imaging services, based upon annual revenue and number of diagnostic imaging systems deployed, and a provider of radiation oncology services. Our principal sources of revenue are derived from magnetic resonance imaging ("MRI") and positron emission tomography/computed tomography ("PET/CT"). Unless the context otherwise requires, the words "we" "us," "our," "Company" or "Alliance" as used in this 10-K refers to Alliance HealthCare Services, Inc. and our direct and indirect subsidiaries. We provide imaging and therapeutic services primarily to hospitals and other healthcare providers on a shared- service and full-time service basis. We also provide services through a growing number of fixed-site imaging centers, primarily to hospitals or health systems. Our services normally include the use of our imaging systems, technologists to operate the systems, equipment maintenance and upgrades and management of day-to-day shared-service and fixed-site diagnostic imaging operations. We also provide non scan-based services, which include only the use of our imaging systems under a short-term contract. We have also leveraged our leadership in MRI and PET/CT to expand into radiation oncology. Our radiation oncology business is operated through our wholly-owned subsidiary, Alliance Oncology, LLC, and includes a wide range of services for cancer patients covering initial consultation, preparation for treatment, simulation of treatment, radiation oncology delivery, therapy management and follow-up care. Our services include the use of our linear accelerators, therapists to operate such systems, administrative staff, equipment maintenance and upgrades, and management of day-to-day operations. We also provide stereotactic radiation oncology services through our wholly-owned subsidiary, Alliance Radiosurgery, LLC.
MRI and PET/CT services generated 47% and 40% of our revenue, respectively, for the year ended December 31, 2009, 54% and 34% of our revenue, respectively, for the year ended December 31, 2008 and 60% and 31% of our revenue, respectively, for the year ended December 31, 2007. The remaining revenue was comprised of radiation oncology revenue, and other modality diagnostic imaging services revenue, primarily computed tomography ("CT"), and management contract revenue. We had 507 diagnostic imaging and radiation oncology systems, including 295 MRI systems and 126 positron emission tomography ("PET") or PET/CT systems, and served over 1,000 clients in 45 states at December 31, 2009. We operated 116 fixed-site imaging centers (three in unconsolidated joint ventures), which constitutes systems installed in hospitals or other medical buildings on or near hospital campuses, including modular buildings, systems installed inside medical groups' offices, and free-standing fixed-site imaging centers, which includes systems installed in a medical office building, ambulatory surgical center, or other retail space at December 31, 2009. Of the 116 fixed-site imaging centers, 91 were MRI fixed-site imaging centers, 16 were PET or PET/CT fixed-site imaging centers, six were other modality fixed-site imaging centers and three were in unconsolidated joint ventures. We also operated 25 radiation oncology centers and stereotactic radiosurgery facilities (including two radiation oncology centers in unconsolidated joint ventures) at December 31, 2009.
Approximately 80%, 79% and 89% of our revenues for the years ended December 31, 2009, 2008 and 2007, respectively, were generated by providing services to hospitals and other healthcare providers, which we refer to as wholesale revenues. Our wholesale revenues are typically generated from contracts that require our clients to pay us based on the number of scans we perform on patients on our clients' behalf, although some pay us a flat fee for a period of time regardless of the number of scans we perform. Wholesale payments are due to us independent of our clients' receipt of retail reimbursement from third-party payors, although receipt of reimbursement from third-party payors may affect demand for our services. We typically deliver our services for a set number of days per week through exclusive, long-term contracts with hospitals and other healthcare providers. The initial terms of these contracts average approximately three years in length for mobile services and approximately five to 10 years in
1
length for fixed-site arrangements. These contracts often contain automatic renewal provisions and certain contracts have cancellation clauses if the hospital or other healthcare provider purchases their own system. We price our contracts based on the type of system used, the scan volume, and the number of ancillary services provided. Pricing is also affected by competitive pressures.
Approximately 20%, 21% and 11% of our revenues for the years ended December 31, 2009, 2008 and 2007, respectively, were generated by providing services directly to patients from our sites located at or near hospitals or other healthcare provider facilities, which we refer to as retail revenue. Our revenue from these sites is generated from direct billings to patients or their third-party payors, including Medicare, which are recorded net of contractual discounts and other arrangements for providing services at discounted prices. We typically charge a higher price per scan under retail billing than we do under wholesale billing.
Fixed-site imaging centers and radiation oncology centers can be structured as either wholesale or retail arrangements. Our contracts for radiation oncology services average approximately 10 to 20 years in length. Revenues from these centers are included in either our wholesale or retail revenues.
Our clients, primarily small-to-mid-sized hospitals, contract with us to provide diagnostic imaging and radiation oncology systems and services in order to:
- •
- take advantage of our extensive diagnostic imaging and radiation oncology project management experience;
- •
- avoid capital investment and financial risk associated with the purchase of their own systems;
- •
- provide access to MRI, PET and PET/CT, radiation oncology and other services for their patients when the demand for these
services does not justify the purchase of dedicated, full-time systems;
- •
- benefit from upgraded imaging systems and technology without direct capital expenditures;
- •
- eliminate the need to recruit, train and manage qualified technologists or therapists and oncologists;
- •
- make use of our ancillary services; and
- •
- gain access to services under our regulatory and licensing approvals when they do not have these approvals.
We were incorporated in the state of Delaware on May 27, 1987 as Alliance Imaging, Inc. On February 17, 2009, we changed our name to Alliance HealthCare Services, Inc.
Significant 2009 Corporate Events
During December 2009, we entered into and completed various debt related transactions in order to expand our borrowing capacity and extend the maturity of our debt (the "Refinance Transaction"). In order to accomplish this, we retired substantially all of our $300.0 million 71/4% senior subordinated notes due 2012 (the "71/4% Notes") through a cash tender offer (the "Tender Offer") and repaid the balance of $351.6 million on our existing Tranche C1 term loan facility (the "Old Term Loan"). In conjunction with the Refinance Transaction we also entered into a new senior secured credit agreement (the "New Credit Facility"), comprised of a $460.0 million term loan (the "New Term Loan") maturing June 2016 and a $120.0 million revolving facility (the "New Revolving Credit Facility") maturing December 2014. Borrowings under the New Term Loan were issued at 98.0% of par, with the discount to par being amortized to interest expense and other, net through the maturity date of the loan. We also issued $190.0 million of 8% senior notes due 2016 (the "8% Notes") in a transaction that was exempt from the registration requirements of the Securities Act of 1933, as amended. The 8% Notes were issued at 98.69% of par, with the discount to par being amortized to interest expense and other,
2
net through the maturity date of the notes. Borrowings under the New Credit Facility bear interest through maturity at a variable rate based upon, at our option, either London InterBank Offered Rate ("LIBOR") or the base rate (which is the highest of the administrative agent's prime rate, one-half of 1.00% in excess of the overnight federal funds rate, and 1.00% in excess of the one-month LIBOR rate), plus in each case, an applicable margin. With respect to the New Term Loan, the applicable margin for LIBOR loans is 3.50% per annum, and with respect to the New Revolving Credit Facility, the applicable margin for LIBOR loans ranges, based on the applicable leverage ratio, from 3.25% to 3.75% per annum, in each case, with a LIBOR floor of 2.00%. With respect to the New Term Loan, the applicable margin for base rate loans is 2.50% per annum, and with respect to the New Revolving Credit Facility, the applicable margin for base rate loans ranges, based on the applicable leverage ratio, from 2.25% to 2.75% per annum. We used the proceeds from these transactions and existing cash to complete the Tender Offer and purchase $294.4 million of the 71/4% Notes at a purchase price equal to 100.125% of the principal amount, together with the accrued interest to the purchase date. We also used the proceeds from these transactions to pay off the Old Term Loan and redeem the remaining $5.6 million of 71/4% notes in January 2010 at a redemption price equal to 100.0% of the principal amount, together with accrued interest to the redemption date. We incurred a loss on extinguishment of debt of $14.6 million related to the Refinance Transaction, which represents the tender premium and consent payment to redeem the 71/4% Notes, write-off of unamortized debt issuance costs related to the retired debt, and other fees and expenses.
Industry Overview
Diagnostic imaging services are noninvasive procedures that generate representations of the internal anatomy and convert them to film or digital media. Diagnostic imaging systems facilitate the early diagnosis of diseases and disorders, often minimizing the cost and amount of care required and reducing the need for costly and invasive diagnostic procedures. Radiation oncology ("RO") is the practice of delivering radiation therapy by radiation oncologists. The market of RO providers is highly fragmented with approximately 70% of services still performed in hospitals.
MRI
MRI technology involves the use of high-strength magnetic fields to produce computer-processed cross-sectional images of the body. Due to its superior image quality, MRI is the preferred imaging technology for evaluating soft tissue and organs, including the brain, spinal cord and other internal anatomy. With advances in MRI technology, MRI is increasingly being used for new applications such as imaging of the heart, chest and abdomen. Conditions that can be detected by MRI include multiple sclerosis, tumors, strokes, infections, and injuries to the spine, joints, ligaments, and tendons. Unlike x-rays and computed tomography, which are other diagnostic imaging technologies, MRI does not expose patients to potentially harmful radiation.
MRI technology was first patented in 1974, and MRI systems first became commercially available in 1983. Since then, manufacturers have offered increasingly sophisticated MRI systems and related software to increase the speed of each scan and improve image quality. Magnet strengths are measured in tesla, and MRI systems typically use magnets with strengths ranging from 0.2 to 1.5 tesla. The 1.0 and 1.5 tesla strengths are generally considered optimal because they are strong enough to produce relatively fast scans but are not so strong as to create discomfort for most patients. Manufacturers have worked to gradually enhance other components of the machines to make them more versatile. Many of the hardware and software systems in recently manufactured machines are modular and can be upgraded for much lower costs than purchasing new systems.
The MRI industry has experienced growth as a result of:
- •
- recognition of MRI as a cost-effective, noninvasive diagnostic tool;
3
- •
- superior soft-tissue image quality of MRI versus that of other diagnostic imaging technologies;
- •
- wider physician acceptance and availability of MRI technology;
- •
- growth in the number of MRI applications;
- •
- MRI's safety when compared to other diagnostic imaging technologies, because it does not use potentially harmful
radiation; and
- •
- increased overall demand for healthcare services, including diagnostic services, for the aging population.
PET, PET/CT and CT
PET is a nuclear medicine procedure that produces images of the body's metabolic and biologic functions. PET can provide earlier detection of certain cancers, coronary diseases or neurologic problems than other diagnostic imaging systems. It is also useful for the monitoring of these conditions. PET can detect the presence of disease at an early stage. The ability of PET technology to measure metabolic activity assists in the identification of lesions and the assessment of organ health. A growing body of clinical research supports PET as a diagnostic tool for cancer diagnosis, staging, and treatment monitoring. Early detection of these conditions enables a broader range of treatments. The expansion of Centers for Medicare & Medicaid Services ("CMS") coverage has driven the growth of PET. Since 1998, CMS has expanded coverage of PET procedures to include the diagnosis, staging, and restaging of lung, esophageal, colorectal, breast, head and neck cancers, lymphoma, and melanoma. Additionally, Medicare covers the use of PET scans for the diagnosis and treatment of dementia and neurodegenerative diseases, as well as for brain, cervical, ovarian, pancreatic, small lung cell, and testicular cancers. Under CMS's current national coverage determination, PET is covered for the detection of pre-treatment metastases in newly diagnosed cervical cancer, as well as for brain, ovarian, pancreatic, small cell lung, and testicular cancers, where provided as part of certain types of clinical trials. In April 2009, CMS adopted a coverage framework that replaces the four-part diagnosis, staging, restaging and monitoring categories with a two-part framework. This new framework differentiates fluorodeoxyglucose ("FDG") PET imaging used to inform the initial treatment strategy from other uses to guide subsequent treatment strategies after the completion of initial treatment. This change applies to all national coverage determinations that address coverage of FDG PET for oncologic conditions.
In CT imaging, a computer analyzes the information received from an x-ray beam to produce multiple cross-sectional images of a particular organ or area of the body. CT imaging is used to detect tumors and other conditions affecting bones and internal organs.
A PET/CT system fuses together the results of a PET and CT scan at the scanner level. The PET portion of the scan detects the metabolic signal of cancer cells and the CT portion of the scan provides a detailed image of the internal anatomy that reveals the location, size and shape of abnormal cancerous growths.
Other Diagnostic Imaging Services
Other diagnostic imaging technologies include: nuclear medicine or gamma camera, ultrasound, mammography, bone densitometry and general x-ray.
Radiation Oncology
Radiation Oncology ("RO") is the practice of delivering radiation therapy by radiation oncologists. RO uses ionizing radiation to treat cancer. In general this radiation is delivered over a period of many days to many weeks. Ionizing radiation damages a cell's DNA that the body then has to repair. Cancer cells are less able to repair the damage than are normal cells. Over the time period during which the
4
radiation is delivered, the cancer cells become more and more damaged while normal cells are able to recover. Eventually, the cancer cells are unable to reproduce and are destroyed while the normal tissue survives.
We estimate that approximately 60% of all new cancer patients are treated with some form of radiation therapy each year. Radiation therapy often is used together with other oncology treatments such as chemotherapy and surgery. A typical radiation oncology department provides a wide range of services for cancer patients. These include: initial consultation; preparation for treatment; imaging, planning, and simulation for the treatment; delivery of radiation therapy treatments; management of the total course of therapy; and follow-up care. The radiation can be delivered by a number of different technologies including linear accelerators and radioactive isotopes.
Our radiation oncology business offers the following treatment options:
- •
- Conventional beam therapy ("CBT"). CBT is a very basic
form of radiation therapy delivered by a linear accelerator. It is the simplest form to plan and deliver and is typically reserved for use in patients where a cure is not envisioned (palliative care).
- •
- 3-D conformal radiation therapy
("3D-CRT"). 3D-CRT uses three dimensional imaging data and three dimensional treatment planning to more
accurately and effectively plan and deliver linear accelerator radiation treatments. It is the basic technology used in most practices supplanted by IMRT and IGRT when the specific case requires it.
- •
- Intensity modulated radiation therapy ("IMRT"). IMRT
entails the use of hundreds to thousands of beams of radiation delivered by a linear accelerator whose intensity is adjusted individually in order to allow the radiation that is delivered to conform
as closely as possible to the three dimensional shape of the tumor. It requires extremely sophisticated and time consuming treatment planning in order to determine what beams should be used and what
their intensities should be, and extensive treatment quality assurance in order to insure that all the beams are modulated and delivered correctly.
- •
- Image guided radiation therapy ("IGRT"). IGRT uses a
number of different types of imaging technologies to localize precisely the patient and the tumor at the time of each treatment delivery in order to ensure that the radiation is delivered to the
correct location. IGRT is not a radiation treatment in and of itself; it is used in support of advanced forms of treatment delivery such as IMRT and SRS.
- •
- Stereotactic radiosurgery ("SRS"). Originally developed
for intracranial applications but now being used in a range of extracranial applications such as spine, lung, liver, prostate, and others, SRS delivers a very high dose of radiation in anywhere from
1 - 5 treatments as opposed to the 20 - 40 treatments used for 3D-CRT and IMRT. SRS needs to be as precisely planned for and delivered
as possible since, because of the reduced number of treatments and the very high dose, it will destroy all cells, cancer and normal alike, that reside within the targeted volume. SRS is delivered with
a range of advanced technologies such as the Cyberknife and the GammaKnife.
- •
- Low dose rate brachytherapy ("LDR"). LDR allows the
radiation oncologist to treat cancer by delivering the dose of radiation from the "inside out." Radioactive isotopes encased in a metal jacket the size of a grain of rice ("seeds") are implanted in
the tumor through needles, with the seeds permanently left in place, gradually treating the cancer over time.
- •
- High dose rate brachytherapy ("HDR"). Like LDR, HDR allows the radiation oncologist to treat cancer by delivering the dose of radiation from the "inside out." Unlike LDR, HDR utilizes temporary seeds that deliver a much higher dose of radiation over a much shorter period of time. These seeds are inserted and removed several times over 24 - 48 hours through needles that are left in place for the entire course of care.
5
Imaging and Radiation Oncology Settings
Diagnostic imaging services and radiation oncology services are typically provided in one of the following settings:
- •
- Hospitals and clinics. Imaging and/or radiation oncology
systems are located in and owned and operated by a hospital or clinic. These systems are primarily used by patients of the hospital or clinic, and the hospital or clinic bills third-party payors, such
as health insurers, including Medicare or Medicaid.
- •
- Independent imaging centers. Imaging and/or radiation
oncology systems are located in permanent facilities not generally owned by hospitals or clinics. These centers depend upon physician referrals for their patients and generally do not maintain
dedicated, contractual relationships with hospitals or clinics. In fact, these centers may compete with hospitals or clinics that have their own systems to provide imaging and/or radiation oncology
services to these patients. Like hospitals and clinics, these centers bill third-party payors for their services.
- •
- Outsourced. Imaging systems, largely located in mobile trailers but also provided in fixed facilities, provide services to a hospital or clinic on a shared-service or full-time basis. Generally, the hospital or clinic contracts with the imaging service provider to perform scans of its patients, and the imaging service provider is paid directly by that hospital or clinic instead of by a third-party payor.
Our Competitive Strengths
A leading national provider of shared-service and fixed-site MRI and PET/CT services
We are a leading national provider of shared-service and fixed-site MRI and PET/CT services, based on annual revenue and number of diagnostic imaging systems deployed. As of December 31, 2009, we had 295 MRI systems, 126 PET or PET/CT systems, and 86 other diagnostic imaging systems in operation. Our size allows us to achieve operating, sourcing and administrative efficiencies, including (i) the ability to maximize utilization through efficient deployment of our mobile systems and (ii) equipment and medical supply sourcing savings and favorable maintenance contracts from equipment manufacturers and other suppliers.
Ability to expand into radiation oncology using our leading national position in MRI and PET/CT services
We have relationships with more than 1,000 hospitals and healthcare providers in 45 states throughout the nation. This national footprint has enabled us to leverage our position as a trusted partner to healthcare providers to expand our services beyond diagnostic imaging and into radiation oncology, transforming us into a more complete outsourced service provider to our clients.
Comprehensive diagnostic and treatment solutions
We offer our clients a comprehensive diagnostic imaging and radiation oncology solution, as well as ancillary services, such as marketing support, education, training and billing assistance. In many cases, we provide services under our regulatory and licensing approvals for clients who lack such authority. We believe that a comprehensive service solution is an important factor when potential clients select a diagnostic imaging or radiation oncology provider.
Exclusive, long-term contracts with a diverse client base
We primarily generate revenues from exclusive, long-term contracts with hospitals and other healthcare providers. These contracts average approximately three years in length for mobile services, approximately five to 10 years in length for fixed-site arrangements and approximately 10 to 20 years in length for radiation oncology contracts. During the year ended December 31, 2009, no single client accounted for more than 2% of our revenue.
6
For the year ended December 31, 2009, we generated approximately 80% of our revenues by billing hospitals and other healthcare providers, which we refer to as wholesale revenues, rather than billing patients or other third-party payors. These payments are due to us regardless of the clients' receipt of payment from patients or reimbursement from third-party payors (including commercial payors, Medicare and Medicaid). Importantly, this contrasts with the vast majority of other diagnostic imaging and radiation oncology providers, who typically collect directly from patients and third-party payors and are therefore directly exposed to reimbursement cuts and higher experiences of bad debt. With our wholesale model, our exposure to patient bad debt is minimized, as evidenced by our bad debt expense of only 0.5% of revenues for the year ended December 31, 2009. Further, short-term exposure to Medicare reimbursement cuts is limited as approximately 4% of our imaging revenues came directly from Medicare for the year ended December 31, 2009.
Stable and significant cash flow generation
We have generated stable and significant cash flows and have maintained attractive margins over a sustained period of time. We attribute our strong cash flows and margins to: (1) comprehensive imaging and treatment solutions, (2) the substantial value proposition for customers, (3) the strength of our customer relationships, (4) the largely wholesale nature of the our revenues and (5) our economies of scale.
Experienced management team
Our senior management team consists of professionals with significant experience within the hospital and healthcare services industry. Our experienced management team includes six senior executive officers who average approximately 25 years of industry experience.
Advanced MRI, PET/CT, and radiation oncology systems
Our technologically advanced imaging systems can perform high quality scans more rapidly and can be used for a wider variety of imaging applications than less advanced systems. Moreover, technological change in this field is gradual and most of our systems can be upgraded with software and hardware enhancements, which should allow us to continue to provide advanced technology without replacing entire systems. Our radiation oncology services utilize the most advanced radiation oncology technology, including IGRT, IMRT and SRS.
Our Services
We provide our outsourcing services on the following bases:
- •
- Shared Service. We offered 59% of our systems on a
part-time basis. These systems are located in mobile trailers which are transported to our clients' locations. We schedule deployment of these mobile systems so that multiple clients can
share use of the same system. The typical shared-service contract averages approximately three years in length. None of our radiation oncology services are offered on a part-time basis.
- •
- Full-Time Service. We offered 31% of our systems on a full-time, long-term basis. These systems are located in either mobile units or buildings located at or near a hospital or clinic. Full-time service systems are provided for the exclusive use of a particular hospital or clinic. We typically offer full-time services under contracts that range from five to 10 years in length. Our relationships with our higher-volume shared-service clients have, from time to time, evolved into full-time arrangements. All of our radiation oncology services are offered on a full-time, long-term basis.
7
- •
- Interim and Rental Services. We offered 10% of our systems to clients on an unstaffed basis. These systems are located in mobile trailers which are transported to our clients' locations. These clients may be unable to maintain the extra capacity to accommodate periods of peak demand for imaging services or may require temporary assistance until they can develop permanent imaging service centers at or near their facilities. Generally, we do not provide technologists to operate our systems in these arrangements. All of our stereotactic radiation oncology services are offered on an unstaffed basis.
Our Strategy
Key components of our strategy include:
Further expand our presence in growth markets. We will continue to operate our mobile, shared-service MRI business to maximize efficiency, clinical excellence and cash flow. However, we are also focused on diversifying and growing our business through the identification of additional services or new technologies which can be deployed on behalf of our hospital and healthcare clients, including:
- •
- PET/CT. We are one of the largest national PET/CT
providers in the United States. In 2008, we added 22 PET and PET/CT systems to our fleet through the acquisition of MOS and SPI and in 2009 we added 12 PET/CT systems to our fleet. At
December 31, 2009 we had 110 mobile systems and 16 fixed-site systems. Modest industry growth in the PET and PET/CT market provides opportunities for us. We anticipate potential for
growth through increases in Medicare-approved procedures and greater physician acceptance of PET procedures.
- •
- Fixed-Site Imaging Centers. Our
fixed-site imaging center contracts generally last for five to 10 years. From January 1, 2003, we have opened or acquired 118 fixed-site imaging centers and
increased fixed-site revenues by 218%. We plan to continue to profitably grow our fixed-site imaging center business line through an aggressive, but disciplined growth strategy
focused on partnerships with hospitals and fact-based, analytical screening processes. On November 5, 2007, we completed the New England Health Enterprises ("NEHE") acquisition,
adding seven fixed-site imaging centers in Maine and Massachusetts.
- •
- Radiation Oncology. Radiation oncology is an established, growing form of treatment that can exhibit strong operating margins and a strong return on investment. RO represents a significant opportunity for us, as PET/CT technology is increasingly used for the early detection of cancer and approximately 60% of new cancer cases are treated with RO each year. On November 2, 2007, we completed the Bethesda acquisition, adding eight radiation oncology centers in Alabama, Mississippi, and Missouri. In March 2008, we acquired six CyberKnife® robotic radiosurgery facilities from Accuray, Inc., which are providing radiosurgery services at hospitals located in California, Maryland, New Jersey and Tennessee. As of December 31, 2009, we operate 25 radiation oncology centers (two in unconsolidated joint ventures). The growth in RO as a part of our business mix is supported by strong demand from hospitals for assistance in upgrading to the latest RO technology (IGRT and IMRT), the increasing incidence of cancer, our PET/CT capabilities and the growing use of PET/CT scans.
Improvement of our Sales Force. We are focused on continuing to improve our sales management and sales support infrastructure to increase the pace of new business. We believe a strengthened sales force will enable us to further diversify our business, pursue growth in low market share territories and focus on converting mature mobile customers to fixed sites. The ability of our sales force to effectively cross-sell mobile and fixed-site MRI, mobile and fixed-site PET/CT and radiation oncology will provide us with future growth and margin enhancement. Some of our sales force initiatives include new training programs, marketing campaigns and account coverage models. We also have designed our commission and incentive programs for our sales managers to align them with our Company's initiatives.
8
Improve Operating Efficiency. We are focused on continuing to reduce our cost structure and improve asset allocation. During 2009, we decreased the number of our business regions from four to three while continuing to standardize certain policies and procedures nationwide. In doing so, we believe we will continue to benefit from our regional managers' direct contact and knowledge of markets we serve, while ensuring quality, consistency and efficiency across all regions. Other initiatives include developing new vendor relationships and actively managing our mobile systems to increase their utilization through improved route efficiency.
Focus on Patient Care and Customer Service. We are dedicated to the highest level of patient care standards and clinical performance improvement. We strive to provide a variety of solutions designed to meet the needs of our customers by developing new surveying tools for both patients and customers. These surveying tools provide performance-driven data to improve levels of satisfaction for all of our products.
As a result of our efforts, we have achieved the highest levels of accreditation. We were the first national provider of shared-imaging services to be awarded accreditation by The Joint Commission on Accreditation of Healthcare Organizations, or JCAHO, in 1998. All of our sites and centers are accredited by The Joint Commission (formerly known as JCAHO) or certified by the American College of Radiology. We have also restructured our marketing function so that our marketing teams are regionally based, enabling us to better understand our patient and customer needs, and thereby improving our service to them.
Selectively Pursue Acquisitions. We intend to manage our market positions by selectively pursuing strategic acquisitions. Changes in the rates or methods of third-party reimbursement for diagnostic imaging services could severely impact our smaller competitors and result in a unique buying opportunity for us. We are particularly focused on acquiring radiation oncology centers, PET/CT providers, both mobile and fixed, and fixed-site imaging providers in Certificate of Need, or CON, regulated states. In some states, a CON or similar regulatory approval is required prior to the acquisition of diagnostic imaging or radiation oncology systems or services, resulting in a barrier to entry for competitors without a CON. In November 2007, we completed the Bethesda Acquisition, adding eight radiation oncology centers, many of which are in CON states, and the NEHE Acquisition, adding seven fixed-site imaging centers located in CON states. In March 2008, we acquired six CyberKnife® robotic radiosurgery facilities from Accuray, Inc., which are providing radiosurgery services at hospitals located in California, Maryland, New Jersey and Tennessee. Also in 2008, we added 22 PET and PET/CT systems to our fleet through the acquisitions of MOS and SPI.
Contracts and Payment
Our typical MRI and PET/CT contract is exclusive, averages approximately three years in length for mobile services and five to 10 years in length for fixed-site imaging center arrangements, and often includes an automatic renewal provision. Most of our contracts require a fee for each scan we perform. With other contracts, clients are billed on a fixed-fee basis for a period of time, regardless of the number of scans performed. These fee levels are affected primarily by the type of imaging system provided, scan volume and the number of ancillary services provided. Our typical radiation oncology contract is exclusive, averages approximately 10 to 20 years in length and often includes an automatic renewal provision.
Wholesale payments under our contracts are due to us independent of our clients' receipt of retail reimbursement from third-party payors. Approximately 80% of our revenues for the year ended December 31, 2009 were generated by providing these services to hospitals and other healthcare providers. To a lesser extent, our revenues are generated from direct billings to patients or their medical payors. Approximately 20% of our revenues for the year ended December 31, 2009 were
9
generated by providing services directly to patients or their medical payors. We typically reserve the right to reduce a client's number of service days or terminate an unprofitable contract.
Systems
As of December 31, 2009, we had 507 diagnostic imaging and radiation oncology systems, including 295 MRI systems, 126 PET or PET/CT systems, and 86 other systems, substantially all of which we own. We operated 116 fixed-site imaging centers (three in unconsolidated joint ventures), which are classified into three categories. The first category is hospital-based fixed-site imaging centers, which includes systems installed in hospitals or other buildings on hospital campuses, including modular buildings. The second category is physician-based fixed-site imaging centers, which includes systems installed inside medical groups' offices, most of which are owned by hospitals. The third category is free-standing fixed-site imaging centers, which includes systems installed in a medical office building, ambulatory surgical center, or other retail space. Of the consolidated fixed-site imaging centers, 70 were hospital-based fixed-site imaging centers, 24 were physician-based fixed-site imaging centers, and 19 were free-standing fixed-site imaging centers. Of the 116 fixed-site imaging centers we operated at December 31, 2009, 91 were MRI fixed-site imaging centers, 16 were PET or PET/CT fixed-site imaging centers, six were other modality fixed-site imaging centers, and three were in unconsolidated joint ventures. We have made significant investments in our systems in an effort to ensure that we maintain the newest, most advanced imaging systems that meet our clients' needs. Moreover, because we can upgrade most of our current MRI and PET/CT systems, we believe we have reduced the potential for technological obsolescence.
We purchase our imaging systems from major medical equipment manufacturers, primarily General Electric Medical Systems, Siemens Medical Systems and Philips Medical Systems. Generally, we contract with clients for new or expanded services prior to ordering new imaging systems in order to reduce our system utilization risk. As one of the largest commercial purchasers of MRI and PET/CT systems in the United States, we believe we receive relatively attractive pricing for equipment and service contracts from these equipment manufacturers.
Regional Structure
We divide our operations into three geographic regions. We have a local presence in each region, none of which accounts for more than 42% of our revenues. None of our revenues for the years ended December 31, 2009, 2008 and 2007 was derived from business outside the United States. We believe we will continue to benefit from our regional managers' direct contact with and knowledge of the markets we serve, which allows us to address the specific needs of each local operating environment. Each region continues to market, manage and staff the operation of its imaging and radiation oncology systems and is run as a separate profit center responsible for its own revenues, expenses and overhead. To complement this regional arrangement, we continue to have standardized contracts, operating policies and other procedures, which are implemented nationwide in an effort to ensure quality, consistency and efficiency across all regions. For the purposes of Financial Accounting Standards Board ("FASB") Accounting Standards Codification ("ASC") 280, "Segment Reporting" (formerly Statement of Financial Accounting Standards ("SFAS") No. 131, "Disclosures About Segments of an Enterprise and Related Information," ("SFAS 131")) the results of our three geographic regions represent one reportable segment.
System Management and Maintenance
We actively manage deployment of our imaging systems to increase their utilization through the coordinated transportation of our mobile systems using 184 power units. We examine client requirements, route patterns, travel times, fuel costs and system availability in our deployment process. Our shared-service MRI and PET/CT systems are currently scheduled for as little as one-half day and
10
up to seven days per week at any particular client, with an average usage of 1.6 days per week per client. Drivers typically move the systems at night and activate them upon arrival at each client location so that the systems are operational when our technologists arrive.
Timely, effective maintenance is essential for achieving high utilization rates of our systems. We contract with the original equipment manufacturers for comprehensive maintenance programs on our systems to minimize the period of time the equipment is unavailable. System repair typically takes less than one day but could take longer, depending upon the nature of the repair. During the warranty period and maintenance contract term, we receive guarantees related to equipment operation and availability.
Sales and Marketing
As of December 31, 2009, our national sales and business development force and sales support staff consisted of 33 members who identify and contact potential clients. We also had 32 marketing representatives, as of that date, who are focused on increasing the number of scans or treatments performed with our systems by educating physicians and radiation oncologists about our new imaging and radiation oncology applications and service capabilities. The sales force is organized regionally under the oversight of regional vice presidents and senior management. Furthermore, certain of our executive officers and regional vice presidents also spend a portion of their time participating in contract negotiations.
Competition
The markets for diagnostic imaging and radiation oncology services are highly fragmented and have few national service providers. We believe that the key competitive factors affecting our business include:
- •
- the quality and reliability of service;
- •
- the quality and type of equipment available;
- •
- the availability of types of imaging, radiation oncology and ancillary services;
- •
- the availability of imaging center locations and flexibility of scheduling;
- •
- pricing;
- •
- the knowledge and service quality of technologists;
- •
- the ability to obtain regulatory approvals;
- •
- the ability to establish and maintain relationships with healthcare providers and referring physicians; and
- •
- access to capital.
We are, and expect to continue to be, subject to competiti on in our targeted markets from businesses offering diagnostic imaging and radiation oncology services, including existing and developing technologies. There are many companies engaged in the shared service and fixed-site imaging market, including two national competitors and many smaller regional competitors. These competitors include RadNet, Inc., InSight Health Services Corp., and several smaller regional competitors, including Medquest, Inc., Medical Resources, Inc., Shared Medical Services, Kings Medical Company Inc. and DMS Health Group. While we believe that we had a greater number of diagnostic imaging systems in operation at December 31, 2009 than our principal competitors and also had greater revenue from diagnostic imaging services during the year ended December 31, 2009 than they did, some of our competitors may now or in the future have access to greater resources than we do. We
11
compete with other mobile providers, independent imaging centers, physicians, hospitals and other healthcare providers that have their own diagnostic imaging systems, and original equipment manufacturers that sell or lease imaging systems to healthcare providers for mobile or full-time use. There are many competitors in the radiation oncology market as well, including Radiation Therapy Services, Inc., Oncure Medical Corp., Vantage Oncology, Inc., and US Oncology, Inc., and many other smaller regional competitors. Throughout our entire business, we may also experience greater competition in states that currently have certificates of need laws should these laws be repealed, thereby reducing barriers to entry in that state.
Employees
As of December 31, 2009, we had 1,956 employees, of whom 1,413 were trained diagnostic imaging technologists, patient coordinators, drivers or other technical support staff. The drivers in a portion of one of our regions, approximately 26 employees, are represented by the Teamsters union as their collective bargaining agent. We believe we have good relationships with our employees, based on the annual Team Member survey, which indicates Team Member satisfaction.
Regulation
Our business is subject to extensive federal and state government regulation. This includes the federal Anti-Kickback Law and similar state anti-kickback laws, the Stark Law and similar state laws affecting physician referrals, the federal False Claims Act, the Health Insurance Portability and Accountability Act of 1996, as amended by the Health Information Technology for Economic and Clinical Health Act of 2009, or HITECH Act, and similar state laws addressing privacy and security, state unlawful practice of medicine and fee splitting laws and state certificate of need laws. Although we believe that our operations materially comply with the laws governing our industry, it is possible that non-compliance with existing laws or the adoption of new laws or interpretations of existing laws could adversely affect our financial performance.
Fraud and Abuse Laws; Physician Referral Prohibitions
The healthcare industry is subject to extensive federal and state regulation relating to licensure, conduct of operations, ownership of facilities, addition of facilities and services and payment for services.
In particular, the federal Anti-Kickback Law prohibits persons from knowingly and willfully soliciting, receiving, offering or providing remuneration, directly or indirectly, to induce either the referral of an individual, or the furnishing, recommending, or arranging for a good or service, for which payment may be made under a federal healthcare program such as the Medicare and Medicaid programs. The definition of "remuneration" has been broadly interpreted to include anything of value, including for example gifts, discounts, the furnishing of supplies or equipment, credit arrangements, payments of cash, waivers of payments, ownership interests, and providing anything at less than its fair market value. In addition, there is no one generally accepted definition of intent for purposes of finding a violation of the Anti-Kickback Law. For instance, one court has stated that an arrangement will violate the Anti-Kickback Law where any party has the intent to unlawfully induce referrals. In contrast, another court has opined that a party must engage in the proscribed conduct with the specific intent to disobey the law in order to be found in violation of the Anti-Kickback Law. The lack of uniform interpretation of the Anti-Kickback Law makes compliance with the law difficult. The penalties for violating the Anti-Kickback Law can be severe. These sanctions include criminal penalties and civil sanctions, including fines, imprisonment and possible exclusion from the Medicare and Medicaid programs.
12
The Anti-Kickback Law is broad, and it prohibits many arrangements and practices that are lawful in businesses outside of the healthcare industry. Recognizing that the Anti-Kickback Law is broad and may technically prohibit many innocuous or beneficial arrangements within the healthcare industry, the U.S. Department of Health and Human Services issued regulations in July of 1991, which the Department has referred to as "safe harbors." These safe harbor regulations set forth certain provisions which, if met in form and substance, will assure healthcare providers and other parties that they will not be prosecuted under the federal Anti-Kickback Law. Additional safe harbor provisions providing similar protections have been published intermittently since 1991. Our arrangements with physicians, physician practice groups, hospitals and other persons or entities who are in a position to refer may not fully meet the stringent criteria specified in the various safe harbors. Although full compliance with these provisions ensures against prosecution under the federal Anti-Kickback Law, the failure of a transaction or arrangement to fit within a specific safe harbor does not necessarily mean that the transaction or arrangement is illegal or that prosecution under the federal Anti-Kickback Law will be pursued. In addition, the Office of Inspector General of the Department of Health and Human Services, or OIG, issued a Special Advisory Bulletin on Contractual Joint Ventures in April 2003. The OIG Bulletin stated the Department's concerns regarding the legality of certain joint contractual arrangements between providers and suppliers of health care items or services. The OIG Bulletin identified characteristics of arrangements the OIG may consider suspect, and focused on arrangements in which a health care provider expands into a related service, through a joint contractual arrangement with an existing supplier of the related service, to service the health care provider's existing patient population. The OIG noted that such arrangements may be suspect when the provider contracts out all or nearly all aspects of the new venture, including the management, to the existing supplier, and provides only an existing patient base. In the OIG Bulletin, the OIG asserted that the provider's return on its investment in such circumstances may be viewed as remuneration for the referral of the provider's federal health care program patients to the supplier, and thus may violate the Anti-Kickback Law.
Although some of our arrangements may not fall within a safe harbor, we believe that such business arrangements do not violate the Anti-Kickback Law because we are careful to structure them to reflect fair market value and ensure that the reasons underlying our decision to enter into a business arrangement comport with reasonable interpretations of the Anti-Kickback Law. However, even though we continuously strive to comply with the requirements of the Anti-Kickback Law, liability under the Anti-Kickback Law may still arise because of the intentions or actions of the parties with whom we do business. In addition, we may have Anti-Kickback Law liability based on arrangements established by the entities we have acquired if any of those arrangements involved an intention or actions to exchange remuneration for referrals covered by the Anti-Kickback Law. While we are not aware of any such intentions or actions, we have only limited knowledge regarding the intentions or actions underlying those arrangements. Conduct and business arrangements that do not fully satisfy one of these safe harbor provisions may result in increased scrutiny by government enforcement authorities such as the OIG.
Many states have adopted laws similar to the federal Anti-Kickback Law. Some of these state prohibitions apply to referral of patients for healthcare services reimbursed by any source, not only the Medicare and Medicaid programs. Although we believe that we comply with both federal and state anti-kickback laws, any finding of a violation of these laws could subject us to criminal and civil penalties or possible exclusion from federal or state healthcare programs. Such penalties would adversely affect our financial performance and our ability to operate our business.
In addition, the Ethics in Patient Referral Act of 1989, commonly referred to as the federal physician self-referral prohibition or Stark Law, prohibits physician referrals of Medicare and Medicaid patients for certain designated health services (including MRI and other diagnostic imaging services) to an entity if the physician or an immediate family member has any financial arrangement with the entity
13
and no statutory or regulatory exception applies. The Stark Law also prohibits the entity from billing for any such prohibited referral. Initially, the Stark Law applied only to clinical laboratory services and regulations applicable to clinical laboratory services were issued in 1995. Earlier that same year, the Stark Law's self-referral prohibition expanded to additional goods and services, including MRI and other imaging services. In 1998, CMS (formerly known as the Health Care Financing Administration), published proposed rules for the remaining designated health services, including MRI and other imaging services, and in January of 2001, CMS published the first phase of the final rule covering the designated health services. Phase one of the final rule became effective on January 4, 2002, except for a provision relating to certain physician payment arrangements, which became effective July 26, 2004. CMS released phase two of the Stark Law final rule as a final rule comment period on March 23, 2004, with an effective date of July 26, 2004. On September 5, 2007, CMS released phase three of the Stark Law final rule which became effective on December 4, 2007. Finally, on August 19, 2008, CMS finalized additional changes to the Stark Law which became effective on October 1, 2009.
A person who engages in a scheme to circumvent the Stark Law's referral prohibition may be fined for each such arrangement or scheme. In addition, any person who presents or causes to be presented a claim to the Medicare or Medicaid program in violation of the Stark Law is subject to civil monetary penalties per bill submission, an assessment of up to three times the amount claimed, and possible exclusion from participation in federal healthcare programs. Bills submitted in violation of the Stark Law may not be paid by Medicare or Medicaid, and any person collecting any amounts with respect to any such prohibited bill is obligated to refund such amounts.
Several states in which we operate have enacted or are considering legislation that prohibits physician self-referral arrangements or requires physicians to disclose any financial interest they may have with a healthcare provider to their patients when referring patients to that provider. Possible sanctions for violating these state law physician self-referral and disclosure requirements include loss of license and civil and criminal sanctions. State laws vary from jurisdiction to jurisdiction and have been interpreted by the courts or regulatory agencies infrequently.
We believe our operations comply with these federal and state physician self-referral prohibition laws. We do not believe we have established any arrangements or schemes involving any service of ours which would violate the Stark Law or the prohibition against schemes designed to circumvent the Stark Law, or any similar state law prohibitions. Because we have financial arrangements with physicians and possibly their immediate family members, and because we may not be aware of all the financial arrangements such physicians and their immediate family members may have with entities to which they refer patients, we rely on physicians and their immediate family members to avoid making prohibited referrals to us in violation of the Stark Law and similar state laws. If we receive a prohibited referral which is not permitted under an exception to the Stark Law and applicable state law, our submission of a bill for the referral could subject us to sanctions under the Stark Law and applicable state law. Any sanctions imposed on us under the Stark Law or any similar state laws could adversely affect our financial results and our ability to operate our business.
The Health Insurance Portability and Accountability Act of 1996, or HIPAA, as amended by the Health Information Technology for Economic and Clinical Health Act of 2009, or HITECH Act, created new federal statutes to prevent healthcare fraud and false statements relating to healthcare matters. The healthcare fraud statute prohibits knowingly and willfully executing a scheme to defraud any healthcare benefit program, including private payors. A violation of this statute is a felony and may result in fines, imprisonment or exclusion from government sponsored programs such as the Medicare and Medicaid programs. The false statements statute prohibits knowingly and willfully falsifying, concealing or covering up a material fact or making any materially false, fictitious or fraudulent statement in connection with the delivery of or payment for healthcare benefits, items or services. A violation of this statute is a felony and may result in fines or imprisonment or exclusion from government sponsored programs.
14
Both federal and state government agencies are continuing heightened and coordinated civil and criminal enforcement efforts. As part of announced enforcement agency work plans, the federal government will continue to scrutinize, among other things, the billing practices of hospitals and other providers of healthcare services. The federal government also has increased funding to fight healthcare fraud, and it is coordinating its enforcement efforts among various agencies, such as the U.S. Department of Justice, the U.S. Department of Health and Human Services Office of Inspector General, and state Medicaid fraud control units. The trend towards increased funding is also seen most recently in President Obama's budget for fiscal year 2011. We believe that the healthcare industry will continue to be subject to increased government scrutiny and investigations.
Federal False Claims Act
Another trend affecting the healthcare industry is the increased use of the federal False Claims Act and, in particular, actions under the False Claims Act's "whistleblower" provisions. Those provisions allow a private individual to bring actions on behalf of the government alleging that the defendant has defrauded the federal government. After the individual has initiated the lawsuit, the government must decide whether to intervene in the lawsuit and to become the primary prosecutor. If the government declines to join the lawsuit, then the individual may choose to pursue the case alone, in which case the individual's counsel will have primary control over the prosecution, although the government must be kept apprised of the progress of the lawsuit. Whether or not the federal government intervenes in the case, it will receive the majority of any recovery. If the litigation is successful, the individual is entitled to no less than 15%, but no more than 30%, of whatever amount the government recovers. The percentage of the individual's recovery varies, depending on whether the government intervened in the case and other factors. Recently, the number of suits brought against healthcare providers by private individuals has increased dramatically. In addition, various states are considering or have enacted laws modeled after the federal False Claims Act. Under the Deficit Reduction Act of 2005, or DRA, states are being encouraged to adopt false claims acts similar to the federal False Claims Act, which establish liability for submission of fraudulent claims to the State Medicaid program and contain whistleblower provisions. Even in instances when a whistleblower action is dismissed with no judgment or settlement, we may incur substantial legal fees and other costs relating to an investigation. Future actions under the False Claims Act may result in significant fines and legal fees, which would adversely affect our financial performance and our ability to operate our business.
When an entity is determined to have violated the federal False Claims Act, it may be liable for damages and civil penalties. Liability arises, primarily, when an entity knowingly submits a false claim for reimbursement to the federal government. Simple negligence should not give rise to liability, but submitting a claim with reckless disregard of its truth or falsity could result in substantial civil liability.
Although simple negligence should not give rise to liability, the government or a whistleblower may attempt and could succeed in imposing liability on us for a variety of previous or current failures, including for example:
- •
- Failure to comply with the many technical billing requirements applicable to our Medicare and Medicaid business.
- •
- Failure to comply with Medicare requirements concerning the circumstances in which a hospital, rather than we, must bill
Medicare for diagnostic imaging services we provide to outpatients treated by the hospital.
- •
- Failure of our hospital clients to accurately identify and report our reimbursable and allowable services to Medicare.
- •
- Failure to comply with the Anti-Kickback Law or Stark Law.
15
- •
- Failure to comply with the prohibition against billing for services ordered or supervised by a physician who is excluded
from any federal healthcare programs, or the prohibition against employing or contracting with any person or entity excluded from any federal healthcare programs.
- •
- Failure to comply with the Medicare physician supervision requirements for the services we provide, or the Medicare
documentation requirements concerning such physician supervision.
- •
- The past conduct of the companies we have acquired.
Further, on May 20, 2009, President Obama signed into law the Fraud Enforcement and Recovery Act of 2009 ("FERA"), which greatly expanded the types of entities and conduct subject to the FCA. We strive to ensure that we meet applicable billing requirements. However, the costs of defending claims under the False Claims Act, as well as sanctions imposed under the Act, could significantly affect our financial performance.
Health Insurance Portability and Accountability Act of 1996
In addition to creating the new federal statutes discussed above, HIPAA also establishes uniform standards governing the conduct of certain electronic health care transactions and protecting the security and privacy of individually identifiable health information maintained or transmitted by certain covered entities, including health care providers, health plans and health care clearinghouses. As a covered entity, we must comply with the Standards for Privacy of Individually Identifiable Health Information, which restrict our use and disclosure of certain individually identifiable health information. We have been required to comply with the Privacy Standards since April 14, 2003. We must also comply with the Standards for Electronic Transactions, which establish standards for common health care transactions, such as claims information, plan eligibility, payment information and the use of electronic signatures. We have been required to comply with these standards since October 16, 2003. We must also comply with the Security Standards, which require us to implement security measures to protect the security and integrity of certain electronic health information. We have been required to comply with these standards since April 21, 2005. One other standard relevant to our use of medical information has been promulgated under HIPAA. CMS has published a final rule, which required us to adopt Unique Health Identifiers for use in filing and processing health care claims and other transactions by May 23, 2007. While the government intended this legislation to reduce administrative expenses and burdens for the health care industry, our compliance with this law may entail significant and costly changes for us. The American Recovery and Reinvestment Act of 2009, commonly referred to as the economic stimulus package signed into law on February 17, 2009, included the HITECH Act, which dramatically expanded, among other things, (1) the scope of HIPAA to also now apply directly to "business associates," or independent contractors who receive or obtain protected health information ("PHI") in connection with providing a service to the covered entity, (2) substantive security and privacy obligations, including new federal security breach notification requirements to affected individuals and DHHS and potentially media outlets, of breaches of unsecured PHI, (3) restrictions on marketing communications and a prohibition on covered entities or business associates from receiving remuneration in exchange for PHI, and (4) the civil and criminal penalties that may be imposed for HIPAA violations, increasing the annual cap in penalties from $25,000 to $1.5 million per year. We believe that we are in compliance with all of the applicable HIPAA standards, rules and regulations, as amended by the HITECH Act. If we fail to comply with these standards, we could be subject to criminal penalties and civil sanctions.
In addition to federal regulations issued under HIPAA, some states have enacted privacy and security statutes or regulations that, in some cases, are more stringent than those issued under HIPAA. In those cases it may be necessary to modify our operations and procedures to comply with the more stringent state laws, which may entail significant and costly changes for us. We believe that we are in
16
compliance with such state laws and regulations. However, if we fail to comply with applicable state laws and regulations, we could be subject to additional sanctions.
Unlawful Practice of Medicine and Fee Splitting
The marketing and operation of our business is subject to some states' laws prohibiting the practice of medicine by non-physicians. We believe that our imaging operations do not involve the practice of medicine because all professional medical services relating to our imaging operations, including the interpretation of scans and related diagnoses, are separately provided by licensed physicians not employed by us. Some states have laws that prohibit any fee-splitting arrangement between a physician and a referring person or entity that would provide for remuneration paid to the referral source on the basis of revenues generated from referrals by the referral source. We believe that our operations do not violate these state laws with respect to fee splitting.
Certificate of Need Laws
In some states, a certificate of need or similar regulatory approval is required prior to the acquisition of high-cost capital items, including diagnostic imaging systems or provision of diagnostic imaging services by us or our clients. Certificate of need regulations may limit or preclude us from providing diagnostic imaging services or systems. Revenue from states with certificate of need regulations represented greater than 50% of our total revenue for the year ended December 31, 2009.
Certificate of need laws were enacted to contain rising healthcare costs, prevent the unnecessary duplication of health resources, and increase patient access for health services. In practice, certificate of need laws have prevented hospitals and other providers who have been unable to obtain a certificate of need from acquiring new machines or offering new services. Our current contracts will remain in effect even if the certificate of need states in which we operate modify their certificate of need programs. However, a significant increase in the number of states regulating our business through certificate of need or similar programs could adversely affect us. Conversely, repeal of existing certificate of need regulations in jurisdictions where we have obtained a certificate of need, or certificate of need exemption, also could adversely affect us by allowing competitors to enter our markets. Certificate of need laws are the subject of continuing legislative activity.
Reimbursement
We derive most of our revenues directly from healthcare providers, primarily from acute care hospitals, with whom we contract to provide services to their patients. Approximately 80% of our revenues for the year ended December 31, 2009 were generated by providing services to hospitals and other healthcare providers. Some of our revenues come from third-party payors, including government programs such as the Medicare and Medicaid programs, to whom we directly bill. In the year ended December 31, 2009, we derived 20% of our revenues from direct billings to patients and their third-party payors. Services for which we submit direct billings for Medicare and Medicaid patients typically are processed by contractors and paid on a fee schedule basis, and patients are responsible for deductibles and coinsurance.
Our revenues, whether from providers who bill third-party payors directly or from our own direct billings, are impacted by Medicare laws and regulations. Many payors model their reimbursement structure using Medicare's policies. The Medicare payment policies vary depending on the site of service. As a result of federal cost-containment legislation currently in effect, Medicare generally pays for hospital inpatient services under a prospective payment system. For acute hospital services, the prospective payment is generally based on the assignment to a classification upon a patient's discharge, known as Medicare severity diagnosis related groups ("MS-DRGs"). The MS-DRG payments are pre-determined payment amounts for inpatient services. The DRG payment amount generally covers all
17
inpatient operating costs regardless of the number of conditions treated or services furnished or the length of the patient's stay.
For hospital outpatient services, Medicare payment generally is based on the hospital outpatient prospective payment system ("HOPPS"), under which services and items furnished in most hospital outpatient departments are categorized into Ambulatory Payment Classifications ("APCs"). Certain new procedures are classified under new technology APCs, which, unlike clinical APCs, are classifications based solely on hospital costs. After a two to three year period, the procedure classified under the new technology APC is assigned to a clinical APC. Under HOPPS, hospitals are paid based on procedures performed and items furnished during a patient visit. In addition to clinical and new technology APCs, certain of these items and services are paid on a fee schedule, and for certain drugs biologics, and devices, hospitals may be reimbursed pass-through amounts. In addition, because Medicare reimburses a hospital for all services rendered to a Medicare patient (both inpatient and outpatient), a free-standing facility cannot be separately reimbursed for an MRI scan or other procedure performed on the hospital patient. Many state Medicaid programs have adopted similar payment policies. When our diagnostic or radiation oncology services are provided to a hospital patient, the hospital is responsible for Medicare billing.
For those hospitals and other providers with which we contract, the Medicare Prescription Drug, Improvement and Modernization Act of 2003 ("MMA"), changed the way Medicare payments are made in many significant ways. For example, the MMA revised the methodology used to calculate payments for certain drugs, including radiopharmaceutical agents, which were paid as pass-throughs, or additional payment amounts under HOPPS. This change resulted in reduced payments to hospitals for diagnostic scans utilizing radiopharmaceuticals; however, this change did not have a material effect on pricing of our PET contracts with hospitals or our financial performance.
For services for which we bill Medicare directly, we are paid under the Medicare Physician Fee Schedule, which is updated on an annual basis. Under the Medicare statutory formula, payments under the Physician Fee Schedule would have decreased for the past several years if Congress failed to intervene. For example, for 2008, the fee schedule rates were to be reduced by approximately 10.1%. The Medicare, Medicaid and SCHIP Extension Act of 2007 eliminated the 10.1% reduction for 2008 and increased the annual payment rate update by 0.5%. This increase to the annual Medicare Physician Fee Schedule payment update was effective only for Medicare claims with dates of service between January 1, 2008 and June 30, 2008. Beginning July 1, 2008, under the Medicare Improvement for Patients and Providers Act of 2008 ("MIPPA"), the 0.5% increase was continued for the rest of 2008. In addition, MIPPA established a 1.1% increase to the Medicare Physician Fee Schedule payment update for 2009. For 2010, the Centers for Medicare and Medicaid Services ("CMS") are projecting a rate reduction of 21.2% unless Congress intervenes again to avoid the payment reduction. Federal legislative proposals have been introduced to prevent the rate reduction. On December 19, 2009, President Obama signed into law the Department of Defense Appropriations Act, 2010 (H.R. 3326) which includes a zero percent Medicare physician update through February 28, 2010. This was further extended through March 31, 2010 by the Temporary Extension Act of 2010, signed into law by President Obama on March 2, 2010. Currently pending in the Senate is the House of Representatives' Medicare Physician Payment Reform Act of 2009 (H.R. 3961), which would prevent the rate reduction by restructuring the formula that forms the basis of the Medicare Physician Fee Schedule payments. If Congress fails to intervene to prevent the 21.2% rate reduction, the resulting decrease in payment will adversely impact our revenues and results of operations.
MIPPA also modified the methodology by which the budget neutrality formula was applied to the 2009 physician fee schedule payment rates, resulting in an overall reduction in payment rates for services performed by many specialties, including an estimated 3% reduction for radiation oncology and 1% reduction for nuclear medicine. The impact of the payment rates on specific companies depends on their service mix. This resulted in decreases in rates for our radiation oncology business, but we cannot
18
predict the full impact the rate reductions will have on our future revenues or business. Also with respect to MIPPA, the legislation requires all suppliers that provide the technical component of diagnostic MRI, PET/CT, CT, and nuclear medicine to be accredited by an accreditation organization designated by CMS by January 1, 2012. On January 26, 2010, CMS initially approved the following designated accreditation organizations to accredit suppliers furnishing the technical component of all advanced imaging modalities (CT, nuclear medicine, PET and MRI) on or after January 1, 2010: The American College of Radiology (ACR), the Intersocietal Accreditation Commission (IAC) and The Joint Commission. All our facilities are accredited by The Joint Commission.
A number of other legislative changes impact our retail business. For example, the Deficit Reduction Act of 2005 ("DRA") imposed caps on Medicare payment rates for certain imaging services furnished in physician's offices and other non-hospital based settings. The caps impact MRI, PET/CT and certain imaging services performed in conjunction with radiation therapy, including certain IGRT services and diagnostic imaging services used to plan IMRT. Under the cap, payments for specified imaging services cannot exceed the hospital outpatient payment rates for those services. This change applies to services furnished on or after January 1, 2007. The limitation is applicable to the technical components of the diagnostic imaging services only, which is the payment we receive for the services for which we bill directly under the Medicare Physician Fee Schedule. CMS issues on an annual basis the hospital outpatient prospective payment ("HOPPS") rates, which are used to develop the caps. If the technical component of the service established under the Physician Fee Schedule (without including geographic adjustments) exceeds the hospital outpatient payment amount for the service (also without including geographic adjustments), then the payment is to be reduced. In other words, in those instances where the technical component for the particular service is greater for the non-hospital site, the DRA directs that the hospital outpatient payment rate be substituted for the otherwise applicable Physician Fee Schedule payment rate. The implementation of this reimbursement reduction contained in the DRA had a significant effect on our financial condition and results of operations in 2007, whereas the changes in 2008 and 2009 have been limited.
The DRA also codified the reduction in reimbursement for multiple images on contiguous body parts, which was previously announced by CMS. The DRA mandated payment at 100% of the technical component of the higher priced imaging procedure and 50% for the technical component of each additional imaging procedure for multiple images of contiguous body parts within a family of codes performed in the same session. Initially, CMS announced that it would phase in this reimbursement reduction over a two-year period, to include a 25% reduction for each additional imaging procedure on contiguous body parts in 2006 and an additional 25% reduction in 2007. To date, CMS has not yet implemented the additional 25% reduction scheduled for 2007. Federal legislative proposals have been introduced that would change the percentage reduction from 25% to 50%. It is unclear what impact this change would have on our business if the proposal is passed.
Regulatory updates to payment rates for which we bill the Medicare program directly are published annually by CMS. For payments under the Physician Fee Schedule for calendar year 2010, CMS changed the way it calculates components of the Medicare Physician Fee Schedule. First, CMS reduced payment rates for certain diagnostic services using equipment costing more than $1 million through revisions to usage assumptions from the current 50% usage rate to a 90% usage rate. This change applied to MRI and CT scans, but not for radiation therapy and other therapeutic equipment. The OIG has stated that for 2010, it intends to focus on, among other things, the practice expense components, including the equipment utilization rate, for certain imaging services reimbursed under Medicare Physician Fee Schedule to determine whether Medicare payment reflects the actual expenses incurred and whether the utilization rate reflects current industry practices. Moreover, federal legislative proposals have been introduced that would result in lower usage assumptions and, if finalized, would supersede CMS's regulatory changes.
19
Further with respect to its 2010 changes, CMS also reduced payment for services primarily involving the technical component rather than the physician work component, including the services we provide, by adjusting downward malpractice payments for these services. The reductions primarily impact radiology and other diagnostic tests. All these changes to the Medicare Fee Schedule will be transitioned over a four year period such that beginning in 2013, CMS will fully implement the revised payment rates. CMS projects that the combined impact of these changes, when fully implemented will result in a 5% reduction in radiation oncology, 16% reduction in radiology, 23% reduction in nuclear medicine and 34% reduction for all suppliers providing diagnostic tests generally. For the 2010 transitioned payment, CMS estimates the impact of its changes will result in a 1% reduction in radiation oncology, 5% reduction in radiology, 18% reduction in nuclear medicine and 12% reduction for all suppliers providing the technical component of diagnostic tests generally. These impacts are calculated prior to any application of the projected negative update factor of 21.2% related to MIPPA (which may be implemented in April 2010 unless Congress intervenes) and may impact our future revenues. If the CMS 2010 reimbursement rates had been in effect for full year 2009, we estimate that our annualized retail revenue related to MRI and radiation oncology would not have been materially impacted.
In addition to annual updates to the Medical Physician Fee Schedule, as indicated above, CMS also publishes regulatory changes to the HOPPS on an annual basis. These payments are the amounts received by our hospital clients for hospital outpatient services. For 2008, the national Medicare HOPPS payment rate for nonmyocardial PET and PET/CT scans was $1,057 per scan and the national payment rate for myocardial PET scans was $1,400 per scan. Effective January 1, 2008, CMS also bundled the PET and PET/CT payment for radiopharmaceuticals with the payment for the PET and PET/CT scan. In addition, CMS reduced the 2008 national Medicare HOPPS rate for MRI scans by approximately 3%. The 2008 national Medicare HOPPS payment rates for stereotactic radiosurgery treatment delivery services ranged from $1,057 to $8,055, depending on the level of service. For 2009, the payment rate for nonmyocardial PET and PET/CT scans is $1,037 per scan. For myocardial PET procedures, the 2009 payment rate is $1,157 per scan. For stereotactic radiosurgery treatment delivery services, the 2009 payment rates range from $952 to $7,642, depending on the level of service. On October 30, 2009, CMS released its 2010 national Medicare HOPPS payment rates, which went into effect January 1, 2010. For nonmyocardial PET and PET/CT, the 2010 payment rate is $1,037 per scan. For myocardial PET procedures, the 2010 payment rate is $1,433 per scan. For stereotactic radiosurgery treatment delivery services, the 2010 payment rates range from $963 to $7,344, depending on the level of service.
Combined, the DRA and PET and PET/CT Medicare HOPPS rate reductions negatively impacted our 2007 revenue by a total of approximately $14 million. For 2008 and 2009, however, the DRA and the net Medicare rate reductions in HOPPS did not have a material negative effect on revenue and earnings. At this time, however, we cannot predict the impact the rate reductions will have on our future revenues or business.
Furthermore, CMS announced additional performance standards for suppliers of mobile diagnostic services. The final rule requires suppliers of mobile diagnostic services under certain circumstances to enroll in Medicare and bill directly for these services, regardless of where they are performed. An exception was made for services provided to hospital patients under arrangement with that hospital. In those circumstances, the mobile diagnostic facility would be required to enroll in Medicare, but the hospital would bill for the services. On December 15, 2008, CMS issued additional guidance that companies that lease or contract with a Medicare-enrolled provider or supplier to provide only diagnostic testing equipment and/or non-physician personnel are not required to enroll in Medicare. The agency nonetheless indicated that it is continuing to evaluate such arrangements. The new policies have not significantly impacted our business.
20
Over the past few years, the growth rate of MRI industry wide scan volumes has slowed in part due to weak hospital volumes as reported by several investor-owned hospital companies, a growing number of medical groups adding imaging capacity within their practice setting and additional patient-related cost-sharing programs. In addition, there is an increasing trend of third-party payors intensifying their utilization management efforts, for example through benefit managers who require preauthorizations to control the growth rate of imaging services generally. We expect that these trends will continue throughout 2010. Further, a number of payment initiatives are being proposed in the imaging area. President Obama's budget for fiscal year 2010 includes provisions that may require the use of radiology benefit managers to preauthorize certain imaging services for Medicare enrollees. Moreover, healthcare reform under the current administration is a priority. If laws are passed, certain changes could become effective as early as 2010. In addition to the House of Representatives' recently passed Affordable Health Care for America Act (H.R. 3962), the Senate's Patient Protection and Affordable Care Act (H.R. 3590) would substantially change the way health care is financed by both governmental and private insurers and may negatively impact payment rates for certain imaging services. Also, on February 22, 2010, President Obama released a third health care reform proposal, which is currently being considered by Congress. At this time, we cannot predict which of the proposals, if any, will be adopted or if adopted, what effect, if any, these or any other proposals would have on our future revenues or business.
Payments to us by third-party payors depend substantially upon each payor's coverage and reimbursement policies. Third-party payors may impose limits on coverage or reimbursement for diagnostic imaging services, including denying reimbursement for tests that do not follow recommended diagnostic procedures. Coverage policies also may be expanded to reflect emerging technologies. Because unfavorable coverage and reimbursement policies have and may continue to constrict the profit margins of the hospitals and clinics we bill directly, however, we have and may continue to need to lower our fees to retain existing clients and attract new ones. If coverage is limited or reimbursement rates are inadequate, a healthcare provider might find it financially unattractive to own diagnostic imaging or radiation oncology systems, yet beneficial to purchase our services. It is possible that third-party coverage and reimbursement policies will affect the need or price for our services in the future, which could significantly affect our financial performance and our ability to conduct our business.
Environmental, Health and Safety Laws
We are subject to federal, state and local regulations governing the storage, use, transport and disposal of materials and waste products, including biohazardous and radioactive wastes. Our PET service and some of our other imaging services require the use of radioactive materials. While this material has a short half-life, meaning it quickly breaks down into inert, or non-radioactive substances, using such materials presents the risk of accidental environmental contamination and physical injury. Although we believe that our safety procedures for storing, handling, transporting and disposing of these hazardous materials comply with the standards prescribed by law and regulation, we cannot completely eliminate the risk of accidental contamination or injury from those hazardous materials. We maintain professional liability insurance that covers such matters with coverage that we believe is consistent with industry practice and appropriate in light of the risks attendant to our business. However, in the event of an accident, we could be held liable for any damages that result, and any liability could exceed the limits or fall outside the coverage of our insurance. We may not be able to maintain insurance on acceptable terms, or at all. We could incur significant costs and the diversion of our management's attention in order to comply with current or future environmental laws and regulations. We have not had material expenses related to environmental, health and safety laws or regulations to date.
21
How to Obtain Our SEC Filings
All reports we file with the SEC are available free of charge via EDGAR through the SEC website at www.sec.gov. In addition, the public may read and copy materials we file with the SEC at the SEC's public reference room located at 100 F Street, N.E., Washington, D.C. 20549. We also provide copies of our Forms 8-K, 10-K, 10-Q, Proxy, Annual Report and amendments to those documents at no charge to investors upon request and make electronic copies of such reports available through our website at www.alliancehealthcareservices-us.com as soon as reasonably practicable after filing such material with the SEC. The information found on, or otherwise accessible through, our website is not incorporated by reference into, nor does it form a part of, this annual report on Form 10-K, or any other document that we file with the SEC.
Our Investor Relations Department can be contacted at Alliance HealthCare Services, Inc., 100 Bayview Circle, Suite 400, Newport Beach, California 92660, Attn: Investor Relations, tel: (949) 242-5300.
Executive Officers of the Registrant
Set forth below is information regarding our executive officers, including their principal occupations for the past five years and their ages as of March 9, 2010. There are no family relationships between any of our executive officers and any other executive officer or board member. Our executive officers are elected by our board of directors and serve at the discretion of our board of directors.
Name
|
Age | Present Position | |||
|---|---|---|---|---|---|
Paul S. Viviano |
56 | Chairman of the Board of Directors and Chief Executive Officer |
|||
Michael F. Frisch |
52 | President, Alliance Imaging |
|||
Richard J. Hall |
56 | President, Alliance Oncology |
|||
Howard K. Aihara |
46 | Executive Vice President and Chief Financial Officer |
|||
Eli H. Glovinsky |
49 | Executive Vice President, General Counsel and Secretary |
|||
Christopher J. Joyce |
46 | Executive Vice President, Mergers & Acquisitions |
|||
Nicholas A. Poan |
32 | Senior Vice President, Corporate Finance and Chief Accounting Officer |
|||
Paul S. Viviano has been a director since 2003 and the chairman of the Board since November 2003. He served as our president and chief operating officer from January 2, 2003 through April 7, 2003 at which time he became our president and chief executive officer. Effective October 1, 2004, Mr. Viviano became our chairman and chief executive officer. Prior to joining us, Mr. Viviano was chief executive officer of USC University Hospital and USC Norris Cancer Hospital from 2000 to 2002. He was employed by the St. Joseph Health System from 1987 to 2000 and served as its executive vice president and chief operating officer from 1995 to 2000. Mr. Viviano currently serves as the Chairman of the Finance Committee.
Michael F. Frisch has served as president, Alliance Imaging since November 2008, our executive vice president and chief operating officer since January 5, 2007, our senior vice president, southeast region, since September 2004, and our regional vice president, mid-atlantic region from November 2002 to August 2004. From January 1999 through October 2002, Mr. Frisch served as senior vice president-regional operations of American Dental Partners, a dental practice management company.
Richard J. Hall has served as president, Alliance Oncology since November 2008. Mr. Hall's health care background includes more than 25 years experience in both the public and private sectors, including approximately four years as senior vice president of business development and marketing for US Oncology, the nation's largest oncology services provider. Mr. Hall began his career with American
22
Hospital Supply and has also held senior leadership positions with General Medical Corporation, McKesson Corporation, PatientKeeper® and BrightStar Healthcare®.
Howard K. Aihara has served as our executive vice president and chief financial officer since December 2005. Mr. Aihara joined us in September 2000 as our vice president and corporate controller. From 1997 until September 2000, he was vice president, finance, for UniMed Management Company, a physician practice management company in Burbank, California. From 1995 through 1997, he was executive director and corporate controller for AHI Healthcare Systems, Inc. of Downey, California. AHI was a publicly traded physician practice management company. Mr. Aihara began his career at Ernst & Young LLP and is a certified public accountant.
Eli H. Glovinsky has served as our executive vice president, secretary and general counsel since February 2007. Prior to joining Alliance, Mr. Glovinsky served as corporate vice president and chief legal counsel at Premier Inc., a voluntary alliance of hospitals and health systems, representing approximately 1,500 hospitals and 20,000 other health care providers. From 1997 to 2003 Mr. Glovinsky served as Premier's vice president and associate general counsel. Mr. Glovinsky began his career as an associate at the law firm of Konowieki & Rank.
Christopher J. Joyce has served as our executive vice president, mergers and acquisitions since January 1, 2008. He joined us in October 2004 as interim regional vice president of one of our regions and was appointed senior vice president of business development in May 2005. Mr. Joyce held the position of senior vice president, general counsel and secretary from February 2006 through February 2007, and then served as senior vice president of one of our regions until December 2007. Prior to joining Alliance, Mr. Joyce served as chief executive officer of Medical Resources, Inc., a publicly-traded fixed-site imaging center operator with 60 centers in nine states. He joined Medical Resources as its senior vice president and general counsel in May 1998 after leaving Alliance Entertainment Corp., a publicly-traded music distribution enterprise where he served as executive vice president of business affairs and general counsel. Mr. Joyce began his career in 1988 as a corporate associate at the law firm of Willkie Farr & Gallagher.
Nicholas A. Poan has served as our senior vice president, corporate finance since October 2006, and our corporate controller and chief accounting officer since December 2005. Previous to these roles, Mr. Poan served as our director of accounting, assistant controller and as part of our accounting management team since May 2003. Prior to joining us, Mr. Poan worked at Deloitte & Touche LLP from September 2000 through May 2003 and is a certified public accountant.
You should carefully consider the risks described below before investing in our publicly-traded securities. If any of these risks actually occurs, our business, financial condition or results of operations will likely suffer. In that event, the trading price of our common stock could decline, and you may lose all or part of your investment.
23
Changes in the rates or methods of third-party reimbursements for diagnostic imaging services could result in reduced demand for our services or create downward pricing pressure, which would result in a decline in our revenues and harm to our financial position.
We derive approximately 20% of our revenues from direct billings to patients and third-party payors such as Medicare, Medicaid or private health insurance companies, and changes in the rates or methods of reimbursement for the services we provide could have a significant negative impact on those revenues. Moreover, our healthcare provider clients on whom we depend for the majority of our revenues generally rely on reimbursement from third-party payors. If our clients receive decreased reimbursement, this could result in a reduced demand for our services or downward pricing pressures, which could have a material impact on our financial position.
From time to time, changes designed to contain healthcare costs have been implemented, some of which have resulted in decreased reimbursement rates for diagnostic imaging services that impact our retail business. For services for which we bill Medicare directly, we are paid under the Medicare Physician Fee Schedule, which is updated on an annual basis. Under the Medicare statutory formula, payments under the Physician Fee Schedule would have decreased for the past several years if Congress failed to intervene. For example, for 2008, the fee schedule rates were to be reduced by approximately 10.1%. The Medicare, Medicaid and SCHIP Extension Act of 2007 eliminated the 10.1% reduction for 2008 and increased the annual payment rate update by 0.5%. This increase to the annual Medicare Physician Fee Schedule payment update was effective only for Medicare claims with dates of service between January 1, 2008 and June 30, 2008. Beginning July 1, 2008, under MIPPA, the 0.5% increase was continued for the rest of 2008. In addition, MIPPA established a 1.1% increase to the Medicare Physician Fee Schedule payment update for 2009. For 2010, CMS are projecting a rate reduction of 21.2% unless Congress intervenes again to avoid the payment reduction. On December 19, 2009, President Obama signed into law the Department of Defense Appropriations Act, 2010 (H.R. 3326) which includes a zero percent Medicare physician update through February 28, 2010. This was further extended through March 31, 2010 by the Temporary Extension Act of 2010, signed into law by President Obama on March 2, 2010. Currently pending in the Senate is the House of Representatives' Medicare Physician Payment Reform Act of 2009 (H.R. 3961), which would prevent the rate reduction by restructuring the formula that forms the basis of the Medicare Physician Fee Schedule payments. If Congress fails to intervene to prevent the 21.2% rate reduction, the resulting decrease in payment will adversely impact our revenues and results of operations.
MIPPA also modified the methodology by which the budget neutrality formula was applied to the 2009 physician fee schedule payment rates, resulting in an overall reduction in payment rates for services performed by many specialties, including an estimated 3% reduction for radiation oncology and 1% reduction for nuclear medicine. The impact of the payment rates on specific companies depends on their service mix. We estimated slight decreases in rates for our radiation oncology business but cannot predict the full impact the rate reductions will have on our future revenues or business. Also with respect to MIPPA, the legislation requires all suppliers that provide the technical component of diagnostic MRI, PET/CT, CT and nuclear medicine to be accredited by an accreditation organization designated by CMS by January 1, 2012. On January 26, 2010, CMS initially approved the following designated accreditation organizations to accredit suppliers furnishing the technical component of all advanced imaging modalities (CT, nuclear medicine, PET and MRI) on or after January 1, 2010: The American College of Radiology (ACR), the Intersocietal Accreditation Commission (IAC) and The Joint Commission. All our facilities are accredited by The Joint Commission.
A number of other legislative changes impact our retail business. For example, the DRA imposed caps on Medicare payment rates for certain imaging services furnished in physician's offices and other
24
non-hospital based settings. The caps impact MRI, PET/CT and certain imaging services performed in conjunction with radiation therapy, including certain IGRT services and diagnostic imaging services used to plan IMRT. Under the cap, payments for specified imaging services cannot exceed the hospital outpatient payment rates for those services. This change applies to services furnished on or after January 1, 2007. The limitation is applicable to the technical components of the diagnostic imaging services only, which is the payment we receive for the services for which we bill directly under the Medicare Physician Fee Schedule. CMS issues on an annual basis the HOPPS rates, which are used to develop the caps. If the technical component of the service established under the Physician Fee Schedule (without including geographic adjustments) exceeds the hospital outpatient payment amount for the service (also without including geographic adjustments), then the payment is to be reduced. In other words, in those instances where the technical component for the particular service is greater for the non-hospital site, the DRA directs that the hospital outpatient payment rate be substituted for the otherwise applicable Physician Fee Schedule payment rate. The implementation of this reimbursement reduction contained in the DRA had a significant effect on our financial condition and results of operations in 2007, whereas the changes in 2008 and 2009 have been limited.
The DRA also codified the reduction in reimbursement for multiple images on contiguous body parts, which was previously announced by CMS. The DRA mandated payment at 100% of the technical component of the higher priced imaging procedure and 50% for the technical component of each additional imaging procedure for multiple images of contiguous body parts within a family of codes performed in the same session. Initially, CMS announced that it would phase in this reimbursement reduction over a two-year period, to include a 25% reduction for each additional imaging procedure on contiguous body parts in 2006 and an additional 25% reduction in 2007. To date, CMS has not yet implemented the additional 25% reduction scheduled for 2007. Federal legislative proposals have been introduced that would change the percentage reduction from 25% to 50%. It is unclear what impact this change would have on our business if the proposal is passed.
For HOPPS rates, effective January 1, 2009, CMS established three HOPPS imaging families according to modality—one for ultrasound, one for CT and CTA, and one for MRI and MRA services. CMS then established five composite Ambulatory Payment Classifications, or APCs, based on these HOPPS imaging families, splitting the families for CT and CTA, and MRI and MRA, into two separate composite APCs each to reflect whether the procedures are performed with or without contrast. CMS will provide a single APC payment when two or more imaging procedures using the same imaging modality are reported on a single date of service. If a with and without contrast procedure are reported together, they are paid at the higher with contrast payment category. The implementation of this new payment methodology did not have a material impact on our consolidated financial position or results of operations.
Regulatory updates to payment rates for which we bill the Medicare program directly are published annually by CMS. For payments under the Physician Fee Schedule for calendar year 2010, CMS changed the way it calculates components of the Medicare Physician Fee Schedule. First, CMS reduced payment rates for certain diagnostic services using equipment costing more than $1 million through revisions to usage assumptions from the current 50% usage rate to a 90% usage rate. This change applied to MRI and CT scans, but not for radiation therapy and other therapeutic equipment. The OIG has stated that for 2010, it intends to focus on, among other things, the practice expense components, including the equipment utilization rate, for certain imaging services reimbursed under Medicare Physician Fee Schedule to determine whether Medicare payment reflects the actual expenses incurred and whether the utilization rate reflects current industry practices. Moreover, federal legislative proposals have been introduced that would result in lower usage assumptions and, if finalized, would supersede CMS's regulatory changes.
Further with respect to its 2010 changes, CMS also reduced payment for services primarily involving the technical component rather than the physician work component, including the services we
25
provide, by adjusting downward malpractice payments for these services. The reductions primarily impact radiology and other diagnostic tests. All these changes to the Medicare Fee Schedule will be transitioned over a four year period such that beginning in 2013, CMS will fully implement the revised payment rates. CMS projects that the combined impact of these changes, when fully implemented will result in an estimated 5% reduction in radiation oncology, 16% reduction in radiology, 23% reduction in nuclear medicine and 34% reduction for all suppliers providing diagnostic tests generally. For the 2010 transitioned payment, CMS estimates the impact of its changes will result in a 1% reduction in radiation oncology, 5% reduction in radiology, 18% reduction in nuclear medicine and 12% reduction for all suppliers providing the technical component of diagnostic tests generally. These impacts are calculated prior to any application of the projected negative update factor of 21.2% related to MIPPA (which may be implemented in April 2010 unless Congress intervenes) and may impact our future revenues. If the CMS 2010 reimbursement rates had been in effect for full year 2009, we estimate that our annualized retail revenue related to MRI and radiation oncology would not have been materially impacted.
In addition to annual updates to the Medicare Physician Fee Schedule, as indicated above, CMS also publishes regulatory changes to the HOPPS on an annual basis. These payments are the amounts received by our hospital clients for hospital outpatient services. For 2008, the national Medicare HOPPS payment rate for nonmyocardial PET and PET/CT scans was $1,057 per scan and the national payment rate for myocardial PET scans was $1,400 per scan. Effective January 1, 2008, CMS also bundled the PET and PET/CT payment for radiopharmaceuticals with the payment for the PET and PET/CT scan. In addition, CMS reduced the 2008 national Medicare HOPPS rate for MRI scans by approximately 3%. The 2008 national Medicare HOPPS payment rates for stereotactic radiosurgery treatment delivery services ranged from $1,057 to $8,055, depending on the level of service. For 2009, the payment rate for nonmyocardial PET and PET/CT scans is $1,037 per scan. For myocardial PET procedures, the 2009 payment rate is $1,157 per scan. For stereotactic radiosurgery treatment delivery services, the 2009 payment rates range from $952 to $7,642, depending on the level of service. On October 30, 2009, CMS released its 2010 national Medicare HOPPS payment rates, which went into effect January 1, 2010. For nonmyocardial PET and PET/CT, the 2010 payment rate is $1,037 per scan. For myocardial PET procedures, the 2010 payment rate is $1,433 per scan. For stereotactic radiosurgery treatment delivery services, the 2010 payment rates range from $963 to $7,344, depending on the level of service.
At this time, we cannot predict the impact the DRA and PET and PET/CT Medicare HOPPS rate reductions will have on our future revenues or business. In addition, we cannot predict whether or the extent to which proposed or future statutory or regulatory changes will affect the demand for our services. For example, President Obama's budget for fiscal year 2010 includes provisions that may require the use of radiology benefit managers to preauthorize certain imaging services. Moreover, healthcare reform under the current administration is a priority. If laws are passed, certain changes could become effective as early as sometime in 2010. In addition to the House of Representatives' Affordable Health Care for America Act (H.R. 3962), the Senate's Patient Protection and Affordable Care Act (H.R. 3590) would substantially change the way health care is financed by both governmental and private insurers and may negatively impact payment rates for certain imaging services. Also, on February 22, 2010, President Obama released a third health care reform proposal, which is currently being considered by Congress. At this time, we cannot predict which of the proposals, if any, will be adopted or if adopted, what effect, if any, these or any other proposals would have on our future revenues or business. Future requirements limiting access to or payment for radiology or radiation oncology services may negatively impact our future revenues or business.
26
We may experience competition from other medical diagnostic and radiation oncology companies and equipment manufacturers and this competition could adversely affect our revenues and our business.
The market for diagnostic imaging and radiation oncology services and systems is competitive. Our major diagnostic imaging competitors include RadNet, Inc., InSight Health Services Corp., Medquest, Inc., Medical Resources, Inc., Shared Medical Services, Kings Medical Company Inc. and DMS Health Group. Our major radiation oncology competitors include Radiation Therapy Services, Inc., Oncare Medical Corp., Vontage Oncology, Inc., and US Oncology, Inc. In addition to direct competition from other imaging and radiation oncology providers, we compete with independent imaging centers and referring physicians with diagnostic imaging systems in their own offices, as well as with original equipment manufacturers, or OEMs, that aggressively sell or lease imaging systems to healthcare providers for full-time installation. In recent years we have seen an increase in activity by OEMs' sale of systems directly to a certain number of our clients. Typically, OEMs target our higher scan volume clients. This increase in activity by OEMs has resulted in overcapacity of systems in the marketplace, especially related to medical groups adding imaging capacity within their practice settings. This has caused an increase in the number of our higher scan volume clients deciding not to renew their contracts. We replace these higher volume scan clients typically with lower volume clients. Our MRI revenues decreased during the year ended December 31, 2009 compared to 2008 due to a decrease in demand. We believe that MRI revenues will continue to decline in future years.
There are many competitors in the imaging sector we find ourselves competing with to gain business. If we are unable to successfully compete, our client base would decline and our business and financial condition would be harmed.
Our revenues may fluctuate or be unpredictable and this may impact our financial results.
The amount and timing of revenues that we may derive from our business will fluctuate based on:
- •
- variations in the rate at which clients renew their contracts;
- •
- the extent to which our mobile shared-service clients become full-time clients;
- •
- changes in the number of days of service we can offer with respect to a given diagnostic imaging system due to equipment
malfunctions or the seasonal factors discussed below; and
- •
- the mix of wholesale and retail billing for our services.
In addition, we experience seasonality in the sale of our services. For example, our revenues typically decline from our third fiscal quarter to our fourth fiscal quarter. First and fourth quarter revenues are typically lower than those from the second and third quarters. First quarter revenue can be affected primarily by inclement weather, the results of which are fewer patient scans during the period. Fourth quarter revenue is affected primarily by holiday and client and patient vacation schedules and inclement weather, the results of which are fewer patient scans during the period. As a result, our revenues may vary significantly from quarter to quarter, and our quarterly results may be below market expectations. We also experience fluctuations in revenues generated due to acquisition activity and general economic conditions, including recession or economic slowdown. We may not be able to reduce our expenses, including our debt service obligations, quickly enough to respond to these declines in revenue, which would make our business difficult to operate and would harm our financial results.
We may be unable to renew or maintain our client contracts, which would harm our business and financial results.
Upon expiration of our clients' contracts, we are subject to the risk that clients will cease using our imaging services and purchase or lease their own imaging systems or use our competitors' imaging
27
systems. During the year ended December 31, 2009, we continued to experience a high rate of contract terminations partially due to stepped up marketing, sales and attractive financing alternatives being offered by original equipment manufacturers to our clients. A portion of our clients can execute early termination clauses and discontinue service prior to maturity. As a result, our MRI revenues for 2009 declined compared to 2008 levels due to a decrease in demand and we believe that MRI revenues from our shared-service operations will continue to decline in future periods. If these contracts are not renewed, it could result in a significant negative impact on our business. It is not always possible to immediately obtain replacement clients, and historically many replacement clients have been smaller facilities which have a lower number of scans than lost clients.
Managed care organizations may prevent healthcare providers from using our services which would cause us to lose current and prospective clients.
Healthcare providers participating as providers under managed care plans may be required to refer diagnostic imaging tests to specific imaging service providers depending on the plan in which each covered patient is enrolled. These requirements currently inhibit healthcare providers from using our diagnostic imaging services in some cases. The proliferation of managed care may prevent an increasing number of healthcare providers from using our services in the future which would cause our revenues to decline.
We may be unable to effectively maintain our imaging and radiation oncology systems or generate revenue when our systems are not working.
Timely, effective service is essential to maintaining our reputation and high utilization rates on our imaging and radiation oncology systems. Repairs to one of our systems can take up to two weeks and result in a loss of revenue. Our warranties and maintenance contracts do not fully compensate us for loss of revenue when our systems are not working. The principal components of our operating costs include depreciation, salaries paid to technologists and other clinical staff, drivers, annual system maintenance costs, insurance and transportation costs. Because the majority of these expenses are fixed, a reduction in the number of scans or treatments performed due to out-of-service equipment will result in lower revenues and margins. Repairs of our equipment are performed for us by the equipment manufacturers. These manufacturers may not be able to perform repairs or supply needed parts in a timely manner. Thus, if we experience greater than anticipated system malfunctions or if we are unable to promptly obtain the service necessary to keep our systems functioning effectively, our revenues could decline and our ability to provide services would be harmed.
Our ability to maximize the utilization of our diagnostic imaging equipment may be adversely impacted by harsh weather conditions, which may affect our ability to generate revenue.
Harsh weather conditions can adversely impact our operations and financial condition. To the extent severe weather patterns affect the regions in which we operate, potential patients may find it difficult to travel to our centers and we may have difficulty moving our mobile systems along their scheduled routes. As a result, we would experience a decrease in scan volume during that period. Our equipment utilization, scan volume or revenues could be adversely affected by similar conditions in the future.
Adverse changes in general domestic and worldwide economic conditions and instability and disruption of credit markets could adversely affect our operating results, financial condition, or liquidity.
We are subject to risks arising from adverse changes in general domestic and global economic conditions, including recession or economic slowdown and disruption of credit markets. Recent global market and economic conditions have been unprecedented and challenging with tighter credit conditions and recession in most major economies continuing into 2010. Continued concerns about the
28
systemic impact of potential long-term and wide-spread recession, inflation, energy costs, geopolitical issues, the availability and cost of credit, the United States mortgage market and a declining real estate market in the United States have contributed to increased market volatility and diminished expectations for the United States economy. Added concerns fueled by the United States government financial assistance to certain companies and other federal government's interventions in the United States financial system has led to increased market uncertainty and instability in both United States and international capital and credit markets. These conditions, combined with volatile oil prices, declining business and consumer confidence, increased unemployment, increased tax rates and governmental budget deficits and debt levels have contributed to volatility of unprecedented levels. We believe our MRI and PET/CT scan volumes have been impacted during 2009 and will continue to be impacted in 2010 by rising unemployment rates, the number of under-insured or uninsured patients and other conditions arising from the global economic conditions described above. At this time, it is unclear what impact this might have on our future revenues or business.
As a result of these market conditions, the cost and availability of credit has been and may continue to be adversely affected by illiquid credit markets and wider credit spreads. Concern about the stability of the markets generally and the strength of counterparties specifically has led many lenders and institutional investors to reduce, and in some cases, cease to provide funding to borrowers.
Continued turbulence in the United States and international markets and economies may adversely affect our liquidity and financial condition, and the liquidity and financial condition of our customers. If these market conditions continue, they may limit our ability, and the ability of our customers, to timely replace maturing liabilities, and access the capital markets to meet liquidity needs, resulting in adverse effects on our financial condition and results of operations.
We may not receive payment from some of our healthcare provider customers because of their financial circumstances.
Some of our healthcare provider customers do not have significant financial resources, liquidity or access to capital. If these customers experience financial difficulties they may be unable to pay us for the equipment and services that we provide. We have experienced, and expect to continue to experience, write-offs of accounts receivables from healthcare provider customers that become insolvent, file for bankruptcy or are otherwise unable to pay amounts owed to us. A significant deterioration in general or local economic conditions could have a material adverse affect on the financial health of certain of our healthcare provider customers. As a result, we may have to increase the amounts of accounts receivables that we write-off, which would adversely affect our financial condition and results of operations.
Natural disasters could adversely affect our business and operations.
Our corporate headquarters is located in California and we currently operate in various geographic regions across 45 states, subject to varying risks for natural disaster, including but not limited to, hurricanes, blizzards, floods, earthquakes and tornados. Depending upon their severity, these natural disasters could damage our facilities and systems or prevent potential patients from traveling to our centers. Damage to our equipment or any interruption in our business would adversely affect our financial condition and could result in the loss of the capital invested in the damaged facilities or systems or anticipated future cash flows from those facilities or imaging systems.
Technological change in our industry could reduce the demand for our services and require us to incur significant costs to upgrade our equipment.
We operate in a competitive, capital intensive and high fixed-cost industry. The development of new technologies or refinements of existing ones might make our existing systems technologically or
29
economically obsolete, or reduce the need for our systems. MRI, PET and PET/CT, radiation oncology and other diagnostic imaging systems are currently manufactured by numerous companies. Competition among manufacturers for a greater share of the MRI, PET and PET/CT and other diagnostic imaging systems market has resulted in and likely will continue to result in technological advances in the speed and imaging capacity of these new systems. Consequently, the obsolescence of our systems may be accelerated. Should new technological advances occur, we may not be able to acquire the new or improved systems. In the future, to the extent we are unable to generate sufficient cash from our operations or obtain additional funds through bank financing or the issuance of equity or debt securities, we may be unable to maintain a competitive equipment base. In addition, advancing technology may enable hospitals, physicians or other diagnostic service providers to perform procedures without the assistance of diagnostic service providers such as ourselves. As a result, we may not be able to maintain our competitive position in our targeted regions or expand our business.
High fuel costs would harm our operations.
Fuel costs constitute a significant portion of our mobile operating expenses. Historically, fuel costs have been subject to wide price fluctuations based on geopolitical issues and supply and demand. Fuel availability is also affected by demand for home heating oil, diesel, gasoline and other petroleum products, as well as overall economic conditions. Because of the effect of these events on the price and availability of fuel, the cost and future availability of fuel cannot be predicted with any degree of certainty. In the event of a fuel supply shortage or further increases in fuel prices, a curtailment of scheduled mobile service could result. There have been significant increases in fuel costs and continued high fuel costs or further increases will harm our financial condition and results of operations.
Because a high percentage of our operating expenses are fixed, a relatively small decrease in revenues could have a significant negative impact on our financial results.
A high percentage of our expenses are fixed, meaning they do not vary significantly with the increase or decrease in revenues. Such expenses include, but are not limited to, debt service and capital lease payments, rent and operating lease payments, salaries, maintenance, insurance and vehicle operation costs. As a result, a relatively small reduction in the prices we charge for our services or procedure volume could have a disproportionate negative effect on our financial results.
We may be subject to professional liability risks, which could be costly and could negatively impact our business and financial results.
We may be subject to professional liability claims. Although there currently are no known hazards associated with any of our scanning or therapy delivery technologies directly related to the physical equipment when used properly, hazards may be discovered in the future. Furthermore, there is a risk of harm to a patient during an MRI if the patient has certain types of metal implants or cardiac pacemakers within his or her body. Although patients are screened to safeguard against this risk, screening may nevertheless fail to identify the hazard. There also is potential risk to patients treated with therapy equipment secondary to inadvertent or excessive over- or under exposure to radiation—a topic on which the U.S. House of Representatives Committee on Energy and Commerce Subcommittee on Health held a hearing on February 26, 2010. We maintain professional liability insurance with coverage that we believe is consistent with industry practice and appropriate in light of the risks attendant to our business. However, any claim made against us could be costly to defend against, result in a substantial damage award against us and divert the attention of our management from our operations, which could have an adverse effect on our financial performance.
30
Loss of key executives and failure to attract qualified managers and sales persons could limit our growth and negatively impact our operations.
We depend upon our management team to a substantial extent. In particular, we depend upon Mr. Viviano, our Chief Executive Officer and Chairman of our Board of Directors for his skills, experience and knowledge of our Company and industry contacts. We do not have key employee insurance policies covering any of our management team. The loss of Mr. Viviano or other members of our management team could have a material adverse effect on our business, results of operations or financial condition.
We require field managers and sales persons with experience in our industry to operate and sell our services for diagnostic imaging and radiation oncology. It is impossible to predict the availability of qualified field managers and sales persons or the compensation levels that will be required to hire them. The loss of the services of any member of our senior management or our inability to hire qualified field managers and sales persons at economically reasonable compensation levels could adversely affect our ability to operate and grow our business.
Loss of, and failure to attract, qualified employees, technologists and other clinical staff could limit our growth and negatively impact our operations.
Our future success depends on our continuing ability to identify, hire, develop, motivate and retain highly skilled personnel for all areas of our organization. Competition in our industry for qualified employees is intense. In particular, there is a very high demand for qualified technologists who are necessary to operate our systems, particularly PET and PET/CT technologists. We may not be able to hire and retain a sufficient number of technologists, therapists, physicists and dosimetrists and we expect that our costs for the salaries and benefits of these employees will continue to increase for the foreseeable future because of the industry's competitive demand for their services. Our continued ability to compete effectively depends on our ability to attract new employees and to retain and motivate our existing employees.
Our positron emission tomography and positron emission tomography/computed tomography, or PET and PET/CT services, and some of our other imaging services require the use of radioactive materials, which could subject us to regulation-related costs and delays and potential liabilities for injuries or violations of environmental, health and safety laws.
Our PET and PET/CT services and some of our other imaging services require radioactive materials. While this radioactive material has a short half-life, meaning it quickly breaks down into inert, or non-radioactive substances, storage, use and disposal of these materials present the risk of accidental environmental contamination and physical injury. We are subject to federal, state and local regulations governing storage, handling and disposal of these materials and waste products. In spite of our safety procedures for storing, handling and disposing of these hazardous materials, we cannot completely eliminate the risk of accidental contamination or injury from those hazardous materials. We maintain professional liability insurance with coverage that we believe is consistent with industry practice and appropriate in light of the risks attendant to our business. However, in the event of an accident, we could be held liable for any damages that result, and any liability could exceed the limits or fall outside the coverage of our insurance. We may not be able to maintain insurance on acceptable terms, or at all. We could incur significant costs and the diversion of our management's attention in order to comply with current or future environmental, health and safety laws and regulations.
We may not be able to achieve the expected benefits from future acquisitions, which would adversely affect our financial condition and results.
We have historically relied on acquisitions as a method of expanding our business. In addition, we will consider future acquisitions as opportunities arise. If we do not successfully integrate acquisitions,
31
we may not realize anticipated operating advantages and cost savings. The integration of companies that have previously operated separately involves a number of risks, including:
- •
- demands on management related to the increase in our size after an acquisition;
- •
- the diversion of management's attention from the management of daily operations to the integration of operations;
- •
- difficulties in the assimilation and retention of employees;
- •
- potential adverse effects on operating results; and
- •
- challenges in retaining clients.
We may not be able to maintain the levels of operating efficiency acquired companies have achieved or might achieve separately. Successful integration of each of their operations will depend upon our ability to manage those operations and to eliminate redundant and excess costs. Because of difficulties in combining operations, we may not be able to achieve the cost savings and other size-related benefits that we hoped to achieve after these acquisitions, which would harm our financial condition and operating results.
Two of our stockholders and their affiliates beneficially own almost half of our outstanding shares of common stock and have the contractual right to designate members of our board of directors and board committees, and will therefore be able to exert significant influence over us, including with respect to change of control transactions.
As of December 31, 2009, funds managed by Oaktree Capital Management, LLC and MTS Health Investors, LLC (collectively the "Oaktree Parties") beneficially owned approximately 47.1% of our outstanding shares of common stock. So long as they beneficially own at least 35% of our outstanding shares of common stock, the Oaktree Parties will have the right to designate three of the members of our board of directors.
As a result of the arrangements described above, the Oaktree Parties have the ability to exert significant influence on our management and operations, as well as matters requiring stockholder approval, including approving mergers, consolidations or sales of all or substantially all of our assets. In addition, beginning in April 2010, provisions of a standstill agreement we entered into with the Oaktree Parties limiting their ability to acquire more than 49.9% of our outstanding common stock will terminate. The interests of the Oaktree Parties may conflict with your interests.
Possible volatility in our stock price could negatively affect us and our stockholders.
The trading price of our common stock on the New York Stock Exchange has fluctuated significantly in the past. During the period from January 1, 2007 through December 31, 2009, the trading price of our common stock fluctuated from a high of $12.03 per share to a low of $4.84 per share. In the past, we have experienced a drop in stock price following an announcement of disappointing earnings or earnings guidance. Any such announcement in the future could lead to a similar drop in stock price. The price of our common stock could also be subject to wide fluctuations in the future as a result of a number of other factors, including the following:
- •
- changes in expectations as to future financial performance or buy/sell recommendations of securities analysts;
- •
- our, or a competitor's, announcement of new products or services, or significant acquisitions, strategic partnerships,
joint ventures or capital commitments; and
- •
- the operating and stock price performance of other comparable companies.
32
In addition, the U.S. securities markets have experienced significant price and volume fluctuations. These fluctuations often have been unrelated to the operating performance of companies in these markets. Broad market and industry factors may lead to volatility in the price of our common stock, regardless of our operating performance. Moreover, our stock has limited trading volume, and this illiquidity may increase the volatility of our stock price.
In the past, following periods of volatility in the market price of an individual company's securities, securities class action litigation often has been instituted against that company. The institution of similar litigation against us could result in substantial costs and a diversion of management's attention and resources, which could negatively affect our business, results of operations or financial condition.
Provisions of the Delaware General Corporation Law and our organizational documents may discourage an acquisition of us.
In the future, we could become the subject of an unsolicited attempted takeover of our Company. Although an unsolicited takeover could be in the best interests of our stockholders, our organizational documents and the General Corporation Law of the State of Delaware both contain provisions that will impede the removal of directors and may discourage a third-party from making a proposal to acquire us. For example, the provisions:
- •
- permit the board of directors to increase its own size and fill the resulting vacancies;
- •
- provide for a board composed of three classes of directors with each class serving a staggered three-year
term;
- •
- authorize the issuance of additional shares of preferred stock in one or more series without a stockholder vote; and
- •
- establish an advance notice procedure for stockholder proposals to be brought before an annual meeting of our stockholders, including proposed nominations of persons for election to the board of directors.
Moreover, these provisions can only be amended by the vote of 662/3% or more of our outstanding shares entitled to vote. Furthermore, we are subject to Section 203 of the Delaware General Corporation Law, which could have the effect of delaying or preventing a change in control.
Risks Related to Government Regulation of Our Business
The regulatory and political framework is uncertain and evolving.
Healthcare laws and regulations may change significantly in the future which could adversely affect our financial condition and results of operations. We continuously monitor these developments and modify our operations from time to time as the legislative and regulatory environment changes.
Currently, there are a number of pending federal legislative proposals that would substantially change the way health care is financed by both governmental and private insurers and may negatively impact payment rates for imaging services. On November 7, 2009, the House of Representatives passed the Affordable Health Care for America Act (H.R. 3962), which, among other things, would require payment rates for services using imaging equipment that costs over $1 million to be calculated using revised equipment usage assumptions and would reduce payment rates for imaging services paid under the Medicare Part B fee schedule. The current 50% usage assumption rate would be replaced with a 75% usage rate for such equipment (compared to CMS's usage rate of 90%, discussed below). In addition, on December 24, 2009, the Senate passed the Patient Protection and Affordable Care Act (H.R. 3590) which would similarly revise the equipment usage assumption for advanced diagnostic imaging services (which includes MRI, CT and PET). The Senate bill would replace the current 50%
33
usage assumption rate with a 65% usage rate for such equipment for 2010 through 2012. The rate would be further increased to 70% beginning in 2013 and 75% beginning in 2014. Both H.R. 3962 and H.R. 3590 would change the technical component discount on imaging of contiguous body parts during a single imaging session from 25% to 50%. Also, on February 22, 2010, President Obama released a third health care reform proposal, which is currently being considered by Congress. We are unable to predict whether any of these proposals will become law or in what form, whether any additional or similar changes to statutes or regulations (including interpretations) will occur in the future, or what effect any such legislation or regulation would have on our business. The federal government may, however, have greater involvement in the healthcare industry than in prior years, and such greater involvement may adversely affect our financial condition and results of operations.
Complying with federal and state regulations is an expensive and time-consuming process, and any failure to comply could result in substantial penalties.
We are directly or indirectly through our clients subject to extensive regulation by both the federal government and the states in which we conduct our business, including the federal Anti-Kickback Law and similar state anti-kickback laws, the Stark Law and similar state laws affecting physician referrals, the federal False Claims Act, the Health Insurance Portability and Accountability Act of 1996, as amended by the Health Information Technology for Economic and Clinical Health Act of 2009, and similar state laws addressing privacy and security, state unlawful practice of medicine and fee splitting laws, state certificate of need laws, the Medicare and Medicaid statutes and regulations, the Medicare Prescription Drug, Improvement and Modernization Act of 2003, and requirements for handling biohazardous and radioactive materials and wastes.
Both federal and state government agencies have heightened and coordinated civil and criminal enforcement efforts as part of numerous ongoing investigations of health care companies, as well as their executives and managers. These investigations relate to a wide variety of matters, including referral and billing practices. The Office of the Inspector General of the Department of Health and Human Services ("DHHS") and the Department of Justice ("DOJ") have, from time to time, established national enforcement initiatives that focus on specific billing practices or other suspected areas of abuse. Some of our activities could become the subject of governmental investigations or inquiries.
If our operations are found to be in violation of any of the laws and regulations to which we or our clients are subject, we may be subject to the applicable penalty associated with the violation, including civil and criminal penalties, damages, fines and the curtailment of our operations. Any penalties, damages, fines or curtailment of our operations, individually or in the aggregate, could adversely affect our ability to operate our business and our financial results. Our risk of being found in violation of these laws and regulations is increased by the fact that many of them have not been fully interpreted by the regulatory authorities or the courts, and their provisions are open to a variety of interpretations. Any action against us for violation of these laws or regulations, even if we successfully defend against it, could cause us to incur significant legal expenses and divert management's attention from the operation of our business. For a more detailed discussion of the various state and federal regulations to which we are subject see "Business—Regulation," "Business—Reimbursement" and "Business—Environmental, Health and Safety Laws."
34
Federal and state anti-kickback and anti-self-referral laws may adversely affect our operations and income.
Various federal and state laws govern financial arrangements among health care providers. The federal Anti-Kickback Law prohibits the knowing and willful offer, payment, solicitation or receipt of any form of remuneration in return for, or to induce, the referral of Medicare, Medicaid or other federal healthcare program patients, or in return for, or to induce, the purchase, lease or order of items or services that are covered by Medicare, Medicaid or other federal healthcare programs. Many state laws also prohibit the solicitation, payment or receipt of remuneration in return for, or to induce, the referral of patients in private as well as government programs. Violation of these laws may result in substantial civil or criminal penalties and/or exclusion from participation in federal or state healthcare programs. We believe that we are operating in compliance with applicable laws and believe that our arrangements with providers would not be found to violate the federal and state anti-kickback laws. However, these laws could be interpreted in a manner that could have an adverse effect on our operations.
The Stark Law prohibits a physician from referring Medicare or Medicaid patients to any entity for certain designated health services (including MRI and other diagnostic imaging services) if the physician has a prohibited financial relationship with that entity, unless an exception applies. Although we believe that our operations do not violate the Stark Law, our activities may be challenged. If a challenge to our activities is successful, it could have an adverse effect on our operations. In addition, legislation may be enacted in the future that further addresses Medicare and Medicaid fraud and abuse or that imposes additional requirements or burdens on us.
A number of states in which our diagnostic imaging centers are located have adopted a form of anti-kickback law and/or Stark Law. The scope of these laws and the interpretations of them vary from state to state and are enforced by state courts and regulatory authorities, each with broad discretion. A determination of liability under the laws described in this risk factor could result in fines and penalties and restrictions on our ability to operate in these jurisdictions.
In addition, under the DRA, states are encouraged to adopt false claims acts, similar to the federal False Claims Act, which establish liability for submission of fraudulent claims to the State Medicaid program and contain qui tam or whistleblower provisions. States enacting such false claims statutes will receive an increased percentage of any recovery from a State Medicaid judgment or settlement. Adoption of new false claims statutes in states where we operate may impose additional requirements or burdens on us.
Healthcare reform legislation and regulations could impact our operations or limit the prices we can charge for our services, which would reduce our revenues and harm our operating results.
In addition to extensive existing government healthcare regulation, there have been and continue to be numerous initiatives at the federal and state levels for reforms affecting the payment for and availability of healthcare services, including proposals that would significantly limit reimbursement under the Medicare and Medicaid programs. Limitations on reimbursement amounts and other cost containment pressures have in the past resulted in a decrease in the revenue we receive for each scan we perform. For example, the DRA, which was signed into law on February 8, 2006, contains provisions affecting Medicare payment for imaging services furnished in a number of settings.
Regulations published in November 2006 by CMS identify 14 supplier standards applicable to independent diagnostic testing facilities, or IDTFs, which include some of our facilities. CMS designed these standards to ensure that minimum quality standards are met to protect Medicare beneficiaries. If an IDTF fails to meet one or more of the standards at the time of enrollment or re-enrollment, then its application will be denied or the agency will revoke an IDTF's billing privileges. These standards went into effect on January 1, 2007, and IDTFs must meet these standards to obtain or retain
35
enrollment in the Medicare program. CMS published additional regulatory provisions in November 2007 and November 2008 that revised the existing IDTF standards and also created several additional standards. These changes went into effect on January 1, 2008 and January 1, 2009, respectively. To the extent that CMS publishes interpretations of these standards that are more restrictive than the standards described in the agency's published rules, our business could be adversely impacted. At this time, we cannot predict the impact that these new standards will have on our business.
It is also not clear at this time what existing or future proposals, if any, will be made or adopted and, if adopted, what effect these proposals would have on our business. Healthcare reform under the current administration is a priority. If laws are passed, certain changes could become effective as early as 2010. In addition to the House of Representatives' Affordable Health Care for America Act (H.R. 3962), the Senate's Patient Protection and Affordable Care Act (H.R. 3590) would substantially change the way health care is financed by both governmental and private insurers and may negatively impact payment rates for certain imaging services. Also, on February 22, 2010, President Obama released a third health care reform proposal, which is currently being considered by Congress. At this time, we cannot predict which of the proposals, if any, will be adopted or if adopted, what effect, if any, these or any other proposals would have on the demand for our services or the revenue per procedure that we can collect.
The application or repeal of state certificate of need regulations could harm our business and financial results.
Some states require a certificate of need or similar regulatory approval prior to the acquisition of high-cost capital items, including diagnostic imaging systems or provision of diagnostic imaging services by us or our clients. Twenty-one of the 45 states in which we operate require a certificate of need and more states may adopt similar licensure frameworks in the future. In many cases, a limited number of these certificates are available in a given state. If we are unable to obtain the applicable certificate or approval or additional certificates or approvals necessary to expand our operations, these regulations may limit or preclude our operations in the relevant jurisdictions.
Conversely, states in which we have obtained a certificate of need may repeal existing certificate of need regulations or liberalize exemptions from the regulations. For example, Pennsylvania, Nebraska, New York, Ohio and Tennessee have liberalized exemptions from certificate of need programs. The repeal of certificate of need regulations in states in which we have obtained a certificate of need or a certificate of need exemption would lower barriers to entry for competition in those states and could adversely affect our business.
If we fail to comply with various licensure, certification and accreditation standards, we may be subject to loss of licensure, certification or accreditation which would adversely affect our operations.
All of the states in which we operate require that the imaging technologists that operate our computed tomography, single photon emission computed tomography and positron emission tomography systems be licensed or certified. Also, each of our retail sites must continue to meet various requirements in order to receive payments from the Medicare program. In addition, we are currently accredited by The Joint Commission, an independent, non-profit organization that accredits various types of healthcare providers such as hospitals, nursing homes and providers of diagnostic imaging services. In the healthcare industry, various types of organizations are accredited to meet certain Medicare certification requirements, expedite third-party payments and fulfill state licensure requirements. Some managed care providers prefer to contract with accredited organizations. Any lapse in our licenses, certifications or accreditations, or those of our technologists, or the failure of any of our retail sites to satisfy the necessary requirements under Medicare could adversely affect our operations and financial results.
36
Risks Related to Our Indebtedness
Our substantial indebtedness could restrict our operations and make us more vulnerable to adverse economic conditions.
We are highly leveraged. As of December 31, 2009, we had $667.9 million of outstanding debt, excluding letters of credit, and approximately $115.5 million was available for borrowing under our New Revolving Credit Facility. Our substantial indebtedness could have important consequences for our stockholders. For example, it could:
- •
- require us to dedicate a substantial portion of our cash flow from operations to payments on our indebtedness, thereby
reducing the availability of our cash flow to fund working capital, capital expenditures and acquisitions and for other general corporate purposes;
- •
- increase our vulnerability to economic downturns and competitive pressures in our industry;
- •
- place us at a competitive disadvantage compared to our competitors that have less debt in relation to cash flow; and
- •
- limit our flexibility in planning for, or reacting to, changes in our business and our industry.
If there is a default under the agreements governing our material indebtedness, the value of our assets may not be sufficient to repay our creditors.
Our property and equipment, which make up a significant portion of our tangible assets, had a net book value of $340.1 million as of December 31, 2009 and $357.2 million as of December 31, 2008. The book value of these assets should not be relied on as a measure of realizable value for such assets. The realizable value may be lower than such net book value. The value of our assets in the event of liquidation will depend upon market and economic conditions, the availability of buyers and similar factors. A sale of these assets in a bankruptcy or similar proceeding would likely be made under duress, which would reduce the amounts that could be recovered. Furthermore, such a sale could occur when other companies in our industry also are distressed, which might increase the supply of similar assets and therefore reduce the amounts that could be recovered. Our goodwill and other intangible assets had a net book value of $294.4 million as of December 31, 2009 and $304.2 million as of December 31, 2008. These assets primarily consist of the excess of the acquisition cost over the fair market value of the net assets acquired in purchase transactions, customer contracts and costs to obtain certificates of need. The value of goodwill and other intangible assets will continue to depend significantly upon the success of our business as a going concern and the growth in future cash flows. As a result, in the event of a default under the agreements governing our material indebtedness or any bankruptcy or dissolution of our Company, the realizable value of these assets will likely be substantially lower and may be insufficient to satisfy the claims of our creditors.
The financial condition of our assets will likely deteriorate during any period of financial distress preceding a sale of our assets. In addition, much of our assets consist of illiquid assets that may have to be sold at a substantial discount in an insolvency situation. Accordingly, the proceeds of any such sale of our assets may not be sufficient to satisfy, and may be substantially less than, amounts due to our creditors.
Despite current indebtedness levels, we and our subsidiaries may still be able to incur substantially more indebtedness, which could increase the risks described above.
We and our subsidiaries may be able to incur substantial additional indebtedness in the future. The terms of the New Credit Facility and the indenture governing the notes permit us or our subsidiaries to incur additional indebtedness, subject to certain restrictions. Further, the New Credit Facility and the
37
indenture governing the notes allow for the incurrence of indebtedness by our subsidiaries, all of which would be structurally senior to the notes. In addition, as of December 31, 2009, our New Credit Facility permitted additional borrowings of up to approximately $115.5 million under the New Revolving Credit Facility subject to the covenants contained in the New Credit Facility, and all of those borrowings would be senior to the notes to the extent of the assets securing the New Credit Facility. If new debt is added to our or our subsidiaries' current debt levels, the risks discussed above could intensify.
If we are unable to generate or borrow sufficient cash to make payments on our indebtedness or to refinance our indebtedness on acceptable terms, our financial condition would be materially harmed, our business may fail and you may lose all of your investment.
Our ability to make scheduled payments on or to refinance our obligations with respect to our debt will depend on our financial and operating performance, which will be affected by general economic, financial, competitive, business and other factors beyond our control. As a result of the recent global market and economic conditions, the cost and availability of credit and equity capital have been severely impacted. We cannot assure you that our business will generate sufficient cash flow from operations or that future borrowings will be available to us in an amount sufficient to enable us to service our debt or to fund our other liquidity needs. If we are unable to meet our debt obligations or fund our other liquidity needs, we may need to restructure or refinance all or a portion of our debt on or before maturity or sell certain of our assets. We cannot assure you that we will be able to restructure or refinance any of our debt on commercially reasonable terms, if at all, which could cause us to default on our debt obligations and impair our liquidity. Any refinancing of our debt could be at higher interest rates and may require us to comply with more onerous covenants, which could further restrict our business operations.
We may not be able to finance future needs or adapt our business plan to changes because of restrictions placed on us by our credit facility, our notes, the indentures governing our notes and instruments governing our other indebtedness.
The indenture governing the notes and our New Credit Facility contain affirmative and negative covenants which restrict, among other things, our ability to:
- •
- incur additional debt;
- •
- sell assets;
- •
- create liens or other encumbrances;
- •
- make certain payments and dividends; or
- •
- merge or consolidate.
All of these restrictions could affect our ability to operate our business and may limit our ability to take advantage of potential business opportunities as they arise. A failure to comply with these covenants and restrictions would permit the relevant creditors to declare all amounts borrowed under the relevant borrowing, together with accrued interest and fees, to be immediately due and payable. If the indebtedness under the credit facility or the notes is accelerated, we may not have sufficient assets to repay amounts due under the credit facility, the notes or on other indebtedness then outstanding. If we are not able to refinance our debt, we could become subject to bankruptcy proceedings, and you may lose all or a portion of your investment because the claims of certain of our creditors on our assets are prior to the claims of holders of the notes.
38
Increases in interest rates could adversely affect our financial condition.
An increase in prevailing interest rates would have an effect on the interest rates charged on our variable rate debt, which rise and fall upon changes in interest rates. At December 31, 2009, approximately $460.0 million of our debt was at variable interest rates.
Increases in interest rates would also impact the refinancing of our debt. If interest rates are higher when our debt becomes due, we may be forced to borrow at the higher rates. If prevailing interest rates or other factors result in higher interest rates, the increased interest expense would adversely affect our cash flow and our ability to service our debt. As a protection against rising interest rates, we may enter into agreements such as interest rate swaps, caps, floors and other interest rate exchange contracts. These agreements, however, carry the risks that the other parties to the agreements may not perform or that the agreements could be unenforceable. Within 180 days after the closing date of the New Credit Facility, which occurred December 1, 2009, we are required to enter into agreements such as interest rate swaps, caps, floors and other interest rate exchange contracts that would have the effect of fixing the rate of a specified percentage of our variable rate debt for periods to be determined.
Item 1B. Unresolved Staff Comments.
Not applicable.
We lease approximately 36,634 square feet of space in Newport Beach, California for our executive and principal administrative offices. We also lease 20,000 square feet of space in Canton, Ohio for our retail billing operations. We have 15,900 square feet of space for a large regional office in Andover, Massachusetts, in addition to other small regional offices throughout the country. We also lease a 15,600 square foot operations warehouse in Orange, California and a 9,000 square foot operations warehouse in Childs, Pennsylvania.
From time to time, we are involved in routine litigation incidental to the conduct of our business. We believe that none of this litigation pending against us will have a material adverse effect on our business.
In connection with our acquisition of MOS, LLC in the third quarter of 2008, we subsequently identified a Medicare billing practice related to a portion of MOS, LLC's retail billing operations that raised compliance issues under Medicare reimbursement guidelines. The practice was in place prior to the acquisition and was discontinued when we became aware of it. In accordance with our corporate compliance program, we have entered into discussions with representatives of the federal government to advise them of the issue and seek guidance on appropriate next steps. The discussions are ongoing and no resolution has yet been reached. Although the government may seek repayment and penalties relating to the billing practice, we do not expect that such repayment and penalties, if imposed on us, would have a material impact on our results of operations, cash flows or financial position because we believe the amounts we would owe will be substantially or fully off-set by recoveries under the indemnification provisions of the MOS, LLC acquisition purchase agreement.
39
Item 5. Market for Registrant's Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities.
Our common stock is traded on the New York Stock Exchange under the symbol "AIQ". The high and low sales prices as reported on the NYSE are set forth below for the respective time periods. As of March 7, 2010, there were 48 stockholders of record of our common stock and approximately 3,000 beneficial holders of our common stock.
| |
2009 | 2008 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |
High | Low | High | Low | |||||||||
First Quarter |
$ | 9.79 | $ | 6.28 | $ | 11.00 | $ | 8.16 | |||||
Second Quarter |
$ | 9.00 | $ | 6.41 | $ | 9.46 | $ | 7.59 | |||||
Third Quarter |
$ | 7.38 | $ | 4.84 | $ | 12.03 | $ | 8.08 | |||||
Fourth Quarter |
$ | 6.47 | $ | 5.06 | $ | 10.25 | $ | 6.15 | |||||
We have never paid any cash dividends on our common stock and have no current plans to do so. We intend to retain available cash to provide for the operation of our business, including capital expenditures, fund future acquisitions and repay indebtedness. Our New Credit Facility and the indenture related to our notes restrict the payment of cash dividends on our common stock. In December 2009, we withheld 333,772 shares from certain employees to pay taxes related to restricted stock awards that vested. These shares are included in treasury stock and are valued at $5.71 per share. See "Management's Discussion and Analysis of Financial Condition and Results of Operations—Liquidity and Capital Resources."
All stock option plans under which our common stock is reserved for issuance have previously been approved by our shareholders. The following table provides summary information as of December 31, 2009 for all of our stock option plans:
| |
Number of shares of Common Stock to be issued upon exercise of outstanding options |
Weighted average exercise price of outstanding options |
Number of shares of Common Stock remaining available for future issuance (excluding shares reflected in column 1) |
|||||||
|---|---|---|---|---|---|---|---|---|---|---|
Stock option plans approved by shareholders |
4,417,550 | $ | 6.87 | 3,347,587 | ||||||
Stock option plans not approved by shareholders |
— | — | — | |||||||
|
4,417,550 | $ | 6.87 | 3,347,587 | ||||||
40
STOCK PERFORMANCE GRAPH
The following graph sets forth the cumulative return on our common stock from December 31, 2004 through December 31, 2009, as compared to the cumulative return of the S&P 500 Index and the cumulative return of the S&P Healthcare Index. The graph assumes that $100 was invested on December 31, 2004 in each of (1) our common stock, (2) the S&P 500 Index and (3) the S&P Healthcare Index and that all dividends (if applicable) were reinvested.
COMPARISON OF THE CUMULATIVE TOTAL RETURN AMONG
ALLIANCE HEALTHCARE SERVICES, INC., THE S&P 500 INDEX, AND
THE S&P HEALTHCARE INDEX
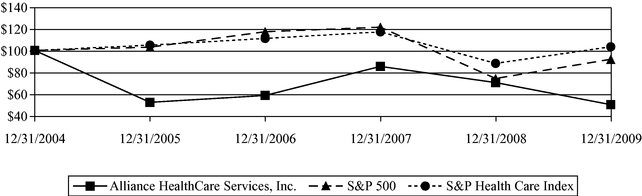
| |
12/31/04 | 12/31/05 | 12/31/06 | 12/31/07 | 12/31/08 | 12/31/09 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
Alliance HealthCare Services, Inc. |
100.00 | 52.89 | 59.11 | 85.51 | 70.84 | 50.76 | |||||||||||||
S&P 500 |
100.00 | 103.00 | 117.03 | 121.16 | 74.53 | 92.01 | |||||||||||||
S&P Healthcare Index |
100.00 | 104.85 | 110.92 | 116.90 | 88.28 | 103.35 | |||||||||||||
This graph and the accompanying text are not "soliciting material," are not deemed filed with the SEC and are not to be incorporated by reference in any filing by us under the Securities Act of 1933, as amended, or the Securities Exchange Act of 1934, as amended, whether made before or after the date hereof and irrespective of any general incorporation language in any such filing.
41
Item 6. Selected Consolidated Financial Data.
The selected consolidated financial data shown below has been taken or derived from the audited consolidated financial statements of the Company and should be read in conjunction with "Management's Discussion and Analysis of Financial Condition and Results of Operations" and our consolidated financial statements and related notes included herein (in thousands, except per share data).
| |
Year Ended December 31, | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |
2005 | 2006 | 2007 | 2008 | 2009 | ||||||||||||
Consolidated Statements of Operations Data: |
|||||||||||||||||
Revenues |
$ | 430,788 | $ | 455,775 | $ | 444,919 | $ | 495,834 | $ | 505,513 | |||||||
Costs and expenses: |
|||||||||||||||||
Cost of revenues, excluding depreciation and amortization |
226,294 | 244,254 | 235,471 | 261,753 | 270,381 | ||||||||||||
Selling, general and administrative expenses |
48,077 | 53,955 | 57,049 | 62,728 | 67,579 | ||||||||||||
Transaction costs |
— | — | — | — | 893 | ||||||||||||
Employment agreement costs |
366 | — | — | — | — | ||||||||||||
Severances and related costs |
826 | 745 | 682 | 636 | 1,404 | ||||||||||||
Loss on extinguishment of debt |
— | — | — | 61 | 14,600 | ||||||||||||
Depreciation expense |
82,505 | 83,397 | 82,703 | 87,728 | 94,918 | ||||||||||||
Amortization expense |
3,954 | 4,933 | 5,195 | 8,696 | 11,000 | ||||||||||||
Interest expense and other, net |
34,203 | 41,078 | 42,362 | 48,392 | 45,894 | ||||||||||||
Other (income) and expense, net |
(399 | ) | 45 | (579 | ) | (872 | ) | (1,178 | ) | ||||||||
Total costs and expenses |
395,826 | 428,407 | 422,883 | 469,122 | 505,491 | ||||||||||||
Income before income taxes, earnings from unconsolidated investees and noncontrolling interest, net of tax |
34,962 | 27,368 | 22,036 | 26,712 | 22 | ||||||||||||
Income tax expense |
14,758 | 12,032 | 11,644 | 11,764 | 308 | ||||||||||||
Earnings from unconsolidated investees |
(3,343 | ) | (5,371 | ) | (7,567 | ) | (4,605 | ) | (3,831 | ) | |||||||
Net income |
23,547 | 20,707 | 17,959 | 19,553 | 3,545 | ||||||||||||
Less: Net income attributable to noncontrolling interest, net of tax |
(1,718 | ) | (2,075 | ) | (1,727 | ) | (3,030 | ) | (3,064 | ) | |||||||
Net income attributable to Alliance HealthCare Services, Inc. |
$ | 21,829 | $ | 18,632 | $ | 16,232 | $ | 16,523 | $ | 481 | |||||||
Earnings per common share attributable to Alliance HealthCare Services, Inc.: |
|||||||||||||||||
Basic |
$ | 0.44 | $ | 0.37 | $ | 0.32 | $ | 0.32 | $ | 0.01 | |||||||
Diluted |
$ | 0.43 | $ | 0.37 | $ | 0.31 | $ | 0.32 | $ | 0.01 | |||||||
Weighted average number of shares of common stock and common stock equivalents: |
|||||||||||||||||
Basic |
49,378 | 49,780 | 50,563 | 51,296 | 51,738 | ||||||||||||
Diluted |
50,262 | 50,335 | 51,582 | 52,159 | 52,155 | ||||||||||||
Consolidated Balance Sheet Data (at end of period): |
|||||||||||||||||
Cash and cash equivalents |
$ | 13,421 | $ | 16,440 | $ | 120,892 | $ | 73,305 | $ | 111,884 | |||||||
Total assets |
675,342 | 664,526 | 849,807 | 883,723 | 887,836 | ||||||||||||
Long-term debt, including current maturities |
579,582 | 529,425 | 670,796 | 662,562 | 667,890 | ||||||||||||
Stockholders' (deficit) equity |
(35,856 | ) | (12,598 | ) | 8,079 | 28,993 | 34,762 | ||||||||||
42
Item 7. Management's Discussion and Analysis of Financial Condition and Results of Operations.
Overview
We are a leading national provider of outpatient diagnostic imaging services, based upon annual revenue and number of diagnostic imaging systems deployed, and are a provider of radiation oncology services. Our principal sources of revenue are derived from magnetic resonance imaging ("MRI") and positron emission tomography/computed tomography ("PET/CT"). We provide imaging and therapeutic services primarily to hospitals and other healthcare providers on a shared- service and full-time service basis. We also provide services through a growing number of fixed-site imaging centers, primarily to hospitals or health systems. Our services normally include the use of our imaging systems, technologists to operate the systems, equipment maintenance and upgrades and management of day-to-day shared-service and fixed-site diagnostic imaging operations. We also provide non scan-based services, which includes only the use of our imaging systems under a short-term contract. We have also leveraged our leadership in MRI and PET/CT to expand into radiation oncology. Our radiation oncology business is operated through our wholly-owned subsidiary, Alliance Oncology, LLC ("AO"), and includes a wide range of services for cancer patients covering initial consultation, preparation for treatment, simulation of treatment, actual radiation oncology delivery, therapy management and follow-up care. Our services include the use of our linear accelerators, therapists to operate such systems, administrative staff, equipment maintenance and upgrades, and management of day-to-day operations. We also provide stereotactic radiation oncology services through our wholly-owned subsidiary, Alliance Radiosurgery, LLC.
MRI and PET/CT services generated 47% and 40% of our revenue, respectively, for the year ended December 31, 2009, 54% and 34% of our revenue, respectively, for the year ended December 31, 2008 and 60% and 31% of our revenue, respectively, for the year ended December 31, 2007. Our remaining revenue was comprised of radiation oncology revenue and other modality diagnostic imaging services revenue, primarily computed tomography ("CT") and management contract revenue. We had 507 diagnostic imaging and radiation oncology systems, including 295 MRI systems and 126 positron emission tomography ("PET") or PET/CT systems and served over 1,000 clients in 45 states at December 31, 2009. We operated 116 fixed-site imaging centers (three in unconsolidated joint ventures), which constitutes systems installed in hospitals or other medical buildings on or near hospital campuses, including modular buildings, systems installed inside medical groups' offices, and free-standing fixed-site imaging centers, which includes systems installed in a medical office building, ambulatory surgical center, or other retail space at December 31, 2009. Of the 116 fixed-site imaging centers, 91 were MRI fixed-site imaging centers, 16 were PET or PET/CT fixed-site imaging centers, six were other modality fixed-site imaging centers and three were in unconsolidated joint ventures. We also operated 25 radiation oncology centers and stereotactic radiosurgery facilities (including two radiation oncology centers in unconsolidated joint ventures) at December 31, 2009.
Approximately 80%, 79% and 89% of our revenues for the years ended December 31, 2009, 2008 and 2007, respectively, were generated by providing services to hospitals and other healthcare providers, which we refer to as wholesale revenues. Our wholesale revenues are typically generated from contracts that require our clients to pay us based on the number of scans we perform on patients on our clients' behalf, although some pay us a flat fee for a period of time regardless of the number of scans we perform. Wholesale payments are due to us independent of our clients' receipt of retail reimbursement from third-party payors, although receipt of reimbursement from third-party payors may affect demand for our services. We typically deliver our services for a set number of days per week through exclusive, long-term contracts with hospitals and other healthcare providers. The initial terms of these contracts average approximately three years in length for mobile services and approximately five to 10 years in length for fixed-site arrangements. These contracts often contain automatic renewal provisions and certain contracts have cancellation clauses if the hospital or other healthcare provider purchases their
43
own system. We price our contracts based on the type of system used, the scan volume, and the number of ancillary services provided. Pricing is also affected by competitive pressures.
Approximately 20%, 21% and 11% of our revenues for the years ended December 31, 2009, 2008 and 2007, respectively, were generated by providing services directly to patients from our sites located at or near hospitals or other healthcare provider facilities, which we refer to as retail revenue. Our revenue from these sites is generated from direct billings to patients or their third-party payors, including Medicare, which are recorded net of contractual discounts and other arrangements for providing services at discounted prices. We typically charge a higher price per scan under retail billing than we do under wholesale billing.
Fixed-site imaging centers and radiation oncology centers can be structured as either wholesale or retail arrangements. Our contracts for radiation oncology services average approximately 10 to 20 years in length. Revenues from these centers are included in either our wholesale or retail revenues.
For services for which we bill Medicare directly, we are paid under the Medicare Physician Fee Schedule, which is updated on an annual basis. Under the Medicare statutory formula, payments under the Physician Fee Schedule would have decreased for the past several years if Congress failed to intervene. For example, for 2008, the fee schedule rates were to be reduced by approximately 10.1%. The Medicare, Medicaid and SCHIP Extension Act of 2007 eliminated the 10.1% reduction for 2008 and increased the annual payment rate update by 0.5%. This increase to the annual Medicare Physician Fee Schedule payment update was effective only for Medicare claims with dates of service between January 1, 2008 and June 30, 2008. Beginning July 1, 2008, under the Medicare Improvement for Patients and Providers Act of 2008 ("MIPPA"), the 0.5% increase was continued for the rest of 2008. In addition, MIPPA established a 1.1% increase to the Medicare Physician Fee Schedule payment update for 2009. For 2010, the Centers for Medicare and Medicaid Services ("CMS") are projecting a rate reduction of 21.2% unless Congress intervenes again to avoid the payment reduction. On December 19, 2009, President Obama signed into law the Department of Defense Appropriations Act, 2010 (H.R. 3326) which includes a zero percent Medicare physician update through February 28, 2010. This was further extended through March 31, 2010 by the Temporary Extension Act of 2010, signed into law by President Obama on March 2, 2010. Currently pending in the Senate is the House of Representatives' Medicare Physician Payment Reform Act of 2009 (H.R. 3961), which would prevent the rate reduction by restructuring the formula that forms the basis of the Medicare Physician Fee Schedule payments. If Congress fails to intervene to prevent the 21.2% rate reduction, the resulting decrease in payment will adversely impact our revenues and results of operations.
MIPPA also modified the methodology by which the budget neutrality formula was applied to the 2009 physician fee schedule payment rates, resulting in an overall reduction in payment rates for services performed by many specialties, including an estimated 3% reduction for radiation oncology and 1% reduction for nuclear medicine. The impact of the payment rates on specific companies depends on their service mix. We estimated decreases in rates for our radiation oncology business, but cannot predict the full impact the rate reductions will have on our future revenues or business. Also with respect to MIPPA, the legislation requires all suppliers that provide the technical component of diagnostic MRI, PET/CT, CT, and nuclear medicine to be accredited by an accreditation organization designated by CMS by January 1, 2012. On January 26, 2010, CMS initially approved the following designated accreditation organizations to accredit suppliers furnishing the technical component of all advanced imaging modalities (CT, nuclear medicine, PET and MRI) on or after January 1, 2010: The American College of Radiology (ACR), the Intersocietal Accreditation Commission (IAC) and The Joint Commission. All our facilities are accredited by The Joint Commission.
A number of other legislative changes impact our retail business. For example, the Deficit Reduction Act of 2005 ("DRA") imposed caps on Medicare payment rates for certain imaging services furnished in physician's offices and other non-hospital based settings. The caps impact MRI, PET/CT
44
and certain imaging services performed in conjunction with radiation therapy, including certain image guided radiation therapy ("IGRT") services and diagnostic imaging services used to plan intensity modulated radiation therapy ("IMRT"). Under the cap, payments for specified imaging services cannot exceed the hospital outpatient payment rates for those services. This change applies to services furnished on or after January 1, 2007. The limitation is applicable to the technical components of the diagnostic imaging services only, which is the payment we receive for the services for which we bill directly under the Medicare Physician Fee Schedule. CMS issues on an annual basis the hospital outpatient prospective payment ("HOPPS") rates, which are used to develop the caps. If the technical component of the service established under the Physician Fee Schedule (without including geographic adjustments) exceeds the hospital outpatient payment amount for the service (also without including geographic adjustments), then the payment is to be reduced. In other words, in those instances where the technical component for the particular service is greater for the non-hospital site, the DRA directs that the hospital outpatient payment rate be substituted for the otherwise applicable Physician Fee Schedule payment rate. The implementation of this reimbursement reduction contained in the DRA had a significant effect on our financial condition and results of operations in 2007, whereas the changes in 2008 and 2009 have been limited.
The DRA also codified the reduction in reimbursement for multiple images on contiguous body parts, which was previously announced by CMS. The DRA mandated payment at 100% of the technical component of the higher priced imaging procedure and 50% for the technical component of each additional imaging procedure for multiple images of contiguous body parts within a family of codes performed in the same session. Initially, CMS announced that it would phase in this reimbursement reduction over a two-year period, to include a 25% reduction for each additional imaging procedure on contiguous body parts in 2006 and an additional 25% reduction in 2007. To date, CMS has not yet implemented the additional 25% reduction scheduled for 2007. Federal legislative proposals have been introduced that would change the percentage reduction from 25% to 50%. It is unclear what impact this change would have on our business if the proposal is passed.
Regulatory updates to payment rates for which we bill the Medicare program directly are published annually by CMS. For payments under the Physician Fee Schedule for calendar year 2010, CMS changed the way it calculates components of the Medicare Physician Fee Schedule. First, CMS reduced payment rates for certain diagnostic services using equipment costing more than $1 million through revisions to usage assumptions from the current 50% usage rate to a 90% usage rate. This change applied to MRI and CT scans, but not for radiation therapy and other therapeutic equipment. The OIG has stated that for 2010, it intends to focus on, among other things, the practice expense components, including the equipment utilization rate, for certain imaging services reimbursed under Medicare Physician Fee Schedule to determine whether Medicare payment reflects the actual expenses incurred and whether the utilization rate reflects current industry practices. Moreover, federal legislative proposals have been introduced that would result in lower usage assumptions and, if finalized, would supersede CMS's regulatory changes.
Further with respect to its 2010 changes, CMS also reduced payment for services primarily involving the technical component rather than the physician work component, including the services we provide, by adjusting downward malpractice payments for these services. The reductions primarily impact radiology and other diagnostic tests. All these changes to the Medicare Fee Schedule will be transitioned over a four year period such that beginning in 2013, CMS will fully implement the revised payment rates. CMS projects that the combined impact of these changes, when fully implemented will result in an estimated 5% reduction in radiation oncology, 16% reduction in radiology, 23% reduction in nuclear medicine and 34% reduction for all suppliers providing diagnostic tests generally. For the 2010 transitioned payment, CMS estimates the impact of its changes will result in a 1% reduction in radiation oncology, 5% reduction in radiology, 18% reduction in nuclear medicine and 12% reduction for all suppliers providing the technical component of diagnostic tests generally. These impacts are
45
calculated prior to any application of the projected negative update factor of 21.2% related to MIPPA (which may be implemented in April 2010 unless Congress intervenes) and may impact our future revenues. If the CMS 2010 reimbursement rates had been in effect for full year 2009, we estimate that our annualized retail revenue related to MRI and radiation oncology would not have been materially impacted.
In addition to annual updates to the Medicare Physician Fee Schedule, as indicated above, CMS also publishes regulatory changes to the HOPPS on an annual basis. These payments are the amounts received by our hospital clients for hospital outpatient services. For 2008, the national Medicare HOPPS payment rate for nonmyocardial PET and PET/CT scans was $1,057 per scan and the national payment rate for myocardial PET scans was $1,400 per scan. Effective January 1, 2008, CMS also bundled the PET and PET/CT payment for radiopharmaceuticals with the payment for the PET and PET/CT scan. In addition, CMS reduced the 2008 national Medicare HOPPS rate for MRI scans by approximately 3%. The 2008 national Medicare HOPPS payment rates for stereotactic radiosurgery treatment delivery services ranged from $1,057 to $8,055, depending on the level of service. For 2009, the payment rate for nonmyocardial PET and PET/CT scans is $1,037 per scan. For myocardial PET procedures, the 2009 payment rate is $1,157 per scan. For stereotactic radiosurgery treatment delivery services, the 2009 payment rates range from $952 to $7,642, depending on the level of service. On October 30, 2009, CMS released its 2010 national Medicare HOPPS payment rates, which went into effect January 1, 2010. For nonmyocardial PET and PET/CT, the 2010 payment rate is $1,037 per scan. For myocardial PET procedures, the 2010 payment rate is $1,433 per scan. For stereotactic radiosurgery treatment delivery services, the 2010 payment rates range from $963 to $7,344, depending on the level of service.
Combined, the DRA and PET and PET/CT Medicare HOPPS rate reductions negatively impacted our 2007 revenue by a total of approximately $14 million. For 2008 and 2009, however, the DRA and the net Medicare rate reductions in HOPPS did not have a material negative effect on revenue and earnings. At this time, however, we cannot predict the impact the rate reductions will have on our future revenues or business.
Furthermore, with respect to the final Medicare Physician Fee Schedule Rule for calendar year 2009, CMS announced additional performance standards for suppliers of mobile diagnostic services. The final rule requires suppliers of mobile diagnostic services under certain circumstances to enroll in Medicare and bill directly for these services, regardless of where they are performed. An exception was made for services provided to hospital patients under arrangement with that hospital. In those circumstances, the mobile diagnostic facility would be required to enroll in Medicare, but the hospital would bill for the services. On December 15, 2008, CMS issued additional guidance that companies that lease or contract with a Medicare-enrolled provider or supplier to provide only diagnostic testing equipment and/or non-physician personnel are not required to enroll in Medicare. The agency nonetheless indicated that it is continuing to evaluate such arrangements. The new policies have not significantly impacted our business.
Over the past few years, the growth rate of MRI industry wide scan volumes has slowed in part due to weak hospital volumes as reported by several investor-owned hospital companies, a growing number of medical groups adding imaging capacity within their practice setting and additional patient-related cost-sharing programs. In addition, there is an increasing trend of third-party payors intensifying their utilization management efforts, for example through benefit managers who require preauthorizations, to control the growth rate of imaging services generally. We expect that these trends will continue throughout 2010. Further, a number of payment initiatives are being proposed in the imaging area. President Obama's budget for fiscal year 2010 includes provisions that may require the use of radiology benefit managers to preauthorize certain imaging services for Medicare enrollees. Moreover, healthcare reform under the current administration is a priority. If laws are passed, certain changes could become effective as early as 2010. In addition to the House of Representatives'
46
Affordable Health Care for America Act (H.R. 3962), the Senate's Patient Protection and Affordable Care Act (H.R. 3590) would substantially change the way health care is financed by both governmental and private insurers and may negatively impact payment rates for certain imaging services. Also, on February 22, 2010, President Obama released a third health care reform proposal, which is currently being considered by Congress. At this time, we cannot predict which of the proposals, if any, will be adopted or if adopted, what effect, if any, these or any other proposals would have on our future revenues or business.
We have experienced and continue to experience an increase in the competitive climate in the MRI industry, resulting in an increase in activity by original equipment manufacturers, or OEMs, selling systems directly to certain of our clients. Typically, OEMs target our higher scan volume clients. This increase in activity by OEMs has resulted in overcapacity of systems in the marketplace. This has caused an increase in the number of our higher scan volume clients deciding not to renew their contracts. We replace these higher volume clients typically with lower volume clients. Our non-scan based MRI business has been impacted by a decline in the number of hospital construction projects, driven by a decrease in new MRI systems being added by hospitals in their facilities and a decrease in the number of equipment upgrades occurring in the hospital market. Our MRI revenues decreased in 2009 compared to 2008 due to the factors described above, and we believe that MRI revenues will continue to decline in future years.
Recent global market and economic conditions have been unprecedented and challenging with tighter credit conditions and recession in most major economies continuing into 2010. Continued concerns about the systemic impact of potential long-term and wide-spread recession, inflation, energy costs, geopolitical issues, the availability and cost of credit, the United States mortgage market and a declining real estate market in the United States have contributed to increased market volatility and diminished expectations for the United States economy. Added concerns fueled by the United States government financial assistance to certain companies and other federal government's interventions in the United States financial system has led to increased market uncertainty and instability in both United States and international capital and credit markets. These conditions, combined with volatile oil prices, declining business and consumer confidence, increased unemployment, increased tax rates and governmental budget deficits and debt levels have contributed to volatility of unprecedented levels. We believe our MRI and PET/CT scan volumes have been impacted during 2009 and will continue to be impacted in 2010 by rising unemployment rates, the number of under-insured or uninsured patients and other conditions arising from the global economic conditions described above. At this time, it is unclear what impact this might have on our future revenues or business.
As a result of these market conditions, the cost and availability of credit has been and may continue to be adversely affected by illiquid credit markets and wider credit spreads. Concern about the stability of the markets generally and the strength of counterparties specifically has led many lenders and institutional investors to reduce, and in some cases, cease to provide funding to borrowers. Continued turbulence in the United States and international markets and economies may adversely affect our liquidity and financial condition, and the liquidity and financial condition of our customers. If these market conditions continue, they may limit our ability to timely access the capital markets to meet liquidity needs, resulting in adverse effects on our financial condition and results of operations.
The principal components of our cost of revenues are compensation paid to technologists and drivers, system maintenance costs, medical supplies, system transportation and technologists' travel costs. Because a majority of these expenses are fixed, increased revenues as a result of higher scan volumes per system significantly improves our margins while lower scan volumes result in lower margins.
The principal components of selling, general and administrative expenses are sales and marketing costs, corporate overhead costs, provision for doubtful accounts, and share-based payment.
We record noncontrolling interest and earnings from unconsolidated investees related to our consolidated and unconsolidated subsidiaries, respectively. These subsidiaries primarily provide shared-service and fixed-site diagnostic imaging and therapeutic services.
47
We experience seasonality in the revenues and margins generated for our services. First and fourth quarter revenues are typically lower than those from the second and third quarters. First quarter revenue is affected primarily by fewer calendar days and inclement weather, typically resulting in fewer patients being scanned during the period. Fourth quarter revenues are affected by holiday and client and patient vacation schedules, resulting in fewer scans during the period. The variability in margins is higher than the variability in revenues due to the fixed nature of our costs. The Company also experiences fluctuations in the revenues and margins generated due to acquisition activity and general economic conditions, including recession or economic slowdown.
Kohlberg Kravis Roberts & Co Acquisition and Disposition
On November 2, 1999, Viewer Holdings L.L.C., an affiliate of Kohlberg Kravis Roberts & Co ("KKR"), acquired approximately 92% of Alliance in a recapitalization merger. Viewer is owned by two investment funds sponsored by KKR. The KKR acquisition consisted of a recapitalization merger in 1999 in which a wholly-owned subsidiary of Viewer was merged with and into Alliance. Upon the consummation of the KKR acquisition, Viewer owned approximately 92% of Alliance.
On November 27, 2006, affiliates of KKR sold 9.2 million shares of our common stock in an underwritten secondary public offering. Following completion of the offering, KKR beneficially owned approximately 52% of our outstanding shares of common stock. We did not sell any shares and did not receive any proceeds from the sale of shares in the public offering.
On April 16, 2007, funds managed by Oaktree Capital Management, LLC ("Oaktree") and MTS Health Investors, LLC ("MTS") purchased approximately 24.5 million shares of our common stock from KKR. Upon completion of the transaction, Oaktree and MTS owned in the aggregate approximately 49.7% of the outstanding shares of our common stock. Subsequently, KKR sold its remaining shares on the open market. At December 31, 2009, Oaktree and MTS owned in the aggregate approximately 47.1% of the outstanding shares of common stock of the Company.
Recent Transactions
Effective October 1, 2007, we purchased the assets of Diagnostic Radiology Systems, Inc., a mobile provider of MRI and PET/CT, with operations in a certificate of need state. The purchase price consisted of $8.6 million in cash and transaction costs. The acquisition was financed using internally generated funds. As a result of this acquisition, we recorded goodwill of $2.1 million and acquired intangible assets of $2.2 million, of which $1.5 million was assigned to customer contracts, which is amortized over eight years, $0.5 million was assigned to the non-compete agreement, which was amortized over one year, and $0.2 million was assigned to certificates of needs, which have indefinite useful lives and are not subject to amortization. The intangible assets were recorded at fair value at the acquisition date. All recorded goodwill and intangible assets are capitalized for tax purposes and amortized over 15 years. The preliminary values above were subject to adjustment for up to one year after the close of the transaction due to additional information that could result in changes in the original valuation of assets acquired and liabilities assumed. During the year ended December 31, 2008, the adjustments to goodwill as a result of changes in the original valuation of assets acquired and liabilities assumed were not material. The year ended December 31, 2007 included three months of operations from this acquisition. We have not included pro forma information as this acquisition did not have a material impact on our consolidated financial position or results of operations.
Effective November 2, 2007, we purchased the assets of eight radiation oncology centers in Alabama, Arkansas, Mississippi, and Missouri from Bethesda Resources, Inc., a wholly-owned subsidiary of Sonix, Inc. ("the Bethesda transaction"). Many of these centers are sole community providers and are located on or near hospital campuses. Several of these radiation oncology centers
48
operate under certificates of need. The purchase price consisted of $36.5 million in cash and $0.8 million in assumed liabilities and transaction costs. The acquisition was financed using internally generated funds and capital leases. As a result of this acquisition, we recorded goodwill of $4.2 million and acquired intangible assets of $31.2 million, of which $2.2 million was assigned to the physician referral network, which is amortized over seven years and $29.0 million was assigned to certificates of need, which have indefinite useful lives and are not subject to amortization. The intangible assets were recorded at fair value at the acquisition date. All recorded goodwill and intangible assets are capitalized for tax purposes and amortized over 15 years. During the year ended December 31, 2008, we decreased goodwill by $0.1 million as a result of changes in the original valuation of assets acquired and liabilities assumed. The year ended December 31, 2007 included approximately two months of operations from this acquisition. We have not included pro forma information as this acquisition did not have a material impact on our consolidated financial position or results of operations.
Effective November 5, 2007, we purchased all of the outstanding shares of the New England Health Enterprises Business Trust and all of the outstanding membership interests of New England Imaging Management, LLC, a fixed-site provider of MRI and CT, collectively referred to as New England Health Enterprises, or NEHE. NEHE operated seven fixed-site imaging centers and one mobile MRI system in Maine and Massachusetts. The purchase price consisted of $44.6 million in cash, $2.3 million in cash which is being held in an escrow account, and $4.6 million in assumed liabilities and transaction costs. The acquisition was financed using internally generated funds, borrowings under an Acquisition Credit Facility and capital leases. We recorded total goodwill of $19.3 million, which includes $10.9 million of goodwill related to deferred tax liabilities recorded for basis differences in intangible assets as a result of the acquisition. None of the goodwill recorded is deductible for tax purposes. We acquired intangible assets of $29.0 million, of which $15.7 million was assigned to the physician referral network, which is amortized over 15 years, $3.8 million was assigned to the non-compete agreement, which is amortized over five years, and $9.5 million was assigned to certificates of need held by NEHE, which have indefinite useful lives and are not subject to amortization. These assets were recorded at fair value at the acquisition date. At the date of acquisition, the acquisition included $2.3 million for a contingent payment which was being held in an escrow account, pending the resolution of claims for indemnification and contingent consideration based on certain performance target requirements, which were resolved over the one to three years following the acquisition date. During the year ended December 31, 2009, these contingencies were resolved and we recorded a decrease to goodwill of $0.6 million. We received $2.9 million from escrow during 2009. All contingencies have been resolved and all escrow amounts have been distributed as of December 31, 2009. The year ended December 31, 2007 included approximately two months of operations from this acquisition. We have not included pro forma information as this acquisition did not have a material impact on our consolidated financial position or results of operations.
On December 4, 2007, we issued an additional $150 million of our 71/4% Senior Subordinated Notes due 2012 (the "new 71/4% Notes") in a transaction exempt from the registration requirements of the Securities Act of 1933, as amended. The new 71/4% Notes were issued at a discount of 8.5%, which was being amortized to interest expense through the maturity date of the notes. The new 71/4% Notes have terms that were substantially identical to our original 71/4% Notes, but were issued under a new indenture and are therefore a separate series of notes. We used a portion of the net proceeds from the issuance of the new 71/4% Notes to repay and terminate an Acquisition Credit Facility entered into to finance the NEHE acquisition (as described in Note 9 of the Notes to Consolidated Financial Statements for the year ended December 31, 2008). The remaining net proceeds were used for general corporate purposes, including acquisitions. The 71/4% Notes were substantially redeemed in December 2009, in conjunction with our Refinance Transaction, as discussed below. At December 31, 2009, $5.6 million of the 71/4% Notes were outstanding. The remaining balance of the 71/4% Notes was redeemed at par in January 2010.
49
In the first quarter of 2008, we purchased six CyberKnife® robotic radiosurgery facilities from Accuray, Inc ("the CyberKnife transaction"). The radiosurgery systems are currently providing radiosurgery services at hospitals located in California, Maryland, New Jersey and Tennessee. The purchase price totaled $10.3 million in cash and $0.7 million in transaction costs. The acquisition was financed using proceeds from the issuance of the new 71/4% Notes in December 2007. As a result of this acquisition, we recorded acquired intangible assets of $1.5 million, which was assigned to customer contracts and will be amortized over seven years. The intangible assets were recorded at fair value at the acquisition date. All recorded intangible assets are capitalized for tax purposes and amortized over 15 years. The year ended December 31, 2008 included approximately nine months of operations from this acquisition. We have not included pro forma information as this acquisition did not have a material impact on our consolidated financial position or results of operations.
In the third quarter of 2008, we purchased all of the outstanding membership interests of Medical Outsourcing Services, LLC ("MOS"), a mobile provider of PET/CT, based in Naperville, Illinois. MOS currently operates in nine states, including, Illinois, Indiana, Iowa, Michigan, Missouri, New Jersey, Ohio, Pennsylvania, and Wisconsin. The purchase price consisted of $17.3 million in cash, $2.5 million in cash which is being held in an escrow account, and $4.6 million in assumed liabilities and transaction costs. We financed this acquisition using internally generated funds and proceeds from the issuance of the new 71/4% Notes in December 2007. As a result of this acquisition, we recorded goodwill of $3.3 million and acquired intangible assets of $12.5 million, of which $3.9 million was assigned to the physician referral network, which is amortized over five years, $6.1 million was assigned to customer relationships, which is amortized over 10 years and $2.5 million was assigned to a non-compete agreement, which is amortized over three years. The intangible assets were recorded at fair value at the acquisition date. All recorded goodwill and intangible assets are capitalized for tax purposes and amortized over 15 years. The acquisition included $2.5 million for a contingent payment which is being held in an escrow account, pending the resolution of claims for indemnification, which is expected to be resolved over the three years following the acquisition date. When the contingencies are resolved and consideration is distributable from the escrow account, we will record the fair value of the consideration as additional purchase price to goodwill. During the year ended December 31, 2009, we increased goodwill by $0.1 million as a result of changes in the original valuation of assets acquired and liabilities assumed. The year ended December 31, 2008 included six months of operations from this acquisition. We have not included pro forma information as this acquisition did not have a material impact on our consolidated financial position or results of operations. Please also see further discussion in Note 12 of the Notes to the Consolidated Financial Statements.
In the third quarter of 2008, we purchased all of the outstanding membership interests of RAMIC Des Moines, LLC ("RAMIC"), a single modality center providing MRI services in West Des Moines, Iowa. The purchase price consisted of $7.2 million in cash, $0.6 million in cash which is being held in an escrow account, and $0.1 million in assumed liabilities and transaction costs. We financed this acquisition using internally generated funds and proceeds from the issuance of the new 71/4% Notes in December 2007. As a result of this acquisition, we recorded goodwill of $2.9 million and acquired intangible assets of $2.6 million, of which $1.8 million was assigned to the physician referral network, which is amortized over five years and $0.8 million was assigned to certificates of need held by RAMIC, which have indefinite useful lives and are not subject to amortization. The intangible assets were recorded at fair value at the acquisition date. All recorded goodwill and intangible assets are capitalized for tax purposes and amortized over 15 years. The acquisition included $0.6 million for a contingent payment which was being held in an escrow account, pending the resolution of claims for indemnification. All contingencies have been resolved and all escrow amounts have been distributed as of December 31, 2009. During the year ended December 31, 2009, $0.6 million was released from escrow, which was recorded to goodwill as additional purchase price. The year ended December 31, 2008 included approximately five months of operations from this acquisition. We have not included pro
50
forma information as this acquisition did not have a material impact on our consolidated financial position or results of operations.
In the fourth quarter of 2008, we purchased all of the outstanding membership interests of Shared PET Imaging, LLC ("SPI"), a mobile and fixed-site provider of PET and PET/CT, based in Canton, Ohio. SPI serves approximately 90 clients in thirteen states, including Ohio, Michigan, Indiana, Illinois, Florida, Pennsylvania, New York, Tennessee and South Carolina. The purchase price consisted of $34.1 million in cash, $2.0 million in cash which is being held in an escrow account, and $9.1 million in assumed liabilities and transaction costs. We financed this acquisition using internally generated funds and proceeds from the issuance of the new 71/4% Notes in December 2007. As a result of this acquisition, we recorded goodwill of $6.9 million and acquired intangible assets of $9.4 million, of which $0.5 million was assigned to the physician referral network, which is amortized over five years, $5.4 million was assigned to customer relationships, which is amortized over 13 years, $3.2 million was assigned to a non-compete agreement, which is amortized over three years, and $0.3 million was assigned to certificates of need held by SPI, which have indefinite useful lives and are not subject to amortization. The intangible assets were recorded at fair value at the acquisition date. All recorded goodwill and intangible assets are capitalized for tax purposes and amortized over 15 years. The acquisition included $2.0 million for a contingent payment which is being held in an escrow account, pending the resolution of claims for indemnification, which will be resolved over the 18 months following the acquisition date. When the contingencies are resolved and consideration is distributable from the escrow account, we will record the fair value of the consideration as additional purchase price to goodwill. During the year ended December 31, 2009, we increased goodwill by $0.4 million as a result of changes in the original valuation of assets acquired and liabilities assumed. The year ended December 31, 2008 included one month of operations from this acquisition. We have not included pro forma information as this acquisition did not have a material impact on our consolidated financial position or results of operations.
Also in the fourth quarter of 2008, we purchased the remaining 20% minority interest in AO. The total purchase price was $6.5 million, which consisted entirely of cash. We financed this acquisition using internally generated funds. As a result of this acquisition, we recorded goodwill of $4.5 million. All recorded goodwill is capitalized for tax purposes and amortized over 15 years.
During December 2009, we entered into and completed various debt related transactions in order to expand our borrowing capacity and extend the maturity of our debt (the "Refinance Transaction"). In order to accomplish this, we retired substantially all of our $300.0 million 71/4% senior subordinated notes due 2012 (the "71/4% Notes") through a cash tender offer (the "Tender Offer") and repaid the balance of $351.6 million on our existing Tranche C1 term loan facility (the "Old Term Loan"). In conjunction with the Refinance Transaction we also entered into a new senior secured credit agreement (the "New Credit Facility"), comprised of a $460.0 million term loan (the "New Term Loan") maturing June 2016 and a $120.0 million revolving facility (the "New Revolving Credit Facility") maturing December 2014. Borrowings under the New Term Loan were issued at 98.0% of par, with the discount to par being amortized to interest expense and other, net through the maturity date of the loan. We also issued $190.0 million of 8% senior notes due 2016 (the "8% Notes") in a transaction that was exempt from the registration requirements of the Securities Act of 1933, as amended. The 8% Notes were issued at 98.69% of par, with the discount to par being amortized to interest expense and other, net through the maturity date of the notes. Borrowings under the New Credit Facility bear interest through maturity at a variable rate based upon, at our option, either London InterBank Offered Rate ("LIBOR") or the base rate (which is the highest of the administrative agent's prime rate, one-half of 1.00% in excess of the overnight federal funds rate, and 1.00% in excess of the one-month LIBOR rate), plus in each case, an applicable margin. With respect to the New Term Loan, the applicable margin for LIBOR loans is 3.50% per annum, and with respect to the New Revolving Credit Facility, the applicable margin for LIBOR loans ranges, based on the applicable leverage ratio, from 3.25% to
51
3.75% per annum, in each case, with a LIBOR floor of 2.00%. With respect to the New Term Loan, the applicable margin for base rate loans is 2.50% per annum, and with respect to the New Revolving Credit Facility, the applicable margin for base rate loans ranges, based on the applicable leverage ratio, from 2.25% to 2.75% per annum. We used the proceeds from these transactions and existing cash to complete the Tender Offer and purchase $294.4 million of the 71/4% Notes at a purchase price equal to 100.125% of the principal amount, together with the accrued interest to the purchase date. We also used the proceeds from these transactions to pay off the Old Term Loan and redeem the remaining $5.6 million of 71/4% notes in January 2010 at a redemption price equal to 100.0% of the principal amount, together with accrued interest to the redemption date. We incurred a loss on extinguishment of debt of $14.6 million related to the Refinance Transaction, which represents the tender premium and consent payment to redeem the 71/4% Notes, write-off of unamortized debt issuance costs related to the retired debt, and other fees and expenses.
Results of Operations
The table below shows the components in our consolidated statements of operations as a percentage of revenues:
| |
Year Ended December 31, | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| |
2007 | 2008 | 2009 | ||||||||
Revenues |
100.0 | % | 100.0 | % | 100.0 | % | |||||
Costs and expenses: |
|||||||||||
Cost of revenues, excluding depreciation and amortization |
52.9 | 52.8 | 53.5 | ||||||||
Selling, general and administrative expenses |
12.8 | 12.6 | 13.4 | ||||||||
Transaction costs |
— | — | 0.2 | ||||||||
Severance and related costs |
0.1 | 0.1 | 0.2 | ||||||||
Depreciation expense |
18.6 | 17.7 | 18.7 | ||||||||
Amortization expense |
1.2 | 1.7 | 2.2 | ||||||||
Interest expense and other, net |
9.5 | 9.8 | 9.1 | ||||||||
Loss on extinguishment of debt |
— | 0.1 | 2.9 | ||||||||
Other (income) and expense, net |
(0.1 | ) | (0.2 | ) | (0.2 | ) | |||||
Total costs and expenses |
95.0 | 94.6 | 100.0 | ||||||||
Income before income taxes, earnings from unconsolidated |
|||||||||||
investees and noncontrolling interest, net of tax |
5.0 | 5.4 | — | ||||||||
Income tax expense |
2.6 | 2.4 | 0.1 | ||||||||
Earnings from unconsolidated investees |
(1.7 | ) | (0.9 | ) | (0.8 | ) | |||||
Net income |
4.1 | 3.9 | 0.7 | ||||||||
Less: Net income attributable to noncontrolling interest, net of tax |
(0.4 | ) | (0.6 | ) | (0.6 | ) | |||||
Net income attributable to Alliance HealthCare Services, Inc. |
3.7 | % | 3.3 | % | 0.1 | % | |||||
As noted previously, we have seen a continued decrease in our scan-based MRI revenues and we believe that scan-based MRI revenues from our shared- service operations will continue to decline in
52
future years. The table below provides MRI statistical information for each of the years ended December 31:
| |
2007 | 2008 | 2009 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
MRI statistics |
|||||||||||
Average number of total systems |
307.9 | 303.7 | 280.1 | ||||||||
Average number of scan-based systems |
252.8 | 254.1 | 241.0 | ||||||||
Scans per system per day (scan-based systems) |
9.29 | 9.18 | 8.82 | ||||||||
Total number of scan-based MRI scans |
645,711 | 630,875 | 567,624 | ||||||||
Price per scan |
$ | 364.78 | $ | 380.54 | $ | 383.58 | |||||
Over the past three years we have seen an increase in PET and PET/CT revenues. The table below provides PET and PET/CT revenue statistical information for each of the years ended December 31:
| |
2007 | 2008 | 2009 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
PET and PET/CT statistics |
|||||||||||
Average number of systems |
72.3 | 86.8 | 116.2 | ||||||||
Scans per system per day |
6.30 | 6.13 | 5.97 | ||||||||
Total number of PET and PET/CT scans |
115,870 | 141,513 | 180,824 | ||||||||
Price per scan |
$ | 1,195 | $ | 1,178 | $ | 1,098 | |||||
Following are the components of revenue (in millions) for each of the years ended December 31:
| |
2007 | 2008 | 2009 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
Total MRI revenue |
$ | 265.3 | $ | 269.4 | $ | 238.5 | ||||
PET/CT revenue |
139.7 | 167.7 | 201.5 | |||||||
Radiation oncology, other modalities and other revenue |
39.9 | 58.7 | 65.5 | |||||||
Total |
$ | 444.9 | $ | 495.8 | $ | 505.5 | ||||
| |
Year Ended December 31, |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| |
2007 | 2008 | 2009 | |||||||
Total fixed-site imaging center revenue (in millions) |
$ | 78.1 | $ | 102.7 | $ | 113.1 | ||||
Year Ended December 31, 2009 Compared to Year Ended December 31, 2008
Revenue increased $9.7 million, or 2.0%, to $505.5 million in 2009 compared to $495.8 million in 2008 due to an increase in PET/CT revenues, radiation oncology, other modalities and other revenue, partially offset by a decrease in MRI revenues. PET/CT revenue in 2009 increased $33.8 million, or 20.2%, compared to 2008. Total PET and PET/CT scan volumes increased 27.8% to 180,824 scans in 2009 from 141,513 scans in 2008, primarily as a result of the acquisition of SPI in the fourth quarter of 2008, the acquisition of MOS in the third quarter of 2008 and growth in our core PET business. The average number of PET and PET/CT systems in service increased to 116.2 systems in 2009 from 86.8 systems in 2008. These PET and PET/CT increases were partially offset by a 6.8% decline in the average price per PET and PET/CT scan, to $1,098 per scan in 2009 compared to $1,178 per scan in 2008. The decline in the average price per PET and PET/CT scan was primarily related to the SPI acquisition, which was largely wholesale in nature and had a lower average price per scan on acquired customer contracts, as well as normal levels of pricing pressure from our wholesale customers. Scans per system per day also decreased 2.6%, to 5.97 scans per system per day in 2009 from 6.13 scans per system per day in 2008. Radiation oncology, other modalities and other revenue increased $6.8 million,
53
or 11.3%, to $65.5 million in 2009 compared to $58.7 million in 2008 primarily due to an increase in the number of radiation oncology centers on operation. MRI revenue decreased $30.9 million in 2009, or 11.4%. Scan-based MRI revenue decreased $22.4 million in 2009, or 9.3%, to $217.7 million in 2009 from $240.1 million in 2008. Scan-based MRI scan volume decreased 10.0% to 567,624 scans in 2009 from 630,875 scans in 2008, primarily due to a decrease in client demand. Scan-based systems in service decreased to 241.0 systems in 2009 from 251.4 systems in 2008. Average scans per system per day also decreased by 3.9% to 8.82 in 2009 from 9.18 in 2008. These decreases were partially offset by an increase in the average price per MRI scan. The average price per MRI scan increased to $383.58 per scan in 2009 from $380.54 per scan in 2008. Non-scan based MRI revenue decreased $8.5 million in 2009 compared to 2008 primarily due to a decline in the number of hospital construction projects and a decrease in the number of equipment upgrades occurring in the hospital market, both of which impact the demand for our non-scan based MRI business. Included in the revenue totals above is fixed-site imaging center revenues, which increased $10.4 million, or 10.1%, to $113.1 million in 2009 from $102.7 million in 2008.
We had 295 MRI systems at December 31, 2009 compared to 301 MRI systems at December 31, 2008. We had 126 PET and PET/CT systems at December 31, 2009 compared to 114 PET and PET/CT systems at December 31, 2008. We operated 116 fixed site imaging centers (including three in unconsolidated joint ventures) at December 31, 2009, compared to 105 fixed site imaging centers (including four in unconsolidated joint ventures) at December 31, 2008. We operated 25 radiation oncology centers (including two in unconsolidated joint ventures) at December 31, 2009, compared to 21 radiation oncology centers (including two in unconsolidated joint ventures) at December 31, 2008.
Cost of revenues, excluding depreciation and amortization, increased $8.6 million, or 3.3%, to $270.4 million in 2009 compared to $261.8 million in 2008. Medical supplies increased $5.8 million, or 24.6%, primarily as a result of an increase in the number of PET and PET/CT scans, which use a radiopharmaceutical as a component of the PET and PET/CT scan. Maintenance and related costs increased $5.7 million, or 10.6%, due to an increase in service costs related to an increase in the number of PET/CT systems in operation and the addition of radiation oncology systems. Compensation and related employee expenses increased $2.2 million, or 1.8%, primarily as a result of an increase in average headcount related to acquisitions completed in the second half of 2008. Fuel expenses decreased $2.7 million, or 34.0%, primarily due to a decrease in the average price per gallon of diesel fuel costs. Equipment rental costs decreased $2.2 million, or 43.8%, primarily due to a lower number of rental systems in use to support current clients as a result of improved system utilization. All other cost of revenues, excluding depreciation and amortization, decreased $0.2 million, or 0.7%. Cost of revenues, as a percentage of revenue, increased to 53.5% in 2009 from 52.8% in 2008 as a result of the factors described above.
Selling, general and administrative expenses increased $4.9 million, or 7.7%, to $67.6 million in 2009 compared to $62.7 million in 2008. Compensation and related employee expenses increased $4.2 million, or 11.7%, as a result investments in the infrastructure of the oncology division and an increase in average headcount related to acquisitions completed in the second half of 2008. Office expenses increased $0.8 million, or 14.6%, due to an increase in information technology expenses and other office expenses. Professional services expenses increased $0.8 million, or 9.4%, due to an increase in legal and other professional fees. Share-based payment increased $0.7 million, or 14.0%, due to new equity awards granted in 2009. The provision for doubtful accounts decreased $1.9 million, or 44.3%, primarily due to the collections of aged wholesale receivables and a reduction in bad debt related to our retail receivables. The provision for doubtful accounts, as a percentage of revenue, was 0.5% of revenue in 2009 compared to 0.9% in 2008. All other selling, general and administrative expenses increased $0.3 million, or 6.5%. Selling, general and administrative expenses as a percentage of revenue were 13.4% and 12.7% in 2009 and 2008, respectively.
Transaction costs were $0.9 million due to acquisition-related costs, which are now required to be expensed.
54
We recorded severance and related costs of $1.4 million in 2009 compared to $0.6 million in 2008.
Depreciation expense increased $7.2 million, or 8.2%, to $94.9 million in 2009 compared to $87.7 million in 2008 as a result of fixed assets acquired in connection with our acquisitions in the second half of 2008.
Amortization expense increased by $2.3 million, or 26.5%, to $11.0 million in 2009 compared to $8.7 million in 2008, primarily due to the incremental amortization expense for intangible assets acquired in conjunction with our acquisitions in the second half of 2008.
Interest expense and other, net, decreased $2.5 million, or 5.2%, to $45.9 million in 2009 compared to $48.4 million in 2008. This decrease was primarily due to lower average rates on our credit facility.
We recorded a loss on extinguishment of debt of $14.6 million in 2009 related to the Refinance Transaction, compared to $0.1 million in 2008.
Income tax expense was $0.3 million and $11.8 million in 2009 and 2008, respectively, resulting in effective tax rates of 39.0% and 41.6% in 2009 and 2008, respectively. Our effective tax rates were higher than the federal statutory rates principally as a result of various permanent non-deductible tax items, including share-based payments, unrecognized tax benefits and other permanent differences.
Earnings from unconsolidated investees decreased by $0.8 million, or 16.8%, to $3.8 million in 2009 compared to $4.6 million in 2008 due to a decrease in earnings from our unconsolidated investees.
Net income attributable to noncontrolling interest increased $0.1 million, or 1.1%, to $3.1 million in 2009 compared to $3.0 million in 2008, due to an increase in earnings from our consolidated subsidiaries.
Net income attributable to Alliance HealthCare Services, Inc. was $0.5 million, or $0.01 per share on a diluted basis, in 2009 compared to $16.5 million, or $0.32 per share on a diluted basis, in 2008.
Year Ended December 31, 2008 Compared to Year Ended December 31, 2007
Revenue increased $50.9 million, or 11.4%, to $495.8 million in 2008 compared to $444.9 million in 2007 due to an increase in PET/CT revenues, radiation oncology, other modalities and other revenue, and MRI revenues. PET/CT revenue in 2008 increased $28.0 million, or 20.0%, compared to 2007. Total PET and PET/CT scan volumes increased 22.1% to 141,513 scans in 2008 from 115,870 scans in 2007, primarily as a result of the acquisition of MOS in the third quarter of 2008, growth in our core PET business, and the acquisition of SPI in the fourth quarter of 2008. The average number of PET and PET/CT systems in service increased to 86.8 systems in 2008 from 72.3 systems in 2007. These PET and PET/CT increases were partially offset by a 1.4% decline in the average price per PET and PET/CT scan, to $1,178 per scan in 2008 compared to $1,195 per scan in 2007. Scans per system per day also decreased 2.7%, to 6.13 scans per system per day in 2008 from 6.30 scans per system per day in 2007. Radiation oncology, other modalities and other revenue increased $18.8 million, or 47.1%, to $58.7 million in 2008 compared to $39.9 million in 2007 primarily due to an increase in radiation oncology revenue generated by the Bethesda transaction and the CyberKnife transaction. MRI revenue increased $4.1 million in 2008, or 1.5%. Scan-based MRI revenue increased $4.5 million in 2008, or 1.9%, to $240.1 million in 2008 from $235.6 million in 2007. This increase is primarily a result of the acquisition of NEHE, which generates retail revenue, which resulted in an increase in the average price per MRI scan from $380.54 per scan in 2008 compared to $364.78 per scan in 2007. Scan-based systems in service increased to 254.1 systems in 2008 from 252.8 systems in 2007. These increases were partially offset by a 2.3% decrease in our scan-based MRI scan volume. Scan-based MRI scan volume decreased to 630,875 scans in 2008 from 645,711 scans in 2007, primarily due to a decrease in client demand. Average scans per system per day also decreased by 1.2% to 9.18 in 2008 from 9.29 in 2007. Non-scan
55
based MRI revenue decreased $0.4 million in 2008 compared to 2007. Included in the revenue totals above is fixed-site imaging center revenues, which increased $24.6 million, or 31.5%, to $102.7 million in 2008 from $78.1 million in 2007.
We had 301 MRI systems at December 31, 2008 compared to 310 MRI systems at December 31, 2007. We had 114 PET and PET/CT systems at December 31, 2008 compared to 79 PET and PET/CT systems at December 31, 2007. We operated 105 fixed site imaging centers (including four in unconsolidated joint ventures) at December 31, 2008, compared to 88 fixed site imaging centers (including five in unconsolidated joint ventures) at December 31, 2007. We operated 21 radiation oncology centers (including two in unconsolidated joint ventures), compared to 12 radiation oncology centers (including two in unconsolidated joint ventures) at December 31, 2007.
Cost of revenues, excluding depreciation and amortization, increased $26.3 million, or 11.2%, to $261.8 million in 2008 compared to $235.5 million in 2007. Compensation and related employee expenses increased $10.6 million, or 9.4%, primarily as a result of an increase in average headcount related to acquisitions completed in the fourth quarter of 2007 and the last half of 2008. Medical supplies increased $4.6 million, or 24.1%, primarily as a result of an increase in the number of PET and PET/CT scans, which use a radiopharmaceutical as a component of the PET and PET/CT scan. Maintenance and related costs increased $4.2 million, or 8.5%, due to an increase in service costs related to the addition of radiation oncology systems and an increase in the number of PET/CT systems in operation. Fuel expenses increased $1.8 million, or 30.5%, primarily due to an increase in the average price per gallon of diesel fuel costs. Site fees increased $1.8 million, or 42.4%, primarily as a result of an increase in the average number of retail fixed-site imaging centers in operation. Outside medical services increased $0.9 million, or 10.3%, primarily as a result of an increase in radiologist service costs associated with the NEHE acquisition. License, taxes and other fees increased $0.7 million, or 15.9%, primarily due to an increase in property taxes related to an increase in PET/CT and radiation oncology systems in use. Equipment rental costs increased $0.5 million, or 11.7%, primarily due to an increase in the number of rental PET/CT systems in use related to the MOS acquisition. Marketing costs increased $0.2 million, or 49.5%, as a result of increased marketing campaigns. All other cost of revenues, excluding depreciation and amortization, increased $1.0 million, or 3.8%. Cost of revenues, as a percentage of revenue, decreased to 52.8% in 2008 from 52.9% in 2007 as a result of the factors described above, offset by a decrease in total fixed costs as a percentage of revenue, due to an increase in revenue.
Selling, general and administrative expenses increased $5.7 million, or 10.0%, to $62.7 million in 2008 compared to $57.0 million in 2007. Compensation and related employee expenses increased $2.8 million, or 8.5%, primarily as a result of an increase in average headcount related to acquisitions completed in the fourth quarter of 2007 and the last half of 2008. Share-based payment increased $1.4 million, or 36.7%, in 2008 from 2007 due to new equity awards granted in 2008. The provision for doubtful accounts increased $0.3 million, or 6.7%, due to an increase in the provision for doubtful accounts related to increased retail revenue generated from acquisitions completed in the fourth quarter of 2007 and third quarter of 2008. The provision for doubtful accounts, as a percentage of revenue, was 0.9% in both 2008 and 2007. All other selling, general and administrative expenses increased $1.2 million, or 7.5%. Selling, general and administrative expenses as a percentage of revenue were 12.7% and 12.8% in 2008 and 2007, respectively.
We recorded severance and related costs of $0.6 million in 2008 and $0.7 million in 2007.
Depreciation expense increased $5.0 million, or 6.1%, to $87.7 million in 2008 compared to $82.7 million in 2007 as a result of fixed assets acquired in connection with our acquisitions in the fourth quarter of 2007 and 2008.
56
Amortization expense increased by $3.5 million, or 67.4%, to $8.7 million in 2008 compared to $5.2 million in 2007, primarily due to the incremental amortization expense for intangible assets acquired in conjunction with our acquisitions in the fourth quarter of 2007 and the last half of 2008.
Interest expense and other, net, increased $6.0 million, or 14.2%, to $48.4 million in 2008 compared to $42.4 million in 2007. This increase was primarily related to incremental interest expense associated with the $150.0 million 71/4% Senior Subordinated Note offering completed in the fourth quarter of 2007 and a $2.4 million non-cash fair value adjustment related to our interest rate swap agreement with LCPI, partially offset by lower interest rates.
Income tax expense was $11.8 million and $11.6 million in 2008 and 2007, respectively, resulting in effective tax rates of 41.6% and 41.8% in 2008 and 2007, respectively. Our effective tax rates were higher than the federal statutory rates principally as a result of state income taxes and various permanent non-deductible tax items, including share-based payments, unrecognized tax benefits and other permanent differences.
Earnings from unconsolidated investees decreased by $3.0 million, or 39.1%, to $4.6 million in 2008 compared to $7.6 million in 2007, primarily due to a $2.0 million gain on sale from a sale/leaseback transaction in one of our unconsolidated investees, as well as a $0.5 million gain on the sale of real estate during 2007.
Net income attributable to noncontrolling interest increased $1.3 million, or 75.5%, to $3.0 million in 2008 compared to $1.7 million in 2007, due to an increase in earnings from our consolidated subsidiaries.
Net income attributable to Alliance HealthCare Services, Inc. was $16.5 million, or $0.32 per share on a diluted basis, in 2008 compared to $16.2 million, or $0.31 per share on a diluted basis, in 2007.
Liquidity and Capital Resources
Our primary source of liquidity is cash provided by operating activities. We generated $139.1 million and $130.1 million of cash flow from operating activities in 2009 and 2008, respectively. Our ability to generate cash flow is affected by numerous factors, including demand for MRI, PET/CT, other diagnostic imaging and radiation oncology services. Our ability to generate cash flow from operating activities is also dependent upon the collections of our accounts receivable. The provision for doubtful accounts decreased by $1.9 million for the year ended December 31, 2009 compared to the year ended December 31, 2008. Our number of days of revenue outstanding for our accounts receivable was 48 days and 49 days as of December 31, 2009 and 2008, respectively, which we believe is favorable compared to other diagnostic imaging and radiation oncology providers.
We used cash of $60.5 million and $151.3 million for investing activities in 2009 and 2008, respectively. Investing activities in 2009 and 2008 includes cash used for acquisitions of $0.8 million and $75.2 million, respectively. Investing activities in 2009 include $2.9 million provided by a decrease in cash in escrow, while investing activities in 2008 include $5.1 million in cash used by an increase in cash in escrow. We expect to continue to use cash for acquisitions in the future. Other than acquisitions, our primary use of capital resources is to fund capital expenditures. We incur capital expenditures for the purposes of:
- •
- purchasing new systems;
- •
- replacing less advanced systems with new systems; and
- •
- providing upgrades of our MRI, PET and PET/CT, and radiation oncology systems and upgrading our corporate infrastructure for future growth.
57
Capital expenditures totaled $73.8 million and $66.2 million for the years ended December 31, 2009 and 2008, respectively. During 2009 we purchased 22 MRI systems and 16 PET/CT systems. We traded-in or sold a total of 55 systems during 2009. Our decision to purchase a new system is typically predicated on obtaining new or extending existing client contracts, which serve as the basis of demand for the new system. We expect to purchase additional systems in 2010 and finance substantially all of these purchases with our available cash, cash from operating activities, our revolving line of credit, and equipment leases. Based upon the client demand described above, which dictates the type of equipment purchased, we expect cash capital expenditures to total approximately $65 to $75 million in 2010.
At December 31, 2009, we had cash and cash equivalents of $111.9 million. This available cash and cash equivalents are held in accounts managed by third party financial institutions and consist of invested cash and cash in our operating accounts. The invested cash is invested in interest bearing funds managed by third party financial institutions. These funds invest in high-quality money market instruments, primarily direct obligations of the government of the United States. To date, we have experienced no loss or lack of access to our invested cash or cash equivalents; however, we can provide no assurances that access to our invested cash and cash equivalents will not be impacted by adverse conditions in the financial markets.
At December 31, 2009, we had $106.9 million in our accounts that are with third party financial institutions which exceed the Federal Deposit Insurance Corporation ("FDIC") insurance limits. While we monitor daily the cash balances in our operating accounts and adjust the cash balances as appropriate, these cash balances could be impacted if the underlying financial institutions fail or could be subject to other adverse conditions in the financial markets. To date, we have experienced no loss or lack of access to cash in our operating accounts.
In connection with the 1999 acquisition of Alliance by an affiliate of KKR, we entered into a $616.0 million credit agreement consisting of a $131.0 million Tranche A Term Loan Facility, a $150.0 million Tranche B Term Facility, a $185.0 million Tranche C Term Loan Facility and a Revolving Loan Facility. On June 11, 2002, we entered into a second amendment to the credit agreement and completed a $286.0 million refinancing of our Tranche B and C term loan facility. Under the terms of the amended term loan facility, we received proceeds of $286.0 million from a new Tranche C term loan facility, and used the entire amount of the proceeds to retire $145.5 million and $140.5 million owed under Tranche B and C of our existing term loan facility, respectively. The new Tranche C borrowing rate was decreased to LIBOR plus 2.375%.
In December 2004, we entered into a third amendment to our credit agreement which revised our Tranche C term loan facility ("Old Term Loan") resulting in incremental borrowings of $154.0 million and decreased the maximum amount of availability under our existing revolving loan facility from $150.0 million to $70.0 million. We applied the proceeds from the amendment to retirement of $256.4 million of our $260.0 million 103/8% Senior Subordinated Notes due 2011 ("the 103/8% Notes") through a cash tender offer (the "2004 Tender Offer", as described in Note 9 of the Notes to Consolidated Financial Statements). The amended Old Term Loan borrowing rate decreased to LIBOR plus 2.250%. On December 19, 2005 we entered into a fourth amendment to our Credit Agreement which revised our maximum consolidated leverage ratio covenant to a level not to exceed 4.00 to 1.00 as of the last day of any fiscal quarter until the expiration of the agreement. Prior to the fourth amendment, our maximum consolidated leverage ratio covenant was 3.75 to 1.00 as of the last day of any fiscal quarter beginning March 31, 2006 to the expiration of the agreement. The fourth amendment also required us to maintain a maximum consolidated senior leverage ratio covenant at a level not to exceed 3.00 to 1.00 as of the last day of any fiscal quarter. The amendment increased the Old Term Loan LIBOR margin from an annual rate of 2.250% to 2.500%. In connection with the amendment, we incurred an amendment fee of $0.6 million.
58
In December 2004, we completed the 2004 Tender Offer and redeemed $256.4 million of our outstanding 103/8% Notes. During 2008, we paid the remaining balance of $3.5 million related to the 103/8% Notes, which had an original balance of $260.0 million. In 2008, we used cash flow from operating activities to pay down $15.0 million under the Old Term Loan.
In December 2009, we entered into a new senior secured credit agreement (the "New Credit Facility"), comprised of a $460.0 million term loan (the "New Term Loan") maturing June 2016 and a $120.0 million revolving facility (the "New Revolving Credit Facility") maturing December 2014. Borrowings under the New Term Loan were issued at 98.0% of par, with the discount to par being amortized to interest expense and other, net through the maturity date of the loan. We used the proceeds from the New Term Loan to retire $351.6 million of our Old Term Loan. Borrowings under the New Credit Facility bear interest through maturity at a variable rate based upon, at our option, either London InterBank Offered Rate ("LIBOR") or the base rate (which is the highest of the administrative agent's prime rate, one-half of 1.00% in excess of the overnight federal funds rate, and 1.00% in excess of the one-month LIBOR rate), plus in each case, an applicable margin. With respect to the New Term Loan, the applicable margin for LIBOR loans is 3.50% per annum, and with respect to the New Revolving Credit Facility, the applicable margin for LIBOR loans ranges, based on the applicable leverage ratio, from 3.25% to 3.75% per annum, in each case, with a LIBOR floor of 2.00%. With respect to the New Term Loan, the applicable margin for base rate loans is 2.50% per annum, and with respect to the New Revolving Credit Facility, the applicable margin for base rate loans ranges, based on the applicable leverage ratio, from 2.25% to 2.75% per annum.
At December 31, 2009, we did not have any borrowings outstanding under the New Revolving Credit Facility. As of December 31, 2009, we had $115.5 million of available borrowings under our New Revolving Credit Facility. In addition to other covenants, the New Credit Facility places limits on our and our subsidiaries' ability to, declare dividends or redeem or repurchase capital stock, prepay, redeem or purchase debt, incur liens and engage in sale-leaseback transactions, make loans and investments, incur additional indebtedness, amend or otherwise alter debt and other material agreements, make capital expenditures, engage in mergers, acquisitions and asset sales, transact with affiliates and alter the business conducted by us and our subsidiaries. The New Credit Facility also contains financial covenants requiring us to maintain (i) a maximum ratio of consolidated total debt to consolidated adjusted EBITDA that ranges from 4.75 to 1.00 to 4.00 to 1.00 and (ii) a minimum ratio of consolidated adjusted EBITDA to consolidated interest expense of 2.75 to 1.00. Within 180 days after the closing date of the New Credit Facility, which occurred December 1, 2009, we are required to enter into agreements such as interest rate swaps, caps, floors and other interest rate exchange contracts that would have the effect of fixing a specified percentage of our variable rate debt for periods to be determined.
As of December 31, 2009, we are in compliance with all covenants contained in our New Credit Facility and expect that we will be in compliance with these covenants in 2010. However, if we are unable to generate sufficient Consolidated Adjusted EBITDA, as defined in our credit agreement, or manage our indebtedness to sufficient levels, we could be out of compliance with our maximum consolidated leverage ratio and maximum consolidated senior leverage ratio. Our failure to comply with these covenants could permit the lenders under the credit agreement to declare all amounts borrowed under the agreement, together with accrued interest and fees, to be immediately due and payable. If the indebtedness under the New Credit Facility is accelerated, we may not have sufficient assets to repay amounts due under the credit facility. If we are not able to refinance our debt, we could become subject to bankruptcy proceedings.
In December 2004, we issued $150.0 million of our 71/4% Senior Subordinated Notes due 2012 (the "original 71/4% Notes") in a transaction exempt from the registration requirements of the Securities Act of 1933, as amended, and applied the proceeds to repayment of a portion of our 103/8% Notes. The original 71/4% Notes were subsequently registered. On December 4, 2007, we issued an additional
59
$150.0 million of our 71/4% Senior Subordinated Notes due 2012 (the "new 71/4% Notes") in a transaction exempt from the registration requirements of the Securities Act. The new 71/4% Notes were subsequently registered. The new 71/4% Notes were issued at a discount of 8.5%, which was being amortized to interest expense through the maturity date of the notes. The new 71/4% Notes have terms that were substantially identical to our original 71/4% Notes, but were issued under a new indenture and are therefore a separate series of notes. We used a portion of the net proceeds from the issuance of the new 71/4% Notes to repay and terminate an Acquisition Credit Facility we entered into the previous month to finance the NEHE acquisition (as described in Note 9 to the Notes to Consolidated Financial Statements). The remaining net proceeds were used for general corporate purposes, including acquisitions. The original 71/4% Notes and the new 71/4% Notes are collectively referred to as the "71/4% Notes."
In December 2009, we issued $190.0 million of 8.0% senior notes due 2016 (the "8% Notes") in a transaction that was exempt from the registration requirements of the Securities Act of 1933, as amended. The 8% Notes were issued at 98.690% of par, with the discount to par being amortized to interest expense and other, net through the maturity date of the notes. We used the proceeds from this transaction, the New Term Loan and existing cash to complete a Tender Offer and purchase $294.4 million of the 71/4% Notes at a purchase price equal to 100.125% of the principal amount, together with the accrued interest to the redemption date. We also used the proceeds from these transactions to redeem the remaining $5.6 million of 71/4% notes in January 2010 at a redemption price equal to 100.0% of the principal amount, together with accrued interest to the redemption date.
The indenture governing the 8% Notes contains covenants limiting our and most of our subsidiaries' ability to pay dividends and make other restricted payments, incur additional indebtedness or issue disqualified stock, create liens on our assets, merge, consolidate, or sell all or substantially all of our assets, and enter into transactions with affiliates, among others. The 8% Notes are unsecured senior obligations and are equal in right of payment to all existing and future senior debt, and rank senior in right of payment to all of our existing and future subordinated debt. The 8% Notes are effectively subordinated in right of payment to all of our existing and future secured indebtedness, including indebtedness under our New Credit Facility, to the extent of assets securing such indebtedness, and are effectively subordinated in right of payment to all obligations of our subsidiaries. As of December 31, 2009, we were in compliance with all covenants contained in the 8% Notes and forecast that we will be in compliance with these covenants in 2010. Our failure to comply with these covenants could permit the trustee under the indenture relating to the 8% Notes and the note holders to declare the principal amounts under the 8% Notes, together with accrued and unpaid interest, to be immediately due and payable. If the indebtedness under the 8% Notes, or any of our other indebtedness, is accelerated, and we are not able to refinance our debt, we could become subject to bankruptcy proceedings.
During 2004, we entered into interest rate swap agreements, with notional amounts of $56.8 million, $46.8 million and $48.4 million to manage the future cash interest payments associated with a portion of our variable rate bank debt. These agreements matured during 2007. We recorded changes in the fair value of the swaps through interest expense.
In the first quarter of 2005, we entered into multiple interest rate collar agreements for our variable rate bank debt. The total underlying notional amount of the debt was $178.0 million. Under these arrangements we purchased a cap on the interest rate of 4.00% and sold a floor of 2.25%. We paid a net purchase price of $1.5 million for these collars. These agreements were two and three years in length and matured at various dates between January 2007 and January 2008. We designated these collars as cash flow hedges of variable future cash flows associated with our long-term debt and recorded changes in the fair value of the collars through comprehensive income during the period these instruments were designated as hedges.
60
During the first quarter of 2008, we entered into two interest rate swap agreements with notional amounts of $92.7 million each, to hedge future cash interest payments associated with a portion of our variable rate bank debt ("the 2008 swaps"). Under the terms of these agreements, we receive three-month LIBOR and pay a fixed rate of 3.15%. The net effect of the hedges is to record interest expense at a fixed rate of 5.65%, as the debt incurred interest based on three-month LIBOR plus 2.50%. These agreements are three years in length and mature in 2011. See below for additional information regarding the 2008 swaps. As discussed below, we elected to terminate and replace one of the 2008 swaps in the first quarter of 2009.
On September 15, 2008, LHI filed for bankruptcy protection under Chapter 11 of the United States Bankruptcy Code. On October 6, 2008, LCPI filed for bankruptcy protection under Chapter 11 of the United States Bankruptcy Code. One of our 2008 swaps with a notional amount of $92.7 million, which expires January 31, 2011, is with LCPI ("the Lehman Swap"). As of September 12, 2008 hedge accounting was terminated and all further changes in the fair market value of the Lehman Swap are being recorded in interest expense and other. Comprehensive income (loss) related to effective unrealized gains or losses on the fair value of the Lehman Swap through September 12, 2008 remain in accumulated comprehensive income (loss) on the balance sheet and will be amortized into interest expense and other as the underlying interest payments are recognized in earnings. The Lehman Swap was valued using the income approach with observable Level 2 market expectations at the measurement date and standard valuation techniques to convert future amounts to a single discounted present amount. The fair market value of the Lehman Swap at September 30, 2008 was an asset of $0.7 million, which was adjusted to zero as collectability was deemed uncertain due to the LHI bankruptcy filing. We included the write down of the asset in interest expense and other for the year ended December 31, 2008.
During the first quarter of 2009, we replaced the Lehman Swap with an interest rate swap agreement which has a notional amount of $92.7 million (the "2009 Swap Replacement") and has been designated as a cash flow hedge of variable future cash flows associated with a portion of our long term debt. Under the terms of this agreement, which matures in January 2011, we receive three-month LIBOR and pay a fixed rate of 3.15%. The net effect of the hedges is to record interest expense at a fixed rate of 5.65%, as the debt incurs interest based on three-month LIBOR plus 2.50%.
Additionally, during the first quarter of 2009, we entered into an interest rate swap agreement which had a notional amount of $56.8 million to hedge future cash interest payments associated with a portion of our variable rate bank debt (the "New 2009 Swap"). Under the terms of this agreement, which was to mature in November 2011, we received three-month LIBOR and paid a fixed rate of 2.07%. The net effect of the hedge was to record interest expense at a fixed rate of 4.57%, as the debt incurred interest based on three-month LIBOR plus 2.50%.
We elected to terminate one of the 2008 swaps and the New 2009 Swap in December 2009 in connection with entering into the Refinance Transaction on December 1, 2009. As a result of the Refinance Transaction, we de-designated the 2008 swap, the 2009 Swap Replacement and the New 2009 Swap and hedge accounting was terminated and all further changes in the fair market value of the terminated swaps are being recorded in interest expense and other. Comprehensive income (loss) related to effective unrealized gains or losses on the fair value of the terminated swaps through September 30, 2009 remain in accumulated comprehensive income (loss) on the balance sheet and will be amortized into interest expense and other as the underlying interest payments are recognized in earnings. The terminated swaps were valued using the income approach with observable Level 2 market expectations at the measurement date and standard valuation techniques to convert future amounts to a single discounted present amount.
61
The maturities of our long-term debt, including interest, future payments under our operating leases and binding equipment purchase commitments as of December 31, 2009 are as follows:
Contractual Obligations
|
2010 | 2011 | 2012 | 2013 | 2014 | Thereafter | Total | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |
|
|
|
(in millions) |
|
|
|
|||||||||||||||
New Term Loan |
$ | 30.0 | $ | 29.7 | $ | 29.4 | $ | 29.1 | $ | 28.9 | $ | 470.9 | $ | 618.0 | ||||||||
8% Senior Notes |
15.2 | 15.2 | 15.2 | 15.2 | 15.2 | 220.5 | 296.5 | |||||||||||||||
71/4% Senior Subordinated Notes |
0.4 | 0.4 | 6.0 | — | — | — | 6.8 | |||||||||||||||
Equipment Loans |
8.1 | 5.9 | 4.7 | 4.2 | 3.3 | 1.6 | 27.8 | |||||||||||||||
Operating Leases |
4.5 | 3.1 | 2.6 | 1.5 | 1.4 | 3.4 | 16.5 | |||||||||||||||
Letters of Credit |
4.5 | — | — | — | — | — | 4.5 | |||||||||||||||
Equipment Purchase Commitments |
18.8 | — | — | — | — | — | 18.8 | |||||||||||||||
Total Contractual Obligation Payments |
81.5 | 54.3 | 57.9 | 50.0 | 48.8 | 696.4 | 988.9 | |||||||||||||||
Less Amount Representing Interest |
(42.4 | ) | (41.7 | ) | (41.1 | ) | (40.2 | ) | (39.7 | ) | (64.5 | ) | (269.6 | ) | ||||||||
Present Value of Future Contractual Obligations |
$ | 39.1 | $ | 12.6 | $ | 16.8 | $ | 9.8 | $ | 9.1 | $ | 631.9 | $ | 719.3 | ||||||||
The remaining $5.6 million of 71/4% notes were redeemed in January 2010 at a redemption price equal to 100.0% of the principal amount, together with accrued interest to the redemption date.
Our liability for unrecognized tax benefits of $1,329 at December 31, 2009 has been omitted from the above table because we cannot determine with certainty when this liability will be settled. It is reasonably possible that the amount of liability for unrecognized tax benefits will change in the next twelve months; however, we do not expect the change will have a material impact on our consolidated financial statements.
We believe that, based on current levels of operations, our cash flow from operating activities, together with other available sources of liquidity, including borrowings available under our revolving line of credit, will be sufficient over the next one to two years to fund anticipated capital expenditures and potential acquisitions and make required payments of principal and interest on our debt. Under current tax law, we expect to utilize all of our net operating loss carryforwards ("NOLs") by 2010, and therefore anticipate being in a tax paying position with respect to a portion of our income in 2010. However, legislation is currently pending which may extend the federal "bonus depreciation" deduction through December 31, 2010. If extended, we may have NOL carryforwards into 2011. We may require or choose to obtain additional financing. Our ability to obtain additional financing will depend, among other things, on our financial condition and operating performance, as well as the condition of the capital markets at the time we seek financing. We cannot assure you that additional financing will be available to us on favorable terms when required, or at all. If we raise additional funds through the issuance of equity, equity-linked or debt securities, those securities may have rights, preferences or privileges senior to the rights of our common stock, and our stockholders may experience dilution. If we need to raise additional funds in the future and are unable to do so or obtain additional financing on acceptable terms in the future, it is possible we would have to limit planned activities or sell assets to obtain liquidity.
Off-Balance Sheet Arrangements
As of December 31, 2009, we were a party to interest rate swap agreements related to $92.7 million of outstanding principal on our variable rate debt. See Item 7A "Quantitative and Qualitative Disclosures about Market Risk."
62
Critical Accounting Policies
The preparation of financial statements in conformity with accounting principles generally accepted in the United States of America requires management to make estimates and assumptions that affect the amounts reported in the financial statements and accompanying notes. Actual results could differ from those estimates. The significant accounting policies which we believe are the most critical to aid in fully understanding and evaluating our reported financial results include the following:
Revenue Recognition
The majority of our revenues is derived directly from healthcare providers and is primarily for imaging services. To a lesser extent, revenues are generated from direct billings to patients or their medical payors which are recorded net of contractual discounts and other arrangements for providing services at less than established patient billing rates. Revenues from direct patient billing amounted to approximately 11%, 21% and 20% of revenues in the years ended December 31, 2007, 2008 and 2009, respectively. We continuously monitor collections from direct patient billings and compare these collections to revenue, net of contractual discounts, recorded at the time of service. While such contractual discounts have historically been within our expectations and the provisions established, an inability to accurately estimate contractual discounts in the future could have a material adverse impact on our operating results. As the price is predetermined, all revenues are recognized at the time the delivery of imaging service has occurred and collectability is reasonably assured, which is based upon contract terms with healthcare providers and negotiated rates with third-party payors and patients.
Accounts Receivable
We provide shared and single-user diagnostic imaging and radiation oncology equipment and technical support services to the healthcare industry and directly to patients on an outpatient basis. Substantially all of our accounts receivable are due from hospitals, other healthcare providers and health insurance providers located throughout the United States. Services are generally provided pursuant to long-term contracts with hospitals and other healthcare providers or directly to patients, and generally collateral is not required. Receivables generally are collected within industry norms for third-party payors. We continuously monitor collections from our clients and maintain an allowance for estimated credit losses based upon any specific client collection issues that we have identified and our historical experience. While such credit losses have historically been within our expectations and the provisions established, an inability to accurately estimate credit losses in the future could have a material adverse impact on our operating results.
Goodwill and Long-Lived Assets
ASC 350, "Intangibles—Goodwill and Other" (formerly SFAS No. 142, "Goodwill and Other Intangible Assets") requires that goodwill and intangible assets with indefinite useful lives not be amortized, but instead be tested for impairment at least annually. In accordance with ASC 350, we have selected to perform an annual impairment test for goodwill and intangible assets with indefinite lives based on the financial information as of September 30, or more frequently when an event occurs or circumstances change to indicate an impairment of these assets has possibly occurred. Goodwill and intangible assets with indefinite lives are allocated to our various reporting units, which are our geographical regions. ASC 350 requires us to compare the fair value of the reporting unit to its carrying amount on an annual basis to determine if there is potential impairment. If the fair value of the reporting unit is less than its carrying value, an impairment loss is recorded to the extent that the implied fair value of the goodwill and intangible assets with indefinite lives within the reporting unit are less than the carrying value. The fair value of the reporting unit is determined based on discounted cash flows, market multiples or appraised values as appropriate. We comply with periodic impairment test procedures. In 2007, 2008 and 2009 we concluded that the fair value of each reporting unit exceeds
63
its carrying value, indicating no goodwill or intangible asset impairment was present. No triggering events occurred during the fourth quarters of 2007, 2008 and 2009 which required an additional impairment test as of December 31, 2007, 2008 or 2009. ASC 350 also requires intangible assets with definite useful lives to be amortized over their respective estimated useful lives to their estimated residual values and reviewed for impairment in accordance with ASC 360, "Property, Plant, and Equipment" (formerly SFAS No. 144, "Accounting for the Impairment or Disposal of Long-Lived Assets"). In 2007, 2008 and 2009 we concluded that no impairment was present in our intangible assets with definite useful lives.
Deferred Income Taxes
Deferred income tax assets and liabilities are determined based on the temporary differences between the financial reporting and tax bases of assets and liabilities, applying enacted statutory tax rates in effect for the year in which the differences are expected to reverse. Future income tax benefits are recognized only to the extent that the realization of such benefits is considered to be more likely than not. We regularly review our deferred income tax assets for recoverability and establish a valuation allowance based on historical taxable income, projected future taxable income and the expected timing of the reversals of existing temporary differences. If we are unable to generate sufficient future taxable income, or if there is a material change in the actual effective income tax rates or time period within which the underlying temporary differences become taxable or deductible, we could be required to significantly increase our valuation allowance, resulting in a substantial increase in our effective tax rate.
Recent Accounting Pronouncements
For a discussion of recent accounting pronouncements, please refer to Note 2 of the Notes to Consolidated Financial Statements.
Cautionary Statement Pursuant to the Private Securities Litigation Reform Act of 1995
Certain statements contained in Management's Discussion and Analysis of Financial Condition and Results of Operations, particularly in the section entitled "Liquidity and Capital Resources", and elsewhere in this annual report on Form 10-K, are "forward-looking statements," within the meaning of the safe harbor provisions of the Private Securities Litigation Reform Act of 1995.
In some cases you can identify these statements by forward looking words, such as "may," "will," "should," "expect," "plan," "anticipate," "believe," "estimate," "predict," "seek," "intend" and "continue" or similar words. Forward looking statements may also use different phrases. Forward looking statements address, among other things, our future expectations, projections of our future results of operation or of our financial condition and other forward looking information.
Statements regarding the following subjects, among others, are forward-looking by their nature: (i) future legislation and other healthcare regulatory reform actions, and the impact of such legislation and other regulatory actions on our business, (ii) our expectations with respect to future MRI and PET/CT scan volumes and revenues, (iii) the impact of seasonality on our business, (iv) expectations with respect to capital expenditures in 2010, and (v) the impact of recent accounting pronouncements on our results of operations and cash flows or financial position.
We believe it is important to communicate our expectations to our investors. However, there may be events in the future that we are not able to accurately predict or that we do not fully control that cause actual results to differ materially from those expressed or implied by our forward looking statements, including:
- •
- our high degree of leverage and our ability to service our debt;
- •
- factors affecting our leverage, including interest rates;
- •
- the risk that the counter-parties to our interest rate swap agreements fail to satisfy their obligations under these agreements;
64
- •
- our ability to obtain financing;
- •
- the effect of operating and financial restrictions in our debt instruments;
- •
- the accuracy of our estimates regarding our capital requirements;
- •
- intense levels of competition in our industry;
- •
- changes in the rates or methods of third-party reimbursements for diagnostic imaging and radiation oncology services;
- •
- fluctuations or unpredictability of our revenues, including as a result of seasonality;
- •
- changes in the healthcare regulatory environment;
- •
- our ability to keep pace with technological developments within our industry;
- •
- the growth in the market for MRI and other services;
- •
- the disruptive effect of hurricanes and other natural disasters;
- •
- adverse changes in general domestic and worldwide economic conditions and instability and disruption of credit markets;
- •
- our ability to successfully integrate acquisitions; and
- •
- other factors discussed under "Risk Factors" in this annual report on Form 10-K.
This Form 10-K includes statistical data that we obtained from public industry publications. These publications generally indicate that they have obtained their information from sources believed to be reliable, but do not guarantee the accuracy and completeness of their information. Although we believe that the publications are reliable, we have not independently verified their data.
Item 7A. Quantitative and Qualitative Disclosures About Market Risk.
We provide our services exclusively in the United States and receive payment for our services exclusively in United States dollars. As a result, our financial results are unlikely to be affected by factors such as changes in foreign currency exchange rates or weak economic conditions in foreign markets.
Our interest expense is sensitive to changes in the general level of interest rates in the United States, particularly because the majority of our indebtedness has interest rates which are variable. The recorded carrying amount of our long-term debt under our New Credit Facility approximates fair value as these borrowings have variable rates that reflect currently available terms and conditions for similar debt. To decrease the risk associated with interest rate increases, we have entered into multiple interest rate swap and collar agreements for a portion of our variable rate debt. These swaps and collars are designated as cash flow hedges of variable future cash flows associated with our long-term debt. Within 180 days after the closing date of the New Credit Facility, which occurred December 1, 2009, we are required to enter into agreements such as interest rate swaps, caps, floors and other interest rate exchange contracts that would have the effect of fixing a specified percentage of our variable rate debt for periods to be determined.
During 2004 we entered into interest rate swap agreements which had notional amounts of $56.8 million, $46.8 million and $48.4 million. Under the terms of these agreements, we received three-month LIBOR and paid a fixed rate of 3.15%, 3.89%, and 3.69%, respectively. The net effect was to record interest expense at fixed rates of 5.65%, 6.39% and 6.19% respectively, as the debt incurred interest based on three-month LIBOR plus 2.50%. For the year ended December 31, 2007, we received a net settlement amount of $1.2 million. The swap agreements matured during the second and fourth quarters of 2007.
65
During 2005 we entered into multiple interest rate collar agreements which had an aggregate notional amount of $178.0 million. Under the terms of these agreements, we purchased a cap on the interest rate of 4.00% and sold a floor of 2.25%. For the years ended December 31, 2008 and 2007, we received a net settlement amount of $0.3 and $2.0 million, respectively, on these collar agreements. The collar agreements matured at various dates between January 2007 and January 2008.
During the first quarter of 2008, we entered into two interest rate swap agreements with notional amounts of $92.7 million each, to hedge future cash interest payments associated with a portion of our variable rate bank debt (the "2008 swaps"). Under the terms of these agreements, we receive three-month LIBOR and pay a fixed rate of 3.15%. The net effect of the hedges is to record interest expense at a fixed rate of 5.65%, as the underlying debt incurred interest based on three-month LIBOR plus 2.50%.For the years ended December 31, 2009 and 2008, we paid net settlement amounts of $1.5 million and $0.2 million, respectively, on these swap agreements. The 2008 swaps are three years in length and mature in 2011. See below for additional information regarding the 2008 swaps. As discussed below, we elected to terminate and replace one of the 2008 swaps in the first quarter of 2009.
The collar agreements and the 2008 swaps have been designated as cash flow hedges of variable future cash flows associated with our long-term debt. In accordance with ASC 815 (formerly SFAS 133, "Accounting for Derivative Instruments and Hedging Activities"), the collars and the 2008 swaps are, and will be, recorded at fair value. On a quarterly basis, the fair value of the collars and swaps will be determined based on quoted market prices and, assuming perfect effectiveness, the difference between the fair value and the book value of the collars will be recognized in comprehensive income, a component of shareholders' equity. On a quarterly basis, the fair value of the 2008 swaps will be determined based on the income approach using observable Level 2 inputs under ASC 825 (formerly SFAS No. 157, "Fair Value Measurements" ("SFAS 157")). The fair market value of the 2008 swaps will be recorded on the balance sheet as assets or liabilities with all effective changes deferred in comprehensive income. Any ineffectiveness of the collars and 2008 swaps is required to be recognized in earnings. The collars outstanding at December 31, 2007 matured during January 2008, and all counterparty obligations were met.
On September 15, 2008, LHI filed for bankruptcy protection under Chapter 11 of the United States Bankruptcy Code. On October 6, 2008, LCPI filed for bankruptcy protection under Chapter 11 of the United States Bankruptcy Code. One of our 2008 swaps with a notional amount of $92.7 million, which expires January 31, 2011, is with LCPI ("the Lehman Swap"). As of September 12, 2008 hedge accounting was terminated and all further changes in the fair market value of the Lehman Swap are being recorded in interest expense and other. Comprehensive income (loss) related to effective unrealized gains or losses on the fair value of the Lehman Swap through September 12, 2008 remain in accumulated comprehensive income (loss) on the balance sheet and will be amortized into interest expense and other as the underlying interest payments are recognized in earnings. The Lehman Swap was valued using the income approach with observable Level 2 market expectations at the measurement date and standard valuation techniques to convert future amounts to a single discounted present amount. The fair market value of the Lehman Swap at September 30, 2008 was an asset of $0.7 million, which was adjusted to zero as collectability was deemed uncertain due to the LHI bankruptcy filing. We included the write down of the asset in interest expense and other for the year ended December 31, 2008. For the last three quarters of 2008, we included $2.4 million in interest expense and other, net related to the fair value adjustment for this swap as we did not expect LCPI to fulfill their obligations under the swap agreement. As a result, we terminated the Lehman Swap in February 2009. We paid $2.2 million for the remaining fair market value of the swap at the date of termination.
During the first quarter of 2009, we replaced the Lehman Swap with an interest rate swap agreement which has a notional amount of $92.7 million (the "2009 Swap Replacement") and has been designated as a cash flow hedge of variable future cash flows associated with a portion of our long term
66
debt. Under the terms of this agreement, which matures in January 2011, we receive three-month LIBOR and pay a fixed rate of 3.15%. The net effect of the hedge is to record interest expense at a fixed rate of 5.65%, as the debt incurs interest based on three-month LIBOR plus 2.50%. We received $2.2 million in cash based on the terms of the agreement. For the year ended December 31, 2009, we paid a net settlement amount of $1.5 million on this swap agreement.
Additionally, during the first quarter of 2009, we entered into an interest rate swap agreement which has a notional amount of $56.8 million, to hedge future cash interest payments associated with a portion of the our variable rate bank debt (the "New 2009 Swap"). Under the terms of this agreement, which was to mature in November 2011, we received three-month LIBOR and paid a fixed rate of 2.07%. The net effect of the hedge was to record interest expense at a fixed rate of 4.57%, as the debt incurred interest based on three-month LIBOR plus 2.50%. For the year ended December 31, 2009, we paid net a settlement amount of $0.5 million on this swap agreement.
We elected to terminate one of the 2008 swaps and the New 2009 Swap in December 2009 in connection with entering into the Refinance Transaction on December 1, 2009. As a result of the Refinance Transaction, we de-designated the 2008 swap, the 2009 Swap Replacement and the New 2009 Swap and hedge accounting was terminated and all further changes in the fair market value of the terminated swaps are being recorded in interest expense and other. We paid $3.3 million and $1.4 million for the remaining fair market value of the 2008 swap and the New 2009 Swap, respectively, at the date of termination. Comprehensive income (loss) related to effective unrealized gains or losses on the fair value of the terminated swaps through September 30, 2009 remain in accumulated comprehensive income (loss) on the balance sheet and will be amortized into interest expense and other as the underlying interest payments are recognized in earnings. The terminated swaps were valued using the income approach with observable Level 2 market expectations at the measurement date and standard valuation techniques to convert future amounts to a single discounted present amount.
Also during the first quarter of 2009, we entered into a diesel fuel swap agreement which has a notional quantity of 1,008,000 gallons, or 84,000 gallons per month, to hedge future cash payments associated with our purchases of diesel fuel for the mobile fleet. Under the terms of this agreement, which matures in February 2010, we receive the Department of Energy published monthly average price per gallon and pay a fixed rate of $2.63 per gallon. For the year ended December 31, 2009, we paid a net settlement amount of $0.1 million on this swap agreement. For the year ended December 31, 2009, amounts recognized in other (income) and expense were not material.
The swaps expose us to credit risk in the event that the counterparties to the agreements do not or cannot meet their obligations. The notional amount is used to measure interest to be paid or received and does not represent the amount of exposure to credit loss. The loss would be limited to the amount that would have been received, if any, over the remaining life of the 2008 swaps. On a quarterly basis, the counterparties are evaluated for non-performance risk. Additionally, the credit crisis could have an impact on our other interest rate swap agreement if that counterparty files for bankruptcy or is otherwise unable to perform its obligations. See Note 11 to the Consolidated Financial Statements for additional details. The collars outstanding at December 31, 2007 matured during January 2008, and all counterparty obligations were met.
Our interest income is sensitive to changes in the general level of interest rates in the United States, particularly because the majority of our investments are in cash equivalents. We maintain our cash equivalents in financial instruments with original maturities of 90 days or less. Cash and cash equivalents are invested in interest bearing funds managed by third party financial institutions. These funds invest in high-quality money market instruments, primarily direct obligations of the government of the United States. At December 31, 2009, we had cash and cash equivalents of $111.9 million, of which $106.9 million was held in accounts that are with third party financial institutions which exceed
67
the FDIC insurance limits. At December 31, 2008, we had cash and cash equivalents of $73.3 million, of which $68.7 million was held in accounts that are with third party financial institutions which exceed the FDIC insurance limits. We held investments in marketable securities during 2007, which consisted primarily of investment grade auction rate securities and debt securities, all classified as available-for-sale with original maturities greater than 90 days. We did not have any marketable securities at December 31, 2007, 2008 and 2009.
The recorded carrying amounts of cash and cash equivalents and marketable securities approximate fair value due to their short-term maturities.
The table below provides information about our financial instruments that are sensitive to changes in interest rates. For long-term debt obligations, the table presents principal cash flows and related weighted average interest rates by expected (contractual) maturity dates. All amounts are in United States dollars.
| |
Expected Maturity as of December 31, 2009 | |||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |
2010 | 2011 | 2012 | 2013 | 2014 | Thereafter | Total | Fair Value | ||||||||||||||||||||
| |
(dollars in millions) |
|||||||||||||||||||||||||||
Liabilities: |
||||||||||||||||||||||||||||
Long-term debt: |
||||||||||||||||||||||||||||
Fixed rate |
$ | 12.3 | $ | 4.9 | $ | 4.0 | $ | 3.8 | $ | 3.1 | $ | 191.4 | $ | 219.5 | $ | 206.2 | ||||||||||||
Average interest rate |
6.83 | % | 6.86 | % | 7.15 | % | 7.51 | % | 7.70 | % | 5.65 | % | 5.85 | % | 7.98 | % | ||||||||||||
Variable rate |
$ | 4.6 | $ | 4.6 | $ | 4.6 | $ | 4.6 | $ | 4.6 | $ | 437.0 | $ | 460.0 | $ | 460.0 | ||||||||||||
Average interest rate |
5.53 | % | 5.50 | % | 5.50 | % | 5.50 | % | 5.50 | % | 5.50 | % | 5.50 | % | 5.50 | % | ||||||||||||
68
Item 8. Financial Statements and Supplementary Data.
ALLIANCE HEALTHCARE SERVICES, INC.
INDEX TO CONSOLIDATED FINANCIAL STATEMENTS
69
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
The
Board of Directors and Stockholders of
Alliance HealthCare Services, Inc.
Newport Beach, California
We have audited the accompanying consolidated balance sheets of Alliance HealthCare Services, Inc. and subsidiaries (the "Company") as of December 31, 2009 and 2008, and the related consolidated statements of operations and comprehensive income, cash flows, and stockholders' (deficit) equity for each of the three years in the period ended December 31, 2009. Our audits also included the consolidated financial statement schedule listed in the Index at Item 15(a)(2). These consolidated financial statements and the consolidated financial statement schedule are the responsibility of the Company's management. Our responsibility is to express an opinion on the consolidated financial statements and the consolidated financial statement schedule based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. An audit includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements. An audit also includes assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, such consolidated financial statements present fairly, in all material respects, the financial position of Alliance HealthCare Services, Inc. and subsidiaries as of December 31, 2009 and 2008, and the results of their operations and their cash flows for each of the three years in the period ended December 31, 2009, in conformity with accounting principles generally accepted in the United States of America. Also, in our opinion, such consolidated financial statement schedule, when considered in relation to the basic consolidated financial statements taken as a whole, presents fairly, in all material respects, the information set forth therein.
As discussed in Notes 1 and 2 to the consolidated financial statements, the accompanying consolidated financial statements have been retrospectively adjusted for the 2009 adoption of Accounting Standards Codification ("ASC") 810, "Consolidation" (formerly Financial Accounting Standards Board ("FASB") Statement No. 160, "Noncontrolling Interests in Consolidated Financial Statements—an amendment of ARB No. 51") and ASC 260, "Earnings Per Share" (formerly FASB Staff Position Emerging Issues Task Force No. 03-6-1, "Determining Whether Instruments Granted in Share-Based Payment Transactions Are Participating Securities").
We have also audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States), the Company's internal control over financial reporting as of December 31, 2009, based on the criteria established in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission and our report dated March 9, 2010 expressed an unqualified opinion on the Company's internal control over financial reporting.
/s/ Deloitte & Touche LLP
Costa
Mesa, California
March 9, 2010
70
ALLIANCE HEALTHCARE SERVICES, INC.
CONSOLIDATED BALANCE SHEETS
(in thousands, except per share amounts)
| |
December 31, 2008 |
December 31, 2009 |
||||||
|---|---|---|---|---|---|---|---|---|
ASSETS |
||||||||
Current assets: |
||||||||
Cash and cash equivalents |
$ | 73,305 | $ | 111,884 | ||||
Accounts receivable, net of allowance for doubtful accounts of $9,178 in 2008 and $8,930 in 2009 |
67,147 | 61,912 | ||||||
Deferred income taxes |
17,719 | 19,058 | ||||||
Prepaid expenses and other current assets |
10,272 | 9,184 | ||||||
Other receivables |
7,902 | 4,197 | ||||||
Total current assets |
176,345 | 206,235 | ||||||
Equipment, at cost |
836,842 | 863,804 | ||||||
Less accumulated depreciation |
(479,609 | ) | (523,748 | ) | ||||
Equipment, net |
357,233 | 340,056 | ||||||
Goodwill |
193,430 | 194,243 | ||||||
Other intangible assets, net of accumulated amortization of $39,526 in 2008 and $50,526 in 2009 |
110,720 | 100,188 | ||||||
Deferred financing costs, net of accumulated amortization of $7,633 in 2008 and $514 in 2009 |
7,173 | 17,143 | ||||||
Other assets |
38,822 | 29,971 | ||||||
Total assets |
$ | 883,723 | $ | 887,836 | ||||
LIABILITIES AND STOCKHOLDERS' EQUITY |
||||||||
Current liabilities: |
||||||||
Accounts payable |
$ | 21,468 | $ | 23,888 | ||||
Accrued compensation and related expenses |
18,575 | 17,311 | ||||||
Accrued interest payable |
3,642 | 3,789 | ||||||
Other accrued liabilities |
38,446 | 32,887 | ||||||
Current portion of long-term debt |
7,743 | 16,902 | ||||||
Total current liabilities |
89,874 | 94,777 | ||||||
Long-term debt, net of current portion |
365,323 | 463,455 | ||||||
Senior subordinated notes |
289,496 | — | ||||||
Senior notes |
— | 187,533 | ||||||
Other liabilities |
7,901 | 3,737 | ||||||
Deferred income taxes |
102,136 | 103,572 | ||||||
Total liabilities |
854,730 | 853,074 | ||||||
Commitments and contingencies (Note 12) |
||||||||
Stockholders' equity: |
||||||||
Preferred stock, $0.01 par value; 1,000,000 shares authorized and no shares issued and outstanding |
||||||||
Common stock, $0.01 par value; 100,000,000 shares authorized; shares issued and outstanding—51,519,033 at December 31, 2008 and 52,025,014 at December 31, 2009 |
514 | 516 | ||||||
Less: treasury stock, at cost—52,931 shares at December 31, 2008 and 386,703 shares at December 31, 2009 |
(430 | ) | (2,333 | ) | ||||
Additional paid-in capital |
4,606 | 10,652 | ||||||
Accumulated comprehensive loss |
(2,159 | ) | (2,392 | ) | ||||
Retained earnings |
20,996 | 21,477 | ||||||
Total stockholders' equity attributable to Alliance HealthCare Services, Inc. |
23,527 | 27,920 | ||||||
Noncontrolling interest |
5,466 | 6,842 | ||||||
Total stockholders' equity |
28,993 | 34,762 | ||||||
Total liabilities and stockholders' equity |
$ | 883,723 | $ | 887,836 | ||||
See accompanying notes.
71
ALLIANCE HEALTHCARE SERVICES, INC.
CONSOLIDATED STATEMENTS OF OPERATIONS
AND COMPREHENSIVE INCOME
(in thousands, except per share
amounts)
| |
Year ended December 31, |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| |
2007 | 2008 | 2009 | ||||||||
Revenues |
$ | 444,919 | $ | 495,834 | $ | 505,513 | |||||
Costs and expenses: |
|||||||||||
Cost of revenues, excluding depreciation and amortization |
235,471 | 261,753 | 270,381 | ||||||||
Selling, general and administrative expenses |
57,049 | 62,728 | 67,579 | ||||||||
Transaction costs |
— | — | 893 | ||||||||
Severance and related costs |
682 | 636 | 1,404 | ||||||||
Depreciation expense |
82,703 | 87,728 | 94,918 | ||||||||
Amortization expense |
5,195 | 8,696 | 11,000 | ||||||||
Interest expense and other, net of interest income of $2,122 in 2007, $2,364 in 2008 and $132 in 2009 |
42,362 | 48,392 | 45,894 | ||||||||
Loss on extinguishment of debt |
— | 61 | 14,600 | ||||||||
Other (income) and expense, net |
(579 | ) | (872 | ) | (1,178 | ) | |||||
Total costs and expenses |
422,883 | 469,122 | 505,491 | ||||||||
Income before income taxes, earnings from unconsolidated investees, and noncontrolling interest, net of tax |
22,036 | 26,712 | 22 | ||||||||
Income tax expense |
11,644 | 11,764 | 308 | ||||||||
Earnings from unconsolidated investees |
(7,567 | ) | (4,605 | ) | (3,831 | ) | |||||
Net income |
17,959 | 19,553 | 3,545 | ||||||||
Less: Net income attributable to noncontrolling interest, net of tax |
(1,727 | ) | (3,030 | ) | (3,064 | ) | |||||
Net income attributable to Alliance HealthCare Services, Inc. |
$ | 16,232 | $ | 16,523 | $ | 481 | |||||
Comprehensive income, net of taxes: |
|||||||||||
Net income attributable to Alliance HealthCare Services, Inc. |
$ | 16,232 | $ | 16,523 | $ | 481 | |||||
Unrealized loss on hedging transactions, net of related tax effects of $769 in 2007, $1,558 in 2008 and $144 in 2009 |
(1,151 | ) | (2,364 | ) | (233 | ) | |||||
Comprehensive income |
$ | 15,081 | $ | 14,159 | $ | 248 | |||||
Earnings per common share attributable to Alliance HealthCare Services, Inc.: |
|||||||||||
Basic |
$ | 0.32 | $ | 0.32 | $ | 0.01 | |||||
Diluted |
$ | 0.31 | $ | 0.32 | $ | 0.01 | |||||
Weighted-average number of shares of common stock and common stock equivalents: |
|||||||||||
Basic |
50,563 | 51,296 | 51,738 | ||||||||
Diluted |
51,582 | 52,159 | 52,155 | ||||||||
See accompanying notes.
72
ALLIANCE HEALTHCARE SERVICES, INC.
CONSOLIDATED STATEMENTS OF CASH FLOWS
(dollars in thousands)
| |
Year Ended December 31, | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| |
2007 | 2008 | 2009 | ||||||||
Operating activities: |
|||||||||||
Net income |
$ | 17,959 | $ | 19,553 | $ | 3,545 | |||||
Adjustments to reconcile net income to net cash provided by operating activities: |
|||||||||||
Provision for doubtful accounts |
4,013 | 4,282 | 2,387 | ||||||||
Share-based payment |
3,860 | 5,276 | 6,080 | ||||||||
Depreciation and amortization |
87,898 | 96,424 | 105,918 | ||||||||
Amortization of deferred financing costs |
2,677 | 2,310 | 2,384 | ||||||||
Accretion of discount on long term debt |
194 | 2,051 | 2,220 | ||||||||
Adjustment of derivatives to fair value |
1,726 | 2,426 | (4,035 | ) | |||||||
Distributions (less than) greater than undistributed earnings of investees |
(138 | ) | 1,453 | (106 | ) | ||||||
Deferred income taxes |
7,690 | 9,919 | (894 | ) | |||||||
Excess tax benefit from share-based payment arrangements |
(592 | ) | (216 | ) | (12 | ) | |||||
Gain on sale of assets |
(579 | ) | (872 | ) | (1,277 | ) | |||||
Loss on extinguishment of debt |
— | 61 | 14,600 | ||||||||
Changes in operating assets and liabilities, net of the effects of acquisitions: |
|||||||||||
Accounts receivable |
(9,068 | ) | (4,589 | ) | 2,925 | ||||||
Prepaid expenses and other current assets |
(1,031 | ) | (3,646 | ) | 2,090 | ||||||
Other receivables |
1,635 | 708 | 1,724 | ||||||||
Other assets |
2,878 | (333 | ) | (209 | ) | ||||||
Accounts payable |
719 | (1,278 | ) | 4,095 | |||||||
Accrued compensation and related expenses |
458 | (287 | ) | (1,264 | ) | ||||||
Accrued interest payable |
592 | (1,281 | ) | 147 | |||||||
Income taxes payable |
(637 | ) | 44 | (488 | ) | ||||||
Other accrued liabilities |
(2,215 | ) | (3,670 | ) | (622 | ) | |||||
Other liabilities |
1,665 | 1,789 | (77 | ) | |||||||
Net cash provided by operating activities |
119,704 | 130,124 | 139,131 | ||||||||
Investing activities: |
|||||||||||
Equipment purchases |
(65,252 | ) | (66,204 | ) | (73,830 | ) | |||||
Decrease (increase) in deposits on equipment |
9,657 | (8,365 | ) | 3,733 | |||||||
Purchases of marketable securities |
(39,850 | ) | — | — | |||||||
Proceeds from sales of marketable securities |
39,850 | — | — | ||||||||
Acquisitions, net of cash received |
(88,979 | ) | (75,268 | ) | (760 | ) | |||||
(Increase) decrease in cash in escrow attributable to acquisitions |
(2,270 | ) | (5,077 | ) | 2,947 | ||||||
Investment in unconsolidated joint ventures |
— | — | (240 | ) | |||||||
Proceeds from sale of assets |
4,329 | 3,590 | 7,698 | ||||||||
Net cash used in investing activities |
(142,515 | ) | (151,324 | ) | (60,452 | ) | |||||
73
ALLIANCE HEALTHCARE SERVICES, INC.
CONSOLIDATED STATEMENTS OF CASH FLOWS (Continued)
(dollars in thousands)
| |
Year Ended December 31, | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| |
2007 | 2008 | 2009 | ||||||||
Financing activities: |
|||||||||||
Principal payments on equipment debt |
(5,295 | ) | (6,083 | ) | (8,218 | ) | |||||
Proceeds from equipment debt |
138 | 872 | 1,469 | ||||||||
Principal payments on term loan facility |
(600 | ) | (15,000 | ) | (351,600 | ) | |||||
Proceeds from term loan facility |
— | — | 450,800 | ||||||||
Principal payments on revolving loan facility |
(57,000 | ) | — | — | |||||||
Proceeds from revolving loan facility |
57,000 | — | — | ||||||||
Principal payments on senior subordinated notes |
— | (3,541 | ) | (294,418 | ) | ||||||
Proceeds from senior subordinated notes |
137,250 | — | — | ||||||||
Proceeds from senior notes |
— | — | 187,511 | ||||||||
Principal payments on margin loan facility |
(15,000 | ) | — | — | |||||||
Proceeds from margin loan facility |
15,000 | — | — | ||||||||
Principal payments on bridge loan |
(50,000 | ) | — | — | |||||||
Proceeds from bridge loan |
50,000 | — | — | ||||||||
Payments of debt issuance costs |
(4,190 | ) | (1,023 | ) | (17,794 | ) | |||||
Payments of debt retirement costs |
— | (61 | ) | (757 | ) | ||||||
Noncontrolling interest in subsidiaries |
(1,680 | ) | (1,987 | ) | (5,428 | ) | |||||
Proceeds from share-based payment |
1,109 | 589 | 229 | ||||||||
Purchase of treasury stock |
(61 | ) | (369 | ) | (1,906 | ) | |||||
Excess tax benefit from share-based payment arrangements |
592 | 216 | 12 | ||||||||
Net cash provided by (used in) financing activities |
127,263 | (26,387 | ) | (40,100 | ) | ||||||
Net increase (decrease) in cash and cash equivalents |
104,452 | (47,587 | ) | 38,579 | |||||||
Cash and cash equivalents, beginning of year |
16,440 | 120,892 | 73,305 | ||||||||
Cash and cash equivalents, end of year |
$ | 120,892 | $ | 73,305 | $ | 111,884 | |||||
Supplemental disclosure of cash flow information: |
|||||||||||
Interest paid |
$ | 39,434 | $ | 45,331 | $ | 41,198 | |||||
Income taxes paid, net of refunds |
4,372 | 6,243 | (553 | ) | |||||||
Supplemental disclosure of non-cash investing and financing activities: |
|||||||||||
Net book value of assets exchanged |
$ | 1,737 | $ | 295 | $ | 2,132 | |||||
Capital lease obligations related to the purchase of equipment |
6,688 | 4,865 | 9,703 | ||||||||
Equipment debt transferred |
— | — | (707 | ) | |||||||
Comprehensive loss from hedging transactions, net of taxes |
(1,151 | ) | (2,364 | ) | (233 | ) | |||||
Equipment debt assumed in connection with acquistions |
2,996 | 8,602 | — | ||||||||
Equipment purchases in accounts payable |
5,183 | 5,883 | 4,205 | ||||||||
Non-cash contribution of equipment |
— | — | 3,781 | ||||||||
See accompanying notes.
74
ALLIANCE HEALTHCARE SERVICES, INC.
CONSOLIDATED STATEMENTS OF STOCKHOLDERS' (DEFICIT) EQUITY
(dollars in thousands)
| |
|
|
|
|
|
|
|
Stockholders' (Deficit) Equity Attributable to |
|
||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |
Common Stock | Treasury Stock | Additional Paid-In (Deficit) Capital |
|
Accumulated (Deficit) Retained Earnings |
Total Stockholders' (Deficit) Equity |
|||||||||||||||||||||||||
| |
Accumulated Comprehensive Income (Loss) |
Alliance HealthCare Services, Inc |
Noncontrolling Interest |
||||||||||||||||||||||||||||
| |
Shares | Amount | Shares | Amount | |||||||||||||||||||||||||||
Balance at January 1, 2007 |
49,906,832 | $ | 499 | — | $ | — | $ | (7,070 | ) | $ | 1,356 | $ | (11,759 | ) | $ | (16,974 | ) | $ | 4,376 | $ | (12,598 | ) | |||||||||
Exercise of common stock options |
339,370 | 4 | 1,099 | — | — | 1,103 | 1,103 | ||||||||||||||||||||||||
Issuance of common stock under directors' deferred compensation plan |
33,744 | — | — | — | — | — | — | ||||||||||||||||||||||||
Issuance of restricted stock |
625,000 | 6 | — | — | — | 6 | 6 | ||||||||||||||||||||||||
Issuance of common stock under stock bonus award |
22,305 | — | — | — | — | — | — | ||||||||||||||||||||||||
Purchase of treasury stock |
— | — | (6,569 | ) | (61 | ) | — | — | — | (61 | ) | (61 | ) | ||||||||||||||||||
Share-based payment |
3,860 | — | — | 3,860 | 3,860 | ||||||||||||||||||||||||||
Directors' deferred compensation |
— | — | 49 | — | — | 49 | 49 | ||||||||||||||||||||||||
Stock option income tax benefit |
592 | — | — | 592 | 592 | ||||||||||||||||||||||||||
Unrealized loss on hedging transaction, net of tax |
— | (1,151 | ) | — | (1,151 | ) | (1,151 | ) | |||||||||||||||||||||||
Net contributions/(distributions) |
(1,680 | ) | (1,680 | ) | |||||||||||||||||||||||||||
Net income |
— | — | — | — | — | — | 16,232 | 16,232 | 1,727 | 17,959 | |||||||||||||||||||||
Balance at December 31, 2007 |
50,927,251 | 509 | (6,569 | ) | (61 | ) | (1,470 | ) | 205 | 4,473 | 3,656 | 4,423 | 8,079 | ||||||||||||||||||
Exercise of common stock options |
123,795 | 1 | 584 | — | — | 585 | 585 | ||||||||||||||||||||||||
Issuance of common stock under directors' deferred compensation plan |
59,217 | — | — | — | — | — | — | ||||||||||||||||||||||||
Issuance of restricted stock |
283,300 | 3 | — | — | — | 3 | 3 | ||||||||||||||||||||||||
Issuance of common stock under stock bonus award |
125,470 | 1 | — | — | — | 1 | 1 | ||||||||||||||||||||||||
Purchase of treasury stock |
— | — | (46,362 | ) | (369 | ) | — | — | — | (369 | ) | (369 | ) | ||||||||||||||||||
Share-based payment |
5,276 | — | — | 5,276 | 5,276 | ||||||||||||||||||||||||||
Stock option income tax benefit |
216 | — | — | 216 | 216 | ||||||||||||||||||||||||||
Unrealized loss on hedging transaction, net of tax |
— | (2,364 | ) | — | (2,364 | ) | (2,364 | ) | |||||||||||||||||||||||
Net contributions/(distributions) |
(1,987 | ) | (1,987 | ) | |||||||||||||||||||||||||||
Net income |
— | — | — | — | — | — | 16,523 | 16,523 | 3,030 | 19,553 | |||||||||||||||||||||
Balance at December 31, 2008 |
51,519,033 | 514 | (52,931 | ) | (430 | ) | 4,606 | (2,159 | ) | 20,996 | 23,527 | 5,466 | 28,993 | ||||||||||||||||||
Exercise of common stock options |
64,400 | 1 | 224 | — | — | 225 | 225 | ||||||||||||||||||||||||
Issuance of common stock under directors' deferred compensation plan |
41,016 | — | (164 | ) | — | — | (164 | ) | (164 | ) | |||||||||||||||||||||
Issuance of restricted stock |
313,000 | 3 | — | — | — | 3 | 3 | ||||||||||||||||||||||||
Issuance of common stock under stock bonus award |
87,565 | 1 | — | — | — | 1 | 1 | ||||||||||||||||||||||||
Purchase of treasury stock |
— | (3 | ) | (333,772 | ) | (1,903 | ) | — | — | — | (1,906 | ) | (1,906 | ) | |||||||||||||||||
Share-based payment |
6,080 | — | — | 6,080 | 6,080 | ||||||||||||||||||||||||||
Share-based payment income tax detriment |
(135 | ) | — | — | (135 | ) | (135 | ) | |||||||||||||||||||||||
Unrealized loss on hedging transaction, net of tax |
— | (233 | ) | — | (233 | ) | (233 | ) | |||||||||||||||||||||||
Net contributions/(distributions) |
41 | 41 | (1,688 | ) | (1,647 | ) | |||||||||||||||||||||||||
Net income |
— | — | — | — | — | — | 481 | 481 | 3,064 | 3,545 | |||||||||||||||||||||
Balance at December 31, 2009 |
52,025,014 | $ | 516 | (386,703 | ) | $ | (2,333 | ) | $ | 10,652 | $ | (2,392 | ) | $ | 21,477 | $ | 27,920 | $ | 6,842 | $ | 34,762 | ||||||||||
75
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
DECEMBER 31, 2009
(dollars in thousands, except per
share amounts)
1. Description of the Company and Basis of Financial Statement Presentation
Description of the Company Alliance HealthCare Services, Inc. and its subsidiaries, formerly known as Alliance Imaging, Inc., (the "Company") provides diagnostic imaging services and therapeutic services primarily to hospitals and other healthcare providers on a shared-service and full-time service basis. The Company also provides services through a growing number of fixed sites, primarily to hospitals or health systems. The Company's services normally include the use of its systems, technologists and other clinical staff to operate the systems, equipment maintenance and upgrades and management of day-to-day shared-service and fixed-site diagnostic imaging and radiation oncology operations. The Company also offers ancillary services including marketing support, education, training and billing assistance. The Company operates entirely within the United States and is one of the largest providers of shared service and fixed-site magnetic resonance imaging ("MRI") and positron emission tomography and positron emission tomography/computed tomography ("PET and PET/CT") services in the country. The Company also operates 25 radiation oncology centers at December 31, 2009. For the year ended December 31, 2009, MRI and PET/CT services generated 47% and 40% of the Company's revenue, respectively.
Principles of Consolidation and Basis of Financial Statement Presentation The accompanying consolidated financial statements of the Company include the assets, liabilities, revenues and expenses of all majority-owned subsidiaries over which the Company exercises control. Intercompany transactions have been eliminated. The Company records noncontrolling interest related to its consolidated subsidiaries which are not wholly owned. Investments in non-consolidated investees are accounted for under the equity method. The consolidated financial statements have been prepared in accordance with generally accepted accounting principles ("GAAP") in the United States of America.
On January 1, 2009, the Company adopted Financial Accounting Standards Board ("FASB") Accounting Standards Codification ("ASC") 805, "Business Combinations" (formerly Statement of Financial Accounting Standards ("SFAS") No. 141(R) (Revised 2007), "Business Combinations"), ASC 810, "Consolidation" (formerly SFAS No. 160 "Noncontrolling Interests in Consolidated Financial Statements—An Amendment of Accounting Research Bulletin No. 51") and ASC 260, "Earnings Per Share" (formerly FASB Staff Position ("FSP") Emerging Issues Task Force No. 03-6-1, "Determining Whether Instruments Granted in Share-Based Payment Transactions Are Participating Securities"). As a result of the adoption of ASC 805, the Company is presenting transaction costs as a line on the statement of operations. The adoption of ASC 810 changed the presentation of noncontrolling interest to a component of stockholders' equity, rather than a liability, at December 31, 2009, and the corresponding amount as of December 31, 2008 has been reclassified. In addition, ASC 810 required the presentation of net income attributable to noncontrolling interest, rather than minority interest expense, for the years ended December 31, 2009, 2008 and 2007. In conformity with the current year presentation, the Company has reclassified Noncontrolling interest in subsidiaries from the operating section to the financing section of the Statement of Cash Flows for the years ended December 31, 2007 and 2008. The adoption of ASC 260 changed the calculation of basic earnings per share requiring restricted stock awards that have previously been included in the Company's diluted weighted-average shares to be included in basic weighted-average shares. Earnings per share for prior periods has been recalculated to conform to the current year presentation.
76
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
2. Summary of Significant Accounting Policies
Cash and Cash Equivalents The Company classifies short-term investments with original maturities of three months or less as cash equivalents.
Accounts Receivable The Company provides shared and single-user diagnostic imaging and radiation oncology equipment and technical support services to the healthcare industry and directly to patients on an outpatient basis. Substantially all of the Company's accounts receivables are due from hospitals, other healthcare providers and health insurance providers located throughout the United States. A substantial portion of the Company's services are provided pursuant to long-term contracts with hospitals and other healthcare providers or directly to patients. Accounts receivable generally are collected within industry norms for third-party payors. Estimated credit losses are provided for in the consolidated financial statements and losses experienced have been within management's expectations.
Concentration of Credit Risk Financial instruments which potentially subject the Company to a concentration of credit risk principally consists of cash, cash equivalents and trade receivables. The Company invests available cash in cash equivalents and money market securities of high-credit-quality financial institutions. The Company had cash and cash equivalents in the amount of $68,705 and $106,923 as of December 31, 2008 and 2009, respectively, in excess of federally insured limits. At December 31, 2008 and 2009, the Company's accounts receivable were primarily from clients in the healthcare industry and third-party payors. To reduce credit risk, the Company performs periodic credit evaluations of its clients, but does not generally require advance payments or collateral. Credit losses to clients in the healthcare industry have not been material. The provision for doubtful accounts was 0.9% of revenues in 2007, 0.9% of revenues in 2008 and 0.5% of revenues in 2009, respectively.
Equipment Equipment is stated at cost and is depreciated using the straight-line method over an initial estimated life of three to 10 years to an estimated residual value, between five and 10 percent of original cost. If the Company continues to operate the equipment beyond its initial estimated life, the residual value is then depreciated to a nominal salvage value over three years.
Routine maintenance and repairs are charged to expense as incurred. Major repairs and purchased software and hardware upgrades, which extend the life of or add value to the equipment, are capitalized and depreciated over the remaining useful life.
With the exception of a relatively small dollar amount of office furniture, office equipment, computer equipment, software and leasehold improvements, substantially all of the property owned by the Company relates to diagnostic imaging and radiation oncology equipment, power units and mobile trailers used in the business.
Goodwill and Intangible Assets ASC 350, "Intangibles—Goodwill and Other" (formerly SFAS No. 142, "Goodwill and Other Intangible Assets") requires that goodwill and intangible assets with indefinite useful lives not be amortized, but instead be tested for impairment at least annually. In accordance with ASC 350, the Company has selected to perform an annual impairment test for goodwill and intangible assets with indefinite useful lives based on the financial information as of September 30, or more frequently when an event occurs or circumstances change to indicate an impairment of these assets has possibly occurred. Goodwill and intangible assets with indefinite useful lives are allocated to the Company's various reporting units, which are its geographical regions. ASC
77
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
2. Summary of Significant Accounting Policies (Continued)
350 requires the Company to compare the fair value of the reporting unit to its carrying amount on an annual basis to determine if there is potential impairment. If the fair value of the reporting unit is less than its carrying value, an impairment loss is recorded to the extent that the implied fair value of the goodwill and intangible assets with indefinite useful lives within the reporting unit is less than the carrying value. The fair value of the reporting unit is determined based on discounted cash flows, market multiples or appraised values as appropriate. The Company complies with periodic impairment test procedures. In 2007, 2008, and 2009 the Company concluded that the fair value of each reporting unit exceeded its carrying value, indicating no goodwill or indefinite-lived intangible asset impairment was present. No triggering events occurred during the fourth quarters of 2007, 2008 and 2009 which required an additional impairment test as of December 31, 2007, 2008, or 2009. ASC 350 also requires intangible assets with definite useful lives to be amortized over their respective estimated useful lives to their estimated residual values and reviewed for impairment in accordance with ASC 360, "Property, Plant, and Equipment" (formerly SFAS No. 144, "Accounting for the Impairment or Disposal of Long-Lived Assets"). In 2007, 2008 and 2009 the Company concluded that no impairment was present in its intangible assets with definite useful lives.
Impairment of Long-Lived Assets The Company accounts for long-lived assets in accordance with the provisions of ASC 360. ASC 360 requires that long-lived assets be reviewed for impairment whenever events or changes in circumstances indicate that the carrying amount of an asset may not be recoverable. Recoverability of assets to be held and used is measured by a comparison of the carrying amount of an asset to undiscounted future net cash flows expected to be generated by the asset. If the carrying amount of an asset exceeds its estimated future cash flows, an impairment charge is recognized by the amount by which the carrying amount of the asset exceeds the fair value of the asset. Assets to be disposed of are reported at the lower of the carrying amount or fair value less costs to sell. In 2007, 2008 and 2009 the Company concluded that no impairment was present in its long-lived assets.
Revenue Recognition The majority of the Company's revenues are derived directly from healthcare providers and are primarily for imaging services. To a lesser extent, revenues are generated from direct billings to third-party payors or patients which are recorded net of contractual discounts and other arrangements for providing services at less than established patient billing rates. Revenues from billings to third-party payors and patients amounted to approximately 11%, 21% and 20% of revenues for the years ended December 31, 2007, 2008 and 2009, respectively. No single customer accounted for more than 2% of consolidated revenues in each of the years ended December 31, 2007, 2008, and 2009, respectively. The Company recognizes revenue in accordance with ASC 600, "Revenue" (formerly Staff Accounting Bulletin No. 104, "Revenue Recognition"). As the price is predetermined, all revenues are recognized at the time the delivery of service has occurred and collectibility is reasonably assured which is based upon contract terms with healthcare providers and negotiated rates with third party payors and patients. The Company also records revenue from management services that it performs based upon management service contracts with predetermined pricing. Revenues from these services amounted to approximately 9%, 6% and 5% of total revenue for the three years ended December 31, 2007, 2008 and 2009, respectively. These revenues are recorded in the period in which the service is performed and collections of the billed amounts are reasonably assured in accordance with ASC 600.
78
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
2. Summary of Significant Accounting Policies (Continued)
Share-Based Payment ASC 718, "Compensation—Stock Compensation" (formerly SFAS No. 123(R) (revised December 2004), "Share-Based Payment"), requires that the fair value at the grant date resulting from all share-based payment transactions be recognized in the financial statements. Further, ASC 718 requires entities to apply a fair-value based measurement method in accounting for these transactions. This value is recorded over the vesting period. Under ASC 718, the Company records in its consolidated statements of operations (i) compensation cost for options granted, modified, repurchased or cancelled on or after January 1, 2006 under the provisions of ASC 718 and (ii) compensation cost for the unvested portion of options granted prior to January 1, 2006 over their remaining vesting periods using the amounts previously measured under ASC 718 for pro forma disclosure purposes.
Derivatives The Company accounts for derivative instruments and hedging activities in accordance with the provisions of ASC 815, "Derivatives and Hedging" (formerly SFAS No. 133, "Accounting for Derivative Instruments and Hedging Activities" and SFAS No. 138, "Accounting for Certain Derivative Instruments and Hedging Activities", an amendment of SFAS 133). On the date the Company enters into a derivative contract, management may designate the derivative as a hedge of the identified exposure. The Company formally documents all relationships between hedging instruments and hedged items, as well as the risk-management objective and strategy for undertaking various hedge transactions. In this documentation, the Company specifically identifies the firm commitment or forecasted transaction that has been designated as a hedged item and states how the hedging instrument is expected to hedge the risks related to the hedged item. The Company formally measures effectiveness of its hedging relationships, both at the hedge inception and on an ongoing basis, in accordance with its risk management policy. The Company would discontinue hedge accounting prospectively (i) if it is determined that the derivative is no longer effective in offsetting change in the cash flows of a hedged item, (ii) when the derivative expires or is sold, terminated or exercised, (iii) because it is probable that the forecasted transaction will not occur, (iv) because a hedged firm commitment no longer meets the definition of a firm commitment, or (v) if management determines that designation of the derivative as a hedge instrument is no longer appropriate. The Company's derivatives are recorded on the balance sheet at their fair value. For derivatives accounted for as cash flow hedges any unrealized gains or losses on fair value are included in comprehensive income (loss), net of tax, assuming perfect effectiveness. Any ineffectiveness is recognized in earnings.
Income Taxes The provision for income taxes is determined in accordance with ASC 740, "Income Taxes" (formerly SFAS No. 109, "Accounting for Income Taxes"). Deferred tax assets and liabilities are determined based on the temporary differences between the financial reporting and tax bases of assets and liabilities, applying enacted statutory tax rates in effect for the year in which the differences are expected to reverse. Future income tax benefits are recognized only to the extent that the realization of such benefits is considered to be more likely than not. The Company regularly reviews its deferred tax assets for recoverability and establishes a valuation allowance, when it is more likely than not that such deferred tax assets will not be recoverable, based on historical taxable income, projected future taxable income, and the expected timing of the reversals of existing temporary differences. Effective January 1, 2007, the Company adopted the provisions of ASC 740 pertaining to the accounting for uncertainty in income taxes (formerly FASB Interpretation No. 48, "Accounting for
79
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
2. Summary of Significant Accounting Policies (Continued)
Uncertainty in Income Taxes—an Interpretation of SFAS 109"). These provisions clarified the accounting for uncertainty in income taxes recognized in an enterprise's financial statements. The provisions prescribe a recognition threshold and measurement attribute for the financial statement recognition and measurement of a tax position taken or expected to be taken in a tax return. These provisions of ASC 740 also provides guidance on derecognition, classification, interest and penalties, accounting in interim periods, disclosure, and transition.
Fair Values of Financial Instruments The carrying amount reported in the balance sheet for cash and cash equivalents approximates fair value based on the short-term maturity of these instruments. The carrying amounts reported in the balance sheet for accounts receivable and accounts payable approximate fair value based on the short-term nature of these accounts. The carrying amount reported in the balance sheet for long-term debt under the Company's New Credit Agreement (as discussed in Note 5 to the Consolidated Financial Statements) approximates fair value, as these borrowings have variable rates that reflect currently available terms, credit spreads and conditions for similar debt. The fair value of the Company's senior subordinated notes, senior notes and its equipment loans was $266,349 and $206,167 compared to the carrying amount reported on the balance sheet of $310,962 and $216,993 as of December 31, 2008 and 2009, respectively. The fair value of the Company's senior subordinated notes was based upon the bond trading prices at December 31, 2008 and 2009, respectively. The fair value of the equipment loans was estimated using discounted cash flow analyses, based on the Company's current incremental rates for similar types of equipment loans.
Use of Estimates The preparation of financial statements in conformity with accounting principles generally accepted in the United States of America requires management to make estimates and assumptions that affect the amounts reported in the financial statements and accompanying notes. Actual results could differ from those estimates.
Comprehensive Income (Loss) The Company reports comprehensive income (loss) in accordance with ASC 220, "Comprehensive Income" (formerly SFAS No. 130, "Reporting Comprehensive Income"). For the years ended December 31, 2007, 2008 and 2009, the Company had entered into multiple interest rate swap agreements and interest rate collar agreements, as discussed in Note 11 to the Consolidated Financial Statements. Assuming perfect effectiveness, any unrealized gains and losses related to the swaps and collars that qualify for hedge accounting are classified as a component of comprehensive income (loss), net of any tax. Any ineffectiveness is recognized in earnings.
Segment Reporting The chief operating decision maker ("CODM") reviews the operating results of the Company's geographic regions for the purpose of making operating decisions and assessing performance. Based on the aggregation criteria in ASC 280, "Segment Reporting" (formerly SFAS No. 131, "Disclosures about Segments of an Enterprise and Related Information"), the Company has aggregated the results of its geographic regions into one reportable segment. During 2009, the Company created two separate divisions, an Imaging Division and an Oncology Division, which constitute separate operating segments as defined by ASC 280. However, for the year ended December 31, 2009, the Oncology Division did not meet the quantitative thresholds for separate reporting. Additionally, the Company does not consider its wholesale revenue and retail revenue
80
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
2. Summary of Significant Accounting Policies (Continued)
sources to constitute separate operating segments as discrete financial information does not exist and is not provided to the CODM.
Recent Accounting Pronouncements FASB ASC 805, "Business Combinations" (formerly SFAS 141(R)) significantly changes the accounting for business combinations. Under ASC 805, an acquiring entity is required to recognize all the assets acquired and liabilities assumed in a transaction at the acquisition-date fair value with limited exceptions. ASC 805 changes the accounting treatment for certain specific items, including:
- •
- Acquisition costs will be generally expensed as incurred;
- •
- Noncontrolling interests (formerly known as "minority interests"—see ASC 810 discussion below) will generally
be valued at fair value at the acquisition date;
- •
- Restructuring costs associated with a business combination will generally be expensed subsequent to the acquisition date;
and
- •
- Changes in deferred tax asset valuation allowances and income tax uncertainties after the acquisition date generally will affect income tax expense.
ASC 805 also includes a substantial number of new disclosure requirements. ASC 805 applies prospectively to business combinations for which the acquisition date is on or after the beginning of the first annual reporting period beginning on or after December 15, 2008. Earlier adoption is prohibited. The Company adopted ASC 805 on January 1, 2009. The adoption of ASC 805 did not have a material impact on the Company's results of operations, cash flows or financial position for the year ended December 31, 2009, except for the presentation of transaction costs as a line in the statements of operations.
FASB ASC 805 (formerly FSP No. FAS 141(R)-1, "Accounting for Assets Acquired and Liabilities Assumed in a Business Combination That Arise from Contingencies") is effective for contingent assets or contingent liabilities acquired in business combinations for which the acquisition date is on or after the beginning of the first annual reporting period beginning on or after December 15, 2008. The adoption of this standard did not have a material impact on the Company's results of operations, cash flows or financial position for the year ended December 31, 2009.
FASB ASC 810, "Consolidation" (formerly SFAS 160) establishes new accounting and reporting standards for the noncontrolling interest in a subsidiary and for the deconsolidation of a subsidiary. Specifically, this statement requires the recognition of a noncontrolling interest (minority interest) as equity in the consolidated financial statements and separate from the parent's equity. The amount of net income attributable to the noncontrolling interest is included in consolidated net income on the face of the income statement. ASC 810 clarifies that changes in a parent's ownership interest in a subsidiary that do not result in deconsolidation are equity transactions if the parent retains its controlling financial interest. In addition, this statement requires that a parent recognize a gain or loss in net income when a subsidiary is deconsolidated. Such gain or loss will be measured using the fair value of the noncontrolling equity investment on the deconsolidation date. ASC 810 also includes expanded disclosure requirements regarding the interests of the parent and its noncontrolling interest.
81
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
2. Summary of Significant Accounting Policies (Continued)
The Company adopted ASC 810 on January 1, 2009. The adoption of ASC 810 did not have a material impact on the Company's results of operations, cash flows or financial position for the year ended December 31, 2009; however, there may be an impact on future transactions. The adoption of ASC 810 changed the presentation of noncontrolling interest to a component of stockholders equity, rather than a liability, at December 31, 2009, and the corresponding amount as of December 31, 2008 was reclassified. In addition, ASC 810 required the presentation of net income attributable to noncontrolling interest, rather than minority interest expense, for the years ended December 31, 2007, 2008 and 2009. In conformity with the current year presentation under ASC 810, the Company has reclassified Noncontrolling interest in subsidiaries from the operating section to the financing section of the Statement of Cash Flows for the years ended December 31, 2007 and 2008.
FASB ASC 815, "Derivatives and Hedging" (formerly SFAS No. 161, "Disclosure about Derivative Instruments and Hedging Activities—An Amendment of FASB Statement No. 133") enhances the current guidance on disclosure requirements for derivative instruments and hedging activities. This statement requires that objectives for using derivative instruments be disclosed in terms of underlying risk and accounting designation. Specifically, ASC 815 requires disclosure about (a) how and why an entity uses derivative instruments, (b) how derivative instruments and related hedged items are accounted for under ASC 815 and its related interpretations, and (c) how derivative instruments and related hedged items affect an entity's financial position, financial performance, and cash flow. This statement requires qualitative disclosure about the objectives and strategies for using derivatives in terms of the risks that the entity is intending to manage, quantitative disclosures about fair value amounts of gains and losses on derivative instruments in a tabular format, and disclosures about credit-risk-related contingent features in derivative agreements to provide information on potential effect on an entity's liquidity from using derivatives. The derivative instruments shall be distinguished between those used for risk management purposes and those used for other purposes. ASC 815 is effective for fiscal years, and interim periods within those fiscal years, beginning after November 15, 2008, with early application encouraged. The Company adopted the provisions of ASC 815 on January 1, 2009. The adoption of ASC 815 did not have a material impact on the Company's results of operations, cash flows or financial position for the year ended December 31, 2009.
FASB ASC 260, "Earnings Per Share" (formerly FSP 03-6-1) addresses whether instruments granted in share-based payment transactions are participating securities prior to vesting and therefore need to be included in the earnings allocation in calculating earnings per share under the two-class method described in ASC 260. ASC 260 requires companies to treat unvested share-based payment awards that have non-forfeitable rights to dividend or dividend equivalents as a separate class of securities in calculating earnings per share. ASC 260 is effective for fiscal years beginning after December 15, 2008 and is to be applied retrospectively. The Company adopted the provisions of ASC 260 on January 1, 2009. The Company granted and expects to continue to grant restricted stock awards to its officers and non-employee directors that contain non-forfeitable rights to dividend and dividend equivalents. Such awards are considered participating securities under ASC 260. As such, the Company is required to include these awards in the calculation of the Company's basic earnings per share and will need to calculate basic earnings per share using the two-class method. Restricted stock awards have previously been included in the Company's dilutive earnings per share calculation using the treasury
82
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
2. Summary of Significant Accounting Policies (Continued)
stock method. The two-class method of computing earnings per share is an earnings allocation formula that determines earnings per share for each class of common stock and participating security according to dividends declared (or accumulated) and participation rights in undistributed earnings. The Company has historically not paid and does not expect to pay dividends in the foreseeable future; however, the Company must still allocate undistributed earnings between common shareholders and participating securities based on the contractual rights of each security, as if all the earnings for the period have been distributed. Since the adoption of ASC 260 was applied retrospectively, the earnings per share for prior periods was recalculated to conform to the current year presentation. The weighted-average number of shares used in the basic earnings per share calculation for the years ended December 31, 2007 and 2008 have been recalculated using the two-class method to conform to the current year presentation.
FASB ASC 825, "Financial Instruments" (formerly FSP No. FAS 107-1 and Accounting Principles Board ("APB") Opinion No. 28-1, "Interim Disclosures about Fair Value of Financial Instruments") requires disclosures about the fair value of financial instruments in interim financial statements as well as in annual financial statements. ASC 825 is effective for periods ending after June 15, 2009. The Company adopted ASC 825 during the interim period ended June 30, 2009.
FASB ASC 855, "Subsequent Events" (formerly SFAS No. 165, "Subsequent Events") enhances the current guidance on accounting and disclosure requirements for subsequent events. This statement requires the disclosure of the date through which an entity has evaluated subsequent events and the basis for that date, that is, whether that date represents the date the financial statements were issued or were available to be issued. ASC 855 is effective for interim periods and annual financial periods ending after June 15, 2009. The adoption of ASC 855 did not have a material impact on the Company's results of operations, cash flows or financial position for the year ended December 31, 2009.
Accounting Standards Update ("ASU") No. 2009-17 ("ASU 2009-17") (formerly SFAS No. 167, "Amendments to FASB Interpretation No. 46 (R)") enhances the current guidance on disclosure requirements for companies with financial interest in a variable interest entity. ASU 2009-17 replaces the quantitative-based risks and rewards calculation for determining which enterprise, if any, has a controlling financial interest in a variable interest entity with an approach focused on identifying which enterprise has the power to direct the activities of a variable interest entity that most significantly impact the entity's economic performance and (a) the obligation to absorb losses of the entity or (b) the right to receive benefits from the entity. ASU 2009-17 requires an additional reconsideration event when determining whether an entity is a variable interest entity when any changes in facts and circumstances occur such that the holders of the equity investment at risk, as a group, lose the power from voting rights or similar rights of those investments to direct the activities of the entity that most significantly impact the entity's economic performance. It also requires ongoing assessments of whether an enterprise is the primary beneficiary of a variable interest entity. ASU 2009-17 requires additional disclosures about an enterprise's involvement in variable interest entities. ASU 2009-17 is effective for fiscal years beginning after November 15, 2009, with early application prohibited. The Company adopted the provisions of ASU 2009-17 on January 1, 2010. The adoption of ASU 2009-17 did not have a material impact on the Company's results of operations, cash flows or financial position.
83
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
2. Summary of Significant Accounting Policies (Continued)
FASB ASC 105, "Generally Accepted Accounting Principles" [formerly SFAS No. 168, "The FASB Accounting Standards Codification and the Hierarchy of Generally Accepted Accounting Principles"] is the single source of authoritative GAAP in the United States. The previous GAAP hierarchy consisted of four levels of authoritative accounting and reporting guidance levels. The ASC eliminated this hierarchy and replaced the previous GAAP with just two levels of literature: authoritative and non-authoritative. The ASC was effective as of July 1, 2009.
3. Transactions
On November 27, 2006, affiliates of Kohlberg Kravis Roberts & Co ("KKR") sold 9,200,000 shares of the Company's common stock in an underwritten secondary public offering. Following completion of this offering, KKR beneficially owned approximately 52% of the Company's outstanding shares of common stock. The Company did not sell any shares and did not receive any proceeds from the sale of shares in the public offering.
On April 16, 2007, funds managed by Oaktree Capital Management, LLC ("Oaktree") and MTS Health Investors, LLC ("MTS") purchased 24,501,505 shares of the Company's common stock from a fund managed by an affiliate of KKR. Upon completion of the transaction, Oaktree and MTS owned in the aggregate approximately 49.7% of the outstanding shares of the Company's common stock. At December 31, 2009, Oaktree and MTS owned in the aggregate approximately 47.1% of the outstanding shares of common stock of the Company.
Effective October 1, 2007, the Company purchased the assets of Diagnostic Radiology Systems, Inc., a mobile provider of magnetic resonance imaging ("MRI") and positron emission tomography/computed tomography ("PET/CT"), with operations in a certificate of need state. The purchase price consisted of $8,620 in cash and transaction costs. The acquisition was financed using internally generated funds. As a result of this acquisition, the Company recorded goodwill of $2,148 and acquired intangible assets of $2,240, of which $1,520 was assigned to customer contracts, which is amortized over eight years, $510 was assigned to the non-compete agreement, which was amortized over one year, and $210 was assigned to certificates of needs, which have indefinite useful lives and are not subject to amortization. The intangible assets were recorded at fair value at the acquisition date. All recorded goodwill and intangible assets are capitalized for tax purposes and amortized over 15 years. The preliminary values above were subject to adjustment for up to one year after the close of the transaction due to additional information that could result in changes in the original valuation of assets acquired and liabilities assumed. During the year ended December 31, 2008, the Company increased goodwill by $35 as a result of changes in the original valuation of assets acquired and liabilities assumed. The year ended December 31, 2007 included three months of operations from this acquisition. The Company has not included pro forma information as this acquisition did not have a material impact on its consolidated financial position or results of operations.
Effective November 2, 2007, the Company purchased the assets of eight radiation oncology centers in Alabama, Arkansas, Mississippi, and Missouri from Bethesda Resources, Inc., a wholly-owned subsidiary of Sonix, Inc (the "Bethesda Transaction"). Many of these centers are sole community providers and are located on or near hospital campuses. Several of these radiation oncology centers
84
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
3. Transactions (Continued)
operate under certificates of need. The purchase price consisted of $36,500 in cash and $800 in assumed liabilities and transaction costs. The acquisition was financed using internally generated funds and capital leases. As a result of this acquisition, the Company recorded goodwill of $4,246 and acquired intangible assets of $31,230, of which $2,230 was assigned to the physician referral network, which is amortized over seven years and $29,000 was assigned to certificates of need, which have indefinite useful lives and are not subject to amortization. The intangible assets were recorded at fair value at the acquisition date. All recorded goodwill and intangible assets are capitalized for tax purposes and amortized over 15 years. During the year ended December 31, 2008, the Company decreased goodwill by $72 as a result of changes in the original valuation of assets acquired and liabilities assumed. The year ended December 31, 2007 included approximately two months of operations from this acquisition. The Company has not included pro forma information as this acquisition did not have a material impact on its consolidated financial position or results of operations.
Effective November 5, 2007, the Company purchased all of the outstanding shares of the New England Health Enterprises Business Trust and all of the outstanding membership interests of New England Imaging Management, LLC, a fixed-site provider of magnetic resonance imaging ("MRI") and computed tomography ("CT"), collectively referred to as New England Health Enterprises, or NEHE. NEHE operated seven fixed-site imaging centers and one mobile MRI system in Maine and Massachusetts. The purchase price consisted of $44,635 in cash, $2,270 in cash which has been held in an escrow account, and $4,592 in assumed liabilities and transaction costs. The acquisition was financed using internally generated funds, borrowings under an Acquisition Credit Facility and capital leases. The Company recorded total goodwill of $19,341, which includes $10,947 of goodwill related to deferred tax liabilities recorded for basis differences in intangible assets as a result of the acquisition. None of the goodwill recorded is deductible for tax purposes. The Company acquired intangible assets of $29,000, of which $15,700 was assigned to the physician referral network, which is amortized over 15 years, $3,800 was assigned to the non-compete agreement, which is amortized over five years, and $9,500 was assigned to certificates of need held by NEHE, which have indefinite useful lives and are not subject to amortization. These assets were recorded at fair value at the acquisition date. At the acquisition date, the acquisition included $2,270 for a contingent payment which was placed in an escrow account, pending the resolution of claims for indemnification and contingent consideration based on certain performance target requirements, which were resolved over one to three years following the acquisition date. During the year ended December 31, 2009, these contingencies were resolved and the Company recorded a decrease to goodwill of $570. The Company received $2,825 from escrow during 2009. All contingencies have been resolved and all escrow amounts have been distributed as of December 31, 2009. The year ended December 31, 2007 included approximately two months of operations from this acquisition. The Company has not included pro forma information as this acquisition did not have a material impact on its consolidated financial position or results of operations.
On December 4, 2007, the Company issued an additional $150,000 of its 71/4% Senior Subordinated Notes due 2012 (the "new 71/4% Notes") in a transaction exempt from the registration requirements of the Securities Act of 1933, as amended. The new 71/4% Notes were subsequently registered. The new 71/4% Notes were issued at a discount of 8.5%, which was being amortized to interest expense through
85
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
3. Transactions (Continued)
the maturity date of the notes. The new 71/4% Notes have terms that were substantially identical to the Company's original 71/4% Notes, but were issued under a new indenture and are therefore a separate series of notes. The Company used a portion of the net proceeds from the issuance of the new 71/4% Notes to repay and terminate an Acquisition Credit Facility entered into to finance the NEHE acquisition (as described in Note 9 of the Notes to the Consolidated Financial Statements). The remaining net proceeds were used for general corporate purposes, including acquisitions. The 71/4% Notes were substantially redeemed in December 2009, in conjunction with our Refinance Transaction, as discussed below. At December 31, 2009, $5,582 of the 71/4% Notes were outstanding. The remaining balance of the 71/4% Notes was redeemed at par in January 2010.
In the first quarter of 2008, the Company purchased six CyberKnife® robotic radiosurgery facilities from Accuray, Inc. The radiosurgery systems are currently providing radiosurgery services at hospitals located in California, Maryland, New Jersey and Tennessee. The purchase price totaled $10,287 in cash and $732 in transaction costs. The acquisition was financed using proceeds from the Company's issuance of the new 71/4% Notes. As a result of this acquisition, the Company recorded acquired intangible assets of $1,459, which was assigned to customer contracts and is being amortized over seven years. The intangible assets were recorded at fair value at the acquisition date. All recorded intangible assets are capitalized for tax purposes and are being amortized over 15 years. The year ended December 31, 2008 included approximately nine months of operations from this acquisition. The Company has not included pro forma information as this acquisition did not have a material impact on its consolidated financial position or results of operations.
In the third quarter of 2008, the Company purchased all of the outstanding membership interests of Medical Outsourcing Services, LLC ("MOS"), a mobile provider of positron emission tomography/computed tomography ("PET/CT"), based in Naperville, Illinois. MOS operated in nine states, including, Illinois, Indiana, Iowa, Michigan, Missouri, New Jersey, Ohio, Pennsylvania, and Wisconsin. The purchase price consisted of $17,271 in cash, $2,500 in cash which is being held in an escrow account, and $4,564 in assumed liabilities and transaction costs. The Company financed this acquisition using internally generated funds and proceeds from the Company's issuance of the new 71/4% Notes. As a result of this acquisition, the Company recorded goodwill of $3,303 and acquired intangible assets of $12,450, of which $3,850 was assigned to the physician referral network, which is being amortized over five years, $6,100 was assigned to customer relationships, which is being amortized over 10 years, and $2,500 was assigned to a non-compete agreement, which is being amortized over three years. The intangible assets were recorded at fair value at the acquisition date. All recorded goodwill and intangible assets are capitalized for tax purposes and are being amortized over 15 years. The acquisition included $2,500 for a contingent payment which is being held in an escrow account, pending the resolution of claims for indemnification, which is expected to be resolved over the three years following the acquisition date. When the contingencies are resolved and consideration is distributable from the escrow account, the Company will record the fair value of the consideration as additional purchase price to goodwill. During the year ended December 31, 2009, the Company increased goodwill by $67 as a result of changes in the original valuation of assets acquired and liabilities assumed. The year ended December 31, 2008 included six months of operations from this acquisition. The Company has not included pro forma information as this acquisition did not have a material impact on its
86
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
3. Transactions (Continued)
consolidated financial position or results of operations. Please also see further discussion in Note 12 of the Notes to the Consolidated Financial Statements.
In the third quarter of 2008, the Company purchased all of the outstanding membership interests of RAMIC Des Moines, LLC ("RAMIC"), a single modality center providing MRI services in West Des Moines, Iowa. The purchase price consisted of $7,216 in cash, $605 in cash which is being held in an escrow account, and $114 in assumed liabilities and transaction costs. The Company financed this acquisition using internally generated funds and proceeds from the Company's issuance of the new 71/4% Notes. As a result of this acquisition, the Company recorded goodwill of $2,899 and acquired intangible assets of $2,600, of which $1,850 was assigned to the physician network, which is being amortized over five years, and $750 was assigned to certificates of need held by RAMIC, which have indefinite useful lives and are not subject to amortization. The intangible assets were recorded at fair value at the acquisition date. All recorded goodwill and intangible assets are capitalized for tax purposes and are being amortized over 15 years. The acquisition included $605 for a contingent payment which was being held in an escrow account, pending the resolution of claims for indemnification. During the year ended December 31, 2009, $550 was released from escrow, which was recorded to goodwill as additional purchase price. All contingencies have been resolved and all escrow amounts have been distributed as of December 31, 2009. The year ended December 31, 2008 included approximately five months of operations from this acquisition. The Company has not included pro forma information as this acquisition did not have a material impact on its consolidated financial position or results of operations.
In the fourth quarter of 2008, the Company purchased all of the outstanding membership interests of Shared PET Imaging, LLC ("SPI"), a mobile and fixed-site provider of PET and PET/CT, based in Canton, Ohio. SPI served approximately 90 clients in thirteen states, including Ohio, Michigan, Indiana, Illinois, Florida, Pennsylvania, New York, Tennessee and South Carolina. The purchase price consisted of $34,092 in cash, $2,000 in cash which is being held in an escrow account, and $9,102 in assumed liabilities and transaction costs. The Company financed this acquisition using internally generated funds and proceeds from the Company's issuance of the new 71/4% Notes. As a result of this acquisition, the Company recorded goodwill of $6,895 and acquired intangible assets of $9,350, of which $500 was assigned to the physician referral network, which is being amortized over five years, $5,350 was assigned to customer relationships, which is being amortized over 13 years, $3,150 was assigned to a non-compete agreement, which is being amortized over three years, and $350 was assigned to certificates of need held by SPI, which have indefinite useful lives and are not subject to amortization. The intangible assets were recorded at fair value at the acquisition date. All recorded goodwill and intangible assets are capitalized for tax purposes and are being amortized over 15 years. The acquisition included $2,000 for a contingent payment which is being held in an escrow account, pending the resolution of claims for indemnification, which is expected to be resolved over the 18 months following the acquisition date. When the contingencies are resolved and consideration is distributable from the escrow account, the Company will record the fair value of the consideration as additional purchase price to goodwill. During the year ended December 31, 2009, the Company increased goodwill by $383 as a result of changes in the original valuation of assets acquired and liabilities assumed. The year ended December 31, 2008 included one month of operations from this acquisition. The Company has
87
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
3. Transactions (Continued)
not included pro forma information as this acquisition did not have a material impact on its consolidated financial position or results of operations.
Also in the fourth quarter of 2008, the Company purchased the remaining 20% minority interest in Alliance Oncology ("AO"). The total purchase price was $6,524, which consisted entirely of cash. The Company financed this acquisition using internally generated funds. As a result of this acquisition, the Company recorded goodwill of $4,537. All recorded goodwill is capitalized for tax purposes and amortized over 15 years.
During December 2009, the Company entered into and completed various debt related transactions in order to expand its borrowing capacity and extend the maturity of its debt (the "Refinance Transaction"). In order to accomplish this, the Company retired substantially all of its $300,000 71/4% senior subordinated notes due 2012 (the "71/4% Notes") through a cash tender offer (the "Tender Offer") and repaid the balance of $351,600 on its existing Tranche C1 term loan facility (the "Old Term Loan"). In conjunction with the Refinance Transaction, the Company also entered into a new senior secured credit agreement (the "New Credit Facility"), comprised of a $460,000 term loan (the "New Term Loan") maturing June 2016 and a $120,000 revolving facility (the "New Revolving Credit Facility") maturing December 2014. Borrowings under the New Term Loan were issued at 98.0% of par, with the discount to par being amortized to interest expense and other, net through the maturity date of the loan. The Company also issued $190,000 of 8.0% senior notes due 2016 (the "8% Notes") in a transaction that was exempt from the registration requirements of the Securities Act of 1933, as amended. The 8% Notes were issued at 98.69% of par, with the discount to par being amortized to interest expense and other, net through the maturity date of the notes. Borrowings under the New Credit Facility bear interest through maturity at a variable rate based upon, at the Company's option, either London InterBank Offered Rate ("LIBOR") or the base rate (which is the highest of the administrative agent's prime rate, one-half of 1.00% in excess of the overnight federal funds rate, and 1.00% in excess of the one-month LIBOR rate), plus in each case, an applicable margin. With respect to the New Term Loan, the applicable margin for LIBOR loans is 3.50% per annum, and with respect to the New Revolving Credit Facility, the applicable margin for LIBOR loans ranges, based on the applicable leverage ratio, from 3.25% to 3.75% per annum, in each case, with a LIBOR floor of 2.00%. With respect to the New Term Loan, the applicable margin for base rate loans is 2.50% per annum, and with respect to the New Revolving Credit Facility, the applicable margin for base rate loans ranges, based on the applicable leverage ratio, from 2.25% to 2.75% per annum. The Company used the proceeds from these transactions and existing cash to complete the Tender Offer and purchase $294,418 of the 71/4% Notes at a purchase price equal to 100.125% of the principal amount, together with the accrued interest to the redemption date. The Company also used the proceeds from these transactions to pay off the Old Term Loan and redeem the remaining $5.6 million of 71/4% notes in January 2010 at a redemption price equal to 100.0% of the principal amount, together with accrued interest to the redemption date. The Company incurred a loss on extinguishment of debt of $14,600 related to the Refinance Transaction, which represents the tender premium and consent payment to redeem the 71/4% Notes, write-off of unamortized debt issuance costs related to the retired debt, and other fees and expenses.
88
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
4. Share-Based Payment
The Company adopted ASC 718, "Compensation—Stock Compensation" (formerly SFAS No. 123(R) (revised December 2004), "Share-Based Payment" ("SFAS 123(R)")) in the fiscal year beginning January 1, 2006, using the modified prospective application transition method. Under ASC 718, the Company records in its consolidated statements of operations (i) compensation cost for options granted, modified, repurchased or cancelled on or after January 1, 2006 under the provisions of ASC 718 and (ii) compensation cost for the unvested portion of options granted prior to January 1, 2006 over their remaining vesting periods using the amounts previously measured under ASC 718 for pro forma disclosure purposes.
The Company has elected to follow the alternative transition method as described in ASC 718 (formerly FSP FAS123R-3, "Transition Election to Accounting for the Tax Effects of Share-Based Payment Awards") for computing its beginning additional paid-in capital pool. In addition, the Company treats the tax deductions from stock options as being realized when they reduce taxes payable in accordance with the principles and timing under the relevant tax law.
Stock Option Plans and Awards
In November 1999, the Company adopted an employee stock option plan (the "1999 Equity Plan") pursuant to which options and awards with respect to a total of 6,325,000 shares of the Company's common stock became available for grant. On May 30, 2007, the Company adopted an amendment to the 1999 Equity Plan which increased the number of shares available to be awarded to 8,025,000 shares. On May 27, 2009, the Company adopted an amendment to the 1999 Equity Plan which increased the number of shares available to be awarded to 11,025,000 shares. As of December 31, 2009, a total of 3,347,587 shares were available for grant under the 1999 Equity Plan. Options are granted with exercise prices equal to fair value of the Company's common stock at the date of grant, except as noted below. All options have 10-year terms. Options granted after January 1, 2008 are time options which vest 25% each year, over four years. For options granted prior to January 1, 2008, initial stock option grants were comprised 50% of "time options" and 50% of "performance options." The time options have a five-year vesting schedule, vesting 20% per year. The performance options cliff vest after eight years; however, in the event certain operating performance targets are met, up to 20% of the performance options may vest each year, accelerating the vesting period up to five years. During the year ended December 31, 2009, there were no options in which vesting was accelerated. Prior to January 1, 2008, subsequent stock options granted under the 1999 Equity Plan to employees were always time options which vest 5% in the first year, 20% in the second year and 25% in years three through five.
In November 2000, the Company granted stock options to certain employees at exercise prices below the fair value of the Company's common stock, of which 35,000 options were outstanding at December 31, 2009. The exercise prices of these options and the fair value of the Company's common stock on the grant date were $5.60 and $9.52 per share, respectively.
The Company uses the Black-Scholes option pricing model to value the compensation expense associated with share-based payment awards. The fair value of each option award is estimated on the date of grant using the Black-Scholes option pricing model that uses the assumptions noted in the table
89
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
4. Share-Based Payment (Continued)
below. In addition, forfeitures are estimated when recognizing compensation expense and the estimate of forfeitures will be adjusted over the requisite service period to the extent that actual forfeitures differ, or are expected to differ, from such estimates. Changes in estimated forfeitures will be recognized through a cumulative catch-up adjustment in the period of change and will also impact the amount of compensation expense to be recognized in future periods. The Company records share-based payments for stock options granted with exercise prices below the fair value of the Company's common stock at the date of grant and for certain stock options subject to amended performance targets under the 1999 Equity Plan, as discussed below.
The following weighted average assumptions were used in the estimated grant date fair value calculations for stock option awards:
| |
Year Ended December 31, | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| |
2007 | 2008 | 2009 | |||||||
Risk free interest rate |
4.74 | % | 3.40 | % | 1.98 | % | ||||
Expected dividend yield |
0.00 | % | 0.00 | % | 0.00 | % | ||||
Expected stock price volatility |
60.3 | % | 53.2 | % | 60.1 | % | ||||
Average expected life (in years) |
6.60 | 6.25 | 6.25 | |||||||
The expected stock price volatility rates are based on a blend of the historical volatility of the Company's common stock and peer implied volatility. The risk free interest rates are based on the U.S. Treasury yield curve in effect at the time of grant for periods corresponding with the expected life of the option or award. The average expected life represents the weighted average period of time that options or awards granted are expected to be outstanding, as calculated using the simplified method described in ASC 718 (formerly Securities and Exchange Commission Staff Accounting Bulletin No. 107), as the Company does not have sufficient historical exercise data to provide a reasonable basis upon which to estimate the expected term.
90
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
4. Share-Based Payment (Continued)
The following table summarizes the Company's stock option activity:
| |
Number of Shares |
Weighted- Average Exercise Price |
Weighted- Average Remaining Contractual Term |
Aggregate Intrinsic Value |
||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
Outstanding at January 1, 2007 |
4,094,325 | $ | 5.93 | |||||||||||
Granted |
668,500 | 7.32 | ||||||||||||
Exercised |
(339,370 | ) | 3.24 | |||||||||||
Canceled |
(617,535 | ) | 6.24 | |||||||||||
Outstanding at December 31, 2007 |
3,805,920 | 6.36 | ||||||||||||
Granted |
505,000 | 9.20 | ||||||||||||
Exercised |
(123,795 | ) | 4.73 | |||||||||||
Canceled |
(172,950 | ) | 8.08 | |||||||||||
Outstanding at December 31, 2008 |
4,014,175 | 6.70 | ||||||||||||
Granted |
835,000 | 7.95 | ||||||||||||
Exercised |
(64,400 | ) | 4.46 | |||||||||||
Canceled |
(367,225 | ) | 7.85 | |||||||||||
Outstanding at December 31, 2009 |
4,417,550 | $ | 6.87 | 5.92 | $ | 1,709 | ||||||||
Vested and expected to vest in the future at December 31, 2009 |
3,968,666 | $ | 6.85 | 5.82 | $ | 1,552 | ||||||||
Exercisable at December 31, 2009 |
2,463,875 | $ | 6.31 | 4.50 | $ | 1,307 | ||||||||
91
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
4. Share-Based Payment (Continued)
The following table summarizes information about all stock options outstanding at December 31, 2009:
| Options Outstanding |
Exercise Price |
Weighted Average Remaining |
Options Exercisable |
Exercise Price |
|||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Contractual Life (years) |
|||||||||||||||
| 2,500 | $ | 3.55 | 3.65 | 2,500 | $ | 3.55 | |||||||||
| 184,025 | 3.67 | 4.01 | 184,025 | 3.67 | |||||||||||
| 19,250 | 4.04 | 4.42 | 19,250 | 4.04 | |||||||||||
| 497,450 | 4.19 | 6.09 | 244,550 | 4.19 | |||||||||||
| 13,000 | 4.95 | 3.37 | 13,000 | 4.95 | |||||||||||
| 99,500 | 5.19 | 3.04 | 99,500 | 5.19 | |||||||||||
| 20,000 | 5.25 | 9.62 | — | — | |||||||||||
| 1,000,000 | 5.27 | 3.01 | 1,000,000 | 5.27 | |||||||||||
| 165,000 | 5.56 | 6.26 | 112,500 | 5.56 | |||||||||||
| 35,000 | 5.60 | 0.84 | 35,000 | 5.60 | |||||||||||
| 50,000 | 6.26 | 6.95 | 25,000 | 6.26 | |||||||||||
| 5,000 | 6.28 | 6.57 | 2,500 | 6.28 | |||||||||||
| 50,000 | 6.42 | 6.64 | 25,000 | 6.42 | |||||||||||
| 26,950 | 6.46 | 6.64 | 9,450 | 6.46 | |||||||||||
| 2,500 | 6.94 | 4.77 | 2,500 | 6.94 | |||||||||||
| 235,000 | 7.05 | 7.09 | 94,000 | 7.05 | |||||||||||
| 287,500 | 7.41 | 7.12 | 74,200 | 7.41 | |||||||||||
| 200,000 | 7.49 | 6.87 | 100,000 | 7.49 | |||||||||||
| 1,000 | 7.75 | 5.77 | 1,000 | 7.75 | |||||||||||
| 1,000 | 7.91 | 6.77 | 1,000 | 7.91 | |||||||||||
| 716,000 | 8.06 | 9.00 | — | — | |||||||||||
| 35,000 | 8.24 | 6.79 | 17,500 | 8.24 | |||||||||||
| 1,000 | 8.57 | 8.77 | 333 | 8.57 | |||||||||||
| 55,000 | 8.74 | 8.78 | 13,750 | 8.74 | |||||||||||
| 320,000 | 9.26 | 8.01 | 81,500 | 9.26 | |||||||||||
| 50,000 | 9.60 | 5.22 | 40,000 | 9.60 | |||||||||||
| 1,000 | 9.74 | 7.77 | 667 | 9.74 | |||||||||||
| 329,875 | 12.35 | 5.01 | 250,150 | 12.35 | |||||||||||
| 15,000 | 13.00 | 1.59 | 15,000 | 13.00 | |||||||||||
| 4,417,550 | $ | 6.87 | 5.92 | 2,463,875 | $ | 6.31 | |||||||||
The weighted average grant-date fair value of options granted during the years ended December 31, 2007, 2008, and 2009 was $4.59 per share, $5.03 per share, and $4.57 per share, respectively. The total intrinsic value of options exercised during the years ended December 31, 2007, 2008 and 2009 was $1,574, $759, and $129, respectively. The total cash received from employees as a
92
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
4. Share-Based Payment (Continued)
result of stock option exercises was $1,109, $589, and $225 for the years ended December 31, 2007, 2008, and 2009, respectively.
The following table summarizes the Company's unvested stock option activity:
| |
Shares | Weighted Average Grant Date Fair Value |
||||||
|---|---|---|---|---|---|---|---|---|
Unvested at December 31, 2008 |
1,916,115 | $ | 4.20 | |||||
Granted |
835,000 | 4.57 | ||||||
Vested |
(593,879 | ) | 4.01 | |||||
Canceled |
(203,561 | ) | 4.59 | |||||
Unvested at December 31, 2009 |
1,953,675 | $ | 4.37 | |||||
At December 31, 2009, the total unrecognized fair value share-based payment related to unvested stock options granted to both employees and non-employees was $4,631, which is expected to be recognized over a remaining weighted-average period of 2.16 years. The valuation model applied in this calculation utilizes highly subjective assumptions that could potentially change over time, including the expected forfeiture rate and performance targets. Therefore the amount of unrecognized share-based payment noted above does not necessarily represent the amount that will ultimately be realized by the Company in the statements of operations. The total fair value of shares vested during the years ended December 31, 2007, 2008, and 2009 was $2,966, $2,305, and $2,381, respectively.
Restricted Stock Awards
The 1999 Equity Plan, as amended and restated, permits the award of restricted stock, restricted stock units, stock bonus awards and performance-based awards. During 2007 and 2008, the Company granted 625,000 and 290,000 restricted stock awards ("awards"), respectively, to certain employees of the Company. During 2009, the Company granted 310,000 awards to certain employees and 66,016 awards to non-employees of the Company. These awards cliff vest after one or five years provided that the employee remains continuously employed and the non-employee continues service through the issuance date. On December 31, 2008, the Company granted restricted stock awards to three non-employee directors of the Company who are unaffiliated with Oaktree and MTS ("unaffiliated directors") equal to 11,318 shares of common stock each. These awards to unaffiliated directors cliff vest after one year based on the unaffiliated directors' continued service with the Company through that date. During the year ended December 31, 2009, 4,558 of these shares vested due to a change in one of the unaffiliated directors in May 2009. For the years ended December 31, 2007, 2008 and 2009 the Company recorded share-based payment related to these grants of $1,006, $1,932 and $2,876, respectively. The weighted average grant-date fair value of restricted stock awards granted during the years ended December 31, 2007, 2008 and 2009 was $6.65, $8.46 and $6.20 per share, respectively.
93
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
4. Share-Based Payment (Continued)
The following table summarizes the Company's unvested restricted stock activity:
| |
Shares | Weighted Average Grant Date Fair Value |
||||||
|---|---|---|---|---|---|---|---|---|
Unvested at December 31, 2008 |
938,954 | $ | 7.25 | |||||
Granted |
376,016 | 6.20 | ||||||
Vested |
(691,954 | ) | 6.79 | |||||
Canceled |
(22,000 | ) | 7.51 | |||||
Unvested at December 31, 2009 |
601,016 | $ | 7.11 | |||||
At December 31, 2009, the total unrecognized fair value share-based payment related to the restricted stock awards granted to employees was $2,795, which is expected to be recognized over a remaining weighted-average period of 2.22 years. At December 31, 2009, the total unrecognized fair value share-based payment related to the restricted stock awards granted to unaffiliated directors was $240, which is expected to be recognized over a remaining weighted-average period of 1.00 year. The unaffiliated directors will each receive a restricted stock award on December 31, 2010 and each December 31 thereafter (the "Grant Date") of the number of shares of common stock having a value equal to $80, rounded down to the nearest whole share, and calculated using the average share price of the Company's stock over the fifteen-day period preceding the Grant Date. Such restricted stock awards will fully vest one year after the Grant Date based on the continued service of the non-employee director through the vesting date. The valuation model applied in this calculation utilizes highly subjective assumptions that could potentially change over time, including the expected forfeiture rate. Therefore the amount of unrecognized share-based payment noted above does not necessarily represent the amount that will ultimately be realized by the Company in the statements of operations.
Restricted Stock Units
On December 31, 2007, the Company granted restricted stock units to three unaffiliated directors equal to 8,421 shares of common stock each. This number of shares represents the number of shares of the Company's common stock having a value equal to $80, rounded down to the nearest whole share, and calculated using the average share price of the Company's stock over the fifteen-day period preceding December 31, 2007. These restricted stock units vested on December 31, 2008.
Stock Bonus Award
During 2006 and 2007, the Company granted stock bonus awards to certain employees of the Company. On the issuance date, the Company issued a number of shares of the Company's common stock ("shares"), equal to the award divided by the fair market value of the shares at that time, provided that the employee remained continuously employed through the issuance date. During the year ended December 31, 2009, the Company issued 125,470 shares related to the stock bonus awards granted in 2006. In January 2010, the Company issued 87,565 shares related to the stock bonus awards
94
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
4. Share-Based Payment (Continued)
granted in 2007. For the years ended December 31, 2007, 2008 and 2009, the Company recorded share-based payment related to these grants of $541, $500 and $167, respectively.
Directors' Deferred Compensation Plan
Effective January 1, 2000, the Company established a Directors' Deferred Compensation Plan (the "Director Plan") for all non-employee directors. Each of the non-employee directors has elected to participate in the Director Plan and have his annual fee of $25 deferred into a stock account and converted quarterly into Phantom Shares. During 2007, the annual fee was increased to $35. If the director elects to have his annual fee converted into Phantom Shares, then each such director has the option of being paid cash or issued common stock for his Phantom Shares, which is paid or issued upon retirement, separation from the Board of Directors, or the occurrence of a change in control. The unaffiliated directors also have the option to have their annual fee paid in quarterly cash installments. This election is made once a year. On April 16, 2007, in connection with the purchase of the Company's common stock by Oaktree and MTS from KKR, the directors who are affiliated with Oaktree and MTS ("affiliated directors") elected not to participate in the Director Plan, and instead received annual cash compensation equal to $35, which is paid quarterly to an investment fund, not to the affiliated directors, as specified by each affiliated director. In addition, on December 31 of each year, the affiliated directors also receive additional cash compensation of $80 in consideration of their Board service during the prior fiscal year. Upon separation from the Board of Directors on April 16, 2007, directors affiliated with KKR were paid cash or issued common stock, based on their applicable election, equal to their respective stock accounts on that date. For the years ended December 31, 2007, 2008 and 2009 the Company recorded director fees of $387, $419, and $509, respectively. For cash payment elections of Phantom Shares in the Director Plan, an increase (decrease) to other accrued liabilities is recorded for the difference between the current fair market value and the original issuance price of the Phantom Shares. For the issuance of common stock elections of Phantom Shares, an increase is made to APIC when director's fees are recorded. All cash elections are accrued in other accrued liabilities until payment is due and payable. At December 31, 2008 and 2009, $694 and $555, respectively was included in other accrued liabilities relating to the Director Plan.
5. Fair Value of Financial Instruments
The Company used the following methods and assumptions in estimating fair value disclosure for financial instruments:
Cash and cash equivalents The carrying amounts reported in the balance sheet approximate fair value due to the short-term maturity or variable rates of these instruments.
Debt The fair value of the Company's publicly traded notes was based on the prices of those notes at December 31, 2008 and 2009. The carrying amount of variable-rate borrowings at December 31, 2009 approximates fair value estimated based on current market rates and credit spreads for similar debt instruments.
Interest rate swaps Fair value was determined based on the income approach and standard valuation techniques to convert future amounts to a single present amount and approximates the net gains and losses that would have been realized if the contracts had been settled at each period-end.
95
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
5. Fair Value of Financial Instruments (Continued)
The estimated fair values of the Company's financial instruments are as follows:
| |
December 31, 2008 | December 31, 2009 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |
Carrying Value |
Fair Value |
Carrying Value |
Fair Value |
|||||||||
Cash and cash equivalents |
$ | 73,305 | $ | 73,305 | $ | 111,884 | $ | 111,884 | |||||
Fixed-rate debt |
289,496 | 246,750 | 193,115 | 184,189 | |||||||||
Variable-rate debt |
351,600 | 351,600 | 450,897 | 450,897 | |||||||||
Derivative instruments—asset position |
— | — | 59 | 59 | |||||||||
Derivative instruments—liability position |
6,008 | 6,008 | 2,409 | 2,409 | |||||||||
The Company adopted ASC 825 (formerly SFAS No. 157, "Fair Value Measurements" ("SFAS 157")) on January 1, 2008. ASC 825 applies to all assets and liabilities that are being measured and reported on a fair value basis. ASC 825 requires disclosure that establishes a framework for measuring fair value in GAAP, and expands disclosure about fair value measurements. This statement enables the reader of the financial statements to assess the inputs used to develop those measurements by establishing a hierarchy for ranking the quality and reliability of the information used to determine fair values. The statement requires that assets and liabilities carried at fair value will be classified and disclosed in one of the following three categories:
Level 1 Quoted market prices in active markets for identical assets or liabilities.
Level 2 Observable market based inputs or unobservable inputs that are corroborated by market data.
Level 3 Unobservable inputs that are not corroborated by market data.
The following table summarizes the valuation of the Company's recurring financial instruments by the above ASC 825 pricing levels as of December 31, 2008:
| |
Total | Quoted market prices in active markets (Level 1) |
Significant other observable inputs (Level 2) |
Significant unobservable inputs (Level 3) |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
Cash and cash equivalents |
$ | 73,305 | $ | 73,305 | $ | — | $ | — | |||||
Interest rate swaps—liability position |
6,008 | — | 6,008 | — | |||||||||
96
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
5. Fair Value of Financial Instruments (Continued)
The following table summarizes the valuation of the Company's recurring financial instruments by the above ASC 825 pricing levels as of December 31, 2009:
| |
Total | Quoted market prices in active markets (Level 1) |
Significant other observable inputs (Level 2) |
Significant unobservable inputs (Level 3) |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
Cash and cash equivalents |
$ | 111,884 | $ | 111,884 | $ | — | $ | — | |||||
Interest rate swaps—liability position |
2,409 | — | 2,409 | — | |||||||||
Fuel swap—asset position |
59 | — | — | 59 | |||||||||
In 2007, 2008 and 2009 the Company concluded that no impairment was present in its intangible assets.
The following table summarizes the Company's fair value measurements of derivative instruments using significant unobservable inputs (Level 3):
Balance as of December 31, 2008 |
$ | — | ||||
Total gains or losses (realized/unrealized) |
||||||
Included in earnings |
13 | |||||
Included in other comprehensive income |
46 | |||||
Balance as of December 31, 2009 |
$ | 59 | ||||
The amount of total gains or losses for the period included in earnings attributable to the change in unrealized gains or losses relating to assets still held at the reporting date |
$ | 13 | ||||
The Company's derivative instruments are primarily pay-fixed, receive- variable interest rate swaps based on LIBOR swap rate. The Company has elected to use the income approach to value these derivatives, using observable Level 2 market expectations at measurement date and standard valuation techniques to convert future amounts to a single present amount assuming that participants are motivated, but not compelled to transact. Level 2 inputs for interest rate swap valuations are limited to quoted prices for similar assets or liabilities in active markets (specifically futures contracts on LIBOR for the first two years) and inputs other than quoted prices that are observable for the asset or liability (specifically LIBOR cash and swap rates at commonly quoted intervals). The Company has identified both a public and a private data source for use in valuing the Department of Energy ("DOE") diesel fuel swap. There appears to be a material difference in the pricing for diesel fuel contracts traded on NYMEX and the pricing that brokers make available to retail clients hedging changes in the DOE average national diesel fuel price as executed by the Company. As a result the Company has elected to use broker data available from its counterparty and informally corroborated by a second broker to fair value the diesel fuel swap. The December 31, 2009 over-the-counter forward rates were compared to the fixed rates executed by the Company for each forward date. The loss on each forward date was
97
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
5. Fair Value of Financial Instruments (Continued)
then present valued at LIBOR plus a credit spread of 4.0%. Mid-market pricing is used as a practical expedient for fair value measurements. ASC 820 states that the fair value measurement of an asset or liability must reflect the nonperformance risk of the entity and the counterparty. Therefore, the impact of the counterparty's creditworthiness and the Company's creditworthiness has also been factored into the fair value measurement of the derivative instruments. For additional information please see Note 11 of the Notes to the Consolidated Financial Statements.
6. Marketable Securities
Investments with original maturities greater than 90 days are accounted for in accordance with ASC 320, "Investments—Debt and Equity Securities" (formerly SFAS No. 115, "Accounting for Certain Investments in Debt and Equity Securities"), and are classified accordingly by the Company at the time of purchase. In accordance with the provisions of ASC 320, the Company's investments in marketable securities are classified as "available-for-sale." During 2007 the Company's investments in marketable securities consisted of investment grade auction rate securities and debt securities. Auction rate securities are variable rate bonds tied to short-term `interest rates with maturities on the face of the securities in excess of 90 days. Auction rate securities have interest rate resets through a modified Dutch auction, at predetermined short-term intervals, usually every 1, 7, 28 or 35 days. Auction rate securities are reported at fair value. Due to the frequent nature of their reset feature, the auction rate securities' market prices approximate their fair value. Debt securities are carried at fair market value, and any unrealized gains or temporary unrealized losses, net of income tax effects, are reported as a component of other comprehensive income. The Company did not recognize any gains or losses associated with the sales of marketable securities during 2007, 2008 and 2009. The Company did not have any marketable securities at December 31, 2008 and 2009.
7. Goodwill and Intangible Assets
Changes in the carrying amount of goodwill are as follows:
Balance at January 1, 2008 |
$ | 175,804 | ||
Goodwill acquired during the period |
18,934 | |||
Adjustments to goodwill during the period |
(1,308 | ) | ||
Balance at December 31, 2008 |
193,430 | |||
Goodwill acquired during the period |
378 | |||
Adjustments to goodwill during the period |
435 | |||
Balance at December 31, 2009 |
$ | 194,243 | ||
98
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
7. Goodwill and Intangible Assets (Continued)
Intangible assets consisted of the following:
| |
December 31, 2008 | December 31, 2009 | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |
Gross Carrying Amount |
Accumulated Amortization |
Intangible Assets, net |
Gross Carrying Amount |
Accumulated Amortization |
Intangible Assets, net |
||||||||||||||
Amortizing intangible assets: |
||||||||||||||||||||
Customer contracts |
$ | 89,853 | $ | (33,818 | ) | $ | 56,035 | $ | 89,708 | $ | (41,701 | ) | $ | 48,007 | ||||||
Other |
14,364 | (5,708 | ) | 8,656 | 16,407 | (8,825 | ) | 7,582 | ||||||||||||
Total amortizing intangible assets |
$ | 104,217 | $ | (39,526 | ) | $ | 64,691 | $ | 106,115 | $ | (50,526 | ) | $ | 55,589 | ||||||
Intangible assets not subject to amortization |
46,029 | 44,599 | ||||||||||||||||||
Total other intangible assets |
$ | 110,720 | $ | 100,188 | ||||||||||||||||
The Company reviews the recoverability of the carrying value of goodwill on an annual basis or more frequently when an event occurs or circumstances change to indicate an impairment of these assets has possibly occurred. Goodwill is allocated to the Company's various reporting units, which represent the Company's geographical regions. The Company compares the fair value of the reporting unit to its carrying amount to determine if there is potential impairment.
The Company uses the estimated useful life to amortize customer contracts, which is a weighted average of 15 years. Other intangible assets subject to amortization are estimated to have a weighted average useful life of four years. Amortization expense for intangible assets subject to amortization was $5,195, $8,696 and $11,000 for the years ended December 31, 2007, 2008 and 2009, respectively. The intangible assets not subject to amortization represent certificates of need and regulatory authority rights which have indefinite useful lives.
Estimated annual amortization expense for each of the fiscal years ending December 31, is presented below:
2010 |
$ | 10,922 | ||
2011 |
10,354 | |||
2012 |
8,693 | |||
2013 |
5,909 | |||
2014 |
4,239 |
99
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
8. Other Accrued Liabilities
Other accrued liabilities consisted of the following:
| |
December 31, 2008 |
December 31, 2009 |
|||||
|---|---|---|---|---|---|---|---|
Accrued systems rental and maintenance costs |
$ | 2,223 | $ | 1,128 | |||
Accrued site rental fees |
1,244 | 1,079 | |||||
Accrued property and sales taxes payable |
14,867 | 16,037 | |||||
Accrued self-insurance expense |
7,380 | 6,095 | |||||
Accrued equipment payments |
4,483 | 380 | |||||
Other accrued expenses |
8,249 | 8,168 | |||||
Total |
$ | 38,446 | $ | 32,887 | |||
9. Long-Term Debt and Senior Subordinated Credit Facility
Long-term debt consisted of the following:
| |
December 31, 2008 |
December 31, 2009 |
|||||
|---|---|---|---|---|---|---|---|
Term loan facility |
$ | 351,600 | $ | 460,000 | |||
Discount on term loan facility of 5.87% |
— | (9,103 | ) | ||||
Senior subordinated notes |
300,000 | 5,582 | |||||
Discount on senior subordinated notes of 8.25% |
(10,504 | ) | — | ||||
Senior notes |
— | 190,000 | |||||
Discount on senior notes of 8.25% |
— | (2,467 | ) | ||||
Equipment debt |
21,466 | 23,878 | |||||
Long-term debt, including current portion |
662,562 | 667,890 | |||||
Less current portion |
7,743 | 16,902 | |||||
Long-term debt |
$ | 654,819 | $ | 650,988 | |||
Bank Credit Facilities On November 2, 1999, the Company entered into a $616,000 Credit Agreement (the "Credit Agreement") consisting of a $131,000 Tranche A Term Loan Facility, a $150,000 Tranche B Term Facility, a $185,000 Tranche C Term Loan Facility, and a Revolving Loan Facility (the "Old Revolving Credit Facility"). On June 11, 2002, the Company entered into a second amendment to its Credit Agreement in order to complete a $286,000 refinancing of its Tranche B and C term loan facility. Under the terms of the amended term loan facility, the Company received proceeds of $286,000 from a new Tranche C term loan facility, and used the entire amount of the proceeds to retire $145,500 and $140,500 owed under Tranche B and C of its existing term loan facility, respectively. The new Tranche C borrowing rate was decreased to the LIBOR plus 2.375%. The borrowing rate under the previously applicable Tranche B borrowing rate had been LIBOR plus 2.750% and the previously applicable Tranche C borrowing rate had been LIBOR plus 3.000%.
100
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
9. Long-Term Debt and Senior Subordinated Credit Facility (Continued)
On December 29, 2004, the Company entered into a third amendment to its Credit Agreement which revised the Tranche C term loan facility ("Old Term Loan") resulting in incremental borrowings of $154,000 and decreased the maximum amount of availability under the existing revolving loan facility from $150,000 to $70,000. The proceeds from the amendment were used to complete a cash tender offer (the "2004 Tender Offer") to retire $256,459 of the $260,000 103/8% Senior Subordinated Notes due 2011, as discussed below. The Old Term Loan borrowing rate decreased to LIBOR plus 2.250%. On December 19, 2005 the Company entered into a fourth amendment to its Credit Agreement which revised the Company's maximum consolidated leverage ratio covenant to a level not to exceed 4.00 to 1.00 as of the last day of any fiscal quarter until the expiration of the agreement. Prior to the fourth amendment, the Company's maximum consolidated leverage ratio covenant was 3.75 to 1.00 as of the last day of any fiscal quarter beginning March 31, 2006 to the expiration of the agreement. The fourth amendment also requires the Company to maintain a maximum consolidated senior leverage ratio covenant at a level not to exceed 3.00 to 1.00 as of the last day of any fiscal quarter. The amendment increased the Old Term Loan LIBOR margin from an annual rate of 2.250% to 2.500%. At December 31, 2008, the Company did not have any borrowings outstanding under the revolving loan facility. In connection with the amendment, the Company incurred an amendment fee of $594.
In December 2009, the Company entered into a new senior secured credit agreement (the "New Credit Facility"), comprised of a $460,000 term loan (the "New Term Loan") maturing June 2016 and a $120,000 revolving facility (the "New Revolving Credit Facility") maturing December 2014. The Company used the proceeds from the New Term Loan to retire $351,600 of its Old Term Loan. Borrowings under the New Term Loan were issued at 98.0% of par, with the discount to par being amortized to interest expense and other, net through the maturity date of the loan. Borrowings under the New Credit Facility bear interest through maturity at a variable rate based upon, at the Company's option, either London InterBank Offered Rate ("LIBOR") or the base rate (which is the highest of the administrative agent's prime rate, one-half of 1.00% in excess of the overnight federal funds rate, and 1.00% in excess of the one-month LIBOR rate), plus in each case, an applicable margin. With respect to the New Term Loan, the applicable margin for LIBOR loans is 3.50% per annum, and with respect to the New Revolving Credit Facility, the applicable margin for LIBOR loans ranges, based on the applicable leverage ratio, from 3.25% to 3.75% per annum, in each case, with a LIBOR floor of 2.00%. With respect to the New Term Loan, the applicable margin for base rate loans is 2.50% per annum, and with respect to the New Revolving Credit Facility, the applicable margin for base rate loans ranges, based on the applicable leverage ratio, from 2.25% to 2.75% per annum.
As of December 31, 2009, the Company had $115,540 of available borrowings under the New Revolving Credit Facility, but did not have any borrowings outstanding. In addition to other covenants, the New Credit Facility places limits on the Company's and its subsidiaries' ability to declare dividends or redeem or repurchase capital stock, prepay, redeem or purchase debt, incur liens and engage in sale-leaseback transactions, make loans and investments, incur additional indebtedness, amend or otherwise alter debt and other material agreements, make capital expenditures, engage in mergers, acquisitions and asset sales, transact with affiliates and alter the business conducted by the Company and its subsidiaries. The New Credit Facility also contains financial covenants requiring the Company to maintain (i) a maximum ratio of consolidated total debt to consolidated adjusted EBITDA that ranges
101
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
9. Long-Term Debt and Senior Subordinated Credit Facility (Continued)
from 4.75 to 1.00 to 4.00 to 1.00 and (ii) a minimum ratio of consolidated adjusted EBITDA to consolidated interest expense of 2.75 to 1.00. Within 180 days after the closing date of the New Credit Facility, which occurred December 1, 2009, the Company is required to enter into agreements such as interest rate swaps, caps, floors and other interest rate exchange contracts that would have the effect of fixing the rate of a specified percentage of the Company's variable rate debt for periods to be determined.
As of December 31, 2009, the Company was in compliance with all covenants under the New Credit Facility. Voluntary prepayments are permitted in whole or in part without premium or penalty. The Company has not made voluntary prepayments on the New Term Loan. As noted in the maturities schedule, principal payments are required annually for the New Term Loan.
The weighted average interest rate of the Old Term Loan at December 31, 2008 was 5.232%. The weighted average interest rate of the New Term Loan at December 31, 2009 was 5.523%. There were no borrowings outstanding under the Old Revolving Credit Facility at December 31, 2008 and there we no borrowings outstanding under the New Revolving Credit Facility at December 31, 2009. The Company pays a commitment fee equal to 0.50% per annum on the undrawn portion available under the New Revolving Credit Facility. The Company also pays variable per annum fees in respect of outstanding letters of credit. At December 31, 2009 the Company had $4,460 of outstanding letters of credit. The New Credit Facility is collateralized by the Company's equity interests in its majority owned subsidiaries, partnerships and limited liability companies and its unencumbered assets, which include accounts receivable, inventory, equipment, and intellectual property. At December 31, 2009, the Company had an unamortized discount of $9,103 related to the New Term Loan.
103/8% Senior Subordinated Notes In December 2004 the Company completed the 2004 Tender Offer for any and all of its outstanding 103/8% Notes. The Company redeemed the 103/8% Notes at a redemption price equal to 113.856% of the principal amount, together with the accrued interest to the redemption date. The Company used the remaining proceeds from the Old Term Loan, proceeds from the sale of the original 71/4% Notes described below, and existing cash to settle the tender premium and consent payment. In April 2008, the Company paid the remaining balance of $3,541 related to the 103/8% Senior Subordinated Notes and recorded $61 in loss on extinguishment of debt.
71/4% Senior Subordinated Notes On December 29, 2004, the Company issued $150,000 of its 71/4% Senior Subordinated Notes due 2012 (the "original 71/4% Notes") in a transaction exempt from the registration requirements of the Securities Act of 1933, as amended, and used the proceeds to repay a portion of its 103/8% Notes. The original 71/4% Notes were subsequently registered on February 1, 2005. On December 4, 2007, the Company issued an additional $150,000 of its 71/4% Senior Subordinated Notes due 2012 (the "new 71/4% Notes") in a transaction exempt from the registration requirements of the Securities Act of 1933, as amended. The new 71/4% Notes were subsequently registered on January 25, 2008 and are fully guaranteed by the Company. No subsidiary of the Company guarantees these Notes. The new 71/4% Notes were issued at a discount of 8.5%, which was being amortized to interest expense through the maturity date of the notes. The new 71/4% Notes have terms that were substantially identical to the Company's original 71/4% Notes, but were issued under a new indenture and are therefore a separate series of notes. The Company used a portion of the net
102
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
9. Long-Term Debt and Senior Subordinated Credit Facility (Continued)
proceeds from the issuance of the new 71/4% Notes to repay and terminate the Acquisition Credit Facility (as described below). The remaining net proceeds were used for general corporate purposes, including acquisitions. The original 71/4% Notes and the new 71/4% Notes are collectively referred to as the "71/4% Notes." The 71/4% Notes contained restrictive covenants which, among other things, limit the incurrence of additional indebtedness, dividends, transactions with affiliates, asset sales, acquisitions, mergers and consolidations, liens and encumbrances, and restrictive payments. The 71/4% Notes were unsecured senior subordinated obligations and were subordinated in right of payment to all existing and future senior debt, including bank debt, and all obligations of its subsidiaries. As of December 31, 2009, the Company was in compliance with all covenants contained in the 71/4% Notes.
In December 2009 the Company completed a cash tender offer (the "2009 Tender Offer") for any and all of its outstanding 71/4% Notes. The Company purchased the 71/4% Notes at a purchase price equal to 100.125% of the principal amount, together with the accrued interest to the purchase date. The Company incurred a loss on extinguishment of debt of $14,600 related to the Refinance Transaction, which represents the tender premium and consent payment to redeem the 71/4% Notes, write-off of unamortized debt issuance costs related to the retired debt, and other fees and expenses. At December 31, 2009, the Company had a remaining balance of $5,582 related to the 71/4% Notes. The remaining balance was redeemed at par, together with accrued interest to the redemption date, in January 2010.
8% Senior Notes In December 2009, the Company issued $190,000 of 8.0% senior notes due 2016 (the "8% Notes") in a transaction that was exempt from the registration requirements of the Securities Act of 1933, as amended. The Company used the proceeds from this transaction, the New Term Loan and existing cash to complete the 2009 Tender Offer and purchase $294,418 of the 71/4% Notes at a purchase price equal to 100.125% of the principal amount, together with the accrued interest to the redemption date. The 8% Notes were issued at 98.690% of par, with the discount to par being amortized to interest expense and other, net through the maturity date of the notes. No subsidiary of the Company guarantees these Notes. The indenture governing the 8% Notes contains covenants limiting the Company's and most of its subsidiaries' ability to pay dividends and make other restricted payments, incur additional indebtedness or issue disqualified stock, create liens on assets, merge, consolidate, or sell all or substantially all of its assets, and enter into transactions with affiliates, among others. The 8% Notes are unsecured senior obligations and are equal in right of payment to all existing and future senior debt, and rank senior in right of payment to all of the Company's existing and future subordinated debt. The 8% Notes are effectively subordinated in right of payment to all of the Company's existing and future secured indebtedness, including indebtedness under the New Credit Facility, to the extent of assets securing such indebtedness, and are effectively subordinated in right of payment to all obligations of the Company's subsidiaries. At December 31, 2009, the Company had an unamortized discount of $2,467 related to the 8% Notes. As of December 31, 2009, the Company was in compliance with all covenants contained in the 8% Notes.
103
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
9. Long-Term Debt and Senior Subordinated Credit Facility (Continued)
Acquisition Credit Facility On November 5, 2007, the Company completed an Acquisition Credit Agreement for a $50,000 six-month term loan facility, maturing May 5, 2008. The proceeds of the term loan facility were incurred to finance the NEHE Acquisition. The facility bore interest at 8.50% for the period the term loan facility was outstanding. The Acquisition Credit Facility was repaid and terminated on December 4, 2007, with the net proceeds from the issuance of the new 71/4% Notes.
The maturities of long-term debt as of December 31, 2009 are as follows:
| |
|
Bank Credit Facilites | |
||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |
New Term Loan | Senior Subordinated Notes |
Senior Notes |
Equipment Loans |
Total | ||||||||||||
Year ending December 31: |
|||||||||||||||||
2010 |
$ | 4,600 | $ | 5,582 | $ | — | $ | 6,720 | $ | 16,902 | |||||||
2011 |
4,600 | — | — | 4,858 | 9,458 | ||||||||||||
2012 |
4,600 | — | — | 3,950 | 8,550 | ||||||||||||
2013 |
4,600 | — | — | 3,755 | 8,355 | ||||||||||||
2014 |
4,600 | — | — | 3,104 | 7,704 | ||||||||||||
Thereafter |
437,000 | — | 190,000 | 1,491 | 628,491 | ||||||||||||
|
$ | 460,000 | $ | 5,582 | $ | 190,000 | $ | 23,878 | $ | 679,460 | |||||||
The remaining $5,582 of the 71/4% notes were redeemed in January 2010 at a redemption price equal to 100.0% of the principal amount, together with accrued interest to the redemption date.
10. Earnings Per Common Share
Effective January 1, 2009, the Company adopted ASC 260 (formerly FSP 03-6-1). ASC 260 addresses whether instruments granted in share-based payment transactions are participating securities prior to vesting and therefore need to be included in the earnings allocation in calculating earnings per share under the two-class method described in ASC 260. ASC 260 requires companies to treat unvested share-based payment awards that have non-forfeitable rights to dividend or dividend equivalents as a separate class of securities in calculating earnings per share. The Company granted and expects to continue to grant restricted stock awards to its officers and non-employee directors that contain non-forfeitable rights to dividends. Such awards are considered participating securities under ASC 260. As such, the Company is required to include these awards in the calculation of the Company's basic earnings per share and calculate basic earnings per share using the two-class method. Restricted stock awards have previously been included in the Company's dilutive earnings per share calculation using the treasury stock method. The two-class method of computing earnings per share is an earnings allocation formula that determines earnings per share for each class of common stock and participating security according to dividends declared (or accumulated) and participation rights in undistributed earnings. The Company has historically not paid and does not expect to pay dividends in the foreseeable future; however, the Company must still allocate undistributed earnings between common shareholders and participating securities based on the contractual rights of each security, as if all the earnings for the period have been distributed. Since the adoption of ASC 260 is to be applied
104
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
10. Earnings Per Common Share (Continued)
retrospectively, the earnings per share for prior periods was recalculated to conform to the current year presentation. The weighted-average number of shares used in the basic earnings per share calculation for the years ended December 31, 2007 and 2008 have been recalculated using the two-class method to conform to the current year presentation.
Basic net income per share is computed utilizing the two-class method and is calculated based on weighted-average number of common shares outstanding during the periods presented, excluding nonvested restricted stock units which do not contain nonforfeitable rights to dividend and dividend equivalents.
Diluted net income per share is computed using the weighted-average number of common and common equivalent shares outstanding during the periods utilizing the two-class method for stock options, nonvested restricted stock and nonvested restricted stock units. Potentially dilutive securities are not considered in the calculation of net loss per share as their impact would be anti-dilutive.
The following table sets forth the computation of basic and diluted earnings per share (amounts in thousands, except per share amounts):
| |
Year Ended December 31, | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |
2007 | 2008 | 2009 | |||||||||
Numerator: |
||||||||||||
Net income attributable to Alliance |
||||||||||||
HealthCare Services, Inc. |
$ | 16,232 | $ | 16,523 | $ | 481 | ||||||
Denominator: |
||||||||||||
Weighted-average shares-basic |
50,563 | 51,296 | 51,738 | |||||||||
Effect of dilutive securities: |
||||||||||||
Employee stock options |
1,019 | 863 | 417 | |||||||||
Weighted-average shares-diluted |
51,582 | 52,159 | 52,155 | |||||||||
Earnings per common share attributable to Alliance HealthCare Services, Inc.: |
||||||||||||
Basic |
$ | 0.32 | $ | 0.32 | $ | 0.01 | ||||||
Diluted |
$ | 0.31 | $ | 0.32 | $ | 0.01 | ||||||
Stock options excluded from the computation of diluted per share amounts: |
||||||||||||
Weighted- average shares for which the exercise price exceeds average market price of common stock |
536 | 927 | 2,428 | |||||||||
Average exercise price per share that exceeds average market price of common stock |
$ | 11.79 | $ | 10.59 | $ | 8.70 | ||||||
105
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
11. Derivatives
The Company accounts for derivative instruments and hedging activities in accordance with the provisions of ASC 815 (formerly SFAS 133, "Accounting for Derivative Instruments and Hedging Activities" ("SFAS 133")). Management generally designates derivatives in a hedge relationship with the identified exposure on the date the Company enters into a derivative contract, as disclosed below. The Company only executes derivative instruments that are economic hedges of exposures that can qualify in hedge relationships under ASC 815. The Company formally documents all relationships between hedging instruments and hedged items, as well as the risk-management objective and strategy for undertaking various hedge transactions. In this documentation, the Company specifically identifies the firm commitment or forecasted transaction that has been designated as a hedged item and states how the hedging instrument is expected to hedge the risks related to the hedged item. The Company formally assesses effectiveness of its hedging relationships, both at the hedge inception and on an ongoing basis, then measures and records ineffectiveness. The Company would discontinue hedge accounting prospectively (i) if it is determined that the derivative is no longer effective in offsetting change in the cash flows of a hedged item, (ii) when the derivative expires or is sold, terminated or exercised, (iii) because it is probable that the forecasted transaction will not occur, or (iv) if management determines that designation of the derivative as a hedge instrument is no longer appropriate. The Company's derivatives are recorded on the balance sheet at their fair value. For additional information please see Note 5 of the Notes to the Condensed Consolidated Financial Statements. For derivatives accounted for as cash flow hedges, any effective unrealized gains or losses on fair value are included in comprehensive income (loss), net of tax, and any ineffective gains or losses are recognized in income immediately. Amounts recorded in comprehensive income (loss) are reclassified to earnings when the hedged item impacts earnings.
Cash Flow Hedges
Interest Rate Cash Flow Hedges
The Company has entered into multiple interest rate swap agreements to hedge the future cash interest payments on portions of its variable rate bank debt. For the years ended December 31, 2008 and 2009, the Company had interest rate swap agreements to hedge approximately $185,438 and $92,719 of its variable rate bank debt, respectively, or 28.3% and 13.9% of total debt, respectively. Over the next twelve months, the Company expects to reclassify $3,882 from accumulated other comprehensive loss to interest expense and other, net.
In the first quarter of 2005, the Company entered into multiple interest rate collar agreements for its variable rate bank debt. The total underlying notional amount of the debt was $178,000. Under these arrangements the Company purchased a cap on the interest rate of 4.00% and sold a floor of 2.25%. The Company paid a net purchase price of $1,462 for these collars. These agreements were two and three years in length and matured at various dates between January 2007 and January 2008. The Company designated these collars as cash flow hedges of variable future cash flows associated with its long-term debt and effective gains or losses were reclassified to interest expense and other, net when the hedged interest was accrued.
106
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
11. Derivatives (Continued)
In the first quarter of 2008, the Company entered into two interest rate swap agreements in accordance with Company policy in order to avoid unplanned volatility in the income statement due to changes in the LIBOR interest rate environment. The swap agreements, with a total notional amount of $185,438, were designated as cash flow hedges of future cash interest payments associated with a portion of the Company's variable rate bank debt (the "2008 swaps"). These agreements are three years in length and mature in January 2011. Under the terms of these agreements, the Company receives three-month LIBOR and pays a fixed rate of 3.15%. The net effect of the hedges was to record interest expense at a fixed rate of 5.65%, as the underlying debt incurred interest based on three-month LIBOR plus 2.50%. See below for additional information regarding the 2008 swaps. As discussed below, the Company elected to terminate and replace one of the 2008 swaps in the first quarter of 2009.
On September 15, 2008, Lehman Brothers Holdings, Inc. ("LHI") filed for bankruptcy protection under Chapter 11 of the United States Bankruptcy Code. On October 6, 2008, Lehman Commercial Paper, Inc. ("LCPI") filed for bankruptcy protection under Chapter 11 of the United States Bankruptcy Code. One of the Company's 2008 swaps with a notional amount of $92,719 was with LCPI (the "Lehman Swap"). As of September 12, 2008, hedge accounting was terminated and all further changes in the fair market value of this swap were recorded in interest expense and other, net. Comprehensive income (loss) related to effective unrealized gains or losses on the fair value of the swap through September 12, 2008 will remain in accumulated comprehensive income (loss) on the balance sheet and will be amortized into interest expense and other, net through 2011 as the underlying interest payments are recognized in earnings. The swap was valued using the income approach with observable Level 2 market expectations at the measurement date and standard valuation techniques to convert future amounts to a single discounted present amount.
During the first quarter of 2009, the Company replaced the Lehman Swap with an interest rate swap agreement which has a notional amount of $92,719 (the "2009 Swap Replacement") that has been designated as a cash flow hedge of variable future cash flows associated with a portion of the Company's long-term debt. Under the terms of this agreement, which matures in January 2011, the Company receives three-month LIBOR and pays a fixed rate of 3.15%. The net effect of the hedge is to record interest expense at a fixed rate of 5.65%, as the debt incurred interest based on three-month LIBOR plus 2.50%.
Additionally, during the first quarter of 2009, the Company entered into an additional interest rate swap agreement which has a notional amount of $56,813 that has been designated as a cash flow hedge of future interest payments associated with a portion of the Company's variable rate bank debt (the "New 2009 Swap"). Under the terms of this agreement, which was to mature in November 2011, the Company received three-month LIBOR and paid a fixed rate of 2.07%. The net effect of the hedge is to record interest expense at a fixed rate of 4.57%, as the underlying debt incurs interest based on three-month LIBOR plus 2.50%.
The Company elected to terminate one of the 2008 swaps and the New 2009 Swap in December 2009 in connection with entering into the Refinance Transaction on December 1, 2009. As a result of the Refinance Transaction, the Company de-designated the 2008 swap, the 2009 Swap Replacement and
107
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
11. Derivatives (Continued)
the New 2009 Swap and hedge accounting was terminated and all further changes in the fair market value of the terminated swaps are being recorded in interest expense and other. Comprehensive income (loss) related to effective unrealized gains or losses on the fair value of the terminated swaps through September 30, 2009 remain in accumulated comprehensive income (loss) on the balance sheet and will be amortized into interest expense and other as the underlying interest payments are recognized in earnings. The terminated swaps were valued using the income approach with observable Level 2 market expectations at the measurement date and standard valuation techniques to convert future amounts to a single discounted present amount.
Diesel Fuel Cash Flow Hedges
The Company is exposed to market fluctuations in diesel fuel prices related to its mobile fleet. During the first quarter of 2009, the Company entered into a diesel fuel swap agreement which has a notional quantity of 1,008,000 gallons, or 84,000 gallons per month, to hedge future cash payments associated with the Company purchasing diesel fuel for its mobile fleet. Under the terms of this agreement, which matures in February 2010, the Company receives the Department of Energy published monthly average price per gallon and pays a fixed rate of two dollars and sixty-three cents per gallon. The Company designated this swap as a cash flow hedge of future cash flows associated with its diesel fuel payments. The swap was designated in a cash flow relationship in the month following execution. The loss from trade date to designation date was recorded in other (income) and expense, net. Post-designation the Company records effective changes in the fair value of the swap through comprehensive income (loss) and reclassifies gains or losses to fuel expense (included in cost of revenues, excluding depreciation and amortization) when the underlying fuel is purchased.
Quantitative information about the Company's derivatives' impact on performance and operations is provided below:
| |
Asset Derivatives as of December 31, 2009 | |||||
|---|---|---|---|---|---|---|
| |
Balance Sheet Location |
Fair Value | ||||
Derivatives designated as hedging instruments |
Other assets | $ | 59 | |||
| |
Liability Derivatives as of December 31, 2009 |
|||||
|---|---|---|---|---|---|---|
| |
Balance Sheet Location |
Fair Value | ||||
Derivatives designated as hedging instruments |
Other liabilities | $ | 2,409 | |||
108
ALLIANCE HEALTHCARE SERVICES, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS (Continued)
DECEMBER 31, 2009
(dollars in thousands, except per share amounts)
11. Derivatives (Continued)